A sightseeing balloon with 9 passengers on board collided with the side of a tree after entering fog during the descent to locate a suitable landing area
The balloon came to rest on the side of the tree, damaging the lower part of the balloon envelope
To reduce the collision risk if a balloon enters an area of visibility less than that permitted by the visual flight rules, pilots should ensure that an immediate recovery is commenced
A sightseeing balloon with 9 passengers on board collided with the side of a tree after entering fog during the descent to locate a suitable landing area, an ATSB investigation report details.
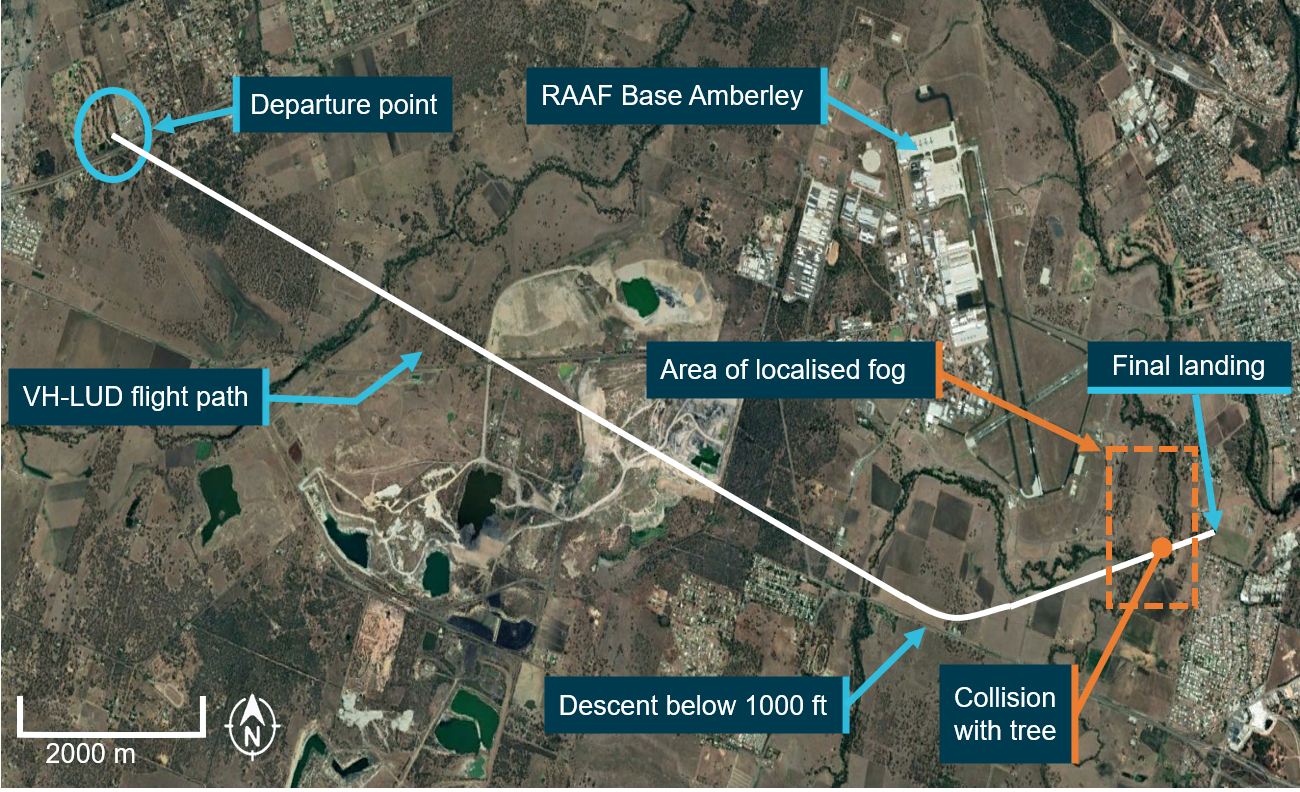
The Floating Images Australia-operated Kavanagh E-240 balloon was conducting a scenic flight near Ipswich, Queensland on the morning of 8 October 2021, with a pilot and the 9 passengers on board.
About 55 minutes into the flight, to the south of the Amberley RAAF Base, the pilot commenced a descent to locate a suitable landing area, during which the balloon entered an area of localised fog where visibility reduced to 10 metres.
The pilot continued the descent into the fog until a tree was observed in the path of the balloon. The pilot attempted to avoid the tree by initiating a climb.
However, due to the 20-30 seconds required before the descent could be arrested and a climb commenced, there was insufficient time for the tree to be avoided.
The balloon came to rest on the side of the tree, damaging the lower part of the balloon envelope.
The pilot subsequently climbed the balloon off the tree and above the fog. The flight continued to an uneventful landing in a nearby paddock that was clear of fog, near the Ipswich suburb of Yamanto.
While there were no injuries, 19 of the balloon’s 480 sewn panels required either repair or replacement.
“The ATSB investigation found that, contrary to the visual flight rules visibility requirement, the pilot entered an area of reduced visibility in which the visibility was 10 metres,” noted ATSB Director Transport Safety Stuart Macleod.
“This did not allow sufficient time to complete an avoidance manoeuvre when an obstacle was observed, as a result the balloon collided with a tree and the balloon envelope was damaged.”
In some circumstances, balloons are permitted to fly in significantly lower visibility than other types of aircraft. While this is mainly due to their inherently low flight speed, it also considerably reduces the available time to see obstacles.
“As balloons can only manoeuvre vertically and significant time may be required to transition from a descent to a climb, they have limited capability to avoid obstacles,” Mr Macleod noted.
“Therefore, to reduce the collision risk if a balloon enters an area of visibility less than that permitted by the visual flight rules, pilots should ensure that an immediate recovery is commenced.”
The ATSB Annual Report 2021-22 outlines performance against the outcome and program structure in the Department of Infrastructure, Transport, Regional Development, Communications and the Arts' Portfolio Budget Statements 2021–22(Opens in a new tab/window)
I am pleased to be able to introduce this annual report on the ATSB activities for 2021–22, a year that continued to present challenges not just for the agency but for the transport sectors we serve due to the ongoing COVID-19 pandemic as well as challenging economic circumstances.
I commenced my term as Chief Commissioner and Chief Executive Officer on 2 September 2021, amidst lockdowns that saw our Canberra, Sydney and Melbourne staff all working from home. It is testament to our staff resilience and flexibility, and the robustness of the ATSB IT systems, that we were able to continue operations with minimal disruptions despite lockdowns, working-from-home requirements, and travel restrictions across the country.
On joining the ATSB I was also well aware that the ATSB is highly respected internationally for its best-practice transport safety investigation, a reputation I will uphold and build upon.
During 2021–22, the ATSB completed and published 60 complex and industry-significant investigation reports into transport accidents and incidents that provided the relevant transport modes with wide-ranging safety learnings. Among the higher profile investigations concluded during the year were:
The runaway and derailment of a loaded iron ore train south of Port Hedland, Western Australia, on 5 November 2018. The ATSB investigation established that the train operator’s risk assessments had limited focus on the potential causes of, and critical controls for preventing, a runaway event.
The evacuation of an A330 passenger aircraft at Sydney Airport, New South Wales, on 15 December 2019 – our investigation highlighted the importance of clear passenger information and commands, and resulted in the airline amending its safety material, cabin crew training, and other procedures as a result of the incident.
The near collision of passenger trains at Park Road Station, Brisbane, on 25 March 2019, following a signal passed at danger (SPAD). Our investigation found that change management relating to the moving or installation of signal aspect indicators, to facilitate the rollout of new rollingstock, did not provide sufficient detail to ensure consistent and conspicuous placement on platforms.
The collision of a fishing vessel with a bulk carrier in darkness near the entrance to Port Adelaide Harbour, South Australia, on 29 February 2020, where we flagged our ongoing concern about collisions between trading ships and small vessels on the Australian coast.
The mid-air collision of 2 twin-engine training aircraft near Mangalore Airport, Victoria, on 19 February 2020, fatally injuring four pilots. The accident was the first mid-air collision in Australia between 2 civilian aircraft operating under instrument flight rules procedures that have been in place for many decades, and our investigation highlighted the potential for ‘ADS-B IN’ technology to improve pilots’ situational awareness in non-controlled airspace.
In addition to ATSB-led investigations, independent investigation agencies in New South Wales and Victoria conduct rail investigations in their jurisdictions on behalf of ATSB under the Commonwealth Transport Safety Investigation Act 2003 (TSI Act). In 2021–22, the ATSB published and promoted 5 rail safety investigations conducted by the New South Wales Office of Transport Safety Investigations (OTSI) and one rail safety investigation conducted by Victoria’s Chief Investigator, Transport Safety (CITS).
The investigations published in 2021–22 identified no fewer than 56 safety issues – factors that if unaddressed have the potential to adversely affect the safety of future operations. Safety issues are characteristic of an organisation or a system, rather than an individual or an operational environment at a specific point in time.
Further, I am pleased to confirm that no changes to published investigation findings were required in 2021–22, evidence of the ATSB central commitment that all published investigations are factually accurate, defendable and evidence-based.
In 2021–22, the ATSB also:
initiated 51 new aviation occurrence investigations, 6 new marine occurrence investigations, and 5 rail occurrence investigations published 15 occurrence briefs, which are short reports that allow us to share safety learnings from a transport safety occurrence that did not meet the threshold of requiring investigation under the TSI Act
received and processed 115 notifications under the REPCON confidential reporting scheme, of which 49 were assessed and classified as meeting the REPCON criteria – during the year, 37 REPCON reports were completed, of which 22 (59%) resulted in safety action being taken by stakeholders
commissioned our new ATSB Investigation Management System (AIMS), a cloud-based IT system used to manage all aspects of our investigations, including logging occurrence notifications, electronic evidence storage and record management for physical evidence, assigning tasks, and recording effort to manage report approvals and distributions
commissioned purpose-built state-of-the-art technical facilities in our Canberra office that will enhance our ability to conduct detailed technical examination of evidence from accident sites.
Outlook
The upcoming 2022–23 period promises to be a year of consolidation as we plan for a more sustainable future for the ATSB. I am aware of the calls stemming from a number of inquiries and associated reports, seeking to extend the ATSB services through an expanded remit. The ATSB will provide input into those inquiries as required.
However, any decisions to change the ATSB remit are a matter for government. It is my immediate priority to address the ATSB existing budgetary challenges – specifically the shortfalls in rail investigation resources resulting from unsustainable funding arrangements outside our core appropriations.
To better position the agency to face the challenges ahead, and to ensure we are making the most effective use of our resources, in 2021–22 I initiated the development of a new strategic plan for the ATSB. This plan, which I intend to publish in early 2023, will set out the ATSB priorities and the actions we will take to ensure we are best positioned to fulfil our responsibilities to government and deliver best practice transport safety investigations for the greatest public benefit.
It will focus on enhancing our best-practice approach to investigations, engaging with stakeholders and influencing improvements in transport safety, fostering our organisational resilience, and affirming our role as the national transport safety investigator.
I look forward to supporting our staff in delivering that plan
I am pleased to present the Australian Transport Safety Bureau’s (ATSB) Corporate Plan, which covers the period 2022-23 to 2025-26.
This Corporate Plan has been prepared consistent with paragraph 35(1)(b) of the Public Governance, Performance and Accountability Act 2013 and the relevant provisions of the Transport Safety Investigation Act 2003 (the TSI Act), which establishes the ATSB. The Corporate Plan is also consistent with the Minister’s revised Statement of Expectations 2021–23 (SOE) for the ATSB, as notified under Section 12AE of the TSI Act. The SOE sets out clear expectations that the ATSB’s resources be used in an efficient, effective, economical and ethical way, following best practice principles and guidelines.
I acknowledge this continues to be a time of great uncertainty for the transport industry in general, and aviation in particular. As an independent safety agency, the ATSB is continuing to apply our safety knowledge and expertise and carefully monitoring the return to safe and reliable transport operations. As an operational agency, the ATSB continues to deploy accident investigation teams where and when necessary during this pandemic.
I look forward to working with the newly elected Federal Government, to ensure the Bureau is well positioned to meet the Minister for Infrastructure, Transport, Regional Development and Local Government’s expectations for the ATSB’s role in improving transport safety. I acknowledge the ongoing uncertainty for Australia’s transport industries operating in an evolving COVID-normal environment and the challenging economic conditions that these sectors face. I am also mindful that such challenges will need to be internally managed to ensure the ATSB maintains its ability to undertake and meet prescribed functions and key deliverables.
I have been the ATSB’s Chief Commissioner for 12 months now. I am aware of the calls stemming from a number of inquiries and associated reports, seeking to extend the ATSB’s services through an expanded remit. The ATSB will provide input into those inquiries as required. However, any decisions to change the ATSB’s remit are a matter for Government. It is my immediate priority to address the ATSB’s existing budgetary challenges – specifically the shortfalls in rail investigation resources resulting from unsustainable funding arrangements outside our core appropriations.
In my time as Chief Commissioner the ATSB has demonstrated itself to me as a highly capable organisation. In the past 12 months we have released a number of complex and industry significant reports that carry wide-ranging safety implications to the relevant transport modes; one such report is the ATSB’s investigation into the mid-air collision near Mangalore Airport in Victoria in 2020. The investigation highlighted the importance of air traffic hazard assessment and the value of aircraft owners installing Automatic Dependent Surveillance-Broadcast (ADS-B) devices to assist pilots with the identification and avoidance of conflicting traffic. Other significant investigations include an investigation into a level crossing accident north-east of Kalgoorlie in Western Australia in 2021 highlighted the risks of driver distraction and the consequences when heavy vehicles and trains operate in the same geographical space and, an investigation into a collision between a bulk carrier and a fishing vessel off the entrance to Port Adelaide in South Australia in 2020 highlighted the need for crew to keep a lookout by all available means including use of radar, radio and automatic identification systems.
As a relatively small operationally-focused agency, the ATSB will need to anticipate change and adapt to ensure we are meeting the needs of government, industry, and the traveling public. Accordingly, I have been working with staff from across the agency to develop a strategic plan that clearly identifies the key objectives, strategies and actions to be given priority over the short to medium term. The plan, to be released this financial year, will have a focus on:
enhancing our products and stakeholder engagement for improving transport safety
fostering organisational resilience
affirming our role as the national transport safety investigator.
An example of the immediate action we are taking, is the greater utilisation of audio-visual content which will increase consumption of our investigation reports and advance important safety messaging. Stakeholders can also expect the ATSB to produce more statistical and research-based outputs ensuring we are making the best use of available data and the specialist capabilities of our people. We will balance these actions with our core occurrence investigation activities which must continue to be managed within our demand/capacity limitations as this will enable us to expedite production and publishing timeframes.
The strategic plan will position the ATSB to be able to provide greater value for persons and organisations seeking to use our products to take safety action.
Based on my recent interactions with a range of prominent overseas safety investigation bodies, it is evident the ATSB is considered a highly reputable agency and world leading. As Chief Commissioner, I am fully committed to continuing to work innovatively and collaboratively with all relevant stakeholders to enhance and amplify our contribution to improving transport safety both domestically and internationally.
The ATSB continues to work towards achieving its new performance measures established in the 2020-21 Corporate Plan. Through revised performance criteria, we are focused on improving our timeliness, demonstrating safety action taken in response to our investigations, ensuring our findings are defendable, and using our resources efficiently and effectively.
To Rollingstock Operators Number: RO-2020-022-SAN-002
Unknown functions in locomotive braking systems
An ongoing investigation, conducted by NSW’s Office of Transport Safety Investigations on behalf of the Australian Transport Safety Bureau, highlights risks associated with misunderstood functionality of locomotive braking systems. Locomotive drivers require a clear understanding of the braking systems on all the locomotives they are operating.
What happened
On 15 December 2020 a loaded grain train derailed whilst descending the 1 in 30 grade rail line between Robertson and Unanderra, NSW.
Runaway locomotives (Source: ATSB)
Why did it happen
During the descent, the train driver lost control of the train. As the train continued to increase speed, the driver did not apply the emergency brake, believing an emergency application of the air brake would disengage the dynamic brake.
The ATSB identified that the locomotives involved had an electronic braking system that allowed the dynamic brake to remain active while the emergency brake was applied. This feature was unknown to the operator and the train driver.
While the specific circumstances of this incident and contributing factors are still under investigation, the ATSB has issued this safety advisory notice to advise rolling stock operators and operational staff of a potential broader industry safety concern.
The ATSB identified similar functional changes on locomotive braking systems more broadly across industry that were also unknown to Rollingstock Operators.
Importantly, dynamic brake functionality is not consistent across all locomotives with electronic braking systems. While some locomotives will disengage the dynamic brake when an emergency brake application is made, in other locomotives the dynamic brake remains functional.
Safety advisory notice
RO-2020-022-SAN-002: The ATSB advises that all Rollingstock Operators (RSO) should review specifications and test locomotives under their control to understand how the braking systems are configured. RSOs must communicate this knowledge through their organisation’s procedures and training material to ensure train crew knowledge and competence in operating various locomotive braking systems.
Ensure understanding of locomotive specifications and operation
Rollingstock Operators must have a complete understanding of the operation of their locomotives. Identifying safety critical information from technical specifications and testing locomotive operations must be completed and used to inform the organisation’s procedural and training material.
In a time of great uncertainty due to the COVID-19 global pandemic, I am proud to report that in 2019–20 the Australian Transport Safety Bureau (ATSB) has been able to continue our focus on improving transport safety through the independent investigation of accidents and incidents, with minimal impact on our productivity and performance.
With many ATSB investigators and operational support staff having come from aviation, rail and marine transport backgrounds, and continuing to maintain those strong industry links, we have great empathy for operators and their respective workforces who are facing an indeterminate future and challenging road to recovery.
Other than the secondment of some staff to Services Australia, we have not been directly involved in the pandemic relief and recovery efforts. However, in support of the transport industry we have continued to apply our safety knowledge and expertise in carefully monitoring the return to operations of safe and reliable transport.
As an operational agency undertaking an essential service, despite the COVID-19 travel restrictions, the ATSB has and will continue to deploy transport safety investigation teams where and when required across the nation during the course of the pandemic. Further, the ATSB’s ICT infrastructure has successfully supported working from home arrangements for our staff. I have worked hard to ensure our staff know that they are supported and feel connected during periods of home-based work and a period of unprecedented uncertainty.
The ATSB has seen a lessening in the number of transport safety occurrences reported to it in the second half of 2019–20, reflective of decreased activity in the aviation industry in particular, due to the COVID-19 pandemic. In addition, we have worked hard as an organisation to reduce the number of active investigations undertaken over time, as we more effectively manage our resources to ensure improved timeliness of report completion.
Nonetheless, during the summer months of 2019–20 we launched a number of complex investigations into significant transport safety accidents, including:
the collision between two freight trains at Jumperkine, Western Australia
the collision with terrain of a C-130 Hercules large air tanker near Cooma, New South Wales
the derailment of an XPT passenger train at Wallan, Victoria
the mid-air collision between two twin-engined training aircraft near Mangalore, Victoria.
Then in early March we launched our investigation into the collision with terrain of a Cessna 404 twin-engine aircraft, with the loss of life of all five on board, near Lockhart River, in far north Queensland.
That long summer of 2019–20 saw the worst bushfire season in Australia’s living memory, which meant a period of high operational tempo for aerial firefighting across Australia. In response to the subsequent Royal Commission into Natural Disaster Arrangements’ request for information, the ATSB produced a safety analysis of aerial firefighting occurrences in Australia, covering the period July 2000 to March 2020. This research report found that estimates of aerial firefighting activity for the 2019–20 bushfire season were around four times higher than other recent bushfire seasons, with more reported occurrences involving aerial firefighting aircraft in Australia in the financial year covering the last bushfire season (between July 2019 and March 2020) than any financial year since July 2000.
The ATSB will continue to examine aviation firefighting safety occurrences with a systemic safety study to commence in 2020–21.
As the COVID-19 pandemic saw a reduction in transport industry activity and transport safety occurrences, in the later months of the year our focus has been on finalising investigations and publishing their final reports. I am pleased to report for 2019–20, we completed and published 47 complex investigations, compared to 34 completed and published complex investigations in 2018–19.
A number of those completed and published complex investigations have led to meaningful improvements in transport safety, and better understandings of transport safety risks. Examples of safety issues raised by ATSB investigations published during 2019–20 concerned upper torso restraints in light aircraft, container ship cargo planning processes, and procedures and guidance for two-driver train operations.
These published investigations, and our new investigations commenced in 2019–20, are consistent with our Minister’s Statement of Expectations, for the period 15 July 2019 to 30 June 2021, which directs us to focus on transport safety as the highest priority, and to give priority to transport safety investigations that have the potential to deliver the greatest public benefit through improvements to transport safety.
These principles guide us in determining which accidents and incidents to investigate, and how best to direct our time and resources, to ensure the best safety outcome for the greatest public benefit. We focus on the public interest where the safety of passengers and workers is concerned, and also on the significant costs to the national economy that can result from an accident.
People and capabilities
It is the skills, professionalism and experience of our people, combined with our highly developed technical expertise and analysis capabilities that enable us to undertake those investigations that have the potential to deliver the greatest public benefit. Right across the agency our staff have broad skillsets, expertise and experience relevant to our role as the nation’s transport safety investigator. And nowhere is that expertise more evident than the ATSB’s governing Commission.
I am very pleased to note that in October 2019, Mr Gary Prosser was appointed to the ATSB Commission. Mr Prosser has 40 years’ experience in the maritime industry, coming from a seagoing career and serving on a wide variety of Australian ships in both the international and domestic trades. More recently, Mr Prosser was the Deputy Chief Executive Officer of the Australian Maritime Safety Authority (AMSA), and he has also served as the Secretary General to the International Organization for Marine Aids to Navigation (IALA).
I am equally pleased to note that Mr Chris Manning was in June 2020 reappointed to the ATSB Commission for a further three years. A former Chief Pilot with Qantas Airways, Mr Manning’s work on the Commission has been exemplary, and we are fortunate to have him with us, working to make transport safer in Australia.
Our Commissioner, Ms Carolyn Walsh also had her tenure extended until September 2020 making her the longest-serving ATSB commissioner.
I would also like to acknowledge and thank Mr Noel Hart for his service to the ATSB Commission and his commitment and passion for improving transport safety since he was first appointed as a Commissioner of the ATSB in July 2009. Mr Hart provided invaluable maritime industry knowledge and experience to countless ATSB investigations.
Also central to the quality of investigations is our ongoing investment in technologies, training and professional development to ensure our investigators have the best available tools and skillsets.
The professional development pathway for our investigators begins with our program of tertiary qualifications the ATSB initiated in partnership with RMIT University in 2019. The inaugural delivery of the Graduate Certificate in Transport Safety Investigation saw 25 participants from both the ATSB and industry gain this coveted tertiary qualification.
The RMIT University partnership will expand to include the development of Graduate Diploma and Masters Programs over time, and is an integral component of our strategy to create a centre of excellence for transport safety investigation in the Asia Pacific region. The ATSB will continue to advance its own safety investigation capabilities through the delivery of these courses, in addition to ensuring that the opportunity exists for industry to do the same.
And we continue to make investments in systems and technologies to ensure our investigators have the best available to effectively undertake their work. Examples include our laser scanning and remotely piloted aircraft systems (RPAS) combined with high accuracy differential GPS data to produce a range of outputs from videos to three-dimensional models of accident sites and vehicles.
Influencing safety action, education and collaboration
Through stakeholder engagement, communication, education and collaboration, the ATSB aims to improve transport safety via influencing safety action. Through our investigations we can identify safety issues but have no powers to make others take safety action. Instead, the ATSB actively engages with stakeholders who are already safety advocates and who may be able to work with us on influencing others to improve safety.
In 2019–20, the ATSB took advantage of a number of key forums and events hosted by industry partners to share priority safety messages and educate key stakeholders as to our role and responsibilities.
In October 2019, we were proud to co-host, alongside the Rail Industry Safety and Standards Board (RISSB) and the Office of the National Rail Safety Regulator (ONRSR), rail safety experts from across the globe at the 29th International Railway Safety Council in Perth.
Also in October, we held our inaugural maritime safety forum, SeaSafe 2019. Following on from the success of our FlySafe 2019 and RailSafe 2019 safety forums delivered in 2018–19, SeaSafe 2019 aligned with the two-day Pacific 2019 International Maritime Exposition in Sydney in order to maximise participation from key stakeholders.
In May 2020, we had planned to host the annual forum of the International Transportation Safety Association (ITSA), for which I am currently the Chair. ITSA is the international network of heads of agencies of independent transport safety investigation authorities from 17 nations, covering aviation, marine, rail and road transport, as well as pipelines and underground infrastructure. This year’s forum, which was to have been held in Sydney, was deferred due to the COVID-19 pandemic.
The mission of ITSA is to improve transport safety in each member country by learning from the experiences of others. It is my hope that that mission can be furthered with our next forum some time in 2021, whether that is held in person in Sydney, or virtually.
And while COVID-19 travel restrictions have placed many conferences and forums on hold, the ATSB has enthusiastically embraced virtual conferences and events to share our safety messages.
Sharing of resources and knowledge is central to our collaboration with our colleagues at the Defence Flight Safety Bureau (DFSB). In January, we were able to exercise the provisions of our Memorandum of Understanding (MoU) with DFSB when they seconded a representative with expertise in the C-130 aircraft to join our investigation team working on the C-130 large air tanker accident.
The ATSB also has in place memoranda of understanding with a number of industry associations that are in a position to reach out to their members with messaging that is tailored to their working environment.
Another example of cooperation was in November, when the ATSB’s communications team hosted media and communications representatives from the AMSA, the Civil Aviation Safety Authority (CASA), Airservices Australia, and the then Department of Infrastructure, Transport, Cities and Regional Development for the first in a series of regular meetings to share details of communications, media and safety promotion activities across the broader group.
This forum will allow the portfolio agencies to work together on promoting and sharing safety issues and education campaigns, such as the ATSB’s ‘Don’t Push it, Don’t Go’ campaign, launched in September 2019 to raise awareness of the dangers of visual flight rules (VFR) for pilots flying into instrument meteorological conditions (IMC).
Outlook
In 2020–21, we will be aligning a new set of performance measures with our Vision 2030 statement. These have been designed to demonstrate our effectiveness against our mission to:
Improve transport safety for the greatest public benefit through our independent investigations and influencing safety action.
Through the revised performance criteria, we are focused on being able to demonstrate the safety action taken in response to our investigations, ensuring that our findings are defendable and timely, and that our resources are being used efficiently.
I intend to publicly release our Vision 2030 statement during 2020–21 at an appropriate time, mindful of and sensitive to the changes occurring within the transport industry.
Another key focus for our agency in 2020–21 will be the replacement of our investigation information management system. This is a significant and essential project utilising cloud technologies and software that will service the ATSB’s investigation information management needs for many years. Investigators will be able to access data and upload evidence to the new system anywhere on any device, while the removal of labour-intensive processes promises to improve our productivity.
From bushfires to a global pandemic, 2019–20 has been a year of unprecedented challenge. I am proud of the ATSB’s staff who have, time and time again, proven themselves resilient and adaptable during this period of uncertainty. Like all Australians, ATSB staff across the nation have had to adapt to changing circumstances during this pandemic. At a professional level they have remained committed to their work, whether this be from the office, home or deploying to transport accident sites across state borders.
Australia’s aviation, rail and marine industries are safer for their efforts.
Carbon monoxide (CO) is a colourless, odourless and tasteless gas found in the exhaust gases of piston‑engine aircraft. Carbon monoxide detectors provide warning to aircraft occupants of the presence of CO levels in the cabin that are above safe concentrations.
What happened
On the afternoon of 31 December 2017, the pilot and five passengers of a DHC-2 Beaver floatplane, registered VH-NOO, boarded the aircraft for a charter flight from Cottage Point to Rose Bay, New South Wales. The aircraft taxied for about 7 minutes. Shortly after take-off, the aircraft deviated from the standard flight path, stopped climbing, and entered a confined area (Jerusalem Bay) below the height of the terrain. The aircraft continued along the bay before making a very steep right turn and colliding with the water. All on board were fatally injured and the aircraft destroyed.
Why did it happen
Toxicological testing of stored blood samples found that the pilot and two of the passengers had elevated levels of carbon monoxide (CO). The levels detected were likely to have adversely affected the pilot’s ability to control the aircraft during the flight.
As it is colourless, odourless and tasteless, CO is generally very difficult to detect. The aircraft was fitted with a disposable CO chemical spot detector. While these type of detectors are commonly used in general aviation aircraft, they have known limitations. They have a limited shelf-life when removed from their original packaging, which may be further affected by factors such as exposure to harsh direct sunlight, cleaning chemicals, and halogens. In addition, they are a passive device, which relies on the pilot regularly monitoring the changing colour of the detector to show elevated levels of CO. In contrast, electronic active CO detectors are designed to attract the pilot’s attention through auditory and/or visual alerts when CO levels are elevated, so are more likely to be effective. These are now inexpensive and widely available. Had the pilot been made aware of the presence of CO, the pilot would have been able to take measures to reduce the risk to those on board. In addition, undetected CO in the cabin is a well‑known risk that has been shown to have contributed to many fatal accidents across the world.
: The use of an attention attracting carbon monoxide detector in the cockpit provides pilots with the best opportunity to detect carbon monoxide exposure before it adversely affects their ability to control the aircraft or become incapacitated. The ATSB strongly encourages operators and owners of piston‑engine aircraft to install a carbon monoxide detector with an active warning to alert pilots to the presence of elevated levels of carbon monoxide in the cabin. If not provided, pilots are encouraged to carry a personal carbon monoxide detection and alerting device.
I am pleased to present the Australian Transport Safety Bureau’s (ATSB) Corporate Plan, which covers the period 2020-2021 to 2023-24. This version of the Corporate Plan, issued in March 2021, is a minor variation of the original plan.
I acknowledge this is a time of great uncertainty for the transport industry in general, and aviation in particular. Many ATSB investigators and operational support staff have come from the aviation, rail and marine transport modes and continue to maintain strong industry links. We have great empathy for operators and their respective workforces who are facing an indeterminate and challenging road to recovery.
The ATSB is not a policy agency, and other than secondment of some staff to Services Australia, we have not been directly involved in the pandemic relief and recovery efforts in support of the transport industry. However, as an independent safety agency, the ATSB is continuing to apply our safety knowledge and expertise in carefully monitoring the return to operations of safe and reliable transport. As an operational agency, the ATSB will continue to deploy accident investigation teams where and when required during the course of this pandemic.
Leading into this new performance period, we have worked hard as an organisation to reduce the number of active investigations undertaken over time. We have managed our resources such that we have teams dedicated to commencing new investigations whilst completing some of the complex, resource intensive investigations we have commenced in recent times. Investigations commenced early in 2020 include the loss of the C-130 firefighting aircraft near Cooma (NSW), the derailment of the XPT near Wallan (Vic), the mid-air collision of two aircraft near Mangalore (Vic), and the loss of five lives in an impact with terrain near Lockhart River (Qld). The ATSB has also responded to the Royal Commission into Natural Disaster Arrangements through the provision of a submission containing an analysis of aviation firefighting safety occurrences.
In this Corporate Plan we have established a new set of performance measures. These are designed to demonstrate our effectiveness against our mission to:
Improve transport safety for the greatest public benefit through our independent investigations and influencing safety action.
Through the revised performance criteria, we are focussed on being able to demonstrate the safety action taken in response to our investigations, ensuring that our findings are defendable and timely, and that our resources are being used efficiently.
The transport safety investigation tertiary qualification which the ATSB initiated in partnership with RMIT University in 2019, will proceed in 2020-2021, despite the impact that the pandemic has had on the tertiary sector. The inaugural delivery of the Graduate Certificate in Transport Safety Investigation in 2019 resulted in 25 graduates from both the ATSB and industry. The RMIT partnership, which will expand to include the development of Graduate Diploma and Masters Programs over time, is an integral component of our strategy to create a centre of excellence for transport safety investigation in the Asia Pacific Region. The ATSB will continue to advance its own safety investigation capabilities through the delivery of these courses, in addition to ensuring that the opportunity exists for industry to do the same.
I am proud of the ATSB’s staff who have, time and time again, proven themselves resilient and adaptable during this period of uncertainty. Like all Australians, ATSB staff across the nation, have had to adapt to changing circumstances during this pandemic. At a professional level they have remained committed to their work, whether this be from the office, home or deploying to transport accident sites across state borders.
This Corporate Plan has been prepared consistent with paragraph 35(1)(b) of the Public Governance, Performance and Accountability Act 2013 and the relevant provisions of the Transport Safety Investigation Act 2003 (the TSI Act), which establishes the ATSB. The Corporate Plan is also consistent with the Minister’s revised Statement of Expectations 2019–21 (SOE) for the ATSB, as notified under Section 12AE of the TSI Act. The SOE sets out clear expectations which, in my capacity as Chief Commissioner and the Accountable Authority, I am committed to meeting in 2020-21 and beyond.
The primary mechanism for the prevention of carbon monoxide exposure to aircraft occupants is to carry out regular inspections of piston-engine exhaust systems to identify and repair holes and cracks, and to detect breaches in the firewall between the engine compartment and the cabin.
What happened
On the afternoon of 31 December 2017, the pilot and five passengers of a DHC-2 Beaver floatplane, registered VH-NOO, boarded the aircraft for a charter flight from Cottage Point to Rose Bay, New South Wales. The aircraft taxied for about 7 minutes. Shortly after take-off, the aircraft deviated from the standard flight path, stopped climbing, and entered a confined area (Jerusalem Bay) below the height of the terrain. The aircraft continued along the bay before making a very steep right turn and colliding with the water. All on board were fatally injured and the aircraft destroyed.
Why did it happen
Toxicological testing found that the pilot and two of the passengers had elevated levels of carbon monoxide (CO) in their blood. The levels detected were likely to have adversely affected the pilot’s ability to control the aircraft during the flight. Carbon monoxide is a colourless, odourless and tasteless by-product found in the exhaust gases of piston-engines.
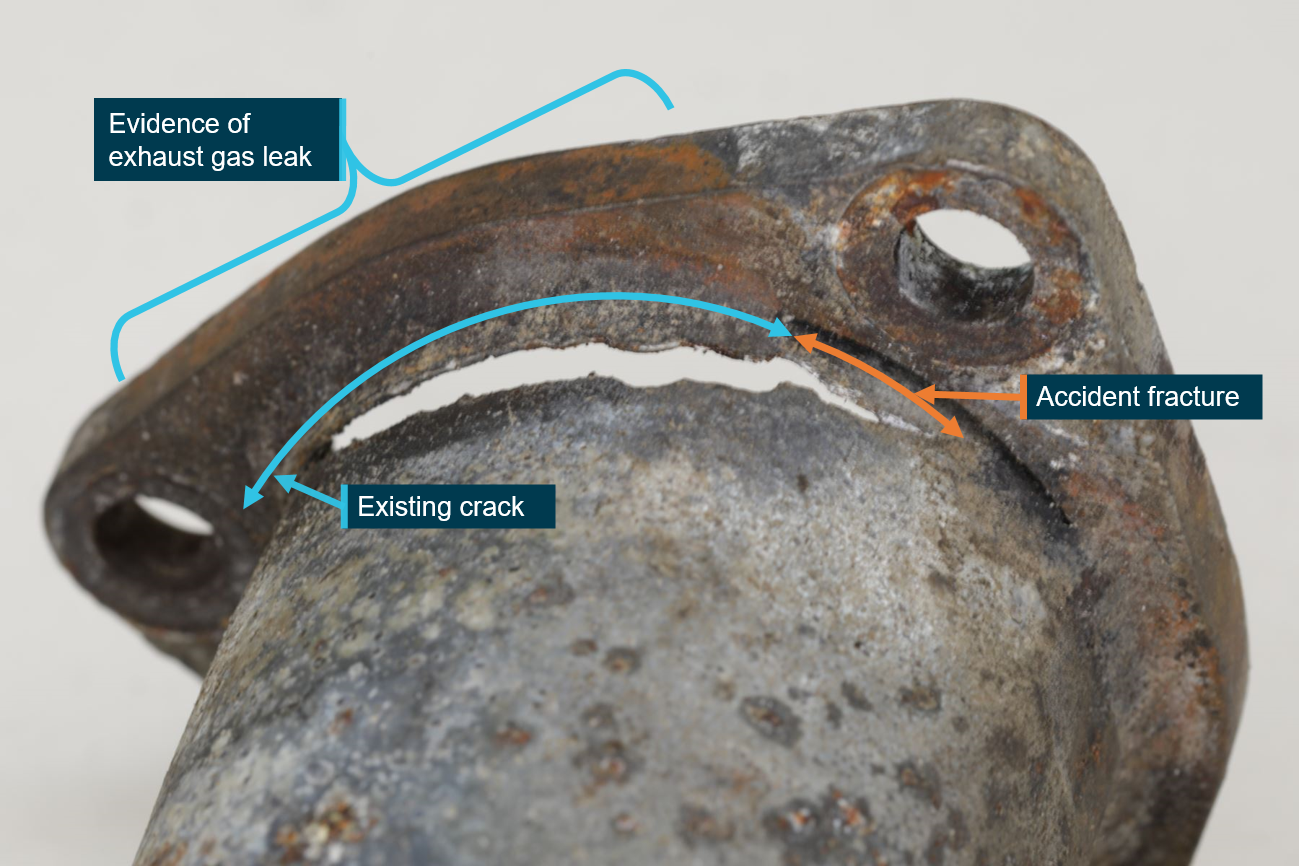
The ATSB conducted a detailed examination of the engine exhaust collector-ring and found evidence of pre‑existing cracking and exhaust leakage into the engine bay.
In addition, three out of eight bolts used to secure the magneto access panels in the firewall under the instrument panel in the cabin were also found to be missing. Any breach in the firewall can allow gases to enter the cabin from the engine bay.
: The thorough inspection of piston-engine exhaust systems and the timely repair or replacement of deteriorated components is the primary mechanism for preventing carbon monoxide exposure. This, in combination with the assured integrity of the firewall, decreases the possibility of carbon monoxide entering the cabin. The ATSB reminds maintainers of the importance of conducting detailed inspections of exhaust systems and firewalls, with consideration for potential carbon monoxide exposure.
Each year, thousands of safety occurrences involving Australian aircraft and foreign‑registered aircraft operating in Australia are reported to the Australian Transport Safety Bureau (ATSB).
This report is part of a series that aims to provide information and statistical data to the aviation industry, manufacturers and policy makers, as well as to the travelling and general public, about these aviation safety occurrences. In particular, the data can be used to determine what can be learned to improve transport safety in the aviation sector.
The study uses information over the 10-year period from 2010–2019 to provide an insight into current and possible future trends in aviation safety.
This statistical report presents interactive web versions of all tables and graphs to allow the user to display aviation occurrence data in the format of their choice.
What the ATSB found
2019
In 2019, 220 aircraft were involved in accidents in Australia, with a further 154 aircraft involved in serious incidents (an incident with a high probability of becoming an accident). There were 35 fatalities from 22 fatal accidents. The number of fatalities was consistent with the average of the previous nine years (32.3 fatalities per year), and the number of fatal accidents was also consistent with its average (23.1 fatal accidents per year).
There have been no fatalities in scheduled commercial air transport in Australia since 2005.
2010 to 2019 accidents and incidents
Between 2010 and 2019, over 90 per cent of accidents and fatal accidents, and around 80 per cent of serious incidents, involved aircraft operating within the general aviation and recreational aviation sectors. In contrast, due to the more stringent reporting requirements for air transport operations, three‑quarters of reported incidents involved aircraft operating within commercial air transport.[1]
Considering all years in the period, the number of general aviation (GA) fatalities and fatal accidents decreased. The number of fatalities and fatal accidents within commercial air transport and recreation aviation remained relatively constant.
Since 2016, remotely piloted aircraft (RPA) have surpassed helicopters to become the second most common aircraft type involved in an accident. Further, the number of manned aircraft experiencing near encounters with an RPA also increased significantly over the study period.
2014 to 2018 accident rates
For the first time, statistics in this report have been organised around the type of aircraft activity being conducted, rather than the operational regulation. Due to the availability of activity data (departures and hours flown data), it was only possible to calculate accident and fatal accident rates over the five‑year period 2014–2018.
Over this period, test and ferry flights, recreational flights involving an aircraft registered with Recreational Aviation Australia (RAAus), followed by pleasure and personal transport, had the highest accident rates. Community services flights, followed closely by test and ferry flights, had the highest fatal accident rates. (However, as there was only one fatal accident involving an aircraft conducting community service flights between 2014 and 2018 there is a high level of statistical uncertainty associated with this rate). For aircraft types, recreational aeroplanes, followed by commercial balloons had the highest accident rates. Also, recreational aeroplanes had the highest fatal accident rate.
Commercial air transport
There were no fatalities within commercial air transport in 2019.
Over the full study period (2010–2019), more than half of all serious incidents and the majority of accidents and fatal accidents for commercial air transport operators involved aircraft conducting non‑scheduled activities, predominantly passenger transport charters. There were no identified increases or decreases in the number of accidents or serious incidents, however, the number of reported incidents for aircraft conducting scheduled international flights and commercial freight increased over the 10 years.
Between 2014 and 2018, around three‑quarters of the hours flown, and approximately one‑half of all departures, within commercial air transport, were operated by scheduled domestic or international operations. Over this period, there was a decrease in the hours flown by scheduled domestic operators; conversely, there was a proportionate increase in the hours for scheduled international operators.
Concerning activities within commercial air transport, passenger transport charters had the highest accident and fatal accident rates.
For specific aircraft types, within commercial air transport, balloons had an accident rate more than 10 times higher than for aeroplanes or helicopters. However, there was only one fatal accident involving a commercial balloon in the 2010 and 2019 timeframe.
Most commercial accidents and serious incidents were operational in nature (typically aircraft control and terrain collisions). The majority of incidents were environmental (mainly birdstrikes).
General aviation
In 2019, there were 17 fatalities in GA.
Over the 10 years, around one‑third of GA accidents and 44 per cent of fatal accidents involved aircraft conducting sport and pleasure flying. Aerial work accounted for a further 37 per cent of GA accidents and 32 per cent of fatal accidents. The number of GA accidents per year increased over the period, with aerial work identified as the primary contributor. Conversely, there was a decrease in the number of fatal accidents, resulting in a decrease of around one fatal accident or 1.4 fewer fatalities per year.
There was also an increase in the number of reported incidents for GA aircraft conducting instructional flying.
Between 2014 and 2018, around 40 per cent of GA hours flown were conducted within aerial work, with instructional flying accounting for a further 30 per cent. Sport and pleasure flying made up around 14 per cent.
The rate of GA accidents decreased over the five years 2014–2018. The main contributors to this decline were sport and pleasure flying, and own business travel. Additionally, there was also a decrease in the rate of fatal accidents for aircraft conducting sport and pleasure flying.
Between 2010 and 2019, there was an increase in the number of GA RPA accidents per year; this primarily resulted from a significant increase in the overall number of survey and photographic accidents.
Overall, there was a decrease in the accident rate for aeroplanes conducting GA flying. The main contributors to this decrease were identified as aeroplanes conducting sport and pleasure flying, and own business travel.
Over the 10 years, the majority of GA accidents, incidents and serious incidents were related to operational or technical issues. Additionally, the majority of fatal accidents were also attributable to operational issues.
Further, the number of GA operational-related accidents and serious incidents, per year, increased over the period. Instructional flying was the main contributor to this operational-related increase. Additionally, there was an increase in the number of accidents and serious incidents of a technical nature; largely attributable to aerial work operations (especially those conducted using an RPA).
Recreational aviation
In 2019, there were 18 fatalities involving an aircraft conducting recreational flying.
The accident rate for recreational flying decreased between 2014 and 2018, with Recreational Aviation Australia (RAAus) registered aircraft having the greatest contribution to this reduction.
Aeroplanes had the highest accident and fatal accident rates of any recreational aircraft type.
Similar to GA, over the full study period (10 years), the majority of recreational accidents and serious incidents were operational (mainly terrain collisions) or technical (primarily engine failure or malfunction) in nature.
The ATSB advises helicopter operators involved in hoist operations that improper stowage of the rescue hoist hook assembly can lead to excessive movement and accelerated wear of the wire rope. If undetected, the wear and associated damage can significantly reduce the cable integrity and operational safety of the hoist system. Should the cable fail while under load during operation, personnel being winched may sustain serious or fatal injuries.
Rescue hoist and hook assembly
Source: NSW Parks and Wildlife Service
What happened
On 4 February 2020, an Airbus Helicopters AS 350 B3 was being operated in support of NSW National Parks and Wildlife Service activities. Winching of personnel and equipment was being conducted when the operating crewman detected a technical issue with the wire rope cable of the hoist system fitted to the helicopter. The outer strands of the cable toward its termination into the hook assembly had loosened in respect of the inner core. Such loosening is known to occur during repeated short length winch deployment and retrieval cycles.
During that conditioning operation, and while under load, the cable fractured at the hook assembly, releasing the ‘dummy’ weight to the ground. There was no damage to the helicopter or injuries to personnel.
Why did it happen
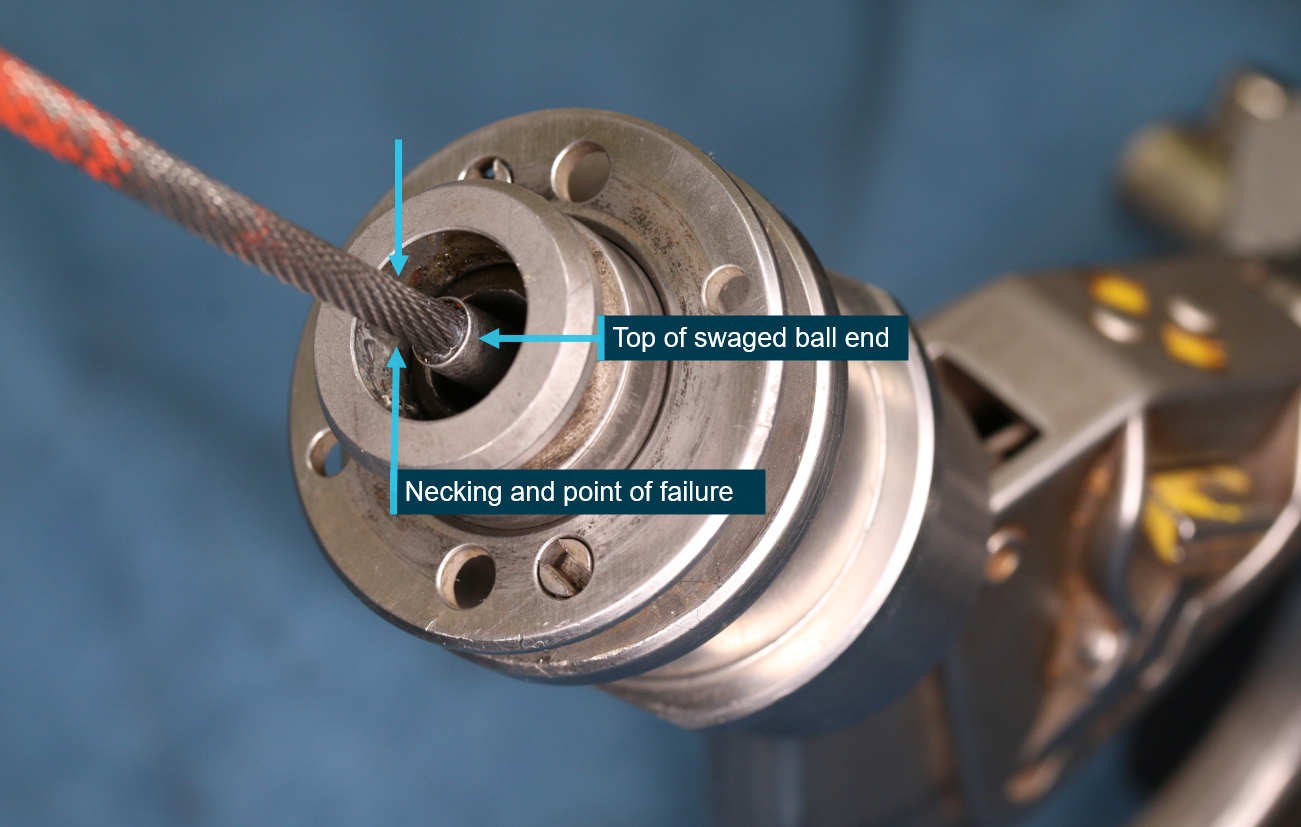
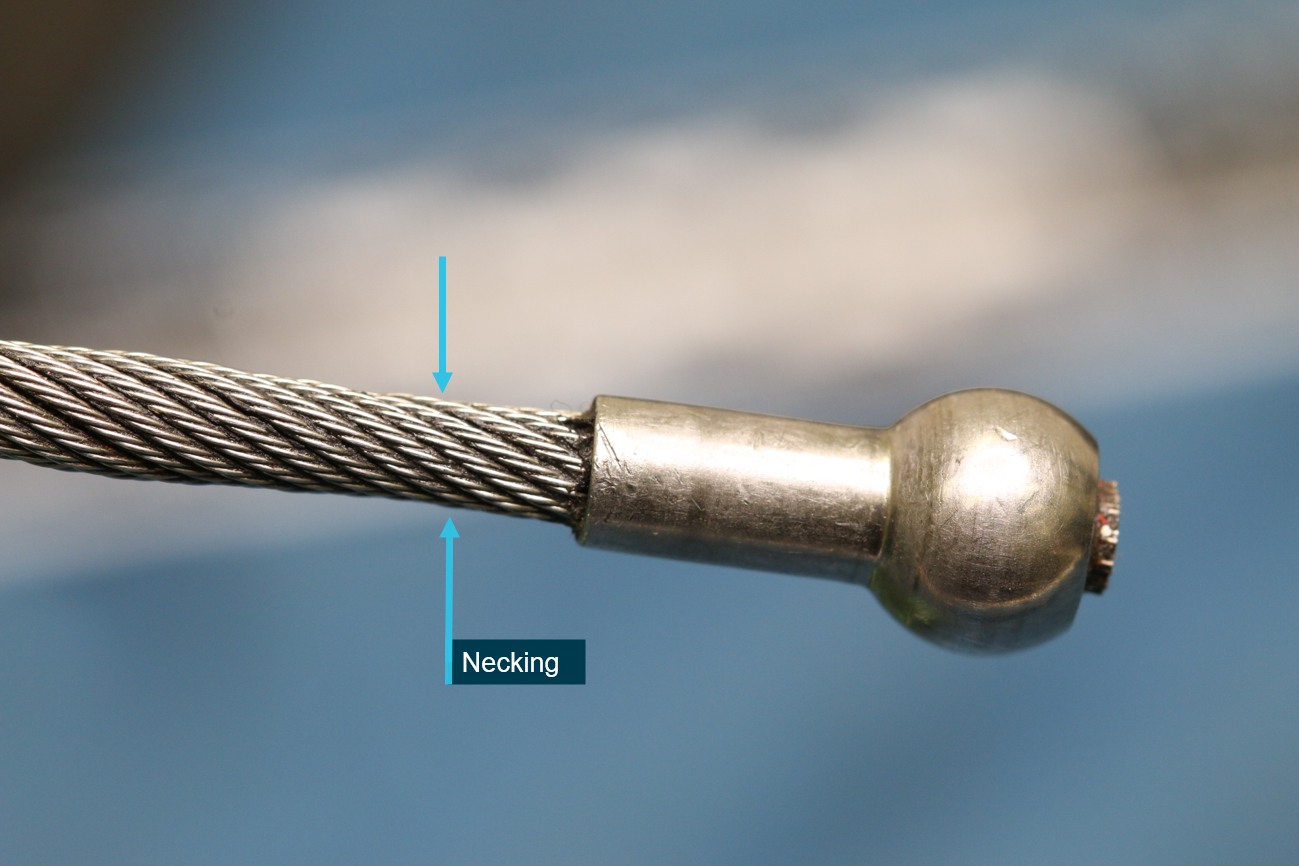
Although the investigation is ongoing, the ATSB’s examination of the helicopter winch system identified that the wire rope cable failed near to the swaged ball-end that terminated into the hook assembly (see images below). Detailed technical examination identified that significant wear had occurred to the individual stainless steel wires comprising the cable, leading to reduced cross-section and an associated gross loss of tensile strength. The cable had accrued just 617 cycles of its 1,500 cycle life-limit. Examination of another rescue hoist from the operator identified similar wear damage had also occurred to that cable.
The ATSB identified that the wear associated with the cable failure probably occurred due to improper stowage of the hook assembly following hoisting operations. A hook that is not firmly seated or with the bump stop spring not sufficiently compressed can move during exposure to airframe vibrations and rotor downwash buffeting during normal helicopter operations. That movement can lead to accelerated wear of the hoist cable close to the ball-end fitting where it enters the hook assembly.
A rescue hoist cable that exhibits ongoing loosening of the outer strands, may have accrued damage from incorrect stowage following hoist operations. If the hook assembly is not firmly seated or is noted to be incorrectly stowed, during the required post-flight inspection particular attention should be paid to the ball-end of the cable for evidence of localised thinning or necking-down, broken wires or deformed strands. Such defects can reduce the cable integrity and compromise the safety of the rescue hoist system.
: The ATSB advises all helicopter operators and flight crew involved in rescue hoist operations to review their current operational practices to ensure hoist operation and hook stowage are in accordance with the hoist manufacturers’ published procedures.
In addition, the ATSB advises those operators, flight crew and maintainers to closely review the pre- and post-flight inspection requirements of the hook and cable assembly, along with any recurring scheduled maintenance of the hoist system, to ensure that they are completed in accordance with the manufacturers’ instructions.