Container ship operator CMA CGM is revising steering guidance across its fleet after ambiguous procedures contributed to one of its ships colliding with a navigational beacon in the Yarra River, an ATSB investigation report notes.
Departing the Port of Melbourne on 25 May 2023 under the conduct of a harbour pilot, container ship CMA CGM Puccini contacted the navigational beacon after swinging wide in a turn when its rudder began responding erratically to helm orders.
The ship was slowed and returned towards the middle of the channel, before being stabilised with tug assistance and then conducted to nearby Webb Dock. While the ship sustained minor hull paint damage, the beacon was significantly damaged.
An ATSB investigation concluded that the erratic steering was the result of a hydraulic bypass valve being left open by crew after an AMSA port state control inspection the day before the incident.
“Notably, the manipulation of steering hydraulics in this way was not required for the demonstration required for the inspection,” Chief Commissioner Angus Mitchell said.
“However, the ship’s responsible officers had an incomplete understanding of how the steering gear operated, and therefore incorrectly configured the steering system hydraulics.”
The ATSB’s investigation identified the risk of this happening was heightened by ambiguous language in CMA CGM’s fleetwide safety management system steering gear procedures.
Specifically, the procedures only referred to ‘steering gear failure’, instead of using common industry terms, such as ‘emergency steering’ and ‘local steering’. In addition, terminology within the guidance was not clearly and explicitly defined.
As a result of the investigation, CMA CGM has advised the ATSB that its fleetwide ‘steering gear failure’ procedure will be amended and titled the ‘emergency steering procedure’, and improved for clarity.
Mr Mitchell welcomed the safety action, noting it had the potential to prevent serious incidents and accidents not only in Australian ports, but overseas.
“Any loss of steering can imperil the safety of the ship, and life at sea,” Mr Mitchell said.
“Unclear or ambiguous operating instructions and terminology should be corrected as soon as they are identified.”
The investigation also found that several officers on board were not as proficient with steering gear operation and change of control modes as was required by international regulations.
“This incident highlights to seafarers and shore management the importance of ensuring shipboard personnel understand and are competent in how the ship’s steering machinery and control systems operate.”
Mr Mitchell also welcomed safety action taken by Ports Victoria in updating the harbour master’s directions for Melbourne to enhance towage requirements in the Yarra River and including advice for the crews of ships that experience a main engine or steering failure while transiting port waters.
“While not associated with any safety issue identified by the investigation, we acknowledge this positive safety action in response to this incident.”
On 23 November 2024, a Cessna 172F aircraft was being used to conduct a recency flight at Lismore Airport, New South Wales. On board was the pilot operating under a private pilot’s licence and a passenger with a recreational instructor rating. The pilot in command decided to conduct various configuration-based scenarios such as short field approaches and landings during the flight.
During a simulated short field landing scenario, the aircraft descended toward the runway and collided with a fence located at the beginning of the tarmac prior to the threshold of runway 15. The aircraft’s propeller, landing gear and engine cowling proceeded to strike the runway resulting in the aircraft rotating 180 degrees on the ground. During the rotation, the rear fuselage impacted the runway, and the aircraft slid on the bitumen for approximately 5 metres before coming to a stop.
The aircraft sustained substantial damage to the fuselage, wing, undercarriage and engine/propeller. The pilot and passenger were uninjured in the accident.
Figure 1: Propeller damage
Source: Aerodrome Operator, annotated by the ATSB
Safety message
Pilots must ensure that they are continually assessing both the aircraft’s profile and airspeed, especially during low-speed operations. Should the aircraft become unstable, conduct a missed approach.
This occurrence also highlights the importance of monitoring and assessing the landing area, taking into consideration all natural obstacles and infrastructure around the aerodrome.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
On 23 August 2024, a Bombardier Dash 8-300 was being operated as a ferry flight, departing Perth Airport, Western Australia to Onslow Airport before refuelling and continuing on to Minderoo aircraft landing area (ALA). On board was a captain, first officer and 2 cabin crew. The aircraft was then operated as a non-scheduled air transport passenger flight on the return leg from Minderoo ALA to Perth Airport.
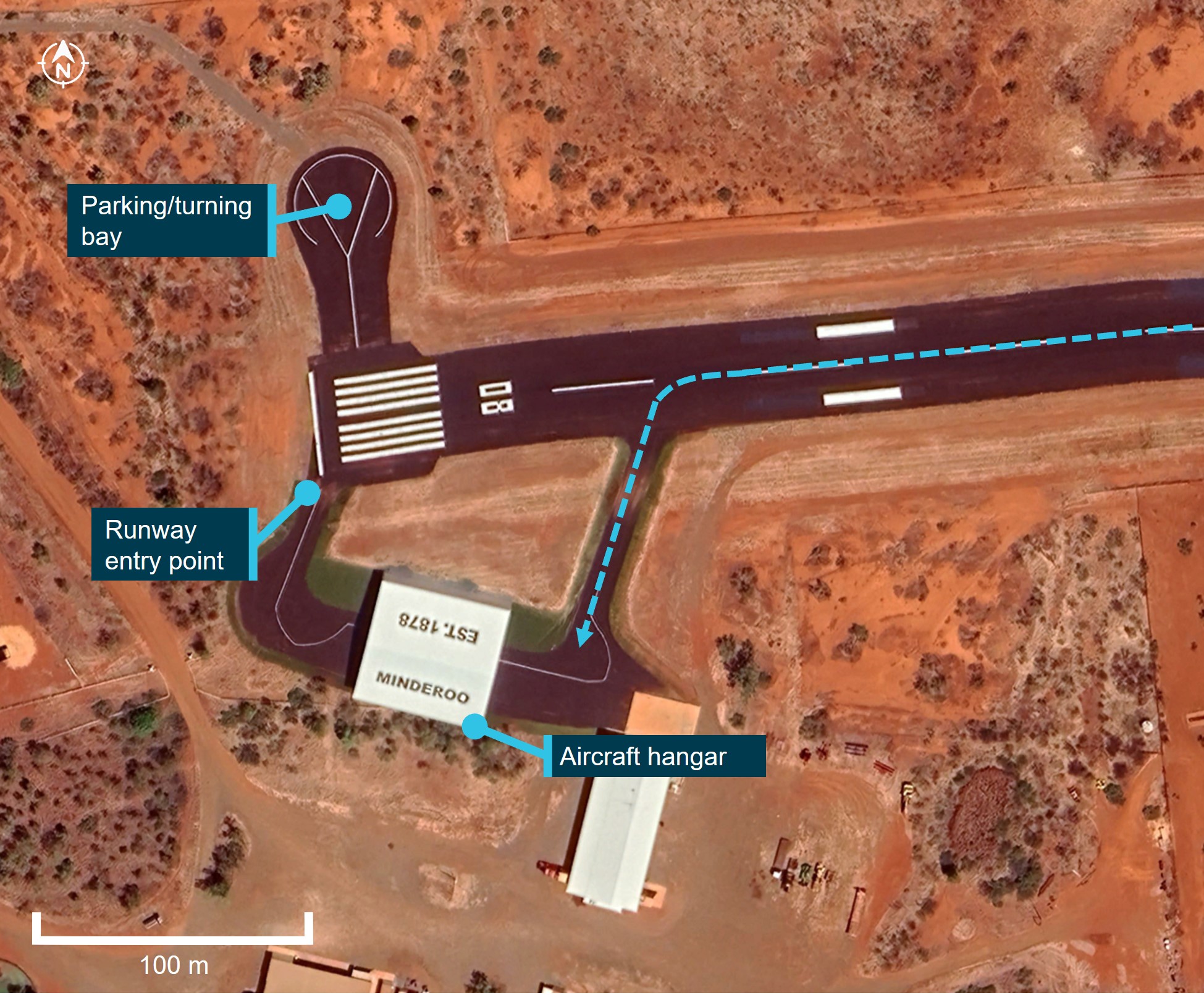
The aircraft departed Onslow at approximately 1402 local time for the 17-minute flight to Minderoo ALA. On approach to Minderoo, the captain made contact with another aircraft which was positioned on the taxiway near the threshold of runway 08, awaiting departure. The crew of this second aircraft instructed the captain to taxi into an open-ended hangar after landing to allow their aircraft to depart on runway 08, as the only other parking bay was occupied by a helicopter. The first officer, who was pilot flying, landed the aircraft on runway 26 and vacated at the first taxiway into a large hangar located on the south side of the runway (Figure 1).
At approximately 1446, the crew completed boarding of 24 passengers for the return leg to Perth inside the hangar. The captain assumed the role of pilot flying, started the engines and began to taxi following the taxi guideline markings[1] painted on the ground through the hangar.
During taxi, both pilots felt a slight drop, which they believed was the right main wheel moving off the taxiway onto the grass. The cabin crew member at the rear of the cabin thought the wing tip may have contacted the hangar as the jolt was greater in the rear of the aircraft. They inspected the wings out of the windows and noted nothing out of the ordinary. The captain continued to taxi towards the entry point of runway 08.
After entering and backtracking on runway 26, the crew aligned the aircraft for departure and final pre-take-off checks. At this time, the captain received a phone call from the operator’s head of flying operations who informed them that a witness reported that the aircraft may have made contact with the hangar during the initial taxi.
The crew shut down the aircraft on the runway and conducted an inspection. The inspection revealed damage to the aircraft’s left elevator (Figure 2). There were no reported injuries, the passengers were disembarked, and the aircraft was moved to the parking bay.
Following the event, the operator commenced an investigation into the occurrence using a third‑party investigator. The hangar was inspected, and no damage was identified (Figure 3).
Since the completion of the independent investigation on the occurrence, the operator has taken the following safety action:
A formal risk assessment for each new port is conducted prior to any operation being conducted regardless of the length of contract. This risk assessment also applies to ad hoc charters.
A risk assessment classification has been included into the aerodromes and routes procedure.
Charter briefs have been updated to include a triple signature sign‑off process to ensure that the head of flying operations (HOFO), head of safety and quality, and operations team lead have conducted all required risk assessments and briefs prior to the flights taking place.
Human factors training has been updated to include new materials related to this accident. This includes a requirement for all flight crew to undertake this training on initial employment and every 2 years thereafter.
The head of safety and quality has conducted a review of the risk assessment and change management process to ensure it is fit for purpose.
Safety message
The ATSB reminds pilots to exercise caution when operating near hangars and avoid taxiing aircraft directly inside. Hangars are confined spaces with limited clearances, increasing the risk of collisions with walls, equipment, or other aircraft. Visibility from the cockpit is often restricted, making it difficult for pilots to accurately judge distances or detect hazards. These factors significantly increase the likelihood of damage to the aircraft or surrounding structures.
To ensure safety, pilots should either stop the aircraft outside the hangar and allow trained ground personnel to tow or manually manoeuvre it into position or organise for a wing walker or marshal to be available during the taxi. This practice provides greater precision and reduces the potential for accidents. In this case, the use of a tug to tow the aircraft through the hanger or the use of a wing walker or marshal would have alleviated these risks.
Operators are also reminded that, even if they have previously used an ALA before, it is important to obtain all relevant information about the ALA prior to flight. ALAs located in remote or rural locations may vary significantly in their condition, dimensions, and available facilities. Operators should ensure they have up-to-date details about the runway surface, obstacles and likely restrictions within the ALA. Additionally, knowledge of available ground support equipment, parking, and turning areas is important for safe operations. Thorough pre-flight planning and communication with the airstrip operator or local contacts can help identify potential hazards and ensure that the aircraft and operation are suitable for the destination.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]A taxi guideline marking consists of a single conspicuous yellow or white line delineating a path for the aircraft to follow.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-004
Occurrence date
23/08/2024
Location
Minderoo Aircraft Landing Area, Western Australia
State
Western Australia
Occurrence class
Accident
Aviation occurrence category
Taxiing collision/near collision
Highest injury level
None
Brief release date
11/02/2025
Aircraft details
Manufacturer
Bombardier Inc
Model
DHC-8-315
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Regional operator Skippers Aviation has taken safety action after a Fairchild Metro 23 twin-turboprop airliner descended below the lowest safe altitude while its crew responded to smoke in the cockpit and a wing overheat indication on a passenger flight from Perth last year.
The serious incident occurred on 15 August 2024, during a flight from Perth to Bronzewing Airport, Western Australia, with 12 passengers and 2 flight crew on board.
Climbing after take-off, the crew observed hot air and smoke from the flight deck air vents. The smoke increased, and the crew initiated the ‘smoke in aircraft’ checklist.
“Required items on the checklist were not completed,” Australian Transport Safety Bureau Director Stuart Macleod said.
“Specifically, the first officer did not don an oxygen mask due to difficulty with its usage, and the left bleed air system was not switched off.”
The ATSB’s final report into the incident notes the hot air and smoke was the result of a failure within the left air cycle machine prior to departure.
The crew commenced preparations for a return to Perth, but with the left bleed air system remaining on, smoke continued to enter the cabin. The left wing overheat light later illuminated, so the crew actioned the ‘wheel well and wing overheat’ checklist.
While actioning this second checklist, the crew did turn the left bleed air system off, and smoke ingress into the cabin ceased.
“However, the crew did not complete the required action of extending the landing gear,” Mr Macleod observed.
“This missed checklist item potentially increased risk, had the wing overheat indication been associated with a brake fire or wheel well overheat issue.”
During the return to Perth, the aircraft deviated both above and below the altitude assigned by air traffic control, including a descent to 639 ft below the lowest safe altitude.
“The ATSB determined the high workload associated with responding to the smoke and wing overheat indication adversely affected the flight crew’s performance,” Mr Macleod said. “This resulted in errors in flight path adherence, checklist completion and decision making.”
The aircraft landed back in Perth without further incident.
Following the occurrence, Skippers Aviation conducted a refresher training course for flight crew on emergency response briefings and a theory examination for flight crew on bleed air, pneumatics, pressurisation and fire warning systems.
Practical training sessions were also held for flight crew on revised emergency procedures and the use of the crew oxygen system.
Skippers also changed its Metro 23 flight crew training program to include a revised Line Oriented Flight Training program, including more comprehensive oxygen system training and a presentation on the Metro 23’s oxygen system.
“This occurrence highlights the importance of careful and methodical checklist completion, particularly during periods of high workload,” Mr Macleod summarised.
“It also emphasises the importance of flight crew being familiar with onboard emergency equipment, and how to use it.”
While not contributing to the occurrence, the ATSB also identified the air traffic controller did not identify or correct a readback error by the first officer during the return to Perth.
Additionally, later when the aircraft first descended below the lowest safe altitude, the crew were advised of the deviation by air traffic control, but the required ‘safety alert’ was not issued.
On 24 January 2025, a Cirrus SR22, VH-DCB, was conducting a private flight from the Gold Coast, Queensland, to Mildura, Victoria with the pilot and one passenger on board.
About 2 hours and 43 minutes into the flight, while approaching the Mitchell Highway to the east of Nyngan, New South Wales, the pilot observed a cautionary alert, advising of low engine oil pressure. The pilot diverted to Nyngan Aerodrome and a short time later, the engine subsequently sustained an in-flight mechanical failure and engine fire. The aerodrome was beyond the aircraft's glide range at the time and the pilot elected not to deploy the Cirrus Aircraft parachute system, but to perform a forced landing on the Mitchell Highway.
The pilot conducted a successful forced landing, both pilot and passenger were uninjured and the aircraft sustained only minor damage.
What the ATSB found
The engine lost oil pressure during flight and sustained an in-flight mechanical failure, prompting the pilot to declare an emergency. The pilot exercised timely and effective decision‑making, which mitigated the risk of injury to the occupants and further damage to the aircraft. The pilot then promptly executed a successful forced landing on a nearby highway, while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin.
Safety message
In-flight engine failures in single-engine aircraft require pilots to exercise effective and timely decision-making to reduce the severity of injuries and damage. These events often result in the pilot experiencing high workload and time pressure, where preparedness is critical.
The ‘aviate, navigate and communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies. Taking action in the appropriate order of priority improves situational awareness and supports coordinated responses in a dynamic environment.
Scenario-based training should reinforce these principles by developing both technical and non-technical skills, helping pilots become familiar with the appropriate responses and techniques required during high‑stress situations.
Decision-making tools also enables pilots to take a structured approach to problem‑solving which enhances safety by minimising the risk of errors during emergencies.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 25 January 2025, the pilot of a Cirrus SR22, registered VH-DCB, planned to conduct a private flight from Gold Coast, Queensland, to Mildura, Victoria. The aircraft departed Gold Coast Airport with the pilot and one passenger at about 0735 AEST.[1]
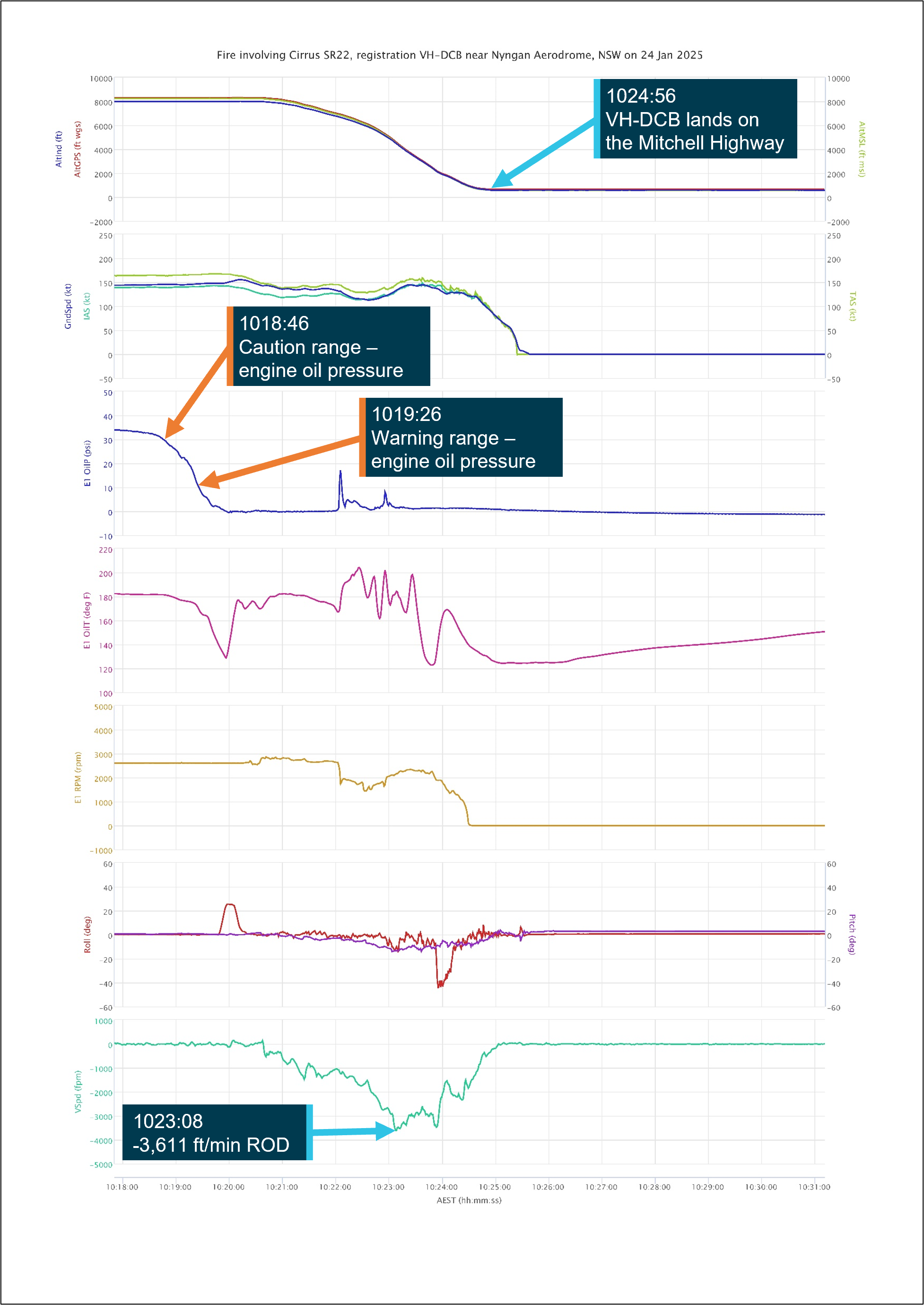
At 1018, while cruising at an altitude of about 8,000 ft above mean sea level (AMSL), the engine oil pressure decreased below the normal operating limits for the engine, 30 pounds per square inch (psi), and the pilot recalled an engine oil pressure alert. The pilot identified that Nyngan Aerodrome was the nearest aerodrome, about 15 NM (28 km) to the north-west. At 1019, the pilot diverted directly to Nyngan with the aid of the autopilot (Figure 1).
Figure 1: VH-DCB flight track and key events taken from recorded data
Source: Google Earth, annotated by the ATSB
The pilot calculated the distance, altitude and glide ratio[2] of the SR22 and concluded that they would likely not make it to Nyngan in the event that the engine failed. They continued towards Nyngan but began to look around for suitable landing sites and identified the Mitchell Highway on the left side of the aircraft.
After checking the engine indications and confirming the engine oil pressure was below normal operating limits and continuing to decrease, the pilot made a PAN PAN[3] broadcast to air traffic control (ATC), advising they were losing engine oil pressure and would be tracking directly to Nyngan. During this broadcast, the pilot recalled the engine began to ‘rev up’ which was followed by an audible ‘bang.’
The pilot then made a MAYDAY[4] broadcast to ATC, advising that the engine had experienced a mechanical failure and they would be making an emergency landing on the highway. As ATC acknowledged the broadcast, the pilot observed flames ‘pouring’ from the top of the cowl.
At 1020 the pilot began a controlled descent towards Nyngan and the Mitchell Highway (Figure 1), and they selected idle power, mixture to cut off and turned off the fuel pump. They attempted to switch the fuel selector lever to off, but they were unable to, recalling that they required both hands to do so. At this time their forward visibility became partially obscured by engine oil on the windscreen.
The pilot reported being concerned that the fire was fuel related and elected to continue with a forced landing rather than deploying the airframe parachute system fitted to the aircraft (see Cirrus airframe parachute system). The pilot was also aware of the increased risk of fire damage to the aircraft rescue system and potential injuries during a parachute‑assisted landing to the passenger, who was pregnant.
At 1023, the pilot commenced a left turn at about 5,000 ft in the direction of the Mitchell Highway. The pilot elected to ‘dive the plane down’ to supress the fire, and increased the rate of descent to over 3,600 ft/min (see Appendix A, Figure A1) and then set up for an immediate forced landing on the highway.
The pilot recalled that the fire appeared to extinguish as the aircraft descended through 4,000 ft and reported they were able to switch the fuel selector off at about 3,250 ft. However, they recalled smoke began to enter the cockpit at about 3,000 ft as the aircraft continued to descend. The pilot selected the first stage of flap and lined up on a section of the Mitchell Highway in a south‑easterly direction. On final approach, the pilot had to adjust the emergency landing flightpath to avoid 2 motor vehicles on the highway and safely conducted the emergency landing, vacating the highway onto a dirt access road at about 1024 (Figure 2).
The pilot recalled that, during the emergency, they had continuously tried to anticipate the next event or action, then evaluated the best course of action and confirmed their decision before proceeding.
The aircraft sustained minor damage to several components on the left wing as a result of colliding with roadside guideposts during the landing roll (Figure 2 right insert) and the pilot and passenger were uninjured. The New South Wales rural fire service attended the scene shortly after the aircraft had safely landed.
Figure 2: VH-DCB alongside Mitchell Highway and minor damage to left wing
Source: Operator, annotated by the ATSB
Context
Pilot information
The pilot held a Commercial Pilot Licence (aeroplane) with an instrument rating and a class 1 aviation medical certificate. They had 3,496 flight hours, including about 1,900 hours on the Cirrus SR22 and had recently logged about 40 hours on type in the last 90 days.
The pilot reported sleeping about 9 hours the night before the occurrence and had been awake for about 5 and a half hours at the time of the occurrence. They further reported that they felt ‘fully alert and wide awake’ on the day of the occurrence and were not tired or fatigued.
Aircraft information
The Cirrus Design Corporation SR22 is a low wing general aviation aircraft with 5 seats and a single piston engine, driving a constant speed propeller. The aircraft was registered as VH-DCB in Australia on 9 November 2018 to the pilot, who was the registered operator. The aircraft was certified for day and night VFR[5] and IFR[6] operations.
Powerplant
The SR22 is equipped with a single Continental Motors Inc. IO-550-N engine. The engine oil used for lubrication and cooling is drawn from an 8-quart capacity sump located in the engine crankcase. The engine had a total time in service of 1,678.5 hours and the manufacturer‑approved time between overhaul[7] was 2,200 hours total time in service.
Engine oil system
The aircraft’s pilot operating handbook required an engine oil level between 6 and 8 quarts for normal operation, with the manufacturer recommending a pre-flight dipstick indication of 7 quarts for extended flights. On the day of the occurrence, the pilot recalled that the engine dipstick was reading 8 quarts prior to departure.
Cirrus airframe parachute system
The Cirrus airframe parachute system (CAPS) was designed to lower the aircraft and its passengers to the ground in the event of a life-threatening emergency and is operated by the pilot. The CAPS system consists of a parachute, a solid-propellant rocket used to deploy the parachute, an activation handle, and a parachute harness embedded within the fuselage structure.
Maintenance history
Immediately prior to the occurrence, the aircraft had undergone a 50‑hour inspection at a Cirrus‑authorised service centre. No engine‑related defects were recorded in the aircraft maintenance certification log.
Prior to that, on 23 October 2024 at the same service centre, the engine had been inspected during an annual inspection and was certified in accordance with approved maintenance data as airworthy at a total time in service of 1,637.6 hours.
All records of inspections and maintenance tasks obtained by the ATSB in the course of the investigation were certified as being conducted in accordance with the latest revisions of the Cirrus airplane maintenance manual and the Continental maintenance manual.
The pilot recalled that they had completed the daily inspection prior to the flight, with no identified issues before certifying the daily inspection on the aircraft maintenance release.
Meteorological information
The Bureau of Metrology aviation meteorological information report, which included the graphical area forecast[8] encompassing Nyngan Aerodrome at the time of the occurrence, contained the following:
visibility greater than 10 km
nil significant weather or cloud
moderate turbulence below 7,000 ft in dust devils and thermals north of Dubbo Airport.
At the time of the occurrence, the pilot stated that the weather was generally fine with good flying conditions and ‘not a cloud in the sky.’
Post-incident inspection
The pilot inspected the aircraft engine after the serious incident and found the crankcase had ruptured adjacent to cylinder 6 (Figure 3 right insert) below the induction duct assembly. They recovered a connecting rod that had separated from the crankshaft (Figure 4) and identified that the air filter was visibly damaged as a result of a fire (Figure 3 left insert). The pilot recalled performing a post‑landing dipstick check and observed that about 6 quarts of oil remained in the engine.
Figure 3: VH-DCB engine bay and damage to the air filter and crankcase
Source: Operator, annotated by the ATSB
Figure 4: Fractured connecting rod recovered from VH-DCB
Source: Operator, annotated by the ATSB
Due to the remoteness of the location, the aircraft was secured on a nearby property and the engine was retained with the fuselage until a replacement was fitted to the aircraft. Following the subsequent removal of the engine, a disassembly and inspection had not been conducted at the time of publication of this report. As a result, the ATSB was unable to determine the root cause for the loss of oil pressure or the mechanical failure of the engine.
Aircraft manufacturer’s emergency procedures
The emergency procedures section of the Cirrus SR22 pilot’s operating handbook (POH) prescribes procedures for handling emergencies and critical flight situations that may occur while operating the aircraft. The POH states:
Although this section provides procedures for handling most emergencies and critical flight situations that could arise in the aircraft, it is not a substitute for proper flight training, thorough knowledge of the airplane, and recognised piloting techniques and standards.
Additionally, the POH recommends 4 basic actions that can be applied to any emergency which include:
maintain aircraft control
analyse the situation
take appropriate action
land as soon as conditions permit.
In cases when a procedure directs a pilot to ‘land as soon as possible’, the POH states:
Land without delay at the first site at which a safe landing can be made. Continued flight beyond an available airfield at which a safe landing can be made will result in increased risk and shall not be attempted.
Loss of engine oil pressure in-flight
When engine oil pressure decreases below 10 psi the aircraft’s crew alerting system[9] (CAS) will annunciate ‘oil pressure’ in red text on the primary flight display which is accompanied by a repeating double chime audio alert. The alert prompts the pilot to carry out the following procedure contained in the emergency procedures section of the POH:
a. Power..........REDUCE TO MINIMUM FOR SUSTAINED FLIGHT
b. Land as soon as possible.
(1) Prepare for potential engine failure
Procedure Complete
Engine fire in-flight
In cases of smoke and fire, the CAS will not alert the pilot to this condition. When a pilot identifies an engine fire in-flight, they must action the following items by memory:
The POH also contained a note which suggested that in the case of a wing fire in-flight, ‘putting the airplane into a dive may blow out the fire.’
During the occurrence, the pilot carried out their actions by memory and stated that they were unable to refer to checklists during the serious incident due to the lack of time. Although the ‘engine fire in-flight’ procedure did not direct the pilot to dive, the pilot decided that diving the aircraft would assist in extinguishing the fire in this case.
The pilot also stated that they encountered difficulty switching off the fuel selector while simultaneously flying the aircraft during the glide approach and managing the emergency. The POH stated ‘to select off, first raise the fuel selector knob release and then rotate the knob to off.’ This is not performed during normal operations which meant the pilot was not familiar with the action. The pilot also recalled turning the ignition switch off after the aircraft had landed.
Cirrus airframe parachute system deployment
The emergency section of the POH contains procedures regarding the deployment of the ballistic parachute in-flight. This section contains the following explanatory notes:
It should also be used in other life threatening emergencies where CAPS deployment is determined to be safer than continued flight and landing. Expected impact in a fully stabilised deployment is equivalent to a drop from approximately 13 feet.
A cautionary note also explains that ‘CAPS deployment will likely result in damage or loss to the airframe.’
The POH identifies several possible scenarios for deploying the CAPS:
midair collision
structural failure
loss of control
landing in inhospitable terrain
pilot incapacitation.
No specific guidance is contained in the POH regarding the use of the CAPS in cases of in-flight smoke and fire.
Recorded information
The Garmin avionics suite installed in the SR22 included a flight data logging feature that automatically stored critical flight and engine data on a removable data card.
The ATSB was provided with the data card installed in the aircraft at the time of the occurrence. The data on the card was downloaded by the ATSB and confirmed to have contained flight data recorded during the occurrence on 24 January 2025.
Recorded data
The recorded flight data captured parameters such as engine parameters, altitude, airspeed, vertical speed, bank angle and various avionics functions (Appendix A – Recorded data). This data enabled a detailed reconstruction of the flight, providing insights into the aircraft’s performance and pilot actions during the occurrence (Figure A1).
Prior to the occurrence, the recorded flight data (Figure A2) indicated that all recorded engine parameters were within normal operating limits outlined in the powerplant limitations section of the pilot’s operating handbook prior to the loss of engine oil pressure. Table 1 depicts the normal and recorded ranges of each engine parameter from the time the aircraft became airborne at 0733:21 until the engine oil pressure decreased below the normal range of 30 psi at 1018:46.
Table 1: Recorded in-flight range prior to loss of engine oil pressure
Recorded in-flight range inclusive of cylinders 1 – 6
[2]Recorded in-flight range inclusive of cylinders 1 – 6
Source: Operator supplied flight data card, tabulated by the ATSB
Related occurrences
The following ATSB investigations highlight the risks associated with encountering engine failures in flight, demonstrating the importance of effective decision‑making.
On 21 November 2012, a Cirrus SR22 aircraft, registered VH‑WYH, departed Emerald, Queensland for Dubbo, New South Wales, on a private flight conducted under instrument flight rules. The pilot and one passenger were on board.
During the flight, the oil pressure annunciation illuminated, and the engine oil pressure indicated 30 pounds per square inch (psi). As the oil pressure continued to slowly drop, the pilot became increasingly concerned and tracked via Gilgandra, New South Wales. They overflew Gilgandra and continued on towards Dubbo, at which point the oil pressure gauge indicated about 12 psi.
Two hours and 39 minutes after the oil pressure light illuminated, the engine failed. When it became evident that a landing at Gilgandra aerodrome was not achievable, the pilot deployed the ballistic parachute. The aircraft impacted the ground and was substantially damaged with the pilot receiving minor injuries while the passenger was uninjured. The pilot reported that the oil pressure indication dropped very gradually giving a false sense of security.
On 6 November 2020, the pilot of a S.E.D.E. Morane-Saulnier MS.893A (Rallye) aircraft, registered VH‑UQI, was conducting a private flight from Moruya, New South Wales, to Archerfield, Queensland. About 22 km south‑west of Archerfield Airport, the engine began running rough before eventually failing.
The pilot elected to conduct a forced landing into an open but slightly undulating paddock. The approach direction resulted in a tail wind landing. The aircraft over‑ran the open area before it impacted with a grove of trees, significantly disrupting the aircraft structure. A post‑impact fire consumed most of the fuselage. The pilot was seriously injured, and the aircraft was destroyed.
The pilot was ferrying the aircraft on behalf of the owner and had limited aircraft type experience and knowledge of its performance capabilities, and it was found that the pre‑flight planning was limited.
Safety analysis
During the investigation, the ATSB was unable to determine the initiating factor that led to the loss of oil pressure and subsequent mechanical failure of the engine. However, the recorded data from the occurrence revealed that all engine parameters were within normal operating limits prior to the loss of engine oil pressure and subsequent in‑flight mechanical failure of the engine.
After observing the oil pressure caution message, the pilot made a timely decision to divert to Nyngan Aerodrome. Being aware of the aircraft’s gliding capabilities and after the oil warning alert, they were immediately able to determine that the aircraft did not have sufficient altitude to safely conduct a forced landing at the aerodrome. They then identified the Mitchell Highway as the most suitable landing site before investigating the engine parameters.
When the engine experienced a mechanical failure, the pilot was able to immediately enact their pre‑planned forced landing procedure, declare the emergency and communicate their intention to land on the Mitchell Highway.
After observing flames and oil coming from the engine cowl, which obscured their visibility, the pilot made a timely decision and elected not to deploy the aircraft’s ballistic parachute. This was due to the pilot’s concern that the fire was fuel‑related and may affect the deployed parachute system as well as the potential risk of injury to the passenger, who was pregnant, and aircraft damage associated with a parachute‑assisted landing.
The pilot began an emergency descent, putting the aircraft into a ‘dive’ in an attempt to put out the fire. Once the fire self-extinguished, smoke entered the cockpit. However, the pilot proceeded to navigate the aircraft to land on the highway among traffic for a successful forced landing with no injuries and only limited damage.
The ATSB research report Engine failures and malfunctions in light aeroplanes, 2009 to 2014 (AR-2013-107) indicated that although engine failures are relatively rare, they do happen. Given the potential severity of the consequences of an engine failure or power loss in a single‑engine aircraft, such occurrences therefore need to be planned for and managed appropriately.
On this occasion, the pilot made effective and timely decisions to manage the evolving emergency and appropriately prioritised their actions. Their decision‑making was likely supported by their experience on the aircraft type and knowledge of the performance capabilities. This enabled prompt and appropriate responses from the pilot, which contributed to a safe outcome.
Additionally, the pilot’s methodical approach during this occurrence highlights the importance of decision-making tools to aid pilots to mitigate the possibility of errors and ensure a considered approach in resolving issues or problems (Civil Aviation Safety Authority, 2019).
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine failure involving Cirrus SR22, VH-DCB, 29 km east-south-east of Nyngan, New South Wales, on 24 January 2025.
Contributing factors
The engine lost oil pressure during flight, leading to an in-flight engine failure and fire.
Other findings
The pilot exercised timely and effective decision making in flight to divert and then identify a safe forced landing area.
The pilot successfully executed an immediate forced landing on a nearby highway while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin. This resulted in no injuries to the 2 occupants and only minor additional aircraft damage.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the serious incident flight
maintenance organisation
Civil Aviation Safety Authority
United States National Transportation Safety Board
Cirrus Design Corporation
Continental Motors Incorporated.
Submissions were received from:
pilot in command/operator
Cirrus Design Corporation
Continental Motors Incorporated.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Recorded data
Figure A1: In-flight data and key events after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Figure A2: In-flight engine parameters after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
An explanation of terminology used in ATSB investigation reports is available here.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Local time was Australian Eastern Standard Time (AEST), which is Coordinated Universal Time (UTC) +10 hours. Times in this report are AEST unless otherwise noted.
[2]Glide ratio: the glide ratio of an aircraft is the distance of forward travel divided by the altitude lost in that distance. The Cirrus SR22 pilot’s operating handbook stated the maximum glide ratio for the aircraft was 8.8:1.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[5]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions
generally clear enough to allow the pilot to see where the aircraft is going.
[6]Instrument flight rules (IFR): rules which allow properly equipped aircraft to be flown under instrument meteorological
conditions
[7]Time between overhaul: is a time limit specified by the engine manufacturer for a specific engine in a specific installation, after which overhaul is either recommended or mandated depending on how the aircraft is used.
[8]Graphical area forecast (GAF) is a combination of graphical and textual information. The graphic is divided into areas that share common weather characteristics which are detailed in an associated table.
[9]Crew alerting system (CAS): aircraft annunciations and alerts are displayed in the CAS window located to the right of the altimeter and vertical speed indicator. Aircraft annunciations are grouped by criticality and sorted by order of appearance with the most recent message on top.
[10]Cylinder head temperature (CHT): CHT is measured by a temperature-sensing probe located at the cylinder head, and it measures heat energy wasted during the power stroke, when the cylinder is under maximum stress from high internal pressures and temperatures.
[11]Exhaust gas temperature (EGT): is a measurement of the temperature of the exhaust gases at the exhaust manifold.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 10 December 2024 an Airbus AS350 B2 (Squirrel) was being operated on a multi-day ferry flight from Caloundra Airport, Queensland to Papua New Guinea (PNG). At about 1000 local time, the helicopter was landed at Gladstone Airport for fuel and then continued north for Cairns Airport. Abeam Rockhampton Airport and about 4 km from the airport control zone boundary, the left front door upper window became detached from the aircraft and was briefly observed by the crew member seated in the left side as falling down and away from the aircraft.
Following the incident the crew aerially searched the area for the window, however, were unable to find it in the dense bushland. Shortly after this the crew landed the aircraft to check for damage to the helicopter. No damage was found and the crew elected to continue to Cairns Airport where a spare window was fitted.
Figure 1: Airbus AS350 B2 left front door upper window before the incident
Source: Operator, annotated by the ATSB
After a repair in Cairns, the helicopter had a post-maintenance flight check before the planned departure.
The remainder of the flight to PNG continued without incident. The crew were reported to be startled by the loud noise that was created as the window detached from the helicopter, however, no injuries were sustained by the crew and no other damage to the helicopter was observed.
The operator advised that, in line with scheduled maintenance of the aircraft, some of the windows had recently been refitted after a period in storage. The operator’s internal review of the incident concluded that the seal on the left-hand door window was installed without sealant and in the incorrect orientation. Further, as depicted in Figure 1, the left front door upper window also displayed a bulge due to theincorrect orientationafter refit. This improper fit reduced the security of the window to stay in place permanently during flight. The review identified that an apprentice aircraft mechanical engineer fitted the window, however, the subsequent inspection and sign‑off process did not identify any problem with the installation.
Safety message
Attention to detail is critical for all aspects of aviation safety, as even small omissions can have serious safety implications. Maintenance manuals for manufacturer and operator procedures should be followed closely. Quality assurance checks to verify compliance following maintenance, and fostering a culture of vigilance in maintenance practices, is essential for preventing inadvertent errors.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Two separate breakaways of container ships berthed at the Port of Brisbane after heavy rains highlight the importance of robust emergency and risk management arrangements, according to an Australian Transport Safety Bureau investigation.
The May 2022 incidents occurred after an unprecedented stretch of rainfall resulted in significant freshwater inflows into the Brisbane River following several controlled water releases from dams located upriver.
This resulted in strong currents through the Port of Brisbane, at the mouth of the river, which added strain to the mooring lines holding ships berthed there.
On 16 May 2022, the container ship OOCL Brisbane broke away from berth 10 at Fisherman Islands. Four days later another container ship, CMA CGM Bellini,broke away from berth 6.
“Fortunately, the ships were brought under control in both cases, and there were no injuries or substantial damage in either incident,” ATSB Chief Commissioner Angus Mitchell said. “But breakaways can have serious outcomes.”
The ATSB investigation found that both breakaways occurred due to the strong currents following the high rainfall combined with the interaction forces created when a second container ships passed alongside and then berthed ahead of, each vessel.
“The high ebb current speeds and the interaction forces introduced by other vessels resulted in the mooring limits for both ships being exceeded,” Mr Mitchell said.
In the case of the OOCL Brisbane, all the ship’s mooring lines parted or paid out, and it moved into the Brisbane River before being assisted by tugs. CMA CGM Bellini’s forward mooring lines parted, and its bow drifted off the wharf before it too was assisted by tugs to be secured alongside.
In the course of its investigation, the ATSB identified that Maritime Safety Queensland (MSQ), the regulator, and the Poseidon Sea Pilots (PSP), Brisbane’s pilotage provider, did not have a process to jointly and effectively identify the hazards to shipping and pilotage that were outside normal environmental conditions, and to properly assess the associated risks.
“These breakaways highlight the importance of robust, properly structured and clearly defined emergency and risk management arrangements for managing port shipping movements outside of normal operating conditions,” Mr Mitchell said.
“Such arrangements must facilitate accurate assessment of all the available information by the involved parties and provide for adequate assessment of all potential risks.”
Mr Mitchell recognised the safety actions taken by both MSQ and PSP in response to these incidents, as well as another breakaway, further upriver and a month prior, which was also investigated by the ATSB.
PSP and MSQ have collaborated with a range of stakeholders to improve extreme weather event planning and response, and to establish a formal channel to identify and risk assess hazards to shipping outside of normal environmental conditions.
This has included the establishment of the Port of Brisbane Maritime Emergency Working Group, with guidelines developed for the group’s role in responding to port emergencies.
Additionally, three additional current meters have been installed in the river, adding to the one installed prior to the incident, and additional meters are planned. Data from these meters will be provided by MSQ to key stakeholders, including PSP.
Finally, PSP has provided input for changes to MSQ’s standard port procedures, including the joint development of procedures for movements to and from various berths under flood conditions, using MSQ’s bridge/ship simulator.