This Corporate Plan sets out the ATSB’s purpose, its strategies for achieving that purpose and how the effect of the strategies and the attainment of the ATSB’s purpose will be measured. It has been prepared in accordance with paragraph 35(1)(b) of the Public Governance, Performance and Accountability Act 2013. The Plan takes account of the relevant provisions of the Transport Safety Investigation Act 2003 (the TSI Act), which establishes the ATSB. It also has regard to the views of the Minister for Infrastructure and Regional Development on the ATSB’s strategic direction as notified under Section 12AE of the TSI Act.
The TSI Act provides that the ATSB’s primary purpose is to improve the safety of aviation, rail and marine transport through accident investigation, data analysis and safety education. It must do so independently, but in cooperation with the other organisations that share responsibility for transport safety, including counterpart organisations in other countries. Successive governments, including the current one, have indicated that, in carrying out its role, the ATSB should give priority to the safety of the travelling public.
The ATSB is required to maintain the people, information and systems to be a world leader in its field. This includes the standing capability to respond immediately to a significant transport safety event, whether it be a major accident or, as is the current case, to undertake a major safety project such as the search for the missing Malaysia Airlines flight MH370. This plan sets out its strategies for doing so in an environment of fast technological advances, constrained resources and significant demographic change in its workforce.
The ATSB has consistently proven itself to be at the forefront internationally in its capability and in its results. I look forward to continuing that achievement as the ATSB implements this Corporate Plan.
The online report includes interactive functionality allowing users to access the report’s safety data to create their own reports specific to their needs.
The purpose of this report
Each year, thousands of safety occurrences involving Australian and foreign-registered aircraft are reported to the Australian Transport Safety Bureau (ATSB) by individuals and organisations in Australia’s aviation industry and by members of the public.
This report is part of a series that aims to provide information to the aviation industry, manufacturers and policy makers, as well as to the travelling and general public, about these aviation safety occurrences. In particular, what can be learned to improve transport safety in the aviation sector.
The study uses information over the ten-year period from 2008-2017 to provide an insight into the current and possible future trends in aviation safety.
What the ATSB found
The majority of air transport operations in Australia each year proceed without incident.
In 2017, nearly 200 aircraft were involved in accidents in Australia, with 203 involved in a serious incident (an incident with a high probability of an accident). There were 40 fatalities in the aviation sector in 2017, which was a significant increase from the 21 fatalities in 2016. There were no fatalities in either high or low-capacity regular public transport (RPT) operations, which has been the case since 1975 and 2010 respectively.
Almost half of all fatalities that occurred in commercial air transport operations during the study period occurred in 2017. During 2017, there were 14 fatalities from 21 accidents in commercial air transport operations, 21 fatalities from 93 accidents in general aviation operations, and five fatalities from 53 accidents in recreational aviation operations.
Terrain collisions were the most common accidents or serious incidents for aircraft involved in general aviation, recreational aviation and remotely piloted aircraft in 2017. Aircraft control, followed by terrain collisions, were the most common occurrence type associated with an accident or serious incident for aircraft involved in air transport operations.
Wildlife strikes, including birdstrikes, were again the most common type of incident involving both commercial air transport and general aviation operations. Runway events and aircraft control incidents were the most common types of incident reported for recreational aviation.
The accident and fatal accident rates for general and recreational aviation reflect their higher‑risk operational activity when compared to commercial air transport operations. They also reflect the significant growth in recreational aviation activity over the last ten years and this sector’s increased reporting culture.
General aviation accounts for one‑third of the total hours flown by Australian-registered aircraft and over half of all aircraft movements across Australia.
The total accident rate, per hours flown, indicates general aviation operations are nine times more likely to have an accident than commercial air transport operations, with recreational operations around twice as likely to experience an accident than general aviation operations.
The fatal accident rate, per hours flown, indicates general aviation operations are around fifteen times more likely to experience a fatal accident than commercial air transport operations, and recreational operations are almost 30 times more likely to experience a fatal accident than commercial air transport operations.
Private/business helicopters followed closely by recreational gyrocopters had the highest fatal accident rate for any aircraft or operation type, whereas recreational aeroplanes had the highest total accident rate. There were no fatal accidents involving general aviation balloons reported during the study period.
Aeroplanes remain the most common aircraft type flown, which is reflected in the proportion of accidents they are involved in. In 2017, 15 of the 22 fatal accidents involved aeroplanes—three gliders, two helicopters, and two weight shift aircraft were also involved in fatal accidents.
Since 2016, the increased availability and use of remotely piloted aircraft (RPA) saw them match helicopters as the second highest aircraft type for reported accidents. However, there were no collisions with other aircraft, fatalities or serious injuries relating to RPA reported to the ATSB. While the consequences of an accident involving an RPA have been low to date, their increased use, and possible interactions with traditional aviation, is an emerging trend in transport safety that will continue to be monitored closely by the ATSB.
Note: Previous editions of Aviation Occurrence Statistics reports contained an error regarding the number of occurrences and subsequently rates for balloons conducting general aviation operations and air transport - charter operations. This error was communicated to the ATSB by the Australian Ballooning Federation. A systemic error was identified and rectified within the reporting system. This report has a decrease in the number of occurrences, and rates, for balloons conducting private operations, and a corresponding increase for balloons conducting charter operations compared to previous editions.
Safety message
This report highlights the importance of effective and timely reporting of all aviation safety occurrences, not just for the potential of initiating an investigation, but also for further study and analysis of aviation transport safety.
While there has been an increase in accident and incident reporting, the limited detail provided for most occurrences, especially by recreational flyers, remains a challenge for the industry and ATSB. This report also highlights the need for improvements in the reporting rates for some areas in general aviation.
By comparing accident and occurrence data across aviation operation types, the ATSB is able to develop a complete picture of the aviation industry to identify emerging trends in aviation transport safety, identify further areas for research and recommend pre-emptive safety actions.
In my second year as Chief Commissioner, the team and I have continued to position the ATSB as a multi-modal, teams-based, world-class transport safety investigation agency. At the start of 2017–18, the Australian Government allocated the ATSB additional funding to address the resourcing challenges encountered in previous years. We have used this funding to put the ATSB on a path of transformation.
We recruited 17 new investigators who are already making an active contribution to transport safety. We are investing significantly in the development of our investigators to position them to be able to disseminate safety findings to industry and the public as quickly as possible. As a team, we have also prioritised the completion of a number of complex investigations, delivering safety outcomes while also freeing up key resources for new investigation priorities. The investment made over the last year will see continued improvement towards the ATSB being able to meet its deliverable targets.
Over the year, we were pleased to bring on board Executive Director Transport Safety, Nat Nagy. Mr Nagy, along with myself and Chief Operating Officer Colin McNamara, constitute the ATSB’s Executive. The Executive are working well with the ATSB’s Commission to build the ATSB up as a world-class investigator for the future. We are fortunate to have the Minister for Infrastructure and Transport reappoint Commissioners Carolyn Walsh, Noel Hart and Chris Manning. The expertise provided by these Commissioners across the aviation, rail and marine transport modes is essential for ensuring we are meeting the interests of our stakeholders with our investigations.
Multi-disciplinary workforce
The ATSB’s greatest resource continues to be its people. We are creating an environment where our employees are empowered. With the multi-disciplinary teams-based approach to our work implemented in 2017–18, we have removed the structural barriers between investigators, researchers and data analysts. The majority of our people are multi-skilling across all these disciplines.
We also have investigators with a background in one particular mode stretching themselves to become involved in investigations from other modes. We are bringing to bear our collective core investigative skills, shared values, passion and drive to improve transport safety.
Building our networks
In 2017–18, we committed to building our networks to deliver our safety messages further. The ATSB was represented at a large number of industry events during the financial year and a number of presentations were provided to stakeholders from the aviation, rail and maritime industries. In May, I presented at Rotortech 2018 on the Sunshine Coast. This provided a platform to launch ‘Don’t Push It, Land It’—a new safety initiative for the helicopter industry, in conjunction with the Australian Helicopter Industry Association and the Civil Aviation Safety Authority. We were also represented by our Executive Director Transport Safety at the RISSB Rail Safety Conference in Sydney. This year I had the honour of being asked by the Royal Aeronautical Society to present the Lawrence Hargrave Memorial Lecture in Melbourne.
In May, I attended the International Transportation Safety Association meeting in Baku, Azerbaijan. This provided a valuable opportunity to exchange information and knowledge with my international counterparts. I was also appointed to the Defence Aviation Safety Council.
We have worked to enhance the mediums through which we communicate. To counter misinformation and provide transparency, we have become more proactive in engaging early with media when there is a transport safety occurrence. We have also been making information more accessible through the use of social media and visual mediums, such as infographics and the production of videos.
Our devotion to making sure that key safety messages are heard is essential for influencing industry and the travelling public towards safe outcomes on the back of our investigative work.
Aviation
During the year, we completed 25 complex aviation safety investigations and 34 short investigations.
The ATSB released the findings from its second investigation into the ditching of an Israel Aircraft Industries Westwind aircraft (VH-NGA) off Norfolk Island in 2009 (AO‑2009‑072). The release of this report demonstrates the diligence of the ATSB in ensuring that it drives safety forward. Thirty-six safety factors were included in the report, with the key message for flight crew, operators and regulators being that unforecast weather can occur at any aerodrome. There is a need for robust and conservative in‑flight fuel management procedures for passenger-transport flights to remote islands and isolated aerodromes.
Another published report relating to weather was the investigation into a collision with terrain involving an Airbus Helicopters EC 135 T1 (VH-GKK) at Cooranbong, New South Wales in 2015 (AO-2015-131). The safety message from this investigation is that avoiding deteriorating weather conditions requires thorough pre-flight planning. Pressing on into instrument meteorological conditions without a current instrument rating carries a significant risk of encountering reduced visual cues leading to disorientation.
Two reports were published covering pilot interaction with automated technology: a collision with terrain involving a Cessna 172 (VH-ZEW) near Millbrook in Victoria in 2015 (AO-2015-105) and a near collision involving Beech Aircraft Corp B200 (VH-OWN and VH-LQR) at Mount Hotham in Victoria in 2015 (AO-2015-108). Pilots need to have a thorough understanding of all systems on board their aircraft and have the skill to provide redundancy when those systems fail, or their performance is reduced.
In addition to completing some significant investigations, a number were also commenced over the year. The collision with water involving a de Havilland Canada DHC-2 Beaver aircraft (VH-NOO) on the Hawkesbury River in New South Wales on New Year’s Eve drew substantial media attention (AO-2017-118). The ATSB response demonstrated our ‘on-call’ readiness at all times. The preliminary factual report was released on 31 January 2018.
Rail
The ATSB completed 13 complex rail safety investigations and three short investigations. Included in these releases is the publication Safe work on track across Australia: Analysis of incident data, 2009–2014 (RI-2014-011). The review of data showed that incidents while maintenance work was being carried out were predominately a result of errors during the implementation or dissolution stage of providing track protection. Protections were either removed incorrectly or prematurely, or key communication exchanges failed to establish the location of the worksite with respect to approaching rail traffic. Improving the levels of safe working on track continues to be an ATSB SafetyWatch priority.
The derailment of train 3MP5 at Rawlinna, Western Australia in 2016 (RO-2016-005) was significant for demonstrating the risks of approaching safety-critical zones at higher speeds. The publication of a report into a signalling control system irregularity at Ballarat, Victoria in 2016 (RO-2016-011) showcased how critical it is for system designers to ensure that the functionality and performance requirements needed to meet all operational scenarios are incorporated within the system. The ATSB found that the train controller had placed a block on the three sets of points, but these ‘blocks’ were ineffective due to design errors within the train control system.
With Queensland coming on board within the national rail safety system, the ATSB commenced eight investigations into rail occurrences in the state over the 2017–18 year. In recognition of the complementary role the regulator and investigator play in the national rail safety system, the Office of the National Rail Safety Regulator and the ATSB signed a new Memorandum of Understanding (MOU) to set out the roles and relationships of the respective organisations. Under the terms of the MOU, in the coming year the ATSB will look forward to receiving a greater range of occurrences information to assist with data analysis and research.
Marine
The ATSB completed four complex marine safety investigations and three short investigations. The published investigations included a loss of propulsion event on the passenger cruise ship Norwegian Star in Bass Strait in February 2017 (MO-2017-003). This investigation highlighted that the operation of newly designed equipment without redundancy increases operational risks. Equipment manufacturers and ship operators must apply extra diligence when designing, installing and operating modified equipment, especially safety-critical equipment.
The ATSB continues to have collisions between trading ships and small vessels reported. A common contributing factor that was present in the investigation into a collision between the container ship Glasgow Express and the fishing vessel Mako in Bass Strait, Victoria in 2017 (MO-2017-007) is the failure to use all available means to accurately appraise a situation and obviate the risk of collision. The ATSB reinforces the importance of a proper lookout by all available means, including radar, to masters, owners, operators and skippers of all vessels.
With the Australian Maritime Safety Authority (AMSA) taking full responsibility for domestic commercial vessels from 1 July 2018, the ATSB invested in seeking to understand the role it can play in the new national maritime safety system. While there is no agreement for an ATSB-funded role, the ATSB committed to a policy to make itself available for major accidents where resources are made available. The ATSB will continue to work with the appropriate Commonwealth and state agencies to clarify its role.
Malaysia Airlines Flight 370—international contribution
On 3 October 2017, the ATSB published its final report into its work coordinating the search for missing Malaysia Airlines Flight 370 (MH370) (AE-2015-054). The search for MH370 has been a complex international program; the largest and most complex search for a missing aircraft in history. The effort of the dedicated ATSB and associated personnel involved in the search is a testament to their ingenuity, adaptability and resilience.
With the finalisation of the ATSB’s work, responsibility for MH370 matters was handed over to the Joint Agency Coordination Centre (JACC) in the Department of Infrastructure, Regional Development and Cities.
Outlook
The ATSB will continue to perform its primary function of ‘improving transport safety’ in an operating environment of continuing growth and change in the aviation, rail and marine transport industries. During the year, I will release a ‘Vision 2025’ statement for the ATSB. The statement will explain the ATSB’s vision to ‘drive safety action in a rapidly changing transport environment’.
Over the next few years, the transport sector is expected to see significant changes in technology, including increased automation (or remotely piloted operation), manufacturing efficiencies and enhanced use of big data to predict future hazards. Workforce challenges are also expected, with shortages of key personnel in some sectors and increased movement of operational staff between employers. From the ATSB’s perspective, we also expect to see opportunities to broaden our jurisdiction across transport modes.
The ATSB must be able to maintain its status as a world leader, implementing best practice in transport safety investigation in this changing environment. It is essential that we are positioned to be able to expose the critical safety issues that others cannot and influence the necessary safety action to provide confidence in our transport systems.
The immediate focus in 2018–19 will be to make progress in addressing some of our key performance indicators around the timeliness for completion of reports. I am confident that we can make good progress, particularly following our recent investigator recruitment exercise. The year will be a positive one, with our team committed to making our aviation, rail and marine modes of transport safer.
This research commenced following receipt of correspondence suggesting that an increase in helicopter engine issues in northern Australia was potentially linked to a change to reduced lead content fuel in these areas. The Civil Aviation Safety Authority (CASA) advised the ATSB that, in December 2015, the colour and branding of fuel supplied to the northern region of Australia changed, from green Avgas 100/130 to blue Avgas 100LL (low lead). Although the maximum permissible lead content reduced with this change, CASA advised that the actual lead content of the supplied Avgas 100/130 fuel had already been below the maximum permitted by the Avgas 100LL standard prior to December 2015.
An analysis of safety occurrence records was conducted to identify if any significant changes to the number of reported engine failures or malfunctions had occurred following the introduction of Avgas 100LL. The analysis found that overall there had been no discernible increase in reported engine failures or malfunctions in northern Australia after the introduction of Avgas 100LL in December 2015. Specifically for helicopters with Lycoming piston engines, there was an increase in reported occurrences of engine failures or malfunctions since 2014, largely dominated by northern Australia. However, occurrence numbers are low so some year-to-year variation from chance alone is expected. Additionally, the increase did not align with the introduction of Avgas 100LL in December 2015.
Potential symptoms of the issues were reported as premature cylinder removals, and a high rate of exhaust valve and guide wear. The analysis found only one incident related to valve wear in northern Australia following the reported fuel change. However, the ATSB found a disproportionate number of engine failures or malfunctions in piston engine helicopters with unidentified failure mechanisms following the change to Avgas 100LL. Although it was not possible to eliminate the introduction of Avgas 100LL fuel as a potential factor in these engine failures, conclusive findings could not be drawn based on the available evidence.
In response to the concerns raised, the Northern Fuels Stakeholder Investigation Group was formed to investigate this issue further. Additionally, CASA has introduced airworthiness bulletin (AWB) 85-024 Issue 1, to raise awareness of an increasing incidence of premature exhaust valve and valve guide wear.
The current legislation does not require commercial operators of aircraft not greater than 5,700 kg maximum take-off weight (MTOW) to provide instructions and procedures for crosschecking the quantity of fuel on board before and/or during flight. This increases the risk that operators in this category will not implement effective fuel policies and training to prevent fuel exhaustion events.
What happened
On 17 July 2016, at about 1039 Central Standard Time, a McDonnell Douglas Corporation 369D helicopter, registered VH-PLY, experienced fuel exhaustion and a collision with terrain while performing powerline inspections 36 km north-west of Hawker, South Australia. There were three crew on board the helicopter. One pilot in the front left seat, one line-worker in the front right seat and one line-worker in the rear left seat. The three crew members were seriously injured and the helicopter was substantially damaged.
Why did it happen
The ATSB found that the pilot was mistakenly told by ground staff that the aircraft had been refuelled and through distraction, omitted a crosscheck of the fuel quantity before flight. The pilot’s monitoring of the fuel in-flight was based on anticipated endurance, which resulted in him not detecting a low fuel level. The ATSB also found the requirements for the development of fuel policy by operators were dispersed throughout the aviation legislation—14 legislative and three guidance material requirements were found—but they did not require the operator to publish procedures for determining fuel on board before and during flight for commercial operators of aircraft not greater than 5,700 kg MTOW.
: From 2003 to 2017, the ATSB has received 26 reports of fuel exhaustion events from Air Operator Certificate holders operating aircraft not greater than 5,700 kg MTOW. Two key contributing factors from these reports are pilots not crosschecking the fuel on board before and/or during flight. Aircraft greater than 5,700 kg MTOW are not represented in the ATSB fuel exhaustion reports. In accordance with CAO 20.2, operators of these aircraft are required to publish instructions and procedures in their operations manuals for the pilot in command to verify the fuel on board before flight. Additionally, CAAP 215-1(2) Appendix B includes guidelines for publishing operations manual procedures for inflight fuel management.
CASA 29/18 – Civil Aviation (Fuel Requirements) Instrument 2018, which contains proposed changes to the current fuel regulations and guidance material is scheduled to commence 8 November 2018. The ATSB considers that the implementation of these changes should address this safety issue.
Until the proposed changes to the current fuel regulations and guidance material are implemented, the ATSB advises Air Operator Certificate holders for aircraft not greater than 5,700 kg MTOW, to consider this safety issue and take action where appropriate.
Read more about this ATSB investigation: AO-2016-078.
Each year, thousands of safety occurrences involving Australian and foreign-registered aircraft are reported to the Australian Transport Safety Bureau (ATSB) by individuals and organisations in Australia’s aviation industry and by members of the general public.
This report is part of a series that aims to provide information to the aviation industry, manufacturers and policy makers, as well as to the travelling and general public, about these aviation safety occurrences. In particular, what can be learned to improve transport safety in the aviation sector.
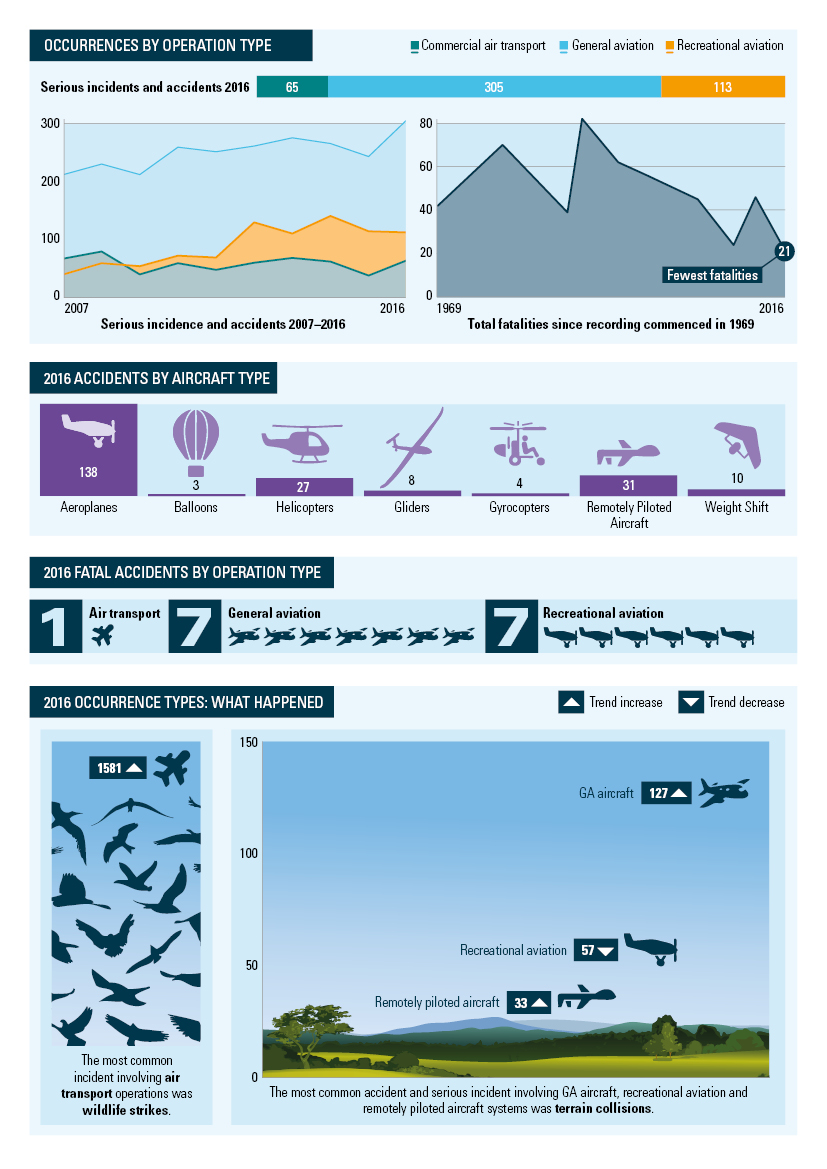
The study uses information over the ten-year period from 2007–2016 to provide an insight into the current and possible future trends in aviation safety, and takes a detailed look at the accidents and incidents in 2016 for each type of aircraft operation.
What the ATSB found
The majority of air transport operations in Australia each year proceed without incident.
In 2016, nearly 230 aircraft were involved in accidents in Australia, with another 291 aircraft involved in a serious incident (an incident with a high probability of an accident). There were 21 fatalities in the aviation sector in 2016, which was fewer than any previous year recorded by the ATSB. There were no fatalities in either high or low-capacity regular public transport (RPT) operations, which has been the case since 1975 and 2010 respectively.
Commercial air transport operations experienced one fatality from 15 accidents; general aviation experienced 10 fatalities from 119 accidents; and recreational aviation had 10 fatalities from 63 accidents.
Collision with terrain was the most common accident or serious incident for general aviation aircraft, recreational aviation and remotely piloted aircraft in 2016. Aircraft control was the most common cause of an accident or serious incident for air transport operators.
Wildlife strikes, including birdstrikes, were again the most common types of incident involving air transport and general aviation operations, with runway events the most common type of incident for recreational aviation.
The accident and fatal accident rates for general and recreational aviation reflect the higher‑risk operational activity when compared to air transport operations. They also reflect the significant growth in recreational aviation activity over the last ten years and this sector’s increased reporting culture.
General aviation accounts for one‑third of the total hours flown by Australian-registered aircraft and over half of all aircraft movements across Australia.
The total accident rate, per hours flown, indicates general aviation operations are 10 times more likely to have an accident than commercial operations, with recreational aircraft around twice as likely to experience an accident than general aviation.
The fatal accident rate, per hours flown, indicates general aviation operations are around 20 times more likely to experience a fatal accident than commercial air transport, and recreational operations are almost 40 times more likely to experience a fatal accident than air transport.
Recreational gyrocopters experienced the highest fatal accident rate for any aircraft or operation type, whereas recreational balloon operations had the highest total accident rate; almost four times as high as any other aircraft operation type. There were no fatal accidents involving recreational balloons reported during the study period.
Aeroplanes remain the most common aircraft type flown which is reflected in their involved in accidents. In 2016, nine of the 15 fatal accidents involved aeroplanes—three helicopters and two powered weight shift aircraft were also involved in fatal accidents.
In 2016, the increased availability and use of remotely piloted aircraft (RPA) saw them surpass helicopters as the second highest aircraft type for reported accidents; however, there were no collisions with other aircraft, fatalities or serious injuries relating to RPA reported to the ATSB that year. While the consequences of an accident involving an RPA have been low to date, their increased use, and possible interactions with traditional aviation, is an emerging trend in transport safety that will continue to be monitored closely by the ATSB.
Safety message
This report highlights the importance of effective and timely reporting of all aviation safety occurrences, not just for the potential of initiating an investigation, but to allow further study and analysis of aviation transport safety.
While there has been an increase in accident and incident reporting, the limited detail provided for most occurrences, especially by recreational flyers, remains a challenge for the industry and ATSB. This report also highlights the need for improvements in the reporting rates for some areas in general aviation.
By comparing accident and occurrence data across aviation operations types, the ATSB is able to develop a complete picture of the aviation industry to identify emerging trends in aviation transport safety, identify further areas for research and recommend pre-emptive safety actions.
The Aviation Short Investigation Bulletin covers a range of the ATSB’s short investigations and highlights valuable safety lessons for pilots, operators and safety managers.
Released periodically, the Bulletin provides a summary of the less-complex factual investigation reports conducted by the ATSB. The results, based on information supplied by organisations or individuals involved in the occurrence, detail the facts behind the event, as well as any safety actions undertaken. The Bulletin also highlights important Safety Messages for the broader aviation community, drawing on earlier ATSB investigations and research.
Issue 61 of the Bulletin features 10 safety investigations:
The Aviation Short Investigation Bulletin covers a range of the ATSB’s short investigations and highlights valuable safety lessons for pilots, operators and safety managers.
Released periodically, the Bulletin provides a summary of the less-complex factual investigation reports conducted by the ATSB. The results, based on information supplied by organisations or individuals involved in the occurrence, detail the facts behind the event, as well as any safety actions undertaken. The Bulletin also highlights important Safety Messages for the broader aviation community, drawing on earlier ATSB investigations and research.
Issue 62 of the Bulletin features 11 safety investigations:
Appointed Chief Commissioner on 1 July 2016, I was honoured to be provided the opportunity to lead a world-class transport safety investigation agency. As the accountable authority, I was acutely aware that the ATSB’s primary function is to improve transport safety with priority given to delivering the best safety outcomes for the travelling public. Having worked in other agencies within the transport portfolio for an extended period of time, I was also cognisant of the agency’s operational environment and the associated challenges. It was within this context that I determined the ATSB needed to be repositioned to face these challenges with courage and determination.
Evolving our capabilities and capacity
The ATSB has undertaken a significant transformation program designed to enable better resource allocation and utilisation across the agency. A number of change imperatives underpinned this program which provided the impetus to refine our business practices and expand our deliverables.
In demonstrating increased effectiveness, we have become more selective in how we allocate resources towards investigating those accidents and serious incidents that have the greatest potential for safety learnings and enhancement. Concurrently, we have expanded our capacity to improve transport safety outside of these traditional investigations, through safety issue investigations, greater interaction with operators and regulators, with data and other intelligence in our possession, and through amplified communications, safety education and promotion.
Key success factors
The ATSB’s greatest resource continues to be “its people” and while there have been changes within our organisational structure—most notably the introduction of multi-disciplined/modal investigator teams—we are well on the way to creating an environment where our employees are empowered. Our people are provided greater opportunities to bring to bear their collective core investigative skills, shared values, passion and drive to improve transport safety. This equally applies to our dedicated and professional operational support staff.
Through the Government’s recent 2017–18 Budget measure “improving transport safety”, the ATSB has been able to re-establish a sound financial position over the next four years. This increase in funding will enable the ATSB to replenish its workforce and re-profile its capital investment strategies to meet its projected needs in essential technical equipment, data warehousing requirements and core enterprise systems.
Core business
The ATSB has committed considerable resources and time to re-engineering its operational model over 2016–17. We did so whilst taking appropriate measures to ensure this did not impact our ability to conduct core business activities, as demonstrated through the range of significant and comprehensive investigations that were either commenced or completed during the financial year.
In relation to other broader functions, the ATSB has completed its transition to becoming the national rail safety investigator, as established through the Council of Australian Governments’ Intergovernmental Agreement on Rail Safety Regulation and Investigation Reform. This milestone coincides with the Queensland Parliament’s agreement to join the national rail safety scheme from 30 June 2017.
Internationally, we have continued an active program of regional engagement with other transport safety agencies within the Asia–Pacific region—most notably with our Indonesian and Papua New Guinean counterparts.
Aviation
During the year, we completed 39 complex aviation safety investigations and 108 short factual investigations.
This year a second interim report was released into the in-flight pitch disconnect of a Virgin Australia Regional Airlines ATR 72 aircraft that occurred about 50 km west-southwest of Sydney Airport, NSW. That report identified a safety issue concerning activation of the aircraft’s pitch uncoupling mechanism with world-wide implications. The ATSB has issued safety recommendations to the aircraft manufacturer, the Civil Aviation Safety Authority (Opens in a new tab/window)(CASA) and the European Aviation Safety Agency(Opens in a new tab/window) to take action to ensure that the aircraft can safely withstand the loads resulting from a pitch disconnect.
A report was also released for an investigation involving the collision with terrain of a parachuting aircraft at Caboolture Airfield, Queensland that fatally injured the five occupants. The ATSB identified that the aircraft aerodynamically stalled at a height from which it was too low to recover control prior to collision with terrain. As a result of that investigation, the ATSB recommended that CASA introduce risk controls to provide increased assurance of aircraft serviceability, pilot competence and adequate regulatory oversight. The ATSB also recommended that CASA work in collaboration with the Australian Parachute Federation to increase the usage of dual point passenger restraints in parachuting aircraft.
Another significant aviation investigation included a traffic management occurrence involving a Jetstar Airbus A320 and a Beech Aircraft Corporation BE-76 Duchess at Ballina/Byron Gateway Airport, NSW. That investigation identified a safety issue relating to the available traffic advisory facilities. The introduction of a certified air/ground radio service to provide weather services and traffic information at the airport in March 2017 is expected to address that safety issue.
The ATSB also released the first research report on Remotely Piloted Aircraft Systems (RPAS). This report showed that there has been a steep rise in the number of RPAS certificate holders in 2016, coinciding with a similar rise in safety occurrences. About half of the 180 occurrences from the past five years related to near encounters with manned aircraft. Of these, 60 per cent were in 2016. Fortunately, there have been no collisions in Australia between RPAS and manned aircraft. The potential consequences of a collision remain uncertain given the limited research available. However, RPAS are an emerging risk that require close monitoring as the number of these aircraft continues to grow.
Rail
During the year, the ATSB completed 16 rail safety investigations. These involved collisions, derailments and failures of safe work practices. Of significance were a level crossing collision between a freight train and a road-train truck near Narromine, NSW, (RO-2015-016) and the derailment of a freight train carrying dangerous goods near Julia Creek, Queensland (RO-2015-028).
The ATSB also continues its focus on occurrences where breaches of safe work practices may place maintenance crews and operators at risk. An investigation has commenced into a fatal collision between a track worker and passenger train near Petrie, Queensland which occurred on 29 May 2017 (RO-2017-003). In addition, our safety issues investigation into safe work on track is nearing completion and will go through a period of public consultation in preparation for final release before the end of 2017.
Marine
The ATSB completed five marine safety investigations in 2016–17. One significant investigation involved a crew member fatality on board the offshore support vessel Skandi Pacific, off the West Australia coast (MO-2015-005). The crew member was crushed while attempting to secure containers during worsening weather conditions.
The investigation complements an ATSB SafetyWatch priority focusing on marine work practices and resulted in a Safety Advisory Notice being issued to highlight the risks posed by open stern vessels in the industry.
The report into the breakaway of the Spirit of Tasmania II from its mooring at Station Pier in Melbourne, Victoria (MO-2016-001) highlighted that all ships, especially those with high windage, are prone to breaking away from moorings during short-term events such as thunderstorms and squalls. The risks this presents to ships with large numbers of people on board means that weather monitoring, mooring systems and procedures need to be regularly checked and verified for changing weather conditions.
Malaysia Airlines Flight 370—international contribution
In January 2017, a Joint Communiqué issued by the Tripartite Governments (Malaysia, Australia, and the People’s Republic of China) formally announced the suspension of the underwater search for missing Malaysia Airlines Flight 370 (MH370) following completion of the 120,000 km2 search area. Should credible new information emerge that can be used to identify the specific location of the aircraft, consideration will be given to determining next steps.
Whilst search operations have been suspended, search area analysis and activities have continued, and an end of search report was released in the third quarter of 2017.
The search for MH370 has been a complex international program, the largest and most complex search for a missing aircraft in history. The effort of the dedicated ATSB and associated personnel involved in the search is a testament to their ingenuity, adaptability and resilience. Consistent with Government policy and direction, the ATSB will continue to provide a supporting role to Malaysia as the country responsible for the investigation into the disappearance of MH370.
Outlook for 2017–18
The ATSB will continue to perform its primary function of “improving transport safety” in an operating environment of continuing growth and change in the aviation, rail and marine transport industries.
In recognising these environmental challenges, the ATSB will adopt and implement a range of strategies designed to further increase its overall efficiency and effectiveness.
Selective investigations
The ATSB will refine its methodologies in selecting the accidents and incidents it investigates, recognising its finite resources, differences in jurisdiction across the modes, and its particular focus on the safety of the travelling public.
Data driven
To position the ATSB to become more proactive in its identification of safety issues, we will continue to build our capability to source data nationally on aviation, rail and marine transport safety occurrences and events, and use that data to identify and communicate safety risks and emerging trends.
We will also deliver a program of safety research and analysis that draws on the results of investigations and the interrogation of safety occurrence datasets.
Stakeholder engagement
To encourage greater safety action, the ATSB will enhance stakeholder relationships, with a particular focus on ensuring a strong culture of reporting safety matters, and through transparent arrangements for the appropriate sharing and use of safety information.
Focused communications
To ensure the targeted delivery of its safety messages, the ATSB will undertake safety communication and education with an emphasis on identifying priority areas where safety risk can be reduced.
We will also increase public awareness of the ATSB’s safety activities by developing a broader range of communication and education products and pursuing their delivery to transport industries and the travelling public through media that interact with a variety of stakeholders.
Workforce capabilities
To enhance its workforce capability the ATSB will complete the implementation of its organisational change program, embedding a multi-discipline teams-based approach to investigations, with the objective of enhancing the agency’s efficiency and effectiveness.
We will expand our resource base through attracting, retaining and developing professional staff as well as developing networks with skilled professionals who the ATSB can work with to fulfil its transport safety functions.
Expanding jurisdictions
While the ATSB has a broad jurisdiction in aviation, there is further work to be done as part of the national rail and marine safety reforms. The ATSB will examine how to best address some of the issues surrounding the independent investigation of serious incidents and accidents in the domestic commercial vessel (DCV) sector consistent with any direction as agreed by governments.
These strategies, the associated deliverables and performance indicators (specifically our commitment to improving the timeliness of our outputs), are detailed and presented in the ATSB’s Corporate Plan 2017–18, published on 31 August 2017.
The 2017–18 year will be a positive and exciting period for the ATSB, and I remain confident that the continued professionalism and capability of our people will ensure the ATSB remains a world-leading transport safety investigation agency.
The Aviation Short Investigation Bulletin covers a range of the ATSB’s short investigations and highlights valuable safety lessons for pilots, operators and safety managers.
Released periodically, the Bulletin provides a summary of the less-complex factual investigation reports conducted by the ATSB. The results, based on information supplied by organisations or individuals involved in the occurrence, detail the facts behind the event, as well as any safety actions undertaken. The Bulletin also highlights important Safety Messages for the broader aviation community, drawing on earlier ATSB investigations and research.
Issue 60 of the Bulletin features 10 safety investigations: