The ATSB is investigating the collision with terrain of a Pitts S1-11X aircraft, registered VH-PVX, at Avalon Airport, Victoria, on 28 March 2025. The pilot, the sole occupant of the aircraft, sustained serious injuries, and the aircraft was substantially damaged.
The pilot, the sole occupant of the aircraft, sustained serious injuries, and the aircraft was substantially damaged. A preliminary report, which detailed factual information established during the evidence collection phase, was released on 9 July 2025 (see the adjacent tab).
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 28 March 2025, at about 1710 local time, the Sky Aces formation aerobatics team, which consisted of 4 Pitts type aircraft operated by Paul Bennet Airshows, became airborne to perform a display at the Australian International Airshow, Avalon Airport, Victoria. The 4 aircraft began their planned routine and flew several aerobatic manoeuvres in 2 and 4 ship[1] configurations.
At about 1715, the pilot of VH-PVX departed the formation, as planned, and began a solo routine while the formation of the 3 remaining aircraft relocated to the south for their next manoeuvre. At about 1717, while conducting their solo routine, the pilot began a ‘triple avalanche’ manoeuvre[2] and entered the aircraft into a loop (example shown in Figure 1, 2 days prior using a smoke system). At the top of the loop and from an inverted position, the pilot performed 3 snap rolls[3] with one wing aerodynamically stalled.[4] The snap rolls were completed and the aircraft returned to stable flight while still inverted. It then entered the back half of the loop, however, the aircraft’s descent rate was unable to be arrested before it collided with terrain. The pilot was seriously injured.
Figure 1: A successful triple avalanche manoeuvre performed by the pilot in VH‑PVX 2 days prior to the accident
Note: This is a still image extracted from a video recording of the validation flight (refer to section titled Flight validation). Source: AMDA Foundation, annotated by the ATSB
Context
Pilot information
The pilot held a valid commercial pilot licence (aeroplane) and class 2 aviation medical certificate. They successfully completed a private instrument rating in August 2023, which satisfied the requirements of a flight review for single-engine aircraft. Additionally, they had the required flight activity and aircraft design feature endorsements to conduct a formation aerobatic display in the Pitts S1-11X aircraft without a minimum altitude limitation. Their formation aerobatics flight activity endorsement was issued in July 2015.
The pilot’s logbook, which was completed up to 17 March 2025, showed a total flying experience of 2,248.6 hours. It recorded multiple aerobatic preparation flights in VH-PVX and evidence of participation in other airshows. The pilot had also conducted practice flights for the Avalon airshow between 17 March 2025 and the accident flight.
Aircraft information
The aircraft was a single-seat aerobatic Pitts S1-11X amateur-built biplane, modified from the Pitts S1-11B and constructed in Germany in 2010 by Wulf (Wolf) Aircraft. It was powered by a Ly-Con AEIO-540-EXP experimental engine and fitted with a 3-bladed, MTV-6 constant-speed propeller of laminated wood construction. The aircraft was a combination of fabric-covered wood and metal, and composite fibre structure and designed for unlimited aerobatics up to +/-10 G.
The aircraft was first registered in Australia in 2015 and issued with a special certificate of airworthiness in the experimental category.[5] It had been operated by Paul Bennet Airshows since that time. The aircraft was to be maintained as per Civil Aviation Safety Authority Schedule 5 and required a periodic inspection every 100 hours or 12 months, whichever came first. The most recent periodic inspection was conducted by an authorised maintenance organisation on 28 February 2025. At the time of the accident the aircraft had accumulated 303 hours total time-in-service, about 5 hours since the previous periodic inspection. There were no defects listed on the aircraft maintenance release.[6]
Meteorological information
The Bureau of Meteorology provided automated weather observations taken at 1-minute intervals at Avalon Airport during the aerobatic display. Between 1710 and 1717, the highest recorded windspeed was 5 kt with gusts up to 6 kt. The temperature was 30°C, visibility greater than 10 km, and the atmospheric pressure ranged 1015–1014 hPa for the period.
Wreckage and impact information
The aircraft collided with terrain on a grassed area west of runway 18/36,[7] in an area of the airport designated as the pyrotechnics box[8] (Figure 2) where multiple pyrotechnics were live and were planned to be used in the show. Additionally, there were many boxes of fuel positioned in the pyrotechnic box that were planned to be ignited during the ‘wall of fire’ display later that evening.
Figure 2: Accident site location
Source: Google Earth, annotated by the ATSB
A ground scar, approximately 95 m long, was on a south-south-west heading (Figure 3). The aircraft came to rest upright and oriented toward north, almost opposite the direction of the impact sequence and debris trail. The initial impact point occurred several metres from the fuel boxes within the pyrotechnics array.
While the ATSB conducted a preliminary examination of the accident site, due to access restrictions for the operational airport and airshow, the aircraft wreckage was relocated to a secure facility for detailed examination.
Figure 3: Accident site overview showing the location of the initial impact mark, pyrotechnics array, and the wreckage of VH-PVX
Source: No 1 Security Forces Squadron, annotated by the ATSB
The aircraft sustained substantial damage from the impact with terrain (Figure 4). Examination of the wreckage at a secure facility identified:
no evidence of pre-impact defects with the flight control system or fuselage structure to the extent that could be determined
the uppermost section of the canopy was fractured and parts of the airframe had departed the main structure
the engine had separated from the airframe
the propeller blades had fragmented, however, the propeller hub remained attached to the engine
the front landing gear was distorted
the upper and lower wings had separated, and the lower fuselage section had sustained compression damage
the rigid outlet lines from the fuel tanks were fractured resulting in post-accident leakage of fuel.
Figure 4: Aircraft wreckage at the accident site
Source: ATSB
Aerobatic manoeuvre
Practice flights
A review of training videos showed that previous triple avalanche manoeuvres performed by the pilot in VH-PVX were started at approximately 200 ft above ground level (AGL)[9] and an airspeed of 165 kt. The recordings showed the aircraft would reach an altitude of approximately 800 ft prior to entering the snap rolls. The aircraft would climb during the rolls to about 1,100 ft before beginning the back half of the loop. After the accident, the pilot reported that their normal minimum altitude for commencing the snap rolls was 1,000 ft.
Accident flight
The ATSB recovered a GoPro video camera from within the cockpit of the aircraft that was forward facing and operating during the accident flight. Flight instruments including the altimeter and airspeed gauges were visible in the recording. The recording identified that the pilot set the altimeter to 0 ft (runway reference height) prior to take-off, in accordance with their standard practice when conducting aerobatic manoeuvres.[10]
During entry to the triple avalanche, the indicated airspeed was approximately 165 kt and the altitude was 100 ft. Just before the aircraft reached its peak altitude, the altimeter was showing 700–800 ft (Figure 5). After this point, the altimeter was blocked from the camera’s view by the pilot’s body position just prior to the collision with terrain.
Figure 5: Still image from the accident flight recording showing the altimeter just prior to the first snap roll during the triple avalanche manoeuvre
Source: ATSB
Figure 6 provides a representation of the triple avalanche manoeuvre, showing the loop with the 3 snap rolls (indicated by inverted triangles) and the approximate position where the image shown in Figure 5 was taken.
Figure 6: Triple avalanche profile and the approximate position in the manoeuvre where the still image from Figure 5 (above) was taken
Source: ATSB
Flight validation
The event organiser required that participants in the airshow successfully complete a flight validation prior to the public display. On 26 March 2025, the formation group satisfied the flight validation requirement, which included the pilot completing the accident manoeuvre in VH-PVX. The event organiser validation report had not noted any concerns about the routine or ability of those involved to successfully perform it on the day of the show.
Emergency response
Due to the location of the accident, the pyrotechnicians were nearby and therefore were first to arrive at the aircraft wreckage and assist the pilot. The pyrotechnicians reported that the pilot was wearing a 5-point safety harness, and the cockpit canopy remained closed. They also reported difficulties opening the canopy as there was not an obvious mechanism or external signage on the aircraft to assist them. The first responders reported smelling fuel and observing it leaking from the aircraft, however, there was no post-impact fire.
The Aviation Rescue Fire Fighting (ARFF) service was notified of the accident at 1718 and arrived onsite at 1721. The ARFF provided 3 tenders, 2 responding from the main southern base and one from the northern temporary base. They reported their response times were increased as, while the pyrotechnicians were busy providing first aid to the pilot, they were unable to be safely guided by the technicians through the pyrotechnics area. Additionally, the northern ARFF response vehicle had to deviate around a passenger-carrying jet aircraft on the northern taxiway. ARFF responders took control of the scene and continued providing first aid to the pilot until an ambulance arrived at 1731. The pilot was subsequently transported to hospital by helicopter.
Further investigation
To date, the ATSB has:
examined the accident site and aircraft wreckage
interviewed the pilot, operator, and first responders
reviewed the meteorological conditions during the display routine
reviewed accident and training video recordings.
The investigation is continuing and will include review of:
components recovered from the aircraft
the aircraft maintenance records
video recordings of the accident flight
the emergency response plan and actions of the responsible organisations
preparation for the display
survivability factors.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Ship: refers to multiple aircraft flying in formation together. The preceding number refers to the number of aircraft in the formation.
[2]The triple avalanche aerobatic manoeuvre is a basic loop with 3 snap rolls at the top of the loop.
[3]Snap roll: is similar to an accelerated horizontal spin and is essentially an autorotation with one wing stalled.
[4]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[5]Experimental category: the Civil Aviation Safety Authority can issue experimental certificates to allow specific operations of aircraft, which are not by their nature type certificated or have modifications incorporated that are not yet approved.
[6]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours’ time in service or 12 months from issue.
[7]Runway number: the number represents the magnetic heading of the runway – in this case, 176° and 356°.
[8]Pyrotechnics box: an area of the airport designated for pyrotechnics which were used during the airshow to be set-up and detonated.
[9]Altitude above ground level: as the altimeter setting is set to 0 ft, the altitudes in this report are given above ground level unless otherwise stated.
[10]Altimeter setting: setting the altimeter to 0 ft on the ground gives the pilot an accurate representation of their altitude above the ground level in that area.
Occurrence summary
Investigation number
AO-2025-017
Occurrence date
28/03/2025
Location
Avalon Airport
State
Victoria
Report release date
09/07/2025
Report status
Preliminary
Anticipated completion
Q2 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: External review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Amateur Built Aircraft
Model
Pitts S1-11X
Registration
VH-PVX
Serial number
UB001
Aircraft operator
Paul Bennet Airshows Pty Ltd
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Sport and pleasure flying-Aerobatics
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Overview
On the morning of 21 March 2025, a pilot was conducting 2 ferry flights of Cessna 150 aircraft that were operated by Norwest Air Work. The first flight, from Shark Bay Airport to Geraldton Airport, Western Australia, involved a Cessna 150M, registered VH‑TDZ. Once at Geraldton Airport, the pilot was to swap aircraft at the maintenance hangar and fly back to Shark Bay Airport in VH‑WWU, the operator’s other Cessna 150M which had been released from maintenance on 18 March 2025.
The pilot was the sole occupant on board both flights. The operator’s senior base pilot was holding SARTIME[1] for both flights.
On the ground at Geraldton Airport
Closed-circuit television (CCTV) showed that the pilot landed VH‑TDZ at 0914:20 local time and taxied the aircraft to the maintenance organisation’s parking bay. At 0922, the pilot texted the senior base pilot informing them of their arrival in Geraldton.
Between 0925 and 0931, the pilot manoeuvred VH‑WWU out of the parking bay and moved VH‑TDZ into it. Once completed, the pilot walked to the maintenance hangar (Figure 1). Witnesses at the airport reported that the pilot appeared unwell and had mentioned having had severe gastroenteritis in the preceding days. Witnesses did not report any apparent speech or physical impairment.
At 0945:15, the pilot left the maintenance hangar, walked to VH‑WWU and conducted a pre‑flight inspection. The aircraft had been refuelled on the morning by the airport refueller. Approximately 2 minutes later the pilot started the engine and taxied the aircraft to the centre apron.
At 0955:16, the pilot reported on the local CTAF[2] that they were lining up and rolling on runway 08. The aircraft lifted off the runway 40 seconds later. At 0957:08 the pilot reported they had departed the runway and were tracking out to the north climbing to 2,500 ft through 600 ft. This was the last recorded call from VH‑WWU on the CTAF. Shark Bay is about 340 km north‑west from Geraldton.
Directly after take‑off, the pilot texted the senior base pilot with the expected arrival time at Shark Bay, which was 1230.
At 1008:52, the pilot took a photo of the aircraft oil temperature gauges. Eight minutes later the pilot sent the photo to a staff member at the maintenance organisation with accompanying text stating ‘WWU flies beautiful, smooth, and tight. Oil temp a little high for a cool day so we might have to look at fitting those coolers back onto WWU. I’d hate to see the rings[3] suffer.’ The maintainer responded via text at 1018, and the message was recorded as delivered (indicating that the pilot’s phone was still functional at that time). The oil temperature shown in the photo was towards the upper end of the normal range but below the 240°F maximum oil temperature limit.
At 1116:43, a call was placed to police by a member of the public stating they had come across aircraft wreckage by the side of a road as they were driving past (Figure 2). The accident was 84 km north‑west of Geraldton Airport, and about 0.5 km right of the direct track. The member of the public stated that although they had been nearby, they had not seen or heard the aircraft or the impact.
Figure 2: Original final position of VH‑WWU at the accident site[4]
Source: Western Australia Police Force
The aircraft was destroyed, and the pilot was fatally injured.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter and aeroplane), with both single and multi‑engine class ratings for aeroplanes and a single engine class rating for helicopters. They held low‑level operational ratings for sling, aerial mustering helicopter and aerial musting aeroplane operations. In addition, the pilot held flight instructor ratings for low‑level flight tests in both aeroplanes and helicopters.
The pilot completed single engine aircraft and low‑level flight reviews on 12 February 2024.
The pilot held a valid class 1 aviation medical certificate which was approved in October 2024. This specified a requirement for the pilot to wear distance vision correction and a headset while flying. It also required reading vision correction to be available.
The pilot logbooks were not available at the time of publication.
Aircraft information
The Cessna 150M is a high‑wing, all metal, 2‑place, unpressurised aircraft with a fixed landing gear. VH‑WWU was manufactured in 1976 and was first registered in Australia on 5 May 1986. It had a single, Continental O‑200‑A reciprocating piston engine driving a fixed-pitch propeller. The aircraft was not equipped with an autopilot.
A periodic and other scheduled inspections were carried out between 6–18 March 2025. The periodic inspection identified minor defects that were subsequently rectified. The aircraft’s engine reportedly had excessive oil consumption, and to address the issue all 4 engine cylinders were removed, honed[5] and refitted along with new piston rings. Additionally, the engine ignition harness was replaced due to it being in poor condition. The engine was tested by carrying out a ground run 3 days before the accident and found to be functioning correctly. At the completion of maintenance, the aircraft had accrued a total time in service of 14,208 hours.
Site and wreckage
The wreckage was located about 20 m south of an east‑west road. The Western Australia Police Force and emergency services attended the site on the day of the accident.
The ATSB commenced the accident site examination on the following day, 22 March. The wreckage trail extended in a north‑easterly direction, about 23 m from the initial impact point to where the main wreckage, including the wings, empennage, engine and propeller had come to rest (Figure 3). There was no fire, and fuel could be smelt in the area.
Ground impact marks and damage to the airframe indicated that the aircraft impacted the terrain in a left wing‑low, steep nose‑down attitude at high speed (Figure 3). All major aircraft components were accounted for at the accident site. The disruption to the airframe from the impact limited the extent to which the aircraft could be examined. Of the components that could be examined, no pre‑impact defects were identified. Bending and damage to the propeller was consistent with the engine running at the time of impact.
A damaged Garmin 296 GPS receiver was recovered from the accident site. There were no available radar or ADS‑B recordings of the flight.
Meteorological information
The graphical area forecast for the accident region forecasted clear conditions for the flight with no forecast cloud and visibility greater than 10 km.
At 1030, the Bureau of Meteorology (BoM) automatic weather station at Geraldton Airport, 85 km south of the accident location, recorded the wind as 5 kt from 121° magnetic. There was no recorded cloud, visibility was greater than 10 km and the temperature was 34°C.
Further investigation
To date, the ATSB has:
examined the wreckage and accident site
recovered the GPS for further examination
conducted interviews with witnesses and the maintenance organisation
collected aircraft, pilot and operator documentation
collected CCTV and CTAF recordings.
The investigation is continuing and will include:
review and examination of any recovered GPS data
collection and review of additional pilot medical information
examination of the aircraft maintenance history.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]SARTIME ('time search action required'): is the time nominated by a pilot for the initiation of search and rescue action.
[2]CTAF (common traffic advisory frequency): a radio frequency used by pilots at non-towered airports to communicate with each other about their position and intentions, ensuring safe and orderly traffic flow.
[3]Likely referring to piston rings, which wear somewhat more quickly at increased temperatures.
[4]Emergency services personnel moved main sections of the aircraft when removing the pilot.
[5]Honing is a process that scratches a crisscrossed (crosshatched) pattern onto the inside of the cylinder. This pattern reduces cylinder wear by allowing oil to be retained in the scratches rather than be removed by the piston rings.
Final report
Investigation summary
What happened
On the morning of 21 March 2025, a pilot was ferrying a Cessna 150M aircraft, registered VH-WWU and operated by Norwest Air Work, from Geraldton Airport to Shark Bay Airport, Western Australia.
Approximately 35 minutes into the flight, the aircraft entered a left turn that transitioned into a spiral dive. The aircraft collided with terrain, the pilot was fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found no evidence of any in-flight failure of the airframe structure or flight control system and the engine was producing power throughout the descent. Based on the pilot’s medical history and sequence of events, it was determined that the pilot likely experienced an incapacitating medical event of an undetermined nature, resulting in a deviation off track and the uncorrected spiral dive.
Safety message
The ATSB recommends that pilots conduct the IMSAFE checklist before every flight. The checklist prompts pilots to self-assess whether factors such as illness, stress or fatigue could affect their performance and compromise flight safety.
The ATSB urges all pilots to integrate the IMSAFE checklist into their pre-flight routine, no matter how routine the flight may seem. Prioritising personal fitness for flight duty helps to reduce the risk not only to the pilot, but also to passengers, crew, and the public.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Overview
On the morning of 21 March 2025, a pilot was conducting 2 ferry flights of aircraft operated by Norwest Air Work. The plan was to fly from Shark Bay Airport to Geraldton Airport, Western Australia, in a Cessna 150M, registered VH‑TDZ. Once at Geraldton Airport, the pilot would swap aircraft at the maintenance hangar and fly back to Shark Bay Airport[1] in VH‑WWU, the operator’s other Cessna 150M, which had been released from maintenance on 18 March 2025.
The pilot was the sole occupant on board both flights. The operator’s senior base pilot was holding SARTIME[2] for both flights.
On the ground at Geraldton Airport
The pilot landed VH‑TDZ at 0914 local time and taxied the aircraft to the maintenance organisation’s parking bay. At 0922, the pilot sent a text message to the senior base pilot informing them of their arrival in Geraldton.
Airport CCTV footage showed that between 0925 and 0931 the pilot manually manoeuvred VH‑WWU out of its parking bay and moved VH‑TDZ into it. Once completed, the pilot walked to the maintenance hangar (Figure 1). Witnesses at the airport reported that the pilot appeared unwell and had mentioned having had severe gastroenteritis in the preceding days. Witnesses did not report any apparent speech or physical impairment. The pilot did not appear to have any difficulty walking around or moving aircraft.
At 0946, the pilot left the maintenance hangar, walked to VH‑WWU, appeared to check the oil level and enter the aircraft. The aircraft had already been refuelled that morning by the airport refueller. At about 0947, the pilot started the engine and taxied the aircraft to the centre apron.
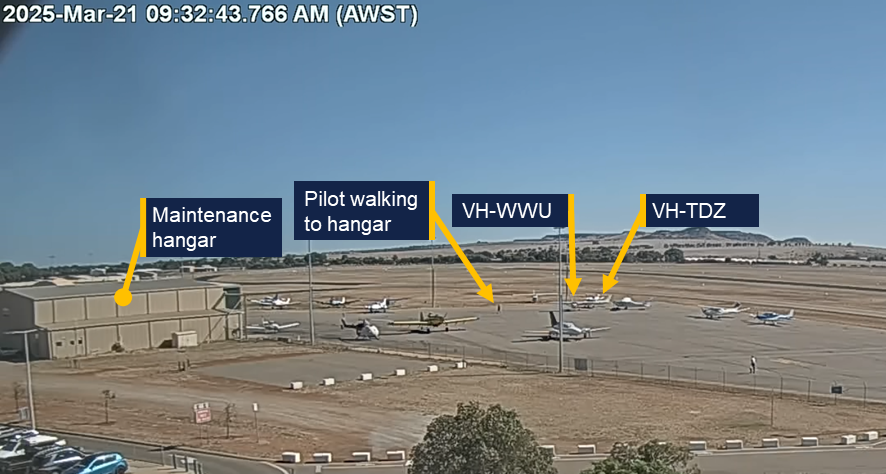
Figure 1: Aircraft changeover
Source: Geraldton Airport, annotated by the ATSB
Geraldton to Shark Bay
At 0956, the pilot broadcast on the local CTAF[3] that they were lining up and rolling on runway 08. The aircraft lifted off the runway 40 seconds later. At 0957 the pilot broadcast they had departed the runway and were tracking out to the north climbing to 2,500 ft through 600 ft. This was the last recorded call from VH‑WWU on the CTAF.
Directly after take‑off, the pilot texted the senior base pilot with the estimated arrival time at Shark Bay of 1230. The aircraft’s flight path from Geraldton is shown in Figure 2.
At 1009, the pilot took a photo of the aircraft oil temperature gauges. Eight minutes later the pilot sent the photo to a staff member at the maintenance organisation with accompanying text stating ‘WWU flies beautiful, smooth, and tight. Oil temp a little high for a cool day so we might have to look at fitting those coolers back onto WWU. I’d hate to see the rings[4] suffer.’ The maintainer responded via text at 1018, and the message was recorded as delivered (indicating that the pilot’s phone was functional at that time). The oil temperature shown in the photo was towards the upper end of the normal range but below the 240°F maximum oil temperature limit.
Figure 2: Flight path overview
Source: Google Earth, annotated by the ATSB
At 1027:12, the aircraft crossed to the right of the direct track to Shark Bay (343°M), while maintaining a track of 347°M (Figure 3). At 1027:47, 25 seconds after crossing the direct track, the recorded data showed a right turn to a track of 011°M.
At 1028:41, while maintaining a track of 011°M, the aircraft commenced a slight descent and 22 seconds later (at 1029:13) entered a shallow left turn. The aircraft then re‑acquired the previous track of 347°M which was maintained for 15 seconds. At 1029:28, another left turn occurred as the slight descent continued. This turn transitioned into a spiral dive with the descent steepening significantly at 1030:12. The spiral dive tightened and steepened until a collision with terrain at 1030:47. The pilot was fatally injured and the aircraft was destroyed.
Figure 3: Track deviation and spiral dive
Source: Google Earth, annotated by the ATSB
At 1116:43, a call was placed to police by a member of the public stating they had come across aircraft wreckage by the side of a road as they were driving past. The wreckage was 84 km north‑west of Geraldton Airport and about 0.5 km right of the direct track. The member of the public stated that although they had been nearby, they had not seen or heard the aircraft or the impact.
Context
Pilot information
Aeronautical experience
The pilot held a commercial pilot licence (helicopter and aeroplane), with both single and multi‑engine class ratings for aeroplanes, and a single engine class rating for helicopters. They held low‑level operational ratings for sling, aerial mustering helicopter and aerial musting aeroplane operations. In addition, the pilot held a flight instructor rating with a low‑level operations training endorsement for both aeroplanes and helicopters.
The pilot most recently completed single engine aircraft and low‑level flight reviews on 12 February 2024.
The pilot’s total aeronautical experience was over 17,000 hours. In the previous 90 days the pilot had flown 28.3 hours (14.2 hours in the Cessna 172, 12.6 hours in the Cessna 206, and 1.5 hours in the Cessna 150).
Medical information
The pilot held a valid Class 1 aviation medical certificate that was revalidated in October 2024. The certificate specified that the pilot was to wear distance vision correction and a headset while flying. It also required reading vision correction to be available and no flying within 24 hours of certain types of medical treatment (which had not been recently provided in this case).
General health
At the time of the accident, the pilot was taking medication for:
gastroesophageal reflux disease, with Barret’s oesophagus – Omeprazole.[5]
All medications taken by the pilot were permissible for use by pilots in accordance with regulatory guidelines. The pilot’s designated aviation medical practitioner (DAME) and general practitioner (GP) both noted the pilot had haemochromatosis.[6]
The pilot last visited their DAME on 31 October 2024, to complete their aviation medical examination.
On 15 January 2025 the pilot completed an exercise stress ECG test. This was triggered due to a raised cardiac risk index score, which takes into account the pilot’s sex, age, blood cholesterol, blood pressure, diabetes status, smoking status and ECG interpretation. The test was valid and was reported by the supervising cardiologist as:
a normal exercise stress test with no significant ST depression during exercise and recovery.[7] Fair exercise tolerance for the patients age. Normal blood pressure at rest and normal blood pressure response to exercise.
On 25 February 2025, the pilot provided the results of a blood test for ferritin and HbA1c completed on 19 February 2025, in response to CASA letters requesting the below items for the pilot’s next medical renewal:
the result of an HbA1c test to monitor if they had progressed from impaired glucose tolerance to diabetes mellitus
the collated results of ferritin levels
other clinically indicated blood tests for the preceding 12 months.
There was no information provided regarding assessment for any other tests.
A colleague at the DAME’s medical practice conducted a tele-consult on 4 March 2025 to discuss slightly raised ferritin[8] from blood samples taken on 19 February 2025 and recommended that the pilot attend their GP to consider venesection.[9] On 4 March 2025, the GP received a letter from a colleague of the pilot’s DAME to consider the venesection. The GP posted the pilot a pathology request form for therapeutic venesection on 12 March 2025. There was no evidence that this venesection was actioned by the pilot before the accident.
The GP, DAME, and pilot’s family reported the pilot was an ex-smoker, however, multiple members of the aviation community who knew the pilot, reported the pilot still smoked. The ATSB was unable to confirm the frequency with which the pilot had been smoking, however the pilot’s smoking status did not change the requirement for or the interpretation of the cardiac risk assessment.
Health leading up to the accident
The pilot’s next of kin (NOK) recalled the pilot had contracted gastroenteritis 5 days prior to the accident. The NOK recalled the pilot stating that they were feeling better the day prior to the accident (20 March) and reminding the pilot to stay hydrated.
The senior base pilot recalled that the pilot had planned to fly the same ferry route as the accident flight on 20 March. However, the pilot reported that they had gastroenteritis and were not well enough to fly.
On the day of the accident while at the maintenance facility in Geraldton, aircraft maintainers noted that the pilot’s skin appeared pale, the pilot had yellow, sunken eyes and appeared to have lost a significant amount of weight. They recalled the pilot stating they had gastroenteritis, had not been eating and had lost 4 kg of weight in the preceding days.
The pilot did not contact either their usual GP, DAME or CASA regarding the gastrointestinal illness. Symptoms usually start within 2–5 days of infection, with full recovery typically within 7–14 days. Symptoms can include diarrhoea, fever, stomach cramps, bloating, nausea and vomiting. Acute complications can include dehydration (signs include scant urine production, dark coloured or concentrated urine, dizziness or light-headedness, low blood pressure, thirst, dry mouth, loss of skin turgor, sunken eyes, acute weight loss).
Pilot health reporting requirements
CASA advised on its website[10] that if a pilot has a medically significant condition that impairs their ability to perform the duties authorised by their licence, they must ground themselves while the condition is present, and check with a DAME and/ or report the condition to CASA. These reporting requirements do not apply for ‘common medical ailments’ including gastroenteritis. It also states that if a medically significant condition lasts longer than 7 days (Class 1)[11], they must notify their DAME and ground themselves until notified by their DAME or CASA that they could continue their licenced duties.
Post-mortem examination and toxicology
Post-mortem examination of the pilot confirmed the presence of bacteria responsible for causing gastroenteritis.
Toxicology results received to date indicated nothing of concern, including that carbon monoxide levels were not significantly raised.
The post-mortem examination was consistent with the pilot wearing the lap portion of the aircraft’s 3-point restraint (see Aircraft information), however it was unable to be determined if the pilot was wearing the upper torso restraint.
Aircraft information
The Cessna 150M is a high‑wing, all-metal, 2‑seat, unpressurised aircraft with a fixed landing gear. VH‑WWU was manufactured in 1976 and first registered in Australia in 1986. It was powered by a Continental O‑200‑A reciprocating piston engine, driving a fixed-pitch propeller. The aircraft was equipped with a 3-point occupant harness.[12] The aircraft was not equipped with an autopilot.
The aircraft was operated until 2016 and then placed in storage. In January 2022, the aircraft was recommissioned which included replacement of the flight control cables and fitment of the engine, which had been overhauled. On 11 April 2024, the aircraft was issued with a maintenance release and commenced operations with Norwest Air Work. At the time, the aircraft had accrued about 13,910 hours total time in service.
A periodic and other scheduled inspections were carried out between 6–18 March 2025. The periodic inspection identified minor defects that were subsequently rectified. The aircraft’s engine reportedly had excessive oil consumption, which was addressed by honing[13] the cylinders and fitting new piston rings. Additionally, the engine ignition harness was replaced. The engine was tested by carrying out a ground run 3 days before the accident and found to be functioning correctly. At the commencement of the accident flight, the aircraft had accrued a total time in service of 14,208 hours.
Site and wreckage
The wreckage was located about 20 m south of an east‑west road. The wreckage trail extended in a north‑easterly direction, about 23 m from the initial impact point to where the main wreckage, including the wings, empennage, engine and propeller had come to rest (Figure 4). There was no fire. Fuel could be smelt in the area.
Figure 4: Overview of VH-WWU accident site
Note: Some of the aircraft had been moved by the first responders at the time this image was captured. Source: ATSB
Ground impact marks and damage to the airframe indicated that the aircraft impacted the terrain in a left wing‑low, steep, nose‑down attitude at high speed (Figure 4). All major aircraft components were accounted for at the accident site. Damage to and deformation of the propeller was consistent with the engine running at the time of impact. There were no identified pre-accident aircraft defects, although disruption to the airframe precluded a full assessment of the aircraft’s serviceability immediately prior to the accident and prevented the ability to measure remaining fuel on board.
Meteorological information
The graphical area forecast for the accident region on 21 March had clear conditions for the flight with no cloud and visibility greater than 10 km.
At 1030, the Bureau of Meteorology (BoM) automatic weather station at Geraldton Airport, 85 km south of the accident location, recorded the wind as 5 kt from 121° magnetic. There was no recorded cloud, visibility was greater than 10 km and the temperature was 34°C. Figure 1 shows the clear conditions at Geraldton during the aircraft changeover.
Recorded data
Flight track
There was no available radar or ADS‑B recording of the flight. However, the ATSB recovered recorded data from a damaged Garmin 296 GPS which was fitted to the aircraft.
From the departure at Geraldton at 0956 until 1027 the flight progressed without any significant events. The ground speeds calculated for this portion of the flight were consistent with normal cruise for a Cessna 150.
The calculated airspeed increased through the spiral dive and reached a maximum of 153 kt to the last recorded data point, which exceeded the aircraft Vne.[14] Analysis from the initial left turn until the collision with terrain indicated that the engine was producing power until impact.
Video
The ATSB obtained video recordings from Geraldton Airport and 3 cameras within the maintainer’s hangar.
The airport camera field of view (Figure 5) covered:
both arrival (runway 14) and departure (runway 08) runways
the parking bay for both Cessna 150s
the maintenance hangar.
Figure 5: Geraldton Airport camera field of view
Source: Google Earth, annotated by the ATSB
Radio communication
Geraldton Airport recorded local area CTAF. At 0957:08 the pilot was heard broadcasting:
Traffic Geraldton, ah, Whisky Whisky Uniform departed runway 08, through, ah, 600. Tracking out to the north, climbing, ah, 2,500. Geraldton traffic.
This was the last call recorded.
There was no mayday call recorded on the Geraldton CTAF or the Melbourne Centre frequencies. A local pilot flying in the area at the time of the accident, stated they heard other aircraft further north of the accident site making radio transmissions on the Geraldton CTAF, however they did not hear anything further from the pilot of VH-WWU.
ATSB analysis of the radio propagation range concluded that, had the pilot made an emergency broadcast at the time of the flight path deviation, it would likely have been heard by nearby aircraft.
Survivability
ATSB analysis indicated that the deceleration forces and aircraft disruption during the collision with terrain exceeded survivability limits.
Related occurrences
Collison with terrain involving Cessna 152, N89059, Tucson, Arizona, United States on 8 February 2013 (National Transportation Safety Board WPR13FA118)
While flying the airport circuit on the base leg (prior to turning and line up for landing), several motorists observed the Cessna 152 aircraft in a steep nose-down attitude and descending rapidly. The aircraft impacted flat terrain about 1.5 miles from the airport. Examination of the airframe and engine did not reveal any pre‑impact anomalies that would have precluded continued engine operation or flight. Review of the air traffic control radar tracking data did not reveal any abnormalities with the departure or flight. The track was observed to conduct a slight right turn before a left turn steepening until collision with terrain.
The NTSB found that the probable cause was the pilot's incapacitation due to their pre‑existing cardiac disease, which resulted in degraded or complete loss of ability to control the aircraft.
Collision with terrain involving Cessna 152, N49278, Naple, Florida, United States on 13 December 1991 (National Transportation Safety Board MIA92FA045)
The Cessna 152 aircraft was observed flying westbound parallel to the runway in the opposite direction to landing. The aircraft suddenly nosed over, rotated to the left slightly, and impacted terrain in near vertical descent. There was no evidence of failure or malfunction of the aircraft structure, flight controls, or engine. The post‑mortem examination of the pilot indicated they had heart disease.
The NTSB found that the probable cause was the pilot became incapacitated due to an undetermined cardiovascular event which resulted in uncontrolled descent into terrain.
Safety analysis
Departure from level flight
Evidence from the accident site, aircraft wreckage, and flight path data identified that the aircraft collided steeply with terrain at high speed and that the accident was not survivable.
Analysis of the flight path data, combined with the aircraft’s recent release from maintenance, prompted examination of several possible factors. These included:
airworthiness related to the post maintenance condition of the aircraft
possibility of control jam affecting flight control functionality
spatial disorientation impacting the pilot
potential medical event.
Airworthiness
Examination of the aircraft’s propeller and analysis of the flight data and aircraft characteristics indicated that the aircraft’s engine was operating at the time of the accident.
Had there been an airworthiness issue with the aircraft, it would have very likely been communicated by the pilot. However, no distress calls or Mayday transmissions were recorded on the common traffic advisory frequency (CTAF), or audible to other aircraft in the vicinity on the same frequency. Analysis of the radio propagation range confirmed that any distress call, if made, would have been within range of detection by nearby aircraft.
The accident site was surrounded by expansive paddocks suitable for an emergency landing, which could have reasonably been utilised in the event of a mechanical or engine issue. The terrain was flat and largely unobstructed, providing viable options for a controlled landing. The absence of any attempt to divert to or land in these paddocks suggests that no mechanical or engine-related emergency necessitated such an action.
Control jam
A control jam in the aircraft would have limited the pilot’s ability to manoeuvre the aircraft. If a primary flight control surface, such as the ailerons, elevator, or rudder, becomes jammed or partially restricted, the pilot may have difficulty controlling the aircraft's attitude and direction. Depending on the severity and type of jam, the pilot may need to rely on secondary or alternative control methods, such as trim adjustments or differential power, to maintain control and safely land the aircraft.
However, the aircraft had been flying in level flight for over 30 minutes prior to the event, demonstrating that the controls were functioning properly during this period. Additionally, the aircraft was equipped with new control cables, and no recent maintenance had been performed on the control surfaces, significantly reducing the likelihood of errors such as improper setup or mechanical failure.
The Cessna 150’s simple design includes backup systems to allows pilots to make adjustments to maintain control even in the event of partial system issues. Although the control continuity could not be fully established at the accident site, these points strongly suggest the accident was not due to a control problem.
Spatial disorientation
Spatial disorientation refers to situation when a pilot fails to correctly sense the position, motion or attitude of the aircraft relative to the ground or the gravitational vertical. This can be particularly hazardous to aviation safety and can be affected by cloud cover, changing weather or light conditions, flight profile (e.g. dynamic high-g manoeuvres or gradual sustained turns), distraction, fatigue and medical conditions.
However, the forecasted weather was for clear flight conditions, with no cloud and visibility greater than 10 km. These favourable conditions provide visual references to the horizon and surrounding terrain minimising the chances of special disorientation.
Additionally, flight data analysis indicated the aircraft entered a left turn followed by a spiral dive, with no recorded corrective control inputs to recover from the manoeuvre. This indicates that the pilot maintained proper orientation, as disorientation typically leads to erratic or incorrect control inputs.
While the pilot is likely to have been unwell, fatigued and distracted from their acute gastrointestinal illness, it is unlikely that these conditions caused spatial disorientation.
Incapacitation event
As discussed above, the aircraft entered a left turn followed by a spiral dive with no corrective control inputs to recover. With the pilot’s significant experience, the lack of any attempt to counteract the spiral dive is highly unusual. As the aircraft was not fitted with an autopilot, no input from the pilot on the controls would likely cause the aircraft to start rolling to the left and the nose dropping causing a left turn with a possible spiral dive or spin.
Further, the absence of response to the spiral dive, in addition to the lack of distress call, are consistent with what would occur if the pilot was incapacitated, preventing them from taking corrective action.
Additionally, the flight path was almost identical to the collision with terrain involving a Cessna 152 in Tucson, Arizona, United States, which concluded a probable cause as pilot's incapacitation due to their pre‑existing cardiac disease.
Given the lack of other reasons, it is therefore likely the pilot was incapacitated.
In considering the likelihood of that incapacitating event being medically related, the ATSB engaged a medical professional to provide specialist analysis of the pilot’s medical history, specifically looking at:
hereditary haemochromatosis
cardiovascular
acute gastroenteritis.
Hereditary haemochromatosis
Haemochromatosis is an inherited genetic disorder in which excess iron builds up in the body. Over time, iron overload may cause symptoms that can be a hazard to flight safety and may cause organ damage. However, the genetic profile of haemochromatosis in this case is usually not associated with significant medical complications and is typically managed with regular blood tests to monitor ferritin levels, and regular clinical assessments to observe for any complications.
There was no indication that the requested venesection was actioned prior to the accident. However, it is noted that the pilot had moderately elevated ferritin results for a long period of time but did not report any signs or symptoms of iron overload. It was not possible to discern whether the pilot’s haemochromatosis condition had any material relevance to the accident.
Cardiovascular
The pilot’s next-of-kin, general practitioner, and designated aviation medical practitioner (DAME), and the Civil Aviation Safety Authority (CASA) understood the pilot to be an ex‑smoker, however colleagues had observed the pilot smoking at times. Smoking is an independent risk factor for cancer, cardiovascular disease (higher blood pressure, heart attack, stroke), respiratory disease (chronic obstructive pulmonary disease) and other conditions which can impact fitness for flight (hypoxia, fatigue, reduced exercise tolerance, higher risk of sudden incapacitation).
The pilot’s hypertension and high cholesterol were also risk factors for cardiovascular disease. The elevated risk of major adverse cardiac event was assessed in accordance with CASA requirements (stress ECG) and the outcome was that there was no safety‑relevant coronary ischaemia detectable. The cardiac assessments do not entirely exclude coronary disease, particularly non-occlusive and non-calcified atheromatous plaque (Jennings et al 2021 and Gray et al, 2019), and it remains possible that this pilot experienced an acute cardiac ischaemic event (or other major adverse cardiovascular event) resulting in acute incapacitation.
Acute gastroenteritis
The pilot’s physical appearance, as noted by the maintenance team, was consistent with the reports that the pilot was suffering from an acute gastrointestinal infection. The fact that the pilot self-excluded from the planned flight on the day prior to the accident, was testament to the extent to which they were afflicted by the illness.
While the pilot reported feeling better ahead of the accident flight, it was very likely that they remained unwell and symptomatic. Gastroenteritis by itself does not cause sudden incapacitation, however it would have reduced the pilot’s physiological reserves and exposed the pilot to the associated complications, including dehydration and electrolyte imbalance, and fatigue. The pilot’s yellow, sunken eyes, weight loss, and reduced food intake indicated it is very likely that the pilot was moderately dehydrated at the time of the accident flight.
There is no evidence that the pilot sought any health advice or treatment from a health care provider for their acute gastrointestinal symptoms. However, for the purposes of this analysis, it could be considered most likely that the pilot continued to take their usual medications (specifically irbesartan for hypertension).
Sudden incapacitation
Dehydration from 5 days of infective gastroenteritis would have increased the pilot’s risk of low blood pressure leading to a syncopal event (faint) and may have caused or contributed to electrolyte imbalances. Additionally, the continued usage of irbesartan would have also reduced blood pressure (van Dijk et al, 2021 and Taylor et al, 2025). While seated in an upright position, a syncopal event (faint) due to low blood pressure was the most likely cause of a rapid incapacitation in this occurrence, with no prospect for timely recovery.
Alternatively, low blood pressure and electrolyte imbalances increase the risk of a major adverse cardiovascular event, such as myocardial infarction (commonly referred to as heart attack), cardiac arrhythmia or stroke, which may also cause a rapid incapacitation.
In conclusion, it is very likely that the pilot experienced an incapacitation event. However, from the evidence available, the exact nature of the incapacitation could not be determined. There were no other factors identified that were likely to have contributed to the accident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 150M, VH-WWU, 40 km north-west of Northampton, Western Australia, on 21 March 2025.
Contributing factors
While in cruise, the pilot likely experienced an incapacitating medical event resulting in a deviation off track, a left-hand spiral dive and subsequent collision with terrain.
The pilot was acutely unwell in the days preceding the accident flight, and was very likely still symptomatic during the accident flight.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Shark Bay Aviation
the next of kin
the senior base pilot of the operator
witnesses who saw the pilot prior to the flight
Civil Aviation Safety Authority
Western Australia Police Service
the maintenance organisation for VH-WWU
Textron Aviation
CCTV footage of the aircraft from Geraldton Airport
recorded data from the GPS unit on the aircraft
the pilot's designated aviation medical examiner
the pilot’s general practitioner
Royal Australian Air Force Institute of Aviation Medicine
ChemCentre Western Australia.
References
Gert van Dijk, J., van Rossum, I A., Roland, D. Thijs,The pathophysiology of vasovagal syncope: Novel insights. Autonomic Neuroscience, Volume 236, 2021https://doi.org/10.1016/j.autneu.2021.102899.
Gray, G, Davenport, E, Bron, D et al The challenge of asymptomatic coronary artery disease in aircrew. Heart 2019; 105: s17-s24
Jennings, G., Audehm, R., Bishop, W., Chow, K., Liaw, S., Liew, D., and Linton, S. National Heart Foundation of Australia: position statement on coronary artery calcium scoring for the primary prevention of cardiovascular disease in Australia. Med J Aust 2021; 214 (9): 434-439. doi: 10.5694/mja2.51039
Neuvonen, P., Niemi, M., & Backman, J. (2006). Drug interactions with lipid-lowering drugs: Mechanisms and clinical relevance. Clinical Pharmacology & Therapeutics, 80(6), 565–581. https://doi.org/10.1016/j.clpt.2006.09.003
Taylor K, Tripathi AK. Adult Dehydration. [Updated 2025 Mar 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555956/
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Shark Bay Aviation
maintenance organisation for VH-WWU
Civil Aviation Safety Authority
Textron Aviation
Royal Australian Air Force Institute of Aviation Medicine
Western Australia Police Force.
Submissions were received from:
Civil Aviation Safety Authority
Royal Australian Air Force Institute of Aviation Medicine.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Shark Bay is about 340 km north‑west from Geraldton.
[2]SARTIME (time search action required): is the time nominated by a pilot for the initiation of search and rescue action.
[3]CTAF (common traffic advisory frequency): a radio frequency used by pilots at non-towered airports to communicate with each other about their position and intentions, ensuring safe and orderly traffic flow.
[4]Likely referring to piston rings, which wear somewhat more quickly at increased temperatures.
[5]The pilot’s use of omeprazole and diagnosis with gastroesophageal reflux disease and Barrett’s oesophagus were medically significant and required ongoing surveillance as part of the medical assessment process, however they were not declared to CASA. The medication is subject to DAME approval, but must also be declared to CASA as part of the medical assessment process.
[6]An inherited genetic disorder in which excess iron builds up in the body. Over time, iron overload may cause symptoms that can be a hazard to flight safety and may cause organ damage (e.g. liver, heart, kidneys).
[7]No significant ECG changes during exercise and recovery.
[8]Ferritin is a blood protein that contains iron.
[9]Venesection, also known as therapeutic phlebotomy, is a medical procedure that involves the controlled removal of blood to reduce excess iron or red blood cells in conditions like hemochromatosis or polycythemia.
[11]A Class 1 medical certificate is required to exercise the privileges of a commercial pilot licence.
[12]A 3-point harness includes a lap belt and upper torso restraint (UTR).
[13]Honing is a process that scratches a crisscrossed (crosshatched) pattern onto the inside of the cylinder. This pattern reduces cylinder wear by allowing oil to be retained in the scratches rather than be removed by the piston rings.
[14]The aircraft’s ‘never exceed speed’ (Vne) was 141 kt. Exceedance of this airspeed may result in structural damage to the aircraft.
On 26 February 2025, a Robinson Helicopter Company R22, with an instructor and a student on board, departed Archerfield Airport, Queensland, to conduct advanced emergency training at Pannikin Island in Moreton Bay, Queensland.
After practising emergency procedures and low-level flying, the student pilot performed several low-level torque turns, a manoeuvre not originally included in the lesson plan. During the final turn, the helicopter entered a low nose attitude and descended rapidly. The instructor attempted to recover, but due to the low height, was unsuccessful. The helicopter impacted the ground and skidded for some distance before rolling and coming to rest on its left side. The instructor sustained serious injuries and the student sustained minor injuries. The helicopter was destroyed.
What the ATSB found
Low‑level torque turns that were not part of the lesson plan, nor a requirement for commercial licence training, were conducted by a student pilot without a formal pre-flight briefing or guidelines. As the manoeuvre fell outside of the syllabus the ad hoc nature of its inclusion and conduct at the end of the lesson relied on an inflight briefing by the instructor to prepare the student for the exercise. Beginning the low-level torque turn exercise at 50 ft AGL rather than starting higher and working down as the student’s capability improved increased operational risk. Due to the low-level conduct of the exercise, this reduced the available safety margin and placed reliance on the instructor as the only risk control to recover from any unexpected mishandling of the sequence.
Although the instructor immediately identified that the helicopter was descending rapidly, and took the controls, their actions were unable to recover the helicopter before colliding with terrain. Environmental conditions may have further reduced the safety margin and complicated the low-level recovery.
The operator had no formal process for monitoring the return of training flights. This would likely delay any search and rescue response and reduce post-impact survivability of the helicopter occupants in the event of life-threatening injuries.
What has been done as a result
The operator reported that SARTIME procedures for the flying school have been revised.
Safety message
Ensuring and maintaining sufficient height for recovery is vital in a training environment when a student has limited experience to manage unexpected aircraft or helicopter behaviour.
All aspects of the lesson should be clearly briefed before flight including planned sequence, risks and hazards to ensure an understanding between instructor and student.
Instructors must rely on conservative in-flight decision‑making to manage risk during flight training operations and to anticipate and be ready to intervene quickly, especially during low-level, or elevated risk manoeuvres.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 26 February 2025, an instructor and a pilot under instruction (student) were conducting an advanced emergency training exercise in a Robinson Helicopter Company R22 (R22), registered VH-8BW, operated by Utility Helicopters, leased from Heliflite. The training commenced from the operator’s company base at Archerfield Airport, Queensland.
At about 0700, the student conducted a daily inspection of the helicopter under the supervision of the instructor. The intended training flight formed part of the requirements for a commercial helicopter pilot licence and the lesson plan intended to cover advanced emergency procedures.
At about 0730 the helicopter, with the student flying, departed Archerfield Airport to the south‑east for a designated training area located in Moreton Bay. After reaching the uninhabited Pannikin Island training area, the emergency training commenced with autorotation[1] and tail rotor failure practise. After about 45 minutes, the student then commenced low-level flying practise, completing several clockwise laps around the island. These were completed between 50–100 ft above ground level (AGL) and at a speed of between 60–70 kt.
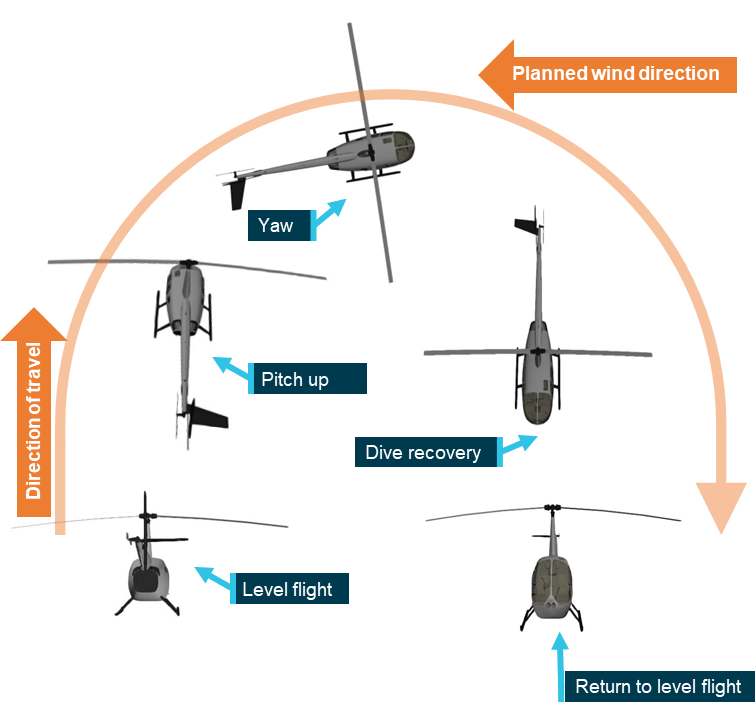
Toward the end of the lesson, the instructor recalled that the student requested to practise some agricultural flying operations, which included torque turns.[2] These manoeuvres were not on the lesson plan for the flight, or part of the commercial flight training syllabus, and there had been no plan to conduct them until this point. The instructor demonstrated the manoeuvre before the student took control and successfully completed 4 torque turns. The instructor reported these were conducted at a height of about 50 ft AGL.
The instructor stated that the low-level turns were conducted across the island roughly in an east–west direction. The exercise was conducted across the prevailing wind direction to avoid a downwind component on each low-level manoeuvre. Torque turns were performed on the eastern side of the island and procedural turns on the western side, with about 4 turns completed at each location. These were executed at a height of about 50 ft AGL.
As the lesson neared completion, they elected to do one more torque turn before returning to base. The instructor recalled noticing the wind had increased a little and had started gusting but stated that these were not considered abnormal conditions and that both he and the student had flown in these conditions before.
The instructor described that at the top of the last torque turn, they were at a height of 100–150 ft AGL when they began to descend to build airspeed and return to level flight. During the recovery, the instructor noticed that the nose of the helicopter was pointing slightly down toward the ground at a height of about 20 ft. The instructor recalled that they were about to correct the student when a sudden gust of wind increased the rate of descent. Aware of the ground proximity,the instructor immediately took over the controls and recalled moving the cyclic[3] aft to arrest the rate of descent. The instructor reported the helicopter shuddering, shaking, and experiencing a jolt in the collective but was unable to prevent the helicopter impacting the ground.
Both occupants recalled that everything happened quickly prior to ground contact and that the estimated speed at impact was about 60–70 kt. The instructor recalled that the helicopter impacted hard in a flared nose high attitude and that the stinger[4] contacted the ground first. The helicopter slid along the ground on its skids for about 40–50 m between mangrove bushes before the left skid dug into the muddy ground and dynamically rolled over.[5] The helicopter came to a stop on its left side after numerous rotations and was destroyed (Figure 1). The instructor recalled that the student remained in the helicopter momentarily after impact and then managed to exit and appeared to have had less injuries than themselves so was able to follow instructions to shut down the machine.
Figure 1: Accident site
Source: Student
The student turned off the battery master and assisted the instructor to exit the helicopter. The instructor was unsure if any staff would be in the office and recalled asking the student to use their mobile phone to call for help. They stated that calling the office would not be as effective as calling their partner, as they were aware that several of the staff were away on business. The company was contacted and another helicopter from the base at Archerfield Airport was then dispatched to collect both occupants. About 25 minutes later they were rescued by a colleague who arrived in another helicopter.
Emergency services were contacted, and an ambulance met the retrieval helicopter on arrival back at Archerfield Airport. Post-accident medical assessment determined that the instructor had sustained serious injuries and the student only minor injuries, both were taken to hospital for treatment.
Context
Aircraft information
The Robinson R22 is a 2-seat, 2-bladed, single-engine, light utility helicopter manufactured by Robinson Helicopter Company in the United States. It has a maximum all up weight of 622 kg. The R22 is powered by a Lycoming O-360 4-cylinder piston engine that is derated to 131 horsepower for take-off and 124 horsepower for cruise at 2,652 RPM. The R22 is mostly used for private operations, rotary wing flight training and agricultural operations.
The instructor reported that there were no mechanical issues identified with the helicopter during the daily inspection and pre-flight that would have precluded normal operation.
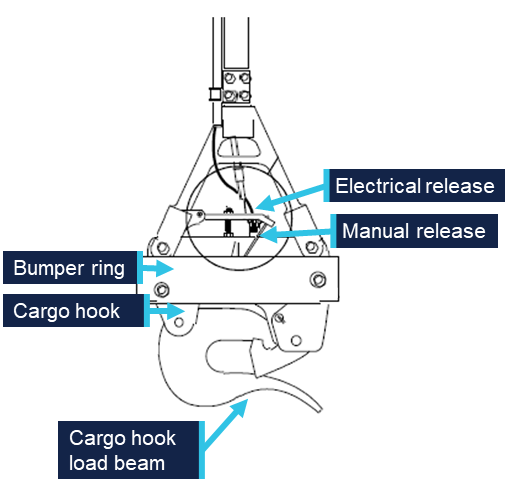
Flight controls
The helicopter was fitted with conventional light helicopter flight controls, such as dual cyclic controls for each seat, and a centre‑mounted collective.[6] The engine throttle is connected to collective inputs through a mechanical linkage; when the collective is raised, the throttle is opened and when lowered, the throttle is closed.
Pilot information
Instructor
The instructor held a commercial pilot licence (CPL-H) helicopter and had been an instructor with the operator for 3 years and 3 months. They began as a grade 3 instructor and progressed to a grade 1 instructor during their employment, logging about 2,800 flying hours. The instructor’s last proficiency check was 29 November 2024. The instructor obtained a low-level rating in 2021 and their low-level flight review for the R22 was valid until 13 November 2025. The instructor held a current Class 1 medical certificate.
Student pilot
The student pilot had been conducting training with the operator for about 3.5 years. Initially training for a private pilot licence (PPL-H) helicopter, they had not finalised the required ground theory or conducted a flight test. Although they did not hold a PPL-H, they continued training to obtain the required flight hours for a CPL-H.
Nearing completion of the commercial flight training, the student scheduled their lessons to coincide with their work commitments and they were not regular, but rather when time permitted. Their last lesson before the accident was conducted on 29 January 2025, about 4 weeks prior. They had previously completed advanced emergency training and the intention was to use the lesson as a refresher for CPL-H competency elements. The student reported they wanted to consolidate their low-level flying skills with a goal of working in the agricultural sector.
At the time of the accident the student had accrued 89 hours of pilot training with the operator. The student reported that about two thirds of all the lessons had been taken with the instructor involved in the accident and the remainder with head of operations (HOO) and one other instructor.
Meteorological information
Minute-by-minute wind data from the Bureau of Meteorology around the time of the accident indicated generally moderate winds with some directional variability.
Brisbane Airport observations recorded winds at 126°–143° with wind speeds of 9–13 kt, gusting to 18 kt. Similarly, Gold Coast Airport recorded winds at 150°– 208° with wind speeds of 9–14 kt, gusting to 18 kt. The accident site which was located between these two reporting stations (Figure 2) was likely subject to similar wind conditions.
Figure 2: Map showing location of weather stations and Pannikin Island
Source: Google Earth, annotated by the ATSB
The instructor stated that they checked the weather conditions before departing, and that the wind direction indicated a south‑easterly wind at about 15 kt. On arrival at Pannikin Island, they recalled that the surface wind was observed to be more southerly in direction and felt slightly stronger than 15 kt.
Downdraught
Downdraught is a vertical atmospheric condition where a current of air sinks rapidly, leading to sudden changes in conditions at ground level and can produce strong surface winds. Downdraughts can pose a significant threat to rotary aircraft, particularly while manuevering at low level. The most common causes of downdraught experienced by helicopter pilots are due to irregular terrain when combined with strong surface winds, mechanical turbulence,[7] temperature inversions or thermal convection movements.
Accident site and wreckage
The operator conducted training over Pannikin Island, a designated training area to the south-east of Archerfield Airport. The island is one of several uninhabited islands located in southern Moreton Bay, about 56 km south-east of Brisbane (Figure 3).
The instructor recalled that the Pannikin Island training area extended from sea level to 3,500 ft. The vegetation on the island is mainly mangrove shrubland, with no buildings or power lines in the vicinity, and for this reason was used for low-level training.
Figure 3: Google Earth image of location of Pannikin Island, Queensland
Source:Google Earth, annotated by the ATSB
The initial ground contact of the helicopter indicated a high‑speed, upright skid contact before further loss of directional control and impact (Figure 4). The student and instructor reported that the speed on touchdown of the helicopter was about 70 kt and was consistent with the skid mark length.
Figure 4: Photograph of impact site
Source: Student
After further impacting mangrove trees, the tail rotor assembly, including tail rotor, gearbox vertical and horizontal stabiliser, separated from the cabin and was reported as being located about 15 m north of the wreckage (Figure 5) and was largely intact.
Figure 5: Photograph of main and tail rotor wreckage at accident site
Source: Student
Post-accident aircraft examination
The operator’s chief engineer carried out an inspection of the helicopter at the accident site before the wreckage was removed. The engineer reported that their examination found no evidence of mechanical issues that could have led to the accident.
Recorded data
There was no onboard data recording on the helicopter to determine the flight control inputs and their effect on the helicopter during the accident.
Recorded radar data was available of the helicopter in the training area, however due to the low-level nature of the operation, this was intermittent.
Helicopter exercises and operator’s procedures
Helicopter pilots are taught a range of manoeuvres as part of their training and licensing requirements. These are typically categorised as either normal, advanced or emergency procedures and are detailed by the Civil Aviation Safety Authority (CASA) for different licence levels and ratings.
In addition to the standard syllabus for advanced emergencies (e.g. autorotation, tail rotor failure), advanced procedures that are not required for the CPL-H may be introduced by flight instructors to extend a student’s capability and confidence. The approved Civil Aviation Safety Regulation (CASR) Part 141 operator exposition did not include torque turns as a requirement to obtain a CPL-H.
Pre-flight briefing
Briefings prior to a flying lesson are an essential part of flight preparation and represent an opportunity to gather, mentally prepare and organise the structure of the upcoming training flight. It is also an opportunity to assess the potential risks and hazards that might arise during normal and emergency operations. Discussion on the procedures to be used in the case of unexpected events disrupting the planned flight operations are also covered, and this prepares and sets student expectations for the lesson.
While pre-flight briefings were normally conducted before each lesson covering the intended lesson sequences, on this occasion the instructor considered a detailed briefing was unnecessary due to the student’s previous experience. Before departure, the instructor and student recalled a brief discussion focused primarily on the weather, but this did not include a formal briefing covering the planned exercises and potential risks.
The intent of the lesson was to consolidate the student’s prior training and both pilots recalled that the session was to refresh and consolidate advanced emergency procedures.
Low-level operations
A low-level operation is defined by regulation 61.010 of CASR as flight at a height lower than 500 ft AGL, other than when taking off or landing, and is not permitted unless the circumstances outlined in sub regulation 91.267(3) of CASR apply to the flight and the pilot is authorised under Part 61 to conduct the operation. Low‑level operations can introduce increased risk for all pilots as the proximity to terrain and reduced margin for recovery intensify the consequences of any deviation from the expected performance. There is also an increased susceptibility to adverse environmental conditions for students with less experience.
Torque turns
A torque turn is an advanced manoeuvre to quickly complete a 180° change in direction of flight (Figure 6). The manoeuvre begins with a pitch upwards to reduce forward airspeed followed by an application of power to increase altitude. As airspeed decreases, aerodynamic stability is reduced and the increased torque induces yaw.[8] This yaw is used to initiate the turn which continues until the helicopter is facing the opposite direction. Once the turn is complete, the pilot regains airspeed, eases out of the dive and resumes level flight in the new direction.
Figure 6: Helicopter torque turn flight sequence
Source: ATSB
The student reported that their request to conduct the torque turn training was driven by their desire to seek employment in the agricultural domain (aerial application and dispensing operations) after obtaining their commercial licence. They recalled completing several turns successfully before the accident turn.
However, in response to the draft report, CASA stated that torque turns are not common and are actually avoided in rotorcraft aerial application and dispensing operations, in favour of accurately flown and coordinated procedure turns (see below).
No official height for conducting torque turns in training is provided by CASA, however general guidance provided for starting more advanced or complex manoeuvres is to begin at higher altitudes and reduce once competence is gained.
Procedure turns
A procedure turn is a standard course reversal manoeuvre used to change the helicopter’s direction. ICAO defines the manoeuvre as a turn made away from a designated track followed by a turn in the opposite direction to permit the aircraft to intercept and proceed along the reciprocal of the designated track. Procedure turns may be designated as being made either in level flight or while descending, according to the circumstances of each individual approach procedure. To commence the turn the aircraft would turn off track, maintain airspeed, conduct the turn and turn onto the reverse of the original course. They are sometimes referred to as ‘P turns’ as the flight track looks like a ‘P’ from above.
The Part 61 Manual of Standards competency standards for unit AA2 – Helicopter aerial application operation, specifically requires procedure turns in element AA2.6 – Manipulate helicopter at low level:
(a) manoeuvres helicopter at all speeds below 500 ft AGL, up to and not beyond the limits of the flight-manoeuvring envelope, without exceeding the operating limitations of the helicopter;
(b) conducts coordinated, smooth procedure (P) turns with varying power settings.
Operator low-level training
In line with the CASA requirements, the operator’s exposition stated that procedure turns were required for advanced low-level training and detailed amongst other manoeuvres that the height range for the conduct of these was between 200 ft and 5 ft AGL. However, no specific minimum height was declared for procedure turns.
There was no reference for torque turns in the operator’s exposition.
Search and rescue
Search and rescue time (SARTIME) is the time nominated by a pilot for the initiation of search and rescue action. Any person deemed to be a responsible person can hold SARTIME for a pilot’s safe arrival.
There was no regulatory requirement for the operator’s local training flights under CASR Part 91 for a SARTIME, however the absence of a formal flight following process during flight training may have implications for the operator’s duty of care during the operation.
The operator’s head of operations (HOO) reported that a range of tracking systems were used across the operator’s fleet, including satellite trackers and transponders. These devices allowed staff to monitor the location of helicopters during flight and, if a helicopter did not return within an expected time, its position could be quickly determined. A television screen located in the operator’s office displayed tracking data, however, no personnel were specifically assigned to monitor return times or to observe the radar feed.
Many of the flight training lessons were conducted from the operator’s base at Archerfield Airport, where staff could maintain direct visual oversight of helicopter movements. However, as the accident flight was early in the morning, there was only one other instructor conducting flight training and the office staff were not yet on duty.
Some helicopters in the fleet were fitted with electronic locator transmitters and others with personal locator beacons. Under CASR regulations these are mandated for flights greater than 50 NM from the departure aerodrome. The accident helicopter was fitted with a manually‑activated personal locator beacon, however the instructor reported that they were dazed immediately after the accident and did not prioritise the activation.
Safety analysis
Introduction
An instructor and a student were conducting advanced emergency training in a Robinson Helicopter Company R22 (R22) helicopter, registered VH-8BW, at Pannikin Island in Moreton Bay, Queensland. Near completion of the commercial helicopter pilot lesson, the instructor and student agreed to conduct torque turns, an advanced helicopter handling manoeuvre that was outside of the training syllabus. After conducting several torque turns, the helicopter entered an increased low nose attitude during recovery at low altitude which resulted in a collision with terrain and dynamic rollover.
This analysis will consider decision‑making of the instructor and student and the instructor’s recovery as factors in the accident.
Decision-making
Instructing is a complex task and flight instructors must balance the benefit to the student’s learning and experience with safe margins of operation in a dynamic and sometimes rapidly changing environment.
The decision to conduct torque turns was only discussed between the instructor and the student during the flight.
Instructors consider several factors such as student performance, recent progress and training objectives when making in‑flight decisions to alter or vary the training flight plan. While instructors can adapt lessons to suit the student’s progress, deviations from planned activities should be underpinned by clear safety considerations, briefings and effective risk management.
Effective instructional decision-making balances educational value with operational risk. The instructor assessed the student to be capable of performing the manoeuvres based on their recent progress and performance during the lesson and having completed many previous training hours together. However, this assessment was done during the training flight, limiting the time available for the instructor to fully consider the benefits and risks (including height to conduct the training – see below).
The benefits of conducting a pre-flight brief of the lesson, especially where training operations are conducted in emergencies is well-established. Such a briefing reaffirms standard operating procedures, promotes predictable behaviour, and sets expectations (Sumwalt and others, 2010).
The torque turns were not part of the syllabus and were not necessary for the lesson. However, if the decision to conduct them had been agreed before flight, this would have allowed for a full ground briefing to establish the torque turn procedures, discuss the conduct of the manoeuvre and ensure a common understanding of how the practise turns would be conducted.
Manoeuvre height
Torque turns were outside of the advanced emergency lesson for the operator’s commercial pilot training syllabus and consequently no procedure was identified in the training materials for conducting them during training. The absence of a defined procedure places the reliance on the instructor to become the risk control. In this case there was an increase in risk as the manoeuvre was conducted at a height that reduced the available safety margin and limited the opportunity for recovery when the helicopter entered an undesired state. By contrast, if the manoeuvre had been initiated at a higher altitude, the increased height would have provided more time for the student and instructor to identify, intervene and recover from the undesired aircraft state. Increased altitude when practising a high-risk manoeuvre with a student would allow time for corrective control inputs from the instructor to avoid collision with terrain.
Beginning the low-level torque turn exercise at 50 ft AGL, rather than starting higher and working down as the student’s capability improved, increased operational risk.
Instructor recovery
During the torque turn, the helicopter exited the manoeuvre in a lower than expected nose attitude. Instructor intervention is a critical control in flight training and is often the final opportunity to regain control of the helicopter. Although the instructor took over control as soon as they recognised the rapid descent rate, the low height on exiting the torque turn limited the time available to arrest the descent before ground contact occurred. Environmental conditions may have further reduced the safety margin and complicated the low-level recovery.
Due to the high speed of the helicopter and approaching vegetation, the instructor likely attempted to slow the helicopter using rear cyclic (as would be normal practice when airborne), however, after skid contact with the ground in an upright attitude, this likely resulted in the main rotor disk flexing and making contact with the tail boom. This resulted in the severing of the tail boom by the main rotor blades, loss of torque control and the front left skid digging into soft soil, leading to a dynamic rollover.
SARTIME
The operator had no formal process for monitoring the return of training flights. While many operations were conducted within line-of-sight or in close proximity to the operator’s base, this informal system provided limited assurance that an overdue returning training flight outside of the airport vicinity would be identified. In this case, had the crew been more seriously injured or rendered unconcious, the lack of formal SARTIME and flight following would likely have delayed the initiation of search and rescue efforts and substantially reduced survivability.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Robinson R22 Beta, VH-8BW, 29 km north of Southport Aerodrome, Queensland, on 26 February 2025.
Contributing factors
While conducting commercial training consolidation for low‑level and emergency procedures, the instructor and student agreed to conduct torque turns, which were outside the lesson plan and training syllabus.
Without a procedure, the instructor conducted the exercise at an inappropriate low height, which increased risk and did not allow for a margin of error.
During the torque turn exercise the helicopter exited the turn in a lower than expected attitude. The instructor assumed control but was unable to prevent a collision with terrain.
Other findings
The operator had no formal process for monitoring the return of training flights. This would delay search and rescue response and reduces post-impact survivability of aircraft occupants in the event of life-threatening injuries.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action addressing SARTIME
The operator has implemented a SARTIME procedure using an application for shared messaging between instructors and staff. For each flight, the instructor records the helicopter registration, flight details and estimated time of arrival back at base. Any delays are communicated through the group and landings are confirmed upon arrival at base or the intended destination. The procedure is documented on the pre-flight board.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
instructor of the accident flight
student pilot
operator CEO and HOO
Civil Aviation Safety Authority
Bureau of Meteorology.
References
Sumwalt, R. L. Lemos, K. A., & McKendrick, R. (2019). The accident investigator’s perspective. In Crew resource management (pp. 489-513). Academic Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
instructor of the accident flight
student pilot
operator CEO and HOO
Civil Aviation Safety Authority.
Submissions were received from:
instructor of the accident flight
operator CEO and HOO
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Autorotation is a condition of descending flight where the main rotor of a helicopter is driven only by aerodynamic forces with no power from the engine due to engine failure or deliberate disengagement.
[2]A torque turn is an advanced manoeuvre involving rapid yaw using engine torque to change direction.
[3]Cyclic: a helicopter control used to tilt the rotor disc allowing the aircraft to move in a particular direction.
[4]A stinger, otherwise known as the tail skid, is a protrusion at the rear of a helicopter that is intended to protect the tail boom when landing.
[5]Dynamic rollover: a helicopter is susceptible to a lateral rolling tendency. It begins when the helicopter starts to pivot laterally around its skid or wheel while in contact with the ground. Once the critical angle, typically around 5–8° is exceeded, the helicopter rolls over, often too quickly for any corrective pilot action.
[6]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[7]Mechanical turbulence occurs when wind flows over obstacles like mountains or buildings, disrupting smooth airflow and creating bumpy flight experiences.
[8]The motion of an aircraft about its vertical or normal axis.
Occurrence summary
Investigation number
AO-2025-011
Occurrence date
26/02/2025
Location
29 km from Southport Aerodrome
State
Queensland
Report release date
04/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Flight control systems, Loss of control, Weather - Other
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-8BW
Serial number
4200
Sector
Helicopter
Operation type
Part 141 Recreational, private and commercial pilot flight training
The ATSB is investigating a loss of control event involving a Bell 412EP, registered VH-VJF, 57 km north-east of Strahan Aerodrome, Tasmania, on 10 March 2025.
The helicopter was being operated by Coulson Aviation for firefighting operations using a sling‑loaded water bucket. While hovering to load the bucket from a river, the helicopter unexpectedly sank about 50 ft. In an attempt to recover, the pilot initiated forward flight but was unable to jettison the load before the longline became taut, causing a sudden stop and an abrupt tail-down motion. This resulted in the external hook and longline making contact with the lower fuselage.
The pilot flew back to the base at Zeehan where inspection identified damage to the helicopter’s fuselage, control tubes for both the engines and the tail rotor. Damage was also identified to the bucket and longline.
To date, the ATSB investigation has included:
interviewing involved parties
retrieving recorded data
the collection of other relevant information
reviewed recorded aircraft information
reviewed the forecast and observed weather conditions
reviewed maintenance documentation for VH-VJF
analysed recorded helicopter information
reviewed pilot training delivered by Coulson Aviation.
An interim report, which detailed factual information established during the course of the investigation, was released on 17 March 2026 (see separate tab).
The continuing investigation will include:
review of Coulson Aviation’s risk controls for bucketing operations in the Bell 412
review of Coulson Aviation’s operational and reporting procedures
review of Tasmanian Fire Service operational and reporting procedures.
In the course of the investigation, the ATSB has identified potential limitations in risk controls that are considered likely to have contributed to the occurrence. Examination of these factors represent a significant increase in the scope of this investigation, and it has been upgraded from Short to Defined as a result (the ATSB's different levels of investigation are detailed here).
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Interim report
This interim report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Prior to the occurrence flight
On 10 March 2025, a Bell 421EP, registered VH-VJF and operated by Coulson Aviation as HT204, was tasked with ground crew support operations on the Canning Peak fire, a sub‑fire of the West Coast fire complex in Tasmania.
At about 0830, the Tasmanian Fire Service briefed pilots on the weather and taskings for the day while at Strahan Airport. The Air Attack Supervisor (AAS) reported that the 2 Bell 412 helicopters were tasked with the insertion of crews into the fireground (HT201) and then firebombing[1] in support of those crews with a 150-ft longline and bucket[2] (HT204).
At about 0900, both helicopters departed Strahan Airport for Tullah, which was the designated staging area[3] for the activities. Approximately 25 minutes later both helicopters arrived at Tullah. The pilot of HT204 reported shutting down the helicopter and waiting until they were required for firebombing operations. The pilot of HT201 reported picking up a crew and completing an insertion into the fireground before returning to Tullah and remaining on standby in case an extraction was required.
First fuel cycle
At about 1215, HT204 was tasked with firebombing operations in direct support of ground crew who were undertaking hot and cold trailing.[4]
At 1226 local time the pilot departed Tullah for hotspots located west of the Murchison River on the south‑east end of the fire. The pilot was the only person on board. The pilot reported that the weather conditions on departure were calm, with a temperature of 22°C and light, variable winds.
When reaching the dip site[5] the pilot completed one fuel cycle, approximately 10 bucket loads, under relatively stable conditions. The pilot described the dip site as a narrow section of river, approximately 50–60 m wide, with tall trees lining the bank (see also Dip site). The drop zone was located approximately 1 km west of the dip site.
The pilot then returned to Tullah to pick up an air crew officer (ACO) at 1400 and continued onto the designated air base in Zeehan, which had a sports oval being used as a refuel base (Figure 1).
Figure 1: First fuel cycle and return to Tullah
White line: flight path of the first fuel cycle and return to Tullah. Purple line: flight path from Tullah to Zeehan. Source: Google Earth, annotated by the ATSB
Zeehan air base
During the approach to Zeehan, the pilot noted a significant weather change, with winds shifting to a westerly direction at approximately 30 knots.
While on the ground, the helicopter was refuelled for the next cycle. At about 1440 the pilot departed Zeehan and returned to the Canning Peak fireground.
Second fuel cycle and occurrence
The pilot recalled that various dip sites along the river looked similar. Flight data (Figure 2) indicated the pilot initially conducted a descent into an incorrect dip site. The pilot recognised this and undertook reconnaissance to find the intended dip site. Once reaching the dip site, the pilot resumed bucketing operations.
Figure 2: Second fuel cycle flight path
Source: Google Earth, annotated by the ATSB
The pilot reported that, at about 1525, while filling the third bucket load of water, the helicopter had been in a stable hover at about 150 ft above the water, when it unexpectedly sank. The pilot recalled the helicopter sinking approximately 50 ft. To recover control, the pilot applied forward cyclic and upward collective inputs to transition to forward flight and stabilise the helicopter, while aiming to avoid an over-torque event.
Prior to this manoeuvre, the pilot reported they were unable to jettison the longline, which they attributed to pressing on the button’s ring guard instead of its centre, and the longline subsequently became taut. The helicopter then came to an abrupt stop and the pilot heard a ‘loud clunking noise’. The pilot then recovered the helicopter to a stable hover approximately 30 ft above the water and initiated rearward flight to release the water and retrieve the bucket from the river. The pilot observed an engine torque split[6] and once the bucket and longline were recovered they initiated a climb to clear the surrounding trees.
The pilot reported that once they had cleared the trees, the torque split levelled back out. They conducted a range of tests to assess controllability and engine performance, including minor adjustments to engine torque. The pilot noted that the tail rotor control pedals felt stiff, however they continued to provide adequate input for sufficient helicopter control.
The pilot contacted the AAS on the fire common traffic advisory frequency (FCTAF) stating they had a bucket issue and a flight control issue.
The air attack pilot (who flew the helicopter with the AAS on board) oriented the helicopter to view HT204. The AAS recalled HT204 gaining altitude and tracking away from the Murchison River, over the fire, heading on a bearing south‑west uphill and back to Zeehan. They noted the helicopter was climbing slowly and appeared to be flying irregularly during this period. They reported they had not seen the occurrence as the dip site HT204 was using was beneath and behind the air attack helicopter.
The AAS contacted the pilot on the FCTAF. The pilot of HT204 reported issues with the helicopter pedals and when asked what their intention was, the pilot reported they were heading back to Zeehan. The AAS acknowledged this and reported they would follow HT204 back.
The pilot of HT204 assessed available landing options but elected to continue toward Zeehan rather than commit to an off-field landing. This decision was influenced by a previous experience where a potential landing site, assessed from approximately 500 ft, had appeared suitable but proved unsuitable upon reaching around 30 ft. The pilot considered that committing to a landing carried the risk of being unable to complete it safely.
The AAS and air attack pilot discussed possible landing options nearby. However, given the impaired controllability of HT204 and the smaller prepared landing areas on the fireground, they agreed the best action would be to return to Zeehan.
Return flight
The pilot of HT204 reported that, during the return flight to Zeehan, airspeed was maintained between 65 and 70 kt[7] due to the tail rotor pedals feeling stiff. This would reduce strain on the tail rotor by operating the helicopter at a lower power setting.
The pilot reported continuing the flight toward Zeehan with a plan that, should the situation deteriorate further, the flight would be changed to Strahan Airport as an alternative. Throughout the remainder of the flight, pedal inputs were minimised in an effort to avoid exacerbating the condition.
The AAS described the helicopter’s flight en route to Zeehan as appearing abnormal. In addition to the notably reduced speed, HT204 appeared to be yawing from side to side and maintained an unusually low height above ground. They reported that due to the pilot sounding stressed they did not contact the pilot further.
The AAS recalled contacting the air base manager at Strahan and the air operations manager and advised them of an unknown mechanical malfunction with HT204. They reported that the pilot was still in control, and that they were following HT204 back to Zeehan.
Landing at Zeehan
At about 1548, the pilot conducted a shallow approach to set up a vertical descent to the oval in Zeehan with the bucket and longline attached. During the landing sequence, the ACO secured the bucket and longline and moved it away and forward of the landing zone.The pilot then released the line and allowed the helicopter to sink, utilising available power, which resulted in what they stated ‘appeared to be a satisfactory landing with minimal pedal input required’.
After landing, during the shutdown procedure, the pilot was unable to roll the engine throttles back to idle. While disconnecting the longline from the hook, the ACO observed significant damage to the helicopter’s fuselage structure aft of the external hook.
The pilot of HT201 recalled that they landed and shut down their helicopter in Zeehan. They observed HT204 still running and the pilot underneath the helicopter assessing damage. They discussed the issue of not being able to roll the engines back and the pilot of HT201 suggested pulling the helicopter’s T-handles.[8] The T-handles were pulled to shut down the engines.
Context
Pilot information
The pilot held a Commercial Pilot (Helicopter) Licence, with a single engine class rating for helicopters. They held type ratings for the Bell 212, 412 and 427. The pilot’s total aeronautical experience was over 3,000 hours of which 120.6 hours were on the Bell 412. In the previous 90 days the pilot had flown 50.3 hours, all on the Bell 412.
The pilot was qualified to conduct helicopter firefighting operations and had low‑level and sling operation ratings.
The pilot last completed an aerial application proficiency check on 11 November 2024, which was valid for 12 months, and a low-level helicopter flight review on 4 December 2023.
The pilot held a valid Class 1 aviation medical certificate, valid to July 2025. The certificate specified that the pilot was to wear distance vision correction while flying, which was being worn on this occasion.
Helicopter information
General information
The Bell Helicopter Company 412EP is a medium‑lift[9] utility helicopter commonly used for firefighting, search and rescue and transport operations. The helicopter had a 4-blade main rotor and 2‑blade tail rotor and was powered by 2 Pratt & Whitney PT6T-3DF turboshaft engines. The helicopter was manufactured in Canada in 2004 and first registered in Australia in 2020. The helicopter was owned by NSW Rural Fire Service (RFS) and operated by Coulson Aviation Australia.
VH-VJF had accumulated about 4,819 flight hours total time in service and had a current certificate of airworthiness and registration. The helicopter’s technical log indicated no outstanding defects at the time of the accident.
The helicopter’s multi-role configuration enabled it to be utilised in a range of aerial firefighting tasks, including reconnaissance, winching operations and firebombing using either a belly tank or external bucket system (Figure 3).
Figure 3: NSW RFS Bell 412 EP VH-VJF
Source: Lesley de Robllard, annotated by the ATSB
On the day of the accident, the helicopter was configured for firebombing operations and was fitted with an external load system, a vertical reference door, and a 150‑ft longline attached to a Bambi bucket[10] (see Bucket and longline information). In addition to these items, the helicopter also had a forward looking infrared (FLIR) camera mounted on the left‑hand side of the helicopter above the skids.
External load system
VH-VJF was equipped with an Onboard Systems International cargo hook suspension system. The system attached to an existing Bell hard point and hung at approximately the centre of gravity. It extended through an opening in the lower fuselage, which was fitted with a protective rubber ring around the edge (Figure 4). This protective ring was used to reduce the risk of damage if the hook hit the edge of the opening.
Figure 4: Onboard Systems International cargo hook suspension system on the Bell 412
Source: Onboard Systems International, annotated by the ATSB
The release of the hook could be initiated electrically or mechanically. Normal release was completed by pilot actuation of a push button on the side of the cyclic (Figure 5, left). The button is guarded by a small ring to prevent inadvertent pilot activation. When this button is pressed the latch of the cargo hook is opened.
In addition to the electrical release, in an emergency a mechanical release can be completed by pushing a small pedal located between the 2 tail rotor pedals at the pilot’s feet (Figure 5, right). This activated a manual release cable attached to the cargo hook.
The cargo hook suspension system was required to be inspected annually or after 100 hours of external load operations, whichever came first. The system was last inspected on 20 February 2025.
Figure 5: Electrical and mechanical external load release systems
Left: the electrical release found on the cyclic grip. Right: mechanical release between the 2 pedals. Source: Coulson Aviation, annotated by the ATSB
Coulson Aviation required pilots to test the electrical and manual release system prior to conducting flights for the day. The pilot recalled testing both the electrical and mechanical release the morning of the accident. They stated that both systems were in working order. In addition to the tests, the pilot recalled that when landing at Zeehan after the accident, the electrical release was used to drop the longline and bucket without issue.
Coulson Aviation reported that both the electrical and mechanical releases of the hook were tested following the accident. Both were reported as serviceable.
Vertical reference door
The Bell 412EP helicopters are usually flown from the right-hand seat. This configuration is used when pilots are conducting either winching or reconnaissance operations. The helicopters can be modified to include a vertical reference door, which is designed to provide the pilot with a side bubble window and instruments for longline operations from the left-hand seat.
VH-VJF was modified with a vertical reference door in accordance with the Transwest vertical reference door supplement type certificate. This included a bubble window, viewing slot, and instruments and warning lights installed in the door (Figure 6).
Figure 6: Instruments and warning lights installed in the vertical reference door
Source: Coulson Aviation, annotated by the ATSB
In addition to the instruments and warning lights, the type certificate required the installation of several systems to be placed on the left side of the helicopter. This included:
a force trim switch, cargo release switch and automatic flight control system (AFCS) release switch mounted on the left cyclic
the torque meter and tachometer from the left-hand instrument panel moved to the vertical reference door
an additional mechanical cargo release pedal between the left side pedals.
During the occurrence flight and other firebombing operations, the pilot was operating the helicopter from the left-hand seat, utilising the left cyclic and referencing the flight instruments through the vertical reference door. While conducting the water collection, the torque indicator was visible through the bubble window and could be monitored during the lift.
Bucket and longline information
The bucket and longline were attached to the external load system via a bow shackle (Figure 7, left).
The bucket was a Bambi Max bucket with a nominal capacity of 240 US gallons (910 L). The empty weight of the bucket was 137 lb (62 kg) and the maximum gross weight was 2,140 lbs (970 kg).
The collapsable bucket was equipped with multiple selectable drop valves. Pilots were able to use the bucket to split water loads into multiple drops (Figure 7, right) and had the capability to shed the load rapidly.
Figure 7: Longline attachment and Bambi Max bucket
Source: Coulson Aviation, annotated by the ATSB
The longline was constructed from high-strength synthetic fibre rope selected for its high tensile strength, low stretch characteristics, light weight, and resistance to heat and abrasion. The line incorporated an electrical cable along the line to control bucket release. The 150-ft length provided vertical separation between the helicopter and the load to reduce rotor downwash disturbance during water pick‑up.
Forward looking infrared (FLIR) camera
FLIR cameras are used on aerial firefighting aircraft to provide thermal imaging of fire grounds, enabling crews to detect heat sources through smoke, darkness, or challenging terrain. This capability allows operators to identify fire hotspots, monitor fire spread, and support decision-making for resource deployment and suppression strategies.
On the Bell 412s, the FLIR camera was mounted on the left side, just above the skids. Coulson Aviation stated that although the cameras could be removed, they would generally be kept on the helicopters throughout all operations, allowing the ability for the crews to be re-tasked for reconnaissance missions. Some pilots indicated to the ATSB that the camera could partially obscure visibility during bucketing.
Helicopter damage
The ATSB did not examine the helicopter or equipment. Coulson Aviation conducted an examination of the helicopter the morning after the occurrence. The following damage was identified:
The #1 engine control tube had sheared at the lower tube end bell crank, resulting in a complete loss of pilot input to the engine.
The #2 engine control tube bell crank attachment bracket had detached from the helicopter structure’s securing rib, restricting pilot control of the engine.
The tail rotor control rod on the right-hand side of the external hook’s bell crank airframe attachment had broken away, with the primary structure also separated.
The main transmission oil cooler pressure line exhibited significant contact damage, however, no splits or leaks were identified.
The fuel tank interconnect braided hoses sustained minor contact damage.
Multiple aft fuselage drain lines were damaged.
Images of the helicopter indicated that the structural fuselage honeycomb aluminium skin, adjacent to and aft of the external hook, was deformed and had separated from the primary structure (Figure 8).
Figure 8: Helicopter aluminium skin damage
Source: Coulson Aviation, annotated by the ATSB
Images revealed indications consistent with contact between the longline and the rear cross tubes of the helicopter. In addition, inspection of the cargo hook and associated bumper stop components identified visible signs of impact damage (Figure 9).
Figure 9: External load system damage
Source: Coulson Aviation, annotated by the ATSB
In addition, the ring in the middle of the Bambi bucket spoke assembly was fractured in 4 places (Figure 10).
Figure 10: Bambi Max damage to spoke assembly
Source: Coulson Aviation, annotated by the ATSB
Multiple instances of cable bruising and stretching were reported to have been observed on the bucket cable wiring and attachment eye ends. The ATSB was unable to substantiate the presence of cable bruising and stretching based on the images provided of the cables.
Weather data
On departure from Strahan Airport, the meteorological aerodrome report (METAR)[11] reported wind west‑north-west at 6 kt, visibility greater than 10 km and no cloud cover.
The Tasmania Fire Service (TFS) incident action plan indicated that weather on the Canning Peak fire would change from north-westerly to west-south‑westerly by mid‑morning with winds reaching 10 kt by the afternoon (Table 1).
Table 1: Canning Peak fire forecast
Local time
Temperature (°C)
Dew point (°C)
Wind direction
Wind speed (kt)
Wind gust (kt)
0800
14
12
N
5
8
0900
17
13
NNW
8
10
1000
19
14
NW
8
14
1100
22
14
WNW
8
14
1200
23
14
W
10
16
1300
25
14
W
10
16
1400
26
13
WSW
10
16
1500
26
13
WSW
8
14
1600
26
13
WSW
8
10
The AAS reported that on the day of the accident the wind was calm, there was no turbulence and ‘great’ visibility. A change in wind direction was noted from mid-morning changing from northerly to south-westerly, however this was expected based on the forecast. They recalled the area in which the aircraft were working in was protected from south‑westerly winds due to the topography. They reported no feedback from pilots regarding the weather or any other environmental conditions on the day.
The pilot of HT201 reported there were blue skies and fairly light winds on the day of the accident. They recalled that although they were not bucketing on this day, during previous bucketing operations in the same valley, the wind conditions were variable and the wind would shift ‘back and forth’.
A weather station atop Mt Inglis, approximately 15 km north of the operating area (Figure 11), recorded south‑south-westerly winds at 5.7 kt gusting to 11.4 kt at the time of the accident.
Figure 11: Canning Peak weather station location to dip site
Source: Google Earth, annotated by the ATSB
Fireground information
The West Coast fire complex originated from 24 individual ignitions sparked by dry lightning strikes on 3 February 2025, across Tasmania’s remote western and north‑western regions. These separate fires were grouped into a single complex for coordinated management due to their proximity, shared weather influences, and overlapping spread patterns.
There were 4 primary firegrounds that accounted for the majority of the burnt area: the Canning Peak fireground, the Yellowband Plain fireground, the Mount Donaldson fireground, and the Corinna Road fireground. Each represented a distinct sector with unique terrain, vegetation types, and behavioural characteristics. These firegrounds collectively contributed to the complex’s total footprint of nearly 95,000 hectares.
Canning Peak fireground
The Canning Peak fireground was located in a more elevated and vegetated zone close to the Cradle Mountain area and in proximity to sections of the Overland Track. This sector featured rugged alpine-influenced terrain that complicated direct ground access, leading to heavy reliance on aerial suppression tactics.
Figure 12: Canning Peak fireground
Black outline indicates area which has been burnt by fire. Source: Tasmania Parks and Wildlife Service, annotated by the ATSB
Day of accident
On the day of the accident HT201 was the designated winching helicopter and HT204 was part of the bucketing helicopters on the fireground. There were 6 helicopters (3 x AS350, 1 x Bell 412 (HT204), 1 x Bell 212, 1 x BK 117) bucketing within a 2 km proximity of each other intermittently. In addition, the air attack helicopter was on scene overhead.
The helicopters were distributed across 4 separate circuits, with 5 separate dip points, seperate individual and shared targets and some shared ground crew.
Dip site
The pilot reported that the general location for a dip site was provided prior to commencing operations on the fireground, with selection of the specific section of river within that area being at their discretion.The pilot advised that they chose this dip site location on the river as it was relatively wider than other areas and they had used this section as a dip site on the days preceding the accident.
HT204’s dip site was approximately 700 m from the next nearest dip site with working helicopters. The dip site was approximately 1 km south‑east of the drop zone, along the Murchison River. Google Earth images indicate the river width at the dip point was approximately 20 m (Figure 13).
Figure 13: Dip site location on Murchison River
Source: Google Earth, annotated by the ATSB
The pilot described the dip site as a narrow section of river, approximately 50–60 m wide, with tall trees lining the bank. They reported that there were limited locations deep enough to operate the bucket, which constrained where they could dip and they stated they had used the same dip point on the days prior.
In addition, the river contained very little water at the time, allowing clear visibility to the riverbed. They stated that they could not recall whether any tree branches or rocks were present in the riverbed during the operation. Despite the presence of tall trees, the pilot indicated that the area was accessible to the aircraft and considered it one of the better dip sites along the river. They also noted that the turnaround time from the dip point to the fireground was approximately one minute.
The AAS described the dip site as a section of river with trees approximately 30–60 m tall on either side. They recalled that the pilot was the only one using the dip point and the only helicopter in the circuit. In previous weeks, when different crews had flown the same helicopter on similar missions, no pilots had reported any problems with the dip point. Based on the dips that were observed, the occurrence pilot appeared to be performing them safely and adequately.
Recorded data
Multiple independent data sources, including TracPlus satellite-based tracking logs, FlightAware ADS-B derived positions, and OzRunways electronic flight bag recordings, were cross‑referenced and correlated to reconstruct the helicopter’s flights throughout the day and to approximate the entry and exit angles into and out of the bucketing site.
TracPlus
The helicopter was fitted with a TracPlus surveillance system, which provided real-time tracking through a satellite or mobile phone network. It reported position, altitude, and speed at set time periods, in this case every 15 seconds.
OzRunways
The OzRunways application recorded the helicopter’s position at regular intervals of approximately 5 seconds throughout the day, capturing parameters including latitude, longitude, groundspeed, track, and truncated altitude (in 100 ft increments) where connectivity permitted. However, no position data was recorded during the bucketing operations (Figure 14). This absence of recorded data was likely attributable to the helicopter operating at very low levels, down to around 150 ft above ground level, while conducting repeated drops in mountainous terrain.
Figure 14: OzRunways flight data
Source: Google Earth, annotated by the ATSB
FlightAware
The FlightAware flight tracking data captured the helicopter’s en route flight to the bucketing site, as well as the subsequent low-level manoeuvres involving repeated water dips and drops. Position reports were recorded at irregular intervals ranging between approximately 8 seconds and 40 seconds[12] during these operations.
In addition to the TracPlus data, FlightAware was incorporated into the data analysis. The differing sampling rates and coverage characteristics of the 2 systems together produced a more complete reconstruction of the helicopter’s flight circuit during the second fuel cycle (Figure 15).
Figure 15: Second fuel cycle data from TracPlus and FlightAware
Pink line: TracPlus data. Blue line: FlightAware data. Source: Google Earth, annotated by the ATSB
Further investigation
To date, the ATSB has conducted the following activities:
interviewed the pilot and other Coulson Aviation personnel
interviewed the air attack supervisor from Tasmania Parks and Wildlife Service
reviewed recorded aircraft information
reviewed the forecast and observed weather conditions
reviewed maintenance documentation for VH-VJF
analysed recorded helicopter information
reviewed pilot training delivered by Coulson Aviation.
The investigation is continuing and includes:
review of Coulson Aviation’s risk controls for bucketing operations in the Bell 412
review of Coulson Aviation’s operational and reporting procedures
review of Tasmanian Fire Service operational and reporting procedures.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Firebombing: The National Aerial Firefighting Centre states that firebombing is the dropping of fire suppressant or fire retardant from an aircraft to assist with the control or suppression of a fire.
[2]Firebombing with a bucket, often known as ‘bucketing’, requires filling the bucket by lowering it into a water source, and emptying it as required at the flame front.
[3]A staging area is a designated location where aircraft and crews temporarily assemble and wait for tasking to active fires.
[4]Hot and cold trailing is a task requiring identification of hotspots along the fire perimeter, opening these areas/smouldering ground fire up with hand tools and directing pilots to drop buckets atop the burning material to prevent further fire spread.
[5]A dip site is a designated water source where helicopters equipped with buckets can collect water for aerial firefighting. These sites can be natural bodies of water, such as lakes, rivers, or ponds, or artificial sources like reservoirs and water tanks. Their key requirements are sufficient water depth, accessibility, and proximity to the fire to maximise efficiency.
[6]Engine torque split in a multi-engine helicopter is where there is an unequal proportion of total main rotor torque shared between each engine through the gearbox.
[8]The T-handles are a red handle which pilots pull in an emergency to shut off fuel, hydraulics, and other systems to an engine while arming the fire extinguishing bottles.
[9]A medium-lift helicopter is one capable of carrying moderate loads, typically between 2,000 kg and 5,000 kg.
[10]A Bambi bucket is a collapsible water bucket suspended beneath a helicopter, used to collect and drop water during aerial firefighting operations.
[11]METAR (Meteorological Aerodrome Report) is a routine aerodrome weather report issued at half‑hourly intervals. The report ordinarily covers an area of 8 km radius from the aerodrome reference point.
[12] This update rate arises from the way FlightAware processes ADS-B data: although equipped aircraft transmit position messages nominally every second, the displayed track depends on signals received by a network of ground stations. In remote hilly terrain, at low altitudes down to around 150 ft AGL, terrain shadowing, ridges, valleys, and line-of-sight limitations can prevent some transmissions from being captured reliably. As a result, FlightAware relies on the most consistent available reports, leading to longer effective intervals of 25–40 seconds or more during intermittent low-level reception.
Occurrence summary
Investigation number
AO-2025-013
Occurrence date
10/03/2025
Location
57 km north-east of Strahan Aerodrome
State
Tasmania
Report release date
17/03/2026
Report status
Interim
Anticipated completion
Q3 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Control issues, Loss of control, Miscellaneous - Other
On the morning of 25 February 2025, an Agusta A109E helicopter was conducting a marine pilot transfer operation on the inbound bulk carrier Star Coral at Blossom Bank pilot boarding ground, about 200 km north‑east of Mackay, Queensland.
At 0901 local time, during take‑off from the ship with 2 pilots on board, the helicopter developed severe vibrations. The pilots discontinued the take-off but their attempts to recover control of the helicopter were unsuccessful. The helicopter came to rest in an upright position on the helideck, having spun more than 90° counterclockwise from its initial heading, and sustaining substantial damage. The pilots and ship’s crew were unharmed.
What the ATSB found
The investigation did not identify any airworthiness issues with the helicopter and it was considered that the loss of control was not attributable to a mechanical issue.
The ATSB found that the vibration was likely the result of the helicopter entering ground resonance, a phenomenon that dissipates when airborne, while it was in the process of departing from the ship. The discontinuation of the take‑off, after the onset of the vibration, probably resulted in the loss of control and subsequent damage to the helicopter.
What has been done as a result
The operator has added new guidelines on ground resonance to its procedures. The guidelines include procedures for recognising and recovering from ground resonance and feature case studies and video resources for training purposes.
The operator has also developed an updated procedure for training and checking flight briefings that will include confirming the roles of each pilot, procedures for transferring aircraft control between pilots, and actions to be followed in the event of an actual emergency.
Safety message
The occurrence highlights the dangers of ground resonance, a potentially catastrophic phenomenon that can occur in helicopters with fully articulated rotor systems. Typically, the onset of ground resonance is sudden and if the pilot does not take immediate corrective action, a loss of control can rapidly occur.
The occurrence also highlights the importance of proper coordination between a helicopter’s pilots when responding to abnormal or emergency situations. This is particularly pertinent for situations where the pilot flying is not the pilot in command. Ideally, the pilots’ individual roles and responsibilities for emergency response and flying duties should be well established prior to the flight.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 0730 local time on 25 February 2025, the 229 m bulk carrier Star Coral arrived at the Blossom Bank pilot boarding ground, about 200 km north‑east of Mackay, Queensland (Figure 1). The ship waited to embark a coastal marine pilot by helicopter for its inbound transit of the Great Barrier Reef via Hydrographers Passage.[1] It was in ballast and bound for Hay Point to load coal.
Figure 1: Blossom Bank pilot boarding ground and Hydrographers Passage
Source: Australian Hydrographic Office, annotated by the ATSB
Meanwhile, at Mackay Airport, a twin‑engine Agusta A109E helicopter, operated by Flyon Helicopters and registered VH‑XUM (XUM), with 2 pilots on board, embarked the marine pilot scheduled to conduct the ship’s pilotage. The marine pilot transfer (MPT) flight to Star Coral was the first scheduled for the helicopter and its pilots that day. These flights were normally conducted as a single‑pilot operation. However, on this occasion, the pilot flying, a pilot recently engaged by the operator under its ‘in‑command‑under supervision’ (ICUS)[2] program, was under the supervision of a company check pilot (pilot supervising).
The pilots’ plan was to transfer Star Coral’s marine pilot and then proceed to a nearby outbound ship to collect its marine pilot for return to Mackay.
At 0759, the helicopter departed Mackay Airport under the control of the pilot flying. En route, the pilots established communication with Star Coral’s master via VHF[3] radio. The master advised that the ship was rolling about 3° on its inbound heading due to a 2 m south‑easterly swell. Subsequently, the pilots requested the master to reposition the ship on a heading[4] of 270° to reduce rolling. At 0853, the pilot flying landed the helicopter on the ship’s helideck, situated on the number 5 cargo hold hatch cover (Figure 2). The marine pilot exited the helicopter and proceeded to the ship’s bridge.
Figure 2: Landing position of VH-XUM aboard Star Coral
This figure is a representation of the helicopter’s orientation relative to the wind during the take‑off. Source: Flyon Helicopters and Star Coral, annotated by the ATSB
Meanwhile, the helicopter remained on the helideck at flight idle[5] while its pilots radioed the outbound ship’s pilot to coordinate the transfer. After some discussion, the pilots elected to keep the helicopter on the deck of Star Coral until the outbound ship had departed the compulsory pilotage area.
After about 5 minutes, as the 2 ships were about to pass each other, the helicopter pilots began conducting their pre‑take‑off checks. The pilots observed a 20 to 28 knot headwind (relative to the helicopter) and noted that the ship was rolling less than 2°. The pilot flying conducted a brief for a performance category 1[6] take‑off, which involved establishing the helicopter in a hover 35 ft above deck height before departing. Both pilots later recalled that everything seemed normal as the take‑off checks were completed.
At about 0900, the pilot flying raised the collective[7] and observed the engine torques increasing through 50%. The pilot flying recalled the aircraft became light on its oleos as though it was ‘right at the point of lifting off’. Meanwhile, the pilot supervising was observing the outbound ship passing. A few seconds later, both pilots felt a sudden and substantial vibration.
The pilot supervising immediately looked down at the controls and recalled that the pilot flying was holding the cyclic[8] in an abnormally aft position. Concerned that the main rotor might have struck the tail boom, the pilot supervising decided to assume control of the helicopter and took hold of the cyclic and collective unannounced. Meanwhile, the pilot flying was still attempting to lift off, unaware of the pilot supervising’s decision to take control. The pilot supervising recalled that the pilot flying had centred the cyclic and ‘must have’ lowered the collective by the time the pilot supervising took hold of the controls. In contrast, the pilot flying stated that the pilot supervising rapidly lowered the collective after the vibration started, causing the aircraft to descend from being light on its oleos and bounce heavily on the helideck.
Moments later, the cyclic became uncontrollable as the vibrations suddenly worsened into a violent, vertical oscillation of the airframe. The pilot supervising tried to stabilise the helicopter but was unable to control the cyclic movement. Subsequently, the pilot supervising elected to shut down the engines.
The pilot supervising initially struggled to reach the engine mode switches (located on the centre console) due to the severe vibrations but subsequently managed to shut down engine number 2. The vibrations slightly eased and moments later, they were able to also shut down engine number 1. The vibration dissipated and the helicopter came to rest in an upright position on the helideck, having spun more than 90° counterclockwise from its initial heading. The sequence, from the attempted take‑off to shut‑down occurred within a period of about one minute.
Soon after, the pilots exited the wreckage and inspected the damage. The tail rotor was separated from the helicopter and had come to rest on the main deck between cargo hatches 4 and 5. Items of debris, including main rotor fragments, laid scattered on the deck along with some hydraulic fluid pooled beneath the substantially damaged fuselage (Figure 3).
Figure 3: Helicopter wreckage
Source: Star Coral
Apart from a thumb sprain to the pilot supervising and some bruising to both pilots’ upper leg areas, where they had been struck by the cyclic, neither were significantly injured and no‑one on board Star Coral was injured.
Context
Helicopter information
The helicopter was an Agusta A109 E variant, manufactured in 2006 and issued serial number 11684. It was registered in Australia in 2006 and began services under the operator’s Air Operator’s Certificate (AOC) in 2023.
The Agusta A109E is a multipurpose helicopter equipped with 2 Pratt & Whitney PW206‑C turbine engines. It has a fully articulated 4‑blade main rotor system, a 2‑blade tail rotor and retractable tricycle landing gear. Able to carry up to 7 occupants, it has a maximum allowable take‑off weight of 2,850 kg.
The helicopter was able to perform flight performance class 1 operations by adherence to Category A procedures[9]. While the helicopter was normally operated from the right crew seat, it was fitted with dual controls. A left seat‑approved pilot in command (PIC) was permitted to occupy either seat during training flights. Each set of controls could not be operated independent of the other.
The helicopter’s wreckage was recovered from the ship 2 days after the incident and transported to a secure hangar at Mackay Airport. Prior to its removal, photographs of the wreckage and the accident area were taken. There were no indications that the main rotor or tail rotor had struck any part of the ship during the accident.
Based on its inspections, the operator advised that no engine faults or exceedance alarms had been recorded by the helicopter’s electronic engine management systems. Additionally, no faults or defects had been reported by any of XUM’s pilots or maintainers leading up to the occurrence flight.
Post-accident activities
There was no recorded flight data available to determine the flight control inputs and their effect on the motion of the helicopter during the occurrence.[10] The pilots’ accounts, a witness statement from the master of Star Coral and photographs of the wreckage were the main sources of evidence.
The ATSB also sought the manufacturer’s input for this occurrence. The manufacturer advised that its preliminary assessment of the available evidence suggested that the helicopter damage appeared consistent with a ground resonance phenomenon (see the section titled Ground resonance).
The licenced maintenance organisation for XUM carried out an examination of the wreckage at the Mackay hangar. On advice from the manufacturer, the examination included inspection of specific components commonly associated with ground resonance. These included main rotor dampers, landing gear struts and tyres. The operator advised the ATSB that the inspection did not identify any airworthiness issues that may have contributed to the occurrence. The operator did not provide the inspection report or findings to the manufacturer for its assessment.
Pilot flying
The pilot flying obtained a New Zealand commercial helicopter licence (CPL) in 2011 and started flying commercially in 2014. They converted their CPL over to an Australian CPL in 2016 and held a grade 2 flight instructor rating and a class 1 aviation medical certificate. They had experience flying both single and twin-engine helicopters in various operations. Prior to joining the operator’s in‑command‑under‑supervision (ICUS) program in September 2024, they had no previous experience on the A109E, or with marine pilot transfers (MPT).
Under the ICUS program, the pilot was required to accrue 200 hours on the A109E before they could be assessed to fly the helicopter unsupervised on daytime VFR[11] MPT operations. At the time of the occurrence, the pilot had completed the operator’s training requirements and accrued around 50 hours flight time on the A109E. They had also been cleared to conduct unsupervised MPT operations on single‑engine Eurocopter AS350 helicopters.
Pilot supervising
The pilot supervising was the operator’s head of flying operations and held an air transport pilot (helicopter) licence, issued in 2014, and a class 1 aviation medical certificate. They were approved under the operator’s training and checking system to conduct check and supervision flights on the A109E.
The pilot supervising had been flying helicopters for 26 years in various operations and had accumulated over 10,000 hours flying time, including 3,800 hours in the A109E. They first started MPT operations in 2007 and commenced working with the operator in December 2016.
Star Coral
Star Coral was built in 2009 by Jansu Newyangzi Shipbuilding, China, registered in The Bahamas and classed with Bureau Veritas. The ship was owned by Panormos Shipping, The Bahamas, and managed and operated by Charterwell Maritime, Greece.
At the time of the occurrence, the 229 m ship had a mean draught of 6.51 m and the helideck height was about 18 m above the waterline.
In a written witness statement, the master reported that:
• shortly after the helicopter started to take off, it began to pound on the helideck before it spun and the tail rotor separated
• during the sequence, the helicopter became airborne for no more than 2 seconds.
Ground resonance
Ground resonance can be defined as a vibration of large amplitude resulting from a forced or self‑induced vibration of a helicopter in contact with the ground.[12] The phenomenon is normally associated with helicopters equipped with fully articulated main rotor systems consisting of 3 or more rotor blades. It is more common on helicopters with sprung landing gear than those with skids. Typically, ground resonance occurs during landing, take‑off and ground manoeuvres.[13]
In fully articulated rotor systems, drag hinges allow each blade to advance or lag in the plane of rotation to compensate for the stresses caused by the acceleration and deceleration of the rotor hub. Such rotor systems are typically fitted with lead‑lag dampers to limit the extent of this movement and help prevent excessive vibrations. However, if for any reason one or more of the blades assumes a dragged position different to the others, the blades will move out of phase and the rotor will become imbalanced, transmitting an oscillation throughout the entire airframe.[14]
The risk of ground resonance arises when the unbalanced forces in the rotor system cause the fuselage to oscillate on its landing gear at or near its natural frequency. Ground resonance will occur if the helicopter’s damping systems are unable to compensate for the oscillation.[15] Unless corrective action is taken, the amplitude of the oscillation will increase until the helicopter becomes uncontrollable.[16] Ground resonance can also be induced when the helicopter is in light contact with the ground, if the landing gear oscillation frequency is in sympathy with the rotor head vibration.[17]
Ground resonance is commonly precipitated by the helicopter making hard or asymmetric contact with the ground, landing on a slope or sudden control movements by the pilot.[18] It can also result from other factors such as improper blade balancing and tracking, or damage to any of the blades.[19] Hard contact with the ground by some part of the landing gear when the main rotor is in an unbalanced state can further aggravate the condition.[20]
Additionally, improper maintenance of the helicopter’s main rotor and fuselage damping systems, or incorrect tyre pressures, can induce or worsen ground resonance.[21]
Flight control inputs that may induce ground resonance typically involve sudden control movements or a mishandling of the cyclic that causes the fuselage to bounce.[22]
The helicopter manufacturer advised that the application of certain cyclic commands, such as extreme aft cyclic input, could theoretically reduce the main rotor damper effectiveness in respect to the damping action on the blades’ regressive lead‑lag dynamic.
Recovery technique
The onset of ground resonance can be recognised by a rocking motion or oscillation of the fuselage while on the ground.[23] The United States Federal Aviation Administration (FAA) Helicopter Handbook[24] documented 2 widely accepted recovery techniques:
• if the condition arises when there is insufficient rotor speed for take‑off, the only option is to lower the collective to reduce the pitch of the blades. The rotor rpm[25] should also be reduced as soon as possible.[26]
• If the rotor speed is in the normal operating range for flight, the Helicopter Handbook recommends lifting the helicopter off the ground to allow the rotor blades to rephase themselves automatically.
Additionally, the FAA cautioned that:
If a pilot lifts off and allows the helicopter to firmly re‑contact the surface before the blades are realigned, a second shock could move the blades again and aggravate the already unbalanced condition. This could lead to a violent, uncontrollable oscillation.
In practice, a pilot experiencing ground resonance typically has seconds to identify the condition and take corrective action.
Similar occurrences
The ATSB reviewed several investigation reports relating to previous A109E accidents attributed to ground resonance. The incidents reviewed occurred outside of Australia between 2006 and 2025 and the contributing factors were found to be operational. Technical factors which may have caused or exacerbated ground resonance were not identified.
Details of the previous incidents bear similarity to the occurrence involving XUM, particularly in respect to subsequent damage to the helicopter (Figure 4).
Figure 4: Previous occurrences of ground resonance involving the Agusta A109E
Source: Leonardo Helicopters
Flight manual procedures
The A109E rotorcraft flight manual (RFM) listed fault conditions and corrective actions for emergencies and malfunctions that might occur during take‑off.
The RFM included the caution below for ground resonance within the normal flight procedure for take‑off. This was not part of the emergency and malfunction procedures.
The RFM procedure for ground resonance was consistent with recovery techniques published by the FAA. The RFM reference to the helicopter being ‘free of ground resonance’ was intended to indicate that, like all helicopters, the A109E was designed and certified to applicable standards so that the rotor and fuselage systems do not vibrate at the same frequency under normal conditions.
Operator procedures
As an AOC holder, the operator maintained a CASA‑approved[27] operations manual/exposition[28] to promulgate general policy and standardised procedures for MPTs on the A109E. The version of the operations manual current at the time of the occurrence was issued by the operator in November 2023.
Ground resonance
The operator’s normal procedures and emergency checklists for the A109E were derived from the RFM and did not contain any procedures related to ground resonance.
Crew coordination in response to abnormal situations
While MPT flights were predominantly conducted by a single pilot, the helicopter was certified for operations with either a single pilot or 2 pilots. In either case, the normal procedure and emergency checklists remained the same, except that 2‑pilot checklist procedures were to be based on challenge and response.
Normal handover and takeover procedures provided that:
In the case where the pilot flying (PF) is not the PIC and the PIC determines that the PF is not maintaining adequate control of the aircraft, the PIC may elect to take control, in which case they will signal their intention by saying ‘I have control’ upon which the PF will immediately relinquish control and the roles will reverse.
In abnormal or emergency situations, the PIC was responsible for ensuring the aircraft was flown and kept under control. The operations manual emphasised the importance of cockpit resource management (CRM) standards throughout the situation, in accordance with the below procedure:
Note: In the above procedures PM stands for ‘pilot monitoring’, NR refers to main rotor speed and IAS means indicated airspeed.
In the context of rapidly escalating emergencies such as ground resonance, pilots have limited time to perform the procedure.
Pilot in command responsibility during training flights
As the holder of a certificate that authorised air transport and aerial work operations, the operator was required to have in place a training and checking system (TACS). A training and checking manual (TACM) sets out policies and procedures for conducting training flights. It provided that a check pilot supervising ICUS training was to be the PIC. Check pilots were to ensure that pilots involved in training exercises were made aware of who was acting as the PIC through proper handover of control procedures.
While an ICUS pilot might be considered the PIC for flight‑time logging purposes, the pilot supervising was deemed the PIC and responsible for the safety of the flight. The TACM stated that in the event of an actual emergency during flight training:
If the flight examiner or check pilot deems it necessary to take physical control of the aircraft at any stage after the occurrence of the emergency, then they shall do so in accordance with the hand‑over and take‑over procedures specified in the Operations Manual - Hand over and take‑over procedures.
The flight examiner or check pilot must be prepared and ready to assume physical control of the aircraft at any stage, particularly during critical manoeuvres such as during take‑off and landing.
As such, beyond the normal handover of control procedures, there were no special provisions in the TACM for the allocation of PIC responsibility and PF duties during ICUS flights.
Briefings
For 2‑pilot operations or training flights, the operator’s procedures did not require pilots to brief who would assume PF duties in the event of an abnormal or emergency situation during critical phases of flight.
Operational limits
Under the operator’s operations manual, the A109E was permitted to conduct daytime MPT operations up to a wind strength of 30 knots, with a maximum crosswind of 20 knots. The operational limit for ship’s pitch was 4° up and 2° down while the maximum permissible roll was 4°. The manufacturer did not have input into these operator‑defined limits.
The pilots reported that the conditions at the time of the occurrence (20–28 knot headwind, 2° roll and minimal pitching) were within the operator’s limits for MPTs.
Safety analysis
Prior to the accident, VH‑XUM (XUM) made an uneventful landing on Star Coral and remained on the deck for several minutes without incident. There was no evidence that the helicopter was operating abnormally or experienced any instability during this period.
Examination of the accident site did not reveal any evidence to suggest that the occurrence resulted from the main rotor or tail rotor striking the ship. Star Coral’s master reported that the tail rotor separated after the helicopter started contacting on the deck, indicating that contact with the tail boom by the main rotor was a consequential rather than causative factor.
In that context, it is most likely that the helicopter encountered ground resonance. Assessment of the damage to the helicopter following the occurrence revealed significant similarities to that seen in previous A109E incidents attributed to this phenomenon.
It is well established that ground resonance only arises when the helicopter is in contact with the ground. Both pilots asserted that the helicopter did not become airborne prior to the vibrations while the master reported that it became airborne for about 2 seconds. However, it is more likely this occurred after the vibration worsened and the helicopter started rebounding on the helideck.
The exact cause of the vibration could not be determined. The possibility of causative operational factors such as flight control inputs or environmental factors could not be ruled in or out.
Similarly, while the operator’s post‑accident inspection of the helicopter (including examination of its rotor and fuselage damping systems) did not reveal any apparent defects, causative technical factors could not be discounted.
However, the sudden lowering of the collective after the onset of the vibration likely aggravated the situation. The helicopter was almost certainly light on its oleos when the vibration began. Therefore, a sudden lowering of the collective would have caused the helicopter to come down firmly on the helideck. The United States Federal Aviation Administration (FAA) Helicopter Handbook describes that such an impact when the rotor is already in an unbalanced state can cause the rotor blades to move further out of phase, resulting in violent uncontrollable oscillations. This description is consistent with the occurrence sequence described by the pilots and the master.
The pilots’ accounts of who lowered the collective differed. The recollection of the pilot flying that their intention was to lift the helicopter off the deck in response to the vibration was not consistent with a lowering of the collective. In contrast, the pilot supervising did not immediately identify the source of the vibration and later shut down the engines, believing the main rotor may have struck the tail boom. In this context, lowering of the collective would be a natural and expected response. Therefore, it is most likely that the pilot supervising lowered the collective while the pilot flying was attempting to lift the helicopter off the helideck.
In isolation, the immediate responses taken by each pilot following the sudden onset of the significant vibration were understandable. However, since the helicopter’s rotor speed was in the normal operating flight range, continuation of the take‑off would probably have resulted in the vibration dissipating (as detailed in the FAA Helicopter Handbook).
The operator had adequate procedures for responding to abnormal and emergency situations. However, the rapidly escalating nature of this occurrence meant that there was virtually no time to implement them. There was no requirement for the pilots to conduct a pre‑flight or pre‑take‑off brief about who would assume flying duties in the event of an emergency on take‑off. Therefore, the normal procedures for handover and takeover of control were assumed to apply.
However, the time between observing the vibrations and the loss of control severely limited the time available for a formal transfer of control between the pilots. As a result, neither of these procedures were followed and each pilot responded to the situation separately.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control during marine pilot transfer operations, involving an Agusta A109E, VH‑XUM and bulk carrier Star Coral, about 200 km north‑east of Mackay, Queensland, on 25 February 2025.
Contributing factors
During take‑off, the helicopter likely experienced ground resonance, resulting in the rapid onset of significant vertical oscillations through the airframe.
Discontinuing the take‑off after the onset of the vibration, with the rotor speed in the flight range, probably resulted in the loss of control and substantial damage to the helicopter.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Flyon Helicopters
Following this occurrence, the helicopter’s operator, Flyon Helicopters, established ground resonance guidelines for its pilots. Forming part of its exposition, the guidelines were purposed to raise awareness of ground resonance and provide information about how to recognise and respond to the phenomenon. They included response procedures and featured case studies and video resources. The procedures were to be implemented into the operator’s training framework for new and current pilots.
Flyon Helicopters advised the ATSB that it also planned to implement an additional briefing procedure in its training and checking manual (TACM). The briefing is to be conducted by the training or checking pilot prior to any training or checking flight. It will include:
the objectives and scope of the flight, including the intended lesson plan or sequence
the training/checking outcomes
the roles of each pilot, including the allocation of aircraft command responsibility
procedures for transferring aircraft control between pilots
actions to be followed in the event of an actual emergency
procedures to be used in the simulation of emergencies
procedures for the conduct of unusual operations
the method to be used to simulate instrument flight conditions, if required
human factors/non‑technical stills and threat and error management.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilots and operator of VH-XUM
the master and manager of Star Coral
the helicopter manufacturer, Leonardo Helicopters
References
Lemmens Y, Troncone E, Dutré S, Olbrechts T. (2012). Identification of Helicopter Ground Resonance with Multi-body Simulation, 28th International Congress of the Aeronautical Sciences
United Kingdom Ministry of Defence, AP3456 Central Flying School Manual of Flying Vol 12 - Helicopters
Salini S N, Haradev G S, Ranjith M. (2020). Ground Resonance: Nonlinear Modelling and Analysis, 6th Conference on Advances in Control and Optimization of Dynamical Systems (ACODS), India
United States Federal Aviation Administration. (2019). Helicopter Flying Handbook
Schafer J. (1980). Helicopter Maintenance
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilots and operator of VH-XUM
the master and manager of Star Coral
the ship’s flag State administration, The Bahamas
the helicopter manufacturer, Leonardo Helicopters
Agenzia Nazionale per la Sicurezza del Volo (ANSV)
Civil Aviation Safety Authority
Australian Maritime Safety Authority
Submissions were received from:
the pilots of VH-XUM
the ship’s flag State administration, The Bahamas
the helicopter manufacturer, Leonardo Helicopters
Agenzia Nazionale per la Sicurezza del Volo (ANSV)
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Hydrographers Passage provides a deep-water shipping route through the Great Barrier Reef between Blossom Bank pilot boarding ground, near the entrance to the passage, and the Cumberland Islands, north-east of Mackay. Pilotage is compulsory through Hydrographers Passage for ships over 70 m, as well as for loaded oil and chemical tankers and gas carriers, irrespective of size.
[2]In-command-under-supervision (ICUS) generally refers to a pilot who is acting as the pilot in command (PIC) for a flight under the supervision of a more experienced pilot.
[4]All ship’s headings are reported in degrees true.
[5]Flight idle refers to the lowest engine power setting that allows the aircraft to maintain stable operations during flight. A flight idle setting when the helicopter is on the ground allows for the engine(s) to go to higher power settings faster and facilitate take-off when collective pitch is raised.
[6]Performance Class 1 (PC1) refers to operations for which, in the event of a critical engine failure, performance is available to enable the helicopter to safely continue the flight to an appropriate landing area.
[7]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical speed.
[8]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[9]Category A (CAT A) operations were those where, in the event of an engine failure, the helicopter has adequate performance to safely continue or reject the take-off or landing.
[10]The aircraft type involved was not required under regulations to carry a cockpit voice recorder (CVR) or flight data recorder (FDR).
[12]United Kingdom Ministry of Defence, AP3456 Central Flying School Manual of Flying Vol 12 – Helicopters.
[13]Lemmens Y, Troncone E, Dutré S, Olbrechts T. (2012). Identification of Helicopter Ground Resonance with Multi-body Simulation, 28th International Congress of the Aeronautical Sciences.
[14]United Kingdom Ministry of Defence, AP3456 Central Flying School Manual of Flying Vol 12 – Helicopters.
[15]Salini S N, Haradev G S, Ranjith M. (2020). Ground Resonance: Nonlinear Modelling and Analysis, 6th Conference on Advances in Control and Optimization of Dynamical Systems (ACODS), India.
[16]United States Federal Aviation Administration. (2019). Helicopter Flying Handbook.
[17]United Kingdom Ministry of Defence, AP3456 Central Flying School Manual of Flying Vol 12 – Helicopters.
[28]‘Exposition’ is a term used in some regulatory domains for a document or set of documents that describe how an organisation will comply with all applicable legislative requirements, and how they will manage the safety of their operations. An exposition is broadly equivalent to an operations manual in other domains.
The ATSB is investigating a misaligned take-off involving a Bombardier Inc DHC-8-315, registered VH-TQM, at Mildura Airport, Victoria, on 25 February 2025.
Just prior to first light, the aircraft was inadvertently lined up with the edge lights for runway 09 rather than the runway centreline. During the take-off roll the aircraft struck and damaged multiple runway edge lights. Once the flight crew identified their incorrect position, they realigned the aircraft with the centreline and continued the take-off. On arrival in Melbourne, it was identified that the aircraft had sustained minor damage.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2025-008
Occurrence date
25/02/2025
Location
Mildura Airport
State
Victoria
Report status
Pending
Anticipated completion
Q1 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: External review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Runway excursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Bombardier Inc
Model
DHC-8-315
Registration
VH-TQM
Serial number
604
Aircraft operator
Eastern Australia Airlines Pty. Limited
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 7 January 2025 a Cessna 208 Caravan Amphibian (floatplane), registered VH-WTY and operated by Swan River Seaplanes, was being utilised for non-scheduled passenger air transport flights to and from South Perth and Rottnest Island, Western Australia.
At about 0840, the pilot and 10 passengers prepared for the flight to Rottnest Island. Prior to boarding at South Perth, passengers watched a safety briefing video and were fitted with life jackets. At 0915 the aircraft departed, before climbing to a cruising altitude of about 1,600 ft. The aircraft orbited to the north of Rottnest Island, then landed in a south-south-west direction on the waters of Thomson Bay at 0926 (Figure 1). Passengers recalled that the flight was uneventful. The passengers alighted the aircraft onto a pontoon and were then conveyed to the island onboard a tender vessel. The aircraft remained at Thomson Bay throughout the day, with the pilot remaining on the island.
Figure 1: Map showing Rottnest Island and key locations in Thomson Bay (inset)
Source: Google Earth, annotated by the ATSB
At 1116, the chief pilot of Swan River Seaplanes sent the pilot a text message stating that winds were forecast to increase that afternoon, and included an image from a weather website, showing that winds at Rottnest Island were 25 kt with gusts to 34 kt.
The pilot responded that they may need to return to South Perth earlier than the planned 1600 departure time. The chief pilot indicated they agreed with this, stating that if necessary the passengers could return via ferry. The pilot responded to this text with a thumbs up.
CCTV recordings showed that at about 1305, the tender vessel used by Swan River Seaplanes to ferry passengers to and from the pontoon in Thomson Bay departed from alongside the aircraft. The video appeared to show the pilot travel north on the vessel from the pontoon. The vessel was then returned to shore where it was docked at a jetty on Rottnest Island at about 1320.
At about 1330, the pilot sent a text message to the chief pilot of Swan River Seaplanes, stating that the wind had reduced but the swell remained high at the normal departure location. The pilot stated they planned to depart taking a quartering crosswind closer to shore, where they perceived conditions were calmer. The chief pilot responded to this message stating they trusted the pilot’s judgement, encouraging the pilot to resist any perceived pressure to depart. Following this exchange, there was no further discussion around rescheduling the departure time.
At about 1500 the pilot requested the coxswain take them out in the tender vessel to the area normally used for floatplane departures from Thomson Bay to inspect the sea conditions. The coxswain recalled perceiving that conditions were rough, with swell about knee to waist high, and wind of at least 30 kt. The coxswain recalled that the pilot determined the conditions to be unsuitable for the planned departure, and requested to be taken closer to the southern shore of Thomson Bay. The coxswain recalled that conditions were calmer in this location, and the pilot had planned to depart on an easterly track towards Phillip Rock.
At 1511, one of the directors of Swan River Seaplanes texted the pilot and asked about the wind conditions. The pilot responded that conditions were ‘ok but rough’, however the swell was ‘not too bad’ closer to shore. The pilot also noted in that text message conversation that the aircraft would be ‘pretty light’ for the departure.
At about 1540, the passengers for the flight from Rottnest Island to South Perth were conveyed via the transfer vessel to the pontoon where the aircraft was moored. There were 6 passengers for the return flight, all of whom had travelled to Rottnest on the flight earlier that morning. Passengers described conditions onboard the vessel and pontoon as rough and windy. Each passenger was fitted with a life jacket before boarding the aircraft.
Once all passengers were boarded, the pilot signalled to the coxswain to release the mooring lines securing the aircraft to the pontoon. The aircraft then drifted before the pilot started the engine and taxied the aircraft to the south then north-west, before lining up for an easterly take‑off (Figure 2). At 1558, while taxiing the aircraft, the pilot was recorded making a broadcast on the Rottnest Island Common Traffic Advisory Frequency, announcing an intention to depart from Thomson Bay to the south-east.
Figure 2: VH-WTY take-off track with approximate location of key events
Source: Google Earth, annotated by the ATSB
Flight data showed at 1600:20 engine power was applied for the take-off. Over the following 32 seconds, the aircraft travelled along the surface of the water in an easterly direction. Witness video and the fight data showed that at 1600:52,[1] as the aircraft approached the western tip of Phillip Rock it became airborne with a high nose attitude. At 1600:58, the aircraft rolled rapidly to the left with the left wingtip and then fuselage impacting the water. Further description of the aircraft behaviour during the take-off sequence is described in Recorded information.
Survivors and other witnesses recalled the aircraft remained partially afloat in a perpendicular orientation, with the aircraft nose resting on the sea floor. The survivors reported that all cabin doors were submerged. The rear windows were not submerged. Four passengers moved into a pocket of air in the rear cabin and one of the passengers opened the top section of the rear right door. They and another passenger exited through this door. The coxswain of the tender vessel broke the rear left aircraft window, and 2 passengers recalled escaping through this broken window.
The pilot and the 2 other passengers remained in the aircraft, which later sank. Western Australia Police Force (WA Police) divers recovered the 3 deceased occupants in the evening of 7 January 2025.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane), with a current single-engine class rating and endorsements including for floatplane operations. The pilot had a current Class 1 medical certificate, with no restrictions.
The pilot had a total aeronautical experience of over 1,900 hours, including almost 1,400 hours on floatplanes and over 2,600 water landings. The pilot had about 700 hours experience in the Cessna 208 Caravan Amphibian, including over 60 hours accrued since commencing with Swan River Seaplanes in October 2024. Since commencing with the operator, the pilot had conducted 102 water landings, 12 of which were at Thomson Bay.
Aircraft information
VH-WTY (Figure 3) was a Cessna 208 Caravan Amphibian[2] floatplane, powered by a single Pratt & Whitney Canada (P&WC) PT6A-114A turboprop engine and a 3-bladed McCauley constant speed propeller. The aircraft was fitted with Wipline Model 8750 amphibious floats which enabled operation from both land and water. It was configured in a 13-seat interior layout. The aircraft was manufactured in the United States in June 2016, then registered in Australia in September 2016. It had accumulated about 1,125 hours total time in service at the time of the accident. Further aircraft information is detailed in VH-WTY maintenance history below.
The aircraft had 2 crew entry doors at the front of the cabin, next to the pilot (left) and copilot (right) seats. The crew entry doors had interior and external handles, which could be set to OPEN, CLOSE and LATCHED positions. The doors were also equipped with separate locks, and with lock override knobs inside the aircraft. To close the door, aircraft operating procedures instructed pilots to place the handle in the CLOSE position and pull the door closed, before rotating the handle to the LATCHED position. When unlocked and in the LATCHED position, the crew entry doors could be opened from either inside or outside the aircraft by rotating the handle to the OPEN position.
There were also 2 doors towards the rear of the cabin, each with a horizontal clamshell opening. Each rear door included separate handles for the upper and lower sections, and the upper section had to be opened first by pulling the handle inwards before rotating it from CLOSED to OPEN. When the lower section of the right rear door opened, a set of integral airstairs deployed. Information about passenger use of these exits following the accident is described in Seating arrangement and occupant injuries below.
Rottnest Island is located 18 km offshore the West Australian coast. The island has a sealed runway with 1,293 m available for the take-off run at Rottnest Island Airport. The runway is oriented east-west.
Thomson Bay is situated on the eastern side of Rottnest Island and is the main landing point for marine vessels visiting the island. Phillip Rock is a rocky outcrop about 400 m offshore the eastern tip of Thomson Bay.
The operator had received approval to conduct water landings and departures into and out of Thomson Bay. Swan River Seaplanes pilots reported that flights to Rottnest Island would normally utilise the sealed runway at the airport, and that Thompson Bay would only be utilised if forecast weather (wind direction and wind speed) would make the sealed runway unsuitable. The approval included a designated landing area, located in the south-eastern end of Thomson Bay, with the south-western area of the landing area subject to a 5 kt marine traffic limitation (Figure 4). Company pilots reported that it was normal practice to depart from Thomson Bay along a southerly track and to become airborne prior to the 5 kt limitation.
An initial review of flight data by the ATSB showed results consistent with these recollections. There were 6 flights which departed from Thomson Bay after Swan River Seaplanes commenced operations with VH-WTY on 2 January, comprising 3 flights on 4 January, 2 flights on 5 January, and the accident flight on 7 January. All these flights departed with a southerly track, except for the accident flight which departed with an easterly track (Figure 5).
Figure 4: Thomson Bay approved floatplane landing area
Figure 5: Recorded departure tracks for VH-WTY within Thomson Bay displaying the difference between the accident flight and the previous flights
Source: Google Earth, annotated by the ATSB
Weather and sea conditions
The Bureau of Meteorology automated weather information service (AWIS) located at Rottnest Island Airport provided meteorological observations at one-minute intervals. At 1600, the AWIS reported winds of 25 kt from 210° (approximately south-south-westerly). The temperature was 24°C.
Witnesses to the accident recalled strong gusty winds in Thomson Bay throughout the afternoon of the accident. Video recordings taken on the afternoon of the accident showed that the sea was calm close to the southern shore of Thomson Bay. Further into the bay, however, waves were larger and more frequent. The sea state around the aircraft during the take-off run was choppy, with some white caps. Video showed that beyond the eastern end of Thomson Bay, sea conditions became significantly worse, with larger and more frequent white caps (Figure 6).
Figure 6: Aerial view shortly after the accident near to the impact point showing the rougher sea state outside of Thomson Bay (top), with surface photography from a vessel in Thomson Bay (bottom left) and a witness on the shore (bottom right) showing conditions shortly before the accident.
Note: The police video (top image) was captured at about 1627, approximately 26 minutes after the accident.
Source: Western Australia Police Force, ferry operator and witness video, modified by the ATSB
Site and wreckage information
Accident site information and wreckage recovery
Analysis of witness video and information recorded by avionics and navigational equipment onboard the aircraft showed that the aircraft collided with the sea approximately 70 m south-east of Phillip Rock. The right float and part of the left float separated from the aircraft after the collision, and these were later recovered by WA Police and members of the public. The rear section of the left float remained tethered to the aircraft by the fly wire and sea rudder control cables.
The aircraft drifted approximately 800 m north of Phillip Rock until being tethered to the sea floor by WA Police divers. Their dive video showed that the main body of the aircraft remained largely intact following the collision (Figure 7). On 9 January 2025, commercial salvors lifted and recovered the aircraft using barges and a crane (Figure 8), before it was transported to a secure storage facility near Perth for further examination.
Figure 7: The aircraft sank inverted onto the sea floor within Thomson Bay
Examination of the aircraft wreckage at the secure facility identified:
The wings, fuselage and floats did not display any physical markings that the aircraft had struck landmass or a submerged object prior to the collision with the sea.
The engine controls were attached to the associated engine components and were free to move through their full range of movement.
The propeller blades were intact and attached to the propeller hub. They could be rotated through 360º about the feathering axis, indicating internal damage to the feathering mechanism. The investigation will include further analysis to determine the significance of this damage.
All 3 propeller blades were significantly bent toward the blade face. The significance of this was not able to be determined due to the propeller assembly resting on the sea floor prior to recovery.
The primary flight controls could not be moved due to structural damage from the accident. The flight pushrods, bellcranks and control cable hardware were examined for continuity and correct assembly. No pre-existing damage or defects were identified.
The flap selector was in the ‘full’ position and the flap position indicator was showing an intermediate position of about 15°. The wing flaps were in the retracted position.
The instrument panel and combing appeared undamaged. All circuit breakers were pushed in except those corresponding to the strobe light and stall warning.
The wings were swept back, with significant damage to both wings outboard of the ailerons. The left wing section, outboard of the aileron pushrods, was separated during the accident sequence and not recovered.
Video footage from WA Police divers for the recovery of the deceased occupants showed that the left (pilot) crew door was in the LATCHED position and the right crew door was in the LATCHED position. The upper section of the right rear door was open but the lower section, incorporating the airstairs, remained closed. Both sections of the left rear door were closed (with ATSB examination showing both handles in the CLOSED position).[3] The ATSB examined the functionality of all doors and determined that they could be unlatched and opened. Some doors were difficult to open, most likely due to structural damage to doorframes following the accident.
Engine examination
P&WC provided an engineering specialist to complete an internal borescope inspection of the engine. No evidence of pre-accident damage was identified.
The engine was removed from the aircraft in preparation for detailed teardown examination at the P&WC facilities in Canada. The ATSB analysis will consider the report from that examination.
The ATSB recovered the Garmin G1000 avionics equipment from VH-WTY. Using the flight data recovered from the G1000, witness video recordings of the accident, and automatic dependent surveillance broadcast (ADS-B) data[4] the following was identified:
Engine power was applied to commence the take-off at 1600:20, with the aircraft about 600 m from the western tip of Phillip Rock, and at a heading of 108°.
Fifteen seconds into the take-off the aircraft had accelerated to 40 kt and was about 400 m from Phillip Rock. The aircraft transitioned onto the step[5] and the nose was lowered. The aircraft heading was manoeuvred on a course between Phillip Rock and the eastern tip of Thomson Bay.
About 200 m from Phillip Rock, and with a recorded airspeed of 46 kt, the aircraft appeared to cross a wave or swell. Video footage showed the aircraft appearing to bounce on the water, becoming airborne momentarily before settling back onto the water.
Over the next few seconds, the left wing rose on 2 occasions as the aircraft approached Phillip Rock, with the left float separating from the water. On each occasion, the aircraft struck waves and the right float did not separate from the water.
There was a gradual reduction in engine power for about 20 seconds, commencing prior to the aircraft becoming airborne.
About 30 m from Phillip Rock, the aircraft had accelerated to a recorded airspeed of 57 kt, and again appeared to strike waves.
At 1600:52, the aircraft then became airborne, with a nose high attitude and on a heading of about 110°. Over the next few seconds, the aircraft maintained a nose-up attitude of between about 15°–18°. The aircraft climbed to about 16 ft above the surface of the water. The right wing then dropped, followed by an apparent aerodynamic stall of the left wing, with the aircraft rolling to the left.
A witness video recording at about the time the aircraft separated from the water showed that the flaps were extended for take-off. The video also indicated the water rudders were extended.
At 1600:56 the engine torque increased rapidly.
At 1600:58 the left wingtip struck the water then followed by the fuselage.
Surviving passengers recalled watching a safety briefing video prior to boarding the flight to Rottnest Island on the morning of the accident, with the pilot providing an additional safety briefing in the aircraft prior to departing from South Perth. Passengers recalled that there was no briefing provided prior to the departure from Thomson Bay, with the pilot asking if the passengers recalled the briefing from the morning. Passengers reported that the safety video and pilot briefing were thorough and provided adequate information on the use of seatbelts and the location and use of the aircraft exits.
One passenger additionally recalled that during boarding the aircraft prior to the departure from Thomson Bay, the pilot requested the passenger assist with closing and latching the left rear door. The passenger considered that the pilot’s instructions for closing the door were crucial for the passenger to subsequently open the right door after the aircraft struck the water.
The ATSB identified multiple safety information cards for the Cessna 208 Caravan in the aircraft wreckage, which showed information including the location of the aircraft exits, and how to unlatch and open the aircraft doors.
Surviving passengers recalled wearing life jackets during the accident flight. The life jackets worn by passengers were designed for constant wear in a pouch, with a belt securing the pouch around the waist. The life jackets were designed to be donned and inflated when required in an emergency. The life jackets could be inflated using a gas-cylinder inflation system or using an oral inflation system.
Surviving passengers recalled that the seating positions (Figure 9) for the accident flight were as follows:
The pilot was seated in the normal position in the front left seat, and there was no passenger seated in the front right (copilot) seat.
Two passengers were seated in the second row, with the central seat vacant. The passenger seated in the left seat was fatally injured in the accident. The passenger in the right seat recalled escaping through the rear left window, which had been broken by the coxswain of the operator’s tender vessel.
Two passengers were seated in the third row, with the central seat vacant. The passenger seated in the right seat was fatally injured in the accident. The passenger seated in the left seat was pulled from the aircraft through the left rear window by the coxswain of the operator’s tender vessel.
Two passengers were seated in the fourth row, with the central seat vacant. Both passengers in the fourth row survived the accident. The passenger seated in the left seat of the fourth row opened the top section of the right rear door, through which they exited the aircraft along with the passenger seated in the left seat of the fourth row.
The investigation will consider the post-mortem examination reports for each of the fatally injured occupants, including in support of analysis of the accident survivability.
Figure 9: Cessna 208 seating plan showing the occupant location for those who survived (green) and those who sustained fatal injuries (red)
Passengers were able to exit the aircraft using the top section of the right rear door (upper inset) and left rear window (lower inset).
Source: Textron Aviation, modified by the ATSB
Swan River Seaplanes
Swan River Seaplanes conducted Part 135 of CASR air transport operations for the purpose of passenger flights from the Swan River to Rottnest Island and Margaret River, Western Australia. It also operated flights around Perth, Western Australia, departing and landing on the Swan River. The operator reported commencing flights to Rottnest Island in October 2017, with operations from Thomson Bay commencing in January 2023.
Swan River Seaplanes had cross-hired VH-WTY, commencing passenger‑carrying flights in the aircraft on 2 January 2025. Swan River Seaplanes operated another Cessna 208, registered VH‑UOZ, however due to maintenance requirements this aircraft had been unavailable for operations since December 2024.
Swan River Seaplanes had 3 line pilots including the chief pilot. Another pilot, who conducted check and training for the operator, had also previously conducted line flights but was not operating in that function at the time of the accident.
The aircraft had been operated in the Whitsunday region of Queensland (Qld) since arrival into Australia. In the period between 29 June 2021 to 20 October 2023, it had not been operated and was inactive at Shute Harbour Airport, Qld.
It was then flown to Caloundra, Qld where it stayed for 31 days, and then flown to Sunshine Coast Airport, Qld where it remained for 37 days. It was not operated during these periods except for a relocation flight where it was flown to Bankstown Airport, New South Wales (NSW) on 3 March 2024.
The aircraft had been inactive at Bankstown, NSW, from 4 March 2024 to 27 December 2024, with no recorded flights. Maintenance releases and logbooks did not show evidence of engine or airframe preservation having been performed for the periods of storage of the aircraft.
On 27 December 2024, a special flight permit was issued by an authorised approver on behalf of the Civil Aviation Safety Authority, for a ferry flight to Jandakot, Western Australia (WA). This permit was required due to the expiry of the maintenance release on 20 October 2024.
Maintenance documentation showed that a new battery was installed in the aircraft at Bankstown on 27 December 2024.
On the morning of 28 December 2024, a 12-minute flight was recorded for the Bankstown Airport flying circuit.
From 28 December to 29 December 2024, the aircraft was flown from Bankstown Airport, NSW to Jandakot Airport, WA.
The aircraft and engine logbooks identified that from 30 December 2024 to 1 January 2025, the airframe, floats and role equipment (life jackets, fire extinguisher and first aid kit) were inspected. From the records, a new elevator pushrod bearing was installed, and new rudder pulleys were installed for the left and right floats. Engine work included a compressor power recovery wash and desalination rinse. Additionally, the chip detector plugs were recorded to have been inspected with no defects listed.
Further investigation
To date, the ATSB has conducted the following activities:
interviewed Swan River Seaplanes personnel and survivors of the accident
examined the aircraft wreckage
reviewed information recorded by avionics equipment onboard VH-WTY
reviewed the forecast and observed weather conditions at Rottnest Island
reviewed video recordings from witnesses, CCTV and other sources.
The investigation is continuing and will include review and examination of:
information recovered from mobile devices
the recorded data from the aircraft engine
the results of the engine teardown by Pratt & Whitney Canada
weather and sea conditions in Thomson Bay on the day of the accident
the information available to the pilot for Thomson Bay operations on the day of the accident
the operator’s procedures and other risk controls for assessing the suitability of planned floatplane departures from Thomson Bay
the history, identification and assessment of Thomson Bay for floatplane operations
the aircraft maintenance history
pilot training records, medical information and recent history
pilot and passenger injuries and post-mortem reports
the safety briefings provided to passengers, the location and availability of exits after the accident, and the performance of the aircraft seatbelts
regulatory oversight and surveillance for the floatplane operations from Thomson Bay and for the maintenance of VH-WTY.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the support of the Western Australian Police Force and those involved with the recovery of VH-WTY.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Witness videos were aligned to the time of events recorded on the flight data, and the synchronisation between these sources has a margin of error of +/- 1 second.
[2]The term amphibian refers to an aircraft equipped to operate from land runways and water.
[3]The ATSB examined the aircraft after the deceased occupants had been recovered by the police. The investigation will include analysis to determine the likely configuration of door control positions during and after the accident sequence.
[4]The ADS-B tracking of VH-WTY on the afternoon of the accident can be viewed at ADSBexchange.com.
[5]The step position is the attitude of the aircraft when the entire weight of the aircraft is supported by hydrodynamic and aerodynamic lift, as it is during high-speed taxi or just prior to take‑off. This position produces the least amount of water drag.
Interim report
This interim report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Events prior to the accident flight
On 7 January 2025 a Cessna 208 Caravan amphibian (floatplane), registered VH‑WTY and operated by Swan River Seaplanes, was being utilised for non-scheduled passenger air transport flights to and from South Perth and Rottnest Island, Western Australia. The flights were conducted using the waters of the Swan River at South Perth and Thomson Bay at Rottnest Island.
At about 0840, the pilot and 10 passengers prepared for the flight to Rottnest Island. Prior to boarding at South Perth, passengers watched a safety briefing video and were fitted with life jackets.
At 0915 the aircraft departed the Swan River, before climbing to a cruising altitude of about 1,600 ft. The aircraft orbited to the north of Rottnest Island then landed in a south‑south‑west direction on the waters of Thomson Bay at 0926 (Figure 1). Passengers recalled that the flight was uneventful.
Figure 1: Rottnest Island (insert) and key locations in Thomson Bay
Source: Google Earth, annotated by the ATSB
The passengers alighted the aircraft onto a pontoon and were then conveyed to the island on board a tender vessel. The aircraft remained at Thomson Bay throughout the day, with the pilot remaining on the island.
At 1116, the Swan River Seaplanes head of flying operations (HOFO)[1] sent the pilot a text message stating that winds were forecast to increase that afternoon. The HOFO sent the pilot an image from a weather website, showing that winds at Rottnest Island were 25 kt with gusts to 34 kt.
The pilot responded that they may need to return to South Perth earlier than the planned 1600 departure time. The HOFO indicated they agreed with this, stating that if necessary the passengers could return via ferry. The pilot responded to this text with a thumbs up.
Closed‑circuit television (CCTV) recordings showed that at about 1305 the Swan River Seaplanes tender vessel departed from alongside the aircraft, with the pilot operating the vessel solo. The video appeared to show the pilot travel north from the pontoon. The tender vessel was then returned to shore where it was docked at a jetty on Rottnest Island at about 1320.
At about 1330, the pilot sent a text message to the HOFO, stating that the wind had reduced but the swell remained high towards the centre of Thomson Bay, from where take-offs were normally commenced (see Thomson Bay departures). The pilot stated they planned to depart taking a quartering crosswind closer to shore, where they perceived conditions were calmer. The HOFO responded to this message stating they trusted the pilot’s judgement, encouraging the pilot to resist any perceived pressure to depart.
At about 1500, the pilot requested the coxswain[2] operate the tender vessel to the area normally used for floatplane take-offs from Thomson Bay, so the pilot could conduct an inspection of the sea conditions. The coxswain recalled that the pilot determined the conditions to be unsuitable for take-off, and requested to be taken closer to the southern shore of Thomson Bay. The coxswain recalled that conditions were calmer in this location, and the pilot had planned to take off eastwards towards Phillip Rock. At the completion of this inspection, the pilot requested to be conveyed to the aircraft.
At 1511, one of the directors of Swan River Seaplanes (who was also the approved safety manager) texted the pilot and asked about the wind conditions. The pilot responded that conditions were ‘ok but rough’, however the swell was ‘not too bad’ closer to shore. The pilot also noted in that text message conversation that the aircraft would be ‘pretty light’ for the take‑off.
At about 1540, the passengers for the flight from Rottnest Island to South Perth were conveyed by the coxswain to the pontoon at which the aircraft was moored. The pilot met the passengers at the aircraft.
There were 6 passengers for the return flight, all of whom had travelled to Rottnest Island on the morning flight. Passengers described conditions on board the vessel and pontoon as rough and windy. Each passenger was fitted with a life jacket before boarding the aircraft (Figure 2).
Figure 2: Passengers boarding VH-WTY at Thomson Bay
Source: Witness
Passengers recalled the pilot told them the departure would be rough. Some passengers recalled the pilot using the term ‘choppy’, and others recalled the pilot said the departure ‘might get a bit bumpy’.
Once all passengers were boarded, the pilot signalled to the coxswain to release the mooring lines securing the aircraft to the pontoon. The aircraft then drifted before the pilot started the engine and taxied the aircraft to the south then north-west, before lining up for an eastwards take‑off. At 1558, while taxiing the aircraft, the pilot was recorded making a broadcast on the Rottnest Island common traffic advisory frequency,[3] announcing an intention to depart from Thomson Bay to the south-east.
Accident flight
Figure 3 shows the track of the aircraft during its take-off from Thomson Bay. Recorded data showed that engine power was applied for take-off at about 1600:20. The aircraft accelerated in the plowing position[4] to about 31 kt groundspeed and 21 kt indicated airspeed (IAS)[5] by 1600:30, and yawed slightly left, on course towards Philip Rock.
The aircraft continued to accelerate, reaching about 37 kt IAS by 1600:34. At about this time, the pilot corrected the track to the south of Philip Rock.
Figure 3: VH-WTY take-off track with approximate location of key events
Source: Google Earth, annotated by the ATSB
At about 1600:38, as the aircraft accelerated to about 43 kt IAS, the pilot manoeuvred the aircraft onto the step.[6]
The aircraft continued to accelerate, reaching 50 kt IAS by 1600:44. As it accelerated on the step, the aircraft encountered sea swell and chop. Passengers recalled the aircraft bumping loudly and forcefully against the water, perceiving this to be much rougher than the take-off from South Perth. Video captured by a passenger on board included the sound of these bumps.
At about 1600:49, as the aircraft accelerated to about 57 kt IAS, it struck swell and became airborne. The aircraft nose attitude increased significantly, reaching a maximum 18° nose up. The aircraft reached a maximum altitude of 16 ft above the surface of the water, before rolling to the left (see Flight data and video).
Impact and passenger escape
The left wing impacted the water, followed by the fuselage and the rest of the aircraft. Surviving passengers and other witnesses recalled the aircraft remained partially afloat in a vertical orientation, with the aircraft nose resting on the sea floor. The surviving passengers reported that all cabin doors were submerged.
The forward section of the cabin rapidly filled with water. Four passengers moved into a pocket of air in the rear cabin. One passenger opened the top section of the rear right door, through which they escaped with another passenger.
The coxswain of the Swan River Seaplanes tender vessel, having observed the collision, piloted the vessel to the crashed aircraft. Upon reaching the aircraft, the coxswain observed a passenger in the rear cabin. This passenger recalled perceiving they were stuck inside the sinking aircraft, as they were unable to exit through the door opened by the other passenger.
The coxswain broke the rear left window, through which 2 passengers recalled escaping. The pilot and the 2 other passengers remained in the aircraft.
Police officers stationed at Rottnest Island responded to the accident, arriving at the aircraft at about 1610. Police body-worn camera footage showed the aircraft was partially submerged in a vertical orientation, with the rear left window above the water surface (Figure 4). Under conditions of uncertainty and potential danger, police and members of the public entered the water and attempted to rescue the occupants. Despite these efforts, none of the remaining occupants were able to be freed from the aircraft. Police who entered the water were not able to open the forward aircraft doors.
Figure 4: VH-WTY inverted in the water shortly after the collision
Source: WA Police
At about 1630 the aircraft began to sink, becoming fully submerged at about 1640.
Police divers recovered the 3 deceased occupants on the evening of 7 January 2025.
Context
Pilot information
Licencing and experience
Licence and experience details for the pilot of VH-WTY are shown in Table 1.
Table 1: Pilot licencing and experience
Licence type
Commercial Pilot Licence (Aeroplane)
Medical certificate
Class 1, valid to October 2025
Total aeronautical experience
1908.5 hours
Total time on type (Cessna 208 amphibian)
708.0 hours
Recent aeronautical experience (90 days)
60.1 hours
Recent aeronautical experience (7 days)
7.8 hours
The pilot obtained a Private Pilot Licence in 2014 and had held a Commercial Pilot Licence (Aeroplane) since June 2019. The pilot obtained a floatplane endorsement in August 2019.
The pilot’s experience included almost 1,400 hours on floatplanes and over 2,600 water landings. Since commencing with the Swan River Seaplanes in October 2024, the pilot had accrued over 60 hours, including 102 water landings.
Recent history
The pilot’s roster for the week prior to the accident (from 1 to 7 January 2025) is shown in Table 2. The pilot had conducted multiple floatplane flights during this week however none involved operating from Thomson Bay.
Table 2: Pilot rostered duties, 1 to 7 January 2025
Date
Shift start-finish time
Total flight hours
1 January
OFF
2 January
0630-1430
1.5
3 January
0630-1430
2.1
4 January
0630-1430
1.8
5 January
0630-1430
2.4
6 January
OFF
7 January
0730-1630
The Swan River Seaplanes incident reporting system included a report from one of these shifts. At about 0800 on 4 January, the pilot was departing from Jandakot, Western Australia,[7] for the first flight of the day when they omitted to retract the aircraft water rudders. The pilot submitted an incident report for this, which identified that the pilot was ‘likely in a fatigued state’.
The pilot’s partner recalled the pilot went to bed at about 2130 on 6 January, before waking at 0645 on 7 January and leaving for work at about 0730. Records from the pilot’s mobile phone were consistent with these estimates, and indicated the pilot had opportunity to sleep from 2124 on January to 0645 on 7 January.
Witnesses recalled that the pilot of VH-WTY appeared happy and alert on the day of the accident. There were no reports of the pilot appearing tired.
Prior flights into Thomson Bay
The system used by Swan River Seaplanes to track flight and duty times showed that the pilot had conducted 12 water landings (and take-offs) at Thomson Bay prior to the day of the accident (Table 3). Flight tracking records from the operator’s aircraft and notes from the flights the pilot conducted under supervision showed only 10 landings at Thomson Bay. It is possible that the pilot conducted touch-and-go landings[8] at Thomson Bay during initial training flights.
All the pilot’s prior landings at Thomson Bay had been conducted in the other Cessna 208 amphibian utilised by Swan River Seaplanes, VH‑UOZ (see Organisational background).
Table 3: Thomson Bay landings conducted by the pilot
Date
Thomson Bay landings
Aircraft crewing information
Recorded wind [1]
1 November 2024
2
Under supervision by the HOFO
13–15 kt SSW
2 November 2024
1
Under supervision by the HOFO
17 kt SSW
9 November 2024
2
Under supervision alternate HOFO (Thomson Bay proficiency check)
20–22 kt SSW
16 November 2024
2
Pilot in command, without supervision
23–28 kt SSW[2]
1 December 2024
3
Pilot in command, without supervision
13–17 kt WNW
Source: Bureau of Meteorology, Rottnest Island weather station
Note: Wind direction information was not available for Rottnest Island weather station at the time of these flights. Wind direction was estimated by averaging the wind direction recorded at other nearby stations.
The Swan River Seaplanes Head of Flying Operations (HOFO) recalled having a positive impression of the pilot’s performance at Thomson Bay. The HOFO’s notes from the flights undertaken on 2 November included that all water landings were conducted well in ‘lumpy conditions’. The Swan River Seaplanes alternate HOFO indicated a similar impression from the flights conducted on 9 November. Flight tracking records showed that all the Thomson Bay take‑offs on 1, 2 and 9 November were conducted on a predominantly southerly track, consistent with the typical water runway used for Thomson Bay take-offs (see Thomson Bay departures). After the flight conducted on 9 November, the pilot was checked to line to conduct flights from Thomson Bay without supervision.
Analysis of the pilot’s subsequent 5 take-offs from Thomson Bay (without supervision) showed that 4 of these were conducted using tracks which were significantly different to the operator’s typical water runway.
The Swan River Seaplanes HOFO stated that they had reviewed the take-offs conducted by the pilot. The HOFO stated that the take-offs from Thomson Bay on 16 November and 1 December did not raise any concerns and were consistent with the wind direction at the time.
Previous cancellations
The HOFO stated the pilot was comfortable making command decisions to cancel flights if conditions were not suitable, and had been supported in these decisions by company personnel.
Records extracted from the pilot’s mobile phone included communication between the pilot and other company personnel, and demonstrated the pilot’s assessment of weather conditions for 2 previous departures:
On 16 November 2024, the pilot sent the HOFO an image of the conditions at Thomson Bay and said 'this is on limits'. The HOFO responded 'Yeah that'd be pretty close to limits… Next one is light. But totally your call’. The pilot texted 'Yeah, we're done for the afternoon…way too rough’. Later that day, a company director (who was also the safety manager) sent a group message stating 'hey guys, great call this afternoon’. The director also said the following flight had been cancelled and passengers had been booked on ferries for their return from Rottnest Island.
On 24 November 2024, the pilot texted the company director and safety manager of Swan River Seaplanes and advised that wind conditions were 26 kt and forecast to increase. The pilot stated they would cancel an afternoon flight due to the winds. The director responded by thanking the pilot.
Aircraft information
General information
VH-WTY was a Cessna[10] 208 Caravan amphibian floatplane, powered by a Pratt & Whitney Canada (P&WC) PT6A-114A turboprop engine and a 3-bladed McCauley constant speed propeller. The aircraft was fitted with Wipline 8750 amphibious floats, manufactured by Wipaire, which enabled operation from both land and water. The aircraft was manufactured in the United States in June 2016, then registered in Australia in September 2016. It had accumulated about 1,125 hours total time in service at the time of the accident.
Operating procedure documentation
The Cessna 208 Pilot’s Operating Handbook (POH) provided normal and emergency operating procedures, performance and aircraft systems information for the Cessna 208 equipped with standard landing gear.[11]
The Wipaire Approved Pilot’s Operating Handbook and Airplane Flight Manual Supplement (AFMS) provided procedures for the Cessna 208 equipped with Wipline 8750 floats.[12]
Weight and balance
The maximum take-off weight (MTOW) for the Cessna 208 equipped with Wipline 8750 floats was 3,968.9 kg (8,750 lb). Considering recorded passenger weights and other information, VH‑WTY was estimated at about 3,206 kg without fuel and about 3,565 kg with fuel at the commencement of the take-off from Thomson Bay. The aircraft was within its centre of gravity envelope.
Water rudders
Most floatplanes are equipped with retractable water rudders to provide for greater manoeuvrability on the water surface while taxiing. The Wipline 8750 floats were equipped with a water rudder steering and retract system, with water rudders fitted to the rear end of each float.
Quadrant friction lock
The Cessna 208 is equipped with a quadrant friction lock, which is a knob located on the side of the pedestal that when rotated adjusts the level of friction on the engine controls. The POHstated that the friction lock was provided ‘to minimise creeping of the engine controls once they have been set’.
Stall warning system
The Cessna 208 was equipped with a vane-type stall warning unit in the leading edge of the left wing. The stall warning unit sensed change in the airflow over the wing, and produced a warning horn if the sensed airspeed was between 5 and 10 kt above the stall speed. The purpose of this system was to provide a warning to the pilot if the aircraft was approaching a stall.[13]
The POH identified that the stall warning system was protected by a pull-off circuit breaker, labelled STALL WARN. This circuit breaker was also provided as a means to shut off the warning horn in the event it became stuck on.
Meteorological and environmental information
Location information
Rottnest Island is located 18 km from the Western Australian coast. Rottnest Island Airport has a sealed runway, which is oriented east-west and provides 1,293 m for take‑off and landing.
Figure 5: Rottnest Island and Thomson Bay
Source: Google Earth, annotated by the ATSB
Thomson Bay is on the eastern side of Rottnest Island and is the main landing point for marine vessels visiting the island. Swan River Seaplanes conducted operations in the south-eastern quadrant of Thomson Bay. This section of the bay extends to the east towards Phillip Point. Phillip Rock is a rocky outcrop about 400 m offshore of the eastern tip of the southern shore.
Swan River Seaplanes maintained a pontoon close to the southern shore of Thomson Bay. A tender vessel was used to ferry passengers from the pontoon to the Rottnest Island Fuel Jetty.
Local climate
The Bureau of Meteorology (BoM) maintained a weather station about 5.5 km south-west of Philip Rock. The weather station was located at an elevation of 43.1 m above sea level, on the side of a hill with exposure to the south-west. BoM records showed the mast anemometer[14] was 10m high and had been replaced in 2016.
Records from the BoM captured the wind direction and speed at 1500 local time, from November 1987 to August 2024 (over 12,000 observations). Southerly winds were recorded on nearly 40 per cent of days, with south-westerly winds recorded on over 20 per cent of days (Figure 6). Recorded winds were regularly over 30 km/h (16 kt).
Figure 6: Climatology data from BoM showing winds recorded at Rottnest Island at 1500 local time, from 1987 to 2024
Source: Bureau of Meteorology
Coastal geography and sea conditions
The terrain surrounding the bay near Phillip Point includes coastal dunes, some small hills and buildings, with elevation to about 16 m above sea level (Figure 7). Maritime charts showed that the sea in Thomson Bay was around 3–4 m deep, whereas past Phillip Point the depth increased significantly (Figure 8).
Figure 7: Overhead photography of Thomson Bay near Phillip Point, with accident flight track of VH‑WTY highlighted
Source: Google Earth, annotated by the ATSB
Figure 8: Maritime chart showing sea depth in Thomson Bay
Source: WA Department of Transport, annotated by the ATSB
Thomson Bay was protected from wind and sea conditions during typical southerly and south‑westerly winds, particularly close to the southern shore. Witnesses familiar with boating at Rottnest Island identified that conditions east of Phillip Rock were typically much rougher than in the bay.
Meteorological forecasts and observations
The BoM issued a grid point wind and temperature forecast for the southern portion of Western Australia (including Rottnest Island) at 0726 on 7 January. This forecast showed that, from 1400, conditions on Rottnest Island were forecast to include south-westerly winds of 21 to 26 kt.
The BoM provided meteorological aerodrome reports (METAR) for Rottnest Island Airport every half hour. The METAR issued at 1600 showed winds from 210° at 25 kt, which was unchanged from the previous report issued at 1530. Table 4 shows the METAR from 1400 to 1600 on the afternoon of the accident.
Table 4: Rottnest Island Airport METAR, 1400 to 1600 on 7 January 2025
Time
Wind speed
Wind direction (º)
Temperature (ºC)
1400
25 kt
210
24
1430
23 kt
210
25
1500
26 kt
210
24
1530
25 kt
210
24
1600
25 kt
210
24
The Western Australia Department of Transport maintained a wave monitoring buoy approximately 17 km south-west of Thomson Bay. Data from this buoy recorded a relatively constant 0.6 m swell[15] with a marked increase in the sea waves[16] from 1 m at 0900 to around 2 m by 1500. At 1600 the wave monitoring buoy recorded a sea wave height of 2 m. The total wave height[17] was 1.2 m at 0900, increasing to 2.1 m at 1600.
Directional wave data showed that the swell and sea waves were from a south-westerly direction (230°).
Witness environmental observations and recorded video
Witnesses recalled strong gusty winds and choppy seas in Thomson Bay on the afternoon of the accident. One witness, who was an experienced mariner, who observed the accident from the shore about 500 m away, estimated the wind at the time of the accident at 25 kt. The witness recalled that the aircraft operated in protected, calmer water at the start of the take-off, with conditions becoming rougher during the take-off run.
The coxswain who operated the Swan River Seaplanes tender vessel recalled that conditions in Thomson Bay included winds of about 30 kt and waist-height (approximately 1 m) waves near the usual floatplane departure location. Conditions closer to the shore were calmer, with waves at about 20 cm high.
Video recordings taken on the afternoon of the accident showed that the sea was calm close to the southern shore of Thomson Bay. Further into the bay, however, waves were larger and more frequent.
Video recorded by the passenger in seat 2A (see Passenger video) showed:
The aircraft encountered waves immediately prior to the application of power for take‑off. These waves may have been influenced by reef in the area. The video showed the waves encountered by the aircraft at this point were perpendicular to its take‑off track (Figure 9, A).
As the aircraft transitioned onto the step, the sea became smoother and continued to improve during the step phase (Figure 9, B).
The aircraft encountered rougher sea conditions later in the step phase, causing it to bounce. Figure 9 (image C) shows the sea conditions at the time the aircraft separated from the water. The video showed that the waves encountered by the aircraft had changed in direction, and were now more reciprocal to the take-off track.
Sea conditions developed east of Philip Rock, with larger waves observed. Figure 9 (image D) shows the sea conditions almost directly beneath the nose of the aircraft when it was about 25 ft above the water surface.
Figure 9: Sea conditions encountered by VH-WTY during take-off
Source: Passenger video and Google Earth, annotated by the ATSB
Flight recorders and other recorded information
Onboard recorders
VH-WTY was not fitted with a flight data recorder or cockpit voice recorder, and nor were these recorders required for the type of aircraft or operation.
The aircraft was fitted with a Garmin G1000 integrated electronic flight instrument system that presented flight instrumentation, position, navigation, communication, and identification information to the pilot through large-format displays.
The G1000 had a flight data logging feature that stored flight and engine parameters onto a secure digital (SD) card at approximately one second intervals while the multi‑function display was powered on. The ATSB retrieved the SD card from VH-WTY after the accident and downloaded data from the SD card. The data comprised of the accident flight and 71 previous flights from 30 December 2024. For the accident flight, the G1000 recorded data up to 1600:54, about 2 seconds before the aircraft impacted the water.
The aircraft was also fitted with a Pratt & Whitney Canada digital aircraft data acquisition system (ADASD) that primarily recorded engine parameters at approximately 0.5 second intervals. The data was extracted by Pratt & Whitney Canada and provided to the ATSB and included the accident flight and previous flights. For the accident flight, the ADASD recorded data up to and after the impact with water.
Passenger video
The passenger in seat 2A recorded a video of the accident flight, including about 35 seconds of footage prior to the aircraft colliding with the sea. The video was mainly focused outside the aircraft, and captured sound including the aircraft moving along the sea during the take-off.
Recorded engine performance
Engine parameters were recorded on both the G1000 and ADASD and showed good agreement. The data showed the following (Figure 10):
The propeller speed was relatively constant, just below the maximum take-off limit of 1,900 RPM. Fuel flow and temperature values were consistent with the recorded engine torque.
At the beginning of the take-off, between 1600:21 and 1600:26, the engine torque was above the maximum take-off limit of 1,865 ft lb. This was below the maximum transient limit of 2,400 ft lb.
Between 1600:29 and 1600:42, the engine torque was relatively stable between about 1,750 ft lb and 1,710 ft lb.
Between 1600:43 and 1600:52, the engine torque reduced from about 1,720 ft lb to about 1,580 ft lb.
At 1600:53, the engine torque increased, exceeding the maximum take-off limit until the aircraft impacted the water. The engine torque did not exceed the maximum transient limit.
Figure 10: Engine torque recorded by ADASD unit on board VH-WTY
Source: ATSB
Flight data and video
Flight data recorded by the G1000 unit on board VH-WTY is displayed in Table 5.
Table 5: VH-WTY selected flight data parameters.
Time
Groundspeed (kt)
Indicated airspeed (kt)
Heading (º)
Pitch attitude (º)
Altitude MSL[1] (ft)
1600:10
8
0
116
6
1
1600:26
23
1
114
10
2
1600:30
31
21
111
12
3
1600:35
39
39
125
9
3
1600:40
48
44
120
10
3
1600:45
55
52
117
9
3
1600:46
56
53
116
11
4
1600:47
57
55
114
10
4
1600:48
59
56
117
14
4
1600:49
61
57
113
9
2
1600:50
61
56
112
16
5
1600:51
62
54
110
17
10
1600:52
62
55
113
16
13
1600:53
62
57
117
18
15
1600:54
62
56
115
17
16
[1] Altitude MSL: Altitude above mean sea level
The flight data and recorded video indicated the following:
The aircraft separated from the sea at about 1600:49 with high pitch angle, increasing to a maximum of 18º.
Video footage indicated the elevator was deflected up and the left aileron was deflected down after the aircraft separated from the sea. The float rudders were also shown to be extended as the aircraft separated from the sea.
The aircraft climbed to about 16 ft above the surface of the water.
At 1600:53, there was a simultaneous reduction in pitch and commencement of left roll which continued until the aircraft impacted the water.
Ongoing investigation focus
Aircraft handling and performance prior to and following the separation from the water.
Wreckage information
Accident site and recovery
Analysis of witness video and recorded information showed that the aircraft collided with the sea approximately 70 m south-east of Phillip Rock. The right float and part of the left float separated from the aircraft after the collision and were later recovered by WA Police and members of the public. The rear section of the left float remained tethered to the aircraft by the fly wire and sea rudder control cables.
The aircraft drifted approximately 800 m north of Phillip Rock until being tethered to the sea floor by WA Police divers. Their dive video showed that the main structure of the aircraft remained largely intact following the collision. Both wings had separated from the fuselage at the leading (forward) edge and had hinged rearward, entering the fuselage at the trailing (aft) edge (Figure 11). The right wing had been pushed back significantly more than the left wing.
On 9 January 2025, the aircraft was recovered from the sea and transported to a secure storage facility for further examination.
Figure 11: VH-WTY submerged in Thomson Bay on 8 January 2025
Source: WA Police, annotated by the ATSB
Wreckage examination
The wreckage examination identified structural damage consistent with a collision with water. The floats had been separated from the aircraft, as had the left wing section outboard of the aileron pushrods. The wings were swept back, with significant damage to both wings outboard the ailerons. The lower surface of the tail had sustained buckling and puncture damage, consistent with damage from impact with the floats during the accident sequence.
The cockpit windscreen was intact, while several of the cabin windows were broken including inboard of the right wing and the rear left window. The wings, fuselage and floats did not display any physical markings to suggest that the aircraft had struck landmass or a submerged object prior to the collision with the sea.
The pilot’s seat was observed in a locked, forward position. The seat rails were firmly attached to the aircraft structure, and the adjusting and locking system were observed to be functional. None of the passenger seats displayed any damage, buckling or failure.
The examination identified that the engine controls were attached to the associated engine components and were free to move through their full range of movement. The propeller blades were intact and attached to the propeller hub. All 3 propeller blades were significantly bent toward the blade face. The significance of this could not be determined due to the propeller assembly resting on the sea floor prior to recovery.
Due to structural damage from the accident, the primary flight controls could not be moved when examined. The flight control pushrods, bell-cranks and control cable hardware were examined for continuity and correct assembly. No pre-existing damage or defects were identified.
The instrument panel appeared undamaged. All circuit breakers were in the pushed-in (power on) position except those corresponding to the strobe light and stall warning which were in the out (power off) position.
Wing ingress into cabin structure
The trailing edge and inboard flap sections of both wings had been forced into the cabin area at the wing rear attachment points. The fuselage was deformed and the passenger windows broken around the wing structure (Figure 12 and Figure 13).
Figure 12: Ingress of left wing into VH-WTY fuselage. Image depicts inverted aircraft facing aft
Source: ATSB
Figure 13: Ingress of right wing into VH-WTY fuselage. Image depicts inverted aircraft facing aft
Source: ATSB
Examination of the wing support structure showed the left and right carry‑through structure[18] had fractured at the wing rear attachment points (Figure 14). The fractured sections of the carry-through structure were forced inwards and downwards into the space normally occupied by passengers seated in row 2 of the cabin.
Figure 14: Internal cabin showing fuselage and wing support structural damage. The image is taken from the rear of the cabin looking towards the cockpit.
Source: ATSB
Wing flap position
The wing flaps were observed in the retracted (0°) position. The flap selector however was in the ‘full’ (extended) position, and the flap position indicator was showing an intermediate position of about 15°. The emergency flap switches were in the guarded position and lockwire was present.
Examination of the flap control system showed that the jack screw which controlled the movement of the wing flaps was in a position indicative of a ‘full’ (extended) flap position. It is very likely that the wing flaps were in the ‘full’ position during the take-off, and that discrepancies between the flap selector, the position indicator and the wing flaps were because of disruption following the collision with the sea.
Additional engine examination
The engine was removed from the airframe and transported to the Pratt & Whitney facilities in Canada for a detailed teardown examination.[19] The report from this examination identified that the engine displayed rotational contact marks to internal engine components, characteristic of the engine developing power at the time of impact. The report further identified that there were no indications of pre-impact mechanical anomalies to the engine components which would have precluded normal operation.
The report also reviewed the data recorded by the digital aircraft data acquisition system (ADASD), noting the data showed the engine was running at high power at the time of impact. ATSB analysis of this data is provided in Recorded engine performance.
Aircraft structure and passenger seating
VH-WTY was configured in a 13-seat layout. This comprised the pilot (left) and copilot (right) seats in the front row, followed by 4 rows of passenger seats. The first 3 rows of passenger seats were configured with 2 seats on the right side of the cabin and 1 seat on the left. The rear row provided 2 seats in a bench layout.
Surviving passengers recalled that the seating positions for the accident flight were as follows (illustrated in Figure 15):
The pilot was seated in the normal position in the front left seat, and was fatally injured in the accident. There was no passenger seated in the front right seat.
Two passengers were seated in the first passenger row (seats 1A and 1C), with the central seat vacant. The passenger seated in the left seat was fatally injured in the accident.
Two passengers were seated in the second passenger row (2A and 2C), with the central seat vacant. The passenger seated in the right seat was fatally injured in the accident.
Two passengers were seated in the third passenger row (3A and 3C), with the central seat vacant. Both passengers in the third row survived the accident.
Figure 15: Cessna 208 seating plan showing the occupant location of those who survived (green) and those who sustained fatal injuries (red)
Source: ATSB
Figure 16 is an illustration showing the ingress of the wing trailing edges into the cabin area and encroaching seats 2A and 2C. It also illustrates how the wings were hinged and rotated on the forward attachment points and wing struts. Figure 17 shows the ingress of the wing structure relative to the position of seats 2A and 2C.
Figure 16: Projected movement of wings inboard into cabin space
Source: ATSB
Figure 17: Right wing ingress into VH-WTY cabin and position of seat 2C
Source: ATSB
Post-mortem and other medical information
Post-mortem examinations of the 3 deceased occupants were conducted by a qualified pathologist, on behalf of the Coroner’s Court of Western Australia. The pathologist’s reports identified the following:
The cause of death for the pilot was drowning. The post-mortem report for the pilot did not identify evidence of significant internal or skeletal injury or the presence of significant natural disease. Toxicological analysis for the pilot was negative for the presence of alcohol and other common drugs.
The cause of death for the passenger in seat 1A was drowning. The report did not identify evidence of significant internal injury or natural disease relevant to the accident.
The cause of death for the passenger in seat 2C was drowning with head injury. The report identified the passenger had sustained a brain injury which was traumatic in nature.
The surviving passengers sustained injuries including:
The passenger in seat 1C sustained bruising and lacerations to the torso.
The passenger in seat 2A sustained bruising and lacerations to their arms and shoulders.
The passenger in seat 3C experienced a significant hand injury.
The ATSB has engaged medical specialists to provide analysis of the post-mortem records and assist the investigation to identify the factors which may have contributed to the non-survival of the pilot and 2 of the passengers.
Aircraft restraints and exits
Restraints
Figure 18 shows the restraints provided for occupants of VH-WTY. The pilot and copilot seat were equipped with 5-point restraint which consisted of 5 webbing straps all connecting to a central release buckle. The buckle released when twisted in either direction.
Figure 18: Types of restraints fitted to VH-WTY and their positions
Source: ATSB
The passenger restraints for the first 3 rows were a 3-point lap-sash design which clicked into place in a buckle with a push-button release, similar to a motor vehicle. The restraints for the bench seat were also 3-point design with lap belt and shoulder strap. These restraints, however, required separate fastening of the shoulder and lap belts.
All surviving passengers recalled wearing their restraint during the flight, and that the deceased passengers were also secured. Three of the surviving passengers recalled successfully disconnecting their restraint, with one recalling that another passenger disconnected their restraint for them. Passenger video showed the pilot secured by the 5-point restraint during the accident flight.
Police video footage from the recovery of the deceased occupants showed that the pilot and 2 passengers were not secured by their restraints. The pilot and the passenger in seat 1A were found near their seats. The passenger in seat 2C was partially outside the aircraft, with their torso through an overwing window that had broken in the accident. The circumstances by which the deceased occupants became released from their restraints, and by which the passenger of seat 2C partially exited the aircraft, has not been determined.
Crew entry doors
The aircraft had 2 crew entry doors at the front of the cabin, next to the pilot (left) and copilot (right) seats. The crew entry doors had interior and external handles, which could be set to OPEN, CLOSE and LATCHED positions. The doors were also equipped with separate locks, and with lock override knobs inside the aircraft. To close the door, aircraft operating procedures instructed pilots to place the handle in the CLOSE position and pull the door closed, before rotating the handle to the LATCHED position. When unlocked and in the LATCHED position, the crew entry doors could be opened from either inside or outside the aircraft by rotating the handle to the OPEN position (Figure 19).
Figure 19: Operation of front door handles on a Cessna 208
Source: Swan River Seaplanes briefing video, annotated by the ATSB
The wreckage examination found the right (copilot) door handle in the LATCHED position. The door sustained significant damage in the accident, rendering it inoperable.
Footage captured by WA Police divers on the evening of 7 January showed the left (pilot) door handle in the LATCHED position. The divers unlatched the left (pilot) door during the recovery of the deceased occupants. When examined by the ATSB, the left (pilot) door handle was in the OPEN position, and the door was free to open. The reason why the door was not unlatched and opened by the pilot immediately following the accident has not been determined.
Passenger doors
There were 2 doors towards the rear of the cabin, each with a horizontal clamshell opening. Each rear door included separate handles for the upper and lower sections. The upper section had to be opened first by pulling the handle inwards before rotating it from CLOSED to OPEN. The lower section was released by pulling up on the inside door handle, rotating the handle to the OPEN position and pushing outwards. When the lower section of the right rear door opened, a set of integral airstairs deployed.
After the collision, the passenger in seat 3A opened the top section of the right rear door. Because the aircraft was inverted, however, the aircraft stairs were extended across the aircraft exit (Figure 20). The passengers in seat 3A and 3C recalled this restricted the opening to a narrow gap, requiring both passengers to swim through the rungs of the aircraft stairs to escape.
The passenger in seat 2A recalled unsuccessfully attempting to open a door in the rear of the aircraft.
Figure 20: VH-WTY right rear door
Source: ATSB
Other information related to passenger escape
Passengers recalled that water filled the aircraft immediately after the collision. The surviving passengers moved to the rear of the cabin, where a small pocket of air was available. The passengers recalled that carry-on bags and a seat cushion had also floated into this air pocket, reducing the space available and hindering their escape.
The passengers in seats 1C and 2A recalled escaping through the rear left window, which had been broken by the coxswain of the operator’s tender vessel.
Other survivability information
Life jackets
The Swan River Seaplanes Aircraft Operations Manual[20] stated that prior to any flight over water, the pilot was to ensure that all persons on board were wearing a life jacket.
Swan River Seaplanes provided passengers pouch-style life jackets which were designed for constant wear, and to be donned and inflated when required in an emergency. The life jackets could be inflated using a gas-cylinder inflation system or using an oral inflation system. Instructions for wearing, donning and inflating the life jackets (as shown in Swan River Seaplanes safety information cards) are depicted in Figure 21.
Figure 21: Passenger life jacket wearing, donning and inflating instructions
Source: Swan River Seaplanes
The pilot and all passengers wore their life jackets during the accident flight.
None of the surviving passengers had donned or inflated their life jackets during the evacuation process. Similarly, the pilot and the 2 deceased passengers were found with their life jackets secured around their waists.
Safety briefings and passenger briefing cards
Part 135 of the Civil Aviation Safety Regulations requires pilots to ensure passengers are provided safety briefings (regulation 135.280). The regulations also require the operator of an aeroplane with more than 2 rows of seats to have a safety briefing card available to each passenger, and that the safety briefing card meets the requirements of the Part 135 Manual of Standards (regulation 135.275).
Swan River Seaplanes utilised a safety briefing video, which was shown to passengers prior to departures from South Perth. The surviving passengers all recalled watching the video on the morning of the accident. The video demonstrated:
the use of the aircraft safety equipment, including the location of the aircraft exits, how to open the front and rear doors and how to don the life jackets
the operation of the seatbelts equipped to the final (rear) row of seats.
The video did not demonstrate the operation of the seatbelts equipped to the forward three passenger rows.
The Swan River Seaplanes Aircraft Operations Manual required that prior to all departures, pilots were to ensure that all passengers had received a briefing that included the proper use and adjustment of restraints, the location and operation of emergency exits, and the proper stowage of luggage. The manual required that for overwater flights, the use of life jackets must be demonstrated. The HOFO reported that Swan River Seaplanes pilots were required to provide a passenger briefing in addition to, and including repeating content provided in, the safety video.
Surviving passengers recalled that prior to the departure from South Perth on the morning of the accident, the pilot instructed them to fasten their seatbelts. Passengers did not recall the pilot providing additional instructions about the aircraft exits prior to the morning departure, however they did perceive the video and briefing were comprehensive.
Surviving passengers recalled that the pilot did not provide a briefing during the boarding and preparation for the return flight from Thomson Bay (the accident flight). The passenger in seat 3A recalled that during the boarding, the pilot requested they assist with closing the rear left door. The passenger recalled the pilot provided detailed instructions on how to operate the 2 sections of the rear door, and requested the passenger push the door closed. The passenger considered that the pilot’s instructions for closing the door were helpful for the passenger to subsequently open the right door after the aircraft collided with the sea.
Ongoing investigation focus
Accident survivability, consistent with the ATSB SafetyWatch priority Reducing the severity of injuries in accidents involving small aircraft. This will include consideration of the crashworthiness of Cessna 208 Caravan aircraft, and the suitability of the emergency equipment and procedures for accidents involving immersion in water.
Aircraft maintenance information
Maintenance procedures
The Textron Aircraft Maintenance Manual (AMM) and the Pratt & Whitney Engine Maintenance Manual (EMM) provided manufacturer procedures for the maintenance of the airframe and engine, respectively. Both manuals specified requirements for preservation for extended periods of inactivity, and for return to service inspection procedures following inactivity.
For periods of inactivity greater than 90 days, the EMM required preservation actions including draining the engine oil, installing numerous caps, covers and plugs, and coating numerous surfaces with preservative oils and compounds. The EMM stated that the preservation requirements for periods of inactivity could be substituted by alternatively ensuring the engine is ground run[21] once a week.
The EMM also provided an engine unpreserved procedure, which was for inspection of engines which had been inactive without preservation. For periods of inactivity greater than 90 days, the procedure required examination of engine components, fuel system flush, engine runs and inspection of the fuel control unit at an approved facility. Pratt & Whitney stated that extended inactivity of PT6 engines without the required preservation carried risks associated with moisture ingress and corrosion, and that the risk of corrosion was exacerbated for aircraft operated in a salt-laden environment. Pratt & Whitney further advised that a PT6 engine inactive for the periods specified in the EMM, which had neither been preserved for inactivity nor inspected following inactivity according to the EMM procedures, would be considered to have been not maintained in accordance with the published instructions for continued airworthiness.
Maintenance history prior to acquisition by Swan River Seaplanes
Maintenance documentation associated with VH-WTY showed that the aircraft had been inactive for extended periods of time from June 2021 until it was leased and operated by Swan River Seaplanes in late December 2024. The aircraft was inactive for 1,265 out of 1,277 days during this period and was only operated for 12 days and for 8.1 hours. The main periods of inactivity are shown in Table 6.
Table 6: VH-WTY periods of inactivity June 2021 to December 2024
Dates
Duration (days)
29 June 2021 – 22 June 2022
358
25 June 2022 – 16 March 2023
263
16 March 2023 – 20 October 2023
217
4 March 2024 – 27 December 2024
298
There was no record the engine was preserved according to the EMM procedures for any of these periods of inactivity. Other than during the first few weeks of the final period of inactivity (discussed in the following paragraph) there was no record of engine runs having been conducted while the aircraft was inactive.
During the final period of inactivity, from March to December 2024, VH-WTY was at Bankstown Airport, New South Wales. Another operator had intended to acquire the aircraft and conducted checks of the airframe and associated maintenance documentation. The aircraft was initially stored in a hangar in Bankstown, and the operator conducted weekly engine runs in the first few weeks after VH-WTY arrived.
The acquisition, however, did not eventuate, and with no ongoing commercial arrangement with the aircraft owner, the Bankstown operator moved VH-WTY to a location outside its hangar in about June 2024. The Bankstown operator discontinued weekly engine runs on VH-WTY in around April 2024.
Ferry and inspection prior to operation by Swan River Seaplanes
VH-WTY was leased by Swan River Seaplanes in late December 2024. On 27 December 2024, a special flight permit was issued by an authorised approver on behalf of the Civil Aviation Safety Authority (CASA), for a ferry flight from Bankstown to Jandakot. This permit was required due to the expiry of the maintenance release on 20 October 2024.
On 28 December, VH-WTY departed Bankstown Airport, and on 29 December arrived at Jandakot Airport. A maintenance organisation at Jandakot then conducted checks to meet the time-expired requirements of the maintenance release. The maintenance documentation showed this included conducting the 12-month, 100‑, 200‑, 400‑ and 800‑hour inspections as described in the AMM. A new elevator pushrod bearing was installed, and new rudder pulleys were installed for the left and right floats. Engine work included a compressor power recovery wash and desalination rinse. A seal kit was installed on the engine, which included a new fuel filter. Additionally, the chip detector plugs were recorded to have been inspected with no defects listed.
The records from these maintenance activities did not include reference to the engine unpreserved procedure. The ongoing investigation will consider the maintenance activities conducted prior to VH-WTY being returned to service on 2 January 2025.
Ongoing investigation focus
VH-WTY aircraft preservation actions and return to service inspection activity.
Aircraft operating procedures
Use of water rudders
The AFMS required that water rudders only be used for taxiing the aircraft. The first item on the before take-off checklist was to retract the water rudders.
Witness video footage from the shore of Thomson Bay showed the water rudders extended while the aircraft taxied, consistent with normal practice. Video showed the water rudders were also extended when the aircraft separated from the water, whereas they should have been retracted by this stage.
It is possible that the water rudders were retracted by the pilot during the take-off, but released back to the extended position as the aircraft moved through sea swell. Operational experience is that the Cessna 208 water rudders can inadvertently deploy in rough swell, and a previous operator of VH-WTY had installed an additional restraint strap to prevent this occurring. The pilot of VH-WTY did not use the additional water rudder restraint strap.
Witness and passenger video recorded the aircraft encounter significant swell during the take-off (see Witness environmental observations and recorded video). Video recorded by a passenger on board the aircraft also captured sounds consistent with the water rudder being retracted at a normal stage for the floatplane departure (the video did not show the operation of the water rudder controls).
The primary reason water rudders were required to be retracted during take-off and flight was to prevent damage to the rudders, which can occur if they are left extended during flight operations. Wipaire stated operational experience was that water rudders extended during take-off had benign influence on performance.
Use of quadrant friction lock
The POH, when describing before take-off procedures, required the pilot to adjust the friction lock. It was not possible to determine the setting of the quadrant friction lock for the accident flight.
Stall warning procedures and Cessna 208 amphibian pilot practices
The POH warned pilots that the circuit breaker must be closed for approach and landing. The POH identified that the stall warning system was required to be installed and operable during flight. It further required that pilots check that all circuit breakers were in the ‘IN’ position prior to engine start.
Video recorded by a passenger on board VH-WTY recorded sound within the cabin as the aircraft approached Philip Rock and became airborne. No stall warning horn was captured on the footage. The stall warning circuit breaker was found in the out (power off) position after the accident.
Cessna 208 amphibian aircraft are used by several Australian operators. Pilots experienced with these operations identified that the stall warning system regularly activates during normal water take-offs. These pilots noted that the stall warning horn was loud and distracting, and caused concern to passengers. The pilots identified it was a common practice for Cessna 208 amphibian aircraft pilots to disable the stall warning system by pulling the circuit breaker to the out (power off) position.
The Swan River Seaplanes HOFO stated they were aware that some C208 amphibian pilots engaged in the practice of disconnecting the stall warning circuit breaker. They stated, however, that this was not a common practice of Swan River Seaplanes pilots, and that the operator's procedures required pilots to operate company aircraft according to the aircraft procedures, including ensuring the stall warning circuit breaker was connected.
Ongoing investigation focus
Cessna 208 Caravan stall warning system configuration and the stall warnings provided to pilots during water take-offs and landings.
Take-off procedures
General background
When compared to land-based operations, floatplane take-offs involve the additional challenge of overcoming hydrodynamic drag, parasite drag and the additional weight of the floats. To achieve this, the pilot accelerates the aircraft through the water in a high nose attitude to build hydrodynamic pressure under the floats. This is known as the 'plow' or ‘plowing’ phase. Once there is sufficient pressure, the weight of the aircraft can be supported by the forward section of the floats with the rear section held out of the water. Modern floats feature a stepped construction to reduce drag and facilitate faster acceleration during this phase of the take-off. When the aircraft weight is supported by this forward section of the floats, the aircraft is said to be 'on the step'. Once on the step, the pilot maintains the aircraft in a ‘planing’ attitude and as airspeed increases, more of the aircraft weight is supported by the aerodynamic lift of the wings. When the airspeed is sufficient for the wings to support all the weight of the aircraft, the aircraft becomes airborne.
In crosswind conditions, seaplane pilots may attempt to use a technique whereby they utilise co‑ordinated control inputs to counter the effect of the crosswind to maintain directional control. A crosswind will generally raise the upwind wing, pushing the downwind float into the water which increases drag. By applying ailerons to lift the downwind wing, this drag is reduced. Coordinated use of rudder to keep the floats tracking straight through the water, and elevator to maintain the correct planing attitude on the step, will further minimise drag and assist with acceleration until the upwind float separates from the water.
Procedures for Wipline 8750 equipped Cessna 208 floatplanes
The Airplane Flight Manual Supplement (AFMS) water take-off procedures instructed the pilot to configure the aircraft with the wing flaps set to either 10 or 20°, and the rudder trim at the floatplane take-off index. The pilot was then required to set the power lever for take-off, before retracting the water rudders. Considering the ambient temperature and altitude of the departure from Thomson Bay, the maximum torque for take-off was 1,865 ft lb.
Once on the step, the procedures required the pilot to maintain the planing attitude to allow the aircraft to accelerate. The procedures stated that once the aircraft reached the take-off speed of between 65–70 kt IAS, the pilot could apply light back pressure on the controls to fly the aircraft off the water smoothly.
Take-off performance
Wind component information
The Rottnest Island weather station recorded winds of 23 to 27 kt (with gusts to 33 kt), at 210–220°, from 1530 to 1600 on the day of the accident. While the weather conditions in Thomson Bay may have differed to those recorded at the weather station (about 5.5 km away, and at an elevation of 43.1m), observations from witnesses indicate conditions were similar to those recorded. Further description of recorded and observed weather is provided in Meteorological and environmental information.
Recorded data showed VH-WTY departed on a heading of about 110°. Assuming the aircraft encountered winds consistent with those recorded at the Rottnest Island weather station at 1600, this indicates a tailwind of about 4.3 kt and a crosswind of about 24.6 kt in the prevailing winds.
Performance information
The AFMS provided guidance on the distance required for a water take-off, including values for the distance required for aircraft to achieve a lift-off speed of approximately 67 kt IAS, when configured for take-off with flaps set to 20° and the engine torque set for maximum continuous power.
Considering the values and guidance provided by the AFMS, for the conditions encountered by VH-WTY during its take-off from Thomson Bay:
The aircraft would require a take-off distance of approximately 756 m (2,482 ft) considering ambient temperature of 24°C and sea-level altitude.[22]
The take-off distance required was extended by 20% (151 m) due to the approximately (mean) 4 kt tailwind.
The take-off distance required was increased by 1% (8 m) due to the pilot setting the inertial separator system[23] to BYPASS.
The take-off distance required, according to the guidance provided in the AFMS, was thus estimated to be about 915.4 m (3,003.2 ft).
As identified in Meteorological forecasts and observations, the recorded wind strength and direction remained relatively constant from 1400, and therefore this calculation is likely to be reflective of the conditions apparent when the pilot inspected Thomson Bay at 1500 (see Assessment of environmental conditions by the pilot of VH-WTY).
The AFMS calculated take-off distances were based on smooth (not glassy) water conditions, and at the maximum take-off weight for the aircraft. The AFMS did not provide methods for adjusting the calculations for variations in water conditions or take‑off weight. The ATSB notes that VH-WTY was operated at less than its MTOW (see Weight and balance), and that the water conditions in Thomson Bay included significant swell and waves (see Witness environmental observations and recorded video).
The calculated take-off distances do not account for variations in wind direction or strength, including gusts, which were present on the afternoon of the accident. The ATSB final investigation report may include additional calculation of the take-off distance required considering these factors.
Regulatory requirements for determining take-off distances
The Civil Aviation Safety Regulations (CASR), Part 135.350, states that the Part 135 Manual of Standards (MOS) may prescribe requirements relating to the take-off performance for a flight of an aeroplane. The Part 135 MOS states that an operator and pilot in command must ensure that the take-off run available for a selected runway does not exceed the factored take-off run for that aircraft. The factored take-off run is the take‑off run required for the aeroplane, multiplied by a standard take-off factor determined by the MTOW of the aircraft. The Part 135 MOS states that for an aeroplane with a MTOW of greater than 3,500 kg a take-off factor of 1.25 must be applied.
The required factored take-off run for VH-WTY was estimated to be about 1,144 m.
Aircraft crosswind limitations
The Cessna 208 was certified under US Federal Aviation Regulations Part 23[24] and approved in October 1984 with ongoing production. Under Part 23 certification testing requirements the manufacturer was required to demonstrate handling characteristics and adequate directional stability and control. The regulations defined the required crosswind handling characteristics as:
A 90 degree cross-component of wind velocity, demonstrated to be safe for taxiing, takeoff, and landing must be established and must be not less than 0.2 VS0.
The published Vs0[25] for the Cessna 208 is 60 kt calibrated airspeed.[26] This means that the aircraft was required to demonstrate adequate handling, stability and control in crosswinds of at least 12 kt.
The AFMS specified the maximum crosswinds in which Cessna 208 aircraft equipped with the Wipline 8750 floats had been demonstrated during certification testing. The AFMS stated that for water take-offs, the maximum demonstrated crosswind was 14 kt. The AFMS further stated that the demonstrated limitation was ‘close to the capabilities of the airplane’.
Aircraft tailwind limitations
The US Federal Aviation Administration (FAA) Floatplane Handbook identifies that downwind take-offs (that is, take-off conducted with a tailwind component) may be necessary or preferred due to water conditions. The FAA Floatplane Handbook notes, however, that this will result in a longer take-off run due to the requirement for the aircraft to first accelerate to the speed of the wind, then to the correct speed to generate lift for take-off.
The FAA Floatplane Handbook notes that during floatplane operations, tailwind has an additional effect to further lengthen the required take-off run due to float drag. It states:
The speed of the floats in the water corresponds to the higher groundspeed required in a landplane, but the drag of the floats increases as the square of their speed. This increase in drag is much greater than the increase in rolling resistance of tires and wheel bearings in a landplane. A tailwind may lengthen the seaplane’s takeoff distance much more dramatically than the same tailwind in a landplane.
There was no maximum tailwind for take-off identified in the AFMS. The AFMS stated that for tailwind up to 10 kt, take-off distance required increased by 10% for every 2 kt of tailwind.
Aircraft wave and sea limitations
Rough water can adversely affect the performance of floatplanes during take-off and landing. The FAA Floatplane Handbook states:
In most cases an experienced seaplane pilot can safely take off in rough water, but a beginner should not attempt to take off if the waves are too high…The advisability of canceling a proposed flight because of rough water depends on the size of the seaplane, wing loading, power loading, and, most importantly, the pilot’s ability. As a general rule, if the height of the waves from trough to crest is more than half the height of the floats from keel to deck, takeoffs should not be attempted except by expert seaplane pilots.
The FAA Floatplane Handbook provides guidance on pilot techniques for rough water take-offs and states:
Fortunately, a takeoff in rough water is generally accomplished within a short time because if there is sufficient wind to make water rough, the wind is also strong enough to produce aerodynamic lift earlier and enable the seaplane to become airborne quickly.
The FAA Handbook does not consider the suitability of conducting a rough-water take-off with headwind and crosswind component.
The AFMS stated that the Cessna 208:
Has been demonstrated to operate satisfactorily in wave heights (trough to crest) of approximately 14 inches [35.6 cm]. This is not considered to be a limitation.
Wipaire identified that the effect of rough wind is not easily quantifiable, and these effects were not directly assessed during certification testing beyond the demonstrated 14‑inch limit noted in the AFMS. Wipaire also noted that very rough water with large swell can cause the aircraft to lift off before intended.
Ongoing investigation focus
Take-off performance requirements and limitations considering environmental conditions.
Swan River Seaplanes Thomson Bay operations
Regulatory context for water aerodromes
The Civil Aviation Safety Authority (CASA) advisory circular AC 139.F-01 provided guidance for the design and operation of water aerodromes for air transport operations. Water aerodromes were defined as:
A defined area, primarily on water, intended to be used either wholly or in part for the arrival, departure and movement of seaplanes, and any building and equipment on ground or water.
AC 139.F-01 noted that the International Civil Aviation Organization (ICAO) recommends that States certify water aerodromes open to public use through an appropriate regulatory framework. AC 139.F-01 stated that as CASA does not require certification of water aerodromes, it has notified a difference with this requirement.
Guidance provided by AC 139.F-01 included that:
The take-off direction of water runways will vary depending on prevailing conditions. AC 139.F-01 stated that floatplane pilots will determine the correct direction at the time of take‑off.
The length of a water runway should be sufficient to meet the requirements of the floatplane with which take-offs are intended to be conducted, considering the conditions in the local operating environment.
The dimensions available for aircraft use should be provided in a suitable format. Any limits or restrictions should be made available to pilots operating to the area.
Regulatory context for use of water runways
The CASR Part 91.410, stated that take-offs and landings must only be conducted at a location if:
The aircraft can land at, or take off from, the place safely having regard to all the circumstances of the proposed landing or take‑off (including the prevailing weather conditions).
The regulations specified that aircraft may take-off or depart from certified aerodromes, or from a place ‘that is suitable for the landing and taking-off of aircraft’. The water alighting area at Thomson Bay was not certified, and therefore the use of the bay for floatplane operations was dependent on the pilot and Swan River Seaplanes determining the area was suitable for the aircraft.
The CASA publication AC 91-02[27] provided advisory guidance to assist pilots when determining the suitability of a place to safely take off and land. The publication stated that pilots have a responsibility to satisfy themselves that an aeroplane can safely take off from, or land at, a location. The publication advised that this requires consideration of the aircraft type and weight, the prevailing weather conditions and the dimensions and other characteristics of the intended landing or take-off location. AC 91-02 recommended that water aerodromes provide a channel of at least 60 m width for day operations, and sufficient depth.[28]
AC 91-02 further stated pilots must resist personal and external pressures to proceed when evidence suggests safety is not reasonably assured. The publication advised that persons involved in operating an aircraft should pre-identify criteria for cancelling an operation (‘no-go decision criteria’). AC 91-02 advised that operations should not be commenced in circumstances where no-go criteria have been met, unless appropriate consideration has been given to safety mitigation and regulatory requirements.
Swan River Seaplanes procedures
The Swan River Seaplanes Air Routes and Aerodromes manual described the aerodromes and water alighting areas regularly used by the operator. The exposition stated that Rottnest Island (Thomson Bay) was a ‘water alighting area’ approved by Swan River Seaplanes for use for CASR Part 135 operations.
The procedures for the Thomson Bay water alighting area provided a water alighting area diagram, which showed a defined ‘suitable landing area’ (Figure 22). The procedures did not describe the dimensions of the suitable landing area, and nor did they indicate the tracks which should be utilised for take-offs and landings in the area.
Figure 22: Swan River Seaplanes water alighting area diagram for Thomson Bay
Source: Swan River Seaplanes
The water alighting area procedures stated that water landings were only to be conducted at Thomson Bay ‘in a clear area with safe available landing and take-off distances. These factors are to be determined by pilot in command’. The procedures also stated that the (red shaded) danger area was to be avoided at all times.
Rottnest Island approvals
The Rottnest Island Authority[29] provided approval for Swan River Seaplanes pilots to conduct water landings and departures from Thomson Bay. Following approval to conduct trial take-offs and landings in January to April 2023, the authority provided and renewed approvals for the operations from October 2023 to June 2025.
The approvals to conduct operations in Thomson Bay specified several conditions, including that landings may only occur in a designated area. The Rottnest Island Authority and Swan River Seaplanes personnel confirmed it was understood that take‑offs were also to only occur in this area. The Swan River Seaplanes HOFO stated that company pilots were permitted to operate outside the designated area if required for safety of flight.
Figure 23: Thomson Bay area of approved operations, as described in Rottnest Island Authority approval
Source: Google Earth, annotated by the ATSB based on information provided by Rottnest Island Authority
Marine vessels were restricted to a maximum 5 kt in parts of Thomson Bay. The Western Australian Department of Transport provided an exemption to this limit for seaplanes during take-off and landing, in a designated section of the bay. The exemption was gazetted in May 2023.
Ongoing investigation focus
Swan River Seaplanes’ identification and assessment of Thomson Bay for floatplane operations.
Thomson Bay departures
The ATSB examined available electronic flight data records of previous take-offs from Thomson Bay by aircraft operated by Swan River Seaplanes since 2023. Swan River Seaplanes operated another Cessna 208 amphibian, registered VH-UOZ, and used this aircraft for all flights conducted in 2023 and 2024.
A flight tracking device equipped to VH-UOZ recorded 95 departures from Thomson Bay in 2023 and 2024. The flight tracking data showed that departures from Thomson Bay typically involved the aircraft taxiing from the pontoon to the north‑east, into the centre of the bay. The take-off run would then typically be conducted on a south-westerly or south‑easterly heading (Figure 24).
Figure 24: Typical tracks recorded for take-offs from Thomson Bay in VH-UOZ
Source: Google Earth, annotated by the ATSB
Flight tracking information from the accident aircraft, VH-WTY, recorded the flights conducted from Thomson Bay on 4 and 5 January under the command of the Swan River Seaplanes HOFO. All of these flights were conducted on a south-easterly track (Figure 25). The pilot of the accident flight had not conducted a take-off from Thomson Bay using VH-WTY prior to the day of the accident.
Figure 25: Recorded departure (including taxiing phase) tracks for VH-WTY within Thomson Bay displaying the difference between the accident flight and the previous flights
Source: Google Earth, annotated by the ATSB
Take-off wind for previous flights
Observations recorded at the Rottnest Island weather station included the wind strength and direction at the time of take-offs from Thomson Bay, as captured in the flight tracking information for VH-UOZ and VH-WTY. Recorded weather and flight tracking information for 30[30] take-offs from Thomson Bay in 2024 and 2025 (including the accident flight) showed the following:
Only 2 flights were conducted from Thomson Bay with a tailwind, with the accident flight being conducted with the highest tailwind (4.3 kt).
The accident flight take-off was conducted with the highest crosswind component (24.6 kt), with only 1 other take-off having a crosswind component of over 18 kt. The majority of the take-offs (25 of 30) were conducted with a crosswind component of less than 13 kt.
Most (25 of 30) take-offs were conducted with a recorded windspeed of less than 20 kt.
Pre-flight assessments
Swan River Seaplanes procedures
The Swan River Seaplanes Aircraft Operations Manual stated that all flights were to be authorised by the HOFO. Prior to authorising flights, the HOFO was to consider whether the pilot in command was rated for the aircraft type and class, had a current flight review and was current for the route. The HOFO was deemed to have authorised a flight when they rostered a pilot onto a flight sector.
The Aircraft Operations Manual stated that once the HOFO had authorised a flight, a pilot with more than 250 water landings may be given ‘a general approval to operate in weather conditions at their discretion’. Such pilots had authority to make decisions regarding whether a flight should proceed, proceed subject to modification, or be cancelled. The manual stated that the HOFO retained the authority to override a pilot’s decision and was still responsible for controlling operations.
The Aircraft Operations Manual stated that within one hour prior to a flight, the pilot in command must study all available information relevant to the flight. This was to include all current weather reports and forecasts for the route, departure and destination aerodromes.
The Aircraft Operations Manual did not provide or suggest any limits for forecast wind conditions.
Ongoing investigation focus
Swan River Seaplanes’ operational oversight practices.
Suitability of alighting areas
The Aircraft Operations Manual stated that water take-offs and landings must be conducted from an area conforming to the recommendations described in Civil Aviation Advisory Publication (CAAP) 92(1).[31] CAAP 92(1) provided similar guidance to that contained in AC 91-02, recommending that water alighting areas provide:
a runway length equal to or greater than that specified in the aeroplane's flight manual or approved performance charts or certificate of airworthiness, for the prevailing conditions is required...
CAAP 92(1) further recommended:
A pilot should not use a landing area without taking all reasonable steps to ensure the physical characteristics and dimensions are satisfactory. For aerial work and charter operations the operator should provide evidence to the pilot on the suitability of a landing area prior to its use.
The Aircraft Operations Manual further required pilots assure themselves that the proposed take-off area provided a suitable water surface that was clear of obstructions. The manual indicated that pilots must assure themselves of the suitability of the water surface. The manual indicated this check was to be conducted from the air, stating:
Pilots shall make judgments when airborne, of the suitability of the sea surface for alighting on the water. If in doubt - do not operate. This shall consider variables such as, wind velocity, turbulence, sea state, tidal flow and natural protection by bays, reefs etc.
Ongoing investigation focus
Swan River Seaplanes’ procedures and other risk controls for Thomson Bay operations, including safety management system functions.
Assessment of environmental conditions by the pilot of VH-WTY
The pilot’s mobile phone and other sources showed that the pilot had access to multiple sources of weather observation and forecast information while preparing for the departure from Thomson Bay. This included:
The HOFO messaged the pilot at 1116, providing an image from a weather website showing that winds at Rottnest Island were 25 kt with gusts to 34 kt.
At 1316, the pilot accessed and saved weather observation and forecast information for Rottnest Island. The image showed that winds had been recorded at 25 kt, gusting to 34 kt, and that actual winds were much stronger than predicted.
At 1525, the pilot accessed the same forecast and saved another image. This showed that winds were still recorded at 25 kt south-south‑west, however the gusts had reduced to 27 kt. The image showed forecast winds increasing (Figure 26).
Figure 26: Rottnest Island wind measurement and prediction obtained by pilot of VH‑WTY at about 1525 on 7 January 2025
Source: Mobile phone records
The tender vessel used by Swan River Seaplanes was equipped with a tracking device, which recorded positional information at approximately 1-minute intervals. Closed‑circuit television (CCTV) recorded the jetty where the tender vessel docked at in Thomson Bay, and showed the times the vessel arrived and departed.
The tracking data and CCTV showed that the pilot operated the tender vessel solo at about 1300, with the tracking data showing the tender vessel operated to about 400 m north-west of Philip Rock. The vessel was recorded at this location at about 1310 on a heading of 55° at 22 kt. The vessel returned to the jetty at about 1320.
Figure 27: Thomson Bay showing farthest (most easterly) recorded positions of the tender vessel during inspection journeys at 1300 and 1500, 7 January 2025
Source: Google Earth, annotated by the ATSB
CCTV recorded the coxswain arrive at the jetty and board the tender vessel with the pilot at about 1450. The tracking data showed the tender vessel was then operated to about 450 m west of Philip Rock, before returning to the fuel jetty. Regarding this journey, the coxswain recalled that:
The tender was navigated along the operator’s normal north-south take-off track.
Both the pilot and the coxswain agreed that conditions along that track were not suitable.
The pilot decided to conduct a crosswind take-off, using an easterly track.
The tender was not operated along this easterly track.
Conditions in Thomson Bay were calm, but were rough beyond Philip Rock. The coxswain did not recall the pilot describing an assessment of the conditions along the easterly departure track, or identifying an intended lift-off point.
Ongoing investigation focus
The pilot of VH-WTY’s assessment of conditions for the take-off from Thomson Bay, including the decision to conduct an eastwards take-off.
Swan River Seaplanes
Organisational background
Swan River Seaplanes commenced flight operations in 2017. The organisation initially conducted flights from the Swan River to Margaret River, Western Australia, using a leased Cessna 208 amphibian. Swan River Seaplanes reported commencing flights to the sealed runway at Rottnest Island Airport in October 2017, with operations from Thomson Bay commencing in January 2023. In addition to operating to Rottnest Island, Swan River Seaplanes conducted scenic flights departing and arriving on the Swan River. The operator also conducted occasional charter flights to Busselton, Western Australia.
Swan River Seaplanes had 2 directors, one of whom founded the organisation and was also the approved chief executive officer for the air operator’s certificate (AOC).[32] The other director was also the approved safety manager for the AOC.
Swan River Seaplanes had a HOFO and alternate HOFO. The HOFO also held the positions of head of training and checking, head of aircraft airworthiness and maintenance control, and conducted line flying duties. The alternate HOFO conducted check and training activities for Swan River Seaplanes. The organisation also employed 2 line pilots, one of whom was the pilot of VH-WTY. The alternate HOFO had previously conducted line flights but was not operating in that function at the time of the accident.
Additionally, Swan River Seaplanes employed several personnel to conduct duties such as operating the company tender vessel and docking company aircraft.
Swan River Seaplanes operated 2 Cessna 208 amphibian aircraft, registered VH-UOZ and VH-WTY. The operator used VH-UOZ for all flights conducted in 2023 and 2024, until the aircraft became unserviceable due to a mechanical problem. The operator leased VH-WTY and commenced operations using the aircraft on 2 January 2025.
Regulatory context
Swan River Seaplanes had a valid AOC with approval to conduct air transport operations under Part 135 of the CASRs. The company also had valid approval to conduct aerial work (Part 138) and to operate a flight check system.
Further investigation
To date, the ATSB has conducted the following activities:
interviewed current and former Swan River Seaplanes personnel and other parties involved in the maintenance of VH-WTY
engaged Pratt & Whitney to conduct a tear-down examination of the aircraft engine, and reviewed the findings from that examination
reviewed information recorded by avionics equipment on board VH-WTY
reviewed video recordings from witnesses, CCTV and other sources
reviewed information recovered from mobile devices
reviewed the forecast and observed weather conditions at Rottnest Island
reviewed maintenance documentation for VH-WTY
reviewed Swan River Seaplanes operational procedures
analysed recorded flight data and weather information for previous take-offs from Thomson Bay
engaged medical specialists to review post-mortem records to support analysis of the cause of the 3 fatalities.
The investigation is continuing and will include review and consideration of:
aircraft handling and performance prior to and following the separation from the water
take-off performance requirements and limitations considering environmental conditions
the pilot of VH-WTY’s assessment of conditions for the take-off from Thomson Bay, including the decision to conduct an eastwards take-off
accident survivability, consistent with the ATSB SafetyWatch priority Reducing the severity of injuries in accidents involving small aircraft; this will include consideration of the crashworthiness of Cessna 208 Caravan aircraft, and the suitability of the emergency equipment and procedures for accidents involving immersion in water
VH-WTY aircraft preservation actions and return to service inspection activity
Cessna 208 Caravan stall warning system configuration and the stall warnings provided to pilots during water take-offs and landings
Swan River Seaplanes’ identification and assessment of Thomson Bay for floatplane operations
Swan River Seaplanes’ operational oversight practices
Swan River Seaplanes’ procedures and other risk controls for Thomson Bay operations, including safety management system functions
regulatory oversight of Swan River Seaplanes and VH-WTY maintenance activities.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The position ‘head of flying operations’ is also commonly referred to as the ‘chief pilot’.
[2]A coxswain is a person in charge of navigating and steering a small water vessel.
[3]A common traffic advisory frequency is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport or within a broadcast area.
[4]A nose high, powered taxi characterised by high water drag and an aftward shift of the centre of buoyancy. The weight of the floatplane is supported primarily by buoyancy, and partially by hydrodynamic lift. Also referred to as the ‘plow’ position.
[5]Indicated airspeed (IAS): the relative velocity between the aircraft and the surrounding air (airspeed), as measured by the equipped airspeed indicator and corrected for instrumentation error.
[6]The aircraft is said to be ‘on the step’ when the weight of the aircraft is supported on the forward portion of the floats by hydrodynamic and aerodynamic lift, as it is during high-speed taxi or just prior to take-off. This position, which is also referred to as the planing position, produces the least amount of water drag.
[7]Swan River Seaplanes stored its aircraft at Jandakot Airport. Prior to the first flight of the day, pilots would position the aircraft from Jandakot to the Swan River.
[8]A ‘touch-and-go’ is a practice landing in which the aeroplane is permitted to touch the landing area briefly.
[9]Wind direction information was not available for Rottnest Island weather station, and was estimated by averaging the wind direction recorded at nearby weather stations.
[10]Cessna is a brand of aircraft owned by Textron Aviation, which is the aircraft manufacturer.
[11]The complete title of this manual was the Pilot’s Operating Handbook and FAA Approved Airplane Flight Manual, Caravan Model 208, 675 SHP – Gamin G1000. This manual was applicable to Cessna 208 aircraft equipped with G1000 avionics equipment. The revision applicable at the time of the accident, and referred to in this report, was Revision 6.
[12]The complete title for this manual was the FAA Approved Pilot’s Operating Handbook and Airplane Flight Manual Supplement for the Cessna Model 208 Caravan (675 Shp Pt6a-114a) with Wipline Model 8750 Amphibious Floats when operated at a Maximum Gross Weight Of 8750 Lbs.
[13]An aerodynamic stall is a rapid decrease in lift and increase in drag caused by the separation of airflow from the wing’s upper surface. A stall occurs when the angle of attack exceeds the wing’s critical angle of attack, resulting in the disruption to the smooth airflow over the wing. This can ordinarily occur at angles of around 16°.
[14]An anemometer is a device that measures wind speed and direction.
[15]Swell - swell waves are the regular, longer period waves generated by distant weather systems. Definition provided by the Department of Transport – WA.
[16]Sea waves – sea waves are generated by the local prevailing wind. Their height depends on the length of time the wind has been blowing, the fetch (the distance the wind has blown over the water), and the water depth. Definition provided by the Department of Transport – WA.
[17]Total wave height is the combined height of the sea waves and the swell. It's also called the combined sea and swell. Definition and method for calculating total wave height obtained from Waves and swell | The Bureau of Meteorology.
[18]The carry-through structure of an aeroplane joins, and transmits loads between, the wings and the fuselage.
[19]Pratt & Whitney examined the engine on 25 to 27 March 2025. The examination was overseen by the Transportation Safety Board of Canada, which is an accredited representative of the ATSB investigation under the provisions of Annex 13 to the Convention on International Civil Aviation.
[20]The formal title of this document was ‘Part 135/138 Exposition: Volume 2A – Aircraft Operations – General’.
[21]Engine ground running is the operation of the aircraft engine while on the ground for the purpose of checking the operation of the engines or other aircraft systems.
[22]The AFMS provided take-off distances for ambient temperatures of 20° and 30°C. The ATSB interpolated between these figures to estimate the distance required for 24°C.
[23]An inertial separator is an engine component designed to prevent foreign objects from entering the engine air intake.
[24]These regulations prescribe the airworthiness standards for Normal category aeroplanes.
[25]Vs0 is an abbreviation of Velocity stall 0. It represents the stall speed of an aircraft configured for landing.
[26]Calibrated airspeed is the aircraft’s speed through the air once non-standard atmosphere (or atmosphere of the day) effects are applied to true airspeed.
[27]The full title of this document was ‘CASA Advisory Circular 91-02 - Guidelines for Aeroplanes not Exceeding 5700 kg MTOW - Suitable Places to Take Off & Land’, dated November 2022.
[28]AC 91-02 recommended ‘ensuring that the depth of water over the whole water channel be 300 mm or greater below the hull or floats when the aeroplane is stationary and loaded to maximum take-off weight.’
[29]The Rottnest Island Authority is a statutory authority responsible for the management of Rottnest Island on behalf of the Western Australian Government.
[30]There were 32 take-offs conducted from Thomson Bay in VH-UOZ in 2024 and 6 conducted in VH-WTY in 2025. Records from several departures were not included due to issues with recorded wind data. For 4 recorded flights, wind direction information was not available for Rottnest Island weather station, and was estimated by averaging the wind direction recorded at nearby weather stations.
[31]Civil Aviation Advisory Publication 92-1. Guidelines for Aeroplane Landing Areas. Note: This publication was discontinued by CASA in 2021.
[32]A certificate issued by CASA under the provisions of the Civil Aviation Act (1998), Part 3, Division 2. The Civil Aviation Safety Regulations, Part 119, require that a valid Australian air transport AOC is required for all air transport operations.
Summary
The ATSB is investigating a collision with water involving a Cessna 208 Caravan Amphibian, registered VH-WTY, near Rottnest Island, Western Australia, on 7 January 2025. On board was one pilot and 6 passengers.
During the water take-off, the aircraft was observed to become airborne then impact the water. The pilot and 2 passengers were fatally injured, and 3 passengers sustained serious injuries.
Preliminary and interim reports, which detailed factual information established during the course of the investigation, have been released (see the adjacent tab).
The ATSB anticipates publishing a substantive interim report, to update industry and the public on the progress of the investigation and to detail areas of continuing investigation, in mid 2026.
A final report will be released at the conclusion of the investigation, and will detail analysis and findings.
However, if at any time during the investigation we discover a critical safety issue, the ATSB will work closely with the relevant stakeholders so action can be taken to address that issue.
Occurrence summary
Investigation number
AO-2025-001
Occurrence date
07/01/2025
Location
Rottnest Island
State
Western Australia
Report release date
19/12/2025
Report status
Interim
Anticipated completion
Q3 2026
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Textron Aviation Inc.
Model
208 Caravan (amphibian)
Registration
VH-WTY
Serial number
20800586
Aircraft operator
Swan River Seaplanes
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Thomson Bay, Rottnest Island, Western Australia
Destination
Elizabeth Quay Aircraft Landing Area, Western Australia
The ATSB assisted the New South Wales Police Force with an investigation into a collision with water involving a TL Ultralight Sting S4, registered 23-1677, 5 km north-west of Scotts Head, New South Wales, on 4 January 2025. This assistance was initiated at the request of Recreational Aviation Australia (RAAus).
While reportedly conducting flying training, the aircraft collided with water resulting in fatal injuries to the 2 occupants. The aircraft was destroyed.
As part of an investigation by the Coroner’s Court of New South Wales, the ATSB provided assistance to the NSW Police by conducting an onsite technical examination of the recovered airframe. The ATSB found that the predominantly composite airframe was significantly disrupted, consistent with a relatively high energy impact with the water. Almost all of the major airframe components, flight controls, linkages, and control surfaces were available and examined by the ATSB, which did not identify any pre-existing defects that could have contributed to a premature, in-flight component failure.
Information on ATSB investigation of sport aviation accidents is available here.
Any enquiries relating to the investigation should be directed to the New South Wales Police Force.
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 4 December 2024, at about 0530 local time, a Robinson R44 Raven II helicopter, registered VH-XIX, departed from Griffith Regional Airport, New South Wales to conduct a ferry flight to a property approximately 50 km east of Young. Onboard were the operator’s Griffith base manager and a loader[1] (acting as pilot for the ferry flight). They arrived at a paddock on the farm at 0744, landing next to a chemical tank. They were met by the farm manager of the property, and the pilot for the day, who had arrived shortly before by motor vehicle from Crookwell. The tasking for the day was the aerial application of herbicide across 2 properties, to be conducted under Part 138 of the Civil Aviation Safety Regulations.
The base manager, pilot, loader and farm manager discussed the day’s work and then prepared the helicopter for spraying operations, including refuelling the helicopter, attaching the spray booms and mixing herbicide. At 0912, the pilot and base manager, who had sprayed the paddocks previously, flew the helicopter on a reconnaissance mission of the intended paddocks returning 5 minutes later.
The helicopter was loaded with herbicide and, at 0921, the pilot departed for application of the first load of the day. The pilot applied 10 loads consecutively. Each load took around 10 minutes to apply, with the pilot returning for the helicopter to be replenished with herbicide, and fuel as required, before immediately departing again.
Toward the end of this activity, the farm manager from an adjacent property arrived and discussed the task for the second property with the base manager. During this time, the pilot departed for the 11th and planned final load of the job on the first farm. After 15 minutes, the base manager realised the helicopter should have returned and tried, unsuccessfully, to contact the pilot via ultra‑high frequency radio in the work vehicle. The base manager then checked a flight tracking application on their mobile phone that showed the helicopter had not moved from its last indicated location for a couple of minutes. The base manager and second farm manager departed in the farmer’s vehicle toward the intended spray area, while the loader stayed to monitor the work vehicle’s radio.
Prior to the flight, high tension powerlines that ran through the middle of the intended spray area had been identified as a hazard to the operation. The base manager and farmer headed to a location near the powerlines but could not find the helicopter. After further searching, they located the wreckage of the helicopter in a gully. They made their way down to the helicopter and found the pilot had exited the helicopter and moved approximately 1 m away but was seriously injured. Emergency services attended, however, the pilot succumbed to their injuries.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter) with a single-engine helicopter class rating. The pilot had 1,035 hours total aeronautical experience, of which 637 hours were on the R44 type. Most of the pilot’s recent flying had been on the R44. The pilot also held a gas turbine design feature endorsement, and numerous piston and turbine type ratings. In addition, the pilot held aerial application, low-level, and sling operational ratings. The pilot had spent approximately 3 years flying agricultural helicopters in New Zealand where they also obtained a mountain flying operational rating.[2]
The pilot held a valid class 1 aviation medical certificate and was reported as appearing well rested and fully alert for the flight.
Helicopter information
The Robinson R44 Raven II is a 4-seat helicopter, powered by a single Textron Lycoming IO‑540‑AE1A5 piston engine driving a 2 blade semi-rigid main rotor system and 2 blade tail rotor system. The helicopter was manufactured in the United States in 2003 and first registered in Australia in May 2003. It was issued with a special certificate of airworthiness in the restricted category in January 2017. The certificate permitted VH-XIX to be used in agricultural operations and aerial surveying, among other similar operations.
A periodic inspection and minor maintenance tasks were carried out on 30 October 2024. At the time of the accident, the helicopter had accumulated about 5,820 hours. The helicopter was configured with an agricultural spray system, which consisted of 2 fibreglass chemical tanks, a flexible hose and stainless-steel tubing distribution system, a petrol‑powered water pump, valving systems, and 2 cantilevered carbon fibre spray booms, one each on either side of the fuselage.
Meteorological information
The closest Bureau of Meteorology weather station was at Young Airport, 50 km to the west of the accident site, which reported winds of 7–8 kt from the north-west and a temperature of 28°C in 30‑minute windows around the time of the accident. Cloud cover[3] was measured as few at 3,500 ft and broken at 4,800 ft. Cowra weather station, 53 km to the north, reported winds of 4–7 kt varying between northerly and westerly and a temperature around 28–30°C. Cloud cover was not recorded.
Wunderground.com is a weather network designed to provide public access to community weather stations. A weather station at Boorowa, 14 km south-south-west of the accident site, reported wind, in 5-minute windows, of 6.8 km/h (3.6 kt) gusting to 7.3 km/h (3.9 kt), from the south‑south‑west and a temperature of 19°C around the time of the accident. Another weather station at Frogmore, 8 km to the north-east, reported wind of 0.9 km/h (0.5 kt) gusting to 1.9 km/h, (1.0 kt) from the north-north-west, with a temperature of 22°C.
Wreckage and impact information
The wreckage was located about 1,200 m south-south-east of the base of operations for that day, in a steep gully towards the southern end of the target spray area. The area was in hilly terrain and contained high dry grass with scattered large alive and dead eucalyptus trees.
The first items in the debris trail were the stabiliser assembly, right side carbon fibre spray boom and broken branches. These items were located next to a dead tree, with freshly broken branches on one side, near the top (Figure 1).
The helicopter was orientated on its left side and facing the direction of the travel. The main fuselage had sustained minor impact damage, with the exception of the cabin, which was significantly disrupted. Outboard sections of both main rotor blades had been liberated during the accident sequence. For the tail rotor assembly, one liberated tail rotor blade, and sections of the tailcone were scattered to the right of the ground path. Despite the disruption, all components of the helicopter were accounted for.
Two ground scars, consistent with the landing gear skids, were located between the tree and the wreckage in the gully. The ground marks were indicative of the upright helicopter sliding along the ground, prior to reaching the edge of the gully.
Figure 1: Wreckage site
Note: Ground scars from the helicopter skids are highlighted red.
Source: ATSB
While the ATSB conducted a preliminary examination of the wreckage at the site, due to access restrictions, the wreckage was relocated to a secure facility for detailed examination. This further examination identified:
no evidence of pre-impact defects with the flight controls or structure
approximately 55 L of low-lead aviation fuel in the fuel system, which was visibly clear of contaminants and tested negative to the presence of water
the engine was able to be rotated, contained oil and there were no obvious defects upon external examination
the fuel gascolator, engine oil, hydraulic fluid, and intake air filters were clear of particles
the air intake hose had no signs of collapse, delamination or restriction
the main and tail rotor gearboxes contained oil, with no metal contamination on the respective chip detectors.[4]
Recorded data
The helicopter had analogue instrumentation and did not record any flight or engine parameters.
A SpotTrace device was carried inside the helicopter, which broadcast the device’s position every couple of minutes when movement was detected. Anybody with access rights could see the position of the tracking device using a computer or mobile phone application. The SpotTrace device broadcast the position of the helicopter from shortly after take‑off that morning, until the helicopter stopped moving, in a position coincident with the collision with terrain.
To assist with aerial application tasks, the helicopter was also fitted with a Tracmap GPS guidance device with recording capability. The flight tracks from the day of the accident were recorded and downloaded, including information about when the spray valve was open (Figure 2 in orange), up until a couple of minutes before the accident. Due to the sudden removal of power, some data collected towards the end of the flight was not able to be downloaded. A chip level recovery[5] was conducted from the device but it contained no further information.
Figure 2: Tracmap spray runs completed
Note: The last few minutes of the flight and spray runs were not recorded.
Source: Google Earth Pro, annotated by the ATSB using operator and onboard data sources
Further investigation
To date, the ATSB has conducted witness interviews, collected documentation and recorded data, and examined the site and wreckage.
The investigation is continuing and will include review and examination of:
witness accounts
recorded data
the wreckage
helicopter documentation
operational records
pilot medical records, qualifications and experience.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance of the Young branch of the NSW Police Force during the onsite stages of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Loader: the term used to denote ground support personnel whose functions include assisting with mixing chemicals, loading and dispatching the aircraft.
[2]A mountain flying rating is not a rating classification available under the Civil Aviation Safety Regulations Part 61 licencing system but is a valid rating in some countries.
[3]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[4]Chip detector: a magnetic device used to gather chips of metal from engine or transmission oil to provide early warning to maintenance personnel of impending engine failure. Depending on the installation, it can be linked to an in-cockpit indicating light to provide immediate advice to aircrew.
[5]Chip level recovery: involves removing (desoldering) the memory integrated circuit (IC) package from the circuit board of the device and, using dedicated hardware and software tools, reading an image of the IC contents directly from the IC.
Summary
The ATSB is investigating a collision with terrain involving Robinson Helicopter Co R44 II, VH‑XIX, about 50 km east of Young Airport, New South Wales, on 4 December 2024.
During aerial spraying operations, the helicopter collided with terrain and was destroyed. The pilot sustained fatal injuries.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
On 7 May 2024, a Cessna 208 amphibian was operating a round-trip sightseeing flight from a floating pontoon facility in Talbot Bay, Western Australia with a pilot in command under supervision, a supervising pilot and 6 passengers on board. The facility had the capacity for up to 4 seaplanes to launch and dock side by side. The aircraft was moored on dock 1, the forward‑most dock.
A strong pushing on[1] tide existed on the day with an easterly 8 kt wind. Two dockhands on the pontoon assisted the flight crew with the launch of the aircraft while the flight crew began the engine start sequence.
The environmental conditions had a greater effect on the aircraft than the crew anticipated, and the tide pivoted the front of the aircraft left around the corner of the dock, while the wind pushed the tail of the aircraft away from the pontoon. Once the aircraft was out of reach of the dock crew, the tidal movement pushed the aircraft through the water towards a houseboat at the front of the pontoon’s configuration.
The crew continued with the engine start and the aircraft started to move forward under its own power. The supervising pilot took over control, increasing engine power and bringing the propeller out of the feathered[2] position. However, the wind continued to rotate the aircraft to the left, and the flight crew was unable to achieve sufficient forward speed through the water before the aircraft collided with the houseboat.
The aircraft’s left wing impacted first, swinging the aircraft into the bow of the houseboat, resulting in a further propellor impact (Figure 1). The aircraft came to rest entangled in the pontoon’s mooring lines. There were no injuries to the flight crew or passengers.
Figure 1: Propeller damage
Source: Operator, annotated by the ATSB
Operator’s procedures
The operator provided a pontoon operating manual which outlined the standard operating procedures and limitations. The manual identified pushing on tides as one potentially hazardous scenario when it could be difficult for dockhands to maintain control of the aircraft. To mitigate the risk in such conditions, a wind limit of 10 kt was stipulated when the prevailing winds were blowing opposite to the tidal flow, and further limitations were to be observed when operating from dock 1 in pushing tides.
The procedures for launching from dock 1 required dockhands to push the aircraft from the pontoon while maintaining control of the aircraft from the rear and pulling on ropes attached to the wing. By positioning the nose downwind of the launch, this procedure allowed the aircraft to be swung into its position while the flight crew conducted the engine start. Once in the correct position, the dockhands would call ‘clear’, notifying the pilot in command that the aircraft was safe to dispatch and launch. The pilot in command would then announce ‘launching’ and commence the engine start and subsequent launch from the pontoon.
The operator’s manual stated that if at any time the dockhands observed anything abnormal related to the dispatch sequence not complying with the standard operating procedures, they were to notify the crew using hand signals or radio contact.
Operator’s comments
The operator advised that mechanical or steering malfunctions that would have precluded the normal operation of the aircraft were ruled out as contributing factors.
The operator determined that the crew’s decision to not abort the launch, while attempting to recover the aircraft, exacerbated the situation by swinging the aircraft back towards the dock.
Safety message
During times of significant workload, effective communication is important when relaying safety critical information. This incident highlights the importance of adhering to operational limitations and defined operating procedures, especially in marginal conditions. It is also a reminder of the importance of conducting regular risk assessments to ensure the safe operation of the aircraft and its crew and passengers.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Pushing on tide: The term ‘Pushing On’ comes from the effect of the tidal currents pushing the aircraft onto the pontoon.
[2]A practice employed by operators where the propeller blades are rotated to an edge-on angle to the airflow to assist in securing the propeller while the aircraft is docked. This reduces the risk of injury and damage to the engine caused by the internal components rotating without a supply of oil.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-024
Occurrence date
07/05/2024
Location
253 km from Broome Airport
State
Western Australia
Occurrence class
Serious Incident
Aviation occurrence category
Collision with terrain
Highest injury level
None
Brief release date
02/12/2024
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
208
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes

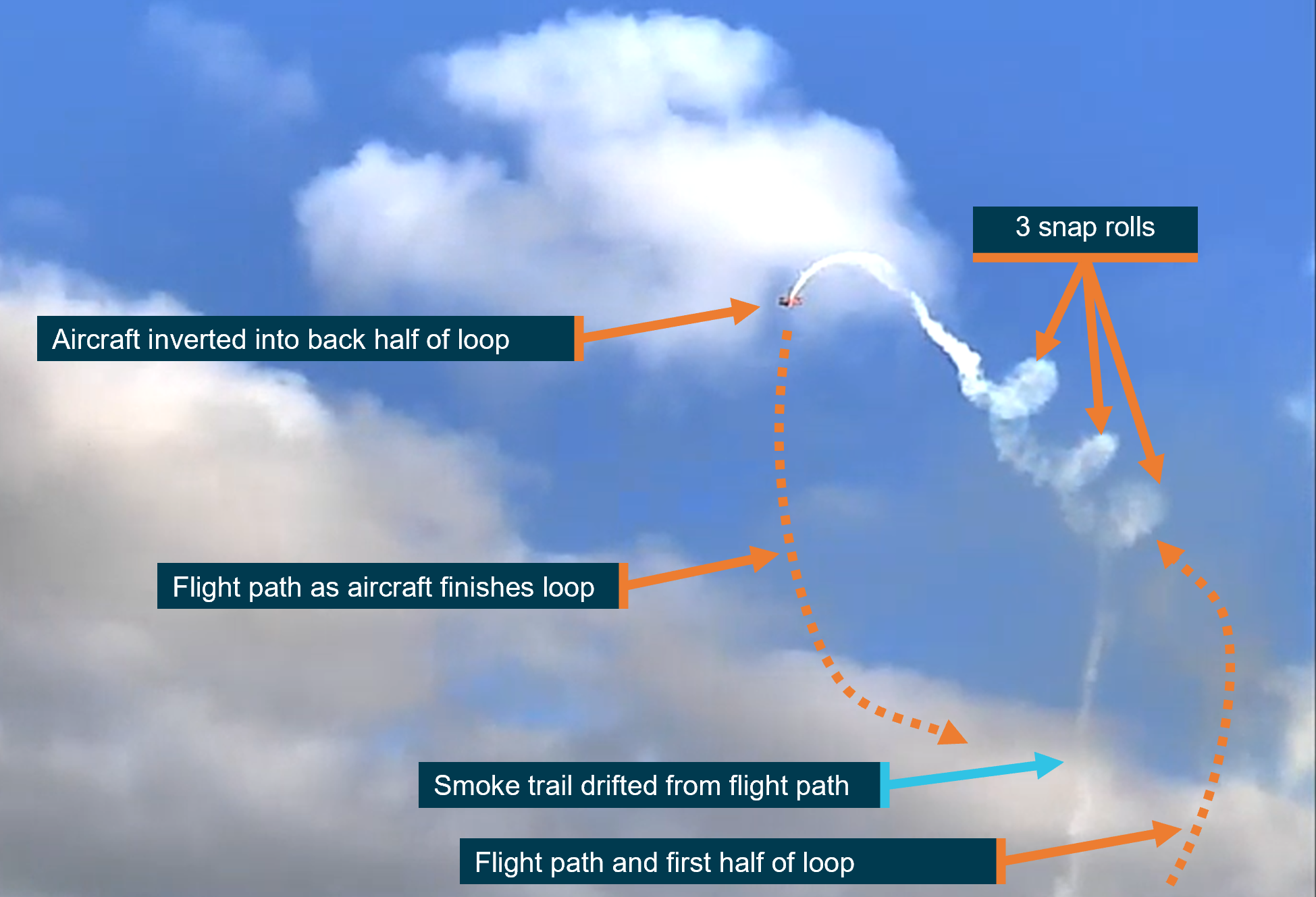






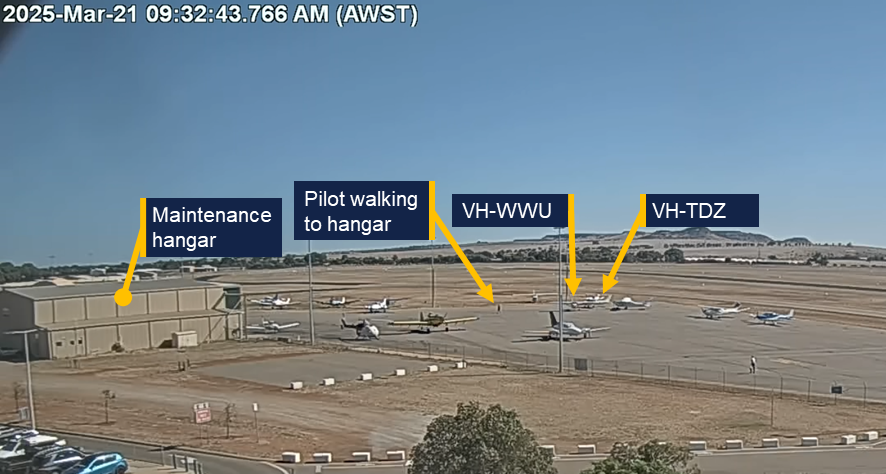
![Figure 2: Original final position of VH‑WWU at the accident site[4]](/sites/default/files/2025-05/AO-2025-014-Figure%20%282%29.png)