
Final report
Report release date: 22/12/2025
Investigation summary
What happened
On 11 March 2022, at about 1050 local time, the pilot of a Bell Helicopter Company B206L-1, registered VH‑BHF and operated by Heli Surveys Pty Ltd, departed Jindabyne aerodrome, New South Wales, to conduct a weed survey task on behalf of the New South Wales National Parks and Wildlife Service (NPWS). On board were the pilot and 4 NPWS officers. At about 1112, at a low level and low speed over the Snowy River, control of the helicopter was lost. While attempting an emergency landing in the river, the helicopter collided with a large boulder. Three of the occupants received serious injuries and 2 received minor injuries. The helicopter was destroyed.
What the ATSB found
The ATSB found that, to conduct the weed survey above the riverbank, the helicopter was flown at low-level, at a slow speed, and yawed to the right by about 45°. It was also noted that the helicopter was operating at a high gross weight and higher density altitude. In combination, these conditions were conducive to the onset of a loss of tail rotor effectiveness. As such, it was likely that a loss of tail rotor effectiveness occurred at an insufficient height to recover and avoid a collision with terrain. Following the collision into the river, the carriage of dedicated emergency locator transmitting devices allowed for a timely response for retrieving the occupants.
Further, one of those on board was not required for the survey task, which unnecessarily exposed them to the risks associated with low-level flight. While the client’s operating procedures referred to ‘essential personnel’, they did not provide a definition or specify the roles and responsibilities of these personnel.
The ATSB also identified that the operator’s risk assessment for low-level operations did not contain the hazard and control measures to avoid the likelihood of loss of tail rotor effectiveness. Further, there was no requirement for its pilots to conduct pre-flight risk reviews to ensure that operations could be conducted without unacceptable safety risk.
What has been done as a result
Heli Surveys conducted a review of its risk management processes and made changes to its operational conduct. Its changes focused on identifying flight‑related hazards that included loss of tail rotor effectiveness and compiling mitigation controls in a dedicated risk assessment. Other changes included the introduction of a ‘Hazardous Flight Conditions’ course for pilots and a requirement for flight crews to ensure that only essential crew were to be on board its helicopters.
The NPWS revised its aviation safety policy and developed an aviation safety management system to enhance safety and manage risk across its aviation activities and operations. To define essential personnel, the NPWS committed to developing detailed task profiles to ensure that the roles and responsibilities of all personnel were clearly defined and committed to the development of task‑specific risk profiles to manage risks associated with its aerial work activities.
Safety message
Survey flights, particularly when performed in alpine environments, are generally conducted at low level and slow speeds. This creates a high-risk operating environment that requires effective risk management. Risk management should include an overarching pre‑operational risk assessment to identify the hazards and risks common to that type of operation. This assessment can then be used to inform the management of risk for specific taskings including a pilot’s pre-flight risk review, to ensure the operation can be conducted safely.
This accident further highlighted the benefits of carrying multiple position transmitting devices. This not only eliminates potential doubt associated with transmissions generated from inadvertent beacon activation but can accelerate an emergency response.
The occurrence
On 11 March 2022, at about 1050 local time, the pilot of a Bell Helicopter Company B206L-1 helicopter, registered VH‑BHF and operated by Heli Surveys Pty Ltd, departed Jindabyne aerodrome, New South Wales, to conduct a low-level English Broom weed[1] survey task on behalf of the New South Wales National Parks and Wildlife Service (NPWS) (Figure 1). On board were the pilot and 4 NPWS officers.[2]
Following departure, the flight tracked north along the western side of Lake Jindabyne and at about 1055, the pilot turned north-west and tracked upstream along the Snowy River before turning south-west towards Island Bend. At about 1102, the helicopter passed overhead Island Bend where a clump of the weed was located. This local infestation provided an opportunity for the NPWS officers to familiarise themselves with spotting the target weed in the local environment, to assist with identification during the survey.
From Island Bend, the flight continued south-west, following the course of the river. At 1110:35, the helicopter approached Guthega (Munyang) hydro‑electric power station where the pilot commenced a left turn, to pass to the east of the power station.
Figure 1: VH-BHF flight path from Jindabyne aerodrome to Guthega power station with inset showing location relative to capital cities
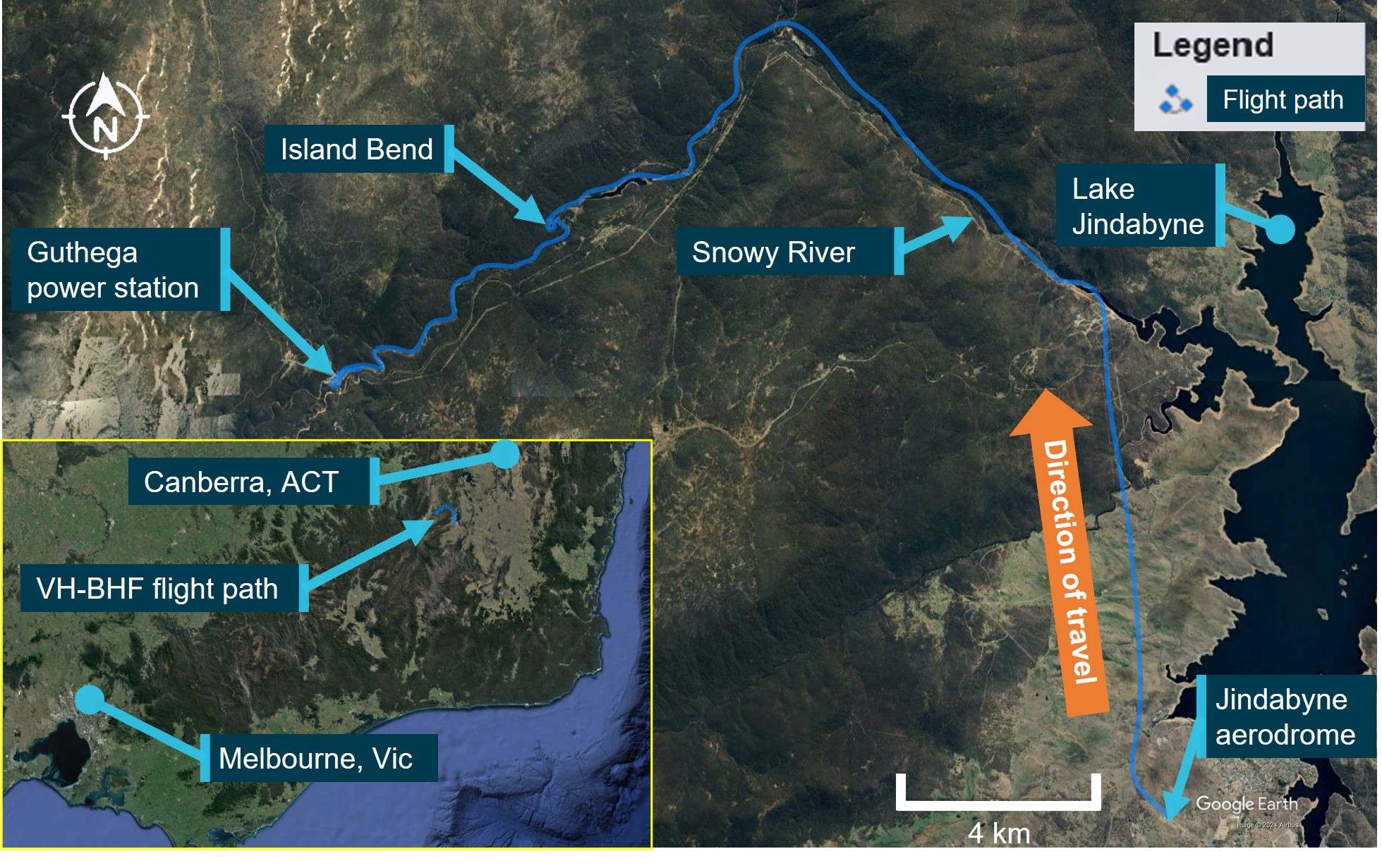
Source: Google Earth and TracPlus data, annotated by the ATSB
At 1110:47, and now south of the power station, the pilot commenced a right, high orbit to remain clear of power lines in the area and return towards the river course.
By 1111:17, the helicopter was heading downstream above the southern riverbank and established in a descent towards the river in preparation for commencing the weed survey (Figure 2).
Corroborating reports from the occupants of the helicopter, which included the pilot, indicated that due to the seating position of the NPWS officers (3 seated on the left side of the helicopter), the later part of the descent was conducted with the nose of the helicopter yawed to the right about 45°. The right yaw was in response to the officers’ request to provide the best view of the riverbanks for them to identify and map the locations of the English Broom weed. The officers reported that they asked the pilot to fly lower and sideways to enhance their view. The pilot reported to the ATSB that, prior to setting up the right yaw position, the helicopter’s speed was about 30 kt and they noted they had sufficient power with no abnormal engine indications.
As the helicopter descended past Pipers Creek, the pilot reported that their vision of trees and other obstacles was obscured by the helicopter’s instrument console. To improve their vision for the final descent to the river, the pilot indicated that they ‘touched’ the left anti-torque pedal[3] to straighten the helicopter ‘a bit’, upon which the helicopter started an uncommanded yaw[4] to the right.
In interview with the ATSB, the pilot stated that they believed they had full and free movement of the anti-torque pedals until the uncommanded yaw to the right started. After the yaw started, they felt that the helicopter did not respond to their pedal inputs, but they could not recall exactly what inputs they made. The pilot did not recollect any shock loading of the tail rotor, such as from a bird or tree strike. The officers reported that, when the uncommanded right yaw started, they thought it was a pilot‑initiated turn and that they were clear of trees and there were no physical knocks or signs of a failure before the yaw commenced.
After the first turn, when the helicopter was facing downstream, the pilot attempted to gain forward speed, but the helicopter continued to yaw right, and the yaw rate started to accelerate. At 1111:58, when about 200 m past Pipers Creek, the pilot reported realising their only landing option was in the river and, to do so, they rolled the throttle to idle, which stopped the yawing motion. The helicopter entered an autorotation[5] with the pilot aiming for a spot in the river. The pilot attempted to cushion the landing but did not see a large boulder in the water at their aim point.
At 1112:04, the helicopter collided with terrain. Three occupants received serious injuries, and 2 sustained minor injuries. The helicopter was destroyed.
Figure 2: Approach to Guthega power station, orbit to the south, descent and collision with terrain
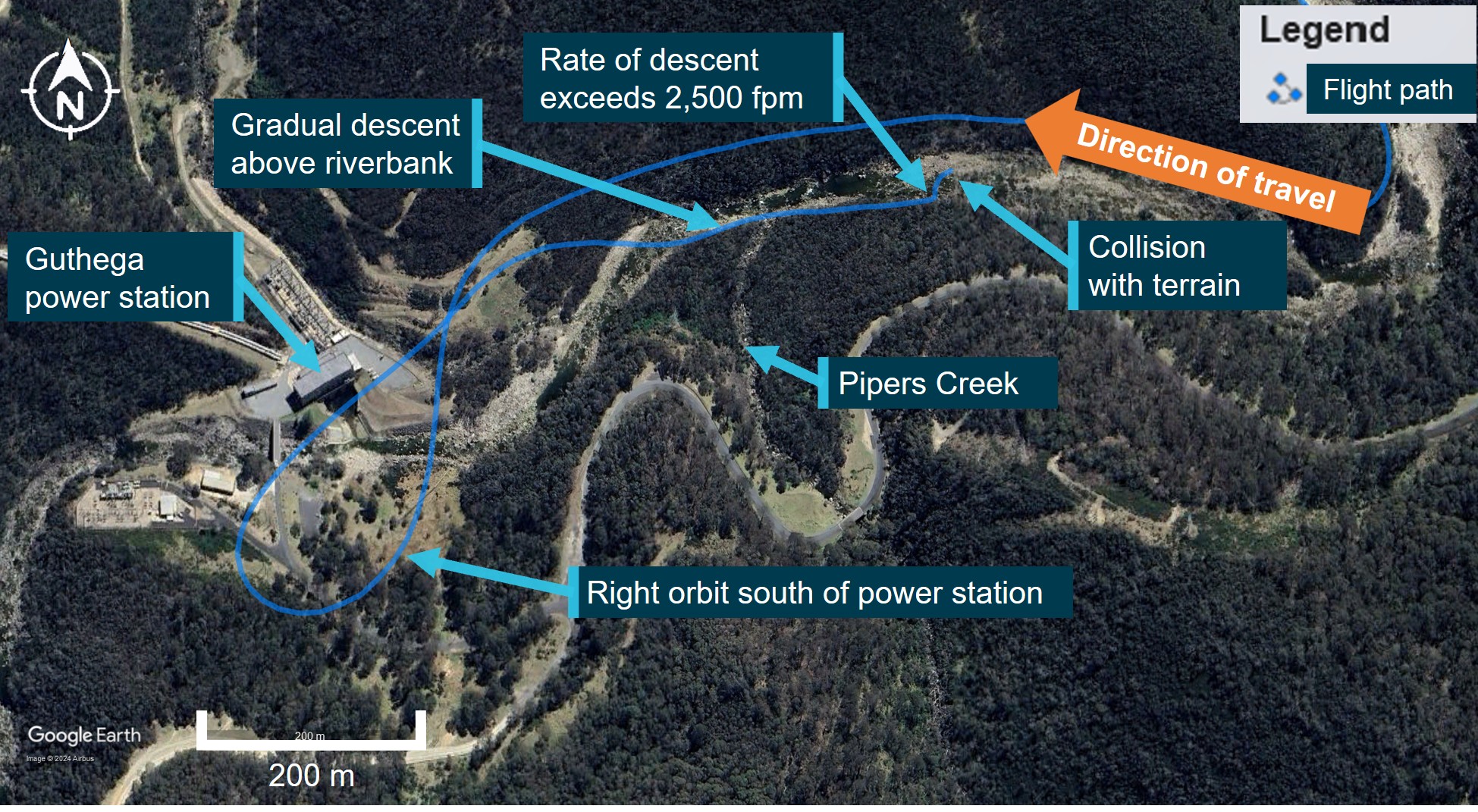
Source: Google Earth and TracPlus data, annotated by the ATSB
At the time of the accident, the operator had another helicopter in the local area conducting sling‑work operations. At around 1130, the pilot of that helicopter, who was also the head of flying operations, received a report[6] of an alert notification from the emergency locator transmitter on VH‑BHF, and a subsequent report of a personal locator beacon activation. Aided by their onboard resources, the pilot identified the last recorded position of VH-BHF that was transmitted by its satellite‑based tracking system (TracPlus) and immediately ceased the sling-work operation and departed for that recorded position. While enroute, the pilot notified emergency services and directed their ground‑based resources in the local area to the expected helicopter location.
The pilot located VH-BHF at about 1138 and confirmed the accurate position with emergency services. While surveying the scene from overhead, they were joined by another of the operator’s helicopters, and that pilot was able to unload an air crew person at the accident site. The air crew person was equipped with a first aid kit and provided a communications link between the ground and the overhead helicopters. At about 1210, the operator’s ground-based staff arrived to provide assistance and reported that emergency services had started to arrive. Following initial treatment, 3 of the injured persons were airlifted to hospital while the remaining 2 were able to walk from the site to awaiting ambulances.
Context
Personnel information
Pilot
Qualifications and experience
The pilot held a valid class 1 aviation medical certificate and a Commercial Pilot’s Licence (Helicopter) with single‑engine helicopter and low‑level rating, and a gas turbine endorsement. The operator’s pilot record sheet, dated 2 November 2021, indicated the pilot had accrued 900 hours turbine experience from a total of 2,065 flying hours experience. The pilot had also logged 530 hours aerial work and low flying, and 20 hours mountain flying. In the 28 days prior to the accident, the pilot had accrued 47.1 hours flight time, and 98.7 hours in the previous 90 days. In total, the pilot had 145 hours experience on the Bell 206L-1 helicopter, which included 9.3 hours in the previous 90 days.
Operator training
The pilot joined the operator, Heli Surveys, in early November 2021. On 21, 22 and 23 October 2021 they completed 6 pre-employment check flights on the AS350 helicopter with a contracted training and checking organisation. The syllabus for the checks included low flying within the normal procedures and tail rotor malfunction, autorotation, fire, jammed controls and system failures within the emergency procedures.
The pilot reported that a loss of tail rotor effectiveness (LTE) (refer to section titled Loss of tail rotor effectiveness) would have been covered in their training history at some stage but could not recall any specific occasion, and that they had never experienced it before in flight. The operator’s head of flying operations (HOFO) reported that they conducted a flight with the pilot before they were released to line and was impressed with their attention and focus on control of the helicopter during take-off and landing. The HOFO did not specifically discuss LTE during their flight with the pilot but did discuss mountain and survey operations. They further reported that they considered LTE a component of the low-level flying conducted in the pilot’s pre‑employment check flights.
National Parks and Wildlife Service officers
The National Parks and Wildlife Service (NPWS) team on board consisted of:
- A task coordinator who had the lead role in terms of liaising with the pilot and the other officers and was logging the location of the English Broom weed on a hand-held electronic device.
- Two officers designated as primary observers (spotters). Their role was to look for the weed, and when a plant was identified, advise the coordinator. One of these observers was logging the position of the weed on a hand-held electronic device.
- Another NPWS officer had joined the group given their employment as the area ranger. The survey task had provided the opportunity for the officer to familiarise themselves with the area from the air and observe the conduct of the weed survey task. While the officer did not have a specific function to perform for the survey, they assisted the team in locating the English Broom weed.
Helicopter information
General
VH-BHF was a Bell Helicopter Company B206L-1 powered by a Rolls-Royce model 250‑C30P gas turbine engine driving a 2‑blade main and tail rotor system. It was manufactured in the United States in 1979 and assigned serial number 45164. The helicopter was issued with an Australian Certificate of Airworthiness on 7 April 1987 and first registered in Australia on the same date. Including the pilot, the helicopter provided seating for 7 occupants. At the time of the accident, the helicopter had accumulated about 11,849 hours, total time in service.
Recent maintenance history
At the last 100-hour periodic inspection on 27 November 2021, a maintenance release was issued, permitting night visual flight rules[7] operations. The maintenance release showed that an engine hot start defect had been recorded in December 2021. Rectifications for that included the replacement of the engine turbine assembly, and post‑repair power assurance checks that were certified as completed on 14 February 2022, deeming the engine serviceable. The maintenance release also showed that:
- other than items that would be addressed during a daily inspection, no maintenance was due
- there were no defects that required rectification before the next flight
- the helicopter had been flown for about 22 hours from when the maintenance release was issued prior to the accident.
Modifications
The helicopter was fitted with Van Horn Aviation 2062200-101/-301 tail rotor blades with a United States Federal Aviation Administration (FAA) approved rotorcraft flight manual supplement (206L1‑FMS‑901). The supplement stated that the tail rotor blade design increased the stall margin, thereby improving high altitude performance:
Satisfactory stability and control has been demonstrated in relative winds of 30 MPH (26 knots) sideward and rearward at all loading conditions…
The helicopter was also fitted with main rotor yoke part number 206-011-149-101 allowing flight operations up to a gross weight limit of 1,882 kg (4,150 lb), up from 1,837 kg (4,050 lb) as stated on the type certificate data sheet.
Weight and balance
The ATSB completed weight and balance calculations for the helicopter, considering the pilot and 4 NPWS officers on board. Including fuel, baggage and cargo, the helicopter all‑up weight at take‑off was determined to be about 1,842 kg, 40 kg below its gross weight limit of 1,882 kg, and within its centre of gravity limits. Accounting for fuel burn-off, the helicopter’s all-up weight at the time of the accident was about 1,799 kg, 83 kg below its gross weight limit.
Meteorological information
The Bureau of Meteorology grid point wind and temperature forecast (relevant to the accident) for 1100 on 11 March 2022 was 5 kt of wind from the west (280°) and a temperature of 8°C at 5,000 ft. The graphical area forecast, valid from 1000, was for visibility greater than 10 km with scattered[8] stratus cloud between 2,000 ft and 3,500 ft until 1100.
The nearest aerodrome with an automatic weather information service was Cooma, New South Wales, located 50 km east of the accident site at an elevation of 3,106 ft. The recorded conditions at Cooma at 1100 were a wind of 9 kt from 030°, visibility greater than 10 km, no cloud detected, a temperature of 13°C and QNH[9] at 1021.
The pilot reported fine weather conditions with light winds from the south-west of no more than 5 kt when in the vicinity of the power station, dropping to nearly nil wind conditions once below treetop height on descent towards the river. The NPWS officers reported that the weather was calm. One of the first responders provided a similar report of light and variable winds, as they noted that the wind conditions allowed each rescue helicopter to assume a different heading while hovering as the injured persons were winched on board.
A similar report regarding local weather conditions was received from the operator who maintained an airborne presence during the initial discovery of the wreckage and throughout the rescue operation. They described the conditions on the day as very good with visibility greater than 10 km and wind speed predominantly below 5 kt. They added that there was a very light wind flowing in the downstream direction of the river at the accident site.
Recorded data
A TracPlus™ RockAIR tracking device was recovered from the helicopter following the accident. The device recorded global positioning system tracking information at a frequency of 1 Hz on a removable micro-SD card. ATSB analysis of the recorded data for the last 60 seconds of the flight is shown in Figure 3 for illustrative purposes.
For a period of about 32 seconds before the helicopter started to yaw, the recorded data indicated that its groundspeed was below 25 kt and further decreased below 20 kt about 5 seconds before the yaw began. About 3 seconds after the yaw commenced, and from a height of about 200 ft above ground level, the helicopter’s rate of descent (vertical speed) increased and reached a peak of about 2,500 ft/min, consistent with the pilot rolling off the throttle and entering an autorotational descent. The data indicated that the yaw lasted for about 5 seconds and was arrested within about 3 seconds of the start of the descent. When the yaw stopped, the helicopter’s height was about 65–100 ft above ground level.
Figure 3: Ground positioning system flight tracking data over the last 60 seconds of recording
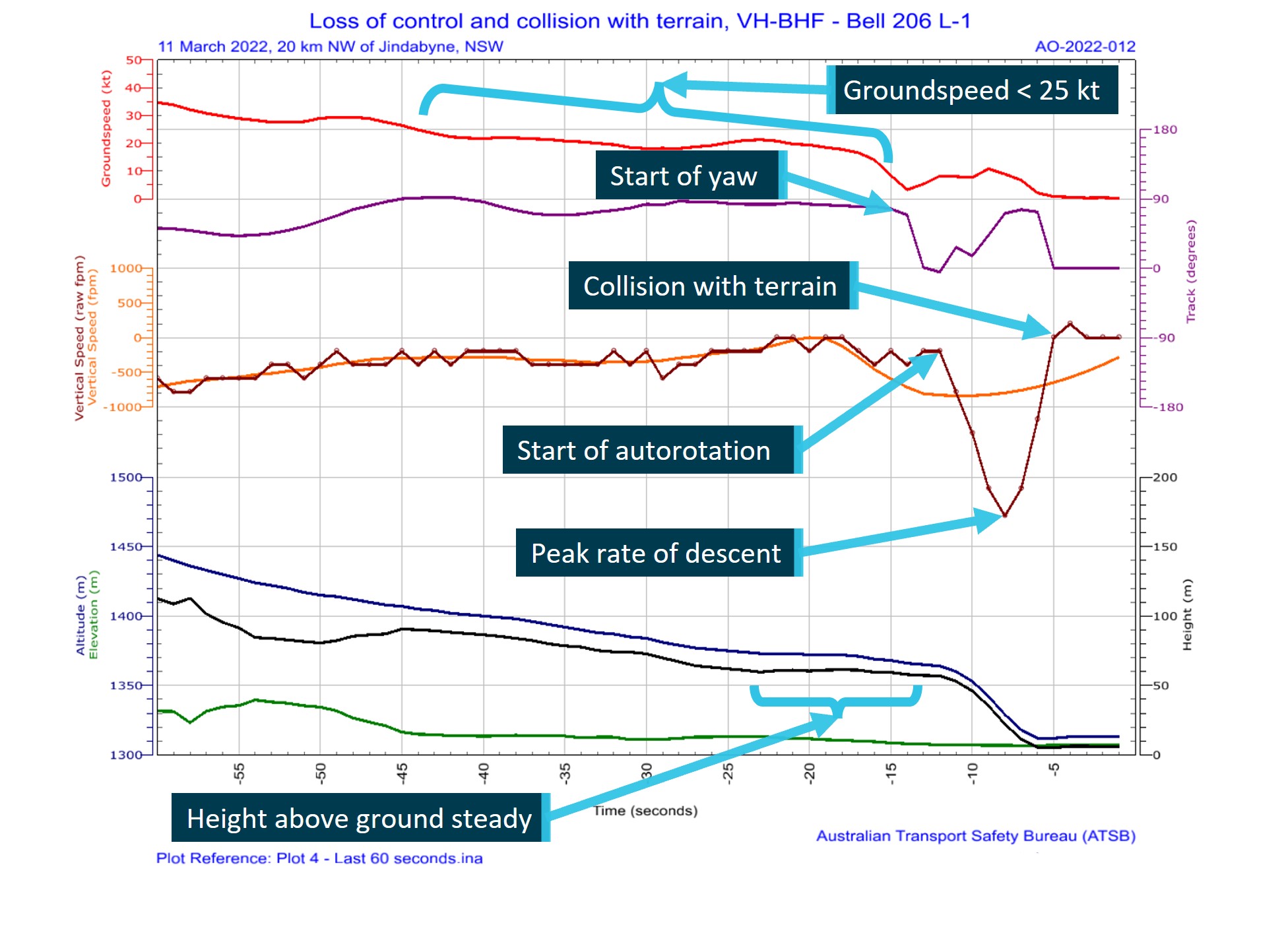
Graphical representation of flight data showing helicopter forward and vertical speeds, altitude, height above terrain and helicopter track with descriptive comments added. Source: TracPlus data, accessed and annotated by the ATSB
Wreckage and impact information
The accident site was located less than 600 m downstream from the Guthega power station (Figure 2) and 20 km north-west of Jindabyne, New South Wales. The helicopter landed on top of a large boulder in the shallows of the Snowy River and came to rest on a heading of 310°, with the fuselage canted significantly to the right (Figure 4).
The helicopter struck the boulder at a point forward of the external cargo hook fuselage mount and slightly aft of the forward skid gear cross tube. The impact with the boulder structurally damaged the helicopter, breaking the forward cockpit section from the cabin area, and resulted in the tailboom partially fracturing near its fuselage attachment point.
The tailboom fracturing and subsequent deflection likely resulted in a tail rotor ground strike and loss of a portion of a tail rotor blade, which was not recovered from the site. Apart from the missing section of tail rotor blade, the rest of the helicopter was present at the accident site. No evidence of a bird or in-flight tail rotor strike was identified and there was no post‑impact fire.
The location of the helicopter in the riverbed and the surrounding environment precluded a complete examination of the wreckage at the accident site. The operator reported receiving advice that anticipated water inflows at Guthega Dam would result in increased water levels downstream of the dam from water exiting the uncontrolled spillway. In response, the wreckage was removed from the accident site at the earliest opportunity, airlifted from the riverbed and relocated to a secure site in Cooma for detailed examination.
Figure 4: VH-BHF following collision with terrain against large boulder in the Snowy River, New South Wales
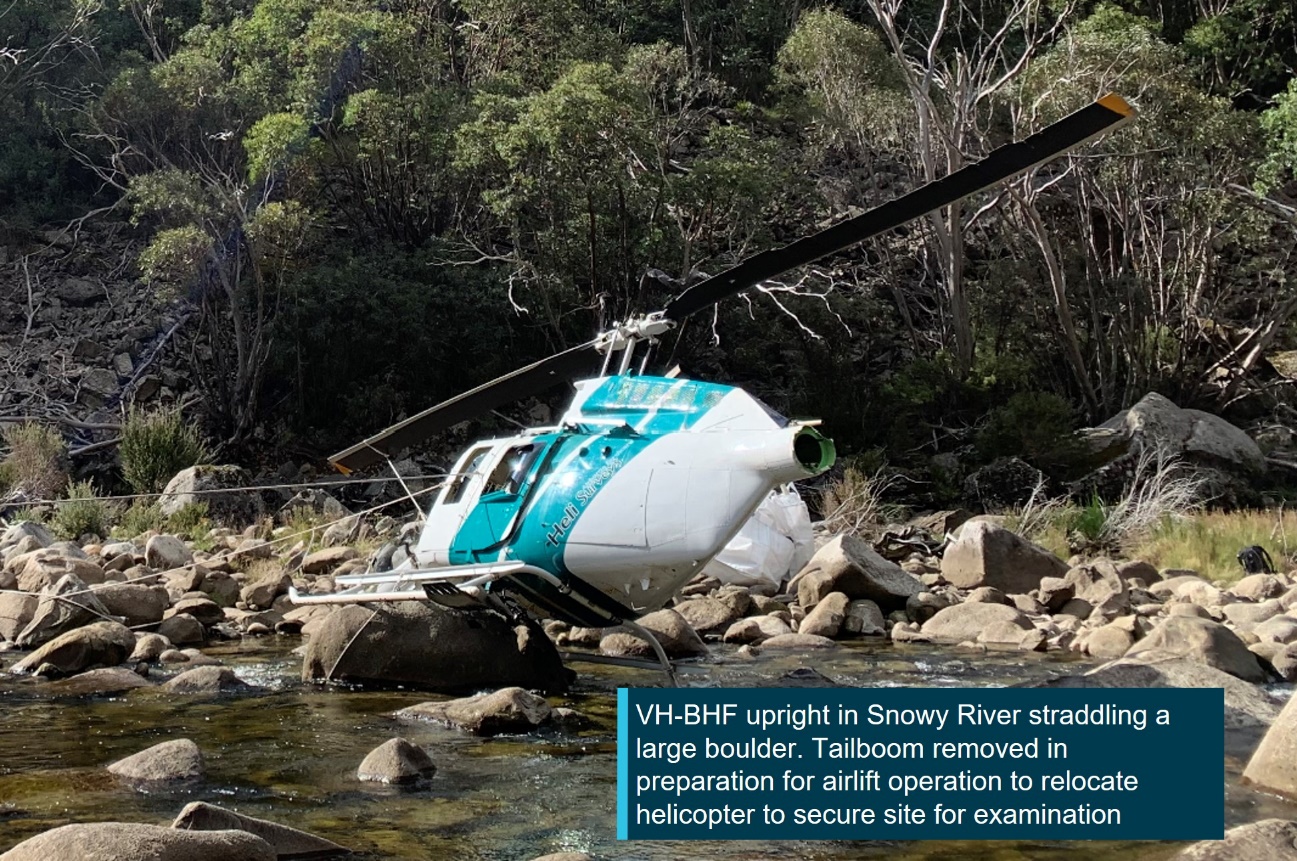
Source: ATSB
The ATSB’s site examination did not reveal any pre-existing defects that may have affected the operation of the helicopter or its systems. The detailed examination of the flight control systems in Cooma did not identify any pre-existing defects that may have affected the control of the helicopter.
Where evidence of structural fractures and breaks were identified, the failures were found to be fresh and were attributed to being either collision‑related, or as the result of torsional overload forces. Of note was the torsional overload of the tail rotor driveshaft at the tail rotor gear box location. This indicated that the driveshaft was driving the tail rotor when the tail rotor experienced a sudden stoppage (Figure 5).
The engine presented as intact, securely mounted, and with controls functional but with restricted movement due to fuselage damage. The compressor and turbine were found to spin freely. No defects were identified with the supply, delivery and quality of the fuel that was available to the engine.
Figure 5: Tail rotor drive shaft showing torsional overload

Source: ATSB
Survival aspects
Seating layout
The seating configuration of the helicopter consisted of 2 cockpit seats and, in the cabin section, a centre row of 2 aft-facing seats and a rear row of 3 forward‑facing seats. For the accident flight, the pilot was in the front right seat with an NPWS officer (coordinator/recorder) in the front left seat, another officer (area ranger – observer) in the centre row left seat (facing rearwards), and the 2 remaining officers in the left (observer/recorder) and right (observer) seats of the rear row (Figure 6). Each seat was equipped with a 4-point restraint harness.
Figure 6: VH-BHF cockpit and cabin seating layout and NPWS officers’ functional positions
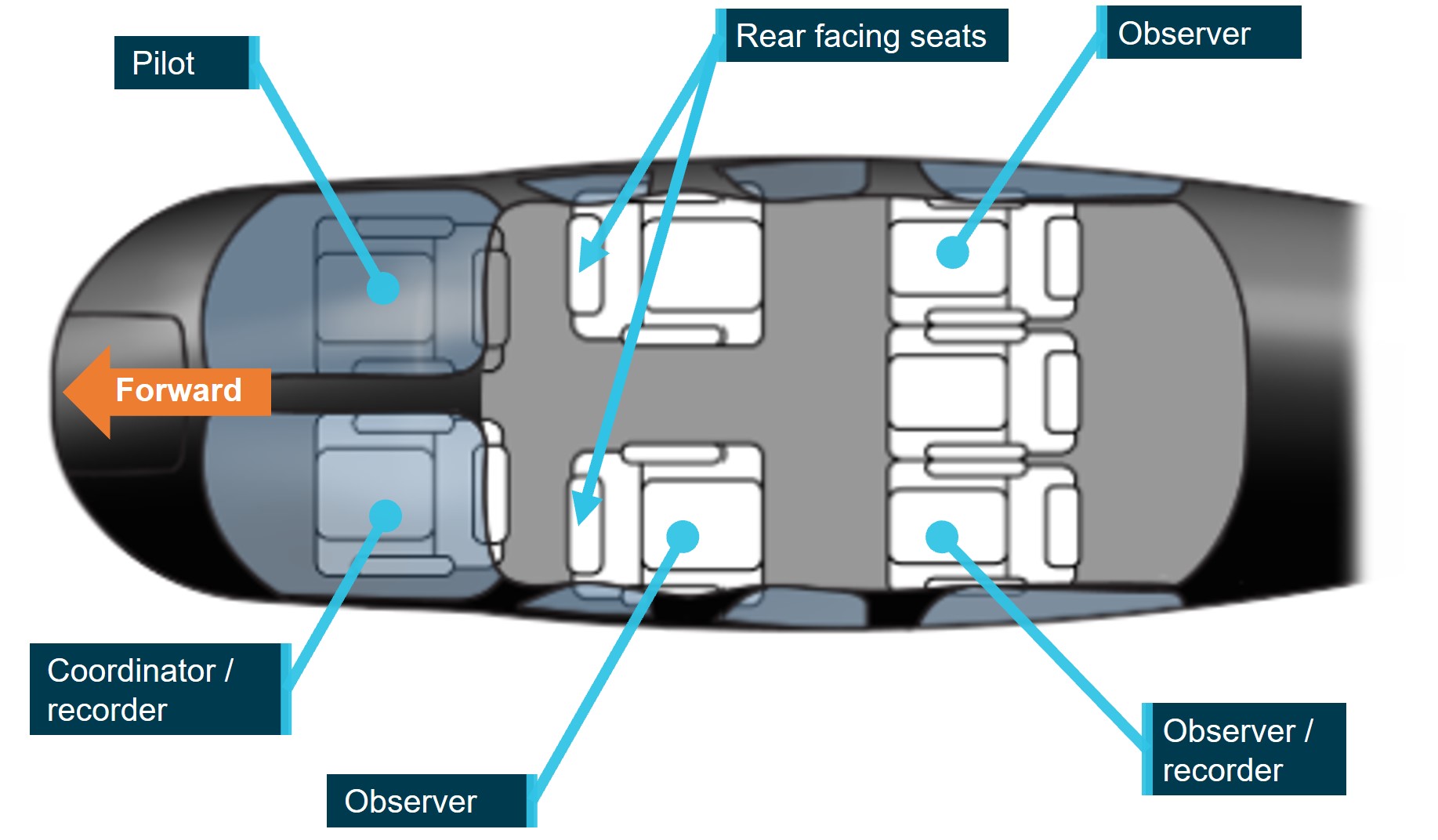
Bell 206 LongRanger III seating layout adopted for illustrative purposes only. Source: FlyFlapper.com annotated by the ATSB
Injuries
The pilot, task coordinator, and observer in the rear‑facing cabin seat sustained serious injuries. The 2 observers in the rear row received minor injuries.
Evacuation
While airborne above the accident site, the HOFO reported they contacted the power station and advised them of the accident downstream of their location and for consideration of the possible impact on power generation commitments. They were advised that power generation would be postponed, however, water levels downstream of Guthega Dam were dependent on natural inflows and outflows from the dam.
At interview, 2 of the NPWS officers advised that they were aware that the water level would likely rise in response to power generation activity. As a precaution, after assisting the injured with evacuating from the helicopter, they were immediately moved to higher ground.
Survival equipment
The NPWS aviation standard operating procedure for low-level flying specified that, when engaged in such activities, helicopters were to carry an emergency locator transmitter (ELT) and be fitted with a tracking system that could be tracked by the agency. As such, the helicopter was equipped with an ELT, and a survival pack that included a personal locator beacon (PLB), a first aid kit and a satellite phone. A TracPlus RockAIR device was also mounted on the instrument console, which provided real-time location tracking of the helicopter through GPS technology. The tracking device was designed to transmit an alert if a sudden impact of 16g or more for a period greater than 10 milliseconds was detected.
ELT and PLB emergency radio beacons are used to provide a location fix on a person, aircraft or other vehicle (ATSB, 2013). ELTs are usually fixed in an aircraft and are designed to activate automatically during an impact, typically by a g-force[10] activated switch but can also be wired to be manually activated by a cockpit-located switch usually mounted within reach of the pilot or a front‑seat passenger. PLBs are designed for personal use and may be carried on the person or carried as part of a survival kit. They are manually activated and may be used as an alternative to a fixed ELT, provided certain requirements are met.
In the event of an accident followed by beacon activation, the aircraft wreckage and its occupants can be located quickly by search and rescue authorities. Finding the aircraft wreckage quickly not only increases the chance of survival of the occupants but also reduces the risk to pilots of search and rescue aircraft who commonly need to operate in marginal weather conditions and over mountainous terrain (ATSB, 2013).
The collision resulted in both the ELT and tracking device activating. The collision alerts were received by the operator (HOFO) and were followed by a third report of a PLB that was manually activated by one of the NPWS officers. This allowed the HOFO to promptly identify the last known position of VH-BHF and commence an emergency response. The operator reported that the multiple transmissions from independent sources provided the surety that a distress situation existed.
Operational information
Helicopter performance
The out-of-ground effect performance chart in the B206L-1 rotorcraft flight manual indicated the helicopter had the performance required to hover out-of-ground effect at the elevation and temperature conditions for the accident. The accident site was located at an altitude of 4,308 ft. Accounting for temperature and QNH, the density altitude for the flight just prior to the accident was calculated to be about 4,500 ft.
The recorded data for the flight indicated that the groundspeed had dropped below 20 kt before the loss of control, and accounting for density altitude influence, this equated to a calibrated[11] airspeed of about 1–2 kt below the groundspeed in nil wind. The height and airspeed of the helicopter at this time placed it inside the avoid area of the height-velocity diagram[12] (Figure 7 – left). The helicopter’s weight and density altitude also placed the operation outside of the weight-altitude limit for the height-velocity diagram (Figure 7 – right).
Consequently, the helicopter was operating in a region of the flight envelope where there was no assurance that a safe autorotation could be made without damage and injuries to occupants. At interview, the operator advised that flight operations in the avoid area was common practice, and necessary to effectively and accurately conduct a weed survey task.
Figure 7: B206L-1 flight manual performance charts showing operational caution zones and VH-BHF relative position in preparation for survey task
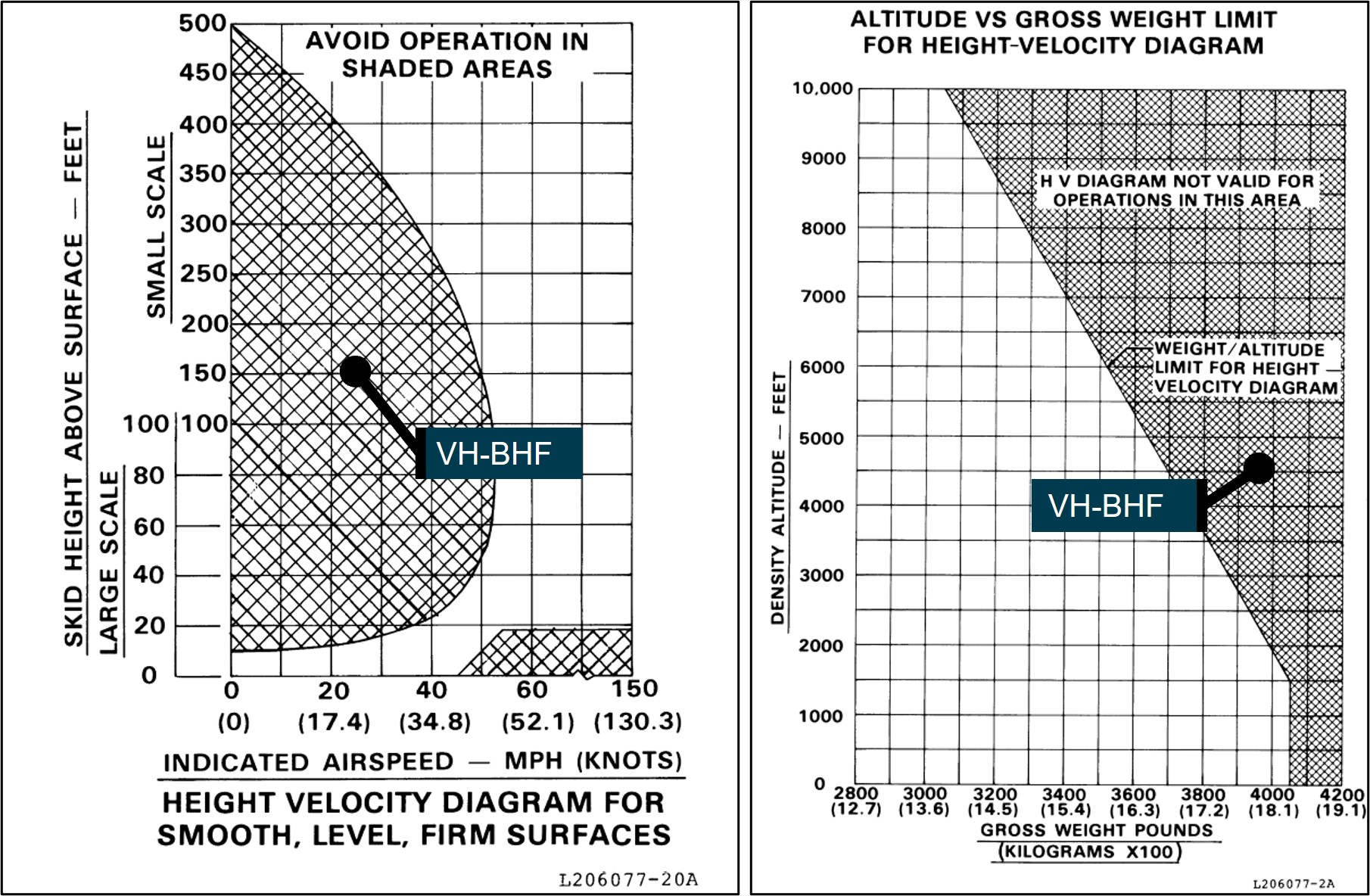
Source: Bell Helicopter Company, annotated by the ATSB
Aerial work operations
Heli Surveys
Heli Surveys Pty Ltd was approved by the Civil Aviation Safety Authority (CASA) to conduct various flight operations including Civil Aviation Safety Regulation (CASR) Part 138 aerial work operations. Its aerial work operations were varied and included roles associated with feral animal control and survey flights of pest animals, weeds and power lines.
Part 138 aerial work operations
CASR Part 138 and the Part 138 (Aerial Work Operations) Manual of Standards (MOS) addressed the certification, operational and safety risk management requirements for operators engaged in aerial work operations (CASA, 2021e). At the time of the accident, aerial work encompassed the core activities of external load operations, dispensing operations or task specialist operations.[13] Advisory circular AC 138-01 v1.0 Part 138 core concepts defined task specialist operations as:
carrying out a specialised activity using an aircraft in flight and includes training for such an activity. An example of a task specialist operation is a low level weed survey or pipeline inspection.
Additional guidance for aerial work operations applicable at the time of the accident was provided in advisory circular AC 138-05 v1.1 Aerial work risk management (July 2021b) and the Part 138 Acceptable means of compliance and guidance material – Aerial work operations v2.2 (December 2021f).
Conducting the survey flight
At interview, the HOFO described the accident task as an ad hoc type survey in which the helicopter would be flown up-valley and then down-valley to view both sides of the river and that the airspeed, direction and height was not prescribed. The HOFO expressed the view that the optimum profile for survey flights was a height of 300 ft and airspeed of 55 kt. However, if adopting that profile, it would make it impractical to identify English Broom weed in surveys of the Snowy River.
The HOFO reported that, from experience, they did not consider that it was unusual when the client presented with 4 NPWS officers for the conduct of the survey flight. In terms of managing client requests, all pilots are provided with a ‘stop work authority’ and can therefore decline a client request if they perceive a safety of flight issue.
The NPWS officers indicated that, on the morning of the accident flight, they discussed their English Broom weed survey plan while waiting for the pilot and helicopter to return from a prior task. After the pilot arrived, they completed the operator’s online induction and a safety brief with the pilot and then briefed the pilot on their plan for the weed survey.
None of the officers had previously met the pilot who they understood was new to the company and had not previously done the English Broom weed survey task with them. They reported that the pilot was operating in a cautious manner and appeared to be safety‑conscious, advising them all to speak-up if they identified any hazards during the flight. On departure, the pilot made a radio call to their NPWS contact for flight‑following purposes, and they conducted a hazard identification for wires during the flight upstream to the Guthega Power Station.
Persons permitted on board during aerial work operations
For aerial work operations conducted under Part 138, CASA advisory circular 138-01 specified that persons who were permitted on board must be categorised as either:
- crew members (including flight crew, air crew and task specialists)
- passengers that meet the requirement to be aerial work passengers.
The advisory circular further defined an air crew member, task specialist and aerial work passenger as:
Air crew member
An air crew member…includes crew members who carry out a function during the flight relating to the safety of the aircraft.
Task specialist
A task specialist … includes crew members who carry out a function for the flight relating to the aerial work operation (as distinct from a safety related role).
Examples of a task specialist would include a camera operator that operates an external camera pod, or an aerial shooter used in an animal culling operation.
A task specialist will require training to be inducted into the operation and to ensure they are competent in carrying out their assigned function as a member of the operator's crew.
Aerial work passenger
…are persons who are closely associated with the purpose of the aerial work operation. Their presence in the aircraft must not be for mere convenience or enjoyment.
Examples of such persons would include: Personnel involved in carrying out or supporting a mustering activity carried on a positioning flight before or after the mustering operation, such as ground based personnel to assist with refuelling or for opening and closing of gates etc. and yarding of stock for the mustering operation…
In most circumstances aerial work passengers do not require training before their carriage on an aerial work operation or a positioning flight, but they will in all cases (except for some notable situations, such as a person being rescued) require a safety briefing prior to the flight...
On the accident day, as the helicopter was being used to conduct a low-level weed survey activity, it met the definition of a task specialist operation. In terms of the roles as defined above, the pilot was the only flight crew member and there were no air crew members. The 3 NPWS officers with the roles of task coordinator and primary observers would be classed as task specialists. While the area ranger assisted with the task, they reported that they were on the flight as an opportunity for familiarisation of the survey area.
Operational hazards
CASA flight crew licencing uses a competency-based training and assessment system for pilots. Various competencies are required to be demonstrated by pilots during both initial and recurrent licence testing. The competencies vary by aircraft type and licence type.
For pilots to achieve their helicopter rating, they are required to demonstrate that they have the skills and underpinning knowledge to manage abnormal and emergency situations in helicopters (CASA, 2021c). The range of situations include, but are not limited to:
- key hazards – underpinning knowledge of their causal factors, contributing operational situations, avoidance and recognition of symptoms and recovery techniques that include:
- the impact of high gross weight and high-density altitude on key hazards
- techniques for how to avoid a potentially hazardous situation whilst in flight.
These competencies were consistent with the list of hazards detailed in the jointly developed CASA and Civil Aviation Authority of New Zealand helicopter flight instructor manual, issue 3 (CASA, 2012). The instructor manual differentiated hazards from emergencies, which are the technical failures particular to the helicopter model and addressed in the flight manual emergency procedures section.
To be licensed for low-level helicopter operations, pilots must demonstrate skills to safely conduct low‑level operations include managing variable terrain and weather, surface conditions, loose objects and personnel. The required underpinning knowledge related to critical operational conditions that included retreating blade stall,[17] vortex ring state, over pitching and loss of anti‑torque or tail rotor effectiveness (CASA, 2021c).
The ATSB reviewed the emergencies and hazards chapter of the FAA Helicopter Flying Handbook (2019) and found key operational hazards presented were the same as those that CASA required pilots to demonstrate. The FAA handbook provided a thorough description of each of the key hazards, which included techniques for avoidance and recovery. The FAA handbook also reported the following about LTE events:
Certain flight activities lend themselves to being more at high risk to LTE than others. For example, power line and pipeline patrol sectors, low-speed aerial filming/photography as well as in the Police and Helicopter Emergency Medical Services (EMS) environments can find themselves in low and slow situations over geographical areas where the exact wind speed and direction are hard to determine.
Loss of tail rotor effectiveness
Introduction
Loss of tail rotor effectiveness (LTE) or unanticipated yaw is a phenomenon that can occur in single main rotor, tail rotor-equipped helicopters. It is a condition that occurs when the air flow through a tail rotor is changed in some way, by altering the angle or speed at which the air passes through the rotating blades of the tail rotor disc (FAA, 2019). If uncorrected, LTE can result in loss of control of the helicopter and serious to fatal occupant injuries. In 1995, the FAA published advisory circular 90-95 Unanticipated right yaw in helicopters, which described a loss of tail rotor effectiveness as:
…a critical, low-speed aerodynamic flight characteristic which can result in an uncommanded rapid yaw rate which does not subside of its own accord and, if not corrected, can result in the loss of aircraft control.
Any manoeuvre which requires the pilot to operate in a high-power, low-airspeed environment with a left crosswind or tailwind creates an environment where unanticipated right yaw may occur.
LTE is not related to a maintenance malfunction and may occur in varying degrees in all single main rotor helicopters at airspeeds less than 30 knots.
Single-rotor helicopters manufactured in the US, such as the Bell 206, have main rotors that rotate anticlockwise when viewed from above. When powered, their rotation produces a torque reaction or tendency of the helicopter to turn in the opposite direction, which is a right yawing motion from the pilot’s view. The tail rotor thrust provides the anti‑torque control. An effective tail rotor relies on a stable and relatively undisturbed airflow in order to provide a steady and constant anti-torque reaction (FAA, 2019).
The FAA AC described 3 wind conditions conducive to the onset of LTE. One of these conditions refers to the relative wind[18] azimuth of 285° to 315°, which can produce ‘main rotor disc vortex interference’ with the tail rotor (Figure 8) and is described as:
As the main rotor vortex passes the tail rotor, the tail rotor angle of attack is reduced. The reduction in the angle of attack causes a reduction in thrust and a right yaw acceleration begins. The thrust reduction will occur suddenly and, if uncorrected, will develop into an uncontrollable rapid rotation about the [main rotor] mast.
The relative wind from the critical quadrant may present when the nose of the helicopter is pointing forward (Figure 8), or the condition is generated when the helicopter is flown with the nose sufficiently yawed to the right.
Figure 8: Main rotor disc vortex interference with tail rotor
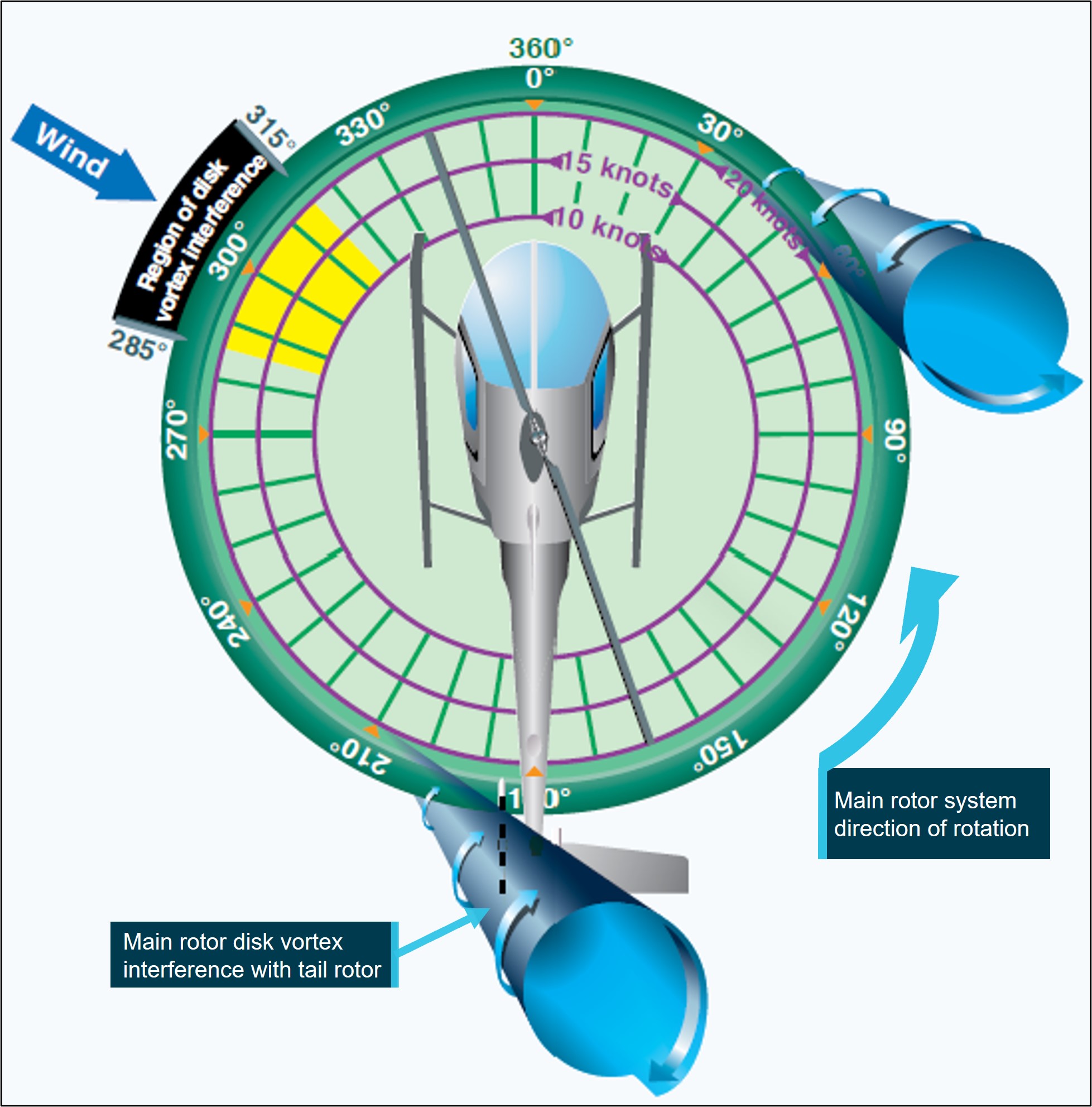
Source: FAA Helicopter Flying Handbook (FAA, 2019), annotated by the ATSB
Factors affecting loss of tail rotor effectiveness
Other than main rotor blade action affecting the quality of the airflow about the tail rotor disc and impacting its ability to provide useful thrust, additional factors are also considered when discussing LTE. According to the FAA Helicopter Flying Handbook (2019):
The design of main and tail rotor blades and the tailboom assembly can affect the characteristics and susceptibility of LTE but will not nullify the phenomenon entirely.
FAA AC 90-95 also identifies other factors that influence the severity of the onset of LTE including:
Gross Weight and Density Altitude. An increase in either of these factors will decrease the power margin between the maximum power available and the power required to hover. The pilot should conduct low-level, low-airspeed manoeuvres with minimum weight.
Recovery technique
The Bell 206L-1 rotorcraft flight manual revision 14 did not have an emergency procedure for LTE but did have a procedure for a complete loss of thrust under the heading tail rotor control failure, which was a mechanical failure. Following the procedure for a complete loss of thrust, pilots were to reduce the throttle to idle and immediately enter an autorotation while maintaining a minimum airspeed of 52 kt during the descent.
The FAA AC 90-95 recommended recovery technique from LTE was:
a. If a sudden unanticipated right yaw occurs, the pilot should perform the following:
(1) Apply full left pedal. Simultaneously, move cyclic[19] forward to increase speed. If altitude permits, reduce power.
(2) As recovery is effected, adjust controls for normal forward flight.
b. Collective[20] pitch reduction will aid in arresting the yaw rate but may cause an increase in the rate of descent. Any large, rapid increase in collective to prevent ground or obstacle contact may further increase the yaw rate and decrease rotor rpm.
c. The amount of collective reduction should be based on the height above obstructions or surface, gross weight of the aircraft, and the existing atmospheric conditions.
d. If the rotation cannot be stopped and ground contact is imminent, an autorotation may be the best course of action. The pilot should maintain full left pedal until rotation stops, then adjust to maintain heading.
Heli Surveys operations manual
The Heli Surveys Operations Manual volume 10 – Specialist operations, prescribed the operator’s general low flying requirements. Paragraph 0.7.3, under Conduct of flight during low flying stated the following:
Pilots shall be aware of recovery techniques and avoid flight configurations which could include:
• Vortex ring/ settling with power.
• Tail rotor vortex ring or loss of tail rotor effectiveness.
• Downwind operations outside the aircraft performance envelope.
• Loss of close visual cues to indicate actual aircraft relative movement and out of wind operations (particularly over water), leading to possible unanticipated control difficulties.
The operations manual did not include any avoidance or recovery procedures for LTE nor any reference material to address this condition.
Safety risk management
Aerial work risk management
Pre-operational risk assessment
CASR Part 138 required an operator conducting aerial work to undertake risk assessments of its operations. The Part 138 MOS and corresponding advisory circular (AC 138-05 v1.1) detailed a layered approach to risk assessments. One of the key requirements was that an operator should undertake an overarching assessment (pre‑operational risk assessment) to consider and evaluate the risks associated with its proposed operations, in this case, low-level helicopter survey. This assessment recognised the underlying principles of CASR Part 138, where the risks and hazards associated with a type of aerial work operation are common to that type of operation. The MOS indicated that the matters to be considered for such an assessment included:
• the operation and its particular characteristics
• the location of the operation and its particular characteristics
• the aircraft to be used in the operation, its particular characteristics, and its performance
• the qualifications and experience of the crew members to be used in the operation
• the hazards, external to the aircraft, that may be met in the course of the operation.
The operator is required to gather data for inclusion in the pre-operational risk assessment using a range of sources. Acknowledging that certain risk factors may be common to all operators, may be particular to the aircraft type operated or may be unique to the operator; potential sources include, but are not limited to (CASA, 2021b):
- CASA ‘sector risk profiles’ for the varying types of operations
- ATSB incident and accident reports
- industry association safety reports
- manufacturers' safety bulletins and advisory notices
- input from experienced pilots and other operators.
Once the pre-operational risk assessment has been populated, it should be updated over time to include lessons learnt from previous operations. It should also form part of the operator’s operations manual.
Flight risk management plan
The results of the pre-operational risk assessment were to be considered when preparing the flight risk management plan, which was specific to an individual flight or task within the type of operation. The plan should outline the specific mitigators or risk controls that were to be used during the flights.
Pre-flight risk review
The next step was for the pilot, on behalf of the operator, to conduct a pre-flight risk review, with reference to the pre‑operational risk assessment, flight risk management plan, and the most recent data for the operation. The review was to be completed prior to the commencement of the operation and was to consider the conditions and circumstances that existed at the site or area at the time of the proposed activities. This ensured that the operation could be conducted without unacceptable safety risk.
Operator risk management
As per CASR Part 138, Heli Surveys was required to undertake risk assessment and mitigation processes and include those processes in its suite of operational documents. The Heli Surveys Operations Manual described that the operator would address its risk management obligations via the use of Safe Work Method Statements (SWMS).
The Heli Surveys Safety Management Systems Manual further detailed how risk was identified, controlled and documented. Their safety risk management process started with hazard identification, which included internal sources and external sources. A hazard was defined in their SWMS as ‘what could result in harm’ and was used to describe both the hazard and associated risk.
Internal sources for hazard identification included, but were not limited to:
- safety assessments of systems and operations
- voluntary and mandatory safety reports
- inspections and audits.
Its list of external sources included, but was not limited to:
- accident and incident reports
- safety information bulletins, safety alerts and other safety publications from CASA, Airservices Australia, the ATSB and other authorities worldwide.
The operator had prepared SWMSs to comply with the CASR Part 138 requirements which was equivalent to a pre-operational risk assessment. As the accident flight was a low‑level survey operation in the Snowy Mountains, the 2 SWMS relevant to the flight were Low level surveys and aerial photography (henceforth referred to as Low-level surveys) and Alpine operations.
The SWMS documents provided the means to record the specific tasking event, the equipment and approvals that were relevant, and any specific checks or personal protective equipment required to perform the task. A risk matrix was also included. The risk matrix described the likelihood and consequence of each identified hazard and provided the means to assess the initial and residual risk level following the implementation of suitable risk controls.
The ATSB reviewed the SWMSs that were developed by the operator. A summary of the internal and external hazards that were identified by the operator are below (Table 1).
Table 1: Summary of hazards related to Safe Work Method Statements for low-level survey tasking and alpine operations
| Low-level survey hazards | Alpine operations hazards |
| intercom failure | adverse weather events |
| high communication workload/distraction | inadvertent flight into instrument meteorological conditions |
| loose articles exiting aircraft | collision with powerlines/aerials |
| collision with objects while airborne | heavy landing – exceeding power requirements |
| inadvertent flight into instrument meteorological conditions | exposure – inappropriate dress for conditions |
| restraint harness issues | |
| aircraft door issue | |
| turbulence/windshear |
The heavy landing hazard associated with the alpine operations SWMS was assessed by the ATSB to be related to the CASA flight crew licensing competency requirement to manage the hazard associated with overpitching. The SWMS provided some control measures, such as a power check, landing into wind and monitoring environmental conditions between a landing and take-off.
With the exception of the relationship between overpitching and the operator’s heavy landing hazard in its alpine operations SWMS, the ATSB did not find references to hazards associated with abnormal situations and emergencies specific to the operator’s unique activities in its SWMS. Of note, there was no reference to LTE and vortex ring state, and the impact of flight regimes and operations at high gross weights and density altitudes that may affect such hazards.
The operator reported that pilots were required to have read and understood the suite of SWMS documents, which were provided during their induction process and at scheduled intervals thereafter. However, there was no requirement for pilots to conduct a pre-flight risk review for low-level survey operations and reference the relevant SWMS when conducting pre-flight tasks in preparation for the activity. As such, the pilot had not conducted a review prior to the accident flight.
Client risk management
The NPWS (the client) had contracted Heli Surveys to conduct the weed survey operation. Its Aviation Safety Policy and related documents were provided to the ATSB. The policy identified a range of aviation operations that utilised rotary wing aircraft.
The policy adopted a risk management approach to aviation operations and safety. Key elements of the policy were the development and observance of aviation‑related standard operating procedures and the use of a job safety analysis (JSA).[21] The JSA assessed the risks associated with each task, which was equivalent to a flight risk management plan.
Regarding vegetation‑related activities that necessitated low-level flight operations, the NPWS provided several task-related JSA documents that identified specific hazards. The documents also detailed the control measures to be implemented to manage the associated risks. The JSA documents that were provided related to low-level flying in general, low-level flying when undertaking Scotch (English) Broom survey and aerial application (spraying) activities.
When engaging in those activities, a key control measure specified in the JSA advised that only ‘essential personnel’ were to be on board the operating helicopter. The NPWS reported that the suite of documents supporting aviation operations did not provide a definition of essential personnel nor was there a procedure on record that detailed the roles and responsibilities of NPWS personnel reflected in the JSA control measure.
Related occurrences
Loss of tail rotor effectiveness
Between 2013 and 2022, the ATSB received 16 notifications where the reporter advised of an LTE or unanticipated yaw event. Of the 16 notifications, 12 were investigated by the ATSB. Most of these resulted in nil to minor injuries to those involved and one serious injury and one fatality. Some of these investigations are described below.
ATSB investigation AO-2013-016
On 19 January 2013, a Bell 206B3 helicopter was being operated on an aerial filming task over hilly terrain on the north-eastern outskirts of Perth, Western Australia. After hovering and manoeuvring at about 500 ft above ground level to allow the camera operator to record footage of a truck accident, the pilot conducted a right orbit to complete filming and depart the area. The pilot had initiated the turn when the nose of the helicopter moved left, then suddenly and rapidly to the right as the helicopter yawed and developed a rotation of about 5 revolutions.
The ATSB found that, when the pilot turned to the right to commence the orbit, the helicopter was exposed to a crosswind from the left while at an airspeed around the 30 kt threshold value for susceptibility to LTE, precipitating an unanticipated right yaw and temporary loss of control. The pilot regained sufficient control for a forced landing.
ATSB investigation AO-2015-091
On 20 July 2015, the pilot of a Bell 206L3 (LongRanger) helicopter, registered VH-BLV, conducted a charter flight from Essendon Airport to Falls Creek, Victoria, with 5 passengers on board. The helicopter took off from Essendon close to its maximum take‑off weight.
When at 700 ft above ground level and tracking from the north-west, the pilot conducted a shallow approach towards the helipad at Falls Creek. As the helicopter descended to about 50 ft above ground level, the pilot found that significantly more power was required to conduct the approach than anticipated. The pilot assessed that there was insufficient power available to continue to land and elected to abort the approach. The pilot pushed forward on the cyclic to increase the helicopter’s airspeed and conducted a left turn.
As the helicopter turned left, it started to yaw rapidly towards the right. The pilot applied full left anti-torque pedal to counteract the yaw, but the helicopter continued to yaw. The helicopter turned through one and a half revolutions, as the pilot lowered the collective. Lowering the collective reduced the power demand of the power rotor system, thereby increasing the ability of the anti‑torque pedals to stop the right yaw. The combination of lowering collective and applying forward cyclic to gain forward airspeed, allowed the pilot to regain control of the helicopter. The pilot then conducted a left turn towards the helipad and made an approach to the helipad from an easterly direction. The helicopter landed following the second approach without further incident.
The ATSB’s report highlighted the importance for pilots to understand and avoid conditions that are conducive to unanticipated yaw or LTE and noted that pilots can reduce their exposure to LTE by maintaining awareness of the wind and its effect on the helicopter. Further, if a pilot encounters unanticipated yaw, quick application of the correct response is essential to recover control of the helicopter.
Carriage of additional personnel
ATSB investigation AO-2019-008
On 28 January 2019, the crew of a Sikorsky S-64E Skycrane helicopter was conducting firebombing activities when it collided with water at Woods Creek Dam, Victoria. The collision occurred following an approach to the dam to fill an external tank with water. The helicopter was crewed by 2 pilots, and a maintenance crew chief was also on board. Following the collision, all the occupants were able to exit the helicopter and swim to shore. One crewmember was seriously injured and 2 were uninjured. The helicopter was substantially damaged.
The ATSB found that the helicopter was placed in a steep flare, which contributed to the helicopter entering vortex ring state when on approach to the dam.
It was also noted that the operator’s operations manual stated that only flight crew and crew essential to the operation could be carried aboard the aircraft during firefighting operations. The operation could be conducted without the crew chief, and not all company crew chiefs were on board their aircraft during firefighting operations. While the crew chief had significant system and task knowledge, they were not required to be on board the helicopter.
On this occasion, their presence on board subjected them to the significant hazards associated with underwater egress. More generally, the carriage of additional personnel during specialised operations like firefighting exposes them to unnecessary risk.
ATSB investigation AO-2019-025
On 21 May 2019, while engaged in a planned cull of feral animals in Kakadu National Park, Northern Territory, a crew of 3 were using a Bell 206B3 JetRanger helicopter for aerial platform shooting. While the helicopter was operating at about 50 ft above the ground, the engine decelerated to idle, resulting in an immediate loss of power, and subsequent collision with terrain. The 3 occupants (pilot, shooter and spotter) were seriously injured.
The investigation identified that it was normal practice across industry that an aerial culling task was performed with just 2 persons on board the helicopter, the pilot and a shooter. Experienced aerial shooters interviewed after the accident expressed a preference for carrying just the pilot and shooter on board to reduce risk to crew, carry more fuel to improve endurance and to complete more work. In 2016, the aerial culling task was redesigned for 3 crew, including a spotter. There was no formal risk analysis of the inclusion of the spotter position, or consideration of the potential benefits of improved data collection when weighed against operational difficulties in recording data, reduced efficiencies in operation, and increased exposure of employees to risk.
The investigation identified that, given the increased complexity and risk in low-level operations, the number of crew should be kept to a minimum. That is, only personnel essential for conducting the task should be carried.
Safety analysis
Introduction
On the morning of 11 March 2022, a Bell B206L-1 helicopter, registered VH-BHF, departed Jindabyne aerodrome, New South Wales, to conduct a weed survey task on behalf of the National Parks and Wildlife Service (NPWS). On board were the pilot and 4 NPWS officers. While descending towards the riverbed in the vicinity of the Guthega power station, the helicopter started an uncommanded yaw to the right. The pilot was able to stop the yaw but was unable to arrest the descent before the helicopter collided with terrain. The helicopter was destroyed. Three occupants received serious injuries, and the remaining 2 occupants received minor injuries.
The following analysis will discuss the uncommanded yaw, and the carriage of persons on the flight. It will also consider the risk management practices of both the operator and its client and discuss the emergency response following notification of the accident.
Helicopter position
The weed survey task was a low-level, low-speed flight activity. On the accident flight, in addition to the pilot seated in the front right seat, there was an NPWS officer in the front left seat and 3 NPWS officers in the cabin area with 2 seated on the left of the helicopter. With 3 of the NPWS officers seated on the left, the pilot was asked if the helicopter could be flown sideways to provide the best view of the target vegetation for those officers. In response, the pilot yawed the helicopter about 45° to the right of their track. Forward flight with the helicopter yawed 45° to the right, in calm wind conditions, produced a relative wind opposite to the motion of the helicopter, from an angle of about 315°.
Weight and balance data indicated that with the 5 occupants on board, the helicopter was operating within 100 kg of its maximum all-up weight. It was also operating at a density altitude of about 4,500 ft. As weight and density altitude increase, the margin between the power available and power required for the flight is reduced. Further, the flight data identified that the groundspeed of the helicopter was below 25 kt and further reduced to less than 20 kt for several seconds prior to the uncommanded right yaw. As there was little wind, the airspeed was close to the recorded groundspeed.
As described by the United States Federal Aviation Administration in its Helicopter Flying Handbook and advisory circular 90-95, there are certain conditions that can change the air flow through a tail rotor, subsequently resulting in a loss of tail rotor effectiveness (LTE). In this case, the combination of a low speed and right yaw placed the helicopter inside the region of main rotor disc vortex interference with the tail rotor, a condition conducive to the onset of LTE. The severity of the onset of LTE was further influenced by the high gross weight and density altitude.
Contributing factor The sideways movement of the helicopter during the weed survey operation, combined with the high-density altitude, high gross weight, and low airspeed, were conditions conducive to the onset of a loss of tail rotor effectiveness. |
Loss of tail rotor effectiveness
The pilot’s description of flying the helicopter with a significant amount of right yaw at about 30 kt was consistent with the recorded data at the start of their run from the Guthega power station. However, the speed slowly decayed below 20 kt just prior to an uncommanded right yaw when the pilot applied some left anti-torque pedal to straighten the helicopter and improve their vision on their approach to the river below. After the helicopter started yawing to the right, the pilot identified a forced landing site in the river and rolled the throttle back to idle, which stopped the yawing motion. The cessation of the yawing motion when the engine power was reduced indicated the yaw was being driven by the reaction to the engine torque applied to the main gearbox and there was insufficient anti-torque to prevent it.
The ATSB determined that there was no evidence of a pre-existing mechanical issue, and the helicopter had the performance capability to operate at the altitude of the survey area. However, the helicopter was positioned in the region of main rotor disc vortex interference with the tail rotor just prior to the loss of control. As such, the ATSB concluded that the uncommanded right yaw was likely an LTE event.
At the time of the event, the helicopter was operating at about 150 ft above ground level in the avoid area of the height-velocity diagram, in addition to which, it was also outside the weight-density altitude limits for the height‑velocity diagram. Therefore, there was no assurance a safe forced landing with minimal damage and injuries could be achieved from the height that the autorotation was commenced.
Contributing factor It was likely that a loss of tail rotor effectiveness occurred at a height that was insufficient for the pilot to recover before the helicopter impacted the ground. |
Operator’s risk management
As a Part 138 operator, Heli Surveys was required to adopt a layered approach to risk management. This approach included conducting a pre-operational risk assessment, which considered all the generic risks and hazards common to the type of operation, in this case, low‑level survey. Heli Surveys achieved this requirement through the Safe Work Method Statements (SWMS).
To inform the pre-operational risk assessment, a range of internal and external data sources could be used that considered the risks common to all low-level survey operators, particular to the aircraft type operated, or unique to the operator. For example, for low-level helicopter operations this may include hazards such as a high-density altitude, retreating blade stall, LTE, vortex ring state and over pitching. Therefore, it was foreseeable that hazards influenced by the particular operating environment would be included in the operator’s SWMS for both Low-level surveys and Alpine operations.
The ATSB reviewed the SWMS accounting for the circumstances of the accident. The SWMS incorporated heavy landings, adverse weather events, collisions with obstacles and hazards associated with the carriage of passengers and task specialists. In consideration of the operation and activities, which included the carriage of passengers and task specialists, the hazards identified by the operator appeared to be relevant. However, their SWMS did not address LTE, although this was identified in its operations manual as a condition specific to low flying and is a known hazard as discussed by the Civil Aviation Safety Authority and the United States Federal Aviation Administration.
The English Broom weed survey operation was conducted at low level and low speed, which were conditions conducive to the onset of LTE. Therefore, and in establishing the context for the operation, LTE was relevant. However, while the risk of LTE was not considered in the SWMS, the accident pilot was familiar with LTE and indicated that it had been covered in their training at some point. As a result, the ATSB was unable to determine if having LTE identified in the SWMS would have influenced the accident outcome. That said, the absence of this consideration did not allow for formal mitigation strategies to be implemented, nor provide assurance that the risk level associated with LTE was as low as reasonably practical. Consequently, there was a reliance on the underpinning knowledge and operational experience of the individual pilot to manage the risk of LTE.
In addition, as a requirement for Part 138 operators, the pre-operational risk assessment, or in this case the SWMS, was to inform the pre-flight risk review. This review was to be performed by a pilot, on behalf of the operator, before a flight commenced. The operator reported that such a review was not conducted for its low-level survey operations nor was one performed by the accident pilot. The merits of this process would have provided the operator an opportunity to validate the SWMS against the proposed operation and allow pilots to determine that the operation could be conducted without unacceptable safety risk.
Documenting and detailing known hazards and the associated risk controls in a dedicated SWMS, reviewed pre-flight, would complement a pilot’s underpinning knowledge. In turn, this would raise immediate awareness of the possibility of encountering hazards such as LTE when conducting a low-level survey task. Further, the pre-flight risk review would provide the means for all the participants involved to consider these critical operational conditions and associated controls. This would complement the safety briefing provided by the pilot in conjunction with the NPWS officers as they prepared for the accident flight.
Other factor that increased risk The Heli Surveys safe work method statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre‑flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low-level survey operations were as low as reasonably practicable. (Safety issue) |
Helicopter occupants
There were 5 occupants on the helicopter, including the pilot. It was very likely that the weed survey could have been completed with just the NPWS coordinator in the front left seat and 2 officers in the left and right rear forward‑facing seats. As such, they would meet the criteria of a task specialist as described under Part 138. If not required as a task specialist, and excluding the pilot, all others on board would be regarded as aerial work passengers and would not be permitted. As such, it was likely that the additional NPWS officer on board (the area ranger) was not fulfilling the role of a task specialist. The additional person’s presence appeared to be motivated by opportunity, and while it was acknowledged that they could contribute as a survey team member, their involvement was not essential to a successful task outcome.
Given the nature of the task and the operating conditions under which it was being conducted, the inclusion of personnel who were not essential to fulfilling the task outcomes exposed them to the risks of low-level helicopter flight and, in the event of an accident or incident, potential injury. On this occasion, the occupant who did not have a specific role to perform, for either the spotting or logging activity, was seriously injured in the accident when operating at low level with limited landing options available due to the surrounding terrain.
Contributing factor The carriage of an additional person on board the helicopter who was not essential to the tasking, exposed them to risks associated with low flying operations over inhospitable terrain. |
Client’s risk management
The client (NPWS) arranged for the survey flight to be undertaken, and its officers presented at Jindabyne to board the helicopter on the appointed day. Risk assessments covering low-level flying operations and weed survey tasks in the form of a job safety analysis were on record, and a key risk control measure advised that only essential personnel were to be on board. However, no definition of essential personnel was available to potentially limit the number of persons that would be exposed to the identified risks. Defining essential personnel would also support informed distinctions between those who would appropriately fulfil roles as task specialists and those who were aerial work passengers.
Further, the procedure and roles of the persons conducting the survey were not documented. This likely allowed a degree of discretion to be applied by the participants, which resulted in others participating alongside task specialist(s) whose presence may, on occasion, be unnecessary. For example, for this accident one of the NPWS officers who did not have a specific role received serious injuries.
The client was also engaged in other activities such as aerial spraying and culling, both of which likely involved helicopter operations at low level. Having a definition of essential personnel and documenting their respective roles and responsibilities as task specialists would provide the necessary information for determining who should be involved. This would potentially confine the numbers to the minimum required to conduct the task thereby minimising risk exposure.
Contributing factor The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities. (Safety issue) |
Accident notification
The helicopter was equipped with a fixed emergency locator transmitter and an electronic flight tracking device (TracPlus), which provided active monitoring of the helicopter’s position. Additionally, a personal locator beacon and a satellite phone were carried on board as part of the operator’s survival kit.
Within a very short time of the accident occurring there were reports of the helicopter's fixed emergency locator transmitter activating, the TracPlus unit transmitting the helicopter’s last recorded position and manual activation of a personal locator beacon. The multiple reports removed any doubt of a spurious transmission from any of the units and, as a result, the operator and emergency services were able to respond with minimal delay.
The timely alerts also provided the means for the power station to be alerted to the presence of injured persons on the riverbank who required urgent medical assistance. Their recovery would likely have been impacted by an increase in water level and provided the opportunity for decisions to be made regarding water discharge into the river via the power station.
The extraction of the damaged helicopter from the Snowy River was also influenced following advice of water storage buildup and possible uncontrolled discharge from the Guthega Dam spillway. The early notification likely provided sufficient time to plan for and safely airlift the helicopter wreckage from the river for detailed examination and removed a potential environmental issue.
Other finding The activation of the on-board emergency locator transmitter and a flight monitoring device, and manual activation of a personal locator beacon, resulted in an immediate emergency response. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Bell 206L-1, VH-BHF, 20 km north-west of Jindabyne, New South Wales, on 11 March 2022.
Contributing factors
- The sideways movement of the helicopter during the weed survey operation, combined with the high-density altitude, high gross weight, and low airspeed, were conditions conducive to the onset of a loss of tail rotor effectiveness.
- It was likely that a loss of tail rotor effectiveness occurred at a height that was insufficient for the pilot to recover before the helicopter impacted the ground.
- The carriage of an additional person on board the helicopter who was not essential to the tasking, exposed them to risks associated with low flying operations.
- The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities. (Safety issue)
Other factors that increased risk
- The Heli Surveys safe work method statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre‑flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low-level survey operations were as low as reasonably practicable. (Safety issue)
Other findings
- The activation of the on-board emergency locator transmitter and a flight monitoring device, and manual activation of a personal locator beacon, resulted in an immediate emergency response.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Operator's risk assessment
Safety issue number: AO-2022-012-SI-01
Safety issue description: The Heli Surveys Safe Work Method Statements for low-level survey and alpine operations did not identify the operational factors that could affect the control of the helicopter. There was also no requirement for its pilots to conduct a pre-flight risk review for low-level survey operations. Combined, this limited the operator’s ability to manage the possibility of loss of tail rotor effectiveness and ensure that the risks associated with low‑level survey operations were as low as reasonably practicable.
Client’s risk assessment
Safety issue number: AO-2022-012-SI-02
Safety issue description: The New South Wales National Parks and Wildlife Service operating procedures referred to, but did not define, ‘essential personnel’, or specify their roles and responsibilities as task specialists when performing aerial work activities.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action taken by Heli Surveys
In addition to the safety action detailed above, Heli Surveys has revised its risk register detailing both flight-based and ground‑based threats in its operations and associated risk controls. It has also introduced a ‘Hazardous Flight Conditions’ ground-based course that was proactively developed in response to this accident. The intent of the course was to refamiliarize pilots with such conditions (for example, loss of tail rotor effectiveness) to ensure currency and assist with informed decision‑making and is to be completed every 12 months. The flying aspects discussed in the course will be covered in operator proficiency checks.
Additionally, Heli Surveys has defined ‘essential crew’ in its operations manual. It has also added a requirement that, prior to flight, the pilot in command is to confirm that when undertaking Part 138 operations, all persons on board are deemed essential and each person has a relevant and specific task.
Glossary
| AC | Advisory circular |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| ELT | Emergency locator transmitter |
| FAA | Federal Aviation Administration (United States) |
| HOFO | Head of flying operations |
| JSA | Job safety analysis |
| LTE | Loss of tail rotor effectiveness |
| NPWS | National Parks and Wildlife Service |
| MOS | Manual of Standards |
| PLB | Personal locator beacon |
| SWMS | Safe Work Method Statement |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot
- New South Wales National Parks and Wildlife Service officers
- Heli Surveys Pty Ltd
- New South Wales National Parks and Wildlife Service
- Bureau of Meteorology
- Civil Aviation Safety Authority
- New South Wales Police Force
- recorded data – TracPlus unit.
References
ATSB. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents (AR-2012-128). Australian Transport Safety Bureau, Canberra, ACT, Australia.
CASA. (2012). Helicopter Flight Instructor Manual, Issue 3. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021a). Advisory Circular: Part 138 core concepts (AC 138-01 V1.0). Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021b). Advisory Circular: Aerial work risk management (AC 138-05 V1.1). Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021c). Part 61 Manual of Standards Instrument 2014. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021d). Part 91 (General Operating and Flight Rules) Manual of Standards 2020. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021e). Part 138 (Aerial Work Operations) Manual of Standards 2020. Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2021f). Acceptable means of compliance and guidance material, (Aerial work operations - Part 138 of CASR). Civil Aviation Safety Authority, Canberra, ACT, Australia.
CASA. (2023). Multi-part Advisory Circular: AC 91-30, AC 121-12, AC 133-03 and AC 135-14 V1.0, Emergency locator transmitters. Civil Aviation Safety Authority, Canberra, ACT, Australia.
FAA. (1995). Advisory Circular: Unanticipated right yaw in helicopters (AC 90-95). U.S. Department of Transportation, Federal Aviation Administration, Washington, D.C., USA.
FAA. (2019). Helicopter Flying Handbook (FAA-H-8083-21B). U.S. Department of Transportation, Federal Aviation Administration, Oklahoma City, OK, USA.
NSW Government. (2023). Scotch broom, www.environment.nsw.gov.au accessed July 2024.
NTSB. (2017). Safety Alert SA-062: Loss of tail rotor effectiveness in helicopters. National Transportation Safety Board, Washington, D.C. USA.
Weeds Australia. (2019). Broom, English Broom, Scotch Broom, Common Broom, Scottish Broom, Spanish Broom, www.weeds.org.au accessed July 2024.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot of the accident flight
- Heli Surveys Pty Ltd
- National Parks and Wildlife Service officers
- National Parks and Wildlife Service
- Civil Aviation Safety Authority
- Transportation Safety Board of Canada.
Submissions to the report were received from the following parties:
- Civil Aviation Safety Authority
- Heli Surveys Pty Ltd
- National Parks and Wildlife Service
- National Parks and Wildlife Service officers.
The submissions were reviewed and where appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] English Broom: also known as Broom, Scotch Broom, Common Broom or Spanish Broom and is a highly invasive, environmental weed of national significance that favours cooler, higher rainfall regions.
[2] Officers: denotes NPWS personnel and their job titles and includes officers, rangers and other staff members.
[3] Anti-torque control pedals: a primary helicopter flight control that changes the pitch of tail rotor blades to control thrust around the yaw axis. Acts to counterbalance the main rotor torque reaction and provides heading control in the hover and balanced flight when the helicopter is in forward motion.
[4] Yaw: the motion of an aircraft about its vertical or normal axis.
[5] Autorotation: a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[6] The operator reported that, as the registered owner of the beacons, the Australian Maritime Safety Authority contacted the nominated person and the head of flying operations was subsequently advised of the beacon activations.
[7] Visual flight rules: a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[8] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
[9] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[10] The force needed to accelerate a mass. G-force is normally expressed in multiples of gravitational acceleration (normal gravity = 1g).
[11] For flight operations at low airspeeds, there is a negligible difference between calibrated and indicated airspeed.
[12] The height-velocity diagram shows the combinations of indicated airspeed and height above the ground which will allow an average pilot to successfully complete a landing after an engine failure. By carefully studying the height-velocity diagram a pilot can avoid the combinations of altitude and airspeed that may not allow sufficient time or altitude to enter a stabilised autorotative descent (FAA, 2019).
[13] As of July 2025, the carriage of fireground personnel was also classified as an aerial work operation core activity.
[14] Vortex ring state describes an aerodynamic condition where a helicopter may be in a vertical descent with 20% up to maximum power applied, and little or no climb performance (FAA, 2019).
[15] Overpitching occurs when collective pitch is increased to a point where the main rotor blade angle of attack creates so much drag that all available engine power cannot maintain or restore normal operational revolutions per minute (ICAO, 2024).
[16] When a helicopter is hovering, some of the air passing through the main rotor disc is recirculated back into the disc from the top. This phenomenon is common to all airfoils and is known as tip vortices. As long as the tip vortices are small, their only effect is a small loss in rotor efficiency. However, operating in close proximity to obstructions can lead to an increase in recirculation and loss of performance (FAA, 2019).
[17] In forward flight, the relative airflow through the main rotor disc is different on the advancing and retreating side of the rotor blades. The relative airflow over the advancing side is higher due to the forward speed of the helicopter, while the relative airflow on the retreating side is lower. To generate the same amount of lift across the rotor disc, the advancing blade flaps up while the retreating blade flaps down. This causes the angle of attack to increase on the retreating blade, which increases lift. At some point, as forward speed increases, the low blade speed on the retreating blade, and its high angle of attack will result in a stall and loss of lift (FAA, 2019).
[18] Relative wind: the airflow relative to an aerofoil created by movement of an aerofoil through the air.
[19] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[20] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[21] Job safety analysis: a form of risk assessment that details, step-by-step, how a task is to be performed safely.
Occurrence summary
| Investigation number | AO-2022-012 |
|---|---|
| Occurrence date | 11/03/2022 |
| Location | 20 km north-west of Jindabyne |
| State | New South Wales |
| Report release date | 22/12/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Loss of control |
| Occurrence class | Accident |
| Highest injury level | Serious |
Aircraft details
| Manufacturer | Bell Helicopter Co |
|---|---|
| Model | 206L-1 |
| Registration | VH-BHF |
| Serial number | 45164 |
| Aircraft operator | Heli Surveys Pty Ltd |
| Sector | Helicopter |
| Operation type | Aerial Work |
| Departure point | Jindabyne aerodrome, New South Wales |
| Destination | Jindabyne aerodrome, New South Wales |
| Damage | Destroyed |