On 10 November 2022, SCT Logistics freight train 4PM9 departed Perth, Western Australia for Melbourne, Victoria. At about 0450 on 14 November, the train was travelling at about 80 km/h when it passed over a culvert located to the east of the township of Inverleigh in Victoria. Soon after, there was a loss of brake pipe pressure, and the leading end of the train came to a stop across the Hamilton Highway level crossing. The embankment supporting the track at the location of the culvert had collapsed and 16 wagons had derailed. Ten of the original 55 wagons were still attached to the leading 5 locomotives.
Victoria's Chief Investigator Transport Safety is conducting the investigation under the Transport Safety Investigation Act 2003 (Cth), under a collaboration agreement with the ATSB.
A preliminary report into the incident was published on the ATSB website on 06 February 2023. See below.
The drafting of the final investigation report has been completed and is currently being internally reviewed.
Preliminary report
Report release date: 24/02/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Passage of freight train 4PM9
On 10 November 2022, SCT Logistics freight train 4PM9 departed Perth, Western Australia for Melbourne, Victoria. The train left Adelaide, South Australia on 13 November and consisted of 5 locomotives hauling 55 wagons[1] and was about 1800 m in length. The train was operating on the Australian Rail Track Corporation (ARTC) standard gauge network.
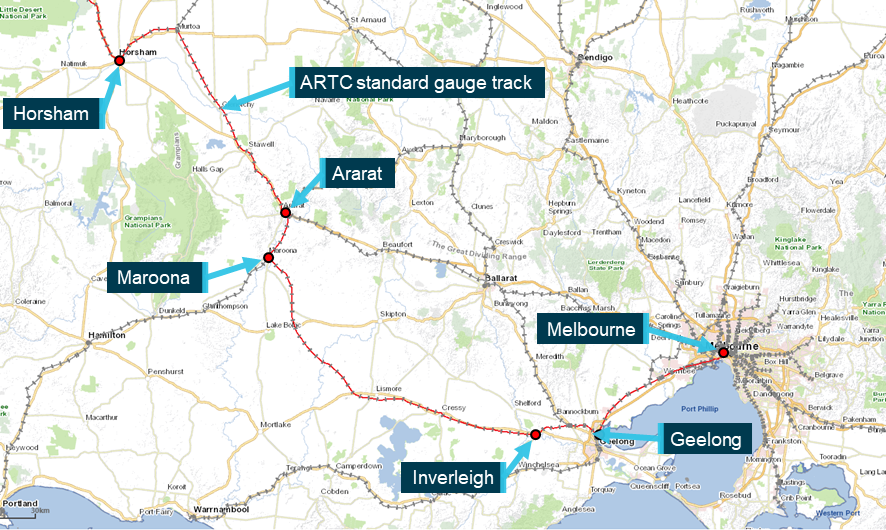
The train arrived in Horsham, Victoria at about 2320[2] on 13 November. A crew change occurred in Horsham and the train resumed its trip to Melbourne that would take it through Ararat, Maroona and then Inverleigh (Figure 1).
Figure 1: Standard gauge route from Horsham to Melbourne
Source: e-way Electronic Street Directory Version 2.2 (c) Copyright Melway Publishing Pty. Ltd. annotated by Chief Investigator, Transport Safety
At about 0450 on 14 November, train 4PM9 travelling at about 80 km/h passed over a culvert located to the east of the township of Inverleigh. Soon after, there was a loss of brake pipe pressure[3] and the leading end of the train came to a stop across the Hamilton Highway level crossing. Ten of the original 55 wagons were still attached to the leading 5 locomotives. The next 16 wagons were derailed including 7, 5-pack articulated wagons (Figure 2).
Figure 2: Aerial view of derailed train 4PM9
Source: Aerial footage provided by ABC News, annotated by CITS
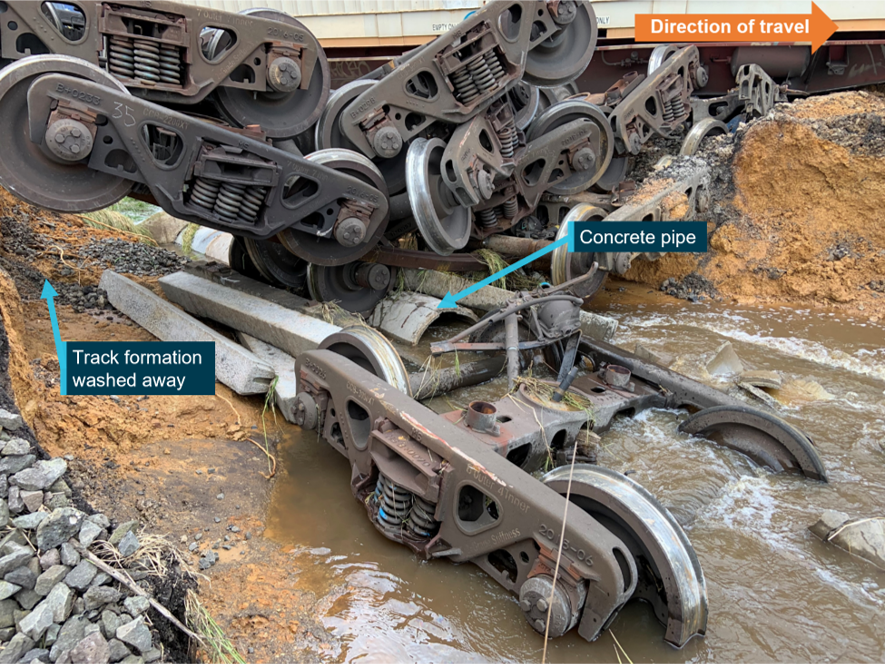
The embankment supporting the track at the location of the culvert had collapsed (Figure 3).
Figure 3: The pipe culvert and the collapsed track formation
Source: Chief Investigator, Transport Safety
Context
Location
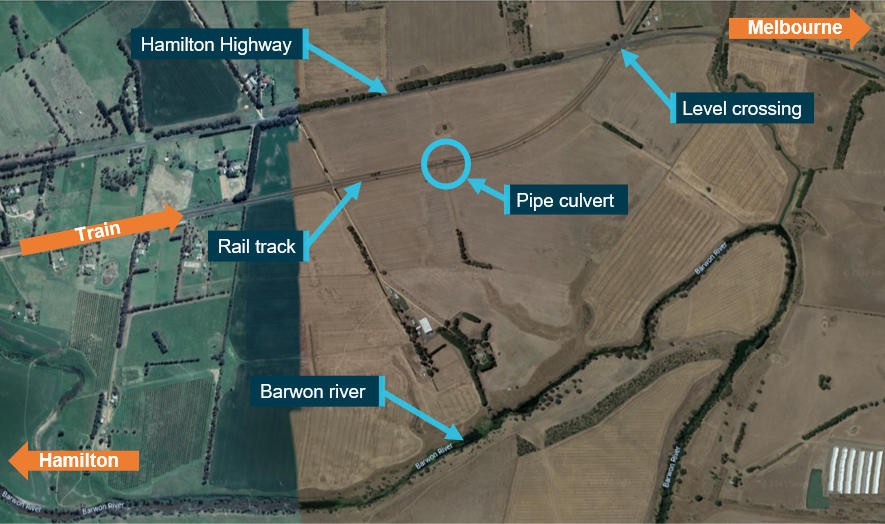
The derailment occurred about 3 km east of the township of Inverleigh on a section of track located between the Hamilton Highway and the Barwon River (Figure 4). Travelling in an easterly direction, the track ran parallel to the Hamilton Highway before curving towards and across the highway. The derailment occurred within the Mid Barwon catchment area that made up part of the Barwon drainage basin. The agricultural land on either side of the rail reserve generally sloped from the highway down towards the Barwon River. Therefore, run-off from rainfall flowed from the north side of the track through culverts (below the track) towards the Barwon River.
Figure 4: Derailment site of train 4PM9
Source: Google maps, annotated by the Chief Investigator, Transport Safety
Track infrastructure
The standard gauge track at Inverleigh was a single, bi-directional line, and consisted of 60 kg/m rail fastened to concrete sleepers. The track through the location was carried on an embankment that was at a height of about 3 m at the location of the wash-away (at the culvert). This culvert was located at the 96.805 track km mark[4] and comprised of a 750 mm diameter concrete pipe embedded at the base of the embankment carrying the track.
Rainfall
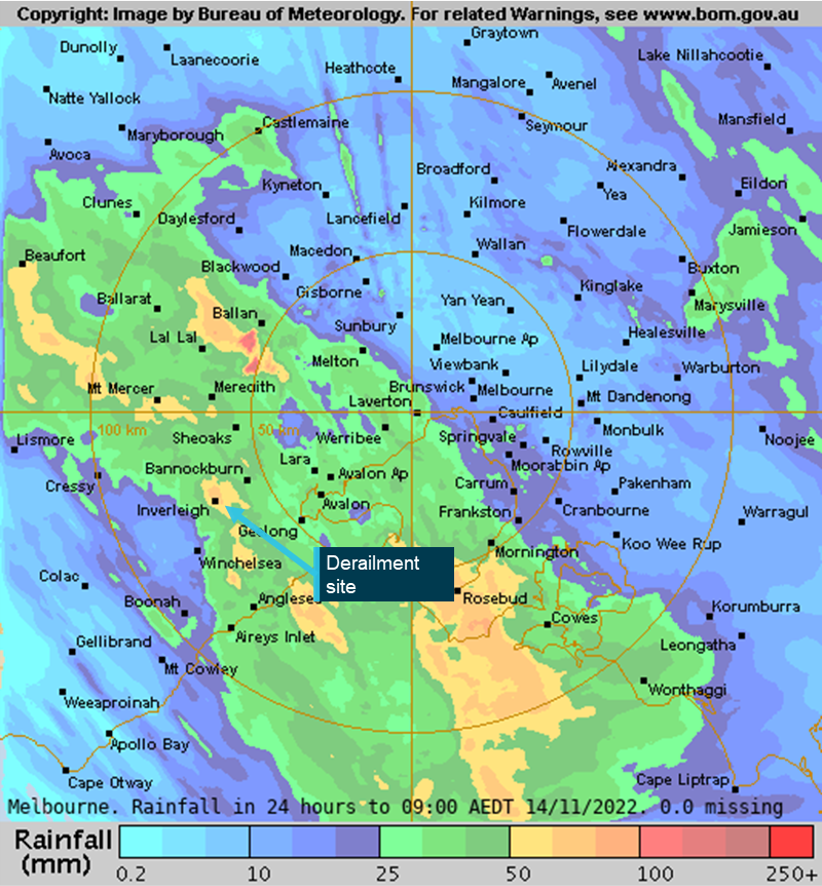
Heavy rain fell in Inverleigh from the late evening of 13 November and through the early hours of the morning of 14 November. A weather monitoring station at Gnarwarre[5], located about 12 km from Inverleigh recorded about 42 mm of rain in the 12-hour period[6] before the derailment, and local weather stations in Inverleigh recorded rainfall of around 70 mm.
Bureau of Meteorology (BoM) radar-derived[7] rainfall accumulations estimated that between 50 and 100 mm of rain fell at Inverleigh in the 24 hours to 0900 on 14 November 2022 (Figure 5).
Figure 5: Radar-derived rainfall accumulations
Source: Bureau of Meteorology, annotated by Chief Investigator, Transport Safety
Further investigation
To date, CITS has:
attended and completed derailment site inspections
examined drainage in the waterway catchment area and commenced hydrology studies
examined train consist and operational information
interviewed the driver of train 4PM9
commenced collection of other relevant information
The investigation is continuing and will include review and examination of:
the train consist and operation of the train
the waterway catchment area, including local catchment features
the effect of prior rainfall on soil moisture and catchment flow
culvert design including capacity
track infrastructure including inspection and maintenance
weather warnings
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Australian Transport Safety Bureau
About the ATSB
The ATSB is an independent Commonwealth Government statutory agency. It is governed by a Commission and is entirely separate from transport regulators, policy makers and service providers.
The ATSB’s purpose is to improve the safety of, and public confidence in, aviation, rail and marine transport through:
independent investigation of transport accidents and other safety occurrences
safety data recording, analysis and research
fostering safety awareness, knowledge and action.
The ATSB is responsible for investigating accidents and other transport safety matters involving civil aviation, marine and rail operations in Australia, as well as participating in overseas investigations involving Australian-registered aircraft and ships. It prioritises investigations that have the potential to deliver the greatest public benefit through improvements to transport safety.
The ATSB performs its functions in accordance with the provisions of the Transport Safety Investigation Act 2003 and Regulations and, where applicable, international agreements.
Rail safety investigations in Victoria
Most transport safety investigations into rail accidents and incidents in Victoria and New South Wales (NSW) are conducted in accordance with the Collaboration Agreement for Rail Safety Investigations and Other Matters between the Commonwealth Government of Australia, the State Government of Victoria, and the State Government of New South Wales. Under the Collaboration Agreement, rail safety investigations are conducted and resourced in Victoria by the Chief Investigator, Transport Safety (CITS) and in New South Wales by the Office of Transport Safety Investigations (OTSI), on behalf of the ATSB, under the provisions of the Transport Safety Investigation Act 2003.
The Chief Investigator, Transport Safety(CITS) is a statutory position established in 2006 to conduct independent, no-blame investigation of transport safety matters in Victoria. CITS has a broad safety remit that includes the investigation of rail (including tram), marine and bus incidents.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available on the ATSB website. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
[1] Of the 55 wagons, 10 were ‘5-pack’ articulated skeletal container flat wagons.
[7] The BoM rainfall accumulation images are made by blending measurements from rain gauges (accurate point data) and radar. Radar data is calibrated with rain gauge data and is used to fill in the "gaps" between rain gauges.
On 19 November 2022, the pilot of a Robinson Helicopter Company R44, registered VH-TKI, was conducting a private flight from a nearby property to a function centre at Forresters Beach, New South Wales with 2 passengers onboard. The proposed landing site was the carpark of the venue. During the approach, the pilot reported an uncommanded yaw to the right which was unable to be recovered. Following a loss of control, the helicopter struck powerlines before colliding with terrain. The occupants received minor injuries and the helicopter sustained substantial damage.
What the ATSB found
The ATSB found that during approach to a confined area landing site, the helicopter experienced a loss of tail rotor effectiveness and accompanying right yaw. The pilot’s response was ineffective at recovering control, however, with the position of the aircraft on approach to the confined area it could not be established if the control of the aircraft could have been recovered before the helicopter collided with powerlines and terrain.
Safety message
Helicopter pilots should remain cognisant of the factors that may induce unanticipated yaw, especially the relative wind direction, and either avoid or manage their influence on the helicopter’s anti‑torque system by maintaining positive control of the yaw rate. If unanticipated yaw is encountered, prompt and correct pilot response is essential. Depending on the yaw rate recovery may not be immediate, but maintaining the recovery control inputs is the most effective way to stop the yaw.
A prompt response is especially important for confined area operations where the physical characteristics of the landing site may limit the options available to the pilot in the event of an unanticipated yaw or emergency landing.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 19 November 2022, the pilot of a Robinson Helicopter R44, registered VH-TKI, was conducting a private flight to take 2 passengers from a nearby property to a function centre at Forresters Beach, New South Wales (Figure 2).
At about 1800 local time, the pilot commenced the first of 2 approaches to the proposed landing site, located in the carpark of the function centre. The pilot reported that the approach was towards the north-east, with the wind coming from 10º to the left of the nose and that all indications were normal.
After experiencing instability in the hover over the landing area, the pilot elected to conduct a missed approach (see Video 1). During the second approach, as the helicopter slowed to an airspeed of approximately 20 kt and approached the tree line at approximately 100 ft above ground level, the pilot reported the helicopter began an uncommanded yaw to the right that could not be corrected with full left pedal input.
Recognising the helicopter’s proximity to the people gathered at the venue and in the street below, the pilot attempted to manoeuvre the helicopter away from the landing site towards a clearing on the opposite side of the road. However, the rate of rotation increased, with the helicopter making two and a half revolutions before striking powerlines and colliding with terrain. The pilot and both passengers sustained minor injuries and the helicopter was substantially damaged (Figure 1).
Figure 1: Accident site
Source: ATSB
Context
Pilot information
The pilot held a valid commercial pilot license (helicopter) with a class 2 medical certificate.
At the time of the accident, the pilot had about 190 hours of aeronautical experience, with most of this experience in the R44. Since obtaining their license in 2016, they had accrued approximately 90 hours of flying. The pilot also completed a low-level rating in an R44 on 1 October 2022. This operational rating also counted as a flight review.
The low-level rating included low-level emergencies and autorotations,[1] however, unanticipated yaw, (see the section titled Unanticipated yaw) was not covered. The pilot did recall receiving classroom-based training in relation to the recognition of the onset of loss of tail rotor effectiveness (LTE) during their license training and recalled conducting loss of tail rotor emergency training as part of a previous flight review.
Helicopter information
The R44 is a 4-place helicopter that is primarily all metal construction with a 2-blade main and tail rotor system powered by a 6-cylinder Lycoming piston engine. VH-TKI was manufactured in the United States in 1994 and issued serial number 0040. It was registered in Australia in 2021. The helicopter was maintained in accordance with the manufacturer’s maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever came first. The maintenance release indicated that VH-TKI had accumulated a total of 1,582.9 hours in service at the time of the occurrence.
The helicopter had flown 3.8 hours since the last periodic inspection, and no outstanding defects were noted in the maintenance release. The helicopter was within the weight-and-balance and centre-of-gravity limits. The co-pilot controls had been removed and were stored under the pilot’s seat for the flight.
Weather
The pilot advised that as part of their pre-flight planning, they had obtained the weather forecast and prior to departure continued to monitor the observations, at Williamtown Aerodrome, located about 75 km to the north-north-east of the landing site. Williamtown was the closest aerodrome on the coast with briefing and NOTAM[2] services available.
The weather forecast for Williamtown indicated the conditions expected for the planned time of arrival would be CAVOK[3] with winds from the north-east at 12 kt. Conditions throughout the flight were reportedly as forecast and provided smooth flying conditions.
The nearest Bureau of Meteorology weather observation site was located at Gosford, 10 km south-south-west of the landing site. Weather data recorded at about the time of the occurrence showed the wind from the north-east at 6–10 kt.
The ATSB received video footage of both approaches (see video 1 and 2) which showed the palm trees at the edge of the landing area moving in the wind. The pilot advised that flags positioned by the road at the front of the venue were used to ascertain the local wind direction. Eye-witness reports did not provide a clear indication of the wind speed, but confirmed the wind was coming from the north-east.
The approaches
The Robinson R44 Pilots Operating Handbook stated that in-ground effect hover controllability had been demonstrated to 17 kt wind from all directions. While a limiting figure was not provided for an out of ground effect[4] hover, the pilot advised that a power assurance check conducted prior to commencing the approach confirmed that out of ground effect power existed.
In the video footage of the first approach, (Video 1) taken from the edge of the landing site, the helicopter became unstable in the final stages of the approach, with the nose yawing to the right. The yaw was arrested by the pilot, but sideways drift was evident as the approach continued. Upon terminating into a hover over the landing site, the tail again began yawing from side to side before the pilot conducted a missed approach.
Video 1: First approach
Source: Witness
The data extracted from the onboard GPS (Figure 2), indicated the track for both approaches was approximately south‑east.
Figure 2: Final approach path
The flight track extracted from the helicopter GPS is shown in red. The inset shows the proximity of the obstacles (power lines and palm trees) under the approach to the planned landing area. The relative wind can be seen to be almost perpendicular to the track from the left, an area of known hazard for the onset of LTE.
Source: Google Earth with GPS data, annotated by ATSB
Video footage of the second approach (Video 2) showed that the helicopter approached at approximately 100 ft above ground level before suddenly yawing to the right. The rate of rotation could be seen to accelerate, and the radius of turn tighten as the helicopter rotated through two and a half revolutions. Directional control of the helicopter was not recovered, and the rotational speed of the main rotor blades could be heard to decrease as the helicopter began to descend. The rotating descent continued until the helicopter struck powerlines and then collided with terrain.
Video 2: Accident sequence
Source: Witness
Proposed landing site
The pilot had been in contact with the venue’s management and visited the location twice prior to the flight, to confirm the dimensions and the suitability of the carpark as the landing site. Civil Aviation Safety Regulations (CASR) 1998, 91.410 Use of aerodromes required that an aircraft take-off or land from
a place that is suitable... and the aircraft can land at, or take off from the place safely having regard to all the circumstances of the proposed landing or take-off (including the prevailing weather conditions)
The venue was located on a main road in a built-up suburban area (Figure 2). The approach to the carpark was planned to overfly a clearing on the opposite side of the road to the venue before passing over powerlines along the road, and palm trees at the perimeter of the carpark (Figure 3). The helicopter would be required to enter an out of ground effect hover at approximately 50 ft above ground level, before conducting a vertical descent to the ground.
CASA guidance in Advisory Circular AC 91-29 Guidelines for helicopters – suitable places to take off and landacknowledges that as a private operation, the safety margins that would otherwise be expected to be applied to performance calculations when conducting commercial operations do not apply.
There is no legal obligation on helicopter pilots operating solely under Part 91 to apply safety margins to the take-off or landing distance, take-off performance and obstacle avoidance ability which has been determined when using the helicopter manufacturer's data.
Additionally, AC 91-29 detailed when a particular landing site was considered to be a confined area and the obligations of the pilot when selecting the particular landing site.
An unprepared landing site that has obstructions that require a steeper than normal approach, where the manoeuvring space in the ground cushion is limited, or whenever obstructions force a steeper than normal climb-out angle is often defined as ‘Confined Area’. While a pilot can land at a Confined Area, they still have to apply all the basic principles.
While not having landed at this location before, the pilot had operated into other confined area landing sites on previous flights.
Figure 3: Planned landing site looking in the direction of the approach
Source: ATSB
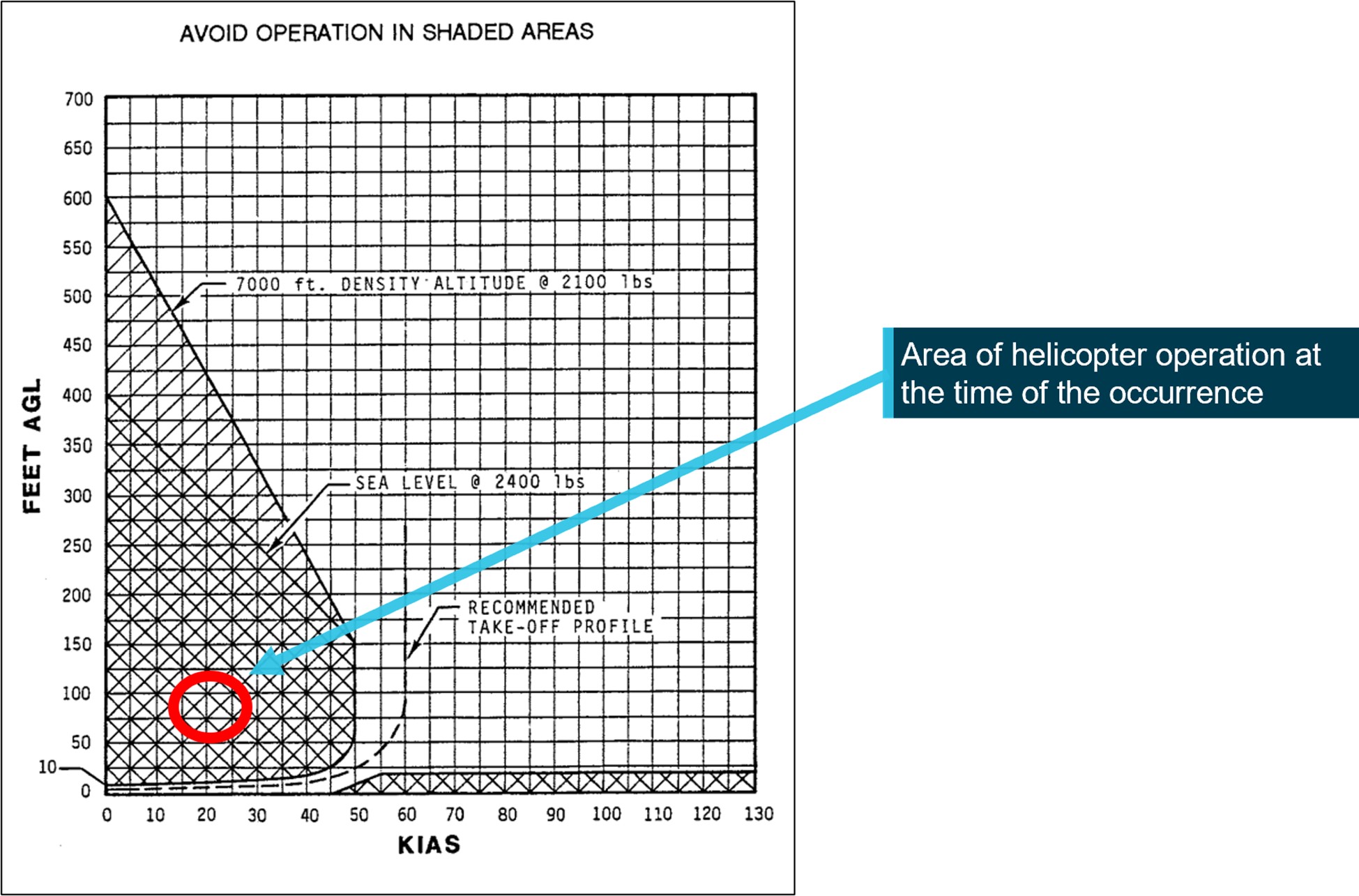
Where a site is considered to be a confined landing area, CASA guidance in Advisory Circular AC 91-29 Guidelines for helicopters – suitable places to take off and land recommended that in addition to aircraft performance, ‘the height velocity diagram should also be carefully considered before operating from these areas’. The R44 flight manual included a height-velocity diagram, which defined the conditions from which a safe power-off landing could be made. A notation on the diagram encouraged pilots to avoid operation in the shaded area. The approximate speed and height at which the aircraft was flown during the occurrence with respect to the height-velocity diagram is shown in Figure 4.
The FAA Helicopter Flying Handbook Chapter 11: Helicopter emergencies and hazardsstated that loss of tail rotor effectiveness (LTE) is ‘an uncommanded rapid yaw towards the advancing blade’. It ‘is an aerodynamic condition and is the result of a control margin deficiency in the tail rotor’. Tail rotor thrust is affected by numerous factors, including relative wind, forward airspeed, power setting and main rotor blade airflow interfering with airflow through the tail rotor.
Several wind directions relative to the nose of the helicopter, shown in Figure 5, are conducive to LTE when single rotor helicopters fitted with counterclockwise rotating main rotor blades such as the R44, are flown at speeds of less than 30 kt. The wind directions that were of relevance during VH-TKI’s approach included the following:
210–330°, tail rotor vortex ring state. Turbulent air produced by the tail rotor blade vortices recirculate through the tail rotor leading to the development of unsteady airflow through the tail rotor and fluctuations in tail rotor thrust. The change in thrust means that the airflow around the tail rotor will vary in direction and speed, requiring an increase in rudder pedal workload to maintain directional control. The loss of this tail rotor efficiency increases the power demand and there is an additional antitorque requirement.
285–315°, main rotor disc vortex interference. Winds at velocities of 10–30 kt from the left front cause the main rotor blade vortices to enter the tail rotor disc producing turbulent airflow that interferes with the tail rotor. High power settings generate an associated increase in main rotor downwash and blade tip vortices. The turbulent airflow increases the likelihood of main rotor disc vortex interference as illustrated in Figure 5.
Figure 5: Azimuths[5] of concern for loss of tail rotor effectiveness
Any manoeuvre which requires the pilot to operate in a high-power, low-airspeed environment with a left crosswind or tailwind creates an environment where unanticipated right yaw may occur.
It also provides guidance on how to avoid the onset of LTE and advised pilots to avoid the following flight conditions when operating below 30 kt:
tailwinds
out of ground effect hovers and high-power demand situations such as downwind turns
hovering out of ground effect in winds of about 8–12 kt.
The Robinson Helicopter Company advised that to avoid unanticipated yaw, pilots should be aware of conditions that may require large or rapid pedal inputs. They recommend practising slow, steady-rate hovering pedal turns to maintain proficiency in controlling yaw.
Recovery from unanticipated yaw
In addition to providing guidance on how to avoid the sudden onset of unanticipated yaw, AC 90‑95 provided the following recovery technique:
apply full left pedal while simultaneously moving cyclic[6] control forward to increase speed.
if altitude permits, reduce power.
as recovery is affected, adjust controls for normal forward flight.
The pilot stated that the yaw to the right was uncommanded and unexpected. As the rotation began, the pilot applied full left anti-torque pedal input to arrest the rotation and manoeuvred towards a clearing on the opposite side of the road. While maintaining left pedal input, they also applied forward cyclic to increase the helicopter’s forward speed. These inputs were consistent with the recovery guidance for unanticipated yaw.
The pilot further advised that they probably raised the collective in an attempt to fly away. As the collective is raised, there is a simultaneous and equal increase in pitch angle of all main rotor blades. An increase in pitch angle also results in increased drag on the main rotor blades. To counter this adverse effect, the R44 has a throttle correlator mechanism attached to the collective control that increases the throttle when the collective is raised.
A condition known as overpitching exists when the collective is raised to a point where the main rotor blade angle of attack creates so much drag that all available engine power cannot maintain or restore normal operation rotor RPM.[7] Beyond this point, any further attempt to raise the collective will result in a reduction of main rotor RPM as the engine has no remaining power margin to overcome the drag on the blades. With a reduction of the main rotor RPM, there will be a reduction in lift being produced and a disproportionate reduction in the amount of anti‑torque thrust available to the tail rotor. In explaining the reduction in tail rotor thrust, Robinson stated:
Since thrust of the rotor is proportional to the square of RPM, and the tail rotor is operating at roughly 6 times the RPM of the main rotor, a small reduction in main rotor RPM leads to a large reduction in tail rotor thrust.
Overpitching can also occur if the pilot raises the collective lever at a rate that is faster than the correlator will open the throttle, while not compensating for the increased drag by manually increasing the throttle.
The pilot was confident that the throttle was set to 100% for the approach, however, they were not certain if the throttle was manipulated in the avoidance manoeuvre. The recommended technique for recovery from unanticipated yaw is to lower the collective to reduce torque and simultaneously increase throttle to over-ride the correlator, which would otherwise decrease the throttle when the collective is lowered.
Maintaining maximum available engine RPM ensures that the maximum power is available to the anti-torque system. During both approaches, the helicopter could be seen to drift with the wind. AC 90-95 advised that drifting with the wind results in a reduction in the effective translational lift[8] and a corresponding increase in the power demand and anti-torque requirements. This again could result in a decrease in the main rotor RPM and the corresponding anti‑torque thrust available.
Accident site
The ATSB attended the site and conducted an inspection of the wreckage (Figure 1). The helicopter had struck high and low-voltage power lines during the descent and came to rest on its left side, spanning a drainage culvert.
Inspection of the cockpit showed that there was full left pedal input. While the pedals could not be moved, a subsequent examination found this was due to airframe deformation attributed to the impact. Once adjusted, the pedals moved freely. The drive belts were intact and in place. Once the clutch was released, the main rotor rotated freely, and drive continuity was followed to the tail rotor.
The tail boom skin was disrupted in 2 locations but was still attached to the helicopter. The fracture surfaces on the drive shaft were consistent with overstress and attributed to the impact with terrain. Similarly, damage to the tail rotor gearbox housing showed evidence of uniform overstress attributed to the impact. A review of witness videos showed no evidence of tail boom disruption in flight and the engine could be heard to operate normally.
The main rotor blades showed evidence of low rotational energy with both blades still intact and connected to the hub. Additionally, no major ground scars were observed on-site. The pilot advised that the low rotor RPM horn sounded at approximately the same time the helicopter struck the powerlines.
The positions of the collective and the throttle were examined during the on-site inspection and the collective was found lowered with the half throttle set. It could not be determined from the onsite inspection what control inputs were applied prior to descent and it is likely that these controls were disrupted following the collision with terrain as the pilot fell in that direction across the controls.
Assessment of damage
No anti-torque, cyclic or collective control faults or other mechanical issues were found with the helicopter. Continuity in the anti-torque system and drive train were consistent with pilot report of no mechanical issues with the helicopter.
On 17 May 2017, the pilot of a Robinson Helicopter R44 II, registered VH-MNU, was conducting aerial work at Moreton Island, Queensland with one passenger on board. The pilot departed for a local flight at about 1005 local time. At about 1130, the helicopter was operating at approximately 50 ft above ground level and tracking in a south-westerly direction, at an airspeed of about 10 kt (and groundspeed of about 20 kt), when the pilot commenced a right turn. The pilot felt a loss of tail rotor effectiveness as the helicopter continued to yaw to the right and reported that they were unable to arrest the yaw with left pedal input.
The pilot applied forward cyclic to try to increase the helicopter’s forward speed and some right cyclic to try to follow the turn. As the helicopter turned back into wind and rotated through about 110°, the rate of yaw started to increase. The pilot then raised the collective in an attempt to increase the helicopter’s height above trees, which further increased the yaw rate due to the increase in torque. The helicopter completed about 2 full rotations and reached about 80 ft above the ground, when the low rotor RPM warning horn sounded. The pilot immediately lowered the collective and the helicopter descended. As the helicopter neared treetop height, the pilot deployed the emergency floats and the pilot raised the collective to cushion the impact. The pilot and passenger sustained minor injuries and the helicopter was substantially damaged.
Safety analysis
The pilot planned to land at a confined area that required them to approach the landing site over powerlines and a row of trees. This required the helicopter to be flown out of ground effect with a high-power setting and at slow forward air speed.
Considering the recorded Gosford weather observations of the wind from the north-east at 10 kt, the approach track placed the wind from a direction and at a speed known to be conducive to the onset of loss of tail rotor effectiveness (LTE) via both tail rotor vortex ring state and main rotor disc vortex interference (Figure 5). The yaw fluctuations experienced during the first approach were consistent with the onset of an unanticipated yaw but were not identified by the pilot.
Video footage of the accident sequence showed a right yaw with accelerating rotation, also consistent with the symptoms of an unanticipated yaw event.
Flying out of ground effect at a slow forward airspeed in proximity to obstacles placed the aircraft in a scenario that did not easily allow for recovery. It is likely that the initial actions by the pilot were consistent with the recommended recovery techniques. However, while setting 100% throttle provided maximum power-on rotor RPM and ensured the maximum anti‑torque thrust was available, it would also have maintained the torque inducing the yaw.
Further, consistent with the pilots account of the low rotor RPM horn activation and the audible reduction in main rotor RPM present in the video footage, raising of the collective to avoid obstacles during the attempted recovery, probably over-pitched the main rotor blades. The resulting decrease in both the main and tail rotor speed reduced the available anti‑torque thrust and increased the rate of descent.
In a situation where the time to respond is reduced, such as during an approach, following the recommended recovery technique greatly improves the likelihood of recovering controlled flight. However, based on the available height above obstacles and uncertainty around the actual control inputs made by the pilot, it could not be determined if application of the recommended recovery technique would have been effective in recovering the helicopter or if a collision was unavoidable.
The FAA helicopter flying handbook stated that a recovery path must always be planned, especially when terminating to an out of ground effect hover and executed immediately if an uncommanded yaw is evident. Terrain, obstacles, and people in the undershoot limited the available forced landing options to the pilot on this occasion.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving VH-TKI on 15 November 2022.
Contributing factors
During approach to a confined area landing site, the helicopter experienced unanticipated right yaw, resulting in collision with powerlines and terrain.
Other findings
It could not be established if control of the aircraft was recoverable from the point in the approach that the unanticipated right yaw occurred.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
chief pilot of Skyline Aviation
Bureau of meteorology
Robinson Helicopter Co. R44 Pilot Operating Handbook
accident witnesses
video footage of the accident flight
recorded data from the GPS unit in VH-TKI.
References
Civil Aviation Safety Authority. (2022). Advisory Circular AC 91-29 v1.1 Guidance for helicopters – suitable places to take-off and land. Civil Aviation Safety Authority.
Civil Aviation Safety Authority. (2019). Civil Aviation Safety Regulations 1998 - Part 91 (General operating and flight rules) Australian Government.
International Civil Aviation Organization. (2011). Manual of Aircraft Accident and Incident Investigation Part III: Investigation, Doc 9756, ICAO, Montréal.
Federal Aviation Administration. (1995). Advisory Circular AC 90-95–Unanticipated right yaw in helicopters. Federal Aviation Administration.
Federal Aviation Administration. (2019). Helicopter flying handbook. U.S Department of Transportation.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
the chief pilot of Skyline Aviation
Robinson Helicopter Company
United States National Transportation Safety Board.
Submissions were received from:
the chief pilot of Skyline Aviation
Robinson Helicopter Company
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Autorotation: Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[2] Notice to Airmen (NOTAM): A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[3] Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[4] Out of ground effect: helicopters require less power to hover when in ‘ground effect’ then when out of ‘ground effect’ due to the cushioning effect created by the main rotor downwash striking the ground. The height of ‘ground effect’ is usually defined as more than one main rotor diameter above the surface.
[5] Azimuth: An azimuth is an angle measured clockwise from the south or north.
[6] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[7] International Civil Aviation Organization (ICAO) Manual of Aircraft Accident and Incident Investigation. Chapter 15: Helicopter investigation.
[8] Effective translational lift: Increase in the efficiency of a rotor achieved as it clears its own tip vortices and enters undisturbed air. The increased efficiency of the blade results in an increase in lift with an associated reduction in power demand on the antitorque system.
Typically, the ATSB safety reporting team receives more than 17,000 notifications of safety occurrences each year, spread over aviation, marine and rail.
While there may be duplicate notifications of the same occurrence and many of the notifications submitted are about matters not required to be reported under the Transport Safety Investigation Act 2003, each one is reviewed and recorded.
The TSI Act requires any responsible person who has knowledge of any accident or serious incident (or any immediately reportable matter) to report it as soon as it is reasonably practicable.
Immediately reportable matters also require a written notification within 72 hours, as do safety incidents (or routine reportable matters).
While the terms of this requirement may seem broad, the Transport Safety Investigation Regulations 2021 (TSI Regulations) provide a list of persons who, by the nature of their qualifications, experience or professional association, would be likely to have knowledge of an immediate or routine reportable matter for their mode of transport.
In addition, responsible persons are not required to report a transport safety matter if they believe, on reasonable grounds, that another responsible person has already reported, or is in the process of reporting, that matter.
The ATSB maintains a 24-hour service to receive notifications, including a toll-free telephone number (for immediately reportable matters).
In marine, both immediately reportable and routine reportable matters are reported to the ATSB via AMSA(Opens in a new tab/window).
While not all reported occurrences are investigated, the details of each occurrence are retained within the ATSB occurrence database. These records are a valuable resource, providing a detailed portrait of transport safety in Australia. The searchable public version of the aviation occurrence database is available on the ATSB website and contains data from July 2003 onwards. The online database is used by industry, academics, the media and regulators to search and research past events.
The ATSB prioritises the investigation of transport safety matters that have the highest potential to yield improvements to transport safety for the greatest public benefit.
Our focus on the greatest public benefit reflects the contribution the ATSB makes to preventing loss of life, as well as avoiding significant local, state and national economic costs that can be associated with an accident.
The ATSB is not resourced to investigate every single accident or incident that is reported to us but allocates priorities within the transport modes to ensure that investigation effort achieves the best outcomes for safety improvement.
We recognise that there is often more to be learned from serious incidents and patterns of incidents, and we give focus to these investigations, as well as specific accident investigations.
When assessing and prioritising accidents and incidents for investigation we consider a broad range of factors including ATSB resource availability and, in no particular order:
the anticipated safety value of an investigation, including the likelihood of furthering the understanding of the scope and impact of any safety system failures
the likelihood of safety action arising from the investigation, particularly of national or global significance
the existence and extent of fatalities/serious injuries and/or structural damage to transport vehicles or other infrastructure
the unique value an ATSB investigation will provide over any other investigation by industry, regulators or police
the obligations or recommendations under international conventions and codes
the nature and extent of public interest – in particular, the potential impact on public confidence in the safety of the transport system
the existence of supporting evidence, or requirements, to conduct a special investigation based on trends
the relevance to identified and targeted safety programs
the risks associated with not investigating – including consideration of whether, in the absence of an ATSB investigation, a credible safety investigation by another party is likely
the timeliness of notification
the training benefit for ATSB investigators.
For information on investigation prioritisation within our three transport modes, see:
The ATSB will release a final report at the conclusion of an investigation, detailing contributing factors, safety issues and other findings. However, at any time during the course of an investigation, should we uncover safety critical information we will immediately share that with relevant parties so they can take appropriate safety action.
Depending on the complexity of the occurrence and the scope of the investigation, the ATSB may also publish preliminary and interim reports.
Preliminary reports detail factual information determined in an investigation’s initial evidence collection phase and areas of ongoing investigation. They are typically released 1–4 months after the initial occurrence.
Interim reports detail more extensive factual information and outline areas of ongoing investigation.
During the course of an investigation, the ATSB also provides brief factual updates on an investigation's progress on our website.
Either in conjunction with a report release or at any time during an investigation, the ATSB may also issue a safety advisory notice to relevant organisations and industry sectors to highlight a safety issue or concern and advising that relevant parties take safety action where appropriate.
Final report structure
ATSB occurrence investigation final reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports normally contain the following sections:
Investigation summary—summarises the occurrence (or other transport safety matter), the investigations findings, any safety action taken as a result, and highlights broader safety messages.
The occurrence—describes the sequence of events related to the occurrence and, if relevant, the consequences in terms of injuries and damage.
Context—details the evidence collected during the investigation that is necessary to help the reader understand the occurrence and safety analysis, or the broader safety issues for research purposes.
Safety analysis—outlines how the evidence justifies the investigation findings.
Findings—the contributing factors, other factors that increased risk and other findings identified during the investigation and discussed in the safety analysis.
Safety issues and actions—a summary of the safety issues identified during the investigation and details of what safety action has been taken, or is planned to be taken, by relevant parties to address those issues.
Appendices—additional information that supports the report, for example, specialist reports on materials failure or flight data analysis.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
Ownership of intellectual property rights
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in ATSB investigation reports is owned by the Commonwealth of Australia.
This allows for the distribution, remixing, adaption, and building upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly
Naming organisations in reports
ATSB policy provides for identifying most organisations in its transport safety investigations. Most organisations directly involved in any aviation occurrence investigated by the ATSB are identified in the report and on the investigation web page.
The policy ensures the ATSB’s compliance with the International Civil Aviation Organization’s recommended practices. It also ensures that the ATSB has a consistent and transparent approach across all of its aviation, rail and marine safety investigations.
Operators and other organisations can be assured that it is not a function of the ATSB to apportion blame or determine liability. Including the name of the organisation does not imply any adverse inferences.
Which organisations are identified
For aviation, all operators and regulators are identified.
For marine, all ship owners, ship management companies and the regulator are identified.
For rail, rail transport operators (rail infrastructure managers and/or rolling stock operators) and regulators are identified.
Other large organisations that contributed substantively to the occurrence will also be mentioned. The exception to the above policy will be where the operator is an individual or an individual’s name is the company name. Consistent with the Transport Safety Investigation Act 2003, the ATSB does not name individuals in its final reports.
Are there any exceptions?
If an operator or organisation had a passive or third-party involvement in an occurrence, the ATSB will not name that operator in the investigation report or published information.
Operators and other organisations will not be named in investigation report titles.
This policy applies to safety occurrences investigated by the ATSB from 1 July 2017. Any incident or accident that occurred before 1 July 2017 was treated under the previous policy.
How will an organisation know if they’re named?
The ATSB provides advance copies of its investigation reports to all organisations involved in a transport safety occurrence. This ensures organisations are aware of, and have the opportunity to provide feedback on, the report’s contents before it is made public.
Gender-neutral language in ATSB reports
All ATSB reports are de-identified. On the basis that gender‑specific language can lead to the identification of individuals, in 2020 the ATSB Commission adopted a policy of using gender‑neutral language in ATSB investigation reports.
In the report writing process, care is taken to ensure context and meaning are not lost.
ATSB occurrence investigations are scoped according to the anticipated scale of work required to determine the contributing factors to a safety occurrence.
Scope also generally also reflects not only the level of resources and/or time they require, but their complexity.
Our four levels of investigation scope build on the previous level and comprise:
Short
Short investigations provide a summary and analysis of commonly occurring transport safety accidents and incidents. Investigation activity includes sourcing imagery and documentation of any transport vehicle damage and/or accident site, conducting interviews with involved parties, and the collection of documents such as procedures and internal investigations by manufacturers and operators.
Short investigation reports include a description of the sequence of events, limited contextual factual information, a short analysis, and findings. Findings include safety factors (the events and conditions that increased the risk of incident or accident happening) but only examine the actions and conditions directly relating to the occurrence and any proactive safety actions taken.
Defined
Defined investigations look at transport safety accidents and incidents of a more complex nature than short investigations, and seek to identify systematic safety issues that reveal underlying causes of an occurrence. They involve several ATSB resources and may involve in-the-field activity or be an office-based investigation. Evidence collected can include recorded flight and event information, multiple interviews, analysis of similar occurrences, and a review of procedures and other risk controls related to the occurrence.
Defined investigation reports include an expanded analysis to support the broader set of findings within the report and may include safety factors not relating directly to the occurrence. Defined investigations may also identify safety issues (safety factors with an ongoing risk) relating to ineffective or missing risk controls. The report also identifies safety issues, along with proactive safety action taken by industry and ATSB safety recommendations.
Systemic
Systemic investigations can involve in‑the‑field activity, and a range of ATSB and possibly external resources. They have a broad scope and involve a significant effort collecting evidence across many areas. The breadth of the investigation will often cover multiple organisations. Occurrences and sets of transport safety occurrences investigated normally involve very complex systems and processes.
In addition to investigating failed and missing risk controls, systemic investigations may also investigate the organisational processes, systems, cultures and other factors that relate to those risk controls, including from the operator, regulator, and certifying and standards authorities. Systemic investigations result in substantial reports, often with several safety issues identified.
Systemic investigations were previously known as 'complex' investigations. The change in terminology more accurately reflects the broad scope and systems-level complexities involved in these investigations.
Major
In the event of a significant accident (potentially involving a large number of casualties), the ATSB would conduct a major investigation. Major investigations would likely involve significant ATSB and external resources and potentially require additional one-off government funding.
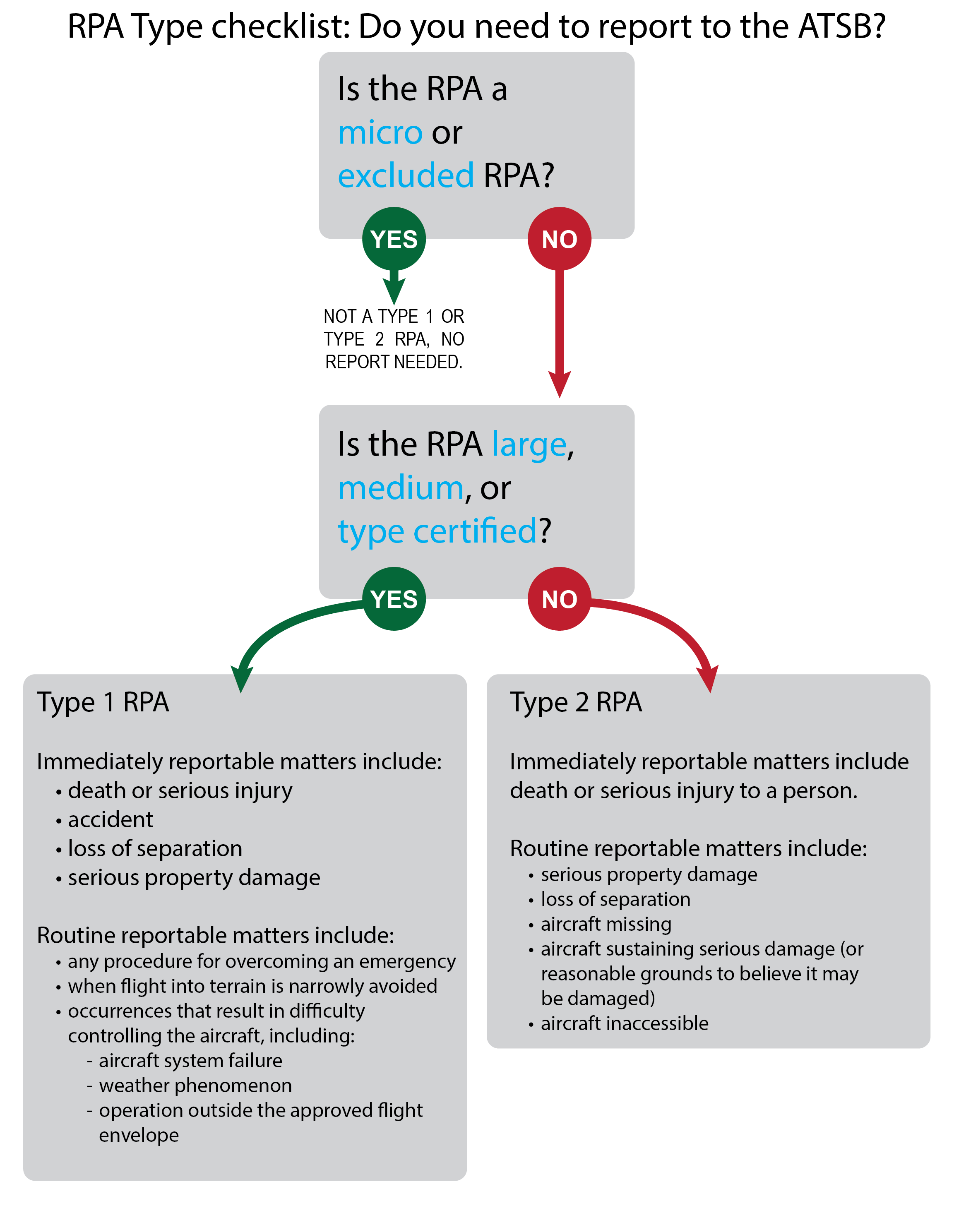
New reporting requirements for safety occurrences involving remotely piloted aircraft (or drones) took effect on 30 September 2021.
The Transport Safety Investigation Regulations 2021(Opens in a new tab/window) require the reporting of certain transport safety occurrences to the ATSB as immediately or routine reportable matters, and introduced updated requirements for operators of certain types of remotely piloted aircraft (RPA) to make reports to the ATSB.
Recognising the range of different types of RPA and their uses, the regulations categorise relevant RPA as type 1 or type 2 RPA.
RPAs that have been certified against relevant airworthiness standards (type certification), large (greater than 150kg) and medium RPAs (more than 25kg but not more than 150kg) are defined as type 1 and are an emerging form of commercial aviation that will benefit from investigation into systemic safety issues to help prevent future accidents.
Type 2 RPA are defined as those RPA that are not type 1, excluded or micro RPA (gross weight of not more than 250 grams) and have fewer reporting requirements. This distinction is made on the basis that ATSB investigations are unlikely for these operations unless there is serious risk of harm to people or significant third-party property.
RPAs that are not type 1 or type 2 including excluded or micro RPA have no reporting requirements.
Mandatory reporting for certain occurrences involving type 1 and type 2 RPA allows the ATSB to properly measure, investigate and report on safety trends in the RPA sector.
Making a report to the ATSB is not a time-consuming process, and the ATSB investigates incidents from a ‘no-blame’ perspective, prioritising improved safety outcomes.
Who is affected?
In order to provide an efficient and effective safety framework, the regulations define two types of RPAs which are subject to specific reporting requirements.
Type 1 RPAs are those which are type certified, large (over 150 kg) or medium (25 kg to 150 kg) RPA.
Type 2 RPAs are those that are not Type 1, and are not an excluded or micro (under 250 g) RPA.
Type 1 operators are required to immediately report to the ATSB RPA occurrences involving:
death or serious injury;
accidents;
loss of a separation standard with aircraft; and,
serious damage to property.
Less serious incidents and occurrences are required to be reported to the ATSB within 72 hours
Occurrences involving Type 2 RPAs generally only need to be immediately report to the ATSB if they involve death or serious injury, while less serious incidents and damage to the RPA will need to be reported within 72 hours.
ATSB policy provides for identifying most organisations in its transport safety investigations. Most organisations directly involved in any aviation occurrence investigated by the ATSB are identified in the report and on the investigation web page.
The policy ensures the ATSB’s compliance with the International Civil Aviation Organization’s recommended practices. It also ensures that the ATSB has a consistent and transparent approach across all of its aviation, rail and marine safety investigations.
Operators and other organisations can be assured that it is not a function of the ATSB to apportion blame or determine liability. Including the name of the organisation does not imply any adverse inferences.
Which organisations are identified
For aviation, all operators and regulators are identified.
For marine, all ship owners, ship management companies and the regulator are identified.
For rail, rail transport operators (rail infrastructure managers and/or rolling stock operators) and regulators are identified.
Other large organisations that contributed substantively to the occurrence will also be mentioned. The exception to the above policy will be where the operator is an individual or an individual’s name is the company name. Consistent with the Transport Safety Investigation Act 2003, the ATSB does not name individuals in its final reports.
Are there any exceptions?
If an operator or organisation had a passive or third-party involvement in an occurrence, the ATSB will not name that operator in the investigation report or published information.
Operators and other organisations will not be named in investigation report titles.
This policy applies to safety occurrences investigated by the ATSB from 1 July 2017. Any incident or accident that occurred before 1 July 2017 was treated under the previous policy.
How will an organisation know if they’re named?
The ATSB provides advance copies of its investigation reports to all organisations involved in a transport safety occurrence. This ensures organisations are aware of, and have the opportunity to provide feedback on, the report’s contents before it is made public.
The Australian Transport Safety Bureau has provided an interim report from its ongoing investigation into the derailment of a freight train north of Queensland’s Sunshine Coast earlier this year.
Aurizon freight train Y279 was substantially damaged, and its driver sustained minor injuries, when the train’s two locomotives, and four of its wagons, derailed on flood-affected track at Traveston, on 23 February 2022.
Today’s interim report details the evidence collected so far in the ATSB’s transport safety investigation.
It notes a remote weather monitoring station, located about 200 m ahead of the derailment site, detected floodwaters had overtopped the track about 40 minutes before the train entered the area.
“While the remote monitoring station transmitted this information to the Queensland Rail asset management protection system, no warning or critical alarm messages were provided to the network control officer, or other relevant operational staff,” ATSB Director Transport Safety Dr Michael Walker said.
“This meant the network control officer and train driver were not alerted that floodwater had overtopped the track ahead of the train.”
Dr Walker noted the ATSB has investigated numerous accidents involving heavy rain events leading to derailments or other adverse outcomes.
This has included the derailment at Julia Creek on the Mount Isa Line in December 2015, the collision with floodwater at Banyan Creek in March 2018 on the North Coast Line, and current investigations into derailments at Nana Glen, New South Wales in February 2021 (conducted on behalf of the ATSB by NSW's OTSI), Traveston in February 2022, and Inverleigh, Victoria early this month (conducted on behalf the ATSB by Victoria's CITS).
“All such events show the importance of rail infrastructure managers having effective processes in place to manage the risk of a heavy rain event affecting the integrity of a rail line prior to a rail movement.”
With the Traveston interim report published, investigators will review and examine Queensland Rail’s integrated asset management protection system, and arrangements for the distribution of weather-related warning and alarm messages generated by the system.
“We will also be looking at procedures in place for the identification and management of a potential hazard from a weather event, and for response to warning and alarm messages,” Dr Walker said.
Procedures and training for drivers will be reviewed, both in terms of identifying and managing weather events, and egressing from a locomotive cab in an emergency.
“Investigators will also look into the training provided to network control staff and the maintenance inspections of cross track drainage systems at Traveston,” Dr Walker added.
In addition to evidence gathered, the interim report details some safety actions already taken by Queensland Rail after the derailment.
“While the ATSB will reserve its findings, and any safety issues and recommendations, for its final report, we welcome the safety action taken so far by the network operator.”
The International Confidential Aviation Safety Systems Group
The International Confidential Aviation Safety Systems (ICASS) Group promotes confidential reporting systems as an effective method of enhancing flight safety in commercial air transport and general aviation operations. The principal objectives of the ICASS Group are:
To provide advice and assistance in the startup and operation of a confidential reporting system.
To facilitate the exchange of safety related information between independent confidential aviation reporting systems.
To identify solutions to common problems in the operation of such systems.
Group membership
Membership to the ICASS Group is by invitation.
Membership - Membership with full voting rights.
Available to Reporting Systems that provide:
Voluntary reporting
Confidential protections
Operating on a regional, national or international level
Observer Status - In attendance by invitation during general business, but may be excluded from sensitive discussions.
Available to interested third party groups, eg. research institutions, airlines, service providers, manufacturers, and representatives of emerging confidential reporting systems.
For more information on confidential reporting and/or membership of ICASS, contact any one of the following programs.
Current Member Programmes
International Confidential Aviation Safety Systems Group





![Figure 5: Azimuths[5] of concern for loss of tail rotor effectiveness](/sites/default/files/inline-images/AO-2022-060%20Figure%205.jpg)