The Australian Transport Safety Bureau has released a preliminary report into its ongoing investigation of a mid-air collision involving two jet trainer aircraft over Port Phillip Bay, south of Melbourne, in November.
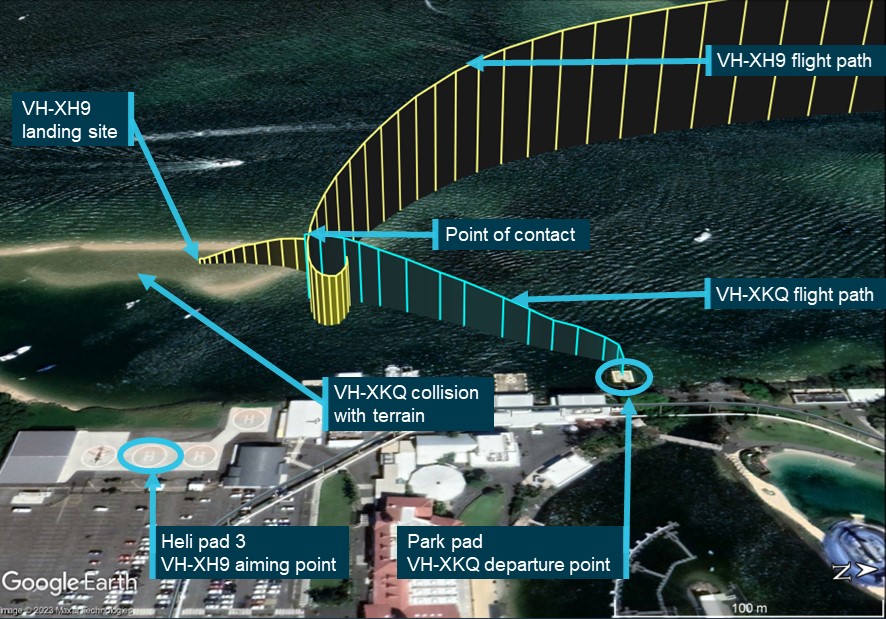
On 19 November 2023, a pair of SIAI Marchetti S-211 aircraft were being used for an aerobatic formation filming flight when they came into contact, with one of the two aircraft subsequently departing controlled flight before colliding with the water below, fatally injuring both occupants.
“Today’s preliminary report provides factual information from the early evidence gathering phase of our ‘no blame’ transport safety investigation,” ATSB Chief Commissioner Angus Mitchell explained.
“It does not include any analysis or findings, which will be detailed in the final report we will release at the conclusion of the investigation.”
The preliminary report notes the S-211s, both ex-military aircraft used for pilot training, had left Essendon in what was designated ‘Viper formation’.
Viper 1, the lead aircraft, was carrying a pilot and safety pilot, while Viper 2 was carrying a pilot and camera operator.
“As discussed in the pre-flight briefing, the pilots’ first planned manoeuvre involved Viper 1 flying inverted, straight and level, so Viper 2 could move alongside it, upright, to then manoeuvre as required to maintain separation and conduct filming,” Mr Mitchell said.
During the second attempt at this manoeuvre, when Viper 1 rolled inverted, the pilot of Viper 2 passed below and to the left of Viper 1.
“The safety pilot in Viper 1 observed Viper 2 pass beneath and alerted the pilot of Viper 1 to the manoeuvre,” Mr Mitchell said.
“Afterwards, the pilot of Viper 2 advised the pilot of Viper 1 that it provided a good filming opportunity, and asked to repeat it.”
After the pilots discussed this manoeuvre, they decided to attempt it again.
“On this next attempt, after Viper 2 passed beneath, it began to pitch up and bank away from Viper 1, and the right wings of each aircraft collided,” Mr Mitchell said.
Video footage taken from fixed cameras on board Viper 1 showed that as the aircraft collided, the outer right wing structure of Viper 2 immediately failed, with deformation to the forward wing spar and separation of the lower wing skin. The right aileron control system also appeared to be significantly damaged.
Witnesses observed Viper 2 impact the water in a near-vertical, nose down attitude at high speed. The aircraft was extensively damaged and came to rest on the floor of Port Phillip Bay at a depth of 24 metres.
Fortunately, Viper 1 was able to return to Essendon, having sustained only minor damage.
“Several impact marks and paint transfers from Viper 2 were present on the upper surface of Viper 1’s right wing, and its landing light cover was shattered,” Mr Mitchell detailed.
As the ATSB’s investigation progresses, it will include consideration of formation flying procedures and practices, further analysis of recorded video and audio, a review of the category of operation, and a range of other investigative activities.
“A final report will be released at the conclusion of the investigation, but if we identify a critical safety issue during the course of the investigation, we will immediately notify relevant parties so appropriate and timely safety action can be taken.”
Twenty-one people were fatally injured in nine aircraft accidents in the last 10 years where pilots had flown into cloud, fog or darkness when they did not have the proficiency to do so, Australian Transport Safety Bureau (ATSB) figures show.
A total of 101 occurrences of visual flight rules (VFR) pilots inadvertently flying into instrument meteorological conditions (IMC) in Australian airspace were reported to the ATSB in the decade from 1 July 2009 to 30 June 2019. Of those occurrences, nine were accidents resulting in 21 deaths.
“These concerning figures taken from the ATSB’s National Aviation Occurrence Database show that almost one in 10 ‘VFR into IMC’ occurrences resulted in fatal accidents,” ATSB Chief Commissioner Greg Hood said.
“Weather-related general aviation accidents remain one of the ATSB’s most significant causes for concern in aviation safety; the often fatal outcomes of these accidents are all the more tragic because they are avoidable.”
To remind VFR pilots of the dangers of flying into IMC and to highlight the actions they can take to avoid a weather-related accident, the ATSB is launching a new safety promotion titled ‘Don’t push it, DON'T GO. Know your limits before flight’.
“‘Don’t push it, DON'T GO’ highlights three key messages: the importance of thorough pre-flight planning and having alternate plans, that pressing on where there is the possibility of entering IMC carries a significant risk of spatial disorientation, and the value of using a ‘personal minimums’ checklist to help manage flight risks,” Chief Commissioner Hood said.
Flying into poor weather without the training and experience to do so can rapidly lead to spatial disorientation.
Flying into poor weather without the training and experience to do so can rapidly lead to spatial disorientation when the pilot cannot see the horizon.
“The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and a resultant loss of control of the aircraft,” ATSB Director Transport Safety Dr Stuart Godley said.
For pilots who fly under VFR, conducting thorough preflight planning and working to a personal minimums checklist aids sound decision-making both prior to take-off and during flight when faced with marginal weather or darkness.
“Pilots without a current instrument rating should always be prepared to amend and delay plans to fly due to poor or deteriorating weather conditions, and not to push on,” Dr Godley said.
“Have alternate plans in case of unexpected changes in weather, and make timely decisions to turn back, divert or hold in an area of good weather.
“Further, setting expectations for your passengers beforehand can take the pressure off continuing with the flight if the conditions exceed your personal minimums.”
Developing a personal minimums checklist is an effective defence against what pilots often term as ‘push-on-itis’ or ‘get-home-itis’, Dr Godley noted.
A personal minimums checklist is an individual pilot’s own set of rules and criteria for deciding if and under what conditions to fly or to continue flying based on your knowledge, skills and experience. As a personal ‘go/no go’ checklist they can help take the stress out of difficult decisions both before and during flight, acting as a safety buffer between the demands of the situation and the extent of a pilot’s skill.
“Discuss your personal minimums with an instructor or a more experienced pilot. Have the discipline to stick to your personal minimums in spite of external pressures. And treat your personal minimums as a line in the sand over which you would not cross,” Dr Godley said.
But if VFR pilots do find themselves in marginal weather, and are becoming disorientated or lost, they should seek whatever assistance is available.
“In particular, air traffic control services may be able to provide assistance, including radar vectoring away from bad weather if the aircraft is in an area of surveillance coverage,” Dr Godley said.
“There have been a number of reported occurrences where this simple action has averted potential disaster.”
Findings from ATSB investigations into aircraft accidents where a VFR pilot flew into IMC makes for sobering reading. A selection of those findings are published in the ATSB’s updated Accidents involving pilots in Instrument Meteorological Conditions publication.
“The ATSB encourages VFR pilots to learn from the experiences of others, to help build a robust understanding of the risks of flying into IMC and just how rapidly such accidents can happen,” Chief Commissioner Hood said.
The ATSB investigation into an Airbus EC130 helicopter accident on Mount Disappointment highlights that the effective management of the risk of inadvertent entry into instrument meteorological conditions (IMC) relies on multiple layers of controls.
The helicopter was one of two EC130s, operated by Microflite, which had departed a helipad at Melbourne’s Batman Park bound for Ulupna in Victoria’s north, on 31 March 2022. The pilots of both helicopters were operating under the visual flight rules (VFR) – regulations that permit a pilot to operate an aircraft only in weather conditions clear enough to allow the pilot to see where the aircraft is going – but had planned and commenced a route for which instrument meteorological conditions were present.
The pilots continued the flight as conditions deteriorated until a rapid change of course was required to avoid entering cloud.
“During the attempted U-turn without visual cues the second helicopter developed a high rate of descent, resulting in the collision with terrain,” said ATSB Chief Commissioner Angus Mitchell.
“Unfortunately, the pilot had no instrument flying experience, and the helicopter was not equipped with any form of artificial stabilisation, albeit neither of which are required for VFR flying.”
All five occupants of the helicopter were fatally injured in the accident.
Mr Mitchell noted that whilst not required by regulations the helicopter operator had not incorporated several available risk controls for their day VFR pilots to mitigate against inadvertent entry into IMC.
“These risk controls may have included inadvertent IMC recovery training and basic instrument flying competency checks during operator proficiency checks.”
The operator had also not introduced an inadvertent IMC recovery procedure for their air transport operations, or a pre-flight risk assessment to trigger an escalation process for marginal weather conditions identified at the pre-flight planning stage.
The investigation report notes that the operator had identified poor weather conditions as a risk, but its management of that risk was limited to the mandated regulatory requirements, and it did not consider ways to enhance pilot recovery from an inadvertent IMC event.
The Civil Aviation Safety Regulations for rotorcraft air transport (Part 133) only require the risk of a VFR inadvertent IMC event to be managed through avoidance.
“While avoidance of inadvertent IMC is important, it is not always assured, and Part 133 does not address the risk of recovery from an inadvertent IMC entry event.”
Mr Mitchell said the ATSB encourages all pilots to develop the knowledge and skills required to manage the risk of inadvertent IMC.
“Decision-making in marginal weather conditions can be supported with the use of a pre-flight risk assessment tool,” he said.
At an organisational level, the risk of helicopter inadvertent IMC should be considered within the context of a company’s operations.
“The effective management of this risk relies on multiple layers of controls to reduce the risk of single point-of-failure accidents.”
This includes training and procedures for both avoidance and recovery, which can be enhanced with equipment, such as autopilots to reduce the risk of loss of control, and terrain awareness and warning systems to reduce the risk of controlled flight into terrain.
Mr Mitchell acknowledged the operator had taken a number of actions as a result of the accident including introducing basic instrument flying training and inadvertent IMC recovery training; updating their proficiency check syllabus to include knowledge and practical skills checks for avoiding and recovering from inadvertent IMC; and upgrading the avionics systems on its helicopter fleet to incorporate synthetic vision, a terrain alerting functionality, and, where available, an autopilot.
The ATSB has also recommended that CASA take further safety action to address the risk of inadvertent IMC events in Part 133 helicopter passenger operations.
On 8 January 2024, a Cessna 208B Grand Caravan, registered VH‑NWJ and operated by East Air, departed Lizard Island Airport, Queensland on a non‑scheduled passenger service to Cairns Airport, with the pilot and 9 passengers on board. During the climb, at approximately 3,400 ft, the pilot observed the engine speed and thrust increase uncommanded, and the engine instrumentation indicated numerous parameters were exceeded or were not indicating at all. The pilot returned to land but due to the uncontrollable excessive power being generated by the engine, they conducted a high‑speed approach, touched down long on a short runway, overran the end, and the aircraft flipped over. All occupants received minor injuries, and the aircraft was substantially damaged.
What the ATSB found
The ATSB determined that the fuel control unit of the Pratt & Whitney Canada PT6A‑114A engine very likely malfunctioned due to internal or external influences. This resulted in the engine speed accelerating uncommanded and exceeding numerous engine limitations, including the gas generator speed and interstage turbine temperature. The ATSB was not able to determine the exact nature of the fault.
In accordance with the aircraft flight manual procedure, pilots of PT6A turbine engine aircraft are trained for ‘roll back to idle’ malfunctions, including the use of the manual override or emergency power lever where fitted. However, there was no such procedure for an uncommanded engine acceleration malfunction or inability to reduce power, although this type of event occurred at a rate higher than any other fuel control unit related malfunction or failure mode. As such, ATSB’s consultation with training organisations for the Cessna Caravan aircraft identified that the nature of the fuel control unit malfunction was not widely understood by pilots, operators or the pilot training industry.
What has been done as a result
As a result of this accident, East Air has published a temporary revision to its Quick Reference Handbook for the Cessna 208B aircraft to include an emergency item for 'Unscheduled power increase during flight (High Torque, Ng, ITT and/or Fuel Flow)'.
The ATSB has issued safety advisory notice AO‑2024‑001‑SAN‑001 in conjunction with this investigation report. The SAN raises awareness of engine acceleration events on PT6A powered aircraft and encourages operators to consider the potential responses to this type of failure for different phases of flight, to document appropriate actions, and to train pilots to ensure that operations are performed correctly and consistently.
Safety message
Procedures are widely recognised as being basic to safe aircraft operations. They are designed to assist with reducing variation within a given process and ensure operations are performed correctly. Without procedures, pilots are required to exercise judgement based on their experience, skills and knowledge. When details regarding certain non‑normal or emergency scenarios are not contained in an aircraft flight manual, air transport operators should consider customising their exposition and providing appropriate training to ensure that their pilots are adequately prepared for such an event.
Summary video
The occurrence
On 8 January 2024, at about 0646 local time, a Cessna 208B Grand Caravan, registered VH‑NWJ and operated by East Air, departed Lizard Island Airport, Queensland on a non‑scheduled passenger service to Cairns. On board the aircraft were the pilot and 9 passengers.
After take-off from runway 12, the pilot turned right, tracked south‑south‑west and made a departure call to Brisbane Centre air traffic control (ATC).[1] At 1,750 ft above mean sea level, the pilot turned left onto the departure track in a cruise climb and engaged the autopilot.
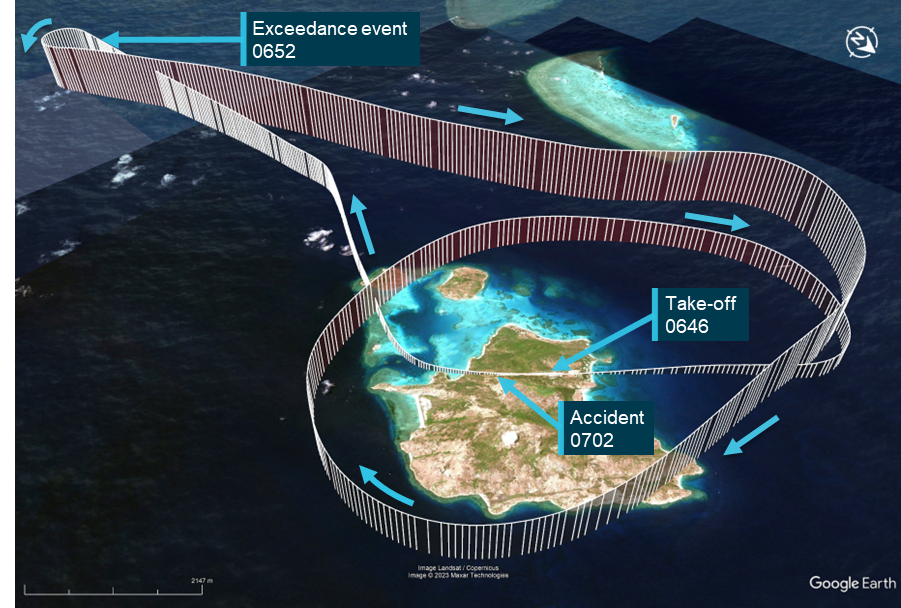
At 0652, passing 3,400 ft at an indicated airspeed of 102 kt, the pilot noted a change to the engine sound and that the aircraft was accelerating (Figure 1, ‘Exceedance event’). The pilot checked the engine gauges on the Garmin G1000 multifunction flight display. They noted the values indicated on both the engine torque and interstage turbine temperature gauges were above the redline and the gas generator speed and fuel flow were not indicating, being marked with a diagonal red cross through the gauge locations. The propeller revolutions per minute was high but within the green operating range.
Within 10 seconds, the pilot initiated a left turn with the purpose of returning to Lizard Island and broadcast a PAN PAN call[2] on the area frequency advising their intentions. Despite trying to arrest it, the aircraft continued to climb and accelerate over the next 2 minutes reaching 4,000 ft and 166 kt.
The pilot started troubleshooting the issue by moving the power, propeller control and emergency power levers with the only response coming from the propeller control lever. The pilot also partially moved the fuel condition lever through the gate[3] from low idle to cut‑off and noted the engine power cutting in and out and returned the condition lever to low idle. At the same time, the pilot conducted a large orbit around the island attempting a shallow descent while the engine continued to produce excessive power. Further manipulation of the propeller control lever somewhat reduced the engine thrust. The pilot updated ATC on their situation and progressively deployed the flaps to create drag in an attempt to slow the aircraft.
After one orbit of the island, the pilot felt they were low enough to attempt a landing with a 2 NM (4 km) final approach to runway 12 and notified ATC of their intentions. The pilot reported they were concerned with the populated resort accommodation and maintenance buildings on the approach end of the runway and the possibility of injury to those on board and on the ground if the aircraft did not have the energy to make the runway. To ensure they cleared potential obstacles, the pilot elected to perform a powered‑on approach.
The pilot continued to adjust the propeller lever in an attempt to reduce the engine thrust. The final approach was started at 147 kt (the pilot operating handbook stated the normal approach speed with full flaps was 75–85 kt). The pilot was able to reduce the airspeed to 123 kt by the runway threshold and reported attempting to shut down the engine. The aircraft floated along the down‑sloping runway, bouncing and touching down at around 100 kt, an estimated two‑thirds of the way along the runway.
The pilot applied maximum braking, but the aircraft exited the end of the runway at 92 kt. The aircraft continued across undulating sandy soil and low vegetation before the left wingtip struck the ground, which spun and flipped the aircraft, coming to rest inverted, 127 m from the end of the runway.
Figure 1: Flightpath of VH-NWJ
Source: Google Earth, annotated by the ATSB
After the aircraft had stopped, most passengers started evacuating the aircraft through the cargo (rear left) door. The pilot, after completing shutdown actions, exited through the front left door, followed by other passengers. Upon exiting, the pilot noticed a small fire had started at the front of the engine. After ensuring the passengers were still evacuating successfully, the pilot returned to the cockpit to retrieve a fire extinguisher, then discharged it into the engine cowling. The fire was extinguished but continued to smoulder.
Once all passengers had evacuated, the pilot moved them to the end of the runway where they were met by Lizard Island resort staff who raised the alarm with emergency services. Concurrently, ATC tried to contact the pilot but received no response. They engaged another pilot flying in the area to make contact, but that pilot was also unsuccessful in receiving a response. ATC then called the island resort and were advised the aircraft had overturned off the end of the runway. ATC then advised the Australian Maritime Safety Authority Joint Rescue Coordination Centre which coordinated the emergency response.
All aircraft occupants were flown to Cairns Hospital with the pilot and 9 passengers receiving minor injuries. The aircraft was substantially damaged.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) with a single-engine class rating and tailwheel, retractable undercarriage, gas turbine engine and manual propeller pitch control design feature endorsements. The pilot had 3,706 hours total aeronautical experience, of which 2,431 hours were on the C208 type. All the pilot’s recent flying had been on the C208B. The pilot held instrument and flight instructor operational ratings.
The pilot held a valid class 1 aviation medical certificate and reported being well rested and fully alert for the flight. The pilot was required to wear distance vision correction.
Airport information
Lizard Island Airport was a restricted access airfield servicing a resort and marine research centre. It had one sealed asphalt 15 m wide runway aligned to 120/300° of 980 m length. The runway rises and falls through approximately 5 m over its length.
Aircraft information
General
The Cessna 208B Grand Caravan was a high‑wing aircraft powered by a single Pratt & Whitney Canada (P&WC) PT6A‑114A turboprop engine and McCauley Propeller Systems feathering 3‑bladed metal propeller. VH‑NWJ was first registered in Australia in April 2023 and had accumulated about 8,765 hours total time in service at the time of the accident. It was configured with a cargo pod and a 14‑seat interior layout.
Engine limitations
The P&WC PT6A-114A turboprop engine is managed by a Honeywell DP‑F2 fuel control unit (FCU) controlling and limiting the gas generator speed (Ng), interstage turbine temperature (ITT) and engine torque. Ng and ITT are controlled by the rate of fuel consumption, while engine torque is controlled by a combination of fuel consumption and propeller pitch. The associated limits for the engine and propeller are listed in Table 1.
Table 1: Powerplant limitations for PT6A-114A as installed in the Cessna 208B
Instrument
Normal operating limit (caution range)
Permitted transient exceedance (time)
Engine power (shaft horsepower)
675
-
Engine torque (ft-lb)
1,865/1,970[1]
2,400 (20 s)
Interstage turbine temperature (°C)
765 (805)[2]
850 (2 s)
Gas generator (% RPM)
101.6
102.6 (2 s)
Propeller speed (RPM)
1,900
2,090 (2 s)
[1] Engine torque has a moving limit. If maximum torque is used, propeller rpm must be set so as not to exceed power limitations.
[2] 5-minute limitation.
Source: Pilot’s operating handbook for Cessna Model 208B G1000 aircraft
Engine controls
In the C208 aircraft, the engine and propeller are controlled principally by 3 levers, the power lever, propeller lever, and fuel condition lever. The power lever primarily controls the amount of power the engine generates. The propeller lever controls the propeller speed (Np) by biasing a constant speed governor. However, in beta mode,[4] the power lever also directly controls the propeller blade angle. The condition lever provides 2 idle speeds for the engine but is there principally as a fuel control to permit starting or stopping the engine.
Engine power is controlled by the power lever that, through FCU fuel scheduling, controls the gas generator speed. Excess energy generated by the engine core is used to turn the power turbine which, via a gearbox, turns the propeller. The propeller thrust generated is controlled by the propeller rotational speed in combination with the propeller blade angle. The propeller blade angle is adjusted by the propeller speed governor to maintain a constant propeller speed that can be biased by the propeller lever.
A fourth control is provided on the C208 for emergency purposes. The emergency power lever (EPL) can be used to manually override control of the FCU, which can be effective during certain fuel control malfunctions[5] (refer to section titled Malfunction conditions).
Fuel control unit basic operation
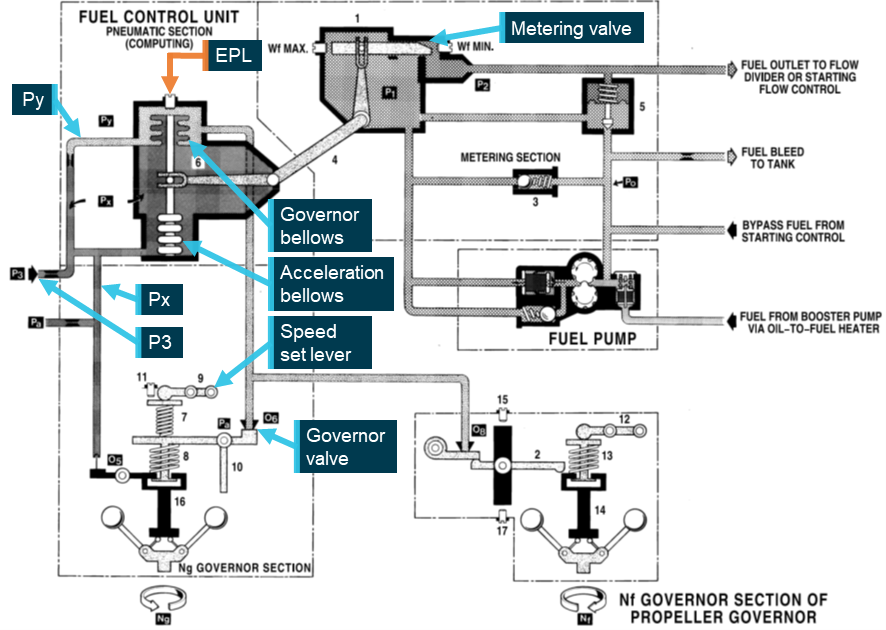
The FCU receives 2 inputs directly from the engine, Ng and compressor discharge air pressure (P3). P3 air passes through 2 metering orifices to the pneumatic section of the FCU. Air from both the first and second pneumatic meterings are used as part of the fuel control and are labelled Px and Py respectively (Figure 2). A flyweight governor driven by the compressor turbine pushes against spring‑loaded levers, which open a bleed valve to Py (governor valve).
The Py and Px air lines connect to the governor bellows, which controls a liquid metering valve in the fuel side of the FCU. Px and an ambient pressure line are connected to a second bellows (acceleration bellows), which also connects to the governor bellows shaft and is used to provide smooth changes to the fuel scheduling.
The fuel side of the FCU is supplied with unmetered fuel from the fuel pump. The metering valve, controlled by the governor and acceleration bellows, meters fuel to the flow divider and fuel nozzles.
Figure 2: Fuel control unit schematic
Source: Pratt & Whitney Canada, annotated by the ATSB
In normal operation when a power increase is requested, the power lever moves the speed set lever in the FCU, which biases the spring pressure to close the governor valve, increasing Py causing the governor bellows to compress, opening the metering valve and increasing fuel flow. As Ng accelerates, P3 increases (and in turn Px and Py) allowing the acceleration bellows to compress, further opening the metering valve. However, the engine does not continue to accelerate as the increase in Ng also increases the flyweight governor force on the governor valve, thereby opening it and reducing Py. This slight reduction finds a new equilibrium in the governor bellows and maintains the metering valve position until another input changes.
In summary, the power lever indirectly controls the fuel flow to the engine. The governor bellows initiates acceleration, deceleration, and controls the Ng steady state. Increasing Py pressure causes Ng to increase, and vice versa, a decrease in Py reduces Ng. The power lever only biases the governor spring and lever to alter the rate of Py bleed.
In the case of an FCU malfunction, an EPL is provided to the pilot to manually override the automated fuel scheduling. In practice, moving the EPL drives a shaft in the FCU, which presses on the end of the governor bellows, compressing it and the acceleration bellows mechanism, which in turn opens the fuel metering valve. As such, the feature is used to maintain engine functionality when the engine experiences a power rollback (usually to idle). As the EPL linkage is not directly attached to the governor bellows and can only push on it, the EPL can only be used to increase fuel flow to the engine above what the FCU is scheduling (either in normal use or during a malfunction). The EPL cannot be used to reduce fuel flow and thus cannot control an engine experiencing an uncommanded engine acceleration event.
Meteorological information
There was no Bureau of Meteorology weather station at Lizard Island. The nearest station was at Cape Flattery, 20 NM (37 km) south‑south‑west, which reported winds of 7 kt at 120° and a temperature of 30°C. The pilot reported there was little cloud and light winds of about 5 to 6 kt from the south‑east. Video taken by a witness of the final approach showed greater than 10 km visibility, few cumulus clouds[6] at lower levels and scattered cirrus cloud at high levels suitable for a visual approach.
Wreckage and impact information
Site information
While there was no evidence of the touchdown point on the runway, a skid mark, identified to be from the right main tyre, started about 110 m before the end of the runway asphalt. The skid mark disappeared and reappeared multiple times towards the end of the runway and was determined to be evidence of wheel brake modulation by the pilot.
Low foliage disruption showed the aircraft track through about 100 m of scrub after it had exited the end of the runway. The aircraft came to rest inverted with the aircraft nose pointing to the west (Figure 3). There was evidence of a small fire on the underside of the engine cowl in the vicinity of the exhaust duct and areas of the engine were found to have a coating of dry powder extinguishant.
Figure 3: Wreckage position in relation to the runway
Source: East Air, annotated by the ATSB
Wreckage examination
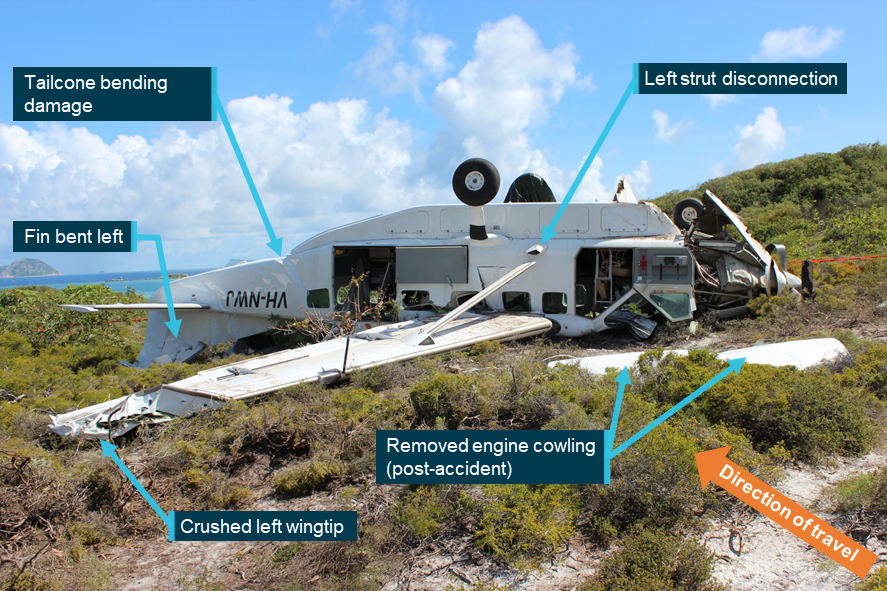
The outboard 1.5 m of the left-wing leading edge was crushed down and back (Figure 4). The left‑wing front spar fuselage attachment had failed in tension and the rear spar fuselage attachment had pushed into the adjacent fuselage wall. In addition, the wing strut had failed at the fuselage end fitting. The vertical stabiliser and rudder were bent to the left with downward bending damage to the tailcone.
The nose wheel strut had collapsed rearward. The propeller blades were bent in a manner that indicated they were in the feathered[7] position at the time of impact with the ground.
The engine cowl side doors had been removed. The engine mount was distorted downwards and to the right, and there was minor creasing of the firewall. All engine controls and rigging, sense lines, piping and hoses were checked and found to be secure and intact. All secured connections were found to be lock wired or pinned. The oil tank lid was latched and secure.
Figure 4: Aircraft wreckage
Source: Queensland Police Service, annotated by the ATSB
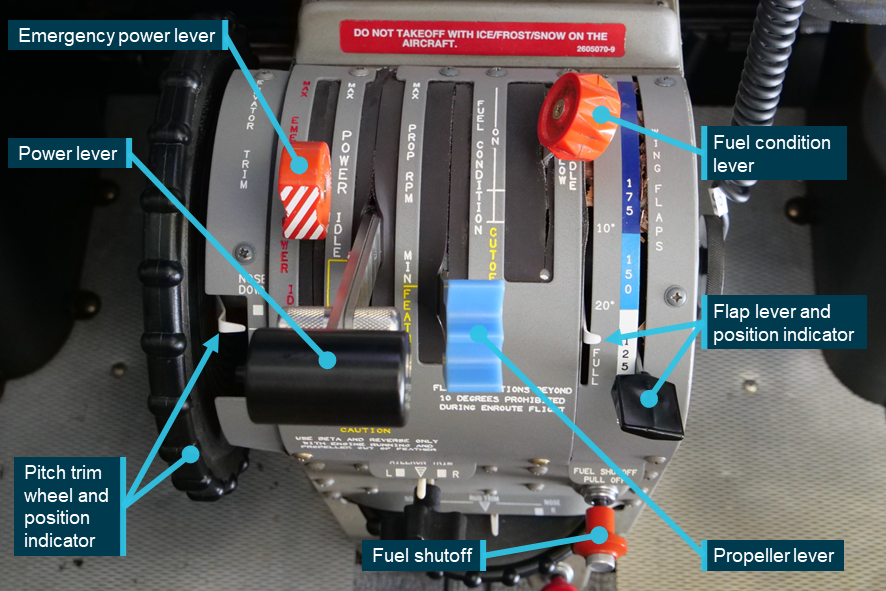
The wing fuel tank selectors were both off. Battery and avionics switches were off, and no circuit breakers were identified as tripped. The following centre console control positions (Figure 5) were found:
fuel shutoff: in (on)
wing flaps selector and indicator: FULL
fuel condition lever: just above LOW IDLE
prop RPM lever: FEATHER
power lever: IDLE
emergency power lever: one third of the way between IDLE and MAX
elevator trim: a quarter from NOSE DOWN.
Cockpit engine controls were exercised and, despite some distortion and damage in the engine bay, moved as expected through their ranges of motion.
Figure 5: Centre console as found after the accident
Source: ATSB
The cabin was intact except for the left wall adjacent to the wing where the incursion of the wing had created slightly reduced space for one passenger in the fourth row. All seats were attached to the floor and not deformed.
Fuel control unit examination
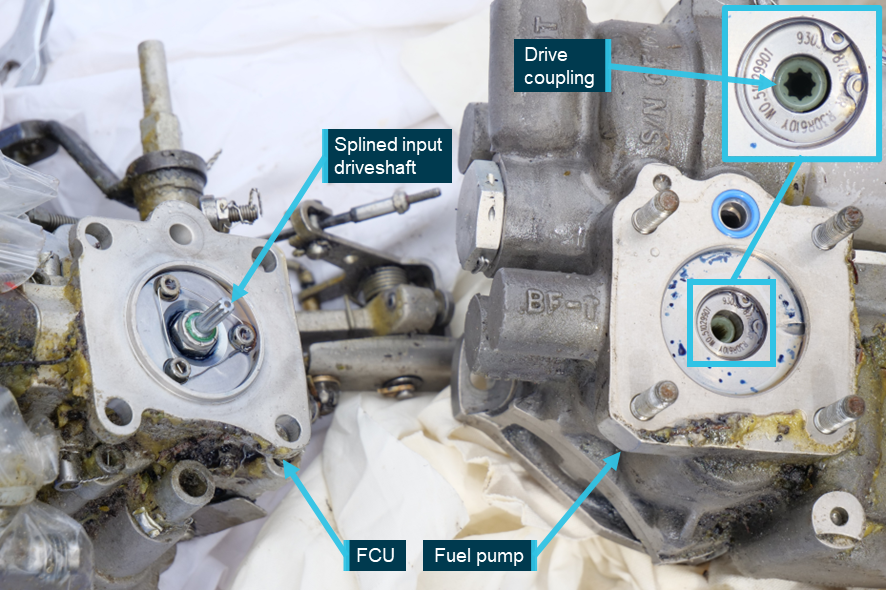
No pre-existing damage or faults were found with the aircraft during the wreckage examination, and so the other plausible explanation for the engine acceleration was an internal issue with the FCU. During ATSB attendance at the accident site, the FCU was retrieved from the engine. The FCU mates with the fuel pump and shares a common driveshaft from the compressor turbine via a gearbox. The FCU and fuel pump were separated to determine the condition of the drive coupling, a possible failure location associated with uncommanded engine acceleration. The input drive shaft to the FCU and the drive coupling were both found serviceable and in good condition (Figure 6).
The P3 compressor discharge air hose and P3 inline filter were checked and found to be clean and clear of debris.
Arrangements were then made for the FCU to undergo a specialised inspection by Pratt & Whitney Canada on behalf of the ATSB. The FCU was dispatched from the ATSB Brisbane office as an international air freight consignment but it was lost in transit. Extensive checking and investigation by the freight provider to locate the tracked consignment was unsuccessful. Consequently, any internal mechanical faults, such as component failures, material degradation, or contamination of pneumatic passageways in the FCU could not be determined. Should the FCU ever be recovered, this report will be amended to reflect any findings of the subsequent analysis.
The FCU had been removed from the aircraft and sent to TAE Aerospace 3 weeks before the accident. Work packs showed the unit was bench flow tested to confirm the operator‑reported high cut‑off angle and was adjusted. The FCU was not disassembled during the procedure.
Figure 6: Fuel control unit and fuel pump
Source: ATSB
Recorded data
Garmin G1000
The aircraft was fitted with a Garmin G1000 electronic flight instrument system consisting of 2 primary flight displays and one multi-function display. The G1000 had a 58 channel, 1 Hz, flight and engine parameter, flight data logging capability. Crew alerting system messages were not recorded in the flight data log. An SD memory card was retrieved from the device, which contained recorded data from multiple flights, including the accident flight.
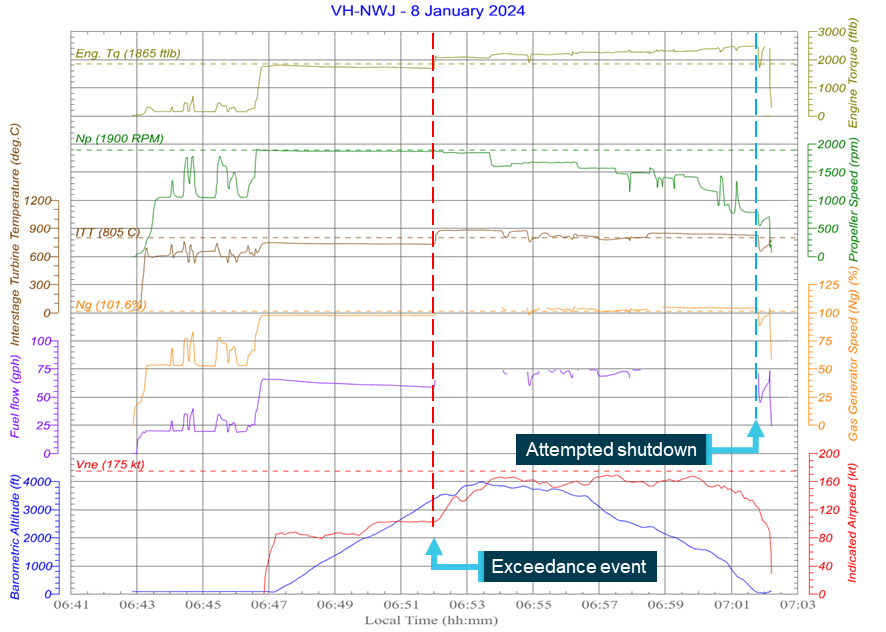
The data indicated at 0652:00 there was a sudden change in fuel flow and consequential increase in Ng, ITT and engine torque (the exceedance event). There was an associated momentary 25 rpm increase in Np but it returned to its prior setting of ~1,868 rpm immediately (Figure 7). After the exceedance event, fuel flow and Ng both appeared to increase to such an extent that the values went outside the range of sensor capabilities. This aligned with the pilot’s recollection that these parameter indications blanked on the G1000 display and were replaced by a red cross indication.
While flight and engine control positions were not recorded, engine parameter changes could be associated with certain inputs of the propeller and condition levers. Particularly, on short finals when the aircraft was approaching the runway threshold, a marked reduction in fuel flow, Ng, ITT, propeller speed and engine torque over 6 seconds was identified, indicative of an attempted engine shutdown. However, all these parameters then slowly increased over the next 18 seconds until about the time the aircraft overturned. The engine manufacturer could not understand the slow response without inspecting the FCU and advised that in throttle slam testing, the PT6A takes approximately 3–4 seconds to reach maximum power.[8]
Figure 7: Garmin G1000 recorded data for accident flight
Source: ATSB
Powerplant parameters
A review of the data showed that for the exceedance event, engine torque, ITT, and Ng all exceeded the upper limits including permitted transient periods and values. The variation in all 3 parameters were characterised by a step change in value over a 3 second period.
The Ng parameter recorded periods of valid and invalid data. Analysis of the data appeared to indicate periods where sensor values surpassed the limits of the recordable range. This interpretation would indicate Ng exceeded 105.16% for 2 minutes initially, with additional shorter exceedance periods also noted. Hence, the maximum Ng during the flight could not be determined. Regardless, assuming the invalid data were out‑of‑range values, the Ng exceeded the normal operating limit for a total period of more than 8 minutes.
ITT exceeded the normal operating limit from the exceedance event until approximately the time of the flare for landing (almost 10 minutes). The maximum recorded temperature was 885°C.
At the time of the exceedance event, engine torque increased from 1,700 ft-lb to ~2,080 ft-lb. In an attempt to control the engine and reduce propeller thrust, the pilot progressively coarsened the propeller pitch. This had the effect of increasing engine torque. The maximum engine torque recorded was 2,483 ft-lb.
Propeller speed was within limits for the entire flight except for a small, permitted transient event that occurred during initial power application at the start of the take‑off. Other engine parameters such as oil pressure and temperature remained within limits for the entire flight.
Fuel control unit
Malfunction conditions
There are at least 3 ways in which an FCU malfunction is known to affect engine performance:
engine power rolls back to idle
an inability to change the power setting, or
induce uncommanded engine acceleration.
A roll back to idle can result from Py leaks or governor spring failures. The EPL is provided for this situation and if used, can command more fuel as described above.
An inability to change power usually results from a control (power lever) disconnect. If more power was required than what was set at the time of the disconnect, the EPL could be used to achieve that. However, there is no way to reduce power other than to shut down the engine, that is, zero power.
An uncommanded acceleration can result from multiple sources in either the pneumatic or fuel side of the FCU. In the pneumatic side of the FCU, cap bearing distress, a sheared drive coupling, Py bleed blockage (multiple causes), drive body contamination, or split governor bellows can result in engine acceleration. The fuel side of the FCU includes possible failures such as splitting of the metering valve seat or bypass valve seal failure. Such failures will command the equivalent of pushing the power lever fully forward, or for some failure modes, possibly higher power levels.
Malfunction rates
FCU failure and malfunction rate information of PT6A engines was sought from the engine manufacturer. P&WC reported 13 uncommanded acceleration or the inability to reduce power events over a 10‑year period (2014–2024) for the C208/C208B Caravan and 19 similar events for other single‑engine aircraft types using a similar FCU configuration. The manufacturer also supplied 5‑year (2019–2024) malfunction rate data shown in Table 2. The data provided events in different classifications as well as malfunction rates over an equivalent period for power rollback events.
It was shown that half of all reported Honeywell FCU malfunctions on single‑engine aircraft, including the Cessna Caravan, were uncommanded engine acceleration or inability to reduce power situations. While this malfunction rate met acceptable levels of reliability for component part certification, the rate for uncommanded engine acceleration or inability to reduce power situations was higher than any other type of event and equated to 0.9 events per million flight hours as shown in Table 2 for PT6A‑114/114A engines fitted to the Cessna Caravan.
Table 2: 5-year malfunction rate (events per million flight hours)
Event type
All PT6A equipped with Honeywell FCU single‑engine
PT6A‑114/114A (Cessna Caravan)
All FCU events
2.2
1.8
Power roll back to idle
0.3
0.2
Uncommanded acceleration/ inability to reduce power
1.1
0.9
Source: Pratt & Whitney Canada
Operational information
Operator information
The aircraft operator, East Air, was conducting a non‑scheduled passenger service under Part 135 of the Civil Aviation Safety Regulations (1998) ‘Australian air transport operations – smaller aeroplanes’. The operator conducted multiple flights most days between Cairns and Lizard Island carrying passengers as required to and from the resort island.
Engine emergency scenarios
All Cessna 208/208B pilot’s operating handbooks and flight manuals incorporate emergency checklists and expanded procedures that include engine scenarios such as engine fire or engine failure. Specifically, the flight manual for the accident aircraft included engine failure emergency checklist procedures for 4 different phases of flight.
The manual also included 3 engine malfunction procedures including ‘Loss of Oil Pressure’, ‘Fuel Control Unit Malfunction in the Pneumatic or Governor Sections (Engine Power Rolls Back To Idle)’, and ‘Emergency Power Lever not Stowed’ at engine start, along with some related fuel system procedures. The FCU malfunction in the pneumatic or governor sections provided instruction, among other things, on the use of the EPL.
There was no procedure for an uncommanded engine acceleration or inability to reduce power. The ATSB sought the aircraft manufacturer’s (Textron Aviation) advice as to why there was no procedure for this type of malfunction. Textron Aviation advised that at the time of the aircraft’s certification, the flight manual was reviewed and approved by the United States Federal Aviation Administration and subsequently accepted by the Civil Aviation Safety Authority. It also advised that it was not aware of any single‑engine aircraft with a procedure for what to do if a pilot finds that they do not have control over an engine.
The ATSB sought the engine manufacturer’s (Pratt & Whitney Canada) advice as to why there was no procedure for an uncommanded engine acceleration or inability to reduce power malfunction. P&WC advised that, while it is the engine manufacturer, the aircraft manufacturer is responsible for developing the aircraft handling procedures, which are documented and approved through the aircraft flight manual. P&WC advised it would support any manufacturer in the development of suitable procedures.
The ATSB reviewed pilot operating handbooks and aircraft flight manuals for many PT6A powered single‑engine aircraft as well as those powered by other makes of turbine engines. While some aircraft types had propeller overspeed procedures, the only PT6A powered single‑engine aircraft identified that had a procedure that mentioned excessive power was the PA46‑600TP. This procedure stated that, for excess power when performing a manual [fuel] override operation, pitch up and deploy the landing gear and flaps. This was followed by an instruction to land as soon as possible and when landing was assured, to bring the condition lever to cut‑off/feather.
The C208B flight manual emergency procedures for engine failure and engine fire, as well as the normal procedure for engine shutdown, all called for the propeller to be feathered before the fuel condition lever was moved to the cut‑off position. In the event of an uncommanded engine acceleration, feathering a propeller prior to moving the fuel condition lever to cut‑off would increase the risk of overstressing the engine or airframe structures.
Training requirements
Parts 119 and 135 of the Civil Aviation Safety Regulations (1998) and the Part 135 Manual of Standards contained requirements for operator training of flight crew including proficiency checks in non‑normal and emergency procedures. As a Part 135 operator using a prescribed single‑engine aeroplane[9] they were required to have procedures in their exposition for engine malfunction or failure for certain phases of flight, for example, during the take‑off roll, take‑off below turnback height, and take‑off above turnback height. The standards also required procedures for other phases of flight in visual[10] and instrument meteorological conditions,[11] and further delineated between phases of flight above and below 1,000 ft above ground level.
Most relevant, the operator had to establish procedures to address certain defined engine failure and malfunction scenarios including ‘the exceeding of an engine performance parameter’. Advisory circular 135‑13 v1.0 Prescribed single‑engine aeroplanes, further explained this requirement and advised that these items would normally be addressed in the aircraft’s flight manual. However, if the detail in the flight manual was insufficient, operator customisation of their exposition was encouraged, provided that the mandatory matters of the flight manual were still included in the correct order.
The operator reported that it was previously unaware that the PT6A engine could malfunction in such a way as to produce an uncommanded acceleration. Hence, no training was conducted within the organisation for that type of failure, nor was there a procedure in the company’s exposition for the C208 aircraft.
Industry knowledge of uncommanded acceleration events
An ATSB review of selected training organisations in Australia conducting initial and conversion training for the Cessna Caravan, and similar types, identified limited industry knowledge of this type of engine malfunction. Those organisations had a range of knowledge on uncommanded engine acceleration malfunctions varying from:
no knowledge of the malfunction and thus no inclusion in their training syllabus
some knowledge of certain events and included a ‘discussion’ during class‑based training
knowledge of multiple events and inclusion of a procedure to follow in such situations.
Only one training organisation covered an uncommanded acceleration malfunction as part of its training syllabus. Its inclusion was based on the organisation having experienced such an event with one of its own aircraft. The emergency procedure was developed by the organisation and was based on its incident experience.
The pilot of this accident reported they had no knowledge that an uncommanded engine acceleration was a possible malfunction of the FCU, and they had subsequently talked to other pilots who also had not heard of such malfunctions.
Passenger safety
A passenger survey was conducted post‑accident with a 66% response rate. All respondents reported they received a safety briefing from the pilot before the flight, which included information about lifejackets, seatbelts, exits and fire extinguishers. Most respondents reported that they were aware of exit locations because of the briefing. Passengers were also asked about seatbelt fitment, with all of those that responded advising that they wore both the lap belt and shoulder harness. Two passengers reported the belts were ‘snug’. One passenger reported the shoulder harness was difficult to fit initially but was resolved and fitted correctly prior to take‑off.
The pilot recalled that, when the engine malfunction occurred, they turned to the passenger behind them and said, ‘we've got an engine issue, we've got to go back to Lizard [Island]’. While a passenger at the front of the aircraft reported they were alerted to an issue by the pilot, and they passed that information to some passengers behind, other passengers did not realise there was a problem until the aircraft was coming into land.
Three passengers reported that the pilot told them to brace for impact. After stopping, one passenger reported difficulty releasing their seatbelt due to them being upside down. Four respondents reported they were instructed to leave the aircraft, and 2 passengers reported the pilot gave instructions to move away from the wreckage once they had evacuated. Three passengers reported they left the aircraft by the rear left exit, which was opened by one of those passengers, and it was identified that 3 other passengers left by following the pilot out the front left door. One passenger got stuck exiting via the pilot’s door and required assistance from other passengers. Estimations by the passengers on time to evacuate ranged from ‘approximately 30 seconds’ to ‘less than a couple of minutes’.
Injuries reported by the passengers included bruising, cuts and abrasions, stiffness and soreness to joints and muscles. One reported receiving a seatbelt burn to their left shoulder. The most severe passenger injury was a laceration to the side of the head.
Related occurrences
A review of the ATSB’s aviation occurrence database between 2010 and 2024 involving aircraft with P&WC PT6A engines showed that there was one related occurrence during that period. Additionally, the Transport Canada Web Service Difficulty Reporting System[12] was also searched for power runaway events between 2014 and 2024. One defect in this system was also identified on the Transportation Safety Board of Canada investigation website. The following occurrences are a selection of those found as part of this search.
ATSB occurrence (OA2011-08920)
On 23 December 2011, while in cruise flight, the engine of a Cessna Caravan went uncommanded to full power and was unresponsive to power lever inputs. The aircraft was climbed to a safe height and the crew shut down the engine and glided to the destination airport. Recorded data indicated at times the ITT exceeded 920°C, Ng exceeded 112% and engine torque exceeded 2,300 ft‑lb. While the fault could not be replicated in bench tests of the FCU, an inspection revealed non‑required grease on the P3 air adapter mating face could have made its way to, and temporary blocked, the Py air bleed orifice, leading to the metering valve moving towards the maximum fuel stop.
Transport Canada defect report (20140908003)
The pilot of a Cessna 208 reported that, while flying, the power lever was moved to the idle position but there was no change in engine power. Engine torque stayed between 1,250 and 1,400 lbs. The FCU manufacturer found a cracked governing bellows.
Transport Canada defect report (20141218004)
On 4 December 2014, a Cessna C208B, experienced a runway overrun upon landing and came to rest in water. The aircraft sustained substantial damage, and the 6 occupants on board were not injured. The engine was reported to have had an uncommanded and uncontrollable acceleration.
Transport Canada defect report (20141218009)
After landing, during the engine shutdown procedure, the pilot of a Cessna 208B reported that the engine remained at flight [sic] idle even when the fuel condition lever was placed at ground idle [sic]. When they slightly moved the power lever, the engine experienced an uncommanded acceleration. After some manipulation of the condition and power levers, the pilot successfully shut down the engine.
Transport Canada defect report (20171103016)
During taxi, the pilot moved the fuel condition lever from low to high and noticed engine torque and Ng reached the upper limit, with the ITT crossing the red line. The pilot returned the condition lever back to the initial position, but the engine did not respond, with no changes to the indicated parameters. The crew attempted to maintain control but due to the aircraft’s speed, the aircraft flew to 100 ft off the ground. The crew elected to shut down the engine and landed uneventfully.
Transport Canada defect report (20190906001)
On 25 August 2019, while the aircraft was on approach for landing, the pilot reduced the power lever and reported that the torque did not reduce. The pilot elected to perform an in‑flight shutdown and landed uneventfully. The maintenance repair overhaul service provider performed an engine ground run, which was found satisfactory and elected to perform a flight test. During the flight test, the engine behaved as previously, and the pilot elected to perform a second in‑flight shutdown and landed again uneventfully. The failed part was reported as a cracked bellows in the FCU.
Transport Canada defect report (20210721007)
On 15 June 2021, when climbing through 2,500 ft above ground level, the engine tone on a Cessna 208 aircraft changed, and all engine parameters started increasing. The power lever was retarded, but the engine parameters such as propeller speed, engine torque, and ITT all increased continuously. All indications on the primary flight display for the engine turned red. The pilot declared an emergency and made a 180° turn back to the runway. To prevent damage to the engine, or possible catastrophic failure, the engine was shut down and a safe landing was made down wind.
Transportation Safety Board of Canada (A24C0004)
On 10 January 2024, the pilot of a De Havilland DHC‑3T Turbo Otter was unable to reduce engine power shortly after take‑off. The pilot activated the emergency power lever, but it had no effect. The pilot initiated a climb in an attempt to manage the airspeed. The flight proceeded to its destination, however, the airspeed increased to over 140 miles per hour, and the pilot’s side window shattered. When within range of the airport at approximately 4,000 ft, the pilot shut down the engine with the condition lever. The aircraft decelerated more quickly than anticipated and struck trees on final approach. The aircraft came to a stop beside the runway, sustained substantial damage but there were no injuries.
Safety analysis
Introduction
On 8 January 2024, a Cessna 208B Grand Caravan with a pilot and 9 passengers on board departed Lizard Island Airport to Cairns, Queensland. Shortly after take‑off, the aircraft experienced an uncommanded and uncontrolled engine acceleration. The pilot elected to return to Lizard Island where a high‑power, high‑speed landing was conducted that resulted in a runway overrun and the aircraft flipping over.
This analysis reviews the reason for the engine acceleration and the resulting effect on the flight. It also examines the aircraft procedures for Pratt & Whitney Canada PT6A engines, and industry awareness and training on experiencing an uncommanded engine acceleration event.
Uncommanded engine acceleration
Shortly after take-off, the engine experienced an uncommanded acceleration, which was detected by the pilot as a change to the engine sound and that the aircraft was accelerating. The pilot confirmed a malfunction by the available engine parameter displays, which were either beyond limits or not indicating. The pilot attempted to diagnose the malfunction but had no ability to correct the situation and thus elected to return to the departure airport. Recorded data reviewed by the ATSB confirmed the engine malfunction and engine parameter exceedances.
With no other pre-existing damage or faults found with the aircraft, the fuel control unit (FCU) was the only component that could produce such a malfunction. It was removed from the aircraft wreckage for further examination. The ATSB determined that the input drive shaft and drive coupling was serviceable. Unfortunately, further analysis by the manufacturer was unable to be conducted. Irrespective, and consistent with other related occurrences, an internal failure or foreign object contamination of the FCU was the only plausible explanation for the uncommanded engine acceleration, although the definitive reason for the malfunction could not be determined.
Contributing factor
Shortly after departure, the fuel control unit very likely malfunctioned resulting in an uncommanded engine acceleration event beyond limits, necessitating a return to the airport.
Runway overrun
The pilot, faced with an aircraft producing excessive power and thrust, inhospitable terrain, populated areas under the approach path, and a short runway, elected to perform a power on approach to land to enable them to control their final flightpath.
The pilot reported moving the fuel condition lever to cut‑off when the aircraft was on short finals and making the runway was assured. While the recorded data showed the engine parameters dropped significantly, the engine then accelerated slowly over the next 18 seconds to again exceed limits. The pilot recalled attempting to shut the engine down, however, the emergency power and condition levers were not found in their expected positions post‑accident. This, in addition to the flight data, showed that the engine had not been successfully shut down as intended. The slow response of the engine returning to excessive power could not be explained and was possibly associated with an FCU malfunction.
Due to the excessive speed and the downslope of the runway, the aircraft touched down about two‑thirds along the runway. Despite brake application, the aircraft left the end of the runway crossing uneven terrain with low foliage before a wingtip caught the ground and the aircraft flipped upside down.
Contributing factor
The engine power was unable to be reduced and the engine was not successfully shut down on final approach. As a result, the aircraft could not be slowed sufficiently to prevent a runway overrun.
Limited pilot and operator awareness
While the aircraft flight manual provided a procedure for scenarios such as an engine failure and FCU malfunction resulting in a roll back to idle power, there was no equivalent procedure for an uncommanded engine acceleration. Therefore, there was no documented procedure or troubleshooting information available to the pilot for this type of malfunction. Instead, the procedural options available were for an engine failure or fire, or the normal procedure for engine shutdown. However, for an uncommanded engine acceleration event, the steps in an engine shutdown procedure would have to occur in a different order so as not to overstress the engine or airframe structures.
Both the pilot and operator indicated that, prior to the event, they were not aware the FCU could malfunction in such a manner. There was also a mixed understanding from the flight training organisations consulted. While one organisation specifically trained for uncommanded engine acceleration malfunctions (based on directly having experienced the problem), the majority did not, though some did informally discuss the issue with trainees while not providing a procedure for handling the situation.
For Pratt & Whitney Canada PT6A engines, data provided by the manufacturer showed an uncommanded engine acceleration or inability to reduce power event occurred at a rate of 0.9 events per million flight hours. While this malfunction rate met acceptable levels of reliability for component part certification, the rate for uncommanded engine acceleration or inability to reduce power situations was higher than any other type of event, including roll back to idle events, for which a specific procedure existed. It is acknowledged that every type of event cannot be accounted for in an aircraft flight manual or the pilot’s operating handbook. However, given the likelihood of this type of event, it is important that pilots are aware that the event can occur and how best to manage such a situation.
As the pilot had intended to shut down the engine, it could not be determined if a lack of procedure and training influenced the accident. However, awareness and training for an uncommanded engine acceleration event will prepare pilots, ensure operations are performed correctly and consistently, and should result in a better outcome. As noted in the Civil Aviation Safety Authority advisory circular for prescribed single‑engine aeroplanes, it would also be beneficial for operators to develop strategies to manage this type of malfunction in the absence of a flight manual procedure. Otherwise, without formal procedures, pilots are required to exercise judgement and innovate in a highly stressful situation, based on their experience, skills and knowledge.
Other factor that increased risk
While uncommanded engine acceleration or inability to reduce power events occur at a higher rate than any other type of fuel control unit malfunction in Pratt & Whitney Canada PT6A single‑engine aircraft, there were no flight manual procedures addressing this type of occurrence. Consequently, there was limited awareness by pilots and operators on how to identify and safely respond to an uncommanded engine acceleration event.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine malfunction and runway overrun involving Cessna 208, VH-NWJ, at Lizard Island, Queensland on 8 January 2024.
Contributing factors
Shortly after departure, the fuel control unit very likely malfunctioned resulting in an uncommanded engine acceleration event beyond limits, necessitating a return to the airport.
The engine power was unable to be reduced and the engine was not successfully shut down on final approach. As a result, the aircraft could not be slowed sufficiently to prevent a runway overrun.
Other factors that increased risk
While uncommanded engine acceleration or inability to reduce power events occur at a higher rate than any other type of fuel control unit malfunction in Pratt & Whitney Canada PT6A single‑engine aircraft, there were no flight manual procedures addressing this type of occurrence. Consequently, there was limited awareness by pilots and operators on how to identify and safely respond to an uncommanded engine acceleration event.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions will be provided separately on the ATSB website on release of the final investigation report, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website after the release of the final report as further information about safety action comes to hand.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by East Air
As a result of this accident, East Air published a temporary revision to its Quick Reference Handbook for the Cessna 208B to include an emergency item for 'Unscheduled power increase during flight (High Torque, Ng, ITT and/or Fuel Flow)'.
Safety advisory notice to operators of PT6A engine aircraft
SAN number:
AO-2024-001-SAN-01
SAN release date:
22 August 2025
In the absence of a flight manual procedure and with limited industry awareness, the ATSB encourages operators of single‑engine PT6A powered aircraft to consider potential responses to an uncommanded engine acceleration event for different phases of flight, and to document and train pilots on appropriate actions to ensure operations are performed correctly and consistently.
Glossary
ATC
Air traffic control
EPL
Emergency power lever
FCU
Fuel control unit
ITT
Interstage turbine temperature
Ng
Gas generator speed. The rotational speed (depicted as a percentage of nominal speed) of the core compressor in a turbine or turboprop engine.
Np
Propeller speed. The rotational speed (depicted in revolutions per minute) of the propeller of a turboprop engine.
P&WC
Pratt & Whitney Canada
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passengers
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
Transport Canada
Transportation Safety Board of Canada
Queensland Police Service
recorded data from the primary flight display unit on the aircraft.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
United States National Transportation Safety Board
Transportation Safety Board of Canada.
Submissions were received from:
the pilot
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
Transport Canada Civil Aviation.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
[1]The Australian flight information region is split into 2 geographical areas each controlled by Brisbane Centre and Melbourne Centre. Each centre provides regional air traffic services.
[2]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[3]A gate is a second motion, additional lever or button that is required to be actioned in order to progress the movement of the lever. It is designed to prevent inadvertent progression of a lever to a position usually commanding a mode change or exceeding a limit.
[4]Beta mode is a range of propeller pitch angles that typically result in zero to negative thrust. Beta is used selectively for all ground operations aside from take-off.
[6]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
[7]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[8]Throttle slam testing involves moving the power lever from the idle position to maximum power position rapidly, and measuring the response time of the engine.
[9]Prescribed single-engine aeroplanes (PSEA) are single-engine aeroplanes that are approved, if suitably equipped, to perform passenger carrying air transport operations under instrument flight rules or visual flight rules at night. Pre‑2 December 2021, these aircraft were referred to as approved single-engine turbine powered aeroplanes (ASETPA).
[10]Visual meteorological conditions: an aviation flight category in which visual flight rules flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[11]Instrument meteorological conditions: weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules, rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[12]This system contains reports submitted to Transport Canada, the United States Federal Aviation Administration and the Civil Aviation Safety Authority defect reporting systems. It also contained defects occurring in countries outside these systems as P&WC submitted defects reported to them by operators worldwide.
Occurrence summary
Investigation number
AO-2024-001
Occurrence date
08/01/2024
Location
Lizard Island Airport
State
Queensland
Report release date
22/08/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Engine failure or malfunction, Runway excursion
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
208B
Registration
VH-NWJ
Serial number
208B2161
Aircraft operator
Townsville Airlines Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
The ATSB is investigating the collision between an A-double truck (road train) and an intermodal freight train near Cutana, South Australia, on 31 December 2023.
At about 1015 local time, the truck, travelling towards Broken Hill, entered the Barrier Highway level crossing into the path of Pacific National train 7SP5 travelling from Sydney, New South Wales to Perth, Western Australia. The collision between the lead locomotive and the second trailer of the truck resulted in the derailment of 2 locomotives, and several trailing wagons from the train. The locomotives, several trailing wagons and the trailer from the truck were destroyed. The crew of 7SP5 sustained fatal injuries. The truck driver received minor injuries and was transported to hospital.
A preliminary report, which detailed factual information established during the evidence collection phase, was released on 29 May 2024. See below.
To date, the ATSB investigation has included:
truck driver actions
collision dynamics and protection
emergency communications and risk identification
Barrier Highway level crossing design, compliance, and operation
train loading
truck and train driver fatigue and impairment
locomotive cab crashworthiness and Australian Standards
level crossing safety interface agreements and oversight
managing level crossing risk.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be published at the conclusion of the investigation. Should a critical safety issue be identified during the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 29/05/2024
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 31 December 2023, at about 0902 local time, a truck configured as an A-double[1] road-train (truck) departed Yunta, South Australia on the Barrier Highway in the direction of Broken Hill, New South Wales.
On the same day, following a crew change, the crew of Pacific National train 7SP5 reported to the network control officer that they had departed Broken Hill (towards Yunta) at 0919 (Figure 1).
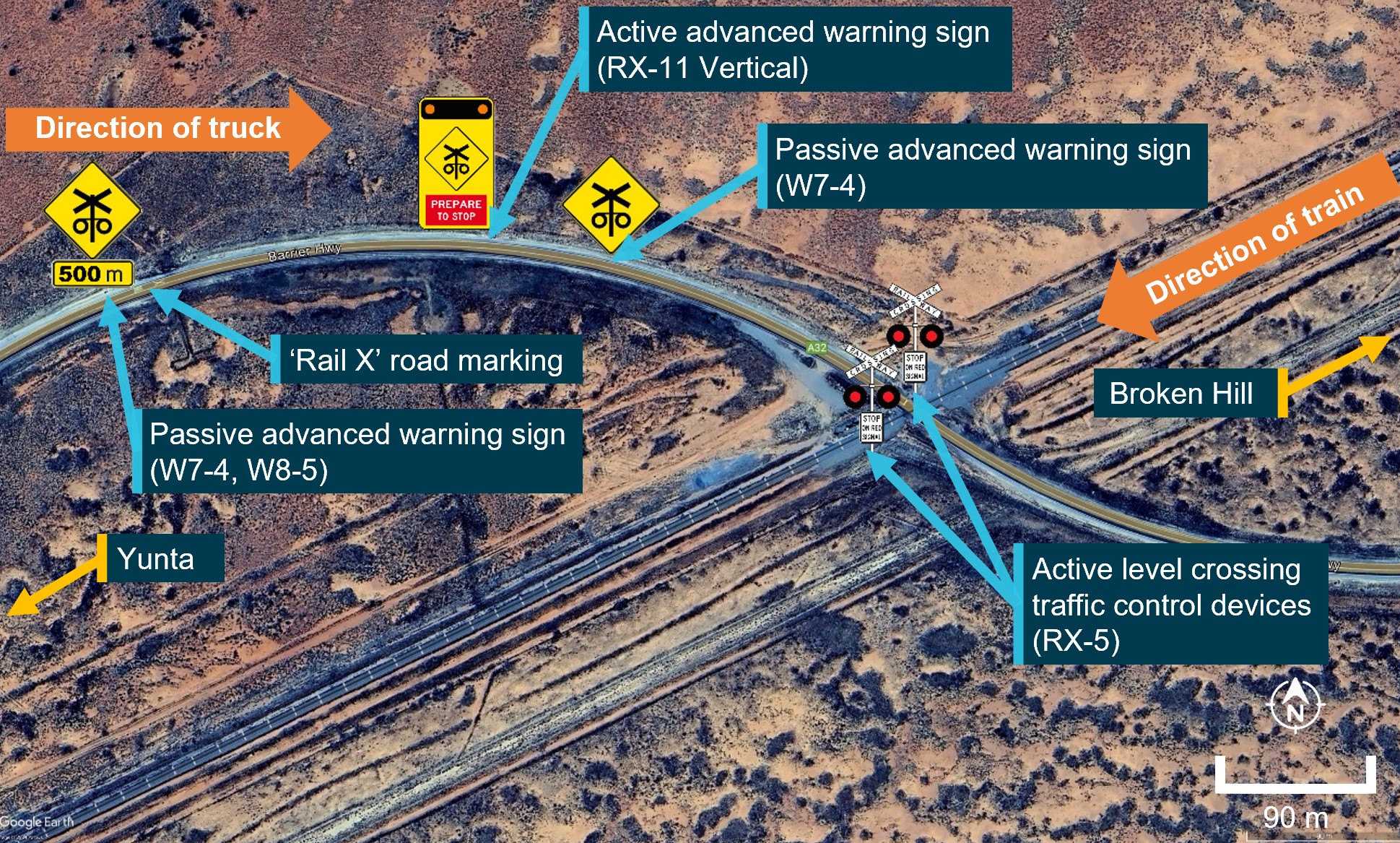
The road approach to the Barrier Highway level crossing near Cutana in the direction the truck was travelling consisted of a sweeping right curve. Passive road surface markings, as well as 2 passive[2] level crossing advanced warning signs, and an active[3] advanced warning sign provided advice to approaching road traffic of a crossing ahead.
The level crossing had active level crossing traffic control devices (flashing red light level crossing controls and bells). Further information about the advanced warning signs and traffic control devices is provided in the Level crossing section.
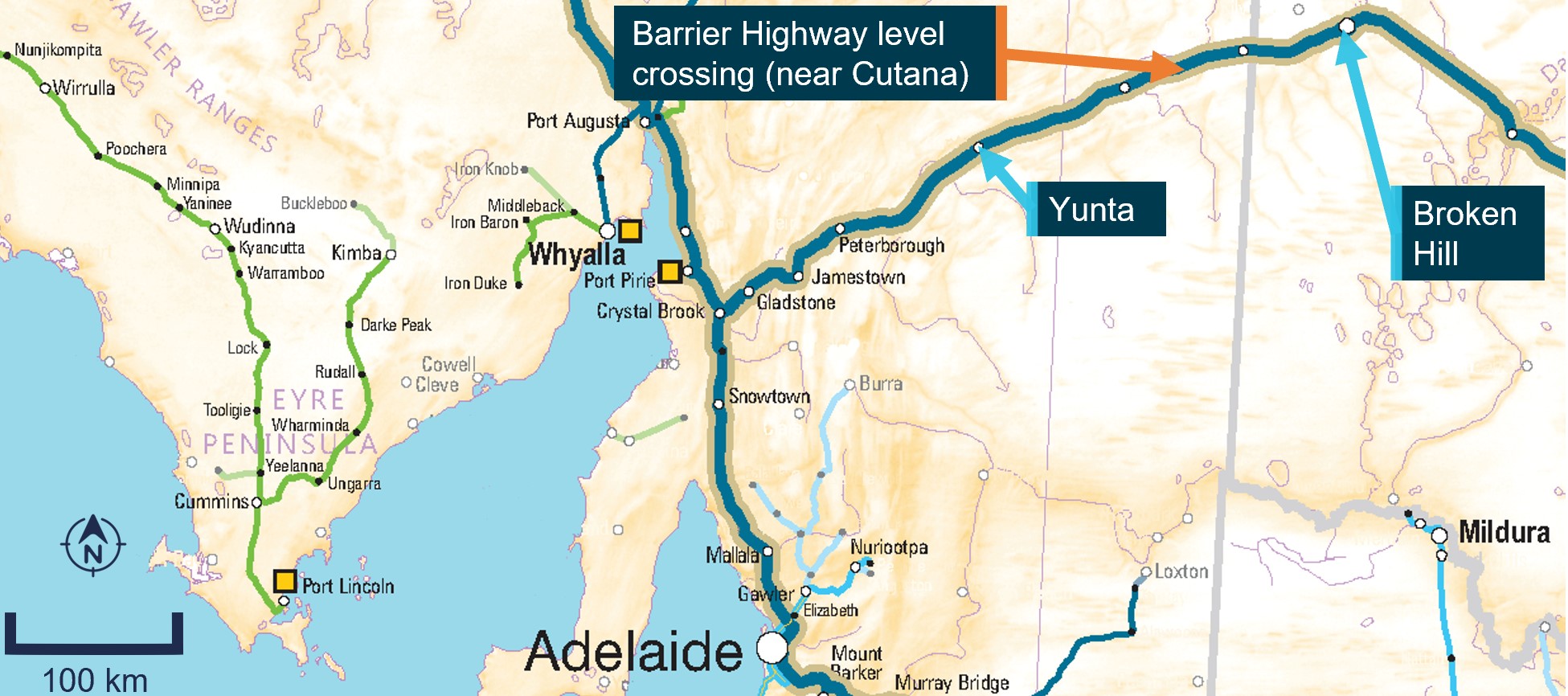
Figure 1: Map showing location of level crossing
Note: The image shows the Barrier Highway level crossing near Cutana, South Australia, in relation to Broken Hill, and Adelaide.
Source: ARA Railways of Australia Map 2014, annotated by the ATSB
As the train approached the level crossing, the active advanced warning sign and level crossing traffic control devices began operating. Recorded video from the truck as it approached the level crossing confirmed that the active advanced warning signs (flashing amber lights) and the active traffic control devices (flashing red lights) were operating. Recorded information from the locomotives confirmed that, during the approach to the level crossing, the headlight was on, the horn[4] was activated and an emergency brake application was made prior to the collision.
At approximately 1015 the truck, travelling at about 90 km/h, entered the activated level crossing into the path of Pacific National train 7SP5. The train, travelling at about 84 km/h, collided with the trailers of the truck, resulting in the derailment of both locomotives and 6 multi-platform 5-pack[5] wagons. The second trailer of the truck, both locomotives and several wagons were destroyed in the collision as well as substantial damage to the track and signal infrastructure, and active level crossing traffic controls (Figure 2). The train drivers received fatal injuries and no injuries were reported for the truck driver.
Figure 2: Overhead image of the accident site
Source: South Australia Police, annotated by the ATSB
At about 1030, the rail infrastructure manager (ARTC) received a number of calls from emergency services querying reports about a collision with a truck and derailment east of Yunta. The ARTC network control officer was unaware of a derailment or collision and commenced calling the crew of train 7SP5 that was known to be in that area.
The network control officer made multiple attempts to contact the crew via the train radio, before contacting Pacific National who then concurrently commenced trying to contact the crew via their personal mobile phones. At about 1124, a member of the public answered one of the train driver’s personal phones and confirmed to Pacific National that both drivers were fatally injured. Pacific National passed this information on to ARTC at about 1130, approximately the same time that the emergency services, despatched from Broken Hill, arrived at the scene.
Context
Truck information
The truck was a 2018 Kenworth T659 prime mover, coupled to 2 FTE3A model refrigerated semi‑trailers in an A-double road train configuration (Figure 3). The combined unloaded weight of the truck and trailer was about 35 t. At the time of the collision, the truck was loaded with avocados and was on a return trip from Perth, Western Australia. The estimated weight of the loaded truck trailer combination was 78 t.
The truck driver was an experienced driver who was familiar with the route along the Barrier Highway and this level crossing.
Figure 3: Truck configuration prior to collision
Source: Main image, Blenners Transport; inset image National Heavy Vehicle Regulator, annotated by the ATSB
Train information
Train 7SP5 was a Pacific National intermodal freight service, crewed by 2 drivers that was scheduled to travel from Sydney, New South Wales to Perth, Western Australia. Train 7SP5 consisted of 2 locomotives, lead locomotive NR41 and trailing locomotive NR79, with 27 loaded multi-platformed wagons. The train was 1,771 m in length, with a total weight of 3,898 t.
The train crew involved in the collision had commenced their driving shift at Broken Hill about an hour before the collision.
Infrastructure information
Road
The Barrier Highway was a sealed road surface and key road transport corridor connecting South Australia and Western Australia to the far and central west of New South Wales. The road manager for the section of the highway, including this level crossing, was the South Australian Department of Infrastructure (DIT).
The Barrier Highway at the location of the level crossing is oriented in a north-east to south-west direction before curving right immediately prior to the level crossing. On the other side of the level crossing, the road returned to a north-east to south-west orientation (Figure 4). The maximum speed limit for road-trains was 90 km/h.
Rail
The rail corridor at this location forms part of the defined interstate rail network, connecting New South Wales to South Australia, Western Australia, and the Northern Territory. The rail infrastructure manager for this section of the rail network was the Australian Rail Track Corporation (ARTC).
The rail infrastructure at the level crossing was a single bi-directional standard gauge line. The line had tangent track[6] with minimal gradient (about 1 in 450). The maximum track speed at the level crossing was 115 km/h.
Level crossing
The level crossing was located on the Barrier Highway, about 114 km north-east of Yunta and 84 km south-west of Broken Hill at the 309.701 km mark (Figure 1).
The land adjacent to the Barrier Highway on the approach to the level crossing was sparsely vegetated with low-lying stubble and minimal trees. There was minimal road gradient, with the road being about the same height as the train line around the vicinity of the rail approach towards the level crossing. On the southern side of the track, the ground surface did fall below the height of the road and rail infrastructure.
The level crossing approaches were fitted with passive road markings, passive advanced warning signs and active advanced warning signs (Figure 4). The placement of these signs from the level crossing, in the direction the truck approached the crossing, was about:
500 m for the first passive advanced warning sign (sign type W7-4 and W8-5)
485 m for the ‘Rail X’ road marking
267 m for the active advanced warning sign (sign type RX-11 vertical)
193 m for the last advanced warning sign (sign type W7-4).
The road manager (DIT) was responsible for the road markings and signage, and the maintenance and operation of the advanced warning signs.
The level crossing was equipped with active level crossing traffic control devices (flashing red light level crossing controls and bells). This consisted of 2 RX-5 style active level crossing traffic control devices on either side of the track and road. The active level crossing traffic control devices were comprised of light-emitting diode type lights with hooded housings and target boards to enhance visibility and were focused to provide warning to each road approach. The rail infrastructure manager (ARTC) was responsible for the maintenance and operation of the active level crossing traffic control devices.
There was an electronic interface between the ARTC and DIT electrical infrastructure at the site to enable coordination of the DIT active advanced warning signs with the ARTC active level crossing traffic control devices.
Figure 4: Aerial view of the level crossing approach and road alignment
Source: Google Earth, annotated by the ATSB
Further investigation
To date, the ATSB has:
attended and completed site inspections
interviewed directly involved parties
undertaken preliminary analysis of a number of sources of recorded data, including from the locomotive, the truck and network control.
The investigation is continuing and will include:
further analysis of the recorded data
review and examination of similar occurrences
analysis of the operation of the truck and train
review and examination of safety interface agreements
analysis of the locomotive human survivability aspects with respect to train crew injuries
review of train emergency alerting and location systems
examination of the road-rail interface infrastructure, design, and environment.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]A-double means a heavy road vehicle combination not longer than 36.5 m consisting of a prime mover towing two trailers in which the first semi-trailer is connected to the prime mover by a roll coupled connection and the second trailer is a dog trailer. A-doubles are sometimes called double road trains.
[2]Passive: warning or control of the movement of vehicular or pedestrian traffic across a railway crossing by signs and devices, none of which are activated during the approach or passage of a train, and which rely on the road user including pedestrians detecting the approach or presence of a train by direct observation.
[3]Active: warning or control of the movement of vehicular or pedestrian traffic across a railway crossing by devices such as flashing signs/signals, gates or barriers, or a combination of these, where the device is activated prior to and during the passage of a train through the crossing.
[4]The operation of the locomotive horn in a NR class locomotive also commences operation of the oscillating ditch lights on the front of the locomotive intended for enhancing the visibility of the leading vehicle of a train from the perspective of a driver of a motor vehicle approaching a level crossing.
[5]5-pack wagon: an articulated wagon comprising 5 platforms.
The Australian Transport Safety Bureau has released an interim report detailing contextual information established as part of its ongoing investigation into the mid-air collision between two helicopters on the Gold Coast one year ago.
The report is intended to update the industry and public on the progress of the ATSB’s independent ‘no blame’ investigation, which is conducted with the goal of improving transport safety.
“To date, the ATSB has undertaken extensive work to understand and recreate the events of the day in order to identify and examine the context and risk controls that existed at the time,” Chief Commissioner Angus Mitchell said.
“The ATSB analysis framework looks at a hierarchy of factors arranged in their relative proximity to an event, and this investigation has so far concentrated on elements closest to the event: individual actions, vehicle/equipment performance, local conditions, and risk controls.”
This work has included interviews with key personnel and witnesses, the examination of both helicopters, maintenance logs, and postmortem information, a review of industry understanding of seat belt fitment, and analysis of ADS-B and radar flight tracking information, CTAF recordings, and video imagery.
“A large amount of the evidence gathered through this work is detailed in today’s interim report, and investigation into and analysis of many of these areas is ongoing,” Mr Mitchell said.
Mr Mitchell noted the evidence includes a toxicology report for the fatally injured pilot, showing a positive result for low levels of cocaine metabolites.
“A forensic pharmacologist engaged by the ATSB has stated that the very low concentrations of these metabolites suggest exposure was not likely to have occurred in the 24 hours prior to the accident, and it is unlikely there would have been impairment of the pilot’s psychomotor skills,” he said.
“It is important to note while this is a substantive and comprehensive interim report, the ATSB is yet to make formal findings as to the contributing factors that led to this accident as we are continuing our analysis of that evidence.”
Moving forward, Mr Mitchell said the investigation would consider whether any systemic factors contributed to, or increased risk in the accident.
“This will include consideration of the design of the operating environment and operating procedures, the onboarding and implementation of aircraft, change management, and the regulatory environment and input,” he explained.
The ATSB’s final report, which will include analysis, findings, and any recommended safety actions, is on track for an anticipated completion in the third quarter of 2024.
“This was a tragic accident, and it is our responsibility to make findings and drive safety actions, which reduce the likelihood of a similar occurrence in the future,” Mr Mitchell said.
The interim report notes several steps which have already been taken in response to the accident.
After reviewing its processes and procedures, Sea World Helicopters has implemented a new ‘pad boss’ traffic advisory role, added air traffic systems to each of its helicopters’ avionic systems, increased communication protocols, and taken steps to make its helicopters more visible.
Separately, the ATSB issued a Safety Advisory Notice in September, targeting aircraft lifejacket manufacturers and national aviation certification authorities.
“During this investigation, our investigators identified a potentially common lack of understanding in the broader helicopter tourism community about how constant wear lifejackets should be worn in conjunction with seatbelts,” Mr Mitchell explained.
“This correlated with a discovery that some passengers’ seatbelts were not fitted correctly in this accident, in part due to interference from their lifejackets – although we have not attributed this to the tragic outcomes in this case.”
The Australian Transport Safety Bureau has commenced a transport safety investigation into the level crossing accident involving a freight train and a truck on the Barrier Highway, South Australia, on Sunday morning.
The ATSB is deploying Adelaide-based transport safety investigators, with experience in train and railway operations, to the accident site.
As part of their evidence collection activities investigators will examine the level crossing infrastructure and rollingstock, interview involved parties and any witnesses, examine truck and train operational information, recover any relevant components for further examination at the ATSB’s laboratories in Canberra, and analyse any recorded information.
The scope of the investigation and its timeframe will be determined as the ATSB builds its understanding of the nature of the accident.
The ATSB will release a final report at the conclusion of the investigation, detailing its analysis and findings.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
Two trams collided at the intersection of Victoria Parade and Nicholson Street in Melbourne, after a set of points turned one tram off its intended course and into the path of the other, a preliminary transport safety investigation report has detailed.
An investigation is ongoing into the collision, which resulted in substantial damage to the lead car of both trams, as well as minor injuries to one driver and five passengers.
The investigation is led by the Office of the Chief Investigator, Transport Safety, which conducts rail investigations in Victoria on behalf of the Australian Transport Safety Bureau.
The preliminary report is released to provide timely information to industry and the public. It does not include analysis or findings, which will be released in a final report at the conclusion of the investigation.
The preliminary report notes the trams were running in opposite directions on route 96, between Brunswick East and St Kilda Beach.
“On this route, the trams should have passed one another on parallel tracks along Nicholson Street, as they crossed Victoria Parade – one from the north and one from the south,” Chief Investigator Mark Smallwood explained.
“However, a set of points was set such that the north-travelling tram turned to the right, down Victoria Parade, and into the path of the south-travelling tram.”
Each tram was travelling at about 20 km/h at the time of the collision, and both derailed.
The preliminary report includes photographs, diagrams and descriptions of the intersection, signals, road markings and infrastructure involved in the incident.
It notes the previous north-travelling tram which travelled through the intersection prior to the accident, had set the points and turned right onto Victoria Street.
The report notes that north-travelling trams do not turn right onto Victoria Street as part of the standard operation of any route, and trams would only turn right if travelling on an amended route, or when being directed to another location.
“As our investigators continue their work, they will review and examine the operation of both trams, and the functioning and operation of their equipment, as well as track infrastructure, signalling, and traffic management systems,” Mr Smallwood said.
“Investigators will also consider the design and arrangement of infrastructure at the intersection, and the management of safety risk associated with trams deviating from their designated route.”
A final report will be released at the conclusion of the investigation.
A transport safety investigation is continuing into the grounding and wreck of the pilot launch PV Corsair off Point Lonsdale, Victoria, with early evidence published in a preliminary report.
Victoria’s Office of the Chief Investigator, Transport Safety is undertaking the investigation in an agreement with the Australian Transport Safety Bureau, under the Commonwealth Transport Safety Investigation Act 2003.
The preliminary report, which does not include analysis or findings, notes the launch was returning after collecting a pilot from an outbound container ship when, just after 11 pm on 5 October 2023, it entered shallow water surrounding Point Lonsdale Reef, and then ran aground.
Fortunately, Corsair’s coxswain and deckhand, and the pilot they had collected, were safely rescued from the vessel by Victoria Water Police about 90 minutes later.
The vessel, however, was destroyed on the reef during the night, and the debris was recovered the following day.
“Point Lonsdale makes up the western side of the Port Phillip Heads – the mouth of Port Phillip, through which all ships visiting the ports of Melbourne and Geelong must pass,” Chief Investigator Mark Smallwood said.
“Point Lonsdale Reef, an outcrop of flat-topped rocks, extends up to about 540 m south-east of Point Lonsdale, and sits west of a defined small craft channel – which itself is to the west of a number of channels suitable for larger ships.
“The extent of the reef’s exposure and its visibility varies with tide and sea conditions.”
To date, the transport safety investigation has included interviews with relevant personnel, vessel inspections, the examination of pilot launch track recordings from the accident and previous transits of the Heads, and a review of relevant communications.
“As it progresses, the investigation will consider the operation of Corsair, including bridge resource management, and will further examine relevant safety management systems and vessel data recordings,” Mr Smallwood said.
A final report will be released at the conclusion of the investigation.
“Relevant parties will be notified immediately, should the investigation identify a critical safety issue before the final report is complete.”
Plan continuation bias probably influenced a pilot’s decision to continue their visual flight rules flight despite forecast unsuitable weather prior to a controlled flight into terrain accident west of Brisbane, an ATSB investigation report explains.
On the morning of 29 August 2022, a Cessna R182 Skylane RG operating an air transport (charter) flight with a pilot and two passengers on board collided with terrain in the D’Aguilar Range, about 36 km north-west of its destination of Archerfield Airport. All on board were fatally injured.
The Cessna had departed from Dalby toward forecast en route weather unsuitable for visual flight, despite the pilot only being qualified for flight in visual conditions.
After crossing a section of the Great Dividing Range below cloud, and with minimal terrain separation, the pilot continued the flight in similar conditions toward the Lake Manchester VFR route, adjacent to the D’Aguilar Range.
“The aircraft very likely entered cloud while manoeuvring in this area, resulting in the pilot losing visual reference with the ground, eventually leading to controlled flight into terrain,” ATSB Chief Commissioner Angus Mitchell said.
“The pilot was probably influenced by plan continuation bias – an internal pressure or desire to get to the destination – to continue the flight, which probably became stronger as they got closer to Archerfield,” Mr Mitchell said.
However, due to a lack of information, the ATSB was unable to determine the reasons why the pilot continued the flight at cruise speed and low level into unsuitable weather in the vicinity of known high terrain. The ATSB considered it unlikely that there was any direct or perceived organisational pressure on the pilot to continue the flight.
As the report notes, the safety risks of visual pilots flying into non-visual conditions are well documented.
“This Christmas period, especially with wet weather around the country, the ATSB urges all VFR pilots to be mindful of the subtle pressures of plan continuation bias,” Mr Mitchell said.
“Be prepared to amend and delay plans to fly due to poor or deteriorating weather and environmental conditions, and not to push on,” he said.
“Have alternate plans in case of unexpected changes in weather, and make timely decisions to turn back, divert or hold in an area of good weather.”
While not determined as a contributing factor in the accident, the ATSB also found the operator’s hazard and risk register did not identify inadvertent entry into non-visual conditions as a hazard.
“Not including inadvertent entry into non-visual conditions in its hazard and risk register – which formed part of the operator’s safety management system – reduced the operator’s ability to effectively manage that risk,” Mr Mitchell explained.
Since the accident, the operator has removed aeroplane operations from its Air Operator’s Certificate and, after a risk assessment, plans to implement two risk controls for its helicopter operations by February 2024.
First, the operator will update its operations manual to include a formal organisational policy for supporting pilots to land or return to a safe landing site if they assess that they will be unable to maintain visual meteorological conditions.
Second, annual operator proficiency checks will include techniques for avoiding, and recovering from, inadvertent entry into non-visual conditions.