Loss of separation
A loss of separation between two Boeing 737s on reciprocal tracks demonstrates the importance of communication and coordination between air traffic controllers operating in separate, yet adjacent airspace, as well as the need for a clear understanding of the responsibility for separation assurance when operating without a shared traffic picture.
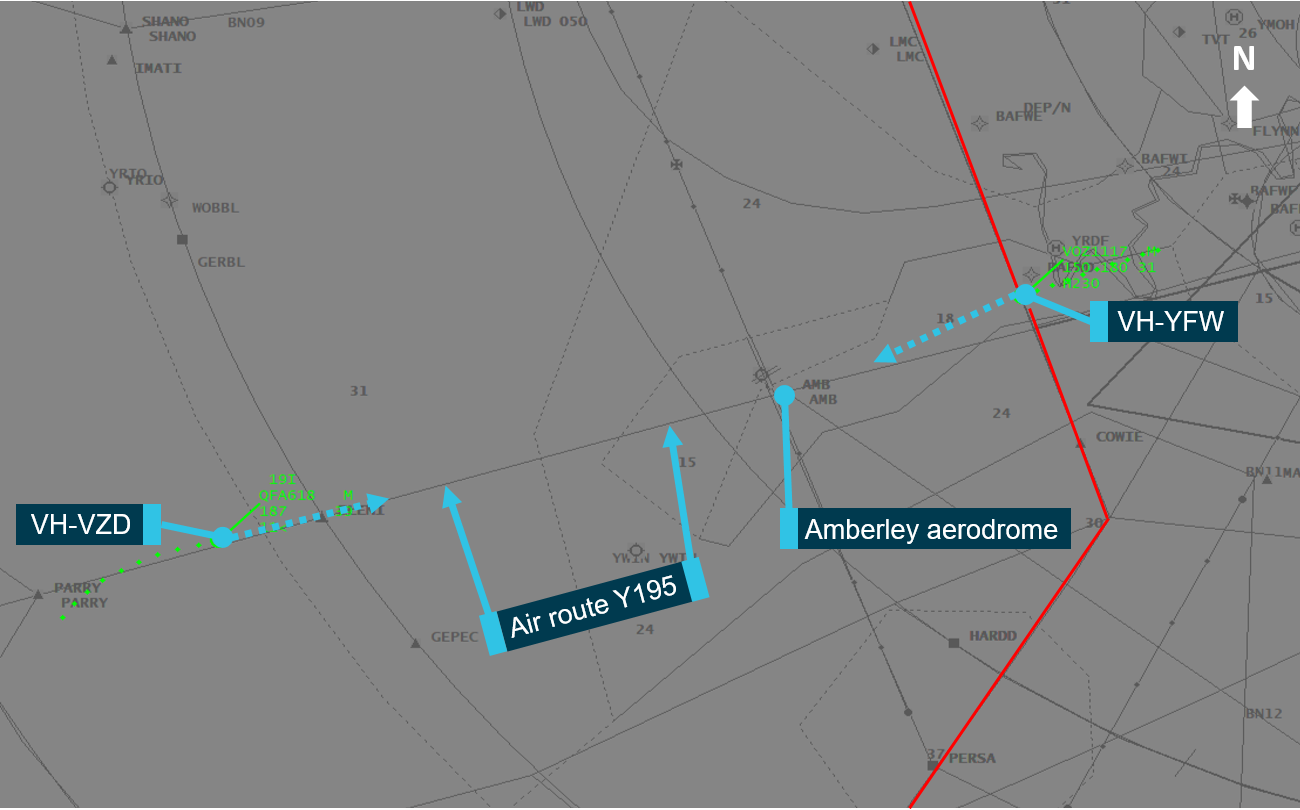
These are the key safety messages from the ATSB’s final investigation report into the 11 October 2018 incident, where a Qantas 737-800, registration VH-VZD, was on descent to Brisbane Airport through military-controlled airspace near Amberley Air Force Base, while a Virgin Australia 737-800, VH-YFW, which had departed Brisbane Airport, was approaching Amberley airspace on a reciprocal track. (Airservices Australia, which operates Australia’s civil air traffic management system, and the Royal Australian Air Force, which is responsible for controlling military airspace, such as around major air bases, currently operate separate air traffic management systems at Brisbane and Amberley. As a result, in this scenario traffic information had to be shared manually.)
Due to thunderstorms in the area, the Virgin aircraft was flying air traffic control (ATC)-assigned radar headings, rather than using a procedural standard instrument departure. As the Virgin aircraft approached Amberley airspace, the Brisbane departures controller (operating from Airservices’ Brisbane terminal control unit at Brisbane Airport) provided an identification of the Virgin aircraft to the Amberley approach controller, who advised that there was an aircraft on an inbound air route. Brisbane replied that the Virgin aircraft would soon be turning right, and thus would avoid Amberley airspace; however when advised to turn right, the crew of the Virgin aircraft replied that due to the weather they wished to continue on their current heading for another 70 or 80 nautical miles.
It was around this time that the Virgin aircraft entered Amberley airspace without a hand‑off from Brisbane ATC and without instructions to the crew to change to Amberley frequency. Prior to this, the Brisbane terminal control unit had not advised Amberley ATC of a changed terminal control unit configuration. This delayed Amberley ATC in being able to contact the correct controller position at the Brisbane terminal control unit to inform them of the inbound aircraft, thus reducing the opportunity for Amberley ATC to resolve the impending conflict.
Once appropriate communication between Amberley and Brisbane ATC was established, the Virgin aircraft was transferred to the Amberley frequency, and the two aircraft were diverted away from each other.
The successful recovery of separation illustrates the effectiveness of the conflict resolution training received by air traffic controllers in loss of separation events.
The ATSB's investigation found the aircraft had incurred a vertical and lateral loss of separation with a minimum-recorded distance between the aircraft of 2.1 nautical miles horizontally and 650 feet vertically, respectively, where the required separation was 3 nautical miles horizontally or 1,000 feet vertically. (Both aircraft were fitted with traffic collision avoidance systems which would have assisted in providing separation instructions to their flight crews in the event ATC were unable to resolve the situation.)
“This investigation highlights the importance of clear communication and coordination between air traffic controllers operating in different, yet immediately adjacent airspace, and the need for a clear understanding of the responsibility for separation assurance, especially when operating without a shared traffic picture,” ATSB Director Transport Safety Dr Stuart Godley said.
As a result of the incident, both Brisbane and Amberley ATC have taken a number of steps to improve communication between their two systems.
“The ATSB welcomes the new dedicated communications pathway between the Amberley approach and Brisbane departures south positions, and the implementation of an airspace release that controls the risk that short notice deviations present across the two non-linked systems.”
Dr Godley also said the successful recovery of separation illustrates the effectiveness of the conflict resolution training received by air traffic controllers in loss of separation events.
Read the final report: Loss of separation involving Boeing 737 aircraft, VH-YFW and VH-VZD, near Amberley, Queensland, on 11 October 2018