The ATSB is investigating a forced landing involving a Cessna 172P, registered VH-CIY, 58 km west of Latrobe Regional Airport, Victoria, on 14 April 2026.
During cruise, the engine failed due to fuel exhaustion and the crew conducted a forced landing in a field. No injuries or damage to aircraft were reported.
To date, the ATSB investigation has included:
interviewing involved parties
retrieving and reviewing policies and procedures
collection of other relevant information.
The ATSB has commenced examination and analysis of the collected evidence.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-072
Occurrence date
14/04/2026
Occurrence time and timezone
04:11 UTC
Location
58 km west of Latrobe Regional Airport
State
Victoria
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Forced/precautionary landing, Fuel exhaustion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172P
Registration
VH-CIY
Serial number
17274321
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the afternoon of 10 March 2026, following completion of a routine 100-hourly maintenance inspection, a commercially licensed and instructor-rated pilot was operating a Cessna 182 on a test flight from Caboolture Aircraft Landing Area, Queensland. The pilot reported that after pre-flight inspections and engine operational checks (‘run ups’), they took off from Caboolture runway 11 before tracking towards Bribie Island to the east and climbing to 2,500 ft AMSL. After conducting a series of steep turns overhead the island, the pilot turned south‑west, back towards the airfield. During the return leg, the pilot reported an uncommanded loss of engine power and commenced troubleshooting checks as the aircraft began to descend, which included moving the fuel selector from the ‘Both’ to ‘Right’ tank selection. Regaining engine power after this action, the pilot climbed back to 1,500 ft and continued tracking toward the airport. An estimated 2 minutes later, the engine again lost power and the pilot configured the aircraft for best glide while continuing troubleshooting attempts.
When engine power could not be restored and the pilot determined the aircraft would not reach Caboolture, they elected to conduct a forced landing into a grassed paddock north of the airfield. After a successful touchdown, the aircraft travelled around 15–20 metres in the landing roll before the nosewheel, then under the full weight of the aircraft, sunk into soft terrain. The aircraft subsequently flipped forward, coming to rest inverted (Figure 1). The pilot was able to climb free from the aircraft, which had sustained substantial damage, and was later conveyed to hospital with minor injuries.
Operator’s investigation
The aircraft operator undertook a detailed investigation into the circumstances of the accident and provided a summary of findings to the ATSB.
Significantly, when interviewed, the pilot indicated that during the pre-flight inspection, they had not used a dipstick to visually verify the amount of fuel remaining in the aircraft’s wing tanks – choosing to rely on the fuel gauges and the aircraft’s fuel log. Further, it was found that the fuel log had not been updated following the last flight prior to the maintenance activities.
In summary, the operator concluded that the engine power loss resulted from fuel exhaustion.
Figure 1: Aircraft after the forced landing
Source: Operator, edited by the ATSB
Safety action
The operator has advised that, following this occurrence and its subsequent internal investigation, a written directive will be issued to all company pilots requiring them to conduct a visual fuel dip before commencement of flight, and to ensure that aircraft fuel quantity gauges are crosschecked against indications from 2 other independent quantity assessment methods.
Safety message
The circumstances of this fuel exhaustion and forced landing occurrence reinforces the critical importance of all pilots – regardless of experience level – verifying available fuel on board the aircraft using multiple, independent methods before flight. Reliance on unverified documentation or uncalibrated instrumentation without independent assurance (through the fuel dip process required by the manufacturer’s operating handbook and CASA Advisory Circular AC 91-15, section 5.2), exposes the pilot to increased risk of inadvertent fuel exhaustion and subsequent forced landing.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-018
Occurrence date
10/03/2026
Location
3.8 km north of Caboolture Aircraft Landing Area
State
Queensland
Occurrence class
Accident
Aviation occurrence category
Forced/precautionary landing, Fuel exhaustion
Highest injury level
Minor
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
182Q
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational - Other general aviation flying - Test flights
The ATSB is investigating a collision with terrain involving a Robinson R44 II, VH-HYR, at Yorke Island Airport, Queensland, on 31 March 2026.
Shortly after take-off at 100 ft AGL, the low rotor RPM horn activated and the pilot conducted an emergency landing on the aerodrome. During the landing, the helicopter collided with terrain resulting in substantial damage. The pilot sustained serious injuries. The investigation is continuing.
The ATSB has commenced the examination and analysis of the initial evidence collected. To date, the ATSB investigation has included:
interviewing the pilot of the occurrence aircraft
examination of maintenance records
examination of independent engineering report
images of the wreckage
reviewing the common traffic advisory frequency recordings
examination of pilot training and records
The wreckage has been moved to an independent maintenance facility for further analysis
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-069
Occurrence date
31/03/2026
Occurrence time and timezone
14:36 Eastern Australia Standard Time
Location
York Island Airport
State
Queensland
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Abnormal engine indications, Collision with terrain, Forced/precautionary landing
The ATSB is investigating a power loss and forced landing involving a Cessna 441, VH-LBZ, 3.6 km east of Broome Airport, Western Australia, on 19 March 2026.
During initial climb from runway 10, it is reported that both engines lost power. The pilots maintained heading and conducted a forced landing in mangroves. Five passengers and 2 pilots were evacuated from the aircraft, which was substantially damaged.
The ATSB deployed a team of transport safety investigators to the accident site with experience in aircraft operations, maintenance, engineering and survivability. As part of the on-site phase of the investigation, ATSB investigators examined the aircraft wreckage and other information from the accident site, examined operator procedures, interviewed witnesses and involved parties, and examined maintenance records and any recorded data.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-068
Occurrence date
19/03/2026
Occurrence time and timezone
03:18 UTC
Location
3.6 km east of Broome Airport
State
Western Australia
Report status
Pending
Anticipated completion
Q3 2026
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
441
Registration
VH-LBZ
Serial number
4410038
Aircraft operator
Skippers Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
Source: Operator
What happened
On 30 January 2026 at about 1205 local time, the pilot and sole occupant of a Cessna U206F departed from an Emu Point aircraft landing area, Northern Territory, en route to Darwin Airport.
Prior to departure the pilot conducted a pre-flight inspection and reported that the aircraft departed with 190 L of fuel. No abnormalities were observed during the take-off or the initial climb. The aircraft levelled off at about 2,000 ft above mean sea level (AMSL) and the pilot conducted the cruise checklist, with no issues identified. Shortly after this, the pilot observed an engine RPM overspeed. The pilot reduced the propellor pitch lever, but this had no effect, so they reduced the throttle to maintain an appropriate RPM.
Shortly after this, the engine began running rough, accompanied by increasing vibration and a reduction in engine power. Almost immediately, smoke began entering the cockpit via the cabin air vents, which the pilot closed. The engine performance continued to degrade to the extent that the aircraft was unable to maintain straight and level flight. The pilot observed smoke and oil spraying onto the airframe and windscreen, reducing forward visibility. They reported that the engine vibrations increased violently, to the point that the entire airframe was shaking.
The pilot selected an area of open grassland interspersed with trees and termite mounds beyond a heavily wooded area and prepared to conduct a forced landing.
Figure 1: Aircraft wreckage
Source: Operator, annotated by the ATSB
Prior to landing, the pilot conducted final checks, unlatched their door and maintained what power was available to assist in clearing the tree line. However, prior to touchdown, the aircraft collided with several trees before rotating left, impacting the ground heavily and coming to a stop (Figure 1).
The pilot reported a brief period of unconsciousness and after ‘coming to’, turned off the ignition and checked that the ELT[1] had activated. The pilot exited through the shattered cockpit windscreen and moved to a safe distance from the wreckage, returning briefly to retrieve a handheld VHF radio and a personal mobile phone. The pilot’s initial attempts to coordinate emergency assistance were unsuccessful. Shortly after, they established radio contact with another aircraft that relayed a MAYDAY call. A rescue aircraft with an emergency response team arrived about one hour later.
The pilot was medically assessed and later admitted to hospital with minor abrasions and a broken collarbone requiring surgery.
The aircraft was significantly damaged and, at the time of publishing, the remote location, terrain and weather conditions have prevented aircraft recovery. Consequently, the likely cause of the reported engine failure remains undetermined.
Safety message
In-flight engine failures and partial power loss in single-engine aircraft require pilots to exercise effective and timely decision-making to reduce the severity of injuries and damage. These events often result in the pilot experiencing high workload and time pressure, where preparedness is critical. Deciding on responses to a partial engine power loss before the flight will reduce your workload during the event and assist you in taking some form of considered action.
When experiencing a rough running engine, pilots should focus on flying the aircraft and continually assess landing options. The ‘aviate, navigate and communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies. Acting in the appropriate order of priority improves situation awareness and supports coordinated responses in a dynamic environment.
recommends that scanning the environment should take 85% of the time available, 10% on checking aircraft attitude including lookout, and 5% of the time scanning of the altitude and airspeed indications.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Electronic Locator Transmitter (ELT): an aviation safety device installed in aircraft that automatically or manually transmits a distress signal via satellites.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-010
Occurrence date
30/01/2026
Location
102 km east-north-east of Port Keats Aerodrome
State
Northern Territory
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Smoke
Highest injury level
Serious
Brief release date
20/02/2026
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
U206F
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Emu Point Aircraft Landing Area, Northern Territory
The ATSB is investigating a main rotor blade strike involving a Leonardo Helicopters AW139, VH-TJF, 41 km south-east of Corryong Airport, New South Wales (NSW), on 5 January 2026.
During preparation for a rescue winch, the main rotor blades struck tree branches. The winch operation was cancelled, and the crew diverted the flight to Perisher Valley, NSW where the helicopter landed. The helicopter sustained minor damage.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-002
Occurrence date
05/01/2026
Occurrence time and timezone
17:25 Australian Eastern Daylight Time
Location
41 km south-east of Corryong Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Approval
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Controlled flight into terrain (CFIT), Forced/precautionary landing
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Leonardo Helicopters
Model
AW139
Registration
VH-TJF
Serial number
31710
Aircraft operator
Helicorp Pty Ltd
Sector
Helicopter
Operation type
Part 133 Air transport operations - rotorcraft
Activity
Commercial air transport-Non-scheduled-Medical transport
Departure point
Southcare Base Helicopter Landing Site, Australian Capital Territory
The ATSB is investigating a collision with terrain involving a Van's RV-8, registered VH-YGY, 40 km west of Gladstone Airport, Queensland, on 23 November 2025.
During initial climb, the aircraft reportedly encountered a mechanical issue and the pilot attempted to land. The aircraft subsequently collided with a tree and was destroyed. The pilot sustained serious injuries.
The ATSB deployed a team of 4 transport safety investigators to the accident site with experience in aircraft operations, maintenance, and engineering. As part of the on-site phase of the investigation, ATSB investigators examined the aircraft wreckage and other information from the accident site, interviewed witnesses and involved parties, and examined maintenance records and recorded data.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2025-068
Occurrence date
23/11/2025
Occurrence time and timezone
09:00 Eastern Australia Standard Time
Location
40 km west of Gladstone Airport
State
Queensland
Report status
Pending
Anticipated completion
Q2 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: External review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Van's Aircraft
Model
RV-8
Registration
VH-YGY
Serial number
80605
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Unknown general aviation flying
The ATSB is investigating suspected rotor drive belt failures involving 2 Robinson R22s, registered VH-8H8 and VH-HFQ, near Argadargada Aerodrome, Northern Territory, and Chillagoe Aerodrome, Queensland, on 15 November 2025 and 23 November 2025.
During cruise for mustering, the pilot and passenger of VH-8H8 noticed a smell of burning rubber and the pilot thought the rotor drive belts had failed. The engine over sped and the pilot conducted an autorotation. The helicopter subsequently collided with terrain resulting in substantial damage.
During cruise on a private flight, the pilot and sole occupant of VH-HFQ detected an airframe vibration and observed an abnormal rotor RPM indication, before conducting an autorotation and forced landing. The helicopter landed hard and the pilot observed a rotor belt on the ground. The helicopter was subsequently destroyed by post‑impact fire.
The ATSB has examined and analysed recovered components, maintenance records, and information from the occurrence pilots, maintenance personnel and the helicopter manufacturer. The evidence collection and analysis phases of the investigation are now complete and the ATSB is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2025-069
Occurrence date
15/11/2025
Occurrence time and timezone
08:30 Australian Eastern Standard Time
Location
Near Argadarga Aerodrome and Chillagoe Aerodrome
State
Northern Territory
Report status
Pending
Anticipated completion
Q2 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Forced/precautionary landing, Powerplant/propulsion - Other
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-8H8
Serial number
3293
Aircraft operator
Georgina Pastoral Company Pty Ltd
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Aerial work-Observation and patrol
Departure point
Argadargada Station, Costello, Northern Territory
Destination
Argadargada Station, Costello, Northern Territory
Injuries
None
Damage
Substantial
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-HFQ
Serial number
4279
Aircraft operator
Sunrise Helicopters Pty Ltd
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Own business travel
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 5 October 2025, the pilot of a Schweizer Aircraft Corp 269C-1 planned a ferry flight from Lake Macquarie Airport (where the helicopter had just received an annual service) to a landing area near Duri, New South Wales.
The pilot’s usual procedure was to conduct a pre-flight inspection of the helicopter prior to departure which included confirming the amount of fuel in the fuel tank with a dipstick. On this occasion, however, the pilot recalled observing the calibrated amount of fuel inside the tanks to be 92 litres. Assuming this amount was correct, the pilot was satisfied with the fuel quantity and proceeded to collect their passenger from the taxiway. Shortly after, the helicopter departed from runway 25.
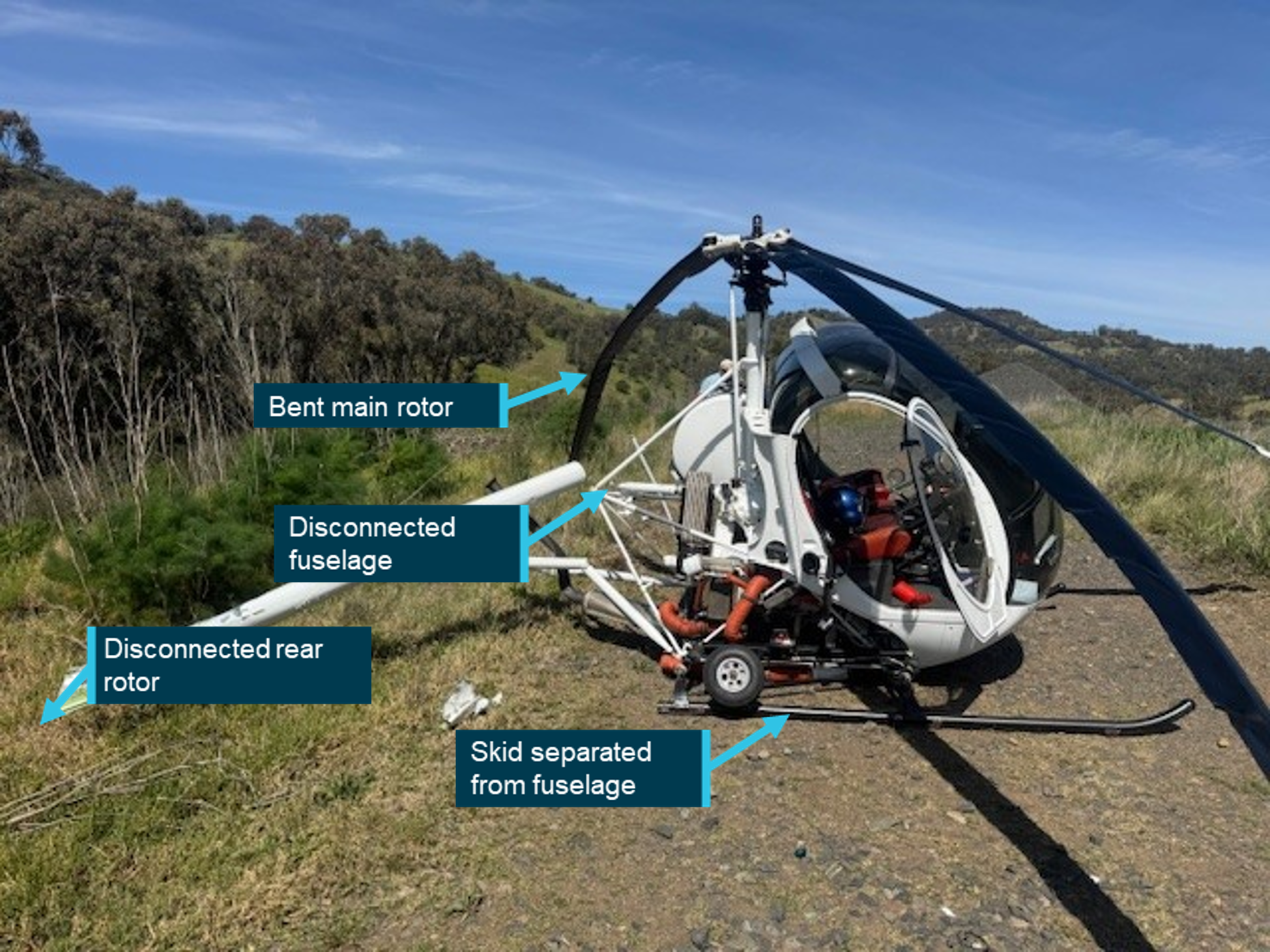
En route to the arranged helicopter landing area about 1.7 hours away, the pilot observed a different fuel burn rate to the calculations that were initially completed. Due to the distance left to travel, the pilot advised the passenger that there would be a precautionary landing conducted to inspect the fuel tank further. The pilot selected a suitable landing area and began to configure the helicopter for landing. However, at 2,500 ft, the engine stopped producing power due to fuel exhaustion and the pilot conducted an autorotation[1] to land at a track beside a train line. The helicopter landed hard, resulting in substantial damage to the skids, rotor blades and tail boom (Figure 1).
Figure 1: Damage to helicopter
Source: Pilot, annotated by the ATSB
Safety message
Pilots are reminded to always check the fuel quantity prior to departure using a known calibrated instrument such as a dipstick.
Pilots are also encouraged to use at least 2 independent verification methods to determine the quantity of fuel on board the aircraft. The Civil Aviation Safety Authority (CASA) advisory publication,
, provides guidance for fuel quantity crosschecking.More specifically, the advisory circular published by CASA, AC 91-15 v 1.2 - Guidelines for aircraft fuel requirements, highlights the importance of pre-flight fuel quantity checks and in-flight fuel management.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-053
Occurrence date
05/10/2025
Location
Kankool
State
New South Wales
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Forced/precautionary landing, Fuel exhaustion
Highest injury level
None
Brief release date
07/11/2025
Aircraft details
Manufacturer
Schweizer Aircraft Corp
Model
269C-1
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Departure point
Lake Macquarie Aircraft Landing Area, New South Wales
On 17 August 2025, a Piper PA-28, registration VH-BUN, was undertaking a navigation training exercise under the visual flight rules from Wollongong (Shellharbour) Airport, New South Wales, with a student pilot and instructor on board.
While flying south along the coast north of Sydney, at around 1,600 ft above mean sea level, the crew heard unusual engine noises and observed a rapid drop in engine RPM. This was accompanied by a period of heavy engine vibration and a smell of oil. As they continued south, the engine RPM progressively reduced. Approximately 6 minutes after the first abnormal engine indications, the instructor determined that the safest option would be to conduct a landing on the Mona Vale golf course.
However, during the final stages of the approach to the golf course, the pilot slowed the aircraft to around 50 kt indicated airspeed before they realised they could not safely land straight ahead, and made a right turn to avoid the club house facilities. The aircraft subsequently landed heavily in a right-wing low attitude. All 3 undercarriage legs detached, and the aircraft slid approximately 45 m before coming to rest. The student pilot received minor injuries while the instructor was uninjured. The aircraft suffered substantial damage.
What the ATSB found
The ATSB found that the exhaust valve of the engine’s number 3 cylinder broke away from its stem and caused extensive damage to the internal surfaces of the cylinder, its piston, and spark plugs. This resulted in a rapid loss of power from the engine, such that the aircraft was unable to maintain level flight. The specific failure sequence of the exhaust valve could not be determined.
The instructor was proactive in maintaining an awareness of potential landing sites throughout the flight. Consequently, they were able to promptly identify a suitable area to conduct a precautionary landing and avoid a more adverse outcome.
What has been done as a result
Following the accident, the operator undertook several safety actions, including:
Revision of the emergency briefing content, and formal re-statement of the requirement for pre-impact and evacuation procedures to be briefed by the instructor, and confirmed by the student, before every flight.
Completion of a review of competency in conducting engine failure procedures for all flight instructors, and implementation of additional training and enhanced supervision where required.
Commencement of a process to check students’ post‑engine failure competencies, including glide path judgement, execution of post‑failure actions, and engine securing checks.
Safety message
This investigation highlights the importance of effective contingency management and decision-making skills in emergency situations.
In a single engine aircraft, a partial engine failure can present more options and decision‑making challenges than a total loss of power. Greater uncertainty of the aircraft’s performance over time makes it more difficult to choose the lowest risk course of action and potentially requires decisions to be revisited and revised. However, certain traits of human cognition, such as confirmation bias, may resist changing decisions which have already been made.
The instructor in this investigation reported they had an awareness of several contingency landing locations along their route prior to the engine malfunction occurring. This subsequently helped them to decide a suitable course of action when the malfunction did occur. Furthermore, as the situation evolved, they recognised the need to re‑evaluate their original choice of landing site. Their timely selection of a different landing site likely minimised the adverse consequences of the occurrence. A previous ATSB investigation (AO-2024-010) highlighted how a delayed decision to land following an engine malfunction in a single engine aircraft led to a more challenging forced landing.
In this case the cause of the exhaust valve failure could not be determined. However, in 1988 Textron Lycoming, the manufacturer of the aircraft’s engine, provided guidance on maintenance practices to reduce the possibility of valve sticking (Service Instruction No. 1425 ASuggested Maintenance Procedures to Reduce the Possibility of Valve Sticking). The guidance noted that engine oil contamination increases the possibility of valve sticking and advised preventative actions, including:
regular changing of oil and oil filters
cleaning of air filters
proper sealing of the air induction system.
The risk of valve sticking is increased for engines operating in hot ambient conditions, and where engines are regularly shut down before they have cooled sufficiently.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 17 August 2025, a Piper PA-28-140, registration VH-BUN, was undertaking a navigation training exercise under the visual flight rules (VFR)[1] from Wollongong (Shellharbour) Airport, New South Wales, with a student pilot and flight instructor on board.
The aircraft departed Wollongong at 1222 local time, initially flying north to Camden Airport. The student flew 3 circuits at Camden before landing and shutting down the aircraft for a brief stop. Departing Camden at 1331, the aircraft continued north to Wisemans Ferry, before turning south-east at Barrenjoey Head. From there the crew had planned to follow the coast south before returning to Wollongong (Figure 1).
At 1413, shortly after the aircraft passed overhead Barrenjoey Head at an altitude of 1,600 ft, the aircraft’s engine suddenly started to produce an unusual noise, accompanied by a brief period of heavy vibration and a smell of oil in the cockpit. The instructor observed the engine RPM indication drop rapidly from the cruise setting of 2,450 to around 2,100. Indications of oil temperature, oil pressure and fuel pressure all remained in the normal range.
The instructor assumed control of the aircraft from the student. The student then followed the instructor’s directive to turn on the fuel pump and switch the fuel selector valve from the right tank to the left tank. The instructor advised they did not select the carburettor heat to ON as they assessed it would further reduce the engine RPM by about 100 and, as they had been flying at cruise power for about an hour, it was unlikely they were experiencing carburettor icing.
The instructor communicated the nature of the engine problems to Sydney terminal air traffic control (ATC) and was informed that the nearest airport to them was Sydney, directly to the south. Shortly after, the instructor reported that they would continue tracking south, but that the engine RPM had fallen further to 1,900. ATC advised that Long Reef golf course was 4 NM (7 km) ahead of the aircraft. The instructor assessed that the engine’s performance was deteriorating, and the aircraft could not maintain level flight. They therefore decided to make a landing at Long Reef golf course, noting that although Mona Vale golf course was closer, its abundance of trees would make landing more challenging.
Shortly after, with the aircraft approximately 1 NM (1.9 km) south-east of the Mona Vale golf course the instructor detected that the engine RPM had reduced further to 1,500. They determined that the aircraft would no longer be able to reach Long Reef and decided that Mona Vale golf course was now the best available option for a landing. The instructor advised ATC of their intention to land at Mona Vale and turned the aircraft north towards it.
Once the instructor felt assured that the aircraft was able to reach the golf course, they began to progressively extend the aircraft’s flaps and reduce the airspeed from the best glide speed, which based on the aircraft’s weight they assessed to be 70 kt, aiming for approximately 55 kt, reducing to 50 kt on touchdown. However, as the aircraft neared the ground, travelling in a north-east direction, the instructor judged that there was insufficient clear area ahead of them to land safely. Consequently, they made a right turn of approximately 90 degrees to avoid the club house facilities and re-aligned the aircraft to land in a south-east, downslope direction. The instructor did not identify the extent of the downslope.
During the turn, the right wing dropped, and the aircraft impacted the golf course heavily. All 3 undercarriage legs detached on impact and the aircraft slid approximately 45 m before coming to rest upright on a section of fairway.
Figure 1: Flightpath of VH-BUN
The image shows the point at which abnormal engine indications were first noticed and the location of the precautionary landing on Mona Vale golf course. Source: Google Earth and Flightradar24, annotated by the ATSB
Fuel began leaking from the underside of the aircraft but there was no fire. Both occupants were able to exit the aircraft soon after, assisted by first responders from the golf club. The aircraft received substantial damage. The student suffered minor injuries during the impact, while the instructor was uninjured. Both were subsequently taken by ambulance to a local hospital for assessment, where the student remained overnight, but the instructor discharged themselves later in the evening.
Context
Flight crew background
The flight instructor held a Commercial Pilot Licence (Aeroplane) and a CASA class 1 aviation medical certificate. At the time of the occurrence, they had accumulated 1,392 flying hours, 305 of which were in the Piper PA-28. The instructor had flown 75 hours in the past 90 days, 31 of which were in the PA-28.
The instructor reported that they had flown the same navigational route many times prior to the occurrence flight. They had developed knowledge of various sites along the route, which could serve as contingency landing locations in the event of an emergency.
The student pilot was undertaking training towards their Private Pilot Licence (Aeroplane) and held a CASA class 2 aviation medical certificate. At the time of the occurrence, they had accumulated a total of 91 hours flying time, 3 of which were in the PA-28.
Aircraft information
General
The aircraft was a Piper PA-28-140 (serial number 28-23228) manufactured in the United States in 1967. The aircraft was fitted with a Textron Lycoming O-320-E2A piston engine and Sensenich fixed pitch propeller. The aircraft was being maintained under the Civil Aviation Safety Authority Schedule 5. The most recent periodic maintenance was a 100‑hour inspection completed on 26 May 2025. At that time the aircraft had accumulated 8,478 hours in service. The next periodic inspection was due on 26 May 2026, or 8,578 hours, whichever occurred first. The aircraft’s total time in service at the time of the occurrence was around 8,509 hours.
A review of the maintenance documentation indicated that the aircraft’s engine was last overhauled in November 1993 and was maintained under Civil Aviation Regulation 42B CASA maintenance schedule using Airworthiness Directive AD/ENG/4 during every periodic inspection. During the last periodic inspection in May 2025, there were no engine discrepancies identified. At the time of the occurrence, the engine had accrued approximately 1,680 hours since overhaul.
Fuel system
The aircraft was equipped with 2 fuel tanks, one in each wing, referred to as the left and right tanks. Each tank had a maximum capacity of 95 litres, providing a total capacity of 190 litres.[2] A fuel tank selector valve in the cockpit could be positioned to control which tank provided fuel to the engine. The selector valve could be positioned to feed fuel from either the left tank or the right tank, or to an off position, where neither tank would provide fuel. It was not possible to supply fuel to the engine from both tanks simultaneously. After the selector valve, fuel passed through a strainer, 2 fuel pumps, and a carburettor before reaching the engine.
Pre-flight inspection
On the morning of the flight, both the instructor and the student pilot conducted independent pre‑flight inspections. This included inspection of the engine compartment where there was no evidence of oil leaks. They checked the oil levels and observed that there was sufficient oil, and it was a normal colour.
Both of the aircraft’s fuel tanks were filled to their maximum capacity shortly before departing Wollongong. The crew started up and taxied out using fuel from the left tank, before switching to the right tank just before take-off. The first flight to Camden was 41 minutes in duration and was flown entirely using the right tank. After landing at Camden, the student pilot inspected the quantity of fuel in each tank using a dipstick. The amount of fuel consumed during the first flight was as expected and there was sufficient fuel on board to perform the second flight as planned, with significant reserves.
Approximately the first 30 minutes of the second flight were flown using the left tank, before the crew switched to using the right tank again, at around 1404, just after passing Wisemans Ferry. The right tank remained selected until the engine began to malfunction. The crew switched back to the left tank as part of their efforts to rectify the engine problems, and the fuel selector valve remained in this position for the rest of the flight.
Post-flight fuel inspection
A post-accident inspection of the aircraft’s fuel system determined that approximately 58 litres of fuel remained in the right tank, but only around 2.5 litres remained in the left tank. The fuel selector valve was positioned to feed fuel from the left tank.
However, the fuel strainer, located on the lower edge of the engine firewall, was ruptured during the impact and a significant quantity of fuel was observed draining from it after the accident. With the fuel selector valve positioned to the left tank, it is therefore likely that the low quantity of fuel observed in the left tank was a result of fuel draining away via the damaged fuel strainer post-accident. The ATSB determined that fuel starvation was not a contributing factor.
Post-flight engine inspection
The ATSB undertook a detailed engineering inspection of the aircraft’s engine following the occurrence. Each of the engine’s 4 cylinders was subject to a compression check, external visual inspection, and internal borescope inspection. Cylinders 1, 2 and 4 exhibited no major defects. However, cylinder 3 showed signs of significant damage.
The exhaust manifold of cylinder 3 was heavily soaked with oil and its valve train components showed signs of exposure to combustion gases. Cylinder 3 provided no compression, and an internal inspection showed its upper surface and piston face to be heavily damaged with multiple strike marks and 2 large holes (Figure 2). The exhaust valve had broken off at its stem and was missing, while the valve guide exhibited a small fracture line. Both of the cylinder’s spark plugs had sustained impact damage to their electrodes.
Figure 2: Borescope images of cylinder 3 showing the missing exhaust valve and damage to the piston face
Source: ATSB
Meteorological information
The Bureau of Meteorology reported the visibility at the time of the occurrence as greater than 10 km. The temperature was around 16°C, with a dew point of around 1°C, and an atmospheric pressure adjusted to mean sea level of 1,017 hectopascals.
Both the instructor and student pilot reported that the weather conditions were favourable for VFR flying, with extensive visibility, little turbulence, and only light southerly winds.
Safety analysis
The ATSB determined that the exhaust valve of cylinder 3 impacted the piston surface multiple times, causing damage to the piston, cylinder and spark plugs. This resulted in a sudden loss of compression and subsequent loss of engine power. It could not be determined if the valve had stuck open, resulting in the piston impact and valve fracture, or if the valve fractured prior to impacting the piston.
Following the loss of power, the instructor identified that an off-airport landing was required. The instructor’s prior knowledge of the area and proactive contingency planning helped them identify possible locations. Furthermore, as the engine’s performance continued to deteriorate, they re-evaluated their decision and changed the plan, including shortly before touchdown when it was assessed that there was insufficient clear area ahead.
While the turn away from obstacles prevented a potentially significant frontal impact, it also led to the aircraft contacting the ground with substantial vertical force due to the low remaining airspeed limiting the instructor’s ability to flare the aircraft. Fortunately, the aircraft absorbed the vertical impact, preventing significant injury to the occupants.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following finding is made with respect to the loss of power and forced landing involving Piper PA-28, VH-BUN, 32 km north-north-east of Sydney Airport, New South Wales, on 17 August 2025.
Contributing factor
An exhaust valve in the aircraft's engine failed, resulting in a significant reduction of power and aircraft performance. Subsequently, the pilot in command conducted a forced landing on a golf course.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety actions by operator
The operator undertook the following safety actions after this accident:
Revised the emergency briefing content and formally re-stated the requirement for pre‑impact and evacuation procedures to be briefed by the instructor and confirmed by the student before every flight.
Completed a review of competency in conducting engine failure procedures for all flight instructors and implemented remedial training and enhanced supervision where required.
Commenced a process to check students’ post‑engine failure competencies, including glide path judgement, execution of post‑failure actions, and engine securing checks.
Implemented Drugs and Alcohol Management Plan (DAMP) policy refresher training and increased the frequency of random Alcohol and Other Drugs (AOD) testing across all employees undertaking safety sensitive aviation activities.
Introduced carburettor icing probability assessment as part of the standard pre-flight preparation activities and provided education on the precautionary use of carburettor heat.
Reviewed the on-boarding process for cross-hired aircraft and is consulting with other industry participants to create internal guidance around the use of aircraft with older engines.
Sources and submissions
Sources of information
The sources of information during the investigation included:
pilots of the accident flight
the aircraft operator
the aircraft owner
the maintenance organisation
the aircraft insurer
Airservices Australia
Civil Aviation Safety Authority
New South Wales Fire and Rescue
the Bureau of Meteorology
video footage of the accident flight and other photographs and videos taken on the day of the accident
ADS-B data from Flightradar24.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots of the accident flight
operator of the accident aircraft
owner of the accident aircraft
Civil Aviation Safety Authority.
Submissions were received from:
one of the accident flight pilots
the operator of the accident aircraft
the owner of the accident aircraft.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]The operator’s documentation noted that of the total 190 litre fuel capacity, only 187 litres were usable.
Occurrence summary
Investigation number
AO-2025-049
Occurrence date
17/08/2025
Occurrence time and timezone
14:00 Australian Eastern Standard Time
Location
32 km north-north-east of Sydney Airport
State
New South Wales
Report release date
22/01/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-140
Registration
VH-BUN
Serial number
28-23228
Aircraft operator
Airspeed Aviation
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Departure point
Wollongong (Shellharbour) Airport, New South Wales
Destination
Wollongong (Shellharbour) Airport, New South Wales