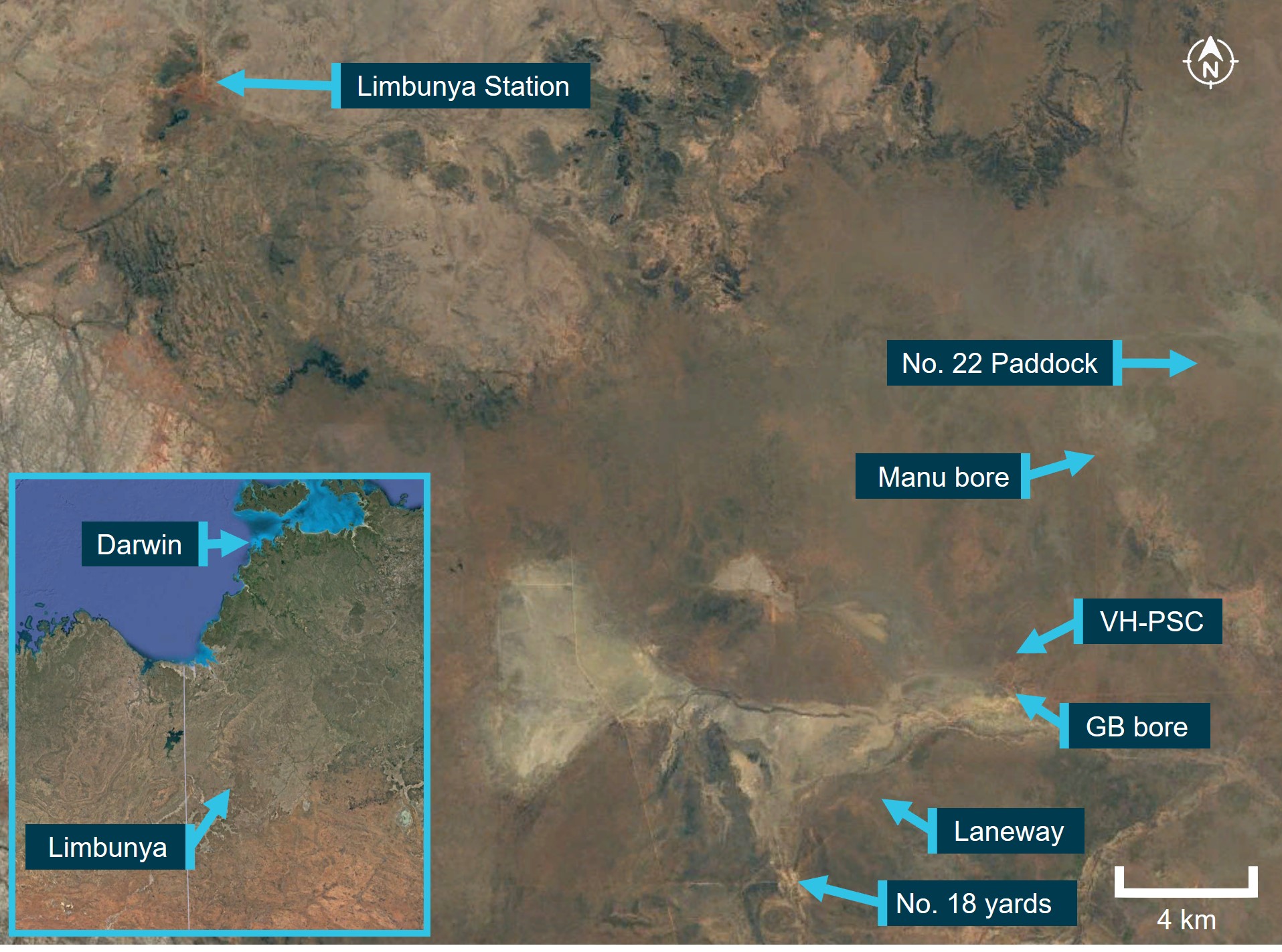
The helicopters arrived at the northern end of the paddock at about 0730 and began pushing cattle south towards the GB bore holding yards. The pilot of PSC then supported the ground mustering party in moving stock from the yards into a fenced laneway. The laneway would guide the stock to the No. 18 holding yards, that were located about 8 km to the south‑west.
At about 0915, when the cattle were moving along the laneway under the control of the ground mustering party, the pilot of PSC was released from that task, and returned to assist the pilot of RSC with completing the mustering task.
At about 0930, the pilot of RCS diverted to Manu bore to refuel the helicopter from drum stock. Following refuelling, the pilot departed back to the small paddock, and at about 0945 acknowledged a departure call from the pilot of PSC who had also completed refuelling at Manu bore.
At about 1000, the pilot of RCS contacted the head musterer via radio to enquire if they had been in contact with the pilot of PSC. The head musterer advised that no contact had occurred since the time PSC had been released. Having received no replies from PSC to their radio calls, the pilot of RCS commenced searching the area around Manu bore, and gradually progressed the search towards GB bore.
At about 1015, the pilot of RCS located the wreckage of PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries.
The pilot held a Commercial Pilot Licence (Helicopter) with the required ratings and endorsements to operate the accident helicopter, and a valid Class 1 Aviation Medical Certificate. The pilot had about 14,000 flying hours on helicopters, including over 3,000 hours on the R22 type. The pilot also held a Commercial Pilot Licence (Aeroplane), with about 2,500 hours logged.
Aircraft information
VH-PSC was a Robinson Helicopter Company R22 Beta helicopter, serial number 4429. It was manufactured in the United States in December 2008 and first registered in Australia in January 2009. The helicopter was fitted with a 4-cylinder Lycoming engine, model O‑360-J2A, serial number L-40927-36C-C-A. On 15 June 2023, the aircraft underwent a 100-hourly/annual inspection, during which the engine was replaced with a newly overhauled unit. A new maintenance release was issued at this time, which stated that the aircraft had accrued 6,300.2 hours total time-in-service.
Meteorological information
Witnesses in the area reported that the weather conditions at the time of the accident consisted of overcast[1] skies with no precipitation, a temperature of about 20-25 °C, and a slight breeze.
Site and wreckage information
The accident site was located in an area that was flat and moderately wooded. The helicopter collided with terrain on an approximate north-west heading. There was a short wreckage trail of about 18 m, with all helicopter parts present at the accident site and no evidence of an in-flight break-up or a post-impact fire.
One main rotor blade tip was liberated in the collision and was found about 40 m to the left of the helicopter. Examination of the flight controls and helicopter structure did not identify any pre‑existing defects. The site examination found that both fuel tanks remained intact and contained fuel. In addition, fuel quality was established through testing of fuel stocks at Manu bore and the homestead.
Recorded information
The helicopter was not fitted with a tracking unit, flight data recorder or cockpit voice recorder, nor was it required to be.
The investigation is continuing and will include further review and analysis of:
electronic data from the pilot’s mobile phone
meteorological data
wreckage information
instruments and components collected from the accident site
aircraft maintenance history
similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB acknowledges the assistance provided by the Northern Territory Police Force, the management and staff at Limbunya Station, and the operator.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘overcast’ indicates that all the sky is covered.
Final report
Executive summary
What happened
On the morning of 27 June 2023, the pilot of a Robinson Helicopter R22 Beta II, registered VH‑PSC and operated by Top End Mustering, was conducting mustering operations in company with a second R22 registered VH-RCS, on Limbunya Station, Northern Territory.
After not hearing from the pilot of VH-PSC for some time, the pilot of VH-RCS attempted to contact VH-PSC with no response received, and the ground mustering crew stated that they had no recent communication either. Subsequently, the pilot of VH-RCS commenced a search and shortly after located the wreckage of VH-PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries.
What the ATSB found
The ATSB found that, for reasons that could not be determined, VH-PSC collided with terrain in a nose and right-side down orientation. The site and wreckage examination identified signatures consistent with low rotor energy and low-to-nil engine power.
There was no evidence of any flight control or mechanical system abnormality that would have prevented the helicopter from operating normally. In addition, in the absence of an identified problem with the helicopter, the reason for the loss of control could not be determined.
The ATSB also identified that the maintenance release contained no endorsements for daily inspection certification, hours flown, total time‑in‑service or engine oil uplift. This was despite VH‑PSC being operated daily since its issue 13 days prior. A scheduled 25-hour engine oil and filter change had reportedly been conducted, however, had not been certified on the maintenance release. Further, the absence of recorded operating hours increased the risk of the helicopter having been operated beyond other scheduled maintenance requirements.
Safety message
Routine low-level flight brings several significant complexities to a helicopter operation including management of emergencies and the conduct of forced landings. Time to respond and the availability of suitable forced landing areas may also be significantly reduced. Main rotor energy management is an important element of maintaining control and safely landing a helicopter.
Aircraft owners and pilots should ensure that the maintenance release is updated at the end of each day’s flying. This will allow all pilots to be aware of the operational status of the aircraft and to avoid unintentional flight beyond scheduled maintenance. In addition, engine oil uplift records assist with trend monitoring of engine condition.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
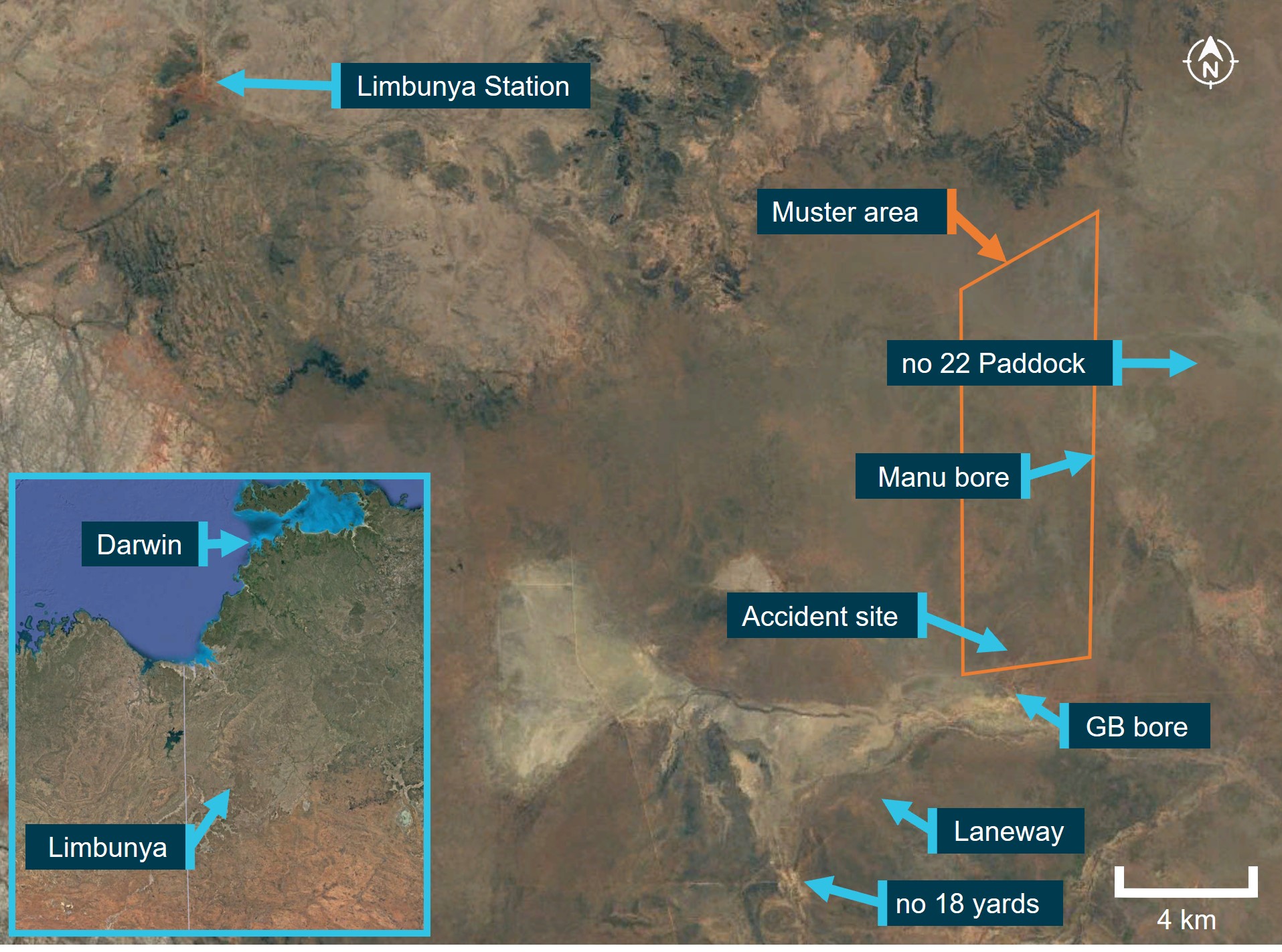
On 27 June 2023, at about 0700 local time,[1] the pilot of a Robinson Helicopter R22 Beta II, registered VH‑PSC (PSC), and operated by Top End Mustering, departed Limbunya Station, Northern Territory, in company with a second R22 registered VH‑RCS (RCS). Their task was to muster stock in a small paddock to the north of ‘GB’ bore, about 29 km to the south-east of the station homestead. In addition, they were to assist the ground mustering crew (on horseback and motorcycles) to move stock that had been mustered the previous day from ‘no 22’ paddock into the GB bore holding yards, to the ‘no 18’ yards (Figure 1). RCS was working the western side of the paddock, with PSC working down the eastern side. The helicopter pilots could communicate with each other via very high frequency (VHF) or ultra high frequency (UHF) band radios, and with the ground mustering crew via UHF.
The helicopters arrived at the northern end of the paddock at about 0730 and began pushing cattle south towards the GB bore holding yards. The pilot of PSC then supported the ground mustering crew in moving stock from the yards into a fenced laneway. The laneway would guide the stock to the no 18 holding yards that were located about 8 km to the south‑west.
At about 0915, when the cattle were moving along the laneway under the control of the ground mustering crew, the pilot of PSC was released from that task, and returned to assist the pilot of RSC with completing the mustering task.
At about 0930, the pilot of RCS diverted to Manu bore to refuel the helicopter from drum stock. After refuelling, the pilot of RCS departed back to the small paddock, and at about 0945 acknowledged a departure call from the pilot of PSC, on VHF radio, who had also completed refuelling at Manu bore.
Following a period of radio silence, the pilot of RCS contacted the head musterer at about 1000, via UHF, to enquire if they had been in contact with the pilot of PSC. The head musterer advised that no contact had occurred since about 0915. Having received no replies from PSC to their radio calls, the pilot of RCS commenced searching the area around Manu bore, and then progressed the search towards GB bore.
After about 15 to 20 minutes, the pilot of RCS located the wreckage of PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries. There were no witnesses to the accident.
Figure 1: Limbunya Station and operational area
Source: Google Earth, annotated by the ATSB
Context
Pilot information
Qualifications and experience
The pilot held a Commercial Pilot Licence (Aeroplane) since 1985, a Commercial Pilot Licence (Helicopter) since 1986 and a valid Class 1 Aviation Medical Certificate. The pilot also held helicopter gas turbine engine and night visual flight rules ratings. Additionally, the pilot held a low‑level aerial mustering (aeroplane and helicopter) rating and helicopter sling operations, valid until 3 April 2025.
On 3 April 2023, the pilot underwent a flight review in an R22, with a helicopter low-level flight review and a company pilot proficiency check also conducted at the same time, at Kununurra, Western Australia. The pilot demonstrated proficiency with emergency procedures and the instructor’s handwritten flight review note stated, ‘all to a good standard. Placed a lot of emphasis on power management’.
The last entry in the pilot’s helicopter logbook was dated 10 July 2021, almost 2 years prior to the accident, with a total helicopter aeronautical experience of 12,288.1 hours. Using several sources of information, the ATSB calculated the pilot had about 14,000 flying hours on helicopters at the time of the accident, including over 3,000 hours on the R22 helicopter type.
Recent history
The pilot relocated to Kununurra and had been operating the R22, R44 and Bell 206-series helicopters across north-western Australia since 3 April 2023. The pilot had operated several helicopters most days from 5 June 2023, and VH-PSC (PSC) exclusively since 21 June 2023.
On 25 June, the pilot ferried PSC to Limbunya Station, arriving around 1800. On 26 June, the pilot conducted mustering operations at the station, with 2 other company R22 helicopters, from about 0630 until about 1300.
The second helicopter pilot and several members of the ground mustering team reported the pilot was in good spirits at dinner the night before the accident and retired to their room about 2130.
The ATSB considered whether the pilot’s activity in the preceding days and months may have led to them being fatigued at the time of the accident. A review of the pilot’s diary indicated they had operated a helicopter for all but 19 days in the preceding 90 days, totalling over 340 hours of duty time.[2] The diary indicated over 170 hours in the preceding 30 days and about 47 hours in the 7 days prior to the accident. The accident occurred on the 14th consecutive day of duty. However, the ATSB noted a short ferry flight on 25 June, the pilot being relieved from duty about midday on 26 June and being on duty for less than 5 hours on the day of the accident. It was possible that the months of extensive work time coupled with high workload operations had the potential to produce cumulative fatigue. However, noting the workload and opportunity for rest in the preceding days, there was insufficient evidence to establish if the pilot was likely experiencing a level of acute fatigue known to affect performance at the time of the accident.
Helicopter information
General
VH-PSC was a Robinson Helicopter Company (RHC) R22 Beta II helicopter, serial number 4429, powered by a Textron Lycoming O-360-J2A, 4-cylinder carburetted piston engine (Figure 2). It was manufactured in the United States in December 2008 and first registered in Australia in January 2009.
The R22 has 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seatbelt and inertia reel shoulder strap, similar to those used in motor vehicles. The helicopter was not fitted with an optional cabin heating system.[3] Typical for mustering activities, the helicopter was being operated with both doors removed.
Figure 2: VH-PSC
Source: Operator
Systems information
Rotor drive system
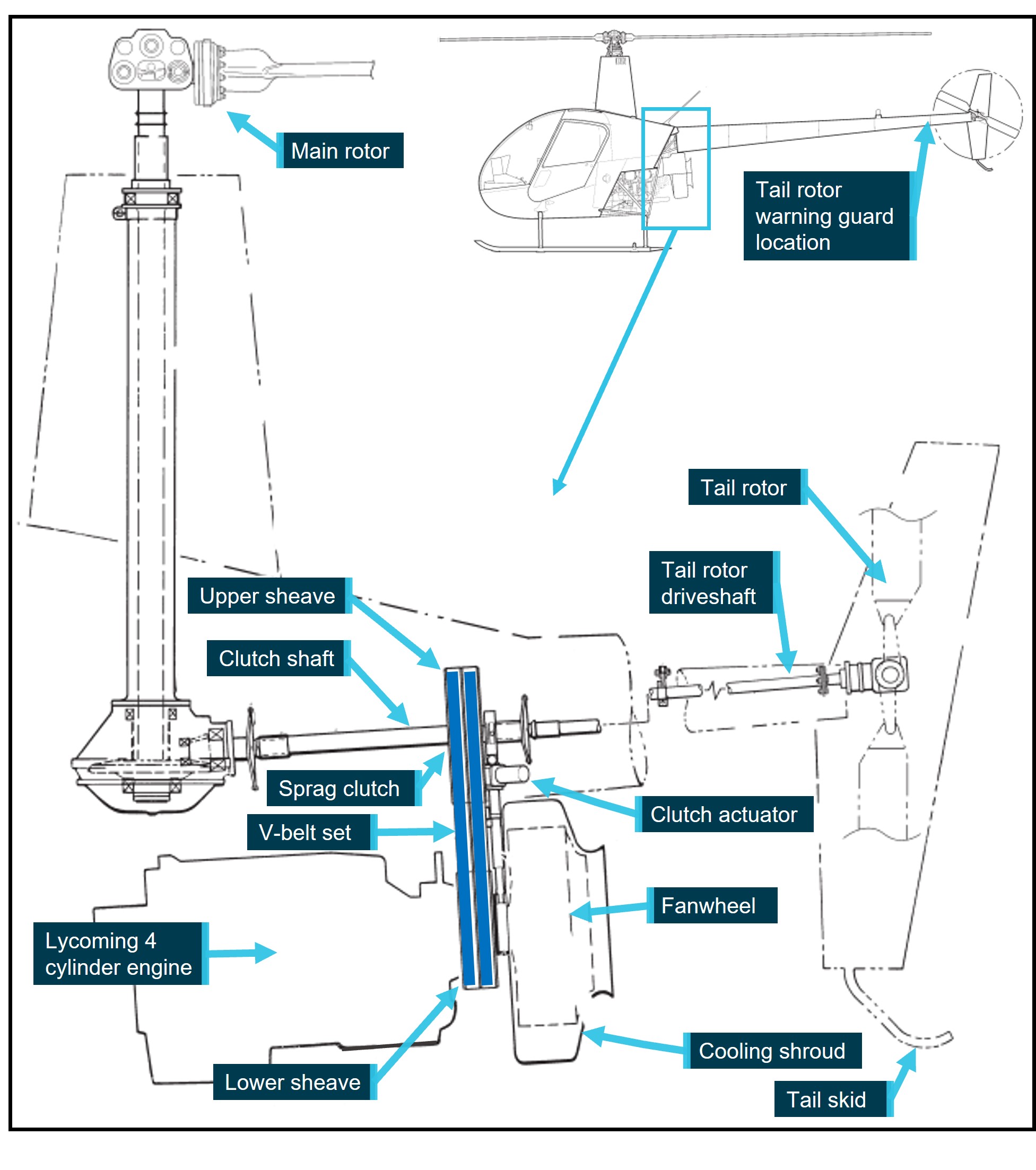
The rotor drive system on the R22 helicopter uses 2 reinforced rubber drive belts (V-belts). The drive belts are double-banded and fitted to upper and lower multi-grooved sheaves. The upper sheave has an overrunning sprag clutch (freewheeling unit)[4] in its hub, which the clutch shaft passes through. The clutch shaft transmits power forward to the main rotor gearbox and aft to the tail rotor driveshaft. The lower sheave is attached directly to the engine crankshaft.
The upper sheave is moved, relative to the lower sheave, by means of an electric clutch actuator, thereby controlling the tension on the drive belts. This allows the engine to be unloaded during startup (drive belts slack) without the rotor system engaged, and then tensioned to allow engine power to be transmitted to the rotor drive (Figure 3).
The fanwheel utilised on the R22 is a commercial product, modified by RHC. Its purpose is to direct cooling air onto the engine. It is constructed of steel, and is comprised of 8 cooling vanes welded to the rear plate (on the engine side) and a support ring on the outer side. The assembly mounts onto the fan shaft, behind the lower sheave, and is enclosed in a fibreglass shroud.
The tail rotor was fitted with a visual warning guard located on the underside of the tailcone, just forward of the tail rotor. Painted with red and white stripes, it provides a visual warning of the tail rotor disc, which can be difficult to see when operating.
Figure 3: Diagram of the R22 rotor drive system
Source: Robinson Helicopter Company, annotated by the ATSB
Low rotor revolutions per minute (RPM) warning
A ‘low RPM’ warning light will illuminate, with an associated horn, when rotor RPM is at or below 97%, regardless of engine RPM.
Fuel system
The fuel system consists of a main tank (left side, when looking from the rear of the helicopter, 69 L) and an auxiliary tank (right side, 37 L). Fuel is gravity-fed via a gascolator to the carburettor.
Engine governor system
Under normal conditions, the governor senses engine RPM and makes adjustments to the throttle control to maintain a constant engine RPM, which leads to a constant rotor RPM in flight. The governor can be selected on or off using the toggle switch on the right seat’s collective.[5] The R22 pilot’s operating handbook (POH) stated that the governor may not prevent over- or under-speed conditions generated by aggressive flight manoeuvres. In the event of malfunction, the pilot can override the governor and manipulate the throttle to maintain engine RPM, until the governor can be selected off, or rendered inoperative by pulling the circuit breaker.
Given the dynamic nature of mustering operations, when compared to flying in cruise (normal flight conditions), the pilot was likely not relying on the governor.
Carburettor heat system
The helicopter was fitted with a carburettor heat system, which directed hot air collected from a scoop installed on the engine exhaust system, via a duct, to the engine induction air box. Within the air box was a sliding guillotine-type valve to proportion the mix of cool and heated air. The pilot could monitor the temperature of the carburettor air using the carburettor air temperature gauge on the instrument panel console.[6] The carburettor heat control knob was situated aft and rear of the cyclic,[7] with ‘down’ being no heat and ‘up’ providing full heat, or anywhere in between as selected by the pilot. This heated air prevented the temperature within the carburettor from dropping to, or below, the freezing point of water.
The helicopter also had a carburettor heat assist system, which automatically applied carburettor heat when lowering the collective, generally for descent, to reduce pilot workload. The pilot could override the heat assist. In addition, a latch was provided at the carburettor heat control knob to lock the heat assist off when not required.
Fuel rotary pump
The operator reported that each helicopter would carry a drum fuel pump, which could be broken down into components with the suction tube (standpipe) capable of being separated into 3 sections. The operator advised the fuel pump components could be stored under the left (passenger) seat or optionally store some, or all, of the pump components in the left seat footwell.
The pilot of RCS used their pump for refuelling from the drum stock at Manu bore.
Airworthiness and maintenance
General
A periodic inspection of the helicopter was to be conducted every 100 hours or 12 months, whichever came first. In addition, the helicopter was subject to an overhaul every 2,200 hours or 12 years. On 15 June 2023, the helicopter underwent a 100-hourly/annual inspection, during which the engine was replaced with a newly overhauled unit.[8] As part of the periodic inspection, the exhaust system was certified as being visually inspected and pressure tested. A new maintenance release was issued at this time, which stated that the helicopter had accrued 6,300.2 hours total time‑in‑service.
Maintenance release
The maintenance release (MR) is a legal document that is part of the ongoing airworthiness requirements of an aircraft and is divided into several parts. Part 1 details any scheduled maintenance that will be required to be completed during the MR period of validity. When a maintenance task has been completed it can be certified for in Part 2 of the MR, or in the aircraft maintenance logbook. The person who performed the maintenance, or the certificate of registration holder is then required to clear the entry in Part 1, making note if the certification was logged in Part 2 or the aircraft logbook. Part 3 of the MR is used to certify for the daily inspection of the aircraft, for recording the daily total flight time, calculating the total time-in-service at the end of each day’s flying and for tracking other events, such as engine oil uplift. The regulations state that, if the certificate of registration holder, the pilot in command or the operator becomes aware the aircraft may be operated beyond any maintenance requirement noted in Part 1, then they must make ‘an endorsement signed by him or her setting out the facts of the situation and stating that the aircraft is unairworthy, and thereupon the maintenance release ceases to be in force’.
The current MR was located at the accident site. An endorsement, in Part 1 of the MR, included that an engine oil and filter change was required at 25, 50 and 75 hours post engine change. Since its issue on 15 June 2023, there were no endorsements for daily inspection certification, hours flown, total time-in-service or engine oil uplift.
Pilot approved maintenance
The civil aviation regulations permitted the pilot to perform some maintenance including changing oil filters and changing or replenishing engine oil. Further, the regulations required that ‘a person who carries out maintenance … must ensure that completion of the maintenance is certified in accordance with … the CASA [Civil Aviation Safety Authority] system of certification of completion of maintenance’.
Engine oil and filter maintenance
Following fitment of any new, rebuilt or overhauled engine, RHC required Lycoming service bulletin 480 be complied with. The bulletin required an oil and filter change after the first 25 hours of engine operation and then an oil and filter change, along with suction screen inspection and cleaning, every 50 hours of operation, or 4 months, whichever came first.[9] In addition, the filter was to be cut open and the filter element carefully inspected for metal contamination. Further, oil uplift was to be recorded to enable monitoring of oil consumption.[10]
A text message from the pilot to the operator on 19 June 2023 stated that the 25-hour oil change on PSC had been conducted. The pilot also commented that the filter looked ‘pretty clean’ and that they had bagged the element (filter) with the intent to provide it to the operator the next day. The MR had not been endorsed to show this inspection had been completed. Neither the operator, or the maintainer, could locate the filter element to verify whether the maintenance had taken place. Text messages to the operator, which aligned with the pilot’s diary, indicated the helicopter may have accumulated an additional 25 hours following the first oil and filter change, prior to 27 June 2023. However, there were no records indicating the 50-hour oil and filter change had become due, nor if it was completed.
Weight and balance
There were no records to indicate fuel quantity onboard PSC following the refuel. The ATSB calculated the helicopter weight for ‘full fuel’ and for the quantity of fuel drained from PSC at the accident site. Both calculations determined that the helicopter was being operated within the approved weight and balance envelope.
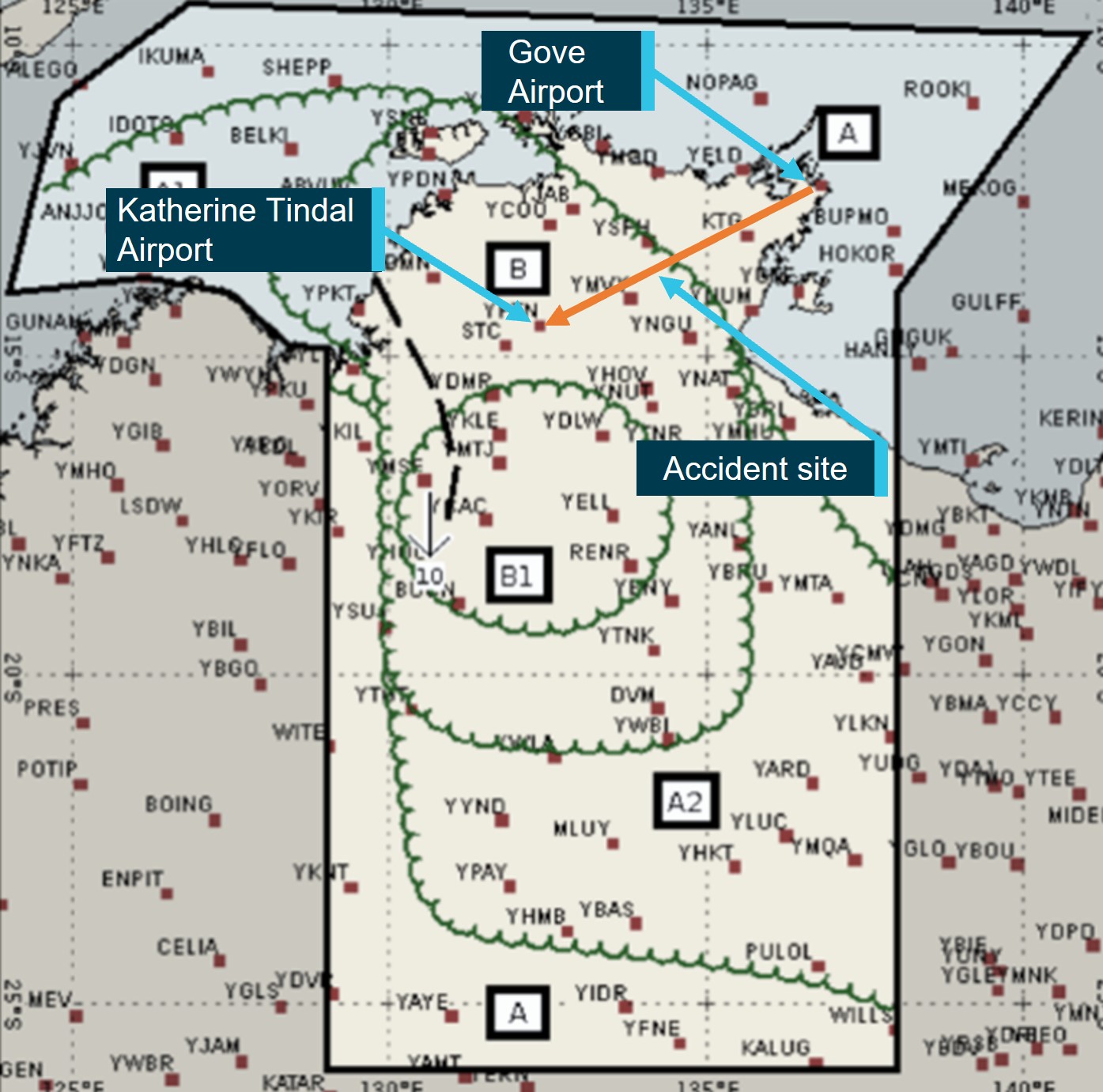
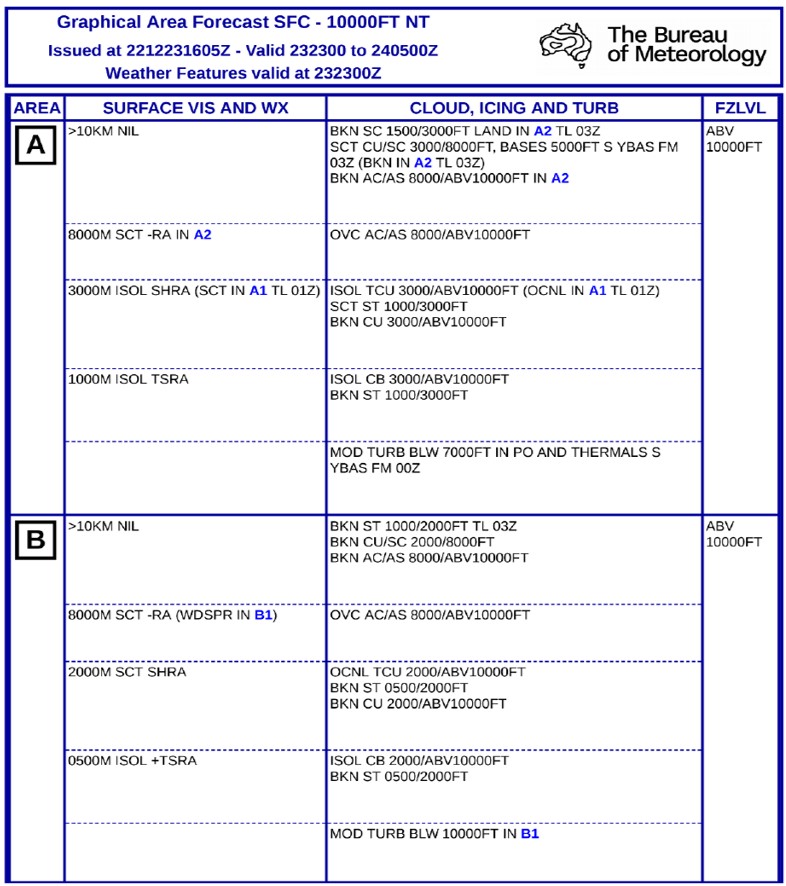
Meteorological information
Witnesses in the area and the pilot of RCS reported that the weather conditions at the time of the accident consisted of overcast[11] cloud well above their operating height with no precipitation, a temperature of about 20–25 °C, and a slight breeze.
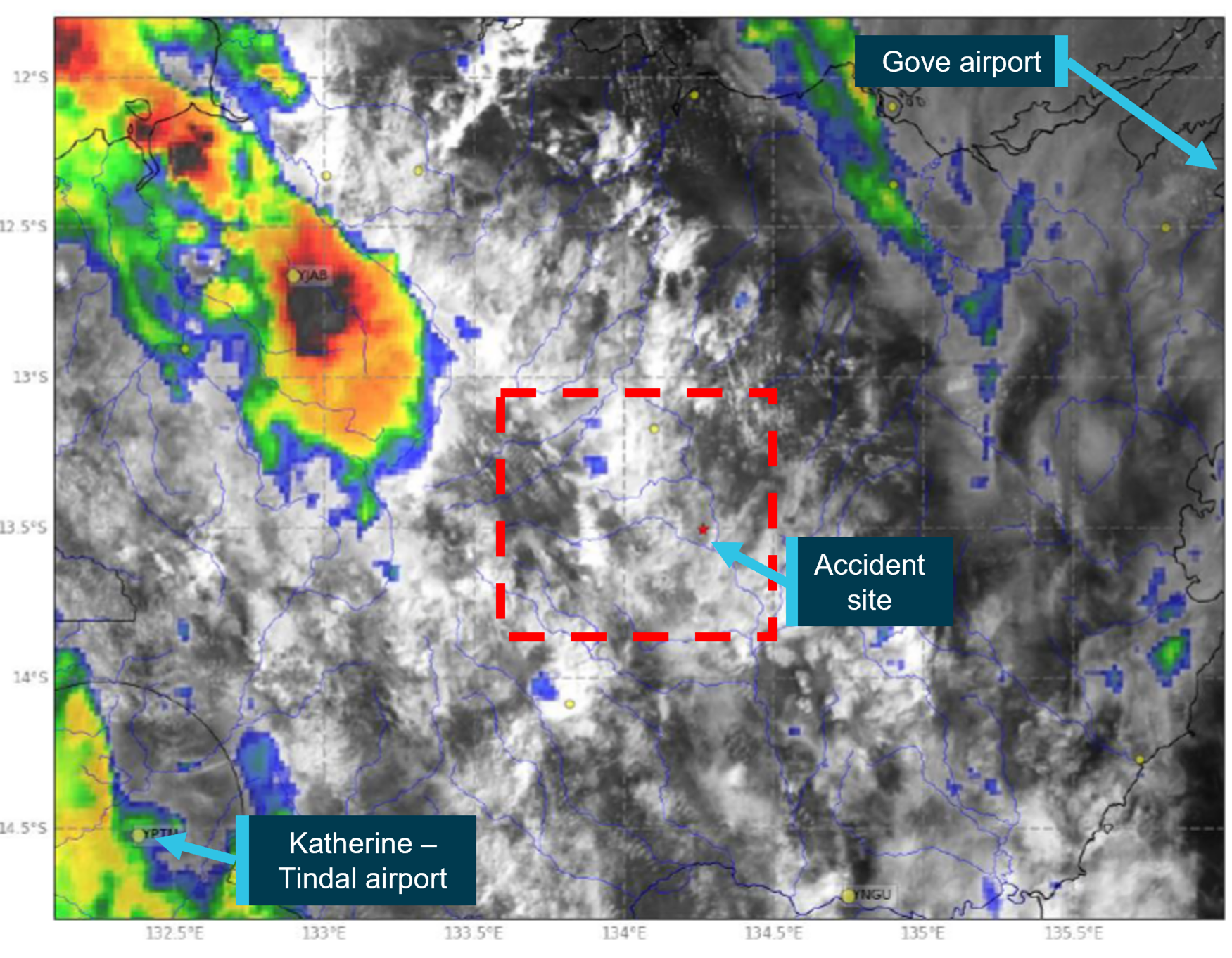
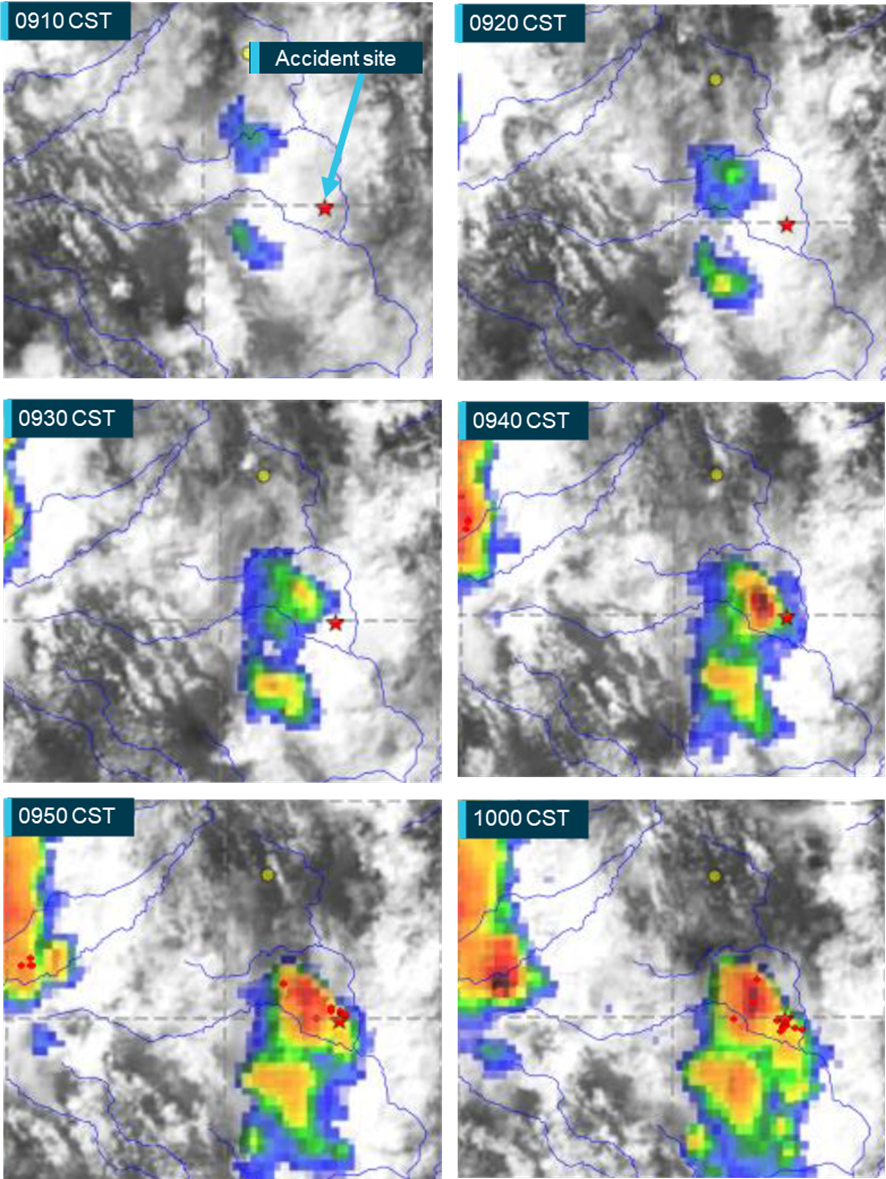
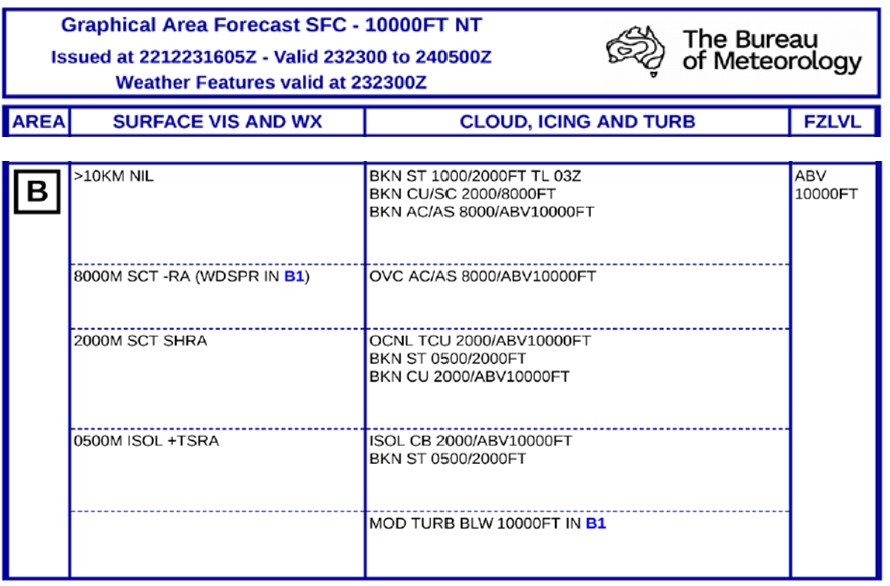
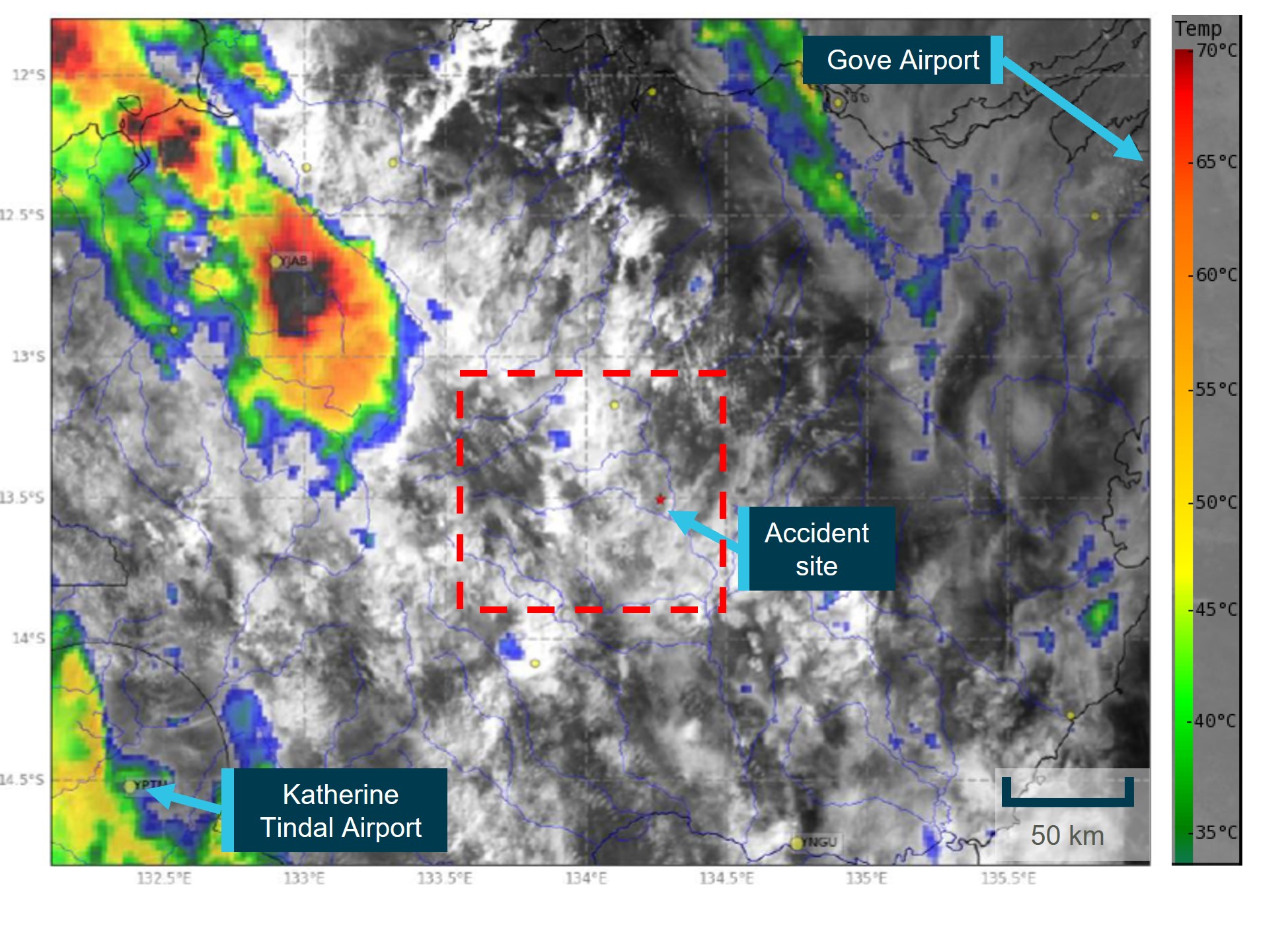
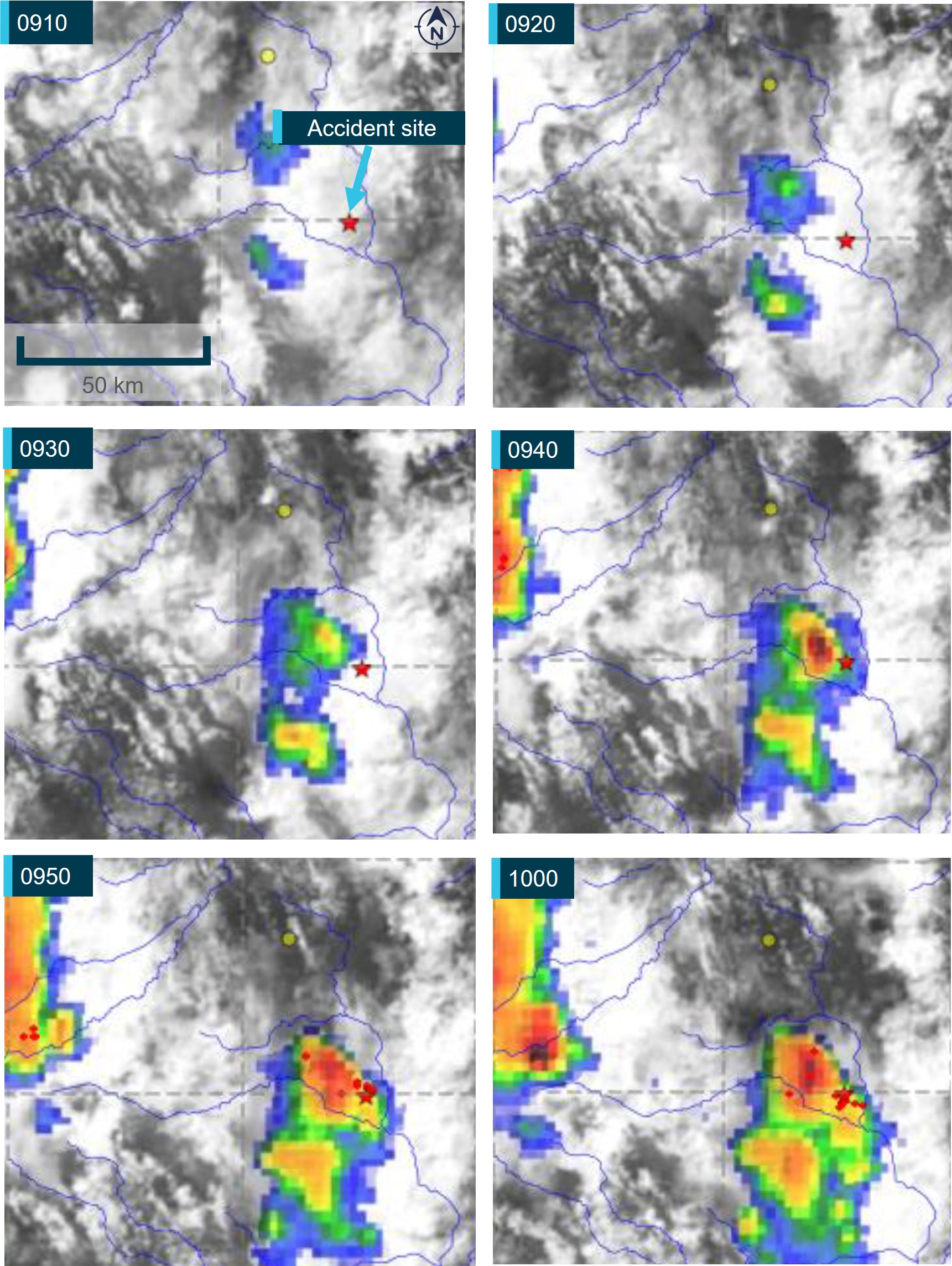
The weather station at Limbunya recorded precipitation only. The nearest Bureau of Meteorology station was located at Victoria River Downs, about 144 km to the north-east. At about the time of the accident, the temperature recorded was 27 °C and the dewpoint[12] was 15 °C. The wind was about 5 kt, variable between north and east-north-east. The graphical area forecast showed the accident site shared similar conditions with Victoria River Downs. The forecast grid point temperature was 2 °C lower. The actual temperature and dew point data was not available for the accident site.
According to the Civil Aviation Safety Authority Carburettor icing probabilitychart, the temperature and dewpoint at Victoria River Downs were on the edge of the ‘serious icing – descent power’ and ‘moderate icing – cruise power’ envelopes. Carburettor ice is formed when the normal process of vaporising fuel in a carburettor cools the carburettor throat so much that ice forms from the moisture in the airflow, which can restrict airflow to the engine. This is more likely to occur at low engine power settings, and may result in reduced power output, rough running and in some cases engine failure. The pilot of RCS advised the ATSB that their assessment of the local conditions was they were not conducive to carburettor icing. Therefore, they did not use carburettor heat and did not encounter any adverse effects to engine operation.
Recorded information
Flight data
The helicopter was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be. In addition, the operator did not utilise electronic tracking of the helicopter.
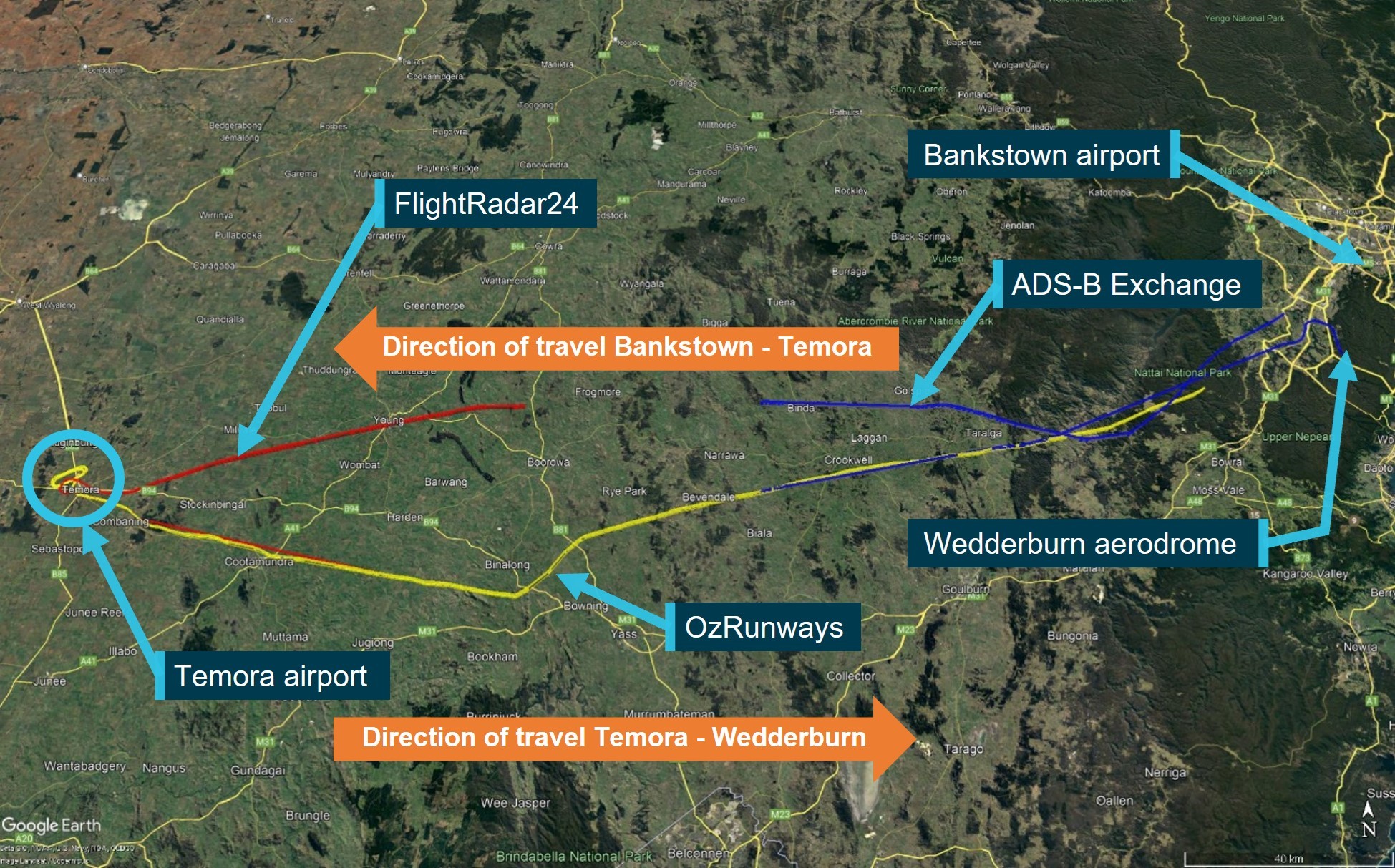
The ATSB obtained flight tracking data from the OzRunways application installed on the pilot’s mobile phone. The application was using the mobile telephone network to transmit data to the OzRunways[13] servers every 5 seconds, which included the current position, track, groundspeed and truncated altitude in increments of 100 ft.
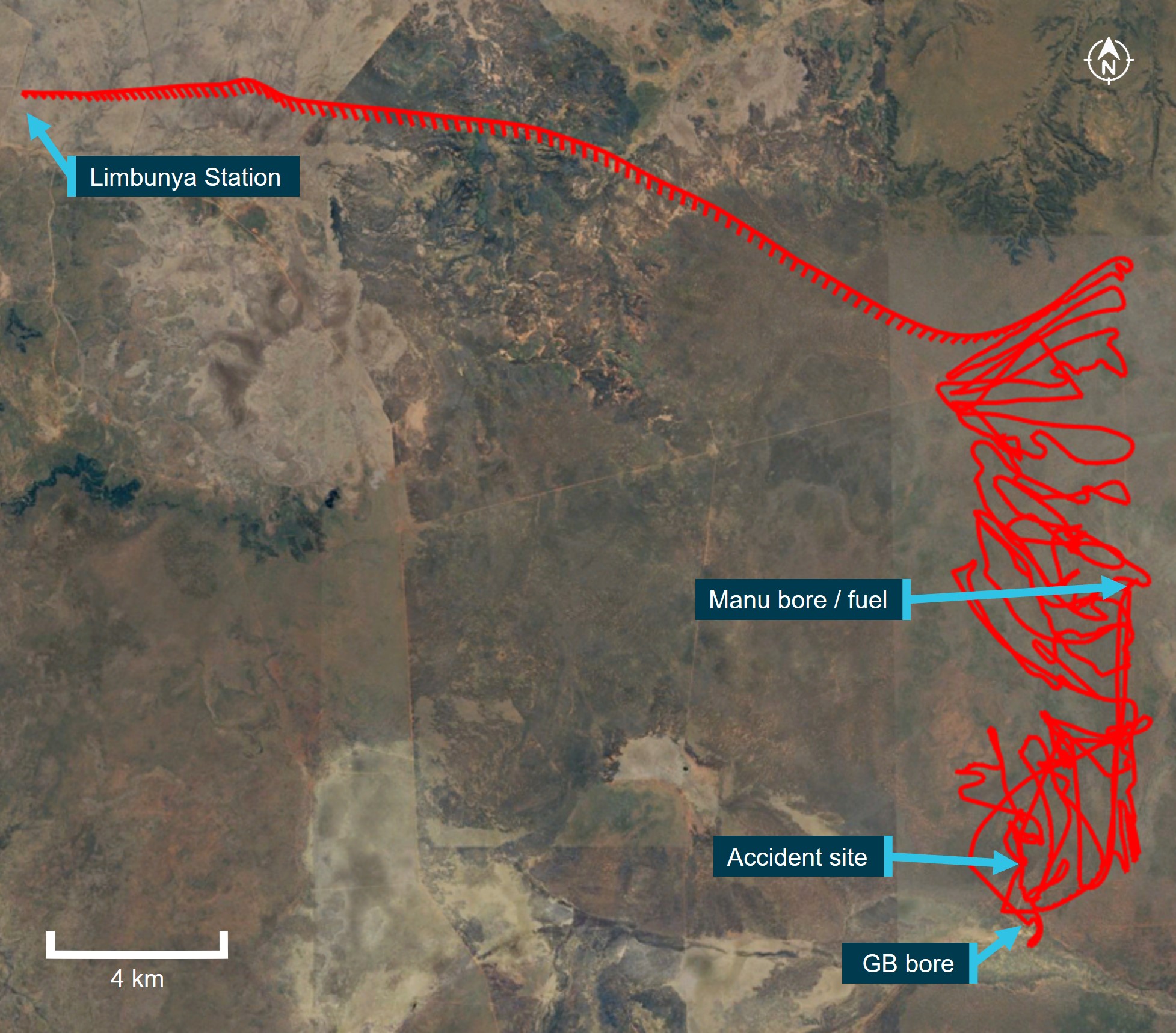
The recorded data showed PSC being operated in a manner consistent with the other pilot’s description of the mustering activities that day. Following the departure from the station homestead, the helicopter was flown direct to the northern end of the paddock and then systematically flown back and forth within the operational area, while gradually heading south to the designated holding area (Figure 4).
The flight profile data showed PSC was operated generally about 300 ft (100 m) above the ground, with extremities between 80 and 800 ft above terrain. Following the refuel, the data showed the helicopter being operated slightly higher than before the refuel. However, this was consistent with the bulk of the cattle having been mustered and the requirement to go to a higher altitude to identify isolated cattle through the timber. The final data points showed a descent of about 750 ft (230 m), followed by about 30 seconds of relatively level flight between 180–345 ft (55–105 m), before the data ceased.
There were several periods of no data being recorded during the day, of between 5 and 10 minutes.[14] The tracking data stopped short of the accident site,[15] at 1011, which prevented analysis of the final stages of flight. It could not be determined if this lack of recorded data was consistent with earlier dropouts, or due to the collision with terrain interrupting normal function.
Figure 4: VH-PSC track data
Image source: OzRunways and Google Earth, annotated by the ATSB
Helicopter recording devices
RHC introduced cockpit video cameras and engine monitoring units/governor (EMU), which are standard on new R22, R44 and R66 helicopters. The forward-facing camera records video (encompassing a view through the windshield, pilot controls and the instrument panel), intercom audio, radio transmission and GPS data. The cameras are an optional retrofit to most in-service helicopters.
The EMU monitors engine speed, rotor speed, engine oil temperature, cylinder head temperature, manifold pressure, ambient pressure, and outside air temperature. If the EMU detects an engine or rotor parameter outside of operating limits, an exceedance record is created and the data is stored.
These recording devices could assist with occurrence investigations by allowing investigators to understand the circumstance/s that precede an accident, particularly when there are no survivors or witnesses. In turn, this aids the identification of important safety issues. VH-PSC was not equipped with a cockpit camera nor EMU, nor was it required.
Wreckage and impact information
Wreckage distribution
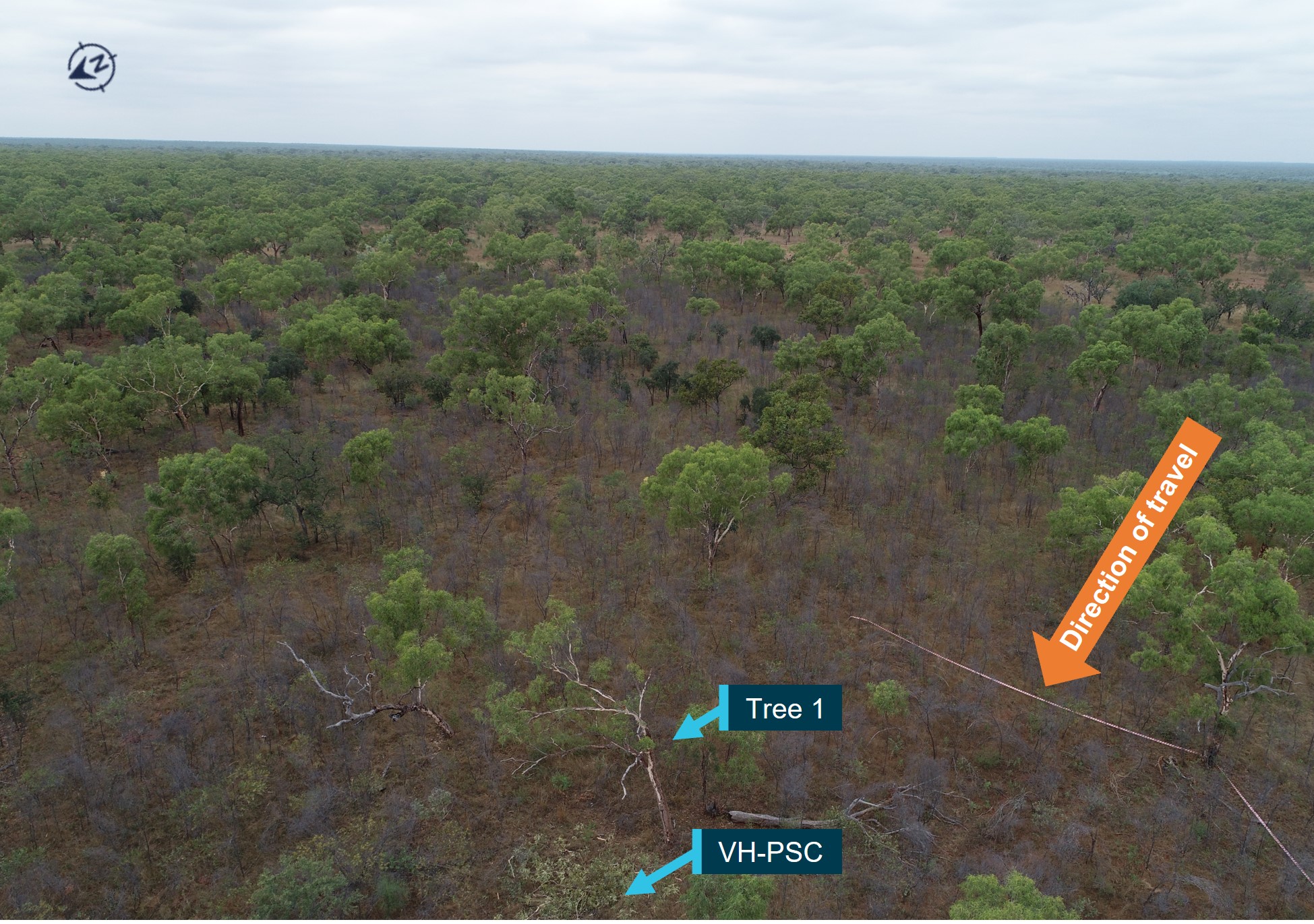
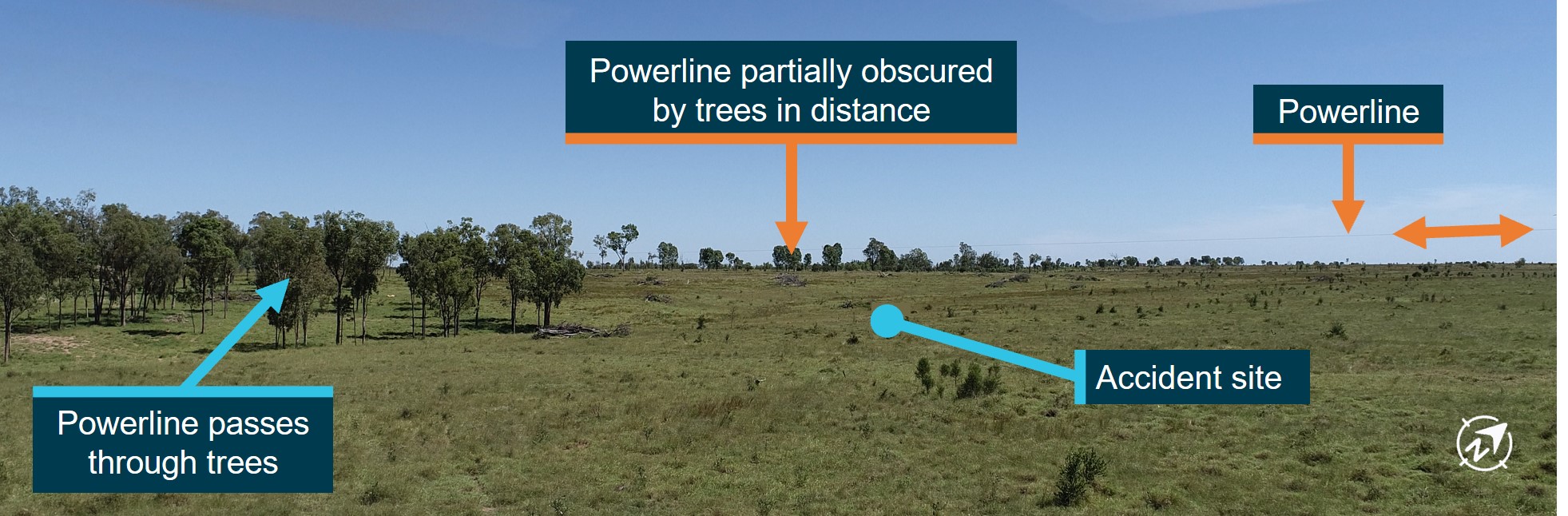
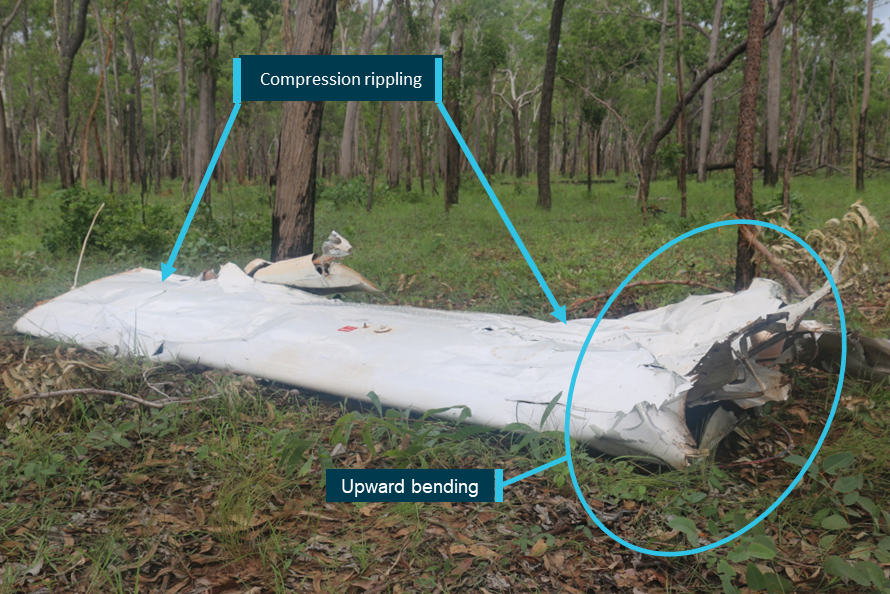
The accident site was located in an area that was flat and moderately wooded (Figure 5). There were no power lines or wires in the surrounding area. The helicopter collided with several branches of a tree (Tree 1) about mid height (5.7 m above the ground). The forward fuselage then impacted terrain in a nose-down, right side low attitude at the base of the second tree (Tree 2). The descent angle through the trees was calculated to be 45–48°. There was a short wreckage trail of about 18 m, on an approximate north-west heading. All helicopter parts were present at the accident site and there was no evidence of an in-flight break-up or a post-impact fire.
Figure 5: Site location, showing surrounding vegetation
Source: ATSB
The stabiliser assembly, with branch impact damage, was located just prior to Tree 2, the base of which exhibited impact damage and black paint transfer consistent with the landing gear. Pieces of windshield, the instrument panel and other forward fuselage components were located in the impact zone at the base of Tree 2. Fallen foliage was cleared from around Tree 2, and a distinct main rotor blade (MRB) ground scar was identified, with tip components embedded at the start. The fuselage came to rest, upright and to the right of a small tree, with the detached tailcone assembly nearby (Figure 6). The outboard section of the other MRB (MRB tip) had liberated during the tree strikes and was located about 40 m to the left of the debris trail. Rotary fuel hand pump components were located in the vicinity of the fuselage.
Figure 6: Site overview
Source: ATSB
Wreckage examination
Detailed examination of the wreckage identified continuity of the flight and engine controls, with all fractures consistent with overstress failure. However, distortion to the fuselage precluded determining engine control position prior to impact. There was nil evidence of birdstrike found in the wreckage or the surrounding area. The examination further identified the following.
Fuselage/cabin area
The collision with terrain compressed the cabin section, resulting in significant disruption of the cockpit area, the cabin structure, and the underfloor flight control mechanism. Police site images showed that the pilot was found to be wearing their seat belt at the time of the accident. Further, tearing of the seat belt webbing was very likely a result of the forces generated by the pilot restrained by the seat belt and being propelled in the direction of impact. The quick-disconnect dual flight controls[16] were not installed for left seat operation. The copilot’s seatbelt was found to be latched with the tongue locked in the buckle.
The mixture knob was in the ‘full-rich’ position with distortion to the fuselage preventing determination of the throttle selection. The throttle and mixture controls were securely connected to the carburettor, however, both linkages had failed in overstress. There was no evidence of a restriction or blockage to any part of the air induction system. Notably, the air intake hose was in good condition and the air box filter was clear.
Main rotor assembly
The main rotor blades had not contacted the cabin or tailcone and there was no evidence of extreme teeter or mast bump.[17] Both main rotor blades remained connected to the rotor head and exhibited rearward bending distortion. All hardware associated with the rotor head, blades and flight controls was secure and both pitch links were measured and found to be within service adjustment limits.[18] The pitch links were secured to the swashplate and main rotor pitch horns, with one pitch horn exhibiting distortion consistent with the main rotor blade ground strike. Overall, the damage to the main rotor blades and head assembly was indicative of low rotational energy at impact with the ground and simultaneous strike to the upper sections of Tree 2.
Landing gear
Vegetation debris on the upper surface of the left skid, forward of the strut, along with distortion to the forward strut was consistent with impact with the base of Tree 2. Fracture of the right skid and distortion to the right side of the landing gear was consistent with the nose and right-side low, impact with the ground.
Drivetrain
Both drive belts were intact, however, the rear belt had dislodged entirely from the upper sheave and the forward belt had jumped one groove forward (with one ‘v’ still engaged) during the accident sequence. There was no evidence of rubbing on either belt or sheave outer rim.[19]
The belt-tensioning clutch actuator extension was consistent with a properly functioning actuator and a relatively new belt set.[20] There was evidence of minor rotational scoring to the actuator body. The upper sheave rear face exhibited some minor surface corrosion of about a quarter to a third of the circumference, consistent with actuator body contact during the accident sequence.
Continuity of the drive train was established, except where the tail rotor drive shaft had fractured and there was tailcone separation. The main and tail gearboxes contained sufficient oil, could be rotated and the respective chip detectors were free of contamination. The freewheeling sprag clutch engaged/disengaged as expected.
Tailcone
The tailcone was securely mounted to the fuselage but had separated where the outer skin had fractured at the forward-most frame rivet line. Distortion to the tailcone just aft of the fractured rivet line was consistent with dynamic deflection occurring at fuselage impact with terrain. This corresponded to the upper left bolt, that secures the tailcone to the upper frame, being sheared. Momentum carried the tailcone forward and it came to rest in front of the fuselage, 180° opposite normal orientation.
The horizontal stabiliser and lower vertical fin exhibited damage consistent with tree branch impact and the mount to the tailcone had fractured in overstress. There was no damage or distortion to the upper vertical fin nor tail skid.[21] The tail rotor assembly was secured to the tailcone and both tail rotor blades exhibited low-energy tree strike damage. There was a small amount of dirt on the end of the tail rotor visual warning guard, consistent with coming into contact with the ground following tailcone separation from the fuselage.
Fuel system
The fuel system was selected to ‘ON’ and the bladder-type fuel tanks contained sufficient fuel for engine operation. The fuel supply from the tanks to the carburettor was intact and no signs of obstructions were noted. In addition, fuel quality was established through testing of fuel stocks at Manu bore and the homestead, and no contamination was found.
Carburettor
The carburettor heat knob was fully down (nil heat) and the heat assist was locked out (not functioning). The carburettor heat slider was in the HEAT selection, however, disruption to the airframe resulted in the control cable pulling the slider before the cable fractured in overstress.
Governor
The governor switch was oriented toward ON, however, impact damage and distortion meant the selection prior to impact could not be determined. The governor control unit was examined and tested by RHC, while being observed by a member of the United States National Transportation Safety Board (on behalf of the ATSB). The governor was within limits for all but one parameter, the ‘duty cycle’, which recorded an exceedance of 0.89%. RHC noted:
Duty cycle is the percentage of power sent to the motor to effect required throttle response. Under normal flight conditions this slight reduction in response speed would not be observable by the pilot.
Engine and fanwheel
The onsite examination identified the engine was intact and securely attached to its mount with all engine accessories securely attached. The engine sump casing had been perforated at impact, with a loss of oil contents.
Examination of the fanwheel identified the ring aft face was perforated between 2 vanes, with the edges of the break displaced aft, and curling of the edges. There was no paint transfer nor vegetation deposits, which may have identified if the damage was from a helicopter component, or tree branch. The dimension of the peeled skin was similar to the diameter of a rotary fuel pump standpipe section.
There was no circumferential scoring or damage to the other vane segments nor the aft face of the fan ring, as would be expected with a rotating fan. Damage to the fan shroud was consistent with ground impact with a stationary fan. Therefore, damage to the fan and shroud indicated that the engine was likely not operating at the time the damage to the fanwheel occurred.
Summary
Typical signatures of high energy (the engine driving the rotor) at the time of a collision with terrain include liberation and/or fragmentation of main rotor blades, fragmentation of the fanwheel and/or shroud, fracture of the main rotor pitch links and severe deformation of driveshaft flex couplings. However, in this instance, both main rotor blades remained connected to the rotor head and only exhibited rearward bending distortion. All hardware associated with the rotor head, blades and flight controls was secure. The pitch links were secured to the swashplate and main rotor pitch horns, with one pitch horn exhibiting distortion consistent with the main rotor blade ground strike. These, and other signatures, were indicative of a collision with terrain in a low rotor energy state (engine not driving the rotor system), where the energy diminishes with main rotor contact with the trees, followed by rotor sudden stoppage at ground strike.
Post onsite examination
The magneto switch was found selected to the BOTH position with the key in the barrel. The switch was examined and tested at the ATSB’s technical facility in Canberra, Australian Capital Territory. The results of the testing indicated that the ignition switch was fully functional and other than some external, physical damage attributed to impact forces, no internal defects that may have affected magneto selection operation were identified.
In January 2024, the engine was disassembled and examined at a CASA‑authorised engine overhaul facility under the supervision of the ATSB. The engine condition was consistent with the engine’s recorded time-in-service since overhaul. No internal or external damage was identified that may have prevented the engine from operating normally prior to the accident. No defects were identified in the induction system components, core engine, or cylinder assemblies that may have affected its pre-accident operation. Both magnetos were operationally tested and returned positive results and then internally examined and resistance tested with nil defects identified.
The carburettor was bench tested and internally examined, with no issues identified.
Medical and pathological information
Medical history
The pilot was known to be health conscious, fit, did not drink alcohol or smoke (cigarettes or vapes) and did not use recreational drugs. A review of the pilot’s medical records noted no medications were prescribed between 27 June 2021 and 27 June 2023.
Due to the pilot’s age, they were required to undergo an electrocardiogram (ECG),[22] and serum lipids (cholesterol) and blood glucose testing for each Class 1 medical certificate renewal. At the pilot’s most recent medical examination (November 2022) it was identified that their cholesterol level had increased. Due to the heightened cholesterol level, the pilot underwent an ECG, a treadmill stress echocardiogram,[23] and a computed tomography (CT) coronary angiogram. Following a review by a consultant cardiologist and the CASA‑designated aviation medical examiner, the pilot’s Class 1 medical certificate was renewed.
Post-mortem and toxicology
A post-mortem examination of the pilot was conducted by a qualified pathologist, on behalf of the Northern Territory Coroner. The pathologist’s report indicated that their examination was impeded due to the elapsed time between the accident and the recovery of the pilot’s body to a suitable mortuary facility. With consideration to these limitations, the report concluded that:
the pilot succumbed to multiple blunt force injuries sustained during the accident sequence
there was no evidence of any natural disease that have may resulted in death or impaired the pilot’s ability to control the aircraft.
Toxicological testing conducted as part of the pilot’s post-mortem examination identified concentrations of alcohol at 0.078% and carboxyhaemoglobin (COHb) at 11%.
The pathologist concluded that the alcohol concentration, while higher than that permitted to operate a vehicle in Australia, was ‘not relevant to death by means of interfering with mood, judgement or coordination’. In addition, the pathologist also noted that the sample location and post‑mortem changes likely affected the alcohol concentration in this instance.
The ATSB engaged an aviation medical specialist to review the pilot’s post-mortem and toxicology examinations (discussed below). Acknowledging the limitations reported by the pathologist due to decomposition, the ATSB’s aviation medical specialist also advised that some causes of death or incapacitation were not always able to be identified post-mortem.
Carboxyhaemoglobin
Carbon monoxide is an odourless, colourless and tasteless gas formed by the incomplete combustion of carbon-containing materials. When inhaled, it preferentially binds to haemoglobin, the oxygen carrying molecule in red blood cells. This creates COHb compounds and prevents oxygen from binding to the molecule and being transported, resulting in oxygen starvation.
ATSB investigation AO-2017-118 found that the physical symptoms of carbon monoxide exposure generally start to occur at COHb levels of around 10%. However, adverse neurobehavioural and cognitive effects can occur at lower levels. These symptoms and effects can include headaches, nausea, dizziness, confusion, and disorientation. These will become more severe with increasing COHb levels and duration.
The toxicology report noted:
Samples other than unpreserved peripheral blood may be unsuitable for accurate carboxyhaemoglobin determination. Results must be interpreted with caution in instances of aged or putrefied blood samples.
Correspondence with the pathologist and the ATSB’s aviation medical specialist determined that, given the time elapsed before sample collection, the sample location, and absence of an accurate determination of fluid versus blood ratio of the sample, resulted in uncertainty as to the accuracy of the COHb concentration level at the time of the accident.
A review of the ATSB aviation occurrence database identified about 60 carbon monoxide occurrences involving aeroplanes between 2010 and 2024. In contrast, only one occurrence was recorded for helicopters between 1991 and 2023:
In 2018, during take-off, the wind blew the exhaust fumes into the cockpit of an R44 resulting in the crew receiving a carbon monoxide warning. The crew returned the helicopter to the aerodrome.[24]
In addition, no accident reports (worldwide) were identified, which discussed elevated COHb levels involving R22 helicopters.
Based on the configuration of the helicopter, with the engine below and behind the cabin, it was considered unlikely for significant exhaust gases to enter the cabin, even with both doors removed.
Pilot injury assessment
According to Campman and Luzi (2007), identifying who was in control of the aircraft at the time of impact may provide valuable insight into the events leading up to the accident. The presence or absence of certain occupant injuries could assist with this determination. In particular, those relating to the upper and lower extremities from manipulating the flight controls and by the forces transmitted through the extremities at the time of impact.
Gradwell and Rainford (2016) stated that although ‘Unequivocal control-type injuries indicate that the pilot was conscious at the time of the crash’, they also highlighted that:
…caution must be exercised in their interpretation as they are neither particularly sensitive nor specific findings. Similar injuries may be seen in passengers if they grasp a solid structure at the time of impact, and if the pilot lets go of the controls in the instant before impact, then control-type injuries will not be seen.
The ATSB’s aviation medical specialist indicated that they would have expected more bone fractures if the pilot had been manipulating the controls at the time of impact. However, it was not possible to determine if the absence of typical control-related injuries identified on the pilot were suggestive of incapacitation prior to impact or rather, letting go of the flight controls during the accident sequence.
Operational information
Mustering operations
The operator’s staff described that the helicopters were typically operated ‘at height’ so that the helicopter ‘noise’ was used to move the cattle, rather than flying low and ‘upsetting’ the cattle. In this method, the helicopters were operated about 700–900 ft above the ground, which allowed the pilots to have a good overview of the area and see down through the timber to locate cattle. They would then gradually descend the helicopter, using the noise to get the cattle moving in the desired direction, before climbing to locate other cattle. The accident pilot was described as ‘careful’ and ‘calm’, when compared with some other pilots.
Quick descent
Where a quick descent is desired, the pilot will lower the collective while simultaneously rolling off throttle, to avoid main rotor overspeed. The descent will typically be steep and in a right turn, to allow the right-seated pilot to maintain forward airspeed and visual contact with their target. The throttle will then be rolled on prior to raising the collective to arrest the descent. This technique is similar to that when practicing an autorotation. The normal procedures section of the R22 POH Practice autorotation – power recovery includes the following caution:
To avoid inadvertent engine stoppage, do not chop throttle to simulate a power failure. Always roll throttle off smoothly. Recover immediately if engine is rough or engine RPM continues to drop.
Autorotation
The R22 POH detailed that a power failure may result from either an engine or drive system failure and will usually be indicated by the low rotor RPM horn. An engine failure may be indicated by a change in noise level, nose left yaw, an oil pressure light, or decreasing engine RPM. A drive system failure may be indicated by an unusual noise or vibration, nose right or left yaw, or decreasing rotor RPM while engine RPM is increasing.
The energy to successfully land (autorotation)[25] a helicopter in an engine off condition, such as an engine failure, comes from a combination of available potential and kinetic energy in the form of height, forward speed and rotor RPM. A pilot can utilise that energy to maintain drive to the main rotor and create lift.
The R22 POH explained the steps to take to enter an autorotation when between 8–500 ft.[26] The procedure stated to lower the collective immediately to maintain rotor RPM. While in a steady descent, adjust the collective to maintain rotor RPM between 97 and 110%. If time permitted, and when an engine restart is not possible, turn off unnecessary switches and close the fuel valve. Prior to landing from an autorotation, at about 40 ft above the ground, the pilot must flare the helicopter in order to reduce forward speed and increase rotor RPM before cushioning the landing.
The conditions from which a safe autorotation could be made were specified in the height-velocity diagram in the POH. A notation on the diagram encouraged pilots to avoid operation in the shaded area. When operating in this area, a pilot may be unable to complete an autorotation landing without damage. The unshaded region of the diagram shows the combinations of airspeed and height above the ground that allows a pilot to successfully complete a landing in a full autorotation without requiring exceptional skill. Recorded data showed that, over the course of the morning, PSC had been operated both in the shaded ‘avoid’ area, as well as in the non-shaded area.
Low rotor RPM and stall
The R22, with its low rotor system mass and relatively high RPM, is described as ‘low inertia’ helicopter. In low inertia systems, rotor RPM is gained and lost very easily. Low rotor RPM occurs when drag on the rotor system exceeds the power available to drive it. Without quick and effective intervention, the rotor RPM decays, it produces less lift, and the helicopter will start to descend. Airflow over the blade changes and the condition deteriorates until one or both of the main rotor blades stall.[27] According to RHC safety notice SN-24Low RPM rotor stall can be fatal, recovery fromrotor stall is ‘virtually impossible’.
Low-rotor RPM can occur at almost any time during power-on and power-off operations and is usually the result of improperly coordinating the collective and throttle, including overpitching or a failure to quickly lower the collective in an emergency such as engine failure or power reduction.
A primary cause of fatal accidents in light helicopters is failure to maintain rotor RPM. To avoid this, every pilot must have his reflexes conditioned so he will instantly add throttle and lower collective to maintain RPM in any emergency.
The low rotor RPM warning lamp and horn will activate when the rotor RPM reduces to 97% or below. The warning lamp is located on the top of the instrument panel and the horn can be heard in the cabin and through the headset. The POH stated that ‘catastrophic rotor stall could occur if the rotor RPM ever drops below 80% plus 1% per 1,000 ft of altitude’. Further, the United States Federal Aviation Administration Helicopter Flying Handbook stated that ‘low inertia rotor systems can become unrecoverable in 2 seconds or less if the RPM is not regained immediately’.
Partial power loss
As discussed in ATSB investigation AO-2022-009, RHC previously advised that a main rotor strike to the ground, a significant tree or structure, could stall (stop) an engine when operating at low power or idle, prior to an impact with the terrain.
Safety analysis
Introduction
On the morning of 27 June 2023, 2 Robinson Helicopter Company R22 helicopters were conducting mustering operations near Limbunya Station, Northern Territory, in conjunction with a ground team on horseback and motorcycles. When the pilot of the second helicopter (VH-RCS) had not heard from the pilot of VH-PSC for some time, they commenced a search and located the accident site after about 15–20 minutes. The helicopter was destroyed, and the pilot was fatally injured.
There were no witnesses and no recorded data to accurately determine the accident sequence, including the time of the accident.
This analysis will discuss the potential reasons for engine power reduction and loss of control. It also considers some aspects associated with the maintenance release.
Occurrence events
Engine power reduction
The wreckage signatures were consistent with the main rotor being in a low energy state. Given this, the ATSB considered how much engine power was being produced at the time of the accident.
Examination of components identified some minor scoring to the drive train belt-tensioning clutch actuator body, consistent with contact with the upper sheave. The corresponding location on the sheave exhibited some minor discolouration from actuator body material deposits that had begun to corrode. While scoring would normally indicate engine rotation at impact, in this instance, the sheave discolouration extended only a quarter to one third of the circumference. This limited scoring may be more representative of a low‑energy main rotor blade being forced backward to the direction of rotation at impact with the ground, rather than engine rotation. However, the non‑rotational damage to the fanwheel was consistent with the engine not operating at the time of impact.
The ATSB considered the potential reasons for the reduction in engine power, which can be broadly categorised as:
engine and associated systems defect
fuel contamination or starvation
carburettor ice
pilot-induced (intentional).
Examination of the engine and associated systems did not identify a fault or condition, which would have prevented normal operation. Nor was any issue found with the fuel quantity or quality. While an intermittent interruption to normal operation could not be completely discounted, there was no observable evidence to indicate this may have occurred.
The meteorological conditions at the nearest Bureau of Meteorology weather station,144 km away, were on the edge of the ‘serious icing – descent power’ and ‘moderate icing – cruise power’ envelopes for carburettor icing. However, the pilot of the other R22 operating in the accident area, reported that local conditions did not require the use of carburettor heat and they did not observe any indications of the formation of carburettor ice.
The ATSB considered the possibility that the pilot intentionally reduced the throttle as part of a quick descent. Inadvertent engine stoppage could occur from the throttle being reduced too quickly, which may have occurred at a height too low to perform a successful engine off landing (autorotation) to clear ground. In addition, the collision with terrain in a nose and right-side low orientation could also be indicative of a quick descent manoeuvre, from which recovery did not occur. Alternatively, as noted by the manufacturer, if the engine was in a low-power state when the main rotor blades impacted the tree and ground, it was possible that this impact stopped the engine.
Loss of control
The ATSB considered other loss of control events that may have preceded the nose and right-side down trajectory through a tree and then the subsequent collision with terrain.
There were no indications of a collision with a bird or other object, such as a wirestrike. Based on the witness observations, there was no evidence to suggest that the weather conditions affected the pilot’s ability to maintain control of the helicopter. As discussed above, there was no observable issue identified with the helicopter nor was there any indication of mast bumping. While it was possible that a loose object in the cabin interfered with the pilot’s flight controls, the disruption to the cabin area precluded identifying any evidence of this. Regardless, this scenario did not account for the low rotor energy (engine not driving the rotor system).
While distractions can occur unexpectedly, the other R22 was not operating in the immediate area to distract the pilot. The engine reduction (if not intentional) could have potentially been a distraction and required the pilot to conduct an autorotation. However, ATSB research has shown that distraction events most often result in an incident rather than accident (ATSB, 2006).
A reduction in engine power, whether operating at low or idle power, or in the event of a complete engine stoppage, requires prompt and effective management of main rotor RPM, above 97%, in order to conduct a successful autorotation.In this instance, the trajectory and orientation of the helicopter was not consistent with what would be expected if the helicopter was being flared, to reduce the rate of descent prior to touching down during a controlled autorotation.
Conclusions
The site and wreckage signatures were consistent with an engine power reduction and loss of control. Further, it could not be determined if the engine was producing low power, or was stopped, and if this was due to an engine issue (unobserved from the wreckage examination) or pilot induced. The pilot was highly experienced in low-level helicopter operations and demonstrated their capability to an instructor during simulated emergency procedures about 3 months prior. However, as there was no recorded data available or witnesses to the final stages of the flight, the pilot’s actions leading up to the accident were unknown.
Without conclusive reasons to explain the accident sequence, the ATSB also considered if it was possible that the pilot experienced some level of incapacitation before (resulting in inadvertent throttle manipulation), or after the reduction in engine power. Incapacitation could also explain the low rotor energy and/or helicopter trajectory into terrain. The absence of a radio transmission, in the event of an autorotation, could be suggestive of an incapacitation event, but could also indicate a sudden event that the pilot did not have time to transmit.
Despite this, a comprehensive review of the pilot’s medical history and general health did not identify any pre‑existing or other condition that could have adversely affected their performance. The post‑mortem did not identify the presence of any natural disease, however, the pathologist reported limitations due to decomposition, including the elevated carboxyhaemoglobin results. Further, analysis of the flight control injuries was inconclusive. Although the ATSB’s aviation medical specialist advised that some causes of death or incapacitation were not always able to be identified post-mortem, incapacitation remained only a possibility as there was insufficient evidence to conclude probability.
Therefore, due to the limited evidence available, the ATSB was unable to determine the reason for the engine power reduction and loss of control, nor the sequence of these events.
Maintenance release no longer in force
The current maintenance release, located at the accident site, had no endorsements showing daily inspections, hours flown each day, calculation of accumulated time-in-service or certification for completion of scheduled maintenance.
The pilot’s diary indicated they had operated VH-PSC every day since the maintenance release was issued (13 days prior to the accident). Text messages between the pilot and operator indicated that the required 25-hour engine oil and filter change had been completed, despite not being certified for on the maintenance release. Without a record of the accumulated total time‑in‑service, the ATSB could not determine if the 50-hour oil and filter change had come due, nor if it had been completed.
In this instance, as the pilot was the sole operator of the helicopter, the absence of endorsements did not hinder other pilots from being aware of the serviceability status. However, the maintenance release is a legal document that is part of the ongoing airworthiness requirements for the helicopter. The lack of certification for the completion of maintenance did not contribute to the accident, however, the helicopter was being operated with a maintenance release that had ceased to be in force and was therefore considered unairworthy.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Robinson R22 Beta II, VH-PSC, near Limbunya Station, Northern Territory, on 27 June 2023.
Contributing factors
While conducting mustering operations, for reasons that could not be determined, there was a reduction in engine power and a loss of control.
Other findings
While not contributory to the accident, the absence of endorsements for daily inspections and nil certification for the completion of scheduled maintenance resulted in VH-PSC being operated with a maintenance release that had ceased to be in force.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the other pilot and members of the ground muster team
the operator and maintainer
Civil Aviation Safety Authority
Northern Territory Office of the Coroner
Northern Territory Police
Western Australia Police
forensic and aviation pathology specialist
Robinson Helicopter Company
Airservices Australia
Bureau of Meteorology
OzRunways data from the pilot’s phone
next of kin and friends of the pilot.
References
Campman, S.C. & Luzi, S.A. (2007). The sensitivity and specificity of control surface injuries in aircraft accident fatalities. The American Journal of Forensic Medicine and Pathology, 28(2), 111‑115.
Gradwell, D. & Rainford, D.J. (Eds.). (2016). Ernsting’s Aviation and Space Medicine (5th ed). Boca Raton, FL: CRC Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
pilot of VH-RCS
the maintenance organisation that conducted the engine overhaul
Civil Aviation Safety Authority
United States National Transportation Safety Board
Robinson Helicopter Company
Bureau of Meteorology
the pathologist and medical subject matter expert.
Submissions were received from:
Robinson Helicopter Company
the operator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]All times provided by the pilot of RCS and members of the ground muster team were estimated (give or take 10-15 minutes each side), however, were sufficiently consistent to develop the timeline of events.
[2]The hours noted in the diary were likely a combination of flight time and duty (or on ground) time.
[3]When installed, the cabin heat system uses air warmed by a shroud surrounding the muffler, which is then directed via ducting to the cabin.
[4]The freewheeling unit automatically disengages any time the engine revolutions per minute become less than rotor revolutions per minute, allowing the rotor system to rotate free of the engine drive system.
[5]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[6]When conditions were conducive to carburettor ice, the POH required the pilot to use carburettor heat as required to keep the needle on the carburettor air temperature gauge out of the yellow arc (-15 to 5 °C). In addition, carburettor heat was to be used with power settings below 18” mercury, regardless of the indicated carburettor air temperature.
[7]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[8]As the engine had been fitted to other aircraft, its overhaul cycle did not align with PSC.
[9]Service bulletin SB 480 also noted that ‘in special circumstances’ the oil and filter change ‘can be extended not more than 5 hours while en route to a place where the oil change can be done’.
[10]High oil consumption and/or a change in oil consumption can be indicative of a developing engine issue.
[11]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘overcast’ indicates that all the sky is covered.
[12]Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to predict the probability of aircraft carburettor icing or the likelihood of fog.
[13]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[14]OzRunways distinguishes one flight from another by identifying that the aircraft is conducting a flight when it is above a threshold speed. Therefore, a ‘flight’ is considered to be when the aircraft is above the threshold speed to when it drops below the threshold speed. Data may not be recorded when the aircraft is below the speed threshold. PSC likely regularly dropped below the threshold speed, probably while at low altitude moving the stock. As such, the OzRunways system thought this was the end of a flight and did not record the data. Data acquisition recommenced when the helicopter was operated above the ‘flight’ thresholds.
[15]The ATSB examined the pilot’s mobile phone in case data had been collected but not yet transmitted, however, no additional information was available.
[16]Quick-disconnect flight controls do not require use of tooling to fit and remove and can therefore be accomplished by the pilot, without the requirement for a licenced aircraft maintenance engineer.
[17]Mast bumping: contact between the main rotor hub/spindle and the rotor mast which, if excessive, could severely damage the mast, or result in the separation of the main rotor system from the helicopter. Damage from mast bumping is indicative of excessive blade flapping and/or excessive tilt of the main rotor disc relative to the mast. As documented in many investigation reports worldwide, scenarios that have been linked to mast bumping include low-g and/or low rotor revolutions per minute/rotor stall, in conjunction with delayed and/or inappropriate flight control inputs.
[18]Main rotor pitch links can be lengthened (to decrease RPM) or shortened (to increase RPM) to obtain optimum autorotation rotor RPM.
[19]Rubbing from contact between a belt and the sheave can be an indication of engine providing power to the drivetrain, however, it is also possible that a dislodged belt may not make contact with the sheave under certain circumstances.
[20]A new drive belt set had been installed during the last periodic inspection.
[21]Tail skid: A guard device attached below the lower vertical fin to protect the tail rotor blades from ground strike.
[22]An ECG detects heart problems by measuring the electrical activity generated by the heart as it contracts. ECGs from healthy hearts have a characteristic shape. If the ECG shows a different shape it could suggest a heart problem.
[23]Stress echocardiogram (stress echo) is a test to assess heart function under physical stress. It uses ultrasound waves (inaudible sound waves) to image the heart and assess its function before and immediately after the exercise to see how the heart muscle pump is working, and sometimes to measure other parameters.
[24]Effects to the flight crew, if any, were not provided to the ATSB in the occurrence notification.
[25]Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[26]For power failure below 8 ft, the pilot was to apply right tail rotor pedal input as required to prevent yaw, allow the helicopter to settle and raise the collective just before touchdown to cushion landing.
[27]Rotor stall, similar to aerodynamic stall in aeroplanes, occurs when increasing rotor blade angle, relative to airflow (angle of attack), reaches a point where airflow separates from the rotor upper surface and becomes turbulent, reducing lift. As the helicopter descends, the upward flow of air further increases the angle of attack until the critical angle of stall in reached, resulting sudden loss of lift and a large increase in drag. The increased drag acts like a rotor brake causing the rotor RPM to rapidly decrease, further increasing the rotor stall.
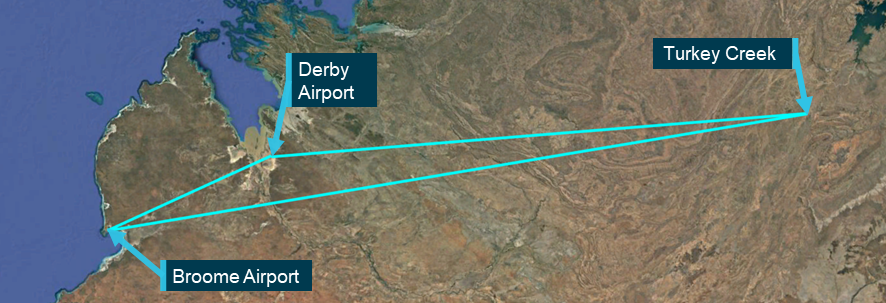
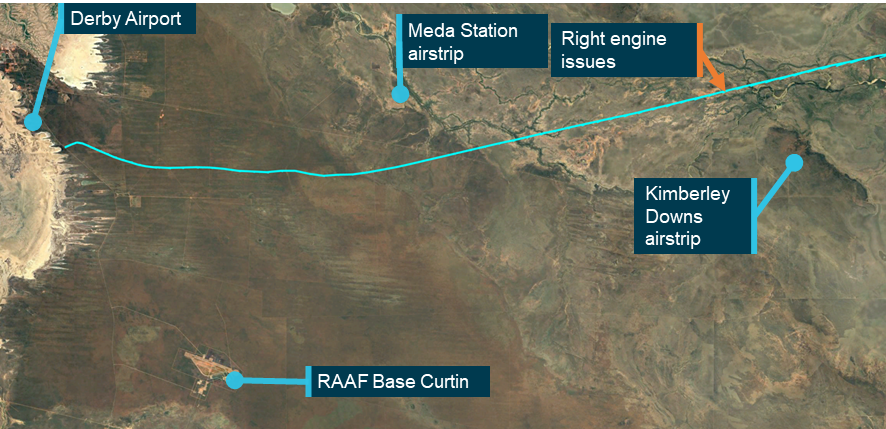
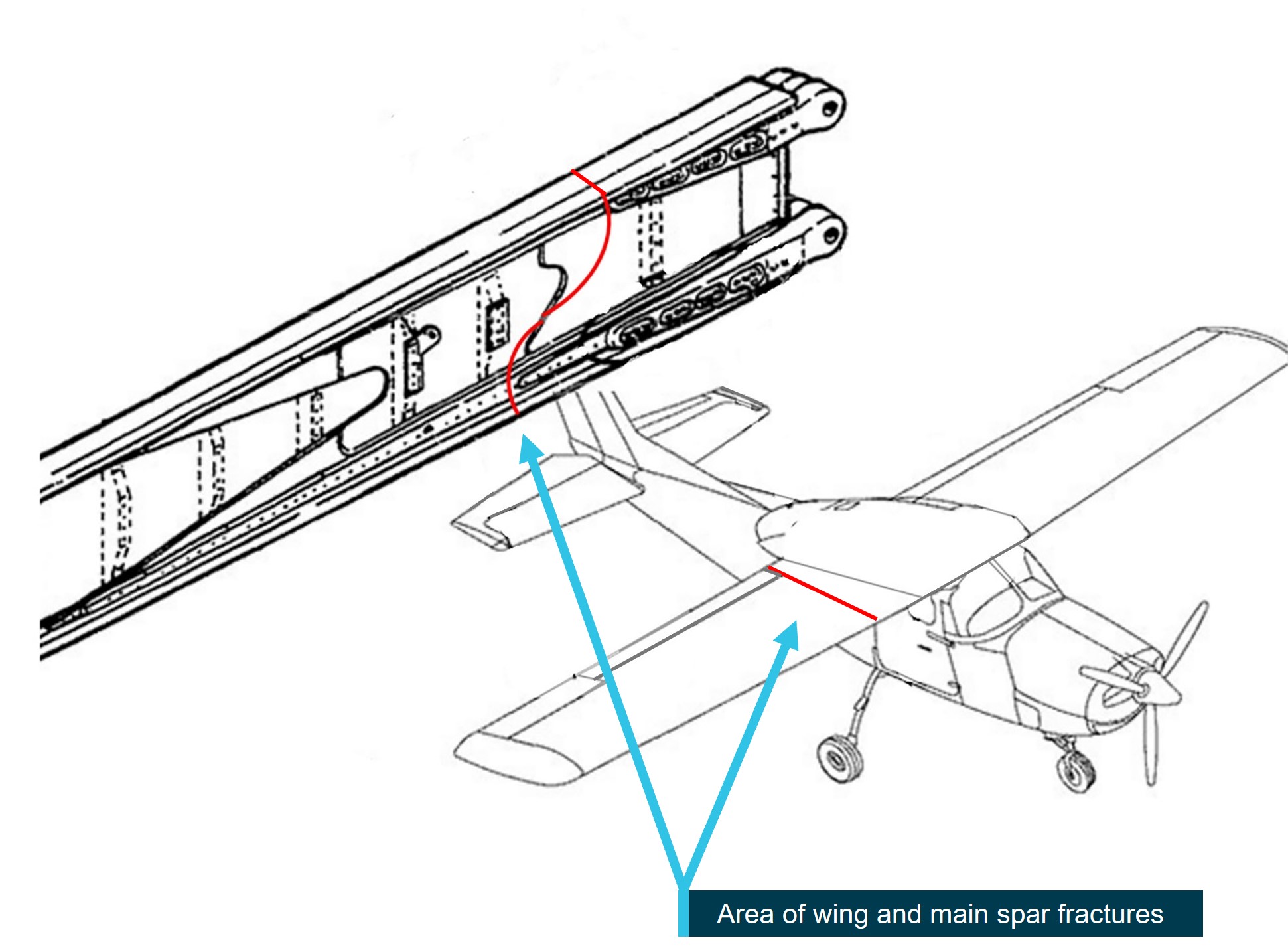
On 20 June 2023, a Cessna 310R, registered VH-DAW and operated by Broome Aviation, was being flown on an air transport operation with a pilot and one passenger from Broome Airport to Turkey Creek, Western Australia (WA) and return. On the return flight, the pilot planned to stop at Derby Airport, to refuel.
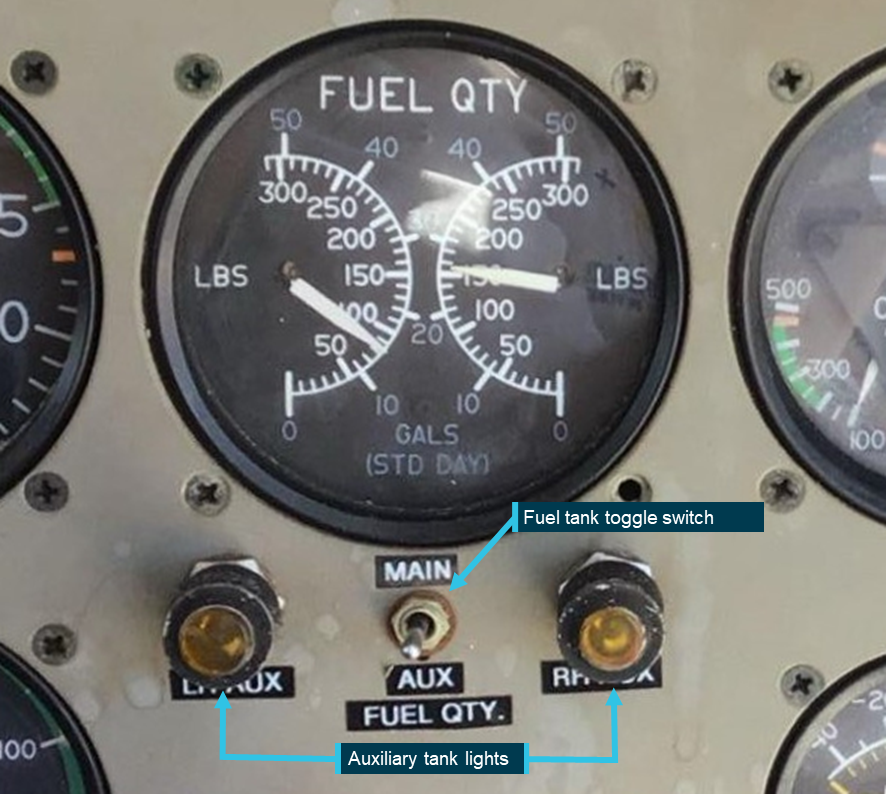
On the return flight from Turkey Creek to Derby, the aircraft’s right engine began surging while being supplied from the auxiliary fuel tank. The pilot changed the tank selection to the right main tank, which had little fuel remaining. The right engine began surging a second time and the pilot determined there was enough fuel in the left main tank to sustain both engines to Derby. The pilot then selected the right engine to cross feed from the left main fuel tank.
Ten minutes later, both engines began surging. The pilot, assessing they had a dual engine fuel starvation, began switching fuel tanks searching for any remaining fuel. Unable to stop the engine surging, the pilot extended the landing gear and banked into a right turn with the intention of landing on the Derby Highway. During the turn, the right wing of the aircraft contacted a tree causing the aircraft to turn 180° and come to an abrupt stop on the edge of the highway.
The pilot sustained serious injuries, and the passenger sustained minor injuries. The aircraft was substantially damaged.
What the ATSB found
The occurrence
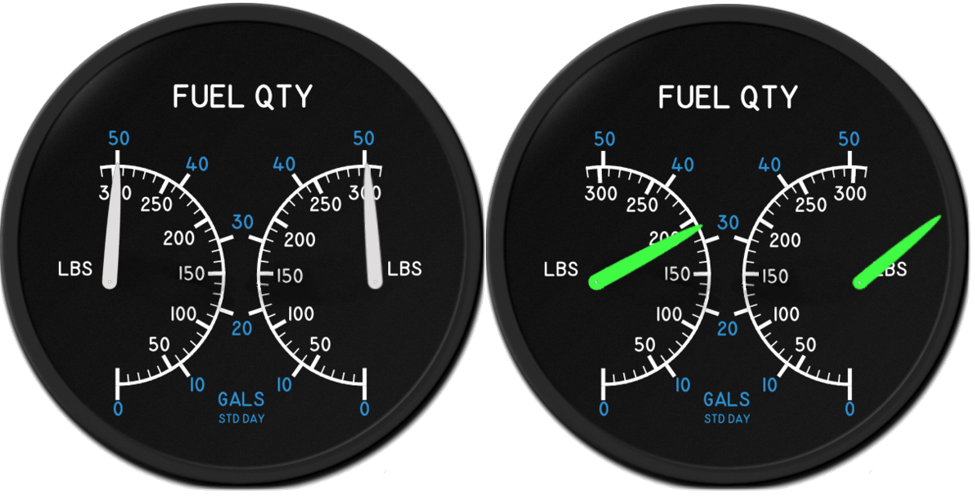
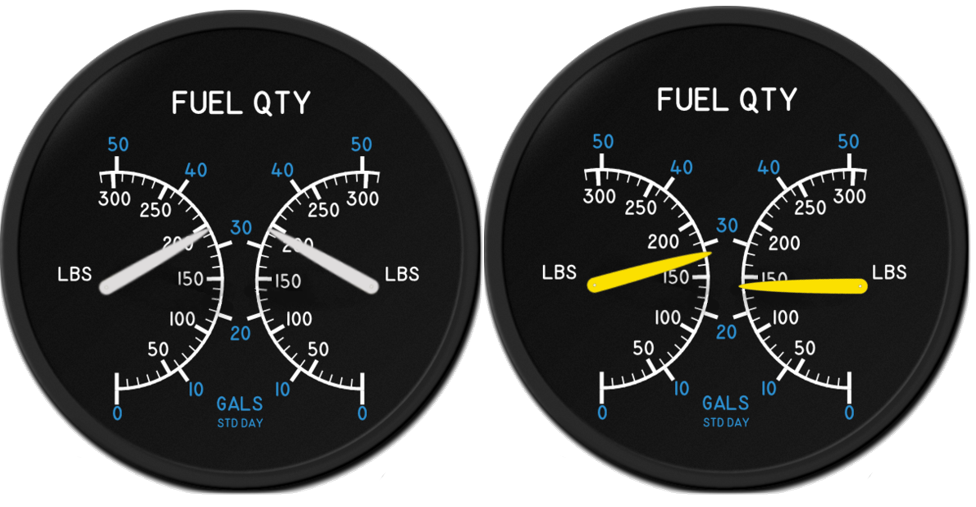
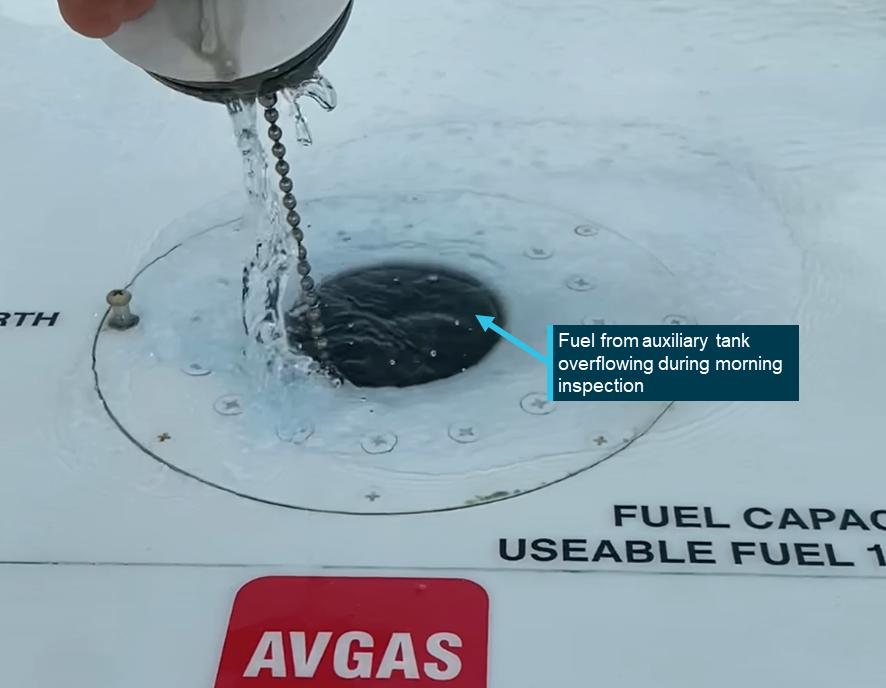
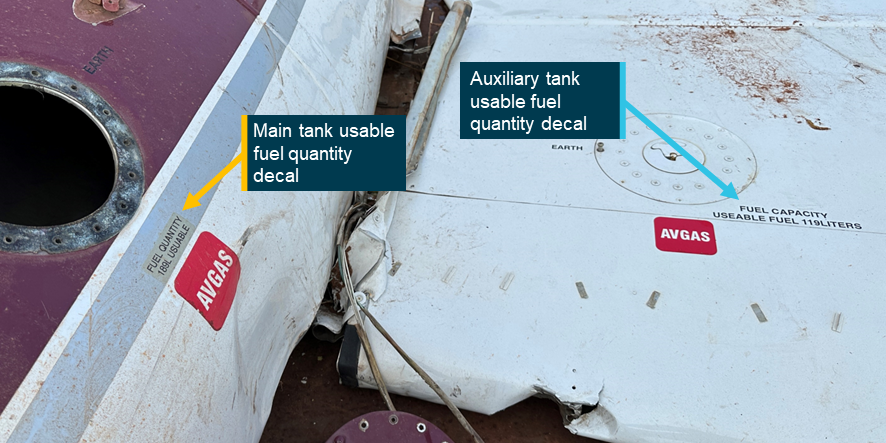
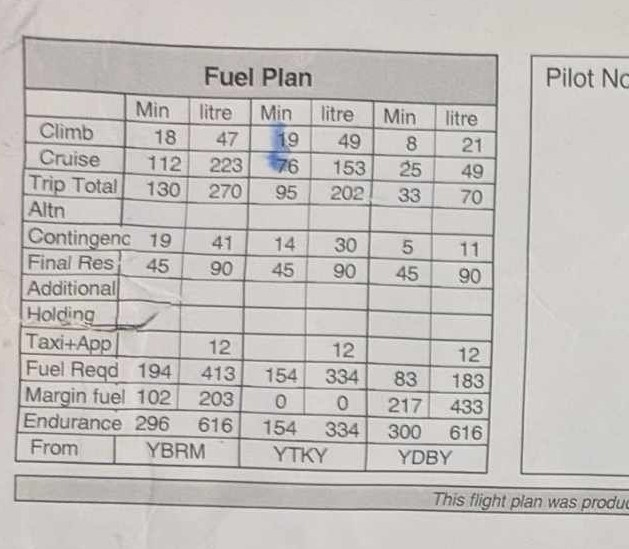
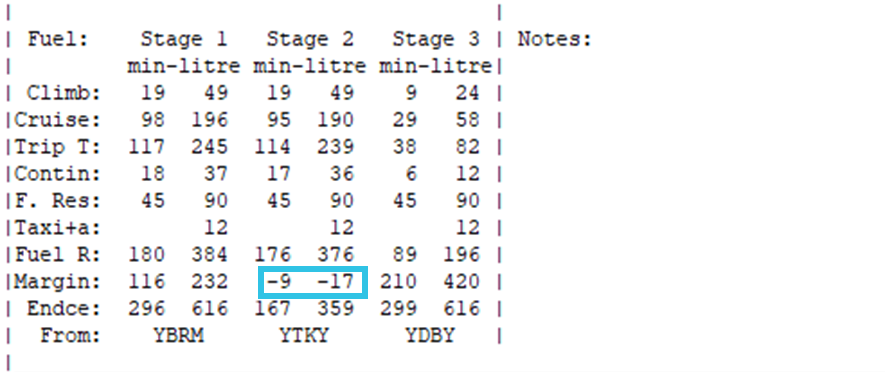
The ATSB found that the planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available. Also, the aircraft fuel gauges did not indicate accurately.
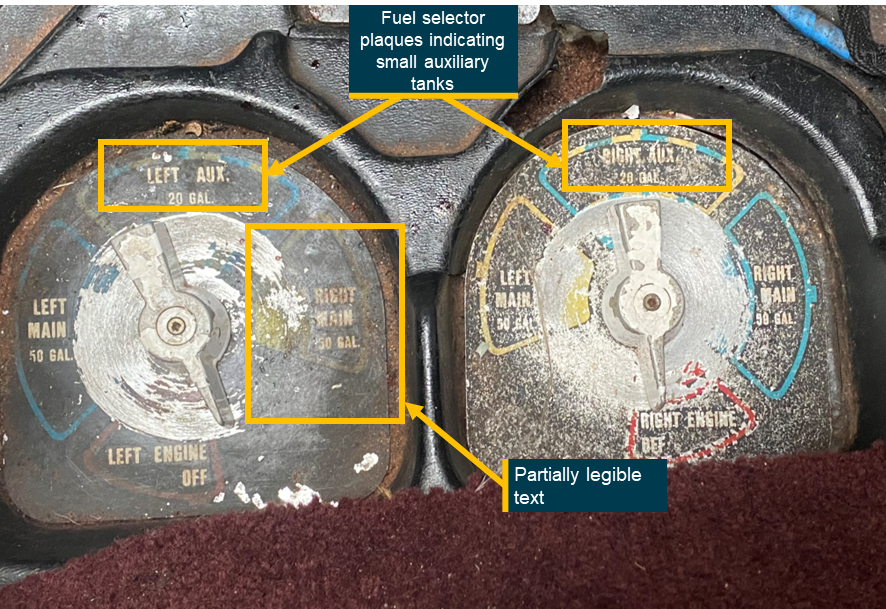
The ATSB also found that the pilot inadvertently did not select the fuel supply to the right engine to the right auxiliary fuel tank during the first leg of the journey and did not manage the fuel in accordance with the pilot's operating handbook requirements. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained.
Further, after the fuel in the right main fuel tank had been used, the pilot did not divert the aircraft to the closest airport, select the left engine to the left auxiliary fuel tank, or maintain altitude to increase their safety margin. Additionally, the pilot was not wearing an upper torso restraint during the forced landing resulting in the pilot receiving serious head injuries during the collision.
The pilot also had a lack of understanding of the aircraft fuel planning, fuel management and emergency procedures, and due to a lack of consolidation training and limited to no operational oversight these issues were not detected.
Operator oversight
The ATSB also found that during the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. In addition, aircraft defects were not being written on the maintenance release, leading to several defects not being rectified or managed.
Further, Broome Aviation pilots experienced pressure to not report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight.
Finally, Broome Aviation’s operations manual did not include a procedure for recording in‑flight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate in‑flight fuel management.
Civil Aviation Safety Authority oversight
The ATSB identified that, following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, the Civil Aviation Safety Authority (CASA) conducted a level 2 surveillance activity on the operator in early June 2023 with a key scope element being to evaluate the complaint. In addition, CASA received further complaints after the accident, that were also added to a level 1 surveillance activity in August 2023. However, the surveillance activity and the associated reports did not assess the subject of the complaints.
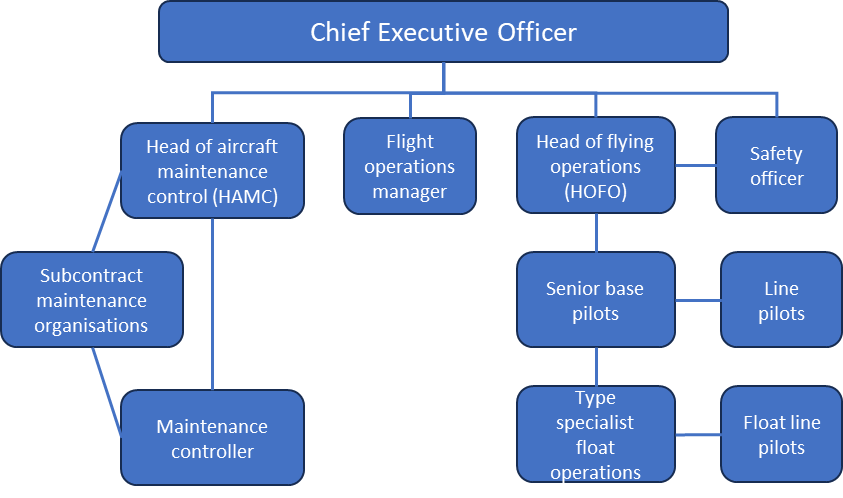
Additionally, CASA approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment as they had already been assessed for another operator and due to an expectation that it was an interim appointment. The person subsequently remained in the position for a much longer period and, when this situation was identified by CASA, the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO was not fully assessed.
What has been done as a result
Broome Aviation updated its operations manual to the new format exposition in response to Civil Aviation Safety Authority (CASA) findings during a level 1 surveillance audit. It now outlines an in‑flight fuel management procedure.
The operator now has both a full-time HOFO and an alternative HOFO, who is also the Safety Manager. The new HOFO reported that all company pilots are fully aware that they are available to address questions or concerns. The operator has also modified its check and training system, implementing a revised check and training procedure and updated documentation to facilitate the tracking of pilot training and competency in line with current Civil Aviation Safety Regulations (CASR).
The new HOFO has changed the defect reporting process to ensure all defects are reported to either the HOFO or the alternative HOFO, and where required noted on the MR. The operator is now using maintenance releases to systematically document defects, ensuring that issues with aircraft in the fleet are properly tracked and addressed.
Finally, Broome Aviation has implemented a safety management system in line with the current CASR in relation to a CASA audit finding. Monthly safety meetings are now being held to address safety concerns.
Safety message
Accidents involving fuel mismanagement are an ongoing aviation safety concern. In addition to the importance of ensuring there is sufficient fuel prior to, and during, flight, this occurrence reinforces the need to:
be fully familiar with the aircraft’s fuel system and capacity
conduct a thorough pre-flight inspection, including verification of the fuel quantity
ensure the appropriate tank selections are made
ensure all aircraft documentation and placarding is up to date and readily available.
This accident and many other previous accidents demonstrate the importance of pilots having knowledge of the aircraft type and its systems, especially when faced with an abnormal situation. Operators, as part of their safety management processes, should provide the opportunity for skill consolidation during and following the initial training on a new aircraft type to reduce safety risk during this transition. This is particularly relevant for types with increased complexity compared to those a pilot has previously flown.
Pilots have a vital role in ensuring maintenance personnel are aware of all aircraft defects to enable prompt rectification and compliance with aviation regulations. This includes documenting aircraft defects on the maintenance release (MR) accurately and without omission. Failing to record defects compromises aircraft airworthiness and safety, placing crew, passengers, and operations at unacceptable risk.
Pilots who perceive serious risks, such as defects not being addressed, management pressure to operate defective aircraft, or being discouraged from documenting defects on the MR, are urged to report these concerns through their organisation’s safety management system (SMS). The SMS is designed to provide a structured and confidential channel for reporting safety issues to enable investigation and resolution.
If internal reporting channels are ineffective or unavailable, pilots are encouraged to report safety concerns confidentially to either the Civil Aviation Safety Authority’s confidential reporting system (Reporting illegal behaviour | Civil Aviation Safety Authority) or the ATSB’s REPCON scheme (REPCON – Aviation Confidential Reporting Scheme | ATSB). These reporting systems ensure the identity of individuals is protected, while enabling critical safety issues to be addressed. Accurate reporting of safety concerns and occurrences is essential to preventing accidents and fostering a strong safety culture.
The occurrence
Overview
On 20 June 2023, a Cessna 310R, registered VH-DAW and operated by Broome Aviation, was being prepared for an instrument flight rules (IFR)[1] air transport operation with a pilot and one passenger from Broome Airport, Western Australia (WA) to Turkey Creek, WA. On the return flight, the pilot planned to stop at Derby Airport to refuel before returning to Broome Airport (Figure 1).
At Broome Airport, the pilot completed flight planning, using software provided by the operator. They then completed the pre-flight checks of the aircraft, including visually confirming all 4 fuel tanks (see the section titled Fuel system) were full. The pilot then delivered a safety briefing to the passenger, which included the use of seatbelts, the location of the emergency locator transmitter (ELT) and the first aid kit.
The aircraft departed Broome at 0542 local time. The pilot supplied fuel to both engines from the main fuel tanks for 60 minutes before selecting the auxiliary fuel tanks. They advised that after 30 minutes, they reselected the main tanks and continued to Turkey Creek.
The pilot indicated that when switching between fuel tanks, they recorded the duration of usage for each tank and calculated the anticipated fuel consumption on a printed flight plan as the operator did not have a formal inflight fuel log.
The aircraft landed at Turkey Creek at 0744. The pilot shut down the engines and left both fuel selectors on the main tanks position. The pilot did not check the total remaining fuel on the gauges at that time. Both the pilot and the passenger left the runway strip for approximately 6 hours. The pilot recalled being able to see the aircraft from the building in which they were waiting for the passenger to complete their business.
Turkey Creek to Derby
Upon returning to the aircraft, the pilot completed a fuel quantity check by dipping the main tanks with a dipstick. They recalled that the left main tank had 110 L of fuel, which was in line with what they expected (see the section titled Pre-flight fuel plan). However, the right main tank contained only approximately 70 L of fuel. The pilot turned on the aircraft battery to compare the dipstick readings to the fuel gauge readings and reported that both main tank fuel gauge indications correlated with the dipstick readings. Upon checking the auxiliary tank gauges, the pilot noted the right auxiliary tank gauge was indicating full, 40 L more fuel than expected, and the left was indicating as expected. Due to the design of the auxiliary fuel tanks, the amount of fuel contained in the tank can only be visually verified when the tank is full. The pilot stated they did not visually confirm the fuel level in the auxiliary tanks at that time as they assumed both auxiliary tanks had been used during the flight to Turkey Creek.
The pilot assumed the difference in fuel distribution between the tanks may have been due to an internal fuel leak from the right main tank to the right auxiliary tank, while they were on the ground at Turkey Creek, which they reported had occurred on a previous occasion (see the section titled Main to auxiliary tank fuel leak). However, the pilot was confident there was enough fuel on board, between all 4 fuel tanks, to fly the second leg of the flight to Derby Airport based off an expected 1.5 hour flight time. The pilot used these revised fuel quantity figures for pre-flight fuel planning and filled in the relevant sections of the journey log. At 1333, the pilot started the engines, taxied out to the runway and at about 1339 departed Turkey Creek with the main tanks selected.
At about 1439, the pilot switched from main fuel tanks to the auxiliary tanks. Approximately 10 minutes later, the pilot changed the fuel tank selection for the left engine to run off the left main tank. The pilot kept the right engine selected to the right auxiliary tank due to the extra 40 L of fuel they had detected during the pre-flight fuel check. Due to belief that they could only draw fuel for 45 minutes from the auxiliary fuel tanks (see the section titled Limited fuel draw from auxiliary tanks), the pilot calculated there was approximately 30 minutes of fuel available for use in the right auxiliary tank.
At about 1454, (15 minutes after they had selected the right auxiliary fuel tank), the right engine began surging. Unsure why they were unable to run the right engine on the right auxiliary tank for longer, the pilot reselected the right main fuel tank, which resolved the surging. The pilot advised that, as the autopilot had difficulty maintaining altitude (see the section titled Autopilot), they selected it to OFF when the engine issues began. Ten minutes later, the right engine began to surge again. The pilot switched back to the right auxiliary fuel tank, however the surging continued. Now at the top of descent for Derby, the pilot deliberated 2 options: shut down the right engine and fly asymmetrically or crossfeed the right engine to the left main tank and run both engines off the left main tank.
After checking the fuel gauges, the pilot determined there was enough fuel in the left main tank (approximately 45 L) to run both engines to Derby. The pilot then selected the right engine to crossfeed from the left main fuel tank and referred to the quick reference handbook for engine failure in flight checklist to determine a possible cause for the surging.
Figure 2: VH-DAW flight path
1. Change from main tanks to auxiliary tanks; 2. Change the left engine from auxiliary tank to main tank; 3. Right engine surge – changed the right engine to right main tank; 4. Right engine surge – crossfeed right engine off left main tank; 5. Inbound call for Derby Airport; 6. Dual engine surge; 7. Mayday call; 8. Accident site. Source: Google Earth, annotated by the ATSB
At 1511, the pilot made an inbound call for Derby Airport on the common traffic advisory frequency. Both engines began surging 3 minutes later. The pilot, assessing they had dual engine fuel starvation, selected the fuel pumps to HIGH and began switching fuel tank selections, searching for any remaining fuel. They advised that after they selected each tank, they waited for a response however, there was no improvement. The pilot advised that the engines did not stop but they could not maintain altitude.
At 1516:40 the passenger began video recording the flight due to its ‘apparent turbulence’, capturing the engines surging. The recording concluded about 30 seconds later, as the pilot initiated a MAYDAY[2] call to Brisbane Centre air traffic control, stating ‘dual engine failure, suspected engine fuel starvation and I have to put it down on the road’. Brisbane Centre acknowledged the MAYDAY, requested the pilot activate their ELT on landing, and requested details on the number of people on board. The pilot did not respond.
The pilot alerted the passenger to the emergency and told them to brace for impact. Approximately 30 seconds later, the pilot extended the landing gear and banked into a right turn with the intention of landing on the Derby Highway. However, during the turn the right wing of the aircraft hit a tree causing the aircraft to turn 180⁰ and come to an abrupt stop on the edge of the highway.
Upon landing, the pilot was temporarily rendered unconscious. The passenger called emergency services and a local passerby stopped to help the pilot and passenger. The passenger recalled the area smelling of fuel when stepping out of the aircraft.
The pilot sustained serious facial injuries and the passenger sustained minor injuries. The aircraft was substantially damaged.
Context
Pilot information
Qualifications and experience
The pilot held a commercial pilot licence (aeroplane), issued in December 2020. They also held a multi-engine aircraft (MEA) class rating (issued on 21 June 2021), and an MEA command instrument rating (issued/renewed on 27 August 2021).
At the time of the accident, the pilot had about 776 hours of total flying experience, with about 613 hours as pilot in command and 43.4 hours as pilot in command of MEA.
The pilot joined the operator in July 2022, commencing operations on the Cessna 210 (C210). After a period of induction and flying in command under supervision (ICUS), the pilot completed a proficiency check with the substantive[3] head of flying operations (HOFO) (see the section titled Head of flying operations) on the C210 and then commenced passenger air transport operations as pilot in command.
Prior to joining the operator, the pilot had accumulated a total of 37.6 hours on MEA, of which 35 hours were dual day flying and 2.6 hours were dual night flying, completed during the pilot’s initial MEA flight training in 2019. Up until that time, the pilot’s MEA experience had all been gained on the Piper Seminole (PA-44).
In November 2022, the pilot and other pilots from the operator hired an external instructor, at their own expense, to complete instrument proficiency checks (IPCs) on MEA, using VH-DAW. CASA did not require pilots to have a type‑specific endorsement for the Cessna 310 (C310).
By the end of November 2022, the pilot had completed online theory training relating to the basic operation of the C310 and IFR theory, including a Civil Aviation Safety Authority (CASA) MEA questionnaire. On this assessment, the pilot had incorrectly stated the size of the C310 auxiliary tanks (see the section titled Fuel system), and the requirement to use the main tanks for 60 minutes prior to using the auxiliary tanks (see the section titled Fuel management). In mid‑December 2022, when the external instructor visited the organisation for the flight component of the IPC, the instructor assessed the MEA questionnaire using the aircraft’s pilot’s operating handbook (POH). They later advised that they noted the errors, and while they did not correct the answer on the questionnaire, they discussed the correct answers with the pilot.
The pilot’s C310 IPC training included general handling skills, stalls, turns, circuit operations, instrument approaches, asymmetric training, and an outline of how the auxiliary tanks were used. The auxiliary tanks were used for no more than 10 minutes during the first flight. The pilot obtained their IPC on 16 December 2022. The instructor noted that, although fuel management was not explicitly covered during the IPC flights, they had an expectation it would be covered during the organisation’s line training.
In total, the pilot gained approximately 8.1 hours ICUS on the C310 by the end of December 2022 (Table 1). The pilot then returned to flying the C210 for the operator.
A check-to-line flight on the C310 was planned to be conducted during a passenger-carrying air transport operation on 21 March 2023, however this flight was cancelled due to a hydraulic malfunction with the aircraft. A shorter, non-air transport operation, check-to-line flight was subsequently conducted by the interim[4] HOFO on 25 March 2023, 130 days after their IPC was issued. The pilot had not flown the C310 in the interim.
The check-to-line flight with the interim HOFO covered various operational aspects, however it was focused on ensuring the pilot was proficient flying under the IFR. The pilot could not recall completing emergency procedures during this flight or using the auxiliary fuel tanks. The pilot was assessed as competent in all areas. At the end of the check-to-line flight, the pilot had accrued 10.5 hours ICUS on the C310.
After completing the check-to-line flight, the pilot alternated between operating the C210 and the C310, accumulating 37 hours on the C210 and 43.4 hours on the C310 prior to the accident. At the time of the accident, the pilot had 53.9 hours experience on the C310, including 43.4 hours in the 90 days prior to the accident.
Recent history
In the 7 days prior to the day of the accident, the pilot completed flights on 14 June (4.6 hours flight time), 15 June (1.9 hours flight time), and 17 June 2023 (5.1 hours flight time). The pilot was rostered off duty on 18 and 19 June. They were within the operator’s flight and duty limitations for maximum cumulative flight and duty times in the 7 days prior to the accident (20 June).
The pilot reported that, on the evening of 19 June, they retired to bed at 2030, woke up at 0300 and began their pre-flight duties at 0500. The pilot noted that they went to bed earlier than normal, due to the early start time, but could not fall asleep straight away. It is likely they obtained about 5–6 hours of sleep.
The operator’s operations manual[5] detailed that, when starting between 0500–0559, pilots had a maximum available flight duty period (FDP) of 9 hours. Due to the pilot being on the ground at Turkey Creek for 6 hours, the operator reported they had organised a suitable sleeping accommodation for the pilot to allow for a split shift. This arrangement allowed the pilot’s FDP to be extended by 4 hours. The pilot was unaware of this facility, stating the operator had never previously given them suitable sleeping accommodation during a long day shift, only when needing to stay overnight. The pilot reported they waited for the client in an air‑conditioned room and had an adequate amount of food.
The pilot reported that they felt somewhat rested during the day of the accident flight and recalled that, although they had gone to bed early, they had not fallen asleep straight away. Based on the available information, the ATSB concluded that the early wake-up time and long duty day were problematic but, overall, there was insufficient evidence to conclude that the pilot was experiencing a level of fatigue known to affect performance.
Medical information
The pilot held a class 1 aviation medical certificate that was current to 3 May 2024. This specified a requirement for the pilot to wear distance vision correction. The pilot stated that they did not have any medical concerns or issues in the period prior to the accident.
Aircraft information
The Cessna 310R is a twin-engine, low-wing, 6-seat, unpressurised aircraft equipped with retractable landing gear and powered by 2 Continental IO-520 piston engines. VH-DAW was manufactured in the United States and first registered in Australia in 1975. Broome Aviation became the registration holder on 12 July 2011.
Fuel system
The C310 fuel system consists of 2 sets of fuel tanks in the wings – main and auxiliary, that supply fuel to each engine independently. Two fuel selectors, one for each engine, are installed on the floor between the pilot seats. These allow selection of main fuel, auxiliary fuel, crossfeed and fuel shutoff (Figure 10). The selector allows fuel to flow from the selected fuel tank to the engine‑driven fuel pump for the selected engine. Figure3 shows the layout of the standard fuel system installed in the aircraft.
1. VH‑DAW was fitted with both optional auxiliary tanks, totalling 31.5 US gallons on each side; 2. The aircraft did not have the optional low level fuel light fitted. Source: C310 POH, annotated by the ATSB
Main tanks
The 2 main fuel tanks for the C310 are integrally‑sealed aluminium tanks located on each wing tip. Each main tank holds 189 L (50 United States (US) gallons) of usable fuel, with approximately 7.5 L of unusable fuel. There are 2 fuel pumps in each main tank, the first (auxiliary fuel pump) is used to provide fuel pressure to prime the engine for start or to provide fuel pressure during an engine‑driven fuel pump failure. The second (transfer pump), operates continuously during flight and allows the transfer of fuel from the nose section to the centre section of the main tank, where the fuel outlet is positioned. The transfer pumps are on the same electrical circuit as the left landing light. The main tanks are vented to atmosphere and if overfilled, fuel will be vented overboard through these vents.
Auxiliary tanks
The auxiliary fuel tanks are bladder‑type tanks and are located in the outboard section of each wing. Each auxiliary tank holds 119 L (31.5 US gallons) of usable fuel. The POH stated that fuel could be drawn from the auxiliary tanks during cruise flight only.
Engine-driven fuel pump
Each engine had an engine‑driven fuel pump that contained a bypass, which continuously returned excess fuel and vapour to their respective main tank.
If auxiliary fuel tanks are to be used, select main fuel for 60 minutes of flight (with 40-gallon auxiliary tanks) or 90 minutes of flight (with 63-gallon auxiliary tanks). This is necessary to provide space in the main tanks for vapor and fuel returned from the engine-driven fuel pumps when operating on auxiliary fuel. If sufficient space is not available in the main tanks for this diverted fuel, the tanks can overflow through the overboard fuel vents.
It also stated:
Since part of the fuel from the auxiliary tanks is diverted back to the main tanks instead of being consumed by the engines, the auxiliary tanks will run dry sooner than anticipated; however, the main tanks endurance will be increased by the returned fuel. The total usable fuel supply is available during cruise flight only. An engine failure or engine driven fuel pump failure results in the auxiliary fuel on the side of the failure to be unusable.
It was recommended that auxiliary fuel was used until either exhausted or the flight phase had reached the top of descent. When questioned by the ATSB, neither the engine nor aircraft manufacturer could provide a fuel flow rate to calculate how much fuel was being returned to the main tank when the auxiliary tank was selected. The POH also advised ‘operation of the auxiliary fuel tanks near the ground (below 1,000 ft) is not recommended’.
The pilot advised that to simplify fuel management, they routinely used the main tanks for 60 minutes on each segment of a flight before selecting auxiliary tanks. They did not mention the reasoning behind using 60 minutes rather than the expected 90 minutes associated with the larger auxiliary fuel tanks (as fitted to VH‑DAW) detailed in the POH. Other pilots within the organisation who flew the C310 also reported using the 60-minute timeframe.
Fuel flow gauge
The fuel flow gauge indicated the approximate fuel consumption of each engine in pounds per hour. The POH stated that the gauge dial is ‘marked with arc segments corresponding to proper fuel flow for various power settings and is used as a guide to quickly set the mixtures. The gauge has markings for take-off and climb, and cruise power settings for various altitudes.’
The pilot advised that they used the fuel flow gauge while leaning the engines to determine the engines were receiving the appropriate fuel flow and to ensure the flow was stable after changing fuel tanks. The pilot reported that this process was completed during the accident flight on all tank changes.
Fuel quantity gauge
One fuel quantity gauge was located above the right-side control column and indicated the weight of the fuel (in both US gallons and pounds) for the left and right fuel tanks on the display. The gauge showed the fuel quantity for the selected tanks (either main or auxiliary) and the fuel quantity in the non-selected tanks could be displayed through the use of a toggle switch below the gauge. There were also 2 yellow indicator lights (one for each side), these illuminated when the auxiliary tank on the selected side was selected (see Figure 7).
The aircraft was not equipped with the optional independent low fuel warning lights for the main fuel tanks.
Vortex generators
VH-DAW was fitted with 88 vortex generators located on the wings and vertical fin with additional strakes mounted on the outboard of each engine nacelle. The Supplemental Type Certificate (STC) for this modification included various amendments to the limitations and performance, including reduced stall and VMCA[6] speeds, and allowed for an increased operating weight.
Site and wreckage
Accident site
The ATSB did not attend the accident site. The site was attended by members of the Western Australia (WA) Police Force on 20 June 2023 and by the aircraft operator the following day. The site inspection was recorded by the police and the video footage was provided to the ATSB, along with photographs taken on the day of the accident (Figure 4).
The wreckage was located on the edge of the road in an area of low foliage, approximately 2.8 NM (5.2 km) east-south-east of Derby Airport. The left main tank and right auxiliary tank were ruptured during the accident sequence.
The left auxiliary tank was reported by the operator as being intact and found to contain about 20 L of fuel, while the right main tank contained negligible amounts of fuel. As both wings displayed visible damage (Figure 5), the ATSB was unable to verify if fuel had leaked from the fuel tanks following the ground collision. The propellers on both engines were not in the feathered position.
Top image – left wing; bottom image – right wing. Source: Western Australia Police Force, annotated by the ATSB
While reviewing the video footage taken by the police onsite, the left landing light circuit breaker was found to have tripped. The ATSB could not verify if this occurred due to ground impact forces or during the flight.
The operator arranged for the wreckage to be transported to a non-secure storage area at Broome Airport, which required the wings and one horizontal stabiliser to be separated from the fuselage.
ATSB examination
On 30 June 2023, the ATSB examined the wreckage focusing on the aircraft fuel system, particularly the right wing, both auxiliary fuel tanks, and the fuel quantity indicating system (FQIS). Despite the disruption during the accident sequence and transportation, no pre-existing defects or fuel system anomalies were identified. The following key components were retained for further examination and testing:
right and left auxiliary interconnect check valves
right and left vapour return check valves
right fuel selector mains inlet port
right fuel selector auxiliary inlet port
FQIS indicator and signal conditioner.
Detailed technical examination of these components identified the following defects in 3 components, which likely existed prior to the accident:
right fuel selector – main tank inlet valve did not seal when closed (i.e. when not selected ON)
the check valve in the right auxiliary tank outlet bleed return line (interconnecting the inboard and outboard fuel cells) did not seal in the reverse flow direction
the right vapour return line (engine driven fuel pump to main tank) check valve did not seal in the reverse flow direction.
Testing of the check valve in the right auxiliary tank vent outlet bleed return line in the reverse direction identified a small leak. However, the testing indicated that the leak rate was significantly less than that required to allow fuel to have transferred from the main tank to the auxiliary tank while the aircraft was on the ground at Turkey Creek in the quantities reported by the pilot.
Civil Aviation Safety Authority (CASA) Airworthiness Bulletin (AWB) 28-010 stated that if this valve was leaking, it could allow the engine‑driven fuel pump to draw air into the fuel system resulting in either engine surging or loss of power. It was reported that this is most likely to occur when the auxiliary tank quantity was less than about half full.
The differential pressure applied to the check valve during testing was likely far lower than expected operating pressures. Therefore, it is possible that during engine operation with the auxiliary fuel tank selected, as the fuel quantity reduced, the increased system pressure affected the leak rate and resulted in an increased reverse flow. This may allow the engine driven fuel pump to draw air in sufficient quantity to effect engine performance.
There was no evidence of defects in the auxiliary tank inlet valve of the right fuel selector or the corresponding check valves from the left fuel system. The left fuel selector was not implicated in the occurrence and was therefore not tested.
The FQIS indicator and signal conditioner were not tested or examined due to difficulty finding a facility capable of testing the signal conditioner. Although testing may have established the serviceability status of these individual components, aircraft accident damage prevented operational testing of the whole system. As such, evidence provided by pilots that the FQIS system was not indicating correctly was relied upon (see section titled Fuel gauge displays).
Aircraft maintenance
Maintenance release
A maintenance release (MR) is required to be carried on an aircraft as an ongoing record of the aircraft’s time-in-service and airworthiness status. The operator’s system of maintenance stated that the MR was valid for 200 hours in service or 12 months from issue, with inspections to be completed at 50, 100, 150 and 200 flight hours.
A daily inspection was required to be carried out and the MR signed to show the inspection had been completed, prior to the first flight of the day. The inspection and certification could be made by any pilot licenced to fly the aircraft, or an appropriately licenced aircraft maintenance engineer. After the last flight of the day and before the aircraft was next flown, the total daily flight time was required to be entered and the progressive total time in service recorded.
The MR is also used to record any maintenance which is due on the aircraft prior to the next periodic inspection, or any defects[7] detected.
The last periodic maintenance inspection was carried out on 11 May 2023 at 150 flight hours. At that time the aircraft total time in service was 18,630 hours. The aircraft had flown 30 hours since this inspection with no defects recorded. The only maintenance issue recorded on the MR was a hydraulic leak in the right main brake, which was rectified and signed off by a maintenance engineer on 24 April 2023.
The ATSB interviewed all 5 pilots who had flown the operator’s C310 during the period from December 2022 to June 2023, as well as other pilots who flew the operator’s C210s. Most of the pilots interviewed stated they were encouraged not to write any defects with aircraft on the MRs. These pilots recounted that if any defects were documented on a MR, they would be reprimanded by the CEO and face a reduction in flight hours on the subsequent roster.
The pilots also reported that the interim HOFO (see the section titled Head of flying operations) exhibited more willingness for defects to be documented on the MR, however they firstly required assurance that the reported matter was a legitimate defect. The pilots had mixed views on the stance of the substantive HOFO, with 3 noting they had been told not to write defects on the MRs. Two pilots stated they had attempted to implement a ‘snag’ recording system as an alternate method of recording defects, however this was never adopted.
Most pilots advised that, to circumvent what they assessed as a restriction on using the MRs to record defects, they utilised a group chat to communicate specific issues they had encountered on different aircraft in the fleet. They also noted they found it easier to directly communicate with engineers in the maintenance facility if they had any issues after they completed a flight. This approach usually resulted in minor defects getting fixed immediately.
The substantive HOFO stated they were unaware of any ongoing defects with the operator’s C310 and were unaware of any instances of the CEO reprimanding pilots due to the recording of defects on the MRs. They also stated that, on occasion, pilots deviated from the standard documented procedure for defect reporting (see the following section titled Defect reporting process).
The interim HOFO also noted that any defects with aircraft in the fleet should have been reported to them and put on the MR, although even if this was not the case then pilots could go straight to the engineers in the maintenance facility to get the matters rectified. In relation to the C310, the HOFO stated the aircraft fuel gauges ‘weren’t fabulous’, however they did not offer an explanation why this was not written up on the MR. They reported being unaware of any other aircraft defects.
The chief engineer advised that all defects would be reported to them by either the HOFO or the CEO using the operator’s defect reporting process. Contrary to the process advised by the pilots, the chief engineer advised that as Broome Air Maintenance was not a part of Broome Aviation, all rectification work had to be requested, and that pilots were not permitted to bypass the request.
The CEO stated that if there was a defect with an aircraft, they would have expected the pilots to follow the company’s policy regarding defects and write them on the MR. When asked about the C310, the CEO recalled having no knowledge of any defects with the aircraft other than the autopilot not holding altitude. No reason was provided as to why this was not written on the MR. The CEO reported that the fleet were maintained to a high standard and that if a pilot found a defect on an aircraft it would be delt with accordingly. They dismissed the reports they would reprimand pilots for reporting defects, noting they were ‘pedantic’ about maintenance.
Defect reporting process
The operator’s operations manual outlined a formal process to report deficiencies detected between periodic inspections, which stated:
Line pilots shall report any deficiencies to the [head of flying operations] HOFO, [head of maintenance control] HAMC and CEO via email; verbal or text message notification may be used as a secondary notification method where appropriate or required.
Once an email was received from a pilot, the process required the HOFO to liaise with the HAMC to determine the steps to investigate and rectify the deficiency. The substantive HOFO advised that if a pilot were to call with an issue, if required, the HOFO would tell the pilot to endorse the issue on the MR and then the HOFO would follow up with engineering personnel.
The chief engineer reported that they did not use the maintenance release to record defects. Rather, if defects were identified either by the operator or by the maintenance organisation, these defects would be rectified and recorded in the aircraft’s Broome Air Maintenance (BAM) worksheets. The ATSB inspected the aircraft logbooks and was unable to identify any unscheduled maintenance. The last unscheduled maintenance recorded in the logbooks was dated 2017.
The interviewed pilots stated that if they detected an aircraft defect, it was easier to talk directly to individual engineers in the maintenance facility, as they were usually in the hangar when returning from a flight and it was more likely to be dealt with.
Reported aircraft issues
The operator’s pilots reported multiple issues with the aircraft to the ATSB, including:
inaccurate fuel gauge displays
an internal fuel leak from the right main tank to the right auxiliary tank
limited fuel draw from the auxiliary tanks
engine surging
inability of the autopilot to accurately maintain an assigned altitude
significant tail flutter.
During an interview with the ATSB, the chief engineer reported that, to their knowledge, the aircraft was fully serviceable with no issues identified. They also advised they were not aware of the issues raised by the pilots.
Fuel calibration cards are aircraft specific and used to enable an accurate assessment of fuel quantity. The aircraft’s dual indicating fuel quantity gauge was last tested and calibrated on 24 June 2020. Pilots reported that the main tank calibration card was disregarded as it was considered inaccurate.
There was no fuel calibration card relating to the auxiliary tanks. The ATSB was unable to confirm if the auxiliary tank calibration had occurred as there was no record in the maintenance worksheets or the aircraft logbook of the results. There was no regulatory requirement to record the results of a fuel gauge calibration test.
The next due date to test and recalibrate the fuel gauges was expected to be in June 2024 in compliance with the CASA Civil Aviation Order (CAO) 100.5 General requirements in respect of maintenance of Australian Aircraft – 2011 and the operator’s system of maintenance.
Pilots who operated the aircraft reported that the fuel gauges displayed significant inaccuracies when the tanks were full. Specifically, when the main tanks were full, the right main tank display would exceed full scale deflection, while the left main tank display would under‑read by approximately 64 L (105 lbs) (Figure 6).
Left image – expected fuel gauge indications for main tanks when full; right image – the reported fuel gauge indications for main tanks when full. Source: Braden Blennerhassett (Air Manager), edited by the ATSB
It was reported that, as fuel was used during the fight, the displays became progressively more accurate, however there was still a large discrepancy between the displays (Figure 7). The expectation was that, when the fuel tank selection was changed from main to auxiliary or vice versa, both sides would be changed at the same time.
Figure 7: VH-DAW main tank fuel gauge indications after supplying the engines for the same time
Both the left and right main tanks had been used for the same amount of time during the flight. Source: Pilot of VH-DAW, annotated by the ATSB
It was reported that when the gauge was selected to the auxiliary tank display, there was also a discrepancy when the tanks were full, although the difference was not as significant as that observed with the main tank display. It was reported that the display for the left auxiliary tank under‑read by approximately 9 L (15 lb), while the display for the right auxiliary tank under‑read by approximately 36 L (60 lb) (Figure 8). Pilots did not indicate that the accuracy of the auxiliary tank gauge displays improved during use. However, it was noted that the auxiliary tanks were never used below about 12 L.
Left image – expected fuel gauge display for auxiliary tanks when full; right image – reported fuel gauge display for auxiliary tanks when full. Source: Braden Blennerhassett (Air Manager), edited by the ATSB
The fuel gauge inaccuracy was reported to be widely known by pilots and informally reported to individual engineers in the maintenance facility, however the defect was not recorded on the aircraft’s MR. Pilots reported that maintenance personnel informed them that the external organisation capable of fixing the gauges indicated that new sensors were needed, and that the process of fixing the gauge was lengthy and the necessary parts were costly and so it was unlikely it would be completed. The CEO stated they were unaware of any issues with the fuel gauges.
The pilots advised that they adopted a time-based approach to track the amount of fuel in each tank during flight, noting there was no other guidance from the interim HOFO or senior management on how to manage the fuel quantity. Pilots stated that the most accurate way to ensure the known quantity of fuel on board prior to take-off was to depart Broome with full main and auxiliary tanks and, where possible, fill the main tanks to full when flying intermediate sectors.
The aircraft minimum equipment list (MEL) allowed 1 display on the gauge to be inoperative[8] providing a reliable means was established to ensure that the fuel quantity on board met the requirements for the intended flight.
The pilot of the accident flight and the supervisor of their first ICUS flight reported there were occasional instances where, having been fully refuelled, the right main tank would be missing approximately 10–30 L of fuel the following day. They further advised that when this occurred, the right auxiliary tank would overflow when the fuel cap was removed (Figure 9). This led the pilots to suspect a fuel leak between the right main and auxiliary tanks.
Figure 9: Auxiliary fuel tank overflowing on morning inspection
Source: Previous operator pilot, annotated by the ATSB
This issue was informally reported to maintenance staff, but not recorded on the MR. The CEO reported being unaware of the issue. After the initial report, the reporting pilot noted that engineers in the maintenance facility were unable to identify a fuel leak. Although the issue reportedly recurred, it was not further reported.
The pilot of the accident flight stated that the auxiliary fuel tanks could only supply the engines for 40–45 minutes before surging occurred. They noted that their initial understanding of the limited fuel draw came from the supervisor of their first ICUS flight. They further advised observing this limitation on their first solo passenger-carrying flight in the aircraft.
This issue was informally reported to individual engineers in the maintenance facility by the supervising pilot, and they recalled that maintenance was unable to identify a cause. The pilot of the accident flight assumed that since the issue had been reported previously, it had been addressed by maintenance. However, both the CEO and the chief engineer advised being unaware of the issue.
Other pilots stated that around the 40-minute mark while using auxiliary tanks, the aircraft’s engines would lightly surge before regaining power. They would then continue to use the fuel from the auxiliary tanks until about 12 L remained, before changing to the main tanks. The HOFO reported there were no issues when using the auxiliary tanks.
Engine surging
Multiple pilots recalled that the engines would surge during flight. The pilot of the accident flight and one other pilot noted the surging generally occurred when operating on auxiliary tanks, which they attributed to the limited fuel draw issue.
Other pilots also recalled the engines surging however, they could not confirm which tanks were selected at the time. These surges were described as minor and intermittent, typically ceasing after a few seconds and did not require the fuel pumps to be selected ON.
The engine surging had been reported to individual engineers in the maintenance facility verbally and had not been documented on the MR. Both the CEO and the chief engineer advised that they were unaware of this issue.
According to pilots who operated VH-DAW, the aircraft’s autopilot maintained an accurate heading, however, despite pre-flight testing of the system reportedly consistently indicating that the autopilot was fully operational, it could not maintain an assigned altitude. There was no evidence or record that this issue was formally or informally reported to the engineers in the maintenance facility, and the chief engineer advised not being aware of the issue. However, the issue was known to the organisation’s CEO, at the time of the occurrence.
An autopilot was considered inoperative if it was unable to maintain both altitude and heading. The aircraft MEL allowed continued operation with the autopilot inoperative under any one of the following conditions:
if flight was operated under IFR rules for RPT, charter[9] or aerial work, the aircraft was equipped with dual controls and had 2 control seats, with one control seat occupied by the pilot in command of the aeroplane and the other seat occupied by a person holding a commercial pilot (aeroplane) licence with an endorsement on the aircraft and an instrument rating
if the flight was operated under IFR rules with a single pilot for RPT, charter or aerial work, the flight was within the period of 3 days commencing on the day on which the autopilot became inoperative provided only one capability of the autopilot system was unserviceable
the flight was operated under VFR rules
the flight was operated for a private flight.
Elevator flutter
Pilots reported the presence of a known elevator flutter[10] on the aircraft, which was attributed to the installation of vortex generators on the elevator. This flutter resulted in challenging handling characteristics at low speeds, particularly during take-off and landing.
The engineers in the maintenance facility had conducted an extensive investigation into the issue in 2018, including the removal and reinstallation of the vortex generators. They concluded that the flutter did not impose stress on the airframe, and the aircraft was returned to service on 13 August 2018. The vibration defect was raised again on the MR on 20 October 2022 and cleared by maintenance personnel on 4 November 2022. There was no information regarding what was completed during the November sign‑off. The pilot of the accident flight stated that the elevator flutter was still present, although not noted on the accident flight.
Aircraft placarding
The fuel selectors had plaques stating the amount of fuel in each tank in US gallons. On inspection, it was noted that the auxiliary tank capacity for both sides incorrectly indicated that small auxiliary tanks (20 US gallons) were fitted to the aircraft (Figure 10).
This contradicted the usable fuel decals next to each filler cap on the airframe, which identified that the auxiliary tanks held 119 litres (31.5 US gallons) (Figure 11).
Just above the fuel selector plaques, there was a requirement for a plaque specifying how long to operate on the main tanks when first taking off with full tanks. For a C310 with the larger auxiliary tanks, the plaque was required to include:
Use main tanks for takeoff, landing and first 90 minutes of flight.
This plaque was missing from the aircraft (Figure 12).
Figure 12: VH-DAW internal placards relating to the fuel system
Top image – VH-DAW internal fuel placarding; bottom image – exemplar internal fuel placarding. Source: Top image – ATSB; bottom image – Textron, annotated by the ATSB
All aircraft placarding was required to be checked under the aircraft system of maintenance every 200 hours for security, presence and legibility. There was no requirement to check the validity of the information presented on the placards. The aircraft had five 200‑hourly maintenance events in the last 5 years, the last being August 2022.
The fuel selector placards had last been replaced on 24 October 2008, prior to the aircraft being registered to Broome Aviation. The installed placards were the incorrect part number and as such displayed the incorrect size of the auxiliary tanks. The ATSB was unable to determine if the plaque relating to the 90 minutes on mains had been removed previously or never installed.
The pilot of the accident flight was unaware that any of the plaques were incorrect, noting that they had not discussed it with the instrument proficiency check (IPC) instructor (see the section titled Qualifications and experience) or HOFO.
Fuel management
Pre-flight fuel plan
The flight plan used by the pilot on the day of the occurrence was destroyed during the accident and was not recorded by the operator’s planning software. During the draft report review process the pilot advised that they had recently found a copy of the flight plan, which they provided to the ATSB. The plan (Figure 13), generated by the flight planning software, showed a zero fuel margin. The pilot stated that they did not input the expected winds for the flight as they were unaware how to. Additionally, they recalled that all their previous flight planning had been conducted with nil wind.
A pre-flight fuel plan was created using the operator’s software (Figure 14). The flight plan software used a 120 L/h fuel burn for cruise and 150 L/h for climb. These figures were extracted from the POH performance tables using the typical operating conditions encountered for different phases of flight when flying out of Broome Airport.[11]
The known winds on the day of the occurrence were used. The fuel plan showed that the aircraft could not legally fly with the required reserves on the return flight to Derby.
Figure 14: Example fuel plan based off reported winds for each sector of the occurrence flight
Trip T – Trip total less taxi fuel; Contin – Contingency fuel (15% of expected trip total); F. Reserve – Fixed reserve; Fuel R – Fuel required for next leg including contingency and fixed reserve; Margin – Endurance subtracting fuel required; Endce – Endurance. Source: Operator, annotated by the ATSB
The ATSB also generated a fuel plan based on the pilot’s understanding of the amount of fuel they could use from the auxiliary tanks. The analysis used:
the flight times calculated by the operator’s software
the pilot’s standard use of 40 minutes from the auxiliary tanks
1.5 x fuel burn rate[12] – the extra fuel was diverted to the main tanks.
This resulted in approximately 120 L of fuel being available for use from the auxiliary tanks (40 L plus the redraw of 20 L = 60 L from each auxiliary tank). Therefore, the pilot’s perceived total available fuel onboard when all tanks were full was 498 L (main tanks 378 L + auxiliary tanks 120 L). As shown in Table 2, such a plan indicated there was insufficient fuel onboard to conduct the flight without fuel starvation.
A previous pilot of the C310 indicated that when flying the same route, on the return leg they would refuel the aircraft at Halls Creek, another base for the operator, as it was 77 NM south-west of Turkey Creek. They would then fly directly from Halls Creek to Broome. This flight route ensured they had enough fuel to complete the flight with reserves intact.
Previous flight
The pilot recalled completing the same flight 4 weeks prior to the occurrence. They stated that they had landed at Derby and refuelled the aircraft for the final leg back to Broome. A retrospective fuel log was created using the known winds on that day and the pilot’s reported timing of the fuel tank changes (Table 3). The ATSB also calculated the average fuel burn for the aircraft during this flight using the fuel added to refuel the aircraft to full after the flight which showed the aircraft used an average of 124 L/h.
The operator’s standard 12 L taxi fuel was used for the first leg of the flight. Due to the prevailing wind, the first leg from Broome to Turkey Creek was recorded as having a duration of 126 minutes, requiring the pilot to use the auxiliary tanks for 40 minutes (66 L draw from auxiliary tanks and 22 L returned to the main tanks on both sides).
The flight time from Turkey Creek to Derby was recorded as 90 minutes. Due to the assumed auxiliary tank issue and having used the auxiliary tanks for 40 minutes on the first leg, the pilot would have likely used main tanks for the entire leg. It is highly probable that the pilot landed at Derby with 21 L of useable fuel remaining in each of the main tanks, equating to about 15 minutes of remaining engine operation before fuel exhaustion.
Table 3: Retrospective fuel log of previous flight Broome – Turkey Creek – Derby on 25 May 2024
FUEL LOG
Broome – Turkey Creek
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
Taxi Broome
119
189
189
119
Departure Broome
119
183
183
119
Change to auxiliary tanks
119
123
123
119
Change to main tanks
59
143
143
59
Estimated fuel on landing
59
117
117
59
Turkey Creek – Derby
Taxi Turkey Creek
59
117
117
59
Departure Turkey Creek
59
111
111
59
Estimated fuel on landing
59
21
21
59
Fuel quantity analysis of the accident flight
The ATSB obtained flight data that was transmitted at regular intervals from a V2 Flight Tracker, which had been installed on the aircraft. A retrospective fuel log for the Turkey Creek to Derby leg (Table 4) was created using:
the pilot’s recalled amount of fuel in each tank on startup
the pilot’s recollection of when they completed tank changes
the operator’s average fuel consumption rate of 120 L/h
a conservative estimate of fuel return (0.5 multiplier) to the main tanks when using auxiliary tanks
a conservative estimate of fuel draw from the left main tank (2.5 multiplier) and return to the right main tank (0.5 multiplier) when cross feeding the right engine.
As such, it is only indicative of the fuel on board in each tank at each change of tank and at the time of the dual engine surging.
Table 4: Retrospective fuel log of remaining fuel in aircraft from Turkey Creek to the point of the dual engine surge using 120 L/h
FUEL LOG
Turkey Creek – Dual engine surge
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
1336: Taxi Turkey Creek (used 6 L each side)
74
110
70
119
1339: Departure Turkey Creek
74
107
67
119
1439: Change to auxiliary tanks
74
44
4
119
1449: Change left auxiliary to main tank
59
49 (44+5)
9 (4+5)
104
1454: Change right auxiliary to main tank
59
44
12 (9+3)
97
1504: Cross feed left main tank
59
34
2
97
1514: Dual engine surging
59
9
7 (2+5)
97
At the point of dual engine surge, it is estimated that the left main tank had approximately 9 L of fuel remaining.
The aircraft manufacturer stated that if the engines were surging while on the main tanks and there were no other issues with the fuel system and fuel available in the auxiliary tanks, the pilot should have been able to use the remaining fuel in the auxiliary tanks to regain full power. At the point of the dual engine surge, the left auxiliary tank had approximately 59 L and the right had approximately 97 L available.
The same calculations were completed using the pilot’s average fuel consumption rate of 124 L/h (see the section titledOperator fuel flow check). Those calculations (Table 5) indicated that about 6 L of fuel remained in the left main fuel tank (supplying both engines) at the point of the dual engine surging.
Table 5: Retrospective fuel log of remaining fuel in aircraft from Turkey Creek to dual engine surge using the pilot’s average 124 L/h
FUEL LOG Turkey Creek – Dual engine surge
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
1336: Taxi Turkey Creek (used 6 L each side)
73
110
70
119
1339: Departure Turkey Creek
73
104
64
119
1439: Change to auxiliary tanks
73
42
2
119
1449: Change left auxiliary to main tank
58
48 (42+6)
8 (2+6)
104
1454: Change right auxiliary to main tank
58
42
10 (8+2)
96
1504: Crossfeed left main tank
58
32
1
96
1514: Dual engine surging
58
6
5 (1+4)
96
Operator fuel planning requirements
Pre-flight
The operator’s procedures required the pilot to complete pre-flight fuel planning using the available electronic flight planning software. However, if the flight planning software was not available, the pilots were required to calculate the fuel required for the flight using the fuel flow guidelines for the aircraft.
The operations manual outlined the fuel figures, specific to the C310, to be used when manually completing fuel planning. The guidelines did not contain a fuel flow rate for climb. However, they did include a block (total) fuel margin of 47 L which was to be available for each sector. The operator advised they were not aware of where the margin of 47 L figure had originated from. The electronic flight planning software did not include this 47 L margin fuel when calculating fuel requirements.
To confirm the amount of fuel on board prior to flight, the operator’s fuel policy required pilots to visually confirm the fuel quantity in each tank using a dip or drip stick when possible, then compare this to the flight plan and fuel gauges. If there was a discrepancy more than an allowable margin with the fuel gauges the pilots were required to inform the HAMC and/or HOFO to determine the possible cause. The allowable margin quantity was not listed in the operator’s fuel policy.
Inflight
The operator’s procedures required pilots to recalculate fuel in flight at 2 specific points:
when reaching cruise
if required to divert.
The procedures outlined that once reaching cruise altitude pilots should:
calculate the remaining quantity of fuel on board for the proposed destination. This must be equal to or above the legal minimum final reserve quantity. If this is not the case, consider using more conservative fuel power settings, change cruise level for more favourable winds or divert to an alternative.
The procedure did not stipulate if this calculation was required to be recorded on any documentation, nor did it outline any requirement for a fuel crosscheck. Additionally, the operator did not have a fuel log or method of monitoring fuel during the flight.
If the pilot was required to divert, inflight fuel replanning was to be carried out using the fuel flow guidelines for the aircraft.
A previous pilot for the operator stated there was no standardised method of completing inflight fuel logs and it was based on pilot preference. They further reported a ‘feeling’ that the organisation had not had any fuel starvation events due to ‘luck’.
Post-flight
The operator’s procedures recommended that pilots conduct a fuel gauge check against the value on the fuel totaliser at the completion of a flight. However, the operator stated that none of its aircraft were fitted with a fuel totaliser. Additionally, the quantity of fuel used was to be checked against the expected burn from the flight plan.
Pilots were required to complete the fuel documentation, including recording on the journey log and manifest the amount of fuel at shutdown. The manifest did not provide the option to indicate the remaining fuel in each tank.
The operator reported that pilots were required to enter the amount of fuel consumed and flight time after each flight into the organisation’s data recording software. The program created a monthly report, which outlined the fuel flow rate for each flight, segregated by aircraft.
The substantive HOFO used this information to determine the average fuel flow for each aircraft, and which pilot completed each flight. If there was an unexpected trend for a particular pilot, the substantive HOFO would use this to discuss how the pilot was configuring the aircraft’s fuel system during flight. If the trend was over multiple pilots, the HOFO would liaise with maintenance to determine the cause.
The substantive HOFO noted there was no indication that the aircraft was burning more than the expected 120 L/h however, they could not confirm if this process was being completed by the interim HOFO while they were on leave. ATSB analysis of the pilot’s flight times and fuel uplift over the previous 10 flights indicated the aircraft was using 124 L/h on average.
Regulatory requirements
Pre-flight fuel planning
According to Civil Aviation Safety Regulation (CASR) Part 135 Australian air transport operations – smaller aeroplanes section 135.205 operators are required to provide pilots with an exposition which provides comprehensive tools, procedures, and guidance for effective pre-flight fuel planning. The exposition must outline step-by-step instructions for calculating fuel requirements to ensure compliance with Australian regulations and operational safety.
According to CASR Part 135.D.6 and the Manual of standards (MOS) Part 135 7.04, pilots must have access to resources for determining fuel needs for each phase of the flight, including:
taxi fuel
trip fuel
holding fuel
destination alternate fuel
contingency fuel
final reserve fuel
There should also be a process outlining:
fuel calculations
determining and recording fuel quantities – pre-flight
recording fuel quantities.
To support these calculations, operators must provide tools such as flight planning software, fuel calculation tables, or automated planning systems. Operators are also responsible for ensuring that pilots are trained to use these resources effectively and can adjust their fuel requirements based on dynamic operational factors, such as deteriorating weather or delays.
Part 135 manual of standards (MOS) Section 7.03 (2) required that the pilot in command must consider the effect of the relevant meteorological reports and forecasts when determining the quantity of useable fuel.
In-flight fuel management
The Part 135 MOS Section 7.05 (2) required that the exposition outline a process for regular inflight fuel checks, which required the pilot to:
determine the amount of fuel remaining
analyse planned fuel consumption against actual consumption
determine there is sufficient fuel on board
calculate the amount of fuel expected to remain at the destination.
According to the CASA Advisory circular 1-02 V4.1 Exposition and operations manual fuel policy guidance Annex D, the exposition should detail what maximum discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure is tolerable, noting that industry practice is a maximum of 3% discrepancy.
Part 135 MOS section 7.03 required that operators must provide pilots with aircraft‑specific fuel consumption. This could be sourced from the aircraft/engine manufacturer or taken from recent historical consumption records. Operators should also require pilots to document any significant deviations in fuel consumption or incidents involving fuel advisories or emergencies. This data enables operators to analyse and improve fuel planning and management procedures.
In addition, Part 135 MOS section 7.06 required that operators must also ensure that the exposition outlines clear procedures for pilots to follow in the event of a low-fuel situation, including:
a minimum fuel state
emergency fuel situation.
Finally, operators should regularly review and update their operational manuals to reflect lessons learned from safety reports and audits, ensuring continuous improvement in fuel management practices.
Operator requirements for training, experience and consolidation on new aircraft types
Induction and minimum qualifications
The operator’s operations manual stated that recruited pilots were to meet the following minimum requirements:
commercial pilot licence with no medical restrictions[13]
current Australian medical certificate
pass of a pre-employment check flight with the HOFO or a delegate.
Once inducted, a new pilot would learn the routes with existing pilots before being checked to line by the HOFO.
The operator’s operations manual stipulated 5 minimum requirements for a pilot in command of the C310 (Table 6).
Table 6: Operator’s 5 minimum requirements for operating the C310
Requirement number
Minimum requirements
1
5 hours on type for VFR operation
2
10 hours on type for IFR operation
3
Minimum of 750 total flying hours
4
Minimum 20 hours in command on MEA for VFR operation
5
A multi engine command instrument rating if flying IFR.
The HOFO was required to conduct a check-to-line flight and, if successful, the pilot would be cleared to conduct air transport operations as pilot in command on the new type. The substantive HOFO stated that generally it would be expected that multiple ICUS flights would occur with either the HOFO or a supervisory pilot before a check-to-line would be conducted. The CEO reported that generally 15–20 hours on type would be sufficient to conduct line operations as pilot in command.
During the draft review process, the CEO reported that the calibre of pilots coming through from flight schools was lower than previously experienced, noting that a lot of the organisation’s time was spent getting pilots up to commercial standard.
After completing the check-to-line flight, the pilot of the accident flight had accrued a total flying time of 740.5 hours. The operator received an exemption from the operator’s insurer for the pilot to undertake air transport operations in the C310 without meeting the specified minimum requirement of 750 hours.
Under CASR 61.650, pilots were required to have completed an IPC in the previous 12 months to fly a multi-engine aircraft under the IFR. The IPC must also be done in a multi-engine aircraft of the same category. The substantive HOFO noted that, once a pilot was checked to line, there was no follow up or specific oversight on their operating capabilities until their next proficiency check in 12 months, in line with the CASR requirements and the operations manual, which stated:
If flying under the IFR, pilots are required to conduct an Instrument Proficiency Check with an authorised Flight Examiner prior to one (1) year from the last day of the month in which it was issued (IFR operations).
There were no specific regulatory requirements for Broome Aviation to provide additional consolidation flights for pilots transitioning to the C310 as, at the time of the accident, the operator was operating under CASA exemption 87/21.[14]
In December 2021, Civil Aviation Safety Regulation (CASR) Part 135 (Australian air transport operations – smaller aeroplanes) commenced. It introduced more stringent requirements for flight crew training and checking for operators conducting air transport operations. However, operators could operate under the exemption that applied to a significant proportion of the previous small charter sector. This meant the operator was not required to conduct line training, a check-to-line, or complete proficiency checks, other than to ensure those proficiency checks and flight reviews mandated by Part 61 of CASR were carried out on their flight crew members.
Supervisory pilots
The CASA‑AMC/GM Part 119 - Australian air transport operators - certification and management v 2.3 noted that some operators have diverse fleets and there are scenarios where the HOFO may not be qualified on every aircraft type or in every role/function performed under its air operator’s certificate (AOC). In this case, operators can elect to use a structure where another pilot is identified to complete that position. In the case of Broome Aviation, the substantive HOFO conducted the check and training for the C210, in addition to nominated supervisory pilots, but for the MEA this position was covered by supervisory pilots. The operator required that supervisory pilots had:
a minimum of 20 hours total time on type
completed training with the HOFO or nominated person (with such training including the use of the line training and check forms)
met the relevant recency or proficiency requirements to act as pilot in command
been nominated, in writing, by the operator to be supervisory pilot and recorded as a named supervisory pilot.
The operator’s supervisory pilot register had not been updated since 1 December 2021. The register contained the name of one pilot who had been approved to conduct supervisory flights for the C310, however this pilot left the operator while the substantive HOFO was on leave. A second pilot had been listed as a supervisory pilot for the C210. The substantive HOFO stated that the second pilot had been assessed to conduct supervisory flights for the C310, however the register had not been updated to include this information. This pilot (detailed below as ‘Pilot 1’) also left the operator while the substantive HOFO was on leave.
During the period between December 2022 and June 2023, 7 pilots flew the operator’s C310, including one who had completed the training but had not been checked to line. Multiple pilots stated that training and guidance on the C310 during this period was limited. Of the 7 pilots:
Pilot 1 – was a senior pilot for the operator who was signed off as a supervisory pilot for the C310. They conducted the check-to-line for Pilot 2. Pilot 1 left the operator at the end of December 2022 and returned for 3 weeks at the end of February 2023.
Pilot 2 – completed no ICUS flights prior to completing a check-to-line flight in November 2022 that lasted 1.1 hours. The pilot was not formally signed off as a supervisory pilot on the C310, although they had extensive instructional time on MEA, prior to assisting with ICUS flights. The pilot left the operator at the end of February 2023.
Pilot 3 – completed 2 ICUS flights, one with the interim HOFO (3.7 hours) and 1 with Pilot 2 (1.6 hours), before completing a check-to-line (1.5 hours) with the interim HOFO a week later in February 2023. The pilot left the operator at the end of March 2023.
Pilot 4 (pilot of the accident flight) – completed 1 ICUS flight with Pilot 2 and 4 IPC flights with the external instructor on the aircraft. They were subsequently checked to line in April 2023, 130 days after their last flight in the aircraft, by the interim HOFO.
Pilot 5 – completed 3 IPC flights with the external instructor and completed no ICUS flights. They were checked to line in May 2023, 162 days after their last flight in the aircraft, by the interim HOFO.
Pilot 6 – completed 3 IPC flights with the external instructor and had not completed any ICUS flights since.
Pilot 7 (interim HOFO) – completed their check-to-line with Pilot 1 (3.6 hours) in December 2022 and completed 1 IPC flight with the external instructor.
At the time of their check-to-line, multiple pilots who conducted C310 operations for the operator during the period from November 2022 to June 2023, did not meet the operator’s minimum requirements 1, 2 and 3 detailed in Table 7. All pilots met requirements 4 and 5. The pilot of the accident flight and Pilot 5 both had limited experience flying MEA (under 50 hours), having not flown another MEA type outside of flight training.
Table 7: Compliance with operator’s minimum requirements on the C310 at the time of check-to-line
Pilot
Minimum 5 hours on type for VFR operation
Minimum 10 hours on type for IFR operation
Minimum of 750 total flying hours
Pilot 2
No
No
Yes
Pilot 3
Yes
No
Yes
Pilot 4 (pilot of the accident flight)
Yes
Yes
No
Pilot 5
Yes
No
No
Pilot 7 (Interim HOFO)
No
No
Yes
Pilot 1 was excluded as their check-to-line was completed prior to November 2022. Pilot 6 was excluded as they had not completed a check-to-line for the operator.
Multiple pilots reported that they had limited training on the C310 and anticipated completing additional ICUS flights before being checked to line. Three pilots assessed that they were tasked with operating the aircraft without adequate training on the fuel system. They expressed concerns about the limited training noting the C310 had a complex fuel system. Multiple pilots reported learning the systems while conducting operational flights.
Emergency procedures
The POH included emergency procedures for inflight engine failure, which included a requirement to check:
fuel flow rate
fuel selector positions
fuel quantity.
After the second surging event on the right engine, the pilot crossfed the left main tank to the right engine and referred to the quick reference handbook. This handbook outlined the ‘engine failure during flight’ checklist. The pilot stated that they referred to the checklist to determine whether any actions could be taken to address the surging, noting that the engine had not completely failed. There was no checklist to address engine surging.
At this point in the flight, the aircraft was located between 2 nearby diversion airstrips of Kimberley Downs Station, located approximately 5 NM to the south‑east, and Meda Station located approximately 16 NM west (Figure 15). The pilot noted they were familiar with the location of the airstrips, however they had never operated from them and were unaware on their suitability and condition. The pilot stated that because of these unknowns that they believed the only suitable airstrip was Derby Airport.
The pilot did not consider diverting to RAAF Base Curtin. Source: Google Earth, annotated by the ATSB
The flight data indicated that the pilot initiated their descent from 10,000 ft at the normal top of descent position, while continuing to track towards Derby Airport, at an average descent rate of 400 ft/min. Approximately 3 minutes into this descent, the pilot crossfed the right engine from the left main tank.
Engine surging
When surging occurred in both engines, the pilot noted that it appeared to be from fuel starvation. The aircraft manufacturer noted that in the event of simultaneous engine power losses or surging, the engine ’Airstart’ checklist could be actioned twice, as only one engine should be restarted at a time. Additionally, the ‘FORCED LANDINGS (Complete Power Loss)’ checklist should be used if pilots were unable to regain power.
The pilot continued tracking to Derby Airport while switching fuel tanks, attempting to draw any remaining fuel. The manufacturer noted that the certification rule, at the time of the aircraft’s certification, required multi-engine aircraft to regain full power and fuel pressure within 20 seconds after switching from an empty tank to a full tank in level flight. The aircraft tracking data indicated that at an altitude of approximately 4,500 ft the descent rate increased to 1,500 ft/min. The aircraft travelled approximately a further 5.5 NM over approximately 3 minutes before a forced landing was conducted (Figure 16).
Figure 16: Aircraft altitude variation with distance to Derby Airport
4. Right engine surge – crossfeed right engine off left main tank; 5. Inbound call for Derby Airport; 6. Dual engine surge; 7. Mayday call; 8. Accident site. Source: ATSB
When the pilot determined they would be conducting a forced landing, they declared a MAYDAY to ATC. The aircraft was at an altitude of approximately 700 ft. The pilot later advised they had insufficient time to complete any checklist items after the MAYDAY call, however they lowered the landing gear as they were aiming to land on the Derby Highway as it was assessed as the best available option. There were approximately 30 seconds between the MAYDAY transmission and the forced landing.
Survivability
Safety briefing
The operator had a safety briefing video for the C310. The video outlined the:
use of:
doors
seatbelts
emergency exits
location of:
life vests
safety briefing card
emergency supplies
installed emergency locator transmitter (ELT)
The pilot noted there were 2 main differences between the aircraft and the information in the video. The location of the emergency supplies was in the nose of the aircraft rather than the wing cargo locker, and the ELT was portable rather than installed (see the section below titled Emergency locator transmitter).
This was the second time the passenger had flown in VH-DAW with the pilot. The passenger noted that on the first time flying in the aircraft they were shown a safety briefing video. On this occasion they were not shown the video and instead were given a briefing while at the aircraft. They recalled the briefing outlined the information regarding the emergency exits and seatbelts, noting there were other topics covered that they could not recall. The passenger recalled that they did not read the safety card while in the aircraft as they flew frequently. The safety card contained information on how to adopt the brace position.
When the passenger was asked to brace by the pilot, they stated they were unsure how to brace properly in the aircraft and reverted to their knowledge of the brace position for larger commercial aircraft.
Seatbelts and upper torso restraints
The pilot seat was fitted with a lap belt and upper torso restraint (UTR),[15] consistent with the regulatory requirements. The pilot stated that they would not wear the UTR portion of the harness during cruise as it limited their ability to view the gauges on the opposite side of the cockpit. The UTR was only worn during take-off and landing. The pilot stated that during the emergency, they did not put on the UTR. The pilot sustained severe facial injuries and a loss of consciousness when the aircraft collided with terrain.
The passenger’s seat was fitted with a lap belt. This was worn by the passenger during the emergency and forced landing. The passenger received minor injuries, including bruising around the abdomen due to the lap belt.
The aircraft was fitted with a portable emergency locator transmitter (ELT).[16] The pilot recalled that on first flying the aircraft they had checked the expiry date of the ELT and noted it was out of date. The portable ELT was subsequently replaced prior to the aircraft’s next flight.
The safety briefing video showed an automatic installed ELT[17] within the aircraft. The pilot noted that during pre-flight briefing with the passenger they explained the location of the ELT was different to the safety briefing video, however they did not explain the process to activate it.
The CASR Part 135 MOS required aircraft that were flown more than 50 NM from the departure aerodrome to carry an automatic ELT. However, this requirement was not applicable to the aircraft until 2 December 2023. Prior to then, the aircraft was operating under regulation 252A of the Civil Aviation Regulations, and subsection 6 of Civil Aviation Order 20.11, which permitted either a portable ELT or an installed ELT in the aircraft.
Due to the pilot being rendered unconscious during the accident sequence, the portable ELT was not activated. The passenger contacted emergency services while still in the aircraft using their phone, identifying the accident location from a passerby who stopped to help.
Operator and management information
Overview
Broome Aviation was re-issued an air operator’s certificate (AOC) on 11 November 2022, to conduct operations under CASR Part 135 ‑ Australian air transport operations – smaller aeroplanes, allowing single and multi-engine piston and single engine turbine air transport operations. At the time of the accident, it operated the following Cessna aircraft:
7 x C210 (single-engine piston)
1 x C310 (multi-engine piston)
1 x C404 (multi-engine piston)
1 x C208 (single-engine turbine).
In addition to a head of flying operations (HOFO), the operator had 7 seasonal pilots in a combination of full-time and casual positions.
Figure 17: Operator’s organisational structure
Source: Broome Aviation
Chief executive officer
The CEO held the positions of flight operations manager[18] and head of maintenance control (HAMC) (Figure 15).[19] They also owned and operated Broome Air Maintenance (BAM). This maintenance facility performed all the maintenance on the Broome Aviation fleet. The facility’s personnel comprised a chief engineer, who was registered as a licenced aircraft maintenance engineer (LAME), and aircraft maintenance engineers (AMEs). The chief engineer began working at BAM in October 2022.
The interim HOFO stated that the CEO had a hands-on approach to the organisation, stating that the CEO would generally create the roster for the pilots, which the interim HOFO would check and approve. The chief engineer stated the CEO would also be the final authority of any maintenance conducted on an aircraft.
The Broome Aviation operations and maintenance manuals contained contradictory information relating to the person nominated in the HAMC position. In the operations manual, the chief engineer of BAM was incorrectly listed as the HAMC, whereas the maintenance manual accurately listed the CEO in the position. The CEO later stated that the chief engineer of BAM was filling a dual role of both chief engineer and HAMC, however this was not communicated to CASA and was not the understanding of the chief engineer.
Head of flying operations
During the period from December 2022 to June 2023, the HOFO position underwent a temporary change. The substantive HOFO took a period of leave, during which a new person assumed the position on an interim basis.[20]
The interim HOFO was employed as a full-time, permanent pilot for another operator (operator 2), which was also based in Broome and only conducted operations in Cessna 208 aircraft. Operator 2 was independent of Broome Aviation. The interim HOFO began to work with Broome Aviation in November 2021 as a casual pilot during operator 2’s off season. They recommenced casual work with Broome Aviation on 13 November 2022, again during operator 2’s off season.
In late November, Broome Aviation asked them if they were willing to fill the position of HOFO to cover the leave period of the substantive HOFO. Having agreed, their application was submitted to CASA on 25 November 2022 (see the section titled Head of flying operations assessment).
The interim HOFO was assessed for the HOFO position by CASA on 7 December 2022 and subsequently approved for that position on 12 December 2022. On the same day, a handover was completed with the substantive HOFO. CASA was informed that the handover had been completed. The interim HOFO was also assessed by CASA (18 November 2022) and approved for the position of ‘alternate’ HOFO with operator 2 in January 2023 (see the section titled Requirements for an alternate HOFO).
At the time of their appointment to the Broome Aviation HOFO position, the interim HOFO held a commercial pilot licence (aeroplane), issued in early 2008, with single and multi-engine aircraft (MEA) class ratings. They had a total flying experience of 5,049 hours, of which approximately 135 hours were on MEA (Table 8). They had flown the C310 once prior to their HOFO assessment, which was a check-to-line flight in VH-DAW on 3 December 2022.
Table 8: Interim HOFO flight hours prior to assessment
Single-engine
ICUS
Dual
Command
Day
Night
Day
Night
Day
Night
184.3
1.4
158.9
13.9
4,542.4
13.3
Multi-engine
13.9
3.8
31.7
1.5
76.4
7.9
The interim HOFO completed an IPC for MEA, in a different aircraft type, on 2 December 2021. It was renewed in the C310 during the external instructor visit to the operator in December 2022. Prior to conducting supervisory or check flights with Broome Aviation pilots, the interim HOFO had gained 20 hours flight time on the C310. This met the operator’s minimum requirements for supervisory pilots.
Check-to-line for the pilot of the accident flight
2.4
The interim HOFO stated that they expected to occupy the position until the end of February 2023, when they were to return to operator 2 and the substantive HOFO was expected to return from leave. This time period was agreed to by operator 2, with the understanding that all flight and duty times for either operator would be recorded in both operators’ systems to ensure flight and duty limits were not exceeded. The interim HOFO stated they were unaware they had been approved and appointed by CASA in the ‘HOFO’ position and assumed they were in the ‘alternate HOFO’ position for Broome Aviation. They advised they only became aware that they were the appointed HOFO during a CASA level 2 surveillance activity (see the section titled Level 2 surveillance – 20 June 2023).
Oversight of operations
Although the assessment CASA completed of the interim HOFO was for a period of one month, they did not contact the operator at the end of this period to consider if the assessment was still appropriate.
At the end of February 2023, the interim HOFO was told that the substantive HOFO’s return would be delayed until the end of June 2023. They advised that they discussed remaining as acting HOFO with the Broome Aviation CEO, however their duties would need to be reduced. These duties were subsequently reduced to check and training, confirmation of rosters (arranged by the CEO), and general availability for pilots requiring assistance. CASA was not informed of this change. The interim HOFO stated that their main responsibility after this time was with operator 2.
At the beginning of March 2023, the interim HOFO completed a 2-week flight instructor rating course for MEA in Darwin, which was funded by operator 2. Following its completion, the interim HOFO then recommenced full-time work with operator 2. They stated that they were still contactable for any pilots at Broome Aviation who needed assistance and noted that 2 ‘senior’ pilots were available during this time (one of these pilots being the pilot of the accident flight).
In March 2023, the management of operator 2 identified that the interim HOFO was still conducting flights for Broome Aviation. In response, they were advised to cease working for Broome Aviation as that work would affect their flight and duty times as they were also in the alternate HOFO position for operator 2. Operator 2’s management was unaware that the interim HOFO continued to conduct flights and remained the HOFO for Broome Aviation after the discussion in March 2023.
While at Broome Aviation, the interim HOFO checked 3 pilots to line on the C310. The interim HOFO had accumulated 23.1 hours on the C310 prior to conducting the check-to-line flight on the pilot of the accident flight. They recalled that, even though they had recently received their instructor rating for MEA at that time, they did not feel comfortable simulating single engine emergencies.
The interim HOFO stated that, after the pilot of the accident flight was checked-to-line, they followed up with them after their first couple of flights. The interim HOFO expressed no concern about the pilot’s operation of the C310 and noted the pilot had not contacted them in relation to issues or questions about the aircraft. The accident pilot confirmed they never contacted the interim HOFO regarding the C310, noting:
I didn’t feel comfortable contacting the HOFO with 310 questions … this was due to their very minimal type knowledge and support within the entire company, so I sought advice from outside the company from more experienced pilots on the 310.
During the 4-month period from March to June 2023, the interim HOFO recorded 33.85 duty hours at Broome Aviation, however they noted that they would often ‘drop in’ after completing flights for operator 2 and did not formally record all the time spent at Broome Aviation. The CEO later advised that the HOFO was available in the afternoons for discussions with pilots however, none of the pilots made use of that opportunity. Comparatively, the interim HOFO recorded 458 duty hours at operator 2 during this period and reported they flew full‑time for the operator, while also conducting check and training for its pilots.
At the time of the accident, the interim HOFO had been in the HOFO position for Broome Aviation for 7 months. A week after the accident flight, the substantive HOFO returned to the operator.
Pilots flying for Broome Aviation stated that, when contacting the interim HOFO between March and June 2023 they would not get an immediate response, noting that the HOFO’s priority was flying for operator 2. The pilot of the accident flight stated that they would generally reach out to another pilot (who had recently left Broome Aviation) for guidance on the C310 rather than the interim HOFO.
Multiple pilots reported that the CEO would monitor each flight using the operator’s online tracking system. If any deviations in flight time or route occurred, the pilot would receive a ‘barrage’ of foul language, be accused of not considering the monetary implications for the organisation, and then face threats of loss of flight hours or potential termination of employment. By contrast, the CEO stated they had little interaction with the pilots as their office was located at the maintenance facility, which was on the opposite side of the airport. They also stated that all communications about aircraft maintenance would be directly from the HOFO.
The interim HOFO reported that, after completing a day’s duties at operator 2, they would pass through Broome Aviation to check the operations for the day. They recalled they would have general conversations with pilots and considered them to be close friends as well as work colleagues. However, the pilots the ATSB spoke to stated that, during this period, they received little to no guidance on flight operations (for all aircraft types).
The substantive HOFO stated that they primarily spent the workday in their office and generally interacted with pilots while they were completing paperwork. Most interactions involving questions or issues occurred over the phone. They also reported that the CEO, whose office was located at the hangar, had more frequent face-to-face interactions with the pilots, often seeing them before and after their flights.
Safety management system
CASR Part 119 (119.190), which commenced on 2 December 2021, included a requirement for an operator conducting operations under CASR Part 135 (Australian air transport operations – smaller aeroplanes) to have a safety management system (SMS). However, at the time of the accident the operator was operating under exemption EX87/21 and was not required to have met the SMS requirement. This exemption applied to a significant proportion of the small charter sector and was not specific to this operator. Despite that, Broome Aviation was required to have completed an SMS implementation plan and submitted the plan to CASA by 4 April 2023. The operator had not completed that process at the time of the accident.
The operator’s nominated safety officer was a line pilot. They left the operator at the end of December 2022 and returned to complete a short 3-week stint at the end of February 2023. The operator did not nominate a new safety officer after this pilot left the organisation and they were not required to do so, as there was no regulatory requirement for them to have one.
While not required, the operator did not have a formal incident or hazard reporting system, or a means of identifying the development of hazardous trends. Interviews with various staff members indicated that, although there were safety meetings involving pilots to identify safety risks, these meetings had not been held since the arrival of the interim HOFO.
Organisational pressures
The ATSB interviewed the 5 pilots who conducted Cessna 310 operations for the operator during the period November 2022 to June 2023, as well as 2 other pilots. During interviews, most of these pilots revealed events in which they were reprimanded or challenged by the CEO, or they witnessed similar treatment to other pilots, for declining a flight due to a maintenance concern. Many pilots stated they had experienced pressure from the CEO to complete flights with aircraft they considered unairworthy.
They stated they were worried about the consequences, such as employment termination or the hindering of their career progression, if they did not complete those flights. Pilots also stated that they felt pressure to ‘get the job done’, with one pilot stating:
…it was always like you just have to do the job. You have to do the job. It's not anything to do with safety or if you have the training for it either…
During the draft report review process, the CEO acknowledged that at times they had reprimanded and challenged pilots. However, they stated that this was in response to pilot actions that they considered imposed unnecessary financial and/or reputational cost on the company.
Complaints received by CASA from pilots and a passenger (see the section titled Complaints to CASA) stated multiple concerns for the safe operation of aircraft. One complaint by a former pilot stated:
… operational pressure from the organisation and their management is forcing pilots to make unsafe decisions in flight. A report to CASA is better than trying to reason with the company. The mentality of not only managers but also the owner isn't conducive to safe aviation practices.
Senior management stated they were unaware of any instances where pilots were reprimanded for not flying an aircraft considered to be unserviceable. All stated that, if there was a defect with an aircraft, the operator’s stance would be to get it rectified before another flight was completed.
During interviews, former pilots expressed concerns for the operator’s future, and one stated:
I knew that either I was going to be involved in something that I shouldn't be or that an incident was going to happen.
Most of the pilots the ATSB spoke to who had left the organisation stated their decision to leave was based on aircraft maintenance issues and/or the unacceptable treatment they received as pilots from senior management.
Civil Aviation Safety Authority oversight
Head of flying operations assessment
Position requirements
Under the CASRs, the HOFO must meet specific requirements, including holding appropriate qualifications, demonstrating substantial operational experience, and having a thorough understanding of regulatory obligations. The HOFO is responsible for overseeing operational standards, managing safety and compliance frameworks, providing leadership to flight crews, and ensuring that all activities align with organisational and regulatory expectations.
Specifically, CASR sub regulation 119.140(1) stated that:
The head of flying operations of an Australian air transport operator must safely manage the flying operations of the operator.
CASR 119.135 required the HOFO to:
• hold a pilot type or class rating for a type or class of aircraft that is used to conduct a significant proportion of the operator’s air transport operations
• have at least 500 hours flight time on a type of aeroplane that is the same as, or substantially similar to the type of aeroplane used to conduct a significant proportion of the operator’s Australian air transport operations
• have at least 6 months experience in the conduct or management of air operations conducted under an AOC or equivalent foreign authorisation.
CASA’s acceptable means of compliance and guidance material (AMC/GM) Part 119 - Australian air transport operators - certification and management v 2.3 outlined recommended minimum hours and experience for a HOFO based on the size and complexity of the operator. For an operator with more than one MEA, such as Broome Aviation, CASA recommended that a HOFO have a minimum of:
Under CASR 119.205, there was a requirement for the operator’s exposition to list the qualifications, responsibilities, and names of key personnel. There was also a requirement to list the names of each person authorised to carry out the responsibilities of the position when the substantive position holder was absent from the position or unable to carry out their responsibilities. These authorised persons were referred to as alternate key personnel.
If an operator wanted to change the specific individual in the alternate key position, CASA approval was required, due to this being considered a significant change. Once approved, this should lead to the insertion of the nominated person into the operator's exposition as an alternate key position holder. Operators working under CASA exemption EX82/21, including Broome Aviation, were not required to name alternate key personnel in the exposition, even if they had an alternate.
The AMC stated that small operators with limited personnel may nominate alternate HOFOs employed by another operator, provided they detailed in their exposition how the alternate HOFO would perform the position effectively. The requirements for an alternate HOFO were the same as the HOFO position. In addition, the alternate HOFO had to have a direct relationship with the operator and sufficient capacity to fulfill their duties. It also stated that dual responsibilities for multiple operators were unlikely to meet this standard.
The operator’s operations manual stated that an alternative HOFO must be approved by CASA. It also stated that:
• a handover form must be completed prior to the transfer of the responsibilities from the HOFO to the alternate HOFO
• the alternate HOFO could not be the acting HOFO of any other operation while acting as the HOFO for Broome Aviation
• the alternative HOFO could only perform the duties of the HOFO during the specified period they had been nominated to act as HOFO
• CASA be informed within 7 days of the transfer being completed.
Assessment process
CASA’s HOFO suitability assessment was a formal process designed to evaluate a candidate’s suitability for the position of HOFO in a CASR Part 135 operator. It aimed to ensure the individual had the necessary qualifications, operational experience, and management skills to oversee flight operations safely and in compliance with CASA regulations. The assessment begins with a review of the candidate’s documentation, including licences, flight experience, and familiarity with the operator’s aircraft and procedures. CASA also examined the candidate’s knowledge of relevant regulations, operational procedures, and safety management principles.
The assessment included an interview where CASA evaluated the candidate’s understanding of key areas such as CASA regulations (Parts 135, 91, and 119), the operator’s exposition and procedures, SMS implementation, and human factors. The candidate was also required to demonstrate the ability to manage compliance, oversee pilot performance, and respond effectively to safety-critical situations. Leadership and decision-making skills were also a focus, as the HOFO must manage teams, promote a strong safety culture, and ensure the organisation adheres to all operational requirements.
The assessment may have also required a practical demonstration of the candidate’s ability to implement operational procedures and manage risk. Based on the assessment, CASA determined whether the candidate was fit for the position or if further experience was needed.
Applicant 1
In October 2022, the operator submitted an application to CASA for its HOFO position, replacing the substantive HOFO as they advised they were resigning from the key personnel position of HOFO for medical reasons on 17 October. It also submitted a change to its operations manual to replace the substantive HOFO with the proposed HOFO candidate. This applicant had 2,327 flight hours with 1,009 multi engine hours, however they did not have any air transport experience and had not been a HOFO with any other operator.
This application was assessed on 14 November 2022 and the CASA flight operations inspector (FOI) deemed the applicant unfit for the position due to:
limited experience in air transport operations
not meeting the 500-hour requirement on aircraft substantially similar to those primarily operated by the operator
an assessment, based on previous dealings with the CEO, that an experienced HOFO was required to ensure pilots were managed professionally and the operation was safe and efficient.
On 21 November, CASA advised the operator that the applicant was unsuitable. In internal CASA correspondence, the FOI noted that the application was to replace the substantive HOFO who would be on leave and would be returning at the end of April 2023. The FOI stated concern for continuity of the operation over this period.
The substantive HOFO continued in the role in a limited capacity.
On 19 July 2022, operator 2 applied to CASA for approval of an alternate HOFO position, with the applicant who was later approved to be Broome Aviation’s interim HOFO being the nominated candidate (Table 10). This application was assessed by the same FOI mentioned in the section above on 18 November 2022. When requested, CASA could not locate the assessment form completed on applicant 2 for this position. The FOI later stated that they had expected to complete a flight test for the interim HOFO during this original assessment, however an internal CASA decision was made that it would be a desktop assessment only.
Following the rejection of its first applicant, Broome Aviation submitted an application for an alternate HOFO position on 25 November 2022, with the interim HOFO being the nominated candidate and an expectation that this person would be acting in the HOFO position for a limited period. This application included changes to the operations manual to update the positions. The same FOI completed this assessment and stated that, because they had recently assessed the applicant as an alternate HOFO for operator 2, the process could be expedited as many of the assessment elements had previously been covered.
The assessment for the interim HOFO for Broome Aviation was completed by the FOI on 7 December 2022. The documentation stated that the assessment was for an ‘alternate’ HOFO position, with a time limitation of 1 month. It was also noted that the applicant had taken leave from their original operator to fulfill this position.
The FOI advised that the 1-month timeframe was due to their understanding that the substantive HOFO would be travelling overseas for this time and would be returning to the operator. However, there was also email evidence indicating that the FOI knew the substantive HOFO would be on leave until April 2023. In discussions with the ATSB, the FOI stated the 1‑month period was the primary timeframe considered for this applicant and as a result they were not assessed in their:
check and training experience
MEA experience
ability to conduct oversight, if working for 2 operators.
On 12 December, CASA formally issued the approval for the applicant to become the HOFO rather than as requested and stated in their own paperwork, the alternate HOFO for Broome Aviation. The updated operations manual specified the applicant was appointed in the alternate HOFO position, instead of the CASA‑approved position of HOFO. It did not change the nominated person for the HOFO position, even though they were on leave for a significant time. There was no explanation in the operations manual of how the alternate HOFO would manage this position if they returned to their original operator. The manual amendment was accepted by CASA. The FOI advised that the operations manual was accepted as the change was for a short time and they did not expect the operator to resubmit the manual when the substantive HOFO returned.
CASA stated that a key personnel position did not come with a time limitation, although one could be imposed by the operator and outlined in its exposition.[21] If this was the case, CASA would note the time limitation on its assessment of the applicant and place a note on file in the CASA system. While CASA’s assessment of the interim HOFO was based on a 1-month period, no note was placed on file.
In February 2023, while preparing for a level 2 surveillance activity, a regulatory oversight flight operations inspector (RO FOI) identified that the interim HOFO had been assessed for the position on the basis of performing that position for one month, however they were still acting in this position 3 months after the assessment had been completed.
The RO FOI contacted the interim HOFO to discuss the situation and was advised that the substantive HOFO would be on leave until June 2023 and the interim HOFO had been conducting HOFO duties. They also were advised that the interim HOFO would be recommencing seasonal work with operator 2 at the beginning of March 2023, with the intention of continuing with Broome Aviation as HOFO on a ‘remote basis’. The RO FOI ensured the interim HOFO was aware of their own requirements for fatigue management, discharge of responsibilities and general oversight of Broome Aviation activities while working with the other operator.
The RO FOI noted that, although there was nothing legislatively preventing this arrangement under CASR Part 119, it was unorthodox and created a level of concern. There was no reassessment of the interim HOFO in relation to their duties, as the RO FOI assumed a full assessment had been completed during the other FOI’s previous assessment in December 2022.
Complaints to CASA
The CASA Surveillance Manual 15.1 required that when CASA received a complaint about an operator, it be classified as a class A–C occurrence and action be taken if it was assessed as class A or B (Table 11). A class A assessment required instigation of a level 2 unscheduled investigation, while a class B assessment could be investigated or added as an item in an upcoming surveillance.
Table 11: CASA complaint occurrence classes and follow‑up action
Class
Occurrence event
Surveillance type
Action Type
A - Critical
Complete loss/failure of the aviation system(s), or a destructive failure, impacting directly on the safe operation of the aircraft
In November 2022, CASA received a complaint about Broome Aviation relating to operational issues. The complainant stated that:
there was an oppressive culture at the organisation, based on bullying and pressure from the CEO that ‘preys on junior pilots’.
It also detailed instances of:
pilots being forced to fly aircraft at night with unserviceable instruments
pilots being advised to fly outside legal operational requirements
comments made to pilots to ignore issues or defects with aircraft.
This information was passed to the CASA surveillance team, where the RO FOI followed up on the complaint by talking to the complainant in February 2023. Although evidence, including copies of text messages, was supplied to CASA, the RO FOI explained to the complainant the importance of reporting an incident (either via the company reporting system or the CASA confidential system), with specific details, at the time it occurred. They also outlined the legal obligations of a pilot in command to record aircraft defects correctly.
After discussing the matter with the complainant, the RO FOI assessed the complaint was either indicative of a ‘disgruntled’ former employee, or there was a cultural issue at the operator. The complaint was added to the scoping document for a June 2023 surveillance activity (see the section titled Level 2 surveillance – 20 June2023), and assessed as a class B.
There was no documentation outlining if the complaint was followed up after the audit.
CASA stated that the complaint it received in November 2022 did not provide sufficient specific information to act upon. The supplied text messages were not considered to be fully contextualised, clear, or related to specific events where additional evidence could be sought.
Following the accident on 20 June 2023, CASA received 2 more complaints. The first complaint was from a pilot who stated that there was operational pressure from management forcing pilots to make unsafe decisions in flight. The complainant stated that they had witnessed this firsthand. No specific examples were provided. The second complaint was from a passenger who stated that on a charter flight from Broome, the twin-engine aircraft experienced a technical fault, and the pilot was instructed by management to continue the flight.
The scope of these complaints was added to a level 1 audit scheduled to be completed in August 2023 (see the section titled Level 1 audit – August 2023).
There was no indication in any of the CASA documentation that the complaints received were followed up during or after either surveillance event.
CASA stated that complaints regarding the safety culture of an organisation that did not have a safety management system (SMS) were difficult to assess, and there was no guidance given to inspectors on what to specifically assess. As such, an assessment, if completed, would be subjective to the person completing it. An in-depth assessment of an organisation’s culture required people to be prepared to talk about specific events or actions to ensure the context of the situation was fully understood.
Surveillance activities
A level 1 CASA audit was a detailed evaluation that assessed an aviation organisation's compliance with regulatory and safety standards. Such an audit encompassed various aspects of the organisation’s operations, including:
the SMS
operational control
maintenance
airworthiness
training
competency
regulatory adherence.
It involved a sample of operational aspects, often including extensive documentation reviews, interviews, and inspections. It aimed to identify both systemic issues and specific non-compliance or safety concerns. Any findings from a level 1 audit required the organisation to implement corrective actions to enhance safety and ensure continuous compliance with aviation regulations. The audit was typically scheduled at regular intervals or when there was a significant change in the organisation’s operations, such as new certifications, major incidents, or regulatory changes. The last level 1 audit on Broome Aviation prior to the accident was conducted on 19 October 2018.
A level 2 CASA surveillance activity was a more focused evaluation conducted to examine specific areas of an organisation's operations. This type of surveillance was typically less comprehensive than a level 1 audit and entailed an examination of aspects such as operational procedures, training programs, or maintenance practices. This surveillance was often conducted in response to a specific incident, identified risks, previous audit findings, or as part of ongoing surveillance and monitoring efforts. The last level 2 surveillance activity on Broome Aviation prior to the accident was conducted on 19 August 2018.
At the beginning of March 2023, the CASA surveillance team approved a level 2 surveillance activity on the operator. This was initiated as a result of:
the complaint received by CASA in November 2022 regarding allegations of operational pressures placed on flight crew by the CEO
the process surrounding the assessment and appointment of a temporary HOFO while the substantive HOFO was on leave.
The surveillance was scoped to cover both topics and involved a site visit conducted by the RO FOI on 14 June 2023, 6 days before the accident. The scoping did not outline how the complaint received by CASA would be assessed during the surveillance and the surveillance report was finalised on 11 July 2023.
During the surveillance, discussions were held with the interim HOFO regarding their position and level of oversight of operations, noting they were working full time for another operator at that stage. It was concluded that the interim HOFO was providing a level of oversight and interaction with personnel, and this was achieved via:
regular discussions with crew
oversight of schedules and flight and duty via the organisation’s systems
conduct of company proficiency flights / line and remedial training with flight crew
some limited formal governance meetings.
The surveillance report noted that no documentation could be supplied to demonstrate that both informal and formal meetings were being conducted during the interim HOFO’s time in the position. CASA issued a safety observation to Broome Aviation to review and update the content of its operations manual to include the governance processes utilised by the HOFO and establish a method and database to record such meetings and their outputs.
CASA reviewed the documentation surrounding the interim HOFO’s flight and duty times at both organisations and assessed that these complied with regulatory requirements.
The RO FOI advised the ATSB that they had concerns about the level of oversight the interim HOFO was providing for Broome Aviation during the time they were concurrently employed as an alternate HOFO at another local operator. They noted the interim HOFO’s view of the position seemed to revolve around being there for a short time. This concern was not documented on the final audit report.
The final surveillance report contained no mention of the November 2022 complaint and how it was assessed during the surveillance activity, and there was no other documentation to explain why the complaint was not mentioned in the report. The RO FOI stated that the complaint gave little information around the specifics of the incident, making it hard to check while at the operator.
When asked if any of the pilots were interviewed regarding the topic of operational pressures, the FOI stated they witnessed pilots coming in and out of the office area while they were conducting the meeting with the interim HOFO and ‘everyone seemed happy’. They also recalled there was no indication there was anything out of the ordinary that would have made them want to talk to any of the pilots. The RO FOI stated that it was generally possible to find a way of talking to pilots during surveillance activities and they had done so on previous occasions (with other operators), but did not see the need to do so on this occasion. There was no indication the operator’s management was aware of the complaint at the time the audit was conducted.
CASA’s processes required that this surveillance report was submitted to the RO FOI’s manager for approval prior to the audit being finalised. The absence of any content about the complaint, one of the 2 reasons for the surveillance activity, was not addressed during the approval process.
A level 1 audit on the operator was conducted in August 2023. The audit’s scope originally covered:
airworthiness assurance
data and documentation
operational support systems
safety assurance
safety risk management.
It was subsequently expanded to include aspects associated with the apparent circumstances of the C310 accident, focusing on the fuel policy, flight planning, and training, and the 2 further complaints submitted to CASA on the operational pressures placed on flight crew. The audit team consisted of 3 inspectors, and included a site visit conducted on 28 August.
The audit found multiple issues with the operator’s operations manual. It noted that, although it met the basic requirements, it had not been updated in accordance with legislative changes. It also noted that the operations manual was not compliant with CASR Part 91/135 fuel and flight planning requirements.
The audit also identified that there was a general weakness with regard to the content and detail of the operations manual, in particular the policy and procedure surrounding the induction, operational training and release to line of junior pilots. The RO FOI stated that, due to the operator sitting under exemption 87/21, the requirements for meeting a training and checking system were not in place at the time. This situation meant no safety finding could be issued regarding the weaknesses in training and checking.
The audit found that, although the operations manual had an extensive section relating to operational use of maintenance releases (MRs), some references were either no longer valid or current legislative references were missing. It also found that Broome Aviation was no longer following the process for monitoring MRs and MELs that it had outlined in its maintenance control manual (MCM). The MRs of aircraft current at the time were not reviewed during this audit.
Previous level 1 audit
During the previous level 1 audit in October 2018, an airworthiness inspector noted various deficiencies with an aircraft during a ramp inspection. These deficiencies had not been entered into the MR or other aircraft documentation. The operator was given a list of these deficiencies in the surveillance report. No other aircraft or MRs were inspected during this event.
After the FOI was informed about the deficiencies on the aircraft, they identified that pilots’ maintenance training was not being conducted in accordance with the MCM or the operations manual. CASA recommended the operator undertake an educational program to provide guidance for the pilots in the following areas:
conducting accurate pre-flight inspections
entering defects into maintenance releases
checking for any potential items that could pose a risk to flight
correct use of maintenance releases.
CASA confirmed that Broome Aviation completed this educational program with all pilots who were employed at the time.
Related occurrences
Numerous fuel management and fuel starvation incidents and accidents have previously been investigated by the ATSB, including:
Engine power loss and forced landing involving Pilatus Britten-Norman Islander BN-2A VH‑WQA, Moa Island, Queensland on 3 October 2022 (AO-2022-046)
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040)
Cessna C310R, VH-HCP, 3 km east of Newman Airport on 26 January 2001 (200100348)
The ATSB found that pilot understanding of, and management of aircraft fuel systems played a crucial role in these occurrences.
Safety analysis
Introduction
On the return leg of a flight from Turkey Creek to Derby, Western Australia, the pilot encountered dual engine surging. The pilot, assessing this was due to fuel starvation, began switching fuel tanks to utilise any remaining fuel. With no resolution, the pilot initiated a MAYDAY call to Brisbane Centre air traffic control, alerted the passenger to the emergency, and told them to brace for impact. During the subsequent forced landing, the right wing of the aircraft hit a tree causing the aircraft to turn 180⁰ and come to an abrupt stop on the edge of the highway.
The pilot sustained serious facial injuries, and the passenger sustained minor injuries. The aircraft was substantially damaged.
This analysis firstly considers the pilot’s fuel management during both the first and second leg of the flight, the response to the emergency, and survivability aspects relating to the injuries of those onboard. It also discusses contextual factors that potentially influenced the pilot’s performance during this period.
The analysis then discusses several other safety factors identified during the investigation related to pilot training and consolidation, operator oversight, organisational aspects and regulatory oversight. These factors either contributed to the accident, or increased aviation safety risk more generally.
The safety factors are discussed under the following topics:
management of fuel
response to the emergency
factors influencing pilot performance
defect reporting
legibility and accuracy of aircraft internal placards
survival aspects
operational pressures
regulatory oversight.
Management of fuel
Pre-flight planning
Pre‑flight planning is vital to ensure there is sufficient fuel for all phases of the flight. This includes accounting for fuel required for taxi, take-off, climb, cruise, descent, landing and the required fuel reserves.
The pilot used the operator’s flight planning software to plan the flight, however they did not know how to input forecast winds and reported that they routinely planned using nil wind. The operator also provided a manual system that would have enabled the pilot to accurately plan the fuel requirements for the flight. A pilot in command is required to ensure the relevant meteorological forecasts are considered when determining the quantity of fuel required for a flight.
Taking into account the known environmental conditions and the aircraft’s fuel consumption, if the pilot had used the available wind data, the flight plan would have identified to the pilot that the planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route.
Pilot perception of fuel available in the auxiliary tank
The pilot conducted all their flights in the Cessna 310 (C310) with the assumption that the auxiliary tanks could not be used for longer than 45 minutes without the engines surging and so used the auxiliary tanks for 40 minutes. While it is likely that this behaviour was due to the reverse leak in the right auxiliary tank check valve, the ATSB was unable to conclusively determine if this was the reason for the engine surging reported by the pilot on the day of the accident.
As a result, the pilot had not intended to use all the usable fuel on board, reducing their actual endurance. However, this was not reflected during flight planning.
Contributing factor
The planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available.
Broome to Turkey Creek
On assessing the remaining fuel following arrival at Turkey Creek, the pilot reported that it was unevenly distributed, with the right auxiliary tank full and less than expected in the right main tank. The ATSB considered the following possibilities to account for this reported distribution:
the pilot did not switch the right main tank to the right auxiliary fuel tank en route to Turkey Creek
the fuel leaked from the main tank to the auxiliary fuel tank on the ground at Turkey Creek.
Testing of the right auxiliary tank check valve indicated that, although there was a leak through the tank vent outlet bleed return line check valve, it is unlikely this leak was large enough to have resulted in the 40 L discrepancy the pilot experienced on the day of the occurrence. In addition, it is very unlikely that the amount of fuel that leaked would have been equal to the amount of fuel which would have been used if the pilot had selected the auxiliary tank during this leg of the flight. As such it was assessed that it was more likely that the pilot did not select the auxiliary tank on the right side during the flight.
This resulted in the pilot having full fuel in the right auxiliary fuel tank at Turkey Creek and 40 L of fuel less in the right main tank than the pilot expected.
Upon returning to the aircraft and completing pre‑flight checks, the pilot did not visually confirm the right auxiliary tank was full. As the fuel gauges in the aircraft were known to be inaccurate, a visual inspection of the auxiliary tank would have verified if it was full.
Return flight leg
The pilot routinely flew the aircraft with the main tanks selected for 60 minutes after take-off on each leg of a flight, rather than the 90 minutes detailed in the pilot’s operating handbook (POH) for the larger tanks fitted to VH‑DAW. While the pilot advised this was how they simplified inflight fuel management, that practice increased the risk of fuel being vented overboard from the main tanks.
When the pilot switched from the main tanks to the auxiliary tanks on the second leg of this flight, it is likely the right main tank had only approximately 4 L of fuel remaining, and the left main tank had approximately 44 L remaining.
The ATSB could not establish why the right engine reportedly surged when selected to the right auxiliary tank, as there should have been approximately 97 L of fuel in the tank, and the reported issue with the check valve occurred when the fuel level in the auxiliary tank was approximately half (60 L).
When the pilot reselected the right main tank in response to the surging, the amount of fuel contained in the tank would have increased to approximately 12 L due to the fuel returned when using the auxiliary tank. After a further 10 minutes, the right engine again surged, this time most likely due to fuel starvation, resulting in pilot crossfeeding to the left main tank, which also had minimal fuel at that stage.
Fuel calculations conducted by the ATSB determined that when the right engine was crossfed to also draw fuel from the left main tank there was approximately 34 L of fuel left in that tank. About 10 minutes later, the engines began surging as the fuel in the left main tank was reduced to approximately 9 L of useable fuel. While it could not be determined why that quantity was insufficient to maintain continuous power, supply issues associated with an inoperative transfer pump (due to the observed tripped circuit breaker) and/or debris and other contaminants in the bottom of the fuel tank were possibilities.
Contributing factor
It is likely that the pilot did not utilise the right auxiliary fuel tank during the first leg of the journey and did not manage usage from the main fuel tanks in accordance with the pilot's operating handbook. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained.
Continued operation with defective fuel gauges
Multiple pilots who flew the aircraft stated that the fuel gauges did not indicate the correct amount of fuel in both the main and auxiliary tanks. Multiple pilots recalled that the gauges would become more accurate as fuel was burnt, however images of the gauge after flights indicated there was a still a large disparity between the 2 sides. The reading for both the main tanks and the auxiliary tanks were determined to be significantly out of tolerance and did not show an accurate amount of fuel on board for most of the flight.
Accurate fuel gauges are crucial in an aircraft to ensure precise monitoring of fuel levels throughout the flight, directly impacting safety and operational efficiency. They provide the pilot with real-time information about the quantity of usable fuel, allowing for informed decision-making during critical phases of flight, such as when a diversion is required or in an emergency. Although the pilot was aware that the fuel gauges were unreliable, they relied on the indicated readings at multiple points in the flight.
CASA guidance stated that an operator’s exposition should detail the maximum allowable discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure, noting that industry practice was a maximum of 3% variation. This percentage was not outlined in the operations manual, and the gauge defects were not recorded on the maintenance release.
However, the ATSB assessed that the gauge display defect did not contribute to the accident as the pilot was able to assess the fuel quantities in the fuel tanks throughout the flight.
Other factor that increased risk
The aircraft fuel gauges did not indicate accurately.
Operator’s procedures for fuel management
Pre-flight
A review of Broome Aviation’s pre-flight planning software identified that it did not include the 47 L block (total) fuel margin required under the operator’s fuel policy. It did however have a fixed fuel flow rate for climb of 150 L/hr. Conversely, the documented fuel planning figures to be used for manual fuel calculations did not include a fuel flow rate to use for climb. Although the operator was unaware of where the 47 L requirement originated from, the ATSB assessed that the margin it provided would cover the additional fuel flow used during climb, despite not being originally intended for that purpose.
Inflight
Broome Aviation’s operations manual required pilots to conduct an inflight fuel check when reaching cruise or if needing to divert. It did not contain guidance on:
conducting fuel checks at regular time intervals
assessing fuel burn rates
verifying the remaining fuel relative to the reserves required for contingencies, alternate routing, and final reserve fuel
the maximum allowable discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure.
This resulted in pilots using a variety of procedures.
Under the Civil Aviation Safety Authority (CASA) Manual of Standards (MOS) 135 Part 7, operators are required to outline inflight fuel management procedures. CASA’s Advisory Circular (AC) 91-15 Guideline for aircraft fuel requirements stated that pilots should have 2 sources of fuel values to crosscheck the available fuel on board. While the operator’s pilots were using a time‑based approach to their fuel calculations in flight, they did not have a viable crosscheck as the fuel gauge was inaccurate. A crosscheck process mitigates the reliance on a single source of information and ensures that any fuel related issues, such as high burn rates or fuel system defects, are promptly detected and managed, reducing the risk of fuel exhaustion.
Although Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations, the pilot completed an inflight fuel record every time they switched tanks. When the right engine surged the second time and crossfeed to the left main tank was selected, the pilot correctly assessed the amount of fuel remaining in the left main tank. They did not however accurately assess the remaining flight duration to Derby and the associated fuel required to fly that distance, considering that the right engine would be returning fuel to the right main tank.
The operations manual also gave little guidance on decision-making frameworks to address fuel‑related issues during flight, nor did it outline clear protocol for pilots to follow in the event of a low-fuel situation, including notification to air traffic services.
Post-flight
The operator’s post‑flight cross check methods could not be completed as there was no fuel totaliser on board the aircraft and the fuel gauges were inaccurate. As such, the remaining fuel at the end of the flight was based on the pilot’s fuel calculations or a visual check by the pilots, which was not required by the operator in the post‑flight process.
Consequently, an accurate record of the fuel remaining in the aircraft was not being documented for the next pilot, nor was it being accurately entered into the operator’s data recording software for fuel flow checks. The pilots were working around this issue by ensuring the fuel tanks were full prior to every flight.
Other factor that increased risk
Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management. (Safety issue)
Response to the emergency
After crossfeeding the right engine to the left main fuel tank, the pilot was confident that the available fuel was sufficient to reach Derby. They did not consider diversion to an alternate airstrip as they were unfamiliar with the condition and suitability of the nearby airstrips. They also did not consider the option of changing the left engine fuel selection to the left auxiliary fuel tank. This would have increased the fuel available in the left tank via the extra fuel return.
In addition, as the aircraft had passed the pilot’s planned top of descent, they initiated a 400 ft/minute descent reducing the available glide altitude. Maintaining the aircraft's potential energy (altitude) is crucial for extending an aircraft's range during an engine failure, providing more landing options and time to manage the emergency effectively.
Contributing factor
After the usable fuel in the right main fuel tank had been exhausted, the pilot did not divert the aircraft to the closest airport, select the left engine selection to the left auxiliary fuel tank, or maintain altitude to increase the safety margin.
Recognising the stress induced by an emergency, indecision during an engine power loss situation reduces the time available for a pilot to plan and conduct an effective forced landing. Delays caused by prolonged troubleshooting, uncertainty over the severity of the issue, or hesitation in selecting a course of action consumes valuable altitude.
Once both engines began surging, the pilotidentified that the left main tank had been drained of fuel and began to switch tanks in an attempt to utilise any remaining fuel. This included attempting to gain fuel from the main tanks a second time. Although the aircraft’s certification stipulated that power must be restored to the engines within 20 seconds in level flight if fuel was depleted from a tank, this requirement applied to level flight conditions and not during a descent phase. In a descent, the restoration of power, potentially extended beyond the 20 second threshold due to gravitational effects and reduced pressure in the fuel system.
At this point, only the auxiliary tanks had enough fuel to sustain engine power, but these tanks did not have fuel pumps to supply fuel to the engines. Textron advised that if the engines remained operating and the auxiliary tanks had been selected, the fuel could have been drawn from these tanks via the engine‑driven fuel pumps. As detailed above, it could not be established why the engines did not continue to operate at that stage as a small quantity of usable fuel remained in the left main tank.
There were 3 minutes between the start of the engine surging and the pilot's MAYDAY transmission. In this timeframe, a pilot who was experienced on the C310 would have had sufficient time to shut down and secure both engines (including feathering the propellers) and establish a glide approach. However, the pilot had limited familiarity with the aircraft fuel system, limited practical emergency procedure training on the C310, and the fuel gauges were faulty. As such, it is likely they struggled to methodically cycle through the fuel tanks while monitoring for engine response under the pressure of an unfolding emergency. During this time, the pilot also opted to continue to track towards Derby Airport, which increased the distance to the highway landing site, and delayed making a MAYDAY broadcast.
While acknowledging that if the pilot had been able to re‑supply the engine/s with fuel and restart at least one of them, they could have continued to Derby, the delay associated with the multiple tanks selections ultimately compromised the safety and control of the forced landing.
Factors influencing pilot performance
A review of the pilot’s activity in the days leading up to the accident identified an early wake-up time and long duty day. However, there was insufficient evidence to conclude that the pilot was experiencing a level of fatigue known to affect performance prior to, or during, the flight. The ATSB examined in detail the potential effects of experience and consolidation of skills around fuel planning and fuel management on the development of the accident.
Pilot experience and consolidation on the Cessna 310
Acquiring new skills, such as learning to fly a new aircraft type, requires training and practice. As the amount of experience on the aircraft increases, generally a pilot’s proficiency will improve, and performing tasks will become more automated and require less attention or mental resources (Wickens and others 2015, Stothard and Nicholson 2001). Prolonged gaps when flying an aircraft type have been known to affect skills, such as familiarity with specific aircraft systems, aircraft handling, and emergency procedures.
After completing their IPC on the C310 in December 2022, the pilot had a 130-day gap before their check-to-line flight in April 2023. This limited the opportunity for skill retention on the aircraft.
In addition, as the interim HOFO did not conduct any flights with the pilot that involved the use of auxiliary fuel tanks, there was no opportunity for the HOFO to see that the pilot was limiting their use of fuel from the auxiliary tanks to 40 minutes and the implications this had for fuel planning. Similarly, there was no opportunity to observe that the pilot was only using the main tanks for 60 minutes on every departure. The pilot also only began flying the C310 operationally after the interim HOFO had returned to their original operator. While the interim HOFO recalled discussing the pilot’s first flights with them, the pilot advised they only discussed operation of the aircraft with a pilot who had left the organisation.
Contributing factor
The pilot had limited understanding of the aircraft fuel planning and inflight fuel management, but due to a lack of consolidation training and limited to no operational oversight these issues were not detected by the operator.
Operator continued oversight and guidance
Pilots at Broome Aviation reported that the interim HOFO was unavailable most of the time between March and June 2023 due to their second job. Although the interim HOFO advised that they were available for any calls and were at the operator’s premises every day informally, the overall impression of pilots was that they were learning on their own and that they received little to no guidance on the operation of the C310.
In addition, the interim HOFO’s recorded flight and duty times indicated that, although they reported that they visited the operator often, there was limited available time to oversee the operation. CASA personnel noted they had concerns about this aspect, and stated they received limited evidence to prove appropriate oversight was being conducted. During a surveillance event conducted shortly after the accident, CASA issued a safety observation to the operator to update the contents of its operations manual to include governance processes to record interactions between the HOFO and the operator’s flight crew.
At the time of the accident, as the operator was operating under an exemption from some Civil Aviation Safety Regulations (CASR) Part 135 (Australian air transport operations – smaller aeroplanes) requirements, there were no specific regulatory requirements for them to provide additional consolidation flights for pilots transitioning to the C310. For many types of transitions, such as to a new single engine aircraft type, consolidation may not be necessary. However, when moving from single-engine to relatively complex multi-engine aircraft, a period of consolidation flights is an effective risk mitigator.
The operator had limited processes in place to ensure pilots with low time and experience on the C310 had the opportunity to effectively consolidate their skills prior to (or after) being checked to line. The substantive HOFO stated that they expected pilots new to the C310 to have completed multiple ICUS flights prior to a check-to-line flight. However, coincident with the substantive HOFO being on leave, several senior pilots left the organisation and the interim HOFO returned to work for their original operator. In combination this left limited capacity to supervise pilots.
Pilots who flew the C310 for the operator between November 2022 and June 2023 reported receiving limited training on the aircraft prior to being checked to line, noting they had expected to have completed more ICUS flights. Of the 7 pilots the ATSB contacted regarding C310 operations, 2 pilots reported they received less than the 5 hours required by the operator to fly under VFR, prior to being checked to line. Most pilots were checked to line with less than 10 hours on type. The pilot of the accident flight and one other casual pilot had limited MEA experience prior to being checked to line, having only flown one other MEA type, which was during their flight training.
Additionally, the interim HOFO had limited hours on MEA and the C310 prior to assuming the position at Broome Aviation. They accumulated a further 57 hours of MEA operation, including 23 hours on the C310, prior to checking the pilot of the accident flight to line. However, it is likely the interim HOFO’s limited experience on the aircraft type impacted the depth and accuracy of operational guidance provided to pilots during line checks, as well as the ongoing oversight of their flying performance.
Due to the relatively complex fuel system on the C310, pilots transitioning to the aircraft type require a thorough understanding of the system’s layout, managing fuel during normal and abnormal operations, and recognising potential problems. While this knowledge can be obtained via ground‑based study of the system, supervised practice helps ensure pilots develop the necessary skills and confidence to operate the system safely and effectively in all conditions. Most pilots who flew the C310 received little to no guidance on its fuel system.
Contributing factor
During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. (Safety Issue)
Defect reporting
Recording defects on a maintenance release (MR) allows for the timely identification, assessment, and rectification of issues that could impact an aircraft’s performance or safety. This process ensures that maintenance personnel have a clear understanding of any outstanding defects requiring attention, thereby reducing the risk of oversight or miscommunication during maintenance activities. It also records important information for pilots operating the aircraft.
Furthermore, documenting defects on a MR creates an auditable maintenance history, which is essential for tracking repairs, modifications, and inspections over the lifecycle of the aircraft. This documentation is also a regulatory requirement, ensuring compliance with regulatory standards.
There were aircraft defects that had not been recorded on the MR, including inaccurate fuel gauges and a partially‑unserviceable autopilot. Although the operator had a process for pilots to report defects, this had generally not been followed by the pilots. The pilots advised that they would often talk to individuals in the maintenance facility after a flight about any defects or issues they had noted. Through this process, straightforward defects would likely be rectified but nothing would be written on the MR. However, defects requiring longer maintenance time and multiple parts, they reported being advised by maintenance personnel that the operator would not pay for the defect to be rectified and so consequently were not reporting them.
This situation meant that when the pilot of the accident flight encountered defects, such as the engine surging, they did not report the concern. Consequently, this reduced the likelihood that the interim HOFO would become aware of the issue and arrange for it to be resolved, or at least communicated to the company pilots.
Of the serviceability‑related issues raised by the pilots, the fuel gauges and the autopilot were assessed to have been inoperable at the time of the flight. The interim HOFO did not themselves report the gauge defects or encourage the pilots to do so.
Contributing factor
Aircraft defects were not written on the maintenance release, leading to several defects not being rectified or managed. (Safety Issue)
Legibility and accuracy of aircraft internal placards
The fuel selector placards fitted to VH‑DAW were incorrectly labelled, with both placards indicating that the aircraft was fitted with the smaller auxiliary tanks. In addition, the placard stating that the main fuel tank should be used for 90 minutes after take-off was missing and some of the internal fuel-related placards within the cockpit of the aircraft were partially illegible.
The ATSB determined that these issues likely did not contribute to the occurrence as the pilot was aware the aircraft had the larger auxiliary tanks, and the pilot did not notice the discrepancy between the size of the tanks and the placard. Despite that, in aircraft like the C310 with specific fuel usage requirements, fuel placarding plays a critical role in ensuring accurate operation of the fuel system.
Survival aspects
Upper torso restraints
A substantial body of research has demonstrated that wearing upper torso restraints (UTRs) in small aircraft significantly reduces the severity of injuries compared to wearing only a lap belt. In particular, UTRs reduce the risk of head, neck and upper body injuries, associated with the person’s upper body flailing forward. An NTSB study published in 2011 found that when wearing a lap belt only, a pilot was 49% more likely to receive a serious or fatal injury, compared to those wearing both the lap belt and UTR.
The pilot of VH-DAW was not wearing the aircraft’s sash-type upper torso restraint (mounted above the pilot’s left shoulder) at the time of the accident. The pilot received significant injuries, when they impacted the dash of the C310.
That injury outcome was consistent with the findings of previous ATSB investigations, which found that pilots or passengers in the front seats of small aeroplanes and helicopters have not always worn the available UTRs, exacerbating the severity of their injuries in many accidents (for example, ATSB investigations 199800442, 200605133, AO-2010-053, AO-2012-083, AO-2012-142, AO-2016-074, and AO-2022-027).
It is very likely that the severity of pilot’s head injuries would have been reduced if they had been wearing the available UTR.
Contributing factor
The pilot was not wearing an upper torso restraint during the accident flight, resulting in the pilot receiving avoidable serious head injuries during the collision.
Emergency locator transmitter
The CASR Part 135 Manual of Standards required aircraft that were flown more than 50 NM from the departure aerodrome to carry an automatic emergency locator beacon (ELT), however at the time of the accident there was an exemption for the aircraft to operate with a portable ELT.
A portable ELT requires manual activation during an emergency landing and on this occasion the pilot was rendered unconscious during the accident sequence and the passenger did not know the exact location of the portable ELT. Therefore it is very likely that if a forced landing of similar severity had occurred in a more remote location, notification of the accident to emergency services would have been significantly delayed. That in turn may have led to a more severe outcome for the aircraft’s occupants.
An effective safety culture relies on open communication channels, where employees can report hazards or errors without fear of reprisal. In this case, pilots reported to the ATSB that they experienced pressure from individuals in senior management to avoid recording defects on the MR, particularly those that could lead to operational delays, and pressure to conduct flights with aircraft that they considered were unsafe for flight. The sample involved several pilots selected by the ATSB based on them performing similar roles to the pilot involved in this accident. All the information they provided was consistent with similar concerns also reported to CASA by other pilots, together with a related complaint from a passenger.
The pressure the pilots reported experiencing led to them regularly flying aircraft with defects. With regards to the C310, pilots developed an understanding that it was normal and approved practice to conduct flights in an aircraft with inaccurate fuel gauges, an autopilot incapable of holding altitude and engines prone to surging.
In addition, the pressure the pilots reported experiencing probably led to them being less likely to formally report defects or discuss them with senior management as they had developed an understanding that they would not be remedied.
Based on the available evidence, management personnel were not fully aware of all the aircraft defects that the pilots were managing. If the defects had been formally reported through the defect reporting process, it is more likely they would have been discussed and, if they could not be rectified, then a more considered approach developed to manage the problem. For example, the issue around fuel supplied from the auxiliary fuel tanks would probably have been investigated further, or a mitigation put in place.
A study completed on the factors influencing the decision‑making of commercial pilots flying in outback Australia found that it was common for them to feel pressured to make risky decisions and commit ‘violations’ due to threat of employment termination. It also noted that career ambition was an important factor, with pilots seeking to build flight time for future employment with major airlines, leading them to take risks while flying (Michalski and Bearman, 2014). The extent to which this situation exists within the small aircraft air transport sector is difficult to determine, however the evidence from this investigation indicates that it existed within this operator.
Contributing factor
Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight. (Safety Issue)
Regulatory oversight
The purpose of regulatory oversight is to ensure operators are meeting regulatory standards and to monitor the ongoing safety, health and maturity of the operators. This oversight is comprised of both regulatory services activities and surveillance activities.
CASA response to complaints
CASA received a complaint in November 2022 regarding operational issues at Broome Aviation. This complaint was included in the scope of a level 2 surveillance activity conducted by CASA in June 2023, the week prior to the accident. The CASA regulatory oversight flight operations inspector (RO FOI) determined there was no reason to question pilots regarding the complaint after noting the pilots seemed ‘happy’. This perception occurred in an open environment where the FOI, the interim HOFO and the CEO were present with the pilots.
As CASA noted, complaints regarding the safety culture of an organisation that does not have a safety management system (SMS) can be difficult to assess. Interviews with pilots can provide valuable information, but the usefulness of that information can be limited if only a small sample size was used (and confidentiality could not be maintained), or corroboration from some form of documentary evidence could not be identified. Although there are clearly challenges with examining these types of topics during surveillance activities, on this occasion it appears an important opportunity was missed when the RO FOI did not discuss these concerns with any of the current pilots or bring it to the attention of the operator.
When the surveillance report was submitted by the RO FOI to their supervisor, the RO FOI was not questioned as to why the complaint had not been assessed, even though it was a key reason for the surveillance activity. This was a second missed opportunity for CASA to assess the safety culture within the operator.
When CASA received 2 further complaints after the accident, it had a further opportunity to examine operational issues which encompassed all 3 complaints. Although the complaints were added to the scoping of the level 1 audit in August 2023, the contents of the audit report indicated that they were again not investigated.
Acknowledging CASA’s difficulty with assessing the safety culture of such an organisation, there were multiple pilots within the organisation who could have provided valuable insights given their extended time and familiarity with the operator. Engaging with these individuals during either of the surveillance activities would have allowed CASA to gather a broader perspective and determine whether the reported organisational issues were systemic or simply reflective of dissatisfaction from potentially disgruntled former employees. As demonstrated during this investigation, there were widespread concerns about these matters within the pilot group.
Contributing factor
Following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, CASA conducted a level 2 surveillance activity on the operator in early June 2023 and following further complaints, a level 1 audit in August 2023, with key scope elements being to evaluate the complaints. Despite that, the surveillance activities and the associated reports did not assess the subject of the complaints.
Head of flying operations assessment
Broome Aviation’s interim HOFO was firstly assessed by CASA for the position of alternate HOFO for another operator (operator 2) and then again for the position of alternate HOFO for Broome Aviation. CASA was unable to provide documentation outlining the specific elements discussed during the first assessment, so it was not possible to confirm what was specifically covered during that process.
The retention of assessment records ensures accountability and transparency in the evaluation process, including a documented trail of decisions. This transparency is important to ensure that any regulatory approval by CASA is supported by clear, justifiable, and objective assessments. Such records also assist CASA with future assessments of the same candidate.
In this case, this first assessment was used as a basis for CASA’s alternate HOFO assessment of the same candidate for Broome Aviation 19 days later, enabling the process to be expedited. The FOI specified that this assessment was for the alternate HOFO position, however the approval given was for the HOFO position. Although CASA advised that the assessment process for an alternate HOFO and a HOFO position was the same, the FOI noted that they did not complete a full assessment of the applicant’s experience due to the expected short timeframe of the appointment.
In addition, although no time limitations for a HOFO position could be recorded on the official approval, CASA accepted Broome Aviation’s operations manual, which nominated the substantive HOFO as the HOFO and the newly assessed HOFO in the alternate HOFO position. The operations manual also did not outline how the alternate was going to manage the dual positions while being employed for operator 2 conducting check and training for its pilots and full-time flying, and fulfil the HOFO duties for Broome Aviation. CASA was aware that the substantive HOFO would be on leave and the alternate HOFO would be the acting HOFO.
CASA did not contact the operator at the end of the month despite only assessing the HOFO for one month. When the operator was advised that the substantive HOFO was extending their leave beyond April, they did not advise CASA of the change in circumstances within 7 days as required.
Upon discovering in February 2023 that the interim HOFO had been conducting the role for longer than the timeframe considered in the assessment, the CASA RO FOI discussed the matter with the interim HOFO. However, CASA did not re-assess the suitability of the interim HOFO to act for an extended period, and to ensure that the interim HOFO was available to effectively oversee Broome Aviation pilots when they returned to operator 2 in March 2023.
The dual arrangement of a pilot serving as HOFO for one operator and full‑time line pilot for another, posed challenges with:
operational priorities
workload management
operational oversight
compliance with regulatory requirements.
In this instance, the interim HOFO reduced their flying duties at Broome Aviation to return to flying and conduct check and training for operator 2. The reduction resulted in the interim HOFO having reduced oversight of Broome Aviation pilots during the March–June 2023 period.
Under CASR regulations, key personnel must demonstrate the capacity to discharge their responsibilities fully and effectively. CASA emphasised that it is ‘highly unlikely’ for key personnel to meet this requirement when performing similar duties for multiple operators simultaneously. If this dual arrangement is pursued, the second operator must clearly outline in its exposition how a HOFO will fulfill their responsibilities. This includes ensuring sufficient availability and capability to respond promptly to operational demands. Although in this case CASA personnel stated concern for the operation and oversight of Broome Aviation at the time, the 4-month period in which the interim HOFO was working for both operators resulted in Broome Aviation effectively having little oversight of its pilots.
Contributing factor
The Civil Aviation Safety Authority approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment due to an expectation that it was an interim appointment, and they had already been assessed. The person subsequently remained in the position for a much longer period. When this was identified by CASA, it did not fully assess the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation and forced landing involving Cessna 310R, VH-DAW, about 5 km south‑east of Derby Airport, Western Australia on 20 June 2023..
Contributing factors
The planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available.
It is likely that the pilot did not utilise the right auxiliary fuel tank during the first leg of the journey and did not manage usage from the main fuel tanks in accordance with the pilot's operating handbook. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained
After the usable fuel in the right main fuel tank had been exhausted, the pilot did not divert the aircraft to the closest airport, select the left engine selection to the left auxiliary fuel tank, or maintain altitude to increase the safety margin.
The pilot had limited understanding of the aircraft fuel planning and in‑flight fuel management, but due to a lack of consolidation training and limited to no operational oversight these issues were not detected by the operator.
During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. (Safety Issue)
Aircraft defects were not written on the maintenance release, leading to several defects not being rectified or managed. (Safety Issue)
The pilot was not wearing an upper torso restraint during the accident flight, resulting in the pilot receiving avoidable serious head injuries during the collision.
Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight. (Safety Issue)
Following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, CASA conducted a level 2 surveillance activity on the operator in early June 2023 and following further complaints, a level 1 audit in August 2023, with key scope elements being to evaluate the complaints. Despite that, the surveillance activities and the associated reports did not assess the subject of the complaints.
The Civil Aviation Safety Authority approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment due to an expectation that it was an interim appointment, and they had already been assessed. The person subsequently remained in the position for a much longer period. When this was identified by CASA, it did not fully assess the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO.
Other factors that increased risk
The aircraft fuel gauges did not indicate accurately.
Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management.
Safety issue description: During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system.
Safety issue description: Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight.
Glossary
AC
Advisory circular
AMC
Acceptable means of compliance
AME
Aircraft maintenance engineer
AOC
Air operators’ certificate
AWB
Airworthiness Bulletin
BAM
Broome Air Maintenance
CAO
Civil Aviation Order
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulation
CEO
Chief executive officer
ELT
Emergency locator transmitter
FDP
Flight duty period
FOI
Flight operations inspector
FOR
Flight operations regulations
FQIS
Fuel quantity indicating system
GM
Guidance material
HAMC
Head of maintenance control
HOFO
Head of flying operations
ICUS
In command under supervision
IFR
Instrument flight rules
IPC
Instrument proficiency checks
LAME
Licenced aircraft maintenance engineer
MCM
Maintenance control manual
MEA
Multi engine aircraft
MEL
Minimum equipment list
MOS
Manual of standards
MR
Maintenance release
POH
Pilot operating handbook
RO FOI
Regulatory oversight flight operations inspector
RPT
Regular public transport
SMS
Safety management system
SOM
System of maintenance
STC
Supplement type certificate
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passenger of the accident flight and multiple other company pilots
the head of flying operations at the time of the accident
the operator and substantive head of flying operations of Broome Aviation
Civil Aviation Safety Authority (CASA)
Western Australia Police Force
Textron Aviation
the maintenance provider for VH-DAW (Broome Air Maintenance)
the maintenance tracking provider and logbook controller for Broome Aviation (Avtrac Maintenance Tracking)
Airservices Australia
video footage of the accident flight and other photographs and videos taken on the day of the accident
Stothard C & Nicholson R 2001, Skill acquisition and retention in training: DSTO support to the army ammunition study, Defence Science and Technology Organisation, report DSTO-CR-0218.
Wickens CD, Hollands JG, Banbury S & Parasuraman R 2013, Engineering psychology and human performance, 4th edition, Pearson Boston, MA.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
other pilots interviewed during the investigation
Broome Aviation
Civil Aviation Safety Authority
Textron Aviation
National Transport Safety Bureau
Broome Air Maintenance
Submissions were received from:
the pilot
other pilots interviewed during the investigation
Broome Aviation
Civil Aviation Safety Authority
Textron Aviation
Broome Air Maintenance
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR) are a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[3]The substantive HOFO held the position with the operator prior to December 2022 and after June 2023.
[4]The interim HOFO held the position from December 2022 to June 2023.
[5]Broome Aviation was in a transitional state to the Civil Aviation Safety regulations Parts 119 and 135 requirements and still used a document known as an operations manual rather than the exposition required by the new regulations.
[6]VMCA: the minimum speed, while in the air, that directional control can be maintained with one engine inoperative.
[7]An imperfection that impairs the structure, composition, or function of an object or system of an aircraft or component.
[8]Inoperative: an item for a flight of an aircraft is inoperative if, due to a defect, the item, or a function of the item, does not accomplish its intended purpose, or consistently function within the operating limits or tolerances mentioned in the approved design for the item or the flight manual for the aircraft.
[9]Under previous legislation, air transport operations were split into regular public transport (RPT) and charter flights.
[10]Elevator flutter: refers to an uncontrolled, rapid oscillation or vibration of the elevator control surface. This phenomenon can occur due to aerodynamic forces, structural dynamics, or a combination of factors.
[11]The Cessna 310R POH detailed numerous fuel flow rates for specific power settings.
[12]This was a conservative rate of fuel burn as the engine manufacturer could not give an expected fuel return rate as this was dependent of the engine power used and the conditions on the day.
[13]Medical restriction, as defined by the operator, was any condition that required the carriage of an additional flight crewmember.
[14]CASA EX87/21 was an exemption instrument providing certain operators with deferrals from specific requirements of the Flight Operation Regulations particularly concerning safety management systems, human factors principles & non‑technical skills, and training & checking. The deferrals applied to certain operators only and were subject to conditions.
[15]Upper torso restraint: a shoulder strap or harness. A shoulder strap, when paired with a lap belt, effectively makes the occupant’s restraint similar to the seatbelt on modern cars.
[16]Portable ELT: An emergency locator transmitter that is manually activated by a pilot or passenger when in distress.
[17]Automatic fixed ELT: An emergency locator transmitter that is permanently attached to the aircraft and designed to stay attached even after a crash to aid Search and Rescue (SAR) teams in locating a crash site.
[18]Flight operations manager: plans, coordinates and controls all operational activities of all aircraft movement.
[19]HAMC: monitors and records aircraft hours, cycles and equipment maintenance and other information relevant to maintenance scheduling. Coordinates defect rectification and unscheduled maintenance activities. Reviews Airworthiness Directives for applicability and compliance.
[20]Under CASR Part 119.080(1)(c) – Conditions of an Australian air transport AOC, the operator was required to fill the HOFO position at all times and the person fulfilling the role was to be approved by CASA (whether the permanent HOFO, a permanent alternate HOFO, or a person temporarily filling the position as an interim HOFO).
[21]Broome Aviation did not have an exposition at this time – the time limitation should have been stated in the operations manual.
Occurrence summary
Investigation number
AO-2023-029
Occurrence date
20/06/2023
Location
about 5 km south-east of Derby Airport
State
Western Australia
Report release date
30/04/2025
Report status
Final
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Forced/precautionary landing, Fuel starvation
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
310R
Registration
VH-DAW
Serial number
310R0148
Aircraft operator
Broome Aviation Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Turkey Creek Aircraft Landing Area, Western Australia
Between June 2023 and April 2024, 3 misaligned take-offs at Perth Airport, Western Australia, were reported to the ATSB. Each incident occurred before first light and involved the pilots inadvertently lining the aircraft up with the edge lighting, rather than the centreline, on runway 06 prior to take-off.
On 12 June 2023, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-IWQ, was being operated on a regular passenger transport flight from Perth, Western Australia, to Sydney, New South Wales. During the take-off roll, the flight crew identified that the aircraft was aligned with the left edge lights of the runway and manoeuvred to the centreline. The flight continued without further incident. A subsequent aircraft and runway inspection did not find any damage.
On 10 August 2023, a Western Sky Aviation Cessna Conquest 441, registered VH‑NSA, was being operated on a passenger charter flight from Perth to Southern Cross, Western Australia. During the take-off roll, the pilot detected an impact with the aircraft. After take‑off, the pilot returned to Perth and a subsequent inspection found no aircraft damage, but identified several damaged runway edge lights.
On 4 April 2024, VH‑NSA was again operating a passenger charter flight from Perth to Southern Cross. During the take-off roll, the pilot (different to the previous incident) heard an unusual noise but believed it originated from inside the cabin. As all engine indications were normal, they continued the departure. A runway inspection conducted by the aerodrome operator later that morning found several damaged runway edge lights. The pilot identified minor damage to the propeller on the right engine after returning to Perth Airport.
What the ATSB found
The ATSB found that, in all 3 incidents, when entering runway 06 from taxiway V, the pilots taxied past the turn onto the centreline and lined the aircraft up along the runway edge lighting on the far side of the runway to where they entered. In each incident, as the pilots believed they had correctly aligned the aircraft with the runway centreline, they commenced the take-off.
Several factors known to increase the risk of a misaligned take-off in the dark were identified as present in all 3 incidents. In terms of the runway environment, there was an unlit and unmarked extended pavement area on each side of runway 06, which made the runway appear wider. In relation to the available airport lighting, the lead-on lights from taxiway V continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway’s centreline; recessed edge lights at the start of runway 06 could be mistaken for centreline lighting, and there was limited ambient airport lighting around taxiway V and runway 06 to enhance visibility. The taxi lighting on one of the aircraft was reported by the pilots as being of limited benefit. Additionally, the required runway markings were reported by 2 of the incident pilots to be difficult to see at night.
One factor specific to the flight crew in incident 1 was their attention was diverted to completing pre-take-off tasks and their take-off clearance while lining up on the runway. This divided their attention between the flight deck and the monitoring of the external environment.
The ATSB also identified differences in how the pilots responded to the misaligned take‑off. In the first incident, the flight crew identified that they had lined up in the incorrect position, manoeuvred the aircraft onto the centreline, and continued the take-off and flight. The pilot of the second incident detected an impact during the take-off roll and decided to conduct a return to Perth for further inspection. The pilot of the third incident was not aware the aircraft was misaligned on the runway edge and damage to the propeller blade was not detected until several flights later.
What has been done as a result
After the incidents in August 2023 and April 2024, Western Sky Aviation distributed notices to its flight crew that included strategies to check runway alignment prior to take‑off, including the use of an electronic flight bag aerodrome chart and integrated landing systems, where available.
Perth Airport requested an update to the Aeronautical Information Publication supplement, effective November 2023, to identify a misaligned take-off hotspot on runway 06, and highlight to pilots that runway 06 did not have centreline lighting and that there was extra pavement on either side of the runway. The En Route Supplement Australia was updated to reflect the misaligned hotspot area in March 2024. Further, in works to repaint the runway markings, completed in April 2024, Perth Airport also painted chevrons on the extra pavement on either side of runway 06 to delineate this area from the useable runway to assist pilots with determining their position prior to commencing take-off.
Following the incident in June 2023, Virgin Australia Airlines completed a number of safety actions, including:
added caution notes to its Perth Airport supplementary port information about centreline misidentification on runway 06
revised the before take-off procedure to reallocate tasks earlier in the taxi to reduce flight crew workload during line-up.
developed case studies involving this event, which were incorporated into non‑technical skills training.
Safety message
The features of airport runways and taxiways can vary, and the combination of these features or lack of guidance to assist pilots to navigate or confirm their aircraft’s position can increase the risk of runway misalignments. Further, this can be exacerbated at night‑time where the amount of visual information available is markedly reduced. These reduced visual cues can affect pilots even when they are familiar with the airport. It is important for all pilots to thoroughly brief themselves with the local conditions to increase their awareness of the environment. Pilots are also encouraged to report any circumstances where they believe they may have conducted a misaligned take-off, to limit the risk to their aircraft and others subsequently using the same runway. This would also allow aerodrome operators to identify any trends or emerging misaligned take-off hotspots to consider mitigations.
Summary video
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrences
Between June 2023 and April 2024, 3 misaligned take-off events occurred at Perth Airport, Western Australia. Each incident occurred prior to first light and involved the pilots inadvertently lining the aircraft up with the runway 06 edge lighting, rather than the centreline, prior to take‑off.
Incident 1
On the morning of 12 June 2023, the captain and first officer (FO) of a Virgin Australia Airlines Boeing 737-800, registered VH-IWQ, prepared for a regular passenger transport flight from Perth, Western Australia, to Sydney, New South Wales.
At 0600 local time, the aircraft was pushed back from the bay and the captain switched on the aircraft navigation lights and logo lights. The FO obtained a taxi clearance from air traffic control, and the captain switched on the taxi lights before taxiing the aircraft to runway 06 using taxiway ‘V’ (Figure 1).[1] Around 12 minutes later, as they approached the holding point[2] on taxiway V from the south, the FO reported to the controller that they were ‘ready’ [for take-off]. At this time, the flight crew commenced the ‘before take-off’ procedure (see Incident 1 Virgin Australia procedures). When they arrived at the holding point, the captain turned off the taxi light to avoid stunning the flight crew of another aircraft on the opposite taxiway.
At 0616, after the controller provided a line-up clearance, the flight crew taxied the aircraft onto runway 06 and switched on the taxi lights, landing lights, and strobe lights. Prior to entering the runway, the flight crew recalled crosschecking the runway number to assist with positioning the aircraft, as per the procedure. The captain did not recall whether there were lead-on lights to the runway.[3]
The FO reported that the markings that would lead into the runway centreline were not followed but believed the captain was trying to maximise the take-off distance on the runway. The captain reported in interview that maximising take-off distance was their general practice. The FO also recalled that they were completing the line-up scan inside the flight deck during the turn onto the runway. Recorded flight data showed the aircraft was taxied past the runway centreline and lined up on the left edge lights of runway 06 (Figure 1). Both flight crew believed they were lined up on the runway centreline lights.
At 0616:50, as the aircraft was lined up, the controller issued a take-off clearance to the flight crew, and the FO focused on preselecting the next radio frequency for departure. At this time, the captain handed over control of the aircraft to the FO, who was the designated pilot flying[4] for the sector. At 0617:18, the captain set take-off thrust. In interview later, the FO reported that, during the commencement of the take-off roll they noticed a raised edge light and realised the aircraft was lined up on the runway edge. In response, they manoeuvred the aircraft toward the centreline as evidenced by the right rudder pedal input at 0617:20. Shortly after, at 0617:24 the aircraft was aligned with the runway centreline. The FO recalled asking the captain to confirm whether to continue with the take-off, which the captain confirmed as they believed they were above the take‑off decision speed.[5]
Figure 1: Overhead of Perth Airport and showing the aircraft’s line up on runway 06 with key events during the take-off for incident 1
Taxi and take‑off roll during the departure is shown in green. Source: APS Aerospace Flight Animation System based on flight data recorder from the aircraft, annotated by the ATSB
The continuation of the take-off and departure was normal. Once airborne, the flight crew discussed the incident. As they believed they did not strike the runway lights they decided to continue the flight and reported the incident after arriving in Sydney around 4 hours later. After the incident, a runway inspection was conducted, which identified no damage to the runway lights. The operator completed an engineering inspection and found there was no damage to the aircraft.
Incident 2
On the morning of 10 August 2023, the pilot of a Cessna 441 aircraft, registered VH-NSA and operated by Western Sky Aviation, prepared for a passenger charter flight from Perth to Southern Cross, Western Australia.
At around 0500, when at a parking bay at the terminal, the pilot completed the taxi checklist, which included switching on the navigation light, taxi light, and beacon light. In interview later, the pilot commented that the environment appeared dark, even with the aircraft lighting on. At 0508, the pilot received a taxi clearance from air traffic control and taxied to taxiway V towards runway 06.
The pilot recalled that, while at the northern runway holding point, lights from what they assumed to be another aircraft stunned them, affecting their vision. Three minutes later, at the runway holding point, the pilot was cleared to line up and wait on runway 06 until another aircraft had departed. Prior to entering the runway, the pilot completed the line‑up checklist, which included switching on the anti‑collision lights and landing lights.
Air traffic control recorded data showed that the aircraft taxied past the centreline of the runway and lined up along the right edge lighting (Figure 2). During interview, the pilot recalled that the runway markings were ‘scuffed’ and difficult to see, but they believed they were lined up on the runway centreline lighting. They also noticed ‘plenty’ of runway to their right and reported not realising there were no centreline lights on runway 06.
At 0512, the aircraft was cleared for take-off. During the take-off roll, the pilot heard an impact outside the aircraft and suspected a birdstrike had occurred. The pilot decided they were above the rejected (decision) take-off speed so continued with the take-off, but manoeuvred the aircraft to the left, toward the centreline. After the aircraft was airborne, the pilot contacted air traffic control to request a return to Perth. A runway inspection identified damage to several runway edge lights. There was no damage to the aircraft.
Figure 2: Overhead of Perth Airport showing the aircraft’s line up and take-off on runway 06 for incident 2
Taxi and take‑off roll during the departure is shown in red. Source: Google Earth, annotated by the ATSB
Incident 3
On the morning of 4 April 2024, VH-NSA was again prepared for a passenger charter flight from Perth to Southern Cross, Western Australia. During preparation, the pilot[6] reviewed the relevant Notices to Airmen[7] that stated, due to runway resealing works the centreline lights on taxiway V, the runway 24 to taxiway V lead-off lights, and taxiway V stop bar[8] were unserviceable. Temporary blue edge lighting was provided on taxiway V while the resealing work was completed.
At around 0500, while at the parking bay at the terminal, the pilot completed their taxi checklist, which included switching on the navigation light, taxi light, and beacon light. In interview, the pilot commented that they felt the aircraft lights did not appear to illuminate the environment well, so they switched the lights off and on again to confirm their operation. At 0509, the pilot taxied to taxiway V, noting that the northern corner between taxiway V and runway 06 appeared darker than usual, and there was little ambient light in the area.
At 0519, the pilot called ‘ready’ [to take off] to air traffic control and 2 minutes later received a clearance to line up on runway 06. Prior to entering the runway, the pilot completed the line‑up checklist, which included switching on the anti-collision lights and landing lights. To assist with runway alignment, the pilot reported that they would normally taxi between the runway number and the gap between the threshold markings (see Markings). The pilot reported they lined up with a white line, which they assumed was the runway centreline marking. They also recalled that the runway markings appeared to be ‘scuffed’ and were difficult to see. They also checked for the runway edge lights on both sides and believed they were aligned with the runway centreline.
Air traffic control recorded data showed that the aircraft taxied past the runway centreline and lined up along the edge lighting on the right side of the runway (Figure 3). At 0523, air traffic control issued the take-off clearance. During the take-off roll, the pilot reported hearing a noise and believed that the sound originated within the cabin, so continued the take-off. They also reported that they checked their engine indications, which were normal. The pilot departed and completed the planned flight.
Figure 3: Overhead of Perth Airport showing the aircraft’s line up and take-off on runway 06 for incident 3
Taxi and take‑off roll during the departure is shown in orange. Source: Google Earth, annotated by the ATSB
The pilot conducted a flight back to Perth from Southern Cross and then flights from Perth to Cue and return. After each of these flights, the pilot conducted a walk around the aircraft. This involved the pilot using the torch from their phone when conducting the aircraft inspection in the dark. The first inspection was conducted in the dark, and the others were during daylight. The inspection involved the pilot walking in a clockwise direction around the aircraft and included an examination of the propellers for damage. A checklist was reviewed afterwards to ensure all the components were checked.
Later in the morning, Perth Airport contacted the operator to advise that several runway edge lights were damaged, which they determined were coincident with the aircraft’s departure based on recorded departures and closed-circuit television footage. At 1208, the aircraft returned to Perth and during the walk around inspection, the pilot noticed damage to one propeller blade on the right engine (Figure 4).
Figure 4: Damage to propeller blade on right engine
Source: Operator
Context
Pilot information
All the pilots held the appropriate licences and qualifications to conduct their respective flights. ATSB analysis of sleep and roster information obtained from each of the pilots found that, despite the early morning departure time, there was a low likelihood any individual was experiencing a level of fatigue known to adversely affect performance.
The ATSB also considered whether pilot familiarity with the airport played a role in the incidents. Both pilots involved in the first incident were based in Sydney. The captain last operated from Perth one month prior to the incident, while the FO last operated from Perth one week prior. The pilots involved in the second and third incidents were both employed by a Perth-based operator, and therefore familiar with the airport. The operator reported that the third incident pilot was advised of the hazards around runway 06 during their line training.
Environmental conditions
During interview, all the pilots described the lighting conditions during the taxi to the runway as dark. Information from Geoscience Australia found that the first incident occurred around 1 hour prior to sunrise and the second and third incidents occurred around 1.5 hours prior to sunrise. All the incidents occurred before morning civil twilight, also known as first light.[9]
Perth Airport information
Runways
Perth Airport has 2 runways, 03/21 and 06/24 (Figure 5). Both runways are 45 m wide but runway 06/24 is shorter than 03/21. All pilots involved in the incidents reported that runway 03/21 was the runway they would use most frequently on departure.
Prior to the construction of taxiway V in 2012, there was a turning bay at the beginning of runway 06 to allow pilots to backtrack their aircraft and line-up to use runway 06. As a result, extra pavement remained on either side of the runway. The width of this extra pavement was 34 m from either side of the runway edge at the widest part, which is where each of the aircraft were aligned. The extra pavement tapers, where the widest part was closest to the runway end. At the time of each of the incidents, this extra pavement was not lit or marked, and there was no regulatory requirement to do so.
Taxiway V crossed the end of runway 06 and could be used to enter the runway from either the right (south) or left side (north). The flight crew from the first incident entered runway 06 from the right of taxiway V, and lined up on the left edge lights, while the pilots from the second and third incidents entered from the left and lined up on the right edge lights.
Figure 5: Perth Airport runways
Source: Google Earth, annotated by the ATSB
Lighting
The Civil Aviation Safety Regulations Part 139 Manual of Standards (MOS) for Aerodromes stated the requirements for runway and taxiway lights and markings for Australian airports.
Runway centreline lights
When installed, runway centreline lights were inset in the runway, and would be white and omnidirectional, apart from lights towards the end of the runway, which were required to be red.
Runway 03/21 was fitted with centreline lights (Figure 6). Runway 06/24 did not have centreline lights, and was not required to as per MOS 139.
Runway edge lights
The MOS stipulated that a permanent runway edge lighting system was required to be installed on runways intended for use at night. The edge lighting system should be comprised of 2 parallel rows of lights, equidistant from the runway centreline. The lights may be elevated (raised) or recessed (inset) and would be situated along the declared edge of the runway to delineate the area available to pilots for landing and take-off at night in reduced visibility. Consistent with the MOS requirements, the runway 06/24 edge lights were white (Figure 6 shows these lights for runway 03). The first 2 edge lights on runway 06 were inset into the runway, and the remainder of the lights were elevated (Figure 7).
Figure 6: Runway centreline lights and edge lights on runway 03
Source: Perth Airport, annotated by the ATSB
Figure 7: Runway 06 edge lighting (left side)
Source: Perth Airport, annotated by the ATSB
Taxiway centreline lights
The MOS also stated that, where taxiway centreline lights were used for both runway exit and runway entry purposes, the colour of the lights viewed by the pilot must be green for entering the runway and alternately green and yellow for exiting the runway. Taxiway V had lights from the centreline of the runway to the centre of the taxiway (Figure 8). These lights were alternating yellow and green unidirectional lights visible only when exiting the runway, known as lead-off lights. Lights visible when entering the runway were known as lead-on lights. Taxiway V did not have lead-on lights that joined from the taxiway to the runway centreline, but there were green bi-directional taxiway centreline lights spanning across the runway threshold in the middle of taxiway V (Figure 8 top and bottom).
Figure 8: Runway centreline lights (top), view from the runway centreline of runway 06 (middle) and view from taxiway V holding point, facing towards the opposite side of the taxiway (bottom)
Source: Google Earth (top image) and Perth Airport (middle and bottom images), all images annotated by the ATSB
Markings
MOS 139 stipulated the characteristics of aerodrome markings, including runway and taxiway markings. Runway markings were required to be white (on paved runways) and included runway designation, runway threshold, centreline markings, and edge markings (also known as side-stripe markings). Runway designation markings were the 2-digit runway number, determined from the approach direction, indicating the magnetic heading of the runway. Runway threshold markings identified the beginning of the runway that was available for landing and take-off using ‘piano key’ markings. They consist of a white line across the width of the runway and a series of white longitudinal stripes of uniform dimensions. Runway centreline markings were a line of uniformly spaced stripes and gaps that identify the centre of the runway and provide the pilot alignment guidance during take-off and landing. Runway edge markings were required to be continuous white lines on both sides of the runway. Taxiway markings were required to be yellow and provided on all sealed, concrete or asphalt taxiways for continuous guidance between the runway and the apron.[10]
Runway 06 had runway markings as per the MOS requirements. The runway edge markings were an unbroken white line and centreline markings were broken white lines. The markings were painted with non-reflective paint. There was no regulatory requirement to use reflective paint for runway markings. All taxiways including taxiway V had continuous yellow taxi centreline markings (Figure 9).
Figure 9: Runway markings on Runway 06 (as of March 2023)
Source: Perth Airport, annotated by the ATSB
Alternate runway markings to assist with visibility
There was no requirement for runway markings to be painted using reflective markings in Australia, but other countries use reflective paint to increase visibility and contrast in the dark. For example, the International Civil Aviation Organization recommended that aerodromes where operations take place at night, pavement markings should be made with reflective materials to enhance the visibility of markings. The United States Federal Aviation Administration (FAA) includes the use of retroreflective airport markings with glass beads in paint to improve conspicuity of markings at night, during low visibility conditions or when the pavement is wet. The Federal Aviation Administration also stated that runway shoulder stripes may be used to supplement runway edge stripes to identify pavement areas contiguous to the runway sides that are not intended for use by aircraft. Runway shoulder stripes were to be painted yellow.
Air traffic control information
Airservices Australia provided the ATSB with the air traffic control data for each of the incidents. The data included a recording of the tower controller’s screen from the Advanced Surface Movement Guidance and Control System, which showed the position of aircraft and ground vehicles. For all 3 of the incidents, the recording showed the respective incident aircraft lining-up and taking off from the edge of runway 06.
When asked whether a tower controller could detect misaligned take-offs, Airservices Australia advised that the scale setting and margin of error on the screens may make it difficult for controllers to detect a misaligned take-off. Further, the tower controller’s role was to look outside, and they may not be using the screen to check the runway alignment of an aircraft.
Operational information
Incident 1
Virgin Australia procedures
The Virgin Australia Policy and Procedures Manual stated that during take-off, flight crew must:
Use all available cues to ensure the aircraft is on the correct runway (including runway numbers, localizer, etc)
Ensure the take-off roll is only commenced when the aircraft is aligned.
The Flight Crew Operations Manual included as part of the ‘before take-off’ procedure a runway verification check, which included runway take-off position (Figure 10).
Figure 10: Excerpt of the ‘before take-off’ procedure
Source: Virgin Australia
Take-off decision speed
Based on the airspeed calculations for the flight on the take-off and landing card, the decision speed (V1) was 139 kt. The flight data showed that, when the aircraft was manoeuvred from the runway edge to the centreline, the groundspeed was 44 kt. As there were no significant winds in the area at the time affecting the aircraft’s speed, it was likely that a rejected take-off could have occurred.
Incidents 2 and 3
The pilots from the 10 August 2023 and 4 April 2024 incidents recalled that they would use the runway markings, including the centreline and runway threshold markings, to assist with alignment. They would also check that the runway edge lights were on either side of the aircraft when lining up on the runway.
Misaligned take-offs
Previous research
When pilots taxi and take-off during daylight conditions, they normally have a wide range of visual cues by which they can navigate and verify their location. At night, however, the amount of visual information available is markedly reduced. Pilots rely more on the taxiway and runway lighting patterns presented to them and what can be seen in the field of the aircraft’s taxi and landing lights.
In 2010, the ATSB published a research report titled Factors influencing misaligned take‑offs at night (AR-2009-033) which reviewed several Australian and international occurrences. The report identified several factors that increased the risk of a misaligned take-off. The most prevalent factors that contributed included environmental factors such as the physical layout of the runway and/or airport. Examples included a wide runway and/or extra pavement near the runway or confusing taxiway marking and/or lighting, such as recessed lighting at the runway’s edge and/or the absence of centreline lighting.
Areas of additional pavement around the taxiway entry and runway threshold area can provide erroneous visual cues at night and pilots can believe that they are in the centre of the runway when they are actually lined up on the edge. Recessed (inset) lighting, particularly at the taxiway entry to the runway, was often quoted as an influencing factor in reports relating to lining up incorrectly. Centreline lighting, when it was present, was always recessed to allow aircraft to safely travel over the centreline during take-off. However, runways will often have recessed lights at the runway edge where the taxiway meets the runway. Therefore, recessed runway edge lighting can act as confirmation that the flight crew have lined up on the centreline, when this is not actually the case. Similarly, the degradation of airport markings can provide erroneous cues to the pilots of the aircraft’s position on the runway.
The next most common factors were human factors such as flight crew distraction (divided attention). Divided attention results in a focus inside the flight deck at the expense of monitoring the external environment. An example was flight crew performing checklist items or setting power/checking instruments/readings. Completing checklists were a normal and necessary part of the departure, however, can be a distraction during a critical time, such as while lining up. Another factor was a lack of familiarity with the runway at night, as it can present an additional demand during taxi and line-up.
The last group of factors were operational factors, such as air traffic control clearances, which can provide a distraction to flight crew depending on the timing. They can also contribute to, precipitate, and/or exacerbate the presence or impact of other factors such as workload, distraction, or a lack of visual cues to assist the crew in lining up the aircraft on the runway centreline.
Previous safety recommendations
Previous investigations conducted by the United Kingdom Air Accident Investigation Branch (UK AAIB) and Dutch Safety Board, involving misaligned take-off incidents in 2015 and 2018 respectively, have included safety recommendations to the International Civil Aviation Organization (ICAO). These recommendations proposed that ICAO should develop runway design standards that would prevent pilots misidentifying runway edge lighting as centreline lighting. ICAO reviewed these safety recommendations and determined that guidance included in the Procedures for Air Navigation Services (PANS) – Aerodromes (Doc 9981) provided strategies to address misaligned take-offs. The guidance included considerations for aerodrome operators, such as conducting safety assessments as part of the risk management process. An example of an item to be considered in this process was aerodrome/runway layout.
In 2021, the Global Action Plan for the Prevention of Runway Excursions was published and included addressing misaligned take-off incidents. Specifically, the report stated there should be measures for preventing visual confusion during line-up between runway edge and centreline lights leading to misalignment with the runway centreline. The measures should also take into account the effects of low visibility and runway contamination and the effect of using various light colours and patterns to differentiate the runway centreline and edge lighting systems.
Related occurrences
A review of the ATSB occurrence database found 3 reported incidents of misaligned take-offs in the 5 years prior to April 2024. These incidents, along with 2 similar international incidents are as follows.
On 20 April 2021, at 1854 local time, the pilot of a Fairchild SA227 aircraft taxied at Townsville Airport for a freight charter flight to Brisbane, Queensland. While lining up for take-off on runway 01, air traffic control advised that the aerodrome QNH[11] had changed. During this time, the pilot became aware that the aircraft had deviated from the lead-on line and started correcting the turn to realign with the centreline. During the take-off roll, the aircraft struck a runway edge light resulting in minor damage to the propeller.
A number of factors that contributed to the misaligned take-off included the wider paved section at the end of the runway, no centreline lights on the runway, recessed edge lighting, and taxiway lead-on lights not visible when entering the runway. It was also found that there was reduced visibility prior to departure due to the rain and time of day.
On 21 July 2023, at 0109 local time, the pilot of a Piper PA-31 aircraft taxied at Essendon Fields Airport, Victoria for a freight charter flight to Bankstown, New South Wales. After reading back their clearance from air traffic control and accepting the departure from runway 26, the aircraft was taxied and prepared for take-off. The pilot was completing checklists, which required attention to be focused within the aircraft. After commencing the take-off run, the pilot heard multiple loud noises, rejected the take-off and exited the runway. Inspection of the aircraft upon return to the apron identified a damaged main landing gear tyre and brake calliper. An inspection of the runway found damage to multiple runway lights and foreign object debris scattered across the runway.
On 13 May 2024, at 0537 local time, the pilot of an Aero Commander 500-S aircraft taxied for departure at Brisbane Airport on a regular scheduled freight flight. The aircraft was cleared for a departure from runway 01 at the intersection of taxiway A7, the pilot taxied to this holding point. While turning onto the runway, the pilot inadvertently lined up along the left side runway edge lighting instead of the runway centreline. During the take‑off roll, the pilot recognised the aircraft was left of the centreline and took corrective action to reposition the aircraft on the runway. The underside of the aircraft had minor damage and several runway lights were also damaged.
The brief highlighted the complexity of the intersection with multiple lead-off lines into the runway as well the runway touchdown zone markings near the runway centreline markings that were both broken white lines.
German Federal Bureau of Aircraft Accident Investigation BFU20-0251-EX
On 27 April 2020, at 0353 local time, the flight crew of a ATR72-212 aircraft prepared for take-off on a freight flight from Cologne Airport, Germany, to Sofa Airport, Bulgaria, in the dark. After receiving their taxi clearance, the flight crew taxied the aircraft to the centreline of runway 24 towards the turn pad (paved area next to the runway for turning) for runway 06 (the reciprocal runway). The flight crew completed the before take-off checklist during taxi. At this time, the flight crew heard a sound in the cockpit and determined it was from the captain’s bag falling from the chair. When the turn pad was reached the aircraft initially followed the yellow taxiway markings to turn 180°. The captain completed the turn and aligned the aircraft with the row of lights ahead, believing they were the centreline lights. During the take-off roll, the flight crew felt and heard an impact to the aircraft, so the captain aborted the take-off. The aircraft had minor damage to the nose landing gear and propeller blades.
Factors identified that contributed to the misaligned take-off related to the runway environment and distraction. The runway edge marking on the turn pad was a broken white line, which was similar to the centreline markings. Due to the viewing angle from the cockpit to the runway edge and centreline lighting they were difficult to differentiate, especially in the dark without any other visual refences. The width of the turn pad including the runway was also identified as a factor. Another factor was flight crew distraction during the turn due to determining the sound in the cockpit. The report had a safety recommendation (07/2020) to ICAO:
The International Civil Aviation Organization (ICAO) should modify the standard recommendations regarding runway edge lighting in Annex 14 Volume 1 Aerodrome Design and Operations to ensure clear distinction of other airport lightings (sic).
Transportation Safety Board of Canada investigation A23F0062
On 16 February 2023, at 1817 local time, the flight crew of a Boeing 737 aircraft taxied to runway 01R in Nevada, United States, to Edmonton, Canada, on a scheduled passenger flight. The flight crew taxied the aircraft along the taxiway centreline until reaching the right runway edge marking, turned to the right and entered and lined up with what was believed to be the runway centreline. The aircraft took off while aligned with the right edge of runway 01R, and its nosewheel contacted 8 runway edge lights. During the take‑off roll, both the flight crew heard sounds and felt vibrations but believed it was the runway centreline lights. The flight crew were unaware of the misaligned take-off and the flight was continued. The aircraft had minor damage to the right tyre on the nose landing gear and there was damage to several runway lights.
The investigation identified several factors that contributed to the misaligned take-off. The factors included the high workload between the flight crew at the time of departure where the FO was focused on a task within the cockpit and the captain’s perceived time pressure to depart. Other factors included the visual cues in the runway environment. The taxiway centreline lighting on the taxiway used for departure terminated at the runway edge markings and the runway did not have centreline lighting.
Safety analysis
Runway environment resulting in the misaligned take-off
On runway 06, there was extra pavement on either side of the runway where each aircraft lined up for take-off. As there were no markings or lighting to delineate this area, there were no visual cues to assist the pilots to identify the extra pavement was adjacent to the runway. Consequently, this area likely appeared to be an extension of the usable runway. This was consistent with the pilot’s observation in incident 2 where they reported seeing ‘plenty’ of runway to their right when lined up on the right runway edge.
Although the runway had all the required markings in accordance with regulations, they were reported by 2 of the pilots as being difficult to see at night and were ‘scuffed’, thereby reducing the contrast and visibility of the markings. It was also noted that, while not required, reflective paint was not used for the markings to improve conspicuity at night.
While there were taxiway centreline markings, there were no lead-on lights from the taxiway to the runway centreline. Although there were lead-off lights, these were unidirectional and designed to only be visible when exiting the runway. Therefore, at night, the pilots had limited cues to assist them while navigating from the taxiway to ensure they would turn the aircraft into the centre of the runway.
Runway 06 did not have centreline lighting. However, the first 2 edge lights on either side were white and inset within the runway, which were the same characteristics for centreline lighting. Given that all the pilots indicated they would use runway 03/21 more frequently for take‑off, which was fitted with centreline lights, this potentially influenced them misidentifying the edge lights as centreline lights.
The pilots of the 2 incidents operating the Cessna 441 also commented that although the aircraft lighting was switched on, the environment appeared dark. One of these pilots also reported that there was limited ambient lighting at the intersection of taxiway V to runway 06. The combination of the reduced visual cues and runway features that can be misidentified may have also given the impression that the aircraft were aligned with the runway centreline and increased the risk of a misaligned take-off. These characteristics were evident in many previous similar investigations.
Consistent with the ATSB’s research, the extra pavement area, the absence of lead-on lights and runway centreline lights, and some degraded markings, were all factors that influence misaligned take-offs at night, where visual information may be markedly reduced. A combination of these factors in each incident supported the pilots’ belief that the aircraft were correctly aligned with the centreline when they were positioned on the runway edge lighting. Confirmation bias is the tendency for people to seek information and cues that confirm the tentatively held hypothesis or belief (Wickens et al 2022). As they believed they were correctly aligned with the runway centreline, the pilots in each occurrence commenced the take-off roll.
Flight crew focus of attention
In incident 1, the flight crew divided their attention between pre-take off tasks being completed in the flight deck and monitoring the environment. Additionally, the flight crew also received their take-off clearance during the turn onto the runway, requiring the FO to communicate with air traffic control. While these are normal and a required part of the departure, they can divert the flight crew’s attention away from the external environment at a critical time, such as while lining up. Barshi and others (2009) state that during busy periods, it is easy for attention to be absorbed in one task, which can divert attention from other important tasks, such as monitoring.
Pilots’ response to the misaligned take-off
The pilots’ responses to each misaligned take-off incident were different. During the take‑off roll, the flight crew in the June 2023 incident identified that they had lined up on the runway 06 edge lighting and manoeuvred the aircraft toward the centreline and continued the take-off. However, believing they had not struck the runway lights, the misalignment of the take-off was not reported to the operator or to airport personnel until the flight had arrived in Sydney, around 4 hours later. Although the subsequent aircraft and runway inspections did not identify any damage, there was the risk that unrecognised debris could have affected the safety of other aircraft using the same runway or the flight continuing with unknown damage.
The pilot in the August 2023 incident detected an impact during take-off, though did not initially notice the aircraft was aligned with the runway edge lighting. As they had detected a problem, the pilot returned to the airport to ensure there was no damage to the aircraft and provided the opportunity for a runway inspection to occur to check for damage. The pilot’s decision was important as damage to the aircraft (which was carrying passengers) and debris on the runway can affect flight safety.
The pilot in the April 2024 occurrence did not identify they had lined up the aircraft on the runway edge lighting and subsequently completed multiple flights. As a result of the misaligned take-off, the aircraft had sustained damage to the right propeller and several runway lights were damaged, which was not detected until later that day. Damage from a foreign body impact to a propeller blade could lead to gouges, dents and deformation, or cracks and blade failure if left undetected (Federal Aviation Administration 2005), although in this instance there was no reported effect on flight from the sustained damage.
Overall, misaligned take-offs can increase the risk of damage to aircraft and lighting given that raised runway lighting, unlike recessed runway lighting, is more likely to sustain an impact. Given the risk, it is important to promptly communicate the incident, for example to air traffic control or airport personnel, to provide the opportunity for inspections to be conducted. The outcome of these inspections allows pilots to make more informed decisions on whether to continue the flight, return or divert to a closer location.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the 3 misaligned take-off occurrences on runway 06 at Perth Airport, Western Australia.
Contributing factors
On runway 06 at Perth Airport, features of the runway environment included extra pavement, degraded markings, and reduced lighting. As a result, the pilots in 3 separate occurrences misidentified this runway's edge lighting for centreline lighting and commenced take-off from this position.
During the turn onto the runway in incident 1, the flight crew were focussed on completing pre-take off tasks within the flight deck, and communicating with the air traffic controller about their take-off clearance. These actions diverted their attention away from monitoring their position on the runway.
Other factors that increased risk
After the misaligned take-offs, the 3 pilots responded differently. This increased the risk of damage, to aircraft or runway lighting, remaining undetected.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Perth Airport Pty Ltd
After the first 2 misaligned take-off incidents, Perth Airport submitted a notice to Airservices Australia requesting an update to the Aeronautical Information Publication about the misaligned take-off risk on runway 06. Subsequently, this update was included in an Aeronautical Information Publication supplement H78/23 effective November 2023 containing an update to the ground and movement charts for Perth Airport. The new aerodrome chart highlighted there was a ‘misaligned take-off hot spot’[12] at the intersection of taxiway V and runway 06. The supplement detailed that runway 06 had wider shoulders due to previously being used as a turn pad, had no centreline lights, and that, when lining-up on the runway from taxiway V, pilots should ensure that the aircraft was aligned with the runway centreline. In March 2024, Airservices Australia updated the En Route Supplement Australia to reflect this change.
Perth Airport conducted airport works in late March to early April 2024 to repaint all markings on the runway and taxiway. As part of this work, they also painted chevron markings on the extra pavement next to runway 06 to prevent future misalignment.
Safety action by Western Sky Aviation
As a result of the incident on 10 August 2024, the operator issued a notice to aircrew to highlight the importance of vigilance by confirming the nominated runway position. For runways with an instrument landing system (ILS), the operator encouraged pilots to line up and tune the ILS and dial up the course to check the course deviation indicator is centred. For runways with no ILS (such as runway 06), the operator encouraged pilots to crosscheck the runway heading with the GPS position of the aircraft overlaid on the aerodrome map display in the OzRunways software on tablets in the aircraft.
After the April 2024 incident, a second notice to aircrew was distributed, emphasising the importance of situational awareness with runway identification when preparing for take‑off. The notice specified that pilots must confirm they are on the runway centreline and ensure the runway number is identified, either through the runway markings or association with the heading displayed by an aircraft instrument. For night take-offs specifically, pilots were instructed to self-brief the expected runway to familiarise with the specific characteristics of the runway such as whether it has centreline lighting or not, and to ensure that they have both the sides of the runway lighting visual before commencing the take-off roll.
Safety action by Virgin Australia Airlines
Virgin Australia Airlines added caution notes to its Perth Airport supplementary port information about centreline misidentification on runway 06 due to the environment, such as no centreline lighting during night or in poor visibility conditions. They also revised the before take-off procedure to reduce flight crew workload during line‑up by reallocating items (setting the weather radar) to earlier in the taxi. Finally, case studies involving this event were incorporated into non-technical skills training.
Sources and submissions
Sources of information
The sources of information during the investigation included:
pilots from the 3 incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Airservices Australia.
References
Airservices Australia. (2023). A pilot’s guide to runway safety, Airservices Australia.
Australian Transport Safety Bureau. (2010). Factors influencing misaligned take-off occurrences at night, Australian Transport Safety Bureau, Australian Government.
Barshi, I., Loukopoulos, L.D. and Dismukes, R.K. (2009). The multitasking myth: Handling complexity in real-world operations. Ashgate Publishing.
Civil Aviation Safety Authority. (2019). Part 139 Manual of Standards for Aerodromes, Civil Aviation Safety Authority, Australian Government.
Federal Aviation Administration. (2005). Advisory Circular AC20-37E Aircraft Propeller Maintenance, US Department of Transportation, United States.
Wickens, C.D., Helton, W.S., Hollands, J.G., and Banbury, S. (2022). Engineering psychology and human performance, 5th edn, Routledge, doi: 10.4324/9781003177616.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots from the 3 incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Airservices Australia
Civil Aviation Safety Authority.
Submissions were received from:
a pilot from one of the incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway (for example, runway 06 is orientated 60º magnetic). The runway identification may include L, R or C as required for left, right or centre. Runways 06/24 were reciprocal runways.
[2]Holding point: designated point for holding on airfield, especially before entering active runway.
[3]Lead-on lights: green unidirectional taxiway centreline lighting that extends into the runway.
[4]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path. On the Boeing 737, the captain taxis the aircraft as the steering is on the left side.
[5]Take-off decision speed (V1): the critical engine failure speed or decision speed required for take-off. Engine failure below V1 should result in a rejected take off; above this speed the take-off should be continued.
[6]The pilot in incident 3 was a different pilot to incident 2.
[7]Notice to Airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[8]Stop bars are a series of unidirectional red lights embedded in the pavement, at right angles to the taxiway centreline, at the associated runway holding point. They are intended to provide additional protection of runway/taxiway intersections to reduce runway incursions.
[9]First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions.
[10]Apron: large paved area of airfield for such purposes as: loading and unloading of aircraft; aircraft turnaround operations; aircraft modification, maintenance or repair; any other approved purpose other than flight operations.
[11]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[12]Hot spot: a location on an aerodrome movement area with a history of potential risk of collision or runway incursion, and where heightened attention by pilots / drivers is necessary.
Occurrence summary
Investigation number
AO-2023-027
Occurrence date
12/06/2023
Location
Perth Airport
State
Western Australia
Report release date
20/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Runway excursion
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8SA
Registration
VH-IWQ
Serial number
44225
Aircraft operator
Virgin Australia Airlines Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Perth Airport, Western Australia
Destination
Sydney Airport, New South Wales
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
441
Registration
VH-NSA
Serial number
441-0087
Aircraft operator
Western Sky Australia Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 12 May 2023, an instructor and student pilot in a Magni M16C Tandem Trainer gyroplane, registered G1850, were conducting wheel balance exercises on runway 07 at Lake Macquarie Airport, New South Wales. Following the sixth of these exercises, the student made a radio broadcast while the instructor turned the gyroplane around and taxied on the runway toward the runway 07 threshold at the western end to repeat the exercise. Meanwhile, the pilot of an Extra EA 300L, registered VH-IOG, taxied from the apron for a scenic flight with one passenger. The Extra pilot made 2 radio broadcasts before entering the runway near the eastern end and taxied towards the runway 07 threshold. At about this time, the gyroplane commenced another exercise and accelerated down runway 07 towards the Extra. As the gyroplane approached the runway midpoint, the instructor and student observed the Extra about 20 m ahead. The instructor manoeuvred to avoid a collision, banking right before colliding with terrain resulting in substantial damage to the gyroplane. The instructor was seriously injured, with the student sustaining minor injuries. The Extra was not damaged, and its occupants were uninjured.
What the ATSB found
The ATSB found that neither aircraft’s pilots heard each other’s radio broadcasts and consequently, aircraft separation became reliant solely upon visual acquisition. The investigation found that the Extra pilot did not see the gyroplane before entering the runway, and subsequently taxied towards it. Also, while accelerating on the runway, the instructor and student in the gyroplane did not see the Extra taxiing towards them until a collision was imminent.
There were several factors that likely reduced the ability of the pilots to identify each other, including the small angular size of each aircraft, the complex background features with low relative contrast, and minimal relative movement between the aircraft.
Additionally, the tailwheel configuration of the Extra limited the pilot’s forward visibility and sun glare likely also affected the pilot’s ability to detect the gyroplane. The gyroplane pilots were likely also influenced by the higher workload associated with the training exercise which probably reduced their available attention for identifying conflicting aircraft.
What has been done as a result
The airport operator released a bulletin to all operators based at Lake Macquarie Airport highlighting the importance of a visual lookout in addition to radio discipline. A runway hold point line was repainted, and radio recording equipment will be purchased to allow radio communications to be periodically reviewed.
The operator of VH-IOG updated operational procedures to require a ground employee to have a hand-held radio switched on and in reach for all operations, and to monitor all departure and arrival radio calls. Pilots are now also required to stop at a hold point line before entering the runway for departure at Lake Macquarie Airport.
The Australian Sport and Rotorcraft Association (ASRA) advised the ATSB of its intent to replace the one-off human factors exam, completed as a requirement of the ASRA pilot certificate, with a recurrent exam, to be completed as part of each biennial flight review.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the collision risk around non-towered airports. This accident highlights the limitations of unalerted see-and-avoid in such an environment. Pilots are reminded of the importance of effective radio communications to increase traffic awareness and to ensure an effective visual scan to identify conflicting traffic.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 12 May 2023, an instructor and student pilot in a Magni M16C Tandem Trainer gyroplane, registered G1850 and operated by Airborne Flight Training, were planning to conduct wheel balance training exercises (see the section titled Operational information) at Lake Macquarie Airport, New South Wales. The airport was located within class G, non‑controlled airspace and had a designated common traffic advisory frequency (CTAF) on which pilots made positional broadcasts to coordinate aircraft separation.
At about 1537, the student and instructor pilots, seated in the front and rear seats respectively, taxied the gyroplane onto the runway near the runway 25[1] threshold and then backtracked[2] towards the runway 07 threshold (Figure 1) to commence the wheel balance training. The training exercise involved the student accelerating the gyroplane on the runway while balancing on the main landing gear until the gyroplane lifted off the ground briefly. The student then handed control to the instructor who would land on the runway, turn the gyroplane around and backtrack towards the 07 threshold before handing control back to the student and repeating the exercise.
At about 1542, the student pilot reported making a ‘rolling' radio call on the CTAF to indicate they were commencing the first wheel balance exercise. About 30 seconds later, after accelerating along the runway and briefly becoming airborne, the gyroplane landed about half-way down runway 07 and turned around. During this turn, the student reported making another radio call to indicate they were backtracking towards the runway 07 threshold.
At about 1543, the pilot of an Extra EA 300L, registered VH-IOG and operated by Inverted Downunder, walked towards the aircraft, which was located on the airport apron near the eastern end of the runway, to prepare for a scenic flight with one passenger. This was to be the pilot’s fifth flight of the day in the Extra.
Figure 1: Lake Macquarie Airport showing G1850 estimated ground track and VH-IOG location
G1850 track estimated using CCTV footage and pilot statements. VH-IOG location based on CCTV footage.
Source: Google Earth, annotated by ATSB
At about 1544, the gyroplane’s student pilot commenced a second wheel balance exercise from the runway 07 threshold. While the gyroplane was undertaking this exercise, airport video footage showed that the pilot of the Extra stepped onto the parked aircraft’s wing to prepare the front seat for the passenger. By about 1545, the gyroplane had travelled towards the end of runway 07, adjacent to the apron area and was slowing down to turn around (Figure 2). The student recalled that during the turn, a backtracking radio call was made. At about the same time, the video footage showed the Extra’s pilot, who was still on the wing, appear to look up for about a second toward the gyroplane. Shortly after, the passenger climbed into the front seat of the Extra, while the gyroplane backtracked towards the runway 07 threshold.
Over the next 8 minutes, the Extra’s pilot secured the passenger in their seat, provided a pre-flight briefing, and then climbed into the rear seat, putting their seatbelt and helmet on. During this time, the instructor and student pilot performed a further 4 wheel balance exercises, with the gyroplane turning around at different locations along the runway (Figure 2), but none as far as during the second wheel balance exercise (near the airport apron). The student pilot and instructor recalled radio calls being made prior to the commencement of, and during the turnaround at the end of, each wheel balance exercise.
At 1554:05, a few seconds after turning around following the sixth wheel balance exercise, the Extra’s pilot started the aircraft’s engine and conducted pre-flight checks which included switching on the aircraft’s radios.
At 1554:39, the Extra’s pilot began to taxi towards the runway while the gyroplane was backtracking along runway 07. At about 1554:53, the Extra’s pilot reported making a radio call on the CTAF that the aircraft was taxiing for runway 07.
At about 1555:09, and for about the next 10 seconds while taxiing, the Extra pilot reported visually looking for aircraft on final approach for runways 25 and 07, and for aircraft on the runway. The pilot recalled that most of their attention during this visual lookout was towards the ‘bad lighting’ at the runway 07 threshold and they recalled not seeing any aircraft. During this time, the Extra pilot made another radio call advising they were entering and backtracking runway 07. Shortly after, the aircraft crossed the hold point line without stopping and turned left onto the runway (Figure 3). The pilot stated that they did not usually stop at this line because they had unobstructed views towards the runway 07 threshold and final approach to runway 25 before this point. At a similar time, the student commenced the seventh wheel balance exercise from the runway 07 threshold. Both gyroplane pilots recalled that they did not see any aircraft on the runway at this time, nor could they recall making a ‘rolling’ radio call prior to this exercise.
As the Extra backtracked runway 07, the student was accelerating the gyroplane along the runway. About 30 seconds later, as the gyroplane approached the midpoint of the runway, the instructor and student observed the Extra about 20 m ahead and backtracking towards them. The instructor took control and banked the gyroplane right to avoid a collision. The rotor blades impacted the runway surface before the gyroplane veered off the runway and collided with terrain, coming to rest on its side. The gyroplane sustained substantial damage to the rotor blades, propeller blades, and landing gear. The instructor was seriously injured, with the student sustaining minor injuries. The Extra pilot saw the gyroplane veer off the runway to the left, stopped their aircraft and exited to provide assistance. The Extra was not damaged and its occupants were uninjured.
Figure 3: G1850 and VH-IOG ground tracks before accident
Labels ‘A’ and ‘B’ are timestamps for the approximate locations of each aircraft.
Source: Google Earth, annotated by ATSB
Context
Pilot information
G1850 pilots
The instructor pilot held an Australian Sport Rotorcraft Association (ASRA)[3] pilot certificate and was approved by ASRA as a chief flying instructor (CFI). They had accrued 2,254 hours of flying time in gyroplanes and about 751 hours on the Magni M16 and Magni M16C Tandem Trainer gyroplane, with 43 of those hours flown in the previous 90 days.
The student held an ASRA pilot certificate and a Private Pilot Licence (aeroplane). The student had accrued about 330 hours of flying time in aeroplanes, and 60 hours in gyroplanes, 10 of which were on the Magni M16C Tandem Trainer gyroplane in the previous 90 days.
The Magni M16C Tandem Trainer is a 2-seat gyroplane with fixed tricycle landing gear (Figure 4). A 4‑cylinder piston engine drives a 3-bladed pusher propeller, with an unpowered rotor to develop lift. The gyroplane has a pre-rotation system linking the engine to the rotor which, when engaged, can drive the rotor to start it spinning without needing forward motion.
The Magni M16C is 4.7 m long, 2.7 m high (fuselage about 1.5 m high), and 1.8 m wide, with a rotor diameter of about 8.5 m. An external landing light was fitted to the front of the fuselage with strobe lights fitted to each side of the fuselage and one on the rear of the mast.
The front seat was instrumented for the pilot in command and was occupied by the student. The rear seat was not fitted with instrumentation but had flight controls, and was slightly higher than the front seat to improve forward visibility. Both seats were fitted with 4-point harnesses and both pilots were wearing them at the time of the accident.
The Extra EA 300L is a low-wing, 2-seat aerobatic monoplane with fixed tailwheel landing gear and the rear seat was instrumented for the pilot in command. A 6-cylinder piston engine drives a 3-bladed tractor propeller. VH-IOG was manufactured in Germany in 1999 and first registered in Australia in June 2005 (Figure 5).
The aircraft is about 7 m in length and 1.8 m high while on the ground with a wheel track of 1.8 m and a wingspan of 8 m. External navigation and strobe lights were fitted to the wingtips.
The gyroplane instructor planned for the student to perform several wheel balance exercises to teach the student the correct pitch attitude for take-off, and the exercise included many similar aspects of a normal take-off. The United States Federal Aviation Administration (FAA) Rotorcraft Flying Handbook[4] described a normal gyroplane take-off as follows:
The normal takeoff for most amateur-built gyroplanes is accomplished by prerotating to sufficient rotor r.p.m. to prevent blade flapping and tilting the rotor back with cyclic control. Using a speed of 20 to 30 m.p.h., allow the rotor to accelerate and begin producing lift. As lift increases, move the cyclic forward to decrease the pitch angle on the rotor disc. When appreciable lift is being produced, the nose of the aircraft rises, and you can feel an increase in drag. Using coordinated throttle and flight control inputs, balance the gyroplane on the main gear without the nose wheel or tail wheel in contact with the surface. At this point, smoothly increase power to full thrust and hold the nose at takeoff attitude with cyclic pressure. The gyroplane will lift off at or near the minimum power required speed for the aircraft.
The instructor stated that if the student obtained the correct pitch attitude, the gyro would lift‑off briefly, before the instructor would take control and land on the runway, turn around, backtrack towards the runway 07 threshold, and repeat.
The instructor also stated that during the acceleration phase of the wheel balance exercise, the workload was high due to the multi-tasking required in monitoring the gyroplane’s attitude, the student’s flight control inputs, and the gyroplane’s response.
The student stated that during the acceleration phase of each wheel balance exercise, they glanced down occasionally to look at the cockpit instrumentation, but their focus was primarily on looking out of the aircraft and monitoring the gyroplane’s pitch attitude.
Meteorological information
The weather at Lake Macquarie Airport at the time of the accident was good with a light easterly wind, visibility greater than 10 km, and no cloud over the airport.
At the time the Extra’s pilot was taxiing towards the runway from the apron (heading north), the sun was positioned at about the 10 o’clock (300°) position,[5] at an elevation of about 12°. This would have placed the sun in the pilot’s field of view while looking towards the runway 07 threshold (Figure 6). It is likely that the gyroplane would have been illuminated by the sun at this time. The Extra pilot stated that as there was a light wind, a take-off from runway 07 was preferable since the sun was getting low in the west making it difficult to look in that direction. The pilot stated that they were wearing a tinted helmet visor, which would have reduced sun glare.
Figure 6: VH-IOG turning left to backtrack runway 07
Source: Airport operator
While the gyroplane was accelerating towards the Extra on runway 07 during the seventh and final wheel balance exercise, the sun was positioned behind the gyroplane at about the 8 o’clock position. The Extra was likely illuminated by the sun while backtracking along the runway towards the gyroplane.
Airport information and procedures
Lake Macquarie Airport was an aircraft landing area,[6] located about 20 km southwest of Newcastle, New South Wales. It had an elevation of 5 ft above mean sea level, and a single, sealed 880 m long and 11 m wide runway designated 07/25, with trees lining each side.
As a non-controlled airport, separation between aircraft was maintained by ‘alerted see-and-avoid’ principles guided by Civil Aviation Safety Authority (CASA) advisory circulars[7]. Unalerted see‑and‑avoid relies on a pilot or crew visually detecting other aircraft without the assistance of other aids or information. This visual detection can be improved through pilots being alerted to an aircraft’s presence by radio, electronic systems, or other means (alerted see‑and-avoid).
At Lake Macquarie Airport, the carriage and use of a radio was required by the airport operator for all operating aircraft. Pilots were required to broadcast their position and intention so that nearby traffic would have an awareness of their aircraft and be able to plan or act accordingly.
All 3 pilots were familiar with the airport operations and had operated at Lake Macquarie for many years. Both aircraft were on the correct CTAF frequency before the accident, with all pilots having 2-way communications with other aircraft. None of the pilots reported hearing the other aircraft’s radio calls. The gyroplane pilots could not recall whether they had made a rolling call at the start of the final wheel balance exercise.
The Extra pilot reported that once they had taxied clear of the apron toward the hold point line, there was nothing obstructing their view of the runway 07 threshold other than the lighting conditions. The gyroplane instructor similarly reported no limitations with visibility of the entire runway when viewed from the runway 07 threshold.
The Extra pilot stated that there had been historically poor radio usage at the airport, and that they needed to use visual lookout ‘aggressively’ and not rely on radio communications. The gyroplane instructor considered radio to be a secondary means of collision avoidance to visual lookout.
Limitations of see-and-avoid
The see-and-avoid principle has been an effective defence in preventing aircraft collisions, but has several limitations (ATSB, 1991).
Workload
See-and-avoid can only be effective when the pilot is looking outside the cockpit. However, many tasks require pilots to direct their attention inside the aircraft, particularly when conducting operations and tasks that involve a high workload.
There was an opportunity for the Extra pilot to become aware of the gyroplane while they were on the Extra’s wing preparing the passenger’s seat, when they looked up briefly toward the gyroplane turning around on the runway. However, the Extra’s pilot recalled being unaware of any other operations being conducted at the airport while on the apron preparing the passenger for the flight. It is possible that the pilot’s focus on preparing the aircraft and passenger for flight resulted in them not detecting the gyroplane despite appearing to look towards it.
Although the Extra had occupied the runway for about 30 seconds before the gyroplane pilots saw the aircraft, the gyroplane pilots’ focus on other traffic in the runway environment was probably limited due to the complex training exercise being conducted. The instructor and student’s attention was primarily focused on the gyroplane’s motion and attitude to ensure the exercise was being conducted appropriately.
Visual search
In daylight, a pilot must look almost directly at an object to see it and it is possible for a pilot to look past an object if they do not see it directly. An FAA advisory circular recommended scanning the entire visual field outside the cockpit with eye movements of 10 degrees or less, with about a second spent on each 10 degree sector, to ensure effective detection of conflicting traffic.[8]
It was estimated that the Extra pilot would have spent about 10 seconds on their visual lookout which included viewing both ends of the runway and associated approaches. While the Extra’s pilot was approaching the runway from the apron, the runway 07 environment would have been captured in a sector about 30 degrees horizontal by 10 degrees vertical. This suggests that the Extra pilot would have required at least 3 seconds for an effective visual scan of the runway (without accounting for any other factors). While the pilot probably spent at least that length of time viewing the runway 07 environment, there were other factors that likely affected their visual scan and their ability to detect the gyroplane in that time.
Cockpit visibility
Items such as window pillars, sun visors, and front seat occupants may impact on the pilot’s ability to see an aircraft. The FAA Airplane Flying Handbook[9] described the reduced forward visibility of tailwheel aircraft:
In the normal nose-high attitude, the engine cowling may be high enough to restrict the pilot’s vision of the area directly ahead of the airplane while on the ground. Consequently, objects directly ahead are difficult, if not impossible to see...In taxiing such an airplane, the pilot should alternately turn the nose from one side to the other (zigzag) or make a series of short S-turns. This should be done slowly, smoothly, positively, and cautiously.
The pilot reported that the Extra EA 300L had limited visibility from inside the cockpit between 11‑1 o’clock directions while on the ground. Their usual procedure at Lake Macquarie Airport was to undertake a ‘zig-zag’ manoeuvre at the half-way point of the runway to allow them to see the runway environment and ensure the final approach was clear of traffic. The manoeuvre was only performed once as the narrow runway required the aircraft to slow down significantly. On this occasion, the accident occurred before the Extra had reached the half-way point on the runway.
Threshold for acuity
The eye’s ability to recognise an object also depends on the relative size of the object and an approaching aircraft might be too small to be seen. Studies have estimated the size an object needs to be for it to be sighted, with estimations of visual angle varying from about 0.02° to detect features of an alphabet letter (Howett, 1983), to at least 0.2° (NTSB, 1988) to reasonably detect an overall object. However, visual acuity varies widely across the retina of the eye and therefore, these values are only of relevance when looking directly at an object. Additionally, these observations were conducted under certain conditions, for example high object contrast with the background and moderate illumination (Howett, 1983), while the particular conditions experienced by the pilots involved in this occurrence were likely different.
With the Extra’s pilot at the hold point line and the gyroplane at the runway 07 threshold lined up with the runway, the estimated angular size of the gyroplane’s fuselage including landing gear would have been between 0.11° (height) and 0.14° (width). If the gyroplane pilots were at the runway 07 threshold and looked towards the runway 25 end with the Extra facing them on the runway, the estimated angular size of the Extra’s fuselage would have been about 0.14° (height and width). While the angular size of the Extra’s wingspan and the gyroplane’s rotor would be larger, these were both thin making them difficult to detect at such a distance compared to each aircraft’s fuselage.
Background features
Detecting an aircraft can become more difficult against a complex background that has different colours, contours, and objects. Aircraft are more easily spotted if they have a high contrast with their background. Images taken from around the midpoint on the runway about 20 minutes after the accident (Figure 7) provided some indication of the background features present at the time of the accident:
The background behind the runway 07 threshold end had some small dark areas of shrub where the gyroplane’s white fuselage illuminated by the sun would have provided good contrast. However, the fuselage and background area covered by the shrub were small, and the light blue of the lake, and lighter terrain areas covered with haze in the distance, would have a presented a lower contrast difference with the white fuselage.
Behind the runway 25 threshold was a highway at the same elevation as the runway, which video footage showed was busy with traffic around the time of the occurrence, with trees illuminated by the sun behind the highway. Although the Extra’s yellow nose and spinner would have been illuminated by the sun during the wheel balance exercise, the background behind the Extra had the sideways motion of traffic at the same level as the Extra creating a more complex scene. In addition, the trees in the background were also illuminated by the sun potentially reducing the contrast of the nose and spinner as the Extra moved closer to the gyroplane.
In regard to aircraft lighting, research has shown that lights are generally ineffective in daylight at making an aircraft more visible, especially against bright sky backgrounds and can be less conspicuous than the aircraft itself, but may make aircraft more visible against terrain or in conditions of low light. The Extra’s strobe lights were off while the aircraft was backtracking runway 07. The gyroplane strobe lights were on at the time of the accident and the landing light was off.
Glare occurs when unwanted light enters the eye. Glare can come directly from the light source or can take the form of veiling glare, reflected from crazing or dirt on the windscreen. The Extra’s pilot reported that the cockpit canopy was cleaned between flights and had some scratches as it was the original canopy fitted from manufacture. Although the pilot was wearing a sun visor to reduce glare, the sun would have been in the pilot’s field of view while looking towards the runway 07 threshold before entering the runway. The associated glare, which may have been exacerbated by the cockpit canopy, would have probably reduced the pilot’s ability to detect the gyroplane.
Additionally, it is difficult to see another aircraft when there is little relative motion between one aircraft and the other, such as when they are moving towards the same location in space. There was little relative movement between the 2 aircraft while (a) the gyroplane pilots were accelerating towards the backtracking Extra and (b) the gyroplane was positioned near the runway 07 threshold while the Extra pilot was visually looking towards that location before turning onto the runway.
Recorded data
Airport video footage from several locations captured the Extra pilot’s pre-flight activities, taxi, and backtrack towards the runway 07 threshold. The footage also showed segments of the gyroplane’s wheel balance exercises when in view from around the middle of the runway towards the runway 25 threshold. Footage of the runway 07 threshold up to the runway midpoint was not captured by any available video camera.
CTAF radio broadcasts were not recorded at Lake Macquarie Airport. Of the airports that operated on the same CTAF, Warnervale Airport (28 km south-west of Lake Macquarie Airport) was the only airport that recorded radio transmissions. Due to distance and line-of-sight limitations, radio calls on or near the ground at Lake Macquarie were not normally received at Warnervale Airport. The ATSB reviewed recorded radio calls from Warnervale while both the Extra and gyroplane were operating at Lake Macquarie Airport, however, no radio calls from either aircraft were recorded. No recorded data was available from either aircraft.
Safety analysis
Radio alerting
The gyroplane student pilot recalled making backtracking radio calls when turning around at the end of every wheel balancing exercise. However, the final backtracking call was made before the Extra pilot had turned the aircraft’s radio on, and therefore, they would not have heard this radio call. Additionally, the gyroplane pilots could not recall making a rolling call at the commencement of the final wheel balancing exercise prior to the accident, and there were no other sources of evidence to assist in establishing whether this call was made. In any event, the Extra pilot reported that they did not hear any call.
The Extra pilot reported making 2 radio calls before entering the runway. However, for reasons that could not be determined, the gyroplane pilots reported that they did not hear these calls. Consequently, neither aircraft’s pilots were alerted to the other’s presence over the radio and therefore, aircraft separation became solely reliant on each aircraft’s pilots seeing each other.
Visual search
The gyroplane was operating on the runway for about 11 minutes while the Extra pilot was on the apron preparing for the flight. During this time, the gyroplane was primarily on an area of the runway some distance from the pilot and not directly in sight, limiting the Extra pilot’s ability to detect it during this time.
The Extra pilot did not sight the gyroplane before entering the runway. The gyroplane pilots also did not sight the Extra at the start of their seventh and final wheel balance exercise, or while accelerating on the runway until a collision was imminent. While the reasons for this could not be determined, there were likely many common factors that reduced the ability of the pilots to identify each other such as the small angular size of each aircraft, the complex and cluttered background with reduced contrast difference, and the minimal relative movement between each aircraft.
The effectiveness of the Extra pilot’s visual scan was likely also affected by sun glare before entering the runway, and the tailwheel configuration of the aircraft which limited forward visibility while backtracking. The gyroplane pilots were likely also influenced by the higher workload associated with the training exercise, which probably reduced their available attention for identifying conflicting aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Magni M16C Tandem Trainer gyroplane, G1850, while avoiding Extra EA 300L, VH‑IOG.
Contributing factors
Before entering the runway, the pilot of VH-IOG did not see G1850 occupying the runway and subsequently backtracked towards G1850. As VH-IOG was a tailwheel aircraft, the pilot was unable to sight G1850 while backtracking.
While accelerating on the runway, the instructor and student in G1850 did not see VH-IOG backtracking towards them until a collision was imminent. While manoeuvring to avoid a collision, G1850 collided with terrain.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Lake Macquarie Airport
In May 2023, the airport operator released a bulletin reminding all operators based at Lake Macquarie Airport of several aspects of safe operational practice highlighted by this event, including that:
aircraft should stop forward motion at the hold point line (or equivalent for helicopters) to ensure a good lookout prior to entering the runway environment
pilots are to ensure they know and use correct radio terminology while operating at the airport and to broadcast their intentions
although radio discipline was required, it cannot be relied upon for safety, and that the visual lookout was paramount
for operations involving a backtrack for runway 07, aircraft should turn through 90° in the turning node at the far end, stop to lookout, then broadcast a radio call on lining up
the runway should only be occupied for the minimum time required to either taxi, take off, or land.
The airport operator also advised that:
the hold point line at the apron end of the runway (near the runway 25 threshold) had been repainted and a hold line also painted at the runway 07 end
CTAF radio recording equipment was purchased and anticipated to be installed in February 2024. This will ensure all communications can be reviewed periodically, and in the event of an incident.
Safety action by Inverted Downunder
The operator of VH-IOG advised the ATSB that operational procedures were updated to include requirements for:
a ground employee to have a hand-held radio, switched on and in reach for all operations, and to monitor any departure and arrival radio calls
pilots to stop at the hold point before entering the runway for departures.
Safety action by Australian Sport Rotorcraft Association
The Australian Sport Rotorcraft Association (ASRA) advised the ATSB that, in response to this accident and other previous sport rotorcraft accidents, ASRA intends to replace the one-off human factors exam, which is completed as a requirement of the ASRA pilot certificate, with an updated exam to be completed recurrently as part of each biennial flight review.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot and passenger of the VH-IOG
instructor and student of G1850
VH-IOG operator photos
New South Wales Police Force photos
CCTV footage from Lake Macquarie Airport and Westpac Rescue Helicopter Service
Howett, G. L. (1983), Size of letters required for visibility as a function of viewing distance and observer visual acuity (National Bureau of Standards Technical Note 1180).
National Transport Safety Board (1988), Aircraft Accident Report - Midair Collision of Skywest airlines Swearingen Metro II, N163SW, and Mooney M20, N6485U, Kearns, Utah, January 15, 1987.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Pilot of VH-IOG
instructor and student of G1850
operators of VH-IOG and G1850
Lake Macquarie Airport
the Australian Sport Rotorcraft Association (ASRA)
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway numbers represent the magnetic heading closest to the runway orientation (for example, runway 25 is oriented 250° magnetic while the reciprocal runway 07 is oriented 070º magnetic).
[2] An airport ground procedure which involves the use of any portion of a runway as a taxiway for an aircraft to taxi in the opposite direction from which it will take off or has landed.
[3] ASRA is a national sport and recreational association, representing people with an interest in building and flying gyroplanes. Under Civil Aviation Safety Authority (CASA) accreditation, ASRA administers sport gyroplanes through the certification of pilots and the listing of gyroplanes in Australia.
[5] O’clock: the clock code is used to denote the direction of an aircraft or surface feature relative to the current heading of the observer’s aircraft, expressed in terms of position on an analogue clock face. For example, twelve o’clock is ahead while an aircraft observed abeam to the left would be said to be at 9 o’clock.
[6] An aircraft landing area is an airfield that has not been certified by CASA. These airfields are non-controlled, unregulated facilities. It is the responsibility of pilots and operators to determine whether these airfields are suitable for use.
On 3 April 2023, the ATSB commenced a transport safety investigation into a fatal accident involving a Piper Aircraft Corp PA-28-180 aircraft, registered VH-PXR, about 26 km west of Lakeside Airpark, Queensland.
On 2 April 2023, at about 1530 local time, the pilot and passenger departed Natal Downs Station for a private flight to the Lakeside Airpark (Figure 1). The automatic dependent surveillance-broadcast data recorded the aircraft climbing to, and cruising between 6,000 ft and 6,500 ft above mean sea level while tracking easterly towards the Clarke Ranges. At about 1633, the aircraft was descended and then maintained an altitude between 2,000 ft and 2,500 ft. At about 1651, when in the vicinity of high terrain, the aircraft was turned onto a south-easterly direction for 1 minute. The final recorded position was about 250 m north-north-east of the accident site at about 2,150 ft (about 250 ft above ground level) (Figure 2).
Figure 1: Map with key locations and flight path (red)
Source: Google Earth and Airservices Australia, annotated by the ATSB
When the aircraft did not arrive at the Lakeside Airpark at the expected time, a search and rescue operation commenced. The following day, the aircraft wreckage was located on a steep slope at 1,913 ft. The pilot and passenger were fatally injured and the aircraft was destroyed.
Pilot information
Experience and qualifications
A review of records established that the pilot did not hold a Civil Aviation Safety Authority (CASA) aeroplane pilot’s licence (either a Recreational Pilot Licence or Private Pilot Licence) required to conduct the flight. The pilot also did not hold a Recreational Aviation Australia pilot certificate.
Records from the flying school where the pilot trained showed that they had completed 30.4 hours of flight instruction (25.4 hours dual and 5.0 hours solo) between November 2021 and November 2022. This included 2.9 hours on the Piper PA-28-180 aircraft type. During this time, the pilot completed the practical requirements to obtain a CASA recreational pilot licence but had not completed the flight or theory tests required to have the licence issued. It was reported by the flying school that the pilot intended to continue with training to attain a CASA Private Pilot’s Licence (Aeroplane), and this was the reason no testing had been completed. The training records also showed that the pilot had completed one navigation theory lesson towards this licence. No further records of flying training or other flying experience was available.
The pilot became the registered owner of VH-PXR in November 2022. The ATSB could not determine how many hours experience the pilot had in the aircraft. Information obtained by the ATSB detailed that the pilot had flown around the area around Natal Downs station in the aircraft. In addition, the automatic dependent surveillance-broadcast data recorded a previous return flight in the aircraft from Natal Downs Station to Lakeside Airpark about 1 week prior to the accident.
In suitable weather conditions, the planned flight from Natal Downs Station to Lakeside Airpark could have been flown in visual flight rules[1] conditions by a pilot holding a CASA Recreational Pilot Licence with a navigation endorsement.
Medical information
The pilot was issued with a Class 2 Aviation Medical Certificate in January 2023. The ATSB reviewed the pilot’s aviation medical records, which noted that they had previous, and ongoing medical conditions. The ATSB corresponded with CASA, who advised that they had considered this information in the issue of the pilot’s medical certificate. They had also conducted a post‑accident review of the pilot’s medical records and remained satisfied that the pilot met the requirements for the issue of the certificate.
Aircraft information
VH-PXR was a Piper Aircraft Corp PA-28-180 Cherokee aircraft, first registered in Australia in August 1968. A periodic inspection was carried out and a maintenance release issued on 24 October 2022 at 10,861.6 hours’ time-in-service. The aircraft was approved for instrument flight rules[2] operation, however, at the time of the accident it was restricted to day visual flight rules only until instrument lighting and glideslope defects were rectified.
The ATSB acquired evidence the pilot had completed maintenance on the aircraft’s pitot-static mast in February 2023 to clear blockages. They did not hold an aircraft maintenance engineer licence or authorisation to perform or certify for maintenance on the aircraft. This type of maintenance could lead to erroneous indications of the airspeed indicator, altimeter, and vertical speed indicator. It could not be determined if this contributed to the accident.
Meteorological information
The flight departed in good conditions suitable for visual flight. However, as was forecast, the conditions deteriorated as the aircraft approached the Clarke Ranges. Information from the Bureau of Meteorology for the accident area (within the Clarke Ranges) indicated that the forecast for all heights above mean sea level was:
generally broken cloud[3] between 2,000 ft and 6,000 ft
scattered showers of rain with broken cloud base of 1,000 ft and visibility reducing to 3,000 m
isolated thunderstorms with bases of 1,000 ft and visibility reducing to 1,000 m.
The conditions over these ranges and toward the coast included significant low cloud, rain, and thunderstorms. All these phenomena led to reduced visibility. Immediately prior to the accident, the weather radar recorded rain in the area.
Images and video taken during the flight showed broken cloud ahead, with the base below the altitude of the aircraft. The ranges where the accident site occurred were obscured by low cloud, with rain visible (Figure 3).
Figure 3: Image taken in-flight of the weather conditions ahead
Source: Supplied
Terrain
The flight was initially conducted over the relatively flat terrain of inland Queensland, with elevations generally ranging between 500 ft and 1,500 ft. The Clarke Range separated the inland areas from the low and flat coastal plains near the destination, Lakeside Airpark, for about 55 km along the intended route. Within the Clarke Range, the topography was substantially more rugged and elevated than the coastal or inland areas, rising in excess of 3,200 ft. The accident occurred within this area at an elevation of 1,913 ft.
Site and wreckage information
Due to the terrain, the ATSB did not attend the accident site. However, photographs and videos were obtained from Queensland Police and the Australian Maritime Safety Authority Joint Research Co-ordination Centre, and examined by the ATSB (Figure 4). Observations of the accident site included:
About 80 m prior to the wreckage, a number of trees sustained damage. This damage was shown to have an increasing angle down towards the wreckage.
The aircraft collided with terrain on a steep slope, and the wreckage was observed to be inverted. It was unknown if the aircraft collided with terrain inverted or became inverted during the accident sequence.
There was minimal spread of the wreckage, and the wings, fuselage, and tail were in their expected positions relative to the structure of the aircraft.
The leading edge of the right wing sustained damage consistent with a tree strike.
The forward fuselage was destroyed by fire.
The propeller was found intact, and showed impact marks and bending consistent with the engine producing power at the time of impact.
Consideration of these factors suggested that an in-flight break-up, engine failure or fuel exhaustion were unlikely to be contributory to the accident. The relatively contained wreckage was representative of a low speed, high angle of attack impact with the ground.
This accident highlights the importance of following the standards for the operation and maintenance of aircraft to ensure the safety of flight. It further demonstrates that weather continues to remain one of the most significant causes of accidents in general aviation. The often‑fatal outcomes of these accidents are usually all the more tragic as they are avoidable. Despite the dangers of visual flight rules pilots flying into instrument meteorological conditions being well recognised, this continues to be a recurring factor in aircraft accidents and has been the focus of numerous previous ATSB reports and publications.
The ATSB publication Avoidable Accidents No. 4, Accidents involving Visual Flight Rules Pilots (VFR) in instrument Meteorological Conditions (IMC) found that weather alone is never the only factor affecting pilot decisions that result in these events. Investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather. The ATSB encourage all pilots, no matter what their experience level, to develop the knowledge and skills required to avoid unintentional operations into adverse weather. This could be aided by having alternate plans in case of unexpected changes in weather, making timely decisions to turn back, divert or hold in an area of good weather, and using a ‘personal minimums’ checklist to help clearly identify risk factors.
Reasons for the discontinuation
The Civil Aviation Safety Authority have put in place regulations designed to ensure pilots are properly trained and qualified to manage challenges likely to be encountered during flying operations. This includes training intended to teach pilots to identify and manage situations presented by adverse weather, both at the pre-flight planning phase and during flight. However, when pilots operate outside these rules, they remove the built-in safety defences. On that basis, the ATSB determined that there was limited safety benefit in continuing to direct resources at this investigation when compared with other priorities and elected to discontinue this investigation.
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[3] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘broken’ indicates that more than half to almost all the sky was covered.
On 4 April 2023, the pilot of a Robinson R44 Raven II helicopter, registered VH-WLH, was conducting aerial mustering operations on at Bingegang, Queensland (about 60 km south-east of Middlemount). The pilot was the only person on board.
While the pilot was reportedly flying to look for straggling cattle the helicopter struck an aerial powerline and collided with terrain. The pilot was fatally injured and the helicopter was destroyed by post-impact fuel-fed fire.
What the ATSB found
The pilot had an operational reason to be in the area at low level at the time of the accident. There was no evidence of pre-existing helicopter defects and the terrain was generally suitable for a landing had an in-flight emergency arisen.
The pilot was reportedly familiar with the property and knew that there was a powerline running across it, although it was not possible to conclusively determine the level of awareness they had of the wire’s presence and location during the flight. The ATSB concluded that the pilot likely lost awareness of, and did not see, the unmarked aerial powerline during low-level aerial mustering.
The powerline was not marked and nor was there a requirement to do so. The helicopter model was not able to be fitted with wirestrike protection equipment.
Safety message
This accident provides another reminder of the dangers posed by aerial powerlines during low-level mustering. There are limits to the extent to which operators can mitigate the risk of wirestrike during low-level operations near powerlines. Helicopter wirestrike protection (WSPS) can provide a last line of defence in the event of a wirestrike. Some aircraft selected for aerial agriculture operations can be configured to include WSPS. However, this technology is not currently available on smaller helicopters such as the Robinson R44.
The ATSB has released, in association with the Aerial Application Association of Australia (AAAA), an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains numerous wirestrike accidents and lessons learned from them.
Electrical power and telecommunications companies in Australia can mark powerlines that are identified as a hazard for low-level flying operations and some have a safety scheme to reduce the costs to property owners.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 4 April 2023, the pilot of a Robinson R44 Raven II helicopter, registered VH-WLH, was conducting cattle mustering operations on a private property at Bingegang, Queensland (about 60 km south-east of Middlemount), owned and operated by the pilot’s family business. The pilot was the only person on board and was reported to be familiar with the property. The weather was clear.
Mustering commenced early in the morning and according to witnesses the pilot took a 60–90 minute break before recommencing at about 1000. At about 1110, after mustering a large mob of cattle into a holding paddock, the pilot flew back to one corner of the lot to look for stragglers. The pilot then radioed for workers on the ground to help with further mustering.
As the workers approached, they saw a plume of smoke and were unable to contact the pilot via radio. They then saw that the helicopter had struck a single-strand aerial powerline and collided with terrain. The wreckage was on fire. The pilot was unresponsive and the workers were unable to remove the pilot due to the increasing intensity of the fire.
The pilot had been fatally injured and the helicopter was destroyed by post-impact fire.
Context
Personnel information
The pilot held a private pilot licence with a class rating for single-engine helicopters and a helicopter low-level operational rating. The pilot held a class 2 civil aviation medical certificate which included the requirement for distance vision correction lenses to be worn and reading correction lenses to be available. It was reported that the pilot always wore glasses, was wearing them on the day of the accident, and that they knew of the presence of the powerline on the property.
Aircraft information
The helicopter was a Robinson R44 Raven II, serial number 14253, manufactured in the United States in 2018 and registered in Australia on 30 October 2018. It was issued with a certificate of airworthiness in the normal category on 16 November 2018.
The R44 is a single-engine, light utility and training helicopter with a semi-rigid, two-bladed main rotor, a two-bladed tail rotor and skid type landing gear. It has an enclosed cabin with two rows of side-by-side seating for a pilot and three passengers. The pilot sat on the right side, and extensive windows at the front of the helicopter afforded generally excellent visibility ahead. The accident helicopter was being flown with the doors fitted.
A wirestrike protection system (WSPS) was not fitted to the accident helicopter. In general, smaller helicopters such as Robinson R22 and R44 series had no structural hard points to fit a wirestrike protection system, were too light, and in many instances travel too slowly for a WSPS to be effective.[1]
Site information
Figure 1 shows an overview of the accident site. The powerline, a single-wire earth return (SWER) wire that ran across the property, was not marked and there was no requirement within the applicable aviation regulations, Australian Standards or elsewhere to do so. The wire was estimated to be at a height of 5.6 m at the point of impact.
The terrain was clear to the right of the helicopter’s flightpath, and there were trees taller than the wire height that would have obscured the wire and pole on the left side.
Source: Google, Queensland Police. Annotated by the ATSB
The helicopter impacted terrain left side down and yawing to the right about 90 m beyond the point of contact with the wire and facing back towards the wire. There was insufficient evidence available to determine the angle and speed of impact with the ground.
Visibility of powerline
Queensland Police officers later returned to the accident site to conduct a simulation using a remotely piloted aircraft system (RPAS) of the helicopter’s approximate flight path and height prior to striking the powerline assuming that it had not turned. The simulation was conducted in conditions similar to those on the day of the accident. Images from the RPAS simulating what the pilot would have seen when approaching the wire showed the wire was difficult to distinguish from the background and the left pole was obscured by trees (Figure 2).
The ATSB examined the aircraft wreckage after it was moved to a secure facility by Queensland Police.
The examination of the wreckage indicated that the impact with terrain was likely not survivable. The helicopter’s cockpit, systems and engine were severely damaged by the impact and post-impact fire. Within the limitations of the available evidence, there were no indications of pre-flight defects, in-flight fire or birdstrike.
The examination found that the wire was struck between the helicopter’s nose and the upper surface of the skids. Additionally, the wire marks on the upper surface of both skids were similar, and in conjuction with the position of the wreckage indicated the helicopter was travelling about perpendicular to the wire.
During the accident sequence, the rotor struck and separated the tail boom. The nature of this damage, and other evidence, indicated that the rotor had high energy at the time.
Marks on the left oil cooler indicated that the engine and ring gear were rotating at the time of impact. Other impact marks indicated that the engine stopped rotating during the impact sequence.
The helicopter’s warning light filaments, including a carbon monoxide warning, were consistent with them not being illuminated at impact.
The helicopter was fitted with a bladder fuel tank, which was breached during the accident sequence. Due to the intense fire, it was not possible to assess how the tank was breached.
Maintenance information
The helicopter’s most recent periodic (100-hourly) inspection was carried out on 6 September 2022, at 660.6 hours in service, after which a maintenance release was issued. A review of all previous maintenance releases identified no discrepancies or significant defects. The most recent maintenance (a tail rotor blade inspection) was carried out at 674.1 hours, on 6 January 2023.
At each periodic maintenance inspection, engine cylinder compression checks were carried out. The tests resulted in satisfactory compression. However, during the most recent test (at 660.6 hours in service), the variation in compression levels was at the lower limit (10–15 psi) of where a re-test should be made within 10 engine operating hours (no later than 670.6 hours in service). There was no record that this was carried out, however, the time in service at the time of the accident could not be determined as the maintenance release was not found and was likely destroyed in the post-impact fire.
Medical and pathological information
A toxicological examination showed the pilot did not have elevated levels of carbon monoxide at the time of the accident and tests for other substances likely to have an effect on performance were negative.
Witnesses reported that the pilot was wearing the helicopter’s three-point harness. The pilot was not wearing a helmet.
A final post-mortem examination report was not available at the time of publication, however, the autopsy certificate for the pilot recorded the cause of death as chest injuries resulting from the accident.
Safety analysis
Within the limitations of the available evidence, there were no indications of pre-impact defects, in-flight fire or birdstrike. Damage to the wire and helicopter were consistent with a wirestrike at a height of about 5.6 m.
The pilot had an operational reason to be in the area at low level at the time of the accident. The pilot was reportedly familiar with the property, which was also owned and operated by the pilot’s family business, and knew that there was a powerline running across it, but it was not possible to conclusively determine the level of awareness they had of the wire’s presence and location during the flight. However, the wire was unmarked and would have been very difficult to see from the air as it was partially obscured by large trees to the left of the helicopter’s flight path and in the distance, and combined with the undulating terrain, deprived the pilot of critical visual cues. Further, the task of visually scanning for cattle that had been separated from the larger mob was a potential distraction. It is therefore likely that any awareness the pilot had of the wire was lost during the flight, and the pilot did not see it at all or in time to avoid the wirestrike.
Helicopter wirestrike protection (WSPS) can provide a last line of defence in the event of a wirestrike. Some aircraft selected for aerial agriculture operations can be configured to include WSPS. However, this technology is not currently available on smaller helicopters such as the R44.
Wreckage examination indicated that the fatal injuries sustained by the pilot probably would not have been prevented through the use of a helmet, and the pilot was wearing a three-point harness which reduces the likelihood of upper body injuries. However, in low-level operations where the risk of an accident is higher, options to improve accident survivability include the wearing of a helmet and the installation and use of a five-point harness.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving Robinson R44 II, VH-WLH on 4 April 2023.
Contributing factors
The pilot likely lost awareness of and did not see an unmarked aerial powerline during low-level aerial mustering.
Other factors that increased risk
The powerline was partially obscured by trees and terrain, depriving the pilot of critical visual cues as to its presence.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Civil Aviation Safety Authority
Queensland Police Service
maintenance organisations for VH-WLH.
References
Australian Transport Safety Bureau 2006, Aviation Research and Analysis Report B2005/0055 Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
Civil Aviation Safety Authority.
A submission was received from the operator. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] ATSB Aviation Research and Analysis Report B2005/0055 Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004 (Re-released September 2006).
On 17 March 2023, the pilot of a Cirrus SR22, registered VH-XGR, was conducting a private flight under the instrument flight rules from Southport, Queensland to Bankstown, New South Wales.
During the landing, the aircraft sunk onto the runway and bounced along the runway for about 5 seconds, then rapidly entered a steep climbing turn to the left. Having reached a maximum height of about 40 ft, the bank angle exceeded 90° and the aircraft dropped onto the left wing and nose.
When emergency services arrived at the site, the aircraft was upside down on the grass between the runways. The left wing had detached, and fuel was leaking from the right side. The pilot was strapped in and conscious but confined in the aircraft.
Once the site had been blanketed with fire suppression foam and the aircraft stabilised with step blocks, ambulance personnel were able to attend to the pilot. Rescue personnel stabilised the wreckage and used a reciprocating saw to cut the left side of the inverted fuselage to extricate the pilot.
When the pilot was extricated, their condition suddenly deteriorated they were taken to hospital in a critical condition and later died from injuries sustained in the accident.
During the rescue process the site commander was advised that the aircraft was equipped with a ballistic parachute. A Cirrus-qualified maintenance engineer then attended to render the ballistic system safe from inadvertent activation.
What the ATSB found
In the early stages of a go-around from an unstable landing, the pilot was unable to counter the substantial torque effect associated with high engine power, low airspeed, and high pitch angle, resulting in loss of control and collision with terrain.
The emergency responders were initially unaware that the aircraft was equipped with a ballistic parachute (CAPS) and initiated the recovery of the pilot with the system still armed. By not securing the CAPS, the risk of inadvertent rocket activation and injury was increased.
Cirrus Aircraft provided training, education, and placards to reduce the risk of inadvertent post‑accident actuation of the ballistic parachute (CAPS) rocket and associated injury. However, the training and education had limited reach, and the placards did not clearly communicate the danger or provide access to safety information.
The ATSB also identified an opportunity for Cirrus to enhance the safety benefit of their go-around related training and educational products, especially in regard to the SR22 models that were equipped with relatively high-power engines.
What has been done as a result
Cirrus Aircraft advised that they had enhanced the external CAPS placarding on 2 new models of aircraft (the SF50, and another in development) to align with current American Society for Testing and Materials (ASTM) standards. The SR2X series of aircraft (the SR20, SR22, and SR22T) were certified prior to the implementation of ASTM standards. At the time of writing, Cirrus was reviewing the possibility of enhancing the placard that was certified with SR2X.
During the draft report review process the ATSB sought input from Cirrus as to whether there was an opportunity to enhance the safety benefit of their go‑around training and educational products, especially in regard to the SR22 models that are equipped with relatively high-power engines during the landing phase.
Cirrus did not advise of any associated safety action.
Safety message
A go-around to recover from an unstable landing is more dynamic and presents a greater challenge than a go-around on approach. Although the procedure for go-arounds generally applies to both scenarios, it requires careful application when implemented in the landing phase.
Pilots of single-engine aircraft with relatively high-power engines, such as the Cirrus SR22, need to be aware of the potential for significant torque effect and loss of control associated with high engine power, low airspeed, and high pitch attitude.
The Cirrus Airframe Parachute System (CAPS) is credited with saving a number of lives but also presents a serious post-accident hazard when it has not been deployed and the aircraft is damaged. If the rocket is inadvertently activated, anyone in its path would be seriously or fatally injured. Cirrus Aircraft advises first responders that it is imperative that the presence of an airframe parachute system be identified as early as possible, and the system disabled to make it safer to work around.
The ATSB directs first responders/emergency services and airport operators to the Advisory Guide For First Responders: Cirrus First Responders (cirrusaircraft.com) to provide awareness and reduce the risk of inadvertent post-accident activation of CAPS and to the ATSB webpage ‘Hazards at aviation accident sites’.
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 17 March 2023, the pilot of a Cirrus SR22, registered VH-XGR, was conducting a private flight under the instrument flight rules[1] from Southport, Queensland to Bankstown, New South Wales.
The aircraft departed Southport at 1211 Eastern Standard Time[2] and tracked initially to the south‑west. After a couple of minutes, the pilot turned the aircraft onto a southerly heading for the relatively direct track to Bankstown. The pilot initially climbed the aircraft to FL 180[3] for a couple of minutes then descended to FL 160 for the remainder of the cruise phase of the flight. All of the flight parameters—track, altitude and groundspeed—indicated normal operation.
At 1504 Eastern Daylight-saving Time,[4] the pilot commenced descent and altered track slightly. There were other minor track changes, consistent with air traffic control (ATC) or airspace requirements, as the flight progressed towards visual flight rules (VFR)[5] reporting point Prospect Reservoir (Figure 1).[6]
Figure 1: Sydney VTC extract showing Prospect Reservoir in top left corner and Bankstown Aerodrome in lower middle of image
Source: Sydney VTC
At 1533, the aircraft was over Prospect Reservoir on descent through 1,900 ft and tracking towards Bankstown Airport (Figure 2). Shortly after, the pilot transmitted on the applicable Bankstown Tower frequency:
Bankstown Tower, Cirrus xray golf romeo (XGR), Prospect, 1,800, inbound with information November, and visual.
In response, the aerodrome controller (ADC) instructed XGR to:
Join final runway 11 Left[7] and report established at 3 miles. VFR traffic about 2 miles is a Tecnam. If you get a bit too close you can expect runway centre.
This was acknowledged by the pilot of XGR.
About 20 seconds later, the ADC advised XGR:
I’ll make that a plan now, join final for runway 11 Centre. Report established 3 miles. Traffic is that Tecnam ahead.
This was acknowledged by the pilot of XGR.
The ADC passed traffic information to the Tecnam with advice that the Cirrus would be overtaking to the right and to shift slightly to the left. This was followed by some traffic guidance to the pilot of XGR:
XGR suggest a slight right turn, the Tecnam is in about your one o’clock at 1 mile.
This was associated with a diversion of track slightly to the right for a minute and 15 seconds.
The pilot then turned left to align the aircraft for final approach to runway 11C. At this point (1535:19), the aircraft was 2.87 NM (5.3 km) from the runway threshold, slowing down through 106 kt groundspeed, and about to descend from 950 ft.
As XGR was being turned onto finals, the ADC advised:
XGR runway centre number 1. Additional traffic is a Diamond late right downwind in the training circuit [runway 11 Right].
This was acknowledged by the pilot of XGR.
At 1535:45, the ADC advised:
XGR runway centre cleared to land
This was promptly read back by the pilot of XGR:
Cleared to land on centre, XGR
That was the last communication with the pilot of XGR. At that point, XGR was 1.9 NM (3.5 km) from the threshold, on descent through 725 ft, and slowing down through 90 kt groundspeed.
As the approach continued, the groundspeed continued to slow until reaching a groundspeed of 60 kt while on descent through 350 ft. The groundspeed varied between 60 and 63 kts until the last data point recorded at 100 ft.
Figure 2: Track from Prospect reservoir to Bankstown Airport
Source: Google Earth, annotated by the ATSB
Although some witnesses noted the speed of the Cirrus was relatively slow, there were no reports of anything abnormal until the landing. The landing was observed by pilots on concurrent approaches to the adjacent runways, and the aerodrome controller. A security camera recorded imagery of the accident sequence.
The instructor in the right seat of the Tecnam (at about 200 ft on final for runway 11 Left) observed the Cirrus touchdown on the runway and bounce into the air to a height of about 10–20 ft. They advised that the aircraft appeared to be very slow, and it bounced again with low energy, with white dust evident from the tail area. It then started to veer to the right, pitched up violently and started to bank steeply to the left (towards runway 11 Left). Concerned about separation, the instructor initiated a go-around. The Cirrus came down on one wing and tumbled onto the roof, stopping quickly.
The instructor in the right seat of the Diamond (on short final for runway 11 Right) observed the Cirrus over the runway in a very high nose attitude and veering right. They advised that it then rolled sharply to the left, dropped the nose, and tracked over the grass between runways 11 Centre and 11 Left. The left wing impacted the ground first, followed by the nose, then flipped over onto the canopy.
The ADC was observing the Cirrus as it was about to touch down. They advised that they saw the aircraft pitch up and reach about 30–40 ft then roll to the left. As the aircraft was crossing over towards runway 11 Left, the ADC issued a safety alert to the Tecnam (1537:38). It appeared to the ADC that the aircraft was accelerating as the left-wing tip impacted the ground followed by the nose.
A camera mounted on the Bankstown Airport passenger terminal[8] recorded low resolution imagery of the accident sequence (Figure 3). It showed the aircraft sinking onto the runway, proceeding along the runway for about 5 seconds, then rapidly entering a steep climbing turn to the left. Having turned through 90° and reached a maximum height of about 40 ft, the bank angle exceeded 90° and the aircraft dropped onto the left wing and nose. This was also recorded by a camera in a different location.
Figure 3: Bankstown Airport terminal CCTV showing sequence from initial touchdown to just before impact (right to left)
Source: Bankstown Airport edited and annotated by the ATSB
Bankstown Tower activated the aerodrome emergency plan, including notification to emergency services and the aerodrome reporting officer. The airport was subsequently closed, and traffic was processed out of the control zone.
New South Wales (NSW) Police Force personnel arrived within 5–8 minutes of the notification, followed by NSW Ambulance. Fire and Rescue NSW (FRNSW) crews arrived about 8.5 minutes from receiving the call. Bankstown Fire Station crews usually responded to incidents at the airport, but they were unavailable so crews from Revesby Fire Station attended.
When emergency services arrived at the site, the aircraft was upside down on the grass between the runways. The left wing had separated, and fuel was leaking from the right side. The pilot was strapped in and conscious but confined in the aircraft.
The responding FRNSW crews did not include technical rescue personnel, so the site commander arranged for that expertise to attend. Once the site had been blanketed with foam and the aircraft stabilised with step blocks, ambulance personnel were able to attend to the pilot.
Before starting the rescue, the crew strapped the rear fuselage to the ground. They then used a reciprocating saw to cut the left side of the inverted fuselage to extricate the pilot. The FRNSW personnel were unaware of any aircraft type-specific hazards and did not notice any no-cut labels on the aircraft.
When the pilot was extricated, their condition suddenly deteriorated, and they were taken to hospital in a critical condition.
About 15 minutes into the rescue process, the FRNSW site commander was advised that the aircraft was equipped with a ballistic parachute. The commander had a general awareness that a ballistic parachute was installed in the tail but found it difficult to get information about its operation. The airport owner arranged for a Cirrus-qualified maintenance engineer to render the ballistic parachute system, known as the Cirrus Airframe Parachute System (CAPS), safe from inadvertent activation.
The maintenance engineer advised that they inserted a pin into the CAPS activation handle located in the cabin ceiling and taped it into place. They inspected the activation mechanism in the rear cargo compartment and found that the activation cable was not under tension and the rocket igniter switch firing pin had not moved. The electrical wires were not disconnected because of concern about the fuel spillage. On the day after the accident, the engineer disconnected a battery in the tail but, due to aircraft damage, was unable to access an additional battery in the front of the aircraft.
Another Cirrus-qualified maintenance engineer who attended the aircraft the day after the accident advised that there was tension on the activation cable, and it was only marginally lower than the force required to move the pin. To render the CAPS safe for recovery of the wreckage, the engineer cut the activation cable and disconnected the electrical leads from the igniter switch.
The pilot died in hospital on 6 April 2023 from injuries sustained in the accident.
Context
Pilot information
The pilot held a private pilot licence (aeroplane), issued in 2011, with a single engine aeroplane rating. In addition, the pilot held a single engine aeroplane instrument rating and Night VFR rating.
In February 2023, the pilot had recorded total flying experience of 860 hours, including 47 hours in the previous 6 months. Almost all of the total experience and all of the recent experience was reported to be operating VH-XGR.
The last training or check completed by the pilot was an instrument proficiency check (IPC) in VH‑XGR. This was attempted on 8 February 2023 but was not successful. The flight examiner advised that during a hand-flown instrument approach the pilot had allowed the aircraft to descend below the glidepath indication and develop a high rate of descent.
As recommended by the flight examiner, the pilot then conducted some VFR flying (without an instructor) and a pre-IPC practice flight with the flight examiner. On 2 March 2023, the pilot attempted the IPC again with the flight examiner and was successful.
The flight examiner recalled that over the course of the 2 recent IPCs, and associated practice flights, the pilot’s general flying, including circuits and landings, was unproblematic. Although those flights included a number of go-arounds that were safely executed, the flight examiner had discussed with the pilot the need to be cautious when applying power during go-arounds to ensure the aircraft remained easy to control.
The flight examiner had completed the Cirrus Standardised Instructor Pilot training in 2020 and been involved in the pilot’s flying training and assessment during the previous 3 years.
The pilot’s last aviation medical examination, conducted on 28 February 2023, was for a Class 2 medical certificate. This was revalidated by the designated aviation medical examiner with continuation of the restrictions that distance vision correction must be worn and reading correction to be available while flying.
At the time of drafting the report, the postmortem report was not available. However, analysis of the radio transmissions made by the pilot to Bankstown Tower showed that these transmissions were appropriate and there were no indications of any abnormalities—slowed/slurred speech patterns or simple errors—which could indicate a medical issue.
Environmental conditions
The aerodrome forecast for Bankstown Airport issued at 1534 local time anticipated that between 1500 and 1700 the wind would be from 130 degrees (True) at 17 kt, visibility would be greater than 10 km with no cloud, temperature over the same time period was forecast to be 28°. At 1530, the wind was reported from 090 degrees (True) at 16 kts and the other conditions were consistent with the forecast.
Wind speed and direction were recorded at Bankstown airport every minute. Those observations in the 2 minutes before and after the accident are presented in Table 1.
Table 1: One-minute wind observations at Bankstown Airport on 17 March 2023
Local Time
Wind speed (kt)
Wind direction (Degrees True)
1536
16
106
1537
15
106
1538*
14
099
1539
17
104
1540
15
100
*The closest observation to the time of the accident was at 1538. At that time, the angle between runway 11 (111° magnetic) and the recorded wind from the left (086° magnetic) was 25°. That provided a crosswind component of 6 kt from the left and headwind component of 13 kt. There was no significant variation in the minute before or after that time.
Operational information for Bankstown Airport in the En Route Supplement Australia (ERSA) cautioned that:
During winds with a southerly direction, building induced mechanical turbulence may be experienced on final for RWY 11C and RWY 11R/29L.
Although the prevailing wind was not from a southerly direction, the ATSB considered the potential for mechanical turbulence. The closest buildings in line with the direction of the wind were no higher than 3 levels and located at least 900 m from the threshold of runway 11 Centre. Given the wind strength and the distance of the buildings, it is unlikely that the buildings had any significant effect on the conditions for landing on runway 11 Centre.
The instructor in the Tecnam advised that on approach and landing to runway 11 Left there was no significant crosswind or mechanical turbulence, and the conditions were relatively smooth. In addition, the ADC did not notice any disturbance to the flight path of aircraft on approach.
Operating procedures
The Cirrus SR22 Pilot’s Operating Handbook included a procedure for balked landing/go-around:
In a balked landing (go around) climb, disengage autopilot, apply full power, then reduce the flap setting to 50%. If obstacles must be cleared during the go around, climb at 80-85 KIAS with 50% flaps. After clearing any obstacles, retract the flaps and accelerate to the normal flaps up climb speed.
Pilot training and operational guidance
Pilot training and assessment
Pilot training and assessing in Australia was carried out in accordance with the CASR Part 61 manual of standards (MOS). The competency standards for the Land Aeroplane unit included elements and performance criteria for conduct of a missed approach and recovery from a missed landing.
For both sequences, the criteria was to make a smooth positively-controlled transition from approach or missed landing to a missed approach including selection of power, attitude and configuration to safely control the aeroplane. The causes of loss of control during landing and contents of the pilot’s operating handbook were part of the underpinning knowledge requirements.
The competency standards for night VFR and instrument approaches included the conduct of missed approaches.
To safely exercise the privileges of a rating, a pilot must have completed a flight review for the rating within the previous 2 years. Once the pilot demonstrated competency in accordance with the Part 61 MOS, the instructor was able to assess it as completed.
An instrument proficiency check (IPC) is an assessment of the pilot’s competency to conduct a flight in actual or simulated instrument meteorological conditions under the IFR to the standards specified in the Part 61 MOS. An IPC included missed approaches in the context of instrument approaches and was valid for 12 months.
Cirrus training and guidance material
Cirrus Aircraft provided an instructor pilot course intended to prepare qualified instructors with SR20/22 experience to provide high-quality standardised training to owner-pilots and students using Cirrus Aircraft-approved resources. The course included the demonstration, teaching, and assessment of landings and go-arounds with an emphasis on flight operations manual (FOM) procedures and use of the TOGA button, and memory items.
Online training and education for pilots was also available through the Cirrus Approach portal. This included the FOM for the SR series aircraft that addressed standard operating procedures applicable to the traffic pattern, stabilised approaches, landings, and go-arounds.
One of the specialty courses was ‘SR series Take-offs and Landings’ and 2 of the shorter presentations hosted on YouTube (Flight Fix) addressed go-arounds and stable approaches.
The following information, selected for relevance to the occurrence, has been adapted from the FOM and online training/education resources.
It was recommended that the autopilot was disconnected prior to entering the traffic pattern (circuit) and the yaw damper was off prior to landing.
For final approach, the target indicated airspeed (IAS) was 80 kt with full flap and engine power as required. One of the common errors on approach was not compensating for ballooning when deploying the flaps, resulting in excessive loss of airspeed and/or altitude gain.
A stabilised approach was defined as constant angle and constant rate of descent approach profile ending near the touchdown point. If this was not achieved, a go-around must be carried out. In addition, a go-around was recommended in situations such as excessive ballooning during landing or excessive bouncing.
A go-around was presented as a 4-part flow comprising:
Power Up – immediately but smoothly apply full power (as for take-off – typically 4–5 seconds), connected right rudder due to significant left turning tendencies (possible strong pitch up), and simultaneously;
Pitch Up – smoothly and initially to level attitude and begin accelerating. If the aircraft has a TOGA button and it is pushed, it provides pitch guidance on the primary flight display (PFD)
Clean Up – retract flaps to 50% then as the aircraft speed increases gently transition to Vx [speed for best angle of climb] or Vy [speed for best rate of climb]. When positive rate of climb and obstacles are cleared above flap retract speed of 80 KIAS, retract flaps to zero
Call Up – communicate as required.
Common errors included not maintaining coordination during the go-around, and improper pitch control resulting in excessive loss of altitude, stall entry, or both. This could occur if the aircraft was climbed out of ground effect before a safe airspeed was reached.
Landing technique including in a crosswind was conventional. Common errors included the pilot flaring too high and creating a stall to hard landing situation.
Rejected landing and go-around aerodynamics
Engine power changes can affect stability. An increase of power may tend to make the nose rise (low thrust line tends to add to nose-up effect of horizontal tail surface). This effect can be exacerbated with full flap.
In a single-engine propeller-driven aircraft, application of engine power will produce ‘torque’ in the form of a twisting or rotating motion around at least one of the 3 axes. For an aircraft with a clockwise rotating propeller (viewed from the cabin) such as the Cirrus SR22, the overall result will be a left turning tendency. This is the combined effect of 4 elements, which are briefly explained in the context of a clockwise rotating propeller.
Torque reaction: as described by Newton’s Third Law of Physics, the revolution of the engine and propeller in one direction produces an equal force trying to rotate the aircraft in the opposite direction. As this induces a roll to the left when the aircraft is airborne, the design will generally compensate for this tendency in cruise (for example, by an offset engine and by provision of aileron trim). During the take-off roll, the increased loading on the left main wheel produces relatively higher drag and a turning moment to the left. The magnitude of the left roll and turn tendency is dependent on:
size and power of the engine
size of propeller and RPM
size of the aircraft
condition of the ground surface.
Corkscrew effect: At high propeller RPM and low forward speed, the spiral or corkscrew rotation of the slipstream exerts a sideways force on the vertical fin, which produces a yawing moment to the left. In addition, the corkscrew flow of the slipstream produces a rolling moment to the right around the longitudinal axis. Although these forces may be counteracting each other, they vary greatly and require the pilot to apply the necessary corrective action.
Gyroscopic action: as a spinning rotor, the propeller is subject to gyroscopic precession when a force is applied to the rim of the plane of rotation. In simple terms, any yawing about the vertical axis results in a pitching moment and any pitching around the lateral axis results in a yawing moment.
Asymmetric loading (P-factor): when an aircraft is flying with a high angle of attack, the effectiveness of the downward moving blade is greater than that of the upward moving blade. This moves the centre of thrust to the right, which results in a yawing moment towards the left around the vertical axis.
Aircraft information
General information
The aircraft was manufactured in 2009 by Cirrus Design Corporation in the United States to a GTS equipment specification and with G3 model features such as a redesigned carbon fibre wing. It was registered in Australia as VH-XGR in the same year.
Although produced as an SR22, which was certified with a normally aspirated Continental Motors Inc. IO-550-N engine, the aircraft engine had been modified during manufacture in accordance with a supplementary type certificate. This involved installation of a Tornado Alley Turbo Inc. Turbonormalizing System that was designed to maintain sea-level performance of 310 hp up to the maximum altitude of 25,000 ft. As such, it was referred to as an SR22TN.
One of the features of the aircraft was a single-lever power control that adjusted engine throttle with automatic adjustment of engine speed through a mechanical linkage to the propeller constant speed unit. The system was set to maintain approximately 2,500 RPM at cruise power settings and 2,700 RPM at full power.
The aircraft was also equipped with an oxygen system to allow the pilot to operate over 10,000 ft in the unpressurised cabin. A fingertip oximeter was located in the cabin after the accident.
Conventional flight controls are operated mechanically by a single-handed side control yoke and rudder pedals. Pitch and roll trim was provided through adjustment of the neutral position of a compression spring cartridge by means of an electric motor in each control system. These were intended to allow easy override of full trim or autopilot inputs by using normal control inputs. Pilot control was effected by movement of a conical trim button on the control yoke.
Yaw trim is provided by a spring cartridge in rudder control system that provided a centralising force, regardless of the direction of rudder deflection. This was not adjustable in flight.
Avionics and instrumentation
The aircraft was equipped with the Cirrus Perspective Integrated Avionics System developed by Garmin. Flight instrumentation, position, navigation, communication, and identification information were displayed through a primary flight display (PFD) and a multifunction display (MFD). An automatic flight control system (AFCS) provided flight director, autopilot, yaw damper, and manual electric trim functions.
Indicated airspeed is displayed on the PFD by a moving tape with a rolling number gauge. The colour-coded tape showed the low-speed range as a red strip up to the low-speed awareness velocity (VLSA). An airspeed trend vector in the form of a variable-length magenta vertical line showed the projected indicated airspeed in 6 seconds (for constant rate of acceleration or deceleration). When selected on, V speeds such as Vx (best angle of climb) and Vy (best rate of climb) were displayed next to the airspeed scale.
Key engine parameters are displayed on the left side of the MFD during normal operations, including analogue style power indication (percentage) and numeric values for power, RPM and manifold pressure.
A carbon monoxide detector generated a CO LVL HIGH annunciation when the carbon monoxide level was greater than 50 ppm.
The aircraft was equipped with an electro-pneumatic stall warning system to provide audible warning of an approach to an aerodynamic stall. At approximately 5 kt above the stall (full flaps, power off, level flight) and slightly higher in turning and accelerated flight, a warning horn will sound and a red stall warning annunciation will illuminate.
Electronic stability and protection is an optional feature to discourage exceedance of attitude, airspeed and angle of attack parameters through corrective control pressures. This will only function above 200 ft above ground level and when the autopilot is off.
An aircraft data logger system acquires serial information from the primary integrated avionics unit and transmits it to the recoverable data module located in the vertical stabiliser. The PFD and MFD had the capability to record flight and engine data on SD cards.
Occupant safety features
A composite roll cage within the fuselage structure provided roll protection for all occupants. The lower firewall was designed to improve crashworthiness. The seat bottoms have an integral aluminium honeycomb core designed to crush under impact to absorb downward loads. Integrated seat belt and shoulder harness assemblies with inertia reels were provided for each occupant. The front seats utilised a 4-point inflatable restraint system.
An inflatable shoulder harness is integral to each front seat harness. In the event of a collision, the sensor evaluates the force pulse and sends a signal to an inflator assembly mounted in the aft seat frame. This signal releases the gas in the inflator and rapidly inflates the airbag within the shoulder harness cover.
As is standard for SR series aircraft, the aircraft was equipped with a Cirrus Airframe Parachute System (CAPS). Cirrus Aircraft reported that there had been 124 CAPS Saves (deployments) that resulted in 254 lives saved. CAPS consisted of the following primary components:
parachute
solid-propellant rocket to deploy the parachute
rocket activation handle and cable
harness embedded in the fuselage structure.
The parachute and rocket were located in a compartment behind the rear baggage compartment. The rocket activation handle was mounted in a cabin ceiling enclosure between the 2 front seats and the cable was routed through the cabin ceiling and angled towards the left side of the CAPS compartment.
To initiate the CAPS, the pilot removes the access cover and pulls the rocket activation handle out and down. Movement of the cable compresses the igniter steel spring and cocks the plunger. When one half-inch of plunger travel is reached, the primary booster is ignited, which then ignites a secondary booster and the rocket motor. For aircraft with electronic ignition for the booster, both aircraft batteries are connected to the system and either can actuate the booster in response to cable movement.
Once ignited, the rocket impacts and dis-bonds the parachute compartment cover situated behind the rear cabin window and pulls the deployment bag from the enclosure. The deployment bag then stages the suspension line deployment and inflation of the parachute.
On the upper fuselage, either side of the CAPS rocket cover was a placard approximately 16.5 cm long (Figure 4).
The last 100-hour/annual inspection was completed on 13 January 2023 when the aircraft total time in service was 857.1 hours. According to the aircraft log book, the annual inspection was carried out in accordance with the Cirrus SR22 aircraft maintenance manual and included:
scheduled inspection of the oxygen system
scheduled inspection and check of the autopilot servos
software update to Perspective Avionics
MFD lower SD card slot and card contacts cleaned (due to supplemental data intermittently unavailable)
scheduled check of the aircraft data logger system (RDM).
The scheduled check of the aircraft data logger system involved accessing the diagnostic LED and confirming that the rate and duration of the LED blinking indicated normal operation. According to the maintenance organisation, this was carried out with nil defects identified.
The only subsequent maintenance was carried out on 15 March 2023 at 887.1 hours total time in service. In response to pilot concern about uneven EGT burn at altitude, the maintenance organisation checked the magneto timing and found it within limits. And as engine data showed a spark plug irregularity, those plugs were cleaned, tested, and reinstalled.
Cirrus first responder information
The aircraft manufacturer produced a comprehensive Cirrus 1st Responder Information Manual to inform emergency services of the potential hazards they may encounter when working on or around a Cirrus aeroplane at an accident site. This focussed on CAPS and addressed other hazards such as oxygen bottles, airbag seatbelts, and composite materials. The manual and other safety information including a video was available at Cirrus First Responders (cirrusaircraft.com). In addition, Cirrus Aircraft advised that they had trained thousands of first responders in on-site and classroom contexts.
According to the manual, it is imperative that the presence of an airframe parachute system be identified as early as possible when responding to an aviation mishap and the system disabled to make it safer to work around. In certain circumstances it may be advisable to secure an accident site and have a Cirrus trained technician attend to disable or disarm the system prior to proceeding with recovery efforts.
Of particular concern is the activation cable routed through the cabin roof that can be altered or stretched during an accident sequence and/or rescue and recovery. This can occur with the activation handle safety pin inserted. On a diagram of the aircraft, the cable route and parachute compartment were identified as a do not cut zone (Figure 5).
Figure 5: Diagram extracted from Cirrus 1st Responder Information Manual - Activation handle and cable hazards
Source: Cirrus 1st Responder Information Manual, Date: July 23, 2018, Revision: 2
If the rocket is launched, it accelerates to over 100 mph (160 kmh) in the first tenth of a second, making it a projectile hazard to anyone in its path. Normal trajectory of the rocket is upward and rearward over the tail but damage to the aircraft and nearby obstacles in the flight path can render the trajectory unpredictable.
For an intact aircraft, CAPS can be secured by inserting a safety pin into the activation handle and handle holder. If an aircraft is not intact, CAPS should be disabled by cutting the activation cable as close to the igniter assembly as practicable (Figure 6). This is a temporary measure that decreases the risk of inadvertent ignition substantially enough to proceed with rescue efforts. Additionally, for an electrically fired system, aircraft batteries can be disconnected, and the igniter wires shunted.
CAPS can be disarmed by trained and authorised technicians, which renders the rocket, igniter, base, and reefing line cutters inert.
In response to ATSB request for data about unintentional post-impact rocket activations, Cirrus Aircraft advised that there was limited data as most of these events were not recorded. A few rocket activations had resulted from exposure to direct flame or heat soaking in post-impact fires.
Figure 6: Image extracted from Cirrus 1st Responder Information Manual showing rear cabin (looking rearward; carpeting and panels removed), warning placard, and cable cutting location
Source: Cirrus 1st Responder Information Manual, Date: July 23 2018, Revision: 2
Accident site and wreckage information
Images of the accident site and wreckage (after recovery of the pilot) were provided to the ATSB. Those images show that the aircraft came to rest on the grass about midway between runway 11 Centre and 11 Left. It was inverted and oriented on the same general heading as the runway.
About 100 m from the threshold of the runway was a white scrape mark on the centreline consistent with a tail strike. A further 230 m along the runway, a series of ground marks started from 30 m to the left of the runway centreline and extended 16 m away from the runway until the main wreckage site. These ground marks were consistent with left wing tip, left wing, and main nose down impact.
The left wing had broken in 2 places and those pieces were detached from the main wreckage at the wing root. The nose of the aircraft was severely damaged, and 2 propeller blades had sheared off at the hub. Although the propeller blades were damaged, there was no plastic deformation that might indicate engine power at impact because the blades were composite material.
Some of the left fuselage was cut away and it is likely there was some alteration to the internal conditions around the pilot’s seat as part of the recovery of the pilot. There was significant intrusion of the instrument panel into the cabin. The cabin space was mostly intact, although there was apparent deformation and reduction of cabin height.
The pilot’s seat was in location but both outboard seat feet had torn the flanges from the outboard seat track at the mid‑seat position due to impact forces and track deformation. The pilot’s seat belt airbags had inflated.
Depending on observer perspective, the CAPS warning placard was visible on the left rear inverted fuselage (Figure 7). Because of the tilt of the wreckage, the right-side placard was not as visible.
Figure 7: Wreckage (inverted) at accident site showing CAPS warning placard on left rear fuselage
Source: NSW Police (annotated by ATSB)
The ATSB examined the wreckage after it was removed from the accident site and secured in a hangar. By that stage the CAPS rocket had been disarmed and removed.
A search for SD cards located 2 Garmin cards and an SD data card from the MFD. The PFD screen had detached from the instrument panel during the accident and no associated SD card was found. The Garmin cards were not designed to record data and the SD data card was not formatted properly to enable storage of information.
The recoverable data module (RDM) was intact and removed from the vertical fin for data recovery. The ATSB connected to the RDM but was unable to download any data. After consultation with Cirrus Aircraft and the National Transportation Safety Board (NTSB), the RDM was sent to the NTSB data recovery specialists. They confirmed the ATSB nil result then transferred the memory chips to a surrogate RDM. This allowed data to be downloaded but the RDM had not been recording data since at least 2012.
Examination of the aircraft identified that the:
elevator trim setting was neutral
wing flap selector was in the 100% down position
oxygen controller was off but there were indications it had been used.
Fire and rescue
Bankstown Airport did not have an aviation rescue fire fighting facility and it was not a regulatory requirement for that airport. The emergency response to an aircraft accident on Bankstown Airport included Fire and Rescue NSW (FRNSW), which is the State Government agency responsible for the provision of fire, rescue and hazmat services in cities and towns across New South Wales. FRNSW advised that all fire and rescue personnel received the same training and had access to guideline support documents that addressed aircraft incidents including ballistic parachutes. In addition, firefighting crews with an aerodrome/airport as part of their risk profile would be familiar with that environment and take part in emergency exercises.
Flight path information
The ATSB obtained automatic dependent surveillance broadcast (ADS-B) data transmitted from the aircraft’s Mode S transponder during the flight. That data included altitude, indicated airspeed, and rate of descent, and the approximate distance to the runway threshold was derived from aircraft coordinates (Table 2).
Table 2: Selected ADS-B data for final approach
Altitude (ft)
Indicated airspeed (kt)
Rate of descent (ft/min)
Distance to runway (NM)
500
98
416
1.51
400
87
448
1.23
300
80
416
0.93
200
83
448
0.71
100
79
352
0.37
50
74
224
Not available
25
73
384
Not available
0*
71–61
416–224
Not available
* There were a number of data points around 0 ft altitude so the range of airspeed and rate of descent around the initial touchdown is provided. Cirrus noted that the last recorded airspeeds were low and may have been a factor in the bounced landing and aircraft response in the go‑around.
Based on the derived distance data, from 500 ft the aircraft was close to a 3° descent profile, which became about 2.5° after 300 ft.
In the landing configuration, the stall speed in steady flight was 62 kt (at unfavourable weight and balance conditions).
Other Cirrus SR22 go-around occurrences
AO-2015-110 Collision with terrain involving a Cirrus SR22, VH-OPX, near Moree, New South Wales, on 17 September 2015.
The pilot was landing at a private airstrip 10 km north of Moree. Based on observations at Moree and the runway direction, the wind was a quartering tailwind/crosswind from the right of up to 20 kt with small gusts up to 22 kt.
After a normal approach and extension of full flap, the pilot commenced the flare for landing at about 80–90 kt. To align the aircraft with the runway, the pilot reported applying almost full left rudder and right aileron due to the crosswind. The right main landing gear touched down first, and the aircraft bounced back into the air. The pilot immediately applied full power to initiate a go‑around. However, the left wing dropped and the aircraft yawed to the left. The aircraft’s left wing and propeller then collided with a dam wall. The aircraft stopped abruptly and spun around. The engine separated from the aircraft and came to rest about 20 m away, the tail broke off and the nose landing gear collapsed. The pilot suffered minor injuries, and the aircraft sustained substantial damage.
AO-2018-038 Loss of control and collision with terrain involving Cirrus SR22, VH-PDC, at Orange Airport, New South Wales, on 15 May 2018.
The pilot (aircraft owner) and flight instructor were conducting night circuits as the first part of training for a night endorsement. Wind conditions were reported as light and variable.
On the second approach, the pilot flared the aircraft a ‘little high’ for the touchdown, and the aircraft bounced twice. The pilot elected to go-around and applied full power before touching down again. The ATSB report identified that as the pilot applied full power to perform the go-around, the aircraft pitched nose-up and rolled to the left.
This report also identified 2 other accidents involving SR22 go-arounds in the United States where the aircraft nose pitched up and the aircraft veered left after full power was applied to the engine. (Report ERA12FA540, and Report NYC07CA010)
Previous CAPS hazard safety action
In the past, the ATSB produced a publication Hazards at Aviation Accident Sites: Guidance for Police and Emergency Personnel which was distributed as a booklet. The printed version is no longer available and at the time of writing the investigation report, a pdf copy was available while a digital version was under development.
When the final report for AO-2018-038 was released the ATSB released a news item with a safety message about the risks associated with post-impact deployment of the CAPS rocket. Flight Safety Australia magazine, produced by CASA, also published an article warning readers to beware of the rocket in the wreckage.
Safety analysis
Attempted landing and loss of control
En route, approach and landing
The flight path from Southport to final approach at Bankstown was steady with no indication of problems and there was no report of any anomalies regarding radio transmissions. Given the oxygen system was used, there is low risk that the pilot was exposed to hypoxia when operating above 10,000 ft.
After reporting inbound at Prospect Reservoir in accordance with standard procedures, the pilot responded appropriately to controller advisories. When the pilot acknowledged the clearance to land, which was the last transmission from the pilot, there was no discernible indication of any stress or impairment.
After joining final approach at 950 ft, the pilot maintained a direct, steady track to the runway and the descent profile was close to a standard 3° approach profile. Although some witnesses reported the aircraft speed was slower than expected on approach, the transmitted data indicated that the aircraft was at the Cirrus‑recommended approach speed of 80 kt (indicated airspeed) by 300 ft. Based on the flight data, the approach was consistent with the Cirrus stabilised approach criteria.
Below 100 ft, the airspeed reduced to between 71 and 61 kt but given the fidelity of the data it is not possible to establish the speed at the initial touchdown or subsequently. As Cirrus indicated, low airspeed just before landing may have been a factor in the occurrence.
In the CCTV imagery, the aircraft appeared to sink onto the runway and witnesses observed the aircraft bounce along the runway. After the initial bounce, the aircraft tail scraped on the runway, which was symptomatic of the unstable landing without any effect on the subsequent controllability of the aircraft.
Although there was a crosswind component, it was well within the capability of the aircraft and expected to be within the capability of the pilot. There was also no indication from the aerodrome forecast and observations, or from other pilots on approach to adjacent runways, of any significant wind gusts or turbulence affecting the landing.
Landings are dynamic, skill-based manoeuvres that rely on pilot judgement of existing and projected energy state with sensitive adjustment of aircraft attitude and engine power. The unstable landing was consistent with a misjudged flare. Pilots can recover by adjusting the aircraft energy and attitude for another attempt to land or by initiating a go-around.
Loss of control
About 5 seconds after the initial touchdown, the aircraft came off the ground and immediately rolled into a climbing steep left turn up to a height of about 40 ft then dropped and impacted the ground on the left wing and nose.
As there was no recorded flight or engine data, there was no direct information about the engine power settings during the accident sequence. The pilot did not transmit his intentions however, in the context of landing difficulties and trying to control the aircraft, a radio call would not be expected.
Based on the CCTV and witness information, the performance of the aircraft as it lifted off and entered the climbing turn was consistent with high engine power. It follows that the pilot had intentionally initiated a go-around as recovery from the unstable landing.
A mild pitch up would be expected in the early stages of go-around from a bounced landing to maintain ground clearance. However, the large pitch up that was observed was not consistent with the recommended go-around procedure to pitch up to a level attitude and begin accelerating to the speed consistent with either Vx (best angle of climb) or Vy (best rate of climb). It is likely that application of high engine power exacerbated the effects of nose-up control inputs. The Cirrus SR22 is equipped with a relatively high-power engine for a 4-place aircraft. Although turbo‑normalising the engine does not increase the maximum rated power of the engine, it was reported that there could be a noticeable ‘surge’ as the throttle was advanced on the ground.
Application of high engine power will produce ‘torque’ that will result in a strong left turning tendency. This effect is magnified by low airspeed and a high pitch angle. The rate of throttle control movement and engine response will also influence torque characteristics and associated controllability.
In normal operational contexts where high or full engine power is applied at the recommended rate, the pilot is able to counteract torque effect through coordinated use of steering (on the ground), and use of rudder and aileron once airborne. However, in this case, the torque effect was probably stronger than experienced during normal operation and the effectiveness of the flight controls was compromised by the low airspeed. Consequently, the pilot lost directional control of the aircraft early in the go-around sequence and was unable to recover.
As the angle of bank increased in the turn away from the runway, the stall speed increased, and the vertical component of lift generated by the wings decreased to zero as the aircraft reached a 90° angle of bank. Consequently, the aircraft dropped out of the turn.
The ATSB investigated 2 previous Cirrus SR22 go-around accidents at Moree in 2015 and Orange in 2018. Although the reports identified other factors that played a role in those occurrences, it is likely that torque effect played a key role in each loss of control.
To summarise: In the early stages of a go-around from an unstable landing, the pilot was unable to counter the substantial torque effect associated with high engine power, low airspeed, and high pitch angle. As a result, when the aircraft came off the ground, it rolled into a climbing steep left turn up to a height of about 40 ft then dropped and impacted the ground on the left wing and nose.
Go-around safety considerations
A go-around is a transition from a low-power condition while descending/landing to a high-power climb. When this occurs during an approach, the aircraft has potential and kinetic energy and in visual conditions there is generally no urgency to carry out the procedure. In contrast, when a pilot does a go-around from an attempted landing, the aircraft is in a low energy state and there is typically some urgency to initiate the procedure to recover from an unstable state on or close to the ground.
Flight training and reviews include go-arounds and the pilot had recently completed an instrument proficiency check that included missed approaches. As this check, and the preceding attempted check with associated training, was carried out by a Cirrus Standardised Instructor Pilot in the pilot’s SR22, the pilot was familiar with the type-specific characteristics of missed approaches. The instructor had also conducted practice go-around sequences at safe altitudes with the pilot.
This training and assessing is essential but has an inherent limitation because it is not feasible to simulate the conditions experienced during recovery from an unstable landing. It is possible that the pilot had not previously encountered a go-around from a rejected landing and was not prepared for the aircraft response to engine power in that context.
The balked landing/go-around procedure in the POH specified a sequence of 5 actions/parameters. Although this was applicable to all phases of flight, it did not provide any guidance for conduct of the procedure in different conditions.
To supplement the POH, Cirrus produced a flight operations manual and training videos that addressed approach, landing, and go‑arounds in SR20/22 aircraft. These resources provided useful guidance that was oriented to go‑arounds during final approach. It is not known if the pilot had referred to the guidance in the flight operations manual and there was no record of the pilot having directly accessed training videos for go-arounds, although some videos were freely available without a subscription.
The Cirrus procedure and the more detailed flow for go-arounds was conventional and applicable to the occurrence scenario with careful implementation from memory so control could be maintained during the recovery and transition into a climb. However, the ATSB noted that the material provided by Cirrus did not highlight the risk of loss of control associated with a go-around during the landing phase, where there was high engine power, low airspeed, and high pitch attitude.
CAPS hazard
Cirrus Aircraft advised that 254 lives have been saved due to the CAPS system. However, notwithstanding the benefits, CAPS also presents a serious post-accident hazard when it has not been deployed and the aircraft is damaged. If the rocket is inadvertently activated, anyone in its path would be seriously or fatally injured.
Cirrus Aircraft had been actively managing this risk by providing training to first responders (in the United States) and producing a detailed manual for first responders that is freely available on a dedicated website. In Australia, the ATSB has published and distributed a booklet for emergency services that addressed the risk of ballistic parachute systems in various aircraft types, including the Cirrus SR20/22. After the Cirrus SR22 accident at Orange in 2018 when the rocket was activated by the post-impact fire, the ATSB produced a video about the CAPS hazard and Flight Safety Australia magazine published a related article.
The only external indication of the CAPS hazard on the aircraft is a warning placard either side of the rocket exit point. These are not prominent and did not feature symbology or colour that are recognised indicators of danger. In addition, there are no markings to identify the no-cut area associated with the activation cable. On this occasion, the placards were not easy to identify or read because the aircraft was inverted.
Despite the availability of online guidance for first responders to a Cirrus aircraft accident, placards on the aircraft, and RFNSW training/education, the emergency services site commander was not aware of the presence of the airframe parachute system until advised after the rescue had started. At that point, while the site commander was aware of the rocket hazard, they did not know how to access information about the activation mechanism and method to secure the system. All first responders from FRNSW should have an awareness that aircraft might be equipped with a rocket propelled parachute system and the associated risks but it is not feasible for them to have type‑specific knowledge.
As the accident was at a major general aviation airport on a weekday and during standard working hours, there were aircraft maintenance personnel with knowledge of Cirrus aircraft that were available to assist with securing of the CAPS. They informed emergency personnel about the activation mechanism and secured the handle, which helped to reduce the risk of rocket activation. The risk could have been reduced further if the system had been secured by cutting the activation cable and, if the conditions had allowed, disconnection of the 2 batteries.
If the rocket had been inadvertently activated while the fuselage was inverted, the path of the rocket would have been uncertain and the release of heat and energy in the presence of fuel would have been a significant fire risk.
Cirrus advised first responders that it is imperative that the presence of an airframe parachute system be identified as early as possible, and the system disabled to make it safer to work around. In support of these imperatives, Cirrus provided training, education, and aircraft placards. However, the ATSB considered that the training and education had limited reach, and the placards did not effectively communicate the danger or provide access to safety information.
The ATSB considered that these limitations increased the risk of injury during the recovery of the pilot in this occurrence. Given no recorded incidents of post-impact rocket activations unrelated to fire, and the variability of aircraft accidents and associated damage, the ATSB did not identify this as a safety issue. Nevertheless, the ATSB supports any enhancement to the post-accident identification of CAPS and disabling of the system to reduce the risk of injury.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Cirrus Design Corporation S22 at Bankstown Airport, New South Wales on 17 March 2023.
Contributing factor
In the early stages of a go-around from an unstable landing, the pilot was unable to counter the substantial torque effect associated with high engine power, low airspeed, and high pitch angle. As a result, when the aircraft came off the ground, it rolled into a climbing steep left turn up to a height of about 40 ft then dropped and impacted the ground on the left wing and nose.
Other factors that increased risk
The first responders were initially unaware that the aircraft was equipped with a ballistic parachute (CAPS) and initiated the recovery of the pilot with the system still armed. By not securing the CAPS, the risk of inadvertent rocket activation and injury was increased.
Cirrus Aircraft provided training, education, and placards to reduce the risk of inadvertent post‑accident actuation of the ballistic parachute (CAPS) rocket and associated injury. However, the training and education had limited reach, and the placards did not clearly communicate the danger or provide access to safety information.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Cirrus Aircraft
Cirrus Aircraft advised that they have enhanced the external CAPS placarding on 2 new models of aircraft (the SF50, and another in development) to align with current American Society for Testing and Materials (ASTM) standards (Figure 8). The SR2X series of aircraft (the SR20, SR22, and SR22T) were certified prior to the implementation of ASTM standards. At the time of writing, Cirrus was reviewing the possibility to enhance the placard that was certified with SR2X.
Figure 8: Example of an ASTM Standard CAPS Placard used on the SF50 Vision Jet
Source: Cirrus Aircraft
During the draft report review process the ATSB sought input from Cirrus as to whether there was an opportunity to enhance the safety benefit of their go‑around training and educational products, especially in regard to the SR22 models that are equipped with relatively high-power engines during the landing phase.
Cirrus did not advise of any associated safety action.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
aerodrome controller
Fire and Rescue NSW onsite commander
Aeria Management Group (Bankstown Airport)
Civil Aviation Safety Authority
Flight examiner
Cirrus Aircraft
maintenance organisation for VH-XGR
Submissions were received from:
Civil Aviation Safety Authority
Cirrus Aircraft
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit a pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[2]Eastern Standard Time (EST): Coordinated Universal Time (UTC) + 10 hours.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 180 equates to 18,000 ft.
[4]Eastern Daylight-saving Time (EDT): Coordinated Universal Time (UTC) + 11 hours.
[5]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[6]An IFR flight can change to a VFR flight for the arrival to Bankstown Airport to enable sequencing with VFR traffic operating in the airspace.
[7]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[8]The distance from the airport terminal to the threshold of runway 11 Centre was 600 m and the distance to the accident site was 350 m.
On 18 February 2023, at 0643 local time, a Textron Aviation CE340A aircraft, registered RP-C2080, departed Bicol International Airport for Ninoy Aquino International Airport, Philippines. A few minutes after departure, air traffic control lost contact with the aircraft, and the wreckage was subsequently found to have collided with terrain on the slope of Mount Mayon. There were 2 Australian citizens on board.
The Civil Aviation Authority of Philippines (CAAP) investigated this occurrence. As Australian citizens were on board the aircraft, the CAAP invited the ATSB to appoint an expert to the investigation. To facilitate this appointment, the ATSB initiated an accredited representative investigation under the provisions of the Transport Safety Investigation Act 2003.
During 2023, an ATSB investigator provided liaison between the Australian passengers' next-of-kin, Australian Federal Police family liaison officers and CAAP as required. The final report into this investigation was released by CAAP on 16 October 2023. The report is available for download on the CAAP website.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Air traffic control audio recorded the aircraft departing Bankstown Airport at about 1003 local time. Flight tracking data (Figure 1 blue line) obtained from ADS-B Exchange and FlightRadar24 (Figure 1 red line) showed the aircraft being flown to Temora, landing at about 1133 on runway 36.[2] The aircraft was then refuelled, with OzRunways data (Figure 1 yellow line) showing that the aircraft conducted 2 circuits from runway 05 between 1229 and 1246. Flight data also indicated that, about an hour later, at 1323, the aircraft departed Temora via runway 18 for Wedderburn.
Figure 1: ADS-B Exchange, FlightRadar24 and OzRunways flight data from N600 on 26 December 2022.
Source: Google Earth, ADS-B Exchange, FlightRadar24 and OzRunways, annotated by the ATSB.
On arrival at Wedderburn, N600 was positioned on a wide circuit and landed on runway 17 at Wedderburn at 1452. For unknown reasons, the aircraft then became airborne again. Eyewitnesses and CCTV at Wedderburn observed the aircraft in a shallow, unstable climb, enough to just clear rising terrain and trees at the end of runway 17. After clearing the trees, the aircraft then disappeared from view and about 2 minutes later collided with terrain about 2.7 km from the end of the runway, approximately 150 m from Appin Road (Figure 2). The wreckage was consumed by a post-impact fire that also started a small bush fire. Both occupants sustained fatal injuries.
Figure 2: ADS-B Exchange flight data showing the landing and go-around at Wedderburn Airport and the location of the collision with terrain. Also shown is the approximate direction of wind based on Bureau of Meteorology reports and CCTV footage.
Source: Google Earth and ADS-B Exchange, annotated by the ATSB.
N600 was a Stoddard Hamilton Aircraft Glasair Super II FT, amateur built aircraft[3] constructed in the United States (US). The aircraft was a conventional two-seat, single-engine, low-wing monoplane with tri-cycle undercarriage, built mostly of fiberglass. The aircraft was fitted with a Subaru EJ-25 automotive engine, modified for aviation use by NSI Propulsion Systems (later Maxwell Propulsion Systems). The first flight was conducted on 4 June 2014 at Chesapeake Regional Airport, US. About 60 hours flight time was accumulated before the aircraft was imported into Australia in 2021.
Prior to leaving the US, the aircraft’s one-piece wing was disassembled to facilitate shipping. Subsequently, upon arrival in Australia, significant work was undertaken to restore the aircraft to an airworthy condition prior to its first flight in Australia on 26 December 2022. The aircraft was not equipped with a flight data recorder or cockpit voice recorder, nor was it required to be.
Meteorological information
Campbelltown and Bellambi are the closest aviation weather reporting sites to Wedderburn Airport, with the accident site being roughly half-way between the two. The Bureau of Meteorology’s routine report of the weather conditions at Campbelltown at 1500 (6 minutes after the accident) showed an east-north-eastly wind at 8 knots, gusting to 15 knots, with an air temperature of 33.2°C and a dew point temperature[4] of 8.6°C. It also showed that no rainfall was recorded since 0900 that morning.
The Bellambi Airport weather report at 1500 local time showed a north‑north-easterly wind at 12 knots, gusting to 16 knots, with an air temperature of 23.7°C and a dew point temperature of 20.0°C. It also showed no rainfall recorded since 0900 local time that morning.
CCTV footage from Wedderburn Airport showed clear skies and a crosswind with an easterly quartering tailwind during the landing and subsequent take‑off.
Wreckage examination
To the extent possible due to the condition of the wreckage, on-site examination of the aircraft’s flight controls, and structure did not identify any pre‑existing faults or failures. However, several components were retained by the ATSB for further examination, including the engine, gearbox, propeller, and electronic devices.
Operational Information
As the aircraft was registered with the Federal Aviation Authority (US), it was operating in Australia under a Civil Aviation Safety Authority (CASA) Special Flight Authorisation Instrument. The CASA instrument was valid until 31 October 2024 and stated that the aircraft must not be operated over a populous area.
the conduct of similar amateur-built experiment flight operations
pilot qualifications, experience and medical information.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] VFR: a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Runway number: the number represents the magnetic heading of the runway.
[3] Aircraft supplied in kit form and is designed to be constructed for the education and recreation of the owner
[4] Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to monitor the risk of aircraft carburettor icing or the likelihood of fog.
Final report
Executive summary
What happened
On 26 December 2022, a Stoddard Hamilton Aircraft Glasair Super II FT, registered N600, departed Temora, for a private flight to Wedderburn aircraft landing area, New South Wales. On arrival at Wedderburn, N600 conducted a landing and go-around on runway 17. During the go‑around, N600 failed to achieve sufficient climb performance and impacted terrain about 2.7 km to the south-west of Wedderburn. The aircraft was destroyed, and the two pilots on board were fatally injured.
What the ATSB found
The ATSB found that N600 conducted an approach to land on runway 17 with a quartering tailwind and subsequently conducted a go-around after touch down. For reasons that could not be determined, N600 did not achieve a sufficient climb performance after take-off which led to a collision with terrain.
The ATSB also found that both pilots on board did not have recent experience in single-engine, automotive engine conversion, amateur-built aircraft or the Glasair in general.
Additionally, the pilots elected to operate the aircraft from Bankstown to Temora for the aircraft’s first flight in Australia, even though the special flight authorisation did not permit operations over built-up areas.
It was also found that N600 was fitted with propeller pitch change rocker switches on the left and right side of the throttle which were reversed in orientation for each flight crew member. This increased the risk that a pilot flying from the right seat could operate the propeller pitch change opposite to the intended selection.
Safety message
Pilots intending to operate amateur-built aircraft should be aware of the potential differences in systems and controls to that of conventional type-certified aircraft. They should also consider transition training onto the same aircraft type, or aircraft with similar design features and performance capabilities.
Pilots attempting to conduct post-maintenance proving flights in amateur-built aircraft are urged to be proficient in the specific aircraft emergency operations, particularly those related to partial power failures. It is also prudent to select an appropriate aerodrome and benign weather conditions to conduct familiarisation flights, to safely expand their operational experience.
When a formal flight plan is not lodged, leaving a flight note with a responsible person who is able to notify the appropriate authorities should the flight become overdue is also an important safety consideration.
Understanding the safety implications of regulatory permissions is vital so that experimental aircraft operations do not adversely affect the safety of third parties, such as other airspace users and people on the ground not associated with the operation of the aircraft.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 26 December 2022, a Stoddard Hamilton Aircraft Glasair Super II FT, registered N600, was operated on a private flight under the visual flight rules (VFR)[1] from Bankstown to Temora, then onto Wedderburn, New South Wales. The aircraft was registered in the US, and this was the aircraft’s first flight in Australia, and its purpose was to reposition the aircraft to Wedderburn. The two pilots were both co-owners of the aircraft. Air traffic control audio recorded the aircraft departing Bankstown at about 1003 local time.
Flight tracking data (Figure 1) showed the aircraft being flown to Temora, landing at about 1133. The aircraft was then refuelled and conducted 2 circuits[2] before departing about an hour later for Wedderburn, which was expected to be its planned destination.
Figure 1: Flight tracking data from N600 on 26 December 2022
Source: Google Earth, ADS-B Exchange, FlightRadar24 and OzRunways, annotated by the ATSB
On arrival at Wedderburn, N600 was positioned on a wide circuit and landed on runway 17[3] at about 1452. The pilot then conducted a go-around[4] and the aircraft became airborne again.
Witnesses at Wedderburn observed the aircraft in a shallow climb, climbing just enough to clear rising terrain and trees at the end of runway 17. After clearing the trees, the aircraft disappeared from view below the ridgeline. About 2 minutes later, N600 collided with terrain about 2.7 km from the end of the runway, and about 150 m from Appin Road (Figure 2), about 1.4 km to the south‑east of Appin township.
The wreckage was consumed by a post-impact fire that also started a small bush fire. Both occupants were fatally injured.
Figure 2: ADS-B Exchange flight data showing the landing and go-around at Wedderburn aircraft landing area and the location of the collision with terrain
Source: Google Earth and ADS-B Exchange, annotated by the ATSB
Context
Pilot Information
For clarity, as there were 2 pilots on board N600, this report will identify them individually as ‘Pilot A’ and ‘Pilot B’. Witnesses confirmed that it was the intention that Pilot B would be in command for the flight from Temora to Wedderburn, however the exact seating positions and pilot in command for the accident flight are unknown due to the nature of the accident sequence.
To operate N600, a pilot was required to hold a valid US licence. Both pilots had obtained their United States Federal Aviation Authority (FAA) qualifications based on their previous Australian pilot licences and aviation medical certificates, however recent flight times and current FAA flight reviews were unable to be located.
Pilot A
Licencing and aeronautical experience
Pilot A was experienced in multi-engine fixed wing operations. They were operating N600 for the first time that day. Their FAA Private Pilot (Aeroplane) Licence was issued on 16 July 2009, however there are no records of an FAA single-engine aeroplane flight review since initial issue of the FAA licence based on their Australian qualification.
They held a Civil Aviation Safety Authority (CASA) Air Transport Pilot (Aeroplane) Licence (ATPL(A)) that was re-issued on 22 January 2015. Recent pilot logbooks were unable to be located, however an electronic logbook file from December 2021 showed a total flying experience of 2,697 hours, of which almost 2,212 hours were in multi-engine aircraft.
The pilot had completed a CASA multi-engine flight review on 7 March 2021, which was valid to 31 March 2023. They had operated N600 for a number of ground runs in preparation for the first flight and was reported to have operated N600 from Bankstown to Temora on the day of the accident. The pilot held an RAAus pilot certificate, however it is unknown how much experience the pilot had with high performance single-engine aircraft. A witness identified that the pilot had previously flown a Glasair aircraft prior to the purchase of N600, however this was unable to be identified in the pilot’s logbook.
Medical
Pilot A held a valid CASA Class 2 aviation medical certificate, which was issued with restrictions that required distance correction and reading correction to be available whilst exercising the privileges of the licence.
Pilot B
Licencing and aeronautical experience
Pilot Bwas also experienced in multi-engine fixed wing operations, and operated N600 for the first time that day at Temora.
They held a CASA ATPL(A) that was issued on 29 April 1991. A recent pilot logbook was unable to be located, however the latest logbook identified (from July 1996 to August 2004) recorded a total flying experience of 6,156 hours, of which only 761 hours were in single-engine aircraft, with the last recorded single-engine flight in September 1999.
FAA records indicate that Pilot B received an FAA Commercial Pilot Certificate on 5 January 1990, based on their Australian licence however there are no records of an FAA single-engine aeroplane flight review since initial issue of the FAA licence based on their Australian qualification. CASA records indicate that the pilot had last completed a multi-engine aeroplane flight review on 7 March 2021 which was valid until 31 March 2023, there was no record of any single-engine flight reviews for either CASA or FAA licences.
Due to limited recorded flight hours for Pilot B, it was unable to be determined if the pilot had flown the aircraft type previously.
Medical
Pilot B previously held a CASA Class 2 aviation medical certificate which had expired on 18 November 2022. The Class 2 was issued with a restriction that reading correction must be available whilst exercising the privileges of the licence.
N600, serial number 2277, was a Stoddard Hamilton Aircraft Glasair Super II FT, amateur-built aircraft[5] constructed in the US. The aircraft was a high performance, conventional two-seat, single-engine, low-wing monoplane with tricycle undercarriage, built mostly of fibreglass. The aircraft was fitted with a Subaru EJ-25 automotive engine, modified for aviation use by NSI Propulsion Systems (later Maxwell Propulsion Systems). N600 had an initial Special Airworthiness Certificate issued on 30 April 2014. The first flight was conducted on 4 June 2014 in the US. About 59 hours flight time was accumulated before the aircraft was imported into Australia in 2021.
Prior to leaving the US, the aircraft was disassembled to facilitate shipping. Subsequently, upon arrival in Australia, significant work was undertaken to restore the aircraft to an airworthy condition.
Airworthiness and Maintenance history
The last recorded maintenance work in N600’s maintenance log was on 12 May 2016. Maintenance had continued to be recorded in the aircraft log up until disassembly on 28 April 2021.
After shipping to Australia in July 2021, N600 was reassembled in Bankstown by a CASA approved maintenance facility. When the maintenance facility was notified by the owners that N600 would remain on the US FAA register, an FAA certified Airframe and Powerplant (A&P) technician performed an airworthiness inspection in accordance with Federal Aviation Regulation 43, Appendix D.
During the disassembly process in the US, several electrical wiring looms were cut to facilitate the removal of the wing from the fuselage. An authorised repair facility performed the electrical reconnection and required inspections. No engine work was performed during the reassembly. The aircraft was released for service on 14 September 2022 by the FAA A&P.
No record of any periodic maintenance was identified since its original test flying and the aircraft had accrued about 59 hours total time in service.
Engine and propeller speed reduction unit
The Subaru EJ-25 is a 4-cylinder, liquid-cooled, fuel-injected automotive engine, fitted with a single electronic ignition. The engine throttle control was controlled by a single cockpit tee handle throttle, mounted in the centre console between the two seats, operating a cable to the fuel control unit (Figure 3).
The propeller speed reduction unit (PSRU) was mounted to the front side of the engine and had a speed reduction gearing of 2.1:1. The PSRU contained a sprag clutch to dampen engine harmonics.
Detailed laboratory examination of the engine and PSRU did not indicate any pre-impact or mechanical abnormalities that may have contributed to the accident. However, due to the fire affected engine components, much of the ignition and electrical system were consumed by the post-accident fire, and therefore were unable to be tested.
Propeller
N600 was fitted with a Maxwell Propulsion Systems CAP-220 two-blade, electric variable pitch propeller, with an alloy hub. The carbon fibre propeller blades were manufactured by Whirlwind Propellers.
Propeller pitch change control (Figure 3) was achieved with two rocker switches (one for each crew seat) mounted on either side of the throttle tee-handle lever, activating the electric pitch change motor. It took about 10 seconds to cycle between the course and fine pitch stops. The rocker switches were identical in their design and operation, in that when viewed directly on, the left side of the switch had the increase pitch selection (+), and the right side had the decrease pitch selection (-). This meant that if the switches were wired in accordance with the ‘+’ and ‘-‘ labelling, the switches would be actuated in opposite directions relative to each pilot’s seated position to achieve the desired propeller pitch change. The switch orientation and wiring was confirmed by the original aircraft builder as being wired correctly to the switch orientation when the aircraft was constructed.
Figure 3: Engine throttle tee-handle lever showing propeller rocker switches mounted to each side
Source: FAA A&P mechanic during inspection, annotated by the ATSB
There was no propeller pitch position indicator fitted to the aircraft. The pitch was set by using engine revolutions per minute (RPM) and manifold pressure indications. Pilot operation of the rocker switch electrically adjusted the propeller blades to achieve an optimal RPM and manifold setting for take-off, climb, cruise, approach, and landing.
ATSB performed a disassembly and examination of the electric in-flight adjustable propeller pitch motor and drive unit, which appeared in good condition. No evidence of pre-impact mechanical defects was identified. Some visible corrosion was found, however this was likely due to water used to extinguish the post-impact fire. The propeller pitch was set to about 19.5° and was consistent with other exemplar propeller pitch settings in the take-off configuration (fine propeller pitch) to allow greater acceleration and initial climb performance.
Fuel
N600 operated on aviation gasoline (AVGAS), and held 151 L in the main wing tanks, 76 L in the wingtip extensions, and an additional 26 L in the header tank. Each tank was fitted with a sump and a fuel drain. A fuel selector (Figure 3) was located on the centre console aft of the throttle. The selector had ‘off’ and ‘on’ positions only, and no option to select an individual tank to supply fuel to the engine.
Fuel records indicate that on 23 December 2022 100 L of AVGAS was uploaded to N600. It is unknown how much fuel N600 had on board at the time of departure from Bankstown, as a number of ground runs had been conducted prior to departing Bankstown for Temora.
On the day of the accident while at Temora, N600 was refuelled with 70.4 L of AVGAS before subsequently departing to Wedderburn.
Fuel residue was unable to be detected at the accident site due to substantial disruption to the airframe and subsequent post-impact fire. Therefore, the amount of fuel on board at the time of the accident was unable to be determined.
Meteorological Conditions
No significant rainfall was observed or recorded within 40 km of Appin around the time of the accident. Closed Circuit Television (CCTV) footage from Wedderburn showed clear skies and an easterly crosswind on runway 17, with a quartering[6] tailwind during the landing and subsequent go-round of N600.
Wreckage information
The accident site was located about 1.2 km to the south-east of Appin township (Figure 4).
N600 entered trees on an approximate heading of 237° and the first tree impact was about 50 ft above ground level (Figure 4) at 833 ft above mean sea level. The left-wing tip (fuel tank) was located to the left of that tree, and a piece of the upper left wing was to the right of the direction of travel, most likely as a result of initial tree impact. The aircraft then continued for about 45 m, hitting further trees, before impacting a large rock. The airframe was upright and facing opposite the direction of travel. The main wreckage was spread along a path of about 90 m and was heavily disrupted and fire affected.
During the accident sequence, the engine and propeller assembly had detached from the airframe and came to rest about 10 m further in the direction of travel, and was heavily affected by fire. Initial propeller contact with trees led to both blades separating from the hub. Most of the wreckage was contained within the fire zone with a small fragment of unburnt propeller blade located about 100 m from the initial tree impact point to the right of aircraft direction of travel.
About 1 hour 23 minutes later, N600 joined a wide right downwind for runway 17 at Wedderburn. Wedderburn aircraft landing area has a single runway with a bitumen surface area of about 950 m in length. At about 1452, N600 touched down about 200 m into runway 17 at about 87 kt ground speed and rolled for about 50 m before becoming airborne again.
CCTV at Wedderburn showed the aircraft in a shallow climb, enough to just clear rising terrain and trees at the end of runway 17. After clearing the trees in the vicinity of the airfield, the aircraft then disappeared from CCTV view. Recorded data indicated that about 2 minutes later, N600 collided with terrain about 2.7 km from the end of the runway, about 150 m from Appin Road (Figure 6).
Image source: Google Earth and ADS-B Exchange, annotated by the ATSB
Other information
Amateur-built aircraft
Pilots and passengers of experimental aircraft in Australia accept the risk that the aircraft may not meet the same airworthiness safety standards as certified aircraft and operate these aircraft on the basis of informed participation.[7]
Transition to unfamiliar aircraft
General competency
For a pilot to operate a different aircraft type already covered by their licence category and class rating, they need only be satisfied that they are competent to conduct all normal, abnormal, and emergency flight procedures for the aircraft. They also need to be able to apply operational limitations, conduct weight and balance calculations, and apply aircraft performance data, including take-off and landing performance data, for the aircraft.
Guidance on transition
While no definitive Australian guidance provided advice on the transition of pilots to unfamiliar aircraft, the FAA advisory circular (AC) AC90-109A – Transition to Unfamiliar Aircraft (U.S. Department of Transportation Federal Aviation Administration, 2015) is a widely recognised and utilised publication providing a sound basis to consider the hazards oftransitioning to unfamiliar types of aircraft, whether certified or experimental amateur-built.
The AC recognises the importance of providing guidance to pilots transitioning between aircraft types, or to experimental aircraft with differing design features to high performance and complex aircraft. It recommends that pilots should develop a training strategy (Figure 7) for mitigating the risks of operation of an unfamiliar aircraft type.
The FAA AC recommends that:
Prior to flying an unfamiliar airplane, all pilots should review the hazards and risks outlined in this AC, and complete the training recommended before operating the airplane. Accident data has shown that there is as much risk in “moving down” in performance as “moving up.” For example, consider a pilot who has substantial experience in high-performance corporate, airline, or military airplanes. The knowledge and skills used to safely fly at high speeds, high altitudes, and over long flights will, by themselves, not prepare the pilot for the challenges of a low-inertia, high-drag airplane.
Figure 7: FAA recommended airplane transition training approach
Source: FAA AC90-109A
The guidance recommends firstly that pilots should consider undertaking flight training with a qualified flying instructor in the proposed transition aircraft, the same make and model or an aircraft that exhibits the same design features or characteristics of the transition type. If instruction is unavailable, seek another experienced pilot to conduct a familiarisation flight. However, if the instructor is unwilling, at least discuss the differences and expected characteristics of the transition aircraft.
The guidance further recommended that pilots take a risk management approach to formally identify the hazards and mitigate any known or elevated risks identified.
These may include, specific type training in the transition aircraft or similar type/design features, the condition, maintenance and history of the transition aircraft, planning transition flights to conservatively build up manoeuvres and aircraft experience and conducting initial flights in benign weather conditions
US registration
It was reported that, to avoid operating under Australian aircraft requirements, the owners decided to leave the aircraft on the US register, and apply on behalf of the registered owner to CASA for a special flight authorisation[8] (SFA) for operations in Australia.
In order for this to occur, the FAA required the registered owner of N600 to have US citizenship. The owners of N600 approached a mutual friend with dual Australian/US citizenship, to act in an administrative role as the registered owner. The owners then applied on behalf of the registered owner to CASA for a SFA in order to operate N600 in Australia.
CASA Special flight authorisation
On 19 October 2022, CASA instrument CASA SA 22/2982 was issued providing a SFA for N600 to operate in Australia under conditions that included that the aircraft be maintained in accordance with the requirements of the FAA. Other operational requirements included that it only be flown in day VFR, must not be operated over populous areas, operated in accordance with CASR Part 91, and only be flown by nominated persons of the registered owner.
Witnesses
A witness at Temora saw N600 at the fuel bowser after conducting circuits, and spoke generally with the pilots by radio about the aircraft. Nothing unusual about the aircraft was observed by the witness prior to its departure from Temora.
The last witness to see the aircraft was at Wedderburn, shortly before the accident, and recalled N600 conducting a go-round after landing and recounted that the aircraft did not climb as expected.
A witness near the accident site just prior to impact recalled the noise of the aircraft reverberating off a nearby water storage tank seconds before impact and described it as ‘revving high and sounded like a machine gun firing’.
Survival aspects
Examination of the aircraft wreckage indicated that the initial impact was in a controlled state at a slow speed, into dense trees. The cabin structure surrounding the cockpit was significantly disrupted during the later stages of the accident sequence, and was not considered survivable.
The carriage of an appropriate emergency locator transmitter (ELT) and/or personal locator beacon (PLB) was a requirement under Civil Aviation Regulation (CAR) 252A unless, among other requirements, the aircraft would be operating within a 50 NM radius from the original point of departure. The ELT fitted to N600 was not compliant with Australian requirements. No crash activation of the ELT was detected or advised by authorities after the accident. A family member identified that one of the pilots was carrying a PLB onboard the aircraft on the day of the accident. However, given the post impact fire and severe degradation of the site, the ATSB was unable to locate the PLB.
Although not legally required, the pilots had not lodged a flight plan or arranged a SARTIME to be held by a responsible person. One of the pilot’s spouses was awaiting the arrival of the aircraft at Wedderburn but was not in receipt of a flight plan or nominated SARTIME.
Safety analysis
On 26 December 2022, a Stoddard Hamilton Aircraft, Glasair Super II FT, registered N600, departed Bankstown, New South Wales for a private flight to Temora, and then onto Wedderburn. N600 conducted a landing and go-around on runway 17 at Wedderburn. However, during the go‑around, N600 failed to achieve sufficient climb performance and impacted terrain about 2.7 km to the south-west of Wedderburn aircraft landing area. The aircraft was destroyed, and the two pilots on board were fatally injured.
This analysis will explore airworthiness considerations pertaining to N600, relating to the engine, reduction gearbox and propeller, the pilots’ experience on the aircraft type, control layout, the approach to land at Wedderburn and general conditions for operation in Australia.
Climb performance
After conducting a landing and go-around from runway 17 at Wedderburn, N600 encountered reduced climb performance and was unable to sufficiently out climb surrounding terrain for about 2 minutes before contacting trees.
Post-accident review of the aircraft engine could not determine any mechanical discontinuity of the engine or gearbox, however due to fire affected components of the electrical and ignition systems, there was not enough evidence to examine these systems definitively.
CCTV footage indicated a fast but controlled landing at Wedderburn prior to the go‑around.
Witness accounts of high engine power leading up to the impact and the degree of post-impact fire indicates sufficient fuel onboard and no evidence of engine stoppage in flight.
Propeller fragments found at the accident site indicated that the propeller had significant rotational speed at initial impact with trees. Propeller pitch settings at the time of the accident were likely in a setting to facilitate take-off power, however the pitch setting at the time of the go-around could not be determined.
Witness indications of a ‘machine gun noise’ may indicate propeller noise, imbalance or damage prior to the impact, however, as post-impact evidence was mostly consumed by fire these possibilities were unable to be further examined.
Therefore, with the limitations of evidence, the ATSB could not determine the reasons why the aircraft was unable to sufficiently out climb surrounding terrain.
Pilot experience on amateur-built aircraft
Both pilots had significant experience in larger multi-engine aircraft and neither had flown N600 prior to the day of the accident. While experienced in larger conventional aircraft operations, there was little evidence to support recent flying experience in light, single-engine, or amateur-built aircraft types.
Each amateur-built aircraft by their very nature is unique. The aircraft builder develops their own systems architecture to accommodate their selected components. This may vary significantly to conventional aircraft configurations and systems.
The absence of previous experience on the aircraft type and recent single-engine flying likely did not prepare the pilots for the challenges of managing an emergency on take-off of a single-engine, experimental amateur-built aircraft with particular design, performance, and control differences.
Special flight permit
The owners of N600 operated the aircraft from Bankstown Airport and over populous areas on the morning of the accident. This was not in accordance with condition 6 as detailed in schedule 2 of the special flight authorisation approved and issued by CASA.
Flight over populous areas in aircraft with a non-certified automotive engine, increases the risk of injury and death to third parties not associated with the operation of the aircraft and reduces the emergency landing options available to pilots if an emergency occurs during take-off.
Non-conventional systems in amateur-built aircraft
Amateur-built aircraft traditionally have different attributes to that of certified aircraft. This can sometimes be evident in the control system layouts and actuation. In the case of N600, the propeller pitch rocker switches were reversed in activation orientation from the left to the right seat. Even with prior knowledge of this control layout, it is likely that operating the aircraft from a different seating position would increase the likelihood of inadvertent pitch change reversal in an emergency during a critical phase of flight, although it could not be determined which seat the aircraft was being operated from at the time of the accident.
The absence of a propeller pitch position indicator or visual references to the pitch settings increases pilot reliance on pre-set throttle and pitch settings prior to take-off, which may not be adequately set during a go-around.
Circuit approach and go-around at Wedderburn
The final approach to land at Wedderburn was conducted after a wide circuit on runway 17 without an overhead circuit join, limiting the appreciation of the wind direction on the ground. This likely led to landing with a quartering left-tailwind in hot and gusty conditions, increasing the aircraft’s ground speed for landing. It is likely that this higher ground speed, downwind landing was a significant factor in pilot decision making to conduct a go‑around.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Stoddard Hamilton Aircraft Glasair Super II FT, N600 near Wedderburn, New South Wales on 26 December 2022.
Contributing factors
For reasons that cannot be determined, N600 did not achieve sufficient climb performance after take-off from Wedderburn, which led to a collision with terrain.
The pilots were not experienced in the characteristics of N600's systems, performance and handling, which limited their ability to effectively manage an in-flight emergency.
Other factors that increased risk
The pilots operated N600 over a built-up area after departing from Bankstown. The special flight permit did not permit operations of experimental aircraft with automotive conversion engines in these areas due to increased risk to third parties and people on the ground.
N600 was likely fitted with reversed in activation orientation propeller pitch change rocker switches on the left and right side of the throttle. This increased the risk that a pilot flying from the right seat would operate the propeller pitch change opposite to the desirable selection.
Other findings
The pilot of N600 conducted a downwind landing on runway 17 which likely prompted the pilot to conduct a go-around.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Federal Aviation Administration
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meterology
No submissions were received from the directly involved parties for changes to the report.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Visual flight rules: a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] A rectangular take-off and landing pattern comprising of upwind, crosswind, downwind, base and final approach legs.
[3] Runway number: the number represents the magnetic heading of the runway.
[5] Aircraft supplied in kit form and is designed to be constructed for the education and recreation of the owner.
[6] Wind coming from behind the aircraft direction, either the left or right side of the aircraft.
[7] Informed participation relies on the premise that before you take part or pay for an activity that you are fully aware of the potential risks and consequences.
[8] A legislative instrument allowing operation of a foreign registered amateur-built aircraft in Australia subject to certain conditions.
On 24 December 2022, a pilot from Katherine Aviation was assigned to operate a Cessna 210N aircraft, registered VH-TFT (TFT), on a charter flight from Gove Airport to Katherine-Tindal Airport, Northern Territory. The fight was arranged to transport a single passenger who was scheduled to be in Katherine over the Christmas period.
At about 0730 local time the aircraft was refuelled with 211 litres of Avgas 100LL. At about 0800 the passenger arrived at the airport in preparation for the flight. Radio transmissions recorded on the Gove common traffic advisory frequency (CTAF) indicated that, at 0812, the aircraft was being taxied for engine run-up checks, and at 0814 the pilot advised that the aircraft had commenced the departure roll on Runway 31. At 0817 a final transmission was recorded on the CTAF indicating that TFT had departed Gove on a direct track to Katherine-Tindal Airport and was on climb to a cruising altitude of 8,500 ft.
At 0841 the operator received a text message from the pilot advising an expected arrival time at Katherine-Tindal Airport of 1024. As the aircraft tracked toward Katherine, mobile phone tower tracing records identified that the aircraft first came into the detectable range of the Bulman cellular tower at 0914.
At 1044 the operator called the pilot’s mobile phone and then at 1058 sent a text message seeking confirmation that the flight had arrived at its destination. When the operator did not receive a response, they checked with another company pilot who was stationed at Gove who confirmed that TFT had not returned to the departure airport. The operator then contacted several station properties along the expected route to check whether TFT had been sighted. At around midday, the operator contacted search and rescue officials and advised that TFT was overdue.
An airborne search and rescue response for the aircraft was commenced by the Joint Rescue Coordination Centre (JRCC) that afternoon. On 25 December 2022, at about 1345, a debris field was located by a search aircraft in a remote area of medium-density bushland, approximately 237 km east-north-east of Katherine (Figure 1). Both occupants were fatally injured and the aircraft was destroyed.
Figure 1: Satellite view of the Northern Territory showing the location of the accident site
The ATSB initiated a field-based investigation following notification from the JRCC that the aircraft wreckage had been located. ATSB investigators attended the accident site on 29 and 30 December 2022. The ATSB’s on-site examination of the wreckage and accident site identified that:
the right wing and its wing tip (which was not attached to the wing) were the first major components in the wreckage trail
the right wing was located approximately 300 m before the primary point of ground contact, indicating that it had separated from the aircraft fuselage during flight (Figure 3)
severed tree branches and ground scars were consistent with the aircraft having a trajectory of approximately 35° down from horizonal immediately before colliding with terrain
almost complete fragmentation of the aircraft structure had occurred on impact with trees and the terrain
aircraft components were spread over a distance of 80 m from the primary ground contact point. The propellor, engine, left wing, carry-through structure, empennage, nose gear and cabin components were all identified in the wreckage trail
the general orientation of the wreckage spread was in a north-east direction, opposite to the intended flight path to Katherine-Tindal
all major sections of the aircraft’s structure were accounted at the accident site
flight control continuity was established where possible
the wing flaps were assessed to have likely been in the retracted position
the landing gear was likely in the retracted position
there was no cockpit voice or flight data recorder, nor was there a regulatory requirement for them to be fitted to an aircraft this size
the aircraft was not fitted with ADS-B out or in-flight satellite tracking equipment and the aircraft was beyond the range of air traffic control radar.
Figure 2: Aerial view of the accident site showing the spread of wreckage
Source: ATSB
Figure 3: As found position of the right wing approximately 300m from the main wreckage
The right wing and its wing tip were the first items located in the wreckage trail. On-site examination of the main wing spar identified that it had fractured diagonally, about 30‑60 cm from the inboard fuselage attachment points (Figure 4).
Figure 4: Illustration of the Cessna 210 and the wing and main spar fracture location
Source: Textron – annotated by the ATSB
Examination of the right wing showed extensive permanent deformation of the wing surface with associated compression rippling to the upper skin. The damage was indicative of substantial upward bending forces applied to the wing prior to its failure and separation from the aircraft (Figure 5).
The inboard end of the right wing-spar remained attached to the fuselage carry-through structure. The left wing remained attached to the carry-through and was located within the primary wreckage area. Examination of the fracture surfaces from the right wing-spar identified evidence of ductile overstress. The on-site assessment did not identify any regions of fatigue cracking or other pre‑existing damage that might have weakened the spar caps, straps, or web.
The outboard tip section from the right wing was found about 70 m from the right wing. Black contact marks on the tip surfaces indicated that the outboard tip impacted the rubberised leading-edge protection on the tail during the break-up sequence.
The inboard end of the right wing-spar and the corresponding fracture surfaces from the separated right wing were retained for further detailed examination at the ATSB technical facilities in Canberra.
Figure 5: Separated right wing assembly showing damage associated with significant upward bending forces
On-site inspection of the propeller identified that the propeller hub had separated from the engine crankshaft due to overstress fracture under predominantly bending loads. One propeller blade had fractured from the hub at its base. All of the blades had sustained forward bending and rotational abrasion damage. One of the blades displayed chordwise twisting and compound bending. The damage signatures indicated that the engine was likely to have been driving the propeller with significant power when the aircraft collided with terrain.
Figure 6: Propeller assembly as removed from the ground impact crater
VH-TFT was a 210N, manufactured in the United States in 1978 by the Cessna Aircraft Company and first registered in Australia in 1989. The aircraft was capable of seating six-people including the pilot and had been designed with a high cantilever wing and a single-engine operating a variable-pitch three-blade propeller. The aircraft was equipped with retractable tricycle landing gear.
The operator’s maintenance records indicated that the aircraft had accrued about 15,100 total flight hours. The most recent scheduled maintenance was a 100-hourly inspection that was completed in accordance with the Civil Aviation Safety Authority maintenance Schedule 5, about 2 months (95 flight hours) prior to the accident. A number of detailed wing inspections were conducted during the last 100 hourly. They included:
Federal Aviation Administration Airworthiness Directive 2012-10-04 (inspection for cracking of the main spar lower cap)
Cessna Special Inspection Document (SID) operation 33 – Inspection of the wing lower spar cap
SID operation 35 – Inspection of the carry through spar lower surface
SID operation 37 – Inspection of the wing spar carry through attachment lugs.
A maintenance release was issued in the night visual flight rules and charter operational categories. The current maintenance release was found in the aircraft wreckage with the daily inspection certified on the day of the accident. No defects or overdue maintenance were recorded on that document.
Weather and environmental information
The Bureau of Meteorology (BoM) advised that, on the morning of 23 December 2022, the day prior to the accident, tropical cyclone Ellie crossed the coastline to the west of Darwin and tracked to the south. Later that evening, Ellie was downgraded to a tropical low, however heavy rain and strong to damaging winds were expected to impact large parts of the greater Northern Territory top-end.
BoM analysis of satellite imagery[1] indicated that on the morning of 24 December 2022, convective cloud started to develop along the expected flight path of the aircraft, near to the accident site. At around 0900, the cloud development strengthened into thunderstorms, with the first observations of lightning recorded between 0940 and 0950. The satellite imagery in the vicinity of the accident site is shown in Figure 7 and Figure 8. That imagery showed the formation of a thunderstorm near to the accident site from about 0910 and its progression through to 1000. The system persisted for several hours after that initial formation.
The BoM further advised in their analysis of the weather conditions that a thunderstorm could result in severe turbulence, severe icing and wind shear with outflows of strong and gusty winds, not only in the immediate vicinity but also at some distance away from the storm. An automated weather station at Bulman, approximately 20 km to the south of the accident site, recorded 12.4 mm of rainfall between 0930 and 1030 that morning.
The development of the severe weather was consistent with the forecast conditions in the Northern Territory Graphical Area Forecast (GAF) that was issued by the BoM at 0135. In the region of the aircraft’s expected flight path the GAF predicted cloud coverage between 5 and 7 oktas[2] at the accident site location around the time of the accident, with an effective ceiling of 1,000 feet above ground level (AGL). There were no breaks predicted between subsequent cloud layers, with cloud tops predicted to be the same as each subsequent cloud base to above 10,000 ft AGL. Further, areas of heavy and moderate rain were predicted with reduced visibility between 500 and 2,000 metres from convective clouds including towering cumulous and cumulonimbus, each with associated severe turbulence.
Figure 7: Weather satellite imagery showing cloud and convective activity over the region of the accident site at 0900. Subsequent changes in convective activity (within the boxed region) are further highlighted in Figure 8
Source: Bureau of Meteorology, annotated by the ATSB
Figure 8: Close-up montage of satellite imagery and convective activity overhead the accident site from 0910 to 1000
Red dots in the above images at 0940 Central Standard Time (CST), 0950 CST and 1000 CST are recorded lightning strikes. The accident site is represented by a red star.
Source: Bureau of Meteorology, annotated by the ATSB
Pilot information
The pilot commenced their flight training in June 2021 and in late January 2022 they obtained a commercial pilot license (aeroplane). The pilot obtained a multi-engine aircraft instrument rating in February 2022. The pilot also held a Class 1 aviation medical certificate, valid until May 2023.
The pilot commenced flight training with Katherine Aviation in August 2022, completing 14 proficiency flights in a Cessna 210 during the induction period and passing the company line check on 20 September. The pilot was then employed by the operator, completing passenger‑carrying charter flights from Katherine-Tindal to remote locations within the Northern Territory top-end (totalling 76 hours). At the start of December, the pilot was restationed to the operators base in Gove, East Arnhem, completing an additional 45 hours until the day of the accident. They had recorded a total of 364 flying hours before the accident flight.
Witness information
The expected track for the flight between Gove and Tindal-Katherine was over remote sections of the Northern Territory. No witnesses to the accident have been identified.
Audio information
Examination of the recorded CTAF radio transmissions for Gove on 24 December 2022 revealed 3 transmissions from the pilot:
during the ground run-up checks
during taxi for departure
shortly after take-off.
No additional recordings regarding the operation of the flight have been identified.
The investigation is continuing and will include further review of the:
aircraft wreckage and recovered electronic devices
environmental influences including analysis of the meteorological data
pilot qualifications, experience, and training
operator training policies and procedures
passenger records
similar occurrences in Australia and internationally.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB acknowledges the assistance provided by the Bureau of Meteorology, Airservices Australia, the Northern Territory Police Force and Heli-Muster Pty Ltd in supporting the ATSB’s onsite team, and for providing information through the evidence collection phase of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Satellite images were processed by the Bureau of Meteorology from the geostationary meteorological satellite Himawari-8 that was operated by the Japan Meteorological Agency
[2] Cloud cover observations are measured in oktas (eighths). A completely clear sky is recorded as zero okta, while a totally overcast sky is 8 oktas. Any trace of blue on an otherwise cloudy sky is recorded as 7 oktas.
Final report
Executive summary
What happened
On 24 December 2022, the pilot of a Cessna 210N aircraft, registered VH-TFT and operated by Katherine Aviation, was conducting a charter flight under the visual flight rules to transport a single passenger from Gove to Katherine, Northern Territory. The aircraft departed Gove at 0814 local time, with an estimated arrival time to Katherine Tindal Airport of 1024. When the aircraft did not arrive, and contact was unable to be made with the pilot, search and rescue activities were initiated by the authorities. At 1204 the following day a wreckage field was found near to the intended flight track at a remote location in East Arnhem, approximately 237 km east-north-east of Katherine. The pilot and passenger sustained fatal injuries.
What the ATSB found
Upon arrival overhead the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm, which probably resulted in exposure to a combination of severe turbulence and reduced visibility for the pilot.
It is probable that a combination of turbulence encountered from the thunderstorm, airspeed, and control inputs led to the excessive structural loading and in-flight separation of the right wing from the fuselage before the aircraft collided with terrain.
It could not be determined with certainty why the pilot flew in close proximity to the storm, however, it is possible that they were in the process of diverting or turning back when the break-up occurred and/or the severity of the storm was not apparent.
What has been done as a result
Shortly following this accident, Katherine Aviation advised that it had:
provided tracking and communication devices for their pilots that enabled real-time satellite‑based tracking and monitoring of their fleet. The devices allowed messages to be exchanged between the company and their pilots in the absence of a mobile telephone signal.
presented the theory component of their wet season training material to their company pilots and updated their exposition with the requirement that all pilots were to complete the briefing program on an annual basis.
developed flight assessment tools to provide their pilots with better decision-making capability when planning for operations during marginal weather.
Safety message
During the Northern Territory wet season, rapidly developing and frequent thunderstorms with associated severe turbulence present pilots with a challenging and hazardous operating environment. Identifying and maintaining adequate clearance from thunderstorms is critical to flight safety.
The United States Federal Aviation Administration recommends that thunderstorms be avoided by at least 20 NM. Weather radar and satellite imagery can assist planning and in‑flight storm avoidance, provided their limitations are understood.
A careful study and understanding of the relevant Bureau of Meteorology (BoM) forecasts, including the graphical area forecasts (GAF), when flight planning will also assist in avoiding hazardous weather. As shown in the example below, GAFs detail the forecast prevailing weather and other weather phenomena over a broad area for a 6-hour period. The forecast is set out in a tabular format, with the first row detailing the forecast prevailing conditions and the subsequent rows forecasting the presence, and effect, of other weather phenomena.
Of note, this format does not mean that the prevailing (first row) conditions and subsequent rows will necessarily co‑exist. Pilots should keep this in mind and the BoM advises that it is not always practical for GAFs to detail the specific timing and likely locations of weather phenomena.
Source: BoM
Contacting the duty BoM forecaster via the phone number on the relevant GAF is the best way for pilots to assess the viability of a planned route, particularly if the forecast is marginal and the weather is changing. The BoM’s online Knowledge Centre for pilots can further assist understanding of the meteorological information that is necessary for safe operations in the wet season.
A range of other education resources are also available for pilots to understand the unique weather challenges of operating during the wet season, including the Civil Aviation Safety Authority’s (CASA) annual Flying in the wet season seminars. CASA also has available online a range of educational resources for managing severe weather-related scenarios.
The occurrence
On 24 December 2022, a pilot from Katherine Aviation was assigned to operate a Cessna 210N aircraft, registered VH-TFT, on a passenger transport flight from Gove Airport to Katherine Tindal Airport, Northern Territory under the visual flight rules[1] (Figure 1).
At about 0730 local time, a Katherine Aviation operations staff member called the pilot advising of a potential delay to the sole passenger’s arrival for the scheduled 0800 departure. With the pilot in attendance, the aircraft was refuelled by the Gove Airport refueler at 0735. The passenger arrived at about 0800 and boarded the aircraft with the pilot.
The pilot’s radio transmissions were recorded on the Gove common traffic advisory frequency (CTAF). The transmissions indicated that at 0812 the aircraft was taxied for engine run-up checks and the take-off roll commenced shortly after at 0814. A witness observed the aircraft depart from runway 31 at about this time. At 0818, a final transmission was recorded on the CTAF, in which the pilot advised that VH-TFT was passing an altitude of 1,700 ft on climb to 8,500 ft and tracking direct to Katherine. No further radio communications from the pilot were identified. At 0841, the operations staff member received a text message from the pilot advising their expected arrival time of 1024 at Katherine Tindal Airport.
At 1058, when the aircraft had not arrived as scheduled, the staff member called the pilot’s mobile phone without answer and then sent a follow-up text message. When no response was received, they checked with another company pilot stationed at Gove, who confirmed that VH-TFT had not returned to Gove. Several station properties were then contacted along the expected route to check whether VH-TFT had been sighted. At around midday, search and rescue officials were contacted by Katherine Aviation advising that VH-TFT was overdue.
Search and rescue
A search and rescue response was commenced by the Australian Maritime Safety Authority’s Joint Rescue Coordination Centre (JRCC), with an airborne search commencing at 1344. The JRCC requested mobile phone tracing records that enabled the search to be refined around the Bulman area (Figure 1). The JRCC advised there was no signal received from the aircraft’s emergency locator transmitter to assist with locating the aircraft.
On 25 December 2022 at 1204, a debris field was sighted from a search aircraft in a remote area of medium-density bushland in East Arnhem. The accident location was 237 km east-north-east of Katherine, approximately 7 km north of the planned track and 18 km north of Bulman. At 1354 first responders arrived at the accident site and confirmed that both occupants were fatally injured and the aircraft was destroyed. There were no known witnesses to the accident.
Figure 1: Satellite view showing the planned direct track, the location of the accident site and its proximity to Bulman
Source: Google Earth, annotated by the ATSB
Context
Pilot and passenger information
Pilot information
The pilot commenced their flight training in June 2021 and obtained a commercial pilot licence (aeroplane) on 24 January 2022. After further flight training, the pilot obtained a multi‑engine aircraft instrument rating that was issued on 19 February 2022. The pilot had accrued 23.6 hours of instrument flying, the last of which was 1.9 hours during the conduct of the instrument rating assessment flight on 19 February 2022. No further instrument hours were recorded in the pilot’s logbook. The pilot held a Class 1 aviation medical certificate, valid until 13 May 2023, with no restrictions and no declared medical conditions.
The pilot’s first commercial flying role commenced in August 2022 with Katherine Aviation, based in Katherine, Northern Territory. On 11 August 2022 the pilot commenced line training through the operator’s in-command-under-supervision (ICUS) program, operating Cessna 210 aircraft under the supervision of either a senior base pilot or the head of flying operations. During that period, the pilot flew to remote communities and station properties throughout the Big Rivers, Top End and East Arnhem regions,[2] including on 3 occasions to the airfield at Bulman. The operator’s training records showed that the pilot undertook 14 ICUS flights totalling 53.1 hours, and passed their company line check on 20 September 2022. The pilot remained in Katherine and completed an additional 76.1 hours conducting passenger‑carrying charter flights under the visual flight rules (VFR) to predominantly remote locations within the Northern Territory.
On 1 December 2022, the pilot relocated to the operator’s base in Gove, East Arnhem and accrued a further 45.2 flight hours prior to the accident day.
The pilot’s logbook and operator’s records showed the pilot had a total flying experience of 364.3 hours, 180.8 of which were in Cessna 210 aircraft. In the 30 and 90 days prior to the accident, the pilot had flown 53.7 and 99.1 hours exclusively in Cessna 210 aircraft.
72-hour history
The operator provided the pilot’s accommodation in Gove. Table 1 summarises the pilot’s flight and duty times for the previous 3 days. The pilot did not fly on 21 or 22 December 2022. On 23 December 2022 they accrued 5.7 hours on a flight to Lake Evella, Groote Eylandt and Elcho Island.
Table 1: Summary of pilot’s duty and flight times
Date
21 December 2022
22 December 2022
23 December 2022
Duty time
0 hours
0700 – 1300 (6 hours)
0730 – 1815 (10.8 hours)
Flight time
0 hours
0 hours
5.7 hours
The ATSB was unable to establish the pilot’s sleep routine in the 3 days prior to the accident, as the pilot lived alone at their Gove accommodation. A company pilot reported that during those 3 days, they saw the pilot intermittently in the office at Gove Airport. They also socialised together as part of pre-Christmas celebrations during the evenings of 22 and 23 December 2022, with each event concluding between 2000 and 2030. No concerns were noted by the co‑worker on the accident pilot’s wellbeing during that period.
At 0615 on the morning of the accident, the pilot sent a text message to the Gove Airport refueller requesting that the aircraft be refuelled. Software login records showed that at 0659 the pilot had commenced their pre-flight flight planning from the airport company office. At about 0735 the refueller met with the pilot while the aircraft was being refuelled. They commented that the pilot did not show any indications of fatigue.
Passenger information
The passenger was being transported to Katherine for a period of respite care over the Christmas and New Year period and was scheduled to return to Gove on 4 January 2023. Katherine Aviation advised that the flight on 24 December 2022 was the third attempt to depart Gove, with the 2 previous attempts being cancelled due to unsuitable weather.
Aircraft information
General overview
The aircraft was manufactured by the Cessna Aircraft Company as a model 210N in the United States in 1979 and was first registered in Australia in 1989. It had seating for 6 people including the pilot and had a high‑cantilever wing with retractable tricycle landing gear. It was powered by a Teledyne Continental IO-520-L46B 6-cylinder engine operating a Hartzell variable-pitch, 3‑blade propeller.
The wing construction comprised a forward spar, main spar, conventional formed sheet-metal ribs and aluminium skin. The inboard section of each wing, forward of the main spar, was sealed to form an integral fuel tank. The aircraft fuel tanks held a combined total capacity of 341 L, of which 337 L was useable. Both wings attached to the central wing spar carry-through structure, which was the primary structural design element for carrying lateral and bending flight loads.
Aircraft maintenance
The maintenance records showed that the aircraft had accrued about 15,100 total flight hours. The engine had been factory overhauled and fitted on 27 March 2022, subsequently accruing 273.5 hours. The propellor had accrued 1,201.8 hours since overhaul.
The aircraft was maintained in accordance with Schedule 5 requirements prescribed by the Civil Aviation Safety Authority (CASA). Schedule 5 is a generic maintenance program developed by CASA that is required to be completed every 100 flight hours or 12 months, whichever comes first.
The most recent scheduled maintenance was a 100-hourly inspection completed on 27 October 2022 at 15,004.9 hours total time in service. During that maintenance, the following detailed inspections for cracking of the wing were completed with no defects found:
Federal Aviation Administration Airworthiness Directive (FAA AD) 2012-10-04– Inspection for cracking of the main spar lower cap
Cessna Special Inspection Document (SID) operation 33 – Inspection of the wing lower spar cap
SID operation 35 – Inspection of the carry through spar lower surface
SID operation 37 – Inspection of the wing spar carry through attachment lugs.
The maintenance release current at the time of the accident was issued in the night visual flight rules and charter categories. It was found in the aircraft wreckage with the daily inspection certified for the day of the accident. There were 3 minor defects listed on the maintenance release that had not been certified as rectified, however they were not considered to have influenced the development of the accident. The defects were:
rear navigation light inoperative
early peaking of exhaust gas temperature in the number-5 cylinder
fuel gauge flickering.
The maintenance release indicated that VH-TFT was due for a 100-hourly inspection at 15,104.9 hours. As the aircraft had less than 5 hours remaining prior to commencement of the accident flight, Katherine Aviation operations personnel arranged with the pilot to exchange VH‑TFT with another Cessna 210 for the return to Gove.
Meteorological information
Wet season
Although variable from year to year, weather in the Northern Territory can generally be divided into the dry season from May to September and the wet season from October to April. In the context of Northern Territory aviation operations, most of the hazardous weather occurs during the wet season. This is a period of unstable atmospheric conditions where tropical cyclones and active monsoon troughs may produce heavy rainfall for prolonged periods, squally winds, and thunderstorms.
Thunderstorms are a very frequent and widespread hazard during the wet season. They are common during the late afternoon and early evening, with a secondary peak in the early morning. They often spread out to form sheets of altostratus and cirrostratus clouds late in their life cycle, bringing steady overnight rain and low cloud persisting into the morning. As a thunderstorm is growing, updrafts in the core can reach over 100 kt. These updrafts can exist alongside downdrafts of similar strength as rain starts to fall out of the storm, resulting in potential for severe turbulence and loss of aircraft control if flying into such conditions (BoM, 2012).
General weather conditions
The Bureau of Meteorology (BoM) advised that, on the morning of 23 December 2022, tropical cyclone Ellie crossed the coastline west of Darwin and tracked south. Later that evening, Ellie was downgraded to a tropical low, however, heavy rain and strong to damaging winds were expected to impact large parts of the greater Northern Territory the next day.
Aerodrome forecasts for Gove and Katherine Tindal
The BoM produces aerodrome forecasts (TAFs) that state the expected meteorological conditions in the airspace within an 8 km radius of the aerodrome reference point. TAFs were available for both Gove and Katherine Tindal Airports for the proposed flight.
Gove Airport conditions after 0830 and until 1130 were predicted to be clear with visibility greater than 10 km, northerly winds at 10 kt, no cloud ceiling below 10,000 feet above ground level (AGL) and no other weather phenomena.
The prevailing weather conditions at Katherine Tindal Airport were forecast to be above the day VFR alternate minima for the entire validity period of the TAF. Notably, the prevailing cloud ceiling was predicted to improve after 0930. However, deteriorating conditions below the alternate minima were predicted for periods up to 1 hour during the expected arrival time of the aircraft. Specifically, thunderstorms, low visibility (1,000 m), strong winds up to 35 kt, and a cloud ceiling at 500 ft AGL were forecast. These conditions required the pilot to plan for at least 60‑minutes holding fuel on arrival at Katherine Tindal, or to plan for an alternate destination aerodrome to land.
Graphical area forecast
The Graphical Area Forecast (GAF) provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text. They are produced for 10 areas across Australia and are broadly state-based (BoM, 2017). Cloud amount is given using the following descriptions (BoM 2018):
For cumulonimbus and towering cumulus, cloud amount is described as:
isolated – individual features which are forecast to affect up to 50% of an area
occasional – well-separated features which are forecast to affect greater than 50% but not more than 75% of an area
frequent – little or no separation between adjacent features forecast to affect greater than 75% of an area.
Embedded is added to these coverage quantifiers to indicate cumulonimbus or towering cumulus clouds are embedded in layers of other cloud and cannot be readily recognised, regardless of whether or not they are protruding from the layer.
Weather coverage is described as:
isolated – individual features which are forecast to affect up to 50% of an area
scattered – well-separated weather features which are forecast to affect greater than 50% but not more than 75% of an area
widespread – features with little or no separation forecast to affect greater than 75% of an area.
When thunderstorms, cumulonimbus or towering cumulus are forecast, it implies severe icing and severe turbulence will be present. Forecast cumulus, stratocumulus and altocumulus imply moderate turbulence. All heights referred in the GAF are above mean sea level (AMSL) (BoM, 2017).
The GAF for the Northern Territory issued at 0135 on 24 December 2022, valid from 0830 to 1430, divided the territory into several areas (Figure 2). Gove was in area A, Katherine in area B and the accident occurred about 25–35 km into area B.
Figure 2: GAF for the Northern Territory with the track from Gove to Katherine Tindal Airport highlighted (upper image) and accompanying weather features (lower table)
Source: Bureau of Meteorology, annotated by the ATSB
For the planned flight in area A, the GAF predicted visibility greater than 10 km when no other weather was present. Visibility was forecast to reduce in 2 weather phenomena, each with isolated coverage of up to 50% of area A. These were moderate showers of rain reducing visibility to 3,000 m, and thunderstorms with moderate rain reducing visibility to 1,000 m. Forecast clouds associated with these phenomena were:
moderate rain – isolated towering cumulous clouds covering up to 50% of the area of reduced visibility with bases at 3,000 ft to above 10,000 ft, scattered stratus clouds covering 25–50% of the area with bases at 1,000 ft and cloud tops at 3,000 ft and broken cumulous clouds covering more than 50% of the area from 3,000 ft to above 10,000 ft.
thunderstorms with moderate rain – broken stratus clouds covering more than 50% of the area from 1,000 ft to 3,000 ft, and isolated cumulonimbus clouds covering up to 50% of the area from 3,000 ft to above 10,000 ft.
In area B, broken cloud, covering more than 50% of the area was forecast from 1,000 ft to above 10,000 ft. Visibility was forecast to be greater than 10 km except in scattered light rain reducing visibility to 8,000 m in 50–75% of the area, scattered moderate showers of rain, reducing visibility to 2,000 m in 50–75% of the area, and isolated thunderstorms with heavy rain, reducing visibility to 500 m in up to 50% of the area. Clouds associated with these weather phenomena were forecast to be:
light rain – overcast alto-cumulous and alto-stratus covering 100% of the area from 8,000 ft to above 10,000 ft.
moderate showers of rain – occasional towering cumulus clouds covering 50–75% of the area from 2,000 ft and to above 10,000 ft. Broken stratus clouds from 500 ft to 2,000 ft and broken cumulus clouds from 2,000 ft to above 10,000 ft covering more than 50% of the area.
thunderstorms of rain – isolated cumulonimbus clouds covering up to 50% of the area from 2,000 ft to above 10,000 ft, and broken stratus clouds covering more than 50% of the area from 500 ft to 2,000 ft.
Grid-point wind and temperature
Grid-point wind and temperature (GPWT)[4] forecasts are issued by the BoM every 3 hours for low‑level operations and display mean wind speed, direction and temperature for a range of altitudes. ATSB’s review of the GPWT chart that was issued at 0330 (local) and valid at 0930 (local) showed a wind direction of 340° and speed of 18 kt at an altitude of 8,500 ft.[5]
En route weather
Analysis of satellite imagery[6], conducted by the BoM, indicated that from 0900 convective cloud developed to the west of the accident site. The cloud developed into thunderstorms with the first observations of lightning recorded between 0940 and 0950. The satellite imagery in the vicinity of the accident site is shown in Figure 3 and the montage in Figure 4. The imagery shows the development of the weather system near the accident location from 0900 to 1000. The system persisted for several hours after 1000. The BoM estimated that the cloud tops in the vicinity of the accident site were between 38,000 ft and 46,000 ft AMSL.
The BoM further advised that the thunderstorms near the accident site may have resulted in severe turbulence,[7] severe icing[8] and wind shear with outflows of strong and gusty winds, not only in the immediate vicinity but also at some distance away from the storm. An automated weather station near Bulman recorded 12.4 mm of rainfall between 0930 and 1030 that morning. The development of the severe weather was consistent with the forecast for isolated thunderstorms in the Northern Territory GAF issued by the BoM at 0135.
The ATSB queried the BoM on whether the term embedded (EMBD) should have been added to the GAF considering the forecast for extensive cloud cover and isolated thunderstorms. The BoM advised that the term embedded indicates that a pilot may encounter cumulonimbus or towering cumulus clouds that they may not be able to readily recognise due to them being contained within other cloud layers.
In their analysis of the satellite imagery the BoM identified that the thunderstorms were not embedded due to discrete scattered to broken convective cloud rather than an overcast, poorly separated layer of cloud as would more likely occur in a rain band. The Bureau further advised that although the forecast prevailing conditions were for extensive cloud cover in area B, there was still a moderate to high likelihood that the convective clouds would have been visible to the pilot. This means that the top, or prevailing weather, row and subsequent weather rows may not necessarily co-exist. Put another way, conditions in area B at any location or point in time would be either the prevailing conditions or one of the subsequent rows in the forecast.
The forecast for area B covered a substantial portion of the Northern Territory, for a 6-hour period, with unstable atmospheric conditions. BoM advised that the predicted coverage was a worst case forecast for each weather row in area B, with conditions predicted to develop at different times and places throughout the period. For example, thunderstorms were predicted to cover up to 50% of area B at some point in time during the validity period of the forecast.
The BoM also advised that it was not practical to include additional detail of the specific timing and likely locations of weather phenomena in the GAF product in scenarios like those predicted for area B. To account for this, in cases where convective weather is forecast, pilots are encouraged to call the meteorologist who produced the GAF for details on the weather phenomena likely to be encountered for a specific route and time period.
A comparison of the overhead satellite imagery and the Katherine–Tindal weather radar is also shown at Figure 5 to Figure 7. After the flight had departed Gove, the data at 0830 that morning identified that while significant thermal activity had developed to the north-west of the planned route, the immediate area along the planned track near to Bulman was clear of rain. At 0930 to 1000, the weather radar identified light to moderate rain, along with increased convective activity, signalling the development of a thunderstorm. The BoM identified that limitations exist to the accuracy of weather radar information, particularly as distances increase from the radar head. As the flight progressed toward Bulman, it remains possible that the weather radar did not completely display the extent of the weather system to the pilot. Optimal coverage of weather radar information is described by the BoM:
Generally, the optimal coverage area extends to approximately 200km away from the radar. Beyond this distance some rainfall echoes may be displayed on the radar image, however these echoes will be from clouds higher up in the atmosphere and will not directly correspond with conditions experienced on the ground.
OzRunways and AvPlan were 2 electronic flight bag (EFB) applications authorised by Katherine Aviation. Each application can display rain radar information to assist pilots with weather‑related decision‑making. The operator reported that it was expected that its pilots would access weather radar information in flight, however they identified that this was dependent on cellular data availability.
It was not possible to determine whether the pilot accessed the weather radar information prior to, or during the accident flight. Furthermore, the location of the accident site surrounding Bulman was beyond the optimal coverage range of the BoM radar. Therefore, as discussed above, even if this information was accessed by the pilot, the rain intensity detected by the BoM weather radar on approach to Bulman may not have accurately represented the conditions at the time.
Figure 3: Weather satellite imagery showing cloud and convective cloud activity relative to the accident site at 0900 on 24 December 2022
The white areas are scattered to broken clouds, and the colours provide an indication of the vertical development of the cloud with temperatures ranging between −35 to −70 ºC. The colours provide an indication of the vertical development of the cloud and in general terms, the colder the cloud top temperature, the higher the top of the cloud. Source: Bureau of Meteorology, annotated by the ATSB
Figure 4: Montage of satellite imagery showing the rapid build-up of convective activity near the accident site from 0910 to 1000 on 24 December 2022
Red dots in the above images at 0940, 0950 and 1000 are recorded lightning strikes. The accident site is represented by a red star. The white areas are scattered to broken clouds, and the colours provide an indication of the vertical development of the cloud. Source: Bureau of Meteorology, annotated by the ATSB
Figure 5: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 0830 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Figure 6: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 0930 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Figure 7: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 1000 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Operational information
Flight planning
The planned track between Gove and Katherine was over remote sections of the Northern Territory in class G non-controlled airspace and, closer to Katherine, RAAF Tindal controlled airspace. Katherine Aviation required its pilots to produce an internal company flight plan using an electronic flight planning tool within one hour prior to departure. The planning tool was also used to access en route and destination weather data, through Airservices Australia’s National Aeronautical Information Processing System (NAIPS).[9] Login files identified that NAIPS was accessed by the pilot’s personal and company accounts 3 times on the morning of the accident flight; at 0659, 0702 and 0712.
The NAIPS records showed that a GPWT forecast had been accessed during these periods, however, due to software limitations it could not be confirmed whether a GAF was accessed by the pilot.
A review of the pilot’s previous flights identified that meteorological information, including the GAF, was used by the pilot for their flight planning. The operator indicated that their pilots were required to submit their flight documents to the senior base pilot at the conclusion of each flight. Documents included the flight plan, passenger information, fuel receipts and meteorological information. Although the loose-leaf flight plan printouts were not located at the accident site, based on previous work practice, the required weather forecasts, including the departure and destination TAFs, were probably accessed by the pilot on the morning of the accident flight.
It was a company requirement that a flight notification be lodged with Airservices prior to departure. This could be accomplished using the NAIPS website, the EFB software, or by telephone if internet access was not available. Airservices advised that a flight notification was not lodged for the accident flight.
During a telephone conversation at about 0730 on the morning of the accident flight, the pilot was reported to have stated to a Katherine Aviation operations staff member that the weather was ‘a bit iffy’. The staff member further stated that pilots were encouraged by Katherine Aviation to remember that there was always the option to divert or return. The pilot had taken off and then turned back, due to unsuitable weather, on a flight a few days prior to the accident.
Requirements for flight under visual flight rules
Visual meteorological conditions are the minimum conditions in which a VFR flight is permitted. These conditions ensure pilots have sufficient visibility to control the aircraft and maintain visual separation from terrain and other aircraft.
The rules require that pilots operating below 10,000 ft have a minimum of 5,000 m flight visibility. Pilots also need to maintain 1,500 m horizontal and 1,000 ft vertical separation from cloud when above the higher of 3,000 ft AMSL or 1,000 ft AGL in non-controlled airspace. When operating at or below the higher of 3,000 ft AMSL or 1,000 ft AGL, the pilot must remain clear of cloud and in sight of the ground or water.
En route
The flight was expected to track directly from Gove to Katherine Tindal Airport. A loose-leaf form used by the operator for engine trend monitoring was located at the accident site. The document was damaged and incomplete, however it identified that the pilot had conducted trend monitoring when the aircraft was stabilised in cruise at 146 kt airspeed and at an altitude of 8,500 ft. Taking into account the climb performance of the aircraft, a forecast 18 kt wind speed at 340°, the cruise speed and a direct track to Katherine, the ATSB assessed that the aircraft would pass north of Bulman and over the accident site at about 0930.
Operational staffing
Due to the approaching Christmas and New Year shutdown period, most Katherine Aviation staff were on leave, including the head of flying operations (HOFO) in Katherine and the senior base pilot at Gove. With only 2 flights scheduled for 24 December 2022, 2 staff remained on duty comprising of a senior pilot and an operations staff member, both in Katherine. The senior pilot had prepared another Cessna 210 aircraft for transfer back to Gove, while waiting for TFT to arrive.
Fuel
The aviation refueller at Gove reported receiving a text message from the pilot at about 0615, requesting full fuel (169 L) in the left wing tank and the right wing tank to be filled to the indicator tab (127 L), totalling 296 L. The fuel receipt showed that 211 L of Avgas 100 low lead fuel was uploaded to the aircraft between 0735 and 0745. Based on the Pilot’s Operating Handbook (POH), 4 L was unusable, therefore there was 292 L usable fuel on board at startup, equating to 210 kg using a specific density of 0.72 for Avgas. Previous flight logs showed the pilot allowed 5 L (3.6 kg) for taxiing. This was consistent with the passenger/cargo manifest located at the accident site, which listed 207 kg fuel on board at take-off.
Weight and balance
The passenger/cargo manifest included a loading summary, which calculated the take-off weight including occupants, cargo and fuel for the aircraft to be 1,415 kg, which was less than the aircraft’s maximum take-off and landing weight of 1,724 kg. The associated weight and balance assessment normally completed by the pilot was not located in the wreckage and the passenger’s seating position was unknown.
Based on the weights listed in the manifest and the information provided in the POH, the ATSB assessed that the aircraft was in the mid-range of the aircraft’s centre of gravity envelope, whether the passenger was seated in the front or centre row. Records from previous flights also showed that the pilot routinely switched between left and right tanks to maintain lateral balance. Therefore, the aircraft was almost certainly within the weight and balance limits throughout the flight.
Design limitations
The Cessna 210N is certified as a normal category aircraft. The airspeed and load limits defined in the Cessna 210N POH are defined in Table 2.
Table 2: Cessna 210N airspeed and load limitations
Never exceed airspeed (VNE)
200 kt (red line on the airspeed indicator)
Maximum structural cruising airspeed (VNO)
165 kt (green line on the airspeed indicator)
Manoeuvring airspeed (VA)
125 kt at 1,724 kg
113 kt at 1,428 kg
101 kt at 1,134 kg
Maximum flight load factors (g)
+3.8 g to −1.52 g (flaps up)
+2.0 g (flaps down)
Manoeuvring airspeed (VA) is the maximum airspeed at which full control travel can be used without exceeding the design load factor. The manoeuvring speed decreases with aircraft weight. Factoring the take-off weight and TFT’s fuel usage, the ATSB calculated that the manoeuvring airspeed at the time of the accident was about 111 kt.
The 4 forces acting on an aircraft in flight are lift, weight, thrust and drag. The ratio of lift force to the aircraft weight is the load factor. Load factors are defined in terms of g-loading, which is a measure of the forces acting on the aircraft structure to produce the accelerations involved in changing speed and direction in flight. In straight and level flight, lift force and aircraft weight are balanced, so the load factor is 1 g. Aircraft structural limits are based on aircraft weight and the load factor, which can be affected by any one or combination of the following:
full control movements above VA which can occur while manoeuvring, as a result of disorientation, or during recovery from an unusual attitude.
windshear, turbulence or gusts – severe turbulence is defined as variations in vertical acceleration greater than 1 g.
An aircraft must be operated within its flight envelope[10] to prevent structural damage, or aerodynamic stall.[11] Exceeding the flight load limit below VA results in a stall, whereas exceeding the flight load limit at a speed above VA can produce structural damage.
Accident site and wreckage examination
Wreckage location
The ATSB initiated a field-based investigation following notification from the JRCC that the aircraft wreckage had been located. ATSB investigators attended the accident site on 29 and 30 December 2022. It was situated within the East Arnhem wilderness region with medium‑density trees and largely flat terrain. The nearest aerodrome was located at Bulman, approximately 18 km south.
Site examination
The ATSB’s onsite examination identified that the right wing and its detached wing tip were the first components in the wreckage trail. The wing tip and right wing were located 370 m and 300 m respectively from the primary point of ground impact, indicating they had separated from the aircraft during flight (Figure 8).
Figure 8: Aerial view of the accident site showing the spread of wreckage
Source: ATSB
Severed tree branches and ground scars were consistent with the aircraft having a trajectory of approximately 35° down from horizontal immediately before colliding with terrain. Almost complete fragmentation of the aircraft structure had occurred on impact leading to aircraft components spreading over about 80 m from the primary ground contact point. The propellor, engine, left wing, carry-through structure, empennage, nose gear and cabin components were all identified in the wreckage trail.
The orientation of the wreckage trail was in a north-east direction, which was about 180° to the intended flight track to Katherine Tindal. The tail and empennage section had broken into several pieces and was partially reassembled to ensure that all the extremities and flight control mass balance weights were identified. Excluding the right wing and wing tip, all key components of the airframe were identified in the wreckage trail with no pre-impact defects identified. The left wing remained attached to the intact wing carry-through structure. The landing gear was assessed to be retracted at impact and the flaps were assessed to be in the retracted position.
Both wing tank filler caps remained fitted to their respective fill ports. There was no remnant smell of fuel in the wreckage when it was examined although there had been significant rain through the region prior to ATSB’s examination of the wreckage. Additionally, yellowing of the small grasses and vegetation surrounding the accident site was consistent with chemical burning, likely from the release of fuel when the aircraft impacted terrain.
Separated right wing
Onsite examination of the right main wing spar identified that it had fractured diagonally, about 30–60 cm from the fuselage attachment points (Figure 9–Figure 11).
The right wing showed extensive permanent deformation and tearing of the internal structure with associated compression rippling to the upper skin. The damage was indicative of substantial upward bending forces applied to the wing prior to its failure and separation from the aircraft. The wing structure at the point of failure contained a permanent deflection of about 30° in the upward direction. The internal main fuel tank had been ruptured during the break-up, with no residual fuel remaining.
The inboard end of the right wing spar remained attached to the fuselage carry-through structure. Examination of the fracture surfaces from the right wing spar presented evidence of ductile overstress. Wood fibres and soil were also embedded throughout the main spar surfaces. The onsite assessment did not identify any regions of fatigue cracking or other pre-existing damage that might have weakened the spar caps, straps, or web structure of the wing.
Black contact marks on the wing tip surfaces indicated that it had probably impacted the rubberised leading-edge protection on the tail during the break-up sequence.
The inboard end of the right wing spar and the corresponding fracture surfaces from the separated right wing were retained for further detailed examination at the ATSB technical facilities in Canberra.
Figure 9: The right wing as it was found approximately 300 m from the main wreckage
Source: ATSB
Figure 10: The right wing showed compression rippling of the upper skin surface and permanent deformation from exposure to upward bending
The wing was permanently deformed by about 30° in the upward direction at the point of failure. Source: ATSB
Figure 11: Illustration of the Cessna 210 and the wing and main spar fracture location
Source: Textron – annotated by the ATSB
Engine
The engine had separated from the airframe and was found several metres from the initial impact point. The engine was examined externally for any type of pre-impact mechanical failure with none identified.
Exhaust system
Only small portions of the exhaust system from the engine were located at the accident site. The left side of the exhaust system containing the muffler section and heater shroud had been liberated from the engine and was not found at the accident site. It is possible they were obscured by debris or buried under the soil within the impact crater. The firewall area that housed the cabin heater inlet was destroyed and unable to be assessed for integrity.
The chief engineer for Katherine Aviation indicated they were unaware of any pre‑existing issues with the exhaust system from VH‑TFT and that it was inspected every 100 hours.
Propeller
The propeller hub had separated from the engine crankshaft due to overstress fracture under predominantly bending loads. One propeller blade had fractured from the hub at its base. All blades had sustained forward bending and rotational abrasion damage from passing through sand/soil. One of the blades displayed chord-wise twisting and compound bending. The damage signatures produced on collision with the terrain were consistent with an operating engine (Figure 12).
Figure 12: Propeller assembly after removal from the ground impact site
Source: ATSB
Emergency locator transmitter
The emergency locator transmitter (ELT) installed in the aircraft was an Artex 406 transmitter fitted to a fixed mounting bracket within the aft fuselage. It was required to be switched to the ARM position for flight so that the g-switch would provide impact-activation in the event of an accident.
The ELT from the aircraft was located within the wreckage trail. The switch was set to the armed position and the front panel light had illuminated, indicating that the inertial switch had activated on impact as designed. Although the unit was likely transmitting, the antenna had been severed, preventing the signal from propagating sufficiently to be received by overflying aircraft and/or satellites.[12]
Technical examination
A limited number of items from the accident site were retained as evidence for further review by the ATSB. They included operational documentation, electronic devices and physical components that were subsequently transported to the ATSB’s technical facilities.
Electronic devices
It was a Katherine Aviation requirement for all pilots to use an electronic flight bag (EFB). The pilot used the OzRunways application on an iPad device. The ATSB’s review of the pilot’s OzRunways account identified a portion of a previous flight to Groote Eylandt on 23 December 2022. The account contained no flight data from the accident flight on 24 December 2022.
The ATSB’s examination of the iPad and 2 mobile phones retrieved from the accident site was completed to establish if electronic data regarding the conduct of the flight could be recovered. Access to the severely damaged passenger’s phone was achieved, however there was no data relating to the accident flight stored on that device. Data recovery from the pilot’s phone and iPad was unsuccessful.
Flight instruments
Portions of 2 flight instruments were recovered from the accident site – a gyroscope from the artificial horizon and the front face of the vertical speed indicator.
Disassembly and examination of the gyroscope identified rotational scoring from contact with the rotor’s housing. The scoring damage indicated that the aircraft’s vacuum system and artificial horizon were likely operating.
Examination of the front face of the vertical speed indicator identified a defined witness mark that was consistent with the needle striking against the instrument face on ground impact. The witness mark showed a descent rate of 2,000 ft per minute. However, because the mark was at the limit of the instrument range, the descent rate of the aircraft may have been higher than indicated when it collided with terrain.
Right wing main spar
A red-brown product was adhered to much of the spar fracture surfaces and was likely a mixture of soil and impacted vegetation. Detailed examination of the main spar fragments identified features typical of ductile overstress. There was deformation and angular tearing throughout the spar cap, shear web and strap structure.
Overstress fracture in ductile materials (including the alloys comprising the wing component) occurs when the structure is loaded beyond its ultimate limit. Several rivets that had secured the straps to the spar cap had sheared during the break-up. The examination did not identify any evidence of pre-existing damage such as fatigue cracking, corrosion or other defects (Figure 13 and Figure 14).
Figure 13: Fractured right wing main spar as received at the ATSB’s technical facilities
Source: ATSB
Figure 14: Close-up of the lower spar cap outboard fracture surfaces
Only ductile overstress features and associated deformation was present through the spar structure fracture surfaces. Source: ATSB
Post-mortem and toxicology information
General
The pilot was described by co-workers and next of kin as active with a high level of health and fitness. They were a non-smoker.
Pilot results
A post-mortem examination conducted on the pilot found they sustained fatal injuries during the impact sequence. Toxicological analysis[13] identified the presence of alcohol and carboxyhaemoglobin (COHb). However, due to chemical changes that occur post‑mortem there was significant doubt over the validity of these results. That is, they were not reliable indications that the pilot was exposed to either alcohol or carbon monoxide prior to the accident.
Passenger results
A post-mortem autopsy examination was performed on the passenger, which found that they sustained fatal injuries during the impact sequence. Toxicology testing was not conducted.
Survivability
The accident was not survivable. Although a product of the accident dynamics, had an ELT signal been received by the search and rescue satellite system this would have resulted in earlier location of the accident site by the search authorities.
Organisational information
General
Katherine Aviation was established in 2006. It held an Air Operator’s Certificate (AOC) and operated 15 Cessna 210, 6 Beechcraft Baron BE58, and 4 Cessna 172 aircraft. At the time of the accident it employed 20 pilots and was the registered operator of VH-TFT. It operated from 6 locations, with Katherine Tindal Airport being their main base, and Gove being one of 5 remote bases. The company conducted operations under Civil Aviation Safety Regulations (CASR) Part 135.[14] It flew to communities and townships throughout the Northern Territory, and its services included general charter, patient transfer, freight and mail delivery, and scenic flights.
Katherine Aviation had a CASA-approved exposition that defined its procedures, activities, and conditions. It did not, and wasn’t required to under the regulations, have a safety management system.
In December 2023, following sale of the business and its assets, Katherine Aviation ceased all charter operations and in January 2024 it cancelled its AOC, de‑registering as an authorised aviation operator.
Key personnel
Katherine Aviation’s key personnel were the chief executive officer (CEO), who was also the head of aircraft airworthiness and maintenance control (HAAMC), and a separate head of flying operations (HOFO). The HOFO commenced their aviation flying career with Katherine Aviation and after several years as a line pilot and performing other duties within the company, was appointed as the HOFO in May 2021. The HOFO role described in the company Exposition was to manage and ensure the safety of flight operations. Duties also included the employment and induction of new pilots into the company, ground training and checking pilots to line.
Line pilots
The organisation’s minimum requirements for pilots was a multi-engine instrument command rating with at least 5 flight hours operating a Cessna 210. Once located at a remote base, it was general practice that a senior base pilot provided supervision, mentoring and advice. Senior base pilots reported to the HOFO.
The HOFO and other company personnel stated that there was never any pressure applied to line pilots to complete a flight. They advised that the company supported the decision of a pilot if they elected to cancel a flight due to bad weather. The HOFO also advised it was an accepted, though not formalised practice, for pilots to depart and ‘go have a look’, when the forecast weather was unfavourable.
In-command-under-supervision training
Katherine Aviation required all pilots joining the company to complete line training as part of their induction. The training program was conducted in-command-under-supervision (ICUS) and provided assurance to the operator that, following a series of reviews, a pilot was proficient to conduct line operations. The HOFO reported that it typically took 25–60 ICUS flight hours before new pilots were checked to line. Elements from the ICUS program included:
aircraft knowledge (aircraft speeds and limitations, pre-flight inspections)
flight planning requirements
flight component (taxi, climb, cruise, circuit and landing)
weather management
passenger briefings
rules and procedures.
The operator advised that competency surrounding weather management and avoidance was assessed during ICUS flights. There was no formal weather examination during the training period, and pilots were expected to deviate, or descend early, to ensure the aircraft did not enter cloud.
Weather hazard management
On 13 October 2022, the operator held a safety meeting, which the pilot attended in preparation for the upcoming wet season. According to the meeting minutes, senior pilots discussed their personal accounts and experiences from flying during a wet season. The minutes from the meeting also identified that the HOFO had addressed the attending pilots, reiterating that:
‘…no pressure to get the job done exists, and that pilots will be supported in their decision making.’
Katherine Aviation had created a specific internal training presentation on the hazards that exist in the Northern Territory during the wet season. That presentation was not delivered at the pilot safety meeting, however it was available for pilots to review on the internal computer network. The operator did not have a record of the accident pilot reviewing the presentation. The training presentation commenced with the following introductory statement:
This course is aimed at providing you with some specific information and guidance to help with decision making processes during the wet season. If you are new to flying in the NT then it is likely that you may not have experienced flying in a wet season. Wet season presents some extreme weather patterns that add to the complexities of planning and carrying out a flight. It is important that you are aware of some of these challenges and are suitability equipped to manage these situations whilst you are flying in the NT.
The presentation included advice on wet season weather phenomena, flight planning, flight into marginal visual meteorological conditions, guidance on the safe operation and control of an aircraft when in turbulence and when to turn back. It also included a case study and lessons learned from a Cessna 210 in-flight break-up that occurred during the 2017 Northern Territory wet season (see the section titled Related occurrences).
Procedure for severe weather
The wet season training identified that it was likely for turbulence to be encountered when flying during a wet season. The presentation offered the following guidance:
• When encountering turbulence your priority is always to CONTROL THE AIRCRAFT
• Determine the intensity of the turbulence
• If the turbulence is of adequate intensity, begin to make corrective actions but do this slowly, (any abrupt changes to control inputs and power can increase G-loading on the aircraft)
• If descending – slowly revert to level flight to reduce airspeed
• Ensure you keep the wings level and do not “chase” attitude adjustments
• Slowly reduce power as appropriate to a minimum of 18 inches to reduce airspeed
• Allow the aircraft to decelerate to below the appropriate turbulent penetration speed for its weight (if applicable)
• If needed, ensure the aircraft is below gear extension speed and lower the gear
• Continue flight or descent in this configuration until you are clear of the turbulence
• DO NOT initiate quick roll manoeuvres or large turns. This may significantly increase G-loading on wings. G-loading limits are assessed on vertical movements of pressure and are not applied to twisting moments on wings. A twisting moment on the wing caused by rapid rolling movements (usually associated with someone attempting to “chase” an attitude) will apply further stresses to the aircraft. If a turn is required to attempt to manoeuvre away from a high turbulence area, ensure that it is made slowly and with minimum bank angle.
• CB’s and developed thunderstorms should be avoided by up to 10-15 nm or more. Some may need to be avoided by up to 40 nm or more!
• If you are diverting around a thunderstorm and it is turbulent then you are probably too close!
Additionally, section 2.19.3 of the operator’s exposition described procedures when encountering severe weather:
To minimise the risk of exceeding aircraft structural limitations due to thunderstorm turbulence, the pilot in command should:
• Ensure the aircraft does not take-off when thunderstorms are active within 10 nm of the aerodrome
• Avoid thunderstorms enroute by diverting by a minimum of 10 nm upwind or 20 nm downwind
• The pilot in command must either hold or divert to an alternate aerodrome if a thunderstorm is in 20 nm of the destination aerodrome.
Forecast and reported areas of turbulence should be avoided whenever possible. If turbulence is anticipated or encountered, the pilot in command should:
• ensure all persons, loose articles and cargo are secured
• maintain turbulence penetration speed or manoeuvring speed (VA)
• maintain attitude control and accept altitude changes and speed variations whilst keeping the attitude within safe limits.
Decision making and perceived pilot pressure
The pilot was described by their co-workers and the HOFO as professional and meticulous with their selection of speed and power settings when operating the Cessna 210 aircraft. They reported that the pilot exercised good en route decision‑making during the ICUS program, particularly in the avoidance of weather. A few days prior to the accident, the pilot turned back during a flight when en route weather conditions were unfavourable. In that instance, the pilot called the operations department and advised of the decision to cancel the flight. The decision not to push on was reflected by the company’s stance on turnback and cancellation decisions during periods of adverse weather.
Perceived (or self-induced pressure) is specific to each pilot and may come from a range of sources. It may not be evident or easily identifiable by the pilot. Not every flight will result in potential for pilots to experience pressure; some pilots may not have experienced pressure due to the flights they have been involved in, and some pilots may not feel pressure in circumstances where other pilots do. In their research, Bearman (2014) reported that outback pilots are more likely to undertake risky behaviour to meet commercial imperatives and gain approval from their management. The desire for career progression by accumulating flight time was also an identified factor to influence risky behaviour for outback pilots.
On the day of the accident, conditions existed that may have led the pilot to experience a level of self-perceived pressure to proceed with the flight. These included:
The aircraft was expected in Katherine for a 100-hourly scheduled maintenance. If the flight had returned to Gove, then it is likely that insufficient hours would remain on the aircraft’s maintenance release to return to Katherine, potentially requiring a maintenance engineer to travel to Gove and complete the necessary maintenance.
The flight was described in the booking as a patient transfer flight. This was the third time that Katherine Aviation had attempted to transfer the passenger for respite care. The previous flights earlier that week had been cancelled due to bad weather.
The accident pilot was seeking to further their commercial flying career. The operator reported that the pilot was always keen to be assigned flight taskings to build flight time.
Balancing the potential for the above conditions, Katherine Aviation had no expectations for company pilots to depart or continue with a flight when confronted with adverse weather conditions. This expectation was outlined in the company Exposition and was supported by statements provided by operational personnel that pilots were accepted if they elected to cancel, divert or turn back. While it could be demonstrated that some aspects of self-perceived pressure were present, there was insufficient evidence available for the ATSB to determine the influence of each of these on the pilot’s decision‑making related to the accident flight.
Recorded data
Radar data
The Royal Australian Air Force (RAAF) provided air traffic control (ATC) recordings from Darwin and Tindal radar towers for the period of the accident flight. A review of the ATC data was completed and VH-TFT was not detected by the radar. In their analysis of the radar coverage, RAAF ATC confirmed that an aircraft operating at an altitude of 8,500 ft overhead the accident site would not have been detected by the Tindal radar system.
Telephone records
A single text message was sent from the pilot’s phone to the operator at 0841, advising of the planned 1024 arrival time to Katherine. Mobile phone call charge records for the pilot and passenger’s mobile phone devices were provided by a telecommunication network provider for the period 0900 to 1130. The data identified that from 0900 as the flight progressed, network connections were established with the cellular towers at Ramingining, Gapuwiyak, Alyangula, Numbulwar, and then to Bulman. The pilot’s phone first came into the detectable range of the Bulman cellular tower at 0914 and the passenger’s phone into range of the Bulman tower at 0915.
At 0929 both phones were again briefly detected on the Ramingining cellular tower, approximately 150 km north of the accident site. The provider advised that mobile networks were designed for ground coverage. Connection to a network from within an aircraft while en route can be unpredictable and may be affected by variables such as climatic conditions, aircraft altitude and radio network traffic within the region. The Ramingining tower connection suggests that the aircraft may have been at a higher elevation and possibly closer to the planned cruise altitude of 8,500 ft, rather than at significantly lower altitudes.
At 1001 the passenger’s phone signal ceased its connection with the Bulman tower, however the data identified that the pilot’s phone remained connected to the cellular network. The passenger’s phone was severely damaged during the accident sequence and had likely stopped operating upon impact with the terrain. In contrast, the pilot’s phone remained relatively undamaged.
Recording devices on VH-TFT
The aircraft was not equipped with either a cockpit voice recorder or a flight data recorder, nor was it required to be. Further, there was no active flight tracking equipment fitted to the aircraft, which may have otherwise been used by the operator to track the aircraft and to assist search authorities to locate the occupants. The was no other device or system fitted to the aircraft that provided flight data.
Onboard recording devices have long been recognised as an invaluable tool for investigators in identifying the factors behind an occurrence and assisting with the identification of important safety issues. However, in many cases, investigations involving light aircraft are hampered by a lack of data about the circumstances that led to the occurrence. This contrasts with the investigation of occurrences involving larger transport aircraft that are required to be fitted with a flight data recorder and cockpit voice recorder.
Two recent ATSB investigations benefited greatly from the availability of recording devices. Although not crash protected, they greatly assisted in determining the contributing safety factors and enabling safety advice to be provided to the aviation industry:
VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD, near Mount Disappointment, Victoria, on 31 March 2022(AO-2022-016),
Loss of control and in-flight break-up involving Robinson R66, VH-KFT, near Hawks Nest, New South Wales, on 26 October 2023(AO-2023-051). Ongoing at the time of writing.
Related occurrences
A search of the ATSB occurrence database identified 5 other fatal accidents involving structural break-up for the Cessna 210 series aircraft in Australia (Table 3). Of these:
One accident from 1976 (Cessna 210L) and one from 2017 (Cessna 210B) were attributed to significant aerodynamic loading, the source of which could not be established with certainty.
The 2019 in-flight break-up and separation of the right wing from a Cessna 210M was identified to be from the fatigue cracking and fracture of the wing carry-through spar. Weather was not a factor to that accident.
Exposure to severe weather was identified to be contributory for 2 accidents, one in 2011 (Cessna 210M) and the other in 2017 (Cessna 210L). These accidents and a serious incident from 2019 involving severe turbulence are briefly discussed below.
Table 3: Cessna 210 in-flight break-ups – Australia
Date
Investigation agency accident ID
Aircraft detail
General location
Detail
11 June 1976
Commonwealth of Australia Department of Transport AAIR 197600023
On 7 December 2011, the owner-pilot of a Cessna 210M was conducting a private flight under visual flight rules from Roma to Dysart in Queensland. Thunderstorms with associated cloud, rain and severe turbulence were forecast for the area. About 30 minutes into the flight, the outer sections of the wings and parts of the tail separated. The aircraft collided with terrain, fatally injuring the pilot.
The ATSB established that the aircraft was structurally sound before the wing and tail sections separated. No aircraft system defects were identified. Ground-based weather radar showed thunderstorms in the vicinity of the accident site, and recorded engine data showed cruise power setting was maintained until recording ceased. Although the precise circumstances leading up to the accident were not known, a combination of aircraft airspeed with the effects of turbulence and/or control inputs generated stresses that exceeded the design limits of the aircraft structure.
On 23 October 2017, a Cessna 210L with 2 pilots on board was conducting a charter flight from Darwin to Elcho Island, Northern Territory. When the flight was diverted to avoid adverse weather, the aircraft entered an area of strong convective activity and rapidly developing precipitating cells, which resulted in it experiencing severe turbulence and possibly reduced visibility for the pilots. While flying in these conditions, a combination of airspeed, turbulence and control inputs probably led to excessive loading on the aircraft’s wings, which separated from the fuselage in-flight before it collided with terrain.
The ATSB found that the pilots had limited experience flying in the ‘build-up’ to the wet season in the Darwin area. Although pairing a supervisory pilot with a pilot new to the company was likely to reduce risk in other instances, in this case it did not adequately address the weather-related risks because neither pilot had experience flying in the region during the wet season.
A serious incident was investigated by the ATSB following the report of passenger injuries and structural damage from exposure to severe turbulence during a charter flight.
On 25 November 2019, a Cessna 210M with four passengers was being flown from Darwin to Tindal, Northern Territory. Soon after departure, the pilot diverted 5 NM right of the planned track to avoid a large storm cell that was 5 NM left of track. Shortly after, the aircraft encountered sudden and sustained severe turbulence.
During the turbulence, the aircraft airspeed could not be controlled for several minutes through changing power settings, and for the most part the airspeed could not be held below 155 kt. For extended periods, the pilot had no control over bank angle, height, or heading. At one stage, the airspeed dropped below 140 kt, and the pilot lowered the landing gear in order to create drag and slow the aircraft down. ATSB’s analysis of the radar data showed that the aircraft ground speed reached 210 kt, a maximum descent rate of 5,000 ft per minute.
International accidents
A search of the accident report databases held by both the Transportation Safety Board of Canada (TSB) and the United States National Transportation Safety Board (NTSB) identified several instances over a 25-year period where the Cessna 210-aircraft type has sustained structural failure during flight (Table 4). There were 8 fatal accidents identified and categorised as private operations and one other categorised as a charter operation. The accidents were further categorised to similarly themed primary and secondary contributing factors, these included: manoeuvring in excess of VA, loss of control, spatial disorientation, continued flight into instrument meteorological conditions and severe weather.
Table 4: Cessna 210 in-flight break-ups – International
Date
Investigation agency accident ID
Aircraft detail
General location
21 Jan 1997
US NTSB CHI97FA056
Cessna 210N
Highland, Michigan
28 July 1997
Canada TSB A97Q0158
Cessna 210L
Milan, Quebec
18 June 2001
Canada TSB A010O165
Cessna 210L
Lake Lavieille, Ontario
4 December 2002
US NTSB FTW03FA057
Cessna 210L
Harrison, Arkansas
7 April 2005
US NTSB LAX05FA132
Cessna T210L
Tranquillity, California
12 August 2007
US NTSB MIA08FA027
Cessna T210N
Bloomfield, Kentucky
7 September 2010
US NTSB CEN10FA520
Cessna T210
Mountain Home, Arkansas
17 November 2014
US NTSB CEN14FA064
Cessna T210M
Cedaredge, Colorado
25 March 2017
US NTSB ERAFA17136
Cessna T210
Hayden, Alabama
Analysis
Introduction
On the morning of 24 December 2022, a Cessna 210N, registered VH-TFT, operated by Katherine Aviation, departed Gove Airport for a charter flight under the visual flight rules (VFR) to Katherine Tindal Airport. The flight departed with one pilot and one passenger on board. After the aircraft did not arrive and contact was unable to be made with the pilot, search and rescue activities were initiated by authorities. A distributed wreckage field was found the following day at a remote location in East Arnhem, approximately 237 km east-north-east of Katherine. Both occupants of the aircraft were fatally injured.
Examination of the accident site and recovered wreckage identified that the aircraft had sustained an in-flight break-up involving separation of the right wing. No pre-existing aircraft defects that had the potential to influence the accident were identified. The emergency locator transmitter fitted to the aircraft had activated from the accident sequence, however physical disruption between the unit and its antenna prevented an alert signal being received by the search authority.
The availability of flight data generally assists in the determination of contributing factors in accidents investigated by the ATSB. In this instance additional data may have provided time‑referenced positional information, airspeed, altitude and heading. Notwithstanding, weather satellite information was gathered that identified the formation of a rapidly developing thunderstorm near to Bulman during the time period the aircraft likely transited the region. The following analysis will examine the flight into adverse weather, the accident time, development of the structural break-up, and aspects related to the operator’s wet season training.
Time of the accident
The ATSB reviewed the aircraft performance, planned flight information and the available telecommunication records to determine a likely accident time. Based on the expected direct flight route conditions and aircraft speed, the aircraft should have arrived overhead the accident site at about 0930. However, the ATSB’s review of the available telecommunication records identified that the passenger’s mobile phone ceased its connection with the Bulman cellular tower at 1001 probably due to damage sustained during the accident sequence.
While there was insufficient information to ascertain the likely accident time more accurately than somewhere between about 0930–1000, possible reasons for the additional flight time to that planned included that the aircraft was slowed en route or diverted due to weather, including possibly being flown beyond Bulman and then turned back towards Gove.
Flight into adverse weather
This was the pilot’s first commercial aviation role and was also their first period operating through a Northern Territory wet season. They had completed their line training with the operator in September 2022 during the dry season and after deployment from Katherine had flown for approximately 3 weeks from the operator’s base in Gove. During that period, they had turned back previously due to unsuitable weather. This showed that the pilot had decision‑making experience flying in convective weather.
The ATSB considered it likely that, while completing flight planning earlier that morning, the pilot had accessed the graphical area forecast (GAF) that described the predicted weather en route to Katherine. Supporting that was the pilot’s previous flight planning records, where all the necessary information had been obtained and documentation completed. The pilot had mentioned in conversation to the Katherine Aviation operations staff member on the morning of the accident that the weather ‘appeared to be a bit iffy’, which also supported that the pilot had obtained and assessed the en route weather forecast.
Though most Katherine Aviation staff were away on leave that day, including the Gove senior base pilot and Head of Flying Operations, there were operational staff in place and on duty at the Katherine Aviation main base for consultation to assist with decision‑making surrounding the conduct of the flight. Additionally, Bureau of Meteorology staff who had produced the forecast remained available as an informed source to provide weather advice.
The prevailing cloud coverage along the flight route near to Bulman were predicted in the GAF to cover between 5 and 7 oktas, with an effective ceiling of 1,000 ft above mean sea level (AMSL). There were no breaks predicted between subsequent cloud layers, with cloud tops predicted to be the same as each subsequent cloud base to above 10,000 ft AMSL. These forecast conditions were unsuitable for a flight under the VFR at an altitude of 8,500 ft. However, BoM analysis of satellite imagery identified that the forecast overcast conditions were not present in the Bulman region in the lead up to the accident.
Increasingly severe weather conditions were predicted to develop from the prevailing cloud coverage during the validity period of the GAF. Visibility was expected to between 500 m and 2,000 m from rain showers, which was significantly below the required visual meteorological conditions. Towering cumulus and cumulonimbus clouds were also forecast to develop from cumulus cloud cells at different times and locations throughout area B during the forecast period.
A review of the available satellite imagery identified that the prevailing cloud coverage around the Bulman region rapidly formed into convective clouds as the aircraft approached the area. The thermal activity depicted in the satellite imagery within the Bulman area was accompanied by lightning strike detections at 0940, which confirmed that the towering cumulus and cumulonimbus clouds had further developed into a thunderstorm. This would have led to areas of moderate to heavy rain, with significantly reduced visibility as forecast in the GAF.
Depending on the proximity to these weather phenomena, it is also likely that the aircraft encountered severe turbulence associated with the convective action. Furthermore, because the satellite imagery confirmed that the prevailing overcast conditions did not exist in the Bulman region in the lead up to the accident, there was probably sufficient separation between the convective cloud formations associated with the developing thunderstorm to have been visible to the pilot. However, the severity of the conditions may not have been visually apparent.
The operator’s procedures required a 20 NM downwind separation from thunderstorms and it was expected practice that a flight was to be diverted upon encountering such phenomena. If severe turbulence was encountered, pilots were to slow the aircraft and to avoid rapid manoeuvres. It was not possible to determine the pilot’s precise actions during this final period of the accident flight. Had they been using the weather radar application on the iPad during the flight, it is possible that the extent of the developing storm near to Bulman was not evident due to the storm’s significant distance from the weather radar head. This may have led to the pilot not perceiving the potential severity of the storm as they approached the Bulman region.
In summary, upon arrival into the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm which probably resulted in exposure to a combination of severe turbulence and reduced visibility for the pilot.
In-flight break-up
The position of the right wing and its control surfaces relative to the remainder of the aircraft at the accident site indicated that an in-flight break-up had occurred. All other control surfaces remained with the aircraft up until the collision with terrain. The main wing spar was critically important to carry the aerodynamic loads encountered during flight. Bending and shear loads were transmitted from the wing spar into the fuselage via the carry-through structure. Without any redundant load paths, aeroelastic upward bending and then fracture of the main spar led to the wing separation and an immediate loss of control. There was only evidence of overstress and associated deformation on the fracture surfaces, with no pre-existing defects or damage that might have otherwise reduced its overall structural integrity.
The single wing separation indicates that the aircraft was likely subject to asymmetric loading at the time of the in-flight break-up consistent with the aircraft being manoeuvred. The limited distance between the separated wing and the primary accident site also indicates that the break‑up occurred at an altitude considerably lower than the initial cruise altitude. The direction of the wreckage trail was toward Gove. It was therefore possible that the aircraft had been, or was being, turned back to Gove prior to the break-up.
Had the aircraft entered an area of reduced visibility this would have likely created an increased risk of the pilot losing visual cues and experiencing spatial disorientation. The pilot’s last recorded flight under instrument flight was about 10 months prior when they obtained their multi-engine endorsement. Though the pilot was rated for flight into instrument meteorological conditions, it was likely that the pilot’s instrument flying proficiency had reduced during the intervening period.
Other previously investigated Cessna 210 accidents have identified structural failure and in-flight wing separation to be associated with conditions that were present near Bulman on the day of the accident. One serious incident from the Northern Territory during the 2019 wet season, also investigated by the ATSB, identified that upon coming within 5 NM of a developed thunderstorm, the pilot was unable to control the aircraft’s attitude, airspeed and descent rate. Although the aircraft was able to be landed, the investigation determined that the structural limits of the airframe were likely approached during that flight.
Based on the available evidence, the ATSB concluded that the most likely explanation for the in‑flight break-up of VH-TFT is that, while operating above the manoeuvring speed, the pilot applied a control input and/or the aircraft encountered severe turbulence that resulted in overloading and separation of the right wing.
Wet season training
New pilots employed by Katherine Aviation were given weather avoidance training during the ICUS period. Supporting that training, Katherine Aviation had specific information contained within its exposition for pilots to avoid thunderstorms as part of their operational requirements. Specifically, while en route pilots were to divert by a minimum of 10 NM upwind or 20 NM downwind of such weather systems. Pilots were to also slow the aircraft to the manoeuvring or turbulence penetration speed (VA) when turbulence from these weather systems was encountered. Due to limited available information, the ATSB was unable to assess the degree those requirements were being applied by the accident pilot prior to the in-flight break-up of VH‑TFT.
In addition to the formal operational requirements, Katherine Aviation had developed a training package that detailed the unique hazards of flying during the wet season. It described the procedures to help pilots mitigate the hazards when operating in that environment. The briefing contained specific advice on wet season weather phenomena that included: flight planning, flight into marginal visual meteorological conditions, safe operation and control of an aircraft when in turbulence, and advice on when to cancel the flight.
The pilot attended a company safety briefing prior to the commencement of the 2022 wet season, where elements of decision making were discussed, including first-hand accounts from senior pilots of their own wet season experiences.
Although the slide pack was not presented at the briefing it was made available for pilots to review after the meeting. Katherine Aviation did not require the training material to be reviewed by its pilots. The absence of a requirement for the training material to be reviewed may have been a lost opportunity for Katherine Aviation to ensure its pilots were further prepared to safely operate during the top end wet season.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the in-flight break-up involving a Cessna Aircraft Company 210N, registered VH-TFT, that occurred 237 km east‑north‑east of Katherine, Northern Territory on 24 October 2022. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Upon arrival in the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm, which probably resulted in exposure to a combination of severe turbulence and reduced visibility.
It is probable that a combination of turbulence from the thunderstorm, airspeed above the aircraft manoeuvring speed, and control inputs led to the excessive structural loading and in‑flight separation of the right wing from the fuselage before the aircraft collided with terrain.
Safety actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Katherine Aviation
Wet season training
On 11 February 2023, Katherine Aviation formally presented its wet season training material to its company pilots. In August 2023, the Katherine Aviation Exposition was updated with the requirement that all pilots were to complete the training on an annual basis.
Flight monitoring
Katherine Aviation advised that, in January 2023, it commenced providing satellite tracking and communication devices for its pilots that enabled real-time satellite-based tracking and monitoring of its fleet. The devices allowed text messaging to be exchanged between the company and its pilots in the absence of a mobile telephone signal.
Operational control
Katherine Aviation advised that it had developed flight assessment tools that were required to be completed by its pilots prior to the conduct of any flights. The requirement to complete the assessments was identified in the August 2023 update to the Katherine Aviation Exposition. The tools were targeted to provide its pilots with better decision-making tools during planning for marginal weather.
A marginal weather decision-making chart was also developed to assist pilots assess the daily conditions. The requirement was communicated during a pilot safety meeting and the flowchart was displayed at all Katherine Aviation bases. Both charts are displayed below.
Glossary
AD
Airworthiness Directive
AGL
Above ground level
AMSL
Above mean sea level
ATC
Air traffic control
BoM
Bureau of Meteorology
CB
Cumulonimbus
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CEO
Chief Executive Officer
CTAF
Common traffic advisory frequency
EFB
Electronic flight bag
ELT
Emergency locator transmitter
EMBD
Embedded
FAA
Federal Aviation Administration
GAF
Graphical area forecast
GPWT
Grid-point wind and temperature
HAAMC
Head of aircraft airworthiness and maintenance control
HOFO
Head of flying operations
ICUS
In-command-under-supervision
JRCC
Joint Rescue Coordination Centre
NAIPS
National Aeronautical Information Processing System
POH
Pilot’s Operating Handbook
RAAF
Royal Australian Air Force
TAFs
Terminal area forecasts
VFR
Visual Flight Rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
Katherine Aviation
Civil Aviation Safety Authority
Northern Territory Police Service
Textron Aviation (Cessna)
Airservices Australia
Royal Australian Air Force
Australian Maritime Safety Authority
Northern Territory Health
Bureau of Meteorology
Champagne PC Services
Telecommunication network provider
OzRunways
witnesses.
References
Australian Transport Safety Bureau. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents. AR-2012-128
Bureau of Meteorology, Graphical Area Forecast & AIRMET User Guide, Version 2.0 July 2018, Commonwealth of Australia
Bureau of Meteorology, Graphical Area Forecast User Guide, A guide for the transition from ARFORs to GAF, Version 1.2 20 October 2017, Commonwealth of Australia
Bureau of Meteorology, Aeronautical Services Handbook, Amendment 213, 1 December 2022, Commonwealth of Australia 2020
Federal Aviation Administration, Advisory Circular No. 00-24C (2013), Thunderstorms, U.S. Department of Transportation
Michalski, D.J., and Bearman, C. (2014). Factors Affecting the Decision Making of Pilots who Fly in Outback Australia. Safety Science, 68, 288-293
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Katherine Aviation
Bureau of Meteorology
Civil Aviation Safety Authority
Airservices Australia
Australian Maritime Safety Authority.
A submission was received from the Bureau of Meteorology.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions in which they have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[2]The Northern Territory is administered through 6 defined regional areas: 1. Darwin, Palmerston and Litchfield, 2. Top End, 3. East Arnhem, 4. Big Rivers, 5. Central Australia, and 6. Barkly.
[3]Cloud cover: cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[5]The wind direction and speed at an altitude of 8,500 ft was calculated by interpolating the wind speed and direction that was provided in the GPWT at altitudes of 7,000 ft and 10,000 ft.
[6]Satellite images were processed by the Bureau of Meteorology from the geostationary meteorological satellite Himawari-8 that was operated by the Japan Meteorological Agency.
[7]Turbulence intensity is specified according to the perceived effect upon aircraft and occupants. Severe turbulence produces large abrupt changes in attitude and/or altitude and momentary loss of control. Unsecured objects are tossed about and occupants violently forced against seatbelts. www.bom.gov.au/aviation/data/education/turbulence.pdf
[8]Severe icing: the rate of accumulation is such that de-icing/anti-icing equipment fails to reduce or control the hazard to the aircraft, and thus an immediate diversion is necessary. www.bom.gov.au/aviation/data/education/icing.pdf
[9]The National Aeronautical Information Processing System (NAIPS) is a multi-function, computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots and the Australian Air traffic Control platform. About NAIPS (airservicesaustralia.com)
[10]Flight envelope: the range of combinations of speed, altitude, angle of attack etc., within which an aircraft is aerodynamically stable.
[11]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.