Spin recovery

Key points:
- Instructor and student were conducting an aerobatic training flight in a Cessna A150 Aerobat to introduce and practice spin entry and recovery;
- Instructor likely intended to practice two spin recovery techniques, one of which has been shown to not recover a Cessna A150 Aerobat established in a spin to the left;
- While experienced in other aerobatic aircraft, the instructor likely had no experience conducting spinning and/or spin instruction in the accident aircraft type or similar variants;
- ATSB has issued a Safety Advisory Notice alerting aerobatic pilots and instructors of the limitations of the Meuller/Beggs spin recovery method for some aircraft types.
he Australian Transport Safety Bureau is advising aerobatic pilots and instructors of the limitations of the Meuller/Beggs spin recovery method for some aircraft types, after an investigation into an aerobatics training flight accident on Queensland’s Sunshine Coast.
During the accident flight on 23 June 2021, an instructor and student were likely intending to practice two methods of spin recovery. One of those techniques, broadly known as the Meuller/Beggs method, has been shown to not recover a Cessna A150 Aerobat established in a spin to the left.
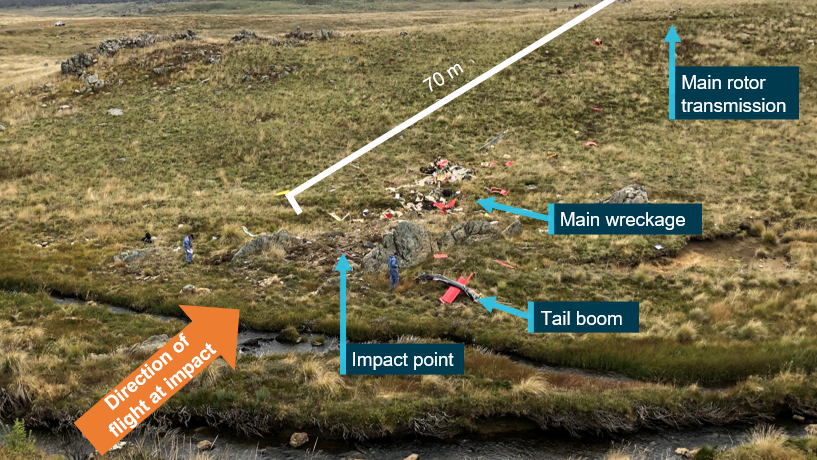
Both occupants were fatally injured when the aircraft collided with bushland near Peachester.
Air traffic control radar data showed that about 20 minutes after take-off the aircraft entered a spin to the left 5,800 ft above ground level, and then impacted the ground 55 seconds later.
The ATSB’s analysis of the accident site established that the aircraft’s forward movement and low angle of entry indicated it was most likely in the process of recovering from the spin when it impacted with terrain.
The aerobatics instructor was experienced in conducting spins, primarily in the Pitts Special aircraft type, for which the Mueller/Beggs method is effective. However, it was likely that they had no experience in spinning a Cessna A150 Aerobat or any similar variant.
“The instructor likely intended to practice two spin recovery techniques, including the Mueller/Beggs recovery method, which has been shown to not recover a Cessna A150 Aerobat established in a spin to the left,” ATSB Director Transport Safety Dr Michael Walker said.
The other method planned to be demonstrated, the generic PARE method typical of most small single-engine aeroplane types, aligned closely with the aircraft’s pilot’s operating handbook (POH) and, if utilised, would recover the aircraft from a spin.
“A second student, who was also to fly the same training flight with the instructor in the Aerobat aircraft later that day, told the ATSB they believed they would be conducting both methods of spin recovery,” Dr Walker said.
“The ATSB therefore concluded it was likely the instructor was either not aware, or did not recall, that the Aerobat would not recover using this method in a spin to the left.”
Dr Walker noted that, based on the available evidence, the ATSB was unable to ascertain which recovery technique or techniques were being utilised at the various stages of the spin recovery preceding the accident. For this reason, the ATSB could not conclude if the use of an inappropriate recovery technique contributed to the accident.
“Nevertheless, this investigation presents a timely reminder that pilots should review the POH of the aircraft type that they intend to operate, and obtain instruction and/or advice in spins and recovery techniques from an instructor who is fully qualified and current in spinning that model,” Dr Walker said.
To highlight this message, the ATSB has issued a Safety Advisory Notice to aerobatic pilots and instructors, flying training organisations and aerobatic aircraft owners to raise awareness of the limitations of the Mueller/Beggs spin recovery method.
“Prior to intentionally spinning an aircraft, pilots should obtain instruction and/or advice in spins and recovery techniques from an instructor who is fully qualified and current in spinning that model,” Dr Walker said.
“All aircraft types do not spin and recover in the same way. Know your aircraft type, what recovery techniques will work and what recovery techniques will not work.”
Read the final report: Collision with terrain involving Cessna A150M, VH-CYO, 5 km west-south-west of Peachester, Queensland, on 23 June 2021