Robinson R22 had returned to camp at end of day’s mustering operations, before engine was restarted;
Wreckage discovered the next day, with pilot found to be fatally injured and the helicopter destroyed;
Preliminary report outlines known order of events and contains no findings or analysis, which will be included in the investigation’s final report.
The Australian Transport Safety Bureau has released a preliminary report from its on-going investigation into a fatal Robinson R22 helicopter accident in the Northern Territory’s East Arnhem Land, on 14 November 2022.
The preliminary report details factual information established in the investigation’s early evidence collection phase, but presents no analysis or findings, which will be detailed in the investigation’s final report.
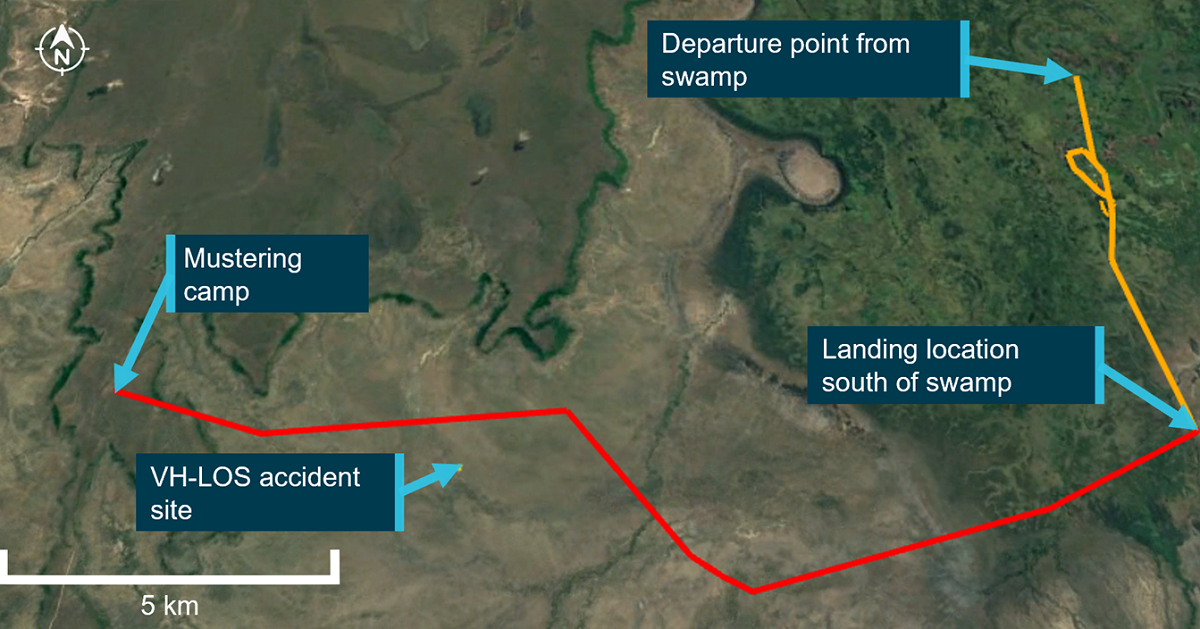
The R22, registered VH-LOS, was being used as part of a multi-vehicle animal mustering operation in the Arafura Swamp, south of Ramingining.
At the end of the day’s work, the land vehicles departed the swamp to return to the mustering camp, about 20 km west.
A witness reported the helicopter remained at the swamp as the others departed, and it was expected the pilot would depart shortly to pick up another member of the group, from the southern edge of the swamp, before continuing to the camp.
Flight tracking information showed the helicopter took off at about 6:00pm, before flying to the south of the swamp and shutting down. It was later reported, however, that they did not pick up the other group member at this time.
“The data then showed the helicopter departing the swamp, tracking to the mustering camp, then landing and shutting down at 6:54pm,” ATSB Director Transport Safety Dr Michael Walker said.
“Later, the data showed the helicopter was started again at 7:21pm, but this tracking ended about one minute later with the helicopter still at the camp.”
There was no data recorded after this time.
The preliminary report notes sunset at Ramingining was at 7:05pm and last light was at 7:27pm, and there was no moon. The pilot was not rated to fly at night, and the helicopter was not equipped for night flight.
The helicopter and pilot were not at the camp when the other members of the mustering party arrived from the swamp. At about 9:00pm they commenced a land-based search, but were unable to find the pilot.
“Some acquaintances attended the area in helicopters the following day to conduct an aerial search, and the accident site was located about 6 km east-south-east of the mustering camp,” Dr Walker said.
The pilot was deceased, and the helicopter destroyed.
To date, the ATSB has examined the accident site and wreckage, interviewed witnesses who were involved in the mustering operations and the search, and collected meteorological data, aircraft maintenance records and pilot records.
“From here, the investigation will further review pilot records, medical information, witness information, and aircraft maintenance and flight records,” Dr Walker said.
“Investigators will also further examine aircraft wreckage, meteorological data, and recorded aircraft tracking data.”
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Dr Walker concluded.
This Airport Safety Week the Australian Transport Safety Bureau (ATSB) and Airservices Australia are again reminding pilots and operators to observe and obey stop bar lights at runway intersections where installed at Australian airports, and not cross a lit stop bar at any time.
Stop bar lights are red when illuminated and are embedded across the taxiway at runway holding points and intersections. They are controlled by Airservices Australia air traffic controllers during operational tower hours as an added safety measure to prevent an aircraft or authorised vehicle unintentionally entering or crossing an active runway.
ATSB Chief Commissioner Angus Mitchell said that since 1 September 2015, more than 100 runway incursions involving stop bars at Melbourne, Sydney, Perth, Brisbane and Canberra airports have been reported to the ATSB, involving aircraft and airside vehicles.
“Fortunately, none of these runway incursions have resulted in any accidents, but they have involved a range of aircraft including airliners and general aviation aircraft as well as authorised airport vehicles, and they have occurred at different times of the day and night, and at different airports and holding points,” Mr Mitchell said.
“This year’s theme for Airport Safety Week is ‘Safety is always our destination’ and gives the ATSB and Airservices Australia the opportunity to remind pilots and operators to ensure they operate in line with all safety instructions regardless of what phase of flight they are in or where or how they are operating at an airport, including taxiways.”
Mr Mitchell said the ATSB’s investigation into a runway incursion and subsequent rejected take-off event at Perth Airport on 28 April 2018 highlighted the need for all pilots, no matter their experience or what aircraft they fly, to always observe for, and comply with the stop bar directions.
“In this occurrence, after landing, a Boeing 737-800 crossed a lit stop bar and entered the active crossing runway where another 737 had commenced its take-off roll,” Mr Mitchell said.
“The Airservices Aerodrome Controller in Perth Tower alerted the departing aircraft to the runway incursion and instructed the 737 to stop. Both aircraft stopped safely and there was no collision.”
Airservices Head of Aerodrome Services, Craig Charker, reinforced that all pilots and authorised airside drivers must only proceed when an air traffic controller has given the appropriate verbal instruction and has also switched off the stop bar lights.
“If you have a verbal clearance to enter the runway but the stop bar lights remain lit, please query this with air traffic control before proceeding,” Mr Charker said.
“For your safety and the safety of others, you cannot cross an illuminated stop bar. I encourage all operators and pilots to include checking the stop bar status as a requirement in their line up and crossing runway checks.”
I am pleased to deliver this annual report for the Australian Transport Safety Bureau (ATSB), my first as Chief Commissioner and Chief Executive Officer.
While continuing to navigate the challenges of the COVID-19 pandemic, 2020–21 saw the ATSB commence, progress and complete a series of complex transport safety investigations; continue to deploy to transport accident sites; develop and implement a new core enterprise investigation information management system; and implement key elements of our strategic property plan.
For this sustained performance in a complex operational environment, I would like to acknowledge the leadership and service of my predecessor, Mr Greg Hood, who retired on 30 June on the completion of his five-year term as Chief Commissioner and Chief Executive Officer.
Mr Hood drove an innovation and transformation agenda at the ATSB, which saw the introduction of world-leading practices like a multi-modal teams approach to investigations, new recruitment practices, a tertiary partnership for transport safety investigator training with RMIT University, and new technologies to support investigations such as remotely piloted aircraft and 3D modelling.
The ATSB has a well-deserved reputation of excellence – and for that I acknowledge Mr Hood’s transformational stewardship. It is without doubt that the ATSB has grown in both stature and importance under his watch.
I would also like to acknowledge and thank our Chief Operating Officer, Mr Colin McNamara, who acted as Chief Commissioner and Chief Executive Officer from Mr Hood’s retirement until my appointment took effect on 2 September 2021. Mr McNamara shouldered a substantial load in acting as Chief Commissioner during an incredibly dynamic and demanding operating environment.
May I also acknowledge the contributions of Ms Carolyn Walsh, who finished her more than 10-year term as an ATSB Commissioner in September 2020. The ATSB benefited greatly from her expertise in transport safety, occupational health and safety, risk management, and regulatory frameworks and governance.
In turn during 2020–21, we welcomed Ms Catherine Scott, who has extensive experience in rail safety and road transport, finance and risk management, and board directorships, with her appointment to the ATSB Commission in September 2020.
I look forward to working with Ms Scott and her fellow Commissioners, Chris Manning and Gary Prosser, to continue to ensure all ATSB staff are resourced and empowered to bring their expertise to the forefront. This then will allow me to deliver on my other responsibility to build on the ATSB’s long-term success by continuing to increase the relevance and value that our work brings to all those whom we are entrusted to deliver safety outcomes.
Achievements
The ATSB continues to work towards achieving our new performance measures established in our 2020–21 Corporate Plan. Through revised performance criteria, we are focused on improving our timeliness, demonstrating safety action taken in response to our investigations, ensuring our findings are defendable, and using our resources efficiently and effectively to achieve the greatest safety outcomes across our multiple modes of transport.
With fewer safety occurrence notifications reported to the ATSB during the year, we were not required to commence as many new investigations when compared to previous years. This allowed the ATSB to focus on, and close, several complex older investigations from early 2020. ATSB investigator resources were also allocated to support the design and build of the new purpose-built investigation management software system. The ATSB’s new Investigation Management System (AIMS) comes online in 2021–22 and is set to deliver significant productivity improvements through the removal of time-intensive manual processes. Additionally, the system’s cloud-based functionality will allow investigators to access data and upload evidence in-the-field on any device.
During 2020–21, the ATSB completed 62 occurrence investigations. Among the higher profile investigations published during the year were:
The collision with water of a de Havilland Canada DHC-2 Beaver aircraft at Jerusalem Bay, Hawkesbury River, New South Wales, on 31 December 2017.
Signal ME45 passed at danger involving suburban passenger train TP43 and near collision with another suburban passenger train, Bowen Hills, Queensland, on 10 January 2018.
The loss of control and collision with water of a Eurocopter EC120B helicopter at Hardy Reef, Whitsundays, Queensland, on 21 March 2018.
The fire on board the self-unloading bulk carrier Iron Chieftain at Port Kembla, New South Wales, on 18 June 2018.
The collision with terrain involving an AS350 helicopter during powerline stringing operations 60 km east of Woomera, South Australia, on 20 March 2019.
ATSB investigations place considerable focus on identifying safety issues that can be addressed by the parties that are ultimately responsible and best positioned for managing risk. This includes both operators and regulators. In 2020–21, 59% of our completed systemic, defined and safety study investigations identified new safety issues.
In all, 60 safety issues were identified in the reporting period, of which the ATSB determined 33 had been adequately addressed by 30 June 2021.
The ATSB is steadfast in its commitment that all published investigations are factually accurate, defendable and evidence-based. Accuracy of investigation findings remain integral to ensuring industry and government confidence in ATSB safety information in order to take action to improve transport safety. Consequently, I am pleased to confirm no changes to published investigations findings were required in 2020–21.
In the delivery of rail safety investigation services in New South Wales and Victoria, the ATSB has a collaboration agreement with independent investigation agencies in those states who conduct investigations under the Commonwealth’s Transport Safety Investigation Act 2003 (TSI Act). In 2020–21, the ATSB published and promoted eight rail safety investigations conducted by the New South Wales Office of Transport Safety Investigations (OTSI) and four rail safety investigations conducted by Victoria’s Chief Investigator, Transport Safety (CITS).
In 2020–21, the ATSB also:
Initiated 49 aviation occurrence investigations, three marine occurrence investigations and five rail occurrence investigations.
Published 39 occurrence briefs (38 aviation occurrences and one marine occurrence). Occurrence briefs are short reports that allow us to share safety learnings from a transport safety occurrence notification where the occurrence has not met the threshold of being subject to a transport safety investigation.
Processed 10,634 aviation transport safety occurrence notifications, 716 marine notifications and 882 rail notifications. From those, the ATSB safety reporting team identified 4,073 aviation and 294 marine accidents, serious incidents and incidents for the year. (In rail, the Office of the National Rail Safety Regulator (ONRSR) is responsible for processing all notifications from industry into occurrences in the Australian national rail occurrence database shared with the ATSB.)
Received and processed 198 notifications under the REPCON confidential reporting scheme, of which 75 were assessed and classified as meeting the REPCON criteria. During the year, 47 REPCON reports were completed, of which 18 (38%) resulted in safety action being taken by stakeholders.
Despite the limitations of the pandemic, participated in 27 key industry engagement events, including the International Confidential Aviation Safety Systems, the Rail Industry Safety and Standards Board’s Rail Safety Conference, and the Australian Association for Unmanned Systems' RPAS in Australian Skies Conference. Former Chief Commissioner, Greg Hood also hosted the International Transportation Safety Association’s Annual Conference.
Managed 361 media inquiries, used our in-house media studio to produce and distribute 32 packages of pre-recorded audio, video and video overlay content for distribution to national radio and TV outlets, and logged the publication and airing of 1,997 stories about the ATSB and its investigation activities by mainstream and transport industry media outlets. Of those, 1,261 stories (approximately 63%) carried safety messaging relating to our investigations.
Promoted a number of safety education campaigns, including highlighting the dangers of CO gas exposure in piston-engined aircraft, reminding pilots of the need to be aware of stop bars at major airports across Australia, and supported the TrackSAFE Foundation’s Rail Safety Week in August 2020 to promote safety for road users and rail passengers when interacting with the rail network.
Published a video to promote the safety messaging from the investigation into Beaver aircraft the collision with water accident on the Hawkesbury River, which included a high-fidelity animation of the aircraft’s flight path. This video has been viewed more than 6,700 times across all of our social media channels.
Continued to support our regional partners build transport safety investigation capacity, in particular via the ongoing involvement in the Australian Government Indonesia Transport Safety Assistance Package (ITSAP), and assisting Papua New Guinea consistent with the Memorandum of Understanding on Cooperation in the Transport Sector.
Supported external agencies by assisting Recreational Aviation Australia and the Civil Aviation Authority of the Philippines – Aircraft Accident Investigation and Inquiry Board to recover and analyse data from damaged recording devices.
Progressed the rationalisation of our accommodation footprint with the leasing of new premises for the Canberra central office and the Melbourne regional office. This ensures we have highly capable technical facilities to support our operational requirements and a more dispersed workforce that will enhance our ability to deploy to transport accident sites throughout Australia.
Established a project to transfer our website onto the GovCMS content management system website platform.
Supported the delivery of the third Graduate Certificate in Transport Safety Investigation course in partnership with RMIT University. The course was delivered online to a cohort of 22 consisting of six ATSB investigators, two investigators from the Office of Transport Safety Investigation NSW, and 14 students from a broad range of industry organisations.
Outlook
In a challenging year for the transport industry, the ATSB continued to focus on improving transport safety through our independent transport safety investigations.
The COVID-19 pandemic has been a time of great uncertainty for the transport industry in general, none more so than aviation. Cognisant of these challenges, I am committed to ensuring that the ATSB continues to effectively apply our safety knowledge and expertise in identifying safety risks in industry, and in monitoring the return to safe and reliable air transport operations as the pandemic eases.
And as an operational agency, the ATSB will continue to deploy accident investigation teams where and when necessary during the pandemic, whenever it is safe to do so.
The challenges experienced by workplaces and workforces across the country over the past year are both generic as well as very individual and personal. One of my key responsibilities and my initial focus as Chief Commissioner and Chief Executive Officer will be to ensure we continue to have a well-supported workforce that delivers world-class transport safety investigations that contribute to a safe and efficient Australian transport industry.
A high-performance aerobatic aircraft’s collision with a helicopter on the runway at Caloundra, Queensland highlights the importance of pilots being aware of the circuit procedures for differing kinds of aircraft, an Australian Transport Safety Bureau investigation report notes.
On 18 September 2020, a two-seat Extra EA-300 aircraft with two experienced pilots onboard was conducting circuits at 1,000 ft (above airport elevation) at Caloundra Airport, a non-towered airport where aircraft self-separate from each other using radio calls on the Common Traffic Advisory Frequency (CTAF). The pilot-in-command occupied the Extra’s front seat, and was conducting a check flight of the rear-seat pilot.
A two-seat Guimbal Cabri G2 helicopter, with a solo student pilot on board conducting a navigation exercise flight from Redcliffe, joined the circuit ahead of the Extra and was conducting a stop-and-go on the active runway.
The Extra landed on the runway behind it, and during the landing roll collided with the rear of the hovering helicopter, resulting in substantial damage to both aircraft. The helicopter sustained multiple propeller strikes underneath the cabin and separation of its right landing skid. The Extra’s wooden propeller was destroyed by the impact with the helicopter’s fuselage and landing skid, which punctured the Extra’s right wing fuel tank. Fortunately there were no injuries.
“The ATSB found the pilots of the Extra did not expect the helicopter to join the 1,000 ft circuit pattern, and did not assimilate the helicopter pilot’s radio calls into their mental models of the current operations at the airport. As a result, they were not aware that the helicopter was ahead of them in the circuit,” said ATSB Director Transport Safety Stuart Macleod.
The ATSB also identified that, on the final leg of the circuit, the pilots of the Extra were focused on a third aircraft in the circuit, which was ahead of the helicopter, and which they had been in radio communications with.
“While the pilots visually scanned the runway prior to landing, they were not aware of the helicopter’s presence, and they perceived a different aircraft to be the next ahead of them in the circuit, which resulted in them not sighting the helicopter and continuing the approach to the runway,” Mr Macleod said.
Further, the tail-dragger Extra’s nose-high attitude during landing obscured the hovering helicopter until immediately before the collision.
During interviews with the ATSB, the rear-seat pilot reported an expectation that helicopters would generally remain clear of circuit traffic, and that they have never known helicopters to hover over runways, while the front-seat pilot noted that helicopters regularly approach Caloundra but most remain clear of the circuit.
Mr Macleod said the accident highlights the importance for pilots of having an awareness of the circuit procedures for different types of aircraft at non-towered airports, including helicopters.
“A helicopter performing a stop-and-go will usually require significantly more time to clear the runway, compared to an aeroplane performing a touch-and-go,” he said.
“Around CTAF and uncontrolled airports there is the possibility of aeroplanes and helicopters conducting movements that might not be considered commonplace. This investigation highlights that multiple options are available to helicopters at non-towered airports, including the active 1,000 ft circuit pattern.”
Although not a factor in this occurrence, due to the speed of the Extra it could be classified as a high-performance aircraft, as it is capable of a downwind speed of greater than 150 kt, allowing it to fly a circuit at 1,500 ft.
“All pilots are reminded that the 1,500 ft circuit height is not just limited to regular passenger transport and turbine aircraft,” Mr Macleod said.
Safety around non-towered airports is one of the ATSB’s eight ‘most wanted’ safety priorities, as part of the SafetyWatch initiative.
“The alerting provided by radio broadcasts at non-towered airports such as Caloundra greatly assists the process of sighting traffic that might be a collision risk,” Mr Macleod noted.
“This accident reinforces that, even for experienced pilots, visual identification of unknown traffic is difficult.”
A train derailment near Koolyanobbing, WA illustrates the value of non-destructive testing, an Australian Transport Safety Bureau investigation highlights.
SCT Logistics train 2PM9 was on a service from Perth to Melbourne on 27 October 2020 when a wheel on the 58th wagon in its consist fractured and disintegrated.
This resulted in derailment of the wagon, and separation of the derailed wagon, and the 10 wagons trailing it, from the front of the train. No other wagons derailed, and there were no injuries.
Detailed material examination identified that, prior to the incident journey, a transverse fatigue crack had initiated in the vicinity of a spalling defect in the wheel tread.
“The crack propagated into the rim and flange of the wheel,” ATSB Director Transport Safety Stuart Macleod explained.
“On the day of the incident, a skidding event at the fatigue crack likely induced rapid brittle cracking in the wheel, resulting in fragmentation of the wheel and, subsequently, derailment of the wagon.”
The wagon in question had experienced various issues with brakes and overheated wheels in the 12 months prior to the derailment, but it is not clear whether any of these issues contributed to the derailment.
The failed wheel had recently been reprofiled, but the maintenance provider’s work instruction did not require non-destructive examination beyond a visual inspection to identify any remaining defects.
“Skids and hotspots may be repairable on wheels in otherwise good condition, but they can induce wheel failure if cracks are present, as in this case,” Mr Macleod said.
“Diligent inspections and non-destructive testing can be useful for detecting and monitoring wheel cracks, which is particularly important as these cracks approach the wheel wear condemning limit.”
Since the derailment, the operator and maintenance provider have developed a process for monitoring wagons that experience repeated issues, such as with braking.
Inspection procedures for thermal cracks and overheated wheels have been refined, and non-destructive testing is being investigated for use in certain wheel inspections.
First officer incorrectly calculated the total fuel on board to be about 340 kg more than the actual quantity;
Aircraft departed Tamworth with inaccurate load, take-off and fuel management data;
Occurrence highlights importance of adhering to standard operating procedures, as well as clear and concise communication, and independent cross checks between pilots.
The Australian Transport Safety Bureau is emphasising the need for adherence to standard operating procedures, after a Dash 8 turboprop airliner departed with incorrect take-off data when a fuel miscalculation was not detected in pre-flight checks.
On 15 January 2021, a QantasLink Dash-8-315 aircraft had landed at Tamworth, New South Wales, and was being prepared for a return to Sydney with two flight crew, two cabin crew, and 29 passengers on board.
In the Dash-8-315, the quantities displayed on fuel tank gauges for Tank 1 and Tank 2 must be manually added together by the flight crew to get a total fuel reading.
While finalising records for the flight which had just been completed, the first officer incorrectly calculated the total fuel on board to be about 340 kg more than the actual quantity.
This error was not detected by the captain during cross checks, and the inaccurate flight record was submitted electronically.
Moving on to pre-flight procedure for the return trip to Sydney, the flight crew then relied on this incorrect mental model of the aircraft’s fuel state, rather than physically verifying the fuel quantity once again.
While going through the ‘before start’ checklist with the first officer, the captain recalled looking at the fuel gauges for the fuel quantity check, but again relied on memory to read out the fuel figure.
This resulted in the aircraft departing Tamworth with inaccurate load, take-off and fuel management data. The error was not detected by the flight crew until the aircraft reached cruise level, when it was corrected, and the flight continued without further incident.
“Thankfully, the data input error did not result in any abnormality during take-off or climb in this case,” ATSB Director Transport Safety Stuart Macleod said.
“But it is a lesson in the importance of adhering to standard operating procedures, as well as clear and concise communication, and independent cross checks between pilots.”
Data input error is one of the ATSB’s eight ‘most wanted’ safety concerns, as part of the SafetyWatch initiative.
“Flight crews can guard against errors by applying effective threat and error management strategies that recognise when such threats may arise and put in place suitable actions to minimise error potential,” Mr Macleod said.
Following the incident, QantasLink provided internal communications to flight crew on checklist usage and cross checking of data. QantasLink also intends using the incident as a case study in its human factors/non-technical skills training program.
Rescue crewman lost footing on deck of sea rescue vessel during helicopter winching exercise, interrupting the normal winching sequence flow;
The pilot reacted to a verbal communication from the winch operator and instinctively moved the helicopter away from the vessel, dragging the rescue crewman overboard.
Incident highlights the importance of effective communication between pilots and crewmen when undertaking winching.
A police air wing operator has taken a range of safety actions in response to a helicopter winch training incident where a crewman was dragged overboard and briefly pulled through the water, an Australian Transport Safety Bureau investigation notes.
During a 29 September 2020 training exercise, a pilot, four tactical flight officers (TFOs) and a TFO instructor on board a Western Australia Police Air Wing Eurocopter AS365 Dauphin helicopter were conducting winching to a sea rescue vessel in waters off the Perth coastal suburb of Swanbourne.
During one exercise phase, a TFO performing the role of rescue crewman lost their footing on the deck of the vessel as it pitched and travelled over a wave, just as winching had commenced to bring them back on board the helicopter.
As the pilot began to separate the helicopter from the vessel, the winch cable became taut and the crewman was pulled overboard and dragged through the water for around six seconds.
Just prior to the crewman’s fall, the winch operator had correctly called ‘winching in’. However, seeing the crewman had fallen on the deck, the winch operator called ‘crewman has fallen’.
The pilot subsequently advised the ATSB they commenced moving the helicopter away from the vessel in response to hearing the ‘winching in’ call, expecting the usual sequence to continue as had occurred on previous occasions that day.
The pilot acknowledged this was not consistent with procedure, which was to wait until the winch operator called ‘clear to move back and left’.
In addition, once the crewman had been pulled overboard, the winch operator called for the helicopter pilot to ‘hold’, intending for the helicopter to hover over the crewman in the water, instead of announcing ‘crewman overboard’, as per the procedure. The pilot interpreted the ‘hold’ message as meaning to hold position with reference to the moving vessel, which resulted in the crewman being dragged through the water. The crewman, once winched into the helicopter, confirmed they were uninjured.
“The ATSB found that, although the winch operator communicated that the crewman had fallen, this was not recognised by the pilot, who expected the usual sequence to continue as had previously occurred on numerous occasions that day during earlier training phases,” said ATSB Director Transport Safety Dr Mike Walker.
“As a result, the pilot instinctively increased the distance between the helicopter and vessel, and the rescue crewman was dragged overboard by the winch cable.”
In addition, the ATSB found that the operator did not regularly brief or practice crewman overboard drills during vessel winching training.
This contributed to a breakdown in communication during the incident, and reduced the crew’s preparedness to respond effectively to such an event.
“Effective communication between pilots and crewmen is critical when undertaking helicopter winching as the pilot is required to safely manoeuvre the aircraft while unable to visually monitor the progress of the activity,” Dr Walker said.
“Even during highly-trained and well-rehearsed operations, human performance limitations such as expectancy and reduced attention associated with a familiar task, together with deviations from standard phraseology, can have undesired outcomes.”
Separately, and though not a factor contributing directly to this event, the ATSB found that changes to sea state limitations – i.e. the severity of sea and swell conditions – that could be allowed during training exercises had been approved without the required review by the operator’s Safety Action Group.
“The absence of that review reduced the opportunity to identify any increased risk associated with the change,” Dr Walker said.
Following an internal investigation in response to the incident, the WA Police Air Wing has introduced a range of safety actions, including amending training and pre-flight briefings to include a crewman overboard scenario, and implementing crewman overboard drills during winch simulation training.
The Police Air Wing also concluded that the inherent risk of open water vessel winching outweighed the operational benefit. Consequently, it will no longer conduct open water winching to small vessels underway. Instead, to conduct an emergency response to a small vessel, it will deploy a rescue raft while winching or helocasting* a rescue crewman to the water.
This eliminates the risk of transferring persons to small vessels underway while still maintaining the same level of rescue capability to the community when required.
* Helocasting is where a crewman jumps from the helicopter at a low altitude and speed into the water.
Locomotive collided with the rear of a stationary coal train on entering a loop;
Locomotive was operating long end leading during route tuition for two drivers;
Preliminary report outlines factual information, investigation is ongoing.
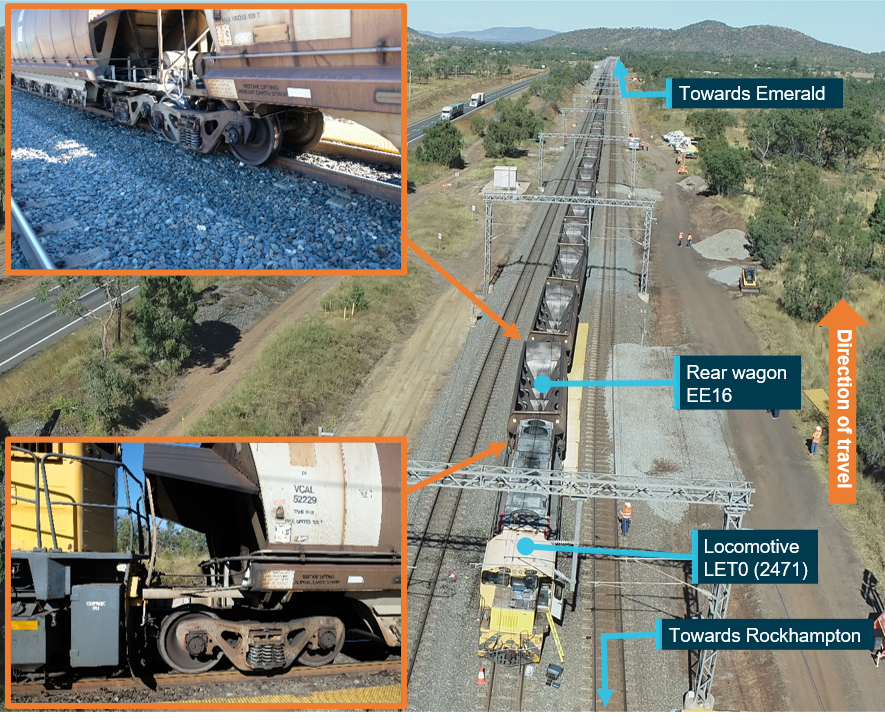
Long end leading operations - where the drivers' cab is to the rear of the locomotive relative to the direction of travel - is one of a number of areas of focus of the Australian Transport Safety Bureau’s on-going investigation into the fatal collision of a locomotive with the rear of a stationary coal train at Westwood, Queensland, on 18 June 2021.
The ATSB has released a preliminary report into the accident, which details factual information from the investigation’s early evidence collection phase but does not contain analysis or findings. The report notes that the single Queensland Rail (QR) 2470 class locomotive (operating as a ‘light engine’ as no rolling stock was attached) had left Rockhampton for Bluff, operating long end leading.
Three drivers were on board the locomotive: one tutor driver and two qualified drivers undergoing route tuition (to learn the signalling, speeds and track dynamics of the route) before being qualified to operate trains between Rockhampton and Bluff. One of the drivers undergoing route tuition was performing the role of driver, the other was performing the role of co-driver, assisting the driver by observing, announcing and confirming signal aspects as they were sighted.
While the route between Rockhampton and Bluff is dual track, maintenance on the Down line to the west of Westwood meant all rail traffic in that area had to use the Up line, and the common loop at Westwood was being used to facilitate passing traffic.
As the locomotive approached Westwood on the Down line, an empty Aurizon coal train was waiting in the crossing loop, and the Network Control Officer (NCO) set the signal interlocking system to show a yellow (caution) aspect at the approach signal and a red (stop) aspect at the signal before the points to enter the Westwood common loop.
The NCO then set the points as planned from the Down line into the loop.
Analysis of the locomotive’s data logger showed a partial application of the independent brake was initiated as the locomotive entered a downhill gradient into the Westwood yard. It entered the 50 km/h turnout from the Down line to the loop at approximately 72 km/h.
In response to a SPAD (signal passed at danger) alarm the NCO made an emergency radio broadcast. There was no response from the locomotive crew.
A full independent braking application was made approximately four seconds after the locomotive entered the turnout, when it was travelling at 60 km/h. The locomotive collided with the rear of the coal train, just past the start of the crossing loop, at a speed of approximately 44 km/h.
The locomotive and the last nine wagons of the coal train sustained significant damage in the collision. The driver was fatally injured, the co-driver sustained serious injuries, and the tutor driver received minor injuries.
“When operating long end leading, the structure of the locomotive and the configuration of the cabin limits vision for the train crew, and as our investigation progresses, the ATSB will review and examine the functionality and cabin ergonomics of the 2470 class locomotive for long end leading operations,” ATSB Chief Commissioner Angus Mitchell said.
“We will also review the nature and extent of the use of long end leading for main line operations, other factors that might have influenced the crew’s performance, and the risk controls in place relating to collisions and authority exceedances, such as SPADs, during long end leading operations.”
The investigation will also review change management and risk management processes applicable to the use of long end leading for route tuition and post incident procedures for managing emergencies on the network.
Since the accident, QR has suspended all mainline long end leading operations, with permitted operations for long end leading limited to shunting, turning of a locomotive, setting back and propelling movements.
Separately, the Office of the National Rail Safety Regulator issued a safety alert(Opens in a new tab/window) on 25 June 2021 that required all infrastructure managers and rolling stock operators to review the risks associated with long end leading operations by the end of July.
The ATSB will release a final report at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Mr Mitchell said.
I am pleased to present the Australian Transport Safety Bureau’s (ATSB) Corporate Plan, which covers the period 2021-22 to 2024-25.
This Corporate Plan has been prepared consistent with paragraph 35(1)(b) of the Public Governance, Performance and Accountability Act 2013 and the relevant provisions of the Transport Safety Investigation Act 2003 (the TSI Act), which establishes the ATSB. The Corporate Plan is also consistent with the Minister’s revised Statement of Expectations 2021–23 (SOE) for the ATSB, as notified under Section 12AE of the TSI Act. The SOE sets out clear expectations that the ATSB’s resources be used in an efficient, effective, economical and ethical way, following best practice principles and guidelines.
I acknowledge this continues to be a time of great uncertainty for the transport industry in general, and aviation in particular. As an independent safety agency, the ATSB is continuing to apply our safety knowledge and expertise and carefully monitoring the return to safe and reliable transport operations. As an operational agency, the ATSB continues to deploy accident investigation teams where and when necessary during this pandemic.
The ATSB Commission and I acknowledge the retirement of Mr Greg Hood as Chief Commissioner and Chief Executive Officer, and sincerely thank him for his leadership, professionalism and guidance in leading the ATSB from 1 July 2016 to 30 June 2021. Mr Hood drove an innovation and transformation agenda at the ATSB during his five-year term, which saw the introduction of world-leading practices including a multi-modal teams approach to investigations, new recruitment initiatives, a tertiary partnership with RMIT University, and new technologies to support investigations. All have helped to further establish the ATSB as a global leader in transport safety investigation and we look forward to yielding the benefits resulting from these advancements over the out-years.
The Deputy Prime Minister, the Hon Barnaby Joyce MP, has appointed Mr Angus Mitchell as the new ATSB Chief Commissioner and Chief Executive Officer, commencing with the agency in early September 2021. I am looking forward to supporting Mr Mitchell in his new role.
Together, Mr Mitchell and I will work to progress the key initiatives prescribed in the 2021-23 SOE. Our immediate focus will be on the continuing rationalisation of our accommodation footprint to ensure we have highly capable technical facilities to support our operational requirements and a more dispersed workforce that will enhance our ability to deploy to transport accident sites throughout Australia.
Consistent with the SOE, the ATSB is also well placed to support the Australian Government’s responses to two inquiries with recommendations concerning the ATSB’s jurisdiction and funding. These are the government responses to the:
Productivity Commission’s final report on its inquiry into the National Transport Regulatory Reforms; and
the Senate Rural and Regional Affairs and Transport References Committee report into the policy, regulatory, taxation, administrative and funding priorities for Australian shipping.
The ATSB continues to work towards achieving its new performance measures established in the 2020-21 Corporate Plan. Through revised performance criteria, we are focused on improving our timeliness, demonstrating safety action taken in response to our investigations, ensuring our findings are defendable, and using our resources efficiently and effectively.
A freight train driver erroneously determined their train to be clear of the track section to the rear when they supplied a release code to a network control officer, who then authorised a road-rail vehicle to enter that occupied block, an Australian Transport Safety Bureau investigation details.
The safeworking irregularity occurred on 28 July 2020 at a section of dual track used for crossing trains at Sellheim Station, North Queensland on the Mount Isa Line.
Travelling from west to east, Aurizon freight train 9261 passed over a set of points to enter the down section of track, and travelled until reaching an information sign that read: ‘Stop at this point unless holding DTC (direct traffic control) authority to Mingela’.
After stopping at the sign, the driver provided network control with a release for the previous section of track.
However, the rear wagons of the train were still foul of the crossing point, occupying the released section.
The network control officer then authorised a road-rail vehicle carrying three people to proceed through the crossing point in the opposite direction, from east to west.
The road-rail vehicle subsequently came to a stop when its driver observed the freight wagons occupying the track ahead.
The ATSB’s investigation into the incident found the advisory signs where the train stopped were 940 metres past the block limit boards at the crossing point, whereas the line allowed for train lengths of up to 1,009 metres. Train 9261 was 997 metres long.
Following noise complaints, the signs had been placed by rail infrastructure operator Queensland Rail (QR) in 2015 to prevent trains from idling too close to nearby residences while waiting for passing traffic. At that time, Aurizon did not operate trains over 940 metres, but a second operator on the line did.
“The investigation found that when installing the information signs, QR did not complete a formal infrastructure change approval process or risk assessment to consider the potential operational implications of the signs,” ATSB Director Transport Safety Dr Mike Walker said.
“The investigation also found that the train driver used the information sign as a reference point for stopping rather than cross-checking the in-cab counter readout against the train comparison length,” Dr Walker said.
The driver had set the in-cab counter when they entered the section of dual track to measure the distance travelled.
The counter’s readout, being lower than the length of the train, would have indicated to the driver that the rear wagons were not clear of the crossing point.
“Subsequently, the driver erroneously provided the network control officer with a release code for the Charters Towers to Sellheim section block.”
Direct train control has limited functionality to verifying the availability of a released block, Dr Walker noted.
“Given these limitations, train crew when stopping at a directional travel station to allow other rail traffic to pass, must ensure their train is in-clear before releasing the section block to network control,” he said.
“In addition, rail infrastructure managers should carefully consider the potential for information signs to be misinterpreted by rail traffic crew, particularly if such signs contain the word ‘Stop’,” Dr Walker noted.
“This occurrence also highlights the importance of rail infrastructure managers conducting appropriate change management and risk assessment processes when introducing changes to their infrastructure.”
Following the incident, QR moved the Sellheim Station information signs approximately 134 metres east, providing about 1,060 metres between the block limit boards and the signs.
QR also started a program of works to find locations on the Mount Isa Line and other lines where inconsistencies exist between infrastructure and the information contained in route maps, signalling arrangement diagrams and the DTC software.