
Final report
Report release date: 04/02/2026
Investigation summary
What happened
On 1 February 2025, a Sikorsky S‑92A helicopter operated by PHI International Australia, departed Exmouth Aerodrome, Western Australia, to conduct night recency flights, including landings and take-offs, at an off-shore drill rig for the 3 crew on board. They departed for the Transocean Endurance drill rig, about 71 km north-north-west of Exmouth Aerodrome.
During the cruise, the copilot was rushed to complete the calculations of the helicopter’s take-off safety speed, a requirement to complete the approach briefing. Unsure of the accuracy of the calculation the crew agreed to use an estimated take-off safety speed and commenced the descent.
At about 1,500 ft, the copilot set the radar altitude hold mode to the circuit height of 660 ft to allow the helicopter’s automation to descend to, and level at, the preset circuit height.
Assuming the helicopter had levelled at the preset circuit height of 660 ft, the captain requested the copilot to check the accuracy of their earlier take-off safety speed estimate, which required the copilot to use the electronic flight bag. At about the same time, the captain elected to activate the helicopter’s moveable searchlight and shifted their focus outside to adjust the position of the searchlight beam.
Unnoticed by the crew, the helicopter continued to descend and, at about 220 ft above the ocean surface, the enhanced ground proximity warning system indicated a terrain caution alert, followed about 4 seconds later by a terrain warning as the aircraft descended through 181 ft. The crew responded to the warning and initiated a climb, the helicopter descended to its lowest point of 152 ft above the water, before climbing away.
What the ATSB found
Both flight crew members had limited experience on the helicopter type at night. The combination of this limited experience and a shorter than normal sector, which reduced the time to plan the approach, resulted in them experiencing a higher than normal workload.
As the helicopter descended through about 1,200 ft, the captain inadvertently mis‑selected the vertical speed mode while attempting to select the helicopter’s autopilot heading hold mode. The mode selection error was not recognised by either flight crew member. The selection cancelled an automation mode that would have levelled the helicopter at a preset circuit height, and instead activated a mode that set up a continuous 500 ft per minute descent until the crew reacted to the EGPWS alerts.
The flight crew had been unable to accurately determine the take-off safety speed prior to their descent for landing. While in the circuit area, the captain requested the copilot calculate the speed, which increased workload and focused them away from their monitoring duties.
While in the circuit area, both flight crew members were preoccupied with additional tasks and therefore not monitoring the helicopter’s altitude as it continued to descend below the preset circuit height until the flight crew reacted to the automated terrain alert.
The operator’s pre-flight operational risk assessment completed by the flight crew did not capture the risks of the flight crew’s limited experience on type at night.
What has been done as a result
PHI International Australia advised that procedural improvements have been implemented, including:
- All initial approaches during night flights to be conducted as an instrument approach, which ensures a more structured process with procedural barriers.
- Night recency flights not to be conducted on a first flight back following any pilots’ period of leave.
- Radar altimeter alert to be set at 500 ft.
PHI International Australia also increased the risk loading on its operational risk assessment for pilots with less than 500 hours on type. Night flights with both pilots with less than 500 hours on type at night now require discussion with the senior base pilot regarding the additional risks relating to inexperience on type.
Learnings from this occurrence have been shared and promoted both internally and externally. These efforts included an internal safety alert and a ‘learning from occurrence’ video detailing what happened and why to the international community through industry body HeliOffshore.
The S‑92A cockpit lighting environment was reviewed by the operator with subject matter experts to consider if an engineered improvement was practicable. A procedural change was implemented by PHI International Australia that required the use of small lights that are worn on the pilot’s fingers to improve visibility of the cockpit environment (such as switches, buttons, and controls) during S‑92A night flights.
Operational procedures regarding multi-crew cooperation, automation mode changes/awareness, and EGPWS alerts were highlighted to all flight crews through internal communications. These points were also highlighted within the training and competency teams as focus areas during both simulator and line training sessions.
Safety message
The incident highlights the importance of disciplined and effective multi-crew cooperation. A deviation by flight crew from operational processes may lead to unrecognised errors and undesired aircraft states. Flight crew are reminded of the risks associated with divided attention in the cockpit and the potential serious consequences of an unmonitored aircraft. Operators are advised to review their guidance on flight crew preoccupation.
All operators of Sikorsky S‑92A helicopters are advised of the potential hazard that exists with differing display versions of the automatic flight control system mode select panel. Due to the lighting design of the panel, distinguishing between hard and soft keys is more difficult at night. More recent versions of the mode select panel include a tactile white finger barrier installed between the rows of hard and soft keys which reduce but do not eliminate the risk of a mode selection error.
The occurrence
On the evening of 1 February 2025, a Sikorsky S‑92A helicopter operated by PHI International Australia and registered VH-IPE, departed Exmouth Aerodrome, Western Australia, to drilling rig Transocean Endurance, located about 38 NM (71 km) to the north‑north-west of Exmouth Aerodrome. On board were 3 crew conducting a night recency flight, the captain was the pilot flying (PF), in the right seat and the copilot was the pilot monitoring (PM)[1] in the left seat. The third pilot was seated in a passenger seat in the main cabin of the helicopter.[2]
The helicopter departed Exmouth at about 1918 local time, with last light occurring at 1933. The purpose of the flight was for each pilot to conduct 3 take-offs and landings so the crew would remain current in case of a night medical emergency evacuation from an offshore drilling rig. The operator routinely used offshore rigs for night recency flights so pilots remained familiar with night helideck landings.
Cruise
On board flight data indicated that following the departure from Exmouth, the helicopter reached the top of climb height of 4,000 ft at 1924 and maintained the cruise altitude for about 9 minutes. During that time the PM completed flight administration tasks that included:
- communication with Melbourne Centre air traffic control (ATC)
- conduct of the cruise checklist
- entering the flight log details with ETA to the rig
- calculation of top of descent
- communication with the drill rig to confirm weather and deck status
- conduct of the descent checklist.
On receiving the updated weather information from the rig, the PM intended to calculate the take-off safety speed (Vtoss) for landing. Vtoss is used by the operator as a minimum target speed in the event that one engine became inoperable during the approach to land. The target airspeed is set on the airspeed indicator with a marker bug for the crew to use as a reference, and is required to be set as part of the approach briefing (see Take‑off safety speed (Vtoss)).
The PM recalled that while trying to obtain the predicted gross landing weight from the onboard flight management system, they had difficulty obtaining an accurate figure. This delayed the input of the weight into the Sikorsky performance application. The PM later reported the process was rushed, and as a result was unsure of the accuracy of the calculated Vtoss for landing prior to the top of descent.
To allow the crew to complete the descent checklist, the PM later reported that the crew agreed to use 45 kt, based on their previous experience in the S‑92A, with the intention of recalculating the speed when time permitted.
Descent
At about 1933 and 11 NM (20 km) south-east of the drill rig and now in darkness (see Meteorological information), the helicopter began a descent to the lowest safe altitude of 1,500 ft (Figure 1). At 1937, the PF requested the PM to engage the radar altimeter (RADALT) hold mode and lower the target altitude capture height to the 660 ft circuit height. This was confirmed by the PM and the helicopter commenced a further descent to the drill rig circuit height. Both flight crew later recalled completing the before landing checklist during the descent.
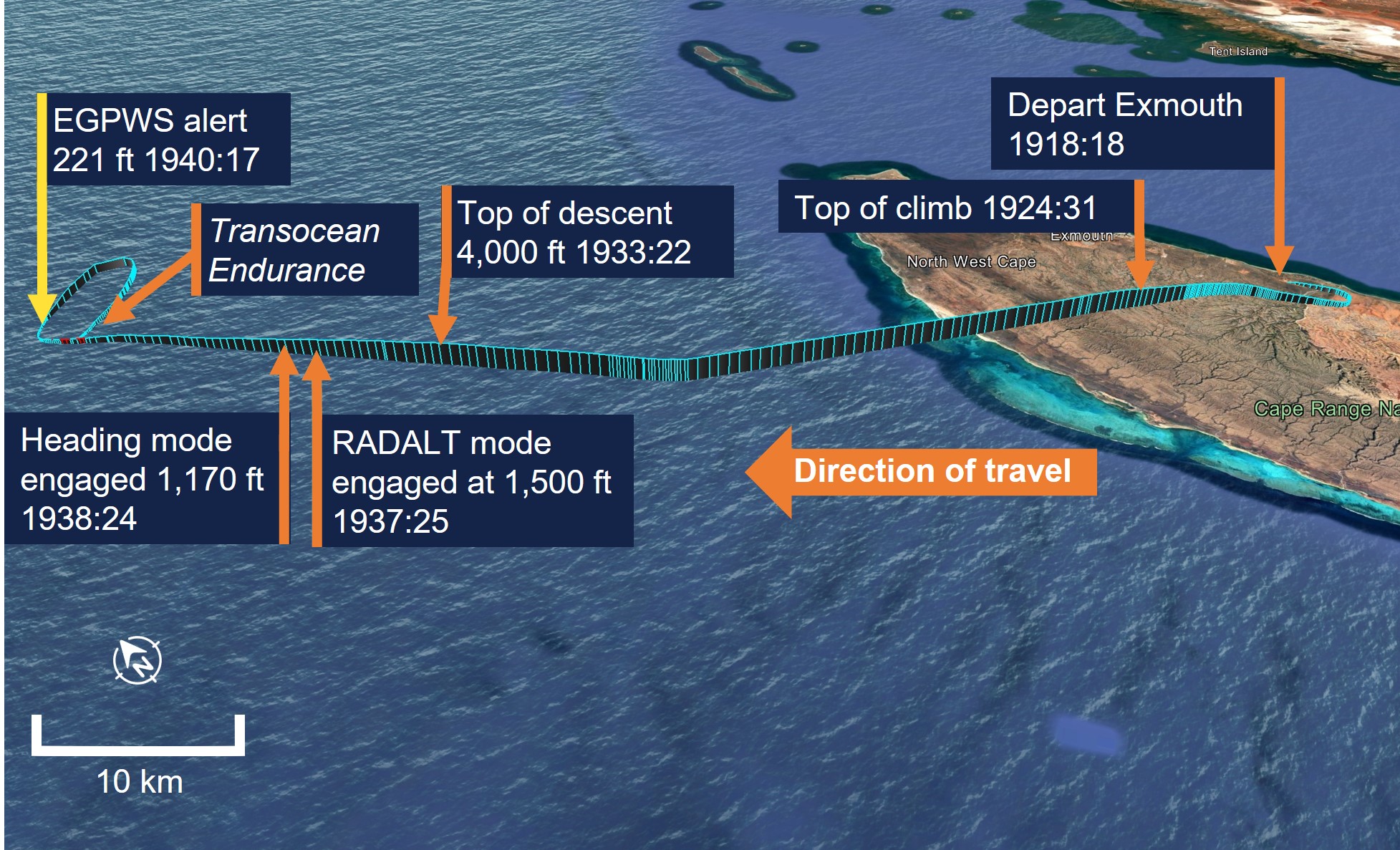
Source: Google Earth, annotated by the ATSB
At 1938:21 and about 1,235 ft, during the descent for a visual approach to the rig (Figure 2), the PF attempted to select the heading mode on the automatic flight control system (AFCS) mode select panel to adjust the heading and avoid flying directly over the rig.
While attempting to press the heading mode button, the PF inadvertently and unknowingly selected the vertical speed button which was directly below it.
The inadvertent selection of the vertical speed hold mode captured the helicopter’s 500 ft per minute rate of descent, and cancelled the RADALT hold mode that would have levelled the helicopter at a preset circuit height of 660 ft above sea level.
The PF noticed the heading button on the AFCS panel was not lit, indicating it was not engaged and presumed the original selection had not registered on the first attempt and reselected the heading mode key. Heading hold mode was engaged at 1938:24, at about 1,200 ft. The PF later recalled confirming the selection with the PM.
During interviews conducted with the ATSB following the occurrence, both flight crew reported they believed their total time and time at night flying the S‑92A likely affected their familiarity with the cockpit and efficiency completing administrative tasks.
Figure 2: VH-IPE flight track from 1,500 ft
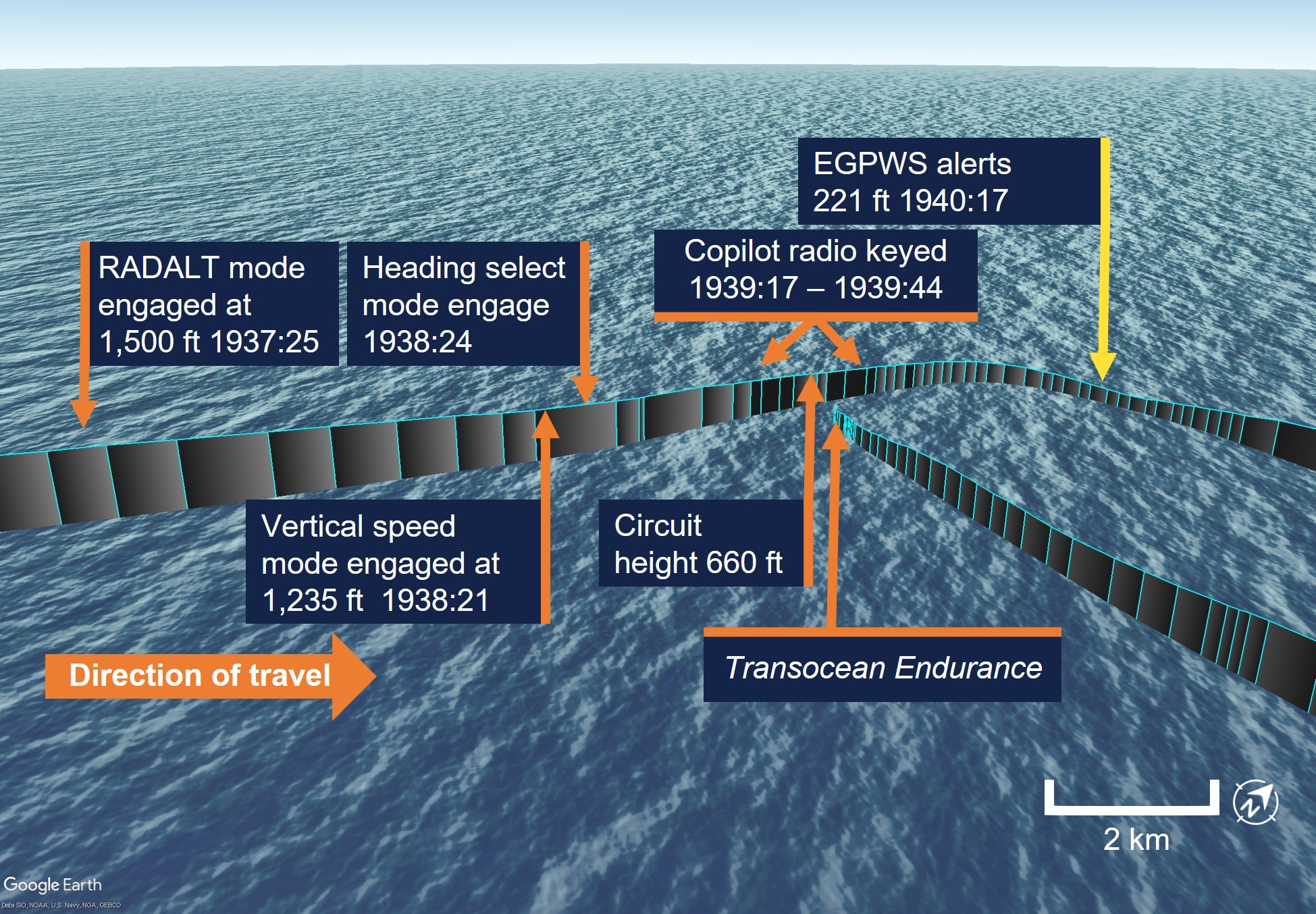
Source: Google Earth, annotated by the ATSB
Circuit
At 1939:00, the helicopter joined a crosswind leg to conduct a right circuit to the rig. This was so the PF could keep the rig visible from their side of the helicopter. While on the crosswind leg, the PM’s radio was keyed several times (see Recorded information). During this time, both crew were unaware that the helicopter had continued descent through the preset circuit height of 660 ft.
At 1939:46 and about 500 ft, the PF commenced a turn onto the downwind leg of the circuit and later stated they were certain the helicopter had levelled at the circuit height. The PF then requested the PM to check the Vtoss for landing, later stating that they thought the estimated speed was too high. This required the PM to use the electronic flight bag (EFB). During an interview the PF recalled at this point they also began to manoeuvre the helicopter searchlight which required them to visually identify that the beam was in the desired direction. The PF later reported they had difficulty finding the searchlight beam due to reflection on the water from the well-lit rig, and therefore setting the beam in the right position took longer than expected.
At 1940:17 and 221 ft, the crew received an EGPWS terrain caution alert and at 1940:21 and 181 ft, this was followed by a terrain warning alert. The crew reacted to the alerts and initiated an emergency climb to the minimum safe altitude of 1,500 ft. At 1940:25, recorded data showed the helicopter had descended as low as 152 ft above the ocean before increasing altitude.
Debrief and continued operations
When the helicopter had reached the minimum safe altitude, the crew discussed the incident and believed that they had identified that the unintended descent was a result of the PF accidently adjusting the RADALT target height as the trim switch is located in close proximity to the searchlight slew toggle on the collective[3] control lever.
The crew agreed they were comfortable to continue with the planned night recency flights and the helicopter landed on the helideck of the rig at 1949.
The 3 crew each completed the 3 required night take-offs and landings from the rig and then returned to Exmouth without incident, landing at 2208.
Context
Personnel information
Captain
The captain held an Air Transport Pilot Licence (Helicopter), issued on 23 June 1995 and a class 1 aviation medical that was valid until 20 June 2025. They had accumulated about 10,240 hours total aeronautical experience, of which 1,100 hours were at night and about 3,530 total hours in multi-engine helicopters. The captain also held an instrument rating valid until 31 May 2026.
The captain joined PHI International Australia (previously Helicopters New Zealand) in 2014 and had operated from its Karratha, Western Australia base, flying AW 109 helicopters for marine pilot transfer operations.
The captain completed crew resource management (CRM) training as part of their operator conversion course for the S‑92A on 31 December 2023 and the CRM command training on 22 August 2024.
The captain had held a command position on the S‑92A with the operator since 8 October 2024 and had accumulated 77 command hours on type. They had previously flown the S‑92A as copilot and were checked to line in that position on 19 July 2024. At the time of the incident, the captain had accumulated 299 hours on type of which 13 hours were at night. The captain’s night hours were a combination of simulator assessments and their initial 5‑night helideck landings which was a minimum requirement for newly type rated flight crew.
The captain had last flown at night during an operational proficiency check flight in a simulator on 8 November 2024 and had completed their initial 5-night helideck landings as required by the operator to be rostered for night standby duty on 2 November 2024 while under supervision.
The captain had been rostered on night standby 5 times during their previous roster period, however had not been required to fly.
The occurrence flight was the captain’s first flight following 4 weeks off duty.
Copilot
The copilot held a commercial pilot licence (helicopter), issued on 20 August 2010 and a class 1 aviation medical valid until 6 June, 2025. The copilot’s total aeronautical experience was about 5,360 hours of which 1,240 were at night and about 2,390 total hours in multi-engine helicopters. The copilot held an instrument rating valid to 31 August 2025.
The copilot joined PHI International Australia in 2023 and had initially flown for the operator from their Karratha, Western Australia base flying the AW 109 for marine pilot transfer operations.
They had completed CRM training as part of their operator conversion course for the S‑92A on 11 November 2024. They were checked to line on the S‑92A on 29 November 2024 and had accumulated a total of 224 hours as copilot, of which 9 hours were at night at the time of the incident.
The copilot had last flown at night on 14 December 2024 during their initial night helideck landings under supervision.
The copilot was rostered for standby night duty 7 times during their previous roster period and also had not been required to fly at night before the occurrence flight.
The copilot began their rostered-on period on 17 January 2025 and had flown 3.6 hours the day prior to the occurrence flight.
Fatigue
The captain recently completed 4 weeks off duty and had travelled from their home in New Zealand to Perth 2 days prior to the occurrence and from Perth to Exmouth the day prior to the occurrence. The captain began their duty period at about 1715 on the afternoon of the occurrence and reported they felt well rested prior to the flight.
The captain reported that they had slept about 9 hours in the last 24 hours and had been awake for 13 hours but reported feeling lively and responsive at the time of the occurrence.
The copilot had commenced an online training course between 0800 and 1430 that day from their accommodation. They stated that they took the opportunity for a lay down to rest for an hour and eat following the course before commencing the second duty period at 1715 and stated they felt fine before the flight.
The copilot reported they had about 8 hours sleep in the last 24 hours and reported feeling okay and somewhat fresh at the time of the occurrence.
The ATSB considered that fatigue was not likely at a level that adversely affected the performance of either pilot.
Aircraft information
General information
The Sikorsky S‑92A is a 2 crew, twin-engine helicopter with a maximum take-off weight of 12,020 kg. With a capacity of 19 passengers it is commonly used for offshore oil and gas industry passenger transport. The S‑92A is powered by twin General Electric CT7‑8A turboshaft engines, producing 1,737 kW during maximum continuous power. The engines power a fully articulated 4-bladed main rotor system.
VH-IPE was manufactured in the United States in 2006 as serial number 920038 and was first registered in Australia in April 2017 by PHI International Australia (then Helicopters New Zealand).
Automation
The rotorcraft flight manual for the S‑92A provided a description of the automatic flight control system:
The Automatic Flight Control System (AFCS) electronically enhances basic aircraft handling qualities through a trim system, Stability Augmentation System (SAS), Attitude Hold (ATT) features, and Coupled Flight Director (CFD). The AFCS is dual redundant in all features except trim actuators. It is controlled via a single AFCS control panel located on the center console and two mode select panels located on each side of the instrument panel. Cyclic and collective switches plus main flight display bezel keys are also used to control the AFCS. The core of the AFCS consists of two separate and identical Flight Control Computers (FCC) which receive data from various aircraft sensors. AFCS control inputs are enabled via electrically powered trim actuators and hydraulically powered SAS servos.
Coupled flight director
The CFD utilised trim actuators to maintain the helicopter on a pilot selected flight path. The following features (Table 1) are available through the CFD.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mode select panel
Two AFCS mode select panels were located on the lower middle section of the helicopter instrument panel (Figure 3). The rotorcraft flight manual described the mode select panel (MSP) functions:
Coupled modes are selected by pressing the appropriate keys on the active MSP. There are four hard keys on top of each MSP. These hard keys allow the pilot to select or deselect the three basic autopilot modes of airspeed, altitude and heading hold. The function of these hard keys does not change. When any of these hard keys are pressed on the active MSP the aircraft will immediately couple the selected parameter and the hard key will light. The standby hard key on the active MSP and the standby button on either cyclic stick will always deselect all flight director functions and decouple the aircraft. Hard keys along the bottom of the MSP allow the pilot to choose CRUISE, APPROACH or TEST menus. The centre display area of the MSP is surrounded by soft keys whose function will change depending on the menu selected. Once a soft key is pressed the mode goes to ARM, CAPTURE or ON. ARM is displayed in white signifying that control inputs are not being made based on this mode. CAPTURE or ON is displayed in green signifying that the mode is now controlling that portion of the CFD.
Figure 3: Sikorsky S‑92A cockpit

Source: Vertical, annotated by the ATSB (occurrence aircraft not depicted)
The manufacturer advised that from aircraft serial number 920057 (built after VH-IPE), the mode select panel was upgraded to incorporate 2 white coloured finger barriers above and below the display screen between the rows of hard and soft keys (Figure 4). The barrier protruded higher than the height of both the soft and hard keys and gave pilots tactile feedback on finger position in relation to the rows of hard and soft keys. The manufacturer advised that the design change was likely due to customer feedback regarding the panel.
Figure 4: Sikorsky S‑92A mode select panels

Source: Lockheed Martin, annotated by the ATSB
VH-IPE featured an MSP without the white finger barriers on the left copilot side of the cockpit but with the revised MSP with the finger barriers on the captain’s right side. In this occurrence, the mis-selection of button below the finger barrier was done by the captain as the pilot flying.
The maintenance manual for the S‑92A advised that it was acceptable to mix versions of the mode select panel within the same helicopter, stating:
It is acceptable to mix and match mode select panels dashes 92900‑01812‑104, 92900‑01812‑105, 92900‑01812‑106, 92900‑01812‑110
Mode select panels 92900-01812-112 can be installed as a replacement unit but is not interchangeable with any other mode select panel part number. The mode select panel 92902‑01812‑112 must be installed in pairs with another 92900‑01812‑112
Mode select panel lighting and display
The top row of hard keys, which included the heading key, were not back lit when the relevant modes were not engaged (Figure 5). The manufacturer identified that the lower row of hard keys featured a lit border on the individual key as those keys were menu keys and changed the function of the lower row of soft keys. The white finger barrier (when installed) separating the hard and soft keys did not illuminate.
Figure 5: Sikorsky S‑92A mode select panel at night
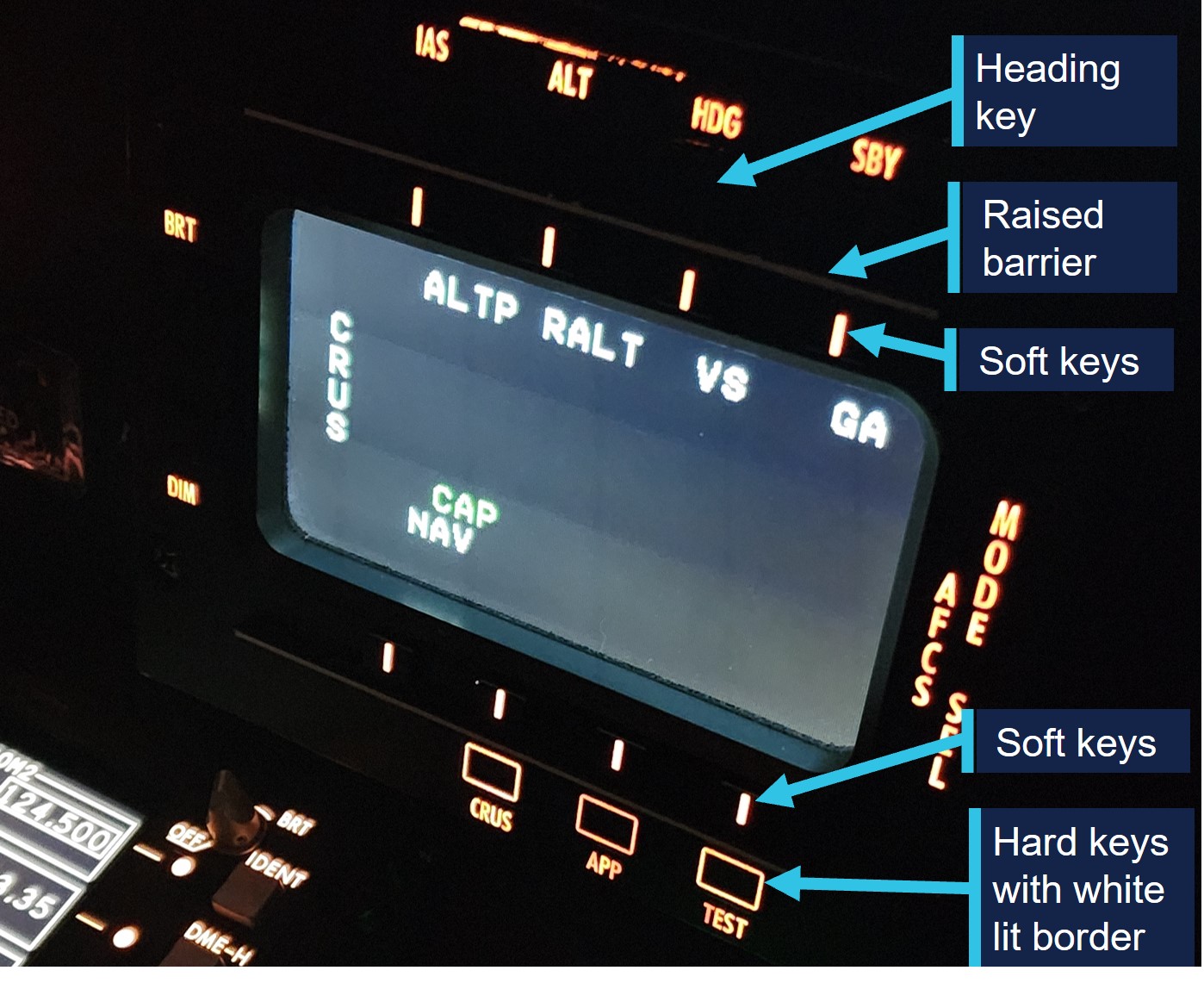
Source: PHI International Australia, annotated by the ATSB
Automation modes controlled by the top row of soft keys were displayed with an ‘ON’ symbol on the MSP display screen below the relevant key. There was no change in colour or lighting to the soft key itself when selected. Active automation modes captured on the AFCS MSP were also displayed on the flight crew’s primary flight display (PFD) (Figure 6).
Figure 6: Sikorsky S‑92A primary flight display

Source: Lockheed Martin, amended and annotated by the ATSB
Primary flight display indications
The letters P (Pitch), R (Roll), and C (Collective) are displayed at the top of each PFD. These letters correspond to the autopilot axis controlling each CFD mode.
- if the helicopter is coupled so that the pitch axis is controlling altitude, ALT is displayed next to the P
- if the helicopter is coupled so that the pitch axis is controlling airspeed and the collective axis is controlling altitude, IAS is displayed next to the P and ALT is displayed next to the C.
Modes that are captured ‘ON’, are displayed on the PFD in green letters signifying that the mode is now controlling that portion of the CFD. Modes that are armed, but not yet captured, are displayed in white letters signifying that control inputs are not being made based on this mode.
The system does not provide audible tones or display alerts when a mode is changed or immediately captured.
The PM stated that the PFD was used to confirm that the correct automation modes had been engaged.
Radar altitude hold
The RADALT hold is engaged using the corresponding soft key on the AFCS MSP.
The RADALT will capture the reference radar altitude height which is displayed on the PFD. The S‑92A rotorcraft flight manual states that a pilot can adjust the reference height using the following methods:
• Depress and hold the collective trim release, manually fly the aircraft to the desired altitude and release the trim button, or
• Use the collective trim beeper to beep to the selected altitude. When increasing radar altitude with the collective beep switch, the aircraft will climb at a maximum of 500 fpm. When decreasing radar altitude with the collective beep switch, aircraft descent rate is predicated on the current radar altitude. When above 500 feet AGL, the aircraft will descend at a maximum of 500 fpm. As the aircraft descends below 500 feet, the descent rate will decrease linearly so that the maximum descent rate at 200 feet AGL and below is 200 fpm.
RADALT mode was engaged to descend the helicopter from 1,500 ft and the PM adjusted the target altitude to the circuit height of 660 ft. The flight crew confirmed the target altitude and the helicopter commenced a descent.
Vertical speed mode
The engagement of the vertical speed (VS) mode will capture the aircraft’s current rate of climb or descent. When the VS mode is engaged, the MSP display will indicate a green ‘ON’ symbol below the VS display. The collective axis display on the PFD would display ‘VS’ to indicate vertical speed mode is now controlling the collective axis and the rate of climb or descent will be displayed on the vertical speed indicator on the PFD.
Heading mode
The heading mode is engaged by selecting the heading button on the AFCS MSP and will immediately turn the helicopter to the reference heading. When engaged the reference heading is adjusted by turning the heading knob on the remote instrument controller or by the lateral beeper switch located on the cyclic control to adjust the heading left or right from the helicopter’s current track.
As the helicopter approached the drill rig using a lateral navigation mode, the captain reported that they engaged the heading mode to cancel the navigation and then adjusted the helicopter track so to avoid flying directly over the top of the rig.
EGPWS
The Honeywell MKII enhanced ground proximity warning system (EGPWS) was installed on the S‑92A helicopter.
The EGPWS purpose is to provide an audio and visual alert to crew when terrain or obstacle clearance is not assured.
The S‑92A rotorcraft flight manual contained the following system description:
The EGPWS computer receives inputs from aircraft sensors to include radar altitude, barometric altitude, airspeed, vertical speed, pitch and roll attitude, magnetic heading, temperature, navigational radios, and FMS GPS. These inputs are combined with internal terrain and obstacle databases to predict when the aircraft will impact terrain or an obstacle. The system is designed to provide a warning to the pilot in sufficient time to take corrective action to prevent CFIT (controlled flight into terrain) while avoiding unnecessary false alarms.
The EGPWS had numerous modes for different stages of flight. The ‘look ahead’ mode used helicopter sensors to determine the helicopter flight path. It compared the helicopter predicted position to the terrain and obstacle database to look for conflicting terrain or obstacles. When the helicopter is approximately 30 seconds from impact with terrain or obstacles, a caution will be given. When the helicopter is approximately 20 seconds from impact, a warning will be given. The pilot will see and hear the caution or warning until the helicopter is manoeuvred away from the hazard (Figure 7).
Look ahead cautions: CAUTION TERRAIN, CAUTION TERRAIN or CAUTION OBSTACLE, CAUTION OBSTACLE aural alert every seven seconds
Look ahead warnings: WARNING TERRAIN or WARNING OBSTACLE continuous aural alert.
The flight crew received a terrain caution alert as the helicopter descended through about 220 ft followed by a terrain warning alert at about 180 ft AGL.
Figure 7: EGPWS look ahead mode
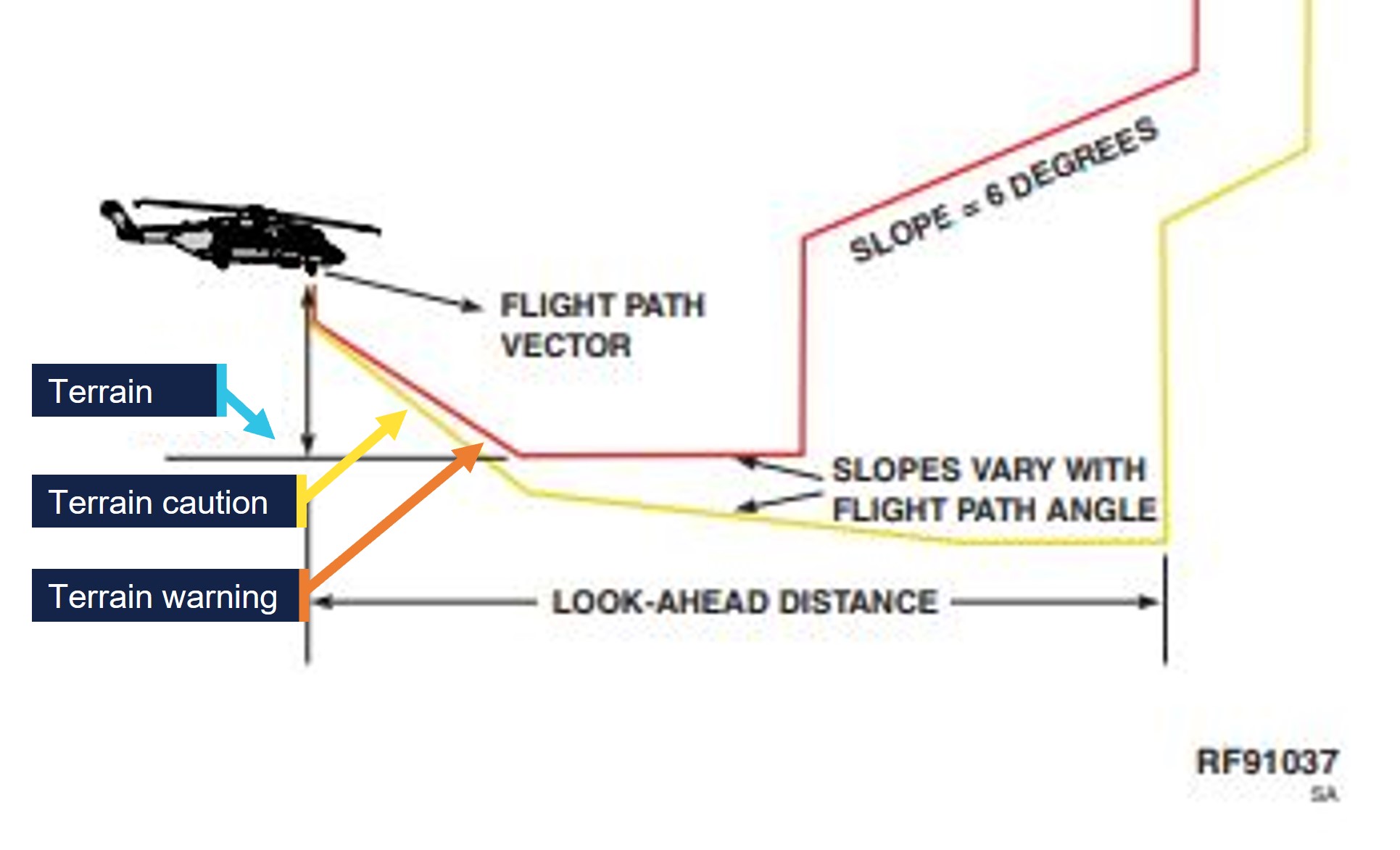
Source: Lockheed Martin, annotated by the ATSB
External lighting
Two 450-watt landing lights were located under the nose of the helicopter. The lights were controlled by the switches located on the exterior light control panel in the cockpit.
In addition to the landing lights, another 450-watt controllable searchlight was located under the right-side nose of the helicopter and was coupled with a directional searchlight control located on the collective controls. The searchlight ON/OFF/STOW switch on the collective moved the light from its stowed position to its operating position and turned the light on. The searchlight can be moved forward through a 120° arc from the stow position. The searchlight slew switch allowed rotation of the light through 360°.
The operator’s before landing checklist required the landing lights to be selected ‘On’, although there was no requirement for the use of the searchlight for landing in the operator’s checklists.
The PF reported that the use of the searchlight was, in the event of a water ditching, to assist the flight crew to visually identify the water’s surface and therefore time control inputs to assist in managing the ditching.
Take‑off safety speed (Vtoss)
The pilot monitoring was required to calculate Vtoss using the Sikorsky performance application on the EFB. The calculation required the input of:
- pressure altitude[4]
- outside air temperature
- gross weight of the helicopter for landing.
The operator’s flight crew operating manual stated that for normal landings:
The airspeed bug should be set at Vtoss/Vblss[5] for all landings. This is so that the crew have a reference speed to accelerate to, and remain above, in the event of engine failure.
Meteorological information
Bureau of Meteorology
The aerodrome forecast (TAF)[6] for Learmonth, about 22 km south of Exmouth, was issued at 1317 and valid between 1400 on 1 February and 1400 on 2 February 2025. The forecast wind after 1700 was from 260° at about 14 kt with a slight directional change after 20000 to 240˚at about 10 kt with CAVOK[7] conditions. The temperature was forecast at 32˚ with a QNH[8] of 1003.
Transocean Endurance weather
A weather report obtained prior to departure for the Transocean Endurance, and valid at 1750, indicated:
- wind 241°/ 07 kt
- visibility 15,000 m
- QNH 1001
- temperature 30°C
- dewpoint 30°C
- cloud 0/8 okta[9]
- present weather – fine.
Last light
Sunset was recorded as 1909 and last light at 1933, with the end of nautical twilight recorded at 2001 at Exmouth.
The crew reported that some residual terrestrial light remained as they approached the rig and allowed them to see the ocean and recalled the wind conditions to be calm with no white caps.
Airport information
The drill rig Transocean Endurance is described as a harsh environment semi‑submersible vessel accommodating up to 130 people (Figure 8). The dimensions of the rig were 116 m x 97 m and had an obstacle height of 343 ft.
The helideck height was 109 ft above the ocean surface and approved to accommodate the S‑92A helicopter.
The operator’s helideck approach guidance indicated a 1,500 ft height for minimum safe altitude above the rig and that the circuit height was 660 ft above mean sea level.
The rig was located 38 NM (71 km) north‑north-west of Exmouth Aerodrome and was being used for the night recency flight due to its proximity.
Figure 8: Drilling rig Transocean Endurance

Source: PHI International Australia Pty Ltd
Recorded information
On board recorded data from the flight data monitoring system was obtained and analysed by the ATSB for the occurrence.
Autopilot mode selection
Following the descent from 4,000 ft, the crew continued descent to the minimum safe altitude height of 1,500 ft in the vicinity of the rig.
- At about 1937:25, while the helicopter maintained 1,500 ft, the PM selected the RADALT hold mode on
- 55 seconds later the vertical speed mode was selected, simultaneously RADALT mode automatically disengaged.
Heading adjustments
During the descent from 1,500 ft:
- At 1938:24, 3.3 seconds after the engagement of vertical speed mode, the heading mode was shown to be engaged at about 1,170 ft (Figure 9).
- At 1938:32, the helicopter heading was adjusted from 348° to 333°.
- The flight track was adjusted to the left and the helicopter passed to the south-west of the drilling rig.
- At 1939:46, as the helicopter descended through about 510 ft, the helicopter heading was again adjusted from 345° to 065° and the helicopter commenced a turn onto the downwind leg of a right circuit to the drilling rig helideck.

Source: ATSB
Pilot monitoring radio keying
At 1939:10, when the helicopter was recorded descending through about 810 ft on the crosswind leg[10] of the circuit the PM’s radio was keyed for a 6‑second period. At 1939:27, and about 675 ft, the PM’s radio was again keyed for a duration of 9 seconds and at 1939:43 a further 1‑second radio key when the helicopter descended through 526 ft.
EGPWS terrain alerts
At 1940:17 as the helicopter descended through 221 ft on the downwind leg[11] of the circuit the EGPWS terrain caution alert was triggered. The caution was followed by an EGPWS terrain warning at 1940:21 and 181 ft.
Cockpit voice recorder
VH-IPE was fitted with a 4‑channel cockpit voice recorder (CVR). The CVR recorded continuously for 120 minutes before being overwritten. Following the occurrence the crew continued with the night recency flights for each of the 3 flight crew. Therefore the CVR from the occurrence was overwritten prior to their return to Exmouth.
Operator information
PHI International Australia Pty Ltd is a global helicopter operator founded in the United States and commenced operations in Australia in 1980, operating from numerous bases on the coast of Western Australia. These operations support the offshore oil and gas industry as well as conducting marine pilot transfers and search and rescue operations.
PHI International Australia operates a fleet of about 20 helicopters that include the following types:
- Augusta Westland AW189
- Augusta Westland AW139
- Augusta Westland AW109
- Airbus H175
- Sikorsky S‑92A.
PHI International Australia’s Exmouth base supports the offshore oil and gas industry, transferring employees to and from offshore fixed installations and mobile drilling rigs. Employee transfers arrive and depart from the Learmonth Airport located about 22 km south of Exmouth. Transfers are typically daytime only operations, however flight crews are rostered on standby each evening for immediate emergency medical evacuations if required.
When flight crew are required to conduct night recency flights, nearby offshore rigs are used to ensure pilots are familiar with the helideck landings at night.
Operational policy and procedures
Multicrew cooperation
The Sikorsky S‑92A helicopter requires a 2-pilot configuration and duties of the crew are divided between the PF and PM. PHI International Australia’s flight operations manual part 2 (FOM 2) described the intention of a coordinated flight crew:
Operating procedures have been developed to achieve the optimum use of both pilots. Many duties may be carried out by either pilot, depending upon which one at the particular time has spare capacity. However, system handling by the PF should never interfere with their main task of flying the aircraft. Particular attention must be given to good crew co-ordination during all phases of flight. A crew briefing must be completed prior to every take-off, approach and landing. Normally the crew briefing will be given by the PF.
Normal checklists
The FOM 2 detailed the operator’s philosophy regarding checklists:
Crews should operate the aircraft, which includes changing the configuration and setting up systems, using the “next event” activity cycle, based around the priorities of "Aviate - Navigate - Communicate - Administrate". The NCL [normal checklist] should be used as the mechanism to confirm that the required actions have been completed and the aircraft is configured correctly for the task ahead. Crews should avoid flying the aircraft by checklist.
Prior to commencing the descent, the crew completed the descent checklist which required them to conduct an approach briefing. The briefing required the crew to confirm the navigation setup for the approach that included:
- clearance
- flight director, bugs, pointers, preview
- navigation source
- radio tuning unit and flight management system.
As the copilot was unable to determine the Vtoss for landing prior to the approach briefing, the crew discussed and bugged an estimated 45 kt Vtoss speed to the airspeed indicator and completed the approach brief and descent checklist.
Crew rostering policy
PHI International Australia’s rostering policy for flight crew minimum experience reflected the guidance of the International Association of Oil and Gas Producers for offshore helicopter operations, which stated:
For ATO [air transport operations], co-pilots with less than 500 hours offshore multi engine and multi-crew should not be rostered with any commander who has less than 100 hours PIC since command appointment on the contracted type.
The captain had less than the 100 hours in command of the S‑92A, however the copilot had significant experience in multi-engine helicopters in offshore operations including operations at night that exceeded the requirement to be paired with a captain with more experience on type (see Personnel information).
No additional rostering restrictions were identified in either the International Association of Oil and Gas Producers guidance or the operator’s policies for flight crews experience for pairing crew night.
Flight crew roles and responsibilities
The FOM 2 detailed that while conducting multi-crew operations and engaging automated flight modes, the PF was to monitor the helicopter’s flight path, anticipate any planned changes to that path and to make changes to flight references and automation modes, or instruct the PM to make the required changes.
Other responsibilities of the PF also included:
- cockpit management
- control of the helicopter
- responding to any immediate actions related to any emergencies
- communicating with the PM in accordance with good CRM practice
- interacting with the PM on checklist procedures
- briefing the PM prior to undertaking any flight procedure or deviation to the planned flight.
The primary role of the PM was to monitor the helicopter’s flight path, the activities of the PF and any other activities designated in the operations manual including radio transmissions.
The FOM 2 further detailed night operations, stating:
During all operations, the priority role of the PM is to monitor the PF, especially below 1000', and not be distracted from the task. Reference to checklists, navigation logs or other manuals is not to be made during these critical flight phases. Essential drills, type specific, may be completed with due consideration for the monitoring tasks.
Crew communication and standard callouts
The FOM 2 provided the standard phraseology for the multi-crew environment and stated that the callouts were designed to promote situational awareness to ensure crew have an understanding of the helicopter system’s status.
These included standard calls for automation mode selection:
It is important to ensure that the flight director modes have been selected, armed and captured correctly. Both crew members should be actively involved in this process.
When the PF performs the ‘action’, the PM is required to check and confirm the status of the actions (Figure 10).
Figure 10: Examples of PHI International Australia standard callouts
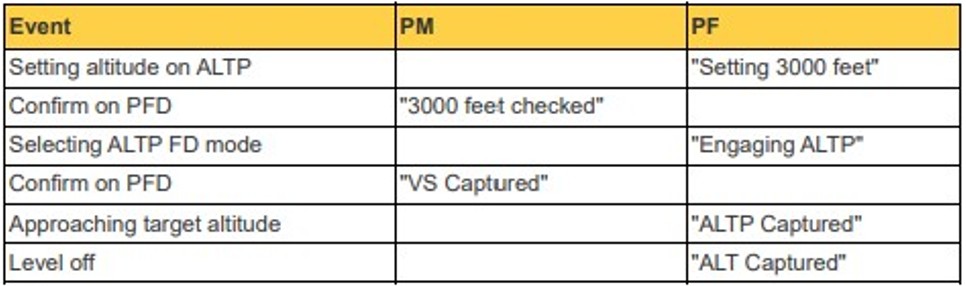
Note: ALTP (altitude preselect), FD (flight director), VS (vertical speed), ALT (altitude). Source: PHI International Australia flight operations manual part 2
Following the selection of the heading mode the PF later stated that they confirmed the mode selection with the PM, however neither crew member recognised the unintended selection of the VS mode.
While the PM was communicating on the radio, the helicopter descended through the intended circuit height of 660 ft and no ‘Alt captured’ call was made by the PF or challenged by the PM.
Pilot monitoring and deviation calls
The FOM 2 detailed that standard crew calls were designed to stimulate early corrective behaviour in response to identified deviations from assigned or briefed flight references and that deviation from the reference should trigger a prompt. The FOM 2 stated that a 100 ft difference from cleared or briefed altitude was considered a deviation.
While in the circuit area and following the radio communication, the PM began using the EFB to calculate the landing Vtoss speed. No deviation call was made by either flight crew member and the helicopter descended below the intended circuit height.
Operational risk assessment
During pre-flight planning, flight crews were required to complete an operational risk assessment relevant to the flight. The operator used aviation management software that generated a risk level for the flight based on algorithms set by the operator.
The risk assessment completed by the crew captured:
- Human factors – illness, medication, stress, alcohol, fatigue and eating.
- Personal recency – flown the helicopter type within the last 30 days, if operating from home base, and if flight crew had accumulated more than 500 hours on the helicopter type.
- Operational factors – type of flight such as routine, training or medevac, planning time, client pressure or any additional factors.
- Environmental factors – day or night, instrument flight rules weather conditions or if adverse weather was anticipated.
- Helicopter factors – minimum equipment list items that may affect the flight.
Operational risk level output categories were classed as:
- Normal operations – Crews were required to complete normal pre-flight planning procedures and briefing.
- Caution – Flight may proceed after the pilot in command and crew discuss the risk factors and record details of the discussion.
- High caution – Flight may proceed after discussion with the senior base pilot.
- Critical safety decision – Pilot in command required specific authorisation prior to flight from the Chief Pilot / Head of Flying Operations.
Both flight crew had not yet accumulated 500 hours on the helicopter type. The crew selected a routine flight type and also indicated that the flight would be conducted at night. The operational risk assessment did not capture the flight crew’s personal recency or experience on type at night.
The completed risk assessment indicated a ‘caution’ risk due to the crews’ experience on the aircraft type and flight at night. The crew recorded that they had discussed the risks involved with their inexperience and night flight during the sortie planning.
The captain also stated that as this was their first flight back following an off-duty period they took additional time to go through pre-flight checklists recalling they did not want to rush.
PHI International Australia advised it was able to customise the aviation management software parameters and could configure the operational risk assessment to assign individual risks and a unique risk score as it deemed suitable for its operation.
Regulatory requirements
The captain had conducted their last flight at night on 8 November 2024 and the purpose of the occurrence flight was so the crew could remain current at night.
Civil Aviation Safety Regulation (CASR) part 61.395 sub regulation (2) states that:
The holder of a pilot licence is authorised to pilot, during take‑off or landing, an aircraft of a particular category carrying a passenger at night only if the holder has, within the previous 90 days, in an aircraft of that category or an approved flight simulator for the purpose, conducted, at night:
(a) at least 3 take‑offs; and
(b) at least 3 landings;
while controlling the aircraft or flight simulator.
Human performance
Workload represents the level of mental and physical demand placed on an individual by the operational environment and the nature of the task. Excessive and insufficient workload can degrade performance.
High workload may lead to errors when task demands exceed the available cognitive or physical resources. As task demand increases beyond certain limits, performance declines even though an individual’s effort may rise.
Slips occur when a person’s understanding of the situation is correct, and the wrong action is executed (Wickens, Helton, Hollands, & Banbury, 2022). Characteristics of this error also occur when people accept a close match for the proper object, something that looks similar, is in the expected location or does a similar job. Slips and lapses (forgetting to do an action) can be reduced through good design of the working interfaces, procedures and environments, however it is impossible to prevent them entirely.
Divided attention refers to the allocation of cognitive resources to several tasks at once. The ability for individuals to attend to multiple stimuli and do various tasks at a time has limits (Dismukes, Berman, & Loukopoulous, 2017). The efficiency of divided attention depends on the task’s complexity and familiarity. Simpler, well-practiced tasks require less cognitive effort and are more easily combined than complex or novel tasks.
Expectations strongly influence where a person will search for information and what they will search for (Wickens & McCarley, 2008), and they also influence the perception of information (Wickens, Hollands, Banbury, & Parasuraman, 2013). For example, pilots frequently set the automation and in almost all situations, the helicopter will perform as the automation was intended.
Crew resource management
Crew resource management (CRM) is the effective use of all available resources for flight crew personnel to assure a safe and effective operation, reducing error, avoiding stress and increasing efficiency. It encompasses a wide range of knowledge, skills and attitudes including communications, situational awareness, problem solving, decision‑making, and teamwork, along with the sub-disciplines which support these areas. CRM helps mitigate human limitations risks discussed above.
Related occurrences
In-flight upset involving Boeing 737-8FE, VH-YQR, 143 km west of Ballina/Byron Gateway Airport, New South Wales (AO‑2023‑042)
On 6 September 2023 the pilot of a Boeing 737 inadvertently input full left rudder trim when they intended to activate the flight deck door switch, resulting in an in-flight upset and a cabin crew member sustaining a minor injury.
Unstable approach involving Embraer 190, VH-UZI, about 4 km north-east of Brisbane Airport, Queensland (AO-2024-030)
On 9 May 2024 following a request from the captain the first officer inadvertently pushed the flight path angle button – a ‘slip’ type error, which unintentionally disengaged the ILS approach mode.
Surprised by the mode change, over the next 10 seconds the flight crew focused on resolving it, rather than conducting a go-around.
During this time, the pilots were not effectively monitoring the aircraft’s flight path, and it exceeded the glideslope limit requirement of the operator’s stabilised approach criteria.
Safety analysis
Introduction
On 1 February 2025 a Sikorsky S‑92A helicopter, registered VH-IPE and operated by PHI International Australia, was conducting a night recency flight to an offshore drilling rig north‑north-west of Exmouth, Western Australia. The captain was the pilot flying (PF) for the outbound flight to the rig and the copilot was the pilot monitoring (PM).
While on descent to the rig the PF intended to activate the heading hold mode on the automatic flight control system mode select panel to adjust the heading to avoid overflying the rig. An inadvertent and unrecognised selection resulted in the cancellation of an automation mode that would have levelled the helicopter at a preset circuit height. The helicopter continued descent below the circuit height until the crew received an enhanced ground proximity warning system (EGPWS) alert at about 220 ft.
This analysis will explore the operational considerations pertaining to flight crew experience, pre-occupation in the cockpit, decision‑making and flight crew coordination.
Flight crew experience and workload
The flight crew were experienced pilots, however, both had limited flight time in the S‑92A at night. As the crew departed Exmouth and flew direct to the drill rig, this decreased the time at cruise altitude by about 5 minutes compared to normal passenger‑carrying flights the crew would usually conduct from Learmonth. This reduced the time available to complete the required cockpit administration and likely contributed to the PM being unable to complete the required tasks prior to top of descent.
Since their initial check to line on the S‑92A in November 2024, the PM had accumulated about 220 hours on the S‑92A, of which about 9 hours were at night. Their total experience on the helicopter type meant it was likely the PM was still becoming familiar with the onboard systems and administration requirements of the helicopter type, especially at night.
The combination of the shorter than usual flight time and the PM’s experience on the helicopter type, resulted in them being rushed to complete the take-off safety speed (Vtoss) calculation prior to the top of descent.
The PF had accumulated about 300 hours flying the S‑92A of which 13 hours was night flying conducted during training and simulator sessions. The PF’s low familiarity with the helicopter type at night likely created an unfamiliar cockpit environment which was compounded by their lack of recency, following a 4-week period off duty. In a complex cockpit environment such as the S‑92A this increased the risk of a selection error.
Contributing factor The flight crew had limited time on type and on type at night which increased risk and due to the short sector were experiencing a higher than normal workload. |
Autopilot mode selection error
During the descent to the rig, it was the PF’s intention to engage the autopilot heading mode to adjust the helicopter track and avoid flying directly over the top of the rig. However, they mistakenly selected the vertical speed key before then reselecting the heading key. The inadvertent selection of the vertical speed mode went unrecognised by the crew.
Both the heading and vertical speed keys are physically close, located one above the other. Further, as the top row of hard keys were not backlit when the mode was not engaged, identification of the correct key is more difficult in a dark cockpit, especially for flight crew who had limited experience flying the S‑92A at night.
This inadvertent selection was consistent with an unintentional slip, which cancelled an automation mode the crew had engaged to level the helicopter when it reached circuit height.
Following the inadvertent activation of the vertical speed mode, the PF confirmed with the PM that the engagement of the intended heading mode was correct as per the operator’s procedures. However, as the PF was unaware they had selected the vertical speed mode, the engagement was not announced to the PM, nor would the PM have any expectation that the vertical speed mode would be engaged at that point of the flight.
The helicopter continued a 500 feet per minute rate of descent that was not recognised by the crew in the mostly dark conditions. The reduced visual reference when combined with the preoccupation of additional tasks resulted in the helicopter’s continued descent until the crew reacted to the EGPWS alert.
Contributing factor During a night recency flight, an autopilot mode selection error was made which the flight crew did not recognise. This cancelled the helicopter levelling off at 660 feet and set up a continuous 500 feet per min rate of descent. |
Captain’s request to calculate safety speed
Following the crew’s estimation of the Vtoss for landing, the PF became concerned that the reference speed was too high. With an expectation the helicopter had levelled in the circuit area, the PF requested the PM to again attempt to calculate the Vtoss for landing which required the PM to use Sikorsky’s performance application in the electronic flight bag.
PHI International Australia flight operations manual detailed that, especially for flight at night and below 1,000 ft, the PM was not to be distracted from their monitoring duties. However, at the PF’s request the PM’s attention became focused on the electronic flight bag, this drew their attention away from their required monitoring duties while the helicopter was below 1,000 ft above ground level (AGL).
Contributing factor Within the circuit area the captain requested the copilot to calculate Vtoss for landing, diverting the copilot’s attention away from their pilot monitoring duties. |
Preoccupation in the circuit area
When focus is diverted to a secondary task, attention can narrow to that task, and so monitoring of other sources degrades (Dismukes, Berman, & Loukopoulous, 2017). This degradation of monitoring can occur without the flight crew realising.
As the helicopter approached the circuit area, it continued to descend through 810 ft AGL as the PM communicated on the radio. At the completion of the radio transmissions, the helicopter was recorded at about 526 ft AGL and below the intended circuit height.
The operator’s standard calls for flight crew required the PF to announce the helicopter had captured the intended altitude and the announcement should then be crosschecked and confirmed by the pilot monitoring. However during this time the PM was communicating on the radio and an ‘altitude captured’ call was not made by the PF.
A short time after the completion of the PM’s radio transmissions, the PF commanded the aircraft to turn onto the downwind leg of the circuit.
While the PF requested the PM to calculate the Vtoss for landing, they also diverted their own attention to activating and manipulating the searchlight beam outside the helicopter.
Consequently, neither flight crew member was monitoring the helicopter’s altitude which contributed to the unidentified descent below the circuit height, triggering a ground proximity alert.
Contributing factor Both flight crew members became preoccupied with additional tasks. Neither crew were monitoring the altitude nor identified that the helicopter had not levelled at the circuit height and continued the descent. |
Pre-flight operational risk assessment
Flight crews were required to complete the PHI International Australia pre-flight operational risk assessment prior to departure. The risk assessment captured the flight crew’s overall experience on the helicopter type and that the flight was being conducted at night, presenting the flight crew with a caution risk level that required a discussion of the elevated risk between themselves.
However, the risk assessment did not capture the flight crew’s experience on the helicopter type at night. Prior to the occurrence flight neither flight crew member had flown the S‑92A helicopter at night outside of their training and simulator sessions and both individually had less than 13 total hours flying the S‑92A at night. However, no additional risk was placed on their limited night experience on type.
The flight crew’s combined experience in the S‑92A at night was not formally risk assessed and no controls were in place to prevent the pairing of flight crew with limited night hours on type. This increased the likelihood of an event due to a lack of familiarity with the helicopter systems and was a missed opportunity to provide further risk controls for the intended night operations.
Contributing factor PHI International Australia Pty Ltd’s operational risk assessment did not capture the risk of the crew’s limited experience on type at night. (Safety Issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the ground proximity alerts involving Sikorsky S‑92A VH-IPE, 71 km north‑north‑west of Exmouth Aerodrome on 1 February 2025.
Contributing factors
- The flight crew had limited time on type and on type at night which increased risk and due to the short sector were experiencing a higher than normal workload.
- During a night recency flight, an autopilot mode selection error was made which the flight crew did not recognise. This cancelled the helicopter levelling off at 660 feet and set up a continuous 500 feet per min rate of descent.
- Within the circuit area the captain requested the copilot to calculate Vtoss for landing, diverting the copilot’s attention away from their pilot monitoring duties.
- Both flight crew members became preoccupied with additional tasks. Neither crew were monitoring the altitude nor identified that the helicopter had not levelled at the circuit height and continued the descent.
- PHI International Australia Pty Ltd’s operational risk assessment did not capture the risk of the flight crew’s limited experience on type at night. (Safety Issue)
Safety issues and actions
Ineffective operational risk assessment
Safety issue number: AO-2025-005-SI-01
Safety issue description: PHI International Australia’s operational risk assessment did not capture the risk of the crew’s limited experience on type at night.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
The S‑92A cockpit lighting environment was reviewed by the operator with subject matter experts to consider if an engineered improvement was practicable. A procedural change was implemented by PHI International Australia that required the use of small lights that are worn on the pilot’s fingers to improve visibility of the cockpit environment (such as switches, buttons, and controls) during S‑92A night flights.
PHI International Australia advised lessons from this occurrence have been shared and promoted both internally and externally. These efforts included an internal safety alert and a ‘learning from occurrence’ video detailing what happened and why to the international community through industry body HeliOffshore.
Operational procedures regarding multi-crew cooperation, automation mode changes/awareness, and EGPWS alerts were highlighted to all flight crews through internal communications. These points were also highlighted within the training and competency teams as focus areas during both simulator and line training sessions.
Glossary
| AFCS | Autopilot flight control system |
| AGL | Above ground level |
| ATPL | Air transport pilot licence |
| ATS | Air traffic services |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| EFB | Electric flight bag |
| EGPWS | Enhanced ground proximity warning system |
| FCOM | Flight crew operations manual |
| IAS | Indicated airspeed |
| MSP | Mode select panel |
| NAV | Navigation |
| PF | Pilot flying |
| PFD | Primary flight display |
| PM | Pilot monitoring |
| RADALT | Radar altitude |
| VS | Vertical speed |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot of the occurrence flight
- the copilot of the occurrence flight
- PHI International Australia Pty Ltd
- Civil Aviation Safety Authority
- Lockheed Martin
- Bureau of Meteorology
- recorded flight data
- International Association of Oil and Gas Producers.
References
Dismukes, R. K., Berman, B. A., & Loukopoulous, L. (2017). The limits of expertise: Rethinking pilot error and the causes of airline accidents. Routledge.
Wickens, C. D., & McCarley, J. S. (2008). Applied attention theory. Boca Raton, FL: CRC Press.
Wickens, C. D., Helton, W. S., Hollands, J. G., & Banbury, S. (2022). Engineering Psychology and Human Performance 5th edition. New York: Routledge.
Wickens, C. D., Hollands, J. G., Banbury, S., & Parasuraman, R. (2013). Engineering Psychology and human performance, 4th edition. Boston, MA: Pearson.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- captain of the occurrence aircraft
- copilot of the occurrence aircraft
- PHI International Australia Pty Ltd
- Lockheed Martin
- Civil Aviation Safety Authority
- Bureau of Meteorology.
Submissions were received from:
- captain of the occurrence aircraft
- copilot of the occurrence aircraft
- PHI International Australia Pty Ltd
- Lockheed Martin.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] The third pilot, seated in the passenger seat could hear and communicate with both crew, however their view of the cockpit and instrumentation was obstructed.
[3] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[4] Pressure altitude: altitude adjusted for air pressure.
[5] Vblss: baulked landing safety speed.
[6] TAF: aerodrome forecast: a statement of meteorological conditions expected in the airspace within a radius of 8 kilometres of the aerodrome reference point.
[7] Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[8] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[9] Okta: an okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[10] The crosswind leg is flown perpendicular to the runway.
[11] The downwind leg is the segment when the aircraft is flying parallel to the runway but in the opposite direction of landing.
Occurrence summary
| Investigation number | AO-2025-005 |
|---|---|
| Occurrence date | 01/02/2025 |
| Location | 71 km north-north-west of Exmouth Airport |
| State | Western Australia |
| Report release date | 04/02/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Aircraft preparation, E/GPWS warning |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Sikorsky Aircraft |
|---|---|
| Model | S-92A |
| Registration | VH-IPE |
| Serial number | 920038 |
| Aircraft operator | PHI International Australia Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Exmouth Aerodrome, Western Australia |
| Destination | Transocean Endurance, Western Australia |
| Damage | Nil |