Rejected take-off involving SAAB 340, VH-ZRC, Flinders Island Airport, Tasmania, on 4 November 2022
Final report
Report release date: 17/05/2023
Executive summary
What happened
On 4 November 2022, a Saab Aircraft Co 340B, registered VH-ZRC and operated by Pel-Air Aviation Pty Limited, was preparing to take-off from Flinders Island, Tasmania. During the take-off roll, the aircraft veered to the left of the runway centreline and the crew detected a decrease in acceleration before rejecting the take-off. After the aircraft came to a stop, the pilots noted significant tyre marks on the runway, a flat spotted tyre, and all main landing gear tyres were deflated.
What the ATSB found
The ATSB found the parking brake handle had likely not been completely seated in the panel when released by the pilot resulting in residual pressure remaining in the brake system. During the taxi to the runway, the residual pressure in the brake system provided a partial application of the brakes allowing heat to generate within the brake system. This resulted in a continual increase in brake application. During the take-off roll, heat generation increased significantly resulting in further application of the brakes and the crew rejecting the take-off. All main landing gear wheel fusible plugs activated deflating the main landing gear wheels.
What has been done as a result
The operator reported a number of safety actions that have been taken as a result of this occurrence. These include the dissemination of a Notice to Aircrew to all company pilots with detailed information on the operation of the parking brake. A review of the ground school information specific to the function and operation of the parking brake. The inclusion of a parking brake function and operation as a check item in the upcoming flight crew cyclic.
The operator also advised an intention to disseminate an occurrence briefing to all flight crew that will include engineering information related to the design and function of the parking brake system and the importance of completely seating the parking brake handle in the panel.
Safety message
This occurrence demonstrates the importance of completing routine tasks in accordance with manufacturer’s instructions. The outcome of this event, no passenger injuries and minimal aircraft damage, was a result of the flight crew’s effective monitoring of the aircraft’s performance and prompt action to reject the take-off when the expected performance was not achieved.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
At 0912 local time on 4 November 2022, a Saab Aircraft Co 340B, registered VH-ZRC and operated by Pel-Air Aviation Pty Limited, departed Melbourne Airport, Victoria for a multi-day, multi-stop charter flight with 25 passengers and 3 crew. The crew consisted of a captain, first officer and a cabin attendant. The first officer was undergoing command training experience and was flying from the left seat, with the captain seated in the right seat. After an uneventful flight the aircraft landed at Flinders Island, Tasmania at approximately 1012 and taxied to the terminal. The passengers disembarked and, along with the cabin attendant, departed the airport for a sightseeing tour of Flinders Island. Both the captain and the first officer remained at the airport to conduct post flight duties and to prepare for the next leg of the charter to Wynyard, Tasmania, scheduled for 1430.
After the cabin attendant and the passengers returned to the aircraft and were boarded, the first officer started the aircraft’s engines and conducted the appropriate checklists. Due to the short taxi required at Flinders Island, the flight crew decided to delay commencement of the taxi until they heard the flight attendant commence the safety briefing.
The first officer released the parking brake and conducted an immediate 180° left turn out of the parking bay (Figure 1). They then proceeded to taxi the aircraft to the threshold of runway 32 via runway 23.[1] The first officer commented that there was no abnormal handling or unusual power settings required to taxi the aircraft. They decided to taxi slowly so the cabin attendant had sufficient time to prepare the cabin for take-off. The first officer also recalled slowing the aircraft with the brakes prior to entering the runways. The aircraft entered runway 32, back tracked and lined up on the runway centreline in preparation for take-off.
The first officer commenced the take-off roll, noting that a crosswind was present from the left. The first officer glanced down after setting power to check the torque gauges. When the first officer looked up again, they noted that they had drifted over to the left of the runway centreline, with the airspeed indicating 46 KIAS.[2] In response, the first officer applied right rudder and brought the aircraft back onto the centreline of the runway. The aircraft continued to accelerate to around 80 knots when the flight crew noted a reduction in the aircraft’s acceleration rate. The first officer called failure, the captain called stop and the take-off was rejected. The aircraft reached a maximum airspeed of 96 knots.
Figure 1: Flinders Island Airport

Source: Google Earth, annotated by the ATSB
When the first officer retarded the power levers the aircraft began to veer to the right of the runway centreline. They then used the nose wheel steering tiller in an attempt to keep the aircraft on the centreline. The first officer also recalled the aircraft felt like it was braking by itself, and that pressure was felt in the brake pedals under their feet.
Just prior to the aircraft coming to a complete stop the Flinders Island Airport Operations Officer (ARO) radioed the flight crew on the Flinders Island Common Traffic Advisory Frequency to advise them of smoke coming from the aircraft’s wheels. The flight crew acknowledged the radio transmission.
The first officer advised the cabin attendant and passengers to remain seated. Melbourne air traffic control was contacted and informed that VH-ZRC was disabled on runway 32 at Flinders Island. The ARO further advised the crew that the smoke had dissipated. The pilots shut down the aircraft and the passengers were disembarked.
The aircraft was inspected by the pilots after the occurrence, with the following observed:
- all 4 main landing gear wheels on both the left and right main landing gear had deflated
- the outboard wheel on the left main landing gear had a flat spot (Figure 2).
Figure 2: Left main landing gear after occurrence
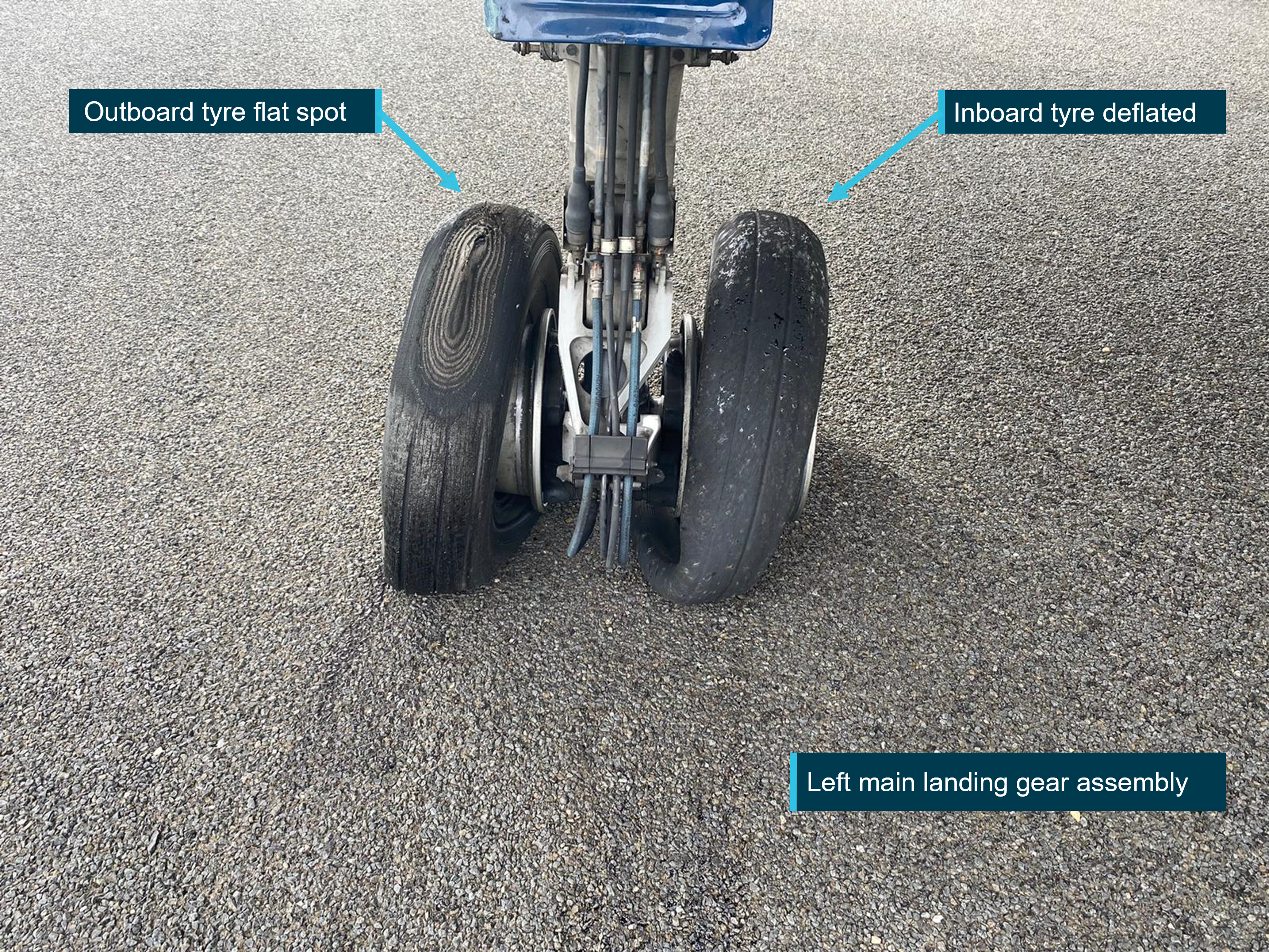
Source: Supplied, annotated by the ATSB
The runway was also inspected by the pilots and the ARO, with the following observed:
- tyre marks were evident commencing 300 m from the runway threshold until the aircraft came to a stop approximately 1,150 m from the runway threshold (Figures 3 and 4)
- initial tyre marks showed a veering to the left of centreline
- final tyre marks displayed a significant veer to the right with a change in tyre markings from a locked tyre to a deflated tyre prior to the aircraft coming to a stop (Figure 5).
Figure 3: Tyre marks on runway
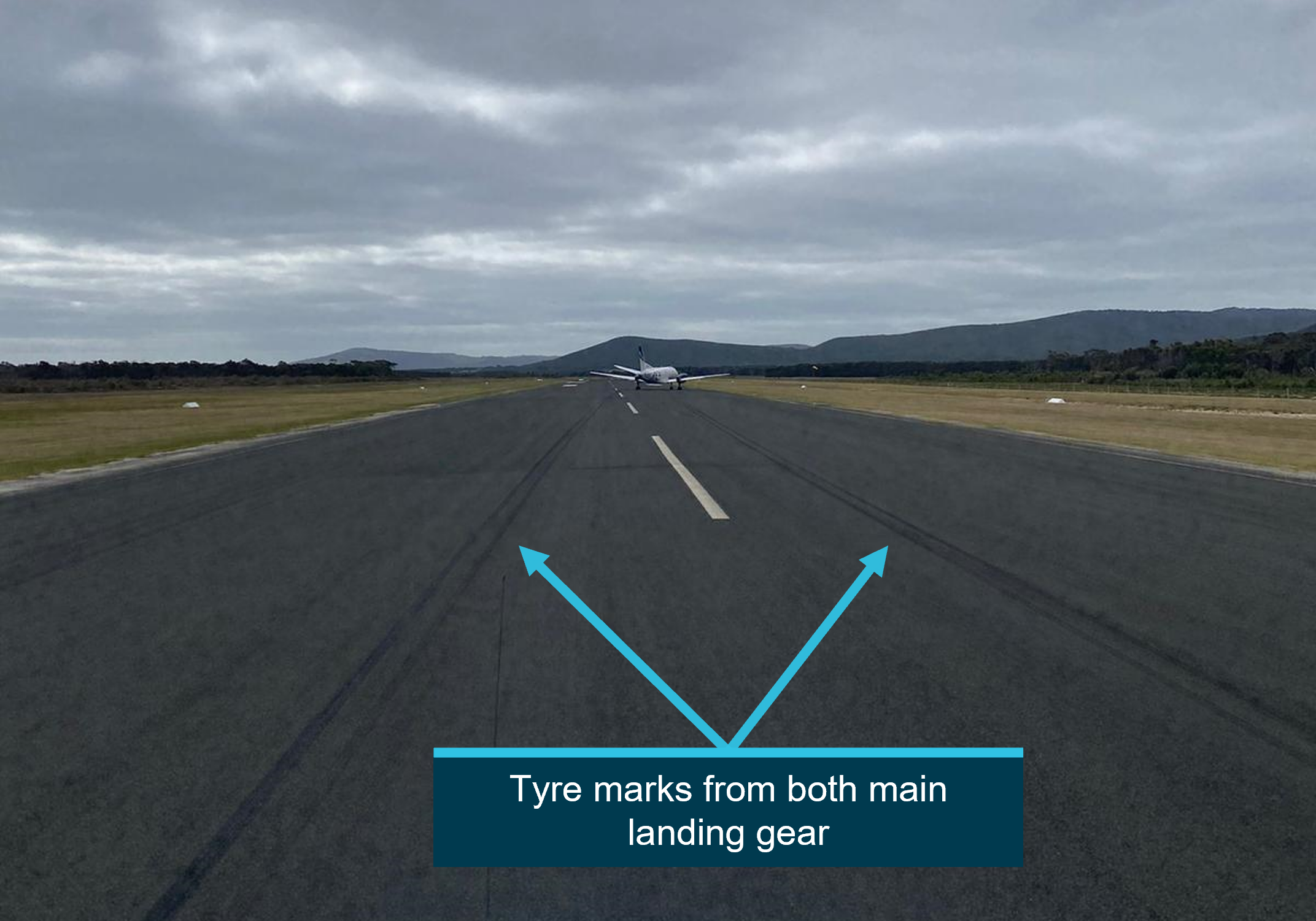
Source: Supplied, annotated by the ATSB
Figure 4: Initial tyre marks from VH-ZRC on runway 32
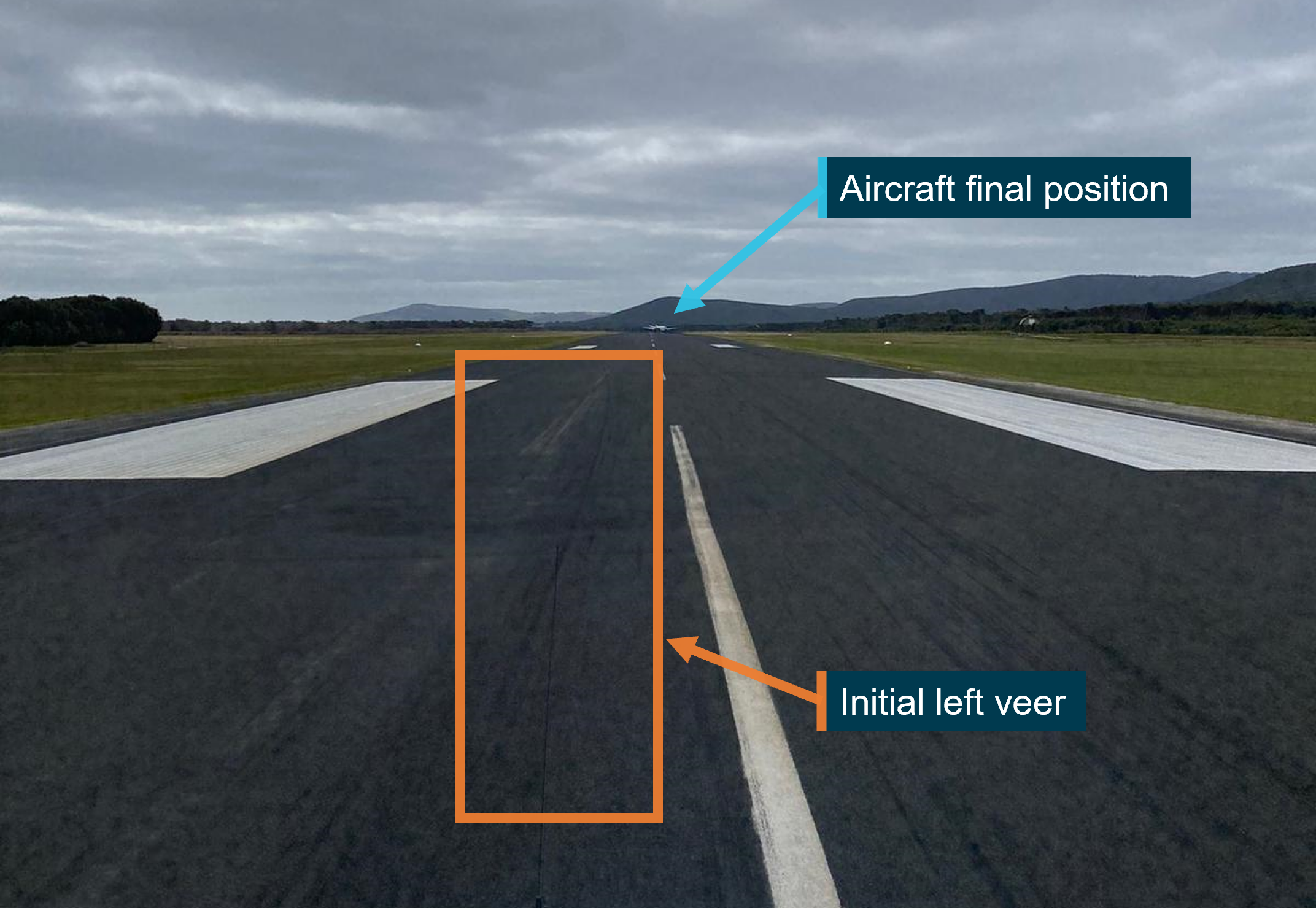
Source: Supplied, annotated by the ATSB
Figure 5: Left main landing gear tyre marks
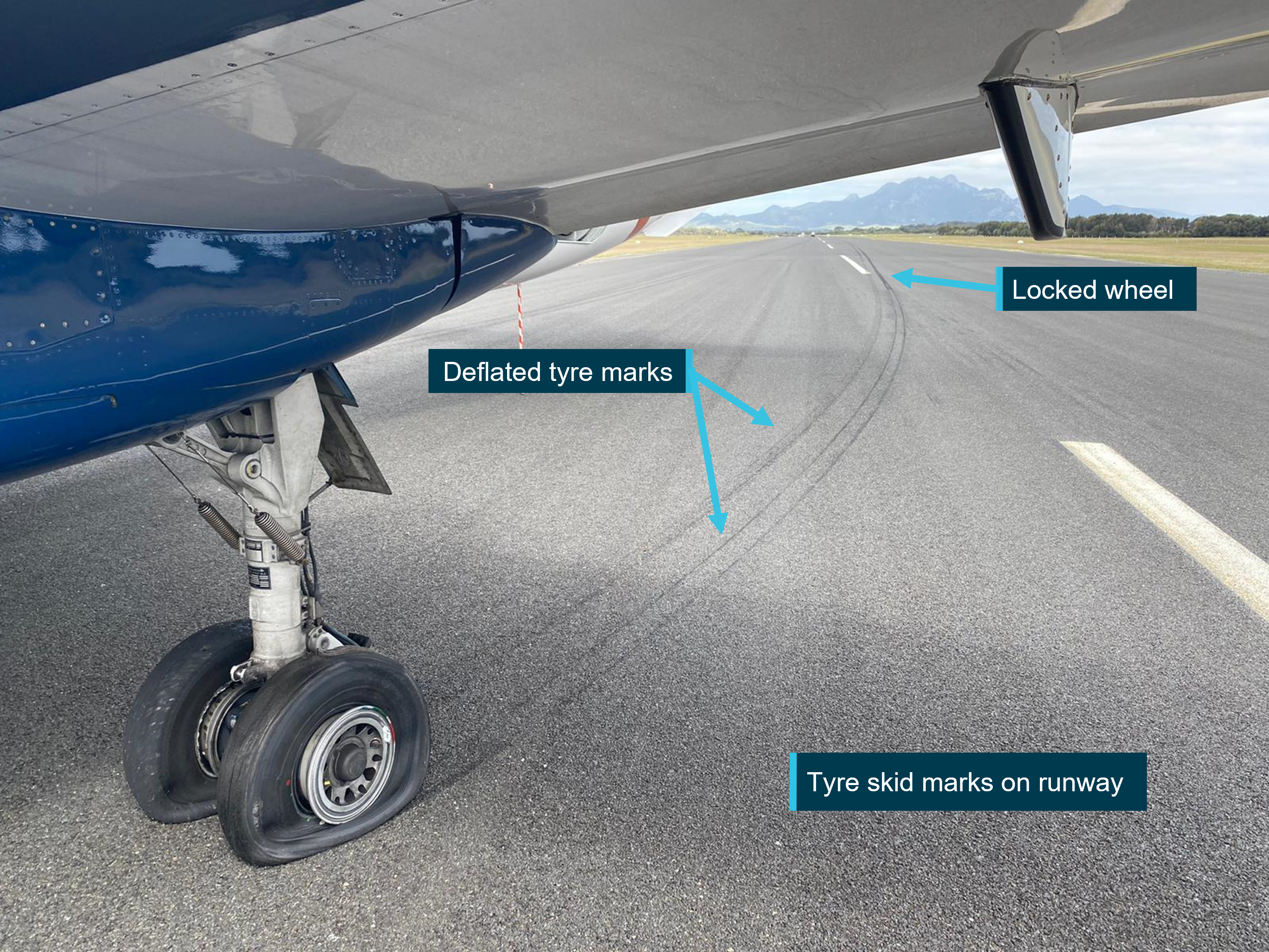
Source: Supplied, annotated by the ATSB
A Rex Airlines engineering crew was flown in to inspect the aircraft. The engineers identified that the main landing gear wheels had deflated due to their fusible plugs activating. All the main landing gear wheels and brakes were replaced. Brake and parking brake testing was carried out with no faults evident, and the aircraft was returned to service.
Context
Pilot information
The captain held an Air Transport Pilot Licence (Aeroplane) and a multi-engine command instrument rating. The captain held a Class 1 aviation medical certificate. The captain had a total flying time of 4,660 flying hours with 4,461 hours on the SAAB-340.
The first officer held a Commercial Pilot Licence (Aeroplane) and a multi-engine command instrument rating. The first officer held a Class 1 aviation medical certificate. The first officer had a total flying time of 2,449.5 flying hours with 2,219 hours on the SAAB-340.
Flinders Island weather
The pilots and ARO reported that the wind during the take‑off roll was from 280° at 16 knots with broken cloud at 3,000 ft above the airport. Visibility was greater than 10 km.
Brake system
The main landing gear wheels are fitted with hydraulic disc brakes. Each landing gear has an inboard and outboard brake assembly which are powered by separate hydraulic circuits, an inboard brake circuit and an outboard brake circuit. Each circuit has its own accumulator that is pressurised, when required, by a demand electrical hydraulic pump. The brake circuits share a common hydraulic return line to the aircraft hydraulic system main reservoir. Independent wheel braking is controlled by toe pedals at the top of the rudder pedals. Each pedal is connected via a cable to its corresponding brake valves.
Figure 6: Brake system schematic
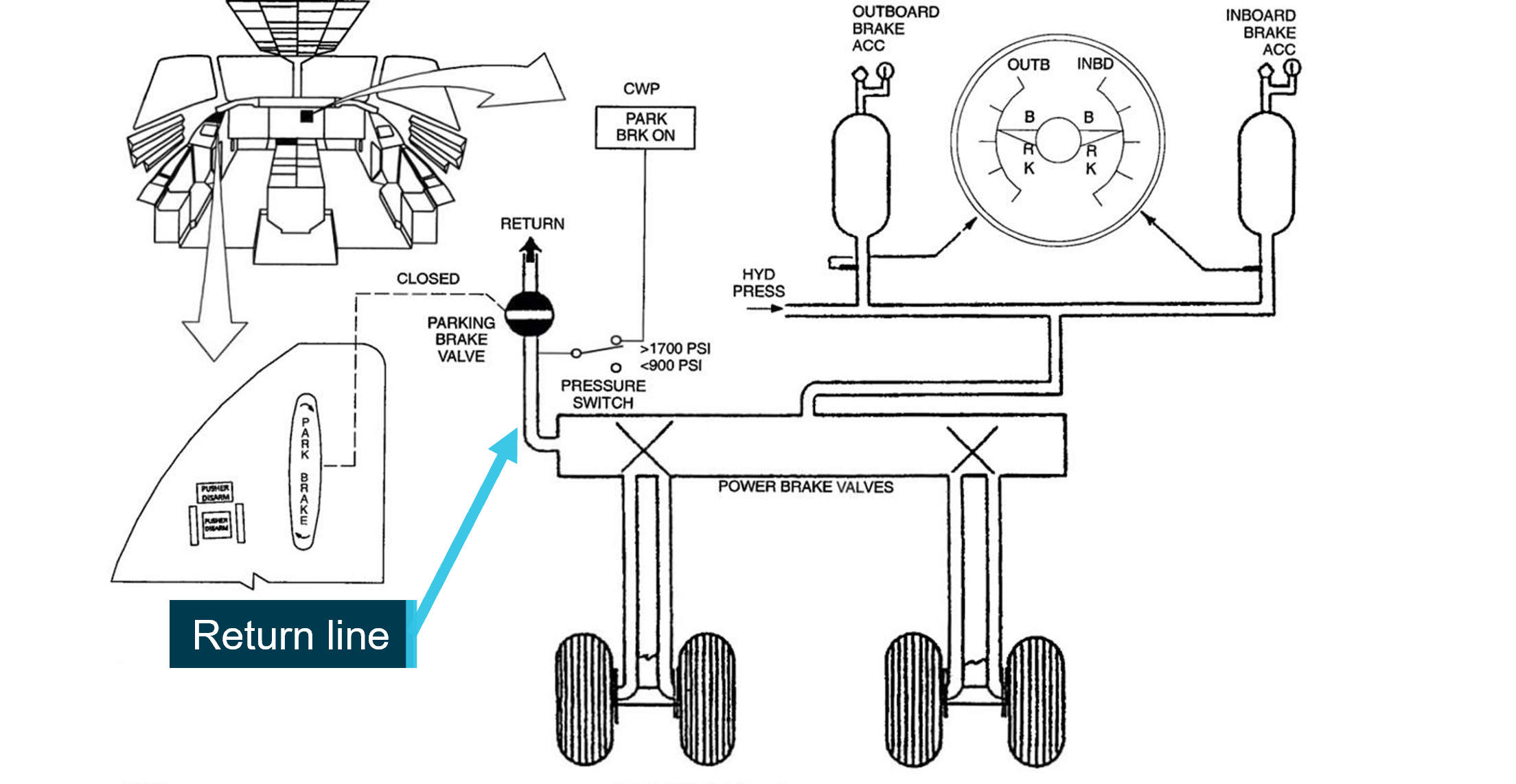
Source: Supplied, annotated by the ATSB
Parking brake
The parking brake is controlled by a handle on the left pilot’s side panel (Figure 6). The handle is attached via a push-pull cable to a parking brake valve located in the brake hydraulic circuit common return line. The parking brake is set by pulling up on the handle whilst depressing the brake pedals. This action closes an internal valve against spring pressure inside the parking brake valve, retaining hydraulic pressure in both brake circuits and maintaining brake application. The handle is then locked in the UP position by rotating the handle 30° clockwise. When the parking brake is set, the pilots reported that it is usual for there to be a firmness felt in the toe brakes on the pedals.
Figure 7: Parking brake valve internal
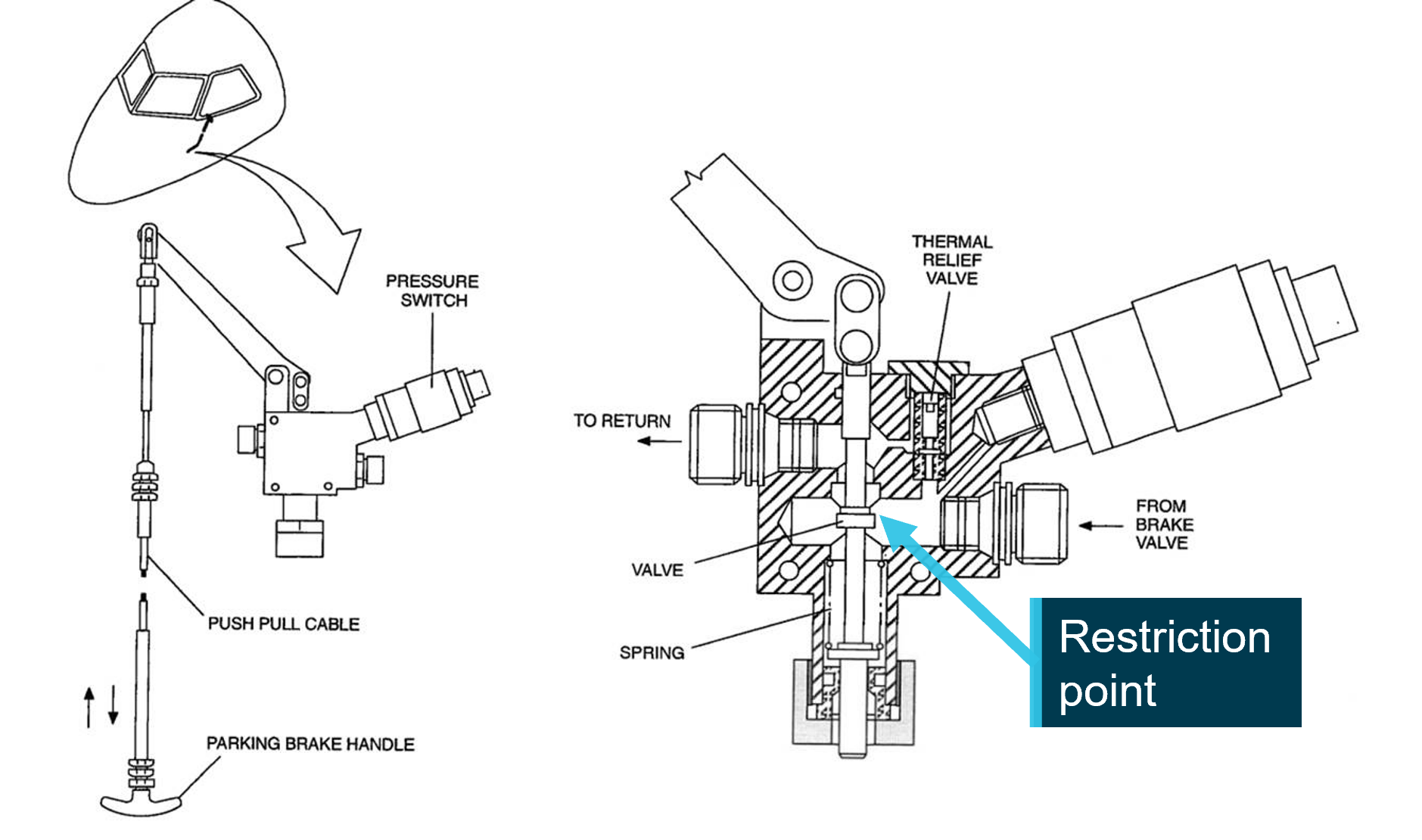
Source: Supplied, annotated by the ATSB
The parking brake is released by turning the handle 30° anticlockwise and pushing the handle down into the panel. This mechanically opens the return line, relieving pressure from the brake circuit, allowing the brakes to release.
The brake system requires an unrestricted hydraulic fluid flow through a single return line within the parking brake valve for normal operation (Figure 7). Any restriction of this return line will increase the time required for brake pressure to be relieved, resulting in a partially applied or dragging of the brakes. A dragging brake will generate heat within the wheel and brake assemblies. This will cause all brake components, including the hydraulic fluid, to expand, further increasing the pressure in the brake circuits. In the event of a restriction, this increase in pressure will transfer directly to an increase in brake application.
Parking brake annunciator
An amber PARK BRK ON annunciator light on the pilot’s Central Warning Panel, located in the centre of the dashboard, illuminates when parking brake hydraulic pressure exceeds 1700 psi (Figure 6). The light goes off when the parking brake handle is pushed down and/or the pressure reduces below 900 psi. The pilots recalled that there were no warnings or cautions on the Central Warning Panel prior to take-off.
Anti-skid system
The Saab 340B is fitted with an anti-skid brake system that maximises braking efficiency by monitoring wheel speed signals across all 4 main wheels. The system modulates brake pressure in the brake hydraulic circuits to prevent a wheel locking. The anti-skid valves are located within the brake circuits, upstream of the parking brake valve, and have no influence on parking brake application.
Fusible plugs
The main landing gear wheels are fitted with 3 fusible plugs each. Should a critical temperature be reached in the wheel assembly, the core of the fusible plug will melt and provide a relief mechanism allowing the tyre to deflate.
Flight data
The flight data recorder was downloaded by the operator and data from the occurrence event and the 2 previous days of flying was provided to the ATSB. ATSB examination of the recorded flight data did not identify any anomalies in relation to engine operation which could have contributed to a loss of acceleration during the event. There were no brake system parameters recorded on the flight data recorder.
Manufacturers response
The manufacturer, Saab Aircraft Co, were contacted for further information about brake system design and operation. Saab stated that due to the mechanical nature of the brake system, with cables between the pedals and the brake valves, and considering that the brake system was inspected with no faults after the occurrence, they could not identify any other system reason that could contribute to brake application other than the parking brake. They further advised that if the parking brake is released properly and the parking brake valve is serviceable, there is no possibility of both brake systems remaining on.
Saab were also asked if they were aware of any similar examples of occurrences with the Saab 340 aircraft, Saab responded that, after a search of their database, they did not find any comparable occurrences.
Post occurrence rectifications
After the occurrence, the following rectifications were carried out prior to the aircraft returning to service:
- all 4 brake assemblies were replaced
- all 4 main landing gear wheel assemblies were replaced
- all 4 main landing gear wheel axles were visually inspected with no defects identified
- the input cables to the brake control valves were visually inspected with no binding or defects evident
- a parking brake control system test was carried out with no defects identified
- a high-speed taxi and brake test was carried out with no faults.
The brake and wheel assemblies were transported to the REX engineering workshops for further examination. The examinations found:
- all 4 brake assemblies were within wear limits and the brake pistons were serviceable. All 4 brake assemblies showed signs of overheating and were removed from service
- all 4 main landing gear wheel assemblies displayed signs of overheating evident with all fusible plugs blown. The wheel assemblies were removed from service for disposal.
Safety analysis
On 4 November 2022, a Saab Aircraft Co 340B operated by Pel-Air Aviation Pty Limited, taxied for runway 32 at Flinders Island Airport. During the take-off roll, the aircraft veered to the left and did not accelerate as expected. The crew rejected the take-off and subsequent inspection identified that one tyre was flat spotted and all the main landing gear tyres were deflated.
Subsequent post occurrence rectification and system testing was carried out. No defects or unusual wear was identified on the replaced components other than signs of overheating. The brake system and parking brake system, including handle operation, was tested with no faults identified. The aircraft was released for service with no further brake related faults reported.
Significant tyre marks, from all 4 main landing gear wheels, were observed on the runway after the occurrence. These tyre marks commenced early in the take-off roll and continued to the disabled aircraft. This evidence, as well as a review of the engine parameters from the flight data recorder and reports from the flight crew, identified that the occurrence was brake‑related and not an issue with aircraft propulsion. The brake system, consisting of 2 separate hydraulic circuits, an inboard and an outboard circuit, share a common return line. For all 4 brakes to be applied and overheat the wheel assemblies, a fault would have had to occur in both systems simultaneously or in the single hydraulic return line.
The pilot conducted an immediate 180° left turn from the hardstand as the taxi commenced. This is evidence that the parking brake was released to the extent necessary for pressure to reduce below 900 psi and the PARK BRK ON annunciator to extinguish. The pilots observed that there were no cautions present prior to the take-off roll. The pilot also noted that the aircraft was able to be taxied with no abnormal handling or any extra engine power required however the pilot also reported taxiing slower than usual, to allow cabin crew to prepare the cabin, which may have masked any brake application.
If the parking brake handle is not completely seated by the pilot, the common return line from both brake hydraulic circuits will be partially obstructed within the parking brake valve. This will restrict hydraulic fluid from flowing out of the brake system, slowing down the rate at which pressure is relieved, resulting in a partial application or dragging of the brakes. During the taxi out, the partially applied brakes created heat due to friction resulting in further brake application to the restricted system as the temperature increased.
As the aircraft commenced the take-off roll, heat from the dragging brakes increased rapidly due to the acceleration of the wheel assemblies. At 46 knots the aircraft veered to the left, likely as a result of the left tyre locking and skidding. The pilot corrected towards the runway centreline and continued with the take-off. At approximately 80 knots the pilots observed that the aircraft’s acceleration rate had reduced and the take-off was rejected.
The pilot commented that, when they reduced power, and prior to manually applying the brakes, the aircraft slowed as though the brakes were applied. This was likely a combination of an application of the brakes and the tyres deflating as identified by the change in runway tyre marks. The tyre marks had changed from a solid tyre mark for the left outboard wheel to a set of parallel lines for each individual wheel. These parallel lines are a result of the weight of the aircraft acting only on the edges of the wheel rim through the tyre to the runway, indicative of a deflated tyre. This is evidence that that the core of the fusible plugs had melted due to a build-up of heat in the wheel assemblies, resulting in the tyres deflating during the latter stage of the take-off roll. The pilot commented that when they then applied the brakes, they felt pressure in the pedals and likened it to the parking brake being set.
Consideration of all the available evidence supports a conclusion that the push-pull parking brake handle was likely not completely seated in the console resulting in the parking brake valve partially restricting the hydraulic return line. This residual pressure allowed a partial application of the brakes, or an incomplete release of the brakes, at the commencement of the taxi, resulting in the brakes dragging. This resulted in the generation of heat in the brake system, a continual increase in brake application and the rejected take-off.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the rejected take-off involving SAAB 340B, VH-ZRC, at Flinders Island Airport, Tasmania on 4 November 2022
Contributing factors
- The parking brake handle was likely not completely reset (seated in the panel) by the pilot, resulting in residual pressure remaining in the brake system.
- Residual pressure in the brake system resulted in a partial application of the brakes during taxi. This allowed heat to generate within the brake system resulting in a gradual increase in brake application.
- The significant and increasing drag associated with the partially applied brakes resulted in a flat spotted tyre and all of the main landing gear wheel fusible plugs activating during the take‑off roll.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Pel-Air
Pel-Air advised that they have taken the following safety actions:
- disseminated a Notice to Aircrew to all company pilots with detailed information on the operation of the parking brake
- reviewed the Flight Operations Training and Checking ground school information specific to the function and operation of the parking brake
- included parking brake function and operation as a focus item in the upcoming flight crew check cycle
- provided ancillary training to the occurrence flight crew.
Pel-Air also advised an intention to disseminate an occurrence briefing to all flight crew that will include engineering information related to the design and function of the parking brake system and the importance of completely seating the parking brake handle in the panel.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the flight crew of VH-ZRC
- the Flinders Island Airport Operations Officer
- Pel-Air Aviation Pty Limited
- Saab Aircraft Company
- Airservices Australia
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the flight crew of VH-ZRC
- the Flinders Island Airport Operations Officer
- Pel-Air Aviation Pty Limited
- Saab Aircraft Company
Submissions were received from:
- the captain of VH-ZRC
- Pel-Air Aviation Pty Limited
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2022-054 |
|---|---|
| Occurrence date | 04/11/2022 |
| Location | Flinders Island Airport |
| State | Tasmania |
| Report release date | 17/05/2023 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Rejected take-off |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Saab Aircraft Co. |
|---|---|
| Model | 340B |
| Registration | VH-ZRC |
| Serial number | 340B-390 |
| Aircraft operator | REGIONAL EXPRESS PTY LIMITED |
| Sector | Turboprop |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Flinders Island, Tasmania |
| Destination | Wynyard, Tasmania |
| Injuries | None |
| Damage | Minor |