On 27 July 2016, at about 0930 Eastern Standard Time (EST), the pilot of a Robinson R22 Beta helicopter, registered VH-HRL (HRL), completed mustering operations at a property about 33 km south of Blackall, Queensland. The helicopter then departed from the property on a ferry flight and tracked towards the pilot’s home about 110 km to the west-northwest. The pilot was the sole occupant of the helicopter.
At about 1002, the pilot’s GPS tracker indicated that the helicopter had stopped moving, about 41 km from its destination and on the helicopter’s direct track. The helicopter had struck a powerline and subsequently collided with terrain. At about 1030, a local landowner notified the energy provider of a power outage. Two line workers from the energy provider later departed from Blackall to determine the source of the power outage.
At about 1500, while inspecting the powerlines in the area, the line workers located the wreckage of HRL. The windshield and right skid of the helicopter had struck the single wire, which was strung east-west across a cleared area, 4.8 m above the ground. The first point of impact of the helicopter was about 31 m beyond the powerline and it then collided with the ground inverted about 18 m further away. During that impact, it appeared that the pilot’s seatbelt sheared through and the pilot was ejected from the helicopter sustaining serious injuries. The wire had been stretched about 30 m, two power poles broke off and another two were pulled out of the ground. The helicopter was destroyed (Figure 1).
The line workers called emergency services using a satellite phone, and remained with the pilot until police and paramedics arrived at about 1700.
Figure 1: Accident site showing damage to VH-HRL
Source: Queensland Police
Accident site
The helicopter struck the powerline in a clearing, mid-span between two power poles about 250 to 300 m apart. The helicopter was travelling across the direction of the powerline.
An aircraft warning marker may be installed on an overhead cable or its supporting structures to warn pilots of their presence. The powerline struck in this incident was not, and was not required to be, marked with aircraft warning markers according to the relevant Australian Standard (AS3891.1).
Based on the forward speed indicated by the distance of the wreckage from the wires, and the marks left in the ground by the helicopter main rotor blades, the helicopter engine was probably producing power at the time it struck the wire.
ATSB comment
Due to the injuries sustained in the accident, the pilot was unable to recall the event or provide any comments for the investigation.
Safety message
Low-level flight carries an increased risk of striking hazards, such as powerlines, many of which are difficult to see in flight. The ability of pilots to detect powerlines depends on many factors, including the physical characteristics of the powerline (such as the spacing of power poles and the orientation of the wire), prevailing weather and light conditions, and the nature of surrounding terrain and vegetation.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 20 July 2016, the pilot of a Schweizer 269C helicopter, registered VH-NTZ, conducted aerial spraying operations near Deloraine, Tasmania.
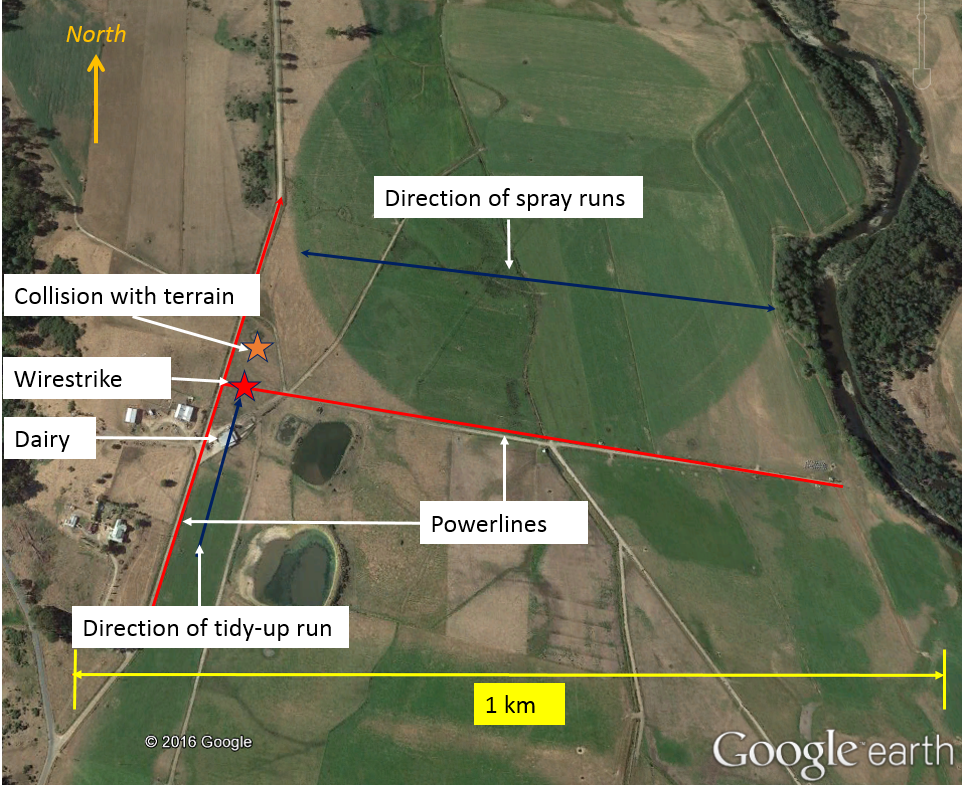
The pilot completed spraying one area, and prior to commencing spraying another, overflew it to assess the site. During that inspection, the pilot sighted two sets of powerlines, one running approximately north-south, and the other branching off to the east. Based on the location of the powerlines and the wind, which was a light northerly, the pilot elected to spray the paddock in an east-west direction (Figure 1). The helicopter was operating north of the powerline running east-west, and in each run, was overflying and remaining clear of the powerlines at the western end of the paddock.
Figure 1: Area of operations showing powerlines
Source: Pilot
At about 1230 Eastern Standard Time (EST), after completing two spray loads, the pilot tracked south over the powerline and turned to conduct a tidy-up run to the north along the road and powerlines running north-south.
After overflying a dairy building, the helicopter descended as the pilot intended to commence spraying. However, the helicopter struck the powerlines running east-west and subsequently collided with terrain.
The pilot, who was the sole occupant of the helicopter, sustained serious injuries and the helicopter was destroyed (Figure 2).
Figure 2: Accident site
Source: Tasmania Police
Pilot comments
Prior to commencing the day’s operations, the pilot had obtained a map of the area and identified hazards including the powerlines. During the aerial inspection of the property prior to commencing spraying, the pilot had sighted those hazards.
The pilot commented that in the tidy-up run they should have been thinking ‘over the dairy and over the powerlines then descend’, but had momentarily forgotten about the powerlines and descended after passing over the dairy. Usually, they overflew the whole paddock again to check for hazards before commencing a tidy-up run, but had omitted to do it on this occasion.
The pilot was wearing a helmet at the time of the accident. The helmet was found some distance from the wreckage and was badly damaged.
Safety message
ATSB research indicates that in 63 per cent of reported wirestrike incidents, pilots were aware of the position of the wire before they struck it.
The Aerial Application Association of Australia (AAAA) suggests a way to keep focus is to ask yourself:
Where is the wire now?
What do I do about it?
Where am I in the paddock?
For further risk management strategies for agricultural operations, refer to the AAAA Aerial application pilots manual.
US military research[1] analysed helicopter accidents that were at least partially survivable. It found that occupants not wearing a protective helmet were significantly more likely to sustain severe and fatal head injuries. The US National Transportation Safety Board (NTSB) also acknowledged that the use of head protection can reduce the risk of injury and death. The NTSB issued Safety Recommendation A-88-009, recommending that crewmembers of emergency medical services helicopters wear protective equipment including helmets.
The ATSB investigation report (AO-2014-058) into an accident involving a Robinson R22 helicopter where the pilot sustained a serious head injury, reminded pilots and operators to consider the benefit of occupants wearing helmets to reduce the risk of head injury.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 25 March 2016, Bell 206B JetRanger helicopter, registered VH-WHU, struck a powerline while spraying cane fields about 5 km south-west of Carmila, Queensland. During the accident sequence, the helicopter’s tail rotor and vertical stabiliser assembly separated from the helicopter. The helicopter collided with terrain and was destroyed by impact forces and a post‑impact fire. The pilot was fatally injured.
What the ATSB found
The ATSB found that the helicopter was equipped with upper and lower wirestrike protection system equipment and four-point safety harnesses. The pilot was wearing an aviation flying helmet. While not preventing fatal injuries on this occasion, these safety enhancements generally reduce risk and increase the possibility of surviving a collision.
The ATSB also found that the inherent difficulty in visually detecting powerlines was exacerbated in this case by the outer two supporting power poles being masked by trees. There was also a low-contrast background that included cane fields, rising terrain and a tree-lined creek. In combination, these features negated a number of visual cues normally associated by pilots with the location of powerlines. This increased the difficulty of the pilot seeing the wires, and reduced the time available to take action once the powerline was located.
Safety message
Aerial application is conducted at low level, where there is an elevated risk of collision with terrain, man-made structures and wildlife. Pilot training, experience, pre-flight preparation and planning and fatigue management are important means to reduce risk.
The Australian aviation industry has invested heavily in an effort to minimise the risk associated with low-level aerial application. This includes the:
the Aerial Application Association of Australia Ltd. (previously Aerial Agricultural Association of Australia Ltd.), which has written a number of manuals (available at www.aerialag.com.au), conducted training in aerial application, facilitated access to available wire databases and taken safety action to increase the high visibility marking of wires
operators, who develop and include risk mitigation strategies in their operations manuals
Civil Aviation Safety Authority, which issues associated regulations, publications (available at www.casa.gov.au), conducts workshops and carries out operator surveillance aimed at addressing the risks associated with low-level aerial application operations
ATSB, which has investigated numerous aerial application accidents and issued public reports in an effort to enhance safety in those operations.
Despite those efforts and requirements, wirestrikes continue to occur in low-level aerial application operations. It is therefore prudent, when planning and/or conducting aerial application operations, for pilots and operators to learn from other occurrences and accidents, and continue to apply that knowledge to reduce risks to their operations.
Photograph VH-WHU
Source: Heli-Central
Sources and submissions
Sources of information
The sources of information during the investigation included the:
operator of VH-WHU
property owner
Civil Aviation Safety Authority
Queensland Police.
References
The Aerial Application Association of Australia Ltd., Application Pilots Manual 3rd edition
Australian Government, Australian Transport Safety Bureau, 2006, Wire-strike accidents in general aviation: Data analysis 1994 to 2004 (Re-released September). Research and Analysis Report – B2005/0055
Gibb, R., Scharff, L. and Gray, R., 2010. Aviation Visual Perception: Research, Misperception and Mishaps (Ashgate studies in human factors for flight operations). Ashgate Publishing Group.
Szczecinski, Dr G. Cable, (date unknown), Aviation Medicine for Aircrew. Royal Australian Air Force Institute of Aviation Medicine.
Veillette, P., 2015. Wire wary: what you don't see can kill, and does. Business and commercial aviation.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the owner of the helicopter, the property owner, the helicopter loader and the Civil Aviation Safety Authority. Submissions from those parties were reviewed and, where considered appropriate, the text of the report was amended accordingly.
The occurrence
History of the flight
At about 1600 Eastern Standard Time[1] on 24 March 2016, the pilot of Bell Helicopter Company 206B JetRanger, registered VH-WHU (WHU), landed at a property 5 km south‑west of Carmila, Queensland in preparation for aerial application agricultural spraying operations. The pilot met the property owner and together they reviewed the proposed operation. This included identifying significant features such as powerlines and property boundaries. A diagram was provided to assist the review.
The pilot and property owner then conducted a 15-minute aerial survey of the area in WHU to locate the features that were previously identified on the diagram. On completion of that flight, the pilot landed, secured the helicopter and retired for the night.
The pilot, property owner and loader[2] for the operation met at the property at about 0545 the next morning. However, local fog delayed the commencement of the application until about 0700. During the intervening period, the helicopter’s hopper was filled with chemicals, the helicopter refuelled and its windows cleaned.
The spraying operations commenced at about 0700 and continued for a total of about 3.5 hours. During this time, the pilot landed and replenished the helicopter with fuel and chemicals 10 times, and was twice observed to leave the helicopter and ‘stretch their legs’. On one occasion, at about 0800, the property owner accompanied the pilot to clarify a section of the property to be sprayed.
At about 1000, the pilot landed and discussed the changing wind conditions with the property owner and loader. It was reportedly agreed during this discussion that the increasing wind would ultimately affect the chemical distribution. The chemicals were again replenished and the pilot decided to suspend operations for the day once the payload on board the helicopter was depleted.
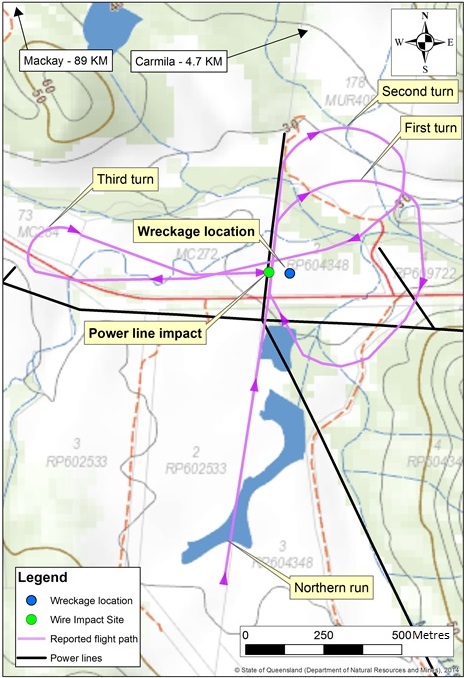
The pilot took off and was observed flying at various locations around the property. The property owner and loader presumed the pilot was conducting ‘clean-up runs’. Shortly prior to the wirestrike, the helicopter was observed flying in a north-north-easterly direction, to the east of and adjacent to the north-south powerline (Figure 1). This line was strung low between three wooden power poles that were located between two sugar cane fields, about 8 m above the ground.
Concerned about the proximity of the helicopter to the powerlines, the loader radioed the pilot and reminded him of their location. The pilot replied ‘powerlines sighted and marked’. The loader continued with the job at hand and the property owner observed the helicopter complete two clockwise circles before tracking to the west, over the north-south powerline. The pilot continued the application to the north and west of the powerlines before turning back towards the east.
At about 1028, the helicopter collided with the north-south powerline (Figure 1).
Initially, the property owner alerted the loader that he thought the pilot was ‘in trouble’. The owner later described the helicopter at that time as being in a nose-up position, ‘hanging’ and making a loud noise. The property owner reported being unsure if the noise was engine or rotor system‑derived. The helicopter then lurched forward and spun clockwise before the property owner lost sight of the helicopter amongst the sugar cane.
The subsequent impact with terrain was not observed by the property owner or loader. There was a post-impact, fuel-fed fire that, despite the efforts of the property owner and loader, could not be readily extinguished. Impact forces and the post-impact fire destroyed the helicopter. The pilot was fatally injured.
Figure 1: WHU’s flight path, as reported by witnesses
Source: State of Queensland (Department of Natural Resources and Mines), modified by the ATSB
Pilot information
It is likely the pilot’s flight logbook was on board the helicopter at the time of the accident and destroyed in the post-impact fire. The operator understood that the pilot had flown 2,870 hours on a number of different helicopter types. An extract of the pilot’s logbook supplied by the operator showed that as of 14 February 2016, the pilot recorded 2,807 flight hours. The extract also showed that the pilot:
undertook ‘Agriculture Rating training’ on the second and third of August 2014 that included 3.7 flight hours of flight time
underwent a 1-hour ‘Agriculture II flight test’ on 4 August 2014
completed a 1-hour ‘Aerial Application rating proficiency check’ on 22 September 2015
performed 3.7 flight hours Aerial Seeding application on 24 September 2015.
The ATSB understood from the operator that the pilot also flew WHU for 4 days preceding the accident including ferry flights and 2 days aerial application of about 110 hectares under the direct supervision of the operator.
It is possible that the pilot flew additional aerial application hours prior to the accident as there was a period of 42 days between the last log book entry and the accident. Given the available evidence, this could not be confirmed.
The pilot held a current Class 1 Civil Aviation Medical Certificate with the following restrictions when exercising the privileges of the pilot’s licence:
distance vision correction was to be worn
reading correction was to be available.
Three pairs of heat-damaged sight correction glasses were identified in the helicopter wreckage. The ATSB could not determine if these included the pilot’s distance correction glasses or whether the pilot was wearing distance correction glasses leading up to the wirestrike.
The ATSB considered the potential for pilot fatigue to have influenced the development of the accident. This included a review of the pilot’s 72-hour history prior to the flight that day. Based on the available information obtained from witnesses and the operator, there was insufficient evidence to assess whether fatigue was a factor.
Weather, terrain and sun position
There was no Bureau of Meteorology weather station in the vicinity of Carmila. The closest aviation weather information was available from Mackay Airport, Queensland, about 85 km to the north of Carmila. Daily automatic weather observations were available from St Lawrence, approximately 50 km to the south of Carmila.
The 0900 observation at St Lawrence on the day of the accident recorded the following data:
temperature – 27.1˚C
relative Humidity – 64 per cent
cloud – Nil
wind Direction and Speed – east-south-easterly at 9 km/hr[3]
mean Sea Level Air Pressure – 1017.9 hPa.
At 1030 that day, the azimuth[4] of the sun was 48°32’20’’ and its altitude[5] 56°05’30”. During the flight, the pilot was wearing an aviation helmet that was fitted with a retractable sun shield. If lowered over the eyes, the sun shield was designed to reduce glare. Although the position of the pilot’s sun shield preceding the wirestrike was unable to be determined, the position of the sun was such that the potential for it to have been a factor in the wirestrike was minimal.
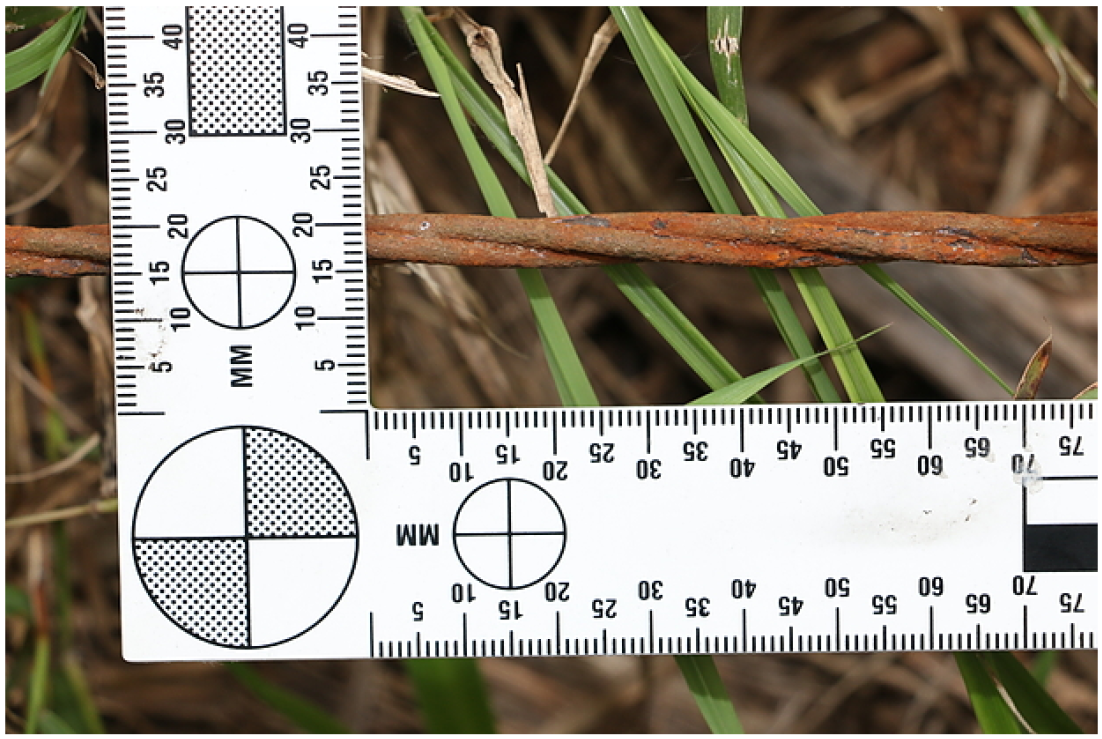
Powerline and poles
The area being sprayed was divided by powerlines that consisted of three cables, each made from three steel wires twisted together (Figure 2). The powerline that was struck by WHU was strung north‑to‑south, rusted and supported by three power poles over a distance of about 386 m (Figure 1). The poles to the north and south were located between tall trees (Figure 3). The centre of these poles was estimated to be about 3–4 m higher than the surrounding cane fields and was situated in a north–south clear area that was used as an access road.
Given the approximate 8 m height of the centre pole, and the normal spraying height of the helicopter, there was the potential for the pole to have been masked by the trees and rising terrain to the east of the powerline. The powerlines were not marked with visibility devices, nor were they required to be by regulation.
Figure 2: Power cable consisting of three steel wires twisted together (note the rust-like discolouration)
Source: Queensland Police, modified by the ATSB
Figure 3: Terrain in the vicinity of the powerline, showing the helicopter’s direction of travel and the powerline and associated poles. Note the power pole that has been pulled down as a result of the wirestrike (centre of the picture) and the tree-lined creek that tracks right to left (located towards the top of the figure)
Source: Queensland police, modified by the ATSB
Guidance to aerial application pilots
The difficulty associated with identifying electrical and other wires and cables during aerial application operations is an acknowledged occupational hazard in the aviation industry. The Aerial Application Association of Australia Ltd.[6] stated in their 3rd edition of the Aerial Application Pilots Manual that:
The pilot usually locates the wires by observing the run of the poles, thus establishing a mental picture of the treatment area in plain view i.e. by looking down on it. However, the actual treatment is undertaken close to ground level, where horizontal views are used to establish relationships between obstacles – an entirely different situation. There is plenty of scope for misjudgment. There is also a limit to the amount of attention a pilot can divert from maintaining a precise flight path to any obstacles, they must also consider. Therefore, great care must be exercised in transferring from ‘plan view’ to ‘elevation view’. In addition, the background to the wires - trees, hills etc. - may be concealed by intervening obstacles or by being so far towards the periphery of the pilot’s visual field that they are not noticed. Thus, to state the obvious, wires are very hard to see and their height and distance is not easily determined.
Human performance at low-level
Visual cues during low-level visual flying
Flight at low-level is widely acknowledged to be a demanding task, particularly in terms of processing the associated visual information. A key influence on the risk of a wirestrike in that environment is the pilot’s visual acuity given the environmental conditions.
A number of variables affect a pilot’s ability at any one moment to see and avoid powerlines. In this regard, Gibb and others (2010) describe the difficulty in seeing objects with varying contrast backgrounds where:
…an object’s visibility is affected by differences in its luminance contrast and differences in texture between the object and its surroundings. In general, more luminous and/or texturally-different objects are easier to discern from their background.
The near invisibility of wires results from a number of factors in addition to their size. These include atmospheric conditions, cockpit ergonomics, viewing angle, sun position, visual illusions, pilot scanning abilities and visual acuity, flight deck workload, and the camouflaging effect of nearby vegetation, among others. Even the condition of the aircraft’s transparencies, whether pitted, deteriorated with age, or dirty from dust or bug strikes, will significantly affect the pilot’s ability to see wires [and] depending on the lighting situation and background, lines can be obvious or invisible, and change from moment to moment.
and that:
Older wires may be difficult to see because their colour often changes with age….A wire that is perfectly visible from one direction may be completely invisible from the opposite. The exact location of specific wires may change throughout the day because of fluctuating ambient temperatures, which may cause wires to sag or tighten. Sagging wires may also be blown by the wind.
Perception and reaction time
Szczecinski (date unknown) listed the following times taken to recognise and react to a hazard:
It takes a finite amount of time for an object to be detected, recognised, a decision made on an action, and then for that reaction to be initiated. Table 1 lists the expected times for these events to happen. It can take up to 5.5 seconds for the process to be completed.
Table 1. Perception and reaction time
Process
Time (Seconds)
Detect, visualise, recognise
1.0
Decide what to do
2.0
Initiate action
2.5
Total
5.5
Aircraft information
The Bell 206B is a single main and tail rotor-equipped helicopter that is powered by a gas turbine engine and has skid-type landing gear. WHU was fitted with chemical spray equipment and a wirestrike protection system.[7]
Wreckage and impact information
The accident occurred in an area where the sugar cane was about 3 m high. The terrain was flat, but rising towards the east, which was the direction of flight leading up to the wirestrike. Trees lined a creek that spanned from the east to the west of the property.
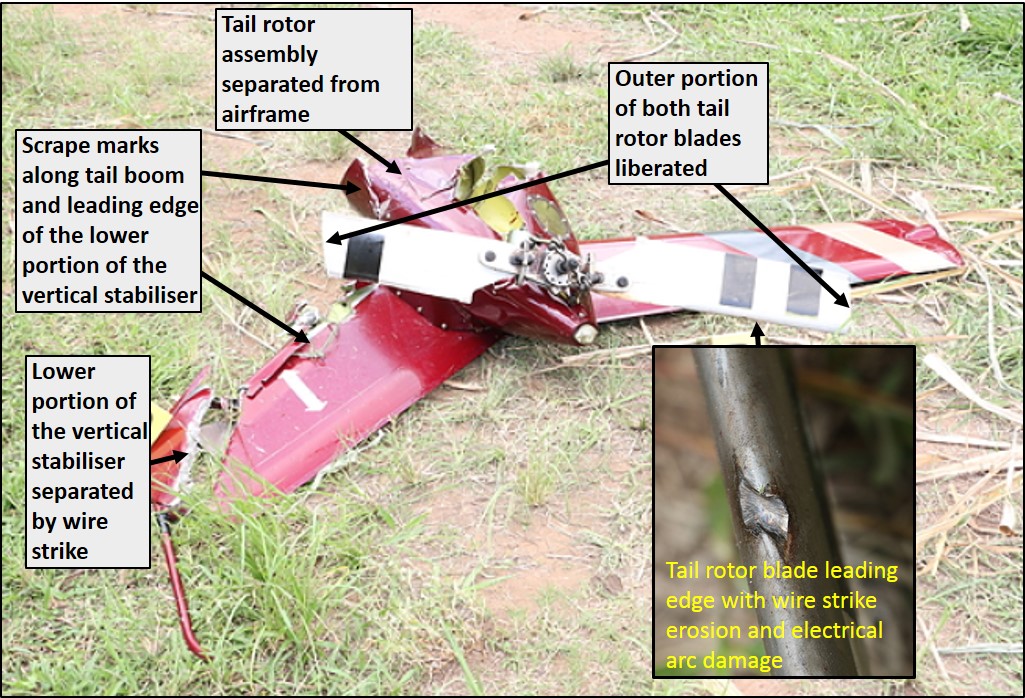
The vertical stabiliser and tail rotor assembly fractured from the boom during the accident sequence and were found about 30 m from the main helicopter wreckage. Scrape marks and gouging identified along and around the tail rotor section was consistent with colliding with a wire.
The lower portion of the vertical stabiliser displayed uneven, high-energy impact damage. The composite structure was abraded, roughened and had separated from the vertical stabiliser assembly. This was consistent with one of the powerline cables ‘pulling through’ the stabiliser during the impact sequence. The outer portions of both tail rotor blades were fractured and gouged, also consistent with colliding with one of the power line cables before separating from the tail rotor assembly (Figure 4). The liberated outer portions of the tail rotor blades were not recovered.
The helicopter’s structure, including the fuselage and cabin, was significantly compromised from the collision with terrain and post-impact fire. However, despite that damage, continuity of the flight control system was established.
An internal examination of the engine and gearbox confirmed continuity of the power and compressor sections of the engine and the drive to the gearbox. Each was likely capable of normal operation prior to the collision.
Evidence of the transmission of engine power from the gearbox to the main and tail rotors was identified. Fracture of the main rotor pitch links and torque twisting and fracture of the tail rotor drive shaft were consistent with the engine driving the rotor system during the impact sequence.
In summary, the damage to the helicopter was consistent with a wirestrike, followed by a collision with terrain and post-impact fire. No pre-existing defects, including cracks or fractures that may have contributed to the accident, were identified.
Figure 4: Separated tail rotor assembly, showing the liberation of the outer portion of both tail rotor blades, electrical arcing to the leading edge of one tail rotor blade (at inset) and the separated lower portion of the vertical stabilizer
Source: Queensland Police, modified by the ATSB
Research
The ATSB Avoidable accidents No.6 Experience won’t always save you, Pilot experience is not always a protection against an accident highlighted that:
Experience alone can never compensate for high-risk activity.
Sound decision-making and experience are not necessarily synonymous.
Using pilot experience as mitigation for potential operational risks is inadvisable. If the risks are unacceptable for a qualified and competent pilot, there should be no reason for an experienced pilot to find it otherwise.
In aviation, pilot’s need to attend to the three Cs- compliance, communication and complacency, and all the other human performance considerations. Experience cannot overcome the mental and physical limitations of humans.
Experienced pilots who accept higher risks may not be as safe as a pilot with much less experience flying comfortably within the limits of his or her competency
In some accidents, the pilot’s vast experience was found to have perhaps even led to decisions that, in hindsight, were riskier than necessary.
On the day prior to the accident, the pilot flew to, and landed VH-WHU (WHU) at the property in preparation for the next day’s aerial application activity. The pilot and property owner used a map to review the area of operations, prominent landmarks and the electrical power distribution network in the area to be sprayed. The pilot and property owner then boarded WHU and surveyed the area from the air.
The pilot was appropriately qualified to command WHU and was endorsed to perform aerial application in the helicopter. However, in respect of the pilot’s aerial application qualification, the ATSB could not establish the pilot’s flight hours and current experience prior to the accident.
The operation that day
After an initial delay due to fog, the pilot flew about 3 hours aerial application in weather conditions that were described as ‘suitable’. This included the relatively light winds that were ideal for distributing the aerial chemicals. The pilot landed WHU about 10 times to replenish the chemicals and fuel. During two of these replenishments, the pilot left the helicopter to stretch their legs. The operator, loader and property owner reported that, before and during the operation, the pilot appeared to be in good health. No issues with the pilot or operation were reported.
About 30 minutes prior to the accident, the pilot landed and discussed the changing wind. It was decided that the next flight load would be the last for the day, as the wind was increasing.
The pilot was aware of the powerlines, having flown along and over them directly before the wirestrike. In addition, the loader alerted the pilot as to the proximity of the powerlines by radio. The pilot acknowledged this call, responding that the ‘powerlines [were] sighted and marked’.
The wirestrike
Despite the pilot’s awareness of the powerlines, as outlined by Veillette (2015), ‘being aware of a wire is still no guarantee of avoiding it’. That is, the pilot’s prior knowledge of the location of the powerlines did not assure their detection, and therefore avoidance, on each approach. Factors likely making visual detection of the wires difficult included that the:
outer supporting power poles were obscured by trees as the pilot approached them, negating one of the visual cues often used by pilots to locate powerlines
luminance of the power cables was reduced by their rust-like discolouration, reducing the likelihood of their detection by the pilot
powerlines were not marked, and were not required to be marked, with visibility devices
contrast in texture between the background and the powerline was decreased, including by a sugarcane field, rising terrain and a tree-lined creek. In combination, these features resulted in a camouflaging effect.
Those factors decreased the likelihood that the pilot would detect the north-south powerline in sufficient time to avoid the wirestrike. The ATSB could not quantify the extent to which the presence of visibility devices might have influenced the earlier detection of the powerline.
Evidence of scraping along the tail boom, the damage to the lower vertical stabiliser and the separation of the outer portion of the tail rotor blades indicated that WHU struck the powerline in a nose-up attitude. This would be consistent with the pilot taking action to avoid a wirestrike, but likely contributed to the wire passing underneath the lower component of the helicopter’s wirestrike protection system and striking the tail rotor and stabiliser assembly. The tail rotor and stabiliser assembly separated from the helicopter’s tail boom, resulting in a loss of directional control and a change in the helicopter’s centre of gravity. This would explain the property owner’s description of the helicopter lurching forward and spinning clockwise, contributing to the loss of control by the pilot.
Findings
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain that occurred about 5 km south-west of Carmila, Queensland on 25 March 2016 and involved Bell 206B helicopter, registered VH-WHU. They should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
During aerial application at low altitude, the helicopter collided with powerlines while in a nose up attitude, consistent with the pilot attempting to avoid the powerlines. The tail rotor and vertical stabiliser assembly separated leading to a loss of control and collision with terrain.
The masking of the outer two power poles by trees and the ‘camouflaging’ effect of the low contrast background cane fields, rising terrain and tree-lined creek reduced the available visual cues on the location of the powerline. This increased the pilot’s difficulty in maintaining visibility of the powerline.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 20 February 2016, the pilot of a Robinson R22 helicopter, registered VH-LYW, was conducting aerial cattle mustering operations on a property about 88 km northeast of Roma, Queensland.
The pilot had mustered in that paddock several times previously, and was aware of a set of high voltage transmission wires that had been erected across the property in the previous 12 months.
Prior to commencing mustering, the pilot overflew the paddock, sighted the powerlines and formed a plan to muster the cattle from north to south, giving due consideration to the wires running east-west. The pilot then mustered the mob from north to south, and the helicopter remained above the wires during that time.
The pilot then saw two bullocks hidden in scrub, near a dam that was situated near to and just south of the powerlines, and returned to muster them up. The helicopter then descended below the level of the wires. The cattle would not turn back, so the pilot radioed a musterer on horseback to assist. The pilot turned the helicopter to leave the area as the horse and rider arrived. The pilot then saw another vegetated area near the dam, where cattle may be hidden from view, and flew the helicopter towards it.
While the pilot’s focus was on searching for cattle in the scrub below, the helicopter neared the powerlines. The pilot’s attention suddenly returned to the wires, and sighting them close in front at the same level, immediately commenced a near-vertical climb to try to avoid them. As the helicopter climbed, the pilot assessed that it was not going to clear the earth wire, and lowered the nose of the helicopter in an attempt to pass below the earth wire and above the other wires. The tail rotor blade struck the earth wire.
The helicopter was vibrating and the pilot turned it away from the wires. The tail rotor then failed and the helicopter yawed around. The helicopter descended rapidly and continued to rotate. The pilot entered an autorotation, and closed the throttle, overriding the governor. As the helicopter neared the ground, the low rotor revolutions per minute warning horn sounded, and the pilot raised collective[1] to try to cushion the landing. The helicopter collided with the ground nearly upright, and sustained substantial damage (Figure 1). The pilot was seriously injured.
Marking of overhead cables
The Australian Standard (AS) 3891.2-2008 Air navigation – Cables and their supporting structures – Marking and safety requirements, specified requirements for permanent and temporary marking of overhead cables and their supporting structure for visual warnings to pilots of aircraft involved in intentional and legal low-flying operations. The AS included examples such as powerlines in areas where aerial agricultural activities took place. An Appendix to the AS stated that markers should be installed where regular low-level flying operations take place, and that the responsibility for requesting their installation rests with the person requesting the planned low-level flying operations.
Additionally, other than for low-level flying, Part 1 of the AS 3891.1Permanent marking of overhead cables and their supporting structures for other than planned low level flying,stipulated that any section of cable that had a height in excess of 90 m above a road, railway or navigable waterway should be marked. Cables above 90 m located in other places should be marked if they had a continuous span greater than 50 m.
Pilot comment
The pilot reported feeling substantial operational pressure to ensure no cattle were missed. They commented that this may have increased focus and attention on looking for cattle, and therefore momentarily lost awareness of the powerlines.
Figure 1: Accident site showing damage to VH-LYW
Source: Queensland Police
Safety message
Pilots and operators are reminded that they can ask the property owner and power company to have a wire marked if it presents a hazard to low-level operations, even if it is not required to be marked according to the Australian Standard due to its height and span.
ATSB research indicates that in 63 per cent of reported wirestrike incidents, pilots were aware of the position of the wire before they struck it. In this instance, the pilot was aware of the powerline, however, the pilot’s attention was diverted to looking for cattle, and they did not maintain awareness of the wires.
The Aerial Agricultural Association of Australia suggests a way to keep focus is to ask yourself:
Where is the wire now?
What do I do about it?
Where am I in the paddock?
For further risk management strategies for agricultural operations, refer to the Aerial Application Pilots Manual.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 14 February 2016, the pilot of a Robinson R44 helicopter, registered VH-HXY, conducted a local private flight from a property about 90 km north of Hughenden, Queensland.
After operating for about 1 hour, the pilot landed near a water trough to check a float. During the approach and landing, the pilot sighted powerlines strung across the trough, and manoeuvred to remain clear of them.
While the helicopter was on the ground, the wind veered from a south-west to a southerly direction, so that to take off into wind, the helicopter would track perpendicular to the powerlines. After completing the pre-take-off checks, the pilot turned his attention to a mob of cattle, to ensure the noise of the helicopter would not send them through a fence.
The helicopter lifted off initially parallel to the powerlines, and the pilot then turned the helicopter to manoeuvre around a tree and climbed to about 20 ft above ground level. The tree momentarily obscured the powerlines and the pilot’s attention was on the cattle.
As the helicopter rounded the tree, at an airspeed of about 50 kt, the skids struck the powerlines. The pilot heard the wires contact the helicopter and it decelerated rapidly. The pilot lowered the collective[1] and pulled back on the cyclic[2] control, but the helicopter rolled forwards over the wires, descended rapidly, and collided with the ground left side down in a nose-down attitude.
The wire was hooked on the helicopter’s right skid, with electrical power still running through it. After the blades stopped turning, the pilot exited the helicopter. The pilot was not injured and the helicopter was destroyed (Figure 1).
Figure 1: Accident site of Robinson R44 helicopter, registered VH-HXY
Source: Helicopter owner
Safety message
ATSB research indicates that in 63 per cent of reported wirestrike incidents, pilots were aware of the position of the wire before they struck it. In this instance, the pilot was aware of the powerline however, they were unable to see the wires from the helicopter’s position on the ground due to a tree. The pilot’s attention was then diverted to the cattle and did not maintain awareness of the wires.
The Aerial Agricultural Association of Australia suggests a way to keep focus is to ask yourself:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 7 February 2016, the pilot of a Kavanagh G-450 balloon, registered VH-RUW, conducted a 30-minute scenic flight from Mareeba, Queensland with 18 passengers on board.
Shortly before 0627 Eastern Standard Time (EST), the balloon approached the target landing area. The pilot referred to his iPad, which showed the location of the balloon and a set of powerlines strung across the paddock. The balloon was then about 30 ft above ground level, travelling at a ground speed of 7 kt, with a descent rate of 50 ft per minute. The pilot confirmed that all the passengers were in the correct landing position.
The pilot sighted two power poles either side of the landing area, but was unable to see the wires. The pilot estimated where the wires would be based on the crossbars on the poles, and assessed that the balloon had sufficient height to pass over the powerlines. The pilot then sighted the powerlines, about half a metre ahead of and below the basket. The pilot applied all four burners to try to climb and avoid the powerlines, but the left side of the basket contacted one wire, breaking it. The pilot heard a loud fizzing noise and immediately realised they had struck a powerline.
The pilot checked that the passengers were all ok and still in the landing position, and checked that there was no evidence of fire. Due to the amount of heat in the balloon, the balloon was climbing. The pilot then conducted a normal controlled descent and landing into a paddock about 500 m beyond the original planned landing site. The balloon landed without further incident and no one was injured. The wicker basket sustained scorching (Figure 1) and a stainless steel cable fixed to the underside of the basket sustained arc damage.
Figure 1: Scorch marks on wicker basket
Source: Balloon operator
Landing site
The balloon operator and the pilot had used the paddock on many occasions for both launching and landing.
The balloon’s track crossed the powerlines at an angle (Figure 2). As the balloon approached the wires, the pilot lost sight of the pole to the left and used the pole on the right to gauge their height. However, the left pole was situated on a hill and higher than the right pole, and the wires sloped upwards from the right pole to the left. The pilot’s assessment of sufficient height was based on the lower pole; consequently, the left side of the basket struck the wires to the high side.
The powerlines were difficult to see as the area was heavily vegetated. The sun was to the right of the balloon and did not affect the pilot’s vision of the wires.
Figure 2: Balloon track and location of powerlines
Source: Balloon operator
Powerlines and markings
The balloon operator used the following strategies to improve powerline awareness:
The operator had developed an iPad application which pilots used in-flight as an early powerline warning system, which showed all of the powerlines on a google earth map, and the balloon’s current location. The energy company provided updates to the location of the powerlines at six monthly intervals.
The operator maintained a map of powerlines identified by the company pilots to be of low visibility. These were highlighted on the application to draw pilots’ attention.
Company pilots were required to visit the site of identified low-visibility powerlines to familiarise themselves with the location of the lines.
In addition, ground personnel were expected to identify from the ground any powerlines in the balloon’s flight path, which may pose a risk to the balloon on approach to land, and to confirm that the pilot was aware of the lines and their location.
The balloon operator had designated the powerlines at the site to be low-visibility, and had paid the energy provider to fit white marker flags with a reflective green centre to the wires to increase the pilot’s ability to see the lines (or flags). Despite being clearly visible from the ground, the pilot was unable to see the flags. This may have been due to the effect of the wind deflecting the flags at an angle, and possibly their colour.
Pilot comments
Two other balloons had already landed in the paddock. The pilot elected to fly on rather than conduct an emergency descent after the wirestrike, because a high rate of descent from that height carried a risk of injury to the pilot and passengers, and to avoid a collision with the balloons that had landed ahead.
Safety action
Balloon operator
As a result of this occurrence, the balloon operator has advised the ATSB that they are taking the following safety actions:
Review of powerline markings
The operator is investigating the installation of more visible three-dimensional powerline markings such as balls.
Communication to company pilots
The operator will circulate a copy of their investigation report and findings to all company pilots. Pilots are reminded to consider the possibility of sloping powerlines and apply an appropriate clearance margin when overflying them.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Aviation Short Investigation Bulletin - AB-2016-044
On 27 July 2015, the pilot of an Eagle DW1 aircraft, registered VH-FHP, was conducting aerial spraying operations on a property about 77 km southeast of Townsville, Queensland. The pilot completed aerial spraying of two paddocks, and then loaded the aircraft with about 450 L of chemical (about half capacity), and half a tank of fuel.
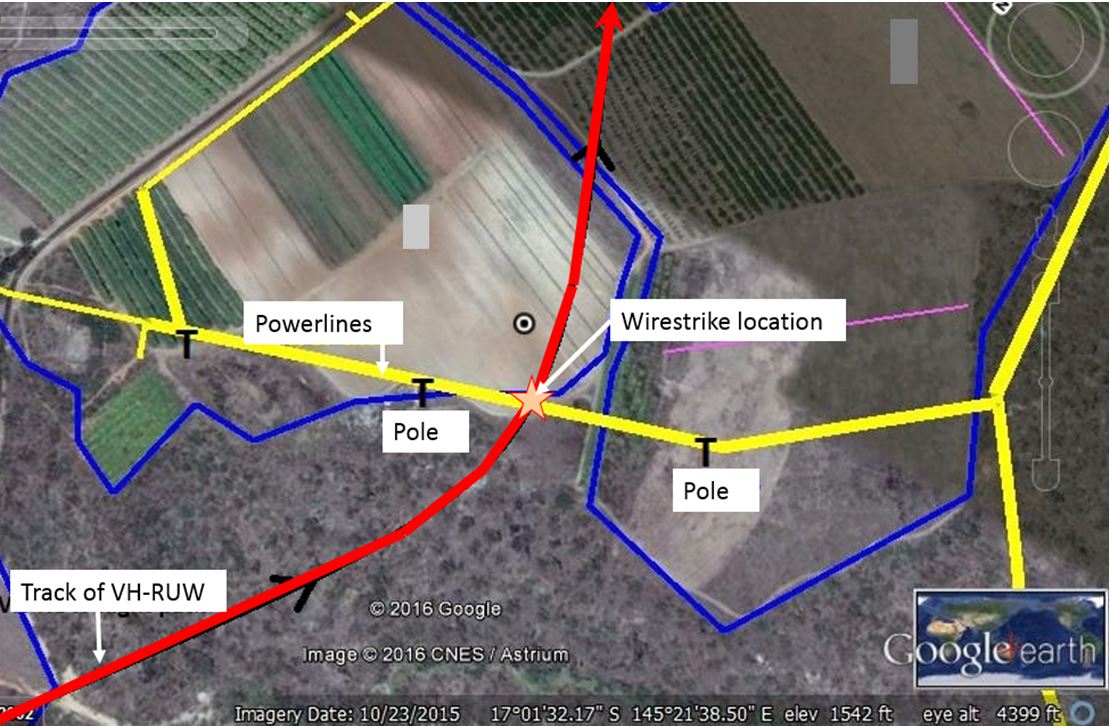
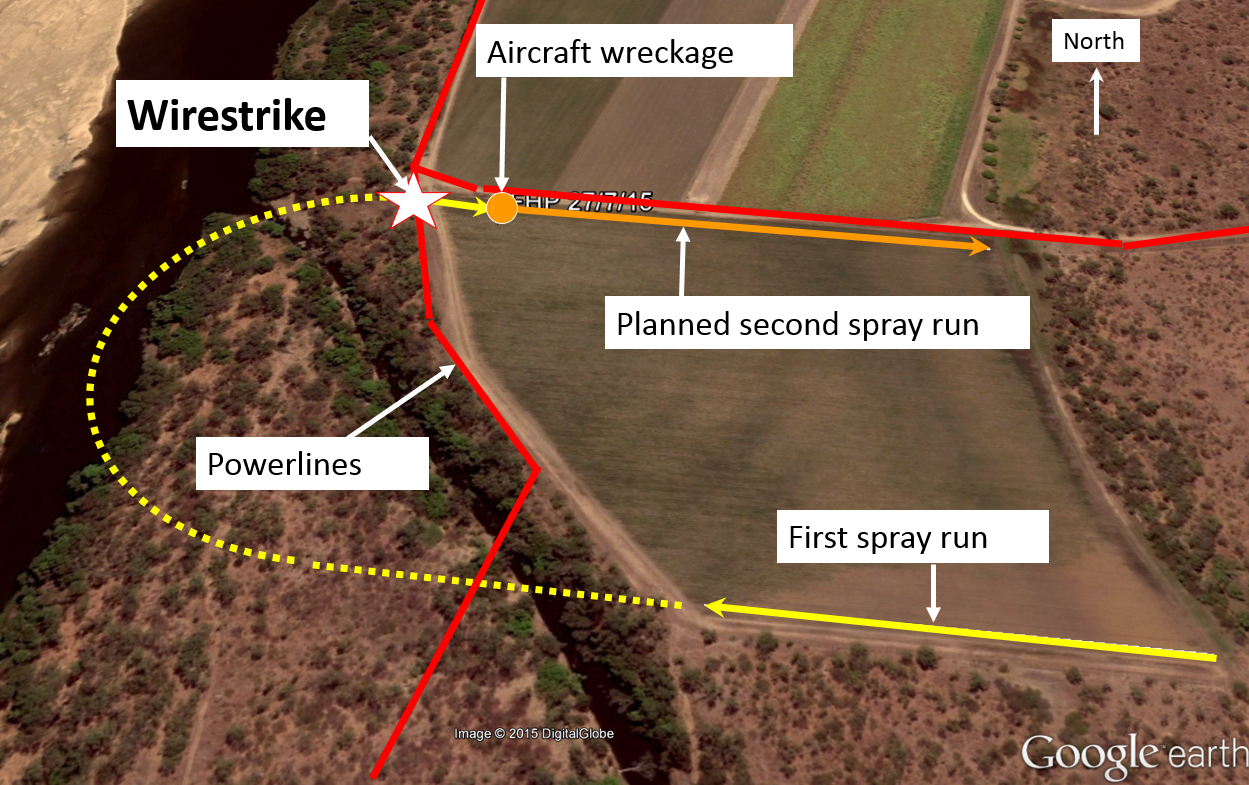
At about 0930 Eastern Standard Time (EST), the pilot took off to spray the third paddock for that day. The pilot overflew the paddock and identified two sets of powerlines. The pilot formed a plan to spray the paddock using a racetrack pattern and flying it in a clockwise direction. One set of powerlines ran parallel to the spray direction, and the other ran across it at the western end. There was a line of trees along the western powerline, which obscured vision of the power poles.
The pilot completed the first spray run towards the western powerline, overflew it, and then turned to line up for the second spray run (Figure 1). A small area of about 30 m of trees had been cleared for a pump installation and the clearing was in line with the start of the second spray run. The pilot noted the powerline ahead, but then diverted their attention to the other powerline, running parallel to the direction of flight, and about 5 m off the left wingtip. The pilot also looked inside at the GPS to check the aircraft’s line for the spray run.
Figure 1: Paddock to be sprayed showing powerlines and wirestrike location
Source: Google earth and the pilot of VH-FHP – annotated by the ATSB
The pilot commenced the descent into the paddock through the clearing in the trees and did not see the powerline at that time. As the aircraft descended, the pilot looked up and suddenly sighted the powerline. The pilot elected to push forwards on the controls to make the aircraft descend. The aircraft then struck the powerline above the propeller on the wing struts.
After the aircraft struck the wires, it yawed violently to the left. The pilot used the right rudder to turn the aircraft away from the other powerlines, and the force of the aircraft pulled the transformer off the power pole on the left. The aircraft then yawed to the right. The force broke the power pole on the right and severed the powerline.
The aircraft decelerated rapidly, and the wires pulled the aircraft towards the ground. The pilot landed the aircraft with the wings level. The landing gear sheared off, the propeller struck the ground and the aircraft ground-looped, coming to rest facing the opposite direction. The pilot sustained minor injuries and the aircraft was destroyed (Figure 2).
Figure 2: VH-FHP at the accident site showing damage to the aircraft and wires
Source: Aircraft operator
Pilot comments
The pilot provided the following comments:
The pilot had sprayed that paddock once previously, and had used an anticlockwise racetrack pattern. On that occasion, as the power poles were on the eastern side of the trees, they were more visible from that direction.
The pilot elected to descend after sighting the powerline, to prevent the landing gear from potentially catching on the wires and flipping the aircraft over.
The aircraft had a wire cutter on the undercarriage and a wire deflector between the top of the wing and the tail, but not on the struts where the wire struck.
The powerlines were three phase.
Safety message
The pilot was aware of the powerline the aircraft collided with, but did not have it front-of-mind at the start of the spray run. The pilot’s attention was diverted to other powerlines, parallel to the direction of flight, and also inside the aircraft to the GPS. The pilot reported that stating aloud ‘powerlines ahead’, would have helped to maintain awareness of the wires.
The Aerial Agricultural Association of Australia suggests a way to keep focus is to ask yourself:
The ATSB research report Aerial application safety: 2014-2015 year in review, stated that aerial application operations have a high accident rate relative to other aviation sectors. These operations involve inherent risks. Those risks include low-level flying, high workloads and obstacles such as powerlines. More than half of the total accidents and serious incidents over the past 10 years were wirestrikes.
The report also stated that it is important to constantly monitor the environment, so the hazards that were identified in pre-planning can be recognised and avoided. If a pilot is not specifically looking for a hazard, it is unlikely they will notice it.
The ATSB investigated a similar accident, involving a Robinson R66 helicopter. A copy of that report is available here: AO-2014-142.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The pilot was spraying a cotton crop with insecticide. Although he had not sprayed the field for about 12 months, he remembered a power line traversing it but could not remember if he had flown over or under the wire previously. On this occasion he elected to fly under it, however, as the aircraft passed under the wire it snagged the rudder. The pilot reported that the aircraft remained controllable, but the rudder was jammed to the right. He slowed the aircraft to 70 knots to reduce the effectiveness of the rudder but was unable to reduce the extreme right yaw.
He decided to return to the town airstrip where better facilities were available and advised the police of his problem by radio. He was subsequently able to land the aircraft without further incident. Inspection later revealed that the rudder horn had been severely damaged, jamming the rudder. The power line was reported to be 3 metres above ground level where the strike occurred.
The pilot reported that the glider collided with power lines during an outlanding, cartwheeled and landed inverted. The pilot was trapped for thirty minutes before being able to free himself. The accident occurred at the end of a 500km distance badge attempt. The pilot, who was visiting from England, had assessed his position over the Warby Hills as being satisfactory for a final glide into Benalla.
After leaving Warby Hills he encountered sink and diverted to land on a known emergency landing strip on the north shore of Lake Mokoan. The sink was heavier and more persistent than expected and the pilot had to manoeuvre to land in a field short of the emergency strip. The pilot noted power lines on the approach, however the sink was such that he was unable to avoid colliding with them.
Significant Factors
The following factors were considered relevant to the development of the accident:
1. The pilot was forced to carry out an outlanding.
2. The pilot misjudged the approach.
3. The pilot was unable to avoid power lines on the approach.
While spraying ICI insecticide known as "Karate" the aircraft collided with a powerline and overturned. At the time of impact, the pilot was flying a swath run at about one metre above the crop in a southerly direction over a 220-acre paddock. Visibility was good. The pilot had no idea that the wire was there. His first knowledge of it was when the aircraft hit the wire.
This wire had not been detected during the initial airborne inspection of the paddock prior to commencement of spraying. Other wires had been detected. The span was about 150 metres. The pilot was splashed in the face with some of the poisonous chemical (S7) but was able to flush his eyes with water very soon after the accident. However, his face did suffer burns similar to sunburn.
Significant factors
The following factors was considered relevant to the development of the accident:
1. The pilot had not detected the powerline during his initial inspection of the paddock prior to spraying.