Taxiway excursion, ground strike and near collision with terrain involving Cessna 172R, VH-EWW, at Gold Coast Airport, Queensland, on 6 February 2024
Final report
Report release date: 17/04/2024
Executive summary
What happened
On 6 February 2024, a student pilot and flight instructor conducted a dual training flight from Gold Coast Airport, Queensland, in a Cessna 172R aircraft, registered VH-EWW. On their return, the student received an initial air traffic control clearance to track direct to runway 32.
About 40 seconds later, the flight crew accepted an amended clearance to track to the shorter runway 35 at ‘best speed’. When VH-EWW was at 1,000 ft and 1.9 NM from the runway 35 threshold, the flight crew were cleared to conduct an approach and maintain ‘best speed all the way in to crossing the runway’. Unsure how to comply with that instruction, the instructor directed the student to reduce the throttle to idle and lower the aircraft’s nose.
The aircraft subsequently passed about 100 ft above the runway threshold at about 25 kt faster than the normal approach speed. As a result, the aircraft floated along the runway before it touched down and bounced once. During the landing roll, as the aircraft approached the end of the runway, the instructor took over control of the aircraft from the student. They attempted to brake and turn the aircraft onto a taxiway beyond the end of the runway. During the turn, the aircraft veered off the taxiway towards a ditch. In response, the instructor applied back pressure on the control column and full power to commence a go-around, during which the rear fuselage and tail struck the ground. A right circuit and landing to runway 32 was then conducted.
What the ATSB found
The ATSB found that the air traffic controller's request to maintain best speed to the runway, combined with the instructor's interpretation of the instruction, resulted in an excessively fast approach. Although the aircraft exceeded both the manufacturer’s approach speed and the operator’s stabilised approach speed, the instructor did not conduct a go-around prior to landing or while on the runway. This resulted in the aircraft landing long and fast.
The excessive landing speed also resulted in reduced braking effectiveness and a loss of control during the turn onto the taxiway. Following the loss of control, a go-around was initiated to avoid a drainage ditch, resulting in a ground strike and near collision with hangars located on the eastern boundary of the airport.
What has been done as a result
The aircraft operator reviewed the company’s standard operating procedures for stabilised and unstable approaches. They also reviewed training material and sequences for instructors and students, including human factors aspects regarding communication, decision making and assertiveness.
Finally, the operator and their instructor team discussed training challenges at Gold Coast Airport with a focus on non-standard air traffic control requests and clearances, including the refusal of clearances considered operationally unacceptable.
Safety message
Although not standard phraseology, air traffic controllers may ask pilots to maintain ‘best speed’. It is up to the pilot to determine what is best in this context and more generally advise if an instruction is unclear or cannot be complied with. An approach must be flown in accordance with the aircraft flight manual and operator’s procedures. Landing with excessive speed is likely to result in the aircraft floating, landing long on the runway, bouncing and/or ballooning, all of which increase the risk of a landing mishap.
When operating in visual meteorological conditions, if an approach is not stabilised by the height specified by the operator (or generally by about 500 ft above the ground), or becomes unstable after that point, a go‑around should be conducted. The Flight Safety Foundation’s briefing note Being prepared to go around, emphasises the importance of being go-around-prepared and go‑around‑minded. This includes being ready to conduct a go‑around during the approach if any desired flight parameter, such as aircraft configuration, vertical speed, airspeed, or attitude cannot be achieved.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 6 February 2024, a student pilot and flight instructor were conducting a dual training flight in a Cessna 172R aircraft, registered VH-EWW. The aircraft took off from Gold Coast Airport, Queensland, at about 1138 local time, and tracked to the locality of Baryulgil, New South Wales (NSW), where the flight crew conducted aerial work overhead. The aircraft then tracked to Casino Aerodrome, NSW, where the student conducted 5 circuits, before departing at about 1354 to return to Gold Coast Airport (Figure 1).
Figure 1: VH-EWW track Gold Coast – Baryulgil – Casino – Gold Coast
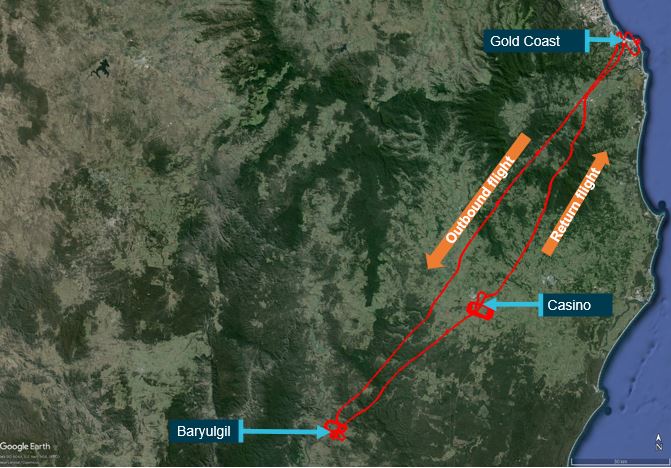
Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
At about 1419, when VH-EWW was about 10 NM south-west of Gold Coast Airport, the student pilot contacted Gold Coast Tower air traffic control. The student pilot advised that they were inbound and requested a clearance to enter controlled airspace. The aerodrome controller (ADC) issued the flight crew a clearance to track direct to the airport at 1,500 ft and advised them to expect runway 32. The ADC subsequently cleared the flight crew to descend to 1,000 ft. At that time, VH-EWW was 6.3 NM from the airport and tracking towards a right base leg[1] for runway 32.
About 40 seconds later, to facilitate sequencing with other aircraft, the ADC asked the VH-EWW flight crew whether they could ‘accept runway 35, best speed’. The student pilot reported looking at the instructor and shaking their head thinking the aircraft was too high and close to that runway. At that time, VH-EWW was 3.9 NM from the threshold of runway 35, which was 582 m long, and significantly shorter than runway 32, at 2,492 m (Figure 2). The student’s assessment was probably due to inexperience, having only landed on runway 35 once before. Had they been cleared to commence the approach from that position, a landing should have been readily achievable, with an approach profile of about 2.4°.
Figure 2: Gold Coast Airport showing runways 32 and 35

Source: Google earth, annotated by the ATSB
The instructor assessed that, as there was a headwind of about 14 kt, the aircraft could land safely on runway 35 from that position, and it would be a good opportunity for the student to practise landing on the shorter runway. The instructor therefore responded ‘affirm’ to the ADC. The ADC then issued a clearance to track for a straight-in approach to runway 35 at ‘best speed’ and advised the flight crew that they would shortly be cleared to descend.
Just over 1 minute later, the ADC cleared the flight crew to conduct a visual approach, and stated, ‘I need best speed all the way in to crossing the runway’. According to radar data, VH-EWW was then 1.9 NM from the runway 35 threshold, at about 1,000 ft and 90 kt ground speed.
The student and instructor later reported that, although on previous flights they had received air traffic control instructions to maintain best speed, these had been up to the commencement of an approach. They had not previously received a clearance for a visual approach and best speed to the runway, and were unsure what was expected.
In an attempt to comply with the clearance, the instructor advised the student to reduce the throttle to idle and lower the aircraft’s nose to maintain best speed. When the airspeed was below 110 kt, the student extended the flaps 10°. Further flap extension required a maximum airspeed of 85 kt. As the airspeed remained at or above 90 kt for the remainder of the approach, the flaps were not subsequently extended to the normal 30° landing configuration.
According to radar data, VH-EWW was about 1 NM from the runway 35 threshold, descending through about 500 ft at 95 kt ground speed, when the ADC cleared the flight crew to land and to ‘continue to taxi into GOLF’ (Figure 3 and Figure 4). This was to reiterate that they were cleared to continue through the runway 32 intersection. As VH-EWW approached the runway, the controller observed that the aircraft appeared to be faster than normal and, expecting the flight crew would conduct a go-around,[2] started planning to re-sequence the aircraft.
Figure 3: VH-EWW track showing positions of key air traffic control communications

Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
The aircraft crossed the runway 35 threshold at about 100 ft and 90 kt indicated airspeed (about 80 kt ground speed). The aircraft floated in ground effect just above the runway for a significant period before it briefly touched down and bounced/ballooned once. The instructor advised the student to continue the landing rather than go around. The instructor reported that this was based on their experience of normal operations on runway 32, which had sufficient runway length to decelerate following a fast approach and long float prior to touchdown. When the aircraft landed long on runway 35 and the student commenced braking, the wheels locked up. The instructor then took over control of the aircraft from the student and reported applying firm back pressure to the control column in an attempt to increase the weight on wheels to assist with the braking. However, the application of heavy braking still resulted in the brakes locking the wheels.
The instructor assessed that the aircraft was still travelling faster than expected. At this stage the aircraft was past the runway 32 intersection and rapidly approaching the end of the runway. Seeing this, the ADC stated, ‘turn up [taxiway] CHARLIE if need be’, to alert the flight crew that they could make a 20° left turn onto that taxiway, instead of a 66° right turn onto GOLF. The instructor heard the call but did not recognise the alternate option, as they were focused on making the turn onto GOLF (Figure 4).
Figure 4: Gold Coast Airport taxiways CHARLIE and GOLF, drainage ditch, hangars and VH-EWW track

Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
During the turn, the aircraft skidded left off the taxiway onto grass and towards a drainage ditch. The instructor then applied full power and back pressure on the control column to clear the ditch, which resulted in a ground strike, damaging the rear fuselage (Figure 5). Having observed the aircraft exit the taxiway, the ADC activated the crash alarm[3] to alert aviation rescue fire fighters.
Figure 5: Ground strike damage to VH-EWW
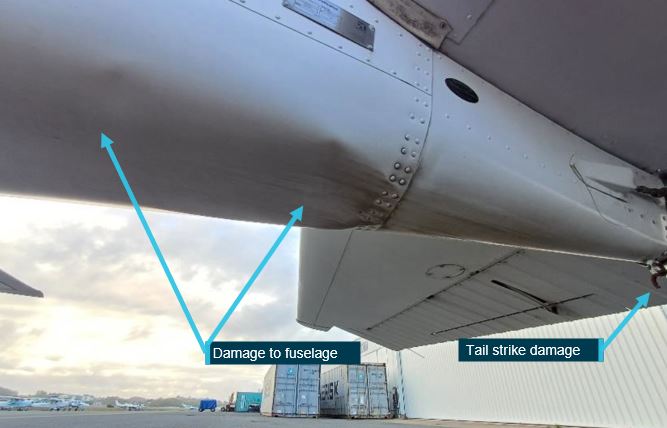
Source: Aircraft operator, annotated by the ATSB
Unaware of the ground strike, the instructor commenced a go-around, with the aircraft climbing towards a row of hangars. The instructor turned the aircraft slightly right towards the lowest roof to maximise the clearance from the buildings. The instructor reported that the stall warning horn[4] was sounding, and therefore they had to lower the aircraft’s nose to prevent a stall, but also maintain a high enough nose attitude for the aircraft to climb above the hangar (Figure 6). The instructor advised the ADC that they ‘just had to make an emergency go-around’.
Figure 6: Image from CCTV footage showing VH-EWW passing close above hangars

Source: Gold Coast Airport Limited, annotated by the ATSB
The ADC handed over aerodrome control duties to another controller, who advised the VH-EWW flight crew they had had a tail strike and confirmed they anticipated being able to conduct a normal approach and landing. The instructor then conducted a right circuit, with a left orbit on downwind as required by air traffic control for spacing, and landed on runway 32 at about 1434.
Context
Approach airspeeds
According to the Cessna 172R Pilot’s Operating Handbook (POH), the aircraft’s power-off stall speed was 47 kt with full (30°) flap and 51 kt with the flaps retracted. The handbook also provided the following approach speeds:
Table 1: Airspeeds for normal operation – approach
| Approach | Indicated airspeed |
| Normal approach, flaps up | 65–75 kt |
| Normal approach, flaps 30° | 60–70 kt |
| Short field approach, flaps 30° | 62 kt |
Landing distance required
The automatic terminal information service current at the time of the accident broadcast the following: temperature 31 °C, QNH[5] 1008 hPa, wind from 010° (magnetic) at 15 kt. For runway 35, this equated to a headwind component of 14 kt and a crosswind of 5 kt. Gold Coast Airport aerodrome elevation is 21 ft above mean sea level. The calculated pressure altitude[6] was 171 ft and the density altitude[7] was 2,091 ft.
The pilot’s operating handbook provided a chart for calculating the landing distance required at the aircraft’s maximum weight. The distances were based on a short field landing technique with flaps 30°, power off, maximum braking, paved level dry runway, nil wind and 62 kt indicated airspeed at 50 ft above the ground. It also advised to decrease distances 10% for each 9 kt of headwind. Further, if landing with flaps up, increase the approach speed by 7 kt indicated airspeed and allow for 35% longer distances. There was no data for landing with flaps 10°, or for landing at a higher indicated airspeed.
At flaps 30°, sea level pressure altitude and 30 °C, the ground roll distance required was 177 m and the total distance required to clear a 50 ft obstacle (on the approach path) was 408 m. The beneficial effect of the 9 kt headwind reduced these distances to 159 m and 368 m respectively. If landing with the flaps retracted, the required approach speed was 69 kt, ground roll 215 m and distance to clear a 50 ft obstacle 496 m.
Speed control
The Airservices Australia Aeronautical Information Publication (AIP) listed standard air traffic control phraseologies, including for speed control. ‘Best speed’ was not a standard phrase however, the AIP also stated that clear and concise plain language should be used where no phraseology was available. In the section regarding speed control for arriving aircraft, the AIP stated that a clearance for a visual approach ‘terminates speed control’. Airservices Australia advised that this meant termination of previous speed instructions but did not preclude a controller issuing subsequent speed control instructions for sequencing. Further, speed control instructions to flight crew conducting visual approaches were frequently issued.
Additionally, the Airservices Australia Manual of Air Traffic Services section Speed control principles included ‘Do not vary the final approach speed’. That manual defined final approach as ‘That part of an instrument approach procedure which…commences at the specified final approach fix or point…ends at a point in the vicinity of an aerodrome from which…a landing can be made; or…a missed approach is initiated’. In response to the draft report, Airservices Australia reiterated that the term final approach only applied to aircraft conducting an instrument approach, therefore was not applicable when flight crew were conducting a visual approach.
The aerodrome controller issued the ‘best speed’ instruction to the VH-EWW flight crew to facilitate traffic flow. The controller estimated that had the flight crew conducted a normal approach, there would probably have been insufficient spacing for VH-EWW to land before an inbound Boeing 737. The controller reported that flight crew of training aircraft sometimes deliberately conducted very slow approaches. Further, that the approach speeds of similar aircraft to the Cessna 172 could vary by 20 to 30 knots, but the landing speed would be essentially the same. In issuing the instruction, the ADC expected that the flight crew would maintain a higher speed until the aircraft was a bit closer to the airfield than normal, and then reduce speed appropriately to make a safe landing.
The AIP Speed control section also included:
5.2 The pilot must request an alternative when an ATC-issued speed control instruction is unacceptable on operational grounds.
The instructor reported that during the approach, they wanted to help the ADC by getting in quickly, and not impeding the Boeing 737. After the incident, the instructor reported that in future they would be more assertive with air traffic control and advise they could not comply with maintaining best speed while conducting a normal approach.
Stabilised approach
The United States Federal Aviation Administration’s (FAA’s) Airplane Flying Handbook defined a stabilised approach as:
one in which the pilot establishes and maintains a constant-angle glide path towards a predetermined point on the landing runway. It is based on the pilot’s judgment of certain visual clues and depends on maintaining a constant final descent airspeed and configuration.
The handbook further stated that for a general aviation piston-engine aircraft, an immediate go‑around should be initiated if an approach became unstable below 300 ft above the ground. The handbook listed criteria for a stabilised approach. These included a criterion for airspeed. For a stable approach, the airspeed was to be within +10 and -5 kt of the recommended landing speed specified in the aircraft flight manual, 1.3 x stalling speed or an approved placard/marking.
The FAA fact sheet Stabilized approach and landing, described an optimum 3° glideslope. The fact sheet referenced a study that found unstable approaches with a glideslope greater than 3° often had high descent rates and approach speeds.
The operator of VH-EWW prescribed stabilised approach criteria in the operations manual. When operating in visual meteorological conditions[8] the criteria were, when below 300 ft:
- in the landing configuration
- on the correct flight path
- only small changes in heading and pitch required to maintain the correct flight path
- speed stabilised at not more than the reference landing speed[9] [in this case 61 kt with full flap and 66 kt with the flaps retracted] plus 10 kt and not less than the reference landing speed
- sink rate of not more than 1,000 feet per minute
- the power setting is appropriate for the aircraft configuration and is not below the minimum power for the approach as defined by the aircraft operating manual.
Safety analysis
When the aerodrome controller cleared the flight crew to conduct a visual approach and to maintain best speed until crossing the runway, their expectation was that the flight crew would initially maintain a higher airspeed, but reduce to normal final approach speed as required for a safe landing. However, the flight crew were uncertain how to comply with the instruction, having previously only been requested to maintain best speed up until the commencement of an approach. Despite that, the flight crew did not seek clarification from the controller, or advise that they were unable to comply with the speed requirement.
When the flight crew were issued the clearance to conduct a visual approach, the aircraft was at about 1,000 ft and 1.9 NM from the runway threshold. A stabilised approach is generally based on a 3° approach profile. In this case the aircraft’s flight path to the threshold was steeper at about 5° (to the horizontal). To achieve that flight path, and maintain what they interpreted as the required airspeed, the crew reduced the throttle to idle and lowered the aircraft’s nose. Those actions resulted in an approach airspeed significantly faster than that published in the POH.
The phrase ‘best speed’ used by the controller was not included in the standard air traffic control phraseology published in Airservices Australia’s Aeronautical Information Publication (AIP). However, controllers could use clear and concise plain language when a standard phrase did not exist. In this instance, the controller’s emphasis to maintain best speed until within the vicinity of the runway contributed to the aircraft’s excessive airspeed.
Based on published landing data, runway 35 was long enough for the aircraft to land at maximum weight, even using a normal landing technique with the flaps retracted. However, VH‑EWW’s 90 kt airspeed when it crossed the runway threshold was 15 kt higher than the upper limit of the flapless approach speed specified in the POH. Additionally, the aircraft’s approach speed exceeded the operator’s stabilised approach criteria for the airspeed to be not more than the reference landing speed (61–66 kt depending on flap setting) plus 10 kt, which should have prompted the flight crew to initiate a go-around.
The instructor’s expectation that they could remedy the effects of the fast approach on the runway, rather than having to go around, was based on usually landing on runway 32, which was more than 4 times the length of runway 35. The flight crew therefore continued the approach, resulting in the aircraft floating above the runway and landing a long way down the runway. Because of the higher airspeed (and possibly the extended flap) reducing the load on the wheels, when the aircraft landed brake application locked the wheels despite the instructor’s application of back pressure on the control column.
Although still travelling at speed, the instructor attempted to turn onto taxiway GOLF. The instructor did not identify the controller’s intent for them to make a much smaller left turn onto taxiway CHARLIE, while focused on trying to achieve the right-hand turn onto GOLF. The turn at speed resulted in the aircraft skidding off the side of the taxiway into grass.
The instructor’s application of full throttle and back pressure to avoid the aircraft nosing forward into a ditch resulted in the fuselage and tail striking the ground. Unaware that the ground strike had occurred, the instructor initiated a go-around from the grass. By that stage, the airspeed had reduced such that the stall warning indicated an impending stall. The instructor’s action to lower the aircraft’s nose prevented the stall but resulted in a low climb gradient and near collision with hangars.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the taxiway excursion, ground strike and near collision with terrain, involving Cessna 172R, VH-EWW, at Gold Coast Airport, Queensland, on 6 February 2024.
Contributing factors
- The air traffic controller's requirement to maintain best speed to the runway, combined with the instructor's interpretation of the instruction, resulted in an excessively fast approach.
- Although the aircraft exceeded the speed for a stabilised approach, the instructor did not conduct a go-around prior to landing or while on the runway.
- The excessive landing speed resulted in reduced braking effectiveness and a loss of control during the turn onto the taxiway.
- Following the loss of control, a go-around was initiated to avoid a drainage ditch, resulting in a ground strike and near collision with hangars located on the eastern boundary of the airport.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. |
The aircraft operator advised that the following safety actions had been taken:
- The safety committee reviewed the company’s standard operating procedures for stabilised and unstable approaches. Company procedures and training were found to be aligned with the United States Federal Aviation Administration Private Pilot – Airplane Airman Certification Standards – Short field approach and landing speed tolerance (+10/-5 knots with gust factor applied) and the Civil Aviation Safety Authority’s Part 61 Manual of Standards Schedule 8, Table 1 Final approach speed tolerance (+5/-0 knots).
- A review of training material and sequences for instructors and students, including human factors aspects regarding communication, decision making and assertiveness.
- Discussions with the instructor team focused on training challenges at Gold Coast Airport for non-standard air traffic control requests and clearances, including refusal of clearances considered operationally unacceptable.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the student pilot, instructor and air traffic controller
- the operator
- Airservices Australia
- video footage of the accident flight.
References
Federal Aviation Administration (2021). Airplane Flying Handbook, FAA-H-8083-3C. US: FAA. Retrieved from: https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/airplane_handbook
Federal Aviation Administration (2022). Stabilized approach and landing, AFS-850 20-04. US:FAA. Retrieved from: Stabilized Approach and Landing (faa.gov)
Flight Safety Foundation (2000). FSF Approach and Landing Accident Reduction Briefing Note 6.1– Being prepared to go around. US:FSF. Retrieved from: https://flightsafety.org/files/alar_bn6 1-goaroundprep.pdf
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the student pilot, flight instructor and air traffic controller
- the aircraft operator
- Airservices Australia
- the Civil Aviation Safety Authority.
Submissions were received from:
- the aircraft operator
- Airservices Australia.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The base leg of the circuit is at a right angle to the final approach leg.
[2] A go-around is an aborted landing of an aircraft that is on final approach or has already touched down.
[3] Crash alarm: an emergency is declared when an aircraft is experiencing problems and there is a reasonable certainty of a threat to the safety of the aircraft.
[4] The Cessna 172R Pilot’s Operating Handbook stated that the stall warning horn sounds between 5 and 10 knots above the stall in all configurations.
[5] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[6] Pressure altitude is the altitude corrected for non-standard pressure.
[7] Density altitude is pressure altitude corrected for temperature.
[8] Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[9] Reference landing speed is usually defined as 1.3 x stall speed for the configuration.
Occurrence summary
| Investigation number | AO-2024-004 |
|---|---|
| Occurrence date | 06/02/2024 |
| Location | Gold Coast Airport |
| State | Queensland |
| Report release date | 17/04/2024 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Ground strike |
| Occurrence class | Accident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 172R |
| Registration | VH-EWW |
| Serial number | 17280090 |
| Aircraft operator | Flight One Australia Pty Ltd |
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Gold Coast Airport, Queensland |
| Destination | Gold Coast Airport, Queensland |
| Damage | Substantial |