Civil aviation safety is based on managing the safety of knowledge of things that can affect the safety of flight. One of these sets of knowledge is confidence that the facilities at the destination will be good enough to give confidence of a safe landing. Weather at the destination can affect the safety of a landing. Detailed historical records are kept of weather observations and weather forecasts. This study has analysed the level of statistical confidence that has been achieved with destination weather forecasts under various conditions. It has also looked at other mechanisms that are or could be used to reduce the risk in addition to the existing methods.
This study provides an overview of aircraft cabin safety communications in Australia, in terms of effectiveness, passenger attitudes to such communications and opportunities that exist for improvement.
Most passengers agreed that paying attention to cabin safety communications is important. However, results revealed that behaviours do not always match this perception. Perceived relevance of safety information and frequency of travel were found to be significant factors affecting passenger attitudes and behaviours. High levels of message recognition, combined with excessive levels of confidence in personal ability to perform safety actions may be key drivers of reduced perceptions of relevance.
Passenger attention levels to safety communications were found to be generally low. Of all communication types tested, the safety briefing was most prone to perceptions of reduced relevance through repeated exposure, while very low attention levels and perceptions of content establish safety cards as being generally ineffective.
Analysis identified that low levels of passenger attention to safety communications results from overconfidence, superficial familiarity with messages, issues relating to the way safety content is presented, perceptions of substitutability between the card and briefing and social norms present in the aircraft cabin.
A framework for cognitive processing of cabin safety communications is presented. The framework identifies that passenger behaviours may be negatively influenced by perceptions that it is socially undesirable to pay attention to safety information. Changing normative and attitudinal beliefs represents the greatest opportunity to improve communication effectiveness.
Key opportunities are identified to improve cabin safety through enhancement of communications. These recommendations include tailoring communications to the needs of specific passenger profiles, providing additional information to passengers, improved design guidelines, regular content variation and use of communications specialists in safety media design.
The 2005-06 financial year continued to have a substantial building element for the ATSB as rail investigation further matured and aviation investigators were trained and prepared for 2006-07 implementation of a new aviation safety database with associated project and risk management.
The Bureau is continuing its commitment to training its investigators through the Diploma of Transport Safety Investigation. In 2005-06, ten staff completed the Transport Safety Investigation (TSI) Diploma and a further 25 were progressing through the coursework and mentoring.
In addition to releasing 93 final aviation investigation reports, ten aviation safety research reports and eight grant reports, substantial work occurred on the fifteen-fatality Lockhart River accident investigation, including the issuing of a number of safety recommendations.
In marine, 13 investigation reports were released including a major report into the loss of the Department of Immigration and Multicultural Affairs vessel Malu Sara in Torres Strait which resulted in five fatalities. The ATSB also continued an education campaign within the fishing industry on commercial fishing vessel safety.
The ATSB's rail safety investigation team released 11 final reports under the TSI Act. In October 2005 the Queensland Minister of Transport released the final report of the joint Queensland Transport/ATSB investigation into the Tilt Train accident which occurred north of Bundaberg in November 2004, and in February 2006 the Victorian Minister for Transport released the final ATSB report on the Benalla level crossing fatal accident.
The ATSB continued to support Ministers with road safety advice and coordinated input with other jurisdictions. In 2005-06 we released 22 road safety research and statistical publications including an Indigenous Road Safety Update. Preparations were also made for a national indigenous road safety forum later in 2006.
There were two areas of particular disappointment in 2005-06. First, there was little progress on a road safety education trial for novice drivers in partnership with NSW and Victorian governments and industry bodies primarily because of finance, risk and governance issues with Victoria.
Second, rail regulators advised the ATSB that even the very basic safety data that had been provided for several years was not accurate or comparable and broader data promised under an April 2005 memorandum of understanding would be significantly delayed. Obtaining quality rail safety data from jurisdictions has been a goal of the ATSB since 1999. The ATSB provided $80,000 late in 2005-06 to rail regulators to support an audit to seek to resolve data issues and provide a basis to make real progress for the future.
On 1 March 2006 I became the Chairman of the International Transportation Safety Association (ITSA), which includes a dozen of the major independent transport safety investigation bodies from around the world. The annual ITSA meeting was held in Canberra later that month and was a very helpful forum for exchanging information and enabling learning from sharing the good (and less good) experiences of colleagues.
A number of valued staff members retired during the year or prior to publication of this Review. I wish to express my particular appreciation for the long term contribution to marine and rail safety by Captain Kit Filor PSM who has been the ATSB's Deputy Director of Surface Transport Investigation since July 1999 and previously the Inspector of Marine Accidents from January 1991. Kit has made an enormous contribution in Australia and internationally.
I am grateful to the Minister for Transport and Regional Services, the Hon. Warren Truss MP, the Minister for Local Government, Territories and Roads, the Hon. Jim Lloyd, MP, and to the Secretary of the Department of Transport and Regional Services, Mr Mike Taylor for their support throughout the year.
Area navigation global navigation satellite system (RNAV (GNSS)) approaches have been used in Australia since 1998 and have now become a common non-precision approach. Since their inception, however, there has been minimal research of pilot performance during normal operations outside of the high-capacity airline environment. Three thousand five hundred Australian pilots with an RNAV (GNSS) endorsement were mailed a questionnaire asking them to rate their perceived workload, situational awareness, chart interpretability, and safety on a number of different approach types.
Further questions asked pilots to outline the specific aspects of the RNAV (GNSS) approach that affected these assessments.
Responses were received from 748 pilots, and answers were analysed based on the aircraft performance category1. For pilots operating Category A and Category B aircraft (predominantly single and twin-engine propeller aircraft), the RNAV (GNSS) approach resulted in the highest perceived pilot workload (mental and perceptual workload, physical workload, and time pressure), more common losses of situational awareness, and the lowest perceived safety compared with all other approaches evaluated, apart from the NDB approach. For pilots operating Category C aircraft (predominantly high-capacity jet airliners), the RNAV (GNSS) approach only presented higher perceived pilot workload and less perceived safety than the precision ILS approach and visual day approach but lower workload and higher safety than the other approaches evaluated. The different aircraft category responses were likely to have been due to high-capacity aircraft having advanced automation capabilities and operating mostly in controlled airspace. The concern most respondents had regarding the design of RNAV (GNSS) approaches was that they did not use references for distance to the missed approach point on the approach chart and cockpit displays. Other problems raised were short and irregular segment distances and multiple minimum segment altitude steps, that the RNAV (GNSS) approach chart was the most difficult chart to interpret, and that five letter long waypoint names differing only by the last letter can easily be misread.
Aircraft performance approach categories are determined by multiplying the aircrafts stall speed in the approach configuration by a factor of 1.3. See Section 3.1.
Producing the annual review is in line with a recommendation of the McGrath report into the former Bureau of Air Safety Investigation released in August 1999 to improve the transparency and accountability of the Bureau.
Creation of the ATSB on 1 July 1999 brought together the safety investigation, statistical analysis, research and safety program management of the Commonwealth's transport safety role in one multi-modal agency within the Department of Transport and Regional Services. ATSB intends to prepare an annual review to provide all stakeholders with an overview of its activities and safety in each transport mode. This first review covers a range of topics including:
Transport accidents are a leading cause of injury, both fatal and non-fatal. The primary purpose of this publication is to provide a broad overview of serious injury due to transport accidents in Australia in the one-year period 2003-04, the latest year for which data are available.
Serious injury is defined for this report as an injury which results in the person being admitted to hospital, and subsequently discharged alive either on the same day or after one or more nights stay in a hospital bed (i.e. deaths are excluded). This report presents estimates of the numbers of persons seriously injured in Australia due to transport accidents in the one-year period 2003-04. All modes, air, sea, road and rail, are included.
Transport accidents are a leading cause of injury, both fatal and non-fatal. The primary purpose of this publication is to provide a broad overview of serious injury due to land transport accidents in Australia in the one-year period 200304, the latest year for which data are available. The main focus is on accidents involving road vehicles travelling on public roads (called travelling in traffic). Road vehicles include motor vehicles, pedal cycles and other road vehicles such as trams, animals or animal-drawn vehicles (when they travel on the road).
Serious injury is defined for this report as an injury which results in the person being admitted to hospital, and subsequently discharged alive either on the same day or after one or more nights stay in a hospital bed (i.e. deaths are excluded).
This report presents estimates of the numbers of persons seriously injured in Australia due to land transport accidents, including road traffic crashes, in the one-year period of 2003-04. Trends in injury rates in road traffic crashes are examined over a five-year period, 1999-00 to 2003-04.
Technical Analysis Report " Short Bros. SD360-300, VH-SUM
EXECUTIVE SUMMARY
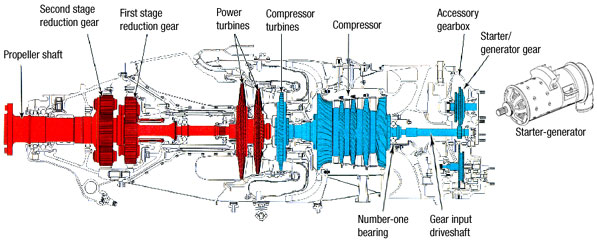
On 13 August 2000, a Shorts SD-360 aircraft (VH-SUM) sustained an in-flight shutdown of the right engine, which was later attributed to the seizure of the gas generator and power sections of the turbine.
Further examination of the engine by the ATSB and Pratt & Whitney Canada showed the seizure to have stemmed from the distress and severe overheating of the engine number one bearing in the compressor section.
Despite the degree of damage to the bearing races, evidence of electrical arcing damage was found on the inner race (non-thrust side) and was subsequently traced back through the accessory gearbox components to the starter-generator input shaft. Intermittent pitting on the starter-generator drive gear and continuous pitting on the driven gear indicated the primary source of electrical potential was within the starter-generator assembly.
Recommendations for safety action stemming from this examination include the further study and testing of the PT6A-67R starter-generator and engine assembly to determine the conditions under which excessive current leakage could result. It was also recommended that the assembly, as installed within VH-SUM be examined to identify the potential influence of other electrical accessory items fitted.
FACTUAL INFORMATION
Introduction
On 13 August 2000, a Shorts SD360-300 aircraft VH-SUM sustained an in-flight uncommanded feathering of the right propeller. The engine was shut down immediately. Examination of the engine showed the gas generator and power sections of the engine to have seized.
Pratt & Whitney Canada (Australasia) subsequently disassembled the engine. The findings of the teardown examination are presented in Pratt & Whitney report number 25885.
To support the investigation of the occurrence, the ATSB carried out an analysis of the following components from the failed engine.
Number-1 bearing and debris. The outer race of the bearing remained within the inlet case (figs. 1 & 2).
Gearbox input shaft and roller bearing assemblies (fig. 3).
Coupling splined hollow shaft (fig. 3).
Starter gear and roller bearing assemblies (fig. 3)
In addition, an unused bearing identical with the engine number-1 bearing was supplied, as well as copies of reports prepared by Pratt & Whitney addressing previous engine failures experienced by the operator.
Component history
The history of the engine was reported as follows (Pratt & Whitney Canada report #25885).
Serial Number: 106223 Time Since New: 6410.9 hrs Time Since Overhaul: 1500.1 hrs Cycles Since New: 9704 Cycles Since Overhaul: 2463 Previous Workshop Visit: 5 June 1999 for routine overhaul
Figures 1, 2 & 3. Components as received.
ANALYSIS
Visual examination
Number-1 Bearing:
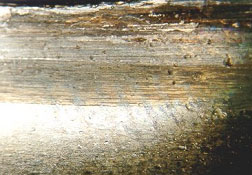
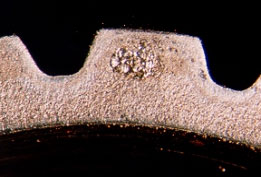
Figure 4 shows the general condition of the bearing as recovered from the engine. All surfaces of the bearing as well as the nearby casing showed heavy discolouration and blackening that is typical of extreme overheating. All the balls and the inner race (fig. 5) showed heavy localised wear and metal flow, signalling the sliding contact of the balls against the inner race.
Figures 4 & 5. Condition of bearing balls and races.
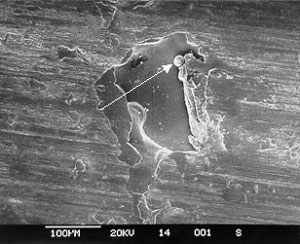
The effects of thrust loads within the operating engine had produced a bias in the wear on the inner race toward the rear inlet casing. Resulting from this loading and the amount of wear experienced, the inlet case of the turbine had come into contact with the adjacent compressor rotor disc. Closer study under the stereomicroscope showed fine pitting towards the inner edge of the non-thrust inner race (fig. 6), although scoring marks obscured much of this. Damage to the outer race was equally severe, with heavy indentation and bruising of the contact surfaces from the ingress of debris (fig. 7).
Figures 6 & 7. Indentation and pitting damage to the inner and outer races.
The bearing cage had experienced multiple radial cracks and cracks around the circumference, with most associated with galling, scoring and other evidence of metal to metal surface contact (fig. 8).
Figure 8. Contact damage and scoring on the external surface of the bearing cage.
Some internal corners of the cage showed shallow fatigue cracks - these had started at areas of heavy surface scoring and metal flow (fig's. 9 & 10).
When compared with the new item, the extent of the damage to the bearing parts was clear (figs. 11, 12 & 13).
Figures 11, 12 & 13. Bearing components compared with new items.
Associated components:
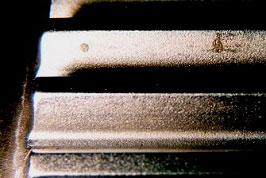
The coupling gear, starter gear and coupling shaft each showed varying levels of gear surface and spline pitting damage. Mostly, the pitting was restricted to localised spots at the gear teeth pitch-line (figs. 14, 15 & 16), although the starter gear showed uniform damage over the whole contact surface (fig. 17).
Figures 14 & 15. Pitting on coupling gear teeth faces.
Figures 16 & 17. Fine pitting found on starter gear teeth.
Studying the overall distribution of pitting on each item revealed the large diameter starter gear showed the most significant damage over two or three teeth in four equally spaced regions around the circumference (fig. 18). The smaller coupling gear which mates with this item showed no suggestion of this intermittent pitting, with damage found uniformly around the entire circumference.
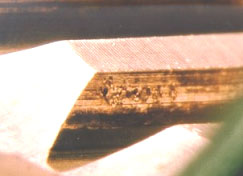
The male and female splined connections showed pitting over both the teeth faces (figs. 19 & 20) and end surfaces (figs. 21 & 22), with the damage appearing similar in all cases.
Figure 18. Starter gear, showing four localised areas of pitting around the diameter.
Figures 19 & 20. Pitting found on coupling gear and shaft spline teeth.
Figures 21 & 22. Pitting on coupling gear and shaft end contact faces.
Electron microscopy
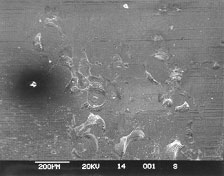
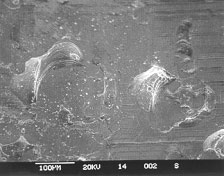
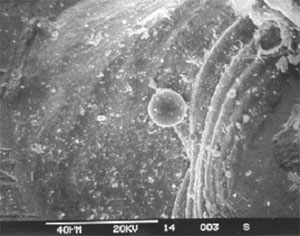
Electron microscope imaging of the pitting identified on the internal bearing race and gear teeth showed many of the pits to have a semicircular form, with a shallow concave profile. Observation at higher magnifications found evidence of localised melting, which presented as small balls of metal within the pit confines. Many of the pits showed a distinctive flattened appearance - typical of the effects, produced by normal rolling surface contact. Figures 23 through to 28 show the typical appearance of the surface pits at various magnifications.
Figures 23 & 24. Pitting on coupling gear faces.
Figure 25. Globules of remelted metal within coupling gear surface pits - typical of electrical arcing damage.
Figures 26 & 27. Pitting damage as found on non-thrust side of the inner race.
Figure 28. Closer view of bearing race pitting, also showing remelted globules.
Metallographic examination
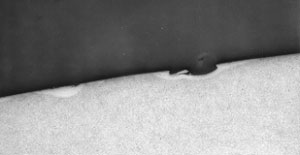
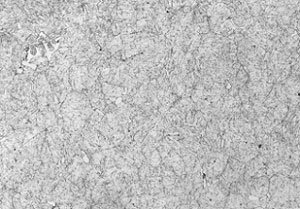
Sections for microscopy were taken through a pitted area on the less damaged, non-thrust section of the inner race and prepared using conventional methods. Etching with a 2% Nital solution revealed several regions along the contact surfaces that displayed locally transformed, untempered martensite associated with the pitting and extending to around 60mm in depth (figures 29 & 30). The general microstructure of the bearing race was fine, lightly tempered martensite with areas of globular massive carbide randomly throughout (figure 31).
Figure 29. Transformed regions surrounding pitting on the inner race (X80).
Figure 30. Closer view of a transformed region (X200).
Figure 31. General tempered martensite and carbide bearing race microstructure.
Hardness tests
The parent metal hardness, as measured away from the pitted surface was around 804 - 810 HV30.
CONCLUSION
Material and manufacture
The number-1 bearing inner race (non-thrust section) showed a microstructure and hardness level that was acceptable for the item and contained no obvious deficiencies that could have affected the bearing's service performance.
Engine failure
The breakdown of the PT6A-67R engine (S/N 106223) as installed within the aircraft VH-SUM was attributed to the failure of the number-1 turbine bearing. The bearing had experienced severe frictional damage and overheating, stemming from the seizure of the balls and the sliding contact against the inner race surfaces. Because the bearing carried a degree of rearward compressor axial thrust loading, the front inner race experienced most of the severe wear and scoring, leaving the rear race comparatively undamaged and able to be closely studied.
Development of the breakdown
Electron microscopy of the non-thrust inner race showed evidence of pitting that resembled damage produced by electrical arcing. Subsequent metallographic examination verified the damage; revealing localised thermally affected regions associated with the surface pits. In the presence of such physical and metallurgical discontinuities, rolling contact fatigue cracking developed and larger spalled areas formed over the contact surfaces. Increases in friction stemming from the spalling and the generation of metallic debris would have raised the vibration and temperature levels, eventually resulting in the thermal runaway of the bearing and the seizure as experienced. Such findings concur with the results of previous examinations conducted on PT6A-67R engines by Pratt & Whitney Canada.
Source of the electrical current
Several other components in the accessory gear train showed electrical arcing effects. The damage was found chiefly around the contact points between the gear teeth. The large diameter starter gear showed four evenly spaced regions around the circumference where the pitting was most severe. In contrast, the smaller mating coupling gear showed uniform pitting around the diameter. This observation led to three direct conclusions -
The electric current flowed from starter gear, through to the coupling gear and into the bearing via the turbine shaft and inner races.
The electric current was steady or continual and not a transient surge.
The current was of an alternating or pulsed nature at a frequency equal to four times the rotational speed of the starter gear.
From the general design of the engine, it appeared that the most likely source of the current was from the starter-generator unit, as the unit coupled directly to the large diameter starter gear. Armature leakage current from the unit would have conducted via the frictional coupling; through to the starter gear and into the bearing via the coupling gear, shaft and turbine shaft.
The ATSB carried out a safety deficiency investigation in accordance with powers under section 19CB (1) (d) of the Air Navigation Act 1920.
SAFETY DEFICIENCY
An allegation was made to the ATSB that Australian registered Boeing 747-300 aircraft operating from Bangkok airport in Thailand were failing to meet take-off performance requirements. A 'specified' flight was cited as demonstrating that the aircraft had not complied.
Comprehensive analysis of data from the 'specified' flight, as well as data from other flights departing Bangkok under similar conditions, was undertaken. Documentation provided by the crew of the 'specified' flight was also analysed. The data included brakes release to VR (take-off rotation speed); VR to VLOF (aircraft lift off speed); VLOF to 35 feet; total distance from brakes release to V2 (take-off safety speed) at 35 feet.
Appropriate sections of the Boeing and the operator's Flight Crew Training Manuals (FCTM) were reviewed and the ATSB concluded that the actual take-off data correlated with the Flight Crew Training Manual information.
For certification, the Boeing 747-300 aircraft is required to be able to sustain an engine failure at or after a specified speed (V1) at its maximum take-off weight and safely climb on the thrust of the remaining three engines. V1 is the decision speed at, and below which take-off can be aborted and the aircraft stopped within the runway confines. It is also the speed at and above which the take-off can safely be continued should the critical engine become inoperative, where the critical engine is the engine that would most adversely affect the performance or handling qualities of the aircraft.
Analysis of the recorded data confirmed that the 'specified' take-off from Bangkok was with four engines operating. No evidence was found to suggest that the aircraft concerned did not meet the certified requirements for take-off performance.
Nothing in the cases examined suggested that the aircraft would not be able to safely climb from the runway on three engines if an engine had failed at or after reaching V1 speed. Had an engine failure occurred before V1, by definition the aircraft would have been able to stop within the runway confines.
Formulae from Boeing Jet Transport Methods were used to derive actual take-off distance of the 'specified' take-off. Digital Flight Data Recorder (DFDR) and Quick Access Recorder (QAR) data were used to establish time from brakes release to rotate, time from rotate to lift-off, time from lift-off to a height of 35 feet by radar altimeter, and to calculate take-off distance. Data from the flights analysed showed the aircraft met the certification requirements for take-off performance.
Calculations by Boeing and the operator were assessed by performance engineers from the Civil Aviation Safety Authority. Subsequent independent review of the data, including comparison with the ATSB's calculations, verified the accuracy of those calculations. Again, no evidence was found to suggest that the aircraft did not meet certified performance requirements.
The ATSB was not able to source any information to quantify any in-service experience with the worldwide Boeing 747-300 fleet to suggest that there has been any deviation from the aircraft performance levels indicated in the approved Aircraft Flight Manual.
There is also no evidence that a dangerous situation as described in the report of the alleged safety deficiency has occurred in the 12-month period to October 2000. The ATSB concluded that Boeing 747-300 aircraft are meeting scheduled performance requirements.
Occurrence Date: 14 NOVEMBER 1999 Registration No: VH-EBX Model: B747-300 Manufacturer: Boeing Co
The partial wreckage of a Cessna 206 aircraft was recovered from an area in the Gulf of Carpentaria, near where an aircraft of this type disappeared on 24-November 1999 (ATSB Occurrence number 199905562).
Photographs and video footage of the wreckage were supplied to the ATSB and reviewed with a view to gathering further detail regarding the accident. The ATSB subsequently requested that the propeller and attitude indicator instrument from the aircraft be shipped to the bureau's Canberra laboratories for further study and analysis. On the basis of damage to several aircraft articles recovered during the initial search, the original investigation concluded that the aircraft had impacted the water at high speed. The findings of the recent study concurred with this. From the attitude indicator and propeller, it was possible to conclude with good probability that the aircraft impacted the water at high speed in an uncontrolled, inverted attitude. Evidence indicated that the propeller was rotating at impact, although it was not possible to determine whether the engine was developing power.
N.R. Blyth Senior Transport Safety Investigator Technical Analysis