Although further analysis is required to establish the contributing factors in this accident, the circumstances as far as they are known at this time suggest that the helicopter encountered turbulence, followed by a low‑g condition immediately prior to the in‑flight break‑up. The ATSB therefore considers it prudent to draw attention to Robinson’s advice regarding flight in turbulent conditions and avoidance/recovery from low‑g flight until such time as the factors that contributed to this accident can be fully established.
Awareness of conditions likely to produce turbulence, and slowing down prior to encountering turbulence, could increase the time available to recognise and respond to a low-g condition in Robinson Helicopters.
What happened
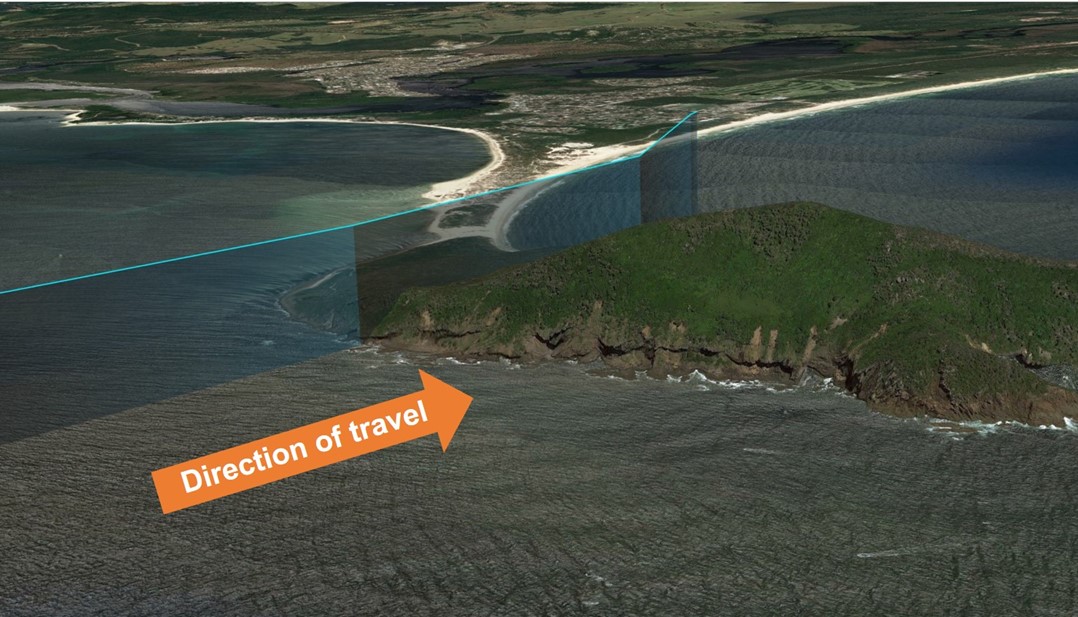
On 26 October 2023, the pilot of a Robinson R66 helicopter encountered mechanical turbulence flying over Yacaaba Headland, NSW, which resulted in a rapid loss of control and subsequent in-flight break-up.
Why did it happen
Prior to encountering turbulence, the aircraft was traveling at an airspeed which may have increased the severity of the aerodynamic effects of the turbulence. This possibly reduced the time available for the pilot to recognise and recover from a low-g condition, and avoid a loss of control.
Safety advisory notice
AO-2023-051-SAN-001: The ATSB advises all operators of Robinson helicopters to be aware of the possibility of mechanical turbulence and avoid it whenever possible. If it is not possible to avoid flying through an area where mechanical turbulence is anticipated, reduce airspeed to 60–70 kt in accordance with Robinson Safety Notice 32, prior to encountering turbulence.
Slow down prior to suspected turbulence
Robinson Helicopters’ handling characteristics in low-g and turbulent conditions are well documented and detailed in Robinson Helicopter Safety Notices SN-11 & SN-32 respectively. In both cases an increased airspeed affects the severity of the resulting aircraft response, and increases the likelihood of mast bumping and in-flight break-up.
It is possible that, at high airspeeds, an encounter with turbulence may produce a reaction that requires an immediate and decisive response from the pilot to ensure the safety of flight. As outlined in Robinson Safety Notice 11, a low‑g (weightless) condition can result in a powerful right roll. In such circumstances, ‘The rotor must be reloaded before lateral cyclic can stop the right roll. To reload the rotor, apply an immediate gentle aft cyclic, but avoid any large aft cyclic inputs.’
As airspeed increases, the time available for the pilot to recognise and respond to undesirable aircraft states is significantly reduced.
Pilots are reminded to remain vigilant at all times and to continuously assess conditions to identify the possibility for turbulence. Where any doubt exists, pilots should reduce airspeed prior to entering an area with potential for turbulence to reduce the effects of, and increase the available response time to, an upset condition.
On 19 March 2024, a Fairchild SA226-TC Metroliner, registered VH-KGX and operated by CASAIR, taxied at Geraldton, Western Australia for runway 03. About one minute later, a Beechcraft A36 Bonanza, registered VH-CKX and operated by Shine Aviation, taxied for runway 14. After reaching their respective runway thresholds, both pilots attempted to contact the other, however, they did not hear each other, nor could they see each other. A third aircraft assisted by relaying information. Based on the information received, the Bonanza and Metroliner pilots commenced their take-off within 3 seconds of each other. The Metroliner crossed runway 14 about 400 m in front of the Bonanza, with a vertical separation of about 250–300 ft.
What the ATSB found
The ATSB found that, when aircraft were positioned at the thresholds of runway 03 and 14 (and 08), they will unlikely be visible to each other due to the position of the airport buildings. Further, they may not be contactable on VHF radio due to potential shielding effects. This resulted in the pilots being unable to verify each other’s position and intentions prior to commencing their take-off.
While the pilot of the third aircraft was attempting to assist, the details provided were inaccurate and incomplete. This inadvertently resulted in misinterpretation by the Bonanza and Metroliner pilots and influenced their decision to take off.
What has been done as a result
CASAIR emphasised to its flight crew that in situations where communication difficulties were identified, flight crew should stop or slow down until completely assured of the situation. Further, to assist in flight preparation and planning, CASAIR amended its aerodrome documentation to include a caution regarding limited visibility and potential VHF shielding at Geraldton.
Shine Aviation highlighted to its pilots the importance of being completely certain of other aircraft’s position and intentions and not making assumptions. It also advised that, when a third party provided assistance, that pilot should take responsibility for accurately communicating all relevant information. Further, although CTAF radio communications were an assessed item for pilot checks, it was not included in their training syllabus, which has since been amended.
Geraldton Airport conducted informal radio checks and identified that, when operating at opposite ends of the aerodrome, VHF shielding was possible. It has submitted an amendment to the En Route Supplement Australia to highlight this possibility.
Safety message
Operations at non-controlled aerodromes require pilots to monitor traffic and maintain separation through the use of VHF radio in conjunction with a vigilant lookout. This principle of alerted see and avoid can be an effective measure against collisions. However, situations may arise where VHF radio communications difficulty is encountered and/or visibility is limited. In this case, it is critical that pilots take all reasonable measures to verify the position and intentions of known traffic. A third party may be available to assist and when doing so, that party must ensure they accurately relay all relevant information. Where necessary, all involved should actively organise a separation plan.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the collision risk around non-towered airports.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 19 March 2024, at about 0803 local time, a Fairchild SA226-TC Metroliner aircraft, registered VH-KGX and operated by CASAIR, began taxiing for runway 03 at Geraldton, Western Australia, for a flight to Cobra Station with the pilot and 9 passengers. A minute later, a Beechcraft A36 Bonanza aircraft, registered VH‑CKX and operated by Shine Aviation, began taxiing for runway 14 for a flight to East Wallabi Island with the pilot and 5 passengers.
The pilots of both aircraft made appropriate broadcasts (refer to section titled CTAF audio recordings) on the common traffic advisory frequency (CTAF),[1] and after reaching their respective runway thresholds, attempted to establish radio contact to ascertain their position and intentions. Both pilots reported that they were unable to establish contact with the other, nor were they able to see the other from their relative positions.
At the same time, VH-MVQ, a Cessna 172 (company aircraft to the Bonanza) was on taxiway Charlie, holding short[2] of runway 14. The pilot attempted to assist by providing traffic information, initially to the Bonanza pilot and later to the Metroliner pilot. The Cessna pilot’s last traffic advice was not addressed to a particular aircraft and advised that both aircraft were holding short for each other.
Both the Bonanza and Metroliner pilots later reported that, following that transmission they believed that they were safe to proceed with their take-off. At 0808:38, the Bonanza pilot broadcast that they were rolling on runway 14, which was followed immediately by the Metroliner pilot broadcasting that they were rolling on runway 03. Neither pilot heard the other pilot’s rolling call. The Metroliner commenced take-off at 0808:52 followed 3 seconds later by the Bonanza (refer to section titled Flight tracking data).
The pilot of a GA-8 Airvan (VH-AVP, another company aircraft to the Bonanza) was waiting in line behind the Cessna and reported that, when they became aware of a potential conflict, they made a transmission to alert the Bonanza pilot. By this time the Bonanza had advanced 100 m along the runway, but the pilot did not hear this transmission and continued their take-off. The Metroliner pilot heard the call, however, as they were past their low speed abort regime, they elected to continue their take-off.
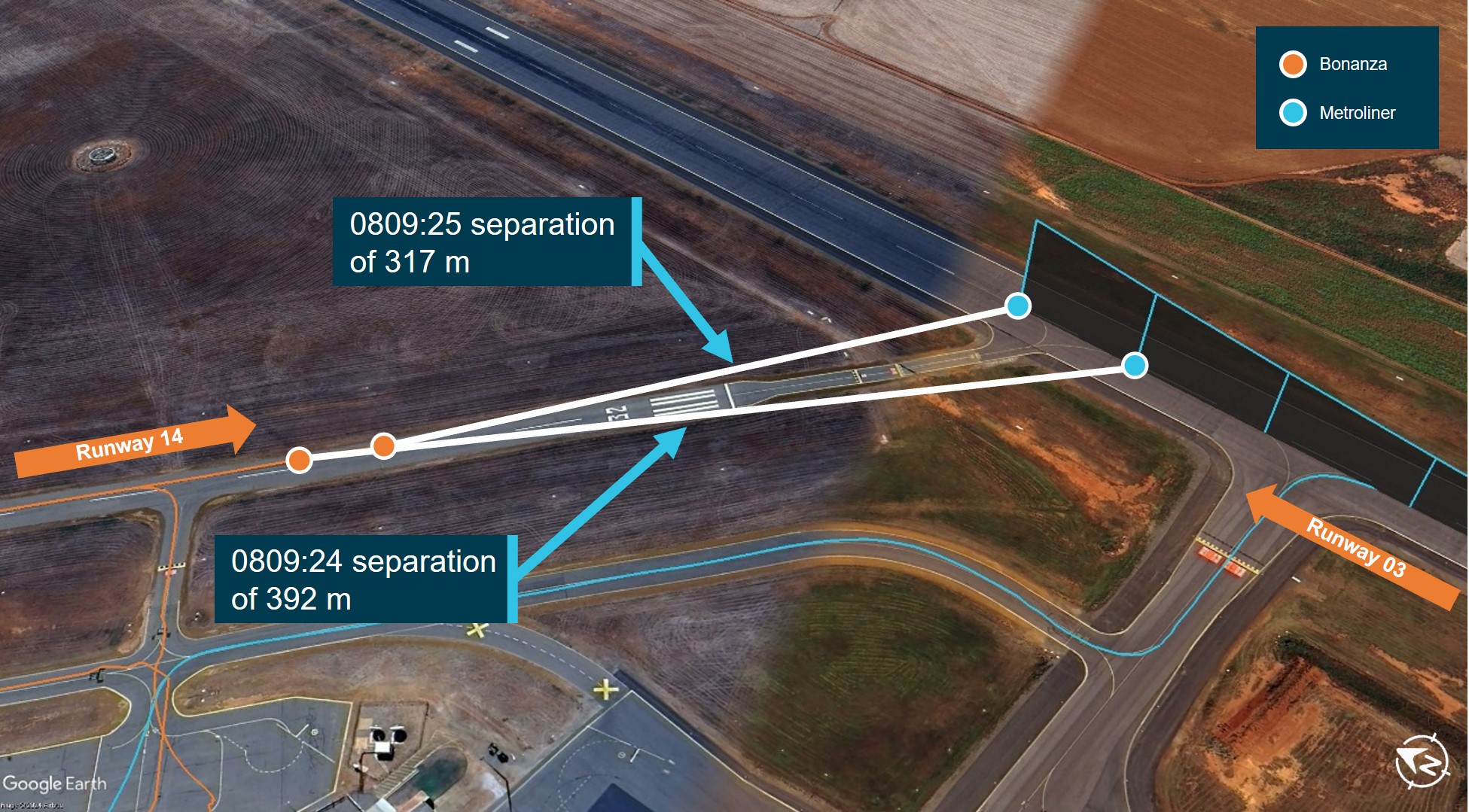
The Metroliner entered the runway 14 strip just before 0809:24, about 400 m ahead of the Bonanza, with a vertical separation of 250–300 ft. The Metroliner cleared runway 14 one second later (Figure 1). Once both the Bonanza and Metroliner were airborne, the pilots were able to establish and maintain effective 2-way radio communications with each other.
Figure 1: Closest position of VH-CKX (Bonanza) and VH-KGX (Metroliner)
Source: Google Earth, with recorded data overlaid and annotated by the ATSB
Context
Pilot information
VH-CKX
The pilot held a commercial pilot licence (aeroplane) and a valid class 1 aviation medical certificate. They reported a total of 2,127 flying hours of which they had flown 155 hours on type. Their last proficiency check was in March 2024.
The pilot reported being familiar with operations at Geraldton having been based there for over 4 years.
VH-KGX
The pilot held an air transport pilot licence (aeroplane) and a valid class 1 aviation medical certificate. They reported a total of 13,092 flying hours, which included 1,632 hours on type. Their last proficiency check was in December 2023.
The pilot reported having operated at Geraldton about 6 times in recent months.
Aircraft information
VH-CKX was a Beechcraft A36 Bonanza single piston-engine aircraft manufactured in the United States in 1974 and was first registered in Australia in 1974. The Bonanza has a maximum seating capacity of 6, including the pilot.
VH-KGX was a Fairchild SA226-TC Metroliner twin turboprop aircraft manufactured in the United States in 1980 and was first registered in Australia in 1997. VH-KGX was configured to carry a maximum of 12 passengers and 2 flight crew.
Meteorological information
The weather at Geraldton at the time of the incident was good with visibility greater than 25 km and no cloud below 10,000 ft. The wind was 140° (south-easterly) at 19 kt, which favoured operations on runway 14 and runway 21. The pilot of the Metroliner initially planned their departure from runway 21 but amended this to runway 03 to allow for an on‑track departure.
Geraldton Airport
General information
Geraldton Airport was a certified, non‑controlled aerodrome located 11.11 km to the east‑south‑east of the city of Geraldton, Western Australia. Its elevation was 122 ft, and it had 2 sealed runways, 03/21[3] and 14/32, with a third gravel runway 08/26.
Geraldton Airport was located within class G uncontrolled airspace. The CTAF was assigned the discrete very high frequency (VHF) 126.8 and it had an aerodrome frequency response unit.[4]
Visual limitations
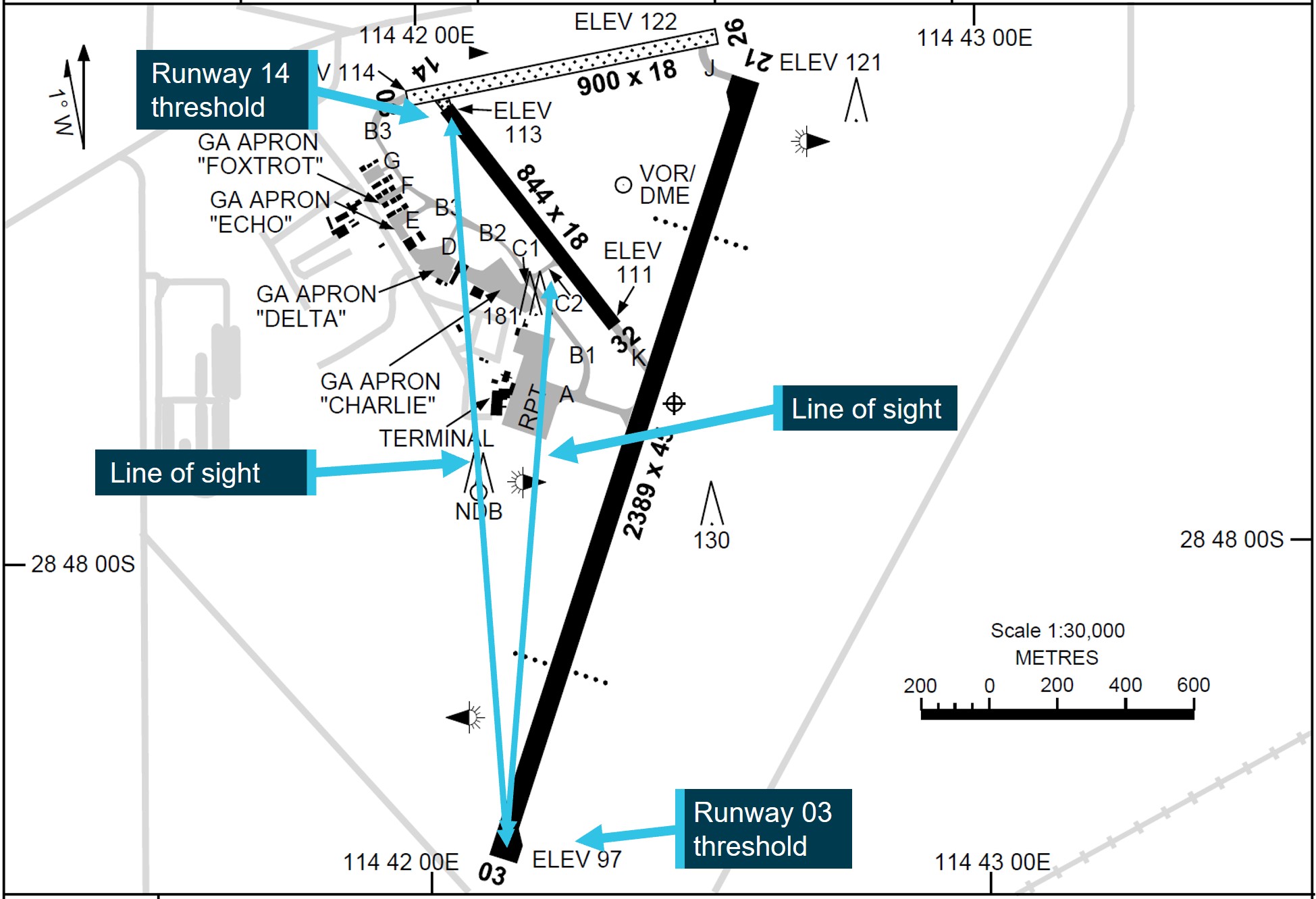
The thresholds of runways 03 and 14 were separated by a distance of 2,168 m and the majority of airport infrastructure such as the terminal, hangars and aprons were situated between those thresholds (Figure 2).
Figure 2: Geraldton Airport chart extract
Source: Airservices Australia, annotated by the ATSB
The En Route Supplement Australia provided information to pilots on the operations specific to each aerodrome. The entry for Geraldton Airport did not include any information about visibility between the thresholds of runways 03 and 14 (or 08).
The pilots involved in this incident reported not being able to see each other from the thresholds of their respective runways and photographs obtained from Geraldton Airport (Figure 3, Figure 4) showed the visibility from the 03 and 14 runway thresholds.
Figure 3: View of runway 14 threshold from runway 03 threshold
Source: Geraldton Airport, annotated by the ATSB
Figure 4: View of runway 03 threshold from runway 14 threshold
Source: Geraldton Airport, annotated by the ATSB
Recorded information
CTAF audio recordings
A recording of the CTAF transmissions at the time of the incident was obtained and a summary of the key transmissions is in Table 1.
Table 1: Geraldton CTAF radio transmissions
Time
Station
Transmission
0804:15
VH-KGX
Geraldton traffic, Metro Kilo Golf Xray entering backtracking amended runway zero three, Geraldton.
0804:31
VH-CKX
and traffic Geraldton, Charlie Kilo Xray taxis runway one four departure to the northwest
0806:48
VH-CKX
Metroliner, Charlie Kilo Xray, your current position please.
0807:13
VH-CKX
Metroliner for runway zero three, Charlie Kilo Xray.
0807:23
VH-CKX
Mike Victor Quebec, Charlie Kilo Xray, do you know Metroliner’s position?
0807:30
VH-MVQ
Charlie Kilo Xray, Mike Victor Quebec, yeah, he’s still on the runway hasn’t departed yet, I’m guessing he’s on centre.
0807:36
VH-CKX
Garbled transmission with interference to begin, then:
Understood.
0807:38
VH-KGX
Kilo Golf Xray is just holding zero three for a moment, Geraldton.
0807:53
VH-KGX
Geraldton traffic for departure on runway one four, say your position please.
0808:01
VH-CKX
Metroliner runway zero three, Charlie Kilo Xray.
0808:15
VH-MVQ
Charlie Kilo Xray, Mike Victor Quebec, ah yeah, I don’t know if you got his last transmission but he's holding short runway zero three.
0808:22
VH-KGX
roger, understand traffic, it's coming through a bit muffled, just understand that you’re holding short confirm.
0808:34
VH-MVQ
ahh right now, ahh you guys are both holding short for each other. (confirmed as VH-MVQ)
0808:38
VH-KGX
Garbled transmission with interference to begin, appears two stations transmitting at same time, then:
Roger.
0808:39
VH-CKX
OK copy that, Charlie Kilo Xray, Metroliner… pause... we're lining up shortly rolling 14 overhead departure outbound to the north-west climbing two thousand five hundred.
0808:50
VH-KGX
Geraldton traffic, Kilo Golf Xray rolling runway zero three.
0809:08
VH-AVP
[Bonanza pilot’s name] he’s rolling.
Flight tracking data
Flight tracking data was retrieved from both the Bonanza and Metroliner. Key locations and associated transmissions/events are shown in Figure 5.
At the time the pilot of the Metroliner transmitted their entering/backtracking call (Figure 5, Label 1), the tracking data showed their position as approaching taxiway A, with the Bonanza located at apron C. When the Bonanza pilot made their taxi call the Metroliner was just entering runway 03 and both aircraft were still within line of sight (Figure 5, Label 2).
At 0806:48 (Figure 5, Label 3), the Bonanza was lined up and holding on runway 14 when the pilot made their first attempt to contact the Metroliner. The Metroliner had not yet reached the threshold of runway 03 and lined up on runway 03 at 0807:30.
At 0808:52, the Metroliner commenced its take-off roll, followed by the Bonanza rolling at 0808:55. When the Airvan pilot attempted to alert the Bonanza at 0809:07, the Bonanza had progressed about 100 m along runway 14. The Metroliner had progressed about 400 m (Figure 5, Label 4).
The Metroliner entered the runway strip of runway 14 just prior to 0809:24, about 400 m in front of the Bonanza, with about 250–300 ft vertical separation (Figure 5, Label 5). It was clear of runway 14 just after 0809:25. The Bonanza reached the centreline of runway 03 at 0809:33 by which time the Metroliner was at a distance of 560 m and climbing away from the Bonanza.
Figure 5: Flight tracking data overlay
Source: Google Earth with recorded data overlaid and annotated by the ATSB
Communication between the aircraft
Interviews with the pilots of the Metroliner, Bonanza and Cessna confirmed that all 3 had recognised some difficulty in communicating. The CTAF audio recordings confirmed that although both pilots attempted to, they did not establish direct contact with each other. There were a number of transmissions that were not responded to and some instances of over transmission or interference in the 2-minute period prior to the incident.
The Bonanza pilot reported that the last radio transmission heard from the Metroliner was their entering/backtracking broadcast.
The Metroliner pilot reported they heard several garbled/muffled transmissions during their taxi for runway 03 but they were only able to understand 2 transmissions, one of which was what they believed was that 4 aircraft were holding for runway 14. The other transmission heard was ‘[Bonanza pilot’s name] he’s rolling’.
Decision to take off
The Bonanza pilot reported that, when they lined up on runway 14, they had expected the Metroliner to have already departed. Although they had asked the Cessna pilot about the Metroliner, they did not request the Cessna pilot to directly contact the Metroliner to confirm their position and intentions. After being advised by the Cessna pilot that both aircraft were holding for each other, the Bonanza pilot reported that they believed this gave them the opportunity to announce they were rolling and commence take-off.
The Metroliner pilot had expressed some mild frustration at being delayed following refuelling at Geraldton, due to having to locate their passengers. They did not report any time pressure but said that they could accept the tailwind on runway 03, which would allow an on track departure. The Metroliner pilot reported that of the radio transmissions that they were able to understand, they believed they heard that 4 aircraft were holding on runway 14. They understood this to be that those aircraft were waiting for the Metroliner allowing them to announce rolling and commence take-off.
Third party assistance
The Cessna pilot reported being able to clearly hear both the Bonanza and the Metroliner pilots, but they could only see the Bonanza. However, from the broadcasts, the Cessna pilot realised there was some confusion as to who was communicating with each other. When making the broadcast stating ‘right now you guys are both holding for each other’, the Cessna pilot stated during interview that this transmission was not directed at a particular aircraft, and they intended to let both know they were holding for each other. By the time they realised both aircraft had commenced take-off, the Cessna pilot assessed it was too late for the Bonanza to stop and therefore did not make an advisory broadcast.
Operations at non-controlled aerodromes
At and around non-controlled aerodromes, pilots are required to be aware of other aircraft by maintaining a listening watch on the appropriate frequency. In accordance with Civil Aviation Safety Regulations Part 91 Manual of Standards Chapter 21, pilots must also make radio broadcasts when reasonably necessary to avoid the risk of collision with another aircraft.
This is the basis of alerted see and avoid. An ‘alerted’ search is one where the pilot is alerted to another aircraft’s presence, typically through radio communications or aircraft based alerting systems. Broadcasting on the CTAF to any other traffic in the vicinity of a non-controlled aerodrome is known as radio-alerted see-and-avoid and assists by supporting the pilot’s situational awareness and visual lookout for traffic with the expectation of visually acquiring the subject in a particular area.
Civil Aviation Safety Authority advisory circulars AC 91-10[5] and AC 91-14[6] provided additional guidance on the recommended broadcasts which focus on the provision of a pilot’s position and intentions to enhance situational awareness. AC 91-10 advised:
8.6.1 Whenever pilots determine that there is a potential for traffic conflict, they should make radio broadcasts as necessary to avoid the risk of a collision or an Airprox event. Pilots should not be hesitant to call and clarify another aircraft’s position and intentions if there is any uncertainty.
8.6.4 In addition to making their own broadcasts, pilots should listen to other broadcasts by other aircraft, an air traffic service or CA/GRS to increase situational awareness.
AC 91-14 advised:
10.1.5 Pilots should be mindful that transmitting information by radio does not guarantee receipt and complete understanding of that information. Many of the worst aviation accidents in history have their genesis in misunderstanding of radio calls, over-transmissions, or poor language/phraseology which undermined the value of the information being transmitted.
10.1.6 Without understanding and confirming the transmitted information, the potential for alerted see-and-avoid is reduced to the less safe situation of unalerted see-and-avoid.
VHF communication at Geraldton Airport
VHF radio requires line of sight between stations in order to maximise transmission quality. Obstacles between stations such as terrain and buildings can attenuate the radio signal, in terms of both strength and clarity. VHF radio is also susceptible to over transmission, where 2 stations transmit at the same time, which may cancel one or both transmissions. Neither the Bonanza nor the Metroliner had any other devices or aids for traffic awareness other than VHF radio.
Following the incident, Geraldton Airport staff conducted informal radio tests at the thresholds of runway 03 and 14 using vehicle mounted VHF radios. They noted a number of factors that could impact radio signal strength, including vehicle height in comparison to aircraft height, radio age/condition and if the radio was handheld or vehicle mounted. However, the testing identified varied levels of VHF radio reception and that there was the possibility of shielding due to the buildings.
On 6 June 2023, a Piper PA-28-161, registered VH-ENL, taxied for runway 36 at Mildura, Victoria. At about the same time, a QantasLink Bombardier DHC-8-315 (Dash 8), registered VH-TQH, began to taxi for runway 09. Both aircraft broadcast their intentions on the local common traffic advisory frequency. The pilot of the PA-28 was aware of the Dash 8, but the crew of the Dash 8 were not aware of the PA-28. Both aircraft commenced their take-off at about the same time and the Dash 8 crossed ahead of the PA-28 at the runway intersection of 09/36 by about 600 m.
The pilot of the PA-28 was unable to visually sight the location of the Dash 8 due to airport buildings and assumed that the Dash 8 was still backtracking on runway 09. They did not directly contact the Dash 8 to positively organise separation. They also incorrectly referred to the runway direction at Mildura Airport as ‘runway 35’ instead of ‘runway 36’.
The Dash 8 crew was focused on obtaining their pre-departure information from air traffic control and had the volume for the radio tuned to the common traffic advisory frequency turned down. An over transmission from air traffic control meant that the Dash 8 crew only received certain elements of the PA-28 pilot’s radio calls. This likely led to an incomplete comprehension of traffic by the Dash 8 crew who believed that the PA-28 was not at Mildura (due to the incorrect reference to runway 35). However, they did not seek further information of the source of the radio calls to positively identify the traffic location.
The investigation found that, due to the topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The Dash 8 crew did not give a rolling call on runway 09, nor were they required to. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off.
Safety analysis
Introduction
On 19 March 2024, a Fairchild SA226-TC Metroliner, registered VH-KGX, commenced a take-off on runway 03 at Geraldton, Western Australia. About 3 seconds later, a Beechcraft A36 Bonanza, registered VH-CKX, began to take off on runway 14. The Metroliner crossed runway 14 about 400 m in front of the Bonanza, with a vertical separation of about 250–300 ft.
This analysis will examine the factors relating to the communication issues regarding the position and intentions of each aircraft, and the location of the airport buildings potentially affecting visibility and radio calls when positioned at the runway thresholds.
Verification of traffic
The configuration of Geraldton Airport meant that when aircraft are operating simultaneously from the runway 03 and 14 (or 08) thresholds, they are likely not visible to each other, obstructed by the airport buildings situated between them. This was consistent with the photographs later taken from the runway thresholds. In this situation, pilots are solely reliant on VHF radio communications for maintaining situational awareness with other aircraft. However, from the informal testing conducted by Geraldton Airport and as shown in a previous ATSB investigation at a different airport, the location of infrastructure may also result in shielding of VHF transmissions, potentially rendering them weak and/or unreadable.
Both the Bonanza and Metroliner pilots were aware of each other’s presence prior to commencing their taxi and attempted to maintain contact in preparation for their departure. However, when at either end of the aerodrome (for runway 03 and 14), they were unable to make direct contact with each other, with several transmissions reported as being weak and unreadable or unheard, as evidenced by the CTAF audio recordings and interviews with both pilots. Further, the pilots were unable to see each other’s aircraft when at the thresholds. Therefore, it was likely that the buildings between the Metroliner and Bonanza aircraft had the effect of radio shielding, preventing the pilots from directly communicating, and limited visibility of their respective positions. Consequently, their only option was to relay information via the Cessna pilot, who was able to communicate with both aircraft, despite only being able to see the Bonanza.
Third-party assistance
The Cessna pilot who attempted to provide assistance did not directly ask either pilot about their intentions prior to each commencing their take-off and therefore did not have all the relevant information to relay. They also mistakenly transmitted an incorrect position for the Metroliner, advising the Bonanza pilot that the Metroliner was holding short of runway 03, instead of holding on runway 03. It was also noted that the Cessna pilot had made a broadcast intended for both pilots advising that were holding for each other.
Both the Bonanza and Metroliner pilots, based on advice from the Cessna pilot, thought that the other was holding, although neither had positively verified with each other or with the intermediary Cessna. Consequently, the advice influenced their understanding that they could safely proceed, announce rolling and commence take-off, which occurred at the same time and increased the potential for a collision.
While the Cessna pilot was not required to communicate what was occurring, nor were they responsible for the decisions made by the other pilots, they were in a position to be able to reduce confusion and increase situational awareness of all parties. As described in the Civil Aviation Safety Authority guidance, the transmission of information by radio does not guarantee that it will be received or understood. Therefore, it is imperative that all parties ensure the accurate transmission of all relevant information and verify receipt when necessary to prevent misunderstandings.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the near collision involving Beechcraft A36, VH-CKX, and Fairchild SA226-TC, VH-KGX, at Geraldton Airport, Western Australia, on 19 March 2024.
Contributing factors
Due to the position of the airport buildings at Geraldton Airport, aircraft on the thresholds of runway 03 and 14 (and 08) are likely not visible to each other and may experience VHF radio shielding. This resulted in the pilots being unable to verify each other’s position and intentions for their take-off.
The pilot of a third aircraft attempted to relay information to the incident pilots to assist with the communication difficulties. However, the details provided inadvertently lead to misinterpretation by the incident pilots, influencing their decision to take off.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by CASAIR (VH-KGX)
Following an internal investigation of the incident, company guidance for operations at Geraldton Airport were revised to notify flight crew that caution was required with multiple aircraft movements on intersecting runways and that communication shielding may obscure any traffic conflict. The revised guidance also included a caution that aircraft operating from runway 03 may not see or hear aircraft operating on runway 08 or 14.
CASAIR also reviewed ground radio selection procedures to ensure optimum communications but found the most effective option based on equipment and antenna installation was already in practice.
CASAIR included discussion of the incident in a flight crew meeting, emphasising the inclusion of airfield limitations in their preparation and planning. Further, where a significant reduction in communications quality was identified, flight crew should stop or slow down until they are completely assured of the situation.
Safety action by Shine Aviation (VH-CKX)
Shine Aviation conducted an internal investigation and scheduled an agenda item for its next flight crew meeting. It would discuss ensuring sufficient 2-way communication was established with any aircraft believed to be operating in the vicinity and where a third party assists that this party should take responsibility for accurately communicating with all involved. The operator also advised that its flight crew must be completely certain of other aircraft position and intentions, and not assume anything prior to proceeding. The operator has also provided its investigation report to Geraldton Airport for review and possible action with regard to potential VHF shielding.
Shine Aviation noted that, while CTAF radio communication and awareness was assessed during line training and any check flights, it was not documented in the line training syllabus and an amendment was actioned to correct this.
Safety action by Geraldton Airport
The Geraldton Airport manager discussed the incident with the pilots and the operator, and believed that the circumstances were relatively rare but has highlighted the possibility of VHF radio shielding to their airport team. Geraldton Airport has also submitted an amendment to the En Route Supplement Australia to alert pilots to the possibility of radio shielding when operating at opposite ends of the aerodrome.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of VH-CKX and other pilots who conducted flights for the operator
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of VH-CKX
the pilot of VH-KGX
the pilot of VH-MVQ
CASAIR
Shine Aviation
the Civil Aviation Safety Authority
Geraldton Airport.
Submissions were received from the:
pilot of VH-KGX
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Common traffic advisory frequency (CTAF): a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome or with a broadcast area.
[2]The term ‘holding short’ typically indicates that the aircraft has stopped at the marked runway holding point and that no part of the aircraft extends onto the runway.
[3]Runway numbering: represents the magnetic heading closest to the runway orientation.
[4]Aerodrome frequency response unit (AFRU): a device that provides an automatic response when the pilot transmits on the traffic frequency (normally a CTAF) for a particular non-controlled aerodrome. This helps pilots to both confirm they are using the right frequency and makes them aware of potential traffic in the area.
A Cirrus SR22 landing accident at Bankstown Airport highlights both the hazards of inadvertent discharge of rocket-propelled parachute recovery systems to first responders and the challenges of conducting a go-around to recover from an unstable landing.
The ATSB investigation report from the accident details that at the end of a private flight from Southport, Queensland on 17 March 2023, the SR22, with a single pilot on board, sank during landing and bounced along the runway for about five seconds, before rapidly entering a steep climbing turn to the left, up to about 40 ft off the ground.
As its bank angle exceeded 90°, the aircraft dropped onto the left wing and nose, coming to a rest upside down on the grass between runways.
The ATSB found that in the early stages of a go-around from the unstable landing, the pilot was unable to counter the substantial torque effect associated with high engine power, low airspeed, and high pitch angle, resulting in loss of control and collision with terrain.
Emergency services extricated the pilot from the wreckage, but the pilot later died in hospital due to injuries sustained in the accident.
“The site commander was initially unaware that the aircraft was equipped with a rocket-propelled parachute, which was subsequently made safe from inadvertent activation by a Cirrus-qualified maintenance engineer,” ATSB Director Transport Safety Stuart Macleod said.
While the aircraft’s Cirrus Airframe Parachute System (CAPS) is credited with saving a number of lives, Mr Macleod noted it presents a serious post-accident hazard where it has not been deployed and the aircraft is damaged.
“If the rocket is inadvertently activated, anyone in its path would be seriously or fatally injured,” he said.
While Cirrus has issued an Advisory Guide for First Responders(Opens in a new tab/window) to provide awareness of CAPS and to reduce the risk of inadvertent post-accident activation, the ATSB found the training and education provided by Cirrus on the hazards of CAPS post-accident had limited reach, and that the placards installed on the accident aircraft type did not clearly communicate the danger or provide access to safety information.
Since the accident, Cirrus has enhanced the external placarding on two new aircraft models (including the SF50). It is also reviewing the possibility of enhancing the placard that was certified with its SR20, SR22 and SR22T aircraft.
Mr Macleod noted the investigation also highlights that a go-around to recover from an unstable landing is more dynamic and presents a greater challenge than a go-around on approach.
“The go-around procedure requires careful and coordinated flight control and power application, in particular when conducted in the landing phase,” he said.
“Pilots should consider the increased challenge presented by making a go-around decision to recover from an unstable landing, rather than an earlier go-around decision made on approach.”
The investigation also highlights that pilots of single-engine aircraft with relatively high-power engines need to be aware of the potential for significant torque effect and loss of control associated with high engine power, low airspeed, and high pitch attitude.
On 8 March 2024, the pilot of an Aero Commander 500-S, registered VH-MEH and operated by GAM Air, was conducting a return cargo transport operation from Bankstown Airport to Parkes Regional Airport, New South Wales with one intermediate stop outbound, and 2 intermediate stops on return.
After landing on the first sector, the pilot found the fuel cap was off and secured only by a retention chain. The pilot re‑secured the cap but after landing at Parkes on the second sector, they again found the fuel cap off, and arranged an inspection by a maintenance engineer. The engineer found a fault that prevented the fuel cap from locking and rectified it.
Later that day, the pilot commenced the return sectors to Bankstown. Shortly after departing Bathurst for the final sector, both engines lost power, and the pilot conducted a forced landing in a field. The aircraft was undamaged and the pilot was uninjured.
What the ATSB found
The ATSB found that for the first 2 sectors, the fuel cap was incorrectly installed with the retention chain lodged in the fuel tank’s anti-siphon valve, resulting in the cap dislodging in‑flight and fuel being siphoned overboard. At Parkes Regional Airport, the pilot identified an unexplained discrepancy between expected fuel remaining and gauge quantity indication but did not refuel to a known quantity or amend the flight log. As a result, the aircraft departed Parkes with the pilot unaware there was insufficient fuel to complete the remaining flights.
After departing Parkes, the pilot likely did not monitor the fuel gauge, continued fuel calculations based on an incorrect fuel quantity, and did not refuel the aircraft to a known quantity at Bathurst Airport. This resulted in fuel exhaustion shortly after the aircraft departed from Bathurst.
The ATSB also found that GAM Air's Quick Turn Around – Pre-Start checklist did not include a fuel quantity check before start, contrary to the aircraft flight manual’s before-start checklist.
What has been done as a result
GAM Air published a pilot notice reinforcing fuel management procedures for Aero Commander 500 series aircraft. The notice highlighted the importance of fuel tank cap security, and the likelihood of fuel loss should a fuel cap become dislodged, despite the anti-siphon valve. The notice also provided instructions and guidance on fuel planning, in-flight fuel calculations and fuel log entries to expand on information in the standard operating procedures.
GAM Air also commenced periodic auditing of pilot fuel calculations and advised an intention to discontinue use of the Quick Turn Around – Pre-Start checklist. The fuel supplier at Bankstown was also reminded of the requirement to let fuel settle when refuelling.
Safety message
A missing or unsecured fuel cap can lead to rapid and substantial fuel loss in‑flight, even when the fuel tank is equipped with an anti-siphon valve. Loss of a fuel cap in‑flight should be considered as an emergency and, if detected, an immediate diversion to the nearest suitable aerodrome should be conducted. In addition, in aircraft with rubber fuel cells or bladders, fuel gauge readings should not be relied upon as siphoning of fuel can lead to collapse and distortion of the cells causing the fuel gauge to overread. Filling to an amount that can be visually confirmed is required to re‑establish an accurate measure of fuel on board.
The Civil Aviation Safety Authority’s Advisory Circular 91-15 – Guidelines for aircraft fuel requirements, stated:
It is of critical importance that the amount of usable fuel on board an aircraft at the commencement of and during a flight is known with the highest level of certainty.
Pre-flight fuel quantity checks should use at least 2 different verification methods to determine the amount of fuel on board. When using computed fuel on board and comparing against gauge readings, it is important that calculations are accurate. If any discrepancy is detected between the 2 methods, another method such as filling to a known quantity is required.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
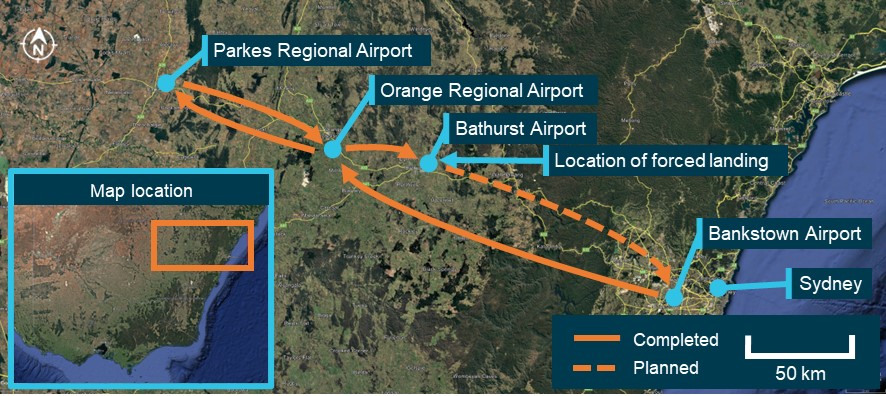
On 8 March 2024, the pilot of an Aero Commander 500-S, registered VH-MEH and operated by GAM Air, was preparing to conduct a return cargo transport operation from Bankstown Airport to Parkes Regional Airport, New South Wales (NSW). The planned flight to Parkes included a stop at Orange Regional Airport to unload a portion of the cargo. The aircraft and pilot were to remain at Parkes for the day before the aircraft was reloaded to return to Bankstown in the afternoon with intermediate stops at Orange and Bathurst airports to load additional cargo (Figure 1). All operations were conducted under instrument flight rules (IFR).[1]
Figure 1: VH-MEH flights on day of incident
Source: Google Earth, annotated by the ATSB
The aircraft had been refuelled 5 days earlier by a contract refueller, with a written instruction to fully refuel the aircraft. Since refuelling, the aircraft had been repositioned on the ground but not flown.
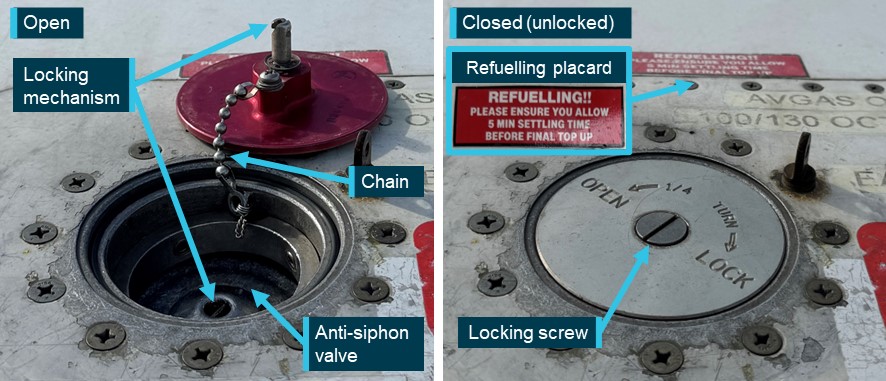
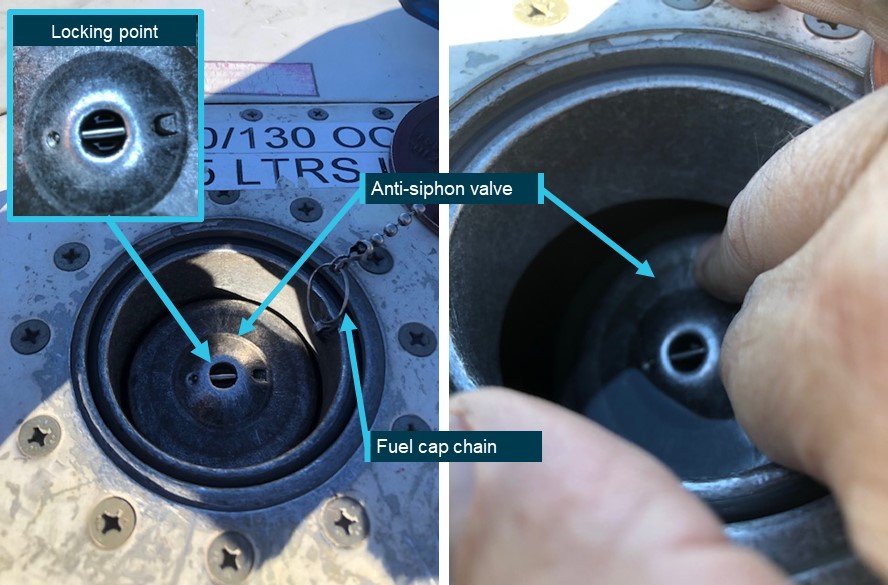
VH-MEH had a single fuel tank that supplied fuel to both engines, accessed through a filler port on the top of the right wing. A spring-loaded anti-siphon valve was installed at the fuel tank opening to mitigate in-flight fuel siphoning.[2] The anti-siphon valve could be pushed open when refuelling or when visually observing the fuel level. The fuel cap was secured to the filler neck by a chain and interlocked with the top of the anti-siphon valve, securing both the fuel cap in place and the anti‑siphon valve in its closed position when the locking screw was turned (Figure 2). To ensure the locking mechanism engaged correctly, pilots were advised to tap the structure around the tank cap once closed. That action should cause the cap to pop open if it was loose or unsecured.
Figure 2: Fuel cap and filling point components (not incident aircraft)
Source: GAM Air, annotated by the ATSB
At about 0610 local time, the pilot conducted a pre-flight inspection of the aircraft, during which they observed the fuel quantity to be 3–4 cm below the anti-siphon valve, which was below the level usually observed when the fuel tank was full. Based on that observation, the pilot estimated that they had 560 L of fuel on board of the total 590 L usable fuel[3] capacity. The pilot also received a weather briefing for the planned flights, which showed no significant wind effect en route (see the section titled Fuel planning).
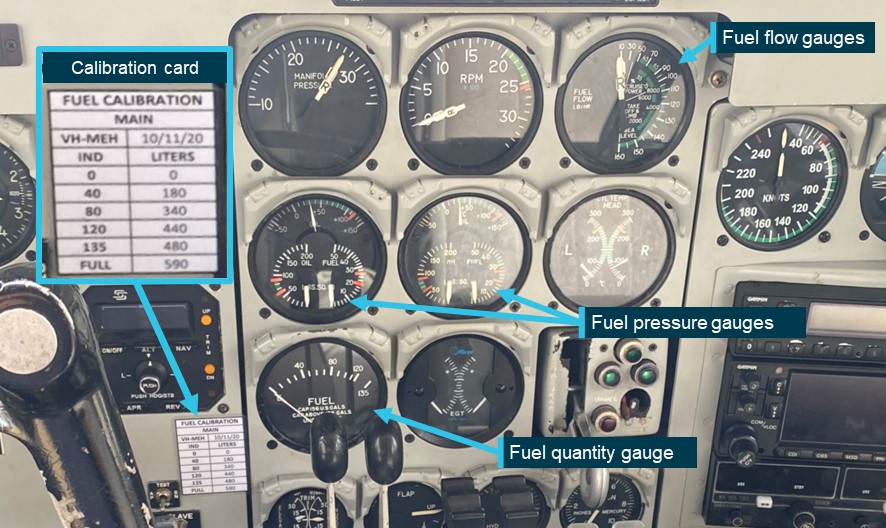
The aircraft had fuel quantity, fuel pressure and fuel flow gauges in the cockpit (Figure 3). A printed calibration card that provided the conversion of fuel gauge readings in US gallons (USG) to usable fuel in litres was affixed adjacent to the fuel quantity gauge. Although full fuel was 159 USG (590 L), the gauge could not indicate a quantity of fuel above 135 USG (480 L). Therefore, prior to commencing the flight, the pilot was unable to confirm the fuel level using the gauge. Because of this gauge limitation, the operator required pilots to begin flights with a fuel quantity that had been visually confirmed.
Figure 3: Cockpit fuel system indicators
Source: GAM Air, annotated by the ATSB
In accordance with the operator’s procedures, the pilot planned to assess the aircraft’s fuel on board by maintaining a log of fuel usage for each sector using a prescribed calculation method (see the section titled Fuel management). The calculated fuel on board would then be regularly compared to the fuel quantity gauge in the cockpit. The pilot used the estimated 560 L of fuel on board as the starting point for their calculations.
The aircraft departed Bankstown at 0658 and landed at Orange Airport at 0735. Upon landing, the pilot calculated that 89 L of fuel had been used. After shutdown, the pilot conducted a post-flight inspection. During the inspection the pilot found that the fuel cap was off, attached only by the chain, which they re‑secured. The pilot reported that they compared the calculated fuel remaining with the fuel quantity gauge reading and determined that there was no discrepancy. Additionally, the pilot reported that they expected the anti-siphon valve would have prevented any fuel loss from the unsecured cap.
The aircraft departed Orange at 0802 and landed at Parkes at 0825. After landing, the pilot calculated that 63 L of fuel would have been used for the sector and calculated the fuel remaining. The pilot conducted a post-flight inspection and again found that the fuel cap was off. They advised the company operations team, who arranged for an aircraft maintenance engineer at Parkes to inspect the fuel cap.
The pilot then identified that the fuel gauge was showing approximately 35–40 L less than the calculated fuel remaining. Due to the discrepancy, the pilot reported recalculating the fuel required for the remaining sectors, based on the fuel gauge indication, and determined that there was adequate fuel on board for the return flight. Specifically, even taking into account the required fuel reserves, the pilot calculated there was almost 1.5 hours excess fuel endurance. However, the pilot did not reduce the calculated fuel remaining on the flight log to reflect the lower gauge quantity indication. The pilot then left the airport.
The maintenance engineer inspected the fuel cap and found that the chain securing the fuel cap to the inside of the filler neck had disconnected from its attachment point and lodged under the anti‑siphon valve, holding it slightly open. This also prevented the fuel cap locking mechanism from engaging. The engineer removed the chain from its lodged position, re‑attached it to the filler neck, and successfully closed and locked the fuel cap. They also observed minor blue fuel dye staining aft of the fuelling point, consistent with Avgas 100 low lead fuel. The engineer later reported that they informed the pilot and the operator’s engineering department of what was found with the fuel cap.
The pilot returned to the airport in the afternoon and the aircraft departed for Orange at 1622, landing at 1644. The pilot calculated that 59 L of fuel had been used for that sector. After loading additional cargo, the aircraft departed Orange at 1702 and landed at Bathurst Airport at 1719, using a calculated 38 L of fuel (see the section titled Fuel monitoring). At that point, the pilot’s calculations determined that 311 L of fuel remained on board. The pilot later reported that they did not recall specific gauge readings at those intermediate stops, but that there were no noted discrepancies.
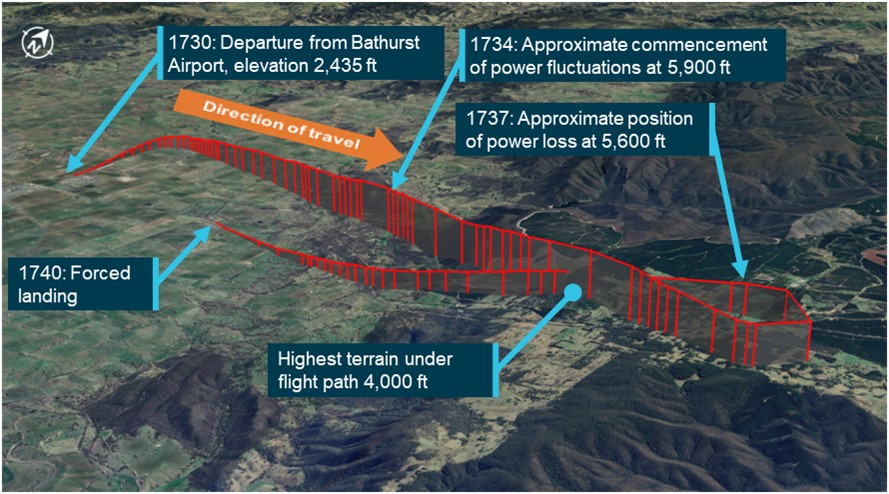
The aircraft departed Bathurst Airport at 1730 for the planned 73 NM flight to Bankstown Airport. At that time, the automated weather observation at the airport indicated no cloud, and wind from the north-east at 10 kt. The aircraft initially tracked north before turning right to track east towards Bankstown (Figure 4).
Figure 4: Incident flight path
Source: FlightRadar24 flight data overlaid on Google Earth, annotated by the ATSB
The pilot reported that, approximately 4 minutes after departure, while climbing through 5,900 ft above mean sea level (AMSL), the aircraft yawed[4] significantly to one side, and then shortly afterwards, yawed to the other side. The pilot recalled performing initial engine failure actions, while using rudder to control the yaw as the engine noise and power fluctuated on both engines.
The pilot observed the fuel flow gauge readings increasing and decreasing in line with the fluctuating engine RPM indication and switched on the fuel boost pumps. The pilot was aware that the terrain below was at approximately 4,000 ft AMSL and the terrain ahead provided few options for a safe forced landing. The pilot advised air traffic control (ATC) of the situation before conducting a 210° left turn to track back towards Bathurst Airport, and towards flatter and lower terrain.
After completing the turn, both engines stopped making power, and the pilot prepared for a forced landing. The pilot selected a large field ahead as a suitable landing area. The pilot elected not to feather[5] the propellors in case partial power was restored and they could continue to the airport. As the aircraft approached the planned landing area, the pilot extended the landing gear prior to manoeuvring below power lines and over a fence. The aircraft landed in the field and came to a stop, after which the pilot advised ATC of their situation before securing the aircraft. The aircraft was undamaged and the pilot was uninjured.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) issued in 2018 and completed an instrument proficiency check[6] in August 2023. A line check and a proficiency check were completed with the operator in September 2023, where the pilot was assessed as competent, and approved to conduct charter flights.
The ATSB obtained the pilot’s experience as of 2 months after the incident, by which time they had accumulated 1,745 total flight hours, 776 hours on multi-engine aircraft, of which 335 hours were logged on Aero Commander 500-type aircraft.
The pilot held a valid Class 1 aviation medical certificate with no restrictions and reported that they were well rested.
Aircraft information
VH-MEH was an Aero Commander 500-S aircraft fitted with 2 Lycoming IO-540-E1B5 290-hp piston engines driving Hartzell 3-bladed constant‑speed propellors. The aircraft was manufactured in the United States in 1975 and first registered in Australia in 1976.
The aircraft had an Australian Supplemental Type Certificate allowing an increased maximum take-off and landing weight of 3,243 kg for IFR operations.
The last periodic inspection was carried out on 13 December 2023, and there were no outstanding items recorded on the aircraft’s maintenance release.[7] At the time of the incident, the aircraft had accumulated 44,963.3 hours total time in service.
There were no onboard recording devices installed on the aircraft that recorded engine indications, gauge readings, fuel flow or fuel levels.
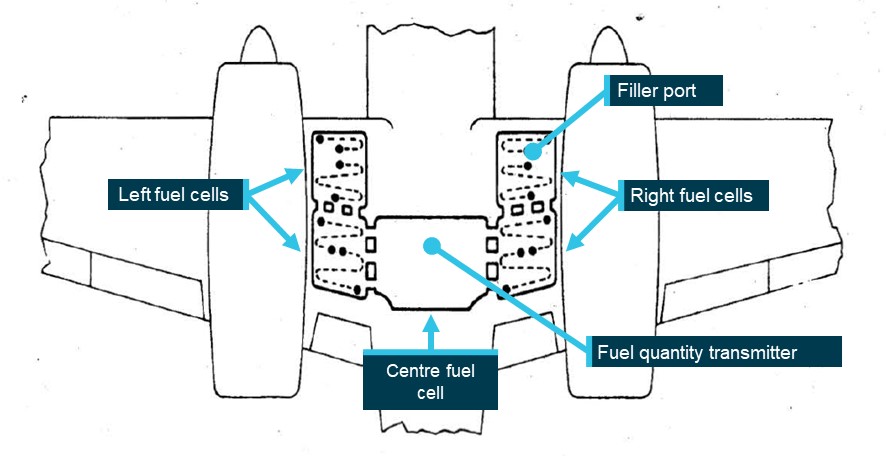
The aircraft’s fuel tank consisted of 5 interconnected synthetic rubber cells installed in the inboard and centre wing sections (Figure 5). A single fuel quantity transmitter was installed in the centre fuel cell and electrically connected to the fuel quantity gauge. Both the operator and the aircraft manufacturer reported that the distribution of the fuel throughout interconnected fuel cells made physical determination of the fuel level using a dipstick impractical. Therefore, the only way to confirm the fuel level was to observe the fuel at a level full or close to full. Additionally, during refuelling, the fuel could take time to settle and allow a reliable visual determination of the fuel level. A placard advising of this was placed adjacent to the filling point on the operator’s Aero Commander aircraft (Figure 2).
Figure 5: Fuel tank internal layout
Source: Aero Commander 500-S maintenance manual, annotated by the ATSB
Post-incident inspection
The ATSB did not attend the incident site. Evidence from approximately 30 minutes after the incident showed the fuel gauge indicating empty when electrical power was turned on. The operator’s maintenance engineers conducted an on-site inspection of the aircraft 6 days later, at which point they reported that the fuel cap was found secured and locked, and the fuel drain points were in the closed position. A small amount of fuel discharged from them when opened, likely to be unusable fuel.[8]
The fuel cap was inspected and tested and was found to attach and remain on, with an observation that the retention spring in the locking screw was noted to be in weak condition, meaning that it could be turned by pressure from a finger or thumb rather than requiring a screwdriver. The fuel cap was replaced as a precautionary measure. Inspection and testing of fuel system components and a general inspection on the aircraft found no issues.
The aircraft was recovered 2 weeks later and taken to Bathurst Airport, where 180 L of fuel was added to the fuel tank, during which the fuel gauge was noted to read correctly and move as expected. Engine ground runs and propellor checks were conducted with all engine parameters observed as normal.
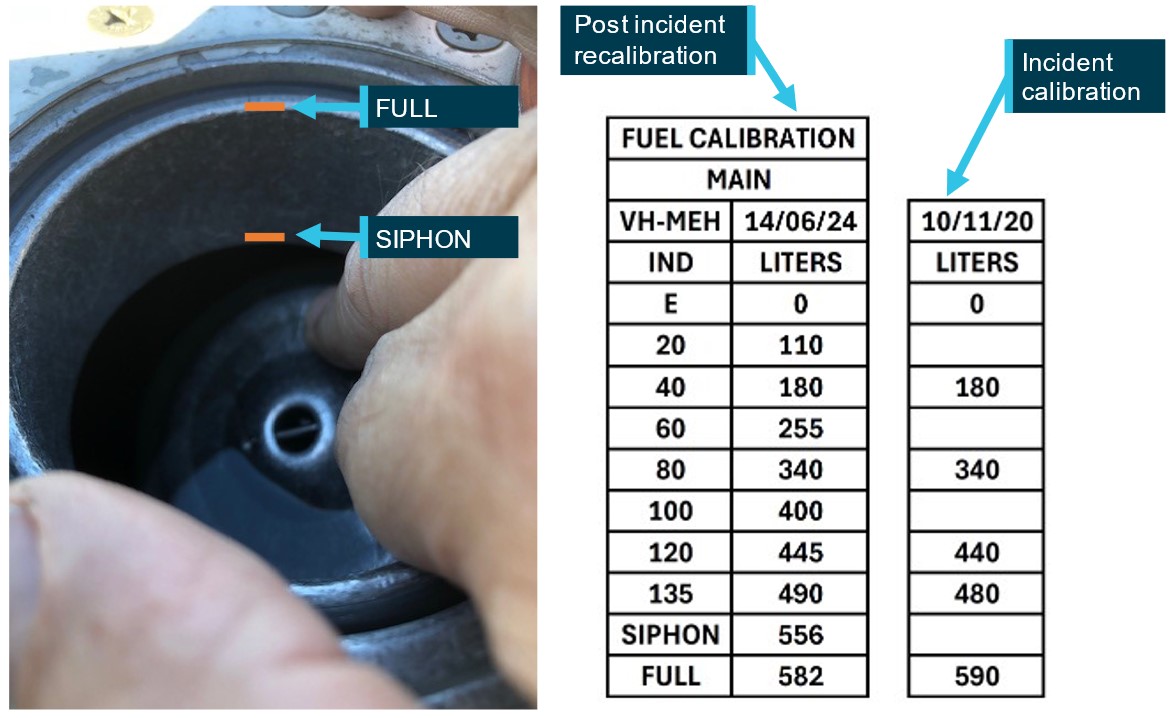
Fuel gauge calibration was required to be conducted every 4 years and prior to the incident was last conducted for VH-MEH on 10 November 2020. Before the aircraft was returned to service, the fuel gauge was recalibrated to verify the correct operation of the fuel indication system, and to fulfil the periodic recalibration requirement. The calibration was expanded to 10 increments from the initial 6. Additionally, a new visual fuel level, annotated as SIPHON, was added. Figure 6 shows how these 2 visible levels were observed and compares the re‑calibration with the calibration values available to the pilot during the incident flight.
Figure 6: Fuel gauge recalibration and observations (photo not VH-MEH)
Source: Parkes Aviation and GAM Air, annotated by the ATSB
Fuel management
Determination of fuel on board
The operator’s fuel policy described the procedures to be conducted to determine fuel on board before each flight. Those procedures stated that fuel quantity gauge readings were required to be crosschecked against either a visual confirmation of the fuel on board, or against calculated fuel on board. This was in line with guidance provided in the Civil Aviation Safety Authority (CASA) Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements:
Unless assured and verified by the PIC that the aircraft fuel tanks are completely full, or a totally reliable and accurately graduated dipstick, sight gauge, drip gauge or tank tab reading can be made, the PIC should endeavour to use the best available cross-check process before engine start. The cross-check should use at least two different verification methods to determine the amount of fuel on board.
As it was not possible to establish the quantity of fuel on board by visual inspection other than when full, a flight log was required to be maintained to calculate fuel usage. This calculated quantity, based on the flight time and maximum altitude of each flight leg, was then deducted from the starting fuel quantity to determine the fuel remaining on board prior to take-off of each flight and compared against the fuel gauge. Table 1 lists the components used in this calculation.
Table 1: Fuel calculation for VH-MEH
Calculation component
Fuel amount
Start, taxi and run-up
5 L
Cruise and descent
115 L/h
Climb Allowance:
- To 3,000 ft
10 L
- 3,000 ft–6,000 ft
15 L
- Above 6,000 ft
20 L
Holding
90 L/h
Instrument approach allowance
30 L
Source: GAM Air
The operator’s fuel policy stated that when a significant or unexplained discrepancy was identified between fuel gauge readings and calculated fuel on board the only way to ensure a known quantity of fuel was to fill the tank to full and confirm visually.
Any significant fuel discrepancy or variation between gauge readings, actual fuel on board (visual) and/or calculated shall be reported to Operations Control.
Where a significant or unexplained discrepancy exists the only way to ensure a known quantity of fuel on board is to fill the tanks full and visually confirm. Should a visual confirmation of actual full tanks not be possible, a flight must not commence unless the Pilot in Command has ensured that the fuel quantity on board has been checked by two separate methods.
Fuel monitoring
The pilot maintained an aircraft flight log as required by the operator’s procedures to keep track of fuel usage. Table 2 compares the pilot’s calculations with the ATSB’s calculations based on the operator’s procedures detailed in Table 1, showing that the pilot underestimated the fuel used by 28 L (11%). The ATSB also reviewed flight log fuel calculations performed for flights on previous operating days of the incident aircraft. Those previous flights were operated by several different pilots, none by the incident pilot, and the calculations sometimes differed from the ATSB’s calculations based on the documented procedures, but to a lesser degree than the incident day flight log.
Table 2: Pilot calculations vs ATSB calculations – incident day
Route
Flight time
Cruise altitude
Pilot calculated fuel
ATSB calculated fuel
Difference
Bankstown – Orange
37 min
8,000 ft
89 L
96 L (71 cruise / 5 taxi / 20 climb)
7 L
Orange – Parkes
24 min
6,000 ft
63 L
66 L (46 cruise / 5 taxi / 15 climb)
3 L
Parkes – Orange
22 min
7,000 ft
59 L
68 L (43 cruise / 5 taxi / 20 climb)
9 L
Orange – Bathurst
14 min
5,000 ft
38 L
47 L (27 cruise / 5 taxi / 15 climb)
9 L
TOTAL
249 L
277 L
28 L (11%)
Fuel planning
The aircraft operator maintained and provided pro forma flight plans and fuel plans for pilots operating their standard routes. The fuel plans calculated fuel required using fuel flow rates applicable to the specific aircraft in the fleet. Pilots were required to adjust the standard flight times and fuel loads for forecast winds.
The pro forma fuel plan required that in nil wind, aircraft conducting the planned Bankstown–Parkes–Bankstown flights including intermediate stops, started with a minimum of 461 L, comprising 278 L of flight fuel, 40 L of taxi allowance, 112 L of mandatory reserves, and an allowance for 31 L for ATC delays. When aircraft conducting that route started the day with full fuel, they typically returned to Bankstown with more than an hour of fuel in addition to required reserves.
The ATSB obtained the weather forecast that would have been available to the pilot prior to departure from Bankstown to determine if forecast winds would have been expected to affect the fuel required. Table 3 shows that the total expected flight time for all sectors would have differed by 1 minute, resulting in an additional 2 L of fuel required.
Table 3: Forecast wind effect on expected flight times
Route
Proforma plan flight time (nil wind)
Forecast Wind
Expected flight time
Bankstown – Orange
40 min
14 kt tailwind
37 min
Orange – Parkes
20 min
8 kt tailwind
19 min
Parkes – Orange
20 min
7 kt headwind
21 min
Orange – Bathurst
12 min
14 kt headwind
13 min
Bathurst – Bankstown
32 min
13 kt headwind
35 min
TOTAL
124 min
125 min
Initial fuel quantity
The pilot estimated the start fuel to be 560 L based on observing the fuel level 3–4 cm below the anti-siphon valve. Post-incident fuel calibration found the siphon level to be 556 L on VH-MEH and 490 L to be the maximum that could be shown on the fuel gauge. Based on that, the ATSB estimated that initial fuel was between 556 L and 490 L, as less than that would have indicated on the fuel gauge prior to departure. This indicated that the pilot overestimated the initial fuel by up to 70 L.
Unaccounted-for fuel
Applying the operator’s fuel calculation method, the ATSB calculated that 305 L of fuel would have been consumed by the engines for the flights conducted on the incident day until fuel exhaustion. Therefore, considering the above range of fuel onboard at the start of the flight, 185–251 L of fuel was unaccounted for (Table 4). The ATSB considered whether a higher rate of fuel consumption by the engines compared to that expected could account for that fuel. However, it was determined that the fuel flow required would have been at least 276 L/h, greater than the maximum continuous power specified in the aircraft flight manual (AFM) and more than the fuel flow gauges could indicate. Therefore, this was not considered to be a possibility. The flight times of each sector were also compared against the operator’s planned flight times and showed no significant differences, indicating that en route winds did not adversely affect fuel calculations.
Table 4: Fuel analysis
Route
Flight time (min)
Start fuel (L)
Fuel used (L)
Unaccounted fuel (L)
End fuel (L)
Bankstown – Orange
37
490–556
96
112–152
282–308
Orange – Parkes
24
282–308
66
73–99
143
Parkes – Orange
22
143
68
75
Orange – Bathurst
14
75
47
28
Bathurst – [Exhaustion]
4
28
28
0
TOTAL
490–556
305
185–251
0
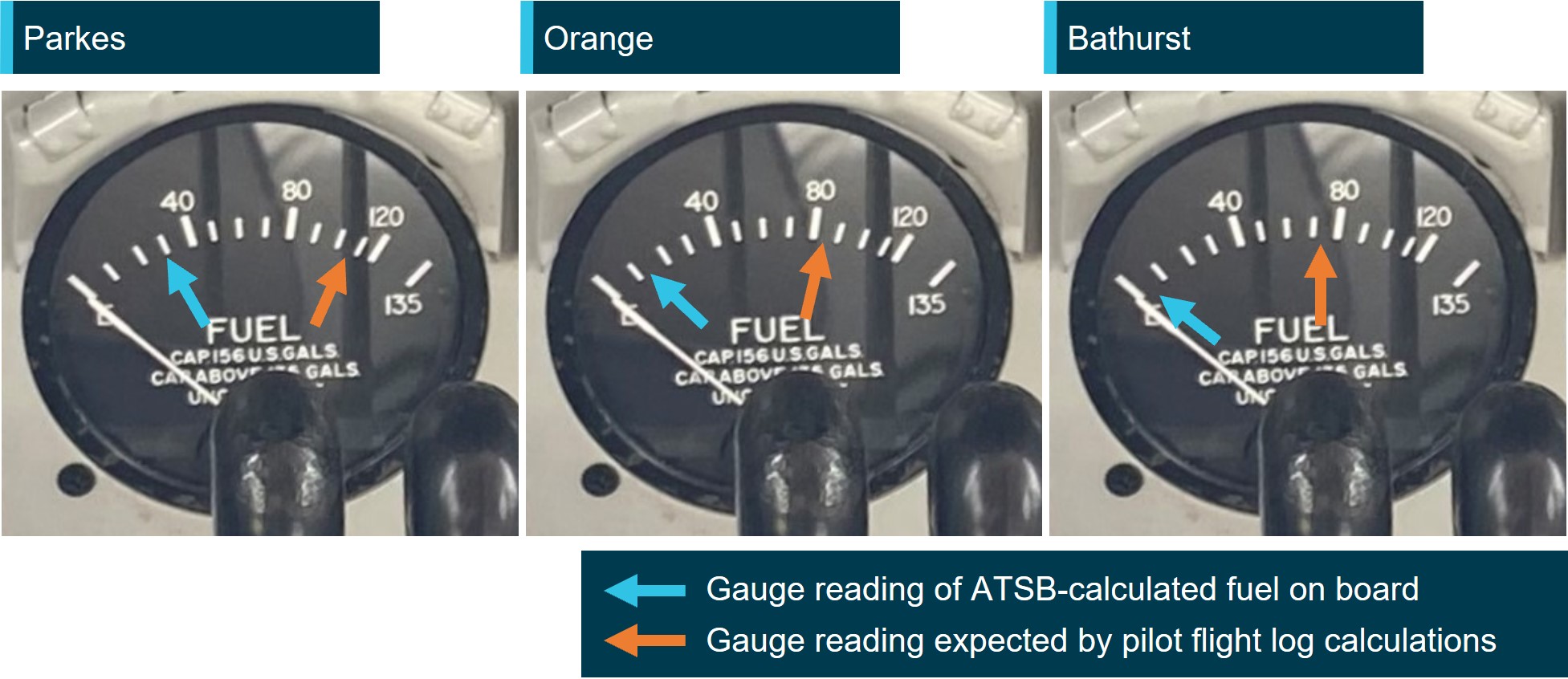
Based on the unaccounted-for fuel, for each of the return sectors, the fuel gauge reading that would have been showing according to the ATSB‑calculated start fuel was compared against the reading expected by the pilot based on their flight log (Figure 7).
Figure 7: Pre-departure fuel gauge indications
Source: GAM Air annotated by the ATSB
Fuel loss and anti-siphon valve
Because the fuel filling point of VH-MEH was located on the top surface of the wing (as on most light aircraft), the low-pressure area on the top surface of the wing created when the aircraft was in‑flight could draw fuel up and out of the fuel tank if the fuel cap become dislodged.
The anti-siphon valve (Figure 8) provided a secondary barrier to fuel venting. The relatively higher pressure inside the fuel tank would act to hold the valve closed and reduce the opportunity for fuel loss without the fuel cap in place.
Any obstruction preventing the anti-siphon valve from closing would provide an opening for fuel to vent should the fuel cap become dislodged. Additionally, the fuel cap locking mechanism would be unable to engage as the locking point of the anti-siphon value would be held away from the locking component of the fuel cap, making it more likely to dislodge.
Figure 8: Anti-siphon valve
Source: Parkes Aviation, annotated by the ATSB
In 2018, the operator circulated a notice to pilots regarding fuel tank cap security in response to 2 incidents involving unsecured fuel caps. One of those incidents was an in-flight fuel siphoning event resulting in the loss of approximately 250 L of fuel. The notice was also issued to the incident pilot as part of their induction. The notice advised that significant fuel loss was possible from Aero Commander aircraft (turbine and piston engine) despite being fitted with an anti-siphon valve, and highlighted the pilot’s responsibility to ensure fuel tank caps were secured. It stated:
During the pre-flight inspection and after each refuelling all Aero Commander pilots will check tank cap security by:
• Ensuring the lock mechanism is secured by using a flat blade screw driver as found in the aircraft fuel drain tool (a 5 cent piece can be used only if no screw driver present)
• Firmly thump/bang the structure immediately around the fuel tank cap. A loose cap may ‘pop’ open if loose. Thumping the tank cap itself will not show if loose.
If there is any doubt about the fuel tank security or integrity pilots will advise Operations Control.
CASA’s Fuel and Oil Safety Advisory Circular (AC) 91-25v1.1 described the importance of maintaining the integrity of fuel caps in preventing in-flight fuel loss including the impact of a trapped fuel cap chain:
In-flight fuel loss by siphoning overboard is primarily attributed to poor maintenance and service practices. Siphoning overboard can be traced to problems such as fuel filler caps incorrectly installed and/or worn fuel filler caps and gaskets. Always check the condition of fuel filler cap O-rings, gaskets, pawls, and springs for evidence of wear and/or deterioration. Deformed or worn pawls may affect the sealing effectiveness of the O-rings or gasket. Similarly, a tank-cap attachment chain or lanyard can be trapped across the seal and defeat its purpose.
In addition to fuel loss, in aircraft where the fuel tanks were comprised of flexible rubber cells, the suction effect created by the low pressure above the wing could cause the fuel cells to collapse upwards from the bottom as fuel is siphoned out. The collapse and deformation of the cells could increase the level of the fuel as the volume of the fuel cells decreased causing the fuel quantity gauge to overread. AC 91-25v1.1 described the potential effect of fuel cell collapse and distortion on fuel quantity indication:
If the fuel gauge apparatus is in the vicinity of the pump and surrounded by relatively solid structure it may not be immediately affected by a tank collapse and could continue to give readings that may at first appear to be credible. It is possible for the indications to temporarily suggest a very low rate of usage or even show a transitory increase in the quantity of fuel in the tank. Whatever the cause or manner of fuel bladder collapse, a dangerous situation will result. CAUTION: Fuel bladder collapse may exaggerate indications of fuel in the tank.
The Flight Safety Australia article Caps tanks and drains: a three pronged attack (CASA, 2016), described the potential consequences of in-flight fuel siphoning due to a loose fuel cap, including the possibility of fuel cell deformation and its effect on fuel gauge readings.
The loose cap exposes the fuel to the low-pressure area over the wing; the fuel then obeys the laws of physics and finds its way out.
If the tank is a rubber fuel cell it will collapse upwards from the bottom, because the top of the rubber fuel cell is secured more firmly to the top wing-tank cavity. This can have at least three effects, all of them bad:
• The bottom of the tank keeps rising. Fuel is thus kept at or near the top of the tank near the cap hole, so that siphoning continues until most or all of the fuel is lost overboard.
• The float of the fuel tank quantity gauge can come into contact with and be supported, or even raised, by the rising of the tank liner bottom. As a result, the cockpit fuel quantity indicator may continue to show full or nearly full, despite the loss of fuel.
• The tank becomes distorted and wrinkled. The tank may not re-shape itself and volume is reduced for the next fill. The valleys now hold lakes and rivers that cannot be drained, until the aircraft is climbing.
Recognising the hazard posed by fuel cell distortion, the aircraft operator and maintainer advised that this was not possible in Aero Commander aircraft as the fuel tanks are interconnected via feed tubes and vent tubes. Additionally, the fuel sender unit is at the bottom of the main tank, and both the sender and the tank are held at the bottom via a large panel and a series of retaining bolts. It would therefore be impossible for the bottom part of the tank to suck up and affect the sender arm to give an erroneous high reading.
The aircraft manufacturer also advised that they would not expect fuel siphoning to lead to fuel gauge overreading.
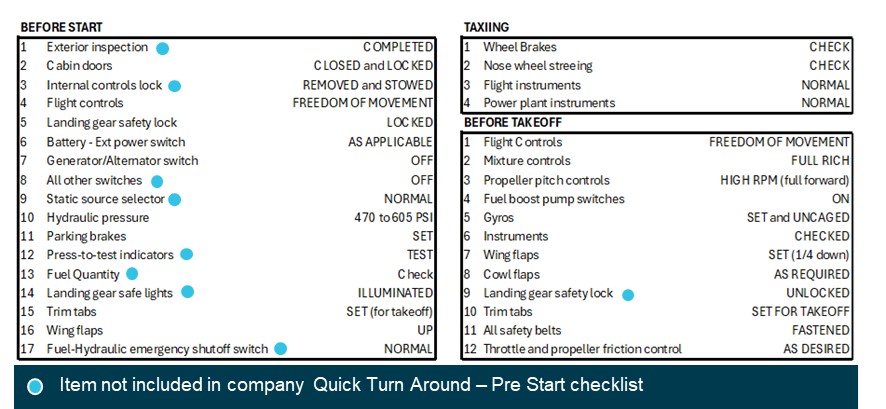
Aircraft checklists
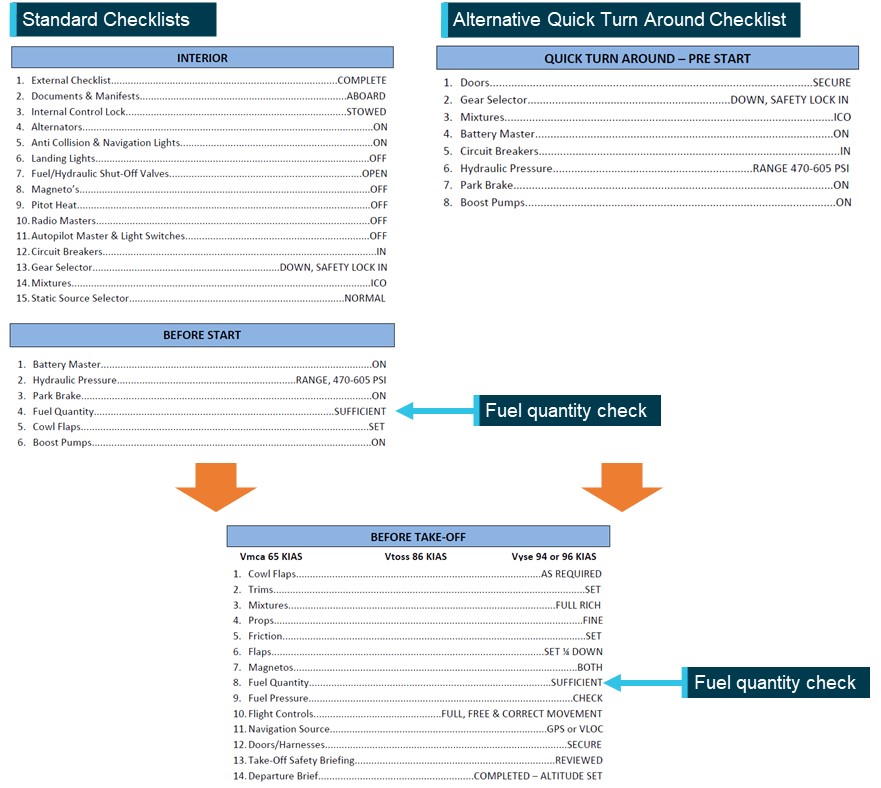
The operator’s checklists (Figure 9) to be used when operating VH-MEH provided points at which the fuel quantity was required to be checked.
Before the aircraft was started, the pilot was required to conduct the INTERIOR checklist, followed by the BEFORE START checklist. This second checklist contained an item to check that the fuel quantity was sufficient, and the gauge was indicating correctly.
To enable expediency during multiple sectors such as cargo operations, the operator provided a QUICK TURN AROUND – PRE-START (QTA) checklist as an alternative to those 2 checklists. The QTA checklist did not include a fuel quantity check. However, regardless of whether the standard or QTA checklists were used before aircraft start, a subsequent fuel quantity check was required to be conducted in the BEFORE TAKE-OFF checklist before the aircraft departed.
Figure 9: GAM Air Aero Commander 500 checklists
Source: GAM Air, annotated by the ATSB
The ATSB compared the operator’s checklists with equivalent checklists in the manufacturer’s aircraft flight manual (AFM) (Figure 10). While standard checklists closely followed the checks included in the AFM, several checks were excluded when a pilot conducted the operator’s QTA Checklist.
Figure 10: AFM checklists
Source: Aero Commander 500-S aircraft flight manual, annotated by the ATSB
Emergency procedures
The operator’s checklists and the AFM did not contain checklists specific to simultaneous power loss from both engines. However, having identified that an engine was inoperative, the checklists instructed the pilot to feather the propellor of the inoperative engine. Feathering the propellor of a failed engine reduces drag and adverse yaw (when only one engine has failed).
In the case of both engines failing, feathering both propellors significantly reduces drag, improves the handling characteristics and flight performance of the aircraft and, by increasing the glide distance, potentially expands options for a forced landing site.
Related occurrences
Australia
Excluding the incident flight, the ATSB occurrence database contained 97 reported occurrences of fuel leaking or venting from non-jet aircraft between 2014 and 2024. Of those occurrences, 7 resulted in fuel starvation or fuel exhaustion. Additionally, in 17 of those occurrences, the fuel cap was incorrectly installed or not secured prior to flight. Those numbers likely under‑represent the total number of incidents of this type, as the ATSB only requires instances of fuel leaking/venting or missing/insecure fuel caps to be reported for commercial passenger transport operations.
The database also contained one occurrence of fuel venting leading to starvation immediately after landing of an Aero Commander 500-S in 1995. Although the ATSB did not investigate the incident, it was reported that a post-landing inspection revealed the main fuel tank filler cap was defective and would not remain locked, allowing fuel to vent overboard in‑flight.
International
The ATSB identified the following occurrences of fuel exhaustion of an Aero Commander 500 aircraft:
Fuel exhaustion of Aero Commander 500 N107DF on 28 January 2023 (NTSB ERA23LA122)
The aircraft lost power to both engines and landed in a field, sustaining substantial damage and seriously injuring the pilot. It was determined that it was likely that the pilot did not visually confirm the aircraft’s initial fuel quantity prior to departing and that the available fuel was exhausted.
Fuel exhaustion of Rockwell 500 N900DT on 28 August 2020 (NTSB ERA20LA297)
The aircraft impacted a building and terrain about 10 minutes after take-off and was destroyed, fatally injuring both pilots. It was determined that this was due to a total loss of engine power due to fuel exhaustion. Contributing to the fuel exhaustion was the fatigue fracture of an electrical wire in the tank unit or fuel transmitter, which likely resulted in an inaccurate fuel quantity indication. It was also determined that the initial fuel quantity on board was not able to be confirmed visually.
Safety analysis
Prior to the day’s flights, the pilot estimated the fuel on board based on a visual assessment of fuel below the anti-siphon valve level. The fuel quantity was less than full due to either the refueller not allowing the fuel to settle during refuelling, ground running to reposition the aircraft, or a combination of both. Although the pilot likely overestimated the fuel quantity by up to 70 L, the aircraft departed Bankstown with enough fuel to complete the planned sectors and return to Bankstown with the required reserves intact, given the forecast winds.
As the pilot found the fuel cap off and replaced it after landing at both Orange and Parkes airports, it was likely that the fuel cap was also unsecured in‑flight during those sectors. The maintenance engineer in Parkes found that the fuel cap chain had been holding the anti‑siphon valve slightly open, preventing the fuel cap locking mechanism from engaging, and reported advising the pilot of that. Significantly, the engineer also detected evidence of fuel dye staining, indicating fuel had leaked from the tank.
After rectification by the maintenance engineer, the fuel cap remained secured including after the forced landing. ATSB analysis indicated that it was very likely that about 200 L of fuel siphoned overboard in‑flight during one or both sectors to Parkes. The loss of fuel en route to Parkes left the aircraft with about 143 L of fuel upon landing at Parkes, which was insufficient for the return sectors to Bankstown.
At Parkes, aware that the fuel cap had been unsecured on the 2 previous sectors, but unable to physically confirm the quantity of fuel in the tank, the pilot identified an unexplained discrepancy between their calculated fuel remaining and the fuel quantity gauge reading.
Due to the discrepancy, the operator’s procedures required the pilot to refuel the tank to full, to visually confirm the quantity of fuel onboard. However, instead of refuelling, the pilot reported recalculating the aircraft’s fuel state based on the gauge reading, although they did not update the flight log, and incorrectly determined that they had sufficient fuel for the remaining flights. Despite being informed of issues found with the fuel cap, the pilot’s decision not to refuel may have been influenced by their expectation that the anti-siphon valve would prevent fuel siphoning overboard and the typical excess of remaining fuel on board when completing the same route.
The ATSB assessed whether the fuel quantity gauge was likely to have been providing erroneous indications to the pilot. This was based on CASA guidance that during in-flight siphoning events in aircraft with rubber fuel cells, it was possible for the rubber to deform and move upwards away from the base of the tank, resulting in overreading of the fuel quantity sender. However, the aircraft operator/maintainer and manufacturer advised that this was not possible in Aero Commander aircraft due to the construction of the fuel cells and sender. There were also no reported issues or defects with the fuel gauge prior to the incident flight.
The fuel gauge was determined to be working correctly after the incident and 2 minor adjustments were made to fuller fuel quantities in the calibration conducted post‑incident. Therefore, the fuel quantity gauge was likely indicating correctly at Parkes and would have shown a significant discrepancy with the pilot’s assessed fuel quantity.
As a result of the pilot’s misunderstanding of the fuel quantity, the aircraft departed Parkes with significantly less fuel than determined by the pilot, and insufficient for the remaining flights. The pilot did not then effectively monitor the fuel state or refuel after landing at Bathurst. Consequently, fuel exhaustion occurred shortly after the aircraft departed from Bathurst.
Although not considered to have contributed to this occurrence, the operator’s Quick Turn Around – Pre-Start checklist was an abbreviated version of the before-start checklist specified in the aircraft flight manual and did not include a fuel quantity check. As there was a fuel quantity check in the operator’s and manufacturer’s before-take-off checklist, the pilot was required to verify the fuel quantity before departure. However, a fuel quantity check before start in accordance with the manufacturer’s procedures would have prompted the pilot to crosscheck the fuel state when workload was lower, and any discrepancy could have been more easily identified and addressed.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel exhaustion involving Aero Commander 500-S, VH-MEH, 6 km east of Bathurst Airport, New South Wales on 8 March 2024.
Contributing factors
For the first 2 sectors, the fuel cap was incorrectly installed with the chain lodged in the fuel tank’s anti‑siphon valve, resulting in the cap dislodging in‑flight and a significant quantity of fuel being siphoned overboard.
At Parkes Regional Airport, the pilot identified an unexplained discrepancy between their calculated fuel remaining and the fuel quantity gauge indication but did not refuel to a known quantity. As a result, the aircraft departed Parkes with the pilot unaware that there was insufficient fuel to complete the remaining flights.
After departing Parkes, the pilot likely did not monitor the fuel gauge, continued fuel calculations based on an incorrect fuel quantity, and did not refuel the aircraft to a known quantity at Bathurst Airport. This resulted in fuel exhaustion shortly after the aircraft departed from Bathurst.
Other factors that increased risk
GAM Air's Quick Turn Around – Pre-Start checklist did not include a fuel quantity check before start, contrary to the aircraft flight manual’s before-start checklist.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by GAM Air
GAM Air published a pilot notice reinforcing fuel management procedures for Aero Commander 500 series aircraft. The notice highlighted the importance of fuel tank cap security, and the likelihood of fuel loss should a fuel cap become dislodged, despite the anti-siphon valve. The notice also provided instructions and guidance on fuel planning, in-flight fuel calculations and fuel log entries to expand on information in the standard operating procedures.
GAM Air also commenced periodic auditing of pilot fuel calculations and advised an intention to discontinue use of the Quick Turn Around – Pre-Start checklist. The fuel supplier at Bankstown was also reminded of the requirement to let fuel settle when refuelling.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot
aircraft operator and maintainer
Civil Aviation Safety Authority
Parkes maintenance engineer
aircraft manufacturer
recorded flight data.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to directly involved parties including the:
pilot
aircraft operator and maintainer
Civil Aviation Safety Authority
Parkes maintenance engineer
aircraft manufacturer.
Submissions were received from the:
aircraft operator and maintainer
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]In-flight fuel siphoning: a phenomenon where fuel escapes from the fuel tank of an aircraft in-flight. On aircraft where the fuel filler point is on top of the wing, the low-pressure area above the wing created when an aircraft is in‑flight can draw the fuel up and out of the fuel tank if it is not sufficiently sealed.
[3]Usable fuel: The amount of fuel which is available in the fuel tanks for supply to the engines.
[4]Yawing: the motion of an aircraft about its vertical or normal axis.
[5]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[6]Instrument Proficiency Check: A 12-monthly assessment with a flight examiner to assess the flying skills and operational knowledge required to conduct flights under the IFR.
[7]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[8]Unusable fuel is the amount of fuel in the tank below which continued running of the engine while performing the most adverse manoeuvre cannot be assured.
Occurrence summary
Investigation number
AO-2024-008
Occurrence date
08/03/2024
Location
6 km east of Bathurst Airport
State
New South Wales
Report release date
19/11/2024
Report status
Final
Anticipated completion
Q4 2024
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Forced/precautionary landing, Fuel exhaustion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Aero Commander
Model
500-S
Registration
VH-MEH
Serial number
3258
Aircraft operator
General Aviation Maintenance Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
The pilot of an R22 helicopter that collided with terrain south of Katherine in December 2023 had taken off after last light without the qualifications to fly at night and their helicopter not being equipped to be flown at night, an ATSB final report details.
A search was initiated at 8:15 pm on the evening of 7 December 2023 after the pilot did not arrive as planned at Gorrie Station, having departed nearby Bloodwood Station 45 minutes earlier.
The wreckage of the destroyed aircraft was subsequently discovered about 6 km away from Gorrie. The pilot was fatally injured.
The ATSB investigation report details that despite being offered a place to stay overnight at Bloodwood Station, the pilot had taken off after last light to return to their own property. The pilot did not hold a night visual flight rules rating but had reportedly completed some night flying training and had arrived home after last light on previous occasions.
“Pilots qualified to only operate under day visual flight rules are at risk of spatial disorientation and loss of control of their aircraft when they operate – intentionally or otherwise – in night conditions, where little to no useable external visual cues can be present,” ATSB Director Transport Safety Stuart Macleod said.
“The visual flight rules require pilots to only operate under daylight conditions, and to plan to land 10 minutes before last light, which provides a reliable method for ensuring there are sufficient external visual references available to safely operate.”
The ATSB report notes the accident helicopter was not equipped for night flight. Notably, it did not have an artificial horizon.
“Without the minimum instruments and training, it was unlikely that the pilot would have been able to orientate the helicopter without external visual references,” Mr Macleod said.
“It is likely that during the return home flight, the helicopter entered a smoke plume associated with bushfires under dark night conditions, and the pilot became spatially disorientated, resulting in a collision with terrain, uncontrolled, at a high speed.”
A Singapore Airlines Airbus A350 was about to be pushed back from the gate at Brisbane’s international terminal on 27 May 2022 when a refueller in an adjacent bay noticed covers were still on the aircraft’s pitot probes, an ATSB investigation final report describes.
Upon being alerted to this, the licenced aircraft maintenance engineer (LAME) responsible for the aircraft’s turnaround returned to the aircraft and removed the pitot covers. The aircraft then proceeded for its planned passenger service to Changi, Singapore, without further incident.
Pitot probes, which provide airspeed data to aircraft systems and flight crew, are routinely covered during turnarounds at Brisbane due to the nesting behaviour of a species of invasive mud wasp, which has been known to block the tubes in as little as 20 minutes. The covers must be removed prior to take-off.
In a serious incident in 2018, a Malaysia Airlines A330 took off from Brisbane with its pitot covers still in place, and its crew had to conduct an emergency return landing without airspeed data.
In this more recent occurrence, the ATSB found Singapore Airlines’ contracted engineering provider at Brisbane, Heston MRO, had not yet implemented an acceptable method for accounting for tooling and equipment prior to aircraft pushback, although that was identified in the ATSB’s investigation into the 2018 occurrence.
“Additionally, the procedural risk controls which were in place for the removal of the pitot probe covers were circumvented when the LAME certified for their removal in the technical log and removed a relevant warning placard from the flight deck, without visually or verbally confirming that they had been removed,” ATSB Chief Commissioner Angus Mitchell said.
“The final walk around inspection of the aircraft was also not conducted by the LAME or the headset operator. That inspection is intended to ensure that the aircraft is correctly configured for flight with all panels and doors closed and all covers removed.
“This incident demonstrates how assumptions and procedural omissions can lead to unsafe conditions; in this case, the potential for an aircraft to take-off with erroneous or absent airspeed indications.”
While the ATSB was not able to formally establish that fatigue contributed to the occurrence, the investigation did note the LAME had reported the workload associated with their dual role of LAME/regional manager had become considerably more demanding following the COVID-19 pandemic.
“The engineering provider did not track the work-related hours of personnel with dual roles like the LAME involved in this incident (who was also the regional manager) for fatigue calculation purposes,” Mr Mitchell said.
“This meant there was an increased risk of a fatigue-related incident with these personnel.”
The report notes that, since the occurrence, Heston MRO no longer requires the Brisbane regional manager position to undertake dual responsibilities, and tracks work hours of all employees for fatigue management purposes.
Also, during the ATSB’s investigation, a review of CCTV footage of pre-flight inspections by Singapore Airlines flight crew for the occurrence flight and others around the same time showed they were truncated, and not undertaken in accordance with company procedures.
“The pre-flight walk-around occurs before the pitot probe covers are to be removed, so this did not contribute to this incident,” Mr Mitchell noted.
“Nonetheless, it was identified in our investigation as a safety issue, which Singapore Airlines has subsequently addressed.”
The airline, the report notes, has communicated with flight crews about the importance of pre-flight walk-around checks to be completed in their entirety and in accordance with the procedures.
The airline has also provided Heston MRO with pitot probe covers with longer streamers, to improve conspicuity.
The pilot of a single-engine Rockwell Commander aircraft that impacted the water following fuel starvation had not completed all pre-take-off checks including fuel tank selection due to distraction, an ATSB investigation has found.
The four-seat Commander 114, with a pilot and three passengers on board, had departed Redcliffe airfield, north of Brisbane, on the morning of 19 December 2021, the investigation report details.
Prior to the flight the aircraft had been stored in a hangar, during which time most of the fuel moved into the right wing tank. The pilot would have been aware of the fuel imbalance from measuring fuel in both tanks via a dipstick before flight. However, it was likely that the fuel tank selection prior to take-off was to the left fuel tank only.
A video of the accident flight taken on a passenger’s mobile phone showed that while conducting the engine run-ups, the pilot perceived a technical difficulty with the aircraft, and the checks were paused. After notifying a ground crew member by phone, the pilot taxied back toward the ground crew who was walking towards the aircraft on the taxiway.
The ground crew member recalled that through hand signals, the pilot identified the issue as misidentification of the mixture control for the propeller pitch control and communicated that they had identified and corrected the problem.
The pilot then taxied again for the runway without continuing or restarting the interrupted pre-take-off checks.
Shortly after take-off, the engine lost power and the pilot elected to return to the airfield. During the return, the aircraft lost altitude and contacted the water, overturning and coming to rest inverted in about 2 m of water. The occupants were unable to escape the aircraft and were fatally injured.
“During preparation for the flight, the perceived engine problem distracted the pilot during the conduct of pre-take-off checks,” said ATSB Director Transport Safety Dr Stuart Godley.
“After rectifying the issue, the pilot did not complete the remaining pre-take-off checks, including fuel tank selection, before departure.”
It was likely that the fuel tank selection prior to take-off was to the left fuel tank only, which led to fuel starvation and engine stoppage soon after take-off, the investigation found.
“Likely experiencing the effects of stress and time pressure following the engine power reduction and then stoppage, the pilot did not conduct initial emergency actions and attempted to return to the runway for landing,” said Dr Godley.
However, the pilot did not maintain glide speed, and the aircraft impacted shallow water prior to reaching the airfield. The extension of the undercarriage for the intended landing then contributed to the aircraft overturning.
This likely resulted in occupant disorientation and added difficulty in operating the exits, reducing their ability to escape. The investigation also notes that it is very likely that the passengers did not receive information about the brace position or actions to be taken in the event of a ditching as part of the pre-flight briefing. Further, in the limited time available inflight after the power loss, the pilot also did not provide an emergency briefing or any instructions to passengers prior to impact with the water.
“This tragic accident highlights the importance of using checklists as they provide pilots with the detailed normal and emergency checks specific to the aircraft type without having to rely on committing these to memory,” Dr Godley said.
“This ensures that aircraft are operated in a way that meets aircraft flight manual requirements and limitations.
“When distracted, restarting an interrupted checklist from the beginning is a means of ensuring that all steps to be performed are done so in order and the checklist is complete.”
The Australian Transport Safety Bureau has released a preliminary report from its ongoing investigation into a Cessna 172 light aircraft accident near Camden Airport, in south-west Sydney in January.
The report details factual information established in the early evidence collection phase of the ATSB’s investigation, but contains no analysis or findings, which will be detailed in the investigation’s final report.
On 24 January 2024, a student pilot was conducting a solo flight in the four-seat Cessna when, toward the end of the downwind leg of a planned circuit around Camden Airport at 1,400 ft, the aircraft descended before colliding with terrain in a paddock.
The pilot was fatally injured, and the aircraft was destroyed.
The ATSB’s preliminary report notes the accident flight was the pilot’s first solo in the Cessna 172 after 6.1 hours in the type with an instructor. The pilot had also completed 51.3 hours of flying under a Recreational Aviation Australia pilot certificate, including 4.1 hours of solo flight in a two-seat, single-engine Skyfox Gazelle.
“The instructor, who flew with the student pilot on flights immediately preceding the accident flight, reported the student demonstrated exceptional aircraft handling proficiency,” ATSB Director Transport Safety Dr Stuart Godley said.
“The instructor assessed them as competent and ready for their first solo in the Cessna 172.”
CCTV footage showed the aircraft collided with terrain at high speed, wings level and with an attitude of about 60° nose-down.
An on-site examination of the wreckage established pre-impact flight control continuity, and that the engine was producing power at impact. There was no evidence of an in-flight break-up or other pre-impact airframe or control defects.
Along with the on-site examination, so far in the investigation the ATSB has recovered aircraft components and other items for further examination and interviewed the operator’s head of flying operations and the student pilot’s instructors.
“As the investigation progresses, the ATSB will examine relevant documentation and aircraft components and other items recovered from the accident site,” Dr Godley explained.
“Further analysis will also examine the flight path information gathered from CCTV recordings and flight data.”
A final report will be released at the conclusion of the investigation.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Dr Godley concluded.
A number of safety advisories and directives have been released, or have come into effect, since a UH-1H ‘Huey’ accident in northern Tasmania in 2022 where the helicopter’s main KAflex drive shaft failed.
On 14 February 2022, a Huey helicopter collided with terrain after losing main rotor drive during waterbombing operations over the Labrina bushfire north of Launceston.
An Australian Transport Safety Bureau investigation found the engine-to-transmission main KAflex drive shaft had partially failed, likely due to the fracture of a flex frame attaching bolt, or a flex frame element during flight.
“This initial failure resulted in the KAflex entering fail-safe mode, which allows for a short period of continued flight, but necessitates landing as soon as possible,” ATSB Director Transport Safety Stuart Macleod explained.
With the KAflex in fail-safe mode, the pilot jettisoned the water from the underslung bucket and diverted toward clear ground but, while the helicopter was descending, the KAflex failed completely, resulting in instantaneous loss of drive to the rotor system.
“Following the loss of main rotor drive, the pilot was unable to complete a survivable autorotative descent and landing, probably due to a critical reduction in main rotor speed,” Mr Macleod said.
The helicopter collided with the ground in a paddock, and was destroyed. The pilot was fatally injured.
During its investigation, the ATSB issued a safety advisory notice to all UH-1H operators, advising them of the details of the accident and to look for evidence of defects in the KAflex driveshaft of their helicopters, if fitted.
Also since the accident the Civil Aviation Safety Authority has updated a previously-released Airworthiness Bulletin, on the subject of pre-flight inspection requirements for the KAflex drive shaft.
Meanwhile, a US Federal Aviation Administration airworthiness directive is now in effect, requiring operators to replace KAflex drive shafts beyond 5,000 hours of use, or where flight hours are unable to be verified.
“A rapid increase in vibration or noise from the transmission area – significantly the commencement of a distinct ‘howling’ or ‘shrieking’ – may signify the KAflex has entered fail-safe mode, and could imminently fail,” Mr Macleod said.
“Pilots should land as soon as possible on detection of such symptoms.”
Mr Macleod said the accident was also a reminder to UH-1H helicopter pilots, operators and maintainers that fatigue cracking can occur on critical flight components.
“Particular vigilance should be applied during the daily or pre-flight inspections of the main transmission driveshaft because it represents an important opportunity to detect for defects such as cracks, and to identify evidence of loose or missing attachment hardware.”
The United States National Transportation Safety Board (NTSB) is investigating an accident involving an amateur-built Beck Michael J Sonex, registered N920MB, near Auburn Municipal Airport, Washington, United States, at about 1130 local time on 16 January 2024.
The pilot reported that while climbing after take-off, a partial engine power loss occurred, and the aircraft began descending. The pilot then planned to conduct a forced landing on a road straight ahead of the aircraft but several seconds later, the engine regained power enabling a climb. About 40 seconds later, the engine lost all power and the pilot turned the aircraft toward the airport. The aircraft then collided with signage structures and terrain and was substantially damaged. The pilot was not injured.
As part of the investigation, the NTSB identified an Australian-manufactured Rotec Aerosport TBI Mk 1 throttle body in the aircraft wreckage and considered it an item of interest. To support the investigation, the NTSB requested assistance and the appointment of an accredited representative from the ATSB to facilitate manufacturer examination and functional testing of the throttle body.
To facilitate this support and to provide the appropriate protections for any relevant information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
To ensure the integrity of the material evidence and to provide independent oversight, ATSB personnel were required to be present for the Australian manufacturer’s examination and testing of the throttle body. However, Rotec Aerosport would not permit ATSB personnel to be present and therefore, the NTSB elected not to proceed with the testing.
As no further involvement has been requested, the ATSB has closed this investigation.