Rail operator Aurizon has taken steps to better identify out-of-gauge loads at its Stuart terminal, after a bridge was damaged in Rockhampton due to an overheight trailer;
The ATSB encourages operators to identify and embrace cost-effective ways to enable rail staff to more accurately identify loads with the potential to cause damage or injury during transit.
A Rockhampton railway bridge was damaged by a tipping trailer that had been loaded onto a freight train despite being too high for the rail network, an Australian Transport Safety Bureau report details.
The tipping trailer was loaded onto the train at the Stuart terminal, near Townsville, on 16 September 2021.
“Stuart terminal was cooperatively operated between Linfox and Aurizon, with Linfox responsible for the movement of road freight to and from the terminal, and Aurizon conducting the loading of rail wagons and rail operations,” ATSB Director Transport Safety Dr Michael Walker explained.
“The tipping trailer was a Linfox asset rather than customer freight and, as such, it was not managed through Linfox’s normal process, which required any non-standard loads to be referred to management for approval.”
The trailer, when loaded onto a rail wagon, reached a height of 4.41 m above the rail – almost 60 cm over the maximum permissible height on the North Coast Line from Townsville to Brisbane.
“This was not identified by the heavy lift (forklift) operator during loading, likely because they did not have a nearby reference and were not expecting the load would be out of gauge,” Dr Walker said.
“The rail operator also did not routinely apply a process at the Stuart terminal to verify that the dimensions of non-standard loads were within the permissible profile.”
During the subsequent journey to Brisbane, the trailer’s hydraulic lifting post collided with the overhead structure of Alexandra Bridge in Rockhampton, resulting in damage to both the bridge and the trailer. There were no injuries or damage to the train.
Since the incident, Aurizon has installed a jangle bar at Stuart terminal, and is assessing options for automated controls.
The rail operator has also updated its freight management system and booking system, and implemented procedures for the identification of non-standard freight.
The ATSB encourages all operators to identify and embrace cost-effective ways to enable rail staff to more accurately identify loads with the potential to cause damage or injury during transit.
“In the absence of measuring equipment, or nearby objects of a known and relevant height, it is difficult to accurately estimate the dimensions of loaded freight, especially when judging the height of tall freight from ground level,” Dr Walker said.
“Tools to alleviate this limitation will be significantly more accurate and come with minimal cost.”
Interim report details investigation’s progress so far;
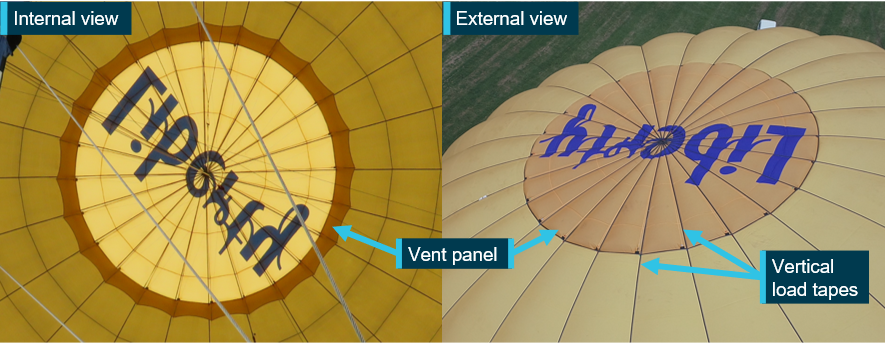
Report details that about 10 minutes into the flight, the pilot noticed a gap between the vent panel and the edge of its vent aperture;
Incident balloon was the only one of its kind with the modified vent design produced by the manufacturer.
The Australian Transport Safety Bureau has provided an update on its ongoing investigation into the collision of a hot air balloon, with 13 passengers and a pilot on board, with buildings in suburban Melbourne.
The interim report details evidence gathered so far in the ATSB’s investigation. It contains no analysis or findings, which will be detailed in the investigation’s final report.
The balloon had departed from Royal Park on the morning of 20 April 2022, for an intended destination of Moorabbin Airport.
“Passenger photos showed the vent panel, designed to control the release of air from the top of the balloon was almost, or already, pushing through its opening at normal operating temperatures,” ATSB Director Transport Safety Stuart Macleod said.
About 10 minutes into the flight, the pilot noticed a gap between the panel and the edge of its vent aperture. The pilot was unable to seal it using the deflation system lines.
“As the flight progressed, the gap between the vent aperture and the vent panel expanded and altitude control became increasingly difficult,” Mr Macleod said.
After an unsuccessful attempt to land in Fawkner Park, the pilot tracked the balloon to the south with the intent to land at Elwood Beach. Before reaching the beach, however, with the pilot unable to maintain altitude, the balloon would land outside the entrance of an apartment building in Elwood.
Three passengers sustained minor injuries.
The interim report notes the accident flight was the balloon’s first since manufacture, and that prior to its manufacture in 2021, the balloon’s operator requested a larger vent (both the vent aperture and panel) to increase the balloon’s descent performance.
As such, the incident balloon was the only one of its kind with the modified vent design produced by the manufacturer.
Following the incident, the ATSB arranged for the balloon’s deflation system to be tested. During that testing, the balloon was tethered to the ground and its envelope inflated.
“During the test, at an internal envelope temperature of about 90 °C, which was below the maximum allowable temperature of 124 °C, edges of the vent panel between the vertical load tapes pushed up through the aperture creating many gaps for internal envelope air to vent out,” Mr Macleod noted.
“Attempts to seal the gaps using the parachute vent line and white line were unsuccessful, and at higher temperatures, the gaps became larger and more numerous.”
According to the pilot of the incident flight, who witnessed the testing, and an analysis of passenger video, the vent gaps were very similar to those observed during the incident flight.
Mr Macleod noted that as the investigation continues the ATSB will examine the balloon manufacturer’s processes and procedures for modifying the balloon’s design, and the balloon’s acceptance into service.
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.”
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
The occurrence
On the afternoon of 14 November 2022, a Boeing 737-800 aircraft (B737), registered VH-IWQ was being operated by Virgin Australia on a passenger air transport flight between Melbourne, Victoria and Sydney, New South Wales. The flight from Melbourne had been uneventful and the flight crew of the B737 were given a clearance by the aerodrome controller (ADC)[1] to land on runway 25 at Sydney and vacate the runway at taxiway Yankee. After vacating the runway, the flight crew contacted the surface movement controller east (SMCE)[2] and were issued a clearance to taxi to their assigned parking bay on the domestic apron via taxiway Golf, and to cross runway 34 left (34L). The SMCE deactivated the taxiway stop bar[3] for the B737 to cross the runway.
At the time the clearance was issued for the B737 to cross the runway, an Airbus A380-841 (A380) aircraft, registered 9V‑SKQ and operated by Singapore Airlines, had just commenced its take-off on runway 34L and was accelerating through a groundspeed of about 40 kt. The B737 was on taxiway Golf and about 300 m from runway 34L when its flight crew saw the A380 on initial climb. They remarked to each other that this was unusual and thought they had been instructed to cross runway 34L ahead. They contacted the SMCE and received confirmation they were clear to cross the runway and taxied to their parking bay. The B737 did not infringe on the 34L runway strip and there was no runway incursion.
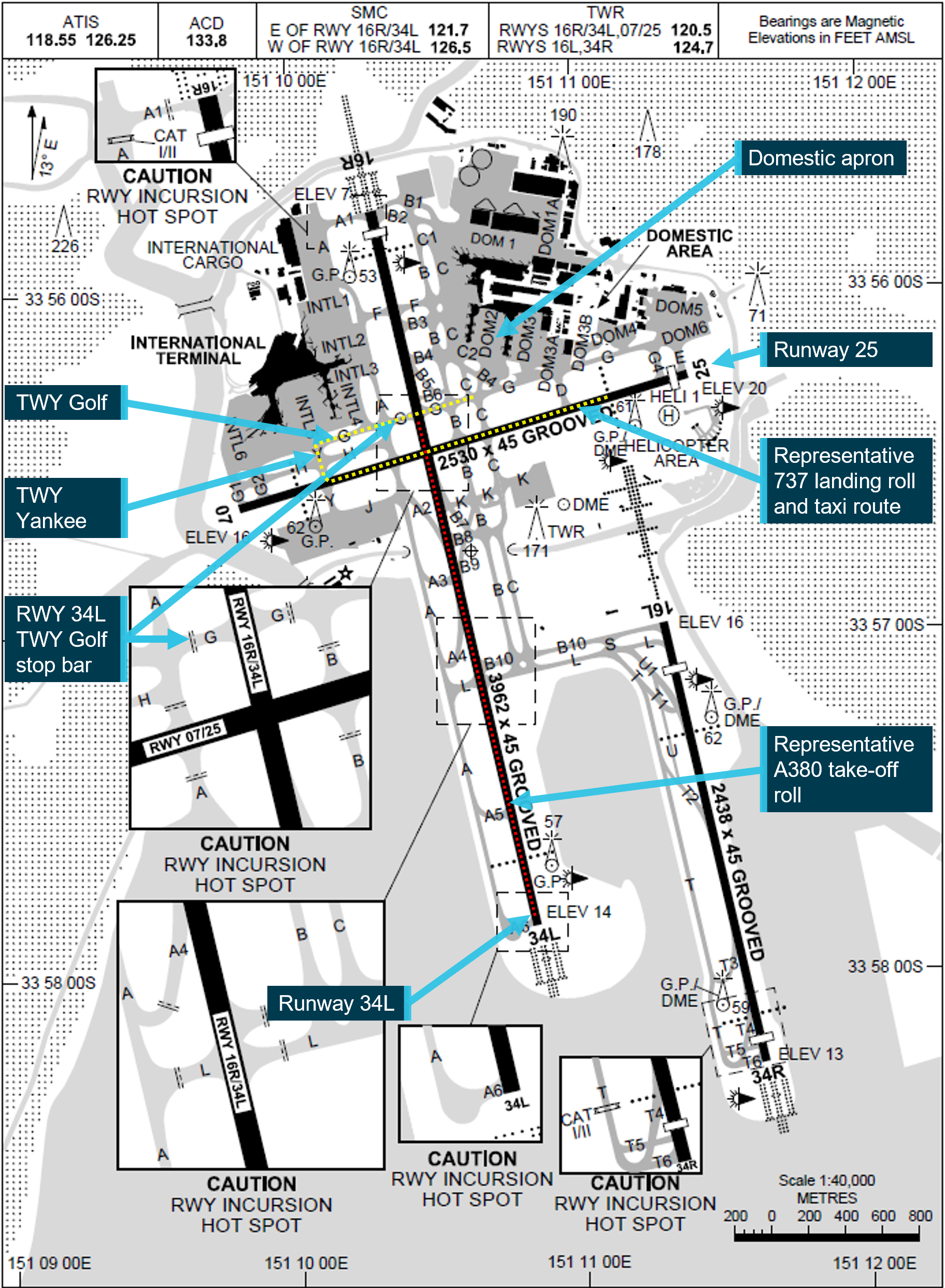
Figure 1 depicts the relative locations between runways 25 and 34L, representative ground tracks for the B737 and A380 together with the location of taxiways Yankee and Golf.
Figure 1: Extract from Sydney Airport aerodrome chart with runway (RWY) orientation and taxiway (TWY) layout
Source: Airservices Australia, annotated by the ATSB
Runway and taxiing operations
Strong westerly winds prevailed during the afternoon, with runway 25 being used as the duty runway for both arriving and departing aircraft. For aircraft requiring the use of a longer runway, 34L was available on request but was deactivated when not operationally required.
With runway 25 being used for arrivals, flight crews of landing domestic jet aircraft were typically required to vacate via taxiway Yankee or if operationally required, taxiway Alpha. The flight crew were then to contact the SMCE, who would issue the taxi clearance to the domestic apron, including the clearance to cross runway 34L.
Similarly, the surface movement controller west (SMCW) was responsible for coordinating taxi clearances for aircraft using the international apron. The SMCW had provided approval for the flight crew of the A380 to push back from their parking bay and issued the clearance to taxi to the runway threshold for 34L.
Activation of runway 34L and take-off of the A380
The ADC had activated runway 34L using the tower control and monitoring system. Soon after, the flight crew of the taxiing A380 had called ready for take-off. With the activation of the runway, the responsibility for separating aircraft and vehicles using that runway transferred to the ADC, including approving requests to cross or enter the active runway.
The SMCE and SMCW were alerted to the runway activation by notification chimes at their controller positions, which required their acknowledgement and insertion of a ‘34L ACTIVE’ strip in their flight progress strip board.[4] The SMCW and SMCE in turn used their hotline to the ADC to acknowledge the changed status of the runway and provide relevant details for aircraft or vehicles operating on that part of the aerodrome’s movement area. When the SMCE acknowledged the runway activation and placed the relevant status strip into their flight progress strip board, they requested (and were issued) clearance from the ADC, for an aircraft under tow to cross runway 34L.
After activating the runway, the ADC instructed the flight crew of the A380 to line-up and hold position. Soon after, the B737 flight crew were transferred to the tower frequency and established contact with the ADC. About a minute later, the ADC issued the B737 flight crew a landing clearance and passed information about the A380, which was lining-up on the crossing runway to hold position. The ADC issued the A380 flight crew their clearance to take-off as the B737 passed through 34L during its landing roll.
After landing and vacating the runway, the B737 flight crew transferred to the SMCE frequency. The SMCE subsequently issued the B737 flight crew their taxiing instructions and clearance to cross runway 34L, without coordinating the crossing of the active runway with the ADC.
Sighting limitations
The B737 operator required its flight crews to scan the runway approach path and runway environment prior to entering any runway, to identify potential traffic that could conflict with their safe crossing. Flight crew and airside vehicle drivers crossing runway 34L in the vicinity of taxiway Golf had several sighting limitations along the runway to the south, principally due to reprofiling of terrain that had occurred with the construction of General Holmes Drive (which passes under the airport south of taxiway Golf).
The ATSB examined any sighting limitations based on the time a B737 flight crew would have been scanning the runway environment as they approached the taxiway hold position and the performance of the A380 on its take-off roll. The ATSB found that the lower fuselage, wings and landing lights of an A380 would be shielded by terrain during the first part of the take-off roll and not visible to flight crew or vehicle operators approaching runway 34L along taxiway Golf. In addition, the oblique viewing angle of an A380 upper fuselage and tail at the maximum sighting range made it harder to identify aircraft during the early stages of the take-off roll.
Stop bar lighting and procedures
Operating the stop bars and runway guard lighting
The airport’s ground-based infrastructure included runways, taxiways and the associated airfield lighting systems, which were maintained by Sydney Airport Corporation Limited. The intersections of taxiways with runways were equipped with stop bar lighting, runway guard lighting[5] and movement area guidance signs. Those systems were intended to help reduce the incidence of runway incursions.[6]
Local procedures at Sydney required taxiway stop bars to be illuminated at all runway crossing points, irrespective of runway status.[7] Consequently, an air traffic controller was required to deactivate the taxiway’s stop bar for every clearance issued for a runway crossing or entry by taxiing aircraft or authorised vehicles. The responsible controller selected and deselected the taxiway’s stop bar using the airfield ground lighting (AGL) panel.[8] The location of the stop bar at the intersection of taxiway Golf with runway 34L is depicted in Figure 1.
As noted previously, when runway 34L was active, the ADC was responsible for separating aircraft and vehicles, and for operating the stop bars. When runway 34L was inactive and the runway had been released by the ADC, the SMCE in this case was responsible for both deactivating the stop bars and issuing the runway crossing clearance to flight crews of aircraft taxiing to the domestic terminal.
Advanced surface movement guidance and control system
Sydney Airport was equipped with an advanced surface movement guidance and control system (A-SMGCS) that provided tower controllers a surveillance picture of the airport’s surface movement areas. The A‑SMGCS interfaced with several related systems, including the airport surveillance radar, flight data system and AGL systems.
Data was shown on the A-SMGCS controller’s working position display, which included a map of the airport environment (runways, taxiways and apron/ramp), together with the position/identification of aircraft/vehicles and information about the status of the various related systems. The system also had several safety logic functions that included closing/opening a runway, airport configuration, operator role (including control over runways) and runway alerts and warnings. The safety logic detection parameters would activate an alert or warning when detecting a conflict between tracks on the runway. In this instance, a safety alert was not generated due to the B737 not entering the runway strip while the A380 was on its take-off roll.
Manual of Air Traffic Services procedures
The Manual of Air Traffic Services (MATS) procedures required that all runways in use were controlled by the relevant ADC and activation of all stop bars at the holding positions associated with that runway (where installed). The ADC controlling the runway was responsible for issuing clearances to cross or enter the runway and temporarily deactivating the stop bar at that relevant holding position to indicate the traffic may proceed. Stop bars were installed on the runways at Brisbane, Canberra, Melbourne, Perth and Sydney airports.
At Canberra, Melbourne and Brisbane, the stop bars were only activated when the runway was in use. When runways at those airports were not in use, the stop bars were deactivated and the inactive runway did not need to be released to the SMC.[9] This was consistent with the guidance provided in MATS.
For Sydney and Perth airports, stop bars were continuously active irrespective of the runway status. When a runway was not in use, the ADC released the runway to the SMC who was then responsible for authorising flight crews or vehicle drivers to cross/enter the runway and also operated the stop bar lighting system.[10] While this was inconsistent with MATS, Airservices Australia, the airport operators and local users had implemented local procedures to facilitate the activation of stop bars on all runways, irrespective if they were in use and under the control of an ADC.
Operational standards review
Airservices Australia’s Sydney tower unit had been subject to a routine national check and standardisation supervisor review in June 2022, covering the period from completion of the last review in May 2019. The purpose of review was to ensure that the unit was meeting required documentation and operational standards, together with consideration of any local unit procedures that could be considered for national implementation.
The review identified that Sydney tower operated stop bars differently to other airports, including their use when the runway was not being used, when stop bar activation was not required. That finding was not identified to be safety critical but recommended that the process for stop bar operation should be standardised. The actions identified to address the finding included a clarification to MATS that the controller with control of the runway was to have sole ownership of the associated stop bars and that the stop bar procedures for Sydney were to be aligned to the national standardised practice.
The revised procedures were subsequently implemented in March 2024. In addition, in July 2024, the AGL system was updated, enabling the jurisdictional transfer of stop bar operation to the ADC at times the runway was in use and at those times, the stop bars could not be deactivated by the SMC.
Surface movement controller east information
The controller performing SMCE duties at the time of the incident had more than 30 years’ experience and had worked in Sydney Tower for most of that period. The controller was rated for all positions in Sydney Tower and previously held ratings for training, checking and supervising tower operations. They had successfully completed 2 days of their regular scenario based tower simulator training about 10 days prior to the incident and their 6-month proficiency check in August 2022.
The SMCE had signed on for duty at 1320 and felt they were adequately rested and fit for their duty. The controller had occupied 2 other positions (with 30-minute breaks between each position) prior to commencing the SMCE duties. At the time of the incident, the controller had been performing SMCE for about 1 hour 15 minutes and recalled feeling 4-a little tired, less than fresh.[11] The ATSB reviewed the controller’s roster for a 6-week period, however, there was insufficient evidence to suggest that the controller’s performance was affected by fatigue.
The incident flight was the first activation of runway 34L for a departing or arriving aircraft while the controller was in the SMCE position. Prior to this, the SMCE had cleared the flight crew of about 18 landed jet aircraft to taxi to the domestic terminal. These all included a clearance to cross the inactive runway 34L and deselection of the stop bars. This was in addition to the SMCE’s other workload, which included coordinating ground movements for arriving turboprop aircraft, departing aircraft (including approving pushbacks from the parking bay), and other vehicles operating on the airport.
ATSB observations
The ATSB made the following observations regarding the incident:
When the flight crew of the B737 landed and contacted the SMCE for taxiing instructions and a clearance to their parking bay, the SMCE did not correctly recall the changed status of runway 34L. Subsequently, they deactivated the stop bar and issued a clearance for the B737 to cross the active runway. However, as the runway was active, those actions were the responsibility of the ADC.
Although the SMCE was using the runway 34L active strip in the flight progress strip board, clearing landed jet aircraft to the domestic apron, deselecting the stop bar lighting in the AGL panel and crossing them through the inactive runway 34L was a repetitive task and familiar in nature. This increased the likelihood that if a change to the runway status was overlooked, it would result in the deactivation of the stop bar lighting and the issuing of an incorrect clearance.
The design of the AGL panel at the time of the incident enabled the SMCE to deactivate a stop bar of an active runway, for which they did not have responsibility for.
At the time of publication for this notice, only 5 Australian airports were fitted with stop bars. The procedures for using stop bars on inactive runways varied between these airports.
The routine use of stop bars on an inactive runway was inconsistent with the procedures indicated in MATS. This influenced the SMCE deactivating the stop bars and issuing the clearance for the B737 flight crew to cross the runway while it was being used for take-off by the A380. Alternately, if the stop bars were only used when the runway was in use, the stop bars would have been activated by the ADC when resuming control for the runway. Even if the SMCE had incorrectly assessed the status of the runway and issued a clearance to cross (what they thought was an inactive runway), the stop bars would have remained illuminated, indicating to the flight crew they could not cross.
Safety action
Procedural changes to the stop bar operation at Sydney Airport and implemented since this incident are as follows:
If runway 34L is inactive and the ADC has not released the runway to the SMC, the ADC retains stop bar ownership and is required to approve all runway crossings of the inactive runway. The SMC is unable to operate the stop bar lighting controls in the AGL panel.
If runway 34L is inactive and the ADC has released the runway to the SMC, access for the SMC to operate the stop bars is enabled in the AGL panel when the ADC selects the relevant runway mode. The SMC is responsible for issuing runway crossing clearances and operates the stop bars without requiring coordination with the ADC.
When runway 34L has been released to the SMC and the ADC takes ownership back, the ADC amends the operating mode in the AGL panel and the SMC is then unable to operate the stop bar lighting controls in the AGL panel. The SMC coordinates runway crossings with the ADC, who operates the stop bars.
When runway 34L is active, the ADC retains stop bar jurisdiction and the SMC is unable to operate the stop bar controls in the AGL panel. The SMC requests clearances for runway crossings from the ADC, and when the ADC approves the crossing and deselects the stop bar, the SMC issues the clearance for the aircraft or authorised vehicle to cross the runway.
Safety message
Although stop bars were principally introduced to help reduce runway incursions by taxiing aircraft and authorised airside vehicles during periods of low visibility, they are also used effectively at other times to help reduce the risk of an incursion on an active runway. The ATSB also notes that, at Australian airports where stop bar lighting is only activated at times the runway is active, the associated procedure introduces an additional risk control by removing the coupling between an SMC’s deactivation of stop bars and their issuing of clearances to cross the inactive runway. This reduces the potential for an SMC to deactivate stop bars and issue an incorrect clearance to cross an active runway, with taxiing flight crew and vehicle drivers required to stop at all illuminated stop bars.
Reasons for the discontinuation
Based on a review of the available evidence and the implementation of safety action by Airservices Australia and Sydney Airport Corporation Limited, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues or important safety lessons.
The ATSB strives to use its limited resources for maximum safety benefit, and considers that in this case, the change to stop bar procedures at Sydney Airport and the change to the airfield ground lighting system has likely reduced the risk of a similar incident occurring. Consequently, the ATSB discontinued the investigation.
[1]The function of aerodrome control for the purpose of aircraft taking-off, landing and transiting the airspace associated with the control zone was provided by air traffic controllers located in the airport’s control tower. At Sydney Airport, there was provision for several aerodrome control positions, depending on the number of runways in use and any additional coordination that was required for arriving and departing aircraft.
[2]The function of airport surface movement control was provided by an air traffic controller located in the airport’s control tower. At Sydney Airport, there were 2 surface movement control positions (east and west). The surface movement controller coordinated the ground movement of aircraft and vehicles.
[3]When activated, the stop bars comprise a row of red lights inset into the surface of the taxiway, at an angle of 90° to the taxiway centreline. The inset lighting was augmented with a red above ground light either side of the taxiway, abeam the stop bar position. Aircraft or authorised vehicles must not cross the stop bars without both an air traffic control clearance and the red stop bar lights being extinguished.
[4]The flight progress strip board formed part of the controller’s scan when issuing clearances to cross inactive runways.
[5]Runway guard lighting comprised pairs of above ground flashing amber lights on each side of the taxiway, which continuously flashed to indicate a runway was ahead. Each amber light in the pair flashed alternately so that one light in each pair was always illuminated. Runway guard lighting installations are also known as ‘wig wags’.
[6]Stop bar and runway guard lighting was initially designed to reduce the risk of runway incursions during periods of low visibility. Those lighting systems are also used more generally to help mitigate the risk of runway incursions that could occur at other times.
[7]When not being used operationally, a runway could be inactivated and responsibility for aircraft and vehicles using that part of the movement area transferred to the surface movement controllers.
[8]The airfield ground lighting system was part of the airport’s operating infrastructure, which was provided/maintained by Sydney Airport Corporation Limited.
[9]At Canberra airport, stop bars were activated when runways were closed by NOTAM. In addition, when the tower was closed overnight, the stop bars were deactivated and flight crews were responsible for their operations at the uncontrolled aerodrome.
[10]At Perth and Sydney airports, stop bars were also activated when runways were closed by NOTAM.
[11]The score is based on the Samn-Perelli 7-point fatigue scale, where 1 indicates fully alert and 7 indicates completely exhausted.
Occurrence summary
Investigation number
AO-2022-062
Occurrence date
14/11/2022
Location
Sydney Airport
State
New South Wales
Report release date
30/01/2025
Report status
Discontinued
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Discontinued
Mode of transport
Aviation
Aviation occurrence category
ANSP info/procedural error
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8SA
Registration
VH-IWQ
Serial number
44225
Aircraft operator
Virgin Australia Airlines
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On the afternoon of 30 November 2022, the student pilot of a Hughes Helicopters 269C, registered VH-OBK, was returning to Moorabbin following the pilot’s second solo navigation training flight.
As the helicopter approached the landing area, the approach became unstable, and the pilot commenced a go‑around. As the helicopter climbed to about 650 ft above ground level, the pilot commenced a right turn onto the downwind leg of the circuit to position for a second approach for landing. Shortly after, the pilot noticed reduced performance and decided to continue the turn back toward the airport.
The helicopter continued to lose height and, recognising that a forced landing was required, the pilot turned the helicopter left toward a school ground to attempt an autorotation landing. The helicopter subsequently collided with the rooftops of 2 houses just short of the school ground. The pilot sustained serious injuries and the helicopter was substantially damaged.
What the ATSB found
The ATSB found that as the helicopter climbed to about 650 ft above ground level, the engine lost power. The reason for the engine power loss was not determined.
The power loss was not immediately recognised which limited the opportunities for a safe forced landing. During the forced landing, the helicopter did not have sufficient height to reach the selected landing area and collided with rooftops.
Safety message
This accident highlights the challenges pilots face when confronted with a loss of engine power at low level and with few suitable landing areas available.
…before conducting a take-off from any aerodrome, pilots of single-engine helicopters make themselves aware of the areas that would be suitable, from the lift-off point to a safe manoeuvring height, to conduct a forced landing in the event of engine failure after take-off.
These challenges of managing a power loss are increased for an inexperienced student pilot. While in this case, the selected landing location was unable to be reached, importantly, the pilot maintained control of the helicopter to maximise survivability.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 1100 local time on the morning of 30 November 2022, the student pilot of a Hughes Helicopters 269C, registered VH-OBK, departed Moorabbin Airport, Victoria for the pilot’s second solo navigation training flight.
The navigation exercise was conducted without incident and at 1255, the helicopter returned to Moorabbin where air traffic control provided the pilot with clearance to conduct a visual approach to the southern apron.
At 1300, the helicopter approached the apron to land. At a height of about 20 ft above ground level (AGL), the approach became unstable, and the pilot accelerated the helicopter slightly to stabilise the approach. The acceleration moved the helicopter further along the apron where the pilot judged that insufficient space remained to conduct a safe landing so they commenced a go‑around.
During the go-around, the pilot observed factories located immediately south of the apron and made a left turn, opposite to the right circuit direction, to provide sufficient room to climb over the factories (Figure 1). This left turn unintentionally took the helicopter toward the departure path of the active runway 17 right, and air traffic control instructed the pilot to make an immediate right turn. The pilot turned the helicopter right and continued climbing on the crosswind leg of the circuit.
Figure 1: Go-around flight path of VH-OBK (Moorabbin airport)
Source: Google Earth, annotated by the ATSB
As the helicopter climbed to about 650 ft AGL, the pilot commenced a right turn onto the downwind leg of the circuit.[1] During the turn, the pilot noted reduced helicopter performance and decided to continue the right turn to take the helicopter back toward the airport.
The pilot recalled that there were no unusual engine sounds or vibrations but that regular communications between air traffic control and other aircraft limited their ability to hear the engine. The pilot reviewed the instrumentation to attempt to identify a reason for the performance loss. The pilot observed the helicopter’s airspeed had increased from the climb speed of 55 kt to between 70‑80 kt and that the manifold pressure had increased above the targeted 24 inches of mercury (Hg) to 29 inches Hg. The engine RPM reading was not checked.
The pilot then adjusted the pitch attitude of the helicopter to that which normally provided a climb speed of 55 kt and lowered the collective[2] slightly to reduce the observed high manifold pressure reading. Following these actions, the helicopter continued descending as it tracked toward the airport.
As the aircraft descended to about 100 ft AGL, the pilot recognised that the descent rate had increased, and a forced landing was required. At that time, a football oval was likely positioned under or slightly ahead and to the right of the helicopter, but the pilot did not see it possibly because it was obscured by the airframe or instrument panel. The pilot identified a water catchment and a school ground as suitable areas for a forced landing and turned the helicopter left toward the school ground to attempt an autorotation[3] landing (Figure 2). The helicopter did not have sufficient height to reach the school ground and collided with the rooftops of 2 houses. The pilot sustained serious injuries and the helicopter was substantially damaged.
Figure 2: Flight path of VH-OBK
Source: Google earth, annotated by the ATSB
Context
Meteorology
A meteorological report for Moorabbin Airport, recorded at 1300, included a south-westerly wind of 11 kt, visibility greater than 10 km, no cloud, a temperature of 17 °C, and a mean sea level air pressure of 1,018 hectopascals.
The estimated air pressure at 650 ft above mean sea level (600 ft AGL) was 996 hectopascals (29.4 inches Hg).[4]
Aircraft details
VH-OBK was a 3-seat Hughes Helicopters 269C helicopter, manufactured in 1980. The helicopter was powered by a 190 horsepower Textron Lycoming HIO-360-D1A, four-cylinder, fuel injected piston engine. Engine power was transmitted via a belt drive transmission to the main transmission and tail rotor drive shaft. The belt drive assembly incorporated an overrunning clutch to permit autorotation without driving the belts or engine.
The helicopter was not fitted with a low rotor RPM aural warning system, nor was it required to be.
Using information provided by the aircraft operator, the ATSB calculated that the autorotative range from 650 ft AGL was about 0.26 nm (490 m) with no wind and about 0.32 nm (590 m) with a 11 kt south-westerly tail wind.
Site and wreckage information
The helicopter impacted 2 houses immediately adjacent to the school ground targeted for the forced landing (about 600 m from the estimated position of the power loss). The helicopter came to rest embedded in the roof of one of the houses. After recovery of the wreckage, an inspection of the helicopter’s fuel tanks found at least 60 litres of fuel on board.[5]
Figure 3: Accident site
Note: The forward section of the fuselage was cut away by first responders to facilitate removal of the pilot.
Source: Victoria Police, annotated by the ATSB
A detailed examination of the airframe or engine was not performed. However, a visual inspection of the engine cooling fan and fan shroud indicated that the engine was not running at the time of the accident. The degree of damage to the rotor blades also indicated that the engine was providing little or no power.
Witness information
Two Moorabbin air traffic controllers observed the accident. One was located within the control tower, and the other was on a break, walking about 650 m north-east of the accident site. The controller on break noted that prior to the accident, the helicopter’s descent path was shallower than that of a normal autorotation and no engine noise was heard. The controller in the tower also noted the shallow descent path.
Safety analysis
As the helicopter turned from crosswind to downwind after the go-around, the pilot recognised a reduction in performance. The pilot did not identify a change in the engine sound or vibration, however multiple radio broadcasts around this time reduced the pilot’s ability to do so. A review of the engine manifold pressure indications showed that it was significantly higher than expected and consistent with ambient conditions. Furthermore, the distance travelled during the descent was consistent with that expected for an autorotation. Both factors indicate that the engine was very likely not producing power at that time.
The shallower‑than‑expected descent profile observed by the witnesses familiar with the helicopter’s autorotative descent profile, may have been due to the beneficial effect of the pilot pitching the helicopter up to reduce the airspeed from 70‑80 kt to the target airspeed of 55 kt. After the accident, a visual inspection of the engine cooling fan and shroud identified no rotational damage, similarly indicating that the engine was not running at the time of the accident.
There were no reported actions made that may have led to the power loss and the helicopter had sufficient fuel on-board. There were no other reported indications of a fault with the engine. A detailed examination of the engine and airframe was not performed, limiting the ability to identify the reason for the power loss.
The engine power loss occurred at low height over a densely populated area presenting a challenging scenario for the inexperienced student pilot. The pilot did not immediately identify that power was lost and attempted to return to the airport while troubleshooting the reduced helicopter performance. During this time, the helicopter passed 2 suitable forced landing sites (Figure 4).
Figure 4: Flight path of VH-OBK following the engine power loss
Source: Google Earth, annotated by the ATSB
When the pilot recognised that a forced landing was required, the football oval was likely the closest suitable area, but the pilot did not identify the oval, possibly due to it being obscured by the airframe or instrument panel. The pilot identified the school ground and attempted a landing there. However, the helicopter did not have sufficient height to reach the selected site and the helicopter collided with rooftops. While the helicopter did not reach the intended area, the pilot maintained sufficient control of the helicopter and rotor RPM to conduct an autorotation landing into the rooftops, which maximised survivability.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Hughes Helicopters 269C, VH-OBK near Moorabbin Airport, Victoria on 30 November 2022.
Contributing factors
As the helicopter climbed to about 650 ft above ground level, the engine lost power. The reason for the power loss was not determined.
The power loss was not immediately recognised which limited the opportunities for a safe forced landing. During the forced landing, the helicopter did not have sufficient height to reach the selected landing area and collided with rooftops.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
pilot’s instructor
operator
Airservices Australia
Bureau of Meteorology
aircraft manufacturer
air traffic controllers
video footage of the accident flight.
References
Civil Aviation Safety Authority 2022, Advisory Circular AC 91-29 v1.1 Guidelines for helicopters -suitable places to take off and land, July 2022.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
operator
pilot’s instructor
pilot
air traffic control witnesses.
Submissions were received from the:
operator
pilot’s instructor
pilot.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] The altitude for the downwind leg of the circuit for helicopters at Moorabbin Airport was 700 ft above mean sea level (650 ft AGL).
[2] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[3] Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[4] The International Standard Atmosphere (ISA) provides hypothetical standard temperatures and pressures at specified altitudes. ISA conditions are used as a datum for calculating aircraft performance data. The ISA states that air pressure reduces by 1 hectopascal for each 30 ft increase in altitude.
[5] The helicopter was fitted with a main and auxiliary fuel tank. These tanks were interconnected and acted as one fuel tank.
Occurrence summary
Investigation number
AO-2022-063
Occurrence date
30/11/2022
Location
Near Moorabbin Airport
State
Victoria
Report release date
30/03/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Hughes Helicopters
Model
269C
Registration
VH-OBK
Serial number
1190855
Aircraft operator
The Helicopter Group
Sector
Helicopter
Operation type
Part 141 Recreational, private and commercial pilot flight training
The ATSB collects, holds and uses a range of information for the purposes of improving transport safety. The ATSB is a part of Australia's aviation safety system, and the information gathered by the ATSB may be provided to other agencies for the specific purpose of maintaining and improving aviation safety. It is an additional legislative function for the ATSB to cooperate with these agencies.
Mandatory reporting
A principal source of safety information is the mandatory reporting scheme established under the Transport Safety Investigation Act 2003 (TSI Act). The scheme gathers information on occurrences which endanger or could endanger aviation safety. The information is gathered so that it can be used by those with responsibilities within the safety system to discharge their responsibilities to maintain and improve aviation safety.
The scheme requires 'responsible persons' (including aircraft crew, owners, operators, air traffic controllers, licensed aircraft maintenance engineers, ground crew and airport operators) to notify the ATSB of accidents and safety incidents ('safety occurrences').
Where the duty to report rests with an individual, it can be fulfilled by the individual notifying the operator who employs them. The operator then has a duty to pass the information on to the ATSB.
Use of safety information by the ATSB
The ATSB uses safety information to assist in its determination of what to investigate for the purposes of improving safety.
Any information that is the subject of an ATSB investigation will only be used in accordance with the provisions of the TSI Act which provides significant protections to information acquired by the Bureau in the course of its investigation.
The ATSB also uses safety information for the purposes of safety research and analysis. The results of research and analysis are generally made public, but in such a way that either the information is either de-identified or is otherwise protected.
ATSB and CASA information sharing
The Civil Aviation Safety Authority (CASA) is constituted under the Civil Aviation Act 1988 (CA Act). The primary object of the CA Act is to establish a regulatory framework for maintaining, enhancing and promoting the safety of civil aviation, with particular emphasis on preventing aviation accidents and incidents. CASA's primary function under the CA Act is to conduct the safety regulation of civil air operations in Australia and the operation of Australian aircraft outside Australian territory.
Consistent with the objective of maintaining and improving aviation safety under the Australian aviation safety framework, the ATSB recognises CASA needs access to a range of information about aviation safety occurrences that is collected and held by the ATSB.
What information is shared
The ATSB informs CASA about accidents and serious incidents as soon as the ATSB is informed. The information may contain details such as operator names, registration numbers, times, dates, locations and a description of the event. The ATSB aims, wherever possible, to avoid directly identifying individuals.
CASA is also provided daily with a redacted report of all occurrences entered into the ATSB database. The report contains standard information about occurrences notified to the ATSB, including aircraft registration, so that CASA has enough detail to gather its own information about the occurrence. It does not contain a detailed narrative.
An automated weekly transfer of summaries of information entered in the ATSB's database during that week is also provided to CASA. The aggregate summary does not include identifying information such as aircraft registration, but provides enough information for CASA to be able to analyse safety trends, and to identify actual or potential safety risks to which more immediate attention needs to be directed. Since 1 July 2023, the de-identified occurrence database is being shared via the centralised Aviation Safety Data Sharing Platform.
Aviation Safety Data Sharing Platform
The aviation safety data sharing platform is a collaboration between the ATSB and the Bureau of Infrastructure and Transport Research Economics (BITRE), CASA and Airservices Australia.
Aviation data was already being shared between aviation safety agencies on a regular and ad-hoc basis. The Aviation Safety Data Sharing Platform will streamline and modernise this process to provide this same data in a consistent real-time format, while incorporating additional security controls and privacy measures.
The information shared to the platform between aviation authorities will enable better decisions to be made for policy development, regulatory settings and safety outcomes for the aviation industry and general public.
All agencies involved in this project are ensuring that data shared or analysed within the platform will not be used to identify individuals or firms, or for regulatory and compliance purposes. The existing legislative restrictions on data sharing continue to apply, and agency-specific user access controls are in place in line with relevant privacy and confidentiality standards.
Purpose of information sharing
CASA uses safety information from the ATSB principally for two purposes: to have sufficient information about an occurrence to decide whether to initiate its own, independent regulatory inquiries; and to have access to a database of occurrence information so that trends in aviation safety can be detected and, where necessary, safety action can be taken.
Limits on use of information by CASA
CASA may use information reported under the mandatory scheme as the basis for informing its need to initiate its own inquiries in the interests of safety. However, CASA will not rely on the report in taking action unless it is necessary to do so in the demonstrable interests of safety and where there is no alternative source of the information practicably available to CASA.
CASA will not normally recommend the institution of criminal proceedings in matters which come to its attention only because they have been reported under ATSB's mandatory reporting scheme. The exceptions will be in cases of conduct that should not be tolerated, such as where a person has acted intentionally, knowingly, recklessly or with gross negligence.
In taking any action, CASA will afford affected individuals and organisations natural justice.
This policy is consistent with contemporary practice in leading aviation States. It is also in line with the new ICAO Annex 19 – Safety Management. Standard 5.1.1 of the Annex requires that:
Each State shall establish a mandatory incident reporting system to facilitate collection of information on actual or potential safety deficiencies.
Recommended practice 5.3.1 states:
State authorities responsible for the implementation of the State Safety Program should have access to appropriate information available in the incident reporting systems.
The regulator and the accident investigator both have responsibilities with respect to the implementation of the State Safety Program. This policy outlines what each agency requires accident and incident information for in order to be able to perform their respective complementary functions. It also makes clear what limitations currently govern the use of information by CASA. Having regard to international developments, the ATSB and CASA will seek the views of industry participants and the wider Australian aviation community on the implementation and further development of this policy.
On 18 September 2022, a Jabiru J230-C, registration 24-5067 collided with terrain at Lucyvale, Victoria.
The pilot was fatally injured, and the aircraft was destroyed. Recreational Aviation Australia requested technical assistance from the ATSB to assist in its investigation.
The ATSB was requested to download and recover flight data from the GPS. To facilitate this assistance, the ATSB initiated an external investigation under the provisions of the Transport Safety Investigation Act 2003.
The ATSB has completed its work downloading the recorded flight path data from the supplied Garmin GPS Map 296 unit. A copy of the data and a report detailing the work undertaken by the ATSB was provided to RAAus on 22 December 2022.
On 16 November 2022, a non-scheduled passenger transport flight was conducted in a Cessna Citation Mustang, registered VH-IEQ, between Young Airport and Bankstown Airport, New South Wales. On board were a pilot and one passenger.
As the aircraft approached Bankstown Airport to land under the instrument flight rules, about 10 minutes after last light, the pilot established contact with air traffic control (ATC), where a ‘visual’ approach was requested. ATC approved the pilot to fly directly toward final approach for runway 11 centre. Immediately after this clearance, the pilot started tracking toward final approach for this runway and descended to a height of 1,000 ft, which was about 800 ft below the lowest safe altitude for the area. ATC subsequently issued a terrain safety alert. An uneventful landing was conducted at 2020 local time.
What the ATSB found
The ATSB found that the pilot had submitted a flight plan earlier in the day for an arrival after last light, when more stringent rules applied than day operations. However, the pilot followed the rules applicable to day operations as there was still some ambient light available to allow features on the ground to be visually identified and avoided. This resulted in the pilot descending below the lowest safe altitude applicable for operations at night.
Safety message
This incident highlights the importance of planning, particularly around times when rules change, such as the transition from day to night. In this case, the pilot reported that flying a published instrument approach procedure, rather than declaring ‘visual’ would have been a more suitable plan for this flight.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
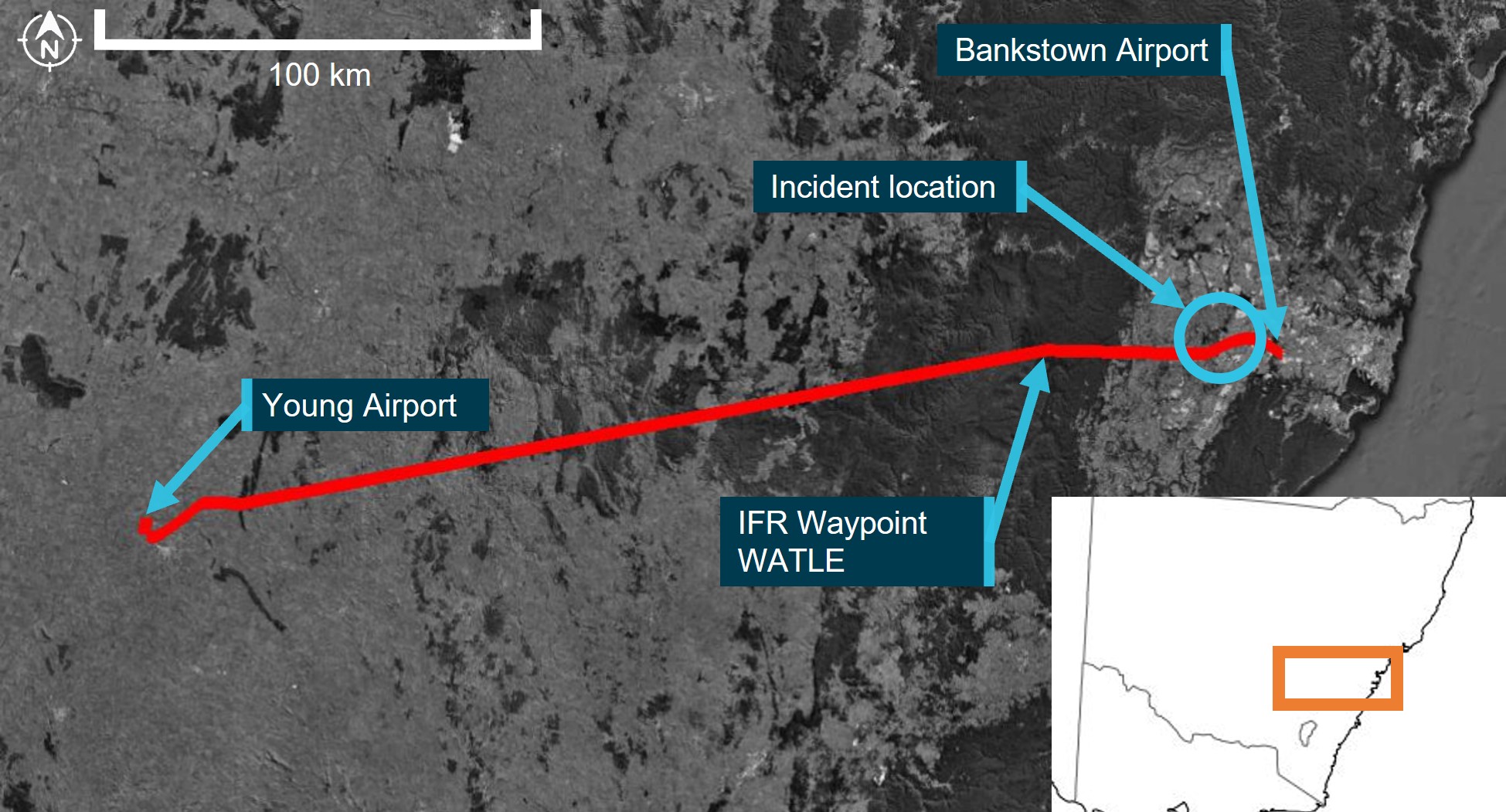
In the late afternoon of 16 November 2022, a non-scheduled passenger transport flight was conducted in a Cessna Citation Mustang, registered VH-IEQ (IEQ) between Young Airport and Bankstown Airport, New South Wales (Figure 1). On board were a pilot and one passenger.
This was the fourth and final flight of the day, with the pilot completing 3 earlier flights in the aircraft. National Airspace Information Planning System records indicated that the pilot submitted all flight plans for these flights at about 0448 local time, with this plan showing a planned departure from Young at about 1945 for the incident flight. This flight was planned to follow flight routes under the instrument flight rules (IFR)[1] and arrive at Bankstown at about 2014.
Figure 1: Flight path of VH-IEQ and incident location
Image showing flight path of aircraft (red line) on a map, with take-off, arrival and location of flight below lowest safe altitude.
Source: Google Earth and Geoscience Australia, annotated by the ATSB
Flight data recorded by the GPS navigation unit onboard the aircraft indicated that a take-off was commenced from Young on runway 19 at about 1946. After take-off, the aircraft started tracking to the east and climbed to a cruising altitude of flight level (FL)[2] 230 by about 1956.
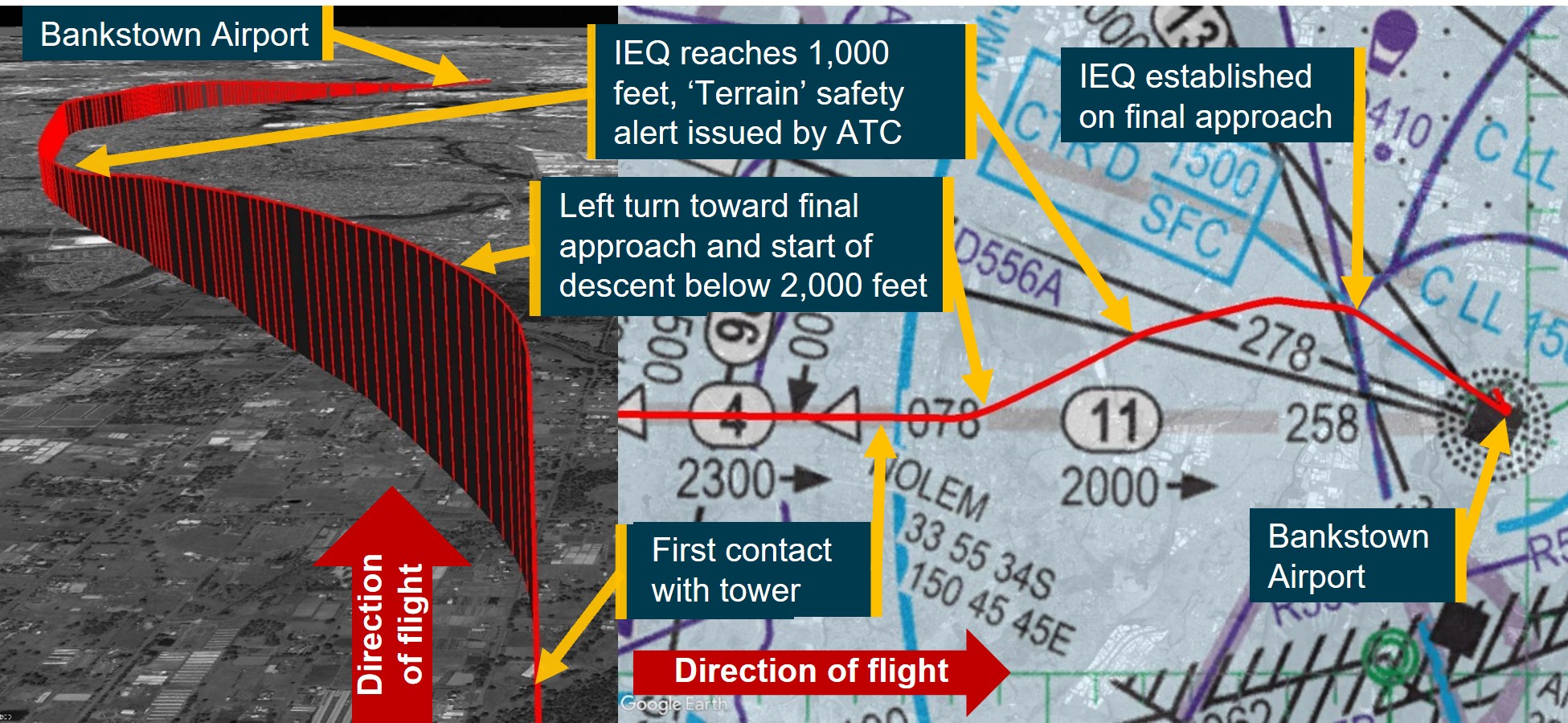
At about 2001, the aircraft started to descend, continuing to track toward IFR waypoint WATLE. During this descent, at about 2004, last light[3] for Bankstown occurred. Six minutes later, the aircraft arrived overhead WATLE and proceeded to follow the planned IFR route denoted ‘Y20’, directly toward Bankstown Airport, 28 NM (52 km) to the east. At 2014:48, at waypoint NOLEM (Figure 2), the aircraft levelled out at 2,000 ft[4] above mean sea level and continued to track toward Bankstown. At this time, the pilot established first contact with Bankstown Tower air traffic control (ATC) near waypoint NOLEM (Figure 2), with the following communication exchange:
2014:48 IEQ: ‘Bankstown tower IEQ is 11 miles west 2,000 with Quebec visual inbound’
2014:59 BANKSTOWN TOWER: ‘IEQ BK TWR Join Final Runway 11 centre’
2015:08 IEQ: ‘Join Final 11 centre IEQ’
Immediately after responding to ATC, flight data indicated that the aircraft began a left turn onto a track of approximately 060° (true). Near the completion of the left turn, at 2015:22, the aircraft began to descend from 2,000 ft (labelled ‘left turn toward final approach and start of descent below 2,000 feet’ in Figure 2). The aircraft continued to descend on this track, levelling out at 1,000 ft at 2016:20. Around this time, ATC identified that the aircraft was ‘too low’, and issued a ‘Terrain’ safety alert at the location marked in Figure 2. The communication exchange for the safety alert between ATC and the pilot were as follows:
2016:30 BANKSTOWN TOWER: ‘IEQ Safety Alert Terrain QNH[5] is 1012’
2016:38 IEQ: ‘Roger copy 1012 IEQ I'm ahh visual’
2016:43 BANKSTOWN TOWER: ‘IEQ’
At the time the safety alert was issued and while maintaining at 1,000 ft, flight track data showed that the aircraft started to change track to the right by 15° to 075° for about 2 NM (3.7 km). The aircraft then changed track again to the right toward the intersection of the Bankstown Airport control zone and the extended centreline of runway 11 centre. Just prior to entering the control zone at 2017:55, Bankstown Tower provided the aircraft with a clearance to land, which was acknowledged by the pilot. At this time, the aircraft turned toward runway 11 centre and started to descend from 1,000 ft. An uneventful landing on runway 11 centre was conducted at 2019:56.
Figure 2: Flight path of VH-IEQ showing descent to 1,000 ft and approach to land
Note: Image showing flight path of aircraft (red line) on a low level enroute chart (right) and from the perspective of the approach from the NOLEM waypoint (left).
Source: Google Earth and Airservices Australia, annotated by the ATSB
Context
Meteorological information
The meteorological report (METAR)[6] for Bankstown Airport released at 2000 local time indicated the following weather conditions for the aircraft’s arrival:
winds at 6 kt from the north-west
visibility greater than 10 km
3 layers of cloud, comprising scattered[7] at 5,100 ft and at 7,000 ft, and broken at 8,200 ft above the ground
the QNH was 1012 hPA.
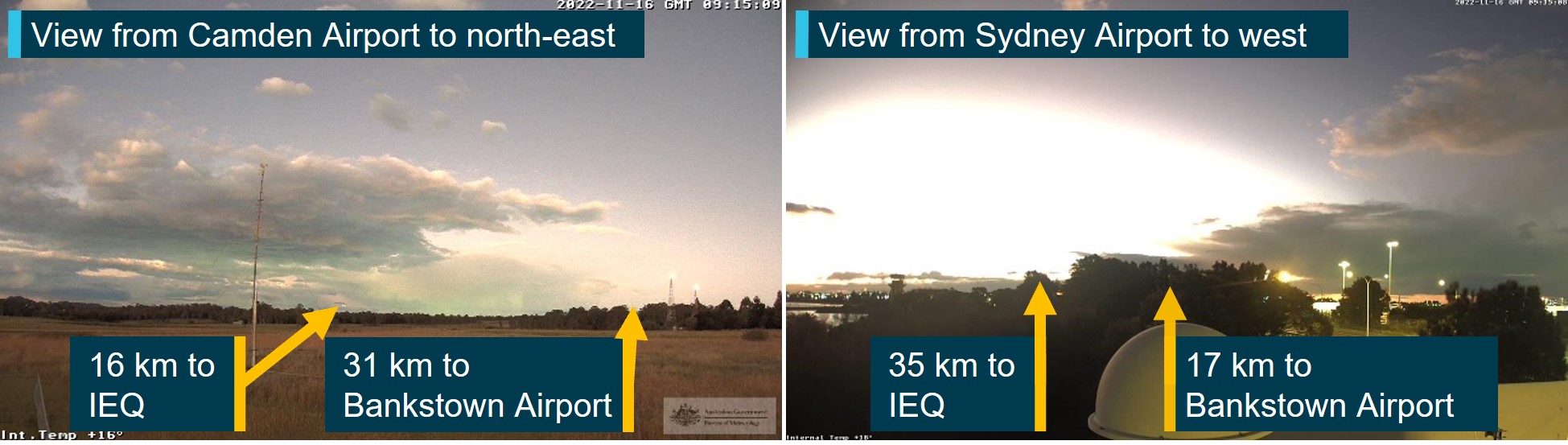
Images from weather cameras at the time of the incident located at Camden and Sydney Airports facing the direction of the aircraft and Bankstown Airport are shown in Figure 3. The images show that less than half of the sky is covered by cloud, with the cloud tops illuminated by the sun. There were no weather cameras operating at Bankstown Airport.
The Bureau of Meteorology advised that these weather cameras were configured 'to work in low light and will use the light available to provide the best image’, that is, the images shown in Figure 3 ‘look brighter than the actual conditions experienced by the pilot’. However, relatively clear atmospheric conditions are shown by the images, with well-defined silhouettes of ground‑based features.
Figure 3: Images from weather cameras at Camden and Sydney Airports
Source: Bureau of Meteorology, annotated by the ATSB
Visual approach to Bankstown Airport
During the approach, the pilot advised ATC that they were ‘visual’. This transmission signified that the requirements for a visual approach under the IFR could be met. ATC responded providing an instruction to ‘join final 11 centre’, which constituted a clearance to enter the Bankstown control zone on the centre line of runway 11 centre, tracking toward that runway.
As last light was at 2004 and this instruction was provided at 2014, this meant that the visual approach requirements for IFR flights by night applied.
To assist with conducting the visual approach, runway 11 centre was equipped with a precision approach path indicator system.[8]
Required actions by pilot following instructions from ATC
AIP ENR 1.1 paragraph 2.2.7.2[9] (Operations in Class D Airspace)[10] stated that in circumstances where ATC responds with the aircraft callsign and instructions, the pilot must comply with ATC instructions. It also states that ‘when no level instruction is issued’, the pilot may ‘descend as necessary to join the aerodrome traffic circuit’. In this case, ATC had instructed the pilot to join final runway 11 centre without a level instruction. The instructions meant that the pilot was required to fly the aircraft to enter the Bankstown control zone on the extended centreline for runway 11 centre. However, minimum height requirements applied to the flight as discussed in the next section.
Minimum height requirements during a visual approach for an IFR flight at night
During a visual approach at night, subparagraph 91.305(3)(b)(i) of the Civil Aviation Safety Regulations 1998 (CASR 91.305(3)(b)(i)) allowed an IFR flight to descend below minimum stipulated heights if the aircraft was being flown in accordance with:
…requirements relating to visual approach or departure procedures published in the authorised aeronautical information for the flight.
AIP ENR 1.5 section 1.14 articulated these requirements. AIP ENR 1.5 paragraph 1.14.6(b)[11] was relevant to this flight and included the provision that the pilot may visually approach the aerodrome by night when at an altitude not below the lowest safe altitude (LSALT)[12] or minimum sector altitude (MSA)[13] for the route segment, if the aircraft was established:
(1) clear of cloud;
(2) in sight of ground or water;
(3) with a flight visibility not less than 5,000M; and
(4) subsequently can maintain (1), (2) and (3) at an altitude not less than:
…
(ii) one of the following:
Route segment LSALT/MSA; or…
Based on the reported weather conditions, clauses 1, 2 and 3 noted above were achieved when the request for a visual approach was made by the pilot to ATC. Further, the AIP stipulated one of the conditions allowing an aircraft to descend below LSALT was when the aircraft was:
Within 5NM (7NM for a runway equipped with an ILS/GLS) of the aerodrome, aligned with the runway centreline and established not below “on slope” on the T-VASIS or PAPI;
Based on the ATC clearance provided to the pilot, and runway 11 centre being equipped with a PAPI, this meant that the aircraft could descend below LSALT once aligned with the runway centreline and not below on-slope of the PAPI and within 5 NM (9.3 km) of the PAPI.
Calculation of the lowest safe altitude
Flight data showed that after the initial climb from Young Airport, the aircraft had been above the published LSALT for the duration of the flight until reaching waypoint NOLEM.
AIP GEN 3.3 section 4 defined how to calculate the LSALT. Specifically, paragraph 4.2 stated:
For routes and route segments not shown on AIP aeronautical charts, the lowest safe altitude must not be less than that calculated in accordance with para 4.3 within an area defined in the following paras 4.6, 4.7, 4.8 and 4.9.
For this flight, paragraph 4.3 clause 4.3(a) stated the LSALT was to be calculated using the following method:
Where the highest obstacle is more than 360FT above the height determined for terrain, the LSALT must be 1,000FT above the highest obstacle; …
Additionally, paragraph 4.5 stated:
If the navigation of the aircraft is inaccurate, or the aircraft is deliberately flown off-track, or where there is a failure of any radio navigation aid normally available, the area to be considered is a circle centred on the DR position, with a radius of 5NM plus 20% of the air distance flown from the last positive fix.
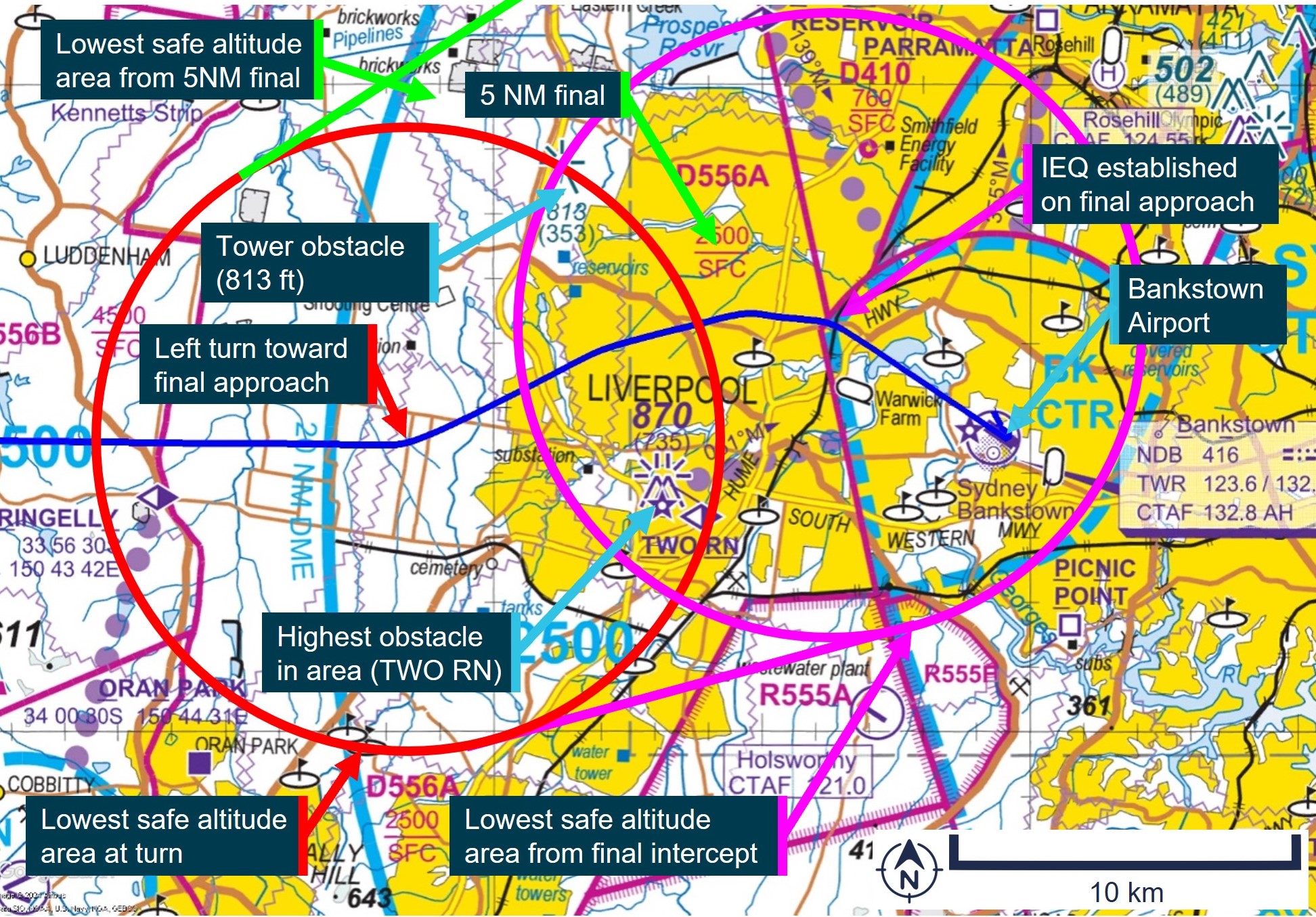
Paragraph 4.5 applied to the incident flight after the pilot intentionally flew off-track toward final approach for runway 11 centre with the last positive fix being the waypoint NOLEM. Based on this, the ATSB calculated the LSALT for the aircraft between NOLEM and being aligned with runway 11 centre. An extract of the visual terminal chart applicable to the area is shown inFigure 4.
The aircraft was equipped with an approved global navigation satellite system, which was being used for navigation under RNP 2[14] meaning that the aircraft remained with a positive fix for the duration of the flight. For RNP 2 operations, AIP GEN 3.3 paragraph 4.7 required the following area to be considered for LSALT calculations:
…within an area of 5NM [9.3km] surround and including the departure point, the destination and each side of the nominal track.
This area is shown for the incident between the red circle labelled ‘Lowest safe altitude area at turn’ and the magenta circle labelled ‘Lowest safe altitude area from final intercept’ inFigure 4. Calculations were also performed in the circumstance where the aircraft flew to an extended 5 NM final for runway 11 centre, the earliest point of descent when using the PAPI, and this is depicted by the green circle labelled ‘Lowest safe altitude area from 5 NM final’ in Figure 4.
Figure 4 also shows 2 charted obstacles in the area. This indicated that paragraph 4.3(a) from AIP GEN 3.3 applied to this part of the flight. The highest obstacle in the area to be considered for LSALT was the tower ‘TWO RN’ at 870 ft above mean sea level, located about 2.5 NM (4.6 km) to the right of track, as labelled in Figure 4. Another tower was present about 2.5 NM (4.6 km) to the left of track at a height of 813 ft. Based on this, the LSALT for the aircraft during this segment of the flight was 1,870 ft.
Figure 4: Area applicable to lowest safe altitude calculations for VH-IEQ between flight path deviation and the extended centreline of runway 11 centre at Bankstown Airport
Source: Airservices Australia, annotated by the ATSB
Lowest safe altitude for a visual approach during the day
AIP ENR 1.5 section 1.14 paragraph 1.14.6(b) stipulated the same requirements for a visual approach by an aeroplane in the day, except for clause (4)(ii), which required pilots to maintain an altitude not less than:
The minimum height prescribed by CASR 91.265 or 91.267 as relevant to the location of the aircraft.
For the location of this incident, regulation 91.265 for flights over ‘populous areas and public gatherings’ applied. This stipulated that the aeroplane must be flown more than 1,000 ft above the highest feature or obstacle within a horizontal radius of 600 m of the point on the ground or water immediately below the aeroplane. Based on this, the height flown by the aircraft was above that required for an IFR visual approach during the day.
Decision to descend below lowest safe altitude
During an interview with the ATSB, the pilot recalled the following observations about the navigation conditions during the approach:
It was a light evening with plenty of twilight allowing the ground to be seen clearly.
The light was sufficient to see a clear horizon.
Ground features were able to be clearly seen, sufficient to identify the aircraft’s precise position.
All known obstacles could be seen.
Based on these observations, the pilot reported deciding to ‘call visual’.
The pilot’s description of the weather conditions was consistent with those recorded by the Bureau of Meteorology.
The pilot stated that, during a self-briefing prior to departure, the time of last light had been recorded for Young Airport and not Bankstown Airport as intended. The pilot also reported reviewing the last light time prior to descent to Bankstown Airport. Last light at Young Airport occurred about 12 minutes later than Bankstown Airport due to it being further west. The pilot later stated that recording the last light time for Young instead of Bankstown in the briefing sheet possibly contributed to the decision to descend and conduct the approach flown.
The pilot stated that descending to 1,000 ft assisted with meeting the stabilised approach criteria, which was:
“in a landing configuration with gear down, full flap, the sink rate … under 1,000 feet per minute and the checklists … completed…by 1,000 feet”.
The pilot stated that a challenge with using the PAPI was not being able to descend until 5 NM (9.3 km) from the runway, and that this was up to 1,000 ft higher than the ideal glideslope of about 1,600 ft at that location if the minimum sector altitude of 2,500 ft was used. The pilot also stated:
“the aircraft will then give you a lot of warnings about sink rate and terrain which can be very stressful… for passengers”.
For these reasons, the pilot stated:
“that is why I elected to descent to make sure that I was able to get that stabilised approach criteria. And …, it only worked because I had such good visibility in the twilight, I was able to see the ground, and I was able to see visually where I was.”
The pilot also stated that a motivation for declaring visual was to ‘fit in’ with the other traffic in the Bankstown area. However, the pilot stated that, on reflection, flying an instrument approach (specifically the RNP approach, rather than declaring visual) would have been a better solution for arriving close to or after last light for the aircraft stating:
“the only way to do it to achieve the stabilised approach is by the RNP”.
Fatigue considerations
The ATSB evaluated the likelihood that the pilot was fatigued at the time of the incident. Some areas of increased risk of fatigue potentially relevant related to:
continued period of wakefulness/length of duty period
split duty and efficacy of naps
quantity of sleep, particularly relating to early starts.
The pilot reported obtaining 7.5 hours of sleep immediately prior to the incident, and 8 hours for each of the 2 nights prior to that. The pilot submitted a flight plan at 0448 and was likely awake for some time prior to this. The pilot’s flight duty period (FDP) for the day started at 0630,[15] had a split duty rest period between 1030 and 1730 that included a 1-hour nap, and then was on duty again until 2100. As the incident occurred at 2016, the pilot’s total FDP was 14 hours and 30 minutes, which was 30 minutes over the maximum allowed under Appendix 4 of Civil Aviation Order 48.1 for single-pilot air transport operations, or to an approved fatigue risk management system. However, section 5.3 of Appendix 4 stated:
Despite the FDP limits provided in the operations manual, in unforeseen operational circumstances at the discretion of the pilot in command, the FDP limits in the operations manual may be extended by up to 1 hour.
The pilot reported having a discussion with the chief pilot about extending the FDP limits due to floods in the area delaying the departure time for the flights. However, the final flight of the day arrived within 5 minutes of the planned time.
Based on the reported sleep obtained, the pilot was likely not fatigued at the time of the incident.
Safety analysis
After last light, the pilot contacted Bankstown Tower declaring that they were ‘visual’ at 2,000 ft. This signified to ATC that requirements for a visual approach at night under the IFR could be achieved. The controller’s subsequent instruction to join final runway 11 centre indicated that the pilot could track toward the extended centreline for that runway.
The clearance from ATC did not specify an altitude, allowing the pilot to descend to the LSALT until established within 5 NM (9.3 km) of the PAPI for runway 11 centre. However, immediately after this clearance, the pilot descended to 1,000 ft, below the LSALT of 1,870 ft. This LSALT applied due to the 2 towers in the area rising to a height of 870 ft about 2.5 NM (4.6 km) from the aircraft. Analysis by the ATSB showed that flight above the LSALT could have been achieved by maintaining altitude between the point of diversion until being aligned with the extended centreline of runway 11 centre within 5NM (9.3 km) of the PAPI.
The pilot reported that the actual approach flown was as they had planned and declared ‘visual’ as they could ‘see the obstacles’. Weather camera imagery showed that the conditions were consistent with the pilot’s description. However, the camera imagery was likely brighter than that experienced by the pilot from altitude looking down on the obstacles and terrain. In this case, the flight path flown by the pilot was applicable and suitable for operations in the day. However, both the planned and actual times when the flight below LSALT occurred were after last light, based on the elapsed time between first contact with ATC and landing. Further, the pilot also reported incorrectly recording a later time for last light than actual, based on Young instead of Bankstown. The additional perceived duration of usable light possibly contributed to the decision to conduct the approach flown. The pilot reported that, on reflection, a better option would have been to fly an instrument approach procedure when planning to arrive at Bankstown just prior to or after last light. This indicated that these requirements could have been considered prior to the flight and represented a missed opportunity during flight planning.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight below minimum altitude involving Cessna Citation 510, VH-IEQ, 13 km west of Bankstown Airport, New South Wales, on 16 November 2022.
Contributing factors
While conducting a visual approach to Bankstown Airport, the aircraft descended 800 ft below the lowest safe altitude for operations at night, reducing the assurance for separation from terrain and ground-based obstacles.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
Airservices Australia
recorded data from the GPS unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Navair Flight Operations Pty Ltd
the Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from:
the pilot
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 230 equates to 23,000 ft.
[3]Last light is defined as the end of evening civil twilight, marking the commencement of night. The end of evening civil twilight occurs when the Sun’s centre is 6° below the horizon.
[4]This was also the published lowest safe altitude between IFR waypoint NOLEM and Bankstown Airport.
[5]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[6]METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[7]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
[8]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach.
[9]AIP ENR 1 GENERAL RULES AND PROCEDURES, section 1.1 GENERAL RULES, subsection 2 OPERATIONS IN CONTROLLED AIRSPACE, sub subsection 2.2 Air Traffic Control Clearances and Instructions
[10]Class D: This is the controlled airspace that surrounds general aviation and regional airports equipped with a control tower. All flights require ATC clearance.
[11]AIP ENR 1 General Rules and Procedures, section 1.14 Visual Approach Requirements for IFR flights, subsection 6, sub subsection 6(b) Visual approach by Night, dated 02 DEC 2021.
[12]Lowest safe altitude (LSALT): The lowest altitude that provides safe terrain clearance at a given place.
[13]Minimum sector altitude (MSA): The lowest altitude that will provide a minimum clearance of 1,000 ft above all objects located in an area contained within a circle or a sector of a circle of 25 NM (46 km) or 10 NM (19 km) radius centred on a significant point.
[14]Required navigation performance (RNP) levels refer to the performance required from the navigation system. RNP 2 is primarily used in continental airspace where there is some ground navigation aid infrastructure.
[15]A flight duty period starts when ‘a person is required by an AOC [Air Operator’s Certificate] holder to report for a duty period in which 1 or more flights as an FCM [flight crew member] are undertaken’. The flight plan submission at 0448 was therefore not counted as duty (only time awake).
Occurrence summary
Investigation number
AO-2022-061
Occurrence date
16/11/2022
Location
15 km west of Bankstown Airport
State
New South Wales
Report release date
05/06/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Flight below minimum altitude
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Textron Aviation Inc.
Model
510
Registration
VH-IEQ
Serial number
510-0462
Aircraft operator
NAVAIR FLIGHT OPERATIONS PTY LTD
Sector
Jet
Operation type
Part 135 Air transport operations - smaller aeroplanes
ATSB has released a second weather-related investigation final report from a fatal general aviation accident this month;
It is highly likely cloud and visibility conditions resulted in the pilot experiencing a loss of visual reference and probably becoming spatially disoriented;
Pushing on into cloud and low visibility when you do not hold the appropriate rating and experience in an aircraft that is not appropriately equipped carries a significant risk of severe spatial disorientation.
Weather-related accidents remain one of the most significant causes of fatal accidents in general aviation, says Australian Transport Safety Bureau Chief Commissioner Angus Mitchell.
Mr Mitchell reiterated the concern with the release of the ATSB’s final report from the investigation into a fatal helicopter accident in Kosciuszko National Park on 3 April this year.
One of 7 helicopters taking part in a flying tour, a Bell 206L-4 LongRanger, registered VH-PRW, departed with a pilot and passenger on board, for a visual flight rules (VFR) flight from a private property at Majura, near Canberra, to Mangalore, Victoria, with a planned refuelling stop in Tumut.
The weather forecast indicated low cloud, rain and associated reduced visibility on the planned route, and 2 of the helicopters diverted to Wagga Wagga, due to weather while 4 others landed near Wee Jasper, to Canberra’s north-west.
The pilot of VH-PRW elected to continue until they encountered poor weather conditions and landed in open terrain alongside Long Plain Road in the Brindabella region, west of Canberra and to the south of Wee Jasper, shortly before noon, the investigation report details (pictured).
About three hours later, at 1453 local time, the helicopter departed the interim landing site at low level, in overcast conditions with low cloud and light rain.
At about 1525, recorded data showed that the helicopter commenced a rapid climb and shortly after, entered a steep left descending turn which continued until it impacted terrain at an elevation of 4,501 ft.
A search was initiated the next day with the accident site located later that evening. The helicopter was destroyed, and both occupants were fatally injured.
The pilot held a private pilot licence (helicopter) and did not hold an instrument rating, and the helicopter was not approved for instrument flight.
“The pilot initially made the right decision and landed the helicopter,” noted Mr Mitchell.
“However, you’re only as safe as your last decision, and the pilot’s then decision to launch again and push on – for reasons that we will never fully comprehend – put the helicopter into a dangerous environment with powerful and misleading orientation sensations and no visual cues.
“It is highly likely these cloud and visibility conditions resulted in the pilot experiencing a loss of visual reference and probably becoming spatially disoriented. Tragically, this led to a loss of control of the helicopter and an unsurvivable collision with terrain.”
This investigation report is the second the ATSB has released this month into an accident where a VFR pilot likely encountered low visibility conditions, before becoming spatially disorientated leading to a loss of control of their aircraft.
In 2018, following the final report release into another fatal helicopter accident involving VFR into IMC conditions, the ATSB, in conjunction with CASA and the Australian Helicopter Industry Association launched the ‘Don’t Push it, LAND IT – when it’s not right in flight’ safety campaign encouraging helicopter pilots to conduct a precautionary landing rather than push on into abnormal situations.
“Pushing on into cloud and low visibility when you do not hold the appropriate rating and experience carries a significant risk of severe spatial disorientation and can affect any pilot, no matter what their level of experience.”
In the decade from 1 November 2012 to 1 November 2022, 97 VFR into IMC occurrences in Australian airspace were reported to the ATSB. Of those, 11 were accidents resulting in 22 fatalities.
Mr Mitchell stressed the importance of planning ahead to avoid deteriorating weather.
“Ensure you have alternate plans in case of an unexpected deterioration in the weather and make timely decisions to turn back or divert,” he said.
“And know your limits. As a visual flight rules pilot the use of a ‘personal minimums’ checklist helps to control and manage flight risks through identifying risk factors that include marginal weather conditions.
“The ATSB continues to see this category of accident happening,” Mr Mitchell noted.
“In fact, this is the second final report we’ve published this month into a fatal accident where a visually rated pilot has likely become spatial disorientated and collided with terrain.
“Please, only fly in environments that do not exceed your capabilities, and most importantly, don’t push it, land it. Or, just don’t go.”