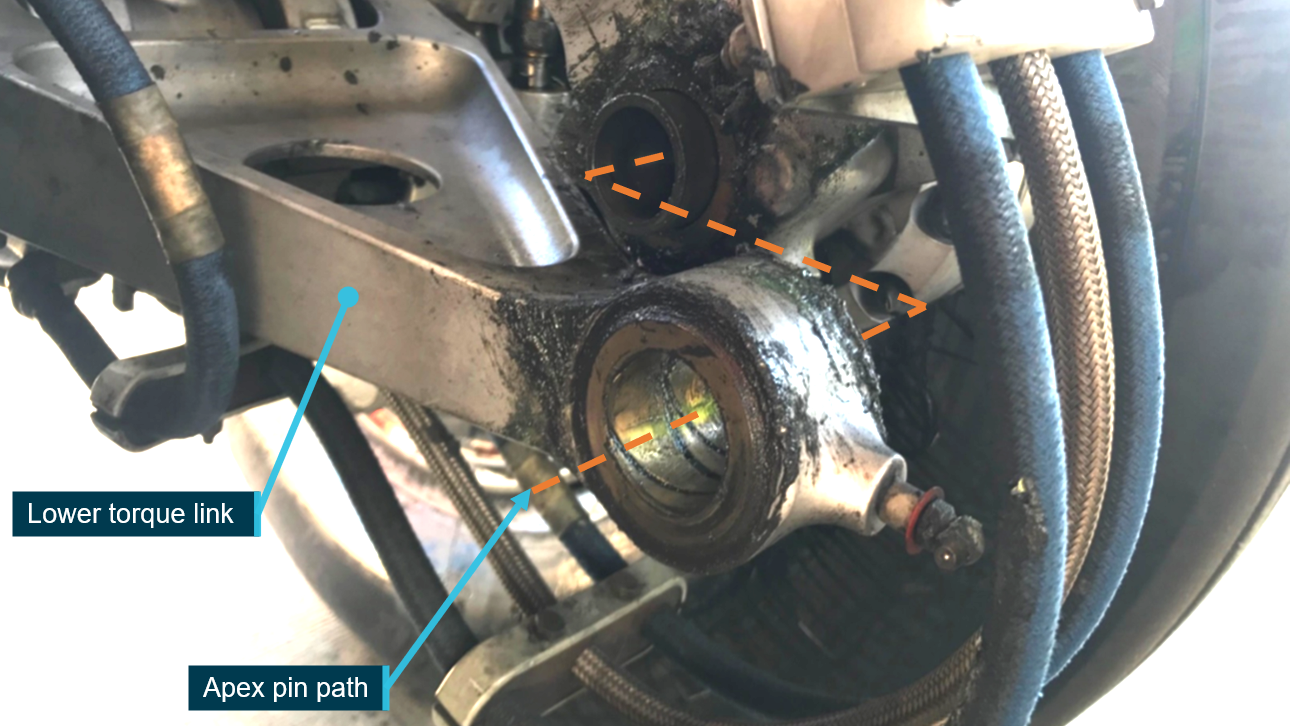
Apex pin failure
The main landing gear of an Airbus A320 could not be fully retracted due to the fatigue failure of a pin in the aircraft’s left main landing gear, an ATSB investigation report details.
The Jetstar Airways-operated A320 was departing Sydney to operate a scheduled passenger service to the Gold Coast on the morning of 1 August 2019.
After take-off and on selecting retraction of the undercarriage, the flight crew received multiple warnings of the undercarriage not retracting completely. The flight crew informed air traffic control of the issue and requested vectors to an area where they could troubleshoot the problem where they then cycled the undercarriage to the extended and then retracted positions, however, the issue remained.
Meanwhile, the crew of another aircraft taxiing at Sydney Airport identified an object on the ground which they reported to the air traffic control (ATC) Ground controller.
The debris was collected by an airport ground car and determined to be an aircraft part that was subsequently identified as an A320 main landing gear component.
The ATC Departures controller notified the A320’s flight crew that an aircraft part had been found on the runway, subsequently informing them ‘they believe it might be a part of the landing gear’. Separately, Jetstar engineering communicated to the flight crew that the part had not yet been positively identified and advised them to follow their standard operating procedures.
When all appropriate checks were completed, the flight crew elected to return to land at Sydney, requesting the airport’s emergency services be put on a local standby.
While the landing was uneventful, further damage to the left main landing gear occurred including the loss of brakes and the severing of electrical sensors.
The flight crew had made the decision to return and land after seeking and assessing information relating to the landing gear malfunction, the ATSB’s investigation notes.
However, at that time the operator’s engineering personnel were gathering and analysing additional information about the failed component.
“Despite the failed part and aircraft being positively identified by elements within Jetstar, a message was unable to be conveyed to the flight crew before they returned for landing,” said ATSB Director Transport Safety Stuart Macleod.
“As such, the flight crew was unaware of the true nature of the undercarriage defect and the associated risks, and that additional information would have better informed crew decision making.”
Without the apex pin in place, the main landing gear axle could rotate out of alignment. This both prevented the landing gear from retracting, and caused damage to other landing gear components and systems during the taxi, take-off and landing, including disabling the left side main landing gear’s brakes.
While the disconnected torque link reduced the directional stability and braking performance, the degradation was manageable and the aircraft landed safely.
“Investigations determined that the fatigue failure of the apex pin was the result of a crack that initiated during the quench step of the heat treatment process at manufacture,” Mr Macleod noted.
The failed apex pin shank was sent to A320 aircraft main landing gear manufacturer Safran Landing Systems, which concluded the cracks were initiated during the manufacturing process and were not caused by environmental effects in service.
Following the incident Airbus issued an alert to A320 operators requiring the recall or inspection of 1,988 apex pins – as a result 19 pins were removed from service due to cracking.
Safran had previously revised its manufacturing processes for the apex pin.
Also in response to the incident, Jetstar clarified its non-normal operational communication guidance for ground crews in the Airport Operations Manual. This included dedicated phraseology for gaining priority on airband frequencies to relay high priority messages.
“This investigation highlights the importance of ensuring that operational processes permit coordinated, accurate and timely flow of information between ground personnel and flight crew to assist airborne decision making,” said Mr Macleod.
Read the final report: Landing gear malfunction involving Airbus A320, VH-VFN, Sydney Airport, New South Wales, on 1 August 2019