Collision with terrain involving Robinson R22 helicopter, 38 km south-west of Tindal Airport, Northern Territory, on 4 January 2018
Brief
| Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. |
What happened
On 4 January 2018, at about 0900 Central Daylight-saving Time (CDT), a Robinson R22 helicopter departed from a private property in Katherine, Northern Territory. The pilot, who was the sole occupant, was conducting a private flight to obtain GPS coordinates of structures on a property 38 km south-west of Tindal, NT.
The pilot landed the helicopter alongside a fence line in long grass. The pilot remained in the helicopter, with the engine running and obtained coordinates as required. The pilot then manoeuvred the helicopter into a low hover and with the breeze coming from the north-east, commenced to move out of the hover and felt the helicopter move to translational lift.[1] The pilot lifted the power to maximum take-off while easing the cyclic[2] forward to take advantage of the headwind.
As the helicopter straightened, about 3 ft above ground level (AGL), it dipped suddenly, pivoting on the front left-hand skid. The pilot attempted to pull the cyclic back but the helicopter rolled to the left and the main rotor blades contacted the ground at full power, almost severing them at the blade roots. The main rotor blades cut the tail boom into three pieces, lodging the tail rotor and assembly into the ground about 5 m in front of the fuselage. The fuselage came to rest on the left side.
Although hanging from his seatbelt, the pilot was able to shut off the master; however, was unable to reach the fuel shut off valve. The pilot’s seat base dislodged and fell off once the pilot released himself from the seatbelt.
Post-accident observation
The pilot observed two old barbed wires leading from the fence line at a 45-degree angle One wire appeared to have broken with impact and the other wire was entangled around the front left-hand skid.
The wires were half buried in the ground and below the grass top level, making them invisible.
Figure 1: Accident site showing fence wire
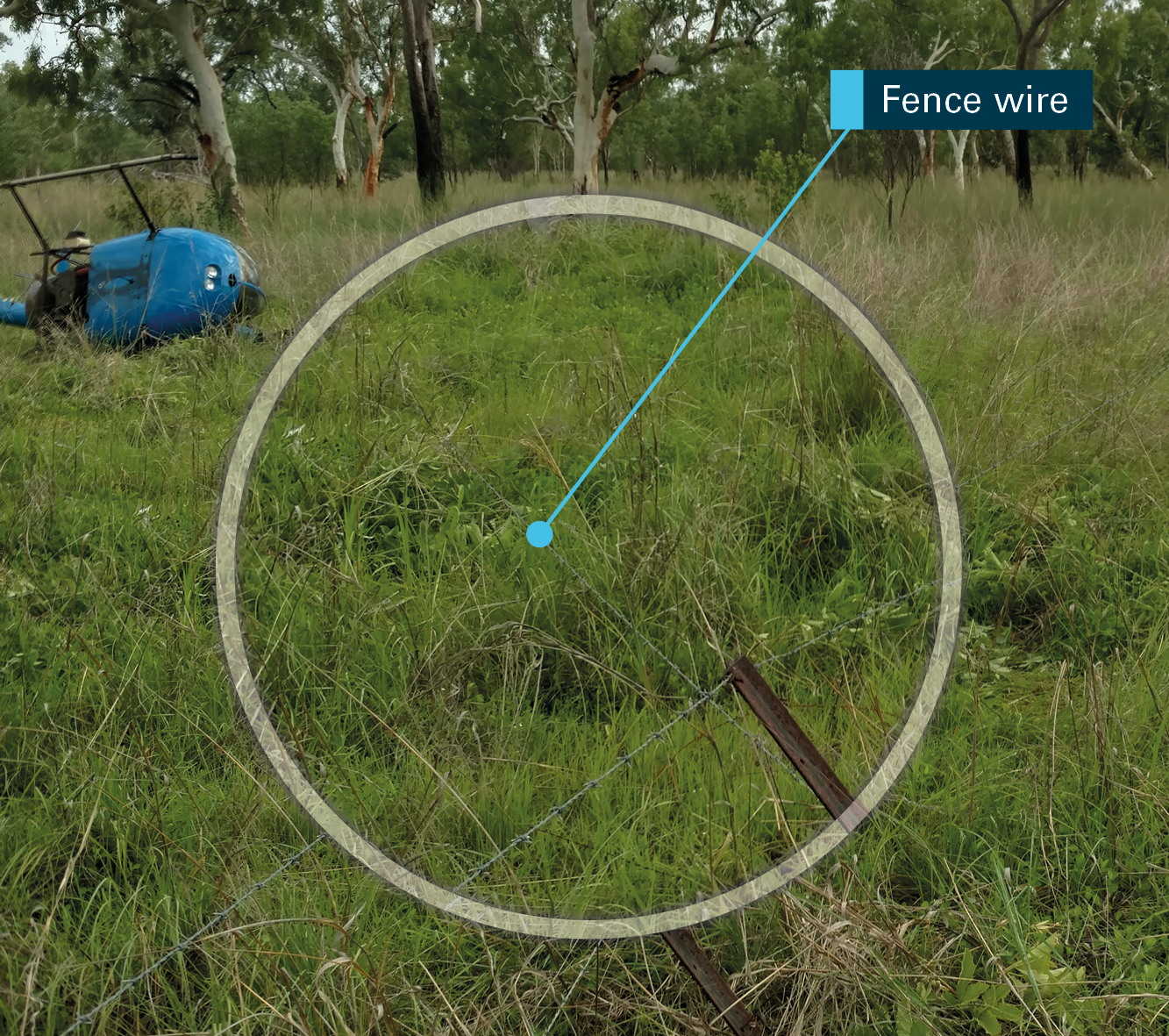
Source: Operator
Safety action
As a result of this occurrence, the pilot has advised the ATSB that they are taking the following safety actions:
- avoid landing in grass any higher than skid tube height
- conduct a thorough visual inspection when lifting off around fences.
Safety message
This incident provides a reminder to pilots to conduct a thorough visual inspection to confirm wire locations and other hazards.
This accident highlights the value of restraints and safety helmets for pilots to prevent more serious injury.
ATSB report AO-2014-058 provides an account of a serious head injury to an R22 pilot who was not wearing a helmet. In a later ATSB report, AO-2015-134, the operator commented that the pilot of an R22 accident would have sustained more serious head injuries if he was not wearing a helmet.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
__________
- Translational lift occurs when clear, undisturbed air, flows through the rotor system from wind or forward speed.
- Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2018-001 |
| Occurrence date | 04/01/2018 |
| Location | 38 km SW Tindal |
| State | Northern Territory |
| Occurrence class | Accident |
| Aviation occurrence category | Collision with terrain |
| Highest injury level | None |
| Brief release date | 28/03/2018 |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 |
| Sector | Helicopter |
| Damage | Substantial |