Misaligned take-off involving Bombardier DHC-8-315, VH-TQM, Mildura Airport, Victoria, on 25 February 2025
Final report
Report release date: 12/05/2026
Investigation summary
What happened
On 25 February 2025, a QantasLink DHC-8-315 aircraft, registered VH-TQM, was being operated on a scheduled passenger transport flight from Mildura to Melbourne Airport, Victoria. The flight crew commenced taxiing the aircraft prior to first light. The aircraft was backtracked on runway 09 and taxied past the threshold into the starter extension bypass pad to turn around and line up. The flight crew inadvertently lined up the aircraft with the right runway edge lights and commenced taking off from this position.
During the take-off roll, the nose landing gear contacted and damaged 5 runway edge lights. Although the flight crew heard some external noises, neither recognised this as contact with the runway edge lights. The captain, however, identified that the aircraft was not on the centreline and manoeuvred towards the centreline and continued the take-off. During the initial climb, the flight crew realised that the aircraft had contacted the runway edge lights.
The flight crew conducted a low pass at Melbourne to facilitate a visual inspection of the landing gear by air traffic control. This did not identify any issues and the aircraft landed without incident. An inspection of the aircraft found minor damage to the nose landing gear, fuselage and right propeller blade.
What the ATSB found
The ATSB found that the incident took place in dark ambient conditions and that the taxi guidance line markings were not followed for the turn to line up. Instead, the aircraft was turned tighter, which positioned it closer to the right edge of the runway. Also, the flight crew’s attention was focused on conducting checks during the turn and on completion of the turn. However, as the flight crew believed they were correctly aligned with the runway centreline, they commenced the take-off roll.
It was also established that, when conducting the low pass of the Melbourne air traffic control tower, the aircraft was not maintained at the briefed height of 200 ft above ground level and descended to 134 ft for a short period. It was noted that the flight crew did not seek advice on the low pass nor did the operator provide supporting procedures for this.
Further, during post‑incident drug and alcohol testing, the captain tested positive for a non-prescribed medication. However, impairment was not expected given the reported dosage and time elapsed since taken.
What has been done as a result
QantasLink advised that human factors and non-technical skills training on the threat awareness of factors that have contributed to misaligned take-offs was included for wider flight crew recurrent training. Supporting documentation for Mildura Airport was updated to include information on the runway 09 starter extension for increased awareness along with education material being distributed regarding flight crew briefings and identifying relevant threats.
A safety alert was issued to prohibit the conduct of checks during runway end turns. This was incorporated into the Flight Crew Operating Manual. QantasLink also introduced policy aligned with Qantas Group operators regarding the risks associated with air traffic control tower fly pasts.
Safety message
A number of factors known to influence misaligned take-off occurrences were identified in this investigation. Dark ambient conditions have been consistently identified in similar occurrences and can reduce the visual cues available. This may limit the ability of flight crew to identify their position when lining up.
Although the completion of checks are a necessary part of a flight, they may result in a diversion of attention towards the checks at the expense of another task such as lining up. Pilots must consider the timing for conducting checks in situations where monitoring their external environment is important.
The incident further highlighted that, in non-normal situations for which there is no documented procedure, pilots should consult all available sources including their operator for assistance. Lastly, pilots should exercise caution when taking any medications and should be discouraged from taking prescription medications without medical supervision. Many prescription (and non-prescription) medications are not safe for use while conducting aviation activities and are therefore not permitted for use.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
Flight schedule
On 24–25 February 2025, a QantasLink DHC-8-315 (Dash 8) aircraft, registered VH‑TQM, was operated on scheduled passenger transport flights over the 2 days, which consisted of 5 sectors on the first day and 3 sectors the following morning.1 The crew consisted of 2 flight crew and 2 cabin crew.
On 24 February, the flight crew signed on at 1040 local time in Melbourne, Victoria, and completed 2 return flights to Devonport, Tasmania, and Wagga Wagga, New South Wales. For the final sector to Mildura, Victoria, the aircraft departed Melbourne at about 1922 and arrived at 2045. The crew signed off from duty at 2100 and arrived at their accommodation about 15 minutes later.
On 25 February, at about 0545, the crew departed their accommodation and signed on for duty at 0600 for a 0630 scheduled departure from Mildura to Melbourne. The captain was the pilot flying (PF) and the first officer (FO) was the pilot monitoring2 for this sector. There were 50 passengers on board.
Taxi to runway 09
The captain commenced taxiing the aircraft before first light at about 0631. Closed-circuit television (CCTV) footage showed the aircraft taxi light was on, illuminating a portion of the tarmac ahead of the aircraft. The captain reported that they had also selected the approach lights to ‘on’ to provide greater illumination of the runway surface during the taxi. CCTV footage also showed that the taxiway, runway and starter extension bypass pad3 lighting was active.
After entering the runway, the aircraft was backtracked along the centreline. CCTV footage showed that, when the aircraft approached the runway 09 threshold, the approach lights were selected on. The aircraft was taxied past the threshold and into the runway starter extension bypass pad to turn the aircraft around and line up. The captain reported that the starter extension was not required for performance, but their preference was to use the full runway length where possible. They also stated that the wider extension area would provide more room for the turn around.
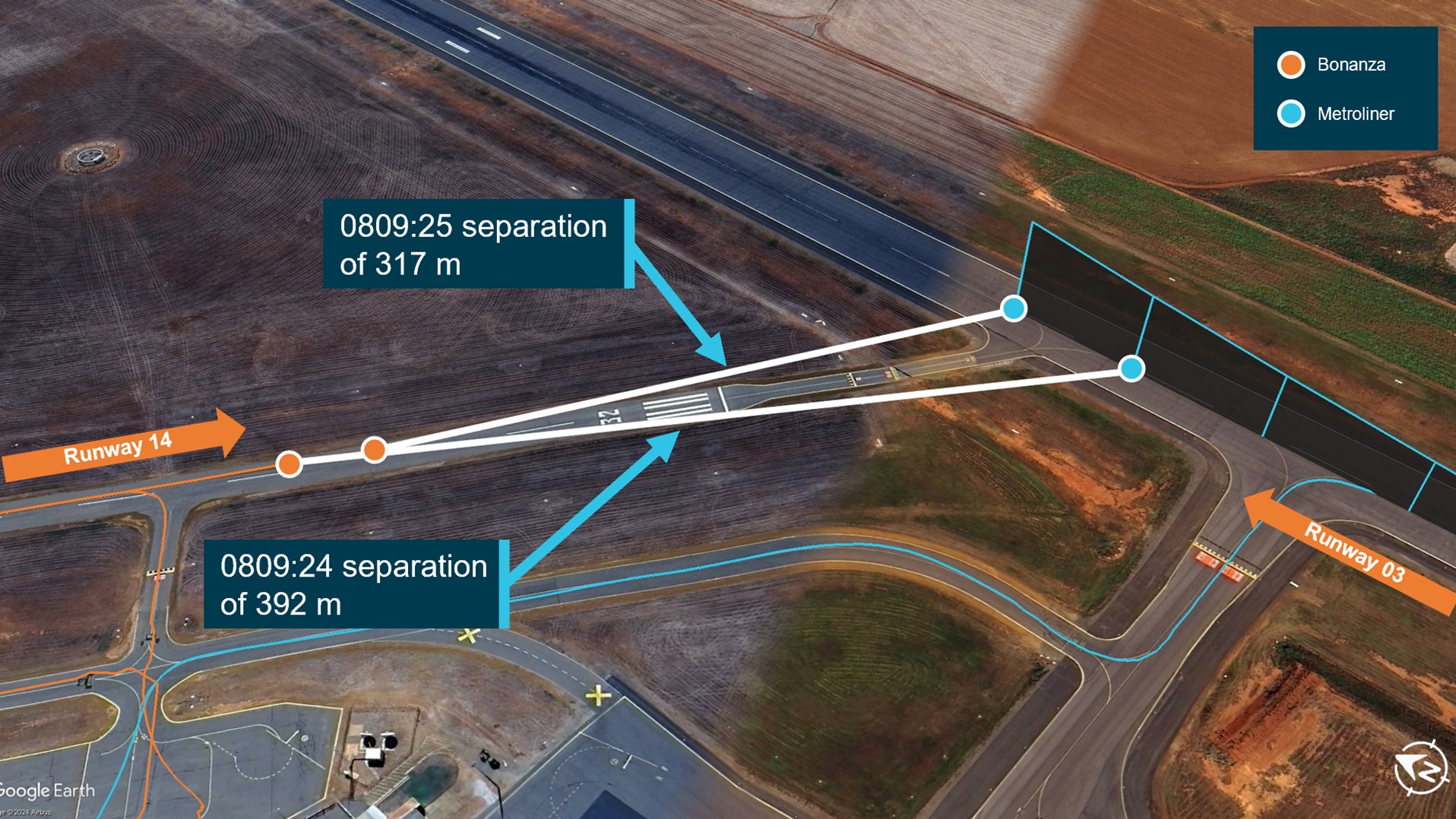
The recorded flight data4 showed that the aircraft path followed the taxi guideline marking into the starter extension but was turned right, prior to the end, and away from the guideline, which led to the extended centreline. The captain explained that their initial intent was to use the complete starter extension. However, once established in the extension, they chose not to do so to avoid inadvertently exiting the pavement in the dark conditions. The FO reported that this was not communicated to them at the time nor were they aware that the aircraft had been turned earlier. The aircraft path during the turn remained to the right of the extended centreline, resulting in it being positioned close to the right edge of the runway (Figure 1).
During the turn, the flight crew conducted the ‘ready checks’ and the associated checklist, during which time they both reported being focused within the flight deck on the conduct of the checks. The captain also reported being distracted by either smoke or mist outside the left window. On completion of the turn, the captain stated they were drawn to the white right runway edge lights, believing them to be runway centreline lights. The captain also indicated that the flight director and heading bug confirmed that the aircraft was aligned with the runway direction. The FO reported that they observed the runway 09 threshold markings, which they equated as the aircraft being in the correct position to line up. They did not recall noticing any lights ahead of their position. Once lined up, both flight crew believed they were aligned on the centreline of runway 09.
Take-off on runway 09
The captain recalled that, when they commenced the take-off roll, they advanced the power levers as close to the required power setting as possible, then called ‘set power’. At this point, the FO checked the power setting and adjusted the levers to ensure the exact power required was set. The FO reported their attention was predominantly focused inside the flight deck from this time. The captain identified that the take-off roll was ‘rough’, explaining that this was not unusual for an early morning first flight of the day for that aircraft type.
The captain recalled that, about the time the FO called ‘70 kt’, the sounds and sensations became more intense and identified that the aircraft was on the runway edge (Figure 1). They then manoeuvred the aircraft to its correct position along the centreline.
The FO reported hearing ‘1 or 2 thuds’ at about the time that they called ‘70 kt’. The FO also explained becoming momentarily distracted with the storm light5 on their side of the flight deck, which had unexpectedly turned on. The FO continued their scan between airspeed and ahead of the aircraft and shortly after made the calls ‘V1’ and ‘rotate’.6
The FO stated that they had not become aware of the misaligned take-off until after the captain had already begun manoeuvring the aircraft toward the runway centreline.
The captain continued the take-off, recalling that the aircraft had operated normally, and that the abnormal sounds and sensations had ceased. Once airborne, the ‘after take-off’ procedures were completed, as required.
Figure 1: Flight tracking data for the take-off with the starter extension inset

The aircraft track (within the inset) at the end of the starter extension shows a sharply clipped turn, which is due to the fidelity of the data. Source: Google Earth, with aircraft flight data overlaid and annotated by the ATSB
During the initial climb, the flight crew realised that they may have contacted the runway edge lights. The FO contacted the Mildura Airport aerodrome reporting officer and advised them of this. They requested the area be inspected and for them to report back on any debris located. The flight crew were subsequently advised that there was damage to 5 lights on the right edge of runway 09 (Figure 2). No aircraft debris was identified.
Figure 2: Damaged runway edge lights (inset) on runway 09
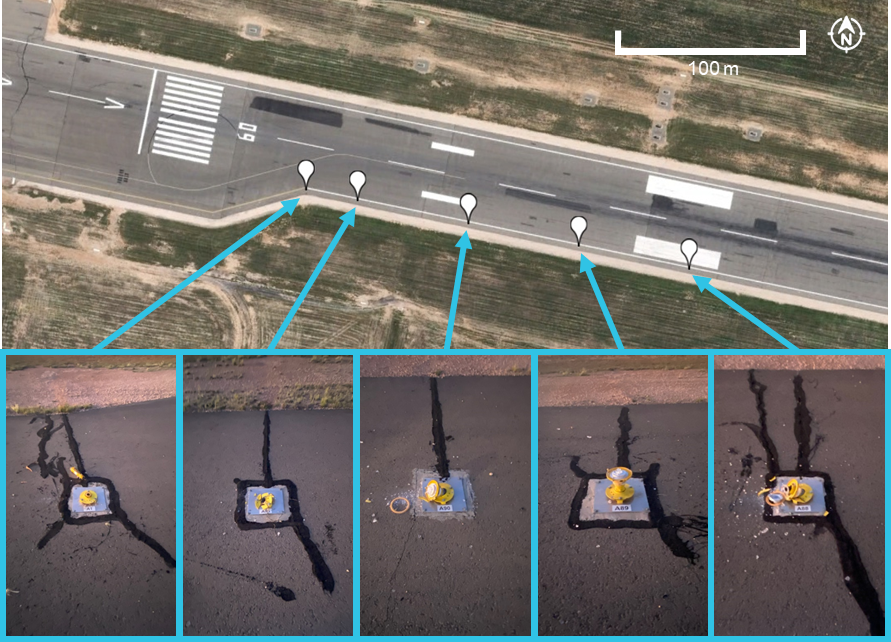
Source: Google Earth and Mildura Airport, annotated by the ATSB
After take-off inspections
The flight crew reported that following discussion about what had occurred, they considered the possibility that the landing gear had not been damaged as the remainder of the take-off roll occurred normally and the landing gear retracted without fault. They consulted the Quick Reference Handbook, however, there was no procedure to assist them with assessing the landing gear status. They then discussed and assessed the potential risks for landing with potential damage to the aircraft, and that a visual inspection of the landing gear would be required.
The captain explained that after the landing gear was extended, the main gear would become visible from the passenger cabin. The captain had briefed a cabin crew member that the landing gear would be extended earlier than normal for them to inspect. The captain asked them to check for any signs of fluid or tyre damage and whether the gear had deployed correctly. The cabin crew were to use the cabin ready button to signal if the landing gear appeared okay, otherwise they were to call the captain if they had concerns. Although the cabin crew were able to inspect the main landing gear, they could not view the nose landing gear. QantasLink advised that, during this time there was no contact for assistance between the flight crew and its operations centre.
The FO contacted Melbourne Centre air traffic control (ATC) and requested to conduct a low pass on their arrival at Melbourne Airport to facilitate a visual inspection of the landing gear. ATC was requested to focus their inspection on the nose landing gear. On advice from ATC, the flight crew briefed to complete the pass at approximately 200 ft above ground level (AGL), which would place the aircraft at an equivalent level to the controller who was in the control tower. The captain set the radar altimeter to 150 ft AGL to assist them in maintaining the aircraft at 200 ft AGL. As the landing gear and flaps would be extended, the captain planned to fly the aircraft at 120–130 kt. During the low pass, the captain reported that the height was adjusted to enable ATC to inspect the landing gear and that they received a minimums audio alert, signifying that the aircraft had descended below 150 ft AGL. The flight data identified the aircraft had descended at its lowest to a height of 134 ft AGL at which point the speed was 122 kt.
The inspection of the main landing gear was completed by a cabin crew member and they pushed the cabin ready button to advise the flight crew that the gear appeared satisfactory. Similarly, ATC did not observe any anomalies of the landing gear, advising the flight crew that the gear appeared correctly aligned and the tyres appeared in satisfactory condition. Following the low pass, the landing gear was raised and a missed approach conducted. The flight crew completed another approach, and the aircraft was landed without further incident.
Context
Flight crew information
Qualifications and experience
The captain held an Air Transport Pilot Licence (Aeroplane) and a valid class 1 aviation medical certificate. They had a total of 19,000 hours flying experience of which 935 hours were on the Dash 8. The captain had flown 107 hours on the Dash 8 in the previous 90 days.
The FO held a Commercial Pilot Licence (Aeroplane) and a valid class 1 aviation medical certificate. They had a total of 3,386 hours flying experience of which 773 hours were on the Dash 8. The FO had flown 45 hours on the Dash 8 in the previous 90 days.
The captain’s logbook identified they had operated at Mildura on numerous occasions in the previous few months. None of those flights were at night or before first light. The FO reported they last operated in similar light conditions at Mildura in September 2024.
Flight crew fatigue assessment
The captain reported going to bed at around 2230 after arriving in Mildura and waking at around 0500 the next morning. The noise from the hotel had interrupted their sleep and they recalled feeling ‘a little tired, less than fresh’, to, ‘moderately tired’7 at the time of the incident. In total, the captain reported obtaining around 6 hours sleep in the previous 24 hours and around 13 hours in the previous 48 hours.
The FO reported they went to sleep at around 2200, woke around 0500, and obtained a ‘good’ sleep. During interview, the FO described that they did not feel ‘match fit’, as they had not operated a 5-sector overnight duty for some time. They also reported feeling ‘okay, somewhat fresh’7 at the time of the incident. In total, the FO reported obtaining around 7 hours sleep in the previous 24 hours and around 14.5 hours in the previous 48 hours.
Aside from the usual workload associated with a take-off in the dark, neither of the flight crew reported any additional fatigue‑related factors on the incident flight.
The ATSB assessed the flight crew’s sleep opportunity, actual sleep obtained, and quality of sleep leading up to the flight as well as other fatigue‑related factors. A number of factors were present that could have increased the risk of fatigue, including a minimum rest period that was provided after a 5-sector day, and a slight reduction of sleep hours and poor-quality sleep in the previous 24 hours (for the captain). However, given the total hours of sleep obtained, time awake, time on duty, and time of the incident, it was unlikely the flight crew was experiencing a level of fatigue known to have an adverse effect on performance.
Drug and alcohol test results
In accordance with the QantasLink drug and alcohol management plan, the flight crew underwent a post-incident alcohol breath test and urine drug test. The FO returned a negative result, however, the captain’s drug test was non-negative. When the test was administered the captain declared that on consecutive days during the prior weekend they had taken a prescription medication that was not prescribed to them.
As there was a non-negative result, a second test of the sample was conducted at a laboratory. The presence of a testable substance above the cut-off level was confirmed.
QantasLink confirmed that the captain had returned a positive test result and that they had been stood down pending further assessment in accordance with company policy. Their medical review officer explained that, while the test result confirmed the presence of a testable substance above the cut-off level, the testing could not indicate when or what dosage was taken, nor could it indicate if there were any effects. They further explained that the medication was not currently permitted for use by pilots, it had an effective period of about 10 hours, and there would be no lingering effects expected unless there was an adverse reaction.
The captain reported to the ATSB they did not experience any effect from the medication at the time it was taken, nor did they experience any side effects. The FO and cabin crew members reported not noticing anything of concern regarding the captain nor their fitness for duty on that morning.
The ATSB engaged a forensic pharmacologist to review the test results. They stated that the concentration detected was consistent with the reported dosage self-administered by the captain on the weekend prior to the incident flight.
The pharmacologist noted numerous potential adverse effects of the medication that included: insomnia, loss of appetite, restlessness, euphoria, dizziness, dyskinesia (involuntary, repetitive and or jerky movements), tremor, dysphoria and with higher doses personality changes, irritability, hyperactivity and psychosis. It may produce peripheral effects such as increasing blood pressure and heart rate, palpitations, increased sweating and hyperthermia (increased temperature). The manufacturer’s consumer medication information stated that the medication should not be taken by persons with known cardiovascular disease. Additionally, the information advised consumers to not drive or operate machinery until they know how the medication affects them. The pharmacologist advised it was possible that the non-therapeutic use of the medication could result in some impairment and potentially, in some cardiovascularly susceptible persons, serious harm.
The pharmacologist further noted it was not possible to determine the likelihood of impairment from a urine sample. There were no studies that have established any relationship between urine concentration of the medication and psychomotor skills performance. For a person using a non-prescribed medication and who has not developed a tolerance, they indicated that impairment could not be excluded as being possible. However, based on the reported dosage, the specialist assessed that impairment would not have been expected on the day of the incident.
Aircraft information
General
The aircraft was a Bombardier DHC-8-315 (Dash 8) twin turbo-propeller regional aircraft capable of carrying 50 passengers and normally crewed by 2 flight crew and 2 cabin crew. It was manufactured in 2004 (serial number 604) and first registered in Australia in 2004.
Post‑incident maintenance
Following the incident, the operator conducted a towing assessment and general visual inspection of the aircraft, with particular attention paid to the landing gear, engines, propellers and fuselage. More detailed inspections of the nose and right main landing gear also took place. In addition, the aircraft manufacturer requested an unscheduled engine inspection.
Damage was identified to the nose landing gear, including both tyres, the cover for the weight on wheels sensor, and the trailing arm (Figure 3). The lower fuselage skin sustained minor impact damage (to 17 areas) and there was minor impact damage to the leading edge sheath of a right propeller blade. Both tyres, the weight on wheels sensor cover and the nose landing gear trailing arm were replaced. The remaining damage was assessed to be within the limits in accordance with manufacturer guidance.
Figure 3: Nose landing gear damage

From left to right: trailing arm impact damage, tread cuts and chunking, tyre impact damage, tyre sidewall slice. Source: QantasLink
Meteorological information
The captain described the weather as good with no fog or rain, although it was dark at the time as their departure was before first light. They specifically noted that the conditions were very dark and the area was poorly lit when conducting the turn to line up. Similarly, the FO reported that it was clear but very dark.
Data from the Bureau of Meteorology showed that the weather at Mildura was fine and clear of any cloud or significant phenomena that may have reduced visibility. The aerodrome weather information service recorded visibility in excess of 10 km at the time of the incident. The wind was generally from 170° (southerly) around 5 kt in the 10 minutes prior.
Information from Geoscience Australia identified that the incident was 14 minutes prior to first light and 40 minutes prior to sunrise.8 CCTV footage showed that the conditions were dark and the sun had not yet risen.
Airport information
Mildura Airport was a certified, non-controlled aerodrome and had 2 sealed runways, aligned 09/27 and 18/36. Runway 09/27 was 45 m wide and included a starter extension bypass pad at the western end of the runway. The starter extension bypass pad provided an additional surface of 117 m in length available for take-off from runway 09. It also provided an additional 23 m in width to turn an aircraft around.
The extension included taxi guideline markings with turn guidance to realign the aircraft with the centreline. It also had arrows aligned with the runway centreline and pointing to the runway threshold (Figure 4).
Figure 4: Runway 09 starter extension bypass pad

Source: Google Earth, annotated by the ATSB
The airport was equipped with airfield lighting, which included elevated white omni‑directional runway edge lights, inset green and red bi-directional runway threshold lights9 and elevated blue omni-directional taxiway edge lights on taxiways C and D only. The starter extension also had elevated blue edge lights. Runway 09/27 did not have, nor was it required to have, runway centreline lighting. Runway 09 also included precision approach path indicator10 lighting on both sides of the runway. CCTV footage obtained from Mildura Airport confirmed that the airfield lighting was active at the time of the incident. Although the foreground was not illuminated by an aircraft taxi light, Figure 5 is indicative of the view that was likely available to the flight crew after lining up on the right edge of runway 09.
Figure 5: View of the runway 09 lighting that was available to the flight crew when lined up with the right edge of the runway
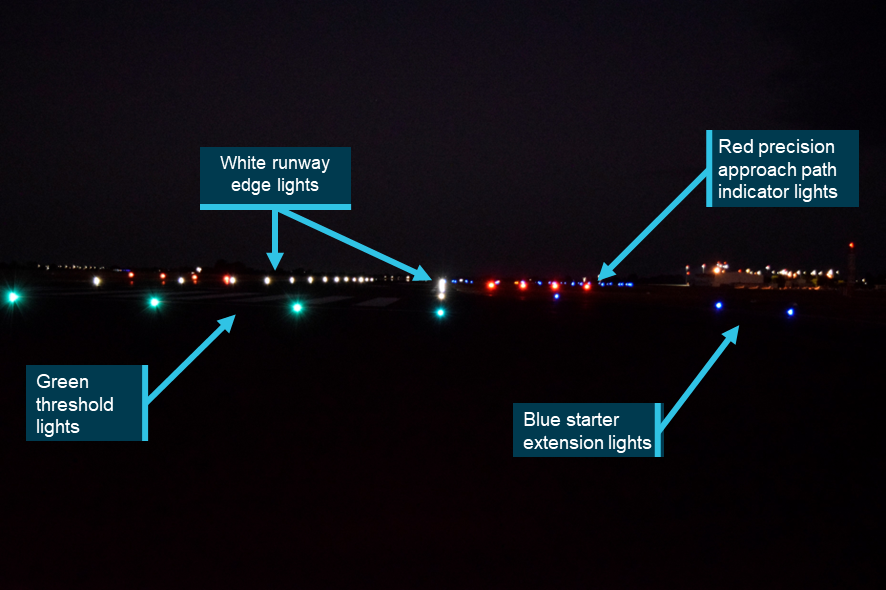
Source: Mildura Airport, annotated by the ATSB
Operational information
Runway alignment
The Operations Manual OM 1 section 6.13.1.2 Navigation and monitoring of taxi routes stated that:
During taxi, the PM is to monitor aircraft location and provide proactive guidance to the PF on the taxi route.
Section 6.13.5.1 Takeoff also required that:
Prior to commencing the takeoff the Pilot in Command and the First Officer shall check the aircraft position is on the runway centreline and either at the correct runway threshold or other designated takeoff position (e.g. intersection).
Similarly, section 2.8 Takeoff of the Flight Crew Operating Manual 300 (FCOM) also indicated that the captain shall align the aircraft with the runway centreline prior to take‑off.
‘Ready’ and take-off procedures
The FCOM included a ‘Ready and Line Up’ procedure. Although it directed flight crew to conduct the associated checks at an appropriate time, the FCOM did not provide detail as to when was appropriate. However, the captain reported that they would not normally conduct the ready checks during a turn to line up, explaining that some runways they operated on were 30 m wide and the tight turn required was not compatible with the conduct of the ready checks. They further explained that runway 09 at Mildura was 45 m wide, with an even wider starter extension, and they felt comfortable that this would allow them the appropriate time and area to conduct the checks concurrent with the turn.
The FCOM also included a rejected take-off procedure in section 3.4.1. The procedure stated that the take-off should be rejected for a critical malfunction (for example, a master warning, engine failure or directional control issue) when between 70 kt and V1. At and after V1, the take-off must be continued. Neither the captain nor FO reported anything meeting the rejected take-off criteria. The captain did, however, discuss in hindsight that they possibly should have rejected the take-off.
Low flying
Section 4.4.4 Low Flying Operations in the Operations Manual OM 1 stated:
A company aircraft shall not be flown below 500’ AGL in day VMC [visual meteorological conditions],11 below LSALT [lowest safe altitude] at night or in IMC [instrument meteorological conditions],12 or below 1000’ over a built up area, unless it is:
• An emergency,
• To takeoff or land,
• Part of a published instrument approach,
• In accordance with ATC instructions, or
• Specifically authorised.
There was no guidance provided on conducting a low pass for the purposes of an external visual inspection of the aircraft.
Airport guidance
Qantaslink provided additional operational guidance for Mildura Airport, which included:
The standard position for RWY [runway] 09 take-off is on the threshold lines. An alternate start position is available which includes the runway starter extension.
However, guidance on how or when flight crew could use the starter extension for runway 09 was not included.
Misaligned take-offs
Previous research
When pilots taxi and take-off during daylight conditions, they normally have a wide range of visual cues by which they can navigate and verify their location. At night, however, the amount of visual information available is markedly reduced. Pilots rely more on the taxiway and runway lighting patterns presented to them and what can be seen in the field of the aircraft’s taxi and landing lights.
The ATSB research report Factors influencing misaligned take-off occurrences at night (AR-2009-033) was published in 2010 following the review of 24 misaligned take-offs that occurred at night in Australia and overseas. The report identified 8 common and recurring factors that contributed to misaligned take-offs at night, as presented below (Figure 6).
Figure 6: Factors contributing to misaligned take-off occurrences
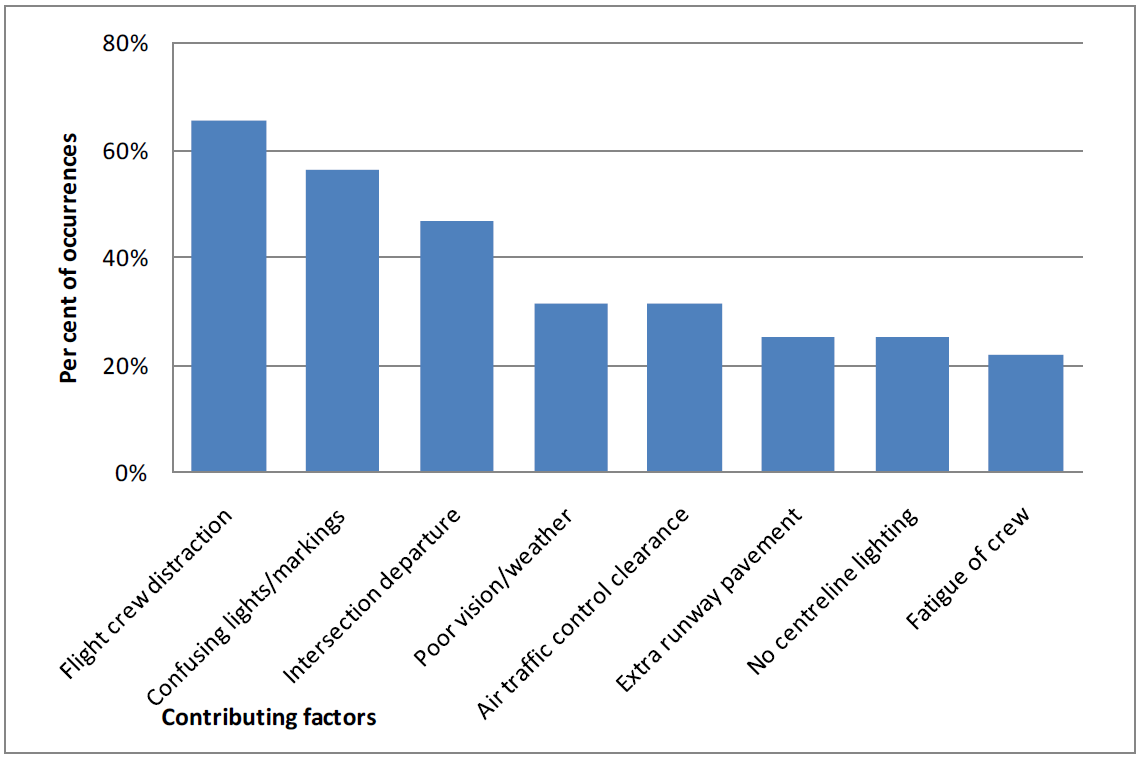
Source: ATSB
Environmental factors were the predominant contributors, which included physical features such as the runway layout, line markings and lighting. Weather and visibility were also considerations. The report identified that confusing runway entry, lighting or taxiway layout/lighting were the most frequent factors and that additional areas of pavement around taxiway entry and runway threshold areas could provide erroneous cues for pilots at night.
Human factors were the next most common contributor, in particular, flight crew distraction, divided attention, workload and fatigue. Flight crew distraction upon entering, or just prior to entering the runway was frequently identified as a factor. The report described distraction as the drawing away or diverting attention, or an action that divided attention. This was reported to have occurred for numerous reasons including the performance of checklists, setting power or checking instruments.
The report explained that:
…distraction comes about when multiple stimuli or tasks make simultaneous demands for attention. Generally, distraction results from one of these competing stimuli or tasks interfering with or diverting attention from the original task or focus of an individual.
Part of the problem with distraction is the resulting divided attention of the flight crew, with a focus on tasks inside the cockpit being at the expense of accurately assessing the external environment. This often occurs during taxi, when flight crew need to be ‘eyes inside’ the cockpit for significant periods of time. That is, instead of maintaining a visual look out from when they enter the runway, their attention is drawn inside for some reason such as checking instruments, confirming aircraft configuration or performing checklist items. While multi-crew operations partially mitigate this risk by articulating and dividing aircraft handling and monitoring roles between the pilots, there are still times when both crew members may not be processing the external environmental cues accurately. This divided attention is often a necessary part of lining up or beginning the take-off roll, but occasionally the attention of the flight crew will be diverted for longer than normal in response to an unusual event or problem. It is often attention to this non-standard action or item that contributes to line-up error events.
Operational factors were also identified such as air traffic control clearances and intersection departures were examples and in some cases they either contributed to, precipitated and/or exacerbated the environmental and human factors that were present.
Related occurrences
A review of the ATSB occurrence database identified a previous QantasLink misaligned take-off, which was investigated by the ATSB in 2009. ATSB investigation AO-2023-027 detailed 3 misaligned take-offs at Perth Airport in 2023 and 2024, and a number of other related occurrences were discussed in that report.
ATSB investigation AO-2009-007
On 11 February 2009, at about 1922 local time, a Bombardier DHC-8-315 aircraft, commenced the take-off roll on runway 01 at Townsville Airport for Cairns, Queensland. During the take-off, the captain realised that the aircraft was aligned with the left runway edge. The aircraft was manoeuvred to the centre of the runway and the take-off rejected. It was later determined that the aircraft’s left mainwheel had damaged a runway edge light. There were no injuries to the 34 passengers or 5 crew members and no damage to the aircraft.
The investigation found a number of factors that may have led to the captain not aligning the aircraft on the runway centreline for the take-off. Those factors included misinterpreting the normal runway cues, time pressure to depart, the weather conditions at Townsville Airport and the associated delays during the aircraft’s arrival, landing and departure.
ATSB investigation AO-2023-027
Between June 2023 and April 2024, 3 misaligned take-offs occurred at Perth Airport, Western Australia. Each occurred before first light and in all 3 incidents, when entering runway 06 from taxiway V, the pilots taxied past the turn onto the centreline and lined the aircraft up along the runway edge lighting on the far side of the runway to where they entered. The investigation found that, in each incident, the pilots believed they had correctly aligned the aircraft with the runway centreline, prior to taking off. Several factors known to increase the risk of a misaligned take-off in the dark were identified from the investigation:
- In terms of the runway environment, there was an unlit and unmarked extended pavement area on each side of runway 06, which made the runway appear wider.
- In relation to the available airport lighting, the lead-on lights from the taxiway continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway’s centreline.
- Recessed edge lights at the start of runway 06 could be mistaken for centreline lighting.
- There was limited ambient airport lighting around taxiway V and runway 06 to enhance visibility.
- The taxi lighting on one of the aircraft was reported by the pilots as being of limited benefit.
- The required runway markings were reported by 2 of the incident pilots to be difficult to see at night.
In one of the incidents, the flight crew’s attention was diverted to completing pre-take-off tasks and their take-off clearance while lining up on the runway. This divided their attention between the flight deck and the monitoring of the external environment.
Safety analysis
Diverted attention
The starter extension included a taxi guideline that curved around towards the extended centreline. The guideline was likely visible to the crew as the flight data showed that the aircraft was taxied along the line from the time it entered the starter extension bypass pad until the time it commenced the right turn to line up on runway 09. The captain reported that, although their intention was to use the full length of the extension, it was not required and due to the dark, ambient conditions, they did not want to continue that plan and risk exiting the pavement. As such, they turned the aircraft early.
The flight crew reported that the ready checks were conducted while turning the aircraft to line up for departure. The Flight Crew Operating Manual stated that ready checks could be conducted at a time appropriate for the anticipated take-off. However, the manual did not provide any guidance as to when an appropriate time was during this process. Therefore, the decision was at crew discretion and dependent on the circumstances at the time.
The FO and captain had predominantly focused their attention inside the flight deck while conducting the ready checks. The captain also reported becoming momentarily distracted looking out the side window. This was at a time when they would also be required to monitor the aircraft’s taxi path. The data showed that the aircraft was turned tightly to the right of the extended centreline and was no longer following the line markings for guidance.
Barshi and others (2009) discuss that it was easy for attention to become absorbed in one or more tasks, allowing another task to drop from awareness. Therefore, it can be concluded that, during the turn to line up, the flight crew's attention was diverted to completing the ready checks, likely reducing their monitoring of the aircraft position within the starter extension, and resulted in it being close to the edge of runway 09. This was consistent with the ATSB research report (2010), which discussed flight crews becoming focused on other tasks upon entering the runway or just prior to entering the runway, and that this was a frequently cited factor in misaligned take-off occurrences.
Misaligned take-off
Although not required for performance, using the starter extension allowed for additional take-off distance and a wider turn than was normally available at airports where the aircraft was mostly operated. However, as identified through ATSB research (2010) and related investigations, additional pavement on one or both sides of the runway has been known to provide erroneous visual cues for pilots. This potentially gives the impression that the additional pavement is part of the runway and that the runway is wider than it is.
Then, following completion of the ready checks and when the aircraft neared completion of the turn to line up, the captain reported being drawn to a row of white lights, believing them to be centreline lights, even though such lights were not fitted to runway 09. With reduced visual cues available due to the dark conditions, a distinct visual indicator such as the white runway edge lights was likely to have been an influence in their belief that it was the runway centreline. Such dark ambient conditions have been consistently cited in the research and similar occurrences. The FO reported looking up but also believed the aircraft was correctly lined up, having associated their observation of the runway threshold markings as being in the correct position to line up.
However, imagery of runway 09 in similar conditions to the incident flight did show that the runway threshold lights, edge lights and right side precision approach path indicator lights would have been visible to the crew from their line‑up position. Confirmation bias is the tendency for people to seek information and cues that confirm their tentatively held hypothesis or belief (Wickens et al, 2022). As the flight crew believed they were correctly aligned with the runway centreline, they commenced the take-off roll.
Low pass
The flight crew noted no indications of a landing gear malfunction or failure, and the gear was retracted without issue following the misaligned take-off. They also received advice from the Mildura Airport aerodrome reporting officer that no aircraft parts or debris were identified along the runway. As the aircraft documentation did not provide guidance for such an incident, and to further assess the condition of the landing gear, the flight crew decided that a visual inspection via a low pass of the Melbourne Airport ATC tower was necessary.
The flight crew did not contact QantasLink operations for assistance regarding the landing gear or the conduct of the low pass. This prevented QantasLink from providing input into the decision-making process. Further, while a visual inspection (using binoculars) by ATC from the tower may give a general assessment of the landing gear, it was not likely to have identified specific damage that would have otherwise been visible at close proximity during a ground inspection.
A flight at low altitude, and at a low speed with the landing gear and flaps extended may introduce a number of risks. Notably, the low pass was conducted lower than the briefed low pass height. As this was not a procedure within the operations manuals, there was no assurance that all potential risks had been identified and mitigated.
Unauthorised/unsupervised use of prescription medication
Post‑incident drug and alcohol screening of the flight crew detected the presence of a medication, which the captain reported was not prescribed to them. The medication had been taken in the days prior to the incident flight, and although the substance was above the permitted threshold for detection, the results could not be used to assess any level of impairment. Independent analysis by a forensic pharmacologist indicated any effects from the medication could not be completely ruled out, however, impairment was not expected given the reported dosage and time elapsed.
The medication taken could only be dispensed with a prescription, and its consumer medicine information sheet highlighted this requirement and several cautions and potential side effects. Although it was a strictly controlled, commercially produced medication, the absence of medical supervision meant there was no assurance that the captain would not experience any adverse effects or impairment that may have impacted their ability to safely operate the aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the misaligned take-off involving Bombardier DHC-8-315, VH-TQM, at Mildura Airport, Victoria, on 25 February 2025.
Contributing factors
- During line‑up, the aircraft was taxied off the starter extension guidance line and the flight crew’s attention was diverted to completing the ready checks. This likely reduced their monitoring of the aircraft's position within the starter extension and resulted in it being positioned close to the right edge of runway 09.
- The flight crew commenced the take-off from a misaligned position resulting in damage to the aircraft and runway edge lights.
Other factors that increased risk
- The flight crew conducted a low pass to facilitate a visual inspection of the landing gear by air traffic control. There were no supporting procedures for the low pass or visual inspection, nor did the flight crew contact the operator to seek assistance.
- The presence of a prescription medication was detected in the captain's post‑incident drug and alcohol test that was not prescribed for them. While they were unlikely to have been impaired by the medication, there was no assurance that the captain would not experience any adverse effects or impairment that may have impacted their ability to safely operate the aircraft.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence. |
Safety action by QantasLink
QantasLink advised the ATSB of the following safety actions:
- Targeted human factors/non-technical skills training on the threat awareness of factors that have contributed to misaligned take-offs has been included in wider flight crew recurrent training.
- Further information and a diagram was added to QantasLink operational documentation for Mildura Airport, specifically for the runway 09 starter extension to improve flight crew familiarity and situation awareness.
- Educational material regarding departure briefings and identifying relevant threats was included in various mediums available to flight crew.
- A safety alert was issued to flight crew soon after the incident with a new policy that prohibits ‘ready checks’ being completed during runway end turns. This was incorporated permanently in the Flight Crew Operating Manual to ensure that during runway turns the flight crew’s attention was not divided externally between aircraft manoeuvring and internally on checklist completion.
- A policy was introduced to outline the risks associated with an ATC tower fly past published in the operations manual and aligned with other operators in the Qantas Group.
- A risk review was conducted on reduced sleep opportunity during overnights, fatigue reporting trends, risk controls and mitigators currently used in fatigue risk management.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the flight crew
- the cabin crew
- QantasLink
- Civil Aviation Safety Authority
- Airservices Australia
- Bureau of Meteorology
- Mildura Airport
- recorded data from the aircraft
- the consultant forensic pharmacologist.
References
Australian Transport Safety Bureau. (2010). Factors influencing misaligned take-off occurrences at night, Australian Transport Safety Bureau, Australian Government.
Civil Aviation Safety Authority. (2024). Civil Aviation Safety Regulations 1998 Part 99- Drug and alcohol management plans and testing, Civil Aviation Safety Authority, Australian Government.
Civil Aviation Safety Authority. (2019). Part 139 Manual of Standards for Aerodromes, Civil Aviation Safety Authority, Australian Government.
Dawson, D., Sprajcer, M., & Thomas, M. (2021). How much sleep do you need? A comprehensive review of fatigue related impairment and the capacity to work or drive safely. Accident Analysis & Prevention, 151, 105955. doi: 10.1016/j.aap.2020.105955.
Goode J.H. (2003). Are pilots at risk of accidents due to fatigue?’ Journal of Safety Research, 34(3), 309–313. doi: 10.1016/s0022-4375(03)00033-1.
Dawson, D., Sprajcer, M., & Thomas, M. (2021). How much sleep do you need? A comprehensive review of fatigue related impairment and the capacity to work or drive safely. Accident Analysis & Prevention, 151, 105955. doi: 10.1016/j.aap.2020.105955.
Loukopoulos, L. D., Dismukes, R. K., & Barshi, I. (2009). The multitasking myth: Handling complexity in real-world operations. Routledge.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- flight crew
- cabin crew
- QantasLink
- Civil Aviation Safety Authority
- consultant forensic pharmacologist.
Submissions were received from:
- the flight crew
- QantasLink.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Footnotes
| 1 | Although the crew was scheduled for 3 sectors the following morning, the captain was only rostered to fly the first sector back to Melbourne. |
| 2 | Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path. |
| 3 | Starter extension bypass pad: a runway starter extension may be established where additional take-off distance, take‑off run or accelerate-stop distance is required (Civil Aviation Safety Authority advisory circular AC 139.C-09 v1.0). It may also incorporate a bypass pad, which resembles a runway turn pad except that it is part of the runway starter extension and allows an aircraft to go around the declared end of the runway and runway end lights before turning around 180° to use the runway in a reciprocal direction. |
| 4 | The flight data for the incident was downloaded by the operator and provided to the ATSB for analysis. The cockpit voice recorder was removed from the aircraft and downloaded by the ATSB. However, a combination of the 1 hour and 45-minute flight time and delays in the isolation of the recorder resulted in the incident flight being overwritten. |
| 5 | The storm light is part of the flight deck lighting, which will illuminate the instrument panel when on. |
| 6 | The 70 kt and V1 calls were procedural calls that served as a confirmation of the indicated airspeed (70 kt) and as a decision point for the flight crew. Below 70 kt, the take-off was to be rejected for any failure, malfunction or caution/warning light. Between 70 kt and V1, the take-off was to be rejected for a critical malfunction or malfunction that was deemed to make the aircraft not flyable. Above V1, the take-off was to be continued. |
| 7 | Responses based on the Samn-Perelli 7-point scale which asks people to rate their fatigue at a point in time: 1 = fully alert, wide awake; 2 = very lively, responsive, but not at peak; 3 = okay, somewhat fresh; 4 = a little tired, less than fresh; 5 = moderately tired, let down; 6 = extremely tired, very difficult to concentrate; 7 = completely exhausted, unable to function effectively. |
| 8 | Morning civil twilight or first light is defined as the instant in the morning when the centre of the Sun is at a depression angle of 6° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible. The brightest stars and planets can be seen and for navigation purposes at sea, the sea horizon is clearly defined. Sunrise is defined as the instant in the morning under ideal meteorological conditions, with standard refraction of the Sun's rays, when the upper edge of the Sun's disk is coincident with an ideal horizon. |
| 9 | Runway threshold lights: When viewed approaching the start of a runway, the threshold lights will be green, with red showing at the end of the runway. |
| 10 | Precision approach path indicator: a ground based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach. |
| 11 | Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft. |
| 12 | Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules, rather than by outside visual reference. Typically, this means flying in cloud or limited visibility. |
Occurrence summary
| Investigation number | AO-2025-008 |
|---|---|
| Occurrence date | 25/02/2025 |
| Occurrence time and timezone | 0636 EDT |
| Location | Mildura Airport |
| State | Victoria |
| Report release date | 12/05/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Runway excursion |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Bombardier Inc |
|---|---|
| Model | DHC-8-315 |
| Registration | VH-TQM |
| Serial number | 604 |
| Aircraft operator | Eastern Australia Airlines Pty Ltd operating as QantasLink |
| Sector | Turboprop |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Activity | Commercial air transport-Scheduled-Domestic |
| Departure point | Mildura Airport, Victoria |
| Destination | Melbourne Airport, Victoria |
| Injuries | None |
| Damage | Minor |