ATSB releases Cessna 182 collision with water near Moreton Island investigation final report
The Australian Transport Safety Bureau has released the final report from its investigation into the collision with water of a Cessna 182 light aircraft near Moreton Island.
The Cessna 182Q aircraft had departed Caloundra Airport at around 3:30pm on 22 January 2020 for a private sightseeing flight over Moreton Island and Flinders Reef, with a pilot and passenger on- board.
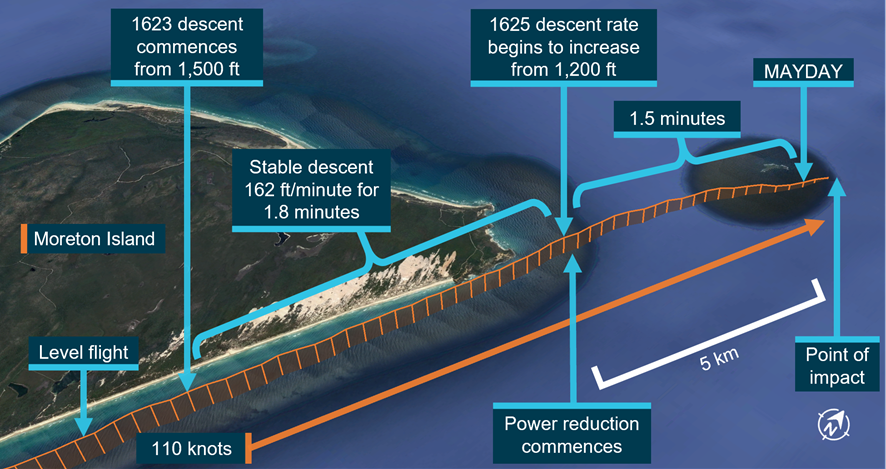
Recorded air traffic control radar data from the flight indicated that the aircraft flew along Moreton Island’s eastern coastline, from south to north, at 1,400—1,500 ft above sea level.
The aircraft then commenced a shallow descent before passing Cape Moreton, at the northern tip of the island, at about 1,300 ft, continuing north-east towards Flinders Reef.
The aircraft rate of descent began to increase, and after approximately 90 seconds, the pilot made a MAYDAY call that identified the aircraft’s callsign but not its position nor the nature of the emergency.
At the time of the MAYDAY, the aircraft was east of Flinders Reef and descending through 300 ft, with a groundspeed of about 115 kt (213 km/h). The aircraft continued north-east for 15–20 seconds, before colliding with water at 4:26pm.
On 29 January the aircraft wreckage was found on the ocean floor at a depth of about 30 m, and about 45 m from the estimated point of impact with water. The pilot and passenger were not located.
On the evidence available, the nature of any in-flight emergency or abnormal situation, and any effect it had on the pilot’s ability to control and configure the aircraft for a ditching on the water, could not be established.
Examination of the wreckage indicated the aircraft was likely destroyed by the collision with water at a moderately high speed and there was no evidence of pre-impact defects or structural failure.
“ATSB investigators found that the engine’s power was reducing over the last period of the flight, for about 100 seconds,” noted ATSB Director Transport Safety Dr Mike Walker.
At the time of the accident flight, weather conditions were conducive to carburettor icing, which is common in the region. The ice build-up within an aircraft engine’s carburettor may result in reduced power output, poor engine performance, rough running, and in extreme cases engine failure. The risk of carburettor icing is significantly increased at partial power settings (for example, when power is reduced during descent), because of the cooling effect of a partly-closed throttle.
“The likely reduction in power in the last 100 seconds of recorded flight could plausibly have been due to carburettor icing,” Dr Walker observed.
“However, a conclusion regarding the possible influence of carburettor icing on the development of the accident could not be drawn with any certainty.
“Carburettor icing conditions are frequently encountered in the region, and carburettor icing can be easily prevented and managed through the use of carburettor heating.”
During the accident flight, the aircraft maintained course away from suitable landing areas at a speed well above the aircraft’s best glide speed.
Although the reduction in power and resulting descent would have been indicated on the aircraft’s instruments, the pilot may have been initially unaware of it because there would have been little or no change in sound and feel.
The investigation also found that the pilot had twice descended over water beyond the glide range of a suitable landing area on a previous flight.
“Although it could not be determined whether the aircraft’s descent out of glide range during the accident flight was intentional, pilots are reminded that the operation of single engine aircraft over water should at all times be conducted with consideration of the aircraft’s glide distance to a suitable landing area,” said Dr Walker.
“Descending over water beyond the glide range of a suitable landing limits a pilot’s options to conduct a forced landing in the event of an emergency, such as an engine failure or partial power loss.”
Read the final report: Collision with water involving Cessna 182, VH-WNR, 6 km north-west of Moreton Island, Queensland, on 22 January 2020