We encourage anyone who doesn’t feel comfortable in reporting an aviation, marine or rail safety concern to their employer, an operator or a service provider to report it to us by using our REPCON confidential reporting scheme.
As our video explains, making a REPCON report ensures that your privacy, and the identity of those involved, always remains completely confidential.
If you see something you think is not quite right and don’t feel comfortable reporting it, make a confidential online REPCON report at atsb.gov.au/voluntary or you can call 1800 020 505.
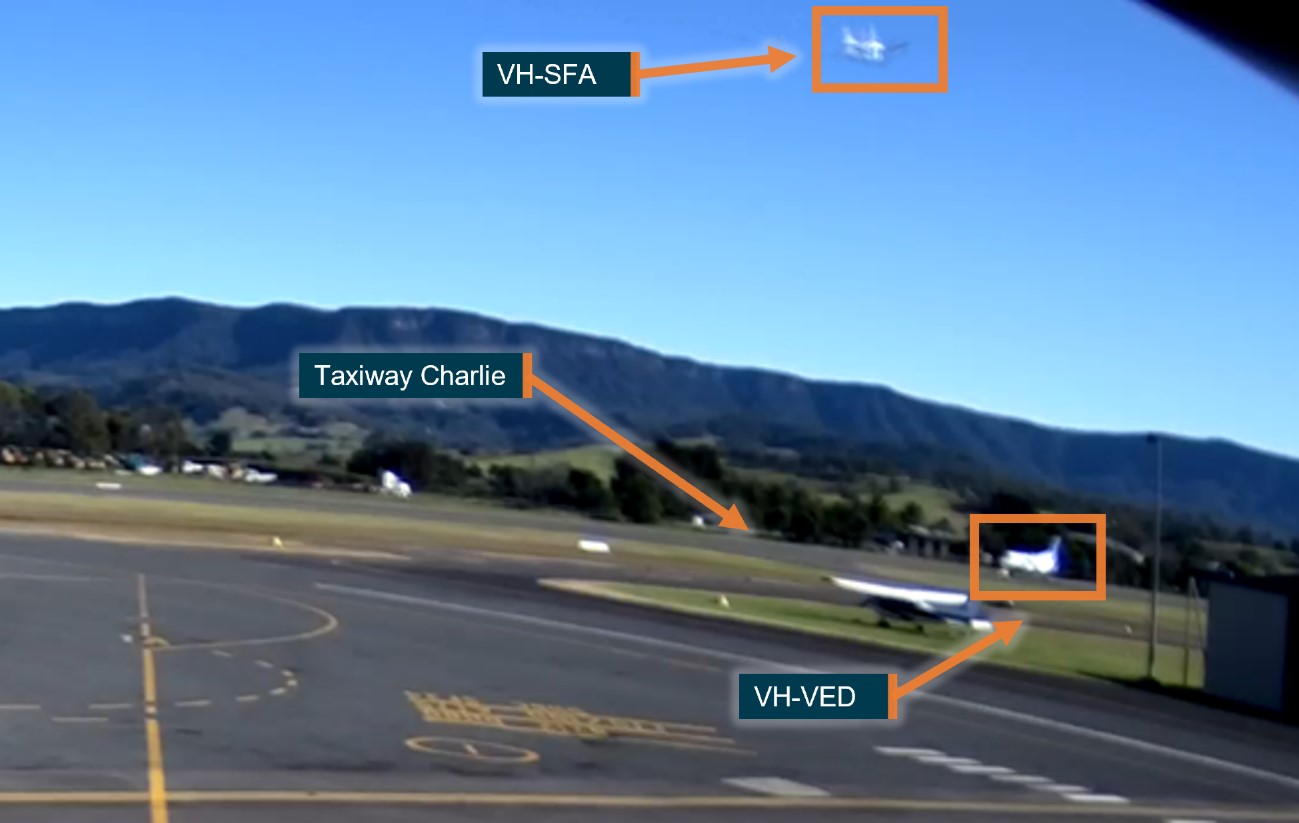
The pilot of a Piper Cherokee that took off over a Saab 340 that was backtracking on the same runway used non-standard radio phraseology and had missed a transmission from the larger aircraft, an ATSB investigation report details.
The Piper pilot began their take-off from runway 34 at Shellharbour, NSW, as part of a solo navigational training exercise on 6 July 2023.
At the same time, a Saab 340 regional airliner was backtracking along the same runway, having just landed on a scheduled passenger service from Brisbane.
As the crew of the Saab saw the Piper conducting its take-off roll towards them, they attempted to contact the Piper pilot on the radio, but were unable to make contact, and veered their aircraft to the edge of the runway.
When the pilot of the Piper saw the Saab, they elected to continue the take-off, passing over the left wing of the Saab at approximately 150 ft above ground level.
“The Piper pilot had incorrectly assumed the Saab would be using the taxiway after landing, and that the runway was clear,” ATSB Manager Transport Safety Derek Hoffmeister said.
“They were unaware that a weight restriction on the taxiway meant the Saab had to use the runway to backtrack, and so when they saw the Saab begin to turn at the end of its landing, they turned their attention to other aircraft in the circuit.”
The ATSB’s investigation found the Piper pilot used non-standard radio phraseology when turning onto runway 34, and then didn’t hear the Saab crew re-state their intention to backtrack on the runway.
“Additionally, the investigation determined that once the Piper pilot saw the Saab, it would have almost certainly been possible for them to reject the take-off,” Mr Hoffmeister said.
“Despite this, they elected to continue the take-off from an occupied runway.”
Mr Hoffmeister said the incident was another reminder of the need for pilots to make clear radio broadcasts, and pay attention to transmissions being made by other pilots, in particular at a non-towered airport like Shellharbour.
“At a non-towered airport, pilots are responsible for maintaining separation between one another,” he said.
Network operator Queensland Rail has taken a number of safety actions after two passenger trains nearly collided with an excavator, which had driven onto an active section of track in Brisbane, an Australian Transport Safety Bureau final investigation report notes.
During preparations for a planned works closure of the rail line between Brisbane’s Thorneside and Birkdale stations on the evening of 7 March 2020, an excavator was driven onto a section of track that was still in operation.
As a Queensland Rail suburban passenger train approached at over 90 km/h, the train driver saw the excavator and applied the emergency brake.
The excavator operator also saw the train, and removed the machine from the tracks, with footage showing the excavator clearing the running line less than one second before the train passed at about 61 km/h.
After the train stopped, it was then approved to proceed by the network control officer (NCO), because the NCO was told the excavator was clear of the tracks, despite it still being within the 3 m danger zone.
Then, once the first train had departed with the excavator in the danger zone, the excavator operator was directed to remove the machine from the danger zone. As the operator began to do this, another suburban passenger train passed through the site.
During this second near collision, the excavator operator jumped clear down an embankment to escape danger.
The ATSB’s investigation concluded a range of factors contributed to the near collision incidents. The final report notes a number of communication processes were limited and unclear, leading some individuals to misinterpret information, and some to unintentionally communicate incorrect information.
Among the contributing factors, the ATSB found the Queensland Network Rules and Procedures did not provide sufficient guidance for rail safety workers to ensure they used standardised, rail-specific terminology when communicating safety-critical information.
Additionally, a number of issues were identified with the work group’s pre-start briefing, including the fact that the lead protection officer (PO), assistant PO and excavator operator were not involved.
“Substandard network pre-start briefings and communication irregularities have been identified as contributors to railway accidents in Australia and abroad,” ATSB Chief Commissioner Angus Mitchell said.
“Despite this being well documented, rail infrastructure managers and track workers continue to experience issues with the application of effective safety-critical communication, and assuring network pre-start briefings are conducted in accordance with procedures designed to manage safety risks.”
Mr Mitchell said it was essential all workers attend pre-start briefings, prior to entering the rail corridor, and fully understand the worksite protection that is in place.
Separately, while Queensland Rail had undertaken significant work in the years prior to the incident targeted at managing the risk of collisions between rail traffic workers and machinery, the ATSB’s investigation found the design of the first-line assurance activities, and the limited use of second-line and third-line assurance activities, meant there was only limited assurance that the worksite protection aspects of pre-start briefings were being conducted effectively.
“The rail corridor is a safety-critical work environment, and work in that corridor fundamentally relies on procedural controls to remain safe,” Mr Mitchell said.
“It is therefore vital that first-line assurance activities are appropriately designed to provide an accurate account of key work practices being assessed, and that sufficient higher level assurance activities are conducted to provide confidence in the results of the first-line assurance activities.”
“The absence of accurate information limits the ability of an organisation to learn and continuously improve safety.”
As a result of the incident, Queensland Rail issued a critical safety alert to all relevant staff, outlining a number of key actions, including that all workers must attend a pre-start briefing prior to entering the rail corridor.
Queensland Rail also entered an enforceable voluntary undertaking with the Office of the National Rail Safety Regulator, committing to 13 initiatives to improve planning processes for track access, and a range of other safety steps.
The Tonga Civil Aviation Office (TCAO) commenced an investigation into a loss of control during taxi, and a subsequent ground collision involving a SAAB 340B, registered A3-PUA, at Fua'amotu International Airport, Tonga, on 8 December 2023. The TCAO requested assistance and the appointment of an accredited representative from the ATSB.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 26 June 2025, the TCAO released its final report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation.
Any enquiries relating to the accident investigation should be directed to the TCAO.
The ATSB has released a preliminary report to detail factual information established as part of its ongoing investigation into an accident involving a Cirrus SR22 light aircraft near Gundaroo, north of Canberra on 6 October 2023.
The report, which does not outline findings nor provide analysis, details that the aircraft had departed Canberra bound for Armidale with a pilot and three passengers on board shortly after 2:30pm, with the pilot operating under the instrument flight rules.
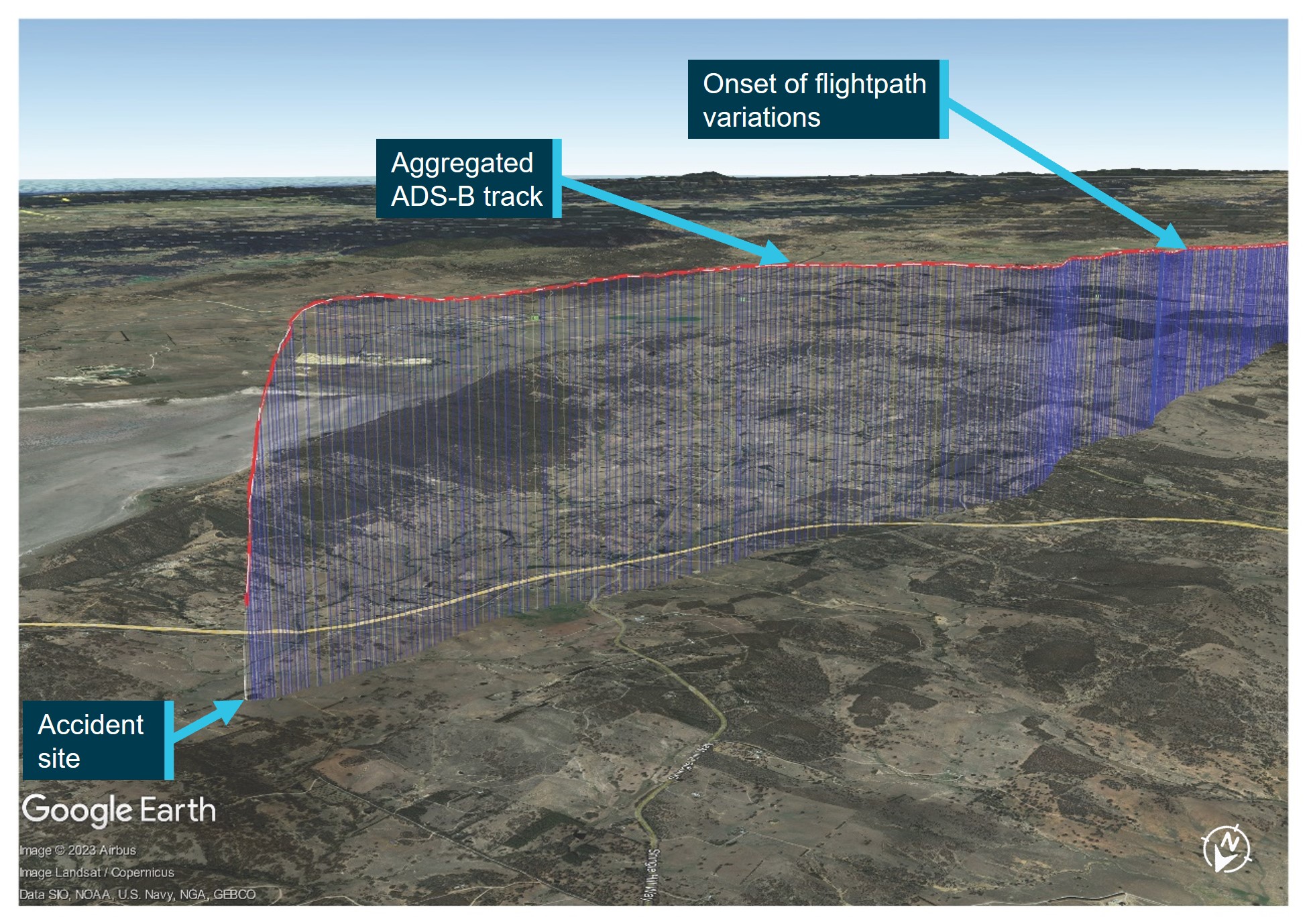
Data from the aircraft’s ADS-B (Automatic Dependent Surveillance Broadcast) transmitter, which broadcasts GPS-derived position and speed information, shows that as it climbed through 7,500 ft up to its planned cruising altitude of 10,000 ft its groundspeed fluctuated and its track varied.
Several people at locations below the aircraft’s flight path during this time reported hearing noises that they described as a rough running or surging light aircraft engine.
“Twelve minutes after take-off, the aircraft was about 25 km north of Canberra, at an altitude of about 10,000 ft, when it abruptly departed from controlled flight and descended steeply towards the ground. Witnesses described the aircraft rotating in a corkscrew motion,” said ATSB Director Transport Safety Kerri Hughes.
The aircraft collided with the ground on a private property in an open field adjacent to a dam. The occupants were fatally injured, and the aircraft was destroyed by a post-impact fire.
“Impact marks and wreckage distribution at the accident site indicated that the aircraft impacted with terrain upright, with a slight nose low attitude and with little forward momentum, suggestive of a spin,” said Ms Hughes.
“Key components of the aircraft’s airframe parachute system were all located within the wreckage, However, based on the available evidence, the ATSB was unable to determine if an attempt had been made by the pilot to deploy the parachute system before the impact.”
Damage to the propeller blades indicated that the engine had low or no power at impact. The report notes that spin recovery, icing, un-porting of fuel tank outlets in a spin, preparation for use of the parachute, and an engine mechanical issue could all be reasons for a power reduction.
The forecast meteorological conditions at the time of the accident included isolated rain showers, broken cumulus/stratocumulus cloud, and a freezing level of 5,000 ft in the south and 8,000 ft in the north, conditions which can imply moderate turbulence and moderate icing.
“As the investigation continues, the ATSB will continue an assessment of the recovered components, review pilot and operator documentation and pilot medical information, and analysis of the aircraft’s performance based on flight track data and meteorological information,” said Ms Hughes.
The ATSB will release a final report, detailing contributing factors and analysis, at the conclusion of the investigation.
“However, if at any stage we identify a critical safety issue, we will immediately alert the relevant parties so that they might take safety actions.”
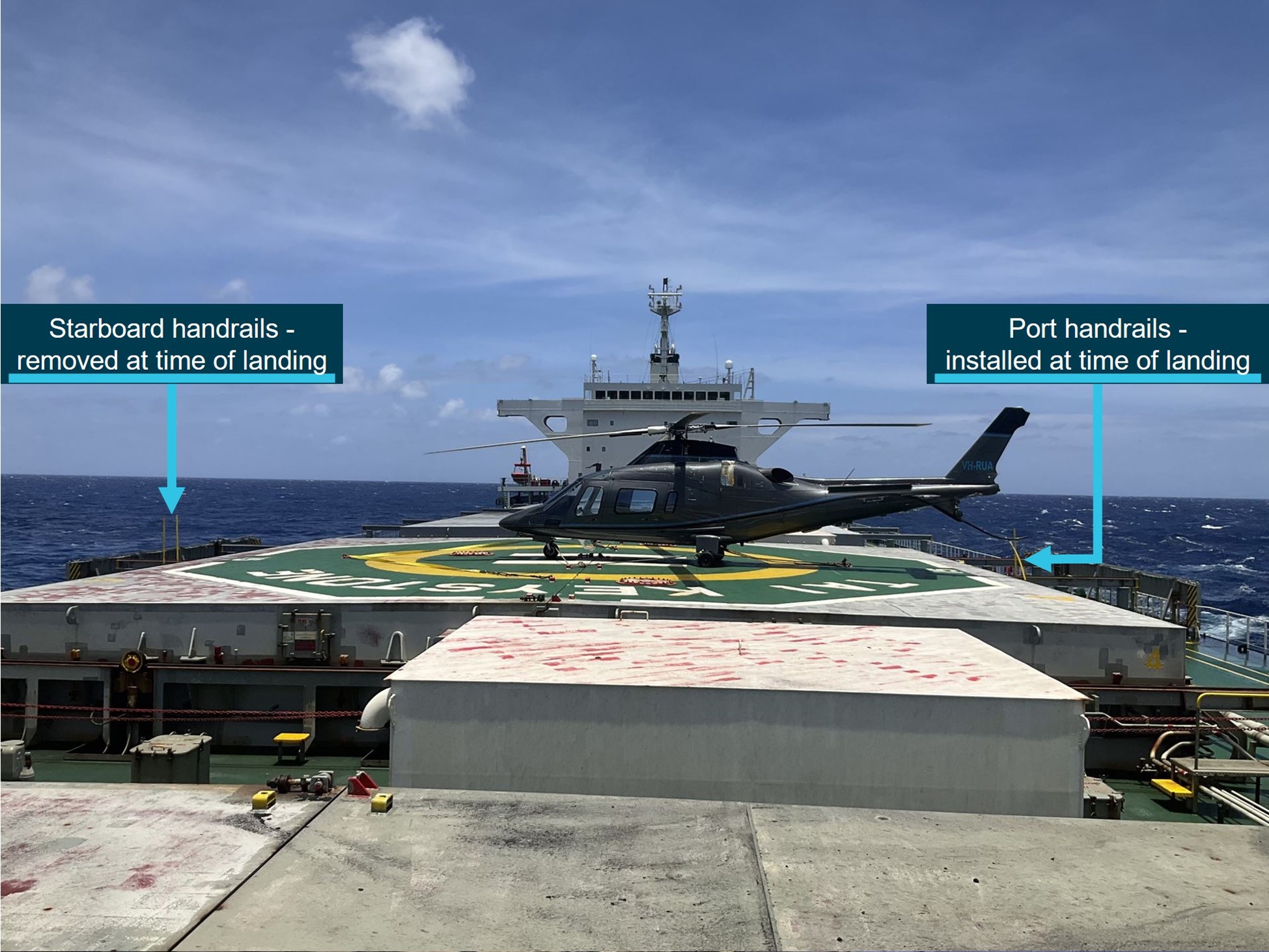
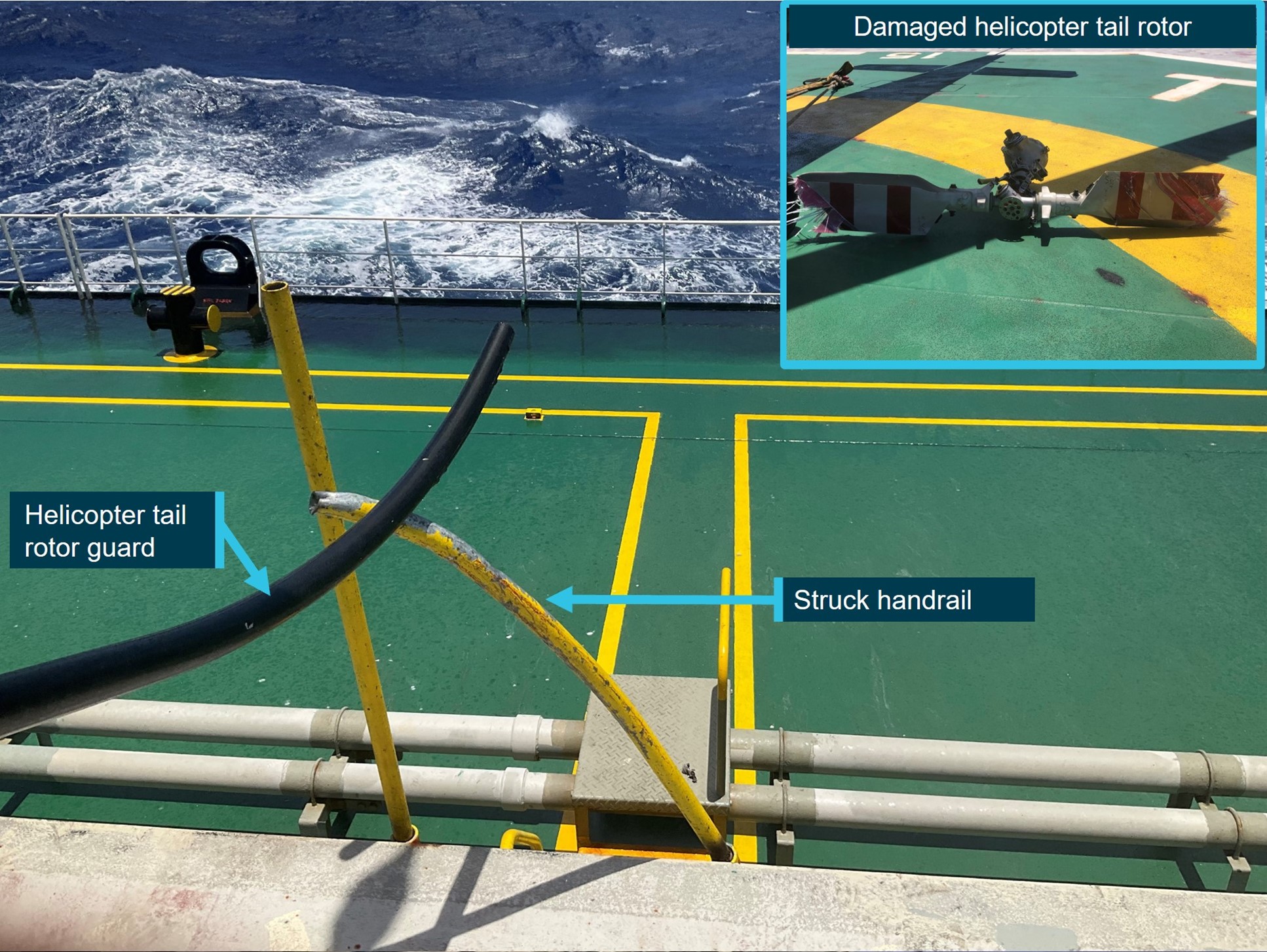
On 7 December 2023, an Agusta A109E helicopter was conducting a marine pilot transfer operation. While landing on the ship Tai Keystone, the aircraft struck a handrail resulting in substantial damage to the tail rotor and minor damage to the vessel.
What the ATSB found
The ATSB found that the handrail had not been removed during the preparation of the helicopter landing site. It was also found that the ship’s crew was using an older version of a checklist which did not require their removal. This item was however included in the latest version of the International Chamber of Shipping Guide to Helicopter/Ship Operations checklist current at the time of the occurrence.
The ATSB also determined that the handrail would have been difficult for the helicopter pilot to detect as it had been painted in a colour which did not contrast with the colours used on the ship deck. This was not in accordance with the guidance for shipboard helicopter landing sites in the International Chamber of Shipping Guide to Helicopter/Ship Operations. Additionally, during the landing, the helicopter was not positioned correctly on the helicopter landing site. This resulted in the tail rotor being outside the obstacle free zone and striking the handrail.
It was also identified that the Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports - design and operation did not include guidance material for the marking of objects, except for wind direction indicators, located on the helicopter landing site.
Finally, the Australian Maritime Safety Authority Marine Order 57 – Helicopter operations referenced an outdated version of the International Chamber of ShippingGuide to Helicopter/Ship Operations.
What has been done as a result
Taiwan Navigation Co. Ltd, have updated their helicopter/ship operation safety checklist to include the following checklist items:
the deck party is aware that a landing is to be made
the operating area is free of heavy spray or seas on deck
the side rails and, where necessary, awnings, stanchions and other obstructions have been lowered or removed
all personnel been warned to keep clear of rotors and exhausts
the ship operator will now be notified of updates to the International Chamber of ShippingGuide to Helicopter/Ship Operations when new versions are published.
Jayrow Helicopters have amended their procedures to ensure that helicopter pilots are provided with visual representation of each individual vessel helicopter landing site prior to departure. They were also developing a new pilot checklist that included a requirement to ensure no obstacles existed in the helicopter landing area.
The Australian Maritime Safety Authority noted the reference to the outdated guide and will include this for correction in a planned review of Marine Order 57.
Safety message
It is the responsibility of the pilot in command to ensure that a landing area is safe. Where possible, helicopter pilots should attempt to gather as much information about the helicopter landing site (HLS) prior to departure and conduct an inspection of the intended landing area before commencing an approach to land. Photographs and obstacle maps of the HLS can be a valuable source of information to assist helicopter pilots with threat identification.
Objects that present a threat to a landing helicopter that are retractable, collapsible or removable should be painted in an appropriate colour to ensure they are visible if forgotten or missed. The use of reflective tape or lighting also increases the visibility of these objects.
Additionally, vessel operators should ensure their procedures and the landing area on the ship are aligned with the relevant guidance material.
The occurrence
On 6 December 2023 at 2015 local time, the merchant vessel Tai Keystone, departed Hay Point, Queensland for Tachibana, Japan. The vessel’s route passed through the Great Barrier Reef via the Hydrographers Passage and due to its size (over 70 m in length), the Tai Keystone required a marine pilot[1] to assist navigating this route.
The Tai Keystone departed Hay Point with the marine pilot on board and reached the start of the compulsory pilotage area for Hydrographers Passage at about 0100 on 7 December. The vessel completed the passage at about 0730 and the marine pilot was relieved of duty. As the marine pilot did not expect to depart the vessel for several hours they left the ship’s bridge to obtain rest in the sleeping quarters.
At about 0830, an Agusta A109E helicopter, registered VH-RUA, departed Mackay, Queensland with just the pilot onboard. The pilot planned to land on the Tai Keystone to retrieve the marine pilot and then proceed to another ship, to conduct a second marine pilot retrieval, before returning to Mackay Airport.
The helicopter was flown north‑east from Mackay and at about 1012 the helicopter pilot attempted to establish communication with the Tai Keystone for the first landing however, this was unsuccessful. Another attempt to establish communication was successful at about 1027, 15 minutes prior to landing.
Due to slope landing limitations, the helicopter pilot requested information on the extent to which the vessel was rolling[2] and the master[3] of the ship advised it was between 3–5°. As this was at the helicopter operator’s limit of 5° for daylight operations, the helicopter pilot requested the marine pilot join the ship’s master on the bridge to give instructions to help reduce the ship’s roll.
The marine pilot arranged for the vessel’s heading to be changed to 340°, which reduced the roll to approximately 2°. The helicopter pilot was informed that the emergency crew was on standby, and that the master had given permission for the helicopter to land.
The helicopter pilot completed their pre-landing checks and, while at 300 ft on approach to the ship, conducted a visual inspection of the shipboard helicopter landing site (HLS).[4] They advised that, while they had not landed on this ship previously, this height was close enough to do an effective reconnaissance of the HLS. The pilot noted red manhole covers, where they would normally land the nose wheel, as the only obstacles inside the landing area. Having assessed that these did not present a threat as the helicopter could land clear of the manholes, they continued the approach.
At about 1042, the helicopter landed on the shipand as the wheels touched the deck, the tail rotor struck an upright handrail that was not identified by the pilot during the approach. The helicopter pilot reported hearing a shredding noise and an increase in the engine pitch before completing the emergency shutdown procedure.
The helicopter sustained substantial damage and was secured to the deck of the Tai Keystone,which then returned to Hay Point to assist with removal of the helicopter from the vessel.
Context
Helicopter Pilot
The pilot of the helicopter held a commercial pilot licence (helicopter) with a multi‑engine helicopter class rating. Their total flight experience at the time of the incident was 4,880 hours with 300.8 hours on the Agusta A109E and they had recently completed both a proficiency check and line check to a satisfactory standard. The helicopter pilot also held a current class 1 medical certificate.
Helicopter
The helicopter was an Agusta A109E, which was manufactured in 2001 and issued serial number 11129. It was registered in Australia in 2010 as VH-RUA and began operations with the operator in 2017. The Agusta A109E is a multi-engine helicopter with 2 Pratt & Whitney PW206-C engines driving a 4-blade main rotor and a 2-blade tail rotor.
The ATSB was provided aircraft flight data from the onboard spider track recording device. The data provided an updated aircraft position at a maximum of 15 second intervals.
Vessel
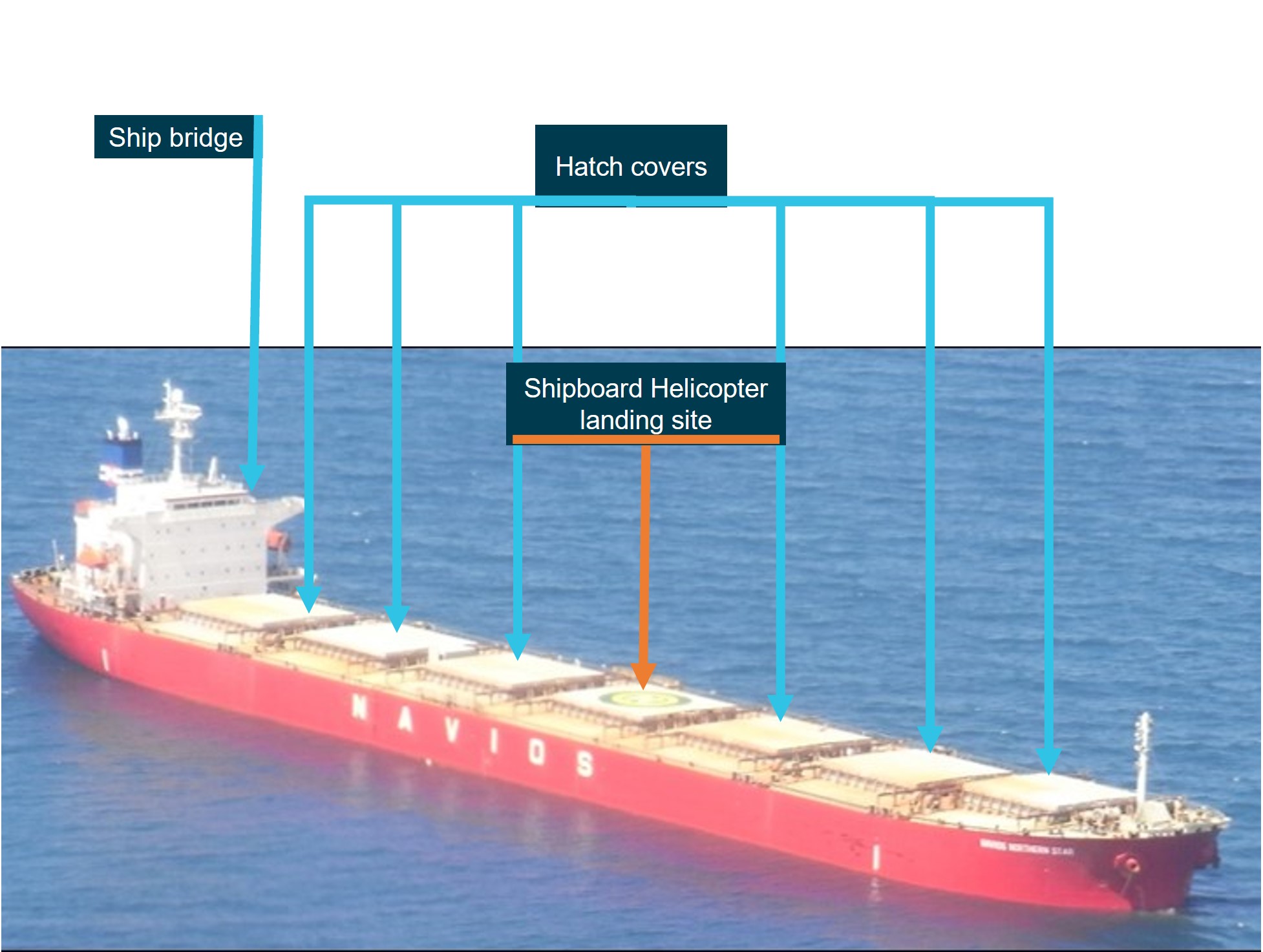
The merchant vessel Tai Keystone was a bulk carrier with an overall length of 228.41 m, it was built in 2017 and provided the unique ship identifier number 9789843 by the International Marine Organisation (IMO). The vessel was operated by the Taiwan Navigation Co Ltd and registered under the Panama flag.
The vessel had several hatch-covers, one of which was used as a shipboard HLS when needed (Figure 1).
Figure 1: Exemplar vessel for reference
Image source: ATSB investigation MO-2016-003 annotated by the ATSB
Handrails
Handrails or stanchions[5] are used as an extension of the ladders installed to gain access to the shipboard HLS (Figure 2). The handrails are removable and usually stowed when the ship is underway. They are normally only installed once the helicopter has landed and removed prior to its departure. The handrails were painted yellow and were about 2.5 cm in diameter by 1 m tall. It was reported that these types of handrails were not considered to be a common feature on vessels.
The marine pilot on board the ship advised they instructed the vessel’s crew to remove the handrails before the helicopter arrived. This request occurred prior to the marine pilot going to the sleeping quarters and when they returned to the bridge, they did not confirm whether this action had been completed.
Figure 2: Starboard[6] handrails (removed at the time of the occurrence)
Image source: helicopter pilot in command
The helicopter pilot reported that, after exiting the helicopter, they observed the vessel’s starboard‑side handrails were removed. However, the port‑side handrails that were struck were still installed (Figure 3).
Figure 3: Handrail positions
Image source: helicopter pilot in command
The HLS was predominantly painted in green with a yellow circle and a white ‘H’. The vessel’s name was also painted in white in the HLS. There was a permanent yellow ladder (Figure 2) leading up to the HLS and yellow painted walkway lines leading to the ladder, on the deck of the ship (Figure 4).
Figure 4: Struck handrail and damaged tail rotor
Image source: helicopter pilot in command
Communication
Once the marine pilot joined the master on the bridge, they advised the helicopter pilot that:
the wind was from 080° at 20 kt
the ship was not pitching
there was no sea spray
emergency crews were on standby
the helicopter had the master’s permission to land.
No information on obstacles was passed to the helicopter pilot.
Helicopter approach
The helicopter pilot advised that they commenced their approach from behind the Tai Keystone on the port[7] side of the vessel as it provided a clear view of the vessel from their position on the right side of the helicopter.
The pilot reported that once the helicopter was turned to align with the HLS, which occurred after they completed their reconnaissance, the instrument panel obscured the undershoot area of the HLS, so they could only see the landing area and not the entire hatch cover. They further advised that, due to the position of the manhole covers, they ensured that during the landing, the nose wheel was slightly back on the ‘H’ on the HLS (Figure 5). It was reported by both the helicopter and marine pilots that it was common for the helicopter tail rotor to hang over the edge of the hatch to avoid other obstacles, such as pipes and vents.
The helicopter pilot also advised that at 300 ft, a narrow yellow pole was almost impossible to detect. In addition, the ladder leading to the poles was painted yellow, there was yellow on the hatch, and yellow lines on the edge of the landing hatch (the yellow walkway) (Figure 4). They advised yellow was a very common colour on a ship and, on this occasion, impeded detection of the port‑side handrails during the approach.
Figure 5: Tai Keystone's helicopter landing site viewed from the bridge
Image source: helicopter pilot in command
Touchdown position
The Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports – design and operation required that an HLS had a helicopter touchdown/positioning marking (TDPM) as follows:
The objective of touchdown/positioning marking (TDPM) is to provide visual cues which permit a helicopter to be placed in a specific position such that, when the pilot’s seat is above the marking, the undercarriage is within the load bearing area and all parts of the helicopter will be clear of any obstacles by a safe margin.
Where there was no limitation on the direction of touchdown/positioning, a touchdown/positioning circle (TDPC) should be used instead. The line width should be at least 1 m.
On this occasion, the helicopter was positioned with the pilot’s seat over the centre of the white ‘H’, rather than as required with the pilot’s seat above the yellow TDPC (Figure 5).
Marine pilot transfer procedures
Helicopter procedures
The operator’s exposition provided the following information on a typical transfer procedure:
…Descend to 500 ft for a recce[8] to confirm wind, obstructions and approach options.
It also stated that this could be amended to suit the variables of weather, pilot experience, type of ship and whether it is day or night.
The exposition also stated that:
• The safety of the helicopter remains at all times the responsibility of the helicopter pilot in command…
• On arrival overhead or approaching each ship a reconnaissance (recce) should be flown. During this recce or circuit, a careful assessment must be made of the relative wind over the deck with particular attention paid to possible obstructions such as stanchions and cranes, etc… For some transfers, several orbits or an approach with overshoot may be required to obtain sufficient information.
• Pilots should exercise caution on final to look for seamen or deck hands who may be in a position on the deck to approach the landing hatch from behind. Look for ladders and/or handrails during the recce and on final. They will have good intention in trying to assist the marine pilot exiting the helicopter but are often over enthusiastic and unaware of the dangers associated with the tail rotor. Therefore, attempt to keep the tail clear of ladders leading to the hatch from the surrounding deck…
The operator advised they did not maintain a database of ships that they regularly worked with, nor did they require the ship operators to provide a copy of the HLS certification. However, prior to each transfer the ship’s master was required to complete a form designed to identify hazards. If any hazardous items were identified, they were to be photographed and the images added to the form. These forms were provided to pilots prior to departure.
The ship’s master completed this form and did not identify any hazards that increased risk for this vessel. Specifically, they advised there were no obstructions higher than 30 cm on the landing hatch.
Vessel procedures
The Hay Point port procedures required that the ship’s master complete a form to show that the ship complied with the Hay Point port procedures. This form was completed and signed by the ship’s master on 19 November 2023 and indicated that there were no obstructions higher than 30 cm on the landing hatch. The form also indicated that the ship would comply with the International Chamber of Shipping Guide to Helicopter/Ship Operations, as per Marine Order 57 (see the section titled International Chamber of Shipping Guide to Helicopter/Ship Operations).
The vessel’s crew completed a helicopter/ship operation safety checklist on 7 December at 0925, prior to the helicopter’s landing. The checklist revision date was 2017 and referenced the International Chamber of Shipping Guide to Helicopter/Ship Operations, for further guidance. This checklist did not include an item to remove handrails/stanchions.
International Chamber of Shipping Guide to Helicopter/Ship Operations
The International Chamber of Shipping Guide to Helicopter/Ship Operations, fifth edition was published in June 2021, the checklist provided in the fifth edition of the guide included:
• Side rails and, where necessary, awnings, stanchions and other obstructions have been lowered or removed.
The guide also included the following additional considerations for helicopter operating areas.
Chapter 4.3.1 General guidance on markings
The recommended colours of the markings reflect current international standards and best practices and promote a standardised approach to helicopter landing area markings. But as the colour of the main deck may vary from ship to ship, there is some discretion in the selection of deck paint schemes, the objective always being to ensure that the markings show up clearly against the surface of the ship and the operating background.
Chapter 4.5 Additional considerations for helicopter operating areas
- Any handrails that exceed the height limitations set out in section 4.1.2 are made retractable, collapsible or removable and do not obstruct access/exit routes. These handrails should be painted in a contrasting colour scheme and procedures should be in place to retract, collapse or remove them before the helicopter arrives.
- Obstructions close to or inside the operating area, which may present a hazard to helicopter operations, need to be readily visible from the air and should be highlighted. Painting of obstructions should follow the scheme set out in Chapter 9 and Appendix E, as appropriate.
Chapter 9.5 Centreline/amidships helicopter landing/operating area plan included a procedure which should be followed when indicating obstructions on the operating area plan.
1. Red and white stripes should be used to mark the location of notifiable objects in either the central clear zone or the obstacle free sector for the breadth of the ship deck…
- Objects in the central clear zone of height exceeding 2.5 cm; and
- Objects around or outside the central clear zone but in the obstacle free sector described as the funnel of approach for the breadth of the ship’s deck of height exceeding 25 cm.
2. Yellow should be used for marking the position of objects in the forward and aft limited obstacle sectors for the width of the ship’s deck to which the attention of the helicopter pilot should be drawn.
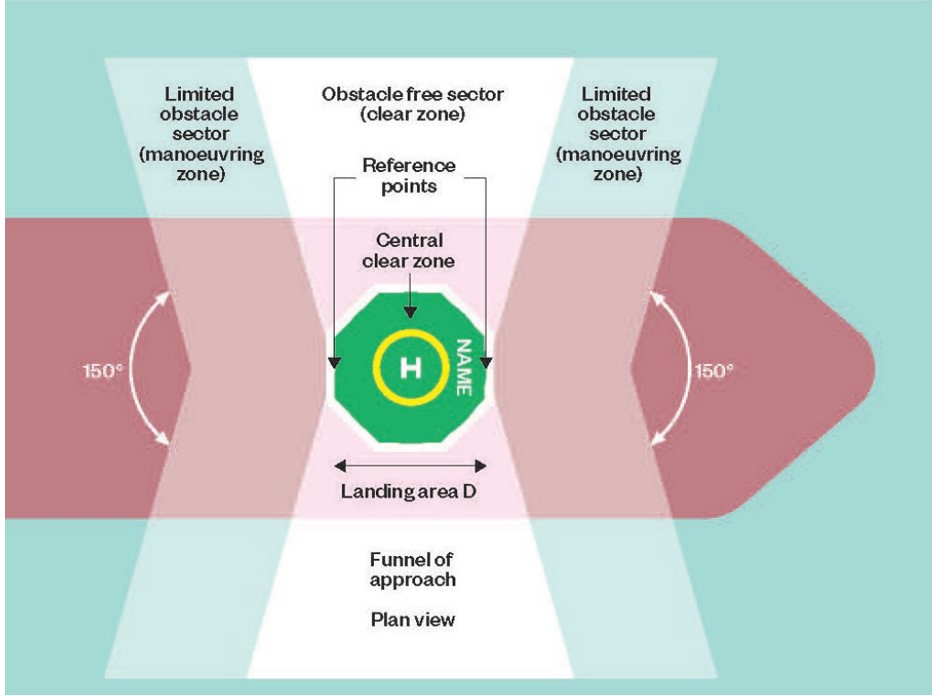
The port‑side handrails were within the obstacle free sector (clear zone) (Figure 6). The clear zone is required to be free of obstacles that present a risk to the helicopter operation.
Figure 6: Landing area terminology
Image source: Civil Aviation Authority UK Civil Aviation Publication 437
Civil Aviation Authority of United Kingdom, Civil Aviation Publication 437
The Civil Aviation Authority (CAA) of United Kingdom published Civil Aviation Publication 437 (CAP 437) Standards for offshore helicopter landing areas. This publication has become an accepted worldwide source of reference for assessing offshore helicopter landing areas.
The CAP 437 provides the same guidance as the International Chamber of Shipping guide for handrails detailed above.
The Australian Civil Aviation Safety Authority published Advisory Circular (AC) 139 Guidelines for heliports design and operation. The AC guidance stated there should be no objects greater than 25 cm or that present a threat to the safe operation of the helicopter on the HLS. However, it did not discuss removable objects, nor a colour to ensure they were visible if accidently left in place.
Australian Marine Safety Authority, Marine Order 57
The Australian Marine Safety Authority, Marine Order 57 specifically defined the International Chamber of Shipping (ICS) guide as the Guide to Helicopter/Ship Operations,fourth Edition (2008), published by Marisec Publications, London, on behalf of the ICS. The fifth edition of this guide was released in June 2021, however Marine Order 57 was not amended to reflect the latest updated/improved document.
Safety analysis
The marine pilot advised that they detected the handrails installed on the helicopter landing site (HLS) and instructed a crew member to remove them prior to the helicopter arriving. The helicopter pilot also advised that only one set of handrails was in place when they landed. As such, it is possible that when the instruction was given to remove the handrails:
one set of handrails was installed, and these were not removed, or
2 sets of handrails were installed, and only one was removed.
The ship’s crew were using an outdated version of the International Chamber of Shipping Guide to Helicopter/Ship Operations checklist, which did not include a specific check for handrails or stanchions. While the ATSB could not identify if the checklist had been completed prior to the marine pilot detecting the installed handrails, it is likely that if the vessel was using the most current version, which included a specific item to check for handrails and stanchions, it would have required a member of the vessel’s crew to actively check the handrails and consequently they would have been removed.
The communication between the helicopter and vessel did not include information regarding obstacles, and because no obstacle information was passed to the helicopter pilot, they believed the HLS would be safe to land on. During the helicopter’s approach to the HLS, the helicopter pilot completed a reconnaissance at 300 ft, which provided an opportunity to identify the obstacle. However, as the handrails were an unusual method of accessing the HLS and due to their size, shape and colour, it is likely they would have been difficult to detect. Since the starboard‑side handrails were not installed, once the pilot aligned the helicopter with the final approach path to the landing site, there were no visual cues alerting them to the possibility that the port‑side handrails had not been removed.
The pilot of the helicopter stated they were aware of the red hatch cover obstacles inside the landing site and decided to avoid them by positioning the helicopter clear of the covers. Consequently, the aircraft was positioned with the pilot’s seat over the white ‘H’ instead of the yellow touchdown/positioning circle. This position put the tail rotor slightly outside the obstacle free sector and resulted in contact with the railing.
The International Chamber of Shipping guide provided guidance that removeable handrails should be painted in a contrasting colour scheme, however it did not identify what the colour should be contrasting with. The guide advised that:
objects in the forward and aft limited obstacle sector should be painted yellow (the handrails were not in this zone)
notifiable objects in the obstacle free sector exceeding 25 cm should be marked in red and white stripes.
However, despite the handrails being within the obstacle free sector, as they were removable, they were not notifiable objects. In addition, the HLS surface was painted green with yellow markings and, the environment surrounding the handrails, including the permanent ladder leading to the handrails, consisted of items which were also mostly painted in yellow. As such, the yellow handrails did not visually stand out to the helicopter pilot.
The helicopter operator’s exposition provided a warning for pilots relating to seamen installing the handrails prior to a helicopter landing. While the main concern was ensuring seamen did not enter the HLS, this indicated that handrails were a known threat. The helicopter pilots were not always provided with a visual representation of HLSs prior to departure. However, they did receive a form completed by the ship’s master which identified if obstacles were present. Often, the first time they saw the landing site was on arrival overhead the vessel, which limited the opportunity to assess possible threats. Despite this, because the handrails were not a notifiable object, it is unlikely that they would have been included in any guidance of the HLS.
The Civil Aviation Safety Authority published Advisory Circular (AC) 139 Guidelines for heliports ‑ design and operation however, when compared with the United Kingdom (UK) Civil Aviation Authority (CAA) Civil aviation publication (CAP) 437 Standards for Offshore Helicopter Landing Areas, it lacked guidance relating to the colour of obstacles inside the HLS clear zone. AC 139 did not encompass the most current guidance available.
As the Tai Keystone was using the guidance from the International Chamber of Shipping guide, despite it being an earlier version, the lack of information in AC 139 was not considered to have contributed to the incident.
The Australian Marine Safety Authority, Marine Order 57 specifically referenced the International Chamber of Shipping guide, however it referred to a superseded version.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the ground strike during a marine pilot transfer, involving an Agusta A109, VH-RUA and ship Tai Keystone, about 240 km north‑east of Mackay Airport, Queensland on 7 December 2023.
Contributing factors
During preparation for the helicopter’s arrival, the port side handrails were not removed.
Prior to the approach, the pilot did not detect the obstacle on the helicopter landing site.
During the landing, the pilot's seat was not positioned over the touchdown/positioning circle resulting in the tail rotor being outside the obstacle clear sector and striking the handrail.
An earlier version of the helicopter operations checklist was used by the crew of the Tai Keystone. That checklist did not include a requirement, present in the version current at the time of the incident, to remove handrails or stanchions from the helicopter landing site. [Safety issue]
The colour of the handrails did not comply with the guidance material provided by the International Chamber of Shipping guide, which increased the difficulty for the helicopter pilot to detect them.
Other factors that increased risk
The Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports – design and operation did not include guidance material for the marking of objects, except for wind direction indicators, located on the helicopter landing site.
The Australia Maritime Safety Authority Marine Order 57 – Helicopter operations, defined the International Chamber of Shipping guide as the fourth edition published in 2008. This was not the latest improved/updated version of the guidance material.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the marine industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action..
Safety issue description: An earlier version of the helicopter operations checklist was used by the crew of the Tai Keystone. That checklist did not include a requirement, present in the version current at the time of the incident, to remove handrails or stanchions from the helicopter landing site.
Safety action not associated with an identified safety issue
Proactive safety action taken by Jayrow Helicopters
Action number:
AO-2023-059-PSA-03
Action organisation:
Organisation name: Jayrow Helicopters Pty. Ltd.
Action status:
Closed
Following this occurrence, Jayrow Helicopters amended their procedures to ensure that helicopter pilots were provided with images of each individual vessel helicopter landing site prior to departure. They were also developing a new pilot checklist that included a requirement to ensure no obstacles existed within the helicopter landing area.
Proactive safety action taken by Australian Maritime Safety Authority
Action number:
AO-2023-059-PSA-04
Action organisation:
Organisation name Australian Maritime Safety Authority (AMSA)
Action status:
Closed
AMSA noted the reference in Marine Order 57 to the 2008 edition of International Chamber of Shipping Guide, not the updated edition 2021. They advised that this outdated information would be noted for correction in its planned review of Marine Order 57.
Glossary
AMSA
Australian Maritime Safety Authority
CAA
Civil Aviation Authority (United Kingdom)
CASA
Civil Aviation Safety Authority
HLS
Helicopter landing site means an aerodrome, including a heliport, intended for use wholly or partly for the arrival, departure or movement of helicopters.
IMO
International Marine Organisation
TDPC
Touchdown/positioning circle
TDPM
Touchdown/positioning marking
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Australian Transport Safety Bureau. (2017). Contact with navigation buoy, Navios Northern Star, Torres Strait, Qld on 15 March 2016. MO-2016-003
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
helicopter pilot
helicopter operator
marine pilot
vessel operator
Tai Keystone Master
Civil Aviation Safety Authority
Australian Maritime Safety Authority
Submissions were received from:
the vessel operator
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Marine pilot is an expert in navigating a ship through specific waters.
[2]Roll: describes the degree to which the vessel tilts from one side to the other about the longitudinal axis.
[3]Master: the person who has command or charge of a vessel, but does not include a marine pilot.
[4]Helicopter landing site: means an aerodrome, including a heliport, intended for use wholly or partly for the arrival, departure or movement of helicopters.
The Australian Transport Safety Bureau has outlined the evidence gathered so far in its ongoing investigation of a fatal light aircraft accident in the Mackay region of Queensland in October.
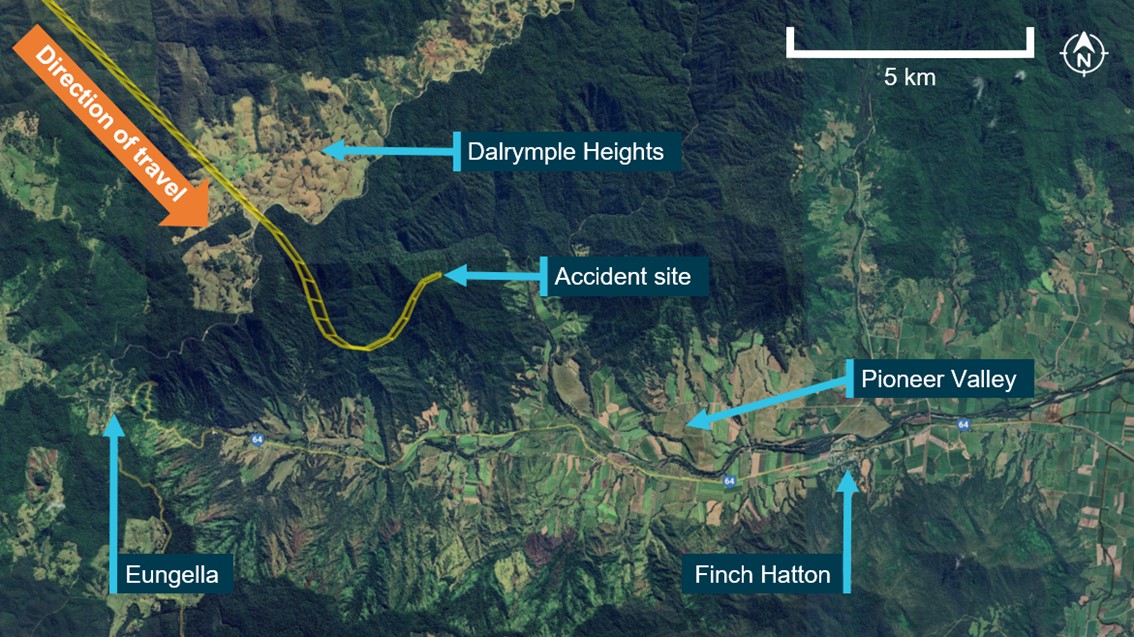
On the morning of 28 October 2023, a SOCATA TB-20 Trinidad single-engine aircraft was destroyed when it collided with terrain near Finch Hatton, west of Mackay. The pilot and passenger on board were fatally injured.
The ATSB’s investigation has so far gathered a range of evidence, which is presented in a preliminary report to provide timely information to industry and public.
Analysis and findings are not included in the preliminary report, and will be detailed in the investigation’s final report.
ATSB investigators were not able to deploy to the accident site, due to its inaccessible location and extreme surrounding terrain, and degradation of the site itself.
However, detailed on-site photographs, provided by Queensland Police Service specialist forensic officers, have provided investigators an understanding of the accident site location and layout, and an appreciation of the level and type of damage to the aircraft’s structure and components.
“The photographs indicate the aircraft’s propeller was under a significant level of power when it impacted with terrain, indicating the engine was almost certainly operational at the time of the accident,” ATSB Director Transport Safety Dr Stuart Godley said.
The evidence-gathering phase of the ATSB’s investigation has also included witness interviews, a review of flight data and air traffic control recordings, and an examination of the aircraft’s maintenance history.
“The accident flight was intended as a private flight from Montpellier aircraft landing area to Palmyra aircraft landing area,” Dr Godley detailed.
About 40 minutes into the flight, the pilot reportedly told a friend, via phone call, that they were at 5,500 ft and above cloud, and asked about weather conditions at Palmyra.
“The pilot stated they were passing Dalrymple Heights and on descent, and that their intentions were to fly along the Pioneer Valley to Palmyra.”
The aircraft’s OzRunways flight track showed, about 20 minutes after the phone call, the pilot made a right turn, followed by a left turn, before the aircraft collided with the northern side of Bull Mountain, at about 1,900 ft above sea level.
“As the investigation progresses, the ATSB will conduct a further review of recorded data and recovered components from the accident site, and will analyse available flight data,” Dr Godley said.
“The investigation will also include analysis of aircraft maintenance and repair information.”
A final report will be released once the investigation is complete.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Dr Godley concluded.
On 7 December 2023, at 1930 local time, a Robinson R22 Beta 2 helicopter, registered VH-DLD, departed from Bloodwood Station, Northern Territory, on a private flight to Gorrie Station, Northern Territory. The helicopter was last seen by witnesses on the ground at about 1945 and a search for the helicopter was initiated at about 2015. The wreckage was found on the afternoon of 9 December. The helicopter was destroyed and the pilot, who was the sole occupant, was fatally injured.
What the ATSB found
The ATSB found that the pilot departed after last light for a return home flight on a dark night but was not qualified to fly at night and the helicopter was not equipped to be flown at night. While it was reported that the pilot had some night flying experience, the helicopter was not fitted with an artificial horizon. Without the minimum instruments and training, it was unlikely that the pilot would have been able to orientate the helicopter without external visual references.
It is likely that during the return home flight, the helicopter entered a smoke plume associated with bushfires under dark night conditions and the pilot became spatially disorientated after losing external visual references. This resulted in the helicopter colliding with terrain uncontrolled at high speed.
Safety message
Night conditions can result in little to no useable external visual cues and in these environments day visual flight rules (VFR) pilots are at risk of spatial disorientation and loss of control of their aircraft. The ATSB’s Avoidable Accidents No 7 - Visual flight at night accidentsprovides further discussion of these risks and how they have contributed to accidents. The requirement to only operate under daylight conditions, and plan to land 10 minutes before last light, provides a reliable method for ensuring there are sufficient external visual references available to safely operate.
In 2022, the Civil Aviation Safety Authority published their advisory circular for the night visual flight rules rating, AC 61-05 v1.1 - Night VFR rating (casa.gov.au), which provides guidance on the requirements for the granting of night VFR ratings, as well as the conduct of operations under night VFR. The advisory circular highlighted the hazards of night flying and provided advice to pilots and others on how to safely conduct night operations. The ATSB encourages everyone involved in night flying or considering night operations to familiarise themselves with the contents of the advisory circular.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
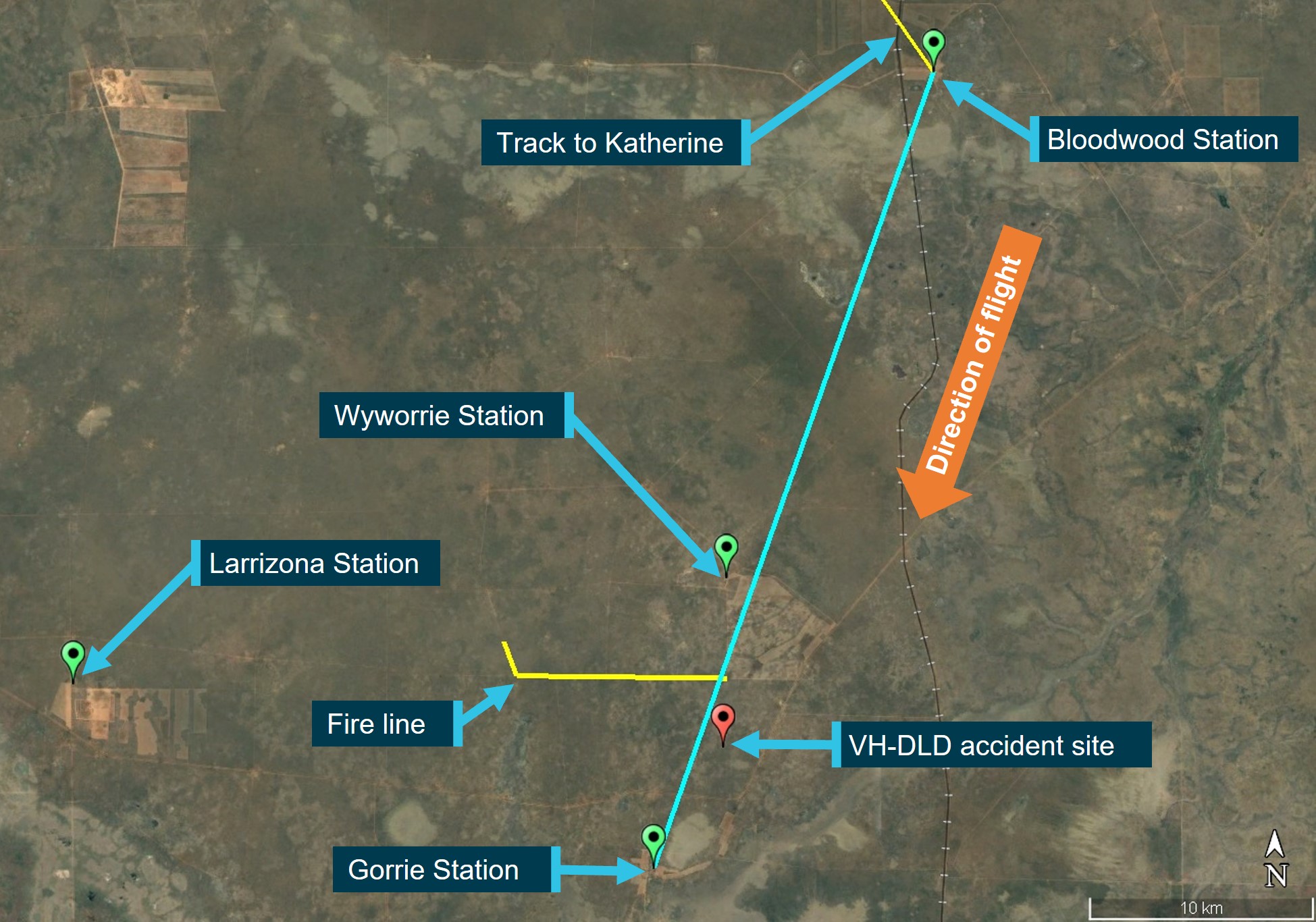
On 7 December 2023, at about 1930[1] local time, a Robinson R22 Beta 2 helicopter, registered VH-DLD, departed from Bloodwood Station, Northern Territory (NT) on a private flight to the pilot’s home at Gorrie Station, NT (Figure 1). The pilot was the sole occupant. Bloodwood was located about 48 NM south-east of Katherine, where last light[2] was at 1924 on 7 December. The flight from Bloodwood to Gorrie was about 21 NM on a direct track of 200° (True).
Figure 1: Direct track from Bloodwood Station to Gorrie Station
The track line from Bloodwood Station to Gorrie Station is representative of a direct track and not the actual flightpath. The position of the fire line was based on a hand drawing by the pilot’s relative based at Wyworrie Station.
Source: Google Earth, annotated by ATSB
Earlier in the evening, just after 1900, the caretaker at Gorrie switched the helicopter hangar lights on to illuminate the helicopter landing pad.[3] The caretaker then received a radio call from the pilot at about 1915 to request the activation of the lights, to which the caretaker replied that the lights were already on. This was about the time the helicopter arrived at Bloodwood where the pilot had stopped for a brief social visit. Just prior to 1930, the owner of Bloodwood advised the pilot that it was getting dark outside and offered the pilot a bed for the night. However, the pilot declined the offer and departed. The owner of Bloodwood reported that it was about a 17-minute flight from Bloodwood to Gorrie in the R22 in calm conditions.
At about 1945, two of the pilot’s relatives, who were sitting outside for dinner at Wyworrie Station (located about 13.5 NM along the track from Bloodwood to Gorrie), observed the silhouette of the helicopter, with the navigation and strobe lights on, pass in front of their homestead, tracking towards Gorrie. They both noted the helicopter was tracking towards smoke from fires located on the southern boundary of Wyworrie. It was at about this time that the pilot made another radio call to the caretaker at Gorrie to confirm the lights were on. The caretaker checked outside and then confirmed that they were on. At this stage, the caretaker started to become concerned because the pilot sounded a ‘little bit disorientated’ and the caretaker could not recall the pilot ever previously challenging the status of the lights.
Residents at Larrizona Station, located 14.7 NM west-north-west of Gorrie, monitored the same radio frequency as Gorrie and Wyworrie. The manager at Larrizona heard the radio calls between the pilot and the Gorrie caretaker about the lights. They reported that the second radio call at 1945 was unusual because the clarity of the call on the Larrizona radio indicated the helicopter was likely close to Gorrie and that the pilot should have been able to see the lights.
At about 2015, the Gorrie caretaker called the pilot’s relatives at Wyworrie to ask if the helicopter had landed there. On being advised that the helicopter had not landed at Gorrie, the pilot’s family initiated the search and rescue process. At about 1730 on 9 December, the helicopter wreckage was found about 4 NM (7.5 km) south of the Wyworrie homestead and 3.3 NM (6.1 km) north‑north‑east of the Gorrie homestead.[4] The pilot was fatally injured.
Context
Pilot information
The pilot was initially issued with a commercial pilot licence (helicopter) on 7 April 2011,[5] and held a class endorsement for single-engine helicopters with a low-level and an aerial mustering rating for helicopters. The pilot completed a Class 1 medical examination on 24 January 2023 and a flight review on 13 February 2023 in a Robinson R44 helicopter. The pilot recorded 6,700 flight hours experience on the medical examination submission and the medical certificate was issued with 2 restrictions – for distance vision correction and for a headset to be worn.
The remains of a headset were found at the accident site and one of the pilot’s relatives reported the pilot always flew with prescription sunglasses and had prescription glasses for driving at night. However, it was unknown if the pilot was wearing the night driving glasses during the flight. The pilot did not hold a night visual flight rules (VFR)[6] rating but had reportedly completed some night flying training and had arrived home after last light on previous occasions.
Helicopter information
The helicopter, registered VH-DLD, was a 2-seat Robinson Helicopter Company R22 Beta 2 helicopter, serial number 3675, powered by a Textron Lycoming O-360-J2A 4-cylinder piston engine (Figure 2). The helicopter was manufactured in the United States in 2004, first registered in Australia on 31 August 2004, and issued with a Certificate of Airworthiness on 7 October 2004.
Figure 2: VH-DLD
Source: Pilot’s relative
The most recent maintenance release was issued on 11 October 2023 for day VFR operations[7] at an aircraft time in service of 7,144.4 hours. The current maintenance release was not recovered from the helicopter and was likely lost or destroyed during the accident sequence. The last 2,200‑hour airframe inspection was completed in February 2021 at 6,457.9 hours, which was 686.5 hours prior to the latest maintenance release. The ATSB’s logbook review did not identify any anomalies with the maintenance of the helicopter.
Environmental conditions
Local observations
At the town of Katherine, located about 48 NM north-north-west of Bloodwood Station, moonset was at 1403, sunset was at 1900 and last light was at 1924. On the afternoon of the accident there were bushfires in the area and back-burning had been initiated on the southern boundary of the Wyworrie Station, between the Wyworrie and Gorrie homesteads, to provide fire breaks. The terrain between the Wyworrie and Gorrie homesteads was described as flat and therefore unlikely to cause terrain shielding effects.
One of the pilot’s relatives at Wyworrie described the conditions at the time the helicopter flew past Wyworrie Station as 'very dark, no moon, and complete nightfall'. There were 2 fires to the south of the Wyworrie homestead with one located about 1 km south of the homestead. The bushfire smoke resulted in hazy conditions, such that it became dark earlier, and the direction the helicopter was flying was towards the smoke. The relative reported that at nightfall the wind became calm, which stopped the smoke drifting away and resulted in it hanging in the air.
The pilot’s other relative at Wyworrie, who was also a helicopter pilot, reported the only hazard that night was the smoke and recalled ‘there was a lot of smoke’. They had flown the same flightpath in the past and reported that the pilot ‘would have flown into the smoke’ based on the direction the helicopter was tracking as it flew past Wyworrie. They also reported that the pilot could have flown around the smoke but that it might have been too dark for the pilot to see the smoke.
The owner of Bloodwood Station reported there was no smoke at their homestead when the helicopter departed but observed a lot of smoke in the vicinity of Gorrie Station later in the night after the search was initiated. The manager of the Larrizona Station reported that the conditions were ‘really dark, no moon’ and that there was smoke blowing across the road between the Larrizona and Gorrie Stations.
Bureau of Meteorology
A graphical area forecast for the NT was issued by the Bureau of Meteorology at 1337 on the day of the accident and valid for the period from 1430 until 2030. The forecast divided the NT into 3 areas: area A, B and C. The location of the accident site was near the boundary of area A, which extended northward, and area B, which extended southward. There was no smoke forecast for area A. However, area B included a forecast for isolated[8] areas of visibility reduced to 5,000 m in smoke below 10,000 ft. Satellite imagery provided by the Bureau of Meteorology revealed smoke in the vicinity of the accident site was present throughout the day. A comparison of the daytime and night-time satellite images revealed the smoke likely became more widespread in the vicinity of the accident site after last light.[9]
Collision and wreckage information
The ATSB did not attend the accident site and the following information was derived from analysis of imagery provided by the NT Police. The imagery included ground-based photography and filming, and aerial photography and filming with a remotely piloted aircraft system.
Accident sequence
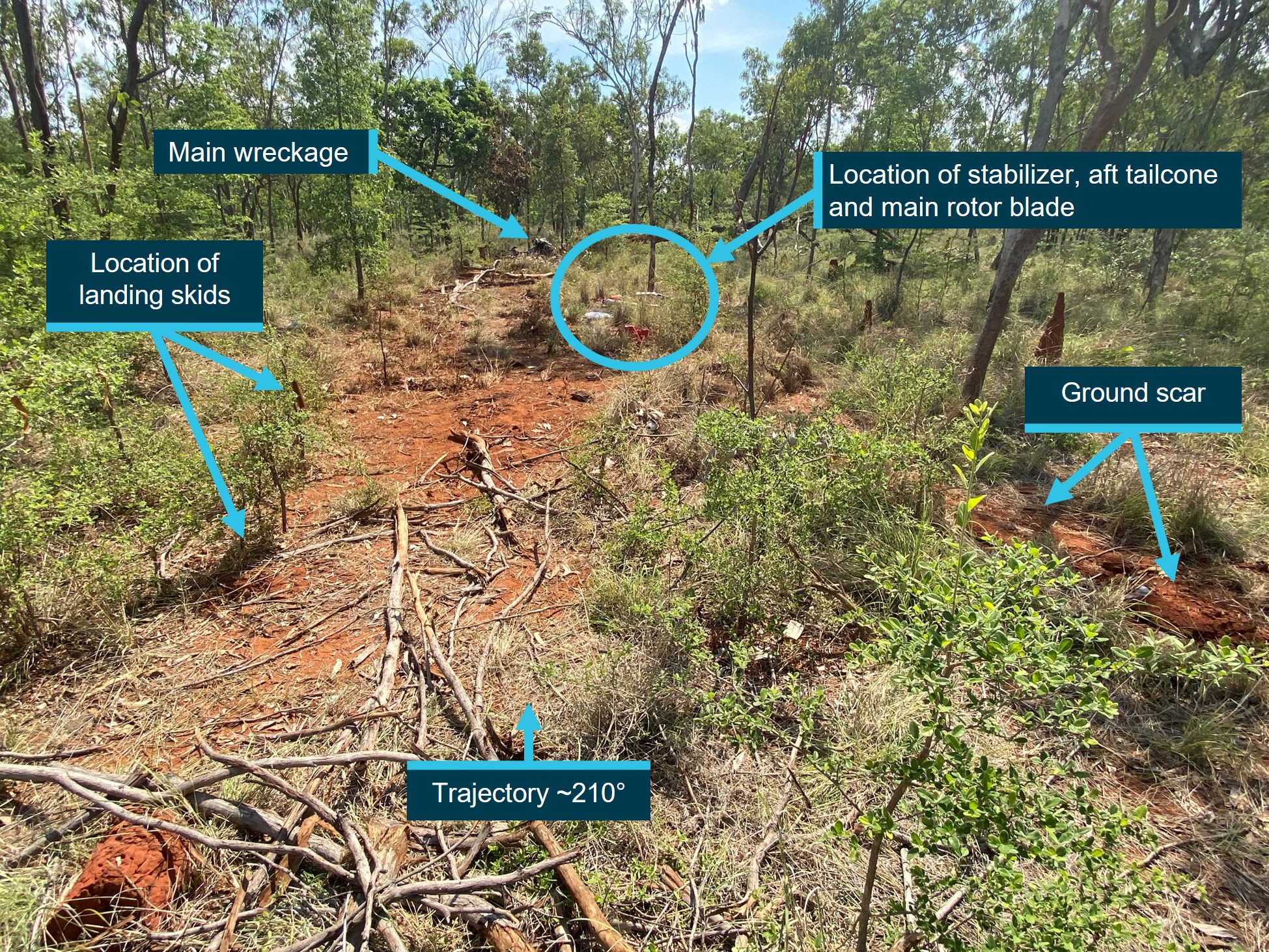
The helicopter initially struck a tall tree, breaking tree branches and the cabin perspex, before impacting the ground. The direction of travel was about 210° (True). There was a prominent ground scar on the right side of the main wreckage trail, which exhibited a pattern of multiple ground strikes and was the start of the ground impact sequence. Two broken sections of the landing skids were found buried in the ground on the left side at the start of the main wreckage trail, one after the other with the second one protruding. They were estimated by the police to be about 8 ft apart (Figure 3).[10] The fronts of the landing skids were otherwise not identified among the images of landing skid debris in the wreckage.
Figure 3: Location of broken landing skids
Source: Northern Territory Police, annotated by ATSB
Following the initial ground contact, subsequent ground contact caused the helicopter to become significantly fragmented. The vertical and horizontal stabilizer assembly separated from the tailcone and were found on the right side of the wreckage trail, followed by the aft section of the tailcone with the tail rotor and driveshaft, followed by one of the main rotor blades. The entire cabin forward of the vertical firewall was destroyed. The trail from the initial tree strike to the main wreckage was estimated by the ATSB to be about 46 m in length (Figure 4).[11]
Figure 4: View of the wreckage trail
Source: Northern Territory Police, annotated by ATSB
The helicopter battery was found beyond the main wreckage at a distance estimated by the police to be about 15-20 m. An outboard section of the attached main rotor blade separated from the rotor blade and was estimated by the police to be about 75 m beyond the main wreckage. The main wreckage was consumed by a post-impact fire that was contained within the immediate area. There was no evidence of fire in the trail leading to the main wreckage site or on any parts separated from the airframe outside the immediate area.
Engine and fuel systems
The engine was lying on its left side (as installed) in the main wreckage. No engine controls were identified. The alternator and exhaust system were present. Of the 2 uppermost cylinders, the induction system was present and the upper and lower spark plugs were noted as fitted with the ignition leads attached. The engine starter ring gear, lower sheave and 2 engine oil coolers were identified in the wreckage and the cooling fan fibreglass shroud had collapsed around the fan assembly. The fuel tanks were not identified and were likely consumed in the post‑impact fire. The engine carburettor, air filter housing and related ducting were not identified.
Flight control system
A review of the images of the helicopter flight control system identified that the pitch link to the separated blade spindle was present, intact, and securely attached to the swashplate rotating ring. The opposite pitch link was not identified. Of the 3 control tubes attached to the swashplate stationary ring, the rod ends were identified and found to be securely attached. The control tubes were consumed in the fire but the jackshaft was identified. The pilot’s collective and cyclic controls were not identified but a portion of the cyclic torque tube and aft bellcrank was identified with control rod ends attached and hardware present. The tail rotor pitch links, and the pitch change mechanism at the tail gearbox were present and connected.
Rotor systems and drive train
One of the main rotor blades separated in the accident sequence while the other remained attached to the rotor head. The detached blade showed evidence of upward and aft bending that presented as a significant upward bend at the blade root and buckling of the trailing edge (Figure 5). The detached blade also lost a small portion of the trailing edge section; however, the blade tip was present and attached. The opposite (attached) main rotor blade exhibited trailing edge buckling and had lost a section of the outer portion including the tip (found about 75 m beyond the main wreckage), which was consistent with the blade striking an object. A strike mark in the shape of a main rotor blade profile was present on the left side of the tailcone and the intermediate flex coupling exhibited significant tension, which indicated the tailcone was probably separated by a main rotor blade strike after the initial ground impact.
Figure 5: Aft tailcone and bent main rotor blade
Source: Northern Territory Police, annotated by ATSB
The tail rotor gearbox and tail rotor assembly were attached to the tailcone and both tail rotor blades were attached to the hub with one blade exhibiting signs of a strike and the other significantly bent near the root. The drive train from the engine to main gearbox was identified with the input yoke, forward flex plate and clutch yoke found to be fastened together. The upper sheave was identified but the drive belts were not visible and likely consumed by fire. The tail rotor drive shaft and damper bearing assembly were identified in the tailcone.
Instruments and electrical systems
The lower instrument panel was located near the start of the wreckage trail. The upper instrument panel was located closer to the main wreckage with the airspeed indicator gauge. The needle in the airspeed indicator indicated about 88 kt. The engine ignition switch was identified and found with the key broken off in the barrel. The position of the switch was aligned with ‘BOTH’, indicating that both magnetos were selected, which is the normal position for flight.
Survivability
During the search and rescue process, the Australian Maritime Safety Authority produced a Timeframe for Survival Briefing Report. The report noted that the pilot was physically fit with no known heart conditions or long-term health issues and there were no mental or physical health concerns held by the pilot’s immediate family, which was consistent with the pilot’s last medical examination report. The pilot had managed the cattle station property since 1988 as well as neighbouring properties at various points in time and was therefore familiar with the area. The impact-activated emergency locator transmitter had been removed from the helicopter and the pilot carried a portable emergency beacon and a satellite phone. The helicopter was fitted with a global positioning system and ultra-high frequency radio and the pilot reportedly always carried a 2 L bottle of water in the helicopter and a larger container of water if mustering.
The NT forensic pathologist post-mortem examination report found that the overall pattern of injuries was consistent with forces sustained in a helicopter accident from a ‘substantial height and/or at high-speed.’ The ATSB’s review of the impact and wreckage trail was consistent with the pathologist’s conclusion and the accident was not considered to be survivable.
Previous accidents
Collision with terrain occurrences at night are often fatal and the ATSB has investigated several Robinson R22 accidents in which the helicopter was not equipped to be operated at night and the pilot was not qualified to fly at night. This accident was the third in the last 3 years. The previous 2 accidents were:
Of the 26 accidents during night visual conditions, half involved a loss of aircraft control, most likely due to the influence of perceptual illusions caused by the lack of visual cues. The other half involved controlled flight into terrain (CFIT), where the pilot probably did not know of the terrain’s proximity immediately before impact.
Civil Aviation Safety Authority advisory circular
In 2022, the Civil Aviation Safety Authority published version 1.1 of their night VFR rating advisory circular, AC 61-05 v1.1 - Night VFR rating (casa.gov.au), in which they described the safety case for the night VFR rating as follows:
Night flying accidents are not as frequent as daytime flying accidents; however, significantly less flying is done at night. Statistics indicate that an accident at night is about two-and-a-half times more likely to be fatal than an accident during the day. Further, accidents at night that result from controlled flight into terrain (CFIT) or uncontrolled flight into terrain (UFIT) are very likely to be fatal accidents. Loss of control by pilots flying under NVFR [night VFR] has been a factor in a significant number of fatal accidents.
The hazards and risks section of the advisory circular included the expected dark adaptation time for the human eye, which can take up to 30 minutes to fully adjust to darkness. It also described ‘black-hole’ operations as those conditions where there are insufficient external visual cues present to allow for aircraft orientation.
There were several sections of the advisory circular specific to night helicopter operations, which included the following information:
6.3.4 Rotorcraft operations
6.3.4.1 The pilot must be able to maintain the rotorcraft's orientation by use of visual external cues as a result of lights on the ground or celestial illumination, unless the aircraft is fitted with an autopilot, stabilisation system or is operated by a two-pilot crew.
6.3.4.2 When flying at night, it is good practice to select a route via high visual cueing areas, such as a populated or lighted area, or a major highway or town that will make navigation easier and offer more options in the event of an emergency.
6.5.5 Requirements for flight
6.5.5.2 In order to conduct operations safely and legally at night in a rotorcraft, the visual cueing environment must be accounted for in the planning and execution of NVFR [night VFR] rotorcraft operations.
Safety analysis
On 7 December 2023, moonset and last light at Katherine, NT, were at 1403 and 1924 respectively, which resulted in dark night conditions. At 1930, the pilot departed Bloodwood Station on a private flight to return home to Gorrie Station. The weather at Bloodwood was described as a clear, moonless night, and the track from Bloodwood to Gorrie was away from the major population centres that might otherwise have provided an artificially illuminated horizon.
A review of the pilot’s qualifications and aircraft logbook found the pilot and helicopter were limited to day VFR conditions. The pilot had some night flying experience but the helicopter was not equipped for night flight, specifically, there was no artificial horizon. Without the necessary instruments and training it was very unlikely that the pilot would have been able to orientate the helicopter without external visual references.
The pilot’s relatives at Wyworrie Station observed the helicopter fly past their homestead, at about 1945, where conditions were very dark with smoke from fires between Wyworrie and Gorrie. This was consistent with the estimated flight time between Bloodwood and Wyworrie and indicated that despite not being night VFR rated, the pilot was able to operate the helicopter at night under clear conditions. However, the relatives also noted the helicopter was flying into the smoke as it tracked towards Gorrie and at this time the pilot was heard making a radio call to the caretaker at Gorrie, questioning if the hangar lights were on. This was a source of lighting the pilot would likely have been able to see under clear conditions from overhead Wyworrie and the caretaker thought that the pilot sounded disorientated. The last radio call from the pilot, dark night conditions, change in weather conditions at nightfall and satellite imagery of the distribution of smoke after last light all suggested the pilot inadvertently flew into the smoke.
The helicopter wreckage was later found about 7.5 km south of the Wyworrie Station homestead, and 6.1 km north-north-east of the Gorrie Station homestead, where it had collided with terrain on a track consistent with the direction towards Gorrie. The forecast reduction in visibility to 5 km in smoke likely resulted in the lights at both Gorrie and Wyworrie being beyond visual range for the pilot at the location of the accident site. It is also possible the pilot’s eyesight may not have fully adapted to the darkness at the time of the accident and the ATSB could not determine whether the pilot was wearing their prescription night driving glasses.
The ground scar to the right of the main wreckage path and discovery of the broken landing skids buried in the ground on the left side of the main wreckage trail followed by the lower instrument panel indicated that the helicopter was likely in a nose down, right roll attitude when it collided with terrain. The discovery of the helicopter battery about 20 m beyond the main wreckage, and an outboard section of one of the main rotor blades about 75 m beyond the main wreckage, indicated a high energy collision in terms of both the helicopter airspeed and rotor speed. The evidence from the witnesses, forecast conditions and the impact and wreckage trail indicated the pilot likely lost external visual references in smoke on a dark night after passing the Wyworrie Station homestead and became spatially disorientated, which resulted in the helicopter colliding with terrain uncontrolled at high speed.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into smoke on a dark night and collision with terrain involving Robinson R22, VH-DLD, 112 km south‑south‑east of Tindal Aerodrome, Northern Territory on 7 December 2023.
Contributing factors
The pilot departed after last light for a return home flight on a dark night but was not qualified to fly at night and the helicopter was not equipped to be flown at night.
It is likely that the pilot became spatially disorientated after the helicopter entered a smoke plume under dark night conditions during the return home flight, which resulted in uncontrolled flight into terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Australian Maritime Safety Authority
Bureau of Meteorology
Civil Aviation Safety Authority
maintenance organisation for VH-DLD
Northern Territory Office of the Coroner
Northern Territory Police
Robinson Helicopter Company
witnesses.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Robinson Helicopter Company
United States National Transportation Safety Board.
A submission was received from the Civil Aviation Safety Authority. The submission was reviewed and, where considered appropriate, the text of the draft report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The owner of Bloodwood Station received a phone call at 1930, as the helicopter departed.
[2]Last light: the time when the centre of the sun is at an angle of 6° below the horizon following sunset. At this time, large objects are not definable but may be seen and the brightest stars are visible under clear atmospheric conditions. Last light can also be referred to as the end of evening civil twilight.
[3]The hangar lighting included internal floodlights and 2 external spotlights, 1 pointed downward onto the pad and the other pointed upward.
[4]It was likely that the continued presence of smoke, degree of damage and accident site located among trees hampered the location of the wreckage.
[5]The pilot was re-issued with a commercial pilot licence (helicopter) on 6 May 2015 in accordance with the new flight crew licencing regulations.
[6]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[7]The helicopter was fitted with instrument lighting but it was not equipped with the minimum instrument requirements for night VFR flight. Specifically, there was no attitude indicator installed to provide the pilot with an artificial horizon.
[8]Isolated: Individual features which affect or are forecast to affect up to 50% of an area.
[9]A night-time temperature inversion could trap smoke and prevent it dispersing but the data was not available for this location to confirm the presence of an inversion.
[10]Paced out by NT Police onsite. The distance between the R22 landing gear skids is 6 ft 4 inches.
[11]This distance was estimated by scaling and overlaying imagery on Google Earth.
The pilots of a BAE 146 freighter aircraft which flew below minimum safe altitude during a night approach to Rockhampton were likely experiencing fatigue and were dealing with a high workload, an Australian Transport Safety Bureau investigation has found.
On the morning of 5 January 2023, two pilots were operating a Pionair Australia BAE 146-200 on a night freight flight from Brisbane to Rockhampton, Queensland.
At about 3:30am the crew began a straight-in, required navigation performance (RNP) approach to Rockhampton’s runway 33, but discontinued due to low cloud.
Following the missed approach, the crew climbed the aircraft to 4,500 ft and entered the holding pattern before descending to the minimum holding altitude of 3,500 ft.
“The captain’s normal practice for a straight-in approach was to have the aircraft descending to cross the initial approach fix at about 5,000 ft, and to continue descending to the next waypoint while remaining above the 3,000 ft minimum safe altitude for that segment of the approach,” ATSB Chief Commissioner Angus Mitchell explained.
“However, prior to this second approach, the flight crew were conducting the holding pattern at 3,500 ft.
“The aircraft subsequently passed through the initial approach fix on its second approach at that lower altitude, but the captain commenced descending as per their normal practice – resulting in the aircraft incorrectly descending along a profile consistent with being one approach segment further along than its actual position.”
The aircraft subsequently descended below the minimum safe altitude for the first two segments of the RNP approach to runway 33.
As the aircraft descended towards the minimum descent altitude in the second segment of the approach, the pilots recognised their low altitude, and commenced another missed approach.
At about the same time, the aircraft’s ground proximity warning system activated.
The ATSB found the captain commenced the second approach descent early, based upon their incorrect application of their preferred regular descent technique.
The first officer did not identify the early descent due to an incorrect mental model of the aircraft’s position in relation to the required flightpath.
“The ATSB found that due to the time of the approaches and inadequate sleep, both flight crewmembers were likely experiencing a level of fatigue known to adversely affect performance,” Mr Mitchell added.
“This, in combination with a period of high workload associated with the missed approach and second approach, led to the early descent and monitoring errors.”
The ATSB also found the operator’s flight crew rosters were within regulations, but they were irregular and disruptive to the flight crew’s sleep patterns.
“This adversely impacted the flight crew’s ability to obtain adequate sleep prior to the incident flight.”
The ATSB’s SafetyWatch initiative, which highlights broad safety concerns stemming from its investigation findings and occurrence data reported by industry, has improving the management of fatigue as one of its priorities.
“Managing fatigue is a shared responsibility. This incident emphasises the importance of operators providing predictable and stable rosters to support pilots in achieving adequate sleep,” Mr Mitchell concluded.
“It is equally important pilots monitor their own health and wellbeing to ensure they are well-rested, especially when conducting overnight operations.”
An Australian Transport Safety Bureau investigation highlights to pilots planning to fly amateur (kit) built aircraft the importance of being aware of potential differences in systems and controls compared to type-certified factory-built aircraft.
Two pilots were fatally injured when their amateur-built Glasair aircraft collided with terrain shortly after a landing and go-around at Wedderburn aircraft landing area, south-west of Sydney, on 26 December 2022.
The aircraft, a Stoddard Hamilton Aircraft Glasair Super II FT, was powered by a Subaru automotive engine modified for aviation use, and was originally assembled from a kit in the United States.
It accumulated about 60 flight hours before being sold by its original owner to the two pilots, who then had it transported to Australia.
Earlier on the day of the accident, the pilots conducted the aircraft’s first flight since it was reassembled, flying from Bankstown to Temora. While at Temora, the pilots conducted two circuits, before landing and then subsequently setting off for Wedderburn about an hour later.
On arrival at Wedderburn, the aircraft landed and conducted a go-around, during which it failed to achieve sufficient climb performance and impacted terrain about 2.7 km to the south-west of Wedderburn airfield. The two pilots on board were fatally injured.
The aircraft wreckage was consumed by a post-impact fire, limiting the evidence available for ATSB examination. As such, the reasons for the insufficient climb performance after take-off could not be determined, however the ATSB’s investigation report highlights key safety messages for amateur-built aircraft pilots.
“Pilots intending to operate amateur-built aircraft should be aware of the potential differences in systems and controls to that of conventional type-certified aircraft,” ATSB Director Transport Safety Dr Stuart Godley said.
“They should also use familiarisation flights to better understand the systems, controls, and emergency operations specific to the aircraft they are flying, and they should use an appropriate aerodrome, and benign weather conditions, for these flights.”
The ATSB’s final report notes the pilots were both highly experienced in multi-engine fixed wing operations, and both held a valid Air Transport Pilot (Aeroplane) Licence, but neither had recent experience in single-engine operations, automotive engine conversions, amateur-built aircraft, or the Glasair in general.
The report also notes the pilots elected to operate the aircraft from Bankstown to Temora for its first flight in Australia, despite the aircraft’s special flight authorisation not permitting operation over built-up areas.
“Understanding the safety implications of regulatory permissions is vital so that experimental aircraft do not adversely affect the safety of third parties, such as other airspace users and people on the ground,” Dr Godley said.