Approach to the wrong runway involving a Diamond Aircraft Industries DA 40, at Coffs Harbour Airport, New South Wales, on 1 May 2018
Brief
| Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. |
What happened
On 1 May 2018, a solo training flight was conducted in a Diamond DA 40 at Coffs Harbour Airport, New South Wales. On returning to Coffs Harbour, air traffic control (ATC) cleared the aircraft for a visual approach to join the final leg of the circuit for runway 21. ATC also instructed the pilot to follow a Piper PA-28, which at that time was on a left base leg for runway 21. The pilot of the DA 40 confirmed that they had sighted the PA-28, and ATC instructed the pilot to follow the PA-28 and report when they joined the final approach leg of the circuit.
As the DA 40 joined the final approach, the pilot advised ATC that they were on a 3 NM final, however the aircraft was unable to be sighted. ATC subsequently observed the DA 40 on final approach to taxiway E5. The controller advised the pilot that the aircraft appeared to be on final for taxiway E5, and that runway 21 location was to their left. The pilot turned left and reported runway 21 in sight. The aircraft landed without further incident.
Figure 1: Coffs Harbour Airport Chart
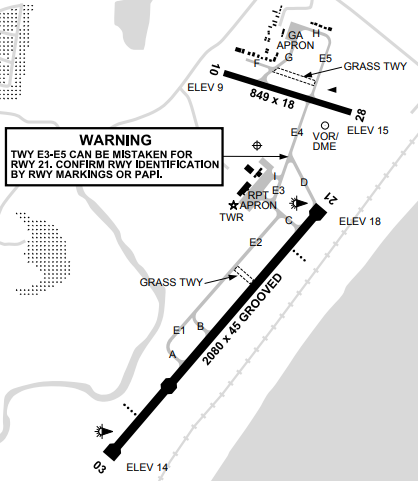
Source: Airservices Australia DAP155 Aerodrome & Procedure Charts
Safety message
Pilots should be aware of the layout of aerodromes and runways they are using. At Coffs Harbour aerodrome, warnings exist in the aerodrome charts regarding the potential confusion of taxiway E5 and runway 21, including a notice on how to avoid this confusion by confirming the presence of a Precision Approach Path Indicator at the end of the runway.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2018-063 |
| Occurrence date | 01/05/2018 |
| Location | Coffs Harbour Airport |
| State | New South Wales |
| Occurrence class | Incident |
| Aviation occurrence category | Runway - Other |
| Highest injury level | None |
| Brief release date | 16/11/2018 |
Aircraft details
| Manufacturer | Diamond Aircraft Industries |
|---|---|
| Model | DA 40 NG |
| Sector | Piston |
| Operation type | Flying Training |
| Departure point | Coffs Harbour Airport, NSW |
| Destination | Coffs Harbour Airport, NSW |
| Damage | Nil |