Fatigue cracking in biplane’s bolts
Key points:
- Biplane aerobatic aircraft sustained an in-flight break-up shortly after departure from Caboolture;
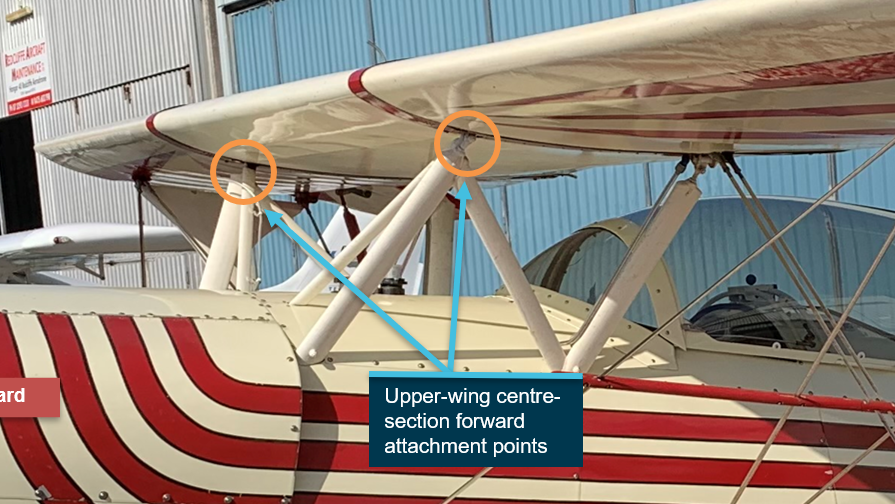
- Preliminary technical examination determined that two of the eye bolts that attached the upper wings to their supporting struts had failed due to fatigue cracking;
- ATSB has issued a Safety Advisory Notice to other owners and operators of the Acroduster aircraft type to raise awareness of the fatigue cracking.
Technical examinations as part of the Australian Transport Safety Bureau’s on-going investigation into the in-flight break-up of an Acroduster aerobatic biplane near Bribie Island on 18 August have determined that two eye bolts used to secure the aircraft’s upper wings had failed due to fatigue cracking.
The two-seat home-built Acroduster aerobatic aircraft had departed Caboolture on the morning of 18 August to conduct an aerobatic flight with the pilot, the sole occupant, on board.
A short time later the crew of a helicopter operating nearby noticed red and white debris falling from the sky before sighting the main wreckage of the biplane inverted in tidal wetlands in the Pumicestone Passage, adjacent to Bribie Island. The pilot was found to have been fatally injured.
Investigators from the ATSB’s Brisbane office deployed to the site later that day.
“It was evident to our investigators once they had arrived on site that the aircraft had sustained an in-flight break-up, with the wreckage trail distributed over a distance of about 2.4 km,” said ATSB Chief Commissioner Angus Mitchell.
The main wreckage consisted of the fuselage and tail as well as the outer-wing sections, which had remained attached to the fuselage by bracing wires. The remainder of the wing sections had separated from the aircraft.
The aircraft was recovered from the accident site by barge and taken to a secure facility for a detailed examination.
“Preliminary examination of the main wreckage revealed that two of the eye bolts that attached the upper wings to their supporting struts had failed due to fatigue cracking,” said Mr Mitchell.
The ATSB has already notified the owner of the only other Acroduster in Australia of the issue, and has advised its counterpart agency in the US, the National Transportation Safety Board, so that the information can be shared with the US Federal Aviation Administration, the US Experimental Aircraft Association and the kit plane design/material provider.
Additionally, the ATSB has also now issued a Safety Advisory Notice to alert pilots, owners and maintainers of the Stolp Acroduster (both the SA-700 Acroduster and SA-750 Acroduster) to check the condition of their aircraft.
“While our investigation is on-going, the Safety Advisory Notice serves to inform operators of this type internationally of this discovery so that they can take appropriate action to ensure that their aircraft remain airworthy,” said Mr Mitchell.
It is not clear how many aircraft may be affected by the Safety Advisory Notice, however approximately 130 Acroduster aircraft have been built since plans for the types were made available in the early 1970s.
The accident aircraft, registered VH-YEL, had been built in the United States from plans supplied in 1976 and first flew in 1981. The aircraft was shipped to Australia in 2003 and had accumulated 717 flight hours at the time of the accident.
Mr Mitchell noted today’s preliminary report details basic factual information determined in the investigation’s early evidence collection phase.
“As the ATSB’s investigation progresses, transport safety investigators will undertake a metallurgical examination of the entire upper-wing attachment hardware and structure; review the aircraft’s operational history and maintenance procedures and inspection requirements; and further analyse radar data,” he said.
A final report, which will detail analysis and findings, will be released at the conclusion of the investigation.
Read the preliminary report: In-flight break-up, Stolp Acroduster II SA-750, VH-YEL, 16 km north-east of Caboolture airfield, Queensland, on 18 August 2021
Read the Safety Advisory Notice: AO-2021-032-SAN-001: Are your wing attachment points serviceable?