On 5 November 2022, an Airborne Australia Edge XT-912-L collided with terrain near Mokuleia, Hawaii. The aircraft was substantially damaged, and 2 people on board were fatally injured.
As the aircraft was Australian manufactured, the United States. National Transportation Safety Board (NTSB) requested that the ATSB appoint an accredited representative to assist in their investigation.
To facilitate this support and to provide the appropriate protections for any information gathered, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 19 November 2024, the NTSB released its final report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation.
Any enquiries relating to the accident investigation should be directed to the National Transportation Safety Board, United States at www.ntsb.gov.
In the early afternoon of 29 September 2023, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-315 (Dash 8) registered VH-TQZ, being operated on a scheduled air transport flight to Melbourne, Victoria, began to taxi at Mildura, Victoria for runway 09. A short time later, an amateur‑built Lancair Super ES registered VH‑VKP, taxied for runway 36 at Mildura for a private flight to Ballarat.
Both aircraft gave taxi, entering and backtracking calls on the local common traffic advisory frequency. Neither the pilot of the Lancair, or the crew of the Dash 8, were aware of each other. The crew of the Dash 8 gave a rolling call and had commenced their take‑off on runway 09 as the pilot of the Lancair gave a rolling call on runway 36, this was received by the Dash 8 crew with an immediate response given to the Lancair to hold on the runway. Another aircraft, taxiing behind the Lancair for runway 36, advised them to hold position while the Dash 8 departed.
The Dash 8 crossed the runway 09/36 intersection while the Lancair remained on the threshold of runway 36.
What the ATSB found
The ATSB’s investigation identified that the Dash 8 crew were actively engaged in organising separation with other airborne traffic. During this time, the pilot of the Lancair made a taxi call, and then an entering and backtracking call which partially over‑transmitted the Dash 8 checking on other airborne traffic. The crew of the Dash 8 heard neither of the Lancair pilot’s calls. This led to a situation where the crew of the Dash 8 had an incomplete comprehension of the ground‑based traffic at Mildura, and had no knowledge of the Lancair until during the take‑off. In addition, due to the position and distance of the Dash 8, the pilot of the Lancair had no awareness of the Dash 8 or its radio calls until another aircraft advised that the Dash 8 was rolling on runway 09.
The ATSB investigation found that the Dash 8 aircraft type had reduced ground‑based radio reception and transmission strength with other airfield users located behind the aircraft, which affected radio call readability. This reduced the situational awareness for the Dash 8 crew and other traffic. Further, the Dash 8 ground‑based transmissions on VHF COM 2 (which used an aerial on the aircraft underbelly) had reduced strength and clarity compared to VHF COM 1 (which used an aerial on the roof). This likely led to situations where other aircraft had difficulty in receiving and understanding radio transmissions, and the Dash 8 not receiving other traffic radio transmissions. Due to topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. This, and the lack of a requirement for mandatory rolling calls, increased the risk of aircraft not being aware of each other immediately prior to take‑off.
The ATSB also identified that the QantasLink radio procedure required Dash 8 crews to use the VHF COM 2 radio to broadcast and receive on local frequencies during operations at all non‑controlled aerodromes. This reduced the ground‑based reception and transmission strength of the Dash 8, and therefore reduced the likelihood of radio calls being received in some circumstances.
Furthermore, the aircraft manufacturer, De Havilland Aircraft of Canada Limited, did not have guidance to operators on the transmission and reception performance limitations of VHF COM 2 radios for ground‑based communications in Dash 8 aircraft.
What has been done as a result
On 6 December 2024, De Havilland Aircraft of Canada Limited issued 2flight operations service letters relating to radio communications, with one covering Dash 8 100‑300 series aircraft and the other covering the Dash 8 400 series aircraft. The service letters remind operators that ground‑based VHF communications are affected by line of sight and can be impacted by buildings, terrain or aircraft structures and that use of VHF COM 1 is more effective for ground‑based communications with other aircraft on the ground.
In support of the De Havilland Aircraft of Canada Limited service letters, the ATSB has issued a safety advisory notice (AO‑2023‑050‑SAN‑01) in conjunction with this report to advise operators ofDash 8 aircraft of the potential for reduced ground‑based communications quality of VHF COM 2 radios. The SAN advises all operators and crew of De Havilland Aircraft of Canada Limited Dash 8 aircraft to consider the use of VHF COM 1 radios for all ground‑based communication while operating at non‑controlled aerodromes.
QantasLink has updated its operations manual to reflect the updated minimum company requirements of a rolling call to be made at all CTAF aerodromes. This is to improve procedural consistency across the pilot group, and to reduce the likelihood of traffic conflict. QantasLink has provided guidance to its pilot group on specifics of potential radio communication degradation on the ground at Mildura Airport between runway 36 and 09 thresholds, including the conduct of rolling calls, and required the clarification of broken, suspicious or ambiguous radio calls from other aircraft prior to departure. QantasLink has also made changes to its operations into Mildura Airport, requiring crews to use VHF COM 1 for ground‑based departure communications, however this does not apply to other non‑controlled aerodromes.
In response to the draft ATSB report, QantasLink provided a bowtie qualitative risk assessment on the proposed adoption of modified CTAF radio panel usage, which focused on additional threats, increased complexities and controls. ATSB acknowledges that the risk assessment identified additional threats. However, QantasLink has not provided an assessment of how these threats may pose a higher risk than the existing aircraft collision risk identified in the safety issue. The ATSB notes that the risk assessment does not address aerodromes other than Mildura that may exhibit similar risk factors, namely, radio shielding, visual obstructions, and/or multiple runways. Furthermore, the risk assessment did not take into account the newly introduced advice from the aircraft manufacturer in 2 flight operations service letters. Notwithstanding, the ATSB has closed the safety issue as partially addressed as the risk has been controlled at Mildura. However, noting that the use of VHF COM 2 at other non‑controlled airports for ground‑based traffic communication currently remains unaddressed, the ATSB expects QantasLink will appropriately apply its safety management system to ensure any similar risk is controlled.
As a result of the potential radio interference at Mildura Airport that was investigated in an ATSB investigation (AO-2023-025) into a similar collision‑risk pairing event about 3 months earlier, Mildura Airport successfully established a permanent notice to airmen for Mildura Airport operations as of 4 April 2024. This included the advice that aircraft are not directly visible to each other on the thresholds of runway 09, 27 and 36 and that mandatory rolling calls are required from all aircraft immediately prior to take‑off due to the increased risk of aircraft not being aware of each other. This permanent notice to airman was subsumed into the En Route Supplement Australia publication for Mildura Airport in the 2406 amendment cycle on 13 June 2024.
Additionally, QantasLink has updated its operations manual to reflect the updated minimum company requirements of a rolling call to be made at all CTAF aerodromes. This was to improve procedural consistency across the pilot group, and to reduce the likelihood of traffic conflict.
Safety message
Communication and self‑separation in non‑controlled airspace is one of the ATSB’s SafetyWatch priorities. Whenever you fly, into either non‑towered or controlled aerodromes, maintaining a vigilant lookout at all times is important. Situational awareness and alerted see‑and‑avoid is an effective defence against collisions, and good airmanship dictates that all pilots should be looking out and not be solely reliant on the radio for traffic separation. Being aware of other nearby aircraft and their operational intentions is important to prevent collisions. Remember that there may be a variety of aircraft of different sizes, flight rules, and performance levels all operating at the same time, in the same airspace.
Pilots can guard against similar issues to those highlighted by this incident by:
making the recommended broadcasts when in the vicinity of a non‑controlled aerodrome
actively monitoring the CTAF while maintaining a visual lookout for other aircraft and constructively organising separation through direct contact with other aircraft
clarifying radio call over‑transmissions to ensure that all stations in the vicinity have the best chance of updating their mental model of potentially conflicting traffic
ensuring transponders, where fitted, are selected to transmit altitude information
ensuring transmissions are made at non‑controlled aerodromes with the radio/antenna that will provide the optimal ground‑based transmission and reception strength.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. This investigation report highlights the safety concerns around Reducing the collision risk around non-towered airports.
The occurrence
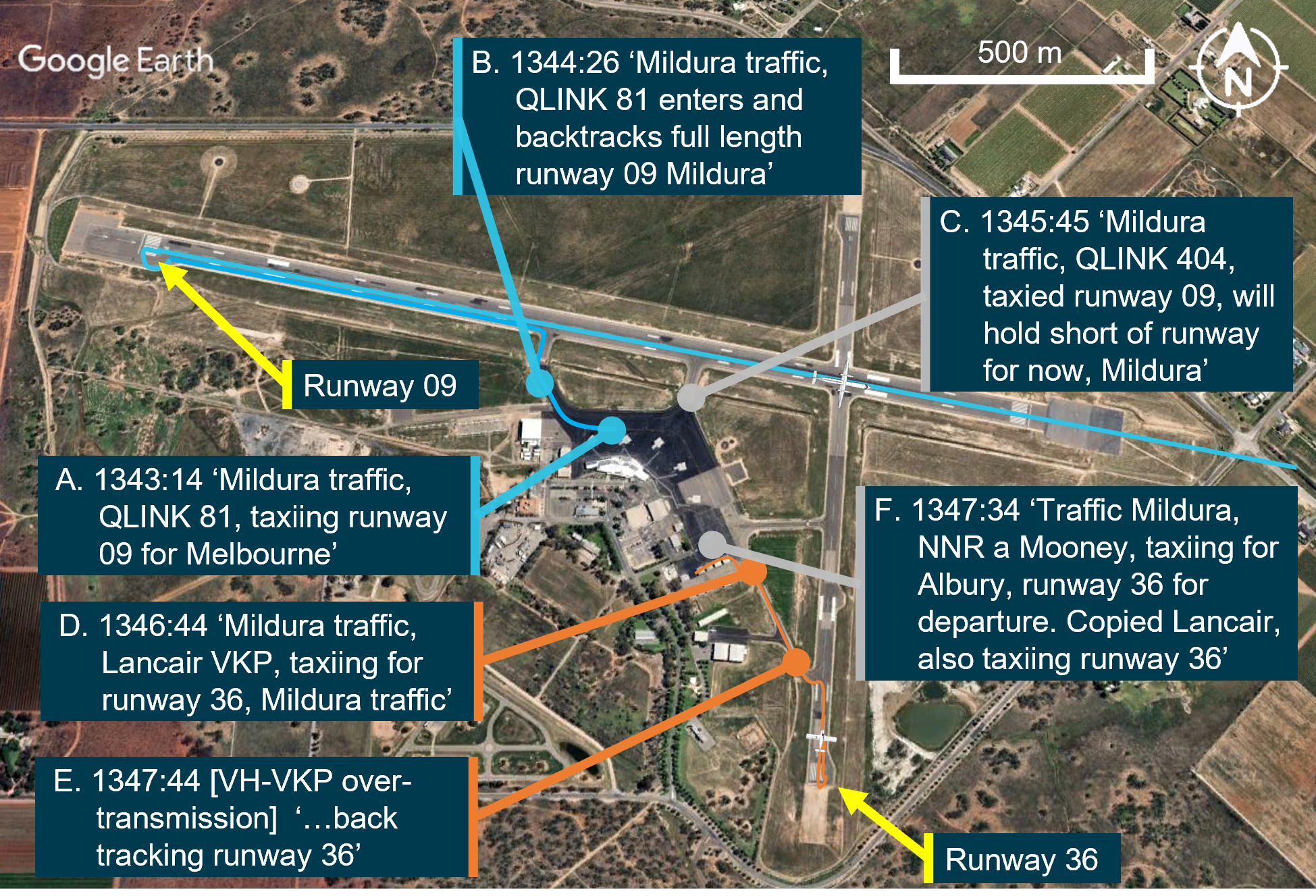
In the early afternoon of 29 September 2023, a De Havilland Aircraft of Canada Limited DHC-8-315 (Dash 8), registered VH‑TQZ, with 4 crew and 50 passengers on board, being operated by QantasLink on a scheduled air transport flight to Melbourne, Victoria, began to taxi at Mildura Airport for runway 090F[1] (Figure 1, blue line). A short time later, an amateur‑built Lancair Super ES aircraft, registered VH-VKP, taxied for runway 36 at Mildura, for a private flight to Ballarat (Figure 1, orange line). The pilot was accompanied by 2 passengers.
Figure 1: Overview of airport showing Dash 8 (blue) and Lancair (orange) ground tracks
Aircraft in the overhead images are not the occurrence aircraft. Source: Google Earth, annotated by the ATSB
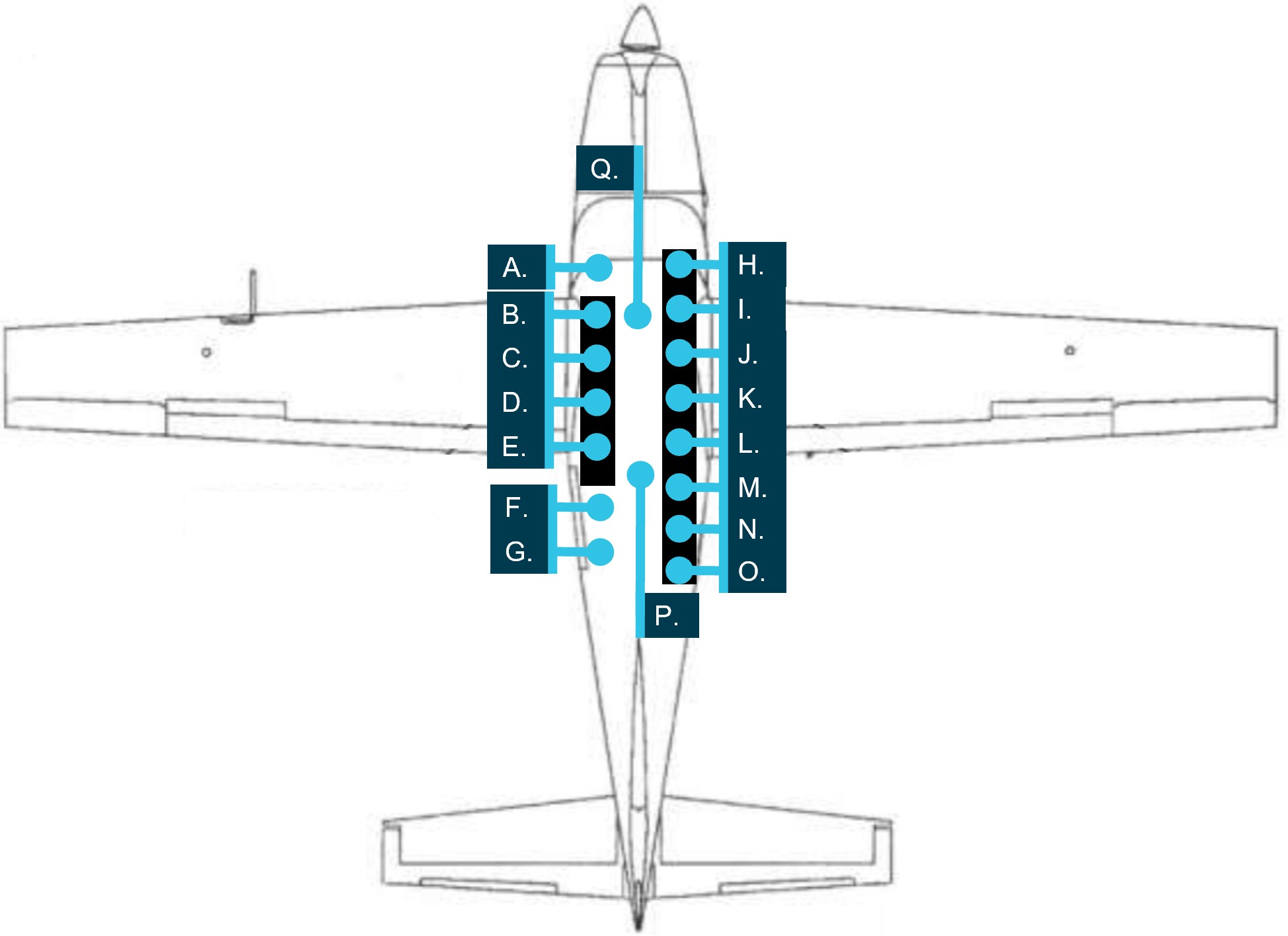
Radio data collected from Mildura Airport CTAF recordings (Appendix A) are overlaid on a Google Earth image of the airfield (Figure 2). These showed that the crew of the Dash 8 (call sign QLINK81) made a taxi call for runway 09 at Mildura (A), with a further entering and backtracking call 72 seconds later (B). The crew of a second Dash 8 (QLINK 404) called taxiing for runway 09 and held short of runway 09 (C).1F[2]
Figure 2: Sequence of events while the Dash 8 and Lancair taxied to their respective runways
Source: Google Earth, annotated by the ATSB
The Dash 8 flight crew were backtracking on runway 09 while making a series of calls with the pilot of a Tecnam aircraft, about 11 km north of Mildura and a Cessna joining the circuit overhead the aerodrome. The Dash 8 flight crew spent about 11 minutes communicating with the Cessna to establish deconfliction. It was during this time that the pilot of the Lancair made their taxi call on the CTAF (D).
The flight crew of the Dash 8 had just begun another call to contact the overhead traffic at the same time as the Lancair pilot transmitted an entering and backtracking call for runway 36 (E). This over-transmission made the first 10 seconds of the Lancair pilot’s call unintelligible.
A Mooney aircraft, departing Mildura for Albury, also gave a call about 70 seconds after the Lancair taxi call, stating that they intended to taxi for runway 36 and that they had copied the Lancair also taxiing for runway 36 (F). According to ATSB interviews with the respective pilots, neither the pilot of the Lancair nor the flight crew of the Dash 8 backtracking on runway 09 were aware of each other at this time.
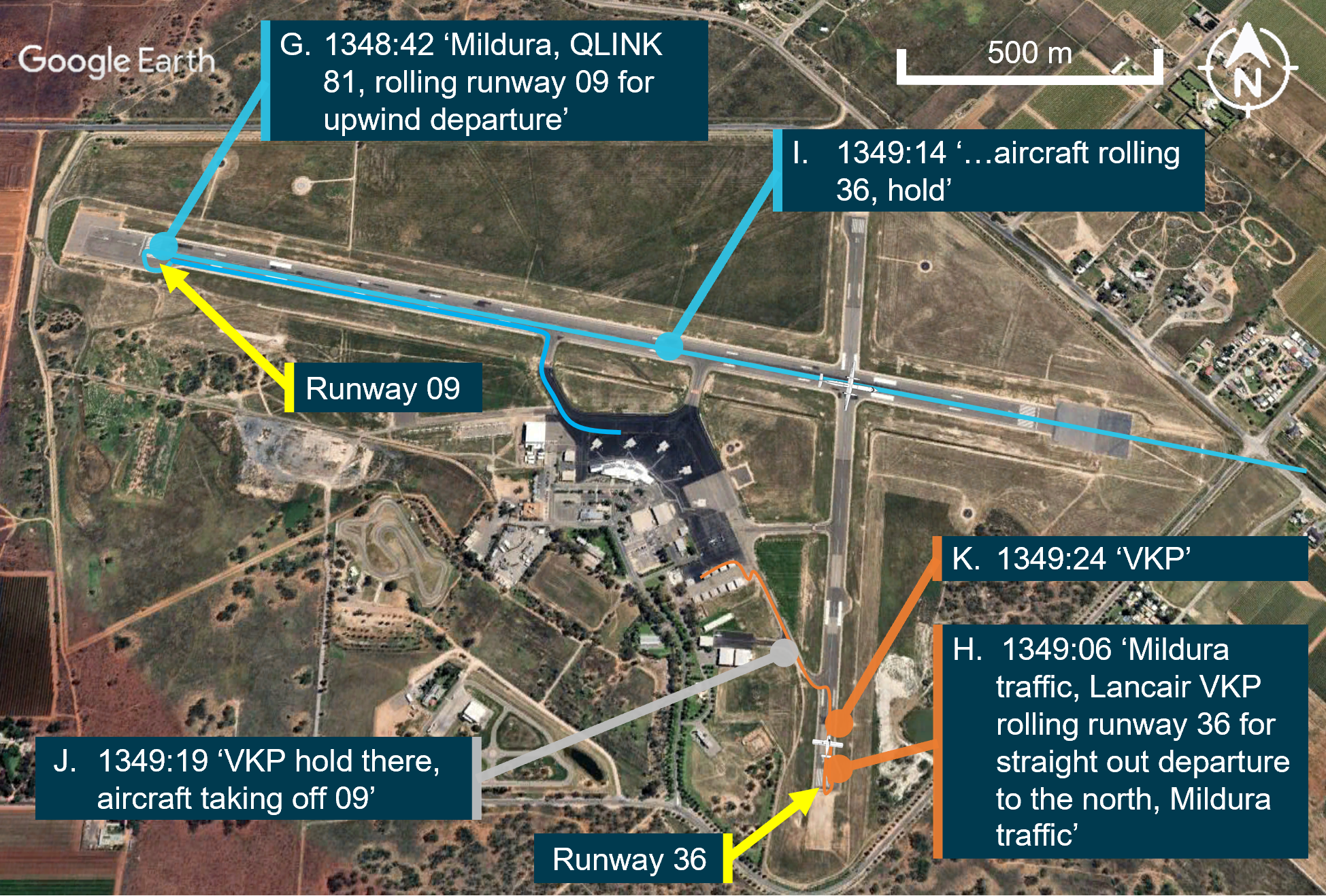
Subsequent events are shown in Figure 3. After reaching the end of the runway, at 1348:42, the Dash 8 gave a rolling call on 09 for departure (G). After a short backtrack along runway 36, the Lancair gave a rolling call on runway 36 at 1349:06 (H). The Dash 8 first officer immediately responded with ‘aircraft rolling 36, hold’ (I). The Lancair pilot did not recall hearing any calls from the Dash 8.
Figure 3: Sequence of events after Dash 8 commenced take-off
Source: Google Earth, annotated by the ATSB
Believing that the Dash 8 crew’s call may not have been heard by the Lancair, the Mooney pilot relayed to the Lancair that there was another aircraft rolling on runway 09 (J). The Lancair pilot acknowledged and aborted their take-off at 1349:24 (K) as they had not yet begun to roll, at which point the Lancair was stationary at the end of runway 36, about 730 m from the runway intersection. As the Dash 8 had already passed V1,2F[3] the flight crew continued the take-off.
Context
Pilot information
Flight crew VH-TQZ (Dash 8)
The captain held an Air Transport Pilot Licence (ATPL) (Aeroplane), a valid class 1 aviation medical certificate and reported a total flying time of about 18,500 hours with about 420 of those being on the Dash 8 and about 60 hours as captain. The captain reported being familiar with Mildura Airport and had operated there regularly in the past and recalled operating into Mildura at least 5 times in 2023, with the last flight being the week before the occurrence.
The first officer (FO) held an ATPL (Aeroplane), a valid class 1 aviation medical certificate, and reported a total flying time of about 3,100 hours, having flown about 700 of those hours in the Dash 8. The FO was familiar with Mildura Airport having regularly operated there over 50 times and had also operated into Mildura the previous week.
Pilot VH-VKP (Lancair)
The pilot held a Private Pilot Licence (Aeroplane) and reported a total flying time of about 200 hours, with about 93 hours on VH-VKP. They held a valid class 2 aviation medical certificate and were familiar with Mildura Airport, however had only operated there 3 or 4 times previously.
Aircraft information
VH-TQZ
The De Havilland Aircraft of Canada Limited DHC-8-315 is a high-wing, pressurised, commuter aircraft powered by 2 turboprop engines. VH-TQZ was manufactured in Canada in 2000 and was first registered in Australia on 29 November 2000. It was registered with Qantas Airways Limited on 8 February 2011, and operated by Eastern Australia Airlines Pty Limited.
VHF radio antenna position and condition
The Dash 8 had 2 VHF antennas installed on the upper and lower fuselage.
Number 1 VHF COM antenna (VHF COM 1) mounted on the roof of the aircraft forward of the wings.
Number 2 VHF COM antenna (VHF COM 2) mounted on the belly of the aircraft (Figure 4).
Figure 4: Dash 8 antenna position
Source: ATSB
The VHF COM 2 antenna was installed onto VH-TQZ on 1 March 2018 with the last reported C‑check3F[4] conducted on VH-TQZ on 1 August 2023. There was no reported corrosion present under the VHF COM 2 antenna and the only recent defects in the previous 6 months related to the VHF COM 2 screen and frequency knob on the head unit inside the cockpit which were subsequently returned to service.
Traffic collision avoidance system
A traffic collision avoidance system (TCAS) was fitted to the Dash 8. A TCAS interrogates the transponders of nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provided a visual representation of this information to the flight crew and issued alerts should a traffic conflict be identified. Other aircraft do not receive TCAS alerts if they are not fitted with TCAS.
These alerts include:
Proximate traffic: an alert issued when another aircraft is within 6 NM range (and 1,200 ft vertically if the traffic is transmitting altitude information).
Traffic advisory (TA): an alert issued when the detected traffic may result in a conflict.
Resolution advisory (RA): a manoeuvre, or a manoeuvre restriction, calculated by the TCAS to avoid a collision (the closest point of separation is approximately 25 seconds away or less). This alert is inhibited (inactive) on the ground.
Due to its method of operation, a TCAS cannot detect aircraft that are not equipped with a transponder or one with a transponder that is switched off. Additionally, the system is unable to issue an alert for traffic that is not fitted with an altitude reporting transponder (mode C or S), or in circumstances where the mode C or S transponder on board the conflicting traffic is not transmitting altitude information.
The crew of the Dash 8 reported that the TCAS was used regularly by the operator as an aid to identify potential conflicting traffic in the vicinity of a non-controlled aerodrome prior to take-off.
QantasLink advised that the use of TCAS was not a formalised procedure for monitoring other aircraft ground movements and that TCAS identification on the ground may be unreliable due to system limitations.
The first officer recalled conducting a check of the TCAS prior to rolling on runway 09 and the TCAS only identified airborne traffic in the vicinity of Mildura Airport.
VH-VKP
VH-VKP was a privately owned amateur‑built aircraft Lancair Super ES, built in New Zealand in 1997. It was first registered in Australia on 26 November 2020 to the pilot. The Lancair is a low wing, fixed undercarriage, piston engine, 4‑seat touring aircraft made from composite materials.
VHF radio antenna position
The primary VHF radio antenna on the Lancair was located underneath the rear of the aircraft empennage and was used to make the required broadcasts on the day of the occurrence. No defects or communication problems, either prior to or after the occurrence at Mildura, were reported by the owner.
Lancair transponder operation
The Lancair was equipped with a mode C transponder and the pilot recalled turning the transponder on (and selecting mode C) before entering the runway at 1347. The pilot believed that the transponder was operating and transmitting positional and altitude information during the take-off. The ATSB was unable to identify any transponder data of the Lancair during its taxi at Mildura.
In September 2024, the Lancair had 2-yearly Civil Aviation Order 100.5 instrument checks conducted and it was found that the transponder was transmitting a weak signal, was considered unserviceable and was replaced. It is unknown if this problem existed with the transponder at the time of the incident at Mildura, however recorded transponder data of the Lancair at the time of the occurrence was unavailable.
Meteorological information
At Mildura Airport around the time of the occurrence, the wind was variable at about 3 kt, with clear conditions and good visibility. Four of the pilots involved remember the wind favouring runway 36 with one stating that the wind at the time of the occurrence was from the north at about 5 kt.
Mildura Airport
Mildura Airport was a certified aerodrome. The aerodrome had an elevation of 167 ft above mean sea level and had 2 sealed runways, orientated in an east-west, north-south direction. The main east-west runway was 1,830 m long and the secondary, north-south runway was 1,139 m long.
The airport was serviced by a number of major aviation carriers and a large international flying school and accommodated aircraft as large as Boeing 737s but regularly operated with lower capacity passenger flights from numerous operators. It also accommodated general and recreational aviation flight training schools, charter operators and private flying. The aerodrome terminal building was upgraded in 1994, with further expansion constructed in 2004 due to increased utilisation and growth. Due to aerodrome expansion in recent years, numerous new buildings had been erected, including the site of an international flight training school and the southern general aviation hangar complex.
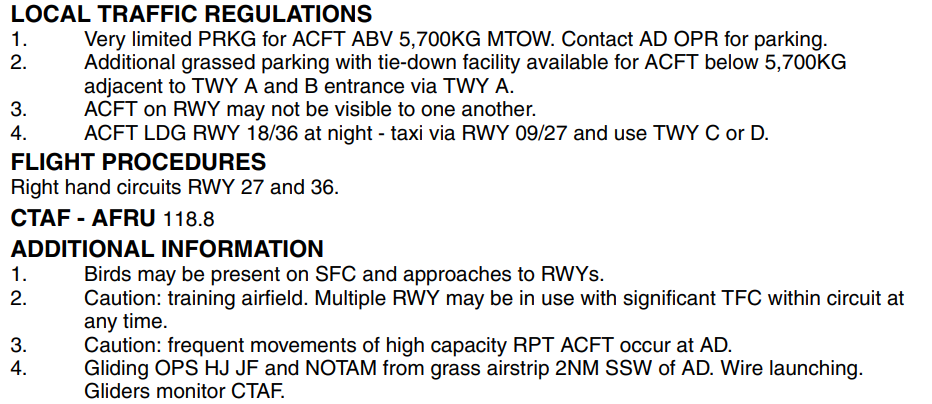
The En Route Supplement Australia (ERSA), promulgated by Airservices Australia, provides information to pilots on the operations specific to each aerodrome. The ERSA entry for Mildura Airport detailed that aircraft may not be visible to one another while on the runway. It also stated that the circuit can be busy due to it being a training airfield with multiple runways in use at any time, in conjunction with frequent high-capacity passenger air transport operations (Figure 5).
Figure 5: Mildura Airport ERSA details
Source: Airservices Australia
Airspace and traffic services
Mildura Airport was located within non-controlled Class G4F[5] airspace and did not have an air traffic control tower. The non-controlled airspace surrounding Mildura Airport was available for use by aircraft operating under visual flight rules (VFR) and instrument flight rules (IFR). No separation service was provided to aircraft operating in this airspace, with pilots responsible for making themselves aware of nearby aircraft and maintaining mutual self-separation. The primary method of traffic separation at Mildura Airport was by visual reference and relied on pilots using ‘alerted see‑and-avoid’5F[6] practices (see Alerted see-and-avoid).
Common traffic advisory frequency
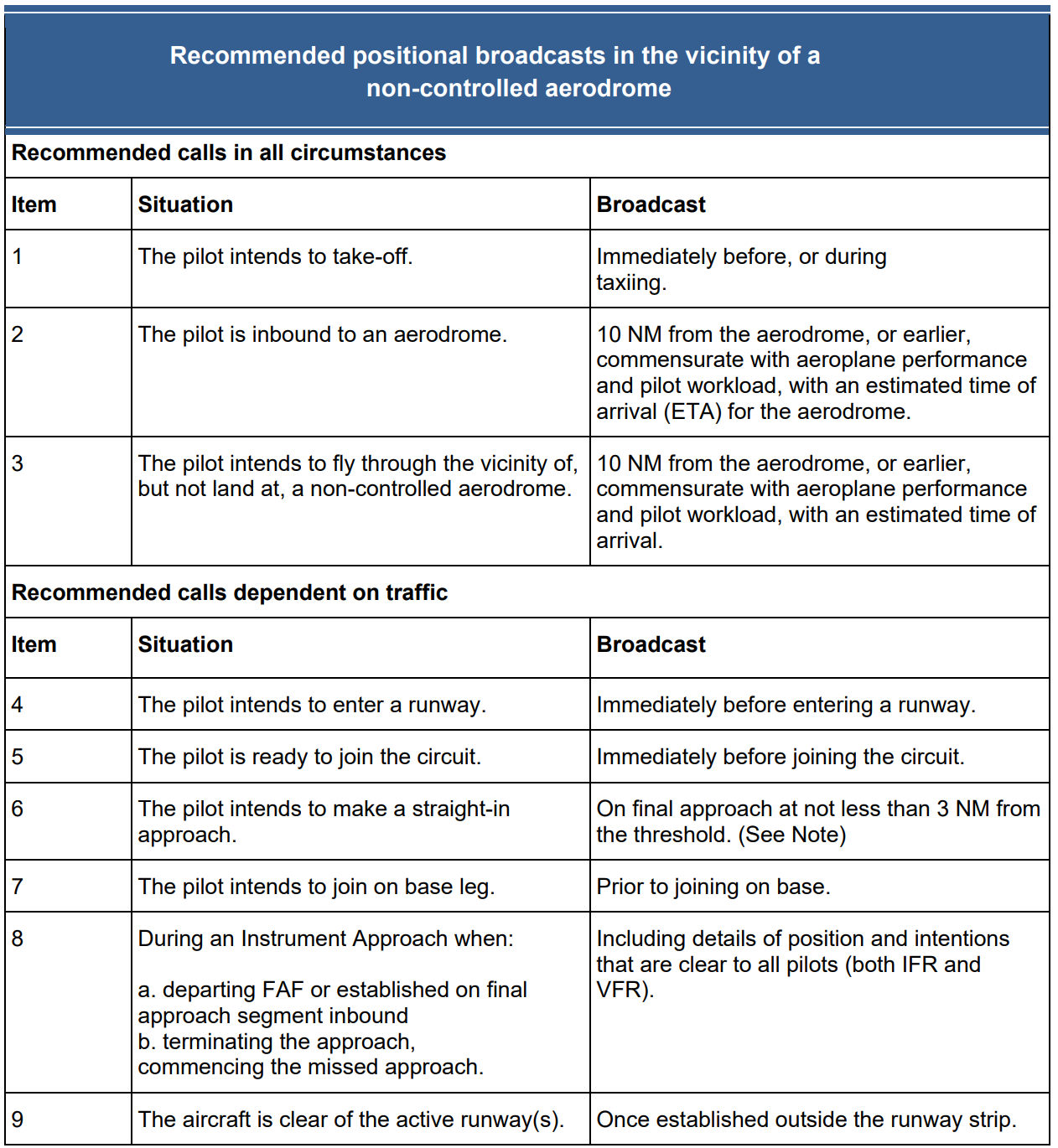
The Mildura Airport CTAF was a designated very high frequency (VHF) radio frequency on which pilots must monitor and make positional broadcasts when operating within a 10 NM radius of the aerodrome. For non-controlled aerodromes, including Mildura, there were a number of recommended VHF radio calls (Table 1) to assist traffic coordination and to enhance the situational awareness of pilots operating within the surrounding airspace.
Visual line of sight limitations
ATSB inspection of Mildura Airport established that from the threshold of runway 36, the threshold of runway 09 was visually obscured by the terminal buildings (Figure 6). The threshold of runway 36 was similarly not visible from the threshold of runway 09.
Figure 6: View from threshold runway 36
Source: Operator, annotated by the ATSB
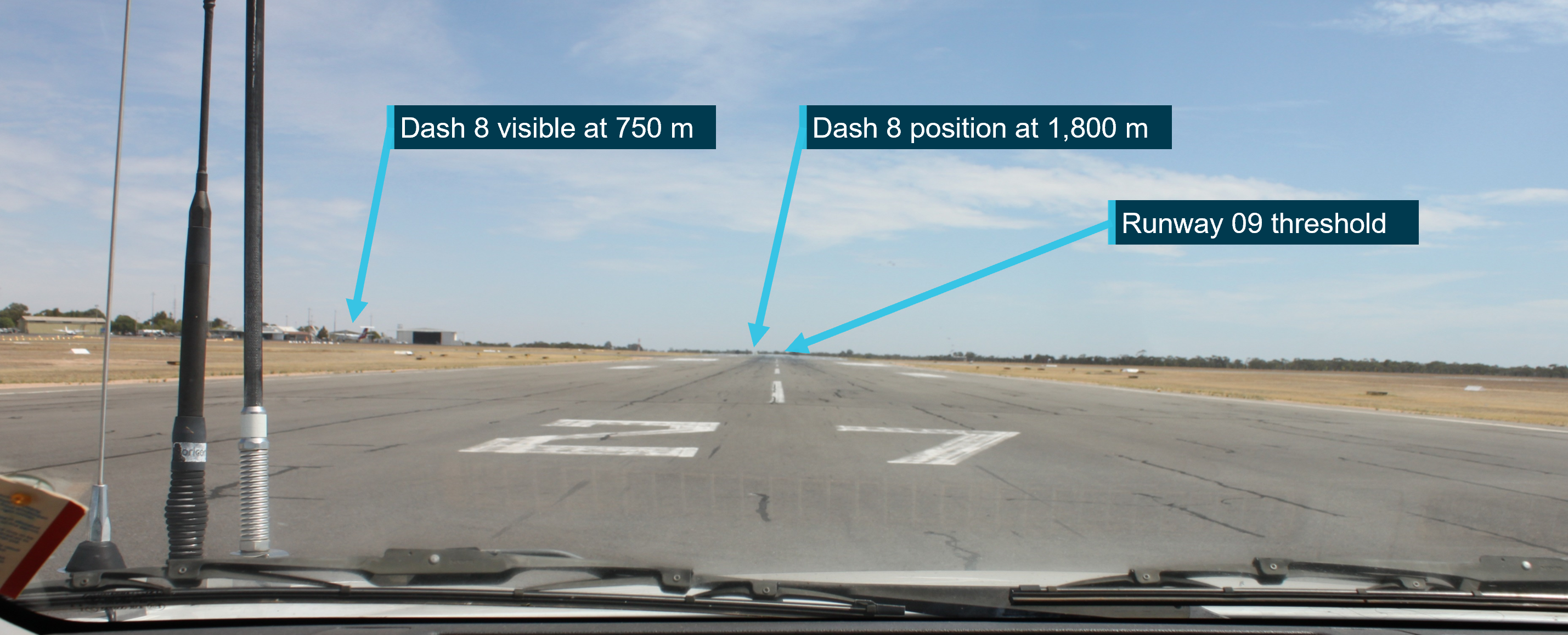
The ATSB site inspection also identified a lack of line of sight between the thresholds of runway 09 and 27 (either end of the same physical runway about 1,800 m away) when viewed from the occupant height of a road vehicle. This was due to raised terrain along the runway between the two ends (Figure 7).
Figure 7: View from threshold of runway 27
Dash 8 not clearly visible at other end of runway. Source: ATSB
Operations in the vicinity of non-controlled aerodromes
At and around non-controlled aerodromes, pilots are responsible for making themselves aware of nearby aircraft and maintaining separation. Safe operations at non-controlled aerodromes relies on all pilots maintaining an awareness of their surroundings and other aircraft, flying in compliance with procedures, while being observant, courteous and cooperative.
VHF radio is the primary communication tool to provide ‘alerted see-and-avoid’ commonly across aviation from sport and recreational flying to air transport. VHF radio allows for the communication of information (in this instance traffic information) to the pilot from other aircraft (Civil Aviation Safety Authority, 2013). Other tools to enhance ‘alerted see‑and-avoid’ include ground radar, automatic dependent surveillance broadcast (ADS-B), and traffic collision avoidance system (TCAS).
Civil Aviation Safety Regulation 91.630 made certain radio calls (listed in the Part 91 Manual of Standards) mandatory for aircraft that are fitted with or carry a radio. Chapter 21 of the Part 91 Manual of Standards prescribed one type of mandatory broadcast that applied at all non-controlled aerodromes, namely:
When the pilot in command considers it reasonably necessary to broadcast to avoid the risk of a collision with another aircraft.
To aid in increasing situational awareness at non-controlled aerodromes, recommended broadcasts are published by the Civil Aviation Safety Authority (CASA) for pilots to alert other traffic to their location and intentions before take-off, inbound to land at, or if intending to overfly a non-controlled aerodrome.
Table 1: Recommended radio calls
Source: CASA advisory circular 91-10 Operations in the vicinity of non-controlled aerodromes
In addition, individual aerodromes can require additional broadcasts due to unique circumstances by adding a requirement into the ERSA entry for their aerodrome. As seen in Figure 5, the ERSA entry for Mildura did not have any additional broadcast requirements.
CASA advisory circular 91-10, Operations in the vicinity of non-controlled aerodromes, provided further guidance on operations at non-controlled aerodromes, including that:
• In addition to making positional broadcasts, pilots should listen to other broadcasts to increase situational awareness
• Whenever pilots determine that there is a potential for traffic conflict, they should make radio broadcasts as necessary to avoid the risk of a collision or an Airprox event. Pilots should not be hesitant to call and clarify another aircraft’s position and intentions if there is any uncertainty.
Alerted see-and-avoid
Issues associated with unalerted see-and-avoid have been detailed in the ATSB research report Limitations of the See-and-Avoid Principles(Hobbs, 1991). The report highlights that unalerted see-and-avoid relies entirely on the pilot’s ability to sight other aircraft. An ‘unalerted’ search is one where reliance is entirely on the pilot searching for, and sighting, another aircraft without prior knowledge of its presence.
An ‘alerted’ search is one where the pilot is alerted to another aircraft’s presence, typically through radio communications or aircraft-based alerting systems. Broadcasting on the CTAF to any other traffic in the vicinity of a non-controlled aerodrome is known as radio-alerted see-and-avoid and assists by supporting the pilot’s situational awareness and visual lookout for traffic with the expectation of visually acquiring the subject in a particular direction. The ATSB research report found that an alerted search is likely to be 8 times more effective than an unalerted search, because knowing where to look greatly increases the chances of sighting traffic.
Positional broadcasts
Traditionally VHF radio broadcasts are made at non-controlled aerodromes in order to provide situational awareness, traffic separation and deconfliction to other traffic in the vicinity of the aerodrome.
However, positional broadcasts rely on the accuracy of the information being broadcast and the ability of other traffic receiving, comprehending and reacting to this information.
Civil Aviation Advisory Publication (CAAP) 166-2(1),Pilots’ responsibility for collision avoidance in the vicinity of non‑controlled aerodromes using ‘see and-avoid’ stated:
11.5 Pilots should be mindful that transmission of information by radio does not guarantee receipt and complete understanding of that information. Many of the worst aviation accidents in history have their genesis in misunderstanding of radio calls, over-transmissions, or poor language/phraseology which undermined the value of the information being transmitted.
11.6 Without understanding and confirmation of the transmitted information, the potential for alerted see-and-avoid is reduced to the less safe situation of unalerted see-and-avoid.
Positional broadcasts are a one-way communication, intended to provide a short and concise broadcast to minimise radio channel congestion. However, they do not imply receipt of information by other parties unless direct radio contact is made between stations to acknowledge the traffic, confirm intentions and if required, discuss measures to provide deconfliction.
The successful broadcast of the information is also subject to limitations of the VHF radio system.
VHF radio line of sight limitations
The VHF radio requires line of sight between both stations in order to function effectively. If an aircraft does not have a clear visual path direct to another in the vicinity, then the radio wave signal strength and clarity can be affected by obstacles. In some cases, terrain, vegetation or buildings can create areas that may shield or substantially reduce radio wave propagation and adversely affect broadcast signal strength and clarity.
At Mildura Airport, VHF radio calls on the CTAF frequency were recorded from an antenna south of the main terminal. Due to its elevated position, this antenna is within line of sight of the entire runway environment.
The Dash 8 operator’s internal investigation report identified that instrument flight rules (IFR) taxi calls and entering backtracking calls were recorded well, however reduced radio strength and clarity existed with broken radio calls and aircraft unable to hear each other when on the thresholds of runway 09/36.
Transponder operation at non-controlled aerodromes
Historically, transponders have usually been switched to the standby mode on engine start‑up and taxi. This was done to prevent clutter or false collision avoidance information to airborne traffic while not an immediate collision risk on the ground. If a transponder was fitted, pilots were required to select the transponder to ‘on’ and if mode C or S (that is, altitude information output) was available, this was to be selected to ‘on’ before entering the runway.
The introduction of Civil Aviation Safety Regulation 1998 (CASR) Part 91 basic operating rules commenced on 2 December 2021 and included a change to the required operation of aircraft fitted with a functioning transponder. This change required the selection of the transponder to a transmitting mode prior to the aircraft moving under its own power for the intention of take-off. This is particularly important in a non-controlled aerodrome environment where any form of enhanced situational awareness to all flight crew is paramount to avoiding the risk of collision.
Witnesses’ recollections
Dash 8 crew at the holding point
The crew of the second Dash 8 (QLINK 404) that taxied to holding point Charlie believed that all radio calls appeared normal, and it was their understanding that all parties seemed to know what was going on. They reported being aware of the 2 aircraft taxiing for runway 36. The FO recalled the Lancair taxi call, and the captain recalled the entering or backtracking call and the lining up call from the Lancair. They both recalled the first Dash 8 organising traffic and their rolling call. The crew of the second Dash 8 described the radio signal strength of the Lancair as ‘staticky’ and ‘scratchy’ with a readability score of 2 out of 5.
Mooney pilot taxiing for runway 36
The pilot of the Mooney that taxied behind the Lancair, noted that they heard all the radio calls made by all aircraft and that they did not believe that their reception was blocked by airport shielding. The pilot recalled that they were holding at the taxiway Alpha holding point as the Dash 8 made their rolling call, at about the same time the Lancair had completed their enter and backtrack. Shortly after that, the Lancair called rolling on runway 09, to which the rolling Dash 8 replied to hold position. Worried that the Lancair had not heard this broadcast, the pilot of the Mooney advised the Lancair of the departing traffic.
Dash 8 operator radio procedure
The QantasLink Dash 8 standard operating procedure for departure from a non-controlled aerodrome, at the time of the occurrence, required VHF COM 1 to be set to the area frequency and VHF COM 2 to be set to the CTAF, as passenger boarding commenced.
Prior to releasing the handbrake to taxi, a call was to be made to the relevant air traffic centre on VHF COM 1 and then followed by a taxi call to the CTAF on VHF COM 2. The departing aircraft was to remain on the CTAF until after departure and clear of the CTAF, only then was the VHF COM 2 selected to 121.5 Mhz.
As a result of a related event on 6 June 2023 (see ATSB investigation report AO-2023-025), the operator provided its crew with a route manual amendment for Mildura on 8 June 2023 with a caution that:
Crew must be extra vigilant when managing the threat of cross-strip operations at Mildura. Aircraft operating on cross runways may not be visible to each other. When operating from runway 09, the runway 36 threshold and touch down zone will not be visible.
Radio wave degradation is likely to occur on the ground due to terrain and obstacle shielding. This radio shielding is most likely to occur when one aircraft is operating on runway 09 (west of Taxiway D), and other aircraft is positioned on runway 36 (south of taxiway A).
Due to reduced visibility and radio wave degradation threats, flight crew are required to:
• Conduct a rolling call for all departures.
• Clarify any broken, suspicious or ambiguous radio calls from other aircraft prior to departure.
In the course of this investigation, QantasLink issued a technical advisory bulletin, effective from 17 July 2024, which changed the VHF communications procedure for Mildura departures. The aim of the change was to improve ground‑to-ground CTAF VHF communication during the taxi phase. The changed procedure required use of the VHF COM 1 system, noting that this was found to have an improvement in both transmission clarity and reception.
Tests and research – radio signal strength and clarity
The ATSB conducted VHF signal strength and readability testing, undertaken on 13–14 March 2024 at Mildura Airport. The aim of the testing was to establish if signal strength degradation was occurring due to line of sight limitations and obstacles on the airport or/and if radio signal strength and clarity was aircraft related.
The testing included numerous stakeholders including expertise provided by Australian Communications and Media Authority (ACMA), Airservices Australia, QantasLink, Mildura Airport management, aerodrome reporting officers (ARO) and a local operator.
ACMA was consulted in the development of the testing schedules and assisted the ATSB during the testing with measuring equipment, by recording radio signal strength data and providing advice. All stakeholders, with the exception of the local operator, were consulted on the testing schedules prior to the conduct of the testing.
The testing comprised of signal strength, readability and clarity assessments to and from various locations on the aerodrome. The testing focused on the circumstances related to the runway incursion, concentrating on the quality of radio transmissions on the airfield and in particular between the threshold of runways 09 and 36.
Testing specific to Dash 8 aircraft was conducted on VH-SBI, provided by the operator. This involved reception signal strength testing of aircraft transmissions.
Test schedules
The testing comprised of 4 schedules:
Schedule 1 involved aerodrome signal reception strength and readability testing. This comprised of measuring the strength and readability of radio transmissions to and from VHF radios in ARO vehicles at relevant points on the airfield (Figure 8).
Schedule 2 involved light aircraft signal reception strength and readability testing. This was achieved by testing transmissions to and from a light aircraft to an ARO vehicle to measure the strength and readability of radio transmissions of both stations.
Schedule 3 included Dash 8 signal strength testing. By transmitting from relevant points on the airfield using the testing Dash 8 aircraft’s VHF radios COM 1 and COM 2, and an ARO vehicle to measure the strength and readability of radio transmissions.
Schedule 4 involved Dash 8 airframe signal strength and shielding testing. This was achieved by recording the test Dash 8 aircraft’s VHF radios COM 1 and COM 2 reception strengths and readability of radio transmissions around the aircraft at about 20 m distance using an 8-point clock code.
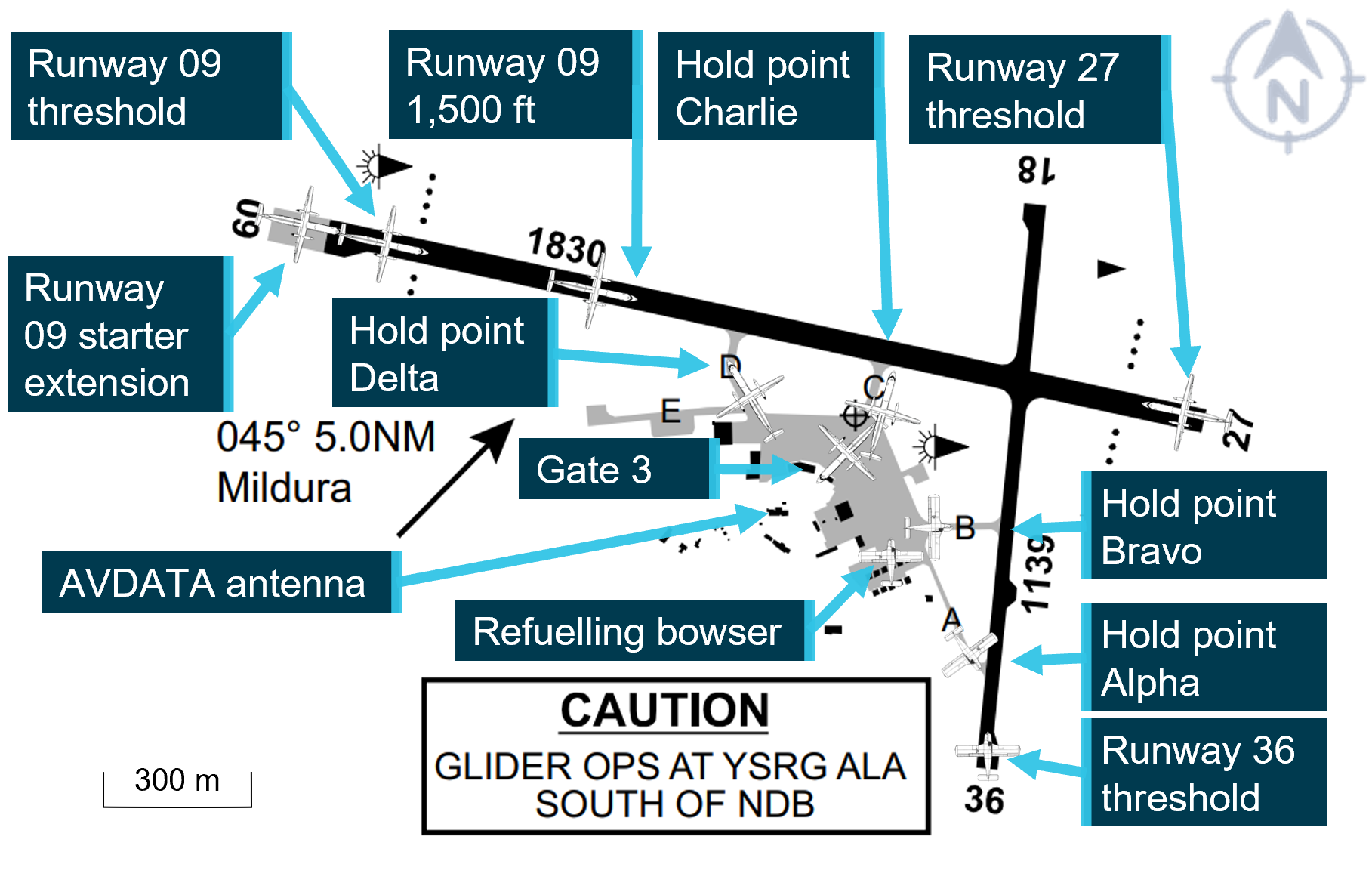
Figure 8: Test locations at Mildura Airport
Source: En Route Supplement Australia, annotated by the ATSB
Signal strengths and readability measurements
The signal strength measurement recorded during the testing was the signal power level received from the radio transmission on the ACMA equipment at various locations remote from the aircraft or vehicle. Signal strength was measured in dBm which represents decibels relative to a milliwatt (mW). This is the power ratio in decibels (dB) of the measured power referenced to one milliwatt.6F[7]
A stronger and acceptable signal is one higher than −70 dBm. A weaker, unreliable signal is less than this towards a level of −100 dBm. Stronger signal strength results in more reliable and clear communications.
ATSB also recorded a radio signal readability test. For this, a qualitative 1–5 readability scale provided by ACMA (Table 2) was recorded at the receiving locations. To avoid subjectivity, these scores were recorded by ATSB, ACMA and Airservices employees and averaged to arrive at an agreed value to accurately represent the call readability.
Table 2: VHF radio readability scale
Scale
Description
5
Perfectly readable
4
Readable with practically no difficulty
3
Readable with considerable difficulty
2
Readable now and then
1
Unreadable
Aerodrome signal strength, shielding and readability testing
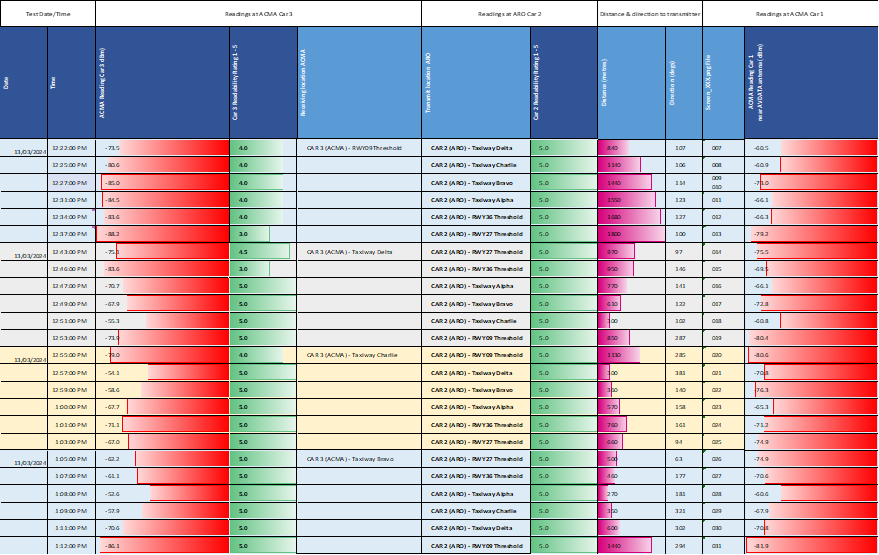
Schedule 1 testing was conducted on the afternoon of 13 March 2024 at about the same time of day as the occurrence. It measured the signal strength and readability during CTAF transmissions from ARO car 2 (ARO and ATSB investigator) transmitting from locations at Mildura Airport (Figure 8). Signal strength measurements and readability assessments were recorded by the ATSB and ACMA staff using ACMA measuring equipment in ARO car 3 which relocated around the aerodrome for the series of tests. Observers of the testing, including Airservices and a Mildura ARO were also in ARO car 3.
Additional signal strength readings were taken by an ACMA officer from their vehicle, designated ACMA car 1, located near the AVDATA antenna at Mildura Airport (Figure 8). ARO car 2 also conducted a readability assessment of ARO transmissions from ARO car 3 and recorded their readability testing.
The testing identified that between the radio transmission points on the aerodrome, the lesser the distance and greater the line of sight, the clearer the radio transmission was with a readability of 4 (readable with practically no difficulty) or more and signal strengths of greater than −70 dBm.
The testing also identified that the most significant reduction in recorded signal strength and readability was received when transmitting greater distances at:
the runway 36 threshold to the threshold of runway 09, which reduced readability to 3 (readable but with considerable difficulty) and had a weaker signal strength of less than −70 dBm
transmitting from the runway 27 threshold to the runway 09, resulting in readability of 3 (readable but with considerable difficulty) and a weaker signal strength of less than −70 dBm
transmitting from the runway 09 threshold with slight general reduction in signal readability across all other runway thresholds and holding points to 4 (readable with practically no difficulty), but a general reduction in signal strength of less than −70 dBm across all readings.
The results of schedule 1 are shown in Appendix B.
Light aircraft signal strength and readability testing
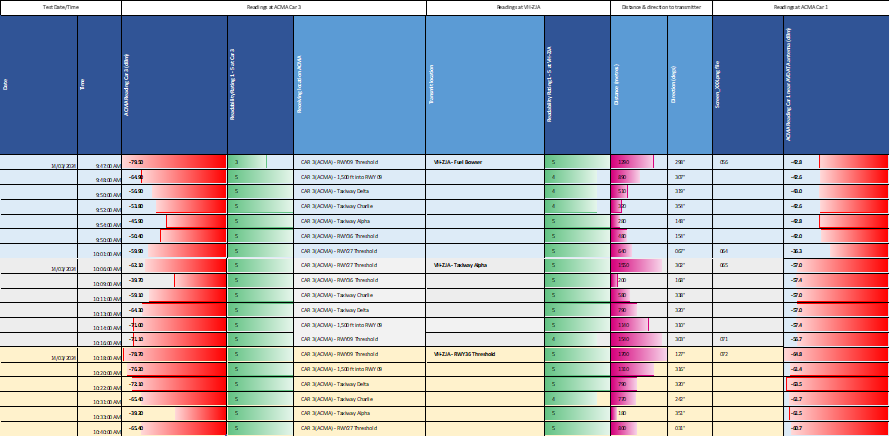
Schedule 2 testing was conducted on the morning of 14 March 2024. However, due to the unavailability of Lancair VH-VKP due to inclement weather, the Aero Dynamic Flight Academy at Mildura provided Cessna 172, VH-ZJA and an instructor to assist with the testing.
Signal strength and readability during CTAF transmissions from VH-ZJA (Instructor and ATSB investigator) were conducted, transmitting from locations at Mildura Airport. Signal strength measurements and readability assessments were recorded by the ATSB and ACMA staff using ACMA measuring equipment in ARO car 3 which also relocated around the aerodrome for the series of tests. Observers of the testing, including Airservices and a Mildura ARO were also in ARO car 3.
The testing identified that between the aircraft radio transmission points on the aerodrome, the lesser the distance and greater the line of sight, the clearer the radio transmission was with a readability of 4 (readable with practically no difficulty) or more and signal strengths of greater than −70 dBm.
The testing also identified that the most significant reduction in recorded signal strength and readability was received when transmitting greater distances at:
transmitting from the Mildura fuel bowser to the threshold of runway 09, which may be indicative of close proximity hangar shielding
when receiving from the fuel bowser, a general reduction in signal strength to taxiway Charlie, Delta and the runway 09 threshold greater than −70 dBm.
However, the readability scores in this testing did not score less than 3 (readable with considerable difficulty).
The results of schedule 2 testing are shown in Appendix 2.
Dash 8 signal strength and readability testing
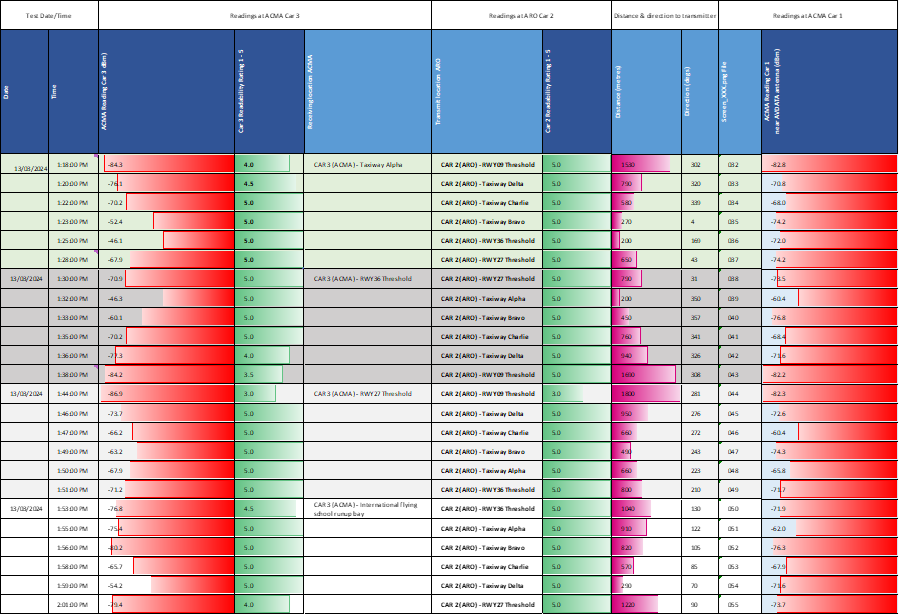
Schedule 3 testing was conducted on the afternoon of 14 March 2024 at around the same time as the occurrence and measured the signal strength and readability during CTAF transmissions from a QantasLink DHC-8-316, Dash 8 aircraft, VH-SBI.
The VHF radios installed in both VH-SBI (test aircraft) and VH-TQZ (occurrence aircraft) were Collins Aerospace VHF Transceiver Model: VHF-22C, Part No: 822-1113-021, with RF Power Output 20W Nominal/16W Minimum. These were installed after being released to service in 2022 in Singapore.
Dash 8 flight crew with an ATSB investigator conducted a modified schedule 1 test using both the No 1 VHF COM antenna (VHF COM 1) mounted on the roof of the aircraft forward of the wings and No 2 VHF COM antenna (VHF COM 2) mounted on the belly of the Dash 8 (Figure 4) to provide comparative ground-based signal strength and readability results. The testing focused on the recorded signal strength and reception of radio signals to and from the Dash 8 to ATSB and ACMA staff using ACMA measuring equipment in ARO car 3 which relocated around the aerodrome for the series of tests.
The purpose of this testing was to ascertain if there were any limitations of the reception and transmission of radio signals that may be affected by attenuation of the signal due to reflection, refraction or shielding from aircraft structure and what limitations this might have on both VHF COM 1 and COM 2.
This testing was conducted by the Dash 8 transmitting on VHF COM 1 first and subsequently from COM 2 from 6 locations around Mildura Airport (Figure 8). These locations were at:
gate 3 (nose in)
hold point taxiway C
hold point taxiway D
starter extension on runway 09
runway 09 threshold
1,500 ft into runway 09.
The ARO vehicle (car 3) with the ACMA staff and test equipment then progressed to various locations around the airport to take transmission and readability measurements. The stationary ACMA vehicle (car 1) recorded measurements of the same VH-SBI transmissions.
The testing identified that between the Dash 8 and the radio reception points on the aerodrome, the lesser the distance and greater the line of sight, the clearer the radio transmission was with a readability of 4 (readable with practically no difficulty) or more and signal strengths stronger than −70 dBm.
The testing also identified that the most significant reduction in recorded signal strength and readability was received when transmitting greater distances at:
receiving and transmitting from the runway 09 starter extension to the runway 36 threshold on VHF COM 2 scored a readability assessment of 2 (readable now and then), and signal strength weaker than the −70 dBm acceptable signal strength limit
receiving and transmitting from the runway 09 threshold to the runway 36 threshold on VHF COM 2 with a readability of 1 (unreadable), and −85 dBm signal strength, 15 dBm weaker than the acceptable signal strength of −70 dBm
receiving transmissions from the 09 threshold or starter extension to taxiway Alpha on VHF COM 2 with a readability of 1 (unreadable), and −85 dBm signal strength, 15 dBm weaker than the acceptable signal strength of −70 dBm
It was identified that transmission and reception from the Dash 8 were considered 1 (unreadable) from the runway 09 threshold to the runway 36 threshold on VHF COM 2, while these were 5 (perfectly readable) to 4 (readable with practically no difficulty) on VHF COM 1.
Testing also identified a significant reduction in recorded signal strength and readability was recorded when the Dash 8 was:
parked at gate 3 (nose in) transmitting and receiving to the threshold of runway 27 on VHF COM 2
transmitting and receiving from holding points Delta and Charlie to the runway 36 threshold and holding point Alpha on VHF COM 2.
General trends identified from schedule 3 testing were that:
Dash 8 VHF radio readability was most adversely affected by stations transmitting from directly behind the Dash 8 on both VHF COM 1 and 2 with slightly reduced readability and increasing signal weakness with increasing distance.
VHF radio readability was adversely affected by increased distance between the ground-based stations, this was more evident on VHF COM 2, leading to unreadable radio signal readability and weaker signal strength.
VHF readability was somewhat adversely affected from the runway 27 threshold to the runway 09 threshold using VHF COM 2, however Dash 8 reception from the runway 09 threshold reduced further to become only 2 (readable now and then).
Dash 8 airframe signal strength and shielding testing
The purpose of schedule 4 testing was to ascertain if there were any limitations of the reception and transmission of radio signals that may be affected by attenuation of the signal due to reflection, refraction or shielding from aircraft structure and what limitations this might have on both VHF COM 1 and COM 2.
The testing was conducted on the Mildura apron, adjacent to parking bay 3, with VH-SBI facing towards the terminal (nose in), simulating the startup position with engines running. An ATSB investigator was also present on the flight deck with operator’s crew. ATSB and ACMA staff conducted a ground-based signal strength and readability test from the tarmac at about 20 m distance from the aircraft at 8 cardinal points around the aircraft (Figure 9). The testing was restricted to close proximity testing and possible results from a greater distance may vary. However, the magnitude of variation even at close distance was considered significant.
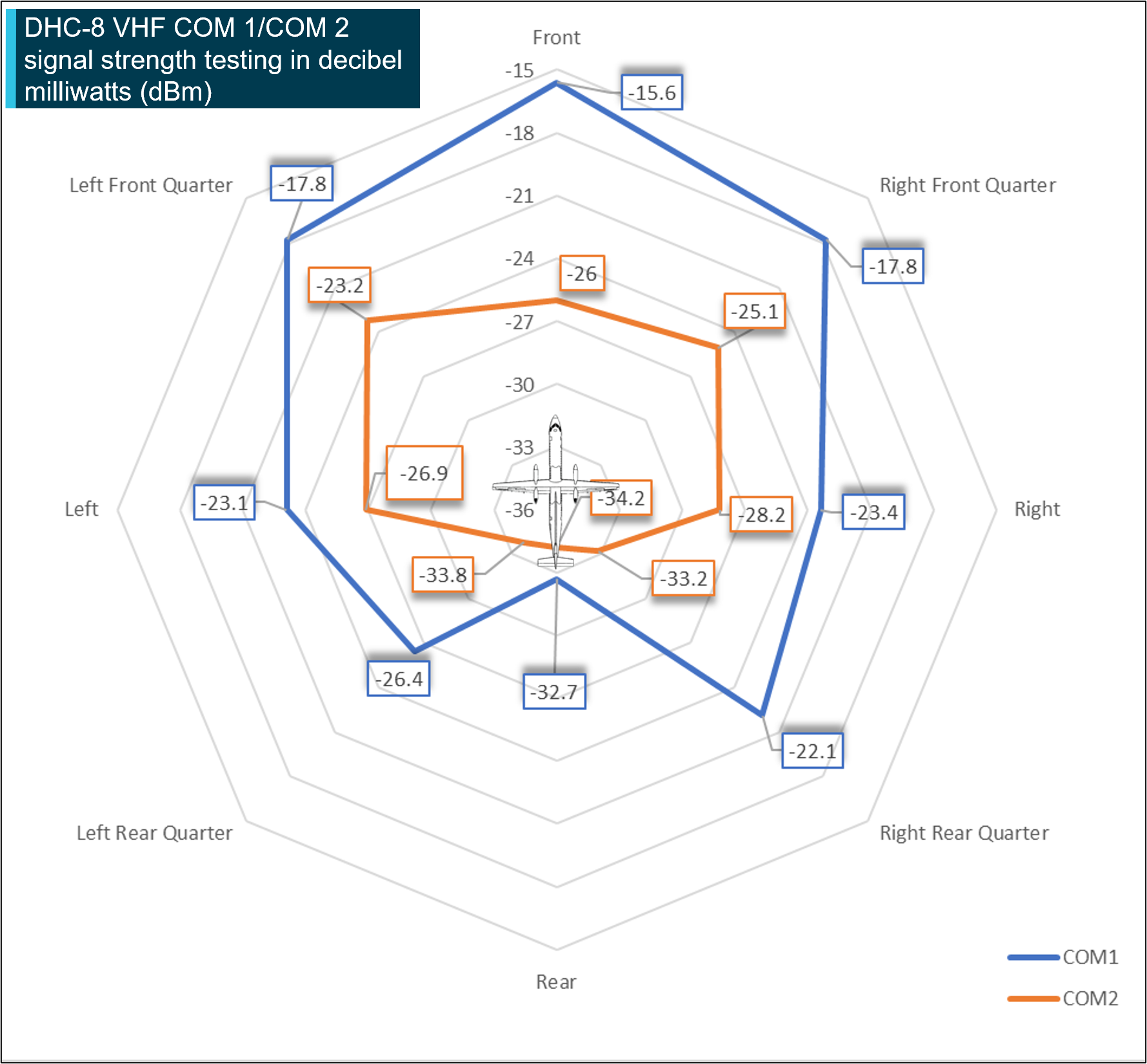
Figure 9: Dash 8 airframe signal strength and shielding testing
It should be noted that when considering these schematics the higher dBm figures (less negative and located on the outside of the antennae radiation pattern) are of a stronger signal strength level with a greater readability. Source: ACMA test data, annotated by the ATSB
Testing identified that:
the signal strength was strongest towards the front of the aircraft and weakest to the rear using VHF COM 1
the signal strength of VHF COM 2 was consistently less (greater than half strength) at all locations with the VHF COM 2 maximum loss (−10 dBm) at the front and right rear quarter most notable.
at the direct rear of the aircraft, the lowest VHF COM 1 strength (−32.7 dBm) was recorded and was consistent with similar levels to VHF COM 2
transmissions on VHF COM 2 on the ground had significantly reduced strength compared to VHF COM 1 and that radio reception and transmission strength to the rear of the aircraft was reduced on both VHF COM1 and VHF COM 2.
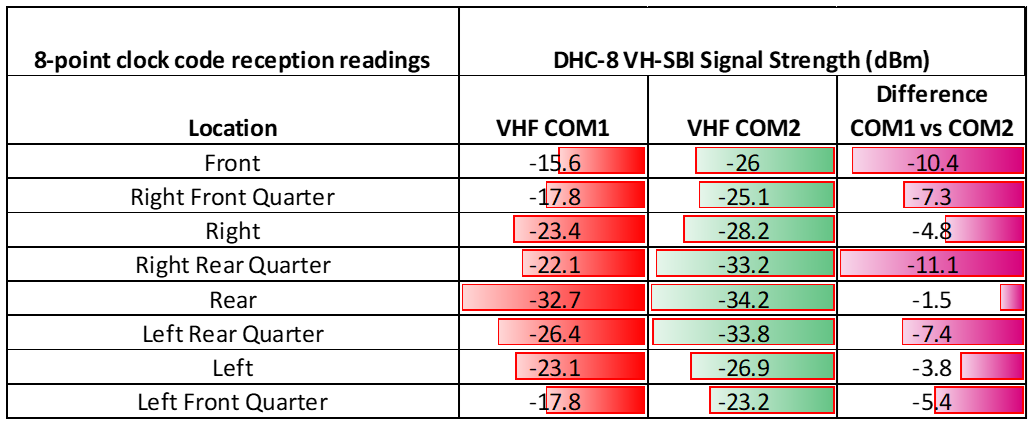
The results of schedule 4 testing are shown at Table 3.
Table 3: 8-point testing VH-SBI
Aircraft antenna installation and condition
The operator identified the VHF COM 2 antenna on the test aircraft, VH-SBI, was installed on 23 March 2020.
The operator’s approved maintenance program included a company derived task to remove the VHF COM antennas at each 7,000 hr ‘C Check’ and to inspect both the fuselage mounting surface, perforated foil gasket and antenna for corrosion and condition.
No defects were identified relating to the antenna or base plate mount, either prior to the testing or after.
No corrosion or foreign object damage to the antenna or mount was identified and the operator was not aware of any directives or advisory information from the manufacturer regarding elevated risk of corrosion in this location.
Dash 8 aircraft communications
VHF radio certification – ground-based testing
The Dash 8 manufacturer, De Havilland Aircraft of Canada Limited, advised that initial ground-based VHF radio testing for original certification was conducted during original certification for the Dash 8 on 29 March 1984, in Downsview, Ontario, Canada and that this involved measuring the field strength intensity of the reception of radio signal of VHF COM 2 in ground-to-ground communications of a single aircraft. The manufacturer confirmed that at the time, there was no requirement for certification to consider the aircraft’s transmission field strength intensity. The testing was recorded by an EMC-25 field intensity meter, connected to the aircraft’s VHF COM 2 antenna on the ground with the aircraft conducting a tight turn while receiving radio transmissions from a ground source located at no less than 2,000 ft (610 m).
At the time of original certification in 1984, De Havilland Aircraft of Canada Limited identified that the Dash 8 aircraft radio installation was a Collins Aerospace Proline II VHF transceiver Model: VHF-22C. The radio had been certified to the required technical standing orders (TSO)-C37b and C38b standards and complied with the US Federal Communications Commission (FCC) Rules and Regulations, Parts 15 and 87 during certification testing.
Ground-based communication limitations
The ATSB supplied the above test results to De Havilland Aircraft of Canada Limited for review and comment. It identified that Dash 8 aircraft have a relatively uniform antenna polar pattern of reception on both VHF COM 1 and 2 whilst airborne and that in the air, radio range was near horizon limits. De Havilland Aircraft of Canada Limited identified that the original certification testing of the VHF COM 2 was performed at close transmitter/transceiver antenna distances and that the 1984 certification testing indicated a satisfactory result.
The De Havilland Aircraft of Canada Limited review of the ATSB Mildura test results identified that the signal strength and readability results appeared consistent with the effects of VHF line of site limitations such as physical obstructions, and intervening airport ground and localised aircraft structures, such as fuselage, wings and the tail.
De Havilland Aircraft of Canada Limited further reported that, due to the physical location of the VHF COM 1 antenna, this would inherently have better line of sight and more reliable performance in ground-based communication with other ground stations when compared to the installation location of the VHF COM 2 antenna
In response to ATSB questions about what guidance has been provided to Dash 8 operators for the use of the 2 communication channels, De Havilland Aircraft of Canada Limited reported that there was no guidance published by them on best practices for VHF radio communication usage. It was De Havilland Aircraft of Canada Limited’s understanding that this was done at the airline, or national level.
In terms of the communications issues apparent in this incident, and an earlier incident at Mildura also involving a Dash 8 (see ATSB investigation AO-2023-025), De Havilland Aircraft of Canada Limited reported that it considered the root cause of both events to be operational and not aircraft related.
De Havilland Aircraft of Canada Limited further identified that due to the lower mounted aerial position of VHF COM 2, that base plate corrosion due to moisture wicking, if not drained correctly, could degrade signal strength. Additionally, antenna damage from foreign objects may also have the same effect.
Related occurrences
Occurrence history
The ATSB reviewed 30 years of recorded occurrences involving Dash 8 aircraft communication difficulties, both in the vicinity of non-controlled aerodromes and during ground-based communications at non-controlled aerodromes from 1995–2024. There were 57 communication occurrences and 51 runway-related occurrences.
Further review identified that of the above radio communication occurrences between a Dash 8 and another station, there were 25 during approach to land and 27 on the ground where the reason for the radio communication issue remained undetermined. At the time of this occurrence, these undetermined ground-based occurrences were identified across 15 different aerodromes in Australia (see Appendix C). Of these aerodromes, 10 involved a secondary runway and at the time, 4 of which also had dedicated CTAF broadcast procedures due to line of sight limitations during ground-based operations.
Ground‑based air traffic services (ATS) were also identified at 9 of those aerodromes, which provides a local ground‑based radio frequency and one circuit‑based frequency to facilitate communication with air traffic control.
Due to the historic nature of these reported occurrences, it is not possible to provide further analysis of the exact contributing factors of the undetermined events; this could be due to numerous factors not related to limitations to line of sight, Dash 8 VHF COM 2 transmissions or reception. However, all led to a breakdown of alerted see‑and‑avoid during operation within the vicinity of a non-controlled aerodrome.
On 6 June 2023, a Piper PA-28-161, registered VH-ENL, taxied for runway 36 at Mildura, Victoria. At about the same time, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-315 (Dash 8), registered VH-TQH, began to taxi for runway 09. Both aircraft broadcast their intentions on the local common traffic advisory frequency. The pilot of the PA-28 was aware of the Dash 8, but the crew of the Dash 8 were not aware of the PA-28. Both aircraft commenced their take-off at about the same time and the Dash 8 crossed ahead of the PA-28 at the runway intersection of 09/36 by about 600 m.
The pilot of the PA-28 was unable to visually sight the location of the Dash 8 due to airport buildings and assumed that the Dash 8 was still backtracking on runway 09. They did not directly contact the Dash 8 to positively organise separation. They also incorrectly referred to the runway direction at Mildura Airport as ‘runway 35’ instead of ‘runway 36’.
The Dash 8 crew was focused on obtaining their pre-departure information from air traffic control and had the volume for the radio tuned to the common traffic advisory frequency turned down. An over‑transmission from air traffic control meant that the Dash 8 crew only received certain elements of the PA-28 pilot’s radio calls. This likely led to an incomplete comprehension of traffic by the Dash 8 crew who believed that the PA-28 was not at Mildura (due to the incorrect reference to runway 35). However, they did not seek further information of the source of the radio calls to positively identify the traffic location.
The investigation found that, due to the topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The Dash 8 crew did not give a rolling call on runway 09, nor were they required to. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off.
On 19 March 2024, a Fairchild SA226-TC Metroliner, registered VH-KGX and operated by CASAIR, taxied at Geraldton, Western Australia for runway 03. About one minute later, a Beechcraft A36 Bonanza, registered VH-CKX and operated by Shine Aviation, taxied for runway 14. After reaching their respective runway thresholds, both pilots attempted to contact the other, however, they did not hear each other, nor could they see each other. A third aircraft assisted by relaying information. Based on the information received, the Bonanza and Metroliner pilots commenced their take-off within 3 seconds of each other. The Metroliner crossed runway 14 about 400 m in front of the Bonanza, with a vertical separation of about 250–300 ft.
The investigation found that, when aircraft were positioned at the thresholds of runway 03 and 14 (and 08), they will unlikely be visible to each other due to the position of the airport buildings. Further, they may not be contactable on VHF radio due to potential shielding effects. This resulted in the pilots being unable to verify each other’s position and intentions prior to commencing their take-off.
While the pilot of the third aircraft was attempting to assist, the details provided were inaccurate and incomplete. This inadvertently resulted in misinterpretation by the Bonanza and Metroliner pilots and influenced their decision to take off.
ATSB investigation (AO-2024-041)
The ATSB is investigating a runway incursion involving a De Havilland Aircraft of Canada Limited DHC-8-402 registered VH‑QOD and a Piper PA-28, registered VH-XDK, at Wagga Wagga Airport, New South Wales, on 15 July 2024.
The De Havilland Aircraft of Canada Limited DHC-8 entered active runway 05 as the Piper PA-28 began its take-off roll. The crew of the DHC-8 was made aware of the PA-28 by another aircraft and stopped, reversing the aircraft clear of the runway.
Both crews report making the appropriate radio calls, however, no radio calls were heard from either aircraft reportedly due to known radio shielding.
The investigation is continuing.
Safety analysis
Introduction
On 29 September 2023, a Lancair, registered VH-VKP (Lancair) lined up for take-off on runway 36 at Mildura, however, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-315 registered VH-TQZ (Dash 8), was just becoming airborne on runway 09 at Mildura. The Lancair stopped on the runway after being alerted to the conflicting traffic by the Dash 8 and another aircraft, the Dash 8 crossed ahead of the Lancair at the runway intersection.
This analysis will explore the operational considerations pertaining to radio calls and communication at Mildura Airport, the flight crew and pilot’s mental models, and factors pertaining to the breakdown of communication.
Communication and local traffic mental models
Succinct and timely radio communication is important to ensure high levels of situational awareness and aids in providing enhanced alerted see-and-avoid safety outcomes. As such, the accuracy of the information broadcast by pilots is also critical in ensuring minimum misunderstanding.
The ATSB investigation considered a range of human factors that could have influenced the decisions and actions of the pilots involved. While both the Dash 8 and the Lancair crews made radio calls in accordance with the applicable regulation and guidance, not being aware of each other meant that they were unable to anticipate the risk of collision and take appropriate action.
Alerted see-and-avoid relies on crew/pilot awareness of all traffic in the vicinity that may be considered a hazard to their operations. Enhanced situational awareness requires the crew/pilot mental model of the location and intentions of nearby traffic being updated in order to form an evolving understanding of the nearby traffic.
Without this information, the likelihood of effective situational awareness is degraded, and the mental model and shared understanding of hazards is compromised.
During one of the busiest parts of passenger transport operations from a non‑controlled aerodrome, the crew of the Dash 8 were managing the co-ordination and deconfliction of a number of other airborne aircraft in the vicinity of Mildura Airport. This added complexity within the busy phase of pre-departure for the Dash 8 crew and likely led to attentional focus on the identified airborne traffic. Reduced Dash 8 ground-based signal reception associated with distance between the stations, aircraft and geographical shielding, likely reduced the clarity of calls on the CTAF. Although the Lancair pilot’s taxi call was not over-transmitted and was likely received by the Dash 8’s radio, its reduced clarity meant it would have required more of the crew’s attention to notice and interpret.
A significant amount of radio use was recorded by the Mildura CTAF prior to the occurrence (Appendix A). Substantial use can introduce difficulty in identifying relevant parties, especially during multiple runway operations. The Dash 8 crew had focussed their concern on the identified overhead aircraft as an increased threat to their operation and, while in the protracted process of organising this separation, was not aware of the Lancair. The phenomenon of inattentional blindness, where an unexpected stimulus is not perceived even though it can be physically seen (Mack & Rock, 1998), also applies to auditory stimulus. Known as inattentional deafness, being focused on something else in the auditory environment reduces the chance of hearing an unexpected but salient auditory event (Dehais and others, 2012). The more a person’s attention is required for other tasks, the higher the chance of missing something unexpected, such as the Dash 8 crew missing the Lancair taxi call while focused on overhead aircraft. At an extreme end of this spectrum is cognitive tunnelling where the person is too focused on the task at hand at the expense of what is happening in the present environment (Mack & Rock, 1998).
Such focus can reduce the chance of hearing and therefore appreciating the relevance of other radio broadcasts. The culmination of the Dash 8 crew’s focus likely led to the Dash 8 crew not being aware that the Lancair was taxiing for a conflicting runway.
Contributing factor
The Dash 8 crew were actively engaged in multiple communications with airborne traffic to ensure separation for departure, and were not aware of the Lancair taxiing for runway 36.
While the Dash 8 was organising separation with another airborne aircraft, the pilot of the Lancair also broadcast their ‘entering and back tracking’ call at the same time, resulting in an over-transmission and only partial receipt of the Lancair call to the CTAF. The over-transmission was not queried by any of the other local traffic.
This was a missed opportunity that could have allowed the Dash 8 crew to update their mental model as they still had no expectation of another aircraft on the ground that had the potential to become a conflict. The Dash 8 crew continued to focus their attention on airborne traffic.
Should over-transmission occur, a request for one or both stations to repeat their last transmission is vital to ensuring position and intentions are well known to all other operators in the vicinity.
Contributing factor
The Lancair pilot's entering and backtracking radio call for runway 36 was partially over‑transmitted. This did not afford an opportunity to alert other aircraft as to their location or intentions.
The pilot of the Lancair did not hear the calls from the Dash 8, and visual identification of the location of the Dash 8 backtracking on runway 09 was not possible from the threshold of runway 36. This likely reduced the effectiveness of the alerted see-and-avoid principle and prevented the Lancair pilot from seeing the other traffic on runway 09.
Analysis of the radio calls made on the CTAF frequency and the traffic at Mildura, identified that both airborne and taxiing traffic did not witness any direct communication, between either the departing Dash 8 crew or the taxiing Lancair. It is highly likely that both the Dash 8 crew and the Lancair pilot did not either receive or recognise each other’s positional broadcasts and therefore were not able to update their mental model of other aircraft in the vicinity of Mildura Airport at the time.
Contributing factor
Neither the Dash 8 nor the Lancair crews heard each other's previous radio calls prior to the Dash 8 taking off on runway 09, and the Lancair giving a rolling call on runway 36.
The Lancair pilot was aware of other airborne traffic and traffic taxiing behind them as they entered and backtracked runway 36.However, during all the time from start up, taxi and entry to runway 36, they were not aware of the Dash 8 backtracking and holding on the threshold of 09, likely a result of weaker signal strength transmission from the VHF COM 2 of the Dash 8 at the threshold of runway 36, there being no visual line of sight between the thresholds of runway 36 and 09, and localised radio transmission effects between these two locations.
The crew of the Dash 8 were not aware of the presence of the Lancair as a threat to their operation. Although visibility was greater than 10 km with no cloud in the area, start-up, taxi direction and entering the runway orientation of the Dash 8, meant that visibility of the GA apron was limited to the Dash 8 crew with it being behind them. Visual searches prior to take-off on runway 09 for other conflicting traffic were likely obscured by obstacles such as trees, hangars and buildings between the threshold of runway 09 and runway 36.
Furthermore, the Dash 8 crew also checked electronic surveillance equipment prior to departure and did not identify any conflicting traffic.
In addition to neither crew hearing radio calls from the other aircraft, the above resulted in both crew of the Dash 8 and the pilot of the Lancair having incorrect mental models of the local traffic at Mildura during their take-off. While each of the pilots made assumptions as to local traffic location and intentions, neither were directly aware of each other to positively ascertain traffic separation, resulting in a missed opportunity to utilise the mitigation of alerted see-and-avoid effectively.
Contributing factor
Both the Dash 8 and Lancair crews had no awareness of each other at any stage until after the Dash 8 was taking off, and the Lancair pilot gave a rolling call.
The Mooney pilot taxiing behind the Lancair, became situationally aware of the departing Dash 8 on runway 36 and identified the potential collision risk as the Lancair gave a rolling call on runway 09. At this time, the Dash 8 requested the Lancair stop their take-off, however fearing that the Lancair may not have understood the import of the call, the pilot of the Mooney advised the Lancair to hold their position, due to the departing traffic. This third-party intervention likely prevented a near miss or collision at the runway 09/36 intersection.
Other finding
Third party intervention by the Mooney pilot prevented the Lancair from rolling on runway 36. The Lancair pilot held on the runway until the Dash 8 departed.
Dash 8 radio reception and transmission
The VHF radio strength and readability testing conducted at Mildura on 14 March 2024 by the ATSB in conjunction with the Australian Communications and Media Authority (ACMA), identified that Dash 8 signal strength reception could be adversely affected by the Dash 8’s orientation relative to the other aircraft or antenna locations. Significant recorded signal reduction on both VHF COM 1 and VHF COM 2 radios was observed when the tail of the aircraft was pointed towards the receiver.
Schedule 3 testing with no geographical or man-made obstructions between stations identified that the Dash 8 with the nose in at the terminal gate and tail pointed to the end of runway 27, recorded a significant drop in readability on VHF COM 2 to the threshold of runway 27 to a readability of 3 (readable with considerable difficulty). Signal strength weakening, over one of the shortest distances tested was also observed. Conversely, testing on VHF COM 2 at the taxiway Charlie holding point to the threshold of runway 27 with almost the same physical distance, but different aircraft orientation at about right angles to the runway 27 threshold, resulted in perfectly readable transmissions and adequate signal strength.
This had the effect of reducing the likelihood that other ground-based airfield users located behind the Dash 8 would either receive the transmission or that the Dash 8 would receive transmissions made by those aft ground-based stations.
This meant that a Dash 8 taxiing from the bay, or at holding points Charlie or Delta, would be orientated with their tail towards the GA parking, refuelling area, taxiway Alpha and the threshold of runway 36. This, coupled with reduced VHF COM 2 strength and readability, significantly reduced the likelihood of transmissions being received and understood by other airfield users, which adversely affected the situational awareness of all operations in the vicinity of the aerodrome.
Contributing factor
The reduced Dash 8 radio reception and transmission strength to the rear of the aircraft affected radio call readability to and from other airfield users. This reduced the situational awareness for the Dash 8 crew and other traffic.
Testing conducted by ATSB and ACMA measured the transmission power pattern of the VHF COM 2 (via the lower antenna) on the ground and identified that signal reception exhibited significant directional variation, with the average signal strength forward of the aircraft being about 8.5 dB stronger than the average signal strength behind and to the side of the aircraft. Depending on the external physical environment and other factors, this can lead to signal degradation or loss.
While geographic obstacles and structures between the stations had the likelihood of reducing signal strength and readability in general, it was identified that a significant reduction in radio signal strength and consequent readability existed when VHF COM 2 was used for ground-based communications when compared with VHF COM 1, even when no geographical or man-made structures were present between the stations. It was further identified that Dash 8, VHF COM 2, radio signal strength also declined significantly depending on the distance between ground-based transmission stations.
VHF COM 2 transmissions made from the starter extension and threshold of runway 09, to a receiver at the threshold of runway 36 or holding point Alpha, lacked the signal strength and readability required for effective communication when compared to the use of VHF COM 1, which had an acceptable level of signal strength and readability despite potential surface-based obstacles that may partially impede VHF radio line of sight.
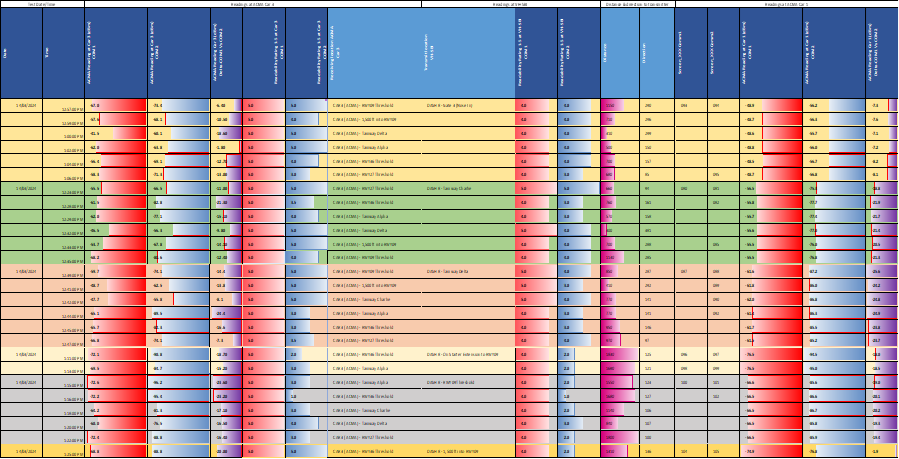
Schedule 3 radio signal strength testing from the Dash 8 and readability testing to and from the Dash 8 (Table 4) at taxiway Delta and Charlie with its tail pointing directly towards the holding point at taxiway Alpha and the runway 36 threshold without significant man-made shielding, had reduced Dash 8 VHF COM 2 readability and this was also reflected in the Dash 8 VHF COM 2 readability from taxiway Delta to the threshold of runway 36.
Table 4: Schedule 3 testing of VHF COM strength and readability
Both these tests with COM 2 indicated recorded strength values 10 to 20 dBm lower than the acceptable level with reduced readability. Comparatively, Dash 8 VHF COM 1 reception at these locations resulted in perfectly readable transmissions with improved signal strength.
Readability at the Dash 8 from taxiway Alpha and the threshold of runway 36 was also found to be significantly reduced on VHF COM 2 with some reduction on VHF COM 1.
Further to this, testing conducted with the Dash 8 at taxiway Charlie, with its tail orientated to the terminal, with a clear line of sight to both taxiway Alpha and the threshold of runway 36, showed reduced Dash 8 VHF COM 2 transmission readability and signal strength readings lower than the acceptable level. Comparatively, the Dash 8 VHF COM 1 reception at this location resulted in perfectly readable transmissions with improved signal strengths.
The readability at the Dash 8 from taxiway Alpha and the threshold of runway 36 was also found to be reduced significantly on VHF COM 2 with some reduction on VHF COM 1 readability.
The reduction of transmission strength and readability of VHF COM 2 broadcasts, coupled with the reduced transmission reception provided to the flight crew, increased the likelihood of the Dash 8 crew and the other operators in the vicinity of a non-controlled aerodrome having communication difficulties.
Given the decades of operation of this aircraft type and related types without widespread reports of radio problems using VHF COM 2 on the ground, and the difficulty in ascertaining and obtaining the applicable standards, the ATSB did not further evaluate certification aspects of the aircraft VHF radio.
Contributing factor
Dash 8 ground-based transmissions on VHF COM 2 had reduced strength and clarity. This likely led to situations where other aircraft had difficulty in receiving and understanding radio transmissions, and Dash 8 aircraft not receiving other traffic radio transmissions.
Rolling calls at Mildura Airport
Prior to take-off, rolling calls at all non-controlled aerodromes were not required when there was no identified traffic. This determination was based on the situational awareness of flight crew and may not always be correct at aerodromes where visual identification of other traffic is limited by buildings, terrain or vegetation. At Mildura Airport, it has been established that when 2 aircraft are at the thresholds of runway 09 and 36, they are not visible to each other due to buildings and trees. Similarly, 2 aircraft at either end of runway 09/27 intending to take off toward each other, may not be visible due to central runway elevation.
While the lack of visibility may be recognised by some pilots and prompt them to make a take-off rolling call, a lack of awareness of another aircraft will not prompt the pilot to consider the possibility of another aircraft. As such, a reliance on an extra broadcast through recognition of the lack of visibility will often be ineffective, especially when there is no expectation of another aircraft.
Aerodromes can mandate additional broadcasts where there is a need, such as a rolling call to improve flight crew situational awareness of conflicting traffic when there are visibility limitations. Although Mildura Airport had recognised that aircraft may not be visible to each other on the runway prior to take‑off and had this noted in the En Route Supplement Australia (ERSA), they had not mandated any additional mitigating radio calls.
The need for further radio calls is exacerbated due to topography and buildings at Mildura Airport, with aircraft not directly visible to each other on the threshold of runways 09, 27 and 36.
Contributing factor
Due to topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off. (Safety issue)
Operator procedures
QantasLink procedures required the use of VHF COM 2 for ground-based communication at non-controlled aerodromes. However, the use of VHF COM 2 for ground-based communications was not required for controlled airspace, where ground-based communications were conducted by VHF COM 1.
Schedule 3 ground-based signal strength testing on Mildura Airport (Table 4) identified a significant and mostly uniform reduction in the Dash 8 VHF COM 2 radio transmission strength and readability compared to the Dash 8 VHF COM 1 system. It was also found that the use of VHF COM 2 reduced ground-based recorded signal strength and call readability to other aerodrome users in comparison with signal strength and readability results from the Dash 8 VHF COM 1 system.
It was also identified that radio call reception at the Dash 8 was significantly reduced while using VHF COM 2. This was particularly evident during transmissions made in the vicinity of the threshold of runway 09 to most of the other tested locations on the airport.
Procedurally required use of the Dash 8 VHF COM 2 radio system for ground-based communications at non‑controlled aerodromes reduced the likelihood of other aircraft receiving and interpreting their calls in some circumstances. Furthermore, the reduced transmission reception also increased the likelihood of Dash 8 crews not receiving strong and readable radio calls from other aerodrome users.
The use of VHF COM 1 in preference to VHF COM 2 to broadcast and receive on local frequencies during ground‑based operations at non-controlled aerodromes would increase the VHF transmission strength and readability, increasing the likelihood of other aircraft and vehicles on the ground receiving a strong and clear transmission from the Dash 8 aircraft.
Radio calls made at runway 09 and 36 thresholds with reduced line of sight and at significant distances, compounded by using VHF COM 2, are less likely to be heard by other aerodrome operators. This likely reduced the situational awareness of the Dash 8 crew and all other traffic at Mildura.
In addition, many regional non-controlled aerodromes into which QantasLink Dash 8 aircraft operate have some, if not all, of the attributes of Mildura Airport. However, regardless of cross runways, non-line of sight communication due to geographical or man-made structures, the reduced transmission strength of the Dash 8 ground-based VHF COM 2 transmissions routinely used at all non-controlled aerodromes added a potential risk to clear communications that may degrade situational awareness for all operators.
ATSB analysis of 30 years of non-controlled aerodrome occurrences involving Dash 8 aircraft communication, identified 25 unresolved radio communication issues during approach and landing and 27 occurrences of radio communication difficulties in ground‑based communication at 15 different aerodromes in multiple Australian states. Some of these exhibit similar characteristics to the occurrence at Mildura.
Contributing factor
The QantasLink radio procedure required Dash 8 flight crews to use the VHF COM 2 radio to broadcast and receive on local frequencies during operations at non-controlled aerodromes. This reduced the ground-based radio transmission and reception strength, and therefore reduced the likelihood of other aircraft receiving calls in some circumstances. (Safety issue)
Manufacturer advice to operators
De Havilland Aircraft of Canada Limited identified that there is no specific guidance provided on the limitations of ground-based communications on VHF COM 2 to operators. Its understanding was that most operators used VHF COM 1 for ground-based communications and that best practice VHF communication usage was conducted at an airline or national level. However, the ATSB identified that without specific knowledge of the nature or limitations of the ground-based communications provided by the manufacturer, including reduced signal strength and clarity, operators would not be in a position to identify and mitigate the risks.
Contributing factor
De Havilland Aircraft of Canada Limited did not publish any guidance to operators of Dash 8 aircraft on the transmission and reception performance limitations of VHF COM 2 radios for ground-based communications.(Safety issue)
Safety advisory notice
The Australian Transport Safety Bureau advises all operators and crew of De Havilland Aircraft of Canada Limited DHC-8 (Dash 8) aircraft to consider the use of VHF COM 1 radios for ground-based communication while operating at non-controlled aerodromes, to improve radio transmission and reception with other stations.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the aircraft separation issue during take‑off involving a Lancair, VH-VKP, and De Havilland Aircraft of Canada Limited DHC‑8-315, VH-TQZ, at Mildura Airport, Victoria, on 29 September 2023.
Contributing factors
The Dash 8 crew were actively engaged in multiple communications with airborne traffic to ensure separation for departure, and were not aware of the Lancair taxiing for runway 36.
The Lancair pilot's entering and backtracking radio call for runway 36 was partially over‑transmitted. This did not afford an opportunity to alert other aircraft as to their location or intentions.
Neither the Dash 8 nor the Lancair crews heard each other's previous radio calls prior to the Dash 8 taking off on runway 09, and the Lancair gave a rolling call on runway 36.
Both the Dash 8 and Lancair crews had no awareness of each other at any stage until after the Dash 8 was taking off, and the Lancair pilot gave a rolling call.
The reduced Dash 8 radio reception and transmission strength to the rear of the aircraft affected radio call readability to and from other airfield users. This reduced the situational awareness for the Dash 8 crew and other traffic.
Dash 8 ground-based transmissions on VHF COM 2 had reduced strength and clarity. This likely led to situations where other aircraft had difficulty in receiving and understanding radio transmissions, and Dash 8 aircraft not receiving other traffic radio transmissions.
Due to topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off. (Safety issue)
The QantasLink radio procedure required Dash 8 flight crews to use the VHF COM 2 radio to broadcast and receive on local frequencies during operations at non‑controlled aerodromes. This reduced the ground-based radio transmission and reception strength, and therefore reduced the likelihood of other aircraft receiving calls in some circumstances. (Safety issue)
De Havilland Aircraft of Canada Limited did not publish any guidance to operators of Dash 8 aircraft on the transmission and reception performance limitations of VHF COM 2 radios for ground-based communications. (Safety issue)
Other finding
Third party intervention by the Mooney pilot prevented the Lancair from rolling on runway 36. The Lancair pilot held on the runway until the Dash 8 departed.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation, industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Due to topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off.
Safety issue description: The QantasLink radio procedure required Dash 8 flight crews to use the VHF COM 2 radio to broadcast and receive on local frequencies during operations at non-controlled aerodromes. This reduced the ground-based radio transmission and reception strength, and therefore reduced the likelihood of other aircraft receiving calls in some circumstances.
Safety issue description: De Havilland Aircraft of Canada Limited did not publish any guidance to operators of Dash 8 aircraft on the transmission and reception performance limitations of VHF COM 2 radios for ground-based communications.
Safety advisory notice to operators and crew of De Havilland Aircraft of Canada Limited DHC-8 aircraft
SAN number
AO-2023-050-SAN-01
The Australian Transport Safety Bureau advises all operators and crew of De Havilland Aircraft of Canada Limited DHC-8 (Dash 8) aircraft to consider the use of VHF COM 1 radios for ground-based communication while operating at non-controlled aerodromes to improve radio transmission and reception with other stations.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by QantasLink addressing CTAF operations
The introduction of rolling calls at all CTAF aerodromes through introduction of changes to their current operations manual.
Pilot group provided further guidance on specifics of potential radio wave degradation on the ground between runway 36 and 09 thresholds at Mildura.
Glossary
ACFT
Aircraft
ATS
Air traffic services
ADS-B
Automatic dependant surveillance - broadcast
ATPL
Air transport pilot licence
ACMA
Australian Communications and Media Authority
ARO
Aerodrome reporting officer
ATSB
Australian Transport Safety Bureau
BCST
Broadcast
CAAP
Civil aviation advisory publication
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulation 1998
CTAF
Common traffic advisory frequency
dBM
Decibels per milliWatt
ERSA
En Route Supplement Australia
FO
First officer
FOSL
Flight operations service letter
IFR
Instrument flight rules
NOTAM
Notice to airmen
RA
RWY
Resolution advisory
Runway
TA
Traffic advisory
TFC
Traffic
THR
Threshold
TWY
Taxiway
TCAS
Traffic collision advisory system
VFR
Visual flight rules
VHF
Very high frequency
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of VH-ENL
the crew of VH-TQH
the crew of QLINK 404
The pilot of VH-NNR
QantasLink
De Havilland Aircraft of Canada Limited
Civil Aviation Safety Authority
Airservices Australia
Mildura Airport
AVDATA
ADSB data
References
Bell, M., Facci, E., & Nayeem, R. (2005). Cognitive Tunnelling, Aircraft-Pilot Coupling Design Issues and Scenario Interuption Under Stress in Recent Airline Accidents. 2005 Inernational Symposium on Aviation Psychology, (pp. 45-49).
Civil Aviation Safety Authority. (2013, December). PIlot's responsibility for collision avoidance in the vicinity of non-controlled aerodromes using 'see-and-avoid'. Canberra, ACT, Australia.
Civil Aviation Safety Authority. (2021, November). Operations in the vicinity of non-controlled aerodromes. Canberra, ACT, Australia.
Dehais, F., Causse, M., Regis, Régis, N., Menant, E., Labedan, P., Tremblay, S. (2012). Missing Critical Auditory Alarms in Aeronautics: Evidence of Inattentional Deafness? Proceedings of the Human Factor and Ergonomics Society Annual Meeting, (p. Vol 56).
Hobbs, A. (1991). Limitations of the see-and-avoid principle. Canberra: Australian Transport Safety Bureau.
Mack, A., & Rock, I. (1998). Inattentional blindness. Cambridge MA: MIT Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Airservices Australia
Mildura Airport
QantasLink
De Havilland Aircraft of Canada Limited
pilot of VH-VKP
crew of VH-TQZ
crew of QLNK 404.
Submissions were received from:
Civil Aviation Safety Authority
QantasLink
De Havilland Aircraft of Canada Limited.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Recorded VHF radio transmissions
Table 5: Recorded VHF radio transmissions
UTC 29 Sept
Origin
Call transcript
1343:14:00
QLINK 81
Mildura traffic QLINK 81, taxi's runway 09 for Melbourne
1344:26:00
QLINK 81
Mildura traffic QLINK 81, enters and backtracks full length runway 09 Mildura
1345:00:00
QLINK404
Midura traffic, QLINK 404, taxies runway 09, will hold short of runway for now, Mildura.
1345:22:00
QLINK*81
Zulu Papa Victor, QLINK 81
1345:32:00
QLINK 81
And 1769, QLINK 81
1345:27:00
Tecnam 1769
QLINK 81, 1769 go ahead
1345:30:00
QLINK 81
We are about to line up and roll on 09, will be making a right turn for departure to Melbourne, can you confirm your current position north of the field?
1345:48:00
Tecnam 1769
Can do, 6 NM to the north of the field at the moment
1345:55:00
QLINK 81
Understood, just need you remain north of the field until we have departed?
1346:00:00
Tecnam 1769
Understood, will remain north of the field until you have departed.
1346:04:00
QLINK 81
Zulu Papa Victor, QLINK 81
1346:23:00
VH-ZPV
Traffic, Zulu Papa Victory passing 2,000 ft, descending to 1,200, going mid-downwind 27, Mildura traffic
1346:44:00
Lancair
Mildura traffic, Lancair Victor Kilo Papa, taxiing for runway 36, Mildura traffic.
Copied, so you’re joining runway 09, is that correct?
1347:06:00
ZPV
Copied that, going crosswind 09, Mildura traffic
1347:25:00
ZPV
Mildura traffic, Zulu Papa Victor, remaining on the dead side, Mildura traffic.
1347:34:00
Mooney
Traffic Mildura CTAF, November November Romeo a Mooney, taxiing for Albury, runway 36 for departure. Copied Lancair, also taxiing runway 36.
1347:47:00
QLINK 81
Zulu Papa Victor just confirm…
1347:51:00
Lancair
(Over‑transmission; QLINK 81 continuing transmission and likely part of Victor Kilo Papa call for entering and backtracking runway 36)
1347:56:00
Lancair
…back tracking runway 36
1347:58:00
ZPV
Zulu Papa Victory, tracking dead side 09, Mildura traffic
1348:24:00
ZPV
Zulu Papa Victory, maintaining dead side 09, Mildura traffic
1348:42:00
QLINK 81
Mildura, QLINK 81, rolling runway 09 for upwind departure.
1349:06:00
Lancair
Mildura traffic, Lancair Victor Kilo Papa rolling runway 36 for straight out departure to the north, Mildura traffic.
1349:14:00
QLINK 81
…aircraft rolling 36, hold.
1349:19:00
Mooney
Victor Kilo Papa hold there, aircraft taking off 09.
1349:24:00
Lancair
Victor Kilo Papa
1349:50:00
Mooney
Good to go now sir
1349:54:00
Lancair
VKP rolling runway 36, departure to the north, VKP, Mildura traffic.
1350:01:00
QLINK 81
Traffic Mildura QLINK 404, Dash 8, entering and backtracking 09 will be for departure to the East, climbing to flight levels.
1350:13:00
Mooney
VKP, your hatch is open sir, on the back of your aircraft
1350:18:00
Lancair
VKP, just caught that
1350:20:00
Mooney
Traffic Mildura, November November Romeo entering and backtracking runway 36 for departure to Albury, copied traffic taxiing runway 09.
Source: Transcribed from Airservices and AVDATA recorded data 29 September 2024
Appendix B – CTAF transmission test results
Schedule 1 test – CTAF transmission testing
Schedule 2 test – CTAF transmission testing from Cessna 172 VH-ZJA
Schedule 3 test – CTAF transmission testing from Bombardier De Havilland Aircraft of Canada Limited DHC-8-315Q VH-SBI
Appendix C – Aerodromes with historical undetermined Dash 8 communication occurrences
Aerodrome
Number of occurrences
Secondary runway
Line of sight limitations procedures
Details/comments
Armidale, NSW
1
Yes
No
Ground based ATS frequency
Bundaberg, Qld
1
Yes
No
Ground based ATS frequency
Gladstone, Qld
3
No
Yes
Limited to ATS contact on ground due to shielding
Horn Island, Qld
3
Yes
Yes
Due to terrain, Take-off runway 14 and land runway 32 not available
Ground based ATS frequency
Mackay, Qld
1
No
No
No details relating to line of sight limitations or ground based ATS frequency
Mildura, Vic
4
Yes
No
Ground based ATS frequency
Procedures implemented from April 2024
Moranbah, Qld
1
No
No
No details relating to line of sight limitations or ground based ATS frequency
Moree, NSW
1
Yes
No
Ground based ATS frequency
Port Lincoln, SA
1
Yes
No
Ground based ATS frequency
Port Macquarie, NSW
1
No
No
Ground based ATS frequency
Roma, Qld
2
Yes
No
Ground based ATS frequency
Toowoomba, Qld
1
Yes
Yes
Due to single lane and obstructed visibility, all TFC using TWY and/or taxilane B or C to check for oncoming ACFT and BCST intentions
Wagga Wagga, NSW
3
Yes
Yes
Light ACFT at THR of RWY 23 not visible to other ACFT on the ground using RWY 05. Radio black spots may result under some conditions
Further procedures implemented from March 2024
Ground based ATS frequency
Williamtown, NSW
2
No
No
No details relating to line of sight limitations or ground based ATS frequency
Whyalla, SA
2
Yes
No
ATS available in the circuit but not on the ground
Appendix D – Flight Operations Service Letters
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. In this case, ‘09’ represents a magnetic heading of 090 degrees.
[2]See Witnesses for the recollections of the crew of this Dash 8 and the pilot of the Mooney, discussed below.
[3]V1: the critical engine failure speed or decision speed required for take off. Engine failure below V1 should result in a rejected take off; above this speed the take-off should be continued.
[4]A detailed operator maintenance check of the aircraft and systems, which occurs about every 18 months to 2 years (depending on type of aircraft) and takes up to 3 weeks.
[5]This airspace is uncontrolled. Both IFR and VFR aircraft are permitted and neither require air traffic control clearance.
[6]Improved visual acquisition by pilots alerted to traffic presence (by radio, electronic conspicuity, or other means).
[7]1 mW = 0 dBm. The dBm scale is logarithmic (so a loss of −3 dBm is half of the signal strength (10-0.3) and −10 dBm is 10 times less than 0 dBm at 0.1 mW, similarly 0.01 mW = −20 dBm. The closer the value was to 0, the stronger the signal. e.g. −56 dBm is a better signal strength than −90 dBm.
[8]Bowtie analysis is a risk analysis methodology that uses a visual representation of threats, hazards, consequences, and risk controls.
[9]When on the ground, pilots often need to communicate with air traffic services that are not located at the airport.
Occurrence summary
Investigation number
AO-2023-050
Occurrence date
29/09/2023
Location
Mildura Airport
State
Victoria
Report release date
30/05/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft separation, Runway incursion
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
Model
DHC-8-315
Registration
VH-TQZ
Serial number
555
Aircraft operator
QantasLink
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
An unstable approach due to excessive height and airspeed contributed to an Airvan charter aircraft overrunning the runway on landing at Rat Island, Western Australia, an ATSB investigation has found.
On the morning of 6 April 2023, the GippsAero GA8 Airvan with a pilot and six passengers onboard departed from Geraldton Airport for Rat Island, part of the Houtman Abrolhos Islands archipelago.
During the landing, the aircraft floated for a significant time and touched down approximately halfway down the runway, with insufficient remaining runway to stop. The pilot reported applying heavy braking, however the aircraft traversed the runway overshoot area and came to rest on the island’s edge, tipping forward into shallow seawater.
Neither the pilot nor the 6 passengers were injured during the landing or when evacuating the aircraft.
ATSB analysis of recorded data from the aircraft and video footage taken from the front passenger seat showed the aircraft was unstable during the approach to land, due to excessive height and airspeed.
“An unstable approach can contribute to the risk of a runway excursion, as occurred in this case,” ATSB Director Transport Safety Stuart Macleod said.
“Pilots should be prepared to conduct a go-around if the stabilised approach criteria are not met.
“The later a go-around is made, the more likely that additional hazards will be present for pilots to manage.”
Since the accident, the operator, Shine Aviation Services, has taken safety actions to improve pilot landing and late-stage go-around training for their single- and multi-engine piston aircraft.
An increased oversight program has also been implemented to provide more regular mentoring for junior flight crew.
On the 22 September 2023, a Bell Helicopters 407, conducting a passenger flight from Sengapi to Gerbrau Airstrip in Madang Province, collided with terrain during the approach to the airstrip. All of the occupants sustained serious injuries and the helicopter was destroyed.
The Accident Investigation Commission (AIC) of Papua New Guinea requested assistance from the ATSB to oversee the data being downloaded from the engine control unit, at a maintenance organisation in Australia.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The ATSB attended the successful download of the aircraft engine control unit data at an Asia Pacific Aerospace facility on 1 November 2023 with a technical representative of Rolls Royce. The data was extracted according to Rolls Royce procedures, however it was not possible to determine whether it contained all the relevant data for the occurrence as it could not be accessed locally. The data was provided to the Rolls Royce technical representative for further analysis. No further assistance was sought by, and further enquiries should be directed to the Papua New Guinea AIC as the investigating agency.
On 20 October 2023 the pilot of a Cessna 208 aircraft, registered VH‑UMV and operated by Experience Co, was conducting parachute operations at Barwon Heads Airport, Victoria with 16 parachutists on board. Passing about 500 ft on climb, the pilot detected a partial power loss consistent with a previously‑encountered transient power reduction.
Expecting the power to return immediately, the pilot did not lower the aircraft’s nose to maintain airspeed. The airspeed continued to reduce until the stall warning horn sounded and, due to the low height, low engine power and low airspeed, the pilot attempted to conduct a forced landing. However, the aircraft collided with water before continuing onto the riverbank and ground for approximately 50 m before coming to rest.
The aircraft was substantially damaged, 6 of the parachutists received serious injuries, 8 sustained minor injuries, and 2 were uninjured. The pilot also sustained minor injuries.
What the ATSB found
The ATSB found that passing about 500 ft on climb, the power reduced likely due to abnormal activation of an engine torque and temperature limiting system. Expecting the power to return quickly and surge, and in preparation for turning off the system, the pilot moved the power lever aft to reduce the power setting and delayed lowering the aircraft’s nose to maintain airspeed, resulting in a stall warning and subsequent collision with water.
The ATSB also found that Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the engine limiting system, but did not specify a minimum safe height at which to do so. This increased the risk of a loss of control and/or ground collision.
Further, the ATSB found that the operator's weight and balance calculation for the accident flight did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity, therefore, although it did not contribute to the accident, the weight and balance was inaccurate for the intended flight. Additionally, the software used to calculate aircraft weight and balance did not provide a warning if individual aircraft zones were overloaded.
Finally, the ATSB found that Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
What has been done as a result
At the time of writing, Experience Co was re‑developing its sport skydivers safety video to include emergency procedures. Additionally, the following proactive safety actions have been taken:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet-wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the single red line/torque and temperature limiter malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed Cessna 208 and Cessna 208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the supplemental type certificate (STC) holder to be followed at or above 1,000 ft above ground level.
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of its aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Finally, the Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Lower the nose to maintain the glide speed of the aircraft. If turning is conducted, keep in mind an increased bank angle will increase the stall speed of the aircraft.
Maintain glide speed and assess whether the aircraft is maintaining, gaining or losing height to gauge current aircraft performance.
Fly the aircraft to make a landing, given the aircraft’s height and performance, and the pre-planned routes for the scenario.
If time permits, moving the power lever through the full range may result in increased power available to climb and/or create the time to diagnose the issue.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. This incident highlights the importance of passengers being appropriately briefed on the brace position and use of emergency exits. It also illustrates the higher injury risk associated with the carriage of parachutists, due to the increased number of occupants and inferior restraints compared to being secured in a certified seat.
The occurrence
Early on the morning of 20 October 2023, the pilot of a Cessna 208 aircraft, operated by Experience Co and registered VH-UMV, refuelled and inspected the aircraft in preparation for parachuting operations from Barwon Heads Airport, Victoria. No defects, including any fuel debris or contaminants, were identified.
The pilot’s first flight of the day was to carry 16 sport parachutists for a parachute jump from 15,000 ft. At about 0750 local time, the parachutists boarded the aircraft. The pilot recalled that the conditions were CAVOK,[1] with a light wind from the north. They taxied the aircraft to runway 36 for a northern departure.
A review of OzRunways[2] flight data, recorded at 5-second intervals, showed the aircraft commenced the take-off roll at 0757. The pilot reported moving the power lever forward until the engine reached 100% torque, and then reducing the power slightly during the take-off roll. Camera footage showed that the aircraft became airborne at 0757:22.
The pilot reported that, as the aircraft climbed and the airspeed increased, they retracted one stage of flap passing through 85 kt and another at about 95 kt. At 0757:47, climbing through about 400 ft, the aircraft reached its maximum recorded ground speed of 95 kt. The pilot reported that as the aircraft approached 500 ft above ground level and they reached for the flap lever to retract the last stage of flap, they heard a reduction in engine noise, and felt a deceleration.
The pilot initially associated the loss of power with activation of the torque and temperature limiter (TTL) (see the section titled Torque and temperature limiter), which they had previously experienced in that aircraft. Consistent with the previous TTL activation, the pilot expected the power to quickly return, and reported reducing power slightly to prevent the engine surging[3] as power was restored.
The reduction in engine power, combined with the climb pitch attitude, resulted in the airspeed reducing and activation of the stall warning horn. On hearing the stall warning, the pilot lowered the aircraft’s nose to reduce the angle of attack[4] and increase the airspeed.
At 0757:57 the aircraft reached the highest recorded altitude of about 700 ft at 88 kt ground speed and, 5 seconds later, had descended to 600 ft and the ground speed reduced to 71 kt, then to 69 kt 5 seconds later. This flight path was consistent with video camera footage of the aircraft’s flight path (Figure 1). At 0758:08 the ADS-B[5] data recorded a descent rate of 3,520 ft/m passing an altitude of approximately 400 ft.
Figure 1: VH-UMV flight path captured by the airport camera
The ATSB combined multiple images together to show the flight path of the aircraft as captured by a local video camera. Source: Airport operator, annotated by the ATSB
The pilot reported that, as the aircraft descended, they observed the engine torque indication reducing through approximately 30% and attempted to switch off the TTL in accordance with the operator’s Engine Power Loss checklist. Due to the aircraft’s low height above the ground, and the pilot’s assessment that there was an engine issue, the pilot then selected a field in which to conduct a forced landing.
The pilot turned to the loadmaster[6] seated beside them and called out ‘gear-up’, to alert parachutists to be ready to exit the aircraft. In response, the loadmaster began directing parachutists to open the roller door, secure their harnesses, and brace for landing. The roller door was opened, but not secured in that position.
The pilot selected a forced landing location in a clearing beyond a river. However, less than 1 minute after becoming airborne and unable to maintain altitude, the aircraft impacted the water short of the clearing, resulting in water entering the cabin and forcing the unsecured roller door closed. The aircraft continued onto the riverbank where the main landing gear detached, then travelled along the ground for about 50 m before coming to rest (Figure 2).
The pilot sustained minor injuries, 6 parachutists sustained serious injuries, 8 sustained minor injuries and 2 were uninjured. The aircraft was substantially damaged.
Figure 2: VH-UMV flight path
Source: ADS-B exchange flight data overlaid on Google Earth and image of accident site provided by operator, annotated by the ATSB
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) and a current class 2 aviation medical certificate. On 19 April 2023, the pilot completed their gas turbine engine design feature endorsement and single engine aircraft flight review in a Cessna 208 aircraft.
At the time of the accident, the pilot had accrued approximately 220 hours of total flight experience, which included 38 hours on the Cessna 208 aircraft type. Of those hours on type, 36 had been accrued in the previous 90 days.
The pilot reported that they were familiar with VH-UMV, having conducted multiple flights in it prior to the accident flight. The pilot was also aware of operator-specific engine operating limitations for VH-UMV, and reported having previously experienced an engine surge at 5,000 ft (see the section titled Engine surging).
Aircraft information
Certification details
The Cessna Aircraft Company 208 (C208) is an all-metal, high-wing aeroplane with tricycle landing gear and designed for general utility usage. The aircraft type certificate data sheet (TCDS) A37CE described the C208 as an ‘11-place closed land monoplane’, and under the heading ‘No. of seats’, provided a centre of gravity range for seating for one or 2 pilot seat locations and referenced the current Pilot’s Operating Handbook (POH) and United States (US) Federal Aviation Administration (FAA) Airplane Flight Manual (AFM) for passenger seat arrangements for seats 3 to 11.
The C208 POH Section 2 – Limitations – Maximum passenger seating limits stated that up to 11 seats, including the pilot’s seat/s, may be installed.
VH-UMV, serial number 20800077, was manufactured in 1986 and first registered in Australia in 2005. At that time, the aircraft was issued 2 certificates of airworthiness, one for normal category[7] operations and one for restricted category[8] operations for the purpose of carrying people for parachute jumping.
Operating in the restricted category required several conditions, including removal of the cabin seats, compliance with a specific engineering order and readily visible restricted category placards, none of which were in place on the accident flight. Additionally, under Civil Aviation Safety Regulations (CASR) current at the time of the accident (CASR 91.845, 91.025, 135.030), aircraft operating in the restricted category were not permitted to conduct air transport operations (carriage of passengers or cargo for hire or reward).
In 2017, the aircraft’s Pratt & Whitney PT6A-114 gas turbine engine was replaced with a Honeywell International Incorporated TPE331-12JR-704TT gas turbine engine that drove a 4‑bladed, constant‑speed, full‑feathering,[9] reversible[10] Hartzell HC-E4N-5KL propeller with hydraulically‑operated variable‑pitch control. The engine modification was completed under the Texas Turbine Conversions supplemental type certificate (STC) SA10841SC, with an associated AFM Supplement. Under the heading ‘Maximum passenger seating limits’, the AFM supplement stated ‘No changes’ (from the C208 AFM).
The aircraft was also modified in accordance with STC SA01180SE, which increased the original maximum take-off weight from 3,628 kg to 3,792 kg. Both STCs were approved by the US FAA and therefore accepted in Australia and taken as having been issued by CASA in accordance with CASR Part 21 regulation 21.114.
Three modifications made to VH-UMV and other aircraft in the operator’s fleet were completed under engineering orders in accordance with the CASR Part 21 regulation 21.437 Grant of modification/repair design approvals—grant by authorised person or approved design organisation:
ESE-C208-25-001—Rework of interior for parachute operations
ESE-C208-25-007—Installation of parachute bench seating
ESE-C208-95-003—Installation of Go-Pro cameras.
Torque and temperature limiter
VH‑UMV was fitted with a switch‑activated torque and temperature limiter (TTL) system designed to prevent these parameters exceeding specified limits. Where an exceedance of the allowable torque or exhaust gas temperature (EGT) was detected, the TTL computer restricted fuel flow to the engine. The maximum allowable fuel reduction of a normally-functioning bypass was about 68 L/hour (125 lbs/hour), resulting in a reduction of the torque output from 100% to about 62% (due to the approximate 25% reduction in fuel flow).
Texas Turbine Conversions advised that, when functioning normally, the system would maintain the lower of the allowable torque or EGT limits and if the TTL bypassed the maximum allowable fuel, it would be felt immediately. In that case, the appropriate pilot response was to switch off the TTL.
The aircraft’s engine monitoring system included a single red line (SRL) controller, associated with the EGT limit. Like the TTL, the SRL was switch‑activated and deselection of the SRL also deactivated the TTL.
The allowable EGT limit was dependent on the phase of flight. Specifically, the operating margin from the EGT limit in the climb phase was reduced in the cruise phase. The phase was dependent on the position of the speed lever. Therefore, if the speed lever was moved aft during take-off or climb, the EGT limit also reduced and could result in activation of the TTL. The operator reported that the speed lever was fully forward throughout the short flight, and therefore the climb EGT limit applied.
Operating limits
The AFM supplement for the Honeywell engine specified operating limits. With the SRL and TTL on, those limits included a maximum EGT of 650 °C, maximum 100% torque and maximum of about 101% RPM during take-off and climb. The supplement also provided an EGT table with limits for operating with the SRL off or inoperative, or ‘manual mode’. The limits were provided for operating at 100% RPM or 96% RPM based on the outside air temperature in 5 °C increments from −60 to +60 °C.
The AFM defined take-off power as the lower of 100% torque or 650 ºC EGT (SRL ON), whichever is reached first at 100% engine RPM.
Engine surging
On 17 October 2023, the pilot submitted an internal safety report relating to an uncommanded engine surge, which they experienced at an altitude of approximately 5,000 ft. The pilot report stated:
Torque roll back for a split second, noticeable reduction in power and deceleration.
The pilot reported reducing the power then slowly increasing it while monitoring engine parameters in response to the event.
Although not recorded on the aircraft’s maintenance release (MR),[11] reportedly due to their transient nature, pilots submitted 7 other internal safety reports between July and October 2023 of engine surging in VH‑UMV, assessed as being due to the TTL.
A review of maintenance recorded in VH-UMV’s engine logbook for the previous 12 months showed that the TTL controller was replaced ‘for fault isolation’ following the first reported surging occurrence on 3 April 2023. A further logbook entry on 18 September 2023 recorded that the EGT harness was replaced in response to reported engine surging at take-off power.
The engine surging safety reports indicated troubleshooting test flights were also conducted. A series of test flights on 7 September 2023 was able to replicate the previously‑reported surging.In addition, a test flight following the EGT harness replacement noted that the surging was still present. One of the experienced surges resulted in a torque value of 62% and fuel flow reduced by approximately 72 L/hour (128 lbs/hour). The MR current at the time of the accident identified that the aircraft operated over 90 flights prior to the next reported surge event on 17 October 2023. On that day, the aircraft operated 6 flights, and one surge occurrence was reported. According to the MR, 12 flights were conducted over the next 2 days (18–19 October), with no reports of engine surging submitted. However, the ATSB was also advised of an engine surge on 18 October, which was not recorded.
The MR current at the time of the accident recorded 257 flights over 3 months, during which there were 6 reported surging events. That frequency illustrated the intermittent nature of the anomaly, which likely hindered troubleshooting.
As a result of the internal reports, on 21 July 2023, pilots were advised to operate VH-UMV under a set of unique operating conditions to avoid the TTL scheduling a significant bypass of fuel and subsequent notable drop in available power. These were limitations of 95% torque and 640 °C EGT.
A review of the operator’s safety reports also identified that surging events were reported on 3 other company aircraft. For those aircraft, maintenance actions rectified the cause of each event and there were no subsequent surging events reported.
Minimum equipment list
Experience Co’s minimum equipment list (MEL) specified permissible unserviceable items with which the aircraft was permitted to operate temporarily under the stated procedures, conditions and limitations. The MEL included that both the SRL computer system and TTL ‘may be inoperative provided inoperative SRL system procedures and limits are observed’. In that case, it was also required that an MEL placard be fitted adjacent to the TTL or SRL switch for the inoperative system/s. There was no MEL placard for the TTL nor was it listed as inoperative at the time of the accident.
Engine power loss checklist
The Texas Turbine Conversions AFM supplement provided checklists for engine failures, but not for partial engine power loss. The operator’s ‘Engine Power Loss’ checklist for the C208 with the Honeywell engine (Figure 3), required pilots to first control the aircraft by moving the elevator control forward to lower the aircraft’s nose if climbing. After completing initial checks, if the RPM was above 60% or the engine was surging, the pilot was to move the power lever to ½ inch (12.7 mm) forward of the flight idle position, in preparation for turning off the TTL, so as not to produce a transient exceedance of the EGT.
Figure 3: Engine power loss checklist
Source: Aircraft operator
Weight and balance
Aircraft moment arms
To enable calculation of the aircraft’s weight and balance, the C208 POH included a 2-place seating option, which divided the cabin into 7 zones (zones 0–6) (Figure 4). The flight manual supplement for the Texas Turbine Conversions STC did not include changes to the zones or seating configuration, therefore the POH applied.
Source: Cessna 208 Pilot’s Operating Handbook, annotated by the ATSB
Accident flight weight and balance
Prior to departure, a member of the parachuting operations team calculated the weight and balance for the proposed flight using the IBIS Technology flight planning module software (Table 1).[12] The moment arms from the POH were used for the calculations. Zone 6 was not used.
Table 1: Planned weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272.152
1,273.672
Zone 0 [1]
3,442
272
936.142
Zone 1
4,277
218
932.386
Zone 2
4,948
318
1,573.464
Zone 3
5,613
173
971.049
Zone 4
6,261
404
2,529.444
Zone 5
6,896
173
1,193.008
Total
3719.152
17,307.075
Centre of gravity
4,653
The operator’s weight and balance used the crew seat arm as the zone 0 arm.
The calculated weight and balance resulted in a take-off weight of approximately 3,719 kg and the aircraft’s centre of gravity located at 4,653 mm aft of the datum. To remain inside the operating limitations, the maximum allowable weight was 3,792 kg. Additionally, the aircraft needed to remain within the centre of gravity envelope, which had an aft limit of 4,680 mm and the forward limit varied with the operating weight. Each zone had a maximum allowable weight limit, and the maximum for zone 0 was 159 kg. However, the calculation software did not provide a warning to notify the user a zonal limit had been exceeded.
Information provided by the parachutists included the position they were seated at the time of the accident. Those positions did not match the original seating positions on the planned weight and balance sheet provided to the pilot prior to departure. The operator calculated a revised weight and balance based on the probable parachutist seating positions, which moved the aircraft’s centre of gravity 5 mm aft, although still within the allowable envelope (Table 2). It also showed that zone 0 was under the allowable weight limit.
Table 2: Revised weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272
1,272.960
Crew seat
3,442
92
316.664
Zone 0
3,472
80
277.760
Zone 1
4,277
349.4
1,494.384
Zone 2
4,948
271.4
1,342.887
Zone 3
5,613
334.4
1,876.987
Zone 4
6,261
197
1,233.417
Zone 5
6,896
233
1,606.768
Total
3,718.2
17,319.746
Centre of gravity
4,658
Aircraft basic empty weight
A weigh of VH‑UMV on 17 October 2017 identified that the aircraft’s basic empty weight was 1,889 kg in the single pilot seat configuration (Figure 5).
Figure 5: VH-UMV configuration on date of reweigh
The image meta-data showed the image was taken on 17 October 2017 – the reweigh date. Source: AeroWeigh.
The aircraft seating configuration at the time of the accident is shown in Figure 6.
Figure 6: VH-UMV cabin seating arrangement
Source: Aircraft operator, annotated by the ATSB
The basic empty weight of the aircraft did not include the flooring, or the 36 kg bench seating installed under engineering order ESE-C208-25-007. The engineering order provided the moment arms and weights shown in Table 3.
Table 3: ESE-C208-25-007 Parachute bench seating options – bench seat weight and arm
Item
Arm (mm)
Weight (kg)
Forward seat & backrest right-hand side only – option 2, without oxygen bottle mount.
3,556
7.82
Centre cabin bench seats both left-hand and right-hand sides (2 x 10.92 kg)
5,003
21.84
Aft bench seat right hand side only
6,553
6.36
Total of unaccounted weight for bench seating
36.02
Using the operator’s revised weight and balance calculation that reflected the likely positions of the parachutists, and the additional weight of the bench seating, the ATSB determined the probable take-off weight was 3,754 kg and the centre of gravity was 8 mm aft of the originally calculated centre of gravity (4,661 mm).
The operator subsequently weighed the aircraft’s jump mat, single point restraints, rubber matting, and portable oxygen tank. The total of these items was 30.2 kg, increasing the probable take-off weight to 3,784 kg.
Weight and balance implications
Regarding the importance of accurate weight and balance, the FAA Pilot’s handbook of aeronautical knowledge stated:
An overloaded aircraft may not be able to leave the ground, or if it does become airborne, it may exhibit unexpected and unusually poor flight characteristics.
Changes of fixed equipment have a major effect upon the weight of an aircraft. The installation of extra radios or instruments, as well as repairs or modifications, may also affect the weight of an aircraft.
Loading in a nose-heavy condition causes problems in controlling and raising the nose, especially during take-off and landing. Loading in a tail-heavy condition has a serious effect upon longitudinal stability and reduces the capability to recover from stalls and spins. Tail heavy loading also produces very light control forces, another undesirable characteristic. This makes it easy for the pilot to inadvertently overstress an aircraft.
Recorded data
The ATSB obtained OzRunways and third-party ADS-B recorded data for the accident flight. That data was compared with flight data for the flight conducted by the same pilot in the same aircraft on 17 October 2023, which was the day the pilot reported engine surging at about 5,000 ft. The comparison did not show significant performance difference from take-off to about 500 ft between the 2 flights.
Although the aircraft had an engineering order to fit GoPro cameras, they were not in place for the accident flight. The operator reported that these were only used during the creation of promotional footage and not during day-to-day operations. There was also no video footage from inside the aircraft, but the airport operator provided video footage from cameras located at the airport. One of those cameras recorded the accident flight footage (Figure 1) and provided audio for analysis.
The recorded audio included the aircraft noise and the nearby road and wind noise. The camera was stationary, therefore as the aircraft departed its sound signature reduced. Analysis of the audio conducted by Honeywell found that the engine RPM was approximately 99% throughout the take-off and initial climb. However, the engine noise was not discernible from the background sounds recorded at the time of the reported engine surge.
Site and aircraft examination
Site assessment
The ATSB did not attend the accident site, but the aircraft operator and Victoria Police attended shortly after the accident and provided the ATSB with photos of the aircraft and cockpit. A review of the images showed that the:
flaps were fully retracted
power lever was in the max reverse position
speed lever was in the minimum position
condition lever was in shutoff/feather position.
Those positions were consistent with the pilot’s reported actions to secure the engine after the impact. Additionally, one image appeared to show the TTL switch ON and the SRL switch OFF, indicating that the pilot may have inadvertently selected the SRL OFF instead of the TTL.
Engine and accessories assessment
The aircraft’s engine was recovered by the operator and sent to the Honeywell Investigation Laboratory in the US. On behalf of the ATSB, the US National Transportation Safety Board (NTSB) arranged independent oversight of the engine examination that was conducted between 3–5 January 2024.
Honeywell and the NTSB subsequently oversighted inspection and testing of removed components at various technical facilities. The Honeywell investigation report, provided to the ATSB and aircraft operator, detailed the observations and findings from the engine and associated component examinations, as follows.
The SRL and TTL were tested on 27 February 2024. Although some test points were not within the specified test tolerances, both units were found to be functional. However, further examination of the fuel bypass valve conducted by Woodward Inc. on 5 November 2024, resulted in a maximum bypass flow of 110 L/hour (194.5 lbs/hour), which exceeded the maximum flow test range of 68–74 L/hour (120–130 lbs/hour). At take-off power, a normal fuel flow was approximately 312 L/hour (550 lbs/hour). Therefore, if a bypass of 110 L/hour occurred during the accident flight with take‑off power set, the fuel flow would have reduced by about 35%.
Initial inspection of the fuel bypass valve’s outer casing revealed impact markings (Figure 7). When the protective cover plate was removed, the pole associated with the impact side was found in contact with the armature. When a 4.5 kg (10 lb) force was applied to each of the poles, there was no visible movement. The armature was cut away from the spade to determine if the armature screws were loose. The armature screws were found to be suitably tightened, and the armature was not bent.
The findings of the inspection showed the out‑of‑limit test results were due to impact damage resulting from the accident. As such, the higher fuel bypass identified in the test was not considered to be contributory.
Figure 7: Fuel bypass valve
Source: Woodward Inc, annotated by the ATSB
The fuel control unit (FCU) was examined and tested between 26–27 March 2024. The FCU tested values were either within specified ranges or marginally outside of tolerance limits for new or overhauled components. The test results may have been affected by procedures for adjusting an in-service FCU defined in the engine maintenance manual.
On 11 January 2024, a computed tomography scan of the propeller governor was conducted by Honeywell. Between 26–27 March 2024, the propeller governor was subject to functional testing by the manufacturer. While there were abnormalities identified with the magnetic pickup voltage and RPM maximum/minimum speeds, no contributing anomalies were noted. It was then disassembled, inspected and reassembled, followed by an additional functional test. The results from both functional tests were consistent with expected parameters of various operational modes.
The fuel pump was functionally tested on 2 May 2024, and found to be operating within specifications.
The Honeywell investigation found that the damage was indicative of an engine that was rotating and operating at the time of impact. It found no pre-existing condition that would have prevented normal operation.
Photos of the propeller were provided to Hartzell for analysis. As the propeller was of composite material, on impact it fractured into parts rather than deforming the propeller shape. From the limited fragments that were retrieved, Hartzell concluded the blades were likely rotating under low power at the time of the accident.
The ATSB considered whether the pilot had moved the power lever to beta range, reversing the propeller, but Hartzell found it likely that the propeller was forced to a low pitch angle during the initial impact.
Carriage of parachutists
Cabin configuration
The aircraft was configured for skydiving such that:
the cargo door was replaced with a vertical sliding door (made of nylon, polycarbonate and aluminium)
the passenger seats and lap belts were removed
bench seating and 17 single point restraints were installed.
The restraints attached to the parachute harness and parachutists could be seated either on the bench seating or floor, facing toward the aft of the aircraft.
The associated flight manual supplements for the parachute configuration were:
cargo doors removed kit
in-flight openable cargo door
in-flight opening of doors
oxygen system
skydiving jump light
external mounted GoPro cameras.
Aircraft modifications
Classification of design changes
CASA stipulated regulations for modification of an aircraft from the original manufacturer specifications. CASA Advisory Circular (AC) 21-12 Classification of design changes provided different processes for modifying aircraft, depending on the type of change being made. These changes were classified as either major or minor.
A minor modification was anything that was not considered to be a major modification and could be completed by a CASA-authorised person under CASR Part 21.M. Any modification with a significant effect on airworthiness – structural, weight and balance, systems, operational or other characteristics, were classified as major. Additionally, any alteration to the type certificate datasheet was classified as a major change.
A major modification was further classified into a substantial change or a significant change. A significant change required a supplemental type certificate application to be completed with CASA’s involvement. A substantial change required a new type certificate application, which also involved CASA. The AC provided the following example of a significant change to a small aircraft:
Changes in types and number of emergency exits or an increase in maximum certificated passenger capacity.
The notes associated with that example were:
Emergency egress certification specifications exceed those previously substantiated. Invalidates assumptions of certification.
CASA advised that the modifications would be considered a major change if the number of persons was increased above that permitted by the aircraft type certificate data sheet. This was consistent with the US FAA Advisory Circular 105-2E – Sport Parachuting, which included:
The approved number of skydivers that each aircraft can carry for parachute operations will most commonly be found on FAA Form 337, Major Repair and Alteration (Airframe, Powerplant, Propeller, or Appliance), used for field approvals, or an aircraft Supplemental Type Certificate (STC).
In its submission to the draft report, CASA advised that it considered that the legal basis for conducting parachuting flights with a greater number of passengers than the TCDS specified may be met if the aircraft was modified appropriately by a suitably authorised person and there was an associated aircraft flight manual supplement.
In determining whether the parachuting configuration modification was major or minor, the CASA‑authorised design engineer assessed that it was minor as it had no significant effect on:
structure
cabin safety
flight
performance or function of:
systems
propellers
engines or powerplant installation
environment.
The engineer also assessed that the design did not:
alter airworthiness or operating limitations
require an adjustment of the type-certification basis
Technical assessment of modifications
Aircraft modifications must meet the airworthiness requirements of the aircraft’s certification basis. According to the type certificate data sheet, VH-UMV was certified under FAR 23 amendments 23-1 through 23-28. Modifications were required to comply with standards from that or subsequent amendments. Technical assessments of the modifications detailed in the engineering orders nominated FAR 23 amendment 62 as the certification basis for the parachuting configuration modifications, including the roller door, bench seating and oxygen system.
The technical assessments included a design compliance matrix, with the following key comments by the design engineer of relevance.
Weight and balance
The engineering order was to include that:
It is the operator’s responsibility to accurately update the aircraft’s load data sheet to reflect the quantity and positioning of oxygen bottles as this may vary dependant on the number of parachutists on a given high altitude drop.
Structure
Standard aircraft hardware is used to secure items of mass installed as part of the parachute fit out modifications. This modification does not alter or effect the strength of the aircraft structure to support all normal aircraft loads. All materials & fasteners used as part of this design package have been selected to have adequate structural properties for their intended use.
Flight loads
The document package includes instructions to ensure the Cessna standard Flight Manual Supplement for operations with the cargo door open/removed is in the Flight Manual.
Oxygen
The engineer assessed the oxygen requirements for conducting flights above 14,000 ft in an unpressurised aircraft, stating:
…The operators (max) occupant capacity for the 208 & 208B model aircraft is x16 & x20 occupants respectively. As such these aircraft must be fitted with a minimum of 2x oxygen dispensing face masks if more than x15 occupants are carried…
Emergency landing conditions
Engineers assessed that the oxygen cylinder restraints were adequate in all load cases. They also rated the seats to at least 170 lb (77 kg) as required by FAR 23.785.
Regarding the installation of the oxygen bottle the engineers provided the following:
…the seat base and surrounding structure is adequate to support the small increase in weight due to the installation…there is no risk of the installation coming loose and inflicting serious injury on the cabin occupants.
Control systems
The design package included instructions for the removal of the copilot control wheel and column in accordance with the aircraft maintenance manual, to configure the aircraft for parachuting operations. There was no change to the design or functionality of the pilot's primary flight controls.
Doors
The number and arrangement of doors was not altered by the modifications. Regarding ‘vibration and buffeting’, the parachute door had a proven service history, with no reported issues since the design was originally implemented in June 2012. Further, the roller-style parachute door was commonly installed on parachuting aircraft and Cessna had an approved roll-up door as part of the production standard design.
Operation of the roller door was ‘simple and obvious’, easily operable from inside and outside the aircraft. The door was held in place by gravity and friction and could not be accidentally opened. Decals specific to the operation of the parachute roller door were installed.
Seats and restraints
The single point restraints for the parachutists were previously approved for use by ‘Air Safety Solutions’.
The aircraft certification did not require dynamic testing of the seats and, although the bench seating was not tested, the design engineer referenced FAA AC 105-2E Sport parachuting, which stated:
1. Straddle benches can offer more occupant crash protection than floor seating since they can be designed to provide significant vertical energy absorption.
Emergency exits
For reference, FAR 23.807 required:
In addition to the passenger-entry door, for an airplane with a total passenger seating capacity of 16 through 19, three emergency exits, as defined in paragraph (b) of this section, are required with one on the same side as the passenger entry door and two on the side opposite the door.
(b) Emergency exits must be movable windows, panels, canopies, or external doors, openable from both inside and outside the airplane, that provide a clear and unobstructed opening large enough to admit a 19-by-26-inch ellipse. Auxiliary locking devices used to secure the airplane must be designed to be overridden by the normal internal opening means. The inside handles of emergency exits that open onward must be adequately protected against inadvertent operation. In addition each emergency exit must:
• be readily accessible, requiring no exceptional agility to be used in emergencies;
• have a method of opening that is simple and obvious;
• be arranged and marked for easy location and operation, even in darkness;
• have reasonable provision against jamming by fuselage deformation; …
(c) The proper functioning of each emergency exit must be shown by tests
The design engineer commented that there was no change to the number of emergency exits and that the ‘steps, handles, bench seats etc. installed for this modification met the requirements for egress in an emergency as specified by this regulation’. Additionally, as there was no change to the door functionality or positioning, no additional emergency testing was required.
The unmodified rear right passenger door met the requirements of the regulation in that a 19" x 26" (48 x 66 cm) ellipse may be passed through the door un-obstructed. However, the rear right bench seat extended across the door at a height of 10” (25.4 cm). The design engineer commented that access to the door handles/operation and decals was not obstructed, and no exceptional agility was required to exit through that door in an emergency.
The roller door was also required to meet the emergency exit criteria, including ‘reasonable provisions against jamming by fuselage deformation’, and that ‘proper functioning of each emergency exit must be shown by tests’. However, this was not documented.
The parachuting configuration detailed in the engineering orders enabled seating and single-point restraints for 17 parachutists, in addition to the fitted pilot seat and 5-point restraint. The design engineer had not intended to explicitly increase the seating capacity above the 11 specified in the TCDS, as the number of parachutists that could be carried was an operational consideration. The design engineer provided comment on a technical assessment provided to CASA in 2017 regarding maximum passenger seating configuration, that the aircraft operator’s understanding was:
it is the pilots [sic] responsibility to ensure the aircraft is loaded within the weight and balance and centre of gravity limitations of the aircraft at all times. From these calculations the maximum safe number of parachutists to carry on the Cessna 208 Caravan is 17...
Regulatory requirements
Part 105 of the CASR came into effect in December 2021 and set out the operational requirements for aircraft used to facilitate parachute descents. Civil Aviation Order (CAO) 20.16.3 paragraph 15 Carriage of parachutists was in force at the time of the accident, and the following regulations were relevant to the aircraft parachuting configuration:
CASR 91.200 Persons not to be carried in certain parts of aircraft permitted a person to be carried in ‘a part of the aircraft that is not designed to carry crew members or passengers’, if the aircraft was being operated for a parachute descent and met the Part 105 MOS.
CAO 20.16.3 required parachutists to wear a seatbelt, shoulder harness or approved single point restraint (except when about to jump). Similarly, CASR Part 105 section 105.105 required parachutists who were not flight crew to be provided with a seatbelt, shoulder harness or approved single-point or dual-point restraint.
The Part 105 Manual of Standards (MOS) came into effect on 2 December 2023, 44 days after the accident, and specified requirements in greater technical detail. CASA advised that the Part 91 Manual of Standards will be amended to remove ambiguity about approved passenger restraints being permitted in lieu of seatbelts.
Maximum passenger seating configuration
In drafting CASR Part 105, the number of parachutists that could be carried was a significant point of discussion between CASA and the parachuting industry.
In 2006, CASA proposed Civil Aviation Safety Regulation 105.140 paragraph 3.5.20 which stated:
Proposed CASR Part 105 seeks to provide clarity to the parachuting industry that operating a parachuting aircraft with more parachutists than the normal published aircraft seating capacity in passenger-carrying operations is acceptable, provided weight and balance and other manufacturer’s limitations for the aircraft are observed.
A subsequent notice of proposed rulemaking indicated that the following may be included in the proposed CASR Part 105.140 – Number of parachutists in aircraft:
(1) A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and…
When the above proposed rule was not incorporated into draft CASR Part 105 or MOS, as detailed in meeting minutes of the technical working group that reviewed the 30 August 2022 draft Part 105 MOS, they proposed to meet with CASA’s Airworthiness and Engineering Branch to discuss:
possible options for parachuting aircraft to operate with seats removed, to carry more passengers than currently permitted by the aircraft’s type certificate or flight manual and regulatory support mechanisms for modifications (doors, handles etc.) that support safe parachuting operations.
The ATSB was unable to determine whether this discussion took place, however no related changes were incorporated into the regulations or MOS, noting that the MOS had not come into effect at the time of the accident.
In response to the ATSB’s request for clarification of CASA’s expectation for the number of parachutists that could be carried, CASA advised that:
The legal basis for conducting parachuting flights with a greater number of passengers than the TCDS is met where the aircraft has been modified appropriately by a suitably authorised person and the aircraft’s flight manual has been modified accordingly.
CASA has been aware for multiple decades that parachuting aircraft were carrying a maximum number of passengers greater than the TCDS maximum number of dedicated passengers.
CASA understood that the increase in passenger capacity for parachuting aircraft was achieved by operators through legitimate aircraft modification processes that removed the normal passenger seats and modified the aircraft for parachute‑specific operations.
CASA did not identify any immediate safety of flight issues.
In its submission to the draft report, CASA advised that it was ‘considering the issue of a legislative instrument to remove any doubt that an approved aircraft modification which replaces normal seating with appropriate alternative seating and restraint arrangements is explicitly permitted’.
Supplemental type certificate application
In April 2017, the design engineer applied to CASA on behalf of the aircraft operator for a supplemental type certificate based on the engineering order for the addition of bench seating. The STC application submitted to CASA included details and images of aircraft that already had modifications completed under an engineering order and did not include an increase in the seating capacity.
After several communications and iterations of the documents provided, in August 2017, CASA highlighted 2 areas directly related to safety of parachutists: the rear exit crashworthiness and the increase of maximum passenger capacity to 17.
In July 2020, the STC application was withdrawn by the applicant.
Other parachuting configuration supplemental type certificates
Cessna 182 models E to R
In 1996, CASA issued STC-214 to the APF. The STC background explained the application was the result of a CASA ramp check, which identified that there were 6 persons on board without single point restraints while conducting parachute operations, where the TCDS stated it was a 4‑seat aircraft.
The STC assessed the floor loading capacity of the aircraft to carry 6 persons (including the pilot) for the purpose of parachute operations. It concluded:
The floor was analysed and substantiated for parachutist loads. The hard points for the approved single point restraints were determined, analysed and substantiated for parachute loads... The aircraft loading is such that no special loading system needs to be devised as the aircraft will always be within the approved centre of gravity range.
The original C182 TCDS 3A13 showed ‘No. of seats 4’.
The amended TCDS for the STC showed ‘No. of seats 1, Parachutist 5’.
Cessna 208, 208B
In 2018, the US FAA issued supplemental type certificate SA04352CH, which incorporated many similar modifications made to model 208 and 208B aircraft certified under A37CE. The modifications included the installation of:
wind deflector
benches
external assist handle
internal assist handle
jump exit control light
external step
wind block (sliding parachute door).
The STC limitations and conditions included:
(3) This modification does not install Title 14 [US Code of Federal Regulations] CFR part 23 compliant seating and is therefore zero occupancy.
(4) The left and right hand benches are compliant as monuments and are not certified to carry any items of mass. Testing performed during certification would be sufficient for gust loading or seven evenly distributed masses of 215 pounds (97.5 kg) each…
Australian Parachute Federation
The APF is the peak body for the administration and representation of Australian Sport Parachuting. With the approval of the Civil Aviation Safety Authority, the APF:
applies the standards of operation
conducts competitions
issues parachuting licences, certifications and instructor ratings
conducts exams
distributes publications to keep its members informed of events and safety standards.
The APF organisation had over 55 group members also known as member organisations, 3,000 licenced members, and engaged with the operators of nearly 100 aircraft conducting parachute operations. As detailed above, the APF held an STC for parachuting operations in Cessna 182 models E through R for parachuting 6‑person operations. The associated supplemental type certificate data sheet amended the aircraft configuration to 1 seat and 5 parachutists from the 4‑seat configuration stated on the type certificate data sheet.
Aircraft operators that conducted parachuting operations as a member of the APF did so in accordance with the APF regulations. This included adhering to the APF Jump Pilot Manual. The Jump Pilot Manual Version 01-2023, in force at the time of the accident, stated:
5.3.3 Loading – Balance/C of G
A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and
(b) any other limitations related to the provision of:
(i) adequate structural support for restraint of occupants; or
(ii) supplemental oxygen for the flight.
For paragraph 5.3.3 (b), the limitations do not include those that are solely related to the number of seats or seating positions that are, or are normally, fitted in the aircraft.
If an aircraft does not have a flight manual, then any information supplied by the manufacturer that relates to the matters mentioned above or is included in the aircraft’s airworthiness certificate, is taken to be the flight manual.
Balance must be a consideration for all aircraft involved in parachuting operations and can be especially critical during climb-out and exit, when changes occur. Know the operational limitations of your aircraft!
Under the Loadmaster’s supervision, the parachutists will normally load the aircraft in the reverse order of the exit.
The Jump Pilot Manual was accepted by CASA and CASA personnel reported having reviewed the manual. Regarding the wording that a parachuting aircraft could carry more occupants than the maximum specified in the AFM, CASA reported that they understood that only applied to Cessna 182 models E through R, for which the APF held a supplemental type certificate that permitted the carriage of 6 persons. CASA personnel also reported that the manual wording was ‘never intended to serve as a quasi-engineering approval’.
At the time of writing, CASA and the APF were engaged in ongoing discussions, including the carriage of occupants in excess of the number detailed in the TCDS without the necessary modification approvals.
Survivability
Passenger briefing requirements
The CASA Multi-Part Advisory Circular – Passenger safety information, stated:
2.1.1 In addition to certification standards for the crashworthiness of the aircraft and cabin crew evacuation procedures, well-informed and knowledgeable passengers contribute to survivability in an aircraft accident or incident. There are multiple factors that affect survivability. Physical factors include adopting the correct brace position for impact, the correct use of seatbelts, as well as the location and operation of all emergency exits.
2.1.2 Accident investigations have shown that survival rates are improved when passengers are provided with accurate and effective information about the correct use of equipment such as seatbelts, and the actions they should take in a life-threatening situation such as how to adopt the brace position.
A pilot in command was in contravention of regulation 91.565 if an aircraft commenced a flight and the passengers had not been given a safety briefing and instructions as prescribed by the Part 91 MOS, unless:
(a)the passenger has been previously carried on the aircraft; and
(b)the passenger has previously been given a safety briefing and instructions in accordance with this regulation; and
(c)in the circumstances it is not reasonably necessary to give the same safety briefing and instructions.
The CASR Part 91 MOS provided a list of items that must be covered in a passenger safety briefing and instructions before an aircraft takes off for a flight. Relevant to this occurrence, the list included:
(c) when seatbelts must be worn during the flight, and how to use them;
(f) how and when to adopt the brace position;
(g) where the emergency exits are, and how to use them;
(s) for a flight of a jump aircraft — the physical location(s) within, or on, the aircraft that the passenger must occupy during the flight in order to ensure the aircraft is operated within the aircraft’s weight and balance limits during the flight.
Operator’s safety briefing
The aircraft operator had 2 videos, one of which was shown to parachutists depending on whether they were conducting a tandem jump or a sport jump. The sport jump video was specific to the Barwon Heads operation and included:
aircraft climb performance
17 single point restraints, which were to be worn up to 2,000 ft
sport jumpers were to listen to the pilot in command in the event of an emergency
location of the door securing clip (but not instructions for use).
The video shown to tandem jump parachutists provided specific aircraft safety information including:
how to approach the aircraft
the use of single point restraints
the location of fire extinguishers
how to brace
how to egress
the requirement not to smoke
the use of life jackets where required.
For the accident flight, the pilot reported that they did not provide a safety briefing, and multiple parachutists reported not having received a safety briefing prior to flight. There was no procedure in the operations manual that waived the pilot’s responsibility to provide parachutists with a safety briefing. The pilot reported that they understood that the drop zone safety officer ensured everyone was briefed on emergency situations before jumping and a video briefing was provided to tandem parachutists.
The operations manual provided the following guidance for providing a safety briefing during an emergency landing with parachutists on board:
It will be the Load Masters responsibility to assist the pilot in ensuring;
1. Parachutists are briefed on and instructed to assume the BRACE position prior to touchdown.
2. Emergency Exits are opened and secured (where possible) prior to touch down.
3. Single point restraints are utilised by all occupants.
The aircraft also had a sign on the rear wall of the internal cabin, detailing the in-flight emergency plan (Figure 8). The sign stated that single point restraints were required as directed by the pilot and at all times below 1,500 ft, differing from the 2,000 ft stipulated in the sport jump video.
The APF Jump Pilot Manual required that restraints were utilised by all occupants below 1,000 ft, or as directed by the pilot.
Figure 8: In-flight emergency plan
Source: Victoria Police and the aircraft operator
Parachutist preparedness
After the accident, in response to an ATSB survey, parachutists reported a lack of awareness of how to brace and the location of emergency exits that were available if the main roller door became damaged and unavailable for use in an evacuation. On this occasion the clip that secured the roller door in the open position was not used, which resulted in it closing on impact. Fortunately, the parachutists were still able to successfully evacuate the aircraft via that door. As detailed further below, several of the parachutists also reported that their restraints were not taut prior to the ground collision.
Some parachutists recalled receiving aircraft-specific emergency information during their initial parachuting training. However, in some cases, several years had passed without receiving a refresher. Furthermore, some had conducted their initial training on different aircraft types.
Injuries and seating positions
The pilot wore a 5-point restraint, and the 16 parachutists each had a single-point restraint attached to their parachute. The probable seating arrangement at the time of the accident was determined based on the recollections of parachutists who responded to ATSB’s request for information (Figure 9). There were 4 parachutists seated on the floor, 4 on the left bench seat and 8 on the right bench seat. The parachutists were facing aft and those on the bench seats were seated between each other’s legs.
Injury information was obtained for the pilot and 14 of the 16 parachutists, with the other 2 assumed to have no injuries (Table 4). The injury mechanisms included deceleration, flail and impact with the aircraft or other occupants.
Figure 9: Seating positions
The seating positions in the image are referenced in Table 4: Injuries sustained. Source: Texas Turbines Cessna 208 pilot operating handbook, annotated by the ATSB
Table 4: Injuries sustained
Image reference
Injuries sustained
ATSB injury classification
Survivability Comments
A. (Pilot)
Cut on forehead, bruising, whiplash, bruised sternum, and difficulty talking/breathing
Minor
5-point safety harness; likely impact with control column/dash
B.
Pulmonary contusion, fifth and sixth rib fractures, psychological trauma, and lower back pain
Serious
Slipped off the end of the bench seat and ended up squashed against the ladder or back of the pilot seat due to a loose restraint
C.
No reported injuries
No injuries
D.
Tears to both rotator cuffs, tear to sternocleidomastoid muscle, and nerve damage to left arm and shoulder
Serious
E.
Broken ribs and internal bleeding to the chest.
Serious
Loose restraint
F.
Whiplash, fractured L4 transverse process, and nerve pain in right shoulder and leg
Serious
Loose restraint, seated on floor; adjacent end of bench seat
G.
Whiplash, bruising, and headaches
Minor
Seated on floor
H. (Loadmaster)
Cut injury to right leg requiring stitches, and sore back
Minor
I.
Strained back, cuts, and bruising
Minor
J.
Whiplash, cuts, and bruising
Minor
Loose restraint
K.
Whiplash, cuts, and bruising
Minor
Loose restraint
L.
Cuts to head, face, internal chest cuts, and bruising
Minor
Tight restraint
M.
Broken tailbone, bruising
Serious
Tight restraint
N.
Concussion, and bruising
Minor
O.
Swollen knee, bruised kidney, bruised vertebrae, and strained neck ligaments
Minor
Loose restraint
P.
Internal abdomen bleeding, Internal hematoma inner right leg, cuts, bruising, whiplash, and back pain.
Serious
Loose restraint; inappropriate structures around/in front
Q.
No reported injuries
No injuries
The single point restraints could not be adjusted, but an occupant could potentially position themselves such that the restraint was taut. Nine parachutists provided information about the tightness of their restraint; 7 reported their restraints were loose and 2 reported tight restraints. Of those with loose restraints, 3 sustained minor injuries and 4 sustained serious injuries. Of the 2 parachutists who reported having tight restraints, one sustained minor injuries and the other sustained serious injuries.
Of the 4 parachutists seated on the floor, 2 sustained serious injuries, one sustained minor injuries, and another was reported to have been uninjured. The other serious injuries were sustained by 2 parachutists on the left bench seat and one on the right bench seat.
The parachutist who sustained the most injuries of the highest severity was at the front of the left bench seat. As that bench seat did not have a seatback, the parachutist came off the forward end of the bench between the bench and pilot seat and contacted the back of the pilot’s seat and/or ladder adjacent to the seat. The injuries were likely also increased by the mass of the 3 other parachutists on that bench moving forward during the impact sequence.
The ATSB compared the injuries sustained by the pilot and parachutists of VH-UMV with those involved in 2 survivable accidents involving C208 aircraft, assessed as likely to have been subjected to similar impact forces (AO-2016-007 and AO-2024-001). In the 2 comparative accidents, some of the occupants sustained minor injuries while others were uninjured. The pilot and front seat passengers had 5-point restraints, and in the 2016 accident the other passengers wore lap belts. In the more recent accident, the other passengers wore 3-point restraints.
ATSB investigation AO-2014-053 found that single point restraints were less effective than dual restraints in mitigating injury for parachutists. This was consistent with the US FAA’s technical report – Evaluation of Improved Restraint Systems for Sport Parachutists, which found that dual straps attached to the parachute harness provided better restraint and produced less flailing and bending of the body than single point restraints (FAA 1988). The following loading of aft‑facing passengers was found to increase restraint effectiveness:
• the person most forward in the cabin should be leaning against a bulkhead or other substantial support to limit flailing and head impact.
• each parachutist’s restraint should be anchored to the floor aft of his/her pelvis (relative the aircraft’s orientation) at a point on the floor near the middle of the thigh. The restraint should be taut to reduce forward motion, and the loads transmitted to the person behind.
• the proper brace for impact position would be to lean toward the front of the aircraft onto the person or bulkhead behind them.
The US FAA AC 105-2E Sport parachuting also stated that single point restraints were ‘not very effective’, and that dual point restraints offered ‘superior restraint’.
The ATSB assessed that the increase in number and severity of injuries of the parachutists compared to passengers seated and restrained in seats, was probably a result of single-point restraints being less effective and less cushioning due to being seated on the floor or bench.
Related occurrences
National Transportation Safety Board Special investigation report
The US National Transportation Safety Board (NTSB), Special investigation report on the safety of parachute jump operations (2008), found that between 1980 and 2008 in the US, 32 accidents involving parachute aircraft resulted in fatal injuries of 172 people, most of whom were parachutists. Acknowledging risks associated with parachuting, the report stated:
Although parachutists, in general, may accept risks associated with their sport, these risks should not include exposure to the types of highly preventable hazards that were identified in these accidents and that the parachutists can do little or nothing to control. Passengers on parachute operations aircraft should be able to expect a reasonable level of safety that includes, at a minimum, an airworthy airplane, an adequately trained pilot, and adequate Federal oversight and surveillance to ensure the safety of the operation.
Of the 32 accidents, 8 involved exceedances of the aircraft’s weight and balance, and 21 resulted from inadequate airspeed or stall situations, and in 6 accidents, both were factors. There was one accident involving a Cessna 208, which resulted in 17 fatalities.
The report also acknowledged that parachuting is typically a revenue operation where a participant pays for a jump and receives the flight as part of that service, it stated:
Most parachute operations flights are operated under the provisions of 14 Code of Federal Regulations (CFR) Part 91 and are typically revenue operations; parachute jump operators provide the flights as part of their services to parachutists who pay to go skydiving, or parachutists pay dues for membership in parachuting clubs. The risks of parachuting are generally perceived to involve the acts of jumping from the aircraft, deploying the parachute, and landing; parachutists are aware of and manage these risks. However, a review of accident reports reveals that traveling on parachute operations flights can also present risks.
The report highlighted the potential for paying participants to be unaware of the risks they were accepting when they boarded a parachute aircraft.
The report identified the following recurring safety issues:
• inadequate aircraft inspection and maintenance;
• pilot performance deficiencies in basic airmanship tasks, such as preflight inspections, weight and balance calculations, and emergency and recovery procedures; and
• inadequate FAA oversight and direct surveillance of parachute operations.
Recent accidents
The following 3 more recent accidents involved aircraft conducting parachuting operations and resulted in injuries to the occupants.
Loss of engine power after take-off involving Cessna 208B, PH-FST, West of International Airport Teuge, Netherlands, on 25 June 2021 (2021062)
On 25 June 2021 at 0932 local time, a Cessna 208B with a pilot and 17 parachutists on board departed from International Airport Teuge. During the initial climb, the aircraft suddenly lost engine power after which the pilot made an emergency landing in a field close to a motorway. The aircraft was substantially damaged, and one parachutist sustained minor injuries.
Accident involving GA8-TC-320 Airvan, SE-MES, Storsandskär, Västerbotten, Sweden, on 14 July 2019 (RL 2020:08e).
The purpose of the flight was to drop 8 parachutists from an altitude of 13,000 ft. On the drop run, the pilot lost control of the aircraft. The parachutists were unable to evacuate the aircraft resulting in fatalities of the 9 persons on board.
The investigation found that control of the aeroplane was probably lost due to low airspeed. Other contributing factors were that the aeroplane was unstable as a result of a tail-heavy loading, weather conditions, and a high workload in relation to the pilot’s knowledge and experience.
Loss of control involving Cessna U206G, VH-FRT, Caboolture Airfield, Queensland, on 22 March 2014 (AO-2014-053)
On 22 March 2014, a Cessna U206G aircraft was being used for tandem parachuting operations at Caboolture Airfield, Queensland. At about 1124 local time, the aircraft took off from runway 06 with the pilot, 2 parachuting instructors and 2 tandem parachutists on board. Shortly after take-off, witnesses at the airfield observed the aircraft climb to about 200 ft above ground level before it commenced a roll to the left. The left roll steepened, and the aircraft then adopted a nose‑down attitude until impacting the ground in an almost vertical, left-wing low attitude. All the occupants on board were fatally injured. A post-impact, fuel-fed fire destroyed the aircraft.
The ATSB identified that the aircraft aerodynamically stalled at a height from which it was too low to recover control prior to collision with terrain. The reason for the aerodynamic stall was unable to be determined. Extensive fire damage prevented examination and testing of most of the aircraft components. Consequently, a mechanical defect could not be ruled out as a contributor to the accident.
A number of safety issues were also identified by the ATSB. These included findings associated with occupant restraint, modification of parachuting aircraft and the regulatory classification of parachuting operations.
Safety analysis
Introduction
On the morning of 20 October 2023, the pilot of a Cessna 208, registered VH-UMV, commenced take-off for a planned climb to 15,000 ft to drop 16 parachutists. Passing about 500 ft on climb, the pilot detected a partial power loss, consistent with an abnormal activation of the torque and temperature limiter (TTL). The pilot reduced the power to prevent the engine surging, but the combination of low power and airspeed resulted in the aircraft colliding with water before continuing into a field.
Six of the parachutists sustained serious injuries and the pilot and 8 parachutists sustained minor injuries. The aircraft was substantially damaged.
This analysis will discuss the TTL activation and response actions. The aircraft’s seating configuration, weight and balance and occupant safety will also be examined. Additionally, the analysis will consider the number of parachutists on board, and operational guidance from the Australian Parachute Federation manual approved by the Civil Aviation Safety Authority (CASA).
Operator’s prescribed actions
Normal operation of the TTL permitted reduction in the fuel flow to the engine to maintain the lower of 100% torque or 650 °C nominal exhaust gas temperature (EGT). However, the TTL manufacturer advised that the limiter was capable of restricting fuel flow sufficiently to reduce the maximum power to about 62% torque. A noticeable power reduction, followed quickly by a power increase, had been reported by the operator’s pilots as engine surging events associated with the TTL. However, maintenance actions had been unable to identify or resolve the cause of 6 reported engine surging events in VH-UMV over a 5‑month period.
Unable to resolve the intermittent excessive TTL response, the aircraft operator had advised pilots to limit torque to 95% and EGT to 640°C to prevent TTL activation. Although well intentioned, that was contrary to the aircraft flight manual supplement, which defined take-off power as 100% RPM and 100% torque or 650°C EGT, whichever was reached first. The operator had not assessed the TTL and single red line (SRL) systems as inoperable, which would have required pilots to manually ensure torque and temperature limits were not exceeded. Power reductions resulting from TTL activations were reported to be momentary and power returned to the previous level after the torque or EGT limit reduced below the limit.
Additionally, in the absence of an aircraft manufacturer’s checklist for partial power loss, the operator had created an engine power loss checklist. The first item was to immediately move the elevator control forward if climbing to prevent airspeed decay. After other initial actions, the checklist then instructed pilots to significantly reduce power if the engine RPM was above 60% or surging, in preparation for switching off the TTL. While that was intended to ensure engine limits would not be exceeded when the pilot subsequently reintroduced power, the operator did not specify a minimum height at which it was appropriate for a power reduction to be made.
Such a significant power reduction close to the ground increased the risk of a loss of control and/or ground collision.
Contributing factor
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Pilot actions
At the commencement of the take-off roll, in accordance with normal and the manufacturer’s procedures, the pilot reported applying full power – initially reaching 100% torque for take-off, before reducing power slightly in an attempt to remain under the operator‑specific torque limit of 95%. Whether the torque or temperature limit were reached during the initial climb could not be determined as these parameters were not recorded. However, the pilot detected a power reduction consistent with an abnormal TTL activation.
As shown by previous safety reports, in the event of TTL activation, the maximum power available may have been approximately 62%. Such a significant power reduction would have required the pilot to lower the aircraft’s nose attitude to prevent an aerodynamic stall, consistent with the operator’s engine power loss checklist.
However, the pilot did not initially lower the aircraft’s nose, instead they moved the power lever aft, reducing the power setting. This was in accordance with the operator’s procedure in preparation for switching off the TTL. Although the as‑found switch positions indicated that the pilot may have inadvertently selected the SRL switch instead of the TTL, in either event the TTL would have been deactivated. However, as the pilot had not lowered the aircraft’s nose, the aircraft approached an aerodynamic stall, and the stall warning horn sounded.
In response, the pilot lowered the aircraft’s nose and, due to the low height above terrain, low airspeed and low power, searched for a suitable field for landing. Although the pilot only reported reducing the power slightly, as the post-accident inspections found the engine was capable of producing normal power, and there were no pre-existing conditions that would have prevented normal operation, the low power was likely a result of the pilot reducing power to a level insufficient to maintain height in the climb attitude, and not restoring it.
At the low height above the ground at which the power loss occurred, the above factors led to the collision with water.
Contributing factor
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Weight and balance
The aircraft had all the aircraft’s certified seating removed other than the pilot’s seat, following which the aircraft was weighed, and a basic empty weight established. However, that weight did not include the bench seating, parachute restraints, floor matting or oxygen bottles which were fitted to the aircraft at the time of the accident. Although the weight and moment arm of the bench seating had been provided with the engineering order, it was not accounted for in the IBIS Technologies weight and balance calculation software used by the operator.
As a result, the bench seating and other aircraft fixtures were not accounted for in the accident flight weight and balance calculation. Additionally, parachutists did not sit in the positions used for the weight and balance calculations for the accident flight. Therefore, the calculated weight and balance was inaccurate.
Although the operator’s post-accident calculations found that the aircraft was almost certainly operating within the weight and balance limitations throughout the flight, an accurate weight and balance assessment prior to take-off to ensure the flight will operate below the maximum take-off weight is essential for the structural integrity of the aircraft. Operating outside the centre of gravity limits increases the risk of a loss of control. Exceeding weight and balance limitations has previously resulted in fatal accidents involving aircraft conducting parachute operations.
Other factor that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
IBIS Technologies flight planning module
When conducting post-accident weight and balance calculations using the operator’s IBIS Technologies flight planning module, the ATSB identified that, while warnings were provided when the aircraft was outside the overall weight or centre of gravity limit, there was no warning when the weight for a zone within the cabin exceeded the limit. This increased the likelihood of an aircraft being loaded contrary to zone limitations.
The lack of an alert did not contribute to this accident and, as noted above, the aircraft was not loaded in accordance with the planned overall or zonal distributions. However, the software used to calculate the aircraft weight and balance was used by many operators and overloading a zone limit could result in damage to the aircraft.
Other factor that increased risk
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Safety briefings
To maximise survivability in the event of an emergency, pilots are required to ensure aircraft occupants receive a safety briefing and instructions including in the correct use of restraints, emergency exits and adopting the brace position. However, a pilot is not required to brief passengers on every flight, if they have previously been on the aircraft and are likely to be familiar with safety information.
The pilot understood that this responsibility had been delegated to the drop zone officer and that the parachutists had received the required safety briefing and information. However, there was no record of which parachutists had been briefed or when. Additionally, as none of the parachutists on board were tandem jump parachutists, they were unlikely to have viewed the operator’s video that included use of single point restraints, how to brace or exit the aircraft in the event of an emergency.
Although some of the parachutists on board had previously received a safety briefing, it had not necessarily been in the accident aircraft type or recently. Additionally, an ‘in-flight emergency plan’ printed on the rear of the cabin advised parachutists to remain seated with single point restraints attached and brace for an emergency landing when below 500 ft, but did not specify how to brace or exit the aircraft. As a result, some of the occupants were unaware of essential safety information regarding brace position and emergency exits.
Although the aircraft’s roller door closed on impact and water entered the cabin, all 17 occupants evacuated with no difficulties reported. The ATSB was unable to determine whether the absence of a safety briefing increased the severity of the injuries sustained by parachutists. However, adopting the correct brace position for impact, the correct use of restraints, and knowledge of the location and operation of all emergency exits, are factors demonstrated to increase survivability.
Other factor that increased risk
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Seating configuration
The operator routinely conducted parachuting operations in Cessna 208 aircraft with the pilot and up to 17 parachutists on board. This was based on the CASA-accepted Australian Parachute Federation Jump Pilot Manual, which stated that the aircraft could carry as many parachutists as there were restraints and provided the aircraft was operated within the weight and balance limitations.
The aircraft’s cabin was configured with a roller door, oxygen system, bench seating and single‑point restraints for parachuting operations under an engineering order by a CASA‑authorised person. Although the configuration nominally provided restraints and seating (including on the floor) for up to 17 parachutists, this was not formally documented in the aircraft flight manual or a supplement. The engineer also assessed and modified the aircraft to supply oxygen for 16 occupants to meet the operator’s requirements of their intended operation.
CASA assessed that increasing the number of persons carried above that stated on the type certificate data sheet (TCDS) required a supplemental type certificate (STC) as it was a major modification. In this case the TCDS stated that the aircraft had a maximum seating capacity of 11, but the aircraft was modified to supply oxygen for an intended 16 occupants. As such, the CASA‑authorised engineer incorrectly assessed that the modifications they were approving were minor and conducted them under engineering orders. The ATSB considered whether conducting the modifications in that manner increased safety risk.
As part of the assessment of an STC application for the same modifications submitted by the design engineer in 2017, CASA questioned the modified rear exit crashworthiness and increased number of occupants. Specifically, it was noted that the effect of increased occupancy on speed and ease of emergency egress had not been established, nor had it been demonstrated that the roller door would be unlikely to jam in the event of fuselage deformation.
As that STC application was never finalised, the safety of egress via the modified exit was not verified. However, in this accident, all the occupants evacuated the aircraft through the roller door after impact. As such, while the STC process was not followed when modifying the aircraft, there was no evidence that it increased the safety risk on this occasion. Additionally, CASA advised that the legislative requirements would likely be met if a modification conducted by an authorised person (under an engineering order) included an associated aircraft flight manual supplement.
The expectation for parachuting operations was that the parachutists would jump from a planned height, or be able to exit the aircraft in the event of an emergency when above a safe height. However, they would be inside the aircraft during take-off, at low level, and if unable to exit in the event of an emergency. In those phases of flight or conditions, increasing the number of occupants increased the number of people exposed to the risk of harm in the event of an accident. In this accident, as the aircraft was too low for parachutists to exit airborne, 15 of the 17 occupants sustained injuries, some of which probably occurred due to impact with each other.
Although the parachuting configuration was assessed as compliant with the required airworthiness standards, parachutists were exposed to greater risk of harm than if they were passengers in certified seats with adequate restraints. Those seated on the floor did not have the benefit of a seat to absorb impact forces and the bench seating had not been shown to optimally absorb impact forces. Additionally, the lack of a seatback on the left bench seat likely increased the injuries sustained by the forward-most parachutist seated on that side. The parachutists were also using single-point restraints, demonstrated to be less effective than dual restraints.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the partial power loss and collision with terrain involving Cessna 208, VH-UMV near Barwon Heads Airport, Victoria on 20 October 2023.
Contributing factors
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Other factors that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety issue description: Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Proactive safety action taken by Experience Co
Experience Co has taken the following proactive safety actions:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet‑wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the SRL/TTL malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed C208 and C208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the STC holder to be followed at or above 1,000 ft above ground level.
Proactive safety action taken by IBIS Technologies
IBIS Technologies amended its software to include an alert that will be flagged to the staff member in charge of manifesting the flight load if a zone exceeds zonal weight limits.
Proactive safety action taken by the Australian Parachute Federation
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of their aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Proposed safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Glossary
AC
Advisory circular
ADS-B
Automatic dependent surveillance broadcast
AFM
Airplane Flight Manual
APF
Australian Parachute Federation
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CAVOK
Conditions and visibility okay
EGT
Exhaust gas temperature
FAA
(United States) Federal Aviation Administration
FCU
Fuel control unit
MEL
Minimum equipment list
NTSB
(United States) National Transportation Safety Board
POH
Pilot’s Operating Handbook
RPM
Revolutions per minute
SRL
Single red line
TCDS
Type certificate data sheet
TTL
Torque and temperature limiter
US
United States
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and sports jump parachutists
Experience Co
Civil Aviation Safety Authority
Australian Parachute Federation
Victoria Police
Textron Aviation
Honeywell International Inc
OzRunways
Barwon Heads Airport
Texas Turbine Conversions
References
Federal Aviation Administration (2023). Pilot’s handbook of aeronautical knowledge. FAA-H-8083-25C.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Textron Aviation
Honeywell International Inc
Texas Turbine Conversions
Bowden Engineering solutions.
Submissions were received from:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Honeywell International Inc.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather (Source: Airservices Australia).
[2]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[3]Engine surging as reported by the pilots of VH-UMV was a power reduction followed quickly by an increase in the power level.
[4]Angle of attack: the relative angle between the chord line of the wing and the relative airflow.
[5]Automatic dependent surveillance-broadcast (ADS-B) is a surveillance system that broadcasts the precise location of an aircraft through a digital data link.
[6]Loadmaster: a person nominated by the drop zone safety officer who is performing duties for a parachute descent.
[7]Normal category applies to aircraft which are intended for non-acrobatic operation, having a seating configuration (excluding pilot seats) of 9 seats or less, and a maximum take-off weight of 5,700 kg or less.
[8]Restricted category applies to aircraft which may carry out certain special purpose operations, but may not carry passengers or cargo for hire or reward.
[9]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[10]The propeller can move to reverse when the engine is operating in beta mode, which results in thrust acting in the opposite direction of the aircraft. In beta mode, the propeller blade pitch is controlled by the power lever.
[11]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[12]The parachutist’s names, weights, and seating locations removed.
Occurrence summary
Investigation number
AO-2023-049
Occurrence date
20/10/2023
Location
Near Barwon Heads Airport
State
Victoria
Report release date
14/03/2025
Report status
Final
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Incorrect configuration, Loading related
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into the forced landing of a Cessna 208 Caravan skydiving aircraft, carrying a pilot and 17 passengers, near Barwon Heads on Friday morning.
During initial climb after take-off from Barwon Heads, the pilot observed an engine malfunction and conducted a forced landing. during which the aircraft was substantially damaged.
ATSB investigators have commenced early evidence collection and assessment activities, including gathering information from first responders and other stakeholders to inform the scope of investigation activities.
The evidence collection phase of the investigation will also involve interviewing witnesses and involved parties, and reviewing recorded data and maintenance records.
The ATSB asks anyone who may have witnessed or has video footage of the aircraft at any phase of the flight to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
On 28 March 2023, the pilot of a Cessna 172N was taking-off from Groote Eylandt, Northern Territory. Shortly after setting take-off power, the engine ran rough and the pilot rejected the take-off. During the subsequent taxi, the engine failed. The post-flight inspection revealed water contamination in the aircraft’s fuel strainer.
During the daily inspection, the pilot had observed that the right fuel filler cap was unsecured and conducted fuel drains which revealed a quantity of water in the tank. The pilot drained further samples from the fuel tank until no further indications of water contamination were present.
The pilot then refuelled the aircraft and conducted further fuel quality checks which did not indicate the presence of water in the fuel system.
Safety message
Pilots should be vigilant in conducting fuel quality checks and may need to re-familiarise themselves with the fuel contamination settling times, especially in cases where contamination is suspected.
If contamination is detected in the fuel system during initial checks, pilots should thoroughly drain all drain locations again, starting at the highest drain location. If repeated samples indicate significant contamination, the aircraft should not be flown until maintenance action is undertaken.
Pilots should consult approved flight manuals and operator procedures to determine the correct procedure for fuel quality checks.
Filler caps and gaskets
Incorrectly installed and worn fuel filler caps and gaskets leave fuel systems vulnerable to contamination. Pilots should check caps for condition, proper sealing, security, and alignment before and after flight. Worn filler caps and gaskets should be replaced.
Agitation and settling time
After refuelling or moving an aircraft, pilots should allow extra time for fuel contaminants to settle toward the draining area. The Civil Aviation Safety Authority (CASA) has published Advisory Circular AC 91-25 – Fuel and oil safety which provides advice and guidance on procedures and practices to ensure the safety of fuelling operations.
Conducting a fuel drain immediately after fuelling or agitating the fuel tanks may not identify the presence of water and other contaminants. Fuel moving in the tank may disperse water and other contaminants which can remain suspended for some time.
When fuel contamination is suspected, pilots should allow for adequate settling time before testing for water. The CASA AC 91-25 provides suggested settling times for different aviation fuel grades.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2023-002
Occurrence date
28/03/2023
Location
Groote Eylandt Airport
State
Northern Territory
Occurrence class
Serious Incident
Aviation occurrence category
Fuel contamination
Highest injury level
None
Brief release date
23/10/2023
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172N
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes