This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
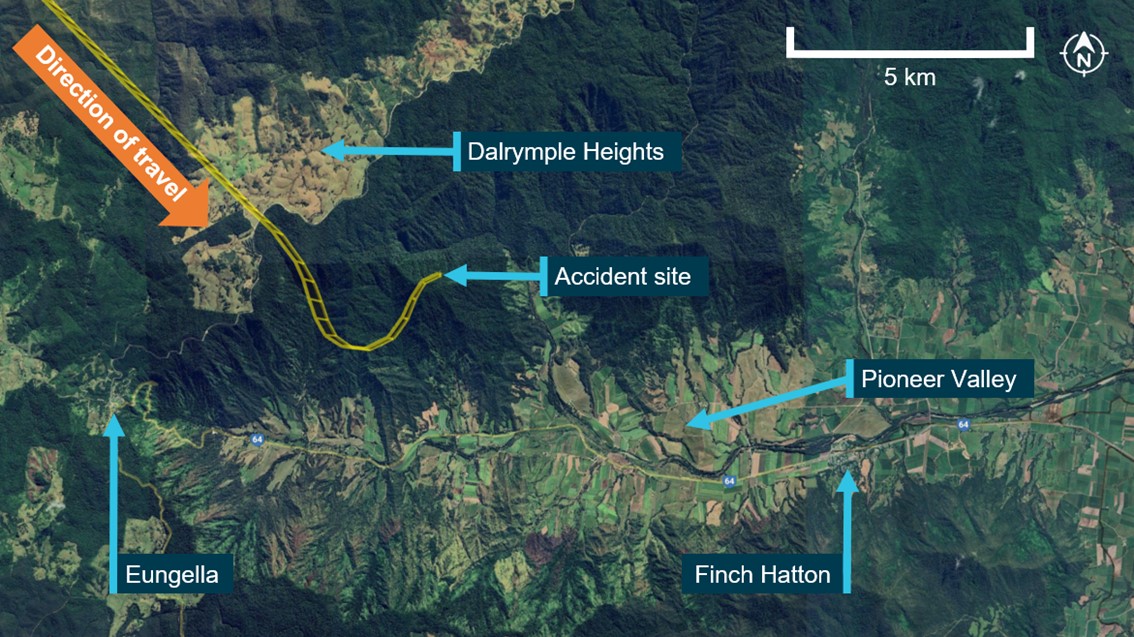
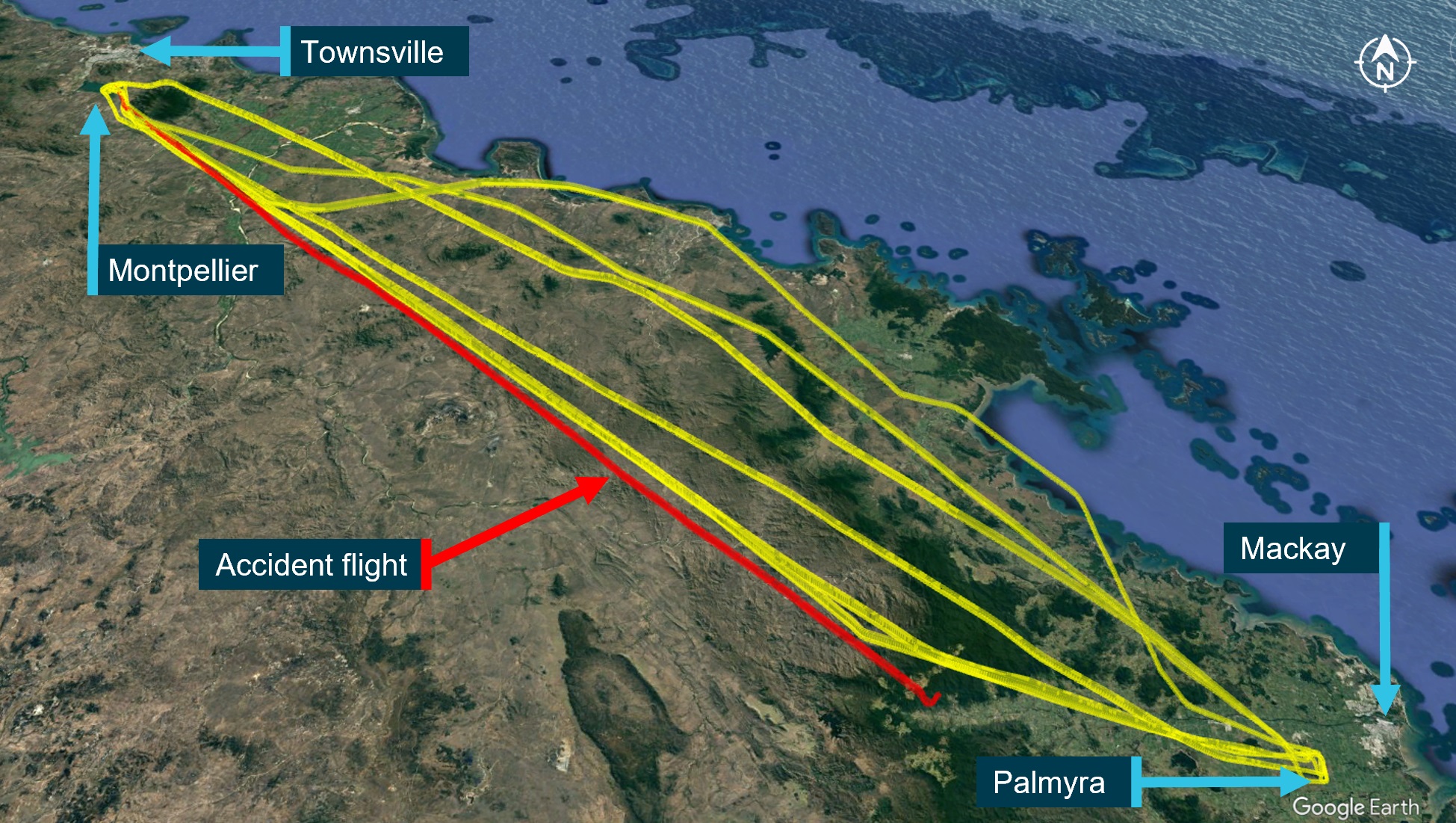
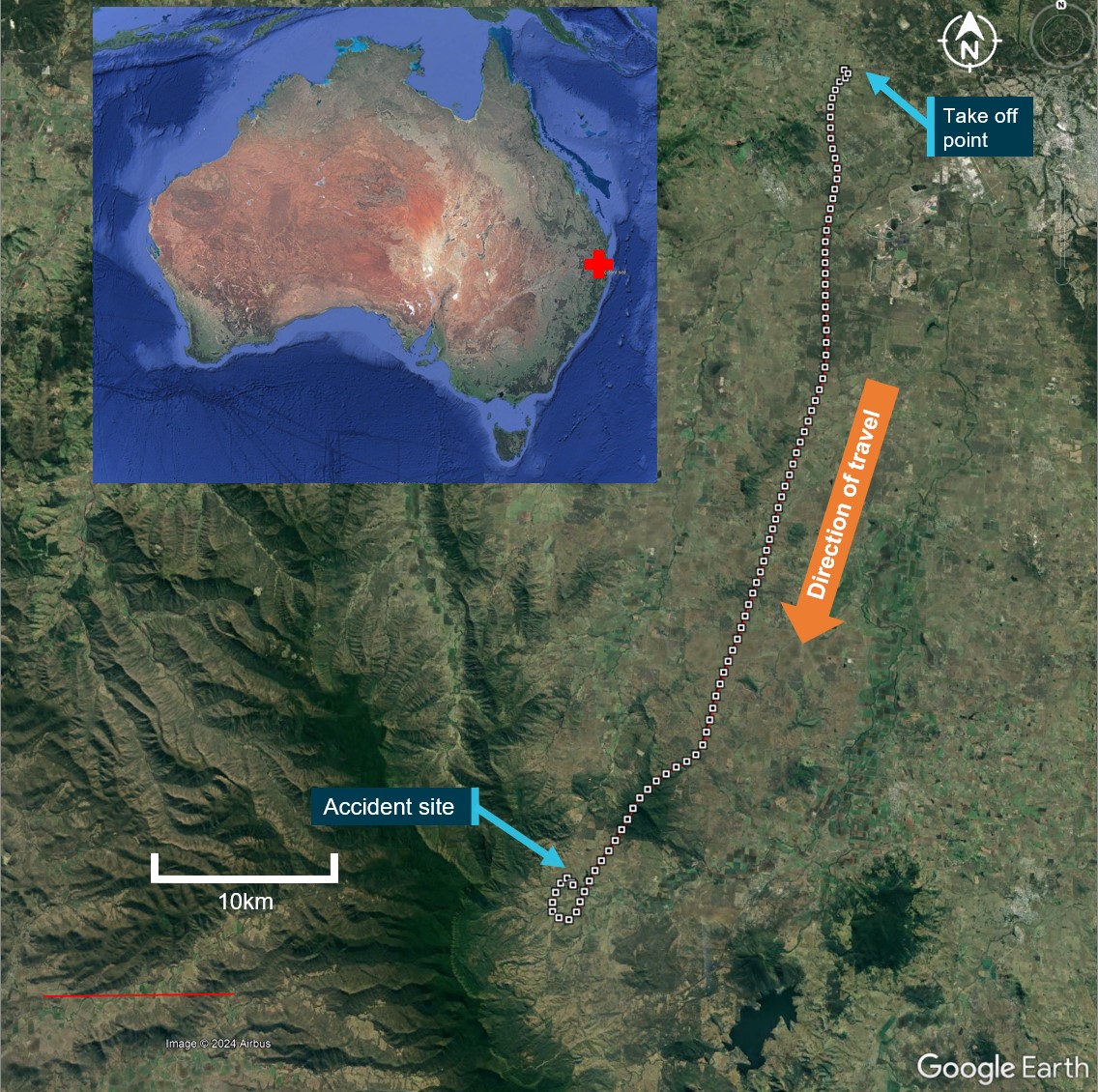
On 28 October 2023, at about 0735 local time, a SOCATA-Groupe Aerospatiale TB-20 (TB-20) registered VH-JTY, departed from Montpellier aircraft landing area,[1] Queensland, for a private flight to Palmyra aircraft landing area[2] (Figure 1). On board was the pilot and a passenger, who was also a pilot.
A friend of the pilot stated that they made a phone call to the pilot at 0814. The pilot stated that they were at 5,500 ft above cloud and asked about weather conditions at Palmyra airfield. The pilot stated they were passing Dalrymple Heights and on descent and that their intentions were to fly along the Pioneer Valley to Palmyra airfield.
At about 0834, the OzRunways[3] flight track (Figure 1) showed that the pilot made a right turn, followed by a left turn before colliding on the northern side of Bull Mountain, at about 1,900 ft above mean sea level. The aircraft was destroyed, and the pilot and passenger were fatally injured.
Figure 1: VH-JTY flight track
Source: Google Earth, OzRunways, annotated by the ATSB
Context
Pilot information
The pilot held a valid Private Pilot Licence (Aeroplane) and a Class 2 aviation medical certificate, valid until October 2024. The pilot held a single engine aeroplane rating, and endorsements for manual propeller pitch control and retractable undercarriage. Their last flight review was conducted in July 2023, and at the time of the accident the pilot had about 2,100 hours total aeronautical experience of which about 1,500 hours were in VH-JTY.
Aircraft information
General information
The TB-20 is an all-metal, 5-place, single engine aircraft with fully retractable landing gear. It was powered by a 6-cylinder Lycoming IO-540 fuel-injected engine, driving a 3-blade constant-speed propeller. VH-JTY was manufactured in France in 1985 and was first registered in Australia in April 1987. The pilot had owned VH-JTY since April 2008 (Figure 2).
The last periodic inspection was conducted on 14 December 2022. In January 2023, VH-JTY sustained rudder and vertical fin damage in a ground handling incident. Structural repairs were carried out and the aircraft returned to service on 25 May 2023. At the time of the accident, it had accrued a total time in service of about 5233.4 hours and had flown about 35 hours since the repairs were carried out.
Figure 2: VH-JTY
Source: Simon Coates, modified by the ATSB
Site and wreckage information
The aircraft wreckage was located in steep mountainous terrain with heavy vegetation, to the north-east of Bull Mountain.
The aircraft fuselage sustained a heavy impact initially with vegetation and then terrain before becoming significantly disrupted with some components sliding downhill and being consumed by fire.
Wreckage examination
Due to the remote location, extreme terrain, and degradation of the accident site, ATSB has not been able to attend the site. However, Queensland Police Service specialist forensic officers have provided detailed on-site photographic evidence. This has assisted the ATSB with gaining an understanding of the accident site location and layout, as well as an appreciation of the level and type of damage to the aircraft’s structure and components.
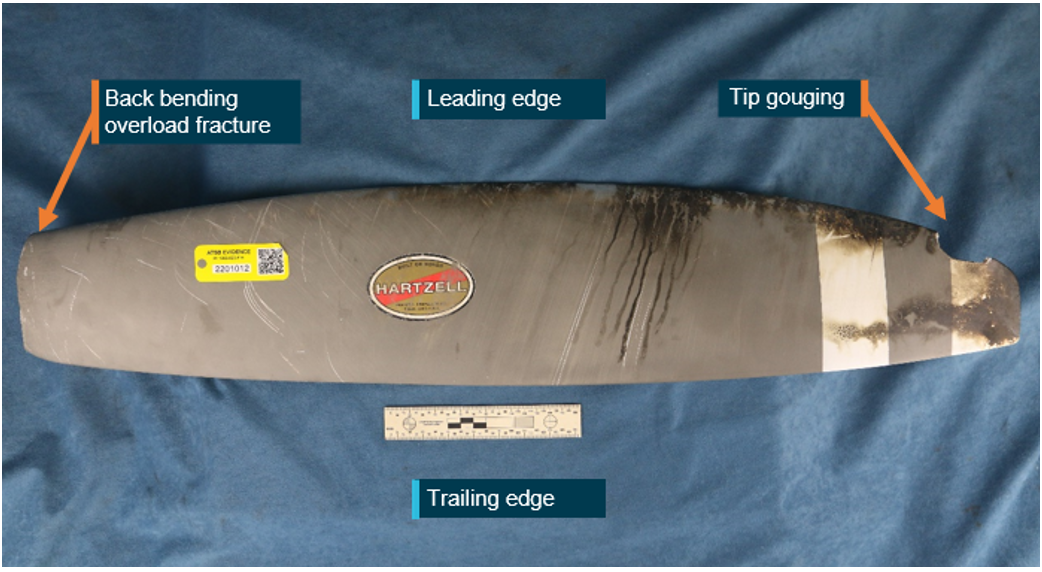
Photographic evidence review of engine and propeller components indicated that the propeller was under a significant level of power when it impacted with terrain, indicating the engine was almost certainly operational at that time.
Further investigation
To date, the ATSB has:
examined photographs of the aircraft wreckage
conducted witness interviews
examined the maintenance history of the aircraft
reviewed historic flight data
reviewed air traffic control recordings.
The investigation is continuing and will include:
further review of recorded data and recovered components from the accident site
analysis of available flight data
analysis of aircraft maintenance and repairs.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance provided by the Queensland Police Service who provided site information and photographs in the course of the on-site phase of this investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Montpellier aircraft landing area is located about 20 km south-south-east of Townsville Airport.
[2] Palmyra aircraft landing area is located about 12 km west-south-west of Mackay Airport.
[3] OzRunways is an electronic mobile application, utilising approved data for electronic maps, and used for navigation.
On the morning of 28 October 2023, a SOCATA-Groupe Aerospatiale TB-20, registered, VH-JTY, departed Montpelier aircraft landing area, Queensland, for a visual flight rules private flight to Palmyra aircraft landing area, Queensland. The flight was to be just over one hour duration and the pilot and their passenger were familiar with the route.
During the flight, the pilot contacted a friend at the destination for an appreciation of the weather. After the friend advised them of the prevailing conditions including cloud, the pilot replied that they would need to go through some cloud before arriving.
Around 30 NM from the destination, shortly after commencing descent for the intended landing, the aircraft began a steep descending turn to the left towards mountainous terrain. During this descent, the aircraft exceeded the airframe’s designed maximum airspeed before pitching up and passing over the top of Bull Mountain. The aircraft then entered a second steep descending turn, this time to the right, before the recorded flight path data ceased.
The wreckage was located nearby in dense forest on the north-east face of Bull Mountain. The accident site indicated that the aircraft had collided with terrain at a steep angle, and with significant forward velocity. The aircraft was destroyed and both occupants received fatal injuries.
What the ATSB found
The ATSB found that, after encountering cloud en route, the pilot elected to continue along the intended flight path through cloud instead of diverting around or remaining on top of it. Shortly after, it is very likely the pilot entered weather conditions not suitable for visual navigation, leading to spatial disorientation and a descent into mountainous terrain.
Safety message
One of the key risk controls for a visual flight rules (VFR) pilot to avoid entering instrument meteorological conditions (IMC) is appropriate pre-flight preparation and planning. Pilots should always obtain up-to-date weather information before and during flight. While forecasts will assist in selecting the route to be flown, pilots should plan an alternate or be prepared to make necessary deviations from the planned route should actual weather conditions indicate the possibility of not being able to comply with the VFR.
For a non-instrument rated pilot, even with basic attitude instrument flying proficiency, maintaining control of an aircraft in IMC by reference to the primary flight instruments alone entails a very high workload that can result in narrowing of attention and loss of situational awareness. While autopilot can be used to reduce workload, it is not infallible and should not be relied upon or used by VFR pilots as a risk mitigator to decide to fly into unsuitable conditions.
Unapproved mobile devices displaying charts and data from an approved data service provider are a useful supplement to navigation, but they cannot be used as a navigation device, and must not be the sole means of navigation when operating under the VFR. Pilots should use navigation equipment approved for aviation and maintain skills in navigating by reference to approved charts.
On 28 October 2023, at about 0735 local time, a SOCATA-Groupe Aerospatiale TB-20 (TB-20) registered VH-JTY, departed from Montpelier (Antill Plains) aircraft landing area,[1] Queensland, for a private flight to Palmyra aircraft landing area,[2] Queensland. The flight was to track via Dalrymple Heights, near Eungella before descending into the Pioneer Valley to the west of Mackay, and then track direct to Palmyra (Figure 1). On board were the pilot and a passenger, who was also a licenced pilot.
Source: Google Earth and OzRunways, annotated by the ATSB
OzRunways[3] data showed the aircraft was flown to 5,500 ft above mean sea level (AMSL) where it maintained a steady track without any significant deviations during the cruise phase of flight.
At 0814, approximately 20 minutes prior to commencing descent for the intended landing at Palmyra, the pilot made a phone call to a friend, another licenced pilot, in Mackay. It was reported that the pilot enquired about the weather at the destination. The friend recalled advising of the presence of cloud at Palmyra and blue sky to the south of the landing area. The pilot replied that they would have to go through some cloud.
The same friend called the pilot at 0833 to confirm their estimated time of arrival so they could meet the pilot in Palmyra. They stated that the pilot reported being over Eungella at 5,500 ft and was about to commence their descent. The friend reported ending the phone call so as not to cause any distraction.
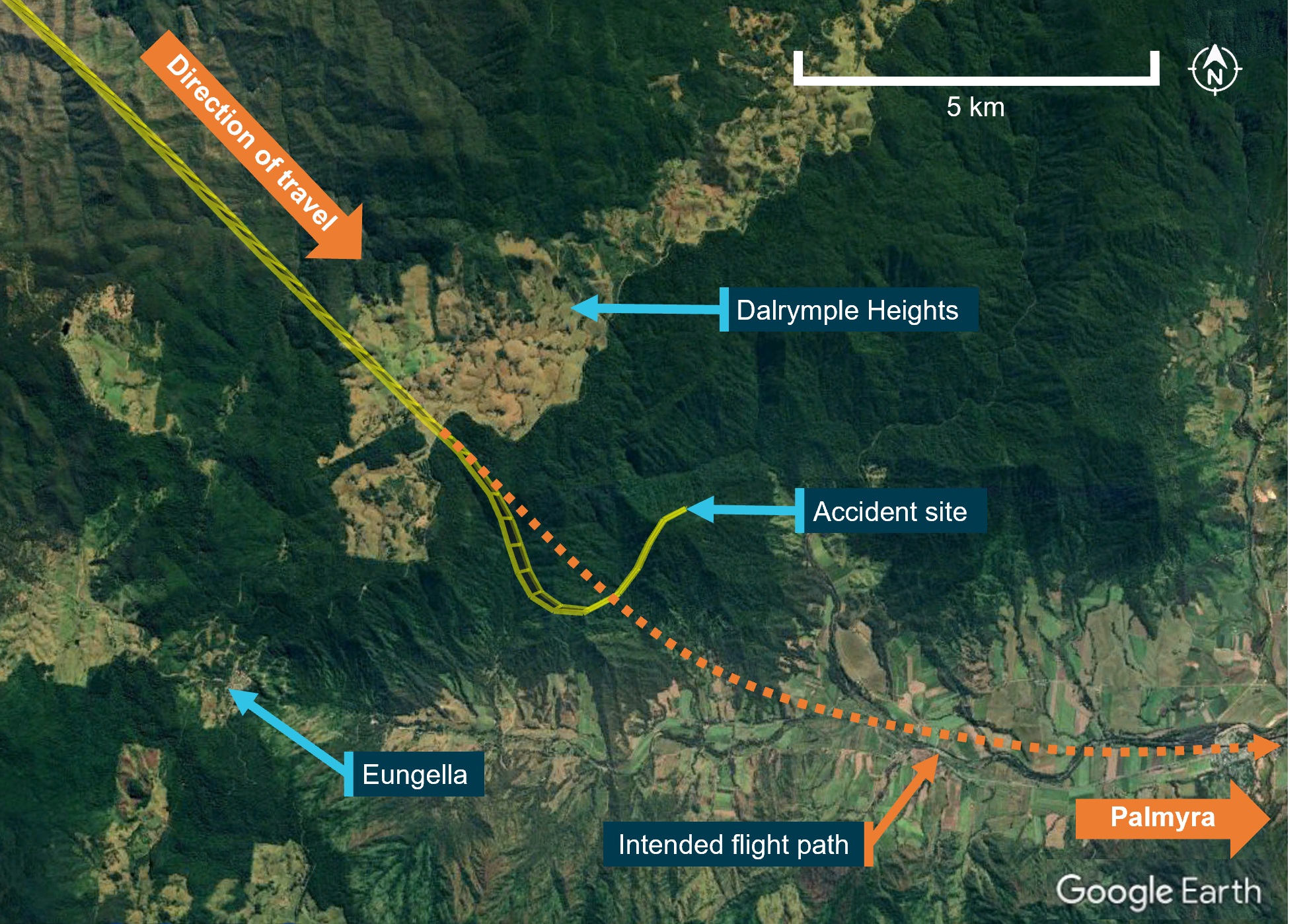
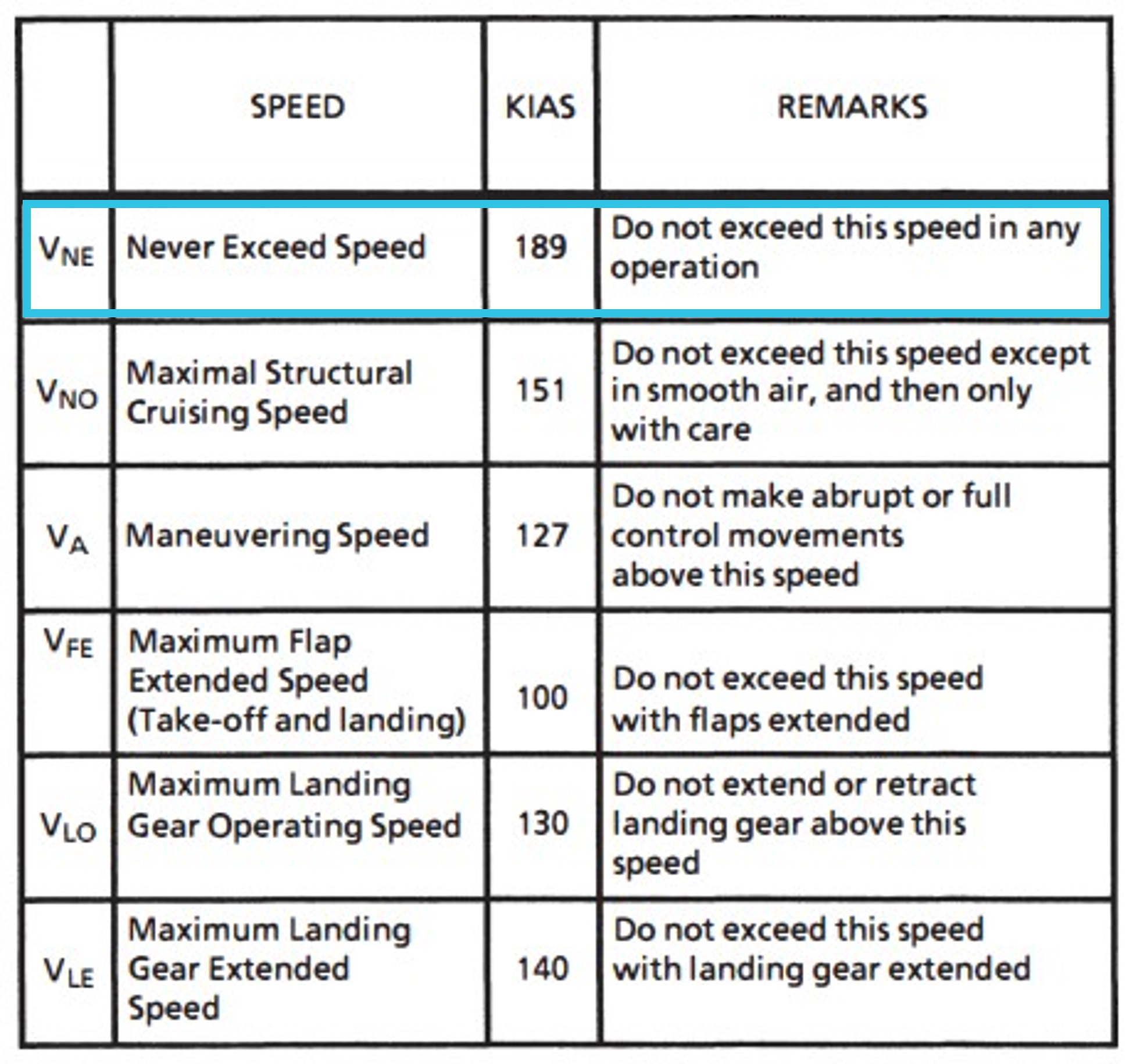
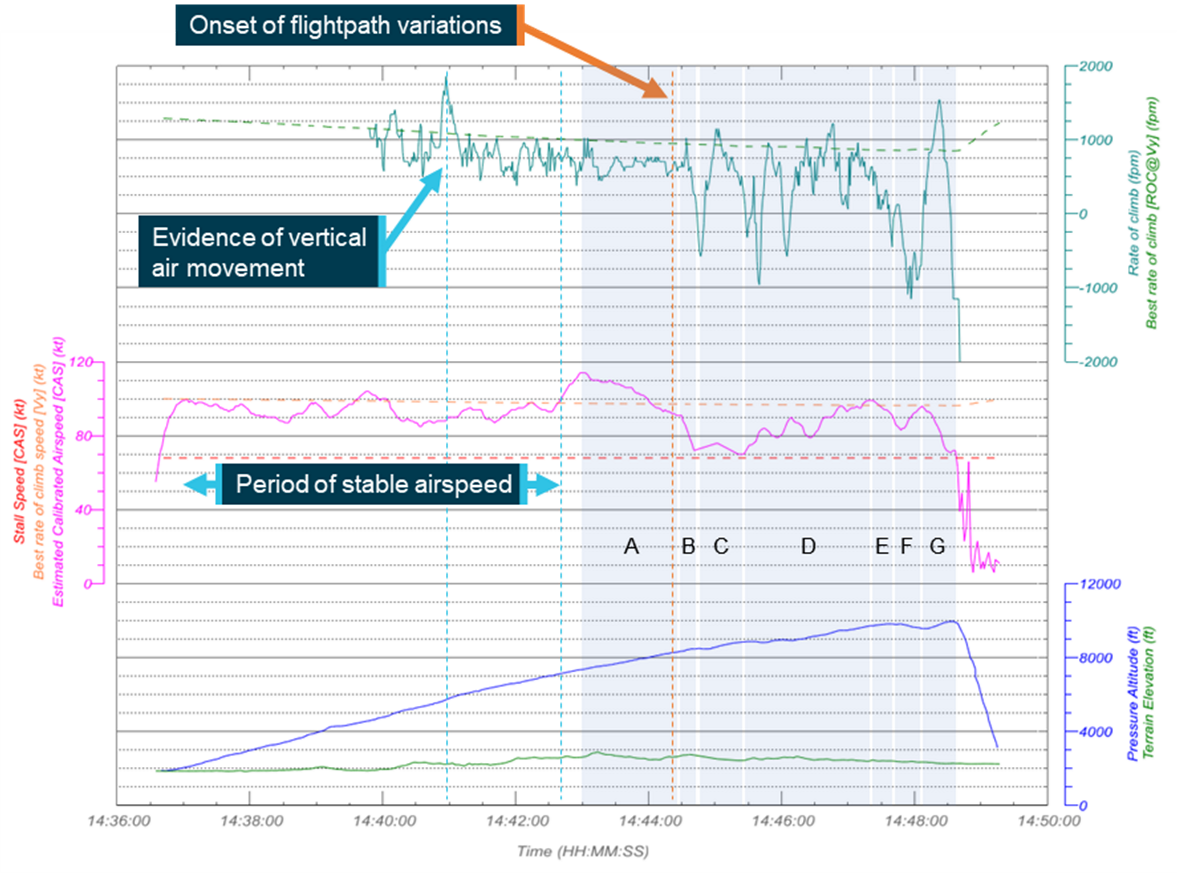
At 08:34, there was a change to the previously stable flight path. The aircraft initially climbed about 100 ft and entered a slight right turn before turning left towards Bull Mountain in a shallow descent. As the turn continued, the aircraft’s descent rate increased, descending about 1,600 ft in 13 seconds (average descent rate of 7,400 ft/min) (Figure 2).
Source: Google Earth with overlaid OzRunways data, annotated by the ATSB
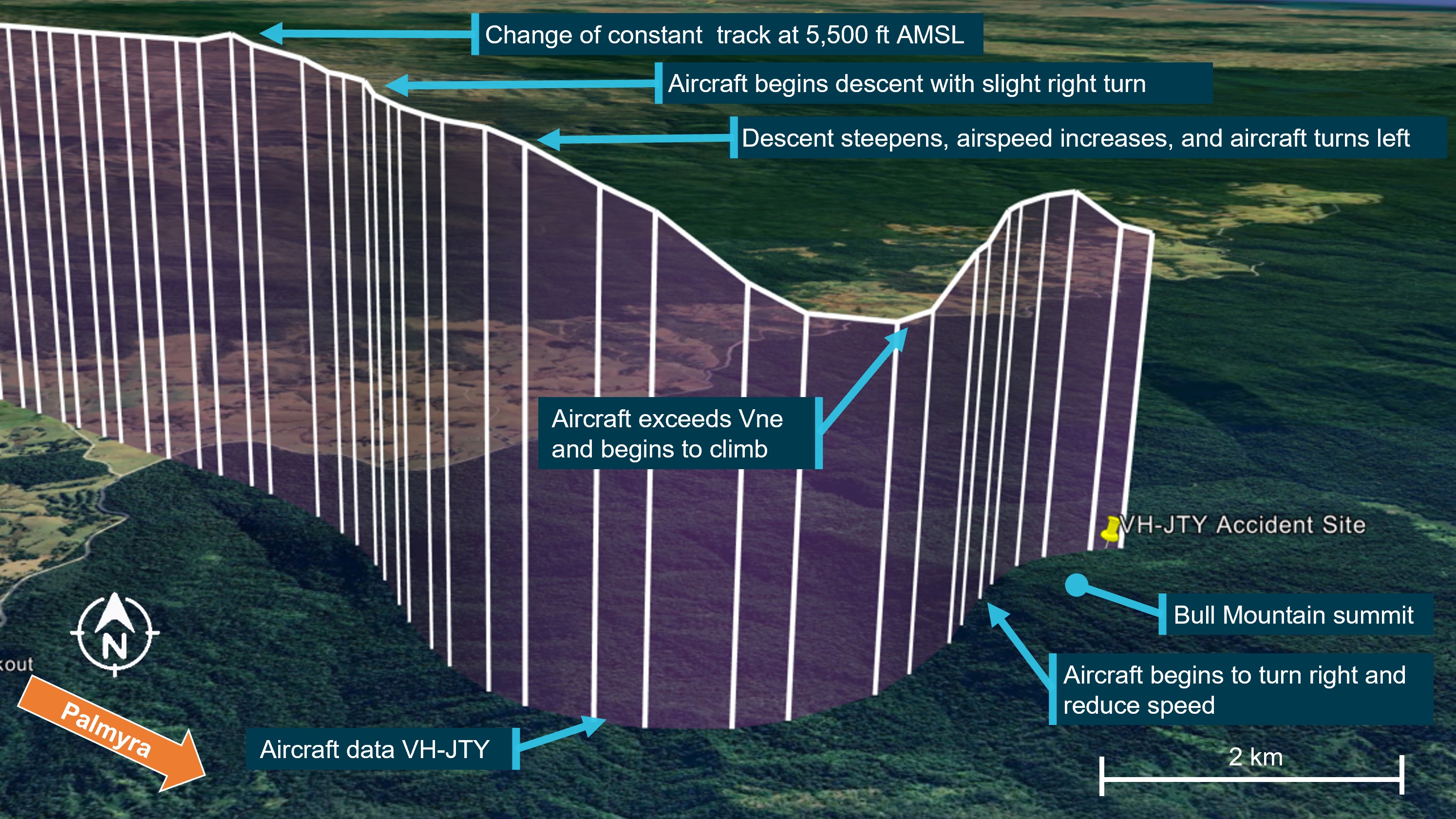
During this descent, the aircraft accelerated to about 218 kt, 29 kt above the aircraft’s published VNE[4] (velocity never exceed) of 189 kt (Figure 3).
Source: Aircraft manufacturer, annotated by the ATSB
In the 10 seconds that followed, the aircraft pitched up steeply, climbed approximately 600 ft, and passed overhead Bull Mountain at 4,200 ft AMSL. The aircraft then slowed to 132 kt before entering a steep descending right turn to the east. The recorded data stopped at 0835, 3,655 ft AMSL with the aircraft estimated to be descending at around 6,000 ft/min in a right turn with 36° angle of bank and increasing roll angle.
The aircraft collided with terrain in dense forest on the north-east face of Bull Mountain 1,900 ft AMSL, not far from where the recorded data stopped. The aircraft was destroyed, and the pilot and passenger were fatally injured.
The pilot was qualified and authorised to fly VH-JTY. They held a valid Private Pilot Licence (Aeroplane), issued on 4 May 2004. In addition, the pilot held a single engine aeroplane rating, and endorsements for manual propeller pitch control and retractable undercarriage. Their last flight review was conducted in July 2023 and valid to 30 September 2025. At the time of the accident the pilot had about 2,100 hours total aeronautical experience of which about 1,500 hours were in VH-JTY.
The pilot held a valid class 2 medical certificate that was issued on 12 December 2022 and valid to 7 October 2024. The class 2 was issued with the restrictions that both distance and reading vision correction was available during flight. A review of the pilot’s medical records showed that a chronic medical condition was being appropriately managed by the pilot and their designated aviation medical examiner (DAME). It required annual review and there were no additional restrictions placed on the pilot’s class 2 medical certificate.
A copy of the coroner’s toxicology and pathology reports were not available to the ATSB at the time of publishing this report.
Passenger information
The passenger was familiar with VH-JTY. While a licensed pilot, they had not renewed their medical certification for flight and had not conducted a recent flight review.
Aircraft information
General information
The TB-20 is an all-metal, 5-place, single engine aircraft with fully retractable landing gear. It was powered by a 6-cylinder Lycoming IO-540 fuel-injected engine, driving a 3-blade constant-speed propeller and equipped[5] for visual flight rules (VFR)[6] (Day) flying only. VH-JTY was manufactured in France in 1985 and was first registered in Australia in April 1987. The pilot had owned VH-JTY since April 2008 (Figure 4).
VH-JTY as it appeared in 2015. The yellow lines and wingtips were later painted dark red.
Source: Simon Coates, modified by the ATSB
Maintenance history
The aircraft was maintained in accordance with the CASA system of maintenance defined in Civil Aviation Regulations 1988 - Schedule 5 and the last periodic inspection was conducted on 14 December 2022. A review of the maintenance records and history for VH-JTY did not show any outstanding defects. The active maintenance release was not recovered from the accident site.
The aircraft was equipped with a Bendix/King KLN 90 GPS navigation system and a Bendix/King KAP 150 2-axis (pitch and roll) autopilot system that had been installed since the aircraft was manufactured. A review of the maintenance history and comments of the approved maintenance organisation showed minor issues with the autopilot consistent with its age. The faults were reported to have resulted in the uncommanded disconnection of the autopilot in flight. The unit was repaired in March 2022 and there were no records of any further maintenance on the autopilot after this date.
In January 2023, a ground handling incident damaged VH-JTY’s vertical fin and rudder. Structural repairs were carried out and following inspection of the flight controls, the aircraft returned to service on 25 May 2023. At the time of the accident, VH-JTY had a total time in service of about 5,233.4 hours and had flown about 35 hours since return to service.
King KAP 150 Autopilot
The pilot information manual supplement for the autopilot did not provide a minimum activation airspeed for the TB-20 but did contain a maximum airspeed limitation of 175 kt for autopilot use. Automatic flight could be activated by pressing the AP ENG (autopilot engage) button on the control panel and disengaged by pressing the AP ENG button again, or by pressing the AP DISC (autopilot disconnect) button on the pilot’s control wheel. When the autopilot is disengaged, an aural alert sounds for 2 seconds to alert the pilot.
The supplement also provided maximum altitude losses that may be encountered following an autopilot malfunction. In a cruise, climb or descent configuration, the maximum altitude loss would be 450 ft.
Recorded data
ADS-B
The aircraft was equipped with a SkyEcho portable automatic dependant surveillance broadcast (ADS-B) antenna capable of receiving information from ADS-B equipped aircraft and transmitting positional information to nearby stations. A review of available flight track history revealed that this antenna did not transmit any positional information during the accident flight.
Mobile devices
There were almost certainly 2 iPads and 2 telephones onboard the aircraft. Queensland Police located and recovered one telephone from the accident site. ATSB data recovery specialists determined that the phone was too heavily damaged to recover the data from the phone’s internal memory. At least 2 mobile devices were running the OzRunways app.
OzRunways data
OzRunways is an electronic flight bag (EFB) provider in Australia that also provides a ‘TX’ service that tracks device location and uploads it to OzRunways servers over the cellular network every 5 seconds. This service displays the device’s location on a user‑selected chart and also plots location data from other aircraft utilising OzRunways. The pilot used the OzRunways application on an iPad for en route planning and navigation. The pilot’s passenger also carried a second iPad with OzRunways when they flew together.
OzRunways is an approved source of aeronautical charts, but it must not be used as a primary means of navigation. The iPad GPS does not meet technical standard order[7] (TSO) specifications for aviation use (OzRunways, 2022). Additionally, there are limitations to the data provided via OzRunways. Altitude information has a resolution of 100 ft, a change in altitude from 190 ft to 210 ft will be displayed as a change from 100 ft to 200 ft. Additionally, filtering applied to smooth the data can affect the accuracy of analysis of small sections of data.
Tracking data obtained from OzRunways provided latitude and longitude as well as time, speed and heading. The last data point was at an altitude of about 1,700 ft above ground level in the vicinity of the accident site (Figure 2). When the OzRunways data ended, the aircraft was shown heading east in a steep descending right turn. The lack of any further data points was probably due to a loss of cellular signal among the mountains.
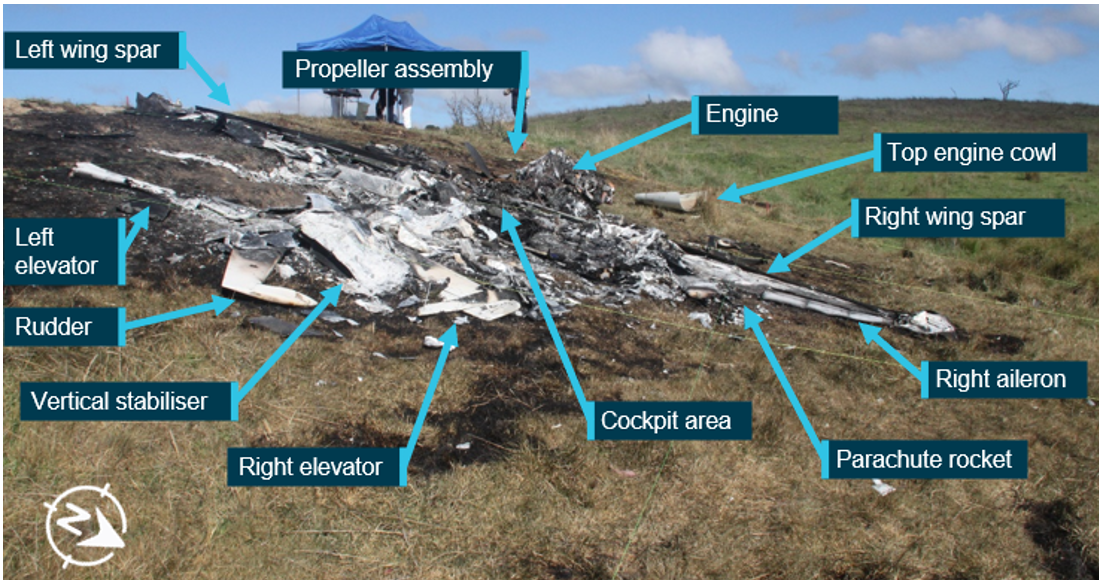
Accident site
The aircraft wreckage was located in heavily vegetated steep mountainous terrain, north-east of Bull Mountain (Figure 5). A Central Queensland Rescue helicopter located the wreckage at 1113 on 28 October and first accessed the site by winch at about 1400 on the day of the accident. The rescue crew confirmed that both occupants were deceased and took preliminary photographs of the wreckage.
The ATSB was unable to access the accident site. ATSB investigators provided a briefing to Queensland Police Service (QPS) forensic officers prior to them attending site on 27 November. With the support of specialists trained in high angle rescue operations the QPS officers collected evidence and provided it to the ATSB.
Source: Central Queensland Rescue, annotated by the ATSB
Wreckage examination
The ATSB’s review of the accident site photographs, and evidence provided by QPS, showed that the aircraft impacted the terrain at a steep angle while tracking 036° (close to north-east). The aircraft was destroyed by the impact and consumed by a post-impact fuel‑fed fire. Several components were buried by shifting soil after the accident.
Source: Queensland Police Service, annotated by the ATSB
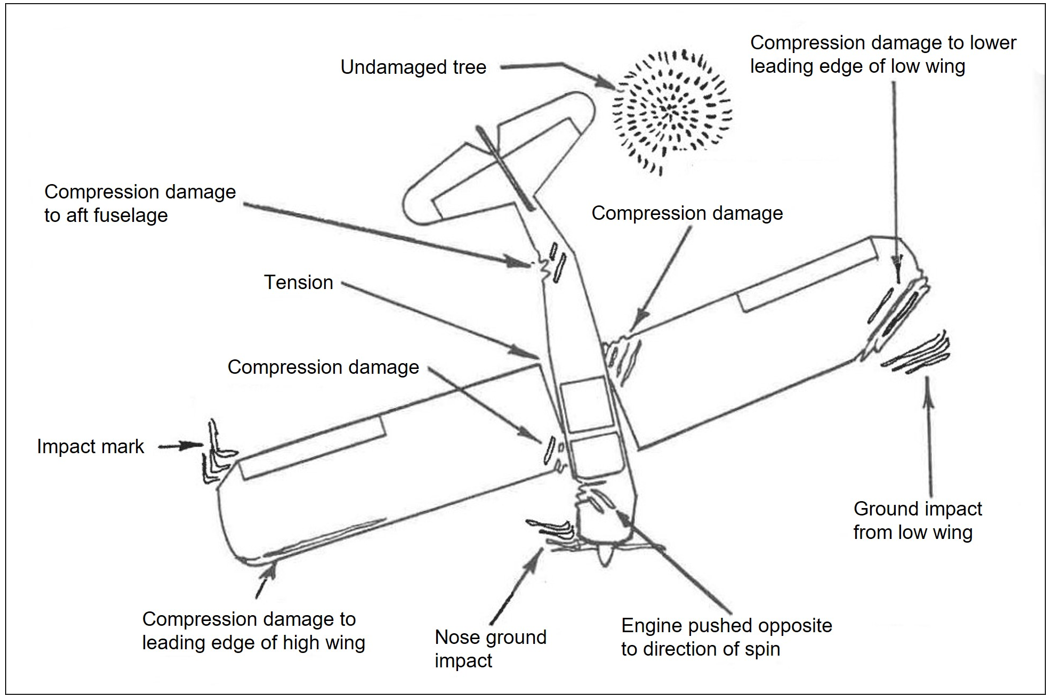
The following observations were made from the wreckage examination:
Impact marks on engine and propeller components indicated that the propeller was turning with power applied when it impacted terrain, indicating the engine was almost certainly operational at that time (Figure 6).
The extremities of the aircraft, the wing tips and stabilator were found at the accident site indicating that the aircraft was complete at the time of collision.
Communications
Police contacted Mackay air traffic control tower following the report of a missing aircraft. The controller confirmed that they did not hear a radio transmission from VH-JTY and that aircraft operating in the area at the time did not hear a distress call from the aircraft.
Operational information
General
Peers of the pilot reported that the pilot would often climb to operate VFR over the top of cloud. The pilot would generally fly the cruise portion of the flight on autopilot and would use the autopilot if they ever had to fly through cloud. While VFR over the top of cloud is permitted under the VFR, a minimum separation from cloud is required when flying under the VFR (see section Visual meteorological conditions).
The Civil Aviation Authority of New Zealand safety publication Vector contained an article called Who’s really flying your aircraft?The article discussed the potential downfalls of relying on automation in the cockpit, and its prevalence in VFR into instrument meteorological conditions (IMC) accidents.
VH-JTY was fitted with an approved GPS. The pilot was not known to program flight plans into the unit, instead relying on OzRunways for navigation. The CASA Visual Flight Guide provided the following note to VFR pilots utilising GPS in their aircraft:
An approved GNSS system may be used under the VFR:
• to supplement map reading and other visual navigation techniques
• to derive distance information for enroute navigation and traffic separation.
The positioning and navigational tools featured in the OzRunways application rely on equipment such as mobile phones or iPads that do not meet the required standard for operational use in aircraft. OzRunways acknowledges this limitation and advises users that the OzRunways application shall not be used as a primary means of navigation. It can, however, be used to supplement traditional visual navigation methods such as map reading.
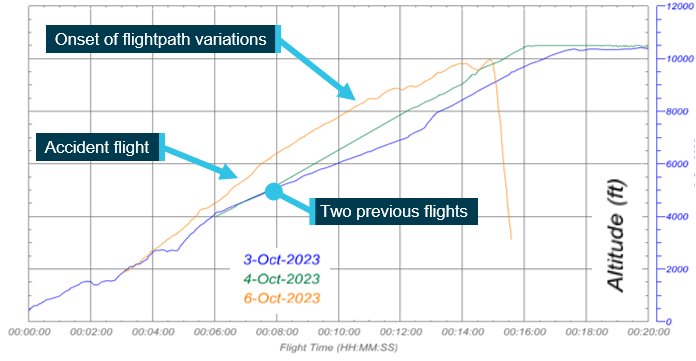
Previous flights
Data obtained for the previous 3 months showed a number of previous flights between the two locations consistent with logged flight records (Figure 7). Each flight took about 1.2 hrs depending on the route taken.
Flights would often depart Palmyra, tracking inland towards Townsville where they would descend outside the Townsville control zone steps and land at Montpelier Airfield. On return to Palmyra, the pilot routinely flew inland past Collinsville and would descend down the Pioneer Valley approaching Palmyra from the west below the Mackay control zone steps.
Source: Google Earth and OzRunways, annotated by the ATSB
Selection of route
The pilot and their passenger were familiar with the route between Montpelier and Palmyra, completing the return journey as often as once a fortnight for the last few years. When they considered the weather unsuitable for flight, they would make the trip by car, and had a vehicle at their disposal in both locations.
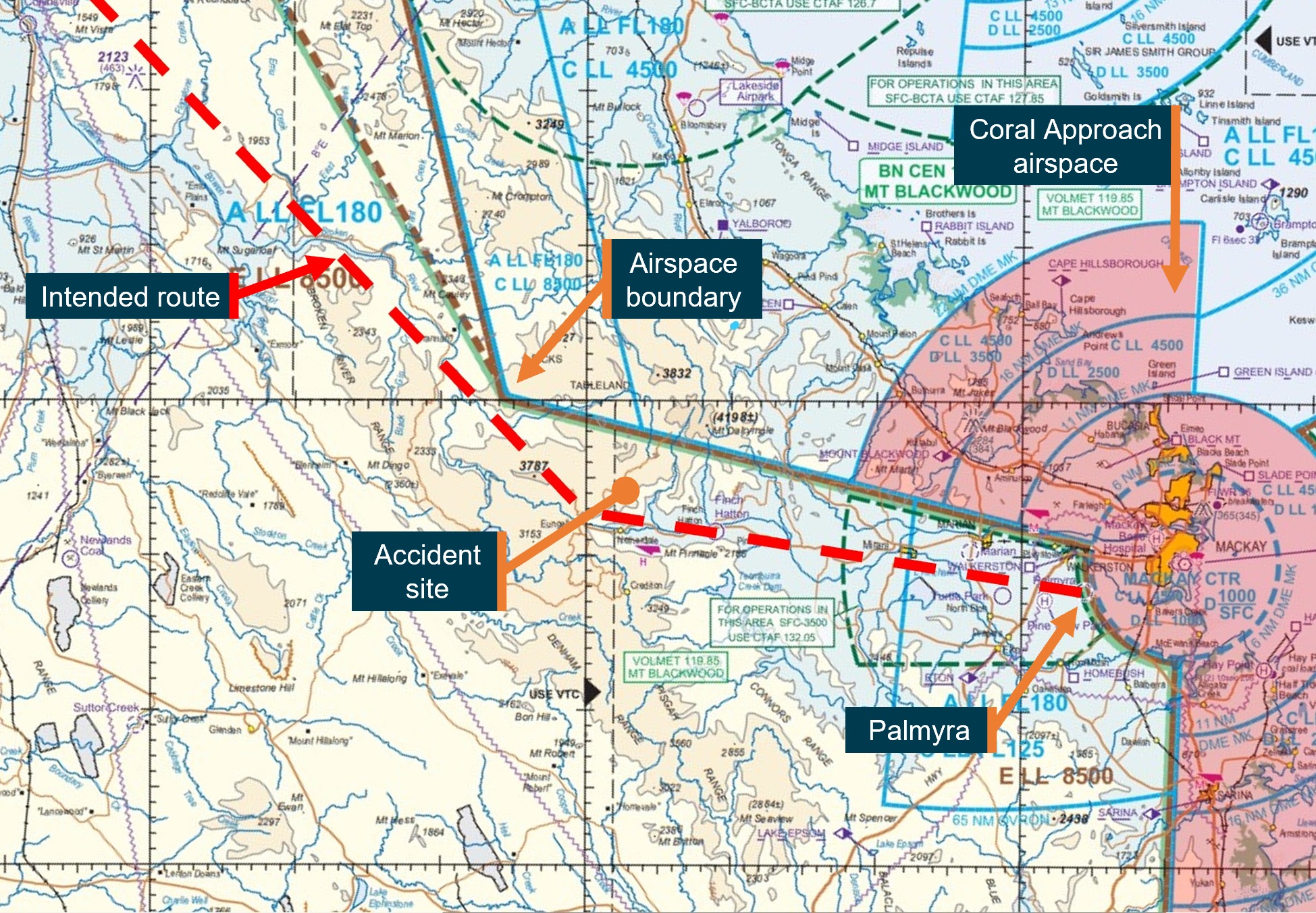
The pilot was known to plan routes that were outside controlled airspace (Figure 8). Witnesses interviewed advised this was common practice among local pilots due to the potential of encountering delays in access to controlled airspace in that region.
Visual meteorological conditions (VMC) are expressed in terms of in-flight visibility and distance from cloud (horizontal and vertical) and are prescribed in the Civil Aviation Safety Regulations (CASR) Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 2.07 VMC criteria. A VFR flight can be conducted above cloud provided VMC can be maintained for the entire flight, including climb, cruise, and descent.[8] The CASA Visual Flight Rules Guide included the following notes for VFR flight:
Pilots should not initiate VFR flight on top of more than SCT [scattered][9] cloud when weather conditions are marginal. Before committing to operate VFR flight on top of more than SCT cloud, pilots should be confident that meteorological information used is reliable and current, and clearly indicates that the entire flight will be able to be conducted in VMC.
And:
When navigating by visual reference to the ground or water, you must positively fix the aircraft’s position by visual reference to features marked on topographical charts at intervals not exceeding 30 minutes.
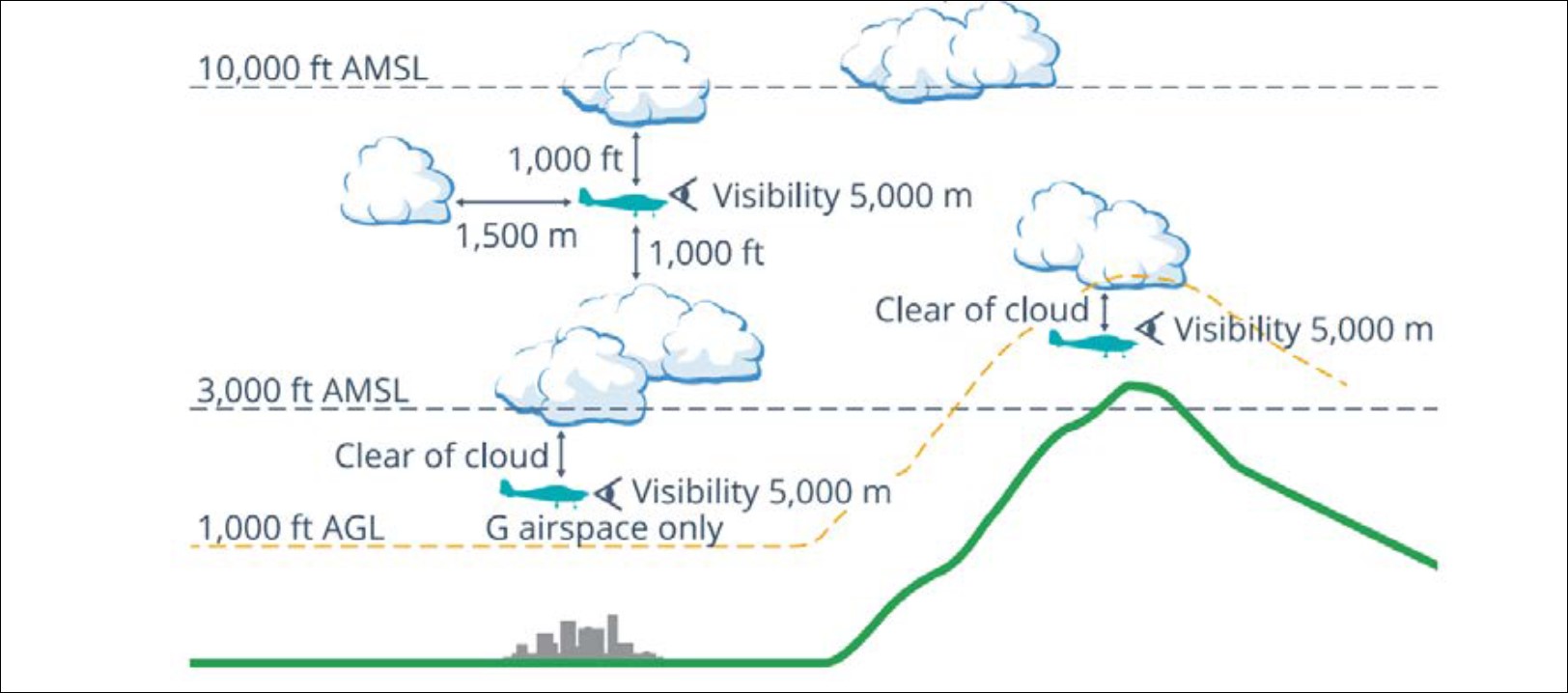
Figure 9, taken from the CASA Visual Flight Rules Guide, provides a visual depiction of the VMC criteria for aeroplanes below 10,000 ft.
According to CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.02 Forecasts for flight planning, an authorised weather forecast must cover the whole period of the flight, and include a wind and temperature forecast and, for a flight at or below 10,000 ft AMSL, a general aviation meteorological area forecast (GAF).
Airservices Australia conducted a review of the pilot’s national aeronautical information processing system (NAIPS)[10] account activity. Two accounts were linked to the pilot. On the day of the flight, one account had expired, and the other had not been accessed since a password update 2 months earlier. Weather requests through OzRunways use the user’s NAIPS login credentials to retrieve the requested information. A third account, linked to the passenger, was last accessed through OzRunways 5 days prior to the flight to obtain an area briefing.
While other third party information such as weather radar overlays, satellite imagery and wind observations are available without an NAIPS login,[11] NAIPS is the only source through which OzRunways obtains weather forecasts for flight planning.
Notwithstanding the requirement of a forecast for flight planning, CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.03 Flights unable to obtain an authorised weather forecast before departure states that a flight can still depart without an authorised forecast provided other conditions are met. These include:
The pilot in command reasonably considers that the weather conditions at the departure aerodrome will permit the aircraft to return and land safely at the departure aerodrome within 1 hour after take-off.
The pilot in command of a Part 91 flight must return to the departure aerodrome if:
(a) the authorised weather forecast required for the planned destination aerodrome is not obtained within 30 minutes after take-off; and
(b) the pilot in command has not nominated a destination alternate aerodrome if required to do so by subsection 8.04 (3).[12]
CASA defined what constituted an approved weather report and a list of who could provide one.[13] Licenced pilots were included in the list. The pilot obtained a weather update for the destination from their friend en route. While the accuracy of the information could not be verified, as a licenced pilot, the weather report provided by the pilot’s friend would have been considered an approved weather report for the destination. Based on the pilot’s phone records, this report was obtained about 39 minutes after departure.
Meteorological information
Forecast weather
The planned flight from Montpelier to Palmyra was within the QLD north (QLD-N) Graphical Area Forecast (GAF)[14] region. Forecast weather conditions in the GAF, valid from 0300 to 0900 on 28 October 2023, included average conditions of greater than 10 km visibility with areas of scattered stratocumulus clouds between 2,000 and 4,000 ft. The cloud was forecast to lift and become scattered cumulus and stratocumulus between 4,000 and 8,000 ft with moderate turbulence below 8,000 ft in thermals later in the day.
The Bureau of Meteorology aerodrome forecast (TAF)[15] for Mackay Airport, issued at 0435 and valid at the time of the accident showed an expected visibility of greater than 10 km, few cloud at 3,000 ft and a wind of 17 kt from the south-east.
Based on the forecasts, local pilots interviewed by the ATSB described the conditions as being conducive to mechanical turbulence around the ranges.
Actual weather
The meteorological aerodrome report (METAR)[16] for Mackay Airport reported wind from the east at 17 kt (100°), visibility greater than 10 km and cloud scattered at 3,300 ft and broken[17] at 5,500 ft. There was no rainfall recorded in the previous 24 hours.
The ATSB requested an assessment of the weather from the Bureau of Meteorology who provided the following observations for the morning of the accident:
• Cloud extended from the coast to the ranges and was clear west of ranges.
• South easterly winds persisted which often bring cloud between 2,000 – 3,000 ft, being lower earlier in the day and climbing as the day warms up.
• Over the accident site, cloud was overcast to broken.
• Cloud extended 25 NM south of accident site.
• Eungella Dam was visible to the west on satellite images.
• Closer to the coast cloud was scattered to broken.
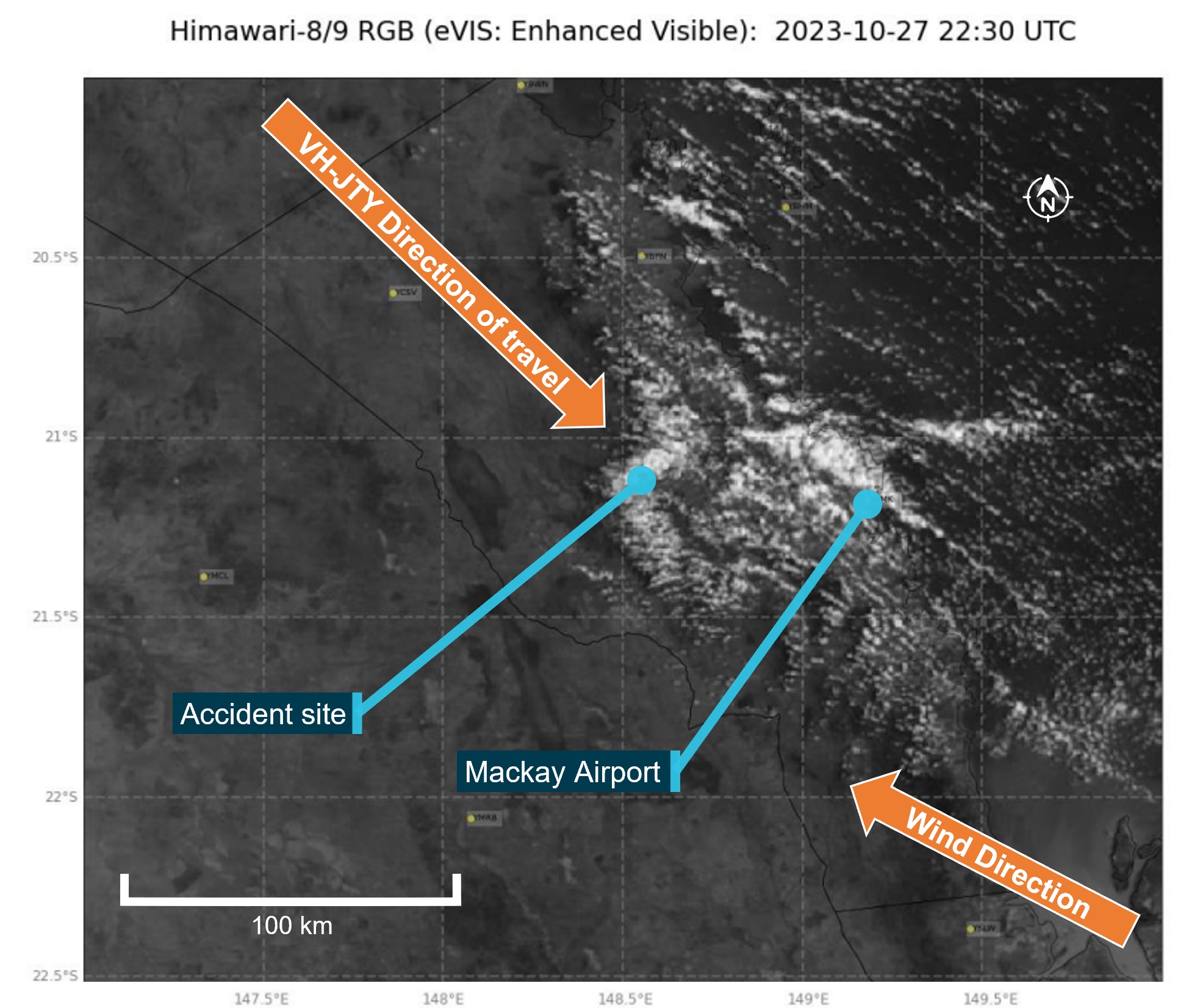
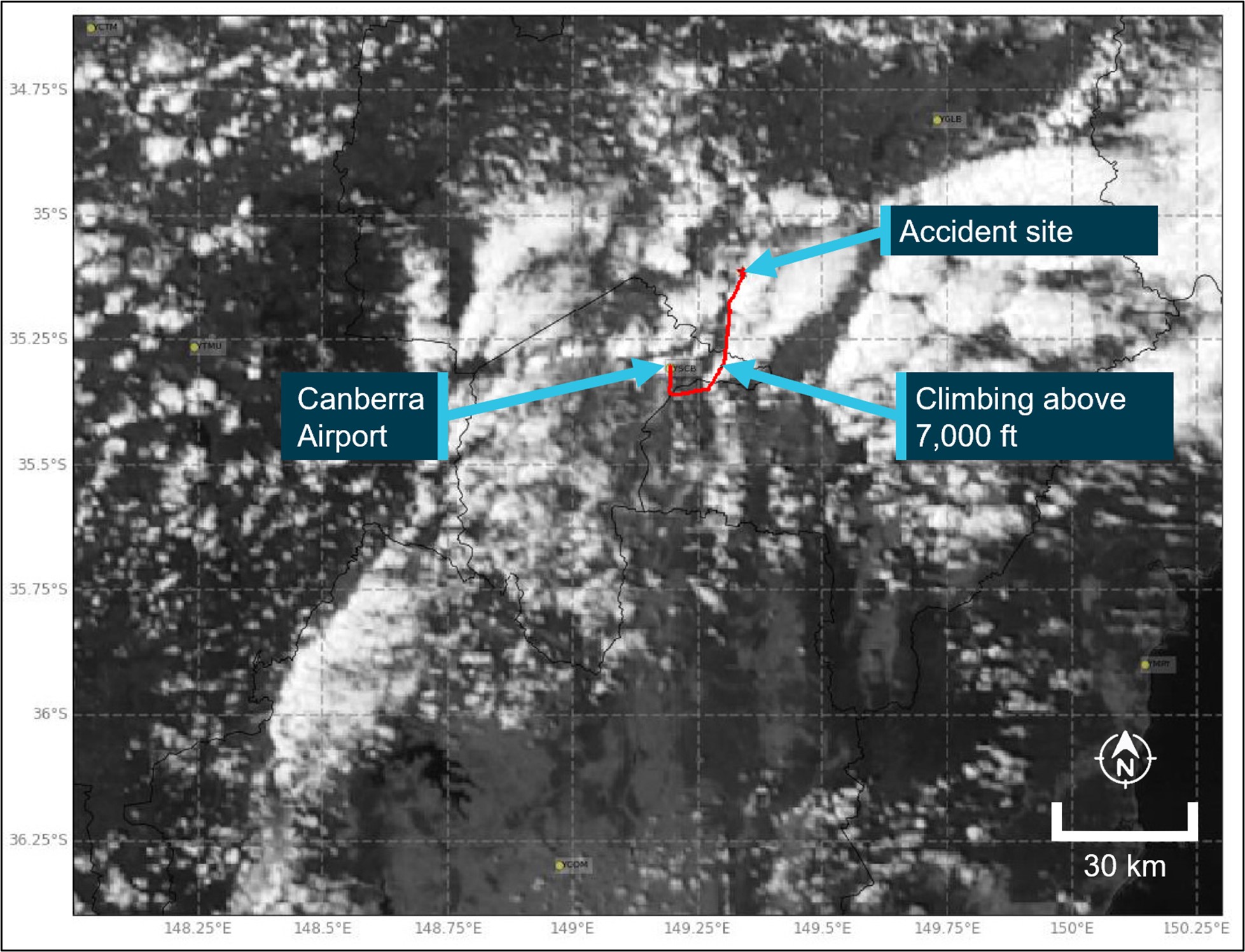
Bureau of Meteorology satellite images showed cloud building in the Pioneer Valley east of the ranges from 0600, covering the mountains to the north of the Pioneer Valley by 0800. Figure 10 shows cloud cover at 0830, 3 minutes before the accident.
Figure 10: Satellite image showing cloud formation on 28 October at 0830 local time
Source: Source: Bureau of Meteorology, annotated by the ATSB
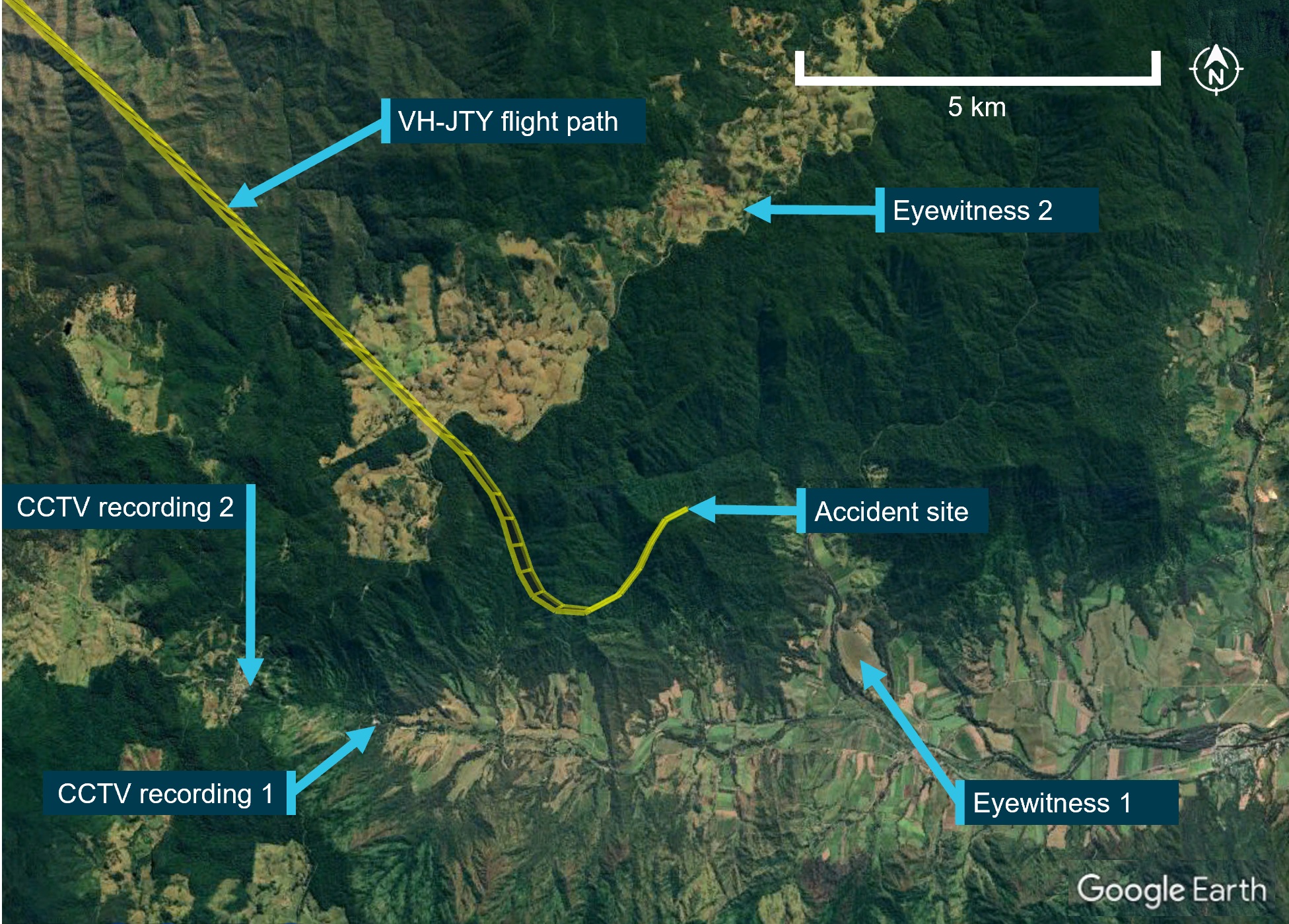
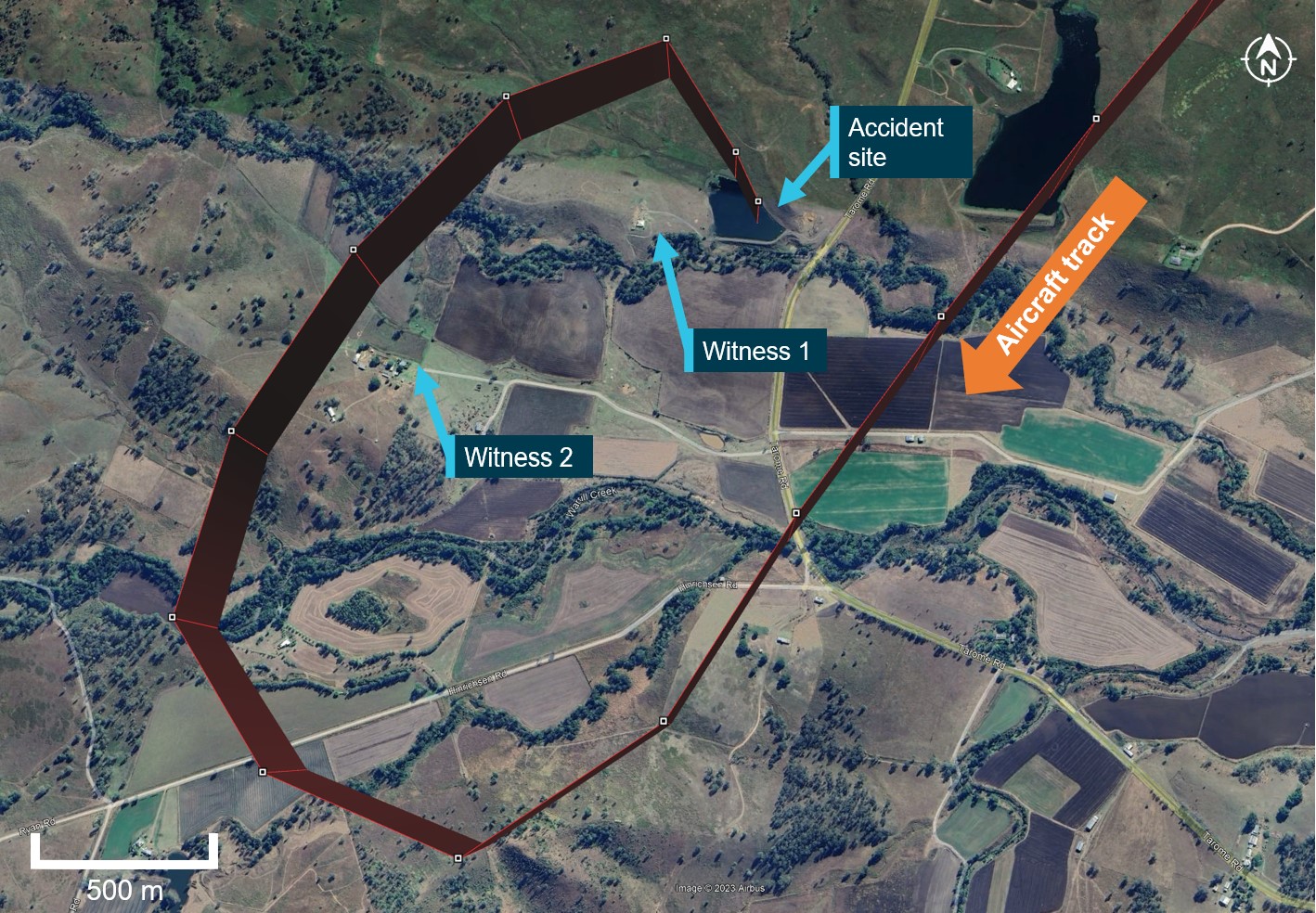
Figure 11 shows the location of witnesses and CCTV recorded at the time of the accident.
Eyewitness 1 located near Bull Mountain heard a low flying aircraft that stopped suddenly. They stated that the top of the mountain was visible around the time of the accident.
Eyewitness 2 described the cloud as being very thick that morning from when they woke at 0500. The cloud started to rise around 0800 but still produced limited visibility of their paddock until around 1000. They also described a ‘good breeze’ on the ground during the morning with occasional gusts but did not recall strong winds on the day. CCTV footage from that location showed low cloud close to where the pilot commenced their descent (Figure 12).
CCTV recording 1 obtained from a business 5 km south-west of the accident site showing diffuse light indicating cloud cover at the time of the accident.
CCTV recording 2 facing north from an elevated position at the head of the valley. That footage showed low cloud to the east and tree movement equivalent to a fresh breeze.
Additionally, a large bushfire around 70 km to the south-east had filled the Pioneer Valley with smoke which was yet to dissipate. The pilot of the rescue helicopter advised that during the search for VH-JTY at around 1000, the cloud base was scattered at 3,000 ft with poor visibility in smoke haze.
Figure 12: Closed circuit footage from Dalrymple Heights
Source: Supplied
Decision making
Flight under the VFR requires minimum conditions of visibility and distance from cloud. Variation from the expected weather conditions en route may prevent a pilot from reaching their destination under this ruleset. Flying into instrument meteorological conditions[18] (IMC) can occur in any phase of flight. However, a 2005 ATSB research publication – General Aviation Pilot Behaviours in the Face of Adverse Weather (B2005/0127) – concluded that the chances of a VFR into IMC encounter increased as the flight progressed, with the maximum chance occurring during the final 20 per cent of the planned flight. It stated:
This pattern suggests an increasing tendency on the part of pilots to ‘press on’ as they near their goal. To turn back or divert when the destination seemed ever closer became progressively more difficult.
The CASA Resource Booklet 7 Decision making contained the following:
A non-instrument rated pilot who proceeds with a flight in marginal weather and ends up in instrument meteorological conditions (IMC) decides to firstly, proceed with the flight and secondly, not turn back when the weather indicated visual flight rules were not able to be maintained
Dejoy (1992, cited in Hunter, 2002) suggests that a person’s propensity to engage in risky behaviour is the result of lower perceived risk in the outcome. Studies have shown that pilots who do not perceive the risks with adverse weather are more likely to engage in higher risk activities when dealing with weather (Cooper, 2003).
A Transportation Safety Board of Canada report A23O0028 into a VFR into IMC accident looked at pilot decision making and the acceptance of unsafe practices.
Pilot decision making is a cognitive process used to select a course of action between alternatives. Several factors, circumstances, and biases can affect pilot decision making, including the flight objective or goal, and the pilot’s knowledge, experience, and training. These factors can lead to situations where pilots might prioritize the achievement of the goal over the management of threats, likely resulting in a reduced safety margin.
A focus on achieving a goal or outcome may lead to a reduced sensitivity to risk, especially when high-risk activities repeatedly result in no negative outcomes. Flight crew members may grow accustomed to these risks, altering their perception and acceptance of such risks over time (Hollenbeck and others 1994).
In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
For non-instrument rated pilots, statistics show they may not be able to recover at all. Research has shown the pilots not proficient in maintaining control of an aircraft with sole reference to the flight instruments will typically become spatially disoriented and lose control of the aircraft within 1 to 3 minutes after visual cues are lost.
The FAA Advisory Circular FAA AC60-4A Pilot’s spatial disorientation discussed the challenges associated with recovering from spatial disorientation. The results of a test conducted with qualified instrument pilots found that it took as much as 35 seconds to establish full control by instruments after the loss of visual reference with the ground or surface.
The ATSB report AR-2011-050 was updated in 2019 and found that in the 10 years prior, there were 101 VFR into IMC occurrences in Australian airspace reported to the ATSB. Of these, 9 were accidents resulting in 21 fatalities. An almost 10% chance of the encounter ending in a fatal accident.
A search of the ATSB Aviation Occurrence Database shows that in the 5 years since 2019, there have been 56 VFR into IMC occurrences reported to the ATSB. Of these, 10 resulted in accidents with 16 fatalities. The dangers of spatial disorientation following a loss of visual cues remains one of the most significant causes of concern in aviation safety.
Similar Occurrences
The risks of visual flight rules (VFR) pilots flying from visual meteorological conditions (VMC) into instrument meteorological conditions (IMC) are well documented, and have been the focus of numerous ATSB reports and publications. VFR pilots flying into IMC is a significant cause of aircraft accidents and fatalities.
AO-2022-016 – VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD, near Mount Disappointment, Victoria, on 31 March 2022
On 31 March 2022, at about 0741 local time, 2 Microflite Airbus EC130 helicopters, registered VH‑WVV and VH-XWD, departed the Batman Park helicopter landing site in Melbourne, for the town of Ulupna, Victoria. Both helicopters were operated in accordance with the VFR and departed in VMC conditions. Cloud was forecast along the route, but the pilots elected to continue to the destination. The helicopters encountered instrument meteorological conditions (IMC) over Mount Disappointment and VH-WVV conducted a U-turn to avoid entering cloud. While also attempting to conduct a U-turn, VH-XWD entered cloud, developed a high rate of descent, and collided with terrain. The helicopter was destroyed, and the 5 occupants were fatally injured.
AO-2021-017 – VFR into IMC and in-flight break-up involving Van's Aircraft RV-7A, VH-XWI 90 km south of Charters Towers, Queensland, on 23 April 2021
On 23 April 2021, a Van’s Aircraft RV-7A, registered VH-XWI, was being operated on a private flight under the visual flight rules (VFR) from Winton to Bowen, Queensland. During the flight, the pilot most likely entered IMC and lost control of the aircraft several times. This led to the airspeed limitations for the aircraft being exceeded and the aircraft sustained an in-flight break-up. The pilot was fatally injured, and the aircraft was destroyed.
, updated in 2019, includes a selection of weather-related general aviation accidents and incidents that show weather alone is never the only factor affecting pilot decisions that result in inadvertent IMC encounters. The documented investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather.
CASA also released a collection of resources related to this type of occurrence on its website titled Preventing VFR into IMC and other related resources on its pilot safety hub under Weather and forecasting.
For more information on VFR into IMC occurrences, recognising inadvertent entry into IMC, and what to do to recover, refer to the following publications:
Civil Aviation Authority United Kingdom: Safety sense booklet VFR flight into IMC
The analysis considers the limited evidence available and discusses possible explanations for the departure from controlled flight:
pilot incapacitation
technical failure or malfunction
decision making
spatial disorientation.
Pilot incapacitation
Pilot incapacitation following a medical event was considered unlikely based on the short timeframe between ending the phone conversation prior to descent and the apparent departure from controlled flight. Medical records indicated that the pilot’s pre-existing condition was being appropriately managed and in the absence of any additional evidence, that was excluded.
Additionally, the passenger was also a pilot, although not current at the time, and they would have been capable of assuming control if the pilot had a medical episode.
Technical malfunction
Structural failure was considered as a possible explanation for the departure from controlled flight. The propeller, wing tips, stabilator, and vertical stabiliser/rudder were all located in site photographs. This was significant in determining that the recent repair to the vertical stabiliser had not failed. With the main components identified at the accident site, the possibility of an in-flight break‑up was excluded. Further, the damage to the engine and propeller indicated the engine was producing power at the time of the accident, eliminating engine malfunction as a possible explanation for the rapid descent.
The autopilot was installed in the aircraft from new and the pilot had owned the aircraft for close to 15 years. The pilot was almost certainly familiar with basic operation of the autopilot. The design of the autopilot servos that moved flight control surfaces incorporated a clutch so a pilot could override the autopilot in the event of a malfunction. The unit also incorporated a design whereby the autopilot would disengage if excessive pitch or roll rates were encountered. The autopilot had been repaired almost a year prior with no record of any additional maintenance, and the nature of the previous autopilot failures would not induce a loss of control.
If a technical malfunction occurred that would have affected the immediate safe continuation of the flight, it is very likely the pilot would have made a radio call declaring an emergency. No radio call was detected.
With no evidence of a failure or malfunction that would have induced uncommanded control inputs, it is considered unlikely that the autopilot contributed to a loss of control.
Pilot decision making
After excluding pilot incapacitation and technical failure, the ATSB considered pilot decision making and the flight path through cloud during the final minutes of the flight.
There was no record that the pilot obtained relevant aviation weather forecasts prior to the flight, and it could not be determined if additional weather information was obtained from other non‑approved sources. However, as the flight was a relatively short distance, and the pilot was very familiar with the route and destination, it is almost certain that they had knowledge and experience of weather behaviour and conditions to be expected. Additionally, the weather report obtained over the telephone while en route provided an accurate assessment of the prevailing conditions along the intended flight path.
Weather observations showed that at the cruising altitude of 5,500 ft, VH-JTY would have been in VMC above cloud before commencing descent. While there was variation in the witness reports concerning the lower level of the cloud, evidence showed there was significant cloud present, and that the pilot planned to pass through it. Witness statements related that it was common practice for the accident pilot to intentionally fly through cloud with the autopilot on. While this action would represent intentional non-compliance with aviation regulations, the main advantage of doing so would be to avoid loss of control following loss of visual references. The hazard being that if the autopilot or any of its input sensors failed or were inadvertently disengaged, loss of control would reasonably ensue.
This behaviour without previous consequence may have affected their perception of the associated risk of continuing through cloud and influenced their decision to continue along the intended flight path instead of diverting around the cloud en route (Cooper, 2003). Personal bias and misperception of the risks associated with VFR flight into IMC (Hollenbeck and others, 1994) is a factor frequently seen in aircraft accidents (Hunter, 2002).
The Bureau of Meteorology assessment of the conditions and analysis of satellite imagery matched the report of the pilot’s friend on conditions at the destination. While cloud existed around to the east of Mackay and around the mountains of the Pioneer Valley, the west and south of the destination were clear of cloud. It was determined that in this context, it is highly likely that the pilot chose to fly through cloud rather than continue visual flight over the top of cloud, divert around weather, or plan flight through controlled airspace.
Spatial disorientation
The flight path from Montpelier to top of descent was compared to previous flights. It was determined to be consistent with the way the pilot would normally conduct cross-country flights in VH-JTY and was almost certainly being flown on autopilot during cruise. The sudden change in flight path prior to descent indicated disconnection of the autopilot and resumption of hand flying.
The weather on the day of the flight was conducive to poor or absent visual cues and turbulence, factors which are known to contribute to spatial disorientation. The pilot was not trained or experienced in flying in low visibility. In these conditions, the pilot would have been required to reference the aircraft’s flight instruments to maintain control. In this case the aircraft was not equipped with the instruments required for flight in IMC.
The accident site showed that the aircraft collided with terrain tracking north-east, indicating that the turn to the right continued after the flight path recording ended. The instability of the flight path with excessive rates of descent and climb are markers commonly observed in spatial disorientation occurrences where pilots are aware of a departure from controlled flight and attempt to correct the unusual flight attitude.
Due to the limited information available, it is not known whether the autopilot disconnect was intentional or why the pilot’s reported strategy of using autopilot when flying through cloud failed on this occasion. Following the commencement of the turn to the left, the significant deviation of pitch attitude during the turn was likely unintentional. The high rate of descent was consistent with the pilot becoming spatially disoriented after flying into weather conditions not suitable for visual navigation. As a result, the aircraft collided with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC, loss of control and collision with terrain involving SOCATA-Groupe Aerospatiale TB-20, VH‑JTY, 65 km west of Mackay Airport, Queensland, on 28 October, 2023.
The visual flight rules pilot very likely entered weather conditions not suitable for visual navigation, leading to spatial disorientation and collision with terrain.
Cooper D. (2003). Psychology, Risk and Safety: Understanding how personality & perception can influence risk taking. Professional Safety. Journal of the American Society of Safety Engineers, November 2003, 39-46.
Hunter DR. (2002), Risk Perception and Risk Tolerance in Aircraft Pilots. Federal Aviation Administration, DOT/FAA/AM-02/17, 2002.
Hollenbeck, J. Ilgen, D. Phillips, J. Hedlund J. (1994) Decision risk in dynamic two-stage contexts: beyond the status quo. Journal of Applied Psychology, Vol.79, Issue 4, pp. 592–598.
OzRunways. (2022). How can OzRunways be used for navigation? On-line, Retrieved 19 August
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
maintenance organisation for VH-JTY
aircraft manufacturer
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meteorology
OzRunways.
Submissions were received from:
the aircraft manufacturer.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Montpelier aircraft landing area is located about 20 km south-south-east of Townsville Airport and is the site of the former military airfield Antill Plains.
[2]Palmyra aircraft landing area is located about 12 km west-south-west of Mackay Airport.
[3]OzRunways is an electronic flight bag app that provides planning, briefing, flight plan filing and moving map navigation services.
[4]VNE (Never Exceed Speed): the speed limit that may not be exceeded at any time. The calculation of this speed is driven by structural or aerodynamic limitations; however, control system flutter is typically one limitation that factors heavily into the calculation of VNE.
[5]The aircraft is equipped with the flight and navigation equipment listed in the aircraft’s flight manual and any additional equipment required for the type of operation in accordance with Civil Aviation Order 20.18.
[6]Visual flight rules (VFR): regulations that permit a pilot to operate an aircraft in conditions whereby navigation and orientation of the aircraft by visual reference is possible.
[7]Technical Standard Order (TSO) – a TSO is a minimum performance standard for specified materials, parts, and appliances used on civil aircraft.
[8]VFR flight above more than 4/8 cloud cover is known as ‘VFR over the top’, as the phrase ‘VFR on top’ is a clearance provided to an instrument flight rules flight to operate at a VFR level in visual conditions.
[9]Scattered: describes cloud covering three or four eighths (oktas) of the sky.
[10]The National Aeronautical Information Processing System (NAIPS) is a multi-function, computerised, aeronautical information system. It processes and stores meteorological information and operational notices and enables the provision of briefing products and services to pilots and the Australian Air Traffic Control platform.
[11]Radar weather overlays and satellite imagery is downloaded from the Bureau of Meteorology. Wind observations obtained through the private company Windy.com are obtained from publicly available weather databases produced by worldwide weather agencies (including the BoM).
[12]CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 8.04 Destination alternate aerodromes — weather.
[13]CASR Part 121 Chapter 9 Division 2 –Dictionary.
[14]GAF (Graphical Area Forecast): provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text.
[15]TAF (Aerodrome Forecast): a statement of meteorological conditions expected for the specified period of time in the airspace within 5 nautical miles (9 km) of the aerodrome reference point.
[16]METAR (Meteorological Aerodrome Report) is a routine aerodrome weather report issued at half hourly time intervals. The report ordinarily covers an area of 8 km radius from the aerodrome reference point.
[17]Broken: used to describe an amount of cloud covering the sky of between 5 and 7 oktas (eighths).
[18]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in conditions of limited visibility.
Occurrence summary
Investigation number
AO-2023-052
Occurrence date
28/10/2023
Location
65 km west of Mackay Airport
State
Queensland
Report release date
02/10/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control, VFR into IMC
On 5 November 2022, an Airborne Australia Edge XT-912-L collided with terrain near Mokuleia, Hawaii. The aircraft was substantially damaged, and 2 people on board were fatally injured.
As the aircraft was Australian manufactured, the United States. National Transportation Safety Board (NTSB) requested that the ATSB appoint an accredited representative to assist in their investigation.
To facilitate this support and to provide the appropriate protections for any information gathered, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 19 November 2024, the NTSB released its final report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation.
Any enquiries relating to the accident investigation should be directed to the National Transportation Safety Board, United States at www.ntsb.gov.
On the 22 September 2023, a Bell Helicopters 407, conducting a passenger flight from Sengapi to Gerbrau Airstrip in Madang Province, collided with terrain during the approach to the airstrip. All of the occupants sustained serious injuries and the helicopter was destroyed.
The Accident Investigation Commission (AIC) of Papua New Guinea requested assistance from the ATSB to oversee the data being downloaded from the engine control unit, at a maintenance organisation in Australia.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The ATSB attended the successful download of the aircraft engine control unit data at an Asia Pacific Aerospace facility on 1 November 2023 with a technical representative of Rolls Royce. The data was extracted according to Rolls Royce procedures, however it was not possible to determine whether it contained all the relevant data for the occurrence as it could not be accessed locally. The data was provided to the Rolls Royce technical representative for further analysis. No further assistance was sought by, and further enquiries should be directed to the Papua New Guinea AIC as the investigating agency.
On 20 October 2023 the pilot of a Cessna 208 aircraft, registered VH‑UMV and operated by Experience Co, was conducting parachute operations at Barwon Heads Airport, Victoria with 16 parachutists on board. Passing about 500 ft on climb, the pilot detected a partial power loss consistent with a previously‑encountered transient power reduction.
Expecting the power to return immediately, the pilot did not lower the aircraft’s nose to maintain airspeed. The airspeed continued to reduce until the stall warning horn sounded and, due to the low height, low engine power and low airspeed, the pilot attempted to conduct a forced landing. However, the aircraft collided with water before continuing onto the riverbank and ground for approximately 50 m before coming to rest.
The aircraft was substantially damaged, 6 of the parachutists received serious injuries, 8 sustained minor injuries, and 2 were uninjured. The pilot also sustained minor injuries.
What the ATSB found
The ATSB found that passing about 500 ft on climb, the power reduced likely due to abnormal activation of an engine torque and temperature limiting system. Expecting the power to return quickly and surge, and in preparation for turning off the system, the pilot moved the power lever aft to reduce the power setting and delayed lowering the aircraft’s nose to maintain airspeed, resulting in a stall warning and subsequent collision with water.
The ATSB also found that Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the engine limiting system, but did not specify a minimum safe height at which to do so. This increased the risk of a loss of control and/or ground collision.
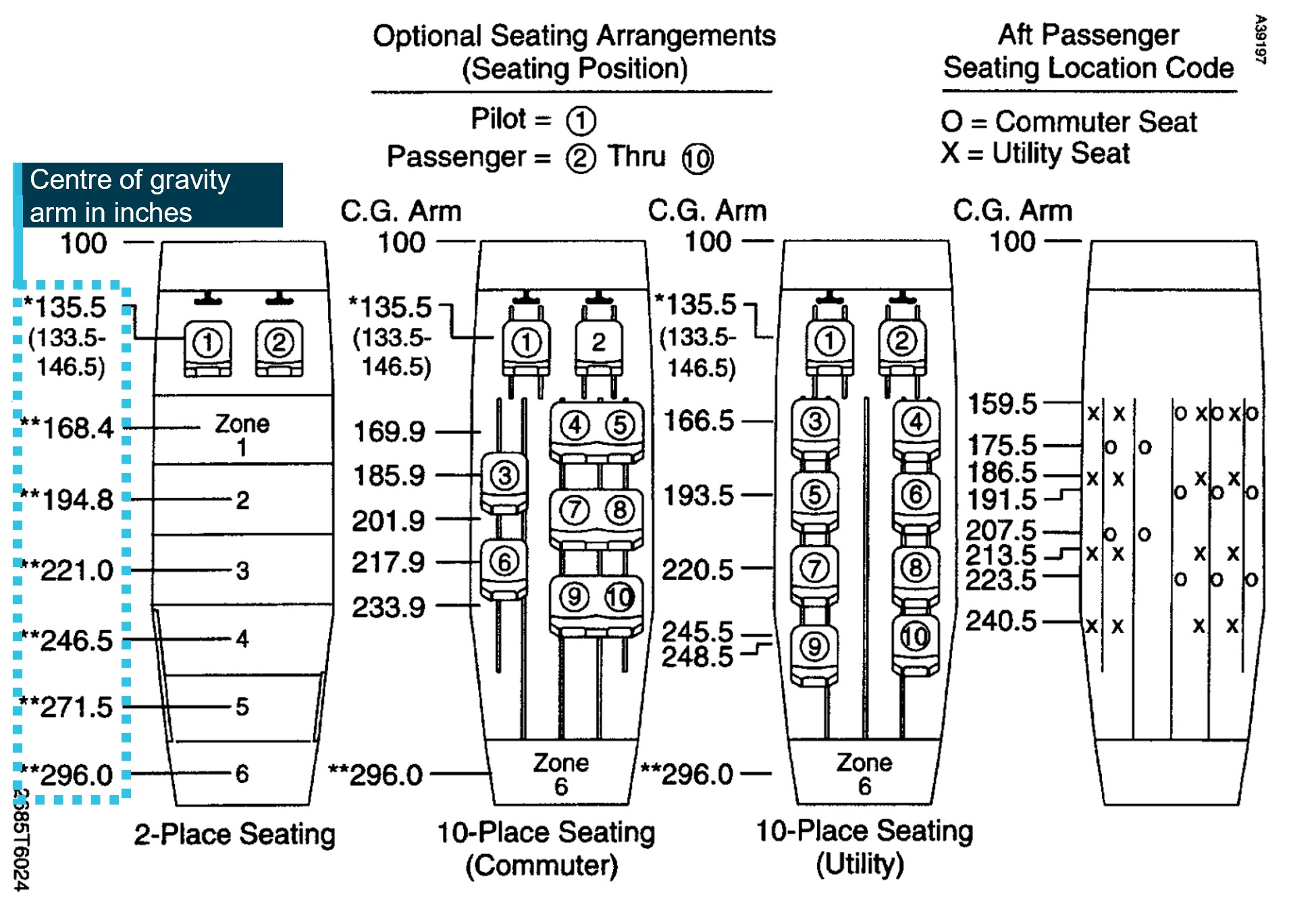
Further, the ATSB found that the operator's weight and balance calculation for the accident flight did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity, therefore, although it did not contribute to the accident, the weight and balance was inaccurate for the intended flight. Additionally, the software used to calculate aircraft weight and balance did not provide a warning if individual aircraft zones were overloaded.
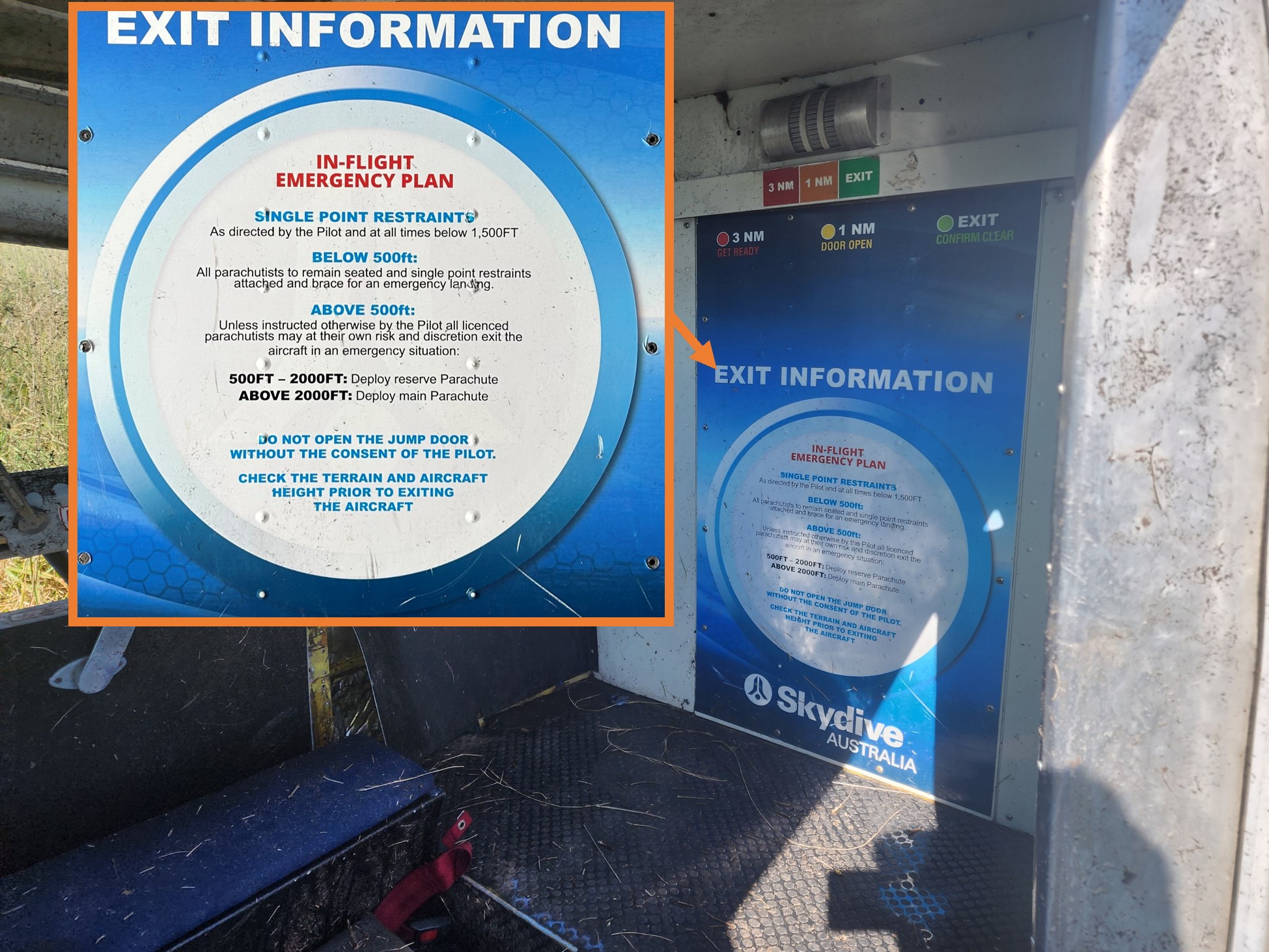
Finally, the ATSB found that Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
What has been done as a result
At the time of writing, Experience Co was re‑developing its sport skydivers safety video to include emergency procedures. Additionally, the following proactive safety actions have been taken:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet-wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the single red line/torque and temperature limiter malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed Cessna 208 and Cessna 208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the supplemental type certificate (STC) holder to be followed at or above 1,000 ft above ground level.
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of its aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Finally, the Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Lower the nose to maintain the glide speed of the aircraft. If turning is conducted, keep in mind an increased bank angle will increase the stall speed of the aircraft.
Maintain glide speed and assess whether the aircraft is maintaining, gaining or losing height to gauge current aircraft performance.
Fly the aircraft to make a landing, given the aircraft’s height and performance, and the pre-planned routes for the scenario.
If time permits, moving the power lever through the full range may result in increased power available to climb and/or create the time to diagnose the issue.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. This incident highlights the importance of passengers being appropriately briefed on the brace position and use of emergency exits. It also illustrates the higher injury risk associated with the carriage of parachutists, due to the increased number of occupants and inferior restraints compared to being secured in a certified seat.
The occurrence
Early on the morning of 20 October 2023, the pilot of a Cessna 208 aircraft, operated by Experience Co and registered VH-UMV, refuelled and inspected the aircraft in preparation for parachuting operations from Barwon Heads Airport, Victoria. No defects, including any fuel debris or contaminants, were identified.
The pilot’s first flight of the day was to carry 16 sport parachutists for a parachute jump from 15,000 ft. At about 0750 local time, the parachutists boarded the aircraft. The pilot recalled that the conditions were CAVOK,[1] with a light wind from the north. They taxied the aircraft to runway 36 for a northern departure.
A review of OzRunways[2] flight data, recorded at 5-second intervals, showed the aircraft commenced the take-off roll at 0757. The pilot reported moving the power lever forward until the engine reached 100% torque, and then reducing the power slightly during the take-off roll. Camera footage showed that the aircraft became airborne at 0757:22.
The pilot reported that, as the aircraft climbed and the airspeed increased, they retracted one stage of flap passing through 85 kt and another at about 95 kt. At 0757:47, climbing through about 400 ft, the aircraft reached its maximum recorded ground speed of 95 kt. The pilot reported that as the aircraft approached 500 ft above ground level and they reached for the flap lever to retract the last stage of flap, they heard a reduction in engine noise, and felt a deceleration.
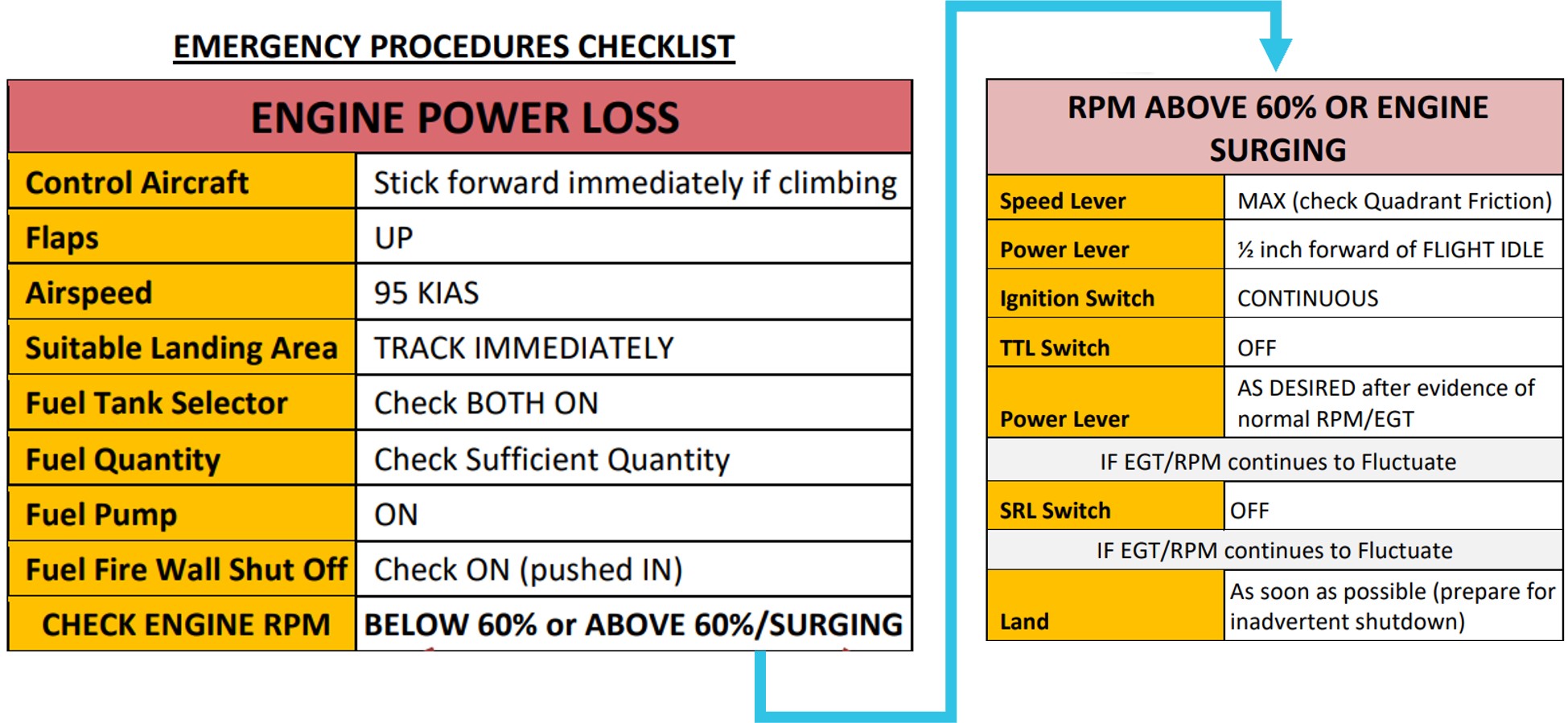
The pilot initially associated the loss of power with activation of the torque and temperature limiter (TTL) (see the section titled Torque and temperature limiter), which they had previously experienced in that aircraft. Consistent with the previous TTL activation, the pilot expected the power to quickly return, and reported reducing power slightly to prevent the engine surging[3] as power was restored.
The reduction in engine power, combined with the climb pitch attitude, resulted in the airspeed reducing and activation of the stall warning horn. On hearing the stall warning, the pilot lowered the aircraft’s nose to reduce the angle of attack[4] and increase the airspeed.
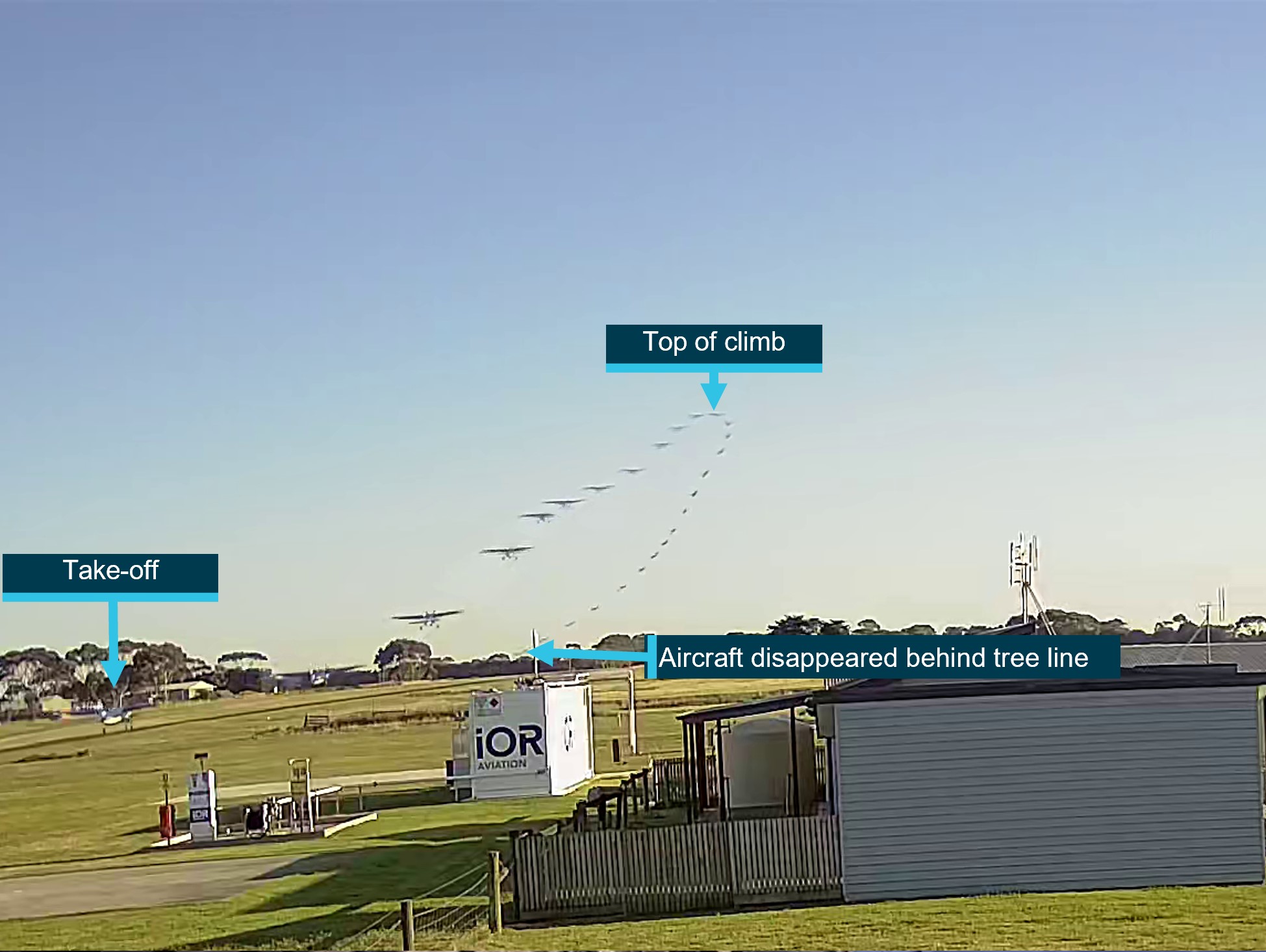
At 0757:57 the aircraft reached the highest recorded altitude of about 700 ft at 88 kt ground speed and, 5 seconds later, had descended to 600 ft and the ground speed reduced to 71 kt, then to 69 kt 5 seconds later. This flight path was consistent with video camera footage of the aircraft’s flight path (Figure 1). At 0758:08 the ADS-B[5] data recorded a descent rate of 3,520 ft/m passing an altitude of approximately 400 ft.
Figure 1: VH-UMV flight path captured by the airport camera
The ATSB combined multiple images together to show the flight path of the aircraft as captured by a local video camera. Source: Airport operator, annotated by the ATSB
The pilot reported that, as the aircraft descended, they observed the engine torque indication reducing through approximately 30% and attempted to switch off the TTL in accordance with the operator’s Engine Power Loss checklist. Due to the aircraft’s low height above the ground, and the pilot’s assessment that there was an engine issue, the pilot then selected a field in which to conduct a forced landing.
The pilot turned to the loadmaster[6] seated beside them and called out ‘gear-up’, to alert parachutists to be ready to exit the aircraft. In response, the loadmaster began directing parachutists to open the roller door, secure their harnesses, and brace for landing. The roller door was opened, but not secured in that position.
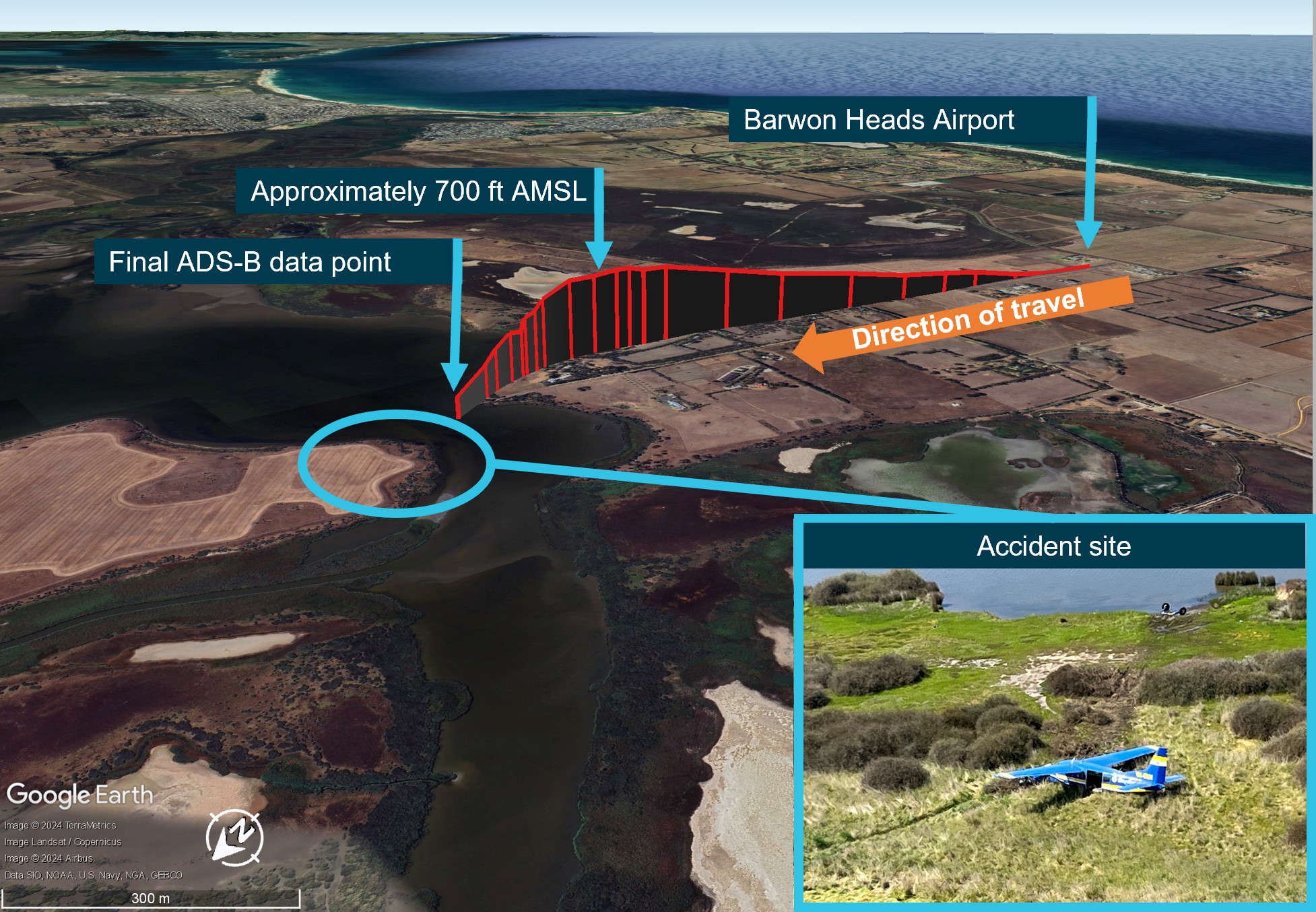
The pilot selected a forced landing location in a clearing beyond a river. However, less than 1 minute after becoming airborne and unable to maintain altitude, the aircraft impacted the water short of the clearing, resulting in water entering the cabin and forcing the unsecured roller door closed. The aircraft continued onto the riverbank where the main landing gear detached, then travelled along the ground for about 50 m before coming to rest (Figure 2).
The pilot sustained minor injuries, 6 parachutists sustained serious injuries, 8 sustained minor injuries and 2 were uninjured. The aircraft was substantially damaged.
Figure 2: VH-UMV flight path
Source: ADS-B exchange flight data overlaid on Google Earth and image of accident site provided by operator, annotated by the ATSB
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) and a current class 2 aviation medical certificate. On 19 April 2023, the pilot completed their gas turbine engine design feature endorsement and single engine aircraft flight review in a Cessna 208 aircraft.
At the time of the accident, the pilot had accrued approximately 220 hours of total flight experience, which included 38 hours on the Cessna 208 aircraft type. Of those hours on type, 36 had been accrued in the previous 90 days.
The pilot reported that they were familiar with VH-UMV, having conducted multiple flights in it prior to the accident flight. The pilot was also aware of operator-specific engine operating limitations for VH-UMV, and reported having previously experienced an engine surge at 5,000 ft (see the section titled Engine surging).
Aircraft information
Certification details
The Cessna Aircraft Company 208 (C208) is an all-metal, high-wing aeroplane with tricycle landing gear and designed for general utility usage. The aircraft type certificate data sheet (TCDS) A37CE described the C208 as an ‘11-place closed land monoplane’, and under the heading ‘No. of seats’, provided a centre of gravity range for seating for one or 2 pilot seat locations and referenced the current Pilot’s Operating Handbook (POH) and United States (US) Federal Aviation Administration (FAA) Airplane Flight Manual (AFM) for passenger seat arrangements for seats 3 to 11.
The C208 POH Section 2 – Limitations – Maximum passenger seating limits stated that up to 11 seats, including the pilot’s seat/s, may be installed.
VH-UMV, serial number 20800077, was manufactured in 1986 and first registered in Australia in 2005. At that time, the aircraft was issued 2 certificates of airworthiness, one for normal category[7] operations and one for restricted category[8] operations for the purpose of carrying people for parachute jumping.
Operating in the restricted category required several conditions, including removal of the cabin seats, compliance with a specific engineering order and readily visible restricted category placards, none of which were in place on the accident flight. Additionally, under Civil Aviation Safety Regulations (CASR) current at the time of the accident (CASR 91.845, 91.025, 135.030), aircraft operating in the restricted category were not permitted to conduct air transport operations (carriage of passengers or cargo for hire or reward).
In 2017, the aircraft’s Pratt & Whitney PT6A-114 gas turbine engine was replaced with a Honeywell International Incorporated TPE331-12JR-704TT gas turbine engine that drove a 4‑bladed, constant‑speed, full‑feathering,[9] reversible[10] Hartzell HC-E4N-5KL propeller with hydraulically‑operated variable‑pitch control. The engine modification was completed under the Texas Turbine Conversions supplemental type certificate (STC) SA10841SC, with an associated AFM Supplement. Under the heading ‘Maximum passenger seating limits’, the AFM supplement stated ‘No changes’ (from the C208 AFM).
The aircraft was also modified in accordance with STC SA01180SE, which increased the original maximum take-off weight from 3,628 kg to 3,792 kg. Both STCs were approved by the US FAA and therefore accepted in Australia and taken as having been issued by CASA in accordance with CASR Part 21 regulation 21.114.
Three modifications made to VH-UMV and other aircraft in the operator’s fleet were completed under engineering orders in accordance with the CASR Part 21 regulation 21.437 Grant of modification/repair design approvals—grant by authorised person or approved design organisation:
ESE-C208-25-001—Rework of interior for parachute operations
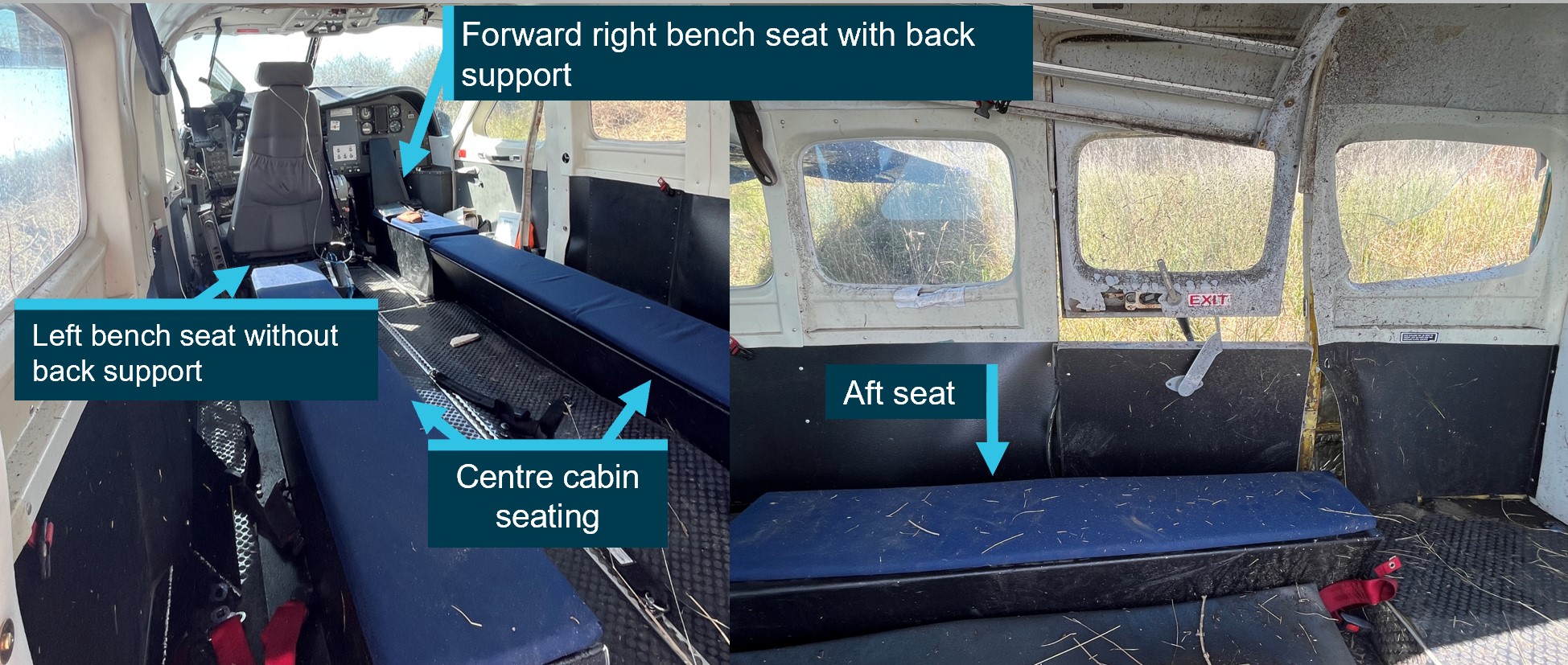
ESE-C208-25-007—Installation of parachute bench seating
ESE-C208-95-003—Installation of Go-Pro cameras.
Torque and temperature limiter
VH‑UMV was fitted with a switch‑activated torque and temperature limiter (TTL) system designed to prevent these parameters exceeding specified limits. Where an exceedance of the allowable torque or exhaust gas temperature (EGT) was detected, the TTL computer restricted fuel flow to the engine. The maximum allowable fuel reduction of a normally-functioning bypass was about 68 L/hour (125 lbs/hour), resulting in a reduction of the torque output from 100% to about 62% (due to the approximate 25% reduction in fuel flow).
Texas Turbine Conversions advised that, when functioning normally, the system would maintain the lower of the allowable torque or EGT limits and if the TTL bypassed the maximum allowable fuel, it would be felt immediately. In that case, the appropriate pilot response was to switch off the TTL.
The aircraft’s engine monitoring system included a single red line (SRL) controller, associated with the EGT limit. Like the TTL, the SRL was switch‑activated and deselection of the SRL also deactivated the TTL.
The allowable EGT limit was dependent on the phase of flight. Specifically, the operating margin from the EGT limit in the climb phase was reduced in the cruise phase. The phase was dependent on the position of the speed lever. Therefore, if the speed lever was moved aft during take-off or climb, the EGT limit also reduced and could result in activation of the TTL. The operator reported that the speed lever was fully forward throughout the short flight, and therefore the climb EGT limit applied.
Operating limits
The AFM supplement for the Honeywell engine specified operating limits. With the SRL and TTL on, those limits included a maximum EGT of 650 °C, maximum 100% torque and maximum of about 101% RPM during take-off and climb. The supplement also provided an EGT table with limits for operating with the SRL off or inoperative, or ‘manual mode’. The limits were provided for operating at 100% RPM or 96% RPM based on the outside air temperature in 5 °C increments from −60 to +60 °C.
The AFM defined take-off power as the lower of 100% torque or 650 ºC EGT (SRL ON), whichever is reached first at 100% engine RPM.
Engine surging
On 17 October 2023, the pilot submitted an internal safety report relating to an uncommanded engine surge, which they experienced at an altitude of approximately 5,000 ft. The pilot report stated:
Torque roll back for a split second, noticeable reduction in power and deceleration.
The pilot reported reducing the power then slowly increasing it while monitoring engine parameters in response to the event.
Although not recorded on the aircraft’s maintenance release (MR),[11] reportedly due to their transient nature, pilots submitted 7 other internal safety reports between July and October 2023 of engine surging in VH‑UMV, assessed as being due to the TTL.
A review of maintenance recorded in VH-UMV’s engine logbook for the previous 12 months showed that the TTL controller was replaced ‘for fault isolation’ following the first reported surging occurrence on 3 April 2023. A further logbook entry on 18 September 2023 recorded that the EGT harness was replaced in response to reported engine surging at take-off power.
The engine surging safety reports indicated troubleshooting test flights were also conducted. A series of test flights on 7 September 2023 was able to replicate the previously‑reported surging.In addition, a test flight following the EGT harness replacement noted that the surging was still present. One of the experienced surges resulted in a torque value of 62% and fuel flow reduced by approximately 72 L/hour (128 lbs/hour). The MR current at the time of the accident identified that the aircraft operated over 90 flights prior to the next reported surge event on 17 October 2023. On that day, the aircraft operated 6 flights, and one surge occurrence was reported. According to the MR, 12 flights were conducted over the next 2 days (18–19 October), with no reports of engine surging submitted. However, the ATSB was also advised of an engine surge on 18 October, which was not recorded.
The MR current at the time of the accident recorded 257 flights over 3 months, during which there were 6 reported surging events. That frequency illustrated the intermittent nature of the anomaly, which likely hindered troubleshooting.
As a result of the internal reports, on 21 July 2023, pilots were advised to operate VH-UMV under a set of unique operating conditions to avoid the TTL scheduling a significant bypass of fuel and subsequent notable drop in available power. These were limitations of 95% torque and 640 °C EGT.
A review of the operator’s safety reports also identified that surging events were reported on 3 other company aircraft. For those aircraft, maintenance actions rectified the cause of each event and there were no subsequent surging events reported.
Minimum equipment list
Experience Co’s minimum equipment list (MEL) specified permissible unserviceable items with which the aircraft was permitted to operate temporarily under the stated procedures, conditions and limitations. The MEL included that both the SRL computer system and TTL ‘may be inoperative provided inoperative SRL system procedures and limits are observed’. In that case, it was also required that an MEL placard be fitted adjacent to the TTL or SRL switch for the inoperative system/s. There was no MEL placard for the TTL nor was it listed as inoperative at the time of the accident.
Engine power loss checklist
The Texas Turbine Conversions AFM supplement provided checklists for engine failures, but not for partial engine power loss. The operator’s ‘Engine Power Loss’ checklist for the C208 with the Honeywell engine (Figure 3), required pilots to first control the aircraft by moving the elevator control forward to lower the aircraft’s nose if climbing. After completing initial checks, if the RPM was above 60% or the engine was surging, the pilot was to move the power lever to ½ inch (12.7 mm) forward of the flight idle position, in preparation for turning off the TTL, so as not to produce a transient exceedance of the EGT.
Figure 3: Engine power loss checklist
Source: Aircraft operator
Weight and balance
Aircraft moment arms
To enable calculation of the aircraft’s weight and balance, the C208 POH included a 2-place seating option, which divided the cabin into 7 zones (zones 0–6) (Figure 4). The flight manual supplement for the Texas Turbine Conversions STC did not include changes to the zones or seating configuration, therefore the POH applied.
Source: Cessna 208 Pilot’s Operating Handbook, annotated by the ATSB
Accident flight weight and balance
Prior to departure, a member of the parachuting operations team calculated the weight and balance for the proposed flight using the IBIS Technology flight planning module software (Table 1).[12] The moment arms from the POH were used for the calculations. Zone 6 was not used.
Table 1: Planned weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272.152
1,273.672
Zone 0 [1]
3,442
272
936.142
Zone 1
4,277
218
932.386
Zone 2
4,948
318
1,573.464
Zone 3
5,613
173
971.049
Zone 4
6,261
404
2,529.444
Zone 5
6,896
173
1,193.008
Total
3719.152
17,307.075
Centre of gravity
4,653
The operator’s weight and balance used the crew seat arm as the zone 0 arm.
The calculated weight and balance resulted in a take-off weight of approximately 3,719 kg and the aircraft’s centre of gravity located at 4,653 mm aft of the datum. To remain inside the operating limitations, the maximum allowable weight was 3,792 kg. Additionally, the aircraft needed to remain within the centre of gravity envelope, which had an aft limit of 4,680 mm and the forward limit varied with the operating weight. Each zone had a maximum allowable weight limit, and the maximum for zone 0 was 159 kg. However, the calculation software did not provide a warning to notify the user a zonal limit had been exceeded.
Information provided by the parachutists included the position they were seated at the time of the accident. Those positions did not match the original seating positions on the planned weight and balance sheet provided to the pilot prior to departure. The operator calculated a revised weight and balance based on the probable parachutist seating positions, which moved the aircraft’s centre of gravity 5 mm aft, although still within the allowable envelope (Table 2). It also showed that zone 0 was under the allowable weight limit.
Table 2: Revised weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272
1,272.960
Crew seat
3,442
92
316.664
Zone 0
3,472
80
277.760
Zone 1
4,277
349.4
1,494.384
Zone 2
4,948
271.4
1,342.887
Zone 3
5,613
334.4
1,876.987
Zone 4
6,261
197
1,233.417
Zone 5
6,896
233
1,606.768
Total
3,718.2
17,319.746
Centre of gravity
4,658
Aircraft basic empty weight
A weigh of VH‑UMV on 17 October 2017 identified that the aircraft’s basic empty weight was 1,889 kg in the single pilot seat configuration (Figure 5).
Figure 5: VH-UMV configuration on date of reweigh
The image meta-data showed the image was taken on 17 October 2017 – the reweigh date. Source: AeroWeigh.
The aircraft seating configuration at the time of the accident is shown in Figure 6.
Figure 6: VH-UMV cabin seating arrangement
Source: Aircraft operator, annotated by the ATSB
The basic empty weight of the aircraft did not include the flooring, or the 36 kg bench seating installed under engineering order ESE-C208-25-007. The engineering order provided the moment arms and weights shown in Table 3.
Table 3: ESE-C208-25-007 Parachute bench seating options – bench seat weight and arm
Item
Arm (mm)
Weight (kg)
Forward seat & backrest right-hand side only – option 2, without oxygen bottle mount.
3,556
7.82
Centre cabin bench seats both left-hand and right-hand sides (2 x 10.92 kg)
5,003
21.84
Aft bench seat right hand side only
6,553
6.36
Total of unaccounted weight for bench seating
36.02
Using the operator’s revised weight and balance calculation that reflected the likely positions of the parachutists, and the additional weight of the bench seating, the ATSB determined the probable take-off weight was 3,754 kg and the centre of gravity was 8 mm aft of the originally calculated centre of gravity (4,661 mm).
The operator subsequently weighed the aircraft’s jump mat, single point restraints, rubber matting, and portable oxygen tank. The total of these items was 30.2 kg, increasing the probable take-off weight to 3,784 kg.
Weight and balance implications
Regarding the importance of accurate weight and balance, the FAA Pilot’s handbook of aeronautical knowledge stated:
An overloaded aircraft may not be able to leave the ground, or if it does become airborne, it may exhibit unexpected and unusually poor flight characteristics.
Changes of fixed equipment have a major effect upon the weight of an aircraft. The installation of extra radios or instruments, as well as repairs or modifications, may also affect the weight of an aircraft.
Loading in a nose-heavy condition causes problems in controlling and raising the nose, especially during take-off and landing. Loading in a tail-heavy condition has a serious effect upon longitudinal stability and reduces the capability to recover from stalls and spins. Tail heavy loading also produces very light control forces, another undesirable characteristic. This makes it easy for the pilot to inadvertently overstress an aircraft.
Recorded data
The ATSB obtained OzRunways and third-party ADS-B recorded data for the accident flight. That data was compared with flight data for the flight conducted by the same pilot in the same aircraft on 17 October 2023, which was the day the pilot reported engine surging at about 5,000 ft. The comparison did not show significant performance difference from take-off to about 500 ft between the 2 flights.
Although the aircraft had an engineering order to fit GoPro cameras, they were not in place for the accident flight. The operator reported that these were only used during the creation of promotional footage and not during day-to-day operations. There was also no video footage from inside the aircraft, but the airport operator provided video footage from cameras located at the airport. One of those cameras recorded the accident flight footage (Figure 1) and provided audio for analysis.
The recorded audio included the aircraft noise and the nearby road and wind noise. The camera was stationary, therefore as the aircraft departed its sound signature reduced. Analysis of the audio conducted by Honeywell found that the engine RPM was approximately 99% throughout the take-off and initial climb. However, the engine noise was not discernible from the background sounds recorded at the time of the reported engine surge.
Site and aircraft examination
Site assessment
The ATSB did not attend the accident site, but the aircraft operator and Victoria Police attended shortly after the accident and provided the ATSB with photos of the aircraft and cockpit. A review of the images showed that the:
flaps were fully retracted
power lever was in the max reverse position
speed lever was in the minimum position
condition lever was in shutoff/feather position.
Those positions were consistent with the pilot’s reported actions to secure the engine after the impact. Additionally, one image appeared to show the TTL switch ON and the SRL switch OFF, indicating that the pilot may have inadvertently selected the SRL OFF instead of the TTL.
Engine and accessories assessment
The aircraft’s engine was recovered by the operator and sent to the Honeywell Investigation Laboratory in the US. On behalf of the ATSB, the US National Transportation Safety Board (NTSB) arranged independent oversight of the engine examination that was conducted between 3–5 January 2024.
Honeywell and the NTSB subsequently oversighted inspection and testing of removed components at various technical facilities. The Honeywell investigation report, provided to the ATSB and aircraft operator, detailed the observations and findings from the engine and associated component examinations, as follows.
The SRL and TTL were tested on 27 February 2024. Although some test points were not within the specified test tolerances, both units were found to be functional. However, further examination of the fuel bypass valve conducted by Woodward Inc. on 5 November 2024, resulted in a maximum bypass flow of 110 L/hour (194.5 lbs/hour), which exceeded the maximum flow test range of 68–74 L/hour (120–130 lbs/hour). At take-off power, a normal fuel flow was approximately 312 L/hour (550 lbs/hour). Therefore, if a bypass of 110 L/hour occurred during the accident flight with take‑off power set, the fuel flow would have reduced by about 35%.
Initial inspection of the fuel bypass valve’s outer casing revealed impact markings (Figure 7). When the protective cover plate was removed, the pole associated with the impact side was found in contact with the armature. When a 4.5 kg (10 lb) force was applied to each of the poles, there was no visible movement. The armature was cut away from the spade to determine if the armature screws were loose. The armature screws were found to be suitably tightened, and the armature was not bent.
The findings of the inspection showed the out‑of‑limit test results were due to impact damage resulting from the accident. As such, the higher fuel bypass identified in the test was not considered to be contributory.
Figure 7: Fuel bypass valve
Source: Woodward Inc, annotated by the ATSB
The fuel control unit (FCU) was examined and tested between 26–27 March 2024. The FCU tested values were either within specified ranges or marginally outside of tolerance limits for new or overhauled components. The test results may have been affected by procedures for adjusting an in-service FCU defined in the engine maintenance manual.
On 11 January 2024, a computed tomography scan of the propeller governor was conducted by Honeywell. Between 26–27 March 2024, the propeller governor was subject to functional testing by the manufacturer. While there were abnormalities identified with the magnetic pickup voltage and RPM maximum/minimum speeds, no contributing anomalies were noted. It was then disassembled, inspected and reassembled, followed by an additional functional test. The results from both functional tests were consistent with expected parameters of various operational modes.
The fuel pump was functionally tested on 2 May 2024, and found to be operating within specifications.
The Honeywell investigation found that the damage was indicative of an engine that was rotating and operating at the time of impact. It found no pre-existing condition that would have prevented normal operation.
Photos of the propeller were provided to Hartzell for analysis. As the propeller was of composite material, on impact it fractured into parts rather than deforming the propeller shape. From the limited fragments that were retrieved, Hartzell concluded the blades were likely rotating under low power at the time of the accident.
The ATSB considered whether the pilot had moved the power lever to beta range, reversing the propeller, but Hartzell found it likely that the propeller was forced to a low pitch angle during the initial impact.
Carriage of parachutists
Cabin configuration
The aircraft was configured for skydiving such that:
the cargo door was replaced with a vertical sliding door (made of nylon, polycarbonate and aluminium)
the passenger seats and lap belts were removed
bench seating and 17 single point restraints were installed.
The restraints attached to the parachute harness and parachutists could be seated either on the bench seating or floor, facing toward the aft of the aircraft.
The associated flight manual supplements for the parachute configuration were:
cargo doors removed kit
in-flight openable cargo door
in-flight opening of doors
oxygen system
skydiving jump light
external mounted GoPro cameras.
Aircraft modifications
Classification of design changes
CASA stipulated regulations for modification of an aircraft from the original manufacturer specifications. CASA Advisory Circular (AC) 21-12 Classification of design changes provided different processes for modifying aircraft, depending on the type of change being made. These changes were classified as either major or minor.
A minor modification was anything that was not considered to be a major modification and could be completed by a CASA-authorised person under CASR Part 21.M. Any modification with a significant effect on airworthiness – structural, weight and balance, systems, operational or other characteristics, were classified as major. Additionally, any alteration to the type certificate datasheet was classified as a major change.
A major modification was further classified into a substantial change or a significant change. A significant change required a supplemental type certificate application to be completed with CASA’s involvement. A substantial change required a new type certificate application, which also involved CASA. The AC provided the following example of a significant change to a small aircraft:
Changes in types and number of emergency exits or an increase in maximum certificated passenger capacity.
The notes associated with that example were:
Emergency egress certification specifications exceed those previously substantiated. Invalidates assumptions of certification.
CASA advised that the modifications would be considered a major change if the number of persons was increased above that permitted by the aircraft type certificate data sheet. This was consistent with the US FAA Advisory Circular 105-2E – Sport Parachuting, which included:
The approved number of skydivers that each aircraft can carry for parachute operations will most commonly be found on FAA Form 337, Major Repair and Alteration (Airframe, Powerplant, Propeller, or Appliance), used for field approvals, or an aircraft Supplemental Type Certificate (STC).
In its submission to the draft report, CASA advised that it considered that the legal basis for conducting parachuting flights with a greater number of passengers than the TCDS specified may be met if the aircraft was modified appropriately by a suitably authorised person and there was an associated aircraft flight manual supplement.
In determining whether the parachuting configuration modification was major or minor, the CASA‑authorised design engineer assessed that it was minor as it had no significant effect on:
structure
cabin safety
flight
performance or function of:
systems
propellers
engines or powerplant installation
environment.
The engineer also assessed that the design did not:
alter airworthiness or operating limitations
require an adjustment of the type-certification basis
Technical assessment of modifications
Aircraft modifications must meet the airworthiness requirements of the aircraft’s certification basis. According to the type certificate data sheet, VH-UMV was certified under FAR 23 amendments 23-1 through 23-28. Modifications were required to comply with standards from that or subsequent amendments. Technical assessments of the modifications detailed in the engineering orders nominated FAR 23 amendment 62 as the certification basis for the parachuting configuration modifications, including the roller door, bench seating and oxygen system.
The technical assessments included a design compliance matrix, with the following key comments by the design engineer of relevance.
Weight and balance
The engineering order was to include that:
It is the operator’s responsibility to accurately update the aircraft’s load data sheet to reflect the quantity and positioning of oxygen bottles as this may vary dependant on the number of parachutists on a given high altitude drop.
Structure
Standard aircraft hardware is used to secure items of mass installed as part of the parachute fit out modifications. This modification does not alter or effect the strength of the aircraft structure to support all normal aircraft loads. All materials & fasteners used as part of this design package have been selected to have adequate structural properties for their intended use.
Flight loads
The document package includes instructions to ensure the Cessna standard Flight Manual Supplement for operations with the cargo door open/removed is in the Flight Manual.
Oxygen
The engineer assessed the oxygen requirements for conducting flights above 14,000 ft in an unpressurised aircraft, stating:
…The operators (max) occupant capacity for the 208 & 208B model aircraft is x16 & x20 occupants respectively. As such these aircraft must be fitted with a minimum of 2x oxygen dispensing face masks if more than x15 occupants are carried…
Emergency landing conditions
Engineers assessed that the oxygen cylinder restraints were adequate in all load cases. They also rated the seats to at least 170 lb (77 kg) as required by FAR 23.785.
Regarding the installation of the oxygen bottle the engineers provided the following:
…the seat base and surrounding structure is adequate to support the small increase in weight due to the installation…there is no risk of the installation coming loose and inflicting serious injury on the cabin occupants.
Control systems
The design package included instructions for the removal of the copilot control wheel and column in accordance with the aircraft maintenance manual, to configure the aircraft for parachuting operations. There was no change to the design or functionality of the pilot's primary flight controls.
Doors
The number and arrangement of doors was not altered by the modifications. Regarding ‘vibration and buffeting’, the parachute door had a proven service history, with no reported issues since the design was originally implemented in June 2012. Further, the roller-style parachute door was commonly installed on parachuting aircraft and Cessna had an approved roll-up door as part of the production standard design.
Operation of the roller door was ‘simple and obvious’, easily operable from inside and outside the aircraft. The door was held in place by gravity and friction and could not be accidentally opened. Decals specific to the operation of the parachute roller door were installed.
Seats and restraints
The single point restraints for the parachutists were previously approved for use by ‘Air Safety Solutions’.
The aircraft certification did not require dynamic testing of the seats and, although the bench seating was not tested, the design engineer referenced FAA AC 105-2E Sport parachuting, which stated:
1. Straddle benches can offer more occupant crash protection than floor seating since they can be designed to provide significant vertical energy absorption.
Emergency exits
For reference, FAR 23.807 required:
In addition to the passenger-entry door, for an airplane with a total passenger seating capacity of 16 through 19, three emergency exits, as defined in paragraph (b) of this section, are required with one on the same side as the passenger entry door and two on the side opposite the door.
(b) Emergency exits must be movable windows, panels, canopies, or external doors, openable from both inside and outside the airplane, that provide a clear and unobstructed opening large enough to admit a 19-by-26-inch ellipse. Auxiliary locking devices used to secure the airplane must be designed to be overridden by the normal internal opening means. The inside handles of emergency exits that open onward must be adequately protected against inadvertent operation. In addition each emergency exit must:
• be readily accessible, requiring no exceptional agility to be used in emergencies;
• have a method of opening that is simple and obvious;
• be arranged and marked for easy location and operation, even in darkness;
• have reasonable provision against jamming by fuselage deformation; …
(c) The proper functioning of each emergency exit must be shown by tests
The design engineer commented that there was no change to the number of emergency exits and that the ‘steps, handles, bench seats etc. installed for this modification met the requirements for egress in an emergency as specified by this regulation’. Additionally, as there was no change to the door functionality or positioning, no additional emergency testing was required.
The unmodified rear right passenger door met the requirements of the regulation in that a 19" x 26" (48 x 66 cm) ellipse may be passed through the door un-obstructed. However, the rear right bench seat extended across the door at a height of 10” (25.4 cm). The design engineer commented that access to the door handles/operation and decals was not obstructed, and no exceptional agility was required to exit through that door in an emergency.
The roller door was also required to meet the emergency exit criteria, including ‘reasonable provisions against jamming by fuselage deformation’, and that ‘proper functioning of each emergency exit must be shown by tests’. However, this was not documented.
The parachuting configuration detailed in the engineering orders enabled seating and single-point restraints for 17 parachutists, in addition to the fitted pilot seat and 5-point restraint. The design engineer had not intended to explicitly increase the seating capacity above the 11 specified in the TCDS, as the number of parachutists that could be carried was an operational consideration. The design engineer provided comment on a technical assessment provided to CASA in 2017 regarding maximum passenger seating configuration, that the aircraft operator’s understanding was:
it is the pilots [sic] responsibility to ensure the aircraft is loaded within the weight and balance and centre of gravity limitations of the aircraft at all times. From these calculations the maximum safe number of parachutists to carry on the Cessna 208 Caravan is 17...
Regulatory requirements
Part 105 of the CASR came into effect in December 2021 and set out the operational requirements for aircraft used to facilitate parachute descents. Civil Aviation Order (CAO) 20.16.3 paragraph 15 Carriage of parachutists was in force at the time of the accident, and the following regulations were relevant to the aircraft parachuting configuration:
CASR 91.200 Persons not to be carried in certain parts of aircraft permitted a person to be carried in ‘a part of the aircraft that is not designed to carry crew members or passengers’, if the aircraft was being operated for a parachute descent and met the Part 105 MOS.
CAO 20.16.3 required parachutists to wear a seatbelt, shoulder harness or approved single point restraint (except when about to jump). Similarly, CASR Part 105 section 105.105 required parachutists who were not flight crew to be provided with a seatbelt, shoulder harness or approved single-point or dual-point restraint.
The Part 105 Manual of Standards (MOS) came into effect on 2 December 2023, 44 days after the accident, and specified requirements in greater technical detail. CASA advised that the Part 91 Manual of Standards will be amended to remove ambiguity about approved passenger restraints being permitted in lieu of seatbelts.
Maximum passenger seating configuration
In drafting CASR Part 105, the number of parachutists that could be carried was a significant point of discussion between CASA and the parachuting industry.
In 2006, CASA proposed Civil Aviation Safety Regulation 105.140 paragraph 3.5.20 which stated:
Proposed CASR Part 105 seeks to provide clarity to the parachuting industry that operating a parachuting aircraft with more parachutists than the normal published aircraft seating capacity in passenger-carrying operations is acceptable, provided weight and balance and other manufacturer’s limitations for the aircraft are observed.
A subsequent notice of proposed rulemaking indicated that the following may be included in the proposed CASR Part 105.140 – Number of parachutists in aircraft:
(1) A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and…
When the above proposed rule was not incorporated into draft CASR Part 105 or MOS, as detailed in meeting minutes of the technical working group that reviewed the 30 August 2022 draft Part 105 MOS, they proposed to meet with CASA’s Airworthiness and Engineering Branch to discuss:
possible options for parachuting aircraft to operate with seats removed, to carry more passengers than currently permitted by the aircraft’s type certificate or flight manual and regulatory support mechanisms for modifications (doors, handles etc.) that support safe parachuting operations.
The ATSB was unable to determine whether this discussion took place, however no related changes were incorporated into the regulations or MOS, noting that the MOS had not come into effect at the time of the accident.
In response to the ATSB’s request for clarification of CASA’s expectation for the number of parachutists that could be carried, CASA advised that:
The legal basis for conducting parachuting flights with a greater number of passengers than the TCDS is met where the aircraft has been modified appropriately by a suitably authorised person and the aircraft’s flight manual has been modified accordingly.
CASA has been aware for multiple decades that parachuting aircraft were carrying a maximum number of passengers greater than the TCDS maximum number of dedicated passengers.
CASA understood that the increase in passenger capacity for parachuting aircraft was achieved by operators through legitimate aircraft modification processes that removed the normal passenger seats and modified the aircraft for parachute‑specific operations.
CASA did not identify any immediate safety of flight issues.
In its submission to the draft report, CASA advised that it was ‘considering the issue of a legislative instrument to remove any doubt that an approved aircraft modification which replaces normal seating with appropriate alternative seating and restraint arrangements is explicitly permitted’.
Supplemental type certificate application
In April 2017, the design engineer applied to CASA on behalf of the aircraft operator for a supplemental type certificate based on the engineering order for the addition of bench seating. The STC application submitted to CASA included details and images of aircraft that already had modifications completed under an engineering order and did not include an increase in the seating capacity.
After several communications and iterations of the documents provided, in August 2017, CASA highlighted 2 areas directly related to safety of parachutists: the rear exit crashworthiness and the increase of maximum passenger capacity to 17.
In July 2020, the STC application was withdrawn by the applicant.
Other parachuting configuration supplemental type certificates
Cessna 182 models E to R
In 1996, CASA issued STC-214 to the APF. The STC background explained the application was the result of a CASA ramp check, which identified that there were 6 persons on board without single point restraints while conducting parachute operations, where the TCDS stated it was a 4‑seat aircraft.
The STC assessed the floor loading capacity of the aircraft to carry 6 persons (including the pilot) for the purpose of parachute operations. It concluded:
The floor was analysed and substantiated for parachutist loads. The hard points for the approved single point restraints were determined, analysed and substantiated for parachute loads... The aircraft loading is such that no special loading system needs to be devised as the aircraft will always be within the approved centre of gravity range.
The original C182 TCDS 3A13 showed ‘No. of seats 4’.
The amended TCDS for the STC showed ‘No. of seats 1, Parachutist 5’.
Cessna 208, 208B
In 2018, the US FAA issued supplemental type certificate SA04352CH, which incorporated many similar modifications made to model 208 and 208B aircraft certified under A37CE. The modifications included the installation of:
wind deflector
benches
external assist handle
internal assist handle
jump exit control light
external step
wind block (sliding parachute door).
The STC limitations and conditions included:
(3) This modification does not install Title 14 [US Code of Federal Regulations] CFR part 23 compliant seating and is therefore zero occupancy.
(4) The left and right hand benches are compliant as monuments and are not certified to carry any items of mass. Testing performed during certification would be sufficient for gust loading or seven evenly distributed masses of 215 pounds (97.5 kg) each…
Australian Parachute Federation
The APF is the peak body for the administration and representation of Australian Sport Parachuting. With the approval of the Civil Aviation Safety Authority, the APF:
applies the standards of operation
conducts competitions
issues parachuting licences, certifications and instructor ratings
conducts exams
distributes publications to keep its members informed of events and safety standards.
The APF organisation had over 55 group members also known as member organisations, 3,000 licenced members, and engaged with the operators of nearly 100 aircraft conducting parachute operations. As detailed above, the APF held an STC for parachuting operations in Cessna 182 models E through R for parachuting 6‑person operations. The associated supplemental type certificate data sheet amended the aircraft configuration to 1 seat and 5 parachutists from the 4‑seat configuration stated on the type certificate data sheet.
Aircraft operators that conducted parachuting operations as a member of the APF did so in accordance with the APF regulations. This included adhering to the APF Jump Pilot Manual. The Jump Pilot Manual Version 01-2023, in force at the time of the accident, stated:
5.3.3 Loading – Balance/C of G
A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and
(b) any other limitations related to the provision of:
(i) adequate structural support for restraint of occupants; or
(ii) supplemental oxygen for the flight.
For paragraph 5.3.3 (b), the limitations do not include those that are solely related to the number of seats or seating positions that are, or are normally, fitted in the aircraft.
If an aircraft does not have a flight manual, then any information supplied by the manufacturer that relates to the matters mentioned above or is included in the aircraft’s airworthiness certificate, is taken to be the flight manual.
Balance must be a consideration for all aircraft involved in parachuting operations and can be especially critical during climb-out and exit, when changes occur. Know the operational limitations of your aircraft!
Under the Loadmaster’s supervision, the parachutists will normally load the aircraft in the reverse order of the exit.
The Jump Pilot Manual was accepted by CASA and CASA personnel reported having reviewed the manual. Regarding the wording that a parachuting aircraft could carry more occupants than the maximum specified in the AFM, CASA reported that they understood that only applied to Cessna 182 models E through R, for which the APF held a supplemental type certificate that permitted the carriage of 6 persons. CASA personnel also reported that the manual wording was ‘never intended to serve as a quasi-engineering approval’.
At the time of writing, CASA and the APF were engaged in ongoing discussions, including the carriage of occupants in excess of the number detailed in the TCDS without the necessary modification approvals.
Survivability
Passenger briefing requirements
The CASA Multi-Part Advisory Circular – Passenger safety information, stated:
2.1.1 In addition to certification standards for the crashworthiness of the aircraft and cabin crew evacuation procedures, well-informed and knowledgeable passengers contribute to survivability in an aircraft accident or incident. There are multiple factors that affect survivability. Physical factors include adopting the correct brace position for impact, the correct use of seatbelts, as well as the location and operation of all emergency exits.
2.1.2 Accident investigations have shown that survival rates are improved when passengers are provided with accurate and effective information about the correct use of equipment such as seatbelts, and the actions they should take in a life-threatening situation such as how to adopt the brace position.
A pilot in command was in contravention of regulation 91.565 if an aircraft commenced a flight and the passengers had not been given a safety briefing and instructions as prescribed by the Part 91 MOS, unless:
(a)the passenger has been previously carried on the aircraft; and
(b)the passenger has previously been given a safety briefing and instructions in accordance with this regulation; and
(c)in the circumstances it is not reasonably necessary to give the same safety briefing and instructions.
The CASR Part 91 MOS provided a list of items that must be covered in a passenger safety briefing and instructions before an aircraft takes off for a flight. Relevant to this occurrence, the list included:
(c) when seatbelts must be worn during the flight, and how to use them;
(f) how and when to adopt the brace position;
(g) where the emergency exits are, and how to use them;
(s) for a flight of a jump aircraft — the physical location(s) within, or on, the aircraft that the passenger must occupy during the flight in order to ensure the aircraft is operated within the aircraft’s weight and balance limits during the flight.
Operator’s safety briefing
The aircraft operator had 2 videos, one of which was shown to parachutists depending on whether they were conducting a tandem jump or a sport jump. The sport jump video was specific to the Barwon Heads operation and included:
aircraft climb performance
17 single point restraints, which were to be worn up to 2,000 ft
sport jumpers were to listen to the pilot in command in the event of an emergency
location of the door securing clip (but not instructions for use).
The video shown to tandem jump parachutists provided specific aircraft safety information including:
how to approach the aircraft
the use of single point restraints
the location of fire extinguishers
how to brace
how to egress
the requirement not to smoke
the use of life jackets where required.
For the accident flight, the pilot reported that they did not provide a safety briefing, and multiple parachutists reported not having received a safety briefing prior to flight. There was no procedure in the operations manual that waived the pilot’s responsibility to provide parachutists with a safety briefing. The pilot reported that they understood that the drop zone safety officer ensured everyone was briefed on emergency situations before jumping and a video briefing was provided to tandem parachutists.
The operations manual provided the following guidance for providing a safety briefing during an emergency landing with parachutists on board:
It will be the Load Masters responsibility to assist the pilot in ensuring;
1. Parachutists are briefed on and instructed to assume the BRACE position prior to touchdown.
2. Emergency Exits are opened and secured (where possible) prior to touch down.
3. Single point restraints are utilised by all occupants.
The aircraft also had a sign on the rear wall of the internal cabin, detailing the in-flight emergency plan (Figure 8). The sign stated that single point restraints were required as directed by the pilot and at all times below 1,500 ft, differing from the 2,000 ft stipulated in the sport jump video.
The APF Jump Pilot Manual required that restraints were utilised by all occupants below 1,000 ft, or as directed by the pilot.
Figure 8: In-flight emergency plan
Source: Victoria Police and the aircraft operator
Parachutist preparedness
After the accident, in response to an ATSB survey, parachutists reported a lack of awareness of how to brace and the location of emergency exits that were available if the main roller door became damaged and unavailable for use in an evacuation. On this occasion the clip that secured the roller door in the open position was not used, which resulted in it closing on impact. Fortunately, the parachutists were still able to successfully evacuate the aircraft via that door. As detailed further below, several of the parachutists also reported that their restraints were not taut prior to the ground collision.
Some parachutists recalled receiving aircraft-specific emergency information during their initial parachuting training. However, in some cases, several years had passed without receiving a refresher. Furthermore, some had conducted their initial training on different aircraft types.
Injuries and seating positions
The pilot wore a 5-point restraint, and the 16 parachutists each had a single-point restraint attached to their parachute. The probable seating arrangement at the time of the accident was determined based on the recollections of parachutists who responded to ATSB’s request for information (Figure 9). There were 4 parachutists seated on the floor, 4 on the left bench seat and 8 on the right bench seat. The parachutists were facing aft and those on the bench seats were seated between each other’s legs.
Injury information was obtained for the pilot and 14 of the 16 parachutists, with the other 2 assumed to have no injuries (Table 4). The injury mechanisms included deceleration, flail and impact with the aircraft or other occupants.
Figure 9: Seating positions
The seating positions in the image are referenced in Table 4: Injuries sustained. Source: Texas Turbines Cessna 208 pilot operating handbook, annotated by the ATSB
Table 4: Injuries sustained
Image reference
Injuries sustained
ATSB injury classification
Survivability Comments
A. (Pilot)
Cut on forehead, bruising, whiplash, bruised sternum, and difficulty talking/breathing
Minor
5-point safety harness; likely impact with control column/dash
B.
Pulmonary contusion, fifth and sixth rib fractures, psychological trauma, and lower back pain
Serious
Slipped off the end of the bench seat and ended up squashed against the ladder or back of the pilot seat due to a loose restraint
C.
No reported injuries
No injuries
D.
Tears to both rotator cuffs, tear to sternocleidomastoid muscle, and nerve damage to left arm and shoulder
Serious
E.
Broken ribs and internal bleeding to the chest.
Serious
Loose restraint
F.
Whiplash, fractured L4 transverse process, and nerve pain in right shoulder and leg
Serious
Loose restraint, seated on floor; adjacent end of bench seat
G.
Whiplash, bruising, and headaches
Minor
Seated on floor
H. (Loadmaster)
Cut injury to right leg requiring stitches, and sore back
Minor
I.
Strained back, cuts, and bruising
Minor
J.
Whiplash, cuts, and bruising
Minor
Loose restraint
K.
Whiplash, cuts, and bruising
Minor
Loose restraint
L.
Cuts to head, face, internal chest cuts, and bruising
Minor
Tight restraint
M.
Broken tailbone, bruising
Serious
Tight restraint
N.
Concussion, and bruising
Minor
O.
Swollen knee, bruised kidney, bruised vertebrae, and strained neck ligaments
Minor
Loose restraint
P.
Internal abdomen bleeding, Internal hematoma inner right leg, cuts, bruising, whiplash, and back pain.
Serious
Loose restraint; inappropriate structures around/in front
Q.
No reported injuries
No injuries
The single point restraints could not be adjusted, but an occupant could potentially position themselves such that the restraint was taut. Nine parachutists provided information about the tightness of their restraint; 7 reported their restraints were loose and 2 reported tight restraints. Of those with loose restraints, 3 sustained minor injuries and 4 sustained serious injuries. Of the 2 parachutists who reported having tight restraints, one sustained minor injuries and the other sustained serious injuries.
Of the 4 parachutists seated on the floor, 2 sustained serious injuries, one sustained minor injuries, and another was reported to have been uninjured. The other serious injuries were sustained by 2 parachutists on the left bench seat and one on the right bench seat.
The parachutist who sustained the most injuries of the highest severity was at the front of the left bench seat. As that bench seat did not have a seatback, the parachutist came off the forward end of the bench between the bench and pilot seat and contacted the back of the pilot’s seat and/or ladder adjacent to the seat. The injuries were likely also increased by the mass of the 3 other parachutists on that bench moving forward during the impact sequence.
The ATSB compared the injuries sustained by the pilot and parachutists of VH-UMV with those involved in 2 survivable accidents involving C208 aircraft, assessed as likely to have been subjected to similar impact forces (AO-2016-007 and AO-2024-001). In the 2 comparative accidents, some of the occupants sustained minor injuries while others were uninjured. The pilot and front seat passengers had 5-point restraints, and in the 2016 accident the other passengers wore lap belts. In the more recent accident, the other passengers wore 3-point restraints.
ATSB investigation AO-2014-053 found that single point restraints were less effective than dual restraints in mitigating injury for parachutists. This was consistent with the US FAA’s technical report – Evaluation of Improved Restraint Systems for Sport Parachutists, which found that dual straps attached to the parachute harness provided better restraint and produced less flailing and bending of the body than single point restraints (FAA 1988). The following loading of aft‑facing passengers was found to increase restraint effectiveness:
• the person most forward in the cabin should be leaning against a bulkhead or other substantial support to limit flailing and head impact.
• each parachutist’s restraint should be anchored to the floor aft of his/her pelvis (relative the aircraft’s orientation) at a point on the floor near the middle of the thigh. The restraint should be taut to reduce forward motion, and the loads transmitted to the person behind.
• the proper brace for impact position would be to lean toward the front of the aircraft onto the person or bulkhead behind them.
The US FAA AC 105-2E Sport parachuting also stated that single point restraints were ‘not very effective’, and that dual point restraints offered ‘superior restraint’.
The ATSB assessed that the increase in number and severity of injuries of the parachutists compared to passengers seated and restrained in seats, was probably a result of single-point restraints being less effective and less cushioning due to being seated on the floor or bench.
Related occurrences
National Transportation Safety Board Special investigation report
The US National Transportation Safety Board (NTSB), Special investigation report on the safety of parachute jump operations (2008), found that between 1980 and 2008 in the US, 32 accidents involving parachute aircraft resulted in fatal injuries of 172 people, most of whom were parachutists. Acknowledging risks associated with parachuting, the report stated:
Although parachutists, in general, may accept risks associated with their sport, these risks should not include exposure to the types of highly preventable hazards that were identified in these accidents and that the parachutists can do little or nothing to control. Passengers on parachute operations aircraft should be able to expect a reasonable level of safety that includes, at a minimum, an airworthy airplane, an adequately trained pilot, and adequate Federal oversight and surveillance to ensure the safety of the operation.
Of the 32 accidents, 8 involved exceedances of the aircraft’s weight and balance, and 21 resulted from inadequate airspeed or stall situations, and in 6 accidents, both were factors. There was one accident involving a Cessna 208, which resulted in 17 fatalities.
The report also acknowledged that parachuting is typically a revenue operation where a participant pays for a jump and receives the flight as part of that service, it stated:
Most parachute operations flights are operated under the provisions of 14 Code of Federal Regulations (CFR) Part 91 and are typically revenue operations; parachute jump operators provide the flights as part of their services to parachutists who pay to go skydiving, or parachutists pay dues for membership in parachuting clubs. The risks of parachuting are generally perceived to involve the acts of jumping from the aircraft, deploying the parachute, and landing; parachutists are aware of and manage these risks. However, a review of accident reports reveals that traveling on parachute operations flights can also present risks.
The report highlighted the potential for paying participants to be unaware of the risks they were accepting when they boarded a parachute aircraft.
The report identified the following recurring safety issues:
• inadequate aircraft inspection and maintenance;
• pilot performance deficiencies in basic airmanship tasks, such as preflight inspections, weight and balance calculations, and emergency and recovery procedures; and
• inadequate FAA oversight and direct surveillance of parachute operations.
Recent accidents
The following 3 more recent accidents involved aircraft conducting parachuting operations and resulted in injuries to the occupants.
Loss of engine power after take-off involving Cessna 208B, PH-FST, West of International Airport Teuge, Netherlands, on 25 June 2021 (2021062)
On 25 June 2021 at 0932 local time, a Cessna 208B with a pilot and 17 parachutists on board departed from International Airport Teuge. During the initial climb, the aircraft suddenly lost engine power after which the pilot made an emergency landing in a field close to a motorway. The aircraft was substantially damaged, and one parachutist sustained minor injuries.
Accident involving GA8-TC-320 Airvan, SE-MES, Storsandskär, Västerbotten, Sweden, on 14 July 2019 (RL 2020:08e).
The purpose of the flight was to drop 8 parachutists from an altitude of 13,000 ft. On the drop run, the pilot lost control of the aircraft. The parachutists were unable to evacuate the aircraft resulting in fatalities of the 9 persons on board.
The investigation found that control of the aeroplane was probably lost due to low airspeed. Other contributing factors were that the aeroplane was unstable as a result of a tail-heavy loading, weather conditions, and a high workload in relation to the pilot’s knowledge and experience.
Loss of control involving Cessna U206G, VH-FRT, Caboolture Airfield, Queensland, on 22 March 2014 (AO-2014-053)
On 22 March 2014, a Cessna U206G aircraft was being used for tandem parachuting operations at Caboolture Airfield, Queensland. At about 1124 local time, the aircraft took off from runway 06 with the pilot, 2 parachuting instructors and 2 tandem parachutists on board. Shortly after take-off, witnesses at the airfield observed the aircraft climb to about 200 ft above ground level before it commenced a roll to the left. The left roll steepened, and the aircraft then adopted a nose‑down attitude until impacting the ground in an almost vertical, left-wing low attitude. All the occupants on board were fatally injured. A post-impact, fuel-fed fire destroyed the aircraft.
The ATSB identified that the aircraft aerodynamically stalled at a height from which it was too low to recover control prior to collision with terrain. The reason for the aerodynamic stall was unable to be determined. Extensive fire damage prevented examination and testing of most of the aircraft components. Consequently, a mechanical defect could not be ruled out as a contributor to the accident.
A number of safety issues were also identified by the ATSB. These included findings associated with occupant restraint, modification of parachuting aircraft and the regulatory classification of parachuting operations.
Safety analysis
Introduction
On the morning of 20 October 2023, the pilot of a Cessna 208, registered VH-UMV, commenced take-off for a planned climb to 15,000 ft to drop 16 parachutists. Passing about 500 ft on climb, the pilot detected a partial power loss, consistent with an abnormal activation of the torque and temperature limiter (TTL). The pilot reduced the power to prevent the engine surging, but the combination of low power and airspeed resulted in the aircraft colliding with water before continuing into a field.
Six of the parachutists sustained serious injuries and the pilot and 8 parachutists sustained minor injuries. The aircraft was substantially damaged.
This analysis will discuss the TTL activation and response actions. The aircraft’s seating configuration, weight and balance and occupant safety will also be examined. Additionally, the analysis will consider the number of parachutists on board, and operational guidance from the Australian Parachute Federation manual approved by the Civil Aviation Safety Authority (CASA).
Operator’s prescribed actions
Normal operation of the TTL permitted reduction in the fuel flow to the engine to maintain the lower of 100% torque or 650 °C nominal exhaust gas temperature (EGT). However, the TTL manufacturer advised that the limiter was capable of restricting fuel flow sufficiently to reduce the maximum power to about 62% torque. A noticeable power reduction, followed quickly by a power increase, had been reported by the operator’s pilots as engine surging events associated with the TTL. However, maintenance actions had been unable to identify or resolve the cause of 6 reported engine surging events in VH-UMV over a 5‑month period.
Unable to resolve the intermittent excessive TTL response, the aircraft operator had advised pilots to limit torque to 95% and EGT to 640°C to prevent TTL activation. Although well intentioned, that was contrary to the aircraft flight manual supplement, which defined take-off power as 100% RPM and 100% torque or 650°C EGT, whichever was reached first. The operator had not assessed the TTL and single red line (SRL) systems as inoperable, which would have required pilots to manually ensure torque and temperature limits were not exceeded. Power reductions resulting from TTL activations were reported to be momentary and power returned to the previous level after the torque or EGT limit reduced below the limit.
Additionally, in the absence of an aircraft manufacturer’s checklist for partial power loss, the operator had created an engine power loss checklist. The first item was to immediately move the elevator control forward if climbing to prevent airspeed decay. After other initial actions, the checklist then instructed pilots to significantly reduce power if the engine RPM was above 60% or surging, in preparation for switching off the TTL. While that was intended to ensure engine limits would not be exceeded when the pilot subsequently reintroduced power, the operator did not specify a minimum height at which it was appropriate for a power reduction to be made.
Such a significant power reduction close to the ground increased the risk of a loss of control and/or ground collision.
Contributing factor
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Pilot actions
At the commencement of the take-off roll, in accordance with normal and the manufacturer’s procedures, the pilot reported applying full power – initially reaching 100% torque for take-off, before reducing power slightly in an attempt to remain under the operator‑specific torque limit of 95%. Whether the torque or temperature limit were reached during the initial climb could not be determined as these parameters were not recorded. However, the pilot detected a power reduction consistent with an abnormal TTL activation.
As shown by previous safety reports, in the event of TTL activation, the maximum power available may have been approximately 62%. Such a significant power reduction would have required the pilot to lower the aircraft’s nose attitude to prevent an aerodynamic stall, consistent with the operator’s engine power loss checklist.
However, the pilot did not initially lower the aircraft’s nose, instead they moved the power lever aft, reducing the power setting. This was in accordance with the operator’s procedure in preparation for switching off the TTL. Although the as‑found switch positions indicated that the pilot may have inadvertently selected the SRL switch instead of the TTL, in either event the TTL would have been deactivated. However, as the pilot had not lowered the aircraft’s nose, the aircraft approached an aerodynamic stall, and the stall warning horn sounded.
In response, the pilot lowered the aircraft’s nose and, due to the low height above terrain, low airspeed and low power, searched for a suitable field for landing. Although the pilot only reported reducing the power slightly, as the post-accident inspections found the engine was capable of producing normal power, and there were no pre-existing conditions that would have prevented normal operation, the low power was likely a result of the pilot reducing power to a level insufficient to maintain height in the climb attitude, and not restoring it.
At the low height above the ground at which the power loss occurred, the above factors led to the collision with water.
Contributing factor
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Weight and balance
The aircraft had all the aircraft’s certified seating removed other than the pilot’s seat, following which the aircraft was weighed, and a basic empty weight established. However, that weight did not include the bench seating, parachute restraints, floor matting or oxygen bottles which were fitted to the aircraft at the time of the accident. Although the weight and moment arm of the bench seating had been provided with the engineering order, it was not accounted for in the IBIS Technologies weight and balance calculation software used by the operator.
As a result, the bench seating and other aircraft fixtures were not accounted for in the accident flight weight and balance calculation. Additionally, parachutists did not sit in the positions used for the weight and balance calculations for the accident flight. Therefore, the calculated weight and balance was inaccurate.
Although the operator’s post-accident calculations found that the aircraft was almost certainly operating within the weight and balance limitations throughout the flight, an accurate weight and balance assessment prior to take-off to ensure the flight will operate below the maximum take-off weight is essential for the structural integrity of the aircraft. Operating outside the centre of gravity limits increases the risk of a loss of control. Exceeding weight and balance limitations has previously resulted in fatal accidents involving aircraft conducting parachute operations.
Other factor that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
IBIS Technologies flight planning module
When conducting post-accident weight and balance calculations using the operator’s IBIS Technologies flight planning module, the ATSB identified that, while warnings were provided when the aircraft was outside the overall weight or centre of gravity limit, there was no warning when the weight for a zone within the cabin exceeded the limit. This increased the likelihood of an aircraft being loaded contrary to zone limitations.
The lack of an alert did not contribute to this accident and, as noted above, the aircraft was not loaded in accordance with the planned overall or zonal distributions. However, the software used to calculate the aircraft weight and balance was used by many operators and overloading a zone limit could result in damage to the aircraft.
Other factor that increased risk
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Safety briefings
To maximise survivability in the event of an emergency, pilots are required to ensure aircraft occupants receive a safety briefing and instructions including in the correct use of restraints, emergency exits and adopting the brace position. However, a pilot is not required to brief passengers on every flight, if they have previously been on the aircraft and are likely to be familiar with safety information.
The pilot understood that this responsibility had been delegated to the drop zone officer and that the parachutists had received the required safety briefing and information. However, there was no record of which parachutists had been briefed or when. Additionally, as none of the parachutists on board were tandem jump parachutists, they were unlikely to have viewed the operator’s video that included use of single point restraints, how to brace or exit the aircraft in the event of an emergency.
Although some of the parachutists on board had previously received a safety briefing, it had not necessarily been in the accident aircraft type or recently. Additionally, an ‘in-flight emergency plan’ printed on the rear of the cabin advised parachutists to remain seated with single point restraints attached and brace for an emergency landing when below 500 ft, but did not specify how to brace or exit the aircraft. As a result, some of the occupants were unaware of essential safety information regarding brace position and emergency exits.
Although the aircraft’s roller door closed on impact and water entered the cabin, all 17 occupants evacuated with no difficulties reported. The ATSB was unable to determine whether the absence of a safety briefing increased the severity of the injuries sustained by parachutists. However, adopting the correct brace position for impact, the correct use of restraints, and knowledge of the location and operation of all emergency exits, are factors demonstrated to increase survivability.
Other factor that increased risk
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Seating configuration
The operator routinely conducted parachuting operations in Cessna 208 aircraft with the pilot and up to 17 parachutists on board. This was based on the CASA-accepted Australian Parachute Federation Jump Pilot Manual, which stated that the aircraft could carry as many parachutists as there were restraints and provided the aircraft was operated within the weight and balance limitations.
The aircraft’s cabin was configured with a roller door, oxygen system, bench seating and single‑point restraints for parachuting operations under an engineering order by a CASA‑authorised person. Although the configuration nominally provided restraints and seating (including on the floor) for up to 17 parachutists, this was not formally documented in the aircraft flight manual or a supplement. The engineer also assessed and modified the aircraft to supply oxygen for 16 occupants to meet the operator’s requirements of their intended operation.
CASA assessed that increasing the number of persons carried above that stated on the type certificate data sheet (TCDS) required a supplemental type certificate (STC) as it was a major modification. In this case the TCDS stated that the aircraft had a maximum seating capacity of 11, but the aircraft was modified to supply oxygen for an intended 16 occupants. As such, the CASA‑authorised engineer incorrectly assessed that the modifications they were approving were minor and conducted them under engineering orders. The ATSB considered whether conducting the modifications in that manner increased safety risk.
As part of the assessment of an STC application for the same modifications submitted by the design engineer in 2017, CASA questioned the modified rear exit crashworthiness and increased number of occupants. Specifically, it was noted that the effect of increased occupancy on speed and ease of emergency egress had not been established, nor had it been demonstrated that the roller door would be unlikely to jam in the event of fuselage deformation.
As that STC application was never finalised, the safety of egress via the modified exit was not verified. However, in this accident, all the occupants evacuated the aircraft through the roller door after impact. As such, while the STC process was not followed when modifying the aircraft, there was no evidence that it increased the safety risk on this occasion. Additionally, CASA advised that the legislative requirements would likely be met if a modification conducted by an authorised person (under an engineering order) included an associated aircraft flight manual supplement.
The expectation for parachuting operations was that the parachutists would jump from a planned height, or be able to exit the aircraft in the event of an emergency when above a safe height. However, they would be inside the aircraft during take-off, at low level, and if unable to exit in the event of an emergency. In those phases of flight or conditions, increasing the number of occupants increased the number of people exposed to the risk of harm in the event of an accident. In this accident, as the aircraft was too low for parachutists to exit airborne, 15 of the 17 occupants sustained injuries, some of which probably occurred due to impact with each other.
Although the parachuting configuration was assessed as compliant with the required airworthiness standards, parachutists were exposed to greater risk of harm than if they were passengers in certified seats with adequate restraints. Those seated on the floor did not have the benefit of a seat to absorb impact forces and the bench seating had not been shown to optimally absorb impact forces. Additionally, the lack of a seatback on the left bench seat likely increased the injuries sustained by the forward-most parachutist seated on that side. The parachutists were also using single-point restraints, demonstrated to be less effective than dual restraints.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the partial power loss and collision with terrain involving Cessna 208, VH-UMV near Barwon Heads Airport, Victoria on 20 October 2023.
Contributing factors
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Other factors that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety issue description: Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Proactive safety action taken by Experience Co
Experience Co has taken the following proactive safety actions:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet‑wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the SRL/TTL malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed C208 and C208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the STC holder to be followed at or above 1,000 ft above ground level.
Proactive safety action taken by IBIS Technologies
IBIS Technologies amended its software to include an alert that will be flagged to the staff member in charge of manifesting the flight load if a zone exceeds zonal weight limits.
Proactive safety action taken by the Australian Parachute Federation
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of their aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Proposed safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Glossary
AC
Advisory circular
ADS-B
Automatic dependent surveillance broadcast
AFM
Airplane Flight Manual
APF
Australian Parachute Federation
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CAVOK
Conditions and visibility okay
EGT
Exhaust gas temperature
FAA
(United States) Federal Aviation Administration
FCU
Fuel control unit
MEL
Minimum equipment list
NTSB
(United States) National Transportation Safety Board
POH
Pilot’s Operating Handbook
RPM
Revolutions per minute
SRL
Single red line
TCDS
Type certificate data sheet
TTL
Torque and temperature limiter
US
United States
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and sports jump parachutists
Experience Co
Civil Aviation Safety Authority
Australian Parachute Federation
Victoria Police
Textron Aviation
Honeywell International Inc
OzRunways
Barwon Heads Airport
Texas Turbine Conversions
References
Federal Aviation Administration (2023). Pilot’s handbook of aeronautical knowledge. FAA-H-8083-25C.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Textron Aviation
Honeywell International Inc
Texas Turbine Conversions
Bowden Engineering solutions.
Submissions were received from:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Honeywell International Inc.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather (Source: Airservices Australia).
[2]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[3]Engine surging as reported by the pilots of VH-UMV was a power reduction followed quickly by an increase in the power level.
[4]Angle of attack: the relative angle between the chord line of the wing and the relative airflow.
[5]Automatic dependent surveillance-broadcast (ADS-B) is a surveillance system that broadcasts the precise location of an aircraft through a digital data link.
[6]Loadmaster: a person nominated by the drop zone safety officer who is performing duties for a parachute descent.
[7]Normal category applies to aircraft which are intended for non-acrobatic operation, having a seating configuration (excluding pilot seats) of 9 seats or less, and a maximum take-off weight of 5,700 kg or less.
[8]Restricted category applies to aircraft which may carry out certain special purpose operations, but may not carry passengers or cargo for hire or reward.
[9]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[10]The propeller can move to reverse when the engine is operating in beta mode, which results in thrust acting in the opposite direction of the aircraft. In beta mode, the propeller blade pitch is controlled by the power lever.
[11]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[12]The parachutist’s names, weights, and seating locations removed.
Occurrence summary
Investigation number
AO-2023-049
Occurrence date
20/10/2023
Location
Barwon Heads
State
Victoria
Report release date
14/03/2025
Report status
Final
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Incorrect configuration, Loading related
On 15 October 2023, the pilot of a Cessna 172M, registered VH-JUA and operated by Air Gold Coast, was conducting a private flight from Gold Coast Airport, Queensland to Murwillumbah, New South Wales.
During the final approach, the pilot estimated that the aircraft was too high for a landing and elected to conduct a go-around. During the go-around, the aircraft did not climb as expected resulting in the pilot conducting a forced landing about 1km north-east of the airport. The aircraft was substantially damaged and the pilot sustained minor injuries.
What the ATSB found
The ATSB found that it was unlikely there was a mechanical fault with the engine and that the pilot’s decision to maintain full flaps in the go-around created a large amount of drag and impaired the aircraft’s climb performance.
The ATSB also found that an unsecured nose-wheel steering tow bar in the aircraft that increased the risk of serious injury to the pilot.
What has been done as a result
Since the accident, the operator has:
updated their quick reference handbook (QRH) to be clearer on balked landings (go-around) procedures
issued an information circular to students and private hire pilots reminding them of the importance to secure items in the baggage area
updated the private hiring agreements with regard to tighter recency requirements.
Safety message
This accident highlights the importance of appropriately actioning checklists and following procedures detailed in the Pilot’s Operating Handbook. The improper or non-use of checklists has been cited as a factor in several aircraft accidents.
Loose items in the baggage area or cockpit can become dangerous projectiles and may cause serious injuries during an abrupt stop, turbulence or an accident sequence. Further, they may hinder an exit in an emergency egress.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 15 October 2023, the pilot, who was the sole occupant, of a Cessna 172M, registered VH-JUA and operated by Air Gold Coast, was conducting a private flight from Gold Coast Airport, Queensland to Murwillumbah, New South Wales.
The aircraft departed Gold Coast Airport at 1100 local time, tracked directly to Murwillumbah Airport and joined the circuit on the downwind leg for runway 01.[1] During the final approach, the pilot estimated that the aircraft was approximately 300–350 ft crossing the threshold, and elected to conduct a go-around.
The pilot started to configure the aircraft for the go-around and recalled selecting the carburettor heat to OFF. When midfield over the runway, the pilot applied full throttle; however, the pilot stated that the engine did not respond with adequate power. The pilot recalled checking that the fuel mixture was rich, master switch was selected to ON, magnetos were selected to BOTH and again ensured the carburettor heat was selected to OFF. The pilot did not verify the engine RPM due to the high workload at the time.
The pilot assessed that the aircraft had insufficient power to climb, and there was insufficient runway remaining to land. They advised that turning around to land on the reciprocal runway was not an option due to the aircraft being at a low height.
Concerned about the possibility of a stall,[2] the pilot advised they decided to keep the flaps at 40 degrees to maintain as much lift as possible and to reduce the stall speed.
The pilot raised the aircraft’s nose to climb over buildings located past the end of the runway, however, this resulted in the speed reducing, and the pilot felt the aircraft begin to buffet[3] in response to an approaching stall. In response, the pilot lowered the nose and selected a field about 1 km to the north of the airport, to conduct a forced landing.
The pilot recalled maintaining control of the aircraft during the landing sequence and commencing a long flare before landing hard, resulting in substantial damage to the aircraft.
The pilot selected the master and magnetos switches to OFF and exited the aircraft unassisted, sustaining only a minor injury from the shoulder strap of the seatbelt they were wearing.
Context
Aircraft
The Cessna 172 was manufactured in the United States in 1976 and registered in Australia in 1989. It was an all-metal high wing aircraft with a Lycoming O-320-D2J piston engine. The operator advised that VH-JUA had an airframe total time of 14,158 hours and the engine had 2,668.4 hours since overhaul. They further advised it had flown 18.4 hours since the last 100-hour inspection, and there were no outstanding maintenance items at the time of the incident.
The post-accident engineering inspection did not reveal any faults with the engine.
Pilot
The pilot obtained a recreational pilot licence in January 2023 and at the time of the accident they had accumulated 107 hours of aeronautical experience, with about 72 hours of that in the accident aircraft. 41 of those hours were in command. The pilot had conducted regular dual and solo flights with the operator since obtaining their licence. However, prior to the accident flight, it had been 121 days since the pilot’s last flight.
Witness
An experienced pilot, who was standing outside a hangar adjacent to the mid-point of the runway, observed the aircraft fly along the runway at approximately 100 ft. The witness advised that the engine sounded as though it was running at a low power setting as it flew along the runway.
At approximately halfway down the runway, adjacent to where the witness was standing, the witness observed the aircraft nose being pushed down, which the witness believed was an attempt to land. Shortly after, they observed the aircraft pitch up and they heard a bang or ‘pop’ sound from the aircraft’s engine which they advised sounded like the throttle was pushed forward too quickly.
Meteorology
Wind
The following weather details were obtained from the Bureau of Meteorology, and taken from the nearest observation station, Gold Coast, Queensland:
Table 1: Weather details
Dew point average
16.7
Temperature average
26.5
Humidity
55%
QNH
1017
Wind direction
037
Wind speed
9 kt
Wind gusts
10 kt
These observations were consistent with both the pilot and witness’s recollections that wind conditions were light and northerly. The pilot stated that there was not much difference between the indicated airspeed and groundspeed on the day and did not consider that the wind had any adverse effect. As such, wind speed and direction were not considered a factor in the accident.
Carburettor icing conditions
The CASA carburettor icing probability chart predicted that serious carburettor icing at descent power was probable (Figure 1). The pilot stated that the engine was performing as expected throughout the approach. However, any loss of power associated with carburettor icing may not have been noticed at low power settings during an approach.
Figure 1: CASA carburettor icing probability chart
Source: CASA annotated by ATSB
Aerodrome information
The Airservices En Route Supplement Australia (ERSA) records Murwillumbah with an elevation of 18ft and runway 01 1,045 m in length.
Recorded data
Data for the flight was obtained from OzRunways, which recorded the aircraft’s location, altitude and speed at 5 second intervals throughout the flight.
When altitude information is transmitted to OzRunways it is truncated to 100 ft increments. This means that the recorded altitude of the aircraft is within a 100 ft altitude band between the altitude recorded and the next 100 ft increment. Altitudes between 0 and 99 ft will be displayed as 0, 100 and 199ft will be displayed as 100 ft and so on.
Taking into account the terrain elevation, the data showed the aircraft crossing the threshold below 80 ft above ground level (AGL) at 58 kts ground speed. The aircraft maintained approximately the same speed and altitude until about halfway down the runway.
The aircraft then commenced a climb, to a maximum height of between 200–280 ft, maintaining approximately 60 kts, before descending towards the cane field (Figure 2).
Figure 2: VH-JUA go-around at Murwillumbah Runway 01
Source: Google Earth with OzRunways data annotated by the ATSB
Go-around procedures
The Pilot’s Operating Handbook for the Cessna 172M states that the procedure for a go-around or 'balked landing' was:
Throttle – full open
Carburettor heat – cold
Wing flaps – 20°
Airspeed – 55 kt
Wing flaps – retract slowly
On most aeroplanes the use of full flaps creates large amounts of drag and impairs climb performance. The FAA airplane flying handbook Chapter 9: Approaches and landings stated that:
flap deflection of up to 15° primarily produces lift with minimal drag… Flap deflection beyond 15 degrees produces a large increase in drag.
In addition, the handbook stated that:
the application of power should be smooth, as well as positive. Abrupt movements of the throttle in some airplanes cause the engine to falter.
Accident site
The ATSB did not attend the accident site and therefore did not conduct a detailed inspection of the wreckage. However, photographs of the site were provided to the ATSB (Figures 3 and 4).
These photographs showed evidence of:
QNH subscale was set to the 1017 hPa
flaps extended to approximately 40 degrees
damage to the left wingtip, fuselage and right wing
nose and right main landing gear collapsed
engine pushed to the right
a nose-wheel steering towbar on the front right seat of the aircraft
The operator advised that the aircraft had full fuel prior to the departure and approximately 70 l of fuel was recovered from the fuel tanks after the accident.
Figure 3: Photos of the aircraft at the accident site
Source: Operator annotated by ATSB
Figure 4: Nose-wheel steering towbar unrestrained in the cockpit
Photograph of the inside of the aircraft after the accident showed the nose-wheel steering towbar on the front passenger seat.
Source: NSW Police annotated by ATSB
The Civil Aviation Safety Regulations 91.600 state that ‘cargo must not be carried in a place where the cargo may damage, obstruct or cause the failure of a control or obstruct or restrict access to an emergency exit’.
While it could not be determined where the towbar was stored prior to the commencement of the flight, the operator’s standard procedure is to put the tow bar under the seat or to be covered by the net in the rear baggage compartment.
Safety analysis
The pilot advised that the aircraft was high on the approach and consequently they conducted a go-around. A go-around is a normal flight manoeuvre and is recommended when a pilot is not comfortable with an approach and as such it was appropriate that the pilot elected to conduct the procedure. However, consistent with the witness’s observations, the flight data indicated that the approach was stable, and that the descent stopped at less than 80 ft above the threshold, which placed the aircraft in a good position to land. It could not be determined why the pilot believed they were at 300–350 ft at this time.
The data further indicates that the aircraft started climbing, consistent with the commencement of a go-around, about half-way down the runway rather than over the threshold as recalled by the pilot.
During the go-around, the pilot advised that the engine did not produce full power. The ATSB could not verify this as there was no recorded data for engine parameters.
However, as the aircraft was able to maintain speed and height across the runway and subsequently climb with full flap, and no faults were found during the engine inspection, it is unlikely that the engine had any mechanical issues or any significant carburettor icing.
The witness’s account of the engine making a loud ‘bang’ as the engine power was applied is consistent with an abrupt forward movement of the throttle, which may have resulted in the engine faltering momentarily.
It is likely that the pilot’s decision to maintain full flap (40 degrees), which creates a large amount of drag and impaired climb performance, resulted in the pilot’s perception that the engine was not performing adequately.
While the nose-wheel steering towbar did not adversely affect the flight or injure the pilot, loose items in the cockpit or baggage area can jam flight controls and become dangerous projectiles and may cause serious injuries during an abrupt stop, turbulence or an accident sequence. Further, they can hinder an emergency evacuation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 172M, VH-JUA, 1km north-east of Murwillumbah, New South Wales on 15 October 2023:
Contributing factors
During the go-around, it is likely the aircraft was incorrectly configured resulting in reduced climb performance.
Other factors that increased risk
The unrestrained object in the aircraft increased the risk of serious injury to the pilot.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Air Gold Coast
Since the accident, the operator has taken the following safety actions:
updated quick reference handbooks (QRH) to be clearer on balked landings (go-around) procedures.
issued an information circular to students and private hire pilots reminding them of the importance to secure cockpit cargo.
updated the private hiring agreements with regard to tighter recency requirements.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
operator
accident witnesses
recorded data from OzRunways
NSW Police
References
Cessna 1972, Pilot’s Operating Handbook, Cessna 176 Skyhawk, model 172M
Federal Aviation Administration, 2022, Airplane Flying Handbook, Chapter 9 – approaches and landings’.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Pilot of the accident flight
Air Gold Coast Pty Ltd
Witness
Civil Aviation Safety Authority
Submissions were received from:
Air Gold Coast Pty Ltd
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway number: the number represents the magnetic heading of the runway.
[2] Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent.
[3] A buffet is an indication of an approaching aerodynamic stall.
Occurrence summary
Investigation number
AO-2023-048
Occurrence date
15/10/2023
Location
1 km north-east of Murwillumbah
State
New South Wales
Report release date
14/02/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172M
Registration
VH-JUA
Serial number
17266434
Aircraft operator
Air Gold Coast Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Prior to departing, the pilot had submitted a flight notification to Airservices Australia, detailing their planned track to Armidale, operating under the instrument flight rules.[1] The pilot was provided an air traffic control clearance to track to Armidale via their flight planned route at an altitude of 10,000 ft above mean sea level.
At 1437 local time, the aircraft departed Canberra. Soon after take-off, the pilot was transferred to, and established radio communication with the approach controller, reporting that they were on climb through 3,400 ft (to their assigned cruise altitude) and turning left onto their assigned radar heading of 070°.
A short time later, the controller instructed the pilot to turn left onto a heading of 010° and the pilot completed readback of the instruction. About 1 minute 30 seconds later, the controller cleared the pilot to resume their own navigation and track direct to waypoint[2] ‘CULIN’. The pilot completed readback of that instruction, which was the last transmission received from the aircraft. Figure 1 illustrates the ground track of the aircraft departing Canberra while assigned radar vectors and the direct track to CULIN.
During the flight, data was being transmitted by the aircraft’s Automatic Dependent Surveillance Broadcast (ADS-B) equipment.[3] A review of that data indicated that the aircraft was climbing through about 7,000 ft as it turned to track towards CULIN. During that turn, the groundspeed increased, over a period of about 30 seconds, from about 110 kt (204 km/h) to 135 kt (250 km/h).
Climbing above 7,500 ft, the data indicated the aircraft’s groundspeed had started to reduce, at an approximately linear rate, with a reduction of about 22 kt (41 km/h) over a 65-second period. At that time, the data showed a relatively constant rate of climb generally between 550–750 ft/min.
Passing through 8,500 ft, a further 21 kt reduction in groundspeed occurred over a 14-second period, which was accompanied by a short increase in the reported rate of climb. The data indicated the groundspeed then started to increase as the aircraft entered a slight descent.
Over the next 4 minutes, the aircraft’s track varied up to 35° and the groundspeed fluctuated between 90 kt and 120 kt (167–222 km/h). During this period, the altitude was generally increasing although at a varying rate, with shorter periods where the altitude and reported rate of altitude change indicated that the aircraft had started to descend. Several people at locations along the aircraft’s flight path during this time reported hearing noises that they described as a rough running or surging light aircraft engine.
Twelve minutes after take-off, the aircraft was about 25.5 km north-north-east of Canberra, at an altitude of about 10,000 ft, when it abruptly departed from controlled flight and descended steeply towards the ground. Two eyewitnesses in the local area described seeing the aircraft at a low altitude, descending rapidly with its nose pitched down and rotating like a corkscrew. One of the witnesses stated that they heard the engine running rough and then stop just before the accident. The other eyewitness was seated on a tractor with the engine running and did not hear the aircraft engine.
The aircraft collided with terrain (at a ground elevation of about 2,250 ft) and was destroyed by impact forces and a post-impact fire. All occupants were fatally injured. The eyewitness on the tractor was the first responder on the scene and notified the emergency services.
Figure 1: Ground track of VH-MSF from take-off to the accident site
Source: OpenStreetMap with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Figure 2 depicts the aircraft’s altitude and ground track during the last part of the flight after the pilot was cleared to resume their own navigation and includes the position where the flightpath variations commenced.
Figure 2: Aggregated ADS-B data for VH-MSF, looking back along the flightpath
Source: Google Earth, with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Context
Pilot information
The pilot held a Private Pilot Licence (Aeroplane), issued in 1985, and with class ratings for single‑ and multi-engine aeroplanes. The pilot was initially issued with a command instrument rating for single-engine aeroplanes in 1987 and their most recent flight review, on 29 August 2023, was an instrument rating proficiency check with an endorsement for multi-engine aeroplanes. The pilot had reportedly accumulated about 800 hours total flying experience.
The pilot held a Class 2 Aviation Medical Certificate valid to 22 October 2023 with 2 restrictions. A requirement for reading and distance vision correction to be worn while flying and that a continuous positive airway pressure (CPAP) system be used for the sleep period before flying. The pilot was reported to have been well rested before the flight and was utilising the CPAP while sleeping as required.
Aircraft information
The Cirrus Design Corporation SR22 is a low wing aircraft with 4 seats and a single piston engine driving a constant speed propeller. It has a ballistic parachute system fitted as standard. The aircraft (S/N 0153) was manufactured in the United States in 2002 as a G1 model. It was purchased as a second-hand aircraft in the United States in 2017 and then placed on the Australian register with the registration VH-MSF. Since then, it has been operated by its owner for private use, community service flights and private charter operations.
Recent maintenance included the completion of a 100-hour/annual inspection and maintenance release issue on 9 November 2022 at an aircraft time-in-service of 2,558.9 flight hours. The Cirrus Airframe Parachute System (CAPS) was inspected, and the parachute and rocket motor assemblies were replaced due to time expiry in January 2023.
The limitations section of the Cirrus SR22 Pilot’s Operating Handbook stated ‘Aerobatic manoeuvres, including spins, are prohibited.’ The note associated with the manoeuvre limits stated, ‘Because the SR22 has not been certified for spin recovery, the CAPS must be deployed if the airplane departs controlled flight.’
The United States Federal Aviation Administration approved the Cirrus SR22 for flight into icing conditions in 2009 based on the introduction of an optional anti-ice system for the wings, windshield, propeller, and vertical and horizontal stabilizer leading edges. This was known as a flight into known icing approval. As VH-MSF was manufactured in 2002, which predated this approval, the aircraft owner confirmed there was no anti-icing system fitted. Therefore, the aircraft was prohibited from flying into known icing conditions. This limitation was documented in both the Pilot’s Operating Handbook and also stated in current aviation regulations.
Meteorological information
Canberra Airport is located near the intersection of 4 areas in the grid-point wind and temperature chart for New South Wales. The chart issued at 1105 on 6 October 2023 and valid from 1400, indicated the freezing level overhead Canberra was forecast to be at about 7,000 ft with south‑westerly winds at 6-17 kt. The graphical area forecast for ‘NSW-East’, issued at 0913 on 6 October 2023, was valid for the period 1000-1600. Canberra Airport and the accident site were in the south of subdivision D1. The forecast for area D, which included subdivision D1, had the following conditions:
visibility greater than 10 km, scattered cumulus/stratocumulus cloud[4] from 5,000 ft to 8,000 ft with broken tops to 10,000 ft in D1
visibility reduced to 3,000 m in isolated showers of rain, with broken stratus cloud from 1,500 ft to 4,000 ft and broken cumulus/stratocumulus cloud from 4,000 ft to above 10,000 ft
freezing level[5] of 5,000 ft in the south and 8,000 ft in the north
cumulus and stratocumulus cloud implies moderate turbulence
cloud above the freezing level implies moderate icing.[6]
Figure 3 illustrates the ADS-B ground track of the aircraft, overlaid on a satellite image of cloud in the local area at 1450, about 1 minute after the accident.
Figure 3: Aircraft flight track overlaid on satellite image
Note: This image depicts the Himawari-8/9 visible satellite imagery just after the accident, including the ADS-B track of VH-MSF and the position which the aircraft climbed above 7,000 ft.
Source: Satellite image originally processed by the Bureau of Meteorology from the geostationary satellite Himawari-8/9 operated by the Japan Meteorological Agency and modified by ATSB and using aggregated ADS-B data from FlyRealTraffic.com
Recorded information
Figure 4 depicts ADS-B altitude data broadcast from the aircraft during the final 5 minutes of the flight. This includes the several relatively minor altitude excursions/descents, together with the larger altitude excursion/descent that occurred immediately before the departure from controlled flight.
Preliminary analysis of the aircraft’s reported groundspeed, together with sources of meteorological data[7] indicated that the aircraft’s calibrated airspeed[8] was about 70 kt (130 km/h) at the time it departed from controlled flight.
The Pilot’s Operating Handbook provided performance data for the aircraft, including information about the aircraft’s aerodynamic stall[9] speeds. At the maximum take-off weight (1,542 kg), idle power and nil wing flap, the published wings-level stall speed was 67-69 kt (124–128 km/h) calibrated airspeed, depending on the centre of gravity position.[10] The Pilot’s Operating Handbook also indicated that the aircraft had conventional stall characteristics, and that power‑on stalls were marked by a high sink (descent) rate at full aft stick.
The altitude and reported rate of altitude change, indicated an accelerating rate of descent, that increased above 13,000 ft/min before reducing back towards 10,000 ft/min prior to the impact with terrain.
Figure 4: Aggregated ADS-B altitude data
Note: The green line at the bottom right corner of the plot depicts the elevation of terrain in vicinity of the accident site.
Source: ATSB, using aggregated ADS-B data from Airservices Australia and FlyRealTraffic.com
Site and wreckage information
The aircraft came to rest on a private property in an open field adjacent to a dam. Although post‑impact fire damage precluded examination of a significant proportion of the aircraft, inspection of the site and wreckage showed that (Figure 5):
The impact marks and wreckage distribution indicated that the aircraft impacted with terrain upright, with a slight nose low attitude and with little forward momentum, suggestive of a spin.[11]
All the aircraft’s extremities and flight controls were present in the immediate area of the accident site.
There were no identified structural defects in the evidence available.
The CAPS cover, deployment system and parachute were all located within the wreckage and had not been deployed before impact. However, based on the available evidence, the ATSB was unable to determine if an attempt had been made by the pilot to deploy the parachute system before the impact.
The damage to the propeller blades indicated that the engine had low or no power at impact. It should be noted though, that spin recovery, icing, un-porting of fuel tank outlets in a spin, preparation for use of the parachute, and an engine mechanical issue could all be reasons for a power reduction.
collected aircraft, pilot, and operator documentation
conducted a preliminary analysis of flight track data.
The investigation is continuing and will include:
examination of recovered aircraft components
further review of aircraft, pilot, and operator documentation
analysis of pilot medical information
an assessment of the aircraft’s performance based on flight track data
analysis of meteorological information
a review of similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the significant assistance provided during the initial investigation response by the New South Wales Fire Service, the accident site property owner and the local community of Gundaroo.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2] The pilot’s flight notification comprised a series of defined geographic positions (waypoints) via which the pilot intended to navigate the aircraft to Armidale. The flight notification’s first waypoint after departing Canberra was CULIN.
[3] The ADS-B equipment transmitted flight data that enabled air traffic service providers to track aircraft when operating outside coverage of conventional air traffic control radar. Airservices Australia recorded the transmissions received by their network of ground-based ADS-B receivers. That data could also be received by other aircraft with suitable equipment and privately-operated ground-based equipment, feeding information to flight tracking websites.
[4] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky and ‘broken’ indicates that more than half to almost all the sky is covered.
[5] The freezing level is the height in feet above mean sea level where the air temperature is 0 °C.
[6] The rate of accumulation of moderate icing is such that even short encounters become potentially hazardous and the use of de-icing/anti-icing equipment or a flight diversion is necessary.
[7] This includes data from the Bureau of Meteorology’s vertical wind profiler at Canberra Airport, wind and temperature data from recorders on an aircraft descending into Canberra close to the time of the accident and data from a similar aircraft that passed overhead Canberra a short time before.
[8] Airspeed was not a parameter transmitted by the aircraft’s ADS-B equipment. The calibrated airspeed was derived from the ADS-B recorded groundspeed and track using the available measurements of wind velocity, atmospheric pressure and temperature.
[9] Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[10] The actual stall speed on any given flight depended on a number of variable factors including the aircraft’s operating weight/centre of gravity, flap setting, engine power, bank angle and/or load factor.
[11] Spin: a sustained spiral descent of a fixed-wing aircraft, with the wing’s angle of attack beyond the stall angle.
Final report
Investigation summary
What happened
On 6 October 2023, a Cirrus Design Corporation SR22 aircraft, registered VH-MSF, was being operated on a private instrument flight rules flight from Canberra, Australian Capital Territory, to Armidale, New South Wales. On board the aircraft were the pilot and 3 passengers.
About 12 minutes after take-off, at an altitude approaching 10,000 ft above mean sea level, the aircraft aerodynamically stalled, departed from controlled flight, entered a high vertical descent developing into a spin, and impacted with terrain. All occupants were fatally injured, and the aircraft was destroyed by a post‑impact fire.
What the ATSB found
The ATSB found that the flight track data showed that, at about 8,000 ft, the aircraft had begun to deviate from its flight track, with heading, altitude and airspeed deviations. Those deviations coincided with reports from ear witnesses located below the aircraft’s flight path of sounds consistent with engine surging.
The data also showed that the aircraft had a high rate of climb (up to 1,500 ft/min) coupled with a low and decreasing airspeed, which led to an aerodynamic stall and rapid descent. Recovery actions from the aerodynamic stall did not occur and the Cirrus aircraft parachute system was not deployed in-flight. It was also noted that no radio calls were received from the pilot to indicate there was a problem prior to the stall.
VH-MSF was not fitted with an anti-icing system and was prohibited from operating in icing conditions. Moderate icing conditions were forecast along the aircraft’s flight path from 7,000 ft to 10,000 ft when in cloud. It was likely that the aircraft had encountered icing conditions prior to the aerodynamic stall. However, the ATSB was unable to determine if these conditions were sufficient to have adversely affected the aircraft’s performance and/or handling.
The ATSB considered several scenarios to establish the reason for the deviations in flight track, subsequent stall and absence of recovery actions. These included in-flight icing, pilot incapacitation and possible aircraft issues. However, due in part to a significant post-impact fire, which limited the collection of evidence, the circumstances preceding the stall and impact with terrain could not be determined.
Safety message
Although it could not be established that icing contributed to the accident, operating in these conditions in aircraft that are prohibited from doing so increases the risk of a loss of control event leading to an accident. Aircraft flying through cloud in sub-freezing temperatures are likely to experience some degree of icing. A pilot can reduce the chance of icing becoming an issue by selecting appropriate flight routes, remaining alert to the possibility of ice formation and knowing how and when to operate de-icing and anti-icing equipment if fitted.
The occurrence
Accident flight details
On 3 October 2023, a Cirrus Design Corporation SR22 aircraft, registered VH-MSF, was operated on a private flight from Redcliffe, Queensland, to Armidale, New South Wales, and then on to Canberra, Australian Capital Territory, the following day.
On 6 October 2023, the return sectors were planned to operate from Canberra to Armidale, with a planned return to Redcliffe. On board the aircraft were the pilot and 3 passengers.
At about 0648 local time, the pilot submitted an instrument flight rules[1] flight plan to Airservices Australia to fly from Canberra to Armidale with an estimated departure time of 1430. The flight planned track was via waypoint[2] ‘CULIN’ (about 31 km west of Goulburn) and Scone, New South Wales, at a cruising altitude of 10,000 ft above mean sea level (AMSL), using RNP 2[3] navigation performance. The lowest safe altitude from Canberra to CULIN was 4,600 ft. While there was no published instrument flight rules route from CULIN to Scone and from Scone to Armidale, the pilot’s flight planning software application provided a lowest safe altitude of 6,000 ft from CULIN to Scone and 6,300 ft from Scone to Armidale using RNP 2 performance.
On contact with Canberra ground air traffic control at 1422, the pilot was provided an airways clearance to track to Armidale via their flight planned route at 10,000 ft.
At about 1437, the aircraft departed Canberra Airport. Soon after take-off, the pilot was transferred to, and established radio communication with, the approach controller, reporting that they were on climb through 3,400 ft (to their assigned cruise altitude) and turning left onto their assigned radar heading of 070°. A short time later, the controller instructed the pilot to turn left onto a heading of 010° and the pilot completed readback of the instruction. About 1 minute 30 seconds later (at about 1442), the controller cleared the pilot to resume their own navigation and track direct to waypoint CULIN. The pilot completed readback of that instruction, which was the last transmission received from the pilot. All transmissions made by the pilot were clear and concise. Flight data showed that the aircraft turned 5° to the left of the direct track to waypoint CULIN.
During the flight, data was being transmitted by the aircraft’s automatic dependent surveillance broadcast (ADS-B) equipment.[4] A review of that data indicated that the aircraft was climbing through about 7,000 ft AMSL as it turned to track towards CULIN. During that turn, the ground speed increased, over a period of about 30 seconds, from about 110 kt (204 km/h) to 135 kt (250 km/h).
Climbing above 7,500 ft, the data indicated the aircraft’s ground speed had started to reduce, at an approximately linear rate, with a reduction of about 22 kt (41 km/h) over a 65‑second period. At that time, the data showed a relatively constant rate of climb generally between 550–750 ft/min.
Passing through 8,300 ft, the somewhat linear flight track altered to an onset of heading, altitude and airspeed variations. The ADS-B data indicated the ground speed then started to increase as the aircraft entered a slight descent. Over the next 4 minutes, the aircraft’s track varied up to 35° and the ground speed fluctuated between 93 kt and 121 kt (172–224 km/h). During this period, the altitude was generally increasing, although at a varying rate, with shorter periods where the altitude and reported rate of altitude change indicated that the aircraft had started to descend.
The ADS-B data showed that, at about 12 minutes into the flight, the aircraft descended by about 250 ft, increased speed by about 13 kts and then climbed at a rate up to about 1,500 ft/min. While in that climb, the airspeed reduced significantly and from a calculated pressure altitude of 9,946 ft, at 1448:37, the aircraft departed controlled flight and descended rapidly towards the ground. For more details on the aircraft’s movements refer to the Recorded information section. About 44 seconds after the onset of the departure from controlled flight, the aircraft collided with terrain (at a ground elevation of about 2,250 ft) and was destroyed by impact forces and a post-impact fire. All occupants were fatally injured. An eyewitness was the first responder on the scene and notified emergency services.
Figure 1 illustrates the ground track of the aircraft departing Canberra while assigned radar vectors and the direct track to CULIN.
Figure 1: Ground track of VH-MSF (in blue) from take-off to the accident site
The aircraft ground track overlaid on this map is referenced to a latitude and longitude grid aligned to true north. The headings assigned by air traffic control are referenced to magnetic north. In the Canberra region, magnetic north is about 12° less than true north. An aircraft’s ground track relevant to the assigned heading can also be affected by wind. Source: OpenStreetMap with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Witness observations
Figure 2 and Table 1 show the witness locations and observations along the aircraft’s flight path; earwitnesses reported hearing aircraft engine noises and 2 eyewitnesses reported seeing the aircraft in its final moments before the impact with terrain.
Four independent ear witnesses (1 through 4 in Table 1) in the local area where the aircraft was climbing through about 8,000 ft described hearing a rough running or surging (revs increasing and decreasing) light aircraft engine, which was likely to be VH-MSF. Another 2 earwitnesses located closer to the accident site reported hearing varying engine sounds (5 and 8 in Table 1).
Two eyewitnesses (6 and 7 in Table 1) in the local area of the accident site described seeing the aircraft at a low altitude, descending rapidly with its nose pitched down and rotating like a corkscrew (spiral descent). One of these witnesses stated that they heard the aircraft approaching with the engine noise fluctuating[5] and the engine running during the descent, but went quiet just before impact. The other eyewitness was seated on a tractor with the engine running and did not hear the aircraft engine.
Table 1: Ear and eyewitnesses summaries with reference to Figure 2
Ear/eyewitness
Description
1 - Earwitness
Heard a light aircraft heading in a north-east direction. It was dropping engine revs and returning to normal revs. I heard this happen several times.
2 - Earwitness
Heard a small aircraft that seemed to be having engine problems overhead. The engine was revving then stuttering – they could not see the aircraft (cloud).
3 - Earwitness
Heard a small aircraft making sounds like it was cutting out and restarting – they could not see the aircraft (cloud).
4 - Earwitness
Engine sounded rough, sputtering. It did not sound like the abrupt silence of a mechanical failure. Sounded like the engine might be starving for fuel – they could not see the aircraft (cloud).
5 - Earwitness
Unusual aircraft noise like engine cutting in and out – they could not see the aircraft (cloud).
6 - Eyewitness
Heard the aircraft approaching with engine noise fluctuating but they could not see the aircraft until it exited below cloud in a steep nose down spiralling descent – the engine was running during the descent but went quiet just before impact.
7 - Eyewitness
Eyewitness to the last couple of steep nose down spiral turns below the cloud before impact. They did not see any smoke coming from the aircraft. Was on a tractor and did not hear the aircraft at any time.
8 - Earwitness
I heard a light plane revs of the engine gradually increasing to its maximum revs and then I heard a loud metal on metal clunking sound and then I heard the explosion about 4 seconds later and saw smoke coming up from a neighbouring property.
Figure 2 shows the aircraft flight track, and the location of each ear/eyewitnesses summarised in Table 1.
Figure 2: Aircraft flight path with ear and eyewitnesses’ locations
Source: Google Earth, with ADS-B data from Airservices Australia, annotated by the ATSB
Context
Pilot information
The pilot held a valid private pilot licence (aeroplane), issued in 1985 (re-issued as a Civil Aviation Safety Regulations Part 61 licence in August 2016), and class ratings for single‑ and multi‑engine aeroplanes. The pilot was initially issued with a command instrument rating for single‑engine aeroplanes in 1987 and their most recent flight review, on 29 August 2023, was an instrument rating proficiency check with an endorsement for multi-engine aeroplanes.
Insurance documentation indicated that the pilot had accumulated about 800 hours total flying experience, with about 180 hours in Cirrus SR22 aircraft, including 12.5 hours in VH‑MSF. The owner of VH-MSF had conducted several flights with the pilot and described them as being a good and careful pilot with no problems entering cloud and utilising the instruments.
Aircraft information
General information
VH-MSF was a Cirrus Design Corporation SR22 low-wing aircraft with 4 seats and a fuel‑injected piston engine driving a constant speed 3‑blade propeller. It had a ballistic parachute system (Cirrus airframe parachute system – CAPS) fitted as standard. The aircraft was fitted with a cabin and windshield heating system, which utilised warm air ducted from the engine exhaust shroud.
The aircraft (S/N 0153) was manufactured in the United States in 2002 as a G1 model. It was purchased by the owner in the United States and first placed on the Australian aircraft register in 2017. It was issued a standard certificate of airworthiness in the normal category. Since then, it had been operated by its owner for private use, community service flights and had been leased to other private pilots (Figure 3).
The current maintenance release was on board the aircraft and was destroyed. A carbon copy of the maintenance release was provided by the aircraft maintainer. It showed that the required 100‑hour/annual inspection was conducted and a maintenance release was issued on 9 November 2022 at an aircraft time-in-service of 2,558.9 flight hours. Inspection of the maintenance release copy, aircraft logbook and worksheet records showed there were 2 items of maintenance that were past their calendar due date. They were a standby compass calibration and an outside air temperature/clock back-up battery replacement, both due about 2 months before the accident. The aircraft owner advised that the overdue maintenance items were an oversight.
The aircraft was certified for use in the private category and for instrument flight rules (IFR) operations. Maintenance documentation showed that the CAPS was inspected, and the parachute and rocket motor assemblies were replaced due to time expiry in January 2023. At the time of the accident flight, the airframe, engine and propeller had accumulated the following hours:
airframe – 2,635.5 hours total time-in-service
engine – 1,192.0 hours’ time since overhaul
propeller – 133.3 hours’ time since overhaul.
It was reported that, in September 2023, the aircraft was hard to start, and the starter motor was replaced, which resolved the issue. The aircraft owner also advised that, in the days prior to the accident flight the pilot had reported that the power lever was stiff to operate. In response to this, the owner checked the lever and determined that the reason for the stiffness was due to the friction adjustment, which had been wound up to a high friction setting. Following readjustment, when the friction was wound off, the power lever was free to move with no issues.
Two and 3 days prior to the accident, post-flight at Armidale and Canberra, the pilot had reported to their family and the owner that the aircraft had operated with no issues. The ATSB did not identify any maintenance issues that may have contributed to the accident.
Flight instrumentation
There were 6 primary flight instruments fitted to the aircraft. They were the airspeed indicator, attitude indicator, altitude indicator, turn coordinator, heading indicator, and vertical speed indicator (Figure 4). The aircraft was fitted with a Sandia SAI-340 model attitude indicator, which also incorporated airspeed, altitude and slip indicators. The unit contained a rechargeable battery capable of providing continued operation in the event of aircraft electrical failure. Maintenance documentation showed that the attitude indicator had been replaced in 2018 with a repaired model that had a software upgrade to include the addition of a vertical speed function.
Figure 4: VH-MSF flight instruments with Sandia attitude indicator top centre
Source: Aircraft owner
The United States Federal Aviation Administration issued an emergency airworthiness directive (AD), AD‑2020‑18‑51, for Sandia attitude indicators in 2020. That directive stated the applicability as being for Sandia attitude indicator part number 306171‑10 and 306171‑20. These attitude indicators may be marked as Bendix King Model KI‑300 or Sandia Model SAI‑340A. They may be installed on aircraft certificated in any category. It also stated that the AD was prompted by reports of 54 failed attitude indicators, which produced erroneous attitude data to the pilot and autopilot, if equipped. The FAA issued the AD to prevent aeronautical decision-making based on erroneous attitude information, which may result in loss of control of the aircraft.
The attitude indicator fitted to VH-MSF was the Sandia SAI-340, part number 306171-00, which was outside the applicability of the emergency AD. Further, the aircraft owner reported that the attitude indicator had not had any issues since it was installed in 2018.
Electric trim control system
The aircraft was fitted with an electric pitch, roll and rudder trim system. Electric trim buttons for pitch and roll were located on the top of each control yoke, while the rudder trim switch was mounted in the console next to the wing flap control switch.
The SR22 Pilot’s Operating Handbook (POH) stated that the pitch trim could be controlled by manually moving the switch forward, which would initiate nose‑down trim and moving the switch aft would initiate nose-up trim. This occurred via an electric motor, which changed the neutral position of the spring cartridge attached to the elevator control horn. The pitch trim also provided a secondary means of pitch control in the event of a primary pitch control failure not involving a jammed elevator. The electric pitch trim was used by the autopilot.
For roll trim, moving the switch left would initiate a left-wing-down trim and moving the switch right would initiate a right-wing-down trim. The trim also provided a secondary means of roll control in the event of a failure with the primary roll control system not involving jammed ailerons. The electric roll trim was also used by the autopilot. The rudder trim was not connected to the autopilot.
Autopilot
The aircraft was equipped with a 2-axis (pitch and roll) S-TEC-55X autopilot system that received roll axis control inputs from an integral electric turn coordinator and altitude information from an altitude transducer connected to the pitot-static system. A multifunction control panel was fitted above the altitude indicator, which provided mode selection, disengage, and turn command functions. The autopilot controller or a button on each control yoke handle could be used to disengage the autopilot. The autopilot features included:
roll stabilisation
turn command
navigation localiser and GPS tracking
altitude hold
vertical speed
GPS steering (GPSS) for smoother turns onto a course or during course tracking.
The limitations section of the SR22 POH stipulated that the autopilot should be disconnected when moderate to severe turbulence was experienced.
According to the aircraft owner, when either the altitude hold or vertical speed modes were selected, the autopilot would not disengage automatically. Also, when in these modes and the flight controls were manually manipulated, the system would apply trim in the opposite direction to maintain the selected altitude or vertical speed.
Electric trim and autopilot failure
The POH indicated that, any failure or malfunction of the electric trim or autopilot could be overridden by manually manipulating the control yoke. Further, if a trim runaway occurred, the pilot was to de‑energise the circuit by pulling the circuit breaker (PITCH TRIM, ROLL TRIM, or AUTOPILOT) and land as soon as the conditions permitted.
Icing protection system
The United States Federal Aviation Administration approved the Cirrus SR22 for flight into icing conditions in 2009 based on the introduction of an optional anti-ice system for the wings, windshield, propeller, vertical and horizontal stabiliser leading edges and the stall warning system. This was known as a FIKI (flight into known icing) approval. The accident aircraft was manufactured in 2002, which predated the FIKI approved modification, and the owner confirmed there was no anti-icing system fitted. Further, pilots were required to undergo an online Cirrus training course in icing awareness and use of the FIKI fitted to the SR22 aircraft before the system could be utilised. The manufacturer confirmed that the pilot of VH-MSF had not undergone that training.
VH-MSF was fitted with windshield defrost, pitot heat[6] and an alternate induction air system, which offered some protection against windshield, pitot and engine air intake icing. Each of those items had to be manually selected on by the pilot as required. According to the SR22 POH, the pitot heat was to be turned on for flight into instrument meteorological conditions, flight into visible moisture, or whenever ambient temperatures were 5 °C or less.
Stall warning system
The aircraft was equipped with an electro-pneumatic stall warning system to provide audible warning of an approach to aerodynamic stall.[7] When a slight negative pressure was sensed by the pressure switch from an inlet in the wing leading edge, a warning horn activated. The warning sounded at approximately 5 kt above the stall with full flaps and power off in wings level flight and at slightly greater margins in turning and accelerated flight.
Cirrus airframe parachute system
The Cirrus airframe parachute system (CAPS) was designed to lower the aircraft and its occupants to the ground in the event of a life‐threatening emergency where activation was determined to be safer than continued flight and landing. The system consisted of the following primary components:
parachute
solid-propellant rocket to deploy the parachute
rocket activation handle and cable
harness embedded in the fuselage structure.
The parachute and rocket were located in the empennage behind the rear baggage compartment. The rocket activation handle was mounted in a cabin ceiling enclosure between the 2 front seats and the cable was routed through the cabin ceiling and angled towards the left side of the CAPS compartment.
A safety pin with a remove before flight flag was fitted to the activation handle when operating on the ground. Part of a pilot’s pre-flight checks included a requirement to remove the safety pin prior to engine start. To initiate the CAPS, the pilot was to remove the access cover on the ceiling and pull the rocket activation handle out and down (Figure 5). Movement of the cable compressed the igniter steel spring and cocked the plunger. When one half inch of plunger travel was reached, the primary booster was ignited, which then ignited a secondary booster and the rocket motor.
Figure 5: Activation handle (top left) and parachute system as fitted to the aircraft
Source: Cirrus Design Corporation, annotated by the ATSB
For aircraft with an electronic ignition for the booster (as was fitted to VH-MSF), both aircraft batteries were connected to the system and either could actuate the booster in response to cable movement. Once ignited, the rocket impacted and dis-bonded the parachute compartment cover situated behind the rear cabin window and pulled the deployment bag from the enclosure. The deployment bag then staged the suspension line deployment and inflation of the parachute.
Meteorological information
Accessing weather information
On the morning of the accident, the pilot submitted a location briefing request at 0615 to the National Aeronautical Information Processing System[8] (NAIPS), which included Canberra and Armidale Airports. This was followed by 5 area briefing requests between 0622 and 0635, which included meteorology information, notices and advisories (NOTAMs),[9] and charts. This would have provided the pilot with the New South Wales east (NSW-E) graphical area forecast (GAF) and the NSW grid point wind and temperature (GPWT) charts.
At 1105, the pilot submitted another NAIPS area briefing request for the same weather information requested previously. This was the pilot’s last briefing request to NAIPS.
Bureau of Meteorology
Initial weather forecast
When the pilot submitted their flight plan at 0648, the current NSW GPWT chart was issued at 0454 and valid from 1100. Canberra was located near the intersection of 4 areas on the chart. Interpolation of the data between these 4 areas indicated the freezing level was forecast to be about 5,500 ft above mean sea level. The current NSW‑E GAF was issued at 0302 and valid from 1000 to 1600, which included the pilot’s planned departure time of 1430. Canberra was in subdivision C1 of area C on the GAF, which included the following weather:
broken[10] stratocumulus cloud from 2,000 ft to 7,000 ft in C1 until 1600
scattered drizzle in C1 with visibility reduced to 3,000 m and overcast stratocumulus cloud from 1,000 ft to 8,000 ft
a freezing level[11] of 4,000 ft in the south and 7,000 ft in the north [Canberra was centrally located within the south region].
The remarks field on the GAF provided additional information of operational relevance and included:
cloud above the freezing level implied moderate icing[12]
stratocumulus cloud implied moderate turbulence.
The estimated freezing level of 5,500 ft at Canberra and forecast broken stratocumulus from 2,000 ft to 7,000 ft, indicated an icing layer of about 1,500 ft overhead Canberra. Armidale was in area B, which included broken cumulus/stratocumulus cloud from 6,000 ft to 9,000 ft from 1300, and a freezing level of 9,000 ft.
Subsequent weather forecast
When the pilot submitted their last NAIPS area briefing request at 1105, the current NSW GPWT chart was issued at 0559 and valid from 1400. It indicated the freezing level overhead Canberra was forecast to be at about 7,000 ft with south‑westerly winds increasing from 6 kt at 5,000 ft to 19 kt at 10,000 ft. The NSW-E GAF was issued at 0913 and valid for the period 1000-1600. Canberra and the accident site were in the south of subdivision D1 of area D. The forecast for area D included the following conditions relevant to the pilot’s departure time of 1430:
visibility greater than 10 km, scattered cumulus/stratocumulus cloud from 5,000 ft to 8,000 ft, with broken tops to 10,000 ft in D1/D2 – the Bureau of Meteorology advised the ATSB that this should be interpreted as being broken cumulus/stratocumulus cloud from 5,000 ft to 10,000 ft in D1/D2
visibility reduced to 3,000 m in isolated showers of rain, with broken stratus cloud from 1,500 ft to 4,000 ft and broken cumulus/stratocumulus cloud from 4,000 ft to above 10,000 ft
freezing level of 5,000 ft in the south and 8,000 ft in the north of area D.
The remarks field stated:
cloud above the freezing level implied moderate icing
cumulus and stratocumulus cloud implied moderate turbulence.
The estimated freezing level of 7,000 ft at Canberra and forecast broken cumulus/stratocumulus from 5,000 ft to 10,000 ft indicated the forecast depth of the icing layer overhead Canberra had increased to 3,000 ft. Figure 6 depicts the NSW-E GAF, current at the time of the pilot’s last NAIPS area briefing request. Information relevant to the flight is labelled and highlighted. This forecast included a freezing level of 9,000 ft for the area containing Scone (area B) and a freezing level of above 10,000 ft for the area containing the destination of Armidale (area A).
Figure 6: Graphical area forecast for New South Wales – East
Source: Bureau of Meteorology, annotated by the ATSB
Assessment of the local conditions
The ATSB requested an analysis of the weather conditions by the Bureau of Meteorology applicable to the aircraft’s track. The following is a summary of that analysis:
Satellite observations at 0400Z [1500 local time] indicated that the IR [infrared] cloud top temperature was ‑7°C which corresponds to a cloud top height of 10,000 ft…Taking the base and cloud top estimates, this gives a depth of cloud of approximately 3,000ft.
The weather conditions observed for the area between Canberra and the accident site were consistent with the forecasts for the afternoon of 6 October 2023. The cloud cover was scattered to broken cumulus/stratocumulus, with a freezing level at approximately 7000ft. Cumulus and stratocumulus cloud were forecast on the GAF and observed on satellite imagery. Showers were forecast and observed over the ranges to the north and northeast of Canberra, including just north of the accident site at 0349Z [1449 local time].
These conditions would have been conducive to moderate icing conditions (most likely of the clear icing type) between approximately 7000ft to 10,000ft above mean sea level. The severity of any icing experienced would depend on how long the aircraft is in the cloud layer between these heights, however, the existence and/or type of airframe icing is very difficult to verify, particularly with the absence of any aircraft icing reports from the area at the time.
Based on Himawari-9 satellite imagery and observations from the aerological diagram at Wagga there is high confidence of moderate icing within the cumulus and stratocumulus field that extended across the Canberra region on 6/10/2023. This is consistent with forecast cloud and weather referenced on the NSW-E GAFs and reinforces the GAF statement (noted on all GAF issued by the Bureau of Meteorology) of "CLD ABV FZLVL implies MOD ICE".
Weather observations
Canberra Airport automatic terminal information service
When the pilot contacted Canberra ground air traffic control for an airways clearance, they reported receipt of the automatic terminal information service[13] ‘Golf’. The recording for information ‘Golf’ stated the following regarding the current weather conditions at Canberra Airport:
Expect instrument approach runway 17, wind 200° 8 kt, visibility greater than 10 km, cloud few 3,000 ft scattered 3,500 ft,[14] temperature 18, QNH[15] 1025.
Camera footage of cloud cover at Canberra Airport
A fixed camera was located about 1.3 km to the west of Canberra Airport showing an aspect to the north-north-east. The footage, coupled with other stills taken around the time the aircraft took off to the south and then tracked to the north-north-east, showed broken cumulous/stratocumulus cloud as per the forecast (Figure 7, taken at 1439).
Figure 7: Footage taken near Canberra Airport with a north-north-east aspect at 1439
Source: Aus Web Cams/myairportcams.com
First responders
Shortly after the accident occurred, first responders took a video around the aircraft in the hope that it could assist with the investigation into the accident. Consistent with the forecast, that video showed broken cloud overhead the accident site to the south-west, which was the direction the aircraft had come from (Figure 8).
Figure 8: Video image taken shortly after the accident viewed to the south-west
Source: Supplied
Pilot report of weather
The pilot of a Cirrus SR22T aircraft fitted with a flight into known icing (FIKI) kit was conducting an IFR flight from Wagga to Moruya, New South Wales, via Canberra on the day of the accident, flight planned at 9,000 ft. The pilot recalled using the anti-icing fluid, first to the west of Canberra when the aircraft was in the tops of the clouds at 9,000 ft. The pilot requested and received a clearance from air traffic control to climb to 10,000 ft to clear the cloud. They turned the anti-icing off and passed overhead Canberra at about 1358 (about 50 minutes prior to the accident) where they entered higher level cumulus cloud. The pilot then turned the anti-icing on again for the leg from Canberra to Moruya.
The pilot observed ice build-up on the aircraft in areas that did not receive the anti-icing fluid directly but did not notice any icing on the wings or any loss of engine performance. The pilot reduced the power and speed for turbulence penetration during the trip and assessed their aircraft was experiencing light icing. They also commented that it would have built up rapidly on an aircraft without an anti-icing system.
The pilot was able to recall one prior experience of icing when on descent into Moruya from Dubbo in their previous SR22, which was not fitted with a FIKI kit. The pilot reported that the ice built up quickly on the wings for about 2,000 ft but dissipated rapidly when the aircraft entered warmer air. They did not notice any loss of engine performance but acknowledged they were using a low power setting for the descent.
Airline flight data
A Virgin Australia Boeing 737-800 aircraft, callsign Velocity 1690, transited and descended through airspace and altitude bands close to the outbound flight track of VH‑MSF and at a similar time.
Velocity 1690 was being operated on a flight from the Gold Coast, Queensland, to Canberra with a landing time of 1445:26, about 4 minutes prior to the accident. Runway 17 was the active runway and Velocity 1690 approached Canberra from the north. On descent, at 1437:03, the aircraft data recorded the engine anti-icing system (ENG COWL ANTI-ICE) being turned on by the flight crew at an altitude of 10,144 ft and an outside air temperature (OAT) of −6.2°C (6°C total air temperature (TAT)).[16] The operator reported that the flight crew could not provide a detailed recollection of the approach but that the selection of the anti-ice would be consistent with the aircraft in cloud above the freezing level during the descent. At 1439:35, the flight crew turned the engine anti-icing off at 6,848 ft and an OAT of 0.2°C (10.5°C TAT). Figure 9 depicts the approach flight path of Velocity 1690 with the times, altitudes and temperatures when the engine anti-icing was turned on and off. The flight path of VH-MSF includes the positions that corresponded with the altitude band (shown in red) in which Velocity 1690 used engine anti‑icing.
Figure 9: Relative positions of Velocity 1690 and VH-MSF
Source: Google Earth and Virgin Australia, annotated by the ATSB
ATSB review of satellite imagery
Introduction
The Bureau of Meteorology provided the ATSB access to various satellite imagery of the Canberra region during the afternoon of the accident, which had been processed from the geostationary satellites Himawari-8 and 9, operated by the Japanese Meteorological Agency. Imaging sensors carried on board the satellite would make progressive scans of the Earth’s full disk at 10-minute intervals.
Cloud coverage
Figure 10 is the enhanced visible satellite image showing cloud coverage for the Canberra region for the 10-minute acquisition period commencing 1440, which was the closest image relative to the time of the accident. The areas of cloud are represented by the lighter pixels, where the darker pixels are areas without (or with less) cloud coverage. This image is overlaid with VH-MSF’s flight track, the direct track to waypoint CULIN, the estimated position and time the aircraft climbed through the 0°C estimated freezing level (at about 14:43 and 7,000 ft).[17] It also showed the aircraft’s position at 8,000 ft where flight path variations commence in relation to cloud coverage.
While this shows cloud coverage along parts of the aircraft’s track, it does not provide information about the depth of the cloud or the height of the cloud tops, and whether those tops were above or below the aircraft’s operating altitude.
Figure 10: VH-MSF track (in red) overlaid on an enhanced visible satellite image, taken close to the time of the accident
Source: Bureau of Meteorology and Japan Meteorological Agency, modified by the ATSB
Temperature of reflective surfaces
To assist with the estimation of cloud heights in the vicinity of the aircraft’s flight path, the Himawari‑8 and 9 RGB infrared enhancement image[18] was reviewed for the same period commencing at 1440. For the infrared images, the colour of the pixels is an indicator of the average temperature of the reflecting surface measured by the infrared imaging sensors.
The lighter coloured pixels represent lower temperature (colder) reflecting surfaces and could reasonably be used to infer higher cloud tops in those regions. The darker pixels were consistent with warmer average temperatures of the reflecting surfaces and could suggest lower cloud tops in those areas. Based on the infrared images, the Bureau of Meteorology assessed the cloud conditions as being scattered to broken with a 3,000 ft cloud band between 7,000 and 10,000 ft, with moderate clear icing likely when in cloud from 7,000 ft.
Figure 11 shows a temperature scale, the flight path, times and altitudes with the position of the aircraft at an estimated freezing level of 7,000 ft. It also shows the point at which the aircraft flight path variations commence and the lighter grey areas indicating cloud tops at 10,000 ft. Based on the infrared image, it was considered likely that the aircraft entered cloud above the freezing level. However, the exact amount of time the aircraft spent in cloud could not be determined.
Figure 11: VH-MSF track overlaid on RGB infrared enhancement image, taken close to the time of the accident
Source: Bureau of Meteorology and Japan Meteorological Agency, modified by the ATSB
Comparison with the airline flight data
The infrared imagery for VH-MSF (Figure 11) was compared with the imagery applicable to the Boeing 737-800 (acquisition period commencing 1430) and the corresponding altitude and temperature data for when this aircraft likely entered cloud during descent into Canberra. This indicated that the lightest coloured pixels in the image represented average temperatures of about −6 °C, with the tops of the reflecting surfaces (clouds) being about 10,000 ft as per the forecast.
Recorded information
General information
The aircraft’s Avidyne multi-function display and EMax engine monitoring system had been significantly damaged by the post-impact fire. Technical assessment and X-ray images of the unit’s compact flash data storage card showed considerable thermal damage, which precluded recovery of onboard recorded data. The aircraft was not equipped with a data transfer unit and recoverable data module, which was available as a fitted option in later models of Cirrus aircraft. Therefore, no onboard recording devices were available for data download to assist the investigation.
Flight data performance assessment
The ATSB obtained digital data that had been broadcast by the aircraft’s automatic dependent surveillance broadcast (ADS-B)[19] equipment and which had been recorded by Airservices Australia and other flight tracking websites.[20] That data included information about the aircraft’s position, ground track, ground speed and altitude.
The ADS-B data transmitted by the aircraft did not include parameters such as airspeed, altitude rate of change, heading or temperature. However, the transmitted data could be integrated with other sources of information (such as wind velocity, air temperature and atmospheric pressure), to derive estimates for other relevant performance data. For the purpose of analysing the ADS-B data and to derive estimates of the aircraft’s calibrated airspeed (CAS)[21] during the accident flight, wind and temperature data was obtained from several sources, which included:
the Bureau of Meteorology’s NSW GPWT chart, valid from 1400, providing wind and temperature forecast data in 1.5 by 1.5° grids
the Bureau of Meteorology’s vertical wind profiler observations (averaged over the preceding 30-minute observation period) for Canberra Airport, issued 1430 and 1500
wind and temperature information from the Boeing 737-800 (Velocity 1690) flight data when transiting through the airspace north of Canberra and passing close abeam the accident site about 10 minutes prior
the United States National Centres for Environmental Prediction global forecast system and global data assimilation system in 0.25 by 0.25° grids, valid at 1400.
Evaluation of those sources demonstrated a reasonable correlation between datasets, particularly during the latter stages of the climb and immediately prior to the departure from controlled flight. For the main analysis task, the investigation used the Canberra Airport vertical wind profiler observations, and the wind velocity and temperature data recorded for Velocity 1690. The estimate for CAS was derived from ADS-B recorded ground speed and ground track, using the sources for wind velocity (from Velocity 1690 data and vertical wind profiler observations), and recorded atmospheric pressure at Canberra Airport and temperature (from Velocity 1690 data).
Further, this information, along with published aircraft performance data was used to determine the required engine power and propellor thrust to meet the performance seen in the recorded data. However, due to the limitations of ADS-B broadcast data (such as position errors, recording resolution, and broadcast dropouts) and at times dynamic manoeuvring of the aircraft, the aircraft trajectory and power required analysis was indeterminate for much of the aircraft’s flight.
Figure 12 depicts the ADS-B data for the accident flight, together with an estimate of the aircraft’s airspeed. The initial climb was conducted on reasonably stable headings and climb rates at airspeeds that were estimated to be generally between 85 kt and 105 kt CAS, to an altitude of about 7,000 ft above mean sea level. At one point during this climb, at about 1441 when approaching 6,000 ft, the aircraft appeared to have passed through an area of rising air (Figure 12 ‘vertical air movement’). This was evidenced by the aircraft substantially exceeding the POH published maximum rate of climb performance while the aircraft additionally accelerated slightly.
At 1442:08, the air traffic controller cleared the pilot to resume their own navigation and track direct to CULIN, where the estimated airspeed increased to about 115 kt. At 1443, the airspeed began to progressively reduce as the aircraft continued to climb. For a full‑page view of Figure 12 refer to Appendix A.
The following provides a summary of the data (in sections A to G, as annotated on Figure 12 and Figure 13) from just prior to passing through 8,000 ft until the departure from controlled flight:
A: Over a period of about 90 seconds, the airspeed reduced by about 25 kt at a relatively linear rate.
B: Climbing through 8,300 ft, the airspeed continued to reduce, with a reduction of about 20 kt occurring over a 15‑second period. The aircraft was estimated to have slowed to around 72 kt, which was 5 kt above the calculated stall speed for the flight.
C: The airspeed recovered slightly but, 40 seconds later, the airspeed reduced again to an estimated 70 kt. During this time, the aircraft was passing overhead several witnesses who had reported hearing unusual revving or stuttering from an aircraft engine.
D: The aircraft then accelerated to the best rate of climb speed for about 45 seconds, and the altitude increased by almost 800 ft. This also included what appeared to be a controlled turn (based on a relatively constant turn radius) to the right, changing heading by about 35° (as shown on Figure 1 and Figure 2).
E: At 1447:20, the aircraft entered a final period of unstable flight. The aircraft decelerated from 100 kt to 94 kt while the climb rate reduced to zero.
F: The airspeed then further decreased by 11 kt, before the aircraft descended 250 ft and recovered to an estimated airspeed of 96 kt. A power required analysis suggested the speed loss and descent were possibly conducted with low or idle power, or due to a downdraft.
G: Over the next 30 seconds, the recorded data showed that the aircraft then climbed above the best rate of climb to about 1,500 ft/min while the airspeed reduced.
At 1448:31–33, about 12 minutes after take-off from Canberra, the aircraft reached a maximum altitude of 9,946 ft at an airspeed of 71 kt. Following this, the flight data showed the aircraft’s airspeed and altitude declined, and rapidly so from 1448:37. The descent rate increased to 13,000 ft/min, the ground speed reduced to less than 32 kt and became erratic, and the aircraft track aligned somewhat with the estimated wind direction, all of which indicated the aircraft had likely entered a spin.[22] As the aircraft passed through about 8,000 ft, the rate of descent started to reduce, which was indicative of the increased drag from an increasing air density as the aircraft descended. When the aircraft had reached ground level the descent rate had reduced to around 10,000 ft/min.
Figure 12: Aggregated ADS-B altitude data for VH-MSF, together with estimated airspeed (CAS)
Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
Figure 13 depicts the aircraft’s flight track looking back along the flight path with A through G labelled to the relevant sections of the flight as shown in Figure 12. As the aircraft climbed through 8,300 ft, the somewhat linear flight track changed, with heading, altitude and airspeed variations commencing.
Figure 13: Aggregated ADS-B data for VH-MSF, looking back along the flight path
Source: Google Earth, with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Performance comparison between flights
Figure 14 illustrates ADS-B altitude data from initial climb to about 10,000 ft for the accident flight and the 2 prior flights (on 3 and 4 October 2023)[23] conducted by the pilot in VH-MSF. The data showed the aircraft climb performance for the accident flight was initially similar or better than the prior flights. During the period of flight path variations, the aircraft performance reduced, potentially due to manoeuvring, but then momentarily returned to comparable performance after passing 9,000 ft.
Figure 14: Comparison of ADS-B altitude data for the accident and 2 prior flights
Flight start times have been adjusted to allow for comparison. Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
The manufacturer was provided a copy of the flight track data for assessment. That assessment was conducted by one of their senior investigators and a senior test pilot. While no definitive conclusions were able to be made based on the data provided, the manufacturer indicated that the aircraft had slowed, aerodynamically stalled and, after a short period of time, entered into a spin.
Wreckage and impact information
Site and wreckage
The aircraft came to rest in an open field adjacent to a dam wall with a 10° downward slope towards the right wing. Although post-impact fire damage precluded examination of a significant proportion of the aircraft, inspection of the site and wreckage showed (Figure 15 and Figure 16):
The impact marks and wreckage distribution indicated that the aircraft impacted with terrain upright, with a slight nose low attitude and no forward momentum. Although the impact evidence was indicative of a spin, it was difficult to ascertain the spin direction.
All of the aircraft extremities (wings and tail section) were accounted for and there was no evidence of an in-flight break‑up.
There were no identified structural defects in the evidence available.
All flight controls systems were inspected to the degree possible with no pre-accident defects identified.
The flap actuator was identified within the wreckage and was in the flap zero position.
The fuel selector was tested and assessed to be in the right tank position.
The fuel tank caps were located and found secured in the filler point opening of each fuel tank.
The engine cowl was located forward of the aircraft outside the fire zone. It did not have any residue to indicate an in-flight loss of oil.
Due to the destruction of the wreckage, cockpit switch settings and circuit breakers, flight/engine control, autopilot or trim positions were unable to be determined.
The engine power lever and mixture control positions could not be determined.
Figure 15: Overview of the accident site and remaining wreckage
Source: ATSB
Figure 16: Aircraft wreckage viewed from the rear showing downslope to the right
Source: ATSB
The cabin heat position was unable to be ascertained, and the engine exhaust and shroud that was utilised for cabin heat was removed so that the exhaust could be examined for pre‑impact defects. No cracks or pre-impact defects were identified in the exhaust that may have led to carbon monoxide[24] being introduced into the cabin by an exhaust leak.
Cirrus aircraft parachute system
The CAPS fuselage cover was located adjacent to the wreckage, but outside the fire zone. Inspection of the cover showed an impact mark on the internal surface at the rocket head location. The cover did not display any thermal or smoke damage (Figure 17). The parachute deployment rocket was not in its original position and was located about 3 m to the right of the fuselage and had dispensed its propellent. The cover and rocket position indicated that the rocket had deployed due to ground impact forces before the post-impact fire had initiated.
The parachute was located in its normal fitted position, remaining in its pack. After an extensive search throughout the remaining wreckage, the parachute deployment handle and safety pin could not be located. Therefore, the ATSB could not establish if an attempt was made to deploy the parachute in-flight.
Figure 17: CAPS external cover showing internal impact mark
Source: ATSB
Propeller and engine examinations
Propeller
The propeller was partially buried at the front of the aircraft. The propeller flange had separated from the engine crankshaft and remained attached to the propeller hub. Two of the 3 propeller blades (Figure 18, blades A and B) were undamaged and showed no signs that they had passed through the ground during the impact with terrain.
Figure 18: Propeller as found at the accident site
Source: ATSB
Propeller blade C was buried in the earth directly under the hub and showed some signs of rotational scoring, some leading-edge gouges, and slight chordwise twisting. A fracture surface at the base of the blade was from back bending overload as a result of the impact with terrain (Figure 19).
Site photographs of the propeller and fractured crankshaft were examined further and blade C was physically examined at the ATSB’s technical facilities in Canberra to determine the level of engine power being produced at the time of impact. The materials failure analysis identified that the propeller hub had fractured from the engine crankshaft at the propeller flange, in a manner consistent with ductile overstress due to bending. The examination determined that propeller blade C exhibited minor compound bending through its section and had a slight twist at the blade tip. Chordwise gouging observed on the front face of the blade was a characteristic of propeller rotation.
With respect to the engine power output, typically, windmilling or an engine at idle power will stop very rapidly when the propeller blades contact the ground. There is often minimal ground entry and little to no distortion to the blade sections. In this case, when blade C entered the ground, the propeller stopped suddenly. Therefore, the ATSB’s analysis concluded that, while there were some signatures that would indicate that the propeller was rotating at the time of impact, there was no evidence of appreciable power being produced by the engine. Rather, the damage to the propeller blades indicated that the engine was operating at low power when it impacted terrain.
Figure 19: Blade C as recovered from the accident site
Source: ATSB
Propeller governor
The propeller governor remained attached to the engine. Impact and fire damage precluded functional testing. The governor was disassembled and inspected at the ATSB’s technical facilities with no pre-impact defects identified.
Engine
The engine was removed from the accident site and taken to an approved engine overhaul facility for disassembly and inspection under the supervision of the ATSB. Sections of the engine were consumed by the intense post-impact fire, which precluded functional testing of specific areas such as the ignition and fuel systems.
The oil filler cap was secured to the crankcase fill adapter. The engine and accessories were completely disassembled. The engine was found to be mechanically sound, with the crankcase section intact and all the cylinders present and securely mounted to the crankcase. No defects were identified in any of the cylinder assemblies that may have provided an indication of a malfunction contributing to a loss of engine power. There was no distress of the main or connecting rod bearings due to oil starvation or loss.
The engine sump was pushed upwards during the impact with terrain, bringing it in contact with the cam shaft drive gear. That contact perforated the sump with gear teeth impressions, indicating that the engine camshaft was not rotating and the engine had stopped by the time the imprints were made (Figure 20).
Figure 20: Camshaft drive gear and impressions made in the engine sump
Source: ATSB
Medical and pathological information
General information
The pilot held a class 2 aviation medical certificate valid to 22 October 2023, with 2 restrictions. These were a requirement for reading and distance vision correction to be worn while flying and that a continuous positive airway pressure (CPAP) machine be used for the sleep period before flying.
The pilot’s last Civil Aviation Safety Authority (CASA) required medical assessment was conducted on 22 October 2021. That documented assessment showed that the pilot had:
been prescribed medication for high cholesterol for over 10 years
an electrocardiogram stress test (heart trace) in 2016 with nil issues reported
their appendix removed in 1980
a computed tomography (CT) angiogram and CT calcium test in 2019 with nil issues reported
a CT chest X-ray in 2019, which was all clear
blood tests in 2016, 2017, 2019 and 2021
a sleep study performed in 2016, which resulted in the use of a CPAP machine (details below).
In 2016, the pilot was identified with moderately severe obstructive sleep apnoea and used a CPAP machine to manage that condition. Downloaded CPAP data showed that the pilot was consistently using the CPAP machine. It was reported that the pilot had their CPAP machine with them during the trip to Canberra and given the previous continuous use it was concluded that the pilot likely utilised the machine during the trip, including the night prior to the accident.
The pilot was reported to have been well rested and had consumed a salmon bowl meal from a local restaurant about 1 hour before the flight. In general, the pilot was reported by their family to be fit and healthy with no known illnesses.
Post-mortem and toxicology results
A full post-mortem[25] of the pilot was conducted. The pilot received extensive thermal injury as a result of the post-impact fire and multiple other injuries from the accident.
The pathologist noted that the pilot had a right coronary artery angulation with an ostium (opening of the artery) that had a slit-like appearance. They stated that it is a rare congenital coronary artery anomaly that, in most cases, does not present with clinical symptoms and may be considered an incidental post-mortem finding in asymptomatic patients. In approximately 20% of cases, the anomaly may result in symptoms such as angina (chest pain), dyspnoea (shortness of breath), syncope (fainting), myocardial ischaemia (reduced blood flow to the heart), ventricular fibrillation (irregular heart rhythm), and sudden death. According to the literature, symptoms generated by congenital coronary artery anomalies are predominantly associated with athlete patients or after intense physical exercise and are rarely present in sedentary individuals.
Toxicology testing was conducted to detect common therapeutic medicines and illicit drug use, and these tests were found to be negative for all substances. The toxicology report noted that a low, insignificant blood alcohol concentration was detected that may have been attributed to post‑mortem decomposition changes (0.006 g per 100 mL). A carbon monoxide saturation level of 2% was also detected in the pilot’s blood, but the report stated that this did not suggest that carbon monoxide poisoning contributed to the accident and death, nor did it suggest a significant survival period after the impact. As previously discussed in ATSB investigation AO‑2017‑118, the physical symptoms and cognitive effects of carbon monoxide exposure generally start to occur at levels of around 10%.
In their concluding remarks the pathologist stated that:
No definite answer can be provided based on the post-mortem findings alone regarding whether the possible sudden incapacitation of the pilot may have contributed to the aviation fatalities. The post‑mortem findings must be correlated carefully with all other available evidence, not least the findings arising from examination of the scene and other relevant evidence as unearthed by detective officers and other investigative authorities.
Specialist medical assessment
Due to the circumstances of the accident and the indeterminate results of the pilot’s post‑mortem, the ATSB requested the assistance of a specialist doctor of forensic pathology to assess the information obtained by the ATSB, which included:
post-mortem and toxicology report
the sequence of events detailed in the ATSB preliminary report
CASA medical records relating to the pilot
Medicare and pharmaceutical benefits scheme records relating to the pilot
compliance and therapy report for the pilot’s ResMed Airsense 10 Elite CPAP machine.
A summary of the specialist’s assessment of the information provided was as follows:
The pilot sustained fatal injuries due to the impact with terrain prior to the post-impact fire.
The blood alcohol level detected was from a sub-optimal sample taken from the chest cavity (often the only choice with severe trauma). Although alcohol consumption could not be ruled out, it was entirely possible that the alcohol was produced post-mortem and could be expected under the given circumstances.
The pilot was known to take rosuvastatin medication for high cholesterol treatment. The drug was not detected in the pilot’s toxicology results and is generally not detectable in routine screening. While it could not be determined if the medication was in the pilot’s blood, the drug would not be expected to have a psychoactive effect or cause incapacitation.
Regarding the identified 3 heart abnormalities in the pilot’s post-mortem, the specialist indicated that:
In the case of the right coronary artery angulation, the specialist indicated that it is an anatomical abnormality in 2% of hearts where one of the 2 main blood vessels suppling the heart muscle is abnormally angled at its origin from the aorta and often presents as a slit‑like opening (as was the case with this pilot), as opposed to the normal opening, which has a round profile. In the majority of cases, it is considered an incidental finding of no clinical significance. In a small percentage of cases, this abnormality is determined to be a cause for heart muscle abnormalities, including the development of cardiac arrhythmias, scarring of heart muscle, and potentially incapacitation and death. It was noted that the pilot had a CT coronary angiogram performed in January 2019, which was reported to be normal. It was considered likely that had a coronary artery abnormality been a clinically significant issue at the time it would have been identified. Also, an absence of fibrosis (scarring) or other changes typical of chronic ischaemia in the distribution of the right coronary artery argues against this being clinically significant in this case.
The second heart abnormality identified was the narrowing of the left anterior descending coronary artery without obvious atherosclerosis. It was considered likely that post‑accident heat effect caused the change rather than natural disease. It was noted again that the pilot had a CT scan in 2019 that was reported as normal, and it would be unlikely that coronary artery disease would have progressed to the extent of being capable of causing incapacitation in that time period.
The third heart abnormality identified was contraction banding in association with lacerations of the heart muscle and was seen in areas supplied by widely patent coronary arteries such as the right coronary artery. In the absence of other indicators, it was considered likely that the contraction banding was a result of the aircraft accident rather than incapacitation due to cardiac disease.
The specialist advised that many natural medical conditions that can result in pilot incapacitation would generally not be detectable from a post-mortem, especially where there have been very extensive injuries, and therefore could not be ruled out. Examples of such conditions include the pilot losing their corrective eyewear at a critical time, the pilot having a coughing fit, the development of many gastrointestinal illnesses including diarrhoea, vomiting, and stomach cramps, and diverse conditions such as fainting spells, kidney stone passage and cardiac arrhythmias.
In conclusion, the specialist stated that it was unlikely that natural disease caused or contributed to the events leading up to the accident. There were no indications of toxicological abnormalities causing incapacitation and/or death. In common with many aircraft accident fatalities, a definitive comment in relation to cause of death could not be made in this case.
Operational information
Icing conditions
The limitations section of the POH stated ‘Flight into known icing conditions is prohibited’. The abnormal procedures section stipulated that, if a pilot inadvertently entered icing conditions, the following abnormal checklist procedure for Inadvertent Icing Encounter was to be applied:
Pitot Heat…ON
Exit icing conditions. Turn back or change altitude.
Cabin Heat…MAXIMUM
Windshield Defrost…FULL OPEN
Alternate Induction Air…ON
The use of alternate induction air was described further in the emergency procedure for Engine Partial Power Loss as follows:
A gradual loss of manifold pressure and eventual engine roughness may result from the formation of intake ice. Opening the alternate engine air will provide air for engine operation if the normal source is blocked or the air filter is iced over.
Aerodynamic stall
A wing generates lift as a result of the pressure differential created by airflow over the wing’s surface. The angle between the incoming or relative air flow and wing chord is known as the angle of attack (AoA). As the AoA increases, lift increases up to a certain angle, known as the critical AoA. At this point, the airflow over the upper surface of the wing becomes separated. This condition is referred to as an aerodynamic stall (or simply a stall) and results in a significant loss of lift and an increase in drag. Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, typically an uncommanded aircraft nose-down pitch results.
Most general aviation aircraft typically have a critical AoA of around 16°. This critical AoA can be exceeded at any airspeed, any (pitch) attitude and any power setting. However, as most small aircraft are not fitted with an AoA indicator, the AoA at which the stall occurs may be referenced to an airspeed.
A loss of altitude also occurs during the recovery from a stall and it is possible to stall with insufficient height above the ground to recover. The POH stated that the altitude loss during a wings level stall may be 250 ft or more.
The Cirrus SR22 performance data showed that, at the maximum weight of 3,400 lbs (1,542 kg) with 0° bank angle and flaps full up, the power-off stall speeds at the forward and aft centre of gravity limits were 70 kt and 68 kt (indicated airspeed) respectively. The calibrated airspeed (CAS) for each limit was 1 kt less than the indicated.
The stall speed was calculated for a mid-centre of gravity position and corrected for an operating weight of 3,300 lb (1,497 kg), generally representative of the accident flight is mid centre of gravity given the take-off weight was close to the maximum take-off weight. The estimated stall speed was 68 kt (indicated) and 67 kt CAS.
The POH normal procedure for stalls stated:
SR22 stall characteristics are conventional. Power-off stalls may be accompanied by a slight nose bobbing if full aft stick is held. Power-on stalls are marked by a high sink rate at full aft stick.
…
When practicing stalls at altitude, as the airspeed is slowly reduced, you will notice a slight airframe buffet and hear the stall speed warning horn sound between 5 and 10 knots before the stall. Normally, the stall is marked by a gentle nose drop and the wings can easily be held level or in the bank with coordinated use of the ailerons and rudder. Upon stall warning in flight, recovery is accomplished by immediately reducing back pressure [on the control yoke] to maintain safe airspeed, adding power if necessary and rolling wings level with coordinated use of the controls.
Spins
A spin can result when an aircraft simultaneously stalls and yaws.[26] A spin is characterised by the aircraft following a downward, corkscrew path and requires significantly more altitude for recovery compared to a wings level stall (Federal Aviation Administration, 2021).
The limitations section of the POH stated ‘Aerobatic manoeuvres, including spins, are prohibited’. The emergency procedures stipulated that the SR22 was not approved for spins and had not been tested or certified for spin recovery characteristics. The only approved and demonstrated method of spin recovery was the activation of the CAPS (refer to the section titled Cirrus aircraft parachute system deployment). Specifically, the POH stated:
If, at the stall, the controls are misapplied and abused accelerated inputs are made to the elevator, rudder and/or ailerons, an abrupt wing drop may be felt and a spiral or spin may be entered. In some cases, it may be difficult to determine if the aircraft has entered a spiral or the beginning of a spin.
…
In all cases, if the aircraft enters an unusual attitude from which recovery is not expected before ground impact, immediate deployment of the CAPS is required.
…
The minimum demonstrated altitude loss for a CAPS deployment from a one turn spin is 920 feet. Activation at higher altitudes provides enhanced safety margins for parachute recoveries. Do not waste time and altitude trying to recover from a spiral/spin before activating CAPS.
Wood and Sweginnis (2006), Aircraft Accident Investigation – 2nd edition, provides the following description of the wreckage from an aircraft that had spun into the ground, with reference to Figure 21:
There is little or no evidence of forward motion. Although the fuselage probably impacted at a steep nose down attitude [spins can be anywhere between nose up, flat, but most commonly nose down], it is likely that there is evidence of a wing tip striking the ground before the nose. The down-going wing will normally strike the ground before the up-going wing, providing one clue as to the direction of the spin. Both the fuselage and the wings will probably have damage which reflects both a high sink rate and yaw. Tall thin objects on the ground, like trees and fence posts, are likely to penetrate the airplane almost from bottom to top, reflecting the almost vertical trajectory of the airplane. Undamaged objects may be found immediately behind the trailing edges, again indicating the vertical path of the airplane.
Figure 21: Example wreckage pattern from a spin
Source: Wood and Sweginnis (2006)
Cirrus aircraft parachute system deployment
Procedures for deployment
For the deployment of the CAPS, the POH stated:
*Warning*
CAPS deployment is expected to result in loss of the airframe and, depending upon adverse external factors such as high deployment speeds, low altitude, rough terrain or high wind conditions, may result in severe injury or death to the occupants. Because of this, CAPS should only be activated when any other means of handling the emergency would not protect the occupants from serious injury.
*Caution*
Expected impact in a fully stabilized deployment is the equivalent to a drop from approximately 13 feet.
*Note*
Several possible scenarios in which the activation of the CAPS would be appropriate are discussed in section 10 – Safety information of this handbook. These include:
- Mid-air collisions
- Structural failure
- Loss of control
- Landing in inhospitable terrain
- Pilot incapacitation.
The POH also noted that the maximum demonstrated deployment speed was 133 kt (indicated airspeed). Once a decision was made to deploy the CAPS, the airspeed should be reduced to the minimum possible, the mixture should be moved to cutoff, the activation handle cover should be removed and the handle pulled down with both hands. Pull forces up to, or exceeding, 45 lbs (20 kg) may be required. After deployment, the fuel selector, fuel boost pump, battery and alternator master switch and ignition switches were to be turned off and the emergency locator transmitter turned on.
In regard to a CAPS deployment altitude, the POH indicated that:
No minimum altitude for deployment has been set. This is because the actual altitude loss during a particular deployment depends upon the airplane’s airspeed, altitude and attitude at deployment as well as other environmental factors. In all cases, however, the chances of a successful deployment increase with altitude. As a guideline, the demonstrated altitude loss from entry into a one-turn spin until under a stabilized parachute is 920 feet. Altitude loss from level flight deployments has been demonstrated at less than 400 feet. With these numbers in mind it might be useful to keep 2,000 feet AGL in mind as a cut-off decision altitude. Above 2,000 feet, there would normally be time to systematically assess and address the aircraft emergency. Below 2,000 feet, the decision to activate the CAPS has to come almost immediately in order to maximize the possibility of successful deployment. At any altitude, once the CAPS is determined to be the only alternative available for saving the aircraft occupants, deploy the system without delay.
Cirrus, in its guidance document CAPS Guide to the Cirrus Airframe Parachute System, advised that, while the POH noted a maximum demonstrated deployment speed, it was possible for the parachute to withstand deployments at higher speeds. The guide provided examples where the CAPS had been deployed at speeds up to 187 kt (indicated airspeed) with a successful outcome. The guidance reiterated that the maximum demonstrated speed was not intended to be a limitation.
Cirrus also encouraged pilots to conduct a take-off briefing that incorporated when to activate the CAPS, as well as the inclusion of a passenger briefing that included the use of the CAPS. The briefing should include:
- Engage the autopilot using the level button (if equipped)
- Attempt to revive the pilot
- Follow the deployment procedures detailed on the CAPS placard
- Prepare for CAPS touchdown
- Follow egress procedures
The ATSB could not confirm what take-off or passenger briefings were undertaken by the pilot on the day of the accident. Further, nor could it be determined with certainty that the passenger seated adjacent to the pilot would have had the physical capability to undertake the required actions if they had received the briefing on the use of the CAPS.
Deployment history
At the time of writing this report, the aircraft manufacturer reported that there had been 126 in‑flight CAPS deployments. They also stated that there had been 3 CAPS anomalies where the parachute failed to deploy. A recent issue where the rocket did not deploy was related to a batch of rocket motor initiating devices (squibs) manufactured in 2015 and 2016 that would not fully ignite. There was a mandatory service bulletin to have those squibs replaced. The squib on VH‑MSF was replaced when the parachute assembly was replaced in its entirety in January 2023.
The ATSB reviewed several aircraft accident reports, which indicated that there had been a number of CAPS deployments above the maximum recommended indicated airspeed of 133 kt resulting in an overload and separation of the chute from the aircraft. Further, there have been a number of documented accidents where the parachute had not been deployed in‑flight but had ground impact initiations of the rocket.
Loss of control
The POH safety information section listed potential reasons for a loss of control and an associated response to such a situation:
Loss of control may result from many situations, such as: a control system failure (disconnected or jammed controls); severe wake turbulence, severe turbulence causing upset, severe airframe icing, or sustained pilot disorientation caused by vertigo or panic; or a spiral/ spin. If loss of control occurs, determine if the airplane can be recovered. If control cannot be regained, the CAPS should be activated. This decision should be made prior to your pre-determined decision altitude (2,000’ AGL).
Engine issue in-flight
In the event of an engine failure in-flight, the POH emergency procedure checklist stipulated:
If the engine fails at altitude, pitch as necessary to establish best glide speed. While gliding toward a suitable landing area, attempt to identify the cause of the failure and correct it. If altitude or terrain does not permit a safe landing, CAPS deployment may be required.
The emergency procedures section of the POH detailed that, for a partial engine power loss, indications of such include fluctuating revolutions per minute, reduced or fluctuating manifold pressure, low oil pressure, high oil temperature, and a rough-sounding or rough-running engine.
The procedure required that, if a partial engine failure permitted level flight, land at a suitable airfield as soon as the conditions allowed. If the conditions did not permit safe level flight, use partial power as necessary to set up a forced landing pattern over a suitable landing field. It was also advised that a pilot should be prepared for a complete engine failure and consider CAPS deployment if a suitable landing site was not available.
To troubleshoot, the POH advised to select the fuel boost pump on, switch fuel tanks, check the engine controls, and cycle the ignition switch left and right to ensure both magnetos were working. Select alternate induction air on, as a gradual loss of manifold pressure and eventual engine roughness may result from the formation of intake ice. Opening the alternate engine air would provide air for engine operation if the normal source was blocked or the air filter was iced over.
Fuel uplift
The aircraft had a total fuel capacity of 318 L (159 L per wing tank) as stipulated in the POH. According to fuel company records, the aircraft was refuelled on 5 October 2023 (one day prior to the accident) at about midday with 110 L of Avgas from a fuel bowser at Canberra Airport. The fuel remaining in each tank before the refuelling commenced was unable to be determined. However, the fuel uplift was close to the estimated fuel consumption of 118 L for the previous flight from Armidale to Canberra. The estimated fuel consumption from Canberra to the accident site was 22 L.
As part of the Canberra Airport fuel company procedures, a sample of fuel was tested for clarity and water content on the morning the aircraft was refuelled and on the afternoon of the accident, with no issues identified. Several other aircraft utilised the same batch of fuel with no issues reported. Therefore, fuel quality and quantity was not considered to be a factor in the accident.
Weight and balance
The aircraft load data sheet indicated that the empty weight was recorded as 1,045 kg and the gross weight limit for the SR22 was 1,542 kg. For the purpose of calculating the weight and balance for the accident flight, the ATSB assumed full fuel and used average weights for each of the occupants and their luggage, based on 4 separate estimates provided by their relatives. This produced an estimated engine start weight of 1,494 kg, which was 48 kg below the gross weight limit. The centre of gravity was within limits for the entirety of the flight.
Flight into icing
Bureau of Meteorology pilot guidance on icing conditions
The accumulation of ice on an aircraft is ‘one of the most significant hazards to the safe and efficient operation of aircraft as it can reduce aircraft performance in a number of ways’ (Bureau of Meteorology, 2015). This includes:
increased stall speed of the aircraft by increasing its weight with the accumulation of ice
difficulty operating control surfaces and landing gear
increased drag and decreased lift due to ice accumulation on the airframe (tests have shown that icing no thicker or rougher than a piece of coarse sandpaper can reduce lift by 30% and increase drag by 40%)
engine power reductions (intake and carburettor icing)
propeller vibrations due to ice accumulation on the blades
errors in instrument readings of airspeed, altitude and vertical speed due to ice contaminated pitot static systems
interference with communications systems (icing on antennas)
reduced visibility due to icing on the windshield and side windows.
The Bureau of Meteorology aviation weather services brochure titled Hazardous Weather Phenomena – Airframe Icing has informative content for pilots. Included in that brochure was a depiction of the icing environment and the various levels of icing risk based on temperature and water content. As shown in the icing environment depiction (Figure 22), aircraft operating within the 0 to −10°C higher risk range if/when in cloud could experience clear ice conditions.
Figure 22: Icing environment depiction
Source: Bureau of Meteorology
The Bureau of Meteorology classifies icing severity as trace, light, moderate or severe. Moderate icing (as identified on the VH-MSF flight route) means the rate of accumulation is such that even short encounters become potentially hazardous, and the use of de‑icing/anti‑icing equipment or a diversion is necessary. An area forecast will include any expectation of moderate or severe icing, while a SIGMET[27] is only required when severe icing is predicted.
There are 4 types of icing which are clear, rime, mixed ice (a combination of clear and rime icing) and hoar frost. Clear ice is formed when supercooled water droplets impact the aircraft. As the droplets freeze, heat is released, slowing the freezing process. This causes some of the water droplets to flow back over the exposed surfaces and freeze as clear ice. Therefore, clear ice tends to cover a large area of the aircraft and can disrupt the airflow and affect the performance of the aircraft. Clear ice forms most readily in temperatures between 0 ºC and −10ºC but can occur, with reduced intensity, at lower temperatures.
Impact of icing on aircraft performance
Baars et al. (2010) conducted research titled A review on the impact of icing on aircraft stability and control. The research stated that:
Structural ice formation on leading edges of wings and control surfaces initiate significant regions of unsteady flow. This change in performance of the lifting surfaces can result in a major change in the handling of aircraft; the aircraft may stall at higher speeds, the stall angle of attack may decrease and irreversible upset events can be initiated.
In the period of 1990-2000, a total of 3,230 aircraft accidents were recorded by the Air Safety Foundation. Twelve percent of those were related to icing.
…
Studies on ice-related accidents of small general aviation aircraft have revealed that in many cases even the most experienced pilots have less than 5 to 8 minutes to escape the harmful icing conditions before their aircraft experience violent upsets. This suggests that in cruise the accumulation of ice, and its effect on stability of aircraft, remain mostly unobserved. Upon changing the attitude of the aircraft, the formation of ice induces unsteady flow phenomena capable of upsetting the aircraft in a catastrophic manner.
United States Federal Aviation Administration – Pilot Guide: Flight in Icing Conditions
The purpose of the United States Federal Aviation Administration’s advisory circular AC 91‑74B, Pilot Guide: Flight in Icing Conditions, was to provide pilots with a convenient reference guide on the principal factors related to flight in icing conditions and the location of additional information in related publications. It included the following information:
Flight planning
If an aircraft is not certificated for flight in icing conditions, each flight should be planned carefully so that icing conditions are avoided…In the event of an inadvertent icing encounter, the pilot should take appropriate action to exit the conditions immediately, coordinating with ATC [air traffic control] as necessary, and declaring an emergency.
Effects of icing on unprotected wings
…The ice causes an increase in drag, which the pilot detects as a loss in airspeed or an increase in the power required to maintain the same airspeed. (The drag increase is also due to ice on other parts of the aircraft). The longer the encounter, the greater the drag increase; even with increased power, it may not be possible to maintain airspeed. If the aircraft has relatively limited power (as is the case with many aircraft with no ice protection), it may soon approach stall speed and a dangerous situation.
Effects of icing on critical systems
Because contamination of the wing reduces lift, even an operational, ice-free stall warning system may be ineffective because the wing will stall at a lower AOA [angle of attack] due to ice on the airfoil. Heated or unheated, if the wing is contaminated in any way, an AOA will become unreliable. The stall onset would occur prior to activation of stall warning devices leading to a potential pitch or roll upset. It is imperative that pilots maintain airspeed and monitor AOA closely when in icing conditions.
Induction icing
Fuel-injected aircraft engines usually are less vulnerable to icing, but still can be affected if the engine’s air source becomes blocked with ice. Manufacturers provide an alternate air source that may be selected in case the normal system malfunctions.
Moderate icing accretion rate
…
The rate of accumulation is such that anything more than a short encounter is potentially hazardous. A representative accretion rate for reference purposes is 1 to 3 inches (2.5 to 7.5 cm) per hour on the unprotected part of the outer wing. The pilot should consider exiting the condition as soon as possible.
General advice
Avoidance - The pilot of an aircraft that is not certificated for flight in icing conditions should avoid all icing conditions. This guide provides guidance on how to do this, and on how to exit icing conditions promptly and safely should they be inadvertently encountered.
Vigilance - The pilot of an aircraft that is certificated for flight in icing conditions can safely operate in the conditions for which the aircraft was evaluated during the certification process, but should never become complacent about icing. Even short encounters with small amounts of rough icing can be very hazardous.
Guidance - The pilot should be familiar with all information in the AFM [airplane flight manual] or POH concerning flight in icing conditions and follow it carefully. Of particular importance are proper operation of ice protection systems and adherence to minimum airspeeds during or after flight in icing conditions. Monitor airspeed, pitch attitude, and do not rely on the airplane’s autopilot or stall warning system in icing conditions. There are some icing conditions for which no aircraft is evaluated in the certification process, such as SLD [supercooled large droplets] conditions within or below clouds, and flight in these conditions can be very hazardous. The pilot should be familiar with any information in the AFM or POH relating to these conditions, including aircraft-specific cues for recognizing these hazardous conditions.
Cirrus SR22 flight in known icing conditions information
Although not fitted to VH-MSF, the approval and specifications for FIKI (flight into known icing) were reviewed as they provided specific guidance for icing on the Cirrus SR22.
The approved POH and airplane flight manual supplement for the FIKI system recommended that the minimum airspeed for flight into known icing conditions was 95 kt (indicated airspeed). The emergency procedures section contained the following information when discussing an observed or suspected failure of the anti-ice system:
An unobserved failure may be indicated by a decrease in airspeed, anomalous handling characteristics, or airframe vibrations.
Note: Significant loss in cruise or climb performance may be an indication of propeller ice accretions that are not visible to the naked eye. Operation of the engine at 2700 RPM [revolutions per minute] will help shed ice in severe icing conditions.
The performance section of the FIKI supplement further stated:
Airplane performance and stall speeds without ice accumulation are essentially unchanged with the installation of the Ice Protection System. Significant climb and cruise performance degradation, range reduction, as well as buffet and stall speed increase can be expected if ice accumulates on the airframe.
Propeller icing
The adverse effects of propeller icing have been explored for several decades, which included the United States National Advisory Committee for Aeronautics producing a report in 1950 (NACA TN 2212), on the subject of The effects of ice formation on propeller performance. Its report included the following observations:
- when a propeller accumulates ice, the resulting changes in propeller performance are reflected in corresponding changes in aircraft performance
- the combined action of centrifugal force and kinetic heating resulting from an increase in propeller rotational speed is often effective in reducing the extent of the ice accumulation
- thus, it appears that in operation of unprotected or inadequately protected propellers in icing conditions, periodic attempts should be made to throw off the accretions by increasing propeller speed.
The propeller manufacturer for VH-MSF, Hartzell, stated on its website that ‘ice typically appears on propeller blades before it forms on the wings, so it’s important to address propeller icing as quickly as possible’. While the NACA (1950) report and the Cirrus FIKI supplement both indicated that increasing the propeller speed was a technique to address propeller icing, another similar technique, published as an online instructional video, was to cycle the propeller lever forwards and backwards. This would vary the propeller blade angle and propeller speed to promote shedding of ice. As the Cirrus aircraft combine the propeller pitch control and engine power control in one lever, the use of propeller blade angle and rotational speed changes to shed ice would be accompanied by associated engine power changes. The ATSB was unable to establish if the pilot was aware of these techniques to remove ice accumulation on the propeller.
Related occurrences
There have been a number of loss of control accidents involving Cirrus SR22 aircraft with contributors including flight in icing conditions, autopilot control issues, pilot incapacitation and loss of control during stall demonstration to name a few. A varied sample of those events is listed below from the United States National Transportation Safety Board (NTSB) and the ATSB.
NTSB investigation (ATL06LA035)
While climbing on autopilot, the airplane entered clouds at 5,000 ft at an airspeed of 120 kt. Upon reaching 7,000 ft, the airplane encountered icing conditions. The pilot informed air traffic control and requested a clearance to climb to 9,000 ft, which was approved. As the airplane reached the cloud tops at 8,000 ft when in visual flight conditions, the airplane began to buffet. The pilot looked at the airspeed indicator and it showed 80 kt. The airplane subsequently aerodynamically stalled, started to spin and re‑entered instrument flight conditions. The pilot deployed the ballistic parachute system and informed the air traffic controller of his actions. The airplane descended under the parachute canopy into the trees.
The NTSB determined the probable cause of the accident to be:
The pilot’s inadequate pre-flight planning, failure to obtain a current weather briefing, and his decision to operate the airplane into known icing outside the airplanes certification standards resulting in the aircraft accumulating ice, loss of airspeed, an inadvertent stall/spin and subsequent collision with trees.
NTSB investigation (ERA20LA129)
While conducting an instrument landing system approach, the airplane flew through the localizer course, and as it passed outside of the outer edge of the localizer, the autopilot turned off. The pilot could not recall turning the autopilot off, and the reason for the autopilot turning off could not be determined from the available evidence. Over the next minute, a series of altitude excursions occurred during which the airplane repeatedly climbed and descended. The pilot reported that, when he added power, he had difficulty maintaining control of the airplane and that it was unstable. Subsequently, the pilot sensed that he was fighting the airplane and in an unusual attitude, he deployed the airframe’s parachute system. The airplane descended under canopy and touched down in the backyard of a house.
While off course with the autopilot engaged and the vertical speed mode selected, the pilot likely applied and held pitch control input that was sensed by the autopilot auto trim system as an out‑of-trim condition. The autopilot auto trim system responded by trimming the airplane, resulting in the corresponding altitude excursions.
The NTSB determined the probable cause of the accident to be:
The pilot’s incorrect use of the autopilot while approaching the initial approach fix and his subsequent improper primary pitch control input while a pitch mode of the autopilot was engaged, which resulted in pitch excursions and subsequent departure from controlled flight.
NTSB investigation (NYC05LA110)
The airplane was in cruise flight at 3,000 ft when the pilot experienced a seizure and lost consciousness. When the pilot awakened, the airplane was in a high-speed descent. In addition, the pilot felt disoriented and numbness in his right leg. The pilot recovered from the descent at an altitude of about 1,700 ft and elected to deploy the CAPS. The airplane descended via the parachute and impacted in a river. The airplane sustained substantial damage to the underside of the composite fuselage. The pilot sustained a fractured vertebra and was able to egress from the airplane before it sank. Subsequent medical examinations on the pilot revealed the presence of a brain tumour.
The NTSB determined the probable cause(s) of this accident to be:
The pilot's physiological condition, which resulted in his incapacitation during the flight, and subsequent loss of aircraft control.
ATSB investigation (AO-2013-126)
The aircraft was being operated on a private flight from Archerfield to Kingaroy, Queensland, with the pilot and one passenger on board. On approach to Kingaroy, at about 500 ft above ground level, the pilot extended the flaps and, shortly after, disconnected the autopilot (AP). Upon disconnecting the autopilot, the pilot reported that the aircraft pitched-up violently due to trim runaway.
The AP pitch trim was trimming the aircraft for a nose-up position, even though the AP was disconnected. This required the pilot to use a large amount of forward physical force to maintain stable flight. The pilot attempted to resolve the problem several times by pressing and holding the autopilot disconnect switch located on the control yoke, however, this had no effect.
The pilot then conducted a go-around. They then used the manual electric trim (MET) hat switch located on the control yoke, in an attempt to trim the aircraft nose-down. As the pilot was using the MET to trim the aircraft, which was going against the AP pitch trim runaway, the trim adjusted at a slow rate.
The pilot was able to regain sufficient control of the aircraft and land safely at Kingaroy. The pilot reported that, upon parking the aircraft and after releasing the MET, the pitch trim was at full nose‑up deflection.
ATSB investigation AO-2014-083
When at about 6,000 ft above ground level, the pilot in command (PIC) was demonstrating the aircraft stall and recovery to a prospective purchaser of the aircraft. They selected 50% flap, rolled the aircraft into a left turn at about 25° angle of bank, reduced the power to idle, and raised the nose. As the aircraft approached the stall, the PIC pointed to the vertical speed indicator. As they did this, the right wing dropped rapidly, and the aircraft entered a spin to the right. The PIC reported that, at this time, they performed their normal recovery procedure for this manoeuvre.
The passenger in the front seat reported that, on about the third rotation of the spin, the PIC said ‘I’m sorry’, and realised that the PIC had lost control of the aircraft.
When at about 2,000 ft, the PIC was unsure whether they had enough height remaining to recover control of the aircraft, so they successfully deployed the CAPS, and the aircraft came to rest in a residential backyard. All 3 occupants were uninjured.
Downloaded flight data indicated that the aircraft stalled at an indicated airspeed of 62 kt and the vertical descent rate in the spin increased to a maximum of 14,000 ft/min before the parachute was deployed.
Safety analysis
Introduction
Flight track data showed that, about 12 minutes after take-off and during the climb phase of the flight from Canberra, Australian Capital Territory, to Armidale, New South Wales, VH‑MSF departed controlled flight and entered a rapid descent just prior to reaching the planned cruising level of 10,000 ft. The aircraft subsequently impacted with terrain. The 4 occupants were fatally injured, and a post-impact fire destroyed the aircraft.
This analysis will consider the events leading up to the departure from controlled flight and the possible explanations for this. It will also consider why the pilot did not recover the aircraft from the rapid descent and the forecast and actual meteorological conditions along the aircraft’s flight track.
Aerodynamic stall
Consistent with the 2 previous flights, the aircraft’s flight tracking data showed a normal, stable take-off and climb out of Canberra Airport towards Armidale until about 7,000 ft above mean sea level. This suggested that the pilot may have been using the aircraft’s autopilot system. Also, up to this point, all radio exchanges between the pilot and air traffic control were clear and readback correctly.
Climbing through about 8,300 ft, the flight track data changed from a relatively steady state to variations in heading, altitude and airspeed. This suggested that the aircraft had likely changed from operating with the autopilot on to manually controlled flight. Potential reasons for this change may have included the avoidance of cloud, turbulence or issues with the autopilot. It was around this time that 4 independent witnesses located below the aircraft’s flight track reported that an aircraft obscured by cloud could be heard making engine surging sounds (see Possible explanations for the contributing factors below for further explanation).
Over the next couple of minutes, while the general trajectory of the aircraft remained in a climb, the aircraft slowed to almost the stall speed on 2 occasions. If working as designed, the stall warning system should have sounded when the aircraft’s airspeed deteriorated to about 5 kt above the stall speed, alerting the pilot to an impending stall condition. Additionally, as a precursor to the stall, a slight buffet might have been felt by the pilot through the airframe. The pilot’s operating handbook (POH) stipulated that, when the stall warning sounds, recovery was accomplished by immediately reducing back pressure on the control yoke to reduce the angle of attack, maintain a safe airspeed, and add power as required. Following these 2 occasions, the flight data showed a slight descent and an increase in airspeed, which may have been representative of a possible pre-stall recovery and then the climb continued.
Following a descent, the performance data indicated a climb rate of up to about 1,500 ft/min and the airspeed decreased from an estimated 96 kt to 70 kt past the point of a pre-stall recovery. At a maximum altitude of 9,946 ft, the airspeed and altitude rapidly decreased, which was consistent with the aircraft aerodynamically stalling and departing controlled flight.
Contributing factor
When approaching 10,000 ft above mean sea level, the aircraft climb rate increased significantly combined with a decreasing airspeed, resulting in an aerodynamic stall and departure from controlled flight.
Recovery actions
The POH procedure for a recovery from an aerodynamic stall required the pilot to reduce back pressure on the control yoke to un-stall the wings and apply power, as necessary, to accelerate the aircraft. However, the flight data showed that, following the stall at about 9,900 ft, the rate of descent increased to about 13,000 ft/min, which was inconsistent with a stall recovery. While descending through around 8,000 ft, the ground speed reduced while the variations in the track became larger, and the rate of descent started to reduce towards 10,000 ft/min by ground level. This, combined with the witness observations, wreckage examination, and manufacturer’s assessment of the flight data, indicated the aircraft had likely entered a spin before the impact with terrain.
The POH stipulated that, following a loss of control when recovery may not be possible, the Cirrus airframe parachute system (CAPS) should be used. The POH further indicated that the only method of recovery from a spin was to deploy the CAPS. The decision to activate the CAPS should be made prior to an altitude of 2,000 ft above ground level. The POH also suggested that when no other survivable options were available, the CAPS should be activated regardless of altitude. That said, the ATSB considered there was adequate time (about 44 seconds) to deploy the CAPS following the departure from controlled flight. However, the inspection of the wreckage indicated that the CAPS had not deployed in-flight, but rather due to ground impact forces. That examination also found that the pre‑deployment procedure of shutting down the engine was not conducted.
It was also determined that a deployment failure was unlikely given the system’s recent replacement, high reliability and the ground impact initiation of the rocket. Therefore, the ATSB was unable to ascertain why the aircraft was not recovered from the stall or if an attempt was made to deploy the CAPS in-flight.
Contributing factor
Following the loss of control, for undetermined reasons, an aerodynamic stall recovery did not occur nor was the Cirrus aircraft parachute system deployed before the impact with terrain.
Possible explanations for the contributing factors
The flight data showed aircraft performance and handling that was beyond what was considered normal, particularly the maintained climb at reducing airspeed leading to the stall. As such, the following section will discuss several scenarios that were considered by the ATSB, which may explain the stall and subsequent loss of control, with no recovery action taken. Those factors include whether there was an aircraft issue, if the pilot had some level of incapacitation, or if in‑flight icing was experienced.
Aircraft issue
There were no reported problems with the aircraft on the 2 flights in the days that preceded the accident. A review of the maintenance documentation revealed 2 items of maintenance that were overdue, which were the standby compass calibration and an outside air temperature/clock back-up battery replacement. However, neither of those items were of significance and should not have contributed to the loss of control. All major aircraft components were identified in the general area of the accident site with an in-flight failure of the airframe structure ruled out. While the post‑impact fire prevented examination of a significant proportion of the aircraft, an inspection of the remaining aircraft structure and flight controls did not identify any pre-accident anomalies.
There have been previous occurrences related to the autopilot and pitch trim systems. However, in this case, the position of the relevant switches and trim could not be established due to the extent of damage.
Witnesses reported hearing surging or a rough running engine along the aircraft flight path in the minutes prior to the departure from controlled flight. If the sound heard was from VH‑MSF, this could potentially suggest an engine issue or alternatively, the pilot manipulating the engine power lever. There were also short periods in the flight track that indicated possible power reductions and loss of altitude, but the general trajectory of the aircraft remained in a climb until the aerodynamic stall.
The engine was disassembled and inspected by the ATSB with no pre-impact mechanical defects identified. The inspection of the propeller damage and crankshaft fracture indicated evidence that the engine was running at low power when it impacted with terrain, although the ATSB was unable to ascertain if the engine controls were set at a low power setting (matching the observed propeller damage). It was also noted that no radio call was received from the pilot advising of a problem, nor had they attempted a diversion to a nearby airfield or return to Canberra, which would be expected if an aircraft issue was experienced.
Therefore, while there were no observable indications of an issue, due to the limited remaining aircraft structure and systems that were available for inspection, an unidentified mechanical failure or anomaly could not be discounted.
Pilot incapacitation
Partial or complete incapacitation can adversely affect a pilot’s psychological and/or physiological capacity to operate an aircraft. Research has shown that pilot incapacitation occurs for a variety of reasons including acute medical conditions (such as food poisoning and gastroenteritis) and pre‑existing medical conditions (such as heart disease, leading to a heart attack). While pilot incapacitation in general aviation accounted for only 13% of all reported occurrences between 2010 and 2014, 70% of those influenced flight operations, namely a return to the departure aerodrome or in the worst case, a collision with terrain (ATSB, 2016). In this accident, indicators of a potential incapacitation were:
the absence of radio calls to indicate a problem or phase of distress
the lack of stall recovery actions with ample altitude and time to recover
the non-use of the CAPS as a procedural recovery action when there was sufficient altitude for deployment.
The pilot’s post-mortem identified a heart anomaly, however, it was noted that in most cases symptoms do not present. Overall, the post-mortem report concluded that the cause of death was undetermined and that an assessment should be made in consideration of the other available evidence to determine if sudden incapacitation may have contributed to the accident.
Therefore, to further examine the possibility of an incapacitating event, the ATSB requested the assistance of an independent doctor of forensic pathology to undertake an assessment of the pilot’s post‑mortem, toxicology and medical history. However, that assessment did not identify any underlying medical conditions, natural disease or toxicological abnormalities that could have led to an incapacitation event.
In addition, records indicated the pilot consistently used a continuous positive airway pressure machine to manage sleep apnoea. As the pilot had taken the machine on their trip, it was likely that they had used it the night before the accident. Also, it was noted that the pilot had lunch just prior to departure, and as the research has shown, gastroenteritis related incapacitation can occur and therefore could not be discounted.
Further, there was no evidence to suggest that the pilot's general health on the day of the accident was degraded. Similarly, the pilot was reported to be fit and healthy and had no identified health conditions that were not being appropriately treated. Consequently, there was insufficient evidence to determine if incapacitation was a contributing factor. That said, medical incapacitation can result for many reasons that may have been undetectable in the post-mortem, toxicology and review of the available medical information.
Icing conditions
The subsequent graphical area forecast accessed by the pilot, which was valid for the flight, indicated broken cloud was expected from 5,000 ft to 10,000 ft along the aircraft’s flight path after departing Canberra. The Bureau of Meteorology’s post-accident analysis concluded that the actual conditions experienced were consistent with the forecast conditions. This analysis estimated a cloud depth of 3,000 ft, with a top height of 10,000 ft, which was the pilot’s nominated cruising altitude. The ATSB’s analysis of the satellite imagery also showed cloud coverage along parts of the aircraft’s track. Likewise, the camera footage and automatic terminal information service at Canberra, and video from first responders at the accident site also noted cloud in the vicinity.
The Bureau of Meteorology’s analysis also determined an approximate freezing level of 7,000 ft. On that basis, it was concluded that the conditions would have been conducive to moderate icing between about 7,000 ft and 10,000 ft, when in cloud. The presence of icing was consistent with pilot observations and data from other aircraft operating in the vicinity of Canberra. The pilot of another Cirrus aircraft reported using the icing protection system when operating at about 9,000 ft. Likewise, the flight data from Velocity 1690 showed that, on descent, the engine anti-ice system had been used from about 10,000 ft down to 7,000 ft, indicating the aircraft was operating in cloud above the freezing level during that time. Therefore, considering the flight path and cruising altitude, VH-MSF likely entered cloud at some point during the flight and was subject to icing conditions.
Operations in icing conditions can lead to performance degradation and changes in aircraft handling due to ice accretion on the wings and control surfaces, and a reduction in engine power due to blocked engine air intakes and ice‑affected propeller blades. It can also result in erroneous airspeed and altitude information due to blocked pitot static systems, loss of visibility due to ice on the windshield, render a stall warning system ineffective, and weaken radio signals due to ice accretion on antennas.
The propeller will likely accumulate ice faster than the airframe and there are techniques for shedding propeller ice, which involve increasing the propeller speed and varying the propeller blade angle. In the Cirrus SR22 aircraft, the propeller lever is combined with the engine power lever and therefore the use of propeller speed and blade angle variations to shed ice would be accompanied by engine power changes. While this technique might have produced the engine power fluctuations heard by witnesses, who were located where the aircraft’s flight path was above the freezing level, the ATSB was unable to determine if the pilot was aware of this technique.
Consistent with the United States Federal Aviation Administration’s guidance, the POH stipulated that, when icing was encountered, the pilot should immediately exit icing conditions by turning back or changing altitude. However, the flight data showed that, overall, the aircraft continued to climb toward the cruising altitude. Also, while there were some variations in the aircraft’s track with a more observable change up to 35° later in the flight, there was no indication of a turnback towards Canberra. Likewise, there was no radio call received from the pilot advising of an intention to change altitude, divert from track or turnback due to icing. Although it was noted that icing has the potential to interfere with communication systems.
The POH also stated that a gradual loss of engine manifold pressure and eventual engine roughness due to intake icing could result, like what was heard by witnesses. However, the ATSB was unable to ascertain if the change in engine sound was from the pilot manipulating the engine control or uncommanded surging of the engine. Despite this, and as previously noted, there was no radio call received from the pilot advising of an engine issue nor was there an attempted diversion or return.
The Federal Aviation Administration’s guidance also indicated that, in moderate icing, a representative accretion rate for reference purposes was about 2.5 to 7.5 cm per hour on the outer wing. If the aircraft was in cloud for the entire period above the freezing level, the maximum amount of time spent in icing conditions before the loss of control would have been about 5 minutes. Therefore, a worst-case scenario was that the aircraft’s outer wings accumulated between 2.1 mm to 6.2 mm of ice. That said, satellite imagery with a flight track overlay showed some flight above the freezing level was likely to have been clear of cloud. Therefore, it was likely that the amount of time spent in icing conditions was less than 5 minutes. However, the exact amount of time spent in these conditions was unable to be determined due to the dynamic nature of the cloud on the day of the accident and the 10‑minute capture between local area satellite images.
When about 1,000 ft above the freezing level, the heading, altitude and airspeed variations had commenced, which might suggest performance effects from icing or cloud avoidance. However, the general trajectory of the aircraft was a climb up to the point of the stall. Also, the aircraft went through a period of about 45 seconds where it achieved the best rate of climb, which was about 1 minute and 30 seconds before the stall. That rate of climb would likely be unachievable if the aircraft had significant icing accretion. Further, as shown in the SR22 ice accretion accident example in this report, if an aircraft was affected by ice the stall speed for the aircraft would likely be much higher than the normal stall speed.
In summary, icing may explain the rough running engine, the variations observed in the flight data, and reduction in airspeed to the point of a stall. However, from the available evidence, it could not be established with a reasonable degree of probability that the aircraft experienced icing for a duration sufficient to result in performance degradation or other known icing issues and, therefore, contributed to the accident. Also, experiencing icing did not explain why the CAPS was not deployed following the loss of control and entry into a spin.
Flight plan
On the morning of the accident, the pilot lodged an instrument flight rules plan with a cruising altitude of 10,000 ft. Canberra Airport was within an area that had a forecast for broken cloud with a layer of moderate icing present below the pilot’s planned cruising altitude. At the time the pilot submitted the flight plan, the cloud tops along the planned route from Canberra to waypoint CULIN were forecast to be 7,000 ft and the layer of icing was expected to be about 1,500 ft deep with the top 3,000 ft below the planned cruising level. However, when the pilot checked the weather later in the morning the cloud tops were forecast to reach 10,000 ft and the icing layer was expected to be about 3,000 ft deep, which could only be avoided if the aircraft remained clear of the broken cloud. The aircraft was not fitted with anti‑icing equipment and was prohibited from operating in icing conditions. Therefore, the only way for the pilot to ensure that icing conditions would be avoided (if they did not amend their planned flight track) was to avoid flying the aircraft in cloud at those levels where icing was forecast.
Noting the lowest safe altitude from Canberra to CULIN was 4,600 ft, the pilot had the opportunity to amend their flight plan to fly this sector at 6,000 ft, below the freezing level. Alternatively, before departing Canberra, the pilot could have requested from air traffic control either a change of cruising altitude and/or a change in track. Likewise, a clearance to manoeuvre left or right of the planned track, or to climb or descend clear of cloud if icing became an issue after take-off, was a possibility. Neither of those options occurred and while the satellite imagery, and recorded images from Canberra and the accident site, indicated there were patches of clear sky, it was considered unlikely that the pilot was able to avoid all cloud above the freezing level.
Noting that the aircraft would have likely been subject to moderate turbulence during the climb, it was possible the pilot was expecting smooth and clear flying conditions on top of the cloud at 10,000 ft. While this might have been a consideration for the pilot’s plan, it could not be confirmed if that was the reason. Despite this, and as discussed above, the ATSB was unable to determine if the aircraft experienced icing to an extent that affected performance and handling.
However, aircraft flying through cloud in sub-freezing temperatures are likely to experience some degree of icing. Operating in these conditions in aircraft that are prohibited from doing so increases the risk of a loss of control event leading to an accident. A pilot can reduce the chance of icing becoming an issue by selecting appropriate routes during the flight planning stage.
Other factor that increased risk
The flight was planned and flown through forecast moderate icing conditions from about 7,000 ft in an aircraft that was prohibited from operating in those conditions. It was therefore likely that the aircraft encountered icing, however, there was insufficient evidence to determine if it was at a level sufficient to affect aircraft performance and/or handling.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Cirrus SR22, VH-MSF, near Gundaroo, New South Wales, on 6 October 2023.
Contributing factors
When approaching 10,000 ft above mean sea level, the aircraft climb rate increased significantly combined with a decreasing airspeed, resulting in an aerodynamic stall and departure from controlled flight.
Following the loss of control, for undetermined reasons, an aerodynamic stall recovery did not occur nor was the Cirrus aircraft parachute system deployed before the impact with terrain.
Other factors that increased risk
The flight was planned and flown through forecast moderate icing conditions from about 7,000 ft in an aircraft that was prohibited from operating in those conditions. It was therefore likely that the aircraft encountered icing, however, there was insufficient evidence to determine if it was at a level sufficient to affect aircraft performance and/or handling.
Glossary
ADS-B
Automatic dependant surveillance broadcast
AGL
Above ground level
AMSL
Above mean sea level
AoA
Angle of attack
CAPS
Cirrus airframe parachute system
CAS
Calibrated airspeed
CPAP
Continuous positive airway pressure
FIKI
Flight into known icing
GAF
Graphical area forecast
GPWT
Grid point wind and temperature forecast
IFR
Instrument flight rules
NAIPS
National Aeronautical Information Processing System
NOTAM
Notice to airmen
NTSB
United States National Transportation Safety Board
POH
Pilot’s operating handbook
RNP
Required navigation performance
Sources and submissions
Sources of information
The sources of information during the investigation included:
Cirrus Design Corporation
the aircraft owner
the maintenance organisation
witnesses
Airservices Australia
Bureau of Meteorology
Civil Aviation Safety Authority
forensic pathology specialist
NSW Police Force
United States National Transportation Safety Board.
References
Australian Transport Safety Bureau. (2016). Pilot incapacitation occurrences 2010-2014 (AR‑2015-096).
National Transportation Safety Board. (2022).Investigation ERA20LA129 - Autopilot issue and loss of control - Cirrus SR22 – Conway, South Carolina USA – March 17, 2020. https://data.ntsb.gov
National Transportation Safety Board. (2006). Investigation ATL06LA035 - Icing conditions and loss of control - Cirrus SR22 – Childersburg, Alabama USA. https://data.ntsb.gov
National Transportation Safety Board. (2006). Investigation NYC05LA110 - Pilot incapacitation and loss of control - Cirrus SR22 - Haverstraw, New York USA – June 30, 2005. https://data.ntsb.gov
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Cirrus Design Corporation
aircraft owner
maintenance organisation
Bureau of Meteorology
Airservices Australia
Civil Aviation Safety Authority
forensic pathology specialist
United States National Transportation Safety Board.
Submissions were received from the:
aircraft owner
Civil Aviation Safety Authority
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix A
VH-MSF aggregated ADS-B altitude data for the accident flight, together with the estimated airspeed.
This image depicts selected ADS-B data and derived estimates of calibrated airspeed and altitude for VH-MSF during the accident flight. The airspeed has been estimated using data from a Boeing 737 descending into Canberra, Australian Capital Territory, a short time prior to the accident. Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]The pilot’s flight plan comprised a series of defined geographic positions (waypoints) via which the pilot intended to navigate the aircraft to Armidale. The flight notification’s first waypoint after departing Canberra was CULIN.
[3]RNP: Required navigation performance for en route use, which can be met with a single global navigation satellite system receiver.
[4]The ADS-B equipment transmitted flight data that enabled air traffic service providers to track aircraft when operating outside coverage of conventional air traffic control radar. Airservices Australia recorded the transmissions received by their network of ground-based ADS-B receivers. That data could also be received by other aircraft with suitable equipment and privately-operated ground-based equipment, feeding information to flight tracking websites.
[5]When an aircraft is in a spin, propeller, engine induction and exhaust will often sound like they are fluctuating due to rotating directional noise sources and the doppler effect, which is the shift in intensity of the sound waves due to relative motion of the wave source and the observer.
[6] Pitot probes provide the flight instruments with airspeed information and are ineffective if covered or blocked.
[7]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[8]The National Aeronautical Information Processing System is a multi-function, computerised, aeronautical information system that allows users, such as pilots, to obtain weather information and submit flight plans into the air traffic system.
[9]Notice to airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[10]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky and ‘broken’ indicates that more than half to almost all the sky is covered.
[11]The freezing level is the height in feet above mean sea level where the air temperature is 0 °C.
[12]The rate of accumulation of moderate icing is such that even short encounters become potentially hazardous and the use of de-icing/anti-icing equipment or a flight diversion is necessary.
[13]ATIS: an automated pre-recorded transmission indicating the prevailing weather conditions at the aerodrome and other relevant operational information for arriving and departing aircraft.
[14]The cloud height broadcast on the automatic terminal information service is above aerodrome elevation.
[15]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[16]Engine cowl anti-ice is activated when the OAT on the ground, or TAT in-flight, is less than 10 °C in visible moisture.
[17]This estimate was based on the forecast and the temperature data from an inbound Boeing 737 to Canberra, which transited through airspace close to the outbound track for VH-MSF.
[18]Composite image produced by composing satellite images coloured in red, green and blue.
[19]The aircraft was fitted with on-board ADS-B equipment, transmitting real-time operational data from the aircraft’s global positioning system and pressure-sensitive altimeter, which enabled air traffic service providers to track aircraft. Airservices Australia recorded the transmissions received by its network of ADS-B receivers. That data could also be received by privately-operated equipment used to feed information to flight tracking websites.
[20]ADS-B data was obtained from various sources, including Airservices Australia, FlyRealTraffic.com and FlightRadar24.
[21]CAS: calibrated airspeed is indicated airspeed corrected for the aircraft’s pitot and static source position errors. Correcting calibrated airspeed for density altitude and air compressibility effects gives true airspeed.
[22]A spin occurs when an aircraft simultaneously aerodynamically stalls and yaws, resulting in a downward, corkscrew path.
[23] The flight on 3 October 2023 was from Redcliffe to Armidale and the flight on 4 October 2023 was from Armidale to Canberra.
[24]Carbon monoxide is a colourless, odourless, tasteless and poisonous gas that is produced as a by-product of burnt fuel. Exposure to a leak from the exhaust of an aircraft engine into the cabin can lead to elevated levels of carbon monoxide, which can impair cognitive function.
[25]A full post-mortem involves a detailed external examination, and a gross and histological examination of organs and tissues contained in the abdominal, thoracic and cranial body cavities. A limited post-mortem is one in which restrictions are placed on the examination, for example, limited to an external examination only with X-rays, computed tomography or magnetic resonance imaging or restricted to an examination of the tissues in only one or 2 body cavities (https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2013_051.pdf).
[26]Yaw: the motion of an aircraft about its vertical or normal axis.
[27]Significant meteorological information (SIGMET): a weather advisory service that provides the location, extent, expected movement and change in intensity of potentially hazardous (significant) or extreme meteorological conditions that are dangerous to most aircraft, such as thunderstorms or severe turbulence.
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Co 204B, registered VH‑EQW, was tasked with fire-fighting operations utilising a 1,200 L bucket with a short line. The helicopter departed from a private property near Amberley, Queensland, and tracked to another property in Tarome, about 26 NM (48 km) away. The pilot was operating the helicopter from the left seat for visibility while conducting the operation.
After arriving at Tarome, the pilot commenced picking up their first load of water from a dam. The pilot reported that, during water collection, they heard an unusual noise and that the helicopter ‘kicked’. Remaining in the hover, the pilot checked that all engine indications were normal and that the bucket and line were in the appropriate place. However, the pilot reported that something still did not feel right. As a result, they elected to dump the water from the bucket and initiate a climb out. Within about 10-15 seconds, as engine power was being applied, and the water was being released from the bucket, the pilot heard what they described as a ‘loud roaring’ sound and the helicopter pitched up, yawed, and subsequently had a reduction in power. The helicopter rolled left and impacted the water at low speed. The pilot sustained minor injuries and the helicopter was destroyed.
Witness observations
The accident was observed by 2 witnesses (Figure 1). ‘Witness 1’ observed the helicopter circle, move towards the dam on their property to collect water, and the entirety of the accident sequence. They photographed and videoed the helicopter’s movements up until a few seconds before the accident (Figure 2). That witness did not see or hear anything unusual before the helicopter impacted the water. ‘Witness 2’ was on an adjacent property; they noted a definitive increase in what they thought may have been engine noise just before the accident occurred.
Figure 1: VH-EQW flight track with accident site and witness locations
Source: Google Earth, modified by the ATSB
Figure 2: VH-EQW picking up water from the dam just prior the accident
Source: Supplied
Pilot egress
Almost immediately after the impact, the helicopter inverted, started to fill with water, and sink rapidly. The pilot removed their seatbelt and helmet, and attempted to open the front left door but could not open it with either the normal or emergency release handles. When the helicopter was almost fully submerged, the pilot swam to the rear of the cabin and tried to open the rear right door but could not open it either, making further attempts to get out by kicking the helicopter windows. The pilot then moved to the rear left door and, utilising considerable force, was able to successfully open it. The pilot noted in interview, that when they initially attempted to open the doors, they may have been trying to move the door handles in the incorrect (opposite) direction due to the helicopter being inverted.
The pilot escaped and swam a few metres to the surface and then to the side of the dam. The pilot stated that familiarity with the helicopter, the open area in the cabin (all seats removed) and HUET (helicopter underwater escape training) all assisted with their ability to successfully escape from the helicopter.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) with ratings for single and gas turbine engine helicopters. Prior to the accident flight, the pilot had accumulated 2,599.4 hours of total flying experience and 220.8 hours on the Bell 204B type helicopter.
The pilot last completed an aerial application proficiency check on 29 June 2023, which was valid until 20 June 2024. The pilot was qualified to conduct helicopter fire-fighting operations and had both low‑level and sling operation ratings.
The pilot held a Class 1 Aviation Medical Certificate, valid to 12 June 2024, with no restrictions.
Aircraft information
The Bell Helicopter Company 204B is the civilian version of the UH-1 Iroquois. It was designed in the mid 1950’s as a utility helicopter. The helicopter had a 2-blade main rotor and 2-blade tail rotor and was powered by an Ozark Aeroworks T53-L-13B turboshaft engine. The accident helicopter (S/N 2038) was manufactured in the United States in 1965. The helicopter was first registered in Australia in 2014 as VH-EQW and had accumulated about 23,515 total time-in-service. It had a current airworthiness certificate and maintenance release with no outstanding defects at the time of the accident.
Wreckage examination
The helicopter was recovered from the dam and taken to a secure facility for detailed examination. The helicopter’s rotor systems, flight controls, exits, and engine were visually examined. No pre‑accident damage was identified. The pilot’s left front door emergency jettison system was tested serviceable.
Further investigation
To date, the ATSB has interviewed the pilot, the witnesses, and conducted a preliminary examination of the helicopter wreckage.
The investigation is continuing and will include review and examination of:
the pilot’s training and records
maintenance documentation
key components of the helicopter.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Company 204B, registered VH‑EQW, was tasked with firefighting operations utilising a 1,230 L (Bambi Max) water bucket with a 5 m line. The helicopter departed on a 25-minute flight from a private property near Amberley, Queensland, and tracked to another property in Tarome, about 48 km to the south‑west.
While picking up a full bucket of water from the dam, the helicopter lost control, impacted the water, and subsequently sank to the bottom of the dam. The pilot extricated themselves with only minor injuries, however, the helicopter was destroyed.
What the ATSB found
The ATSB found that the Bambi Bucket suspension cables were caught over the left rear skid when the helicopter was on approach to the dam and during the water collection into the bucket. As the load of water was lifted, it was almost certain that the helicopter’s centre of gravity moved aft and left due to the tethered weight over the left rear skid. This resulted in asymmetric lift loads, loss of control and collision with water.
The ATSB’s examination of the wreckage did not identify any pre-impact defects with the helicopter. Also, the pilot had completed helicopter underwater escape training (HUET) about 2.5 years prior to the accident.
Safety message
Conducting helicopter external load operations over water is a complex task, with the risk of an accident shown to be over twice as high as private helicopter operations. There can be a lack of visual references, visual illusions over water, limited visibility and vertical reference of the hook and external load through mirrors and bubble windows.
As shown in this accident, fouling of external load suspension cable(s) on the airframe can lead to rapid changes in weight distribution, asymmetric lift and loss of control. This investigation reinforces that correct cable positioning is vital to the safety of external lift operations. Further, this accident highlights the importance of conducting HUET to increase the occupants’ chances of post-accident survival in the event of impact with water.
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Company 204B, registered VH‑EQW, was tasked with firefighting operations utilising a 1,230 L water bucket (Bambi Max) with 5 m cables.
The helicopter departed from a private property near Amberley, Queensland, on a 25-minute flight to another property near Tarome, about 48 km away (Figure 1) with the intention of uplifting water from a dam (dip site) with the water bucket slung under the helicopter for firefighting operations. The flight track data indicated that the helicopter had an average cruise ground speed of about 85 kt (78 kt indicated airspeed (IAS)), with a maximum of 93 kt (85 kt IAS).[1]
After arriving overhead the property, the pilot aligned the helicopter with the dam, descended over the water to the dip site and submerged the bucket. As the pilot began to initiate the bucket lift, control of the helicopter was lost, and it impacted the water surface and sank. The pilot sustained minor injuries, but exited and swam to shore, and the helicopter was destroyed.
Figure 1: VH-EQW flight track from the take-off point to the accident site
Source: Google Earth, modified by the ATSB
Pilot account of events
The pilot was operating the helicopter from the left seat for increased visibility from the bubble window while conducting the external load operation. The pilot recalled that, after arriving at the property at Tarome, they commenced filling their first load of water from a dam. The pilot reported that, during water collection, they heard an unusual noise and that the helicopter ‘kicked a bit’. Remaining in the hover, the pilot checked that all engine indications were normal and that the bucket and line were in the appropriate place. However, the pilot reported that something still did not feel right. As a result, they elected to dump the water from the bucket and initiate a climb out. The pilot stated that, within about 10–15 seconds, as engine power was being applied and the water was being released (dumped) from the bucket, the pilot heard what they described as a ‘loud roaring’ sound and the helicopter pitched up, yawed, rolled left, and impacted the water at low speed.
Witness observations
The accident was observed by 2 witnesses (Figure 2). Witness 1 observed the helicopter circle, move towards the dam on their property to collect water, and observed the entire accident sequence. They also photographed and videoed the helicopter’s movements up until moments before the accident. The witness did not see or hear anything unusual before the helicopter impacted the water. Witness 2 was on an adjacent property; they noted a definitive increase in what they thought may have been engine noise just before the accident occurred.
Figure 2: VH-EQW flight track with accident site and witness locations
Source: Google Earth, modified by the ATSB
Witness video
Recorded video taken by witness 1 just prior to the accident showed the helicopter on approach to the dam. It captured the water bucket suspension cable caught over the rear of the left skid when on the approach (from the start of the video – Figure 3 top) until the helicopter was initiating lift‑off with the external load of water (Figure 3 lower). The video ended as the helicopter started to take the weight of the bucket, which contained a large quantity of water. The helicopter was recorded starting to pitch up and roll left before the video stopped. There was no discernible change in sounds emanating from the helicopter for the duration of the video.
Figure 3: Sequence of water pickup from dam showing bucket cable position from approach (top) to lifting off (lower)
Source: Still photographs taken from witness video, annotated by the ATSB
Pilot egress
The pilot recalled that, after the surface impact, the helicopter almost immediately became inverted, filled with water, and sank to the bottom of the dam. The pilot stated that they removed their seatbelt and helmet and attempted to open the front left door but could not open it with either the normal or emergency release handles. The helicopter was almost fully submerged when the pilot swam to the rear of the cabin and tried to open the rear right door. They made further unsuccessful attempts to egress by kicking the helicopter windows.
The pilot then moved to the rear left door, and applying considerable force, was able to successfully open it. The pilot recalled that, when they initially attempted to open the emergency exits, they may have been trying to operate the door handles in the incorrect (opposite) direction due to the helicopter being inverted.
The pilot escaped the sinking helicopter and swam a few metres to the surface and then to the side of the dam.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) with ratings for single and gas turbine engine helicopters. Prior to the accident flight, the pilot had accumulated 2,599.4 hours of total flying experience. They had 220.8 hours total on the Bell 204/205/UH-1 helicopter. Of this, 22.8 hours was pilot in command of the Bell 204, which was accrued in the 2 months prior.
The pilot was qualified to conduct helicopter firefighting operations and had low‑level and sling operation ratings. The pilot last completed an aerial application proficiency check on 29 June 2023, which was valid until 20 June 2024, and a low-level helicopter flight review on 12 August 2023.
The pilot held a Class 1 Aviation Medical Certificate, valid to 12 June 2024, with no restrictions.
Helicopter information
General information
The Bell Helicopter Company 204B (and 205) is the civilian version of the UH-1 Iroquois. It was designed in the mid‑1950’s as a utility helicopter. The helicopter had a 2-blade main rotor and 2‑blade tail rotor and was powered by an Ozark Aeroworks T53-L-13B turboshaft engine. The helicopter was manufactured in the United States in 1965 and first registered in Australia in 2014 as VH-EQW. It had accumulated about 23,515 flight hours total time in service and had a current certificate of airworthiness and registration. The helicopter’s technical log had no outstanding defects at the time of the accident.
VH-EQW was fitted with an external load hook located directly underneath the main rotor transmission, in line with the helicopter’s centre of lift.
Bucket and suspension cable information
The Bambi Max water bucket fitted to VH-EQW was manufactured by SEI industries and weighed 67 kg empty and 1,300 kg when full, with a capacity of 1,230 L. The bucket was connected to the helicopter’s external load hook by several stainless steel suspension cables, separated fore and aft by a triangular spreader bar (Figure 4). A dump switch on the collective[2] was connected through a black electrical cable to control the dump valve located in the base of the bucket. The suspension cables used on the day had a length of 5.05 m and the total length including the bucket was 6.27 m.
Figure 4: Photo of exemplar Bambi Max bucket in the stored configuration showing the triangular spreader bar and suspension cables
Source: SEI industries, annotated by the ATSB
External load visibility
The helicopter was fitted with 2 rear vision mirrors that were located under each of the Perspex chin bubbles to provide visibility of the external hook, suspension cables and bucket. The bubble window fitted to the pilot’s left door also allowed for better visibility downwards and, to a limited extent, the rear of the helicopter (Figure 5). In response to this draft report, the pilot reported that the mirrors provided a full and clear view of the external hook and bucket.
Source: Operator, annotated by the ATSB
Bear paw modification
The helicopter had a pad like modification to the skids called ‘bear paws’, which are supplied as a kit of 2. The pads fit under and to the rear of each of the skids and are designed for landings off airport, on uneven or unstable terrain, helping with overall landing stability and to prevent the rear of the skids from sinking into soft surfaces. The bear paws are made from a polymer plastic and feature high impact resistance, durability and flexibility. They are secured to the skid utilising 4 metal clamps (Figure 6).
The helicopter was within weight and balance limits during the transit flight to Tarome. However, when lifting the load, with the suspension cables caught over the left rear skid and a full bucket of water (weighing 1,300 kg), the load shifted significantly to the rear and to the left. In this configuration, ATSB calculations showed that the helicopter was outside its balance limitations with the addition of just a 300 kg external load and well outside the balance limitations with the addition of a full bucket of water.
Meteorological information
The weather at the time of the accident was described by the pilot as clear and calm. The Bureau of Meteorology forecast showed visibility was greater than 10 km and the wind was from the north‑west at 11 kt.
The flight was to the south-west and had a calculated tail wind component of about 3 kt. The meteorological conditions were not considered a factor in this event.
Wreckage examination
General engine and airframe examination
The helicopter was retrieved from the dam and taken to a secure facility for detailed examination. The rotor systems, drive shafts, transmissions, flight controls, exits, and engine were visually examined by the ATSB. The fuel control and overspeed governor units were removed from the engine and sent to the engine type certificate holder for functional testing. That testing did not identify any issues with the unit.
The engine drive to main rotor transmission shaft had broken out of its retaining couplings likely due to the impact. The engine manufacturer stated that the damage to the drive couplings was indicative of significant engine power driving the main rotor transmission at the time when the main rotors impacted with water, creating a sudden stoppage.
The pilot’s left front door emergency jettison system was tested and worked as designed by releasing the door from its hinges.
No pre-impact defects in the engine, flight controls or emergency exits were identified.
Skid examination
The left and right skid had their bear paw pads removed to facilitate the transport of the wreckage to the storage facility. The right skid did not have any notable damage. The left skid had several striation type wear marks at the rear of the skid (Figure 7).
Figure 7: Rear of left and right skid sections with the left skid showing wear marks
Source: ATSB
The left bear paw was refitted to the left skid to facilitate inspection as an assembly. It was noted that the bear paw had permanent deformation damage that indicated that it had rotated counterclockwise (viewed from the rear) until it had come into contact with the rear skid support. There was also damage to one of the attachment clamps, which had been forced forward at its upmost point. That clamp was directly in front of the forward set of wear marks on the rear of the skid. There was further abrasion damage that indicated the left bear paw had flexed downward under significant load on its outboard side (Figure 9).
Figure 8: Left rear skid showing corresponding skid and bear paw damage
Source: ATSB
The ATSB conducted testing with string lines and a spreader bar configured in a similar manner to the water bucket suspension cables. It was identified that, if both sets of cables were caught over the left skid, the position of the forward and rear cable positions was consistent with the locations of the striation type wear damage found on the left skid[3].
Figure 9 shows the left rear skid, viewed from an outboard direction, showing projected alignment with the hook, cable spreader and multiple bucket suspension cables. Detail A and B show close‑up wear patterns consistent with numerous stainless-steel cable wear striations that aligned with the direction of the external cargo hook attachment point.
Figure 9: Outboard of left rear skid showing hook position and likely position of spreader with forward and rear cables aligned with wear damage
Source: ATSB
Pre-flight checks with an external load
Wagtendonk (1996), in Principles of Helicopter Flight, stated that:
When a cable or strap has been attached to the helicopter hook it is most important to ensure that the cable does not pass over the skid or undercarriage leg. As the aircraft rises and the strain is taken on the load, this could cause a serious rolling sequence. Use the mirror or look directly at the cable. Sadly, non-compliance with this simple rule continues to cause problems.
Common best practice is for the bucket to be positioned at the front of the helicopter and for the suspension cables to be routed from the hook between the skids to the front. This gives the pilot the best view of the bucket during take-off and reduces the chances of the suspension cables fowling. If the cables are routed and connected from the back of the helicopter, there is potential that the cables can be caught by the skid and not seen during take-off.
The pilot reported that, during their pre-flight check, the bucket was placed at the front of the helicopter and was functionally tested.
Helicopter underwater escape training
Helicopter underwater escape training (HUET) has been in use around the world since the 1940s and is considered best practice in the overwater helicopter operating industry. HUET is designed to improve survivability after a helicopter ditches or impacts into water. Research of such accidents has shown that occupants who survive the initial impact will likely have to make an in‑water or underwater escape, as helicopters usually rapidly roll inverted post-impact due to the position and mass of the engine/s, transmission and main rotor system. The research has also shown that drowning is the primary cause of death following a helicopter accident into water.
Fear, anxiety, panic, and inaction are the common behavioural responses experienced by occupants during a helicopter accident. In addition to the initial impact, in-rushing water, disorientation, entanglement with debris, unfamiliarity with seatbelt release mechanisms and an inability to reach or open exits have all been cited as problems experienced when attempting to escape from a helicopter following an in-water accident (Rice & Greear, 1973).
HUET involves a module (replicate of a helicopter cabin and fuselage) being lowered into a swimming pool to simulate the sinking of a helicopter. The module can rotate upside down and focuses students on bracing for impact, identifying primary and secondary exit points, egressing the wreckage and surfacing. HUET is normally part of a program of graduated training that builds in complexity, with occupants utilising different seating locations, exits and visibility (via the use of ‘blackout’ goggles). This training is conducted in a controlled environment with safety divers in the water.
HUET is considered to provide individuals with familiarity with the crash environment and confidence in their ability to cope with the emergency situation (Ryack et al., 1986).Interviews with survivors from helicopter accidents requiring underwater escape frequently mention they considered that HUET was very important in their survival. Training provided reflex conditioning, a behaviour pattern to follow, reduced confusion, and reduced panic (Hytten, 1989).
The pilot conducted HUET training in March 2021, with a renewal due in 2024. The pilot reported that familiarity with the helicopter, the open area in the cabin (all seats removed) and HUET assisted with their ability to successfully escape from the sinking helicopter.
Helicopter water bucket operation accidents
The helicopter manufacturer stated that, between 1974 and 2017, there were 6 accidents involving Bell Helicopters conducting external lift operations where the suspension cable became entangled with the skids and the helicopter lost control during water uplift. Two of those accidents involved the Bell 204/205 helicopter and 4 were Bell 206s.
The Flight Safety Foundation conducted a study titled External loads, powerplant problems and obstacles challenge pilots during aerial fire-fighting operations. The study utilised data from helicopter accident reports in the United States between 1974 and 1998.
The study showed that, it was over twice as likely for a firefighting helicopter to be involved in an accident when compared to private helicopter flights. Of the 97 accidents studied, 4 instances were due to water bucket cables being caught on the skids leading to a loss of control during uplift. Further, there were 2 instances where the unloaded water bucket or external load cable came into contact with the tail/tail rotor due to excessive speed, turbulence and manoeuvring.
Two recent accidents, one in 2017 (New Zealand Transport Accident Investigation Commission report AO-2017-001) and one in 2019 (French Bureau d'Enquêtes et d'Analyses report 2019‑0023) also involved helicopter buckets coming into contact with the tail rotor. Those accidents were partly attributed to operating at airspeeds above the manufacturers’ velocity never exceed speeds.
Video evidence showed the Bambi Bucket suspension cables were caught over the left rear skid when the helicopter was on approach to the dam and remained attached to the skid during the water uplift. This evidence was consistent with:
The ATSB’s wreckage examination, which identified that the left rear skid and bear paw showed multiple areas of damage including striation marks indicative of contact with the bucket suspension cables.
Testing of the striation marks alignment with the fore and aft cable positions when attached to the external cargo hook with the triangular load spreader.
The video ruled out the capture of the cables over the skid during the water collection phase. However, the ATSB was unable to identify if the cables had become captured due to pre-flight bucket and cable positioning, take-off manoeuvring or during the transit flight to the dam.
Just before the video ceased, it showed the initiation of the full water bucket uplift followed by the helicopter pitching up and rolling left slightly. The ATSB weight and balance calculations concluded that any bucket weight above 300 kg (full is 1,300 kg) acting over the left rear skid, would be sufficient to move the centre of gravity outside of the helicopter’s balance limit. Therefore, it was almost certain that as the load of water was lifted, the helicopter’s centre of gravity moved aft and left as a result of the suspension cables being caught over the skid. The tethered weight created an asymmetric lifting point, which resulted in a rapid loss of control and subsequent collision with water.
Helicopter underwater escape training
The pilot conducted HUET about 2.5 years prior to the accident. This likely assisted their ability to egress the helicopter through a rear door while inverted and underwater. HUET has been shown to significantly increase the chances of survival in the event of collision with water.
No pre-impact defects
The ATSB wreckage examination did not identify any pre-impact mechanical issues with the helicopter. Further, the engine manufacturer concluded that the engine was supplying significant power to the transmission at the time of the impact with water.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with water involving Bell Helicopter Company 204B helicopter, near Tarome, Queensland, on 20 September 2023.
Contributing factors
The Bambi Bucket suspension cables were caught over the left rear skid. Consequently, as the load of water was lifted, it was almost certain that the helicopter’s centre of gravity moved aft and left, the tethered weight over the skid created an asymmetric lifting point. This resulted in a loss of control and the helicopter collided with water.
Other findings
The pilot conducted helicopter underwater escape training 2.5 years prior to the accident. This training increased the pilot's chances of survival when the helicopter became submerged in the dam.
There were no pre-impact defects identified with the helicopter.
Rice, E, V., & Greear, J. F. (1973). Underwater escape from helicopters. In Proceedings of the Eleventh Annual Symposium, Phoenix, AZ: Survival and Flight Equipment Association, 59-60. Cited in Brooks C., (1989). The Human Factors relating to escape and survival from helicopters ditching in water. AGRAD.
Ryack, B. L., Luria, S. M., & Smith, P. F. (1986). Surviving helicopter crashes at sea: A review of studies of underwater egress from helicopters. Aviation, Space, and Environmental Medicine, 57(6), 603-609.
Wagtendonk, W.J. (1996). Principles of Helicopter Flight, Aviation Supplies & Academics, Inc. Washington, USA.
Veillette, P. R. (1999). External loads, powerplant problems and obstacles challenge pilots during aerial fire-fighting operations (Flight Safety Foundation). https://flightsafety.org
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
chief pilot
aircraft maintenance organisation
National Transportation Safety Board
aircraft and engine manufacturers
Civil Aviation Safety Authority.
Submissions were received from the pilot and chief pilot. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The wind information, density altitude and recorded ground speed was used to calculate the indicated airspeed.
[2]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[3]On 27 October 2024 after directly involved party submissions were completed the pilot advised that they were going to carry out their own testing and reenactments on a Bell 204 helicopter with a Bambi Bucket fitted to ascertain what had occurred.
This is a limited-scope technical examination report, based on ATSB examination and analysis using evidence provided to the ATSB by external parties. The ATSB did not attend the accident site or conduct other activities normally associated with an ATSB occurrence investigation. The information contained in this technical examination report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 12 August 2023, an amateur-built gyroplane, registered G‑2468, collided with terrain while conducting circuit training near Allworth, New South Wales. The instructor pilot was fatally injured and the student pilot was seriously injured.
The Australian Sport Rotorcraft Association (ASRA) produced an investigation report into the occurrence which was obtained by the ATSB to assist with this technical examination. The investigation report made a number of observations and findings including that:
The gyroplane had descended inverted, almost vertically through trees.
Other than pieces of the propeller blades, the entire wreckage was located within a 5-metre radius.
The tail unit fitted to the gyroplane was second hand and had previously been repaired due to accident damage.
The rudder post (shaft) was not original and had failed in-flight.
The report concluded that ‘the rudder post failed inflight which initiated sequential failures that resulted in the complete detachment of the majority of the tail unit from the gyroplane’ which rendered the gyroplane uncontrollable.
Purpose of the examination
As part of an investigation by the Coroner’s Court of New South Wales, the New South Wales Police Force requested assistance from the ATSB in the examination of components from the gyroplane’s tailplane. The ATSB conducted an examination and assessment of the fractured rudder shaft and fibreglass structure including previous repairs.
Sources of information
The ATSB was supplied with and examined the following components:
The fibreglass sections of the tailplane that had fractured into several pieces and separated from the keel during the accident sequence
The upper half of the fractured rudder shaft and attachment hardware retained within the base of the rudder.
The ATSB was provided with or obtained the following additional information:
ASRA accident report, which included extracts from the aircraft’s logbook
relevant Magni Gyro design drawings and maintenance documentation.
Context
Tailplane history
Gyroplane G‑2468 was fitted with a tail assembly from a factory-built Magni Gyro M22. In the factory installation, the tail assembly was mounted on an aluminium box section in line with the rest of the keel (Figure 1). The rudder mechanism employed a pulley below the keel that turned a rudder shaft, which passed through the box section and was then bolted longitudinally to a tube fixed within the rudder (Figure 2).
In contrast, when installed to G‑2468, the tailplane was welded to the top of the existing keel, which introduced a second aluminium box section into the structure (Figure 3). The additional box section meant that the original rudder shaft was not long enough for this installation, and a replacement was manufactured.
Figure 3: Tail installation on G-2468, highlighting the modified double-height keel
Source: Aeropedia, modified by the ATSB
The parts supplied for examination are shown in Figure 4. In addition to the requested examination, the ATSB noted that the trim tab on the trailing edge of the rudder was not original and had a larger surface area. Magni Gyro was unable to comment on the influence on flight loads of the rudder trim tab modification.
Figure 4: G‑2468 tailplane as supplied for examination
Source: ATSB
The gyroplane’s logbook indicated it was manufactured in 2009 and had accrued approximately 510 flight hours at the time of the accident. The tail was reported to have undergone fibreglass repairs twice due to rollover accidents; once in 2008 (prior to the manufacture of G-2468) and again in February 2015 at 243 flight hours. The logbook recorded that a new rudder shaft was ‘manufactured and installed’ as part of those repairs. Since that time, the fibreglass structure was repaired twice for observed cracking, at 250 flight hours (November 2016) and 401 flight hours (August 2020).
Tailplane examination
Rudder assembly
The rudder shaft was fractured at the point coincident with the bolt hole for attachment to the outer rudder sleeve (Figure 2, 4). The fracture surface exhibited extensive ‘beach mark’ features consistent with high cycle fatigue[1] crack progression (Figure 5). ATSB examination using optical and scanning electron microscopy identified that cracks had originated at all 4 corners of the bolt hole and progressed across approximately 98% of the cross-sectional area before final fracture.
Note: Concentric beach marks radiating outwards from the corners of the central bolt hole. The inside edges of the bolt hole are not square, and there is a difference in cross sectional area between the two sides of the fracture; The bolt hole is slightly offset to the left of the shaft centreline.
Source: ATSB
There was evidence of severe fretting[2] wear between the bolt and the shaft bolt hole. The shaft bolt hole was enlarged at either end, likely due to material loss from the fretting wear. The hole was slightly offset from the shaft centreline and there were no fillets applied to the hole edges for stress relief.
There was also wear between the shaft and the rudder outer sleeve (Figure 6), and between the outer sleeve and the bolt (Figure 7). The sleeve bolt holes were deformed (‘ovalised’) and one side was fatigue-cracked.
Compared to the original design in Figure 1, the rudder sleeve had been shortened and the bolt hole had been changed from the original longitudinal (fore-aft) orientation to a lateral (left-right) orientation. The original M5 (nominal 5 mm diameter) rudder attachment bolt (Figure 2) had been replaced with a 6.25 mm (1/4 inch) bolt, meaning the bolt hole in the rudder shaft and sleeve were similarly oversized. It was not possible to measure the assembly torque on the nut, due to the shaft fracture, deformation and wear.
Energy dispersive x-ray analysis (EDS) of the fractured rudder shaft showed that it was likely manufactured from a 6xxx-series aluminium rod.[3] The shaft diameter measured 14.85 mm across the unworn area adjacent to the bolt hole. Drawings supplied by Magni Gyro showed that the original rudder shaft was a nominal 15 mm diameter,[4] 2.5 mm thick tube, manufactured from SAE 4130N[5] steel.
Figure 6: Rudder shaft wear from contact with outer sleeve
Scale in millimetres.
Source: ATSB
Figure 7: Rudder sleeve wear from contact with washer, and associated cracking
Source: ATSB
Tail structure
As shown in Figure 4, the majority of damage to the fibreglass tail structure was to the left side. The vertical tip was separated, the lower skin and spar was split from the left horizontal stabiliser and a triangular-shaped piece had fractured from the upper skin. No sections had separated from the right side of the tail, however there were large splits in the upper and lower skins at the leading and trailing edges. The underside of the right horizontal stabiliser, adjacent to the keel, appeared to have been sanded in preparation for painting, however the paint coating had not been applied.
There were 2 areas of paint and fibreglass damage to the leading edge of the left stabiliser upper skin (Figure 8). There was also a cut through the upper skin and a larger puncture spanning both halves of the upper skin sections.
The skin of the tail structure was a sandwich panel consisting of fibreglass skins separated by a foam core. The interior of the left stabiliser had evidence of the reported previous repairs. This included significant amounts of resin fill and drops on the lower skin along the spar (Figure 9). Although there was a considerable amount of resin area at the inboard end of the left spar, none of the upper skin panel remained bonded. There were also areas where the inner fibreglass skin and sections of core were missing and resin had been applied over the top of the damaged structure (Figure 10). One of the larger areas of this type had cracked from one side but was otherwise intact after the accident.
Figure 8: Damage to upper skin of left horizontal stabiliser
Source: ATSB
Figure 9: Evidence of prior repair with large volume of disbonded resin
The fatigue cracking of the rudder shaft was the result of fretting fatigue at the areas of highest stress concentration: the sharp corners of the bolt hole. Compared to plain fatigue, fatigue under fretting conditions results in a significant reduction in fatigue life. The progressive wear of the bolt hole and the rudder sleeve would also have resulted in an abnormal loading condition due to the excessive bolt clearance.
The rudder sleeve was the original part, though had been modified. It had been involved in two reported rollover accidents, the most recent of which required manufacture of a new rudder shaft. The condition of the sleeve at the time could not be established, however it was possible that the sleeve had been damaged in one of these events, resulting in deformation of the bolt holes which would have allowed movement and fretting to occur between the components.
Notwithstanding this possibility, the wear and cracking of the rudder shaft was most likely the result of some of the modifications to the original design of the tail assembly during the fitment to G-2468. The most significant was substitution of the original steel rudder shaft for an aluminium component. Although the aluminium component had a slightly larger cross-sectional area (at the bolt hole) than the original steel tube, the steel component would have had considerably superior mechanical properties, including fatigue resistance.
Using a bolt (and hole) with a 25% larger diameter than specified reduced the normal cross‑sectional area of the rudder sleeve and, ordinarily, the shaft. However, because of the other material and dimensional changes to the rudder shaft, the influence of this on the observed damage to the rudder components was not determined.
Similarly, change to the orientation of the rudder bolt may also have altered the normal loading condition of the assembly, however any actual effect was not determined.
Fibreglass repairs
Damage to the tail assembly was largely to the upper surface of the left stabiliser, which was consistent with the ASRA finding that the gyroplane was inverted as it impacted the trees.
Some of the fibreglass repairs on the tail structure were not carried out to a standard that preserved the integrity of the original part. The missing sections of fibreglass skin and core would be detrimental to the strength and stiffness of the structure. Additionally, the large areas of resin that were disbonded from the substrate suggested that those areas of repair likely had a low adhesive strength, which would similarly be detrimental to the structural integrity of the tail.
The nature of the repairs may have influenced the prevalence of post-repair cracking and/or the degree to which the tail broke up during the impact sequence. However, the report that all of the tail structure ended up within a 5-metre radius indicated that it was unlikely that there was a catastrophic failure of the fibreglass structure prior to the initial tree contact.
Summary
Following the limited-scope technical examination, the following conclusions are made with respect to the examination of tail assembly components from the amateur-built gyroplane G-2468:
The rudder shaft fractured as a result of high cycle fatigue cracking caused by severe fretting.
An aluminium rudder shaft had been substituted for the original steel part, which made the rudder shaft significantly more susceptible to fatigue cracking.
There were several other modifications to the original tail design that had the potential to affect the normal loading of the assembly, however the extent of any influence was not determined.
There was evidence of previous repairs to the fibreglass structure that had not preserved the original structural integrity of the part, however it was unlikely that this resulted in a catastrophic fracture of the tail prior to the impact sequence.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]High-cycle fatigue cracking is associated with cyclic loading of a magnitude that produces deformation that is primarily elastic. Fracture due to high-cycle fatigue is typically greater than 10,000 cycles.
[2]Fretting refers to wear resulting from repeated, small, relative displacements in tight-fitting assemblies.
[3]Aluminium with principal alloying additions of magnesium and silicon.
[4]Tolerance on the diameter at the bolted area was 14.93–14.95 mm.
[5]Society of Automotive Engineers alloy designation. 4130 N is a medium carbon steel in the ‘normalised’ condition, which involves heating the steel above the austenite transformation temperature and air cooling. The result is a part with increased ductility and toughness, and reduced internal stresses.
On 16 July 2023, a Bell 206B‑1 helicopter, registered VH‑ZDI, was being operated on a private flight from a rural property near Tumbarumba to Khancoban, New South Wales, with the pilot and 3 passengers on board. Shortly after take‑off, the pilot brought the helicopter into a hover around 7 ft above the helipad located near a hangar. The pilot then initiated a hovering turn to the left and reported that they were able to complete around 90º of an intended 180º turn before they experienced a shudder, and the helicopter began to rotate to the right. While continuing to rotate to the right for around 2 full rotations, the pilot attempted several pedal control inputs and was unable to regain directional control. The pilot elected to lower the collective, reducing height, and later closed the throttle. As the helicopter descended, the left skid contacted the soft earth beside the pad and broke off. The helicopter rolled over. The occupants were uninjured, and the helicopter was substantially damaged.
What the ATSB found
The helicopter was hovering in ground effect near an obstacle, the hangar. The high all-up weight of the helicopter would have strengthened the recirculation of downwash from the main rotor blades generated by the proximity to the hangar. The hovering left turn, initiated by the pilot, brought the tail of the helicopter from its position away from the hangar, where recirculation would be less, closer to the hangar where recirculation would be greater. It was likely that the flow of air through the tail rotor was disturbed, resulting in a loss of tail rotor effectiveness, which manifested as a right yaw.
The ATSB found that a miscalculation of fuel led to the helicopter being operated about 15 kg above the maximum take-off weight.
The ATSB also noted that the occupants were wearing 4- and 5-point restraints, and a helmet was worn by the pilot. The use of such items reduces the risk of injury to occupants in the event of an accident.
Safety message
Helicopter pilots should remain cognisant of the factors that may induce unanticipated yaw (a loss of tail rotor effectiveness), and that helicopter performance can be adversely affected by the proximity to obstacles, including terrain, vegetation, and buildings. If unanticipated yaw is encountered, prompt and correct pilot response is essential.
This accident also illustrated the importance of operating within the weight and balance limitations prescribed in the flight manual. A weight and balance calculation tool, such as a mobile application, can be a useful way to check hand calculations, but it must be validated to ensure that it accurately reflects the flight manual limitations.
The pilot completed pre‑flight checks and did not identify any defects or outstanding maintenance issues with the helicopter. Following this, the pilot assisted the passengers to board the helicopter and secure their seatbelts. The pilot then briefed the front left seat passenger regarding the seatbelt mechanism and emergency locator transmitter activation. The front passenger had been in the pilot's other helicopter on previous occasions and the pilot stated that the passenger knew not to touch the anti-torque control pedals.[1]
Following a normal engine start, the take‑off commenced at about 1300 local time. As per their normal procedure when departing from this location, the pilot brought the helicopter into a hover around 7 ft, in ground effect,[2] above the helipad facing the hangar. They then initiated a left turn, which initially progressed as the pilot expected. There was no evidence to suggest that the rate of yaw was rapid or deviated from normal. The pilot reported that they were able to complete around 90° of an intended 180° turn before they experienced a shudder, which could be felt through the flight controls and airframe. The helicopter then began to rotate to the right.[3]
In response, the pilot reported that they first applied left, and then both right and left pedal inputs, in an attempt to control the right rotation. They did not recall if either of the left or right pedal stops were reached, nor did they notice any unusual resistance associated with the pedals. The pilot was unable to regain directional control and recalled that ‘nothing could stop’ the right yaw, when describing the pedal control inputs. After about 2 full rotations, the pilot lowered the collective,[4] reducing height, and closed the throttle just prior to the helicopter touching the ground.
Initially, the left skid contacted the soft earth beside the helipad and broke off. The helicopter then rolled over coming to rest on the left side. The pilot reported that they switched the fuel valve into the ‘off’ position as the helicopter contacted the ground. The front passenger was able to exit the helicopter with the assistance of the pilot. They then assisted the rear passengers to exit, whereupon all occupants moved away from the helicopter. The pilot collected fire extinguishers and discharged them into the engine exhaust. There were no injuries. The helicopter was substantially damaged.
The pilot initially reported the accident as a loss of tail rotor effectiveness,[5] but later stated that they believed that there had been a mechanical issue with the helicopter.
The pilot obtained a private pilot licence (helicopter) in 2018. Their flying experience totalled around 300 hours, with about 260 hours on Bell 206 variants. In the 90 days prior to the accident, the pilot had flown 20 hours, all on VH‑ZDI. The pilot’s latest flight review was on 15 March 2023. The pilot reported feeling fully awake immediately preceding the accident, so fatigue was not considered as a contributing factor to the accident.
Helicopter information
VH‑ZDI was a Bell 206B‑1 helicopter, manufactured in 1976, by the Commonwealth Aircraft Corporation Pty Ltd for the Australian Army, powered by a single-engine Allison Gas Turbines 250‑C20 engine. In 2020, a special certificate of airworthiness in the ‘limited category’[6] was issued for the helicopter. At the time of the accident, the total time-in-service was 9,856.5 hours.
The helicopter was maintained in accordance with the Australian Warbirds Association Limited[7] Bell 206B‑1 Kiowa maintenance program. The latest maintenance was performed 15.4 flight hours (20 days) prior to the accident, on 26 June 2023. An engine power assurance check[8] was performed at that time, but the conditions under which this check was conducted could not be validated by the ATSB. The maintainer conducting this check assessed that the minimum acceptable torque requirement was met. A previous engine power assurance check performed on 11 March 2022, 16 months prior to the accident, also indicated the engine was producing above the minimum acceptable torque. No defects were noted in the technical logs.
The helicopter was fitted with an anti-torque control pedal lock‑out kit on the left pedal assembly. The kit is designed to disconnect the passenger pedals without the use of tools, allowing pilots the ability to quickly isolate the pedals to prevent passenger interference with the tail rotor during flight.
Helipad information
The helipad (Figure 2) was a concrete pad, large enough to accommodate the helicopter. It adjoined a hangar, with the terrain sloping downwards to the west, away from it. The centre of the helipad was around 16 m from the hangar. The elevation of the pad was about 1,962 ft.
The method used to conduct a take‑off from the helipad was to push the helicopter out of the hangar tail first (towards the west) and position it such that the tail was over the downhill slope, affording the helicopter the greatest possible clearance from the hangar. The pilot would initiate a hover while facing the hangar, rotate left 180º, before commencing forward flight.
The pilot described experiencing helicopter-building interference from the hangar on other occasions. They stated that they had only experienced interference when they came into land and did not position the helicopter on the ground quickly. They likened the experience to rotor-head shake, bad turbulence, and bad air.
The pilot also stated that, though there was a lot of wildlife around the property, they did not observe any at the time of the accident. Furthermore, they ensured that items were stowed away and clear of the helipad.
Meteorological information
The Bureau of Meteorology analysis of weather observations around the Tumbarumba area found that a large high‑pressure system commonly associated with light winds and clear skies was present. This was consistent with the pilot’s recollections that it was not a windy day, that the wind was barely registering on the windsock, and it was about 15 ºC.
The Bureau of Meteorology did not have observations for Tumbarumba, the nearest airport. Instead, they provided observations for Wagga Wagga and Albury with the note that these airports were located on the same side of the ranges as Tumbarumba and experienced similar weather. Winds were very light, tending to a light to moderate north to north‑easterly and QNH[9] pressure was between 1026 and 1027 hPa. Visibility was greater than 10 km and no significant cloud was detected. Both airports recorded the temperature to be 15 ºC.
Wreckage examination
The ATSB’s examination of the site photographs provided by the pilot and the insurer found that the damage to the helicopter was consistent with a heavy landing and rollover event. The relative locations of the major components were consistent with power being supplied to the main rotor just prior to, or during, impact. The proximity to the ground and integrity of the occupant space contributed to a high probability of occupant survival.
ATSB investigators did not deploy to the site but inspected the wreckage once it was transported to a storage facility. No mechanical issues were identified during that inspection and there was no indication of pre-accident failure. The tail rotor and associated controls were inspected and showed no signs of failure, no restriction of normal operation, and no contact marks indicating a strike with a foreign object or animal. The exception to this was the inspection of the tail rotor control rigging, where system functionality was unable to be confirmed due to the airframe disruption. As a result, the possible contribution of a tail rotor control rigging error could not be eliminated.
While the helicopter was fitted with a pedal lock‑out kit on the left pedal assembly, the kit was not configured such that the passenger was ‘locked-out’. The pilot stated that they had never used the pedal lock‑out kit and were unfamiliar with its use. The passenger side cyclic control[10] was not present and there was no cover. The pilot stated that they removed the cyclic and that there was no cyclic control stub cover available. The passenger side collective was present.
The insurer’s assessment reported that they were not able to confirm the pre‑event serviceability of the tail boom attachment bolts. The tail boom was attached to the fuselage by 4 bolts. Two of the bolts had fractured and laboratory examination conducted by the ATSB identified that the failure of the bolts was consistent with overstress. There was no evidence of pre‑existing flaws or fatigue. Overall, the insurer concluded that the tail boom exhibited damage consistent with impact from a main rotor blade on the left side.
Weight and balance
Limits
The flight manual included forward and aft centre of gravity limits and specified that the maximum take-off weight (MTOW) for the helicopter was 3,200 lbs (1,452 kg). A type‑specific weight and balance assessment was performed on VH-ZDI on 30 June 2020. The resulting load data sheet listed the MTOW as 1,452 kg, the forward centre of gravity limit as 2,672 mm and the aft limit as 2,901 mm (Figure 4).
Calculations by the pilot
The pilot performed a weight and balance assessment prior to commencing the flight. In their handwritten calculations, the pilot included the weight and position of the 4 occupants and 430 lbs of JetA1 fuel. Calculation of the weight and centre of gravity required converting the fuel amount from the indicated units of lbs to kg, as all other amounts were measured in kgs. When converting the fuel from lbs to kg, the pilot mistakenly substituted volume, L, for mass, kg, and believed they had converted 430 lbs to 195 L (with the conversion factor of ÷2.2) (Figure 3). They subsequently converted 195 L to weight (with the conversion factor x0.8), arriving at 156 kg of fuel. This resulted in the pilot calculating the weight of the helicopter to be 1,428 kg (Figure 4). The pilot also listed the MTOW for the helicopter as 1,455 kg. This led the pilot to believe the helicopter was 27 kg under its MTOW.
Source: Airservices Australia, the pilot, annotated by the ATSB
The pilot used a third‑party application (App), iBal Rotary, as a secondary check to ensure that the helicopter was appropriately loaded. The pilot had selected ‘Sample Bell 206B3 (Bell 206B3 Jet Ranger)’ from the available models and input the 4 occupant details and 156 kg for fuel. The pilot was aware that this model selection did not represent VH‑ZDI and, to compensate, included an additional centre aft passenger weighing 100 kg as an adjustment to account for the unrepresentative model selection. The App indicated that the weight and balance of the selected model, which did not reflect the limits specified in the flight manual, was within limits.
According to the developer of the App, a more representative model selection for VH‑ZDI was the ‘Bell OH‑58A/C’.[11] The weight and balance envelope for the App ‘Bell OH‑58A/C’ model was sourced from the Operator's Manual Army Model OH-58 A/C Helicopter (Department of the Army (United States), 1989). This differed to the weight and balance envelope specified in the VH-ZDI flight manual but more closely resembled the flight manual than the model selected by the pilot. When the 4 occupants and 156 kg of fuel was input into the App with ‘Bell OH‑58A/C’ selected, the App indicated that the loading was within MTOW, but that the forward centre of gravity limit was exceeded. When the 4 occupants and 195 kg (430 lbs)[12] of fuel was input into the App, the App indicated that the helicopter loading had exceeded the MTOW.
Calculations by the ATSB
The ATSB performed a weight and balance calculation with the information provided by the pilot and determined the take‑off weight to be 1,467 kg with an associated moment arm of 2,715 mm (Figure 4). This exceeded the MTOW of the helicopter by 15 kg.
Figure 4: VH‑ZDI weight and balance limits and calculations
Source: Flight manual, load data sheet, and pilot, annotated by the ATSB
Operational information
Engine torque required and available
From the flight manual, the minimum engine torque required to hover for the accident conditions was about 61.9 psi and the minimum acceptable torque that the engine should produce under those conditions was about 68.6 psi.
According to the United States Federal Aviation Administration (2019) Helicopter Flying Handbook:
A helicopter’s performance is dependent on the power output of the engine and the lift produced by the rotors, whether it is the main rotor(s) or tail rotor. Any factor that affects engine and rotor efficiency affects performance. The three major factors that affect performance are density altitude,[13] weight, and wind.
An increase in density altitude can affect helicopter performance by reducing the hovering ceiling, operating margins, and rate-of-climb performance. The higher the gross weight, the greater the lift or rotor thrust required for hovering or climbing. Therefore, the margin between the engine power available and the power required to hover at higher weights and density altitudes may often be small for helicopters (Civil Aviation Authority of New of Zealand, 2020). The Helicopter Flying Handbook noted that, while more engine power was required during the hover than in any other phase of flight, if a hover could be maintained, a take-off could also be made.
Recirculation and helicopter-building interference
Recirculation is a type of interference between a helicopter and its surroundings (Royal Air Force (UK), 2010). According to the UK AP3456 Central Flying School (CFS) Manual of Flying, Volume 12 – Helicopters:
Whenever a helicopter is hovering near the ground, some of the air passing through the disc is recirculated and it would appear that the recirculated air increases speed as it passes through the disc a second time (Figure 5). This local increase in induced flow near the tips gives rise to a loss of rotor thrust.
Recirculation will increase when any obstruction on the surface or near where the helicopter is hovering prevents the air from flowing evenly away. Hovering close to a building, wire link fencing or cliff face may cause severe recirculation (Figure 6).
Figure 5: Helicopter hovering near the ground with recirculated air
Source: Royal Air Force (UK) (2010), annotated by the ATSB
Source: Royal Air Force (UK) (2010), annotated by the ATSB
The section of the rotor disc largely affected by recirculation was the side closer to the obstruction (right side of disc in Figure 6). A tail rotor positioned on the far side of the helicopter relative to the obstacle would experience less recirculated air than a tail rotor positioned on the near side.
Łusiak et al. (2009) described wind tunnel testing of a model helicopter with surrounding elements (buildings). Their paper stated:
The phenomenon of interference between the helicopter and the surrounding elements appears with a visible intensity when the helicopter operates at a low speed in the near vicinity of objects with specific geometrical shapes, such as buildings or ship hulls.
All computational analyzes and experimental investigations which were performed in order to study the mutual helicopter-building interaction indicate that in the considered specific situations the phenomenon of aerodynamic interference can seriously disturb the flow around the helicopter and change the loading of some of its elements. Substantial changes in the value of the resulting loads can make the helicopter difficult to control.
Wagtendonk (2011) discussed recirculation within the context of confined area operations, which included the following points:
As rotor downwash strikes the surface it splits, and a large part diffuses horizontally. If obstructions such as buildings or trees interfere with the escaping airflow, it moves vertically up the obstruction and re-enters the disc from above, increasing the induced flow.
The greater the gross weight, the stronger the downwash and the greater the degree of recirculation.
The lower the hover height, the stronger the outbound flow and the greater the degree of recirculation.
The more solid the obstruction, the greater the recirculation. Hovering close to large buildings (such as hangars) creates more recirculation than hovering near trees.
The highest velocity of horizontal outflow escaping from beneath the helicopter occurs at a distance that is roughly 30 percent of the disc diameter beyond the disc tip. For example, with a 30-foot disc the highest velocity occurs about 10 feet away from the tips. Although the velocity beyond that distance decreases sharply, substantial horizontal velocity values can still be encountered.
Recirculation can occur when obstructions are reasonably far away from the disc tip, but in general, the shorter the distance, the greater the risk of recirculation.
The emergency procedures section of the flight manual for VH‑ZDI identified loss of tail rotor effectiveness[14] as an anti‑torque system malfunction. As the main rotor rotated in the anti‑clockwise direction when viewed from above, in instances of anti-torque system malfunction the helicopter will most likely yaw to the right.
a. Tail Rotor Vortex Ring. This condition may be encountered with wind azimuths caused by crosswinds, left sidewards flight, or right pedal turns.
b. Weather Cock Stability. Wind azimuths aft of the beam will cause the helicopter to weather cock.
c. Main Rotor Vortex Interference. Certain wind azimuths will cause the tail rotor to ingest main rotor vortices.
d. Tail Rotor Precessional Flapping. High yaw rates will cause the tail rotor to precess. This, coupled with the pitch change characteristics of the tail rotor flapping hinge, will reduce tail rotor thrust.
e. High Gross Weight. High gross weights require increased torque and reduce tail rotor operating margins.
f. High Density Altitude. High DAs[16] require increased torque and reduce tail rotor operating efficiency.
g. Ground Vortex Interference. Interaction between the main rotor vortex and the ground can reduce tail rotor efficiency.
h. Limited Directional Control Margin. Right relative wind azimuths reduce left pedal travel margins.
i. Governor Droop. Governor droop leads to main rotor RPM droop. This requires increased torque to accelerate the rotor and also reduces tail rotor efficiency.
j. Low Airspeed. The aircraft is dynamically unstable in the yawing plane at low airspeed.
The best recovery technique detailed for ‘Loss of Tail Rotor Effectiveness’ was:
1. Pedal – Full left.
2. Cyclic – Forward.
3. Collective – Reduce if altitude permits.
4. Adjust controls for normal flight as control is regained.
If yaw cannot be controlled and an uncontrolled landing is imminent:
5. Throttle – CLOSED.
6. Collective – Autorotate.
7. Pedal – Full left until yaw stops.
The United States Federal Aviation Administration has produced advisory circular 90-95 that related to loss of tail rotor effectiveness, which they also term ‘unanticipated yaw’. The recommended recovery techniques in the circular were:
a. If a sudden unanticipated right yaw occurs, the pilot should perform the following:
(1) Apply full left pedal. Simultaneously, move cyclic forward to increase speed. If altitude permits, reduce power.
(2) As recovery is effected, adjust controls for normal forward flight.
b. Collective pitch reduction will aid in arresting the yaw rate but may cause an increase in the rate of descent. Any large, rapid increase in collective to prevent ground or obstacle contact may further increase the yaw rate and decrease rotor rpm.
c. The amount of collective reduction should be based on the height above obstructions or surface, gross weight of the aircraft, and the existing atmospheric conditions.
d. If the rotation cannot be stopped and ground contact is imminent, an autorotation may be the best course of action. The pilot should maintain full left pedal until rotation stops, then adjust to maintain heading.
Survival aspects
Seatbelts
The helicopter was fitted with 5‑point turn‑to‑open restraints in the front seats and 4‑point lift‑latch‑to‑open restraints in the rear seats. Zimmermann and Merritt (1989) stated that:
The overall probability of survival in an accident depends to a large extent on the manner of the restraint.
The use of upper and lower torso restraints to prevent such critical body parts as the head and chest from striking surrounding structure can significantly reduce the probability of serious or fatal injury under given accident conditions.
Studies have shown the addition of a shoulder harness greatly reduced injuries from head impacts and maintain proper spinal alignment. The further addition of a lab belt tie down strap (crotch strap on a 5-point harness) may nearly double the tolerance to impact forces.
Helmets
The Flight Safety Foundation (2022) stated that the primary purpose of a helmet was to provide impact protection and thereby reduce the risk of head injury in the event of an accident. The helmet worn by the pilot was damaged (Figure 7), indicating that the helmet sustained an impact during the accident sequence.
Figure 7: Top view of helmet worn by the pilot of VH‑ZDI showing damage
Source: Pilot, annotated by the ATSB
Similar occurrences
A search of the ATSB’s occurrence database for helicopter incidents, serious incidents, or accidents with the occurrence category ‘loss of control’ or ‘control issues’ from 2013 onwards returned 151 results. Eight of these occurrences contained sufficient information to be identified as unanticipated yaw or loss of tail rotor effectiveness. None of the occurrences related to helicopter‑building interference.
The 3 examples detailed below include an occurrence where the pilot was able to recover directional control, one that took place in a confined landing site with nearby obstacles, and an international event where helicopter-building interference was a probable factor.
On 20 July 2015, the pilot of a Bell 206L3 (LongRanger) helicopter, registered VH-BLV, conducted a charter flight from Essendon Airport to Falls Creek, Victoria, with 5 passengers on board. The pilot refuelled at a property near Lake Eildon and departed close to its MTOW.
On approach to the helipad at Falls Creek, the pilot assessed that there was insufficient power available to continue to land and elected to abort the approach. The pilot pushed forward on the cyclic to increase the helicopter’s airspeed and conducted a left turn towards the valley whereupon the helicopter started to yaw rapidly to the right.The pilot applied full left pedal to counteract the yaw, but the helicopter continued to yaw. The helicopter turned through one and a half revolutions, as the pilot lowered the collective. Lowering the collective reduced the power demand of the power rotor system, thereby increasing the ability of the anti-torque pedals to stop the right yaw. The combination of lowering collective and applying forward cyclic to gain forward airspeed, allowed the pilot to regain control of the helicopter. The pilot then conducted a left turn towards the helipad and made an approach to the helipad from an easterly direction. The helicopter landed following the second approach without further incident.
On 19 November 2022, the pilot of a Robinson Helicopter Company R44, registered VH-TKI, was conducting a private flight from a nearby property to a function centre at Forresters Beach, New South Wales with 2 passengers onboard. The proposed landing site was the carpark of the venue and was considered a confined area due to the proximity of roads, powerlines, and palm trees.
During the approach, the pilot reported an uncommanded yaw to the right, which was unable to be recovered. The ATSB found that, during the approach to a confined area landing site, the helicopter experienced a loss of tail rotor effectiveness and accompanying right yaw. The pilot’s response was ineffective at recovering control. The position of the helicopter on approach to the confined area was such that it could not be established if control of the helicopter could have been recovered before colliding with powerlines and terrain. The occupants received minor injuries and the helicopter was substantially damaged.
Federal Safety Investigation Authority (Austria) investigation reference: 2020-0.701.771
On 20 July 2018, a privately‑owned Airbus Helicopters AS350B, registered N36033, was destroyed while the pilot attempted to hover taxi closer to a fuelling station at Wolfsberg airfield in Austria (Aerossurance, 2020; Federal Safety Investigation Authority (Austria), 2020). The pilot, who did not hold a valid licence, sustained a minor leg injury. At the time the wind was 1 to 2 kt.
After lifting into a 1 m hover there were excessive pitching movements forwards and backwards and the helicopter yawed around 90° to the right. The pilot reported feeling turbulence from the side of the fuelling station building, which was a 5.2 m x 5.2 m, flat‑roofed building, 3.2 m high. The Austrian Federal Safety Investigation Authority determined the probable cause was a loss of lateral control during hover in ground effect. The probable factors were:
excessive control inputs
flight crew induced oscillations about the helicopter longitudinal axis
lack of corrective action to stop flight crew induced oscillations
proximity of obstacles
formation of ground effect air vortices in ground effect.
The ATSB considered several reasons to explain the unanticipated right yaw. Although the pilot described a shudder immediately prior to the right yaw, which could have indicated a mechanical issue, examination of the helicopter and maintenance documents did not reveal any anomalies. A wildlife strike or contact with a foreign object was considered but there was no indication of strikes on the rotors, a strike on the hangar, or animal remains to support this hypothesis. Inadvertent interference from the front seat passenger was also explored. This possibility was unlikely as the pilot did not feel any resistance when manipulating the anti-torque pedals.
While the helicopter was loaded above the MTOW, at the estimated density altitude for the time of the accident, the helicopter likely had sufficient power available to sustain a hover in-ground effect. Additionally, the left turn was not likely to be at a rapid yaw rate, and the weather conditions were calm.
During the hover, the helicopter was in a position close to an obstacle, the hangar, where helicopter-building interference was known to have occurred in the past. As described by Wagtendonk (2011), the obstacle would have prevented downwash from the main rotor escaping and the air would have recirculated. This recirculation would have been strengthened by the high all-up weight of the helicopter.
The literature indicated that the side of the main rotor disc closest to the obstruction would be more affected than the side further from the obstruction. Furthermore, recirculation from obstacles, such as buildings, can disturb the airflow though the disc, which can result in random movements and controllability difficulties. The hovering left turn, initiated by the pilot, brought the tail of the helicopter from its position away from the hangar, where recirculation would be less, closer to the hanger where recirculation would be greater. This was a position where the air flow through the tail rotor was more likely to be disturbed. Disturbance to the flow through the tail rotor, to an extent that the anti-torque forces could no longer overcome, likely account for the unanticipated right yaw. The pilot had likened their previous experience to turbulence or ‘bad air’, which could potentially explain the shuddering.
Helicopter-building interference is a variation on one of the contributors to a loss of tail rotor effectiveness described in the flight manual, specifically, ground vortex interference. Instead of the interference being generated from the proximity to the ground, it is generated by close proximity to a building. Therefore, with insufficient evidence to support other potential reasons for the unanticipated right yaw, it was likely that, as the left turn brought the tail rotor closer to the hangar, with recirculation strengthened by the high all-up weight, the flow of air through the tail rotor became disturbed. As a result, a loss of tail rotor effectiveness occurred, and the helicopter began to yaw right.
Once the right yaw initiated, the pilot’s control input included both left and right pedals. This was not consistent with the recommended procedures in the flight manual and advisory circular 90-95 for loss of tail rotor effectiveness, which stated that full and sustained left pedal input was required. This did not give the pilot the best opportunity to regain directional control. Ultimately, the pilot reduced the throttle, but this did not prevent the helicopter from colliding with the terrain.
Maximum take-off weight (MTOW) exceedance
When manually calculating the weight and balance of the helicopter, the pilot inadvertently made an error when converting the fuel load from lbs to kg. Their calculation indicated that the helicopter weight was 27 kg under the MTOW.
When the hand calculation appeared to be acceptable, the pilot used the third-party App for verification. The pilot was aware that the model selected in the App did not represent VH‑ZDI and added an unverified correction factor. Under these conditions, the App confirmed that the loading of the helicopter was within limits. Had the pilot selected the model that the App developer stated more closely reflected VH‑ZDI, the App would have shown that the centre of gravity was beyond the forward limit, even with the fuel conversion error. It is worth noting that third‑party applications are not a controlled source of information, and the flight manual and manufacturer’s documentation is the authoritative source of information.
Applying the required conversion factor, the ATSB weight and balance calculation established that the helicopter was loaded in a way that exceeded the MTOW by around 15kg. Had the pilot not made the conversion error and instead identified that the MTOW was exceeded, it was unlikely that they would have proceeded with the planned flight.
Operation at higher helicopter weights can affect performance and controllability, and potentially exacerbate other conditions such as helicopter-building interference. It is not known what loading configuration would have been sufficiently conservative such that the helicopter-building interference would not have resulted in a loss of control for the conditions. Regardless, compliance with the limitations set out in the flight manual remains vital for safe helicopter operation.
Survivability
The front occupants of the helicopter were wearing 5‑point turn‑to‑open restraints, while the rear occupants were wearing 4‑point lift‑latch‑to‑open restraints. The pilot was also wearing a helmet, on which only minor damage was observed. There was no comparative evidence, such as, one occupant with a seatbelt and one without to determine whether the severity of the accident was such that the occupants would have sustained greater injury if they were not wearing seatbelts. Nevertheless, the literature indicated that the use of upper and lower torso restraints and helmets reduces the risk of injury.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell 206B‑1, VH‑ZDI, 9.3 km south-south‑east of Tumbarumba, New South Wales, on 16 July 2023.
Contributing factors
After lift-off and initiating a hover turn to the left, while operating at a high all-up weight, it was likely that the helicopter’s tail rotor encountered helicopter-building interference from the hangar, which resulted in a loss of tail rotor effectiveness, and a subsequent collision with terrain.
Other factors that increased risk
Errors when calculating the weight and balance for the flight likely resulted in the maximum take-off weight being exceeded by 15 kilograms.
Australian Transport Safety Bureau. (2015). Loss of control involving a Bell 206L3, VH-BLV Falls Creek, Victoria, on 20 July 2015 [ATSB Transport Safety Report](Aviation Occurrence Investigation AO-2015-091). /publications/investigation_reports/2015/aair/ao-2015-091
Australian Transport Safety Bureau. (2023). Collision with terrain involving Robinson Helicopter Company R44, VH-TKI, Forresters Beach, New South Wales on 19 November 2022 [ATSB Transport Safety Investigation Report](Aviation Occurrence Investigation (Short) AO-2022-060). /publications/investigation_reports/2024/report/ao-2022-060
Department of the Army (United States). (1989). Operator's Manual Army Model OH-58 A/C Helicopter [Technical Manual](TM 55-1520-228-10).
Federal Safety Investigation Authority (Austria). (2020). Accident involving the helicopter type AEROSPATIALE AS350B on 20.07.2018 at approximately 06:33 UTC at Wolfsberg airfield, A-9400 Wolfsberg, Carinthia [Investigation report](Reference: 2020-0.701.771).
Łusiak, T., Dziubiński, A., & Szumański, K. (2009). Interference between helicopter and its surroundings, experimental and numerical analysis. Task Quarterly, 13(4), 379-392.
Royal Air Force (UK). (2010). AP3456 The Central Flying School (CFS) Manual of Flying (Volume 12 - Helicopters). Revised November 2013.
Wagtendonk, W. J. (2011). Principals of Helicopter Flight (Second revised ed.). Aviation Supplies & Academics, Inc.
Zimmermann, R. E., & Merritt, N. A. (1989). Aircraft crash survival design guide: Volume I Design criteria and checklists [Final Report](AD-A218 434, TR 89-D-22A). Aviation Applied Technology Directorate.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Anit-torque control pedals: A primary helicopter flight control that changes the pitch of tail rotor blades and thereby affects thrust to provide heading control in the hover and balanced flight when the helicopter is in forward flight.
[2]When hovering within about one rotor diameter of the ground, the performance of the main rotor is affected by ground effect. A helicopter hovering in ground effect requires less engine power to hover than a helicopter hovering out of ground effect. That is, when hovering close to the ground, the air being drawn down through the rotor collects under the helicopter and provides a ‘cushion’ of air, requiring slightly less power than would otherwise be required.
[3]In a single main rotor helicopter, where the main rotor rotates in the anti-clockwise direction when viewed from above, the main rotor generates lift but also generates a torque that causes the body of the helicopter to turn in the nose right direction. A tail rotor is a common means to provide the anti-torque needed to counteract this effect, such that the heading of the helicopter can be controlled.
[4]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[5]Loss of tail rotor effectiveness, also called unanticipated yaw, is a critical, low‑speed aerodynamic flight characteristic, which can result in uncommanded rapid yaw rate that does not subside of its own accord and, if not corrected, can result in the loss of control (United States Federal Aviation Administration, 1995).
[6] The ‘limited category’ permits the use of helicopters (ex-military) in a civil environment with regulations that prescribe how, where, and by whom these helicopters may be operated in order to ensure that public safety is not compromised by their civil operations. (Civil Aviation Safety Authority, 2018).
[7]Australian Warbirds is the administering body for all limited category (ex-military and historic) aircraft operations in Australia. Through delegations granted by the Civil Aviation Safety Authority, Australian Warbirds issues certificates of airworthiness, oversees maintenance systems for limited category aircraft, provides safety guidance, manages adventure flight operations, and facilitates permit index assessments.
[8]Power assurance checks compare the torque gauge reading with the minimum acceptable torque value for the particular power setting, pressure altitude, and temperature. If the torque achieved exceeds the minimum acceptable torque value, then the engine is producing sufficient torque.
[9]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[10]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[11]The Bell 206B‑1 Kiowa was a helicopter acquired by the Australian Army in 1971 (Royal Australian Navy, n.d.), whereas the OH‑58 Kiowa is a different model and was manufactured by Bell Helicopters for the U.S. Army (Vietnam Helicopter Museum, 28 March 2016).
[12]The 430 lbs fuel value was converted to 195 kg and used in the calculation.
[13]Density altitude: the altitude in the standard atmosphere corresponding to a particular value of air density.
[14]While loss of tail rotor effectiveness was included under the heading ‘anti‑torque system malfunctions’, the phenomena is not related to a maintenance malfunction (Federal Aviation Administration, 1995).
On 7 August 2023, a Robinson Helicopter Company R44, registered VH-HRB was departing the Lost City in the Limmen National Park, Northern Territory with 1 pilot and 3 passengers on board. During take-off, the helicopter rolled to the right and collided with terrain resulting in serious injuries to one passenger and minor injuries to the pilot and another passenger.
What the ATSB found
During take-off, the pilot was unaware that the helicopter’s left skid was pressed against a tree root that was partially obscured by sand.
When the pilot applied flight control inputs to raise the helicopter into a hover, it began rolling to the left against the tree root. In response to that unexpected movement, the pilot applied right cyclic input then lowered the collective. However, the pilot was not aware that, while the right cyclic input freed the skid from the tree root, it also led to the helicopter drifting to the right. As such, when the pilot lowered the collective to settle the helicopter on its skids it dynamically rolled over to the right.
Safety message
This accident highlights the importance of smooth and controlled flight control inputs in the critical phases of flight. While a helicopter is in contact with the ground, it is subject to various influences which could result in a dynamic rollover. A thorough understanding of the principles of and contributing factors to dynamic rollover and the recovery methods are essential to conducting safe helicopter take-offs and landings, especially to unprepared areas.
On 7 August 2023, a Robinson Helicopter Company R44, registered VH-HRB and operated by Wellspring Rural Services Pty Ltd, was being used to conduct a series of sightseeing flights from Lorella Springs airstrip to the Lost City in the Limmen National Park, Northern Territory.
On the sixth flight of the day, at approximately 1150 local time, the pilot landed at the Lost City helicopter landing site (HLS) in a southerly direction. In accordance with the operating procedures, the pilot remained in the helicopter with the engine running while 2 passengers were off loaded, and 3 new passengers were loaded by a ground crew member for the return flight to Lorella Springs.
During the subsequent take-off with a prevailing east-south-easterly wind, the pilot applied slight left cyclic[1] to manoeuvre the helicopter into a hover. The pilot advised that the helicopter started rolling to the left, which the pilot thought was the onset of a dynamic rollover (see the section titled Dynamic rollover). In response, they applied right cyclic to counter the roll.
The helicopter subsequently started drifting right, which the pilot later advised they did not recognise, instead believing that the right skid was still on the ground. They lowered the collective[2] in an attempt to settle the helicopter resulting in the helicopter rolling onto its right side (Figure 1).
The ground crew member provided immediate assistance to evacuate those on board, however as they assisted the front left passenger by releasing their seatbelt, the passenger fell and sustained a minor injury. The pilot also sustained a minor injury. The passenger in the rear left seat was uninjured and the passenger seated in the rear right seat sustained a fractured rib.
Source: Operator
Context
Pilot
The pilot held a valid commercial pilot license (helicopter) with a class 2 aviation medical certificate. They obtained their license in May 2023 and the theory of dynamic rollovers was taught during their training.
At the time of the accident, the pilot had accumulated 298 hours of aeronautical experience, with about half of that operating the R44. Since obtaining their license, they had completed around 100 landings at the Lost City HLS and all of those were in VH-HRB.
The pilot had been on duty for 4.5 hours at the time of the accident and stated they were feeling well rested and alert at the commencement of their flying duty that day.
The R44 is a 4-seat helicopter that is primarily all-metal construction with a 2-blade main and tail rotor system powered by a 6-cylinder Lycoming piston engine. VH-HRB was manufactured in the United States in 1994 and issued serial number 104.
The helicopter was maintained in accordance with the manufacturer’s maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever came first. The maintenance release indicated that VH-HRB had accumulated a total of 2,541 hours in service at the time of the occurrence. The helicopter had flown 31 hours since the last periodic inspection, and no outstanding defects were noted in the maintenance release.
The co-pilot controls had been removed and were stored under the pilot’s seat for the flight, and the front doors had been removed. The helicopter was not fitted with an ELT, nor was it required to be.
The ATSB did not attend the accident scene. As such, a detailed examination of the airframe or engine was not performed.
Using information provided by the aircraft operator, the ATSB assessed that the helicopter was operated within the weight and balance requirements for the flight.
Meteorology
The pilot and operator stated east-south-easterly winds were prevailing at the time of the accident, which was typical for the location at that time of day. Two passengers recalled very gusty wind conditions prior to the flight.
Weather data was not available for the accident location; however, a review of weather data from the 3 nearest available locations (Borroloola Airport, Ngukurr Airport and McArthur River Mine Airport) indicated an east-south-easterly wind with a maximum of 15 kt at the time of the accident.
These conditions were within the helicopter’s operating limits and it was reported that the pilot was experienced operating in these conditions. The pilot stated that there was always an option to swap duties with the ground crew member, who was also an experienced pilot, if they had any concerns that the conditions were beyond their personal limits. The pilot did not have any concerns about the wind conditions on the day and did not consider it was a factor in the accident.
Helicopter landing site
The helicopter landing site consisted of a clearing in the national park, approximately 100x30 m, with a sandy surface, scattered with tussocks of spinifex grass. The operator had utilised the landing site for 8 years, and a landing site plan was included in their exposition.
The operator’s procedure for the landing site was to follow a curved departure to the south-east when easterly winds prevailed (Figure 2).
The operator inspected the landing site at the beginning of the tourist season (May) to ensure any hazards were removed or mitigated. While the operator had no specific procedure for regular inspection/maintenance of the landing site, a ground crew member drove to the landing site at the start of each day to wait for the first flight and continued loading and offloading passengers 6–8 times during the day. As such, the ground crew member visually scanned the landing site for hazards, multiple times daily.
Photographs provided by the operator post-accident (Figure 3) depicted a tree root protruding from the sand in close proximity, or pressed against, the helicopter’s left skid.
Figure 3: Left skid indentation against tree root
Source: Operator, annotated by ATSB
Witness observations
The ground crew member was an experienced helicopter pilot and was approximately 50 m from the helicopter during the accident sequence. They later recalled that during the take-off they observed the helicopter pull sharply to the left and then sharply to the right, followed by the helicopter drifting to the right prior to rolling onto its right side.
A rotors-running helicopter resting with one landing skid or wheel on the ground may, without appropriate pilot input, commence rolling around the skid. Under certain circumstances, this roll cannot be controlled and the helicopter will roll over. This condition is known as ‘dynamic rollover’ and is a function of the interaction between the:
horizontal component of the total rotor thrust (or lift) acting about the point of ground contact
weight of the helicopter, initially acting between the helicopter’s skid landing gear or wheels, moving outside the helicopter’s landing gear.
The Federal Aviation Administration Helicopter flying handbook Chapter 11 Helicopter emergencies and hazards stated that dynamic rollover begins when the helicopter starts to pivot laterally around its skid or wheel.
It further stated:
‘This can occur for a variety of reasons, including... the skid or wheel contacts a fixed object while hovering sideward…’
Recovery from dynamic rollover involves smoothly lowering the collective while controlling any tendency to roll in the opposite direction with cyclic to re-establish the helicopter’s weight evenly on the ground. In general, the application of smooth collective inputs is more effective in avoiding rollover issues than using the cyclic control.
Safety analysis
Prior to departing, the pilot was unaware that the helicopter’s left skid was pressed against a tree root, which was not obvious as it was partially obscured by sand. During take-off with prevailing east-south-easterly winds, the pilot applied slight left cyclic to manoeuvre the helicopter into a hover. These inputs pushed the left skid into the tree root, which in turn resulted in the helicopter initially rolling around the left skid.
The pilot recognised this movement and attempted to recover by applying right cyclic then lowering the collective. However, it is likely that before they lowered the collective the helicopter had become light enough on the skids to commence drifting to the right due to the cyclic input. That lateral movement was not detected by the pilot, and when the pilot lowered the collective to settle the helicopter the right skid touched the ground, resulting in a dynamic rollover.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Robinson helicopter R44, registration VH-HRB, 95 km north-west of Borroloola, Northern Territory on 7 August 2023.
Contributing factors
The pilot was unaware that the helicopter's left skid was pushed against a tree root during the take-off, leading to an uncommanded left roll and subsequent dynamic rollover during the attempted recovery.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
operator and the chief pilot of Wellspring Rural Services Pty Ltd
Civil Aviation Safety Authority.
No comments to the draft report were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[2] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.