
Final report
Report release date: 16/10/2025
Investigation summary
What happened
On 6 October 2023, a Cirrus Design Corporation SR22 aircraft, registered VH-MSF, was being operated on a private instrument flight rules flight from Canberra, Australian Capital Territory, to Armidale, New South Wales. On board the aircraft were the pilot and 3 passengers.
About 12 minutes after take-off, at an altitude approaching 10,000 ft above mean sea level, the aircraft aerodynamically stalled, departed from controlled flight, entered a high vertical descent developing into a spin, and impacted with terrain. All occupants were fatally injured, and the aircraft was destroyed by a post‑impact fire.
What the ATSB found
The ATSB found that the flight track data showed that, at about 8,000 ft, the aircraft had begun to deviate from its flight track, with heading, altitude and airspeed deviations. Those deviations coincided with reports from ear witnesses located below the aircraft’s flight path of sounds consistent with engine surging.
The data also showed that the aircraft had a high rate of climb (up to 1,500 ft/min) coupled with a low and decreasing airspeed, which led to an aerodynamic stall and rapid descent. Recovery actions from the aerodynamic stall did not occur and the Cirrus aircraft parachute system was not deployed in-flight. It was also noted that no radio calls were received from the pilot to indicate there was a problem prior to the stall.
VH-MSF was not fitted with an anti-icing system and was prohibited from operating in icing conditions. Moderate icing conditions were forecast along the aircraft’s flight path from 7,000 ft to 10,000 ft when in cloud. It was likely that the aircraft had encountered icing conditions prior to the aerodynamic stall. However, the ATSB was unable to determine if these conditions were sufficient to have adversely affected the aircraft’s performance and/or handling.
The ATSB considered several scenarios to establish the reason for the deviations in flight track, subsequent stall and absence of recovery actions. These included in-flight icing, pilot incapacitation and possible aircraft issues. However, due in part to a significant post-impact fire, which limited the collection of evidence, the circumstances preceding the stall and impact with terrain could not be determined.
Safety message
Although it could not be established that icing contributed to the accident, operating in these conditions in aircraft that are prohibited from doing so increases the risk of a loss of control event leading to an accident. Aircraft flying through cloud in sub-freezing temperatures are likely to experience some degree of icing. A pilot can reduce the chance of icing becoming an issue by selecting appropriate flight routes, remaining alert to the possibility of ice formation and knowing how and when to operate de-icing and anti-icing equipment if fitted.
The occurrence
Accident flight details
On 3 October 2023, a Cirrus Design Corporation SR22 aircraft, registered VH-MSF, was operated on a private flight from Redcliffe, Queensland, to Armidale, New South Wales, and then on to Canberra, Australian Capital Territory, the following day.
On 6 October 2023, the return sectors were planned to operate from Canberra to Armidale, with a planned return to Redcliffe. On board the aircraft were the pilot and 3 passengers.
At about 0648 local time, the pilot submitted an instrument flight rules[1] flight plan to Airservices Australia to fly from Canberra to Armidale with an estimated departure time of 1430. The flight planned track was via waypoint[2] ‘CULIN’ (about 31 km west of Goulburn) and Scone, New South Wales, at a cruising altitude of 10,000 ft above mean sea level (AMSL), using RNP 2[3] navigation performance. The lowest safe altitude from Canberra to CULIN was 4,600 ft. While there was no published instrument flight rules route from CULIN to Scone and from Scone to Armidale, the pilot’s flight planning software application provided a lowest safe altitude of 6,000 ft from CULIN to Scone and 6,300 ft from Scone to Armidale using RNP 2 performance.
On contact with Canberra ground air traffic control at 1422, the pilot was provided an airways clearance to track to Armidale via their flight planned route at 10,000 ft.
At about 1437, the aircraft departed Canberra Airport. Soon after take-off, the pilot was transferred to, and established radio communication with, the approach controller, reporting that they were on climb through 3,400 ft (to their assigned cruise altitude) and turning left onto their assigned radar heading of 070°. A short time later, the controller instructed the pilot to turn left onto a heading of 010° and the pilot completed readback of the instruction. About 1 minute 30 seconds later (at about 1442), the controller cleared the pilot to resume their own navigation and track direct to waypoint CULIN. The pilot completed readback of that instruction, which was the last transmission received from the pilot. All transmissions made by the pilot were clear and concise. Flight data showed that the aircraft turned 5° to the left of the direct track to waypoint CULIN.
During the flight, data was being transmitted by the aircraft’s automatic dependent surveillance broadcast (ADS-B) equipment.[4] A review of that data indicated that the aircraft was climbing through about 7,000 ft AMSL as it turned to track towards CULIN. During that turn, the ground speed increased, over a period of about 30 seconds, from about 110 kt (204 km/h) to 135 kt (250 km/h).
Climbing above 7,500 ft, the data indicated the aircraft’s ground speed had started to reduce, at an approximately linear rate, with a reduction of about 22 kt (41 km/h) over a 65‑second period. At that time, the data showed a relatively constant rate of climb generally between 550–750 ft/min.
Passing through 8,300 ft, the somewhat linear flight track altered to an onset of heading, altitude and airspeed variations. The ADS-B data indicated the ground speed then started to increase as the aircraft entered a slight descent. Over the next 4 minutes, the aircraft’s track varied up to 35° and the ground speed fluctuated between 93 kt and 121 kt (172–224 km/h). During this period, the altitude was generally increasing, although at a varying rate, with shorter periods where the altitude and reported rate of altitude change indicated that the aircraft had started to descend.
The ADS-B data showed that, at about 12 minutes into the flight, the aircraft descended by about 250 ft, increased speed by about 13 kts and then climbed at a rate up to about 1,500 ft/min. While in that climb, the airspeed reduced significantly and from a calculated pressure altitude of 9,946 ft, at 1448:37, the aircraft departed controlled flight and descended rapidly towards the ground. For more details on the aircraft’s movements refer to the Recorded information section. About 44 seconds after the onset of the departure from controlled flight, the aircraft collided with terrain (at a ground elevation of about 2,250 ft) and was destroyed by impact forces and a post-impact fire. All occupants were fatally injured. An eyewitness was the first responder on the scene and notified emergency services.
Figure 1 illustrates the ground track of the aircraft departing Canberra while assigned radar vectors and the direct track to CULIN.
Figure 1: Ground track of VH-MSF (in blue) from take-off to the accident site
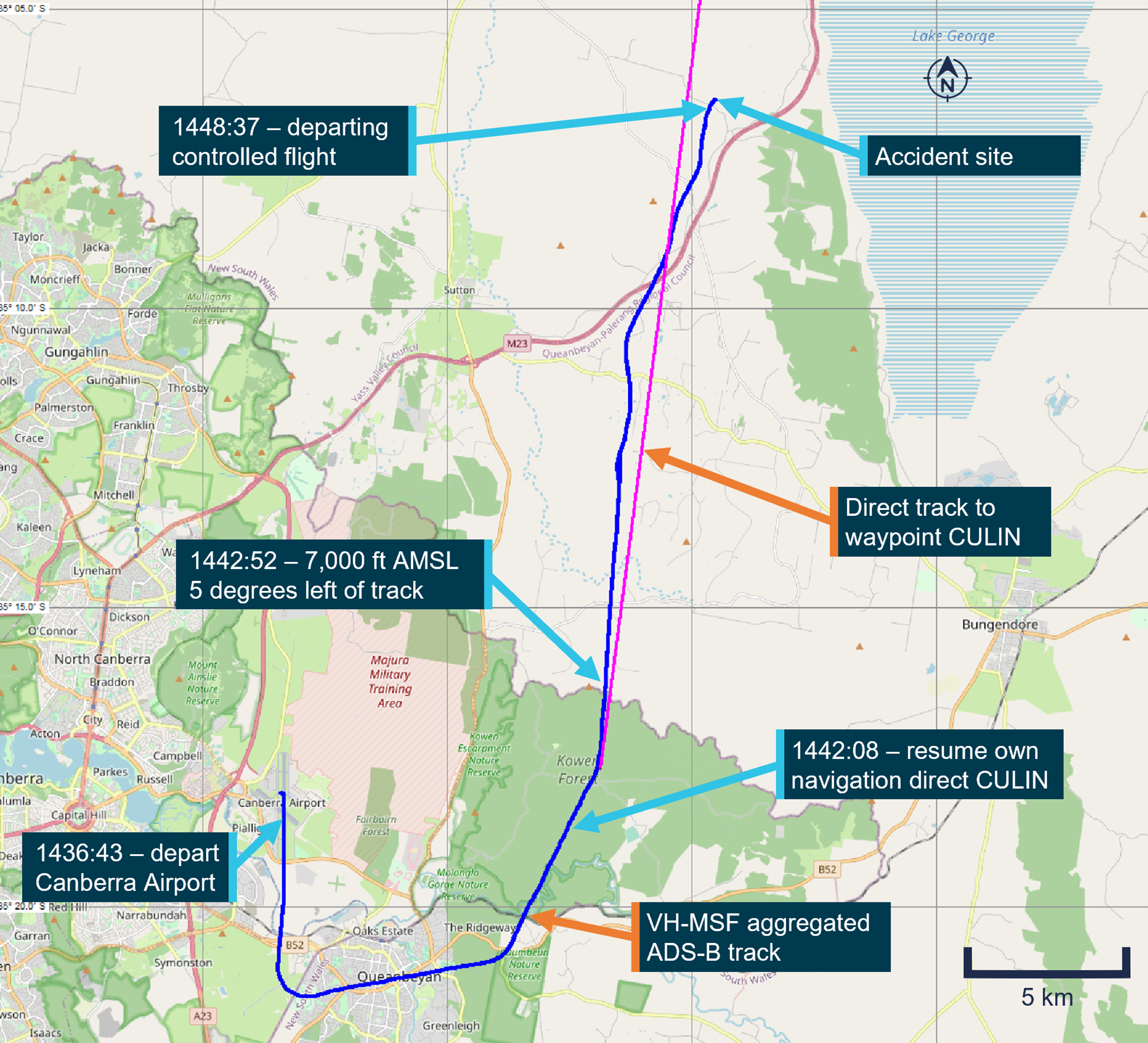
The aircraft ground track overlaid on this map is referenced to a latitude and longitude grid aligned to true north. The headings assigned by air traffic control are referenced to magnetic north. In the Canberra region, magnetic north is about 12° less than true north. An aircraft’s ground track relevant to the assigned heading can also be affected by wind. Source: OpenStreetMap with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Witness observations
Figure 2 and Table 1 show the witness locations and observations along the aircraft’s flight path; earwitnesses reported hearing aircraft engine noises and 2 eyewitnesses reported seeing the aircraft in its final moments before the impact with terrain.
Four independent ear witnesses (1 through 4 in Table 1) in the local area where the aircraft was climbing through about 8,000 ft described hearing a rough running or surging (revs increasing and decreasing) light aircraft engine, which was likely to be VH-MSF. Another 2 earwitnesses located closer to the accident site reported hearing varying engine sounds (5 and 8 in Table 1).
Two eyewitnesses (6 and 7 in Table 1) in the local area of the accident site described seeing the aircraft at a low altitude, descending rapidly with its nose pitched down and rotating like a corkscrew (spiral descent). One of these witnesses stated that they heard the aircraft approaching with the engine noise fluctuating[5] and the engine running during the descent, but went quiet just before impact. The other eyewitness was seated on a tractor with the engine running and did not hear the aircraft engine.
Table 1: Ear and eyewitnesses summaries with reference to Figure 2
| Ear/eyewitness | Description |
| 1 - Earwitness | Heard a light aircraft heading in a north-east direction. It was dropping engine revs and returning to normal revs. I heard this happen several times. |
| 2 - Earwitness | Heard a small aircraft that seemed to be having engine problems overhead. The engine was revving then stuttering – they could not see the aircraft (cloud). |
| 3 - Earwitness | Heard a small aircraft making sounds like it was cutting out and restarting – they could not see the aircraft (cloud). |
| 4 - Earwitness | Engine sounded rough, sputtering. It did not sound like the abrupt silence of a mechanical failure. Sounded like the engine might be starving for fuel – they could not see the aircraft (cloud). |
| 5 - Earwitness | Unusual aircraft noise like engine cutting in and out – they could not see the aircraft (cloud). |
| 6 - Eyewitness | Heard the aircraft approaching with engine noise fluctuating but they could not see the aircraft until it exited below cloud in a steep nose down spiralling descent – the engine was running during the descent but went quiet just before impact. |
| 7 - Eyewitness | Eyewitness to the last couple of steep nose down spiral turns below the cloud before impact. They did not see any smoke coming from the aircraft. Was on a tractor and did not hear the aircraft at any time. |
| 8 - Earwitness | I heard a light plane revs of the engine gradually increasing to its maximum revs and then I heard a loud metal on metal clunking sound and then I heard the explosion about 4 seconds later and saw smoke coming up from a neighbouring property. |
Figure 2 shows the aircraft flight track, and the location of each ear/eyewitnesses summarised in Table 1.
Figure 2: Aircraft flight path with ear and eyewitnesses’ locations
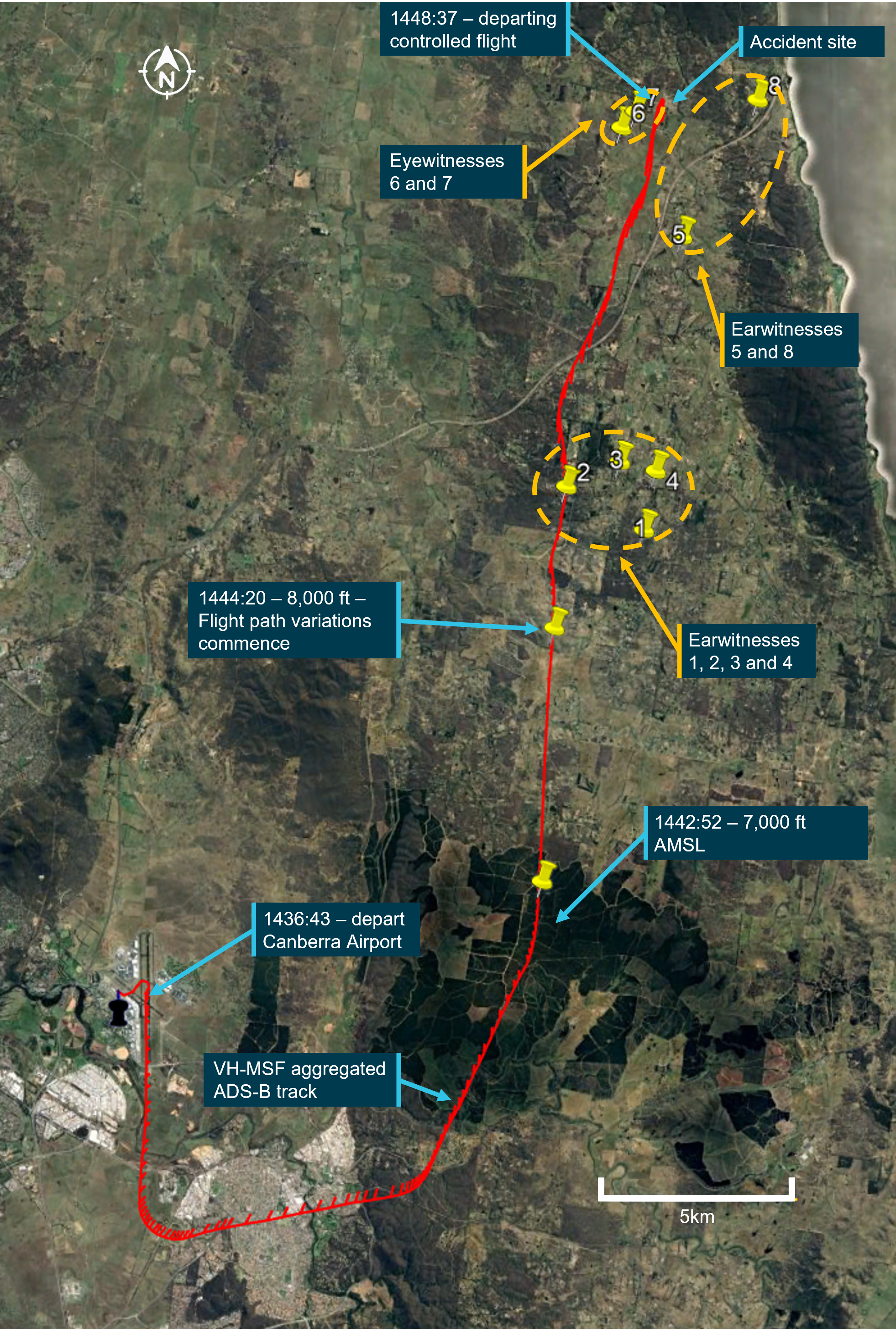
Source: Google Earth, with ADS-B data from Airservices Australia, annotated by the ATSB
Context
Pilot information
The pilot held a valid private pilot licence (aeroplane), issued in 1985 (re-issued as a Civil Aviation Safety Regulations Part 61 licence in August 2016), and class ratings for single‑ and multi‑engine aeroplanes. The pilot was initially issued with a command instrument rating for single‑engine aeroplanes in 1987 and their most recent flight review, on 29 August 2023, was an instrument rating proficiency check with an endorsement for multi-engine aeroplanes.
Insurance documentation indicated that the pilot had accumulated about 800 hours total flying experience, with about 180 hours in Cirrus SR22 aircraft, including 12.5 hours in VH‑MSF. The owner of VH-MSF had conducted several flights with the pilot and described them as being a good and careful pilot with no problems entering cloud and utilising the instruments.
Aircraft information
General information
VH-MSF was a Cirrus Design Corporation SR22 low-wing aircraft with 4 seats and a fuel‑injected piston engine driving a constant speed 3‑blade propeller. It had a ballistic parachute system (Cirrus airframe parachute system – CAPS) fitted as standard. The aircraft was fitted with a cabin and windshield heating system, which utilised warm air ducted from the engine exhaust shroud.
The aircraft (S/N 0153) was manufactured in the United States in 2002 as a G1 model. It was purchased by the owner in the United States and first placed on the Australian aircraft register in 2017. It was issued a standard certificate of airworthiness in the normal category. Since then, it had been operated by its owner for private use, community service flights and had been leased to other private pilots (Figure 3).
Figure 3: Cirrus Design Corporation SR22, registered VH-MSF

Source: Aircraft owner
Aircraft maintenance
The current maintenance release was on board the aircraft and was destroyed. A carbon copy of the maintenance release was provided by the aircraft maintainer. It showed that the required 100‑hour/annual inspection was conducted and a maintenance release was issued on 9 November 2022 at an aircraft time-in-service of 2,558.9 flight hours. Inspection of the maintenance release copy, aircraft logbook and worksheet records showed there were 2 items of maintenance that were past their calendar due date. They were a standby compass calibration and an outside air temperature/clock back-up battery replacement, both due about 2 months before the accident. The aircraft owner advised that the overdue maintenance items were an oversight.
The aircraft was certified for use in the private category and for instrument flight rules (IFR) operations. Maintenance documentation showed that the CAPS was inspected, and the parachute and rocket motor assemblies were replaced due to time expiry in January 2023. At the time of the accident flight, the airframe, engine and propeller had accumulated the following hours:
- airframe – 2,635.5 hours total time-in-service
- engine – 1,192.0 hours’ time since overhaul
- propeller – 133.3 hours’ time since overhaul.
It was reported that, in September 2023, the aircraft was hard to start, and the starter motor was replaced, which resolved the issue. The aircraft owner also advised that, in the days prior to the accident flight the pilot had reported that the power lever was stiff to operate. In response to this, the owner checked the lever and determined that the reason for the stiffness was due to the friction adjustment, which had been wound up to a high friction setting. Following readjustment, when the friction was wound off, the power lever was free to move with no issues.
Two and 3 days prior to the accident, post-flight at Armidale and Canberra, the pilot had reported to their family and the owner that the aircraft had operated with no issues. The ATSB did not identify any maintenance issues that may have contributed to the accident.
Flight instrumentation
There were 6 primary flight instruments fitted to the aircraft. They were the airspeed indicator, attitude indicator, altitude indicator, turn coordinator, heading indicator, and vertical speed indicator (Figure 4). The aircraft was fitted with a Sandia SAI-340 model attitude indicator, which also incorporated airspeed, altitude and slip indicators. The unit contained a rechargeable battery capable of providing continued operation in the event of aircraft electrical failure. Maintenance documentation showed that the attitude indicator had been replaced in 2018 with a repaired model that had a software upgrade to include the addition of a vertical speed function.
Figure 4: VH-MSF flight instruments with Sandia attitude indicator top centre

Source: Aircraft owner
The United States Federal Aviation Administration issued an emergency airworthiness directive (AD), AD‑2020‑18‑51, for Sandia attitude indicators in 2020. That directive stated the applicability as being for Sandia attitude indicator part number 306171‑10 and 306171‑20. These attitude indicators may be marked as Bendix King Model KI‑300 or Sandia Model SAI‑340A. They may be installed on aircraft certificated in any category. It also stated that the AD was prompted by reports of 54 failed attitude indicators, which produced erroneous attitude data to the pilot and autopilot, if equipped. The FAA issued the AD to prevent aeronautical decision-making based on erroneous attitude information, which may result in loss of control of the aircraft.
The attitude indicator fitted to VH-MSF was the Sandia SAI-340, part number 306171-00, which was outside the applicability of the emergency AD. Further, the aircraft owner reported that the attitude indicator had not had any issues since it was installed in 2018.
Electric trim control system
The aircraft was fitted with an electric pitch, roll and rudder trim system. Electric trim buttons for pitch and roll were located on the top of each control yoke, while the rudder trim switch was mounted in the console next to the wing flap control switch.
The SR22 Pilot’s Operating Handbook (POH) stated that the pitch trim could be controlled by manually moving the switch forward, which would initiate nose‑down trim and moving the switch aft would initiate nose-up trim. This occurred via an electric motor, which changed the neutral position of the spring cartridge attached to the elevator control horn. The pitch trim also provided a secondary means of pitch control in the event of a primary pitch control failure not involving a jammed elevator. The electric pitch trim was used by the autopilot.
For roll trim, moving the switch left would initiate a left-wing-down trim and moving the switch right would initiate a right-wing-down trim. The trim also provided a secondary means of roll control in the event of a failure with the primary roll control system not involving jammed ailerons. The electric roll trim was also used by the autopilot. The rudder trim was not connected to the autopilot.
Autopilot
The aircraft was equipped with a 2-axis (pitch and roll) S-TEC-55X autopilot system that received roll axis control inputs from an integral electric turn coordinator and altitude information from an altitude transducer connected to the pitot-static system. A multifunction control panel was fitted above the altitude indicator, which provided mode selection, disengage, and turn command functions. The autopilot controller or a button on each control yoke handle could be used to disengage the autopilot. The autopilot features included:
- roll stabilisation
- turn command
- navigation localiser and GPS tracking
- altitude hold
- vertical speed
- GPS steering (GPSS) for smoother turns onto a course or during course tracking.
The limitations section of the SR22 POH stipulated that the autopilot should be disconnected when moderate to severe turbulence was experienced.
According to the aircraft owner, when either the altitude hold or vertical speed modes were selected, the autopilot would not disengage automatically. Also, when in these modes and the flight controls were manually manipulated, the system would apply trim in the opposite direction to maintain the selected altitude or vertical speed.
Electric trim and autopilot failure
The POH indicated that, any failure or malfunction of the electric trim or autopilot could be overridden by manually manipulating the control yoke. Further, if a trim runaway occurred, the pilot was to de‑energise the circuit by pulling the circuit breaker (PITCH TRIM, ROLL TRIM, or AUTOPILOT) and land as soon as the conditions permitted.
Icing protection system
The United States Federal Aviation Administration approved the Cirrus SR22 for flight into icing conditions in 2009 based on the introduction of an optional anti-ice system for the wings, windshield, propeller, vertical and horizontal stabiliser leading edges and the stall warning system. This was known as a FIKI (flight into known icing) approval. The accident aircraft was manufactured in 2002, which predated the FIKI approved modification, and the owner confirmed there was no anti-icing system fitted. Further, pilots were required to undergo an online Cirrus training course in icing awareness and use of the FIKI fitted to the SR22 aircraft before the system could be utilised. The manufacturer confirmed that the pilot of VH-MSF had not undergone that training.
VH-MSF was fitted with windshield defrost, pitot heat[6] and an alternate induction air system, which offered some protection against windshield, pitot and engine air intake icing. Each of those items had to be manually selected on by the pilot as required. According to the SR22 POH, the pitot heat was to be turned on for flight into instrument meteorological conditions, flight into visible moisture, or whenever ambient temperatures were 5 °C or less.
Stall warning system
The aircraft was equipped with an electro-pneumatic stall warning system to provide audible warning of an approach to aerodynamic stall.[7] When a slight negative pressure was sensed by the pressure switch from an inlet in the wing leading edge, a warning horn activated. The warning sounded at approximately 5 kt above the stall with full flaps and power off in wings level flight and at slightly greater margins in turning and accelerated flight.
Cirrus airframe parachute system
The Cirrus airframe parachute system (CAPS) was designed to lower the aircraft and its occupants to the ground in the event of a life‐threatening emergency where activation was determined to be safer than continued flight and landing. The system consisted of the following primary components:
- parachute
- solid-propellant rocket to deploy the parachute
- rocket activation handle and cable
- harness embedded in the fuselage structure.
The parachute and rocket were located in the empennage behind the rear baggage compartment. The rocket activation handle was mounted in a cabin ceiling enclosure between the 2 front seats and the cable was routed through the cabin ceiling and angled towards the left side of the CAPS compartment.
A safety pin with a remove before flight flag was fitted to the activation handle when operating on the ground. Part of a pilot’s pre-flight checks included a requirement to remove the safety pin prior to engine start. To initiate the CAPS, the pilot was to remove the access cover on the ceiling and pull the rocket activation handle out and down (Figure 5). Movement of the cable compressed the igniter steel spring and cocked the plunger. When one half inch of plunger travel was reached, the primary booster was ignited, which then ignited a secondary booster and the rocket motor.
Figure 5: Activation handle (top left) and parachute system as fitted to the aircraft
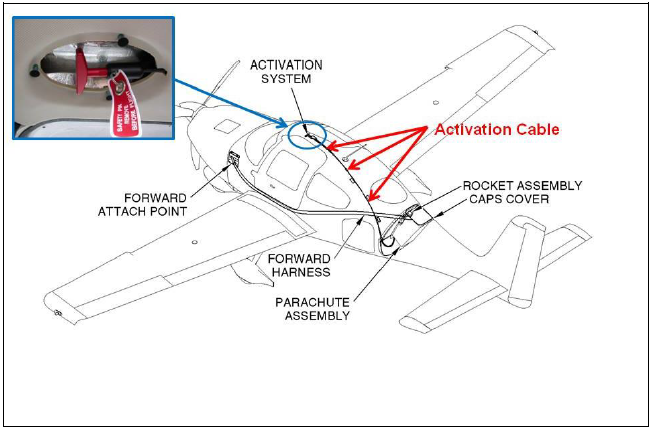
Source: Cirrus Design Corporation, annotated by the ATSB
For aircraft with an electronic ignition for the booster (as was fitted to VH-MSF), both aircraft batteries were connected to the system and either could actuate the booster in response to cable movement. Once ignited, the rocket impacted and dis-bonded the parachute compartment cover situated behind the rear cabin window and pulled the deployment bag from the enclosure. The deployment bag then staged the suspension line deployment and inflation of the parachute.
Meteorological information
Accessing weather information
On the morning of the accident, the pilot submitted a location briefing request at 0615 to the National Aeronautical Information Processing System[8] (NAIPS), which included Canberra and Armidale Airports. This was followed by 5 area briefing requests between 0622 and 0635, which included meteorology information, notices and advisories (NOTAMs),[9] and charts. This would have provided the pilot with the New South Wales east (NSW-E) graphical area forecast (GAF) and the NSW grid point wind and temperature (GPWT) charts.
At 1105, the pilot submitted another NAIPS area briefing request for the same weather information requested previously. This was the pilot’s last briefing request to NAIPS.
Bureau of Meteorology
Initial weather forecast
When the pilot submitted their flight plan at 0648, the current NSW GPWT chart was issued at 0454 and valid from 1100. Canberra was located near the intersection of 4 areas on the chart. Interpolation of the data between these 4 areas indicated the freezing level was forecast to be about 5,500 ft above mean sea level. The current NSW‑E GAF was issued at 0302 and valid from 1000 to 1600, which included the pilot’s planned departure time of 1430. Canberra was in subdivision C1 of area C on the GAF, which included the following weather:
- broken[10] stratocumulus cloud from 2,000 ft to 7,000 ft in C1 until 1600
- scattered drizzle in C1 with visibility reduced to 3,000 m and overcast stratocumulus cloud from 1,000 ft to 8,000 ft
- a freezing level[11] of 4,000 ft in the south and 7,000 ft in the north [Canberra was centrally located within the south region].
The remarks field on the GAF provided additional information of operational relevance and included:
- cloud above the freezing level implied moderate icing[12]
- stratocumulus cloud implied moderate turbulence.
The estimated freezing level of 5,500 ft at Canberra and forecast broken stratocumulus from 2,000 ft to 7,000 ft, indicated an icing layer of about 1,500 ft overhead Canberra. Armidale was in area B, which included broken cumulus/stratocumulus cloud from 6,000 ft to 9,000 ft from 1300, and a freezing level of 9,000 ft.
Subsequent weather forecast
When the pilot submitted their last NAIPS area briefing request at 1105, the current NSW GPWT chart was issued at 0559 and valid from 1400. It indicated the freezing level overhead Canberra was forecast to be at about 7,000 ft with south‑westerly winds increasing from 6 kt at 5,000 ft to 19 kt at 10,000 ft. The NSW-E GAF was issued at 0913 and valid for the period 1000-1600. Canberra and the accident site were in the south of subdivision D1 of area D. The forecast for area D included the following conditions relevant to the pilot’s departure time of 1430:
visibility greater than 10 km, scattered cumulus/stratocumulus cloud from 5,000 ft to 8,000 ft, with broken tops to 10,000 ft in D1/D2 – the Bureau of Meteorology advised the ATSB that this should be interpreted as being broken cumulus/stratocumulus cloud from 5,000 ft to 10,000 ft in D1/D2
- visibility reduced to 3,000 m in isolated showers of rain, with broken stratus cloud from 1,500 ft to 4,000 ft and broken cumulus/stratocumulus cloud from 4,000 ft to above 10,000 ft
- freezing level of 5,000 ft in the south and 8,000 ft in the north of area D.
The remarks field stated:
- cloud above the freezing level implied moderate icing
- cumulus and stratocumulus cloud implied moderate turbulence.
The estimated freezing level of 7,000 ft at Canberra and forecast broken cumulus/stratocumulus from 5,000 ft to 10,000 ft indicated the forecast depth of the icing layer overhead Canberra had increased to 3,000 ft. Figure 6 depicts the NSW-E GAF, current at the time of the pilot’s last NAIPS area briefing request. Information relevant to the flight is labelled and highlighted. This forecast included a freezing level of 9,000 ft for the area containing Scone (area B) and a freezing level of above 10,000 ft for the area containing the destination of Armidale (area A).
Figure 6: Graphical area forecast for New South Wales – East
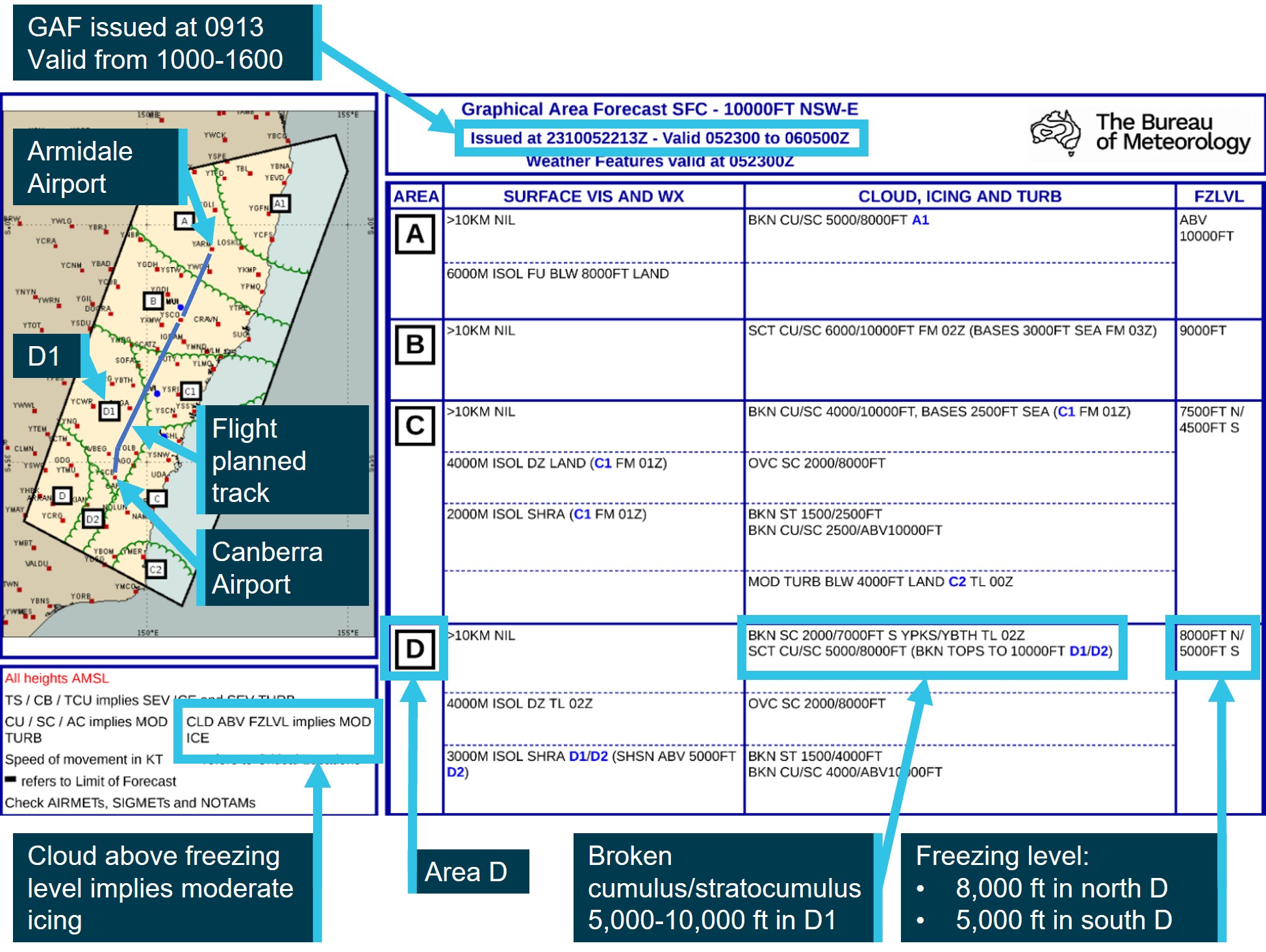
Source: Bureau of Meteorology, annotated by the ATSB
Assessment of the local conditions
The ATSB requested an analysis of the weather conditions by the Bureau of Meteorology applicable to the aircraft’s track. The following is a summary of that analysis:
Satellite observations at 0400Z [1500 local time] indicated that the IR [infrared] cloud top temperature was ‑7°C which corresponds to a cloud top height of 10,000 ft…Taking the base and cloud top estimates, this gives a depth of cloud of approximately 3,000ft.
The weather conditions observed for the area between Canberra and the accident site were consistent with the forecasts for the afternoon of 6 October 2023. The cloud cover was scattered to broken cumulus/stratocumulus, with a freezing level at approximately 7000ft. Cumulus and stratocumulus cloud were forecast on the GAF and observed on satellite imagery. Showers were forecast and observed over the ranges to the north and northeast of Canberra, including just north of the accident site at 0349Z [1449 local time].
These conditions would have been conducive to moderate icing conditions (most likely of the clear icing type) between approximately 7000ft to 10,000ft above mean sea level. The severity of any icing experienced would depend on how long the aircraft is in the cloud layer between these heights, however, the existence and/or type of airframe icing is very difficult to verify, particularly with the absence of any aircraft icing reports from the area at the time.
Based on Himawari-9 satellite imagery and observations from the aerological diagram at Wagga there is high confidence of moderate icing within the cumulus and stratocumulus field that extended across the Canberra region on 6/10/2023. This is consistent with forecast cloud and weather referenced on the NSW-E GAFs and reinforces the GAF statement (noted on all GAF issued by the Bureau of Meteorology) of "CLD ABV FZLVL implies MOD ICE".
Weather observations
Canberra Airport automatic terminal information service
When the pilot contacted Canberra ground air traffic control for an airways clearance, they reported receipt of the automatic terminal information service[13] ‘Golf’. The recording for information ‘Golf’ stated the following regarding the current weather conditions at Canberra Airport:
Expect instrument approach runway 17, wind 200° 8 kt, visibility greater than 10 km, cloud few 3,000 ft scattered 3,500 ft,[14] temperature 18, QNH[15] 1025.
Camera footage of cloud cover at Canberra Airport
A fixed camera was located about 1.3 km to the west of Canberra Airport showing an aspect to the north-north-east. The footage, coupled with other stills taken around the time the aircraft took off to the south and then tracked to the north-north-east, showed broken cumulous/stratocumulus cloud as per the forecast (Figure 7, taken at 1439).
Figure 7: Footage taken near Canberra Airport with a north-north-east aspect at 1439
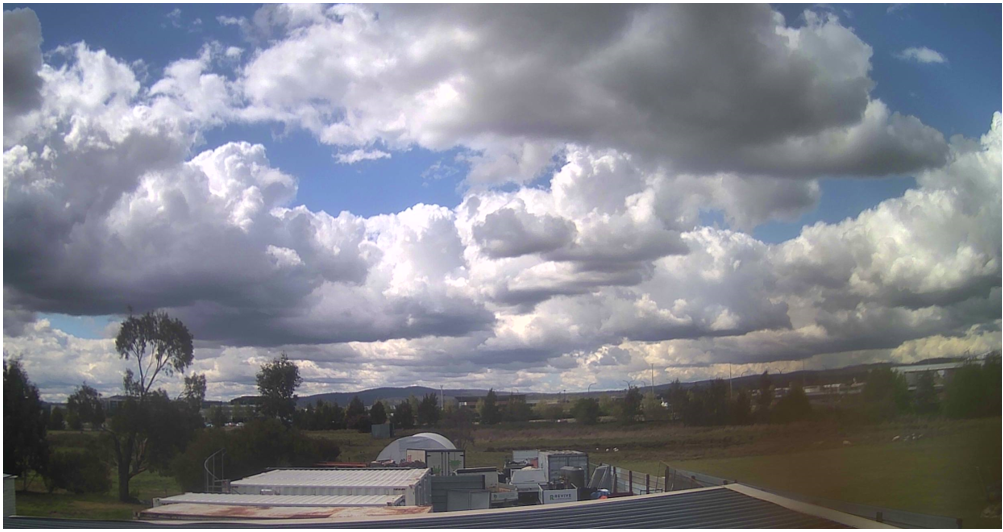
Source: Aus Web Cams/myairportcams.com
First responders
Shortly after the accident occurred, first responders took a video around the aircraft in the hope that it could assist with the investigation into the accident. Consistent with the forecast, that video showed broken cloud overhead the accident site to the south-west, which was the direction the aircraft had come from (Figure 8).
Figure 8: Video image taken shortly after the accident viewed to the south-west

Source: Supplied
Pilot report of weather
The pilot of a Cirrus SR22T aircraft fitted with a flight into known icing (FIKI) kit was conducting an IFR flight from Wagga to Moruya, New South Wales, via Canberra on the day of the accident, flight planned at 9,000 ft. The pilot recalled using the anti-icing fluid, first to the west of Canberra when the aircraft was in the tops of the clouds at 9,000 ft. The pilot requested and received a clearance from air traffic control to climb to 10,000 ft to clear the cloud. They turned the anti-icing off and passed overhead Canberra at about 1358 (about 50 minutes prior to the accident) where they entered higher level cumulus cloud. The pilot then turned the anti-icing on again for the leg from Canberra to Moruya.
The pilot observed ice build-up on the aircraft in areas that did not receive the anti-icing fluid directly but did not notice any icing on the wings or any loss of engine performance. The pilot reduced the power and speed for turbulence penetration during the trip and assessed their aircraft was experiencing light icing. They also commented that it would have built up rapidly on an aircraft without an anti-icing system.
The pilot was able to recall one prior experience of icing when on descent into Moruya from Dubbo in their previous SR22, which was not fitted with a FIKI kit. The pilot reported that the ice built up quickly on the wings for about 2,000 ft but dissipated rapidly when the aircraft entered warmer air. They did not notice any loss of engine performance but acknowledged they were using a low power setting for the descent.
Airline flight data
A Virgin Australia Boeing 737-800 aircraft, callsign Velocity 1690, transited and descended through airspace and altitude bands close to the outbound flight track of VH‑MSF and at a similar time.
Velocity 1690 was being operated on a flight from the Gold Coast, Queensland, to Canberra with a landing time of 1445:26, about 4 minutes prior to the accident. Runway 17 was the active runway and Velocity 1690 approached Canberra from the north. On descent, at 1437:03, the aircraft data recorded the engine anti-icing system (ENG COWL ANTI-ICE) being turned on by the flight crew at an altitude of 10,144 ft and an outside air temperature (OAT) of −6.2°C (6°C total air temperature (TAT)).[16] The operator reported that the flight crew could not provide a detailed recollection of the approach but that the selection of the anti-ice would be consistent with the aircraft in cloud above the freezing level during the descent. At 1439:35, the flight crew turned the engine anti-icing off at 6,848 ft and an OAT of 0.2°C (10.5°C TAT). Figure 9 depicts the approach flight path of Velocity 1690 with the times, altitudes and temperatures when the engine anti-icing was turned on and off. The flight path of VH-MSF includes the positions that corresponded with the altitude band (shown in red) in which Velocity 1690 used engine anti‑icing.
Figure 9: Relative positions of Velocity 1690 and VH-MSF
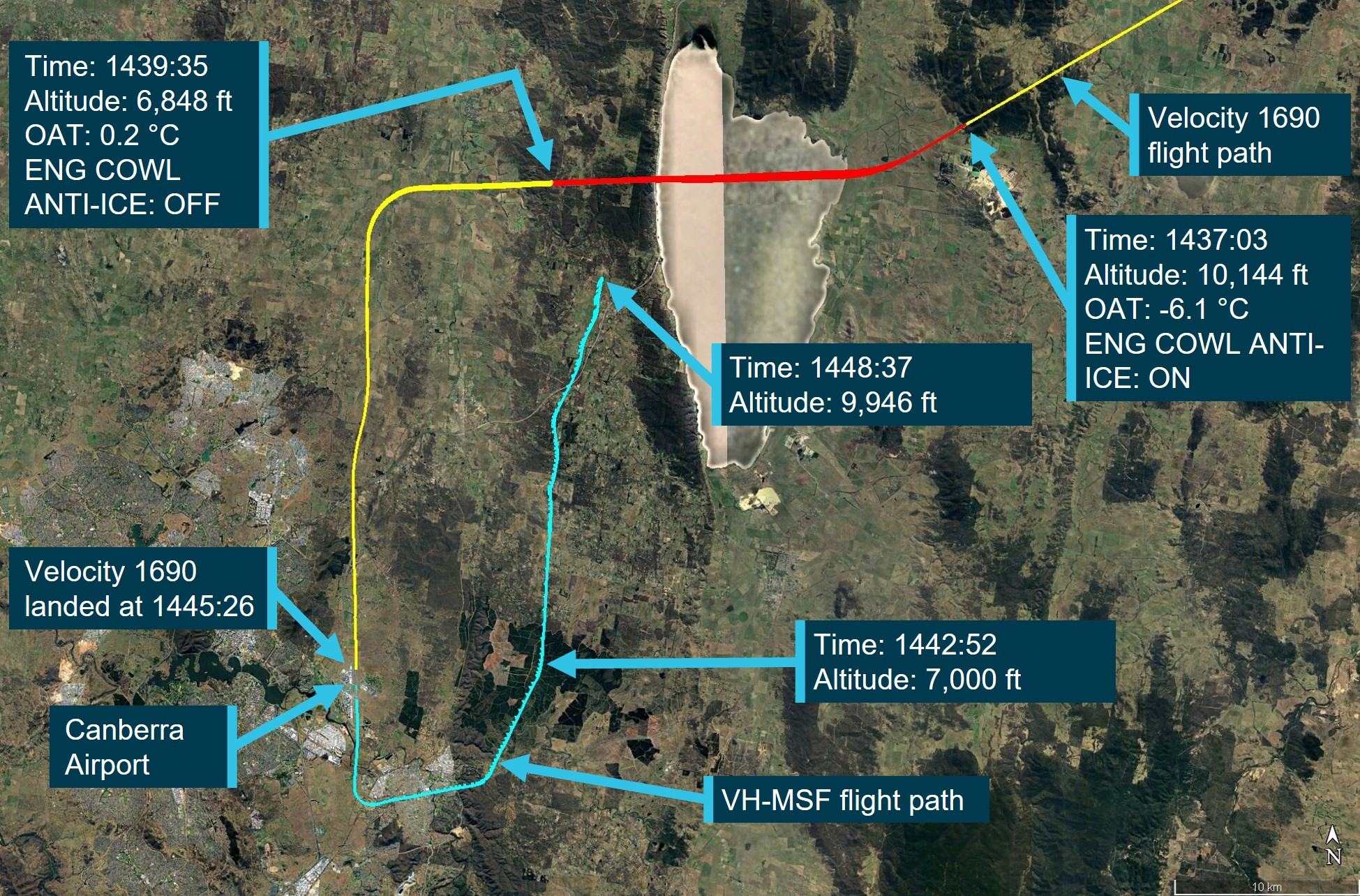
Source: Google Earth and Virgin Australia, annotated by the ATSB
ATSB review of satellite imagery
Introduction
The Bureau of Meteorology provided the ATSB access to various satellite imagery of the Canberra region during the afternoon of the accident, which had been processed from the geostationary satellites Himawari-8 and 9, operated by the Japanese Meteorological Agency. Imaging sensors carried on board the satellite would make progressive scans of the Earth’s full disk at 10-minute intervals.
Cloud coverage
Figure 10 is the enhanced visible satellite image showing cloud coverage for the Canberra region for the 10-minute acquisition period commencing 1440, which was the closest image relative to the time of the accident. The areas of cloud are represented by the lighter pixels, where the darker pixels are areas without (or with less) cloud coverage. This image is overlaid with VH-MSF’s flight track, the direct track to waypoint CULIN, the estimated position and time the aircraft climbed through the 0°C estimated freezing level (at about 14:43 and 7,000 ft).[17] It also showed the aircraft’s position at 8,000 ft where flight path variations commence in relation to cloud coverage.
While this shows cloud coverage along parts of the aircraft’s track, it does not provide information about the depth of the cloud or the height of the cloud tops, and whether those tops were above or below the aircraft’s operating altitude.
Figure 10: VH-MSF track (in red) overlaid on an enhanced visible satellite image, taken close to the time of the accident
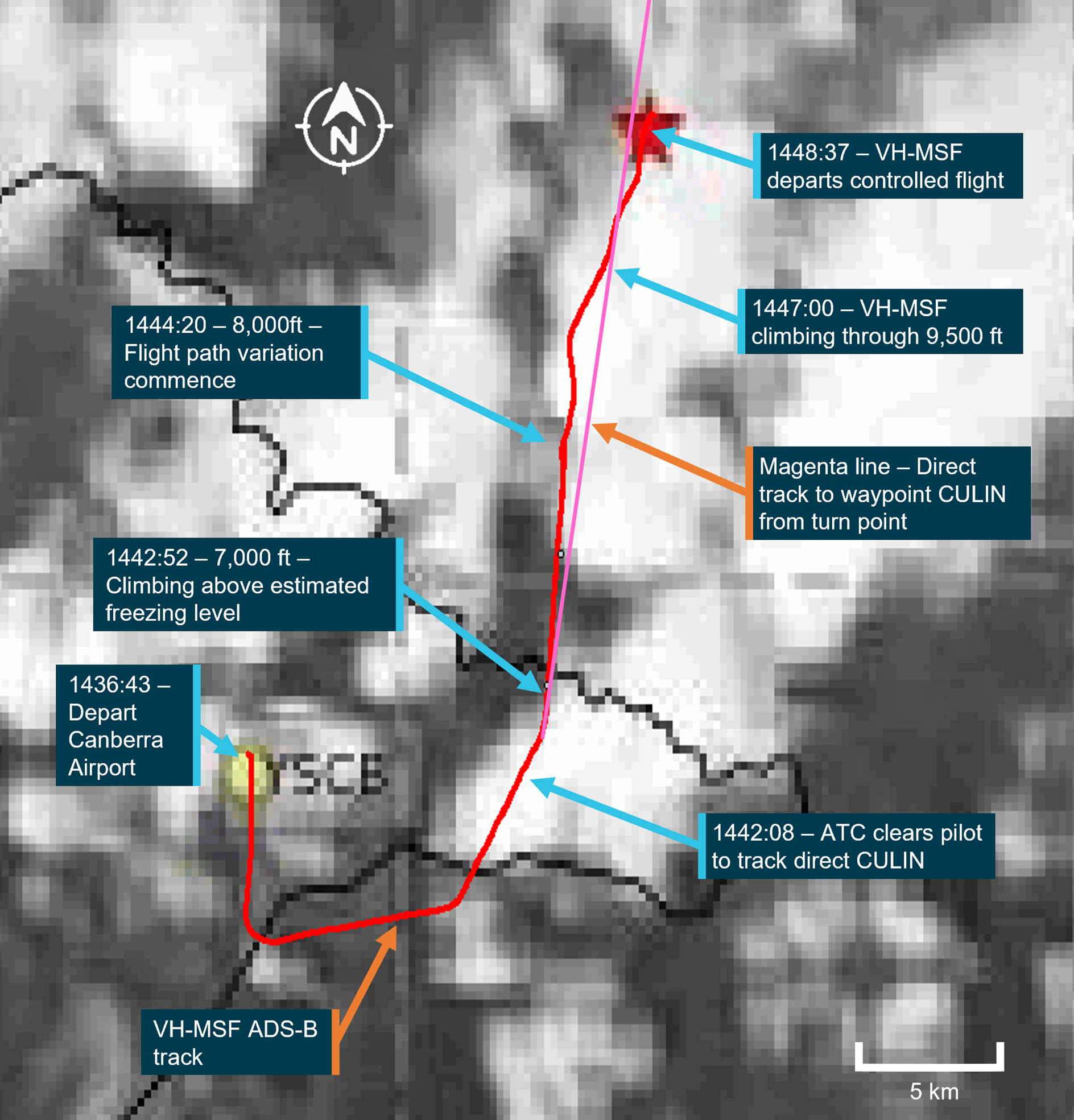
Source: Bureau of Meteorology and Japan Meteorological Agency, modified by the ATSB
Temperature of reflective surfaces
To assist with the estimation of cloud heights in the vicinity of the aircraft’s flight path, the Himawari‑8 and 9 RGB infrared enhancement image[18] was reviewed for the same period commencing at 1440. For the infrared images, the colour of the pixels is an indicator of the average temperature of the reflecting surface measured by the infrared imaging sensors.
The lighter coloured pixels represent lower temperature (colder) reflecting surfaces and could reasonably be used to infer higher cloud tops in those regions. The darker pixels were consistent with warmer average temperatures of the reflecting surfaces and could suggest lower cloud tops in those areas. Based on the infrared images, the Bureau of Meteorology assessed the cloud conditions as being scattered to broken with a 3,000 ft cloud band between 7,000 and 10,000 ft, with moderate clear icing likely when in cloud from 7,000 ft.
Figure 11 shows a temperature scale, the flight path, times and altitudes with the position of the aircraft at an estimated freezing level of 7,000 ft. It also shows the point at which the aircraft flight path variations commence and the lighter grey areas indicating cloud tops at 10,000 ft. Based on the infrared image, it was considered likely that the aircraft entered cloud above the freezing level. However, the exact amount of time the aircraft spent in cloud could not be determined.
Figure 11: VH-MSF track overlaid on RGB infrared enhancement image, taken close to the time of the accident
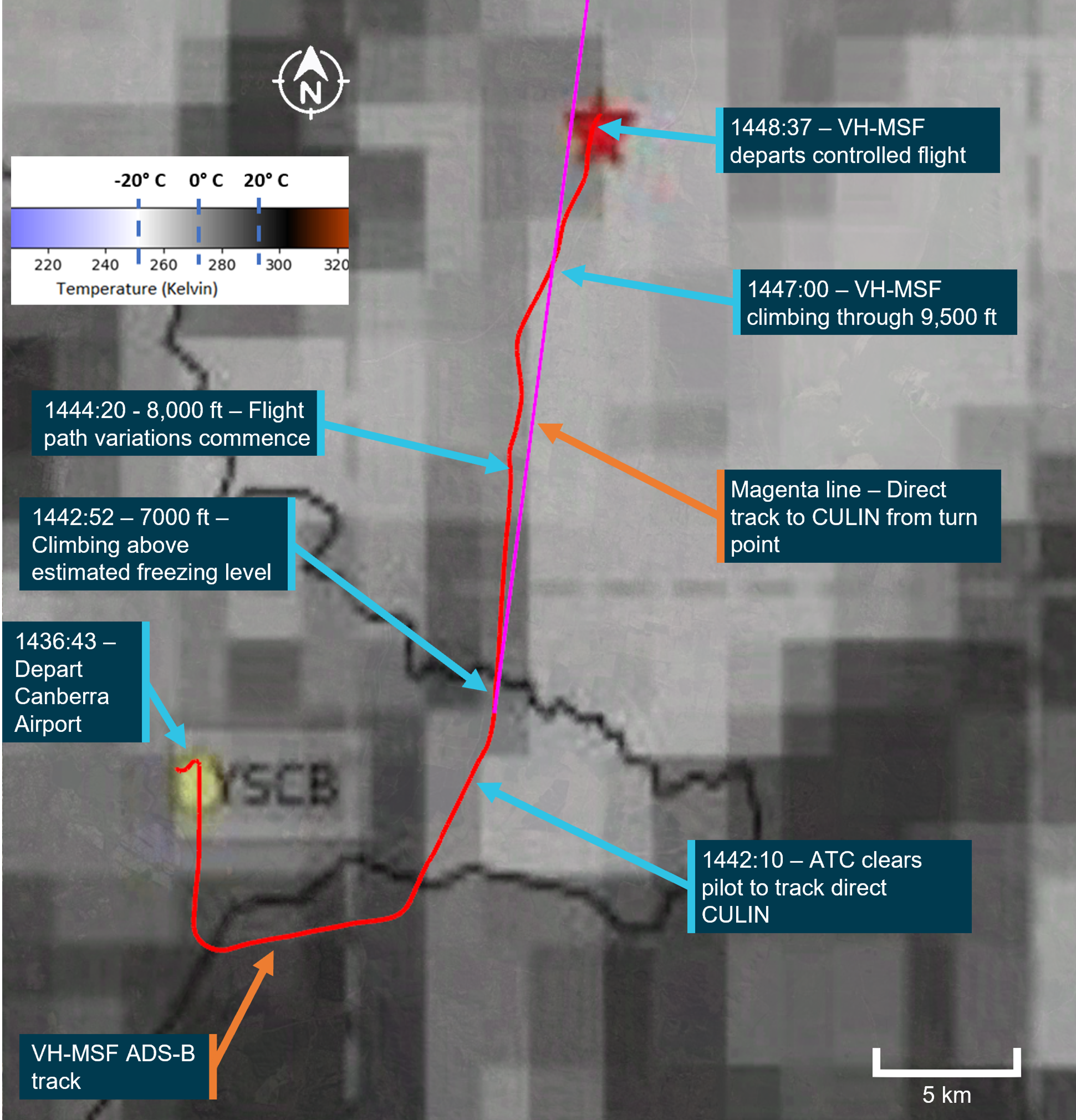
Source: Bureau of Meteorology and Japan Meteorological Agency, modified by the ATSB
Comparison with the airline flight data
The infrared imagery for VH-MSF (Figure 11) was compared with the imagery applicable to the Boeing 737-800 (acquisition period commencing 1430) and the corresponding altitude and temperature data for when this aircraft likely entered cloud during descent into Canberra. This indicated that the lightest coloured pixels in the image represented average temperatures of about −6 °C, with the tops of the reflecting surfaces (clouds) being about 10,000 ft as per the forecast.
Recorded information
General information
The aircraft’s Avidyne multi-function display and EMax engine monitoring system had been significantly damaged by the post-impact fire. Technical assessment and X-ray images of the unit’s compact flash data storage card showed considerable thermal damage, which precluded recovery of onboard recorded data. The aircraft was not equipped with a data transfer unit and recoverable data module, which was available as a fitted option in later models of Cirrus aircraft. Therefore, no onboard recording devices were available for data download to assist the investigation.
Flight data performance assessment
The ATSB obtained digital data that had been broadcast by the aircraft’s automatic dependent surveillance broadcast (ADS-B)[19] equipment and which had been recorded by Airservices Australia and other flight tracking websites.[20] That data included information about the aircraft’s position, ground track, ground speed and altitude.
The ADS-B data transmitted by the aircraft did not include parameters such as airspeed, altitude rate of change, heading or temperature. However, the transmitted data could be integrated with other sources of information (such as wind velocity, air temperature and atmospheric pressure), to derive estimates for other relevant performance data. For the purpose of analysing the ADS-B data and to derive estimates of the aircraft’s calibrated airspeed (CAS)[21] during the accident flight, wind and temperature data was obtained from several sources, which included:
- the Bureau of Meteorology’s NSW GPWT chart, valid from 1400, providing wind and temperature forecast data in 1.5 by 1.5° grids
- the Bureau of Meteorology’s vertical wind profiler observations (averaged over the preceding 30-minute observation period) for Canberra Airport, issued 1430 and 1500
- wind and temperature information from the Boeing 737-800 (Velocity 1690) flight data when transiting through the airspace north of Canberra and passing close abeam the accident site about 10 minutes prior
- the United States National Centres for Environmental Prediction global forecast system and global data assimilation system in 0.25 by 0.25° grids, valid at 1400.
Evaluation of those sources demonstrated a reasonable correlation between datasets, particularly during the latter stages of the climb and immediately prior to the departure from controlled flight. For the main analysis task, the investigation used the Canberra Airport vertical wind profiler observations, and the wind velocity and temperature data recorded for Velocity 1690. The estimate for CAS was derived from ADS-B recorded ground speed and ground track, using the sources for wind velocity (from Velocity 1690 data and vertical wind profiler observations), and recorded atmospheric pressure at Canberra Airport and temperature (from Velocity 1690 data).
Further, this information, along with published aircraft performance data was used to determine the required engine power and propellor thrust to meet the performance seen in the recorded data. However, due to the limitations of ADS-B broadcast data (such as position errors, recording resolution, and broadcast dropouts) and at times dynamic manoeuvring of the aircraft, the aircraft trajectory and power required analysis was indeterminate for much of the aircraft’s flight.
Figure 12 depicts the ADS-B data for the accident flight, together with an estimate of the aircraft’s airspeed. The initial climb was conducted on reasonably stable headings and climb rates at airspeeds that were estimated to be generally between 85 kt and 105 kt CAS, to an altitude of about 7,000 ft above mean sea level. At one point during this climb, at about 1441 when approaching 6,000 ft, the aircraft appeared to have passed through an area of rising air (Figure 12 ‘vertical air movement’). This was evidenced by the aircraft substantially exceeding the POH published maximum rate of climb performance while the aircraft additionally accelerated slightly.
At 1442:08, the air traffic controller cleared the pilot to resume their own navigation and track direct to CULIN, where the estimated airspeed increased to about 115 kt. At 1443, the airspeed began to progressively reduce as the aircraft continued to climb. For a full‑page view of Figure 12 refer to Appendix A.
The following provides a summary of the data (in sections A to G, as annotated on Figure 12 and Figure 13) from just prior to passing through 8,000 ft until the departure from controlled flight:
- A: Over a period of about 90 seconds, the airspeed reduced by about 25 kt at a relatively linear rate.
- B: Climbing through 8,300 ft, the airspeed continued to reduce, with a reduction of about 20 kt occurring over a 15‑second period. The aircraft was estimated to have slowed to around 72 kt, which was 5 kt above the calculated stall speed for the flight.
- C: The airspeed recovered slightly but, 40 seconds later, the airspeed reduced again to an estimated 70 kt. During this time, the aircraft was passing overhead several witnesses who had reported hearing unusual revving or stuttering from an aircraft engine.
- D: The aircraft then accelerated to the best rate of climb speed for about 45 seconds, and the altitude increased by almost 800 ft. This also included what appeared to be a controlled turn (based on a relatively constant turn radius) to the right, changing heading by about 35° (as shown on Figure 1 and Figure 2).
- E: At 1447:20, the aircraft entered a final period of unstable flight. The aircraft decelerated from 100 kt to 94 kt while the climb rate reduced to zero.
- F: The airspeed then further decreased by 11 kt, before the aircraft descended 250 ft and recovered to an estimated airspeed of 96 kt. A power required analysis suggested the speed loss and descent were possibly conducted with low or idle power, or due to a downdraft.
- G: Over the next 30 seconds, the recorded data showed that the aircraft then climbed above the best rate of climb to about 1,500 ft/min while the airspeed reduced.
At 1448:31–33, about 12 minutes after take-off from Canberra, the aircraft reached a maximum altitude of 9,946 ft at an airspeed of 71 kt. Following this, the flight data showed the aircraft’s airspeed and altitude declined, and rapidly so from 1448:37. The descent rate increased to 13,000 ft/min, the ground speed reduced to less than 32 kt and became erratic, and the aircraft track aligned somewhat with the estimated wind direction, all of which indicated the aircraft had likely entered a spin.[22] As the aircraft passed through about 8,000 ft, the rate of descent started to reduce, which was indicative of the increased drag from an increasing air density as the aircraft descended. When the aircraft had reached ground level the descent rate had reduced to around 10,000 ft/min.
Figure 12: Aggregated ADS-B altitude data for VH-MSF, together with estimated airspeed (CAS)
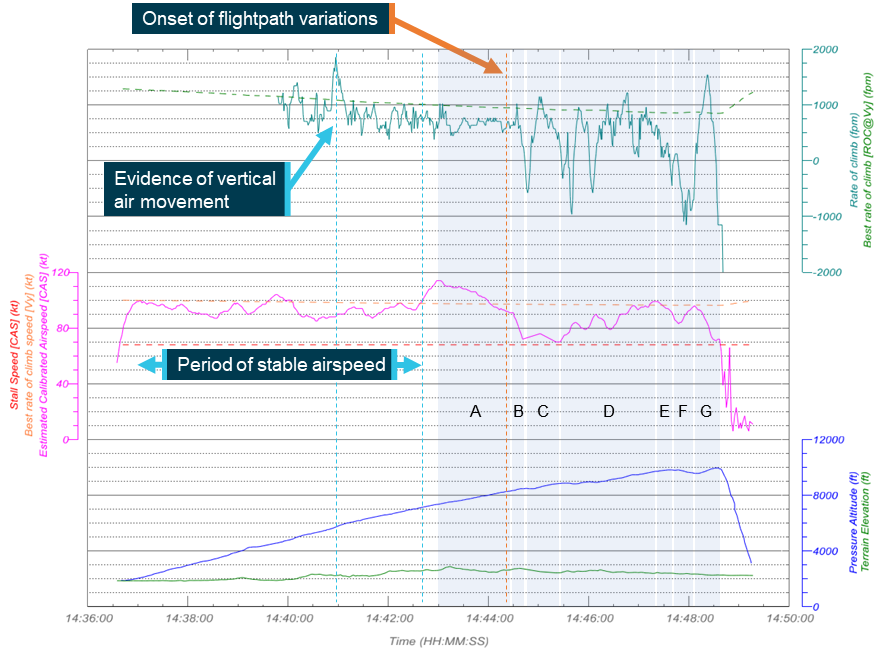
Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
Figure 13 depicts the aircraft’s flight track looking back along the flight path with A through G labelled to the relevant sections of the flight as shown in Figure 12. As the aircraft climbed through 8,300 ft, the somewhat linear flight track changed, with heading, altitude and airspeed variations commencing.
Figure 13: Aggregated ADS-B data for VH-MSF, looking back along the flight path
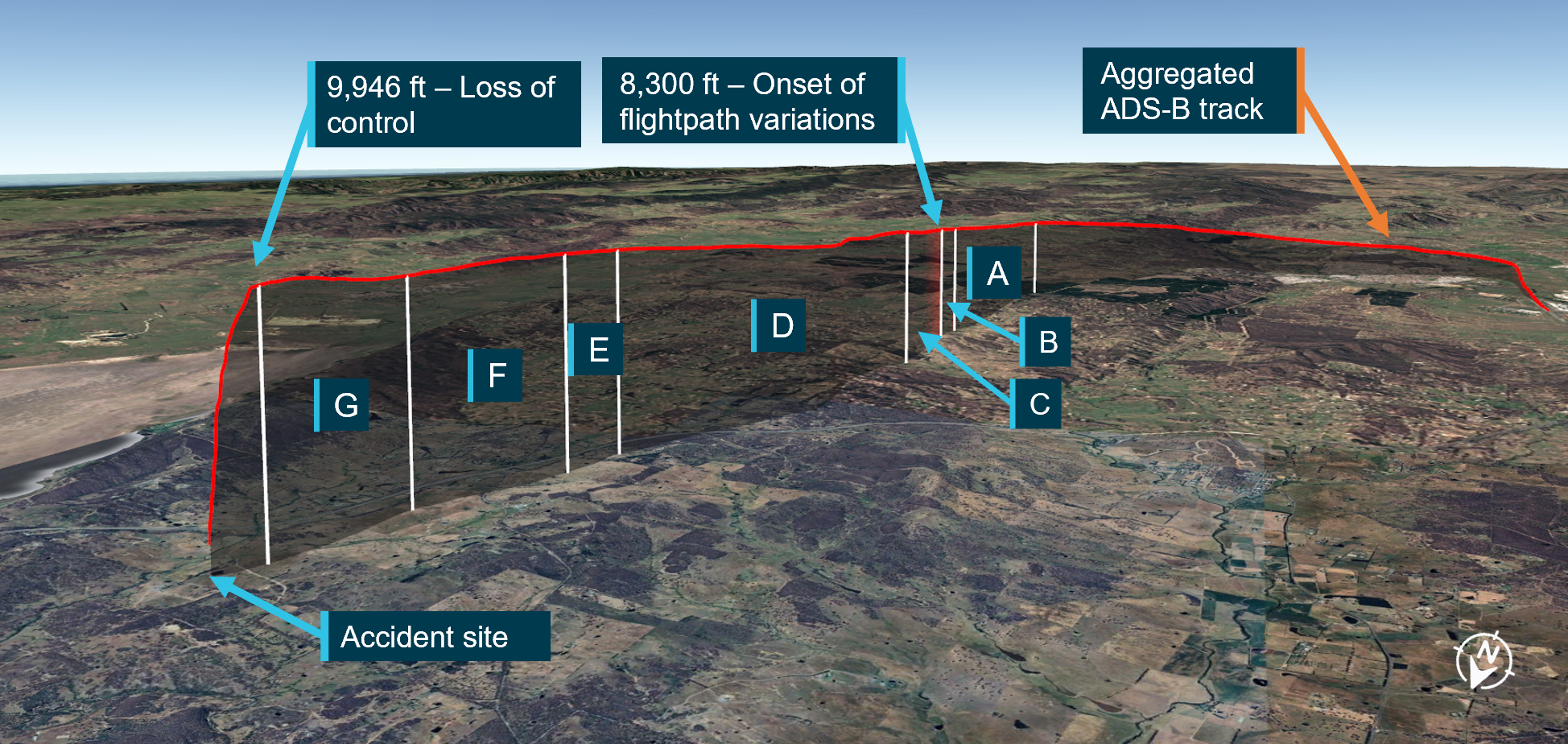
Source: Google Earth, with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Performance comparison between flights
Figure 14 illustrates ADS-B altitude data from initial climb to about 10,000 ft for the accident flight and the 2 prior flights (on 3 and 4 October 2023)[23] conducted by the pilot in VH-MSF. The data showed the aircraft climb performance for the accident flight was initially similar or better than the prior flights. During the period of flight path variations, the aircraft performance reduced, potentially due to manoeuvring, but then momentarily returned to comparable performance after passing 9,000 ft.
Figure 14: Comparison of ADS-B altitude data for the accident and 2 prior flights
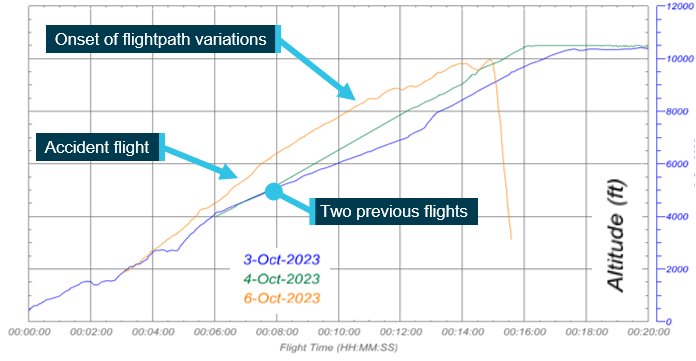
Flight start times have been adjusted to allow for comparison. Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
The manufacturer was provided a copy of the flight track data for assessment. That assessment was conducted by one of their senior investigators and a senior test pilot. While no definitive conclusions were able to be made based on the data provided, the manufacturer indicated that the aircraft had slowed, aerodynamically stalled and, after a short period of time, entered into a spin.
Wreckage and impact information
Site and wreckage
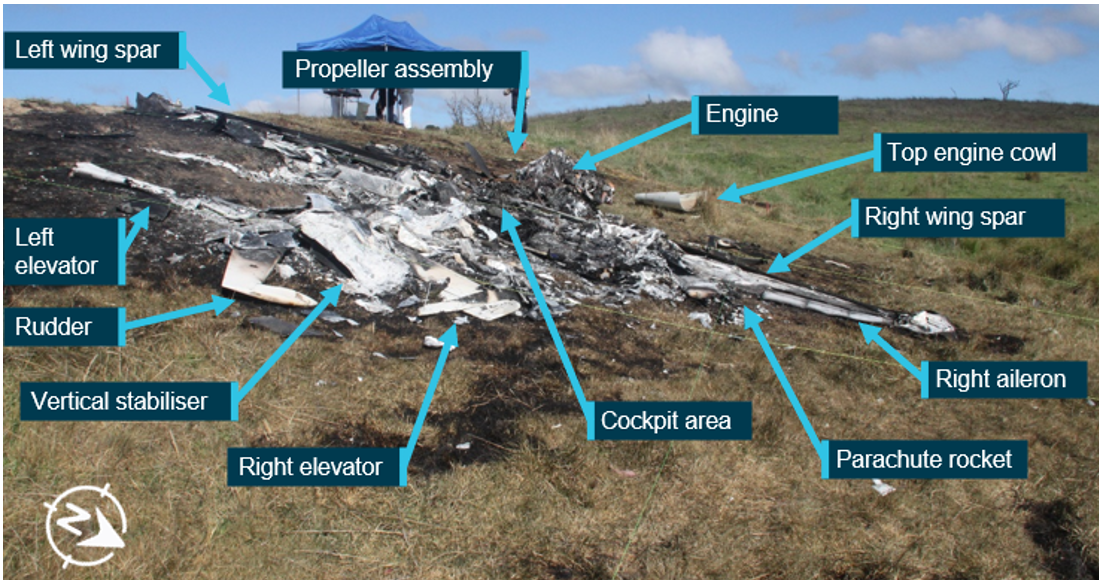
The aircraft came to rest in an open field adjacent to a dam wall with a 10° downward slope towards the right wing. Although post-impact fire damage precluded examination of a significant proportion of the aircraft, inspection of the site and wreckage showed (Figure 15 and Figure 16):
- The impact marks and wreckage distribution indicated that the aircraft impacted with terrain upright, with a slight nose low attitude and no forward momentum. Although the impact evidence was indicative of a spin, it was difficult to ascertain the spin direction.
- All of the aircraft extremities (wings and tail section) were accounted for and there was no evidence of an in-flight break‑up.
- There were no identified structural defects in the evidence available.
- All flight controls systems were inspected to the degree possible with no pre-accident defects identified.
- The flap actuator was identified within the wreckage and was in the flap zero position.
- The fuel selector was tested and assessed to be in the right tank position.
- The fuel tank caps were located and found secured in the filler point opening of each fuel tank.
- The engine cowl was located forward of the aircraft outside the fire zone. It did not have any residue to indicate an in-flight loss of oil.
- Due to the destruction of the wreckage, cockpit switch settings and circuit breakers, flight/engine control, autopilot or trim positions were unable to be determined.
- The engine power lever and mixture control positions could not be determined.
Figure 15: Overview of the accident site and remaining wreckage

Source: ATSB
Figure 16: Aircraft wreckage viewed from the rear showing downslope to the right
Source: ATSB
The cabin heat position was unable to be ascertained, and the engine exhaust and shroud that was utilised for cabin heat was removed so that the exhaust could be examined for pre‑impact defects. No cracks or pre-impact defects were identified in the exhaust that may have led to carbon monoxide[24] being introduced into the cabin by an exhaust leak.
Cirrus aircraft parachute system
The CAPS fuselage cover was located adjacent to the wreckage, but outside the fire zone. Inspection of the cover showed an impact mark on the internal surface at the rocket head location. The cover did not display any thermal or smoke damage (Figure 17). The parachute deployment rocket was not in its original position and was located about 3 m to the right of the fuselage and had dispensed its propellent. The cover and rocket position indicated that the rocket had deployed due to ground impact forces before the post-impact fire had initiated.
The parachute was located in its normal fitted position, remaining in its pack. After an extensive search throughout the remaining wreckage, the parachute deployment handle and safety pin could not be located. Therefore, the ATSB could not establish if an attempt was made to deploy the parachute in-flight.
Figure 17: CAPS external cover showing internal impact mark

Source: ATSB
Propeller and engine examinations
Propeller
The propeller was partially buried at the front of the aircraft. The propeller flange had separated from the engine crankshaft and remained attached to the propeller hub. Two of the 3 propeller blades (Figure 18, blades A and B) were undamaged and showed no signs that they had passed through the ground during the impact with terrain.
Figure 18: Propeller as found at the accident site

Source: ATSB
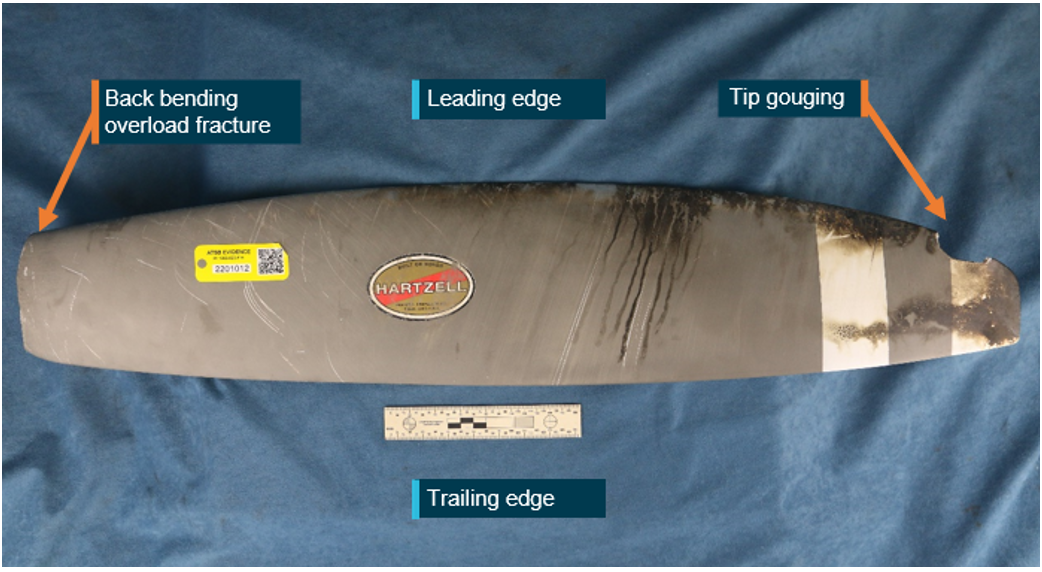
Propeller blade C was buried in the earth directly under the hub and showed some signs of rotational scoring, some leading-edge gouges, and slight chordwise twisting. A fracture surface at the base of the blade was from back bending overload as a result of the impact with terrain (Figure 19).
Site photographs of the propeller and fractured crankshaft were examined further and blade C was physically examined at the ATSB’s technical facilities in Canberra to determine the level of engine power being produced at the time of impact. The materials failure analysis identified that the propeller hub had fractured from the engine crankshaft at the propeller flange, in a manner consistent with ductile overstress due to bending. The examination determined that propeller blade C exhibited minor compound bending through its section and had a slight twist at the blade tip. Chordwise gouging observed on the front face of the blade was a characteristic of propeller rotation.
With respect to the engine power output, typically, windmilling or an engine at idle power will stop very rapidly when the propeller blades contact the ground. There is often minimal ground entry and little to no distortion to the blade sections. In this case, when blade C entered the ground, the propeller stopped suddenly. Therefore, the ATSB’s analysis concluded that, while there were some signatures that would indicate that the propeller was rotating at the time of impact, there was no evidence of appreciable power being produced by the engine. Rather, the damage to the propeller blades indicated that the engine was operating at low power when it impacted terrain.
Figure 19: Blade C as recovered from the accident site
Source: ATSB
Propeller governor
The propeller governor remained attached to the engine. Impact and fire damage precluded functional testing. The governor was disassembled and inspected at the ATSB’s technical facilities with no pre-impact defects identified.
Engine
The engine was removed from the accident site and taken to an approved engine overhaul facility for disassembly and inspection under the supervision of the ATSB. Sections of the engine were consumed by the intense post-impact fire, which precluded functional testing of specific areas such as the ignition and fuel systems.
The oil filler cap was secured to the crankcase fill adapter. The engine and accessories were completely disassembled. The engine was found to be mechanically sound, with the crankcase section intact and all the cylinders present and securely mounted to the crankcase. No defects were identified in any of the cylinder assemblies that may have provided an indication of a malfunction contributing to a loss of engine power. There was no distress of the main or connecting rod bearings due to oil starvation or loss.
The engine sump was pushed upwards during the impact with terrain, bringing it in contact with the cam shaft drive gear. That contact perforated the sump with gear teeth impressions, indicating that the engine camshaft was not rotating and the engine had stopped by the time the imprints were made (Figure 20).
Figure 20: Camshaft drive gear and impressions made in the engine sump
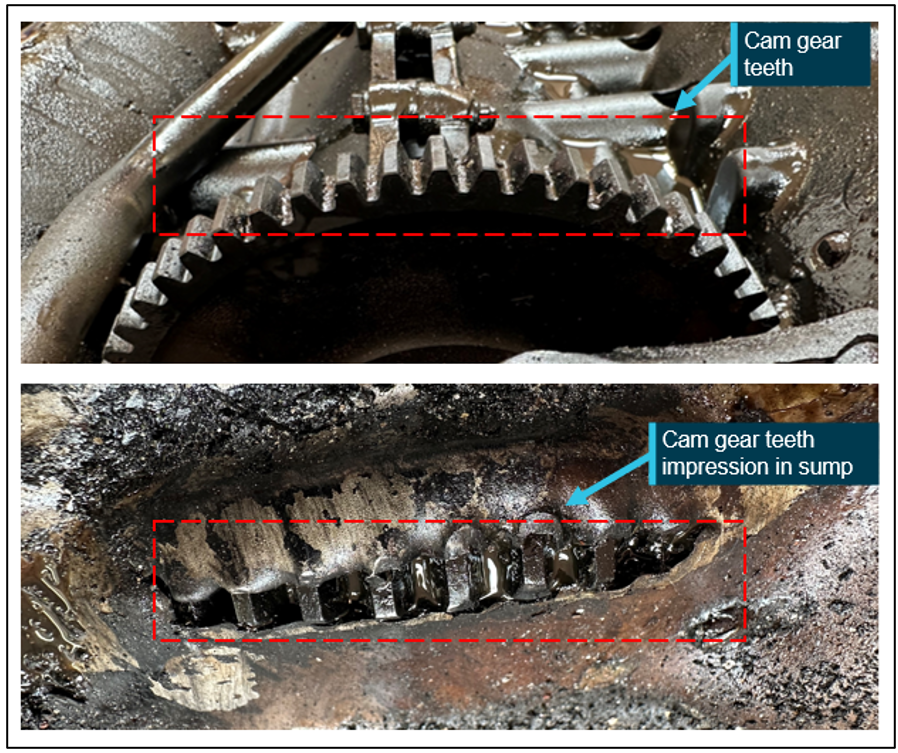
Source: ATSB
Medical and pathological information
General information
The pilot held a class 2 aviation medical certificate valid to 22 October 2023, with 2 restrictions. These were a requirement for reading and distance vision correction to be worn while flying and that a continuous positive airway pressure (CPAP) machine be used for the sleep period before flying.
The pilot’s last Civil Aviation Safety Authority (CASA) required medical assessment was conducted on 22 October 2021. That documented assessment showed that the pilot had:
- been prescribed medication for high cholesterol for over 10 years
- an electrocardiogram stress test (heart trace) in 2016 with nil issues reported
- their appendix removed in 1980
- a computed tomography (CT) angiogram and CT calcium test in 2019 with nil issues reported
- a CT chest X-ray in 2019, which was all clear
- blood tests in 2016, 2017, 2019 and 2021
- a sleep study performed in 2016, which resulted in the use of a CPAP machine (details below).
In 2016, the pilot was identified with moderately severe obstructive sleep apnoea and used a CPAP machine to manage that condition. Downloaded CPAP data showed that the pilot was consistently using the CPAP machine. It was reported that the pilot had their CPAP machine with them during the trip to Canberra and given the previous continuous use it was concluded that the pilot likely utilised the machine during the trip, including the night prior to the accident.
The pilot was reported to have been well rested and had consumed a salmon bowl meal from a local restaurant about 1 hour before the flight. In general, the pilot was reported by their family to be fit and healthy with no known illnesses.
Post-mortem and toxicology results
A full post-mortem[25] of the pilot was conducted. The pilot received extensive thermal injury as a result of the post-impact fire and multiple other injuries from the accident.
The pathologist noted that the pilot had a right coronary artery angulation with an ostium (opening of the artery) that had a slit-like appearance. They stated that it is a rare congenital coronary artery anomaly that, in most cases, does not present with clinical symptoms and may be considered an incidental post-mortem finding in asymptomatic patients. In approximately 20% of cases, the anomaly may result in symptoms such as angina (chest pain), dyspnoea (shortness of breath), syncope (fainting), myocardial ischaemia (reduced blood flow to the heart), ventricular fibrillation (irregular heart rhythm), and sudden death. According to the literature, symptoms generated by congenital coronary artery anomalies are predominantly associated with athlete patients or after intense physical exercise and are rarely present in sedentary individuals.
Toxicology testing was conducted to detect common therapeutic medicines and illicit drug use, and these tests were found to be negative for all substances. The toxicology report noted that a low, insignificant blood alcohol concentration was detected that may have been attributed to post‑mortem decomposition changes (0.006 g per 100 mL). A carbon monoxide saturation level of 2% was also detected in the pilot’s blood, but the report stated that this did not suggest that carbon monoxide poisoning contributed to the accident and death, nor did it suggest a significant survival period after the impact. As previously discussed in ATSB investigation AO‑2017‑118, the physical symptoms and cognitive effects of carbon monoxide exposure generally start to occur at levels of around 10%.
In their concluding remarks the pathologist stated that:
No definite answer can be provided based on the post-mortem findings alone regarding whether the possible sudden incapacitation of the pilot may have contributed to the aviation fatalities. The post‑mortem findings must be correlated carefully with all other available evidence, not least the findings arising from examination of the scene and other relevant evidence as unearthed by detective officers and other investigative authorities.
Specialist medical assessment
Due to the circumstances of the accident and the indeterminate results of the pilot’s post‑mortem, the ATSB requested the assistance of a specialist doctor of forensic pathology to assess the information obtained by the ATSB, which included:
- post-mortem and toxicology report
- the sequence of events detailed in the ATSB preliminary report
- CASA medical records relating to the pilot
- Medicare and pharmaceutical benefits scheme records relating to the pilot
- compliance and therapy report for the pilot’s ResMed Airsense 10 Elite CPAP machine.
A summary of the specialist’s assessment of the information provided was as follows:
- The pilot sustained fatal injuries due to the impact with terrain prior to the post-impact fire.
- The blood alcohol level detected was from a sub-optimal sample taken from the chest cavity (often the only choice with severe trauma). Although alcohol consumption could not be ruled out, it was entirely possible that the alcohol was produced post-mortem and could be expected under the given circumstances.
- The pilot was known to take rosuvastatin medication for high cholesterol treatment. The drug was not detected in the pilot’s toxicology results and is generally not detectable in routine screening. While it could not be determined if the medication was in the pilot’s blood, the drug would not be expected to have a psychoactive effect or cause incapacitation.
- Regarding the identified 3 heart abnormalities in the pilot’s post-mortem, the specialist indicated that:
- In the case of the right coronary artery angulation, the specialist indicated that it is an anatomical abnormality in 2% of hearts where one of the 2 main blood vessels suppling the heart muscle is abnormally angled at its origin from the aorta and often presents as a slit‑like opening (as was the case with this pilot), as opposed to the normal opening, which has a round profile. In the majority of cases, it is considered an incidental finding of no clinical significance. In a small percentage of cases, this abnormality is determined to be a cause for heart muscle abnormalities, including the development of cardiac arrhythmias, scarring of heart muscle, and potentially incapacitation and death. It was noted that the pilot had a CT coronary angiogram performed in January 2019, which was reported to be normal. It was considered likely that had a coronary artery abnormality been a clinically significant issue at the time it would have been identified. Also, an absence of fibrosis (scarring) or other changes typical of chronic ischaemia in the distribution of the right coronary artery argues against this being clinically significant in this case.
- The second heart abnormality identified was the narrowing of the left anterior descending coronary artery without obvious atherosclerosis. It was considered likely that post‑accident heat effect caused the change rather than natural disease. It was noted again that the pilot had a CT scan in 2019 that was reported as normal, and it would be unlikely that coronary artery disease would have progressed to the extent of being capable of causing incapacitation in that time period.
- The third heart abnormality identified was contraction banding in association with lacerations of the heart muscle and was seen in areas supplied by widely patent coronary arteries such as the right coronary artery. In the absence of other indicators, it was considered likely that the contraction banding was a result of the aircraft accident rather than incapacitation due to cardiac disease.
- The specialist advised that many natural medical conditions that can result in pilot incapacitation would generally not be detectable from a post-mortem, especially where there have been very extensive injuries, and therefore could not be ruled out. Examples of such conditions include the pilot losing their corrective eyewear at a critical time, the pilot having a coughing fit, the development of many gastrointestinal illnesses including diarrhoea, vomiting, and stomach cramps, and diverse conditions such as fainting spells, kidney stone passage and cardiac arrhythmias.
In conclusion, the specialist stated that it was unlikely that natural disease caused or contributed to the events leading up to the accident. There were no indications of toxicological abnormalities causing incapacitation and/or death. In common with many aircraft accident fatalities, a definitive comment in relation to cause of death could not be made in this case.
Operational information
Icing conditions
The limitations section of the POH stated ‘Flight into known icing conditions is prohibited’. The abnormal procedures section stipulated that, if a pilot inadvertently entered icing conditions, the following abnormal checklist procedure for Inadvertent Icing Encounter was to be applied:
Pitot Heat…ON
Exit icing conditions. Turn back or change altitude.
Cabin Heat…MAXIMUM
Windshield Defrost…FULL OPEN
Alternate Induction Air…ON
The use of alternate induction air was described further in the emergency procedure for Engine Partial Power Loss as follows:
A gradual loss of manifold pressure and eventual engine roughness may result from the formation of intake ice. Opening the alternate engine air will provide air for engine operation if the normal source is blocked or the air filter is iced over.
Aerodynamic stall
A wing generates lift as a result of the pressure differential created by airflow over the wing’s surface. The angle between the incoming or relative air flow and wing chord is known as the angle of attack (AoA). As the AoA increases, lift increases up to a certain angle, known as the critical AoA. At this point, the airflow over the upper surface of the wing becomes separated. This condition is referred to as an aerodynamic stall (or simply a stall) and results in a significant loss of lift and an increase in drag. Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, typically an uncommanded aircraft nose-down pitch results.
Most general aviation aircraft typically have a critical AoA of around 16°. This critical AoA can be exceeded at any airspeed, any (pitch) attitude and any power setting. However, as most small aircraft are not fitted with an AoA indicator, the AoA at which the stall occurs may be referenced to an airspeed.
A loss of altitude also occurs during the recovery from a stall and it is possible to stall with insufficient height above the ground to recover. The POH stated that the altitude loss during a wings level stall may be 250 ft or more.
The Cirrus SR22 performance data showed that, at the maximum weight of 3,400 lbs (1,542 kg) with 0° bank angle and flaps full up, the power-off stall speeds at the forward and aft centre of gravity limits were 70 kt and 68 kt (indicated airspeed) respectively. The calibrated airspeed (CAS) for each limit was 1 kt less than the indicated.
The stall speed was calculated for a mid-centre of gravity position and corrected for an operating weight of 3,300 lb (1,497 kg), generally representative of the accident flight is mid centre of gravity given the take-off weight was close to the maximum take-off weight. The estimated stall speed was 68 kt (indicated) and 67 kt CAS.
The POH normal procedure for stalls stated:
SR22 stall characteristics are conventional. Power-off stalls may be accompanied by a slight nose bobbing if full aft stick is held. Power-on stalls are marked by a high sink rate at full aft stick.
…
When practicing stalls at altitude, as the airspeed is slowly reduced, you will notice a slight airframe buffet and hear the stall speed warning horn sound between 5 and 10 knots before the stall. Normally, the stall is marked by a gentle nose drop and the wings can easily be held level or in the bank with coordinated use of the ailerons and rudder. Upon stall warning in flight, recovery is accomplished by immediately reducing back pressure [on the control yoke] to maintain safe airspeed, adding power if necessary and rolling wings level with coordinated use of the controls.
Spins
A spin can result when an aircraft simultaneously stalls and yaws.[26] A spin is characterised by the aircraft following a downward, corkscrew path and requires significantly more altitude for recovery compared to a wings level stall (Federal Aviation Administration, 2021).
The limitations section of the POH stated ‘Aerobatic manoeuvres, including spins, are prohibited’. The emergency procedures stipulated that the SR22 was not approved for spins and had not been tested or certified for spin recovery characteristics. The only approved and demonstrated method of spin recovery was the activation of the CAPS (refer to the section titled Cirrus aircraft parachute system deployment). Specifically, the POH stated:
If, at the stall, the controls are misapplied and abused accelerated inputs are made to the elevator, rudder and/or ailerons, an abrupt wing drop may be felt and a spiral or spin may be entered. In some cases, it may be difficult to determine if the aircraft has entered a spiral or the beginning of a spin.
…
In all cases, if the aircraft enters an unusual attitude from which recovery is not expected before ground impact, immediate deployment of the CAPS is required.
…
The minimum demonstrated altitude loss for a CAPS deployment from a one turn spin is 920 feet. Activation at higher altitudes provides enhanced safety margins for parachute recoveries. Do not waste time and altitude trying to recover from a spiral/spin before activating CAPS.
Wood and Sweginnis (2006), Aircraft Accident Investigation – 2nd edition, provides the following description of the wreckage from an aircraft that had spun into the ground, with reference to Figure 21:
There is little or no evidence of forward motion. Although the fuselage probably impacted at a steep nose down attitude [spins can be anywhere between nose up, flat, but most commonly nose down], it is likely that there is evidence of a wing tip striking the ground before the nose. The down-going wing will normally strike the ground before the up-going wing, providing one clue as to the direction of the spin. Both the fuselage and the wings will probably have damage which reflects both a high sink rate and yaw. Tall thin objects on the ground, like trees and fence posts, are likely to penetrate the airplane almost from bottom to top, reflecting the almost vertical trajectory of the airplane. Undamaged objects may be found immediately behind the trailing edges, again indicating the vertical path of the airplane.
Figure 21: Example wreckage pattern from a spin
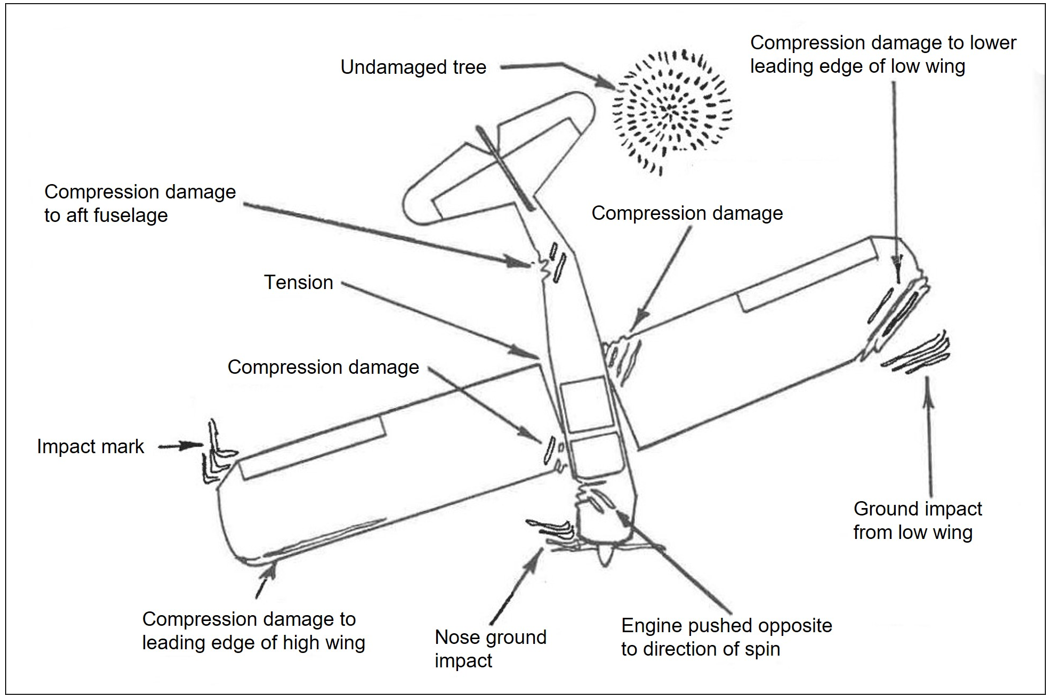
Source: Wood and Sweginnis (2006)
Cirrus aircraft parachute system deployment
Procedures for deployment
For the deployment of the CAPS, the POH stated:
*Warning*
CAPS deployment is expected to result in loss of the airframe and, depending upon adverse external factors such as high deployment speeds, low altitude, rough terrain or high wind conditions, may result in severe injury or death to the occupants. Because of this, CAPS should only be activated when any other means of handling the emergency would not protect the occupants from serious injury.
*Caution*
Expected impact in a fully stabilized deployment is the equivalent to a drop from approximately 13 feet.
*Note*
Several possible scenarios in which the activation of the CAPS would be appropriate are discussed in section 10 – Safety information of this handbook. These include:
- Mid-air collisions
- Structural failure
- Loss of control
- Landing in inhospitable terrain
- Pilot incapacitation.
The POH also noted that the maximum demonstrated deployment speed was 133 kt (indicated airspeed). Once a decision was made to deploy the CAPS, the airspeed should be reduced to the minimum possible, the mixture should be moved to cutoff, the activation handle cover should be removed and the handle pulled down with both hands. Pull forces up to, or exceeding, 45 lbs (20 kg) may be required. After deployment, the fuel selector, fuel boost pump, battery and alternator master switch and ignition switches were to be turned off and the emergency locator transmitter turned on.
In regard to a CAPS deployment altitude, the POH indicated that:
No minimum altitude for deployment has been set. This is because the actual altitude loss during a particular deployment depends upon the airplane’s airspeed, altitude and attitude at deployment as well as other environmental factors. In all cases, however, the chances of a successful deployment increase with altitude. As a guideline, the demonstrated altitude loss from entry into a one-turn spin until under a stabilized parachute is 920 feet. Altitude loss from level flight deployments has been demonstrated at less than 400 feet. With these numbers in mind it might be useful to keep 2,000 feet AGL in mind as a cut-off decision altitude. Above 2,000 feet, there would normally be time to systematically assess and address the aircraft emergency. Below 2,000 feet, the decision to activate the CAPS has to come almost immediately in order to maximize the possibility of successful deployment. At any altitude, once the CAPS is determined to be the only alternative available for saving the aircraft occupants, deploy the system without delay.
Cirrus, in its guidance document CAPS Guide to the Cirrus Airframe Parachute System, advised that, while the POH noted a maximum demonstrated deployment speed, it was possible for the parachute to withstand deployments at higher speeds. The guide provided examples where the CAPS had been deployed at speeds up to 187 kt (indicated airspeed) with a successful outcome. The guidance reiterated that the maximum demonstrated speed was not intended to be a limitation.
Cirrus also encouraged pilots to conduct a take-off briefing that incorporated when to activate the CAPS, as well as the inclusion of a passenger briefing that included the use of the CAPS. The briefing should include:
- Engage the autopilot using the level button (if equipped)
- Attempt to revive the pilot
- Follow the deployment procedures detailed on the CAPS placard
- Prepare for CAPS touchdown
- Follow egress procedures
The ATSB could not confirm what take-off or passenger briefings were undertaken by the pilot on the day of the accident. Further, nor could it be determined with certainty that the passenger seated adjacent to the pilot would have had the physical capability to undertake the required actions if they had received the briefing on the use of the CAPS.
Deployment history
At the time of writing this report, the aircraft manufacturer reported that there had been 126 in‑flight CAPS deployments. They also stated that there had been 3 CAPS anomalies where the parachute failed to deploy. A recent issue where the rocket did not deploy was related to a batch of rocket motor initiating devices (squibs) manufactured in 2015 and 2016 that would not fully ignite. There was a mandatory service bulletin to have those squibs replaced. The squib on VH‑MSF was replaced when the parachute assembly was replaced in its entirety in January 2023.
The ATSB reviewed several aircraft accident reports, which indicated that there had been a number of CAPS deployments above the maximum recommended indicated airspeed of 133 kt resulting in an overload and separation of the chute from the aircraft. Further, there have been a number of documented accidents where the parachute had not been deployed in‑flight but had ground impact initiations of the rocket.
Loss of control
The POH safety information section listed potential reasons for a loss of control and an associated response to such a situation:
Loss of control may result from many situations, such as: a control system failure (disconnected or jammed controls); severe wake turbulence, severe turbulence causing upset, severe airframe icing, or sustained pilot disorientation caused by vertigo or panic; or a spiral/ spin. If loss of control occurs, determine if the airplane can be recovered. If control cannot be regained, the CAPS should be activated. This decision should be made prior to your pre-determined decision altitude (2,000’ AGL).
Engine issue in-flight
In the event of an engine failure in-flight, the POH emergency procedure checklist stipulated:
If the engine fails at altitude, pitch as necessary to establish best glide speed. While gliding toward a suitable landing area, attempt to identify the cause of the failure and correct it. If altitude or terrain does not permit a safe landing, CAPS deployment may be required.
The emergency procedures section of the POH detailed that, for a partial engine power loss, indications of such include fluctuating revolutions per minute, reduced or fluctuating manifold pressure, low oil pressure, high oil temperature, and a rough-sounding or rough-running engine.
The procedure required that, if a partial engine failure permitted level flight, land at a suitable airfield as soon as the conditions allowed. If the conditions did not permit safe level flight, use partial power as necessary to set up a forced landing pattern over a suitable landing field. It was also advised that a pilot should be prepared for a complete engine failure and consider CAPS deployment if a suitable landing site was not available.
To troubleshoot, the POH advised to select the fuel boost pump on, switch fuel tanks, check the engine controls, and cycle the ignition switch left and right to ensure both magnetos were working. Select alternate induction air on, as a gradual loss of manifold pressure and eventual engine roughness may result from the formation of intake ice. Opening the alternate engine air would provide air for engine operation if the normal source was blocked or the air filter was iced over.
Fuel uplift
The aircraft had a total fuel capacity of 318 L (159 L per wing tank) as stipulated in the POH. According to fuel company records, the aircraft was refuelled on 5 October 2023 (one day prior to the accident) at about midday with 110 L of Avgas from a fuel bowser at Canberra Airport. The fuel remaining in each tank before the refuelling commenced was unable to be determined. However, the fuel uplift was close to the estimated fuel consumption of 118 L for the previous flight from Armidale to Canberra. The estimated fuel consumption from Canberra to the accident site was 22 L.
As part of the Canberra Airport fuel company procedures, a sample of fuel was tested for clarity and water content on the morning the aircraft was refuelled and on the afternoon of the accident, with no issues identified. Several other aircraft utilised the same batch of fuel with no issues reported. Therefore, fuel quality and quantity was not considered to be a factor in the accident.
Weight and balance
The aircraft load data sheet indicated that the empty weight was recorded as 1,045 kg and the gross weight limit for the SR22 was 1,542 kg. For the purpose of calculating the weight and balance for the accident flight, the ATSB assumed full fuel and used average weights for each of the occupants and their luggage, based on 4 separate estimates provided by their relatives. This produced an estimated engine start weight of 1,494 kg, which was 48 kg below the gross weight limit. The centre of gravity was within limits for the entirety of the flight.
Flight into icing
Bureau of Meteorology pilot guidance on icing conditions
The accumulation of ice on an aircraft is ‘one of the most significant hazards to the safe and efficient operation of aircraft as it can reduce aircraft performance in a number of ways’ (Bureau of Meteorology, 2015). This includes:
- increased stall speed of the aircraft by increasing its weight with the accumulation of ice
- difficulty operating control surfaces and landing gear
- increased drag and decreased lift due to ice accumulation on the airframe (tests have shown that icing no thicker or rougher than a piece of coarse sandpaper can reduce lift by 30% and increase drag by 40%)
- engine power reductions (intake and carburettor icing)
- propeller vibrations due to ice accumulation on the blades
- errors in instrument readings of airspeed, altitude and vertical speed due to ice contaminated pitot static systems
- interference with communications systems (icing on antennas)
- reduced visibility due to icing on the windshield and side windows.
The Bureau of Meteorology aviation weather services brochure titled Hazardous Weather Phenomena – Airframe Icing has informative content for pilots. Included in that brochure was a depiction of the icing environment and the various levels of icing risk based on temperature and water content. As shown in the icing environment depiction (Figure 22), aircraft operating within the 0 to −10°C higher risk range if/when in cloud could experience clear ice conditions.
Figure 22: Icing environment depiction
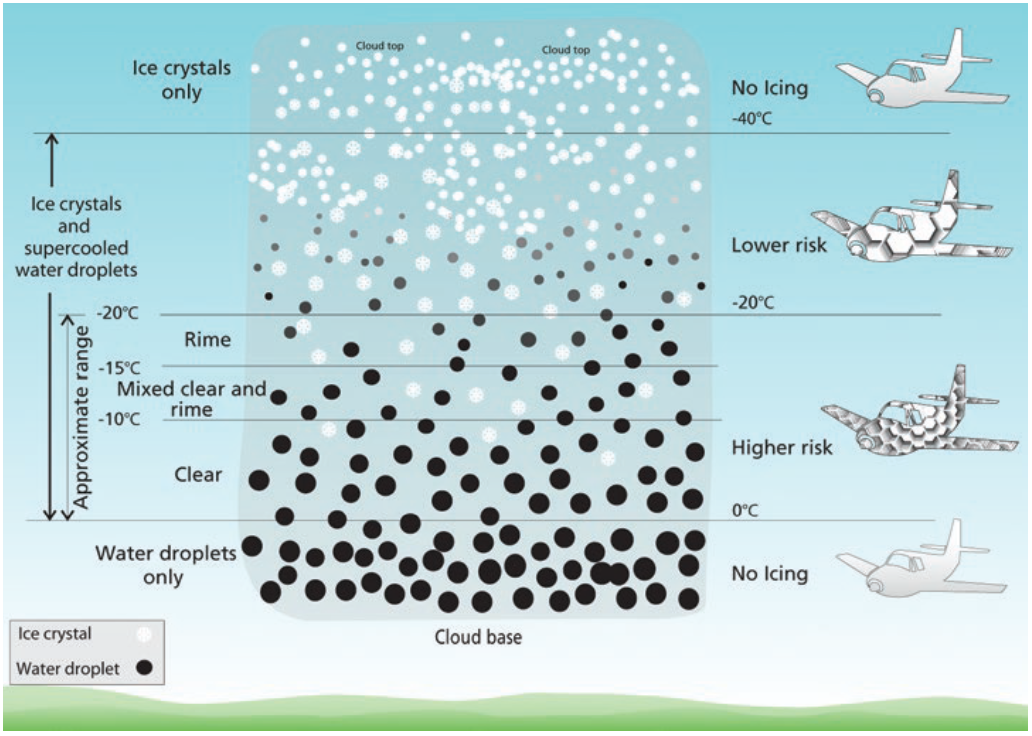
Source: Bureau of Meteorology
The Bureau of Meteorology classifies icing severity as trace, light, moderate or severe. Moderate icing (as identified on the VH-MSF flight route) means the rate of accumulation is such that even short encounters become potentially hazardous, and the use of de‑icing/anti‑icing equipment or a diversion is necessary. An area forecast will include any expectation of moderate or severe icing, while a SIGMET[27] is only required when severe icing is predicted.
There are 4 types of icing which are clear, rime, mixed ice (a combination of clear and rime icing) and hoar frost. Clear ice is formed when supercooled water droplets impact the aircraft. As the droplets freeze, heat is released, slowing the freezing process. This causes some of the water droplets to flow back over the exposed surfaces and freeze as clear ice. Therefore, clear ice tends to cover a large area of the aircraft and can disrupt the airflow and affect the performance of the aircraft. Clear ice forms most readily in temperatures between 0 ºC and −10ºC but can occur, with reduced intensity, at lower temperatures.
Impact of icing on aircraft performance
Baars et al. (2010) conducted research titled A review on the impact of icing on aircraft stability and control. The research stated that:
Structural ice formation on leading edges of wings and control surfaces initiate significant regions of unsteady flow. This change in performance of the lifting surfaces can result in a major change in the handling of aircraft; the aircraft may stall at higher speeds, the stall angle of attack may decrease and irreversible upset events can be initiated.
In the period of 1990-2000, a total of 3,230 aircraft accidents were recorded by the Air Safety Foundation. Twelve percent of those were related to icing.
…
Studies on ice-related accidents of small general aviation aircraft have revealed that in many cases even the most experienced pilots have less than 5 to 8 minutes to escape the harmful icing conditions before their aircraft experience violent upsets. This suggests that in cruise the accumulation of ice, and its effect on stability of aircraft, remain mostly unobserved. Upon changing the attitude of the aircraft, the formation of ice induces unsteady flow phenomena capable of upsetting the aircraft in a catastrophic manner.
United States Federal Aviation Administration – Pilot Guide: Flight in Icing Conditions
The purpose of the United States Federal Aviation Administration’s advisory circular AC 91‑74B, Pilot Guide: Flight in Icing Conditions, was to provide pilots with a convenient reference guide on the principal factors related to flight in icing conditions and the location of additional information in related publications. It included the following information:
Flight planning
If an aircraft is not certificated for flight in icing conditions, each flight should be planned carefully so that icing conditions are avoided…In the event of an inadvertent icing encounter, the pilot should take appropriate action to exit the conditions immediately, coordinating with ATC [air traffic control] as necessary, and declaring an emergency.
Effects of icing on unprotected wings
…The ice causes an increase in drag, which the pilot detects as a loss in airspeed or an increase in the power required to maintain the same airspeed. (The drag increase is also due to ice on other parts of the aircraft). The longer the encounter, the greater the drag increase; even with increased power, it may not be possible to maintain airspeed. If the aircraft has relatively limited power (as is the case with many aircraft with no ice protection), it may soon approach stall speed and a dangerous situation.
Effects of icing on critical systems
Because contamination of the wing reduces lift, even an operational, ice-free stall warning system may be ineffective because the wing will stall at a lower AOA [angle of attack] due to ice on the airfoil. Heated or unheated, if the wing is contaminated in any way, an AOA will become unreliable. The stall onset would occur prior to activation of stall warning devices leading to a potential pitch or roll upset. It is imperative that pilots maintain airspeed and monitor AOA closely when in icing conditions.
Induction icing
Fuel-injected aircraft engines usually are less vulnerable to icing, but still can be affected if the engine’s air source becomes blocked with ice. Manufacturers provide an alternate air source that may be selected in case the normal system malfunctions.
Moderate icing accretion rate
…
The rate of accumulation is such that anything more than a short encounter is potentially hazardous. A representative accretion rate for reference purposes is 1 to 3 inches (2.5 to 7.5 cm) per hour on the unprotected part of the outer wing. The pilot should consider exiting the condition as soon as possible.
General advice
Avoidance - The pilot of an aircraft that is not certificated for flight in icing conditions should avoid all icing conditions. This guide provides guidance on how to do this, and on how to exit icing conditions promptly and safely should they be inadvertently encountered.
Vigilance - The pilot of an aircraft that is certificated for flight in icing conditions can safely operate in the conditions for which the aircraft was evaluated during the certification process, but should never become complacent about icing. Even short encounters with small amounts of rough icing can be very hazardous.
Guidance - The pilot should be familiar with all information in the AFM [airplane flight manual] or POH concerning flight in icing conditions and follow it carefully. Of particular importance are proper operation of ice protection systems and adherence to minimum airspeeds during or after flight in icing conditions. Monitor airspeed, pitch attitude, and do not rely on the airplane’s autopilot or stall warning system in icing conditions. There are some icing conditions for which no aircraft is evaluated in the certification process, such as SLD [supercooled large droplets] conditions within or below clouds, and flight in these conditions can be very hazardous. The pilot should be familiar with any information in the AFM or POH relating to these conditions, including aircraft-specific cues for recognizing these hazardous conditions.
Cirrus SR22 flight in known icing conditions information
Although not fitted to VH-MSF, the approval and specifications for FIKI (flight into known icing) were reviewed as they provided specific guidance for icing on the Cirrus SR22.
The approved POH and airplane flight manual supplement for the FIKI system recommended that the minimum airspeed for flight into known icing conditions was 95 kt (indicated airspeed). The emergency procedures section contained the following information when discussing an observed or suspected failure of the anti-ice system:
An unobserved failure may be indicated by a decrease in airspeed, anomalous handling characteristics, or airframe vibrations.
Note: Significant loss in cruise or climb performance may be an indication of propeller ice accretions that are not visible to the naked eye. Operation of the engine at 2700 RPM [revolutions per minute] will help shed ice in severe icing conditions.
The performance section of the FIKI supplement further stated:
Airplane performance and stall speeds without ice accumulation are essentially unchanged with the installation of the Ice Protection System. Significant climb and cruise performance degradation, range reduction, as well as buffet and stall speed increase can be expected if ice accumulates on the airframe.
Propeller icing
The adverse effects of propeller icing have been explored for several decades, which included the United States National Advisory Committee for Aeronautics producing a report in 1950 (NACA TN 2212), on the subject of The effects of ice formation on propeller performance. Its report included the following observations:
- when a propeller accumulates ice, the resulting changes in propeller performance are reflected in corresponding changes in aircraft performance
- the combined action of centrifugal force and kinetic heating resulting from an increase in propeller rotational speed is often effective in reducing the extent of the ice accumulation
- thus, it appears that in operation of unprotected or inadequately protected propellers in icing conditions, periodic attempts should be made to throw off the accretions by increasing propeller speed.
The propeller manufacturer for VH-MSF, Hartzell, stated on its website that ‘ice typically appears on propeller blades before it forms on the wings, so it’s important to address propeller icing as quickly as possible’. While the NACA (1950) report and the Cirrus FIKI supplement both indicated that increasing the propeller speed was a technique to address propeller icing, another similar technique, published as an online instructional video, was to cycle the propeller lever forwards and backwards. This would vary the propeller blade angle and propeller speed to promote shedding of ice. As the Cirrus aircraft combine the propeller pitch control and engine power control in one lever, the use of propeller blade angle and rotational speed changes to shed ice would be accompanied by associated engine power changes. The ATSB was unable to establish if the pilot was aware of these techniques to remove ice accumulation on the propeller.
Related occurrences
There have been a number of loss of control accidents involving Cirrus SR22 aircraft with contributors including flight in icing conditions, autopilot control issues, pilot incapacitation and loss of control during stall demonstration to name a few. A varied sample of those events is listed below from the United States National Transportation Safety Board (NTSB) and the ATSB.
NTSB investigation (ATL06LA035)
While climbing on autopilot, the airplane entered clouds at 5,000 ft at an airspeed of 120 kt. Upon reaching 7,000 ft, the airplane encountered icing conditions. The pilot informed air traffic control and requested a clearance to climb to 9,000 ft, which was approved. As the airplane reached the cloud tops at 8,000 ft when in visual flight conditions, the airplane began to buffet. The pilot looked at the airspeed indicator and it showed 80 kt. The airplane subsequently aerodynamically stalled, started to spin and re‑entered instrument flight conditions. The pilot deployed the ballistic parachute system and informed the air traffic controller of his actions. The airplane descended under the parachute canopy into the trees.
The NTSB determined the probable cause of the accident to be:
The pilot’s inadequate pre-flight planning, failure to obtain a current weather briefing, and his decision to operate the airplane into known icing outside the airplanes certification standards resulting in the aircraft accumulating ice, loss of airspeed, an inadvertent stall/spin and subsequent collision with trees.
NTSB investigation (ERA20LA129)
While conducting an instrument landing system approach, the airplane flew through the localizer course, and as it passed outside of the outer edge of the localizer, the autopilot turned off. The pilot could not recall turning the autopilot off, and the reason for the autopilot turning off could not be determined from the available evidence. Over the next minute, a series of altitude excursions occurred during which the airplane repeatedly climbed and descended. The pilot reported that, when he added power, he had difficulty maintaining control of the airplane and that it was unstable. Subsequently, the pilot sensed that he was fighting the airplane and in an unusual attitude, he deployed the airframe’s parachute system. The airplane descended under canopy and touched down in the backyard of a house.
While off course with the autopilot engaged and the vertical speed mode selected, the pilot likely applied and held pitch control input that was sensed by the autopilot auto trim system as an out‑of-trim condition. The autopilot auto trim system responded by trimming the airplane, resulting in the corresponding altitude excursions.
The NTSB determined the probable cause of the accident to be:
The pilot’s incorrect use of the autopilot while approaching the initial approach fix and his subsequent improper primary pitch control input while a pitch mode of the autopilot was engaged, which resulted in pitch excursions and subsequent departure from controlled flight.
NTSB investigation (NYC05LA110)
The airplane was in cruise flight at 3,000 ft when the pilot experienced a seizure and lost consciousness. When the pilot awakened, the airplane was in a high-speed descent. In addition, the pilot felt disoriented and numbness in his right leg. The pilot recovered from the descent at an altitude of about 1,700 ft and elected to deploy the CAPS. The airplane descended via the parachute and impacted in a river. The airplane sustained substantial damage to the underside of the composite fuselage. The pilot sustained a fractured vertebra and was able to egress from the airplane before it sank. Subsequent medical examinations on the pilot revealed the presence of a brain tumour.
The NTSB determined the probable cause(s) of this accident to be:
The pilot's physiological condition, which resulted in his incapacitation during the flight, and subsequent loss of aircraft control.
ATSB investigation (AO-2013-126)
The aircraft was being operated on a private flight from Archerfield to Kingaroy, Queensland, with the pilot and one passenger on board. On approach to Kingaroy, at about 500 ft above ground level, the pilot extended the flaps and, shortly after, disconnected the autopilot (AP). Upon disconnecting the autopilot, the pilot reported that the aircraft pitched-up violently due to trim runaway.
The AP pitch trim was trimming the aircraft for a nose-up position, even though the AP was disconnected. This required the pilot to use a large amount of forward physical force to maintain stable flight. The pilot attempted to resolve the problem several times by pressing and holding the autopilot disconnect switch located on the control yoke, however, this had no effect.
The pilot then conducted a go-around. They then used the manual electric trim (MET) hat switch located on the control yoke, in an attempt to trim the aircraft nose-down. As the pilot was using the MET to trim the aircraft, which was going against the AP pitch trim runaway, the trim adjusted at a slow rate.
The pilot was able to regain sufficient control of the aircraft and land safely at Kingaroy. The pilot reported that, upon parking the aircraft and after releasing the MET, the pitch trim was at full nose‑up deflection.
ATSB investigation AO-2014-083
When at about 6,000 ft above ground level, the pilot in command (PIC) was demonstrating the aircraft stall and recovery to a prospective purchaser of the aircraft. They selected 50% flap, rolled the aircraft into a left turn at about 25° angle of bank, reduced the power to idle, and raised the nose. As the aircraft approached the stall, the PIC pointed to the vertical speed indicator. As they did this, the right wing dropped rapidly, and the aircraft entered a spin to the right. The PIC reported that, at this time, they performed their normal recovery procedure for this manoeuvre.
The passenger in the front seat reported that, on about the third rotation of the spin, the PIC said ‘I’m sorry’, and realised that the PIC had lost control of the aircraft.
When at about 2,000 ft, the PIC was unsure whether they had enough height remaining to recover control of the aircraft, so they successfully deployed the CAPS, and the aircraft came to rest in a residential backyard. All 3 occupants were uninjured.
Downloaded flight data indicated that the aircraft stalled at an indicated airspeed of 62 kt and the vertical descent rate in the spin increased to a maximum of 14,000 ft/min before the parachute was deployed.
Safety analysis
Introduction
Flight track data showed that, about 12 minutes after take-off and during the climb phase of the flight from Canberra, Australian Capital Territory, to Armidale, New South Wales, VH‑MSF departed controlled flight and entered a rapid descent just prior to reaching the planned cruising level of 10,000 ft. The aircraft subsequently impacted with terrain. The 4 occupants were fatally injured, and a post-impact fire destroyed the aircraft.
This analysis will consider the events leading up to the departure from controlled flight and the possible explanations for this. It will also consider why the pilot did not recover the aircraft from the rapid descent and the forecast and actual meteorological conditions along the aircraft’s flight track.
Aerodynamic stall
Consistent with the 2 previous flights, the aircraft’s flight tracking data showed a normal, stable take-off and climb out of Canberra Airport towards Armidale until about 7,000 ft above mean sea level. This suggested that the pilot may have been using the aircraft’s autopilot system. Also, up to this point, all radio exchanges between the pilot and air traffic control were clear and readback correctly.
Climbing through about 8,300 ft, the flight track data changed from a relatively steady state to variations in heading, altitude and airspeed. This suggested that the aircraft had likely changed from operating with the autopilot on to manually controlled flight. Potential reasons for this change may have included the avoidance of cloud, turbulence or issues with the autopilot. It was around this time that 4 independent witnesses located below the aircraft’s flight track reported that an aircraft obscured by cloud could be heard making engine surging sounds (see Possible explanations for the contributing factors below for further explanation).
Over the next couple of minutes, while the general trajectory of the aircraft remained in a climb, the aircraft slowed to almost the stall speed on 2 occasions. If working as designed, the stall warning system should have sounded when the aircraft’s airspeed deteriorated to about 5 kt above the stall speed, alerting the pilot to an impending stall condition. Additionally, as a precursor to the stall, a slight buffet might have been felt by the pilot through the airframe. The pilot’s operating handbook (POH) stipulated that, when the stall warning sounds, recovery was accomplished by immediately reducing back pressure on the control yoke to reduce the angle of attack, maintain a safe airspeed, and add power as required. Following these 2 occasions, the flight data showed a slight descent and an increase in airspeed, which may have been representative of a possible pre-stall recovery and then the climb continued.
Following a descent, the performance data indicated a climb rate of up to about 1,500 ft/min and the airspeed decreased from an estimated 96 kt to 70 kt past the point of a pre-stall recovery. At a maximum altitude of 9,946 ft, the airspeed and altitude rapidly decreased, which was consistent with the aircraft aerodynamically stalling and departing controlled flight.
Contributing factor When approaching 10,000 ft above mean sea level, the aircraft climb rate increased significantly combined with a decreasing airspeed, resulting in an aerodynamic stall and departure from controlled flight. |
Recovery actions
The POH procedure for a recovery from an aerodynamic stall required the pilot to reduce back pressure on the control yoke to un-stall the wings and apply power, as necessary, to accelerate the aircraft. However, the flight data showed that, following the stall at about 9,900 ft, the rate of descent increased to about 13,000 ft/min, which was inconsistent with a stall recovery. While descending through around 8,000 ft, the ground speed reduced while the variations in the track became larger, and the rate of descent started to reduce towards 10,000 ft/min by ground level. This, combined with the witness observations, wreckage examination, and manufacturer’s assessment of the flight data, indicated the aircraft had likely entered a spin before the impact with terrain.
The POH stipulated that, following a loss of control when recovery may not be possible, the Cirrus airframe parachute system (CAPS) should be used. The POH further indicated that the only method of recovery from a spin was to deploy the CAPS. The decision to activate the CAPS should be made prior to an altitude of 2,000 ft above ground level. The POH also suggested that when no other survivable options were available, the CAPS should be activated regardless of altitude. That said, the ATSB considered there was adequate time (about 44 seconds) to deploy the CAPS following the departure from controlled flight. However, the inspection of the wreckage indicated that the CAPS had not deployed in-flight, but rather due to ground impact forces. That examination also found that the pre‑deployment procedure of shutting down the engine was not conducted.
It was also determined that a deployment failure was unlikely given the system’s recent replacement, high reliability and the ground impact initiation of the rocket. Therefore, the ATSB was unable to ascertain why the aircraft was not recovered from the stall or if an attempt was made to deploy the CAPS in-flight.
Contributing factor Following the loss of control, for undetermined reasons, an aerodynamic stall recovery did not occur nor was the Cirrus aircraft parachute system deployed before the impact with terrain. |
Possible explanations for the contributing factors
The flight data showed aircraft performance and handling that was beyond what was considered normal, particularly the maintained climb at reducing airspeed leading to the stall. As such, the following section will discuss several scenarios that were considered by the ATSB, which may explain the stall and subsequent loss of control, with no recovery action taken. Those factors include whether there was an aircraft issue, if the pilot had some level of incapacitation, or if in‑flight icing was experienced.
Aircraft issue
There were no reported problems with the aircraft on the 2 flights in the days that preceded the accident. A review of the maintenance documentation revealed 2 items of maintenance that were overdue, which were the standby compass calibration and an outside air temperature/clock back-up battery replacement. However, neither of those items were of significance and should not have contributed to the loss of control. All major aircraft components were identified in the general area of the accident site with an in-flight failure of the airframe structure ruled out. While the post‑impact fire prevented examination of a significant proportion of the aircraft, an inspection of the remaining aircraft structure and flight controls did not identify any pre-accident anomalies.
There have been previous occurrences related to the autopilot and pitch trim systems. However, in this case, the position of the relevant switches and trim could not be established due to the extent of damage.
Witnesses reported hearing surging or a rough running engine along the aircraft flight path in the minutes prior to the departure from controlled flight. If the sound heard was from VH‑MSF, this could potentially suggest an engine issue or alternatively, the pilot manipulating the engine power lever. There were also short periods in the flight track that indicated possible power reductions and loss of altitude, but the general trajectory of the aircraft remained in a climb until the aerodynamic stall.
The engine was disassembled and inspected by the ATSB with no pre-impact mechanical defects identified. The inspection of the propeller damage and crankshaft fracture indicated evidence that the engine was running at low power when it impacted with terrain, although the ATSB was unable to ascertain if the engine controls were set at a low power setting (matching the observed propeller damage). It was also noted that no radio call was received from the pilot advising of a problem, nor had they attempted a diversion to a nearby airfield or return to Canberra, which would be expected if an aircraft issue was experienced.
Therefore, while there were no observable indications of an issue, due to the limited remaining aircraft structure and systems that were available for inspection, an unidentified mechanical failure or anomaly could not be discounted.
Pilot incapacitation
Partial or complete incapacitation can adversely affect a pilot’s psychological and/or physiological capacity to operate an aircraft. Research has shown that pilot incapacitation occurs for a variety of reasons including acute medical conditions (such as food poisoning and gastroenteritis) and pre‑existing medical conditions (such as heart disease, leading to a heart attack). While pilot incapacitation in general aviation accounted for only 13% of all reported occurrences between 2010 and 2014, 70% of those influenced flight operations, namely a return to the departure aerodrome or in the worst case, a collision with terrain (ATSB, 2016). In this accident, indicators of a potential incapacitation were:
- the absence of radio calls to indicate a problem or phase of distress
- the lack of stall recovery actions with ample altitude and time to recover
- the non-use of the CAPS as a procedural recovery action when there was sufficient altitude for deployment.
The pilot’s post-mortem identified a heart anomaly, however, it was noted that in most cases symptoms do not present. Overall, the post-mortem report concluded that the cause of death was undetermined and that an assessment should be made in consideration of the other available evidence to determine if sudden incapacitation may have contributed to the accident.
Therefore, to further examine the possibility of an incapacitating event, the ATSB requested the assistance of an independent doctor of forensic pathology to undertake an assessment of the pilot’s post‑mortem, toxicology and medical history. However, that assessment did not identify any underlying medical conditions, natural disease or toxicological abnormalities that could have led to an incapacitation event.
In addition, records indicated the pilot consistently used a continuous positive airway pressure machine to manage sleep apnoea. As the pilot had taken the machine on their trip, it was likely that they had used it the night before the accident. Also, it was noted that the pilot had lunch just prior to departure, and as the research has shown, gastroenteritis related incapacitation can occur and therefore could not be discounted.
Further, there was no evidence to suggest that the pilot's general health on the day of the accident was degraded. Similarly, the pilot was reported to be fit and healthy and had no identified health conditions that were not being appropriately treated. Consequently, there was insufficient evidence to determine if incapacitation was a contributing factor. That said, medical incapacitation can result for many reasons that may have been undetectable in the post-mortem, toxicology and review of the available medical information.
Icing conditions
The subsequent graphical area forecast accessed by the pilot, which was valid for the flight, indicated broken cloud was expected from 5,000 ft to 10,000 ft along the aircraft’s flight path after departing Canberra. The Bureau of Meteorology’s post-accident analysis concluded that the actual conditions experienced were consistent with the forecast conditions. This analysis estimated a cloud depth of 3,000 ft, with a top height of 10,000 ft, which was the pilot’s nominated cruising altitude. The ATSB’s analysis of the satellite imagery also showed cloud coverage along parts of the aircraft’s track. Likewise, the camera footage and automatic terminal information service at Canberra, and video from first responders at the accident site also noted cloud in the vicinity.
The Bureau of Meteorology’s analysis also determined an approximate freezing level of 7,000 ft. On that basis, it was concluded that the conditions would have been conducive to moderate icing between about 7,000 ft and 10,000 ft, when in cloud. The presence of icing was consistent with pilot observations and data from other aircraft operating in the vicinity of Canberra. The pilot of another Cirrus aircraft reported using the icing protection system when operating at about 9,000 ft. Likewise, the flight data from Velocity 1690 showed that, on descent, the engine anti-ice system had been used from about 10,000 ft down to 7,000 ft, indicating the aircraft was operating in cloud above the freezing level during that time. Therefore, considering the flight path and cruising altitude, VH-MSF likely entered cloud at some point during the flight and was subject to icing conditions.
Operations in icing conditions can lead to performance degradation and changes in aircraft handling due to ice accretion on the wings and control surfaces, and a reduction in engine power due to blocked engine air intakes and ice‑affected propeller blades. It can also result in erroneous airspeed and altitude information due to blocked pitot static systems, loss of visibility due to ice on the windshield, render a stall warning system ineffective, and weaken radio signals due to ice accretion on antennas.
The propeller will likely accumulate ice faster than the airframe and there are techniques for shedding propeller ice, which involve increasing the propeller speed and varying the propeller blade angle. In the Cirrus SR22 aircraft, the propeller lever is combined with the engine power lever and therefore the use of propeller speed and blade angle variations to shed ice would be accompanied by engine power changes. While this technique might have produced the engine power fluctuations heard by witnesses, who were located where the aircraft’s flight path was above the freezing level, the ATSB was unable to determine if the pilot was aware of this technique.
Consistent with the United States Federal Aviation Administration’s guidance, the POH stipulated that, when icing was encountered, the pilot should immediately exit icing conditions by turning back or changing altitude. However, the flight data showed that, overall, the aircraft continued to climb toward the cruising altitude. Also, while there were some variations in the aircraft’s track with a more observable change up to 35° later in the flight, there was no indication of a turnback towards Canberra. Likewise, there was no radio call received from the pilot advising of an intention to change altitude, divert from track or turnback due to icing. Although it was noted that icing has the potential to interfere with communication systems.
The POH also stated that a gradual loss of engine manifold pressure and eventual engine roughness due to intake icing could result, like what was heard by witnesses. However, the ATSB was unable to ascertain if the change in engine sound was from the pilot manipulating the engine control or uncommanded surging of the engine. Despite this, and as previously noted, there was no radio call received from the pilot advising of an engine issue nor was there an attempted diversion or return.
The Federal Aviation Administration’s guidance also indicated that, in moderate icing, a representative accretion rate for reference purposes was about 2.5 to 7.5 cm per hour on the outer wing. If the aircraft was in cloud for the entire period above the freezing level, the maximum amount of time spent in icing conditions before the loss of control would have been about 5 minutes. Therefore, a worst-case scenario was that the aircraft’s outer wings accumulated between 2.1 mm to 6.2 mm of ice. That said, satellite imagery with a flight track overlay showed some flight above the freezing level was likely to have been clear of cloud. Therefore, it was likely that the amount of time spent in icing conditions was less than 5 minutes. However, the exact amount of time spent in these conditions was unable to be determined due to the dynamic nature of the cloud on the day of the accident and the 10‑minute capture between local area satellite images.
When about 1,000 ft above the freezing level, the heading, altitude and airspeed variations had commenced, which might suggest performance effects from icing or cloud avoidance. However, the general trajectory of the aircraft was a climb up to the point of the stall. Also, the aircraft went through a period of about 45 seconds where it achieved the best rate of climb, which was about 1 minute and 30 seconds before the stall. That rate of climb would likely be unachievable if the aircraft had significant icing accretion. Further, as shown in the SR22 ice accretion accident example in this report, if an aircraft was affected by ice the stall speed for the aircraft would likely be much higher than the normal stall speed.
In summary, icing may explain the rough running engine, the variations observed in the flight data, and reduction in airspeed to the point of a stall. However, from the available evidence, it could not be established with a reasonable degree of probability that the aircraft experienced icing for a duration sufficient to result in performance degradation or other known icing issues and, therefore, contributed to the accident. Also, experiencing icing did not explain why the CAPS was not deployed following the loss of control and entry into a spin.
Flight plan
On the morning of the accident, the pilot lodged an instrument flight rules plan with a cruising altitude of 10,000 ft. Canberra Airport was within an area that had a forecast for broken cloud with a layer of moderate icing present below the pilot’s planned cruising altitude. At the time the pilot submitted the flight plan, the cloud tops along the planned route from Canberra to waypoint CULIN were forecast to be 7,000 ft and the layer of icing was expected to be about 1,500 ft deep with the top 3,000 ft below the planned cruising level. However, when the pilot checked the weather later in the morning the cloud tops were forecast to reach 10,000 ft and the icing layer was expected to be about 3,000 ft deep, which could only be avoided if the aircraft remained clear of the broken cloud. The aircraft was not fitted with anti‑icing equipment and was prohibited from operating in icing conditions. Therefore, the only way for the pilot to ensure that icing conditions would be avoided (if they did not amend their planned flight track) was to avoid flying the aircraft in cloud at those levels where icing was forecast.
Noting the lowest safe altitude from Canberra to CULIN was 4,600 ft, the pilot had the opportunity to amend their flight plan to fly this sector at 6,000 ft, below the freezing level. Alternatively, before departing Canberra, the pilot could have requested from air traffic control either a change of cruising altitude and/or a change in track. Likewise, a clearance to manoeuvre left or right of the planned track, or to climb or descend clear of cloud if icing became an issue after take-off, was a possibility. Neither of those options occurred and while the satellite imagery, and recorded images from Canberra and the accident site, indicated there were patches of clear sky, it was considered unlikely that the pilot was able to avoid all cloud above the freezing level.
Noting that the aircraft would have likely been subject to moderate turbulence during the climb, it was possible the pilot was expecting smooth and clear flying conditions on top of the cloud at 10,000 ft. While this might have been a consideration for the pilot’s plan, it could not be confirmed if that was the reason. Despite this, and as discussed above, the ATSB was unable to determine if the aircraft experienced icing to an extent that affected performance and handling.
However, aircraft flying through cloud in sub-freezing temperatures are likely to experience some degree of icing. Operating in these conditions in aircraft that are prohibited from doing so increases the risk of a loss of control event leading to an accident. A pilot can reduce the chance of icing becoming an issue by selecting appropriate routes during the flight planning stage.
Other factor that increased risk The flight was planned and flown through forecast moderate icing conditions from about 7,000 ft in an aircraft that was prohibited from operating in those conditions. It was therefore likely that the aircraft encountered icing, however, there was insufficient evidence to determine if it was at a level sufficient to affect aircraft performance and/or handling. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Cirrus SR22, VH-MSF, near Gundaroo, New South Wales, on 6 October 2023.
Contributing factors
- When approaching 10,000 ft above mean sea level, the aircraft climb rate increased significantly combined with a decreasing airspeed, resulting in an aerodynamic stall and departure from controlled flight.
- Following the loss of control, for undetermined reasons, an aerodynamic stall recovery did not occur nor was the Cirrus aircraft parachute system deployed before the impact with terrain.
Other factors that increased risk
- The flight was planned and flown through forecast moderate icing conditions from about 7,000 ft in an aircraft that was prohibited from operating in those conditions. It was therefore likely that the aircraft encountered icing, however, there was insufficient evidence to determine if it was at a level sufficient to affect aircraft performance and/or handling.
Glossary
| ADS-B | Automatic dependant surveillance broadcast |
| AGL | Above ground level |
| AMSL | Above mean sea level |
| AoA | Angle of attack |
| CAPS | Cirrus airframe parachute system |
| CAS | Calibrated airspeed |
| CPAP | Continuous positive airway pressure |
| FIKI | Flight into known icing |
| GAF | Graphical area forecast |
| GPWT | Grid point wind and temperature forecast |
| IFR | Instrument flight rules |
| NAIPS | National Aeronautical Information Processing System |
| NOTAM | Notice to airmen |
| NTSB | United States National Transportation Safety Board |
| POH | Pilot’s operating handbook |
| RNP | Required navigation performance |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Cirrus Design Corporation
- the aircraft owner
- the maintenance organisation
- witnesses
- Airservices Australia
- Bureau of Meteorology
- Civil Aviation Safety Authority
- forensic pathology specialist
- NSW Police Force
- United States National Transportation Safety Board.
References
Australian Transport Safety Bureau. (2016). Pilot incapacitation occurrences 2010-2014 (AR‑2015-096). https://www.atsb.gov.au/sites/default/files/media/5768970/ar-2015-096
final.pdf
Baars, W.J., Stearman, R.O. & Tinney, C.E. (2010). A review on the Impact of Icing on Aircraft Stability and Control. ASD Journal (2010), 2(1), 35-52.
Bureau of Meteorology. (2015). Hazardous weather phenomena – airframe Icing. www.bom.gov.au/aviation/knowledge-centre
Cirrus Aircraft Corporation (2013) CAPS Guide to the Cirrus Airframe Parachute System.
Federal Aviation Administration. (2021). Airplane Flying Handbook (FAA-H-8083-3C). https://www.faa.gov/sites/faa.gov/files/regulations_policies/handbooks_manuals/aviation/airplane_handbook/00_afh_full.pdf
National Transportation Safety Board. (2022). Investigation ERA20LA129 - Autopilot issue and loss of control - Cirrus SR22 – Conway, South Carolina USA – March 17, 2020. https://data.ntsb.gov
National Transportation Safety Board. (2006). Investigation ATL06LA035 - Icing conditions and loss of control - Cirrus SR22 – Childersburg, Alabama USA. https://data.ntsb.gov
National Transportation Safety Board. (2006). Investigation NYC05LA110 - Pilot incapacitation and loss of control - Cirrus SR22 - Haverstraw, New York USA – June 30, 2005. https://data.ntsb.gov
Wood and Sweginnis. (2006). Aircraft Accident Investigation – 2nd edition. Endeavour Books.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Cirrus Design Corporation
- aircraft owner
- maintenance organisation
- Bureau of Meteorology
- Airservices Australia
- Civil Aviation Safety Authority
- forensic pathology specialist
- United States National Transportation Safety Board.
Submissions were received from the:
- aircraft owner
- Civil Aviation Safety Authority
- Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix A
VH-MSF aggregated ADS-B altitude data for the accident flight, together with the estimated airspeed.
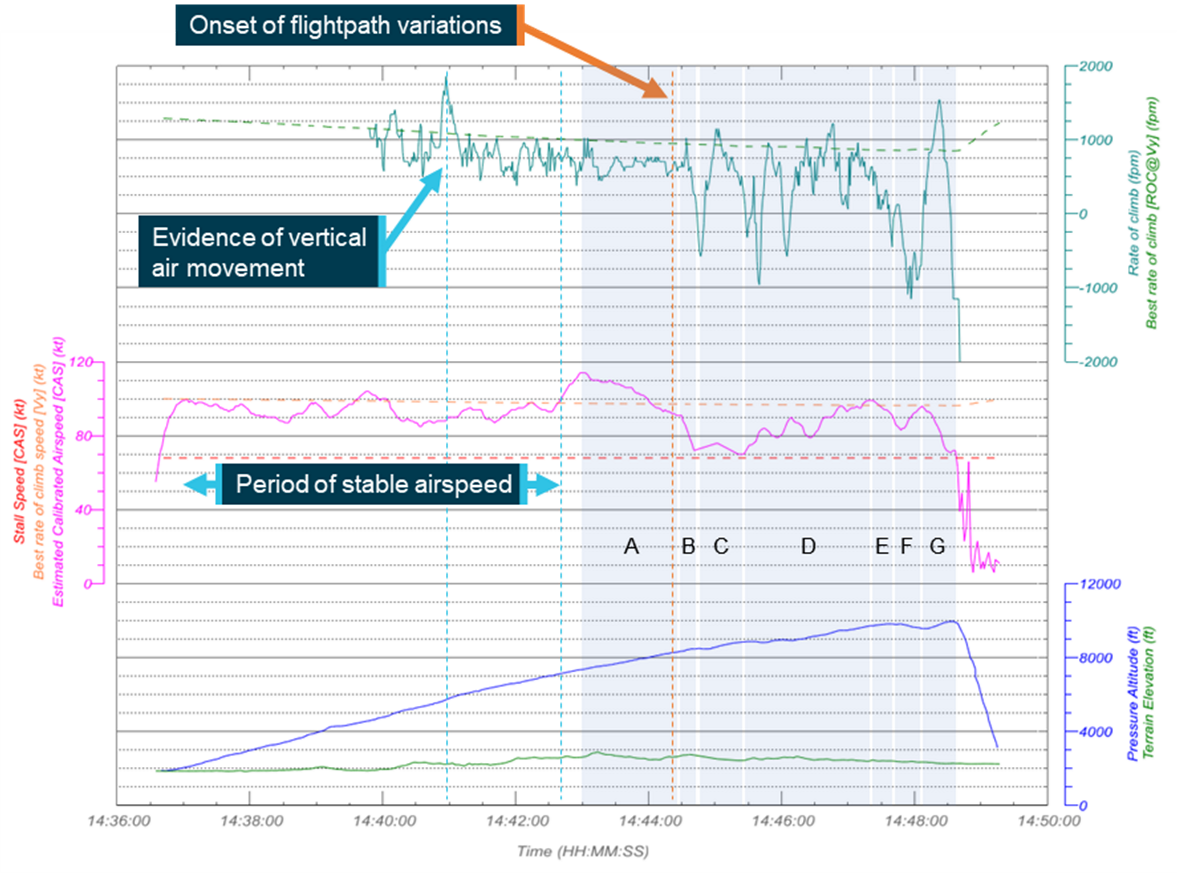
This image depicts selected ADS-B data and derived estimates of calibrated airspeed and altitude for VH-MSF during the accident flight. The airspeed has been estimated using data from a Boeing 737 descending into Canberra, Australian Capital Territory, a short time prior to the accident. Source: ATSB, using ADS-B data aggregated from Airservices Australia and FlyRealTraffic.com
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2] The pilot’s flight plan comprised a series of defined geographic positions (waypoints) via which the pilot intended to navigate the aircraft to Armidale. The flight notification’s first waypoint after departing Canberra was CULIN.
[3] RNP: Required navigation performance for en route use, which can be met with a single global navigation satellite system receiver.
[4] The ADS-B equipment transmitted flight data that enabled air traffic service providers to track aircraft when operating outside coverage of conventional air traffic control radar. Airservices Australia recorded the transmissions received by their network of ground-based ADS-B receivers. That data could also be received by other aircraft with suitable equipment and privately-operated ground-based equipment, feeding information to flight tracking websites.
[5] When an aircraft is in a spin, propeller, engine induction and exhaust will often sound like they are fluctuating due to rotating directional noise sources and the doppler effect, which is the shift in intensity of the sound waves due to relative motion of the wave source and the observer.
[6] Pitot probes provide the flight instruments with airspeed information and are ineffective if covered or blocked.
[7] Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[8] The National Aeronautical Information Processing System is a multi-function, computerised, aeronautical information system that allows users, such as pilots, to obtain weather information and submit flight plans into the air traffic system.
[9] Notice to airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[10] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky and ‘broken’ indicates that more than half to almost all the sky is covered.
[11] The freezing level is the height in feet above mean sea level where the air temperature is 0 °C.
[12] The rate of accumulation of moderate icing is such that even short encounters become potentially hazardous and the use of de-icing/anti-icing equipment or a flight diversion is necessary.
[13] ATIS: an automated pre-recorded transmission indicating the prevailing weather conditions at the aerodrome and other relevant operational information for arriving and departing aircraft.
[14] The cloud height broadcast on the automatic terminal information service is above aerodrome elevation.
[15] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[16] Engine cowl anti-ice is activated when the OAT on the ground, or TAT in-flight, is less than 10 °C in visible moisture.
[17] This estimate was based on the forecast and the temperature data from an inbound Boeing 737 to Canberra, which transited through airspace close to the outbound track for VH-MSF.
[18] Composite image produced by composing satellite images coloured in red, green and blue.
[19] The aircraft was fitted with on-board ADS-B equipment, transmitting real-time operational data from the aircraft’s global positioning system and pressure-sensitive altimeter, which enabled air traffic service providers to track aircraft. Airservices Australia recorded the transmissions received by its network of ADS-B receivers. That data could also be received by privately-operated equipment used to feed information to flight tracking websites.
[20] ADS-B data was obtained from various sources, including Airservices Australia, FlyRealTraffic.com and FlightRadar24.
[21] CAS: calibrated airspeed is indicated airspeed corrected for the aircraft’s pitot and static source position errors. Correcting calibrated airspeed for density altitude and air compressibility effects gives true airspeed.
[22] A spin occurs when an aircraft simultaneously aerodynamically stalls and yaws, resulting in a downward, corkscrew path.
[23] The flight on 3 October 2023 was from Redcliffe to Armidale and the flight on 4 October 2023 was from Armidale to Canberra.
[24] Carbon monoxide is a colourless, odourless, tasteless and poisonous gas that is produced as a by-product of burnt fuel. Exposure to a leak from the exhaust of an aircraft engine into the cabin can lead to elevated levels of carbon monoxide, which can impair cognitive function.
[25] A full post-mortem involves a detailed external examination, and a gross and histological examination of organs and tissues contained in the abdominal, thoracic and cranial body cavities. A limited post-mortem is one in which restrictions are placed on the examination, for example, limited to an external examination only with X-rays, computed tomography or magnetic resonance imaging or restricted to an examination of the tissues in only one or 2 body cavities (https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2013_051.pdf).
[26] Yaw: the motion of an aircraft about its vertical or normal axis.
[27] Significant meteorological information (SIGMET): a weather advisory service that provides the location, extent, expected movement and change in intensity of potentially hazardous (significant) or extreme meteorological conditions that are dangerous to most aircraft, such as thunderstorms or severe turbulence.
Preliminary report
Report release date: 15/12/2023
| This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
On 6 October 2023, a Cirrus Design Corporation SR22 aircraft, registered VH-MSF, was being operated on a private flight from Canberra, Australian Capital Territory to Armidale, New South Wales. On board the aircraft were the pilot and 3 passengers.
Prior to departing, the pilot had submitted a flight notification to Airservices Australia, detailing their planned track to Armidale, operating under the instrument flight rules.[1] The pilot was provided an air traffic control clearance to track to Armidale via their flight planned route at an altitude of 10,000 ft above mean sea level.
At 1437 local time, the aircraft departed Canberra. Soon after take-off, the pilot was transferred to, and established radio communication with the approach controller, reporting that they were on climb through 3,400 ft (to their assigned cruise altitude) and turning left onto their assigned radar heading of 070°.
A short time later, the controller instructed the pilot to turn left onto a heading of 010° and the pilot completed readback of the instruction. About 1 minute 30 seconds later, the controller cleared the pilot to resume their own navigation and track direct to waypoint[2] ‘CULIN’. The pilot completed readback of that instruction, which was the last transmission received from the aircraft. Figure 1 illustrates the ground track of the aircraft departing Canberra while assigned radar vectors and the direct track to CULIN.
During the flight, data was being transmitted by the aircraft’s Automatic Dependent Surveillance Broadcast (ADS-B) equipment.[3] A review of that data indicated that the aircraft was climbing through about 7,000 ft as it turned to track towards CULIN. During that turn, the groundspeed increased, over a period of about 30 seconds, from about 110 kt (204 km/h) to 135 kt (250 km/h).
Climbing above 7,500 ft, the data indicated the aircraft’s groundspeed had started to reduce, at an approximately linear rate, with a reduction of about 22 kt (41 km/h) over a 65-second period. At that time, the data showed a relatively constant rate of climb generally between 550–750 ft/min.
Passing through 8,500 ft, a further 21 kt reduction in groundspeed occurred over a 14-second period, which was accompanied by a short increase in the reported rate of climb. The data indicated the groundspeed then started to increase as the aircraft entered a slight descent.
Over the next 4 minutes, the aircraft’s track varied up to 35° and the groundspeed fluctuated between 90 kt and 120 kt (167–222 km/h). During this period, the altitude was generally increasing although at a varying rate, with shorter periods where the altitude and reported rate of altitude change indicated that the aircraft had started to descend. Several people at locations along the aircraft’s flight path during this time reported hearing noises that they described as a rough running or surging light aircraft engine.
Twelve minutes after take-off, the aircraft was about 25.5 km north-north-east of Canberra, at an altitude of about 10,000 ft, when it abruptly departed from controlled flight and descended steeply towards the ground. Two eyewitnesses in the local area described seeing the aircraft at a low altitude, descending rapidly with its nose pitched down and rotating like a corkscrew. One of the witnesses stated that they heard the engine running rough and then stop just before the accident. The other eyewitness was seated on a tractor with the engine running and did not hear the aircraft engine.
The aircraft collided with terrain (at a ground elevation of about 2,250 ft) and was destroyed by impact forces and a post-impact fire. All occupants were fatally injured. The eyewitness on the tractor was the first responder on the scene and notified the emergency services.
Figure 1: Ground track of VH-MSF from take-off to the accident site
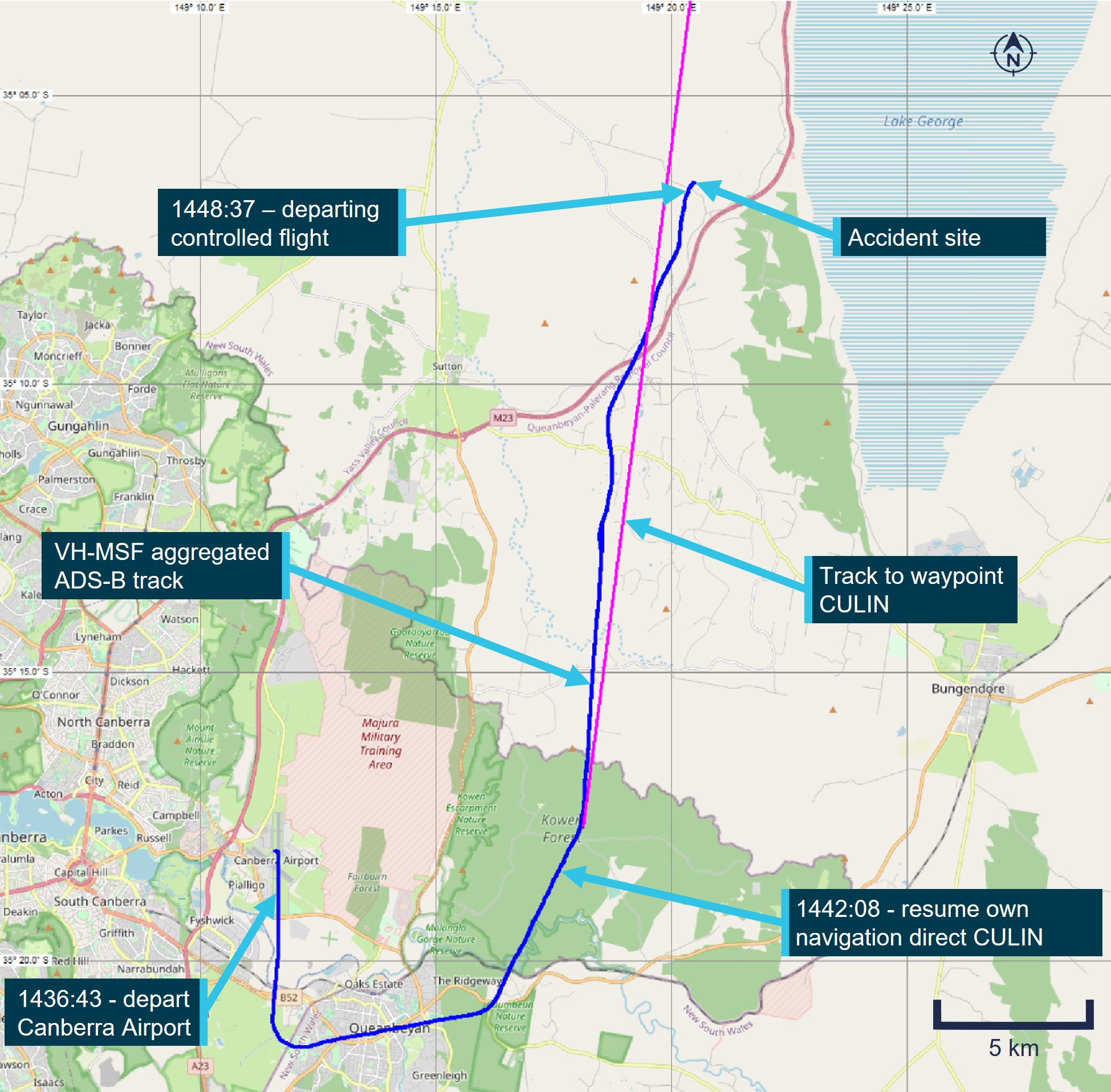
Note: The aircraft ground track overlaid on this map is referenced to a latitude and longitude grid aligned to true north. The headings assigned by air traffic control are referenced to magnetic north. In the Canberra region, magnetic north is about 12° less than true north. An aircraft’s ground track relevant to the assigned heading can also be affected by wind.
Source: OpenStreetMap with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Figure 2 depicts the aircraft’s altitude and ground track during the last part of the flight after the pilot was cleared to resume their own navigation and includes the position where the flightpath variations commenced.
Figure 2: Aggregated ADS-B data for VH-MSF, looking back along the flightpath
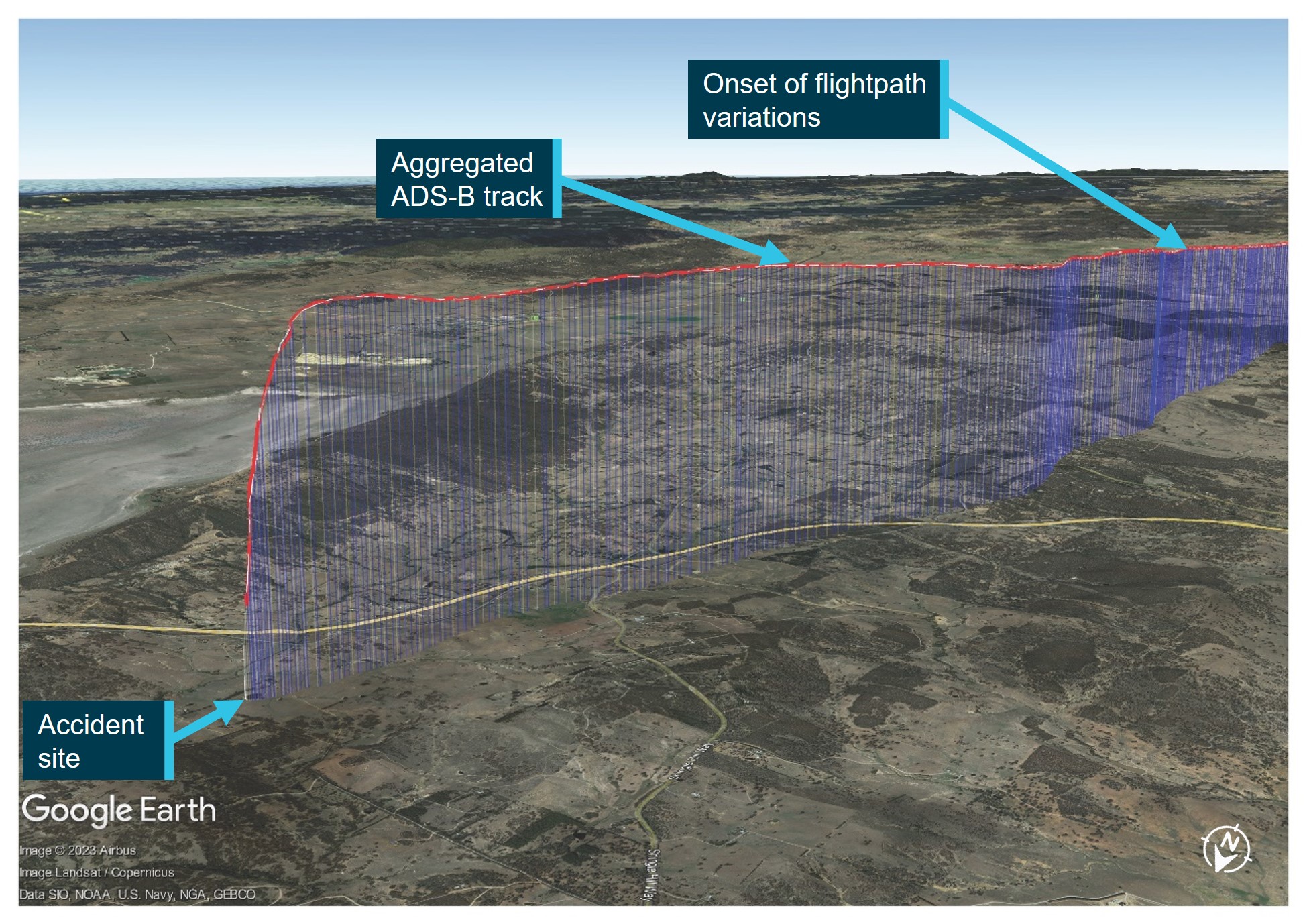
Source: Google Earth, with ADS-B data from Airservices Australia and aggregated ADS-B data from FlyRealTraffic.com, annotated by the ATSB
Context
Pilot information
The pilot held a Private Pilot Licence (Aeroplane), issued in 1985, and with class ratings for single‑ and multi-engine aeroplanes. The pilot was initially issued with a command instrument rating for single-engine aeroplanes in 1987 and their most recent flight review, on 29 August 2023, was an instrument rating proficiency check with an endorsement for multi-engine aeroplanes. The pilot had reportedly accumulated about 800 hours total flying experience.
The pilot held a Class 2 Aviation Medical Certificate valid to 22 October 2023 with 2 restrictions. A requirement for reading and distance vision correction to be worn while flying and that a continuous positive airway pressure (CPAP) system be used for the sleep period before flying. The pilot was reported to have been well rested before the flight and was utilising the CPAP while sleeping as required.
Aircraft information
The Cirrus Design Corporation SR22 is a low wing aircraft with 4 seats and a single piston engine driving a constant speed propeller. It has a ballistic parachute system fitted as standard. The aircraft (S/N 0153) was manufactured in the United States in 2002 as a G1 model. It was purchased as a second-hand aircraft in the United States in 2017 and then placed on the Australian register with the registration VH-MSF. Since then, it has been operated by its owner for private use, community service flights and private charter operations.
Recent maintenance included the completion of a 100-hour/annual inspection and maintenance release issue on 9 November 2022 at an aircraft time-in-service of 2,558.9 flight hours. The Cirrus Airframe Parachute System (CAPS) was inspected, and the parachute and rocket motor assemblies were replaced due to time expiry in January 2023.
The limitations section of the Cirrus SR22 Pilot’s Operating Handbook stated ‘Aerobatic manoeuvres, including spins, are prohibited.’ The note associated with the manoeuvre limits stated, ‘Because the SR22 has not been certified for spin recovery, the CAPS must be deployed if the airplane departs controlled flight.’
The United States Federal Aviation Administration approved the Cirrus SR22 for flight into icing conditions in 2009 based on the introduction of an optional anti-ice system for the wings, windshield, propeller, and vertical and horizontal stabilizer leading edges. This was known as a flight into known icing approval. As VH-MSF was manufactured in 2002, which predated this approval, the aircraft owner confirmed there was no anti-icing system fitted. Therefore, the aircraft was prohibited from flying into known icing conditions. This limitation was documented in both the Pilot’s Operating Handbook and also stated in current aviation regulations.
Meteorological information
Canberra Airport is located near the intersection of 4 areas in the grid-point wind and temperature chart for New South Wales. The chart issued at 1105 on 6 October 2023 and valid from 1400, indicated the freezing level overhead Canberra was forecast to be at about 7,000 ft with south‑westerly winds at 6-17 kt. The graphical area forecast for ‘NSW-East’, issued at 0913 on 6 October 2023, was valid for the period 1000-1600. Canberra Airport and the accident site were in the south of subdivision D1. The forecast for area D, which included subdivision D1, had the following conditions:
- visibility greater than 10 km, scattered cumulus/stratocumulus cloud[4] from 5,000 ft to 8,000 ft with broken tops to 10,000 ft in D1
- visibility reduced to 3,000 m in isolated showers of rain, with broken stratus cloud from 1,500 ft to 4,000 ft and broken cumulus/stratocumulus cloud from 4,000 ft to above 10,000 ft
- freezing level[5] of 5,000 ft in the south and 8,000 ft in the north
- cumulus and stratocumulus cloud implies moderate turbulence
- cloud above the freezing level implies moderate icing.[6]
Figure 3 illustrates the ADS-B ground track of the aircraft, overlaid on a satellite image of cloud in the local area at 1450, about 1 minute after the accident.
Figure 3: Aircraft flight track overlaid on satellite image
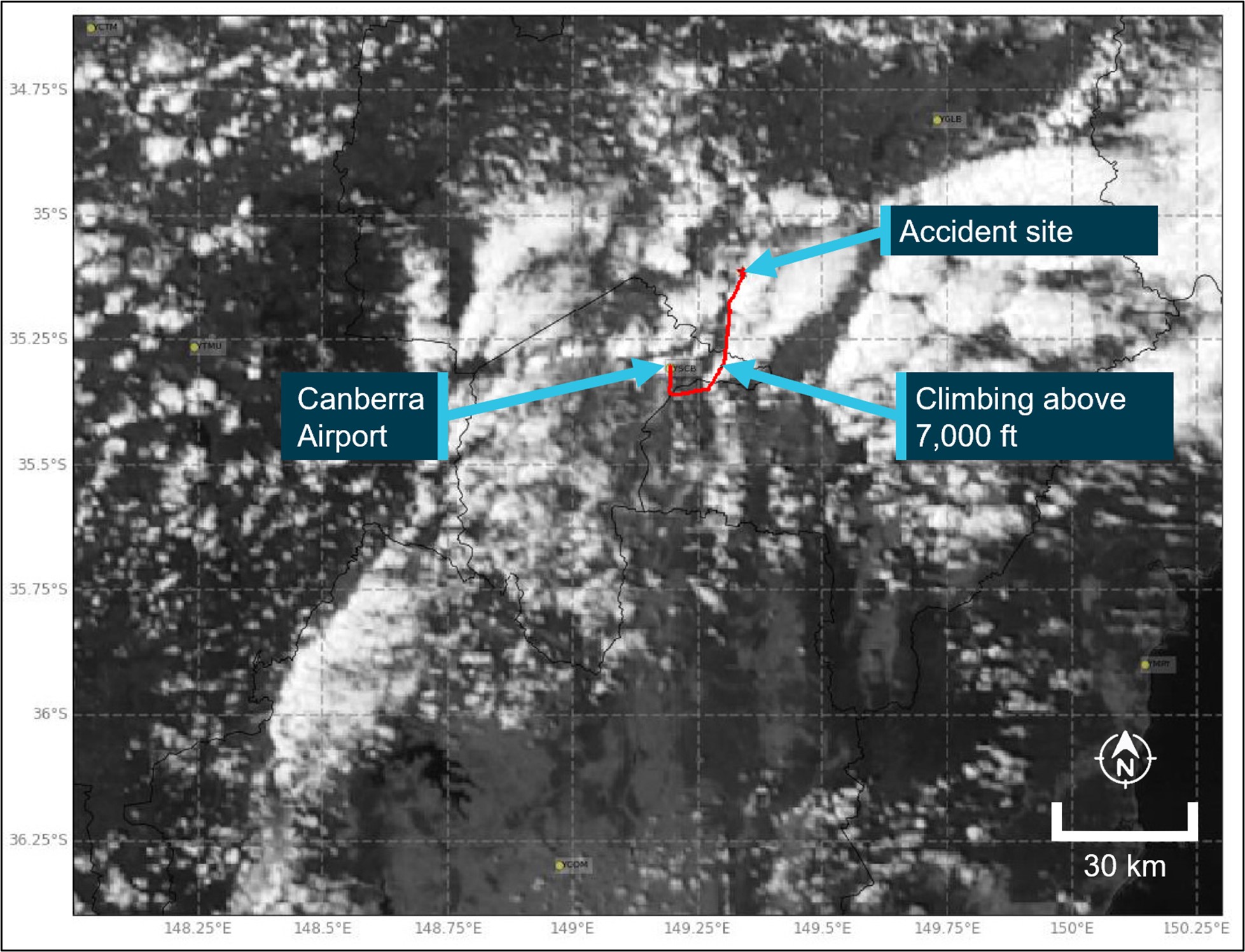
Note: This image depicts the Himawari-8/9 visible satellite imagery just after the accident, including the ADS-B track of VH-MSF and the position which the aircraft climbed above 7,000 ft.
Source: Satellite image originally processed by the Bureau of Meteorology from the geostationary satellite Himawari-8/9 operated by the Japan Meteorological Agency and modified by ATSB and using aggregated ADS-B data from FlyRealTraffic.com
Recorded information
Figure 4 depicts ADS-B altitude data broadcast from the aircraft during the final 5 minutes of the flight. This includes the several relatively minor altitude excursions/descents, together with the larger altitude excursion/descent that occurred immediately before the departure from controlled flight.
Preliminary analysis of the aircraft’s reported groundspeed, together with sources of meteorological data[7] indicated that the aircraft’s calibrated airspeed[8] was about 70 kt (130 km/h) at the time it departed from controlled flight.
The Pilot’s Operating Handbook provided performance data for the aircraft, including information about the aircraft’s aerodynamic stall[9] speeds. At the maximum take-off weight (1,542 kg), idle power and nil wing flap, the published wings-level stall speed was 67-69 kt (124–128 km/h) calibrated airspeed, depending on the centre of gravity position.[10] The Pilot’s Operating Handbook also indicated that the aircraft had conventional stall characteristics, and that power‑on stalls were marked by a high sink (descent) rate at full aft stick.
The altitude and reported rate of altitude change, indicated an accelerating rate of descent, that increased above 13,000 ft/min before reducing back towards 10,000 ft/min prior to the impact with terrain.
Figure 4: Aggregated ADS-B altitude data
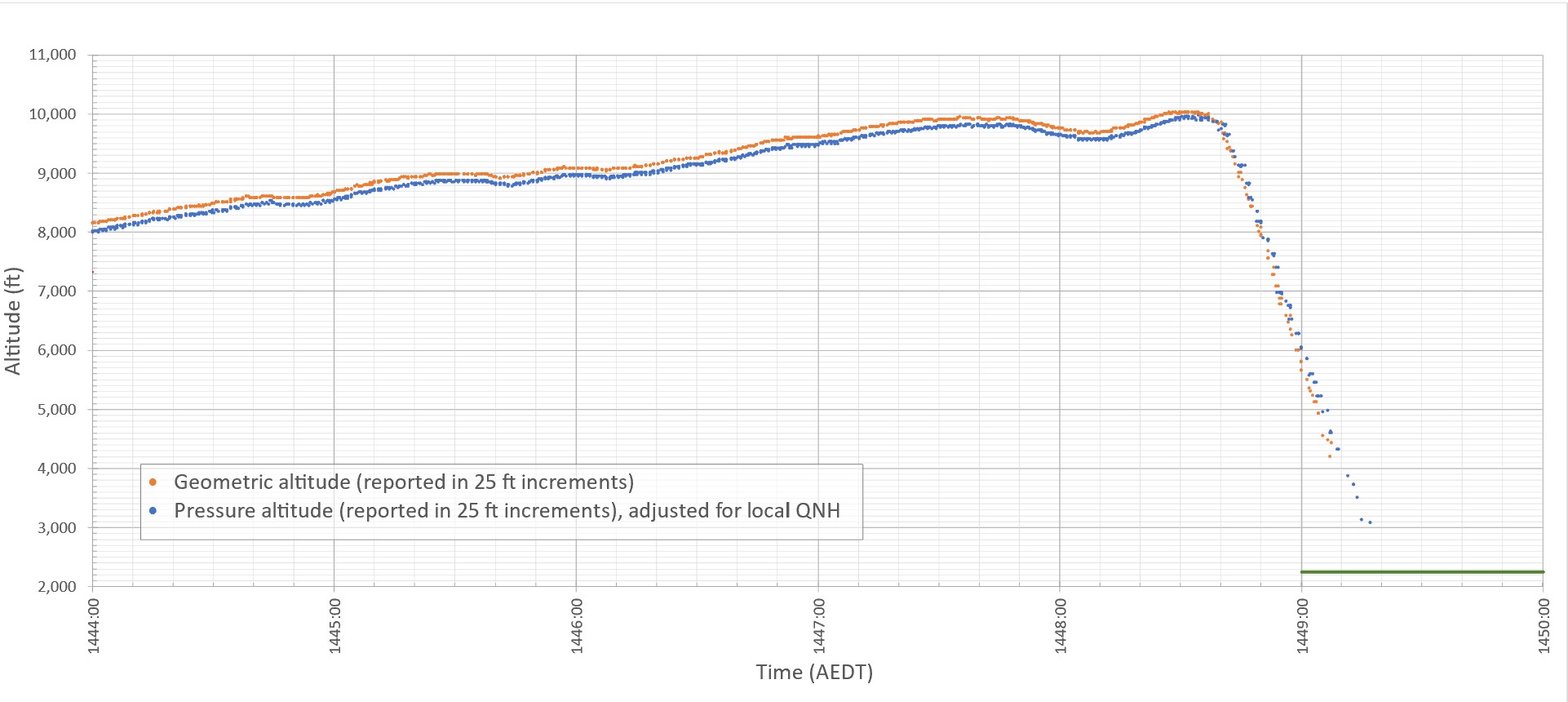
Note: The green line at the bottom right corner of the plot depicts the elevation of terrain in vicinity of the accident site.
Source: ATSB, using aggregated ADS-B data from Airservices Australia and FlyRealTraffic.com
Site and wreckage information
The aircraft came to rest on a private property in an open field adjacent to a dam. Although post‑impact fire damage precluded examination of a significant proportion of the aircraft, inspection of the site and wreckage showed that (Figure 5):
- The impact marks and wreckage distribution indicated that the aircraft impacted with terrain upright, with a slight nose low attitude and with little forward momentum, suggestive of a spin.[11]
- All the aircraft’s extremities and flight controls were present in the immediate area of the accident site.
- There were no identified structural defects in the evidence available.
- The CAPS cover, deployment system and parachute were all located within the wreckage and had not been deployed before impact. However, based on the available evidence, the ATSB was unable to determine if an attempt had been made by the pilot to deploy the parachute system before the impact.
- The damage to the propeller blades indicated that the engine had low or no power at impact. It should be noted though, that spin recovery, icing, un-porting of fuel tank outlets in a spin, preparation for use of the parachute, and an engine mechanical issue could all be reasons for a power reduction.
Figure 5: Overview of the accident site

Source: ATSB
Further investigation
To date, the ATSB has:
- examined the aircraft and accident site
- recovered aircraft components
- interviewed relevant parties
- collected aircraft, pilot, and operator documentation
- conducted a preliminary analysis of flight track data.
The investigation is continuing and will include:
- examination of recovered aircraft components
- further review of aircraft, pilot, and operator documentation
- analysis of pilot medical information
- an assessment of the aircraft’s performance based on flight track data
- analysis of meteorological information
- a review of similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the significant assistance provided during the initial investigation response by the New South Wales Fire Service, the accident site property owner and the local community of Gundaroo.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2] The pilot’s flight notification comprised a series of defined geographic positions (waypoints) via which the pilot intended to navigate the aircraft to Armidale. The flight notification’s first waypoint after departing Canberra was CULIN.
[3] The ADS-B equipment transmitted flight data that enabled air traffic service providers to track aircraft when operating outside coverage of conventional air traffic control radar. Airservices Australia recorded the transmissions received by their network of ground-based ADS-B receivers. That data could also be received by other aircraft with suitable equipment and privately-operated ground-based equipment, feeding information to flight tracking websites.
[4] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky and ‘broken’ indicates that more than half to almost all the sky is covered.
[5] The freezing level is the height in feet above mean sea level where the air temperature is 0 °C.
[6] The rate of accumulation of moderate icing is such that even short encounters become potentially hazardous and the use of de-icing/anti-icing equipment or a flight diversion is necessary.
[7] This includes data from the Bureau of Meteorology’s vertical wind profiler at Canberra Airport, wind and temperature data from recorders on an aircraft descending into Canberra close to the time of the accident and data from a similar aircraft that passed overhead Canberra a short time before.
[8] Airspeed was not a parameter transmitted by the aircraft’s ADS-B equipment. The calibrated airspeed was derived from the ADS-B recorded groundspeed and track using the available measurements of wind velocity, atmospheric pressure and temperature.
[9] Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[10] The actual stall speed on any given flight depended on a number of variable factors including the aircraft’s operating weight/centre of gravity, flap setting, engine power, bank angle and/or load factor.
[11] Spin: a sustained spiral descent of a fixed-wing aircraft, with the wing’s angle of attack beyond the stall angle.
Occurrence summary
| Investigation number | AO-2023-045 |
|---|---|
| Occurrence date | 06/10/2023 |
| Location | Near Gundaroo |
| State | New South Wales |
| Report release date | 16/10/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Loss of control |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Cirrus Design Corporation |
|---|---|
| Model | SR22 |
| Registration | VH-MSF |
| Serial number | 0153 |
| Aircraft operator | Up N Up Aviation Pty Ltd |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Canberra Airport, Australian Capital Territory |
| Destination | Armidale Airport, New South Wales |
| Damage | Destroyed |