This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
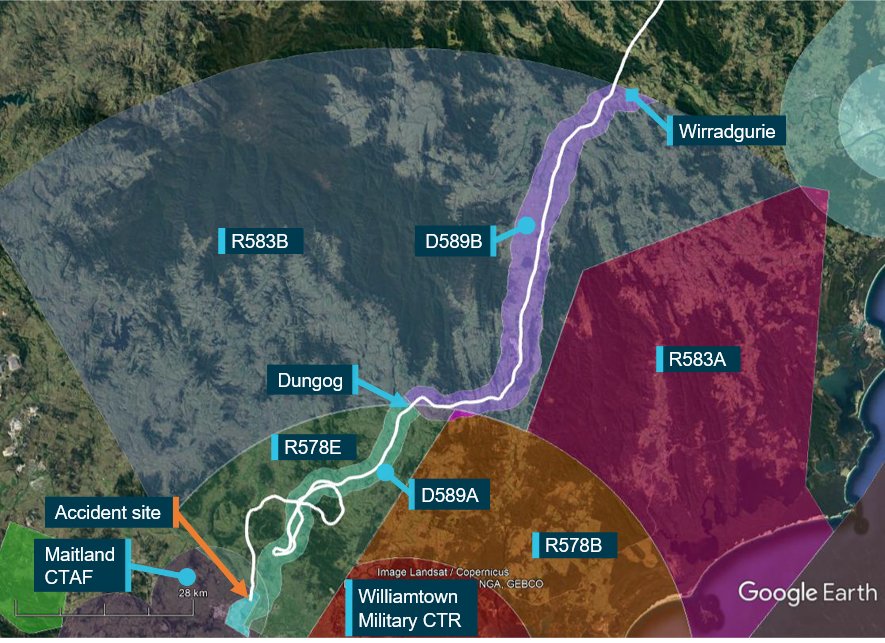
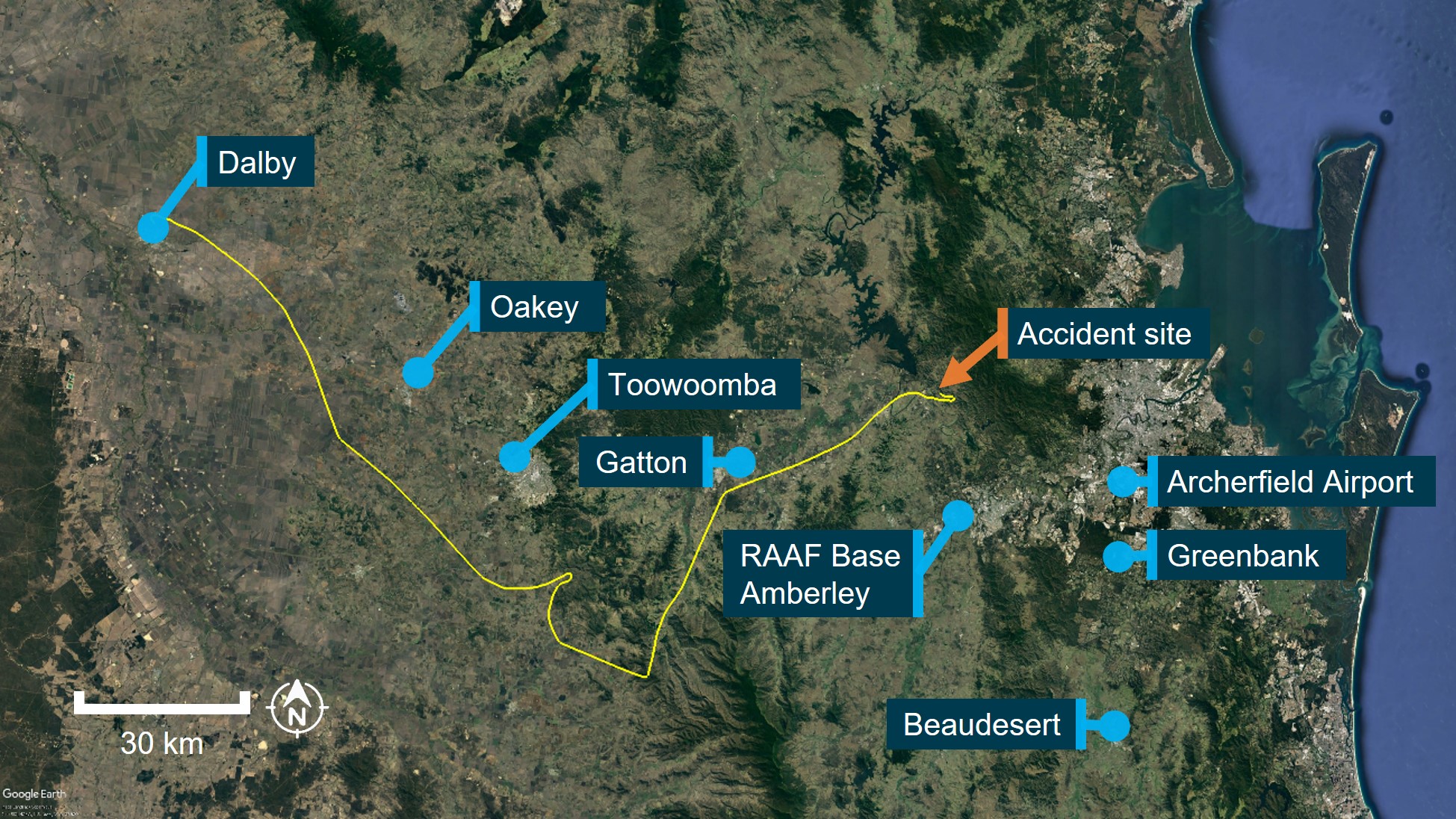
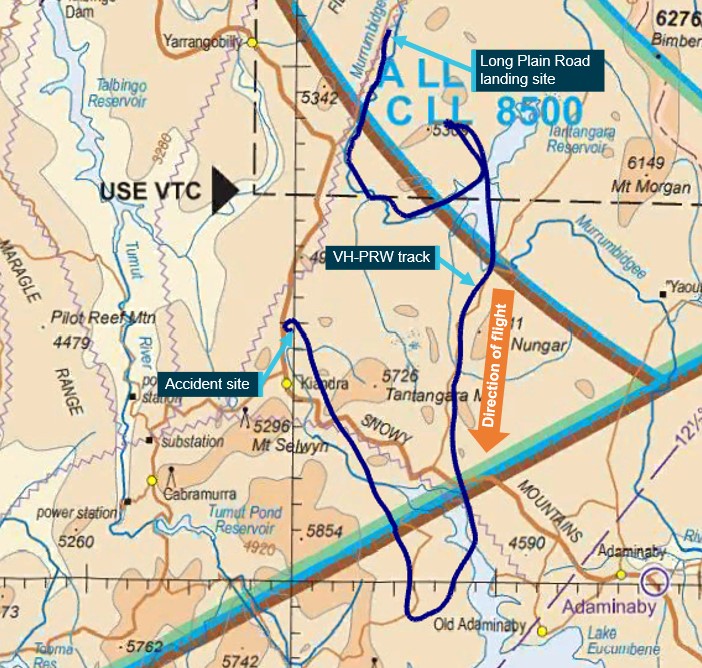
About 1350 local time on 6 October 2022, the pilot of a Bell 206 JetRanger helicopter, registered VH-PHP, departed Casino Airport, New South Wales for a ferry flight to Warnervale, New South Wales. The helicopter was in the process of being returned to its owner after a long‑term repair to correct hail damage and exchange life‑expired items. The pilot was the only person onboard. The aircraft tracked south-south-west, approximately 30-60 km inland of the coast (Figure 1).
Source: Google Earth and OzRunways, annotated by the ATSB
Recorded data indicated that at tracking point Wirradgurie, the pilot followed the inland visual flight rules (VFR) route west of Williamtown Airport through restricted areas R583B and R578E (Figure 2).[1] The VFR lane, designated D589B and D598A, is a 2-3 NM wide corridor under the restricted airspace from ground level to 2,500 ft above mean sea level (AMSL) and ground level to 1,600 ft AMSL, respectively. The VFR lane enables pilots to visually fly under the restricted airspace without requiring permission or monitoring by Williamtown airspace controllers. The VFR route follows the east coast rail line where it passes through the mountainous region between Gloucester and Maitland.
Figure 2: VH-PHP flight track through Williamtown VFR Route D589B and D589A
Source: Google Earth and OzRunways, annotated by the ATSB
At 1547 approaching Dungog, the pilot received a telephone call from a relative enquiring as to their progress. The pilot reported the aircraft was flying well, operations were normal, and they were 5 minutes from Maitland and 20 minutes from Warnervale.
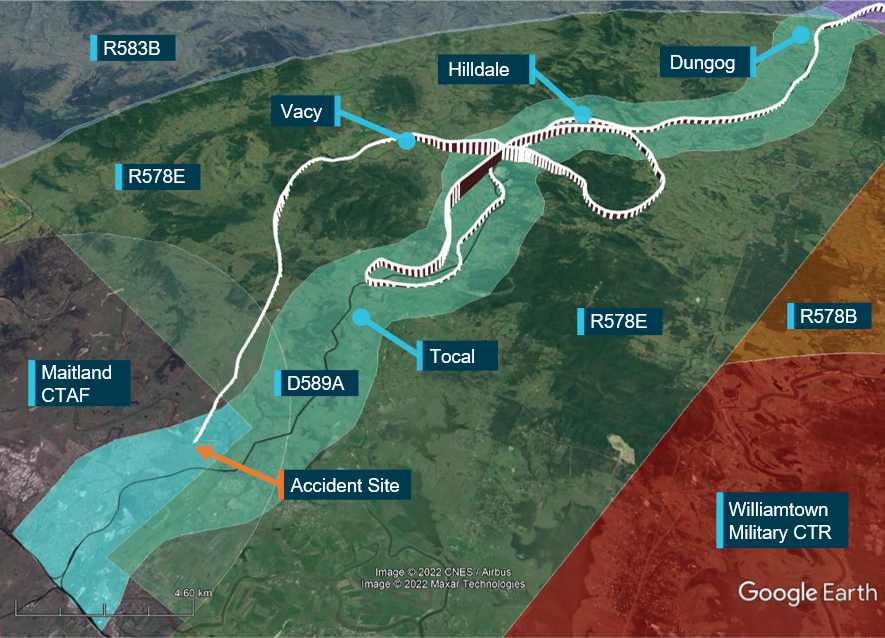
Figure 3: VH-PHP flight track through Williamtown VFR Route D589A
Source: Google Earth and OzRunways, annotated by the ATSB
At 1556 approaching Tocal, approximately 4 NM from the end of the lane, the aircraft started to climb and then conducted a right 180° turn to backtrack northbound. After approximately 2 minutes the helicopter transitioned through the upper limit of the VFR lane and continued climbing to 3,100 ft. The helicopter then descended to 1,100 ft, back into D598A and continued to follow the lane northbound until Hilldale when the aircraft again made a right turn. This time the pilot flew outside the lateral bounds of the lane by conducting a gradual climbing orbit around a hill before crossing from the east to the west of the lane, reaching 2,900 ft during the transition.
The helicopter then descended over the town of Vacy, flying as low as 120 ft above ground level (AGL) before climbing and heading south. The aircraft then descended to low levels travelling parallel to, but just outside, the VFR lane western boundary until it exited the southern border of R578E at Maitland Vale.
At approximately 1616, the helicopter cleared a ridge by approximately 200 ft and descended gradually toward the Hunter River.
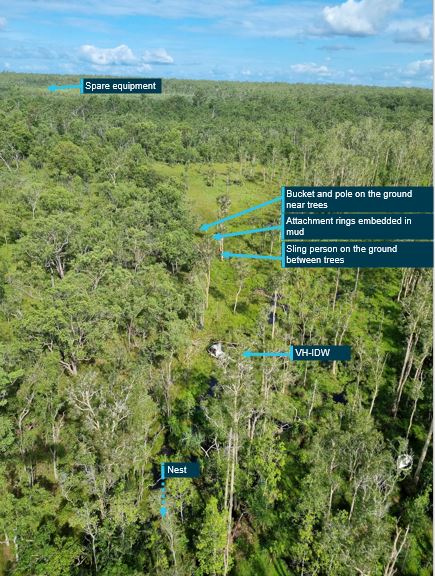
After clearing the ridge, the helicopter was observed by 6 witnesses. Common features of these reports were that the helicopter was heading towards the river, descending slightly, possibly initiating a turn when the helicopter rolled markedly and descended rapidly, colliding with the riverbank. The aircraft came to rest on a muddy river flat approximately 2 m from, and 0.5 m above, the water’s edge. The helicopter was destroyed, and the pilot was fatally injured.
Context
Helicopter information
The accident helicopter was a Bell 206 manufactured in 1970 as an 206A model. The helicopter was first registered in Australia in May 1986. In 1988, the helicopter was rebuilt and converted to a 206B model with fitment of a Rolls Royce/Allison 250-C20 turboshaft engine and the associated uprated transmission, rotor head and other changes.
A maintenance test flight associated with the replacement of components was conducted in Casino the day before the accident flight.
Site and wreckage examination
An initial assessment of the aircraft was conducted in situ after which, due to rising river levels, the wreckage was moved to higher ground and the principal components were moved to a secure location for further examination.
All major aircraft components were accounted for at the accident site. Examination of the aircraft’s flight controls, engine and aircraft structure did not identify any pre-existing defects. Fuel was found spilled at the accident site and fuel in the fuel filter bowl showed no evidence of contamination with water. Multiple sources of evidence indicating engine rotation at impact were identified.
The helicopter struck a tree on the riverbank, prior to impacting the ground. The tree and wreckage damage indicated the helicopter impacted the ground at approximately 80° right angle of bank and 60° nose down pitch.
Several aircraft components were retained by the ATSB for further detailed analysis.
Meteorological information
At 1600 the Bureau of Meteorology Meteorological Terminal Air Report (METAR)[2] for Maitland Airport reported 8 kt of wind with scattered cloud at 4,000 ft and 4,500 ft and overcast cloud at 7,800 ft above the airport.
Witnesses reported the weather at the time and location of the accident to be a mid to high level overcast cloud with no rain. A retired airline pilot reported that the ’Weather was suitable for VFR. A general base layer at 5,000 ft. Scattered cloud with patches to the South’.
Pilot qualifications
The pilot held a Commercial Pilot Licence (helicopter), a valid Class 1 Medical Certificate, a valid flight review, and a low-level helicopter rating.
Further investigation
To date, the ATSB has assessed the aircraft wreckage, interviewed witnesses and collected external data sources related to weather, air traffic communications, and flight tracking.
The investigation is continuing and will include further review and examination of:
aircraft maintenance documentation and operational records
recorded data
weather information
air traffic communications
pilot medical records, qualifications and experience.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the accident site property owners and their extended family for the significant assistance they provided the ATSB with moving, handling and storage of the wreckage away from the rapidly rising floodwaters.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] These restricted zones cover from ground level to an altitude of 10,000 ft radially around Williamtown Airport and are used by military aircraft.
[2] METAR: A meteorological report for an aerodrome at a routine time (half hourly) when conditions are better than specified thresholds
Final report
Executive summary
What happened
On 6 October 2022, the pilot of a Bell 206B JetRanger helicopter, registered VH-PHP, departed Casino Airport, New South Wales for a solo ferry flight to Warnervale. The helicopter flew about 30–60 km inland of the coast before entering the inland visual flight rules route through the Williamtown military restricted area. Before exiting the restricted area, recorded flight data showed that the helicopter deviated from the pilot’s intended track. The helicopter turned around, deviated outside the lane, and the pilot did not respond to radio calls from Brisbane air traffic control.
The pilot then flew south and exited the restricted area below 500 ft above ground level. The helicopter was then observed by multiple witnesses to be heading towards the Hunter River, descending slightly, and was possibly initiating a turn when the helicopter rolled markedly and descended rapidly, colliding with the riverbank. The helicopter was destroyed, and the pilot was fatally injured.
What the ATSB found
Having discounted a number of other scenarios to explain the accident, the ATSB found that it was likely the pilot experienced an incapacitating event.
Less than 12 months prior, the pilot had undergone a review by a cardiologist that determined the pilot had minor coronary artery disease and was at a low to intermediate risk of a cardiac event. However, the pilot’s post-mortem showed they had severe coronary atherosclerosis within all 3 major coronary arteries with at least 80% blockage observed within each artery. While it was not possible to forensically determine if the pilot experienced a heart attack prior to the accident, it remained a significant risk factor for the pilot.
It was also established that the pilot did not declare a significant surgery and was taking numerous prescribed, non-prescribed, and recreational drugs, which had the potential to adversely affect their performance. Further, these were not declared to the Civil Aviation Safety Authority during their aviation medical examination, which prevented a specialist assessment of the aeromedical significance of the surgical outcome, nor the medication’s use and the underlying conditions for which they were prescribed.
Safety message
It is a pilot’s responsibility to declare a full medical history and medication use at the time of an aviation medical examination so that the Civil Aviation Safety Authority and the designated aviation medical examiner can assess a pilot and their medications’ suitability for flying. Alternate medication may be available if current medications for existing conditions are incompatible with flying, thereby permitting the pilot to manage both their own personal risks as well as those to aviation safety.
Pilots should also remain cognisant of health and lifestyle changes and how this may affect their fitness to fly. Do not fly if feeling unwell or until fully recovered from temporary medical conditions and manage chronic conditions in association with your designated aviation medical examiner.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 6 October 2022, at about 1350 local time, the pilot of a Bell 206B JetRanger helicopter, registered VH-PHP, departed Casino Airport, New South Wales for a ferry flight to Warnervale. The helicopter was being returned to the registered operator after a long-term repair to correct hail damage and exchange life-expired parts. The pilot was the only person onboard.
The helicopter tracked south-south-west, about 30–60 km inland of the coast (Figure 1).
Source: Google Earth and OzRunways, annotated by the ATSB
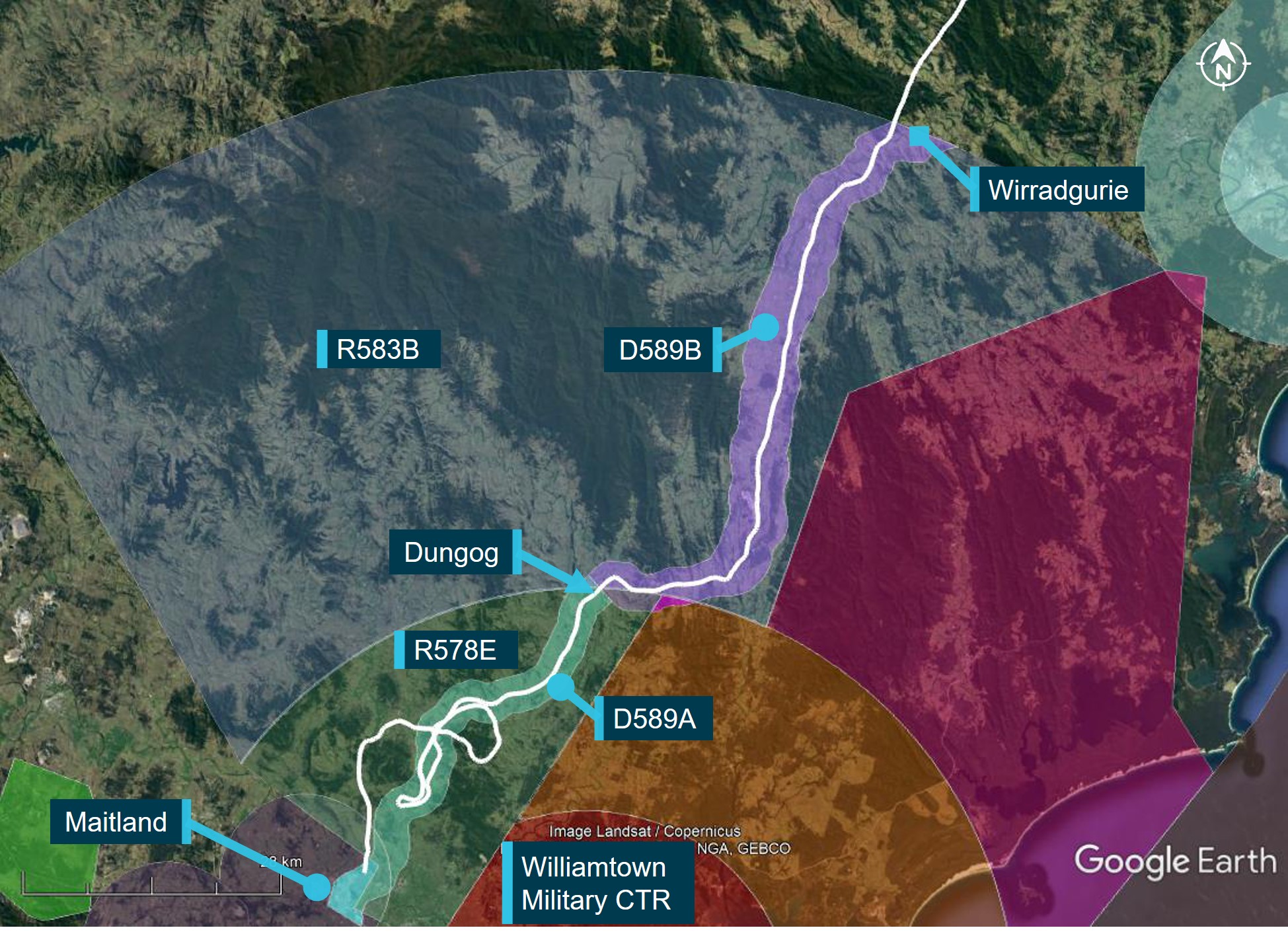
Recorded data indicated that at tracking point Wirradgurie, the pilot followed the inland visual flight rules (VFR)[1] route,[2] D589B and D589A (shaded in purple and green respectively on Figure 2), north of the Williamtown military control area (CTR) through restricted areas R583B and R578E.[3]
At about 1547, when approaching the township of Dungog, the pilot received a telephone call[4] from a family member enquiring as to their progress. The pilot reported the helicopter was flying well, operations were normal, and they were 5 minutes from Maitland and 20 minutes from Warnervale.
Figure 2: VH-PHP flight track (in white) through the Williamtown inland VFR route D589
Source: Google Earth and OzRunways, annotated by the ATSB
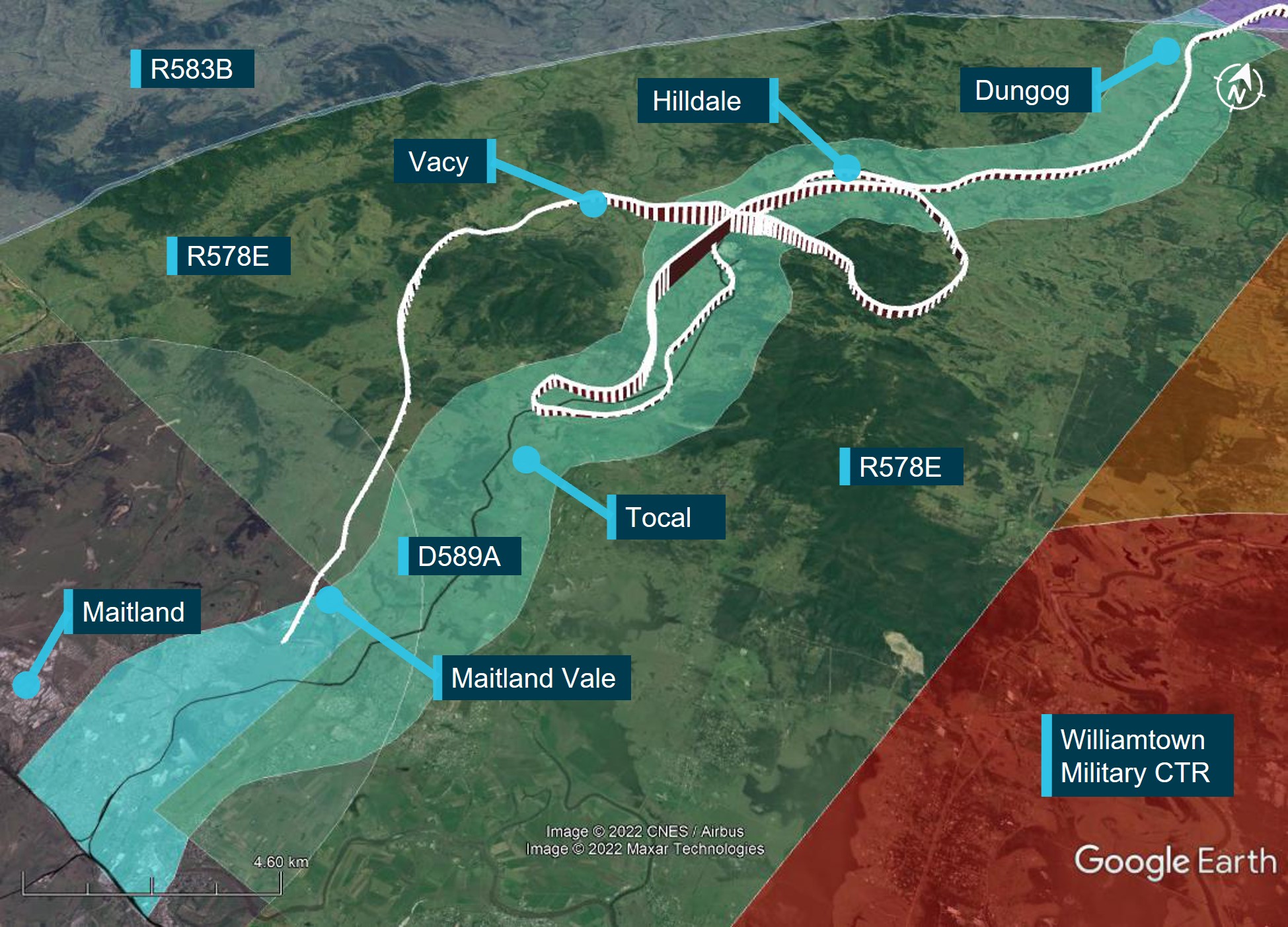
At about 1556, when approaching Tocal (Figure 3), about 4 NM (7 km) from the end of the lane, the helicopter started to climb and then conducted a right 180° turn to track northbound. After about 2 minutes, the helicopter transitioned through the upper limit of the VFR lane (1,600 ft) and continued climbing to 3,100 ft. The helicopter then descended to 1,100 ft, back into D589A and continued to follow the lane northbound until Hilldale when the pilot again made a right turn. This time the pilot flew the helicopter outside the lateral bounds of the lane by conducting a gradual climbing orbit around a hill before crossing from the east to the west of the lane, reaching 2,900 ft during the transition.
At about 1611, the helicopter then descended over the town of Vacy, flying as low as 120 ft above ground level and as slow as 22 kt ground speed before climbing and heading south. The helicopter then descended to low levels travelling parallel to, but just outside, the VFR lane western boundary until it exited the southern border of R578E at Maitland Vale.
Figure 3: VH-PHP flight track (in white) through the Williamtown VFR route D589A
Source: Google Earth and OzRunways, annotated by the ATSB
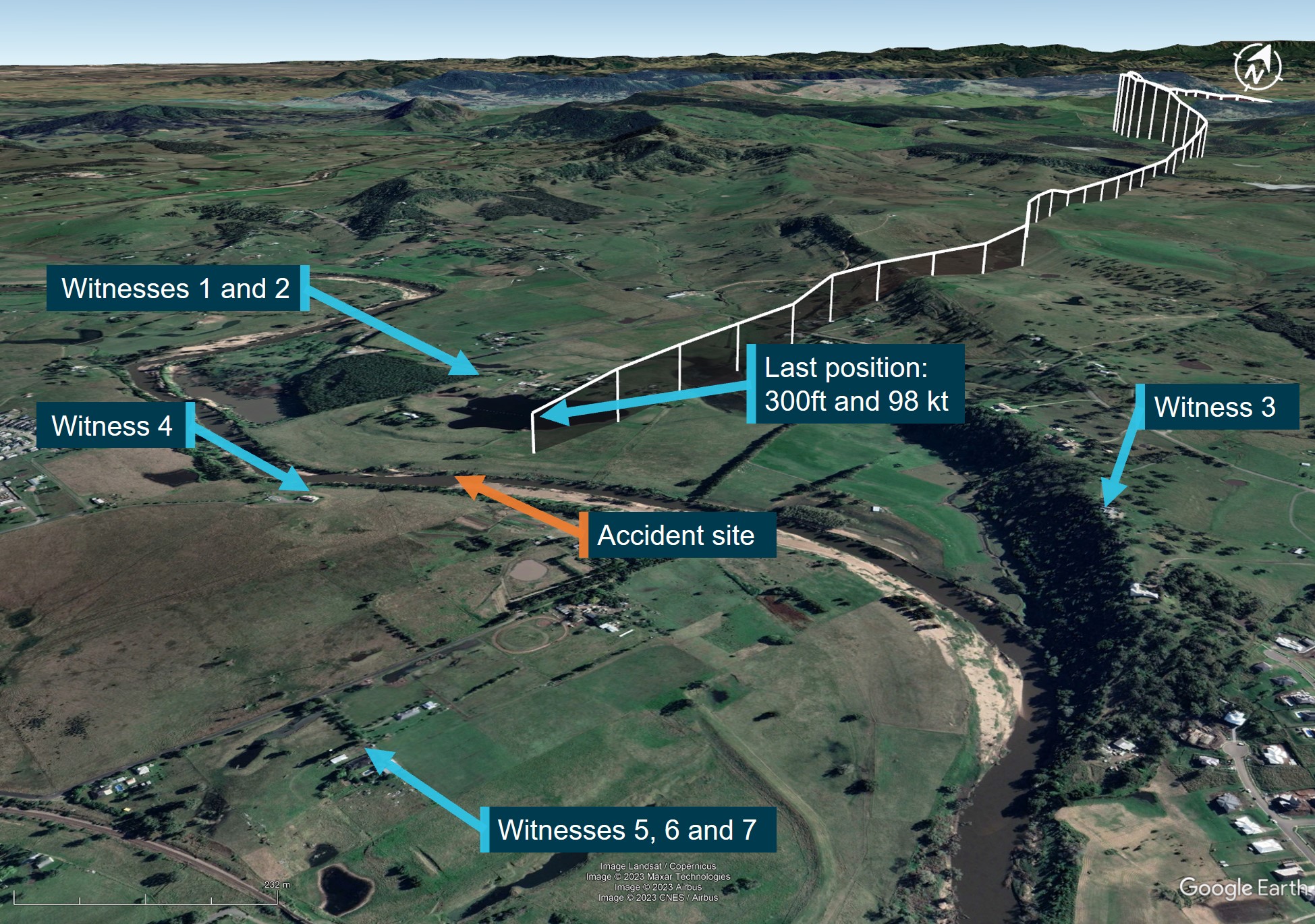
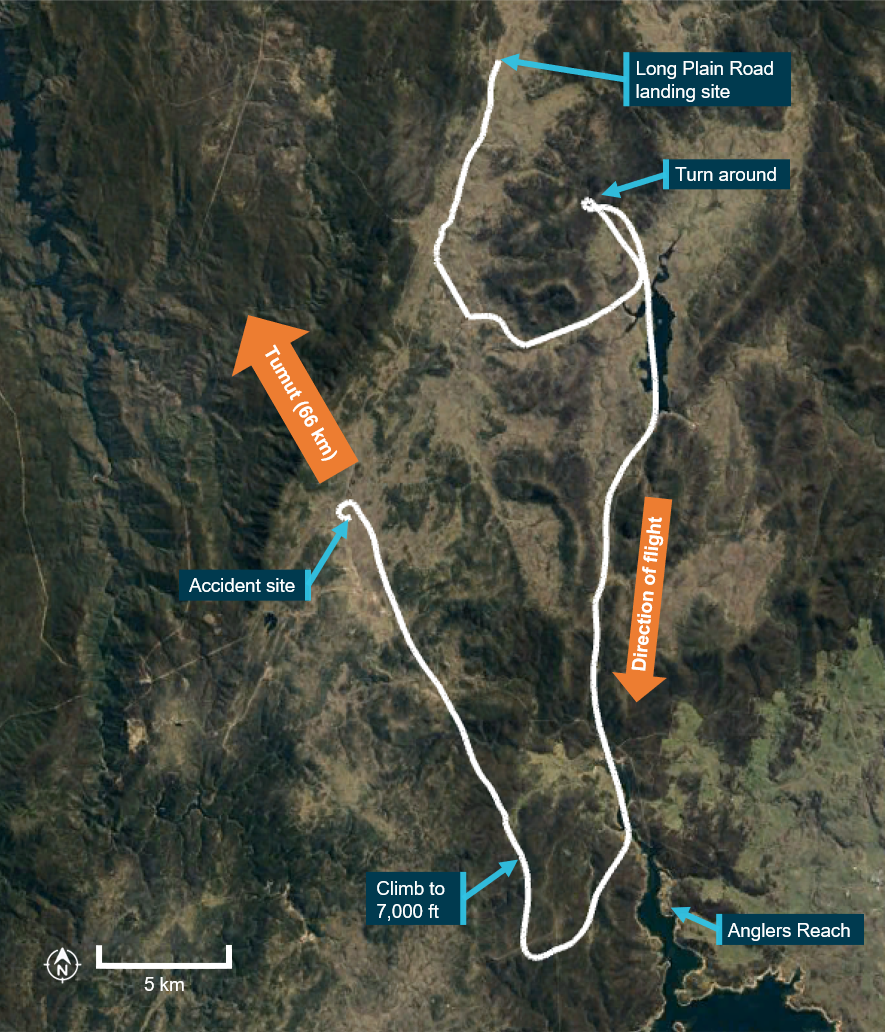
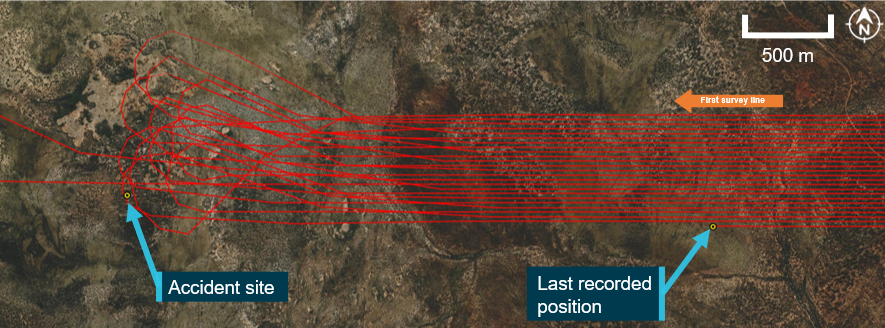
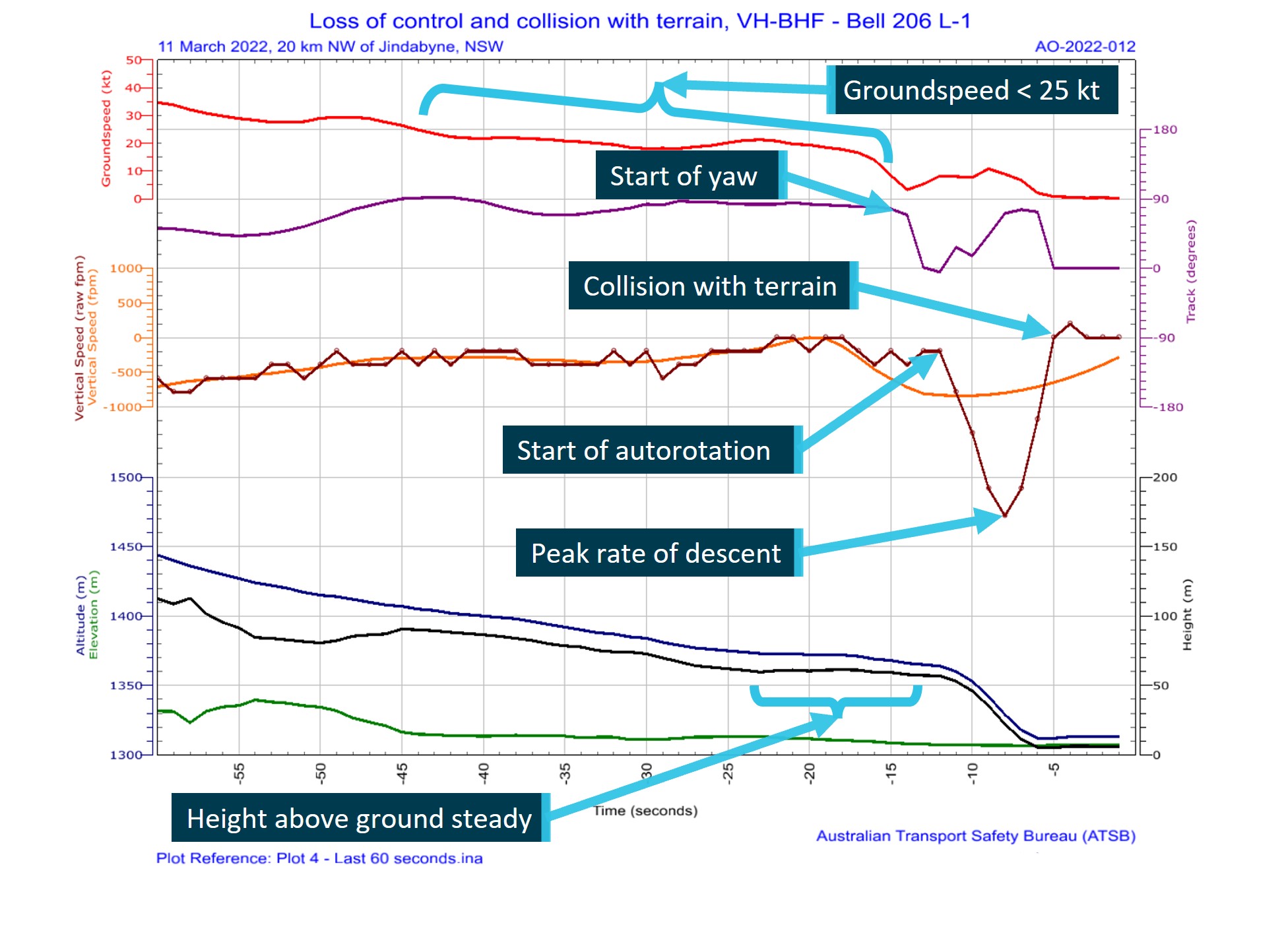
At about 1616, the helicopter cleared a ridge by about 200 ft and descended gradually toward the Hunter River. At the last recorded data position, the helicopter was at 300 ft and 98 kt (Figure 4).[5]
After clearing the ridge, the helicopter was visually observed by 7 witnesses. Common features of these reports were that the helicopter headed towards the river, descended slightly, possibly initiated a turn at which point it rolled markedly, descended rapidly, and collided with the riverbank. Some of those witnesses, as well as others who only heard the helicopter and the impact, reported the helicopter sounded normal or nothing out of the ordinary, while others reported it sounded rough or the engine was ‘screaming’.
The helicopter came to rest on a muddy river flat near the water’s edge. A first responder stated there was smoke coming from an engine fairing grille. They found a fire extinguisher in the cabin, discharged it into the grille and the smoke stopped. The helicopter was destroyed, and the pilot was fatally injured.
Source: Google Earth and OzRunways, annotated by the ATSB
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) and was qualified to fly by day under the visual flight rules (VFR). The pilot’s paper logbook indicated a total of 382.9 hours aeronautical experience, of which 132.5 hours were in various Bell 206 model helicopters. However, the last entry in this logbook was December 2003. No other paper or electronic logbooks could be found. The pilot indicated in their last aviation medical examination in October 2021 that they had 7,200 total flying hours and no hours recorded in the prior 12 months. Prior medical questionnaires recorded hours that appeared to be steadily increasing and rounded to the nearest 100 hours. The pilot had an OzRunways[6] account, which indicated they had accrued 27 hours since May 2017 while using their OzRunways application. The application recorded:
11.6 hours over 11 flights in 2017
1.0 hours over 2 flights in June 2018
11.9 hours over 17 flights in 2022.
In the 90 days prior to the accident, no flights were recorded by the application.
The pilot last conducted a single-engine helicopter flight review on 26 January 2022 that was valid until 31 January 2024. This flight was conducted in the accident helicopter. In interview, the flight instructor stated the pilot was ‘reasonably cautious, not overconfident’ and they were ‘not out of practice’.
The pilot held a Class 1 and Class 2 Aviation Medical Certificate issued by the Civil Aviation Safety Authority (CASA). The Class 1 medical was valid until 26 October 2022 and the Class 2 valid until 26 October 2023. The pilot was required to have reading correction eyewear with them while flying.
The pilot had recently returned from an overseas holiday and had a head cold. A family member reported the pilot had 8 hours sleep the night before the flight and in the morning was in good spirits and appeared to have improved with respect to their head cold.
Helicopter information
VH-PHP was a Bell Helicopter Company, model 206A that was manufactured in 1970 in the United States. The helicopter was first registered in Australia in May 1986. In 1988, the helicopter was rebuilt and converted to a 206B model with fitment of a Rolls Royce/Allison 250-C20 turboshaft engine and the associated uprated transmission, rotor head and other required changes.
In 2019, the helicopter was damaged by hail and repaired over a 3-year period. During this time, other modifications were performed, including correcting issues associated with the A to B model conversion. In April 2022, as part of a maintenance test flight, the helicopter was flown from Warnervale to Casino. During the test flight, a ‘lazy’ power turbine governor was identified. Subsequently, further parts required repair or overhaul, including time-expired parts.
A 30 minute maintenance test flight associated with the replacement of components was conducted and the helicopter was found to be in a satisfactory condition. A maintenance release was issued, and the helicopter flew the following day with the aim of returning to Warnervale (the accident flight).
Meteorological information
In the days before the accident, the east coast of Australia had been under the influence of a low‑pressure system, which had included large quantities of rain in some areas.
The Bureau of Meteorology graphical area forecast, current for the accident flight, indicated greater than 10 km visibility and broken cloud[7] with a base of 4,000 ft above mean sea level on departure from Casino. However, shortly after taking off, the pilot was to fly into an area with isolated rain, 6,000 m visibility and scattered cloud with a 2,000 ft base. Further south along the flight path taken, the weather was forecast to have visibility greater than 10 km but reduced to 5,000 m and 2,000 m in scattered rain and showers. Broken cloud was forecast throughout these varied conditions.
At 1600, the aerodrome meteorological report (METAR)[8] for Maitland Airport (about 6 km west‑south-west from the accident site) recorded 8 kt of wind, visibility greater than 10 km, scattered cloud at 4,000 ft and 4,500 ft, and overcast cloud at 7,800 ft. The air temperature was 21 °C.
Two eyewitnesses separately reported seeing the helicopter, one as it operated down the D589A and the other when it was in the R578E restricted area. These witnesses reported the weather at the time to be a mid to high level overcast cloud with no rain. A retired airline pilot in the area of the accident site stated that the weather was suitable for VFR operations.[9] They observed a general base layer at 5,000 ft, and scattered cloud with patches to the south.
Recorded information
Position data
The helicopter had analogue instrumentation and had no fitted equipment that recorded data. The pilot was using the OzRunways application on their mobile phone. The application sent position information back to a server via a mobile data connection. Position, altitude, and ground speed was recorded for the entire accident flight at about 5 second intervals (refer to Figure 2, Figure 3 and Figure 4).
Radio communications
The Airservices Australia area frequency radio calls were reviewed. The pilot made no calls on the appropriate area frequencies for the flight, nor were they required to do so. At 1605, Brisbane Centre air traffic control made 3 calls trying to contact the pilot in response to the helicopter flying through restricted airspace R578E, with no response received.
No distress calls were made on the area frequency around the time of the accident.
Mobile phone
Mobile phone records showed that the pilot made and received multiple calls during the flight. Some calls were from family members checking on the pilot’s progress. At 1614, the pilot missed a call and received a missed call text. Also at 1614, the pilot received and answered a call from an unknown person for 27 seconds. The call ended about 60 seconds before the accident. Despite numerous attempts, the ATSB was unable to establish contact with this caller to seek any further information on the situation with the pilot at that time.
Wreckage and impact information
An initial assessment of the helicopter was conducted on the riverbank, however, due to rapidly rising river levels, the wreckage was moved to higher ground and the principal components were moved to a secure location for further examination.
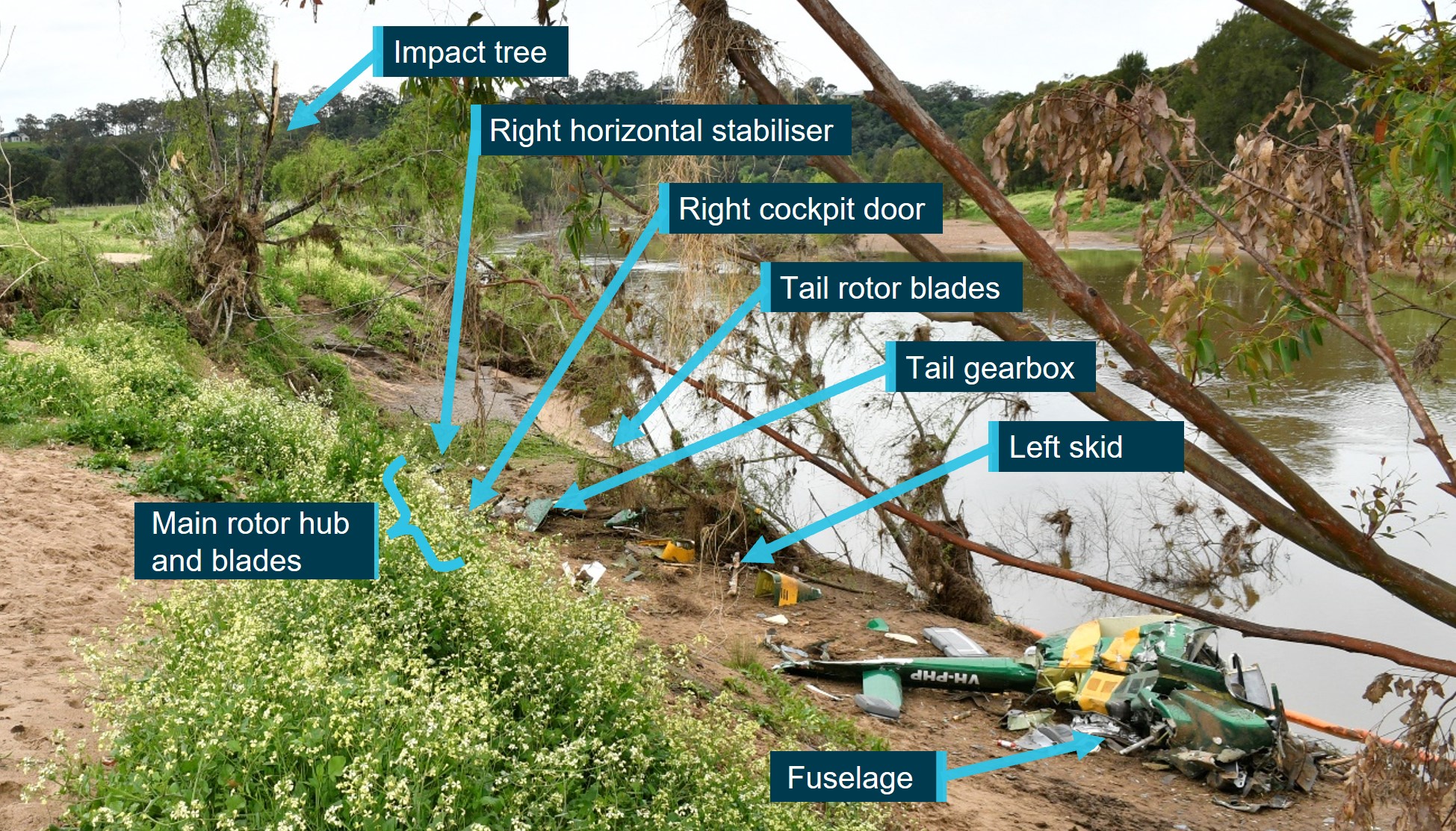
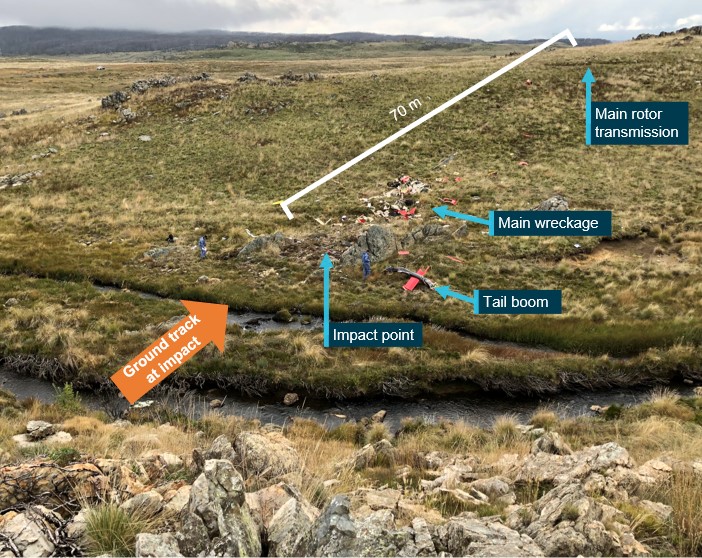
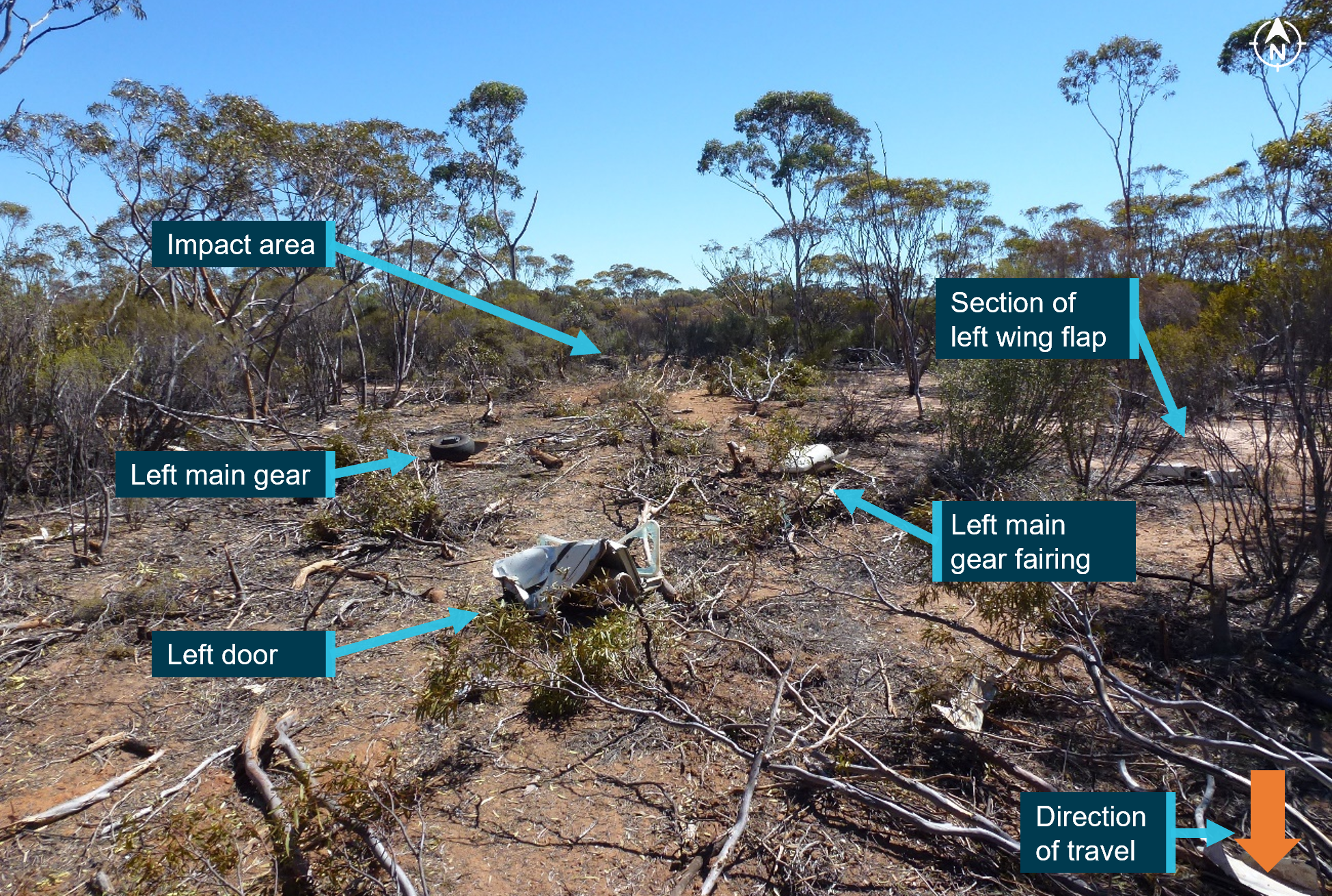
The wreckage trail was about 45° to the right of the last track direction recorded by the pilot’s OzRunways application (Figure 4). Examination of the accident site showed the wreckage trail (Figure 5) had started at a tree and extended along the riverbank for a distance of 33 m on a heading of 210° (magnetic). Figure 5 also shows the location of key components including the main rotor hub and blades, right horizontal stabiliser, right cockpit door, tail rotor blades, tail gearbox, left skid, and the fuselage.
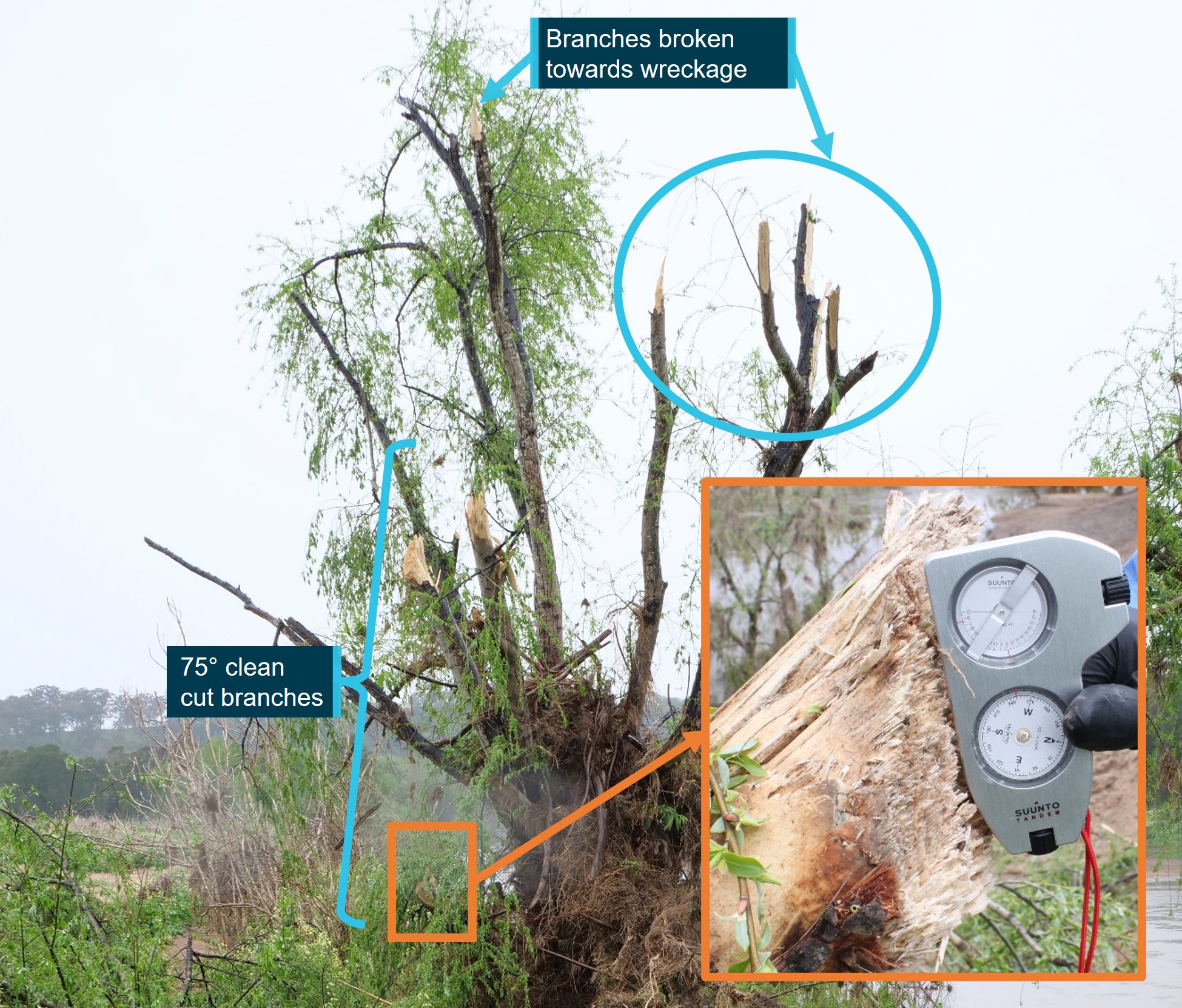
Some lower branches of the tree (Figure 6) were cut at 75° from the horizontal and the multiple cuts were at about 75° to each other suggesting they were cut by the main rotor system. Other branches higher up on the other side of the tree were snapped off in the general direction of the wreckage.
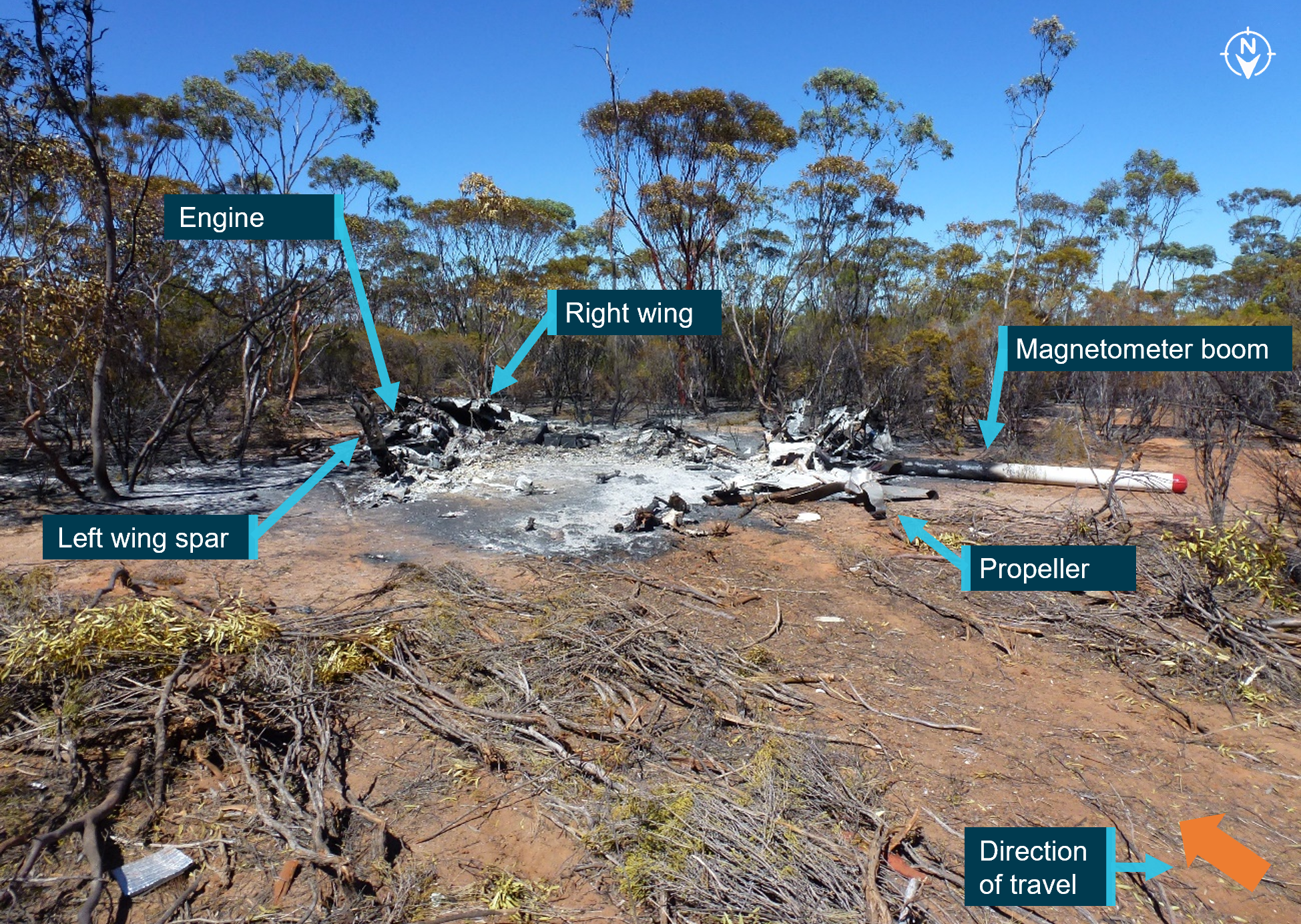
All major aircraft components were accounted for at the accident site except for 2 parts of a main rotor blade. There was no evidence of a birdstrike identified in the wreckage.
The turbine and combustion sections of the engine had partially separated from the gearbox section. The left compressor discharge tube had separated from the compressor section at the compressor output flange. The right compressor tube was partially crushed between the combustion section and compressor section, consistent with the right side of the fuselage impact with terrain. The exhaust pipes were removed and a visual inspection of the output face of the power turbine was carried out with no defects evident. Due to the level of disruption to the engine and compressor casings, rotation of the power turbine and compressor was not possible.
The engine fuel and oil filters were removed and inspected with no unusual contamination found. The engine oil tank was punctured at the bottom of the tank by the tail rotor driveshaft. The puncture exhibited signs of rotation of the driveshaft and remnants of engine oil were found in the tank.
Fuel was found spilled at the accident site and fuel in the fuel filter bowl showed no evidence of contamination with water.
The main rotor hub was intact and attached to the mast section. The mast nut was installed and locked, and there were minimal signs of mast bumping.[10] Both main rotor blades were still attached to the rotor head.
The 2 parts unaccounted for were a 2 ft long outboard section of the main rotor blade leading edge and the associated blade tip weight. It was assessed that the leading edge and tip weight were likely projected into the swollen river during the impact sequence due to the helicopter heading, the pattern of damage, and fracture surfaces of the recovered adjacent leading edge, trailing edge and tip sections.
The main rotor mast was fractured near the main rotor head. The fracture surface was indicative of an overload failure. The main transmission was free and smooth in rotation. No oil was present due to the fracture of the oil filter mount, however, there was residual oil evident in the gearbox and the oil chip detector was removed and inspected with no signs of internal failure evident. The oil filter was opened and inspected with no signs of unusual contamination present.
The upper surface of the main rotor gearbox isolation mount had heavy scoring, caused by the rotating engine driveshaft during the impact sequence and the main gearbox input flange was radially scored through about 225° in a periodic saw-tooth pattern. This indicated that the engine was driving the driveshaft, and the main gearbox input flange were rotating at the time of separation.
In summary, examination of the helicopter’s flight controls, engine and structure did not identify any pre-existing defects that would have affected normal operation.
Survival aspects
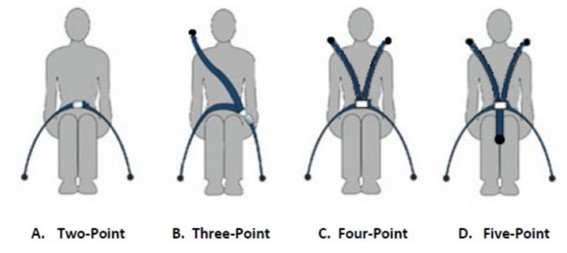
The helicopter cabin underwent severe disruption upon impact with terrain. The front row seats were fitted with a 4-point harness. Evidence showed the pilot was wearing the safety harness correctly but due to the severity of the impact with the ground, the restraint system failed. The pilot was not wearing a helmet.
The accident was not considered survivable, and the pilot received non-survivable injuries.
Operational information
The pilot did not submit a flight plan, nor were they required to do so. The track taken was 30 to 60 km inland from the New South Wales coast, which allowed the pilot to fly under Class E and Coffs Harbour Class C controlled airspace.
At tracking point Wirradgurie, the pilot followed the inland VFR route west of Williamtown (Newcastle) Airport. The VFR route, designated in 2 segments as D589B and D589A, is a 2–3 NM (4–6 km) wide lane under restricted airspace from ground level to 2,500 ft above mean sea level and ground level to 1,600 ft respectively. The VFR lane enables pilots to visually fly under restricted areas R583B and R578E (military flying area) without requiring permission or monitoring by Williamtown airspace controllers.
The 2 eyewitnesses who observed the helicopter in D589A and R578E both reported that it appeared to be operating normally. There were other aircraft in the vicinity operating at higher altitudes both in R578E and in the Class G airspace just to the south of the restricted area. However, VH-PHP was the only aircraft broadcasting a transponder signal in the D589 inland VFR route at the time.
A family member who spoke with the pilot during the flight stated they were not aware of any reason why the pilot would have diverted from the intended track. Based on the assumed flight path and prior cruising ground speed, the estimated times given by the pilot of 5 minutes to Maitland and 20 minutes to Warnervale were broadly correct. However, when the subsequent deviation was included, the ATSB estimated the times to Maitland and Warnervale would have been closer to 29 minutes and 44 minutes respectively.
Medical and pathological information
Post-mortem examination
The forensic pathologist who conducted the post-mortem examination concluded that the pilot received fatal injuries sustained during the accident. However, they also noted severe triple vessel coronary artery disease with at least 80% lumen[11] stenosis[12] observed within each artery. The post-mortem report stated that:
Severe coronary artery disease is a risk factor for sudden death due to myocardial ischaemia[13] and subsequent fatal arrhythmia.[14]
Toxicological results from a post-mortem subclavian blood sample revealed the following medications, which were considered ‘non-fatal’ levels: alprazolam (<0.005 mg/L), diazepam (0.13mg/L), and metabolites nordiazepam, temazepam and oxazepam. Citing Baselt (2020), the forensic pathologist noted that:
Although alprazolam and diazepam were detected at non-lethal levels, they are both central nervous system (CNS) depressant medications which may act synergistically to cause sedation, confusion and incoordination.
Methylecgonine (0.13mg/L) a cocaine metabolite, Levamisole (a common cutting agent of cocaine) and cannabinoids (delta-9-tetrahydrocannabinol (THC) 0.006 mg/L and THC acid 0.004 mg/L) were also detected. Carbon monoxide saturation was less than 1% and no alcohol was detected.
Coronary artery disease
During the post-mortem examination, the pilot’s heart was found to have severe coronary atherosclerosis[16] within all 3 major coronary arteries (the left anterior descending coronary artery, circumflex artery and the right coronary artery) with at least 80% lumen stenosis observed within each artery. Histological examination confirmed the severe atherosclerosis within all 3 main coronary arteries, with 75-90% arterial lumen stenosis observed. Focal perivascular fibrosis[17] and occasional enlarged myocytes[18] were seen, which are both associated with the development of cardiac dysfunction.
In coronary artery disease, one or more of the coronary arteries are partially blocked by plaques. If a plaque breaks open, it can cause a blood clot in the heart, which can lead to a heart attack (also known as a myocardial infarction). They occur when the heart has either a sudden interruption of blood supply, or a longer term reduced blood supply, both of which cause damage to the heart muscle.
Signatures of a heart attack in survivors, such as heart inflammation and fibrosis (scarring) take time to develop and are not normally present in people who immediately succumb to the heart attack or an associated fatal event. Therefore, it may be challenging to identify a heart attack as the reason for an accident when sudden death occurs.
There are 3 types of heart attack. The most severe form is ST segment elevation myocardial infarction. It has the classic symptom of pain in the centre of the chest and may range from discomfort to debilitating. Other symptoms may include shortness of breath or trouble breathing, nausea, heart palpitations, anxiety, sweating, and feeling dizzy, lightheaded, or fainting.
The CASA fact sheet on coronary artery disease, noted that the disease is associated with distracting pain, acute shortness of breath, arrhythmia and sudden death. When considering the effect on flying, CASA indicated that ‘Stressful phases of flight can force the cardiac system to work harder. The sedentary nature of aviation can also be detrimental to this condition.’
The ATSB’s aviation medical specialist’s opinion was the pilot was at risk of a sudden incapacitating cardiac event. They had advanced triple-vessel coronary artery disease, capable of inducing incapacitating and distracting chest pain with or without an arrhythmia, such as ventricular tachycardia[19] or ventricular fibrillation.[20] This can induce severe and incapacitating chest pain leading to distraction and declining consciousness.
Medical history
The pilot had ongoing treatment for chronic insomnia with various medications being prescribed. They underwent a sleep study in 2016 and was found not to suffer from sleep apnoea. At the time of the accident, the pilot was prescribed 2 alternating medications for the insomnia: Alprazolam 2 mg and Amitriptyline hydrochloride 25 mg. Only Alprazolam was found in the pilot’s toxicology. The pilot had also previously been prescribed Stilnox for their insomnia.
The pilot also had a history of elevated blood pressure. Treatment had included medication although this stopped during a period of weight loss. The pilot had since regained weight but had not resumed treatment for high blood pressure.
In 2015, the pilot underwent spinal fusion surgery to correct pain associated with osteoarthritic degeneration of the lumbar spine. In 2020, the pilot underwent re-exploration surgery with the removal of existing intervertebral fusion cages and replacement with new ones. The family advised that this surgery was successful and greatly improved the pilot’s life.
Aviation medical examinations
The pilot had seen the same designated aviation medical examiner (DAME) for many years and medical examinations. In August 2018, the pilot failed a medical examination due to their diastolic blood pressure level.[21] The pilot reapplied for an aviation medical in May 2019 and passed the examination.
In October 2021, their Class 2 aviation medical certificate was due to expire and they attended a consultation with their DAME for a Class 1 and Class 2 medical examination. The pilot passed their examination based on the responses to the pre-medical questionnaire and the testing prescribed by CASA. These tests included an audiogram, a resting electrocardiogram, and a glucose and lipids blood test.
During a Class 1 medical examination, a DAME will enter updated information into the CASA medical record system, which calculates the risk score of an applicant using the CASA coronary heart disease risk factor prediction chart. The chart and an associated formula provide a cardiac risk index. Risk factors include age, high-density lipoprotein and total cholesterol levels, systolic blood pressure, and whether the person is a smoker, has diabetes or left ventricular hypertrophy.[22] A score above 14 triggers the requirement for further investigation starting with a stress electrocardiogram. During their most recent medical examination, the pilot did not score above 14.
The pilot declared in their questionnaire a lower back operation in 2015 and magnetic resonance imaging associated with that operation in 2016. The DAME assessed the pilot’s remaining range of motion to be adequate. In addition, they declared the sleep study undertaken in 2016. The pilot did not declare any ongoing medical issues, recent surgeries, nor that they had taken any prescribed medications in the last 4 years. The DAME had no other resources available to validate the pilot’s response that they were not taking prescription medications.
While the pilot passed their aviation medical exam, in discussions with the DAME, they decided the pilot should be referred for another sleep study and a cardiologist review. This was based on their current job stressors, history of weight fluctuations, history of high blood pressure, high cholesterol, and poor lipid control, and having been 5 years since their previous testing.
The pilot attended an appointment with a cardiologist in November 2021. The cardiologist reported that there was no evidence for significant heart disease and the pilot was at low risk of a significant cardiac event. As the pilot was unable to complete the stress electrocardiogram due to back pain, they were referred for a computed tomography (CT) coronary angiogram. The angiogram report stated a moderate burden of coronary artery calcification with plaques in all areas. In addition, it was reported that the pilot had only minor coronary artery disease (less than 25% narrowing), however, mixed plaque in the proximal third of the left anterior descending artery caused up to 25–49% narrowing. The report also stated the pilot had a poor calcium score of 340, which was in the ninetieth percentile for the pilot’s age and gender.
Civil Aviation Safety Authority requirements
A pilot is required to declare to CASA when they have a medically significant condition that affects them for a period of time and to stop acting as authorised by their licence while that condition continues. If the condition becomes chronic, the DAME, in consultation with CASA, may be able to treat the condition such that the pilot again meets the medical standard. CASA provides guidance for pilots on their website on the process and obligations.
CASA lists the classes of medications that can have side effects, which may impair flying performance and groups them into 4 levels, categories A through D (Table 1).
Category D broadly includes some conditions or classes of medications that can treat conditions such as, but not limited to, angina, cancer, Parkinson’s disease, hypertension, malaria, psychiatric conditions, seizures, smoking cessation aids, steroids and weight loss medications. It also includes Therapeutic Goods Administration Schedule 8 controlled substances.[23]
CASA advised the ATSB that alprazolam, amitriptyline hydrochloride and diazepam are classed as category D. They stated this was due to the side effects of the medications themselves or for the conditions in which they were treating. Alprazolam is a Schedule 8 controlled substance, while diazepam is a Schedule 4D restricted substance.[24] Stilnox is a category B medication, which was approved for use with the restriction of a short no fly period after ingestion.
CASA advised they can access the Medicare Benefits Schedule and Pharmaceutical Benefits Scheme to check an applicant’s history when it has reason to, such as when incomplete medical information is supplied by the applicant, for complex medical certifications, or for monitoring compliance with certain medications.
For the awareness of pilots, CASA publicises a limited list of approved medications, along with a list of medications that are considered hazardous or prohibited in aviation.[25] Medications that are considered as hazardous can only be used with the express clearance of CASA or a DAME.
Pharmacological influence
The post-mortem report was examined by a consultant forensic pharmacologist at the request of the ATSB. The review noted that the detection of THC and THC acid could have only occurred as a result of the use of cannabis. Specifically, the consultant concluded that, with the blood concentration[26] of diazepam and THC detected, some impairment of the high-level psychomotor skills required for flying would be expected and could not be excluded as being factors in the accident.
In 2012, the National Safety Council Committee on Alcohol and Other Drugs stated that it was unsafe to operate a vehicle or other complex equipment while under the influence of cannabis, its primary psychoactive component THC or synthetic cannabinoids with comparable cognitive and psychomotor effects. They reported that studies have demonstrated that cannabis intoxication produces dose-related impairment of cognitive and psychomotor functioning and risk-taking behaviour. They also reported the growing epidemiological evidence that detectable THC concentration in blood is associated with increased motor vehicle crash risk, particularly above THC concentrations of 0.002 mg/L.
The opinion of the forensic pharmacologist was the relative concentration of diazepam to the nordiazepam, oxazepam and temazepam concentrations in the pilot indicated they most likely used diazepam within 12 hours to 24 hours of the accident. The therapeutic range for diazepam is 0.1 to 2.0 mg/L.
Epidemiological and experimental studies have demonstrated benzodiazepines (a class of drug that includes diazepam) impair psychomotor skills performance. There is an epidemiological association between benzodiazepine use, increased motor traffic-accident risk and responsibility of the drivers for the crash (Longo et al., 2001; Bramness et al., 2003; Smink et al., 2008).
The pharmacologist also noted that there was no cocaine or benzoylecgonine (a major metabolite) reported to be present in the pilot’s blood but the cocaine metabolite methylecgonine was detected. They further stated that, while this confirmed the pilot had used cocaine within the previous few days, methylecgonine does not produce impairment although the possibility of impairment due to the ‘crash phase’ or withdrawal phase could not be excluded as being a possible factor in the accident. Cocaine effects on skills performance include risk-taking, inattentiveness and poor impulse control. In the withdrawal phase, the user can experience fatigue, sleepiness and inattention (Couper & Logan, 2014 Revision).
Alprazolam can also impair psychomotor skills (Baselt, 2001) and even at therapeutic blood concentrations, it can cause profound impairment of psychomotor skills required for complex tasks such as driving (Verster et al., 2002; Bramness et al., 2003; Leufkens et al., 2007). However, the pharmacologist indicated that, at the level detected, it was unlikely there would have been impairment of the pilot’s psychomotor functions and it unlikely contributed to the accident.
The ATSB’s aviation medical specialist indicated that the presence and levels of these psychoactive drugs and prescription medications would not have increased the risk of heart attack.
Medical-related accident research
ATSB research report B2006/0170
The ATSB’s research report (B2006/0170) on Pilot Incapacitation: Analysis of Medical Conditions Affecting Pilots Involved in Accidents and Incidents 1 January 1975 to 31 March 2006 (Newman, 2007) found pilot incapacitation due to the effects of a medical condition or a physiological impairment represents a serious potential threat to flight safety. A search of the ATSB’s accident and incident database was conducted for medical conditions and incapacitation events between 1 January 1975 and 31 March 2006. Heart attack was the fourth highest form of pilot incapacitation behind gastrointestinal illness, smoke and fumes, and loss of consciousness.
There were 98 occurrences in which the pilot of the aircraft was incapacitated for medical or physiological reasons and in 10 occurrences (10.2%), the outcome of the event was a fatal accident. All the fatal accidents involved single-pilot operations, and in the majority of cases, heart attack was the cause. The second highest cause was loss of consciousness.
The results of this study demonstrated that the risk of a pilot experiencing an in-flight medical condition or incapacitation event was low. However, if the pilot experienced a heart attack the risk of a fatal accident occurring increased. The report also suggested that the aeromedical certification process must keep pace with the evolving nature of modern medical science to ensure that the risk of in-flight incapacitation remained low.
United States Federal Aviation Administration Office of Aerospace Medicine (DOT/FAA/AM‑18/8)
This study, DOT/FAA/AM-18/8 of Incidental Medical Findings in Autopsied U.S. Civil Aviation Pilots Involved in Fatal Accidents (Ricaurte, 2018) examined incidental medical findings (IMFs) reported in the autopsies of pilots who died in United States aircraft accidents from April 2013 through March 2016. Incidental medical findings are previously undiagnosed medical conditions that were incidentally discovered during the autopsy, which may or may not have been related to the cause of death or of the accident.
Out of the selected pilots, 42% were found with IMFs reported in the autopsy. Cardiovascular abnormalities were the most common IMF (85%). The National Transportation Safety Board determined a medical issue was either the probable cause or a contributory factor in 12.2% of accidents with IMFs. The report noted that, while in commercial operations with 2 pilots, the other pilot carries out the flying duties, in single pilot operations, the outcome of the event is usually catastrophic. Epidemiological studies showed that in 15% of patients with coronary heart disease, sudden cardiac death is the initial coronary event.
On 18 March 2008, a Pitts S-2A aircraft impacted the ground 7 km north-east of Camden, New South Wales, fatally injuring the occupant of the rear cockpit. The occupant of the rear cockpit, an experienced aerobatic pilot, was undergoing a routine flight review with an instructor. During a practice forced landing, the pilot stopped responding to instructions and commands, so the instructor took control of the aircraft. A powerful nose-up force began acting on the control column and the aircraft entered an incipient aerodynamic stall.[27] The instructor recovered the aircraft from the stall but, this came too late to prevent a collision with trees. Post-mortem examination of the pilot found they had severe heart disease. Expert medical opinion considered it likely that the pilot experienced an incapacitating event as a result of their heart disease.
On 22 January 2010, a Victa Airtourer 115/A1 was landed safely on Miles Beach, Bruny Island, Tasmania. The pilot, being the sole occupant, shut down, exited and secured the aircraft before leaving it on the beach and walking away. The pilot was found deceased about 300 m from the aircraft. A post-mortem revealed the pilot had died as the result of a heart attack.
On the afternoon of 17 August 2018, the pilot of a Kawasaki Heavy Industries BK117 helicopter was conducting fire-bombing operations approximately 9 km west of Ulladulla, New South Wales. On the fifth fire-bombing circuit, at this location, the pilot filled the slung Bambi Bucket (bucket) without incident from a nearby dam and departed towards the fire area. Shortly after, the helicopter diverted off course, the bucket and longline became caught in trees and the helicopter collided with terrain. The pilot was fatally injured, and the helicopter was destroyed. The pilot’s post-mortem identified 2 heart conditions, one of which was coronary heart disease that was capable of causing sudden impairment and incapacitation.
On 28 February 2022, the crews of 3 Robinson R44 helicopters were preparing to conduct crocodile egg collection in Arnhem Land, Northern Territory. The crews of 2 of the R44 helicopters collecting crocodile eggs nearby became concerned that they had not heard any communications from the crew of the third helicopter, which they reported was unusual. One of those helicopters returned to the area where they were last seen and found the fatally injured egg collector on the ground and the pilot, having sustained serious injuries, laying beside the helicopter that had collided with terrain.
The pilot’s subsequent toxicology results detected 2 metabolites of cocaine. On the basis that the metabolites indicate exposure to cocaine, the detected levels indicated the pilot had not been exposed to cocaine within the previous 24 hours and may not have been affected by cocaine on the accident day. There was insufficient evidence to enable an assessment of whether the drug contributed to the development of the accident. However, the indication of exposure to cocaine is highlighted, as the effects of cocaine and post-cocaine exposure clearly increase risk to aviation activities. The post-cocaine exposure effects can include fatigue, depression and inattention.
On 2 January 2023, the operator was conducting a series of scenic flights in 2 Eurocopter EC130B4 helicopters. The flights were performed under the visual flight rules from its base with the helicopters operating from separate helipads about 220 m apart. As one helicopter was preparing to land, the other helicopter took off. Shortly after, both helicopters collided. The landing helicopter was able to make a safe landing but the helicopter taking off crashed with the occupants being seriously or fatally injured.
The toxicology report for the fatally injured pilot showed a positive result for cocaine metabolites and the cutting agent levamisole. The ATSB’s interim investigation report found that, although it was unlikely the pilot would have had any psychomotor skill impairment on the day of the accident, it was not known whether post-cocaine exposure effects of the drug, which can include fatigue, depression and inattention, had any effect on the performance of the pilot.
Safety analysis
Introduction
On the afternoon of 6 October 2022, while flying at low level over Maitland Vale, New South Wales, a Bell 206B helicopter, registered VH-PHP, rolled markedly and descended rapidly, colliding with a riverbank. The helicopter was destroyed, and the pilot was fatally injured.
This analysis will consider the possible explanations for why the helicopter deviated from the pilot’s intended track and the final moments of the flight. It will also discuss the importance of disclosing medical information to CASA and the use of psychoactive drugs.
Pilot incapacitation and collision with terrain
The pilot deviated from the defined VFR lane and flew for periods at low level before the helicopter departed controlled flight. The ATSB considered a number of possible reasons to explain these events.
Pilot manoeuvring
The manoeuvring performed when approaching Tocal and the subsequent deviation outside the VFR lane and flight at low level was unexpected given the pilot’s intention to track to Warnervale. At one point during the deviation, the helicopter slowed to 22 kt and descended to 120 ft above ground level, which could be interpreted as an approach to land, but the pilot then climbed away. It was also noted that the pilot did not respond to calls made by air traffic control.
The pilot did not indicate to anyone their intention to deviate from the VFR lane and there was no known reason for the pilot to diverge from the track. To the contrary, the pilot stated to family by phone call just prior that the helicopter was flying well, and they would arrive at their destination in a short amount of time and that time would not have accommodated the deviation. The continued broadcasting by the pilot’s navigation software on their phone throughout the entire flight was evidence the pilot had a functional navigational aid.
Helicopter serviceability
While there were varying accounts by witnesses regarding the engine sound that could not be resolved and the helicopter had been in maintenance, the wreckage examination found no pre‑existing issues (mechanical or structural) that would have prevented normal operation. Numerous signatures of engine and driveshaft rotation were found indicating the powerplant and rotor system were functional. There were minimal signs of mast bumping, and the mast fractured in torsional overload indicating it failed on main rotor blade contact with the ground and the pilot did not excessively manoeuvre the helicopter.
Meteorological conditions
The weather forecast for the flight indicated some areas of low cloud and reduced visibility enroute, which could potentially explain the unexpected manoeuvring when near Tocal. However, an experienced pilot who was in the vicinity of the accident site reported the conditions as suitable for VFR operations. This was consistent with the meteorological equipment observations recorded at nearby Maitland Airport. Other witnesses near the VFR lane also reported weather consistent with these observations. Therefore, there was no evidence to indicate that the weather conditions directly contributed to the flight track deviation or the accident.
Pilot distraction
Distractions can occur unexpectedly, during any phase of flight, but when they have contributed to a safety occurrence, they have most often resulted in an incident rather than an accident (ATSB, 2006). There were no passengers on board, no other aircraft traffic was reported in the area at their altitude, and there was no evidence of any technical issues with the helicopter. While the pilot had been making phone calls, this was through the Bluetooth headset, which has simple handling. In addition, the flight time from Tocal and Vacy to the accident was 15 minutes and 5 minutes respectively, which should have been sufficient time to respond to the distraction and react appropriately. This included conducting a precautionary landing if the pilot had experienced a minor medical event. Therefore, a distraction event that was of sufficient magnitude and duration to result in the pilot losing awareness of their location and flightpath for this amount of time was considered to be unlikely. Further, distraction at the end of the flight was possible but considered unlikely due to the steep angle of pitch and bank prior to impact, which would not go unnoticed by an experienced pilot.
Pilot incapacitation
Pilot incapacitation is operationally defined as (International Civil Aviation Organization, 2012):
…any physiological or psychological state or situation that adversely affects performance.
Incapacitations can be divided into two operational classifications: “obvious” and “subtle”. Obvious incapacitations are those immediately apparent...onset can be “sudden” or “insidious” and complete loss of function can occur. Subtle incapacitations are frequently partial in nature and can be insidious because the affected pilot may look well and continue to operate but at a less than optimum level of performance. The pilot may not be aware of the problem or capable of rationally evaluating it.
ATSB research (ATSB, 2016) has shown that in-flight incapacitation can result from a variety of reasons, including changes in environmental conditions during the flight, the development of an acute medical condition, or the effects of a pre-existing medical condition.
The air temperature at nearby Maitland Airport was not excessive. The pilot had finished a short phone call about 60 seconds before the accident. As such, it was unlikely the pilot had fallen asleep leading up to the accident, although it could not be discounted that this occurred immediately prior to the impact. Also, the pilot was reported to be experiencing a head cold from which they were recovering. However, this was unlikely to be a source of distress enough to not permit continued control of the helicopter.
The pilot had notable changes in health during previous years including weight fluctuations, periods of high blood pressure and high cholesterol, insomnia, and lower back pain, for which the pilot had been prescribed various medications.
In the 12 months prior to the accident, the pilot completed their aviation medical and was found to be below the baseline required for further cardiac assessment. Although, given the pilot’s medical history and job stressors, the designated aviation medical examiner (DAME) and pilot elected to conduct further cardiac testing. The assessment found only minor to moderate cardiac disease and that the pilot was at low risk of a significant cardiac event.
However, the pilot’s post‑mortem examination found severe coronary atherosclerosis within all 3 major coronary arteries with at least 80% lumen stenosis observed. The ATSB’s aviation medical specialist noted that this could result in incapacitating chest pain leading to distraction and declining consciousness. This may possibly explain the unexpected deviation from the pilot’s intended track and the witness observations of the helicopter rolling markedly and descending rapidly before colliding with the riverbank. Nevertheless, it was not possible to forensically determine if the pilot experienced a heart attack prior to the accident. This is consistent with the ATSB research, which indicated it was likely that cardiovascular problems featured more prominently in general aviation accidents, but evidence of this was often difficult to establish with certainty, particularly in fatal accidents (ATSB, 2016).
The pharmacological influence of the medication and controlled substances detected was assessed by a forensic pharmacologist and an aviation medical specialist. While the levels of diazepam and delta-9-tetrahydrocannabinol in the pilot’s blood sample were considered to result in some impairment of cognitive and psychomotor function, they were not at levels likely to exacerbate the pilot’s cardiac condition.
Despite this, in the absence of other reasonable scenarios to explain the unexpected events leading to the collision with terrain, the most plausible explanation was that the pilot likely experienced some level of incapacitation. However, the ATSB could not conclusively determine if this was due to a cardiac event, related to the medication and controlled substances, a combination of both, or for other unknown reasons.
Coronary artery disease
While a previous cardiac assessment identified the pilot had minor to moderate cardiac disease, the post-mortem found severe coronary atherosclerosis within all 3 major coronary arteries. With this level of disease, the ATSB’s aviation medical specialist advised that the pilot was at risk of a sudden incapacitating cardiac event. Similarly, the forensic pathologist also noted that the extent of the disease was a risk factor for sudden death. The post-mortem observations would suggest that the pilot’s cardiac disease had significantly increased in the period leading up to the accident.
Prior accidents and ATSB research have shown that, for fatal accidents with medical-related causes, coronary artery disease is one of the leading reasons for incapacitation, and for single‑pilot operations the majority leads to a fatal accident. Likewise, cardiovascular abnormalities were the most common incidental medical findings identified in pilot autopsies in the United States.
In this case, although it could not be determined if the pilot had experienced a heart attack, it remained a significant risk factor for the pilot. The initiation of a cardiac event can become so debilitating that the pilot becomes physically unable to control their own movements and thus the flightpath of the aircraft, which is particularly crucial in single-pilot operations.
Disclosure of medical information
As the holder of a pilot’s licence, the person is required to apply and obtain a medical certificate of an appropriate class if the person wishes to exercise the privileges of that licence. Aviation medical certificates have a period of validity, depending on their class, and need to be reapplied for at their expiry. As part of the medical process, the pilot is required to answer the DAME’s questions regarding their health and provide historical information so CASA can determine if the pilot meets the relevant medical standard. This includes the pilot completing a pre-medical questionnaire, which is reviewed by the DAME at the medical examination.
The DAME was not aware of the medications the pilot had been prescribed as ongoing treatment for insomnia (Alprazolam and Amitriptyline hydrochloride), as they had not been declared by the pilot during their medical examinations. These 2 medications were classified by CASA as category D drugs, which would have made the pilot ineligible to receive an aviation medical certificate. The Alprazolam, which was found in the pilot’s blood sample, was a Therapeutic Goods Administration Schedule 8 controlled drug.
The pilot also did not declare a spinal operation conducted 12 months before their last aviation medical examination, though the outcome of this was covered by a range of motion tests conducted by the DAME, which the pilot passed.
Medications and chronic conditions declared to a DAME permit medical conditions to be managed appropriately. Where an issue exists, alternative treatments and medications more compatible with aviation can be trialled, thereby permitting the pilot to manage both their own personal risks as well as those to aviation safety. A pilot should not exercise the privileges of their licence while taking a prohibited medication and should consult CASA or their DAME if they are unsure of a medication’s categorisation.
Psychoactive drugs and medications incompatible with aviation
The pilot’s blood sample contained psychoactive drugs, their metabolites and a cutting agent. In addition, the pilot had 2 medications determined by CASA to be incompatible with aviation safety. None of these drugs were permitted to be used in conjunction with flying.
The levels of diazepam detected were considered to be in the therapeutic range.
The family reported that the pilot reported operations were normal during a phone call during the flight. Also, the pilot had been flying for about 2 hours without any apparent issues. Therefore, there was insufficient evidence to enable an assessment of whether the drugs and medications alone contributed to the accident. However, the forensic pharmacologist advised that some of these drugs were at levels where some impairment of the high-level psychomotor skills required for flying would be expected. In addition, at the levels detected for some of these drugs, there is a notable increase in risk-taking.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell Helicopter 206B, VH-PHP, 6.5 km east north-east of Maitland Airport, New South Wales on 6 October 2022.
Contributing factors
While at low level, the pilot likely experienced an incapacitating event, leading to a collision with terrain.
Other factors that increased risk
The pilot had severe coronary artery disease, which is known to reduce the supply of blood to the heart muscle. This can cause chest pain, dizziness, shortness of breath and possible incapacitation.
The pilot did not disclose their use of prescription medicines to the Civil Aviation Safety Authority. This precluded specialist consideration and management of the ongoing flight safety risk the prescribed medications posed.
The presence of metabolites of controlled substances and prescription medications in the pilot's blood stream had the potential to affect their performance and ability to safely operate the helicopter.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Coroner’s Court of NSW
NSW Police Service
NSW Forensic Medicine Service
Civil Aviation Safety Authority
the helicopter owner
the maintenance organisation for VH-PHP
Airservices Australia
OzRunways
Services Australia
Bureau of Meteorology
the pilot’s medical practitioners
the witnesses.
References
Australian Transport Safety Bureau. (2016). Pilot incapacitation occurrences 2010-2014 (AR‑2015-096). Retrieved from /publications/2015/ar-2015-096/
Australian Transport Safety Bureau. (2007). Analysis of Medical Conditions Affecting Pilots Involved in Accidents and Incidents: 1 January 1975 to 31 March 2006. Retrieved from
Baselt, R (2001). Drug effects on Psychomotor Performance. Biomedical Publications, California.
Baselt RC (2017). Disposition of toxic drugs and chemicals in man. 11th Edn. Biomedical Publications,California.
Bramness, J.G., Skurtveit, S. & Morland, J (2003). Testing the benzodiazepine inebriation-relationship between benzodiazepine concentration and simple clinical tests for impairment in a sample of drugged drivers. Eur. J. Pharmacol., 59:593-601.
Couper, F.J. & Logan, B.K. (2014 revision). Drugs and Human Performance Facts Sheets. Technical Report DOT HS 809 725, National Highway Traffic Safety Administration, Washington DC.
Longo, M.C., Lokan, R.J. & White, J.M. (2001). The relationship between blood benzodiazepine concentration and vehicle crash culpability. J. Traffic Med., 29:36-43
Leufkens, T.R., Verneeren, A., Smink, B.E., van Ruitenbeek, P. & Ramaekers, J. G. (2007). Cognitive, psychomotor and actual driving performance in healthy volunteers after immediate and extended release formulations of alprazolam 1 mg. Psychopharmacology (Berl.), 191(4):951-959.
National Safety Council Committee on Alcohol and Other Drugs. (2012). Position on the Use of Cannabis (Marijuana) and driving. J. Anal. Toxicol., 37:47-49
Ricaurte E (2018) DOT/FAA/AM-18/8 Incidental Medical Findings in Autopsied U.S. Civil Aviation Pilots Involved in Fatal Accidents
Smink, B.E., Lusthof, K.J., de Gier, J.J., Uges, D.R.A. & Egberts, A.C.G. (2008). The relation between the blood benzodiazepine concentration and performance in suspected impaired drivers. J. Forensic & Legal Medicine, 15:483-488.
Verster, J.C., Volkerts, E.R. & Verbaten, M.N. (2002). Effects of alprazolam on driving ability, memory functioning and psychomotor performance: a randomized, placebo-controlled study. Neuropsychopharmacology 27(2): 260-269.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
pilot’s medical practitioners
consultant pharmacologist
consultant aviation medical specialist.
Submissions were received from the Civil Aviation Safety Authority and a medical practitioner. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]A VFR route is a designated track usually in an area of high-density traffic or restricted airspace to enable safe separation of VFR traffic. It is also referred to as a VFR lane.
[3]These restricted zones cover from ground level to an altitude of 10,000 ft radially around Williamtown Airport and are used by military aircraft.
[4]The pilot reportedly flew with a Bluetooth enabled aviation headset.
[5]The last position indicated on the track was the last reliable GPS fix. The OzRunways system reported 8 additional points, but these were discarded as being unreliable due to reflected signals.
[6]OzRunways is an electronic mobile application, utilising approved data for electronic maps, and used for navigation.
[7]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[8]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[9]For VFR operations, when flying below the height of 3,000 ft above mean sea level or 1,000 ft above ground level (whichever is the higher) in Class G non-controlled airspace, a pilot is required to have 5,000 m flight visibility and to be clear of cloud.
[10]Mast bumping: abnormal contact between the main rotor hub and the rotor mast which, if excessive, could severely damage the mast, or result in the separation of the main rotor system from the helicopter.
[11]A lumen is the inside space of a tubular structure, such as an artery or intestine.
[12]Stenosis is the abnormal narrowing of a blood vessel or other tubular organ or structure.
[13]Myocardial ischemia occurs when blood flow to the myocardium (the muscular tissue of the heart) is obstructed by a partial or complete blockage of a coronary artery by atherosclerosis.
[14]Arrhythmia, or irregular heartbeat, is an abnormal rate or rhythm of the heartbeat. The heart may beat too quickly, too slowly, or with an irregular rhythm.
[15]Myocardial infarction, colloquially known as ‘heart attack’, is caused by decreased or complete cessation of blood flow to a portion of the myocardium.
[16]Atherosclerosis is the buildup of fats, cholesterol, and other substances in and on artery walls. This buildup is known as plaque. The plaque can cause arteries to effectively narrow, blocking blood flow.
[17]Perivascular fibrosis is the increased amount of connective tissue in the heart vessels, which increases tissue stiffness.
[18]A myocyte is a contractile cell (muscle cell).
[19]Ventricular tachycardia is a type of irregular heart rhythm (arrhythmia) characterised by the lower heart chamber contracting poorly (quivering) but in a coordinated manner resulting in poor pumping function.
[20]Ventricular fibrillation is a type of irregular heart rhythm (arrhythmia) characterised by the lower heart chamber contracting very rapidly but in an uncoordinated manner resulting in poor pumping function.
[21]Diastolic blood pressure is how much pressure the blood is exerting against the artery walls while the heart muscle is resting between contractions.
[22]Left ventricular hypertrophy is thickening of the walls of the lower left heart chamber.
[23]Schedule 8 controlled drugs are substances that should be available for use but require restriction of manufacture, supply, distribution, possession and use to reduce abuse, misuse and physical or psychological dependence (Therapeutic Goods (Poisons Standard - October 2022) Instrument 2022).
[24]Schedule 4 is for prescription only medicine. These are substances, the use or supply of which should be by or on the order of persons permitted by State or Territory legislation to prescribe and should be available from a pharmacist on prescription. However, some prescription medications have further specified controls applying to possession or supply. These are often referred to as restricted drugs or Schedule 4D medications (Therapeutic Goods (Poisons Standard - October 2022) Instrument 2022).
[26]It should be noted that post-mortem blood samples are whole blood samples, but the reported therapeutic ‘blood’ concentrations from clinical studies are generally plasma concentrations. The blood/plasma ratio for diazepam is reported as being about 0.6 (Baselt 2017). Therefore, the reported blood concentration would be very conservative, and a plasma concentration would have been around 40% higher.
[27]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift and increased drag.
The Australian Transport Safety Bureau is investigating the collision with terrain of a Robinson Helicopter R22 Beta, registration VH-CWE at Budgerygar Station, Queensland on 26 September 2022.
During landing, the pilot lost control and the helicopter collided with terrain. The pilot sustained serious injuries and the helicopter was substantially damaged.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
About 1300 local time, on 26 September 2022, the helicopter departed a rural property, with the pilot and one passenger on board, reportedly to perform a weed inspection of that property. While flying at low altitude, the pilot lost control of the aircraft and collided with terrain. The aircraft was substantially damaged, with the pilot sustaining serious injuries, and the passenger receiving minor injuries.
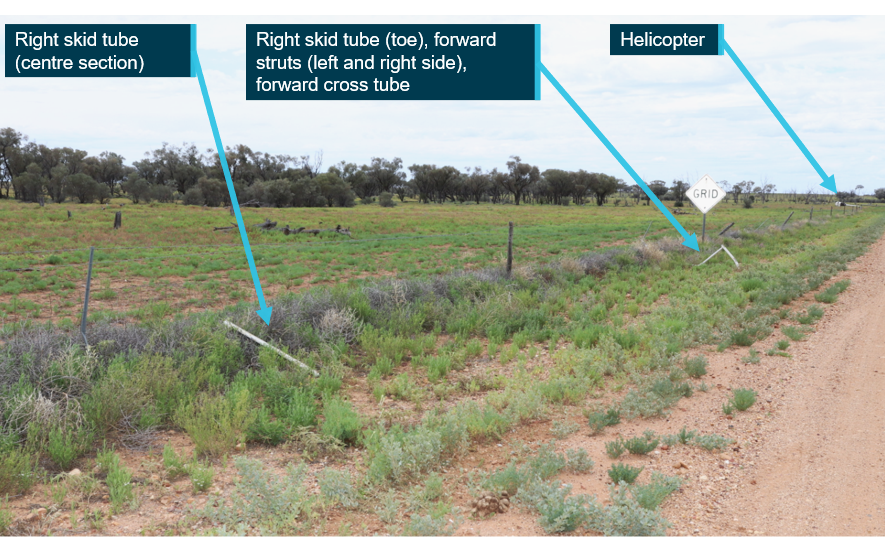
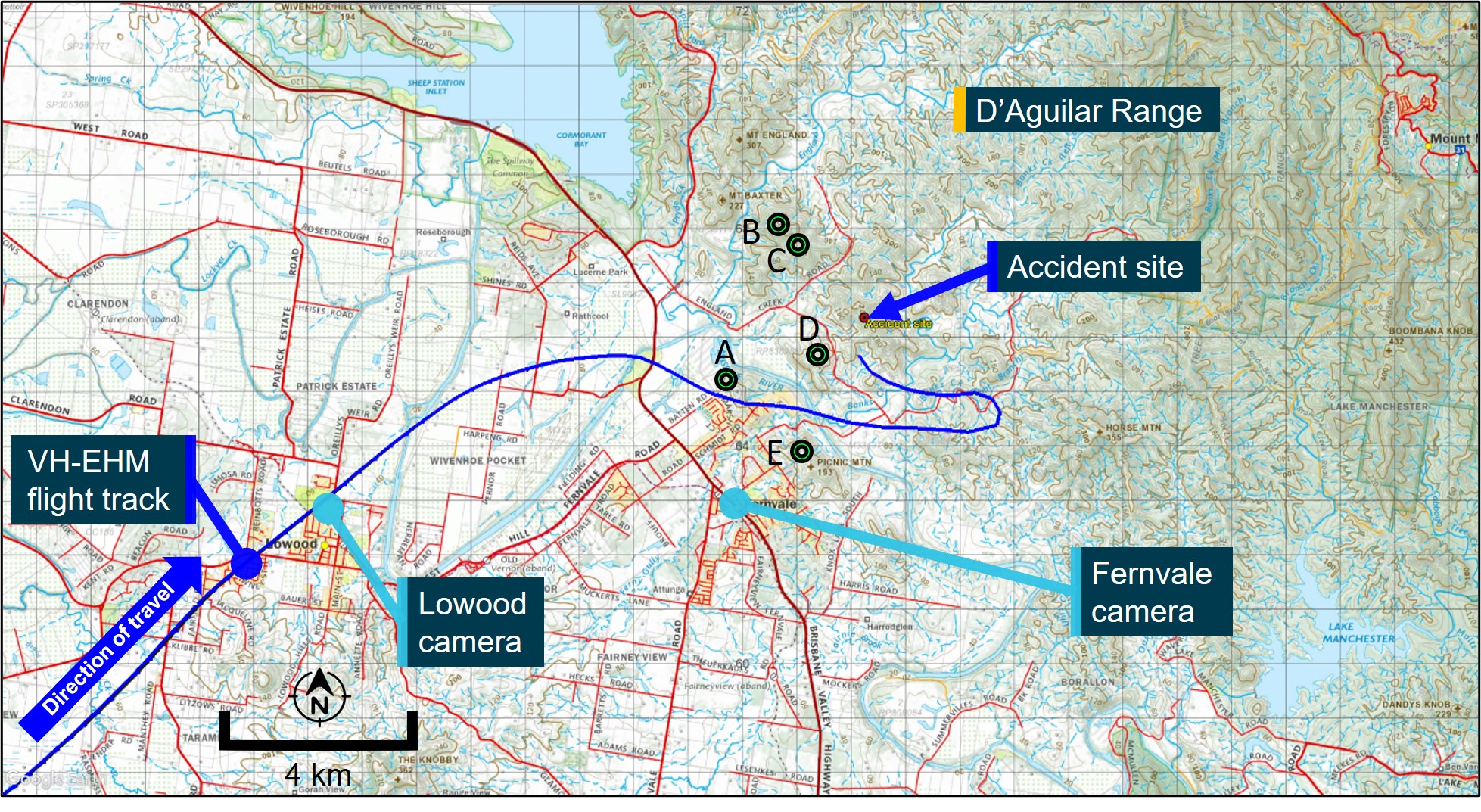
The ATSB evaluated photographic evidence of the wreckage and interviewed the pilot and witnesses. There were no reported problems with the helicopter prior to the collision with terrain. The first items in the wreckage trail were the landing gear, which had separated from the helicopter and had contact marks consistent with impact to the left struts. The main wreckage was located about 400 m away on its side adjacent to the road with no obvious pre‑accident defects (Figure 1 and Figure 2).
Based on the available evidence it is likely that the accident was due to a handling error while operating at low level.
A review of Civil Aviation Safety Authority (CASA) licencing information identified that the pilot held both Commercial and Private Pilot Licences (Helicopter) and a low-level mustering endorsement. However, they did not hold a current medical certificate and CASA had no evidence that the pilot had conducted a flight review within the required period to enable operation of the R22 helicopter. As such, they were not entitled to exercise the privileges of their licence at the time of the accident.
Figure 1: Landing gear assembly components and final helicopter location
Source: Queensland Police, annotated by the ATSB
Figure 2: Helicopter wreckage
Source: Queensland Police
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues or important safety lessons. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any similar occurrences that may indicate a need to undertake a further safety investigation.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
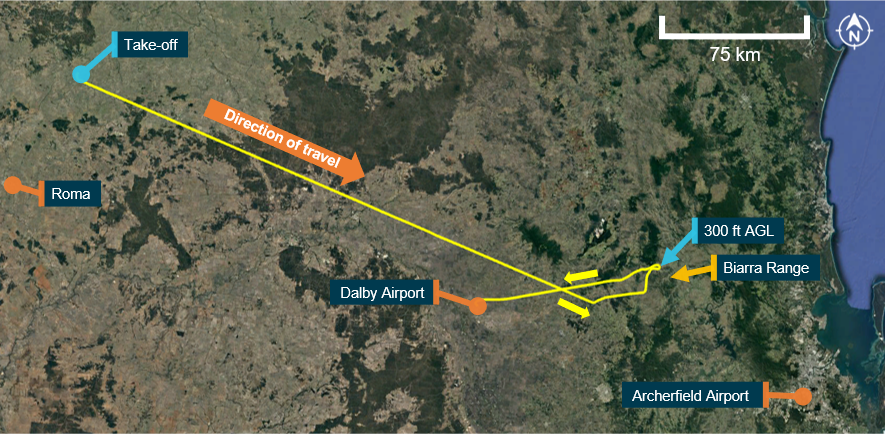
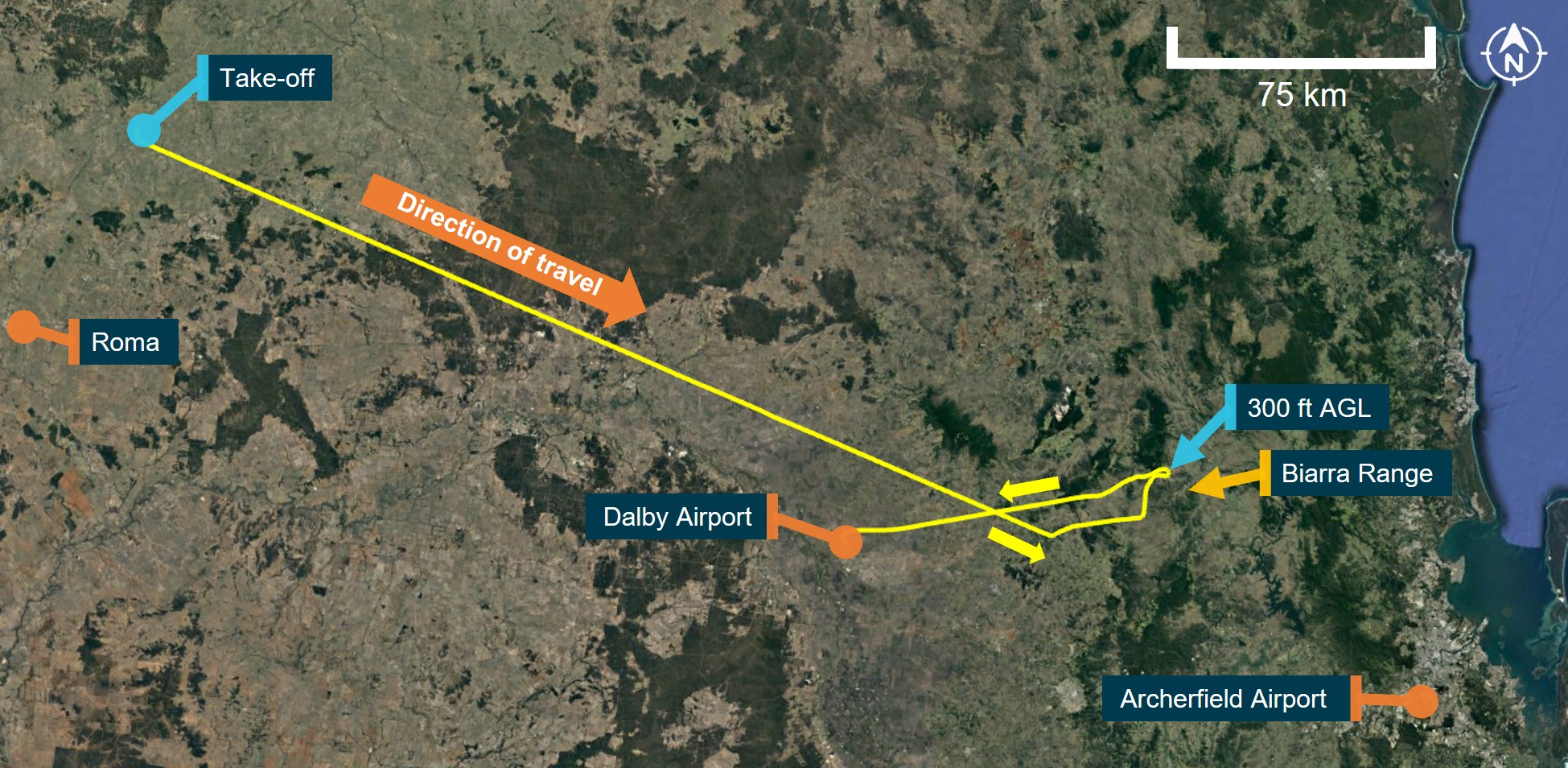
At 1055 local time on 28 August 2022, a Cessna R182 Skylane RG (R182), registered VH-EHM (EHM) and operated by Executive Helicopters, departed Archerfield Airport, Queensland, for an air transport[1] flight under visual flight rules (VFR)[2] to a private property north‑east of Roma, Queensland. The aircraft departed with the pilot and 2 passengers. The aircraft landed at about 1230 and the occupants spent the night at the property.
At 0715 on the following day, the pilot and 2 passengers departed from the property in EHM for a VFR return flight back to Archerfield (Figure 1). Recorded flight tracking data showed the aircraft was initially established on a direct south‑easterly track towards Archerfield at cruise altitudes of between 3,400 ft and 3,900 ft above mean sea level (AMSL). The weather forecast available from the Bureau of Meteorology (BoM) at the time of departure indicated that the route to Archerfield could be affected by low cloud, rain, fog and associated reduced visibility.
At 0828, the aircraft turned left and descended to about 1,800 ft AMSL – 600 ft above ground level (AGL). The flight then tracked north before turning east towards the Biarra Range and into a valley before descending to about 300 ft AGL. Shortly after, the aircraft completed a 180° turn, climbed to 3,900 ft and tracked towards Dalby Airport. At 0901, the aircraft landed at Dalby and was refuelled with about 263 L of fuel.
Source: Google Earth and OzRunways, annotated by ATSB
Recorded data showed the aircraft depart Dalby 11 minutes later, at about 0912, and tracked south‑east, climbing to a cruise altitude of about 2,500 ft (1,300 ft AGL). At 0927, the flight progressed over rising terrain and 3 minutes later was operating at about 400 ft AGL (Figure 2). At 0935, the aircraft turned left towards Main Range before completing a 180° turn between 300‑500 ft AGL. It then tracked south-east, climbing to about 1,000 ft AGL.
At about 0946, the aircraft passed over a mountain ridge at a height of about 200 ft AGL before turning left over another ridge at a height of about 270 ft AGL (2,900 ft AMSL). The aircraft then tracked north‑east, descending down a valley for 8 minutes at an altitude of about 1,200 ft (700 ft AGL).
Source: Google Earth and OzRunways, annotated by ATSB
At about 0955, the aircraft passed to the east of Gatton Airpark and turned right towards Lowood. Eight minutes later, the aircraft passed overhead Lowood and descended to 500 ft AGL before turning east towards Fernvale and the D’Aguilar Range. The flight data showed that at 1005, the aircraft passed over a hill at a height of about 200 ft AGL, before climbing to 700 ft AGL.
The flight progressed down a valley before completing another 180° turn while climbing to 1,000 ft AGL. After the turn, the aircraft descended to 800 ft (600 ft AGL) before turning right, back towards the D’Aguilar Range (Figure 3). During this turn, at 1007, the aircraft impacted terrain at an elevation of about 650 ft AMSL. The aircraft was destroyed, and all occupants were fatally injured.
Source: Google Earth and OzRunways, annotated by ATSB
Search and Rescue
About 30 minutes after departing the private property, the pilot had left a verbal flight note[3] with a person not associated with the operator to expect their arrival ‘late morning’. This person raised concern for the flight after several attempts to contact the pilot were unsuccessful, and notified the operator at 1309 that the pilot was missing. The operator then attempted to contact the pilot and made several calls to other locations to see whether the aircraft had landed at a different location.
At 1331, the operator notified Lowood police and at 1342, arranged for a helicopter from another Archerfield based operator to search for the missing aircraft. At 1344, the operator notified Airservices Australia who coordinated a search and rescue effort with the Joint Rescue Coordination Centre.
At about 1427, the helicopter departed Archerfield and located the wreckage shortly after. The helicopter pilot landed near the wreckage and proceeded to the site on foot, and then reported back to the operator that all of the aircraft’s occupants were deceased. Shortly after, a search and rescue helicopter arrived at the site and paramedics confirmed the fatalities.
Context
Pilot information
The pilot held commercial pilot licences (aeroplane and helicopter), with their last aeroplane flight review being conducted in March 2021 and operational proficiency check last completed in March 2022. The pilot also held an aeroplane instrument rating, but this was not current as the last renewal[4] was completed in October 2002 (valid until October 2003).
The pilot held a night VFR rating (helicopter), but this was also not current as the last proficiency check was completed in May 2019 (valid until May 2021). The pilot held a Class 1 aviation medical certificate, valid until October 2022.
Prior to the accident flight, the pilot had accumulated approximately 13,900 hours of aeronautical experience in helicopters and aeroplanes, of which about 475 hours were in command of the Cessna R182. The pilot also had about 96 hours of instrument flying experience and 22 hours of night VFR experience.
Aircraft information
The Cessna R182 Skylane RG is a 4-seat, high-wing, single‑engine aircraft with retractable landing gear. The accident aircraft was manufactured in the United States in 1978 and first registered in Australia in 1989 as VH-HZU before being purchased by Executive Helicopters in January 2020 and registered as VH-EHM. The aircraft was fitted with a Lycoming O-540 piston engine driving a 3 blade Hartzell constant speed propeller and was equipped for flight under both VFR and instrument flight rules (IFR).[5]
The last periodic maintenance inspection (100-hourly) was completed on 15 July 2022. Since then, the aircraft had accrued about 30 hours of flight time and had about 5,858 hours total time in service.
Terrain
The flight’s track towards Archerfield took the aircraft across the Great Dividing Range to the west of Brisbane with terrain elevations generally between 1,500‑2,000 ft AMSL. This area also contained numerous peaks between 2,000-2,700 ft (Figure 4).
Figure 4: Visual navigation chart extract showing terrain along the flight path
Source: Airservices Australia and OzRunways, modified and annotated by ATSB
Meteorological information
Forecast
The graphical area forecast for the accident region forecast the following cloud conditions at the time of the accident (all heights AMSL):
broken cumulus/stratocumulus between 3,000-7,000 ft
Isolated smoke was forecast below 6,000 ft where the visibility reduced to 6,000 m. Isolated showers were forecast with 3,000 m visibility and the following cloud conditions:
broken stratocumulus between 1,000-2,500 ft
broken cumulus between 2,500-8,000 ft
The grid point wind and temperature chart for the region forecast 1,000 ft easterly winds between 9-13 kt, with temperatures 12-14 °C.
Airservices Australia held three National Aeronautical Information Processing System (NAIPS)[7] login records for the pilot in the 24-hour period before the accident. These were recorded at 0708, 0709 and 0925 on 29 August 2022.
Observations
The following METAR[8] observations from nearby airports were reported at 1000 (about 7 minutes before the accident):
Royal Australian Air Force Base Amberley (24 km south of accident site) – visibility 8,000 m, cloud scattered at 1,400 ft and broken at 2,800 ft[9]
Archerfield Airport (36 km south-east of accident site) – visibility at least 10 km, cloud scattered at 1,900 ft and 2,300 ft, and overcast at 3,300 ft
Several witnesses along the aircraft’s route from Dalby to Fernvale recalled seeing the aircraft flying at low altitude below cloud. One witness in Fernvale reported the aircraft flying at low altitude while heading east towards the D’Aguilar Range with the wings level and undercarriage retracted, before banking left (Figure 3) and disappearing from view as it was obscured by cloud. The witness also reported heavy low cloud, very light rain, and fog covering the Fernvale and surrounding area at the time.
Airspace
The Amberley military control zone extends from ground level up to an altitude of 8,500 ft (Figure 5). The airspace was active from 0800 to 2300 on 29 August and required a clearance to transit. Preliminary information indicated no record of a transit clearance request by the pilot, however, additional information is being collected by the ATSB to verify this.
On-site evidence indicated that the aircraft was in a right turn with an angle of bank of about 47° when it collided with several trees, before impacting terrain about 28 ft vertically below the top of a ridge. The wreckage trail extended about 40 m from the initial impact point to the top of a ridge where most of the wreckage was located, including the engine. The propeller was located about 10 m forward of the main impact point.
On-site examination indicated that the engine was providing power at impact, with the landing gear and flaps in the retracted position. There was no evidence of an in-flight break-up or a pre‑existing defect with the flight controls.
Recorded Data
The aircraft was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be. Recorded data was obtained from various sources:
The flight track data indicated that the aircraft’s ground speed after departing Dalby was generally between 120-140 kt, indicative of normal cruise speeds.
Further investigation
The ATSB has examined the accident site and wreckage, interviewed witnesses, collected meteorological data, pilot and flight records and obtained aircraft tracking data.
The investigation is continuing and will include further review and examination of:
pilot training, qualifications, experience, and medical information
aircraft maintenance and flight records
operator procedures, flight notification practices and management systems
witness accounts
meteorological data
recorded data (CCTV, flight tracking, communications).
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the significant assistance provided by the Queensland Police Service during the onsite investigation phase and initial evidence collection activities.
[1] The flight was operated under Civil Aviation Safety Regulations Part 135 (Air transport operations - smaller aeroplanes).
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[3] Details of the route and timing of a proposed flight provided by the pilot-in-command of an aircraft, other than a notification submitted to Airservices Australia, and which is required to be left with a person who could be expected to notify appropriate authorities if the flight becomes overdue.
[4] Before the introduction of the Civil Aviation Safety Authority (CASA) Part 61 licencing regulations in 2014, under Civil Aviation Regulation 5, pilots maintained instrument currency by completing an instrument ‘renewal’. Under Part 61, pilots maintained this currency by completing an ‘instrument proficiency check’.
[5] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[6] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[7] The National Aeronautical Information Processing System (NAIPS) is a computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots.
[8] METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[9] Cloud heights are reported as above aerodrome elevation. Amberley elevation – 91 ft. Archerfield elevation – 65 ft.
[10] Automatic Dependent Surveillance – Broadcast - A means by which aircraft, aerodrome vehicles and other objects can automatically transmit and/or receive data such as identification, position and additional data, as appropriate, in a broadcast mode via a data link.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Final report
Executive summary
What happened
At 0715 local time on 29 August 2022, a Cessna R182 Skylane RG (R182), registered VH-EHM, and operated by Executive Helicopters, departed a private property (Lighthouse) north-east of Roma, Queensland for an air transport flight under the visual flight rules (VFR) to Archerfield Airport. The aircraft departed with the pilot, 2 passengers, and a passenger’s pet dog on board.
As the aircraft attempted to cross a section of the Great Dividing Range, the pilot encountered forecast low cloud and reduced visibility, and was unable to find a way across. With limited fuel remaining, the pilot diverted to Dalby Airport and refuelled the aircraft before departing once again to find a different location to cross the elevated terrain.
After crossing a section of the Great Dividing Range at low level, the pilot tracked to the north of Amberley below low cloud towards an area adjacent to the D’Aguilar Range. While manoeuvring around the edge of this range, the aircraft collided with terrain during a turn, about 36 km north‑west of Archerfield. All occupants of the aircraft were fatally injured.
What the ATSB found
The ATSB found that the en route forecast available before departing Lighthouse predicted that the flight to Archerfield would be affected by low cloud, rain, fog and associated reduced visibility, particularly around the elevated terrain of the Great Dividing Range. After departing Lighthouse, the pilot encountered and manoeuvred at low level around forecast low cloud over elevated terrain of the range before diverting and landing at Dalby to refuel. An updated weather forecast available while at Dalby predicted similar conditions as previously forecast with additional periods of deteriorating weather around Amberley and Archerfield. However, the low cloud and deteriorating weather were expected to dissipate within the next 2-3 hours. The updated weather was not reviewed by the pilot while on the ground and, after refuelling, they subsequently departed once again toward forecast en route weather unsuitable for visual flight.
The pilot likely reviewed the updated weather forecast in-flight, shortly after take-off, but continued the flight at low level, and at normal cruise speed towards elevated terrain. After crossing a section of the Great Dividing Range below cloud and with minimal terrain separation, the pilot continued the flight in similar conditions toward the Lake Manchester VFR route adjacent to the D’Aguilar Range. While manoeuvring in this area, the aircraft very likely entered cloud resulting in the pilot losing visual reference with the ground and surrounding terrain, eventually leading to controlled flight into terrain.
There was no evidence of any conditions or circumstances likely to induce a medical problem or incapacitation for the pilot. There was also no evidence of any aircraft system or mechanical anomalies that would have influenced the accident. It was also considered unlikely that there was any direct or perceived organisational pressure on the pilot to continue the flight.
The pilot was probably influenced by plan continuation bias – an internal pressure or desire to get to the destination – to continue the flight, which probably became stronger as they got closer to Archerfield Airport. However, due to a lack of information, the ATSB was unable to determine the reasons why the pilot continued the flight at cruise speed and low level into unsuitable weather in the vicinity of known high terrain.
The investigation identified several other factors related to flight notification and fuel planning. Although these factors increased risk, they were not considered contributory to the accident.
Finally, the investigation found that the operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions (IMC) as a hazard, which reduced the ability of the organisation to effectively manage the related risk.
What has been done as a result
The operator advised that they had removed aeroplane operations from their Air Operator's Certificate (AOC) and updated the hazard and risk register to include inadvertent entry into IMC. A risk assessment was conducted with the following risk controls planned to be implemented by February 2024 to minimise the risk of inadvertent entry into IMC for helicopter operations:
the operations manual is to be updated to include a formal organisational policy for supporting pilots to land or return to a safe landing site if they assess that they will be unable to maintain visual meteorological conditions.
annual operator proficiency checks will include inadvertent IMC avoidance and recovery techniques.
Safety message
The safety risks of visual pilots flying into non-visual conditions are well documented. This continues to be a recurring factor in aircraft accidents and has been the focus of numerous previous ATSB reports and publications.
A large amount of reference material is available to pilots for guidance on avoiding VFR flight into adverse weather as well as recovery should inadvertent IMC entry occur. The United States Aircraft Owners and Pilots Association Air Safety Institute website VFR into IMC provides an online course, videos and reference materials to assist pilots in avoiding and managing these scenarios. Additionally, the ATSB publication Avoidable Accidents No. 4, Accidents involving Visual Flight Rules Pilots in instrument Meteorological Conditions provides lessons learned from the analysis of various weather-related accidents and incidents.
Aviation safety risk management can be applied at all levels of aviation to enhance operational safety. For commercial operators, formalised risk management supports individual pilot decision making and provides a systemic approach to safety by introducing layers of controls to reduce single point of failure accidents.
As such, the ATSB strongly encourages operators to specifically assess the risk of inadvertent IMC and implement mitigation strategies commensurate to the level of risk it presents to their pilots and passengers.
The occurrence
On 28 August 2022 a Cessna R182 Skylane RG (R182), registered VH-EHM and operated by Executive Helicopters, flew from Archerfield Airport, Queensland to a private property (Lighthouse) north‑east of Roma, Queensland, with a pilot, 3 passengers, and a passenger’s pet dog on board.
The following day, VH-EHM departed Lighthouse at 0715 local time with the pilot, 2 passengers, and pet dog, for an air transport[1] flight under the visual flight rules (VFR)[2] back to Archerfield (Figure 1). Recorded flight data showed the aircraft was initially established on a direct south‑easterly track towards Archerfield at cruise altitudes between 3,400 ft and 3,900 ft above mean sea level (AMSL).[3] The en route weather forecast valid at the time of departure indicated low cloud, rain, fog and associated reduced visibility (see the section titled Meteorological information).
At 0828, the pilot turned the aircraft left and descended to about 1,800 ft AMSL (about 600 ft above ground level (AGL))[4] before tracking north, then east towards the Biarra Range into a valley. The aircraft was then descended to about 1,200 ft (700 ft AGL), before the pilot completed a 180° turn at 300 ft AGL, climbed to 3,900 ft (2,000 ft AGL) and tracked towards Dalby Airport.
At about 0850, the pilot was contacted by a person via mobile phone. During the conversation, the pilot reported some weather on the range and their intention to refuel at Dalby before attempting to find another way to Archerfield. At 0901, the aircraft landed at Dalby and was refuelled with about 263 L of fuel.
Source: Google Earth and OzRunways, annotated by ATSB
Recorded data showed that VH-EHM departed Dalby at about 0912 and tracked southeast before climbing to a cruise altitude of about 2,500 ft (1,300 ft AGL). By 0927, the flight had progressed over rising terrain and, about 3 minutes later, was operating at about 2,300 ft (400 ft AGL) (Figure 2). At 0935, the pilot turned left towards Main Range, and about 8 km later, completed a 180° turn between 300–500 ft AGL before tracking south-east and climbing to about 2,500 ft (1,000 ft AGL).
At 0946, the aircraft passed over a mountain ridge at about 2,800 ft (200 ft AGL) before conducting a 90° left turn over another ridge at about 2,900 ft (270 ft AGL). VH-EHM then tracked to the north‑east and descended down the range to an altitude of about 1,200 ft (700 ft AGL).
Source: Google Earth and OzRunways, annotated by ATSB
At about 0955, the aircraft passed to the east of Gatton Airpark before tracking towards Lowood. After passing overhead Lowood, VH-EHM descended to about 700 ft (500 ft AGL) before turning east towards Fernvale and the D’Aguilar Range. The flight data showed that at 1005, the aircraft passed over a hill at a height of about 200 ft AGL, before climbing to 900 ft (700 ft AGL).
After passing Fernvale, the flight progressed down a valley before completing another 180° turn while climbing to 1,200 ft (1,000 ft AGL). After completing the turn, the aircraft was then descended to 800 ft (600 ft AGL) before turning right, back towards the D’Aguilar Range (Figure 3) and towards observed low cloud. During this turn, at 1007, the aircraft impacted terrain at an elevation of about 650 ft. The aircraft was destroyed, and the occupants were fatally injured.
Figure 3: Final flight track segment and accident site
Source: Google Earth and OzRunways, annotated by ATSB
Context
Pilot information
Qualifications and experience
The pilot held valid aeroplane and helicopter commercial pilot licences first issued in 1986 and 1990 respectively. The pilot’s last aeroplane flight review was conducted in March 2021 (valid until March 2023) and an annual operator proficiency check was last completed in March 2022 (also valid until March 2023). The pilot obtained a multi-engine command instrument rating in 1992, which was renewed 8 times,[5] with the last renewal completed in October 2002 (valid until October 2003). The pilot also held a helicopter night VFR rating that expired in May 2021, a helicopter low‑level rating,[6] and had completed a flight review for this rating in February 2022 (valid until February 2024).
The pilot first obtained their private pilot licences (aeroplane and helicopter) in 1976 and 1985 respectively and had accumulated experience in both fixed and rotary wing operations. At the time of the accident flight, the pilot had accumulated about 13,900 hours of aeronautical experience with over 12,000 hours in helicopters and over 1,000 hours in aeroplanes, of which about 470 hours were in command of the Cessna R182.
The pilot had about 96 hours of instrument flying experience and about 85 hours of night experience, with the last night flight conducted in April 2018.
The pilot had operated VH-EHM for 32.7 hours in the 30 days before the accident, which included several return flights from Archerfield to Lighthouse.
The pilot had also conducted aerial firefighting tasks throughout their aviation career and in June 2018 reported the following flight hours for different activities and environments:
air attack supervision, reconnaissance, and firebombing – about 200 hours
The pilot’s activities in the week before the accident, and on the day of the accident, were reported as being normal. The pilot’s next of kin stated that the pilot had been sleeping well with about 8–9 hours of sleep obtained each night. Other witnesses stated that the pilot was ‘very fit and healthy’ and not suffering any unusual personal or professional stress.
The day before the accident, the pilot woke at about 0530 and left for Archerfield Airport at about 0600. The pilot and passengers departed Archerfield in VH-EHM at 1055 and arrived at Lighthouse at about 1230. The pilot spoke to next of kin over the phone a few times during the day and had dinner at about 1800. The pilot sent a text message at 1945 indicating they were going to bed, however they also responded to an email at 2130. The next morning, a witness at Lighthouse did not notice anything abnormal during their interaction with the pilot before take-off at 0715. The pilot made and received some phone calls during the accident flight, including one after departing Dalby. The people who spoke to the pilot during the flight reported that they did not notice anything unusual or abnormal during these conversations.
The ATSB found no evidence to indicate that the pilot was experiencing a level of fatigue known to have an effect on performance.
Medical information
The pilot held a Class 1 aviation medical certificate, valid until October 2022. There were no indications of any significant medical problems in the pilot’s aviation medical records.
A post-mortem examination and toxicological analysis indicated no evidence of any pre-existing medical condition that could have contributed to the accident. The pilot’s toxicology report identified that carbon monoxide was present in the pilot’s system, but at a low level that was highly unlikely to cause impairment.
The pilot’s toxicology report also identified the presence of a medication in their system that was not documented on the medical examination questionnaires completed as part of their annual medical certificate renewals. This medication required approval for use by a designated aviation medical examiner (DAME) or by the Civil Aviation Safety Authority (CASA). The approval process required a 1-day ground trial of the medication, during which the pilot’s response to the medication would be assessed. The pilot was first prescribed this medication in 2019 by their DAME (who was also their general practitioner), who recalled that they likely advised the pilot to monitor for any symptoms or side effects. The DAME was unaware at that time that the medication required a ground trial and there was no evidence that this trial was conducted. The medication was not used on an on-going basis but was prescribed for a second time by the DAME in 2021.
The potential side effects of the medication were changes to colour vision, low blood pressure, dizziness, and blurred vision. The medication also had the potential to interact with another documented medication that the pilot had been taking regularly since 2010, although the potential interaction between them was classified as ‘minor’ with no significant interaction indicated by clinical studies. Nevertheless, patients had to be advised of the potential for interaction and were required to contact their doctor if they experienced symptoms such as dizziness, light‑headedness, or fainting.
The DAME reported that the pilot was health conscious and forthcoming in reporting any medical symptoms and that they had not reported any side effects from the use of the medication(s).
The ATSB considers it unlikely that the pilot was experiencing any side effects from the medication during the accident flight as they had probably used the medication previously (since 2019) and had not reported any adverse effects to their DAME. However, had the pilot been experiencing some of the medication’s known symptoms before the accident, it was probably insufficient to affect the ability of the pilot to fly the aircraft because:
the aircraft was under control during the entire flight and very likely so at the time of the accident.
radio calls made during the flight, and video footage of the pilot from Dalby Airport, did not indicate anything abnormal with the pilot.
Therefore, it was considered unlikely that the use of the medication adversely affected their performance during the accident flight. Additionally, while the medication was not documented on the pilot’s CASA medical records, its use was approved by the pilot’s DAME.
Relationship with passengers
There were 2 passengers on board VH-EHM on the day of the accident. The pilot’s next of kin and colleagues reported that the pilot and one of the passengers were close personal friends.
That passenger’s business had utilised the services of the operator (and accident pilot) for several years, and the pilot had flown the passenger to various private properties in Queensland numerous times. The passenger and their business were the operator’s most significant client at the time of the accident and had played a key role in the operator’s growth and success.
Passenger commitments
The passenger had a work-related meeting to attend at 0900 on the morning of the accident flight, however they notified a work colleague that they would not be able to attend the meeting due to the diversion to Dalby. The passenger’s next scheduled meeting was at 1530, which they communicated that they would likely be present for.
The work colleague reported that the passenger was generally not concerned about missing meetings if they could not get there in time. The passenger received business-related phone calls while on the ground at Dalby, and during the accident flight. People who spoke with the passenger during these calls reported that they did not notice anything unusual.
The other passenger on board had been communicating with friends during the flight using internet-based phone applications. Some messages sent by this passenger mentioned the poor weather encountered, the diversion to Dalby, and that they would be late for work. This passenger also contacted their employer at 0903 to advise that they would be late for work.
Aircraft information
The Cessna R182 Skylane RG is a 4-seat, high-wing, single-engine aircraft with retractable landing gear. The accident aircraft (Figure 4) was manufactured in the United States in 1978 and first registered in Australia in 1989. The aircraft was fitted with a Lycoming O‑540 piston engine driving a 3-blade Hartzell constant speed propeller and was equipped and approved for flight under both VFR and instrument flight rules (IFR).[8] The aircraft’s fuel tanks had a total maximum capacity of about 303 L, of which 284 L was useable.
The aircraft was equipped with an autopilot with lateral and vertical modes capable of maintaining altitude, airspeed, track, and wings level. The pilot’s next of kin reported that the pilot was familiar with using the autopilot, including the various modes. The aircraft’s original avionics had been upgraded to include 2 Garmin G5 electronic flight instruments, which provided redundant attitude, altitude, and airspeed information. The original mechanical altimeter and airspeed indicator had also been retained and the aircraft was also fitted with a JP Instruments FS-450, which provided fuel flow, fuel used, and fuel endurance information (Figure 5).
At the time of the accident, the aircraft had accrued about 5,858 hours of time in service. The most recent periodic maintenance inspection (100-hourly) was completed on 15 July 2022 and the aircraft had accrued about 30 hours of flight time since. There were no defects recorded on the aircraft’s current maintenance release,[9] and no scheduled maintenance was due.
The ATSB performed weight and balance calculations for the flight from Dalby based on the fuel quantity from the fuel upload, occupant and aircraft weights, and cargo weight. The calculations showed that the aircraft's take-off weight and centre of gravity were within limits.
Terrain awareness
The aircraft was fitted with a Garmin GTN 750Xi, which operated as both a radio communications unit and Global Navigation Satellite System[10] unit (Figure 5). The GTN 750Xi could operate in different modes and display a significant amount of information relating to management of the flight such as maps, airspace, and terrain.
Source: VH-EHM avionics maintainer, modified by ATSB
While not required to be fitted with a certified terrain awareness and warning system,[11] VH-EHM’s GTN 750Xi unit had a non-certified[12] terrain awareness function capable of predicting hazardous terrain conditions and issuing alerts. Terrain information was advisory only and could include:
display of altitudes of terrain and obstructions relative to the aircraft’s altitude
pop-up terrain alert messages (visual/auditory) issued when flight conditions met parameters set within the terrain system software algorithms. For example, an alert would be generated when the aircraft was above terrain during en route level flight but projected to come within 700 ft vertically of any obstacle, terrain, or powerline below or ahead of the aircraft.
The system also included a ‘terrain inhibit’ mode to deactivate the terrain alert message system.
Alerts from certified or non-certified terrain warning systems can be a nuisance or distraction to pilots when flying at altitudes below the alerting threshold of the system. In March 2023, the United States Federal Aviation Administration advised operators ‘…about the risks associated with distraction and complacency brought about by routine use of the…terrain inhibit feature…[and to] ensure operators understand the importance of having procedures and training for the use of the terrain inhibit aural warning switches associated with nuisance alerts’.[13]
The operator did not have any procedures or training on the use of the terrain awareness and warning system for the Garmin GTN 750Xi. The pilot was reported to usually have the terrain awareness system enabled unless conducting low level visual aerial firefighting operations where the terrain alerts could be a nuisance.
The ATSB was unable to establish whether the terrain awareness function was enabled or inhibited at the time of the accident. Had the terrain awareness system been enabled during the accident flight, the system’s alerting thresholds, coupled with the low-level flying, would likely have produced multiple alerts, potentially distracting the pilot. These factors would have limited the effectiveness of the terrain awareness system in preventing this accident.
Flight following system
All the operator’s aircraft, including VH-EHM, were equipped with a Spidertracks[14] unit with a dash mounted device (Figure 5). The units were fitted primarily to support contracted aerial work and the system was not normally activated for other flights. When powered on, the system entered ‘normal mode’, which would automatically record and transmit the aircraft’s position at regular intervals. A ‘Watch’ function could be manually activated by the pilot so that an alert would be sent out if communication with the aircraft was lost after 10 minutes. The pilot could also manually enable the ‘SOS’ function to signal an emergency or to alert pre‑determined personnel. When the emergency ‘SOS’ function was activated, the system was programmed to send out text messages and emails to operator personnel.
The operator did not receive any Spidertracks alerts from VH-EHM during the accident flight.
Certificate of airworthiness
The aircraft’s certificate of airworthiness (CoA) was issued in 1989 when it was registered VH‑HZU. After purchasing the aircraft in late 2019, the operator requested a change of registration to VH‑EHM, which was approved by CASA in January 2020, effective from 7 February 2020. The CASA approval noted that the aircraft could not be operated beyond 7 February 2020, unless a new CoA bearing the new registration mark was issued.
An application and relevant aircraft documentation was required to be submitted by the operator to CASA for the issue of the new CoA. However, neither the operator, nor CASA possessed any records to indicate that the application for the new CoA had been submitted or that the new CoA was issued. The original CoA was found in the on-site wreckage and showed the old registration mark (VH‑HZU) amended by pen to reflect the new registration mark (VH-EHM).
Terrain
The flight’s planned track toward Archerfield Airport took the aircraft from the low-lying plains of inland Queensland across an area of the Great Dividing Range to the west of Brisbane. Elevations within the range were generally between 1,500–2,000 ft AMSL, with numerous peaks between 2,000–2,700 ft (Figure 6).
Figure 6: Visual navigation chart extract showing terrain along the flight path
Source: Airservices Australia and OzRunways, modified and annotated by ATSB
Meteorological information
Pilot weather requests
CASA regulations[15] required the pilot to review weather forecasts and reports, within 1 hour of commencing a flight, covering the route to be flown, the departure aerodrome, and the planned destination aerodrome. If an authorised weather forecast/report was not available, and the weather conditions at the departure aerodrome would permit the aircraft to return and land safely within 1 hour of take-off, the pilot could take-off without reviewing the weather. However, they were required to obtain the relevant weather information within 30 minutes of take-off or return to the departure aerodrome. The available evidence indicated that the relevant weather forecast information would have been available to the pilot while at Dalby via the internet, or by radio from Brisbane air traffic control.
Data from Airservices Australia indicated that the pilot logged in to the National Aeronautical Information Processing System (NAIPS)[16] 3 times in the 24-hour period before the accident. These were recorded on 29 August 2022 at 0708 and 0709 (shortly before departing Lighthouse), and 0925 (about 13 minutes after departing Dalby).
The data accessed by the pilot in NAIPS included Terminal Area Forecast (TAF)[17] and METAR[18] for aerodromes relevant to the flight (Archerfield, Amberley and Toowoomba). Weather products, such as the graphical area forecast (GAF), and grid point wind and temperature, could also be viewed by the pilot, but access to these were not logged by NAIPS. Therefore, the investigation could not determine whether the pilot reviewed that information.
Forecast
Departure from Lighthouse
Two GAFs[19] issued by the Bureau of Meteorology (BoM) at 0225 on 29 August covered the planned direct route from Lighthouse to Archerfield and were valid from 0300–1500.
The weather forecast from Lighthouse towards the Great Dividing Range was generally suitable for VFR flight. However, from the Great Dividing Range to Archerfield, the forecast included broken[20] stratus cloud from 1,500 ft to 2,500 ft (becoming scattered from 1200), scattered cumulus cloud between 2,500 ft and 6,000 ft, and broken stratocumulus cloud from 5,000 ft to 7,000 ft. Visibility below the cloud layer was greater than 10 km.
Moderate isolated showers of rain were expected to reduce visibility to less than 3,000 m in broken stratus cloud between 1,000 ft and 2,500 ft, and in broken cumulus from 2,500 ft to 8,000 ft. The forecast predicted isolated fog over land areas which would reduce visibility to less than 300 m and was expected to dissipate after 0900. Isolated smoke below 3,000 ft was also forecast with associated reduced visibility of 4,000 m and extending up to 4,000 ft after 0900.
TAFs were also issued for relevant aerodromes along the planned route. Toowoomba had forecast broken cloud at 200 ft AGL (2,303 ft AMSL), mist with 2,000 m visibility, and a 40% probability of fog with 400 m visibility. Amberley had forecast light showers of rain, scattered cloud at 2,000 ft AGL (2,091 ft AMSL), broken at 4,000 ft AGL (4,091 ft AMSL), and greater than 10 km visibility below the cloud layer. Archerfield had forecast light showers of rain, few cloud at 2,000 ft AGL (2,065 ft AMSL), broken at 3,500 ft AGL (3,565 ft AMSL), and greater than 10 km visibility below the cloud layer.
The grid point wind and temperature chart for the region issued at 0359 and valid from 0700–1000 forecast:
easterly winds between 9–13 kt at 1,000 ft, with temperatures of 12–14 °C
easterly winds between 13–21 kt at 2,000 ft, with temperatures of 11–13 °C
north-easterly winds between 8–20 kt at 5,000 ft, with temperatures of 7–10 °C.
Departure from Dalby
An updated GAF was issued at 0819 valid for the period from 0900–1500 with some differences to the previous forecast.
The updated forecast predicted that the previously forecast broken stratus cloud from 1,500 ft to 2,500 ft would reduce to scattered at 1100 and then dissipate by 1200, with broken cumulus and stratocumulus cloud between 3,000 ft and 7,000 ft. Visibility remained greater than 10 km below the cloud layer. The previously forecast moderate isolated showers of rain continued, as did the isolated smoke which extended up to 6,000 ft with an increased visibility of 6,000 m.
An amended TAF was also issued for Amberley at 0851, which included the same rain, cloud, and visibility forecast as the previous TAF but with an INTER[21] period between 0900 and 1100 where visibility reduced to 6,000 m in light showers of rain, with cloud broken at 1,500 ft AGL (1,591 ft AMSL). The Archerfield TAF was also amended at 0831 to include scattered cloud now forecast at 1,500 ft AGL (1,565 ft AMSL), broken at 3,000 ft AGL (3,065 ft AMSL), and an INTER period between 0900 and 1000 where visibility reduced to 4,000 m in moderate showers of rain.
The above forecasts were available when the aircraft was on the ground at Dalby and also when the pilot requested the weather at 0925 – 13 minutes after take-off. At this time, an amended TAF issued at 0914 (after departure from Dalby) was also available for Toowoomba which forecast broken cloud at 100 ft AGL (2,303 ft AMSL), and fog with 300 m visibility.
Observations
The following cloud and visibility observations were recorded or derived at weather stations along the aircraft’s flight path (Figure 7).
Table 1: Cloud and visibility observations
Time
Location
Cloud base
Visibility (m)
0900
Dalby
2,500 ft AMSL (2,500 ft AGL) [1]
- [2]
0930
Oakey
2,531 ft AMSL (1,200 ft AGL)
>10 km
0930
Toowoomba
2,203 ft AMSL (100 ft AGL)
150 m
1000
Gatton
1,542 ft AMSL (1,250 ft AGL)
-
1000
Amberley
1,491 ft AMSL (1,400 ft AGL)
>10 km
1000
Beaudesert
1,657 ft AMSL (1,500 ft AGL)
-
1000
Greenbank
636 ft AMSL (500 ft AGL)
-
1000
Archerfield
1,965 ft AMSL (1,900 ft AGL)
>10 km
1022
Amberley
791 ft AMSL (700 ft AGL)
4,000
[1] The automatic weather stations at Dalby, Gatton, Beaudesert and Greenbank did not have a ceilometer to record cloud base. The cloud base was estimated from the temperature‑dewpoint spread. Dewpoint is the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to monitor the risk of aircraft carburettor icing or the likelihood of fog.
[2] The automatic weather stations at Dalby, Gatton, Beaudesert and Greenbank did not have a visibility meter.
Figure 7: Weather station locations and flight track
Source: Google Earth and Bureau of Meteorology, annotated by ATSB
Video camera footage
Surveillance video cameras from Lowood and Fernvale provided information on the weather around the time of the accident. The field of view of each camera was determined (Figure 8), alongside identifiable mountain peaks (labels A to E).
Figure 8: Map showing camera field of views, identifiable points (A to E), and flight track
Source: Google Earth and Geoscience Australia, modified and annotated by ATSB
The surveillance video camera from Lowood, located about 10.5 km west-south-west of the accident site, captured the aircraft flying overhead below a low-level cloud layer about 4 minutes before the accident. No abnormal engine or propeller sounds were noted. A mountain peak (A) about 7.8 km from the camera location was just visible (Figure 9).
Figure 9: Image from Lowood towards D’Aguilar Range at the time of flyover
Source: Lowood Golf Course, modified and annotated by ATSB
Another surveillance video camera from Fernvale, located about 4.2 km south-west of the accident site, provided video observations of the weather conditions surrounding the accident site. An exemplar image from the video is provided to show identifiable peaks of the D’Aguilar Range and their elevations in clear conditions (Figure 10).
Figure 10: Image from Fernvale showing the D’Aguilar Range in clear conditions
All heights AMSL.
Source: Fernvale Rural Fire Brigade, modified and annotated by ATSB
Video footage of the conditions around the time of the accident[22] (Figure 11) showed low level cloud over the area of the D’Aguilar Range, with mountain peaks B and C, and the accident site, obscured by cloud. The aircraft could not be seen in the footage.
Figure 11: Image from Fernvale around the time of the accident
All heights AMSL.
Source: Fernvale Rural Fire Brigade, modified and annotated by ATSB
Witness observations
Several witnesses along the aircraft’s route from Dalby to Fernvale recalled seeing the aircraft flying at low altitude below cloud. The witness closest to the accident site in Fernvale reported a low flying Cessna heading east towards the D’Aguilar Range with the wings level and undercarriage retracted. They recalled the aircraft banking left and disappearing from view due to cloud. The witness also reported heavy low cloud, light rain, and fog in the Fernvale area at the time.
Visual flight rules
CASA regulations[23] outlined that flight under the VFR could only be conducted in VMC with the criteria provided in the CASR manual of standards and the CASA Visual Flight Rules Guide.
The flight from Dalby, and the location of the accident, were in Class G (non-controlled) airspace. The following VMC were stipulated for flight under the VFR in Class G airspace at or below 3,000 ft or 1,000 ft above ground level (whichever was higher):
clear of cloud and in sight of the ground or water
a flight visibility of 5,000 m.
Amberley was in Class C (controlled) airspace. The following VMC were stipulated for flight under the VFR in Class C below 10,000 ft above ground level:
1,500 m horizontally from cloud
1,000 ft vertically from cloud
a flight visibility of 5,000 m.
Archerfield was in Class D (controlled) airspace. The following VMC were stipulated for flight under the VFR in Class D (all heights):
600 m horizontally from cloud
1,000 ft vertically above cloud, 500 ft vertically below cloud
flight visibility of 5,000 m.
Special VFR
By day, when VMC did not exist, pilots could request, and be issued, a ‘special VFR clearance’ from air traffic control responsible for a control zone (CTR) or control area (CTA). The clearance allowed for flight in a CTR, or in a CTA next to a CTR, for the purpose of entering or leaving a CTR, providing an IFR flight would not be unduly delayed. When operating under a special VFR clearance the pilot was responsible for ensuring that the:
flight could be conducted clear of cloud
visibility was not less than 1,600 m (for aeroplanes).
Requirements for maintaining visual conditions
VH-EHM was an IFR‑equipped aircraft and the pilot had previous instrument flying experience, although not current at the time of the accident. Additionally, passenger air transport flights conducted under CASR Part 135 in single-engine piston-powered aircraft were prohibited from operating under the IFR.[24] Despite that restriction, the aircraft was also in a radar coverage area with air traffic control support available to the pilot from either Amberley or Brisbane in the event emergency assistance due to flight in instrument meteorological conditions (IMC)[25] became necessary. The ATSB was unable to determine the extent to which compliance with the requirement to remain in VMC influenced the pilot’s decision to remain at low level, near terrain, in reduced visibility rather than climbing into cloud at higher altitudes above terrain.
The flight conduct section of the operator’s operations manual stated:
Company aircraft shall not commence a VFR flight unless current meteorological reports and forecasts show that the weather conditions en-route and at the destination are such that the flight can be conducted under the visual flight rules.
If weather conditions begin to deteriorate, the pilot in command must carefully monitor the changes and plan possible alternative action.
Similarly, the emergency procedures section of the operations manual stated:
Company pilots shall divert and land at the nearest suitable aerodrome or return to the departure point if meteorological conditions are encountered which are not suitable for continued flight.
Minimum height
In addition to minimum visibility and distance from cloud requirements, a pilot was also required to maintain a minimum height above the ground. Unless during take-off, landing or other approved low-flying operation, the CASR[26] detailed that a pilot in command must not fly an aeroplane over:
a populous area or public gathering below 1,000 ft above the highest feature or obstacle within a horizontal radius of 600 m of the point on the ground or water immediately below the aeroplane
any other area at a height lower than 500 ft above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the aeroplane.
These minimum heights did not apply if it was essential, through stress of weather or any other unavoidable cause, that a lower height be maintained.
Recorded Data
Recorded data was obtained from various sources during the investigation, as follows:
OzRunways[27] flight track data (altitude, ground speed, heading) was available for the entire flight up until about 8 seconds before the accident.
The pilot made 3 radio broadcasts on the Dalby common traffic advisory frequency[28] during the flight — an inbound call at 0855, left base call at 0859, and a taxi/departure call at 0911. Review of this audio did not indicate anything abnormal with the flight or the pilot.
While at Dalby, airport video footage captured the aircraft’s taxi to the refuel location, refuel, and taxi out to the runway. Once the aircraft had taxied and was stationary near the fuelling location, the pilot remained inside the cockpit for about 20 seconds before disembarking. The pilot spent the next 9 minutes refuelling the aircraft before re‑entering the cockpit, and 30 seconds later, the aircraft taxied back out to the runway.
The aircraft made 4 significant turns during the accident flight including 2 course reversals. Based on flight data, the 2 turns around the Main Range (including a 180° course reversal) had estimated average bank angles of 35° and 39°. The 2 turns near the D’Aguilar Range (including the turn leading up to the accident) averaged 38° and 36° indicating they were made in the course of controlled flight similar to the previous turns (Figure 12).
The aircraft was flown below 500 ft AGL[29] on several occasions during the accident flight, with the lowest being about 200 ft AGL (Figure 13). Since the terrain elevation data did not account for vegetation or structures, it was likely that there were lower vertical clearances during the flight.
The flight track data indicated that the aircraft’s ground speed after departing Dalby was generally between 120–140 kt, about the normal cruise speed for the R182.
Surveillance video footage from a private property in Fernvale, located about 2.3 km south‑west of the accident site, captured the sound of the aircraft as it flew over Fernvale, up to the time of impact with terrain. The sound of the engine and propeller could be heard up to the time of impact with no abnormal engine or propeller sounds noted.
Source: Google Earth and OzRunways, annotated by ATSB
On-board recording devices
The aircraft was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be. There have been numerous investigations undertaken by the ATSB that would have been significantly assisted by the availability of recorded data. Such information would likely have provided additional detail about the events that led to the development of these accidents, and possibly allowed for timely identification and resolution of safety issues.
The ATSB investigation report AO-2017-118 into the collision with water involving de Havilland Canada DHC-2, in Jerusalem Bay, New South Wales in 2017 identified and directed the following safety issue to CASA:
Australian civil aviation regulations did not mandate the fitment of flight recorders for passenger‑carrying aircraft under 5,700 kg. Consequently, the determination of factors that influenced this accident, and other accidents have been hampered by a lack of recorded data pertaining to the flight. This has likely resulted in the non‑identification of safety issues, which continue to present a hazard to current and future passenger-carrying operations.
In October 2021, the ATSB received advice from the International Civil Aviation Organization (ICAO) that the recommendation for fitment of lightweight and airborne image recorders in aircraft less than 5,700 kg used in passenger carrying operations will be referred to an ICAO Working Group for further study and consideration. In May 2023, the coronial inquest relating to the Jerusalem Bay accident recommended that CASA engage with the ATSB on the subject of mandatory fitment of on-board recording devices.
There have been several recent examples of investigations where the use of recording devices, although not required by regulations, has assisted in determining important safety factors related to the incident under investigation. A recent example was the VFR-into-IMC, loss of control, and collision with terrain involving Airbus Helicopters EC130 T2 near Mount Disappointment, Victoria in 2022 which resulted in 5 fatalities, including 4 fare-paying passengers.
The aircraft was fitted with a device that recorded video imagery and audio data from inside the aircraft cabin, as well as GPS inertial and positioning data, which assisted the investigation. Fitment of a similar device to VH-EHM may have been of value to this accident investigation to understand the specific environmental conditions faced by the pilot, insights into the pilot’s weather-related decision making, and any pilot-passenger interactions during the flight.
Site and wreckage information
The accident site was located within the D’Aguilar Range on a steep section of mountainous terrain covered with trees (Figure 14).
There were several initial impact points with numerous trees before the aircraft impacted the ground. These indicated a final flight path descent angle of about 2°, in about a 47° right bank (Figure 15).
Figure 15: Representation of the aircraft’s attitude at time of impact with trees
Source: ATSB
The aircraft impacted terrain at 650 ft AMSL, about 28 ft vertically below the top of the ridge. The wreckage trail extended about 40 m from the initial impact point to the top of the ridge where most of the wreckage, including the engine, was located. The propeller was located about 10 m forward of the main impact point.
On-site examination of the engine did not reveal any pre-impact mechanical damage, while damage to the propeller indicated that the engine was providing high power at impact. The landing gear and flaps were retracted and there was no evidence of an in-flight break-up or a pre‑existing defect with the aircraft. Due to extensive damage, the serviceability of the flight instruments, auto‑pilot, and associated systems could not be determined. The pressure altimeter subscale QNH[30] setting was appropriately set. The fuel tanks ruptured on impact, and an odour of fuel was present at the site. No fuel samples were available for recovery.
A tablet and 3 mobile phones were retrieved from the accident site, however the ATSB was unable to recover any data from these devices due to substantial damage to their internal components.
Survivability aspects
Examination of the aircraft wreckage indicated that the impact was at high speed into steep rising terrain and was not survivable.
Emergency locator transmitters
Emergency locator transmitters (ELT) and/or portable beacons are carried on aircraft so that in the event of an accident in a remote location, the aircraft wreckage and its occupants can be located quickly and efficiently by search and rescue (SAR) operations.
Under CASA regulations,[31] at the time of the accident, the aircraft was required to carry either:
a portable ELT – an emergency position indicating radio beacon (EPIRB), or a personal locator beacon (PLB). These are handheld and usually require manual activation.
an automatic ELT – usually mounted to the airframe and activated automatically during a crash, typically by a g-force[32] activated switch.
A review of the available maintenance documentation identified some inconsistencies regarding the aircraft’s ELT carriage requirements. As part of the aircraft’s maintenance schedule, the automatic ELT’s battery was periodically inspected by the avionics provider and was last replaced in 2019, with replacement due in 2024. The battery condition was last inspected by the avionics provider in July 2022 and was found to be serviceable. However, the aircraft’s maintenance organisation had annotated the aircraft’s current maintenance release to require the carriage of a portable ELT for flight.
The annotation for carriage of a portable ELT first appeared in a maintenance release in March 2020. Of the following 9 maintenance releases, the portable ELT annotation only appeared on 4, with one of those entries crossed out and signed by the maintainer indicating that it was likely annotated in error. The operator similarly understood the annotations on the maintenance releases requiring carriage of a portable ELT to be incorrect as the aircraft was fitted with an automatic ELT and that the pilot had previously spoken to the maintenance organisation to correct this.
During the on-site investigation, an automatic ELT and its antenna were observed to be physically fitted to the aircraft, but its serviceability and whether it was in the armed position was not determined. There were no signals received from the automatic ELT at the time of the accident and no portable ELT (PLB or EPIRB) was able to be located at the accident site.
Data from a 2013 ATSB research report indicated that ELTs function as intended in about 40% to 60% of accidents in which their activation was expected. Various factors can affect activation such as flat batteries, incorrect installation, not arming the ELT, lack of fire protection, and impact damage. The ATSB could not determine why the ELT did not function in this accident.
Flight notification
Requirements
Regulations[33] required pilots conducting VFR air transport flights to follow one of the following flight notification processes:
submit a flight plan to Airservices Australia
nominate a SARTIME[34] for arrival to Airservices Australia
leave a flight note[35] with a ‘responsible person’.
A ‘responsible person’ was required to meet the following requirements:
be over the age of 18 years
have access to at least 2 operative and appropriate means of communicating with SAR (for example, 2 telephones)
satisfy the pilot in command that the person:
knows how to contact the Joint Rescue Coordination Centre (JRCC)
will immediately do so if the pilot in command’s flight is overdue.
The operator’s procedures required that a flight notification be submitted via electronic, verbal or written means for all air transport flights. If the notification was not submitted to Airservices Australia, then a SAR form was to be completed and provided to the operator or a client (passenger) representative who was to be briefed on the SAR procedure.
The SAR form included information such as the route, SARTIME, and a ‘Next Call’ time. Pilots were required to contact the person holding the SAR form by the ‘Next Call’ time or by the SARTIME. If no contact was made within 15 minutes of these times, the person holding the SAR form would contact the operator’s head of flying operations (or their delegate) and the relevant procedures from the operator’s emergency response plan would be initiated, which included contacting JRCC after 30 minutes.
VH-EHM’s operator advised that the pilot would usually either leave the flight notification with the operator’s line pilot if they were on duty, or with a family member who was not associated with the operator. The line pilot was not on duty on the day of the accident.
Accident flight
The aircraft departed Lighthouse at 0715 on 29 August 2022. About 30 minutes after departing, the pilot contacted a family member and advised them to expect their arrival ‘late morning’. The family member was expecting the pilot to arrive at Archerfield between 1030 and 1100, and to receive a call from the pilot upon landing. They stated that they were not provided with any information about what actions to take if the aircraft became overdue.
The family member attempted to contact the pilot on several occasions between 1120 (one hour and 13 minutes after the accident) and 1240 but was unsuccessful. They subsequently raised concern about the flight by notifying the operator via email at 1309 that they were unable to contact the pilot. The operator then attempted unsuccessfully to contact the pilot, and subsequently checked publicly available ADS-B[36] data to check the aircraft’s last recorded position, which was over the Lowood Golf Club. The operator then made several calls to individuals at various nearby locations to see whether the aircraft had landed somewhere other than Archerfield.
At 1331, the operator notified Lowood police and at 1342, arranged for a helicopter from another Archerfield based operator to search for the missing aircraft near the last recorded location. At 1344, the operator notified Airservices Australia who coordinated a SAR effort with the JRCC.
At about 1427 (4 hours and 20 minutes after the accident), the helicopter arranged by the operator departed Archerfield and located the wreckage shortly after. The helicopter was landed near the wreckage and its pilot proceeded to the site on foot, reporting back to the operator that none of the occupants had survived. Shortly after, a SAR helicopter arrived at the site with paramedics confirming the previous report.
Operational information
Fuel planning
The CASR[37] prescribed the fuel requirements for air transport flights conducted under CASR Part 135 which were also reflected in the operator’s operations manual. At a minimum, the aircraft had to carry the following amounts of usable fuel before a flight commenced:
taxi fuel – fuel used before take-off
trip fuel – fuel for take-off, climb, cruise, descent, and landing
contingency fuel – 10% of trip fuel for a piston engine aeroplane
final reserve fuel – 45 minutes flight time for a piston engine aeroplane (between 24–30 L for VH‑EHM)[38]
if required – destination alternate fuel, holding fuel, and additional fuel.
Also, the effect of operational conditions such as the aircraft’s weight, and relevant meteorological reports and forecasts had to be considered during fuel planning.
To determine the required quantity of usable fuel for a flight, fuel consumption data from either the operator’s fuel consumption monitoring system or aircraft manufacturer data could be used. Operators conducting air transport flights under CASR Part 135 were required to complete a ‘journey log’ before and after each flight and include information such as fuel on-board before the flight and after landing. The operator required the quantity of fuel on-board before each flight be determined using 2 independent means.
Fuel records were available for the operator’s helicopters, but no fuel records could be found for VH-EHM. Fuel was available at Lighthouse and was primarily used for filling up helicopters involved in cattle mustering. VH-EHM could be re-fuelled at the property but required some additional effort to set up the fuel drum and pump for fuel delivery. Prior to departure on the morning of the accident flight, VH-EHM was not refuelled at Lighthouse. No information was available about the pilot’s fuel planning for the flight from Lighthouse to Archerfield.
Fuel calculations
After departing Lighthouse and encountering weather on the range, the pilot diverted to Dalby to refuel. An assessment was undertaken to estimate the quantity of fuel on-board the aircraft when it departed Lighthouse, and if that quantity was sufficient for the intended flight to Archerfield (see Appendix – Fuel calculations).
Depending on the fuel flow data used for the calculations, the aircraft was estimated to have had between 100–125 L of useable fuel on‑board (of a total useable capacity of 284 L) before departing Lighthouse. Calculations showed that the aircraft had sufficient fuel on-board to complete the flight to Archerfield (taxi fuel and trip fuel) in ideal weather conditions but was required to land with between 31–39 L of useable fuel (contingency fuel and final reserve fuel). As a result, it was estimated that the aircraft would have landed at Archerfield with between 4–13 L below the minimum required useable fuel in ideal weather conditions.
In addition, even had this minimum required fuel been on-board, it would have been insufficient fuel to account for a weather-related diversion. Weight and balance calculations showed that the aircraft fuel tanks could have been filled completely with the available fuel at Lighthouse while remaining below the allowable maximum take-off weight.
Airspace
The Amberley military control zone extended from ground level up to an altitude of 8,500 ft surrounding Royal Australian Air Force Base Amberley (Figure 16). NOTAMs[39] applicable on the day of the accident established that the Amberley controlled airspace was active from 0800 to 2300 and required an airways clearance to transit. Transit through the Amberley control zone provided the lowest terrain elevations for flights between Archerfield and areas west of the controlled airspace.
In March 2021, Amberley air traffic control notified Archerfield operators that pilots needed to plan flights around the Amberley control zone and should not plan for, or expect to receive, a clearance when departing from or arriving into Archerfield. This was due to an increase in the volume and complexity of traffic in the area, in combination with Brisbane airspace changes.
Flights bound for Archerfield from the west of the Amberley CTR generally tracked around Amberley controlled airspace, either from the north using the Lake Manchester VFR route or from the south using the points of Mount Walker, Flinders Peak, and Spring Mountain (Figure 16). These routes enabled pilots to fly visually under or around restricted airspace without requiring an airways clearance from Amberley air traffic control.
Lake Manchester VFR route
The Lake Manchester VFR route was a corridor under the restricted airspace from ground level to 1,500 ft AMSL (less than 1,000 ft AGL in some sections). The lateral separation from Amberley controlled airspace and elevated terrain reduced to about 1 km at some points, and there was a powerline that passed under a section of the route. Flying south via the mountain peaks required maintaining the aircraft below the 2,500 ft AMSL restriction (associated with the R612B restricted airspace), and above elevated terrain exceeding 600 ft AMSL.
The pilot’s next of kin and a former colleague reported that the pilot had flown the Lake Manchester VFR route, and the route south of Amberley airspace, numerous times in helicopters and aeroplanes and was very familiar with the terrain. The former colleague also reported that the pilot did not recommend using the Lake Manchester VFR route if the weather was poor around the D’Aguilar Range, due to the rising terrain and limited separation from controlled airspace. Transit through the low-lying terrain of the Amberley control zone was preferred in those circumstances.
The operator reported similar concerns associated with the use of the Class G airspace (uncontrolled) surrounding Amberley and the Lake Manchester VFR route, particularly in marginal weather conditions due to the:
rising terrain to the north and east of the Lake Manchester VFR route
limited lateral separation between controlled airspace and rising terrain in some areas of the route
need for aircraft to remain below 1,500 ft while also remaining above the terrain and power lines, with potential for east and west bound traffic
potential for the range to the north of the route to create problematic weather
occurrence of regular airspace infringements in the area.
CASA Office of Airspace Regulation
The CASA Office of Airspace Regulation (OAR) advised that VFR routes, which were usually established following feedback from local airspace users, were only to be used in VMC and generally followed identifiable ground features to ease visual navigation. The OAR further stated that in non‑controlled airspace, pilots were responsible for aircraft separation, terrain clearance, and being appropriately briefed for the flight.
Aeronautical studies and airspace reviews undertaken by the OAR generally involved consultation with the aviation community as well as review of ATSB and Airservices Australia incident data. While there were several reported airspace infringements into the Amberley controlled airspace, in the period from January 2020 to May 2023 there were no CASA aviation safety incident reports recorded relating to the Lake Manchester VFR route, except for the accident involving VH-EHM.
A review of data by the Royal Australian Air Force concluded that infringements of the Amberley controlled airspace were primarily due to pilots not reviewing NOTAMs and an over reliance on electronic flight bags, which in some instances did not accurately display the activity status of military restricted areas.
The OAR considered that the risk associated with defence-related aircraft movements within the Amberley airspace and the segregation of these activities with civil aviation activities was appropriate. The OAR also noted that there was ongoing work by CASA, the Australian Defence Force, and Airservices Australia to reduce airspace infringements by educating pilots on the use of military airspace, including via the publication of guidance material. For example, an infringement from 2017 involved a VFR flight where the pilot was tracking along the Lake Manchester VFR route and requested clearance to transit the Amberley control zone. The clearance was denied by Amberley air traffic control due to other traffic in the area. Unknown to Amberley ATC, the pilot was deviating around weather and subsequently inadvertently entered the Amberley control zone. The Royal Australian Air Force advised pilots facing similar circumstances:
If you are experiencing difficulties (such as bad weather or aircraft issues), advise ATC as early as possible as they may be able to provide you with priority.
Conclusion
The ATSB concluded that there was insufficient evidence to indicate that the structure of the Amberley controlled airspace in relation to the Lake Manchester VFR route contributed to this accident. While acknowledging the narrow lateral and vertical separation between terrain and controlled airspace on the route, it was a published area of airspace intended for use only in VMC.
Furthermore, the route was known to the pilot as being an area to avoid in adverse weather, which existed at the time of the accident, when safety margins would be greatly reduced. In the event of encountering adverse weather along the route making it unsuitable, there remained an alternative in‑flight option of requesting an airways clearance to enter Amberley airspace to either land or transit.
The NAIPS login records indicated that the pilot requested NOTAM information during each NAIPS request and was tracking around Amberley controlled airspace towards the end of the flight. Therefore, the pilot was likely aware it was active at the time, and that it required an airways clearance to transit. However, a review of air traffic control recordings did not identify any radio communications or requests for an airways clearance between VH-EHM’s pilot and Amberley air traffic control.
A pilot previously employed by the operator between January 2021 and June 2022, reported that in their experience, requests to transit Amberley were usually denied. However, there was no information available on the accident pilot's past experience with requesting and being granted/denied Amberley transit clearance, or of their views on the 2021 Amberley notification to Archerfield operators regarding flight planning around the Amberley CTR. Therefore, the investigation was unable to determine whether these considerations influenced their decision not to request a transit clearance.
Organisational information
Executive Helicopters was an Archerfield based operator established in 2008. The pilot joined the operator as chief pilot in 2009 – later retitled head of flying operations (HOFO) – after which commercial helicopter operations commenced. Single-engine piston-powered aeroplane VFR charter[40] (air transport) operations were added to the AOC in 2020 after VH-EHM was purchased.
The operator held an Air Operator’s Certificate (AOC) issued by CASA which was valid at the time of the accident. The AOC authorised the certificate holder to operate various single-engine helicopters, as well as single-engine piston‑powered aeroplane types with a maximum take-off weight not exceeding 5,700 kg, on VFR air transport and aerial work operations.
From 2009 to 2021, the accident pilot was the only full-time pilot conducting operations under the AOC. Over this time, casual pilots were also contracted to undertake flying as required. A second full‑time pilot was employed from January 2021 to June 2022 and a third joined shortly before the accident.
At the time of the accident, the operator’s staff consisted of the HOFO (the accident pilot), one line pilot, an administrative compliance assistant, and the chief executive officer (CEO) who had been involved since the organisation was established in 2008. The accident pilot was also the head of aircraft airworthiness and maintenance control for the operator.
Safety management system
At the time of the accident, CASA regulations did not require the operator to have a safety management system (SMS).[41] However, the operator had voluntarily introduced an SMS in 2020.
ICAO defines an SMS as:
A systematic approach to managing safety, including the necessary organizational structures, accountability, responsibilities, policies and procedures. It is designed to continuously improve safety performance through: the identification of hazards, the collection and analysis of safety data and safety information, and the continuous assessment of safety risks. The SMS seeks to proactively mitigate safety risks before they result in aviation accidents and incidents.
The operator’s SMS manual stated:
Risk management incorporates a decision-making process that enables the company to prioritise the reduction or elimination or hazards. This process removes or reduces risk to acceptable levels.
The SMS manual included several sources of information to aid hazard identification such as previous experience, accident investigations, audits, group discussions, and client feedback. The SMS incorporated a hazard register which included various hazards related to the operator’s flight operations, with the chief pilot being responsible for most of them. The register did not include any hazards related to the loss of visual reference, or inadvertent entry of a VFR flight into IMC.
Pilot training
As part of holding a commercial pilot licence (aeroplane), the pilot was required to complete a flight review every 2 years. The review included competencies related to knowledge of pre-flight weather assessment, maintaining situational awareness and decision making, as well as recognising and managing threats and undesired aircraft states. The review required pilots to perform basic flight manoeuvres using full instrument panel, and to recover from upset situations and unusual aircraft attitudes to straight and level flight while operating under simulated IMC. The pilot had successfully completed this review in March 2021. Biennial flight reviews for the commercial pilot licence (helicopter) could also include an instrument flying component but this was optional.
Operator proficiency checks were conducted annually and involved a ground review and flight review, as well as practical and theoretical components on emergencies. The proficiency check did not include any additional training related to instrument flying or VFR‑into‑IMC prevention and recovery, nor was such training required by CASA.
The operator also conducted annual aeronautical decision-making training based on the non‑technical skills theory within CASR Part 61 (flight crew licencing) although it was not required under CASA regulations at the time of the accident.[42] The training had a slightly different syllabus for each recurrent exercise and was intended to be self-paced, with an estimated duration of 2 hours. The subject matter was based on the CASA resource material – Safety behaviours: human factors for pilots: Resource booklet 7 Decision making. The pilot had completed the initial training in September 2020, which required reading the booklet, watching a CASA video on decision making, and completing a short multiple-choice quiz. The first recurrent training was completed in October 2021 and involved similar tasks.
Regulatory oversight
CASA’s surveillance manual outlined that the surveillance program for Authorisation Holders (AH), such as Executive Helicopters, used a systems and risk-based approach to obtain, record, and analyse results to evaluate safety performance. The scheduling of surveillance events was driven by many factors such as external intelligence, outstanding safety findings, time since the last surveillance event, and safety-related risks specific to each AH.
CASA last conducted a surveillance event on the operator in October 2018. That surveillance was classified as ‘Level 1’[43] and conducted on-site at the operator’s premises. The scope of the surveillance included a review of airworthiness assurance, crew scheduling, and flight operations. The surveillance event resulted in 3 findings regarding crew rostering, navigation logs, and operations manual document control.
The operator responded to each finding with satisfactory corrective action and CASA acquitted the 3 findings in January 2019. Another Level 1 scheduled surveillance event was planned for March 2022 but was not conducted as all CASA surveillance events were postponed due to the flight operations regulations transition.
CASA used an Authorisation Holder Performance Indicator (AHPI) tool to assist with surveillance. The AHPI tool was one of a number of factors used to determine the need for surveillance events. The AHPI tool was a questionnaire-based tool consisting of several factors and sub-factors associated with organisational characteristics and performance commonly thought to affect or relate to safety performance behaviour. The assessment would result in the AH being assigned to either category 1 (higher level surveillance focus required) or category 2 (normal surveillance level appropriate). Since January 2019, 3 AHPI assessments had been conducted on Executive Helicopters — in May 2019, May 2020, and November 2021 — with each resulting in the operator being assigned to category 2 indicating that the normal level of surveillance was appropriate.
VFR-into-IMC
Visual flight rules pilots flying into IMC (VFR-into-IMC) has been a worldwide challenge in aviation and continues to represent a significant portion of fatal accidents. VFR-into-IMC accidents usually involve either loss of control, spatial disorientation, or controlled flight into terrain. A significant number of studies have examined VFR‑into-IMC accidents, and a range of factors are usually involved, of which many are related to decision making.
Decision making
Pilot decision making is a cognitive process used to select a course of action between alternatives. Several factors, circumstances, and biases can affect decision making, including the flight objective or goal, and the pilot’s knowledge, experience, and training (Endsley, 1995).
The CASA Resource booklet 7 Decision making contained the following:
In aviation, decision making is involved in every action a pilot makes before and during a flight, including pre-flight activities, and go/no-go decisions. Every decision will, hopefully, ensure an uneventful, safe flight, but the safety consequences of some poor decisions can be irreversible.
For example…A non-instrument rated pilot who proceeds with a flight in marginal weather and ends up in instrument meteorological conditions (IMC) decides to firstly, proceed with the flight and secondly, not turn back when the weather indicated visual flight rules were not able to be maintained.
Pilots frequently face classic ‘go/no-go’ decision making because of ambiguous or dynamically changing conditions. [Airline] pilots receive intensive training in how to make such decisions, with regular refresher training in these skills in a simulator. For a charter pilot, however, without the intensive, practical training in a simulator, it can be very different. They can be faced with a challenging scenario they have not encountered before, or feel pressured to continue a flight despite changing conditions.
Air transport operations in smaller aeroplanes, such as that conducted by the operator, do not have the same sophistication of systems, processes, and procedures as larger airlines (Harris and others, 2022):
Commercial pilots often fly single-pilot, in remote areas, with limited direct supervision, requiring a greater level of decision making autonomy. These challenges can lead to pilots pushing their own and/or operational limits.
Recent research into general aviation pilots involved in the entry of VFR flights into IMC, noted a distinction between intentional and unintentional VFR-into-IMC (Stanton, 2022), which was normally not considered within previous research. Unintentional or inadvertent VFR‑into‑IMC flight were those where there was no deliberate intention to do so and occurred ‘…due to poor situational awareness or poor interpretation of weather cues whilst operating in a dynamic, sometimes subtly changing environment (Orasanu et al., 2001)’.
Intentional flights were those where the pilots were:
…conscious of the adverse weather (and the associated rules) and yet deliberately decide to continue into the poor conditions and have formed a cognitive behavioural intention to do so.
The violation, in this case, is not malevolent; instead, the person's objective is to adapt, gain efficiencies or achieve goals in complex real-world settings. Violations of this nature are not the action of bad apples or those who are acting irrationally. These intentional actions make sense to the pilots at the time, given the information that they have and the beliefs they hold about themselves and the environment.
A systematic review of the available research into VFR-into-IMC accidents, with a focus on commercial pilots and operations where there was intentional continuation of flight into unsuitable conditions, found the following 2 overarching themes, each with associated personal, social and organisational factors (Harris and others, 2022):
continuation influence
acceptance of risk/normalisation of deviance.
Continuation influence
Research has shown that pilots often continue VFR flights despite deteriorating cues associated with adverse weather conditions. This ‘plan continuation bias’ is an internal pressure or desire to get to the destination and could result from various factors such as previous encounters with IMC or an inability to detect cues of gradually deteriorating conditions while getting closer to the destination.
The ATSB found that the chances of a VFR-into-IMC encounter for general aviation pilots increased until they reached a maximum during the final 20% of the flight distance (ATSB, 2005). This pattern suggested an increasing tendency on the part of pilots to ‘press on’ as they near their goal with a decreasing probability of turning back or diverting as the destination drew closer.
Practical reasons can also play a role, with pilots continuing because the alternative places them in a location with minimal facilities (accommodation, food, communications). Also, the way alternative options are framed can also have an impact (Harris and others, 2022):
When pilots were required to decide between the acceptance of a certain loss (wasting time, losing money, personal hardship, etc.) or risking potential further loss (the chance of having an accident) “the loss frame” vs. framing the decision as a gain, pilots in the loss frame were significantly more likely to elect to continue with the flight.
The presence of passengers or customers on a flight can also directly, or indirectly, place pressure on a pilot to continue the flight, where the pilot does not want to disappoint the passenger(s) and to avoid social disapproval or failure. A review of United States general aviation aircraft accidents between 1990 and 1997 found a significantly greater percentage of VFR‑into‑IMC accident flights carried passengers on board (Goh and Wiegmann, 2001).
At the operator level, pilots can be influenced by time pressures, resource limitations or financial constraints and incentives. An organisation’s safety culture can also affect pilot motivations and decision making. For example, a safety conscious culture could lead to a pilot choosing a safe option (for example, diversion), while a pilot that fears punishment if they divert may lead them to press on into deteriorating weather.
Acceptance of risk/normalisation of deviance
Decision making under uncertainty involves the perception of risk (Harris and others, 2022). Pilots may detect deteriorating weather but perceive the risk of continuing differently based on factors such as personal experience and ability. Pilots that had lower risk perception, or were less risk averse, were more likely to have encountered adverse weather before:
…some pilots may tend to transition into deteriorating weather / IMC deliberately, on the basis that they [are] familiar with or have experienced relatively similar conditions, they perceive the transition into IMC as comparatively less risky, and experience lower levels of anxiety during the encounter.
These findings were supported by another recent study on VFR-into-IMC accidents, where a cycle of repeated and successful VFR-into-IMC encounters could create a pattern of deviation from the rules (Stanton, 2022):
Those pilots who are most at risk are those who mistakenly consider themselves as above average or experts. This cohort is the least likely to have the metacognitive skills required to identify and exit the cycle, driving progressively greater normalised deviance. This cohort of pilots is the most difficult to target for intervention because, according to how they perceive the world, they have already mastered what we want to teach.
This research also found that the perceptions pilots held about what other people, whose opinion they valued, might expect or think about conducting a VFR flight into IMC, and what these people would do in such a situation, was highly influential to forming an intention to conduct VFR flights into IMC (Stanton, 2022).
From an organisational perspective, pilots could become accustomed to risk-taking when instructed to take-off and ‘…see how bad the weather is…’ if it leads to no negative consequences (Harris and others, 2022):
The pilots become accustomed to the risk-taking because that is what’s expected of them. These cultural norms can become the organizational culture and the low organizational safety standards can lead to pilots being willing to take more risks and to reason away risky decisions. The incremental acceptance of progressively lower levels of safety by a group is the definition of the normalization of deviance.
Pilot decision making during the accident flight
The pilot was described as being diligent with weather-related decision making, knowledgeable and experienced with the local terrain surrounding Brisbane. The pilot’s next of kin and a former colleague reported that the pilot always had alternative options in case poor weather was encountered. On 2 separate occasions the pilot had reportedly landed after encountering poor weather, and either waited until the weather cleared, or sought a different method of travel to get to the destination. A review of the ATSB occurrence database did not identify any weather-related occurrences involving the pilot, nor did CASA hold any records of enforcement action taken against the pilot.
In the time leading up to the accident, the pilot was operating the aircraft in regions of elevated terrain at altitudes below the minimum height requirements. While the pilot had substantial experience flying at low level and in mountainous terrain, as well as previous IFR experience, the ATSB was unable to determine whether this previous experience lowered the pilot’s risk perception and influenced the decision to continue the flight.
While the pilot was also described as being very customer focused, a former colleague reported that the pilot never had any urgency to ‘get the job done’ and would not be pressured by anyone to do something they were not comfortable with. On the day of the accident, there was no evidence of schedule-related time pressure for the passengers’ return to Archerfield. Nevertheless, there was insufficient information to determine whether the pilot was under any real or perceived customer-imposed pressure, or self-induced pressure due to the presence of the passengers, to complete the flight.
From an organisational perspective, the accident pilot and the CEO were, for a significant period of time, the only personnel at Executive Helicopters with responsibility and accountability for the safe operation of aircraft. The full-time pilot who was employed by the operator from January 2021 to June 2022 described the CEO as ‘easy going’ with a friendly and open, professional and personal relationship with the accident pilot.
The CEO was not involved in the day to day flying operations of the operator but would receive regular communications from the accident pilot on these matters. The previously‑employed pilot stated that during their time with the organisation they felt 'very comfortable’ with all aspects of operations and did not experience any pressure to complete flights. Based on this information, it was considered unlikely that there was any direct or perceived organisational pressure on the pilot to continue the flight.
Intervention strategies
The commonly documented strategies to avoid entering IMC are appropriate pre-flight preparation and sound decision making. Initial instrument training required for a commercial aeroplane licence, and recurring training as part of biennial flight reviews, can also assist pilots in maintaining aircraft control in IMC and to recover to VMC. Some recent research and information on aspects related to VFR-into-IMC prevention and recovery are outlined below.
Prevention
The dangers of VFR pilots flying into IMC have been recognised for a very long time, yet VFR pilots still fly into deteriorating weather and IMC. Recent research, which applied the ‘theory of planned behaviour’[44] to intentional VFR-into-IMC flights, summarised the historical attempts at preventing these accidents (Stanton, 2022):
The conventional remedy has been to instruct pilots (who care to read the safety journals and magazines) to plan better, pay more attention to the changing weather and to educate pilots more on the potentially tragic outcomes with messages like you have only 178 seconds to live. This approach appears to have achieved little advancement despite the well-intentioned efforts of many.
This research found that pilot’s ‘…beliefs related to the hazardous consequences of conducting VFR flight into IMC (i.e., behavioural beliefs) had limited influence on a pilot’s intentions’ which could explain ‘…why past attempts at intervention have been unsuccessful for so long’.
The research found that the distinction between inadvertent and intentional VFR-into-IMC was likely an important factor when considering intervention strategies:
…there appears limited discussion or application of the interventional distinctions between the intentional and the unintentional cases. Instead, the problem is frequently contemplated simply as a single problem of VFR flights into IMC. The interventions required are likely to be unique between the unintentional and the intentional cases in order to address the respective underlying foundations.
For intentional VFR-into-IMC, the research indicated that ‘…beliefs associated with social pressures and those associated with a pilot’s perception of their skills and ability were the primary influences on behavioural intentions’. The research suggested that intervention strategies be developed by applying behaviour change theories to pilots to alter their beliefs, attitudes, and perceptions. This conclusion was also supported by other research that reviewed VFR-into-IMC from a behavioural economics[45] perspective, which also suggested more comprehensive weather training was required (O’Mahony et al., 2023). The research proposed 3 interventions to facilitate better pilot decision making in the context of VFR-into-IMC:
The first of these is an acceptance by the regulator that the behavioural biases are real and can result in predictable departures from rationality across the spectrum of pilot skill levels and personalities.
Secondly, the educational regime mandated by CASA has a critical role to play. In playing its role, the regime needs to be deeper and more adept at explaining to pilots the psychological factors to which they may fall victim, and we advocate for regulatory intervention to better educate pilots about their own psychology.
Finally, pilots will need better practical (and mandatory) weather training. Currently, the training available to pilots is based around understanding basic weather theory, being able to predict weather using weather-forecasting tools, and understanding the legal requirements of VMC and IMC. As we have shown, environmental literacy often becomes an issue in flight, with pilots struggling to perceive subtle changes in the weather until the weather has deteriorated to dangerous conditions. This practical en route flying training is apt for simulation-based training, a tool which is becoming more common in [general aviation], with the advent of cheaper and more sophisticated software.
IMC recovery
The Cessna R182 pilot’s operating handbook[46] included an emergency procedure for inadvertently entering clouds. The procedure was to execute a standard rate 180° turn using the aircraft’s compass and clock, while maintaining altitude and airspeed.
The 180° turn may not be suitable for all IMC recovery situations and execution of this turn at low altitude has resulted in controlled flight into terrain (CFIT) accidents or a loss of control during the turn. A 2021 United States General Aviation Joint Steering Committee[47] (GAJSC) report into CFIT accidents recommended a task force be created to review IMC recovery events to ‘…make recommendations on revisiting how we teach and train the [IMC] escape response [manoeuvre] to include an initial climb before any heading change, should the data support such a change.’ An Aircraft Owners and Pilots Association (AOPA) article indicated that climbing, rather than turning, was a valid option to consider depending on the situation faced by a pilot:
For years, student pilots have received three hours of training on flight by reference to instruments with the intent that this training will help them get out of the VFR into IMC trap. The 180-degree turn is normally taught as the escape maneuver, and is often the best option. But there are alternatives to consider.
Reviewing two recent VFR into IMC reports, both pilots opted to climb instead of turning around. In one case, the pilot got a low-altitude warning from an aviation app on a mobile device after losing all outside visual references. The pilot climbed to 3,500 feet and continued along the route of flight until finally exiting IMC some 34 miles later. In the other case, the pilot was in a precarious low-altitude VFR into IMC situation where the aircraft was dodging communication towers and entered a cloud. After momentarily experiencing spatial disorientation, the pilot was able to level the aircraft and then began a climb to altitude into the clouds. After a few minutes the airplane broke into clear skies and the pilot continued to the destination VFR.
In both situations the pilots made the decision to climb to avoid a low-altitude encounter with an object. Both pilots maintained straight-ahead, wings-level climbs and did not deviate from their headings. The attitude indicator was the primary instrument for establishing and maintaining the climb, and the other instruments provided supporting information to confirm that climb. Both pilots deliberately focused on the instruments and did not attempt to look outside, to avoid distraction that can cause spatial disorientation.
Instrument training and flying, such as that conducted during flight reviews can assist in maintaining aircraft control and to recover to VMC conditions, although there are limitations to this approach (AOPA, 2022):
In training, you’re instantly put into an IMC scenario. But it’s slightly deteriorating weather, slowly evolving and enveloping you and your airplane, that lures you into the trap.
To resolve this limitation, the 2021 GAJSC report recommended ‘…to improve scenario-based training through the use of [available] advanced view-limiting device technology that simulates inadvertent IMC entry and/or through the use of flight simulators.’
At 0715 local time on 29 August 2022, a Cessna R182 Skylane RG (R182), registered VH-EHM, and operated by Executive Helicopters, departed a private property (Lighthouse) north-east of Roma, Queensland for an air transport flight under visual flight rules (VFR) to Archerfield Airport, Queensland. The aircraft departed with the pilot, 2 passengers, and a passenger’s pet dog on board.
As the aircraft was crossing the elevated terrain of the Great Dividing Range, the pilot encountered forecast low cloud and reduced visibility, and was unable to find a way across that was clear of cloud. With limited fuel remaining, the pilot diverted to Dalby Airport and refuelled the aircraft before departing once again. About an hour later, the aircraft collided with terrain in the D’Aguilar Range about 36 km north-west of Archerfield. All occupants of the aircraft were fatally injured.
The ATSB did not identify any aircraft defects or anomalies that may have contributed to the accident. As such, the following analysis will examine the:
pilot’s pre‑flight planning and decision making.
continuation of the flight into adverse weather.
operator’s risk management.
search and rescue aspects.
Pre-flight planning and diversion to Dalby
Pre-flight weather assessment
While at Lighthouse, the forecast weather at the destination (Archerfield) was suitable for a VFR arrival. However, the en route forecast predicted low cloud, rain, fog and associated reduced visibility, particularly around the elevated terrain of the Great Dividing Range, with cloud down to ground level in some areas. Although the forecast predicted acceptable visibility below the cloud layers, the weather conditions around the elevated terrain of the range – which had to be crossed to reach Archerfield – were unsuitable for visual flight.
About 6 minutes before the flight departed Lighthouse, the pilot requested weather information through the National Aeronautical Information Processing System (NAIPS). This was the pilot’s first NAIPS weather request since their departure from Archerfield the previous day. The exact weather information reviewed by the pilot could not be determined, nor is it not known whether the pilot accessed other non‑approved sources of weather. Nevertheless, the information available as part of the NAIPS request was sufficient for the pilot to assess the weather en route and to inform the pilot’s pre-flight decision making. However, the minimal time between the NAIPS weather request and subsequent take-off (6 minutes), provided limited opportunity for a thorough review of the en route weather and was consistent with a strong motivation to conduct the flight despite the forecast weather conditions.
Fuel planning
Although fuel was available at Lighthouse, and there was sufficient fuel on-board to complete the flight in ideal conditions, there was insufficient fuel to account for weather-related diversions or meet contingency fuel requirements. Furthermore, depending on the fuel flow data used for the calculations, there was also insufficient final reserve fuel on-board.
The limited pre-flight planning information available meant that the investigation was unable to determine the factors considered by the pilot with respect to fuel planning prior to departure.
Flight notification and search and rescue
Civil Aviation Safety Regulations (CASR) required that, before undertaking the flight, the pilot leave details of the flight and arrival time with a ‘responsible person’ who knew when and how to contact the Joint Rescue Coordination Centre (JRCC) and would do so if the flight was overdue.
The operator's documented procedures reflected this requirement and stipulated that this ‘responsible person’ could be someone from the operator or a representative of a client onboard.
The operator reported that the pilot did not always follow this documented procedure and would sometimes provide flight details to a family member, as occurred on the accident flight. Providing the flight note to this family member was still sufficient to meet the regulatory requirement if they were aware of their obligations and expected actions. However, the investigation identified various deficiencies in relation to the pilot’s compliance with this requirement for the accident flight:
The family member was notified about 30 minutes after departure from Lighthouse, limiting search and rescue (SAR) functions during that initial part of the flight.
An unspecific arrival time of ‘late morning’ was provided which was not suitable for the purposes of timely SAR action.
Although the flight diverted to Dalby, the pilot did not notify the family member when there was a change to the flight route and arrival timing.
The pilot had not briefed the family member about the correct actions to take for an overdue flight, resulting in a delay of over 2 hours in notifying the operator that the flight was overdue. This substantially delayed the subsequent emergency SAR response and potential medical attention (in the event of a survivable accident).
The accident was non-survivable, and consequently, a timely SAR response and immediate medical aid would not have altered the outcome. However, in different circumstances, SAR notification and the carriage and use of manually activated emergency beacons would likely have played a key role in increasing the chances of post‑accident survival by facilitating rapid medical aid to treat injuries.
Departure and diversion to Dalby
While the forecast indicated that visual meteorological conditions (VMC) would probably not be maintained while transiting the elevated terrain of the Great Dividing Range, the decision to depart Lighthouse towards Archerfield was in itself reasonable. With adequate fuel on-board and escape routes planned, actual weather conditions could be assessed and managed in‑flight. However, doing so placed additional pressure on the pilot’s in‑flight decision making capabilities.
After encountering the forecast cloud, the pilot continued to manoeuvre to try to find a way through the Great Dividing Range with the aircraft’s fuel running low. The pilot then diverted to Dalby, landing with less than the required final reserve fuel. Although this may have been influenced in part by the aircraft being equipped with instrumentation capable of indicating the fuel state accurately, this indicated that the pilot’s planning before and during the flight was ineffective, and there was likely a motivation to complete the flight even though reduced safety margins existed.
Summary
The operator’s small size, limited flight operation personnel, and single-pilot operations, required the accident pilot to exercise a high level of pre-flight and in-flight decision-making autonomy.
The decision to depart into forecast weather that was not conducive to visual flight, with limited time for pre-flight weather review, insufficient required fuel on-board, and without an appropriate flight notification system, combined to reduce safety margins and presented an increased risk to occupants on board.
Although not contributory to the accident outcome, these factors were indicative of inadequate pre-flight planning. However, having attempted to cross the Great Dividing Range, the pilot did make an effective in-flight decision to return to Dalby to refuel. This provided an opportunity to re‑assess the weather and its suitability for continued flight, as well as providing an opportunity to identify alternative options for the passengers’ continued travel.
Departure from Dalby and continuation of flight
Pre-flight
The updated weather forecast information available to the pilot while at Dalby, predicted en route weather conditions similar to those already experienced but the forecast cloud between 1,500‑2,500 ft was expected to start dissipating within about 2 hours (by 1100), and clear completely by 1200. Also, the forecast deteriorating weather conditions with reduced visibility and low cloud cover at Amberley and Archerfield were also expected to clear by 1100. These deteriorating periods had forecast conditions that were less than the VMC criteria necessary to achieve the minimum height of 1,000 ft AGL required to transit Amberley and land at Archerfield. However, the conditions were within the special VFR criteria which meant that a transit and landing could have been possible had the pilot requested a special VFR clearance from air traffic control at Amberley and Archerfield.
As was the case before departing Lighthouse, although good visibility below the cloud layers was forecast en route, conditions around the elevated terrain of the Great Dividing Range were not suitable for visual flight.
The pilot spent about 10 minutes on the ground at Dalby, almost all of which was spent refuelling, and there were no NAIPS logins recorded during time on the ground. Therefore, it was unlikely that the pilot reviewed the updated forecast either from NAIPS or another source before take-off (for example, via radio), although the pilot likely reviewed it in-flight, shortly after take-off. This suggested that there was little consideration given to alternative means of getting the passengers to their destination (for example, ground transport or waiting until the weather improved as was forecast to occur within the next 2-3 hours). The short time spent on the ground provided further evidence of a motivation to complete the flight despite having already encountered the forecast cloud in-flight.
After departure
Across the Great Dividing Range
The flight track showed that, following departure from Dalby, the pilot attempted to find a different path across a section of the Great Dividing Range to get to the low-lying terrain west of Amberley, this time tracking south of Toowoomba. The pilot requested updated weather through NAIPS about 13 minutes after take-off. However, re-assessing the weather in‑flight removed the ability of the pilot to decide against taking off again. Research indicates that continuing with an initial plan or strategy despite indications that an alternative course of action may be safer can be stronger after take-off, making the decision to discontinue the flight more difficult.
The forecast and observed weather conditions, as well as the pilot’s flight track, indicated that a cloud layer was obscuring terrain on Main Range. The pilot’s first attempt to cross this range was unsuccessful, likely due to cloud, with a 180° turn performed to try to cross at a different location. The pilot then tracked south-east and between 2 peaks at low level, before heading down a long valley towards low-lying coastal terrain.
The flight track suggested familiarity and knowledge of the terrain with the pilot possibly heading towards known locations that presented the best chance of transit. However, the aircraft crossed over the terrain with minimal separation. This was likely indicative of the pilot’s intention and motivation to continue and complete the flight, despite the forecast and observed weather conditions.
Amberley and surrounding area
After crossing Main Range, the pilot descended the aircraft towards Gatton before tracking towards Lowood, following the low-lying terrain below cloud. Weather observations from Gatton, Amberley, and Lowood Golf Course indicated a low cloud base but with good visibility below the layer. However, a weather report about 15 minutes after the accident indicated the forecast deteriorating weather at Amberley had reduced the observed visibility to 4,000 m and lowered the scattered cloud to 700 ft. These conditions would have meant that the area was not suitable for visual flight at that time.
Lake Manchester VFR route
The Lake Manchester VFR route, intended to be used in VMC, had narrow lateral and vertical separation between the hilly terrain of the adjacent D’Aguilar Range and controlled airspace, which increased the difficulty of this route in poor weather. The flight track indicated that the pilot was trying to follow the route to get to Archerfield. However, the adjacent range was obscured by cloud, so it was likely difficult to orientate the aircraft with identifiable ground features to assist with navigation. In addition, the aircraft’s relatively high speed for the conditions reduced the time available for decision making.
After turning east over Fernvale, the aircraft tracked towards a mountain at an altitude below its peak before conducting another 180° turn at about 1,200 ft and less than 2 km from rising terrain. About 10 seconds later, the pilot conducted a right turn at about 140 kt ground speed towards the rising terrain of the D’Aguilar Range, which had low cloud cover obscuring some of the peaks, and shortly after, impacted terrain.
Evidence from the site of the accident and the sound of the aircraft up until the impact indicated:
no abnormal engine or propeller sounds up to the time of impact
no pre-impact issues with the aircraft, engine, or propeller
a relatively high-speed impact
a shallow descent at the time of impact with the trees and terrain
an angle of bank at the time of impact similar to previous turns completed during the flight.
As a result, the ATSB concluded that the aircraft was likely under control during the impact with the pilot very likely unaware of the aircraft’s proximity to the terrain. Although the pilot was knowledgeable and experienced with the location of the D’Aguilar Range relative to Fernvale, the low cloud over the range and the flight track indicated the aircraft was very likely in instrument meteorological conditions (IMC) in the final stages of the flight. The pilot very likely lost visual reference with the ground, limiting the ability to geographically orient themselves and avoid the surrounding hills, eventually leading to a controlled flight into terrain. The high speed would also have limited the pilot’s ability to react and avoid any terrain identified in the final moments of the flight.
Pilot decision making
On the day of the accident, the pilot was conscious of the adverse weather forecast and encountered during the flight prior to landing at Dalby. The pilot then made a deliberate decision to depart Dalby and continue the flight into known unsuitable weather conditions at cruise speed, low altitude, and towards a known area of rising terrain obscured by cloud. This was inconsistent with the prudent judgement, behaviour and decision making capability attributed to them by others. Nevertheless, the available information suggests the pilot was probably influenced by plan continuation bias – an internal pressure or desire to get to the destination – to continue the flight, which probably became stronger as they got closer to Archerfield Airport. However, due to a lack of information, the ATSB was unable to conclusively determine the pilot’s motivations in choosing to continue the flight in unsuitable circumstances with reduced safety margins.
Operator risk management
Although inadvertent IMC was a well-known, high consequence risk, the operator's hazard and risk register, which formed part of the organisation's safety management system (SMS), did not identify this hazard. Consequently, there was no specific assessment of its risk to operations and no specific risk mitigation in place.
Although not documented in the operator’s SMS, the risk of inadvertent IMC was being managed by requiring that pilots not commence flights unless VFR conditions were forecast for the route and at the destination, and to monitor and plan alternative actions in-flight if weather deteriorated. In this accident, the pilot did not follow these procedural controls. The controls relied on an individual pilot’s pre-flight assessment of weather, and on in-flight weather-related decision making, neither of which were addressed by the operator through any specific training, procedures, or review.
In addition, the operator did not have any procedures or training in place beyond the minimum regulatory instrument flying component of fixed wing flight reviews for pilots to recover from an inadvertent IMC encounter. Historically, relying on pilots to avoid IMC has been the primary strategy in preventing inadvertent IMC accidents. However, the continuing occurrence of these accidents demonstrates that this strategy alone is insufficient.
As the hazard of inadvertent entry into IMC was not identified in the risk register, no conclusions could be drawn about the nature and effectiveness of the specific risk controls that might have been implemented, nor whether the pilot would have utilised them. Therefore, while important, the absence of the hazard being identified in the operator’s SMS was not considered contributory to the accident.
On-board recording devices
There was no regulatory requirement for the aircraft to be fitted with on-board recording devices. However, this and numerous other investigations have shown that the lack of such devices limits the ability to understand and determine all of the factors that contributed to an accident. In turn, important safety issues that present a hazard to current and future operations were potentially not identified. Conversely, other investigations where some form of recording device was on board, provided valuable information regarding the accident.
In this investigation, flight track data was available to identify the aircraft’s movement. However, the ATSB was unable to determine why a highly experienced commercial pilot continued the flight into a known area of high terrain obscured by cloud, nor could the circumstances of what was occurring in the cockpit, especially in the final minutes before the accident, be determined. Recorded information may have provided some insights into the pilot’s decision making during the flight and further detail on how the accident developed.
The use of lightweight recorders on smaller aircraft conducting commercial operations has the potential to provide a relatively simple and cost-effective way of achieving many of the benefits that are provided by traditional recorders fitted to larger aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC and controlled flight into terrain involving Cessna R182, VH-EHM, 36 km north-west of Archerfield Airport, Queensland on 29 August 2022
Contributing factors
After encountering and manoeuvring around forecast low cloud, insufficient fuel remained on board the aircraft to complete the flight and the pilot diverted to Dalby to refuel. After refuelling, the pilot departed toward forecast en route weather unsuitable for visual flight.
The pilot continued the flight at low level, at cruise speed, into weather conditions unsuitable for visual flight. This very likely resulted in the pilot experiencing a loss of visual reference leading to controlled flight into terrain.
Other factors that increased risk
Although in this instance the accident was not survivable, several deficiencies were identified that delayed a search and rescue response:
Contrary to operator procedures, the pilot provided flight notification information to a family member not associated with the operator.
The family member was not provided with any information on appropriate actions to be taken in the event of the aircraft being overdue.
The pilot provided flight notification information to the family member about 30 minutes after take-off from Lighthouse which limited search and rescue functions for that time.
The aircraft likely departed Lighthouse for the flight to Archerfield Airport with insufficient fuel to account for weather-related diversions and the required contingency and final reserve fuel.
The operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions as a hazard, which reduced the ability of the organisation to effectively manage the related risk. (Safety issue)
Other findings
While flight tracking data was available, the aircraft was not fitted with an onboard recording device. This could have provided valuable information to better understand the pilot’s in-flight weather-related decision making.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The operator's hazard and risk register, which formed part of the organisation's safety management system, did not identify inadvertent entry into instrument meteorological conditions as a hazard, which reduced the ability of the organisation to effectively manage the related risk.
Glossary
AGL
Above ground level
AMSL
Above mean sea level
AOC
Air Operator's Certificate
AOPA
Aircraft Owners and Pilots Association
ATC
Air traffic control
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CEO
Chief Executive Officer
CoA
Certificate of airworthiness
CFIT
Controlled flight into terrain
CTA
Control area
CTR
Control zone
DAME
Designated aviation medical examiner
ELT
Emergency locator transmitter
EPIRB
Emergency position indicating radio beacon
GAF
Graphical area forecast
GAJSC
General Aviation Joint Steering Committee
HOFO
Head of flying operations
ICAO
International Civil Aviation Organization
IFR
Instrument flight rules
IMC
Instrument meteorological conditions
ISA
International Standard Atmosphere
JRCC
Joint Rescue Coordination Centre
NAIPS
National Aeronautical Information Processing System
PLB
Personal locator beacon
POH
Pilot’s operating handbook
SAR
Search and rescue
SMS
Safety management system
TAF
Terminal area forecast
TAS
True Airspeed
TAWS
Terrain awareness and warning system
VFR
Visual flight rules
VMC
Visual meteorological conditions
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot’s next of kin and former colleagues
the passengers’ friends and colleagues
Bureau of Meteorology
Geoscience Australia
Airservices Australia
Executive Helicopters (operator)
Civil Aviation Safety Authority
OzRunways
Avdata
Fernvale Rural Fire Brigade
Queensland Police Service
witnesses
CCTV video footage of weather near the aircraft’s flight path.
References
Australian Transport Safety Bureau. (2005). General Aviation Pilot Behaviours in the Face of Adverse Weather. B2005/0127
Australian Transport Safety Bureau. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents.
Australian Transport Safety Bureau. (2019). Avoidable Accidents No. 4:Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions.AR-2011-050
Australian Transport Safety Bureau. (2021). Collision with water involving de Havilland Canada DHC-2, VH-NOO. AO-2017-118
Australian Transport Safety Bureau. (2021). VFR into IMC and controlled flight into terrain involving Pilatus Britten-Norman BN2A, VH-OBL. AO‑2018‑078
Australian Transport Safety Bureau. (2023). VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD. AO-2022-016
Harris M.R., Fein E.C. and Machin M.A. (2022). A Systematic Review of Multilevel Influenced Risk-Taking in Helicopter and Small Airplane Normal Operations. Front. Public Health 10:823276. doi: 10.3389/fpubh.2022.823276
International Civil Aviation Organization. (2018). Safety Management Manual (4th ed). ICAO Doc 9859, Montreal
O'Mahony et al. (2023). VFR Into IMC Through the Lens of Behavioral Economics. Journal of Air Law and Commerce. Volume 88, Issue 1, Article 4 https://scholar.smu.edu/jalc/vol88/iss1/4
Stanton A. (2022). 'Gathering Clouds' A Study of Plan Continuation, Risk, Rules, and Pilot Behaviour. https://doi.org/10.25904/1912/4844
Wilson, D.R., & Sloan, T.A. (2003). VFR Flight Into IMC: Reducing the Hazard. Journal of Aviation/ Aerospace Education & Research, 13(1). https://doi.org/10.15394/jaaer.2003.1567
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the aircraft operator and the Civil Aviation Safety Authority.
A submission was received from the aircraft’s operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix – Fuel calculations
Background
An assessment was undertaken to determine the likely quantity of fuel on-board the aircraft when it departed Lighthouse, and if that quantity was sufficient for the intended flight to Archerfield.
Calculations – Fuel on-board at Lighthouse
Using the maximum capacity of the fuel tanks and the fuel uplift data at Dalby, the useable fuel remaining in the tanks on landing at Dalby could be calculated (20.7 L). The total fuel used during the flight (taxi, climb, and cruise) from Lighthouse to Dalby was estimated using the pilot’s operating handbook (POH),[48] the operator’s operations manual, and the forecast weather.
Taxi
Total taxi fuel was calculated from the POH as the difference between the maximum ramp weight (1,411.6 kg) and maximum take-off weight (1,406.1 kg). The operator’s operations manual also provided an estimated taxi fuel amount.
Climb
Climb fuel consumption rate data in the POH was available for maximum aircraft weight, and International Standard Atmosphere (ISA) conditions and for normal climb performance. Similar temperature conditions to International Standard atmosphere (ISA) were forecast. The main cruise altitude from the aircraft’s OzRunways flight track data was 3,400 ft between Lighthouse and Dalby. The POH data provided fuel consumption for 3,000 ft and 4,000 ft so an interpolation calculation was conducted.
Cruise
Fuel consumption from Lighthouse to Dalby was calculated using data provided in the POH, operator’s operations manual, and forecast weather. As the cruise power setting for the flight was not known, cruise fuel consumption rates were calculated for 3 common engine power settings (75%, 65% and 55%). The POH data assumed maximum take-off weight and standard ISA conditions. The most relevant data for the 3,400 ft cruise altitude was contained in the performance chart for 4,000 ft altitude. For calculations conducted using the operations manual data, the provided ‘block fuel flow’ was used as the cruise and climb fuel flow.
Cruise time was based on the OzRunways flight track data after reaching cruise level until landing at Dalby. Although about two-thirds of the flight was at a similar cruise altitude, the remaining third was made up of 2 climbs and 2 descents along with heading changes. It was assumed that the fuel consumption rate during these phases averaged out to be similar to the cruise fuel consumption rate (since a higher fuel consumption rate would occur during climb with a lower rate during descent). Therefore, the cruise fuel consumption rate was used for the flight time between initially reaching cruise altitude and landing at Dalby.
The actual weight of the aircraft at the same power level and operating altitude can affect the cruise speed of the aircraft and thus flight time and total fuel consumption. POH fuel consumption and related true airspeed (TAS) data was provided at maximum weight but the aircraft during the flight was below this weight. The estimated aircraft departure weight based on the operations manual fuel usage was about 1,269 kg. However, the difference in TAS at this weight was considered minimal so no correction to the cruise time was applied.
The estimated fuel on-board at Lighthouse for each scenario is shown in Table 2.
Table 2: Estimated fuel on-board VH-EHM at Lighthouse
Calculations – Fuel required from Lighthouse to Archerfield
The Civil Aviation Safety Regulations defined the fuel requirements for Part 135 operators. The following fuel was required for a Part 135 flight:
taxi fuel – fuel used before take-off
trip fuel – fuel for take-off, climb, cruise, descent, and landing
contingency fuel – 10% of trip fuel for a piston engine aeroplane to compensate for unforeseen factors
final reserve fuel – 45 minutes flight time for a piston engine aeroplane and is useable fuel remaining on completion of final landing at the aerodrome
Destination alternate fuel (if required)
Holding fuel (if required)
Additional fuel (if required)
An estimate on the fuel required to complete the flight from Lighthouse to Archerfield (taxi, climb, cruise) was determined using data available in the POH, operations manual and the forecast wind conditions.
The anticipated ground speed was calculated based on the TAS and forecast wind conditions. The Bureau of Meteorology grid point wind and temperature chart forecast 13‑21 kt wind from 70° at 2,000 ft and 14-20 kt wind from 50-80° at 5,000 ft for most of the planned flight which was on a 115° track. Therefore, an estimated 10 kt headwind was used for the calculations. For the different power settings, the ground speed was used along with the cruise distance to determine the total time and fuel consumption during cruise. For the operations manual fuel flow calculations, the total planned distance to Archerfield was used as the ‘block fuel flow’ accounted for climb, cruise, and descent fuel consumption.
Cruise fuel planning was conducted to overhead the destination aerodrome at cruise level. Manoeuvring and approach fuel consumption was not considered.
Contingency fuel
Contingency fuel was 10% of the calculated trip fuel.
Final reserve fuel
Final reserve fuel was 45 minutes at holding speed, ISA conditions and 1,500 ft. The POH provided a holding fuel of 23.8 L based on 45 minutes at 45 % engine power. The operations manual provided an expected ‘holding’ fuel flow of 40 L per hour (30 L for 45 mins).
Destination alternate fuel, holding fuel, and additional fuel
Either the ‘destination alternate fuel’ or ‘holding fuel’ was required if the destination forecast was below the alternate minima. The relevant Terminal Area Forecast (TAF) for Archerfield forecast conditions above the alternative minima, so no holding or destination alternate fuel was required for the flight. ‘Additional fuel’ was only required for multi-engine aircraft, or aircraft with pressurisation. Since VH‑EHM was a single-engine non-pressurised aircraft, ‘additional fuel’ was not required. The results are shown below in Table 3.
Table 3: Estimated minimum regulatory fuel required for planned flight to Archerfield
Estimated fuel margin
The results of the above calculations are shown below in Table 4 to determine the fuel margin between the useable fuel on-board and the minimum required fuel.
Table 4: Estimated fuel margin for the planned flight to Archerfield
The results are based on forecast ideal weather conditions. As per the general fuel requirements in the CASR, in determining the quantity of useable fuel required, the pilot in command must also consider the effect of relevant meteorological reports and forecasts.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] The flight was operated under Civil Aviation Safety Regulations Part 135 (Air transport operations – smaller aeroplanes).
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[3] GPS altitude from OzRunways, which is truncated to 100 ft increments.
[4] Data used for terrain elevation does not account for vegetation or structures such as power lines, which may protrude some distance above the ground.
[5] Before the introduction of the Civil Aviation Safety Authority (CASA) Part 61 licencing regulations in 2014, under Civil Aviation Regulation 5, pilots maintained instrument currency by completing an instrument ‘renewal’. Under Part 61, pilots maintained this currency by completing an ‘instrument proficiency check’.
[6] A low-level (LL) rating is needed for a low-level flight operation (below 500 feet AGL including low-level aerobatics).
[7] Aerial stock mustering involving the direct use of aircraft for the movement of livestock.
[8] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[9] An aircraft’s maintenance release is a document that provides registered operators and pilots with evidence that an aircraft has had the required maintenance carried out, provides details of any defects that may require rectification before a flight can commence, and also provides essential information about any scheduled maintenance actions that may become due before completion of a planned flight.
[10] Global Navigation Satellite System: A satellite-based radio navigation system that uses signals from orbiting satellites to determine precise position and time.
[11] A TAWS provides visual and aural alerting including a look-ahead terrain function. TAWS is a generic term that also includes a ground proximity warning system (GPWS) with a forward-looking terrain avoidance function. A TAWS is an important tool to help minimise the risk of controlled flight into terrain (CFIT). It provides an independent and unambiguous warning of proximity to the ground or obstacles, regardless of any navigational uncertainty or error such as mis-setting or misreading the altimeter.
[12] The series of Technical Standard Orders (TSO) C151 stipulated the minimum operational performance standards that a terrain awareness and warning system (TAWS) must meet to comply with regulatory requirements for the fitment and use of those systems.
[14] Spidertracks is a subscription aircraft monitoring service that allows operators to track and monitor the location of aircraft at regular intervals. The location is recorded and transmitted by a unit that is fitted to the aircraft.
[15] CASR Part 91 Manual of Standards (MoS), section 7.02.
[16] The National Aeronautical Information Processing System (NAIPS) is a computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots.
[17] A Terminal Area Forecast (TAF) is a statement of meteorological conditions expected for a specified period in the airspace within a radius of 5 NM of the aerodrome reference point.
[18] METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[20] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[21] INTER: an intermittent deterioration in the forecast weather conditions, during which a significant variation in prevailing conditions is expected to last for periods of less than 30 minutes duration.
[22] The timestamp on the video footage was likely accurate within minutes based on comparison with other sources. In any event, the weather conditions shown in the video footage were similar for at least 15 minutes before and after the recorded accident time.
[25] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[27] OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[28] A common traffic advisory frequency is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport, or within a broadcast area.
[29] The height above ground level was based on GPS altitude available from OzRunways (truncated to 100 ft increments), and Geoscience Australia terrain elevation data.
[30] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[31] CASR Part 135 Manual of Standards (MoS), section 11.51.
[32] The force needed to accelerate a mass. G-force is normally expressed in multiples of gravitational acceleration (normal gravity = 1g).
[33] CASR Part 91 Manual of Standards (MoS), section 9.02.
[34] SARTIME: An abbreviation for ‘time search action required’. A SARTIME is the time nominated by a pilot for the initiation of Search and Rescue (SAR) action.
[35] Flight Note: Details of the route and timing of a proposed flight provided by the pilot in command of an aircraft, other than notification submitted to Airservices Australia, and which is required to be left with a person who could be expected to notify appropriate authorities in the event that the flight becomes overdue.
[36] Automatic Dependent Surveillance - Broadcast (ADS-B) is a system in which equipment on board an aircraft automatically broadcasts the precise location of the aircraft. The data can be used by other aircraft and air traffic control to identify the aircraft’s position and altitude without the need for radar.
[37] CASR Part 135 Manual of Standards (MoS), chapter 7.
[38] The Pilots Operating Handbook provided a value of about 24 L compared with 30 L from the operator’s operations manual.
[39] A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[40] The AOC was issued before the CASA flight operation rules changed in December 2021, where the term ‘air transport’ replaced charter, regular public transport, and air ambulance when conducted for hire or reward.
[41] The operator was required to have a CASA-approved SMS by December 2024.
[42] The operator will be required to have a CASA approved program for training and assessing operational safety‑critical personnel in human factors principles and non‑technical skills by a future date to be specified by CASA.
[43] A structured, forward-planned, larger-type, surveillance event, which examined an authorisation holder’s systems, safety risk controls, and processes.
[44] The theory of planned behaviour posits that the most immediate cognitive antecedent to performing a distinct behaviour is the formation of an intention. The theory suggests that behavioural intentions are formed and can be predicted, predominantly from just 3 kinds of beliefs that a person holds in relation to the behaviour: attitude toward the behaviour, social norms, and perceived behavioural control (Stanton, 2022).
[45] Economics has traditionally assumed people always make decisions in their best interests. Behavioural economics challenges this view by providing a more realistic model of human behaviour. It recognises we are systematically biased (for example, we tend to satisfy our present self rather than planning for the future) and can make decisions that conflict with our own interests.
[46] The pilot’s operating handbook (POH) for the aircraft could not be located. Information from the POH of another Cessna R182 Skylane RG with a different serial number was used.
[47] The General Aviation Joint Steering Committee (GAJSC) is a United States based public-private partnership focused on improving the safety of the general aviation industry.
[48] As the aircraft’s POH was damaged during the accident, the POH for a different, but similar, 1978 Cessna R182 Skylane RG aircraft was used (serial number R18200450). The performance related data should be similar or identical to the data for VH-EHM.
Occurrence summary
Investigation number
AO-2022-041
Occurrence date
29/08/2022
Location
36 km north-west of Archerfield Airport
State
Queensland
Report release date
21/12/2023
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
R182
Registration
VH-EHM
Serial number
R18200431
Aircraft operator
EXECUTIVE HELICOPTERS PTY LTD
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 18 April 2022, the pilot of a Cessna 172 aircraft, registered VH-REU, was conducting a private flight at Coonabarabran Aerodrome, New South Wales.
After completing several circuits and touch-and-go landings, the pilot flew a low pass at 15–25 ft above the ground over a tractor that was being used to slash a field adjacent to the aerodrome. During the low pass, the aircraft contacted powerlines over the field and impacted terrain. The pilot received fatal injuries and the aircraft was destroyed
What the ATSB found
No pre-impact defects were identified with the aircraft structure, flight controls or engine, and witnesses stated the aircraft was operating normally on the day of the accident. Although operations at low levels are normal in the vicinity of an airfield during take-off and landing, the aircraft’s flight path just prior to the collision did not align with the runways and was not consistent with any part of a normal circuit pattern. It was therefore very likely that the pilot was conducting an intentional low-level pass over the tractor. The pilot was familiar with the aerodrome and was reported to be aware of the location of the powerlines. The pilot did not have a low-level rating and therefore had not undertaken the required training and assessment required to operate below 500 ft.
The pilot was wearing only the lap portion of the seatbelt during the accident flight, and not the sash-type upper torso restraint that was also fitted. However, it was not possible to determine with certainty whether, if worn, the upper torso restraint would have reduced the severity of injuries.
What has been done as a result
Based on a risk assessment conducted by the electricity provider post-accident, aerial safety markers were fitted to the powerlines in the field adjacent to the aerodrome where the aircraft contacted powerlines.
Safety message
Operations at low height expose an aircraft to several hazards like powerlines, which are typically very difficult to see and present a critical hazard to any low-flying aircraft. As identified in the ATSB publication Avoidable Accidents No. 1 - Low-level flying (atsb.gov.au), research has shown that an awareness of powerline location does not guarantee avoidance. In recognition of these and the other specific risks and hazards of low-level flying, the Civil Aviation Safety Authority requires pilots to receive special training and a specific low-level rating before conducting low-level operations. Even with appropriate training, flying at low-level carries a significant risk and should be avoided when there is no operational reason.
Additionally, research has shown that wearing an upper torso restraint significantly reduces the risk of serious or fatal injury. Therefore, pilots should always wear upper torso restraints when available.
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 18 April 2022, the pilot of a Cessna 172, registered VH‑REU, was conducting a private flight involving circuits[1] and touch-and-go landings[2] at Coonabarabran Aerodrome, New South Wales. The pilot was the only person on board.
The pilot had been at the aerodrome the day prior, and it was reported by a friend (who had known the pilot for a significant period) that a discussion took place about a newly-erected gate, installed to permit access to a field adjacent to the aerodrome. Part of the discussion included the position of the gate, and that it had been installed in a different location than originally decided because of its proximity to overhead powerlines.
On the day of the accident, the pilot arrived at the aerodrome at about 1530 local time. Four other people were at the aerodrome: 3 in a hangar and the friend—who was the person who had talked with the pilot the day before—on a tractor that was towing a slasher in the adjacent field (Figure 1). One of the witnesses in the hangar recalled seeing the pilot take off to the north on runway 29.
The witness on the tractor recalled seeing the pilot do 2 touch-and-go landings on runway 11, before travelling to the north behind the witness, and banking right back towards the aerodrome. At the time, the witness initially thought that the pilot may have been going to conduct an approach to runway 19, but then realised that this was probably not the case as the aircraft was not turning left, which would have been normal for the approach to runway 19.
Inset: En Route Supplement Australia (ERSA) chart of Coonabarabran Aerodrome, showing runway lengths in metres.
Source: Google Earth, annotated by the ATSB. Inset: Airservices Australia
The witness on the tractor recalled that the next time they saw the aircraft, it was about 500 m away and was travelling back towards the field at about 70 ft (or about the same height as some unused navigational aids) (Figure 2). At this time, based on the direction and height of the aircraft, the witness thought that the pilot was likely going to fly directly over the tractor. When the witness turned again, the aircraft was directly behind them, flying straight and level. The witness estimated its speed as about 80–85 kt, or fast enough to maintain control of the aircraft but not at top speed. The witness observed the aircraft contact the powerlines just behind and above the tractor and recalled hearing a whistling and crack as the wires travelled over the tractor cab.
Figure 2: Estimated flight path based on impact with powerlines and witness account
Flight path of VH-REU indicated by blue line.
Source: ATSB
The witnesses inside the hangar recalled hearing the aircraft fly past the back of the hangar with the engine sounding like what one of the witnesses described as ‘high power’. Not long after, electrical power to the hangar was lost.
After the aircraft contacted the powerlines, it impacted the ground at a steep angle, cartwheeling to the right and coming to rest just inside the boundary fence of the aerodrome. The pilot was fatally injured, and the aircraft was destroyed.
The pilot held a valid private pilot licence (aeroplane), issued in 1994 and with class ratings for multi- and single- engine aeroplanes. The pilot did not hold a low-level rating or any other operational ratings. In August 2019, the pilot reported during an aviation medical examination, that they had accumulated 2,655 flight hours. The pilot’s flight hours at the time of the accident could not be determined.
In addition to obtaining their private licence, the pilot had been involved in several aviation activities throughout their career, including involvement in aerial firefighting (in non-piloting aerial support roles) in a rotary-wing context.
The pilot held a class 2 medical certificate, valid to 30 September 2023, with no identified medical conditions. The pilot was required to have reading correction available to exercise the privileges of the licence. There were no issues identified in the post-mortem examination and toxicological results (including carbon monoxide) that may have affected the pilot’s operation of the aircraft. The pilot was also reported to have slept well in the days leading up to the accident and be in good general health.
Aircraft information
The Cessna 172 is a high-wing, all-metal, unpressurised aircraft with a fixed landing gear. VH‑REU had a single, Continental O-300-A piston engine driving a fixed-pitch propeller.
VH-REU was manufactured in 1958 with serial number 46237 and first registered in Australia in 1959. The aircraft had been owned by and registered to the pilot since 2016, and at the time of the accident had accumulated 1,046.3 hours total time in service.
The most recent maintenance for the aircraft was completed in April 2022 with a current maintenance release issued on 6 April 2022. The primary purpose for the maintenance was to complete a periodic (100–hourly) inspection and have a BendixKing Aerocruze autopilot fitted to the aircraft. In the days following installation, 2 flights totalling 2.1 hours were undertaken by the maintenance provider to check and adjust the autopilot. The only subsequent flight was a 0.9-hour flight by the owner on 14 April 2022.
Wreckage and impact information
No pre-impact defects were identified with the aircraft’s engine, flight controls or structure. There was no evidence of fire.
Damage to the aircraft and powerlines indicated that the aircraft had contacted the powerlines and then travelled about 105 m before ground impact. The aircraft impacted the ground about 57° nose-down, skidding to the right, and yawing to the left (Figure 3).
Based on a transfer of material from the airspeed indicator needle to its face, the aircraft likely impacted the ground at about 30 kt (or about 55 km/h) (Figure 4).
Figure 4: VH‑REU airspeed indicator with material transfer
Source: ATSB
The wreckage examination also showed:
damage to the left wing and strut indicated that the aircraft was likely close to level flight (about 11–12° right wing low) when it contacted the powerlines, with one of the powerlines remaining entangled with the left wing and left wing strut (Figure 5)
one of the propeller blades had marks likely from contact with the powerlines, and had a significant forward bend and tip curl, which was consistent with the engine producing power when the aircraft impacted the ground (Figure 6)
the other propeller blade was bent rearwards and had damage consistent with ground impact during the cartwheeling motion of the aircraft
liveable space in the cabin was maintained
the seat tracks were in place and the pilot’s seat was still attached to the aircraft structure
the pilot’s upper torso restraint (shoulder harness) was found stowed.[3]
Figure 6: Damage to propeller from powerlines and ground impact
Source: ATSB
Meteorological conditions
The aerodrome forecast (TAF) for Coonabarabran Aerodrome issued on 18 April 2022 and valid from midday included a forecast wind 350° at 12 kt, visibility more than 10 km, scattered cloud at 3,000 ft and temperature of 22 °C. Actual conditions at about the time of the accident were consistent with the forecast and indicated a temperature of 23° C, wind 360° at 7 kt, nil cloud with visibility greater than 10 km.
Aerodrome information
Coonabarabran Aerodrome was a certified, non-controlled aerodrome. It had a 1520-m long asphalt runway 11/29[4], and a 649-m long grass runway 01/19.
The normal circuits for all runways at Coonabarabran had left-hand patterns (turns made in the circuit were to the left).
Powerline information
The 22-kV powerlines that were struck by the aircraft consisted of a pair of 3-strand galvanised steel wires. The wires spanned across timber poles that were 314 m apart. The powerlines had to be maintained so that the wires had a clearance of 5.5 m from the ground. The powerlines at the aerodrome (including an allowance for catenary) were reportedly compliant with this requirement, and were estimated to be at a height of 21–31 ft (6–9 m) above the ground at the point of impact at the time of the accident. The nearest power pole was a terminus of the line that ran to the aerodrome (Figure 1).
The powerlines were not marked and were not required to be marked by Australian Standards (AS) 3891.1 (Permanent marking of overhead cables and their supporting structures for other than planned low level flying) or AS 3891.2.4 (Marking of overhead cables for planned low level flying operations, addressed the requirements for marking overhead cables, including powerlines).
Separately, the Civil Aviation Safety Authority detailed restrictions in the Civil Aviation Safety Regulations (CASR) Part 139 Manual of Standards (MOS) in relation to obstacles around an aerodrome. The adjacent field was located in the area defined as the aerodrome’s outer horizontal surface. In this area, markings were required on any object that was 150 m or higher. Markings were also required on any object in the take-off or approach path of aircraft. Neither of these requirements applied to the powerlines located at Coonabarabran Aerodrome.
Figure 7, looking west-north-west, shows reinstalled powerlines above the field after the accident.
Figure 7: Reinstalled powerlines in the adjacent field
Source: ATSB
Low-level rating
CASR 91.267 stated that a pilot could not fly below 500 ft (above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the aircraft) unless in certain circumstances. These circumstances included (but were not limited to) the aircraft being in the process of taking off, landing or a missed approach, or the pilot holding an approval to conduct such flights.
The CASR Part 61 MOS required that, for pilots to obtain a low-level rating, which enabled them to undertake certain operations below 500 ft (such as agricultural, aerial survey or aerial firefighting), they must first demonstrate competency against certain performance criteria. In terms of operational techniques, this required (among other things) theoretical knowledge of how to manage obstructions such as powerlines and that a pilot could plan low-level operations, specifically identify hazards, evaluate and manage risks at low level.
Survivability
When assessing whether an aircraft accident is survivable, a number of aspects need to be considered, including:
forces imparted on the aircraft occupants
occupant restraints
liveable space inside the aircraft being maintained.
ATSB analysis indicated that the level of deceleration exerted on the pilot of VH-REU during ground impact was likely to result in severe or fatal injuries.
CASR 90.105 required that the seats in the front row of an aircraft be fitted with an approved safety harness. For small aeroplanes (with maximum take-off weight less than 5,700 kg), the safety harness needed to consist of a lap belt and at least one shoulder restraint (that is, a 3-point restraint).[5]
Upper torso restraints in aircraft serve 2 purposes:
to reduce upper body flailing and subsequent contact with aircraft structures and strike hazards
to distribute acceleration forces across a larger body area to reduce local transmission of force.
Although the upper torso section of a 3-point harness (with a sash-type upper restraint) provides restraint in the forward direction, it may provide very limited lateral restraint (Douglas and others 2007). Furthermore, if the occupant moves in a lateral (side) or diagonal direction away from the shoulder harness upper mounting point, it is possible to slip out of the shoulder harness.
VH-REU was fitted with 3-point restraints in each of the 2 front seats and the 2 rear seats. The pilot’s upper torso restraint was installed to cover the left shoulder. After the initial front-right impact, the pilot remained restrained by the lap belt. The upper torso restraint was not being worn.
Previous occurrences involving low-level flying and wirestrikes
ATSB educational publications discussing occurrences prior to 2013
The 2013 ATSB educational publication Avoidable Accidents No. 1: Low-level flying (AR‑2009‑041) focused on accidents involving unnecessary and unauthorised low flying:
Recognising the risks and hazards of low-level flying, CASA requires pilots to receive special training and endorsements before they can legally conduct low-level flying. In the accidents examined, many of the pilots did not have low-level training or an endorsement to do so, and none had a legitimate reason to be flying below the minimum limits. For most private pilots, there is generally no reason to fly at low levels, except during take-off and landing, conducting a forced or precautionary landing, or to avoid adverse weather conditions.
Another 2013 ATSB publication Avoidable Accidents No. 2: Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028) detailed a wirestrike accident where the pilot was aware of the powerline location:
Studies into ‘inattentional blindness’ have shown that we fail to perceive unexpected objects (even if they appear in the field of vision) if we are not paying attention to them (for example, focusing on another object or task). Without attention, there is no perception. Thus, you are unlikely to notice an approaching wire if you are not looking for it, even if you were previously aware of it. Add to this the inherent difficulty of visually spotting wires, the likelihood of hitting a wire is increased.
AO-2014-068 Wirestrike involving Maule M-5, VH-HOG, 50 km WSW of Casino NSW on 12 April 2014
On 12 April 2014, a Maule M-5 aircraft collided with a powerline spanning the Clarence River west-south-west of Casino, New South Wales. The pilot was accompanied on the private category flight by 2 passengers. The aircraft departed controlled flight after the wirestrike and impacted the water, coming to rest inverted with the cabin submerged. A child passenger was fatally injured.
The ATSB found that the pilot ‘made a spur of the moment decision to fly along an unfamiliar section of a river at very low level and collided with a powerline.’
AO-2014-131 Wirestrike and impact with terrain involving Cessna 182L, VH-TRS at Burrumbuttock, NSW on 20 July 2014
On 20 July 2014, a Cessna 182L aircraft collided with a powerline above a paddock. Prior to hitting the powerline, witnesses observed the aircraft flying at a low height. After hitting the powerline, the aircraft rolled inverted and impacted terrain. The pilot was fatally injured, and the aircraft was destroyed.
The ATSB found that the pilot did not hold an approval to fly at low level and therefore had not received any training in the identification of hazards or in operating techniques for flight close to the ground.
Previous occurrences involving not wearing upper torso restraints
The ATSB has conducted a number of investigations that found that pilots or passengers in the front seats of small aeroplanes that were fitted with upper torso restraints were not wearing the restraint. In all cases this increased the risk of serious or fatal injury and in some accidents, was found to have exacerbated the injuries received. Examples include:
AO-2010-053 Controlled flight into terrain - Cessna 210M, VHTIJ, 59 km NE Norseman WA, 13 July 2010
AO-2012-083 Collision with terrain, Cessna Aircraft Company 182P, VH-WTS, 53 km east-north-east of Cunnamulla, Qld, 19 June 2012
AO-2012-142 Wirestrike involving Cessna 172, VH-TKI, 13 km NE of Bendigo, Victoria, 29 October 2012
AO-2016-074 Loss of control and collision with terrain, Cessna 150, VH-RXU 270 km SE Alice Springs, Northern Territory, on 12 July 2016
AO-2019-002 Loss of power on take-off and forced landing involving Cessna 182, VH-DGF, Tooradin, Victoria on 6 January 2019.
Safety analysis
Intentional low-level flight
An examination of the wreckage found no pre-impact defects involving the aircraft structure, flight controls or engine. There were no recorded issues following flights undertaken to check and adjust the autopilot after its installation, or after the aircraft had returned to Coonabarabran.
Witnesses saw and heard the aircraft operating normally, other than the abnormal flight path. If the pilot had encountered a problem while conducting circuits, there were 2 runways available for an emergency landing. However, the flight path did not align with an approach to either runway. Based on the tractor driver’s observations, the aircraft was heading directly overhead the tractor, flying straight and level at a height of about 70 ft and at a normal speed. Therefore, it was unlikely that a mechanical or other operational problem was involved.
The height of the powerlines was about 21–31 ft (6–9 m) where the impact occurred, and the aircraft was therefore at a height above the ground of about 15–25 ft at the time (allowing about 6 ft for the impact point on the wing). There was no apparent operational reason for the pilot to have been flying at such a low height over the field other than to conduct an intentional overflight of the tractor and its driver. Given the absence of operational reasons or the low flight, and the witness’s observation of the aircraft just prior to the contact with the powerlines, it is likely that the pilot was flying at low-level with an intention of flying directly overhead the friend in the tractor.
Low-level rating
The pilot did not have a low-level rating, which requires specific training on hazard identification and flying techniques when operating at low-level. Generally, a low-level rating is required for occupations or operations where there is a requirement or purpose to be flying below the minimum permitted height, that is below 500 ft. Examples of activities that would require this include agricultural, aerial survey or aerial firefighting and provide a balance between operational necessity and risk.
Although the pilot had previous exposure to low-level flying (aerial firefighting), it was not as a pilot. The pilot did not hold a low level rating and had not undergone the required training and assessment for low level flying which may have better equipped them to identify potential hazards (such as powerlines). Even with the appropriate training, flying at low levels carries a considerable risk and should be avoided when there is no operational reason.
Powerline strike
The pilot was familiar with the aerodrome and had discussed the location of the powerlines the day prior to the accident. However, even if a pilot is aware of powerline locations, this does not guarantee avoidance. There have been several previous accidents whereby pilots who have known the location of powerlines have forgotten about them. Given the difficulty to see powerlines, there is often insufficient time to react and avoid them.
The location and height of the powerlines at Coonabarabran Aerodrome meant that they were not required to be fitted with markers and they would have been very difficult to see from the air. Had markers been fitted, the pilot may have seen the powerlines earlier. Nevertheless, the powerlines were not close to any area that an aircraft would have an operational reason to be operating.
Upper torso restraints and survivability
Research by the United States National Transportation Safety Board (NTSB) and others has shown that pilots wearing the lap portion of a seatbelt only are more likely to receive a serious or fatal injury. An NTSB study published in 2011 examined the effectiveness of upper torso restraints on pilots in small aeroplanes. The study found that a pilot would be 49% more likely to receive a serious or fatal injury when wearing a lap belt only, compared to those wearing both the lap belt and upper torso restraint.
The pilot of VH-REU was not wearing the aircraft’s sash-type upper torso restraint (mounted above the pilot’s left shoulder) at the time of the accident. However, the significant right yaw at impact would have limited the effectiveness of this type of upper torso restraint. Therefore, it was not possible to determine with certainty whether, if worn, the upper torso restraint would have reduced the level of injuries in this case. Nevertheless, in many other types of accident scenarios, wearing an upper torso restraint will significantly reduce the risk of injury.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving Cessna 172, registration VH-REU, on 18 April 2022.
While the pilot was conducting a low pass at a height of 15–25 ft over a field adjacent to the aerodrome, the aircraft contacted powerlines and collided with terrain.
The pilot did not have a low-level rating, which requires specific training on hazard identification and flying techniques when operating at low level.
The powerlines that were contacted by the aircraft were not fitted with a visual marker and given the height and location of the powerlines, there was no requirement for such markers.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Essential Energy
Following the wirestrike accident involving VH-REU and in accordance with its company policy, Essential Energy field workers assessed the risk of another wirestrike to the powerlines that crossed the fields north of Coonabarabran Aerodrome. Subsequently, Essential Energy installed aerial markers to these powerlines.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the witnesses
the NSW Police Force
the Civil Aviation Safety Authority
the maintenance provider for VH-REU
Essential Energy
Warrumbungle Shire Council (aerodrome manager).
References
Douglas CA, Fildes BN, Gibson TJ, Boström O & Pintar FA 2007, ‘Factors influencing occupant-to-seat belt interaction in far-side crashes’, Annual Proceedings of the Association for the Advancement of Automotive Medicine, 51:319–39.
National Transportation Safety Board 2011, Airbag performance in general aviation restraint systems, Safety Study NTSB/SS-11/01.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the Civil Aviation Safety Authority (CASA)
Essential Energy
the maintenance provider for VH-REU
Warrumbungle Shire Council.
Submissions were received from CASA and Essential Energy. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Circuit: the specified path to be flown by aircraft operating in the vicinity of an aerodrome.
[2] Touch-and-go: a manoeuvre in which an aircraft conducts an approach, touches the runway, and immediately takes off again.
[3] The upper torso restraint (shoulder harness) was physically attached to the roof of the cabin at one end, and when in use, the other end is secured to the lap portion of the restraint.
[4] Runway numbering: represents the magnetic heading closest to the runway orientation (for example, runway 29 is oriented 292º magnetic).
[5] The shoulder harness and/or restraint is referred to as an upper torso restraint in this report.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
At 0613 Western Standard Time[1] on 16 April 2022, a Beechcraft B58 Baron (B58), registered VH‑NPT (NPT) and operated by Aviair Pty Ltd, departed Broome Airport, Western Australia, for a regular charter flight to several remote locations in northern Western Australia. The aircraft departed with the pilot, one passenger and 4 boxes of cargo on board. The flight was planned to transit through the East Kimberley Regional Airport at Kununurra (Figure 1) to refuel, then continue to Halls Creek where the passenger was to disembark, Fitzroy Crossing to unload cargo and then return to Broome via Derby.
Figure 1: Flight area
Source: Google Earth annotated by the ATSB
At 0749 WST the pilot called air traffic control (ATC) requesting traffic for a direct track to waypoint Kununurra Whiskey Foxtrot (KNXWF) for approach to runway 12 at Kununurra (Figure 2). At 0817 the pilot of NPT contacted ATC advising that they were leaving their cruising altitude of 9,000 ft on descent for Kununurra.
Figure 2: NPT flight path and Brisbane Centre radio calls
Source: Google Earth and AvPlan annotated by the ATSB
Seventeen minutes later NPT joined a straight in approach to runway 12. The pilot recalled slowing the aircraft, extending the first stage of flaps and attempting to extend the landing gear.
Upon selecting the landing gear handle, the gear down and locked indicators (3 green lights) illuminated immediately. The pilot reported that this was unusual, as normal operation required a few seconds for the landing gear to extend and the lights to illuminate. The pilot also recalled, co‑incident with the landing gear handle activation, that the landing gear warning horn erroneously activated, however no sound was heard from the landing gear motor and no decrease in aircraft performance was felt indicating gear extension. The pilot stated that these unusual indications were followed immediately by an electrical burning smell and smoke emerging from below the left side of the aircraft instrument panel, forward of the pilot’s circuit breaker panel.
About a minute later at 08:35:54 the pilot made a PAN PAN[2] call on the Brisbane Centre frequency advising of smoke and suspected fire in the cockpit. The pilot then activated the SOS[3] function on a dash mounted Spidertracks[4] unit. The pilot recalled switching off the electrical power to the aircraft and by that time flames were emanating from the same location as the previously‑observed smoke.
The pilot then expended the onboard fire extinguisher while continuing a straight in approach to runway 12 (Figure 4). However, the fire almost immediately returned, emanating from the same location, and creating significant smoke in the cockpit. The pilot reported that soon after this they lost visibility of both the instruments and the outside environment. In response, they opened the aircraft’s storm window[5] to attempt to clear the smoke and obtain a visual reference.
Figure 3: NPT approach to East Kimberley Regional Airport
Source: Google Earth, AvPlan and Airservices Australia annotated by the ATSB
Recorded flight data indicated that, at 0837, the aircraft started diverging significantly left of the extended runway centre line, crossing the Ord River at low level approximately 1.5km from the threshold of runway 12. The aircraft subsequently collided with terrain about 600m beyond the river and about 800m from the runway 12 threshold (Figure 4) and was consumed by a significant post‑impact fire.
The pilot sustained serious injuries but was able to extricate themselves and the passenger from the wreckage. The passenger later succumbed to their injuries.
Figure 4: NPT final approach and wreckage location
Source: Google Earth, AvPlan and Airservices Australia annotated by the ATSB
Context
Aircraft Information
NPT was a Beechcraft B58, low-wing, twin engine aircraft. It was manufactured in the United States in 1996 and first registered in Australia in 2012. The aircraft was fitted with 2 Continental IO-550-C piston engines driving 3 blade constant speed propellers.
NPT was acquired by the operator in 2019. It was configured for charter operations with rear club[6] seating for up to 4 passengers and front seating for 2 pilots. The aircraft was configured with dual cockpit controls.
The last 100 hourly inspection was completed 9 days prior to the accident flight. Since this time, and prior to the accident flight, the aircraft had accrued 18.7 hours of flight time.
The B58 is fitted with a fuel‑burning cabin heater in the nose of the aircraft. This heater is fed via a direct line from the left-wing leading-edge fuel tank. The fuel line traverses internally along the lower left fuselage entering the aircraft’s nose-wheel bay where the heater is located. Maintenance records indicated that the heater was infrequently used, and the pilot commented that the heater was not utilised during the accident flight.
Fire Suppression
NPT was fitted with a portable 2 kg halon fire extinguisher for emergency use by the crew. The extinguisher was located centrally between the pilots’ seats and the rearward facing passenger seats. The extinguisher was inspected and reweighed as part of the last 100 hourly inspection in accordance with Civil Aviation Safety Authority requirements.
Site and wreckage information
The initial impact point with terrain was approximately 45 m from the main wreckage location with the aircraft tracking approximately 117° and becoming inverted during the impact sequence.
Despite the aircraft being consumed by a post impact fire some of the aircraft’s contents, including several documents and personal effects were thrown clear during the impact sequence, leaving them largely unaffected.
Due to the severity of the post‑impact fire the ATSB was not able to conduct a complete wreckage examination. However, there was evidence of engine rotation prior to the impact and no evidence found of pre-existing defects in the engines or flight control components that could have contributed to the accident. The landing gear was observed in the stowed position and no landing gear impact marks were visible at the accident site.
Pilot Information
The pilot held a current Commercial Pilot License (Aeroplane) with their last flight review conducted in December 2021. They also held a:
class 1 aviation medical certificate, valid until January 2023
multi engine aircraft instrument rating with retractable undercarriage and manual propellor pitch control endorsements.
Prior to the accident flight, the pilot had accumulated approximately 2,482 hours of aeronautical experience, of which just over 120 hours were in command of the B58. The pilot had completed their most recent operational proficiency check on 9 January 2022 with a line check on the B58 carried out on 25 January 2022.
Recorded Data
The aircraft was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be.
The operator tracked each of their aircraft using a Spidertracks unit. The system consisted of a device located in each aircraft that recorded and transmitted its position at two-minute intervals and allowed the pilot to signal an emergency or alert through a dedicated button on the device.
The operator also utilised the AvPlan electronic flight bag application for pilots to undertake flight planning. The application records position information at 5‑second intervals. The pilot of NPT had a device with the application installed and active for the flight and the ATSB received data for the accident flight. This provided multiple flight parameters including ground speed and tracking details for the aircraft from the time of take-off until it collided with terrain.
In addition, the aircraft was fitted with a transponder that broadcast ADS-B[7] data to ground stations and nearby aircraft fitted with ADS-B IN. The ATSB was able to retrieve the data transmitted by this unit from ground stations operated by both Airservices Australia and other third-party receivers, including one at the East Kimberly Regional Airport.
The ATSB also obtained and reviewed relevant radio communications from the Brisbane Centre and common traffic advisory frequencies.
Meteorological Information
An aerodrome meteorological report (METAR[8] was issued by the automatic weather station at East Kimberley Regional Airport approximately 7 minutes before NPT collided with terrain. The report showed fine weather, with winds from the north at 2 kt, visibility greater than 10 km and nil cloud detected.
The ATSB also reviewed CCTV footage from the East Kimberley Regional Airport. Figure 5 shows the location of a camera covering the regular public transport apron, with the threshold of runway 12 in the background. The camera image showed, consistent with the METAR, a smoke plume rising near-vertically from the accident site approximately 3 minutes after the accident indicating little to no wind immediately after the accident.
Figure 5: Location of CCTV camera
Source: Google Earth annotated by the ATSB
Related occurrence
The ATSB identified another in-flight fire in a BE58 that contained similarities to this occurrence.
On 26 February 2014 at about 1645 local time, a Beech 58 aircraft, registered VH‑SBS, departed Darwin for Gove, Northern Territory, on a private ferry flight with a supervising pilot and pilot in‑command-under-supervision (ICUS) on board.
At about 1815, the pilot detected fumes and smoke emanating from within the cockpit. The pilot flying ICUS saw smoke and flames by their left leg adjacent to the circuit breaker panel and immediately switched off the electrical master switch. The supervising pilot seated in the right seat took control of the aircraft and commenced an immediate descent. The pilot ICUS retrieved the BCF extinguisher from underneath their seat and extinguished the fire
An engineering inspection found electrical wiring had penetrated through the heater supply fuel line causing it to arc out and burn a hole in the fuel line. With an ignition source and fuel, the fire in the cabin was started. Engineers disconnected and capped the heater fuel line and reconnected the vacuum line.
The engineer also reported that the wires had been bundled together and were rubbing on the fuel line. Inspection of the wires prior to the flight would have required the internal panel to be removed and was not a routine inspection item.
Safety advisory notice
Both the heater fuel line and the aircraft wiring of NPT were burnt away by the post impact fire, and an examination was not possible. However, the location, initiation and severity of the fire is similar to the incident detailed in AO‑2014‑040. As such, while the specific circumstances of the fire initiation and development remain under investigation, in the interest of transport safety, the ATSB has issued a safety advisory notice encouraging operators of B58 aircraft to:
note the circumstances of this accident and previous ATSB investigation AO‑2014‑040
conduct a detailed examination of the wiring and fuel line on the left side of the aircraft forward of, and behind, the pilot’s circuit breaker panel.
review the Electrical Wiring Chafing Protection section in Model Communiqué 116
review anti-chafing wiring provisions within the relevant aircraft maintenance manual to ensure serviceability of anti-chafing materials.
Further investigation
The investigation is continuing and will include analysis of recorded flight data and a review of:
the aircraft’s fuel and electrical systems
domestic and international related occurrences.
aircraft records
survivability aspects.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB wishes to acknowledge the assistance provided by the Western Australia Police Force, Helispirit and East Kimberley Regional Airport personnel during the onsite phase of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 16 April 2022, at approximately 0805 local time, the pilot of Beechcraft B58 Baron aircraft registered VH-NPT commenced a straight in approach to runway 12 at the East Kimberley Regional Airport with one passenger and 4 boxes of cargo on-board. The pilot reported that when they attempted to extend the landing gear they received multiple unusual indications, followed by an electrical burning smell, and saw smoke emerge from forward of the pilot’s circuit breaker panel near their left leg.
The pilot made a PAN-PAN call to air traffic control, activated the SOS function on the dash mounted Spider Tracks unit and recalled switching off electrical power. By this time flames were emerging from where the smoke had previously been observed. The pilot then expended the entire contents of a handheld portable fire extinguisher, however the fire quickly returned and intensified.
Flames and thick smoke filled the cockpit preventing the pilot from effectively seeing external visual references or the aircraft’s flight instruments. The aircraft subsequently diverged from the runway centreline track and collided with terrain approximately 800m from the threshold of runway 12.
Following the collision, the pilot extricated themselves from the inverted aircraft. The pilot then re‑entered the aircraft and, with limited assistance from the semi-conscious passenger, extracted them from the aircraft before it was consumed by a significant post impact fire. The passenger succumbed to their injuries and the pilot received serious injuries.
What the ATSB found
The ATSB determined that a fault associated with the landing gear electrical system likely ignited fuel from the cabin heater supply line, resulting in a significant and sustained cockpit fire.
The ATSB also determined that the pilot’s injuries were likely less severe due to the use of a 4‑point restraint. Additionally, while not required by regulation, the use of a rearward facing passenger seat is likely to reduce the severity of frontal impact‑related passenger injuries.
What has been done as a result
In response to this accident the operator reported that they:
commenced a program to install 4-point restraints in the crew seats of all their B58 aircraft
installed an additional fire extinguisher in each of their B58 aircraft
incorporated additional 100-hourly fuel line and wiring inspections in the vicinity of the heater fuel line and circuit breakers adjacent to the pilot’s seat.
The ATSB issued a Safety Advisory Notice encouraging operators of B58 aircraft to conduct a detailed examination of the wiring and heater fuel line on the left side of the aircraft, forward of and below the pilot’s circuit breaker panel.
Safety message
Damaged electrical wiring can pose a range of hazards to the safety of flight, including loss of electrical power, malfunctioning systems, and inflight fire. This hazard is further increased when wiring is proximal to lines carrying flammable liquid. Maintenance organisations and operators should review current practices for the prevention of damage to wiring and ensure that all available steps are being taken. These may include inspections, appropriate stand-offs, and utilisation of anti-chafe sleeving.
The ATSB continues to encourage the utilisation of devices that may increase the survivability in light aircraft accidents.
Four-point restraints, where available, provide increased survivability over 3-point restraints.
Where available and practical, use of rearward facing passenger seats improves frontal impact protection and survivability in an accident.
In the morning of 16 April 2022, the pilot of a Beechcraft B58 Baron (B58) registered VH-NPT (NPT) arrived at Aviair Pty Ltd, at Broome Airport to prepare for a regular charter flight to several remote locations in northern Western Australia. The operator’s duty maintenance officer (maintainer) reported that the pilot contacted them by phone before the flight, reporting a ‘fuel kind of smell’ in the aircraft’s cockpit. The maintainer recalled discussing the basics of the aircraft’s fuel system and asking the pilot to monitor the situation and report back if the smell did not go away.
The flight, with one passenger, seated in the rear right seat, and 4 boxes of cargo onboard, was planned to transit through the East Kimberley Regional Airport at Kununurra (Figure 1), refuel, then continue to Halls Creek where the passenger was to disembark, Fitzroy Crossing to unload cargo and then return to Broome via Derby.
The aircraft departed Broome at 0613 local time and climbed to 9,000 ft while tracking to the north-east. The maintainer, reported that at 0628 the pilot contacted them again, advising that the ’fuel like smell’ detected on the ground was no longer present.
At 0749 the pilot contacted air traffic control (ATC) and requested traffic for a direct track to waypoint Kununurra Whiskey Foxtrot (KNXWF) for an approach to runway 12 at Kununurra (Figure 2). At 0817 the pilot of NPT contacted ATC advising that they were leaving their cruising altitude of 9,000 ft on descent for Kununurra.
Figure 2: NPT flight path and Brisbane Centre radio calls
Source: Google Earth and AvPlan annotated by the ATSB
Seventeen minutes later NPT joined a straight in approach to runway 12. The pilot recalled slowing the aircraft, extending the first stage of flaps, and attempting to extend the landing gear.
Upon selecting the landing gear handle to the down position, the gear down and locked indicators (3 green lights) illuminated immediately. The pilot reported that this was unusual, as normal operation required a few seconds for the landing gear to extend and the lights to illuminate. However, no sound was heard from the landing gear motor and no decrease in aircraft performance was felt that would indicate gear had extended. The pilot also recalled, co‑incident with the landing gear handle activation, that the landing gear warning horn erroneously activated. The pilot stated that these unusual indications were followed immediately by an electrical burning smell and smoke emerging from below the left side of the aircraft instrument panel, forward of the pilot’s circuit breaker panel.
About a minute later, at 0836, the pilot made a PAN-PAN[1] call on the Brisbane Centre frequency advising of smoke and suspected fire in the cockpit. The pilot then activated the SOS[2] function on a dash mounted Spider Tracks[3] unit. The pilot recalled switching off the electrical power to the aircraft, in accordance with the electrical smoke and fire emergency procedure. They also reported switching off the avionics master switch (see the section titled Electrical system) as an additional precaution. By that time flames were emanating from the same location as the previously observed smoke.
The pilot then expended the entire contents of the aircraft’s handheld portable fire extinguisher, while continuing the straight in approach to runway 12 (Figure 3). However, the fire almost immediately returned, emanating from the same location, with flame and significant smoke in the cockpit. The pilot reported difficulty maintaining control of the aircraft as their left hand and leg were exposed directly to the flames and the smoke prevented them seeing both the instruments and the outside environment. In response, they opened the aircraft’s storm window[4] in an attempt to clear the smoke and obtain a visual reference.
Figure 3: NPT approach to East Kimberley Regional Airport
Source: Google Earth, AvPlan and Airservices Australia, annotated by the ATSB
As the aircraft approached the Ord River, multiple airborne witnesses reported that it appeared to be below the standard approach profile and ‘skimming the treetops.’
Recorded flight data indicated that, at 0837, the aircraft started diverging left of the extended runway centre line, crossing the Ord River at low level approximately 1.5 km from the threshold of runway 12. The aircraft subsequently collided with terrain, coming to rest inverted about 600 m beyond the river and about 800 m from the runway 12 threshold (Figure 3) and was consumed by a significant post‑impact fire.
Several pilots who were listening to the Brisbane Centre frequency reported hearing a transmission of static at the approximate time of the collision with terrain.
The pilot reported difficulty in releasing themselves from the restraint and exiting the inverted aircraft. After exiting the aircraft, they attempted to access the passenger through the rear doors but were unable to due to the presence of significant smoke and flame. The pilot then re‑entered the aircraft through the crew door and located the passenger who was still secured in their restraint. The pilot, with limited assistance from the semi‑conscious passenger, undid the restraint and proceeded to extract the passenger from the aircraft. Shortly after the pilot and passenger exited the aircraft, the pilot collapsed, and operator personnel arrived and moved them to a safe distance from the wreckage.
The passenger succumbed to their injuries at the accident site. The pilot suffered serious injuries and was airlifted from the site to East Kimberley Regional Airport for transfer to the Kununurra Hospital before being transferred to Darwin for further treatment.
NPT was a Beechcraft B58, low-wing, twin engine aircraft (Figure 4). It was manufactured in the United States in 1996 and first registered in Australia in 2012. The aircraft was fitted with 2 Continental IO-550-C piston engines, driving 3‑blade constant‑speed propellers.
Figure 4: VH-NPT at the time it was purchased by the operator
Source: Operator
NPT was acquired by the operator in 2019. It was configured for charter operations with seating for up to 4 passengers in a club[5] configuration and seating for 2 pilots. The aircraft was configured with dual flight controls.
Access to the aircraft was through one of 2 doors, a crew door located on the front right of the aircraft next to the co-pilot’s seat, providing access to the front seats. Two rear or ‘barn doors’ on the right side of the aircraft provide access to the rear cabin for the loading of persons and freight (Figure 5). The aircraft was also fitted with an emergency exit window on the left side of the aircraft next to the left rearward facing passenger seat. This window could be opened by a passenger in the event of an emergency. The pilot reported that instruction on its operation was included in the pre-flight briefing to the passenger.
Figure 5: Aircraft schematic identifying location of key elements
Prior to departure the pilot determined that the aircraft would be within weight and balance limitations for each leg of the flight using the operator’s approved spreadsheet for NPT. The ATSB obtained a copy of the approved spreadsheet for NPT and confirmed the pilot’s calculations. This assessment also indicated that for the legs of the flight that the passenger was onboard, the aircraft remained within balance limits irrespective of the seat occupied by the passenger.
In accordance with the manufacturer’s requirements, NPT was fitted with a handheld portable 2 kg halon fire extinguisher for emergency use by the crew. The extinguisher was located centrally between the pilots’ seats and the rearward facing passenger seats. The extinguisher was inspected and reweighed as part of the last 100 hourly inspection in accordance with Civil Aviation Safety Authority requirements.
The pilot commented that, while they were able to access and utilise the extinguisher, its positioning made it more difficult to access in the event of an emergency than in other aircraft within the fleet.
Aircraft power was supplied by a single battery and an alternator fitted to each of the aircraft’s 2 engines. These power sources could be connected and disconnected individually using 3 separate switches on the pilot’s sub‑panel labelled ‘MASTER’ (Figure 6). To protect the avionics from electrical damage when the master switches were being operated, a separate ‘AVIONICS MASTER’ switch (Figure 6) controlled power to these devices. The ‘AVIONICS MASTER’ was dependant on the ‘MASTER’ switches in the control hierarchy, meaning that if the ‘MASTER’ switches were off, the ‘AVIONICS MASTER’ was not able to be powered.
Figure 6: Schematic of the pilot’s subpanel showing master power and landing gear controls
Source: Manufacturer annotated by the ATSB
Electrical power was supplied to several systems including drive motors for the landing gear and flaps, aircraft lighting, avionics and communications. A circuit breaker panel on the pilot’s left side protects the circuits from overload and damage. Wiring was routed from the circuit breaker and instrument panels down along the left side of the aircraft in a series of looms. Figure 7 shows the area forward of the circuit breaker panel and below the pilot’s instrument panel in an exemplar aircraft.
Figure 7: Circuit breaker and instrument panel of an exemplar B58 showing the position of wiring looms.
Source: Operator annotated by the ATSB.
Based on the pilot’s report of the abnormal landing gear behaviour, the ATSB conducted a detailed examination of the system function. The landing gear system consists of:
a motor driving the gear between the extended and retracted positions
an indicating system that identifies to the pilot when the gear is retracted, extended or in transit
an aural alert that the gear is not extended if the aircraft is otherwise configured for landing.
Landing gear motor
The landing gear handle (Figure 6) acts as an electrical switch closing either the retract or extend landing gear motor circuit and powering the motor. Current flows through the switch and landing gear limit switches[6] to the motor relays. They are connected to the pilot’s circuit breaker panel by wiring on the left side of the aircraft and protected by a 5-amp circuit breaker. The relays operate a separate 30-amp circuit providing power directly to the landing gear motor. The switches and relays within the gear motor system provide power, with the motor constantly grounded. The landing gear motor is located below the floor of the aircraft between the crew and passenger seats.
Landing gear indication
The landing gear indication system consists of 4 lights, including one for each of the left, right and nose gears indicating they are in the down and locked position. A fourth light indicates that the gear is in transit. The lights are positioned above the gear handle on the instrument panel on the pilot’s subpanel assembly (Figure 6).
The lights are connected to down-lock and up-lock switches on each of the gear. The in-transit light is illuminated when either the down-lock or up-lock switches on any of the gear are not depressed. Once the down lock switches on each gear is closed, the light for that gear is switched on and once all 3 down lock switches are activated, the in-transit light switches off. These lights are connected to a 5-amp power supply and are switched on by grounding the circuit through these switches.
Landing gear warning
The landing gear warning system warns the pilot if the aircraft is incorrectly configured for landing due to the gear not being extended. The system consists of a warning horn connected to flap, throttle, and landing gear position switches. The horn will activate if the flaps are extended to full and the throttles are retarded while the landing gear is selected up.
The wiring for these systems, and several other electrical systems, are bundled together in the area where the pilot reported the fire started. The ATSB’s review of the aircraft electrical wiring schematics was not able to identify a single point of failure, either through a short between systems or to ground or an open circuit, which could have caused all 3 symptoms that the pilot reported. However, the bundling of multiple wires and the possibility of live circuits contacting one another meant that a multiple point failure in the landing gear, or within other electrical circuits, leading to the symptoms the pilot reported was possible.
After the pilot selected the landing gear to the down position and the fire commenced, the pilot reported switching off the aircraft’s electrical power and that the aircraft’s avionics screens went black. Spider Tracks data (see the section titled Recorded data) ceased shortly after this, however the aircraft’s ADS-B transponder continued to transmit (see the section titled Recorded data) until just before the aircraft collided with terrain. Following the PAN-PAN, no radio transmissions from the aircraft were recorded on the Brisbane Centre frequency. However, multiple pilots operating in the area at the time reported significant static on this frequency at approximately the time the aircraft collided with terrain, possibly indicating that NPT’s radio was powered.
The B58 is fitted with a fuel‑burning cabin heater in the nose of the aircraft (Figure 5). Maintenance records indicated that the heater was infrequently used, and the pilot advised that the heater was not utilised during the accident flight. In the 12 months leading up to the most recent 100 hourly inspection the heater had been used for 102.5 of the aircraft’s accumulated 1,077 hours, of which only 3.3 had been accrued in the last 6 months. The heater’s hour count following the 100 hourly inspection was unable to be determined due to the post impact fire.
The heater is supplied with fuel via a direct line from the left-wing leading-edge fuel tank. The fuel line is attached to the tank at the wing root and traverses internally along the lower left fuselage. It passes through the aircraft cockpit below the pilot’s circuit breaker panel (Figure 6). The line then enters the aircraft’s nose-wheel bay and connects to the heater. The line fills with fuel as the tank is filled and will remain full of fuel at all normal flight attitudes. The line is secured at multiple locations with clamps to prevent damage from contact with the aircraft’s structure.
When the heater is running, fuel flows through the line at a rate of about 4 litres per hour.
The last 100 hourly inspection was completed 9 days prior to the accident flight. Since that time, and prior to the accident flight, the aircraft had accrued 18.7 hours of flight time.
Concurrent with the 100 hourly inspection, additional maintenance tasks were carried out on NPT. One of these tasks was a repair to the leading-edge fuel tank in the aircraft’s left wing. A leak was identified during a post maintenance fuel leak check and traced to a gasket on the tank. Maintenance records indicated that the fuel bladder was manoeuvred to access and replace the leaking gasket. Records did not indicate if the line to the cabin heater was disconnected prior to the maintenance taking place. Following the repair to the gasket a further post maintenance leak check was carried out with nil defects identified. The aircraft manufacturer’s 100 hourly inspection required that the heater be inspected in accordance with the heater manufacturer’s manual. The manual required an operational check of the heater, including at least 2 operational cycles.
The ATSB reviewed the aircraft’s logbook and maintenance release, no references were identified to a fuel leak or a potential fuel smell in the cockpit between the time the 100 hourly was completed and the accident flight.
NPT was fitted with 2 types of restraints, 4-point harnesses for the crew seats and 3-point harnesses for both the forward and rearward facing passenger seats in the main cabin. The 4‑point harnesses fitted to the crew seats were not original equipment and had been retrofitted to the aircraft prior to its purchase by the operator, replacing the existing 3-point harnesses. These restraints were in accordance with or exceeded regulatory requirements (see the section titled Survivability - Restraints).
The B58 was certified under Part 3 of the United States Civil Air Regulations as amended in 1956, which required that materials making up the cabin interior be ’flash resistant’, or ’flame resistant’ if the compartment could be used for smoking.
The type certificate data sheet for the B58 required placarding that the aircraft was non-smoking for serial numbers TH-2173 and later. The interior of NPT, being an earlier serial number, was required to meet the standard for a flame-resistant interior.
Flame resistant materials are required to resist flame advance of more than 4 inches per minute. Flash resistance required average flame advance to be less than 20 inches per minute.
These progression rates are tested under controlled conditions in accordance with FAA advisory circular 23-2A. The tests are conducted on the materials in isolation and do not account for accelerants being present.
The initial collision point with terrain was approximately 45 m from the main wreckage location with the aircraft tracking approximately 117° and becoming inverted during the impact sequence.
Despite the aircraft being consumed by a post impact fire some of the aircraft’s contents, including several documents and personal effects were ejected during the impact sequence, leaving them largely unaffected.
Due to the severity of the post‑impact fire, the ATSB was not able to conduct a complete wreckage examination. However, there was evidence of engine rotation prior to the collision with terrain and no evidence found of pre-existing defects in the engines or flight control components that could have contributed to the accident. The landing gear was observed in the stowed position and no landing gear impact marks were visible at the accident site.
During the impact sequence the aircraft’s windscreen fractured and was liberated from the fuselage in multiple pieces. Some of these pieces, were clear of the post‑impact fire and were located nearby in long grass with their internal surfaces facing down.
The ATSB was able to reassemble almost the entire windscreen on-site (Figure 8). Once reassembled a soot trail was visible on the internal surface of the left side of the windscreen. The trail, emanating from the bottom of the windscreen, was approximately 34 centimetres from the left edge. The soot was of sufficient thickness that a clearly visible trail was able to be wiped into it. At the point where the soot trail initiated, the windscreen material exhibited a different failure mode, likely associated with significant heat.
Due to environmental conditions on-site the soot trail was not easily visible in captured image. The outside surface of the windscreen was subsequently marked on site with yellow paint marker identifying lateral extremities of the soot trail.
Source: ATSB
The upper, aft corner of the pilot’s storm window surround (Figure 9) was located with the outer surface down, closer to the post‑impact fire than the windscreen. Soot was located on both sides with the external surface, consistent with soot being drawn out of the window by the airflow.
Figure 9: Smoke and soot indications on window surfaces adjoining the pilots storm window
Due to fire damage to the flap actuators, the specific position of the flaps at impact was unable to be determined. The aircraft’s flap tracks were recovered for further examination at the ATSB’s technical facilities in Canberra. Impact markings on the flap tracks indicated that the flaps were likely extended to the first of the 2 flap positions (15°) at the time of impact (Figure 10). This corresponded with both the pilot’s report of having extended the flaps one position prior to activating the landing gear and the operator’s procedures that required first stage flap extension as part of the setup of the aircraft for the approach.
Figure 10: Left inboard flap track with markings indicating likely flap position at impact
In response to witness reports that the aircraft skimmed trees prior to the ground collision, the operator conducted an airborne search on the western side of the Ord River. This search identified a grouping of 4 trees in the approach to runway 12 that had damage consistent with aircraft contact.
The trees were approximately 500 m west of the river and 60 m north of the extended runway 12 centreline (Figure 11). Their position was consistent with the aircraft’s approach path, and were close to the lowest point in the aircraft’s flight path data on the western side of the Ord River. Tree damage was between 15 and 20 ft above ground level and the direction of the breaks and fallen limbs were consistent with the aircraft’s direction of travel.
Figure 11: Possible tree strike location
Source: Google Earth, Operator, AvPlan and Airservices Australia, annotated by the ATSB
Other than evidence of a collision with a number of small trees at the accident site, no additional tree strikes were identified, and no evidence of a foliage strike was located on the wreckage, however the significant fire damage prevented a detailed examination.
The pilot held a current Commercial Pilot License (Aeroplane), with their last flight review conducted in December 2021. They also held a:
Class 1 aviation medical certificate, valid until January 2023
multi engine aircraft instrument rating with retractable undercarriage and manual propellor pitch control endorsements.
Prior to the accident flight, the pilot had accumulated approximately 2,482 hours of aeronautical experience, of which just over 120 hours were in command of the B58. The pilot had completed their most recent operational proficiency check on 9 January 2022 and a line check in the B58 was carried out on 25 January 2022.
An aerodrome meteorological report (METAR[7]) was issued by the automatic weather station at East Kimberley Regional Airport approximately 7 minutes before the accident. The report showed fine weather, with winds from the north at 2 kt, visibility greater than 10 km and nil cloud detected.
The ATSB also reviewed CCTV footage from the East Kimberley Regional Airport, which captured the smoke plume from the accident. Figure 12 shows the location of a camera covering the regular public transport apron. The camera image showed a smoke plume rising near-vertically from the accident site approximately 3 minutes after the accident indicating little to no wind immediately after the accident, consistent with the METAR.
In reviewing the survivability aspects of this accident, the ATSB sought expert guidance from the Royal Australian Air Force Institute of Aviation Medicine (IAM). Their report formed the basis of the following section.
Injuries to aircraft occupants arising from traumatic contact with aircraft structure occur at least 5 times more often than acceleration‑related injury. Within small aircraft that have confined interiors, lap belts and upper torso restraints are critical to crash survivability for both crew and passengers. The restraint of the upper body serves 2 purposes:
reducing the likelihood of impacting structures by minimising body flailing
distributing forces more widely across the body, making them more likely to be survivable.
Upper torso restraints can be provided with a single shoulder strap, like that used in a car seatbelt or 2 straps, one over each shoulder. Figure 13, below, shows the difference between 2-, 3- and 4-point restraints. The image also shows a 5-point restraint that has a crotch strap which provides additional protection for the wearer, preventing them from ‘submarining’ or sliding under the lap portion of the restraint.
Figure 13: Aircraft restraint types.
Source: United States Department of the Interior via IAM
Both 3- and 4-point harnesses restrain the upper torso. However, the 3-point only provides lateral restraint in one direction, if the person flails to the unrestrained side they may come out of the shoulder strap rendering it ineffective. Additionally, with only one strap over the torso, the 3‑point restraint has a smaller surface area than the 4-point, increasing the force exerted to the restrained area on the wearer.
In accordance with Civil Aviation Safety Regulation (CASR) 90.105 the flight crew seats must be fitted with a restraint that consists of a lap belt and at least one shoulder strap. Requirements for occupant restraints are outlined in CASR 90.110 and require all occupant seats for aircraft with less than 10 seats and manufactured after 13 December 1986 to be fitted with an approved seat belt and shoulder harness.
It is generally accepted that in the event of a frontal impact a rearward facing seat will increase survivability in two ways.
Spreading the impact force over the entire surface of the back rather than specific areas where a restraint is positioned.
Limiting the movement of the head through flexion and extension of the neck, provided the seat is fitted with an appropriately positioned headrest.
There is no Australian regulatory requirement for the use of rearward facing seats. Their use is subject to availability and based on a range of operational considerations. These include weight and balance, emergency egress, other payload items (cargo), company procedure and passenger and pilot comfort. The ATSB recovered all seat frames from the aircraft wreckage. However, due to the severity of the post‑impact fire the ATSB was not able to conduct a detailed assessment and determine their effectiveness in attenuating impact forces and any subsequent effect on survivability.
IAM reviewed the hospital and post-mortem records of the pilot and passenger respectively and provided a summary of their injuries. Both the passenger and the pilot received injuries attributable to both the fire and the collision with terrain. While there were some similarities in the injury profiles, the passenger’s injuries included more severe burns and trauma to the neck and chest, consistent with a single shoulder restraint and flailing within the aircraft, that the pilot did not suffer.
The last non-SOS Spider Tracks data point, available to the nearest minute was recorded at 0835. Immediately after this, still at 0835, two ’SOS Opened’ data points were recorded, indicating that the SOS function has been activated. No further data was received by the operator.
The SOS function increases the frequency of the data transmissions to 10-15 second intervals rather than the standard 2 minutes. Data from the pilot’s electronic flight bag (EFB) application indicated that the aircraft collided with terrain at 0837. If the Spider Tracks unit had remained powered after the 2 SOS data points at least 8 further transmissions should have been received. If the activation of the SOS function had not triggered the increase in data frequency, then one more point may have been received at 0837, depending on the exact time that the 0835 data point was transmitted.
The operator advised that the Spider Tracks unit was connected to aircraft power and the loss of signal from the Spider Tracks indicated a loss of electrical power to the aircraft.
The operator utilised the AvPlan EFB application for pilots to undertake flight planning tasks, access electronic information, such as charts or relevant documentation and depending on the settings, display nearby traffic. The application can also record aircraft position information at 5‑second intervals. The pilot of NPT had a device with the application installed and active for the flight, for which the ATSB received data. This provided multiple flight parameters including ground speed and tracking details for the aircraft from the time of take-off until it collided with terrain.
The device was powered by an internal battery. However, it could be connected to aircraft power to keep the battery charged. The loss of aircraft power would not reduce the functionality of the device or effect the data recorded while the battery maintained its charge.
The aircraft was fitted with a transponder that broadcast ADS-B[8] data to ground stations and nearby aircraft fitted with ADS-B IN. The ATSB retrieved the data transmitted by this unit from ground stations operated by both Airservices Australia and other third-party receivers, including one at the East Kimberly Regional Airport.
Data obtained from the receivers operated by Airservices Australia and several third-party receivers, recorded the aircraft’s location from Broome until 0835 when the aircraft started the approach to runway 12 at East Kimberley Regional Airport. The signal was then lost, likely due to the aircraft’s descent taking it below the coverage altitude for these receivers.
An ADS-B receiver at the East Kimberley Regional Airport received data from the aircraft between 0834 and 0837. This recorded the aircraft passing KNXWF and commencing the approach to the East Kimberley Regional Airport. The final position report was received at 0836:43. Between 0836:43 and 0837:12 eight more data packets were received containing NPT’s mode S transponder code, however position information was not included.
The aircraft was fitted with a GTX33 ADS-B transponder unit, which was not equipped with an internal backup battery.
The ATSB identified one occurrence in Australia and 3 in the United States that had similarities to this accident. These 4 occurrences involve in-flight fires accelerated by combustible hydrocarbons that were initiated by damaged electrical wiring. Each of these fires were different, with 2 relating to direct feeding fuel and oil gauges (which NPT was not fitted with), one was an engine fire, and one was a cockpit fire that was controllable. While different in detail, they all demonstrate the risks when electrical wiring and combustible hydrocarbons such as fuel and oil are in proximity.
On 26 February 2014 at about 1645 local time, a Beech 58 aircraft, registered VH‑SBS, departed Darwin for Gove, Northern Territory, on a private ferry flight with a supervising pilot and pilot in‑command-under-supervision (ICUS) on board.
At about 1815, the pilot flying ICUS saw smoke and flames by their left leg adjacent to the circuit breaker panel and immediately switched off the electrical master switch. The supervising pilot seated in the right seat took control of the aircraft and commenced an immediate descent. The pilot ICUS retrieved the fire extinguisher from underneath their seat and extinguished the fire.
An engineering inspection found electrical wiring penetrated through the heater supply fuel line causing it to arc and burn a hole in the fuel line. The wires had been bundled together and were rubbing on the fuel line.
Between 1983 and 2022 the NTSB’s public database identified 7 investigations where an inflight fire or explosion was listed as a factor. Of these, 3 were identified to be of particular relevance and are summarised below.
MIA00FA221
On 17 July 2000, approximately 7 minutes after departing Memphis Tennessee, the pilot of a B58 aircraft registered N158MT, serial number TH-1186, contacted ATC reporting that they had an electrical fire and were going to switch off the master. Following two further communications with ATC the aircraft collided with water at Arkabutla Lake. Witnesses reported seeing a ’vapor trail’ or ’dust’ coming from the aircraft. The pilot was fatally injured, and the aircraft was destroyed.
The NTSB investigation identified that the fire was likely the result of arcing of an electrical wire behind the pilot’s instrument panel and associated heat‑related cracking to fuel and oil lines that feed direct reading pressure gauges for fuel and oil pressure in the cockpit. The investigation also identified that the pilot had not switched off the engine alternator switches in accordance with the electrical smoke and fire emergency checklist.
SEA02FA023
During take-off, on 2 January 2002, the pilot of a B58 aircraft registered N132Z, serial number TJ‑284, identified a fire in the aircraft’s left engine. The pilot reduced power and landed the aircraft on the remaining runway. The pilot and the passenger evacuated the aircraft, which sustained substantial damage.
Further inspection identified that an improper clearance had allowed an alternator wire to chafe against a pneumatic line in the engine bay. The exposed wire subsequently arced to the aluminium line igniting fuel vapor. The most probable cause of the accumulated fuel vapor was from a fuel cell leak that had previously been repaired.
ERA11FA312
On 25 May 2011, a B58 aircraft, registered N77AR, serial number TH-757, with a pilot and 3 passengers on board was conducting a flight from Atlanta, Georgia to Hazard, Kentucky. At 1612 local time the pilot contacted ATC to advise they were declaring an emergency due to a fire on board. No further radio transmissions were received. ATC recorded 7 further transponder and 2 primary radar returns. Several witnesses observed the aircraft in its final stages of flight before it collided with terrain at approximately 1613 local time. The 4 occupants were fatally injured, and the aircraft was consumed by a post‑impact fire.
The NTSB investigation identified that an in-flight fire likely initiated in the right front cockpit area forward of the instrument panel and below the glare shield. While the NTSB was unable to conclusively determine the origin of the fire, their analysis notes that the speed of the fire’s advance was consistent with a fuel fed fire. The analysis also identified that the area where the fire was believed to have initiated was an area that is near the direct‑reading oil pressure gauges.
This report noted that B58 and 58A models with serial number TH-001 through TH-1193 were fitted with direct‑reading fuel flow and pressure indicators in the cockpit. Direct‑reading pressure indicators use a direct line from the engine to the cockpit for presentation of engine fuel pressure. The report noted that aircraft with serial number TH-1194 and later (NPT serial number TH-1769) were fitted with remote fuel flow indicators, removing the need for fuel lines to go directly to the cockpit.
At 0834 local time on 16 April 2022, the pilot of B58 Baron aircraft registered VH-NPT commenced a straight in approach to runway 12 at the East Kimberley Regional Airport at Kununurra. During the approach the pilot declared a PAN-PAN to air traffic control reporting smoke and suspected fire in the aircraft’s cockpit.
The pilot continued the approach, diverging from the runway centreline track as they crossed the Ord River. The aircraft collided with terrain on the eastern side of the Ord River approximately 800 m from the runway 12 threshold. The passenger sustained fatal injuries and the pilot sustained serious injuries.
The following analysis will examine the in-flight fire, looking at the sources of initiation and acceleration, the pilot’s loss of visual cues and factors that affected survivability.
The pilot reported that smoke and subsequently flame emerged from below the left side of the instrument panel, below and forward of the circuit breaker panel. The pilot attempted to extinguish the fire with a portable handheld fire extinguisher. The extinguisher suppressed the fire, however once removed, the fire returned vigorously.
Within 90 seconds of the pilot declaring the PAN-PAN, the aircraft had collided with terrain. The pilot sustained serious burns to their left side and the pilot and passenger sustained fire‑related respiratory injuries.
Materials used in the interior trim of NPT were required to be flame-resistant. The fire progressed at a speed greater than what would be expected of flame-resistant materials, consistent with the fire being fuelled by an accelerant.
Several lines and multiple looms of electrical wiring pass through the area where the pilot reported that the fire initiated. The lines contain pitot and static air for instruments, air conditioning system gasses and the fuel line to the aircraft’s cabin heater. Of these, the fuel line to the cabin heater provided the only source for flammable liquid to accelerate the fire.
A breach in the fuel line forward of and below the pilot’s circuit breaker panel would allow fuel to enter the area behind the side wall trim panel, possibly being absorbed by the fibreglass insulation. This would provide a high energy acceleration source capable of overcoming the flammability resistance of the trim materials. A direct examination of the line, surrounding insultation and the trim panel was not possible due to the post impact fire. As a result, the integrity of the heater line was unable to be established.
Two possible scenarios were considered for when a breach in the fuel line may have occurred. The first was that the leak was initiated at the time the pilot detected the smoke. This would show significant similarity to the previous Australian occurrence (AO-2014-040) whereby the breach in the fuel line initiated and provided an accelerant for the fire. However, in the 2014 occurrence, the leak was small, and the fire was comparatively controllable. In the event of a larger breach, or the line fracturing, fuel would be liberated more quickly, decreasing the chances of controlling the fire effectively.
The second scenario considered fuel to have been leaking for some time prior to the initiation of the fire. If the fuel had been leaking previously this would allow accelerant to accumulate behind the trim panel and in the insulation. In this scenario a smaller leak could lead to the same issues controlling the fire as a larger breach occurring due to the accumulated fuel.
The pilot’s report of a ‘fuel like smell’ in the cockpit on the morning of the accident may support the line having been breached at some point prior to the aircraft taking off. However, the pilot reported that the smell was no longer present once airborne. Additionally, there was no reported evidence of fuel spillage on the ground and the aircraft had passed its fuel leak check following maintenance 18 flight hours earlier.
Due to the post impact fire damage the ATSB was unable to determine which of the 2 scenarios were more likely. However, once the fire was initiated, given its location, it would very likely have quickly burned through the heater line liberating fuel that remained in the line further accelerating the fire and contributing to its rapid return after the pilot suppressed it with the portable handheld fire extinguisher.
The electrical burning smell reported by the pilot immediately before the smoke and subsequent flames were observed supports the fire being initiated by a fault in the electrical system. The pilot reported that all systems had been operating normally until the landing gear handle was selected to the down position. Following the operation of the landing gear handle the pilot reported that the landing gear did not extend and there were multiple abnormal landing gear system indications.
Wiring for both the indication and operational systems are contained in wiring looms that pass through the area where the pilot first observed the smoke. These looms run near one another and the aircraft structure. Undetected damage could occur to or within the wiring looms, providing an ignition source from chafing, overheating of wiring or wires shorting to another wire or the airframe. Due to the destruction of the aircraft wreckage the ATSB was not able to determine the exact sequence of events that led to the electrical fault, the initiation of the fire and the other electrical anomalies that occurred.
Despite that, previous occurrences in both Australia and the United States show the danger that damaged electrical wiring can pose in areas with flammable liquid lines.
As the fire advanced it generated a large amount of heat and smoke in the cockpit as reported by the pilot and evidenced by the soot on the internal surfaces of the aircraft windscreen and the pilot’s storm window surround, both of which were separated from the post‑impact fire. The extent of this smoke likely prevented the pilot from being able to see visual cues external to the aircraft or to effectively use the instruments as a reference. That situation, combined with the direct heat of the fire, meant that the pilot was presented with significant difficulty retaining control of the aircraft.
Following the PAN PAN call the aircraft descended below the normal approach profile; however, the pilot was able to maintain the approach track until crossing the Ord River when the aircraft diverged to the left of the extended runway centreline. The pilot was subsequently able to regain the approach heading prior to the aircraft colliding with terrain.
The survivability of the accident can be broken down into the environment within the aircraft prior to and after the collision and the impact forces related to the collision.
The fire generated significant heat and smoke in the aircraft’s cockpit. The reports of the pilot and the respiratory injuries to both occupants indicate that they were unable to effectively vent the smoke.
With the pilot able to self-extract after the collision, the passenger continued to be exposed to the environmental conditions within the aircraft until the pilot was able to re-enter the aircraft to extract them. This likely reduced the passenger’s chances of survival.
The pilot reported that they and the passenger were secured in their restraints at the time the aircraft collided with terrain. The pilot, in the left control seat was in a 4-point harness and the passenger, in the rear right seat, was in a 3-point harness. Generally, the 4-point harness improves survivability in 2 ways. Firstly, it better attenuates the impact forces, by spreading them more broadly over the body. Secondly, it secures the occupant more effectively laterally reducing flailing. This decreases the likelihood of injuries due to contact with obstructions or structure of the aircraft.
The primary difference in injuries between the 2 occupants of the aircraft was the chest and other trauma present in the passenger. This trauma was consistent with the differences between the use of a 3-point and 4-point restraint. The 3-point restraint did not distribute forces as evenly across the body and allowed significant multi-directional movement (flailing) inside the aircraft.
Based on advice from the manufacturer, operator and ATSB research a 4-point restraint is not available for the rear seat of B58 aircraft. However, this accident demonstrates the fitment of the 4-point harness to the crew seats, can improve survivability over the 3-point restraint that is required under the regulations.
NPT was fitted with a club passenger seating configuration, with 2 forward facing and 2 rearward facing seats. As the pilot and passenger were seated in forward facing seats a comparison of injury profiles due to forward or rearward facing seats was not possible. However, the available literature supports that in the event of a frontal impact the rearward facing seat will provide better restraint of the occupant. By both spreading impact force more evenly over the whole back and reducing the potential for flailing by forcing the body into the seat.
For this flight, the ATSB reviewed the weight and balance documentation, determining that the aircraft remained within limits regardless of where the passenger or the cargo were positioned. Additionally, due to the size of the cabin, the passenger’s emergency egress route would not have been altered by changing positions.
Recognising that, when flight planning, pilots have many operational considerations when it comes to passenger positioning, in the event of a frontal impact, such as a collision with terrain, a rearward facing seat will generally better protect the occupant and increase their chances of survival.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the In-flight fire and collision with terrain involving Beechcraft B58 Baron, VH-NPT near East Kimberley Regional Airport, Kununurra, Western Australia on 16 April 2022.
On approach to runway 12 at Kununurra, a fault associated with the landing gear electrical system likely ignited fuel from the cabin heater supply line, resulting in a significant and sustained cockpit fire.
Due to smoke in the cockpit, the pilot lost visual reference to both the instruments and outside environment. This, combined with the direct exposure to flames, led to a divergence from the extended runway centre line and the aircraft impacting terrain off the airfield.
The 4-point harness that was installed for the pilot provided better restraint and attenuation of impact forces compared to the best available option of a 3-point restraint in the rear, leading to less severe impact related injuries.
The aircraft’s passenger cabin had a ‘club’ configuration with 2 forward and 2 rearward facing seats. Although not a requirement, positioning the passenger in rearward facing seat would have likely improved survivability from frontal impact‑related injuries.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Aviair Pty Ltd.
In response to this accident the operator reported that they
commenced a program to install 4-point restraints in the crew seats of all their B58 aircraft
installed an additional fire extinguisher in each of their B58 aircraft,
incorporated additional 100-hourly fuel line and wiring inspections in the vicinity of the heater fuel line and circuit breakers adjacent to the pilot’s seat.
Safety advisory notice to operators of B58 aircraft
In conjunction with the preliminary report released on 21 September 2022, the ATSB issued a Safety Advisory Notice to all B58 operators encouraging them to:
note the circumstances of this accident and previous ATSB investigation AO‑2014‑040
conduct a detailed examination of the wiring and fuel line on the left side of the aircraft forward of, and below, the pilot’s circuit breaker panel.
A copy of the Safety Advisory Notice can be found on the ATSB website here.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
operator
Civil Aviation Safety Authority
aircraft manufacturer
Royal Australian Air Force Institute of Aviation Medicine
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] PAN-PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[2] SOS function is an emergency transmission from the Spider Tracks unit that alerts predetermined personnel via text message that an aircraft is in distress and an emergency response is likely to be required.
[3] Spider Tracks is a subscription aircraft monitoring service that allows operators to track and monitor the location of aircraft at 2 minute intervals. The location is recorded and transmitted by a unit that is fitted to the aircraft. This unit also has ’Watch’ and ’SOS’ functions that allow the pilot to alert predetermined ground-based personnel of a situation requiring monitoring or an emergency situation.
[4] Storm Window is a small window inset in the pilot’s side window allowing ventilation, or visibility in the event it is lost through the forward windscreen
[5] Club configuration – the forward two seats in the rear passenger area are oriented to face the rear of the aircraft while the rear seats face forward.
[6] Landing gear limit switch prevents overdriving of the landing gear motor by disconnecting motor drive to the gear once it reaches the extended or retracted and locked positions.
[7] METAR - a routine aerodrome report of meteorological conditions at an aerodrome, normally issued on the hour and half-hour.
[8] Automatic Dependent Surveillance – Broadcast - A means by which aircraft, aerodrome vehicles and other objects can automatically transmit and/or receive data such as identification, position and additional data, as appropriate, in a broadcast mode via a data link
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the morning of 3 April 2022, a Bell Helicopter 206L-4, registered VH-PRW, departed from a private property at Majura, Australian Capital Territory for a visual flight rules[1] (VFR) flight to Mangalore, Victoria. The flight departed with the pilot and one passenger on board and included a planned refuelling stop in Tumut, New South Wales (NSW). The aircraft was one of 7 helicopters taking part in a flying tour, following a common itinerary but operating independently.
The weather forecast indicated that the planned route could be affected by low cloud, rain and associated reduced visibility. At about 0900 Eastern Standard Time,[2] the tour organiser departed Majura in a helicopter to observe the weather along the planned route. Based on their assessment of the en route weather, the organiser recommended that the flights should track north of the planned route and refuel at Wagga Wagga, NSW.
Recorded flight tracking data showed that at 1021, VH-PRW departed the property at Majura. The helicopter initially tracked south‑east before turning west toward the Brindabella Ranges (Figure 1). The flight then proceeded south over Corin Dam before heading north to Wee Jasper. After passing Wee Jasper, the flight again turned south toward the ranges.
Figure 1: Flight from Majura to Long Plain
Source: Google Earth and OzRunways, annotated by ATSB
During their flights, the occupants of the other helicopters in the tour encountered deteriorating cloud and visibility conditions and landed on a property near Wee Jasper. When VH-PRW did not arrive, authorities were notified and commenced a search for the helicopter.
At 1129, the pilot of VH-PRW landed the helicopter alongside Long Plain Road in the Brindabella region. Shortly after the helicopter landed, a passing motorist on Long Plain Road stopped and approached the aircraft. The motorist transported the pilot to a location that enabled phone contact with other members of the tour. The pilot advised other members of the tour of the safe landing and that the intended destination had been Tumut, not Wagga Wagga as recommended by the tour organiser. The motorist and pilot then returned to the aircraft.
Recorded flight tracking data showed that at 1453, the helicopter departed Long Plain Road with the pilot and passenger on board. Police officers dispatched to locate the helicopter arrived at the landing site just after it became airborne. The motorist and police officers observed the aircraft depart to the south at low level, in overcast conditions with low cloud and light rain.
The flight progressed at heights below 500 ft above ground level (AGL) following geographical features along lower lying terrain. At 1504, the flight turned north‑west and took up a track that corresponded with a direct track to Tumut. Two minutes later, the helicopter encountered higher terrain and turned around to head southward, again following lower lying terrain. At 1517, in the vicinity of Anglers Reach, the flight turned north (Figure 3). Two minutes later, the helicopter turned to the north‑west, again along a flightpath that corresponded with a direct track to Tumut and commenced a climb to 7,000 ft above mean sea level (AMSL) (about 2,500 ft AGL).
Figure 2: Accident flight
Source: Google Earth and OzRunways, annotated by ATSB
The helicopter continued along that track at about 7,000 ft AMSL for 6 minutes until 1525. The helicopter then descended to 6,800 ft, before almost immediately climbing. After reaching 7,400 ft, the helicopter commenced a steep left descending turn. During the turn, the ground speed increased to 134 kt and the descent rate exceeded 3,800 feet per minute.
At 1526, the aircraft impacted terrain at an elevation of 4,501 ft. The helicopter was destroyed, and both occupants were fatally injured.
On the morning of April 4, in response to the aircraft not arriving at Mangalore as expected, a second search was initiated. Poor weather prevented an airborne search. At about 2355, a ground search assisted by aircraft tracking data located the accident site.
Context
Pilot information
The pilot was the aircraft owner and held a valid class 2 medical certificate and a private pilot licence (helicopter).
At the time of the accident, the pilot had about 837 hours of aeronautical experience and did not hold an instrument rating. The pilot’s total flying experience on the Bell 206 was about 532 hours of which about 355 were in the L-4 variant and the remainder in the B-3 variant.
Aircraft information
The Bell Helicopter 206L-4 is a 7‑seat, single‑turboshaft engine helicopter equipped with 2-bladed main and tail rotors. VH-PRW was built in 2008 and first registered in Australia in 2016. At the time of the accident, the helicopter had completed about 830 hours in service and was certified for day VFR flight only.
Meteorological information
The graphical area forecast for the area at the time of the accident indicated broken[3] cumulus/stratocumulus cloud with a base of 2,500 ft AMSL and a top of 10,000 ft AMSL.
At 1530 (4 minutes after the accident), Bureau of Meteorology weather stations at Cabramurra (14 km south‑west of the accident site, elevation 4,864 ft) and Mount Ginini (43 km north‑east of the accident site, elevation 5,774 ft) recorded no rainfall and zero separation between the dew point temperature and air temperature. This indicated cloud was present at both stations, however neither station was equipped to provide more detailed cloud information.
Site and wreckage information
The accident site was located within the Kosciuszko National Park in an area of tussock grass, interspersed by bare protruding rock (Figure 3).
Figure 3: Accident site
Source: ATSB
The helicopter collided with terrain between two rock formations in a descending tight left turn and right side-slip in a northerly direction with a westerly heading. At initial impact, a main rotor blade struck the ground and the tail boom separated. The fuselage then turned left to about a southerly heading. Most of the wreckage was located within 8 m of the impact, but the main transmission, mounts and supporting airframe structure continued a further 70 m up an incline. On-site examination indicated that the engine was providing power at impact. There was no evidence of an in-flight break-up or a pre-existing defect with the drive train or flight controls.
Further investigation
The ATSB investigation to date has examined the accident site and wreckage, interviewed witnesses, collected meteorological data, pilot and flight records and obtained aircraft tracking data.
The investigation is continuing and will include further review and examination of:
pilot records and medical information
aircraft maintenance and flight records
aircraft wreckage and recovered components
emergency locator transmitter functionality
witness information
meteorological data
recorded aircraft tracking data.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 3 April 2022, a Bell Helicopter 206L-4, registered VH-PRW, departed with a pilot and passenger on board, for a visual flight rules (VFR) flight from a private property at Majura, Australian Capital Territory to Mangalore, Victoria, with a planned refuelling stop in Tumut, New South Wales (NSW). The helicopter was one of 7 helicopters taking part in a flying tour that morning and the weather forecast indicated low cloud, rain and associated reduced visibility on the planned route.
Two of the 7 helicopters diverted to Wagga Wagga, NSW due to weather while 4 others landed near Wee Jasper, NSW. The pilot of VH-PRW elected to continue until they encountered poor weather conditions and landed the helicopter in the Brindabella region shortly before noon. At 1453 local time, the helicopter departed once again at low level, in overcast conditions with low cloud and light rain. At about 1525, the helicopter commenced a rapid climb and shortly after, entered a steep left descending turn which continued until the helicopter impacted terrain at an elevation of 4,501 ft. A search was initiated the next day with the accident site located later that evening. The helicopter was destroyed, and both occupants were fatally injured.
What the ATSB found
The ATSB found that, having encountered the forecast low cloud and reduced visibility conditions, the pilot landed the helicopter at an interim landing site. Later that day, the helicopter then departed into cloud and visibility conditions unsuitable for visual flight. It is highly likely these cloud and visibility conditions resulted in the pilot experiencing a loss of visual reference and probably becoming spatially disoriented. This led to a loss of control and an unsurvivable collision with terrain.
In relation to visual flight rules pilots flying into areas of reduced visibility, some key messages to manage risk are:
Know your limits. VFR pilots should use a ‘personal minimums’ checklist to help control and manage flight risks through identifying risk factors that include marginal weather conditions. Only fly in environments that do not exceed your capabilities. For visual flight at night, ensure you are both current and proficient with disciplined instrument flight.
Plan ahead. Avoid deteriorating weather by conducting thorough pre-flight planning. Ensure you have alternate plans in case of an unexpected deterioration in the weather and making timely decisions to turn back or divert.
Don’t press on! Pressing on into instrument meteorological conditions with no instrument rating carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations with no visual cues. Disorientation can affect any pilot, no matter what their level of experience.
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 3 April 2022, a Bell Helicopter 206L-4, registered VH-PRW, was to conduct a visual flight rules[1] (VFR) flight from a private property at Majura, Australian Capital Territory to Mangalore, Victoria with a planned refuelling stop in Tumut, New South Wales (NSW). The helicopter was one of 7 helicopters taking part in a flying tour, following a common itinerary but operating independently.
The weather forecast indicated that the planned route could be affected by low cloud, rain and associated reduced visibility. At about 0900 Eastern Standard Time,[2] two of the helicopters departed Majura. These helicopters encountered low cloud and elected to divert over lower terrain north of the Brindabella Ranges to Wagga Wagga, NSW.
At 1021, VH-PRW, with the pilot and one passenger on board, departed the property at Majura along with the remaining 4 helicopters. Recorded tracking data showed that VH-PRW initially tracked south‑east before turning west toward the Brindabella Ranges (Figure 1). The flight then proceeded south over Corin Dam before heading north to Wee Jasper. As the 5 helicopters approached Wee Jasper, they also encountered deteriorating cloud and visibility conditions. Four of the pilots elected to land on a property near Wee Jasper. The pilot of VH-PRW did not land but continued south to ‘attempt to find a way through to Tumut’.
Source: Google Earth and OzRunways, annotated by ATSB
At 1129, the pilot of VH-PRW encountered poor weather conditions and landed the helicopter alongside Long Plain Road in the Brindabella region, outside of mobile phone coverage.
Shortly after the helicopter landed, a passing motorist stopped and approached the helicopter. The pilot advised the motorist that they had landed to wait for better weather conditions before continuing the flight. The motorist arranged to check on the pilot and passenger during the motorist’s return journey later in the day if the helicopter had not already departed by that time.
At about 1230, when VH-PRW did not return to Wee Jasper and the pilot had not contacted other members of the tour, authorities were notified and a search for the helicopter was commenced.
At about 1415, the motorist returned along Long Plain Road and found that the helicopter had not departed. The motorist transported the pilot to a location that enabled phone contact and the pilot contacted the office of the tour organiser to advise of the safe landing. The pilot also stated that they intended to continue the fight following powerlines at about 50 ft above ground level (AGL). The tour organiser advised against this plan and then notified the other members of the tour and authorities of the landing. The motorist and pilot then returned to the helicopter.
Recorded flight tracking data showed that at 1453, the helicopter departed Long Plain Road, with the pilot and passenger on board. Two minutes later, one of the other pilots in the tour noted the helicopter tracking south on a flight tracking application.
Police officers dispatched to locate the helicopter arrived at the landing site just after it became airborne. The motorist and police officers observed the helicopter depart to the south at low level, in overcast conditions with low cloud and light rain. The police officers stated that the helicopter passed ‘at a similar height or slightly above the powerlines’ before being obscured by low cloud.
The flight then progressed at heights below 500 ft AGL following geographical features along lower lying terrain (Figure 2). At 1504, the flight turned north-west and took up a track that corresponded with a direct track to Tumut. Two minutes later, the helicopter encountered higher terrain and turned around to head southward, again following lower lying terrain. At 1517, in the vicinity of Anglers Reach, the flight turned north. Two minutes later, the helicopter turned to the north-west, again along a flightpath that corresponded with a direct track to Tumut and commenced a climb to about 7,000 ft above mean sea level (AMSL).
The descending turn continued until the helicopter impacted terrain at an elevation of 4,501 ft at about 1526. The helicopter was destroyed, and both occupants were fatally injured.
On 4 April, in response to the helicopter not re-joining the tour as expected, a second search was initiated. At about 2355, a ground search assisted by helicopter tracking data located the accident site.
The pilot held a valid class 2 medical certificate and a private pilot licence (helicopter).
At the time of the accident, the pilot had about 837 hours of aeronautical experience and did not hold an instrument rating. The pilot’s total flying experience on the Bell 206 was about 532 hours of which about 355 were in the L-4 variant and the remainder in the B-3 variant.
The ATSB found no indicators that increased the risk of the pilot experiencing a level of fatigue known to affect performance.
The post-mortem examination and a review of the pilot’s medical history identified no evidence of a medical event or pre-existing condition that likely contributed to the accident.
Aircraft information
The Bell Helicopter 206L-4 is a 7‑seat, single‑turboshaft engine helicopter equipped with 2-bladed main and tail rotors. VH-PRW was built in 2008 and first registered in Australia in 2016. At the time of the accident, the helicopter had completed about 830 hours in service and was certified for day VFR flight only. The helicopter was fitted with an emergency locator transmitter.
The helicopter was also fitted with the HeliSAS stability augmentation system. This used attitude data and electro-mechanical servo actuators connected to the flight controls rods to apply small corrections to the cyclic as required to maintain a reference attitude. The reference attitude could be set as required by the pilot. The system also incorporated a two-axis (pitch and roll) autopilot.
Tour coordination
The flight from Majura to Mangalore was part of an informal multi-day flying tour involving 7 helicopters. This tour was mostly coordinated by a helicopter operator who provided the itinerary and organised logistic details such as accommodation and fuel availability.
The tour organiser also operated a helicopter flying training and transport operation, but this tour was conducted outside of that operation. The tour organiser held no authority or responsibility for the operation of each involved helicopter, this responsibility was held by each pilot in command.
Terrain
The helicopter departed an interim landing site along Long Plain Road in the Brindabella Ranges. The flight then proceeded over rugged alpine areas of the Snowy Mountains with terrain elevations generally higher than 4,000 ft AMSL. Peaks of 5,854 ft AMSL and 5,726 ft AMSL were located near the final flight track (Figure 3).
Figure 3: Visual navigation chart extract showing terrain in the vicinity of the accident
Source: Airservices Australia and OzRunways, annotated by ATSB
Meteorology
Forecast
The graphical area forecast for the accident region provided a forecast icing level of 10,000 ft AMSL and the following cloud and visibility conditions for the time of the accident (all heights AMSL):
Generally greater than 10 km visibility with broken[3] cumulus/stratocumulus cloud between 2,500 ft and 10,000 ft.
Visibility reducing to 4,000 m in scattered rain with broken stratus cloud between 1,500 ft and 6,000 ft. Overlying this, broken altocumulus and altostratus cloud could be expected extending from 6,000 ft to above 10,000 ft.
Visibility reducing to 3,000 m in scattered rain showers with broken stratus cloud between 1,500 ft and 3,000 ft. Overlying this, broken cumulus and stratocumulus could be expected extending from 3,000 ft to above 10,000 ft.
Photograph
A photograph taken 2 minutes prior to the helicopter departing Long Plain Road showed the cloud conditions at that time (Figure 4). The elevation of the landing site was about 4,429 ft AMSL. The peak of the terrain visible behind the helicopter is 4,573 ft AMSL. This peak was obscured by broken cloud indicating that the cloud base was less than 144 ft AGL.
Figure 4: Cloud conditions 2 minutes prior to departure from interim landing site
Source: motorist via NSW Police Force
Recorded observations
At 1530 (4 minutes after the accident), Bureau of Meteorology weather stations at Cabramurra (14 km south-west of the accident site, elevation 4,864 ft) and Mount Ginini (43 km north‑east of the accident site, elevation 5,774 ft) recorded no rainfall and no separation between the dew point temperature and air temperature. This indicated the presence of very low-level cloud, likely down to ground level at both stations. Neither station was equipped to provide more detailed cloud information.
Visual flight rules
Visual meteorological conditions
The Civil Aviation Safety Regulation (CASR) 91.280 outlined that flight under the visual flight rules (VFR) can only be conducted in visual meteorological conditions (VMC). The criteria are provided in the CASR Part 91 Manual of Standards Table 2.07 (3) and the CASA Visual Flight Rules Guide:
The flight, and the location of the accident, were in Class G (non-controlled) airspace. The following VMC were stipulated for flight under the VFR in Class G airspace when below 10,000 ft and above 3,000 ft or 1,000 ft above ground level (whichever is higher):
a minimum vertical distance of 1,000 ft and horizontal distance of 1,500 m from cloud
a flight visibility of 5,000 m.
For helicopter operations in Class G airspace at or below 3,000 ft or 1,000 ft above ground level (whichever is higher), the following minimum conditions were stipulated:
clear of cloud and in sight of the ground or water
a flight visibility of 5,000 m or, if operated by day at a speed that allows the pilot to see obstructions or other traffic in sufficient time to avoid collision, 800m.
Minimum height
In addition to minimum visibility and distance from cloud requirements, a pilot is also required to maintain a minimum height above the ground. Unless during take-off, landing or other approved low-flying operation, CASR 91.265 and 91.267 detail that a pilot in command must not fly a helicopter over:
any city, town, or populous area at a height lower than 1,000 ft above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the helicopter; or
any other area at a height lower than 500 ft above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the helicopter.
The investigation identified no evidence to indicate that the pilot intended to undertake an approved low-flying operation.
Recorded data
On-board the helicopter was a mobile device with the OzRunways electronic flight bag application installed. The application had an option for live flight tracking enabled that transmitted the device’s position and altitude. This data was also obtained by the ATSB.
The data showed that at 1519:22 the helicopter turned to a track that corresponded with the direct track to Tumut and 15 seconds later commenced a climb from low level to about 6,600 ft. At 1522:02, a further climb commenced, reaching 7,000 ft at 1522:42. The helicopter continued to track generally toward Tumut at groundspeeds of 105‑115 kt, corresponding to a normal cruise speed for the helicopter. During this segment of the flight, track variations of up to 21° and altitude variations of up to 300 ft were recorded.
At 1525:22, the helicopter descended from 7,000 ft, reaching 6,800 ft about 20 seconds later. From 6,800 ft, a climb was commenced and a further 20 seconds later, the helicopter reached 7,400 ft (at climb rate of 1,800 ft per minute) with a groundspeed of 60 kt. The helicopter then entered a steep left descending turn. During the turn, the groundspeed increased to 137 kt and the descent rate exceeded 3,800 feet per minute (Figure 5).
Figure 5: Aircraft flight path leading up to the accident
Source: Google Earth and OzRunways, annotated by ATSB
Site and wreckage information
The accident site was located within the Kosciuszko National Park in an area of tussock grass, interspersed by bare protruding rock (Figure 6).
The helicopter collided with terrain between two rock formations in a descending tight left turn and right side-slip in a northerly direction with a westerly heading. At initial impact, a main rotor blade struck the ground and the tail boom separated. The fuselage then turned left to about a southerly heading. Most of the wreckage was located within 8 m of the impact, but the main transmission, mounts and supporting airframe structure continued a further 70 m up an incline. On-site examination indicated that the engine was providing power at impact. There was no evidence of an in-flight break-up or a pre-existing defect with the drive train or flight controls.
The emergency locator transmitter (ELT)[4] antenna separated from the unit during the impact sequence. The ELT was examined at the ATSB’s technical facilities in Canberra and was found to have activated during the accident. However, the separation of the antenna prevented a signal from being broadcast. While this delayed search and rescue efforts, it did not alter the outcome as the accident was not survivable.
Risks of flying in areas of reduced visual cues
The safety risks of VFR pilots flying from VMC conditions into instrument meteorological conditions[5] are well documented. This has been the focus of numerous ATSB reports and publications, as VFR pilots flying into IMC represents a significant cause of aircraft accidents and fatalities. In 2013, the ATSB Avoidable Accidents series was re-published. Of these publications, the booklet titled Accidents involving pilots in Instrument Meteorological Conditions outlined that:
In the 10 years to July 2019, 101 VFR into IMC occurrences in Australian airspace were reported to the ATSB. Of those, 9 were accidents resulting in 21 fatalities. That is, about 1 in 10 VFR into IMC events result in a fatal outcome.
Spatial disorientation
Spatial disorientation is a type of loss of situation awareness, and is different to geographical disorientation, or incorrectly perceiving the aircraft’s distance or bearing from a fixed location. Spatial disorientation occurs when pilots do not correctly sense their aircraft’s attitude, airspeed, or altitude in relation to the earth’s surface. In terms of an aircraft’s attitude, spatial disorientation is often described simply as the inability to determine ‘which way is up’, although the effects can often be more subtle than implied by that description.
Spatial disorientation occurs when the brain receives conflicting or ambiguous information from the sensory systems. It is likely to happen in conditions in which visual cues are poor or absent, such as in adverse weather or at night. Spatial disorientation presents a danger to pilots, as the resulting confusion can often lead to incorrect control inputs and resultant loss of aircraft control. The flight control sensitivity and relative instability of helicopters compared to aeroplanes increases the risk of such a control loss.
Related occurrences
There have been many accidents relating to VFR pilots flying into reduced visibility conditions. The ATSB publication listed above identifies a number of similar occurrences. Of note is investigation AO-2015-131.
At about 5.30 pm on 7 November 2015, the owner-pilot of an Airbus Helicopters (Eurocopter) EC135 departed Breeza, NSW, on a VFR private flight with two passengers on board to Terrey Hills, NSW.
Witnesses observed the helicopter land in a cleared area in a valley. After 40 minutes on the ground, the pilot, who did not hold an instrument rating and was limited to visual flight operations, departed to the east towards rising terrain in marginal weather conditions. About seven minutes later, and approximately 9 km east of the interim landing site, the helicopter collided with terrain resulting in fatal injuries to all occupants.
The ATSB found that the pilot likely encountered reduced visibility conditions leading to loss of visual reference leading to the collision with terrain.
Safety analysis
While en-route from Majura, Australian Capital Territory, to Tumut, New South Wales, a group of 5 helicopters including a Bell Helicopter 206L-4, registered VH-PRW, encountered deteriorating cloud and visibility conditions. The pilots of 4 of the helicopters landed at Wee Jasper, but the pilot of VH-PRW continued south into the Brindabella Ranges. After encountering further low cloud and poor visibility, the pilot of VH-PRW landed the helicopter alongside Long Plain Road in the ranges.
At 1453, the pilot decided to depart the interim landing site and continue the flight. The flight progressed for 32 minutes until the helicopter commenced a rapid climb and then a descending left turn which continued until the helicopter collided with terrain.
Site and wreckage examination did not identify any defects or anomalies that might have contributed to the accident. Additionally, there was no evidence to support the pilot being incapacitated. Therefore, this analysis will focus on the examination of the factors that led to a visual flight rules (VFR) pilot operating in an area of reduced visibility and losing control of the helicopter.
Departure into unsuitable conditions
Low cloud and poor visibility conditions were forecast across the Brindabella Ranges on the day of the accident. The pilot, having encountered these conditions, landed the helicopter alongside Long Plain Road at 1129. The pilot and passenger then waited for conditions to improve sufficiently to depart the interim landing site.
Despite no such improvement eventuating, after about 3 hours and 24 minutes, the pilot elected to depart and continue to Tumut at about 50 ft above ground level. Photographs, along with police and witness reports, showed that at the time of the departure the cloud and visibility conditions were unsuitable for visual flight. The broken cloud base of less than 144 ft did not allow the pilot to maintain the helicopter both, clear of cloud as required by visual meteorological conditions (VMC) and at the minimum height above terrain of 500 ft.
Departing into unsuitable cloud and visibility conditions, particularly in the vicinity of mountainous terrain at very low level carried significant risk of both losing visual reference and of collision with terrain.
Loss of control
After departing the interim landing site, the flight proceeded at very low level for 26 minutes until the pilot turned the helicopter to a more direct track toward Tumut and climbed to about 7,000 ft above mean sea level (AMSL).
Observations recorded at meteorological stations in the vicinity of the flight indicated that it was highly likely that there was low cloud in the area of the accident. In addition, significant cloud was forecast and observed from ground level to above 10,000 ft AMSL along the flown track. In these conditions it was highly likely that VMC could not be maintained and that reduced visual cues were encountered by the pilot.
Over the next 6 minutes, minor tracking and altitude variations were recorded. It is possible these variations resulted from attempts to manoeuvre around, or in, cloud or rain showers with associated reduced visibility. Additionally, this manoeuvring indicates that the autopilot was not being used during this part of the flight. It could not be determined if the stability augmentation system was being used.
The flight at about 7,000 ft continued until 1525:42 when a rapid climb of about 1,800 ft per minute was commenced. This was immediately followed by a steep descending left turn. This manoeuvring was inconsistent with normal helicopter operation and was indicative of a loss of control.
The pilot did not hold an instrument rating and the helicopter was certified for day visual flight only. This greatly increased the risk of the pilot being affected by special disorientation and it is unlikely the pilot could have maintained control without visual reference for an extended period. Given the forecast and observed conditions, it is likely that during the 6 minutes the helicopter was operating at the higher level, it encountered poor weather. This likely led to the pilot experiencing spatial disorientation which resulted in a loss of control and the collision with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell Helicopter 206L-4, VH-PRW, on 3 April 2022.
Having landed the helicopter at an interim landing site due to encountering forecast low cloud and reduced visibility conditions, the pilot subsequently departed into cloud and visibility conditions unsuitable for visual flight.
It is highly likely that cloud and visibility conditions resulted in the pilot experiencing a loss of visual reference and probably becoming spatially disoriented. This led to a loss of control and an unsurvivable collision with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
NSW Police Force
the occupants’ next of kin
Civil Aviation Safety Authority
tour organiser.
Submissions were received from:
Civil Aviation Safety Authority
the passenger’s next of kin
tour organiser.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Eastern Standard Time (EST): Coordinated Universal Time (UTC) + 10 hours.
[3] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered.
[4] Emergency locator transmitter (ELT): a radio beacon that transmits an emergency signal that may include the position of a crashed aircraft, activated either manually or in the crash.
[5] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
The ATSB has commenced a transport safety investigation into a hard landing involving a Kavanagh E-240 balloon, registered VH-ZON, at Moorabbin Airport, Victoria on 27 March 2022.
On the morning of 27 March 2022, the balloon was being operated on a scenic passenger flight between Reservoir and Moorabbin Airport, Moorabbin, Victoria with a pilot and 10 passengers on board. The pilot reported that there were strong winds on approach, and just before landing, the balloon passed through an inversion. The balloon rotated horizontally so that it did not land normally with the passengers facing rearwards. The balloon landed hard, with the basket coming to rest in a culvert at the end of the runway.
As a result of the hard landing and the orientation of the basket, 1 passenger was seriously injured and 2 passengers received minor injuries.
The investigation is continuing. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Discontinuation
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
On 28 March 2022, the ATSB commenced an investigation into a hard landing involving a E-240 Kavanagh balloon, registration VH-ZON, which occurred at Moorabbin Airport, Victoria, on 27 March 2022.
The balloon was being operated on a scenic passenger flight between Reservoir and Moorabbin Airport with a pilot and 10 passengers on board. The pilot provided the operator’s standard safety briefing to the passengers before take-off, while the passengers were in the basket, to explain and demonstrate the position to adopt during normal landings and emergencies. The position was facing opposite to the landing direction, standing with slightly bent knees, holding on to the rope handholds in front, and back rested against padding on the basket. Passengers were to remain in that position until the basket stopped.
There were several other balloons operating the same scenic flight route, and the pilots had collectively decided the departure point and that the weather was suitable for their respective flights (all along the same route). The pilots reviewed several sources of weather information, including the Bureau of Meteorology aerodrome forecasts (TAF) for Melbourne, Essendon and Moorabbin. The Moorabbin TAF forecast the wind to be 11 kt from the north-east at the time the balloons were due to land.
The pilots had also obtained information about the actual wind conditions prior to departure by releasing 2 piballs[1] in different locations to assess the speed and direction of the wind at different levels. Following this assessment, the balloons departed at about 0700 local time.
The pilot had about 30 years experience as a balloon pilot and had been operating balloons in the area for about 18 years, with extensive knowledge of the planned route.
On approach to Moorabbin Airport, VH-ZON was travelling in a south-easterly direction and was about 500 m to the west of the other balloons. The pilot obtained automatic terminal information by radio for Moorabbin, and it advised of a 4-kt north-easterly surface wind.
The pilot reported that they had commenced the descent into Moorabbin Airport after the other balloons and found the wind to be faster at the lower levels than expected. Data collected via another balloon pilot’s navigation equipment post-accident showed the wind was about 38 kt at 1,400 ft and 35 kt at 1,000 feet, which was significantly faster than the pilots had anticipated. This meant that the pilot had to conduct a faster than usual descent to ensure they could land the balloon in a suitable area.
When the balloon reached 300–400 ft, it travelled through a temperature inversion (where temperature increases with altitude, which is a reversal of typical atmospheric conditions) and the balloon rotated 120°. Although the passengers had been instructed to adopt the landing position, the pilot did not have time to rotate the balloon to the correct orientation (with the passengers facing opposite to the landing direction) before reaching the ground. On landing, the balloon impacted the front right corner of the basket and bounced. The basket was then dragged for a short distance, coming to rest in a culvert at the end of a runway within the airport boundary.
As a result of the hard landing and the orientation of the basket, 1 passenger was seriously injured and 2 passengers received minor injuries.
As part of its investigation, the ATSB interviewed the pilot and passengers and reviewed:
weather information including observations and forecasts used by the pilot
air traffic control recordings
recorded navigation information used in-flight by one of the other balloon pilots (data could not be retrieved from the equipment used on the accident balloon)
the operator’s procedures for passenger briefings
photographs taken in-flight by the balloon operator and others that were provided by passengers and a witness on the ground.
The ATSB notes that, due to unexpected wind speed on descent (which was much higher than the surface wind information that the pilot had previously obtained), and the limited landing site options, the pilot decided to land as soon as possible. This resulted in a faster and harder landing than normal. The balloon’s abnormal orientation after passing through the temperature inversion meant that although the passengers were in the correct position for landing, there was a greater risk of injury.
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues or important safety lessons from this specific occurrence. Consequently, the ATSB has discontinued this investigation.
However, the ATSB is concerned about the number of accidents that have been occurring in commercial balloon operations and has listed the reduction of passenger injuries in commercial ballooning operations as one of its Safety Watch items. The evidence collected during the investigation involving VH-ZON will be used in a safety study further examining these types of accidents.
[1] Piball: an abbreviation of ‘pilot balloon’, which is a small, helium-filled free balloon with a light attached. It is released and visually tracked to determine the wind at different altitudes.
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 3 March 2022, a Cessna U206G, registered VH-JVR, was being operated by MAGSPEC Aviation for low-level, geophysical survey flights to the west of Norseman, Western Australia.
At about 1200 WST,[1]the aircraft departed Kalgoorlie, Western Australia, for the survey block about 120 km west of Norseman. The pilot was the sole occupant on board the aircraft.
Weather conditions in the survey area were fine with light southerly winds. Earlier in the morning, another company pilot had flown the aircraft on a survey flight. That pilot had conducted a confirmatory reconnaissance flight, noting no major obstacles or issues other than a few taller trees. This information was passed to the pilot of the accident flight before they departed.
The survey lines were parallel to each other at 25 m spacing in an east-west orientation. The survey lines were to be flown at a height of 25 m (82 ft) above ground level (AGL).
The pilot commenced the first survey line at about 1252. At 1343, the GPS tracking device recorded the aircraft was on a westerly heading at a speed of 116 kt and a height of 1,398 ft (GPS height).[2] This was the last position recorded and the height was consistent with the intended survey height above ground level.
The aircraft did not return to Kalgoorlie by the pilot’s nominated estimated time of arrival of 1630, and the operator commenced its emergency response. The operator had another aircraft and pilot at Norseman, which was dispatched to VH-JVR’s last known position; however, that pilot was not able to locate the aircraft.
The Joint Rescue Coordination Centre (JRCC) initiated a search operation after it was advised by the operator at 1700 that the aircraft was overdue. A search aircraft located the aircraft wreckage at 1852, approximately 3.2 km west of its last recorded position (Figure 1). That aircraft’s crew were not able to establish communications with the pilot of the accident flight. The JRCC also deployed a rescue helicopter to the site, and its crew confirmed that the pilot had been fatally injured.
Figure 1: VH-JVR's accident site and last recorded position
The first survey line was flown in a westerly direction. The direction of flight was reversed on each subsequent line.
Source: Recorded flight path data and Google Earth, annotated by the ATSB
Context
Pilot information
The pilot held a valid commercial pilot licence (aeroplane) with a multi-engine command instrument and low-level ratings. Their last flight review was completed in June 2021 and their class 1 medical was valid until June 2022. The pilot had held a low-level rating since June 2021 and had completed the operator’s low-level survey training in July 2021.
The pilot had previously worked as a flight instructor and high-level survey pilot. At the time of the accident, the pilot had about 1,772 hours total, of which about 557 hours was with the operator.
Aircraft information
General
VH-JVR was a Cessna U206G Stationair, which was a single-engine, fixed landing gear aeroplane powered by a Continental IO-520-F piston engine (Figure 2). It was manufactured in 1978 with serial number U20604795 and was first registered in Australia in 1998. Its last periodic inspection was in March 2022 and it had accrued almost 8,000 hours total time in service.
Modifications
VH-JVR had been modified to conduct geophysical survey flights. A magnetometer boom was installed at the rear of the aircraft and associated survey equipment was in the rear cabin. The survey equipment had its own separate power supply. The aircraft also had a GPS tracking device.
The aircraft had also been modified with a fuel selector valve from a C210, which enabled the selection of both fuels tanks to supply the engine at same time.
Figure 2: VH-JVR
Source: Jarrod Swanwick (via www.jetphotos.com), modified by the ATSB
Site information
The aircraft was located in dense bushland 124 km west of Norseman. Access to the site was difficult with the nearest vehicle-accessible track only reaching to within 4 km of the accident site. An additional track was cleared through bushland to enable vehicle access to the accident site.
Damage at the point of impact indicated that the aircraft initially struck trees in an upright but relatively steep nose-down attitude. The impact caused the left wingtip and aileron to separate from the aircraft. The aircraft then impacted the ground on its left side and continued through the bush in a southerly direction, coming to rest about 45 m from the initial point of impact (Figure 3).
The aircraft felled a number of trees and several parts had separated from the main body, including the nose gear assembly, left main gear, left door, windscreen and sections of the lower engine cowling and lower engine components (Figure 4). There was no indication of fire in the wreckage trail, either in the bushland or aircraft components. However, the remainder of the aircraft was almost entirely destroyed by a post-impact fire. The propeller had separated from the engine and was located towards the rear of the wreckage and the engine had been detached from its mounts. The right wing was relatively intact as was the magnetometer boom, albeit damaged by fire (Figure 5).
Figure 3: Wreckage trail looking south towards the main wreckage
Source: ATSB
Figure 4: Wreckage trail looking north towards the impact area
Source: ATSB
Figure 5: Main wreckage
Source: ATSB
Wreckage examination
The wreckage was examined on-site and to the extent possible (given the post-impact fire). The following observations were made:
all components of the aircraft were accounted for at the site
there were no indications of pre-impact structural failures
flight control continuity was established
propeller damage and propeller strike marks observed in the trees were indicative of the engine producing power at the time of impact
there were no indications of pre-impact damage or defects to the engine
the flaps were fully retracted (although only the right wing was able to be examined due to fire damage)
there was no indication of a pre-impact, inflight fire (although the extent that this was able to be verified was limited due to the post-impact fire).
Further investigation
To date, the ATSB has:
examined the wreckage
recovered aircraft components and other items for further analysis
interviewed relevant parties
collected aircraft and operator documentation
collected the pilot’s records.
The investigation is continuing and will include:
further review of aircraft and operator documentation
further review of the pilot’s records
further review and examination of aircraft components and other items recovered from the accident site
further analysis of flight path information from the aircraft’s GPS tracking device
review of the risk controls in place for low-level survey work.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the significant assistance provided by the Western Australia Police Force and Poseidon Nickel Ltd during the onsite investigation phase.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 3 March 2022, the pilot of a Cessna U206G, registered VH-JVR and operated by MAGSPEC Aviation Pty Ltd, was conducting a low-level geophysical survey, about 120 km west of Norseman, Western Australia. Recorded data showed the first survey line commenced at 1252 local time, and the aircraft’s last recorded position occurred at 1343, in the survey area.
At about 1430, the ground operator observed that the satellite tracking system was no longer reporting the aircraft’s position, and they were subsequently unable to contact the pilot. When the aircraft failed to return to Kalgoorlie by its estimated arrival time of 1630, a search was initiated. At about 1852, the wreckage was located 3.2 km west of the aircraft’s last recorded position. The injured pilot had extricated themselves from the wreckage but shortly after succumbed to their injuries. The aircraft was destroyed.
What the ATSB found
The ATSB found it was likely that, during a manoeuvre to intercept the next survey line, for undetermined reasons, control of the aircraft was lost at a height from which recovery was not possible. While an aerodynamic stall situation was a plausible explanation for the loss of control, this remained only a possibility due to the lack of recorded data beyond the last known position of the aircraft and no witness observations.
Although the aircraft’s satellite tracking system had stopped at 1343, an emergency response was not initiated until 1700. This was in accordance with the operator’s emergency response plan, in which a search and rescue response was to commence 30 minutes after the estimated time for arrival. However, an earlier response was very unlikely to have altered the outcome due to the extent of the pilot’s injuries. Minimising the time for a search and rescue is essential to increasing the chances of a successful outcome in the event of an accident.
In accordance with the operator’s training, its pilots routinely used high angle of bank (45–60°) turns at low level to manoeuvre between survey lines. Steep turns at low level increases the risk of an aerodynamic stall from which a recovery may not be possible. ATSB analysis of the available satellite tracking data identified that, although the pilot was conducting steep turns, they had flown the previous 24 turns without incident.
The pilot was not wearing any protective clothing or a helmet nor were they required to do so by the operator. Wearing of such items has been recommended by industry bodies, as they may offer some protection in the event of an accident, particularly from fire but also as environmental protection following an accident.
The ATSB identified that the operator’s risk management processes did not include a pre‑operational risk assessment that considered the generic risks and hazards common across their low‑level survey operations. Further, a risk register was not maintained, which limited the operator’s ability to track, monitor, and mitigate all known hazards, and assess the effectiveness of the existing risk controls.
Also, the operator trained its pilots to routinely fly survey patterns utilising steep turns at low level. However, the procedures or limitations specific to these manoeuvres were not included in the operations manual. It was also noted that, the operator’s aircraft were fitted with a satellite tracking system, but there was no requirement nor supporting procedures to confirm the set‑up and functionality of the system prior to flight.
Although not contributory, the ATSB identified that the regulatory oversight of the operator had not specifically examined the primary activity of low‑level geophysical survey flights or the processes and procedures designed to mitigate any associated risks.
What has been done as a result
MAGSPEC Aviation has consolidated its manuals, with its health, safety and environmental management system manual incorporated into its operations manual. In addition, it has implemented a range of measures regarding its low‑level survey operations including:
an updated job safety analysis, which provides for the consideration of likelihood, consequence and details of any risk mitigations
procedures for the use of satellite tracking including a requirement for a pre-flight check
conduct of procedure turns including how the turns should be flown, with minimum speeds indicated and what to do if those speeds could not be achieved
the requirement for fixed emergency locater transmitters on all aircraft, and limitations for flight if the unit is unserviceable or not present
updating its low-level training syllabus to include specific parameters (which mimic its previous practical training), so that competency can be formally assessed against those parameters.
MAGSPEC Aviation has also advised it no longer operates at survey heights below 30 m above ground level and it provides its pilots with an individually registered portable locator beacon, which they are required to wear on their person. It is also progressing operational amendments to enable Flight Safety Foundation’s Basic Aviation Risk Standard accreditation. Just prior to final publication of this report, the operator advised that it had been awarded the Basic Aviation Risk Standard accreditation.
Safety message
Geophysical survey operations are generally conducted at low level, necessitated by the requirement for high quality, accurate data acquisition. This creates a high‑risk operating environment that requires effective risk management.
Risk management should include a pre‑operational risk assessment to consider hazards and risks common to an operation. This can then be used to inform the management of risk for specific taskings and assist in developing appropriate mitigations. Tools such as a risk register can assist an organisation to effectively monitor its risk profile and continually improve its risk mitigation strategies.
Policy and procedures form part of effective risk mitigation strategies and will establish safety and the operating standards to be met and maintained. Documented policies and procedures can ensure the correct set‑up and functionality of operating equipment and systems. It can also minimise opportunities for deviation from an operator’s expectations and the erosion of safety margins.
This accident further highlighted that regulatory oversight activities should ensure that an operator’s primary activity is examined in sufficient detail. Not doing so potentially limits the opportunity to assess an operator’s ability to manage the risks associated with its proposed operations.
The occurrence
On 3 March 2022, a Cessna Aircraft Company U206G aircraft, registered VH-JVR, was being operated by MAGSPEC Aviation Pty Ltd for low-level, geophysical survey flights of an area about 120 km west of Norseman, Western Australia (Figure 1).
The aircraft was based at Kalgoorlie for this survey task along with 2 pilots and a ground operator. One pilot would operate the aircraft in the morning and the other in the afternoon. The ground operator was responsible for the technical and logistical aspects of the survey.
At about 1125 local time, at the completion of the morning survey flight, the aircraft was returned to Kalgoorlie. The second pilot commenced their pre‑flight preparations at about 1130 and discussed the morning survey flight with the returning pilot. That pilot advised of a minor concern about a fuel imbalance that developed during the approximate 4‑hour flight, however, they did not report any impact on aircraft handling or engine operation.
The ground operator prepared the survey equipment and assisted the pilot to fully fuel the tanks.
Figure 1: VH-JVR's operating area in proximity to Kalgoorlie and Norseman
Source: Operator’s satellite tracking data, overlaid on Google Earth, annotated by the ATSB
At about 1200, the aircraft departed for the survey area with the pilot as the sole occupant. Recorded GPS data showed that the first survey line was commenced at about 1252, picking up where the morning survey flight had been completed. The last position uploaded to the tracking system was at 1343, which showed the aircraft was on a westerly heading at a ground speed of 116 kt and a GPS height of 1,398 ft above mean sea level in the target survey area.
At about 1430, the ground operator checked the satellite tracking system for VH‑JVR and noted that the aircraft’s position was no longer being reported on the system.The satellite tracking system had the ability to automatically alert the operator 15 minutes after tracking data was no longer being uploaded to the system’s servers. The operator reported they did not receive an automatic alert.
The ground operator then attempted unsuccessfully to call and text the pilot’s mobile phone. Although the aircraft carried a satellite phone as part of its survival kit, it was not routinely switched on during operations. The ground operator then advised the operations manager, who directed them to continue the attempts at making contact and prepare the ground vehicle for a potential response. Further attempts at contact were unsuccessful and the operations manager directed that no further action could be taken other than to monitor the situation and wait until the aircraft’s estimated time of arrival at Kalgoorlie.
The aircraft did not return to Kalgoorlie by the estimated time of arrival of 1630. At 1700, in accordance with its emergency response plan, the operator contacted the Australian Maritime Safety Authority’s Joint Rescue Coordination Centre (JRCC). Another company aircraft and pilot that was at Norseman was dispatched by the operator to VH-JVR’s last known position, however, the pilot was not able to locate the aircraft.
The JRCC initiated a search and rescue operation at 1739. The aircraft wreckage was located at 1852, approximately 3.2 km west of its last recorded position (Figure 2). The search aircraft’s crew were unable to establish communications with the pilot of VH‑JVR. The JRCC also deployed a rescue helicopter to the site, and at 0042, they found the pilot, fatally injured a short distance from the wreckage.
Figure 2: VH-JVR's accident site location and last recorded position
Source: Operator’s satellite tracking data, overlaid on Google Earth, annotated by the ATSB
Context
Pilot information
Qualifications and experience
The pilot held a commercial pilot licence (aeroplane) issued in 2014 and a valid class 1 aviation medical certificate. They held a multi‑engine aeroplane instrument rating and a grade 3 instructor rating, although neither were current, nor were they required to be.
At the time of the accident, the pilot had about 1,822 hours total aeronautical experience, of which about 570 hours were with the operator, primarily in Cessna 210 aircraft. The pilot had accrued over 350 hours on Cessna 206 aircraft prior to joining the operator and had about 12 hours on VH‑JVR.
The pilot commenced and completed a low‑level (aeroplane) rating in June 2021, which comprised 6.7 hours of dual training in a Cessna 152 aircraft, including a flight test. In July 2021, the pilot then commenced low‑level survey training with the operator in a Cessna 210 aircraft. The pilot’s logbook detailed 5 initial training survey flights totalling 18.6 hours. These were followed by about 21 hours of solo low‑level survey, culminating in a check flight of 5.6 hours.
The chief pilot (CP) conducted the pilot’s low‑level survey training and their geophysical survey operations check flight. The CP reported that the pilot ‘was one of those pilots who picked it up very quickly’ and was ‘very switched on’. In total, the pilot had conducted about 500 hours of low‑level survey operations.
Although the pilot had previously flown high‑level surveys, MAGSPEC Aviation was the first operator that the pilot had flown low‑level surveys for. The operator also reported that the pilot had been recently offered and had accepted the role of deputy chief pilot/deputy head of operations.
Recent history
The pilot had been on leave since 23 February 2022. The pilot’s partner reported that, on 1 March 2022, the pilot woke at about 0700, went to bed at about 1930–2000 and did not fly that day. On 2 March 2022, the day prior to the accident, the pilot woke at 0400 and arrived at Perth Airport at 0500 to take a scheduled passenger flight to Geraldton, where VH‑JVR had been undergoing scheduled maintenance. The pilot then ferried the aircraft about 700 km to Kalgoorlie, arriving around midday. Later that day, the pilot accompanied the second company pilot assigned to the survey area on a 30–40 minute local flight to familiarise the second pilot with VH‑JVR, as they had not previously flown that aircraft.
The pilot’s partner received a text message from the pilot at 1922, advising that they were cooking dinner in their accommodation and had no plans to go out that night. There was no further evidence of the pilot’s activities prior to the accident flight, but the pilot usually woke around 0600–0630, exercised and studied in the mornings before conducting the afternoon survey flight.
The day of accident was the first day of that survey task. Neither the other pilot nor the ground operator expressed any concern for the pilot. Based on the available recent history, there was no evidence the pilot was likely experiencing a level of fatigue at the time of the accident.
Aircraft information
General
The Cessna Aircraft Company U206G Stationair was a high‑wing, fixed tricycle undercarriage aircraft powered by a single Continental IO‑520‑F piston engine, with a 3‑bladed constant speed propeller. VH‑JVR was manufactured in 1978 in the United States and was first registered in Australia in 1998. The aircraft was acquired by the operator in 2021.
Factory fitted standard equipment included:
a vane‑type aerodynamic stall[1] warning system in the leading edge of the left wing designed to activate the audible warning horn 5–10 kt above the stall speed in all configurations
2 vented fuel wing tanks, which were an integral part of the metal wing structure[2] and supplied fuel via gravity feed to 2 reservoir tanks, and a fuel selector valve with selections for LEFT, RIGHT and OFF
3-point safety harness restraints.
Modifications
In October 2021, VH‑JVR had been modified and equipped to conduct geophysical survey operations in accordance with engineering orders approved by a Civil Aviation Safety Authority (CASA) authorised aeronautical engineer and supplemental type certificates.[3] These modifications included:
A magnetometer boom installed at the rear of the aircraft and associated survey equipment, with its own power supply, mounted in the rear cabin.
A fuel selector valve, which enabled the selection of LEFT/BOTH/RIGHT with a pull‑out fuel shut off valve installed to cut off fuel flow.
A survey data acquisition and navigation system, which included flight path guidance via a digital display mounted on top of the instrument panel, allowing the pilot to monitor aircraft position in relation to the pre-programmed survey lines.[4]
A 4-point inertia safety restraint harness.
Maintenance
The aircraft was being maintained by an approved maintenance organisation in accordance with the CASA maintenance schedule 5 and regulatory requirements. The last periodic inspection was completed on 2 March 2022 at 7,982.4 hours total time‑in‑service. The current maintenance release was not recovered and likely destroyed in the post‑impact fire. A review of previous maintenance releases and maintenance records did not identify any major repairs or recurring airworthiness issues with the aircraft.
Emergency locator transmitter
Civil Aviation Safety Regulations (CASR) 1998 Part 91 General operating and flight rules Manual of Standards (MOS) required that VH‑JVR carry an emergency locator transmitter (ELT) or a survival ELT for its intended operation. At the time of the accident, VH‑JVR was not fitted with an ELT but carried a survival ELT (refer to section titled Emergency beacons).
Weight and balance
The CP provided a recreated weight and balance sheet of the accident flight to the ATSB. The morning pilot witnessed the aircraft depart with full fuel in the survey configuration. The weight and balance sheet identified that VH‑JVR weighed about 1,488 kg on departure, about 150 kg below the maximum take‑off weight of 1,636 kg. The centre of gravity on take‑off was near the centre of the allowable range. Therefore, it was very likely that VH‑JVR was within the weight and balance limits at the time of take‑off.
Meteorological information
The pilot who flew the morning survey flight reported that the weather at that time was fine with good visibility, except for some light turbulence.
The Bureau of Meteorology forecast for the area, valid from 1300, was for visibility to be greater than 10 km and no significant weather for the time of the accident. Winds were forecast to be southerly at about 15 kt. Satellite imagery indicated no cloud cover over the survey area. The nearest weather stations to the accident site were at Norseman (124 km east) and Hyden (158 km west‑south‑west). There was no significant weather reported at either location. Recorded winds at 1330 were south‑westerly at about 14 kt at Norseman and south‑easterly at 10 kt gusting to 17 kt at Hyden.
According to Geoscience Australia’s geodetic calculator, the sun azimuth was north‑west at about 56° elevation about the time of the accident. This was relatively high in the sky and sun glare affecting the pilot was considered not likely.
Recorded data
Spidertracks data
A Spidertracks Spider X tracking system was installed on the aircraft, which provided near real‑time tracking via satellite and/or cellular networks, recording position, altitude, track heading and groundspeed at 15‑second intervals, increasing during aircraft manoeuvring. The data was transmitted to Spidertracks servers once every minute. The Spidertracks system also had an automatic watch function whereby an alert would be sent via text and email to a nominated person(s) in the event that the data transmissions from the device were not received for a period of 15 minutes.
Spidertracks data was able to be recovered for analysis due to its cloud‑based operation. The physical unit, and other possible data sources of recorded data identified in the wreckage, including personal electronic devices, the engine data monitoring device and the geophysical survey data equipment, were all damaged in the post‑impact fire, preventing data recovery.
The last known position transmitted by Spidertracks was about 3.2 km east, and approximately 1 minute away (at the last recorded speed) from the accident site (Figure 3). Position data was recorded by Spidertracks once every 15 seconds, increasing to about once every 3 seconds during a turn. However, as the data was only transmitted once every minute, it was likely that the accident occurred before Spidertracks was able to transmit the last data packet to the cloud storage.
The recovered data showed that the pilot had conducted procedure turns (refer to section titled Survey pattern) at the end of each of the completed 24 survey lines, over a period of about 50 minutes. Although all turns were observed to be conducted in a similar manner, one particular turn commenced at a greater distance away from the survey area. During interview, the CP suggested that the pilot may have done so in order to have a drink or attend to a flight‑related task. The ATSB noted no evidence to suggest any concern with this particular turn. The aircraft was on the 25th survey line when the data stopped, and the accident site was in the vicinity of the expected 25th procedure turn (Figure 3).
The recorded data showed the survey lines were being conducted in an east‑west orientation, with left turns conducted to the west and right turns to the east. The average survey line speed was 114 kt at an average height of about 78 ft above ground level (AGL).
Figure 3: Recorded flight path (excluding transit from Kalgoorlie)
Source: Operator’s satellite tracking data, overlaid on Google Earth, annotated by the ATSB
Procedure turn analysis
The available Spidertracks data was analysed to assess the aircraft handling during the accident flight. The recorded ground speed data and forecast wind and direction were used to estimate the true airspeed during the survey flight. Based on the available atmospheric conditions, true airspeed was assumed equal to indicated airspeed and is used throughout the following analysis.[5]
Using the available recordings, the average bank angle, rate of turn and G load for each turn for the accident flight were calculated. These calculations assumed steady coordinated turns, at constant altitude and airspeed, with a constant wind speed and direction.
The ATSB’s analysis of the Spidertracks data from the aircraft identified that during the procedure turns:
The angle of bank ranged from 43° to 60° and was typically between 50° to 60°.
The rate of turn ranged from 10° to 18° per second and was typically between 14° to 18° per second.
The G load[6] ranged from 1.3 G to 2 G and was typically about 1.7 G to 1.8 G.
The indicated airspeed ranged from 89 kt to 109 kt and was typically between 94 kt to 104 kt.
The altitude during turns were between 150 ft to 300 ft AGL, with the average being 200 ft.
Comparison flights
Spidertracks data from 2 previous flights for the accident pilot, which were in VH‑JVR, as well as the morning survey flight conducted in VH‑JVR by another pilot were made available to the ATSB. These were analysed for comparison to the accident flight.
Morning flight
The morning flight conducted by the other pilot consisted of 50 survey lines and 49 procedure turns. These survey lines were typically flown at 85 ft AGL and 120 kts. This set of survey lines were immediately adjacent to the accident flight survey, with the procedure turns occurring in a similar area. Analysis of these procedural turns identified:
The angle of bank ranged from 24° to 56° and was typically between 40° and 50°.
The rate of turn ranged from 4° to 16° per second and was typically between 10° and 13° per second.
The G load ranged from 1.1 G to 1.8 G and was typically between 1.3 G and 1.5 G.
The airspeed ranged from 92 kt to 109 kt and was typically between 95 kt and 104 kt.
The altitude during the turns varied between 210 ft and 550 ft, with the average being 320 ft AGL.
These turns, while generally comparable with the accident pilot’s turns, and considered steep turns,[7] were typically flown at lower angle of banks, rates of turn and G load, and at higher heights above ground level. The ATSB noted that the morning pilot had recently completed their survey training with the accident pilot on the Cessna 210. This was their first low‑level survey flight in the Cessna 206.
Previous flights (accident pilot)
Spidertracks data from 2 prior survey flights in VH‑JVR for the accident pilot were available. These flights were conducted in a different location, over undulating terrain with dense vegetation, with a higher average survey height of about 140 ft AGL at about 113 kt. Each flight consisted of just over 50 procedure turns and survey lines. A summary of the analysis of these procedural turns is contained in Table 1 below (refer flights 2 and 3), with comparison to the accident flight, and the morning pilot (flight 1).
Table 1: Comparative turn analysis results
Accident flight
Flight 1
Flight 2
Flight 3
Averaged turn radius (m)
197
277
280
248
Averaged angle of bank (°)
54
45
47
46
Averaged turn rate (°/s)
15
11
11
12
Averaged G load (G)
1.7
1.4
1.5
1.5
The ATSB’s analysis of the Spidertracks data from the pilot’s previous survey flights identified that those turns were flown at slightly lower angles of bank, rates of turn and G load when compared with the accident flight. While the pilot was operating at a different location, which may have influenced the way they conducted their turns, the reason for the differences was not able to be determined from the evidence available.
Wreckage and impact information
Wreckage distribution
The aircraft was located in moderately dense scrubland with small to medium trees. The terrain was relatively flat, with some low ridges in the surrounding area.
The distribution of the wreckage indicated that the aircraft initially struck trees in an upright orientation, with an approximate 20° left angle of bank, and a nose‑down attitude at about a 30° angle of impact. The initial tree strike resulted in the left wingtip and aileron separating from the aircraft. The aircraft then impacted the ground on its left side and continued through the bush in a southerly direction, coming to rest about 45 m from the initial point of impact, where it was consumed by a post‑impact fire.
The wreckage trail consisted of a number of felled trees and aircraft components, including the nose gear assembly, left main gear and fairing, left door, section of the left wing flap, windscreen and sections of the lower engine cowling and lower engine components. There was no indication of fire in the wreckage trail or detached aircraft components (Figure 4).
Figure 4: Wreckage trail looking north towards the impact area
Source: ATSB
The propeller had separated from the engine and was located towards the rear of the wreckage and the engine was upside down and detached from its mounts. Although the left wing was significantly affected by fire, the wing spar was still distinguishable. The right wing was relatively intact as was the magnetometer boom, albeit damaged by fire (Figure 5).
Figure 5: Main wreckage
Source: ATSB
Wreckage examination
Although post‑impact fire damage precluded examination of a significant proportion of the aircraft, inspection of the site and wreckage found:
no evidence of any pre‑existing structural, mechanical or flight control defects that would have prevented normal operation
the wing flaps were in the fully up (retracted) position
a small, yet intense fire zone indicative of a significant amount of fuel, with ignition occurring from the left‑wing integral fuel tank rupturing during the accident sequence
the fuel selector was in the ‘BOTH’ orientation
damage to the propeller indicated that the engine was producing power at the time of the impact.
Extensive fire damage to all instruments and avionics resulted in no useful switch position information. The windscreen, located part way along the debris trail, did not exhibit signs of birdstrike, nor were feather or bird remains identified in the area. In addition, the morning pilot reported that, while they had observed bird activity on survey flights, none had been sighted that day.
The reason for the fuel imbalance noted by the morning pilot could not be determined from the wreckage examination.
Medical and pathological information
Post-mortem examination
A post-mortem examination of the pilot was undertaken by a qualified pathologist on behalf of the Western Australia Coroner. The pathologist determined that the pilot’s cause of death was a result of a combination of traumatic injuries (both soft tissue injuries and multiple fractures) and the effects of fire from significant thermal injury and smoke inhalation. There were multiple fractures to the nasal bones but none to the skull or pelvis.
The pathologist assessed that the traumatic injuries sustained were potentially survivable with immediate medical assistance, but those injuries were compounded by the thermal injury and smoke inhalation. The ATSB’s aviation medical specialist also advised that the impact injuries were likely not fatal, however, they would have been severely incapacitating. The extensive thermal injury and, in particular, the smoke inhalation was likely to have rendered the pilot unconscious within minutes. They also stated that immediate intervention would have been required but the sustained thermal injuries were likely not survivable.
The post-mortem report indicated that the pilot did not have any significant natural disease. Further, toxicological analysis did not detect the presence of alcohol or common drugs and carbon monoxide[8] levels were not significantly raised (at less than 5% saturation).
The pilot was reported by their partner to be fit and healthy with no known illnesses.
Survival aspects
Impact protection
Due to extensive fire damage to the fuselage, there was limited evidence available about the survivable space/intrusions, or seat and seatbelt condition. Therefore, the ATSB was not able to determine survivability with regard to the cabin area. The left (pilot) door indicated an intrusion/compression and the left main landing gear leg was detached, consistent with high impact forces and the injuries sustained to the pilot.
Post-impact fire
Metal fuel tanks are prone to rupturing during an accident impact, allowing fuel to escape and increasing the risk of a post‑impact fire. To improve crashworthiness, the addition of fuel bladders and fuel cells that have been constructed of flexible materials have proven less prone to rupturing during an impact. They are able to withstand greater deformation and puncture less readily and are less likely to expand or tear to form a larger opening from which fuel can escape. Such systems may provide occupants with more time to egress the aircraft and/or reduce the risk of any fire‑related injury.
, extensively discussed post‑impact fire safety and referenced studies by the United States National Transportation Safety Board and Transport Safety Board of Canada. Those studies concluded that post‑impact fire had been shown to contribute significantly to injuries and fatalities in accidents that were otherwise potentially survivable. A potentially survivable accident is one in which the impact forces are within the limits of occupant tolerance, the aircraft structure preserves the required survival space, and the occupant restraint is adequate.
As a result of investigation AO‑2021‑052, the ATSB identified that the aircraft (an Air Tractor AT‑400) was not required to be fitted with a crash‑resistant fuel system under United States Federal Aviation Regulations. A safety issue was raised and the ATSB recommended that the United States Federal Aviation Administration take action to address certification requirements for crash‑resistant fuel systems for fixed‑wing aircraft, in an effort to reduce the risk of post‑impact fire. At the time of writing this report, the ATSB recommendation remained open and the Federal Aviation Administration had advised that the results of a study into post‑crash fire accidents was being reviewed to determine their next action (AO‑2021‑052‑SI‑01).
Protective clothing and helmets
For the accident flight, the pilot was reported to be wearing a t‑shirt, shorts and trainer type shoes and was not using a helmet. The operator did not require its pilots to wear protective clothing or helmets, nor were they required to do so by regulations. The CP explained that this decision took into account temperature, fatigue and pilot comfort balanced against mitigating the potential risks. In addition to comfort and fatigue factors, the bulk of a helmet may not be suitable to the smaller cockpit of the aircraft. However, the CP stated that no formal risk assessment had been completed to support this decision. The operator reported that it issued each pilot (including the accident pilot) with company polo shirts made of 100% cotton as a measure of fire protection and the use of other protective clothing and helmets was left to individual pilots’ discretion. The CP indicated that some of their pilots did wear such items. It could not be determined if the accident pilot was wearing the company polo shirt. The ATSB noted that the operator’s job safety analysis (refer to section titled Job safety analysis) included consideration of protective equipment and clothing as methods of reducing risk factors.
The ATSB’s aviation medical specialist advised that if protective clothing and an appropriate helmet was worn, in most general circumstances, this would have reduced the severity of injury in an accident. However, they were unable to comment on the effectiveness of these items for this accident and noted that protective clothing and a helmet would not have prevented any smoke inhalation injury.
The International Airborne Geophysics Safety Association (IAGSA – refer to section titled International Airborne Geophysics Safety Association) recommended that appropriate clothing should be worn by all flight crew involved in geophysical surveys to minimise the immediate risk of fire in the event of an accident and for protection from exposure in a survival situation. These include:
cotton undergarments covered by long trousers and long‑sleeved shirt or an appropriate flying suit
closed shoes
have gloves available at all times
layers of clothing appropriate for the conditions
cold weather clothing should include felt lined boots, down parka with attached hood and large mittens.
IAGSA also recommended that for fixed‑wing operations, each individual operator should determine the appropriateness of the use of an industry approved helmet. A case by case, risk assessed approach should be adopted, taking into account the relevant variables for each specific survey task.
The Flight Safety Foundation’s Basic Aviation Risk Standard[9] is a set of risk‑based aviation industry standards. The standard covers a wide variety of aviation applications of which airborne geophysical survey operations were included. The standard implementation guidelines for survey operations also recommended appropriate clothing for crew such as non‑synthetic long trousers and pants or flying suit. It also recommended that helmets should be worn when operating below 500 ft AGL unless a risk assessment stated otherwise.
Flight following
Satellite tracking
Operator requirements
The operator had implemented flight following through use of the Spidertracks satellite tracking system installed on each of its aircraft. The company operations manual stated:
In addition to the required safety equipment the Company equips all aircraft with a real-time satellite monitoring system with a refresh rate of at least every 5 minutes and automatic alerting (to company mobile phone and email) in the event of an emergency.
Should the satellite monitoring system alert be inadvertently activated by the pilot an “ops normal” call should be made to the company as soon as practicable.
The ground operator assigned to each survey job was the primary person responsible for flight following. They were to monitor the aircraft’s location via the tracking system and initiate an emergency response, if required.
The morning pilot could not recall any specific pre‑flight requirements for the Spidertracks device and another company pilot reported that there were not any checks required, the device turned on once the aircraft’s electrical system was on.
The operations manual did not include flight following as a specific duty for the ground operator or any other staff member. Further, the manual did not detail procedures for the conduct of flight following, nor were there procedures or guidance to confirm that the tracking system was correctly configured and operating as expected prior to flight.
Automatic watch function
The operator was surprised that a Spidertracks automatic alert was not received during the accident and advised that, on a number of occasions, their satellite tracking had experienced dropouts. On some of those occasions, contact was made with the pilot and a system reset restored normal function. On other occasions, when contact with the pilot was not possible, the aircraft returned by the nominated estimated time of arrival (ETA). The operator had not contacted Spidertracks about the dropouts or conducted any other troubleshooting.
Spidertracks advised the ATSB that the automatic watch function on the aircraft’s device had not been activated on the accident flight, nor was it active for earlier flights on 2 and 3 March 2022. They further advised that there was no indication of any service‑related issues, confirming that up to the loss of data, the aircraft’s device was operating as expected. Diagnostic logs for the device were not available due to this data only being transmitted via mobile phone networks. Spidertracks confirmed that the length of time with no transmissions received, or a data loss or delay was not typical and could be indicative of a power or device failure, transmission interference or installation issue. Spidertracks found no recorded issues with the satellite service or their cloud platform at the time of, or leading up to, the accident.
Emergency response plan
The operator had a phased emergency response plan, predicated on an elapsed time since the aircraft’s ETA. Each phase was commensurate with an escalating level of concern. Satellite tracking was referred to in the plan, within the section Phase 1 - Uncertainty. Phase 1 commenced 0–15 minutes after the aircraft’s ETA had expired. The plan directed a check of the satellite tracking and if there was an abnormal or no indication in the system, the next step was to attempt contact with the crew. If contact with the crew was not possible and overall operations were assessed as not normal, the plan directed that the operations manager, as primary contact, to be notified, then the chief executive officer and CP as alternates.
The plan did not elaborate any further on required actions for an abnormal or no indication in the system prior to advancing to the next step, which was Phase 2 - Alert. Phase 2 commenced 15–30 minutes after the ETA had expired and directed the primary or alternate contacts to establish the final status of the aircraft via the tracking system. It included a note that, if there was no contact with company operations then the ground operator was to contact the Australian Maritime Safety Authority’s Joint Rescue Coordination Centre or local search and rescue services direct. Commencement of Phase 3 - Distress was at 30 minutes after ETA had expired or whenever the aircraft was confirmed as missing.
The operator commenced phase 3 at 1700, 30 minutes after the ETA for VH‑JVR had expired and then contacted the Joint Rescue Coordination Centre.
Emergency beacons
Emergency locator transmitter
The company operations manual stated that all company aircraft were to be fitted with an approved ELT or a portable ELT if the fixed device was inoperative or otherwise not serviceable. The operator was not able to determine why VH‑JVR was not fitted with an ELT.
The ATSB research report (AR‑2012‑128) discussed the potential safety benefits of an approved, fitted ELT, which were designed to automatically activate following an impact normally associated with a collision. While the research noted some limitations with the effectiveness of ELTs, the fitment of a crash‑activated ELT greatly increases the early notification for search and rescue efforts and arrival of potentially life‑saving medical treatment especially when occupants or crew are incapacitated.
Personal locator beacon
The CP and morning pilot stated that a personal locator beacon (PLB) was carried in the aircraft as part of a survival kit, which was secured to the passenger seat. The PLB was routinely carried in the aircraft, and not as an alternative to an ELT but as an additional item. In accordance with regulations, the PLB was classed as a survival ELT, and an alternative to a fixed ELT. However, the PLB was not identified in the wreckage and was likely consumed by fire.
The ATSB research report (AR‑2012‑128) suggested that carrying a PLB will most likely only be beneficial to safety if it is carried on the person, rather than being fixed or stowed elsewhere in the aircraft. The CASR Part 91 MOS stated that a survival ELT must be carried either on the person of a crew member, in or adjacent to a life raft, or adjacent to an emergency exit.
Operational information
Airborne geophysical survey flights
Airborne geophysical survey flights are conducted by a variety of rotary and fixed‑wing aircraft which have been specifically modified and equipped with geophysical sensors. Survey flights were normally flown below 500 ft AGL over the desired area via a pre‑determined pattern and at heights designed to maximise the quality of the data captured. The data provides a detailed below ground composition of the surveyed area, primarily to inform mining and resource industry activities.
Requirement for CASA low‑level rating
Operations requiring flight below 500 ft AGL, such as geophysical surveys, required a pilot to hold a CASA Part 61 low‑level rating. A low‑level rating is specific to various types of flying operations (such as aerial survey, firefighting or agricultural), however, the training and testing is not specific to any one type of operation. To obtain a low‑level rating a pilot must demonstrate competency in certain operational techniques, which included, but were not limited to, steep, maximum rate and minimum radius turns, procedure turns, recovery from approach to stalls (level and turning). In addition to holding a low‑level rating, MAGSPEC Aviation required prospective pilots to have a minimum of 500 hours as pilot in command. MAGSPEC Aviation then provides training specific to its operational requirements.
International Airborne Geophysics Safety Association (IAGSA)
The IAGSA is an international industry association comprised of airborne geophysical survey organisations with an overall objective to promote and enhance safety in the airborne geophysics survey industry. IAGSA publishes a safety manual for its member organisations, which details its standards and recommended safety practices.
IAGSA is a non-regulatory body and holds no authority to compel its members to follow its standards and recommended practices, which are not a replacement for the regulatory requirements that each individual organisation may operate under. However, members have agreed under the terms of membership to follow those standards and practices where they are more stringent or not covered by regulations, except where they have filed a notification of difference. Members are also required to complete an annual self‑audit. At the time of the accident, MAGSPEC Aviation’s most recent self‑audit outlined a number of differences to IAGSA standards and practices. Although IAGSA had requested it, it had not received a formal notification of differences from the operator.
Survey height
The operator was issued a CASA instrument in 2017, which allowed it to conduct operations at a height lower than that permitted by Civil Aviation Regulation (CAR) 157.[10] The instrument was last renewed in 2021 and was valid until 2024.
The instrument did not specify the lowest height that could be flown. The CP stated that survey flights would often be flown at 30 m (100 ft) AGL, although a standard or minimum height was not documented in the operations manual. Rather, the survey height would be requested by the client.
The CP explained that the requested survey height was assessed during the planning stage, through a review of maps of the survey area and the conduct of a reconnaissance flight. A detailed guide on how to conduct a reconnaissance flight was included as an appendix to the operations manual. This process would confirm if the survey could be flown at the requested height. The operator stated that, on numerous occasions this process resulted in the survey being flown at heights higher than requested.
The client for the accident survey specified a height of 25 m (82 ft) AGL.
The IAGSA safety manual acknowledged that there were increased risks associated with low flying and that operating at such heights can ‘aggravate the consequences of mechanical malfunctions or human error’. When discussing minimum safe survey heights, and while recognising that lower heights may improve the quality of survey data, they noted many differences of opinion among its members.
Having a predetermined height had been debated among the members, however, they concluded that ‘no single universal “minimum safe survey height” can be designated given the wide variety of survey conditions and aircraft characteristics’. As such, IAGSA indicated that the safety issue was not necessarily the survey height, but more importantly, could the survey be safely flown at the requested survey height. Consequently, IAGSA recommended that:
Clients specify the maximum clearance height possible, consistent with the objectives of the survey to be flown and that operators, prior to commencing a survey, conduct a detailed risk analysis in accordance with an internationally recognized procedure considering, but not limited to, the following factors and Appendix IV of this manual:
From the recorded data, the accident survey flight was flown in a back‑to‑back pattern, which was a series of consecutive parallel lines followed by a procedure turn used to establish the aircraft onto the next line in the reciprocal direction (Figure 6). This was the routine pattern used by the operator in its geophysical surveys. The client had specified 25 m spacing on east‑west survey lines.
The CP explained that procedure turns consisted of an initial climbing turn to establish the aircraft at about 300 ft AGL and about 400–500 m lateral offset from the next line. After this, a level turn would be commenced (into wind) at a 45–60° angle of bank (referred to as a steep turn) to intercept the next line. Descent to the survey height commenced once the aircraft wings were established straight-and-level.
Figure 6: Back-to-back pattern and procedure turns
Source: Aerial Application Association of Australia, annotated by the ATSB
IAGSA highlighted the risks associated with turns at low level:
Turns at low level present a considerable hazard, particularly if the terrain presents visual illusions; the aircraft descends in the turn, airspeed is low, or the angle of bank is steep. An excessive angle of bank, often resulting from close line spacing or drifting in strong crosswind conditions, is insidious as the stall speed of the aircraft increases with the angle of bank (assuming a level turn) whilst at the same time the aircraft’s speed is reduced from increased drag.
During straight and level flight there may be a significant margin above the stall speed, however in a steep turn the stall speed may be reached quickly with little warning and a stall in the turn at low level will likely result in a fatal accident.
For manoeuvring at low level, IAGSA recommended:
All turns at low level should be limited to a maximum angle of bank of 30 degrees and be done at a constant altitude. No climbs or descents should be carried out during the turn. If the terrain dictates that a climb is necessary the aircraft should be climbed to the required height prior to commencing the turn and any descent back to survey height should only be done after established in a wings level attitude.
The CP explained that the back‑to‑back pattern with procedure turns was the most efficient method and enabled the capture of higher quality survey data. They reported that flying consecutive lines was less workload intensive for their pilots, especially regarding obstacle hazard avoidance. This allowed a pilot to deal with a particular hazard for a short period as they moved away from it.
Operations manual – Special operations
Volume 2 of the operations manual, valid at the time of the accident, discussed aircraft operations and included a section titled Part 2D Special Operations specific to survey operations. It included sub sections on low flying, survey tolerances and safety considerations during surveys. However, there was limited detail with regard to the process or procedures for the conduct of low‑level survey flights.
As previously discussed, a standard or minimum survey height was not included in the operations manual.
In Part 2D1.1 Low Flying, height was discussed in terms of a minimum height when overflying occupied structures, vehicles or livestock but it did not include reference to other obstacles such as terrain, vegetation canopy or masts/antennas.
Part 2D1.4 Survey Tolerances stated:
Track, height and groundspeed tolerances for the survey will be established by the client and should be adhered to as closely as possible. Significant deviations will require the line to be re-flown.
Client established survey tolerances, although important to data accuracy, remain secondary to safety and pilots should disregard them as necessary to ensure the safety of aircraft, personnel, equipment, and environment.
Part 2D1.5 Safety considerations during survey, required a minimum survey speed to be established for each aircraft type operated by MAGSPEC Aviation. This was to be the greater of the 130% of clean stall speed (wing flaps up and landing gear up if retractable), 110% of the best single‑engine climb speed or 110% of the take‑off safety speed.
Although procedure turns and a back‑to‑back survey pattern were taught to, and routinely flown by all company pilots, the special operations section did not refer to these manoeuvres. The CP stated that there was no other reference document that outlined how the operator expected its pilots to conduct the procedure turns, nor were there any documented limitations such as a maximum angle of bank or minimum height AGL prior to commencing the procedure turn.
Aerodynamic stall
A wing generates lift as a result of the pressure differential created by airflow over the wing’s surface. The angle between the incoming or relative air flow and wing chord is known as the angle of attack (AoA). As the AoA increases, lift increases up to a certain angle, known as the critical AoA. At this point, the airflow over the upper surface of the wing becomes separated. This condition is referred to as an aerodynamic stall (or simply a stall) and results in a significant loss of lift and an increase in drag. Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, typically an uncommanded aircraft nose‑down pitch results.
A loss of altitude also occurs during the recovery from a stall and it is possible to stall with insufficient height above the ground to recover. The pilot’s operating handbook (POH) for the U206G stated that the maximum altitude loss during a stall recovery may be as much as 240 ft in power off conditions and straight and level flight. The U206G has a stall warning vane[11] and warning horn to alert the pilot of an impending stall.
Most general aviation aircraft typically have a critical AoA of around 16°. This critical AoA can be exceeded at any airspeed, any (pitch) attitude and any power setting. However, as most small aircraft are not fitted with an AoA indicator, the AoA at which the stall occurs may be referenced to an airspeed.
When banking or turning an aircraft, it is necessary to increase the amount of lift generated to ensure that the aircraft does not descend. This increases the AoA resulting in lift and drag greater than normal straight and level flight. This increases the load factor on the aircraft above 1 G. As the angle of bank increases, the lift required to maintain a constant altitude also increases, requiring the pilot to apply back pressure on the control column. The effect is, as the angle of bank and load factor increases, the stall speed increases. At 45° angle of bank, the load factor is 1.41. This results in an almost 19% increase in the wings level stall speed. At 60° angle of bank, the load factor is 2, resulting in an increase in stall speed of 41%.
The U206G POH provided the stall speeds at maximum weight with power off, flaps up, various angles of bank (up to the POH limit of 60°) and centre of gravity (CoG) positions (Table 2Table 2).
Table 2: U206G stall speeds (extracted from the POH)
Angle of bank
0°
30°
45°
60°
Stall speed (forward CoG)
55 kt
59 kt
65 kt
78 kt
Stall speed (rear CoG)
41 kt
44 kt
49 kt
58 kt
Recovery from a stall requires reducing the AoA by moving the control column forward, which normally means lowering the aircraft nose (pitching down).
Organisational and management information
MAGSPEC Aviation
MAGSPEC Aviation Pty Ltd commenced operations in 2017 to provide airborne geophysical survey services across Australia. It operated a fleet of 2 Cessna 206 and 2 Cessna 210 aircraft. At the time of the accident, they operated under a CASR Part 138 (aerial work) air operator’s certificate. Part 138 came into effect on 2 December 2021. Since commencing low‑level survey operations, the operator had experienced the following occurrences:
In 2018, the engine of a Cessna 210 failed necessitating a forced landing. The pilot was uninjured, however, the aircraft was substantially damaged. It was identified that sufficient fuel had not been transferred from the aircraft’s tip tanks to the main fuel tanks. The operator undertook action to review training and to reinforce fuel management procedures.
In 2019, a Cessna 210 struck a powerline and the aircraft sustained minor damage. The aircraft was safely flown back to its departure point. The operator reported that the aircraft had been flown on north‑south lines due to the sun’s position before transitioning to east‑west lines after the sun was no longer a factor. Following this, the pilot had flown 50 m from the powerline before making contact on the reciprocal heading. Subsequently, the operator incorporated a national database of powerlines into its pre‑survey assessment process.
In 2020, the engine of a Cessna U206G lost partial power and the pilot conducted a forced landing, resulting in substantial damage to the aircraft. The pilot was uninjured. Fuel starvation was determined as the reason for the engine power loss. It was identified that the aircraft had been operated with only one fuel tank selected instead of both. The operator updated checklists to incorporate the requirement for fuel tank selection to BOTH and amended the survey data acquisition system to provide periodic fuel check messages as a reminder to pilots.
Following the 2018 occurrence, the ATSB completed an occurrence brief (AB-2018-058). This was a short summary report and not an investigation, to allow for greater industry awareness of potential safety issues and possible safety actions. The ATSB did not investigate the other occurrences. CASA conducted 2 surveillance events following the 2018 occurrence. In response to the draft report, on 28 January 2025, the operator reported that they had requested assistance from CASA after the other occurrences but reported no assistance was provided. The ATSB reviewed CASA records, which indicated no action had been taken following the 2019 or 2020 occurrences (refer to section titled Regulatory oversight activity.
Safety management system
Managing safety
According to the International Civil Aviation Organization (ICAO, 2018), a safety management system is a systematic approach to managing safety that seeks to proactively mitigate risks before they result in an accident or incident. This includes defining the necessary organisational structures, accountabilities, responsibilities, policies and procedures.
At the time of the accident, there was no CASA regulatory requirement for the operator to have a safety management system. However, the operator had implemented a Health, Safety and Environmental Management System (HSEMS), for the purpose of describing:
…the process by which MAGSPEC aviation manages risks has been developed to meet the Civil Aviation Safety Authority SMS requirements in addition to providing more generalized guidance on the management of risk within the organisation.
Specifically, one of the operator’s policy commitments was to:
…minimize the risks associated with operational activity to a point that is as low as reasonably practicable/achievable…
While the HSEMS was submitted to CASA, a review of CASA records found that it had not been assessed, nor was there a requirement to do so.
Safety risk management
Risk management is a key component of safety management and includes hazard identification, safety risk assessment, safety risk mitigation and risk acceptance. It is an ongoing process as the aviation system is constantly changing, with new hazards introduced, and some hazards and associated risks changing over time (ICAO, 2018).
CASR Part 138 required an operator conducting aerial work to undertake risk assessments of its operations. This was a new requirement introduced with Part 138. The Part 138 MOS detailed a layered approach to risk assessment and that before conducting an operation:
(a) the operator’s operations manual must contain:
(i) pre-operational risk procedures [refer below] for risk assessments and mitigation processes applicable to the operation; and
(ii) procedures for post-flight risk review; and
(b) the operator must have a flight risk management plan based on a pre-operational risk assessment in accordance with the procedures; and
(c) the operator must ensure that the operator and each crew member is satisfied, in a pre-flight risk review, that the flight risk management plan will eliminate, reduce or mitigate risks and hazards to the extent that it is safe to conduct, and continue, the operation without unacceptable risk to the crew members, any aerial work passengers, the aircraft or any other person or property.
The MOS further specified what was to be included in an operator’s pre‑operational risk procedures:
a. processes for identifying, reporting and recording hazards;
b. processes for analysing identified hazards and assessing the risks they may pose, including for pre-flight, in-flight and post-flight stages of operations;
c. processes to mitigate the risks or control the risks, including processes for the incorporation of risk controls into standard operating procedures;
d. the creation and management of:
i. a risk register; and
ii. records of dedicated risk assessments performed to address each type aerial work operation that is to be conducted, including details of the risk assessors;
e. procedures to ensure that the pilot in command and the other crew members are familiar with the pre-operational risk assessment and the associated standard operating procedures (SOP);
f. in-flight procedures for the pilot in command and the other crew members to consider and manage the risks associated with aerial work operations.
The operator’s HSEMS stated that safety risk management begins with hazard identification and then assessing the risks associated with the hazard in terms of likelihood and severity. The manual further stated that, once the level of risk was identified, appropriate remedial or mitigation measures could be implemented to reduce the risk to as low as reasonably practicable. The risk management process detailed in the HSEMS followed a 5‑stage process:
Stage 1 - Identify the hazard and associated risks
Stage 2 - Assess the risk in regard to severity and likelihood
Stage 3 - Evaluate risk tolerability
Stage 4 - Treat/mitigate the risk
Stage 5 - Monitoring
Stage 1 of the process listed sources for hazard identification and stated that the safety manager was to use the Donesafe[12] system to manage and record these hazards. It also noted that:
Due to the varying nature of MAGSPEC Aviation’s operating environment a separate Operational Job Safety Analysis (JSA) (see appendix 3) was undertaken by the Chief Pilot or his designee to assess site-specific risks prior to each job provide an overall risk rating for the job.
Where non-site-specific items are identified as part the JSA or field crew safety meeting these will be reported to the HSEMS system via the DONESAFE “Hazards” report tab.
Each survey task, including the risks associated with that task, were assessed via the job safety analysis (JSA). Any risks identified in the JSA that were not specific to the survey tasking location were entered into the Donesafe system. The risks specific to the location were not captured in the system.
Pre-operational risk assessment
One of the key requirements for managing risk was that an operator should undertake an overarching assessment (pre‑operational risk assessment) to consider and evaluate the risks associated with its proposed operations, in this case, low‑level geophysical survey. This assessment recognised the underlying principles of CASR Part 138, where the risks and hazards associated with a type of aerial work operation are common to that type of operation. The matters to be considered in the assessment included, but were not limited to the (CASA, 2023):
− nature of the intended operation and its particular characteristics
− location (if known) of the intended operation and its particular characteristics
− aircraft to be used in the intended operation and their performance profile and impacts of serviceability status
− qualifications and experience of the FCMs [flight crew members] and support personnel to be used in the intended operation
− generic or known hazards particular to the type of aerial work operation, external to the aircraft, that may be met during the operation.
CASA advisory circular 138‑05 v2.1 Aerial work risk management, stated that an operator should use data from the risk register and dedicated risk assessments to inform the pre‑operational risk assessment. Once populated, the assessment should then be updated over time and from operational experience, to incorporate lessons learnt from previous operations. Further, to ensure it is readily available to all crew members, it should form part of the company’s operations manual.
The ATSB’s review of the HSEMS and operations manual did not identify any requirement for a pre‑operational risk assessment to be completed.The CP also confirmed that, at the time of the accident, such an assessment had not been conducted.
Risk register
Safety risk management activities should be documented, including any assumptions underlying a risk assessment, decisions made, and risk controls implemented. A risk register could be used to ensure identified hazards and risks that emerged during planning or day‑to‑day operations were tracked and mitigated as part of formal risk management processes. An operator’s risk register can also be incorporated into the pre‑operational risk assessment. The register could include the hazard, potential likelihood and consequences, assessment of the associated risks, when or where it applied, and any controls put in place to mitigate the risk. Notably, (ICAO, 2018):
Maintaining a register of identified hazards minimizes the likelihood that the organization will lose sight of its known hazards. When hazards are identified, they can be compared with the known hazards in the register to see if the hazard has already been registered, and what action(s) were taken to mitigate it.
The CP reported that a risk register was not maintained for the company’s operations. Although it was noted that the operator did retain a fatigue risk register.
Flight risk management plan
The results of the pre‑operational risk assessment were to be considered when preparing a flight risk management plan, which was specific to an individual flight or task within the type of operation. The plan should outline the specific mitigators or risk controls that were to be used during the flights. The flight crew should also have sufficient time to review and confirm the plan prior to the commencement of the operation.
Job safety analysis
Components
As required by the company operation’s manual, the JSA was the documented risk management process designed to address the safety concerns with each project the operator conducted, that is, for each specific survey task. The ATSB’s interpretation of the Part 138 risk assessment requirements was that the JSA was equivalent to the flight risk management plan, as discussed above. The JSA consisted of 5 parts:
Part A - Pre-survey risk assessment: This assessment was to be completed by the operations manager at the time a tasking was quoted and included details on the activity, hazards, hazard effects, initial risk score, risk mitigators, residual risk, and a final risk score. This used a pre‑populated risk matrix with 14 hazard areas, each of which were assigned a descriptor and risk score of 1 (negligible) to 5 (unacceptable). The total risk score determined if any further action was required, such as a need for additional risk controls or stopping the tasking until the risk was reduced.
Part B - Operational job safety analysis. This was to be completed by the CP or other suitable person prior to commencing the survey task. This considered any operational limitations relating to aircraft performance, obstacles and human performance, whether any hazards affected the safety or technical performance of the survey, and if any changes were required. The risk level for the task was assessed using a pre-populated matrix with 27 hazards, but with instructions to add more as appropriate. The final risk level determined if the survey could proceed as planned (low risk), or if the survey could proceed with approval from the CP and amendments to the plan or additional risk mitigators (medium risk), or if the survey was not to proceed as currently planned (high risk).
Part C - Field crew safety meeting: The meeting was to be completed by operational personnel at the survey site, prior to commencing survey operations and every crew change. This section was a yes/no answer sheet covering a range of operational areas designed to assess any additional hazards and risks not identified in Parts A and B. At the direction of the CP, a reconnaissance flight could also be performed to assess the survey area for any additional risks or hazards not already identified in the original JSA.
Part D - Post-survey field crew meeting: This meeting allowed the operator to better understand any issues faced on the job and if anything needed to be accounted for, either at that specific location or for an ongoing basis.
Part E - Emergency response plan: This plan was to be reviewed during the field crew safety meeting and crew members were to ensure that the contact and procedure details were correct.
Neither Part A nor Part B referred to consideration of previous JSAs for any applicable risk information that may be relevant to the current JSA.
Survey task assessment
Parts A-C of the JSA completed for the accident flight survey task are discussed in the following paragraphs.
Part A was completed by the operations manager and listed hazards including the 25 m survey height, which was assessed with the highest risk score of 5. It did include mitigating factors of carrying a portable personal ELB and portable GPS, conducting operations with satellite flight following and a comprehensive pilot briefing including maps.
Several elevated risk areas were identified on the matrix, such as operations below 100 ft AGL and operating in hot conditions between 35–40 °C. Overall, the initial risk rating for the survey task was determined to be low, based on a score of 36 (Figure 7)Figure 8.
Figure 7: Part A – Initial pre-survey risk assessment for the accident task
Source: MAGSPEC Aviation, annotated by the ATSB
The CP and operations manager approved Part B of the JSA, identifying that the survey height and antenna/masts, and the survey location with regard to other aircraft activity were concerns. When considering if there were any hazards that would affect safety or the technical performance of the survey, the survey height of 25 m was noted, and the possibility of trees, powerlines and masts in the area were low still but still a risk. As such, it was determined that a detailed reconnaissance flight was to be conducted.
The final risk level was assessed as low, with 4 hazards identified (Figure 8Figure 9). The ATSB noted that the hazard of ‘terrain clearance less than 30 metres’ had not been ticked. However, if it had been selected, the final risk level would have remained at low.
Figure 8: Part B – Hazards risk matrix for the accident tasking
Source: MAGSPEC Aviation
Part C had been originally completed by another pilot and the ground operator. That pilot had conducted a reconnaissance flight of the survey area and signed part C noting that no additional risks had been identified. That pilot was subsequently assigned to another task.
The ATSB noted that the survey height was referred to in the question, Can the job be flown at the suggested survey height? and this was answered as yes with no amplifying comments.
The day prior to the accident, the ground operator met with the accident and morning pilot to conduct another field crew safety meeting. They discussed the JSA, and the ground operator reported that they advised the pilots about some taller trees in the area, which had been identified in the reconnaissance flight (but not noted in Part C).
Text messages between the accident pilot and CP showed that conducting another reconnaissance flight was discussed. The CP suggested that another could be done if the pilot felt it was required but there was no direction from the CP to do so. The morning pilot completed another reconnaissance of the survey area prior to commencing their survey.
In reference to the utility and sufficiency of the JSA, the operator advised on 28 January 2025 in response to the draft report that they considered the JSA to be their risk assessment process and was a combined risk register, pre‑operational risk assessment, flight risk management plan and record of the crew meeting. The operator further advised that the JSA was reviewed by CASA during the transition to Part 138 and:
This risk assessment was approved by CASA during the 2nd December 2021, Part 91 / 138 AWK [aerial work] changes. It has been accepted and approved by multiple third-parties, including those that represent BARS [Flight Safety Foundation’s Basic Aviation Risk Standard].
The ATSB sought clarification from CASA to determine if the JSA met the requirement of Part 138 and whether it had been approved by CASA. On 1 May 2025, CASA advised:
The JSA as described in the report does not meet the requirement of a pre-operational risk assessment.
The reasons for this advice are:
• The ATSB report outlined that Part A of the JSA had a pre-populated risk matrix with 14 hazard areas and Part B of the JAS had a pre‑populated matrix with 27 hazards and instructions to add more as necessary.
• CASA’s AC 138-05 identifies how a risk register is a critical component to the creation of a pre‑operational risk assessment and CASA notes that the ATSB report mentions that the operator’s Chief Pilot (CP) “reported that a risk register was not maintained for the company’s operations” which supports that a pre-operational risk assessment was not produced.
• CASA agrees with the ATSB that this activity is not specifically considering or evaluating the risks associated with the type of aerial work operation to be conducted, i.e. the JSA process is basically done on a per task basis, which is not the same as the pre-operational risk assessment as the pre‑operational risk assessment is intended to be an enduring document that is regularly updated from risk register updates and post-flight risk reviews (see the first sentence of CASA AC 138‑05 paragraph 4.2.5).
• Effectively, the JSA Part A is potentially covering elements of risk assessments that would support the updating of the pre-operational risk assessment but is not creating the pre-operational risk assessment itself.
• CASA further advised:
• The accident occurred 3 months after the commencement of the new flight operations regulations, of which Part 138 of CASR and its supporting Manual of Standards was one element.
• Under the transitional rules in Subpart 202.EAA of CASR, holders of AOCs authorising aerial work under the pre-2 December 2021 paragraph 206(1)(a) of CAR, where the AOC was in force immediately before 2 December 2021, had these AOCs recognised as legally being an aerial work certificate and such operators were required to ensure their operations manuals complied with Part 138 of CASR and contained all necessary content to enable that compliance.
• As the operator was the holder of an AOC authorising aerial work under the pre-2 December 2021 rules, the content of their operations manual would have been approved by CASA as part of them holding that AOC. Compliance with the new flight operations regulations for all such operators would be reviewed at the next appropriate CASA oversight event.
Regulatory oversight activity
Regulatory framework
CASA was responsible, under the provisions of Section 9 of the Civil Aviation Act 1988, for the safety regulation of civil aviation in Australia and of Australian aircraft outside of Australia. Section 9(1) stated the means of conducting the regulation included:
(c) developing and promulgating appropriate, clear and concise aviation safety standards;
(d) developing effective enforcement strategies to secure compliance with aviation safety standards…
(e) issuing certificates, licences, registrations and permits;
(f) conducting comprehensive aviation industry surveillance, including assessment of safety‑related decisions taken by industry management at all levels for their impact on aviation safety…
The 2 primary means of oversighting a specific operator’s aviation activities were:
assessing applications for the issue of, or variations to its air operator’s certificate (AOC) and associated approvals (including approvals of key personnel)
conducting surveillance of its activities.
CASA was required by Section 28 of the Civil Aviation Act 1988 to satisfy itself about various matters when processing an application for the issue of, or variation to, an AOC. The matters included whether the organisation was suitable and whether it had suitable procedures and practices to ensure that AOC operations were conducted safely.
CASA provided records related to their assessment of MAGSPEC Aviation’s initial AOC and low flying applications.
Initial issue of air operator’s certificate
The CASA entry control process involved assessing an application for the issue of a new AOC or a variation to an existing AOC. The worksheet used by CASA for an AOC assessment was intended to be used in conjunction with the AOC Process Manual, AOC Handbook, other relevant technical assessor handbooks and applicable legislation. This worksheet contained the criteria required for an assessor to undertake a technical assessment. It focused on generic regulatory requirements applicable to most operators and there was no specific criteria that referred to assessing an operator’s primary activity, in this case, low‑level survey operations. Although the assessment process confirmed that the operator had processes and procedures to support its operations, there was no evidence that these were examined in any detail for their suitability for the proposed operations.
However, the CASA officer processing the AOC application acknowledged that, while it was a new operation, the organisation included personnel from a previous operator, and that these personnel had experience and exposure to low‑level survey operations. The officer further stated that this experience was evident during the assessment, interview, and inspection phases of the assessment.
As part of the AOC application, CASA was to also approve the appointment of the CP. The CP’s records included an assessment paper, interview record, and notes from an assessment flight. The assessment focused on the CP’s ability to manage the regulatory requirements of an AOC holder, yet did not indicate how the operator would conduct its low‑level survey operations. The assessment flight did not include any low‑level flying as CASA did not permit its officers to undertake low flying.
The AOC was issued to the operator on 3 October 2017.
In December 2021, CASA amended its AOC entry control procedures to include more emphasis on assessing the proposed primary activity. A specific worksheet was introduced for assessing a Part 138 application and included reviewing the processes that allow an operator to safely conduct and manage its aerial work operation in compliance with the regulations.
Low flying approval
The AOC Handbook acknowledged that low flying was an operational requirement and that an application for low flying under CAR 157(4)(b) was required. This assessment was conducted at the same time as the initial AOC application.
The worksheet for the AOC application did not record any assessment undertaken by CASA to approve the operator to undertake low flying below the levels permitted in CAR 157. However, the assessing officer indicated that a key component of issuing the low flying approval was that the operator had a legitimate requirement and that its CP and line pilots held the required low‑level rating. There was no record of any in depth assessment of how the operator would address the risks associated with low flying. Further, the AOC Handbook did not provide any guidance or instruction on how such an application should be assessed.
The low flying instrument was issued to the operator on 22 September 2017.
Surveillance post‑AOC issue (pre‑accident)
Post‑authorisation review
As at 2017, following the issue of an initial AOC, CASA was to conduct a post‑authorisation review (PAR) of the operator to ensure that all the entry control requirements were being met. This surveillance activity was to be conducted within 6–15 months following the initial issue.[13] As described in the CASA Surveillance Manual, a PAR was a type of level 1 surveillance, which was a structured, forward planned larger surveillance event.
The CASA records showed that a PAR, as defined in its surveillance manual, had not been undertaken on the operator.
In response to the draft report on 3 February 2025, CASA advised the ATSB that:
At the time of the accident CASA conducted its surveillance planning under the National Surveillance Selection Process (NSSP), which was a risk-based methodology for the selection and prioritisation of surveillance events. Under the NSSP an operator such as this did not require a post authorisation review. CASA has since implemented a multi-year surveillance approach whereby all Aerial Work Operators undergo surveillance on a regular basis, irrespective of the degree of risk that CASA has assessed. This multi-year surveillance approach is one of many core elements of CASA’s National Oversight Plan.
On 3 April 2025, the ATSB and CASA had a follow‑up briefing to seek clarification on its responses to the draft report. CASA advised that the obligation for a PAR could also be achieved through an alternative activity, and in this case had been accomplished through the conduct of a level 2 surveillance event. CASA indicated that the level 2 surveillance, conducted in July 2018 (discussed below), was noted in its surveillance system as ‘post authorisation’ and would likely have been similarly scoped to a PAR. Therefore, this was considered an equivalent activity at the time. CASA had not provided the ATSB any supporting documentation indicating that an equivalent activity was permitted, or what should have been considered if this was to be undertaken.
Surveillance in 2018
A level 2 surveillance event was a less formal interaction with an operator and could be in the form of checklist-based compliance and product checks of a specific section of its systems. A level 2 surveillance event took place in July 2018, after the operator’s first occurrence. The planned scope included airworthiness assurance, fuel load control, operational standards, and safety assurance. Nil findings were issued, and the CASA surveillance team noted that the operator was still in the process of reviewing its operating procedures with changes to be reviewed at the next surveillance event scheduled for later in 2018. It was not evident to what extent that low‑level survey operations were examined.
A second level 2 surveillance took place in October–November 2018. The planned scope included the same areas as the previous surveillance with the additional items of:
airworthiness control
implementation of the drug and alcohol management plan
crew scheduling
flight systems
safety risk management
assessments
training infrastructure
training management.
Three safety findings and 7 safety observations were issued as a result of that surveillance. The surveillance team noted that the operator was actively trying to mitigate some of the operational risks, but the operations manual was lacking some of the procedures followed by the operator. The findings related to non‑conformance with operations manual procedures, uncontrolled documents, and aircraft defect management.
Observations were not required to be actioned by the operator, although CASA did encourage them to do so. One observation related to fuel load control and procedures for addressing discrepancies in fuel quantity. Another observation related to limited procedures for the completion of the JSA. The surveillance report did not make any findings or observations on overall processes or procedures for low‑level survey operations.
Periodic assessment tool
The authorisation holder performance indicator (AHPI) was a questionnaire‑based tool used by CASA to assess ‘the apparent risk to safety presented by an authorisation holder [operator]’. The AHPI tool consisted of a number of factors and sub‑factors associated with organisational characteristics and performance, commonly thought to affect or relate to safety performance behaviour. This was used by CASA to assist with determining whether any risk‑based surveillance of an organisation was required, and to scope the areas for that assessment.
A number of AHPI assessments had been completed by CASA and 5 out of the 6 AHPIs did not trigger any higher priority for surveillance. The last AHPI prior to the accident was completed in February 2022. CASA noted that there was no record in its system of a formal PAR being conducted, and there was no record of action following the 2019 and 2020 occurrences. The CASA officer recommended surveillance take place at the earliest possible convenience.
Transition to Part 138 regulations
In response to the draft report, on 1 May 2025, CASA advised the ATSB that the accident occurred about 3 months after the commencement of the new flight operations regulations, which included Part 138. Under the transitional arrangements to the new regulations, current holders of an AOC authorising aerial work before 2 December 2021 had this certificate legally recognised as being an ‘aerial work certificate’. These operators were required to ensure that the operations manual complied with Part 138 and contained all the necessary content to enable that compliance.
In this case, as the operator held an AOC prior to 2 December 2021, the content of its operations manual would have been approved by CASA. The operator’s compliance with Part 138 was to be reviewed at the next appropriate CASA oversight event.
While operators were not required to submit their entire operations manual for assessment prior to 2 December 2021, as part of the transition, CASA required operators (no later than 60 days prior) to submit extracts from their operations manual covering 2 key measures. These included change management and procedures for the carriage of aerial work passengers required under Part 138. CASA only required operators to submit their entire updated operations manual immediately before the commencement date of the new regulations.
On 27 September 2021, MAGSPEC provided CASA with its complete operations manual, the HSEMS, including the change management and carriage of aerial work passenger procedures. CASA notified MAGSPEC via email in April 2022 that its initial submissions related to these 2 aspects were not yet compliant. Following a further submission by the operator, on 18 August 2022 CASA advised via email that these areas were ‘compliant’. CASA did not provide any advice related to an assessment of any other parts of the operations manual including those related to operational risk management.
Surveillance post-accident
Shortly after the accident, CASA conducted an initial review to determine if further surveillance of the operator was required. The CASA officer noted that the operator had never undergone a level 1 surveillance event or had a PAR conducted. The officer recommended that a response surveillance event should be scheduled.
On 31 August 2023, the ATSB briefed CASA on the draft investigation findings, which included discussion on the operator’s risk management processes in place at the time of the accident. A similar briefing had also been provided to the operator on 19 July 2023. CASA completed a level 1 systems audit of the operator in September 2023. This level of surveillance is a structured, larger-type event that considers the specific activities conducted by the operator. The audit included a review and follow-up of this accident. The scope included:
airworthiness and maintenance aspects
aircraft and passenger loading control
crew scheduling and fatigue management
operational standards, and data and documentation
authorised activities
flight systems and operational support systems
safety assurance and safety risk management.
The audit identified 6 safety findings and one observation for the operator related to maintenance documentation, fatigue management, and operations manual compliance. Specifically, one finding regarding the operations manual noted that it did not include all the content as required by the regulations. This included limited detail regarding:
processes and procedures relating to low‑level operations and manoeuvring and role specific equipment usage (data acquisition system)
processes and procedures relating to the training of operational and handling procedures with regards to low‑level operations and manoeuvring and role specific equipment usage (data acquisition system).
There were no other findings or observations made regarding the operational risk management processes and procedures.
At the time of the audit, the operator advised CASA that it was waiting for the completion of the ATSB’s investigation prior to initiating any changes to its processes or procedures. However, it was noted that, while the audit was not an investigation, a number of potential latent issues existed, including:
• No active or consistent fatigue monitoring of flight crew during operations other than the required recording of flight and duty records.
• Limited detail in operational risk assessments pertaining to operations in general and the additional fatigue obligations as required by legislation.
• Limited documented operational procedures and associated training relating to low level flight techniques and procedures including the use of operational equipment utilised during survey operations [as detailed above].
• Limited documented process and procedure, and subsequent detail established when conducting internal investigation following operational incidents.
Similar occurrences
Regulatory oversight
Regulatory oversight of air operations has been discussed in detail in previous ATSB investigation reports. These included a fatal Cessna 172 accident at Agnes Waters, Queensland in 2017 (AO‑2017‑005), a fatal Eurocopter EC120B helicopter accident at Hardy Reef, Queensland in 2018 (AO‑2018‑026), and a fatal Eurocopter EC135 helicopter accident at Port Hedland, Western Australia in 2018 (AO‑2018‑022).
These investigations identified that CASA’s regulatory oversight activities had not specifically examined the nature of the operator’s primary activities. The findings were as follows:
The Civil Aviation Safety Authority’s procedures and guidance for scoping a surveillance event included several important aspects, but it did not formally include the nature of the operator’s activities, the inherent threats or hazards associated with those activities, and the risk controls that were important for managing those threats or hazards. (safety issue AO-2017-005-SI-08)
Although the operator’s primary helicopter activity was conducting charter flights to pontoons at Hardy Reef, regulatory oversight activity by the Civil Aviation Safety Authority had not specifically examined the operator’s procedures and practices for conducting operations to these helicopter landing sites.
Although the operator’s primary helicopter activity was conducting marine pilot transfers, regulatory oversight activity by the Civil Aviation Safety Authority had not specifically examined the operator’s procedures and practices for conducting approaches and landings to ships at night in degraded visual cueing environments.
In response to safety issue AO-2017-005-SI-08, CASA amended its surveillance and scoping form to require consideration of current activities. Further, it proposed the addition of an operator profile report to provide current, contextual information on an operator with a view to provide a more effective audit scoping process in which consideration and documentation of an operator’s activities was mandatory.
In response to the draft report, on 3 February 2025, CASA advised the ATSB that:
CASA’s Surveillance activities do not include specific checks of the suitability or effectiveness of the processes and procedures in these specific areas. However, under CASR [Civil Aviation Safety Regulation] Part 138.370, the operator is required to conduct risk assessments and mitigation processes before conducting any particular aerial work operation (that is, they must consider the risk of the specific operation and introduce appropriate mitigants). Surveillance is carried out under set scope of 138 operators under this regulation to ensure the operations are suitably risk assessed.
Based on the actions in response to AO-2017-005-SI-08, the ATSB was of the understanding that an operator’s primary activity was considered in entry control processes and surveillance scope. As such, the above comment was also discussed at the ATSB‑CASA meeting on 3 April 2025. CASA advised that an operator’s primary activity is considered, and when assessing a Part 138 operator it uses a standardised worksheet to ensure there is a consistent approach to that assessment and to maintain a record of the decision‑making process.
Low-level accidents
There has been a number of ATSB investigations into fatal accidents that resulted from a loss of control at low altitude, from which a recovery was not possible.
On 29 April 2012, the owner-pilot of a Cessna 150 aircraft, registered VH‑UWR, was aerial stock mustering on a cattle station about 55 km north‑east of Bourke, New South Wales. The aircraft was observed circling over an area (where cattle were not moving), then entered a steep descent followed by the sound of an impact. The aircraft was substantially damaged, and the pilot sustained fatal injuries.
The ATSB found that, while manoeuvring at low level, the pilot inadvertently allowed the aircraft to aerodynamically stall, resulting in a high rate of descent and collision with terrain. There was insufficient information about pilot control inputs to establish the factors that precipitated the stall.
On 29 December 2014, a Cessna 172S aircraft, registered VH‑PFT, departed Cambridge Airport, Tasmania to photograph yachts participating in the 2014 Sydney Hobart race. On board the aircraft were the pilot and a photographer.
At about 1815 local time, the aircraft commenced low-level photographic runs on yachts to the east of Cape Raoul. Shortly after completing a run on one yacht at a height of about 50 ft, the aircraft entered a steep climbing turn. The aircraft had almost completed a 180° turn when the upper (right) wing dropped sharply while the aircraft’s nose pitched down to almost vertical. The aircraft impacted the water’s surface in an almost vertical nose‑down attitude with wings about level. Both aircraft occupants were fatally injured, and the aircraft was substantially damaged.
As a result of the steep climbing turn, the aircraft’s upper wing aerodynamically stalled, resulting in a rapid rotation out of the turn. The steep pitch attitude indicated that, due to the stalled upper wing, the aircraft entered a spin. There was insufficient height for the pilot to recover the aircraft.
On 13 April 2021, a Cessna R172K aircraft, registered VH-DLA, departed Canberra Airport, Australian Capital Territory, with a pilot and an observer on board to conduct powerline survey work to the north of Sutton township, New South Wales.
About 3 hours into the flight, while conducting a powerline inspection in the vicinity of Tallagandra Lane, nearby witnesses observed the aircraft flying low above the trees before commencing a left turn that continued into a steep descent and collision with terrain. The pilot and observer were fatally injured, and the aircraft was destroyed.
The ATSB found that, while manoeuvring to align the aircraft to inspect a powerline, the aircraft aerodynamically stalled and entered a spin at a height that was insufficient for recovery prior to the collision with terrain.
On 4 December 2021, the pilot of an Air Tractor AT‑400 aircraft, registered VH‑ACQ, was conducting aerial spraying operations on a property 75 km west‑south‑west of Moree, New South Wales.
At 0632 local time, the aircraft took off from the property’s airstrip with the first spray load. The pilot then completed 10 spray loads, each time returning to the airstrip to replenish its load.
Prior to departing with the 11th load, the aircraft was refuelled to full and its spray load refilled. The aircraft then returned to the western side of the target block, but after descending to recommence spraying towards the south, the aircraft climbed and turned away to track north and overfly a flood-affected area. The pilot radioed the company operations manager expressing concern about the weather conditions and the potential for chemical to drift onto a neighbouring property. About 5 minutes later, the aircraft returned to the target block, this time on the eastern boundary.
The pilot then conducted 2 ‘smoker’ runs to assess the drift, followed by 5 back‑to‑back (parallel) spray runs. At the end of the 5th spray run, the aircraft was observed to climb then enter a right procedure turn. During the turn, the aircraft descended rapidly, collided with terrain, and was subsequently destroyed by fire. The pilot sustained fatal injuries.
The ATSB found that the aircraft was too close to the start of the spray run during the turn, which probably resulted in the pilot tightening the turn. This almost certainly resulted in an aerodynamic stall at a height too low to recover before colliding with the ground.
Safety analysis
Introduction
In the afternoon of 3 March 2022, a Cessna U206G, registered VH‑JVR, was being operated on a low‑level geophysical survey flight. When on the 25th survey line, the aircraft collided with terrain and was destroyed in the post‑impact fire. The pilot was fatally injured.
This analysis will discuss the potential reasons for the loss of control and the initiation of the emergency response. The angle of bank regularly used for procedure turns, and the benefits of protective clothing and helmets are also examined. It will also consider the operator’s risk management processes and supporting procedures for low‑level geophysical survey flights, and regulatory oversight of these activities.
Loss of control
The last recorded position of the aircraft was on a survey line consistent with the planned survey parameters. Likewise, a comparison of the available flight data indicated that the aircraft’s location was in a similar position to that of previous procedure turns. Therefore, it was likely that the aircraft was being manoeuvred onto the next survey line at the time of the accident.
The wreckage examination determined that the aircraft impacted the trees in a left angle of bank, with a steep angle of impact and a nose‑down attitude, indicative of a loss of control. The ATSB considered several reasons for the loss of control. There was no evidence to suggest any airborne impact with a bird nor that the weather conditions affected the pilot’s ability to maintain control of the aircraft. To the extent possible, the ATSB determined that the aircraft was structurally intact, there was no flight control malfunction, and the engine was producing power at the time of impact. Further, the pilot did not have any reported health issues, and the post‑mortem and toxicology examinations did not identify the presence of any natural disease or substances. While some causes of incapacitation may not always be identified post‑mortem, there was no evidence to suggest that the pilot had become incapacitated during flight.
The pilot had previously conducted 24 survey lines with no apparent issues identified from the recorded data. Based on the ATSB’s analysis, the aircraft’s airspeed had remained above the aerodynamic stall speed during the procedure turns. Therefore, there was no indication of a near or actual stall on the previous turns. Although, the data identified that the procedure turns were consistently conducted at heights below which a recovery from a stall and loss of control may not be possible. A stall situation was a plausible explanation, as found in previous ATSB investigations into low‑level accidents. However, in this case, this remained only a possibility due to the lack of recorded data beyond the last known position and no witness observations, making it difficult to determine the precise circumstances that led to the loss of control and collision with terrain.
Contributing factor
It was likely that, during a manoeuvre to intercept the next survey line, for undetermined reasons, control of the aircraft was lost at a height from which recovery was not possible, resulting in a collision with terrain.
Delayed emergency response
The operator had a phased emergency response plan, predicated on an elapsed time since the aircraft’s estimated time of arrival (ETA). Each phase was commensurate with an escalating level of concern. Unless there was a notification of an accident by other means, the distress phase would commence at 30 minutes past the ETA, at which point the Joint Rescue Coordination Centre (JRCC) would be contacted to initiate search and rescue activity. Each phase of the plan required accessing the satellite tracking system to ascertain the location of the aircraft.
When the satellite tracking data stopped at 1343, the automatic watch function did not send an alert to the operator after 15 minutes had elapsed, as this function had not been activated. This was not noticed until 1430 when the ground operator conducted a periodic check. While the operator reported previously experiencing dropouts of the satellite tracking system, Spidertracks confirmed that up to the loss of data, the device was functioning as expected and that there were no recorded system outages.
The ground operator was not able to contact the pilot via mobile phone and there was no emergency beacon activation. The ATSB noted that, while the aircraft was not fitted with an emergency locator transmitter, a personal locator beacon was carried in the aircraft. However, as this was not worn by the pilot, this was not readily accessible following the accident.
As such, the status of the pilot and aircraft could not be established. The operations manager then advised the ground operator to follow the emergency response plan and wait until the ETA. When the aircraft did not arrive at the ETA of 1630, about 3 hours after the accident, in accordance with the plan the operator contacted the JRCC at 1701.
The JRCC promptly initiated search and rescue procedures, and an aircraft departed at 1739 and located the aircraft wreckage at 1852. A search and rescue helicopter crew physically located the pilot at 0042. With the time taken to access the pilot, whose injuries required immediate medical care, it was very likely that even if the search and rescue activities had commenced when the satellite tracking data was lost, the pilot would have succumbed to the injuries received.
When an accident occurs and any injuries that result are potentially survivable, a timely response is essential. Minimising the time for search and rescue and enabling emergency services to respond as quickly as possible may increase the chances of a successful outcome.
Other factor that increased risk
An emergency response was not initiated until 30 minutes after the aircraft's estimated time of arrival, which was 3 hours after satellite tracking had stopped and attempts to contact the pilot had been unsuccessful. Although an earlier response was very unlikely to have altered the outcome in this case, minimising the time for search and rescue and enabling emergency services to respond as quickly as possible may increase the chances of a successful outcome.
Low-level manoeuvring
The operator’s pilots routinely used high angle of bank procedure turns to manoeuvre between consecutive survey lines. This back‑to‑back pattern was described by the chief pilot (CP) as the most efficient method and it also reduced pilot workload, especially for obstacle and hazard avoidance.
The CP stated that procedure turns were trained to be at about 300 ft above ground level and a 45–60° angle of bank (known as a steep turn). Analysis of the accident flight indicated that the pilot was flying high angle of bank procedure turns consistent with the operator’s training. However, they were turning at an average of about 200 ft, lower than what was explained by the CP.
The ATSB noted that, during the preceding 24 turns, the pilot had maintained sufficient margin above the stall speeds listed in the pilot’s operating handbook. However, as aircraft data was not available up to the loss of control it was not possible to determine if the aircraft stalled nor the exact circumstances that existed.
The similar occurrences discussed involved a loss of control that was preceded by a stall at very low heights. The U206G pilot’s operating handbook stated that up to 240 ft may be required to recover from a stall, but this height was based on flight testing in controlled conditions and that significantly more height may be required.
High angle of bank turns at low level present a significant risk and International Airborne Geophysics Safety Association (IAGSA) recommended that the angle of bank should be limited due to the stall speed increasing with increasing angles of bank, thus reducing the safety margins available. These margins can be quickly eroded if a pilot tightens the turn to ensure they intercept the survey line, which can increase the load factor further, resulting in reaching the stall speed quicker.
Other factor that increased risk
In accordance with the operator’s training, pilots routinely used increased angle of bank (45–60°) turns at low altitude to position the aircraft onto survey lines. This increased the risk of an aerodynamic stall at altitudes from which recovery may not be possible.
Protective clothing and helmets
At the time of the accident, the pilot was not wearing any protective clothing or a helmet. The use of such equipment was not required by the regulator, or the operator having considered environmental, comfort, and cockpit space aspects. Instead, it was left to the individual pilot’s discretion.
The ATSB’s aviation medical specialist indicated that protective clothing and helmets may reduce the magnitude of injuries in an accident. While they were unable to comment on the effectiveness of these items for this accident, it was acknowledged that these items would not have protected the pilot from smoke inhalation.
In some cases, occupants survive an accident only to succumb to hazards such as fire, drowning or environmental elements such as heat and cold (Shanahan, 2004). IAGSA recommended that survey pilots/crew wear protective clothing, not just as fire protection in the event of an accident but to also provide coverage from the elements while waiting for rescue or in a survival situation. Similarly, the Basic Aviation Risk Standard also recommended that all flight and aircrew wear protective clothing during operations. It is therefore important that these hazards have been considered to enable the best opportunity for survival in the event of an accident.
Other factor that increased risk
The operator did not require its pilots to wear protective clothing or helmets during low‑level survey operations, nor were they required to do so by regulations. However, the use of such has been recommended by industry to improve survivability in the event of an accident.
Risk management
In August 2019, MAGSPEC Aviation implemented a health, safety and environmental management system (HSEMS), which was intended tomeet theCivil Aviation Safety Authority (CASA) safety management system (SMS) requirements. It also provided more generalised guidance on the management of risk within the organisation. However, as an SMS was not required by regulation, it was not assessed by CASA. The ATSB acknowledges that an operator’s SMS, in this case HSEMS, will evolve and mature with time. Significant events like accidents provide an opportunity to assess if the system is operating in a way that assures the highest level of safety given the nature of their operations.
Acknowledging the CASR Part 138 requirements for aerial work operators to undertake risk assessments, which came into effect about 3 months prior to the accident, the ATSB reviewed the safety risk management component of the HSEMS. The HSEMS manual had detailed the 5‑stage process for risk management. However, there was no requirement in the operator’s manuals, as required by Part 138, to conduct a pre‑operational risk assessment nor had one been completed, as confirmed by the CP.
The absence of a pre‑operational risk assessment did not allow formal mitigation strategies, nor provide assurance that the risk level associated with low‑level survey operations was as low as reasonably practical. For example, the operator reported that the survey flights were often flown at about 30 m (100 ft) above ground level. While low operating heights were specified in the job safety analysis (JSA), there was no formalised risk controls referred to in the JSA. The accident survey flight had been flown at 25 m (85 ft) and this had been accepted on the basis of the reconnaissance flight, without any formal identification and implementation of supporting risk controls. While IAGSA acknowledged that stipulating a fixed minimum safe survey height was not practical given differences in survey conditions and aircraft characteristics, a pre‑operational risk assessment for operations at a reasonably anticipated operating height may have provided a foundation from which to adequately assess any variations to this height.
Further, the operator routinely flew consecutive survey lines, which used increased (steep) angle of bank procedure turns (45–60°) to manoeuvre between the lines. There was no assessment to identify any risks associated with conducting higher angle of bank turns at low-level to ensure that reasonable mitigations were implemented, and appropriate safety margins were applied.
The HSEMS further outlined that non‑site‑specific hazards were reported in their online SMS program, but due to the varying nature of operations, a separate site‑specific assessment of each survey job would be completed using the JSA. With the JSA, each survey task was assessed in isolation, with no reference to previous JSAs to ensure that applicable risk controls continued to be applied and/or were appropriate. Also, the JSA did not benefit from being informed by an overarching pre‑operational risk assessment. Therefore, as the predominant method for assessing operational risk, the JSA did not provide assurance that all hazards would be identified, and the associated risks would be assessed and mitigated.
As noted by the International Civil Aviation Organization (2018), safety risk management activities should be documented and the Part 138 Manual of Standards stipulated that the operator’s pre‑operational risk procedures were to include the use of a risk register. The CP reported that an operational risk register was not being maintained as part of their HSEMS at the time of the accident. While non‑site‑specific hazards would be recorded and assessed in the online SMS program, there was a missed opportunity to record the site‑specific hazards identified from the individual JSAs. Therefore, without a risk register, the operator’s ability to track, monitor, and mitigate all known hazards, and assess the effectiveness of existing risk controls was limited.
In interactions with CASA during the transition phase to Part 138 and the level 1 surveillance event post‑accident, there was no commentary related to the adequacy of the operator’s operational risk management processes. On that basis, the operator was of the understanding that the JSA met the risk assessment requirements of Part 138 inclusive of a pre‑operational risk assessment. However, CASA has since advised the ATSB that the JSA did not meet the requirements of a pre‑operational risk assessment.
Other factor that increased risk
MAGSPEC Aviation's safety risk management processes did not include a pre‑operational risk assessment that recognised the generic risks and hazards common across that type of operation nor was a risk register maintained. Consequently, there was limited assurance that all the risks had been identified and that all reasonable mitigations had been applied. (Safety issue)
Survey manoeuvres
As emphasised by IAGSA, conducting steep turns at low level can present challenges for fixed‑wing aircraft as any margin above the stall speed can quickly diminish and there may be limited height within which to respond to an unexpected situation. The ATSB’s analysis of the flight data showed there was some variation in the angle of bank used during the procedure turns on the accident flight, ranging from 43° up to the Cessna U206G angle of bank limit of 60°. At this limit, the stall speed increases by about 40%. The data also indicated that the procedure turns were conducted at an average of about 200 ft above ground level, which was lower than what was explained by the CP.
Similarly, a review of the morning pilot’s flight and discussions with other company pilots identified that there were differences in the individual turn techniques, demonstrating variations of the procedure turns.
While 45–60° angle of bank procedure turns were being taught, the operations manual did not include any policy or procedure for this manoeuvre. Further, there were no specific limits identified, such as a minimum turn height or maximum angle of bank, to establish appropriate safety margins such as that recommended by IAGSA.
ATSB research investigation report B2004/0337 discussed the importance of operational procedures:
The absence, deficiency or inappropriateness of operating procedures for operators may increase the risk to aviation safety.
The absence of standardised procedures means there may be considerable differences in the techniques used by different operators and contracting organisation staff to conduct tasks. Processes that are used to accomplish a particular task will evolve through a process of experience and passing on this information, often by word of mouth. There will be inconsistencies in how the task is accomplished, as different staff and operators will have differing levels of competence and experience, and different solutions to the same problem will have naturally evolved. The organisation that is managing the operation in such an uncontrolled environment will not be in full control or fully aware of how its tasks are being accomplished and therefore will have less control over the safety of the operation.
While the ATSB was unable to determine the circumstances that led to the loss of control, an operator’s expectations and desired safety margins should be documented to minimise variation and ensure operations are performed safely. Otherwise, without formal procedures, pilots are required to exercise judgement based on their experience, skills and knowledge.
Other factor that increased risk
The operator’s pilots were trained to, and routinely flew survey patterns utilising steep turns at low level. However, procedures or limitations specific to these manoeuvres were not included in the operations manual, which increased the risk of inconsistencies in the application of those manoeuvres and reducing the safety margins available.
Flight following
Survey flights are often conducted over remote, inhospitable terrain where regular communication services may not be available. Therefore, the use of satellite‑based flight following services are essential for providing real‑time monitoring of an aircraft’s location and for an efficient search and rescue response.
The operator had installed Spidertracks to all its aircraft and there was an expectation that an automatic alert would be received from the system in the event of emergency. However, there was no requirement and supporting procedure to check the functionality of the system prior to each flight. In this case, the alert function had not been activated for multiple flights, including the accident flight, which potentially influenced the delayed emergency response. Also, while the ground operator assigned to each tasking was responsible for providing flight following services, there was no expected schedule for checking the satellite tracking nor any procedure detailing the expectations of this role. Despite this, given the severity of the pilot’s injuries, it was very unlikely that a prompt emergency response would have changed the outcome.
It is important that an emergency response plan clearly identifies the notification and escalation triggers to avoid delays. Satellite tracking systems are useful in their ability to provide early notification of an emergency, especially in cases where the occupants have been incapacitated or otherwise unable to raise an alarm. However, their usefulness can only be realised if, when installed, they are correctly configured and operating as expected, otherwise increasing the risk of a delayed response.
Other factor that increased risk
While the operator’s aircraft were fitted with a satellite‑based flight following system, there was no requirement nor were there supporting procedures to confirm the set‑up and functionality of the system prior to flight or to monitor the system during flight. This increased the risk of the system not operating as expected and not providing early notification of an emergency.
Regulatory oversight activity
Since 2019, 3 ATSB investigations have been published identifying that regulatory oversight did not formally include the nature of the operator’s primary activities, the inherent threats or hazards associated with those activities, and the risk controls for managing those threats or hazards.
The ATSB acknowledges that CASA’s regulatory oversight activities were subject to normal constraints of time and resources, which may limit an ability to identify issues. Therefore, regulatory surveillance cannot examine every aspect of an operator’s activities, nor identify all the limitations associated with these activities.
The initial air operator’s certificate assessment of the operator and CP focused on the generic regulatory requirements and there were no criteria to evaluate their primary activity of low‑level survey operations. Although CASA had considered the operator and its key personnel as being suitable to conduct the proposed operations, there was no evidence that the processes and procedures for the primary activity had been specifically examined.Likewise, while the operator’s pilots held the appropriate low-level rating, there were no records to indicate that a detailed assessment of how the operator would address the risks associated with low flying had been conducted as part of the low flying approval.
Prior to this accident, the operator had undergone surveillance twice in 2018, following the first occurrence. Operational standards were included in the scope for both surveillance events but there were no related findings made by CASA nor was there any indication to what extent the operator’s low-level survey operations were examined.
The last AHPI review in early 2022 also noted that no post‑authorisation review (PAR) had been conducted following the initial issue of the air operator’s certificate (AOC) and there were no CASA records of action following the 2019 and 2020 occurrences. Consequently, it was recommended that a surveillance activity take place. The same recommendation was also made following this accident. The subsequent surveillance event in 2023 identified that the operator had limited documented operational procedures and training related to low‑level flight techniques.
CASA advised that a PAR (a type of level 1 surveillance) was likely to have been covered by an alternative level 2 surveillance event. The ATSB noted that a level 1 event was more comprehensive than a level 2, and for a PAR, was intended to ensure that the entry control requirements were being met following the initial issue of an AOC. As the CASA officers had made comments about a PAR having never been conducted, it was unclear whether the level 2 was sufficient to have been considered as having met the requirement of a PAR.
While none of CASA’s activities specifically focused on topics related to low‑level survey operations, for example survey patterns and heights, it was difficult to determine whether additional focus, through the conduct of a level 1 PAR for example, would have identified the specific aspects as found in the post‑accident surveillance event. However, CASA has since strengthened its AOC entry control procedures and surveillance planning and scoping to include more emphasis on assessing the primary activity including the use of a specific worksheet that highlights areas specific to Part 138 operators. Consideration of the primary activity provides a level of assurance that operators continue to meet the established requirements and function at the level of competency and safety required to undertake the activity for which they have been approved to perform.
In addition to the above, and as previously discussed, the ATSB identified deficiencies with the operator’s risk management processes. As the requirement for risk assessments only came into effect about 3 months prior to the accident, with the introduction of Part 138, there was limited opportunity for CASA to review these processes within that period. It was also noted that CASA had intended to look at the operator’s Part 138 compliance at the next scheduled surveillance event.
The 2023 surveillance event, which was also a review and follow-up to the accident, was a level 1 surveillance and included risk management within the scope of that activity. However, there were nil findings or observations identifying that there was no pre‑operational risk assessment and risk register, although required under Part 138. As an unintended consequence of this and the transition process to Part 138, the operator was of the understanding that the JSA satisfied this requirement. However, CASA has since indicated to the ATSB that the JSA did not meet the requirement of a pre‑operational risk assessment. While post‑accident, the 2023 surveillance event was a missed opportunity for CASA to identify the deficiencies in processes and inform the operator’s understanding of their risk assessment obligations under Part 138.
Other factor that increased risk
The Civil Aviation Safety Authority regulatory oversight of the operator had not specifically included the primary activity of low‑level survey flights, or the processes and procedures designed to reduce the risks associated with that activity.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain, involving a Cessna U206G registered VH-JVR, 124 km west of Norseman, Western Australia, on 3 March 2022.
Contributing factors
It was likely that, during a manoeuvre to intercept the next survey line, for undetermined reasons, control of the aircraft was lost at a height from which recovery was not possible, resulting in a collision with terrain.
Other factors that increased risk
An emergency response was not initiated until 30 minutes after the aircraft's estimated time of arrival, which was 3 hours after satellite tracking had stopped and attempts to contact the pilot had been unsuccessful. Although an earlier response was very unlikely to have altered the outcome in this case, minimising the time for search and rescue and enabling emergency services to respond as quickly as possible may increase the chances of a successful outcome.
In accordance with the operator’s training, pilots routinely used increased angle of bank (45–60°) turns at low altitude to position the aircraft onto survey lines. This increased the risk of an aerodynamic stall at altitudes from which recovery may not be possible.
The operator did not require its pilots to wear protective clothing or helmets during low‑level survey operations, nor were they required to do so by regulations. However, the use of such has been recommended by industry to improve survivability in the event of an accident.
MAGSPEC Aviation's safety risk management processes did not include a pre‑operational risk assessment that recognised the generic risks and hazards common across that type of operation nor was a risk register maintained. Consequently, there was limited assurance that all the risks had been identified and that all reasonable mitigations had been applied. (Safety issue)
The operator’s pilots were trained to, and routinely flew survey patterns utilising steep turns at low level. However, procedures or limitations specific to these manoeuvres were not included in the operations manual, which increased the risk of inconsistencies in the application of those manoeuvres and reducing the safety margins available.
While the operator’s aircraft were fitted with a satellite-based flight following system, there was no requirement nor were there supporting procedures to confirm the set‑up and functionality of the system prior to flight or to monitor the system during flight. This increased the risk the system not operating as expected and not providing early notification of an emergency.
The Civil Aviation Safety Authority regulatory oversight of the operator had not specifically included the primary activity of low-level survey flights, or the processes and procedures designed to reduce the risks associated with that activity.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: MAGSPEC Aviation's safety risk management processes did not include a pre‑operational risk assessment that recognised the generic risks and hazards common across that type of operation nor was a risk register maintained. Consequently, there was limited assurance that all the risks had been identified and that all reasonable mitigations had been applied.
Safety recommendation to MAGSPEC Aviation Pty Ltd
The ATSB makes a formal safety recommendation, either during or at the end of an investigation, based on the level of risk associated with a safety issue and the extent of corrective action already undertaken. Rather than being prescriptive about the form of corrective action to be taken, the recommendation focuses on the safety issue of concern. It is a matter for the responsible organisation to assess the costs and benefits of any particular method of addressing a safety issue.
Safety recommendation description: The Australian Transport Safety Bureau recommends that MAGSPEC Aviation Pty Ltd develops and maintains a pre-operational risk assessment and risk register that is separate to its existing job safety analysis process. This should encompass the generic risks and hazards common across its operations and allow it to fully consider operational risks beyond individual survey tasks.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by MAGSPEC Aviation Pty Ltd
In response to this accident, MAGSPEC Aviation has taken the following safety action:
The JSA has been revised to include the selection of consequence and likelihood to determine a risk for each identified hazard. It also recorded mitigations that would be applied. The operator advised the overall and highest risk scores determined whether the survey could proceed and/or if it was likely to increase the fatigue and safety of the operation to unacceptable levels.
The health, safety and environmental management system has been incorporated into the operations manual as an appendix.
The emergency response plan was revised to clarify initiation triggers and accounted for a satellite tracking system failure. The operator has also equipped its operations room with 2 dedicated monitors for the sole purpose of tracking aircraft.
The operations manual now includes a minimum speed versus angle of bank section and pilot actions if an aircraft cannot achieve or maintain the required speed.
Guidance on procedural turns has been formalised in the operations manual. Although there is a description of how to conduct the turn, the manual also explains that this was the desired turn method and may not always be possible (due to terrain, obstacles, block shape et cetera).
The operations manual has been amended to clearly state that an aircraft was required to have a fixed emergency locator transmitter. If this becomes unserviceable or has to be removed, the aircraft can only be flown for the purpose of having the issue rectified.
Each pilot has been issued with a personal locator beacon, individually registered with the Australian Maritime Safety Authority. Pilots are required to keep the device on their person while operating company aircraft. The operations manual also states that the personal locator beacon cannot be carried/used if not tested.
Follow-up with Spidertracks is to be made on each occurrence of dropout, service interruption or delay in tracking updates and numerous improvements made to the interface. The operator advised that the SOS automatic watch function and alert has been investigated and rectified. A checklist item has been added to ensure Spidertracks is correctly functioning prior to departure.
They no longer operate at survey heights below 30 m.
The operator identified that its low‑level training syllabus was lacking parameters to mark a pilot as competent, especially in critical phases of flight. This has been formalised to match what had been done practically.
Its operations manual is currently under review by CASA. This includes items to enable Flight Safety Foundation’s Basic Aviation Risk Standard accreditation. Just prior to final publication of this report, the operator advised that it had been awarded the Basic Aviation Risk Standard accreditation.
Glossary
AGL
Above ground level
AHPI
Authorisation holder performance indicator
AoA
Angle of attack
AOC
Air operator’s certificate
CAR
Civil Aviation Act
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CoG
Centre of gravity
CP
Chief pilot
ETA
Estimated time of arrival
ELT
Emergency locator transmitter
G
Gravity
GPS
Global positioning system
HSEMS
Health, safety and environmental management system
IAGSA
International Airborne Geophysics Safety Association
JRCC
Joint Rescue Coordination Centre
JSA
Job safety analysis
MOS
Manual of Standards
PLB
Personal locator beacon
POH
Pilot’s operating handbook
SMS
Safety management system
Sources and submissions
Sources of information
The sources of information during the investigation included:
MAGSPEC Aviation Pty Ltd
other pilots who conducted flights for the operator
recorded data from the satellite tracking device
the maintenance organisation
aviation medical specialist
Pathwest Laboratory Medicine WA
Civil Aviation Safety Authority
Bureau of Meteorology
Western Australia Police Force
Australian Maritime Safety Authority Joint Rescue Coordination Centre
Spidertracks Ltd.
References
Australian Transport Safety Bureau. (2005). Aviation Research Investigation Report B2004/0337 Risks associated with aerial campaign management: Lessons from a case study of aerial locust control. Retrieved from /publications/2005/aerial_locust_control/
Australian Transport Safety Bureau. (2013). ATSB Research Investigation AR-2012-128 A review of effectiveness of emergency locator transmitters in aviation accidents. Retrieved from /publications/2012/ar-2012-128
International Airborne Geophysics Safety Association. (2017). Safety Policy Manual (v2017-1201). Retrieved from https://iagsa.ca/
International Civil Aviation Organization. (2018). Safety Management Manual, fourth edition, Montréal: International Civil Aviation Organization.
Shanahan, D.F. (2004). Human tolerance and crash survivability. RTO HFM Lecture Series on ‘Pathological Aspects and Associated Biodynamics in Aircraft Accident Investigation’. Madrid, Spain.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
MAGSPEC Aviation Pty Ltd
other pilots who conducted flights for the operator
Civil Aviation Safety Authority.
Submissions were received from:
MAGSPEC Aviation Pty Ltd
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[2]Integral fuel tanks are part of the aircraft structure. They are manufactured by assembling parts of the aircraft structure with sealant to form a fuel-tight compartment, most commonly in the wings.
[3]A supplemental type certificate is a type certificate issued when an applicant has received regulatory approval to modify an aeronautical product from its original design. The supplemental type certificate, which incorporates by reference the related type certificate, approves not only the modification but also how that modification affects the original design.
[4]The system was pre-programmed by the ground operator prior to departure, minimising any manipulation required by the pilot during flight.
[5]From the pilot’s operating handbook, the calibrated airspeed and indicated airspeed in the range of interest were within 1 kt, so for the purposes of the analysis were considered equivalent. The term indicated airspeed is used throughout the analysis.
[6]G load: the nominal value for acceleration. In flight, G load represents the combined effects of flight manoeuvring loads and turbulence and can have a positive or negative value.
[7]A steep turn is one greater than a 45° bank angle.
[8]Carbon monoxide is a colourless, odourless, tasteless, and poisonous gas that is produced as a by-product of burnt fuel. Exposure to a leak from the exhaust of an aircraft engine into the cabin can lead to elevated levels of carbon monoxide, which can impair cognitive function.
[10]CAR 157 (2) requires that an aircraft shall not fly over a populous area at a lower height than 1,500 ft or any other area at a lower height than 500 ft. CAR 157 (4)(b) states that the provisions of CAR 157 (2) shall not apply if the aircraft is engaged in aerial work operations and the operator has a permit from the authority (CASA) to do so.
[11]As the wing to which the stall warning vane is mounted approaches the critical AoA, the relative air flow changes direction and will push the vane up, closing a switch in the device. This will activate a warning horn.
[12] Donesafe is a web and application‑based safety management system tool.
[13]This timeframe has since changed with the most recent being 12-18 monthsfollowing the initial issue, depending on the type of authorisation issued (CASA Surveillance Manual version 5.2 ‑ May 2024).
On 11 March 2022, at about 1050 local time, the pilot of a Bell Helicopter Company B206L-1, registered VH‑BHF and operated by Heli Surveys Pty Ltd, departed Jindabyne aerodrome, New South Wales, to conduct a weed survey task on behalf of the New South Wales National Parks and Wildlife Service (NPWS). On board were the pilot and 4 NPWS officers. At about 1112, at a low level and low speed over the Snowy River, control of the helicopter was lost. While attempting an emergency landing in the river, the helicopter collided with a large boulder. Three of the occupants received serious injuries and 2 received minor injuries. The helicopter was destroyed.
What the ATSB found
The ATSB found that, to conduct the weed survey above the riverbank, the helicopter was flown at low-level, at a slow speed, and yawed to the right by about 45°. It was also noted that the helicopter was operating at a high gross weight and higher density altitude. In combination, these conditions were conducive to the onset of a loss of tail rotor effectiveness. As such, it was likely that a loss of tail rotor effectiveness occurred at an insufficient height to recover and avoid a collision with terrain. Following the collision into the river, the carriage of dedicated emergency locator transmitting devices allowed for a timely response for retrieving the occupants.
Further, one of those on board was not required for the survey task, which unnecessarily exposed them to the risks associated with low-level flight. While the client’s operating procedures referred to ‘essential personnel’, they did not provide a definition or specify the roles and responsibilities of these personnel.
The ATSB also identified that the operator’s risk assessment for low-level operations did not contain the hazard and control measures to avoid the likelihood of loss of tail rotor effectiveness. Further, there was no requirement for its pilots to conduct pre-flight risk reviews to ensure that operations could be conducted without unacceptable safety risk.
What has been done as a result
Heli Surveys conducted a review of its risk management processes and made changes to its operational conduct. Its changes focused on identifying flight‑related hazards that included loss of tail rotor effectiveness and compiling mitigation controls in a dedicated risk assessment. Other changes included the introduction of a ‘Hazardous Flight Conditions’ course for pilots and a requirement for flight crews to ensure that only essential crew were to be on board its helicopters.
The NPWS revised its aviation safety policy and developed an aviation safety management system to enhance safety and manage risk across its aviation activities and operations. To define essential personnel, the NPWS committed to developing detailed task profiles to ensure that the roles and responsibilities of all personnel were clearly defined and committed to the development of task‑specific risk profiles to manage risks associated with its aerial work activities.
Safety message
Survey flights, particularly when performed in alpine environments, are generally conducted at low level and slow speeds. This creates a high-risk operating environment that requires effective risk management. Risk management should include an overarching pre‑operational risk assessment to identify the hazards and risks common to that type of operation. This assessment can then be used to inform the management of risk for specific taskings including a pilot’s pre-flight risk review, to ensure the operation can be conducted safely.
This accident further highlighted the benefits of carrying multiple position transmitting devices. This not only eliminates potential doubt associated with transmissions generated from inadvertent beacon activation but can accelerate an emergency response.
The occurrence
On 11 March 2022, at about 1050 local time, the pilot of a Bell Helicopter Company B206L-1 helicopter, registered VH‑BHF and operated by Heli Surveys Pty Ltd, departed Jindabyne aerodrome, New South Wales, to conduct a low-level English Broom weed[1] survey task on behalf of the New South Wales National Parks and Wildlife Service (NPWS) (Figure 1). On board were the pilot and 4 NPWS officers.[2]
Following departure, the flight tracked north along the western side of Lake Jindabyne and at about 1055, the pilot turned north-west and tracked upstream along the Snowy River before turning south-west towards Island Bend. At about 1102, the helicopter passed overhead Island Bend where a clump of the weed was located. This local infestation provided an opportunity for the NPWS officers to familiarise themselves with spotting the target weed in the local environment, to assist with identification during the survey.
From Island Bend, the flight continued south-west, following the course of the river. At 1110:35, the helicopter approached Guthega (Munyang) hydro‑electric power station where the pilot commenced a left turn, to pass to the east of the power station.
Figure 1: VH-BHF flight path from Jindabyne aerodrome to Guthega power station with inset showing location relative to capital cities
Source: Google Earth and TracPlus data, annotated by the ATSB
At 1110:47, and now south of the power station, the pilot commenced a right, high orbit to remain clear of power lines in the area and return towards the river course.
By 1111:17, the helicopter was heading downstream above the southern riverbank and established in a descent towards the river in preparation for commencing the weed survey (Figure 2).
Corroborating reports from the occupants of the helicopter, which included the pilot, indicated that due to the seating position of the NPWS officers (3 seated on the left side of the helicopter), the later part of the descent was conducted with the nose of the helicopter yawed to the right about 45°. The right yaw was in response to the officers’ request to provide the best view of the riverbanks for them to identify and map the locations of the English Broom weed. The officers reported that they asked the pilot to fly lower and sideways to enhance their view. The pilot reported to the ATSB that, prior to setting up the right yaw position, the helicopter’s speed was about 30 kt and they noted they had sufficient power with no abnormal engine indications.
As the helicopter descended past Pipers Creek, the pilot reported that their vision of trees and other obstacles was obscured by the helicopter’s instrument console. To improve their vision for the final descent to the river, the pilot indicated that they ‘touched’ the left anti-torque pedal[3] to straighten the helicopter ‘a bit’, upon which the helicopter started an uncommanded yaw[4] to the right.
In interview with the ATSB, the pilot stated that they believed they had full and free movement of the anti-torque pedals until the uncommanded yaw to the right started. After the yaw started, they felt that the helicopter did not respond to their pedal inputs, but they could not recall exactly what inputs they made. The pilot did not recollect any shock loading of the tail rotor, such as from a bird or tree strike. The officers reported that, when the uncommanded right yaw started, they thought it was a pilot‑initiated turn and that they were clear of trees and there were no physical knocks or signs of a failure before the yaw commenced.
After the first turn, when the helicopter was facing downstream, the pilot attempted to gain forward speed, but the helicopter continued to yaw right, and the yaw rate started to accelerate. At 1111:58, when about 200 m past Pipers Creek, the pilot reported realising their only landing option was in the river and, to do so, they rolled the throttle to idle, which stopped the yawing motion. The helicopter entered an autorotation[5] with the pilot aiming for a spot in the river. The pilot attempted to cushion the landing but did not see a large boulder in the water at their aim point.
At 1112:04, the helicopter collided with terrain. Three occupants received serious injuries, and 2 sustained minor injuries. The helicopter was destroyed.
Figure 2: Approach to Guthega power station, orbit to the south, descent and collision with terrain
Source: Google Earth and TracPlus data, annotated by the ATSB
At the time of the accident, the operator had another helicopter in the local area conducting sling‑work operations. At around 1130, the pilot of that helicopter, who was also the head of flying operations, received a report[6] of an alert notification from the emergency locator transmitter on VH‑BHF, and a subsequent report of a personal locator beacon activation. Aided by their onboard resources, the pilot identified the last recorded position of VH-BHF that was transmitted by its satellite‑based tracking system (TracPlus) and immediately ceased the sling-work operation and departed for that recorded position. While enroute, the pilot notified emergency services and directed their ground‑based resources in the local area to the expected helicopter location.
The pilot located VH-BHF at about 1138 and confirmed the accurate position with emergency services. While surveying the scene from overhead, they were joined by another of the operator’s helicopters, and that pilot was able to unload an air crew person at the accident site. The air crew person was equipped with a first aid kit and provided a communications link between the ground and the overhead helicopters. At about 1210, the operator’s ground-based staff arrived to provide assistance and reported that emergency services had started to arrive. Following initial treatment, 3 of the injured persons were airlifted to hospital while the remaining 2 were able to walk from the site to awaiting ambulances.
Context
Personnel information
Pilot
Qualifications and experience
The pilot held a valid class 1 aviation medical certificate and a Commercial Pilot’s Licence (Helicopter) with single‑engine helicopter and low‑level rating, and a gas turbine endorsement. The operator’s pilot record sheet, dated 2 November 2021, indicated the pilot had accrued 900 hours turbine experience from a total of 2,065 flying hours experience. The pilot had also logged 530 hours aerial work and low flying, and 20 hours mountain flying. In the 28 days prior to the accident, the pilot had accrued 47.1 hours flight time, and 98.7 hours in the previous 90 days. In total, the pilot had 145 hours experience on the Bell 206L-1 helicopter, which included 9.3 hours in the previous 90 days.
Operator training
The pilot joined the operator, Heli Surveys, in early November 2021. On 21, 22 and 23 October 2021 they completed 6 pre-employment check flights on the AS350 helicopter with a contracted training and checking organisation. The syllabus for the checks included low flying within the normal procedures and tail rotor malfunction, autorotation, fire, jammed controls and system failures within the emergency procedures.
The pilot reported that a loss of tail rotor effectiveness (LTE) (refer to section titled Loss of tail rotor effectiveness) would have been covered in their training history at some stage but could not recall any specific occasion, and that they had never experienced it before in flight. The operator’s head of flying operations (HOFO) reported that they conducted a flight with the pilot before they were released to line and was impressed with their attention and focus on control of the helicopter during take-off and landing. The HOFO did not specifically discuss LTE during their flight with the pilot but did discuss mountain and survey operations. They further reported that they considered LTE a component of the low-level flying conducted in the pilot’s pre‑employment check flights.
National Parks and Wildlife Service officers
The National Parks and Wildlife Service (NPWS) team on board consisted of:
A task coordinator who had the lead role in terms of liaising with the pilot and the other officers and was logging the location of the English Broom weed on a hand-held electronic device.
Two officers designated as primary observers (spotters). Their role was to look for the weed, and when a plant was identified, advise the coordinator. One of these observers was logging the position of the weed on a hand-held electronic device.
Another NPWS officer had joined the group given their employment as the area ranger. The survey task had provided the opportunity for the officer to familiarise themselves with the area from the air and observe the conduct of the weed survey task. While the officer did not have a specific function to perform for the survey, they assisted the team in locating the English Broom weed.
Helicopter information
General
VH-BHF was a Bell Helicopter Company B206L-1 powered by a Rolls-Royce model 250‑C30P gas turbine engine driving a 2‑blade main and tail rotor system. It was manufactured in the United States in 1979 and assigned serial number 45164. The helicopter was issued with an Australian Certificate of Airworthiness on 7 April 1987 and first registered in Australia on the same date. Including the pilot, the helicopter provided seating for 7 occupants. At the time of the accident, the helicopter had accumulated about 11,849 hours, total time in service.
Recent maintenance history
At the last 100-hour periodic inspection on 27 November 2021, a maintenance release was issued, permitting night visual flight rules[7] operations. The maintenance release showed that an engine hot start defect had been recorded in December 2021. Rectifications for that included the replacement of the engine turbine assembly, and post‑repair power assurance checks that were certified as completed on 14 February 2022, deeming the engine serviceable. The maintenance release also showed that:
other than items that would be addressed during a daily inspection, no maintenance was due
there were no defects that required rectification before the next flight
the helicopter had been flown for about 22 hours from when the maintenance release was issued prior to the accident.
Modifications
The helicopter was fitted with Van Horn Aviation 2062200-101/-301 tail rotor blades with a United States Federal Aviation Administration (FAA) approved rotorcraft flight manual supplement (206L1‑FMS‑901). The supplement stated that the tail rotor blade design increased the stall margin, thereby improving high altitude performance:
Satisfactory stability and control has been demonstrated in relative winds of 30 MPH (26 knots) sideward and rearward at all loading conditions…
The helicopter was also fitted with main rotor yoke part number 206-011-149-101 allowing flight operations up to a gross weight limit of 1,882 kg (4,150 lb), up from 1,837 kg (4,050 lb) as stated on the type certificate data sheet.
Weight and balance
The ATSB completed weight and balance calculations for the helicopter, considering the pilot and 4 NPWS officers on board. Including fuel, baggage and cargo, the helicopter all‑up weight at take‑off was determined to be about 1,842 kg, 40 kg below its gross weight limit of 1,882 kg, and within its centre of gravity limits. Accounting for fuel burn-off, the helicopter’s all-up weight at the time of the accident was about 1,799 kg, 83 kg below its gross weight limit.
Meteorological information
The Bureau of Meteorology grid point wind and temperature forecast (relevant to the accident) for 1100 on 11 March 2022 was 5 kt of wind from the west (280°) and a temperature of 8°C at 5,000 ft. The graphical area forecast, valid from 1000, was for visibility greater than 10 km with scattered[8] stratus cloud between 2,000 ft and 3,500 ft until 1100.
The nearest aerodrome with an automatic weather information service was Cooma, New South Wales, located 50 km east of the accident site at an elevation of 3,106 ft. The recorded conditions at Cooma at 1100 were a wind of 9 kt from 030°, visibility greater than 10 km, no cloud detected, a temperature of 13°C and QNH[9] at 1021.
The pilot reported fine weather conditions with light winds from the south-west of no more than 5 kt when in the vicinity of the power station, dropping to nearly nil wind conditions once below treetop height on descent towards the river. The NPWS officers reported that the weather was calm. One of the first responders provided a similar report of light and variable winds, as they noted that the wind conditions allowed each rescue helicopter to assume a different heading while hovering as the injured persons were winched on board.
A similar report regarding local weather conditions was received from the operator who maintained an airborne presence during the initial discovery of the wreckage and throughout the rescue operation. They described the conditions on the day as very good with visibility greater than 10 km and wind speed predominantly below 5 kt. They added that there was a very light wind flowing in the downstream direction of the river at the accident site.
Recorded data
A TracPlus™ RockAIR tracking device was recovered from the helicopter following the accident. The device recorded global positioning system tracking information at a frequency of 1 Hz on a removable micro-SD card. ATSB analysis of the recorded data for the last 60 seconds of the flight is shown in Figure 3 for illustrative purposes.
For a period of about 32 seconds before the helicopter started to yaw, the recorded data indicated that its groundspeed was below 25 kt and further decreased below 20 kt about 5 seconds before the yaw began. About 3 seconds after the yaw commenced, and from a height of about 200 ft above ground level, the helicopter’s rate of descent (vertical speed) increased and reached a peak of about 2,500 ft/min, consistent with the pilot rolling off the throttle and entering an autorotational descent. The data indicated that the yaw lasted for about 5 seconds and was arrested within about 3 seconds of the start of the descent. When the yaw stopped, the helicopter’s height was about 65–100 ft above ground level.
Figure 3: Ground positioning system flight tracking data over the last 60 seconds of recording
Graphical representation of flight data showing helicopter forward and vertical speeds, altitude, height above terrain and helicopter track with descriptive comments added. Source: TracPlus data, accessed and annotated by the ATSB
Wreckage and impact information
The accident site was located less than 600 m downstream from the Guthega power station (Figure 2) and 20 km north-west of Jindabyne, New South Wales. The helicopter landed on top of a large boulder in the shallows of the Snowy River and came to rest on a heading of 310°, with the fuselage canted significantly to the right (Figure 4).
The helicopter struck the boulder at a point forward of the external cargo hook fuselage mount and slightly aft of the forward skid gear cross tube. The impact with the boulder structurally damaged the helicopter, breaking the forward cockpit section from the cabin area, and resulted in the tailboom partially fracturing near its fuselage attachment point.
The tailboom fracturing and subsequent deflection likely resulted in a tail rotor ground strike and loss of a portion of a tail rotor blade, which was not recovered from the site. Apart from the missing section of tail rotor blade, the rest of the helicopter was present at the accident site. No evidence of a bird or in-flight tail rotor strike was identified and there was no post‑impact fire.
The location of the helicopter in the riverbed and the surrounding environment precluded a complete examination of the wreckage at the accident site. The operator reported receiving advice that anticipated water inflows at Guthega Dam would result in increased water levels downstream of the dam from water exiting the uncontrolled spillway. In response, the wreckage was removed from the accident site at the earliest opportunity, airlifted from the riverbed and relocated to a secure site in Cooma for detailed examination.
Figure 4: VH-BHF following collision with terrain against large boulder in the Snowy River, New South Wales
Source: ATSB
The ATSB’s site examination did not reveal any pre-existing defects that may have affected the operation of the helicopter or its systems. The detailed examination of the flight control systems in Cooma did not identify any pre-existing defects that may have affected the control of the helicopter.
Where evidence of structural fractures and breaks were identified, the failures were found to be fresh and were attributed to being either collision‑related, or as the result of torsional overload forces. Of note was the torsional overload of the tail rotor driveshaft at the tail rotor gear box location. This indicated that the driveshaft was driving the tail rotor when the tail rotor experienced a sudden stoppage (Figure 5).
The engine presented as intact, securely mounted, and with controls functional but with restricted movement due to fuselage damage. The compressor and turbine were found to spin freely. No defects were identified with the supply, delivery and quality of the fuel that was available to the engine.
The seating configuration of the helicopter consisted of 2 cockpit seats and, in the cabin section, a centre row of 2 aft-facing seats and a rear row of 3 forward‑facing seats. For the accident flight, the pilot was in the front right seat with an NPWS officer (coordinator/recorder) in the front left seat, another officer (area ranger – observer) in the centre row left seat (facing rearwards), and the 2 remaining officers in the left (observer/recorder) and right (observer) seats of the rear row (Figure 6). Each seat was equipped with a 4-point restraint harness.
Figure 6: VH-BHF cockpit and cabin seating layout and NPWS officers’ functional positions
Bell 206 LongRanger III seating layout adopted for illustrative purposes only. Source: FlyFlapper.com annotated by the ATSB
Injuries
The pilot, task coordinator, and observer in the rear‑facing cabin seat sustained serious injuries. The 2 observers in the rear row received minor injuries.
Evacuation
While airborne above the accident site, the HOFO reported they contacted the power station and advised them of the accident downstream of their location and for consideration of the possible impact on power generation commitments. They were advised that power generation would be postponed, however, water levels downstream of Guthega Dam were dependent on natural inflows and outflows from the dam.
At interview, 2 of the NPWS officers advised that they were aware that the water level would likely rise in response to power generation activity. As a precaution, after assisting the injured with evacuating from the helicopter, they were immediately moved to higher ground.
Survival equipment
The NPWS aviation standard operating procedure for low-level flying specified that, when engaged in such activities, helicopters were to carry an emergency locator transmitter (ELT) and be fitted with a tracking system that could be tracked by the agency. As such, the helicopter was equipped with an ELT, and a survival pack that included a personal locator beacon (PLB), a first aid kit and a satellite phone. A TracPlus RockAIR device was also mounted on the instrument console, which provided real-time location tracking of the helicopter through GPS technology. The tracking device was designed to transmit an alert if a sudden impact of 16g or more for a period greater than 10 milliseconds was detected.
ELT and PLB emergency radio beacons are used to provide a location fix on a person, aircraft or other vehicle (ATSB, 2013). ELTs are usually fixed in an aircraft and are designed to activate automatically during an impact, typically by a g-force[10] activated switch but can also be wired to be manually activated by a cockpit-located switch usually mounted within reach of the pilot or a front‑seat passenger. PLBs are designed for personal use and may be carried on the person or carried as part of a survival kit. They are manually activated and may be used as an alternative to a fixed ELT, provided certain requirements are met.
In the event of an accident followed by beacon activation, the aircraft wreckage and its occupants can be located quickly by search and rescue authorities. Finding the aircraft wreckage quickly not only increases the chance of survival of the occupants but also reduces the risk to pilots of search and rescue aircraft who commonly need to operate in marginal weather conditions and over mountainous terrain (ATSB, 2013).
The collision resulted in both the ELT and tracking device activating. The collision alerts were received by the operator (HOFO) and were followed by a third report of a PLB that was manually activated by one of the NPWS officers. This allowed the HOFO to promptly identify the last known position of VH-BHF and commence an emergency response. The operator reported that the multiple transmissions from independent sources provided the surety that a distress situation existed.
Operational information
Helicopter performance
The out-of-ground effect performance chart in the B206L-1 rotorcraft flight manual indicated the helicopter had the performance required to hover out-of-ground effect at the elevation and temperature conditions for the accident. The accident site was located at an altitude of 4,308 ft. Accounting for temperature and QNH, the density altitude for the flight just prior to the accident was calculated to be about 4,500 ft.
The recorded data for the flight indicated that the groundspeed had dropped below 20 kt before the loss of control, and accounting for density altitude influence, this equated to a calibrated[11] airspeed of about 1–2 kt below the groundspeed in nil wind. The height and airspeed of the helicopter at this time placed it inside the avoid area of the height-velocity diagram[12] (Figure 7 – left). The helicopter’s weight and density altitude also placed the operation outside of the weight-altitude limit for the height-velocity diagram (Figure 7 – right).
Consequently, the helicopter was operating in a region of the flight envelope where there was no assurance that a safe autorotation could be made without damage and injuries to occupants. At interview, the operator advised that flight operations in the avoid area was common practice, and necessary to effectively and accurately conduct a weed survey task.
Figure 7: B206L-1 flight manual performance charts showing operational caution zones and VH-BHF relative position in preparation for survey task
Source: Bell Helicopter Company, annotated by the ATSB
Aerial work operations
Heli Surveys
Heli Surveys Pty Ltd was approved by the Civil Aviation Safety Authority (CASA) to conduct various flight operations including Civil Aviation Safety Regulation (CASR) Part 138 aerial work operations. Its aerial work operations were varied and included roles associated with feral animal control and survey flights of pest animals, weeds and power lines.
Part 138 aerial work operations
CASR Part 138 and the Part 138 (Aerial Work Operations) Manual of Standards (MOS) addressed the certification, operational and safety risk management requirements for operators engaged in aerial work operations (CASA, 2021e). At the time of the accident, aerial work encompassed the core activities of external load operations, dispensing operations or task specialist operations.[13] Advisory circular AC 138-01 v1.0 Part 138 core concepts defined task specialist operations as:
carrying out a specialised activity using an aircraft in flight and includes training for such an activity. An example of a task specialist operation is a low level weed survey or pipeline inspection.
Additional guidance for aerial work operations applicable at the time of the accident was provided in advisory circular AC 138-05 v1.1 Aerial work risk management (July 2021b) and the Part 138 Acceptable means of compliance and guidance material – Aerial work operations v2.2 (December 2021f).
Conducting the survey flight
At interview, the HOFO described the accident task as an ad hoc type survey in which the helicopter would be flown up-valley and then down-valley to view both sides of the river and that the airspeed, direction and height was not prescribed. The HOFO expressed the view that the optimum profile for survey flights was a height of 300 ft and airspeed of 55 kt. However, if adopting that profile, it would make it impractical to identify English Broom weed in surveys of the Snowy River.
The HOFO reported that, from experience, they did not consider that it was unusual when the client presented with 4 NPWS officers for the conduct of the survey flight. In terms of managing client requests, all pilots are provided with a ‘stop work authority’ and can therefore decline a client request if they perceive a safety of flight issue.
The NPWS officers indicated that, on the morning of the accident flight, they discussed their English Broom weed survey plan while waiting for the pilot and helicopter to return from a prior task. After the pilot arrived, they completed the operator’s online induction and a safety brief with the pilot and then briefed the pilot on their plan for the weed survey.
None of the officers had previously met the pilot who they understood was new to the company and had not previously done the English Broom weed survey task with them. They reported that the pilot was operating in a cautious manner and appeared to be safety‑conscious, advising them all to speak-up if they identified any hazards during the flight. On departure, the pilot made a radio call to their NPWS contact for flight‑following purposes, and they conducted a hazard identification for wires during the flight upstream to the Guthega Power Station.
Persons permitted on board during aerial work operations
For aerial work operations conducted under Part 138, CASA advisory circular 138-01 specified that persons who were permitted on board must be categorised as either:
crew members (including flight crew, air crew and task specialists)
passengers that meet the requirement to be aerial work passengers.
The advisory circular further defined an air crew member, task specialist and aerial work passenger as:
Air crew member
An air crew member…includes crew members who carry out a function during the flight relating to the safety of the aircraft.
Task specialist
A task specialist … includes crew members who carry out a function for the flight relating to the aerial work operation (as distinct from a safety related role).
Examples of a task specialist would include a camera operator that operates an external camera pod, or an aerial shooter used in an animal culling operation.
A task specialist will require training to be inducted into the operation and to ensure they are competent in carrying out their assigned function as a member of the operator's crew.
Aerial work passenger
…are persons who are closely associated with the purpose of the aerial work operation. Their presence in the aircraft must not be for mere convenience or enjoyment.
Examples of such persons would include: Personnel involved in carrying out or supporting a mustering activity carried on a positioning flight before or after the mustering operation, such as ground based personnel to assist with refuelling or for opening and closing of gates etc. and yarding of stock for the mustering operation…
In most circumstances aerial work passengers do not require training before their carriage on an aerial work operation or a positioning flight, but they will in all cases (except for some notable situations, such as a person being rescued) require a safety briefing prior to the flight...
On the accident day, as the helicopter was being used to conduct a low-level weed survey activity, it met the definition of a task specialist operation. In terms of the roles as defined above, the pilot was the only flight crew member and there were no air crew members. The 3 NPWS officers with the roles of task coordinator and primary observers would be classed as task specialists. While the area ranger assisted with the task, they reported that they were on the flight as an opportunity for familiarisation of the survey area.
Operational hazards
CASA flight crew licencing uses a competency-based training and assessment system for pilots. Various competencies are required to be demonstrated by pilots during both initial and recurrent licence testing. The competencies vary by aircraft type and licence type.
For pilots to achieve their helicopter rating, they are required to demonstrate that they have the skills and underpinning knowledge to manage abnormal and emergency situations in helicopters (CASA, 2021c). The range of situations include, but are not limited to:
key hazards – underpinning knowledge of their causal factors, contributing operational situations, avoidance and recognition of symptoms and recovery techniques that include:
the impact of high gross weight and high-density altitude on key hazards
techniques for how to avoid a potentially hazardous situation whilst in flight.
These competencies were consistent with the list of hazards detailed in the jointly developed CASA and Civil Aviation Authority of New Zealand helicopter flight instructor manual, issue 3 (CASA, 2012). The instructor manual differentiated hazards from emergencies, which are the technical failures particular to the helicopter model and addressed in the flight manual emergency procedures section.
To be licensed for low-level helicopter operations, pilots must demonstrate skills to safely conduct low‑level operations include managing variable terrain and weather, surface conditions, loose objects and personnel. The required underpinning knowledge related to critical operational conditions that included retreating blade stall,[17] vortex ring state, over pitching and loss of anti‑torque or tail rotor effectiveness (CASA, 2021c).
The ATSB reviewed the emergencies and hazards chapter of the FAA Helicopter Flying Handbook (2019) and found key operational hazards presented were the same as those that CASA required pilots to demonstrate. The FAA handbook provided a thorough description of each of the key hazards, which included techniques for avoidance and recovery. The FAA handbook also reported the following about LTE events:
Certain flight activities lend themselves to being more at high risk to LTE than others. For example, power line and pipeline patrol sectors, low-speed aerial filming/photography as well as in the Police and Helicopter Emergency Medical Services (EMS) environments can find themselves in low and slow situations over geographical areas where the exact wind speed and direction are hard to determine.
Loss of tail rotor effectiveness
Introduction
Loss of tail rotor effectiveness (LTE) or unanticipated yaw is a phenomenon that can occur in single main rotor, tail rotor-equipped helicopters. It is a condition that occurs when the air flow through a tail rotor is changed in some way, by altering the angle or speed at which the air passes through the rotating blades of the tail rotor disc (FAA, 2019). If uncorrected, LTE can result in loss of control of the helicopter and serious to fatal occupant injuries. In 1995, the FAA published advisory circular 90-95 Unanticipated right yaw in helicopters, which described a loss of tail rotor effectiveness as:
…a critical, low-speed aerodynamic flight characteristic which can result in an uncommanded rapid yaw rate which does not subside of its own accord and, if not corrected, can result in the loss of aircraft control.
Any manoeuvre which requires the pilot to operate in a high-power, low-airspeed environment with a left crosswind or tailwind creates an environment where unanticipated right yaw may occur.
LTE is not related to a maintenance malfunction and may occur in varying degrees in all single main rotor helicopters at airspeeds less than 30 knots.
Single-rotor helicopters manufactured in the US, such as the Bell 206, have main rotors that rotate anticlockwise when viewed from above. When powered, their rotation produces a torque reaction or tendency of the helicopter to turn in the opposite direction, which is a right yawing motion from the pilot’s view. The tail rotor thrust provides the anti‑torque control. An effective tail rotor relies on a stable and relatively undisturbed airflow in order to provide a steady and constant anti-torque reaction (FAA, 2019).
The FAA AC described 3 wind conditions conducive to the onset of LTE. One of these conditions refers to the relative wind[18] azimuth of 285° to 315°, which can produce ‘main rotor disc vortex interference’ with the tail rotor (Figure 8) and is described as:
As the main rotor vortex passes the tail rotor, the tail rotor angle of attack is reduced. The reduction in the angle of attack causes a reduction in thrust and a right yaw acceleration begins. The thrust reduction will occur suddenly and, if uncorrected, will develop into an uncontrollable rapid rotation about the [main rotor] mast.
The relative wind from the critical quadrant may present when the nose of the helicopter is pointing forward (Figure 8), or the condition is generated when the helicopter is flown with the nose sufficiently yawed to the right.
Figure 8: Main rotor disc vortex interference with tail rotor
Source: FAA Helicopter Flying Handbook (FAA, 2019), annotated by the ATSB
Factors affecting loss of tail rotor effectiveness
Other than main rotor blade action affecting the quality of the airflow about the tail rotor disc and impacting its ability to provide useful thrust, additional factors are also considered when discussing LTE. According to the FAA Helicopter Flying Handbook (2019):
The design of main and tail rotor blades and the tailboom assembly can affect the characteristics and susceptibility of LTE but will not nullify the phenomenon entirely.
FAA AC 90-95 also identifies other factors that influence the severity of the onset of LTE including:
Gross Weight and Density Altitude. An increase in either of these factors will decrease the power margin between the maximum power available and the power required to hover. The pilot should conduct low-level, low-airspeed manoeuvres with minimum weight.
Recovery technique
The Bell 206L-1 rotorcraft flight manual revision 14 did not have an emergency procedure for LTE but did have a procedure for a complete loss of thrust under the heading tail rotor control failure, which was a mechanical failure. Following the procedure for a complete loss of thrust, pilots were to reduce the throttle to idle and immediately enter an autorotation while maintaining a minimum airspeed of 52 kt during the descent.
The FAA AC 90-95 recommended recovery technique from LTE was:
a. If a sudden unanticipated right yaw occurs, the pilot should perform the following:
(1) Apply full left pedal. Simultaneously, move cyclic[19] forward to increase speed. If altitude permits, reduce power.
(2) As recovery is effected, adjust controls for normal forward flight.
b. Collective[20] pitch reduction will aid in arresting the yaw rate but may cause an increase in the rate of descent. Any large, rapid increase in collective to prevent ground or obstacle contact may further increase the yaw rate and decrease rotor rpm.
c. The amount of collective reduction should be based on the height above obstructions or surface, gross weight of the aircraft, and the existing atmospheric conditions.
d. If the rotation cannot be stopped and ground contact is imminent, an autorotation may be the best course of action. The pilot should maintain full left pedal until rotation stops, then adjust to maintain heading.
Heli Surveys operations manual
The Heli Surveys Operations Manual volume 10 – Specialist operations, prescribed the operator’s general low flying requirements. Paragraph 0.7.3, under Conduct of flight during low flying stated the following:
Pilots shall be aware of recovery techniques and avoid flight configurations which could include:
• Vortex ring/ settling with power.
• Tail rotor vortex ring or loss of tail rotor effectiveness.
• Downwind operations outside the aircraft performance envelope.
• Loss of close visual cues to indicate actual aircraft relative movement and out of wind operations (particularly over water), leading to possible unanticipated control difficulties.
The operations manual did not include any avoidance or recovery procedures for LTE nor any reference material to address this condition.
Safety risk management
Aerial work risk management
Pre-operational risk assessment
CASR Part 138 required an operator conducting aerial work to undertake risk assessments of its operations. The Part 138 MOS and corresponding advisory circular (AC 138-05 v1.1) detailed a layered approach to risk assessments. One of the key requirements was that an operator should undertake an overarching assessment (pre‑operational risk assessment) to consider and evaluate the risks associated with its proposed operations, in this case, low-level helicopter survey. This assessment recognised the underlying principles of CASR Part 138, where the risks and hazards associated with a type of aerial work operation are common to that type of operation. The MOS indicated that the matters to be considered for such an assessment included:
• the operation and its particular characteristics
• the location of the operation and its particular characteristics
• the aircraft to be used in the operation, its particular characteristics, and its performance
• the qualifications and experience of the crew members to be used in the operation
• the hazards, external to the aircraft, that may be met in the course of the operation.
The operator is required to gather data for inclusion in the pre-operational risk assessment using a range of sources. Acknowledging that certain risk factors may be common to all operators, may be particular to the aircraft type operated or may be unique to the operator; potential sources include, but are not limited to (CASA, 2021b):
CASA ‘sector risk profiles’ for the varying types of operations
ATSB incident and accident reports
industry association safety reports
manufacturers' safety bulletins and advisory notices
input from experienced pilots and other operators.
Once the pre-operational risk assessment has been populated, it should be updated over time to include lessons learnt from previous operations. It should also form part of the operator’s operations manual.
Flight risk management plan
The results of the pre-operational risk assessment were to be considered when preparing the flight risk management plan, which was specific to an individual flight or task within the type of operation. The plan should outline the specific mitigators or risk controls that were to be used during the flights.
Pre-flight risk review
The next step was for the pilot, on behalf of the operator, to conduct a pre-flight risk review, with reference to the pre‑operational risk assessment, flight risk management plan, and the most recent data for the operation. The review was to be completed prior to the commencement of the operation and was to consider the conditions and circumstances that existed at the site or area at the time of the proposed activities. This ensured that the operation could be conducted without unacceptable safety risk.
Operator risk management
As per CASR Part 138, Heli Surveys was required to undertake risk assessment and mitigation processes and include those processes in its suite of operational documents. The Heli Surveys Operations Manual described that the operator would address its risk management obligations via the use of Safe Work Method Statements (SWMS).
The Heli Surveys Safety Management Systems Manual further detailed how risk was identified, controlled and documented. Their safety risk management process started with hazard identification, which included internal sources and external sources. A hazard was defined in their SWMS as ‘what could result in harm’ and was used to describe both the hazard and associated risk.
Internal sources for hazard identification included, but were not limited to:
safety assessments of systems and operations
voluntary and mandatory safety reports
inspections and audits.
Its list of external sources included, but was not limited to:
accident and incident reports
safety information bulletins, safety alerts and other safety publications from CASA, Airservices Australia, the ATSB and other authorities worldwide.
The operator had prepared SWMSs to comply with the CASR Part 138 requirements which was equivalent to a pre-operational risk assessment. As the accident flight was a low‑level survey operation in the Snowy Mountains, the 2 SWMS relevant to the flight were Low level surveys and aerial photography (henceforth referred to as Low-level surveys) and Alpine operations.
The SWMS documents provided the means to record the specific tasking event, the equipment and approvals that were relevant, and any specific checks or personal protective equipment required to perform the task. A risk matrix was also included. The risk matrix described the likelihood and consequence of each identified hazard and provided the means to assess the initial and residual risk level following the implementation of suitable risk controls.
The ATSB reviewed the SWMSs that were developed by the operator. A summary of the internal and external hazards that were identified by the operator are below (Table 1).
Table 1: Summary of hazards related to Safe Work Method Statements for low-level survey tasking and alpine operations
Low-level survey hazards
Alpine operations hazards
intercom failure
adverse weather events
high communication workload/distraction
inadvertent flight into instrument meteorological conditions
loose articles exiting aircraft
collision with powerlines/aerials
collision with objects while airborne
heavy landing – exceeding power requirements
inadvertent flight into instrument meteorological conditions
exposure – inappropriate dress for conditions
restraint harness issues
aircraft door issue
turbulence/windshear
The heavy landing hazard associated with the alpine operations SWMS was assessed by the ATSB to be related to the CASA flight crew licensing competency requirement to manage the hazard associated with overpitching. The SWMS provided some control measures, such as a power check, landing into wind and monitoring environmental conditions between a landing and take-off.
With the exception of the relationship between overpitching and the operator’s heavy landing hazard in its alpine operations SWMS, the ATSB did not find references to hazards associated with abnormal situations and emergencies specific to the operator’s unique activities in its SWMS. Of note, there was no reference to LTE and vortex ring state, and the impact of flight regimes and operations at high gross weights and density altitudes that may affect such hazards.
The operator reported that pilots were required to have read and understood the suite of SWMS documents, which were provided during their induction process and at scheduled intervals thereafter. However, there was no requirement for pilots to conduct a pre-flight risk review for low-level survey operations and reference the relevant SWMS when conducting pre-flight tasks in preparation for the activity. As such, the pilot had not conducted a review prior to the accident flight.
Client risk management
The NPWS (the client) had contracted Heli Surveys to conduct the weed survey operation. Its Aviation Safety Policy and related documents were provided to the ATSB. The policy identified a range of aviation operations that utilised rotary wing aircraft.
The policy adopted a risk management approach to aviation operations and safety. Key elements of the policy were the development and observance of aviation‑related standard operating procedures and the use of a job safety analysis (JSA).[21] The JSA assessed the risks associated with each task, which was equivalent to a flight risk management plan.
Regarding vegetation‑related activities that necessitated low-level flight operations, the NPWS provided several task-related JSA documents that identified specific hazards. The documents also detailed the control measures to be implemented to manage the associated risks. The JSA documents that were provided related to low-level flying in general, low-level flying when undertaking Scotch (English) Broom survey and aerial application (spraying) activities.
When engaging in those activities, a key control measure specified in the JSA advised that only ‘essential personnel’ were to be on board the operating helicopter. The NPWS reported that the suite of documents supporting aviation operations did not provide a definition of essential personnel nor was there a procedure on record that detailed the roles and responsibilities of NPWS personnel reflected in the JSA control measure.
Related occurrences
Loss of tail rotor effectiveness
Between 2013 and 2022, the ATSB received 16 notifications where the reporter advised of an LTE or unanticipated yaw event. Of the 16 notifications, 12 were investigated by the ATSB. Most of these resulted in nil to minor injuries to those involved and one serious injury and one fatality. Some of these investigations are described below.
On 19 January 2013, a Bell 206B3 helicopter was being operated on an aerial filming task over hilly terrain on the north-eastern outskirts of Perth, Western Australia. After hovering and manoeuvring at about 500 ft above ground level to allow the camera operator to record footage of a truck accident, the pilot conducted a right orbit to complete filming and depart the area. The pilot had initiated the turn when the nose of the helicopter moved left, then suddenly and rapidly to the right as the helicopter yawed and developed a rotation of about 5 revolutions.
The ATSB found that, when the pilot turned to the right to commence the orbit, the helicopter was exposed to a crosswind from the left while at an airspeed around the 30 kt threshold value for susceptibility to LTE, precipitating an unanticipated right yaw and temporary loss of control. The pilot regained sufficient control for a forced landing.
On 20 July 2015, the pilot of a Bell 206L3 (LongRanger) helicopter, registered VH-BLV, conducted a charter flight from Essendon Airport to Falls Creek, Victoria, with 5 passengers on board. The helicopter took off from Essendon close to its maximum take‑off weight.
When at 700 ft above ground level and tracking from the north-west, the pilot conducted a shallow approach towards the helipad at Falls Creek. As the helicopter descended to about 50 ft above ground level, the pilot found that significantly more power was required to conduct the approach than anticipated. The pilot assessed that there was insufficient power available to continue to land and elected to abort the approach. The pilot pushed forward on the cyclic to increase the helicopter’s airspeed and conducted a left turn.
As the helicopter turned left, it started to yaw rapidly towards the right. The pilot applied full left anti-torque pedal to counteract the yaw, but the helicopter continued to yaw. The helicopter turned through one and a half revolutions, as the pilot lowered the collective. Lowering the collective reduced the power demand of the power rotor system, thereby increasing the ability of the anti‑torque pedals to stop the right yaw. The combination of lowering collective and applying forward cyclic to gain forward airspeed, allowed the pilot to regain control of the helicopter. The pilot then conducted a left turn towards the helipad and made an approach to the helipad from an easterly direction. The helicopter landed following the second approach without further incident.
The ATSB’s report highlighted the importance for pilots to understand and avoid conditions that are conducive to unanticipated yaw or LTE and noted that pilots can reduce their exposure to LTE by maintaining awareness of the wind and its effect on the helicopter. Further, if a pilot encounters unanticipated yaw, quick application of the correct response is essential to recover control of the helicopter.
On 28 January 2019, the crew of a Sikorsky S-64E Skycrane helicopter was conducting firebombing activities when it collided with water at Woods Creek Dam, Victoria. The collision occurred following an approach to the dam to fill an external tank with water. The helicopter was crewed by 2 pilots, and a maintenance crew chief was also on board. Following the collision, all the occupants were able to exit the helicopter and swim to shore. One crewmember was seriously injured and 2 were uninjured. The helicopter was substantially damaged.
The ATSB found that the helicopter was placed in a steep flare, which contributed to the helicopter entering vortex ring state when on approach to the dam.
It was also noted that the operator’s operations manual stated that only flight crew and crew essential to the operation could be carried aboard the aircraft during firefighting operations. The operation could be conducted without the crew chief, and not all company crew chiefs were on board their aircraft during firefighting operations. While the crew chief had significant system and task knowledge, they were not required to be on board the helicopter.
On this occasion, their presence on board subjected them to the significant hazards associated with underwater egress. More generally, the carriage of additional personnel during specialised operations like firefighting exposes them to unnecessary risk.
On 21 May 2019, while engaged in a planned cull of feral animals in Kakadu National Park, Northern Territory, a crew of 3 were using a Bell 206B3 JetRanger helicopter for aerial platform shooting. While the helicopter was operating at about 50 ft above the ground, the engine decelerated to idle, resulting in an immediate loss of power, and subsequent collision with terrain. The 3 occupants (pilot, shooter and spotter) were seriously injured.
The investigation identified that it was normal practice across industry that an aerial culling task was performed with just 2 persons on board the helicopter, the pilot and a shooter. Experienced aerial shooters interviewed after the accident expressed a preference for carrying just the pilot and shooter on board to reduce risk to crew, carry more fuel to improve endurance and to complete more work. In 2016, the aerial culling task was redesigned for 3 crew, including a spotter. There was no formal risk analysis of the inclusion of the spotter position, or consideration of the potential benefits of improved data collection when weighed against operational difficulties in recording data, reduced efficiencies in operation, and increased exposure of employees to risk.
The investigation identified that, given the increased complexity and risk in low-level operations, the number of crew should be kept to a minimum. That is, only personnel essential for conducting the task should be carried.
Safety analysis
Introduction
On the morning of 11 March 2022, a Bell B206L-1 helicopter, registered VH-BHF, departed Jindabyne aerodrome, New South Wales, to conduct a weed survey task on behalf of the National Parks and Wildlife Service (NPWS). On board were the pilot and 4 NPWS officers. While descending towards the riverbed in the vicinity of the Guthega power station, the helicopter started an uncommanded yaw to the right. The pilot was able to stop the yaw but was unable to arrest the descent before the helicopter collided with terrain. The helicopter was destroyed. Three occupants received serious injuries, and the remaining 2 occupants received minor injuries.
The following analysis will discuss the uncommanded yaw, and the carriage of persons on the flight. It will also consider the risk management practices of both the operator and its client and discuss the emergency response following notification of the accident.
Helicopter position
The weed survey task was a low-level, low-speed flight activity. On the accident flight, in addition to the pilot seated in the front right seat, there was an NPWS officer in the front left seat and 3 NPWS officers in the cabin area with 2 seated on the left of the helicopter. With 3 of the NPWS officers seated on the left, the pilot was asked if the helicopter could be flown sideways to provide the best view of the target vegetation for those officers. In response, the pilot yawed the helicopter about 45° to the right of their track. Forward flight with the helicopter yawed 45° to the right, in calm wind conditions, produced a relative wind opposite to the motion of the helicopter, from an angle of about 315°.
Weight and balance data indicated that with the 5 occupants on board, the helicopter was operating within 100 kg of its maximum all-up weight. It was also operating at a density altitude of about 4,500 ft. As weight and density altitude increase, the margin between the power available and power required for the flight is reduced. Further, the flight data identified that the groundspeed of the helicopter was below 25 kt and further reduced to less than 20 kt for several seconds prior to the uncommanded right yaw. As there was little wind, the airspeed was close to the recorded groundspeed.
As described by the United States Federal Aviation Administration in its Helicopter Flying Handbook and advisory circular 90-95, there are certain conditions that can change the air flow through a tail rotor, subsequently resulting in a loss of tail rotor effectiveness (LTE). In this case, the combination of a low speed and right yaw placed the helicopter inside the region of main rotor disc vortex interference with the tail rotor, a condition conducive to the onset of LTE. The severity of the onset of LTE was further influenced by the high gross weight and density altitude.
Contributing factor
The sideways movement of the helicopter during the weed survey operation, combined with the high-density altitude, high gross weight, and low airspeed, were conditions conducive to the onset of a loss of tail rotor effectiveness.
Loss of tail rotor effectiveness
The pilot’s description of flying the helicopter with a significant amount of right yaw at about 30 kt was consistent with the recorded data at the start of their run from the Guthega power station. However, the speed slowly decayed below 20 kt just prior to an uncommanded right yaw when the pilot applied some left anti-torque pedal to straighten the helicopter and improve their vision on their approach to the river below. After the helicopter started yawing to the right, the pilot identified a forced landing site in the river and rolled the throttle back to idle, which stopped the yawing motion. The cessation of the yawing motion when the engine power was reduced indicated the yaw was being driven by the reaction to the engine torque applied to the main gearbox and there was insufficient anti-torque to prevent it.
The ATSB determined that there was no evidence of a pre-existing mechanical issue, and the helicopter had the performance capability to operate at the altitude of the survey area. However, the helicopter was positioned in the region of main rotor disc vortex interference with the tail rotor just prior to the loss of control. As such, the ATSB concluded that the uncommanded right yaw was likely an LTE event.
At the time of the event, the helicopter was operating at about 150 ft above ground level in the avoid area of the height-velocity diagram, in addition to which, it was also outside the weight-density altitude limits for the height‑velocity diagram. Therefore, there was no assurance a safe forced landing with minimal damage and injuries could be achieved from the height that the autorotation was commenced.
Contributing factor
It was likely that a loss of tail rotor effectiveness occurred at a height that was insufficient for the pilot to recover before the helicopter impacted the ground.
Operator’s risk management
As a Part 138 operator, Heli Surveys was required to adopt a layered approach to risk management. This approach included conducting a pre-operational risk assessment, which considered all the generic risks and hazards common to the type of operation, in this case, low‑level survey. Heli Surveys achieved this requirement through the Safe Work Method Statements (SWMS).
To inform the pre-operational risk assessment, a range of internal and external data sources could be used that considered the risks common to all low-level survey operators, particular to the aircraft type operated, or unique to the operator. For example, for low-level helicopter operations this may include hazards such as a high-density altitude, retreating blade stall, LTE, vortex ring state and over pitching. Therefore, it was foreseeable that hazards influenced by the particular operating environment would be included in the operator’s SWMS for both Low-level surveys and Alpine operations.
The ATSB reviewed the SWMS accounting for the circumstances of the accident. The SWMS incorporated heavy landings, adverse weather events, collisions with obstacles and hazards associated with the carriage of passengers and task specialists. In consideration of the operation and activities, which included the carriage of passengers and task specialists, the hazards identified by the operator appeared to be relevant. However, their SWMS did not address LTE, although this was identified in its operations manual as a condition specific to low flying and is a known hazard as discussed by the Civil Aviation Safety Authority and the United States Federal Aviation Administration.
The English Broom weed survey operation was conducted at low level and low speed, which were conditions conducive to the onset of LTE. Therefore, and in establishing the context for the operation, LTE was relevant. However, while the risk of LTE was not considered in the SWMS, the accident pilot was familiar with LTE and indicated that it had been covered in their training at some point. As a result, the ATSB was unable to determine if having LTE identified in the SWMS would have influenced the accident outcome. That said, the absence of this consideration did not allow for formal mitigation strategies to be implemented, nor provide assurance that the risk level associated with LTE was as low as reasonably practical. Consequently, there was a reliance on the underpinning knowledge and operational experience of the individual pilot to manage the risk of LTE.
In addition, as a requirement for Part 138 operators, the pre-operational risk assessment, or in this case the SWMS, was to inform the pre-flight risk review. This review was to be performed by a pilot, on behalf of the operator, before a flight commenced. The operator reported that such a review was not conducted for its low-level survey operations nor was one performed by the accident pilot. The merits of this process would have provided the operator an opportunity to validate the SWMS against the proposed operation and allow pilots to determine that the operation could be conducted without unacceptable safety risk.
Documenting and detailing known hazards and the associated risk controls in a dedicated SWMS, reviewed pre-flight, would complement a pilot’s underpinning knowledge. In turn, this would raise immediate awareness of the possibility of encountering hazards such as LTE when conducting a low-level survey task. Further, the pre-flight risk review would provide the means for all the participants involved to consider these critical operational conditions and associated controls. This would complement the safety briefing provided by the pilot in conjunction with the NPWS officers as they prepared for the accident flight.
Other factor that increased risk
The Heli Surveys safe work method statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre‑flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low-level survey operations were as low as reasonably practicable. (Safety issue)
Helicopter occupants
There were 5 occupants on the helicopter, including the pilot. It was very likely that the weed survey could have been completed with just the NPWS coordinator in the front left seat and 2 officers in the left and right rear forward‑facing seats. As such, they would meet the criteria of a task specialist as described under Part 138. If not required as a task specialist, and excluding the pilot, all others on board would be regarded as aerial work passengers and would not be permitted. As such, it was likely that the additional NPWS officer on board (the area ranger) was not fulfilling the role of a task specialist. The additional person’s presence appeared to be motivated by opportunity, and while it was acknowledged that they could contribute as a survey team member, their involvement was not essential to a successful task outcome.
Given the nature of the task and the operating conditions under which it was being conducted, the inclusion of personnel who were not essential to fulfilling the task outcomes exposed them to the risks of low-level helicopter flight and, in the event of an accident or incident, potential injury. On this occasion, the occupant who did not have a specific role to perform, for either the spotting or logging activity, was seriously injured in the accident when operating at low level with limited landing options available due to the surrounding terrain.
Contributing factor
The carriage of an additional person on board the helicopter who was not essential to the tasking, exposed them to risks associated with low flying operations over inhospitable terrain.
Client’s risk management
The client (NPWS) arranged for the survey flight to be undertaken, and its officers presented at Jindabyne to board the helicopter on the appointed day. Risk assessments covering low-level flying operations and weed survey tasks in the form of a job safety analysis were on record, and a key risk control measure advised that only essential personnel were to be on board. However, no definition of essential personnel was available to potentially limit the number of persons that would be exposed to the identified risks. Defining essential personnel would also support informed distinctions between those who would appropriately fulfil roles as task specialists and those who were aerial work passengers.
Further, the procedure and roles of the persons conducting the survey were not documented. This likely allowed a degree of discretion to be applied by the participants, which resulted in others participating alongside task specialist(s) whose presence may, on occasion, be unnecessary. For example, for this accident one of the NPWS officers who did not have a specific role received serious injuries.
The client was also engaged in other activities such as aerial spraying and culling, both of which likely involved helicopter operations at low level. Having a definition of essential personnel and documenting their respective roles and responsibilities as task specialists would provide the necessary information for determining who should be involved. This would potentially confine the numbers to the minimum required to conduct the task thereby minimising risk exposure.
Contributing factor
The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities. (Safety issue)
Accident notification
The helicopter was equipped with a fixed emergency locator transmitter and an electronic flight tracking device (TracPlus), which provided active monitoring of the helicopter’s position. Additionally, a personal locator beacon and a satellite phone were carried on board as part of the operator’s survival kit.
Within a very short time of the accident occurring there were reports of the helicopter's fixed emergency locator transmitter activating, the TracPlus unit transmitting the helicopter’s last recorded position and manual activation of a personal locator beacon. The multiple reports removed any doubt of a spurious transmission from any of the units and, as a result, the operator and emergency services were able to respond with minimal delay.
The timely alerts also provided the means for the power station to be alerted to the presence of injured persons on the riverbank who required urgent medical assistance. Their recovery would likely have been impacted by an increase in water level and provided the opportunity for decisions to be made regarding water discharge into the river via the power station.
The extraction of the damaged helicopter from the Snowy River was also influenced following advice of water storage buildup and possible uncontrolled discharge from the Guthega Dam spillway. The early notification likely provided sufficient time to plan for and safely airlift the helicopter wreckage from the river for detailed examination and removed a potential environmental issue.
Other finding
The activation of the on-board emergency locator transmitter and a flight monitoring device, and manual activation of a personal locator beacon, resulted in an immediate emergency response.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell 206L-1, VH-BHF, 20 km north-west of Jindabyne, New South Wales, on 11 March 2022.
Contributing factors
The sideways movement of the helicopter during the weed survey operation, combined with the high-density altitude, high gross weight, and low airspeed, were conditions conducive to the onset of a loss of tail rotor effectiveness.
It was likely that a loss of tail rotor effectiveness occurred at a height that was insufficient for the pilot to recover before the helicopter impacted the ground.
The carriage of an additional person on board the helicopter who was not essential to the tasking, exposed them to risks associated with low flying operations.
The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities. (Safety issue)
Other factors that increased risk
The Heli Surveys safe work method statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre‑flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low-level survey operations were as low as reasonably practicable. (Safety issue)
Other findings
The activation of the on-board emergency locator transmitter and a flight monitoring device, and manual activation of a personal locator beacon, resulted in an immediate emergency response.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Heli Surveys Safe Work Method Statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre-flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low‑level survey operations were as low as reasonably practicable.
Safety issue description: The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define, ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by Heli Surveys
In addition to the safety action detailed above, Heli Surveys has revised its risk register detailing both flight-based and ground‑based threats in its operations and associated risk controls. It has also introduced a ‘Hazardous Flight Conditions’ ground-based course that was proactively developed in response to this accident. The intent of the course was to refamiliarize pilots with such conditions (for example, loss of tail rotor effectiveness) to ensure currency and assist with informed decision‑making and is to be completed every 12 months. The flying aspects discussed in the course will be covered in operator proficiency checks.
Additionally, Heli Surveys has defined ‘essential crew’ in its operations manual. It has also added a requirement that, prior to flight, the pilot in command is to confirm that when undertaking Part 138 operations, all persons on board are deemed essential and each person has a relevant and specific task.
Glossary
AC
Advisory circular
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
ELT
Emergency locator transmitter
FAA
Federal Aviation Administration (United States)
HOFO
Head of flying operations
JSA
Job safety analysis
LTE
Loss of tail rotor effectiveness
NPWS
National Parks and Wildlife Service
MOS
Manual of Standards
PLB
Personal locator beacon
SWMS
Safe Work Method Statement
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
New South Wales National Parks and Wildlife Service officers
Heli Surveys Pty Ltd
New South Wales National Parks and Wildlife Service
Bureau of Meteorology
Civil Aviation Safety Authority
New South Wales Police Force
recorded data – TracPlus unit.
References
ATSB. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents (AR-2012-128). Australian Transport Safety Bureau, Canberra, ACT, Australia.
CASA. (2021c). Part 61 Manual of Standards Instrument 2014. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021d). Part 91 (General Operating and Flight Rules) Manual of Standards 2020. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021e). Part 138 (Aerial Work Operations) Manual of Standards 2020. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021f). Acceptable means of compliance and guidance material, (Aerial work operations - Part 138 of CASR). Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2023). Multi-part Advisory Circular: AC 91-30, AC 121-12, AC 133-03 and AC 135-14 V1.0, Emergency locator transmitters. Civil Aviation Safety Authority, Canberra, ACT, Australia.
FAA. (1995). Advisory Circular: Unanticipated right yaw in helicopters (AC 90-95). U.S. Department of Transportation, Federal Aviation Administration, Washington, D.C., USA.
FAA. (2019). Helicopter Flying Handbook (FAA-H-8083-21B). U.S. Department of Transportation, Federal Aviation Administration, Oklahoma City, OK, USA.
NTSB. (2017). Safety Alert SA-062: Loss of tail rotor effectiveness in helicopters. National Transportation Safety Board, Washington, D.C. USA.
Weeds Australia. (2019). Broom, English Broom, Scotch Broom, Common Broom, Scottish Broom, Spanish Broom,www.weeds.org.au accessed July 2024.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
Heli Surveys Pty Ltd
National Parks and Wildlife Service officers
National Parks and Wildlife Service
Civil Aviation Safety Authority
Transportation Safety Board of Canada.
Submissions to the report were received from the following parties:
Civil Aviation Safety Authority
Heli Surveys Pty Ltd
National Parks and Wildlife Service
National Parks and Wildlife Service officers.
The submissions were reviewed and where appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]English Broom: also known as Broom, Scotch Broom, Common Broom or Spanish Broom and is a highly invasive, environmental weed of national significance that favours cooler, higher rainfall regions.
[2]Officers: denotes NPWS personnel and their job titles and includes officers, rangers and other staff members.
[3]Anti-torque control pedals: a primary helicopter flight control that changes the pitch of tail rotor blades to control thrust around the yaw axis. Acts to counterbalance the main rotor torque reaction and provides heading control in the hover and balanced flight when the helicopter is in forward motion.
[4]Yaw: the motion of an aircraft about its vertical or normal axis.
[5]Autorotation: a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[6]The operator reported that, as the registered owner of the beacons, the Australian Maritime Safety Authority contacted the nominated person and the head of flying operations was subsequently advised of the beacon activations.
[7]Visual flight rules: a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[8]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
[9]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[10]The force needed to accelerate a mass. G-force is normally expressed in multiples of gravitational acceleration (normal gravity = 1g).
[11]For flight operations at low airspeeds, there is a negligible difference between calibrated and indicated airspeed.
[12]The height-velocity diagram shows the combinations of indicated airspeed and height above the ground which will allow an average pilot to successfully complete a landing after an engine failure. By carefully studying the height-velocity diagram a pilot can avoid the combinations of altitude and airspeed that may not allow sufficient time or altitude to enter a stabilised autorotative descent (FAA, 2019).
[13]As of July 2025, the carriage of fireground personnel was also classified as an aerial work operation core activity.
[14]Vortex ring state describes an aerodynamic condition where a helicopter may be in a vertical descent with 20% up to maximum power applied, and little or no climb performance (FAA, 2019).
[15] Overpitching occurs when collective pitch is increased to a point where the main rotor blade angle of attack creates so much drag that all available engine power cannot maintain or restore normal operational revolutions per minute (ICAO, 2024).
[16]When a helicopter is hovering, some of the air passing through the main rotor disc is recirculated back into the disc from the top. This phenomenon is common to all airfoils and is known as tip vortices. As long as the tip vortices are small, their only effect is a small loss in rotor efficiency. However, operating in close proximity to obstructions can lead to an increase in recirculation and loss of performance (FAA, 2019).
[17]In forward flight, the relative airflow through the main rotor disc is different on the advancing and retreating side of the rotor blades. The relative airflow over the advancing side is higher due to the forward speed of the helicopter, while the relative airflow on the retreating side is lower. To generate the same amount of lift across the rotor disc, the advancing blade flaps up while the retreating blade flaps down. This causes the angle of attack to increase on the retreating blade, which increases lift. At some point, as forward speed increases, the low blade speed on the retreating blade, and its high angle of attack will result in a stall and loss of lift (FAA, 2019).
[18]Relative wind: the airflow relative to an aerofoil created by movement of an aerofoil through the air.
[19]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[20]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[21]Job safety analysis: a form of risk assessment that details, step-by-step, how a task is to be performed safely.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 28 February 2022, the crew of three Robinson R44 helicopters were preparing to conduct crocodile egg collection in Arnhem Land, Northern Territory. The egg collection was conducted under contract to Wildlife Harvesting (Northern Territory).
Each helicopter had two crewmembers – one nominated pilot in command and one egg collector. Two of the helicopters were operating under a Civil Aviation Safety Authority Instrument. The instrument authorised the pilot in command to operate with a person outside the aircraft in a harness system attached to the helicopter for the purpose of collecting crocodile eggs. The authorisation was subject to a number of conditions, which included fitment of equipment under an Engineering Order or a Supplemental Type Certificate and an associated flight manual supplement.
The two helicopters used for sling operations were fitted with dual external cargo hooks, which attached to rings on a 100 ft long line. This enabled the egg collector (‘sling person’) to be slung 100 ft below the helicopter to access the nests. The line could be released by the pilot via a quick release system for the cargo hooks. The cargo hooks were fitted with primary and back-up dual quick release systems, to reduce the likelihood of inadvertent pilot activation and provide redundancy in case of failure. One of those two helicopters was an R44 Raven II, registered VH-IDW, operated by Helibrook Pty Ltd. The third helicopter was primarily to be used for transporting eggs, although both its pilot and collector also collected eggs on foot and wore a harness so they could be slung under either of the other two helicopters as needed.
At about 0703 Central Standard Time,[1] the three helicopters departed from Noonamah, for a 90-minute flight to a site where fuel drums had been pre-positioned en route to the collect sites. Fuel was available at Noonamah and the drum site, however, there were no accurate records of fuel uplift for VH-IDW.
The helicopters departed from the drum site at about 0830 and tracked to the King River staging area, where the crews prepared to commence egg collection operations (Figure 1). Recorded OzRunways[2] data for two of the helicopters recorded their arrival at the staging area at 0850. The pilot and sling person of VH‑IDW planned to start the egg collection from a nest located close to the staging area. At about 0900, the other two helicopters departed the staging area for their crew to commence collecting eggs about 12 km to the north-east. Data recorded for the egg collection showed that the crew of those two helicopters collected eggs from nine nests between 0911 and 1014.
By 1014, the four crewmembers operating to the north-east became concerned that they had not heard any radio communications from the crew of VH-IDW since departing the staging area. As a result, one of the pilots elected to return to the area they expected VH-IDW to be operating in. At 1036, the pilot located the wreckage of VH-IDW and landed near the accident site (Figure 1). They found the helicopter substantially damaged having collided with trees and terrain. The sling person was deceased, and the pilot had sustained serious injuries. After providing reassurance to the pilot of VH-IDW, the other pilot returned to their helicopter and took off briefly to get mobile reception and call for assistance. A Careflight helicopter arrived on site at about 1230 and airlifted the pilot to Maningrida, where they were transferred to an aeroplane and flown to Darwin.
The location of the accident was in the vicinity of the first target nest for egg collection by the crew of VH-IDW. No eggs had been collected, indicating that the accident probably occurred about 90 minutes before it was found. A handheld emergency position indicating radio beacon and the helicopter’s emergency locator transmitter, which was not mounted in the installed airframe rack or armed in case of emergency, were subsequently found in helicopter. Neither was activated to alert rescue personnel at the time of the accident.
Figure 1: Accident area including King River, staging area, accident site and the approximate tracks of the other two helicopters
Source: Google earth overlaid with positions obtained from OzRunways and collection data
Context
Site and wreckage
The accident site was located in a paperbark swamp approximately 300 m from the staging area. Preliminary analysis of the site indicated that the accident sequence had occurred in a north‑westerly direction. The sling person was found approximately 40 m prior to the main wreckage. The long line attachment rings were not connected to the helicopter cargo hooks. Although the pilot reported that they had been wearing the 4‑point seat restraint, the pilot had egressed the helicopter and lay beside it.
The helicopter’s main rotor blade had struck and cut through the trunk of at least one tree at multiple points before the helicopter collided with terrain upright, facing north-east (Figure 2). The helicopter’s skids had splayed and fractured, and the base of the pilot’s seat had crushed as designed to absorb impact forces.
Figure 2: VH-IDW accident site
Source: Careflight
Initial assessment indicated that the engine was stopped when the helicopter collided with the ground. There was no visible damage to the tail rotor blades and continuity of the drive system and flight controls was established.
The two fuel bladder tanks were intact despite breaches of the surrounding metal tanks and there was no fire. However, the fuel system was compromised in the accident, and it was possible fuel escaped into the creek that flowed beneath the wreckage. After initial assessment, the helicopter wreckage was retrieved from the site. ATSB investigators subsequently drained about 250 ml of blue fuel from the main tank’s bladder.
Engine examination
The engine and associated components were taken to CASA-authorised maintenance facilities for examination under supervision of the ATSB. The examinations did not identify defects of the engine likely to result in engine stoppage.
Pilot qualifications and experience
The pilot held a Class 1 Medical Certificate, a Commercial Pilot Licence (helicopter) and a low-level helicopter rating. At the time of the accident, the pilot had a total aeronautical experience of about 2,500 hours.
Weather
The weather recorded at 0900 at the two nearest Bureau of Meteorology weather stations was:
Warruwi (Goulburn Island) 30 km north of the accident site: west-north-westerly wind at 13 km/hr, QNH 1009.6 hPa, temperature 28.8 °C.
Maningrida 90 km east of the accident site: westerly wind at 6 km/hr, QNH 1009.1, temperature 27.5 °C.
At sea level QNH 1009 hPa and 28 °C, the density altitude is 1,680 ft.
Further investigation
The investigation is continuing and will include review and examination of:
electronic components retrieved from the accident site
fuel system components
refuelling practices
fuel quality
maintenance records
operational documentation
regulations
survivability aspects.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB would like to acknowledge the assistance of Careflight, the Northern Territory Police and Nautilus Aviation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Updated 31/10/2023: The ATSB is in receipt of directly involved parties’ submissions with their comments on the draft report, including information on any safety actions they have taken. As such the investigation is now in the ‘final report: approval’ phase, where the submissions are being assessed and the report is being prepared for final review and approval for public release by the ATSB Commission. Once approved by the Commission, the final report will be prepared for publication and dissemination. Public release is currently anticipated by the end of November.
Updated 04/10/2023:The ATSB has agreed to a brief further extension of the period afforded to directly involved parties to review and provide comment on the ATSB’s draft final report.
The ATSB will provide an update on timing for the public release of the report by the middle of October once all submissions from directly involved parties have been reviewed. The ATSB does not anticipate providing any further extensions to the involved parties review process.
The ATSB provides draft reports to directly involved parties to allow them to check the report’s factual accuracy and to ensure natural justice.
Updated 05/09/2023:Following receipt of the draft report as part of the ‘final report: external review’ phase, some extensions to the 14 day review period have been provided.
Given the complexity of this systemic-level investigation, the ATSB has agreed to extension requests commensurate with the interests of the involved parties.
An update on timing for the publication of the report will be provided at the end of September when the ATSB will have had an opportunity to review submissions.
Updated 28/08/2023: The ATSB’s investigation into the collision with terrain involving Robinson R44, VH-IDW, King River, Northern Territory, on 28 February 2022, is now in the ‘final report: external review’ phase.
After the draft final report was reviewed by ATSB management, the ATSB Commission approved providing the draft report to directly involved parties (DIPs) to allow them to check the report’s factual accuracy and to ensure natural justice.
DIPs are individuals or organisations who possess direct knowledge of the circumstances surrounding the accident.
The draft report was provided to DIPs under Section 26(1)(a) of the Transport Safety Investigation Act 2003. Under Section 26, the report may only be copied and disclosed for the purpose of taking safety action or providing comment to the ATSB. Anyone who receives a copy for these purposes is also bound by the confidentiality requirements.
Disclosure of the draft report in any other circumstance may constitute a criminal offence.
ATSB draft reports may contain information that is subject to change as a result of internal and external review and consideration of further evidence. In its draft form, copying or disclosing the report may unjustly affect reputations. This in turn could potentially impede and discourage the crucial, future free flow of safety information to the ATSB.
Directly involved parties have been provided 14 days to provide any comments on the draft report and to present evidence in support of their comments.
Any submissions from directly involved parties will then be reviewed and, where considered appropriate, the text of the report will be amended accordingly.
The report will then be reviewed by ATSB management before approval by the ATSB Commission for public release.
Once approved, the final report will be prepared for publication and dissemination and released to DIPs prior to its public release.
The ATSB conducts 'no-blame' investigations for the purpose of improving transport safety. ATSB investigations are independent of other investigations, including those conducted by the Civil Aviation Safety Authority and the Northern Territory Police Force.
What happened
On 28 February 2022, at about 0900 local time, a pilot and an egg collector were preparing to commence crocodile egg collection activities near King River, Northern Territory, using a Robinson R44 Raven II helicopter, registered VH-IDW and operated by Helibrook. The activity was conducted under a Civil Aviation Safety Authority (CASA) instrument authorising the pilot to carry a sling person (egg collector) on a 100 ft line attached to the helicopter.
At 1024, the crews of 2 other R44 helicopters collecting crocodile eggs nearby became concerned that they had not heard any communications from the crew of VH-IDW, which they reported was unusual. One of those helicopters returned to the area where VH-IDW was last seen and, at 1036, the search pilot found the fatally injured egg collector on the ground, wearing their harness and attached to the sling line, which was disconnected from the helicopter. The helicopter had collided with terrain 44 m beyond the sling person, and the pilot lay beside the helicopter having sustained serious injuries.
The ATSB referred matters concerning possible offences under the Transport Safety Investigation Act 2003 relating to the status of evidence available to the ATSB for the purposes of its 'no-blame' safety investigation to the Australian Federal Police for investigation. The referral did not concern the circumstances of the accident itself. The Australian Federal Police referred the matters to the Northern Territory Police as part of its broader investigations.
What the ATSB found
The ATSB found that the helicopter was likely not refuelled at the en route fuel depot, which was about three quarters of the way between the departure location on the outskirts of Darwin and a clearing near King River where the helicopter and crew were to commence crocodile egg collecting. The pilot did not identify the reducing fuel state before the helicopter’s engine stopped in flight due to fuel exhaustion. During the subsequent autorotation, the pilot released the egg collector above a likely‑survivable height, fatally injuring them. The pilot then completed the autorotation to the ground, but there was insufficient main rotor energy to cushion the landing. This resulted in serious injuries to the pilot and substantial damage to the helicopter.
The ATSB found that Helibrook’s CASA-approved safety management system was not being used to systematically identify and manage operational hazards. As a result, the risks inherent in conducting human sling operations, such as carriage of the egg collector above a survivable fall height, were not adequately addressed.
The ATSB also found that CASA did not have an effective process for assuring an authorisation would be unlikely to adversely affect safety. As a result, CASA delegates did not use the available structured risk management process to:
identify and assess risks
ensure suitable mitigations were included as conditions of the instrument
assess the effects of changes on the overall risk.
This resulted in removal of instrument conditions limiting the height, speed and exposure for the sling person, which permitted carriage of the egg collector at a non‑survivable fall height.
In addition to the above contributing factors to the accident, the ATSB identified the following factors that increased risk but there was insufficient evidence to show they contributed to the accident or severity of the consequences, or to another contributing safety factor. The ATSB identified that CASA's lack of effective process resulted in the continued operation of piston engine helicopters for human sling operations without adequate mitigations. This included the issue of a 3-year instrument to Helibrook shortly prior to the commencement of improved regulations that would require a turbine engine helicopter for human slinging operations. Although conducting the operation with a piston helicopter increased the overall risk of the activity compared with use of a turbine helicopter, previous accident data showed fuel exhaustion was as likely to occur in a piston as it was in a turbine engine helicopter.
Although not likely to result in sudden power loss, engine defects present at the time of the accident likely affected the engine’s maximum power output and fuel consumption. Additionally, Helibrook had likely overrun the helicopter's maintenance, inspection and overhaul periods, which increased the likelihood of the helicopter experiencing a technical failure or malfunction.
The ATSB also found that the pilot’s exposure to cocaine within the previous few days increased the likelihood of fatigue, depression and inattention, however there was insufficient evidence to determine whether these effects occurred.
Finally, the ATSB found that the helicopter's emergency locator transmitter had been removed from its mount prior to the accident. Therefore, it could not activate automatically, which likely delayed the emergency response.
What has been done as a result
CASA implemented significant changes to its internal processes to ensure that the assessment and management of safety risks of new aviation activities (and associated approvals) were standardised in accordance with the CASA Risk Management Manual and that decision-making was appropriately documented. Additionally, CASA developed an ‘exemption protocol suite’ of documents, which detailed the principles, protocols and work instructions for CASA’s regulatory exemption process. CASA also completed and provided exemplar bowtie and aviation safety risk assessments using the structured process.
Following this accident, Helibrook advised that it had ceased operation and the helicopter fleet was being sold. In addition, the chief executive officer/chief pilot was no longer involved with the operation. CASA confirmed that as Helibrook no longer had the required key personnel, it was considered to be suspended from operation. Under those circumstances, the operator’s safety management system was no longer in use.
Safety message
The contributing factors to this fatal accident highlight the significant influence that the actions and decisions of pilots, operators and the regulator can all have on aviation safety.
Fundamentally, this occurrence illustrates the importance of effective fuel management. It is vital to use all available means, including accurate fuel records and quantity cross‑checks, to ensure that pilots accurately know their aircraft’s fuel state. This is especially critical when operating a helicopter where a fuel‑related power loss offers few safe options, such as inside the height-velocity avoid area with a vulnerable human external load. Pilots also should understand the functionality and limitations of any installed low fuel warning systems.
At the operator and regulatory level, effective safety management processes that identify and safely manage hazards are vital to preventing future accidents.
On 28 February 2022, the crews of 3 Robinson R44 helicopters were preparing to conduct crocodile egg collection in Arnhem Land, Northern Territory. Each helicopter was operated by a different aircraft operator, contracted to Wild Harvest Northern Territory, and crewed by a pilot and an egg collector.
One of the helicopters was an R44 Raven II, registered VH-IDW, operated by Helibrook. The method of egg collection included slinging the collector underneath the helicopter, in a harness attached to a 100 ft ‘long line’ (see the section titled R44human external cargo operations).[1]
The pilot of VH-IDW reported that they arrived at Helibrook’s hangar at Noonamah, on the outskirts of Darwin, Northern Territory at about 0530 local time, conducted the daily inspection of the helicopter and found no defects.
The other 2 R44 helicopters involved in the egg collection on the accident day arrived at Noonamah at about 0645. Their crews reported briefing together with the VH-IDW crew. The briefing involved discussing the day’s plan, including who was collecting from which nests, and where they would meet to refuel. The plan was to refuel at Mount Borradaile en route to King River, then collect eggs from about 15 nests located between King River and Maningrida, which was 90 km beyond King River (Figure 1). The crews then planned to refuel at Maningrida, before continuing south-east to collect additional eggs.
At about 0703, the 3 helicopters departed Noonamah for Mount Borradaile, 205 km east-north-east, where fuel drums had been pre-positioned. At 0743, having travelled 111 km from Noonamah, a photo was taken in the cockpit of VH-IDW. The image showed the accident pilot as the passenger, seated in the left front seat, and the egg collector piloting the helicopter from the right seat. Based on the time taken to reach that point, the helicopter probably arrived at Mount Borradaile at about 0816.
Source: Google Earth with OzRunways data, annotated by the ATSB
The 3 R44 helicopters landed at Mount Borradaile for the planned refuelling, where the crews intended to ‘hot refuel’[2] each helicopter from fuel drums. A witness reported that the 3 R44 helicopters departed Mount Borradaile at about 0830 to track towards King River. One helicopter continued past King River to the north-east and commenced collecting eggs. OzRunways[3] data for the other 2 helicopters, including VH-IDW, recorded their arrival near King River at 0850.
At a clearing near King River, 60 km beyond Mount Borradaile, the second helicopter’s crew retrieved a harness from VH-IDW. Two witnesses reported that the accident pilot was in the left passenger seat and the egg collector was in the pilot seat and flew VH-IDW to King River, where the dual controls were removed. However, the accident pilot and one other egg collector reported that the dual controls had been removed at Mount Borradaile and the pilot had swapped to the pilot seat and flown VH-IDW from Mount Borradaile to King River. While VH-IDW was still on the ground, the second helicopter departed to commence collecting eggs about 12 km to the north-east. Data recorded from an egg collection application showed that the crew of the 2 helicopters, other than VH‑IDW, conducted operations from 9 nests (Figure 2) between 0911 and 1014.
Figure 2: Accident area including King River, accident site and nests
Source: Google earth overlaid with nest collection data, annotated by the ATSB
At 1036, they located the accident site closest to the first planned nest and landed nearby. They found the sling person (egg collector) fatally injured. VH-IDW was located 44 m beyond the sling person, substantially damaged having collided with trees and terrain (Figure 3). The accident pilot had sustained serious injuries and was found lying beside the helicopter. After providing reassurance to the pilot of VH-IDW, the other pilot returned to their helicopter and briefly became airborne to get mobile reception and call for assistance. The first call to emergency services was received at 1046.
The second helicopter and remaining crew arrived at the site about 1 hour later. They found spare egg collection equipment from VH-IDW in the clearing where VH-IDW was last seen before the accident. The accident site was between the clearing and the closest of 3 nests that were to be collected by VH-IDW’s crew. No eggs had been collected.
Based on photos and reports from those who attended the site on the accident day, the egg collector’s bucket and pole were the first items in the accident trail (Figure 4). The pole was vertical with one end embedded in the ground. About 4 m beyond the pole, the long line attachment rings were found, also embedded in wet ground, with the long line loosely coiled over about 8 m. The egg collector was found wearing a harness, which was intact, firmly secured and attached to the long line, and their helmet was on the ground nearby. The long line was not connected to the helicopter.
Following notification of the accident, a CareFlight rescue helicopter departed Darwin at 1122, arrived at the accident site at 1232, and departed with the injured pilot at 1310. As they departed the site, another Helibrook R44 helicopter arrived with Helibrook’s chief pilot, a Wild Harvest Northern Territory representative and an off-duty Northern Territory Police Force officer.
A CareFlight nurse remained at the site until the rescue helicopter returned at 1532 to retrieve the deceased egg collector, departing about 20 minutes later. The crews of the other 3 helicopters reported departing about 20 minutes after the rescue helicopter.
The pilot held a commercial pilot licence (helicopter) with low-level and sling ratings. At the time of the accident, the pilot had recorded about 2,500 hours total aeronautical experience. The pilot’s most recent flight review was on 21 May 2021. The pilot had recorded 340.1 hours of sling experience, the most recent of which was gained in May 2021. The pilot had been contracting to Helibrook for 8–9 years, including for crocodile egg collection. In addition, the pilot operated their own R44 helicopters and contracted to other operators. According to the pilot’s logbook, they had first conducted slinging of human external cargo (HEC) for crocodile egg collection on 13 December 2017. Their last recorded HEC sling time was in March 2020, but the pilot reported having also conducted human slinging for egg collection in the wet season from December to May of 2020–2021 and 2021–2022.
Documents provided by the operator indicated that the pilot had completed a proficiency check flight with the Helibrook chief pilot on 3 August 2021 in the pilot’s R44 II helicopter, which was not fitted with dual hooks. The pilot had recorded a flight time of 0.8 hours in their logbook with no reference to conducting sling operations, whereas the Helibrook Rotary Pilot Competency Check form stated the flight time as 1.1 hours. According to the form, the pilot had demonstrated competency in pre-flight tasks, normal and emergency procedures and the following specialised tasks:
search and rescue
charter
sling operations
croc egg harvesting
aerial advertising – banner towing
supply dropping
surveillance
hover exit entry.
The pilot was also a licenced aircraft maintenance engineer and the head of aircraft airworthiness and maintenance control (HAAMC) for Helibrook.
Medical and toxicology
The pilot held a class 1 aviation medical certificate with no restrictions, valid to 27 May 2022.
A blood sample was taken from the pilot at 1638 on the accident day, 11 minutes after the pilot’s arrival at Royal Darwin Hospital. Toxicology results from the sample identified several substances administered by CareFlight and Royal Darwin Hospital medical staff. Additionally, the results detected 2 metabolites of cocaine – ecgonine methyl ester and benzoylecgonine – at low levels (less than 0.01 mg/L). These results were identified using mass spectrometry and considered to be reliable indications of previous cocaine exposure. These metabolites can be detected in the blood up to 3–4 days after exposure (see the section titled Cocaine metabolites).
Cocaine itself is generally detectable in blood tests for up to 1–2 days after exposure and was not detected in the pilot’s blood.
The pilot had no reported medical conditions and in the self-disclosure section of their aviation medical application, they had advised not using any drugs or recreational substances within the last 5 years. The pilot also advised the ATSB that they did not use cocaine.
Anticonvulsant medication levetiracetam was also identified in the pilot’s toxicology results. There was no evidence of this having been administered by CareFlight or Royal Darwin Hospital medical personnel, although it was consistent with emergency treatment for the pilot's injuries. There was also no evidence obtained to indicate that the pilot had recently visited a doctor, had a condition requiring the medication, or obtained a prescription for it. A pharmacological expert advised the ATSB that even if it had been present before the accident, it was one of the least likely anticonvulsant drugs to interfere with cognitive process as there was evidence of its widespread positive effects on cognition. It was also less likely to produce ataxia[4] and dizziness than other antiepileptic drugs.
Recent history
The pilot reported having limited recollection of events leading up to, and including, the accident sequence. Despite that, the ATSB was able to identify the following activity in the days leading up to the accident.
On 24 February 2022, the pilot was operating a Robinson R22 helicopter (not associated with Helibrook) to locate crocodile nests, when an engine valve failed, requiring the pilot to conduct a forced landing. The pilot reported feeling ‘pretty rattled’ by it.
The next day, after repairs were conducted on the R22, its engine again lost power during take-off. Additionally, the day’s egg collection activities were suspended due to rain and the pilot’s partner reported that they spent a quiet evening at home together.
On 26 February, the pilot was involved in crocodile egg collection activities, which were again suspended due to rain. The pilot consumed alcohol that evening and reportedly attended a party, returning home between 0100 and 0200 the following morning. The pilot left again before their partner awoke between 1000 and 1100 on 27 February. Rideshare records from the pilot’s phone indicated that a car was used between 0243 and 0306, and again at 1040, with no end time recorded.
Information obtained from the pilot’s phone showed that later that day, the pilot started operating VH-IDW at 1545 and conducted crocodile egg collection about 60 km south‑west of Darwin, until 1810. This was consistent with information subsequently provided by the helicopter operator. The pilot’s partner reported that the pilot went to bed at about 2130 that evening and left for work at about 0445 on the accident morning.
The ATSB considered whether the pilot’s activity in the preceding days may have led to them being fatigued at the time of the accident. Specific factors that potentially increased fatigue risk included:
the pilot likely experienced a high level of stress following 2 engine power losses, leading to an unscheduled overnight stay at accommodation away from the pilot’s home
the pilot’s usual sleep pattern was significantly disrupted on one night, getting to sleep around 6 hours after the usual reported sleep time
over the previous 4 nights, the pilot slept in 3 different locations, which had the potential to affect sleep quality
the pilot only had 6–7 hours sleep opportunity on each of the 2 nights before the accident, meaning that the pilot was probably carrying some level of sleep debt at the time of the accident
on the day of the accident the pilot awoke during the window of circadian low, which also has the potential to affect the pilot’s sleep debt
consumption of alcohol or exposure to recreational drugs is known to reduce sleep quality
hot, humid weather conditions, such as those in the Northern Territory in February, are associated with reduced sleep quality and quantity.
While a number of these factors could combine to increase likelihood, there was insufficient evidence to establish if the pilot was likely experiencing a level of fatigue known to affect performance at the time of the accident. In a statement provided to the ATSB in response to the draft report, the pilot reported that they were not tired or affected by alcohol or drugs on commencing the operation of the helicopter.
Wild Harvest Northern Territory (WHNT) held a suite of documents for crocodile egg collection, which included safe work method statements[5] and procedures. WHNT engaged multiple helicopter operators each season to undertake crocodile egg collection. At the start of each egg collection season, those intending to conduct egg collection, including pilots and collectors, attended a WHNT ground-based training and administration day. Both the accident pilot and the egg collector attended this training on 1 December 2021, and had signed safe work method statement sign-on sheets for:
ground operations for croc egg collecting, including:
equipment checks
personal protective equipment
safety around helicopters
firearm safety
selecting and collecting nests
human sling operations (see the section titled Operator risk assessment)
VH-IDW was a 4-seat Robinson Helicopter Company (Robinson) R44 Raven II (R44 II) helicopter, certified in accordance with United States (US) Federal Aviation Regulations (FAR) Part 27 and manufactured in the US in 2008. The helicopter was first registered in Australia in July 2008 and had a standard certificate of airworthiness and was to be operated in the normal category.[6] The helicopter was powered by a 6-cylinder Textron Lycoming IO-540-AE1A5 engine derated to 205 brake horsepower (BHP) with a maximum 5-minute take-off power of 245 BHP.
In December 2009, at 62.2 total hours in service, the helicopter was involved in a dynamic rollover that resulted in sudden stoppage/damage to the main/tail rotor and the engine. The aircraft was returned to Robinson for overhaul, including the engine. The hour meter was reset to zero, and the helicopter was returned to service in May 2012.
Helibrook commenced operating VH-IDW on 15 October 2020 and, as the registered operator, was responsible for the continuing airworthiness of the helicopter. VH-IDW was to be maintained in accordance with the airframe and engine manufacturers’ maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever occurred sooner. The engine and airframe were subject to overhaul at 2,200 hours or 12 years, whichever occurred first. Additionally, any instructions for continued airworthiness on approved modifications, such as cargo hooks, were to be complied with. The helicopter was fitted with an hour meter activated by a combination of oil pressure and an electrical switch on the collective.[7] The hour meter was an acceptable means of recording time in service, however it could be disconnected, which would prevent flight hours being recorded.
On 22 October 2020, shortly after the helicopter was purchased by Helibrook, a 100‑hourly inspection was carried out on VH-IDW, at which time the helicopter’s total time in service, recorded in the maintenance records was 1,577.9 hours and the hour meter read 1515.75. The maintainer reported that in November 2021, the hour meter was rolled forward 62.2 hours to match the helicopter’s total time in service for ease of record-keeping. At the accident site, the helicopter hour meter read 2,070.05 hours, which equated to 2,007.85 hours since overhaul.
A maintenance release is required to be carried on an aircraft as an ongoing record of the aircraft’s time-in-service and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours in service or 12 months from issue.
A daily inspection was required to be carried out and the maintenance release signed to show the inspection had been completed, prior to the first flight of the day. The inspection and certification could be made by any pilot licenced to fly the aircraft, or an appropriately licenced aircraft maintenance engineer. After the last flight of the day and before the aircraft was next flown, the total daily flight time was required to be entered and the progressive total time in service recorded.
VH-IDW’s maintenance release, current at the time of the accident, was provided to the ATSB on 3 March 2022. It had been issued on 7 February 2022, with 2,036.3 hours total time in service recorded. The accident pilot’s signature was on the maintenance release for 8, 9 and 10 February, with 7.6, 4.3 and 1.5 hours recorded respectively.
The accident pilot’s signature was on the maintenance release for the accident day. The pilot initially reported having conducted the daily inspection of VH-IDW on the morning of the accident, found no defects and signed the maintenance release. However, the pilot subsequently reported being unsure when they had signed the maintenance release for the accident day’s flight.
No defects had been recorded on part 2 of the maintenance release. Additionally, there were no entries on part 2 of the maintenance releases from when the fuel calibration was certified on 1 May 2020 to the accident day to indicate any issue with the fuel calibration, calibration card or fuel quantity indication.
On 15 January 2022, due to a pilot reporting that the engine was ‘low on power’, the maintainer adjusted the magneto engine timing and renewed the spark plugs.
On 7 February 2022, the maintenance organisation completed a periodic inspection of VH-IDW. During that inspection, the No. 6 cylinder was replaced due to failed compression, however, there was no documentation supporting that a post-replacement compression check had been conducted. Other maintenance items completed at that time included replacement of the engine-driven fuel pump and the tail rotor assembly.
On 11 February 2022, with 2,050.09 hours recorded in the engine logbook, a Helibrook pilot had reported an ‘intermittent miss in flight’ to the maintainer. The maintainer identified that the left magneto had a failed drive bearing and replaced it with an overhauled magneto. The right magneto timing was also adjusted. The worksheet stated ‘compression test ok’ but no figures were recorded. The maintainer reported checking compression during troubleshooting for the intermittent miss but did not record the figures as they were satisfactory. The maintainer then recorded conducting a post-maintenance flight of 0.8 hours with no issues identified.
The pilot’s logbook did not contain any entries relating to the operation of VH-IDW, and the pilot’s last logbook entry was in their own helicopter on 12 February 2022. Additionally, and despite the pilot reporting conducting egg collecting using VH‑IDW in previous seasons, the earlier VH-IDW maintenance releases covering the previous egg collection season did not contain any entries by the accident pilot. However, this did not preclude the pilot having flown VH-IDW after another person conducted the daily inspection and signed the maintenance release.
The pilot reported that VH-IDW had flown significantly more hours than were recorded and that the hour meter was never operating when they flew it, although they could not recall whether the hour meter was operating on the accident morning. The pilot estimated that they had flown VH‑IDW for about 70 hours in the 2021–22 crocodile egg collection season and had also flown it during 2020–21. The ATSB obtained invoices that indicated the pilot had conducted over 36 full days of egg collection in 2020–21 and 2021–22 seasons, all of which were reported to have been in VH‑IDW. Due to the apparent discrepancy in operating hours, the ATSB compared the hours recorded on VH-IDW’s maintenance releases from November 2020 to the accident day with:
the pilot’s time (in units of days/half days) invoiced for crocodile egg collection
spreadsheets recording hours for helicopters (by operator and helicopter type) and day/half‑day rates for personnel involved in crocodile egg collection
the pilot’s phone records of start and stop times for VH-IDW
recorded egg collection data (see the section titled Crocodile nest data)
fuel uplift records
evidence of VH-IDW being operated for a purpose other than egg collecting.
There were 21 days identified when VH-IDW was operating and there was no entry on the maintenance release, some of which were recorded as 10 to 11 hours of helicopter operation. For all other entries for crocodile egg collection, only a portion of the spreadsheet time was recorded – including as little as 10% of the hours recorded on the spreadsheet on single days. On those days, collected nests were recorded on the crocodile egg collection application and for many of them, the pilot had retained a record of VH-IDW start and stop times consistent with the spreadsheet’s recorded hours. The review of the spreadsheets and comparison with VH-IDW’s maintenance release hours included consideration of whether multiple Helibrook R44s were operating on a given day.
The accident pilot reported that the helicopter had not ‘missed a beat this season’, then subsequently described VH-IDW’s performance as good and that it flew well, but that it was nearing the end of its overhaul life and had problems in the weeks prior to the accident. These included a damaged inlet valve, a loose induction tube and fuel injector. The latter 2 items were recorded as rectified on the maintenance release on 14 December 2021. There was no documented recent inlet valve replacement identified but the No. 2 cylinder exhaust valve was replaced on 22 April 2021. When questioned whether there was any indication that the helicopter was overrunning the 100-hour inspection intervals, the maintainer reported that it was difficult to determine whether a helicopter had done 100 or more hours when it arrived for maintenance.
A maintainer who previously maintained Helibrook helicopters from June 2016 to January 2020, reported that they had previously found a Helibrook R44’s hour meter disconnected. In addition, the operator had leased a helicopter from the maintainer and a comparison of recorded GPS flight data with documented flight times showed that the hour meter had been disconnected and about 4 hours of the 14 hours flown during the cross-hire period were not recorded on the maintenance release.
A Civil Aviation Safety Authority (CASA) airworthiness inspector produced a report as part of CASA’s review of this accident. The report identified that VH-IDW’s engine-driven fuel pump had been replaced at reducing hours since new: 733.4 in 2017, 651.9 in January 2020, then, after purchase by Helibrook, at 387.8 hours in April 2021 and 263.2 hours in February 2022. The report stated this was indicative of flight hours not being accurately recorded.
The R44 II POH stated that for tanks fitted with bladders (including VH‑IDW), the main fuel tank capacity was 115 L, of which 112 L was usable, and the auxiliary tank capacity was 65 L, of which 64 L was usable. Of the combined 180 L capacity, the total usable fuel was 176 L. The POH defined usable fuel as the fuel available for flight planning.
Unusable fuel is the amount of fuel in the tank/s below which continued running of the engine while performing the most adverse manoeuvre cannot be assured. Below this level, there is the potential to un-port[8] the fuel tank outlet due to fuel movement. In straight and level flight, some of the unusable fuel is likely to reach the engine. In the R44 II, the main tank to engine fuel union is located on the inboard side of the tank, forward and near its base.
Calibration of the main and auxiliary tank fuel gauges was required every 48 months. The last calibration was conducted by a CASA‑authorised maintainer in May 2020. The calibration is shown in Figure 5. The associated placards for the main and auxiliary tank gauge calibration were affixed in the cockpit, but the auxiliary tank placard was damaged and illegible (Figure 6).
Figure 5: Fuel tank gauge calibration as recorded in May 2020
Source: Supplied
Figure 6: VH-IDW cockpit photo showing fuel gauges and placards
Source: ATSB
The main tank placard stated that the low fuel warning light would illuminate when 20 L total fuel (usable and unusable) remained (Figure 6). According to the maintenance manual, the low fuel warning switch was not subject to calibration. The organisation that conducted the fuel calibration reported that, to establish the 20 L figure, they drained the tank, checked the low fuel light was illuminated, then added fuel until the low fuel light went out. The pilot reported that the light would illuminate with 18 L total fuel remaining. Both those figures differed from the POH, which stated that the low fuel warning light would illuminate with approximately 3 US gallons (11 L) of usable fuel remaining (14 L total fuel in the main tank) (Figure 7).
Source: Robinson R44 II Pilot’s Operating Handbook
The Robinson R44 II POH included Safety Notice SN-15 – Fuel exhaustion can be fatal, which advised pilots never to rely solely on the fuel gauge or low fuel warning light but to always record the hour meter reading each time the fuel tanks were filled. This enabled pilots to monitor fuel consumption and endurance. In addition, the POH required the pilot to visually check fuel quantity at each tank during the pre-flight. VH‑IDW was also fitted with a fuel flow transducer and an associated Fuel Scan (totaliser) instrument in the cockpit. The instrument could display fuel flow and other parameters including fuel used and fuel or time remaining. However, the display of accurate fuel quantity relied on the correct amount of fuel to be entered following engine start and the in-flight photograph taken en route from Noonamah for Mount Borradaile identified that the Fuel Scan instrument display was not visible.
Maximum continuous power manifold pressure limits were prescribed in the POH (Figure 8).
Figure 8: R44 II Maximum continuous power, manifold pressure limits
The red square depicts the limit for the conditions at the time the in-flight photo was taken.
Source: Robinson Helicopter Company, annotated by the ATSB
Flying with a higher manifold pressure than the prescribed limit may exceed the approved torque for the rotor drive system. Robinson advised that if excessive power was held continuously, the helicopter would exceed the normal flight envelope, likely causing stress to drive system components that were not designed for such loads.
Robinson safety notice SN-37 – Exceeding approved limitations can be fatal, stated:
Every second the limitations are exceeded, more stress cycles occur and additional fatigue damage can accumulate within the metal. Eventually, a fatigue crack will begin and grow until a sudden failure occurs…Do not operate the engine above its placarded manifold pressure limits…
Robinson also advised that higher‑than‑normal manifold pressure for a given airspeed could also indicate an engine issue. If one or more cylinders were not operating correctly, higher manifold pressure would be required to produce the same power. In this case, the higher manifold pressure may not exceed the approved torque for the rotor drive system.
The main rotor flight controls are hydraulically boosted to eliminate cyclic[9] and collective feedback forces. The hydraulic system operates at a pressure between 450–500 psi and consists of a pump, 3 servos, a reservoir, and interconnecting lines. The pump is mounted on, and driven by, the main rotor gearbox. A servo is connected to each of the 3 push-pull tubes that activate the main rotor swashplate. The reservoir is mounted on the steel tube frame behind the main rotor gearbox and includes a filter, pressure relief valve, and pilot-controlled pump bypass valve. A sight gauge for pre-flight fluid level checks is incorporated in the reservoir, which has a vented filler cap.
The pump bypass valve is solenoid-actuated and controlled by the hydraulic switch on the cyclic. When selected to HYD (on), the solenoid is deactivated. This fail-safe ensures hydraulic assist is retained in the event of a loss of electric system power. The switch should be on from start-up to shutdown, except during the hydraulic system check or simulated hydraulic failure training. When selected to off, power is applied to the solenoid and high-pressure hydraulic fluid is returned to the reservoir, removing hydraulic assist from the controls.
Robinson reported being unaware of any instances of the solenoid actuating in flight and causing a loss of hydraulic assist in the controls. The ATSB occurrence database contained 3 hydraulic related occurrences in R44 helicopters since 1997, none of which resulted in a loss of control or an accident. The first was the result of the pilot inadvertently switching off the hydraulic master switch in flight, the second was a failure of the hydraulic pump, and the third was a hydraulic leak.
Robinson advised that there had been several accidents in which a pilot had inadvertently induced an engine stoppage by rolling off the throttle too fast. This had occurred in flight training when simulating an engine failure and in response to abnormal situations such as rapid engine RPM changes or discrepancy between engine and rotor RPM.
The helicopter had previously been fitted with floats, which had been removed, but the skid extenders necessary for float fitment remained fitted to the helicopter.
The helicopter had a factory mount for an emergency locator transmitter (ELT) and associated wiring in the main rotor gearbox bay however no ELT was fitted to VH‑IDW, nor was one required to be. When fitted, the ELT is connected to an external antenna. The ELT had an arm/on/off switch, and a remote switch was located next to the cyclic, with a default position of ‘armed’.
A pannier for the carriage of egg collection equipment was fitted on the left side of VH-IDW. This had been approved by a CASA-authorised aeronautical engineer under an engineering order, although the associated rotorcraft flight manual supplement (RFMS) was not inserted in the POH.
VH-IDW was originally fitted with dual hooks for HEC under an engineering order. The engineering order required that the hook system be maintained in accordance with the instructions for continued airworthiness and operated in accordance with the associated flight manual supplement. The engineering order was replaced by a CASA-approved supplemental type certificate (STC)[10] in 2021. The system and hook part numbers and the maintenance requirements were unchanged, and the only change was a reduction in the maximum allowable hook weight from 150 to 129 kg (and the associated placard). This was to provide a greater safety margin for HEC operations for the same hook and its strength rating.
The STC approved nominated R44 and R44 II helicopters to be:
modified with a dual Onboard Systems International cargo hook kit for HEC operations in accordance with Master Document List R5106-07-R5 (28 July 2021)
maintained in accordance with Instructions for Continued Airworthiness (ICA) R5106-09-R11 (21 July 2021)
operated in accordance with RFMS R5106-25-R13 (11 June 2021), which was required to be inserted in the POH. The associated RFMS was not contained within VH-IDW’s POH.
The dual hooks could attach to rings on a 100 ft long line, enabling the carriage of a person below the helicopter. The 2 hooks could be released by the pilot by pressing 2 independent buttons of the primary quick release system (PQRS) or pulling 2 manual handles of the back-up quick release system (BQRS). In addition to 2 independent actions, the PQRS buttons were recessed into a housing to further reduce the likelihood of inadvertent pilot activation. The dual hook and release systems were designed to provide redundancy in case of failure.
Following electrical or manual activation, the hook arm would remain open, until it was manually relatched by pushing the hook up by hand to the closed/locked position (Figure 9). (Note: the red component in Figure 9 is the manual release lever).
Figure 9: Onboard Systems hook open and closed/locked (same part number as those installed on VH-IDW)
Source: Onboard Systems
Serviceability
The Onboard Systems HEC dual hook system was installed on VH-IDW on 23 October 2020. The ICA required the external load operation hours to be recorded when the primary hook, or both hooks, were used for external load operations in flight.[11] There was no evidence that external load operation hours were recorded on either hook. There was also no record in the aircraft maintenance documentation of the required 100-hourly/annual checks having been conducted. Finally, one of the hooks had been removed from another helicopter prior to being installed on VH‑IDW and had exceeded its 3 years in‑service limit.
The RFMS included the requirement for the pilot to conduct a functional check of the quick release systems prior to commencing the day’s HEC operations. The pilot reported that their normal procedure was to test that the primary and back-up quick releases were functional before the sling person hooked up but could not recall whether they had done so on the accident day.
The helicopter departed Noonamah on the accident morning at about 0703. The weather conditions at the time included a light northerly wind and scattered low cloud. At 0743, the helicopter was en route, 60 NM beyond Noonamah and 50 NM from Mount Borradaile. The nearest Bureau of Meteorology weather station was at Point Stuart (Figure 1), where, at 0800, the wind was a north-north-westerly at 10–14 kt, the temperature was 27.5 °C and the QNH[12] 1008 hPa.
The Bureau of Meteorology weather station nearest the accident site was South Goulburn Island Airport (Warruwi), 29 km north-north-west. At 0930, the recorded meteorological conditions were westerly wind at 6 kt, temperature 29 ⁰C, dewpoint 24 ⁰C, QNH 1010 hPa and no cloud. Similar conditions were recorded at Oenpelli, 63 km south-west, and Maningrida, 90 km east-south-east of the accident site.
Recognising that the winds at these recording stations were light and the actual accident time unknown, the accident trail was consistent with it being approximately into wind. At the sea level elevation of the accident site, with QNH 1010 hPa and temperature 29 ⁰C, the calculated pressure altitude was 90 ft and density altitude[13] was 1,770 ft.
There was a mobile telephone and an iPad on board the helicopter at the time of the accident with the potential to contain data relevant to the accident sequence. The ATSB was able to recover information from the pilot’s phone pertaining to their activities in the days prior to the accident, records of hours the pilot operated VH-IDW and previous maintenance release practices. However, no data directly relevant to the accident flight was able to be recovered.
The egg collector’s phone had been operating in the vicinity of the accident site, but was missing and could not be obtained by the ATSB for analysis and the iPad was severely damaged in the accident impact, rendering any stored data unrecoverable.
Phone records show the last mobile data session before the accident, commenced on the pilot’s phone at 0847:37 and the egg collector’s phone at 0858:16. The egg collector was sent a text message at 0923:44 but the message was not received. This indicated that the phone was either out of mobile range, which occurred below about 300 ft in the vicinity of the accident site, or was off/not powered.
A georeferenced in-flight photo was taken at 0743 on the accident morning, 111 km beyond Noonamah and 94 km prior to the Mount Borradaile refuelling stop, on a direct track between the 2 locations (Figure 10). The photo showed:
the fuel gauges reading just below three quarters full
the Fuel Scan instrument was not operating
the manifold pressure about 24 inches of mercury (inHg)
an indicated airspeed 90 kt
the engine and rotor RPM about 103%
a chronometer indicating 00:45.
The photo also showed the accident pilot seated in the left seat as a passenger and the egg collector piloting the helicopter from the right seat.
Figure 10: Cut-out of in-flight photo taken at 0743 showing cockpit indications
Source: Northern Territory Police, annotated by the ATSB
As detailed in VH-IDW’s POH, for the pressure altitude at sea level and temperature 30 °C, the maximum continuous power was 23.1 inHg manifold pressure (red box in Figure 8). Based on the aircraft’s height, temperature and QNH at Point Stuart and interpolating the POH table, the maximum continuous power was about 23 inHg. Robinson advised that exceeding the manifold pressure limits with an engine functioning normally would be expected to result in a higher airspeed or rate of climb than depicted in the photo.
Assuming VH-IDW departed Noonamah at 0703, which was the time one of the other R44s departed, it averaged 90 kt ground speed to the in-flight photo location.
A custom-built iPad application named ‘Crocpad’ was used to record the collection of eggs and nest locations. In the week prior to the accident, pilots (including the accident pilot) had conducted flights to locate the nests and entered each nest’s location into Crocpad.
The Crocpad data included fields for the device name, status, created date and modified date. The device name was that used by the person who located the nest (for example, ‘my iPad’). The created date contained the date and time the nest was located, at which time the nest’s status was set to LOCATED. When a nest was subsequently either COLLECTED or DELETED, the modified date was amended with the date and time this occurred. This did not need to be the same person or Crocpad that located the nest. The device name was not updated when a nest was collected or deleted, and remained as the device name that had been used to locate the nest. The Crocpad data would update to the server when in mobile range, which the accident site was not. The iPad that was running Crocpad in VH-IDW had not updated the server with any information before it was severely damaged in the accident impact. The 9 nests amended on 28 February are shown in Table 1 and Figure 11.
Figure 11: Crocpad data showing nests recorded as collected or deleted on 28 February 2022
Source: Crocpad data overlaid on Google Earth, annotated by ATSB
On the accident morning, after departing the King River set-down area, the pilots and egg collectors of the 2 helicopters other than VH-IDW, reported meeting at a patch of 3 nests (No.1 to No. 3), then one helicopter went to a single nest (No. 4), before re-joining the crew of the other helicopter at another patch of nests (No. 5 to No. 9).
OzRunways flight path data was obtained for 2 of the R44 helicopters, including VH-IDW. The data contained tracks commencing about halfway between Mount Borradaile and the King River, and ceasing near the clearing where VH-IDW and its crew were last seen prior to the accident (Figure 13). The data for VH-IDW was recorded on the egg collector’s iPhone from 0841:28 to 0850:13 local time and uploaded to the OzRunways server. The data covered about 15 NM, equating to a ground speed of about 100 kt. The other track was from 0840:22 to 0850:15, indicating the 2 helicopters were operating in company.
Figure 13: Recorded OzRunways tracks of VH-IDW and another R44 helicopter
Source: OzRunways data overlaid on Google Earth, annotated by ATSB
No OzRunways data was retrieved from the accident pilot’s phone and no data had uploaded to the server from the pilot’s phone or iPad. The pilot reported that they generally used landmarks to navigate for the ferry flight, and would only use OzRunways, in combination with Crocpad, for the egg collection.
The egg collector carried a UHF radio to enable communication with the pilot. It was reported that as the egg collector usually held a bucket in one hand and a pole in the other, it was difficult for them to press the transmit button to talk to the pilot, so they would usually use hand signals to communicate. The accident pilot subsequently reported that egg collectors could easily hold the crate and pole in one hand, making the radio accessible. Additionally, the accident pilot reported that as the helicopter radio was selected to VHF at the time of the accident, they could not have quickly communicated with the egg collector as it would have required switching the radio selector to UHF.
The pilot who was first on the accident site estimated that the accident occurred at about 0922 while they were on the ground and out of radio range. This estimation was based on the pilot not hearing an unintelligible radio transmission, later attributed to IDW, that was reported to have been heard by the crew of the other R44 which was airborne at the time.
The ATSB attended the accident site on 2 March 2022. The site was in a paperbark swamp approximately 440 m east of the clearing where spare equipment was found and where VH-IDW was last seen. From the egg collector to the helicopter, the accident trail lay in an approximately north‑westerly direction towards, and about 150 m before, a nest that was assigned to the crew of VH-IDW.
Assuming a direct transit from the clearing towards the first nest, the trees between where the helicopter probably took off, and where the egg collector was released, were 12–15 m tall. The trees in the vicinity of the target crocodile nest were at least 18 m tall. The bucket and pole were reported to have been found on the ground between trees about 4 m prior to the long line attachment rings. The egg collector was located about 8 m beyond the attachment rings and between 2 trees (Figure 14). On the first tree in the direction of flight, a section of bark had peeled away, about 4–5 m above the ground. While this may have been evidence of possible recent impact, no associated bark was found on the equipment or egg collector.
Source: Northern Territory Police annotated by ATSB
The helicopter impacted the ground upright 44 m beyond the sling person, with the fuselage oriented on a heading of about 060° (Figure 15). The main rotor blades had struck one tall slender tree 3 times, indicating a vertical descent through the tree. The tree was about 9 m tall, with 2 distinctive upper branches that forked from the main trunk about 5 m above the ground. One rotor blade severed one upper branch 8 m above the ground, where the branch diameter was 35–40 mm). A blade then severed the trunk at the fork, 5 m above the ground, where the branch diameter was 50–55 mm. The final cut of the main trunk occurred 1.1 m above the ground, which was below the normal main rotor blade height above the ground in a level attitude.
The severed main tree stump (diameter 150 mm) was 2.4 m in front of the helicopter’s nose, leaning about 55° in the direction of main rotor rotation. The helicopter was facing over 90° right of the apparent direction of travel, consistent with rotation of the fuselage due to the main rotor blade’s impact with the tree trunk or pilot pedal input. During the accident sequence, one main rotor blade fractured about 1 m inboard from the blade tip, with the fragment located 45–50 m north‑west of the wreckage. It was noted that the main rotor pitch control link associated with this blade had fractured in overstress, with no damage to the other pitch link.
Figure 15: Site overview, with the orange arrow showing approximate direction of the accident trail
Source: Northern Territory Police, annotated by the ATSB
In addition to multiple rotor strikes to a single tree, indications of a mostly vertical descent, slightly right and nose-down attitude and a heavy impact included:
the landing gear had splayed almost to horizontal, and fractured
the forward cross tube was pushed up into the cabin, significantly reducing the available space in the rear cabin, resulting in empty egg crates in the middle of the back seats being distorted and wedged up against the internal cabin roof
both skids had fractured forward of the front struts
deformation to the nose was more pronounced to the right of the landing lights
the pilot’s seat was collapsed towards the front right corner.
The base of the pilot’s seat had crushed, as designed, to absorb impact forces. The pilot’s restraint had reportedly been cut by those first on site and used in providing first aid to stabilise their injuries.
All the helicopter components were located in the vicinity of the accident site, indicating that there was no in-flight breakup. The forward doors were not installed, and the rear doors had been ejected on impact but were reportedly moved and placed under the pilot for support.
The helicopter was in a black dirt swamp and surrounded by water, up to about 0.5 m deep. The swamp had a gentle flow away from the helicopter, in a northerly direction, toward a nearby creek that was part of the King River system. When the ATSB attended the site 2 days after the accident, both fuel tank caps were correctly fitted, there was no fuel smell, no fuel in the auxiliary tank and a very small quantity of fuel at the bottom of the main tank.
The impact forced the right side of the transmission deck up to contact the underside of the auxiliary tank, such that the fuel drain could not be accessed. There was no evidence of fuel leaks on the transmission deck, from either tank or associated fuel lines. The right-side low orientation of the helicopter would have directed any fuel in the main tank to the engine fuel hose union near the base of the inboard side of the tank. Any fluid that leaked from the helicopter would have flowed downstream and away from the site.
The first person to arrive at the site could not recall checking the fuel tanks, but 2 others who arrived in the second Helibrook helicopter reported having observed the first person to arrive look in one tank and advise that there was fuel visible. In addition, the Helibrook chief pilot who was on board the second Helibrook helicopter reported looking in one tank and seeing a shimmer of fluid however, they did not dip the tanks to check the quantity. The first person to arrive at the accident site reported that there had been a fuel smell, but subsequently reported that the fuel smell may have been from a damaged jerry can that had been behind the pilot’s seat at the time of the accident.
A CareFlight first responder who arrived at 1232 reported that there was no smell or indication of fuel, only hydraulic fluid, which created a sheen on the water. A photo taken at 1555 on the accident day showed a slick on the water near the accident site. It was unknown whether that was from hydraulic fluid, fuel or another source. The ATSB obtained images of the site taken in June 2022, 4 months after the accident, in which there was no evidence of vegetation dieback that can indicate fuel contamination. However, 206.2 mm of rainfall had been recorded at the nearest Bureau of Meteorology weather station (Warruwi Airport) since the accident, reducing the likelihood that vegetation dieback would be evident.
The first person to arrive at the accident site also reported that there was no power to the aircraft when they arrived, but they switched off the electrical system master and alternator switches as a precaution, and rotated the main rotor blades to provide shade for the pilot. They further reported the fuel mixture control was in the full rich position and the magnetos were selected to ‘Both’, consistent with positions identified by the ATSB on site. The engine RPM governor switch, located at the forward end of the collective, was found in the OFF position. The hour meter read 2070.05. The stowage space under both forward seats was inspected, with nothing being located under the left seat and several small items, including a damaged headset, under the pilot’s seat. The POH and maintenance release were not in the helicopter.
No oil was found in the hydraulic system, however, hydraulic fluid was observed on the main transmission deck. The hydraulic switch was selected ON at the cyclic. Flight control continuity from the tail rotor to the main rotor head, above the transmission deck, was established. The fuses for the belt tensioning actuator, in-use and spare, were noted to be the correct amperage and undamaged. All 4 drive belts were present. The distorted pannier prevented easy access to the left side of the engine and the underside of the helicopter was not accessible due to the collapsed landing gear and distortion to the engine cowls. On-site images indicated that the engine was probably above the water level, however, water may have entered the cowls on impact.
The tail cone remained connected to the fuselage. There was no damage to the upper vertical fin and horizontal stabiliser. The tail cone and the lower vertical fin displayed compression damage consistent with terrain impact.
The tail rotor assembly was secure and rotated freely. Oil was evident in the tail rotor gearbox sight glass and the chip detector was clear of metal contamination. The tail rotor blades were in new condition and undamaged, with some light wood debris at the tip on the leading edge of one tail rotor blade. There was some corresponding minor scuffing to a partially submerged, sodden tree branch immediately under the tail rotor, consistent with contact following a vertical descent.
The ELT’s mount was located in the main rotor gearbox bay however, the ELT was not installed. The ELT harness, which included a quick disconnect socket, and antenna cable, were secured with cable-ties. The ELT end of the antenna cable was secured to the helicopter frame with tape. The remote switch, located next to the cyclic, was in the default ‘armed’ position.
Following on-site examination, VH-IDW was slung from the site by another helicopter. People on the ground when VH-IDW was lifted from the accident site did not report observing any fuel leaking from the helicopter. During the retrieval, VH-IDW was lifted multiple times, and also put down heavily en route to Jabiru, Northern Territory due to a technical issue with the slinging helicopter. At Jabiru, VH-IDW was loaded upright onto a truck and transported 252 km by road to a secure facility in Darwin for detailed examination. The switch positions identified on site were not altered during the retrieval and arrived in the same positions.
The hook electric and manual release systems could not be functionally tested due to impact damage. However, both manual release T handles were found in the down position (not activated) and visual inspection did not identify any faults with the dual hook system. The hooks were found in the ‘up and locked’ position when the wreckage was lifted during retrieval from the accident site. Following activation, the hook arm would normally remain open, until manually relatched by pushing the hook up to the closed/locked position. In this instance, having had to open to release the egg collector, they were likely closed by the subsequent helicopter ground impact.
Continuity of the drivetrain was established from the main rotor gearbox to the tail rotor gearbox, including all flex couplings. There was some distortion to the main rotor gearbox input driveshaft yoke and flex coupling, along with minor scraping on the transmission deck under the intermediate flex plate which was consistent with an unpowered rotor system (see the section titled Autorotation) during a heavy impact.
The main rotor gearbox could be rotated without restriction and the oil level was in the middle of the sight glass. Several main rotor gearbox mounts were fractured and the chip detector was damaged from perforating the transmission deck but was clear of debris. There was no indication of overheating of the main gearbox or clutch assemblies.
The clutch assembly was disassembled with no obvious damage to the sprags or race surface, consistent with the helicopter being in autorotation during multiple tree strikes before impacting the ground.
The belt tensioning actuator assembly had fractured in overstress at the connection to the upper bearing assembly and at the actuating rod. The actuator rod extension was consistent with properly engaged belts, which included assessment of expected stretch typical of their time in service. The drive belts were intact and appeared in reasonable condition although they were displaced from their respective sheave grooves, which was typical of heavy impact and actuating rod failure.
Flight control continuity was established throughout. Many control tubes had fractured due to overstress associated with impact, but the corresponding rod ends were secured to bell cranks. The left seat quick-disconnect (dual) controls were not installed and the cyclic boot was in place. The collective friction device had fractured due to impact forces. There was some movement in the collective, but it was restricted due to damaged control tubes. The overtravel spring was bent in a manner consistent with impact damage.
A power source was applied to the governor motor. The motor operated in both directions with no evidence of interference. The governor wiring loom connector was secure and there was no evidence of loose or deformed pins. The governor switch was functional, with the governor itself sent to Robinson for testing under supervision of the US National Transportation Safety Board and found serviceable.
The aft servo return line tee union was found to have fractured in overstress. The filter was clear with no sediment and the pump was secure. The solenoid that actuated the pressure shut-off valve was also tested and found functional.
As detailed above, on-site examination identified that no ELT was fitted to the helicopter. The ATSB was subsequently provided with an ELT by the helicopter operator, who reported that they had removed it from the site after the accident. They advised that it was typically carried under one of the seats, otherwise it would get wet and erroneously activate. The produced ELT was registered to a former Helibrook chief pilot and not associated with any aircraft registration. It appeared intact, in reasonable condition, was switched off and its battery was due to expire in August 2022.
The Australian Maritime Safety Authority confirmed that previous unintended ELT activations had occurred due to water ingress and identified one record of activation of the ELT associated with VH-IDW, which occurred on 28 December 2021. A company representative for VH-IDW had advised the authority that the ELT had self-activated, likely due to water making contact with the ELT while collecting crocodile eggs. That ELT was not the one provided to the ATSB.
All warning and caution lights were inspected, and electrical continuity confirmed. The filaments of the low rotor, low fuel, alternator and governor warning lamps were subsequently inspected under a microscope with none found stretched or broken as sometimes occurs if illuminated at impact. However, due to variables that affect the rate of acceleration applied to the filament, the absence of filament stretch does not enable a conclusion regarding whether or not the light was illuminated.
The helicopter battery was found out of the battery box but still connected to the helicopter by the battery leads. The alternator control unit was secure and connected.
One of the 2 electrical connections at the back of the hour (Hobbs) meter was found finger tight. Despite that, the connector would not move freely and had a lock washer under the nut to prevent it from coming loose during operation. However, only a small amount of hand pressure was needed to move the connection, consistent with it having been tightened by hand rather than with a spanner or socket.
There were no indications of engine rotation at impact, evidenced by:
no rotational damage to the engine cooling fan or housing
no slippage to the cooling fan retention nut alignment mark
no evidence of rotational scoring to the alternator housing or cooling fan and backing plate.
Significantly, impact damage and bending to the upper sheave forward end, lower surface was consistent with impact with the starter ring gear, and showed defined teeth impact marks, with no smearing (Figure 17).
This strongly supported the ring gear being stationary (engine stopped) when the helicopter collided with terrain.
Figure 17: Upper sheave damage from impact with non-rotating starter ring gear
External examination found no evidence of a catastrophic engine failure. The throttle butterfly was fully open at the fuel control unit, however as the impact forces would have tended to pull it open, the throttle position prior to impact could not be determined.
Oil
The engine oil cap and dipstick were secure, and the sump plug was relatively clean. The ATSB drained 8.6 L of oil from the engine with no significant debris found in the oil. The recommended maximum engine oil quantity was 9 quarts (8.5 L). Although the oil level slightly exceeded the maximum recommended capacity, it would not have affected the engine’s performance. The oil filter was opened and inspected with nil contamination identified on the filter element.
Air
Induction air enters through an opening on the right side of the fuselage and passes through the air filter within the air box. Air then passes along a flexible sceet duct, through the fuel control unit and into the engine. The air intake was damaged consistent with accident impact, but there was no evidence of blockage or ingestion of foreign material. The air box casing was distorted, also consistent with accident damage, though the filter was clean and there was no sign of blockage. The induction sceet hose had been crushed consistent with impact forces. The induction hose was also checked for delamination, due to a previously-identified issue with some induction hoses, and none was evident.
Engine examination
The engine was shipped to a CASA-authorised maintenance facility for examination under ATSB’s supervision. Differential compression checks were carried out on the assembled engine. Cylinders No. 3 and No. 6 were below the limit of 60/80, which the engine manufacturer advised was the point that removal and overhaul should be considered (Table 2). However, cylinder compression is normally checked on a warm engine, as a cold engine may not provide reliable results.
Table 2: Compression checks of assembled engine – red denotes below limit
Cylinder No.:
1
2
3
4
5
6
Compression
78/80
70/80
45/80
60/80
78/80
0/80
The cylinders were then removed from the engine and subjected to a second, differential compression check on a test bench. During testing, the valves were tapped to ensure any debris was not preventing a good seal. All cylinders then reached or exceeded 70/80 except cylinder No. 6, which only attained 5/80. The leak from cylinder No. 6 was visually identified as coming from both valve seats.
The valves from cylinder No. 6 were removed and the seating surface contact was examined. The seating faces were uneven (nonconcentric), particularly on the intake, and the exhaust seat had a low spot consistent with the valve not sealing properly (Figure 18). The poorly seated valves would have accounted for the low compression although the valves appeared in good condition with no evidence of carbon build-up. The No. 6 cylinder had been overhauled in 2016 and a vacuum pressure test was reportedly conducted at the time to check for leaking, however the results weren’t recorded. After overhaul, the cylinder was stored until installation in VH-IDW in 2022.
Figure 18: No. 6 cylinder intake and exhaust seats showing nonconcentric valve seating and low spot
Source: ATSB
The engine examination also found corrosion in all intake tubes, consistent with post-accident moisture from the impact in the swamp.
Prior to removing the cylinders, the valve trains were removed, and the hydraulic plungers were returned to a dry/deflated condition. After reassembly, the rocker arm to valve clearances were checked and only 5 of the 12 clearances were found to be within the engine manufacturer’s service limits. Table 3 shows the resulting clearances, with those out of service limits highlighted in red. Valve clearances were set on installation of the cylinder and can vary with wear. Insufficient clearance may prevent the valve from closing properly and excessive clearance can reduce valve lift and duration.
Table 3: Rocker arm to valve clearance – red denotes outside limits (0.28–0.80”)
Cylinder No.
Intake valve
Exhaust valve
1
0.110
0.047
2
0.022
0.024
3
0.032
0.036
4
0.016
0.095
5
0.000
0.052
6
0.000
0.047
The low compression in cylinder No. 6 would reduce the maximum power output and at any achievable power output, the fuel consumption would be higher than an engine with compressions within service limits. No defects were identified that should have resulted in sudden power loss or engine stoppage.
The ATSB also obtained an expert opinion from the engine manufacturer, regarding the engine and specifically the low compression result. They advised that low compression in the cold test scenario was not necessarily representative of results obtained from a warm engine. They also stated that the low compression would not result in a significant power reduction or sudden engine stoppage.
Loose B nut
At the engine examination, it was identified that the ‘B’ nut[14] on the fuel control unit (FCU) was loose – about 1.5 turns from tight. This was not indicative of its security at the time of the accident as it was loosened by an ATSB investigator during engine removal prior to shipping for examination.
Ignition system
The engine data plate recorded the engine-to-magneto timing as 20° before top dead centre. The left magneto[15] timing to the engine was found at about 35° and the right magneto timing at 23°. The incorrect timing of the left magneto was assessed as having resulted from impact forces, which resulted in mount fracture and anticlockwise rotation of the magneto that advanced the timing. The external oil filter impacted the right magneto.
Testing of spark plugs and visual inspection of the ignition leads found no defects of the ignition system.
The magnetos were functionally tested and internally inspected at a CASA-authorised electrical and instrument maintenance facility, under the supervision of the ATSB. The magnetos were run on a test bench and both functioned throughout the normal operating range, with nil faults. The magnetos were then partially disassembled for internal examination and testing including points gap and continuity, internal timing, coil and capacitor serviceability. Both magnetos were found to be in normal operating condition.
The fuel system includes one main and one auxiliary tank, a gascolator, and a shut-off valve, with the associated pilot control knob located between the front seats. The fuel shut-off selector knob was found separated from the control tube and free to rotate however, the valve position was consistent with the fuel selected to the on position. The auxiliary tank was correctly interconnected with the main tank and, due to it being mounted higher than the main tank, would empty first while fuel remained in the main tank. The inter-tank flexible hose assembly was found clear of obstructions.
The fuel tank bladders remained intact despite splitting along riveted joins and punctures to the outer aluminium tanks. The aluminium tanks showed impact damage and subtle deformation (Figure 19 and Figure 20). Robinson assessed that the deformation of the fuel tanks was consistent with ‘lower fuel quantity’ but could not determine whether the deformation was due to impact damage, bulging of internal contents, or a combination of both. Robinson provided an image of an auxiliary tank that was known to have been nearly full at impact for comparison, which presented severe bulging over the entire tank (Figure 20). When compared with the exemplar image, the damage to VH-IDW’s fuel tanks was assessed as representative of the high vertical impact resulting in severe distortion to the airframe around the tanks, with little or no fuel within. This was also consistent with an ATSB investigation into a previous Robinson R22 accident, in which the tank was half-full on impact and displayed distinctive bulging from the internal contents that was not evident in the deformation of VH-IDW’s tanks.
Figure 19: VH-IDW’s auxiliary and main tanks showing subtle deformation and compression damage
Source: ATSB
Figure 20: An exemplar auxiliary tank known to be nearly full at impact and VH-IDW’s
Source: RHC, annotated by the ATSB
All remnant fuel was drained from the main tank on arrival at Darwin. It comprised about 250 ml of blue fuel (Figure 25), contained minimal debris/sediment and was tested clear of water. No fuel was found in the auxiliary tank. Noting as detailed previously (see the section titled Fuel capacity, calibration and indications) that the helicopter’s fuel system had 4 L of unusable fuel, the relatively small recovered quantity indicated that fuel had either been removed from the tanks after the accident or, considered more likely, had leaked out following the accident and/or during the transport from the accident site to Darwin.
Pressurised fuel system
The pressurised fuel system includes an engine-driven fuel pump, an electric (auxiliary) fuel pump and a fuel return line, which allows pump supply in excess of engine demand to return to the fuel tanks. If pressure from the electric pump is low in flight, a pressure switch illuminates the auxiliary fuel pump caution light. Return fuel passed through the fuel pressure relief valve (FPRV) and then flowed to a tee junction connected to the auxiliary tank. The return fuel jet and tee assembly were found to be installed correctly.
The FPRV was tested on a rig, to simulate both fuel return and static leak from the tank back into the engine fuel system. The FPRV fully opened at about the expected parameter however, a small bypass at lower pressures was noted. Robinson reported that the flow curve was similar to other FPRVs they have seen with significant time in service, and advised that:
We have done extensive testing, with [US Federal Aviation Administration] FAA involvement, on valves with variations in their flow curves, and found that they have very little to no effect on engine operation, both with and without the electric (auxiliary) pump operating and not operating. We found that the only FPRV valve condition that had any effect on the engine operation was a valve that was simulated as being stuck in an excessively open position, and in that case the stuck valve resulted in illumination of the auxiliary fuel pump caution light in idle and run-up (as well as at flight power levels).
The electric fuel pump was connected to a power source and operated. The pump was then disassembled, and the pump vane could be rotated manually. The electric motor was worn, with brushes almost down to the leads and the commutator grooved (Figure 21).
Figure 21: Electric fuel pump showing worn brush and commutator
Source: ATSB
There was no sign of particulate contamination or water in the fuel system.
The mechanical (engine-driven) fuel pump serial number matched that recorded as being installed on 7 February 2022. The pump was not blocked, and no defects were found. In addition, function of the driving plunger was observed with engine rotation.
Fuel control unit examination
The FCU was examined by a specialist at a CASA-authorised maintenance facility, overseen by the ATSB. There was no fuel found in the FCU, and the finger filter was clear. The throttle arm was distorted and there was damage to the FCU body, near the mixture control lever, consistent with impact forces. The nozzles were all visually clear and were bench tested. The fuel flow was within the service limits for overhauled nozzles (31.4–32.6 lb/h) except No. 6, which was slightly low (31.0 lb/h). The fuel system specialist advised the slightly reduced flow would not stop the engine from operating.
On the test bench, the FCU tested slightly high (running slightly rich) at the lower power setting, and within limits at all other settings including maximum power. The specialist advised that it was not uncommon for the low-test point to become overly rich. During the testing, flushed fuel was passed through a filter membrane with no contaminants collected. The FCU diaphragm was in good condition and there was no evidence of water contamination in the FCU. Throughout the examination and disassembly no seals or O-rings were found to be failed or damaged. The throttle mechanism was functional.
Fuel system disruption
The fuel lines, flow divider and gascolator were all clean, and empty of fuel. The gascolator drain valve was found depressed against the firewall when examined at the Darwin hangar but reset when manipulated. Upward forces during impact distorted the aircraft structure around the drain assembly resulting in the drain extender tube, used to compress the drain valve, bending and splitting (Figure 22).
Following removal from the accident site, yellow sand was observed in the end of the tube, which was consistent with the site where the helicopter was set down during the wreckage retrieval. The sand likely entered the tube as the skids were removed prior to extrication of the wreckage from the swamp, leaving the tube as the lowest point below the fuselage. The gascolator bowl was dry and the filter screen was clear. Examination of the cowls did not identify any discolouration or staining that would be associated with leaking fuel, either prior to, or after the accident.
Figure 22: Gascolator, drain valve and tube, and R44 II Illustrated Parts Catalog extract
The flow divider was opened and noted to be dry and clean, and there were no contaminants or restrictions that would have prevented fuel flowing through each of the nozzles and into the cylinders.
Figure 23: Fractured fitting between transducer and flow divider
The fuel gauges and low fuel switch were independent systems, in that the low fuel switch would illuminate the low fuel warning lamp, independently of the fuel sender position. The float-operated low fuel switch assembly, located in the main tank, was electrically tested, while manipulating the float up and down, and found to be functional. Additionally, the low fuel switch and lamp were signed off as having been tested by the maintainer on 7 February 2022, as part of the periodic inspection.
The ATSB removed the fuel quantity senders from both tanks and tested the sender calibration in Darwin in June 2022. Further testing of the main tank senders and gauge was conducted by Northern Territory Police on behalf of ATSB in August 2023.
Both senders moved smoothly throughout the operating range. The R44 Maintenance Manual fuel quantity sender check specified positioning the float arm at 4 noted heights and measuring the resistance at each point to verify it was within the specified tolerance. The main tank sender could not be positioned to the up stop height and at the down stop was slightly below the down stop height for the testing, and measured slightly above the resistance range at the intermediate heights. When the fuel gauge was connected to the sender and a power source, the fuel quantity indicator needle moved smoothly from empty to full. The 4 sender test heights corresponded to the gauge indications at Empty, 1/4,1/2 and Full. As a result of the sender float arm position, the gauge very slightly overread (within a needle-width) at the lower 3 indications.
The results were sent to Robinson for expert assessment. Robinson advised that the testing indicated the main tank gauge would have been reading slightly higher than what was actually in the main tank, but ‘nowhere near’ the calibration sticker figures, which indicated the main tank gauge was underreading.
Examination of the auxiliary tank sender base plate identified a slight bend to the sender pole and that the strainer and siphon assemblies were distorted. It could not be determined if the distortion was associated with the fuselage impact forces, or pre-existing. Regardless, the strainer distortion would not have affected fuel flow to the tank interconnect hose. In addition, the siphon, part of the fuel tank drain system would have no effect on fuel supply to the engine. The ATSB determined that the auxiliary tank sender was within the required resistance range at the up and down stops.
Partial power loss
Robinson advised that main rotor blade strike, or strikes, to a tree could stall an engine at low power or idle, prior to impact with the terrain. The ATSB assessed all available evidence against the engine manufacturer’s troubleshooting tables for Low power and uneven running and Failure of engine to develop full power. In addition, the 29 items on Robinson’s troubleshooting checklist for low power were reviewed. All applicable items were tested where possible, within the constraints of damage. Nothing was identified that would likely result in a sudden onset of low power.
The placard adjacent to the auxiliary fuel tank stated that the procedure to fill the tanks to full fuel entailed filling the main tank, then the auxiliary tank, then topping up the main tank. This procedure was required due to the self-levelling of the interconnected tanks.
The Helibrook operations manual included a procedure for hot refuelling (with the engine running). The manual stated that Robinson helicopters were not to be refuelled with the engine running,
unless a person remained at the controls and an authorised person who has undertaken training recorded on the Aircraft Refuelling Training Record Form 16 is available to carry out the refuel.
The Helibrook safety manager advised that they did not have a completed form for the pilot or the egg collector of VH-IDW, and there was no other evidence to indicate whether they had undertaken the training. The egg collector in the second helicopter to land at Mount Borradaile previously flew and collected eggs for Helibrook and was the only person present who had completed the required training to hot refuel a Helibrook R44 helicopter.
Noonamah
Based on interviews with the helicopter operator, pilot and fuel supplier, and the 2 most recently delivered fuel batch receipts, the Noonamah fuel storage tank contained blue 100 low lead (LL) Avgas. A total fuel quantity of 440 L was recorded as being taken from the Noonamah tank on 28 February, but there were no records of the quantity uplifted to individual helicopters. As well as VH-IDW, at least one of the other 2 R44 helicopters was reportedly refuelled when they arrived at Noonamah at about 0645 and several jerry cans were also filled from the Noonamah storage tank. The Helibrook R44 helicopter that flew to the site after the accident may also have used fuel included in that total.
The quantity and source of fuel remaining in VH-IDW prior to refuelling on the accident morning could not be determined. The accident pilot reported that they would have filled the helicopter to full at Noonamah, in accordance with normal procedures. They also stated that their usual practice was to set the chronometer to zero after fuelling the helicopter. Other pilots reported that normal practice was to ensure sufficient fuel to get to Mount Borradaile, but not necessarily to fill both tanks.
In a submission provided to the ATSB following review of the draft report, one of the egg collectors operating on the accident day reported that VH-IDW was filled with 100 LL fuel at a Helibrook base near Sweets Lagoon, 33 NM from Noonamah at the end of the previous day’s activities. They further reported that they were present at the hangar on the accident morning and had not observed VH-IDW being fuelled. Based on that account, if the helicopter was not refuelled at the hangar on the accident morning it would have departed Noonamah with 23-25 L less than the full fuel tank capacity.
As detailed previously, based on the georeferenced in-flight photograph, VH-IDW probably arrived at Mount Borradaile at about 0816. This time was consistent with the departure and arrival time recorded on a GPS device on the third R44 helicopter to arrive at Mount Borradaile that morning.
There were no records of the fuel uplifted at Mount Borradaile. Those present at Mount Borradaile reported that the R44 helicopters were hot refuelled. The accident pilot reported that their normal action was to always fill the helicopter to full at Mount Borradaile.
An Airbus/Eurocopter AS350 helicopter, with a pilot and crewman onboard, had landed at Mount Borradaile before the three R44 helicopters arrived. The helicopter was associated with the crocodile egg collection and its pilot was waiting for the pilot of the third R44 helicopter, who was the operator of the AS350, to assist with a maintenance issue with the AS350.
In preparation for the R44 refuelling, the AS350 crewman rolled 2 200 L drums out, checked they were marked WHNT, and verified they were labelled 100/130 green Avgas. They further recalled that the first drum had been partly used, and its lid was on tightly and difficult to open.
The helicopter crews reported that VH-IDW arrived first of the 3 R44s at Mount Borradaile. There were consistent recollections that the egg collector was in the pilot seat of VH‑IDW, and the accident pilot was in the passenger seat of VH-IDW, when it arrived. Pilot 2 (P2) and egg collector 2 (E2) were in the second helicopter and pilot 3 (P3) and egg collector 3 (E3) in the third.
When P3 arrived, they reportedly went immediately to the AS350 and did not witness the refuelling. The accident pilot could not confidently recall the refuelling events at Mount Borradaile, other than that they got into the third R44 and moved it up to the fuel drum. P2 reported that there was no drum pump carried in VH-IDW that day, and the pump used for refuelling was from the second helicopter. P2 and E2 reported that the pump from their helicopter was used by the accident pilot to put fuel into the main tank of VH-IDW, before the second helicopter moved to the drum. A submission to the ATSB following review of the draft report included a statement made in April 2023 by E2. In their statement, E2 reported that they had not seen VH-IDW being refuelled at Mount Borradaile.
In a statement to the ATSB in March 2022, E3 reported that when they arrived in the third helicopter at Mount Borradaile, they went to hold the hose for the accident pilot, who was getting ready to fuel VH‑IDW. They recalled that the third helicopter was refuelled next, and the second helicopter was still refuelling when the other 2 helicopters departed Mount Borradaile. However, in a subsequent statement in September 2022, E3 stated that they observed the egg collector partially fuelling VH-IDW before they took over and personally filled VH-IDW to full after first helping to refuel the third helicopter.
The AS350 crew reported that the 3 R44 helicopters left Mount Borradaile at 0830, which was consistent with the OzRunways recorded data for 2 of the 3 helicopters.
Based on the planned fuel figures, each R44 would have consumed about 80–90 L of fuel to reach Mount Borradaile. They therefore needed at least 80–90 L to fully fill at Mount Borradaile (noting that would have resulted in a minimum of 50% of the fuel in the tanks being 100/130 Avgas). The pump transferred about 1 L per revolution from the drum to the tank. After refuelling, the standard operating procedure required pilots to conduct fuel drains from 3 points on each helicopter to check for water and other contaminants. It was possible to fill each helicopter within a few minutes, particularly as several people capable of pumping fuel and conducting fuel drains were at Mount Borradaile.
The WHNT fuel drums at Mount Borradaile contained green-coloured 100/130 ‘leaded’ fuel.[16] The same person who rolled out the 2 fuel drums for the R44 pilots to refuel on the accident day, subsequently identified those drums and provided samples to the ATSB for testing. The person identified that as the drums had been reused, they had old 100 LL labels on the side, and the current 100/130 fuel labels on the top (Figure 24). WHNT was also clearly painted on the drums. The person checked the labels and seals, and recalled that the fuel in the drums was green.
Figure 24: WHNT fuel drum at Mount Borradaile showing distinct paint and labels. Inset: Fuel sample
Source: Supplied, annotated by the ATSB
The first drum rolled out was emptied on the accident morning then placed upside down by the AS350 crewman. As a result, when that crew person subsequently obtained fuel samples on behalf of the ATSB, the drum was distinctive as it had mud on the lid from having stood inverted. It was identified as the drum most likely to have been used first on the accident morning and VH‑IDW was reportedly the first helicopter to land at Mount Borradaile that morning. Samples from all 4 WHNT 100/130 drums at Mount Borradaile were taken to Darwin by WHNT and the ATSB arranged for the fuel to be tested.
The ATSB was subsequently advised that there were many empty fuel drums at Mount Borradaile, including some containing 100 LL located near the 100/130 drums. This raised the possibility that the drums used on the day of the accident may have been misidentified when samples were subsequently collected on behalf of the ATSB. However, a photo of one of those drums showed it was not painted with WHNT but was labelled with a different crocodile farm name and had a fuel expiry date of 13 October 2021. Additionally, the owner of the fuel supply reported that due to the remoteness and the criticality of having fuel available, they would not expect pilots to use fuel purchased for other operators and had not been advised of any fuel being wrongly taken.
Testing of the fuel drained from VH-IDW found it was consistent with 100 LL fuel, partially evaporated due to handling post-accident (see Appendix A – Fuel analysis). Gas chromatography with mass spectrometry testing of the VH-IDW sample found that it comprised less than approximately 1% 100/130 Avgas (1% was the testing limit of distinguishing between 100 LL and 100/130). There was also no evidence of contamination with Jet A-1, diesel, premium 98 petrol (car fuel) or Opal (low-aromatic car fuel used in the Northern Territory).
Samples from the 4 drums at Mount Borradaile containing green 100/130 fuel supplied by WHNT were obtained. The fuel from the 2 drums identified as having been used on the accident morning, were tested and found to meet the specifications of 100/130 fuel in accordance with the supplied batch test results. Figure 25 shows the colour of the Mount Borradaile sample compared with the remaining fuel recovered from VH‑IDW.
Figure 25: Comparison of Mount Borradaile sample and VH-IDW fuel
Images provided to the ATSB from first responders at the accident site showed 2 jerry cans in VH‑IDW, one behind each of the front seats. The jerry cans were subsequently removed from the helicopter and were not at the site when the ATSB arrived, nor subsequently provided to verify their contents. Those first on site and the accident pilot reported that both were full at the time of the accident and had probably been filled at Noonamah that morning. The jerry can behind the pilot seat was reportedly damaged on impact and may have leaked fuel, although no one reported detecting fuel leaking at the time.
The ATSB considered the potential effect of interference with the site in relation to the laboratory fuel testing results. The only plausible scenario that permitted both the described full refuelling at Mount Borradaile with 100/130 fuel and the residual 100 LL identified in testing was if 40 L of 100 LL fuel was poured from the jerry cans into VH-IDW after the accident and then most of it subsequently leaked away before the ATSB assessed the tank fuel quantity on arrival at the accident site. To dilute the 100/130 fuel component to less than the tested 1%, there would have to have been less than approximately 800 ml of fuel remaining in tank at the time prior to the addition of 100 LL from the jerry cans, comprised of approximately 50% 100/130 and 50% 100 LL fuel.
No one at the site, including the first to arrive, who was there until 1555, reported seeing anyone pour fuel into, or drain fuel from, VH-IDW. It was also reported that fuel from the 2 jerry cans was emptied into other helicopters that attended the site prior to their return to Darwin. Further, the empty jerry cans were then reportedly used to transfer fuel from a fuel drum to a helicopter at Mount Borradaile on the return to Darwin.
The Helibrook operations manual required pilots to use a fuel flow rate of 60 L/h for flight planning purposes for R44 II helicopters for ‘normal, specialised and holding’, and a fixed reserve of 20 minutes (20 L). In a submission to the ATSB draft report, the pilot stated that VH‑IDW’s normal fuel burn was 60 L/h. The operator reported that VH-IDW normally consumed about 65–70 L/h.
Robinson does not publish fuel flow rates for their helicopters. They provide a planning fuel flow of 60 L/h and guidance including to record the hour meter reading each time fuel tanks are filled, check the fuel level in the tanks visually, continually check hour meter and fuel gauges, and to refuel before the main tank fuel gauge reads less than 1/4 full.
With 176 L of usable fuel (full fuel) with no reserves, VH-IDW would have the following endurance:
2 hours 56 minutes at 60 L/h
2 hours 42 minutes at 65 L/h
2 hours 31 minutes at 70 L/h.
Required engine power, and therefore fuel flow, is highest during take-off, landing and while hovering. As such, when conducting low‑speed flight while carrying an external load, the engine would be operating at high power and fuel flow rate.
Low compression in one cylinder results in less power produced compared to the other cylinders. Therefore, a higher power setting and increased overall fuel usage would be required to achieve the same airspeed as a fully serviceable engine. The actual increase in fuel consumption on the accident day due to low compression in the number 6 cylinder could not be quantified as the specific compression was unknown.
Regarding in-flight fuel re-planning and quantity measurement, the Helibrook operations manual stated:
Single-pilot low-level aerial work activities undertaken by this company are such that the priority of maintaining control of the aircraft and awareness of their surroundings prevents more than a visual scan of the fuel quantity gauges. For these operations where the recording of fuel figures may be detrimental to safe flight, fuel state will be managed using visual gauge checks, watches and reference to elapsed flight time.
The pilot reported never using the fitted fuel flow meter and the display was not visible in the in‑flight photo.
The RFMS required that the weight and centre of gravity be checked to verify the helicopter remained within the approved limits throughout each flight. Although not required to be documented, there was no evidence that a weight and balance assessment had been conducted on the accident day.
Based on photos, interviews, and evidence from the accident site, when the helicopter departed Noonamah on the accident morning with the pilot and egg collector on board, its contents included:
slinging equipment
6 to 10 egg collecting buckets and poles
2 x 20 L jerry cans filled with 100 LL Avgas fuel
8 x 1 quart (0.95 L) engine oil cartons
fishing rod/s, firearms, drink bottles, ammunition and personal effects.
The ATSB did not have access to many of these items and it is unknown if other items may have been on board but removed from the site. Therefore, the helicopter’s exact total weight at the time of the accident could not be calculated. However, based on the available information, the helicopter was likely operating below the maximum allowable weight of 1,134 kg at the time of the accident.
In addition to the gross weight limit, it was also a requirement of the RFMS for HEC operations that the aircraft was operated at a weight at which the helicopter could hover out of ground (OGE) effect[17] at least 3,000 ft above the ground. Due to the above uncertainty associated with the helicopter’s actual weight (including its fuel quantity), and the identified low engine cylinder compression, it was not possible to determine whether OGE performance existed at the time of the accident. However, in the ambient conditions at the time of the accident, the helicopter would not have met the 3,000 ft out of ground effect hover capability requirement at its maximum gross weight (1,134 kg).
The RFMS also stated that the maximum weight permitted on the dual hooks was 129 kg including the sling person, line, harness, equipment, bucket and crocodile eggs. At the time of the accident, the egg collector with equipment weighed 118 kg and the line weighed 26 kg. The total weight on the hooks was therefore 144 kg plus the bucket, pole and small items that were not weighed. Although this exceeded the permitted weight, there was no evidence the hooks or associated equipment had failed.
In the event of an engine power loss, drive is no longer supplied to the rotor system and the pilot must lower the collective and sometimes conduct an initial flare to maintain sufficient rotor RPM while establishing autorotation. In an autorotation, the rotor blades are driven solely by the upward flow of air through the main rotor. The total energy available for an autorotation in the event of a power loss comes from the kinetic energy of the rotor blades and airspeed, and potential energy, which is directly proportional to the height.
Several factors affect the rate of descent in autorotation: bank angle, density altitude, gross weight, rotor RPM, trim condition, and airspeed. Two aspects pilots commonly use for managing distance travelled and rate of descent, are airspeed and rotor RPM.
In an autorotation in an R44 II, the rate of descent is high at zero airspeed, lowest at 55 kt, and increases again at higher airspeeds. The only energy available to arrest the descent rate for landing is the forward speed of the helicopter and the rotational kinetic energy stored in the rotor blades. Maintaining adequate rotor RPM is essential to ensure sufficient energy to flare the helicopter for landing. The flare is a critical manoeuvre that ensures safe completion of a power-off landing. The flare simultaneously decreases forward speed and rate of descent while increasing rotor RPM. Flaring too far away from the ground will leave the helicopter without sufficient energy to cushion the landing.
The R44 II POH stipulated that in the event of complete power loss, the pilot was to immediately lower the collective to enter autorotation. The specific procedure for power failure between 8 and 500 ft above ground level was:
Lower collective immediately to maintain rotor RPM.
Adjust collective to keep RPM between 97 and 108% or apply full down collective if light weight prevents attaining above 97%.
Maintain airspeed until ground is approached, then begin cyclic flare to reduce rate of descent and forward speed.
At about 8 feet AGL, apply forward cyclic to level ship and raise collective just before touchdown to cushion landing. Touch down in level attitude and nose straight ahead.
The minimum rate of descent during an autorotation was about 1,350 ft per minute at an airspeed of 55 kt and rotor RPM 97% when below 500 ft.
A height-velocity (H/V) diagram is required for single-engine helicopters certified under FAR Part 27. The diagram:
defines an envelope of airspeed and height above the ground from which a safe power-off or one engine inoperative (OEI) landing cannot be made (FAA, 2014).
The Robinson R44 II Pilot’s Operating Handbook (POH)[18] included the H/V diagram for R44 II helicopters, including VH-IDW (Figure 26).
Figure 26: Robinson R44 II height-velocity diagram
Source: Robinson Helicopter Company R44 II POH
When operating at low speed in the shaded (or ‘avoid’) area on the left side of the diagram, in the event of a power loss, a pilot may have insufficient height to accelerate to the speed required to autorotate successfully (autorotation speed).[19] Above a certain height above the ground, at least 400 ft for the R44 II depending on the density altitude, it is possible for a pilot to achieve autorotation speed even from a high hover (FAA, 2019). In the shaded area on the lower right side of the diagram, the combination of faster airspeed and proximity to the ground provides limited reaction time for the pilot in the event of in-flight emergencies. The FAA Helicopter Flying Handbook (FAA, 2019), stated:
the shaded areas should be avoided, as the pilot may be unable to complete an autorotation landing without damage.
The unshaded region of the diagram shows the combinations of airspeed and height above the ground that allows a pilot to successfully complete a landing in a full autorotation without requiring exceptional skill. At low heights (below about 10 ft) with low airspeed, such as a hover taxi, the helicopter is in a safe part of the H/V diagram. There, a pilot can use the kinetic energy from the rotor disc to cushion the landing with collective, converting rotational inertia to lift. An increase in height without a corresponding increase in airspeed puts the helicopter above a survivable un‑cushioned impact height, until a height is reached from which rotor inertia and gravitational potential energy can be converted to sufficient lift to reduce the vertical velocity at impact to a survivable value (FAA, 2019).
A requirement of certification of the dual hooks for HEC was to have the appropriate limitations and procedures for conducting human external cargo operations incorporated in the rotorcraft flight manual supplement (RFMS). The first draft of the RFMS associated with the STC for the hooks system was developed in 2013, and revision 13 of the R44 RFMS for HEC Dual Hook was approved by CASA, along with the STC, in July 2021.
The CASA-approved rotorcraft flight manual supplement
The CASA-approved RFMS and associated STC were specifically for the activity of collecting crocodile eggs, and some operational procedures were included in the RFMS. The RFMS Introduction stated that it was only valid if the operator also had ‘CASA approved operational procedures for use of the HEC Dual Hook system’.
The RFMS Section 1 General, contained a warning of elevated risk to aircrew ‘and particularly the Human External Cargo (HEC)’ involved in helicopter crocodile egg collection operations. The elevated risks included:
a. Any failure in the attachment of the line to the helicopter, lines and harness, including accidental release actuation, inevitably results in injury or death of the HEC.
b. In any malfunction of the helicopter resulting in an emergency landing, the HEC does not have the protection of the airframe structure and restraint harness.
c. The helicopter is operating most of the time in the corner of the speed/height diagram for which a safe landing may not be possible.
d. Operating the aircraft to safely position the HEC in relation to the ground and obstacles is a high skill, high workload operation.
It then detailed additional risks including the:
‘use of a low powered single piston engine helicopter’
lack of a ‘spotter’ in the aircraft due to R44 weight restrictions
isolated nature of crocodile egg collection
potential for crocodile attack.
Section 2 Limitations included:
a maximum airspeed of 60 kt during HEC operations
maximum 15 kt wind
no operations within 5 NM of lightning
a weight limit such that the helicopter has out-of-ground-effect hover capability at least 3,000 ft above ground level
maximum 129 kg down weight: combined weight carried on the hooks including the HEC person, line, harness, equipment, crocodile eggs and their container
HEC line length between 48 and 105 ft (15–32 m).
The RFMS Section 3 Emergency procedures stated:
Survivability of HEC personnel during an in-flight emergency is best accomplished by having suspended personnel remain attached to the aircraft as it makes an emergency landing. Apart from exceptional circumstances, release of the HEC line is not an operational consideration while human external cargo (HEC) is attached beneath the aircraft. In case of an aircraft emergency, the pilot will normally conduct a landing with HEC attached to the short-haul line. The only exception is the HEC or line snagging on terrain, or the probability that this may happen. The choice by the HEC person to cut away from the line is a personal decision depending on the circumstances and best chance for survival.
WARNING
Short-haul operations are inherently dangerous and could be fatal. This must be discussed in detail during training, re-currency and mission pre-flight briefings.
NOTE
It is imperative that potential emergency scenarios, actions and reactions likely required of all involved personnel are discussed as thoroughly as possible prior to flight.
PQRS [PRIMARY QUICK RELEASE SYSTEM] OPERATION
Emergency use of the PQRS is restricted to circumstances where the pilot judges that the consequences for the HEC person are outweighed by the reduction in risk for the aircraft and aircrew.
…
ENGINE POWER LOSS
In addition to the procedures defined in the [Rotorcraft Flight Manual] RFM
1. Roll away, upwind if possible, away from the HEC person.
2. Attempt to touch down level and clear of the HEC person. If insufficient clearance from HEC person, touch down banked so the rotor will be away from the HEC person.
NOTE
HEC person is to rapidly unhook or cut the lines and lay prone on ground to minimize injury risk from the helicopter.
GRADUAL ENGINE POWER LOSS
1. If obstacles permit, place the HEC person on the ground if possible.
2. Attempt to touch down level and clear of the HEC person. If insufficient clearance from HEC person, touch down banked so the rotor will be away from the HEC person.
NOTE
HEC person is to rapidly unhook or cut the lines and lay prone on ground to minimize injury risk from the helicopter.
In establishing the emergency procedures, the design engineer advised that considerations of the line disconnecting (uncommanded) resulting in release of the HEC, were addressed by the hooks’ compliance with FAR certification standards for hooks for HEC. They reported that it was recognised that engine failure was the biggest risk. In managing this risk, the expectation was that an engine would rarely stop suddenly – usually running rough and degrading over a period of 30–60 seconds before stopping. It was considered that expected behaviour should give a pilot time to manoeuvre the helicopter away from the HEC, preferably downwind.
Furthermore, the design engineer advised that the emergency procedures were based on minimising risk to the HEC because the sling person was unprotected, whereas the pilot had a seat, restraint, and airframe as protection. Jettisoning the HEC from higher than 10 to 15 ft above ground would likely result in fatality, therefore keeping the HEC on the line while the helicopter autorotated, was assessed as offering a better overall outcome. The design engineer reported that at the time of the STC approval, the FAA advised that they could see ‘almost no circumstances in which the pilot would release the HEC’, but that more recently FAA’s emphasis had changed to requiring a very high degree of engine and systems reliability.
The US Department of the Interior (DOI) defined the transport of one or more people suspended beneath a helicopter as ‘short-haul’. The DOI Helicopter Short-Haul Handbook outlined minimum policies, procedures, qualifications, training requirements and equipment for helicopter short-haul programs, and was accepted as ‘best-practice’ guidance material.
Preplanning for emergency procedures is a critical component of risk management. Accordingly, each short-haul program must evaluate and discuss potential scenarios and actions that may best mitigate any associated hazards. Training for effective crew resource management should be a part of this process.
It is imperative that everyone involved in short-haul understand how instantaneously an in-flight emergency may occur. Survival of short-haul personnel during an in-flight emergency is best accomplished by having suspended personnel remain attached to the rope while the pilot attempts emergency landing. Examples of formalized emergency planning procedures are outlined below.
WARNING: Short-haul operations are inherently dangerous and could be fatal. This must be discussed in detail during training and recurrency. Release of the short-haul line is a possible consideration while human external cargo (HEC) is attached beneath the aircraft. In case of an aircraft emergency, the pilot may attempt to land with HEC attached to the short-haul line. The decision of any short-hauler to cut away from the line is a personal choice depending on the circumstances and best chance for survival.
The only difference between this text and the CASA-approved RFMS Emergency procedures, was that the DOI Handbook stated that ‘Release of the short-haul line is a possible consideration’, whereas the RFMS stated ‘Apart from in exceptional circumstances, release of the HEC line is not an operational consideration’, while HEC is attached beneath the aircraft. Both documents stated that the HEC survival was best assured by the sling person remaining attached to the line in the event of an emergency landing.
Other dual hooks for HEC RFMS
There were no STCs for dual hooks for HEC for R44 helicopters in Canada or the US. The ATSB reviewed the RFMS and STCs for dual hooks for HEC (using single turbine engine helicopters) that were approved in Canada and the US. Those STCs were used for multiple activities, unlike the R44 dual hooks with HEC for crocodile egg collection, which were only approved for that activity.
In Canada, single turbine engine HEC was only approved for rescue and similar activities considered to be in the public interest, that is, where there is a value of life consideration. The RFMS approved by Transport Canada incorporated only emergency procedures as they related to failure of the hook system. For example, a Transport Canada-approved RFMS for Bell 206L‑series helicopters HEC dual hook system Emergency/malfunction procedures section consisted of:
the need to release both hooks to jettison HEC
actions in the event of (hydraulic) failure of the PQRS to open the HEC hook
uncommanded release of either hook system.
An FAA-approved RFMS for Bell 206L/407 had emergency procedures for the event of electrical failure of the hooks, plus the following statement:
Engine Failure
The presence of an external load may further complicate a failed engine condition. In an emergency, land the rotorcraft as soon as practical.
An FAA-approved RFMS for MD Helicopters MD 369 Emergency procedures stated:
If any aircraft emergency occurs during flight with HEC, the operations should be terminated by landing HEC in the nearest safe area. If during an emergency the aircraft must be landed immediately due to engine failure, or catastrophic control failure, HEC may need to be jettisoned.
1. Land HEC safely to the ground as soon as possible.
2. Release empty long line as required…
3. Refer to basic flight manual Emergency and Malfunction Procedures.
In summary, a Transport Canada-approved test pilot advised that an RFMS associated with an STC for dual hooks for HEC would document how to release a load, and procedures in the event of failure of the hooks or quick release system (QRS), but would not address particular operational scenarios. The expectation was that these would generally be contained in an operator’s standard operating procedures approved by the Operational Authority.
Helibrook held an air operator’s certificate issued 2 April 2020, with an expiry date of 31 July 2022. Under the certificate, Helibrook was permitted to conduct charter and aerial work operations, including sling load operations. At the time of the accident, Helibrook had one Bell 206L and 3 Robinson R44 II helicopters.
The 3 key positions at Helibrook were the head of aircraft airworthiness and maintenance control (HAAMC), who was the accident pilot of VH-IDW, the chief executive officer (CEO), who was also the chief pilot, and the safety manager.
The accident pilot was a licenced aircraft maintenance engineer and had held the role of Helibrook’s HAAMC since 12 July 2019. The Helibrook operations manual defined the HAAMC role as follows.
The safety of aircraft airworthiness and maintenance of aircraft is delegated to the HAAMC. The responsibilities and duties of the HAAMC include, but are not limited to ensuring that appropriate arrangements are made for:
1. Maintenance scheduling
2. Monitoring and recording of aircraft hours, cycles and other information relevant to Maintenance scheduling
3. Monitoring and scheduling of maintenance due and deferred maintenance actions (including deferred defects)
4. The review of Airworthiness Directives for applicability and compliance
5. Defect rectification and unscheduled maintenance
6. Investigation and reporting of defects.
The HAAMC is accepted by CASA under a letter of acceptance and is responsible for ensuring that the aircraft operated are airworthy and maintained in accordance with CASA regulations and directions and liaise directly with the maintenance provider – ultimate responsibility remains with the registered operator.
The chief pilot was responsible to CASA for all operational matters affecting the safety of flying operations. The chief pilot’s responsibilities listed in Helibrook’s operations manual included:
safe and efficient operation of the aircraft
monitoring operational standards
maintaining training records and supervising the training and checking of pilots and crew including of equipment used
ensuring pilot flight and duty times were accurately recorded
ensuring the aircraft were appropriately maintained.
Prior to holding the chief pilot role, the Helibrook CEO had been subject to CASA enforcement action. As a result, CASA imposed a variation on the pilot’s helicopter licence. The variation required the CEO to attend aviation theory remedial training and testing, and complete four 6‑monthly flight reviews with a CASA-approved examiner. These were aimed at ensuring ongoing proficiency in making appropriate safety judgements.
The CEO reported completing the first of those flight reviews and aviation theory training on 6 July 2019. On the same day, the CEO submitted an application to CASA for approval to become Helibrook’s chief pilot. The applicant’s previous breaches meant they did not meet one of the criteria for the chief pilot appointment, which required the person to have ‘maintained a satisfactory record in the conduct or management of flying operations’. CASA offered the applicant the opportunity to demonstrate an acceptable means of compliance with that requirement and submit a safety case stating how they would manage the risks.
Having provided a response to CASA, the chief pilot applicant was required to conduct 2 flights with a CASA flight operations inspector and complete associated ground activities. The CEO conducted the first CASA assessment flight on 6 August 2019 and was assessed satisfactory. The activities assessed were a charter flight and simulated crocodile egg collection. The examiner identified some gaps in knowledge of recent legislation, which the applicant was reported to be working to address. The examiner’s notes described an experienced pilot with a good safety focus.
The CEO’s second chief pilot assessment flight and ground activity was conducted on 25 November 2019. The examiner commented that the CEO demonstrated the ability to supervise and mentor other pilots and was assessed as suitable for consideration for appointment as chief pilot of Helibrook.
CASA subsequently approved the CEO as Helibrook’s chief pilot on 20 January 2020. Additionally, the CEO was provided with an exemption removing the requirement for the previously imposed 6-monthly flight review checks. As part of the process for the CEO to conduct the chief pilot role, Helibrook introduced a safety management system (SMS) and appointed a safety manager.
The safety manager was recruited by the Helibrook CEO in August 2019. The safety manager was also assigned the roles of operations manager and drug and alcohol management plan (DAMP) officer for Helibrook. Apart from a short period in 2020, when the safety manager worked for Helibrook in the Northern Territory, including as a helicopter charter pilot, the safety manager lived interstate and conducted the safety manager, operations manager, and DAMP officer roles remotely.
Documented key responsibilities of the safety manager included:
maintaining the safety management system and ensuring it was relevant to the operations
Attributes of a safe organisation include a healthy safety culture with appropriate risk management processes, which achieves safety objectives through internal responsibility rather than relying on regulatory compliance (CASA, 2019). The International Civil Aviation Organization (ICAO, 2018) defined an SMS as:
A systematic approach to managing safety, including the necessary organizational structures, accountability, responsibilities, policies and procedures.
It is designed to continuously improve safety performance through the identification of hazards, collection and analysis of safety data and safety information, and continuous assessment of safety risks. An SMS seeks to proactively mitigate safety risks before they result in aviation accidents and incidents.
The Helibrook SMS manual version 1.0 was issued on 1 August 2019 and accepted by CASA on 22 November 2019. Although not generally required by CASA regulations at the time, it was introduced to demonstrate a commitment to safety and thereby aid in obtaining CASA’s approval of the chief pilot. The SMS manual outlined the company’s safety policy, objectives, and responsibilities for supporting the SMS and reporting of incidents, risks and hazards. It stated:
HELIBROOK will identify hazards and safety risks to minimise risk to innocent people, clients, contractors, employees, other airspace users and aircraft. It will also maintain the health of all stakeholders, and continually improve safety; these goals will be accomplished through a Safety Management System (SMS).
Helibrook’s SMS manual stated that it was to be updated annually, by the CEO in collaboration with the safety manager, and that safety meetings were to occur monthly and involve the safety manager, CEO/chief pilot and HAAMC.
Safety risk management
Safety risk management includes hazard identification, and safety risk assessment, mitigation and risk acceptance (ICAO, 2018). The safety risk management process is continuous and risk mitigation strategies must be monitored to determine whether they are effective. Helibrook’s SMS manual stated the aim of risk management was ‘to treat or control risks to as low as reasonably practicable’. Their stated risk management tools included a documented risk assessment, evaluation and treatment process, a master risk register, and a regular hazard and risk review process.
Hazard identification
According to ICAO (2018), a hazard can be considered as a dormant potential for harm, which is present in one form or another within the system or its environment. Therefore, hazard identification is the first step in the safety risk management process. The intention is to proactively identify hazards before they lead to accidents, incidents, or other safety‑related occurrences. Hazard identification may also consider hazards that are generated outside of the organisation and outside their direct control, such as weather (ICAO, 2018).
The Helibrook SMS manual listed several means of identifying hazards including reporting systems, audits, staff input, and experience.
Helibrook hazards
The Helibrook hazard register, titled Hazards and Risks, listed items under 7 headings: organisation, operational, helicopter, pilot and flight crew, operating environment, weather and egg collecting. The following 2 lists are relevant to this investigation:
Helicopter:
(a) Preflight checklist
(b) Safety equipment – EPIRB, helmets, life jackets, satellite phone and flares
(c) Equipment lists, equipment and checks
(d) Fuel
(e) Inspection – MRs
(f) Maintenance and status
(g) Inspection and status
(h) Time to rebuild/overhaul
(i) Communications – headsets/radio
(j) Weight/centre of gravity
(k) Fuel margins and range limits
(l) Sling Equipment / Harness equipment PPE
Egg collecting:
(a) Crocodile activity
(b) Terrain
(c) Weather
(d) Pilot and crew performance
On 30 September 2019, in response to a request from CASA, the safety manager identified 13 hazards ‘that have the potential to cause harm to pilots and passengers’ and proposed actions to mitigate associated risks. None were associated with crocodile egg collection operations.
Risk assessment
A risk assessment is a process where hazards and the chances of an adverse event happening due to the hazard were identified, analysed, and evaluated (CASA, 2021). This evaluation was expressed in terms of likelihood and consequence and should highlight the risks to be considered before and while carrying out an operation.
Organisations should have multiple layers of controls or defences in place to manage their identified hazards (CASA, 2014). Risk assessments should be carried out across all levels of an organisation and at different stages in the operation. These could consist of a formal, documented process or a continuous ongoing mental assessment carried out by a pilot, or a combination of both. An example of a formal risk assessment would be an operational risk assessment conducted by the operator to consider and evaluate the risks associated with the type of work being undertaken.
The Helibrook operations manual stated that the ability to identify hazards and assess risks was an important component of their continuous safety improvement process. It stated that if a risk assessment was required, the chief pilot would conduct and document the process, which included assessing the risk, developing risk control strategies and implementing them, then assessing those controls. The Helibrook operations manual standard operating procedure for crocodile egg harvesting included that in the event of an aircraft failure:
the sling person must have a clear understanding of the risk and implications of such an emergency
the risk of injury will be reduced providing all height and speed limitations are adhered to
prior to slinging, the pilot must advise the sling person of the high risk nature of the operation and what steps shall be taken to reduce the risk.
Risk register
Safety risk management activities should be documented, including any assumptions underlying the probability and severity assessment, decisions made, and risk controls implemented (ICAO, 2018). A tool such as a risk register could be used to ensure identified hazards were tracked and mitigated as part of a formal risk management process of prioritisation, documentation, and assessment. The register could include the hazard, potential consequences, assessment of the associated risks, and any controls put in place to manage the risk (ICAO, 2018).
Safety reporting system
The effectiveness of a safety reporting system partly relies on the promotion of a positive reporting culture and proactive identification of safety deficiencies. One way of achieving this is by clearly stating that reported information will be used solely to support the enhancement of safety (International Civil Aviation Organization, 2018). This also included a culture where people can report without fear of punishment (Reason, 1998). The Helibrook SMS described a formal reporting system as a key element of the SMS.
Safety culture
CASA SMS booklet 2 – Safety policy and objectives stated that good safety management ‘is not about having an SMS manual on the shelf…it needs context to be effective’. Further, that the ‘ultimate responsibility for safety rests on the shoulders of senior managers’, who should demonstrate a commitment to safety. This included maintaining a positive safety culture.
Safety culture has been defined as 'the set of enduring values, behaviors and attitudes regarding safety, shared by every member at every level of an organization' (SM ICG, 2019). More simply, it is ‘what goes on when no-one is watching’ (EASA, n.d.). Additionally, the effectiveness of a safety management system has been shown to be dependent on the safety culture (SM ICG, 2019).
The Hudson Ladder defined 5 steps, or maturity levels, in the evolution of safety culture (Figure 27). The first step – pathological (‘who cares as long as we’re not caught’) – was not really a culture of safety (Hudson, n.d.). The second step, a reactive safety culture, was one in which safety was a burden imposed by the regulator. In a reactive culture, action was only taken in response to an incident, and often involved blame or punishment. In a poor safety culture, ‘not everyone takes safety seriously, are not watchful, are complacent and compromise too readily’ (ARPANSA, n.d.). In contrast, a positive safety culture ensures operations are conducted as safely as practicable, which reduces the risk of accidents occurring.
CASA described safety culture elements, in which an example ‘enabler’ of a positive safety culture was that an ‘effective method of hazard identification has been established’. The converse example ‘disabler’ of a positive safety culture was ‘no effort is spent on hazard identification’ (CASA, 2021).
Helibrook’s SMS manual had not been amended since initial issue and no meetings had been conducted since the introduction of the SMS. The safety manager described their role as ‘lacking’ and reported that most of their time was devoted to managing day-to-day operations (in their other role as Helibrook’s operations manager).
The safety manager also described the Helibrook hazard register as ‘a bit lacking’, with many of the listed items not actually hazards. Additionally, there was no assessment of risks, controls or mitigation strategies. Helibrook did not have or maintain a formal risk register, or any alternate means to track and identify hazards and associated controls for their operation. The safety manager also reported that no risk assessment had been conducted of any of Helibrook’s approved activities, including crocodile egg collection (an activity which the safety manager had not actually observed). The CASA instrument that approved human external cargo operations stipulated that human slinging could only be conducted if it was assessed as reducing the risk of heat exhaustion and/or crocodile attack. Despite that, there was no documented means of assessing the relative risks.
Safety equipment, maintenance and time to rebuild/overhaul were listed on the hazard register relating to ‘Helicopter’, however no risks had been identified with VH-IDW. The safety manager also reported being unaware that VH-IDW’s ELT was not installed.
The safety manager described Helibrook’s reporting culture as ‘not great’, with only one incident in Helibrook’s safety reporting system – a hard landing involving VH-XHB, which occurred on 30 August 2020, while the safety manager was at the site. In relation to that occurrence, the safety manager submitted an incident report to ATSB on 1 September 2020.
The report stated the pilot was the only person on board at the time of the accident. However, the ATSB obtained footage taken by one of 3 passengers on board at the time. The safety manager was nearby at the time of the accident and, despite the detail on the incident report, reported being unaware how many people were on board. The safety manager was also the Helibrook DAMP officer and had not requested drug and alcohol testing of the pilot following that incident, as they did not think the incident was sufficiently serious to warrant it. In response to that incident, the safety manager reported proposing a windsock be put in the area to assist pilots identifying the wind direction, as misidentification of the wind direction was assessed as a factor contributing to the incident.
The safety manager did not conduct an internal investigation into the accident involving VH‑IDW and several months after the accident reported that they did not know what happened, had not seen the aircraft or been able to obtain any information about it. As the DAMP officer, the safety manager had also not requested testing of the accident pilot.
CASA first assessed and accepted the Helibrook operations manual in December 2016. The Helibrook operations manual version 7.3 was accepted by CASA on 28 February 2020. The manual included a standard operating procedure (SOP) for crocodile egg harvesting. That SOP was approved by CASA on 11 June 2020. CASA’s approval of the slinging operation was based on reducing the overall risk of crocodile attack and heat exhaustion. The SOP stated that the primary reason for slinging personnel was to:
reduce the risk of heat exhaustion of personnel in extremely difficult terrain and high humidity temperatures.
It further stated:
Should heat exhaustion or fatigue be a factor in collecting the nest then the nest shall be collected by other means other than using a Sling person.
The intent of the latter statement appeared to be to avoid operating in and around a helicopter if personnel were affected by fatigue.
One requirement of the procedure was for the chief pilot to have briefed the pilot before the pilot was permitted to conduct HEC sling loads. The briefing was to include a minimum 30-minute oral brief, a minimum 30-minute equipment demonstration/inspection and a minimum of 1 hour flying time. This was to be documented on a pilot competency check form. There was no record this had been conducted for the accident pilot.
Additionally, Helibrook did not have documented training for the pilot to conduct HEC slinging operations, or evidence that the pilot had trained in Helibrook’s emergency procedures for HEC slinging. The pilot reported having demonstrated some criteria and conducted ergonomic testing of the switches with CASA, but could not recall specific training by the operator. At the start of each season, the pilot completed annual administration and recurrency with WHNT but no helicopter-based training specifically for the activity.
The pilot reported that they did not generally practise emergency procedures for slinging. In their most recent operator proficiency check, the pilot recalled conducting autorotations and other emergencies. They did not practise releasing the sling load, as the pilot reported doing it ‘every day’ and it was ‘just two pushes of the buttons’. The chief pilot reported that it was ‘too dangerous to put yourself in an autorotation in that scenario to practise’, but they did general emergencies/autorotations as part of the training.
The SOP included ‘Safety aspects to consider before approaching a nest’. It required pilots and sling persons to assess slinging access to the nest including consideration of timber, trees and obstacles. It stated: ‘Should there be obstacles that will affect the safe operation then the sling option will be abandoned’.
Pilots were also required to be ‘fully conversant’ with the CASA instrument (approving use of HEC for crocodile egg collection) including the conditions and limitations. The requirement for the pilot to brief the crew/sling person on the emergency procedures was included.
The SOP included the following section titled Emergency procedures:
The pilot shall brief the crew on the emergency procedures in the event of an aircraft failure. The pilot, crew and Sling Person shall together discuss that in the event of an engine failure, aircraft strike or any other type of incident the pilot may need to release the Sling Person. The Sling Person shall have a clear understanding of the risk involved and the implications of such an emergency. Providing all height and speed limitations are being adhered to the risk of injury in the event of an emergency will be reduced.
Both the pilot and Sling Person shall carry personnel emergency locator transmitters during all operations. The aircraft shall have a satellite phone on board at all times and all personnel are to be briefed on its use.
Prior to any Sling Person being slung, the pilot in command must advise the Sling Person of the high risk nature involved in sling operations with an aircraft in the high hover state and the potential for injury or death should there be an equipment failure.
In addition to the Company standard passenger brief the Chief Pilot or approved pilot in command shall brief the Sling Person on the possibility of an emergency happening and what steps shall be taken to reduce the risk to persons involved.
The following emergency procedures were then specified:
Partial engine failure malfunction
The pilot in command shall attempt to place the Sling Person on the nearest safe area and release the strops from the aircraft
The aircraft shall proceed to land at the nearest suitable area
Complete engine failure
The pilot in command shall release the Sling Person as close to the ground as practicable and attempt the cushioning of the aircraft onto the ground, forward of the Sling Person and clear
Note:
At any time that a Sling Person is on the strop (long-line) he / she shall not be any more than five (5) m above the immediate ground and or vegetation
Should an engine failure occur the aircraft will already be in the high hovering state which is outside a safe auto-rotational envelope therefore the pilot will only be able to cushion the aircraft the best he / she can
The Sling Person shall do his / her best to move away from the aircraft or where the aircraft is coming to rest
Training in emergency procedures
Planning for emergency procedures is a critical component of risk management in HEC operations (DOI, 2010). A study into the human factors aspects of human external loads recommended that all HEC crewmembers be initially and continually trained and practised in emergency procedures (Shehab, Schlegel & Palmerton, 1998). For any in-flight emergency, training is essential to ensure a pilot responds quickly and appropriately. The FAA General Aviation Joint Steering Committee’s Safety Enhancement Topic – Emergency Procedures Training (FAA, 2013), stated:
Every pilot needs to prepare for the unexpected. Engine failures and inflight emergencies have a nasty habit of cropping up at the most inopportune times. However, with the right training and preparation, you can be ready for any hazardous situation that comes your way.
In the event of an engine power loss while operating in the H/V avoid area, a safe outcome is not always possible, and a pilot has very limited time to respond to achieve the most effective autorotation possible. In the event of a power loss with an external load, the decision to release a load is dependent on the load characteristics. For non-HEC, the load would be jettisoned to reduce aircraft weight, prevent the load from interfering with controllability and increase survivability of the helicopter’s landing.
For HEC, the pilot must decide whether to put the sling person on the ground or to release them. If the sling person is placed on the ground at a speed that minimises their risk of injury, the helicopter will descend rapidly from the height of the length of the sling line, increasing the pilot’s injury risk. The pilot’s injury risk is reduced as the impact velocity decreases. The minimum rate of descent of an R44 II helicopter in an autorotation is achieved at 55 kt airspeed. A sling person would be unlikely to survive an autorotation to the ground with that combination of vertical and horizontal velocity.
Although the Helibrook SOP permitted a sling person to be carried up to 5 m above vegetation (including trees), releasing the sling person more than 5 m above the ground is likely to result in fatal injuries. Additionally, release of the sling person with any horizontal velocity may make it difficult for them to remain erect, increasing the risk of landing other than feet first and increased injury severity.
Release of the sling person
The CASA-approved RFMS stated that survivability of HEC personnel during an in-flight emergency was best accomplished by having the sling person remain attached to the helicopter, unless they were snagged on terrain or likely to become so. However, the Helibrook emergency procedure in the event of engine failure stated that the pilot ‘shall release the sling person as close to the ground as practicable’.
CASA’s instrument approving HEC for crocodile egg collection required pilots to comply with both the RFMS and the company operations manual, and the onus was on the helicopter operator to ensure there was no discrepancy between the 2 documents. When asked about the discrepancy between the RFMS emergency procedure to keep the HEC attached to the line and Helibrook’s emergency procedure to release the HEC, the accident pilot reported that the RFMS stated it was the pilot’s discretion whether to jettison the HEC in the event of an engine failure.
The pilot commented that they ‘did not agree with’ the RFMS procedure to leave the sling person connected in the event of emergency, as that was ‘not a good method at all’. The pilot further commented that with a complete engine failure when operating above trees, if they left the HEC attached to the helicopter, the helicopter would either descend 100 ft vertically on top of the sling person, or the sling person would be dragged through the trees.
The chief pilot advised that in the event of an issue with the helicopter with HEC the pilot would flare the helicopter to try to ‘get the sling person off safely’, and in doing so, sacrifice themselves (and the helicopter) because they would lose rotor RPM. They further stated that in the event of engine failure while slinging, they would likely have their head out the door (watching the sling person) and would look in at the cockpit instruments and identify what had happened. The pilot reported that if they had forward speed, they would flare to release the sling person as safely as possible, then nose forward to try to regain airspeed before flaring the helicopter onto the ground.
Operating height
The Helibrook emergency procedure stated that the HEC ‘shall not be more than 5 m above the ground and or vegetation’. The accident pilot reported that when slinging with HEC, they tried to minimise the height and distance, and the sling person would usually be just above the treetops. The chief pilot also reported that they would go over trees and another pilot who had previously conducted crocodile egg collection reported that the SOP requirement to be not more than 5 m above the ground or vegetation was interpreted to include not more than 5 m above 30.5 m (100 ft) trees. One of the other operators conducting crocodile egg collection reported that they had normalised operating above treetop height, and had removed the height reference from their operations manual. The amendment to that operations manual had been accepted by CASA.
Operating above trees increased both the height of the fall if the sling person was released and the likelihood of having to release the sling person to prevent entanglement with vegetation rather than place them on the ground.
A CASA-authorised aeronautical (design) engineer first issued an engineering order approval for installation of a hook system on an R44 helicopter in December 2007, to enable slinging of an egg collector onto a crocodile nest to facilitate egg collection. However, the approval for fitment of the hook system did not in itself provide approval to conduct external load operations. To make it clear that operational approval was also required, the RFMS associated with the engineering order for the hooks system stipulated that use of the hooks was limited to the commercial collection of crocodile eggs in accordance with CASA-approved operational procedures.
Civil Aviation Regulations 151 and 250, which were in force throughout the 2007–2021 period of instrument approvals, did not permit a person to be picked up or carried outside a helicopter without CASA’s authorisation and permission. For crocodile egg collection, CASA issued instruments to helicopter operators that authorised the pilot in command to pick up a person under Civil Aviation Regulation 151(3) and permitted the pilot to carry that person in a harness system attached to the R44 helicopter under Civil Aviation Regulation 250(2). Civil Aviation Safety Regulations Part 11 applied to this authorisation. Specifically, CASR 11.055 (1)(d)[20] stated that CASA may grant the authorisation only if ‘granting the authorisation would not be likely to have an adverse effect on the safety of air navigation’ (CASR, 2010).
For the helicopter and pilot (and any other occupants), the key risk that results from carrying (slinging) a person under the helicopter is an event in which the HEC becomes entangled or a similar scenario that may cause a loss of control to the helicopter. Additionally, slinging involves operation in the H/V avoid area, and carries similar hazards to the helicopter and occupants as any other operation in that flight regime.
As the sling person is outside the protection of the helicopter, consideration is required of the likelihood of any scenario where they may collide with an obstacle or the ground, such as a fall resulting from deliberate or inadvertent release of the hooks.
In 2013, CASA identified that the hooks that were being used for crocodile egg collection operations were not certified for HEC. The premise for the certification of any jettisonable external load was that it could be released, without exceptional pilot skill, to prevent hazard to the aircraft, such as causing a loss of control. For HEC, in addition to the need to be able to rapidly release the load to avoid a hazard to the aircraft, it was also necessary to minimise the probability of inadvertent release.
The design engineer then commenced a process to enable the hooks to be approved for HEC by meeting the certification requirements of US FAR 27.865. Compliance was demonstrated except for the requirement that the hooks would not open uncommanded and release the HEC or fail to release, due to electromagnetic interference (EMI). Given limited time until the crocodile egg collection season started that year (December 2013), CASA approved the design engineer to continue to authorise installation of the dual hooks under the engineering order with an interim approval exempting compliance with the FAR EMI requirement until March 2014. The operation continued to be conducted in accordance with a separate CASA operational approval (instrument).
Equivalent level of safety
About 12 months later (after the March 2014 deadline had passed), the design engineer advised CASA that the EMI testing had not been carried out and sought an equivalent safety determination[21] for the requirement. The basis for the proposed equivalent level of safety was that the operational limitations for HEC specific to the egg collection role ‘reduce the risk to equivalent or less than that of a system showing compliance’. That is, there would not be an unacceptable level of risk to the sling person if the hooks released due to EMI while the sling person was on the line, or to the pilot and helicopter if the hooks failed to release due to EMI.
A suite of supporting documents was supplied to CASA, including one that documented operational conditions to reduce exposure to EMI. Another key document proposed limitations to the height the HEC could be carried, to reduce the consequences in the event of release of the sling person due to EMI.
HEC height limitations
In approving crocodile egg collection operations with HEC, CASA had imposed speed and height limitations – that the HEC was to be carried at walking pace and not more than 5 m above the ground or obstacles. The HEC height limitations document relating to EMI risk proposed that those conditions already in place would provide an equivalent level of safety to compliance with the requirement that EMI must not result in release of the hooks. The report concluded that the proposed limitations provided ‘a strictly controlled level of risk for the HEC person in crocodile egg collection operations’. The proposed limitations included ‘a speed not exceeding walking pace’ and that:
a height limitation of 5 metres be imposed. In the alternative if this is unacceptable to CASA a height limitation of 5 meters above water or swampy terrain and a height of 3.3 meters above hard ground be imposed.
The report referenced scientific studies into injuries and mortality due to falls from heights. These studies identified a significant increase in the likelihood of mortality associated with:
falls from heights above 5 m
increased age
landing other than feet first
head injury.
Based on these factors, the report noted 4 conditions associated with crocodile egg collection that mitigated against the risk of injury in falls from heights. These were that:
only fit, young persons were employed
any release would have the person in the best orientation, normally erect, and a maximum of three body lengths above the ground, minimising the time for the orientation to be upset
In October 2015, a new hook wiring design was bench tested and the 28 Volt electrical system was found compliant with the EMI requirement. At that time, CASA requested the design engineer lodge an application for the hooks to be fitted under an STC.
In the same month, the design engineer provided CASA with a compliance report detailing assessment of the R44 dual hook for HEC installation with FAR 27.865 – External loads. Demonstration of the reliability of the system included completion of a Failure Modes and Effects Analysis,[23] showing that all potential failure modes of the QRS that may result in catastrophic failures, serious injuries or fatalities were extremely improbable (in the order of 10-9 or less), and any less significant failures were improbable (in the order of between 10-7 and 10-9). The FAA Advisory Circular (AC) 27-1B regarding Reliability of the external load system, including QRS, stated:
(ii) Any failure mode of the external load system (including QRS, hook and attachments to the rotorcraft) leading to a loss of the HEC should be considered a Catastrophic event….
In meeting all requirements of FAR 27.865, failure of the hooks resulting in the release of the HEC or failing to release were assessed as extremely improbable. These therefore met the defined acceptable (tolerable) level of safety. Having conducted the analysis for failure modes of the hooks, the design engineer described helicopter engine or control loss as ‘the most significant risk for this operation and can only partly be ameliorated’. Further, that the ‘only amelioration which can be applied is’:
5.2.1. Maintaining a high level of airworthiness of the helicopter. CASA have specified a power check prior to each operation, but it is possible stricter control of maintenance processes mat [sic] assist.
5.2.2. Training of persons involved, although options for personnel control of events are extremely limited in this failure mode.
In granting an authorisation to conduct HEC, CASA could specify conditions that were required to be complied with when operating under the authorisation. These were stipulated in an authorisation instrument. CASA delegates stated that the instrument conditions were designed to mitigate the risks of the activity.
Previous CASA instrument conditions
The first CASA authorisation instrument for R44 HEC for crocodile egg collection, was reported to have been issued in 2007 associated with the first fitment of a hook system to an R44 helicopter for HEC. CASA was unable to find any record of instruments issued prior to 2010 or any documented safety case or risk assessment associated with the first instruments that were issued for the activity.
The ATSB obtained instruments issued to several operators from 2010 to 2021 and interviewed several CASA delegates who had approved instruments for the activity, or were involved in the approval process from 2013 onwards.
The 2010 instrument was issued for both R44 and Bell 206 helicopters. All subsequent instruments were for R44 (and R44 II) helicopters only. The 2010 instrument listed 20 conditions, most of which appeared in all subsequent instruments. Included in the conditions were limitations to the height, speed and distance the sling person could be carried. Appendix C – HEC height, speed and distance/time conditions 2010–2021 includes a table of the HEC limitation conditions in the instruments issued from 2010 to 2021.
For the instruments issued from 2010 to 2013 (inclusive), these conditions were:
The person is not lifted to a height of greater than 5 metres above the ground or obstacles.
The aircraft is not flown at a ground speed greater than walking pace when the person is carried under the helicopter.
The maximum distance the person is carried under the helicopter is 500 metres for each pick up.
Request for changes to conditions
In 2013, one operator requested an amendment to the conditions, including replacing HEC height, speed and distance limits with pilot-assessed safe height, speed, and distance. In response, CASA asked the operator to conduct a risk assessment.
That operator provided CASA with an assessment of risks identified for human sling operations for crocodile egg collection. The assessment was derived from a WHNT safe work method statement provided to all operators involved in the crocodile egg collection. The assessment detailed 7 steps in the job sequence. For each of those, it identified ‘What can go wrong’, assessed the initial risk, proposed control measures and assessed the resulting risk.
The job sequence ‘Lift collector and transit to crocodile nest’ obtained an initial risk rating of ‘catastrophic’. The likelihood was assessed as ‘very possible – will probably occur in most circumstances’; the consequences were assessed as ‘extreme – fatality or multiple fatalities’.
The list of hazards for that risk included equipment failure, falling from height and external load limitations (along with crocodile attack, adverse weather, fatigue/heat exposure/exhaustion, flora and fauna). The risk was reduced to ‘high’: unlikely – could happen sometime, with extreme consequences of one or multiple fatalities, with the following proposed mitigations:
• First Aid/trained personnel
• Medivac
• Pilot is spotter for people on ground, must ensure direct line of sight to human sling person at all times
• Collection crews in 1-2 man teams – lookout
• Pre-start inspections include belly hook & longline test
• Collecting crew to inspect harnesses, helmets, radios
• Training/Experience
• Rehydration available
• Lift register
Engine mechanical failure and fuel exhaustion/starvation were not included in the hazards for the slinging component therefore no relevant mitigations were included. Engine mechanical failure was however identified as a hazard in the non-slinging job sequences ‘Start aircraft and take-off’, Fly/Ferry to collection areas’ and ‘Return to base/ferry to next job’. Mitigations for engine mechanical failure included the daily inspection, emergency training and rescue plans, adherence to helicopter limitations, and pilot training/experience.
The CASA delegate who assessed the provided risk assessment described it as basic and the requested condition changes were not granted. However, there was no documentation provided that correlated the risk assessment with CASA’s retention of the conditions in the instrument.
2014 and 2015
The 2014 and 2015 instruments were valid from December to the following May, consistent with the crocodile egg collection season. In 2014, the 2013 condition that limited the HEC height to 5 m above the ground or obstacles was amended to:
The person is not to be lifted to a height of greater than 5 metres above the ground or water. To remove doubt this instrument does not permit lifting of a person to a height greater than 5 metres above an obstacle. The height restriction is in reference to the ground or water in all instances.
No documented reason for amendment to the operating height conditions was provided. The delegate who made that amendment reported that the purpose was to make it clearer and avoid ambiguity. The delegate also amended the speed condition to be less prescriptive and provide ‘flexibility to operate more safely’. The HEC speed limitation was changed from ‘walking pace’ to:
The aircraft is to be flown at speed that is considered by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the total forward speed of the person over the ground.
A new condition was also added in the 2014 instrument, which stated that the sling person must be provided with a copy of the instrument and ‘made aware, in writing, that the hook system is not certified for human use’. That condition was retained in all subsequent instruments.
2016
In 2016, the CASA delegate was invited to a demonstration of human slinging for simulated crocodile egg collection. Following the demonstration, the height condition was amended to provide the operators ‘some relief to be able to go over obstacles that might be in their flight path to go from one point to another’ as follows:
The person is only to be lifted to a height above the ground or water that enables the person and aircraft to safely traverse over natural obstacles. In all other instances, the person is not to be lifted more than 5 metres above the ground or water. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the height the aircraft is operated above the ground or water at any particular time.
When asked how lifting the HEC above the nominal survivable height of 5 m affected the activity risk, the delegate commented that it was not un-survivable because ‘the operator had an obligation to conduct the operation in a safe manner’. Additionally, in 2016, the 500 m distance limit the HEC could be carried was amended to:
The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person.
In 2016, Helibrook received their first instrument for R44 HEC for crocodile egg collection. The chief pilot had previously been involved in conducting the same operation for different AOC holders.
2017 and 2018
The ATSB obtained instruments issued to 3 operators in 2017, including Helibrook. As Helibrook was oversighted by a different CASA regional office to the other operators, multiple delegates were involved in the instrument approvals.
Late in 2016, the EMI test report demonstrating compliance of the hook system was completed. As a result, the HEC height limit was removed from the RFMS for the hooks, which was only required to consider failure of the hook system, not failure of the helicopter and associated operational safety limitations. A 60 kt speed restriction was included in the RFMS, based on reported feedback from an egg collector stating that was a suitable operating speed. It was noted at the time the amendments were made to the RFMS, that operational limitations specified in CASA’s operational instrument would be ‘overarching and could contain more conservative limitations’. However, when CASA asked for advice regarding limitations, the design engineer advised that additional limitations were unnecessary as the system was now HEC compliant.
The 2017 delegates and their CASA subject matter experts – airworthiness/engineering and the previous delegate – agreed that as the height limitation had been removed from the RFMS, it could also be removed from the CASA instrument, because inadvertent release was now extremely unlikely as the hook system was compliant. It was also assessed that there was no longer any purpose in stipulating a speed limit because ‘at 500 ft above ground level…forward speed will have no bearing on the HEC’s chances of survivability’. Therefore, the height limitation condition and the clause in the speed condition regarding minimisation of injury to the HEC were removed from the 2017 instrument conditions. However, the pilot-assessed safe speed and minimum distance conditions were retained.
The delegates reported that they relied on information provided by the subject matter experts and assessed that there were reasonable mitigations in place with the conditions. One delegate reported that they had accessed relevant files and had conversations with other delegates. They therefore assessed that the activity presented an acceptable risk, particularly as the instrument was a renewal for an activity that had been conducted without accident or serious incident for at least 5 years.
Although the height and speed limit conditions were removed once the hooks were HEC compliant, the instrument condition advising that the hooks were not certified for human use was retained. The delegate reported that their understanding was that the hooks were satisfactory and fit for purpose but not certified or approved by CASA.
The instrument delegate responsible for the instrument issued to Helibrook assessed that the activity was high risk, but accepted by CASA. Further, they considered that the removal of the height limitation was ‘a small change’ and nothing significant that would affect the operation.
From 2018, the instruments were issued for a 12-month period from December.
2019 and 2020
The CASA flight operations inspector responsible for oversighting Helibrook was assigned as the delegate for Helibrook’s instrument renewal in 2019 and 2020. The delegate assessed that the Helibrook operations manual had reasonable procedures for the activity, the sling equipment was approved, and the chief pilot and/or pilots involved had sling approval and relevant experience.
The delegate assessed that as it was a renewal, the procedures were in place and if they continued doing what they were doing previously, there was probably no reason not to allow them to continue what was an established activity. They also assessed that minimisation of exposure was included in the operator’s procedures. The delegate did not identify any discrepancies between the operations manual, RFMS and the instrument conditions.
In an email to the ATSB, CASA reported that there was no ‘granular documented process’ for approving instruments like the R44 Dual Hooks for HEC for Crocodile Egg Collection authorisation. The CASA Air Operator’s Certificate (AOC) Process Manual included a section on CASA approvals and exemptions, with a process map and the administrative steps required. Additionally, CASA’s Air Operator’s Certificate Handbook provided detailed information for assessing and issuing an AOC, including:
process overview
assessment criteria, methodology and link to checklists for AOC approvals
operational personnel
inspection of specialised equipment fitted to aircraft
assessing an operations manual
volume 2 provided guidance for assessing an application to include an aerial work purpose on an AOC, which included appropriate operations manual content, inspection of specialised equipment and review of the chief pilot's experience and qualifications
volume 4 included assessing safety management systems with a sub-section on safety risk management, which included guidance to assure an acceptable level of safety existed.
The CASA delegates approached by the ATSB reported that the AOC‑related documents provided broad or generic guidance, and while similar principles could be used for assessing a request for an authorisation and permission instrument, they did not contain specific relevant guidance.
To determine how CASA delegates assessed that safety was preserved when issuing authorisations, the ATSB requested detail of any risk assessments associated with the instruments. In response, CASA advised that they could not locate any risk assessments and that they had not conducted any specific testing or assessment of the risk profile for the activity of R44 HEC for crocodile egg collection. Specifically, CASA also advised that they had no evidence of any risk assessments associated with the instruments issued to Helibrook between 2016 and 2021.
CASA required a request for an authorisation to be made in writing and when assessing a request, delegates relied on the advice of other CASA personnel with subject matter expertise and experience. This advice was generally communicated by emails, some of which were filed in the records management system, or by telephone. The assessment was then made based on judgement of the activity’s reasonableness, but there was no documented acceptable risk level.
Although they reported not having seen a CASA risk assessment for the activity, the involved delegates assumed that a safety case would have been provided with the first operator’s request for approval for the activity (sometime prior to 2013) and that had been assessed and accepted by CASA. The activity was understood to be high risk, but delegates believed that CASA accepted that risk level. In particular, as the 2013 instruments were signed by a senior CASA manager, this was interpreted as an endorsement that it was appropriate to continue issuing the approvals.
Additionally, the annual approvals for operators were considered to be reissues of instruments for a previously accepted activity, albeit to varying helicopter operators. All the operators conducting crocodile egg collection each season received essentially the same instrument, although some conditions varied from one year to another. Prior to issuing Helibrook’s first instrument in 2016, a CASA inspector verified that the operator had:
a procedure for conducting the activity
appropriately experienced personnel
relevant documentation and sling equipment.
For an annual issue of an instrument to an operator who had previously held the authorisation, the delegate’s primary check was whether there had been changes to procedures or personnel since the previous issue. The delegates reported that if there had been no changes to procedures, and no enforcement action taken against an operator, they had no reason not to reissue the instrument. Additionally, as mentioned above, they assessed that the activity was being done safely as there had been no reported accidents or serious incidents.
The delegates all reported that the instrument conditions were intended to mitigate the risks associated with the activity, and that they assessed there were sufficient conditions and procedures in place to mitigate the risk to a reasonable level. Additionally, they considered that there was an onus on the operators to act safely and to advise CASA, via their operating procedures, how they were going to reduce the associated risks.
In August 2013, a CASA project was initiated to consider existing HEC regulations and propose amendments to Civil Aviation Order (CAO) 29.6, which only applied to non-human sling operations. The project identified that permissions being issued by CASA regional offices were not issued on the basis of a risk assessment or reflective of international standards. Specifically, in the US, United Kingdom and Canada, HEC was not permitted with piston engine rotorcraft and, CASA had assessed that the use of piston engine helicopters increased the risks to HEC compared with turbine engine rotorcraft. Additionally, in 2013, helicopter operators involved in the powerline industry had approached CASA for HEC approval using turbine engine rotorcraft, consistent with international requirements.
As a result of the project, in October 2013, the then CASA Director of Aviation Safety (DAS) signed an internal minute that recommended CASA restrict HEC operations to the following requirements:
single engine turbine powered rotorcraft with a usage monitoring system
out of ground effect hover performance with a performance buffer
restrictions on who could be carried
an attachment means certified for the carriage of humans.
The minute also recommended that the proposed standard be communicated to CASA field officers for consideration in all authorisation/permission approvals, while the proposed amendment to CAO 29.6 to reflect the policy was being drafted.
As a component of the project, a CASA risk workshop on crocodile egg collection using HEC was held on 20 November 2013. While no minutes were recorded from the meeting, a draft risk management plan (RMP) provided to the ATSB formed the basis of the discussions.
to examine the risk indicators in HEC operations in a piston engine rotorcraft in an Australian operational context of crocodile egg harvesting.
The RMP was drafted by a senior standards officer with significant helicopter and HEC expertise using a CASA general aviation operations template. The scope included that the assessment:
…considers isolated factors specific to piston engine rotorcraft, single engine turbine rotorcraft and multi-engine turbine rotorcraft. Risks relevant to the task of HEC beneath any rotorcraft are examined for context and amplification. A limitation to scope is that the cumulative effect of the individual risks should they be realised in combination is not considered. It would be prudent to conduct analysis of this eventuality should the risk assessment be furthered.
The assumptions listed in the RMP were:
• Permitted operators must have a proven safety and compliance record underpinned by a robust Safety Management System that could be leveraged for continued operation with strict regulatory oversight.
• CASA will exercise additional oversight of approved operators should an approval be granted that is strictly limited in scope and will result in removal of the operators [sic] approval should any non‑compliance be identified.
• The risk exposed by utilizing an external load assembly not approved for HEC provides a residual risk rating that is acceptable for a finite period of six months.
The overall operational risk of the activity was assessed with an initial risk rating of high (7), which ‘needs senior management attention’, and the residual risk (with controls in place) of medium (5), requiring ‘management responsibility’.
CASA’s General aviation operations group risk matrix utilised to assess the operational risk is depicted in Appendix B – CASA operational group risk matrix (2013). Extreme and high risks were required to be reported to senior management and have detailed treatment plans, ‘which reduce the risk in accordance with the ALARP [as low as reasonably practicable] principle’. CASA AC 138-05 – Aerial work risk management defined ALARP as ‘the point where the costs of introducing further safety measures to lower a risk outweigh the safety benefit. However, a risk should be tolerated only if there is a clear benefit such as a compelling operational need’ (CASA, 2022).
The broad risk categories considered in assessing the risk associated with HEC operation were:
engine failure/malfunction inside the H/V envelope with HEC attached
insufficient excess power available for role and environment
equipment/hardware failure of rotorcraft system or subsystem
human error while undertaking HEC operation.
Potential risk controls were:
preference of multi engine turbine rotorcraft with [one engine inoperative] OEI accountability
preference to single engine turbine rotorcraft
usage monitoring systems of pertinent parameters
equipment standards to HEC design criteria
limitation of exposure measured in time, distance, speed and height [above ground level] AGL
CASA increased surveillance of operations whilst under limited conditions
CASA mandated minimum experience level and qualification to conduct HEC
increased engine and critical component inspection criteria
mandated excess power margin requirements for [hover out of ground effect] HOGE conditions
limitations in environmental conditions including wind azimuth, velocity, humidity.
The RMP identified 26 individual hazards, all of which were assessed as initially not ALARP. Some of the documented hazards were linked to the R44 POH and Robinson Safety Notices. Proposed operational mitigations included additional regulatory oversight to ensure procedures were followed and maintenance/overhaul requirements were adhered to.
For the hazard of single engine piston rotorcraft engine failure while operating in the H/V envelope, the likelihood was assessed as rare – 1 in 10,000 to 1 in 100,000, with severe consequences – multiple life-threatening injuries/less than 10 fatalities, and an overall medium risk. Suggested mitigations to reduce the residual risk, still rated as medium, included:
minimise exposure time for HEC and enforce conservative limits of distance, height and time
require engine usage monitoring system
use fuel injected models only
require single engine turbine to reduce failure rate, or multi-engine rotorcraft with one engine inoperative accountability; or in consultation with the manufacturer increase inspection requirements including engine compression checks, and reduce overhaul period.
There was no assessment of the hazard of fuel exhaustion, but fuel starvation or contamination was assessed. For these, the initial risk was assessed as unlikely, and the consequences were severe with an overall high risk rating. With mitigations including fuel checks, minimum fuel requirements, fuel usage policy and turbine engine, the residual risk was medium, requiring CASA management responsibility.
The author of the RMP subsequently advised the ATSB that the omission of fuel exhaustion as a hazard was unintended, and that the proposed mitigations were also applicable to fuel exhaustion.
CASA’s Flight Standards Branch advised the ATSB that the RMP was never finalised, and the risk controls proposed to mitigate the risks of continuing R44 HEC for a further 6-month period were not implemented. The draft RMP was however used by CASA Flight Standards Branch to propose HEC standards, first for an amendment to Civil Aviation Order 29.6, which was subsequently discontinued (in 2016), and then for the development of CASR Part 138.
CASA also advised that the RMP was used to consider the potential viability of allowing single engine piston helicopter HEC operations based on an equivalent level of safety. This would have required demonstration that the piston engine helicopter had a similar in-flight failure rate as a turbine engine helicopter with a usage monitoring system. Members of CASA’s Flight Standards Branch presented this option to operators in 2014, however, no operator attempted to demonstrate this equivalence.
On 6 December 2013, CASA’s operations division sent a letter to an operator that had previously been authorised to conduct R44 HEC operations. The letter included the proposed future position requiring single engine turbine power rotorcraft with a usage monitoring system and other requirements as per the revised policy position approved by the then DAS. The letter stated that CASA had:
reviewed a number of risks and hazards in human external cargo operations, particularly when conducted by single-engine piston rotorcraft that resulted in unacceptable risks particularly to the person being slung.
The letter then detailed the relative risks of single engine piston rotorcraft compared with single engine turbine rotorcraft. This included detail that in the US from 2004–2008, the accident rate of single engine piston rotorcraft on average exceeded 1 per 10,000 flight hours and was more than 3 times that of single engine turbine rotorcraft. Engine failure inside the H/V envelope was identified as one of the main risks related to single engine rotorcraft. It also listed other known failure modes of R44 rotorcraft that had been identified in the RMP.
In summary, the letter advised the operator that CASA intended to renew the authorisation with some changes to the conditions for one more season before turbine engine rotorcraft would be required. At the time, the cargo hooks were not certified for HEC and a proposed condition was that the authorisation did not override engineering or airworthiness limitations.
The design engineer responsible for the hooks system responded to CASA’s letter on behalf of operators that conducted crocodile egg collection. The response disputed the safety data referenced in CASA’s letter, requested coordination between CASA’s certification/airworthiness and operations personnel and continued R44 operation for one more season to allow operators time to address the proposed requirements.
In response, a CASA regional manager made a documented recommendation to a senior manager within CASA that R44 HEC operations continue. The recommendation outlined CASA’s authorisations of R44 HEC operations for crocodile egg collection, the 2013 DAS decision to establish formal policy (including the use of turbine powered rotorcraft for human sling load operations) and that since that decision, CASA had undertaken work regarding the appropriateness of piston engine rotorcraft to carry human external cargo.
The recommendation also advised that that operator had requested reissue of the authorisation to continue to operate until CAO 29.6 changes were finalised. In support of the request for continued R44 HEC operations, the design engineer provided their comparative analysis of Bell 206 (turbine helicopter) and R44 engine failure data. Additionally, the regional manager proposed that extra conditions be included in the instrument to ‘mitigate those risks further’. Key additional conditions from the precedent instrument (which was valid from 2 December 2011 to 31 December 2013) were:
the hooks are to be certified for use in human sling load operation
engineering orders must confirm that all things attached to the hook systems are fit for purpose
the aircraft is to be operated in accordance with the approved FMS
daily inspection includes sling system/equipment
the pilot is required to verify the engine is capable of normal rated power with no defects evident and to certify this on the maintenance release
only persons employed or contracted for egg collection can be carried.
The reasons given for the recommendation were that:
the overall risk to safety of the egg collector could be reduced by the use of the R44 aircraft type
other operational activities permitted by CASA possessed ‘equal hazards and risks, such as mustering operations, night agricultural operations, and parachuting activities’.
The senior manager agreed with the recommendation and signed instruments authorising continued R44 HEC operations for crocodile egg collection to the end of April 2014 for 2 operators.
The CASA delegate who approved the following year’s instrument assumed that one reason the 2013 instruments were signed by a senior manager was to demonstrate that CASA senior management was aware of the operational approvals process and was satisfied it was appropriate to issue the instruments.
In 2016, the then DAS agreed with a proposal from CASA Flight Standards Division to close the existing project to amend CAO 29.6, as it had been ‘superseded by Part 138’. The finalisation of Part 138 was reported to be ‘imminent’, with a proposed effective date of September 2018. The proposal included that crocodile egg collection would ‘continue as per current exemptions until such time as Part 138 is made and the regulation commences’.
At the time of the accident, Helibrook and other operators were conducting crocodile egg collection under their AOC as an aerial work operation. From 2 December 2021, crocodile egg collection required a CASR Part 138 Certificate (instead of an AOC) to authorise the operation. The crocodile egg collection operation (carriage of a person outside a rotorcraft) was categorised as an aerial work class D external load operation under CASR Part 138.[24] Chapter 15 of the Part 138 manual of standards (MOS) – Rules for external load operations, applied to the activity.
Section 15.06(3)(e) applied to rotorcraft that cannot hover out of ground effect with one engine inoperative, requiring section 9.05(b), (c), (d) and (e) of the MOS to be complied with. This required the rotorcraft to have:
a turbine engine
a usage monitoring system
control to be maintained in all phases of flight in the event of a hydraulics failure or alternatively dual hydraulics
redundant means of controlling fuel flow to the engine.
CAR 151 and 250 were repealed on 2 December 2021. An authority under CAR 151(3) and a permission under CAR 250(2) applied to CASR Part 138. The Part 138 requirements were more onerous than the existing instrument issued to Helibrook for crocodile egg collection, which permitted use of a piston-engine helicopter without a usage monitoring system. In order to permit continued egg collection using the R44 an exemption was granted under Division 11.F.1, including CASR 11.170(3), which stated:
In making its decision, CASA must regard the preservation of a level of aviation safety that is at least acceptable as paramount.
Despite the intended safety improvement associated with the introduction of Part 138 requirements, Helibrook’s instrument was issued on 9 September 2021, with a 3‑year validity period. Under the transitional legislation, it would cease at the earliest of the:
expiry of the instrument (31 December 2024)
second anniversary of the instrument commencement (7 September 2023)
day the operator’s AOC expired (31 July 2022, extended to July 2023 after the accident).
Considering these criteria, Helibrook would be required to comply with CASR Part 138 and Part 138 MOS when its AOC expired.
In July 2021, an internal briefing note to a senior CASA manager stated that:
When Part 138 of CASR commences on 2 December 2021, operators conducting crocodile egg collection operations will need to replace their Robinson R44 helicopters with a helicopter that has improved reliability.
The briefing note outlined the risk assessment and subsequent work, which had concluded that HEC operations were very high risk for the sling person. It stated that the risk could be substantially mitigated through the use of a turbine engine helicopter with a usage monitoring system. Additionally, the hook system needed to provide redundancy in the case of failure of the hooks/system.
The Background section of the briefing note included that CASA’s previous permission instruments had not been issued on the basis of a risk assessment, and that the risk had been assessed in 2013 as unacceptable without mitigation. Further, that CASA’s authorisation of R44 HEC operations was not reflective of international standards and significantly differed from the FAA, Transport Canada and EASA. At that time these organisations generally required multi turbine engine helicopters with one engine inoperative accountability for commercial operations, with the use of high-reliability single turbine engine helicopters permitted for limited specified operations.
The Way Forward section of the document noted that some helicopter operators were already conducting powerline maintenance work using a single engine turbine helicopter for HEC, based on the CASR Part 138 standards.
The 2020 instruments were valid until 31 December 2021. On 2 September 2021, the Helibrook safety manager emailed CASA’s Regulatory Services requesting a renewal of the instrument with the 2020 instrument attached to the email. After payment, the task was assigned to the delegate on 9 September 2021, who recalled that it was relatively urgent. The delegate reported being unaware of the history of the authorisation, but was aware of the general risk of the operation and that it had been assessed by multiple sections within CASA.
The delegate reviewed the file relating to the most recent instruments and emailed the previous approver asking whether there were any concerns regarding reissue of the instrument to Helibrook. The previous approver advised that:
the STC for the hooks had been issued on 30 July 2021
there had been no changes to Helibrook’s equipment or procedures that they were aware of
CASR Part 138 was not yet in force
considering the above, they saw no reason why a new instrument should not be issued.
They also commented that they did not believe there was a compelling statistical argument to justify the higher cost of a turbine engine helicopter that would be required under Part 138.
The delegate then signed the instrument on 9 September 2021 with an expiry date of 31 December 2024. There was no change to the conditions from the previous year’s instrument. The references to the now redundant EO were not removed. Condition 23 stated that when the STC is approved, ‘all aircraft previously certified to the [engineering order] EO will be shown to be compliant with and certified to the STC within 14 days of the STC being approved, after which time aircraft certified only to the EO may no longer undertake this work’. Helibrook did not update the hook installation on VH-IDW to the STC. The delegate reported that they were unsure about whether the hooks had been certified. The delegate also reported being unaware of the implications of the impending Part 138 requirements when they issued the instrument for a 3-year period.
At the time of the accident, VH-IDW was operating under CASA Instrument CASA.CARRY.0163 Revision 1, issued to Helibrook and dated 7 September 2021 (2 days prior to it being assigned to the delegate).
There were 34 listed conditions that Helibrook and the pilot in command were required to comply with (Appendix D – Instrument conditions). There was no limitation specified for the HEC carriage height. Key conditions discussed previously included:
The pilot in command and sling person were required to have completed a course of training for the activity promulgated in the helicopter operator’s operations manual. The operator’s training course was to include not less than 1 hour of flight time and 1 hour of ground instructional time.
A thorough pre-flight briefing was to include actions to be taken by crew members during possible emergencies – the briefing was to be conducted in accordance with the briefing procedures in the operations manual.
The helicopter was required to be compliant with the STC SVR 541 and to be operated in accordance with the FMS, which details normal and emergency procedures associated with the activity.
The pilot and operator were required to comply with the relevant procedures in the company operations manual.
The pilot was required to have continuous and clear radio communications with the sling person throughout.
The pilot was required to fly the helicopter at a ‘safe speed’ and to carry the sling person ‘for the minimum distance and time required in order to safely conduct the activity’.
The sling person was required to wear an Australian Standard helmet (‘appropriate to the risks encountered during the activity’).
Prior to commencement of the activity each day, the pilot was required to verify that the engine was producing normal rated power output, and that no defects were evident which could lead to power reduction during those operations.
The sling person must be made aware, in writing, that the hook system is not certified for human use.
Data based on the Lycoming Service Reporting Database, National Transportation Safety Board Aviation Accident Database, FAA Service Difficulty Reports, and FAA Accident and Incident Database System from 31 December 2016 to 31 December 2021, found power loss rate (incidents per 100,000 flight hours) were 0.54 for the R44 and 0.11 for the R44 II. These helicopter types therefore met the EASA requirements[25] for ‘Helicopter operations without an assured safe forced landing capability’ engine in-service sudden power loss rate requirement of not more than 1 per 100,000 (1 x 10-5) engine hours in a 5-year moving window. For that data, where the cause of the engine failure was unknown, or where maintenance was identified as the reason for the failure, they were counted as 0.5 and 0 events respectively.
A review of R44 and R44 II engine failure occurrences reported to the ATSB,[26] compared with flight hours for the period 2011 and 2020 showed the average engine failure rate was 4.4 per 100,000 flight hours. Unlike the power loss rate data above, these did not consider whether the failure resulted from maintenance or an unknown reason, which may account for the higher engine failure rate in Australia. Fuel exhaustion and fuel starvation were not coded as engine failures.
In addition to engine failures, the ATSB identified R44/R44 II accidents and serious incidents that occurred during the same period, which would likely result in injury to the sling person if they occurred during slinging operations. These were primarily losses of control and occurred at a rate of 2.8 per 100,000 flight hours. The combined rate of engine failure and other occurrence types likely to result in injury to the sling person was 7.2 per 100,000 flight hours.
To quantify the risk of the activity, it was necessary to approximate the amount of time HEC was being conducted each year in Australia under a CASA authorisation. In the 2020–21 and 2021–22 seasons, 3 helicopter operators had CASA authorisation for R44 HEC operations to conduct crocodile egg collection. Of those, 2 contracted to WHNT and one operator supplied a different crocodile farm. WHNT provided total invoiced hours for 3 R44 helicopter operators for those seasons, one of which did not have a CASA instrument for HEC, but the ATSB obtained evidence from February 2021 showing dual hooks installed on their helicopter. In the 2020–21 season, 566.1 hours were invoiced and 507.3 in the following season, in which activities were suspended following the accident. This included the accident pilot, operating VH-IDW as one of the 2 HEC helicopters for WHNT, who had invoiced 21.5 full days of conducting crocodile egg collection for the 2021–22 season to 22 February 2022 (approximately 200 hours).
WHNT initially estimated that they were generally slinging about half the total engine-running time, and later revised this to about 20% of the total time for the 3 helicopters operating for WHNT. The other (non-WHNT) operator estimated they did about 15 hours of HEC each season.
Based on the information and approximations provided, the ATSB assessed the effect of slinging a person under an R44 helicopter for 200 hours per year. On average, an engine failure or in-flight emergency likely to result in an accident, would occur once every 69 years while slinging a person.
Exceeding maintenance, inspection and overhaul limits, increases the probability of an in-flight engine failure. The Robinson R44 Maintenance Manual stated that it ‘is the operator’s responsibility to maintain a record of time in service for the airframe, engine and life-limited components…[an] hour meter is an acceptable means of recording time in service’. The manual included the warning that:
Components with mandatory overhaul times or life limits whose time in service is not reliably documented cannot be considered airworthy and must be removed from service.
Lycoming Service Instruction 1009BE – Time between overhaul (TBO) schedules included the warning that ‘Operation of an engine in a non-airworthy condition could result in loss of life, serious injury, and damage to property’. Additionally, the Lycoming operator’s manual included:
Neglecting to follow the operating instructions and to carry out periodic maintenance procedures can result in poor engine performance and power loss. Also, if power and speed limitations specified in this manual are exceeded, for any reason, damage to the engine and personal injury can happen.
On 11 May 2022, a Bell Helicopter Textron Canada 407 helicopter was conducting HEC training in Livermore, California, US. The helicopter was about 175 ft above ground level with a sling person on a 60-ft long line when the engine lost power. The pilot manoeuvred the helicopter and partially raised the collective when the sling person was about 15 ft above the ground (AGL) and cushioned them onto the ground. The sling person was uninjured.
The pilot then manoeuvred the helicopter away from the sling person and when about 10 ft AGL, raised collective and released the sling line. The helicopter landed hard resulting in substantial damage to the helicopter and serious injury to the pilot, who had to be extricated from the wreckage. At the time of publication of this report, the US NTSB investigation was ongoing however, the occurrence showed that in a helicopter with more main rotor inertia than an R44, it is possible to cushion the HEC onto the ground, but the ensuing autorotative landing can result in serious injuries to the pilot.
Fuel exhaustion happens when there is no usable fuel remaining to supply the engine/s.
Fuel starvation happens when the fuel supply to the engine/s is interrupted although there is adequate fuel on board.
The report stated that the ATSB received an average of 21 reports of fuel exhaustion or starvation occurrences each year. Fuel exhaustion occurrences were normally either the result of an error in pre-flight fuelling, or a number of seemingly minor aspects of fuel planning and management during the flight. Consideration of different fuel consumption rates depending on the activity being conducted and flight conditions is a key component of fuel planning.
The chance of fuel exhaustion is reduced if a pilot accurately determines the amount of fuel on board prior to starting, by cross-checking from multiple sources. These include fuel quantity gauges, dipsticks, totalisers/flow meters and calculations from previous refuels and fuel usage regularly checked for accuracy.
ATSB fuel exhaustion occurrences 2011–2020
The ATSB occurrence database held 54 fuel exhaustion occurrences for the 10-year period 2011‑2020. Considering the involved engine types, 49 were piston, 4 were turbine and 1 engine type was unknown. However, of the total aircraft, only 5 were helicopters, 3 of which had turbine engines and 2 were piston engine helicopters. Neither of the piston helicopters were an R44, but one of the occurrences involved a piston engine R22 Beta helicopter conducting mustering operations. Given the small data set, there was no significant difference in engine type for helicopter fuel exhaustion occurrences.
For 14 of the 54 occurrences, the total flight time of at least one pilot was recorded. Table 4 details the number of occurrences, the number of those where the total flight time of one pilot was known, and the median total flight time. The median total flight time of a pilot involved in a fuel exhaustion occurrence was 1,227 hours with a range of 20 to 14,500 hours. This suggests that experience is not a mitigation against fuel exhaustion occurrences.
Table 4: Fuel exhaustion occurrences 2011–2020, engine type (1 unknown), median and range of pilot total flight time (TT)
On 4 October 2010, a Robinson R22 Beta helicopter collided with the ground while conducting cattle mustering operations. The pilot was fatally injured, and the helicopter sustained substantial damage. The investigation found that the collision with terrain was probably a result of engine stoppage due to fuel exhaustion, while operating at low altitude. The investigation also found that:
The nature of mustering operations had the potential to divert the pilot's attention away from other safety-critical tasks, such as monitoring the helicopter's fuel state.
Long line fuel exhaustion accident
In 2012, the US National Transportation Safety Board investigated an MD Helicopters 500D helicopter accident, in which the engine lost power while a utility worker was suspended on a long line attached to the helicopter. The investigation analysis included the following:
The helicopter was in a hover about 120–150 feet above the ground while a utility worker performing a long-line operation worked on a transmission tower. After the loss of power, the helicopter spun and descended during which the worker was pulled off the tower by the attached long line. The pilot performed an autorotation that resulted in a hard landing. The pilot sustained serious injuries and the worker sustained fatal injuries.
Post accident examination of the helicopter revealed no usable fuel on board, and fuel quantities between the fuel tank and engine were consistent with fuel exhaustion. The examination revealed that the electrical wire to the start pump was not secured, which allowed for the possibility of it interfering with the fuel quantity transmitter float mechanism, thus providing erroneous cockpit fuel quantity indications to the pilot. The examination also revealed that the low fuel quantity annunciator was inoperative due to separation of the fuel quantity transmitter’s low-level fuel whisker.
The National Transportation Safety Board determined the accident to be a result of improper maintenance resulting in erroneous fuel gauge indications, combined with the pilot’s inadequate fuel management. The investigation also found there were no written company procedures or fuelling records to track fuel loading and time-based fuel consumption.
The post-mortem examination of the egg collector found multiple blunt force injuries resulting from a fall from a height. The examination identified that there were numerous head, neck, and torso (or trunk) injuries. There was also external evidence of blunt force trauma to the upper and lower limbs, but there were no underlying skeletal injuries. No obvious evidence of fuel was found on the egg collector’s clothing to indicate a fuel leak prior to the accident, but the clothing was not specifically tested for the presence of fuel. Additionally, no bark residue, indicative of tree contact, was identified.
Three studies conducted on patients presenting to an emergency or trauma centre following a fall from height analysed injuries sustained and the height of the fall (Icer and others, 2013, Liu and others, 2008, Nau and others, 2021). The studies found that the overall injury severity was higher with increasing fall height. With increased height of the fall, there was a significantly higher severity of thoracic and pelvic injuries, whereas the severity of head injuries and spinal fractures did not increase with fall height. Life-threatening injuries were more likely the higher the fall height, and falls greater than 18 m were usually fatal (Nau and others, 2021).
In one study, the mean fatal fall height was 6.61 m, noting that the study excluded people who had died before arriving at the hospital. About 30% of people who fell from 10 m or higher died, which was twice the percentage of those who fell from 6–9.9 m and nearly 3 times that of those who fell from 3.1–6 m. Of those fatally injured, 91% sustained head injuries. The study found haemopneumothorax[27] and subarachnoid haemorrhage[28] were the most important factors affecting mortality (Icer and others, 2013). Another study also found severe head injury was a significant prognostic factor for mortality in people who fell from heights of at least 6 m (Liu and others, 2009).
These research findings were consistent with a retrospective study of autopsy reports (Abder-Rhman, Jaber, & Al-Sabaileh, 2018), which found that internal injuries were directly proportional to the height of the fall. Head injury was the most common fatal injury in all heights, chest injuries and skull base fractures were more prevalent in falls from above 3 m, and abdominal injuries were mainly prominent in heights above 9 m.
The Civil Aeromedical Research Institute of the US FAA report Human survivability of extreme impacts in free-fall, analysed factors affecting survivability in individuals who survived falls from heights of up to 84 m (275 ft) (Snyder, 1963). Among other factors, the study found that orientation of the body was important. The initial impacts were feet-first in 10 of the 12 cases of survived falls from over 33 m (100 ft). The impact force was found to be greatly attenuated by bending and flexion of the leg muscles.
The sling person’s harness is designed to keep them in an upright position. Keeping the sling person attached during an emergency landing would allow them to remain upright and impact the ground feet first, decreasing the mortality risk. When the sling person is released, they have no means of orientating themselves and are more likely to tumble, increasing the likelihood of landing other than feet first, thereby potentially increasing risk of fatal injury.
A forensic pathologist assessed the egg collector’s injuries and found that there was evidence of significant head injury due to ground impact. In assessing the height from which the sling person was likely released, the pathologist referenced research showing that higher mortality is found in falls from greater heights and that the threshold for suffering major trauma from a fall from a height is at least 6.1 m (20 ft). Further, that pelvic fractures occur significantly more often if the fall height is at least 6 m, and chest trauma is more common the higher the height of the fall.
Based on the research and the egg collector’s extensive pelvic, spinal, and chest fractures, the forensic pathologist assessed that they likely fell from a height above 5 m.
The egg collector’s helmet was found nearby, and the helmet’s clasp receptacle had fractured.
The instrument issued to Helibrook for picking up and carrying a sling person under an R44 helicopter for crocodile egg collection stipulated that the sling person was to wear a helmet that ‘meets the Australian standard appropriate to the risks encountered during the activity’. The sling person’s helmet had a sticker showing compliance with American National Standard for Industrial Head Protection ANSI/ISEA Z89.12009 Type I Class C. This standard was amended (in 2014) to Z89.1-2014.
The standard stated that Type I helmets were ‘intended to reduce the force of impact resulting from a blow only to the top of the head’. (The Class C (‘conductive’) helmets also provided no electrical protection). In contrast, Type II helmets met additional requirements for lateral impact protection (front, back and sides) and chin strap retention. In this accident, a Type II helmet would not have reduced the severity of the egg collector’s injuries to a survivable level.
The pilot sustained swelling and bleeding on the brain indicative of rapid deceleration and acceleration. Although the pilot was not wearing a helmet, it would likely not have reduced the severity of head injury in this accident as no head impact occurred. The pilot reported always wearing the 4-point restraint and could not recall how they exited the helicopter.
R44 helicopter seats are designed to crush and absorb impact forces. Under the seat is a stowage area marked with a weight limit and a limitation for storage of soft articles only. The pilot reported that they normally had the following under their seat: lunch, water bottle, satellite phone, first aid kit and a raincoat. A broken headset and other small items were found under the pilot seat and photos from the site showed other items that were removed before ATSB arrived that may also have been stored under the seat.
Impact forces crushed the seat into the storage area, with the seat box and support structure collapsing. Additionally, the fuselage belly pushed upwards after the undercarriage skids exceeded their capability. The floor also pushed up to the level of the collapsed seat pan.
This indicated that the energy absorption capability of the airframe with respect to the seat installation had been exceeded. The seat probably collapsed onto the contents of the stowage compartment and may have contributed to the pilot’s injuries.
In Australia, cocaine is classed as a ‘Schedule 8 – controlled drug’. Cocaine is a central nervous system stimulant and an illicit drug, unless there is evidence it is used for medical purposes. In a dilute solution, it is used as a topical anaesthetic for limited purposes and is listed as an unrestricted Schedule 8 substance in Northern Territory hospitals. A deputy director at Royal Darwin Hospital advised that cocaine was not stocked in the Emergency Department and was not administered to the pilot at Royal Darwin Hospital. CareFlight NT’s Medical Director advised that their aircraft did not carry topical cocaine.
In the context of aviation safety, detrimental effects of cocaine can occur in the hours immediately after use, and depending on the regularity and dose used, there may also be longer-term effects. Immediate effects of a moderate dose of cocaine on skills performance can include risk-taking, inattentiveness and poor impulse control. During the ‘crash phase’, which lasts 9 hours to 4 days following cocaine use, the user can feel depressed, agitated, irritable, and there can be significant fatigue and lack of energy (Isenschmid, 2002). As the effects of cocaine wear off, the user can suffer fatigue, depression, sleepiness, and inattention (Couper and Logan, 2014).
Cocaine is metabolised in the body to benzoylecgonine and ecgonine methyl ester. Blood concentration of cocaine decreases rapidly and is typically detectable in blood 1–2 days after use. Cocaine metabolites benzoylecgonine and ecgonine methyl ester may be detectable for at least 3–4 days after cocaine use. The presence of benzoylecgonine and other cocaine metabolites in blood in the absence of cocaine usually indicates the cocaine exposure did not occur immediately prior to the blood sampling (Isenschmid, 2002). A toxicological pharmacologist advised the ATSB that it was extremely difficult to correlate blood cocaine concentration with the timing and quantity of exposure to the drug. They also assessed that the pilot’s toxicological results were indicative of exposure to cocaine possibly up to about 4 days prior, but not in the previous 24 hours.
CASR 91.520 detailed that a crew member is unfit for duty if their ability to perform the duty is likely to be impaired because they have used a psychoactive substance such as cocaine. Pilots are required to declare recreational drug use to a designated aviation medical examiner.
From about 0850 on 28 February 2022, the crew of Robinson R44 II helicopter, VH-IDW, were preparing to conduct crocodile egg collection, near King River, Northern Territory. The helicopter was operating under a Civil Aviation Safety Authority (CASA) instrument that authorised the pilot to operate with a person in a harness system (‘sling person’) outside and attached to the helicopter, for the purpose of collecting crocodile eggs. The authorisation was subject to conditions that were intended to mitigate the risks of the operation.
After hearing no communications from the pilot of VH-IDW for more than one hour, another pilot conducting egg collection nearby commenced a search. They found the accident site about 150 m from the first nest they expected VH-IDW’s crew to collect eggs from. The egg collector lay fatally injured on the ground, wearing their harness and attached to one end of the sling. The attachment rings at the other end of the sling were not connected to the helicopter, which had collided with the ground upright, 44 m from the egg collector, and was substantially damaged. The pilot sustained serious injuries.
There were no witnesses to the accident and the accident pilot had no recollection of the accident and limited recollection of the hours leading up to it. No recorded data to accurately determine the accident sequence, including the time of the accident, was recoverable.
There was no fuel present in the helicopter’s auxiliary tank and a very small quantity in the main tank. Assessment of the helicopter indicated that the engine was stopped before the helicopter impacted the ground. Additionally, there was no evidence of failure of the harness, sling, attachments or the hooks system. There was also no evidence of failure or defects to the airframe or the helicopter’s systems likely to have contributed to the accident.
This analysis will discuss:
fuel uplift
the pilot’s awareness of the helicopter’s fuel state
potential reasons for the in-flight engine stoppage
the circumstances relating to the release of the sling person and the helicopter’s collision with terrain.
The influence of the helicopter operator’s safety management system and the Civil Aviation Safety Authority’s (CASA’s) process for issuing authorisation instruments will also be analysed. Finally, the potential contribution of the helicopter’s state of airworthiness, presence of cocaine metabolites in the pilot’s toxicology results and lack of emergency location transmitter fitted to the helicopter will also be considered.
After reportedly being filled with fuel, the helicopter departed from the operator’s hangar at Noonamah on the outskirts of Darwin at about 0703 in company with 2 other R44 helicopters. Fuel receipts showed that the Noonamah fuel tank contained only blue‑coloured 100 low lead (LL) Avgas fuel and there was no record of the quantity of fuel uplifted to VH-IDW at Noonamah on the accident morning. An in-flight photo taken en route to Mount Borradaile showed the chronometer reading 45 minutes, which the pilot reported usually setting to zero after refuelling.
A subsequent report that VH-IDW was filled the evening prior to the accident and not on the accident morning, suggested that VH-IDW departed with less than full fuel (151–153 L usable). However, the in-flight photo showed the gauges reading slightly below 3/4, consistent with the helicopter having departed Noonamah at or near full, based on the reported fuel flow rate of about 65 L/h.
Based on flight data, witness accounts and evidence from the in-flight photo, the 3 helicopters probably arrived at the en-route fuel depot at Mount Borradaile at around 0816. The accident pilot reported that they always left Mount Borradaile with full fuel tanks and their intention had been to refuel there. However, they were unable to confidently recall the specific fuelling activities at Mount Borradaile or events thereafter.
There were consistent recollections from others present at Mount Borradaile that VH-IDW was the first helicopter to arrive and that it did not have a fuel drum pump on board to transfer fuel from the drum stock. However, there were also differing recollections of the order in which the R44s were refuelled, with each helicopter being repositioned in turn close to the drums and the entire activity being undertaken without shutting any of the aircraft down. Two people reported seeing the accident pilot pumping fuel, including into VH-IDW. However, in a submission following review of the draft report, one of those reported not having seen anyone fuel VH-IDW. One other person reported assisting the pilot to pump fuel. However, that person’s recollection subsequently changed to having observed the egg collector partially fuelling VH-IDW before taking over to finish the fuelling themselves.
In the approximately 14 minutes the helicopters were at Mount Borradaile, there was probably sufficient time to refuel 3 helicopters given the number of people available to assist. Two witnesses reported that the egg collector was flying VH-IDW, from the right seat, when it departed Mount Borradaile, and that the accident pilot removed the dual controls after arriving at King River. However, the accident pilot and another egg collector reported that the accident pilot had flown VH-IDW from Mount Borradaile, having removed the dual controls there.
The ATSB’s assessment, based on the consistent accounts of the first 2 witnesses and recorded GPS data transmitted to a server from the egg collector’s phone indicating they were using an electronic flight bag application to navigate between Mount Borradaile and King River, was that it was more likely that the egg collector flew VH-IDW from Mount Borradaile to King River.
The person who prepared the 2 fuel drums for the R44 crews on the accident morning at Mount Borradaile had a detailed recollection of which drums were used and subsequently obtained fuel samples from those drums for ATSB testing. The samples were confirmed as green‑coloured 100/130 fuel in accordance with the relevant specifications and the delivered batch test data.
The first person to arrive at the accident site, reported that there was a fuel smell but later assessed that may have been from a leaking jerry can stored behind the pilot’s seat. The first emergency responder on site reported the absence of a fuel smell, but noted leaking hydraulic fluid that created a sheen on the water. The Helibrook chief pilot also reported that there was no fuel smell when they arrived. As the helicopter wreckage was in a swamp, with water slowly running downstream, it was possible for fuel to also drain away, although no one observed that occurring. There were also varying reports that people who attended the site after the accident looked in one or both fuel tanks and detected fuel, but no one attempted to measure the quantity.
When ATSB investigators arrived at the accident site 2 days after the accident, there was no fuel present in the auxiliary tank and only a small quantity of fuel in the main fuel tank. Although it was not possible to accurately measure the quantity in the main fuel tank on‑site, it was assessed by the ATSB investigators to be significantly less than the documented unusable quantity of 4 L. Recognising that the worst‑case helicopter orientation is used to arrive at that unusable fuel quantity, it is possible to consume some of the published 4 L in‑flight. However, it was considered unlikely that the small remaining quantity observed by the ATSB on‑site would have sustained the engine. As such, following the ground collision some fuel was either removed from the helicopter or was able to drain away.
Examination of the helicopter identified that it was possible for fuel to drain under gravity from the tanks through the fuel system and out via either a fractured fitting between the fuel flow transducer and flow divider, or through the drain at the gascolator. However, the loose organic black soil from the accident site that filled the fractured transducer fitting would likely have been flushed out if fuel had drained through that route. There was also no fuel staining on the cowls, but this may have been due to water ingress into the cowls at the accident site. Images taken of the site 4 months after the accident showed no evidence of vegetation dieback that would be indicative of significant fuel leakage, however over 200 mm of rain had fallen in the intervening period.
The helicopter manufacturer assessed that the deformation of the fuel tanks was consistent with a lower fuel quantity, but was unable to distinguish between some or no usable fuel remaining, or between impact damage and possible bulging due to internal contents. However, the degree of tank deformation indicated that the helicopter was not filled with any significant amount of fuel at Mount Borradaile unless the accident occurred at about the time the helicopter was located. This was considered unlikely because the accident occurred between the clearing and the first target nest in the direction of travel that morning. Other than the egg collector’s phone briefly contacting a cell tower at 0858, there was no evidence the crew planned to go anywhere other than the 3 nests they had been allocated to collect, and no eggs had been collected. There was no communication between the cell tower and the pilot’s phone at that time.
Scientific testing of the fuel drained from VH-IDW after the accident found that it was 100 LL Avgas and likely contained no more than 1% 100/130 fuel, consistent with residue from previous fuelling. This physical evidence opposed any significant quantity of 100/130 fuel being added to the tank at Mount Borradaile. Although it was later reported that it was possible for other drums at Mount Borradaile containing 100 LL to have been used, the distinct drum markings and reported general usage of the fuel location made that unlikely.
The potential effect of interference with the site was considered in relation to the removal of the jerry cans and the fuel testing results. The only plausible scenario that permitted both refuelling at Mount Borradaile to occur and the sole presence of 100 LL when chemically tested was if 40 L of 100 LL fuel was poured from the jerry cans into VH-IDW after the accident and then subsequently largely leaked away.
While it was possible that the addition of 40 L of 100 LL from the jerry cans could produce the attained test results, there was no evidence that occurred. Conversely, those on‑site reported that one of the jerry cans was damaged on impact and fuel from the jerry cans out of VH-IDW was used to fuel one of the other helicopters before departing the accident site. This was consistent with reports of empty jerry cans being used at Mount Borradaile to transfer fuel from a drum to a helicopter on the return trip. Additionally, the lack of fuel smell, cowl staining and soil lodged in the fractured transducer fitting also indicated that 40 L of fuel was not poured through the system.
Considering the relatively greater strength of the technical evidence, the ATSB concluded that the helicopter was probably not refuelled at Mount Borradaile prior to the commencement of the egg collecting activity.
The sources of information for the pilot regarding the helicopter’s fuel state were the chronometer, fuel totaliser, fuel log, fuel gauges and low fuel warning system.
The pilot’s normal practice, consistent with the in-flight photo was to reset the chronometer to zero following refuelling. The chronometer did not store data and therefore its reading at the time of accident could not be determined. The pilot reported that they did not use the totaliser, which was not visible in the in-flight photo. Further, there were no records of fuel uplifted to VH-IDW for the accident day.
When tested, the main tank indication overread within a needle-width at empty, a quarter and half full. The auxiliary tank gauge indicated very close to the actual fuel level. The placard below the main fuel tank gauge, from the last fuel calibration, indicated the main tank gauge would significantly underread. Therefore, had the pilot been relying on the calibration placard’s quantity to interpret the gauges, there would have been less fuel in the main tank than expected, other than when full or empty. However, based on the in-flight photo showing the fuel gauges, and testing of the gauge senders and gauges, the gauges would likely have been reasonably accurate.
The calibration placard also stated the low fuel warning light would illuminate with 20 L fuel total remaining and the pilot recalled that it would illuminate with 18 L remaining. However, according to VH-IDW’s Pilot’s Operating Handbook, the low fuel warning light would illuminate with 11 L of usable fuel remaining, which would be 14 L total. It is therefore likely that, if the light illuminated in flight, the pilot would think there was more fuel remaining than the POH indicated. The accident pilot also reported that their normal practice was to depart Mount Borradaile with full fuel. This expectation may have influenced the degree to which the pilot focused on the fuel quantity.
The low fuel warning system was found to be functional. However, it is possible that, if the low fuel light and/or fuel gauges were indicating low fuel, the accident pilot may have dismissed these cues as they would not have been consistent with their expectation. Additionally, had the low fuel light illuminated, the pilot may have thought there was more fuel remaining than actual.
A previous ATSB investigation into a Robinson R22 accident that occurred during mustering operations, found that the nature of the operation potentially diverted the pilot’s attention away from monitoring the helicopter’s fuel state. This resulted in probable fuel exhaustion and stoppage of the engine in flight. This potential also existed in conducting slinging operations, as the pilot would have had their head out the door, looking down at the sling person, and not at the instrument panel or gauges. This limitation of monitoring gauges was included in the Helibrook operations manual and suggested pilots conducting low-level aerial work operations also monitor elapsed flight time. However, had the chronometer been reset to zero at Mount Borradaile but the helicopter not refuelled, this would have provided an erroneous indication of time since refuelling.
Had the pilot detected a low fuel situation, there were 2 jerry cans of 100 LL fuel in VH-IDW that could be used for refuelling and multiple landing sites were available. Ultimately, while indications of the in-flight fuel state should have been available to the pilot, the pilot may have not observed them, dismissed them as erroneous or misinterpreted them. In any case, it is likely that the pilot did not recognise the helicopter’s fuel state.
In assessing whether the pilot’s experience as a helicopter pilot and in slinging operations would mitigate the risk of fuel exhaustion, the ATSB reviewed fuel exhaustion occurrences in the 10-year period 2011–2020. The median total experience of pilots involved in fuel exhaustion occurrences reported to the ATSB in that period was 1,227 hours. This illustrates that experience alone does not mitigate fuel exhaustion.
The ATSB analysed what in-flight event occurred that led to the egg collector dropping their equipment, the pilot releasing them, and the subsequent helicopter collision with terrain. The orientation of the accident trail was consistent with the route between the clearing and the nest most likely to be collected first. There was no evidence of snagging of the sling line or egg collector that led the pilot to release them. There was also no evidence of in-flight breakup or damage to the helicopter airframe due to failure, bird strike, or consistent with a manoeuvring error or mishandling.
Significantly, there was physical evidence that the engine was stationary when the helicopter impacted the ground, and no evidence that supported engine rotation was identified. Based on advice from the helicopter manufacturer, the ATSB assessed whether the engine had stopped in flight or because of the main rotor blade striking the tree while the engine was producing low power. The damage to the main rotor blade, including one broken pitch link, was consistent with a tree strike in a low rotor energy state. The diameter of the branches struck on the first 2 strikes was assessed as too small to stop the engine. The last tree strike was more substantial but occurred below the main rotor blade height, indicating the helicopter impacted the ground prior to that strike. On balance it was therefore considered likely that the engine stopped in flight.
The ATSB assessed the possibility of inadvertent pilot-induced engine stoppage in the context of the pilot’s logged total helicopter flight experience of about 2,500 hours and more than 300 hours of sling time. Robinson advised that there had been several accidents in which a pilot had inadvertently induced an engine stoppage by rolling off the throttle too fast. This had occurred in flight training when simulating an engine failure and as an incorrect response to abnormal situations such as a sudden change in engine RPM or discrepancy between engine and rotor RPM.
It was considered very unlikely that the pilot would have simulated an engine failure at any stage during the accident flight. Although it could not be determined whether there was another situation that led to the pilot quickly rolling off the throttle, this would be a highly unlikely response of an experienced pilot, while conducting human external cargo (HEC) operations.
The ATSB conducted extensive airframe and component examinations. Independent experts were engaged to conduct engine and fuel system examinations, overseen by the ATSB and other involved parties. The results were also analysed by manufacturers of the helicopter and engine, and other specialists. There was no evidence of a defect that could have led to sudden stoppage of the engine, of any critical component of the engine, fuel, or other helicopter system. Examination of the engine and fuel system found:
no evidence of any issue with air intake to the engine or the exhaust system
low static compression in one cylinder, but the actual compression was probably higher when the engine was running and warm, which was unlikely to have resulted in sudden in-flight complete or substantial power loss
several valve clearances were out of service limits
no evidence of any issue with the spark plugs, ignition leads or magnetos
no fuel remaining in the system other than the main fuel tank, no evidence of fuel contamination with debris, water, or wrong fuel, no defects in the fuel system and no condition likely to prevent usable fuel reaching the engine.
The out‑of‑limit valve clearances and low cylinder compression probably reduced the power that the engine was able to produce. However, the accident was not consistent with insufficient power available to lift the sling person, as the maximum power required would have occurred during the lift and before forward speed (consistent with the accident trail) was achieved. The ATSB assessed VH-IDW for all the possible reasons for an engine problem listed by the engine and helicopter manufacturer. The aircraft, engine and fuel system examinations did not identify any failure or condition, other than an absence of fuel throughout the system, that would likely result in sudden complete or substantial engine power loss.
The helicopter had not been shut down between when it was started before 0700 and last seen at a clearing near King River at about 0855. No recorded data was available to indicate the helicopter’s movements after 0900, including at the time of accident. However, the egg collector’s phone was momentarily in range of the nearest phone tower at 0858 and the accident pilot’s phone was not. As mobile phone reception was only in range when about 300 ft above the accident site, this may indicate that the egg collector was briefly airborne in the helicopter at that time.
As described above, the accident occurred between the clearing and VH-IDW’s first target nest, and no eggs had been collected. Additionally, no communication had been made with VH-IDW since about 0900, and it was considered unusual for the crew not to communicate for over an hour.
The operator reported VH-IDW’s normal fuel flow was 65–70 L/h, equating to a fuel endurance between 2 hours 31 minutes and 2 hours 42 minutes. Had the helicopter not been refuelled since 0658 at Noonamah, the helicopter would have exhausted usable fuel between 0929 and 0940. Furthermore, if the helicopter had been refuelled the previous evening and then travelled for about 23 minutes to Noonamah, and was not fuelled prior to the start of the accident day, fuel exhaustion was possible from 0904. Low cylinder compression evident in the No. 6 cylinder at engine examination, and high power settings, as evident in the in-flight photo, increase fuel consumption. Fuel exhaustion was therefore possible earlier than 0929. This was consistent with the search pilot’s estimation that the accident occurred at about 0922, when they were on the ground and out of communication range, and other crew heard a static radio transmission that may have been from VH-IDW.
The helicopter’s hour meter read 2070.05 at the accident site and the maintenance release recorded 2067.6 at the end of the previous day. This indicated the helicopter had a flight time of 2.45 hours (not including time on the ground), which would also support fuel exhaustion. However, this was considered unreliable evidence as the pilot reported that the hour meter was never running when they operated VH-IDW, in which case the maintenance release did not reflect actual hours flown.
There was no evidence of a failure of the hooks system or sling equipment. The pilot reported that they always checked both quick release systems were functional before slinging. Had the experienced egg collector not attached themselves correctly, it was unlikely the pilot would have been able to lift them into the air attached to the helicopter and traverse above trees before they were released. By design and certification, inadvertent release of the hooks by the pilot was extremely improbable. Furthermore, inadvertent release of the egg collector would not have resulted in the subsequent helicopter ground collision without an additional failure/malfunction or mishandling. Therefore, the pilot almost certainly released the sling person, consistent with their stated procedure in the event of an engine failure or malfunction in the vicinity of trees.
Due to a lack of recorded data or recollection from the pilot, an assessment could not be made of the height and speed of the helicopter when the engine stopped or the egg collector was released. The trees between where the helicopter probably took off and the vicinity of the accident site were between 12–15 m tall, with taller trees up to 18 m tall closer to the crocodile nest site. The pilot’s reported procedure was to remain within about 5 m above the vegetation and therefore, if following their stated practice, the egg collector was likely about 20 m above the ground when the power loss occurred. Considering the length of the sling line, that would have positioned the helicopter about 50 m (164 ft) above the ground.
To estimate the height from which the egg collector was released, their injuries were assessed by a forensic pathologist using survivability research into falls from heights. Based on the injuries sustained, the pathologist assessed that the egg collector likely fell from at least 5 m above the ground. Additional research reviewed by the ATSB that considered how specific injuries varied with height indicated a likelihood that the egg collector was released from above 9 m, from which most falls are fatal.
Based on the pilot’s reported normal practice to minimise height and speed while slinging, the helicopter was likely operating within the ‘avoid’ area of the helicopter’s height-velocity graph. In that area, the combination of height and airspeed was such that a pilot may have been unable to complete an autorotation landing without damage. This was consistent with the low rotor energy and crushing of the fuselage evident in the damage sustained by VH-IDW.
The helicopter’s vertical descent through at least the last 8 m (24 ft), which was the height of the tree that the main rotor blade struck 3 times, was consistent with an attempt to avoid the obstacles ahead (due to densely growing tall trees) relative to the direction of travel.
Helibrook had introduced a CASA-accepted safety management system (SMS) in conjunction with CASA’s approval of the Helibrook chief pilot. This included purchase of a third‑party produced SMS manual and assigning the operations manager to also perform the safety manager role. The SMS manual stated that through the SMS, Helibrook would identify hazards and risks, with the goals of minimising risk, maintaining the health of stakeholders, and continually improving safety.
An assessment of the operator’s SMS following the accident quickly identified that in the 2 years since its approval, Helibrook had not implemented the system described in the SMS manual. Time or resources had not been allocated to safety management tasks, and the safety manager’s priority had been to fulfill their other role as operations manager. There was no evidence of a maturing safety culture, in which effective hazard identification enabled actions to proactively manage risks and prevent accidents. No formal, documented risk assessment had been conducted for any of Helibrook’s approved activities, including human external cargo (HEC) operations. As an operator conducting a specialised high-risk activity, application of the SMS would have assisted the identification of hazards and risk controls to reduce the risk of harm to operating crew.
CASA’s approval to conduct HEC operations required the pilot and egg collector to assess that the risk of heat illness and crocodile attack outweighed the risks of slinging. A structured risk process would have provided a means for this assessment to be made as well as identifying occasions when slinging was unacceptably risky. The same process should also have identified mitigations to reduce the:
likelihood of an emergency event occurring, such as:
good maintenance practices and adherence to operating limitations to ensure ongoing helicopter airworthiness
ensuring that required pilot briefing and training in HEC operations were conducted, including fuel management
consequences of an in-flight emergency, such as height and speed limits for carrying the sling person, and fitting the helicopter with an emergency locator transmitter.
In not using their SMS, Helibrook did not identify the risks associated with conducting human external cargo operations, particularly the carriage of the egg collectors at non‑survivable fall heights, and ensure they were adequately managed.
Picking up and carrying a person outside a helicopter was not permitted without specific authorisation. CASA could only grant such an authorisation, if doing so would be unlikely to have an adverse effect on safety. To ensure safety was preserved, CASA could impose conditions set out in an authorisation instrument.
Guidance was available for the administrative side of processing a request for an authorisation. However, there were no guidance or tools for conducting the safety assessment to determine whether an authorisation and its conditions assured the preservation of safety. Flight operations considerations for approving an aerial work activity were detailed in the Air Operator’s Certificate (AOC) Handbook, but this did not include the management of risk. The AOC handbook also contained safety management and risk assessment guidance for assessing an AOC holder's SMS, but the CASA delegates contacted by the ATSB as part of this investigation did not consider this relevant to the instrument approval process.
The first approval instrument to conduct HEC operations for the purpose of crocodile egg collection was reported to have been issued in 2007, and subsequently reissued generally on an annual basis. CASA was unable to locate records of instruments issued before 2010, any assessment as to whether the authorisation was likely to adversely affect safety, or how the imposed conditions mitigated the risks. The first instrument obtained by the ATSB was for 2010 and listed 20 conditions. These included a requirement that hooks were fitted to the helicopter under an appropriate design approval and limitations to the height, speed and distance the sling person could be carried.
The CASA delegates who issued authorisation instruments for R44 HEC for crocodile egg collection from 2013–2021 incorrectly assumed a risk assessment had been performed when the first instrument was issued. The delegates also assumed previous approvals meant that the risks of HEC operations had been assessed as acceptable by CASA, and that the conditions included in the instrument mitigated the risks. However, none of the delegates had sighted a risk assessment for the activity, nor did they conduct one, including when changing or removing instrument conditions. Additionally, although the instrument only permitted operators to conduct HEC if there was an overall safety advantage in reducing the risk of crocodile attack and heat illness, CASA did not ensure that the operators had a process for assessing the relative risks.
In the absence of a formal risk assessment process, delegates based their approval of the activity and the imposed conditions on the advice of CASA flight operations and airworthiness inspectors, and a reasonableness test. Additionally, delegates considered the instruments were reissues of an existing approval even when removing or amending conditions. Therefore, if there were no changes to procedures and no accidents, they assessed that there was no reason not to issue an authorisation, as the level of safety was considered not to have changed.
A draft HEC in piston engine rotorcraft risk management plan (RMP) using a CASA general aviation template was prepared by CASA Flight Standards Branch personnel and presented to CASA executive in 2013. The RMP and associated template was a formal risk assessment tool. The RMP assessed that HEC operations in single engine piston (R44) and turbine helicopters was an unacceptable risk without mitigations to improve helicopter reliability, and speed, height and duration limitations for carrying the HEC.
The RMP formed the basis of CASA’s proposed standard to cease issuing approvals for HEC with the R44 and to require a single engine turbine helicopter with a usage monitoring system. This was due to the associated higher risk of in-flight power loss and additional failure modes of an R44. The turbine engine requirement aligned with US and European regulations and was to be included as an amendment to Civil Aviation Order 29.6. That amendment was abandoned in 2016, due to planned implementation in 2018 of the same ruleset incorporated in Civil Aviation Safety Regulations Part 138. However, regulatory change took longer than anticipated, and Part 138 was implemented in December 2021. None of the delegates involved in approving instruments after 2013 reported having seen the RMP.
As the instrument conditions were described as risk mitigations, a formal risk assessment would have enabled delegates to quantify the change in overall risk associated with changes to, or removal of, conditions. Without a formal risk management process, CASA delegates were unable to show in a structured way that an authorisation did not adversely affect safety or that the conditions included in an authorisation were sufficient to achieve the required level of safety.
Once the hooks met the required certification standard, failure of the hooks was extremely improbable. As a result, CASA approved amendments to the rotorcraft flight manual supplement associated with the dual hooks. These included the removal of limits for the height and distance a sling person could be carried and an increase of the maximum slinging speed to 60 kt. However, this did not consider circumstances that could result in release of the sling person, other than failure of the hooks.
CASA delegates then removed the HEC limitations from CASA’s instrument conditions. It is unclear why these conditions were removed. However, as a formal risk assessment was not performed it was not identified that there were other failure conditions likely to result in release of the sling person and that the removal of height and speed limits for carrying the sling person significantly increased the overall risk.
Falls from greater than 5 m above the ground are more likely to result in a fatality. CASA’s removal of those limitations meant that an operator could both operate within an authorisation instrument’s conditions and permit an avoidable fatal outcome for a sling person in the event of an emergency release, such as occurred during this accident.
As CASA delegates had not formally assessed the operational risk of using an R44 helicopter they continued to approve R44 HEC for crocodile egg collection without assurance that aviation safety was preserved. Although CASA’s RMP assessed that a single turbine engine helicopter with a usage monitoring system had a higher reliability and less likelihood of engine failure than an R44 helicopter, it did not consider or compare the hazard of fuel exhaustion.
Having formally assessed the risks for the RMP in 2013, the following year, CASA Flight Standards Branch personnel engaged with operators who conducted HEC for crocodile egg collection and advised of CASA’s intent to require a turbine helicopter with a usage monitoring system for improved helicopter reliability. CASA personnel then drafted the relevant legislation and engaged with the industry before it was finalised. Although operators had been notified and engaged during the rulemaking process, shortly prior to commencement of the regulations in 2021, a CASA delegate issued Helibrook with a 3-year instrument approving continued use of an R44 helicopter for human slinging operations. This resulted in continuation of what CASA had assessed as an unacceptable ongoing risk.
There was insufficient data available of helicopter fuel exhaustion accidents to indicate an increased risk in piston engine helicopters compared with turbine engine helicopters. There was also insufficient evidence from which to assess the difference in outcome between an autorotation in a single engine turbine helicopter and in an R44. Single engine turbine helicopters, with a higher inertia rotor than the R44, may provide more opportunity to place the sling person on the ground, as occurred in a Bell 407 accident in the US in 2022, and reduce the consequences for the pilot in an autorotative landing. However, operating in any helicopter's height-velocity avoid area does not ensure a safe landing can be made.
Without adequate height and speed limitations to protect the sling person, there is no evidence that the use of a single turbine engine helicopter would have altered the outcome in this accident.
The low compression in one cylinder and valve clearances out of service limits increased the likelihood that the engine's maximum power output was reduced. Although the engine was derated, to counter the reduction in performance at higher density altitudes, the defects increased the risk of having insufficient performance for the helicopter to hover out of ground effect, essential to conduct slinging operations.
The higher-than normal fuel flow for slinging operations was unlikely to have affected the pilot’s assessment of fuel endurance. This was because the pilot had conducted slinging in VH-IDW the day prior to the accident and the fuel flow would unlikely have changed since then. The in-flight photo taken on the accident morning showed the helicopter operating above the manifold pressure limit at the time, which may have been symptomatic of reduced engine performance.
The approval to conduct HEC operations required that the engine was capable of making maximum rated power and able to hover out of ground effect 3,000 ft above the ground. Poor engine condition increased the likelihood of insufficient power available to conduct safe slinging operations and of an in-flight failure. However, there was no evidence of any failure or condition that would have suddenly stopped or significantly reduced engine power.
Accurate recording of time in service is required to ensure helicopter components are inspected, overhauled or replaced within life limits. Exceeding the life limits increases the probability of component failure and renders the helicopter unairworthy.
VH-IDW was to be maintained in accordance with the airframe and engine manufacturers’ maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever occurred sooner, and was subject to overhaul at 2,200 hours or 12 years, whichever occurred first. Based on a review of VH-IDW’s maintenance releases, at the periodic inspections, the helicopter’s hour meter matched the time in service recorded on the maintenance release.
Based on the hour meter reading at the accident site, VH-IDW had about 192 hours until overhaul. The ATSB found the hour meter connected, but one of the 2 connections was only finger tight, consistent with having been connected by hand. Additionally, the hour meter had almost certainly been disconnected for periods, resulting in under-recording of the hours in operation. Based on a comparison of the hours recorded on VH-IDW’s maintenance releases with hours recorded in spreadsheets and on the pilot’s phone, it was likely the helicopter had been overrunning the 100-hour maintenance intervals and had exceeded its overhaul life. This was also supported by a CASA airworthiness inspector’s review of maintenance records, which identified the engine-driven fuel pump being replaced at decreasing recorded hourly intervals, as VH-IDW approached its end of overhaul life and while being operated by Helibrook.
In-use hours for the hooks were independent from total helicopter hours but were also not being recorded. Additionally, one hook was overdue for overhaul based on calendar time and the hooks had not been maintained as required, but there was no evidence these had failed.
Although overrunning maintenance, inspection and overhaul periods increased the likelihood of component failure, there was no evidence of an engine, airframe or hook component failure that resulted in the engine stoppage, helicopter accident or increased severity of injuries or damage. Despite that, while operating in the height-velocity avoid area, a successful autorotation was not guaranteed. Therefore, high reliability of the helicopter and systems was necessary to mitigate the risks to the pilot and the sling person. In stopping the hour meter and exceeding maintenance, inspection and overhaul limits, the operator increased the likelihood of a catastrophic component failure of the helicopter. This posed an unnecessary increase in risk for the pilot and particularly sling crew conducting HEC operations.
Cocaine is an illicit drug and can have deleterious effects on pilot performance. Possible effects include risk-taking, inattentiveness and poor impulse control. Although the pilot reported that they did not use cocaine, very low levels of cocaine metabolites were found in the pilot’s toxicology results.
On the basis that the metabolites indicate exposure to cocaine, the detected levels indicated the pilot had not been exposed to cocaine within the previous 24 hours and may not have been affected by cocaine on the accident day. There was insufficient evidence to enable an assessment of whether the drug contributed to the development of the accident. However, the indication of exposure to cocaine is highlighted, as the effects of cocaine and post-cocaine exposure clearly increase risk to aviation activities. The post-cocaine exposure effects can include fatigue, depression and inattention.
The helicopter's emergency locator transmitter was not mounted and did not activate in the accident impact. Although the actual time of the accident could not be established, there is a high likelihood that it was a significant time before the helicopter was located. Therefore, had the emergency locator transmitter been fitted and activated on impact, emergency medical care may have arrived sooner.
Immediate notification to rescue medical services can have a significant effect on the outcome for occupants of a serious aircraft accident. Although prompt medical attention would not have altered the outcome for the egg collector, the pilot’s condition likely worsened over time since the accident. The actions of the individual to search for VH‑IDW and alert emergency services contributed to the pilot’s survival, but more timely initiation of medical assistance would have reduced the risks of exacerbating the pilot’s injuries and deterioration of their condition.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’. In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
At the time this report was published there were ongoing police investigations concerning the status of evidence at the accident site. Acknowledging this, the following findings are made with respect to the collision with terrain involving Robinson R44 II, VH-IDW, at King River, Northern Territory, on 28 February 2022 on the evidence obtained by the ATSB.
Following likely not refuelling at Mount Borradaile, the pilot did not identify the reducing fuel state before the helicopter engine stopped, probably due to fuel exhaustion.
During the autorotation, the pilot released the egg collector above a likely survivable height, resulting in their fatal injuries.
The pilot continued the autorotation to the ground but there was insufficient main rotor energy to cushion the landing, resulting in serious injuries to the pilot and substantial damage to the helicopter.
Helibrook’s approved safety management system was not being used to systematically identify and manage operational hazards. As a result, risks associated with conducting human external cargo operations such as carriage of the egg collector above a survivable fall height were not adequately addressed. (Safety issue)
The Civil Aviation Safety Authority (CASA) did not have an effective process for assuring an authorisation would be unlikely to have an adverse effect on safety. As a result, CASA delegates did not use the available structured risk management process to identify and assess the risks, ensure appropriate and adequate mitigations were included as conditions of the approval, or assess the effects of changes on the overall risk. (Safety issue)
CASA's lack of effective process for assuring an authorisation would be unlikely to have an adverse effect on safety resulted in the removal of height, speed, and exposure limits, which permitted carriage of the egg collector above a survivable fall height.
CASA's lack of effective process for assuring an authorisation would not have an adverse effect on safety resulted in the continued operation of piston engine helicopters for human sling operations without adequate mitigations and the issue of a 3-year instrument to Helibrook shortly prior to the commencement of improved regulations, which would require a turbine engine helicopter for human slinging operations.
Several engine defects were present at the time of the accident. Although there was no defect likely to result in sudden power loss, these factors likely affected the engine maximum power output and fuel consumption.
Helibrook had likely overrun the helicopter's maintenance, inspection and overhaul periods, which increased the likelihood of the helicopter experiencing a technical failure or malfunction.
The presence of cocaine metabolites in the pilot’s blood sample indicated the pilot had been exposed to cocaine within the previous few days, increasing the likelihood of fatigue, depression and inattention.
The helicopter's emergency locator transmitter had been removed from its mount prior to the accident. Therefore, it could not activate automatically, which likely delayed the emergency response.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Civil Aviation Safety Authority (CASA) did not have an effective process for assuring an authorisation would be unlikely to have an adverse effect on safety. As a result, CASA delegates did not use the available structured risk management process to identify and assess the risks, ensure appropriate and adequate mitigations were included as conditions of the approval, or assess the effects of changes on the overall risk.
Safety issue description: Helibrook’s approved safety management system was not being used to systematically identify and manage operational hazards. As a result, risks associated with conducting human external cargo operations such as carriage of the egg collector above a survivable fall height were not adequately addressed.
Abder-Rhman, H., Jaber, M.S., & Al-Sabaileh, S.S. (2018). Injuries sustained in falling fatalities in relation to different distances of falls. Journal of Forensic and Legal Medicine 54:69-73.
Couper, F.J. and Logan, B.K. (2014 revision). Drugs and Human Performance Facts Sheets. Technical Report DOT HS 809 725, National Highway Traffic Safety Administration (NHTSA), Washington DC.
Department of Defence, Defence Science and Technology Group (2022). Fuel analysis for ATSB Investigation AO-2022-009 involving Robinson R44, VH-IDW. DSTG-CR-2022-0060.
Department of the Interior (2010). Helicopter short-haul handbook. US DOI 351 DM 1
European Union Aviation Safety Agency (n.d) Safety culture, EU-South East Asia Aviation Partnership Project (EU-SEA APP), EASA.
Icer, M., Guloglu, C., Orak, M., Ustundag, M. (2013). Factors affecting mortality caused by falls from height. Ulus Travma Acil Cerr Derg, November 2103, 19(6):529-535 doi:10.5505/tjtes.2013.77535
Isenschmid, D.S. (2002), Cocaine – Effects on human performance and behavior. Forensic Science Review, 14:61; 2002.
Liu, C.-C., Wang, C.-Y., Shih, H.-C., Wen, Y.-S., Wu, J.-K., Huang, C.-I., . . . Huang, M.-S. (2009). Prognostic factors for mortality following falls from height. Injury – International Journal of the Care of the Injured, 40, 595-597.
Nau, C., Leiblein, M., Verboket, R.D., Hörauf, J.A., Sturm, R., & Marzi, I. (2021). Falls from Great Heights: Risk to Sustain Severe Thoracic and Pelvic Injuries Increases with Height of the Fall. Journal of Clinical Medicine, 10(2307):1-9. doi:https://doi.org/10.3390/jcm10112307
Papdimitriou-Olivgeris, M., Panteli, E., Koutsileou, K., Boulovana, M., Zotou, A., Marangos, M., Fligou, F. (2021). Predictors of mortality of trauma patients admitted to the ICU: a retrospective observational study. Brazilian Journal of Anesthesiology. 71:23-30.
Reason, J., 1998. Achieving a safe culture: theory and practice. Work & Stress, 12(3), pp. 293-306.
Shehab, R.L., Schlegel, R.E., and Palmerton, D.A., (1998). A human factors perspective on human external loads, The university of Oklahoma and FAA Civil Aeromedical Institute. Federal Aviation Administration. DOT/FAA/AM-98/13
Snyder, R.G. (1963). Human survivability of extreme impacts in free-fall. Civil Aeromedical Research Institute, Aeromedical Research Division. Oklahoma City: Federal Aviation Administration.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of VH-IDW
helicopter operator
helicopter maintainer
helicopter manufacturer
helicopter engine manufacturer
Civil Aviation Safety Authority
United States National Transportation Safety Board
Wild Harvest Northern Territory
emergency responders
other people involved in the egg collection operation
various subject matter experts.
Submissions were received from:
pilot of VH-IDW
helicopter operator
helicopter maintainer
helicopter manufacturer
Civil Aviation Safety Authority
Wild Harvest Northern Territory
emergency responders
other people involved in the egg collection operation
various subject matter experts.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
The ATSB drained the remaining fuel from VH-IDW after it was relocated to a hangar in Darwin. The observed blue colour of the fuel was consistent with 100 low-lead (LL) fuel. The fuel was stored in an unsealed container overnight resulting in some evaporation. The remaining 235 mL of fuel was sent to Intertek for testing to determine the fuel type. The initial tests requested were for fuel density and aromatics as these are key distinguishing properties between fuel types.
The density of the VH-IDW sample was 729.1 kg/m3 and contained 11.8 % v/v aromatics, see column 4 in Table 5.
The ATSB then obtained the invoices, fuel release notes and certificates of quality for the 100/130 Avgas fuel drums delivered to Mount Borradaile and the 2 most recent (prior to the accident day) batches of 100 LL Avgas delivered to the storage tank at Helibrook’s Noonamah base. In a submission provided following review of the ATSB draft report, Helibrook advised that VH‑IDW had been filled the night before the accident from its base at Sweets Lagoon, which also had 100 LL fuel. Fuel receipts showed 100 LL Avgas with batch density 718.3 kg/m3.
The fuel batch delivered in the drums to Mount Borradaile was green, had a density of 693.7 kg/m3 and 0.7% v/v aromatics, see column 3 in Table 5. The 100 LL fuel delivered to the Noonamah tank was blue, had a density of 715.4 and aromatics of about 15%, based on certificates of quality of recent fuel batches delivered to Darwin Port, see column 2 in Table 5.
The ATSB arranged for samples to be taken from 4 WHNT drums at Mount Borradaile, including the 2 identified as the drums used to refuel the R44 helicopters on the accident day. The first drum rolled out on the day was reportedly not full and its density was slightly higher than the batch testing as shown in column 5 of Table 5. The second drum closely matched the delivered batch results.
The initial comparison between the VH-IDW sample and 100 LL fuel indicated that the sample was consistent with partially evaporated 100 LL fuel. However, it was postulated that the reduction in aromatics could also result from a mixing of 100 LL and 100/130 fuel.
To determine whether the VH-IDW sample contained a proportion of 100/130 fuel, or any other fuel type, the ATSB liaised with 2 fuel experts – one from Viva energy, involved in the supply of the 100 LL Avgas, and the other in distribution of the 100/130 Avgas. The Viva expert suggested the ATSB request a distillation of the VH-IDW sample. The distillation process separates the sample into its component hydrocarbons. The sample would be heated then put into a distillation column where different products boil off at different temperatures. However, insufficient fuel remained from the VH-IDW sample to conduct that test. As an alternative, the Viva expert recommended conducting a simulated distillation, which only uses a very small quantity of fuel.
Intertek conducted the simulated distillation, which involved using a method for crude oil, with the results shown in column 4 of Table 5. The final boiling point obtained for the VH-IDW sample was significantly higher than the values stated in the certificates of quality for the batches of 100 LL and 100/130 fuels, and that obtained by using the normal fuel distillation method on the Mount Borradaile sample, all shown in row 9 of Table 5.
* Distillation for VH-IDW was done with incorrect method (used for crude oils not Avgas)
** Different TEL g-Pb/L values were obtained with 3 separate tests
The ATSB again consulted the Viva expert to understand the implications of the high final boiling point. They advised that, among other fuels, Jet A1 (kerosene) and unleaded car petrol have higher final boiling points than Avgas. This prompted further testing to determine whether the VH‑IDW sample was contaminated with another fuel type.
The Viva expert then liaised with Intertek on the ATSB’s behalf to conduct a gas chromatography test to analyse the hydrocarbons and compare the VH-IDW sample with Jet A1, unleaded petrol and 100 LL Avgas. They advised that the chromatogram of VH-IDW showed no traces of Jet A1, or unleaded petrol, but was consistent with partial evaporation of 100 LL Avgas. While this ruled out contamination with an unsuitable fuel type, it did not enable a determination of whether the VH‑IDW sample contained a significant proportion of 100/130 fuel.
As the lead content of 100/130 fuel is nearly twice that of the 100 LL, the Viva expert recommended that ATSB request Intertek conduct testing of the tetraethyl lead (TEL) content of the VH-IDW sample. The first test of the VH-IDW sample resulted in a value (1.370 g-Pb/L) which exceeded the test method upper limit of detection of > 1.3 g-Pb/L. Consequently, the ATSB requested Intertek retest the sample. Intertek conducted 2 subsequent tests of the VH-IDW sample and obtained values of 0.969 and 0.558 g-Pb/L.
Intertek was unsure why the results were inconsistent, and their final report stated they were unable to report a value due to the lack of a consistent result. Additionally, Intertek advised the ATSB that following the third TEL test, the colour of the VH-IDW fuel sample unexpectedly turned from blue to yellow-green. The ATSB then engaged the Defence Science and Technology Group (DSTG) for independent expert advice and provided all remaining fuel samples to DSTG.
The Viva expert’s assessment of the test results was that the VH-IDW sample was consistent with 100 LL Avgas that had undergone significant evaporation of the lighter boiling components. They assessed that there was no kerosene or road grade petrol in the sample. Based on the colour, prior to the sample turning yellow-green, they assessed that there was no more than 5% v/v of 100/130 fuel in the VH-IDW sample.
Defence Science and Technology Group analysis
Gas chromatography with mass spectrometry
DSTG conducted gas chromatography with mass spectrometry (GC-MS) analysis of the VH-IDW fuel and samples of blue 100 LL and green 100/130 Avgas fuel. The 3 resulting GC-MS traces were overlaid on each other for comparison. This showed that the VH‑IDW sample was missing, or had a very low concentration of, low boiling point compounds, consistent with evaporation. The DSTG report referenced a study performed by Canada’s Environmental agency, which found that a 33% evaporation of Avgas 100 LL resulted in a density change from 714.3 to 725.8 kg/m3 (CETC, 2022). Additionally, evaporation skews results such as distillation profile, TEL and total aromatics content. The evaporation skewed the trace for VH‑IDW towards the heavier side, exaggerating those peaks, including the peak for TEL. Tetraethyl lead was readily identified by DSTG using GC-MS, which showed a high concentration that could be attributed to evaporation and/or residual elements in the fuel tank.
The VH-IDW trace was more consistent with 100 LL than 100/130 fuel, although some extremely low concentrations overlapped with 100/130. This suggested that remnant fuel from previous days may have been detected in the GC-MS analysis. A comparison of the VH-IDW sample with the Mount Borradaile drum sample showed distinct differences in the GC-MC traces, and the VH-IDW sample had a significant number of peaks found only in 100 LL Avgas.
Ultraviolet-visible spectroscopy
The VH-IDW sample was blue when drained from the fuel bladder by the ATSB and when it arrived at Intertek. Following testing for TEL at Intertek, it turned a yellow-green colour. On arrival at DSTG, they described the VH-IDW sample as visually a deeper yellow-green than the 100/130 Avgas sample from Mount Borradaile and lacked the blue that was observed by ATSB investigators. DSTG therefore conducted ultraviolet-visible (UV-Vis) spectroscopy to compare VH‑IDW sample with 100 LL and 100/130 Avgas and, if possible, determine the source of the colour change.
Dyes were isolated using solid phase extraction and evaporated then dissolved in heptane prior to analysis. The UV-Vis spectra of the VH-IDW sample found blue dyes common to the Avgas 100 LL and 100/130 (batch and Mount Borradaile) samples. However, the VH-IDW sample did not contain a yellow dye found in the 100/130 samples. The absence of the yellow dye indicated 100/130 Avgas was not present in the VH-IDW sample at any significant concentration. DSTG subsequently assessed that there was likely less than 1% of 100/130 fuel in the VH-IDW sample.
The compounds contributing to the yellow-green colour were not in 100 LL or 100/130 Avgas and were not attributed to an approved yellow Avgas fuel dye. Further analysis to determine the likely source of the colour was ongoing at the time of the publication of this report.
Findings
The DSTG report found that the VH-IDW sample was consistent with Avgas 100 LL that had partially evaporated. The GC-MS trace of the VH-IDW sample significantly overlapped with the 100 LL sample. The UV-Vis spectra absorptions of the VH-IDW sample closely matched the dye for 100 LL Avgas. The 100/130 levels in the VH-IDW sample were assessed as trace volumes, subsequently approximated at less than 1% of otherwise 100 LL fuel. This was evidence that there was no refuelling of VH-IDW with 100/130 prior to the accident.
There was no evidence of Opal, premium 98 petrol, diesel or Jet A-1 fuel in the VH-IDW sample. The distillation method used by Intertek, although undertaken due to the small available volume of fuel, was for crude oil and not valid for other fuels. Consequently, the resultant high final boiling point was consistent with an incorrect test method rather than an accurate representation of the distillation profile.
At the time of writing, the nature of the colour contamination that occurred at Intertek was still under investigation.
The person is not lifted to a height of greater than 5 metres above the ground or obstacles
The aircraft is not flown at a ground speed greater than walking pace when the person is carried under the helicopter
The maximum distance the person is carried under the helicopter is 500 metres for each pick up
2014-2015
The person is not lifted to a height of greater than 5 metres above the ground or water. To remove doubt, this instrument does not permit lifting of a person to a height greater than 5 metres above an obstacle. The height restriction is in reference to the ground or water in all instances
The aircraft is to be flown at speed that is consider by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the total forward speed of the person over the ground
The maximum distance the person is carried under the helicopter is 500 metres for each pick up
2016
The person is only to be lifted to a height above the ground or water that enables the person and aircraft to safely traverse over natural obstacles. In all other instances, the person is not to be lifted more than 5 metres above the ground or water. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the height the aircraft is operated above the ground or water at any particular time
The aircraft is to be flown at speed that is consider by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter. Minimisation of injury to the person in the event of hook release (whether planned or inadvertent release) must be considered in the context of the total forward speed of the person over the ground
The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person
2017-2021
N/A
The aircraft is to be flown at a speed that is considered by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter
The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person
This instrument is subject to the condition that the pilot in command and the operator must each ensure that:
1. The flying operations for the purpose of the activity are only done so utilising the Robinson Helicopter Company R44 helicopter type and only where the person and pilot in command both determine there is an overall safety advantage to the operation by reducing the risk of crocodile attack and heat exhaustion to the person; and
2. Persons other than crew members essential to the activity are not carried; and
3. Life jackets are worn by all crew members for all flights where the takeoff, positioning flights or approach path is so disposed that, in the event of a mishap occurring during operations, it is reasonably possible that the aircraft would be forced to land onto water; and
4. The pilot in command and the person have successfully completed a course of training for the activity promulgated in the operator’s operations manual which includes not less than 1 hour of actual flight time and 1 hour of ground instructional time; and
5. All crew, including the person being slung, have been inducted into the operator’s organisation, and have been included in the operator’s Drug and Alcohol Management Plan requirements; and
6. No pilot shall undertake the activity unless he or she has a minimum of 100 hours experience in helicopter external sling load operations; and
7. Only one person is carried below the aircraft at any one time; and
8. The chief pilot has personally authorised the flight program for the day associated with operations under this instrument; and
9. A thorough preflight briefing specifically related to each flight is conducted by the pilot in command to all personnel associated with the particular flight and is to include actions to be taken by crew members during possible emergencies encountered during the activity. The briefing is to be in accordance with, but not limited to, the activity briefing procedures promulgated in the operator’s operations manual; and
10. The pilot in command has continuous and clear radio communications with the person throughout the activity; and
11. The aircraft is to be flown at a speed that is considered by the pilot in command to be a safe speed, taking into consideration the prevailing wind direction, wind speed, and aircraft performance when the person is carried under the helicopter; and
12. Wind conditions, including wind gusts, for the area of proposed operation, must not exceed 15 knots; and
13. Operations not to be conducted within 5 kilometres of thunderstorm activity or observed lightning strikes. Should thunderstorm activity or lightning strikes be observed, activities under this instrument are to be terminated as soon as safely possible; and
14. The person is only to be carried for the minimum distance and time required in order to safely conduct the activity, taking the possible effects of suspension trauma on the person into consideration. To avoid any ambiguity, the intent of this condition is that the person is not to be carried for the purpose of positioning flights over landing sites where it would be possible to conduct the safe donning or removal of the person from the strop used to carry the person; and
15. The person wears a helmet that meets the Australian standard appropriate to the risks encountered during the activity; and
16. The person must wear an Australian Standard harness (designed for lifting a person) connecting them to the strop at all times during flight to and from the crocodile egg collection site. The person may be released from the strop during the actual process of crocodile egg collection; and
17. The person carries a readily accessible harness knife capable of cutting the lifting strop or harness in an emergency; and
18. All legislative requirements pertaining to the conduct of sling load operations are complied with; and
19. All normal and emergency equipment utilised for the conduct of the activity are serviceable; and
20. The helicopter carries a portable satellite phone with all crew members trained in its use; and
21. The person carries, and is trained to activate, a portable emergency location transmitter; and
22. Prior to the approval of CASA STC SVR 541, the aircraft must have been modified in accordance with, and remain compliant with, Engineering Order (EO) TDE5106-04-R2, dated 12/12/17 or later approved revision.
23. When CASA STC SVR 541 is approved, all aircraft previously certified to the EO will be shown to be compliant with and certified to the STC within fourteen (14) days of the STC being approved, after which time aircraft certified only to the EO may no longer undertake this work. Further aircraft to be used after the STC approval date will only be certified in accordance with the STC; and
24. Aircraft approved under EO TDE5106-04-R2 or later approved revision are to have the HEC Lines and harnesses installed and maintained in accordance with the EO approved data; and
25. Aircraft approved under STC SVR 541 are to have the HEC Lines and harnesses installed and maintained in accordance with the STC approved data; and
26. Other hook down equipment, such as collection basket/cages, helmets and other things will be determined by the Operator as being fit for purpose and meeting any required workplace or industrial standard; and
27. Aircraft operated under the EO TDE5106-04-R2 or later approved revision, are to be operated in accordance with an approved aircraft flight manual supplement R5106-101-R2 or later approved revision which details normal and emergency procedures associated with the activity; and
28. Aircraft operated under STC SVR 541 are to be operated in accordance with an approved aircraft flight manual supplement R5106-25-R9 or later approved revision which details normal and emergency procedures associated with the activity; and
29. The daily inspection schedule for each aircraft utilised for the activity incorporates detailed requirements for the inspection of any component, part or system utilised as part of human sling load operations; and
30. Prior to the commencement of the activity each day, the pilot in command has verified the aircraft engine is producing normal rated power output, and that no defects are evident which could lead to power reduction during those operations; and
31. Only persons employed or contracted for the purposes of the activity are carried. To avoid any ambiguity, this instrument does not permit persons who have provided consideration of any nature to any party to conduct egg collection activities or to be slung from the aircraft involved in such activities; and
32. The person must be provided with a copy of this instrument and must be made aware, in writing, that the hook system is not certified for human use; and
33. The operator and the pilot in command must comply with all applicable instructions relating to the activity contained within the operator’s operations manual. The operator must not, without the prior written consent of CASA, revise any part of its operations manual relating to the authorisation and permission given under this instrument.
Any breach of the conditions of this instrument will result in the instrument being immediately cancelled by CASA.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Long lines are lightweight, high‑strength, low‑stretch ropes used for carrying loads underneath a helicopter.
[2] Refuelling conducted while the engine(s) are operating and the rotors are turning.
[3] OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[4] Loss of coordination of the muscles, especially of the extremities (Macquarie Dictionary).
[5] Safe work method statement (SWMS): a document that sets out high risk activities, the hazards associated with the activities and measures required to be in place to control the risks to an acceptable level.
[6] Normal category rotorcraft have a maximum take-off weight (MTOW) up to 3,175 kg and up to 9 passenger seats.
[7] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[8] Manoeuvring with low fuel levels can result in fuel flowing away from the fuel tank outlet, or port, to the engine. This disrupts the engine fuel supply, resulting in power fluctuations and/or engine stoppage.
[9] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[10] A supplemental type certificate (STC) is a type certificate (TC) issued when an applicant has received regulatory approval to modify an aeronautical product from its original design. The STC, which incorporates by reference the related TC, approves not only the modification but also how that modification affects the original design.
[11] The primary hook could be used for non-human cargo lifting operations and, as such, could accrue more operational hours than the secondary hook (required for HEC operations).
[12] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[13] The altitude in the International Standard Atmosphere at which a given air density is found.
[14] B nut - threaded sleeve nut that provides clamping force to ensure an effective/good seal to fuel, air and oil lines.
[15] Due to engine installation orientation, the engine right magneto is located on the left side of the helicopter. Further, the engine right magneto contains a second set of points that provided a signal to the governor and engine tachometer.
[16] The lead content of 100/130 is about 0.732 g Pb/L and the lead content of 100 LL fuel is approximately 0.38 g Pb/L.
[17] Out of ground effect: helicopters require less power to hover when in ‘ground effect’ than when out of ‘ground effect’ due to the cushioning effect created by the main rotor downwash striking the ground. The height of ‘ground effect’ is usually defined as more than one main rotor diameter above the surface.
[18] The Pilot’s Operating Handbook (POH) incorporates the US Federal Aviation Administration-approved Rotorcraft Flight Manual.
[19] Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[20] This was CASR 11.055 (1)(d) in 2010 and CASR 11.055 (1A)(e) in 2013, but the wording is the same in both.
[21] Equivalent level of safety means an alternative action taken provides a level of safety equal to that provided by the requirements for which equivalency is being sought.
[22] The parachute landing fall is used to spread the forces of impact across various parts of the body to reduce the risk of injury. The landing position is with the knees slightly bent and feet together. The feet and toes contact the ground first, followed by a sideways roll onto the legs and torso then the back. (ParachutingInjuries_FS_12-006-1115.pdf (army.mil))
[23] A Failure Modes and Effects Analysis is a systematic method of identifying the failure modes and the failure outcome. The assessment may be quantitative or qualitative.
[24] Part 138 MOS definition: Class D external load means a load that is a person, carried external to the rotorcraft, by a rotorcraft in an external load operation.
[26] Transport Safety Investigation Regulation 2.4 (2)(e) and (2)(f)(i) specified that these occurrences were required to be reported if they occurred when the aircraft was boarded for flight and it involved the use of any procedure for overcoming an emergency or resulted in difficulty controlling the aircraft.
[27] Haemopneumothorax is the condition of having air and blood in the chest cavity.
[28] Subarachnoid haemorrhage is bleeding in the space that surrounds the brain.
Occurrence summary
Investigation number
AO-2022-009
Occurrence date
28/02/2022
Location
30 km south of South Goulburn Island (King River), Northern Territory