
A330 engine failure incident
Engine failure incident highlights importance of following procedures.
The flight crew of an AirAsia X Airbus A330 did not follow proper procedures when faced with an engine oil pressure warning, attempting to restart the affected engine even after it had failed, as well as electing to divert to Melbourne when the aircraft was considerably closer to two other airports.
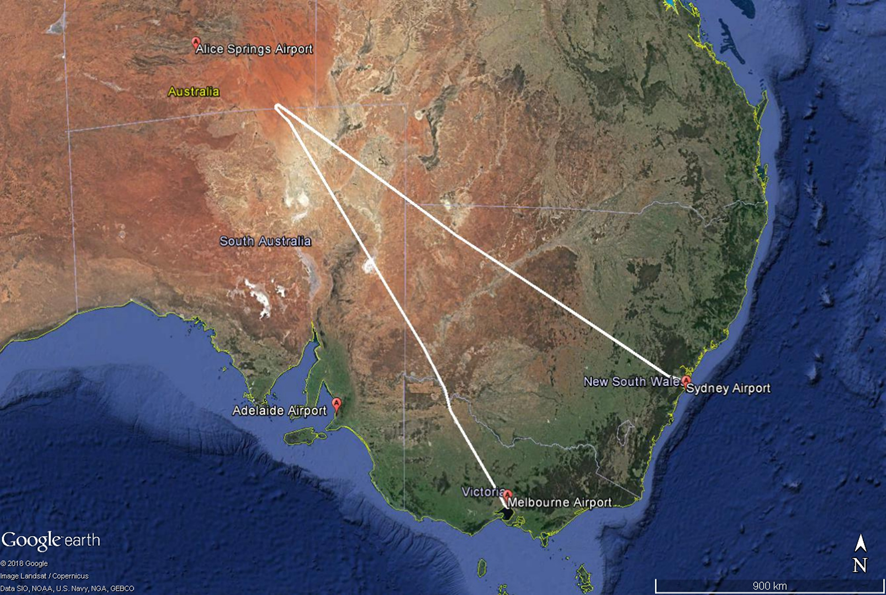
The engine oil pressure warning and subsequent engine failure occurred during a 16 August 2016 scheduled flight from Sydney to Kuala Lumpur, with two flight crew, eight cabin crew and 234 passengers on board. While in cruise near Alice Springs the flight crew received an ‘Engine 2 oil low pressure’ failure alert message, which the ATSB’s subsequent investigation of the event established was due to a shaft failure in the engine’s oil pressure pump.
That alert required immediate crew action comprising of reducing thurst on the affected Rolls-Royce Trent 700 engine to idle and then, in accordance with the Airbus procedure, ‘if [the] warning persists’, shutting down the engine.
Procedures need to be designed with clarity
However, the flight crew probably misinterpreted the term ‘persists’ as requiring they wait a certain period of time to determine if the condition was persisting. As a result, they continued to troubleshoot the failure, rather than shut down the engine.
After monitoring the engine the flight crew formed the view that the warning was the result of a gauge failure. With the intent of further trouble shooting, the crew then increased the engine’s thrust. This led to the engine stalling and ultimately failing.
However, despite evidence to the contrary, the flight crew determined that the failed engine was not damaged and could be restarted. Consequently, and contrary to the operator’s procedures, the flight crew made two attempts to restart the failed engine, even though there was no safety risk to the aircraft that demanded a restart attempt. Both attempts failed.
Also contrary to the operator’s procedures, the flight crew elected to divert to Melbourne following the engine failure, rather than to closer suitable airports in Alice Springs and Adelaide. Although twin-engined airliners such as the A330 are designed to fly safely on a single engine, this decision increased the time that the aircraft was operating in an elevated risk environment of single-engine operations.
“There are three key safety messages from this investigation,” noted ATSB Director Transport Safety Dr Stuart Godley.
“Not only does this occurrence demonstrate the importance of flight crews adhering to standard operating procedures when responding to aircraft system alerts, it also highlights that those procedures need to be designed with clarity,” Dr Godley said.
“Further, the investigation report identifies that where there is not a need for an immediate response, that flight crews look at the full contextural and available information before deciding on a plan of action.”
Since the incident, AirAsia X restated the operational requirements for flight crews for engine restarts and diversion decision making. Further, the airline has also used the occurrence as the basis for a training package for responding to engine failures, restarting failed engines, and diversion decision making.
Read the final report: Engine failure involving Airbus A330, 9M-XXD, 445 km south-east of Alice Springs, South Australia, on 16 August 2016







