REPCON is a voluntary and confidential reporting scheme. REPCON allows any person who has an aviation safety concern to report it to the ATSB confidentially. Protection of the reporter's identity and any individual referred to in the report is a primary element of the scheme.
Who can make a report?
Anyone can report a safety concern confidentially to the ATSB. This means members of the travelling public or people involved in aviation.
Some examples of who has made a REPCON report in the past include:
an employee or contractor of an aviation transport operator who reported a matter under the operator’s Safety Management System (SMS) but does not believe it will be properly dealt with.
a person who has not reported under the SMS because they believe they will suffer retribution. (When submitting a report please ensure that you cannot be identified within your organisation by not copying any other person in to the report).
What may be reported?
Each of the following concerns (reportable safety concerns) in relation to the safety of aircraft operations to which the Regulations apply are examples of what may be reported under REPCON. The list is not exhaustive:
a) an incident or circumstance that affects or might affect the safety of aircraft operations;
b) a procedure, practice or condition that a reasonable person would consider endangers, or, if not corrected, would endanger, the safety of air navigation or aircraft operations, for example:
(i) poor training, behaviour or attitude displayed by an aircraft operator, airport operator or air traffic control service provider; or
(ii) insufficient qualifications or experience of employees of the aircraft operator, airport operator or air traffic control service provider; or
(iii) scheduling or rostering that contributes to the fatigue of employees of the aircraft operator, airport operator or air traffic control service provider; or
(iv) an aircraft operator, airport operator or air traffic control service provider bypassing safety procedures because of operational or commercial pressures; or
(v) inadequate airport facilities for safe operations; or
(vi) unsafe passenger, baggage or cargo management; or
(vii) inadequate traffic or weather information;
c) any other matter that affects, or might affect the safety of or aircraft operations not reportable under a mandatory reporting scheme.
If you are in any doubt whether the matter you wish to report is covered by the REPCON scheme or a mandatory reporting scheme please call us.
What is not a reportable safety concern?
To avoid doubt, the following matters are not reportable safety concerns and are not guaranteed confidentiality
matters relating to a serious and imminent threat to a person’s health or life
industrial relations matters
conduct that constitutes a criminal offence
terrorist acts. If you wish to provide information about terrorist activity you should call the National Security Hotline on 1800 123 400.
Matters which must be reported under a mandatory reporting scheme should not be reported under REPCON. This will not discharge your reporting obligations under a mandatory reporting scheme.
If you believe it would be necessary to act on information about an individual referred to in your report then you should report this directly to the Civil Aviation Safety Authority (CASA) on 1800 074 737 or the aircraft operator
What is confidential?
Personal information about the reporter and any person referred to in the report is confidential. Even if you are not concerned about keeping your identity confidential, do not copy in personnel from within or outside your organisation to the report. The integrity of the confidentiality of the reporter is the main concern of the REPCON system. If this occurs we cannot process the report within the REPCON framework.
If you think it’s necessary to act on information about a person referred to in your report, you should report this directly to the Civil Aviation Safety Authority on 1800 074 737.
Is an anonymous report acceptable?
REPCON does not accept anonymous reports. REPCON staff cannot contact an anonymous reporter to verify the report or to seek additional information. Further, REPCON staff must be satisfied that the reporter's motivation for reporting is aviation safety promotion, and that the reporter is not attempting to damage a rival or pursue an industrial agenda.
How are reports processed?
REPCON staff will assess reports for clarity, completeness and significance for aviation safety and to ensure it meets the requirements of a Reportable Safety Concern (RSC) for aviation.
The report will be de-identified to remove all personal details of the reporter and any individual named in the report. This will be passed to the reporter who must authorise the content before the REPCON can proceed further.
The de-identified text is then forwarded to the relevant organisation that is best placed to address the RSC. The organisation’s response will then be forwarded to the regulatory bodies, such as CASA, for further action as deemed necessary.
REPCON may use the de-identified version of the report to issue an information-brief or alert bulletin to a person or organisation, including CASA, which is in a position to take safety action in response to the safety concern.
What are the possible outcomes from report?
The desired outcomes are any actions taken to improve aviation safety in response to the identified concern. This can include variations to standards, orders, practices, procedures or an education campaign.
Why is REPCON important?
REPCON reports can serve as a powerful reminder that, despite the best of intentions, well-trained and well-meaning people are still capable of making mistakes. The de-identified stories arising from these reports may serve to reinforce the message that we must remain vigilant to ensure the ongoing safety of ourselves and others.
ASRS or REPCON?
REPCON is a separate scheme to the Aviation Self Reporting Scheme (ASRS). The ASRS allows for self-reports of unintentional regulatory breaches by pilots who are seeking to claim protection from administrative action by CASA. A reporter seeking protection from administrative action by CASA should consider reporting under the ASRS and whether they meet its criteria.
REPCON is a much broader reporting scheme designed to capture a wide range of aviation safety concerns from a large pool of potential reporters.
Submission of information known by the reporter to be false or misleading is a serious offence under section 137.1 of the Criminal Code. Aiding, abetting, counseling, procuring or urging the submission of false or misleading information is also a serious offence.
On 16 November 2022, a Regional Express (Rex) Saab 340B, registered VH-ZLJ, was prepared for a scheduled air transport flight from Cairns Airport, Queensland, to Bamaga, Queensland, as flight number ZL5538.
As the crew taxied the aircraft to the runway, an engineer on a nearby parking bay noticed something hanging from the aircraft and contacted the tower. The air traffic controller visually confirmed the engineer’s observations and alerted the crew, who returned the aircraft to the bay.
Aircraft parked overnight at Cairns were required to be fitted with an operator-designed bung installed in the horizontal stabiliser trim actuator cove to prevent bird nesting. The inspection revealed the horizontal stabiliser bungs had not been removed and were still installed in the left trim actuator cove.
What the ATSB found
The investigation found that the horizontal stabiliser bung was not detected during pre-flight preparations, resulting in the aircraft being dispatched with the bung still installed.
The ATSB also found that there was no procedure for the storage and accountability of the bungs after they had been removed, which differed from other bungs and covers used on Rex aircraft. Additionally, the operator did not consider aspects that would ensure the identification of an installed bung, or the safe operation of the aircraft if the bungs were not removed prior to flight.
What has been done as a result
The operator has commenced a risk assessment to formalise the procedures around the use of the horizontal stabiliser bungs. To support this, an engineering order was obtained to document and approve the manufacture of the bungs.
However, these actions did not address the issues around the storage and accountability of the bungs when they are removed or the aspects around the identification of an installed bung or the safe operation of the aircraft if the bungs were not removed. As such, the ATSB issued two safety recommendations and will continue to monitor the safety issues and provide website updates.
Safety message
‘Remove before flight’ conspicuity flags are a visual reminder to remove covers prior to flight. Failure to remove these devices may have the potential to foul or jam aircraft flight controls. In certain circumstances, the flags may not hang freely, which can reduce their visibility. Targeted inspection of locations and components, rather than relying on flags, which may not always be visible, can help to identify when these covers or devices have not been removed.
Further, when a missed item has the potential to affect the safety of flight, a secondary means of assuring the item has been removed should be employed. Similar to procedures employed for other covers on the aircraft, a means to account for what equipment has been removed from the aircraft before being stowed or retained by ground agents will provide the crew with another opportunity to detect when a bung or cover has not been removed.
The occurrence
On 16 November 2022, a Regional Express (Rex) Saab 340B, registered VH-ZLJ (ZLJ), was prepared for a scheduled air transport flight[1] from Cairns Airport, Queensland, to Bamaga, Queensland, as flight number ZL5538.
Ground handling services for the operator’s aircraft based at Cairns, were contracted to a third‑party provider. As part of this contract, 2 ground handlers were assigned to dispatch an aircraft, however, on the day of the occurrence one ground handler was unavailable. This meant that there were times when the available ground handler (ground handler 1) was assisted by a duty manager, prior to another ground handler commencing at 1300.
The aircraft had been parked overnight at Cairns Airport, which required the installation of horizontal stabiliser bungs (bungs) (see the section titled Use of horizontal stabiliser bungs) to prevent birds nesting in the elevator trim actuator coves. This was the first flight of the day for ZLJ, and at 1116 local time, ground handler 1 commenced removing the pitot covers, propeller straps, engine bungs and the wheel chocks from the aircraft and loaded the catering for the flight. It is likely they also attached the tail stand before leaving to dispatch another aircraft at 1131.
They returned to ZLJ at 1231 with the duty manager and continued the aircraft’s preparations, including connecting the ground power unit and the air-conditioning unit to the rear of the aircraft. Both ground crew then left to meet the ground handler who started work at 1300 (ground handler 2). Ground handler 2 was assigned to load luggage on to the aircraft and was occupied with this task until passengers boarded the aircraft at 1400.
The ground handling agent also provided check-in and customer services for the operator. Following a discrepancy with the number of bags checked-in for this flight, ground handler 1 left the aircraft to assist with checking-in the remaining passengers and locating the missing bag. Ground handler 1 was occupied with these tasks until returning to the aircraft at 1357 to load bags and finalise preparations.
At 1330, the flight crew arrived at the aircraft and commenced the pre-flight inspection[2] of the aircraft. The captain initially conducted an external check, walking around the aircraft. The first officer (FO) was completing their final check to line on this flight. They completed an external inspection of the aircraft as part of the aircraft’s daily inspection, in accordance with the flight crew operating manual (FCOM). They advised they paid particular attention to the rear of the aircraft, including inspecting the:
de-icing boots on the front of both sides of the horizontal stabiliser
5 static wicks on the rear of the horizontal stabiliser
depressurisation port to ensure there were no bird’s nests.
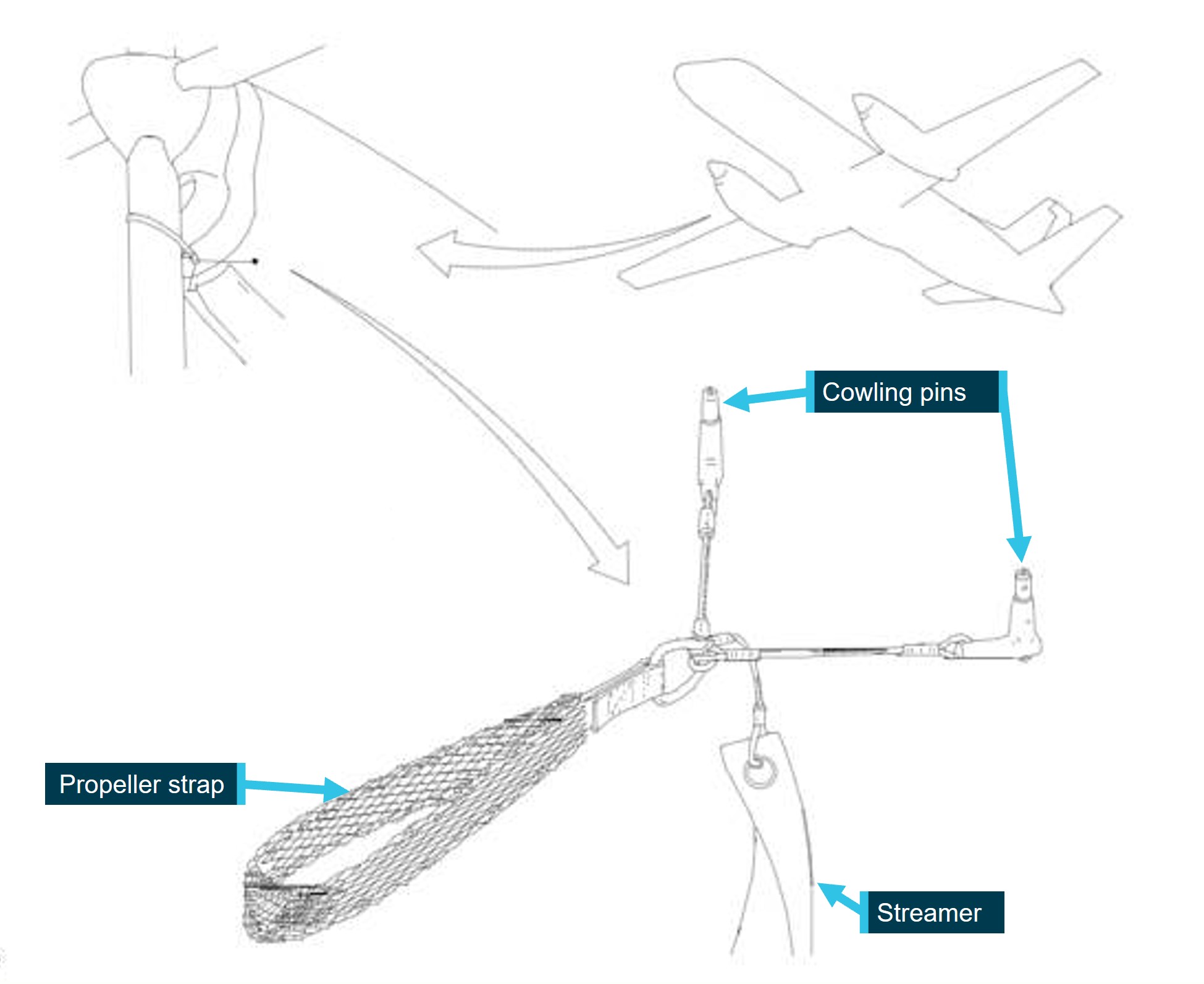
Both flight crew reported that during these checks they did not detect the tether rope with the ‘remove before flight’ conspicuity flag (Figure 2), which attached to each bung and hung under the back fuselage as a visual cue that the bungs were in place (Figure 1). The flight crew completed the internal and external checks prior to passengers arriving. At 1404, the FO completed the final external inspection.
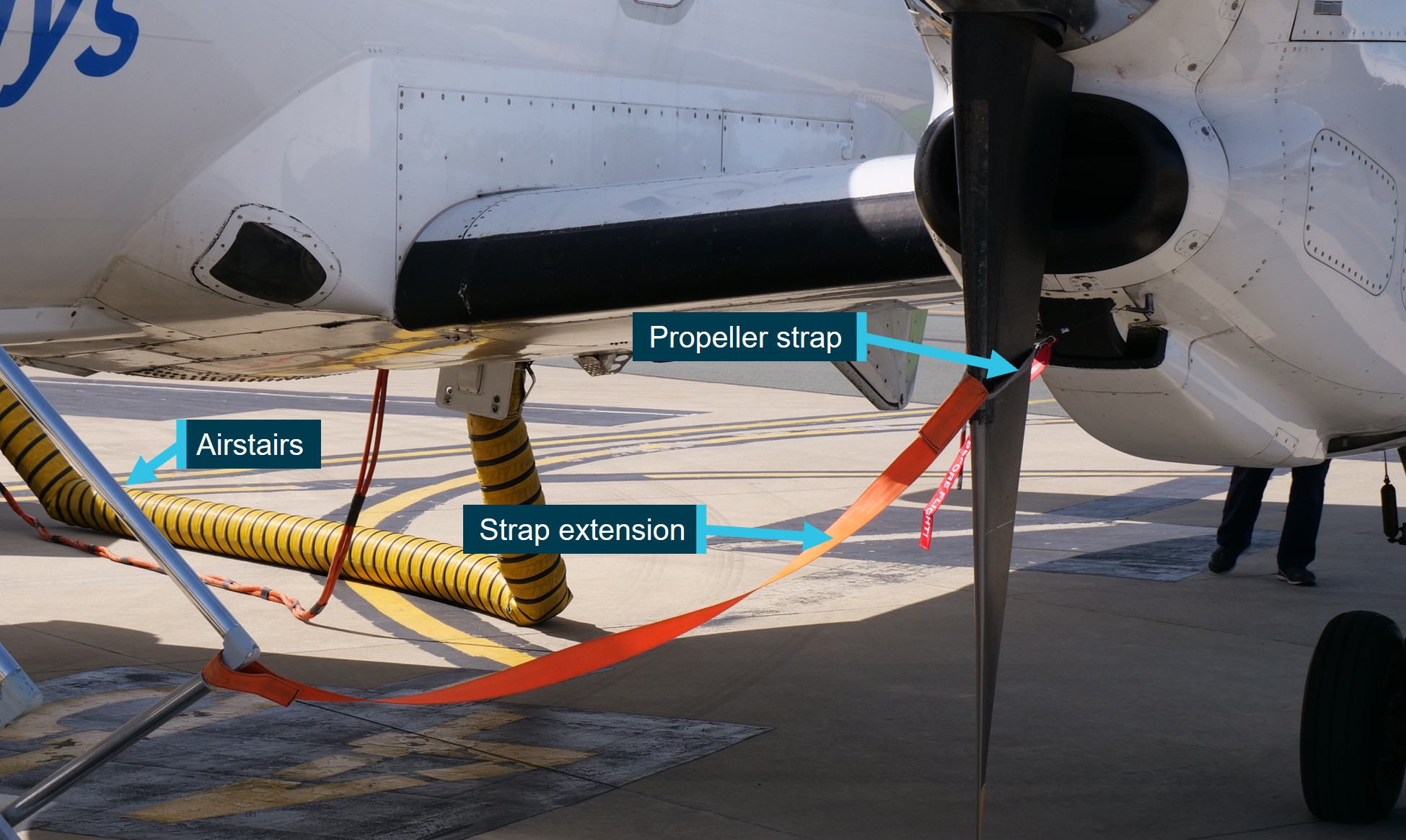
Normally, the air conditioner[3] would have already been removed at this stage, but on this occasion, the FO observed that it was still attached to the aircraft. The ground crew were occupied with the discrepancy on the passenger list and the decision had been made to leave the air conditioner attached until the matter was resolved. The discrepancy was identified to be an administration error and the air conditioner was subsequently removed. The FO then walked under the fuselage of the aircraft to remove the tail stand and placed this in the cargo hold. During this inspection, and before closing the cargo door located at the rear of the aircraft, all straps and bungs to be retained on the aircraft were confirmed as having been removed and accounted for. The FO recalled that prior to entering the aircraft, they removed the guide strap that connected from the propeller to the passenger stairs, and the propeller guard. They also conducted a visual inspection to ensure there was nothing hanging underneath the aircraft.
As the aircraft taxied to the runway, an engineer on a nearby parking bay noticed something hanging from ZLJ and contacted the tower controller. The air traffic controller confirmed that something appeared to be hanging form the tail of the aircraft and alerted the crew who returned the aircraft to the bay.
The subsequent inspection revealed the horizontal stabiliser bungs had not been removed. The right bung was found hanging from the tail, still attached to the left bung installed in the trim actuator cove by the tether rope.
Context
Horizontal stabiliser bungs
Use of horizontal stabiliser bungs
The procedure for the use of horizontal stabiliser bungs (bungs) was implemented by the operator in March 2017 at both Cairns and Townsville Airports. This followed an increase in the number of occurrences where birds had nested in the tail section of aircraft parked overnight during the warmer, humid months. The operator’s engineering department devised a solution with the design and fabrication of bungs to be installed in the elevator trim actuator coves on the upper surface of the horizontal stabilisers (Figure 1).
Figure 1: Horizontal stabiliser bungs
Source: Regional Express Pty Ltd annotated by the ATSB
The horizontal stabiliser bungs (Figure 2) were listed as site-specific equipment for use at both Townsville and Cairns. They consisted of a foam pad, which fitted into the actuator cove, attached to a board for both the right and left elevator. They were connected by a tether rope which had a conspicuity flag marked ‘remove before flight’.
Figure 2: Horizontal stabiliser bungs
Source: Regional Express Pty Ltd
Training
The operator advised that all staff were trained and assessed in the use of the bungs prior to the bungs’ introduction. A training package was developed for contracting agents that included a presentation to familiarise ground staff with the new bungs. The training was delivered by a member of the operator’s airport services ground training department and involved the ground handler operating under supervision to obtain on-the-job training. Once assessed as competent, the ground handler would be approved for unsupervised operations. No additional training was provided by the ground handling agent because the procedure was governed by the airline.
The operator advised that the use of bungs was also covered as part of the induction training for pilots new to type.
Ground handling procedures
The contractor provided ground handling services for the operator at both ports where the bungs were used. They advised that the operator’s procedures for the use of bungs were defined in the operator’s airport services manual (ASM). There was no checklist for these tasks, but ground staff followed the operator’s ASM procedures.
A presentation used by the operator’s ground training department for these pre‑ and post‑flight duties, advised ground agents that:
The horizontal stabilizer bung will be retained by the agent who will be responsible for the fitting of the bung upon termination. Similarly, the ground agent will be responsible for the removal of the bung prior to aircraft operation.
This procedure typically saw the bungs installed after the flight crew had left the aircraft and removed prior to the flight crew arriving at the aircraft the following morning.
Storage of bungs
The ground handling pre-flight duties section in the ASM provided the following guidance:
Remove bungs and propeller straps and store in designated positions in the cargo hold.
During interview, the flight crew advised that this procedure did not apply to site‑specific equipment such as the horizontal stabiliser bungs. It referred to the general instructions for the storage of items such as the pitot tube covers and engine inlet bungs, where specific storage locations were defined on the aircraft. Ground handling staff confirmed that the operator’s ASM procedures did not specify where the bungs were to be stored and that the agent stored these bungs in a container next to the parking bay. These containers were used to store several sets of bungs and were not allocated to a specific parking bay or airframe. Once the bungs were placed in the container, there was no way of knowing which bungs had been removed from what aircraft.
The training presentation, used to familiarise ground handling staff with the bungs, included the use of engine exhaust bungs (exhaust bungs) at Cairns. These exhaust bungs were also retained by the ground handling agent, however, the presentation included guidance for where these bungs should be stored (Figure 3). Similar to the horizontal stabiliser bird bungs, multiple sets were stored together in the designated storage bins.
Figure 3: Exhaust bung storage bins
Source: Regional Express Pty Ltd annotated by the ATSB
Flight crew awareness
The first officer (FO) completed their induction and commenced line training in March 2022. While familiar with the bungs at the time of the occurrence, the FO did not recall being briefed on their use during their induction. They also advised that their first exposure to the bungs was after seeing them installed on other aircraft at Cairns. Additionally, they reported having never handled the bungs before the day of the occurrence.
The airline’s primary means of communicating the use of bungs to flight crew was through the route manual where the following delegation of responsibilities appeared:
The ground agent will be responsible for the removal of the horizontal stabilizer bung prior to aircraft operation. As part of pre-flight duties, the crew MUST ensure the horizontal stabilizer bungs are removed prior to pre-flight inspections.
Additionally, the bungs appeared in the FCOM where they were listed as a check item in the external inspection of the tail area.
Both flight crew were aware of the information relating to the bung in the route manual but also believed that a company notice to air crew (NOTAC) would be provided to crew when the bungs were in use during summer months.[4] In the absence of a NOTAC on this flight, the crew believed that the bungs were not being used, although they had noticed the sporadic presence of the bungs fitted to aircraft at Cairns prior to the occurrence. The operator confirmed that while the route manual referred to the increased risk of bird nesting during the summer months, the manual also stated that the ground agent would install the bungs upon termination of service indicating that they would be used throughout the year. During interview, the ground handler confirmed that the bungs were installed every night.
The information available to the flight crew did not require them to handle the bungs but stressed that they must ensure the bung was removed before the pre-flight inspection. However, there were no instructions provided on how the crew should ensure the bungs had been removed. The flight crew advised the bungs could not be seen from the ground as the horizontal stabiliser fairings (Figure 1) obscured the bung when they conducted an external inspection, unless they moved further from the tail than would otherwise be required when completing the external inspection. In addition, the bungs could not be removed from the ground and required the crew to notify a ground handler if they were found installed during the external inspection.
Pre-flight preparations
Ground crew
The tasks required to dispatch a Rex Saab 340 aircraft were defined in the ground handling section of the company’s ASM. Access to operational information was provided to all ground handling agents to ensure the latest information was utilised with control of the documents remaining with the operator’s training department.
ZLJ terminated at Cairns the evening prior to the occurrence. The ground handling agent confirmed that while the post-flight duties were completed in accordance with the ASM, the operator’s procedures did not require a record of the installation of the bungs, and no additional details were available. As such, it could not be determined if the bung was installed correctly, or by whom, on the evening of 15 November 2022.
Video footage of ZLJ parked on the bay on the day of the occurrence, revealed that ground handling staff passed the rear of the aircraft multiple times while completing the pre-flight duties. During interview, the ground handler in charge advised that neither the bungs nor the tether rope were visible at any time. Further, they advised that they were easily detected when installed correctly and could not be missed with the conspicuity tag normally hanging below the tail and next to the rear cargo door (Figure 1).
Flight crew
Flight crew pre-flight procedures are documented in the company FCOM. The horizontal stabiliser bungs were identified in the external inspection, which formed part of the daily inspection. As this was the first flight of the day for ZLJ, the daily inspection of the tail area included visual checks of the following:
static dischargers
tail lights
ELT antenna
confirmation that the horizontal stabiliser bung had been removed.
Both crew members conducted external checks of the aircraft. The captain initially walked around the aircraft and noted that the bungs and associated tether rope were not visible. The FO then conducted the required external inspection in accordance with the FCOM and advised that they did not see the bungs, despite passing the tail area of the aircraft on several occasions.
Additional checks that may have identified the bungs
The Saab 340 is fitted with a gust lock system. When the handle in the cockpit is engaged, it mechanically locks the elevator, ailerons, and rudder to prevent damage in windy conditions. The gust lock is released while a stall test is conducted. The stall check is completed by the captain prior to the aircraft’s first flight of the day. During this check, the captain would release the gust lock, apply back pressure to the control column and test the stall recognition and recovery protection systems. This is achieved by applying and maintaining aft control column pressure then holding the test button to check that the stickshaker, aural alert and stick pusher activate. Once the test is complete, the gust lock is re-engaged.
The captain was unable to recall if this was the first flight of the day for the aircraft and could not confirm if this check was completed.
An additional flight control check was part of the line-up checklist and would normally have been completed prior to runway entry. It involved a co-ordinated response from the crew to release the gust lock and then check the flight controls. The captain would check the rudder and the FO would manipulate the control column to ensure full and free movement of the aileron and elevator controls. The crew confirmed that the tower controller notified them of the hanging bung before this check had been completed.
During analysis of the airport CCTV footage (Figure 4), the bung was not visible while the aircraft was being prepared, nor was it visible as the aircraft taxied away from the bay. However, the aircraft was not clearly visible in the footage. Later, when the bung was observed hanging from the aircraft, the left bung was still inserted into the trim actuator cove and the tether rope and right bung was hanging from the left horizontal stabiliser.
Figure 4: Airport CCTV footage
Source: Cairns Airport Pty Ltd
Design and considerations
The operator’s engineering department designed and had the bungs manufactured. They determined that because the design did not require alteration of the airframe, a CASA approved‑ engineering order was not required.
The ATSB contacted the aircraft manufacturer to ascertain if the elevator trim actuator cove had been identified as a known area for similar nesting occurrences. Saab advised that they had only received one other report of bird nesting, and a handful of reports involving spider or insect nesting, from Australian operators. Additionally, Saab did not manufacture protection for this particular area of the aircraft, and they had not been involved in the design and manufacture of such a device. Significantly, the manufacturer provided a list of considerations that they felt would be appropriate for such a device. These included:
checklist and visual indicators to aid in identification
consequences if the cover was forgotten with regards to jamming or fouling of flight controls.
The operator confirmed that while a risk assessment had not been completed specifically for the bird bungs themselves, the decision to implement the bird bung procedure was to address the bird nesting safety concern and reduce the potential risk to passengers, crew, and the aircraft itself. There were no reports, prior to this occurrence, of aircraft dispatched with bungs installed in the trim actuator coves. However, it was reported that bungs had previously fallen out of the trim actuator cove in wind and were later found in nearby parking bays.
Safety analysis
Installation of the horizontal stabiliser bung
On the morning of the occurrence, there were significant distractions for the ground handling agent. Despite this, there were no significant time pressures during the early part of the day when the aircraft preparations began, and the ground handler removed the pitot and other aircraft covers. During this time, and later in the aircraft preparation, they were working around the rear of the aircraft on a number of occasions and the horizontal stabiliser bungs (bungs) were not detected.
In addition, while the flight crew were not expecting that the bungs would be installed, they both conducted external inspections of the aircraft, with the first officer (FO) stating they paid particular attention to the rear of the aircraft. The FO also removed the tail stand from under the tail of the aircraft where the bung conspicuity flag would have been hanging prior to entering the aircraft after the external inspection was completed. Neither pilot detected the bungs.
The ATSB analysis of the CCTV footage also did not detect the bungs while the aircraft was parked at the bay, nor as the aircraft taxied to the runway. Together, this would indicate that the bung was not installed correctly or possibly the tether rope with the ‘remove before flight’ conspicuity flag was not hanging from the horizontal stabiliser, as designed.
Procedures to ensure the removal of the bungs
The training package provided to the ground handling agent indicated that the horizontal stabiliser bird bungs were to be retained by the agent, but did not specify how or where the bungs were to be stored. As the containers utilised by the agent stored multiple sets of bungs together, it could not be determined what equipment had been removed from what aircraft. This prevented any positive assurance check by ground handlers or flight crew that the bungs had been removed. This was also the case for the engine exhaust bungs.
Existing airline checklist procedures ensured that flight crew account for other covers and bungs that had been removed from the aircraft during pre-flight inspections. However, there was no pre‑flight procedure on how to check the aircraft for the installation of the horizontal stabiliser bird bungs. In the absence of a prescribed method of assurance, the flight crew walkaround inspection procedures relied on visual confirmation that the bungs had been removed by ensuring that the conspicuity flag was not visible. In this instance, when the conspicuity flag was not detected by both ground crew and flight crew, both parties would most likely have continued preparations with the belief that the bungs were not installed.
This occurrence revealed the potential for the horizontal stabiliser bungs to go undetected if incorrectly installed or not displaying as designed and identified a gap in the assurance procedures for the operator.
Risk assessment
While a risk assessment of the bird nesting hazard led to the implementation of the procedure to install the horizontal stabiliser bungs, the operator did not conduct a separate risk analysis of the potential hazard a control surface bung could induce. Although the design incorporated features to aid in the recognition of the bungs when they were installed correctly, the evidence indicated that the design allowed for an incorrectly installed bung or one not displaying as designed to go undetected.
Existing procedural checks designed to detect fouled or jammed controls did not identify the incorrectly installed bung and there was no documented consideration given to assuring that a bung would be ejected prior to take-off, after which time it could have had the potential to adversely affect the safety of a flight.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the aircraft preparation event involving Saab 340B, registration VH-ZLJ, at Cairns Airport, Queensland on 16 November 2022.
Contributing factors
The horizontal stabiliser bungs were most likely incorrectly installed or possibly the tether rope with the ‘remove before flight’ conspicuity flag was not hanging from the horizontal stabiliser as designed. This resulted in them not being detected during pre-flight preparations and the aircraft being dispatched with the bung installed.
There were no formal procedures for the storage and accountability of horizontal stabiliser bungs after they were removed from the aircraft. (Safety issue)
The design of the horizontal stabiliser bungs did not consider aspects that would ensure the identification of an installed bung, or the safe operation of the aircraft if the bungs were not removed prior to flight. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: There were no formal procedures for the storage and accountability of horizontal stabiliser bungs after they were removed from the aircraft.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Regional Express Pty Ltd continues reviewing the use of horizontal stabiliser bungs and takes action to address the limitations associated with the current procedures around the storage and accountability of equipment removed from an aircraft.
Safety issue description: The design of the horizontal stabiliser bungs did not consider aspects that would ensure the identification of an installed bung, or the safe operation of the aircraft if the bungs were not removed prior to flight.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Regional Express Pty Ltd further reviews the horizontal stabiliser bungs design and pre-flight procedures to ensure that installed bungs are readily identifiable and will not adversely affect the continued safe operation of the aircraft if not removed prior to flight.
Glossary
ASM Airport Services Manual
CASA Civil Aviation Safety Authority
CCTV Closed-circuit television
FCOM Flight crew operations manual
FO First officer
NOTAC Notice to air crew
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-ZLJ
Regional Express Pty Ltd
Aus Flight Handling
Cairns Airport Pty Ltd
Saab Aircraft Co.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew of VH-ZLJ
Regional Express Pty Ltd
Aus Flight Handling
Saab Aircraft Co
Swedish Accident Investigation Authority
Civil Aviation Safety Authority.
A submission was received from:
Regional Express Pty Ltd
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[2] The roles and responsibilities of each crew member when completing the required daily internal and external inspections were defined in the flight crew operating manual.
[3] The portable air conditioner was an item of ground service equipment used to provide cool air to the cabin of the aircraft before engine start.
[4] Summer months was defined in the Rex airport services manual as the period between November and March.
Occurrence summary
Investigation number
AO-2022-058
Occurrence date
16/11/2022
Location
Cairns Airport
State
Queensland
Report release date
26/10/2023
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-ZLJ
Serial number
340B380
Aircraft operator
REGIONAL EXPRESS PTY LIMITED
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
At the conclusion of the investigation into a runaway and derailment in Devonport, Tasmania, the ATSB is strongly advising operators and developers of complex rail systems to apply system safety methodologies so that they can have a high level of confidence in the overall safety of the system
Final report details more than a dozen safety actions taken to address ATSB findings.
The Australian Transport Safety Bureau has released a final report detailing more than a dozen safety actions which address findings from its investigation into the runaway and derailment of a cement train in Devonport, Tasmania.
On 21 September 2018, a driver was using remote control equipment to position a TasRail train for cement loading at a siding in Railton, south of Devonport, when the train stopped responding to commands.
After a series of uncommanded emergency brake applications and releases, the train began to roll away with no-one on board.
This began a 23-minute runaway, through ten active and three passive public level crossings, beneath a highway overpass, and through five sets of points, mostly at speeds greater than the maximum track speed.
TasRail’s network control diverted the train away from public areas to a siding in Devonport Yard, where it collided with a concrete footing and surrounding fences. Fence debris struck two pedestrians nearby, resulting in minor injuries to both. Nobody else was injured.
ATSB Chief Commissioner Angus Mitchell praised the actions of TasRail network control and other staff, as well as the prompt response by Tasmania Police to keep key level crossings clear as the train passed.
The subsequent ATSB investigation found 11 contributing factors for the accident, and highlighted ten distinct safety issues (ongoing safety concerns).
“Throughout this complex and in-depth investigation, the ATSB has worked with various stakeholders and encouraged them to take safety actions aimed to ensure this type of accident does not occur again,” Mr Mitchell said.
“Pleasingly, the final report details more than a dozen safety actions taken to address these issues, by the operator TasRail, the remote control equipment
manufacturer, the rail standards board, and the regulator. All the identified safety issues either have been addressed, or are being addressed.”
Among other actions, TasRail has installed catch points at Railton to prevent uncontrolled train movements from reaching the main line, and has improved its emergency response procedures.
The ATSB found the remote control system, which is no longer in use, had several safety-related design and integration problems that were readily identifiable.
Accordingly, the ATSB’s final report emphasises the need for organisations involved in the development or operation of systems that are performing safety-critical functions to follow ‘system safety’ methodologies.
“These are techniques that can be applied throughout the design and operation of complex systems to prevent the systems from behaving in undesired ways,” Mr Mitchell said.
“Since the remote control system was designed, there have been substantial improvements in the quality and availability of systems safety guidance for complex rail systems in Australia.
“However, it is important this accident serves as a reminder for a heightened focus on systems safety from all transport operators and manufacturers, into the future.”
The report specifically notes new standards, guidance, and fact sheets published by the Rail Industry Safety and Standards Board (RISSB) in recent years, to assist rail transport operators in systems safety, systems engineering and change management.
The report also notes the Office of the National Rail Safety Regulator (ONRSR)’s enhanced focus on the importance of a system engineering approach, including a safety message published in March 2019, and two related fact sheets released in 2020, emphasising the need for a systems engineering approach in rail projects.
“The ATSB strongly advises operators and developers of complex rail systems to follow this guidance, so that they can have a high level of confidence in the overall safety of the system,” Mr Mitchell said.
On the afternoon of 14 November 2022, a Robinson Helicopter R22 Beta, registered VH-LOS, was being operated near the Arafura Swamp, Northern Territory. The helicopter was being used as part of an animal mustering operation, which also included multiple land vehicles.
After the mustering operation had concluded for the day, recorded data indicated that the helicopter returned to the mustering camp. When members of the mustering operation returned to the camp, the pilot and the helicopter were not there. Realising that the pilot was missing and becoming increasingly concerned about the pilot’s welfare, the mustering group commenced a search using land vehicles.
On the morning of 15 November members of the mustering operation organised an aerial search. The wreckage of VH-LOS was located at about 1300, about 6 km from the mustering camp. The pilot was deceased, and the helicopter was destroyed.
What the ATSB found
The ATSB found that the pilot of VH-LOS operated the helicopter after the end of nautical twilight in cloudy conditions and away from the direction of sunset. There was no celestial or terrestrial lighting, and as such the flight occurred in dark night conditions. The pilot did not have an appropriate qualification, and the helicopter was not suitably equipped, for night flight. While flying in dark night conditions, the pilot likely became spatially disoriented which led to a collision with terrain.
A pathologist’s report found that the injuries sustained by the pilot in the collision were probably not fatal, and that the pilot probably succumbed to environmental exposure. VH-LOS was equipped with a manually activated personal locator beacon. However, the beacon was secured to the inside of the helicopter, and the pilot was probably unable to access it once outside the helicopter after the collision.
When members of the mustering operation identified that the pilot and the helicopter were missing, they considered that the pilot may have landed and would either return the following day, or would be waiting nearby. As a result, they did not contact emergency services. In combination with the absence of a distress signal from the personal locator beacon, this led to delays in initiating a formal search and rescue response and subsequent location of the accident site.
The ATSB found that the combination of the personal locator beacon not being activated and authorities not being notified when the aircraft was missing resulted in a delay to the pilot being located before succumbing to environmental exposure after sustaining survivable injuries in the accident.
Safety message
Various ATSB research and investigation reports refer to the dangers of flying after last light without the appropriate qualifications and equipment. Day visual flight rules (VFR) pilots should carefully consider the timing of last light when planning flight near the end of the day. The Civil Aviation Safety Authority Visual Flight Rules Guide provides guidance to pilots on methods for determining the timing of last light, and pilots should also consider the influence of nearby weather that may cause the onset of darkness to be earlier than expected. The requirement to only operate under the VFR in daylight conditions, and to return 10 minutes before last light, provides a reliable method for ensuring visual cues are available for safely operating an aircraft.
Dark night conditions provide no useable external visual cues and in these environments all VFR pilots, including those with endorsement to operate under the night VFR, will experience an increased risk of spatial disorientation. The ATSB’s Avoidable Accidents publication Visual flight at night accidentsprovides further discussion of these risks and how they have contributed to other accidents. The ATSB encourages all VFR pilots to take note of the tragic consequences associated with dark night flight in this accident.
The accident also highlights that when operating in remote locations, there is an increased risk of fatal consequences from otherwise survivable accidents. Pilots operating in remote locations should carefully consider the use and location of equipment such as a personal locator beacon, to maximise the likelihood it will be accessible to them in the event of an accident. The Visual Flight Rules Guide provides guidance on the use of emergency locator beacons.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 14 November 2022, a Robinson Helicopter Company R22 Beta, registered VH-LOS, was being operated in the Arafura Swamp, about 30 km south of Ramingining Aerodrome, Northern Territory (Figure 1). The helicopter was being used as part of an animal mustering operation, which also included multiple land vehicles.
Figure 1: Map of the Northern Territory showing the location of the accident site and nearby locations
Source: Google Earth, locations labelled by ATSB
At about 1800 local time, the mustering operation concluded for the day. The pilot of VH-LOS instructed a member of the mustering group to drive a grader vehicle to the southern edge of the swamp. The pilot planned to collect the grader driver and fly them back to the mustering camp, located about 20 km to the west.
Other members of the mustering operation departed the swamp in land vehicles, heading towards the camp. A witness recalled that VH-LOS was on the ground when the group departed, and they expected the pilot would depart soon after they left.
Flight tracking information showed VH-LOS took off from the swamp at 1803, flew around the swamp before tracking to the south, landing at the edge of the swamp at 1818. The helicopter was then started at 1837, and tracked to the mustering camp, landing and shutting down at 1854. The track of these flights is shown in Figure 2. The flight tracking information showed the helicopter was started again at 1921, before the flight tracking record ended about 1 minute later while the helicopter was still at the camp. The flight tracking device deactivated at 1925 after the helicopter had remained idle at the camp location and the device had lost external power (see Recorded information).
Figure 2: Map of Arafura Swamp and key locations, and track of VH-LOS
The yellow track shows the flight departing from Arafura Swamp at 1803 and shutting down south of the swamp at 1818. The red track shows the flight from the edge of the swamp to the mustering camp departing at 1837 and landing at 1854.
Source: Google Earth, with aircraft tracking plots overlayed by ATSB based on records obtained from recorder onboard VH-LOS
The grader driver travelled from the swamp towards the planned meeting point, which took about 30 minutes. They waited for about 10 minutes before deciding to return to camp on the grader when the helicopter did not arrive. The grader did not have a radio capable of communicating with the helicopter.
The other members of the mustering operation arrived back at the camp and noticed that neither the helicopter pilot nor the grader driver were there. One witness recalled it took about an hour to return to camp, and that the group arrived when it was close to dark, but not ‘pitch black’. Another group member recalled that they arrived after dark, at about 1945 to 2000.
The grader driver arrived at the camp at about 2100. Members of the mustering operation became increasingly concerned about the wellbeing of the helicopter pilot and commenced a search using land vehicles from about 2100 until 0100 on 15 November.
Early on 15 November, members of the mustering operation phoned an acquaintance who had access to the aircraft flight tracking information. The internet-based display showed VH-LOS at the mustering camp, having not moved since the previous evening.
The mustering group members then contacted some acquaintances who attended the area in helicopters and commenced an aerial search from about 1100. The helicopter wreckage was located at about 1300, about 6 km from the mustering camp. The pilot was deceased, and was found outside and resting against the helicopter. The helicopter was destroyed.
Context
Pilot information
Licence and experience
The pilot held a Commercial Pilot Licence (Helicopter) and a valid Class 1 aviation medical certificate. The pilot also held a single engine helicopter rating, and a low level rating with aerial mustering (helicopter) and sling endorsements. The pilot did not hold an instrument rating or a night visual flight rules (VFR) rating.
The pilot’s logbook recorded over 6,200 hours total aviation experience, however no records had been made of flights conducted after March 2022.
Events prior to the accident
The pilot flew VH-LOS to Ramingining on 10 November 2022 and operated around the Arafura Swamp in the days prior to the accident. Aircraft tracking records showed that the helicopter was operated until 1859 on 11 November and until 1931 on 12 November. It is likely that these flights were conducted near or after the end of civil twilight (see Celestial illumination information).
Post-mortem examination and medical information
A post-mortem examination of the pilot was conducted by a qualified pathologist, on behalf of the Northern Territory Coroner. The pathologist’s report indicated that their examination was impeded due to the elapsed time between the accident and the recovery of the pilot’s body to a suitable mortuary facility. Only limited toxicology analysis could be performed, and although a high concentration of alcohol was detected the analysis could not determine if some or all of the measured alcohol (0.18%) was the result of post-mortem changes.
The pathologist’s report identified that the pilot sustained multiple injuries, including a fracture to the left femur, however the injuries were likely survivable. The report found that death was most likely the result of environmental exposure following the collision, with the left femur fracture contributing to reduced mobility.
The pathologist also observed no obvious evidence of injury consistent with being caused by a harness or seatbelt.
Witnesses recalled that the pilot was fit and healthy prior to the accident, and there were no indications that the pilot was experiencing any unusual stress. No witnesses recalled the pilot consuming alcohol or other drugs in the days before the accident.
Aircraft information
VH-LOS was a Robinson Helicopter Company R22 Beta helicopter, serial number 1715, powered by a Textron Lycoming, O-320-B2C, 4-cylinder piston engine. It was manufactured in the United States in 1991, and first registered in Australia in January 1995, and was equipped and maintained to a day VFR standard. The R22 has 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seat belt and inertia reel shoulder strap, similar to those used in motor vehicles. VH-LOS did not have doors fitted at the time of the accident.
Recorded information
VH-LOS was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be.
The operator of VH-LOS tracked the aircraft using a system configured for the TracPlus tracking service. The system consisted of a RockAir device located in the helicopter, which was capable of transmitting the aircraft location using satellite and cellular networks. Registered users could log into the TracPlus website to view the aircraft track and position.
At the accident site, the ATSB found the RockAir unit outside the helicopter. A data card recovered from inside the unit included records showing the recorded tracks of VH-LOS on the afternoon of 14 November, as well as log files for the RockAir system. The files showed the final recorded position of VH-LOS was at the mustering camp location at 1925.
The manufacturer of the RockAir reviewed the log file from the day of the accident and noted the following:
The pilot of VH-LOS did not manually deactivate the aircraft tracker.
The RockAir was performing normally on the day of the accident.
The device was in a mode where it would deactivate if external power was removed, unless it detected the aircraft was moving above a speed threshold.
The RockAir automatically deactivated at 1925 when the device lost power.
There were 36 other instances on the day of the accident where the device lost power for 2-5 seconds, however the unit reverted to battery power because the aircraft was moving.
It was not possible to determine the reason for the power supply interruptions, with mechanical movement of the power supply being a possibility.
Weather and environment
Weather
Members of the mustering operation recalled that conditions were fine while they were operating around the Arafura Swamp on the afternoon of 14 November, with no storms overhead. The grader driver recalled conditions as being cloudy, and that it was dark that night.
An analysis prepared by the Bureau of Meteorology (BOM) identified a thunderstorm to the east of the accident site at about 1730, which moved west during the evening. The analysis stated that outflow from the thunderstorm could have produced variable direction winds with gusts up to 35 kt. Near the thunderstorm, heavy rainfall with reduced visibility and broken low cloud were possible.
BOM also supplied observations for the evening of 14 November and the morning and afternoon of 15 November, at Milingimbi (about 60 km north of the accident site) and Bulman (about 130 km south-west of the accident site). BOM advised that these observations should be used as an estimate only for conditions at the accident site. These observations showed it was a hot and humid night in north-east Arnhem land, with temperatures from 27 to 33°C and humidity of 35 to 90% recorded.
Conditions became hotter and less humid during the day on 15 November. At 1300, when the helicopter wreckage and pilot were found, Milingimbi and Bulman recorded 33°C and 55-60% humidity. Witnesses recalled that conditions that day were hot.
Celestial illumination information
Sunset at the location of the mustering camp on 14 November 2022 was 1835 and the end of civil twilight (last light)[1] was 1858. Nautical twilight[2] was 1924 and astronomical twilight[3] was 1951.
The moon was a waning gibbous, rising at 2337 on 14 November with about 71.3% of the visible disk illuminated. There was no environmental lighting in the vicinity of the accident site.
Accident site and wreckage information
The accident site was located 6 km east of the mustering camp, in a flat clearing scatted with small trees and anthills. There were no sources of terrestrial light. None of the trees had damage consistent with a helicopter rotor strike, and there was no evidence of a bird strike or indications of a post-impact fire.
The helicopter was found on its left side, with significant compression of the nose and underside of the forward left section of the fuselage (Figure 3). The compression damage indicated that the helicopter collided with terrain at about 45° nose-down, and 30° left side low. There was a short wreckage trail extending about 13 m, with all helicopter parts present at the accident site and no evidence of an in-flight break-up.
Figure 3: VH-LOS wreckage
Source: ATSB
Indentations on the terrain nearby indicated a main impact point about 6 m aft and 4 m right of where the helicopter was found. Anthills forward of the main impact point showed damage consistent with having been struck by the rotor blades, and both rotor blades presented with evidence of ground strikes. One main rotor blade was liberated as the result of a ground strike, and was found about 30 m to the right of the wreckage trail. The cockpit windscreen had shattered and remnants were scattered around the accident site along with the contents of the aircraft.
The tail cone and tail rotor assembly remained connected to the fuselage, however presented as deflected down and curled under the helicopter. Site examination showed that both of the bladder-type fuel tanks remained intact and contained fuel. Examination of the helicopter’s flight control system and drive train did not indicate any pre-existing defects that could have affected the control or function of the helicopter. Damage signatures to engine rotating components indicated that the engine was operating at the time of the collision with terrain.
The pilot was found in a reclined position on the north-western side of the aircraft (next to the right helicopter seat), with their head rested against the helicopter. There was a large water bottle on the ground nearby. The screw-cap lid had been removed and the drinking spout exposed, suggesting it was likely the pilot was capable of opening and drinking from the water bottle after the accident.
Helicopter restraints
Both helicopter seatbelts were found to be buckled. The lap belt was in its normal secured position at the base of the seat, while the shoulder belt (which connected from the top right to the lower left), was pulled behind the seat base.
The seatbelt assembly had three anchor points, with the two lower anchor points connected to the pilot’s seat frame. The pilot’s seatbelt was found to be secured to its anchor points. The pilot’s seat had been significantly disrupted, pulled in the direction of impact away from the helicopter structure. The separation of the seat structure was very likely a result of the forces generated by the pilot restrained by the seat belt and being propelled in the direction of impact.
Regulatory information and guidance
Visual flight rules
Flight under the VFR must be conducted in conditions that enable the pilot to determine the aircraft’s position by visual features in the external environment. VFR flights are only permitted at night if:
the pilot in command is authorised to conduct a flight under the instrument flight rules or at night under the VFR, and
the aircraft is appropriately equipped for flight at night.
The CASA VFR guide stated that ‘night is that period between the end of evening civil twilight and the beginning of morning civil twilight... last light (is) the end of civil twilight’. The guide further stated that cloud cover or poor visibility may cause daylight to end at a time earlier than the forecast time, and allowance should be made for these factors when planning a flight near last light.
Civil Aviation Order 20.18 described the requirements for helicopters operating under the instrument flight rules (IFR) or at night under the VFR. Among other requirements, for a helicopter operating at night where attitude cannot be maintained using visual external surface cues, the helicopter must also either equipped for IFR flight with an autopilot or automatic stabilisation system, or be operated by a qualified 2 pilot crew. VH-LOS was not equipped for night flight under the VFR.
A member of the mustering operation who had flown with the pilot did not recall the pilot using procedures or routines for determining a ‘last flight’ time to avoid flying in the dark. They recalled that the pilot had emphasised the importance of having a visible horizon while flying in near dark conditions, to provide a reference for the position of the terrain.
Additional guidance for night VFR flight in dark night conditions
Dark night conditions exist when there is little or no celestial illumination, in locations where no significant ground lighting is available.
The CASA advisory circular Night VFR rating provided guidance to pilots conducting operations under the night VFR (NVFR). This guidance highlighted that while suitably endorsed pilots may safely fly visually in night conditions where there is adequate celestial illumination or other sources of light, visual flight is significantly more hazardous in dark night conditions.
There may be times when there is bright moonlight or extensive ground lighting available, making a night operation only a little more difficult than flying in daylight. However, there may be dark night conditions (i.e. without moonlight or significant ground lighting) that can make it very difficult to discern the natural horizon and maintain control of the aircraft by reference to external visual references.
The absence of a visible horizon during dark night conditions is a particular hazard. As highlighted by Gibb and others (2010), seeing a horizon is ‘crucial for orientation of the pilot’s sense of pitch and bank of the aircraft’. The Night VFR rating advisory circular identified this risk, noting:
CASA strongly recommends that NVFR operations take place only in conditions that allow the pilot to discern a natural visual horizon or where the external environment has sufficient cues for the pilot to continually determine the pitch and roll attitude of the aircraft.
The ATSB’s Avoidable Accidents publication Visual flight at night accidentsidentified that of 26 accidents during night visual meteorological conditions (VMC),[4] almost all occurred on dark nights. Visual flight at night accidents highlighted that:
When flying over land or oceans without light sources, on dark nights with no visible moon, visual flight at night is essentially the same as instrument flight.
Requirements for emergency locator transmitters
An emergency locator transmitter (ELT) is designed to send a distress signal to a network of satellites in an emergency. The Civil Aviation Safety Regulations Part 91 (General Operating and Flight Rules) Manual of Standards (MOS) required aircraft to be fitted with an ELT. For flights such as that conducted by VH-LOS, aircraft may be equipped with an automatic ELT, which is fixed to the aircraft and designed to automatically activate in the event of a severe impact (g) forces. Alternatively, the ELT can be a manually activated and removable survival ELT, also referred to as personal locator beacons (PLB). The MOS required that if an ELT is a PLB, the pilot in command must ensure it is carried either on their person, in or adjacent to a life raft, or adjacent to an emergency exit.
VH-LOS was equipped with an ACR ResQLink 400 PLB. To activate the ResQLink, the user needed to first lift the antenna and expose the on/off button, then press the on/off button for 2 seconds.
The ATSB observed that the PLB remained inside the helicopter post-accident, and was attached to the helicopter's centre console. There was no apparent damage to the unit, and the battery was in-date. The antenna was in the folded-down position with the on/off button covered. There was not evidence that the pilot had attempted to operate the PLB after the accident.
Figure 4: ResQLink activation instructions (left) and condition in-situ at VH-LOS accident site (right). The image on the right shows the antenna and power button guard remained in the down position
Requirements for search and rescue notification
The Part 91 MOS required that for VFR flights conducted in a designated remote area, the pilot must submit a flight plan, nominate a SARTIME (search and rescue time) for arrival, or leave a flight note with a responsible person. The Airservices Australia publication En Route Supplement Australia showed designated remote areas within Australia. The Arafura Swamp, the accident site, and all other areas the helicopter was operating in in the days prior to the accident were within a designated remote area.
The Part 91 MOS described the requirements of the holder of a flight note, including that they must immediately contact the Joint Response Coordination Centre (JRCC) if the flight becomes overdue.
The pilot of VH-LOS did not leave a formal flight note, however, it was understood the pilot would meet the grader driver at a particular location. When the helicopter did not meet the grader driver or return to the camp on the evening of 14 November, it was understood by the members of the mustering operation that the pilot was overdue. However, they did not contact any authority that night. The first call to emergency services (a 000 call) was made after the helicopter wreckage had been found on the afternoon of 15 November.
One member of the mustering operation recalled that it was not uncommon for the pilot of VH-LOS to arrive later than expected, as the pilot sometimes conducted additional unplanned flights. They also recalled that there had been occasions that the pilot had landed in an out-location and not returned until the following day.
When the helicopter did not return as expected on 14 November, members of the mustering group considered the possibility that the pilot had landed and were hopeful of the pilot returning the following day. They also considered the possibility that the pilot encountered problems and landed, and would be waiting to be found by road vehicles. In this context, members of the mustering group reported that they did not become highly concerned about the pilot until the morning of 15 November.
Related occurrences
Since the 2013 publication of Visual flight at night accidents, the ATSB has investigated multiple fatal accidents involving light helicopter pilots operating on dark nights in areas that did not contain any local ground lighting. Examples include:
AO-2014-144: The ATSB found that the pilot, who did not hold a night VFR rating or instrument rating, continued flying towards the destination after last light (end of civil twilight), then in dark night conditions without local ground lighting, inadvertently allowed the helicopter to descend into terrain.
AO-2016-031: The ATSB found that the pilot, who was only qualified to operate in day-VFR conditions, departed on a night flight and continued towards the destination in deteriorating visibility until inadvertently allowing the helicopter to descend into water.
AO-2021-006: The ATSB found that the pilot, who did not hold a night VFR rating or instrument rating, continued flying towards their destination after last light, through the period of civil twilight and into astronomical twilight. In dark night conditions without local ground lighting the pilot inadvertently allowed the helicopter to descend into terrain.
Safety analysis
Flight after last light
The helicopter collided with terrain sometime after 1925 on 14 November 2022. There was no indication of any mechanical problem contributing to the collision with terrain, the helicopter had sufficient fuel on board, and there was no evidence of collision with a bird or another objects. A post-mortem examination indicated the pilot probably survived the accident, and there was no evidence of medical factors that would have resulted in the pilot becoming suddenly incapacitated.
Although the timing of the accident could not be precisely determined, aircraft tracking records indicate that the accident flight took place after nautical twilight. The pilot did not have a rating to fly at night under the VFR. VH-LOS was not equipped for flight by reference to the aircraft instruments, and the pilot did not have a rating for flight under the instrument flight rules.
The accident occurred in an extremely remote location with no nearby terrestrial lighting. On the evening of the accident, the moon rose late and provided no illumination for the accident flight. Depending on how long the aircraft flew prior to the collision with terrain, conditions would have become darker later in the evening, and cloudy conditions associated with a westerly-moving storm system may have further reduced visibility. Considering the last recorded position of the aircraft and the accident location, it is likely that the accident flight was in an easterly direction, meaning sunset was behind the direction of travel. As such, the ATSB concluded that the accident flight was conducted in dark night conditions due to the absence of both celestial and terrestrial lighting.
Spatial disorientation describes the phenomenon of a pilot becoming unable to correctly perceive the position, movement and orientation of their aircraft. When flying under the VFR, pilots rely on external visual cues to maintain spatial awareness, including the orientation of the aircraft (which way is up), and the proximity to terrain. In dark night conditions, when there is no celestial illumination and no nearby terrestrial lighting, there are no external visual cues available to pilots. In such circumstances, spatial disorientation is highly likely unless pilots have access to and utilise aircraft instrumentation. This risk was highlighted in Visual flight at night accidents:
In very dark environments, VMC is essentially the same as IMC[5] in terms of available external visual information. The only real difference is that lights on the ground may be seen in VMC. In remote areas where there are no lights or ambient illumination, there is essentially no difference. Pilots cannot see the ground and have no external visual cues available to assist with their orientation.
The decision by the day VFR qualified pilot to operate a helicopter which was not equipped for night flight after last light was inherently unsafe and increased the risk of unintentional collision with terrain. The dark night conditions on the night of the accident meant that regardless of the pilot’s ability to fly using external visual cues at night, there were none. In these conditions, the pilot likely became spatially disoriented, and unintentionally allowed the helicopter to descend into the terrain.
The significant nose-down and left-side down attitude of the aircraft wreckage, and the short wreckage trail, were consistent with the pilot flying at slow speed and developing an unusual aircraft attitude in the moments prior to collision. The wreckage, being only 6 km from the last known position of the helicopter, indicates that the disorientation and collision occurred soon after the commencement of the flight in dark night conditions.
Survivability
The post-mortem examination identified that the pilot was probably not fatally injured by the collision with terrain. The damage to the helicopter seat indicated that the pilot was at least partially restrained by the seatbelt during the collision. However, considering to the absence of observed bruising associated with a seatbelt, it is possible that the pilot was either only partially restrained (by the lap belt only), or slipped out of the seatbelt in the collision. The direction of impact (lower left) and shoulder belt orientation (top right to lower left), are consistent with the latter explanation. After the collision, it is likely the pilot manoeuvred out of the buckled restraint, outside of the damaged helicopter which was laying on its side. With injuries reducing the pilot’s mobility, the pilot likely planned to wait for rescue.
The post-mortem report further identified it was likely that the pilot succumbed to environmental exposure. There were up to 17.5 hours from when the helicopter collided with terrain and when the pilot was found deceased the following day. Although the pilot likely had a water bottle available and was shaded by the helicopter on the morning of 15 November, conditions were hot and humid. Therefore, this analysis examined the safety systems that could have led to the earlier recovery of the pilot.
Personal locator beacon
The mandatory carriage of emergency locating equipment is a risk control used to facilitate the prompt identification of aircraft accidents, and the timely and accurate response by emergency services. VH-LOS was equipped with a manually-activated PLB, however the pilot did not activate this beacon following the accident. Had the pilot activated the PLB, it is almost certain that a search and rescue response would have located the aircraft, increasing the likelihood the pilot would have survived the accident.
To ensure the PLB is accessible after a collision, regulations require the PLB is carried on the person of the flight crew or adjacent to an emergency exit. The PLB carried in VH-LOS was secured to the centre console, which, in a small helicopter such as a Robinson R22, is nearby the aircraft exits and the pilot’s seated position.
When the helicopter collided with terrain, conditions were dark and the pilot may not have been able to locate the PLB. Once outside the helicopter, in poor visibility and with limited mobility (due to the significant leg injury), the location of the PLB inside the helicopter was effectively inaccessible to the pilot. This highlights the advantage of carrying a PLB on the person of pilots, particularly in one-person operations.
VH-LOS was not equipped with an automatically activated ELT. As in this accident, manually activated PLBs may not be effective in situations where a pilot survives an accident but is incapacitated or is otherwise unable to access the PLB. An automatic ELT will provide another opportunity to alert search and rescue authorities in these situations.
Notification to emergency services
Regulations within the aviation industry require pilots to notify responsible persons of the details of flights, including a planned departure and landing time. The requirements then follow that the Joint Response Coordination Centre (JRCC) should be notified of a potentially missing aircraft, so that a search and rescue response should be initiated.
In this instance, members of the mustering operation at Ramingining became increasingly concerned about the wellbeing of the pilot during the night of 14 November. They conducted a land-based search on the night of 14 November, hoping that the pilot had landed and could be seen from the road. Becoming significantly concerned on 15 November, they requested some acquaintances to conduct an aerial search, which led to the identification of the deceased pilot. Throughout this time, no calls were made to appropriate authorities.
When the pilot was first identified as missing, the level of concern and the perceived urgency of the situation was influenced by previous experiences where the pilot had returned much later than expected. The mustering operations, being conducted in an extremely remote environment, involved a necessity to frequently resolve problems without the assistance of formal authorities. Furthermore, the members of the mustering operation (other than the pilot) had limited engagement with aviation systems and regulation.
While noting the circumstances which contributed to emergency services not been immediately notified in this instance, a prompt formal notification of a missing aircraft is the most effective action personnel on the ground can take. Emergency calls will result in the JRCC being notified, and the JRCC are capable of deploying very capable assets for finding a missing aircraft with minimal delay or at first light the next day.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Robinson R22 Beta, VH-LOS, near Ramingining, NT on 14 November 2022.
Contributing factors
The pilot operated the helicopter after nautical twilight. However, the pilot did not have an appropriate qualification, and the helicopter was not suitably equipped, for night flight.
The flight was conducted in dark night conditions due to the absence of both celestial and terrestrial lighting. As a result, the pilot likely became spatially disorientated which led to a collision with terrain.
The pilot did not activate the personal locator beacon, which was probably inaccessible to the pilot once they left the helicopter after the accident. In addition, authorities were not notified when the aircraft was missing. In combination, this resulted in a delay to the pilot being located before succumbing to environmental exposure after sustaining survivable injuries in the accident.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
persons involved in the mustering operation at Arafura swamp
crew of the helicopters who searched for the helicopter after the accident
Civil Aviation Safety Authority
Northern Territory Police Force
aircraft manufacturer
recorded data from the flight tracking device on the aircraft.
References
Australian Transport Safety Bureau, 2013, Avoidable Accidents No. 7 – Visual flight at night accidents: What you can’t see can still hurt you. Australian Government, Canberra
Gibb, R., Gray, R. and Scharff, L., 2010. Aviation visual perception: Research, misperception and mishaps. Routledge.
Civil Aviation Safety Authority, 2022, Advisory Circular AC 65-05 v1.1 - Night VFR rating. Australian Government, Canberra.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the aircraft owner and operator
the aircraft manufacturer
the aircraft tracking device manufacturer
the aircraft tracking service provider
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Geoscience Australia (GA) defined the ending of civil twilight as the instant in the evening when the centre of the sun is at a depression angle of 6° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible.
[2] GA defined the ending of evening nautical twilight as the instant in the evening when the centre of the sun is at a depression angle of 12° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, it is dark for normal practical purposes.
[3] GA defined the ending of astronomical twilight as the instant in the evening when the centre of the sun is at a depression angle of 18° below an ideal horizon. At this time the illumination due to scattered light from the sun is less than that from starlight and other natural light sources in the sky.
[4] Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[5] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
Preliminary report
Report release date: 06/02/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 14 November 2022, a Robinson Helicopter Company R22 Beta, registered VH-LOS, was being operated near the Arafura Swamp, approximately 30 km south of Ramingining Aerodrome (YRNG), Northern Territory (Figure 1). The helicopter was being used as part of an animal mustering operation, which also included multiple land vehicles.
Figure 1: Map showing location of Ramingining and accident site of VH-LOS
Source: Google Earth, annotated by the ATSB
At approximately 1800 local time, the mustering operation concluded for the day. While the land vehicles departed the swamp and headed to a camp location approximately 20 km to the west, the pilot of VH-LOS remained at the swamp with the helicopter. A witness recalled that they expected the pilot to depart the swamp soon after the land vehicles left. The pilot was expected to collect another member of the mustering operations from a location near the swamp, before returning to the mustering camp.
Meanwhile, the mustering group member who planned to meet the helicopter travelled from the swamp towards the planned meeting point, which was south of the swamp. They recalled it took about 30 minutes to reach the planned meeting point. They waited for about 10 minutes, before deciding to return to camp in their land vehicle when the helicopter did not arrive.
Flight tracking information showed VH-LOS took off from the swamp at 1803, and was flown around the swamp before tracking to the south and shutting down at 1812. The helicopter was then started at 1837, and was flown to the mustering camp, landing and shutting down at 1854. The track of these flights is shown in Figure 2. The flight tracking information showed the helicopter was started at 1921, before the flight tracking record ended about 1 minute later when the helicopter was still at the mustering camp.
Figure 2: Map of Arafura Swamp and key locations, and track of VH-LOS
The yellow track shows the flight departing from Arafura Swamp at 1803 and landing south of the swamp at 1812. The red track shows the flight from the edge of the swamp to the mustering camp departing at 1837 and landing at 1854.
Source: Tracplus and Google Earth, annotated by the ATSB
When the land-based vehicles arrived at the camp, the helicopter was not there. Members of the mustering operation became increasingly concerned and commenced a land-based search at approximately 2100.
The following day, members of the mustering operation contacted some acquaintances who attended the area in helicopters and commenced an aerial search. The helicopter wreckage was located approximately 6 km from the mustering camp. The pilot was deceased, and the helicopter was destroyed.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) and a valid Class 1 Aviation Medical Certificate. The pilot did not hold an instrument rating or a night visual flight rules rating. The pilot’s logbook recorded over 6,000 hours total aviation experience.
Aircraft information
VH-LOS was a 2-seat Robinson Helicopter Company R22 Beta helicopter, serial number 1715, powered by a Textron Lycoming, O-320-B2C, 4-cylinder piston engine. It was manufactured in the United States in 1991, and first registered in Australia in January 1995. The helicopter was not equipped for night flight under the visual flight rules.
Weather and environment
Witnesses involved in the mustering operations at the Arafura Swamp on the afternoon of 14 November recalled that conditions were clear. They reported that there was thunderstorm activity to east of where the group were operating, however no storms passed overhead. An analysis prepared by the Bureau of Meteorology also identified a thunderstorm to the east of the accident site, moving westward during the evening.
Sunset at Ramingining on 14 November 2022 was 1905 and the end of civil twilight (last light)[1] was 1927. Civil nautical twilight[2] was 1953 and astronomical twilight[3] was 2020. The moon was a waning gibbous, rising at 2337 with about 71.3% of the visible disk illuminated.
Site and wreckage
Examination of the wreckage indicated that VH-LOS collided with terrain at approximately 45° nose-down pitch and 30° left angle of bank. There was a short wreckage trail of about 13 m, with all helicopter parts present at the accident site and no evidence of an in-flight break-up. One main rotor blade was liberated in the collision and was found about 30 m to the right of the wreckage trail.
The tail cone and tail rotor assembly remained connected to the fuselage, however presented as deflected down and curled under the helicopter. Site examination showed that both fuel tanks remained intact and contained fuel. Damage signatures to engine rotating components indicated that the engine was operating prior to the collision with terrain. There was no post-impact fire.
Recorded data
The helicopter was fitted with an aircraft tracking unit, which recorded and transmitted the position of the aircraft to a server. The ATSB obtained records showing the recorded tracks of VH-LOS on the afternoon of 14 November, and on other dates prior to the accident. The final recorded position of the helicopter was at the mustering camp, and the aircraft tracking unit did not record the position of the helicopter prior to it colliding with the terrain at the accident site.
The ATSB recovered a handheld GPS unit from the wreckage. Preliminary analysis indicated this unit did not capture the flight on the afternoon of 14 November.
The aircraft was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be.
Further investigation
To date, the ATSB has examined the accident site and wreckage, interviewed witnesses who were involved in the mustering operations and the search of VH-LOS, and collected meteorological data, aircraft maintenance records and pilot records.
The investigation is continuing and will include further review and examination of:
pilot records and medical information
aircraft maintenance and flight records
aircraft wreckage
witness information
meteorological data
recorded aircraft tracking data.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgement
The ATSB wishes to acknowledge the support provided by the Northern Territory Police Force during the ATSB deployment to the accident site. The accident site was in a very remote location and the Northern Territory Police Force provided substantial logistical support to facilitate ATSB access to the accident site and the activities at the site.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Geoscience Australia (GA) defined the ending of civil twilight as the instant in the evening when the centre of the sun is at a depression angle of 6° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible.
[2] GA defined the ending of evening nautical twilight as the instant in the evening when the centre of the sun is at a depression angle of 12° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, it is dark for normal practical purposes.
[3] GA defined the ending of astronomical twilight as the instant in the evening when the centre of the sun is at a depression angle of 18° below an ideal horizon. At this time the illumination due to scattered light from the sun is less than that from starlight and other natural light sources in the sky.
The Australian Transport Safety Bureau has released a preliminary report from its on-going investigation into a fatal helicopter accident near Maitland last month.
On 6 October 2022, the pilot and sole occupant of a single-engine, five-seat Bell 206 JetRanger was conducting a ferry flight from northern New South Wales to Warnervale, on the Central Coast.
About two and a half hours into the flight, the helicopter collided with terrain, coming to rest on a muddy river flat east of Maitland. The pilot was fatally injured and the helicopter was destroyed.
ATSB investigators attended the scene and conducted an initial assessment of the aircraft in situ, before it was moved to higher ground for further examination due to rising water levels.
“Today’s preliminary report details factual information established in the investigation’s early evidence collection phase,” ATSB Director Transport Safety Stuart Macleod said.
“It has been prepared to provide timely information to the industry and public, and contains no analysis or findings, which will be detailed in the final report.”
The preliminary report notes recorded data indicated the pilot was following the inland visual flight rules (VFR) lane west of Williamtown Airport when, approaching Tocal, the aircraft started to climb, and conducted a right 180‑degree turn.
“Data showed that over the next 20 minutes, the helicopter conducted a number of turns, a climb up to 3,100 ft, and a descent to around 120 ft above ground level, and exited and re-entered the VFR lane on a number of occasions,” Mr Macleod said.
“It was then observed by six witnesses, who reported it heading towards the Hunter River, descending slightly, and possibly initiating a turn when it rolled markedly and descended rapidly, colliding with the riverbank.”
ATSB investigators were able to account for all major aircraft components at the accident site, and examination of the aircraft’s flight controls, engine and structure did not identify any pre-existing defects.
Bureau of Meteorology data for Maitland Airport 15 minutes before the accident reported 8 kt of wind with scattered cloud at 4,000 ft and 4,500 ft, and overcast cloud at 7,800 ft above the airport.
“To date, the ATSB has assessed the wreckage, interviewed witnesses and collected external data sources related to weather, air traffic communications, and flight tracking,” Mr Macleod said.
“Moving forward, the investigation will include further review and examination of aircraft maintenance documentation and operational records, recorded data,
weather information, air traffic communications, and the pilot’s medical records, qualifications, and experience.”
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Mr Macleod concluded.
On 8 November 2022, a De Havilland Canada DHC-8-202 aircraft, registered VH‑TQS and operated by QantasLink, was conducting a passenger flight from Lord Howe Island to Sydney, New South Wales. During the descent, the flight crew noticed failures of the traffic alert and collision avoidance system, the ground proximity warning system as well as the radio altimeter.
During landing, the beta lockout system horn activated and then both engine manual warnings illuminated. With the engines in manual mode, the captain advanced the power levers to maintain the propeller speed above their restricted range. After stopping at a holding point about halfway through the taxi, the captain noticed a degradation in the braking performance. Braking performance continued to deteriorate as the aircraft was taxied and the brakes failed and ignited. The captain initiated an evacuation, during which no-one was injured.
What the ATSB found
The ATSB found that the failure of the radio altimeter led to the subsequent failures of the traffic alert and collision avoidance system and the ground proximity warning system, as these systems rely on data from the radio altimeter. The radio altimeter failure also resulted in the beta lockout system relying solely on the weight on wheels sensors. This meant that, when the weight on wheels indicated a momentary ‘in-air’ indication during landing, the beta lockout was triggered. The beta lockout activation resulted in a dual engine manual condition. With the engines in manual mode, the captain had to manually advance the power levers to avoid the ground operating restricted range of the propellers. This increased the amount of wheel braking required, combined with a long taxi of over 5 km, resulted in the brakes overheating, failing and igniting.
Operational guidance contained in the Quick Reference Handbook did not adequately inform the flight crew of the flow-on implication of the radio altimeter failure on the beta lockout system. Nor did it adequately provide guidance on responding to a dual engine manual condition.
Although not contributory, it was also found that the Bromo Chloro di-Fluoromethane (BCF) fire extinguisher was used on the high temperature brake fire, potentially increasing the risk of exposure to hazardous by-products.
What has been done as a result
QantasLink has advised they have made changes to both the DHC-8-200 Quick Reference Handbook and Flight Crew Operating Manual, including:
providing further information about the beta lockout system
new checklists for a radio altimeter failure and dual engine manual condition scenario.
The operator also published a technical advisory bulletin to DHC-8-200/300 flight crew outlining this event and learnings from this event.
Safety message
This occurrence highlights the importance of appropriate operational guidance, particularly in modern aircraft with complex integrated systems. Procedures for managing an equipment failure should consider factors that may influence the performance of other operational systems. In this occurrence, the flow-on effects of the radio altimeter failure on the beta lockout system. Fortunately, the flight crew were able to successfully troubleshoot the system errors and carry on the flight safely. Increased safety margins in procedural documentation can also help ensure flight crew make appropriate decisions when managing unexpected events. In this case, even a one second change in the timing of retarding the power levers could have prevented the occurrence.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Approach to Sydney
On 8 November 2022, a QantasLink De Havilland Canada DHC-8-202 aircraft, registered VH‑TQS departed Lord Howe Island on a scheduled passenger flight to Sydney, New South Wales with 3 crew and 23 passengers on board. The first officer (FO) was the pilot flying (PF)[1] and the captain was the pilot monitoring (PM).
At about 1658 local time, while descending through flight level (FL)[2] 175 on approach to Sydney (Figure 1), the flight crew were alerted to a failure of the traffic alert and collision avoidance system (TCAS)[3] as well as the ground proximity warning system (GPWS).[4] Shortly after, they noticed the radio altimeter (RadAlt) had also failed.
Figure 1: ADS-B[5] derived flight data showing the approximate location of the radio altimeter failure on approach to Sydney
Source: FlightRadar24 and Google Earth, annotated by the ATSB
The FO continued flying the aircraft while the captain consulted the Quick Reference Handbook (QRH) for the GPWS, TCAS and RadAlt failure procedures. The flight crew then informed air traffic control of the TCAS failure, and the FO continued with a visual approach to runway 34R[6] at Sydney.
Landing and taxi
After touching down, the FO retarded the power levers into beta range[7] to use the propellers to help slow the aircraft, as was standard procedure. When this happened, the beta lockout warning horn sounded. The power levers were brought forward to flight idle, which silenced the horn. Shortly after, the captain took over as PF as the aircraft’s nose-wheel steering tiller is located on the left (captain’s) side of the cockpit.
As they vacated the runway, the flight crew noticed that the GPWS and TCAS faults were resolved, but also identified that both the #1 and #2 engine manual caution lights were now illuminated, indicating that the electronic control units (ECU) of both engines were now in manual mode. The ECU normally controls the under-speed governing of the propellers during ground operations. However, when in manual mode, the power levers must be manually advanced by the flight crew to control the propeller speed and avoid the prohibited range[8] below 780 revolutions per minute (RPM). It also meant that reverse thrust would not be available to assist with slowing the aircraft during landing and the taxi.
As the captain advanced the power levers to maintain the propeller speed above 780 RPM, they noted that additional wheel braking was required to maintain a normal taxi speed. While the captain was taxiing the aircraft, the FO consulted the QRH checklist for the engine manual warnings, however, the checklist was prescribed for only a #1 or #2 engine manual caution light, not both simultaneously.
After about 3.3 km of taxiing, the aircraft reached the bravo 8 holding point (Figure 2). The captain brought the aircraft to a stop as air traffic control had instructed them to hold. While stopped, the flight crew contacted engineering support seeking advice on the dual engine manual condition. However, engineering was unable to provide advice within the available timeframe.
Once permitted, the taxi continued towards the domestic terminal. From this point, the taxi had a slight downhill slope and the captain started to notice the response from the brakes reducing. The braking performance continued to deteriorate, and during the final turn into the domestic 1A area (Figure 2), after about 5.5 km of taxiing, there was no braking response and the captain verbalised, ‘We’ve lost brakes’. The captain manoeuvred their aircraft to avoid colliding with another aircraft that was turning into a bay, and then brought the aircraft to a stop. At that time, the cabin crew reported via the interphone that there was fire, including visible flames, from both sides of the aircraft. The captain initiated an evacuation at which point the FO referenced the checklist in the QRH. They then exited the aircraft with the fire extinguisher. As the passengers disembarked, the FO went to both landing gear and attempted to extinguish the fires. A short time later, emergency services arrived and extinguished both fires using foam fire retardant.
No crew or passengers were injured during the evacuation.
Post-flight inspection
Following the occurrence, the aircraft was inspected by maintenance personnel. That inspection identified that all 4 main wheels and brakes were heat affected. Several of the brake and wheel components were replaced as a result of the brake fires. Maintenance testing could not replicate the RadAlt fault and the reason for its failure remains unknown.
Figure 2: ADS-B derived flight data showing the track of the aircraft on the ground at Sydney and the location of the brake failure
Source: FlightRadar24 and Google Earth, annotated by the ATSB
Context
Flight crew information
The captain had been flying for over 10 years and had about 5,000 hours of aeronautical experience with 2,272 hours on DHC-8 aircraft. The FO had been flying for about 9 years and had about 2,400 hours of aeronautical experience, of which 1,734 were on the DHC-8.
Aircraft information
General
VH-TQS was a high-wing, pressurised aircraft manufactured by De Havilland Canada in 1995. It was powered by 2 Pratt & Whitney Canada PWC123D turboprop engines, each driving a Hamilton standard 14-SF-23 4-blade, feathering and reversible, constant speed propeller. QantasLink had been operating the aircraft since 2011.
Radio altimeter
The aircraft was fitted with a radio altimeter (RadAlt). The RadAlt measures the height of the aircraft above terrain immediately below the aircraft, known as the radio altitude, and typically has an operating range of between 0 and 2,500 ft. The RadAlt system on the DHC-8-200 consists of a transmitter/receiver unit mounted under the cabin floor and 2 antennas on the underside of the fuselage. It is integral to the operation of the TCAS and GPWS, as well as the beta lockout system.
Beta lockout system
The power levers on the DHC-8-200 operate in 2 zones, flight mode and beta mode. In flight mode, the levers control engine speed between flight idle and take-off power. While in beta mode, the power levers control propeller pitch directly. The beta range is used for ground operations such as slowing the aircraft after landing and for ground manoeuvring. While in beta range, the ECUs regulate power to provide under-speed governing of the propellers.
As the levers are retarded in the flight mode towards flight idle, a flight idle gate prevents unintentional movement of the levers into the beta region. The gate is overridden by raising gate release triggers, allowing the power levers to be moved further aft to the ‘DISC’ detent. At this point, the propeller blade angle is at +1.5° which is used to slow the aircraft after touchdown. For ground manoeuvring, the levers can be retarded further to maximum reverse, at which point the propeller angle reaches -11.0°.
To ensure the beta condition is not activated in-flight, the system is disabled by the beta lockout while the aircraft is airborne. The beta lockout system is disabled from ground to 50 ft above ground level by the radio altimeter, or from an on-ground indication from the weight on wheels (WoW) system. Both the RadAlt and WoW are interlinked to the beta lockout system to prevent activation of beta lockout in the event that the aircraft bounces slightly during landing.
Weight on wheels system
The WoW system on the DHC-8-200 consists of proximity sensors on each of the landing gear and prevents the gear from retracting while on the ground. The proximity sensors register an on‑ground condition when the suspension compresses due to the weight of the aircraft. The beta lockout system requires the consensus of the main landing gear sensors, whereas the flight data recorder requires the consensus of all 3 gear (both main and nose) to provide a WoW indication in the recorded flight data. Further, it is possible for a sensor to record an in-air condition due to a decompression of the landing gear suspension, even when the wheel remains in contact with the ground.
Engine control unit
On the DHC-8-200, each aircraft engine is fitted with an ECU. The primary function of the ECU is for fuel flow regulation and torque management to optimise performance while protecting the engine from operational hazards such as exceedances of certain engine parameters, including temperature and RPM. In the event of a fault, the ECU will drop offline, and engine management will revert to manual control, as indicated by the illumination of the ECU manual light on the caution panel. In manual mode the flight crew must manually control fuel flow and there will normally be a difference between the 2 engine power lever positions for the same torque.
There are limitations on the use of lower power lever settings, particularly after landing, as the ECU normally controls the engine under-speed governor. With this, in manual mode, the flight crew must manually advance the power levers to maintain the propeller RPM above the ground operating restricted zone. Consequently, reverse thrust is no longer available for the affected engine.
Operational information
Landing procedures – power levers
The QantasLink Flight Crew Operating Manual (FCOM) contains landing procedures. Regarding the setting of the power levers during landing, the FCOM stated that:
Set the power levers to disc after touchdown.
Quick Reference Handbook guidance
The DHC-8-200 QRH did not have guidance in the event of a failure of the radio altimeter. Neither was there any information regarding the implications that the failure would have on the beta lockout system. There was some pertinent guidance available in other manuals. For example, the Operating Data Manual stated:
If the RADALT is inoperative or scrolling ensure positive WOW prior to the selection of discing on touchdown
However, the flight crew would not be expected to access this manual during this phase of flight.
The QRH contained guidance on the GPWS and TCAS failures, but there was no reference to radio altimeter failures. In addition, the QRH contained no information for a dual engine caution condition, however, it did include guidance on an individual #1 or #2 engine manual caution.
Evacuation procedures
Both the Aircrew Emergency Procedures Manual and the QRH contained guidance on actions and flight crew responsibilities in the event of an evacuation. Both documents required the FO to exit the aircraft with a fire extinguisher and torch.
Fire extinguishers
The DHC-8-200 was fitted with a Chubb Bromo Chloro di-Fluoromethane (BCF) fire extinguisher. The Aircrew Emergency Procedures Manual, available in the flight crew’s electronic flight bag, contained guidance on the use of the BCF, which was for general use on most fires except some burning metals. The manual specifically stated that:
Warning: Some metals react adversely with BCF extinguishant (e.g. titanium and magnesium) however they need to [be] at extreme temperatures to react adversely, e.g. brake fire on the Q200/Q300).
The Chubb material safety data sheet stated that hazardous decomposition products:
May evolve bromine, chlorine, fluorine, halogen acids and carbonyl halides when heated to decomposition.
In response to a draft of this report, the operator advised that their annual emergency procedures training for flight crew covers BCF extinguisher description, serviceability, operation and precautions. This included a discussion on the warning, as noted above, and that the extinguisher can be used on in-flight fires.
Flight crew comments
During interview, both flight crew stated that they had never used a BCF fire extinguisher before. Both recalled from their training that the BCF extinguisher should not be used on some metal fires. However, they could not recollect that they were not to be used on brake fires on the DHC-8-200 aircraft. After the evacuation, the FO considered whether to use the BCF extinguisher on the brake fires. Aware that passengers were evacuating, and as the response time of the emergency services was unknown at that point, they elected to deploy the extinguisher on both fires.
Recorded flight data
The aircraft was fitted with an L3[9] FA2100 flight data recorder and L3 FA2100 cockpit voice recorder. Both units were transferred to the ATSB technical facilities in Canberra for download. Figure 3 shows a portion of the flight data recorded during the touchdown phase of the flight.
The data showed that the WoW system indicated an on-ground condition on initial touchdown (black track in Figure 3). One second later, the system recorded an in-air condition for one second, before returning to the on-ground condition for the remainder of the landing sequence. In that one second period in which the WoW returned to the in-air state, the data showed (red and green traces in Figure 3) that both propellers were placed into the beta mode. Coincident with this, the data showed the master caution (orange trace) activating.
Figure 3: Recorded flight data showing the timing of weight on wheels indication in relation to when the propellers were placed into beta mode
Source: ATSB
Safety analysis
Radio altimeter failure
Both the TCAS and GPWS relied on data from the RadAlt. Thus, the failure of the RadAlt resulted in the subsequent failures of the TCAS and GPWS. Further, the beta lockout system was interlinked with both the RadAlt and WoW systems to prevent the beta range from activating in‑flight. This meant that once the RadAlt had failed, the beta lockout system was relying solely on the WoW indication.
Weight on wheels
The flight data showed that, in the same second the power levers were retarded to beta range, the WoW sensors recorded a momentary ‘in-air’ condition. With the system registering an ‘in-air’ condition while the power levers were in beta range, the beta lockout system activated. The activation of the beta lockout resulted in engine manual caution warnings for both engines as the ECUs reverted to manual mode. Consequently, as the ECUs were not providing the under-speed governing during ground operations, this meant that reverse thrust was not available to slow the aircraft during the landing and subsequent taxi.
Brake failure
With both engines in manual mode and the requirement to avoid the ground operating restricted range, the flight crew had to manually advance the power levers on both engines to an increased propeller speed above 780 RPM. This subsequently increased the amount of wheel braking required.
The flight crew were able to safely stop the aircraft at the bravo 8 holding point, after about 3.3 km of taxiing. It was only after this point the braking performance deteriorated, eventually failing, igniting and initiating the evacuation. The combination of the additional burden placed on the brakes due to the increased thrust required to avoid the restricted propeller speed, as well as the length of the taxi with a downhill component, likely both contributed to the brakes overheating then failing, and igniting.
Operator guidance – engine manual warning and RadAlt
After the failures of the GPWS, TCAS and RadAlt, the flight crew consulted the DHC-8-200 QRH finding guidance for the TCAS and GPWS failures, but none for the RadAlt failure. Had the QRH contained information regarding the flow on effects of the RadAlt failure on the beta lockout system, it was likely the flight crew would have delayed the movement of the power levers into beta range during the landing until weight on wheels was assured.
Similarly, when the flight crew observed the engine manual caution warnings on both engines, they again consulted the QRH, finding guidance for only a #1 or #2 engine manual warning. Had the QRH provided additional guidance on dual engine manual cautions, the flight crew could have safely terminated the taxi at the bravo 8 holding point, or at any point prior, likely avoiding the brake failure, fire, and subsequent evacuation.
Fire extinguisher usage
Before evacuating the aircraft, the FO consulted the QRH and in accordance with the checklist exited the aircraft with the BCF fire extinguisher. Cognisant of the proximity of evacuating passengers, and unaware of the response time of the emergency services, the FO elected to deploy the BCF on both brake fires. Although no-one was adversely affected in this occurrence by the use of the BCF fire extinguisher, their use on high temperature metal fires (such as a brake fire on the DHC-8-200 as noted in the Aircrew Emergency Procedures Manual), can result in the production of a number of toxic fumes.
Guidance on the use of the BCF extinguisher was provided in the Aircrew Emergency Procedures Manual, however, it was unlikely that flight crew would review this manual during an emergency evacuation. This information was not covered in the QRH, which was reviewed by the flight crew immediately prior to the evacuation. While the FO exited with the extinguisher, they could not specifically recall that it was not to be used on this type of fire. Therefore, it was likely that, in this occurrence, additional guidance in the QRH could have prevented the use of the BCF on the high temperature brake fire.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the brake failure and fire involving DHC-8-202, VH-TQS, Sydney Airport, New South Wales, on 8 November 2022.
Contributing factors
The radio altimeter failure led to the beta lockout system relying solely on the weight on wheels to prevent the activation of the beta lockout system.
During the touchdown, in accordance with standard operating procedures, the power levers were moved into the beta range. As this occurred when the weight on wheels sensors momentarily recorded an in-air condition, the beta lockout system and engine manual condition activated. This meant that reverse thrust would not be available to assist in decelerating the aircraft during the landing and taxi.
The increased power setting required to avoid the restricted zone while in engine manual mode combined with the long taxi, increased the amount of wheel braking required, resulting in the brakes overheating, failing and igniting.
The operator did not provide adequate guidance on how to respond to a dual engine control unit or radio altimeter failure on the de Havilland Canada DHC-8-200 aircraft, leaving flight crew without sufficient resources to appropriately deal with such failures.
Other factors that increased risk
During the evacuation of the aircraft, the Bromo Chloro di-Fluoromethane (BCF) fire extinguisher was used on a high temperature brake fire, increasing the risk of exposure to hazardous by-products.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by QantasLink
In response to this occurrence, on 4 October 2023, the ATSB was advised by QantasLink that the following actions had been undertaken:
They published a technical advisory bulletin to DHC-8-200/300 flight crew outlining the event and learnings from the event, including relevant technical explanations, such as the radio altimeter failure and the flow-on implications with the beta lockout system.
Further information about the beta lockout system will be added to the DHC‑8‑200/300 Flight Crew Operating Manual Section 4 in an upcoming amendment.
A new QRH checklist is also being produced for a radio altimeter failure. This new QRH checklist will assist to identify a radio altimeter failure and will provide appropriate actions and considerations. In particular, it will include the following note from the De Havilland Operating Data Manual:
If the Radio Altimeter is inoperative or scrolling, ensure positive WOW prior to the selection of Discing on touchdown.
They are developing a new QRH checklist for a ‘#1 ENG MANUAL and #2 ENG MANUAL (Caution Lights)’ scenario. This new checklist will provide guidance in the event both engines operate in manual mode, including considerations such as maintaining propeller RPM outside the prohibitive range and limiting taxi duration, with consideration given to being towed to the bay (where possible). Specifically:
After landing, shutdown both engines as soon as practical. Taxi duration must be limited to avoid excessive braking caused by high power settings.
Additional guidance regarding the use of brakes has been added to the Flight Crew Operating Manual.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
QantasLink
De Havilland Aircraft of Canada Limited
recorded data from the flight data recorder
audio recordings from the cockpit voice recorder
ADS-B data from FlightRadar24.
References
Gunston, B. (2004). The Cambridge aerospace dictionary. Cambridge University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
QantasLink
De Havilland Aircraft of Canada Limited
Civil Aviation Safety Authority
The Transportation Safety Board of Canada
Transport Canada.
Submissions were received from QantasLink. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 175 equates to 17,500 ft.
[3] Traffic alert and collision avoidance system: a type of airborne collision avoidance system (ACAS).
[4] Ground proximity warning system: a system designed to alert pilots if their aircraft is in immediate danger of flying into the ground or an obstacle.
[5] ADS-B: Automatic dependent surveillance–broadcast is a surveillance technology in which an aircraft determines its position via satellite navigation and periodically broadcasts it, enabling it to be tracked.
[6] Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[7] In beta range, the power lever directly controls propeller blade angle during ground operations. Beta range of operation consists of power lever positions from flight idle to maximum reverse.
[8] During ground operations, the propeller speeds must be maintained above 780 RPM to avoid resonance in the propellers, which can result in excessive airframe vibrations.
[9] L3: now L3Harris Technologies, Inc. Melbourne, Florida, USA.
Occurrence summary
Investigation number
AO-2022-056
Occurrence date
08/11/2022
Location
Sydney Airport
State
New South Wales
Report release date
20/02/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Fire
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
Model
DHC-8-202
Registration
VH-TQS
Serial number
418
Aircraft operator
EASTERN AUSTRALIA AIRLINES PTY LTD
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
During an interrupted engine start procedure for the left engine, flame and smoke were visible
Interim report details factual information to provide timely information to the industry and public
Subsequent safety action taken by the operator includes the provision of a training package and guidance to ground staff about dispatch procedures and hand signals.
The ATSB has released an interim report from its ongoing investigation into an incident where passengers were evacuated from a Saab 340 after flame and smoke were briefly observed from the rear of the aircraft’s left engine during an interrupted engine start.
The aircraft, operated by Regional Express, was being prepared for departure on the morning of 5 April 2022 for a flight from Melbourne to King Island, with two pilots, a flight attendant and 23 passengers on board.
“Drawing upon a preliminary review of CCTV footage, on-board recordings and interviews with the crew, the report details the incident’s sequence of events during the engine start-up sequence,” said ATSB Director Transport Safety Dr Mike Walker.
After the right engine was started, and as the crew began to start the left engine, a ground staff member disconnected the ground power unit from the aircraft prior to receiving the signal from the flight crew to do so, the report details. This interrupted the start-up sequence.
The captain then initiated the interrupted engine start procedure for the left engine, which included motoring (using its starter to rotate the engine with fuel and ignition switched off) to remove any residual fuel from inside the engine.
As the left engine propeller began to rotate, flame and smoke were visible coming from the rear of the left engine for about 3 seconds.
A marshaller, positioned at the front of the aircraft, noticed the flames and began to signal to the flight crew to stop the engine start using the appropriate hand signal. However, the marshaller could not recall the hand signal for fire and instead communicated to the flight crew by mouthing the words ‘smoke’ and ‘flame’ and gesturing to the left engine.
The captain ceased motoring the left engine. At about this time, the flight crew noted that the left engine interstage turbine temperature (ITT) was still rising and in response the captain decided to make a second attempt at motoring. At this time, the marshaller continued to signal to the flight crew that there was a problem.
The report then details the actions of the flight crew, including actioning the engine fire emergency checklist and commanding an evacuation.
Two passengers received minor injuries in the evacuation, which took about 4 minutes.
The report details safety action taken by the operator as a result of the incident, including the development of a new hand signal to indicate an interrupted engine start, and providing ground staff with a training package about dispatch procedures and hand signals.
“This interim report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public,” said Dr Walker.
“It contains no analysis or findings, which will be detailed in the investigation’s final report.”
The continuing investigation will include a review and examination of flight crew failure management procedures, crew communication and coordination; flight crew, flight attendant and ground staff recurrent training; and on-board recordings.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Dr Walker noted.
The ATSB conducts a Privacy Impact Assessment (PIA) for all high privacy risk projects. A project may be a high privacy risk if it has a significant impact on the privacy of individuals.
On 10 November 2022, a Link Airways (Link) Saab 340B, registered VH-VEQ, was being prepared for a commercial air transport flight. The aircraft was operating as VA633, scheduled from Canberra, Australian Capital Territory, to Sydney, New South Wales.
During the aircraft preparation process, the first officer (FO) did not attach the strap extension between the stairway and the left propeller. The strap extension was used by some operators to guide passengers onto the aircraft and would prevent the cabin door being closed without its removal. Once passengers had boarded and during the final inspection, the FO did not remove the propeller strap—used to prevent propeller windmilling—from the left engine.
The dispatch coordinator (dispatcher), who was employed and trained by the ground handling company Swissport, did not conduct another walk-around or follow the FO. Prior to engine startup the propeller strap was not noticed by the captain or the dispatcher. During the startup sequence there was a delay between the commencement of engine start and the propeller spinning due to the pins securing the strap to the engine cowling. Once these failed, the propeller began turning normally and the aircraft was cleared to depart with the strap still attached to the left propeller but not visible due to the propeller’s rotation.
At about the time the aircraft became airborne, the propeller strap was thrown free of the blade and into the fuselage. Passengers recalled hearing an extremely loud bang, and could see that an object had penetrated the cabin. The strap itself became embedded in the fuselage, but the failed cowling pins broke free of the strap and entered the cabin. One fragment struck the leg of a passenger, resulting in a minor injury (bruising).
From the flight deck, the flight crew did not see or hear the propeller strap penetrate the fuselage. The cabin manager (CM) realised what had happened, but waited until the aircraft was no longer in a critical phase of flight before contacting the flight crew. The CM stated that there was an emergency in the cabin, and that someone was hit, but did not elaborate beyond expressing a need to return to Canberra and that an ambulance would be required. The flight crew, believing the emergency to be only passenger-related, did not seek any additional information. The aircraft landed safely in Canberra and emergency services assessed the injured passenger.
What the ATSB found
The ATSB found several factors that may have contributed to the propeller strap not being noticed or removed by the FO, captain or dispatcher. Most importantly:
The strap extension was not fitted. Because the cabin door could not be closed with the strap extension in place, its correct fitment would almost certainly have prevented the flight from proceeding with the propeller strap attached. A review of other departures out of Canberra found that some other flights were boarded without the strap extension being attached.
The propeller strap did not have a visibility aid (streamer) fitted in accordance with the manufacturer’s design. Link conducted an inspection of its Saab 340B fleet and found the condition of propeller straps to be significantly variable.
Guidance provided by Link Airways for training of Swissport dispatchers did not explain the appearance, function and importance of the propeller straps.
In addition, while not found to have contributed to this occurrence, Swissport did not ensure that the implemented dispatcher training and audits for operations involving the Link Airways Saab 340B dispatches incorporated all of the elements required for pre-departure walk-arounds in its own ground handling manual. This increased the overall risk to the flight.
Similarly, risk was increased by the flight crew not being informed of the fuselage penetration, although this did not contribute to the outcome of the occurrence.
What has been done as a result
Link advised that it had updated the flight crew and cabin crew operating manuals to include additional preflight checks for the presence of the propeller strap and strap extension. Additional clarity was provided to cabin crew regarding contacting the flight deck during emergencies. Propeller strap discrepancies were rectified within Link’s Saab 340B fleet, and regular inspections and maintenance were added to procedures.
Link amended training guidance to Swissport, including more details on the use of propeller straps and strap extensions, as well as the dispatcher’s role in checking for the strap. Link has planned audits of Swissport dispatches to ensure the procedures are correctly implemented.
Swissport informed all ramp staff (including dispatchers and trainers) that walk-arounds were required on Saab aircraft. It consulted with Link to better define dispatcher responsibilities and expectations, and planned refresher training on the walk-around described in Swissport’s procedures.
Safety message
For those directly involved in aircraft operations, this occurrence highlights the importance of vigilance. When there are multiple risk controls in place and multiple responsible parties, it is easy to become complacent from an expectation that earlier checks have been done correctly and that future checks elsewhere in the system will likely catch anything missed.
From an organisational perspective, the occurrence illustrates the importance of strong communication and harmonised procedures. The use of external ground handling services has become increasingly common in aviation. The relationship between carrier and ground handler can add complexity to ground handling operations. In this instance, differences in expectations and understanding of ground handler responsibilities led to a dispatch procedure that was not effective in confirming that the aircraft was clear for engine start-up. It is critical that all involved parties have a complete understanding of their roles and responsibilities, and how they fit together to create a safe and functional operating environment.
Summary video
The occurrence
On the morning of 10 November 2022, a Saab 340B, registered VH-VEQ, was being prepared for a scheduled air transport flight from Canberra Airport, Australian Capital Territory to Sydney Airport, New South Wales. The flight was being operated by Link Airways (Link), with flight number VA633. The flight was to be conducted with 2 flight crew, a cabin manager (CM), and 29 passengers.
It was the first flight of the day for the aircraft and both members of the flight crew. Both propellers had been restrained overnight to prevent windmilling using propeller straps that secured a propeller blade to the engine cowling. At 0718, as part of the aircraft preparation process, the first officer (FO) began the external portion of the daily aircraft inspection[1] (see Use and stowage). As part of this inspection, the FO removed the right propeller strap and inspected the right engine in accordance with Link’s Flight crew operating manual (FCOM). The FO then ‘dressed’ the propeller, rotating it 45° from its restrained ‘T’ position to an ‘X’ position, as an indication that the propeller was free to spin.
After continuing the walk-around, the FO removed the left propeller strap to inspect the engine, then reattached the strap so that passengers could safely board without the propeller windmilling. The procedures required the attachment of a strap extension[2] from the left propeller strap to the airstairs[3] (see Propeller straps). The strap extension was designed to prevent passengers from walking under the aircraft, and its presence also prevented the cabin door from being closed without first removing it. The strap extension was in its normal stowage location in the flight deck behind the door but the FO did not remove the strap extension from the flight deck.
At 0754, after the passengers had boarded, the FO commenced a final external check of the aircraft, which involved a walk-around starting at the nose and moving clockwise around the aircraft confirming that the aircraft was generally prepared for flight, including that hatches were closed and ground service equipment had been removed. The FO closed the cargo bay door, and proceeded to board the aircraft via the airstairs, instructing the CM to close the cabin door. Prior to boarding the aircraft, the FO inadvertently did not remove the left propeller strap.
The dispatch coordinator (dispatcher)[4] tasked with dispatching the aircraft later reported that they observed the FO closing the cargo bay door and entering the aircraft, and this was supported by available closed-circuit television (CCTV) footage, which showed the dispatcher near the cargo bay door at the time. However, the dispatcher did not follow the FO during the entire walk-around (see Dispatcher training and procedures).
The dispatcher moved to the nose of the aircraft in accordance with procedures, so that the captain could be signalled when engines were clear to start. The dispatcher reported that they did not look for, or notice, the strap fitted to the left propeller. However, from the dispatcher’s perspective, the sun was behind and just above the aircraft, which reportedly reduced the aircraft’s visibility.
The captain signalled that the right engine would be started, and the dispatcher signalled all clear. The captain started the right engine, and then signalled that the left engine would be started. The dispatcher once again signalled all clear.
The captain commenced starting the engine, and CCTV showed the left propeller move slightly, then stop. Neither the captain or dispatcher noticed this brief movement, and neither noticed the propeller failing to rotate as it normally would.[5] Seated on the right side, the FO could not observe the left propeller.
The engine continued to build torque with the propeller restrained, and 33 seconds after the initial movement the propeller began to turn. Subsequent investigation established that the propeller torque caused the pins securing the strap to the engine cowling to fail with the strap remaining secured to one of the blades.
In a subsequent interview, the dispatcher reported that while the delay between the signal for ‘all clear’ and the propeller’s rotation was unusual, sometimes pilots would complete other tasks between signalling an engine start and commencing it. The dispatcher therefore did not believe it needed to be brought to the attention of the captain.
The rest of the aircraft dispatch process was completed without incident. At 0803 the flight crew taxied the aircraft to the runway and took off.
During the take-off, about the time the aircraft became airborne (according to the CM’s recollection), the propeller strap was thrown free of the blade and into the fuselage (Figure 1). The strap itself became embedded in the fuselage, but the two failed cowling pins that were attached to the strap broke free and entered the cabin. One fragment struck the leg of the passenger in seat 2A, resulting in a minor injury (bruising).
Figure 1: Part of the left propeller strap that entered the fuselage adjacent to seat 2A
Source: ATSB
Passengers recalled hearing an extremely loud bang, and were able to see immediately that an object had penetrated the cabin. From the flight deck, the flight crew did not see or hear the strap penetrate the fuselage. The CM recalled that they recognised the propeller strap and realised what had occurred, but did not immediately contact the flight crew. In a subsequent interview, the CM stated that this was due to sterile cockpit procedures (see Cabin procedures).[6]
Approximately 25 seconds after take-off, the CM signalled to the flight crew using the emergency call button, which activated an aural and visual indication on the flight deck. When the flight crew contacted the CM, the response that was recorded was the CM stating ‘Emergency. Somebody… we need to get back to the airport.’ The flight crew then informed Canberra tower and prepared to return the aircraft to Canberra.
After 2.5 minutes, the flight crew contacted the CM again to ask if emergency services were required. The CM replied ‘Yes… a passenger was hit.’ Further communication between the CM and flight crew related to taxi procedures and provision of emergency services. There was no further communication about the nature of the emergency. The flight crew continued the flight under the impression that the emergency was only related to a medical condition of a passenger.
The aircraft landed at 0816 without further incident and the passengers were disembarked. The injured passenger was assessed by the emergency services in attendance.
The aircraft was quarantined in Canberra pending the ATSB’s attendance. A remnant of the propeller strap was recovered from the fuselage (Figure 1) where it had caught on a stringer.[7] The cowling pins were no longer attached to the strap. Sections of both cowling pins were still secured in the engine cowling following the occurrence (Figure 2). Other parts breached the fuselage and were recovered from the cabin floor (Figure 3). A small section of one cowling pin was not located. The strap extension was still stowed on the flight deck.
Figure 2: Cowling pin sections that remained secured in the engine cowling, and the damaged propeller strap shown in the normal fitment location after being recovered from the fuselage
Source: ATSB
Figure 3: Parts of the cowling pins recovered from the cabin floor and the engine cowling
Source: ATSB
Context
Personnel information
The captain held an Air Transport Pilot Licence (Aeroplane) and a multi-engine command instrument rating. The captain held a Class 1 aviation medical certificate and had a total flying time of 4,836.2 flying hours with 1,423.3 hours on the Saab 340.
The first officer (FO) held an Air Transport Pilot Licence (Aeroplane) and a multi-engine command instrument rating. The FO held a Class 1 aviation medical certificate and had a total flying time of 834 flying hours with 436 hours on the Saab 340.
Both flight crew members were within duty limits as prescribed by Civil Aviation Order 48.1 Appendix 3. In a subsequent interview, the FO noted feeling fatigued on the morning of the occurrence due to flight duties and home life.
The cabin manager (CM) had 18 years of cabin crew experience and began working on Saab 340B aircraft in early 2022.
Propeller straps
Function and design
The propeller strap assembly, also referred to as the ‘propeller restraining bridle’ by Saab, was intended for use in preventing propeller movement when the aircraft was parked. The strap assembly provided by Saab consisted of a loop to slide over the propeller blade, two cables with pip pins for securing to the engine cowling, and a streamer to aid visibility (Figure 4).
Figure 4: Propeller strap assembly as issued by Saab
Source: Saab, annotated by the ATSB
The propeller strap could only be fitted with the propeller in the ‘T’ position, with 2 blades vertical and 2 horizontal. Without the strap, the propeller can be rotated.[8]
The propeller strap involved in the occurrence had bright orange webbing. Closed-circuit television (CCTV) footage showed that there was no ‘remove before flight’ streamer attached to it.
Following the occurrence, Link Airways (Link) conducted a fleet-wide review of its propeller straps and found significant variation in serviceability. Link found that:
…several prop straps fitted to the fleet did not have a hi vis [high visibility] streamer attached, or if they were attached were discoloured with age and not effective.
Link also found that the orange webbing of the propeller straps was dull or faded with age in some instances.
Link also used a strap extension, made with fluorescent webbing and connecting between the handrail on the airstairs and the left propeller strap. The strap extension was not designed or supplied by the aircraft manufacturer, but a similar product was used by other Saab 340B operators. According to the Link Flight crew operating manual (FCOM), it was intended to ‘provide a visual indication of a restricted area around the propeller’ and a ‘safety mechanism restricting the passenger door stairs from being closed without removing the extension and prop strap.’ An example of the fitment of a strap extension in accordance with the FCOM is shown in Figure 5.
Figure 5: Exemplar strap extension fitted between airstairs and propeller strap
Source: ATSB
Use and stowage
During aircraft departures, procedures for the propeller straps and strap extension differed slightly depending on whether the aircraft was being prepared for the first flight of the day, or if it was following a previous flight.
Prior to a first flight, Link’s FCOM required a line check, known as a ‘Line Check 1’ or ‘LC1’, to be performed by one of the pilots. Both propeller straps would already be fitted (from the night before), with the strap extension stowed in the flight deck. As part of the line check, FCOM procedures required the pilot to remove the propeller straps in order to properly inspect both engines. The responsible pilot was then required to replace the left propeller strap and fit the strap extension. Prior to the occurrence flight, which was the first flight of the day, the FO removed both straps and replaced the left propeller strap during the inspection, but did not fit the strap extension.
For aircraft preparations following a previous flight, the right propeller strap was not to be fitted. The left propeller strap and strap extension should already be in place, because prior to passenger disembarkation, procedures required the flight crew to fit the connected propeller strap and strap extension to the propeller blade and airstairs, respectively.
For all departures, once passengers boarded, the FCOM required a ‘final external check’ by the flight crew. This list included the following items:
• Remove right Prop Strap and dress the propeller to 45°.
• Remove left Prop Strap and extension and dress the propeller to 45°.
Pilots did not generally separate the strap extension from the propeller strap when they were removed from the engine. They would remove the cowling pins and slide the propeller strap, along with the strap extension, off the blade. The other end of the extension would then be disconnected from the airstairs.
Prior to the occurrence flight during the final external check, the FO did not remove the left propeller strap, and therefore could not ‘dress’ the propeller (moving it from the ‘T’ to the ‘X’ position). The right propeller strap had been removed and the right propeller was dressed as part of the previous inspection. In a subsequent interview, the FO did not recall seeing the propeller strap, their actions after closing the cargo bay door, nor whether any distractions might have affected the walk-around. Available CCTV footage did not reveal any observable distractions, although the FO might have spoken with the CM waiting at the top of the airstairs at the point when the propeller strap would normally be removed.
At the end of the final external check, upon entering the flight deck, the pilot was required to stow the propeller strap and strap extension behind the flight deck door, and confirm with the other pilot using the following phrase as an example:
Pogo[9] stowed, Cargo Door closed, Prop Strap stowed, waiting for confirmation of 22 PAX
A review of cockpit voice recordings found that the FO did not advise the captain of door closure and equipment stowage.
Start-up procedures
Following the final external check, the Link FCOM required the flight crew to complete the engine start checklist and stated:
• Before starting any engine, the LP [left seat pilot, usually the captain] shall check propeller area is clear, the prop tie has been removed and fuel cap is on, then call ‘Clear left’.
• The RP [right seat pilot, usually the first officer] shall check propeller area is clear, the prop tie has been removed, the fuel cap is on and the fuel door is closed, then call ‘Clear right’.
Once the checklist was completed, the start procedure could be commenced. The captain was to signal to the dispatch coordinator (dispatcher) which engine was to be started using hand signals. After receiving the dispatcher’s signal that the specified engine was clear of obstructions and safe to be started, the pilot could start the engine. The FCOM required the captain to monitor the engine instruments, including checking for propeller rotation, during the start process. Although the propeller begins to rotate within a few seconds of the start, the rotation speed is not shown on the instruments until the captain cuts the starter, about 40 seconds after the start is commenced.
In a subsequent interview, the captain recalled checking the left engine area for obstructions before start-up. Seeing that nobody was near the propellers, the captain determined the engine was safe to start, but did not notice the propeller strap or the position of the propeller in the ‘T’ position rather than the ‘X’ position (see Use and stowage).
Ground handling
Ground handling arrangements
The occurrence flight was being operated by Link on behalf of Virgin Australia (Virgin); part of an arrangement that commenced in January 2022. Ground handling services for all Virgin flights at Canberra Airport, including those operated by Link, were handled by Swissport through a Standard ground handling agreement (SGHA). These services included ramp support, equipment, towing/pushback of aircraft, and coordinating dispatches.
The use of third-party ground handling services has become increasingly common in Australia as well as globally. Many of these arrangements, as with the one between Virgin and Swissport, implement a variation on the SGHA that is controlled and distributed by the International Air Transport Association.
Article 5 of the SGHA applying to this arrangement outlined the standard of work to be performed by the handling company (Swissport). It stated:
The Handling Company shall carry out all technical and flight operations services as well as other services having a safety aspect, for example, load control, loading of aircraft and handling of dangerous goods, in accordance with the Carrier’s instructions…
Among the services agreed to be provided was the following ‘safety measure’:
Perform visual external safety/ground damage inspection of (a) doors and panels and immediate surroundings (b) other inspection items as specified in Carrier's Manuals …immediately prior departure
This SGHA subsequently stated:
In the case of absence of instructions by the Carrier, the Handling Company shall apply its own standard practices and procedures…
Dispatcher training and procedures
Information provided by Link to Swissport
Prior to Swissport commencing ground handling duties for Link flights, Link provided Swissport with various documents including its Scheduled air transport ground handling manual (SATGHM), so that Swissport trainers could train its own employees on dispatching Link’s Saab 340B aircraft. The SATGHM included a basic familiarisation of the aircraft and associated hazards, procedures for loading baggage into the aircraft, and procedures for aircraft marshalling.
Within the aircraft familiarisation information, the propeller strap was noted as an item that the flight crew fitted prior to passenger disembarkation. No further information was provided to Swissport about propeller straps. There was also no information about the dressing of propellers. A Swissport trainer reported that they were told by Link staff that walk-arounds were the duty of the flight crew and not dispatchers.
However, Link also provided a practical training checklist for aircraft ramping and dispatch duties. This included a list item requiring the trainee to ‘complete [a] visual check of aircraft in final walk around’. The associated procedure stated:
Confirm by visual and/or touch that all doors and other opening are closed flush with the fuselage
Link provided no additional information to Swissport regarding dispatcher walkaround procedures for Saab 340B dispatches.
Swissport procedures
Swissport’s Ground operations manual (GOM) provided all dispatchers and ground crew with general instructions for tasks such as aircraft dispatches. These were designed to cover a wide variety of aircraft types and did not contain information specific to Saab 340B dispatches or any specific operators. The manual stated:
The purpose of this manual is to provide clear direction to all airport staff and staff contracted to Swissport Pacific on their responsibilities and work procedures relating to airport activities, wherever a client does not have specific procedures relating to the tasks being carried out.
This manual included a requirement for a walk-around for ‘all dispatches’, stating (original emphasis):
SAFETY NON-NEGOTIABLE: The walk-around is extremely important, it is the last physical and visual check of the aircraft prior to departure and is critical to ensuring the safety of passengers and crew. It must always be completed in full, with all due care and attention and without deviation. This is a safety non-negotiable.
This walk-around was to be performed by the dispatcher once all other dispatch preparation had been completed, such as loading and boarding. The GOM instructed dispatchers to walk clockwise from the nose around the aircraft’s perimeter, and provided a 10-point list of check items such as:
open or protruding doors and panels
signs of leaks and damage
‘remove before flight’ streamers on the landing gear or flight data sensors
remaining ground support equipment or foreign object debris on the apron.
There was no specific instruction to look for a propeller strap or objects secured to the propellers/engine cowling.
The manual included a second, 15-point list of specific items to check during the dispatcher walk‑around. Dispatchers were to confirm ‘no signs of visible damage or fluid leaks on the tarmac’ around the engine area, and ‘no signs of “remove before flight” streamers … around the door and panel areas on the fuselage.’ None of the list items related to the propellers or propeller straps.
Following the occurrence, a Swissport internal investigation report stated that because Link had not provided a standard operating procedure for a dispatcher walk-around, it was the flight crew’s responsibility to complete a final walk-around, not the dispatcher.
Swissport training
All dispatchers and other ground crew completed training modules provided by Swissport for general employment procedures, such as work health and safety. The specific training provided by Swissport for Link’s Saab 340B dispatches used a combination of information provided by Link and Swissport’s procedures. This took the form of in-person presentations by the trainer, as well as practical training and assessment. The training did not refer to Swissport’s GOM, or instruct dispatchers to refer to it. Dispatchers seeking additional information were instead directed to Link’s SATGHM.
The ATSB sought interviews with several trainers and dispatchers of Saab 340B aircraft. Both a trainer and a dispatcher confirmed that dispatchers were taught that the final walk-around was the flight crew’s responsibility. Dispatchers were not trained to complete a full walk-around, but were trained to follow the pilot from the cargo bay door to the airstairs during the final external check. Dispatchers were trained to ensure that doors and hatches were flush with the fuselage, and that the pogo stick was stowed. Once the pilot conducting the final walk-around was aboard and the cabin door closed, dispatchers were trained to move to the nose of the aircraft to assist the captain with the engine start procedure (see Start-up procedures).
One dispatcher stated that previous Swissport training for other operators had also not required a walk-around. It was reported that, at the time of the occurrence, some dispatchers were not aware of the requirement in Swissport’s GOM that walk-arounds were be conducted for all dispatches.
It was reported by a trainer and a dispatcher that the training did not provide any information on the use of propeller straps, and did not require dispatchers to look for propeller straps or strap extensions during the aircraft dispatch. Similarly, the training did not discuss the significance of a propeller in the ‘T’ position or the ‘X’ position.
One trainer reported that while they knew that the Saab 340B had some form of propeller restraint, the trainer assumed that the propeller strap and strap extension were inseparable, and therefore that the cabin door could not be closed while the propeller strap was in place. The trainer therefore did not consider the strap an item that should be checked by dispatchers.
Audits on aircraft dispatches
Swissport conducted routine audits of some aircraft dispatches across all of its associated carriers. In March 2022, Swissport agreed to dispatch Link’s Saab 340B aircraft as part of an existing arrangement between Swissport and Virgin. Between March and the occurrence in November 2022, 4 audits on dispatches of Link aircraft were conducted. These audits were conducted by the same people who trained staff on Saab 340B dispatches. There were no adverse findings for 3 of the 4 audits, while the other audit had one finding relating to correct operation of the ground power unit.
Cabin procedures
Link’s Cabin crew operating manual (CCOM) provided cabin crew with a list of tasks to be completed prior to departure. At the time of the occurrence, the cabin crew had no responsibilities relating to the propeller strap or strap extension.
The CCOM contained procedures for various potential emergency scenarios, but there was no guidance specific to an object penetrating the fuselage. The CCOM section describing cabin crew responsibilities in the event of an emergency stated the following:
Reporting of any event or circumstance which may affect the safety or security of passengers, crew members or aircraft to the PIC [pilot in command] must be considered an immediate priority and shall be accomplished through the most expedient means available, even if to do so requires the interruption of the PIC in his duties.
The manual also described sterile flight deck procedures, stating that a sterile flight deck was in place during take-off until the seatbelt sign was turned off. Sterile flight deck (also known as sterile cockpit) procedures are a requirement of the Civil Aviation Safety Regulations and, among other things, limit the timing and reasons for cabin crew communications with the flight crew during certain critical periods of flight, including take-off. Regarding emergencies during the sterile flight deck phase, the CCOM stated:
For an emergency or abnormal situation during the sterile flight deck phase, and no contact period, Cabin Crew may make a call to Flight Crew by pressing EMERG CALL button at any time. Flight Crew will receive aural and visual indications on the Flight Deck.
The manual subsequently stated that ‘Cabin Crew must, as soon as practical, ensure Flight Crew are made aware of what emergency or abnormal situation is happening in the cabin.’
Review of previous flights
CCTV footage was retrieved from Canberra Airport, capturing 8 separate flight preparations and dispatches involving Link Saab 340B aircraft from the day of the occurrence and the days prior. The propeller strap was used on all 8 occasions. Due to the position and quality of the footage, the condition of the individual propeller straps could not be determined. The strap extension was not attached between the propeller strap and airstairs during boarding for 2 out of the 8 observed departures, both of which were the first flight of the day.
Various Swissport staff were observed dispatching aircraft in the recordings. In each recorded departure, the duty dispatcher did not conduct a walk-around around the aircraft’s entire perimeter as prescribed in Swissport’s GOM. While the pilots walked from the cargo bay door to the airstairs, the actions of the dispatchers varied between departures. Some dispatchers were already at the nose of the aircraft, or walking towards it at the time. Others were driving the tug away from the aircraft after loading luggage. One dispatcher out of the 8 appeared to be walking around to the front of the aircraft, observing the pilot between cargo bay door and airstairs, but the dispatcher did not follow the pilot directly.
Safety analysis
Introduction
The aircraft was released for flight with the propeller strap still attached to the left propeller. Rotational torque during the engine start broke the 2 pins securing the strap to the engine cowling, leaving the strap webbing (with broken fragments of the pins still connected) attached to the propeller blade. The partial strap assembly was flung off the propeller during the take-off, penetrating the fuselage and injuring one passenger.
There were several opportunities for the first officer (FO), captain and dispatch coordinator (dispatcher) to recognise that the propeller strap was still attached prior to departure, but the strap’s presence on the left engine was not noticed. In the following sections, this analysis discusses the various factors associated with:
pre-flight and engine start procedures
ground handling and aircraft dispatching
the use of strap extensions
fleetwide propeller strap serviceability
dispatcher training facilitated by Link Airways (Link) and Swissport
interactions between the flight crew and cabin manager.
Pre-flight procedures
The Link Flight crew operating manual (FCOM) required the right seat pilot—the FO in this case—to conduct a final external check (walk-around) of the aircraft before departure. As part of the check, the FCOM required the FO to ‘remove left prop strap and extension and dress the propeller to 45° (the ‘X’ position). In this occurrence, the FO did not see and remove the propeller strap during the final external check, and did not notice that the strap extension was not present at the time. It is likely that the absence of the strap extension contributed to the FO not seeing and removing the propeller strap, since this larger and more obvious strap would serve as a reminder that the propeller strap was still present. Further, the propeller strap streamer was missing, which is specifically designed to attract attention and therefore reduce the chance that someone could miss the presence of the propeller strap (with or without the extension). There was insufficient evidence to determine whether distraction contributed to the FO not seeing or removing the strap.
There was also an opportunity for the flight crew to notice the fact that the propeller strap had not been brought into the flight deck. The FCOM specified that the FO should tell the captain that the propeller strap had been stowed, but it was not done in this instance. If the FO had remembered to confirm strap stowage with the captain, one of the crew members might have noticed its absence. While the FO noted feeling fatigued on the morning of the occurrence, there was insufficient evidence to establish if the pilot was likely experiencing a level of fatigue known to affect performance at the time of the occurrence.
Engine start
During the engine start sequence, there was an opportunity for the captain to notice the propeller strap was still attached prior to start-up. The FCOM required the captain to check the propeller was clear and that the ‘prop tie’ (propeller strap) had been removed. In an interview, the captain recalled checking the left engine area prior to start, but did not notice the strap.
The captain would not have been expecting the strap to still be present, and was probably focusing on ensuring that no people or obstructions were near the propeller rather than the condition of the propeller itself. As discussed in Propeller strap condition, if the propeller strap streamer was present, it would have increased the chance of the captain noticing the strap was still in place.
The captain was not required to check (and did not notice) whether the propeller was in the ‘X’ position or the ‘T’ position, which was used to indicate the presence of the propeller strap. However, sufficiently high winds can rotate an unrestrained propeller to a different orientation prior to engine start, so the propeller orientation would not necessarily alert a pilot to a potential issue.
As part of the engine start, the FCOM required pilots to monitor the instruments for propeller rotation along with other engine instruments. In this occurrence, there was 33 seconds between the propeller moving slightly (indicating engine start) and the cowling pins failing, allowing the propeller to rotate freely. By the time the propeller rotation could be monitored using the instruments (approximately 40 seconds after the start had commenced), the propeller would have been rotating normally. Given that the captain’s attention would have been on the instruments, it is likely that this aspect of the start sequence was not noticeably unusual to the flight crew.
Once the engine start was complete the propeller was likely spinning too fast to see that the propeller strap was still attached to the propeller.
Ground handling and dispatch
The dispatcher did not notice that the propeller strap was still attached to the aircraft during the FO’s final walk-around. The dispatcher was positioned near the cargo bay door during the walkaround, and reported observing the FO moving from the cargo bay door to the airstairs. The dispatcher did not follow the FO during this process, despite it being part of the practical training. Following the FO or performing a full walk-around in accordance with Swissport procedures (see Swissport dispatcher procedures and training) would have provided a better opportunity for the dispatcher to look for the kind of hazards described in the Ground operations manual (GOM), such as open panels, ‘remove before flight’ streamers and ground service equipment. It should be noted that dispatchers were not trained to look for propeller straps (seeDispatchers not familiar with propeller straps or propeller dressing).
While at the nose of the aircraft for the engine start procedure, the dispatcher did not see the strap when checking the engine was clear. The dispatcher also did not notice the slight movement of the propeller at the beginning of the engine start sequence. In addition to the strap visibility and lack of instruction regarding the strap, the position of the sun behind the aircraft could have limited the dispatcher’s view.
Use of strap extensions
The strap extension was to be fitted between the propeller strap and airstairs, and served to indicate the restricted area around the propeller during boarding. Since it was much larger than the propeller strap, it also served as an additional visual indication that the propeller strap was still fitted. Most critically, the strap extension prevented the cabin door being closed without first removing it from the airstairs.
In this occurrence, being the first flight of the day, the strap extension was not already attached from a previous flight. When leaving the flight deck to begin the line check, the FO did not take the strap extension from behind the flight deck door and attach it between the propeller strap and airstairs following the left engine inspection, as required by the FCOM. If the strap extension had been fitted, the cabin manager (CM) would have been unable to close the cabin door after boarding and the flight would have almost certainly not proceeded without removal of the propeller strap.
An examination of closed-circuit television (CCTV) footage at Canberra Airport showed other Link flights where the strap extension was not fitted prior to departure. Out of 8 observed departures, in addition to the occurrence flight, the strap extension was not fitted twice, including one that was the first flight of the day. It is likely that the differences in aircraft preparation for a first flight of the day compared to a turnaround increased the likelihood of the strap extension not being fitted for departure. As 3 of the 9 Link departures (occurrence flight and 8 previous departures) showed the extension strap not being used during boarding, it is evident that its non-use for the occurrence flight was not an isolated event by a single pilot.
Propeller strap condition
The propeller straps designed and supplied by the aircraft manufacturer included a streamer to aid visibility. However, the propeller strap that was provided for the occurrence aircraft did not have a streamer attached. The presence of a ‘remove before flight’ streamer would have increased the likelihood of the FO, captain and dispatcher noticing the propeller strap prior to departure.
Link’s subsequent investigation found variations in the condition of propeller straps within the Saab 340B fleet. The missing, discoloured or damaged streamers that were still in service would have reduced the likelihood of flight crew and dispatchers seeing and removing these propeller straps. Similarly, the straps with faded or discoloured webbing would have been more difficult to see against black propeller blades. This evidence indicates that the condition of propeller straps within Link’s Saab 340B fleet was not effectively managed, increasing the risk to associated flights.
Dispatchers not familiar with propeller straps or propeller dressing
The training material that Link provided to Swissport for dispatcher training did not include any specific requirements for dispatchers to check for propeller straps or the strap extension. Link’s ground handling manual only noted ‘prop straps’ as an item the flight crew fitted to the cabin door prior to disembarkation. The material did not include any further description of the propeller strap or its function and usage by Link. There was also no information regarding Link’s use of a strap extension, which was used by some operators for Saab 340B aircraft. Consequently, the Swissport trainers (and therefore the dispatchers that were trained) would not necessarily have been familiar with flight crew procedures regarding the propeller strap and strap extension. This would have reduced the effectiveness of dispatchers to notice departures from procedure such as a propeller strap not being removed, or a strap extension not being fitted before boarding.
A trainer thought that the strap extension was permanently connected to the propeller strap. Since the cabin door would not be closeable while the strap extension was connected, it would be reasonable for dispatchers to believe that there was no need for them to look for a propeller strap, since the attached strap extension would prevent the flight from proceeding. Beyond guidance on looking for broad problems like ‘remove before flight’ streamers on the landing gear or flight data sensors, dispatchers would not know to look for attached propeller straps during the dispatch process.
Training material from Link did not mention propeller dressing, or the significance of a propeller in the ‘T’ position (indicating the strap was attached) versus one in the ‘X’ position (free to spin). Training dispatchers to ensure propellers were in the correct orientation would provide an additional, albeit indirect, method of checking for the presence of a propeller strap.
Swissport dispatcher procedures and training
Under the ground handling agreement in place between Swissport and Virgin, and by extension between Swissport and Link, dispatches of Link aircraft were to be carried out in accordance with Link’s instructions. In the absence of such instructions, the agreement stated that Swissport was to ‘apply its own standard practices and procedures.’ Similarly, Swissport’s GOM stated that it applied ‘wherever a client does not have specific procedures relating to the tasks being carried out.’
Link provided Swissport with information for the training of dispatchers to provide ground handling services for Link Saab 340B aircraft. Regarding walk-arounds, there was no detailed procedure provided for dispatchers, although a training checklist provided by Link included the need for a ‘final walk-around’ to ‘confirm … that all doors and other opening[s] are closed flush.’ A Swissport trainer reported they were told by Link staff that walk-arounds were the duty of the flight crew, not the dispatcher. However, the training material provided by Link was for aircraft ramping and dispatch duties, not flight crew duties. The training information provided by Link did not provide any detail relating to propeller straps or their use.
In its investigation report into the occurrence, Swissport stated that a dispatcher walk-around was not required since no standard operating procedure for a dispatcher walk-around had been provided by Link. However, both the Standard ground handling agreement (SGHA) and Swissport’s GOM stated that Swissport’s procedures should be applied in the absence of ‘instructions’ or a ‘specific procedure’ from Link.
If this were to be the case, Swissport’s GOM stated that a walk-around was required for all aircraft dispatches, which was to be a check around the entire aircraft perimeter immediately prior to departure. On the other hand, if Link’s instructions had clearly specified that Swissport staff were not to conduct a walkaround, then complying with this would be consistent with the GOM.
Regardless of obligations under the SGHA, Swissport’s GOM strongly emphasised the need for a dispatcher walk-around, and the walk-around prescribed had more detail than in the training material Link provided. In contrast to Swissport GOM procedures, the training actually given to Swissport ground staff did not require a full-perimeter walkaround, and only required them to observe flight crew moving from the cargo bay door into the cabin, to ensure that doors and hatches were flush with the fuselage, and to ensure that the pogo stick was stowed. CCTV footage from Canberra Airport confirmed that a full-perimeter walk-around was not generally done. Including a complete dispatcher walk-around in the dispatch process would provide a second check that nothing critical has been missed before departure.
It is important to note that in this occurrence, since the GOM did not mention propeller straps, it is not certain that the dispatcher would have noticed the strap if Swissport’s full-walkaround had been implemented.
Audits can be an effective method to detect non-compliance with standard procedures and training. In this case, dispatch audits were conducted by the same Swissport personnel that conducted the dispatcher training. These audits might have been sufficient to prevent dispatchers deviating from the training, but it is not likely that they would detect when the training (and dispatcher actions) deviated from Swissport’s GOM or, more importantly, from the operator’s specific requirements.
Flight crew not informed of fuselage penetration
After realising that an object had penetrated the fuselage, the CM did not inform the flight crew immediately, because this would disrupt the sterile flight deck. Link’s Cabin crew operating manual (CCOM) required cabin crew members to inform flight crew of cabin emergencies as an immediate priority, even with sterile flight deck procedures in place. However, the time between the occurrence (at around the time the aircraft became airborne) and the CM contacting the flight deck (25 seconds after take-off) was not unreasonable, given the unexpected nature of the occurrence, and there being no apparent critical danger requiring an immediate response.
After this, however, the CM spoke to the flight crew several times but did not communicate the nature of the emergency (primarily being an object that had penetrated the fuselage) and this type of information was not sought by the flight crew. This left the flight crew under the impression that the emergency related only to the medical condition of a passenger, rather than the state of the aircraft. In accordance with the CCOM, cabin crew were required to ensure flight crew were made aware of the nature of an emergency or abnormal situation as soon as was practical.
Based on the understanding that a passenger was injured, the flight crew responded quickly and appropriately, returning the aircraft to Canberra Airport. In this case, the flight crew would likely not have done anything differently if they had known more about the nature of the emergency. However, the CM had no way of knowing whether there was unidentified damage to the propeller or engine, which could be anticipated if the debris is recognised as being from a propeller strap. The CM also would not have been able to identify damage to other systems, which is a reasonable possibility when any object penetrates the fuselage. If unidentified damage had occurred, the flight crew’s response to any consequential events would have been affected by their assumption that the emergency was not related to the aircraft itself.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the aircraft preparation and foreign object damage event involving Saab 340B VH-VEQ at Canberra Airport, Australian Capital Territory, on 10 November 2022.
Contributing factors
The aircraft was released for flight with the propeller strap still attached to the left propeller. Parts of the strap assembly subsequently penetrated the fuselage during take-off, injuring one passenger.
The first officer did not remove the propeller strap as part of the final external check (walk‑around) of the aircraft.
The captain did not notice the propeller strap or the incorrect propeller position prior to engine start.
The dispatch coordinator did not notice the propeller strap or, during the engine start, the unusual propeller motion.
On one-third of the Link Airways Saab 340B flights for which video surveillance was examined, including the occurrence flight, the flight crews did not fit the strap extension between the propeller strap and the airstairs. As the cabin door could not be closed with the strap extension in place, its correct fitment would almost certainly prevent a flight from proceeding with a propeller strap fitted. (Safety issue)
The propeller strap did not have a high-visibility streamer attached, and Link Airways did not effectively manage the condition of propeller straps for its Saab 340B fleet. This affected the visibility of the straps during ground operations. (Safety issue)
Guidance provided by Link Airways for training of Swissport dispatch coordinators did not explain the appearance, function and importance of the propeller straps.(Safety issue)
Other factors that increased risk
Swissport did not ensure that the implemented training and audits for Link Airways Saab 340B dispatches incorporated all of the elements required in its Ground operations manual for pre-departure walk-arounds. (Safety issue)
The cabin manager did not tell the flight crew that an object had penetrated the fuselage. While this had no bearing on the outcome, it limited the information available to the flight crew if aircraft systems had been damaged.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: On one-third of the Link Airways Saab 340B flights for which video surveillance was examined, including the occurrence flight, the flight crews did not fit the strap extension between the propeller strap and the airstairs. As the cabin door could not be closed with the strap extension in place, its correct fitment would almost certainly prevent a flight from proceeding with a propeller strap fitted.
Safety issue description: The propeller strap did not have a high-visibility streamer attached, and Link Airways did not effectively manage the condition of propeller straps for its Saab 340B fleet. This affected the visibility of the straps during ground operations.
Link training guidance lacked details regarding propeller straps
Safety issue description: Guidance provided by Link Airways for training of Swissport dispatch coordinators did not explain the appearance, function and importance of the propeller straps.
Safety issue description: Swissport did not ensure that the implemented training and audits for Link Airways Saab 340B dispatches incorporated all of the elements required in its Ground operations manual for pre‑departure walk-arounds.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future.
Additional safety action by Link Airways
In addition to the safety action described above, Link Airways took the following safety action:
The Cabin crew operating manual was amended to provide additional clarity regarding the need for the cabin manager to contact the flight crew in the event of an emergency.
A risk assessment was conducted for the potential adoption of an intercom system between pilot and dispatcher, in order to improve communication (on the basis of this risk assessment, such a system was not implemented).
Additional safety action by Swissport
In addition to the safety action described above, Swissport planned to review its Ground operations manualregarding positioning of the dispatcher.
Glossary
CCTV
Closed-circuit television
CCOM
Cabin crew operating manual
CM
Cabin manager
FCOM
Flight crew operating manual
FO
First officer
GOM
Ground operations manual
SATGHM
Scheduled air transport ground handling manual
SGHA
Standard ground handling agreement
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew, cabin manager, dispatcher, and dispatch trainers
Link Airways
Virgin Australia
Swissport
Saab
Canberra Airport
the Civil Aviation Safety Authority
aircraft cockpit voice recorder and flight data recorder.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain, first officer, cabin manager, and dispatcher
dispatch trainers
Link Airways
Virgin Australia
Swissport
Civil Aviation Safety Authority
Saab
Swedish Accident Investigation Authority.
Submissions were received from Link Airways and Swissport.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]This inspection was a ‘Line Check 1’ (or LC1) daily inspection.
[2]Also referred to as a prop (propeller) strap extension.
[3]Airstairs are a passenger and crew stairway that form an integral part of the aircraft and, after use, are hinged up and stowed on board.
[4]A ground handling person who coordinates and performs various activities during dispatch. In this case, the role did not have any direct regulatory or airworthiness responsibilities.
[5]The core engine speed can differ from the propeller speed, as the two are not mechanically linked. When the engine is running, the exhaust flow exerts a rotational force on the propeller via a turbine.
[6]Sterile cockpit procedures are part of the Civil Aviation Safety Regulations and require pilots to only perform duties essential to the aircraft’s safety during certain critical phases of flight, including take-off.
[7]Stringers are structural components that run the length of an aircraft fuselage.
[8]After the prop straps are removed, the propeller is to be moved to the ‘X’ position with the blades at a 45° angle. See Use and stowage.
[9]The tail strut, or ‘pogo stick’ supports the tail of the aircraft during loading/unloading and refuelling. It is stowed in the cargo bay of Saab 340B aircraft.
Occurrence summary
Investigation number
AO-2022-055
Occurrence date
10/11/2022
Location
Canberra Airport
State
Australian Capital Territory
Report release date
09/05/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation
Occurrence class
Serious Incident
Highest injury level
Minor
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
Saab 340B
Registration
VH-VEQ
Serial number
340B-424
Aircraft operator
VEE H AVIATION PTY LTD (operating as Link Airways)
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
On 19 October 2022, a Boeing 737-8FE aircraft, registered VH-YFT and operated by Virgin Australia, departed Brisbane, Queensland on a scheduled passenger flight to Sydney, New South Wales. After the aircraft reached top of descent, the crew contacted air traffic control (ATC) and were issued a clearance for a standard arrival to land on runway 34L in Sydney. However, runway 16L was operational at the time. When the crew transferred to Sydney Approach, they were instructed to expect runway 16L. While this initially led to some confusion between the crew and ATC, the correct runway was established, and the crew performed an independent visual approach to runway 16L.
What the ATSB found
The ATSB found that an incorrect clearance was verbally communicated to VA942, which was not identified by the enroute air traffic controller or the crew during the read-back or hear-back. This error likely occurred due to momentary interference of related, coinciding information about the assigned flight level (FL 340) and the runway (34L).
However, the information entered into the air traffic management system was correct. Consequently, the approach controller identified and rectified the error with the crew of VA942, well before an undesirable state for landing had the opportunity to develop.
Safety message
Slips in verbal communication can happen at any time. They can pose a threat to safe operations if the content of the message is inaccurate, and then not identified during the read-back or hear‑back process.
Pilots and air traffic controllers are reminded to seek verification when there is confusion or a misunderstanding on any information in a clearance that conflicts with other information they have previously received and understood.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 19 October 2022, at 0148 Coordinated Universal Time (UTC), a Boeing 737-8FE aircraft, registered VH-YFT and operated by Virgin Australia as flight number VA942, departed Brisbane Airport, Queensland, on a domestic scheduled passenger flight to Sydney, New South Wales (Figure 1).
At about 0220, the flight crew contacted air traffic control and advised they were maintaining FL 340.[1] The enroute controller issued the flight crew a BOREE 3 ALPHA standard instrument arrival (STAR)[2] for runway 34L.[3] The flight crew read this clearance back to the controller, including runway 34L.
The enroute controller later advised the flight crew that the Sydney Airport automatic terminal information service (ATIS)[4] had been amended. However, both the original and amended ATIS indicated that runways 16L and 16R were in operation for arrivals and departures.
During the descent, the crew contacted Sydney Approach, informing them they were on descent to 10,000 ft and acknowledged receipt of the current ATIS. At this point, the aircraft was at about 17,275 ft and 6 NM from waypoint[5] BOREE. The approach controller replied, confirming runway 16L and to expect an independent visual approach[6] via the STAR to 6,000 ft.
Immediately, the crew questioned the runway assignment informing the approach controller they had been assigned 34L, rather than 16L. The approach controller confirmed that runways 16L and 16R were in operation, and that 16L had been assigned. The flight crew accepted runway 16L, and the approach controller advised the crew that ‘…if you do need some extra track miles to get down to let me know [to] give you some vectors.’ The aircraft continued as cleared and joined the approach as normal.
At about 0245, the approach controller contacted the enroute controller and notified them that VA942 had been incorrectly issued runway 34L. The enroute controller then checked their recorded radio transmissions. They then verified with another aircraft, also recently issued the BOREE 3A Arrival, that they had been assigned 16L, as intended.
Figure 1: Flight path of VA942 with respect to when the runway was assigned.
Source: FlightAware and Google Earth, annotated by ATSB.
Context
Enroute controller
The enroute controller had about 24 years’ experience and was rated, endorsed, and fulfilled all recency requirements. They were responsible for 2 adjacent sectors during their shift.
Work schedule
The enroute controller reported fit for duty for their planned 8-hour shift at 0530 local time, with a scheduled shift end time of 1330. In the previous 3 weeks, the enroute controller had accepted some additional overtime shifts and extended shifts. They reported obtaining good quality 6‑7 hours sleep the night before, and their usual sleep in the previous 72 hours.
The error occurred approximately 10 minutes prior to their scheduled shift end time, and the controller reported feeling ‘fully alert’ at the time. After the occurrence, the work scheduling software indicated that the shift had a predicted fatigue level of high.[7] However, fatigue was not considered to be a contributing factor.
Workload
It was reported that the sector was fully staffed that day, with provision for in-shift relief breaks. The controller advised they were ‘relatively busy’ and were communicating with 10 other aircraft around the time of the occurrence. They estimated that they were operating at a capacity of about ‘six out of ten’. Overall, the workload across the 2 sectors was manageable at the time of the occurrence, and not considered to be a contributing factor.
Issuing of clearance
The enroute controller for this sector provided initial sequencing, STAR clearances, and initial descent instructions for aircraft bound for Sydney Airport from the MAESTRO system. MAESTRO is a tactical traffic sequencing software used for aircraft arrivals at Sydney Airport, and other domestic airports across Australia. It uses actual position and speed information of aircraft to determine the landing order and displays this information to air traffic controllers. This information can then be used to inform decisions about aircraft speed control, vectoring or holding to maintain an orderly traffic flow.
When the enroute controller issues a clearance to aircraft, they check the runway allocation in MAESTRO, then select the aircraft designator on the air situation display (ASD), which opens a drop-down list of runways. The controller then selects the issued runway on the ASD and during the hear-back process, checks that all the information is correct. The aircraft designator also displays other information, including the aircraft's flight level.
At the time of the occurrence, the ASD and MAESTRO displayed flight VA942 assigned for runway 16L and maintaining FL 340. The enroute controller issued the clearance using the standard phraseology, and reported they were looking at the flight level in the aircraft designator when they did this.
Standard Terminal Arrival Route (STAR) clearance
The BOREE 3A arrival positioned aircraft to receive radar vectors to final for all Sydney Airport runways, including 16L and 34L. Waypoint BOREE is the initial approach fix, and the track then later branches for the different runways at waypoint OVILS (Figure 2). The crew reached waypoint BOREE about one minute after the correct runway was confirmed, which required that the approach be re-briefed by the crew. In this case, the change to the approach required that the aircraft fly the procedure as briefed to OVILS where radar vectors would then be provided by ATC.
Figure 2: BOREE 3A Arrival STAR Chart
Source Airservices Australia, annotated by ATSB.
Virgin Australia procedures
Virgin Australia’s flight procedures for the verification of weather and terminal information included a requirement for flight crew to independently review information from the ATIS during arrival preparations.
Virgin Australia did not specifically mandate flight crews to conduct a cross check between the clearance and ATIS. They reported that this would be difficult to implement due to several factors:
STARs can be issued at various distances depending on the destination
STARs can be received before the ATIS information is received
ATIS can’t be specified at set distances, due to the operational mix of aircraft communication addressing and reporting system (ACARS)[8] and non-ACARS aircraft
dynamic runway changes can occur without notice, or without it highlighted in the ATIS information (e.g., ’from time XXX expect RWY xx’)
During the enroute phase of the flight, the enroute controller notified the crew of the ATIS update from ‘X‑ray’ to ‘Yankee’. Both transmissions listed ‘RWY: 16L AND R FOR ARRS AND DEPS’.
The enroute controller later advised they were ‘surprised’ that the crew did not question the runway assignment during the read-back process, because the assigned runway was different to that stated in the ATIS.
Safety analysis
The enroute controller reported that when the crew of VA942 initially made contact and the STAR was provided, runway 16L was selected from the available runways as intended. However, they were looking at the flight level (FL 340) on the ASD, when they issued the clearance for 34L. This skill-based error most likely occurred because of the interference of information between FL 340 and 34L. Verbal slips of this nature are more likely to occur when there is a high degree of similarity between the presentation of simultaneous, related information, while performing a familiar and repetitive action.
The read-back and hear-back procedure was the opportunity for both parties to detect the error before it propagated further. However, on this occasion the error went undetected. The radio recordings confirmed that the standard phraseology was used during the communication, and the flight crew correctly read-back the assigned runway 34L, and this was acknowledged by the enroute controller.
There was information available to the crew in the ATIS indicating that runway 34L was not in operation. This provided an opportunity to identify and question the conflicting clearance and ATIS information between themselves, but the evidence obtained by ATSB showed that they did not enquire further with ATC until they were in contact with the approach controller, who correctly assigned 16L.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the air traffic control error involving Boeing 737, VH-YFT, near Sydney Airport, New South Wales on 19 October 2022.
Contributing factors
The enroute controller verbally issued the clearance to the flight crew to land on runway 34L instead of 16L, which was not identified during readback. This slip was likely due to the similarity between the flight level (FL 340) and runway 34L.
Other findings
The flight crew did not enquire further with ATC about the runway assignment of 34L until the approach controller provided runway 16L.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the involved air traffic controllers
FlightAware
Airservices Australia
Virgin Australia Airlines Pty Ltd
VATPAC ATC Standard Operating Procedures Hub
References
Safety behaviours: human factors for pilots 2nd edition. Resource booklet 4 Communication. Civil Aviation Safety Authority
Air Traffic Flow Management: Harmony for ANSPs. Briefing Paper for Pilots. Version 5. Air Services Australia 2016.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the involved air traffic controllers
Airservices Australia
Virgin Australia Airlines Pty Ltd
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Flight level: At altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 340 equates to 34,000 ft.
[2] Standard instrument arrival (STAR): A designated IFR arrival route linking a significant point, normally on a ATS route, with a point from which a published instrument approach procedure can be commenced.
[3] Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[4] Automatic Terminal Information Service (ATIS): A continued and repetitive voice frequency broadcast, which contains standard operational information such as the type of approaches to expect, the runways in use, and weather conditions. Updated ATIS information is labelled in terms of ascending phonetic code letters and pilots confirm with ATC that they have received and understood the most up to date information.
[5] Waypoint: A defined position of latitude and longitude coordinates, primarily used for navigation.
[6] Independent visual approach (IVA): A procedure to parallel or near-parallel runways which allows a visual approach to one runway independently of approaches occurring on an adjacent parallel or near parallel runway.
[7] ‘Predicted Fatigue Level’ is defined in the Air Traffic Services (ATS) Fatigue Risk Management Procedure, and includes current and future predicted fatigue level, based upon tactical roster management principals.
[8] Aircraft Communications Addressing and Reporting System (ACARS): digital data link system for the transmission of messages between aircraft and ground stations.
Occurrence summary
Investigation number
AO-2022-052
Occurrence date
19/10/2022
Location
Near Armidale
State
New South Wales
Report release date
06/06/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8FE
Registration
VH-YFT
Serial number
41028
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes

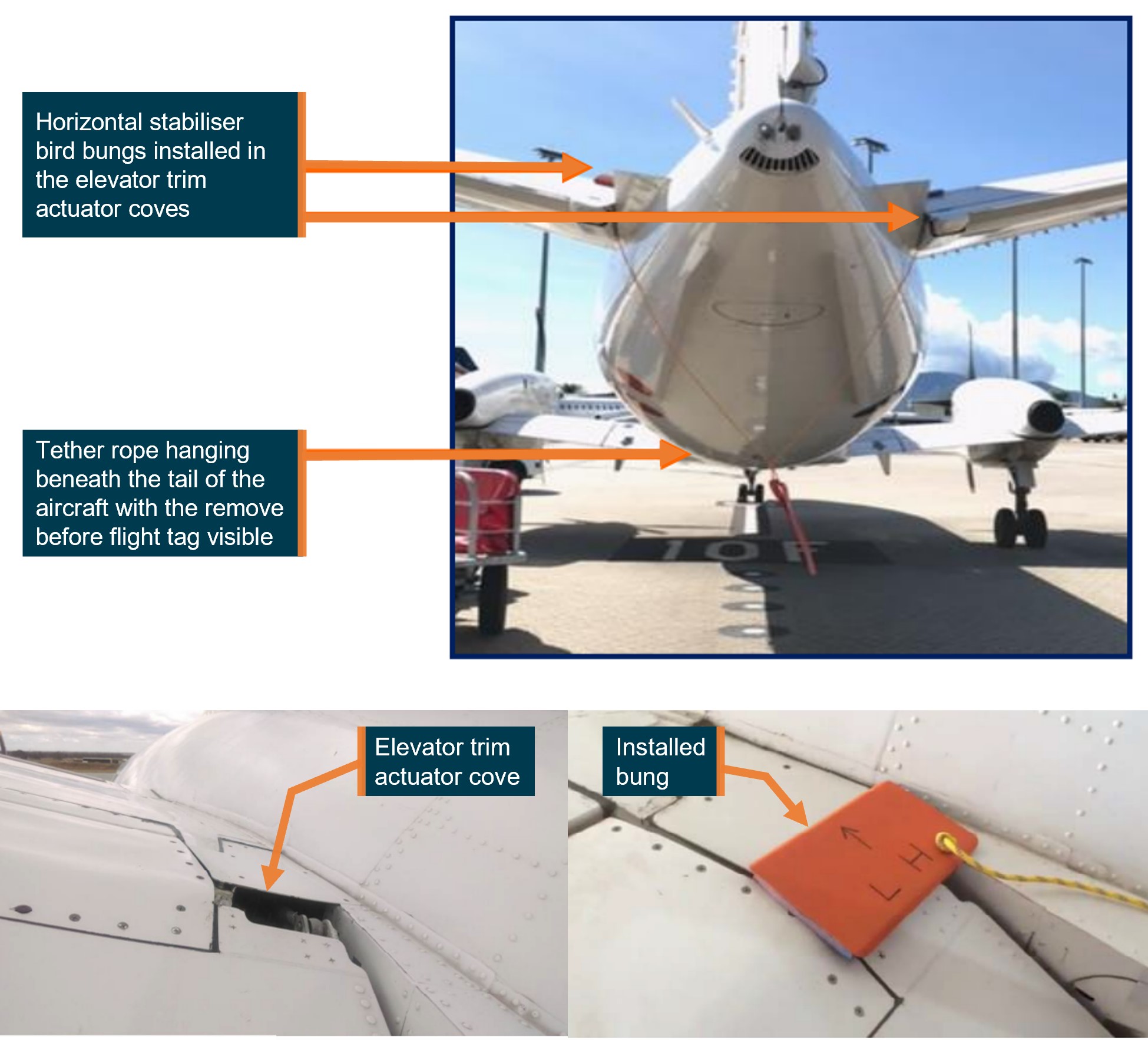
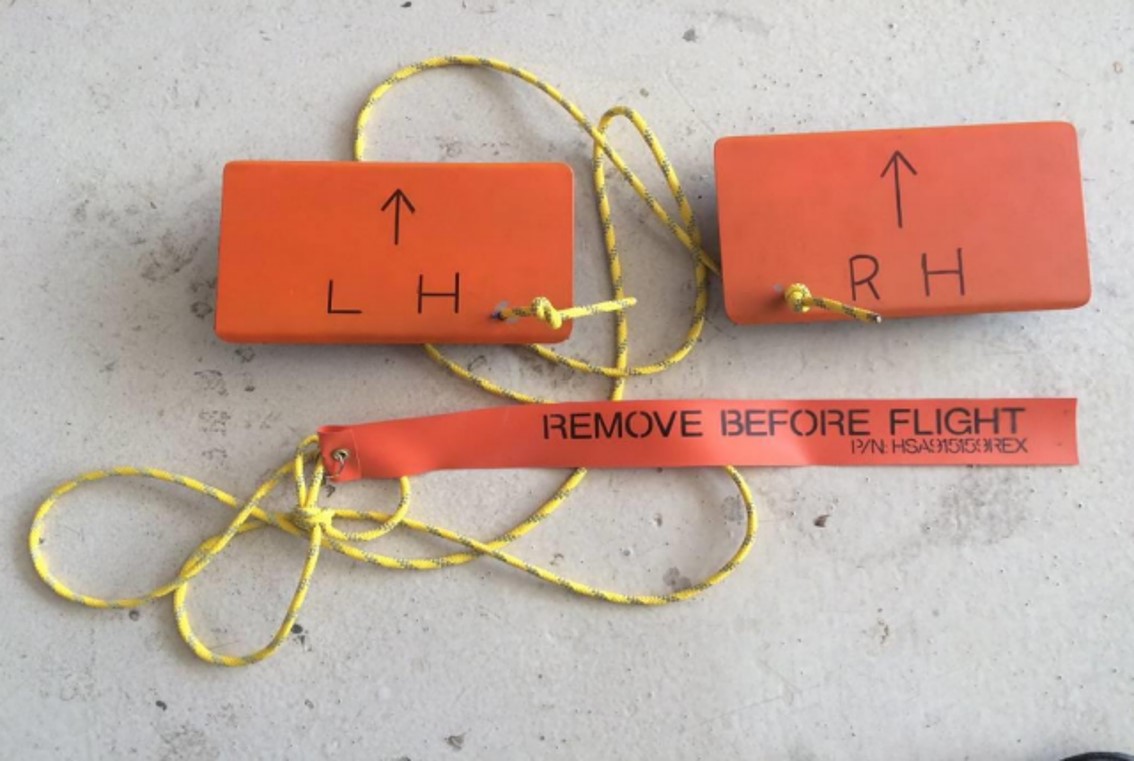
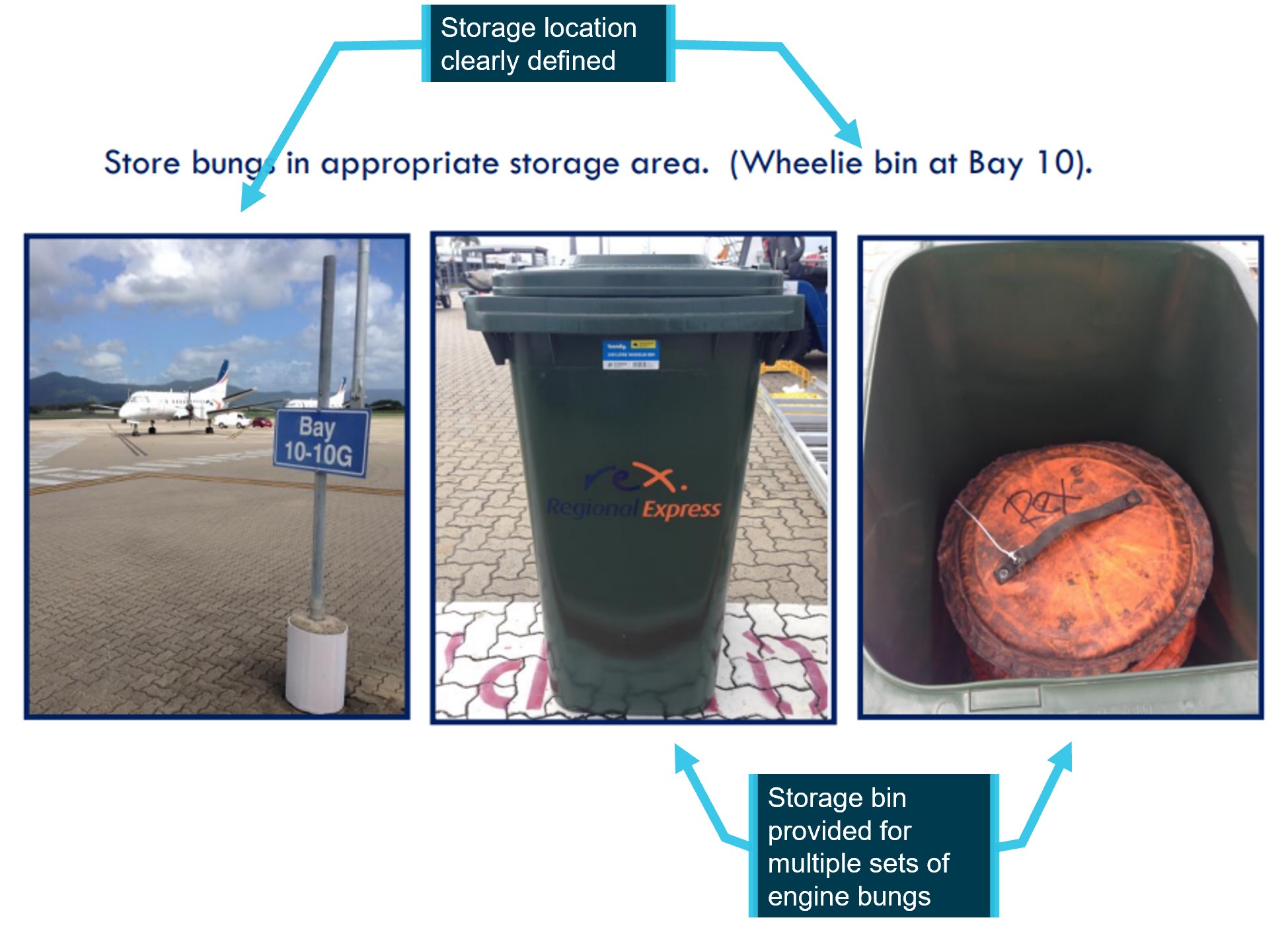




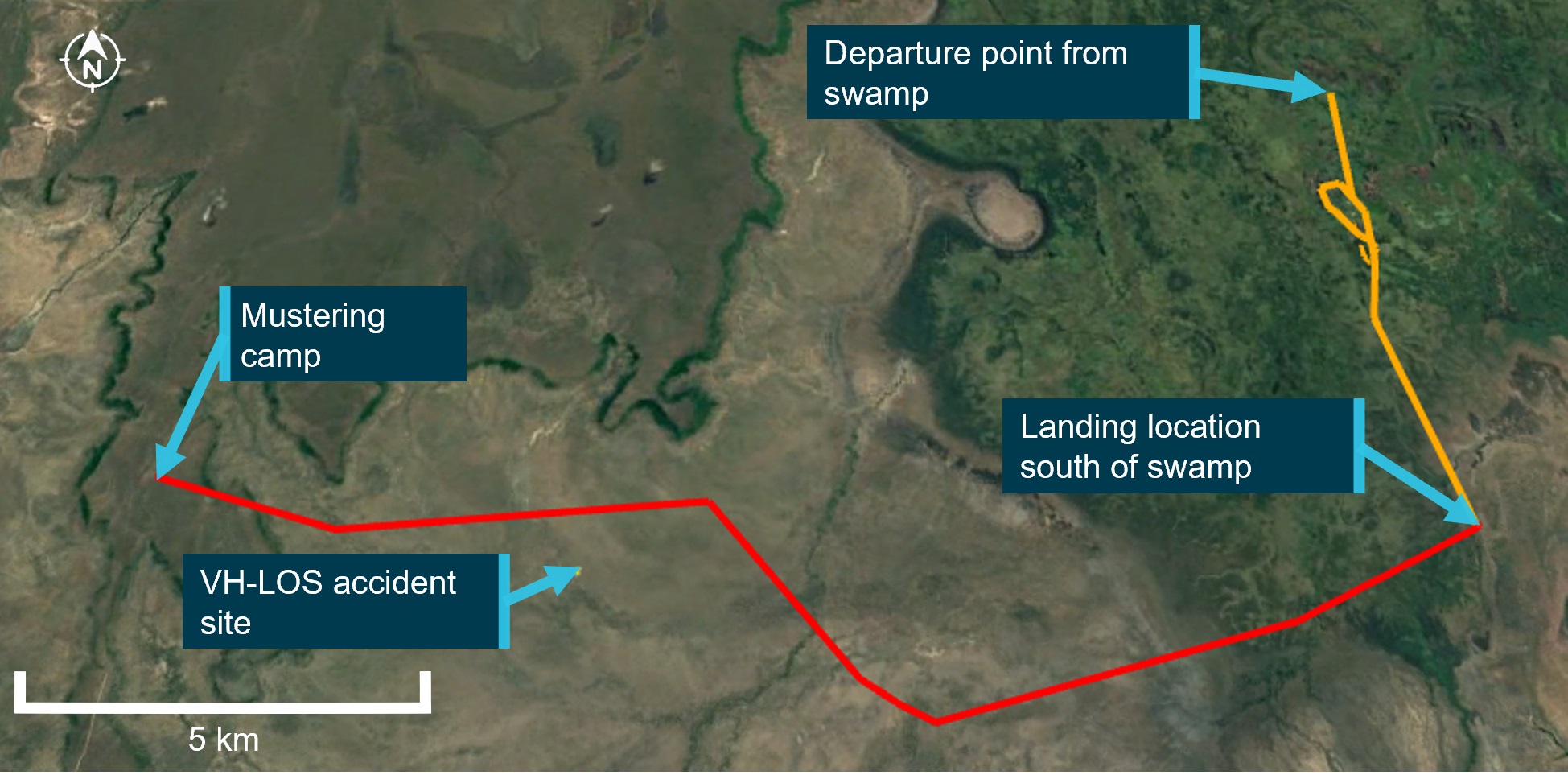



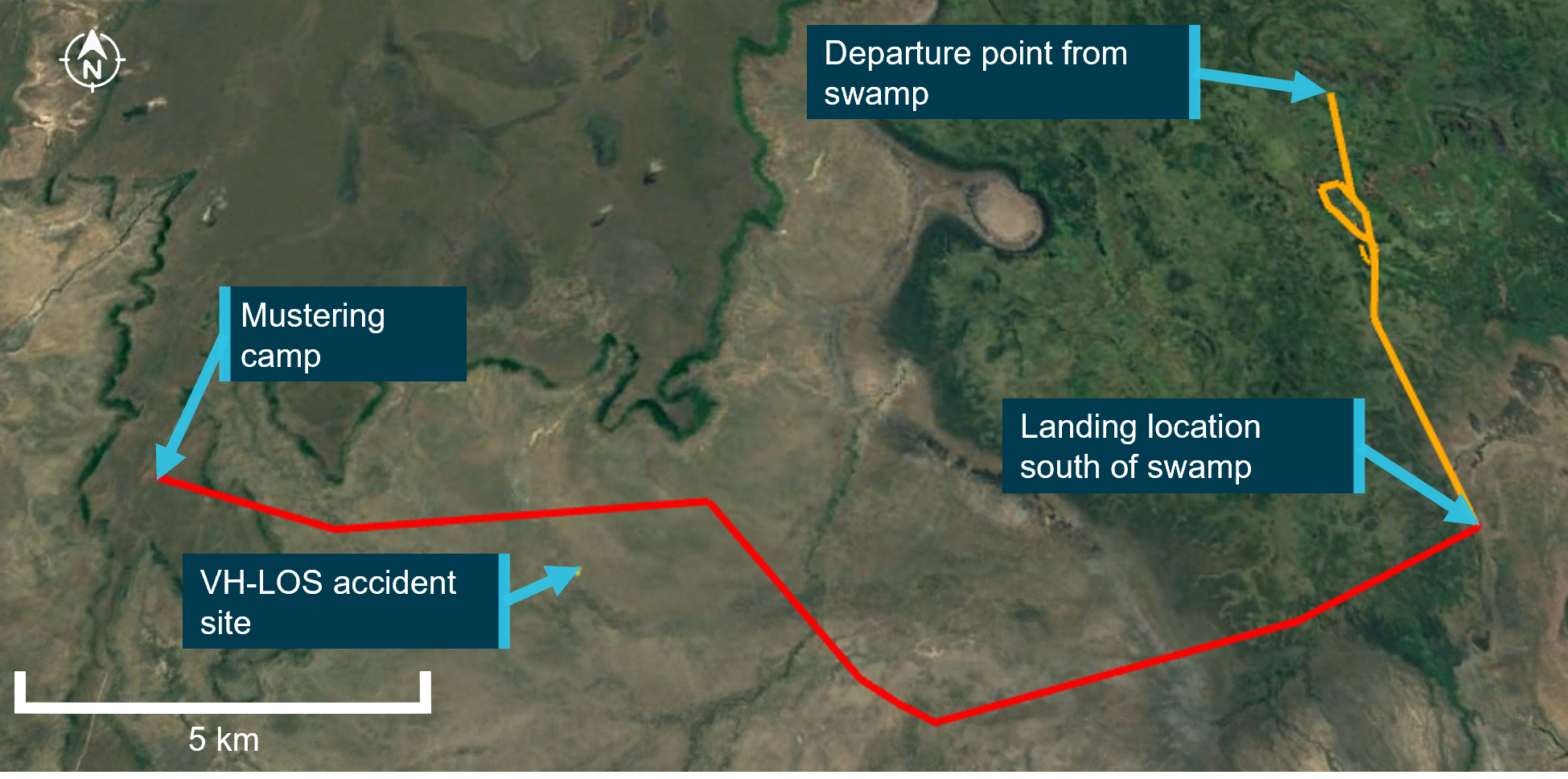
![Figure 1: ADS-B[5] derived flight data showing the approximate location of the radio altimeter failure on approach to Sydney](/sites/default/files/inline-images/AO-2022-056%20Figure%201.jpg)