Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 28 June 2025, a Bell Helicopter 47G-5 was conducting a ferry flight from Clare Valley Aerodrome, South Australia to Sydney, New South Wales. The pilot and passenger departed Clare Valley at about 0900 local time for an intended fuel stop at Renmark Airport, South Australia.
At about 0950, while in cruise flight at about 800 ft above ground level, the pilot felt a ‘couple of small kicks’ (in yaw[1]) and a ‘small shake’ alerting them to a problem. The pilot started to reduce power and altitude and scan the instruments and recalled that the carburettor[2] air temperature indicated the highest temperature on the gauge, although no carburettor heat was being applied. The engine then subsequently failed and the pilot conducted an autorotation[3] into a nearby field.
A run-on landing was conducted with forward speed, before the starboard side skid gear collapsed, causing the cabin to dig into the dirt whereby the helicopter tipped nose forward. As a result, the windscreen bubble ruptured, the advancing blade then struck the ground and severed the tail boom, with the helicopter coming to rest in an upright position, but substantially damaged (Figure 1).
Figure 1: Helicopter damage
Source: Operator
The pilot reported securing the cabin, switching the magnetos[4] and battery off and shutting off fuel (closing the fuel cut-off value). On exiting, the starter motor was smoking, the starter vibrator was buzzing, and the battery relay was chattering. The pilot then disconnected the battery which de-energised the starter system.
No injuries were reported by pilot or passenger.
Engineering inspection
Prior to the aircraft being recovered, engineers confirmed that the battery relay was energising, and the starter vibrator was also receiving power with the master switch in the OFF position when the battery was connected.
A subsequent engineering assessment detected heat damage in the main canon plug connector (connecting the cabin wiring loom with the airframe wiring loom) under the cabin floor, and heat damage in the wiring.
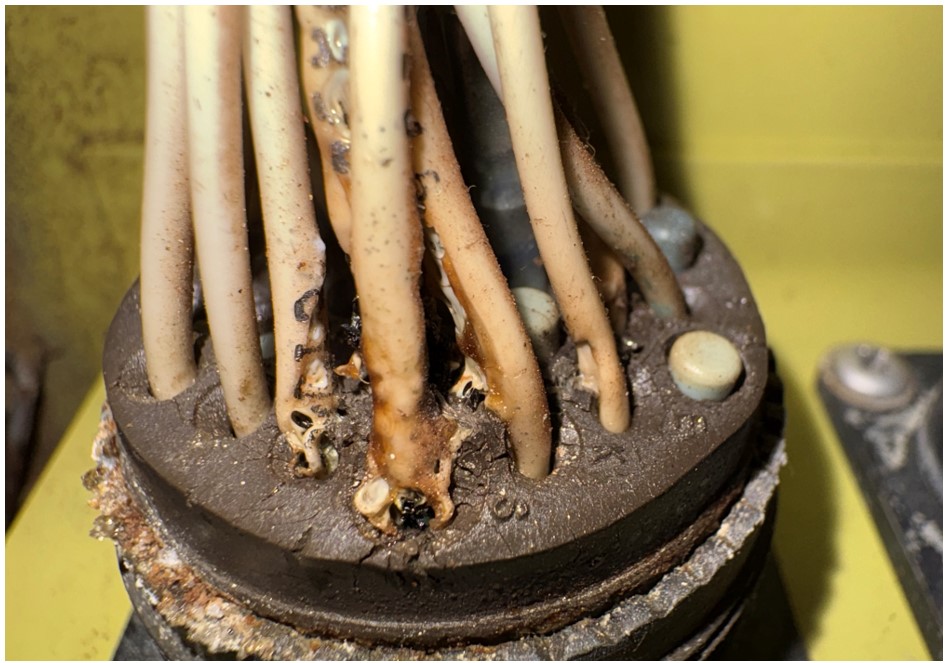
The assessment determined that corrosion in the plug wiring pins (Figure 2) has likely caused resistance to electrical current, and heat build-up. This likely resulted in several wires melting and creating a short circuit for the battery relay, starter vibrator, and instrument cluster.
The operator reported that the short circuit energised the starter vibrator and provided grounding to the magnetos which affected engine operation.
Figure 2: Corrosion in the plug wiring pins
Source: Iconic Helicopters Maintenance Pty Ltd
Safety message
Precise positioning and energy maintenance is required for a successful autorotation landing. Autorotation is a high-risk skill requiring the pilot to descend the helicopter by lowering the collective lever so that the resultant airflow provides the driving force to turn the blades. Thorough and regular training in emergency procedures is crucial for all pilots.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]The motion of an aircraft about its vertical or normal axis.
[2]Device for continuously supplying the engine with optimum combustible mixture.
[3]Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[4]A type of electric generator using permanent magnets to supply an electric current for engine ignition.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-027
Occurrence date
28/06/2025
Location
51 km from Waikerie
State
South Australia
Occurrence class
Accident
Aviation occurrence category
Abnormal engine indications, Collision with terrain, Engine failure or malfunction, Forced/precautionary landing
Highest injury level
None
Brief release date
08/08/2025
Aircraft details
Manufacturer
Bell Helicopter Co
Model
47G-5
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Departure point
Clare Valley Aircraft Landing Area, South Australia
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 31 May 2025 at around 12:50 EST, the pilot of an amateur‑built Van’s RV-8 aircraft was carrying out a documented flight test program to qualify the aircraft for a Special Certificate of Airworthiness in the Experimental category. The flight was being operated in the vicinity of the Jervis Bay Aerodrome, Jervis Bay Territory, when the pilot reported that during a level turn, preparing for an accelerated stall test at approximately 3,500 ft AMSL, the engine lost all power and failed. After attempts at restarting the engine were unsuccessful, the pilot was able to configure the aircraft for a glide approach and safe landing on runway 15 at Jervis Bay.
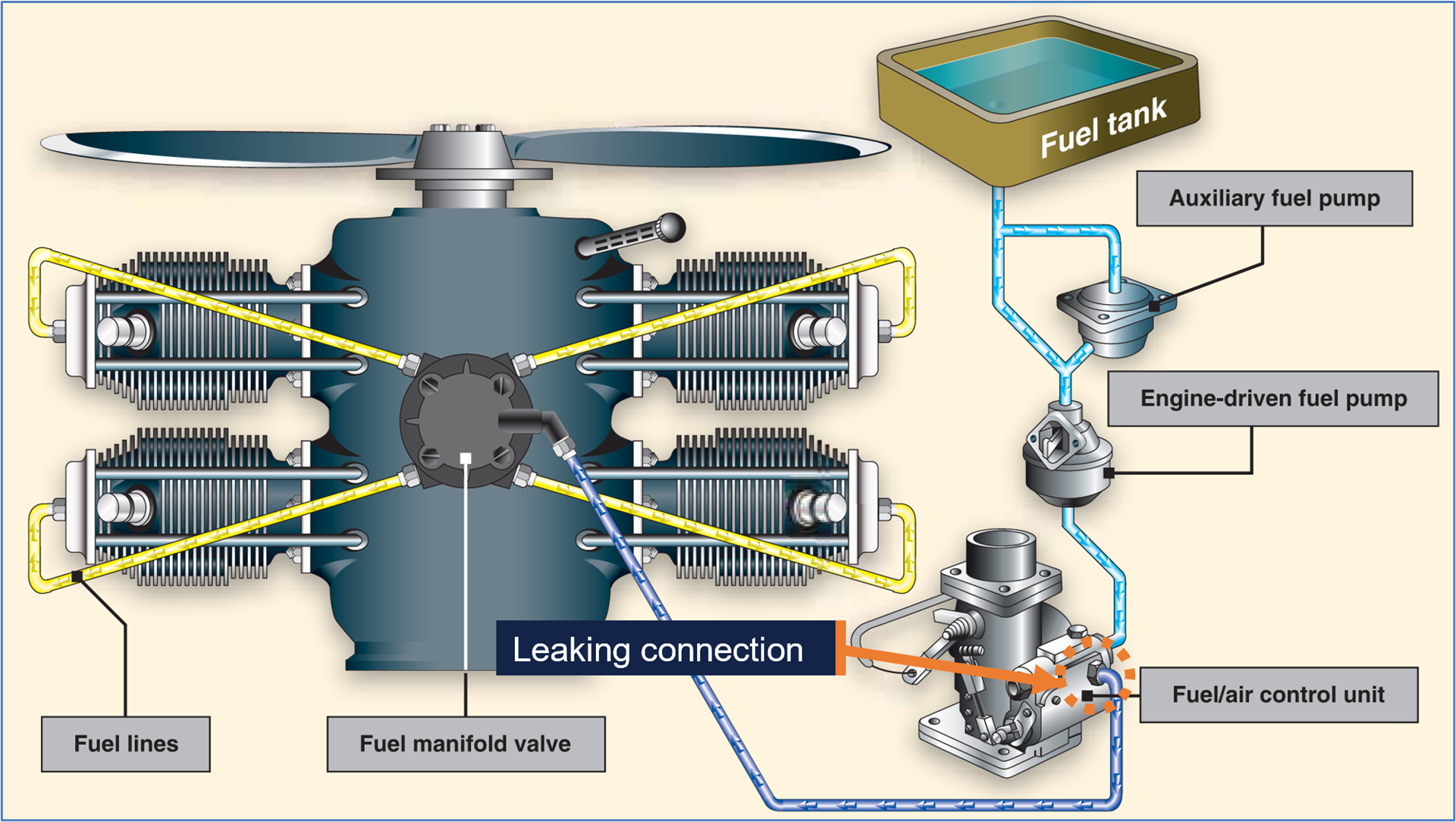
The RV‑8 aircraft was fitted with a Textron Lycoming IO‑360‑M1B four‑cylinder fuel‑injected aeronautical engine. Inspections carried out on the engine and systems after the failure identified a loose and leaking fuel connection between the fuel/air control unit (fuel servo) and the fuel manifold valve (Figure 1). A loss of integrity of the fuel line at this point would result in the engine being starved of fuel and the power loss as sustained.
The pilot reported that since the engine’s assembly in 2023 there had been no maintenance or other activity around the fuel supply connection – leading to the conclusion that the leaking fitting may have been inadequately fastened at that time.
Figure 1: IO-360 fuel system - diagrammatical illustration
An ATSB research report Amateur-built aircraft Part 2: Analysis of accidents involving VH-registered non-factory-built aeroplanes 1988-2010found that across this period, amateur‑built aircraft had an accident rate that was 3 times higher than comparable factory‑built certified aircraft conducting similar flight operations. Further, over half of the accidents were precipitated by partial or complete engine failures – these being significantly more common when compared with factory‑built aircraft.
Considering these findings, this well‑managed safety occurrence provides a direct reminder, to all pilots and crew of sports and general aviation aircraft, of the importance of being prepared for an unexpected partial or complete loss of power during any phase of flight. In this instance, the pilot’s operation at an altitude and position in respect of the Jervis Bay Airport provided some assurance of the ability to conduct a safe unpowered descent and landing after the engine failure occurred.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-024
Occurrence date
31/05/2025
Location
Near Jervis Bay Airport
State
Australian Capital Territory
Occurrence class
Serious Incident
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Fuel systems
On the morning of 14 July 2025, a Bell 206L-3 helicopter, registered VH-JMM, was being operated on multiple passenger charter flights around the Arnhem region in the Northern Territory. On board was a pilot and one passenger.
During the fourth leg of the day at approximately 1338, while looking down and to the left out of the helicopter, the pilot heard a loud bang. The pilot saw a large bird laying between the 2 occupants, and what appeared to be serious injuries to the passenger’s upper body. The pilot reached over to the passenger to check for a pulse but was unable to feel one. Noting the passenger required immediate attention, they decided it would be better for the passenger to receive medical attention at Lake Evella Aerodrome where a police station was next to the airport.
Police, a local nurse and doctor attended to the passenger, however the passenger had succumbed to injuries. The helicopter sustained minor damage.
What the ATSB found
While cruising at about 900 ft AMSL, the helicopter struck a white bellied sea eagle which passed through the windshield and impacted the passenger.
The pilot had limited opportunity to detect the bird as they were looking down and to the left of the helicopter’s trajectory, reducing the pilot’s ability to see the bird and change the helicopter’s flight path in time, and likely rendering the collision unavoidable under the circumstances.
The passenger was not wearing a helmet at the time, nor was there an aviation regulatory requirement for them to do so. In this case, the location of the bird strike on the passenger was such that wearing a helmet probably would not have reduced the level of injury.
Safety message
Birdstrike is an almost unavoidable and relatively common hazard for all aviation operations. While these strikes typically result in minor or no damage to an aircraft and no injuries to occupants, this is the third fatal birdstrike accident in Australia in recent years.
Pilots are reminded that maintaining effective lookout will assist in maintaining better situational awareness in flight, and also assist in providing better outcomes to see‑and‑avoid not only birds, but other airspace users.
Additionally, pilots should maintain situational awareness, especially when flying over waterways or wetlands. It is relatively common for large birds, such as eagles, hawks, and gulls, to attack helicopters and drones, often perceiving them as threats or territorial intruders. These birds may display aggressive behaviour during nesting or breeding seasons, diving at or striking the aircraft in an attempt to drive it away. Helicopter operators should consider whether available occupant protections, such as the wearing of flight helmets and the fitment of impact-resistant aircraft windshields, are appropriate for their operations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 14 July 2025, a Bell 206L-3 helicopter, registered VH‑JMM, was being operated by Nautilus Aviation on multiple air transport (passenger charter) flights around the Arnhem region in the Northern Territory. On board was a pilot and a passenger.
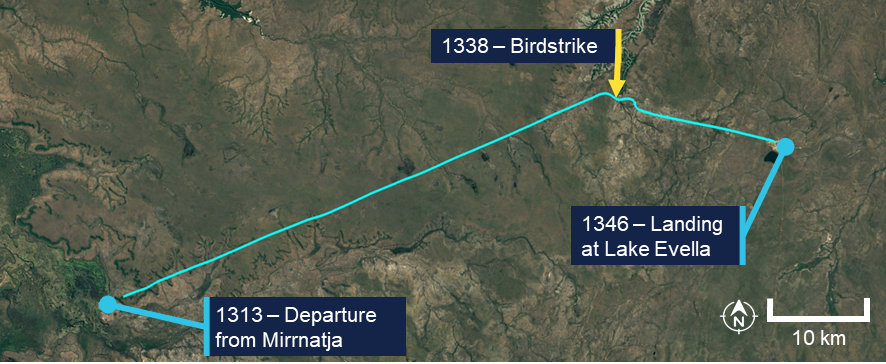
At approximately 0928 local time the helicopter departed Gove Airport for Donydji. The pilot reported that from Donydjii, they flew to ‘Nyquist tower’[1] and then on to Mirrnatja before departing for Burrum, which would be the last stop of the day before returning to Gove (Figure 1).
Figure 1: Flight path overview
Source: Google Earth, annotated by the ATSB
The flight departed for Burrum at 1313 (Figure 2) and the pilot established a cruise altitude of about 900 ft above ground level. The pilot recalled having a conversation with the passenger about a waterway which they were flying near, and was familiar to the passenger. The pilot recalled slightly deviating off track to view the waterway. At approximately 1338, while looking down to the left out of the aircraft, the pilot recalled hearing a loud bang.
The pilot saw a large bird laying between the 2 occupants, and what appeared to be serious injuries to the passenger’s upper body. The pilot reached over to the passenger to check for a pulse, but was unable to feel one. Noting the passenger required immediate attention, the pilot deliberated whether to land nearby and attempt resuscitation, and initially began to descend. However, considering the logistical issues with getting medical attention in a remote location, they decided it would be better for the passenger to receive medical attention at Lake Evella Aerodrome where a police station was next to the airport.
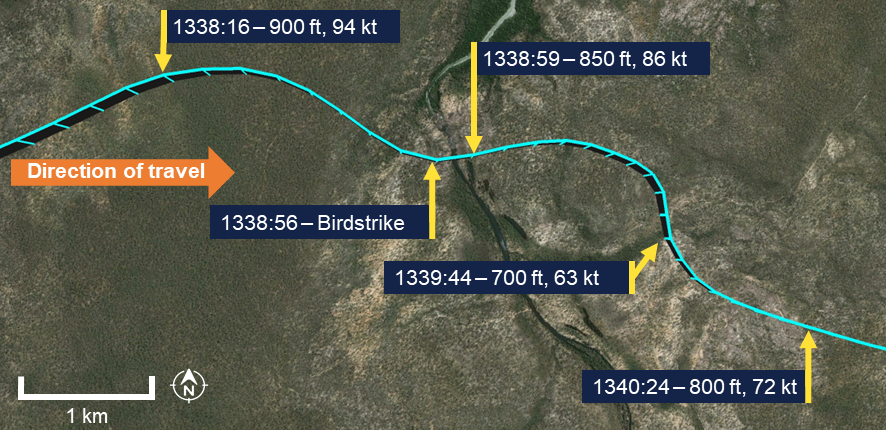
Figure 2: Accident flight overview
Source: Google Earth, annotated by the ATSB
The pilot landed the helicopter at Lake Evella Aerodrome at approximately 1346. They stated they attempted to call emergency services on 000, however the call did not connect. They decided not to attempt the call a second time and ran to the police station for assistance instead.
Police, a local nurse and doctor attended to the passenger, however the passenger had succumbed to injuries. The aircraft sustained minor damage (see Helicopter damage).
Context
Pilot information
The pilot held a valid Class 1 Aviation Medical Certificate and a Commercial Pilot Licence (Helicopter). The pilot had accumulated 2,553 hours of aeronautical experience, of which 1,319 hours was on the Bell 206L.
The pilot had been with the operator since September 2024 and had regularly flown these routes to remote communities as part of their employment.
Passenger information
The passenger was a frequent passenger on the routes operated on the day and had travelled by helicopter regularly to remote communities as part of their employment since 1995.
The pilot reported to having flown this passenger to remote communities on multiple occasions. Familiar with the aviation environment, the pilot reported the passenger would assist with monitoring for birds during flights, as they were aware they presented a hazard in flight.
The post-mortem examination report indicated the passenger was hit between the lower jaw and the upper chest, sustaining fatal injuries to the neck, chin, lower jaw and the right side of the chest.
Helicopter information
General
VH-JMM was a Bell Helicopter Company B206L‑3 Long Ranger, S/N 51400, manufactured in Canada in 1990. It was first registered in Australia in June 2017. The aircraft was registered to the operator in January 2024.
VH-JMM was a helicopter with two‑bladed main rotor and tail rotor systems, powered by a single Rolls-Royce 250‑C30P gas turbine engine.
At the time of the accident, the helicopter had completed 13,250 hours in service and had a current maintenance release.
Helicopter damage
The helicopter sustained damage to the passenger side windshield. There was no other reported damage to the aircraft (Figure 3).
Figure 3: Helicopter damage
Source: Northern Territory Police Force, annotated by the ATSB
Helicopter windshields
VH-JMM was fitted with standard acrylic windshields, which were not rated for impact resistance.
In 2016 Bell Helicopter Company introduced polycarbonate windshields, through a supplemental type certificate (STC) for the Bell 206 series, including the 206L. These were available as an additional option for current owners, offering higher impact resistance compared to traditional acrylic, reducing the risk of breaches from birdstrikes or other impacts. These were rated to United States regulatory requirements of a 2.2 lb (1 kg) bird traveling at VNE (the helicopter’s never-exceed speed).[2]
Despite having a higher impact resistance than acrylic, polycarbonate windshields are more sensitive to scratches, and reportedly susceptible to clouding or hazing due to ultraviolet light exposure, resulting in loss of optical clarity and necessitating more frequent replacements.
Weather information
The terminal aerodrome forecast for the accident region forecasted clear conditions for the flight with scattered cloud above 3,500 ft and visibility greater than 10 km.
At 1530, the weather station at Elcho Island Airport, 48 km north of the accident location, recorded the wind as 4 kt from 110° magnetic. There was scattered cloud at 1,000 ft, visibility was greater than 10 km and the temperature was 23°C.
The pilot reported that the weather varied depending on where they were flying, however it was mostly clear with some areas of cloud. They reported the clouds were above their cruise height.
Recorded data
The aircraft was fitted with a Spidertracks flight tracking unit and the pilot used OzRunways electronic flight bag software; both recorded flight data. Flight data indicated that the aircraft was cruising at 900 ft above ground level at a groundspeed of 94 kt at the approximate time the bird was struck. The data showed an initial deceleration to 86 kt groundspeed and a decrease in altitude of 50 ft, followed by a secondary decrease in altitude of approximately 150 ft (likely associated with the pilot’s consideration of whether to land). The track showed that the helicopter then climbed to 800 ft and increased groundspeed to about 70 kt (Figure 4).
Figure 4: Recorded flight track
Source: Google Earth, annotated by the ATSB
Bird information
Recovered biological specimens of the bird, including wing feathers and residue from the carcass, were found both inside the helicopter and on the passenger. Through images of the bird, the ATSB determined the species to be a white‑bellied sea eagle.
The white-bellied sea eagle (Haliaeetus leucogaster) (Figure 5) is a large raptor commonly found in coastal regions of Australia, recognised for its distinctive white head, belly, and tail contrasted by dark greyish‑brown wings and back. Adults measure approximately 66–85 cm in length, with a wingspan of 1.8–2.2 m (Debus, 2017). Adult males typically weigh between 1.8–3 kg, while females average 2.5–4.5 kg (Marchant & Higgins, 1993). The weight and sex of the bird in this accident was unknown.
Figure 5: Some of the bird remains retrieved from the helicopter
Source: Northern Territory Police Force
These eagles are often observed soaring over coastlines, estuaries, or inland waterways, preying on fish, seabirds, or carrion, and can reach heights of up to 1,000 m (about 3,300 ft) (Ferguson‑Lees & Christie, 2001). Their activity increases during the June to January period in Australia, which is their breeding season (Debus, 2017).
It is relatively common for large birds, such as eagles, hawks, and gulls, to attack helicopters and drones, often perceiving them as threats or territorial intruders. These birds may display aggressive behaviour during nesting or breeding seasons, diving at or striking the aircraft in an attempt to drive it away (Washburn & others, 2015).
Limitations of see-and-avoid
The human visual system is inherently limited in detecting small objects such as birds at distances. Hobbs (1991) notes that effective visual scanning requires systematic eye movements across the visual field, yet pilots often employ unsystematic techniques, resulting in unsearched areas. Furthermore, the cognitive process of identifying a threat, assessing its collision risk, deciding on evasive action, and executing control inputs requires time that is often unavailable in low‑altitude, high‑speed scenarios.
Birds present unique challenges to the see‑and‑avoid principle due to their relatively small size, unpredictable flight paths, and speed difference compared with aircraft.Unlike aircraft, birds cannot be tracked electronically, meaning pilots must rely solely on visual identification.
Survivability
Restraints
The helicopter was fitted with 4‑point harnesses in the front seats. The pilot reported both they and the passenger had been fastened into the seats by the aircraft’s 4‑point harnesses.
Helmets
The pilot reported wearing a flight helmet[3] and reported wearing a helmet whenever possible, noting that helmets had saved lives in the past. The pilot recalled previously having a discussion with the passenger about helmets and the benefits of them.
The passenger was not wearing a helmet at the time, nor was there an aviation regulatory requirement for them to do so. Nautilus Aviation stated that there was no requirement for passengers to wear a helmet and the decision on their use rested with the passengers themselves or their employers.
Telstra helicopter charters
The passenger was on board the aircraft as part of their work for Telstra, a telecommunications company. Telstra reported that its employees took about 630 helicopter charters on average per year, a mix of passenger charter (transit) and aerial work.
The employer had an operational framework for chartering aircraft that addressed many risks typically associated with helicopter flights, outlining expectations for the aircraft operator. These included the requirement for the aircraft operator to perform a risk assessment ‘prior to the first flight of any new operation by the Charter operator.’
Telstra did not have prescribed or recommended personal protective equipment for employees travelling or working on helicopters. Telstra advised that it relied on the licenced and accredited aviation providers that it engages to advise on safety of flight aspects including the use of personal protective equipment (PPE).
Related occurrences
Global data
Birdstrikes are a recognised hazard in aviation and there are mitigators in place at certified airports, however, there are challenges when operating outside of these areas.
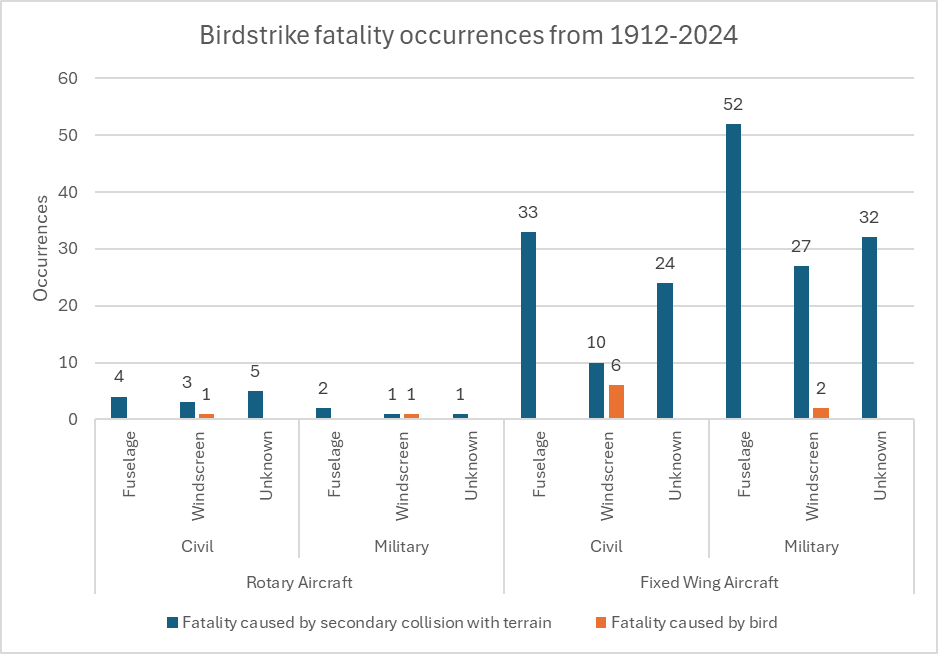
A review of Australian and internation data was conducted using the Avisure serious accident database. Between 1912 and 2024, birdstrikes have resulted in 763[4] reported aviation occurrences worldwide that involved serious or fatal injuries, of which 204 were fatal. Among these fatal cases, 18 involved rotary‑wing aircraft such as helicopters. These 18 accidents comprised 13 civil and 5 military rotary‑wing aircraft (Figure 6).
Figure 6: Global birdstrike data resulting in fatalities
Data does not include this occurrence (AO-2025-039). Source: Avisure
United States data
In the United States, a total of 13,667 bird strike occurrences were reported to the Federal Aviation Administration (FAA) in operations involving aircraft (fixed-wing and rotary-wing) under 5,700 kg maximum take‑off weight from 2014 to 2024. Of these, 60 occurrences resulted in non-fatal injuries, and 11 were fatal.
A subset of 334 occurrences involved birds striking and damaging the aircraft windshield, with 48 of these occurrences (14.4%) resulting in serious injuries and 6 (1.8%) leading to fatal injuries.
Of the total, 3,001 occurrences involved rotary-wing aircraft, which equated to a birdstrike every 285,390 flight hours (Table 1). These included 201 recorded windshield strikes, that resulted in 28 (13.9%) serious injuries and 2 (1.0%) fatalities.
Flight hours per birdstrike to windshield resulting in damage
Australia
412
39,690
8,819
United States
3,001
285,390
19,026
In comparison to the most frequently struck aircraft component, the wings, with 1,171 occurrences, only 6 (0.5%) resulted in injuries including 1 with fatal injuries (0.09%), indicating that the proportion of serious and fatal outcomes from windshield strikes is unexpectedly high relative to other aircraft parts.
Australian data
Birdstrikes in Australia
Between 2014–2024 the ATSB aviation wildlife dashboard indicated there were 17,060 reported birdstrikes reported to the ATSB across all aircraft types (including fixed‑ and rotary-wing). There were 412 reported birdstrikes during helicopter operations (Table 2), which equated to a birdstrike every 39,690 flight hours. The data did not include what component was struck unless the component was damaged, so it was not possible to determine the proportion of windshields struck that were penetrated or damaged. Of the 412 reported birdstrikes to helicopters, 17 had damage to the windshield.
Table 2: Reported helicopter birdstrikes within Australia 2014–2024
Total reported incidents
Injury level
Aircraft damage
Nil
Minor
Fatal
Nil
Minor
Substantial
Destroyed
Unknown
412
411
0
1[1]
352
37
2
2
19
This figure does not include this occurrence
ATSB records indicate there were 2 fatal accidents in civil aircraft in Australia due to birdstrike. Additionally, there was 1 serious accident involving a bird entering through the windshield. These investigations are described in the following subsections.
Birdstrike involving Glasair Sportsman GS‑2, N666GM, near Bathurst, New South Wales, on 24 December 2015 (
During take-off the aircraft collided with a wedge‑tailed eagle (Aquila audax), penetrating the windscreen and causing significant damage to the propeller and engine, while also striking the pilot, who sustained serious facial injuries and was temporarily unable to see. The pilot, who was wearing a headset and spectacles (both dislodged and damaged during the impact), managed to land safely.
Birdstrike and in-flight break-up involving a Bell 206L‑1, VH‑ZMF, near Maroota, New South Wales, on 9 July 2022 (AO‑2022‑034)
Shortly after departing from a private helipad, the helicopter was struck by a wedge‑tailed eagle (Aquila audax) just below the front left windscreen. The pilot, likely startled by the birdstrike and distracted by sun glare and a required radio frequency change, made abrupt control inputs that caused the main rotor to sever the tail boom, resulting in an in‑flight breakup and collision with terrain. The pilot, who was the sole occupant, was fatally injured.
Birdstrike and collision with terrain involving Air Tractor AT‑502B, VH‑KDR, 32 km east‑north‑east of Chinchilla Airport, Queensland, on 19 September 2022 (AO‑2022‑043)
During low-level aerial spraying at about 8 feet above ground, the aircraft was struck by a large Australian bustard (Ardeotis australis), which shattered the right windshield. The bird entered the cockpit, likely impairing the pilot’s ability to control the aircraft. The aircraft continued for approximately 310 m before colliding with terrain, resulting in the pilot being fatally injured and destruction of the aircraft.
Safety analysis
Birdstrike
Images from the accident site showed that the aircraft collided with a white‑bellied sea eagle (Haliaeetus leucogaster). The pilot had limited opportunity to detect the bird as they were looking down and to the left of the helicopter’s trajectory, so it was probably in their peripheral vision where detection of small objects is very limited. Even if they had been looking ahead at the time, they may not have been able to see the bird in time to avoid it due to the inherent limitations of the see-and-avoid principle. The closure rate to the soaring bird would have been around 94 kt and the difference in speed between them would have also made the relative trajectory almost direct. These factors further reduced the pilot’s ability to see the bird and change the helicopter’s flight path in time, likely rendering the collision unavoidable under the circumstances.
Considerations for aircraft operators and employers
Windshield impact resistance
The analysis of bird strike data highlights the significant safety risks posed to windshields. In windshield impacts in the United States, 14.4% caused serious injuries and 1.8% caused fatalities. Australia’s occurrences included 3 fatal and 3 serious injuries. Comparison of the United States and Australian data indicated that there was a higher chance of both birdstrike and the strike resulting in windshield damage per flight hour in Australia.
There is an elevated risk for helicopter operations due to low‑altitude operations and often less robust windshield designs. This is because if a bird penetrates the windshield, it can directly impact occupants, causing injury or incapacitation of flight crew, which may lead to loss of aircraft control or further operational hazards. While advancements in windshield design, such as laminated materials and reinforced structures, have mitigated many impacts, the data highlights vulnerabilities in extreme cases.
Manufacturers like Robinson and Bell have both released birdstrike‑rated windshields that provide higher impact resistance and significantly decrease the likelihood of objects breaching the windshield upon impact. However, these windshields have been rated to withstand a 1 kg bird strike at the aircraft’s never‑exceed speed, and the occurrence scenario involving a 3 kg bird colliding with the helicopter would likely exceed the windshield’s design limits. Nevertheless, and noting there are some disadvantages of impact‑resistant windshields, operators are encouraged to consider installing impact‑resistant windshields if operating in areas with a high probability of birdstrike.
Helmets
Helicopter pilots often wear helmets as a safety measure due to their frequent exposure to the dynamic conditions of rotary‑wing flight, where turbulence, rapid manoeuvres, and potential accidents pose risks of head injury. In contrast, passengers often do not wear helmets, as the risk is lower for occasional travellers, particularly considering the other safety measures associated with commercial passenger transport operations.
Passengers who travel frequently in helicopters fall between these 2 extremes. They are naturally exposed to a higher risk (over the occasional passenger) simply due to the increased number of flights. While the pilot reported being a helmet advocate and had previously discussed the potential benefits with the passenger, the decision whether to wear a helmet was ultimately left to the passenger’s discretion.
Helmets provide an additional layer of protection against birdstrikes, particularly in aviation scenarios like the Glasair Sportsman GS‑2 incident (AO‑2016‑001). A helmet, often equipped with a sturdy visor, can shield the face and head from small‑object impacts, reducing the risk of injury from a shattered windshield. Additionally, a helmet, especially one designed for aviation, is engineered to absorb and disperse kinetic energy from impacts with larger objects such as a bird potentially mitigating the severity of injuries like those sustained by the pilot of the Glasair, who was not wearing a helmet and suffered serious facial injuries. The helmet’s hard outer shell and padded inner liner work together to reduce the force transmitted to the skull, significantly lowering the risk of traumatic brain injuries, concussions, or skull fractures.
A helmet would not have prevented the passenger’s injuries in this case due to the impact location. Nevertheless, wearing a helmet as standard practice would provide some protection against a range of other potential hazards.
Pilot response
The pilot maintained control of the aircraft despite the sudden disruption and potential aerodynamic effects of the compromised windscreen. They promptly identified the nearest suitable landing site with access to medical facilities and executed a controlled descent and landing.
The pilot’s effective response and adherence to emergency procedures ensured the injured passenger was positioned for immediate medical response, highlighting sound decision‑making under extreme circumstances.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the birdstrike involving Bell 206L‑3, VH‑JMM, 16 km west-north-west of Lake Evella Aerodrome, Northern Territory, on 14 July 2025.
Contributing factors
While cruising at about 900 ft above mean sea level, the helicopter struck a white‑bellied sea eagle, which passed through the windscreen and impacted the passenger.
Other factors
Despite the injuries to the passenger and the damage to the aircraft, the pilot demonstrated composure and maintained control of the aircraft, enabling a calm and controlled return to a location where medical assistance could be provided.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
Nautilus Aviation
Northern Territory Police Service
recorded data from the Spidertracks unit on the helicopter
OzRunways.
References
Australian Transport Safety Bureau (2002). The Hazard Posed to Aircraft by Birds. Canberra: ATSB.
Debus, S. J. S. (2017). Australasian Eagles and Eagle-like Birds. CSIRO Publishing.
Ferguson-Lees, J., & Christie, D. A. (2001). Raptors of the World. Christopher Helm.
Hobbs, A. (1991). Limitations of the See-and-Avoid Principle. Canberra: ATSB.
Marchant, S., & Higgins, P. J. (Eds.). (1993). Handbook of Australian, New Zealand and Antarctic Birds: Volume 2 - Raptors to Lapwings. Oxford University Press.
Washburn, B. E., Begier, M. J., & Wright, S. E. (2015). Wildlife strikes to civil helicopters in the United States, 1990–2011. Wildlife Society Bulletin, 39(1), 115‑120.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Nautilus Aviation
Telstra
Civil Aviation Safety Authority
Northern Territory Police Force
TSB Canada.
Submissions were received from:
Nautilus Aviation
Telstra
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Antenna tower with designation NYQUIST NT 0822.
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory, with a pilot and one passenger on board. As the helicopter neared the destination, the pilot felt the onset of severe airframe vibration. The pilot elected to conduct a precautionary landing in an area of open farmland, resulting in a hard landing. The pilot and passenger were uninjured, and the helicopter sustained minor damage.
What the ATSB found
The helicopter’s engine was found to have suffered a mechanical failure due to in-service loosening of the nuts on the connecting rod bolts, leading to separation of one of the connecting rods from the crankshaft. The reason the nuts became loose was not determined.
While there was no indication of influence on this occurrence, independent inspection of the connecting rod attaching hardware performed during the overhaul of the engine did not involve a physical torque check of the connecting rod bolts. While the inspection was not a regulatory requirement, this was a missed opportunity to verify the installation torque.
During the most recent periodic inspection the helicopter maintenance provider did not refit the spark plugs using new gaskets, as required by the spark plug manufacturer. It was also found that the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent in this respect.
What has been done as a result
The Civil Aviation Safety Authority acknowledged the inconsistent information contained within the 2 airworthiness bulletins. CASA advised that Airworthiness Bulletin AWB 20‑001 is scheduled for cancellation and Airworthiness Bulletin AWB 85-023 is to be amended to reflect current recommendations.
The helicopter maintenance provider advised the ATSB it now installs new gaskets when refitting spark plugs.
Safety message
This incident highlights the importance of managing inflight anomalies through a comprehensive understanding of aircraft systems and the application of emergency procedures. The pilot’s timely actions following the onset of the vibrations ensured a safe outcome for the occupants and resulted in minimal damage to the helicopter.
The incident also emphasises the importance of adhering to manufacturer requirements when installing aircraft components, as well as the additional assurance provided by a thorough independent inspection of completed work.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
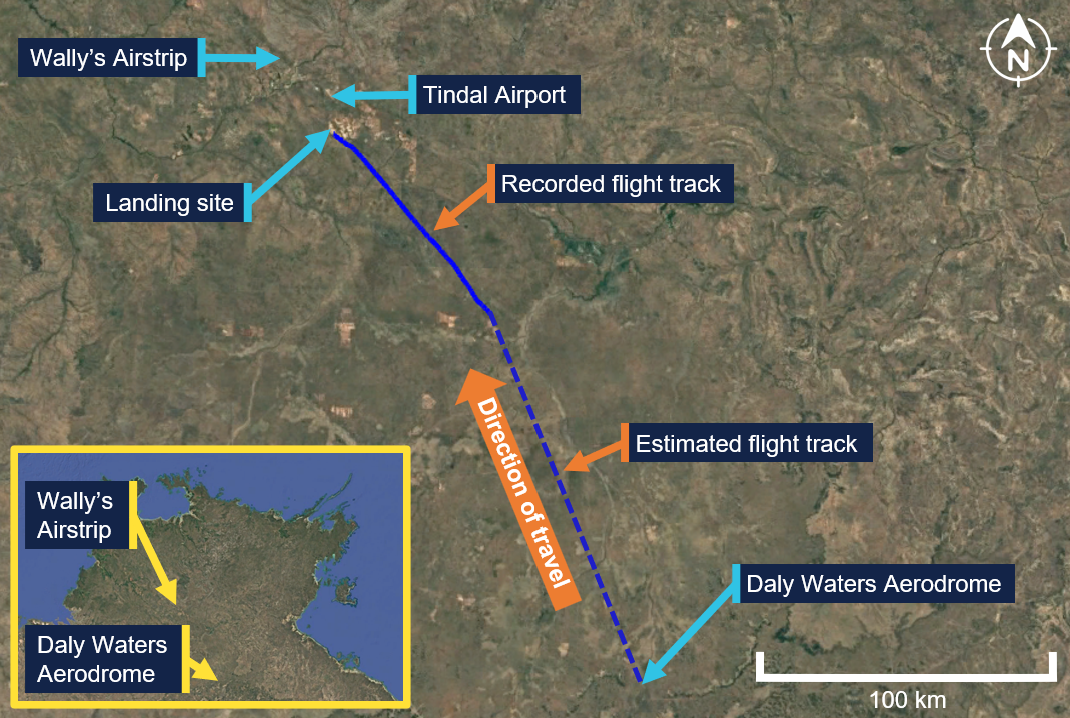
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight with a pilot and one passenger on board. The flight was conducted under the visual flight rules,[1] and the planned route was from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory (NT) (Figure 1).
On the morning of the flight, the pilot completed their pre-flight inspection and refuelled the helicopter. Shortly after starting the engine, the pilot recalled sensing an unusual sound and vibration through the helicopter, but it resolved when the engine speed was increased. The pilot completed their pre-take-off checks, and the helicopter departed Daly Waters Aerodrome at about 0900 local time. The pilot did not recount any issues with the helicopter’s performance during the take-off, climb or initial cruise.
Figure 1: VH-OOE flight track
Source: Google Earth, annotated by the ATSB
At about 1015, when the helicopter was about 46 km to the south‑east of Wally’s Airstrip, the pilot contacted Tindal Airport air traffic control (ATC). Several exchanges with Tindal Airport ATC took place, during which the pilot was instructed to follow a railway line and maintain an altitude not above 1,500 ft above mean sea level. The pilot complied with these instructions and continued towards their destination. At about 1020, when the helicopter was at an altitude of about 1,100 ft, the pilot felt the onset of severe airframe vibration. They recalled initially thinking the helicopter tail may had been struck but later discounted that possibility when they identified they still had directional control. The pilot was unable to diagnose the cause of the vibration and decided to undertake a precautionary landing.
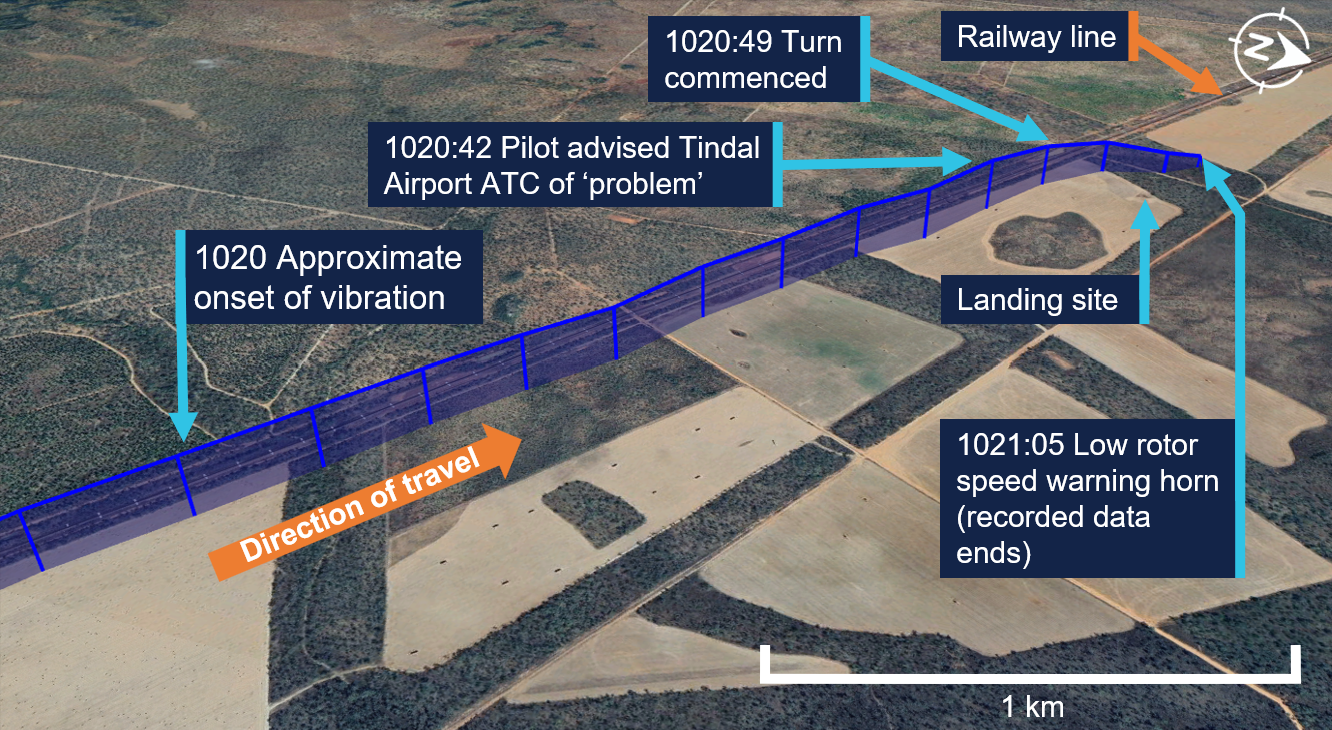
At 1020:42, and an altitude of about 1,100 ft, the pilot alerted Tindal Airport ATC that they had a ‘problem’ (Figure 2). The pilot selected a paddock for the landing that had recently been harvested of its crop and commenced a right turn towards the landing location at 1020:49. At 1020:52, they communicated that operations were not normal, and at 1021:00 they advised Tindal Airport ATC that they would be landing immediately. The pilot recalled noting the engine gauges and the rotor and engine speed indications at that time were normal.
Figure 2: VH-OOE flight path from the onset of vibrations until landing
Source: Google Earth, annotated by the ATSB
At 1021:05, and an altitude of 700 ft, the pilot made a transmission to Tindal Airport ATC during which a low speed warning horn could be heard in the background (see Low rotor speed). The pilot did not recall hearing the horn. At about 150 ft above ground level, the pilot recalled noting a low oil pressure light on the helicopter’s caution warning panel (see Oil warning caution light). They continued the approach and, as the helicopter slowed for landing, they observed smoke blowing forward from the rear and recalled having concerns about a fire.
The helicopter landed heavily in the paddock. The pilot recalled that the landing was probably completed ‘quicker’ and with a lower tail position than normal, due to their concerns about a fire. Once the helicopter had landed, the pilot instructed the passenger to exit and run forward. They then shut down the helicopter’s engine, and at 1021:41 advised Tindal Airport ATC that they had landed and were safe. The pilot then exited the helicopter. Both occupants were uninjured, and the helicopter sustained minor damage.
Context
Pilot information
The pilot held a valid Commercial Pilot Licence (Helicopter) with single engine and low‑level ratings. The licence was issued on 6 June 2025 following the successful completion of a commercial pilot licence flight test in May 2025. The pilot had held a Private Pilot Licence (Helicopter) since October 2023. They also held a current class 1 aviation medical certificate valid to 6 August 2025. At the time of the incident, they had a total flying time of 194 hours of which 118 hours were on the Robinson R44.
Helicopter information
General information
The Robinson R44 Raven I is a 4-place helicopter with a 2-bladed main rotor system and a conventional 2-bladed tail rotor. VH-OOE was manufactured in the United States in 2008 and first registered in Australia in July 2008. At the time of the incident, the helicopter had accumulated 1,995 hours total time in service.
It was powered by a Lycoming O-540-F1B5, 6-cylinder, horizontally opposed piston engine that is naturally aspirated and rated at 235 horsepower. The overhauled engine was installed in September 2022 and had operated for 291 hours at the time of the incident, with a total time of about 1,614.6 hours. The last periodic inspection was undertaken on 6 May 2025, and the helicopter had flown about 25 hours since that inspection.
Airworthiness and maintenance history
Recent maintenance
The last periodic inspection was undertaken by Platinum Helicopters on 6 May 2025. During the inspection, the Champion REM38E spark plugs fitted to the engine were removed, inspected and then refitted by the maintenance engineer. The maintenance engineer recalled that it was not their practice to fit new spark plug washers (gaskets) when refitting the spark plugs, instead electing to use annealed[2] gaskets (see Spark plug maintenance).
Engine overhaul
In September 2022, VH-OOE underwent a 12 year/2,200 hour inspection. During the inspection, the engine was removed and an overhauled engine was fitted to the helicopter. This engine had been salvaged from a Robinson R44, and was overhauled by South West Aviation, a CASA‑approved maintenance organisation.
During the overhaul of the engine, additional components were used to replace some aspects, including:
6 new cylinder kits
new connecting rod hardware (bolts and nuts) with parts manufacturer approval[3]
a crankshaft that had been salvaged from a different Robinson R44.
Records show all salvaged components were inspected and tested to assess serviceability prior to fitment. Once the engine overhaul had been completed, it underwent ground runs and checks prior to being installed in VH-OOE.
Records show that independent inspections were undertaken during the engine overhaul of the engine fitted to VH-OEE. The purpose of an independent inspection is to verify that a maintenance task has been completed correctly. The inspection is undertaken by an appropriately authorised person who did not undertake the original activity. While there was no regulatory requirement for the independent inspection of maintenance work carried out on engine systems, South West Aviation had included these inspections as part of the organisation’s worksheets for engine overhaul.
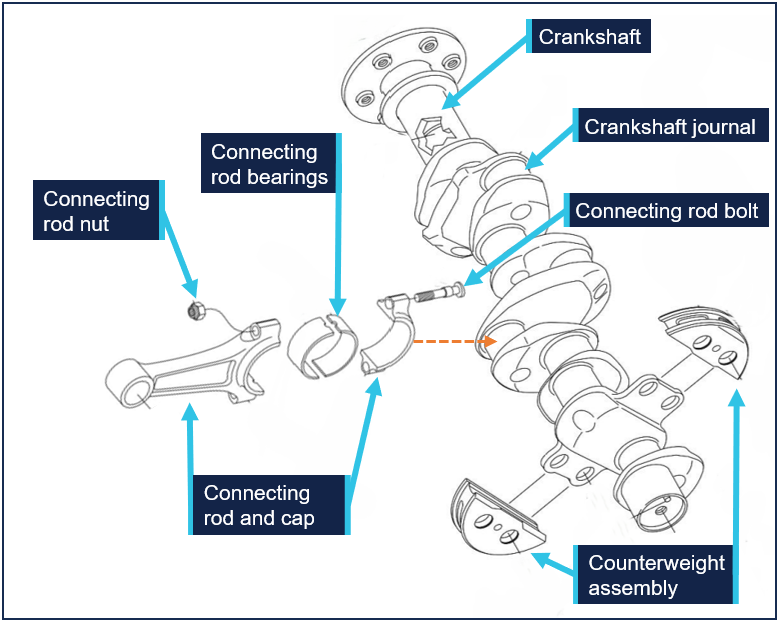
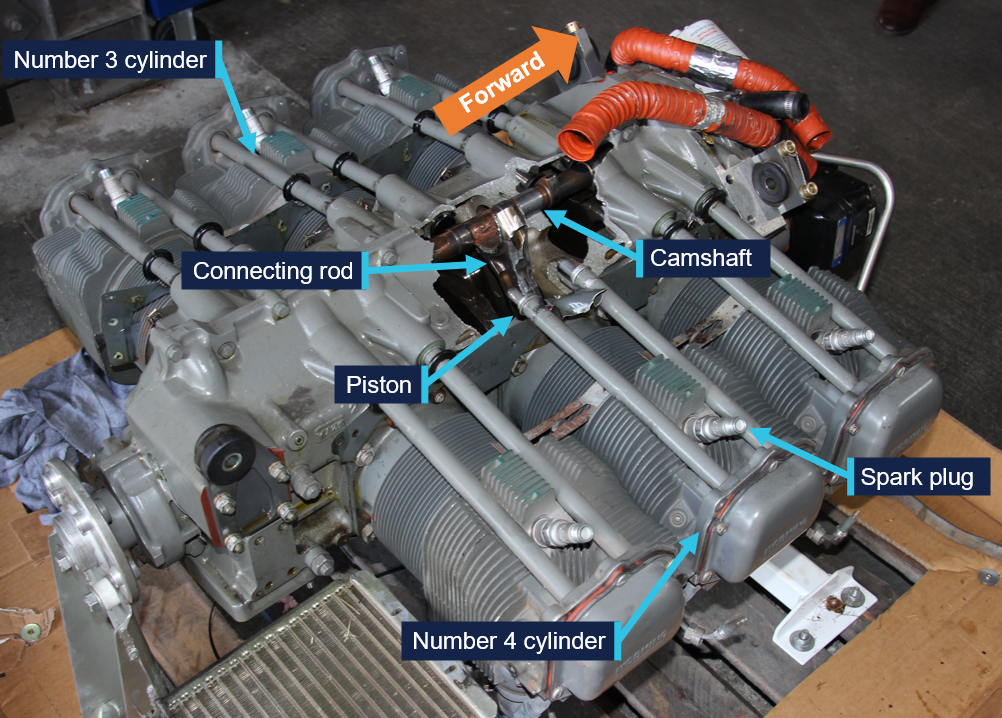
The worksheets for the engine overhaul stated that an independent inspection of the engine sub-assembly was completed during the engine rebuild. Figure 3 shows the sub‑assembly of the crankshaft and the connecting rods, which were secured to the crankshaft by 2 connecting rod bolts and nuts. The crankshaft has 2 dynamic counterweight assemblies fitted, which assist in removing torsional vibration during engine operation.
Figure 3: O-540 crankshaft and connecting rod sub-assembly
Source: Lycoming O-540-F1B5 Illustrated Parts Catalogue, annotated by the ATSB
During interview, when asked about a torque check of the connecting rod nuts, the engineer who conducted the independent inspection stated they would check the torque was set correctly on the tooling that had been used, but it was not their normal procedure to physically check the torque on each nut. South West Aviation did not have a documented procedure that detailed how the independent inspection of the connecting rod hardware should be conducted.
Helicopter systems and procedures
Vibration
The Robinson R44 pilot operating handbook (POH) contained advice for the management of vibration, and stated:
A change in the sound or vibration of the helicopter may indicate an impending failure of a critical component. If unusual sound or vibration begins in flight, make a safe landing and have the aircraft thoroughly inspected before flight is resumed.
Low rotor speed
The helicopter was fitted with a low rotor speed horn. The activation of the horn indicated that rotor speed may be below safe limits (97%). Power available from the engine is directly proportional to rotor speed. With less power the helicopter will start to sink. If the collective is raised to stop it from descending, the rotor speed will reduce even further causing the helicopter to sink faster. To restore rotor speed, the Robinson R44 POH stated that a pilot should lower the collective, roll throttle on and, in forward flight, apply aft cyclic.
Oil warning caution light
The helicopter was fitted with an oil warning caution light. The illumination of the light indicated a loss of engine power or oil pressure. The Robinson R44 POH stated the actions to take in response should be to check the engine tachometer for power loss and the oil pressure gauge. If oil pressure loss was confirmed, the POH stated the pilot should land immediately. Continued operation without oil pressure causes serious engine damage and engine failure can occur.
Spark plug maintenance
The Champion Aviation Service Manual,[4] which included recommended service, handling and reconditioning practices for Champion spark plugs stated:
Always install both new and reconditioned Champion aviation spark plugs with a new copper gasket.
Gaskets that have become too hard with normal usage won’t “hold torque” correctly, and spark plugs can come loose with disastrous results. An annealed gasket will not meet new specifications.
The maintenance engineer stated they carried out the periodic inspection in accordance with the Lycoming O-540 Operator’s Manual.[6] However, this manual, which covered both the O-540 and IO-540 engines, contained no information regarding spark plug gasket fitment. The guidelines for the installation of spark plugs were contained in Lycoming service instruction 1042 Approved Spark Plugs, which stated:
Always install a spark plug with a new gasket.
The Civil Aviation Safety Authority (CASA) had produced 2 advisory airworthiness bulletins (AWBs) that included information on spark plug fitment. However, the advice within these 2 documents was not consistent.
AWB 20-001 Spark Plug Care, issued in September 2001, stated:
Most modern spark plugs have a solid copper gasket that requires annealing prior to spark plug installation to ensure a tight, gas sealed fit. The maintainer should check that the spark plug has only one washer, is of correct dimensions and is annealed. If the engine is equipped with a thermocouple probe in the form of a spark plug gasket, a normal gasket is not required.
Whereas AWB 85-023 Piston Engine Spark Plug Cracking, issued in June 2021, stated:
Always install a new spark plug gasket when servicing spark plugs or installing new spark plugs. Failure to install a new spark plug gasket may result in incomplete sealing of the combustion chamber, loss of heat transfer with spark plug overheating leading to possible pre-ignition.
Meteorological information
The weather at the time of the incident, recorded at Tindal Airport around 13 km to the north of the landing site, captured a wind of between 9–13 kt from the east, clear skies and a temperature of 23°C.
Recorded information
The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the incident flight, data was being transmitted by the helicopter’s transponder. This data, recorded by ground-based receivers, captured the aircraft’s position, altitude, and groundspeed during the final 25 minutes of the flight. All radio communications made and received by Tindal Airport ATC throughout the flight were recorded.
Helicopter damage
The ATSB did not attend the landing site. A post-incident inspection of the helicopter was completed by a maintenance organisation located at Wally’s Airstrip, NT. This inspection identified:
damage to the engine with scattered material within the cowling
damaged and displaced drive belts
impact damage to the engine oil cooler caused by engine material
engine oil on external areas of the engine and airframe
the skid landing gear was spread outwards (Figure 4).
The engine and a selection of components were removed for a detailed examination by the ATSB.
Figure 4: VH-OOE shortly after landing showing oil leak and smoke haze
Source: Supplied, annotated by the ATSB
Engine examination
The engine was disassembled and examined at a CASA‑approved engine overhaul facility under the supervision of the ATSB. The examination found that the number 4 connecting rod had separated from the crankshaft journal, resulting in mechanical damage to the internal engine components and fracture of the adjacent crankcase. Both connecting rod bolts had been fractured, with one connecting rod nut missing and the other unwound (see Component examination). There were also witness marks from impact between the number 4 piston crown and cylinder head.
Prior to removal of the remaining connecting rods, the nuts were checked for torque. The check found that the number 3 cylinder connecting rod nuts were at 20 ft/lb, while numbers 1, 2, 5 and 6 connecting rod nuts were at the correct torque of 40 ft/lb.
The number 4 cylinder spark plugs were found loosened, but the spark plug leads were attached tightly. Subsequent testing of the spark plugs found both were serviceable. Figure 5 depicts the engine prior to disassembly.
Figure 5: Engine assembly showing damage
Source: ATSB
Component examination
Several components were retained from the engine disassembly and were examined at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
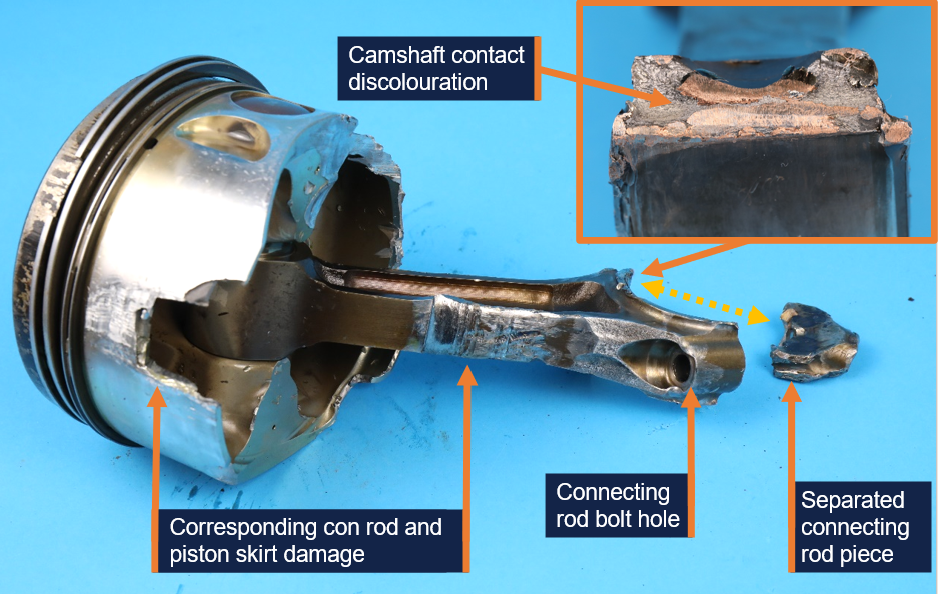
Extensive deformation and fracture of the number 4 connecting rod (Figure 6) and deformation of the crankshaft journal, was consistent with initial separation of the connecting rod, followed by repeated impacts to the connecting rod by the still-rotating crankshaft.
Figure 6: Number 4 cylinder connecting rod and piston
Source: ATSB
This resulted in significant damage to the adjacent cylinder wall, piston skirt, camshaft and the hole in the crankcase. The fractured connecting rod showed no evidence of fatigue cracking or other defect.
The number 4 connecting rod bearings were deformed due to contact with the moving internal engine components but were found to be the correct parts and did not exhibit any abnormal signs of wear. Bearings from some of the other connecting rods displayed minor surface wear, which was attributed to low engine oil volume during the final part of the flight.
There were visibly fewer combustion deposits on the number 4 piston crown, compared to the remaining pistons. However, a considerable amount of sand-like contamination was recovered from the number 4 cylinder during engine disassembly, which was found to be chemically similar to the piston deposits. There was no evidence of destructive combustion issues such as pre-ignition or significant detonation.
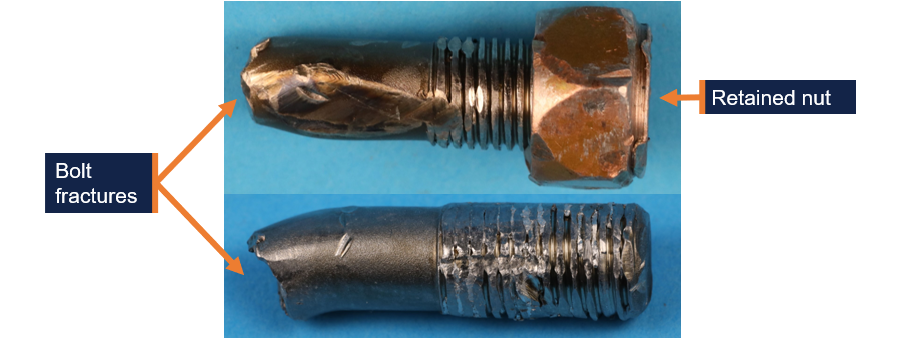
The connecting rod was secured to the crankshaft by 2 connecting rod bolts (Figure 3). Both number 4 cylinder connecting rod bolts were fractured in approximately the same location (Figure 7). The fracture surface features of both bolts and deformation of the adjacent shank were consistent with overstress failures.
Figure 7: Cylinder number 4 connecting rod bolts
Source: ATSB
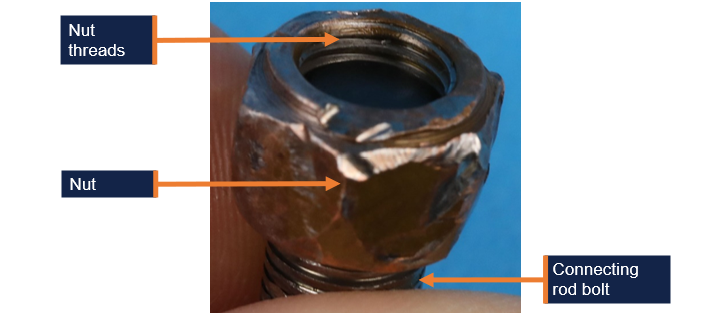
One of the cylinder 4 connecting rod bolts had no nut and heavily damaged threads. The nut was not located. The other connecting rod bolt had a partially unwound nut retained on the threads (Figure 8).[7] The exposed threads were damaged. The nut could not be further unwound by hand, likely due to impact damage. The bolts and nut material was in accordance with their specification. The extent of deformation precluded a detailed inspection of the threads; however, the threads were not stripped and the remnants of a compound consistent with thread lubricant was identified.
Figure 8: Number 4 cylinder connecting rod bolt showing position of retained nut
Source: ATSB
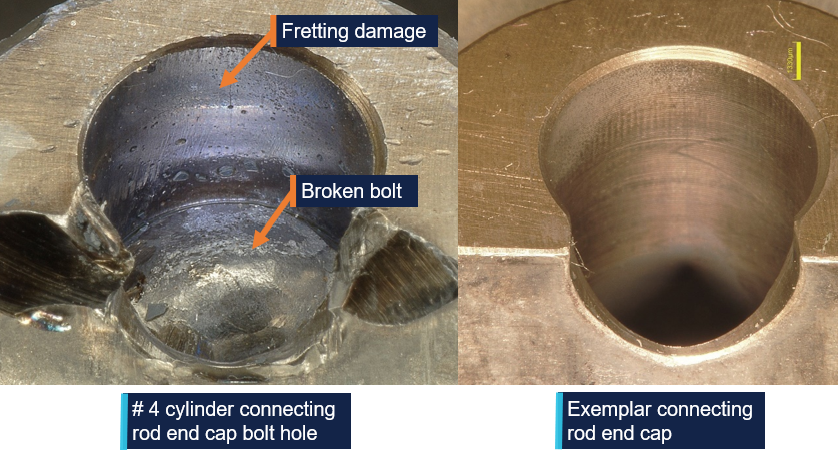
The examination also identified evidence of abnormal fretting[8] wear in the number 4 cylinder connecting rod bolt holes. A comparison between the number 4 cylinder and number 6 cylinder connecting rod bolt holes is depicted in Figure 9.
Figure 9: Number 4 cylinder connecting rod end cap bolt hole fretting wear and exemplar
Source: ATSB
The abnormal fretting wear indicated relative movement (micro-slip) between the bolted surfaces during operation, which would occur if the bolt tension was insufficient to restrain movement under normal operational loads. The missing nut from one of the bolts, and the other nut retained in an improper position on the fractured bolt, was also an indicator that the nuts had loosened in-service.
Possible mechanisms that could result in the in-service loosening of the nuts included:
Abnormal loading or vibration from engine overspeed or abnormal combustion that could lead to bolt stretch and nut loosening.
Variations in thread condition or installing the threads dry versus lubricated could produce a lower bolt stress than desired.
Unintended deformation due to improper or defective parts leading to reduced bolt stress over time.
Microscopic surface deformation and fretting at contact interfaces could reduce clamping force by a small margin over time, which could then make the nut susceptible to further loosening during service.
Inadequate torque applied to the nuts during installation that could lead to relative movement between the clamped surfaces and nut loosening during normal operation.
Related occurrences
In 2007, the ATSB published a research and analysis report (B20070191) into aircraft reciprocating (piston) engine failures. The report examined 20 high-power[9] piston engine structural failure occurrences in Australia, between 2000 and 2005. The report focused on failures of the combustion chamber, connecting rods and crankshaft assemblies. It included several engine failure investigations, including investigation 200105866 (below).
On 14 December 2001, a Piper PA31-350 aircraft, registered VH-JCH, was in cruise flight at 8,000 ft when the flight crew noticed that the propellers went out of synchronisation. Adjustments were made to correct the problem but were unsuccessful. Following right engine speed fluctuations, the crew shut the engine down, feathered the propeller and conducted a single‑engine landing.
During the subsequent disassembly of the engine, the crankshaft was noted to have fractured at the number 6 connecting rod journal, and the number 6 connecting rod big end had separated from the crankshaft and impacted the camshaft. The separation of the number 6 big end permitted the piston to strike the top of the combustion chamber with sufficient force to deform the top of the piston.
The number 6 connecting rod disconnection from the crankshaft was due to the loosening of the nuts on the connecting rod bolts, and eventual loss of one nut. Evidence of nut loosening, leading to fretting wear damage, was observed on the bolt threads and the connecting rod cap bolt hole locations. The reason for the loosening of the number 6 connecting rod nuts could not be determined.
The damage of these components was almost identical to the damage noted in the engine from VH-OOE.
Safety analysis
The ATSB examination of the engine components determined that the engine failure resulted from mechanical damage caused by the separation of the number 4 cylinder connecting rod from the crankshaft.
The initiating factor of the separation was almost certainly the in-service loosening of the connecting rod nuts of the number 4 cylinder. This was evidenced by the fretting wear in the connecting rod bolt holes, which was illustrative of engine operation after a loss of bolt tension, allowing relative movement between the bolts and holes. The absence of one of the associated nuts, and the opposite one mostly unwound was also evidence of the nuts loosening prior to the engine failure. There was also an absence of fatigue cracking of the number 4 bolts or connecting rod that might otherwise account for the component fractures and separation of the connecting rod.
Of the possible mechanisms identified that could have led to the connecting rod nuts loosening:
Abnormal loading or vibration: there was no evidence of engine overspeed, or of piston melting or structural damage consistent with severe abnormal combustion. There was no evidence that the spark plugs, found loose during the disassembly, had any negative impact on the engine performance.
Variation in thread condition and lubrication: this could not be fully assessed due to thread damage and the absence of one of the nuts.
Improper or defective parts: the connecting rod bolts and nut material was correct; however, a full assessment of their original condition was not possible.
Embedding (microscopic deformation): it is possible that the initial bolt tension reduced by a small margin due to microscopic deformation of the clamping or thread surfaces, which would then make the nut more susceptible to further loosening during service.
Inadequate installation torque: like the above, it was possible that the nuts were slightly under-torqued during installation and progressively loosened during the subsequent 291 hours of operation. The number 3 connecting rod nuts being found at the incorrect torque value during the engine disassembly further supports this scenario.
Given most of the possibilities above could not be definitively ruled out, the reason for the nuts loosening was ultimately not determined.
Despite this, it was identified that during the overhaul of the engine fitted to VH-OOE, the independent inspection of the engine sub-assembly did not involve a torque check of the connecting rod nuts. While there was no evidence of influence on this occurrence and while the inspection was not a regulatory requirement, the ATSB considered it a missed opportunity to positively verify the installation torque.
Additionally, during the engine examination, both spark plugs in the number 4 cylinder were found to be loose. The reason for the loose spark plugs was not determined and, as above, there was no evidence identified to indicate influence on the engine failure. However, it was identified that during the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the engine and spark plug manufacturer.
On the same subject, the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances.
The unusual sound and vibration noted by the pilot during engine start was possibly a precursor to the eventual failure inflight, however the vibration disappeared when engine speed was increased. In response to the onset of severe vibration inflight, the pilot assessed the controllability of the helicopter and noted there were no abnormal engine indications at that time. In accordance with the Robinson R44 POH, the pilot conducted a precautionary landing in a suitable location. They also communicated the issue to Tindal Airport ATC, which increased the likelihood of a timely emergency response had one been necessary.
During the late stages of the approach, the low rotor speed warning horn and low oil pressure caution light activated. Both indicated a reduction in power, almost certainly due to the mechanical failure, resulting in less power than normal to arrest the rate of descent in the final stages of landing. This, in combination with the pilot’s concern about a possible fire and recollection of landing ‘quicker’ than normal, likely resulted in the helicopter landing heavily which spread the landing gear skids.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine failure and forced landing involving Robinson R44, VH-OOE, 13 km south of Tindal Airport, Northern Territory, on 11 June 2025.
Contributing factors
In-service loosening of the connecting rod nuts resulted in the eventual separation of the connecting rod from the crankshaft and the mechanical failure of the engine. The reason for the nuts loosening was not determined.
During the engine overhaul, the torque on the connecting rod nuts was not physically checked as part of the independent inspection of the engine assembly. This was a missed opportunity to verify that the installation of the connecting rod nuts had been completed correctly.
Other findings that increased risk
During the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the spark plug manufacturer. This increased the risk of loosened spark plugs, insufficient heat transfer and pre-ignition.
The Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances. The inconsistency in this guidance could have led to incorrect procedures being performed which were not in accordance with spark plug maintenance requirements.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Civil Aviation Safety Authority
The Civil Aviation Safety Authority acknowledged the inconsistency between Airworthiness Bulletin AWB 20-001 (that stated that annealed gaskets could be used) and Airworthiness Bulletin AWB 85-023 (that stated new gaskets must be used in all circumstances) and advised the ATSB that AWB 20-001 will be cancelled and AWB 85‑023 will be amended to reflect current recommendations.
Safety action by Platinum Helicopters
Platinum Helicopters advised the ATSB that new spark plug gaskets are now fitted each time spark plugs are reinstalled.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Australian Government (2021), Aircraft Reciprocating-Engine Failure: An Analysis of Failure in a Complex Engineered System, Australian Transport Safety Bureau, Canberra, ACT. /publications/2007/b20070191
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of VH-OOE
Civil Aviation Safety Authority
the maintenance provider
the engine overhaul organisation
Textron Lycoming
Robinson Helicopters
National Transportation Safety Board (NTSB).
Submissions were received from:
the pilot of VH-OOE
the maintenance provider
the engine overhaul organisation
Textron Lycoming
Robinson Helicopters.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]Annealing: the process of heating a metal to a cherry red colour and them immersing into water to soften the material.
[3]A parts manufacturer approval (PMA) is a combined design and production approval for modification and replacement articles. It allows a manufacturer to produce and sell these articles for installation on type certificated products.
[4]Champion Service Manual AV6-R, revised August 2014.
[5]Champion Aviation Technical Bulletin 95-11, Aviation Spark Plugs – New and Reconditioned Should Always be Installed with a New Gasket, published November 1995.
[7]When installed correctly, 2–3 bolt threads would protrude from the edge of the nut. In this case 2–3 nut threads were visible on the end of the bolt.
[8]Fretting refers to wear involving small amplitude relative movement or vibration between contact surfaces.
[9]The high-power engines analysed as part of the study were Lycoming TIO-540 and IO-540, and Continental TSIO-520 and GTSIO-520 engines.
Occurrence summary
Investigation number
AO-2025-029
Occurrence date
11/06/2025
Location
13 km south of Tindal Airport
State
Northern Territory
Report release date
30/03/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Smoke
At 1021 on 7 April 2025, a Bankstown Helicopters Robinson R44 helicopter, registered VH‑EWM (EWM), with a pilot and 2 passengers on board, departed from Bankstown Airport, New South Wales, for a local scenic flight around Sydney Harbour. Shortly after 1028, as EWM was entering the Parramatta River helicopter lane behind an EC120 helicopter, the occupants of EWM experienced a sudden onset of turbulence followed by an uncontrolled descent.
In response, the pilot applied full collective, which resulted in a low rotor speed condition as the helicopter descended towards the water. The pilot was able to manoeuvre the helicopter and complete a forced landing on the river shoreline.
What the ATSB found
The ATSB found that it is likely that EWM entered the rotor wake from a preceding heavier EC120 helicopter, which resulted in the control difficulties, an uncontrolled descent, low rotor speed warning and the forced landing.
What has been done as a result
Following review of the draft report, the Civil Aviation Safety Authority undertook proactive safety action to improve existing guidance about helicopter wake vortices in Advisory Circular 91-16. The updated advisory circular was released on 17 July 2025 and can be found at the link: AC 91-16 v1.2 - Wake turbulence.
Safety message
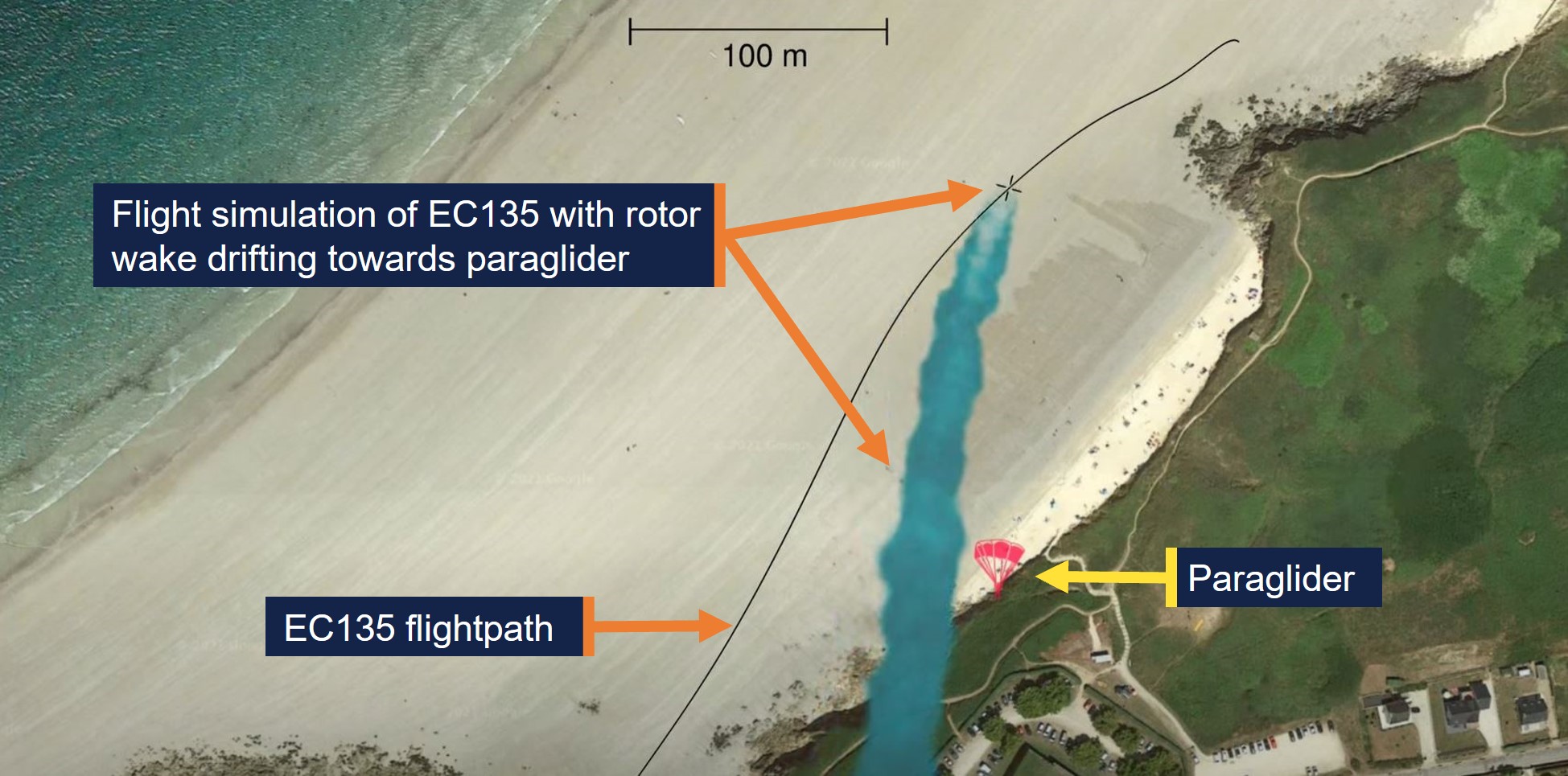
Flight tests have demonstrated that helicopter wake turbulence is comparatively larger and less predictable in its behaviour than for aeroplanes of the same weight. Helicopter rotor vortices can descend, remain level or climb, and the duration of their persistence can increase significantly in conducive weather conditions. The United States Helicopter Safety Team website recommends remaining 3 rotor disks clear of a hovering or taxiing helicopter and allowing 3 NM and/or 2 minutes for the rotor wake from a preceding helicopter to dissipate.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At 1021 local time on 7 April 2025, a Bankstown Helicopters Robinson R44 Raven 1 helicopter, registered VH‑EWM (EWM), with a pilot and 2 passengers on board, departed from Bankstown Airport, New South Wales for a local scenic flight around Sydney Harbour. Bankstown Tower air traffic control (TWR) cleared EWM to depart via ‘Choppers West’, which was a standard procedure for helicopters departing to the north when runway 29 was active at Bankstown.
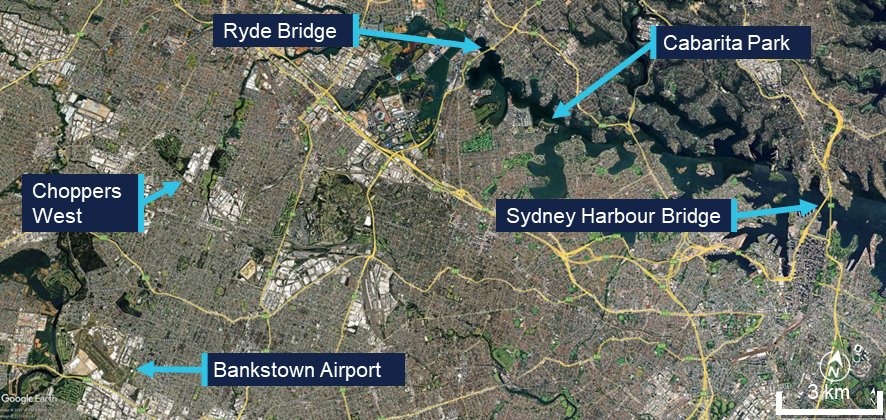
The pilot reported that they climbed to about 1,000 ft above mean sea level.[1] The pilot’s plan was to join the Parramatta River on the west side of the Ryde Bridge and descend to 500 ft to follow the helicopter lane[2] along the south side of the river to Sydney Harbour (Figure 1).
Figure 1: Key locations
Source: Google Earth, annotated by the ATSB
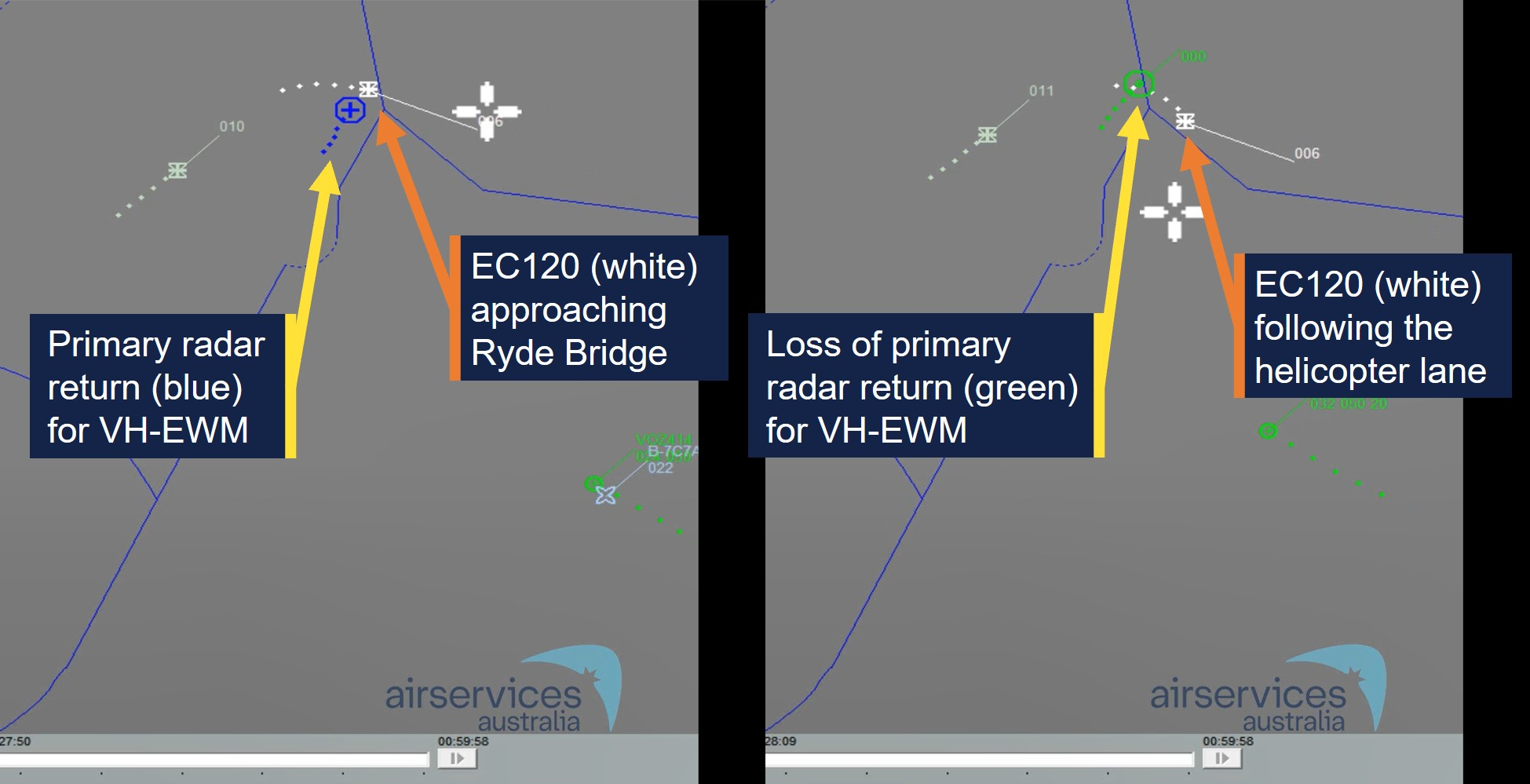
About 1 minute after EWM departed, an Airbus EC120B helicopter departed Bankstown, also following the Choppers West departure. Shortly after the EC120 departed, TWR advised the EC120 pilot that there was ‘R44 traffic 1 NM ahead’, to which the EC120 pilot reported that they had the traffic sighted. Bankstown TWR then advised the pilot of EWM that they were not receiving their transponder data, which the pilot acknowledged. The pilot of EWM then turned their transponder off and on in an attempt to transmit transponder information, but no data was received from it throughout the incident flight.
As the 2 helicopters tracked north towards the Parramatta River, the EC120 flew to the west of EWM and passed it before reaching the river. The EC120 then turned right to join the Parramatta River helicopter lane, tracking towards the Ryde Bridge and Sydney Harbour, and passed over the Ryde Bridge at a recorded radar altitude of 600 ft.
The pilot of EWM reported that they descended the helicopter to 500 ft as they approached the river. Just before the pilot turned EWM right to join the helicopter lane, another larger helicopter (the EC120) suddenly appeared in front of them (Figure 2). The pilot of EWM estimated the EC120 was about 500–600 ft (150–180 m) in front of them and about 100 ft above them. While there was no recorded altitude for EWM, primary radar data indicated that EWM entered the lane about 9 seconds behind the EC120.[3] Primary radar data for EWM was lost about 10 seconds later, just after 1028, indicating it had descended below radar coverage.
Figure 2: Primary radar return (left) and loss of primary radar return (right) for VH‑EWM
Source: Airservices Australia, annotated by the ATSB
The pilot of EWM made a radio broadcast that they were entering the helicopter lane as they crossed the Ryde Bridge behind the EC120. They then experienced what they described as very strong turbulence from a vertical motion in the atmosphere. A passenger later described it as ‘like heavy turbulence … rolling left and right’ followed by ‘diving towards the water’.
The pilot noted that the helicopter was descending through 400 ft and responded by raising the collective lever.[4] However, the helicopter continued descending towards the water as it tracked behind and below the EC120. A passenger recalled the pilot announced ‘brace for impact’ as the helicopter approached the water. The pilot applied full collective to avoid the water, which caused the rotor speed to decay sufficiently for the low rotor speed warning horn to activate. They also reported feeling that they could not escape what they believed to be the rotor wake from the EC120. The pilot then sighted a suitable forced landing area at Cabarita Park and, using the helicopter’s remaining airspeed and rotor speed, manoeuvred the helicopter to the shoreline for a landing.
Following the landing, the pilot rolled the engine throttle back to idle and proceeded through their after‑start checks and confirmed normal operations on the ground. The pilot then conducted a hover check and again confirmed normal operations. The pilot attempted radio contact with their operations base but received no reply. They then conducted a return flight to Bankstown without further incident.
Context
Pilot information
The pilot held a commercial helicopter pilot licence, issued on 26 November 2024, with a single‑engine helicopter class rating and low‑level rating. The pilot held a class 1 aviation medical certificate with no restrictions and expiration date of 30 May 2025. The pilot had accumulated about 112 hours flying experience and the incident flight was the pilot’s first commercial flight.
Helicopter information
The incident helicopter, EWM, was a piston‑engine 2‑bladed Robinson Helicopter Company R44 Raven 1 with a maximum take‑off weight of 1,089 kg. The weight and balance data provided by the operator indicated it was within limits for the flight.
The Airbus EC120B was a turbine-engine 3‑bladed helicopter with a maximum take‑off weight of 1,715 kg. Therefore, the EC120 was about 57% heavier than EWM at their respective maximum take‑off weights.
The maintenance release for EWM indicated the helicopter was operated by Bankstown Helicopters in the operational category of Part 133 Air Transport. The maintenance release current at the time of the incident was issued on 3 April 2025 at 4,349 hours total time in service with an expiry date of 3 April 2026 or 4,400 hours. A maintenance test flight was certified on the maintenance release as conducted on 3 April with ‘nil defects evident.’
After the incident, the operator’s maintenance organisation inspected the helicopter and found no defects. As the flight hours remaining on the helicopter were close to the next overhaul, the operator elected to remove the helicopter from service and have the maintenance organisation complete the overhaul.
Meteorological information
The METAR[5] recordings for Bankstown Airport at 1000 and 1030 indicated that the wind was westerly at a speed of 9 kt at 1000 and 7 kt at 1030. No cloud was detected. These conditions were consistent with the Bankstown Airport forecast for 8 kt westerly winds. The pilot reported their assessment of the weather was 5 kt of variable wind and CAVOK[6] conditions, but when they encountered the turbulence over the Ryde Bridge it felt like 40 kt of wind.
Rotor wake turbulence
In 1996, the United States Federal Aviation Administration (FAA) produced a report on the subject of Flight test investigation of rotorcraft wake vortices in forward flight. They used a laser doppler velocimeter to measure the vortices and small probe aircraft to test the actual flying conditions. Smoke generation was used to visualise the wake vortices for the probe aircraft. Their investigation concluded that:
The measured vortex circulation diminished with decreasing airspeed for helicopter airspeeds below 40 knots. At these lower speeds, the wake vortex structure begins to break down and changes to a distinct downwash.
Vortex duration depends strongly on ambient weather conditions and a variance of 300% was observed on those days most conducive[7] to vortex persistence and duration compared with those observed on typical days.
Typically, helicopters with higher gross weight, larger rotor diameters, and larger numbers of rotor blades generated vortices of larger core diameters.
Probe tests revealed that helicopter vortices did not descend in the same predictable manner as for fixed‑wing aircraft. Some vortices descended; some remained level; and some initially descended, levelled off, and then ascended above the altitude of the generating helicopter.
Figure 3: Rotor wake vortices visualised with smoke generators
Visualisation of the wake vortices behind an S‑76A helicopter in forward flight with smoke generators from the FAA (1996) flight tests. Source: Reddit
Meiris (n.d.) provided an article for the United States Helicopter Safety Team website, on the subject of Avoiding helicopter wake turbulence. The article referenced the FAA 1996 flight test report and provided the following recommendations:
As a result of these findings and the studies conducted regarding helicopter downwash in a hover, a few guidelines have been developed to increase awareness around helicopter wake turbulence:
• For hovering flight or a hover taxi, stay three rotor diameters away.
• For forward flight, a minimum of 3 nm [NM] separation is recommended, especially from larger helicopters. The investigation we discussed previously discovered that even at 3nm [NM], the planes encountered uncommanded pitch and roll oscillations.
• Leave 2 minutes for the rotor vortices to dissipate behind a helicopter in forward flight.
Related occurrences
The French Bureau of Enquiry and Analysis for Civil Aviation Safety investigation BEA2019-0234, Accident to a paraglider involving the Airbus - EC135 - T2 PLUS registered F-HTIN, examined a fatal paraglider accident in 2019. The paraglider’s wing collapsed after encountering the rotor wake from an Airbus EC135 helicopter, which drifted with the wind from the helicopter’s flightpath onto the paraglider (Figure 4).
Figure 4: Simulation of rotor wake drifting onto the paraglider
Source: YouTube – Bureau of Enquiry and Analysis for Civil Aviation Safety, annotated by ATSB
The 2022 United States National Transportation Safety Board investigation WPR22LA072 found that the pilot of a Cessna 120 attempted a go‑around about 20 seconds behind the passage of a Bell UH‑1H helicopter. During the go‑around the Cessna encountered wake turbulence, resulting in a loss of control and collision with terrain (Figure 5). The report indicated light wind conditions of 4 kt at the airport.
Figure 5: Loss of control accident from rotor wake
Source: YouTube – Aviation Safety Network, annotated by ATSB
Safety analysis
Primary radar data and the pilot’s report indicated that EWM entered the Parramatta River helicopter lane and passed over the Ryde Bridge about 9 seconds behind and slightly below the EC120 helicopter. At this point, EWM encountered heavy turbulence, an uncontrolled descent and a low rotor speed when the pilot applied full collective to avoid a collision with the water.
The uncontrolled descent and low rotor speed condition resulted in the pilot conducting a forced landing on the shoreline of the Parramatta River.
The incident occurred under relatively calm wind conditions and EWM operated in a serviceable condition for the return flight. Subsequent maintenance inspections of the helicopter found no fault. Furthermore, EWM passed overhead the Ryde Bridge in sufficient proximity to a preceding heavier 3‑bladed helicopter to be subject to a rotor wake induced upset. Therefore, the ATSB concluded that the sudden onset of turbulence and uncontrolled descent were likely the result of EWM encountering rotor wake turbulence from a preceding EC120 helicopter.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wake turbulence encounter and forced landing involving Robinson R44, VH-EWM, about 15 km north‑east of Bankstown Airport, New South Wales, on 7 April 2025.
Contributing factors
It is likely that the incident helicopter entered the rotor wake from a preceding heavier helicopter, which resulted in control difficulties, an uncontrolled descent, low rotor speed warning and a forced landing.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by the Civil Aviation Safety Authority
Following review of the draft report, the Civil Aviation Safety Authority undertook proactive safety action to improve existing guidance about helicopter wake vortices in Advisory Circular 91-16. The updated version of the advisory circular was released on 17 July 2025 and can be found at the link: AC 91-16 v1.2 - Wake turbulence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
Civil Aviation Safety Authority
the operator and maintenance organisation for VH-EWM
the pilot and passengers of the incident flight
References
Bureau of Enquiry and Analysis for Civil Aviation Safety. (2021). Accident to a paraglider involving the Airbus - EC135 - T2 PLUS registered F-HTIN on 11 May 2019 at Le Conquet (Finistère).https://bea.aero/fileadmin/user_upload/BEA2019-0234.en.pdf
Federal Aviation Administration. (1996). Flight test investigation of wake vortices generated by rotorcraft in forward flight (DOT/FAA/CT-94/117). https://apps.dtic.mil/sti/tr/pdf/ADA318103.pdf
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
the maintenance organisation for VH-EWM
the operator and pilot of the incident flight.
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]All heights in the report are altitudes unless stated otherwise.
[2]The helicopter lane from Ryde Bridge to Sydney Harbour Bridge was contained within Restricted Area R405A.
[3]Radar data did not display speed for the helicopters, but this would correspond to a separation of 556 m at 120 kt.
[4]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor and engine power. Collective input is the main control for vertical velocity.
[5]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[6]Ceiling and visibility okay (CAVOK): Visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[7]Studies have shown that atmospheric turbulence hastens wake breakup, while other atmospheric conditions can transport wake horizontally and vertically (FAA, 2023).
Occurrence summary
Investigation number
AO-2025-018
Occurrence date
07/04/2025
Location
About 15 km north-east of Bankstown Airport
State
New South Wales
Report release date
18/07/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Control issues, Forced/precautionary landing, Turbulence/windshear/microburst, Warning devices
On 26 November 2024, an instructor was conducting training operations with a student pilot in a Piper PA-28-180 Cherokee aircraft. Activities involved general aircraft handling in the Parafield Airport training area, South Australia, before returning to the aerodrome for circuit operations on runway 26L.
Around 1345 local time, as the aircraft was descending through about 600 ft on final approach to the runway, the student advanced the throttle to correct the descent profile when the engine did not respond. The instructor assumed aircraft control and began troubleshooting actions while managing the descent. At about 300 ft, when it was evident that the engine would not respond, the instructor committed to an emergency landing on the grassed area to the east of runway 21L. The landing was uneventful, and the student and instructor evacuated the aircraft without injury. The aircraft was undamaged.
Examination of the aircraft’s systems after the landing found that the fuel selector was in the left tank position – being the tank that was selected before the flight commenced. On inspection, the left tank contained no usable fuel.
Aircraft information
The Piper PA-28-180 aircraft has two independent fuel tanks within the wings, which feed the engine via a ‘Left-Right-Off’ selector valve located on the cockpit left side. The quantity of fuel in each tank is indicated by dash-mounted gauges. A fuel pressure gauge is co-located with the quantity gauges.
The aircraft manufacturer’s Pilot’s Operating Handbook (POH) lists the following actions in the event of a loss of engine power in-flight:
Fuel Selector – switch to another tank containing fuel
Electric Fuel Pump – On
Mixture – Rich
Carburettor Heat – On
Engine Gauges – check for an indication of the cause of Power Loss
Primer – Check Locked
If no fuel pressure is indicated, check tank selector position to be sure it is on a tank containing fuel.
Safety action
Following the occurrence, the operator’s Head of Operations reviewed the known details of the incident flight with all instructors, highlighting the absence of a ‘both tanks’ fuel selection on the PA-28 aircraft and reinforcing the requirement to use calculated fuel logs that are cross‑referenced against the aircraft gauges at periodic intervals during flight.
Safety message
All general aviation pilots must ensure they are fully familiar with the control and operation of the fuel system/s of the aircraft they are operating. This includes actions in the event of engine power loss at any phase of flight, where timely and appropriate responses to possible fuel flow interruptions can be critical to a safe outcome. Emergency checklists should be readily accessible and periodically reviewed to ensure pilots remain familiar with the appropriate actions in the event of fuel-related engine power loss.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-047
Occurrence date
26/11/2024
Location
Parafield Airport
State
South Australia
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Fuel starvation
Highest injury level
None
Brief release date
18/02/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-180 Cherokee
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On 24 January 2025, a Cirrus SR22, VH-DCB, was conducting a private flight from the Gold Coast, Queensland, to Mildura, Victoria with the pilot and one passenger on board.
About 2 hours and 43 minutes into the flight, while approaching the Mitchell Highway to the east of Nyngan, New South Wales, the pilot observed a cautionary alert, advising of low engine oil pressure. The pilot diverted to Nyngan Aerodrome and a short time later, the engine subsequently sustained an in-flight mechanical failure and engine fire. The aerodrome was beyond the aircraft's glide range at the time and the pilot elected not to deploy the Cirrus Aircraft parachute system, but to perform a forced landing on the Mitchell Highway.
The pilot conducted a successful forced landing, both pilot and passenger were uninjured and the aircraft sustained only minor damage.
What the ATSB found
The engine lost oil pressure during flight and sustained an in-flight mechanical failure, prompting the pilot to declare an emergency. The pilot exercised timely and effective decision‑making, which mitigated the risk of injury to the occupants and further damage to the aircraft. The pilot then promptly executed a successful forced landing on a nearby highway, while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin.
Safety message
In-flight engine failures in single-engine aircraft require pilots to exercise effective and timely decision-making to reduce the severity of injuries and damage. These events often result in the pilot experiencing high workload and time pressure, where preparedness is critical.
The ‘aviate, navigate and communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies. Taking action in the appropriate order of priority improves situational awareness and supports coordinated responses in a dynamic environment.
Scenario-based training should reinforce these principles by developing both technical and non-technical skills, helping pilots become familiar with the appropriate responses and techniques required during high‑stress situations.
Decision-making tools also enables pilots to take a structured approach to problem‑solving which enhances safety by minimising the risk of errors during emergencies.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 25 January 2025, the pilot of a Cirrus SR22, registered VH-DCB, planned to conduct a private flight from Gold Coast, Queensland, to Mildura, Victoria. The aircraft departed Gold Coast Airport with the pilot and one passenger at about 0735 AEST.[1]
At 1018, while cruising at an altitude of about 8,000 ft above mean sea level (AMSL), the engine oil pressure decreased below the normal operating limits for the engine, 30 pounds per square inch (psi), and the pilot recalled an engine oil pressure alert. The pilot identified that Nyngan Aerodrome was the nearest aerodrome, about 15 NM (28 km) to the north-west. At 1019, the pilot diverted directly to Nyngan with the aid of the autopilot (Figure 1).
Figure 1: VH-DCB flight track and key events taken from recorded data
Source: Google Earth, annotated by the ATSB
The pilot calculated the distance, altitude and glide ratio[2] of the SR22 and concluded that they would likely not make it to Nyngan in the event that the engine failed. They continued towards Nyngan but began to look around for suitable landing sites and identified the Mitchell Highway on the left side of the aircraft.
After checking the engine indications and confirming the engine oil pressure was below normal operating limits and continuing to decrease, the pilot made a PAN PAN[3] broadcast to air traffic control (ATC), advising they were losing engine oil pressure and would be tracking directly to Nyngan. During this broadcast, the pilot recalled the engine began to ‘rev up’ which was followed by an audible ‘bang.’
The pilot then made a MAYDAY[4] broadcast to ATC, advising that the engine had experienced a mechanical failure and they would be making an emergency landing on the highway. As ATC acknowledged the broadcast, the pilot observed flames ‘pouring’ from the top of the cowl.
At 1020 the pilot began a controlled descent towards Nyngan and the Mitchell Highway (Figure 1), and they selected idle power, mixture to cut off and turned off the fuel pump. They attempted to switch the fuel selector lever to off, but they were unable to, recalling that they required both hands to do so. At this time their forward visibility became partially obscured by engine oil on the windscreen.
The pilot reported being concerned that the fire was fuel related and elected to continue with a forced landing rather than deploying the airframe parachute system fitted to the aircraft (see Cirrus airframe parachute system). The pilot was also aware of the increased risk of fire damage to the aircraft rescue system and potential injuries during a parachute‑assisted landing to the passenger, who was pregnant.
At 1023, the pilot commenced a left turn at about 5,000 ft in the direction of the Mitchell Highway. The pilot elected to ‘dive the plane down’ to supress the fire, and increased the rate of descent to over 3,600 ft/min (see Appendix A, Figure A1) and then set up for an immediate forced landing on the highway.
The pilot recalled that the fire appeared to extinguish as the aircraft descended through 4,000 ft and reported they were able to switch the fuel selector off at about 3,250 ft. However, they recalled smoke began to enter the cockpit at about 3,000 ft as the aircraft continued to descend. The pilot selected the first stage of flap and lined up on a section of the Mitchell Highway in a south‑easterly direction. On final approach, the pilot had to adjust the emergency landing flightpath to avoid 2 motor vehicles on the highway and safely conducted the emergency landing, vacating the highway onto a dirt access road at about 1024 (Figure 2).
The pilot recalled that, during the emergency, they had continuously tried to anticipate the next event or action, then evaluated the best course of action and confirmed their decision before proceeding.
The aircraft sustained minor damage to several components on the left wing as a result of colliding with roadside guideposts during the landing roll (Figure 2 right insert) and the pilot and passenger were uninjured. The New South Wales rural fire service attended the scene shortly after the aircraft had safely landed.
Figure 2: VH-DCB alongside Mitchell Highway and minor damage to left wing
Source: Operator, annotated by the ATSB
Context
Pilot information
The pilot held a Commercial Pilot Licence (aeroplane) with an instrument rating and a class 1 aviation medical certificate. They had 3,496 flight hours, including about 1,900 hours on the Cirrus SR22 and had recently logged about 40 hours on type in the last 90 days.
The pilot reported sleeping about 9 hours the night before the occurrence and had been awake for about 5 and a half hours at the time of the occurrence. They further reported that they felt ‘fully alert and wide awake’ on the day of the occurrence and were not tired or fatigued.
Aircraft information
The Cirrus Design Corporation SR22 is a low wing general aviation aircraft with 5 seats and a single piston engine, driving a constant speed propeller. The aircraft was registered as VH-DCB in Australia on 9 November 2018 to the pilot, who was the registered operator. The aircraft was certified for day and night VFR[5] and IFR[6] operations.
Powerplant
The SR22 is equipped with a single Continental Motors Inc. IO-550-N engine. The engine oil used for lubrication and cooling is drawn from an 8-quart capacity sump located in the engine crankcase. The engine had a total time in service of 1,678.5 hours and the manufacturer‑approved time between overhaul[7] was 2,200 hours total time in service.
Engine oil system
The aircraft’s pilot operating handbook required an engine oil level between 6 and 8 quarts for normal operation, with the manufacturer recommending a pre-flight dipstick indication of 7 quarts for extended flights. On the day of the occurrence, the pilot recalled that the engine dipstick was reading 8 quarts prior to departure.
Cirrus airframe parachute system
The Cirrus airframe parachute system (CAPS) was designed to lower the aircraft and its passengers to the ground in the event of a life-threatening emergency and is operated by the pilot. The CAPS system consists of a parachute, a solid-propellant rocket used to deploy the parachute, an activation handle, and a parachute harness embedded within the fuselage structure.
Maintenance history
Immediately prior to the occurrence, the aircraft had undergone a 50‑hour inspection at a Cirrus‑authorised service centre. No engine‑related defects were recorded in the aircraft maintenance certification log.
Prior to that, on 23 October 2024 at the same service centre, the engine had been inspected during an annual inspection and was certified in accordance with approved maintenance data as airworthy at a total time in service of 1,637.6 hours.
All records of inspections and maintenance tasks obtained by the ATSB in the course of the investigation were certified as being conducted in accordance with the latest revisions of the Cirrus airplane maintenance manual and the Continental maintenance manual.
The pilot recalled that they had completed the daily inspection prior to the flight, with no identified issues before certifying the daily inspection on the aircraft maintenance release.
Meteorological information
The Bureau of Metrology aviation meteorological information report, which included the graphical area forecast[8] encompassing Nyngan Aerodrome at the time of the occurrence, contained the following:
visibility greater than 10 km
nil significant weather or cloud
moderate turbulence below 7,000 ft in dust devils and thermals north of Dubbo Airport.
At the time of the occurrence, the pilot stated that the weather was generally fine with good flying conditions and ‘not a cloud in the sky.’
Post-incident inspection
The pilot inspected the aircraft engine after the serious incident and found the crankcase had ruptured adjacent to cylinder 6 (Figure 3 right insert) below the induction duct assembly. They recovered a connecting rod that had separated from the crankshaft (Figure 4) and identified that the air filter was visibly damaged as a result of a fire (Figure 3 left insert). The pilot recalled performing a post‑landing dipstick check and observed that about 6 quarts of oil remained in the engine.
Figure 3: VH-DCB engine bay and damage to the air filter and crankcase
Source: Operator, annotated by the ATSB
Figure 4: Fractured connecting rod recovered from VH-DCB
Source: Operator, annotated by the ATSB
Due to the remoteness of the location, the aircraft was secured on a nearby property and the engine was retained with the fuselage until a replacement was fitted to the aircraft. Following the subsequent removal of the engine, a disassembly and inspection had not been conducted at the time of publication of this report. As a result, the ATSB was unable to determine the root cause for the loss of oil pressure or the mechanical failure of the engine.
Aircraft manufacturer’s emergency procedures
The emergency procedures section of the Cirrus SR22 pilot’s operating handbook (POH) prescribes procedures for handling emergencies and critical flight situations that may occur while operating the aircraft. The POH states:
Although this section provides procedures for handling most emergencies and critical flight situations that could arise in the aircraft, it is not a substitute for proper flight training, thorough knowledge of the airplane, and recognised piloting techniques and standards.
Additionally, the POH recommends 4 basic actions that can be applied to any emergency which include:
maintain aircraft control
analyse the situation
take appropriate action
land as soon as conditions permit.
In cases when a procedure directs a pilot to ‘land as soon as possible’, the POH states:
Land without delay at the first site at which a safe landing can be made. Continued flight beyond an available airfield at which a safe landing can be made will result in increased risk and shall not be attempted.
Loss of engine oil pressure in-flight
When engine oil pressure decreases below 10 psi the aircraft’s crew alerting system[9] (CAS) will annunciate ‘oil pressure’ in red text on the primary flight display which is accompanied by a repeating double chime audio alert. The alert prompts the pilot to carry out the following procedure contained in the emergency procedures section of the POH:
a. Power..........REDUCE TO MINIMUM FOR SUSTAINED FLIGHT
b. Land as soon as possible.
(1) Prepare for potential engine failure
Procedure Complete
Engine fire in-flight
In cases of smoke and fire, the CAS will not alert the pilot to this condition. When a pilot identifies an engine fire in-flight, they must action the following items by memory:
The POH also contained a note which suggested that in the case of a wing fire in-flight, ‘putting the airplane into a dive may blow out the fire.’
During the occurrence, the pilot carried out their actions by memory and stated that they were unable to refer to checklists during the serious incident due to the lack of time. Although the ‘engine fire in-flight’ procedure did not direct the pilot to dive, the pilot decided that diving the aircraft would assist in extinguishing the fire in this case.
The pilot also stated that they encountered difficulty switching off the fuel selector while simultaneously flying the aircraft during the glide approach and managing the emergency. The POH stated ‘to select off, first raise the fuel selector knob release and then rotate the knob to off.’ This is not performed during normal operations which meant the pilot was not familiar with the action. The pilot also recalled turning the ignition switch off after the aircraft had landed.
Cirrus airframe parachute system deployment
The emergency section of the POH contains procedures regarding the deployment of the ballistic parachute in-flight. This section contains the following explanatory notes:
It should also be used in other life threatening emergencies where CAPS deployment is determined to be safer than continued flight and landing. Expected impact in a fully stabilised deployment is equivalent to a drop from approximately 13 feet.
A cautionary note also explains that ‘CAPS deployment will likely result in damage or loss to the airframe.’
The POH identifies several possible scenarios for deploying the CAPS:
midair collision
structural failure
loss of control
landing in inhospitable terrain
pilot incapacitation.
No specific guidance is contained in the POH regarding the use of the CAPS in cases of in-flight smoke and fire.
Recorded information
The Garmin avionics suite installed in the SR22 included a flight data logging feature that automatically stored critical flight and engine data on a removable data card.
The ATSB was provided with the data card installed in the aircraft at the time of the occurrence. The data on the card was downloaded by the ATSB and confirmed to have contained flight data recorded during the occurrence on 24 January 2025.
Recorded data
The recorded flight data captured parameters such as engine parameters, altitude, airspeed, vertical speed, bank angle and various avionics functions (Appendix A – Recorded data). This data enabled a detailed reconstruction of the flight, providing insights into the aircraft’s performance and pilot actions during the occurrence (Figure A1).
Prior to the occurrence, the recorded flight data (Figure A2) indicated that all recorded engine parameters were within normal operating limits outlined in the powerplant limitations section of the pilot’s operating handbook prior to the loss of engine oil pressure. Table 1 depicts the normal and recorded ranges of each engine parameter from the time the aircraft became airborne at 0733:21 until the engine oil pressure decreased below the normal range of 30 psi at 1018:46.
Table 1: Recorded in-flight range prior to loss of engine oil pressure
Recorded in-flight range inclusive of cylinders 1 – 6
[2]Recorded in-flight range inclusive of cylinders 1 – 6
Source: Operator supplied flight data card, tabulated by the ATSB
Related occurrences
The following ATSB investigations highlight the risks associated with encountering engine failures in flight, demonstrating the importance of effective decision‑making.
On 21 November 2012, a Cirrus SR22 aircraft, registered VH‑WYH, departed Emerald, Queensland for Dubbo, New South Wales, on a private flight conducted under instrument flight rules. The pilot and one passenger were on board.
During the flight, the oil pressure annunciation illuminated, and the engine oil pressure indicated 30 pounds per square inch (psi). As the oil pressure continued to slowly drop, the pilot became increasingly concerned and tracked via Gilgandra, New South Wales. They overflew Gilgandra and continued on towards Dubbo, at which point the oil pressure gauge indicated about 12 psi.
Two hours and 39 minutes after the oil pressure light illuminated, the engine failed. When it became evident that a landing at Gilgandra aerodrome was not achievable, the pilot deployed the ballistic parachute. The aircraft impacted the ground and was substantially damaged with the pilot receiving minor injuries while the passenger was uninjured. The pilot reported that the oil pressure indication dropped very gradually giving a false sense of security.
On 6 November 2020, the pilot of a S.E.D.E. Morane-Saulnier MS.893A (Rallye) aircraft, registered VH‑UQI, was conducting a private flight from Moruya, New South Wales, to Archerfield, Queensland. About 22 km south‑west of Archerfield Airport, the engine began running rough before eventually failing.
The pilot elected to conduct a forced landing into an open but slightly undulating paddock. The approach direction resulted in a tail wind landing. The aircraft over‑ran the open area before it impacted with a grove of trees, significantly disrupting the aircraft structure. A post‑impact fire consumed most of the fuselage. The pilot was seriously injured, and the aircraft was destroyed.
The pilot was ferrying the aircraft on behalf of the owner and had limited aircraft type experience and knowledge of its performance capabilities, and it was found that the pre‑flight planning was limited.
Safety analysis
During the investigation, the ATSB was unable to determine the initiating factor that led to the loss of oil pressure and subsequent mechanical failure of the engine. However, the recorded data from the occurrence revealed that all engine parameters were within normal operating limits prior to the loss of engine oil pressure and subsequent in‑flight mechanical failure of the engine.
After observing the oil pressure caution message, the pilot made a timely decision to divert to Nyngan Aerodrome. Being aware of the aircraft’s gliding capabilities and after the oil warning alert, they were immediately able to determine that the aircraft did not have sufficient altitude to safely conduct a forced landing at the aerodrome. They then identified the Mitchell Highway as the most suitable landing site before investigating the engine parameters.
When the engine experienced a mechanical failure, the pilot was able to immediately enact their pre‑planned forced landing procedure, declare the emergency and communicate their intention to land on the Mitchell Highway.
After observing flames and oil coming from the engine cowl, which obscured their visibility, the pilot made a timely decision and elected not to deploy the aircraft’s ballistic parachute. This was due to the pilot’s concern that the fire was fuel‑related and may affect the deployed parachute system as well as the potential risk of injury to the passenger, who was pregnant, and aircraft damage associated with a parachute‑assisted landing.
The pilot began an emergency descent, putting the aircraft into a ‘dive’ in an attempt to put out the fire. Once the fire self-extinguished, smoke entered the cockpit. However, the pilot proceeded to navigate the aircraft to land on the highway among traffic for a successful forced landing with no injuries and only limited damage.
The ATSB research report Engine failures and malfunctions in light aeroplanes, 2009 to 2014 (AR-2013-107) indicated that although engine failures are relatively rare, they do happen. Given the potential severity of the consequences of an engine failure or power loss in a single‑engine aircraft, such occurrences therefore need to be planned for and managed appropriately.
On this occasion, the pilot made effective and timely decisions to manage the evolving emergency and appropriately prioritised their actions. Their decision‑making was likely supported by their experience on the aircraft type and knowledge of the performance capabilities. This enabled prompt and appropriate responses from the pilot, which contributed to a safe outcome.
Additionally, the pilot’s methodical approach during this occurrence highlights the importance of decision-making tools to aid pilots to mitigate the possibility of errors and ensure a considered approach in resolving issues or problems (Civil Aviation Safety Authority, 2019).
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine failure involving Cirrus SR22, VH-DCB, 29 km east-south-east of Nyngan, New South Wales, on 24 January 2025.
Contributing factors
The engine lost oil pressure during flight, leading to an in-flight engine failure and fire.
Other findings
The pilot exercised timely and effective decision making in flight to divert and then identify a safe forced landing area.
The pilot successfully executed an immediate forced landing on a nearby highway while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin. This resulted in no injuries to the 2 occupants and only minor additional aircraft damage.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the serious incident flight
maintenance organisation
Civil Aviation Safety Authority
United States National Transportation Safety Board
Cirrus Design Corporation
Continental Motors Incorporated.
Submissions were received from:
pilot in command/operator
Cirrus Design Corporation
Continental Motors Incorporated.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Recorded data
Figure A1: In-flight data and key events after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Figure A2: In-flight engine parameters after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
An explanation of terminology used in ATSB investigation reports is available here.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Local time was Australian Eastern Standard Time (AEST), which is Coordinated Universal Time (UTC) +10 hours. Times in this report are AEST unless otherwise noted.
[2]Glide ratio: the glide ratio of an aircraft is the distance of forward travel divided by the altitude lost in that distance. The Cirrus SR22 pilot’s operating handbook stated the maximum glide ratio for the aircraft was 8.8:1.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[5]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions
generally clear enough to allow the pilot to see where the aircraft is going.
[6]Instrument flight rules (IFR): rules which allow properly equipped aircraft to be flown under instrument meteorological
conditions
[7]Time between overhaul: is a time limit specified by the engine manufacturer for a specific engine in a specific installation, after which overhaul is either recommended or mandated depending on how the aircraft is used.
[8]Graphical area forecast (GAF) is a combination of graphical and textual information. The graphic is divided into areas that share common weather characteristics which are detailed in an associated table.
[9]Crew alerting system (CAS): aircraft annunciations and alerts are displayed in the CAS window located to the right of the altimeter and vertical speed indicator. Aircraft annunciations are grouped by criticality and sorted by order of appearance with the most recent message on top.
[10]Cylinder head temperature (CHT): CHT is measured by a temperature-sensing probe located at the cylinder head, and it measures heat energy wasted during the power stroke, when the cylinder is under maximum stress from high internal pressures and temperatures.
[11]Exhaust gas temperature (EGT): is a measurement of the temperature of the exhaust gases at the exhaust manifold.
On 13 October 2024, a Robinson R44 helicopter was being used to conduct a private flight from Tooma to Moree, New South Wales with a pilot and 3 passengers on board. The intention was to conduct a scenic flight in the local area prior to continuing towards the destination.
The pilot’s phone, which the pilot was using for navigation, was secured in a commercial mount attached to the interior of the helicopter. During the flight, the phone became dislodged from the mount and fell to the floor near the pilot’s feet. Concerned that the loose phone would interfere with the flight controls, the pilot elected to conduct a precautionary landing so that it could be retrieved and resecured.
The pilot selected a nearby landing site at an elevation of approximately 6,300 ft. As they approached to land, the pilot applied power but due to the high density altitude associated with the elevation of the selected landing site they were unable to arrest the descent rate. The pilot performed a run-on landing,[1] during which a skid caught on a tussock of grass and the helicopter turned 180° and tipped on its side. During the accident sequence the tail rotor contacted the ground resulting in the boom breaking and separating the tail section from the fuselage. The helicopter was substantially damaged (Figure 1), and the pilot and passengers evacuated without injuries.
Loose items in an aircraft can cause a significant distraction for the pilot and can potentially interfere with flight controls, leading to a loss of control. They can also become dangerous projectiles causing serious injuries during an abrupt stop, turbulence or an accident sequence. All loose items should be stowed prior to departure. When using portable devices as an electronic flight bag (EFB), pilots must ensure that they are securely attached or stowed during flight. The Civil Aviation Safety Authority’s Advisory Circular 91-17 – Electronic flight bags contains requirements for mounting and stowing of EFBs in aircraft.
This occurrence also highlights the importance of inspecting and evaluating the suitability of a landing area before conducting a precautionary landing. This includes considering the effect of elevation and density altitude on aircraft performance and the risks involved in landing on an unprepared surface.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Run-on landing: A manoeuvre used to transition from forward flight to a landing when there may not be sufficient power available to sustain a hover.
On the afternoon of 11 September 2024, the pilot of a Kawasaki 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting a scenic flight over Nitmiluk (Katherine) Gorge, Northern Territory with 2 passengers on board.
About 13 minutes into the flight, while entering the mouth of the gorge, the pilot reported experiencing an engine power loss and lack of response from the engine. Due to inhospitable terrain in the area, the pilot identified a clear landing spot some distance away and attempted a forced landing at that location, during which time the aircraft collided with terrain.
The pilot and both passengers were uninjured in the incident, however, the aircraft was substantially damaged.
What the ATSB found
Several possibilities were considered during the investigation in relation to the reported engine power loss. While the ATSB did not conduct a physical inspection of the engine in this instance, a post‑incident inspection revealed that a large crack had developed in the engine exhaust pipework. Being a turbocharged engine, the escape of exhaust gases through the crack during operation has likely resulted in an engine power loss during flight due to the loss of boost pressure.
The ATSB also identified that the pilot was unable to cushion the landing during termination of the autorotation, likely due to low main rotor RPM, resulting in the helicopter colliding with terrain.
Safety message
Helicopter operations over harsh terrain offer limited safe emergency landing options. Autorotation to a suitable area in such circumstances requires accurate helicopter positioning and energy maintenance (airspeed and rotor RPM). This makes thorough and regular training in emergency procedures crucial for pilots operating in these demanding environments. The prompt action taken by the pilot, in identifying a suitable landing site, was instrumental in ensuring the safety of all personnel on board.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 11 September 2024, the pilot of a Kawasaki Heavy Industries 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting scenic flights over Nitmiluk (Katherine) Gorge, Northern Territory.
During the morning, the pilot conducted the required daily checks on the helicopter and completed a passenger flight over the gorge (Figure 1). After returning to base, the pilot refuelled the helicopter and completed short, uneventful ferry flights to Katherine Museum and return.
That afternoon, the pilot met 2 passengers at the operator’s base, and then completed the flight manifest including the passengers’ weight details, based on verbal information provided by the passengers. The pilot carried out their pre-departure checks, including a flat‑pitch check,[1] which were all normal. A safety briefing was also undertaken with both passengers, which reportedly included:
use of seatbelts
in‑flight procedures
operation of the doors and emergency exits
actions to be taken in case of an emergency.
At around 1451 local time, the helicopter departed and after making a turn towards the north, the pilot gradually climbed to about 1,000 ft above mean sea level (AMSL), proceeding north‑easterly along the Katherine River in the direction of the gorge.
About 10 minutes later, the pilot climbed further to a height of about 1,400–1,500 ft AMSL to fly neighbourly[2] while approaching the escarpment bordering Nitmiluk National Park (Figure 2). The pilot then arranged separation with the pilot of a second helicopter in the area, using the common traffic advisory frequency (CTAF).
Figure 2: View from helicopter of Nitmiluk National Park
Source: Passenger photograph, annotated by the ATSB
Approximately 3 minutes later, as the helicopter was entering the mouth of the gorge, the pilot noticed that the engine did not respond when they increased the throttle, and that the helicopter was decelerating and losing height. Due to being overhead undulating rocky terrain, the pilot commenced a right turn in search of a suitable landing site, in case they had to conduct a landing (Figure 3).
The pilot reported that the ensuing events occurred extremely quickly. While turning around, the helicopter kept slowing and the engine did not respond to throttle movements. They noticed a significant change in the engine noise, described as a low‑pitched ‘whir’ sound, and reported feeling stiffness in the pedals. Not knowing what was wrong with the engine, the pilot lowered the collective[3] and entered autorotation (see the section titled Autorotation).
During the descent, the pilot glanced at the instruments and noted that the engine RPM needle was split[4] from the main rotor RPM needle and again tried unsuccessfully to increase the throttle. The pilot later advised that the main rotor RPM was well below the green arc on the gauge, and the engine RPM was just below idle. The pilot reported identifying a landing site in a clearing about 400–500 m to the west of their location and broadcast a MAYDAY[5] call on the CTAF.
The helicopter proceeded downwind towards the clearing, attaining a maximum groundspeed in excess of 83 kt. Given the prevailing wind, that equated to an airspeed of about 70 kt, which was higher than the recommended autorotation speed for the helicopter type (see the section titled Autorotation). However, during the final approach to the selected landing site, the groundspeed, and given the crosswind approach, also airspeed was reduced to about 50 kt.
Figure 3: Helicopter flight path with identified elevation and ground speed
Source: OzRunways data on Google Earth, annotated by the ATSB
The passengers reported that during the descent, communication from the pilot was minimal. They were not advised by the pilot to brace for impact; however, upon hearing the MAYDAY call and seeing the pilot attempt an unexpected landing, both passengers suspected that an emergency situation had developed, and chose not to interrupt the pilot or distract them from their actions.
The pilot reported that, on nearing the landing site, they attempted to flare the helicopter but there was minimal flare effect, which they assessed was most likely due to low main rotor RPM. Consequently, the pilot attempted a run‑on landing, during which the helicopter collided with terrain, damaging its tail rotor/shaft and skids (Figure 4).
Figure 4: Helicopter accident site
Source: Operator
After landing, the pilot shut off the fuel, magnetos and battery. After checking on the passengers, the pilot disembarked the aircraft, ensured it was safe to exit with the main rotor blades still rotating, and then instructed the passengers to evacuate the aircraft. The pilot of the other helicopter operating in the area repeated the MAYDAY call on the area frequency and then circled overhead the accident site. A rescue crew arrived onsite shortly after and the pilot and both passengers were evacuated uninjured.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter) and a class 1 aviation medical certificate. At the time of the incident, they had accumulated about 380 hours total aeronautical experience. All the pilot’s training and most of their flying experience has been obtained operating Robinson R44 helicopters. They had been flying for Katherine Helicopters for about 3 months.
While at Katherine Helicopters, the pilot received their Bell 47 endorsement after undergoing about 3 hours of training with an instructor that included the conduct of emergency procedures. The pilot also performed about 10 hours of in command under supervision (ICUS)[6] training with the operator.
Operator information
The operator was a helicopter tour operator based in Katherine, Northern Territory. It operated 2 Bell/Kawasaki 47 Helicopters and offered tour flights throughout northern Australia.
Previous incidents
The pilot had been involved in another engine failure incident on a second helicopter of the same type with the operator in July 2024, wherein an engine cylinder failed. The pilot completed a successful autorotation and there were no reported injuries. While this matter was reported to the ATSB, it was not investigated.
In addition to the incident above, the other helicopter operated by the operator was involved in a third off field landing, arising from an engine fault, in February 2024.
Helicopter information
The helicopter was a Kawasaki Heavy Industries 47G3B‑KH4, manufactured in 1969 in Japan by Kawasaki Heavy Industries and first registered in Australia on 20 June 1996. At the time of the accident, VH‑BEU had about 7,495 hours total time in service and had flown about 40 hours since its last periodic service inspection.
Engine and turbocharger system
VH‑BEU was powered by a Textron Lycoming TVO‑435, 6‑cylinder, vertical direct drive, horizontally opposed, turbocharged engine. The turbocharger increases the density of the carburettor inlet air to maintain the available power as altitude increases.
During operation, the exhaust gases expelled from the 3 cylinders on either side of the engine are merged into a single pipe, through which the gases are diverted either to the turbocharger or to the exhaust bypass valve (waste gate), or both (Figure 5).
As the engine power is increased, oil pressure builds up in the exhaust bypass valve assembly and the waste gate in the exhaust system is closed. This diverts the exhaust gas to the turbocharger turbine wheel, compressing the intake air and increasing the available engine power output.
Figure 5: Schematic diagram of engine and turbocharger operation
Source: Lycoming Operator’s Manual, annotated by the ATSB
Maintenance history
As part of the investigation, the ATSB requested the maintenance logs and component log cards for the aircraft. Although the provided information was incomplete, the maintenance history was able to be inferred from the supplied documents as follows:
Lycoming engine TVO‑435, S/N: L‑751‑52 was installed February 2000 at 6,752 airframe hours. The engine component control card showed a number of zero‑hour components at the time of engine installation, indicating that this engine was likely either a new or overhauled unit. Lycoming Service Instruction No. 1009BE specified a 12‑year, 1,000 hour time between overhauls (TBO). This interval was correctly annotated in the engine log card.
The engine was removed on 24 February 2014 (+14 years) at 7,088 airframe hours (+336 engine hours), and was bulk stripped in lieu of being overhauled, to satisfy the requirements of CASA air worthiness bulletin (AWB) 85‑5 Issue 1.[7] The same engine was refitted on 20 March 2014.
The information supplied to the ATSB showed that prior to November 2022, the aircraft flew only limited hours, having recorded 425 airframe hours in 22 years (at an average of 19.3 hours/year). Depending on how these hours were flown,the aircraft may have required special maintenance actions and/or storage procedures. If these actions were not taken, corrosion, or contamination of components may affect serviceability. No record of storage or preservation penalty maintenance was identified in the provided records.
Autorotation
When an engine failure occurs in a single‑engine helicopter such as the Kawasaki 47GB3‑KH4, the pilot must immediately lower the collective and enter autorotation to reduce rotor drag sufficiently to maintain normal rotor RPM. This is a power‑off manoeuvre wherein the engine is disengaged from the main rotor and the rotor blades are driven solely by the upward flow of air through the rotor during descent. The most common reasons for an autorotation are an engine or drive system failure. If the engine fails, the freewheeling unit[8] automatically disengages the engine from the main rotor, allowing it to rotate freely. The tail rotor, still driven by the main rotor transmission, continues to provide yaw control via the anti‑torque pedals.
The United States Federal Aviation Administration Helicopter Flying Handbook noted that the rate of descent during autorotation is influenced by various factors, including:
bank angle
density altitude
gross weight
main rotor RPM
trim condition
airspeed.
Pilots control the autorotative descent rate using airspeed and main rotor RPM. Airspeed is managed with the cyclic[9] pitch control, similar to normal powered flight. The descent angle can range from vertical to a minimum angle for maximum horizontal range. The rate of descent is highest at zero airspeed, reaches its minimum at approximately 50–60 kts (depending on the helicopter and conditions), and increases again at higher speeds.
During an autorotative landing, the kinetic energy associated with the helicopter’s airspeed and rotating main rotor blades are used to arrest the descent and cushion the landing. Termination of the autorotation usually involves initially flaring the helicopter to reduce the airspeed, rate of descent and, if necessary, increase the rotor RPM. The degree of flare effect is influenced by both the airspeed at the time aft cyclic is applied, as well as the rate of cyclic application.
Autorotative terminations at very low airspeeds are more challenging than those performed at the minimum rate of descent airspeed as they offer minimal flare effect. In that case, cushioning the landing using the stored rotor energy requires more precise collective application.
The Kawasaki 47G3B-KH4 flight manual stated that, in the case of an engine failure, the pilot must:
execute a normal autorotative descent and establish a level attitude prior to ground contact. At a height of approximately 10 feet above the ground, apply collective pitch in sufficient quantity to stop descent as ground contact is made. The best descent speed is 55 mph [48 kt].
Meteorological information
At the time of incident, visibility was in excess of 10 km, with scattered cloud[10] well above the aircraft operating height, no precipitation and an east‑south‑easterly wind at 11 kt.
The meteorological conditions reported by the pilot at the time of incident were consistent with the Bureau of Meteorology observations, which recorded a temperature of 36°C and dew point[11] of 11°C at the incident location.
The process of vaporising fuel in a carburetted engine can cool the airflow sufficiently to permit ice formation in the carburettor throat that restricts airflow to the engine. According to the Civil Aviation Safety Authority Carburettor icing probability chart, the probability of carburettor icing, based on the prevalent temperature and dewpoint at Katherine Gorge was on the outer limit of the ‘light icing – cruise or descent power’ zone. Of note however, the turbocharger compressor used in the Kawasaki 47G3B‑KH4 heats the inlet air to the carburettor, significantly reducing the potential for carburettor icing.
Operating weight
The passenger manifest completed by the pilot prior to take‑off recorded the empty weight of the aircraft, the pilot and both passengers, plus fuel. An allowance of 100 kg was made for the weight of fuel. The passenger weights were only verbally requested, and not physically checked by the pilot. However, the calculated total take‑off weight was well below the maximum take‑off weight so any inaccuracy in passenger weights was unlikely to have resulted in the aircraft being overloaded.
Aircraft fuel
The operator conducted an examination of the fuel in the aircraft following the incident and reported to the ATSB that there was adequate fuel remaining in the tank.
The operator also stated that the aircraft had been refuelled with premium 130 octane fuel by the pilot prior to take‑off, and that a post‑incident examination of the fuel quality did not reveal any signs of contamination or leakage.
Engine examination
Following the incident, the operator started the Lycoming TVO‑435 engine and observed that the wastegate did not operate. Thereafter, they removed the engine and delivered it to a third party maintenance facility for examination. As depicted in Figure 6, the post‑incident inspection of the engine revealed the presence of an approximately 6.5 cm crack on the right exhaust collector, with no other defects identified.
The exhaust system of the aircraft engine attains extremely high operating temperatures. The consequent widening of the crack due to heat expansion would result in the escape of exhaust gases from the defective section, resulting in inadequate drive pressure for the turbocharger compressor and reduced power output. Information provided by the engine manufacturer supported that conclusion. As such, exhaust gas bleed from the crack before the turbocharger resulted in the wastegate remaining closed.
The ATSB did not undertake a metallurgical analysis of the exhaust pipe, however, exhaust systems are generally prone to metal fatigue over time due to continuous vibration under corrosive conditions and a cyclical pattern of constant heating and cooling with extreme thermal fluctuations.[12]
While it could not be established when the exhaust crack occurred, the maintenance facility that conducted the post‑accident engine examination assessed that, based on the location and appearance of the defect, it was likely not impact‑related. They further stated that, as the helicopter did not have an engine cowl, the leaking exhaust gases would not have left a residue. This would have made the crack more difficult to detect during a pre‑flight inspection when the engine was cold.
Figure 6: Cracked exhaust collector pipe
Source: the maintenance facility that conducted the engine strip down inspection, annotated by the ATSB
Safety analysis
Engine power reduction
The sequence of events described by the pilot and passengers were consistent with a loss of aircraft engine power during flight, necessitating an emergency landing. The ATSB considered the following potential reasons for the reduction in engine power:
weather conditions, including carburettor icing
fuel contamination or starvation
handling‑related issues
engine and/or associated systems defect.
The evidence gathered by the ATSB during the investigation indicated that the 3 initial possibilities were unlikely.
However, based on information from the engine manufacturer and the personnel that conducted the post‑accident engine examination, a pre‑existing crack in the exhaust collector likely reduced the engine power output during the flight.
Helicopter maintenance
The ATSB identified that low utilisation of the helicopter may have required special maintenance actions and/or storage procedures to be undertaken to prevent component corrosion or contamination. While there was no evidence that such maintenance was undertaken, it was not possible to determine whether its absence contributed to the crack in the exhaust system.
Autorotation
Analysis of flight data identified that the helicopter was over inhospitable terrain at the time of the power loss. After turning towards a suitable landing site, the pilot commenced an autorotation to that location. The helicopter proceeded downwind, initially attaining a maximum airspeed of about 70 kt. The airspeed was then reduced to close to the target minimum rate of descent airspeed of 48 kt, providing good potential flare effect to both slow the helicopter prior to touchdown and increase the rotor RPM if necessary.
Despite that, the pilot reported there was minimal flare effect when they approached the landing site, likely due to low rotor RPM. As a result, the pilot was unable to prevent the helicopter colliding with terrain during the termination. Importantly however, none of the occupants were injured.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Kawasaki 47G, VH‑BEU, 24 km north of Katherine Tindal Airport, Northern Territory on 11 September 2024.
Contributing factors
The right exhaust collector was found to have developed a significant crack, which likely resulted in engine power loss during flight.
The pilot was unable to cushion the landing during termination of the autorotation, likely due to low rotor RPM, resulting in the helicopter colliding with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passengers of the accident flight
the operator
the maintainer for VH-BEU
Civil Aviation Safety Authority
accident witness
OzRunways data from the pilot’s iPad
Bureau of Meteorology
Kawasaki Heavy Industries
the maintenance facility that conducted the post‑accident engine examination.
References
U.S. Department of Transportation Federal Aviation Administration Helicopter Flying Handbook, FAA‑H‑8083‑21B (2019).
Lycoming Service Instruction No. 1009BE (2020).
Reciprocating engine and exhaust vibration and temperature levels in general aviation aircraft, U.S. Department of Transportation Federal Aviation Administration (1968).
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
the operator
the maintainer for VH‑BEU
Civil Aviation Safety Authority
Kawasaki Heavy Industries
Textron Lycoming
United States National Transportation Safety Board
Japan Transport Safety Bureau
Submissions were received from:
the pilot of the accident flight
the operator
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
[1]The flat pitch is the power it takes to run the helicopter at 100% rotor RPM on the ground with the collective lever fully lowered. A helicopter flat pitch check is performed pre‑flight to identify any engine performance trends by monitoring manifold pressure.
[2]Flying neighbourly is a concept aimed at minimising the noise impact of helicopter operations on local communities.
[3]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[4]The term used to describe the position of the 2 needles on the combined engine/rotor tachometer when the 2 needles are not superimposed. When a helicopter enters autorotation, either due to an engine failure or during practice, the needles split as the rotor system drive disengages from the engine. This indicates that the main rotor is no longer being powered by the engine and is instead being driven by the upward airflow through the rotor disc.
[5]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[6]ICUS (In Command Under Supervision) operations enable pilots having the relevant aircraft type endorsement to gain command experience and accumulate flight hours when performing pilot‑in‑command duties under supervision.
[7]The AWB provided guidance on engine bulk strip for the purpose of extending calendar life, in instances where engine calendar life limit was reached before reaching the hourly TBO.
[8]The freewheeling unit is a mechanism that automatically disengages the engine from the main rotor when engine RPM falls below rotor RPM, allowing continued rotor rotation during autorotation.
[9]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[10]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – scattered indicates cloud covering between a quarter and a half of the sky.
[11]Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to predict the probability of aircraft carburettor icing or the likelihood of fog.
[12]US Department of Transport FAA Report No. NA‑68‑27.
Occurrence summary
Investigation number
AO-2024-050
Occurrence date
11/09/2024
Location
24 km north of Katherine Tindal Airport
State
Northern Territory
Report release date
09/05/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales. The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. There was a pilot and one passenger on board.
During the approach, the engine stopped and while looking for a suitable landing place, the pilot saw a taxiway on the airport and decided to aim for that. To successfully reach the airport, the pilot elected to leave the flap retracted and gear up. This was done to reduce drag and achieve maximum glide range. Once the aircraft was assured of a landing on the airport, the gear was lowered. However, it did not successfully lock into place due to the limited time available before touchdown. The aircraft landed wheels-up resulting in minor damage and both occupants were uninjured.
What the ATSB found
The ATSB determined that, while the aircraft departed with sufficient fuel to complete the intended flight, it is likely that the amount of fuel reduced to a level that, in combination with unbalanced flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
The ATSB also determined that the pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Safety message
Fuel starvation occurrences can often be prevented by conducting thorough pre-flight fuel quantity checks combined with inflight fuel management. Pilots are reminded to check fuel quantities prior to departure using a known calibrated instrument such as a dipstick. In addition, comparing the expected fuel burn with actual fuel remaining after a flight, will give a validated fuel burn for the aircraft and ensure the measuring equipment is accurate. Pilots should familiarise themselves with the Civil Aviation Safety Authority, Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in‑flight fuel management.
Practising forced landings from different altitudes under safe conditions can help pilots prepare for an emergency situation, should one arise. Some components of the aircraft such as flap and gear, increase drag and reduce the glide range. Being familiar with emergency checklists and your aircraft’s systems will assist in an emergency when identifying and managing an engine failure.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales (NSW). The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. As the pilot had not previously operated to Bankstown Airport, they elected to carry a passenger, who was also a helicopter pilot, to assist with navigation and radio communication.
At 1313 local time, with the left fuel tank selected for take-off, the aircraft departed from runway 23[1] and tracked south. The pilot reported that about 4 minutes into the flight (while passing abeam Cessnock) they selected the fuller right tank, which they thought would reduce workload when entering Bankstown airspace. The aircraft entered the Visual Flight Rules (VFR) route[2] between Brooklyn Bridge and Prospect Reservoir at 1336 at approximately 2,000 ft.
Figure 1: Sequence of events
The image shows the sequence of events leading up to and during the forced landing, it highlights relevant places and reference times. Source: OzRunways flight data overlay on Google Earth.
The aircraft arrived overhead Prospect Reservoir at 1346 (Figure 1) and the aerodrome controller (ADC) instructed VH-MYW to maintain 1,500 ft and join the downwind leg of the circuit for runway 29R. An approximate 25° angle of bank turn was conducted to track toward a downwind join for runway 29R.
At 1347, the pilot reported joining downwind for 29R and the ADC instructed them to maintain 1,500 ft and provided them with updated Automatic Terminal Information Service (ATIS) [3] information ‘Foxtrot’. The pilot confirmed receipt of the new information by reading back the new QNH.[4]
The pilot recalled that, at about the time of that radio transmission, with the aircraft about 4.5 km north-west of Bankstown Airport, the propeller RPM increased, and they felt a braking sensation. They recalled that, in response they attempted to reduce drag on the propeller, changed fuel tank selection and briefly selected the electric fuel boost pump to ON. They then aimed to maintain glide speed while looking for a place to land.
At 1348, the pilot transmitted a MAYDAY call on the Bankstown Tower radio frequency stating they were having engine problems. The ADC advised that all runways were available, and they could track as required. The ADC continued to coordinate traffic to assist VH-MYW.
The pilot reported that while they were looking for a place to conduct a forced landing, they saw a taxiway on the airport and decided to try to land there. They advised that, during the approach the aircraft clipped the top of a tree and they raised the aircraft’s nose at the last minute to avoid a building on the airport perimeter. They decided not to deploy landing gear or flap until they were assured of reaching the airport.
At 1350, a helicopter operating in the area, reported that the aircraft had landed at the intersection of taxiway November 1 and taxiway Lima.
Both occupants of the aircraft were uninjured, and the aircraft sustained minor damage.
Context
Pilot
The pilot held a private pilot licence (aeroplane) issued in 2014 with a single‑engine class rating. They were appropriately endorsed to fly the Cessna 210 with design features for manual propeller pitch control and retractable undercarriage. The pilot also held a current class 2 aviation medical certificate.
They had accrued a total flight experience of approximately 222 hours, of which 15 hours were on the Cessna 210. In addition, they had previously flown other aircraft in this range including the Cessna 206 and Cessna 177. The pilot’s licence showed an entry for a single‑engine flight review conducted on 31 May 2023.
Weather
At the time of the incident, the Automatic Terminal Information Service information ‘Foxtrot’ was current, which indicated CAVOK[5] conditions, temperature 22°C, wind direction variable at 5 kt, and runway 29R in use for arrival and departures.
Aircraft
The aircraft was a Cessna Aircraft Company T210M manufactured in 1978 and issued serial number 21062277. It was powered by a fuel‑injected Continental Motors Inc TSIO-520-R piston engine driving a 3‑bladed, constant‑speed McCauley Propeller.
The aircraft was purchased from South Africa where it was previously registered as ZS-MYV and was shipped to Australia where it was reassembled and placed on the Australian register on 19 March 2021 as VH-MYW.
Maintenance
The aircraft was issued a maintenance release in November 2022 for private operations however, this expired in November 2023. At the time of the incident the aircraft was being ferried to Bankstown for completion of the maintenance required to return the aircraft to service.
As the maintenance release had expired, a special flight permit (SFP) was issued for the purpose of completing this ferry flight. The SFP was issued by the Civil Aviation Safety Authority (CASA) on 14 May 2024. The permit expired on 31 May 2024 and was subject to the following conditions:
Essential operating crew only to be carried.
Daily inspection and flight times are to be recorded on the Maintenance Release.
Day VFR, non-commercial operation by the most direct route practical and permitted by weather.
Operation shall be conducted in accordance with the approved flight manual / cockpit placards for the aircraft.
A copy of this SFP to be carried on-board and filed with the aircraft logbooks.
The permit also stated the flight was permitted to depart Maitland and arrive at Bankstown.
The last daily inspection signed on the aircraft maintenance release was completed on 2 November. The pilot advised that they had completed the daily inspection prior to the flight, but this was not recorded on the maintenance release.
The aircraft maintenance release also carried 2 endorsements for defects. These included the wing flaps not extending equally and hail damage. The flap defect was addressed by a third party, however, the hail damage was assessed by the aircraft owner in accordance with the CASA Airworthiness Bulletin 51-010 Assessment of hail damage.
Airworthiness Bulletin 51-010 recommended having a person who was appropriately qualified under Civil Aviation Safety Regulations 21.M to inspect the aircraft.
The pilot reported the aircraft had a tendency to fly right wing down. There was insufficient evidence available to the ATSB to determine whether either of the aircraft defects contributed to the flight characteristics described by the pilot.
Aircraft systems
Trim
The aircraft was fitted with elevator and rudder trim. Rudder trimming was accomplished via a wheel mounted in the cockpit (Figure 2). Setting the rudder trim left of centre would result in the aircraft maintaining the nose left of the flight path and remaining in that position until the wheel was manipulated, or the rudder pedals were manipulated. To maintain the desired track with that trim configuration, the aircraft would need to be flown in an uncoordinated state with the right wing low.
The aircraft’s pilot operating handbook stated:
Unusable fuel is at a minimum due to the design of the fuel system. However, when the fuel tanks are ¼ full or less, prolonged uncoordinated flight[6] such as slips or skids can uncover the fuel tank outlets, causing fuel starvation and engine stoppage. Therefore, with low fuel reserves, do not allow the airplane to remain in uncoordinated flight for periods in excess of one minute.
Cessna advised this was originally added to the Cessna 210 model D owner’s manual and was carried through as the aircraft developed into different models. Cessna did not have the available data to assess the likelihood of uncoordinated flight contributing to fuel starvation.
The pilot stated the rudder trim had been set left of centre since the aircraft was re‑assembled in Australia and that the trim wheel was not manipulated in flight.
Figure 2: Aircraft control pedestal post-incident
The image shows the fuel gauge level and the rudder trim. The image was taken on 6 June 2024, several days after the incident. However, the person responsible for recovering the aircraft stated, no fuel was added prior to this photo and the trim was set as found on the day of the incident. Source: Engineer responsible for aircraft recovery.
Fuel system
The Cessna 210 fuel system consists of a main fuel tank located in each wing. Each tank capacity is 171 L, of which 169 L is usable fuel. Each tank gravity fed a smaller fuel reservoir tank of approximately 1.9 L through fuel collector ports, which were located at the forward and aft inboard side of the main fuel tank (Figure 3Figure 3 and Figure 4).
Figure 3: Cessna 210M fuel schematic
Source: Cessna 210M pilot operating handbook, annotated by the ATSB
The fuel selector valve had 3 positions – left, right, and off – and so fuel could only be drawn from either the left or right tank. Cessna advised that at a low cruise power setting, if no fuel was being fed to the smaller fuel reservoir tank, it could supply fuel to the engine for between 1.5–3.5 minutes. The pilot advised that, at the time of the power loss the fuel selector was selected to the right fuel tank.
The fuel system has an engine-driven fuel pump and an auxiliary fuel pump, which is electrically driven. The pilot operating handbook states the following:
If it is desired to completely exhaust a fuel tank quantity in flight, the auxiliary fuel pump will be needed to assist in restarting the engine when fuel exhaustion occurs.
Cessna stated that during testing, the electric auxiliary fuel pump was required to operate for 4 seconds to restart the engine.
Figure 4: Fuel tank design
The above image shows the location of the fuel collector ports and the openings that are located in the rib support structure. The fuel cell image shown is for later serial numbers of the Cessna 210. However, it is the most descriptive image of fuel collector ports. Further images provided by Cessna show the aft collector port is located in a similar location to the above image. Source: Cessna 210 illustrated parts catalogue model 210 & T210 series 1981–1986, annotated by the ATSB.
The fuel tank design included an internal rib support structure (Figure 4). Each rib had an enlarged centre opening for fuel to freely flow through the tank, with small openings at the base of each rib, ensuring useable fuel could not become trapped. Cessna stated, ‘The small, if any, amount of fuel caught behind any structure would be part of the unusable fuel level determined during certification.’
Propeller
A control lever was used to set aircraft RPM by changing the propeller blade pitch. When the control lever is pushed inward, the propeller increases RPM (low blade pitch). When the control lever is pulled outward, the propeller RPM decreases (high blade pitch). This is achieved by a propeller governor which relies on engine oil pressure to move the propeller toward a high blade pitch (low RPM).
The combination of an internal spring and centrifugal force, twists the blades toward a low pitch (high RPM) setting when oil pressure at the propeller hub is relieved.
Engine Failure During Flight checklist
The pilot operating handbook provided the following checklist to be conducted in the event of an engine failure during flight:
airspeed – 85 [kt indicated airspeed] KIAS
fuel quantity – check
fuel selector valve – fuller tank
mixture – rich
auxiliary fuel pump – on for 3-5 seconds with throttle ½ open; then off
ignition switch – both (or start if propeller is stopped)
throttle advance slowly.
Flight data
The ATSB obtained flight data from an electronic flight bag (EFB) used by the pilot. The data provided aircraft position, time, altitude, and ground speed.
The flight data was analysed by the ATSB to obtain the approximate position when the engine stoppage occurred. This was determined to be at 1348 as there was a significant reduction in ground speed at that time.
Flight planning and fuel usage
The pilot reported that during the cruise, the manifold pressure was set near the top of the green (approximately 25 inches) and RPM at 2,200. A fuel flow reading was noted by the pilot of 14 gallons per hour (53 L/hr).
The pilot advised that they normally dipped the tank during the pre-flight inspection using the aircraft’s fuel dipstick. During the pre-flight they estimated 150 L of fuel on board, 60 L in the left tank and 90 L in the right tank (see the section titled Fuel system). Using that fuel quantity and recorded flight data, Table 1 details the expected consumption throughout the flight.
Table 1: Estimated fuel burn based on flight data
Sector
Start time
Block time
(min)
Estimated fuel burn (L) at 53 L/hr
Total
Comments
Departing Maitland
1313
0
5
145
Pilot stated, they departed on left tank (5 L allowed for taxi)
Abeam Cessnock
1317
4
4
141
Climbing phase, fuel burn was likely higher than 53 L/hr.
Near Warnervale
1325
8
8
133
Pilot stated, at approximately overhead Cessnock, they swapped to right fuller tank.
Brooklyn Bridge
1336
11
10
123
Prospect Reservoir
1346
10
9
114
Estimated engine stop
1348
2
2
113
Total
35
38
Totals have been rounded up
Post-incident inspection
The ATSB did not attend the site. A video of the aircraft, provided by 9News Australia showed fuel leaking from the right fuel tank vent. The aerodrome operator who attended the incident site stated that the fuel which leaked from the vent was no more than 2–4 litres, of which most was funnelled into a jerrycan. While the ATSB could not verify how long the fuel was leaking, based on the observations of the aerodrome operator, it was unlikely to have significantly affected the amount of fuel in the tank. There was no evidence of fuel leaking from the left tank.
Figure 5: Fuel leak from right tank vent
Source: 9News Australia
The aircraft was recovered, and an initial inspection was completed. The fuel level was checked using the on-board fuel gauges and dipstick. The left tank was estimated to hold between 0–5 L and the right tank was estimated between 40–50 L.
The aircraft’s damaged propeller was removed, and a suitable test propeller was fitted to the aircraft. The engine was started and was able to draw fuel from the remaining fuel in both tanks, the test continued for approximately 5 minutes on each tank. However, high power settings similar to in‑flight conditions were not tested.
The aircraft had undergone a fuel calibration and the placard above the fuel gauges was no longer relevant however, it was not removed (Figure 2). The placard was not considered to have contributed to the incident as the fuel on board was likely less than the 4 hours stated on the placard. The onboard fuel dipstick used was labelled C210 dipstick and was marked with the aircraft’s previous registration, ZS-MYV.
Related occurrences
Fuel management and fuel starvation incidents and accidents continue to occur with single and twin-engine aircraft. Examples of other ATSB investigations of similar occurrences include:
Fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023 (AO-2023-017)
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021)
Fuel starvation and forced landing involving Pilatus Britten-Norman Islander BN2A, VH-WQA, Moa Island, Queensland, on 3 October 2022 (AO-2022-046).
Safety analysis
The pilot reported that, during approach to Bankstown Airport, they noted an increase in propeller RPM and could not maintain altitude. This behaviour was consistent with an engine failure, with the associated loss of oil pressure resulting in the propeller moving to a finer pitch (increased RPM). The post-incident aircraft inspection did not identify an engine malfunction, and the engine was able to run at low power on the remaining fuel in both tanks. As there was no evident malfunction of the engine, the most probable reason for the inflight power loss was fuel starvation.
The pilot reported that the aircraft departed with 90 L in the right tank and 60 L in the left tank (150 L total). They also advised the right tank was selected for most of the flight. If this was the case, there should have been approximately 61 L in the right tank and 51 L in the left tank. However, given the total fuel on board after the incident occurred (maximum 59 L), it was unlikely that approximately 91 L was burnt during the 35-minute flight. Therefore, it was unlikely that the amount of fuel the pilot stated was on board at the commencement of the flight was actually in the aircraft. Significantly however, there was sufficient total fuel on board for the flight.
The post-incident inspection revealed between 40–50 L remaining (which equated to approximately 1/4 full tank) in the right tank, with about 2–4 L reportedly leaking after the landing. The pilot operating handbook (POH) stated that if there was less than 1/4 fuel in the tank and the aircraft was in uncoordinated flight, the fuel pick-ups could uncover, and fuel starvation could occur.
The post-incident inspection also revealed between 0–5 L remaining in the left fuel tank. If the engine was being supplied from the left tank, during an uncoordinated left turn at Prospect Reservoir at 1346, it is possible the fuel drained away from the fuel pick-ups and the engine continued to draw fuel from the left header tank until 1348 when the engine stopped. This was consistent with Cessna’s advice that the header tank can supply fuel for 1.5–3.5 minutes at low cruise power.
In summary, irrespective of which tank was supplying the engine, the quantities of fuel remaining, when combined with the uncoordinated flight, were conducive to fuel starvation in accordance with the POH.
The pilot’s initial response during the emergency was largely focused on attempting to reduce drag created by the propeller, despite the aircraft not having this ability, and they did not complete the engine failure during flight checklist. If the checklist had been followed, the pilot would have increased the likelihood of restarting the engine in flight. During the extended period where the aircraft was resting on the ground and positioned right-wing low, it is likely the fuel remaining in the left tank drained into the left header tank. Even though this fuel was sufficient to run the engine at low power, it may not have been available during approach or sufficient for the power required in flight.
The pilot’s decision to minimise the aircraft’s drag during the glide, by keeping the gear up and flaps retracted, combined with managing the airspeed, resulted in the aircraft achieving the required performance to land safely inside the airport environment. However, due to the distance the aircraft needed to glide and obstacles that needed to be cleared, by the time the landing gear was selected down, there was not enough time to extend and lock in place before the aircraft collided with the ground resulting in a wheels-up landing.
Finally, the CASA special flight permit was issued for the purpose of ferrying the aircraft for maintenance. The conditions put in place were to minimise the consequences if an incident occurred during flight which was conducted outside of the normal aircraft operation. Although their reported purpose was to assist with navigation and radio communication, the pilot’s decision to allow a passenger to fly on board the aircraft unnecessarily exposed them to a risk of injury and consequently was another factor that increased risk.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation involving Cessna T210M, VH-MYW, 4 km north-west of Bankstown Airport, New South Wales, on 26 May 2024.
Contributing factors
While the aircraft departed with sufficient fuel to complete the intended flight, low usable fuel quantities, in combination with probable uncoordinated flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
Other factors that increased risk
The pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot
aerodrome operator
engineer responsible for aircraft recovery
aircraft manufacturer and insurer
Civil Aviation Safety Authority
Airservices Australia
OzRunways recorded data
video footage of the incident flight and other imagery taken on the day of the incident.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
engineer responsible for aircraft recovery
Civil Aviation Safety Authority
aircraft manufacturer.
Submissions were received from the:
pilot
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]VFR route: A pre-defined laneway for aircraft traffic to remain clear of airspace and enter or exit high traffic areas such as Bankstown Airport.
[3]Automatic terminal information service: The provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations. See Automatic terminal information service (ATIS).
[4]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[5]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[6]Uncoordinated flight occurs when the aircraft skids or slips, this is most commonly associated with a turn, but a skid can occur when the ailerons and rudder are used in opposite directions during normal flight.
Occurrence summary
Investigation number
AO-2024-033
Occurrence date
26/05/2024
Location
4 km north-west of Bankstown Airport
State
New South Wales
Report release date
11/10/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Wheels up landing