High workload decision making

The propellers of a Beech King Air operating a charter flight with one pilot and seven passengers on-board contacted the runway during an attempted landing at Mount Gambier Airport when the aircraft’s landing gear had not extended.
An ATSB investigation into the 8 December 2018 event found that the pilot decided to continue an approach to land shortly after having elected to commence a go-around and retracting the landing gear. The pilot had decided to conduct the go-around as he did not have the runway in sight due to cloud at the minimum descent altitude.
“After retracting the landing gear, the pilot subsequently sighted the runway and decided to continue the approach, but inadvertently did not re-extend the landing gear,” ATSB Director Transport Safety Stuart Macleod said.
The aircraft touched down with the landing gear retracted, with the propellers contacting the runway.
“As a consequence, the aircraft touched down with the landing gear retracted, with the propellers contacting the runway twice before the pilot initiated a go‑around.”
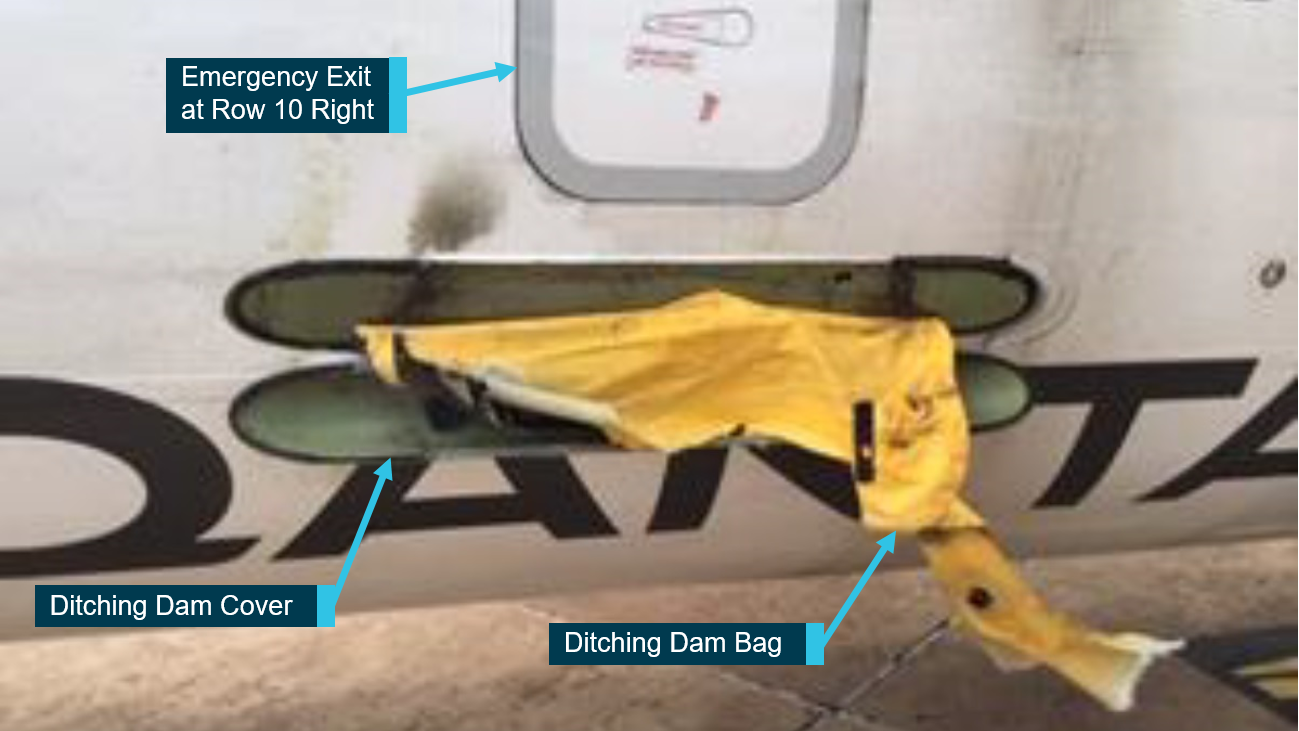
During the landing attempt both propellers were damaged, with fragments of the left propeller penetrating the left side of the fuselage. The left engine also failed upon the application of power for the go-around, however, the aircraft then landed without further incident.
The pilot and passengers, one of whom was a commercial pilot licence holder seated on the flight deck next to the pilot acting as an observer, were uninjured.
“The pilot's expectation of the landing gear position, possibly coupled with the effects of the now increased workload, probably led to him not detecting the retracted landing gear before the aircraft contacted the runway,” said Mr Macleod.
The ATSB investigation notes the decision to conduct a go-around resulted from the pilot’s misunderstanding of the situation and assessment that a runway overrun was imminent.
“There are hazards associated with spontaneous decision-making, particularly during a high‑workload phase of flight in a complex aircraft,” Mr Macleod said.
“Research on unexpected changes in workload during flight has found that pilots who encounter abnormal or emergency situations experience a higher workload with an increase in the number of errors compared to pilots not experiencing these situations.”
Mr Macleod noted that the pilot and his youngest son sadly lost their lives in a bushfire on Kangaroo Island in January 2020.
“The ATSB acknowledges the contribution the pilot made to the aviation and outback tourism industries, and thanks his family for their cooperation during the final stages of this investigation during a very difficult time.”
Read the final report: Wheels-up landing involving Beech Aircraft Corporation B200, VH-ODI, Mount Gambier Airport, South Australia, on 8 December 2018