The ATSB is investigating an engine fuel starvation event involving a Piper PA-32R-301, registered VH-LPW, about 9 km south of Bacchus Marsh Aerodrome, Victoria, on 1 May 2026.
While in cruise at 8,000 ft during a flight from Stawell Airport, Victoria, to Essendon Airport, the engine began running roughly. The pilot actioned emergency procedures including switching fuel tanks and diverted the aircraft to Bacchus Marsh where the aircraft landed without further incident. The investigation is continuing.
The ATSB has commenced the examination and analysis of the initial evidence collected.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-076
Occurrence date
01/05/2026
Occurrence time and timezone
06:16 UTC
Location
About 9 km south of Bacchus Marsh Aerodrome
State
Victoria
Report status
Pending
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Engine failure or malfunction, Fuel starvation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-32R-301
Registration
VH-LPW
Serial number
32R-8113095
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Own business travel
The ATSB is investigating a fuel starvation event involving a Piper PA-32, VH-JFC, near Rottnest Island Airport, Western Australia, on 1 May 2026.
Shortly after take-off, at an altitude of about 1,000 ft, the pilot detected a partial power loss and elected to return to Rottnest Island Airport. The pilot reported initiating troubleshooting checks, which included activating the fuel pump and selecting the right fuel tank. Engine power was restored and the pilot proceeded to land on runway 27 at Rottnest Island Airport.
The evidence collection phase of the investigation will involve:
interviewing involved parties
retrieving and reviewing recorded data
collection of other relevant information.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-075
Occurrence date
01/05/2026
Occurrence time and timezone
16:30 Australian Western Standard Time
Location
Near Rottnest Island
State
Western Australia
Report status
Pending
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Engine failure or malfunction, Fuel starvation
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-32-260
Registration
VH-JFC
Serial number
32-7100025
Aircraft operator
Wadjemup Aerial Service Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
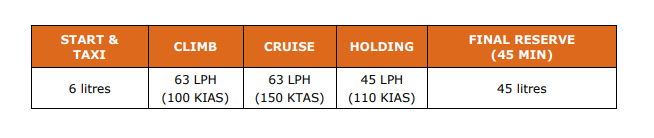
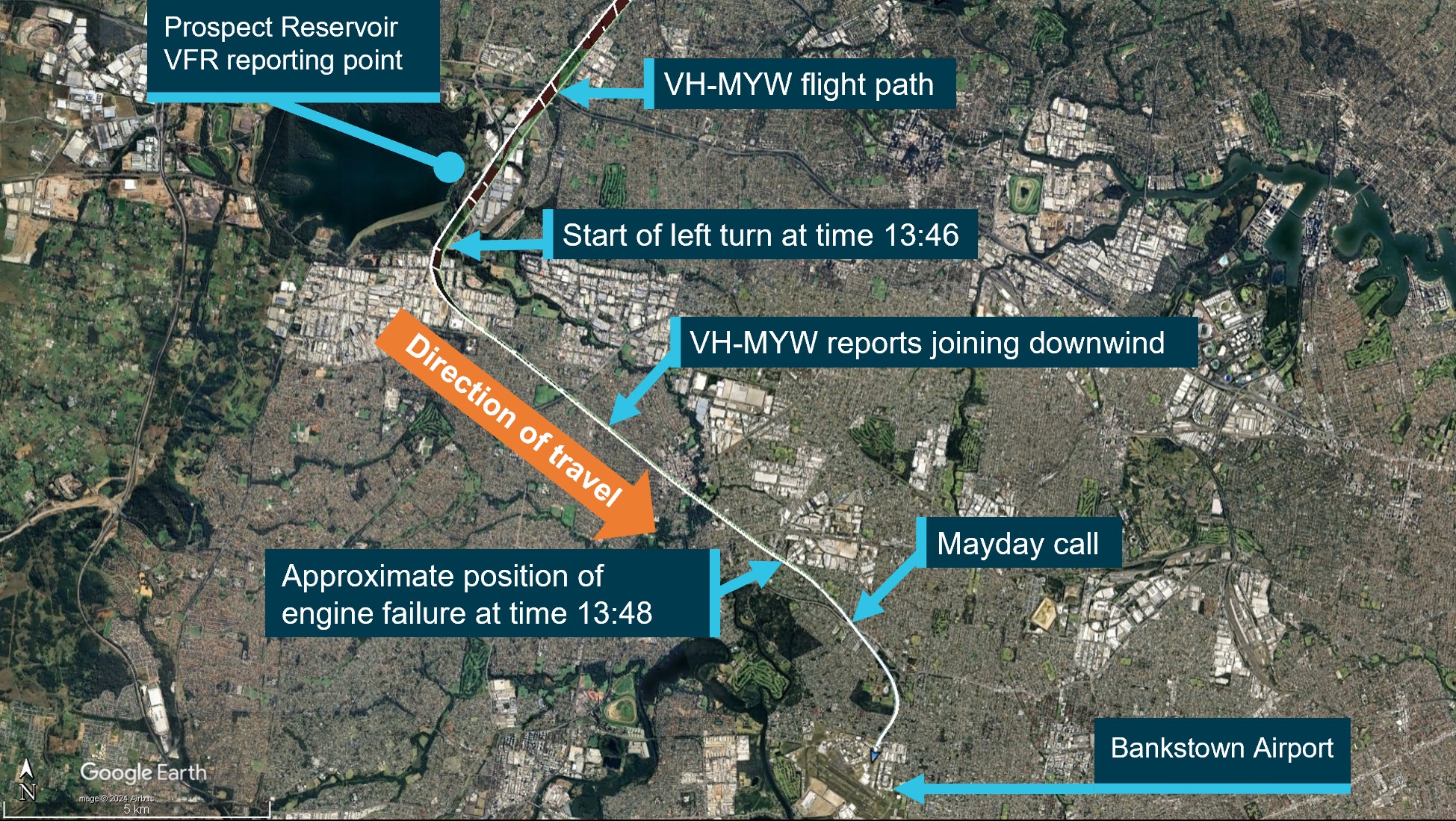
On the evening of 8 September 2025, a Cessna T210M, registered VH-LLM, was conducting night take-offs and landings at Darwin Airport, Northern Territory. On board was an instructor from a training organisation and a student who was doing their first night training flight and owned the aircraft. After completing several take-offs and landings, the instructor directed the student to conduct a go-around. Shortly after turning downwind, the aircraft lost power. The student handed control of the aircraft to the instructor and made a MAYDAY call.
The instructor initiated troubleshooting checks and determined that the fuel selector was set on the right tank and was likely empty. The instructor activated the electric fuel pump before selecting the left tank which restored engine power and the aircraft was recovered into a climb. The student resumed control and proceeded to land safely at Darwin Airport.
What the ATSB found
Fuel was not selected to the fullest tank during multiple circuits resulting in a loss of power.
The student did not effectively conduct the pre-landing checks to monitor the fuel state of the aircraft. This was likely due to an increased workload during their first night flight in controlled airspace. In addition, the configuration of the primary flight display was changed to show airport maps, resulting in a smaller fuel gauges display in a different location, unfamiliar to the student.
The instructor had identified that the student had not changed tanks during previous circuits (a requirement to land on the fullest tank) and had intended to discuss this. However, the instructor later became focused on monitoring the student’s performance and forgot to brief the student on changing to the fuller tank.
In addition, before the flights, the student did not visually inspect the quantity of fuel on board the aircraft prior to departure and relied on the instructor’s recollection the aircraft had adequate fuel for the training session.
Safety message
Fuel starvation occurrences can often be prevented by conducting thorough pre-flight fuel quantity checks combined with in‑flight fuel management.
Although pre-landing checks are routine, they must never become perfunctory. Pilots must understand the purpose behind each check, ensuring the aircraft is properly configured for landing according to the aircraft guidance.
Pilots are reminded to independently visually check fuel quantities prior to departure and use a known calibrated instrument such as a dipstick in addition to fuel gauge readings.
Pilots should familiarise themselves with the Civil Aviation Safety Authority, Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in‑flight fuel management.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the evening of 8 September 2025, a Cessna T210M, registered VH-LLM, was being used to conduct night visual flight rules (NVFR) training circuits[1] at Darwin Airport, Northern Territory. The student was a licensed pilot who owned VH-LLM, and also on board was an instructor from the training organisation, Flight Standards.
The day before the flight, the student refuelled the aircraft to capacity and flew it from Emkaytee aerodrome, Northern Territory, to Darwin Airport. On the morning of the training session, the instructor, who had not previously flown a turbo Cessna 210, took the aircraft for a familiarisation flight, accompanied by Flight Standards’ chief flying instructor. The student reported that they had given permission for the flight but were unaware of the route taken or the amount of fuel used.
The instructor recalled dipping the fuel tanks after completing the familiarisation flight that morning, recording a total of about 55 L in the left tank and 75 L in the right tank. The instructor assessed that the total remaining fuel quantity was sufficient for the planned night circuit training session.
The student arrived at the airport at about 1800 local time[2] and conducted a pre-flight check with the instructor. The student asked whether there was sufficient fuel in the aircraft for the flight and received confirmation from the instructor that there was sufficient fuel. Subsequently, no visual inspection of the aircraft fuel quantity was carried out by the student.
For the flight, the student occupied the left seat with the primary flight display (PFD) directly in front of them and the instructor sat on the right. The student reported noticing that the instructor had altered the configuration of the PFD from their normal set up of engine instruments, to a split screen with a map of Darwin Airport taxiways on the right of the screen.
As this was the student’s first night flight the instructor reported spending additional time briefing the student on night circuits after engine start, which included aircraft lighting and other general information for night flying, before the student conducted engine run-ups at about 1914. During this time, the fuel selector was positioned on the left tank.
The aircraft pilot operating handbook (POH)[3], as well as the training organisation’s flight crew operating manual (FCOM), stated that it was a requirement to take off and land on the fullest tank. The student reported that at the beginning of the flight, this was the right tank. Before handing control to the instructor to demonstrate the first circuit, the student switched from the left to the right tank.
After completing the demonstration, while on the runway, the instructor briefed the student on the focus of the next circuit before the student took control from the left seat.
At about 1952, on completion of the student’s first landing, the instructor noticed that the student had conducted the pre-landing fuel check using a non-standard mnemonic checklist and identified that the student did not turn on the landing lights and that the flaps were not at the correct position. The student did not change the fuel selector from the right tank. As the instructor believed there was more fuel in the right tank at that time, they were comfortable with the student’s actions and did not direct them to change tanks before continuing with the next circuit. The instructor reported they debriefed the student on checklist discipline.
The fuel selector was not changed on the student’s second or third circuit. The instructor noted that the student’s use of a mnemonic checklist was not completely effective in ensuring that the actions in the checklist were completed for landing. In particular, this included that the student’s checklist did not cover the challenge/response to the fuel check as per the POH to ensure that the fuel selector was set to the fullest tank. The student reported their increased concentration on flying the aircraft at night detracted from monitoring the fuel gauge in the altered position. The instructor reported they had planned to request the tanks be changed on the next downwind leg.
At about 2030, during the student’s fourth circuit, the instructor directed the student to conduct a go-around[4] while on the final approach due to an aircraft behind them. The instructor recalled that the go-around was not completed proficiently and mentally noted to brief the student at the next opportunity to change the fuel selector to the left tank.
At 2032:57, recorded data showed that the right fuel tank indicated zero fuel before conducting the go-around, but the aircraft engine continued running using fuel in the lines and header tank (Figure 1).
At 2037:32, after turning onto the downwind circuit leg, the engine began to lose power and, realising that a return to the airport was not achievable, the student handed control to the instructor. The instructor conducted troubleshooting while the student declared an emergency to air traffic control (ATC).
The instructor identified that the aircraft fuel selector was positioned on the right fuel tank and realised that the tank, which had not been changed since beginning the circuits, was likely empty. They followed the POH procedure to change tanks, activated the auxiliary fuel pump and changed the fuel selector to the left tank. This restored engine power and they initiated a climb. The aircraft was at 600 ft above ground level at this time, and the crew heard an alert from ATC. The student responded and cancelled the emergency with the tower.
Once established in the climb, the student assumed control, recovered the aircraft back into the circuit and landed safely at Darwin Airport without further incident.
Post-flight inspection by maintenance personnel reported no mechanical defects with the aircraft fuel system or engine.
Figure 1: Graphical depiction of the occurrence circuit
Source: Google Earth, annotated by the ATSB
Context
Pilot information
Instructor
The instructor attained their Commercial Pilot Licence (Aeroplane) in 2021 with class ratings for single and multi-engine aircraft. They completed their Grade 2 instructor qualifications in December 2024. They held an NVFR endorsement and had a total of about 1,270 flying hours, of which about 800 hours were instructional. The instructor reported that at the time of the occurrence they had accrued 27.6 hours of night flight experience. Their most recent night flying activity prior to the occurrence was a flight instructor rating flight test conducted on 28 July 2025. The instructor was subsequently approved by the operator to carry out instructional flights at night, and the occurrence flight was the first instance of this.
The instructor had about 70 hours experience in non‑turbocharged models of Cessna 210 aircraft. The instructor held a current Class 1 medical certificate.
They reported sleeping for 8 hours the night before the occurrence and identified that they had slept for about 4 hours that afternoon. They reported their level of alertness as a ‘3‑ Okay somewhat fresh’ on a scale of 1–7 where, 1 is fully alert and 7 is completely exhausted.
Student
The student held a Private Pilot Licence (PPL) for a single‑engine aeroplane issued in 2018, held a current Class 1 medical certificate and had a total experience of about 412 hours of which 123.5 hours were completed in VH-LLM. They had completed 2 NVFR training sessions in the Flight Standards’ simulator prior to the occurrence. The student had flown day VFR for several years and wished to obtain a NVFR endorsement along with practice in procedures for Class C controlled airspace.
The student reported having a normal amount of sleep the night before and following their usual routine of breakfast and a light lunch. They worked a busy but uneventful day from about 0800 before arriving at the airport for the lesson at 1800. The student indicated they were fully alert on a scale of 1–7, where 1 is fully alert and 7 is completely exhausted.
Aircraft information
The aircraft was a Cessna Aircraft Company T210M, 6‑seat, high-wing aircraft manufactured in 1977. It was powered by a Teledyne Continental Motors Inc TSIO-520 turbocharged, fuel‑injected piston engine driving a 3-bladed, constant-speed McCauley propeller. The cockpit consisted of side-by-side seating for the pilot/student on the left and instructor/passenger on the right. The aircraft was initially registered on 6 June 1989 and then transferred to the current owner on 27 March 2023.
Glass cockpit
The cockpit of VH-LLM had been retrofitted with a customisable Garmin G3X suite (GI 275) glass cockpit.[5] The student reported that on the night of the training session the instructor had changed the screen from the configuration that the student was previously used to. This included a change to the location of the fuel gauge which was positioned at the far left of the screen rather than on the right (Figure 2).
Figure 2: Photograph of VH-LLM Garmin G3X screen configuration changes
Source: Aircraft owner, annotated by the ATSB
The instructor reported that there were no audio or visual fuel‑related alerts associated with low fuel quantities or reminders to switch the fuel tank selection in the display. The instructor reported that the location of the fuel gauge was difficult to see from their seat position on the right-side of the aircraft.
Both the student and instructor reported that the fuel gauge was less visually prominent in the new screen configuration and more difficult to monitor.
Fuel
The Cessna 210 fuel system consists of 2 main fuel tanks, 1 in each wing. Each tank has a capacity of 171 L, of which 169 L is usable. The fuel selector valve had 3 positions – left, right and off. Fuel could only be drawn from either the left or right tank during normal operations. The fuel system has an engine-driven fuel pump and an electrically‑driven auxiliary fuel pump. The pilot operating handbook (POH) stated:
If it is desired to completely exhaust a fuel tank quantity in flight, the auxiliary fuel pump will be needed to assist in restarting the engine when fuel exhaustion occurs.
The POH stated that a final 45 L reserve fuel should be available for operations. The chief pilot observed that 47 L remained in the left tank after landing.
Training organisation’s procedures for flight planning and fuel usage
The instructor reported that the training organisation’s fuel management guidance for circuit operations stated that circuit flights must plan to land with greater than final fuel reserve.[6]
The training organisation’s FCOM for the Cessna 210 (Section 2.5) stated that it was a requirement to take off and land on the fullest tank, with guidance in Section 7.1 stating:
For take-off and the first 30 minutes of flight, the fullest tank is selected and then tanks are cycled every 60 minutes thereafter, with the fullest tank selected for landing.
Section 5.3 provided typical fuel usage guidance in a table for fuel planning purposes (Figure 3).
Figure 3: Table provided for fuel management from the operator’s Cessna 210 FCOM
Source: Operator
The instructor commented that they were aware that the turbocharged 210 model had a slightly higher fuel burn, but they considered the amount of fuel available as adequate for the planned training session.
Meteorological information
The weather forecast for Darwin Airport indicated good flying conditions with no significant weather, no cloud below 5,000 ft, and visibility greater than 10 km. The automated observation at Darwin Airport for 2030 reported no cloud detected, visibility greater than 10 km, north‑easterly winds at 5 kt, temperature of 27°C and no rainfall.
Airport information
Darwin Airport is a joint civil and military facility. It services domestic and international air traffic and has 2 runways. The airport has an elevation of 103 ft above mean sea level (AMSL). The control tower provides a Class C controlled airspace around the airport, while outside of this area is class G uncontrolled airspace.
Recorded information
Flight data
The Garmin G3X avionics suite recorded to a secure digital (SD) card which was analysed by the ATSB (Figure 4).
Recorded data indicated that during the last circuit, the aircraft had descended from about 1,200 ft to 479 ft AMSL before then climbing.
Figure 4: Data obtained from the VH-LLM Garmin G3X SD card
Source: ATSB
Fuel data
The recorded fuel data identified that fuel from the right tank had been fully used at 2032:57, prior to commencement of the go-around. Due to the residual fuel in the system and header tanks, the engine power loss occurred about 5 minutes later at 2037:32. After conducting engine troubleshooting, the power was restored at 2038:11.
Fuel starvation
Fuel starvation refers to where the fuel supply to the engine is interrupted, although adequate fuel remains on board the aircraft. Fuel exhaustion refers to where the aircraft has depleted all useable fuel.
An ATSB study Avoidable Accidents No. 5 Starved and exhausted: Fuel management aviation accidents (AR-2011-112) regarding fuel starvation accidents found that in addition to accurate knowledge of fuel quantity at the start of a flight, the risks for fuel starvation are increased when pilots forget to change tanks during periods of low workload, or when pilots forget to select the appropriate tank prior to the approach to land. Although tank selection for approach and landing is often specified in the aircraft flight manual, following this procedure will only be successful if the pilot has also ensured that there is sufficient fuel in the required tank for landing.
Cognitive resources
Cognitive ability is a finite resource to pilots, and the limit of its availability plays a role in determining how effectively a pilot maintains adequate performance. Workload is a term used to describe the ‘cost’ for a human to fulfil certain task requirements. This cost can be reflected in the depletion of cognitive resources, the inability to conduct additional activities, emotional stress, fatigue or decreased performance (de Souza Borges and others, 2023). Workload and performance are intricately related as task demands are actively managed through resource allocation and strategy change (Loft and others, 2023).
An intention to perform a task at some future time is known as a prospective task. Prospective memory involves remembering, and sometimes forgetting, to perform tasks that must be deferred (Dismukes, 2010; Harrison and others, 2014).
In aviation, individuals typically must manage several concurrent tasks and consequently are often forced to postpone or interrupt tasks and attempt to remember to perform the deferred tasks later. A significant issue in prospective memory is not retention of the content of intentions, but retrieval of those intentions at the appropriate moment, which is often vulnerable to failure. Typically, if queried after forgetting to perform an action, an individual can recall what they intended to do.
Related occurrences
Fuel starvation occurrences highlight the critical importance of proper fuel management and pre‑flight planning. Fuel management and fuel starvation incidents and accidents have regularly occurred with single and twin-engine aircraft. Examples of other similar ATSB investigations include:
Fuel starvation and forced landing involving Piper PA-28, VH-BDB, 15 km west‑south‑west of Bankstown Airport, New South Wales, on 19 September 2017 (AO‑2017‑094).
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040).
Fuel starvation and forced landing involving Pilatus Britten-Norman Islander BN2A, VH‑WQA, Moa Island, Queensland, on 3 October 2022 (AO-2022-046)
Fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023 (AO-2023-017).
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021).
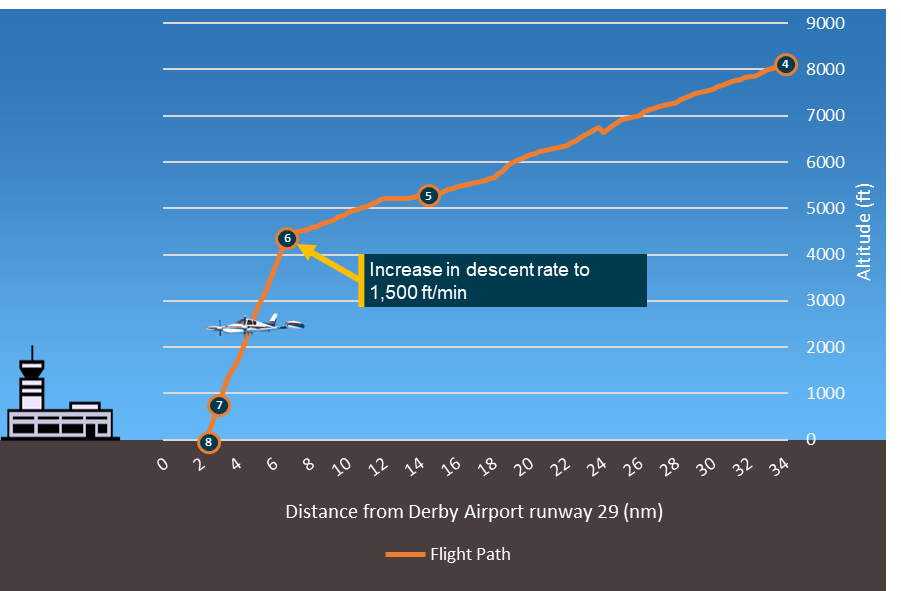
Fuel starvation and forced landing involving Cessna 310R, VH-DAW, about 5 km south-east of Derby Airport, Western Australia, on 20 June 2023 (AO-2023-029).
Fuel starvation involving Cessna T210M, VH-MYW, 4 km north-west of Bankstown Airport, New South Wales, on 26 May 2024 (AO-2024-033).
Safety analysis
The flight crew of VH-LLM experienced a loss of engine power during a night training flight. The instructor took command of the aircraft and quickly diagnosed that the fuel selector was on the right-wing tank and had not been changed for the duration of the circuits. The instructor activated the electric fuel pump and changed to the left tank which restored fuel and engine power to the aircraft.
This analysis will look at the use of appropriate checklists and the management of fuel prior to and during flight.
Fuel management
Student
The student did not visually verify the fuel quantity in the aircraft when conducting pre‑flight checks, instead they relied on the instructor’s confirmation that the aircraft had sufficient fuel on board but without informing the student how much fuel was in each of the tanks.
The student reported not monitoring the fuel gauge (which had been relocated on the primary flight display) due to the screen configuration change from the display that they normally used. Although the student used a mnemonic for pre-landing checks which included the fuel, the check was not completed with the required response that the fuel selector was set to the fullest tank in accordance with the pilot operating handbook.
In addition, the student reported the fuel gauge checks were a consequence of their need to concentrate on flying the aircraft in the night environment. Night flying increases cognitive and perceptual workload due to the decreased visual cues, the requirement for increased instrument monitoring and the risk of spatial disorientation (Biernacki and others, 2024). Further, this was the first time operating at night in controlled airspace for the student. The additional workload likely limited the student’s capacity for systematic visual scanning of cockpit instruments.
Instructor
The instructor reported noticing the student not switching tanks for the first circuit but was satisfied with the student’s decision as the tank in use was the fullest tank at that point. The instructor intended to monitor this on further landings and brief the requirement if it continued. However, during subsequent circuits, their focus shifted to monitoring the student’s performance and other demands such as other aircraft and the execution of the go-around.
As this was the instructor’s first instructional flight at night, this would have increased the demands on their ability to effectively monitor all aspects of the flight and student. The focus on monitoring other aspects of the student’s performance led them to forget to brief the student on switching to the fullest fuel tank as they had intended. Research on attention (Harrison and others, 2014) indicates that demands of competing tasks can narrow attention to the task perceived as most important at the time, reducing the likelihood of recalling or completing other intended actions.
The instructor reported that their ability to monitor the fuel status was influenced by their restricted view of the fuel gauge which was not clearly visible during a normal visual scan.
Missed opportunities by the crew to effectively monitor the fuel status led to fuel starvation and engine power loss beyond glide range of the airport. This increased the risk of having to conduct an off airfield forced landing at night.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation event involving Cessna T210M, VH-LLM, near Darwin Airport, Northern Territory, on 8 September 2025.
Contributing factor
Fuel was not selected to the fullest tank at all during multiple circuits resulting in a loss of power.
The student did not effectively conduct the pre-landing checks to monitor the fuel state of the aircraft, likely due to an increased workload during their first night flight in controlled airspace and the change in configuration of the primary flight display.
The instructor identified that student had not changed tanks during previous circuits however became focused on monitoring the student’s performance and did not brief the student on changing to the fuller tank.
Other factors that increased risk
The student did not conduct a visual check of the fuel quantity prior to departure, relying instead on the instructor’s recollection of sufficient fuel being available.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Biernacki, M. P., & Lewkowicz, R. (2024). The role of visual conditions and aircraft type on different aspects of pilot workload. Applied Ergonomics, 118, 104268.
de Souza Borges, S. F., de Morais, P., Bovo, M. G., Castilho, D. S., & Junior, M. M. C. (2023). Evaluation of workload for operators in the aeronautical sector. Proceedings of the 33rd European Safety and Reliability Conference (ESREL 2023) Edited by Mário P. Brito, Terje Aven, Piero Baraldi, Marko Čepin and Enrico Zio
Dismukes, R. K. (2010). Remembrance of things future: Prospective memory in laboratory, workplace, and everyday settings. Reviews of human factors and ergonomics, 6(1), 79-122.
Loft, S., Tatasciore, M., & Visser, T. (2023). Managing workload, performance, and situation awareness in aviation systems. In Human factors in aviation and aerospace (pp. 171-197). Academic Press.
Harrison, T. L., Mullet, H. G., Whiffen, K. N., Ousterhout, H., & Einstein, G. O. (2014). Prospective memory: Effects of divided attention on spontaneous retrieval. Memory & Cognition, 42(2), 212-224.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the instructor
the student
the operator
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
the instructor
the student
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Circuit: a standard flight path that aircraft follow when taking off and landing at an airfield, ensuring safe and orderly aircraft management.
[2]Local time was Australian Central Standard Time (ASCT) which is Coordinated Universal Time (UTC) + 9.30 hours.
[3]Pilot Operating Handbook: contains specific information about a particular aircraft, such as the equipment installed and weight and balance information. Manufacturers are required to include the serial number and registration on the title page to identify the aircraft to which the manual belongs
[4]Go-around: a manoeuvre where a landing approach is discontinued followed by a climb for another approach.
[5]The term ‘glass cockpit’ refers to a flat panel LCD display system that replaces the conventional analogue flight instruments in an aircraft. In this system primary flight information is presented on one or more integrated electronic flight displays.
[6]Usable fuel to reach the destination and then fly for at least 45 minutes after, at normal cruising power.
Occurrence summary
Investigation number
AO-2025-054
Occurrence date
08/09/2025
Location
Near Darwin Airport
State
Northern Territory
Report release date
28/01/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Fuel starvation
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
T210M
Registration
VH-LLM
Serial number
21061937
Aircraft operator
Howard Springs Veterinary Clinic Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
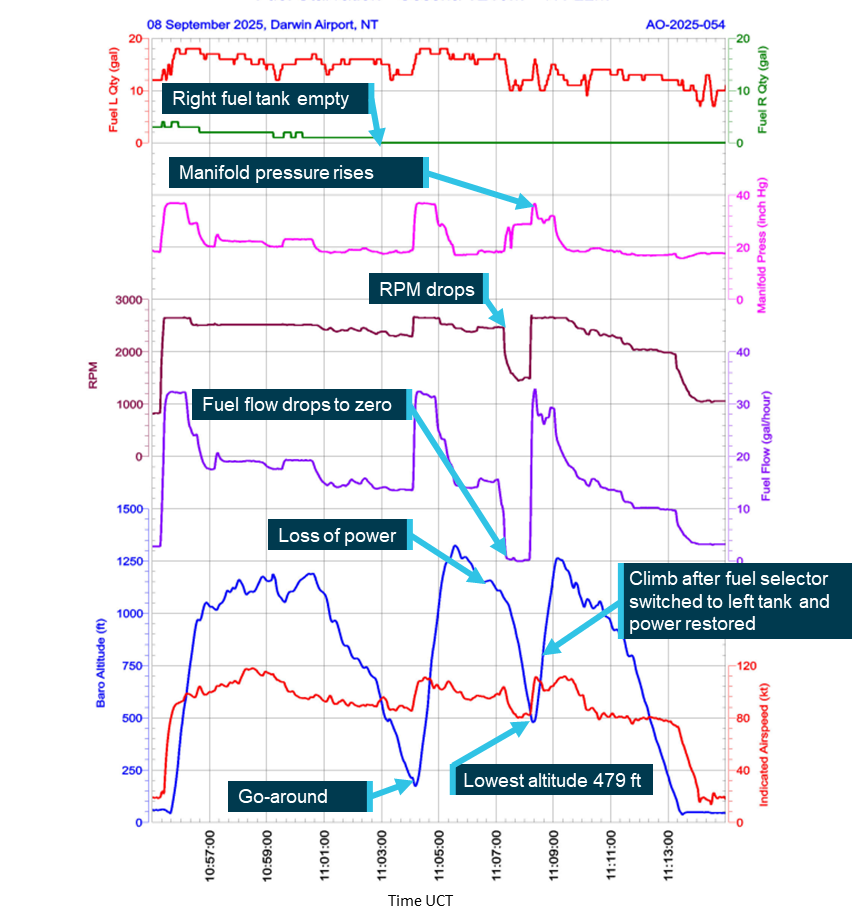
On 31 May 2025 at around 12:50 EST, the pilot of an amateur‑built Van’s RV-8 aircraft was carrying out a documented flight test program to qualify the aircraft for a Special Certificate of Airworthiness in the Experimental category. The flight was being operated in the vicinity of the Jervis Bay Aerodrome, Jervis Bay Territory, when the pilot reported that during a level turn, preparing for an accelerated stall test at approximately 3,500 ft AMSL, the engine lost all power and failed. After attempts at restarting the engine were unsuccessful, the pilot was able to configure the aircraft for a glide approach and safe landing on runway 15 at Jervis Bay.
The RV‑8 aircraft was fitted with a Textron Lycoming IO‑360‑M1B four‑cylinder fuel‑injected aeronautical engine. Inspections carried out on the engine and systems after the failure identified a loose and leaking fuel connection between the fuel/air control unit (fuel servo) and the fuel manifold valve (Figure 1). A loss of integrity of the fuel line at this point would result in the engine being starved of fuel and the power loss as sustained.
The pilot reported that since the engine’s assembly in 2023 there had been no maintenance or other activity around the fuel supply connection – leading to the conclusion that the leaking fitting may have been inadequately fastened at that time.
Figure 1: IO-360 fuel system - diagrammatical illustration
An ATSB research report Amateur-built aircraft Part 2: Analysis of accidents involving VH-registered non-factory-built aeroplanes 1988-2010found that across this period, amateur‑built aircraft had an accident rate that was 3 times higher than comparable factory‑built certified aircraft conducting similar flight operations. Further, over half of the accidents were precipitated by partial or complete engine failures – these being significantly more common when compared with factory‑built aircraft.
Considering these findings, this well‑managed safety occurrence provides a direct reminder, to all pilots and crew of sports and general aviation aircraft, of the importance of being prepared for an unexpected partial or complete loss of power during any phase of flight. In this instance, the pilot’s operation at an altitude and position in respect of the Jervis Bay Airport provided some assurance of the ability to conduct a safe unpowered descent and landing after the engine failure occurred.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-024
Occurrence date
31/05/2025
Location
Near Jervis Bay Airport
State
Australian Capital Territory
Occurrence class
Serious Incident
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Fuel systems
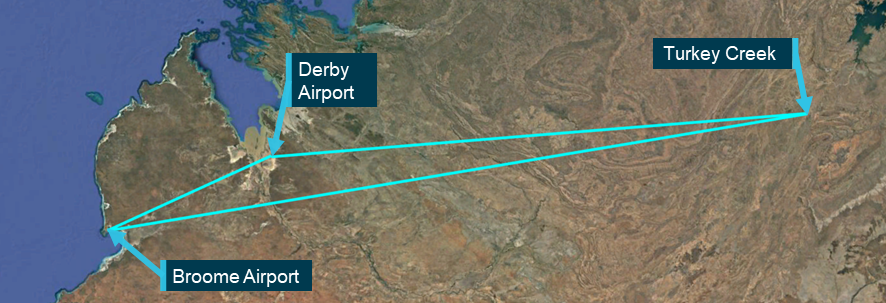
On the morning of 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg return passenger transport operation from Geraldton Airport via Carnarvon Airport and Meekatharra Airport, Western Australia. After refuelling in Carnarvon, VH-PGO departed for Meekatharra with the pilot and 2 passengers on board.
The flight was being conducted under instrument flight rules. During the instrument approach to Meekatharra, the right low fuel flow warning light illuminated. Shortly after, the right boost pump inoperative warning illuminated, and the right engine commenced surging with associated aircraft yaw. The pilot performed the engine failure checks, feathered the propeller, and continued the approach. The aircraft landed without further incident.
What the ATSB found
The ATSB found that the pilot did not check that the fuel caps were secured after refuelling, as required by the pilot’s operating handbook and company procedures. This resulted in the aircraft departing with the right inboard fuel cap incorrectly secured. The incorrectly secured fuel cap led to fuel siphoning overboard in flight. Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in the fuel tank quantity gauge overreading its contents.
The ATSB also found that the pilot was unaware of the actions to be taken on illumination of the right low fuel flow warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Additionally, the ATSB found that Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light.
What has been done as a result
Following the occurrence, Shine Aviation reminded company pilots of the significance of the PA-31 low fuel flow warning and associated procedures. The operator also revised its training programs to strengthen coverage of abnormal and emergency scenarios, with particular emphasis on fuel system management. This included increasing the number of questions in the PA-31 theory examination. In addition, the general competency training syllabus was updated to expand instruction on fuel loading and verification processes, in‑flight fuel management practices, and aircraft type-specific emergency procedures, including detailed guidance on PA-31 annunciator panel warning lights and their operational significance.
Following a repeat incorrect cap fitment in October 2025, Shine Aviation elected to replace the fuel cap as a precaution, with no further incidents reported.
Safety message
An unsecured or incorrectly installed fuel cap can result in significant fuel loss in-flight, potentially leading to an abnormal or emergency situation. Checks of fuel system security including fuel caps should be conducted by the pilot during pre-flight, turnarounds and after refuelling to ensure correct fitment. Fuel cells will collapse if tanks are not sufficiently vented when in use; a collapsed fuel cell can result in a fuel quantity gauge overreading and providing a false indication to the pilot.
Civil Aviation Safety Regulations require pilots to be competent to the standards specified for the aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures. An awareness and understanding of cautions, warnings, and limitations contained in the pilot’s operating handbook enables pilots to identify and respond to any problems that may arise, prior to them escalating further. In this case, had the pilot taken the documented action in response to the warning, it would have prevented an emergency situation arising. However, when the engine stopped during approach while in cloud, the pilot took immediate action to feather the propeller and ensure a safe landing.
Operators also play an important role in pilots achieving the competency requirements. This includes ensuring pilots receive comprehensive training that develops and reinforces aircraft specific system knowledge, particularly regarding manufacturer warnings and cautions, and decision-making skills.
CASA Advisory Circular 91-25 Fuel and oil safety provides advice and guidance on procedures and practices to ensure the safety of fuelling operations. Included in this guidance are recommendations associated with fuel caps and vents to prevent in‑flight fuel loss and starvation.
The occurrence
On 5 June 2025, the pilot of a Piper Chieftain PA-31-350, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg passenger transport operation under the instrument flight rules.1 At 0650 local time, the aircraft departed Geraldton Airport, Western Australia (WA), with the pilot and 3 passengers on board, and all 4 fuel tanks full – left and right, inboard and outboard. Stops were planned at Carnarvon and Meekatharra, WA, where the pilot planned to refuel, before a return flight to Geraldton (Figure 1).
Figure 1: Flight path of VH-PGO
Source: Google Earth, annotated by the ATSB
At 0817, the aircraft landed at Carnarvon Airport. The pilot then escorted the 3 passengers to the terminal building, where one passenger left the airport. The pilot returned to the aircraft to supervise refuelling and conduct a post-flight, external visual inspection of the aircraft. The local fuel supplier, on the pilot’s request, filled VH-PGO to full and then replaced the fuel caps on all 4 tanks. The refueller informed the pilot that a total of 240 L had been added to the aircraft. The pilot calculated, from the previous flight’s fuel usage, that the total fuel on board was now 688 L, which was consistent with full fuel tanks. The pilot recalled that they visually inspected but did not physically check the fuel caps for security after refuelling, and that all fuel cap latches appeared ‘down’ and in the ‘locked’ position.
The pilot assisted the 2 remaining passengers to board the aircraft, removed the chocks and then boarded the aircraft. As the pilot climbed onto the left wing to enter the aircraft, they reported giving the fuel caps ‘one last look’ and noted that they appeared correctly installed.
At 0851, VH-PGO departed Carnarvon Airport. The pilot selected the inboard fuel tanks for departure as per company and the pilot’s operating handbook (POH)2 procedures. The aircraft climbed to 9,000 ft above mean sea level (AMSL), where the pilot selected the outboard fuel tanks for the cruise to Meekatharra. At that time, the pilot calculated a fuel total of 636 L, using the onboard digital fuel flow indicator (see the section titled Fuel flow indicators). The fuel consisted of a combined 348 L in the inboard tanks and 288 L in the outboard fuel tanks. The pilot recalled that the fuel quantity gauges were indicating expected fuel quantities and fuel flow to both engines was stable throughout the take-off, climb, and into the cruise phase of flight.
During the cruise, the pilot obtained the weather at Meekatharra Airport via the aerodrome weather information service3 over VHF radio. The pilot noted that the wind was from 210° at 10 kt, cloud was overcast with a base of 800 ft above ground level (AGL), and visibility was 25 km, with no significant weather present. Based on this information, the pilot planned to conduct a landing on runway 27.4
The pilot selected the inboard tanks prior to the top of descent, in accordance with procedures. The pilot noted that the fuel quantity indication for the right inboard fuel tank was reading slightly lower than the left gauge but reported that they considered it ‘within an acceptable discrepancy for the PA-31’. The pilot calculated that 348 L remained in the inboard tanks and 118 L of fuel remained in the outboard tanks, totalling 466 L of fuel remaining on board.
The pilot descended the aircraft to 1,700 ft AGL and levelled off in accordance with the instrument approach procedure, before commencing the final approach to runway 09 with the intention of conducting a circling approach to runway 27. During this segment the R LOW FUEL FLOW warning light illuminated on the annunciator panel (see Figure 2 and the section titled Fuel system).
Figure 2: Right low fuel flow annunciator illumination during approach to Meekatharra
Source: Pilot, annotated by the ATSB
The pilot scanned the engine indications and noted they were normal, with no discrepancies between the engines. The pilot reported observing that the left and right fuel flow gauges were stable and indicating similar values, the fuel pumps were selected on, the engine mixtures were set to full rich, and the fuel boost pump circuit breakers were in and not tripped. The pilot also checked the fuel quantity gauges and stated that, while they did not recall the exact readings, nothing appeared abnormal or suggested that a tank was empty. The pilot continued the approach to Meekatharra. On the final approach segment, the aircraft entered instrument meteorological conditions (IMC).5 After entering IMC, the R FUEL BOOST INOP warning light (see the section titled Fuel system) illuminated, followed by the right engine surging and associated aircraft yaw.
The pilot conducted their memory item initial engine failure checks and feathered the right propeller. At this time, the aircraft exited IMC and was about 800 ft AGL. The pilot elected to abandon the planned circling approach to land on runway 27 and instead accepted a 5 kt tail wind to conduct a straight-in approach to runway 09, landing without further incident.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) and an instrument rating. The pilot also held a class 1 aviation medical certificate, valid until February 2026. At the time of the occurrence, the pilot had a total flying time of 1,381 hours, with 104 hours on the PA‑31 aircraft type. The pilot had flown 47.8 hours in the last 90 days which included 45.4 hours on PA‑31 aircraft.
The pilot commenced work with the operator in January 2025 and since then, had flown approximately 250 hours, including 220 hours in multi-engine aeroplanes, prior to the occurrence.
Aircraft information
General information
VH-PGO was a Piper Aircraft Corporation PA‑313‑50, twin‑engine, 10‑seat aircraft manufactured in the United States in 1978 and first registered in June 1979. The aircraft was powered by 2 Textron Lycoming engines: a TIO‑540‑J2BD on the left and an LTIO‑540‑J2BD on the right, each driving a Hartzell 3‑bladed constant speed propeller.
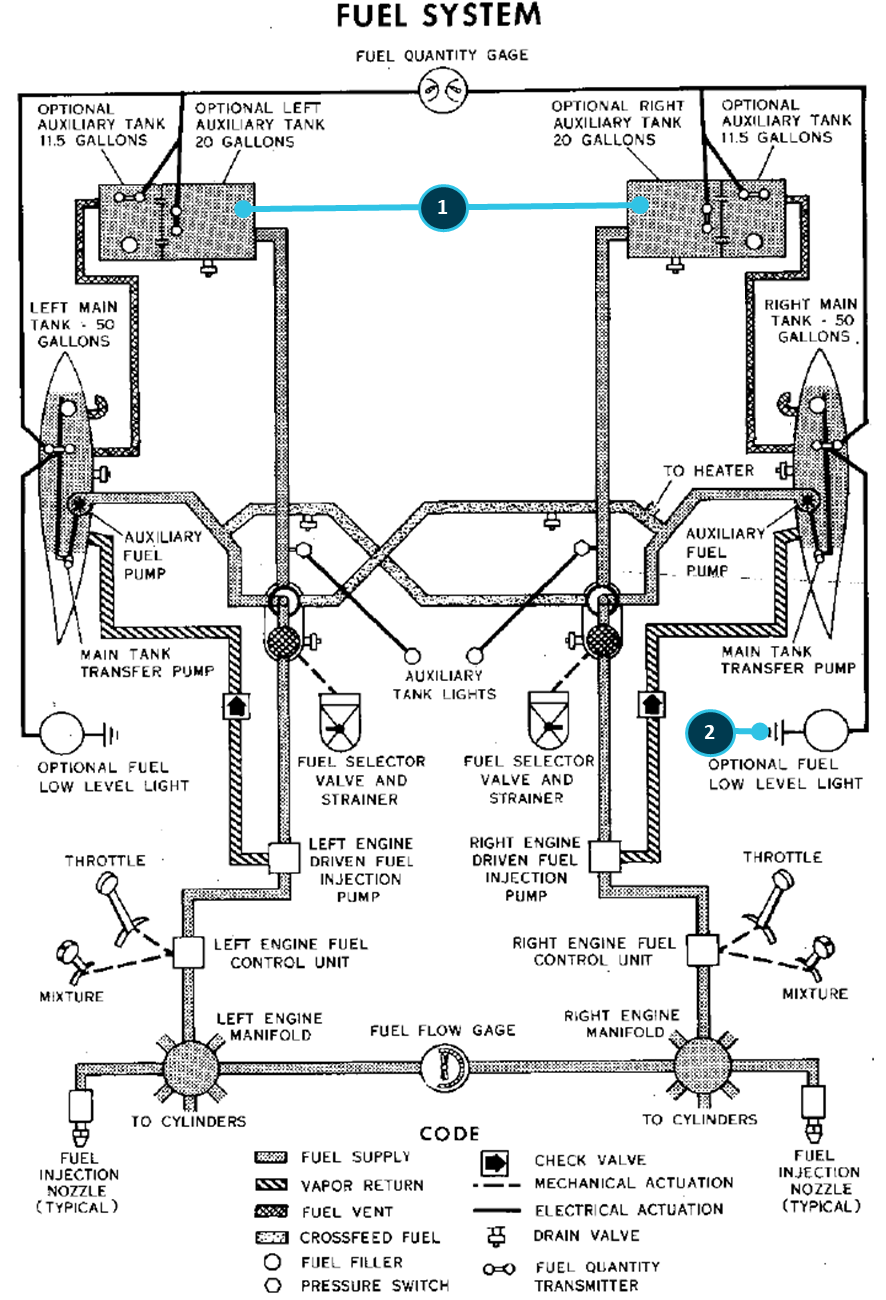
Fuel system
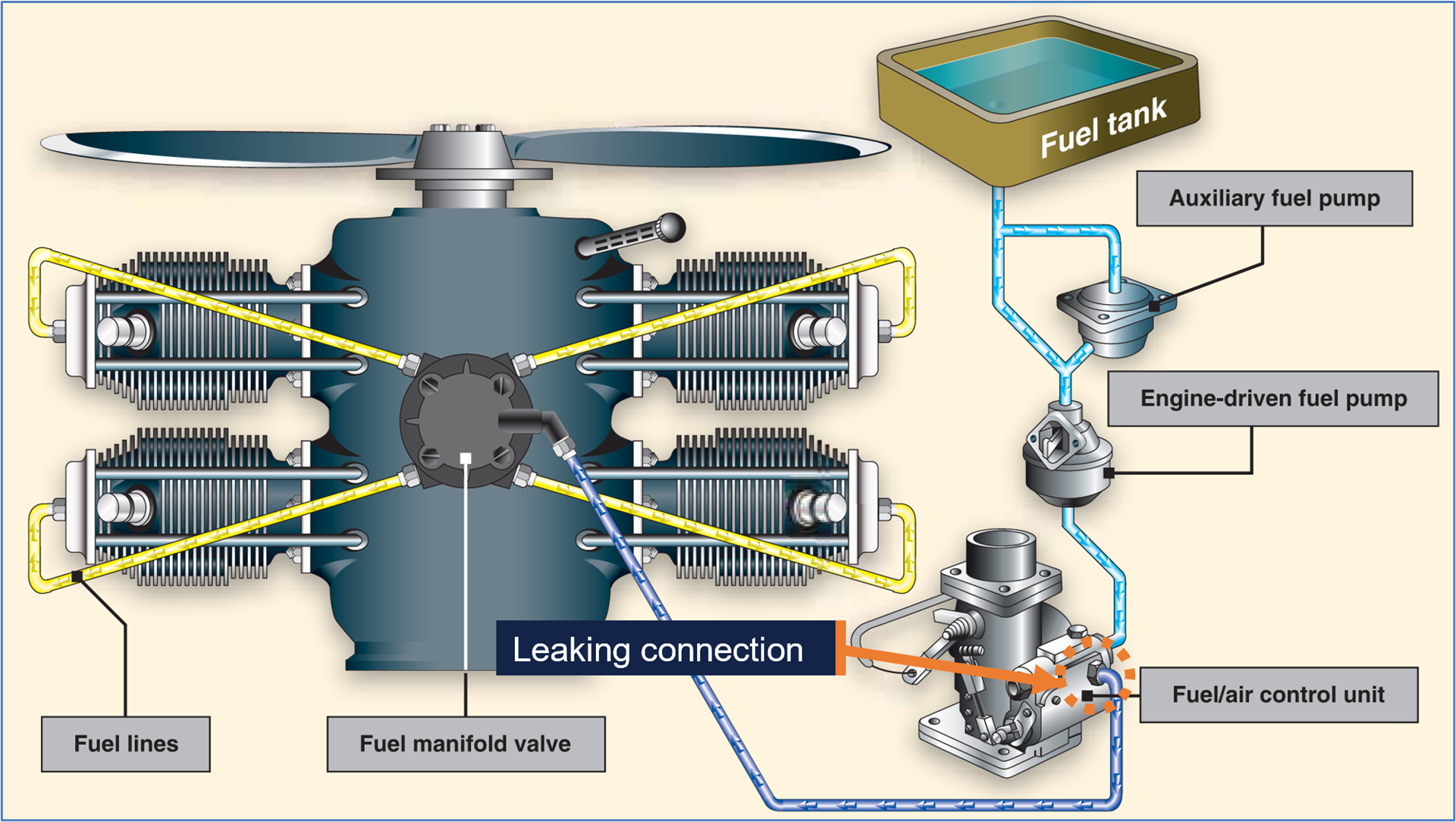
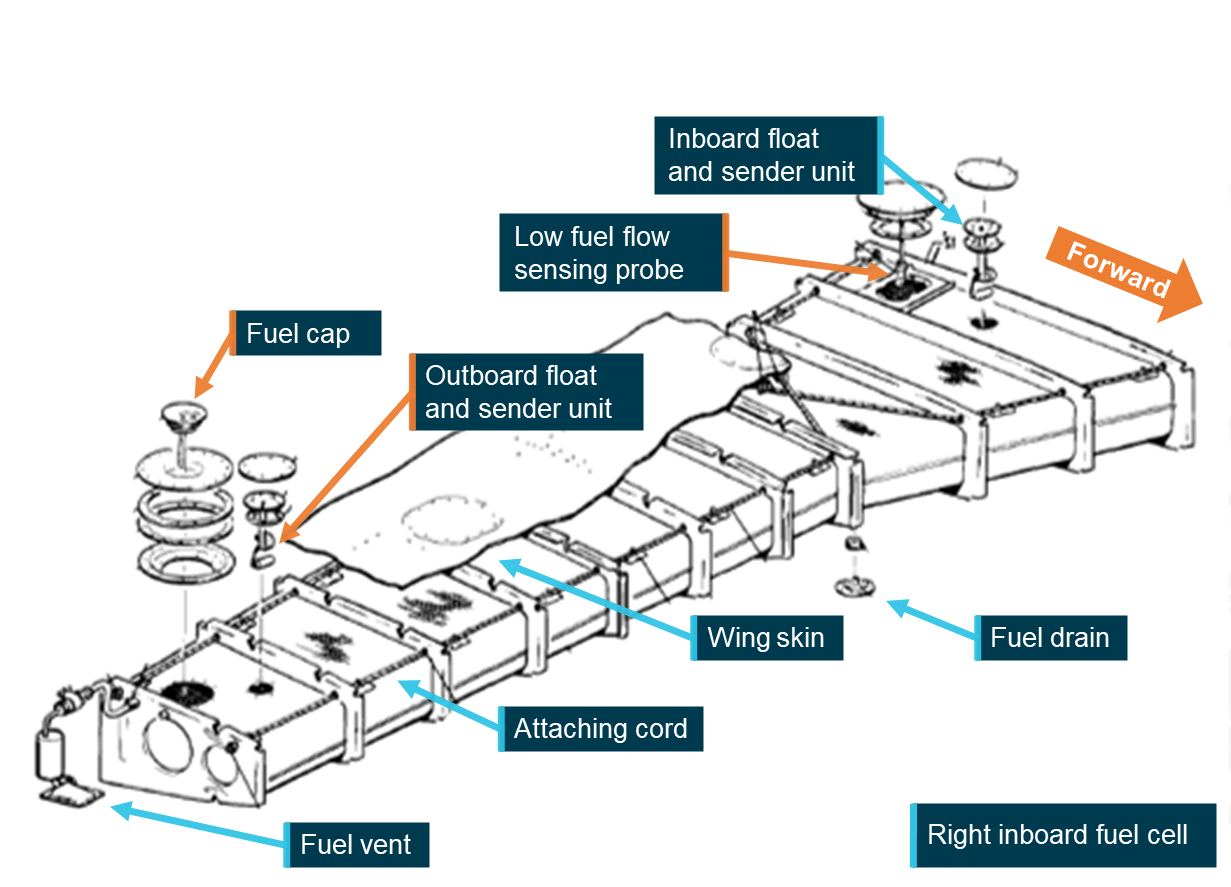
In PA-31 aircraft, fuel is stored in 4 flexible fuel cells, 2 in each wing. The fuel cell is attached to the upper inside of the wing by a cord running around the top section of the cell (Figure 3). The inboard cells hold 212 L each and the outboard cells hold 151 L each, totalling 726 L, of which 689 L are usable fuel.6
Figure 3: Right inboard fuel cell
Source: Operator, annotated by the ATSB
A fuel vent is located on each cell and is designed to maintain each tank at atmospheric pressure by allowing air to enter the tanks as fuel is consumed and as fuel volume changes with temperature and altitude. This is designed to prevent the development of a vacuum in the tanks and ensures a continuous and reliable supply of fuel to the engines. The vent also provides for slight positive pressure in flight. A restriction or blockage of the vent system can result in reduced fuel flow and fuel starvation despite usable fuel remaining in the tanks.
The fuel control panel is located at the base of the central control pedestal and contains the fuel tank selectors, fuel shutoffs and crossfeed controls. During normal operation each engine is supplied with fuel from its own respective fuel system. The fuel controls on the right control the fuel from the right cells to the right engine and the controls on the left control the fuel from the left fuel cells to the left engine. In emergencies, fuel from one system can supply the opposite engine through a crossfeed system.
Fuel is routed from the fuel cells to the selector valves where, dependent on valve position, fuel from either the inboard or outboard tank is routed to the engine. Fuel leaving the selector travels through a fuel filter, a fuel boost pump, the emergency fuel pump, a firewall shutoff valve, and then to the engine-driven fuel pump and engine fuel system.
The emergency fuel pumps are installed for emergency use in case of an engine-driven fuel pump failure. They are also used for take-off and landing and, when necessary, to prime the engines. Control switches for the emergency fuel pumps are located on the overhead switch panel to the right of the fuel gauges.
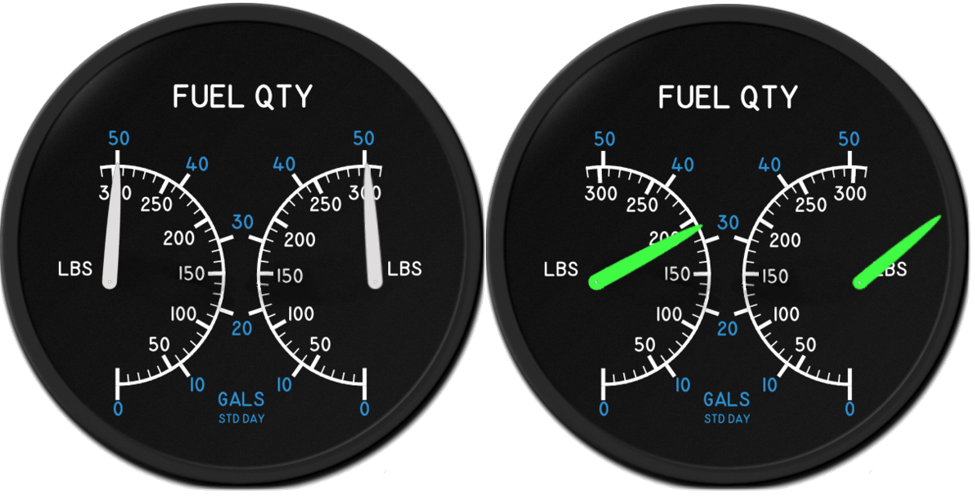
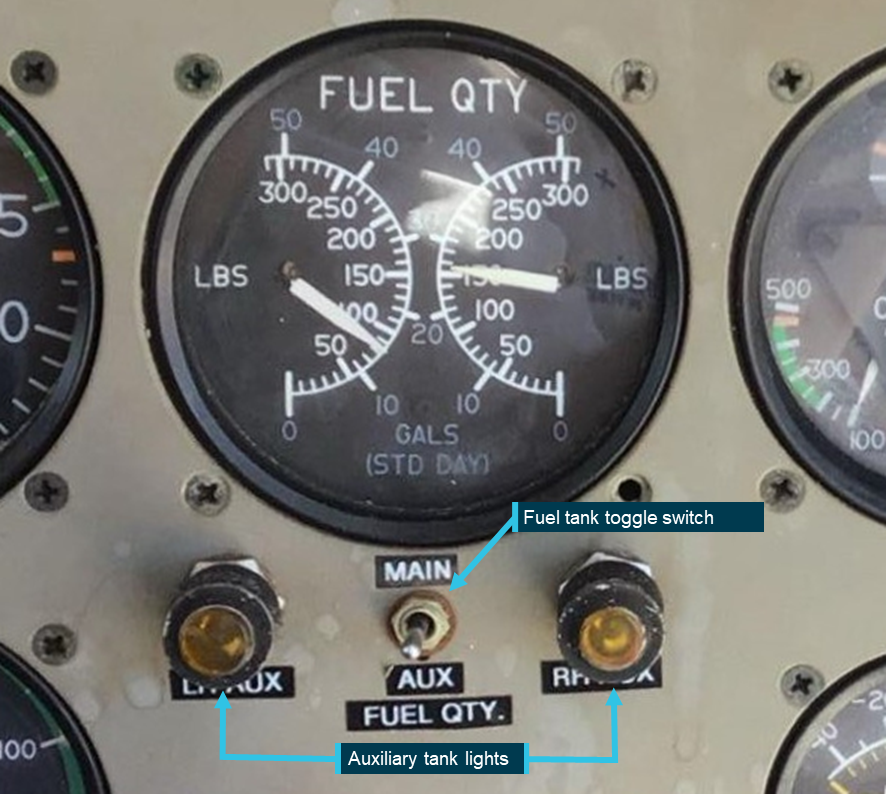
Two electric fuel quantity gauges are also mounted on the overhead switch panel (Figure 5). These indicate the fuel tank level from float-style sender units in each tank. The gauges indicate left inboard or outboard tank, and right inboard or outboard fuel tank quantities dependent on selector valve position. The inboard tanks contain 2 sender units each, one near the wing root and one near the filler cap (Figure 3).
The fuel boost pumps are operated continuously and are provided to maintain fuel under pressure to the engine‑driven fuel pump. There are no fuel boost pump control switches or pressure gauges.
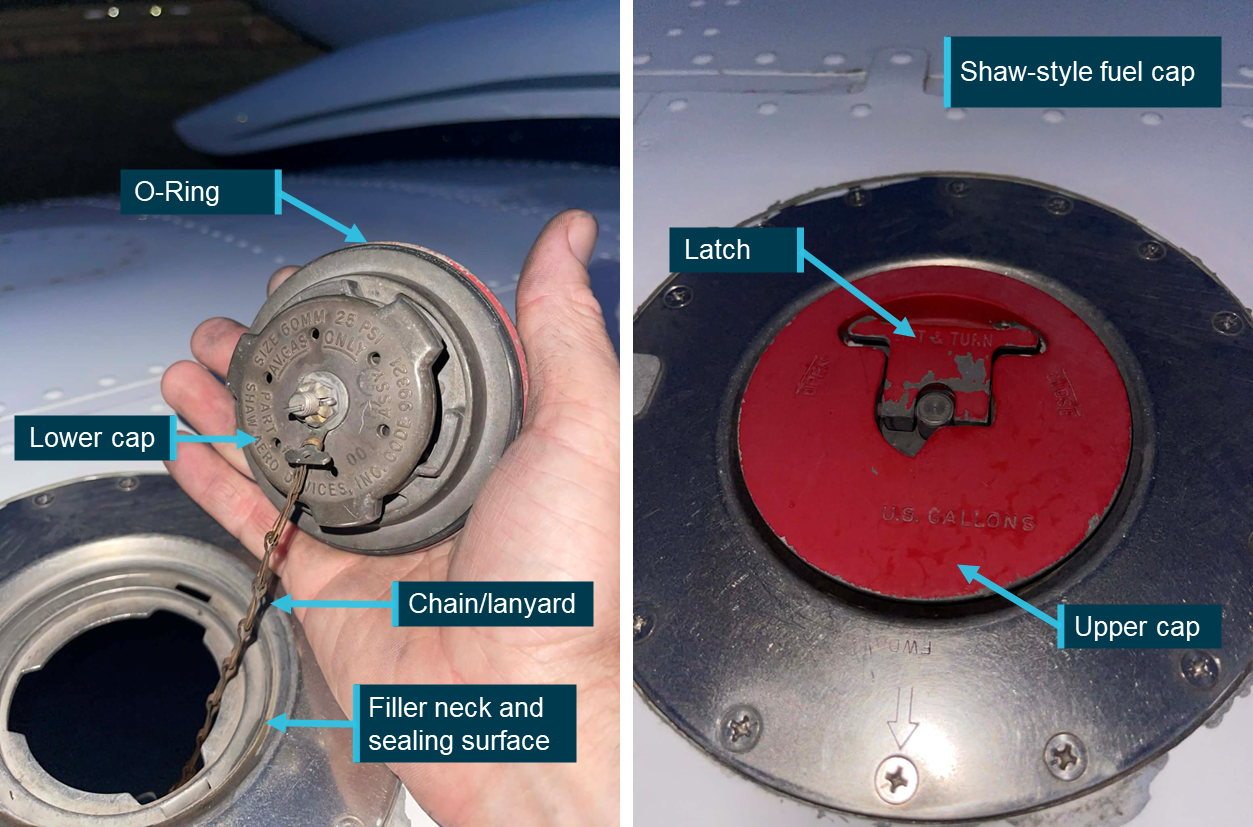
Each tank has a separate Shaw-style fuel cap for servicing (Figure 4). The inboard tank caps are located on the upper centre section of each wing and the outboard tank caps are on the upper outboard section of each wing. The right inboard fuel cap is not visible from the pilot’s seated position. The fuel caps are installed on the filler neck of each tank and utilise a twist‑to‑lock cam mechanism. As the latch is rotated, the upper and lower sections are drawn together, compressing the O‑ring seal against the filler neck to form a secure, fuel- and water-tight closure. The lower cap lugs engage under the filler neck flange to hold the cap in place against vibration, pressure changes, and airflow that is encountered in flight. The caps are also attached to the wing by a lanyard.
Figure 4: Shaw-style fuel cap
Source: Toby Dorn, annotated by the ATSB
Fuel flow indicators
Analogue fuel flow gauges located on the instrument panel indicate fuel flow to the engines in US gallons per hour. An FS-450 fuel flow indicator is also located on the instrument panel and digitally displays real-time fuel flow in litres per hour, fuel used, fuel remaining, and time-to empty. It is used to assist pilots in fuel management, however, it records fuel flowing through the fuel flow indicator transducer into the engine fuel system and would not detect a leak upstream such as a fuel tank leak.
Fuel system warning lights
Right and left fuel flow warning lights are mounted on the annunciator panel and illuminate to warn the pilot of an impending fuel flow interruption from the inboard tanks. The lights are activated by a probe that is mounted near each inboard fuel tank outlet (Figure 3). In the event of the fuel level near the tank outlet dropping to a point where a fuel flow interruption could occur, the LOW FUEL FLOW warning light will illuminate.
The pilot’s operating handbook contains the following warning:
WARNING
If either the right or left fuel flow warning light illuminates and the fuel gauge indicates fuel remaining in the corresponding inboard tank, this will indicate a malfunction of the flapper door in the inboard tank. Immediately select the outboard tank or select crossfeed to avoid fuel flow interruption.
This warning indicates a possible flapper door malfunction within the inboard fuel tank.7 In this condition, the fuel flow warning light may illuminate despite sufficient fuel remaining in the affected tank, as the malfunction may restrict fuel flow to the tank outlet. The procedure directs the pilot to immediately select the outboard tank or crossfeed to maintain fuel supply and prevent fuel flow interruption.
Left and right FUEL BOOST PUMP INOP warning lights are also mounted on the annunciator panel, and they illuminate when the fuel boost pressure to the associated engine fuel pump is less than 3 PSI. An illumination of a fuel boost pump inoperative warning light will occur immediately prior to that engine being starved of fuel.
Post‑occurrence
Pilot actions
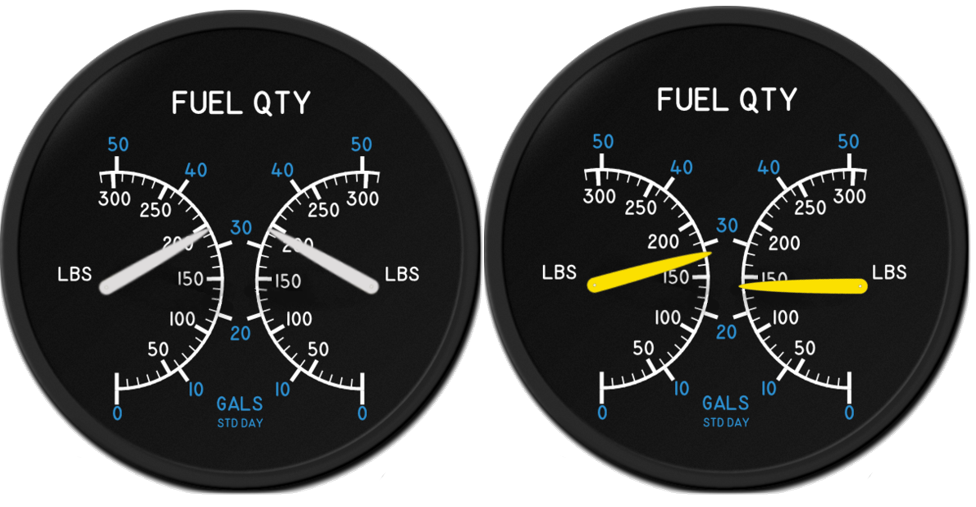
After landing and shutting down the left engine, the pilot escorted the passengers to the terminal, reported the occurrence to Shine Aviation, and then returned to the aircraft. The pilot then applied battery power and noted that the right inboard tank fuel quantity gauge was indicating just above a quarter full, and the left inboard tank fuel quantity gauge was indicating half a tank (Figure 5). The pilot recalled that this was unusual and was more significant than the minor discrepancy observed at the top of descent.
Figure 5: Inboard tank quantity discrepancy after landing
Source: Pilot, annotated by the ATSB
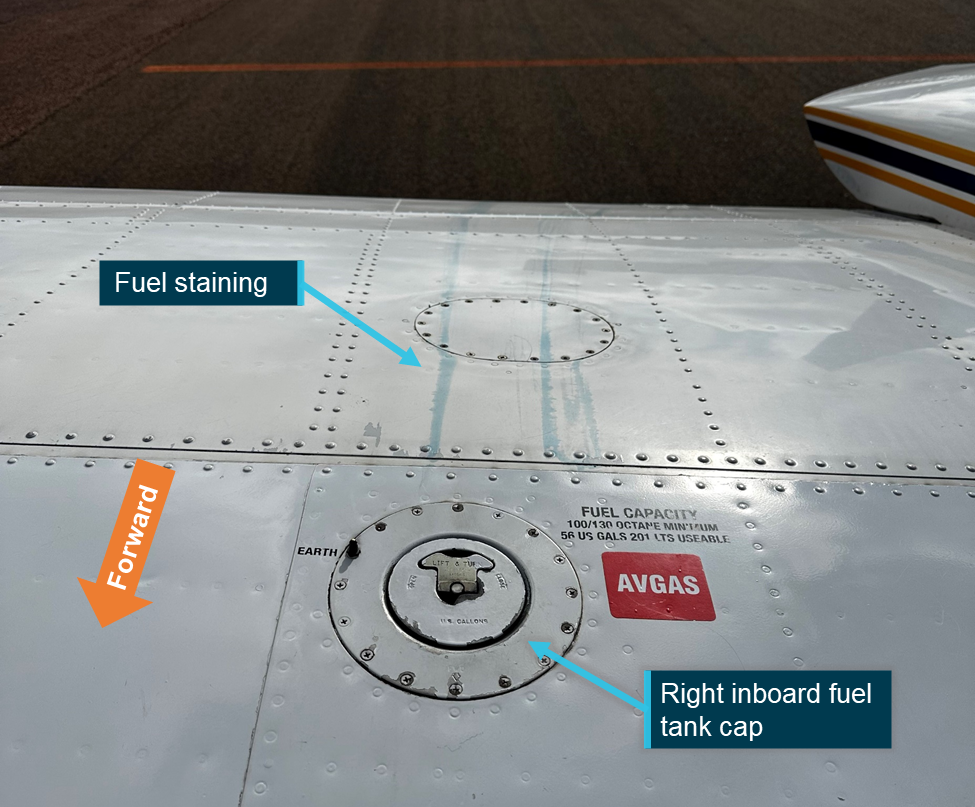
The pilot then conducted a visual inspection of the right wing area and noted blue fuel streaks behind the right inboard fuel cap (Figure 6). After attempting to drain fuel out of the right inboard fuel tank without success, the pilot then removed the right fuel cap to see if any fuel was present. The pilot noted that the fuel cap latch was ‘extremely’ difficult to unlatch and required the use of both hands. Upon looking in the tank, the pilot observed that it was empty, and the bottom of the fuel cell had been sucked up towards the fuel filler area. The pilot then reinstalled the cap, commenting that the cap latched normally and without difficulty.
Figure 6: Fuel staining aft of right inboard fuel cap
Source: Pilot, annotated by the ATSB
At hourly intervals, the pilot reapplied battery power noting that it took 2.5 hours after landing for the right inboard tank fuel gauge to read zero.
Engineering inspection
The company’s chief engineer arrived about 3.5 hours after the occurrence to commence troubleshooting. They reported that there was no evidence of a leak source around the right inboard fuel tank aside from the fuel staining aft of the fuel cap. Although the pilot had already removed and refitted the fuel cap, an inspection of the fuel cap was conducted with no defects noted including the O‑ring being found serviceable. The chief engineer replaced the cap O‑ring seal and re-tensioned the cap’s latch mechanism as a precaution. They also commented that there was a possibility of the fuel cap lanyard interfering with the cap’s fitment however no damage to the cap or the lanyard was identified.
The chief engineer observed that the bottom of the fuel cell had been drawn up towards the fuel cap and required manual reseating. They filled the inboard tanks to maximum capacity; 67 L was required to fill the left inboard tank, and 204 L was required to fill the right inboard tank. The chief engineer stated that they were satisfied that the fuel cell had reseated correctly within the fuel tank cavity.
The engines had been operated alike up to the right engine starvation. The ATSB estimated that the left engine consumed 6 L of fuel after the right engine stopped. Therefore, about 131 L had been siphoned and lost overboard from the right tank through the fuel cap during flight.
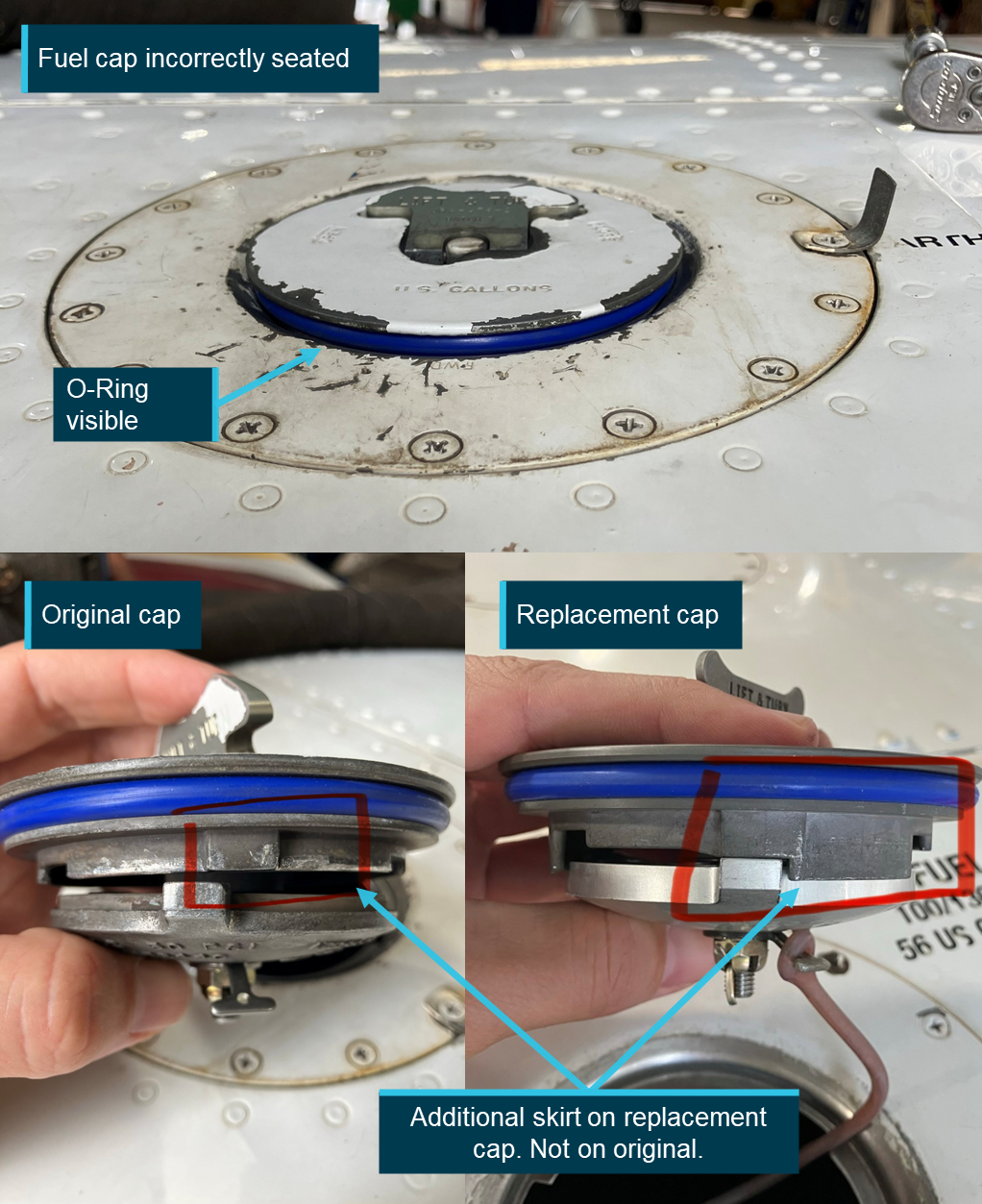
During the draft report review process, the ATSB was informed of a repeat incorrect fitment of VH-PGO’s right inboard fuel cap that resulted in fuel leaking during flight. The operator advised that this occurred on 6 October 2025, 4 months and an estimated 60–70 refuels after the initial occurrence. However, the chief engineer was able to observe the cap in its incorrectly fitted state where they determined that the cap had not been seated correctly prior to being latched. This resulted in the upper and lower portions of the cap clamping on the filler neck of the wing (Figure 7). Following the second occurrence, the chief engineer elected to replace the fuel cap as a precaution.
Upon receipt of the new fuel cap the chief engineer noted that a skirt had been incorporated into the design of the replacement cap therefore limiting the ability of the upper and lower portions of the cap to clamp on the filler neck of the wing (Figure 7). The ATSB contacted the manufacturer for further information on the apparent design change. However, at the time of publication no response had been received.
Figure 7: Incorrect fitment on 6 October 2025
Source: Operator, annotated by the operator and the ATSB
Flight testing
Followingthe inspection, the aircraft was ferried back to Geraldton (without passengers) by the head of flying operations, with the chief engineer seated in a position that allowed full view of the right inboard fuel tank cap.
During climb out of Meekatharra Airport, they observed that the FS-450 fuel flow indicator for the right engine was displaying a significantly lower fuel flow than expected for the selected power and mixture setting, and it was lower than the corresponding analogue fuel flow gauge. The FS-450 indicated approximately 70 L/h, compared to the expected value of about 120‑L/h. However, the right engine exhaust gas temperatures, oil temperature, manifold pressure and cylinder head temperature were within normal limits for that power setting and comparable to the left engine. On that basis, they assessed that the FS‑450 indication was erroneous and not representative of the actual fuel flow to the engine, with the chief engineer stating that the engine would not be able to run with that fuel flow for that power setting. The engineer advised the head of flying operations to use the analogue fuel flow gauges for engine management for the remainder of the flight.
The occurrence pilot reported that they had not observed any irregularities with any of the engine indications prior to the occurrence. This was supported by a review, conducted by the operator’s head of safety and quality assurance, of VH‑PGO’s previous 8 flight logs, which found that fuel usage data was normal and within acceptable parameters for the PA‑31‑350.8 In addition, a review of the flight logs for flights conducted after the occurrence identified no abnormalities.
The chief engineer later commented that the FS‑450 unit’s calibration may have been inadvertently altered by the occurrence pilot after the event during their initial troubleshooting.
During the return flight to Geraldton, the chief engineer did not observe any fuel leaking from the right inboard fuel tank cap, and a post‑flight inspection confirmed that no fuel leakage was present. The aircraft was subsequently flown that evening and the following morning, with no further leaks or related issues identified.
Refueller
The refueller who uplifted fuel to the aircraft at Carnarvon and secured the fuel caps before the occurrence flight later recalled that the right inboard fuel cap was slightly difficult to close. However, based on their familiarity with the aircraft, they believed the cap was properly secured. They also stated that if they had any concerns about the aircraft, they would have informed the pilot.
Pre-flight and refuelling
The pre-flight inspection detailed in the POH stated that the fuel supply should be checked visually, and a check was required to ensure the fuel caps are securely in place. To visually check the fuel supply, the cap would have to be removed and therefore a physical check of security is performed when the caps are installed.
Shine Aviation’s Policy and Procedures manual provided instructions regarding refuelling and fuel caps, additional to the POH procedures. The instructions included:
When fuelling is complete, sufficient airspace must remain in each fuel tank to allow for anticipated fuel expansion, and the PIC must ensure that all fuel and oil tank caps have been securely refitted.
PA-31 training
Regulatory requirements
Shine Aviation operated as a Civil Aviation Safety Regulation (CASR) Part 135 operation (Australian Air Transport Operations - Smaller Aeroplanes) and held a Part 135 Air Operator’s Certificate (AOC). Section 12.05 of the Part 135 Manual of Standards stated the following:
• The flight crew member must have successfully completed the operator’s conversion training, and flight crew member proficiency check, for the aeroplane.
• The training must deal with the following:
- training in the duties and responsibilities for the flight crew member’s position;
- training in the standard operating procedures for the type or class of aeroplane used for the flight;
- training in the normal, non-normal and emergency procedures for an aeroplane of that type or class;
- training in any flight procedures or manoeuvres, conducted in an aeroplane of that type or class, for which the operator holds an approval under regulation 91.045, or 135.020, of CASR;
Note: Examples of approvals issued under regulation 91.045, or 135.020, of CASR include approvals to conduct low visibility operations and flights using certain PBN navigation specifications.
- training in the procedures for any other operations conducted by the operator in an aeroplane of that type or class that the flight crew member has not previously experienced, for example, precision runway monitor operations or land and hold short operations.
Under CASR Part 61.385 Limitations on exercise of privileges of pilot licences – general competency requirement, a pilot may only exercise the privileges of their licence if they are competent to the standards specified for the relevant aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures for that aircraft.
Company flight training
Shine Aviation was approved by CASA as a CASR Part 141 training organisation, enabling it to conduct in-house pilot training and competency assessments in support of pilot qualification for operations under the organisation’s Part 135 Air Operator’s Certificate.
Pilots underwent conversion training onto company aircraft in 2 parts: a ground-based theory component, followed by a flying component. The ground-based theory component consisted of self-paced study of the POH prior to undergoing a multiple-choice theory exam. The theory examination consisted of 25 PA-31 specific questions, automatically generated from a question bank of 82, including topics relating to weight and balance, aircraft performance, and systems knowledge.9
The flying component involved the pilot conducting 2 non-revenue (no passengers) training flights with a company flight instructor. Shine Aviation’s General Competency Training syllabus included the following competencies for the pilots to demonstrate:
departure and arrival (including appropriate engine management for turbocharged aircraft)
stalling
steep turning
different cruise configurations
upper air asymmetric where applicable
normal circuit
flapless circuit
crosswind circuit
engine failure on take-off
engine failure elsewhere in circuit
single engine go‑around
discussion on differences in standard practice between engine models (oil uplift, engine monitoring etc)
any other multi engine or single engine class rating competencies as deemed necessary by instructor.
Although this syllabus contained specific competencies for other types of aircraft Shine Aviation operated, it did not contain any specific PA-31 competencies. However, it did contain an ‘underpinning knowledge’ section in which ‘Instrument failure and warning systems fitted to the aeroplane’ was listed.
Following satisfactory demonstration of the required flying competencies, the pilot was required to act as a copilot for approximately 30 hours of normal company operations prior to conducting single pilot operations.
The pilot in this occurrence completed their ground component and 2 non-revenue training flights, involving 3 hours of flight and 4 hours of briefing time, in January 2025. The pilot then conducted approximately 30 hours of flying as a copilot in the PA-31, including 13.5 hours in VH-PGO, prior to being assessed and approved for single pilot operations. The pilot completed an instrument proficiency check in January 2025 in the PA-31 with a company examiner.10
In May 2025, the pilot successfully completed 2 recurrent flight training exercises in the company’s approved synthetic training device.11 These exercises involved various emergency and abnormal scenarios consisting of adverse weather, engine failures, single engine approaches, instrument failures and flight planning exercises.
Training regarding low fuel flow warning light
The theory examination contained the following question related to the LOW FUEL FLOW warning light:
Illumination of a LOW FUEL FLOW annunciator:
a) Indicates that outboard fuel quantity has decreased to a point where engine power loss could occur
b) Indicates low fuel quantity in the inboard tanks
c) Indicates that a fuel boost pump has failed
d) a and c
The correct answer is (b), however this question pertains to the function of the warning light but does not cover the published warning or the actions to be taken by the pilot upon its illumination (see the section titled Fuel system warning lights). Regardless, the theory examination that was generated for the occurrence pilot did not include this question.
Shine Aviation’s head of training for the PA-31 stated that the LOW FUEL FLOW warning light was likely discussed during the flight training component when the annunciator panel was covered. However, they also stated that not every annunciator panel indication was examined in detail.
The incident pilot advised that the LOW FUEL FLOW warning light was not specifically addressed during initial or copilot training and that, although they understood that it related to a fuel flow issue to the affected engine, they were not aware of, or could not recall, the required immediate actions that are directed by the warning in the POH.
Related occurrences
Excluding the incident flight, the ATSB occurrence database contained 49 reported occurrences of fuel leaking or venting from a fuel cap on non-jet aircraft between 2014 and 2025. Of those occurrences, 8 resulted in fuel starvation or fuel exhaustion. Those numbers likely under‑represent the total number of incidents of this type, as the ATSB only required instances of fuel leaking/venting or missing/insecure fuel caps to be reported for commercial passenger transport operations.
ATSB occurrence brief AB-2021-009 was published following a fuel starvation event involving a PA-31-350 in 2021:
On 21 March 2021 a Piper PA-31-350 aircraft was operating a scheduled freight flight from Moorabbin, Victoria to Devonport, Tasmania. During approach, the low fuel flow and low boost pump warning lights illuminated. The right engine stopped shortly after. The pilot in command confirmed the fuel selector was in the correct position and observed that the fuel gauges indicated three-quarters full, which was as expected. The pilot then attempted to cross-feed fuel from the left engine, which was unsuccessful. By this time, the aircraft was on mid-final and, once assured of making the runway, the pilot stopped troubleshooting and concentrated on landing the aircraft.
After landing, the pilot inspected the fuel cap, which appeared to be secured correctly. However, blue stains were evident on top of the wing consistent with fuel venting out of the fuel cap. The fuel system was subsequently inspected by maintenance personnel with nil defects found with the fuel cap and no blockages in the fuel tank vents.
The pilot later advised that the rubber bladder containing the fuel within the tank was sucked up against the top of the wing as the tank emptied, providing a false indication of the fuel remaining in the tank.
ATSB occurrence investigation AO-2024-008 was published following a fuel exhaustion event in 2024:
On 8 March 2024, the pilot of an Aero Commander 500-S, registered VH-MEH and operated by GAM Air, was conducting a return cargo transport operation from Bankstown Airport to Parkes Regional Airport, New South Wales with one intermediate stop outbound, and 2 intermediate stops on return.
After landing on the first sector, the pilot found the fuel cap was off and secured only by a retention chain. The pilot re-secured the cap but after landing at Parkes on the second sector, they again found the fuel cap off. They arranged an inspection by a maintenance engineer, where a fault was found that prevented the fuel cap from locking and rectified it.
Later that day, the pilot commenced the return sectors to Bankstown. Shortly after departing Bathurst for the final sector, both engines lost power, and the pilot conducted a forced landing in a field. The aircraft was undamaged and the pilot was uninjured.
The ATSB found that the fuel cap retention chain had lodged within the fuel tanks anti siphon valve. This allowed fuel to be siphoned overboard during flight.
CASA Advisory Circular 91-25 Fuel and oil safety, section 6, highlighted recommendations associated with fuel caps and vents. In particular, the circular advised of the possibility of fuel siphoning overboard due to a cap attachment chain or lanyard becoming trapped across a fuel cap seal. The advisory circular also identified that an insufficiently vented tank may collapse the fuel bladder and exaggerate indications of fuel within the tank.
Safety analysis
Introduction
On 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO, and operated by Shine Aviation, was conducting a passenger transport operation from Carnarvon to Meekatharra, Western Australia. During the approach to Meekatharra Airport, the R LOW FUEL FLOW warning light illuminated, followed shortly by the R FUEL BOOST INOP warning light and surging of the right engine. The pilot conducted their memory item initial engine failure checks and feathered the right propeller. The pilot continued the approach and landed without further incident.
Fuel siphoned overboard
Photographs taken by the pilot after landing at Meekatharra Airport show fuel staining immediately aft of the right inboard fuel cap, consistent with fuel leaking from the cap in flight. This staining, in conjunction with the pilot’s observation that the right inboard tank was emptied earlier than expected based on calculated consumption, and that the tank cell collapsed upwards towards the cap, all indicate that fuel had likely been siphoned through the cap in flight. The pilot also reported that the fuel cap latch was difficult to lift, suggesting the cap may not have been correctly seated.
During the post-occurrence inspection, the chief engineer found no evidence of any other fuel leaks around the right inboard tank. The pilot had removed and reinstalled the cap prior to this inspection, therefore the chief engineer could not determine exactly how the cap was incorrectly fitted. The chief engineer was also unable to reproduce an incorrect installation. However, the chief engineer considered it likely that the fuel cap had been incorrectly secured, including the possibility of the attaching lanyard interfering with the cap and seal. No damage was observed to the cap, seal, or lanyard and the chief engineer replaced the O-ring on the cap as a precaution, although they considered the removed O‑ring serviceable. Subsequent flights, including the immediate post‑occurrence flight with the chief engineer observing the cap, did not reproduce the leak. As the leak did not recur, it was almost certain the fuel cap was incorrectly secured in Carnarvon.
As part of the troubleshooting, the chief engineer refuelled the right inboard tank with 204 L, while the left tank required only 67 L to fill. Given that both tanks had been selected for use at similar times during the flight, and accounting for fuel used by the left engine after the right had stopped, the discrepancy indicated that approximately 131 L of fuel had been lost through the fuel cap from the right inboard tank.
Contributing factor
The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight.
Fuel cap installation
Shine Aviation’s Policy and Procedures manual required the pilot in command to ensure that fuel caps were securely fitted. While this did not explicitly require the pilot to remove and reinstall the caps, the pilot’s operating handbook specified that the pilot in command must visually check the fuel supply and confirm that the fuel caps are secure. Checking the fuel quantity required the pilot removing the caps and physically handling the fuel caps to verify correct fitment.
Although the pilot stated that they visually inspected the fuel cap, a closer inspection or physical check of the cap would likely have aided the pilot in identifying the incorrect installation. Consequently, the pilot did not detect that the right inboard fuel tank cap was incorrectly secured.
Contributing factor
The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured.
False gauge reading
During flight, the rate of fuel being siphoned through the fuel cap was likely sufficient to overcome the vent’s ability to equalise pressure in the fuel tank. This resulted in negative pressure collapsing the fuel cell as observed by both the pilot and the chief engineer during their post-occurrence inspections. As the fuel cell was secured by a single cord around the upper perimeter, the collapse of the fuel cell resulted in the base of the cell lifting towards the filler port.
As one of the right inboard fuel tank float-style sender units was located near the fuel filler port, it is likely that the upwards lifting of the fuel cell floor toward the filler port, raised the outboard sender unit’s float. This resulted in an overreading of the cockpit fuel quantity gauge. ATSB occurrence brief AB-2021-009 identified a similar failure mechanism where the fuel cell collapsed resulting in the fuel gauge overreading its contents. The Civil Aviation Safety Authority’s advisory circular (AC) 91-25 Fuel and oil safety, section 6, also contained information about collapsing fuel cells interfering with the accuracy of fuel gauge readings.
During the subsequent flight, the onboard fuel flow indicator was incorrectly and significantly underreading the right engine fuel flow. However, the pilot reported it was functioning normally during the flight to Meekatharra. Engineers assessed the instrument had probably been inadvertently recalibrated during post-incident fault finding.
When the pilot changed from the outboard tanks to the inboard tanks at the top of descent, they noticed that the right inboard tank quantity gauge was reading a slightly lower quantity than the left inboard, however they assessed that this was an acceptable discrepancy related to VH-PGO. It is likely that the right inboard tank was almost empty at that stage of flight as the R LOW FUEL FLOW warning light illuminated shortly after.
Contributing factor
Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents.
Response to warning
The warning in the pilot’s operating handbook (POH) stated that if the right or left LOW FUEL FLOW warning light illuminated, and the fuel gauge indicated fuel remaining in the corresponding inboard tank, this indicated a malfunction of the flapper door in the inboard tank. The prescribed action was to immediately select the outboard tank or select crossfeed to avoid fuel flow interruption. While a flapper door malfunction did not occur in this instance, compliance with the warning actions would likely have restored fuel supply.
The pilot was unaware of the required immediate actions and therefore did not respond to the R LOW FUEL FLOW warning light as directed by the POH. The pilot was also unaware that a fuel starvation event was developing, until the subsequent illumination of the right FUEL BOOST INOP warning light and associated engine surging.
The sequential activation of the R LOW FUEL FLOW warning followed by the right FUEL BOOST INOP warning was a progressive indication that fuel flow to the right engine would be interrupted. As the pilot did not restore fuel flow following either warning, the right engine became starved of fuel, resulting in the engine surging and a corresponding yaw of the aircraft.
Contributing factor
The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Training regarding low fuel flow warning light
As part of the Civil Aviation Safety Regulations (CASR) limitations on the privileges of a pilot licence, pilots were required to be competent in conducting all normal, abnormal and emergency flight procedures for the aircraft. This required the pilot to be aware of the POH warnings and associated instructions included in emergency procedures. Additionally, under CASR Part 135, operators were also required to ensure that flight crew were trained in the normal, non-normal and emergency procedures for the aircraft they were operating.
Shine Aviation PA-31 pilots independently studied the POH and subsequently undertook a theory examination. This examination consisted of 25 PA-31 specific questions that were automatically generated from a question bank of 82. Although there was one question regarding the illumination of the LOW FUEL FLOW warning light, this question did not evaluate the immediate response required. Furthermore, this question was not included in the occurrence pilot’s automatically generated examination.
Shine Aviation’s head of PA-31 training advised that the LOW FUEL FLOW annunciator and associated warning were likely addressed to some extent during practical line training. However, the occurrence pilot did not recall this topic being covered. Shine Aviation’s General Competency syllabus required a general knowledge of the warning systems, however, it did not specifically require demonstration of the appropriate response to a LOW FUEL FLOW warning. In this case, the training was ineffective at ensuring the incident pilot was competent in responding to the warning.
Contributing factor
Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation involving Piper PA-31, VH-PGO, 28 km west of Meekatharra Airport, Western Australia, on 5 June 2025.
Contributing factors
The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight.
The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and the company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured.
Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents.
The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Low fuel flow warning light and subsequent actions not highlighted in training
Safety issue description: Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow annunciator light.
Glossary
AMSL
Above mean sea level
AGL
Above ground level
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
IFR
Instrument flight rules
IMC
Instrument meteorological conditions
POH
Pilot’s Operating Handbook
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
the operator of VH-PGO
Civil Aviation Safety Authority
Airservices Australia.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the operator of VH-PGO
Civil Aviation Safety Authority.
Submissions were received from:
the pilot
the operator of VH-PGO.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
^Pilot’s operating handbook: a manufacturer-produced manual that provides pilots with all the essential information needed to safely operate the aircraft.
^Aerodrome weather information service (AWIS): actual weather conditions, provided via telephone or radio broadcast, from Bureau of Meteorology (BoM) automatic weather stations, or weather stations approved for that purpose by the BoM. Winds are in degrees magnetic.
^Runway number: the number represents the magnetic heading of the runway to the nearest 10 degrees.
^Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
^Usable fuel: the amount of fuel in a fuel tank that can reliably be supplied to the engine in all operating conditions. This excludes fuel that cannot be used due to aspects such as tank geometry and fuel pickup locations.
^A flapper door is installed in each inboard tank to keep fuel around the tankoutlet by preventing it from flowing away during manoeuvring, climb, descent, turbulence, or uncoordinated flight.
^The pilot records fuel quantity prior to start, fuel quantity used via the FS-450, and fuel quantity after shutdown for each sector in a flight log. This allows the operator to monitor fuel usage for individual aircraft.
^Following the occurrence, Shine Aviation increased the number of questions in the PA-31 theory examination to 30.
^Instrument proficiency check (IPC): A required annual flight test to ensure that a pilot maintains the necessary skills and knowledge to safely operate an aircraft under instrument flight rules (IFR). It involves demonstrating competency in tasks such as navigation, communication, and handling the aircraft in various conditions, all while relying on instruments rather than visual references.
^Recurrent training: Shine Aviation conducts recurrent training for all its instrument rated pilots every 6 months. Training is delivered in a synthetic flight training device and consists of simulated IFR flights that include operational and decision-making scenarios tailored to the individual pilot. This recurrent training is in addition to regular instrument proficiency checks as required every 12 months under CASR Part 61.
Occurrence summary
Investigation number
AO-2025-026
Occurrence date
05/06/2025
Occurrence time and timezone
1031 Australian Western Standard Time
Location
28 km west of Meekatharra Airport
State
Western Australia
Report release date
04/06/2026
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Fuel starvation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-31-350
Registration
VH-PGO
Serial number
31-7852109
Aircraft operator
Shine Aviation
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
On 26 November 2024, an instructor was conducting training operations with a student pilot in a Piper PA-28-180 Cherokee aircraft. Activities involved general aircraft handling in the Parafield Airport training area, South Australia, before returning to the aerodrome for circuit operations on runway 26L.
Around 1345 local time, as the aircraft was descending through about 600 ft on final approach to the runway, the student advanced the throttle to correct the descent profile when the engine did not respond. The instructor assumed aircraft control and began troubleshooting actions while managing the descent. At about 300 ft, when it was evident that the engine would not respond, the instructor committed to an emergency landing on the grassed area to the east of runway 21L. The landing was uneventful, and the student and instructor evacuated the aircraft without injury. The aircraft was undamaged.
Examination of the aircraft’s systems after the landing found that the fuel selector was in the left tank position – being the tank that was selected before the flight commenced. On inspection, the left tank contained no usable fuel.
Aircraft information
The Piper PA-28-180 aircraft has two independent fuel tanks within the wings, which feed the engine via a ‘Left-Right-Off’ selector valve located on the cockpit left side. The quantity of fuel in each tank is indicated by dash-mounted gauges. A fuel pressure gauge is co-located with the quantity gauges.
The aircraft manufacturer’s Pilot’s Operating Handbook (POH) lists the following actions in the event of a loss of engine power in-flight:
Fuel Selector – switch to another tank containing fuel
Electric Fuel Pump – On
Mixture – Rich
Carburettor Heat – On
Engine Gauges – check for an indication of the cause of Power Loss
Primer – Check Locked
If no fuel pressure is indicated, check tank selector position to be sure it is on a tank containing fuel.
Safety action
Following the occurrence, the operator’s Head of Operations reviewed the known details of the incident flight with all instructors, highlighting the absence of a ‘both tanks’ fuel selection on the PA-28 aircraft and reinforcing the requirement to use calculated fuel logs that are cross‑referenced against the aircraft gauges at periodic intervals during flight.
Safety message
All general aviation pilots must ensure they are fully familiar with the control and operation of the fuel system/s of the aircraft they are operating. This includes actions in the event of engine power loss at any phase of flight, where timely and appropriate responses to possible fuel flow interruptions can be critical to a safe outcome. Emergency checklists should be readily accessible and periodically reviewed to ensure pilots remain familiar with the appropriate actions in the event of fuel-related engine power loss.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-047
Occurrence date
26/11/2024
Location
Parafield Airport
State
South Australia
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Fuel starvation
Highest injury level
None
Brief release date
18/02/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-180 Cherokee
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On 29 September 2024, at about 1225 local time, an Intermountain Manufacturing Co A-9A (A-9) was conducting glider towing operations at Lake Keepit aircraft landing area, New South Wales (NSW).
It was reported that, prior to the flight, the aircraft had a minor fuel leak on the left fuel tank drain port. Due to the leak, club policy was to only operate the left fuel tank on the ground, thereby minimising the potential fuel leakage from the left-wing tank.
Operations commenced at approximately 1030 local time and following the completion of the fourth tow and glider release at about 1224, the aircraft conducted a descent from the north-west of the landing area, intending to join a crosswind[1] for runway 20 (Figure 2).
During a slow left banked turn, on the northern side of the airfield at about 1,500 ft, the engine experienced a sudden loss of power. The pilot attempted to troubleshoot, however was unable to restore normal power to the engine.
The pilot made the decision to close the throttle and conduct a glide approach, broadcasting a PAN-PAN call with intentions to land on runway 14. The engine continued to operate at idle power during the subsequent descent and landing.
The aircraft landed without incident before clearing the runway and taxiing to a suitable parking area. The engine was reported to be operating normally at this time and a normal shutdown was conducted.
Figure 2: Approach path of aircraft
Source: Google earth, annotated by the ATSB
The operator reported that the loss of power in the engine was due to fuel starvation from an incorrect fuel tank selection. The left tank was being operated in flight, with the pilot believing that the fuel was being sourced from the right fuel tank.
The pilot reported having 233 hrs of total time of which 6.9 hrs were on type.
The fuel selector switch in the A-9 is non-traditional to that of some other conventional aircraft types, such asCessna, Piper, Beechcraft. In those aircraft, the handle is used to indicate the selector (for example, a Cessna 172 is shown in Figure 3, right). In comparison, in the A-9 (Figure 3, left), the fuel selector switch points to the selection so that the longer handle is placed on the opposite side of the tank to which the pilot wishes to select. (There are only left, right and 2 off positions for the selector.)
Figure 3: Fuel selector for the A-9 (left) and as a comparison, a Cessna 172 (right)
Source: Operator photos annotated by the ATSB
Safety message
Accidents involving fuel mismanagement are an ongoing aviation safety concern and pilots are reminded of the importance of understanding an aircraft’s fuel supply system and being familiar and proficient in its use.
Pilots should familiarise themselves with the Civil Aviation Safety Authority publication Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in-flight fuel management.
Practising forced landings from different altitudes under safe conditions can help pilots prepare for an emergency situation, should one arise. Being familiar with emergency checklists and your aircraft’s systems will assist in an emergency when identifying and managing an engine failure.
Examples of other ATSB investigations covering starvation related occurrences include:
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021).
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040).
Fuel starvation involving Cessna 206, 3.5 NM NE of Aldinga, South Australia, on 3 February 2019 (AB-2019-004).
Fuel starvation and forced landing involving Piper PA-28, VH-BDB, 15 km WSW of Bankstown Airport, New South Wales, on 19 September 2017 (AO-2017-094).
The 2013 ATSB publication AR-2011-112 details accidents involving fuel starvation due to fuel management. Ensuring a constant fuel supply to the engine/s during flight relies on the pilot’s knowledge of the aircraft’s fuel system and being familiar and proficient in its use, especially if the system is different to traditional aircraft.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]When arriving and intending to join the circuit from overhead, descend on the non-active side of the circuit so that the aircraft is established at its circuit altitude as it crosses the runway centreline on crosswind, between midfield and the departure end of the runway.
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales. The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. There was a pilot and one passenger on board.
During the approach, the engine stopped and while looking for a suitable landing place, the pilot saw a taxiway on the airport and decided to aim for that. To successfully reach the airport, the pilot elected to leave the flap retracted and gear up. This was done to reduce drag and achieve maximum glide range. Once the aircraft was assured of a landing on the airport, the gear was lowered. However, it did not successfully lock into place due to the limited time available before touchdown. The aircraft landed wheels-up resulting in minor damage and both occupants were uninjured.
What the ATSB found
The ATSB determined that, while the aircraft departed with sufficient fuel to complete the intended flight, it is likely that the amount of fuel reduced to a level that, in combination with unbalanced flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
The ATSB also determined that the pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Safety message
Fuel starvation occurrences can often be prevented by conducting thorough pre-flight fuel quantity checks combined with inflight fuel management. Pilots are reminded to check fuel quantities prior to departure using a known calibrated instrument such as a dipstick. In addition, comparing the expected fuel burn with actual fuel remaining after a flight, will give a validated fuel burn for the aircraft and ensure the measuring equipment is accurate. Pilots should familiarise themselves with the Civil Aviation Safety Authority, Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in‑flight fuel management.
Practising forced landings from different altitudes under safe conditions can help pilots prepare for an emergency situation, should one arise. Some components of the aircraft such as flap and gear, increase drag and reduce the glide range. Being familiar with emergency checklists and your aircraft’s systems will assist in an emergency when identifying and managing an engine failure.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales (NSW). The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. As the pilot had not previously operated to Bankstown Airport, they elected to carry a passenger, who was also a helicopter pilot, to assist with navigation and radio communication.
At 1313 local time, with the left fuel tank selected for take-off, the aircraft departed from runway 23[1] and tracked south. The pilot reported that about 4 minutes into the flight (while passing abeam Cessnock) they selected the fuller right tank, which they thought would reduce workload when entering Bankstown airspace. The aircraft entered the Visual Flight Rules (VFR) route[2] between Brooklyn Bridge and Prospect Reservoir at 1336 at approximately 2,000 ft.
Figure 1: Sequence of events
The image shows the sequence of events leading up to and during the forced landing, it highlights relevant places and reference times. Source: OzRunways flight data overlay on Google Earth.
The aircraft arrived overhead Prospect Reservoir at 1346 (Figure 1) and the aerodrome controller (ADC) instructed VH-MYW to maintain 1,500 ft and join the downwind leg of the circuit for runway 29R. An approximate 25° angle of bank turn was conducted to track toward a downwind join for runway 29R.
At 1347, the pilot reported joining downwind for 29R and the ADC instructed them to maintain 1,500 ft and provided them with updated Automatic Terminal Information Service (ATIS) [3] information ‘Foxtrot’. The pilot confirmed receipt of the new information by reading back the new QNH.[4]
The pilot recalled that, at about the time of that radio transmission, with the aircraft about 4.5 km north-west of Bankstown Airport, the propeller RPM increased, and they felt a braking sensation. They recalled that, in response they attempted to reduce drag on the propeller, changed fuel tank selection and briefly selected the electric fuel boost pump to ON. They then aimed to maintain glide speed while looking for a place to land.
At 1348, the pilot transmitted a MAYDAY call on the Bankstown Tower radio frequency stating they were having engine problems. The ADC advised that all runways were available, and they could track as required. The ADC continued to coordinate traffic to assist VH-MYW.
The pilot reported that while they were looking for a place to conduct a forced landing, they saw a taxiway on the airport and decided to try to land there. They advised that, during the approach the aircraft clipped the top of a tree and they raised the aircraft’s nose at the last minute to avoid a building on the airport perimeter. They decided not to deploy landing gear or flap until they were assured of reaching the airport.
At 1350, a helicopter operating in the area, reported that the aircraft had landed at the intersection of taxiway November 1 and taxiway Lima.
Both occupants of the aircraft were uninjured, and the aircraft sustained minor damage.
Context
Pilot
The pilot held a private pilot licence (aeroplane) issued in 2014 with a single‑engine class rating. They were appropriately endorsed to fly the Cessna 210 with design features for manual propeller pitch control and retractable undercarriage. The pilot also held a current class 2 aviation medical certificate.
They had accrued a total flight experience of approximately 222 hours, of which 15 hours were on the Cessna 210. In addition, they had previously flown other aircraft in this range including the Cessna 206 and Cessna 177. The pilot’s licence showed an entry for a single‑engine flight review conducted on 31 May 2023.
Weather
At the time of the incident, the Automatic Terminal Information Service information ‘Foxtrot’ was current, which indicated CAVOK[5] conditions, temperature 22°C, wind direction variable at 5 kt, and runway 29R in use for arrival and departures.
Aircraft
The aircraft was a Cessna Aircraft Company T210M manufactured in 1978 and issued serial number 21062277. It was powered by a fuel‑injected Continental Motors Inc TSIO-520-R piston engine driving a 3‑bladed, constant‑speed McCauley Propeller.
The aircraft was purchased from South Africa where it was previously registered as ZS-MYV and was shipped to Australia where it was reassembled and placed on the Australian register on 19 March 2021 as VH-MYW.
Maintenance
The aircraft was issued a maintenance release in November 2022 for private operations however, this expired in November 2023. At the time of the incident the aircraft was being ferried to Bankstown for completion of the maintenance required to return the aircraft to service.
As the maintenance release had expired, a special flight permit (SFP) was issued for the purpose of completing this ferry flight. The SFP was issued by the Civil Aviation Safety Authority (CASA) on 14 May 2024. The permit expired on 31 May 2024 and was subject to the following conditions:
Essential operating crew only to be carried.
Daily inspection and flight times are to be recorded on the Maintenance Release.
Day VFR, non-commercial operation by the most direct route practical and permitted by weather.
Operation shall be conducted in accordance with the approved flight manual / cockpit placards for the aircraft.
A copy of this SFP to be carried on-board and filed with the aircraft logbooks.
The permit also stated the flight was permitted to depart Maitland and arrive at Bankstown.
The last daily inspection signed on the aircraft maintenance release was completed on 2 November. The pilot advised that they had completed the daily inspection prior to the flight, but this was not recorded on the maintenance release.
The aircraft maintenance release also carried 2 endorsements for defects. These included the wing flaps not extending equally and hail damage. The flap defect was addressed by a third party, however, the hail damage was assessed by the aircraft owner in accordance with the CASA Airworthiness Bulletin 51-010 Assessment of hail damage.
Airworthiness Bulletin 51-010 recommended having a person who was appropriately qualified under Civil Aviation Safety Regulations 21.M to inspect the aircraft.
The pilot reported the aircraft had a tendency to fly right wing down. There was insufficient evidence available to the ATSB to determine whether either of the aircraft defects contributed to the flight characteristics described by the pilot.
Aircraft systems
Trim
The aircraft was fitted with elevator and rudder trim. Rudder trimming was accomplished via a wheel mounted in the cockpit (Figure 2). Setting the rudder trim left of centre would result in the aircraft maintaining the nose left of the flight path and remaining in that position until the wheel was manipulated, or the rudder pedals were manipulated. To maintain the desired track with that trim configuration, the aircraft would need to be flown in an uncoordinated state with the right wing low.
The aircraft’s pilot operating handbook stated:
Unusable fuel is at a minimum due to the design of the fuel system. However, when the fuel tanks are ¼ full or less, prolonged uncoordinated flight[6] such as slips or skids can uncover the fuel tank outlets, causing fuel starvation and engine stoppage. Therefore, with low fuel reserves, do not allow the airplane to remain in uncoordinated flight for periods in excess of one minute.
Cessna advised this was originally added to the Cessna 210 model D owner’s manual and was carried through as the aircraft developed into different models. Cessna did not have the available data to assess the likelihood of uncoordinated flight contributing to fuel starvation.
The pilot stated the rudder trim had been set left of centre since the aircraft was re‑assembled in Australia and that the trim wheel was not manipulated in flight.
Figure 2: Aircraft control pedestal post-incident
The image shows the fuel gauge level and the rudder trim. The image was taken on 6 June 2024, several days after the incident. However, the person responsible for recovering the aircraft stated, no fuel was added prior to this photo and the trim was set as found on the day of the incident. Source: Engineer responsible for aircraft recovery.
Fuel system
The Cessna 210 fuel system consists of a main fuel tank located in each wing. Each tank capacity is 171 L, of which 169 L is usable fuel. Each tank gravity fed a smaller fuel reservoir tank of approximately 1.9 L through fuel collector ports, which were located at the forward and aft inboard side of the main fuel tank (Figure 3Figure 3 and Figure 4).
Figure 3: Cessna 210M fuel schematic
Source: Cessna 210M pilot operating handbook, annotated by the ATSB
The fuel selector valve had 3 positions – left, right, and off – and so fuel could only be drawn from either the left or right tank. Cessna advised that at a low cruise power setting, if no fuel was being fed to the smaller fuel reservoir tank, it could supply fuel to the engine for between 1.5–3.5 minutes. The pilot advised that, at the time of the power loss the fuel selector was selected to the right fuel tank.
The fuel system has an engine-driven fuel pump and an auxiliary fuel pump, which is electrically driven. The pilot operating handbook states the following:
If it is desired to completely exhaust a fuel tank quantity in flight, the auxiliary fuel pump will be needed to assist in restarting the engine when fuel exhaustion occurs.
Cessna stated that during testing, the electric auxiliary fuel pump was required to operate for 4 seconds to restart the engine.
Figure 4: Fuel tank design
The above image shows the location of the fuel collector ports and the openings that are located in the rib support structure. The fuel cell image shown is for later serial numbers of the Cessna 210. However, it is the most descriptive image of fuel collector ports. Further images provided by Cessna show the aft collector port is located in a similar location to the above image. Source: Cessna 210 illustrated parts catalogue model 210 & T210 series 1981–1986, annotated by the ATSB.
The fuel tank design included an internal rib support structure (Figure 4). Each rib had an enlarged centre opening for fuel to freely flow through the tank, with small openings at the base of each rib, ensuring useable fuel could not become trapped. Cessna stated, ‘The small, if any, amount of fuel caught behind any structure would be part of the unusable fuel level determined during certification.’
Propeller
A control lever was used to set aircraft RPM by changing the propeller blade pitch. When the control lever is pushed inward, the propeller increases RPM (low blade pitch). When the control lever is pulled outward, the propeller RPM decreases (high blade pitch). This is achieved by a propeller governor which relies on engine oil pressure to move the propeller toward a high blade pitch (low RPM).
The combination of an internal spring and centrifugal force, twists the blades toward a low pitch (high RPM) setting when oil pressure at the propeller hub is relieved.
Engine Failure During Flight checklist
The pilot operating handbook provided the following checklist to be conducted in the event of an engine failure during flight:
airspeed – 85 [kt indicated airspeed] KIAS
fuel quantity – check
fuel selector valve – fuller tank
mixture – rich
auxiliary fuel pump – on for 3-5 seconds with throttle ½ open; then off
ignition switch – both (or start if propeller is stopped)
throttle advance slowly.
Flight data
The ATSB obtained flight data from an electronic flight bag (EFB) used by the pilot. The data provided aircraft position, time, altitude, and ground speed.
The flight data was analysed by the ATSB to obtain the approximate position when the engine stoppage occurred. This was determined to be at 1348 as there was a significant reduction in ground speed at that time.
Flight planning and fuel usage
The pilot reported that during the cruise, the manifold pressure was set near the top of the green (approximately 25 inches) and RPM at 2,200. A fuel flow reading was noted by the pilot of 14 gallons per hour (53 L/hr).
The pilot advised that they normally dipped the tank during the pre-flight inspection using the aircraft’s fuel dipstick. During the pre-flight they estimated 150 L of fuel on board, 60 L in the left tank and 90 L in the right tank (see the section titled Fuel system). Using that fuel quantity and recorded flight data, Table 1 details the expected consumption throughout the flight.
Table 1: Estimated fuel burn based on flight data
Sector
Start time
Block time
(min)
Estimated fuel burn (L) at 53 L/hr
Total
Comments
Departing Maitland
1313
0
5
145
Pilot stated, they departed on left tank (5 L allowed for taxi)
Abeam Cessnock
1317
4
4
141
Climbing phase, fuel burn was likely higher than 53 L/hr.
Near Warnervale
1325
8
8
133
Pilot stated, at approximately overhead Cessnock, they swapped to right fuller tank.
Brooklyn Bridge
1336
11
10
123
Prospect Reservoir
1346
10
9
114
Estimated engine stop
1348
2
2
113
Total
35
38
Totals have been rounded up
Post-incident inspection
The ATSB did not attend the site. A video of the aircraft, provided by 9News Australia showed fuel leaking from the right fuel tank vent. The aerodrome operator who attended the incident site stated that the fuel which leaked from the vent was no more than 2–4 litres, of which most was funnelled into a jerrycan. While the ATSB could not verify how long the fuel was leaking, based on the observations of the aerodrome operator, it was unlikely to have significantly affected the amount of fuel in the tank. There was no evidence of fuel leaking from the left tank.
Figure 5: Fuel leak from right tank vent
Source: 9News Australia
The aircraft was recovered, and an initial inspection was completed. The fuel level was checked using the on-board fuel gauges and dipstick. The left tank was estimated to hold between 0–5 L and the right tank was estimated between 40–50 L.
The aircraft’s damaged propeller was removed, and a suitable test propeller was fitted to the aircraft. The engine was started and was able to draw fuel from the remaining fuel in both tanks, the test continued for approximately 5 minutes on each tank. However, high power settings similar to in‑flight conditions were not tested.
The aircraft had undergone a fuel calibration and the placard above the fuel gauges was no longer relevant however, it was not removed (Figure 2). The placard was not considered to have contributed to the incident as the fuel on board was likely less than the 4 hours stated on the placard. The onboard fuel dipstick used was labelled C210 dipstick and was marked with the aircraft’s previous registration, ZS-MYV.
Related occurrences
Fuel management and fuel starvation incidents and accidents continue to occur with single and twin-engine aircraft. Examples of other ATSB investigations of similar occurrences include:
Fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023 (AO-2023-017)
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021)
Fuel starvation and forced landing involving Pilatus Britten-Norman Islander BN2A, VH-WQA, Moa Island, Queensland, on 3 October 2022 (AO-2022-046).
Safety analysis
The pilot reported that, during approach to Bankstown Airport, they noted an increase in propeller RPM and could not maintain altitude. This behaviour was consistent with an engine failure, with the associated loss of oil pressure resulting in the propeller moving to a finer pitch (increased RPM). The post-incident aircraft inspection did not identify an engine malfunction, and the engine was able to run at low power on the remaining fuel in both tanks. As there was no evident malfunction of the engine, the most probable reason for the inflight power loss was fuel starvation.
The pilot reported that the aircraft departed with 90 L in the right tank and 60 L in the left tank (150 L total). They also advised the right tank was selected for most of the flight. If this was the case, there should have been approximately 61 L in the right tank and 51 L in the left tank. However, given the total fuel on board after the incident occurred (maximum 59 L), it was unlikely that approximately 91 L was burnt during the 35-minute flight. Therefore, it was unlikely that the amount of fuel the pilot stated was on board at the commencement of the flight was actually in the aircraft. Significantly however, there was sufficient total fuel on board for the flight.
The post-incident inspection revealed between 40–50 L remaining (which equated to approximately 1/4 full tank) in the right tank, with about 2–4 L reportedly leaking after the landing. The pilot operating handbook (POH) stated that if there was less than 1/4 fuel in the tank and the aircraft was in uncoordinated flight, the fuel pick-ups could uncover, and fuel starvation could occur.
The post-incident inspection also revealed between 0–5 L remaining in the left fuel tank. If the engine was being supplied from the left tank, during an uncoordinated left turn at Prospect Reservoir at 1346, it is possible the fuel drained away from the fuel pick-ups and the engine continued to draw fuel from the left header tank until 1348 when the engine stopped. This was consistent with Cessna’s advice that the header tank can supply fuel for 1.5–3.5 minutes at low cruise power.
In summary, irrespective of which tank was supplying the engine, the quantities of fuel remaining, when combined with the uncoordinated flight, were conducive to fuel starvation in accordance with the POH.
The pilot’s initial response during the emergency was largely focused on attempting to reduce drag created by the propeller, despite the aircraft not having this ability, and they did not complete the engine failure during flight checklist. If the checklist had been followed, the pilot would have increased the likelihood of restarting the engine in flight. During the extended period where the aircraft was resting on the ground and positioned right-wing low, it is likely the fuel remaining in the left tank drained into the left header tank. Even though this fuel was sufficient to run the engine at low power, it may not have been available during approach or sufficient for the power required in flight.
The pilot’s decision to minimise the aircraft’s drag during the glide, by keeping the gear up and flaps retracted, combined with managing the airspeed, resulted in the aircraft achieving the required performance to land safely inside the airport environment. However, due to the distance the aircraft needed to glide and obstacles that needed to be cleared, by the time the landing gear was selected down, there was not enough time to extend and lock in place before the aircraft collided with the ground resulting in a wheels-up landing.
Finally, the CASA special flight permit was issued for the purpose of ferrying the aircraft for maintenance. The conditions put in place were to minimise the consequences if an incident occurred during flight which was conducted outside of the normal aircraft operation. Although their reported purpose was to assist with navigation and radio communication, the pilot’s decision to allow a passenger to fly on board the aircraft unnecessarily exposed them to a risk of injury and consequently was another factor that increased risk.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation involving Cessna T210M, VH-MYW, 4 km north-west of Bankstown Airport, New South Wales, on 26 May 2024.
Contributing factors
While the aircraft departed with sufficient fuel to complete the intended flight, low usable fuel quantities, in combination with probable uncoordinated flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
Other factors that increased risk
The pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot
aerodrome operator
engineer responsible for aircraft recovery
aircraft manufacturer and insurer
Civil Aviation Safety Authority
Airservices Australia
OzRunways recorded data
video footage of the incident flight and other imagery taken on the day of the incident.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
engineer responsible for aircraft recovery
Civil Aviation Safety Authority
aircraft manufacturer.
Submissions were received from the:
pilot
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]VFR route: A pre-defined laneway for aircraft traffic to remain clear of airspace and enter or exit high traffic areas such as Bankstown Airport.
[3]Automatic terminal information service: The provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations. See Automatic terminal information service (ATIS).
[4]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[5]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[6]Uncoordinated flight occurs when the aircraft skids or slips, this is most commonly associated with a turn, but a skid can occur when the ailerons and rudder are used in opposite directions during normal flight.
Occurrence summary
Investigation number
AO-2024-033
Occurrence date
26/05/2024
Location
4 km north-west of Bankstown Airport
State
New South Wales
Report release date
11/10/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Wheels up landing
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 8 March 2024, at about 1304 local time, the pilot of a Beech Super King Air 200 departed King Island Airport, Tasmania, on a private ferry return flight to Moorabbin Airport, Victoria. The pilot was the only person on board.
Passing FL160[1] on climb, the left fuel pressure and left oil pressure warning lights illuminated, and the left engine stopped shortly after. The pilot levelled off and conducted initial actions for an engine failure, secured the left engine and advised air traffic control of the engine failure. Due to the unknown fuel state onboard, the pilot conducted a return to King Island.
On descent, the pilot began to troubleshoot and identified that the engine failure was due to fuel starvation and cross-fed fuel from the right fuel system to the left engine nacelle tank, and successfully restarted the left engine. The pilot reported only using low power settings for the left engine due to concern that there would be insufficient fuel for a go-around if a higher power setting was used. The pilot conducted a normal visual approach and landing at King Island. Upon landing, the pilot checked the fuel quantity and confirmed the fuel reserves were intact.
Fuelling history
The pilot received a late roster change the previous evening which prevented them from ordering fuel for the next day. This resulted in the pilot using a company bowser in the morning which did not contain enough fuel for the planned flying that day. The pilot planned to use the remaining 700 litres of fuel in the bowser to add 350 litres to each wing. However, due to a higher than expected fill rate from the bowser, 450 litres was inadvertently added to the right fuel tanks leaving only 250 litres to add to the left fuel tanks. This resulted in a difference of 200 litres between the left and right tanks, which was within the permitted fuel discrepancy published in the pilot operating handbook. When refuelling later in the day, the pilot added 150 litres of fuel per side, however, did not correct the fuel imbalance of 200 litres.
During the flight from Moorabbin to King Island prior to the occurrence flight, the pilot detected an issue with the left fuel gauge which displayed erroneous figures. An MEL[2] was applied for the unserviceable gauge with the use of right fuel gauge only for the return sector to Moorabbin. The pilot made the decision to rely on mirroring the right fuel gauge for flight planning and inflight fuel calculations, omitting the 200 litre fuel difference.
Beech Super King Air 200 fuel system
The Super King Air 200 fuel system comprises two separate systems (one in each wing) connected by a valve-controlled cross-feed line. Within each fuel system, fuel is automatically transferred from the main and auxiliary tanks into a collector nacelle tank located directly behind the engine. In the event that one of the fuel systems is empty, fuel can be cross-fed directly to the engine from the nacelle tank in the opposite wing’s fuel system.
Safety message
Fuel starvation occurs when the fuel supply to the engine(s) is interrupted although there is usable fuel on board.
This incident reinforces the need to:
verify pre-flight fuel quantity to determine usable fuel available
use a fuel log during flight to provide a record of fuel consumption from each tank and assess remaining fuel on board when refuelling
be fully familiar with the fuel system’s operation.
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]FL – Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL370 equates to 37,000 ft.
On 20 June 2023, a Cessna 310R, registered VH-DAW and operated by Broome Aviation, was being flown on an air transport operation with a pilot and one passenger from Broome Airport to Turkey Creek, Western Australia (WA) and return. On the return flight, the pilot planned to stop at Derby Airport, to refuel.
On the return flight from Turkey Creek to Derby, the aircraft’s right engine began surging while being supplied from the auxiliary fuel tank. The pilot changed the tank selection to the right main tank, which had little fuel remaining. The right engine began surging a second time and the pilot determined there was enough fuel in the left main tank to sustain both engines to Derby. The pilot then selected the right engine to cross feed from the left main fuel tank.
Ten minutes later, both engines began surging. The pilot, assessing they had a dual engine fuel starvation, began switching fuel tanks searching for any remaining fuel. Unable to stop the engine surging, the pilot extended the landing gear and banked into a right turn with the intention of landing on the Derby Highway. During the turn, the right wing of the aircraft contacted a tree causing the aircraft to turn 180° and come to an abrupt stop on the edge of the highway.
The pilot sustained serious injuries, and the passenger sustained minor injuries. The aircraft was substantially damaged.
What the ATSB found
The occurrence
The ATSB found that the planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available. Also, the aircraft fuel gauges did not indicate accurately.
The ATSB also found that the pilot inadvertently did not select the fuel supply to the right engine to the right auxiliary fuel tank during the first leg of the journey and did not manage the fuel in accordance with the pilot's operating handbook requirements. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained.
Further, after the fuel in the right main fuel tank had been used, the pilot did not divert the aircraft to the closest airport, select the left engine to the left auxiliary fuel tank, or maintain altitude to increase their safety margin. Additionally, the pilot was not wearing an upper torso restraint during the forced landing resulting in the pilot receiving serious head injuries during the collision.
The pilot also had a lack of understanding of the aircraft fuel planning, fuel management and emergency procedures, and due to a lack of consolidation training and limited to no operational oversight these issues were not detected.
Operator oversight
The ATSB also found that during the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. In addition, aircraft defects were not being written on the maintenance release, leading to several defects not being rectified or managed.
Further, Broome Aviation pilots experienced pressure to not report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight.
Finally, Broome Aviation’s operations manual did not include a procedure for recording in‑flight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate in‑flight fuel management.
Civil Aviation Safety Authority oversight
The ATSB identified that, following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, the Civil Aviation Safety Authority (CASA) conducted a level 2 surveillance activity on the operator in early June 2023 with a key scope element being to evaluate the complaint. In addition, CASA received further complaints after the accident, that were also added to a level 1 surveillance activity in August 2023. However, the surveillance activity and the associated reports did not assess the subject of the complaints.
Additionally, CASA approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment as they had already been assessed for another operator and due to an expectation that it was an interim appointment. The person subsequently remained in the position for a much longer period and, when this situation was identified by CASA, the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO was not fully assessed.
What has been done as a result
Broome Aviation updated its operations manual to the new format exposition in response to Civil Aviation Safety Authority (CASA) findings during a level 1 surveillance audit. It now outlines an in‑flight fuel management procedure.
The operator now has both a full-time HOFO and an alternative HOFO, who is also the Safety Manager. The new HOFO reported that all company pilots are fully aware that they are available to address questions or concerns. The operator has also modified its check and training system, implementing a revised check and training procedure and updated documentation to facilitate the tracking of pilot training and competency in line with current Civil Aviation Safety Regulations (CASR).
The new HOFO has changed the defect reporting process to ensure all defects are reported to either the HOFO or the alternative HOFO, and where required noted on the MR. The operator is now using maintenance releases to systematically document defects, ensuring that issues with aircraft in the fleet are properly tracked and addressed.
Finally, Broome Aviation has implemented a safety management system in line with the current CASR in relation to a CASA audit finding. Monthly safety meetings are now being held to address safety concerns.
Safety message
Accidents involving fuel mismanagement are an ongoing aviation safety concern. In addition to the importance of ensuring there is sufficient fuel prior to, and during, flight, this occurrence reinforces the need to:
be fully familiar with the aircraft’s fuel system and capacity
conduct a thorough pre-flight inspection, including verification of the fuel quantity
ensure the appropriate tank selections are made
ensure all aircraft documentation and placarding is up to date and readily available.
This accident and many other previous accidents demonstrate the importance of pilots having knowledge of the aircraft type and its systems, especially when faced with an abnormal situation. Operators, as part of their safety management processes, should provide the opportunity for skill consolidation during and following the initial training on a new aircraft type to reduce safety risk during this transition. This is particularly relevant for types with increased complexity compared to those a pilot has previously flown.
Pilots have a vital role in ensuring maintenance personnel are aware of all aircraft defects to enable prompt rectification and compliance with aviation regulations. This includes documenting aircraft defects on the maintenance release (MR) accurately and without omission. Failing to record defects compromises aircraft airworthiness and safety, placing crew, passengers, and operations at unacceptable risk.
Pilots who perceive serious risks, such as defects not being addressed, management pressure to operate defective aircraft, or being discouraged from documenting defects on the MR, are urged to report these concerns through their organisation’s safety management system (SMS). The SMS is designed to provide a structured and confidential channel for reporting safety issues to enable investigation and resolution.
If internal reporting channels are ineffective or unavailable, pilots are encouraged to report safety concerns confidentially to either the Civil Aviation Safety Authority’s confidential reporting system (Reporting illegal behaviour | Civil Aviation Safety Authority) or the ATSB’s REPCON scheme (REPCON – Aviation Confidential Reporting Scheme | ATSB). These reporting systems ensure the identity of individuals is protected, while enabling critical safety issues to be addressed. Accurate reporting of safety concerns and occurrences is essential to preventing accidents and fostering a strong safety culture.
The occurrence
Overview
On 20 June 2023, a Cessna 310R, registered VH-DAW and operated by Broome Aviation, was being prepared for an instrument flight rules (IFR)[1] air transport operation with a pilot and one passenger from Broome Airport, Western Australia (WA) to Turkey Creek, WA. On the return flight, the pilot planned to stop at Derby Airport to refuel before returning to Broome Airport (Figure 1).
Figure 1: VH-DAW flight plan
Source: Google Earth, annotated by the ATSB
Broome to Turkey Creek
At Broome Airport, the pilot completed flight planning, using software provided by the operator. They then completed the pre-flight checks of the aircraft, including visually confirming all 4 fuel tanks (see the section titled Fuel system) were full. The pilot then delivered a safety briefing to the passenger, which included the use of seatbelts, the location of the emergency locator transmitter (ELT) and the first aid kit.
The aircraft departed Broome at 0542 local time. The pilot supplied fuel to both engines from the main fuel tanks for 60 minutes before selecting the auxiliary fuel tanks. They advised that after 30 minutes, they reselected the main tanks and continued to Turkey Creek.
The pilot indicated that when switching between fuel tanks, they recorded the duration of usage for each tank and calculated the anticipated fuel consumption on a printed flight plan as the operator did not have a formal inflight fuel log.
The aircraft landed at Turkey Creek at 0744. The pilot shut down the engines and left both fuel selectors on the main tanks position. The pilot did not check the total remaining fuel on the gauges at that time. Both the pilot and the passenger left the runway strip for approximately 6 hours. The pilot recalled being able to see the aircraft from the building in which they were waiting for the passenger to complete their business.
Turkey Creek to Derby
Upon returning to the aircraft, the pilot completed a fuel quantity check by dipping the main tanks with a dipstick. They recalled that the left main tank had 110 L of fuel, which was in line with what they expected (see the section titled Pre-flight fuel plan). However, the right main tank contained only approximately 70 L of fuel. The pilot turned on the aircraft battery to compare the dipstick readings to the fuel gauge readings and reported that both main tank fuel gauge indications correlated with the dipstick readings. Upon checking the auxiliary tank gauges, the pilot noted the right auxiliary tank gauge was indicating full, 40 L more fuel than expected, and the left was indicating as expected. Due to the design of the auxiliary fuel tanks, the amount of fuel contained in the tank can only be visually verified when the tank is full. The pilot stated they did not visually confirm the fuel level in the auxiliary tanks at that time as they assumed both auxiliary tanks had been used during the flight to Turkey Creek.
The pilot assumed the difference in fuel distribution between the tanks may have been due to an internal fuel leak from the right main tank to the right auxiliary tank, while they were on the ground at Turkey Creek, which they reported had occurred on a previous occasion (see the section titled Main to auxiliary tank fuel leak). However, the pilot was confident there was enough fuel on board, between all 4 fuel tanks, to fly the second leg of the flight to Derby Airport based off an expected 1.5 hour flight time. The pilot used these revised fuel quantity figures for pre-flight fuel planning and filled in the relevant sections of the journey log. At 1333, the pilot started the engines, taxied out to the runway and at about 1339 departed Turkey Creek with the main tanks selected.
At about 1439, the pilot switched from main fuel tanks to the auxiliary tanks. Approximately 10 minutes later, the pilot changed the fuel tank selection for the left engine to run off the left main tank. The pilot kept the right engine selected to the right auxiliary tank due to the extra 40 L of fuel they had detected during the pre-flight fuel check. Due to belief that they could only draw fuel for 45 minutes from the auxiliary fuel tanks (see the section titled Limited fuel draw from auxiliary tanks), the pilot calculated there was approximately 30 minutes of fuel available for use in the right auxiliary tank.
At about 1454, (15 minutes after they had selected the right auxiliary fuel tank), the right engine began surging. Unsure why they were unable to run the right engine on the right auxiliary tank for longer, the pilot reselected the right main fuel tank, which resolved the surging. The pilot advised that, as the autopilot had difficulty maintaining altitude (see the section titled Autopilot), they selected it to OFF when the engine issues began. Ten minutes later, the right engine began to surge again. The pilot switched back to the right auxiliary fuel tank, however the surging continued. Now at the top of descent for Derby, the pilot deliberated 2 options: shut down the right engine and fly asymmetrically or crossfeed the right engine to the left main tank and run both engines off the left main tank.
After checking the fuel gauges, the pilot determined there was enough fuel in the left main tank (approximately 45 L) to run both engines to Derby. The pilot then selected the right engine to crossfeed from the left main fuel tank and referred to the quick reference handbook for engine failure in flight checklist to determine a possible cause for the surging.
Figure 2: VH-DAW flight path
1. Change from main tanks to auxiliary tanks; 2. Change the left engine from auxiliary tank to main tank; 3. Right engine surge – changed the right engine to right main tank; 4. Right engine surge – crossfeed right engine off left main tank; 5. Inbound call for Derby Airport; 6. Dual engine surge; 7. Mayday call; 8. Accident site. Source: Google Earth, annotated by the ATSB
At 1511, the pilot made an inbound call for Derby Airport on the common traffic advisory frequency. Both engines began surging 3 minutes later. The pilot, assessing they had dual engine fuel starvation, selected the fuel pumps to HIGH and began switching fuel tank selections, searching for any remaining fuel. They advised that after they selected each tank, they waited for a response however, there was no improvement. The pilot advised that the engines did not stop but they could not maintain altitude.
At 1516:40 the passenger began video recording the flight due to its ‘apparent turbulence’, capturing the engines surging. The recording concluded about 30 seconds later, as the pilot initiated a MAYDAY[2] call to Brisbane Centre air traffic control, stating ‘dual engine failure, suspected engine fuel starvation and I have to put it down on the road’. Brisbane Centre acknowledged the MAYDAY, requested the pilot activate their ELT on landing, and requested details on the number of people on board. The pilot did not respond.
The pilot alerted the passenger to the emergency and told them to brace for impact. Approximately 30 seconds later, the pilot extended the landing gear and banked into a right turn with the intention of landing on the Derby Highway. However, during the turn the right wing of the aircraft hit a tree causing the aircraft to turn 180⁰ and come to an abrupt stop on the edge of the highway.
Upon landing, the pilot was temporarily rendered unconscious. The passenger called emergency services and a local passerby stopped to help the pilot and passenger. The passenger recalled the area smelling of fuel when stepping out of the aircraft.
The pilot sustained serious facial injuries and the passenger sustained minor injuries. The aircraft was substantially damaged.
Context
Pilot information
Qualifications and experience
The pilot held a commercial pilot licence (aeroplane), issued in December 2020. They also held a multi-engine aircraft (MEA) class rating (issued on 21 June 2021), and an MEA command instrument rating (issued/renewed on 27 August 2021).
At the time of the accident, the pilot had about 776 hours of total flying experience, with about 613 hours as pilot in command and 43.4 hours as pilot in command of MEA.
The pilot joined the operator in July 2022, commencing operations on the Cessna 210 (C210). After a period of induction and flying in command under supervision (ICUS), the pilot completed a proficiency check with the substantive[3] head of flying operations (HOFO) (see the section titled Head of flying operations) on the C210 and then commenced passenger air transport operations as pilot in command.
Prior to joining the operator, the pilot had accumulated a total of 37.6 hours on MEA, of which 35 hours were dual day flying and 2.6 hours were dual night flying, completed during the pilot’s initial MEA flight training in 2019. Up until that time, the pilot’s MEA experience had all been gained on the Piper Seminole (PA-44).
In November 2022, the pilot and other pilots from the operator hired an external instructor, at their own expense, to complete instrument proficiency checks (IPCs) on MEA, using VH-DAW. CASA did not require pilots to have a type‑specific endorsement for the Cessna 310 (C310).
By the end of November 2022, the pilot had completed online theory training relating to the basic operation of the C310 and IFR theory, including a Civil Aviation Safety Authority (CASA) MEA questionnaire. On this assessment, the pilot had incorrectly stated the size of the C310 auxiliary tanks (see the section titled Fuel system), and the requirement to use the main tanks for 60 minutes prior to using the auxiliary tanks (see the section titled Fuel management). In mid‑December 2022, when the external instructor visited the organisation for the flight component of the IPC, the instructor assessed the MEA questionnaire using the aircraft’s pilot’s operating handbook (POH). They later advised that they noted the errors, and while they did not correct the answer on the questionnaire, they discussed the correct answers with the pilot.
The pilot’s C310 IPC training included general handling skills, stalls, turns, circuit operations, instrument approaches, asymmetric training, and an outline of how the auxiliary tanks were used. The auxiliary tanks were used for no more than 10 minutes during the first flight. The pilot obtained their IPC on 16 December 2022. The instructor noted that, although fuel management was not explicitly covered during the IPC flights, they had an expectation it would be covered during the organisation’s line training.
In total, the pilot gained approximately 8.1 hours ICUS on the C310 by the end of December 2022 (Table 1). The pilot then returned to flying the C210 for the operator.
A check-to-line flight on the C310 was planned to be conducted during a passenger-carrying air transport operation on 21 March 2023, however this flight was cancelled due to a hydraulic malfunction with the aircraft. A shorter, non-air transport operation, check-to-line flight was subsequently conducted by the interim[4] HOFO on 25 March 2023, 130 days after their IPC was issued. The pilot had not flown the C310 in the interim.
The check-to-line flight with the interim HOFO covered various operational aspects, however it was focused on ensuring the pilot was proficient flying under the IFR. The pilot could not recall completing emergency procedures during this flight or using the auxiliary fuel tanks. The pilot was assessed as competent in all areas. At the end of the check-to-line flight, the pilot had accrued 10.5 hours ICUS on the C310.
Table 1: Pilot ICUS hours
Date
Location
Flight type
Flight time
12/12/2022
Halls Creek → Broome
ICUS (air transport operation)
2.0
13/12/2022
Broome → Broome
ICUS (IPC)
1.8
14/12/2022
Broome → Broome
ICUS (IPC)
1.9
15/12/2022
Broome → Broome
ICUS (IPC)
1.2
16/12/2022
Broome → Broome
ICUS (IPC)
1.2
25/04/2023
Broome → Derby → Broome
ICUS
Check-to-line
2.4
After completing the check-to-line flight, the pilot alternated between operating the C210 and the C310, accumulating 37 hours on the C210 and 43.4 hours on the C310 prior to the accident. At the time of the accident, the pilot had 53.9 hours experience on the C310, including 43.4 hours in the 90 days prior to the accident.
Recent history
In the 7 days prior to the day of the accident, the pilot completed flights on 14 June (4.6 hours flight time), 15 June (1.9 hours flight time), and 17 June 2023 (5.1 hours flight time). The pilot was rostered off duty on 18 and 19 June. They were within the operator’s flight and duty limitations for maximum cumulative flight and duty times in the 7 days prior to the accident (20 June).
The pilot reported that, on the evening of 19 June, they retired to bed at 2030, woke up at 0300 and began their pre-flight duties at 0500. The pilot noted that they went to bed earlier than normal, due to the early start time, but could not fall asleep straight away. It is likely they obtained about 5–6 hours of sleep.
The operator’s operations manual[5] detailed that, when starting between 0500–0559, pilots had a maximum available flight duty period (FDP) of 9 hours. Due to the pilot being on the ground at Turkey Creek for 6 hours, the operator reported they had organised a suitable sleeping accommodation for the pilot to allow for a split shift. This arrangement allowed the pilot’s FDP to be extended by 4 hours. The pilot was unaware of this facility, stating the operator had never previously given them suitable sleeping accommodation during a long day shift, only when needing to stay overnight. The pilot reported they waited for the client in an air‑conditioned room and had an adequate amount of food.
The pilot reported that they felt somewhat rested during the day of the accident flight and recalled that, although they had gone to bed early, they had not fallen asleep straight away. Based on the available information, the ATSB concluded that the early wake-up time and long duty day were problematic but, overall, there was insufficient evidence to conclude that the pilot was experiencing a level of fatigue known to affect performance.
Medical information
The pilot held a class 1 aviation medical certificate that was current to 3 May 2024. This specified a requirement for the pilot to wear distance vision correction. The pilot stated that they did not have any medical concerns or issues in the period prior to the accident.
Aircraft information
The Cessna 310R is a twin-engine, low-wing, 6-seat, unpressurised aircraft equipped with retractable landing gear and powered by 2 Continental IO-520 piston engines. VH-DAW was manufactured in the United States and first registered in Australia in 1975. Broome Aviation became the registration holder on 12 July 2011.
Fuel system
The C310 fuel system consists of 2 sets of fuel tanks in the wings – main and auxiliary, that supply fuel to each engine independently. Two fuel selectors, one for each engine, are installed on the floor between the pilot seats. These allow selection of main fuel, auxiliary fuel, crossfeed and fuel shutoff (Figure 10). The selector allows fuel to flow from the selected fuel tank to the engine‑driven fuel pump for the selected engine. Figure3 shows the layout of the standard fuel system installed in the aircraft.
Figure 3: VH-DAW Fuel System
1. VH‑DAW was fitted with both optional auxiliary tanks, totalling 31.5 US gallons on each side; 2. The aircraft did not have the optional low level fuel light fitted. Source: C310 POH, annotated by the ATSB
Main tanks
The 2 main fuel tanks for the C310 are integrally‑sealed aluminium tanks located on each wing tip. Each main tank holds 189 L (50 United States (US) gallons) of usable fuel, with approximately 7.5 L of unusable fuel. There are 2 fuel pumps in each main tank, the first (auxiliary fuel pump) is used to provide fuel pressure to prime the engine for start or to provide fuel pressure during an engine‑driven fuel pump failure. The second (transfer pump), operates continuously during flight and allows the transfer of fuel from the nose section to the centre section of the main tank, where the fuel outlet is positioned. The transfer pumps are on the same electrical circuit as the left landing light. The main tanks are vented to atmosphere and if overfilled, fuel will be vented overboard through these vents.
Auxiliary tanks
The auxiliary fuel tanks are bladder‑type tanks and are located in the outboard section of each wing. Each auxiliary tank holds 119 L (31.5 US gallons) of usable fuel. The POH stated that fuel could be drawn from the auxiliary tanks during cruise flight only.
Engine-driven fuel pump
Each engine had an engine‑driven fuel pump that contained a bypass, which continuously returned excess fuel and vapour to their respective main tank.
Fuel management
The POH stated:
If auxiliary fuel tanks are to be used, select main fuel for 60 minutes of flight (with 40-gallon auxiliary tanks) or 90 minutes of flight (with 63-gallon auxiliary tanks). This is necessary to provide space in the main tanks for vapor and fuel returned from the engine-driven fuel pumps when operating on auxiliary fuel. If sufficient space is not available in the main tanks for this diverted fuel, the tanks can overflow through the overboard fuel vents.
It also stated:
Since part of the fuel from the auxiliary tanks is diverted back to the main tanks instead of being consumed by the engines, the auxiliary tanks will run dry sooner than anticipated; however, the main tanks endurance will be increased by the returned fuel. The total usable fuel supply is available during cruise flight only. An engine failure or engine driven fuel pump failure results in the auxiliary fuel on the side of the failure to be unusable.
It was recommended that auxiliary fuel was used until either exhausted or the flight phase had reached the top of descent. When questioned by the ATSB, neither the engine nor aircraft manufacturer could provide a fuel flow rate to calculate how much fuel was being returned to the main tank when the auxiliary tank was selected. The POH also advised ‘operation of the auxiliary fuel tanks near the ground (below 1,000 ft) is not recommended’.
The pilot advised that to simplify fuel management, they routinely used the main tanks for 60 minutes on each segment of a flight before selecting auxiliary tanks. They did not mention the reasoning behind using 60 minutes rather than the expected 90 minutes associated with the larger auxiliary fuel tanks (as fitted to VH‑DAW) detailed in the POH. Other pilots within the organisation who flew the C310 also reported using the 60-minute timeframe.
Fuel flow gauge
The fuel flow gauge indicated the approximate fuel consumption of each engine in pounds per hour. The POH stated that the gauge dial is ‘marked with arc segments corresponding to proper fuel flow for various power settings and is used as a guide to quickly set the mixtures. The gauge has markings for take-off and climb, and cruise power settings for various altitudes.’
The pilot advised that they used the fuel flow gauge while leaning the engines to determine the engines were receiving the appropriate fuel flow and to ensure the flow was stable after changing fuel tanks. The pilot reported that this process was completed during the accident flight on all tank changes.
Fuel quantity gauge
One fuel quantity gauge was located above the right-side control column and indicated the weight of the fuel (in both US gallons and pounds) for the left and right fuel tanks on the display. The gauge showed the fuel quantity for the selected tanks (either main or auxiliary) and the fuel quantity in the non-selected tanks could be displayed through the use of a toggle switch below the gauge. There were also 2 yellow indicator lights (one for each side), these illuminated when the auxiliary tank on the selected side was selected (see Figure 7).
The aircraft was not equipped with the optional independent low fuel warning lights for the main fuel tanks.
Vortex generators
VH-DAW was fitted with 88 vortex generators located on the wings and vertical fin with additional strakes mounted on the outboard of each engine nacelle. The Supplemental Type Certificate (STC) for this modification included various amendments to the limitations and performance, including reduced stall and VMCA[6] speeds, and allowed for an increased operating weight.
Site and wreckage
Accident site
The ATSB did not attend the accident site. The site was attended by members of the Western Australia (WA) Police Force on 20 June 2023 and by the aircraft operator the following day. The site inspection was recorded by the police and the video footage was provided to the ATSB, along with photographs taken on the day of the accident (Figure 4).
Figure 4: Accident site
Source: Western Australia Police Force
The wreckage was located on the edge of the road in an area of low foliage, approximately 2.8 NM (5.2 km) east-south-east of Derby Airport. The left main tank and right auxiliary tank were ruptured during the accident sequence.
The left auxiliary tank was reported by the operator as being intact and found to contain about 20 L of fuel, while the right main tank contained negligible amounts of fuel. As both wings displayed visible damage (Figure 5), the ATSB was unable to verify if fuel had leaked from the fuel tanks following the ground collision. The propellers on both engines were not in the feathered position.
Figure 5: Left and right wing damage
Top image – left wing; bottom image – right wing. Source: Western Australia Police Force, annotated by the ATSB
While reviewing the video footage taken by the police onsite, the left landing light circuit breaker was found to have tripped. The ATSB could not verify if this occurred due to ground impact forces or during the flight.
The operator arranged for the wreckage to be transported to a non-secure storage area at Broome Airport, which required the wings and one horizontal stabiliser to be separated from the fuselage.
ATSB examination
On 30 June 2023, the ATSB examined the wreckage focusing on the aircraft fuel system, particularly the right wing, both auxiliary fuel tanks, and the fuel quantity indicating system (FQIS). Despite the disruption during the accident sequence and transportation, no pre-existing defects or fuel system anomalies were identified. The following key components were retained for further examination and testing:
right and left auxiliary interconnect check valves
right and left vapour return check valves
right fuel selector mains inlet port
right fuel selector auxiliary inlet port
FQIS indicator and signal conditioner.
Detailed technical examination of these components identified the following defects in 3 components, which likely existed prior to the accident:
right fuel selector – main tank inlet valve did not seal when closed (i.e. when not selected ON)
the check valve in the right auxiliary tank outlet bleed return line (interconnecting the inboard and outboard fuel cells) did not seal in the reverse flow direction
the right vapour return line (engine driven fuel pump to main tank) check valve did not seal in the reverse flow direction.
Testing of the check valve in the right auxiliary tank vent outlet bleed return line in the reverse direction identified a small leak. However, the testing indicated that the leak rate was significantly less than that required to allow fuel to have transferred from the main tank to the auxiliary tank while the aircraft was on the ground at Turkey Creek in the quantities reported by the pilot.
Civil Aviation Safety Authority (CASA) Airworthiness Bulletin (AWB) 28-010 stated that if this valve was leaking, it could allow the engine‑driven fuel pump to draw air into the fuel system resulting in either engine surging or loss of power. It was reported that this is most likely to occur when the auxiliary tank quantity was less than about half full.
The differential pressure applied to the check valve during testing was likely far lower than expected operating pressures. Therefore, it is possible that during engine operation with the auxiliary fuel tank selected, as the fuel quantity reduced, the increased system pressure affected the leak rate and resulted in an increased reverse flow. This may allow the engine driven fuel pump to draw air in sufficient quantity to effect engine performance.
There was no evidence of defects in the auxiliary tank inlet valve of the right fuel selector or the corresponding check valves from the left fuel system. The left fuel selector was not implicated in the occurrence and was therefore not tested.
The FQIS indicator and signal conditioner were not tested or examined due to difficulty finding a facility capable of testing the signal conditioner. Although testing may have established the serviceability status of these individual components, aircraft accident damage prevented operational testing of the whole system. As such, evidence provided by pilots that the FQIS system was not indicating correctly was relied upon (see section titled Fuel gauge displays).
Aircraft maintenance
Maintenance release
A maintenance release (MR) is required to be carried on an aircraft as an ongoing record of the aircraft’s time-in-service and airworthiness status. The operator’s system of maintenance stated that the MR was valid for 200 hours in service or 12 months from issue, with inspections to be completed at 50, 100, 150 and 200 flight hours.
A daily inspection was required to be carried out and the MR signed to show the inspection had been completed, prior to the first flight of the day. The inspection and certification could be made by any pilot licenced to fly the aircraft, or an appropriately licenced aircraft maintenance engineer. After the last flight of the day and before the aircraft was next flown, the total daily flight time was required to be entered and the progressive total time in service recorded.
The MR is also used to record any maintenance which is due on the aircraft prior to the next periodic inspection, or any defects[7] detected.
The last periodic maintenance inspection was carried out on 11 May 2023 at 150 flight hours. At that time the aircraft total time in service was 18,630 hours. The aircraft had flown 30 hours since this inspection with no defects recorded. The only maintenance issue recorded on the MR was a hydraulic leak in the right main brake, which was rectified and signed off by a maintenance engineer on 24 April 2023.
The ATSB interviewed all 5 pilots who had flown the operator’s C310 during the period from December 2022 to June 2023, as well as other pilots who flew the operator’s C210s. Most of the pilots interviewed stated they were encouraged not to write any defects with aircraft on the MRs. These pilots recounted that if any defects were documented on a MR, they would be reprimanded by the CEO and face a reduction in flight hours on the subsequent roster.
The pilots also reported that the interim HOFO (see the section titled Head of flying operations) exhibited more willingness for defects to be documented on the MR, however they firstly required assurance that the reported matter was a legitimate defect. The pilots had mixed views on the stance of the substantive HOFO, with 3 noting they had been told not to write defects on the MRs. Two pilots stated they had attempted to implement a ‘snag’ recording system as an alternate method of recording defects, however this was never adopted.
Most pilots advised that, to circumvent what they assessed as a restriction on using the MRs to record defects, they utilised a group chat to communicate specific issues they had encountered on different aircraft in the fleet. They also noted they found it easier to directly communicate with engineers in the maintenance facility if they had any issues after they completed a flight. This approach usually resulted in minor defects getting fixed immediately.
The substantive HOFO stated they were unaware of any ongoing defects with the operator’s C310 and were unaware of any instances of the CEO reprimanding pilots due to the recording of defects on the MRs. They also stated that, on occasion, pilots deviated from the standard documented procedure for defect reporting (see the following section titled Defect reporting process).
The interim HOFO also noted that any defects with aircraft in the fleet should have been reported to them and put on the MR, although even if this was not the case then pilots could go straight to the engineers in the maintenance facility to get the matters rectified. In relation to the C310, the HOFO stated the aircraft fuel gauges ‘weren’t fabulous’, however they did not offer an explanation why this was not written up on the MR. They reported being unaware of any other aircraft defects.
The chief engineer advised that all defects would be reported to them by either the HOFO or the CEO using the operator’s defect reporting process. Contrary to the process advised by the pilots, the chief engineer advised that as Broome Air Maintenance was not a part of Broome Aviation, all rectification work had to be requested, and that pilots were not permitted to bypass the request.
The CEO stated that if there was a defect with an aircraft, they would have expected the pilots to follow the company’s policy regarding defects and write them on the MR. When asked about the C310, the CEO recalled having no knowledge of any defects with the aircraft other than the autopilot not holding altitude. No reason was provided as to why this was not written on the MR. The CEO reported that the fleet were maintained to a high standard and that if a pilot found a defect on an aircraft it would be delt with accordingly. They dismissed the reports they would reprimand pilots for reporting defects, noting they were ‘pedantic’ about maintenance.
Defect reporting process
The operator’s operations manual outlined a formal process to report deficiencies detected between periodic inspections, which stated:
Line pilots shall report any deficiencies to the [head of flying operations] HOFO, [head of maintenance control] HAMC and CEO via email; verbal or text message notification may be used as a secondary notification method where appropriate or required.
Once an email was received from a pilot, the process required the HOFO to liaise with the HAMC to determine the steps to investigate and rectify the deficiency. The substantive HOFO advised that if a pilot were to call with an issue, if required, the HOFO would tell the pilot to endorse the issue on the MR and then the HOFO would follow up with engineering personnel.
The chief engineer reported that they did not use the maintenance release to record defects. Rather, if defects were identified either by the operator or by the maintenance organisation, these defects would be rectified and recorded in the aircraft’s Broome Air Maintenance (BAM) worksheets. The ATSB inspected the aircraft logbooks and was unable to identify any unscheduled maintenance. The last unscheduled maintenance recorded in the logbooks was dated 2017.
The interviewed pilots stated that if they detected an aircraft defect, it was easier to talk directly to individual engineers in the maintenance facility, as they were usually in the hangar when returning from a flight and it was more likely to be dealt with.
Reported aircraft issues
The operator’s pilots reported multiple issues with the aircraft to the ATSB, including:
inaccurate fuel gauge displays
an internal fuel leak from the right main tank to the right auxiliary tank
limited fuel draw from the auxiliary tanks
engine surging
inability of the autopilot to accurately maintain an assigned altitude
significant tail flutter.
During an interview with the ATSB, the chief engineer reported that, to their knowledge, the aircraft was fully serviceable with no issues identified. They also advised they were not aware of the issues raised by the pilots.
Fuel gauge displays
Fuel calibration cards are aircraft specific and used to enable an accurate assessment of fuel quantity. The aircraft’s dual indicating fuel quantity gauge was last tested and calibrated on 24 June 2020. Pilots reported that the main tank calibration card was disregarded as it was considered inaccurate.
There was no fuel calibration card relating to the auxiliary tanks. The ATSB was unable to confirm if the auxiliary tank calibration had occurred as there was no record in the maintenance worksheets or the aircraft logbook of the results. There was no regulatory requirement to record the results of a fuel gauge calibration test.
The next due date to test and recalibrate the fuel gauges was expected to be in June 2024 in compliance with the CASA Civil Aviation Order (CAO) 100.5 General requirements in respect of maintenance of Australian Aircraft – 2011 and the operator’s system of maintenance.
Pilots who operated the aircraft reported that the fuel gauges displayed significant inaccuracies when the tanks were full. Specifically, when the main tanks were full, the right main tank display would exceed full scale deflection, while the left main tank display would under‑read by approximately 64 L (105 lbs) (Figure 6).
Figure 6: VH-DAW main tank fuel gauges
Left image – expected fuel gauge indications for main tanks when full; right image – the reported fuel gauge indications for main tanks when full. Source: Braden Blennerhassett (Air Manager), edited by the ATSB
It was reported that, as fuel was used during the fight, the displays became progressively more accurate, however there was still a large discrepancy between the displays (Figure 7). The expectation was that, when the fuel tank selection was changed from main to auxiliary or vice versa, both sides would be changed at the same time.
Figure 7: VH-DAW main tank fuel gauge indications after supplying the engines for the same time
Both the left and right main tanks had been used for the same amount of time during the flight. Source: Pilot of VH-DAW, annotated by the ATSB
It was reported that when the gauge was selected to the auxiliary tank display, there was also a discrepancy when the tanks were full, although the difference was not as significant as that observed with the main tank display. It was reported that the display for the left auxiliary tank under‑read by approximately 9 L (15 lb), while the display for the right auxiliary tank under‑read by approximately 36 L (60 lb) (Figure 8). Pilots did not indicate that the accuracy of the auxiliary tank gauge displays improved during use. However, it was noted that the auxiliary tanks were never used below about 12 L.
Figure 8: VH-DAW auxiliary tank fuel gauges
Left image – expected fuel gauge display for auxiliary tanks when full; right image – reported fuel gauge display for auxiliary tanks when full. Source: Braden Blennerhassett (Air Manager), edited by the ATSB
The fuel gauge inaccuracy was reported to be widely known by pilots and informally reported to individual engineers in the maintenance facility, however the defect was not recorded on the aircraft’s MR. Pilots reported that maintenance personnel informed them that the external organisation capable of fixing the gauges indicated that new sensors were needed, and that the process of fixing the gauge was lengthy and the necessary parts were costly and so it was unlikely it would be completed. The CEO stated they were unaware of any issues with the fuel gauges.
The pilots advised that they adopted a time-based approach to track the amount of fuel in each tank during flight, noting there was no other guidance from the interim HOFO or senior management on how to manage the fuel quantity. Pilots stated that the most accurate way to ensure the known quantity of fuel on board prior to take-off was to depart Broome with full main and auxiliary tanks and, where possible, fill the main tanks to full when flying intermediate sectors.
The aircraft minimum equipment list (MEL) allowed 1 display on the gauge to be inoperative[8] providing a reliable means was established to ensure that the fuel quantity on board met the requirements for the intended flight.
Main to auxiliary tank fuel leak
The pilot of the accident flight and the supervisor of their first ICUS flight reported there were occasional instances where, having been fully refuelled, the right main tank would be missing approximately 10–30 L of fuel the following day. They further advised that when this occurred, the right auxiliary tank would overflow when the fuel cap was removed (Figure 9). This led the pilots to suspect a fuel leak between the right main and auxiliary tanks.
Figure 9: Auxiliary fuel tank overflowing on morning inspection
Source: Previous operator pilot, annotated by the ATSB
This issue was informally reported to maintenance staff, but not recorded on the MR. The CEO reported being unaware of the issue. After the initial report, the reporting pilot noted that engineers in the maintenance facility were unable to identify a fuel leak. Although the issue reportedly recurred, it was not further reported.
Limited fuel draw from auxiliary tanks
The pilot of the accident flight stated that the auxiliary fuel tanks could only supply the engines for 40–45 minutes before surging occurred. They noted that their initial understanding of the limited fuel draw came from the supervisor of their first ICUS flight. They further advised observing this limitation on their first solo passenger-carrying flight in the aircraft.
This issue was informally reported to individual engineers in the maintenance facility by the supervising pilot, and they recalled that maintenance was unable to identify a cause. The pilot of the accident flight assumed that since the issue had been reported previously, it had been addressed by maintenance. However, both the CEO and the chief engineer advised being unaware of the issue.
Other pilots stated that around the 40-minute mark while using auxiliary tanks, the aircraft’s engines would lightly surge before regaining power. They would then continue to use the fuel from the auxiliary tanks until about 12 L remained, before changing to the main tanks. The HOFO reported there were no issues when using the auxiliary tanks.
Engine surging
Multiple pilots recalled that the engines would surge during flight. The pilot of the accident flight and one other pilot noted the surging generally occurred when operating on auxiliary tanks, which they attributed to the limited fuel draw issue.
Other pilots also recalled the engines surging however, they could not confirm which tanks were selected at the time. These surges were described as minor and intermittent, typically ceasing after a few seconds and did not require the fuel pumps to be selected ON.
The engine surging had been reported to individual engineers in the maintenance facility verbally and had not been documented on the MR. Both the CEO and the chief engineer advised that they were unaware of this issue.
Autopilot altitude hold
According to pilots who operated VH-DAW, the aircraft’s autopilot maintained an accurate heading, however, despite pre-flight testing of the system reportedly consistently indicating that the autopilot was fully operational, it could not maintain an assigned altitude. There was no evidence or record that this issue was formally or informally reported to the engineers in the maintenance facility, and the chief engineer advised not being aware of the issue. However, the issue was known to the organisation’s CEO, at the time of the occurrence.
An autopilot was considered inoperative if it was unable to maintain both altitude and heading. The aircraft MEL allowed continued operation with the autopilot inoperative under any one of the following conditions:
if flight was operated under IFR rules for RPT, charter[9] or aerial work, the aircraft was equipped with dual controls and had 2 control seats, with one control seat occupied by the pilot in command of the aeroplane and the other seat occupied by a person holding a commercial pilot (aeroplane) licence with an endorsement on the aircraft and an instrument rating
if the flight was operated under IFR rules with a single pilot for RPT, charter or aerial work, the flight was within the period of 3 days commencing on the day on which the autopilot became inoperative provided only one capability of the autopilot system was unserviceable
the flight was operated under VFR rules
the flight was operated for a private flight.
Elevator flutter
Pilots reported the presence of a known elevator flutter[10] on the aircraft, which was attributed to the installation of vortex generators on the elevator. This flutter resulted in challenging handling characteristics at low speeds, particularly during take-off and landing.
The engineers in the maintenance facility had conducted an extensive investigation into the issue in 2018, including the removal and reinstallation of the vortex generators. They concluded that the flutter did not impose stress on the airframe, and the aircraft was returned to service on 13 August 2018. The vibration defect was raised again on the MR on 20 October 2022 and cleared by maintenance personnel on 4 November 2022. There was no information regarding what was completed during the November sign‑off. The pilot of the accident flight stated that the elevator flutter was still present, although not noted on the accident flight.
Aircraft placarding
The fuel selectors had plaques stating the amount of fuel in each tank in US gallons. On inspection, it was noted that the auxiliary tank capacity for both sides incorrectly indicated that small auxiliary tanks (20 US gallons) were fitted to the aircraft (Figure 10).
Figure 10: VH-DAW fuel selector plaques
Source: Operator, annotated by the ATSB
This contradicted the usable fuel decals next to each filler cap on the airframe, which identified that the auxiliary tanks held 119 litres (31.5 US gallons) (Figure 11).
Figure 11: VH-DAW fuel decals
Source: ATSB
Just above the fuel selector plaques, there was a requirement for a plaque specifying how long to operate on the main tanks when first taking off with full tanks. For a C310 with the larger auxiliary tanks, the plaque was required to include:
Use main tanks for takeoff, landing and first 90 minutes of flight.
This plaque was missing from the aircraft (Figure 12).
Figure 12: VH-DAW internal placards relating to the fuel system
Top image – VH-DAW internal fuel placarding; bottom image – exemplar internal fuel placarding. Source: Top image – ATSB; bottom image – Textron, annotated by the ATSB
All aircraft placarding was required to be checked under the aircraft system of maintenance every 200 hours for security, presence and legibility. There was no requirement to check the validity of the information presented on the placards. The aircraft had five 200‑hourly maintenance events in the last 5 years, the last being August 2022.
The fuel selector placards had last been replaced on 24 October 2008, prior to the aircraft being registered to Broome Aviation. The installed placards were the incorrect part number and as such displayed the incorrect size of the auxiliary tanks. The ATSB was unable to determine if the plaque relating to the 90 minutes on mains had been removed previously or never installed.
The pilot of the accident flight was unaware that any of the plaques were incorrect, noting that they had not discussed it with the instrument proficiency check (IPC) instructor (see the section titled Qualifications and experience) or HOFO.
Fuel management
Pre-flight fuel plan
The flight plan used by the pilot on the day of the occurrence was destroyed during the accident and was not recorded by the operator’s planning software. During the draft report review process the pilot advised that they had recently found a copy of the flight plan, which they provided to the ATSB. The plan (Figure 13), generated by the flight planning software, showed a zero fuel margin. The pilot stated that they did not input the expected winds for the flight as they were unaware how to. Additionally, they recalled that all their previous flight planning had been conducted with nil wind.
Figure 13: Accident flight fuel plan
Source: The accident pilot
A pre-flight fuel plan was created using the operator’s software (Figure 14). The flight plan software used a 120 L/h fuel burn for cruise and 150 L/h for climb. These figures were extracted from the POH performance tables using the typical operating conditions encountered for different phases of flight when flying out of Broome Airport.[11]
The known winds on the day of the occurrence were used. The fuel plan showed that the aircraft could not legally fly with the required reserves on the return flight to Derby.
Figure 14: Example fuel plan based off reported winds for each sector of the occurrence flight
Trip T – Trip total less taxi fuel; Contin – Contingency fuel (15% of expected trip total); F. Reserve – Fixed reserve; Fuel R – Fuel required for next leg including contingency and fixed reserve; Margin – Endurance subtracting fuel required; Endce – Endurance. Source: Operator, annotated by the ATSB
The ATSB also generated a fuel plan based on the pilot’s understanding of the amount of fuel they could use from the auxiliary tanks. The analysis used:
the flight times calculated by the operator’s software
the pilot’s standard use of 40 minutes from the auxiliary tanks
1.5 x fuel burn rate[12] – the extra fuel was diverted to the main tanks.
This resulted in approximately 120 L of fuel being available for use from the auxiliary tanks (40 L plus the redraw of 20 L = 60 L from each auxiliary tank). Therefore, the pilot’s perceived total available fuel onboard when all tanks were full was 498 L (main tanks 378 L + auxiliary tanks 120 L). As shown in Table 2, such a plan indicated there was insufficient fuel onboard to conduct the flight without fuel starvation.
Table 2: Fuel calculation comparison
ATSB calculated Leg 1
ATSB calculated Leg 2
Start fuel
498 L
241L
Trip fuel (climb + cruise + taxi)
257 L
251 L
Expected remaining fuel onboard at destination
241 L
-10 L
Contingency fuel
37 L
36 L
Fixed fuel reserve
90 L
90 L
Fuel margin
114 L
-136 L
A previous pilot of the C310 indicated that when flying the same route, on the return leg they would refuel the aircraft at Halls Creek, another base for the operator, as it was 77 NM south-west of Turkey Creek. They would then fly directly from Halls Creek to Broome. This flight route ensured they had enough fuel to complete the flight with reserves intact.
Previous flight
The pilot recalled completing the same flight 4 weeks prior to the occurrence. They stated that they had landed at Derby and refuelled the aircraft for the final leg back to Broome. A retrospective fuel log was created using the known winds on that day and the pilot’s reported timing of the fuel tank changes (Table 3). The ATSB also calculated the average fuel burn for the aircraft during this flight using the fuel added to refuel the aircraft to full after the flight which showed the aircraft used an average of 124 L/h.
The operator’s standard 12 L taxi fuel was used for the first leg of the flight. Due to the prevailing wind, the first leg from Broome to Turkey Creek was recorded as having a duration of 126 minutes, requiring the pilot to use the auxiliary tanks for 40 minutes (66 L draw from auxiliary tanks and 22 L returned to the main tanks on both sides).
The flight time from Turkey Creek to Derby was recorded as 90 minutes. Due to the assumed auxiliary tank issue and having used the auxiliary tanks for 40 minutes on the first leg, the pilot would have likely used main tanks for the entire leg. It is highly probable that the pilot landed at Derby with 21 L of useable fuel remaining in each of the main tanks, equating to about 15 minutes of remaining engine operation before fuel exhaustion.
Table 3: Retrospective fuel log of previous flight Broome – Turkey Creek – Derby on 25 May 2024
FUEL LOG
Broome – Turkey Creek
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
Taxi Broome
119
189
189
119
Departure Broome
119
183
183
119
Change to auxiliary tanks
119
123
123
119
Change to main tanks
59
143
143
59
Estimated fuel on landing
59
117
117
59
Turkey Creek – Derby
Taxi Turkey Creek
59
117
117
59
Departure Turkey Creek
59
111
111
59
Estimated fuel on landing
59
21
21
59
Fuel quantity analysis of the accident flight
The ATSB obtained flight data that was transmitted at regular intervals from a V2 Flight Tracker, which had been installed on the aircraft. A retrospective fuel log for the Turkey Creek to Derby leg (Table 4) was created using:
the pilot’s recalled amount of fuel in each tank on startup
the pilot’s recollection of when they completed tank changes
the operator’s average fuel consumption rate of 120 L/h
a conservative estimate of fuel return (0.5 multiplier) to the main tanks when using auxiliary tanks
a conservative estimate of fuel draw from the left main tank (2.5 multiplier) and return to the right main tank (0.5 multiplier) when cross feeding the right engine.
As such, it is only indicative of the fuel on board in each tank at each change of tank and at the time of the dual engine surging.
Table 4: Retrospective fuel log of remaining fuel in aircraft from Turkey Creek to the point of the dual engine surge using 120 L/h
FUEL LOG
Turkey Creek – Dual engine surge
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
1336: Taxi Turkey Creek (used 6 L each side)
74
110
70
119
1339: Departure Turkey Creek
74
107
67
119
1439: Change to auxiliary tanks
74
44
4
119
1449: Change left auxiliary to main tank
59
49 (44+5)
9 (4+5)
104
1454: Change right auxiliary to main tank
59
44
12 (9+3)
97
1504: Cross feed left main tank
59
34
2
97
1514: Dual engine surging
59
9
7 (2+5)
97
At the point of dual engine surge, it is estimated that the left main tank had approximately 9 L of fuel remaining.
The aircraft manufacturer stated that if the engines were surging while on the main tanks and there were no other issues with the fuel system and fuel available in the auxiliary tanks, the pilot should have been able to use the remaining fuel in the auxiliary tanks to regain full power. At the point of the dual engine surge, the left auxiliary tank had approximately 59 L and the right had approximately 97 L available.
The same calculations were completed using the pilot’s average fuel consumption rate of 124 L/h (see the section titledOperator fuel flow check). Those calculations (Table 5) indicated that about 6 L of fuel remained in the left main fuel tank (supplying both engines) at the point of the dual engine surging.
Table 5: Retrospective fuel log of remaining fuel in aircraft from Turkey Creek to dual engine surge using the pilot’s average 124 L/h
FUEL LOG Turkey Creek – Dual engine surge
Phase
Left
Right
Auxiliary
Main
Main
Auxiliary
1336: Taxi Turkey Creek (used 6 L each side)
73
110
70
119
1339: Departure Turkey Creek
73
104
64
119
1439: Change to auxiliary tanks
73
42
2
119
1449: Change left auxiliary to main tank
58
48 (42+6)
8 (2+6)
104
1454: Change right auxiliary to main tank
58
42
10 (8+2)
96
1504: Crossfeed left main tank
58
32
1
96
1514: Dual engine surging
58
6
5 (1+4)
96
Operator fuel planning requirements
Pre-flight
The operator’s procedures required the pilot to complete pre-flight fuel planning using the available electronic flight planning software. However, if the flight planning software was not available, the pilots were required to calculate the fuel required for the flight using the fuel flow guidelines for the aircraft.
The operations manual outlined the fuel figures, specific to the C310, to be used when manually completing fuel planning. The guidelines did not contain a fuel flow rate for climb. However, they did include a block (total) fuel margin of 47 L which was to be available for each sector. The operator advised they were not aware of where the margin of 47 L figure had originated from. The electronic flight planning software did not include this 47 L margin fuel when calculating fuel requirements.
To confirm the amount of fuel on board prior to flight, the operator’s fuel policy required pilots to visually confirm the fuel quantity in each tank using a dip or drip stick when possible, then compare this to the flight plan and fuel gauges. If there was a discrepancy more than an allowable margin with the fuel gauges the pilots were required to inform the HAMC and/or HOFO to determine the possible cause. The allowable margin quantity was not listed in the operator’s fuel policy.
Inflight
The operator’s procedures required pilots to recalculate fuel in flight at 2 specific points:
when reaching cruise
if required to divert.
The procedures outlined that once reaching cruise altitude pilots should:
calculate the remaining quantity of fuel on board for the proposed destination. This must be equal to or above the legal minimum final reserve quantity. If this is not the case, consider using more conservative fuel power settings, change cruise level for more favourable winds or divert to an alternative.
The procedure did not stipulate if this calculation was required to be recorded on any documentation, nor did it outline any requirement for a fuel crosscheck. Additionally, the operator did not have a fuel log or method of monitoring fuel during the flight.
If the pilot was required to divert, inflight fuel replanning was to be carried out using the fuel flow guidelines for the aircraft.
A previous pilot for the operator stated there was no standardised method of completing inflight fuel logs and it was based on pilot preference. They further reported a ‘feeling’ that the organisation had not had any fuel starvation events due to ‘luck’.
Post-flight
The operator’s procedures recommended that pilots conduct a fuel gauge check against the value on the fuel totaliser at the completion of a flight. However, the operator stated that none of its aircraft were fitted with a fuel totaliser. Additionally, the quantity of fuel used was to be checked against the expected burn from the flight plan.
Pilots were required to complete the fuel documentation, including recording on the journey log and manifest the amount of fuel at shutdown. The manifest did not provide the option to indicate the remaining fuel in each tank.
Operator fuel flow check
The operator reported that pilots were required to enter the amount of fuel consumed and flight time after each flight into the organisation’s data recording software. The program created a monthly report, which outlined the fuel flow rate for each flight, segregated by aircraft.
The substantive HOFO used this information to determine the average fuel flow for each aircraft, and which pilot completed each flight. If there was an unexpected trend for a particular pilot, the substantive HOFO would use this to discuss how the pilot was configuring the aircraft’s fuel system during flight. If the trend was over multiple pilots, the HOFO would liaise with maintenance to determine the cause.
The substantive HOFO noted there was no indication that the aircraft was burning more than the expected 120 L/h however, they could not confirm if this process was being completed by the interim HOFO while they were on leave. ATSB analysis of the pilot’s flight times and fuel uplift over the previous 10 flights indicated the aircraft was using 124 L/h on average.
Regulatory requirements
Pre-flight fuel planning
According to Civil Aviation Safety Regulation (CASR) Part 135 Australian air transport operations – smaller aeroplanes section 135.205 operators are required to provide pilots with an exposition which provides comprehensive tools, procedures, and guidance for effective pre-flight fuel planning. The exposition must outline step-by-step instructions for calculating fuel requirements to ensure compliance with Australian regulations and operational safety.
According to CASR Part 135.D.6 and the Manual of standards (MOS) Part 135 7.04, pilots must have access to resources for determining fuel needs for each phase of the flight, including:
taxi fuel
trip fuel
holding fuel
destination alternate fuel
contingency fuel
final reserve fuel
There should also be a process outlining:
fuel calculations
determining and recording fuel quantities – pre-flight
recording fuel quantities.
To support these calculations, operators must provide tools such as flight planning software, fuel calculation tables, or automated planning systems. Operators are also responsible for ensuring that pilots are trained to use these resources effectively and can adjust their fuel requirements based on dynamic operational factors, such as deteriorating weather or delays.
Part 135 manual of standards (MOS) Section 7.03 (2) required that the pilot in command must consider the effect of the relevant meteorological reports and forecasts when determining the quantity of useable fuel.
In-flight fuel management
The Part 135 MOS Section 7.05 (2) required that the exposition outline a process for regular inflight fuel checks, which required the pilot to:
determine the amount of fuel remaining
analyse planned fuel consumption against actual consumption
determine there is sufficient fuel on board
calculate the amount of fuel expected to remain at the destination.
According to the CASA Advisory circular 1-02 V4.1 Exposition and operations manual fuel policy guidance Annex D, the exposition should detail what maximum discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure is tolerable, noting that industry practice is a maximum of 3% discrepancy.
Part 135 MOS section 7.03 required that operators must provide pilots with aircraft‑specific fuel consumption. This could be sourced from the aircraft/engine manufacturer or taken from recent historical consumption records. Operators should also require pilots to document any significant deviations in fuel consumption or incidents involving fuel advisories or emergencies. This data enables operators to analyse and improve fuel planning and management procedures.
In addition, Part 135 MOS section 7.06 required that operators must also ensure that the exposition outlines clear procedures for pilots to follow in the event of a low-fuel situation, including:
a minimum fuel state
emergency fuel situation.
Finally, operators should regularly review and update their operational manuals to reflect lessons learned from safety reports and audits, ensuring continuous improvement in fuel management practices.
Operator requirements for training, experience and consolidation on new aircraft types
Induction and minimum qualifications
The operator’s operations manual stated that recruited pilots were to meet the following minimum requirements:
commercial pilot licence with no medical restrictions[13]
current Australian medical certificate
pass of a pre-employment check flight with the HOFO or a delegate.
Once inducted, a new pilot would learn the routes with existing pilots before being checked to line by the HOFO.
The operator’s operations manual stipulated 5 minimum requirements for a pilot in command of the C310 (Table 6).
Table 6: Operator’s 5 minimum requirements for operating the C310
Requirement number
Minimum requirements
1
5 hours on type for VFR operation
2
10 hours on type for IFR operation
3
Minimum of 750 total flying hours
4
Minimum 20 hours in command on MEA for VFR operation
5
A multi engine command instrument rating if flying IFR.
The HOFO was required to conduct a check-to-line flight and, if successful, the pilot would be cleared to conduct air transport operations as pilot in command on the new type. The substantive HOFO stated that generally it would be expected that multiple ICUS flights would occur with either the HOFO or a supervisory pilot before a check-to-line would be conducted. The CEO reported that generally 15–20 hours on type would be sufficient to conduct line operations as pilot in command.
During the draft review process, the CEO reported that the calibre of pilots coming through from flight schools was lower than previously experienced, noting that a lot of the organisation’s time was spent getting pilots up to commercial standard.
After completing the check-to-line flight, the pilot of the accident flight had accrued a total flying time of 740.5 hours. The operator received an exemption from the operator’s insurer for the pilot to undertake air transport operations in the C310 without meeting the specified minimum requirement of 750 hours.
Under CASR 61.650, pilots were required to have completed an IPC in the previous 12 months to fly a multi-engine aircraft under the IFR. The IPC must also be done in a multi-engine aircraft of the same category. The substantive HOFO noted that, once a pilot was checked to line, there was no follow up or specific oversight on their operating capabilities until their next proficiency check in 12 months, in line with the CASR requirements and the operations manual, which stated:
If flying under the IFR, pilots are required to conduct an Instrument Proficiency Check with an authorised Flight Examiner prior to one (1) year from the last day of the month in which it was issued (IFR operations).
There were no specific regulatory requirements for Broome Aviation to provide additional consolidation flights for pilots transitioning to the C310 as, at the time of the accident, the operator was operating under CASA exemption 87/21.[14]
In December 2021, Civil Aviation Safety Regulation (CASR) Part 135 (Australian air transport operations – smaller aeroplanes) commenced. It introduced more stringent requirements for flight crew training and checking for operators conducting air transport operations. However, operators could operate under the exemption that applied to a significant proportion of the previous small charter sector. This meant the operator was not required to conduct line training, a check-to-line, or complete proficiency checks, other than to ensure those proficiency checks and flight reviews mandated by Part 61 of CASR were carried out on their flight crew members.
Supervisory pilots
The CASA‑AMC/GM Part 119 - Australian air transport operators - certification and management v 2.3 noted that some operators have diverse fleets and there are scenarios where the HOFO may not be qualified on every aircraft type or in every role/function performed under its air operator’s certificate (AOC). In this case, operators can elect to use a structure where another pilot is identified to complete that position. In the case of Broome Aviation, the substantive HOFO conducted the check and training for the C210, in addition to nominated supervisory pilots, but for the MEA this position was covered by supervisory pilots. The operator required that supervisory pilots had:
a minimum of 20 hours total time on type
completed training with the HOFO or nominated person (with such training including the use of the line training and check forms)
met the relevant recency or proficiency requirements to act as pilot in command
been nominated, in writing, by the operator to be supervisory pilot and recorded as a named supervisory pilot.
The operator’s supervisory pilot register had not been updated since 1 December 2021. The register contained the name of one pilot who had been approved to conduct supervisory flights for the C310, however this pilot left the operator while the substantive HOFO was on leave. A second pilot had been listed as a supervisory pilot for the C210. The substantive HOFO stated that the second pilot had been assessed to conduct supervisory flights for the C310, however the register had not been updated to include this information. This pilot (detailed below as ‘Pilot 1’) also left the operator while the substantive HOFO was on leave.
During the period between December 2022 and June 2023, 7 pilots flew the operator’s C310, including one who had completed the training but had not been checked to line. Multiple pilots stated that training and guidance on the C310 during this period was limited. Of the 7 pilots:
Pilot 1 – was a senior pilot for the operator who was signed off as a supervisory pilot for the C310. They conducted the check-to-line for Pilot 2. Pilot 1 left the operator at the end of December 2022 and returned for 3 weeks at the end of February 2023.
Pilot 2 – completed no ICUS flights prior to completing a check-to-line flight in November 2022 that lasted 1.1 hours. The pilot was not formally signed off as a supervisory pilot on the C310, although they had extensive instructional time on MEA, prior to assisting with ICUS flights. The pilot left the operator at the end of February 2023.
Pilot 3 – completed 2 ICUS flights, one with the interim HOFO (3.7 hours) and 1 with Pilot 2 (1.6 hours), before completing a check-to-line (1.5 hours) with the interim HOFO a week later in February 2023. The pilot left the operator at the end of March 2023.
Pilot 4 (pilot of the accident flight) – completed 1 ICUS flight with Pilot 2 and 4 IPC flights with the external instructor on the aircraft. They were subsequently checked to line in April 2023, 130 days after their last flight in the aircraft, by the interim HOFO.
Pilot 5 – completed 3 IPC flights with the external instructor and completed no ICUS flights. They were checked to line in May 2023, 162 days after their last flight in the aircraft, by the interim HOFO.
Pilot 6 – completed 3 IPC flights with the external instructor and had not completed any ICUS flights since.
Pilot 7 (interim HOFO) – completed their check-to-line with Pilot 1 (3.6 hours) in December 2022 and completed 1 IPC flight with the external instructor.
At the time of their check-to-line, multiple pilots who conducted C310 operations for the operator during the period from November 2022 to June 2023, did not meet the operator’s minimum requirements 1, 2 and 3 detailed in Table 7. All pilots met requirements 4 and 5. The pilot of the accident flight and Pilot 5 both had limited experience flying MEA (under 50 hours), having not flown another MEA type outside of flight training.
Table 7: Compliance with operator’s minimum requirements on the C310 at the time of check-to-line
Pilot
Minimum 5 hours on type for VFR operation
Minimum 10 hours on type for IFR operation
Minimum of 750 total flying hours
Pilot 2
No
No
Yes
Pilot 3
Yes
No
Yes
Pilot 4 (pilot of the accident flight)
Yes
Yes
No
Pilot 5
Yes
No
No
Pilot 7 (Interim HOFO)
No
No
Yes
Pilot 1 was excluded as their check-to-line was completed prior to November 2022. Pilot 6 was excluded as they had not completed a check-to-line for the operator.
Multiple pilots reported that they had limited training on the C310 and anticipated completing additional ICUS flights before being checked to line. Three pilots assessed that they were tasked with operating the aircraft without adequate training on the fuel system. They expressed concerns about the limited training noting the C310 had a complex fuel system. Multiple pilots reported learning the systems while conducting operational flights.
Emergency procedures
The POH included emergency procedures for inflight engine failure, which included a requirement to check:
fuel flow rate
fuel selector positions
fuel quantity.
After the second surging event on the right engine, the pilot crossfed the left main tank to the right engine and referred to the quick reference handbook. This handbook outlined the ‘engine failure during flight’ checklist. The pilot stated that they referred to the checklist to determine whether any actions could be taken to address the surging, noting that the engine had not completely failed. There was no checklist to address engine surging.
At this point in the flight, the aircraft was located between 2 nearby diversion airstrips of Kimberley Downs Station, located approximately 5 NM to the south‑east, and Meda Station located approximately 16 NM west (Figure 15). The pilot noted they were familiar with the location of the airstrips, however they had never operated from them and were unaware on their suitability and condition. The pilot stated that because of these unknowns that they believed the only suitable airstrip was Derby Airport.
Figure 15: Diversion locations
The pilot did not consider diverting to RAAF Base Curtin. Source: Google Earth, annotated by the ATSB
The flight data indicated that the pilot initiated their descent from 10,000 ft at the normal top of descent position, while continuing to track towards Derby Airport, at an average descent rate of 400 ft/min. Approximately 3 minutes into this descent, the pilot crossfed the right engine from the left main tank.
Engine surging
When surging occurred in both engines, the pilot noted that it appeared to be from fuel starvation. The aircraft manufacturer noted that in the event of simultaneous engine power losses or surging, the engine ’Airstart’ checklist could be actioned twice, as only one engine should be restarted at a time. Additionally, the ‘FORCED LANDINGS (Complete Power Loss)’ checklist should be used if pilots were unable to regain power.
The pilot continued tracking to Derby Airport while switching fuel tanks, attempting to draw any remaining fuel. The manufacturer noted that the certification rule, at the time of the aircraft’s certification, required multi-engine aircraft to regain full power and fuel pressure within 20 seconds after switching from an empty tank to a full tank in level flight. The aircraft tracking data indicated that at an altitude of approximately 4,500 ft the descent rate increased to 1,500 ft/min. The aircraft travelled approximately a further 5.5 NM over approximately 3 minutes before a forced landing was conducted (Figure 16).
Figure 16: Aircraft altitude variation with distance to Derby Airport
4. Right engine surge – crossfeed right engine off left main tank; 5. Inbound call for Derby Airport; 6. Dual engine surge; 7. Mayday call; 8. Accident site. Source: ATSB
When the pilot determined they would be conducting a forced landing, they declared a MAYDAY to ATC. The aircraft was at an altitude of approximately 700 ft. The pilot later advised they had insufficient time to complete any checklist items after the MAYDAY call, however they lowered the landing gear as they were aiming to land on the Derby Highway as it was assessed as the best available option. There were approximately 30 seconds between the MAYDAY transmission and the forced landing.
Survivability
Safety briefing
The operator had a safety briefing video for the C310. The video outlined the:
use of:
doors
seatbelts
emergency exits
location of:
life vests
safety briefing card
emergency supplies
installed emergency locator transmitter (ELT)
The pilot noted there were 2 main differences between the aircraft and the information in the video. The location of the emergency supplies was in the nose of the aircraft rather than the wing cargo locker, and the ELT was portable rather than installed (see the section below titled Emergency locator transmitter).
This was the second time the passenger had flown in VH-DAW with the pilot. The passenger noted that on the first time flying in the aircraft they were shown a safety briefing video. On this occasion they were not shown the video and instead were given a briefing while at the aircraft. They recalled the briefing outlined the information regarding the emergency exits and seatbelts, noting there were other topics covered that they could not recall. The passenger recalled that they did not read the safety card while in the aircraft as they flew frequently. The safety card contained information on how to adopt the brace position.
When the passenger was asked to brace by the pilot, they stated they were unsure how to brace properly in the aircraft and reverted to their knowledge of the brace position for larger commercial aircraft.
Seatbelts and upper torso restraints
The pilot seat was fitted with a lap belt and upper torso restraint (UTR),[15] consistent with the regulatory requirements. The pilot stated that they would not wear the UTR portion of the harness during cruise as it limited their ability to view the gauges on the opposite side of the cockpit. The UTR was only worn during take-off and landing. The pilot stated that during the emergency, they did not put on the UTR. The pilot sustained severe facial injuries and a loss of consciousness when the aircraft collided with terrain.
The passenger’s seat was fitted with a lap belt. This was worn by the passenger during the emergency and forced landing. The passenger received minor injuries, including bruising around the abdomen due to the lap belt.
Emergency locator transmitter
The aircraft was fitted with a portable emergency locator transmitter (ELT).[16] The pilot recalled that on first flying the aircraft they had checked the expiry date of the ELT and noted it was out of date. The portable ELT was subsequently replaced prior to the aircraft’s next flight.
The safety briefing video showed an automatic installed ELT[17] within the aircraft. The pilot noted that during pre-flight briefing with the passenger they explained the location of the ELT was different to the safety briefing video, however they did not explain the process to activate it.
The CASR Part 135 MOS required aircraft that were flown more than 50 NM from the departure aerodrome to carry an automatic ELT. However, this requirement was not applicable to the aircraft until 2 December 2023. Prior to then, the aircraft was operating under regulation 252A of the Civil Aviation Regulations, and subsection 6 of Civil Aviation Order 20.11, which permitted either a portable ELT or an installed ELT in the aircraft.
Due to the pilot being rendered unconscious during the accident sequence, the portable ELT was not activated. The passenger contacted emergency services while still in the aircraft using their phone, identifying the accident location from a passerby who stopped to help.
Operator and management information
Overview
Broome Aviation was re-issued an air operator’s certificate (AOC) on 11 November 2022, to conduct operations under CASR Part 135 ‑ Australian air transport operations – smaller aeroplanes, allowing single and multi-engine piston and single engine turbine air transport operations. At the time of the accident, it operated the following Cessna aircraft:
7 x C210 (single-engine piston)
1 x C310 (multi-engine piston)
1 x C404 (multi-engine piston)
1 x C208 (single-engine turbine).
In addition to a head of flying operations (HOFO), the operator had 7 seasonal pilots in a combination of full-time and casual positions.
Figure 17: Operator’s organisational structure
Source: Broome Aviation
Chief executive officer
The CEO held the positions of flight operations manager[18] and head of maintenance control (HAMC) (Figure 15).[19] They also owned and operated Broome Air Maintenance (BAM). This maintenance facility performed all the maintenance on the Broome Aviation fleet. The facility’s personnel comprised a chief engineer, who was registered as a licenced aircraft maintenance engineer (LAME), and aircraft maintenance engineers (AMEs). The chief engineer began working at BAM in October 2022.
The interim HOFO stated that the CEO had a hands-on approach to the organisation, stating that the CEO would generally create the roster for the pilots, which the interim HOFO would check and approve. The chief engineer stated the CEO would also be the final authority of any maintenance conducted on an aircraft.
The Broome Aviation operations and maintenance manuals contained contradictory information relating to the person nominated in the HAMC position. In the operations manual, the chief engineer of BAM was incorrectly listed as the HAMC, whereas the maintenance manual accurately listed the CEO in the position. The CEO later stated that the chief engineer of BAM was filling a dual role of both chief engineer and HAMC, however this was not communicated to CASA and was not the understanding of the chief engineer.
Head of flying operations
During the period from December 2022 to June 2023, the HOFO position underwent a temporary change. The substantive HOFO took a period of leave, during which a new person assumed the position on an interim basis.[20]
The interim HOFO was employed as a full-time, permanent pilot for another operator (operator 2), which was also based in Broome and only conducted operations in Cessna 208 aircraft. Operator 2 was independent of Broome Aviation. The interim HOFO began to work with Broome Aviation in November 2021 as a casual pilot during operator 2’s off season. They recommenced casual work with Broome Aviation on 13 November 2022, again during operator 2’s off season.
In late November, Broome Aviation asked them if they were willing to fill the position of HOFO to cover the leave period of the substantive HOFO. Having agreed, their application was submitted to CASA on 25 November 2022 (see the section titled Head of flying operations assessment).
The interim HOFO was assessed for the HOFO position by CASA on 7 December 2022 and subsequently approved for that position on 12 December 2022. On the same day, a handover was completed with the substantive HOFO. CASA was informed that the handover had been completed. The interim HOFO was also assessed by CASA (18 November 2022) and approved for the position of ‘alternate’ HOFO with operator 2 in January 2023 (see the section titled Requirements for an alternate HOFO).
At the time of their appointment to the Broome Aviation HOFO position, the interim HOFO held a commercial pilot licence (aeroplane), issued in early 2008, with single and multi-engine aircraft (MEA) class ratings. They had a total flying experience of 5,049 hours, of which approximately 135 hours were on MEA (Table 8). They had flown the C310 once prior to their HOFO assessment, which was a check-to-line flight in VH-DAW on 3 December 2022.
Table 8: Interim HOFO flight hours prior to assessment
Single-engine
ICUS
Dual
Command
Day
Night
Day
Night
Day
Night
184.3
1.4
158.9
13.9
4,542.4
13.3
Multi-engine
13.9
3.8
31.7
1.5
76.4
7.9
The interim HOFO completed an IPC for MEA, in a different aircraft type, on 2 December 2021. It was renewed in the C310 during the external instructor visit to the operator in December 2022. Prior to conducting supervisory or check flights with Broome Aviation pilots, the interim HOFO had gained 20 hours flight time on the C310. This met the operator’s minimum requirements for supervisory pilots.
Check-to-line for the pilot of the accident flight
2.4
The interim HOFO stated that they expected to occupy the position until the end of February 2023, when they were to return to operator 2 and the substantive HOFO was expected to return from leave. This time period was agreed to by operator 2, with the understanding that all flight and duty times for either operator would be recorded in both operators’ systems to ensure flight and duty limits were not exceeded. The interim HOFO stated they were unaware they had been approved and appointed by CASA in the ‘HOFO’ position and assumed they were in the ‘alternate HOFO’ position for Broome Aviation. They advised they only became aware that they were the appointed HOFO during a CASA level 2 surveillance activity (see the section titled Level 2 surveillance – 20 June 2023).
Oversight of operations
Although the assessment CASA completed of the interim HOFO was for a period of one month, they did not contact the operator at the end of this period to consider if the assessment was still appropriate.
At the end of February 2023, the interim HOFO was told that the substantive HOFO’s return would be delayed until the end of June 2023. They advised that they discussed remaining as acting HOFO with the Broome Aviation CEO, however their duties would need to be reduced. These duties were subsequently reduced to check and training, confirmation of rosters (arranged by the CEO), and general availability for pilots requiring assistance. CASA was not informed of this change. The interim HOFO stated that their main responsibility after this time was with operator 2.
At the beginning of March 2023, the interim HOFO completed a 2-week flight instructor rating course for MEA in Darwin, which was funded by operator 2. Following its completion, the interim HOFO then recommenced full-time work with operator 2. They stated that they were still contactable for any pilots at Broome Aviation who needed assistance and noted that 2 ‘senior’ pilots were available during this time (one of these pilots being the pilot of the accident flight).
In March 2023, the management of operator 2 identified that the interim HOFO was still conducting flights for Broome Aviation. In response, they were advised to cease working for Broome Aviation as that work would affect their flight and duty times as they were also in the alternate HOFO position for operator 2. Operator 2’s management was unaware that the interim HOFO continued to conduct flights and remained the HOFO for Broome Aviation after the discussion in March 2023.
While at Broome Aviation, the interim HOFO checked 3 pilots to line on the C310. The interim HOFO had accumulated 23.1 hours on the C310 prior to conducting the check-to-line flight on the pilot of the accident flight. They recalled that, even though they had recently received their instructor rating for MEA at that time, they did not feel comfortable simulating single engine emergencies.
The interim HOFO stated that, after the pilot of the accident flight was checked-to-line, they followed up with them after their first couple of flights. The interim HOFO expressed no concern about the pilot’s operation of the C310 and noted the pilot had not contacted them in relation to issues or questions about the aircraft. The accident pilot confirmed they never contacted the interim HOFO regarding the C310, noting:
I didn’t feel comfortable contacting the HOFO with 310 questions … this was due to their very minimal type knowledge and support within the entire company, so I sought advice from outside the company from more experienced pilots on the 310.
During the 4-month period from March to June 2023, the interim HOFO recorded 33.85 duty hours at Broome Aviation, however they noted that they would often ‘drop in’ after completing flights for operator 2 and did not formally record all the time spent at Broome Aviation. The CEO later advised that the HOFO was available in the afternoons for discussions with pilots however, none of the pilots made use of that opportunity. Comparatively, the interim HOFO recorded 458 duty hours at operator 2 during this period and reported they flew full‑time for the operator, while also conducting check and training for its pilots.
At the time of the accident, the interim HOFO had been in the HOFO position for Broome Aviation for 7 months. A week after the accident flight, the substantive HOFO returned to the operator.
Pilots flying for Broome Aviation stated that, when contacting the interim HOFO between March and June 2023 they would not get an immediate response, noting that the HOFO’s priority was flying for operator 2. The pilot of the accident flight stated that they would generally reach out to another pilot (who had recently left Broome Aviation) for guidance on the C310 rather than the interim HOFO.
Multiple pilots reported that the CEO would monitor each flight using the operator’s online tracking system. If any deviations in flight time or route occurred, the pilot would receive a ‘barrage’ of foul language, be accused of not considering the monetary implications for the organisation, and then face threats of loss of flight hours or potential termination of employment. By contrast, the CEO stated they had little interaction with the pilots as their office was located at the maintenance facility, which was on the opposite side of the airport. They also stated that all communications about aircraft maintenance would be directly from the HOFO.
The interim HOFO reported that, after completing a day’s duties at operator 2, they would pass through Broome Aviation to check the operations for the day. They recalled they would have general conversations with pilots and considered them to be close friends as well as work colleagues. However, the pilots the ATSB spoke to stated that, during this period, they received little to no guidance on flight operations (for all aircraft types).
The substantive HOFO stated that they primarily spent the workday in their office and generally interacted with pilots while they were completing paperwork. Most interactions involving questions or issues occurred over the phone. They also reported that the CEO, whose office was located at the hangar, had more frequent face-to-face interactions with the pilots, often seeing them before and after their flights.
Safety management system
CASR Part 119 (119.190), which commenced on 2 December 2021, included a requirement for an operator conducting operations under CASR Part 135 (Australian air transport operations – smaller aeroplanes) to have a safety management system (SMS). However, at the time of the accident the operator was operating under exemption EX87/21 and was not required to have met the SMS requirement. This exemption applied to a significant proportion of the small charter sector and was not specific to this operator. Despite that, Broome Aviation was required to have completed an SMS implementation plan and submitted the plan to CASA by 4 April 2023. The operator had not completed that process at the time of the accident.
The operator’s nominated safety officer was a line pilot. They left the operator at the end of December 2022 and returned to complete a short 3-week stint at the end of February 2023. The operator did not nominate a new safety officer after this pilot left the organisation and they were not required to do so, as there was no regulatory requirement for them to have one.
While not required, the operator did not have a formal incident or hazard reporting system, or a means of identifying the development of hazardous trends. Interviews with various staff members indicated that, although there were safety meetings involving pilots to identify safety risks, these meetings had not been held since the arrival of the interim HOFO.
Organisational pressures
The ATSB interviewed the 5 pilots who conducted Cessna 310 operations for the operator during the period November 2022 to June 2023, as well as 2 other pilots. During interviews, most of these pilots revealed events in which they were reprimanded or challenged by the CEO, or they witnessed similar treatment to other pilots, for declining a flight due to a maintenance concern. Many pilots stated they had experienced pressure from the CEO to complete flights with aircraft they considered unairworthy.
They stated they were worried about the consequences, such as employment termination or the hindering of their career progression, if they did not complete those flights. Pilots also stated that they felt pressure to ‘get the job done’, with one pilot stating:
…it was always like you just have to do the job. You have to do the job. It's not anything to do with safety or if you have the training for it either…
During the draft report review process, the CEO acknowledged that at times they had reprimanded and challenged pilots. However, they stated that this was in response to pilot actions that they considered imposed unnecessary financial and/or reputational cost on the company.
Complaints received by CASA from pilots and a passenger (see the section titled Complaints to CASA) stated multiple concerns for the safe operation of aircraft. One complaint by a former pilot stated:
… operational pressure from the organisation and their management is forcing pilots to make unsafe decisions in flight. A report to CASA is better than trying to reason with the company. The mentality of not only managers but also the owner isn't conducive to safe aviation practices.
Senior management stated they were unaware of any instances where pilots were reprimanded for not flying an aircraft considered to be unserviceable. All stated that, if there was a defect with an aircraft, the operator’s stance would be to get it rectified before another flight was completed.
During interviews, former pilots expressed concerns for the operator’s future, and one stated:
I knew that either I was going to be involved in something that I shouldn't be or that an incident was going to happen.
Most of the pilots the ATSB spoke to who had left the organisation stated their decision to leave was based on aircraft maintenance issues and/or the unacceptable treatment they received as pilots from senior management.
Civil Aviation Safety Authority oversight
Head of flying operations assessment
Position requirements
Under the CASRs, the HOFO must meet specific requirements, including holding appropriate qualifications, demonstrating substantial operational experience, and having a thorough understanding of regulatory obligations. The HOFO is responsible for overseeing operational standards, managing safety and compliance frameworks, providing leadership to flight crews, and ensuring that all activities align with organisational and regulatory expectations.
Specifically, CASR sub regulation 119.140(1) stated that:
The head of flying operations of an Australian air transport operator must safely manage the flying operations of the operator.
CASR 119.135 required the HOFO to:
• hold a pilot type or class rating for a type or class of aircraft that is used to conduct a significant proportion of the operator’s air transport operations
• have at least 500 hours flight time on a type of aeroplane that is the same as, or substantially similar to the type of aeroplane used to conduct a significant proportion of the operator’s Australian air transport operations
• have at least 6 months experience in the conduct or management of air operations conducted under an AOC or equivalent foreign authorisation.
CASA’s acceptable means of compliance and guidance material (AMC/GM) Part 119 - Australian air transport operators - certification and management v 2.3 outlined recommended minimum hours and experience for a HOFO based on the size and complexity of the operator. For an operator with more than one MEA, such as Broome Aviation, CASA recommended that a HOFO have a minimum of:
• 1,000 hours total flight time
• 200 hours in command of MEA.
Requirements for an alternate HOFO
Under CASR 119.205, there was a requirement for the operator’s exposition to list the qualifications, responsibilities, and names of key personnel. There was also a requirement to list the names of each person authorised to carry out the responsibilities of the position when the substantive position holder was absent from the position or unable to carry out their responsibilities. These authorised persons were referred to as alternate key personnel.
If an operator wanted to change the specific individual in the alternate key position, CASA approval was required, due to this being considered a significant change. Once approved, this should lead to the insertion of the nominated person into the operator's exposition as an alternate key position holder. Operators working under CASA exemption EX82/21, including Broome Aviation, were not required to name alternate key personnel in the exposition, even if they had an alternate.
The AMC stated that small operators with limited personnel may nominate alternate HOFOs employed by another operator, provided they detailed in their exposition how the alternate HOFO would perform the position effectively. The requirements for an alternate HOFO were the same as the HOFO position. In addition, the alternate HOFO had to have a direct relationship with the operator and sufficient capacity to fulfill their duties. It also stated that dual responsibilities for multiple operators were unlikely to meet this standard.
The operator’s operations manual stated that an alternative HOFO must be approved by CASA. It also stated that:
• a handover form must be completed prior to the transfer of the responsibilities from the HOFO to the alternate HOFO
• the alternate HOFO could not be the acting HOFO of any other operation while acting as the HOFO for Broome Aviation
• the alternative HOFO could only perform the duties of the HOFO during the specified period they had been nominated to act as HOFO
• CASA be informed within 7 days of the transfer being completed.
Assessment process
CASA’s HOFO suitability assessment was a formal process designed to evaluate a candidate’s suitability for the position of HOFO in a CASR Part 135 operator. It aimed to ensure the individual had the necessary qualifications, operational experience, and management skills to oversee flight operations safely and in compliance with CASA regulations. The assessment begins with a review of the candidate’s documentation, including licences, flight experience, and familiarity with the operator’s aircraft and procedures. CASA also examined the candidate’s knowledge of relevant regulations, operational procedures, and safety management principles.
The assessment included an interview where CASA evaluated the candidate’s understanding of key areas such as CASA regulations (Parts 135, 91, and 119), the operator’s exposition and procedures, SMS implementation, and human factors. The candidate was also required to demonstrate the ability to manage compliance, oversee pilot performance, and respond effectively to safety-critical situations. Leadership and decision-making skills were also a focus, as the HOFO must manage teams, promote a strong safety culture, and ensure the organisation adheres to all operational requirements.
The assessment may have also required a practical demonstration of the candidate’s ability to implement operational procedures and manage risk. Based on the assessment, CASA determined whether the candidate was fit for the position or if further experience was needed.
Applicant 1
In October 2022, the operator submitted an application to CASA for its HOFO position, replacing the substantive HOFO as they advised they were resigning from the key personnel position of HOFO for medical reasons on 17 October. It also submitted a change to its operations manual to replace the substantive HOFO with the proposed HOFO candidate. This applicant had 2,327 flight hours with 1,009 multi engine hours, however they did not have any air transport experience and had not been a HOFO with any other operator.
This application was assessed on 14 November 2022 and the CASA flight operations inspector (FOI) deemed the applicant unfit for the position due to:
limited experience in air transport operations
not meeting the 500-hour requirement on aircraft substantially similar to those primarily operated by the operator
an assessment, based on previous dealings with the CEO, that an experienced HOFO was required to ensure pilots were managed professionally and the operation was safe and efficient.
On 21 November, CASA advised the operator that the applicant was unsuitable. In internal CASA correspondence, the FOI noted that the application was to replace the substantive HOFO who would be on leave and would be returning at the end of April 2023. The FOI stated concern for continuity of the operation over this period.
The substantive HOFO continued in the role in a limited capacity.
Applicant 2
On 19 July 2022, operator 2 applied to CASA for approval of an alternate HOFO position, with the applicant who was later approved to be Broome Aviation’s interim HOFO being the nominated candidate (Table 10). This application was assessed by the same FOI mentioned in the section above on 18 November 2022. When requested, CASA could not locate the assessment form completed on applicant 2 for this position. The FOI later stated that they had expected to complete a flight test for the interim HOFO during this original assessment, however an internal CASA decision was made that it would be a desktop assessment only.
Following the rejection of its first applicant, Broome Aviation submitted an application for an alternate HOFO position on 25 November 2022, with the interim HOFO being the nominated candidate and an expectation that this person would be acting in the HOFO position for a limited period. This application included changes to the operations manual to update the positions. The same FOI completed this assessment and stated that, because they had recently assessed the applicant as an alternate HOFO for operator 2, the process could be expedited as many of the assessment elements had previously been covered.
The assessment for the interim HOFO for Broome Aviation was completed by the FOI on 7 December 2022. The documentation stated that the assessment was for an ‘alternate’ HOFO position, with a time limitation of 1 month. It was also noted that the applicant had taken leave from their original operator to fulfill this position.
The FOI advised that the 1-month timeframe was due to their understanding that the substantive HOFO would be travelling overseas for this time and would be returning to the operator. However, there was also email evidence indicating that the FOI knew the substantive HOFO would be on leave until April 2023. In discussions with the ATSB, the FOI stated the 1‑month period was the primary timeframe considered for this applicant and as a result they were not assessed in their:
check and training experience
MEA experience
ability to conduct oversight, if working for 2 operators.
On 12 December, CASA formally issued the approval for the applicant to become the HOFO rather than as requested and stated in their own paperwork, the alternate HOFO for Broome Aviation. The updated operations manual specified the applicant was appointed in the alternate HOFO position, instead of the CASA‑approved position of HOFO. It did not change the nominated person for the HOFO position, even though they were on leave for a significant time. There was no explanation in the operations manual of how the alternate HOFO would manage this position if they returned to their original operator. The manual amendment was accepted by CASA. The FOI advised that the operations manual was accepted as the change was for a short time and they did not expect the operator to resubmit the manual when the substantive HOFO returned.
Table 10: HOFO assessment timeline
Date
Event
Operator
19/07/22
Request for applicant to be alternate HOFO
Operator 2
18/11/22
Applicant assessment
Operator 2
25/11/22
Request for applicant to be alternate HOFO
Broome Aviation
07/12/22
Applicant assessment
Broome Aviation
12/12/22
CASA approval for HOFO position
Broome Aviation
24/01/23
CASA approval for alternate HOFO position
Operator 2
CASA stated that a key personnel position did not come with a time limitation, although one could be imposed by the operator and outlined in its exposition.[21] If this was the case, CASA would note the time limitation on its assessment of the applicant and place a note on file in the CASA system. While CASA’s assessment of the interim HOFO was based on a 1-month period, no note was placed on file.
In February 2023, while preparing for a level 2 surveillance activity, a regulatory oversight flight operations inspector (RO FOI) identified that the interim HOFO had been assessed for the position on the basis of performing that position for one month, however they were still acting in this position 3 months after the assessment had been completed.
The RO FOI contacted the interim HOFO to discuss the situation and was advised that the substantive HOFO would be on leave until June 2023 and the interim HOFO had been conducting HOFO duties. They also were advised that the interim HOFO would be recommencing seasonal work with operator 2 at the beginning of March 2023, with the intention of continuing with Broome Aviation as HOFO on a ‘remote basis’. The RO FOI ensured the interim HOFO was aware of their own requirements for fatigue management, discharge of responsibilities and general oversight of Broome Aviation activities while working with the other operator.
The RO FOI noted that, although there was nothing legislatively preventing this arrangement under CASR Part 119, it was unorthodox and created a level of concern. There was no reassessment of the interim HOFO in relation to their duties, as the RO FOI assumed a full assessment had been completed during the other FOI’s previous assessment in December 2022.
Complaints to CASA
The CASA Surveillance Manual 15.1 required that when CASA received a complaint about an operator, it be classified as a class A–C occurrence and action be taken if it was assessed as class A or B (Table 11). A class A assessment required instigation of a level 2 unscheduled investigation, while a class B assessment could be investigated or added as an item in an upcoming surveillance.
Table 11: CASA complaint occurrence classes and follow‑up action
Class
Occurrence event
Surveillance type
Action Type
A - Critical
Complete loss/failure of the aviation system(s), or a destructive failure, impacting directly on the safe operation of the aircraft
In November 2022, CASA received a complaint about Broome Aviation relating to operational issues. The complainant stated that:
there was an oppressive culture at the organisation, based on bullying and pressure from the CEO that ‘preys on junior pilots’.
It also detailed instances of:
pilots being forced to fly aircraft at night with unserviceable instruments
pilots being advised to fly outside legal operational requirements
comments made to pilots to ignore issues or defects with aircraft.
This information was passed to the CASA surveillance team, where the RO FOI followed up on the complaint by talking to the complainant in February 2023. Although evidence, including copies of text messages, was supplied to CASA, the RO FOI explained to the complainant the importance of reporting an incident (either via the company reporting system or the CASA confidential system), with specific details, at the time it occurred. They also outlined the legal obligations of a pilot in command to record aircraft defects correctly.
After discussing the matter with the complainant, the RO FOI assessed the complaint was either indicative of a ‘disgruntled’ former employee, or there was a cultural issue at the operator. The complaint was added to the scoping document for a June 2023 surveillance activity (see the section titled Level 2 surveillance – 20 June2023), and assessed as a class B.
There was no documentation outlining if the complaint was followed up after the audit.
CASA stated that the complaint it received in November 2022 did not provide sufficient specific information to act upon. The supplied text messages were not considered to be fully contextualised, clear, or related to specific events where additional evidence could be sought.
Following the accident on 20 June 2023, CASA received 2 more complaints. The first complaint was from a pilot who stated that there was operational pressure from management forcing pilots to make unsafe decisions in flight. The complainant stated that they had witnessed this firsthand. No specific examples were provided. The second complaint was from a passenger who stated that on a charter flight from Broome, the twin-engine aircraft experienced a technical fault, and the pilot was instructed by management to continue the flight.
The scope of these complaints was added to a level 1 audit scheduled to be completed in August 2023 (see the section titled Level 1 audit – August 2023).
There was no indication in any of the CASA documentation that the complaints received were followed up during or after either surveillance event.
CASA stated that complaints regarding the safety culture of an organisation that did not have a safety management system (SMS) were difficult to assess, and there was no guidance given to inspectors on what to specifically assess. As such, an assessment, if completed, would be subjective to the person completing it. An in-depth assessment of an organisation’s culture required people to be prepared to talk about specific events or actions to ensure the context of the situation was fully understood.
Surveillance activities
A level 1 CASA audit was a detailed evaluation that assessed an aviation organisation's compliance with regulatory and safety standards. Such an audit encompassed various aspects of the organisation’s operations, including:
the SMS
operational control
maintenance
airworthiness
training
competency
regulatory adherence.
It involved a sample of operational aspects, often including extensive documentation reviews, interviews, and inspections. It aimed to identify both systemic issues and specific non-compliance or safety concerns. Any findings from a level 1 audit required the organisation to implement corrective actions to enhance safety and ensure continuous compliance with aviation regulations. The audit was typically scheduled at regular intervals or when there was a significant change in the organisation’s operations, such as new certifications, major incidents, or regulatory changes. The last level 1 audit on Broome Aviation prior to the accident was conducted on 19 October 2018.
A level 2 CASA surveillance activity was a more focused evaluation conducted to examine specific areas of an organisation's operations. This type of surveillance was typically less comprehensive than a level 1 audit and entailed an examination of aspects such as operational procedures, training programs, or maintenance practices. This surveillance was often conducted in response to a specific incident, identified risks, previous audit findings, or as part of ongoing surveillance and monitoring efforts. The last level 2 surveillance activity on Broome Aviation prior to the accident was conducted on 19 August 2018.
Level 2 surveillance – 20 June 2023
At the beginning of March 2023, the CASA surveillance team approved a level 2 surveillance activity on the operator. This was initiated as a result of:
the complaint received by CASA in November 2022 regarding allegations of operational pressures placed on flight crew by the CEO
the process surrounding the assessment and appointment of a temporary HOFO while the substantive HOFO was on leave.
The surveillance was scoped to cover both topics and involved a site visit conducted by the RO FOI on 14 June 2023, 6 days before the accident. The scoping did not outline how the complaint received by CASA would be assessed during the surveillance and the surveillance report was finalised on 11 July 2023.
During the surveillance, discussions were held with the interim HOFO regarding their position and level of oversight of operations, noting they were working full time for another operator at that stage. It was concluded that the interim HOFO was providing a level of oversight and interaction with personnel, and this was achieved via:
regular discussions with crew
oversight of schedules and flight and duty via the organisation’s systems
conduct of company proficiency flights / line and remedial training with flight crew
some limited formal governance meetings.
The surveillance report noted that no documentation could be supplied to demonstrate that both informal and formal meetings were being conducted during the interim HOFO’s time in the position. CASA issued a safety observation to Broome Aviation to review and update the content of its operations manual to include the governance processes utilised by the HOFO and establish a method and database to record such meetings and their outputs.
CASA reviewed the documentation surrounding the interim HOFO’s flight and duty times at both organisations and assessed that these complied with regulatory requirements.
The RO FOI advised the ATSB that they had concerns about the level of oversight the interim HOFO was providing for Broome Aviation during the time they were concurrently employed as an alternate HOFO at another local operator. They noted the interim HOFO’s view of the position seemed to revolve around being there for a short time. This concern was not documented on the final audit report.
The final surveillance report contained no mention of the November 2022 complaint and how it was assessed during the surveillance activity, and there was no other documentation to explain why the complaint was not mentioned in the report. The RO FOI stated that the complaint gave little information around the specifics of the incident, making it hard to check while at the operator.
When asked if any of the pilots were interviewed regarding the topic of operational pressures, the FOI stated they witnessed pilots coming in and out of the office area while they were conducting the meeting with the interim HOFO and ‘everyone seemed happy’. They also recalled there was no indication there was anything out of the ordinary that would have made them want to talk to any of the pilots. The RO FOI stated that it was generally possible to find a way of talking to pilots during surveillance activities and they had done so on previous occasions (with other operators), but did not see the need to do so on this occasion. There was no indication the operator’s management was aware of the complaint at the time the audit was conducted.
CASA’s processes required that this surveillance report was submitted to the RO FOI’s manager for approval prior to the audit being finalised. The absence of any content about the complaint, one of the 2 reasons for the surveillance activity, was not addressed during the approval process.
Level 1 audit – August 2023
A level 1 audit on the operator was conducted in August 2023. The audit’s scope originally covered:
airworthiness assurance
data and documentation
operational support systems
safety assurance
safety risk management.
It was subsequently expanded to include aspects associated with the apparent circumstances of the C310 accident, focusing on the fuel policy, flight planning, and training, and the 2 further complaints submitted to CASA on the operational pressures placed on flight crew. The audit team consisted of 3 inspectors, and included a site visit conducted on 28 August.
The audit found multiple issues with the operator’s operations manual. It noted that, although it met the basic requirements, it had not been updated in accordance with legislative changes. It also noted that the operations manual was not compliant with CASR Part 91/135 fuel and flight planning requirements.
The audit also identified that there was a general weakness with regard to the content and detail of the operations manual, in particular the policy and procedure surrounding the induction, operational training and release to line of junior pilots. The RO FOI stated that, due to the operator sitting under exemption 87/21, the requirements for meeting a training and checking system were not in place at the time. This situation meant no safety finding could be issued regarding the weaknesses in training and checking.
The audit found that, although the operations manual had an extensive section relating to operational use of maintenance releases (MRs), some references were either no longer valid or current legislative references were missing. It also found that Broome Aviation was no longer following the process for monitoring MRs and MELs that it had outlined in its maintenance control manual (MCM). The MRs of aircraft current at the time were not reviewed during this audit.
Previous level 1 audit
During the previous level 1 audit in October 2018, an airworthiness inspector noted various deficiencies with an aircraft during a ramp inspection. These deficiencies had not been entered into the MR or other aircraft documentation. The operator was given a list of these deficiencies in the surveillance report. No other aircraft or MRs were inspected during this event.
After the FOI was informed about the deficiencies on the aircraft, they identified that pilots’ maintenance training was not being conducted in accordance with the MCM or the operations manual. CASA recommended the operator undertake an educational program to provide guidance for the pilots in the following areas:
conducting accurate pre-flight inspections
entering defects into maintenance releases
checking for any potential items that could pose a risk to flight
correct use of maintenance releases.
CASA confirmed that Broome Aviation completed this educational program with all pilots who were employed at the time.
Related occurrences
Numerous fuel management and fuel starvation incidents and accidents have previously been investigated by the ATSB, including:
Engine power loss and forced landing involving Pilatus Britten-Norman Islander BN-2A VH‑WQA, Moa Island, Queensland on 3 October 2022 (AO-2022-046)
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040)
Cessna C310R, VH-HCP, 3 km east of Newman Airport on 26 January 2001 (200100348)
The ATSB found that pilot understanding of, and management of aircraft fuel systems played a crucial role in these occurrences.
Safety analysis
Introduction
On the return leg of a flight from Turkey Creek to Derby, Western Australia, the pilot encountered dual engine surging. The pilot, assessing this was due to fuel starvation, began switching fuel tanks to utilise any remaining fuel. With no resolution, the pilot initiated a MAYDAY call to Brisbane Centre air traffic control, alerted the passenger to the emergency, and told them to brace for impact. During the subsequent forced landing, the right wing of the aircraft hit a tree causing the aircraft to turn 180⁰ and come to an abrupt stop on the edge of the highway.
The pilot sustained serious facial injuries, and the passenger sustained minor injuries. The aircraft was substantially damaged.
This analysis firstly considers the pilot’s fuel management during both the first and second leg of the flight, the response to the emergency, and survivability aspects relating to the injuries of those onboard. It also discusses contextual factors that potentially influenced the pilot’s performance during this period.
The analysis then discusses several other safety factors identified during the investigation related to pilot training and consolidation, operator oversight, organisational aspects and regulatory oversight. These factors either contributed to the accident, or increased aviation safety risk more generally.
The safety factors are discussed under the following topics:
management of fuel
response to the emergency
factors influencing pilot performance
defect reporting
legibility and accuracy of aircraft internal placards
survival aspects
operational pressures
regulatory oversight.
Management of fuel
Pre-flight planning
Pre‑flight planning is vital to ensure there is sufficient fuel for all phases of the flight. This includes accounting for fuel required for taxi, take-off, climb, cruise, descent, landing and the required fuel reserves.
The pilot used the operator’s flight planning software to plan the flight, however they did not know how to input forecast winds and reported that they routinely planned using nil wind. The operator also provided a manual system that would have enabled the pilot to accurately plan the fuel requirements for the flight. A pilot in command is required to ensure the relevant meteorological forecasts are considered when determining the quantity of fuel required for a flight.
Taking into account the known environmental conditions and the aircraft’s fuel consumption, if the pilot had used the available wind data, the flight plan would have identified to the pilot that the planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route.
Pilot perception of fuel available in the auxiliary tank
The pilot conducted all their flights in the Cessna 310 (C310) with the assumption that the auxiliary tanks could not be used for longer than 45 minutes without the engines surging and so used the auxiliary tanks for 40 minutes. While it is likely that this behaviour was due to the reverse leak in the right auxiliary tank check valve, the ATSB was unable to conclusively determine if this was the reason for the engine surging reported by the pilot on the day of the accident.
As a result, the pilot had not intended to use all the usable fuel on board, reducing their actual endurance. However, this was not reflected during flight planning.
Contributing factor
The planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available.
Broome to Turkey Creek
On assessing the remaining fuel following arrival at Turkey Creek, the pilot reported that it was unevenly distributed, with the right auxiliary tank full and less than expected in the right main tank. The ATSB considered the following possibilities to account for this reported distribution:
the pilot did not switch the right main tank to the right auxiliary fuel tank en route to Turkey Creek
the fuel leaked from the main tank to the auxiliary fuel tank on the ground at Turkey Creek.
Testing of the right auxiliary tank check valve indicated that, although there was a leak through the tank vent outlet bleed return line check valve, it is unlikely this leak was large enough to have resulted in the 40 L discrepancy the pilot experienced on the day of the occurrence. In addition, it is very unlikely that the amount of fuel that leaked would have been equal to the amount of fuel which would have been used if the pilot had selected the auxiliary tank during this leg of the flight. As such it was assessed that it was more likely that the pilot did not select the auxiliary tank on the right side during the flight.
This resulted in the pilot having full fuel in the right auxiliary fuel tank at Turkey Creek and 40 L of fuel less in the right main tank than the pilot expected.
Upon returning to the aircraft and completing pre‑flight checks, the pilot did not visually confirm the right auxiliary tank was full. As the fuel gauges in the aircraft were known to be inaccurate, a visual inspection of the auxiliary tank would have verified if it was full.
Return flight leg
The pilot routinely flew the aircraft with the main tanks selected for 60 minutes after take-off on each leg of a flight, rather than the 90 minutes detailed in the pilot’s operating handbook (POH) for the larger tanks fitted to VH‑DAW. While the pilot advised this was how they simplified inflight fuel management, that practice increased the risk of fuel being vented overboard from the main tanks.
When the pilot switched from the main tanks to the auxiliary tanks on the second leg of this flight, it is likely the right main tank had only approximately 4 L of fuel remaining, and the left main tank had approximately 44 L remaining.
The ATSB could not establish why the right engine reportedly surged when selected to the right auxiliary tank, as there should have been approximately 97 L of fuel in the tank, and the reported issue with the check valve occurred when the fuel level in the auxiliary tank was approximately half (60 L).
When the pilot reselected the right main tank in response to the surging, the amount of fuel contained in the tank would have increased to approximately 12 L due to the fuel returned when using the auxiliary tank. After a further 10 minutes, the right engine again surged, this time most likely due to fuel starvation, resulting in pilot crossfeeding to the left main tank, which also had minimal fuel at that stage.
Fuel calculations conducted by the ATSB determined that when the right engine was crossfed to also draw fuel from the left main tank there was approximately 34 L of fuel left in that tank. About 10 minutes later, the engines began surging as the fuel in the left main tank was reduced to approximately 9 L of useable fuel. While it could not be determined why that quantity was insufficient to maintain continuous power, supply issues associated with an inoperative transfer pump (due to the observed tripped circuit breaker) and/or debris and other contaminants in the bottom of the fuel tank were possibilities.
Contributing factor
It is likely that the pilot did not utilise the right auxiliary fuel tank during the first leg of the journey and did not manage usage from the main fuel tanks in accordance with the pilot's operating handbook. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained.
Continued operation with defective fuel gauges
Multiple pilots who flew the aircraft stated that the fuel gauges did not indicate the correct amount of fuel in both the main and auxiliary tanks. Multiple pilots recalled that the gauges would become more accurate as fuel was burnt, however images of the gauge after flights indicated there was a still a large disparity between the 2 sides. The reading for both the main tanks and the auxiliary tanks were determined to be significantly out of tolerance and did not show an accurate amount of fuel on board for most of the flight.
Accurate fuel gauges are crucial in an aircraft to ensure precise monitoring of fuel levels throughout the flight, directly impacting safety and operational efficiency. They provide the pilot with real-time information about the quantity of usable fuel, allowing for informed decision-making during critical phases of flight, such as when a diversion is required or in an emergency. Although the pilot was aware that the fuel gauges were unreliable, they relied on the indicated readings at multiple points in the flight.
CASA guidance stated that an operator’s exposition should detail the maximum allowable discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure, noting that industry practice was a maximum of 3% variation. This percentage was not outlined in the operations manual, and the gauge defects were not recorded on the maintenance release.
However, the ATSB assessed that the gauge display defect did not contribute to the accident as the pilot was able to assess the fuel quantities in the fuel tanks throughout the flight.
Other factor that increased risk
The aircraft fuel gauges did not indicate accurately.
Operator’s procedures for fuel management
Pre-flight
A review of Broome Aviation’s pre-flight planning software identified that it did not include the 47 L block (total) fuel margin required under the operator’s fuel policy. It did however have a fixed fuel flow rate for climb of 150 L/hr. Conversely, the documented fuel planning figures to be used for manual fuel calculations did not include a fuel flow rate to use for climb. Although the operator was unaware of where the 47 L requirement originated from, the ATSB assessed that the margin it provided would cover the additional fuel flow used during climb, despite not being originally intended for that purpose.
Inflight
Broome Aviation’s operations manual required pilots to conduct an inflight fuel check when reaching cruise or if needing to divert. It did not contain guidance on:
conducting fuel checks at regular time intervals
assessing fuel burn rates
verifying the remaining fuel relative to the reserves required for contingencies, alternate routing, and final reserve fuel
the maximum allowable discrepancy between the actual fuel on board (gauge / visual) and calculated (journey log) figure.
This resulted in pilots using a variety of procedures.
Under the Civil Aviation Safety Authority (CASA) Manual of Standards (MOS) 135 Part 7, operators are required to outline inflight fuel management procedures. CASA’s Advisory Circular (AC) 91-15 Guideline for aircraft fuel requirements stated that pilots should have 2 sources of fuel values to crosscheck the available fuel on board. While the operator’s pilots were using a time‑based approach to their fuel calculations in flight, they did not have a viable crosscheck as the fuel gauge was inaccurate. A crosscheck process mitigates the reliance on a single source of information and ensures that any fuel related issues, such as high burn rates or fuel system defects, are promptly detected and managed, reducing the risk of fuel exhaustion.
Although Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations, the pilot completed an inflight fuel record every time they switched tanks. When the right engine surged the second time and crossfeed to the left main tank was selected, the pilot correctly assessed the amount of fuel remaining in the left main tank. They did not however accurately assess the remaining flight duration to Derby and the associated fuel required to fly that distance, considering that the right engine would be returning fuel to the right main tank.
The operations manual also gave little guidance on decision-making frameworks to address fuel‑related issues during flight, nor did it outline clear protocol for pilots to follow in the event of a low-fuel situation, including notification to air traffic services.
Post-flight
The operator’s post‑flight cross check methods could not be completed as there was no fuel totaliser on board the aircraft and the fuel gauges were inaccurate. As such, the remaining fuel at the end of the flight was based on the pilot’s fuel calculations or a visual check by the pilots, which was not required by the operator in the post‑flight process.
Consequently, an accurate record of the fuel remaining in the aircraft was not being documented for the next pilot, nor was it being accurately entered into the operator’s data recording software for fuel flow checks. The pilots were working around this issue by ensuring the fuel tanks were full prior to every flight.
Other factor that increased risk
Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management. (Safety issue)
Response to the emergency
After crossfeeding the right engine to the left main fuel tank, the pilot was confident that the available fuel was sufficient to reach Derby. They did not consider diversion to an alternate airstrip as they were unfamiliar with the condition and suitability of the nearby airstrips. They also did not consider the option of changing the left engine fuel selection to the left auxiliary fuel tank. This would have increased the fuel available in the left tank via the extra fuel return.
In addition, as the aircraft had passed the pilot’s planned top of descent, they initiated a 400 ft/minute descent reducing the available glide altitude. Maintaining the aircraft's potential energy (altitude) is crucial for extending an aircraft's range during an engine failure, providing more landing options and time to manage the emergency effectively.
Contributing factor
After the usable fuel in the right main fuel tank had been exhausted, the pilot did not divert the aircraft to the closest airport, select the left engine selection to the left auxiliary fuel tank, or maintain altitude to increase the safety margin.
Recognising the stress induced by an emergency, indecision during an engine power loss situation reduces the time available for a pilot to plan and conduct an effective forced landing. Delays caused by prolonged troubleshooting, uncertainty over the severity of the issue, or hesitation in selecting a course of action consumes valuable altitude.
Once both engines began surging, the pilotidentified that the left main tank had been drained of fuel and began to switch tanks in an attempt to utilise any remaining fuel. This included attempting to gain fuel from the main tanks a second time. Although the aircraft’s certification stipulated that power must be restored to the engines within 20 seconds in level flight if fuel was depleted from a tank, this requirement applied to level flight conditions and not during a descent phase. In a descent, the restoration of power, potentially extended beyond the 20 second threshold due to gravitational effects and reduced pressure in the fuel system.
At this point, only the auxiliary tanks had enough fuel to sustain engine power, but these tanks did not have fuel pumps to supply fuel to the engines. Textron advised that if the engines remained operating and the auxiliary tanks had been selected, the fuel could have been drawn from these tanks via the engine‑driven fuel pumps. As detailed above, it could not be established why the engines did not continue to operate at that stage as a small quantity of usable fuel remained in the left main tank.
There were 3 minutes between the start of the engine surging and the pilot's MAYDAY transmission. In this timeframe, a pilot who was experienced on the C310 would have had sufficient time to shut down and secure both engines (including feathering the propellers) and establish a glide approach. However, the pilot had limited familiarity with the aircraft fuel system, limited practical emergency procedure training on the C310, and the fuel gauges were faulty. As such, it is likely they struggled to methodically cycle through the fuel tanks while monitoring for engine response under the pressure of an unfolding emergency. During this time, the pilot also opted to continue to track towards Derby Airport, which increased the distance to the highway landing site, and delayed making a MAYDAY broadcast.
While acknowledging that if the pilot had been able to re‑supply the engine/s with fuel and restart at least one of them, they could have continued to Derby, the delay associated with the multiple tanks selections ultimately compromised the safety and control of the forced landing.
Factors influencing pilot performance
A review of the pilot’s activity in the days leading up to the accident identified an early wake-up time and long duty day. However, there was insufficient evidence to conclude that the pilot was experiencing a level of fatigue known to affect performance prior to, or during, the flight. The ATSB examined in detail the potential effects of experience and consolidation of skills around fuel planning and fuel management on the development of the accident.
Pilot experience and consolidation on the Cessna 310
Acquiring new skills, such as learning to fly a new aircraft type, requires training and practice. As the amount of experience on the aircraft increases, generally a pilot’s proficiency will improve, and performing tasks will become more automated and require less attention or mental resources (Wickens and others 2015, Stothard and Nicholson 2001). Prolonged gaps when flying an aircraft type have been known to affect skills, such as familiarity with specific aircraft systems, aircraft handling, and emergency procedures.
After completing their IPC on the C310 in December 2022, the pilot had a 130-day gap before their check-to-line flight in April 2023. This limited the opportunity for skill retention on the aircraft.
In addition, as the interim HOFO did not conduct any flights with the pilot that involved the use of auxiliary fuel tanks, there was no opportunity for the HOFO to see that the pilot was limiting their use of fuel from the auxiliary tanks to 40 minutes and the implications this had for fuel planning. Similarly, there was no opportunity to observe that the pilot was only using the main tanks for 60 minutes on every departure. The pilot also only began flying the C310 operationally after the interim HOFO had returned to their original operator. While the interim HOFO recalled discussing the pilot’s first flights with them, the pilot advised they only discussed operation of the aircraft with a pilot who had left the organisation.
Contributing factor
The pilot had limited understanding of the aircraft fuel planning and inflight fuel management, but due to a lack of consolidation training and limited to no operational oversight these issues were not detected by the operator.
Operator continued oversight and guidance
Pilots at Broome Aviation reported that the interim HOFO was unavailable most of the time between March and June 2023 due to their second job. Although the interim HOFO advised that they were available for any calls and were at the operator’s premises every day informally, the overall impression of pilots was that they were learning on their own and that they received little to no guidance on the operation of the C310.
In addition, the interim HOFO’s recorded flight and duty times indicated that, although they reported that they visited the operator often, there was limited available time to oversee the operation. CASA personnel noted they had concerns about this aspect, and stated they received limited evidence to prove appropriate oversight was being conducted. During a surveillance event conducted shortly after the accident, CASA issued a safety observation to the operator to update the contents of its operations manual to include governance processes to record interactions between the HOFO and the operator’s flight crew.
At the time of the accident, as the operator was operating under an exemption from some Civil Aviation Safety Regulations (CASR) Part 135 (Australian air transport operations – smaller aeroplanes) requirements, there were no specific regulatory requirements for them to provide additional consolidation flights for pilots transitioning to the C310. For many types of transitions, such as to a new single engine aircraft type, consolidation may not be necessary. However, when moving from single-engine to relatively complex multi-engine aircraft, a period of consolidation flights is an effective risk mitigator.
The operator had limited processes in place to ensure pilots with low time and experience on the C310 had the opportunity to effectively consolidate their skills prior to (or after) being checked to line. The substantive HOFO stated that they expected pilots new to the C310 to have completed multiple ICUS flights prior to a check-to-line flight. However, coincident with the substantive HOFO being on leave, several senior pilots left the organisation and the interim HOFO returned to work for their original operator. In combination this left limited capacity to supervise pilots.
Pilots who flew the C310 for the operator between November 2022 and June 2023 reported receiving limited training on the aircraft prior to being checked to line, noting they had expected to have completed more ICUS flights. Of the 7 pilots the ATSB contacted regarding C310 operations, 2 pilots reported they received less than the 5 hours required by the operator to fly under VFR, prior to being checked to line. Most pilots were checked to line with less than 10 hours on type. The pilot of the accident flight and one other casual pilot had limited MEA experience prior to being checked to line, having only flown one other MEA type, which was during their flight training.
Additionally, the interim HOFO had limited hours on MEA and the C310 prior to assuming the position at Broome Aviation. They accumulated a further 57 hours of MEA operation, including 23 hours on the C310, prior to checking the pilot of the accident flight to line. However, it is likely the interim HOFO’s limited experience on the aircraft type impacted the depth and accuracy of operational guidance provided to pilots during line checks, as well as the ongoing oversight of their flying performance.
Due to the relatively complex fuel system on the C310, pilots transitioning to the aircraft type require a thorough understanding of the system’s layout, managing fuel during normal and abnormal operations, and recognising potential problems. While this knowledge can be obtained via ground‑based study of the system, supervised practice helps ensure pilots develop the necessary skills and confidence to operate the system safely and effectively in all conditions. Most pilots who flew the C310 received little to no guidance on its fuel system.
Contributing factor
During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. (Safety Issue)
Defect reporting
Recording defects on a maintenance release (MR) allows for the timely identification, assessment, and rectification of issues that could impact an aircraft’s performance or safety. This process ensures that maintenance personnel have a clear understanding of any outstanding defects requiring attention, thereby reducing the risk of oversight or miscommunication during maintenance activities. It also records important information for pilots operating the aircraft.
Furthermore, documenting defects on a MR creates an auditable maintenance history, which is essential for tracking repairs, modifications, and inspections over the lifecycle of the aircraft. This documentation is also a regulatory requirement, ensuring compliance with regulatory standards.
There were aircraft defects that had not been recorded on the MR, including inaccurate fuel gauges and a partially‑unserviceable autopilot. Although the operator had a process for pilots to report defects, this had generally not been followed by the pilots. The pilots advised that they would often talk to individuals in the maintenance facility after a flight about any defects or issues they had noted. Through this process, straightforward defects would likely be rectified but nothing would be written on the MR. However, defects requiring longer maintenance time and multiple parts, they reported being advised by maintenance personnel that the operator would not pay for the defect to be rectified and so consequently were not reporting them.
This situation meant that when the pilot of the accident flight encountered defects, such as the engine surging, they did not report the concern. Consequently, this reduced the likelihood that the interim HOFO would become aware of the issue and arrange for it to be resolved, or at least communicated to the company pilots.
Of the serviceability‑related issues raised by the pilots, the fuel gauges and the autopilot were assessed to have been inoperable at the time of the flight. The interim HOFO did not themselves report the gauge defects or encourage the pilots to do so.
Contributing factor
Aircraft defects were not written on the maintenance release, leading to several defects not being rectified or managed. (Safety Issue)
Legibility and accuracy of aircraft internal placards
The fuel selector placards fitted to VH‑DAW were incorrectly labelled, with both placards indicating that the aircraft was fitted with the smaller auxiliary tanks. In addition, the placard stating that the main fuel tank should be used for 90 minutes after take-off was missing and some of the internal fuel-related placards within the cockpit of the aircraft were partially illegible.
The ATSB determined that these issues likely did not contribute to the occurrence as the pilot was aware the aircraft had the larger auxiliary tanks, and the pilot did not notice the discrepancy between the size of the tanks and the placard. Despite that, in aircraft like the C310 with specific fuel usage requirements, fuel placarding plays a critical role in ensuring accurate operation of the fuel system.
Survival aspects
Upper torso restraints
A substantial body of research has demonstrated that wearing upper torso restraints (UTRs) in small aircraft significantly reduces the severity of injuries compared to wearing only a lap belt. In particular, UTRs reduce the risk of head, neck and upper body injuries, associated with the person’s upper body flailing forward. An NTSB study published in 2011 found that when wearing a lap belt only, a pilot was 49% more likely to receive a serious or fatal injury, compared to those wearing both the lap belt and UTR.
The pilot of VH-DAW was not wearing the aircraft’s sash-type upper torso restraint (mounted above the pilot’s left shoulder) at the time of the accident. The pilot received significant injuries, when they impacted the dash of the C310.
That injury outcome was consistent with the findings of previous ATSB investigations, which found that pilots or passengers in the front seats of small aeroplanes and helicopters have not always worn the available UTRs, exacerbating the severity of their injuries in many accidents (for example, ATSB investigations 199800442, 200605133, AO-2010-053, AO-2012-083, AO-2012-142, AO-2016-074, and AO-2022-027).
It is very likely that the severity of pilot’s head injuries would have been reduced if they had been wearing the available UTR.
Contributing factor
The pilot was not wearing an upper torso restraint during the accident flight, resulting in the pilot receiving avoidable serious head injuries during the collision.
Emergency locator transmitter
The CASR Part 135 Manual of Standards required aircraft that were flown more than 50 NM from the departure aerodrome to carry an automatic emergency locator beacon (ELT), however at the time of the accident there was an exemption for the aircraft to operate with a portable ELT.
A portable ELT requires manual activation during an emergency landing and on this occasion the pilot was rendered unconscious during the accident sequence and the passenger did not know the exact location of the portable ELT. Therefore it is very likely that if a forced landing of similar severity had occurred in a more remote location, notification of the accident to emergency services would have been significantly delayed. That in turn may have led to a more severe outcome for the aircraft’s occupants.
An effective safety culture relies on open communication channels, where employees can report hazards or errors without fear of reprisal. In this case, pilots reported to the ATSB that they experienced pressure from individuals in senior management to avoid recording defects on the MR, particularly those that could lead to operational delays, and pressure to conduct flights with aircraft that they considered were unsafe for flight. The sample involved several pilots selected by the ATSB based on them performing similar roles to the pilot involved in this accident. All the information they provided was consistent with similar concerns also reported to CASA by other pilots, together with a related complaint from a passenger.
The pressure the pilots reported experiencing led to them regularly flying aircraft with defects. With regards to the C310, pilots developed an understanding that it was normal and approved practice to conduct flights in an aircraft with inaccurate fuel gauges, an autopilot incapable of holding altitude and engines prone to surging.
In addition, the pressure the pilots reported experiencing probably led to them being less likely to formally report defects or discuss them with senior management as they had developed an understanding that they would not be remedied.
Based on the available evidence, management personnel were not fully aware of all the aircraft defects that the pilots were managing. If the defects had been formally reported through the defect reporting process, it is more likely they would have been discussed and, if they could not be rectified, then a more considered approach developed to manage the problem. For example, the issue around fuel supplied from the auxiliary fuel tanks would probably have been investigated further, or a mitigation put in place.
A study completed on the factors influencing the decision‑making of commercial pilots flying in outback Australia found that it was common for them to feel pressured to make risky decisions and commit ‘violations’ due to threat of employment termination. It also noted that career ambition was an important factor, with pilots seeking to build flight time for future employment with major airlines, leading them to take risks while flying (Michalski and Bearman, 2014). The extent to which this situation exists within the small aircraft air transport sector is difficult to determine, however the evidence from this investigation indicates that it existed within this operator.
Contributing factor
Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight. (Safety Issue)
Regulatory oversight
The purpose of regulatory oversight is to ensure operators are meeting regulatory standards and to monitor the ongoing safety, health and maturity of the operators. This oversight is comprised of both regulatory services activities and surveillance activities.
CASA response to complaints
CASA received a complaint in November 2022 regarding operational issues at Broome Aviation. This complaint was included in the scope of a level 2 surveillance activity conducted by CASA in June 2023, the week prior to the accident. The CASA regulatory oversight flight operations inspector (RO FOI) determined there was no reason to question pilots regarding the complaint after noting the pilots seemed ‘happy’. This perception occurred in an open environment where the FOI, the interim HOFO and the CEO were present with the pilots.
As CASA noted, complaints regarding the safety culture of an organisation that does not have a safety management system (SMS) can be difficult to assess. Interviews with pilots can provide valuable information, but the usefulness of that information can be limited if only a small sample size was used (and confidentiality could not be maintained), or corroboration from some form of documentary evidence could not be identified. Although there are clearly challenges with examining these types of topics during surveillance activities, on this occasion it appears an important opportunity was missed when the RO FOI did not discuss these concerns with any of the current pilots or bring it to the attention of the operator.
When the surveillance report was submitted by the RO FOI to their supervisor, the RO FOI was not questioned as to why the complaint had not been assessed, even though it was a key reason for the surveillance activity. This was a second missed opportunity for CASA to assess the safety culture within the operator.
When CASA received 2 further complaints after the accident, it had a further opportunity to examine operational issues which encompassed all 3 complaints. Although the complaints were added to the scoping of the level 1 audit in August 2023, the contents of the audit report indicated that they were again not investigated.
Acknowledging CASA’s difficulty with assessing the safety culture of such an organisation, there were multiple pilots within the organisation who could have provided valuable insights given their extended time and familiarity with the operator. Engaging with these individuals during either of the surveillance activities would have allowed CASA to gather a broader perspective and determine whether the reported organisational issues were systemic or simply reflective of dissatisfaction from potentially disgruntled former employees. As demonstrated during this investigation, there were widespread concerns about these matters within the pilot group.
Contributing factor
Following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, CASA conducted a level 2 surveillance activity on the operator in early June 2023 and following further complaints, a level 1 audit in August 2023, with key scope elements being to evaluate the complaints. Despite that, the surveillance activities and the associated reports did not assess the subject of the complaints.
Head of flying operations assessment
Broome Aviation’s interim HOFO was firstly assessed by CASA for the position of alternate HOFO for another operator (operator 2) and then again for the position of alternate HOFO for Broome Aviation. CASA was unable to provide documentation outlining the specific elements discussed during the first assessment, so it was not possible to confirm what was specifically covered during that process.
The retention of assessment records ensures accountability and transparency in the evaluation process, including a documented trail of decisions. This transparency is important to ensure that any regulatory approval by CASA is supported by clear, justifiable, and objective assessments. Such records also assist CASA with future assessments of the same candidate.
In this case, this first assessment was used as a basis for CASA’s alternate HOFO assessment of the same candidate for Broome Aviation 19 days later, enabling the process to be expedited. The FOI specified that this assessment was for the alternate HOFO position, however the approval given was for the HOFO position. Although CASA advised that the assessment process for an alternate HOFO and a HOFO position was the same, the FOI noted that they did not complete a full assessment of the applicant’s experience due to the expected short timeframe of the appointment.
In addition, although no time limitations for a HOFO position could be recorded on the official approval, CASA accepted Broome Aviation’s operations manual, which nominated the substantive HOFO as the HOFO and the newly assessed HOFO in the alternate HOFO position. The operations manual also did not outline how the alternate was going to manage the dual positions while being employed for operator 2 conducting check and training for its pilots and full-time flying, and fulfil the HOFO duties for Broome Aviation. CASA was aware that the substantive HOFO would be on leave and the alternate HOFO would be the acting HOFO.
CASA did not contact the operator at the end of the month despite only assessing the HOFO for one month. When the operator was advised that the substantive HOFO was extending their leave beyond April, they did not advise CASA of the change in circumstances within 7 days as required.
Upon discovering in February 2023 that the interim HOFO had been conducting the role for longer than the timeframe considered in the assessment, the CASA RO FOI discussed the matter with the interim HOFO. However, CASA did not re-assess the suitability of the interim HOFO to act for an extended period, and to ensure that the interim HOFO was available to effectively oversee Broome Aviation pilots when they returned to operator 2 in March 2023.
The dual arrangement of a pilot serving as HOFO for one operator and full‑time line pilot for another, posed challenges with:
operational priorities
workload management
operational oversight
compliance with regulatory requirements.
In this instance, the interim HOFO reduced their flying duties at Broome Aviation to return to flying and conduct check and training for operator 2. The reduction resulted in the interim HOFO having reduced oversight of Broome Aviation pilots during the March–June 2023 period.
Under CASR regulations, key personnel must demonstrate the capacity to discharge their responsibilities fully and effectively. CASA emphasised that it is ‘highly unlikely’ for key personnel to meet this requirement when performing similar duties for multiple operators simultaneously. If this dual arrangement is pursued, the second operator must clearly outline in its exposition how a HOFO will fulfill their responsibilities. This includes ensuring sufficient availability and capability to respond promptly to operational demands. Although in this case CASA personnel stated concern for the operation and oversight of Broome Aviation at the time, the 4-month period in which the interim HOFO was working for both operators resulted in Broome Aviation effectively having little oversight of its pilots.
Contributing factor
The Civil Aviation Safety Authority approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment due to an expectation that it was an interim appointment, and they had already been assessed. The person subsequently remained in the position for a much longer period. When this was identified by CASA, it did not fully assess the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation and forced landing involving Cessna 310R, VH-DAW, about 5 km south‑east of Derby Airport, Western Australia on 20 June 2023..
Contributing factors
The planned flight from Broome to Turkey Creek and return to Derby with the required fixed reserve and contingency fuel could not be achieved without refuelling the aircraft en route. In addition, the pilot did not intend to use all the available fuel in the auxiliary tanks and did not take this into consideration in their pre-flight planning, further reducing the amount of fuel available.
It is likely that the pilot did not utilise the right auxiliary fuel tank during the first leg of the journey and did not manage usage from the main fuel tanks in accordance with the pilot's operating handbook. This resulted in the depletion of fuel in the main tanks to a level where continuous engine operation could not be maintained
After the usable fuel in the right main fuel tank had been exhausted, the pilot did not divert the aircraft to the closest airport, select the left engine selection to the left auxiliary fuel tank, or maintain altitude to increase the safety margin.
The pilot had limited understanding of the aircraft fuel planning and in‑flight fuel management, but due to a lack of consolidation training and limited to no operational oversight these issues were not detected by the operator.
During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system. (Safety Issue)
Aircraft defects were not written on the maintenance release, leading to several defects not being rectified or managed. (Safety Issue)
The pilot was not wearing an upper torso restraint during the accident flight, resulting in the pilot receiving avoidable serious head injuries during the collision.
Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight. (Safety Issue)
Following a complaint by a former Broome Aviation pilot regarding management pressure on pilots to operate unserviceable aircraft, CASA conducted a level 2 surveillance activity on the operator in early June 2023 and following further complaints, a level 1 audit in August 2023, with key scope elements being to evaluate the complaints. Despite that, the surveillance activities and the associated reports did not assess the subject of the complaints.
The Civil Aviation Safety Authority approved a head of flying operations (HOFO) for Broome Aviation in early December 2022 via an abbreviated assessment due to an expectation that it was an interim appointment, and they had already been assessed. The person subsequently remained in the position for a much longer period. When this was identified by CASA, it did not fully assess the HOFO’s ability to continue undertaking the position when returning to work for another operator full time as a line pilot and alternate HOFO.
Other factors that increased risk
The aircraft fuel gauges did not indicate accurately.
Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Broome Aviation’s operations manual did not include a procedure for recording inflight fuel calculations. As a result, pilots adopted varying methods for fuel monitoring, leading to reduced assurance of accurate fuel management.
Safety issue description: During the 8-month period from November 2022 until the accident, Broome Aviation provided its pilots transitioning to operating the Cessna 310 with limited supervision, guidance and support, including management of the fuel system.
Safety issue description: Broome Aviation pilots experienced pressure not to report aircraft defects on maintenance releases, and many pilots also experienced or observed pressure from individuals within the company management to conduct flights in aircraft with defects that they considered made the aircraft unsafe for flight.
Glossary
AC
Advisory circular
AMC
Acceptable means of compliance
AME
Aircraft maintenance engineer
AOC
Air operators’ certificate
AWB
Airworthiness Bulletin
BAM
Broome Air Maintenance
CAO
Civil Aviation Order
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulation
CEO
Chief executive officer
ELT
Emergency locator transmitter
FDP
Flight duty period
FOI
Flight operations inspector
FOR
Flight operations regulations
FQIS
Fuel quantity indicating system
GM
Guidance material
HAMC
Head of maintenance control
HOFO
Head of flying operations
ICUS
In command under supervision
IFR
Instrument flight rules
IPC
Instrument proficiency checks
LAME
Licenced aircraft maintenance engineer
MCM
Maintenance control manual
MEA
Multi engine aircraft
MEL
Minimum equipment list
MOS
Manual of standards
MR
Maintenance release
POH
Pilot operating handbook
RO FOI
Regulatory oversight flight operations inspector
RPT
Regular public transport
SMS
Safety management system
SOM
System of maintenance
STC
Supplement type certificate
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passenger of the accident flight and multiple other company pilots
the head of flying operations at the time of the accident
the operator and substantive head of flying operations of Broome Aviation
Civil Aviation Safety Authority (CASA)
Western Australia Police Force
Textron Aviation
the maintenance provider for VH-DAW (Broome Air Maintenance)
the maintenance tracking provider and logbook controller for Broome Aviation (Avtrac Maintenance Tracking)
Airservices Australia
video footage of the accident flight and other photographs and videos taken on the day of the accident
recorded data from the GPS unit on the aircraft.
References
National Transportation Safety Board 2011, Airbag performance in general aviation restraint systems, Safety Study NTSB/SS-11/01.
Stothard C & Nicholson R 2001, Skill acquisition and retention in training: DSTO support to the army ammunition study, Defence Science and Technology Organisation, report DSTO-CR-0218.
Wickens CD, Hollands JG, Banbury S & Parasuraman R 2013, Engineering psychology and human performance, 4th edition, Pearson Boston, MA.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
other pilots interviewed during the investigation
Broome Aviation
Civil Aviation Safety Authority
Textron Aviation
National Transport Safety Bureau
Broome Air Maintenance
Submissions were received from:
the pilot
other pilots interviewed during the investigation
Broome Aviation
Civil Aviation Safety Authority
Textron Aviation
Broome Air Maintenance
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR) are a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[2]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[3]The substantive HOFO held the position with the operator prior to December 2022 and after June 2023.
[4]The interim HOFO held the position from December 2022 to June 2023.
[5]Broome Aviation was in a transitional state to the Civil Aviation Safety regulations Parts 119 and 135 requirements and still used a document known as an operations manual rather than the exposition required by the new regulations.
[6]VMCA: the minimum speed, while in the air, that directional control can be maintained with one engine inoperative.
[7]An imperfection that impairs the structure, composition, or function of an object or system of an aircraft or component.
[8]Inoperative: an item for a flight of an aircraft is inoperative if, due to a defect, the item, or a function of the item, does not accomplish its intended purpose, or consistently function within the operating limits or tolerances mentioned in the approved design for the item or the flight manual for the aircraft.
[9]Under previous legislation, air transport operations were split into regular public transport (RPT) and charter flights.
[10]Elevator flutter: refers to an uncontrolled, rapid oscillation or vibration of the elevator control surface. This phenomenon can occur due to aerodynamic forces, structural dynamics, or a combination of factors.
[11]The Cessna 310R POH detailed numerous fuel flow rates for specific power settings.
[12]This was a conservative rate of fuel burn as the engine manufacturer could not give an expected fuel return rate as this was dependent of the engine power used and the conditions on the day.
[13]Medical restriction, as defined by the operator, was any condition that required the carriage of an additional flight crewmember.
[14]CASA EX87/21 was an exemption instrument providing certain operators with deferrals from specific requirements of the Flight Operation Regulations particularly concerning safety management systems, human factors principles & non‑technical skills, and training & checking. The deferrals applied to certain operators only and were subject to conditions.
[15]Upper torso restraint: a shoulder strap or harness. A shoulder strap, when paired with a lap belt, effectively makes the occupant’s restraint similar to the seatbelt on modern cars.
[16]Portable ELT: An emergency locator transmitter that is manually activated by a pilot or passenger when in distress.
[17]Automatic fixed ELT: An emergency locator transmitter that is permanently attached to the aircraft and designed to stay attached even after a crash to aid Search and Rescue (SAR) teams in locating a crash site.
[18]Flight operations manager: plans, coordinates and controls all operational activities of all aircraft movement.
[19]HAMC: monitors and records aircraft hours, cycles and equipment maintenance and other information relevant to maintenance scheduling. Coordinates defect rectification and unscheduled maintenance activities. Reviews Airworthiness Directives for applicability and compliance.
[20]Under CASR Part 119.080(1)(c) – Conditions of an Australian air transport AOC, the operator was required to fill the HOFO position at all times and the person fulfilling the role was to be approved by CASA (whether the permanent HOFO, a permanent alternate HOFO, or a person temporarily filling the position as an interim HOFO).
[21]Broome Aviation did not have an exposition at this time – the time limitation should have been stated in the operations manual.
Occurrence summary
Investigation number
AO-2023-029
Occurrence date
20/06/2023
Location
About 5 km south-east of Derby Airport
State
Western Australia
Report release date
30/04/2025
Report status
Final
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Forced/precautionary landing, Fuel starvation
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
310R
Registration
VH-DAW
Serial number
310R0148
Aircraft operator
Broome Aviation Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Turkey Creek Aircraft Landing Area, Western Australia