Level crossing collision
The driver of a road-train truck had been distracted by reaffixing their mobile phone mount to their vehicle’s windscreen before the truck entered an active level crossing and collided with a freight train, an Australian Transport Safety Bureau investigation has found.
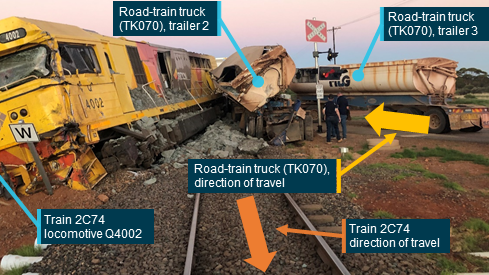
The road-train, comprising a prime mover and 3 tipper trailers, entered the Yarri Road, Parkeston level crossing in front of an Aurizon freight train, north-east of Kalgoorlie, Western Australia, on 22 February 2021.
The two train crew (a driver and tutor driver) sustained serious injuries in the subsequent collision. Both the truck and locomotive were substantially damaged, with the locomotive derailing and coming to a rest about 40 m from the impact point. The truck driver was shaken, but otherwise uninjured.
“Approaching the Yarri Road level crossing from the south, drivers need to look ahead and across a curve to see the active crossing lights,” ATSB Director Transport Safety Dr Michael Walker said.
“Because of the effects of distraction, the truck driver was probably only looking at the section of road directly ahead of their vehicle, contributing to them not identifying the flashing lights until it was too late to stop.”
While approaching the crossing, the truck driver was reattaching a dash-mounted mobile phone cradle, and placing a mobile phone in the cradle.
Consequently, the truck driver’s attention was diverted from the road ahead for critical periods of the approach to the level crossing where the flashing light level crossing controls were visible and there was sufficient distance to stop.
“The Yarri Road level crossing design was consistent with the applicable Australian standard and provided sufficient opportunity for attentive drivers to identify the flashing light level crossing controls and stop,” said Dr Walker.
The investigation notes the truck driver was familiar with the route, but had never encountered a train at that level crossing, meaning a low expectancy of encountering a train possibly contributed to the truck driver allocating a low level of attention to the crossing.
The truck driver only noticed the flashing lights, indicating the oncoming train, when it was too late to prevent the collision. When the train crew saw the truck and identified that it was not going to stop for the crossing, it was too late for them to stop their train or reduce the severity of the impact.
“Given the size and weight of most trains, the onus to take action to avoid a level crossing collision rests almost entirely on the road vehicle user,” Dr Walker said.
“Distraction can significantly impair driving safety,” Dr Walker continued.
“Even though it may be possible to occasionally glance at the road ahead while engaged in another task, critical information from the broader road environment may not be effectively perceived and comprehended, particularly on curved road approaches to level crossings.”
There were 11 collisions between heavy road vehicles and trains at level crossings across Australia between July 2020 and June 2021, and 23 such collisions over the previous 5 years.
“Accordingly, in 2021, the ATSB commenced a safety study into level crossing collisions involving trains and heavy road vehicles in Australia,” Dr Walker said.
“The study, which is on-going, includes a review of previous collisions to determine their characteristics and circumstances, and also determine if there are any unidentified systemic safety issues or learning opportunities that could enhance the safety of future transport operations.”
Read the final report: Level crossing collision between freight train 2C74 and road-train truck, Yarri Road, Parkeston, Western Australia, on 22 February 2021