
Weather a consideration in on-going investigation of light aircraft accident west of Brisbane
Key points
- Preliminary report details factual information established in the investigation’s early evidence collection phase;
- Aircraft was operating under visual flight rules and was attempting to return to Archerfield from a property near Roma;
- Weather forecast indicated that the route could be affected by low cloud, rain, fog and associated reduced visibility;
- Witnesses recalled seeing the aircraft flying at low altitude below cloud.
The Australian Transport Safety Bureau (ATSB) has released a preliminary report from its on-going investigation into a fatal light aircraft accident west of Brisbane in August.
On 28 August 2022, the Cessna R182 Skylane RG, operated by Executive Helicopters, was returning to Archerfield Airport from a private property north-east of Roma, with a pilot and two passengers on board, flying under visual flight rules (VFR).
When the aircraft did not arrive as expected, a search was coordinated by Airservices Australia and the Australian Maritime Safety Authority. The wreckage was located later that afternoon within the D’Aguilar Range on a steep section of wooded mountainous terrain. The aircraft was destroyed and all occupants were fatally injured.
“Today’s preliminary report details factual information established in the investigation’s early evidence collection phase,” ATSB Director Transport Safety Stuart Macleod said.
“It has been prepared to provide timely information to the industry and public, and contains no analysis or findings, which will be detailed in the final report.”
To date the ATSB has examined the accident site and wreckage, interviewed witnesses, collected meteorological data, aircraft maintenance and pilot records, and obtained flight tracking data.
The weather forecast available from the Bureau of Meteorology at the time of the aircraft’s departure indicated that the route to Archerfield could be affected by low cloud, rain, fog and associated reduced visibility.
Flight tracking data showed the aircraft attempted to pass over the Biarra Range at a low height above the ground. Shortly after, the aircraft made a 180° turn, climbed and flew to Dalby Airport where it landed and refuelled. It departed again for Archerfield 11 minutes later.
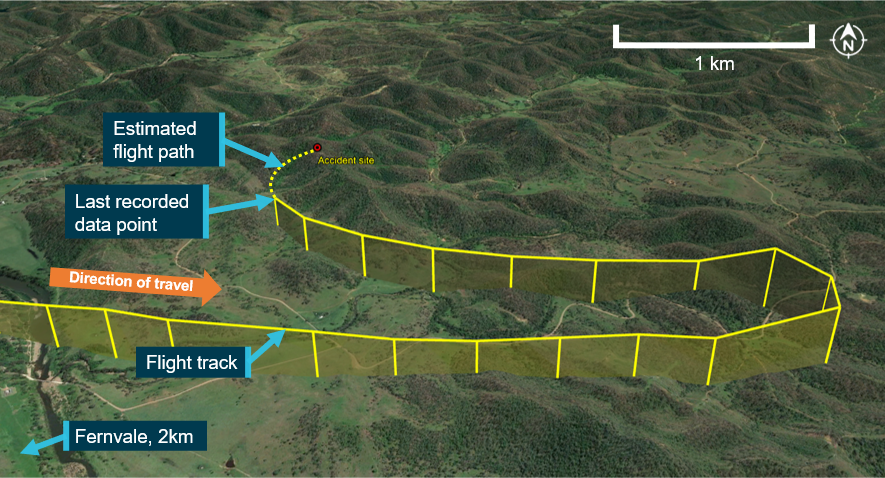
The preliminary report then details the aircraft’s flight path over the subsequent 55 minutes, during which it passed over rising terrain, mountain ridges and a hill at heights as low as 200 ft above ground level (AGL).
Prior to the collision with terrain, the aircraft had progressed down a valley near Fernvale, completing another 180° turn while climbing to 1,000 ft AGL. After the turn, the aircraft descended to 600 ft AGL before turning right, back towards the D’Aguilar Range. It was during this turn that the aircraft impacted terrain.
“The aircraft was equipped for flight under both VFR and instrument flight rules, and the pilot previously held an aeroplane instrument rating, but this was not current as the last renewal was completed in October 2002,” Mr Macleod said.
Several witnesses along the aircraft’s route from Dalby recalled seeing the aircraft flying at low altitude below cloud.
One witness at Fernvale reported the aircraft flying at low altitude while heading east towards the D’Aguilar Range with the wings level and undercarriage retracted, before banking left and disappearing from view as it was obscured by cloud. The witness also reported heavy low cloud, very light rain, and fog covering Fernvale and the surrounding area at the time.
The ATSB’s on-site examination indicated the aircraft’s engine was providing power at impact, with the landing gear and flaps in the retracted position. There was no evidence of an in-flight break-up or a pre-existing defect with the flight controls.
“The investigation is continuing and will include a further review and examination of pilot records and medical information, aircraft maintenance and flight records, operator procedures, meteorological data and recorded data,” Mr Macleod said.
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified at any time during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.”
Read the preliminary report: Collision with terrain involving Cessna R182, VH-EHM 36 km north-west of Archerfield Airport, Queensland, on 29 August 2022
Mentone helicopter accident
Released: Wednesday 30 November 2022
The following statement can be attributed to ATSB Chief Commissioner Angus Mitchell:
“The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into an accident involving a Hughes 269C helicopter at Mentone, in Melbourne’s south-east, on Wednesday.
“The helicopter was reported to have been conducting a missed approach (go-around) procedure from Moorabbin Airport when it collided with the roof of a house.
“As part of its investigation, the ATSB will interview the pilot and any witnesses, and obtain and review recorded data, weather information, aircraft information and maintenance records.
“The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
“However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.”
//Ends

Separation issues involving a Cessna 404 and an American Champion 8KCAB, 8 NM south-east of Moorabbin Airport, Victoria, on 3 November 2022
Brief
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On the morning of 3 November 2022, a Cessna 404 was conducting a freight charter flight from Devonport, Tasmania to Moorabbin, Victoria, operating under instrument flight rules (IFR). While on descent at about 8 NM from Moorabbin in instrument meteorological conditions (IMC), the pilot received traffic information from Moorabbin tower air traffic control (ATC) on an American champion 8KCAB operating under visual flight rules (VFR) on a converging track, departing to the training area (Figure 1). The pilot of the Cessna 404 located the traffic on the aircraft’s traffic advisory system (TAS) and made an initial assessment that the aircraft appeared to be at about the same altitude, climbing between clouds. The pilot increased the descent rate in an effort to increase the separation between the aircraft.
The flight tracks show that both aircraft were in the descent when the Cessna 404 pilot became visual with the American champion 8KCAB. The pilot estimated the other aircraft to be about 300 ft above and slightly right of track at the point of becoming visual.
Figure 1: Image showing both aircraft tracks

Source: Google earth with flightradar24 track overlays, annotated by ATSB.
Safety message
ATC provides traffic information to IFR aircraft even when operating outside controlled airspace (OCTA), however, VFR traffic operating OCTA may change locations, altitudes and intentions without informing ATC. This incident highlights the importance of establishing two-way communication with traffic in the local area and using systems such as the TAS and ADS-B to ensure separation between aircraft is maintained in reduced visibility environments. The ATSB safety study, Aircraft performance and cockpit visibility study supporting investigation into the mid-air collision involving VH-AEM and VH-JQF near Mangalore Airport, Victoria on 19 February 2020 (AS-2022-001) discusses this in more detail. In this instance, the pilot was able to utilise the aircraft’s systems to improve situational awareness and build a mental model of where the other aircraft was located to increase separation.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2022-017 |
| Occurrence date | 03/11/2022 |
| Location | 8 NM south-east of Moorabbin Airport |
| State | Victoria |
| Occurrence class | Incident |
| Aviation occurrence category | Aircraft separation |
| Brief release date | 16/12/2022 |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 404 |
| Sector | Piston |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Devonport, Tasmania |
| Destination | Moorabbin, Victoria |
| Damage | Nil |
Aircraft details
| Manufacturer | American Aircraft Corp |
|---|---|
| Model | 8KCAB |
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Moorabbin, Victoria |
| Destination | Moorabbin, Victoria |
| Damage | Nil |
Failure to pressurise, Beech Aircraft Corp B200T, 34 km west-south-west of Northam, Western Australia, on 27 September 2022
Brief
| Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. |
What happened
On 27 September 2022 at 0845 local time, the pilot of a Beech Aircraft Corp B200T was conducting a ferry flight from Jandakot to Kalgoorlie-Boulder, Western Australia. Prior to departure, the pilot conducted engine run-up and cabin pressurisation checks confirming serviceability. During the initial climb, the pilot conducted the after take-off checks, including to ensure the bleed air valves[1] were open and the cabin was pressurising. This was confirmed by a positive rate of climb indication on the pressurisation vertical speed indicator. Normal operation of the pressurisation system was confirmed again passing 10,000 ft on climb.
At an altitude between flight level (FL) 180[2] and FL 200, the pilot observed the illumination of the altitude warning annunciator (Figure 1) and the master warning. The pilot noticed the cabin altitude and aircraft altitude gauges matching and then observed the passenger oxygen masks in the cabin had dropped.
The pilot donned an oxygen mask and commenced an emergency descent to 10,000 ft. During the descent, the pilot was unable to get oxygen due to the oxygen mask’s microphone dislodging from its mount. The pilot increased the oxygen flow rate and conducted a return to Jandakot.
The engineering inspection revealed the door seal was not inflating correctly.
Figure 1: Pilots are alerted to pressurisation faults via an illuminated alert

Source: Operator, annotated by ATSB
Pilot comments
The pilot reported feeling unwell and noted a longer than usual response time for actioning the descent.
Safety action
The operator advised the ATSB that pilots will undergo a revision briefing for pressurisation system faults and recognising the signs of hypoxia. The operator will also ensure pilots check the serviceability of oxygen masks as part of the first flight of day checks.
Safety message
This incident highlights the importance of ensuring crew oxygen masks are checked for serviceability as part of the daily inspection. This incident further highlights the importance for pilots to have a thorough understanding of the pressurisation system, in particular recognising and reacting to faults in a timely manner. The Beech B200T aircraft alerts the pilot of pressurisation faults with a visual alert only in the form of an illuminated light on the annunciator panel.
Mild hypoxia is not known to impair complex cognition but it has been found to increase fatigue and decrease vigour. Further information about hypoxia can be found in the ATSB research report Depressurisation, Accidents and Incidents Involving Australian Civil Aircraft, and in the Flight Safety Australia article Do not go gentle: the harsh facts of hypoxia.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1] An automatic bleeding valve or air release valve (ARV) is a plumbing valve used to automatically release trapped air from a heating system.
[2] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 370 equates to 37,000 ft.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2022-014 |
| Occurrence date | 27/09/2022 |
| Location | 34 km west south-west of Northam, |
| State | Western Australia |
| Occurrence class | Serious Incident |
| Highest injury level | None |
| Brief release date | 16/12/2022 |
Aircraft details
| Manufacturer | Beech Aircraft Corp |
|---|---|
| Model | B200T |
| Operation type | Part 138 Aerial work operations |
| Departure point | Jandakot, Western Australia |
| Destination | Kalgoorlie, Western Australia |
| Damage | Nil |
Large bird carcass found at Chinchilla aerial application aircraft accident site

Key points
- Air Tractor aircraft was conducting spraying operations typically about 2 metres above the ground;
- A large bird carcass, later identified as an Australian bustard, was found in the cockpit;
- Preliminary report contains no analysis or findings but details information from the investigation’s early evidence collection phase.
A large bird carcass was found in the cockpit of an Air Tractor aerial application aircraft which had collided with the ground during spraying operations on a property near Chinchilla, Queensland, a preliminary report from the ATSB’s on-going investigation details.
The preliminary report contains no analysis or findings but details information from the investigation’s early evidence collection phase, and notes that the Air Tractor AT-502B had been conducting spray runs on the morning of 19 September 2022.
Around 1200, the loader at the private airstrip about 24 NM (44 km) south-east of Chinchilla from where the Air Tractor had been operating attempted to call the pilot to ask whether they needed more fuel.
Concerned with having received no response, the loader phoned the operations manager, who in turn contacted nearby farmers to assist with locating the aircraft.
At about 1215, a local farmer found the aircraft in the paddock where the pilot had been spraying. The pilot was fatally injured and the aircraft was destroyed.
“An ATSB examination of the accident site found that the aircraft had impacted terrain with the fuselage in a near vertical attitude, with its propeller and engine buried in the soft earth, and the wreckage contained to a small area,” said ATSB Director Transport Safety Dr Stuart Godley.
Ground scars and damage to the left wing indicated that the wing struck the ground at about 30° to the horizontal, and examination of the propeller and engine indicated that the engine was delivering power at the time of the impact.
There was no post-impact fire.
“A large bird carcass was found in the cockpit and the bird’s wings were located about 300 m north of the wreckage, in-line with the aircraft’s track,” said Dr Godley.
Biological residue from the bird was found outside the right cockpit window.
“At the request of the ATSB, the Australian Centre for Wildlife Genomics at the Australian Museum analysed biological specimens of the bird, identifying them as being from an Ardeotis australis, commonly known as an Australian bustard or Plains turkey.”
The Australian bustard is a large bird, 80 to 120 cm in height, with an average weight for an adult of 4.5 kg, with males weighing up to 8 kg. They are capable of flying but are mostly ground dwelling.
“The aircraft operator advised that for the field where the accident occurred, they expected that it would be sprayed at a height of about 2 m (6 ft) above the ground, to be just above the weeds.”
Dr Godley noted that the investigation is continuing, and will include research into the nature of birdstrikes and similar occurrences.
“Bird strikes resulting in fatal aircraft accidents are very rare, however, the ATSB is currently investigating a separate accident where a wedge-tailed eagle bird carcass was located near the accident site of a Bell LongRanger helicopter, which experienced an in-flight break-up near Maroota, New South Wales on 9 July 2022.”
The continuing investigation into the Chinchilla accident will include further review and examination of electronic components recovered from the accident site, operational documentation and maintenance records.
A final report will be published at the conclusion of the investigation
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Dr Godley said.
Read the preliminary report: Birdstrike and collision with terrain involving Air Tractor AT-502B, VH-KDR, 32 km east-north-east of Chinchilla Airport, Queensland, on 19 September 2022
Safety action taken after near miss on Sydney Trains network

Key points
- Workers had to jump out of the path of an oncoming passenger train when a signaller incorrectly removed track protections while a freight train was being reversed into a siding;
- Sydney Trains has taken a number of actions to address the issues identified in the subsequent transport safety investigation.
Sydney Trains has taken numerous safety actions in response to a near miss, which resulted in injuries to one rail worker, a transport safety investigation report notes.
On 8 January 2021, a Pacific National freight train with a driver, assistant driver, and trainee onboard, was travelling on the main line south toward Sydney, when it entered a steep section of track near Cowan Station and began to fail due to wheel slip.
Sydney Trains network control directed the crew to propel the train back down the slope, toward a siding at Hawkesbury River.
The assistant and trainee had to walk to the rear of the train, so they could direct the driver over radio throughout the movement. Due to the terrain, they had to walk on the opposite track throughout this procedure.
To protect the workers, the Sydney Trains signaller applied rail signals to prevent another train from entering the section of track, while the assistant driver and trainee were walking to the rear of the train.
When the driver reported the movement was beginning, the signaller removed the protection from the track. The signaller was not familiar with the terrain or the scenario and mistakenly believed the workers were clear of the track.
This meant a passenger train was allowed to enter the section where the workers were walking.
Seeing the lights of a train approaching, the assistant driver and trainee both jumped clear to an adjacent cess area, with one sustaining an injury.
An investigation by the Office of Transport Safety Investigation (OTSI), which conducts rail investigations in NSW on behalf of the Australian Transport Safety Bureau, detailed a range of contributing factors, safety issues, and safety actions that have been taken as a result of the incident.
“Training and competence management regimes for rail safety workers need to provide relevant and meaningful content, such as scenario-based training and site-based network familiarisation, to allow workers to perform safely and effectively,” OTSI Chief Investigator Dr Natalie Pelham said.
“The Sydney Trains signaller and the driver of the train did not observe the requirements of the relevant Train Working Network Rules and Procedures for protecting workers on track with in-service rail traffic.”
The investigation also notes Sydney Trains’ assurance and audit processes for signal box management had failed to detect non-conformances to procedure in the past.
“In this case, the signaller did not report this incident as per the relevant rule – it was only noted when the trainee worker reported their injury,” Dr Pelham said.
“To provide confidence that rules and procedures are being followed and they are effective in managing relevant risks, rail operator assurance processes need to detect non-conformances.”
As a result of this incident, Sydney Trains has taken a range of actions, including re-introducing safety refresher training for signallers, providing signallers with a pair of Safe Tracks alerts, a new Operating Instruction for propelling movements at Cowan Bank, a communications cue card, and an e-learning course on the use of the relevant Network Rule.
The operator has also instructed all signallers to report each use of the relevant Network Rule to their line manager, and all line managers have been instructed to submit an audio compliance request for all reported uses for review.
Read the final report: Safeworking irregularity and near miss with crew of train 5936, at Hawkesbury River, New South Wales, on 8 January 2021
Ship’s fittings in poor condition prior to loss of 50 containers off Sydney

Key points
- ATSB found fixed container securing arrangements on APL England were in poor state of repair and corroded, prior to loss of 50 containers in heavy seas off Sydney;
- APL has reviewed and repaired container fittings on APL England and across the rest of its container fleet;
- APL has implemented safety action regarding passage planning and navigation in bad weather; procedures were not followed during this incident.
A final report into the loss of containers from a ship off Sydney in 2020 notes the importance of vessel fixtures being regularly maintained to ensure they are secure and stable.
Container ship APL England was making way down the east coast of Australia on 24 May 2020 when, in adverse weather, it underwent a series of heavy rolls that resulted in the loss of 50 containers overboard, and shutdown of the main engine.
The Australian Transport Safety Bureau’s investigation found the ship’s fixed container securing arrangements on deck were in a poor state of repair and the strength of many securing fixtures was severely reduced by corrosion.
“Our investigators found this condition would have taken several years of poor maintenance to develop,” ATSB Chief Commissioner Angus Mitchell said.
“This showed the ship had not received the scrutiny from crewmembers, shore management, or other agencies that a ship of its age or condition required.”
In addition, the investigation found procedures for adverse weather were not followed.
“Had these procedures and associated assessment tools been used, navigational and operational decisions could have been made, which would have better prepared the ship for the conditions encountered,” Mr Mitchell said.
Since the incident, fixtures on the APL England were repaired, and deck and container fittings on all other vessels in the APL fleet were inspected and repaired as required.
APL also implemented additional safety action regarding planning and navigation in heavy weather.
“This incident should be a reminder to all ship masters and crews of the importance of adhering to the cargo securing manual, and of following specific procedures and guidance material ahead of – and during – adverse weather,” Mr Mitchell said.
Mr Mitchell also welcomed an update in July 2022, from shipping classification society DNV, to include a new section in the relevant Class Guideline providing requirements on the allowable wear and tear of container supporting structures and container securing equipment.
Read the final report: Loss of containers overboard from APL England, 46 NM south-east of Sydney, New South Wales, on 24 May 2020
Engine fire during start-up involving a Piper PA-28-161, Moorabbin, Victoria, on 11 October 2022
Brief
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 11 October 2022 at 0950 local time, a student pilot prepared a Piper PA-28-161 for a solo navigation exercise at Moorabbin, Victoria. Prior to the flight, the instructor had inspected the aircraft and signed the maintenance release. The student then conducted their own inspection of the aircraft noting there were no defects, which was consistent with the instructor’s assessment.
The student actioned the pre-start checklist but reported difficulty starting the engine after using the electric prime for approximately 5 seconds on the first attempt, and another 3 seconds on the second attempt. On the third attempt, a loud ‘pop’ was heard from the engine, and the student elected to exit the aircraft and ask for help. At this time, smoke was observed emanating from the engine cowling and, upon opening, a fire was found around the carburettor. A fire extinguisher was obtained and the student returned to the aircraft and extinguished the flames. The aircraft sustained minor damage to the engine and surrounding airframe.
Figure 1: Burnt engine cowling

Source: Operator
Safety action
The operator’s pre-start checklist called for an engine fire brief prior to starting, which requires fuel isolation and continued engine cranking to ingest and extinguish a fire. In this case, the student had not suspected an engine fire until after exiting the aircraft. The operator has raised the matter at a recent safety training day for students.
The operator is also reviewing the aircraft pre-start checklist which will include monitoring of the fuel pressure after application of the fuel pump to determine possible malfunctions of the carburettor.
Safety message
Different start procedures may be required for cold and hot starts, and therefore pilots should have an understanding of what these differences mean in terms of engine management and possible consequences. Checklists are a prompt to ensure the required steps are taken to achieve a desired configuration or process. Aircraft manuals are a valuable source of information when it comes to normal starting procedures, and further guidance may be available through company operating procedures. The Aircraft Owners and Pilots Association (AOPA) publication Aircraft Fires - AOPA discusses multiple aircraft fire types. The section regarding engine fires on start notes it as a very common occurrence, which highlights the importance of remaining vigilant during engine starts.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2022-013 |
| Occurrence date | 11/10/2022 |
| Location | Moorabbin |
| State | Victoria |
| Occurrence class | Serious Incident |
| Aviation occurrence category | Fire |
| Brief release date | 16/12/2022 |
Aircraft details
| Model | Piper PA-28-161 |
|---|---|
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Moorabbin, Victoria |
| Destination | Moorabbin, Victoria |
| Damage | Minor |
Ground injury involving Cessna 182, Lower Light, South Australia, on 10 July 2022
Brief
| Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. |
What happened
On 10 July 2022, a group of skydivers were preparing for a jump that was to be filmed by an instructor.
At about 0850 local time, the pilot of the Cessna 182 taxied the aircraft to the passenger emplaning area and prepared to hot load[1] the skydivers. The proposed jump had an instructor positioned either side of the student in the doorway and a third instructor located outside the aircraft to capture the groups freefall. The group conducted a practice exit before the instructor filming repositioned themselves in front of the wing strut to show the student where they would be located when they completed the jump.
The pilot, recognising the instructor’s proximity to the spinning propeller, attempted to get their attention. The instructor filming was focussed on the jumpers and took a small step backwards towards the propeller at which point the pilot immediately shut down the engine. The instructor took another step backwards and away from the fuselage of the plane to simulate their own freefall and their hand was struck by the propeller. Although the engine had been shut down, the propeller was still spinning. The instructor received serious injuries to their hand.
Guidance on hot loading
Hot loading is a common practice in skydiving operations. Guidance provided by the Australian Parachuting Federation[2] (APF) to its members in the
Jump Pilot Manual V01-2023.pdf
(1.89 MB)
, included the warning that:The jump pilot faces a greater risk of having someone walk into the propeller than does a pilot working in any other environment.
To mitigate the risk of this happening, the manual suggested that skydivers and staff should approach the aircraft from the rear where possible. Skydivers and instructors were taught to be propeller aware with posters from the APF warning of the dangers associated with spinning propellers. Additional procedures for movement around aircraft were left to the operator. In this instance, the operator’s procedures specified that any task that required a person to be positioned forward of the wing strut was to be conducted on a mock-up airframe or with the engine shutdown.
Regulatory changes
The loading of passengers with engines running and the requirement to brief passengers for this particular activity was previously covered in Civil Aviation Orders section 20.9.5 (CAO). Following CASA’s regulatory framework reform, numerous CAO were incorporated into Part 91—General operating and flight rules and Part 138—Aerial work operations, of the Civil Aviation Safety Regulations 1998 (CASR). Part 105 of the CASR set out the operational requirements for aircraft used to facilitate parachute descents. These were in addition to Part 91 which also applied to parachuting operations.
While hot loading was covered in Part 138, there were no regulations that applied to the loading of passengers with engines running during skydiving operations in Part 91 or Part 105. CASA advised the ATSB that while less prescriptive than the previous regulation set, the practice of hot loading would be accepted if certain requirements were met:
CASR 91.055 is of general application and requires the pilot in command to not create a hazard to other aircraft, persons, or property. The hazards of loading passengers while the engines are running are significant and CASA would not see this activity as being able to be safely achieved without creating a hazard unless it was conducted by an operator with the organisational structure and procedures to adequately manage those hazards in the context of the operation.
The APF produced guidance material for parachuting operators with the requirements for safety on the ground contained within a number of manuals, including the Training Operations Manual and the Jump Pilots Manual.
Safety action
The operator advised the ATSB that they have taken the following safety action in response to this accident:
- Banned jumpers from conducting practice exits from the aircraft while the engine is running.
- Mock-up aircraft cabin is planned for refurbishment to facilitate practice exits.
- Ground control officer has been made responsible for supervising the boarding of aircraft
- Safe routes to the loading area have been defined.
- Signage refurbished and placed in prominent areas warning of the dangers associated with propellers.
- Conducted briefings with all regular jumpers and staff about the seriousness of this incident and re-iterated the importance of remaining vigilant in the vicinity of aircraft.
Safety message
Hot loading is a common practice in parachuting operations and the commercial benefits of not shutting down an aircraft’s engines needs to be measured against the increased risk to the proposed activity. Clear and workable procedures are critical in ensuring the risk is reduced to as low as reasonably practicable.
In this accident, the instructor was in a hazard-rich environment completing a task that did not necessitate the engine to be running at the time. In addition to a knowledge and understanding of risks present in the operational environment, crew must be especially vigilant in the vicinity of operating aircraft.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2022-005 |
| Occurrence date | 10/07/2022 |
| Location | Lower Light |
| State | South Australia |
| Occurrence class | Accident |
| Aviation occurrence category | Ground operations - Other |
| Highest injury level | Serious |
| Brief release date | 16/12/2022 |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 182H |
| Operation type | General Aviation |
| Departure point | Lower Light, South Australia |
| Destination | Lower Light, South Australia |