Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 6March 2026 at 0915 local time, a Bell 206L-3 was being used for dispensing operations (agricultural spraying) at a location 40 km north-west of Orange Airport, New South Wales, with only a pilot on board.
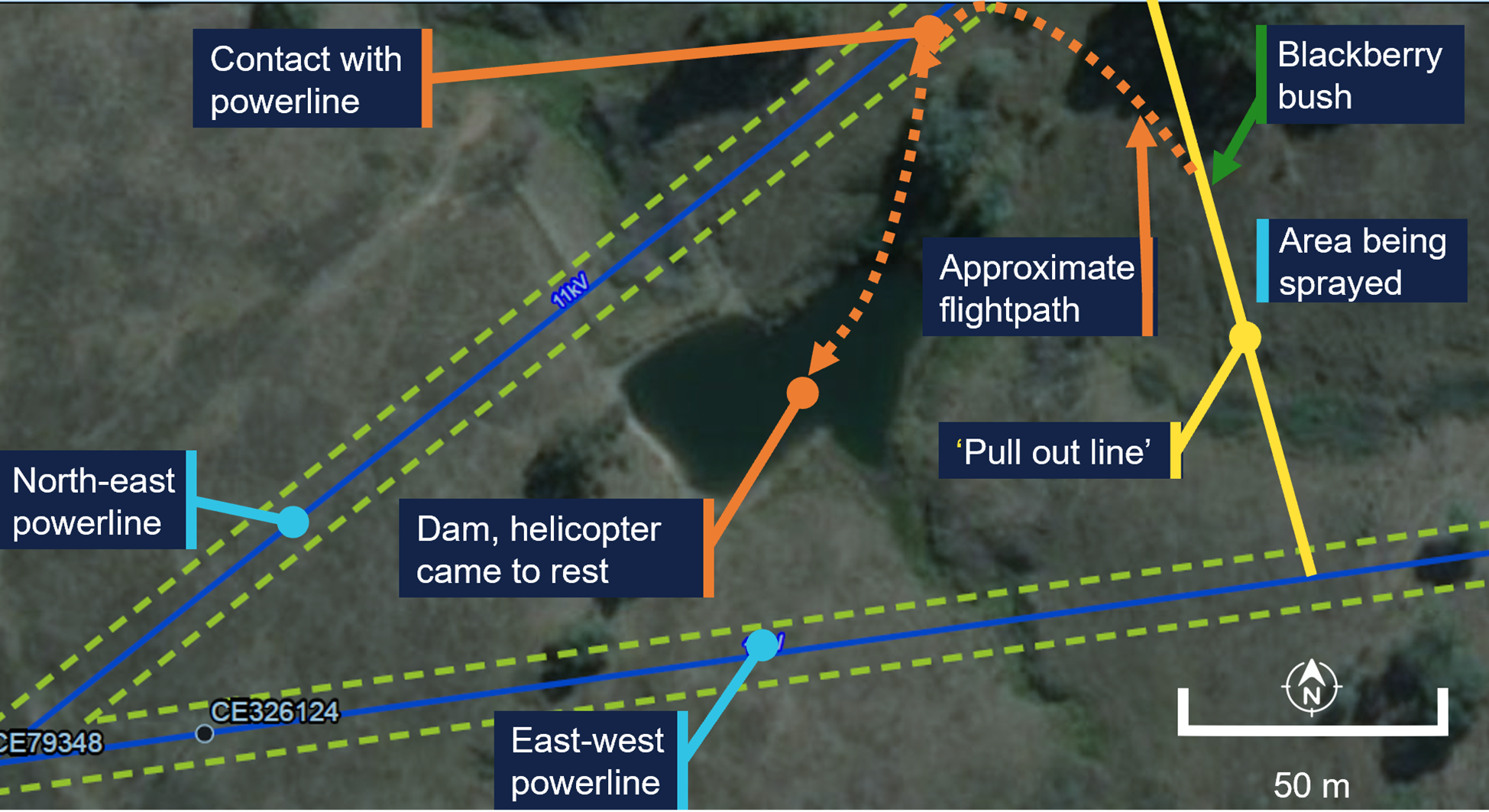
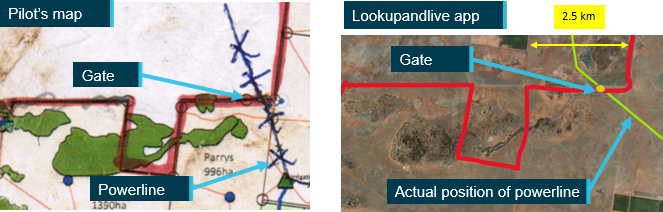
The spraying was being conducted in proximity to unmarked powerlines orientated east‑west and north-east (Figure 1). The area to be sprayed was to the east of a designated ‘pull out line’ that acted as a planned limit of operations. The pilot had identified the location of both the powerlines prior to commencing operations.
Figure 1: Area of operation
Green dotted lines mark the exclusion zone, as defined by the infrastructure owner. Source: Earthstar Geographics, annotated by the ATSB
The pilot reported that during dispensing, they deviated from the planned spray path to conduct an unplanned task: to spray some nearby blackberries they had identified.
Once this unplanned task was completed the pilot commenced a turn and the helicopter made contact with the north-east powerline, which had 3 wires.
The wire cutting kit fitted to the helicopter successfully cut 2 of the 3 wires. However, the third wire struck the main rotor and tail boom. The helicopter descended with some controllability until approximately 5 m above the ground, at which point controllability became difficult. The pilot reported their focus was on keeping the helicopter level and ensuring it did not roll over. The pilot was unable to reach a suitable emergency landing area and conducted a partially controlled ditching into a nearby dam.
Once the helicopter came to rest in the dam it began to roll towards an inverted position. The pilot exited the aircraft as it was rolling and swam to the edge of the dam.
The pilot’s helmet was struck during the accident, and the pilot was not injured. The helicopter sustained substantial damage (Figure 2).
Figure 2: Damage to helicopter, shown after recovery from the water
Source: Helicopter operator, annotated by the ATSB
Safety message
Pilots and operators need to be aware that when a plan is changed new risks can be introduced. This is especially critical for low level operations where previously identified hazards may be subsequently overlooked.
Aerial powerlines pose an ongoing threat to flying operations. In Queensland, New South Wales, Victoria, and South Australia, the Look up and live website or app can be used by pilots to plan flying operations in proximity of overhead powerlines.
Electrical power and telecommunications companies in Australia can mark powerlines that are identified as a hazard for low-level flying operations. The ATSB has released an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028AR-2011-028). This booklet contains several examples of wirestrike accidents and lessons learned from them.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-016
Occurrence date
06/03/2026
Location
41 km north-east of Orange Airport
State
New South Wales
Occurrence class
Accident
Aviation occurrence category
Ditching, Wirestrike
Highest injury level
None
Aircraft details
Manufacturer
Bell Helicopter Co
Model
206L-3
Sector
Helicopter
Operation type
Part 138 Aerial work operations
Activity
General aviation / Recreational-Aerial work-Agricultural spreading / spraying
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the morning of 3 September 2025, a Eurocopter AS 350 was conducting agricultural spraying operations in the Holbrook, New South Wales, area.
In preparation for the second run for the day, the pilot conducted a hazard reconnaissance of a 14‑hectare paddock and identified wires to the west, a road to the east and livestock in the corners of neighbouring paddocks.
The helicopter was fitted with a GPS navigational system which also featured a wire detection system designed to alert the pilot when the aircraft is approaching a mapped wire. The wire was correctly mapped in the aircraft GPS system.
Once spraying operations had commenced, the pilot reported that they were focusing on the spray as well as the stock in the neighbouring property which was at the end of their run. This resulted in them losing sight of the already identified wires in the spraying run overshoot area. Shortly after the dispensing had been completed, the pilot entered the neighbouring paddock and saw the wires. However, with little time to respond, the helicopter’s skids struck a wire resulting in damage to the tail rotor. The helicopter then began vibrating violently and rotated to the left, entering multiple 360° turns before it collided with terrain, rolled onto its right side and caught fire. The pilot was able to exit the passenger door of the helicopter and sustained minor burn injuries. The helicopter was destroyed by post-impact fire (Figure 1).
Figure 1: Post-impact damage
Source: NSW Police
Safety message
Despite the hazard assessment and the systems in place to warn about the wires, in this occurrence the distraction of the stock in the neighbouring paddocks diverted the pilot’s attention resulting in them losing sight of the wires.
Research by the ATSB has shown that 63% of pilots were aware of the position of the wire before they struck it.[1]
In association with the Aerial Application Association of Australia (AAAA), the ATSB released an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains details of multiple wirestrike accidents, lessons learned, and a number of strategies to help agricultural pilots manage the ongoing risk of wirestrikes during spraying operations. The booklet notes that focusing attention on non‑operational tasks or focusing on operational tasks at the wrong time can affect pilots’ hazard avoidance, detection and reaction times, and that all pilots, no matter the level of experience, can get distracted.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]ATSB research and analysis report B2005/0055, Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004, available at www.atsb.gov.au.
The ATSB is investigating a wirestrike and collision with terrain involving an Air Tractor AT-502, registration VH-CJY, 19 km south-east of Lake Cargelligo Airport, New South Wales, on 18 July 2024.
During aerial agricultural spraying operations, the aircraft struck a wire and subsequently collided with terrain resulting in substantial damage. The pilot was fatally injured.
The ATSB deployed a team of transport safety investigators to the accident site with experience in aircraft operations, engineering, and human factors. As part of the on-site phase of the investigation, ATSB investigators examined the aircraft wreckage and other information from the accident site, interviewed witnesses and any involved parties, and examined maintenance records and any recorded data. The ATSB has commenced the examination and analysis of the initial evidence collected.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2024-042
Occurrence date
18/07/2024
Occurrence time and timezone
12:56 Australian Eastern Standard Time
Location
19 km south-east of Lake Cargelligo Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Wirestrike
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Air Tractor Inc
Model
AT-502
Registration
VH-CJY
Serial number
502-0093
Aircraft operator
Thomson Airborne Pty Ltd
Sector
Turboprop
Operation type
Part 137 Aerial application operations
Activity
General aviation / Recreational-Aerial work-Agricultural spreading / spraying
On the afternoon of 8 October 2023, a Cessna 172N, registered VH-RSB, took off from private property near Merriton, South Australia for a private flight with the pilot and one passenger on board.
At about 1612, when the aircraft arrived back at the property and was heading west in line with a pre-prepared runway, it struck a single‑wire aerial powerline. The aircraft collided with terrain and an intense fuel-fed fire broke out.
Rescuers removed the pilot and passenger from the wreckage, sustaining non‑life‑threatening burns as a result. The passenger had been fatally injured and the pilot later succumbed to injuries. The aircraft was destroyed.
What the ATSB found
The pilot likely lost awareness of and did not see the powerline running across the approach path near the runway’s eastern threshold during approach to land.
The pilot was the owner of the aircraft and the property where it landed. The 700 m runway had been positioned in a paddock such that one end was near an oblique powerline. Positioning the end of the runway close to the powerline increased the risk of a wirestrike. Landing to that end of the runway meant that the powerline was in the path of the approaching aircraft unless aiming to land about halfway down the runway (which was well within the landing distance required for the aircraft).
Powerlines, especially single wires, are difficult to see from the air. The powerline was not marked in a manner sufficient to enhance visibility of the powerline to pilots using the runway, nor was there a requirement to do so. The powerline had been marked previously near the pole adjacent to the runway, however this was to alert pilots flying along it to the presence of another powerline crossing above or below, rather than when on approach to the runway.
Further, when passing a powerline that has been seen, its oblique orientation relative to the runway can also increase the chance of a wirestrike from a pilot misjudging the point where the aircraft would be in conflict with the wire.
Safety message
Aerial powerlines pose an on‑going threat to flying operations, more so when landing and taking off nearby. The location of private runways on rural properties needs to be separated from powerlines, even when the strip is only planned to be used by pilots familiar with the wires.
In Queensland, New South Wales, Victoria, and South Australia, the Look up and live website or app can be used by pilots to plan flying operations in proximity of overhead powerlines.
Additionally, electrical power and telecommunications companies in Australia can mark powerlines that are identified as a hazard for low-level flying operations. The principal electricity distributor in South Australia, SA Power Networks, advised that property owners can request a quote for the installation of powerline markers and, if installed, will be maintained into perpetuity. Some companies, such as those in Queensland and New South Wales, have a safety scheme to reduce the costs to property owners.
In association with the Aerial Application Association of Australia, the ATSB has released an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains numerous wirestrike accidents and lessons learned from them.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 8 October 2023, at a time that could not be established precisely, a Cessna 172N, registered VH-RSB, took off from private property near Merriton, South Australia for a private flight with the pilot and one passenger on board. It was reported that the pilot may have intended to fly to Kangaroo Island, about 1.9 flying hours away, but the actual destination(s) or route could not be confirmed.
At about 1612, the aircraft arrived back at the property and was heading west, in line with a pre‑prepared runway, when it struck a single‑wire aerial powerline about 8.5 m (28 ft) above ground level. During the accident sequence the powerline ruptured the fuel tank in the right wing. The aircraft collided with terrain and an intense fuel-fed fire broke out.
A local resident and a nearby driver hurried to the accident site and removed the pilot and passenger from the wreckage. Both rescuers sustained non‑life-threatening burns as a result. The passenger had been fatally injured and the pilot later succumbed to injuries. The aircraft was destroyed.
Context
Pilot information
Around 2020, the pilot commenced flying training with Recreational Aviation Australia (RAAus) before attaining a Civil Aviation Safety Regulation Part 61 recreational pilot licence in May 2023 with a class rating for single engine aeroplanes. The pilot held a valid class 2 civil aviation medical certificate with no restrictions and was not required to wear vision correction when flying.
The pilot had reportedly accumulated about 15 hours flight time in VH-RSB since taking ownership in June 2023. Their exact aeronautical experience could not be established as the logbook was on board the aircraft and was destroyed. The pilot had no reported significant medical conditions, and a toxicology and post-mortem examination report was not available at the time of publication.
Aircraft information
The Cessna 172N is a high‑wing, all-metal, unpressurised aircraft with a fixed landing gear. VH‑RSB had a single, Lycoming O‑320‑H2AD reciprocating piston engine driving a fixed‑pitch propeller. VH-RSB was manufactured in 1980 and was first registered in Australia in the same year.
The aircraft had long periods of inactivity since 2019 and the pilot had been the registration holder since 9 June 2023. In 2019 the aircraft was flown twice, and the previous owner advised the aircraft was run occasionally (without flying) to maintain the engine.
A periodic inspection and minor maintenance tasks were carried out in July 2023. The total hours flown since that time could not be determined accurately as the maintenance release was destroyed in the post-impact fire. Recorded data from OzRunways[1] showed that the aircraft had flown at least 5.9 hours, but this service was not used on all flights (see Recorded data). In conjunction with the OzRunways data and interviews conducted during the investigation, it was estimated the aircraft had flown about 15 hours since its periodic inspection.
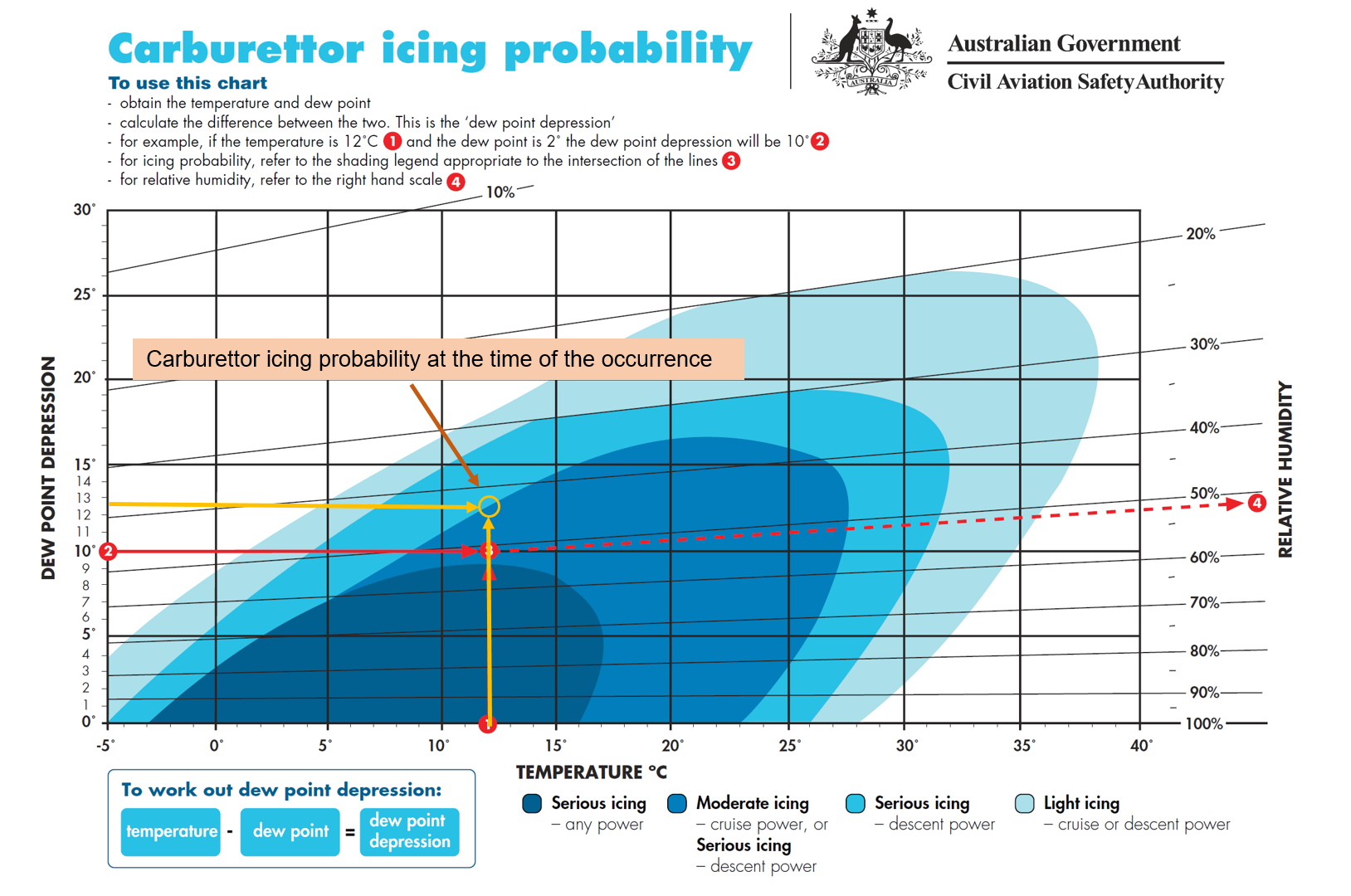
Meteorological information
At 1610, about 2 minutes before the accident, a BoM automatic weather station at Port Pirie, 35 km north of the collision location, recorded the surface wind as 12 kt gusting to 16 kt from 236° true, temperature 24°C, and dew point 1°C. There was no detected cloud or reduced visibility at the nearest weather station with that capability (Whyalla Airport, 74 km north‑west of the accident site).
The burn pattern of a small grass fire that ignited at the accident site shortly after the aircraft collided with terrain indicated the local surface wind at the time was likely from the southwest.
Willy‑willies[2] were reported to be common in the area and were observed at the accident site by ATSB investigators in similar weather conditions to the time of the accident on the days following the accident.
Runway information
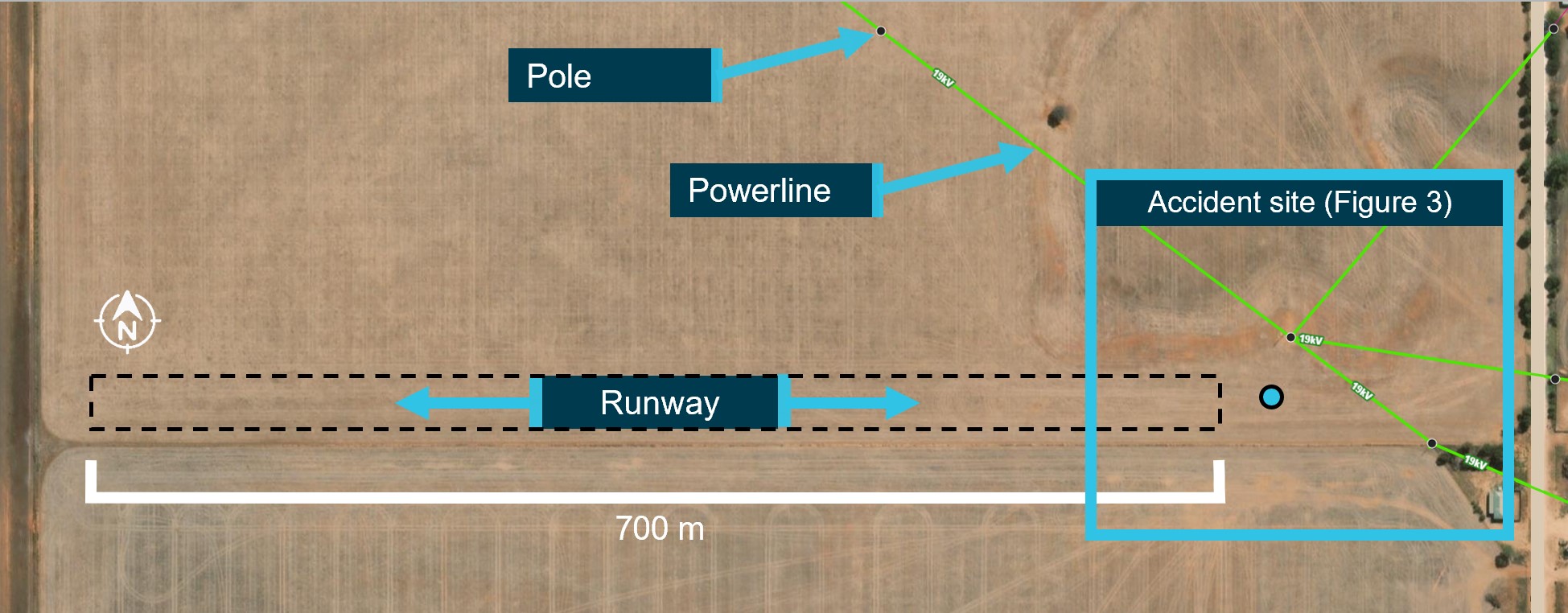
The runway was a private strip on the aircraft owner’s land and they lived less than 1km away. To prepare the runway, the aircraft owner had slashed crops in a relatively flat section of open farmland (Figure 1). It ran in an east–west direction adjacent to a fence line and was about 700 m in length. There were vehicle track marks running the length of the runway, and it was otherwise unmarked.
Figure 1: Runway looking west
Image source: ATSB.
The extents of the runway were not clearly visible during the post-accident survey, and are illustrated in the following figures as an indication of its approximate location (Figure 1 and Figure 2).
Figure 2: Runway overview
Powerlines are highlighted in green.
Image source: Lookupandlive.com.au, annotated by the ATSB.
At the time of the accident there were cattle grazing in the paddock, though it is not known if they were in the vicinity of the runway. The terrain around the runway was also relatively flat, open farmland, and there was reportedly another runway prepared in the same paddock running north–south.
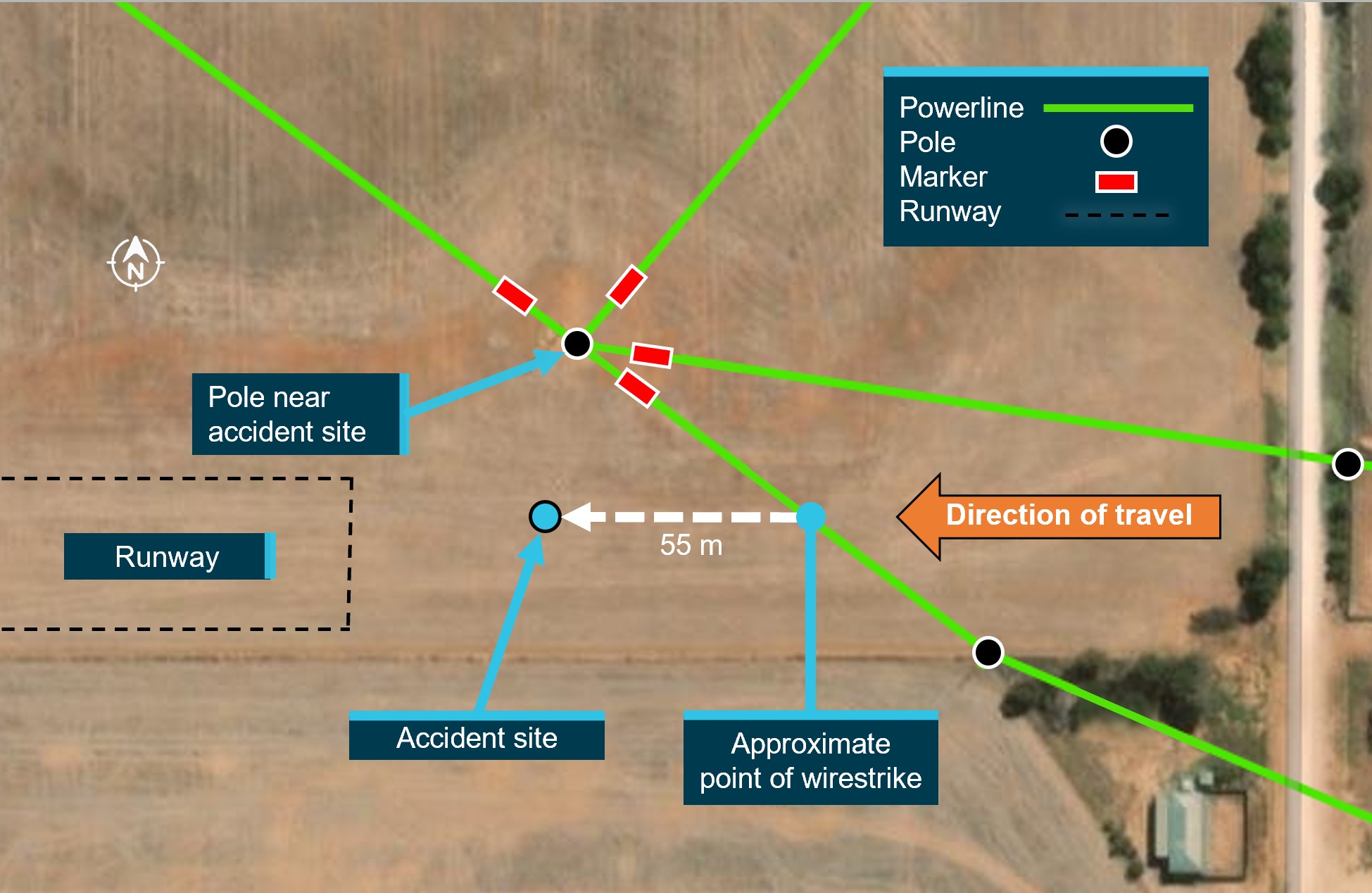
The 19 kV powerlines in the vicinity of the eastern threshold of the runway were of the single-wire earth return (SWER) type. The powerline was estimated to be at a height of 8–8.5 m (26–28 ft) at the point of impact.
Civil Aviation Safety Authority (CASA) Advisory Circular AC 91‑02 v1.2 Guidelines for aeroplanes with MTOW not exceeding 5700 kg - suitable places to take off and land (Civil Aviation Safety Authority, 2022) recommends that pilots have a thorough awareness of the obstacles in the approach and climb‑out flight paths. The ATSB estimated that an aircraft heading west with a typical approach angle of 3° would be in conflict with the powerline at any touchdown point less than about 162 m from it. To be at least 15 m (50 ft) clear of the powerline during landing, the touchdown point would need to be at least 453 m from the powerline, leaving about 420 m of runway for the landing roll.
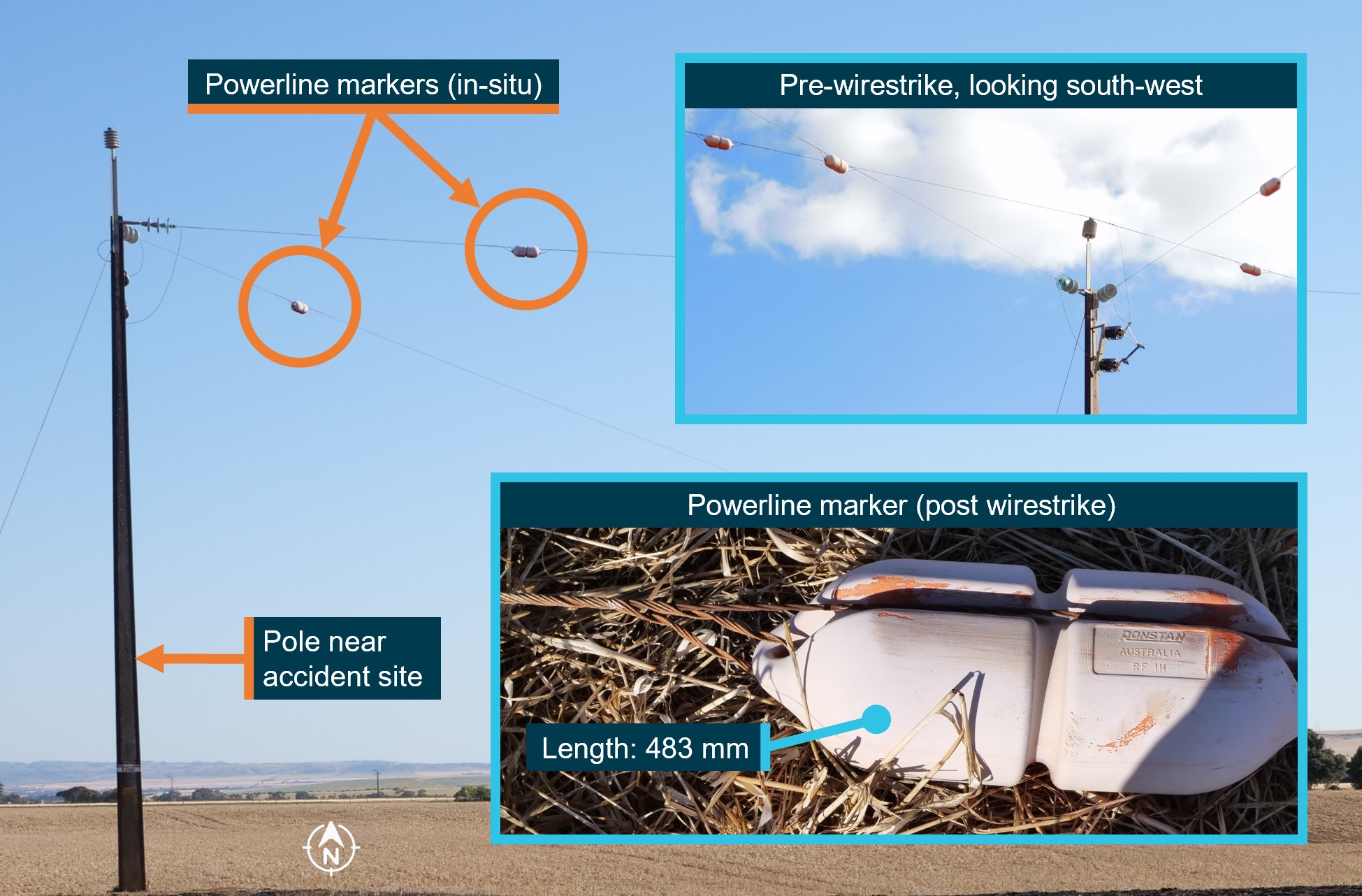
Powerline markers had been fitted to each of the 4 powerlines about 4 m from the pole nearest to the accident site (Figure 3). The markers were marine buoys that had been repurposed as powerline markers. Originally, they would have been bright red, but had faded considerably (Figure 4).
The owner of this infrastructure, SA Power Networks, advised the line markers had been installed in November 2000. They were installed to alert helicopter pilots flying along a powerline for annual pre‑bushfire patrols to the presence of another powerline crossing above or below.
As the runway was not a certified aerodrome or authorised landing area, there was no requirement within the applicable aviation regulations, Australian Standards or elsewhere to mark the powerlines for pilots using the runway.
Figure 3: Accident site and location of powerlines
Image source: Lookupandlive.com.au, annotated by the ATSB.
Figure 4: Powerline markers
Image source: ATSB, SA Power Networks, annotated by the ATSB.
The pilot was very familiar with the property and the position of the powerlines and had flown from the runway about 4 or 5 times in VH-RSB. In about June 2023, the pilot had previously indicated an intention to use the part of the runway that was opposite to the wires and so was not concerned about the wires.
Recorded data
The pilot intermittently used OzRunways for flight and navigation information. The available data showed a flight in July 2023 from Port Lincoln to a neighbour’s property near the owner’s home (the accident site). In August 2023 the aircraft flew from the same neighbour’s property to Kangaroo Island, South Australia, and returned the following day to the neighbour’s property.
The available data also showed a flight in September 2023 where the aircraft took off and landed 3 times from the owner’s runway (the accident site) and flying in the vicinity (mainly circuits). On these flights, the aircraft always landed heading east. On one occasion it took off to the east, over the powerlines.
There was no OzRunways data for the flight from the neighbour’s property to the owner’s runway, for the accident flight on 8 October 2023, or any other flights.
Wreckage information
The aircraft’s cabin, wings, and fuselage were severely damaged by the intense post‑impact fire, limiting the extent to which pre-impact defects could be identified (Figure 5). However, from the evidence available:
the wreckage position, damage to the left wing strut, and the marks from the powerline on the propeller, engine cowl, and right wing was consistent with the aircraft striking the oblique powerline heading west
the aircraft impacted terrain steeply and inverted, probably right wing and engine first
the propeller had indications that the engine was running at low power at the time of impact
the flap actuator extension was consistent with a flap setting of 10° (see Cessna 172N flap settings).
Figure 5: VH-RSB at the accident site
Image source: ATSB.
Survival aspects
When assessing whether an aircraft accident is survivable, a number of aspects are considered, including:
occupant restraints
forces imparted on the aircraft occupants
liveable space inside the aircraft being maintained
post‑impact fire.
It could not be determined whether the occupants were wearing the aircraft’s upper torso restraints. However, ATSB analysis indicated that the level of deceleration exerted on the occupants of VH-RSB during the collision with terrain was likely to result in serious or fatal injuries. Additionally, the fire significantly reduced the likelihood of the accident being survivable.
Additional information
Cessna 172N flap settings
The Cessna 172N flap system includes a single flap actuator located in the right wing. When a flap setting (0°, 10°, 20°, 30°, or 40°) is selected by the pilot, a jackscrew is driven by an electric motor to that setting.
The normal procedures in the pilot’s operating handbook (POH) for the Cessna 172N state that the flaps should be up (0°) for take‑off, however the approved take‑off range is 0°−10°. For landing, POH states that the flaps can be set as desired and suggests 0°−10° for airspeeds less than 110 kt indicated airspeed (KIAS) and 10°−40° for airspeeds less than 85 KIAS.
Cessna 172N take-off and landing information
Take-off and landing distances for a Cessna 172N vary with a number of factors including the local temperature, wind direction and speed, the elevation of the landing area, and the aircraft’s weight. At sea level, about 290 m can be required for the take-off roll (with additional distance required for obstacle clearance), and the landing roll distance can be around 172 m.
Aerial operations around overhead powerlines
The 2013 ATSB educational publication Avoidable Accidents No. 2: Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028) noted that:
…many pilots report that it is almost impossible to see a wire by itself.
Research has shown that it takes between 5.5 and 12.5 seconds for an object to be detected, recognised as a hazard, a decision made on an action, then for that action to be initiated, and the aircraft to respond to that action. Thus, given the inherent difficulty in visually detecting a powerline and the travelling speed of the aircraft, in most cases you will not have enough time to avoid a powerline by the time it can be seen.
The ability of pilots to detect powerlines depends on the physical aspects of the wire, such as the spacing of power poles and the sag of the wire, the orientation of the wire, and the effect of weather (especially visibility). In many cases, the powerline and/or the power pole will blend into the background vegetation or will be obscured by trees etc.
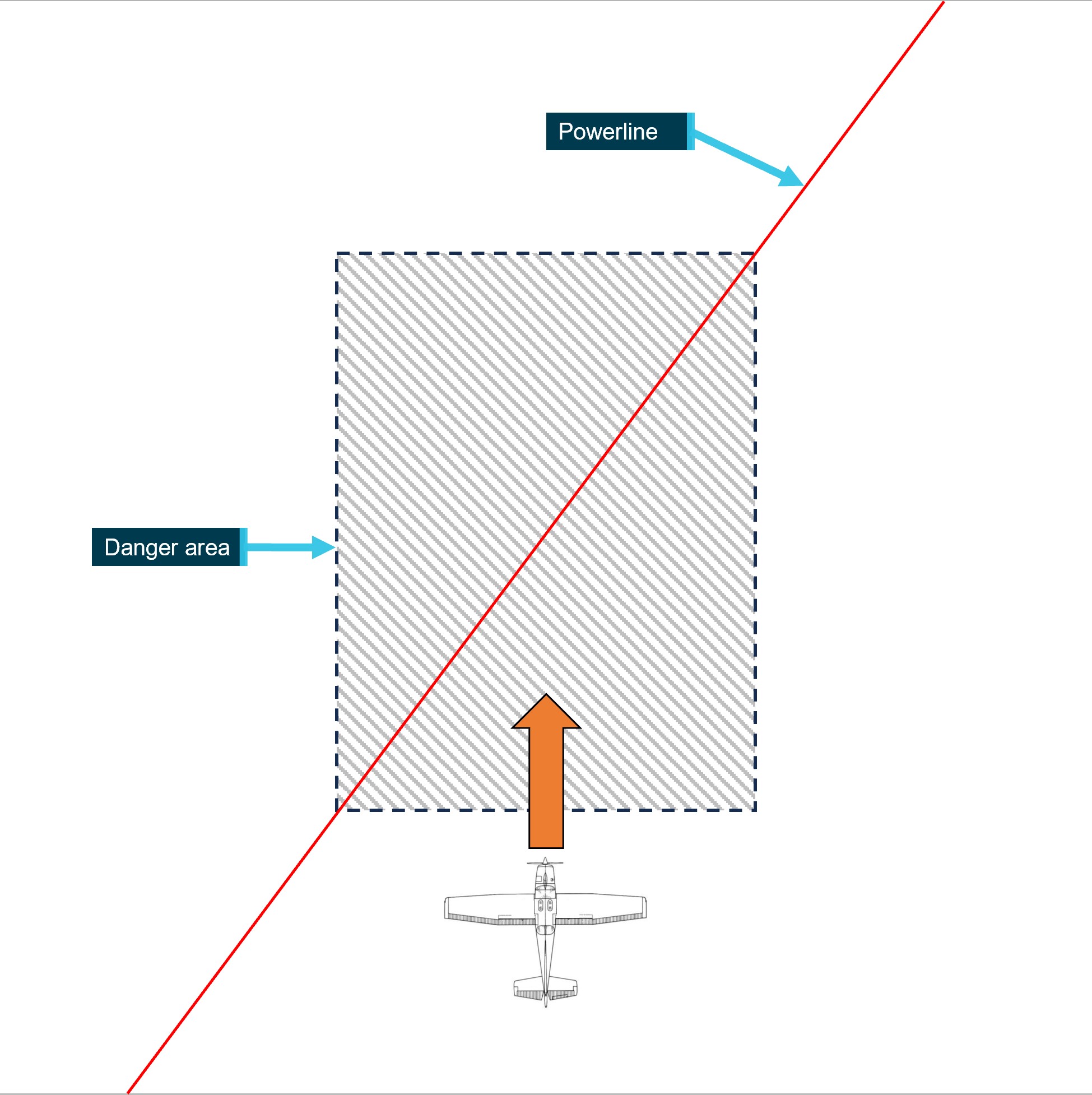
The publication also detailed a number of wirestrikes where aircraft struck a powerline that was known to the pilot. The publication outlines a number of strategies developed by the Aerial Application Association of Australia (AAAA) to help manage the risks associated with aerial operations around overhead powerlines. Regarding aircraft approaching oblique powerlines (as was the case on the accident flight, see Figure 6), the AAAA pilot’s manual states:
Crossing a line of wires at an oblique angle [compared to at a right angle] provides a slower rate of closure with the line as a whole and will allow more time to see it. However, the actual speed of crossing a point directly ahead will of course be the same as if it were crossed at right angles.
The danger here is that the pilot’s preoccupation with this point may lead to a lack of appreciation of the fact that the aircraft’s wing tip will reach the point directly ahead of it slightly earlier. In other words, the pilot may base his [sic] judgement on the wrong section of the wire.
…
A crossing at right angles is to be preferred wherever possible as this reduces the danger area to the thickness of the wire.
Figure 6: Likely approach of VH-RSB to the powerline
Image source: ATSB, based on a diagram from Aerial Application Association of Australia.
Visual illusions associated with sloping terrain
About 4.5 km to the west of the accident site and runway, the terrain rises up from relatively flat, open farmland to a ridgeline (Figure 7).
As outlined in the US Federal Aviation Administration (FAA) publication AM-400-00/1 – Spatial Disorientation Visual Illusions (Federal Aviation Administration, 2011), runways that are positioned on up- or down‑sloping terrain can produce a visual illusion during the approach to landing. For down‑sloping runways, it can result in the pilot believing their approach is low, pitching up, and inadvertently making a steeper approach. Conversely, for up‑sloping runways, it can result in the pilot believing their approach is high, pitching down, and inadvertently making a shallower approach.
This can be more pronounced if the up‑slope occurs beyond the runway. Pilots may unknowingly move their perception of the horizon toward the top of the rising terrain and create the same visual illusion as an up‑sloping runway, resulting in a shallower approach (Previc and others 2004).
Figure 7: Terrain to the west of the runway
Image source: ATSB.
Safety analysis
Wirestrike
The post‑impact fire limited the extent to which any pre‑impact defects could be identified. However, the available evidence indicates the aircraft was very likely heading west on approach to land when it came into contact with the powerline. Evidence supporting this included:
the wind direction (as evidenced by the burn direction of the post‑accident fire in the paddock) favoured a landing in that direction
the indications that the engine was running at a low power setting as would be expected for a final approach to land
the flaps were extended to a landing setting
the height of the aircraft when it struck the powerline, which was likely too low for an effective visual inspection of the runway
the position of the wreckage.
While it could not be established if the pilot had landed on the runway in a westerly direction in the past, the pilot was familiar with the property, the runway and the position of the powerline. Powerlines, especially single wires, are difficult to see from the air, and the pilot likely lost awareness of the powerline and then did not see it when on final approach.
The visual illusions associated with sloping terrain can also occur with up‑sloping terrain in the distance. In this case, the rising terrain beyond the runway could produce this visual illusion. Had this occurred, the pilot may have mistakenly corrected to a shallower approach, putting the aircraft in conflict with the powerline.
Willy-willies were reportedly common in the area and may have been present on the day of the accident. While they can pose a threat to light aircraft and helicopters during low-level operations (such as take‑off and landing), there was no way to determine if a willy-willy was a factor in the accident. In any case, however, the aircraft’s approach path would not have been a sufficient distance from the powerline to assure separation in the event of even a small deviation.
Runway position and powerline marking
The runway was about 700 m long, more than twice the take-off and landing distances required for a Cessna 172N. Moving the runway’s eastern threshold away from the powerline would have reduced the chance of conflict. Even with the existing threshold location, using the end furthest from the powerline for take-off and landing would have reduced the risk of potential conflict.
Recorded data from a day in the month before the accident indicated that the pilot may have intended to reduce the risk of wirestrike when operating from the runway: on that day, 5 of the 6 landings and take-offs used the runway end opposite the wire (and the only exception was a take‑off, which typically provides more clearance over a hazard than a landing the opposite way). However, pilots can forget about hazards, and the thresholds of the runway were not marked, so a pilot could inadvertently revert their aim point for a landing to the east to the start of the runway, putting the aircraft in potential conflict with the powerline.
While there were no powerline markers in line with the runway, the markers adjacent to the nearby pole could alert or remind a pilot to the presence of the powerline. However, their original purpose was to alert pilots flying along a powerline to the presence of another powerline crossing above or below, rather than for a pilot using the runway, and their visibility and location was not optimal for landing on the runway in their locations.
Further, the powerline’s oblique orientation relative to the runway can also increase the chance of a pilot misjudging the point where the aircraft was in conflict, increasing the risk of a wirestrike.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving Cessna 172N, VH-RSB, near Merriton, South Australia on 8 October 2023.
Contributing factors
The pilot likely lost awareness of and did not see the aerial powerline during approach to land.
The runway was positioned near an oblique powerline, and the powerline was not marked in a manner sufficient to enhance visibility of the wire to pilots using the runway.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Aerial Application Association of Australia
Airservices Australia
Civil Aviation Safety Authority
SA Power Networks
South Australia Police
maintenance organisation for VH-RSB
accident witnesses
recorded data from OzRunways.
References
Australian Transport Safety Bureau 2006, Aviation Research and Analysis Report B2005/0055 Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004.
Aerial Agriculture Association of Australia 2011, Aerial Application Pilots Manual (3rd edition).
Civil Aviation Safety Authority 2022, AC 91‑02 v1.2 – Guidelines for aeroplanes with MTOW not exceeding 5700 kg - suitable places to take off and land.
Federal Aviation Administration AM‑400‑00/1 Spatial Disorientation Visual Illusions, rev. 2/11. Washington DC: U.S. Department of Transportation Federal Aviation Administration.
Previc FH 2004 ‘Visual illusions in flight’, in FH Previc & R Ercoline (Eds) Spatial disorientation in aviation, American Institute of Aeronautics and Astronautics, Reston VA.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
SA Power Networks
Civil Aviation Safety Authority.
There were no submissions received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]OzRunways: An electronic flight bag application providing subscriber flight information and navigation service.
[2]Willy-willies (also known as dust devils) are revolving masses of air resulting from local atmospheric instability, such as that caused by intense heating of the air mass adjacent to the ground by the sun on a hot day. They can be 3–100 m in diameter and up to 300 m high. Wind speeds inside the vortex reach a maximum of 100 km/h.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
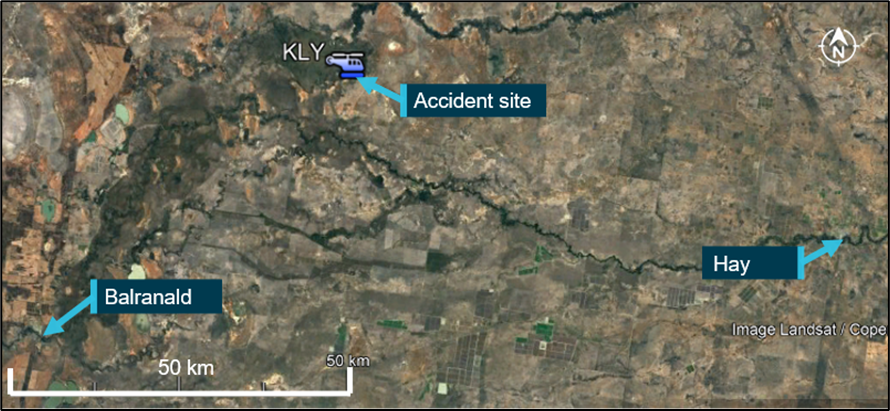
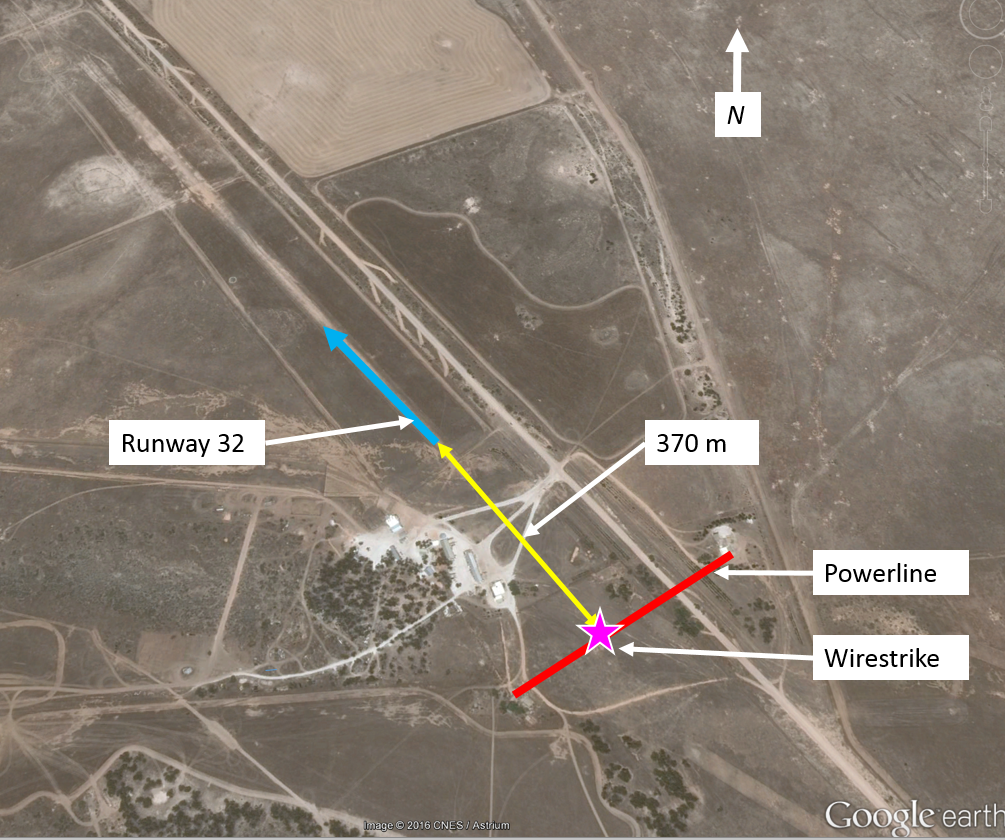
On 26 May 2021, the pilot of a Robinson R22 Beta helicopter, registered VH-KLY (KLY) and operated by Stock & Station Aviation, was conducting mustering operations on a property 75 km west‑north-west of Hay, New South Wales (Figure 1). The pilot was the only person on board.
Figure 1: Accident location
Source: Google maps annotated by the ATSB
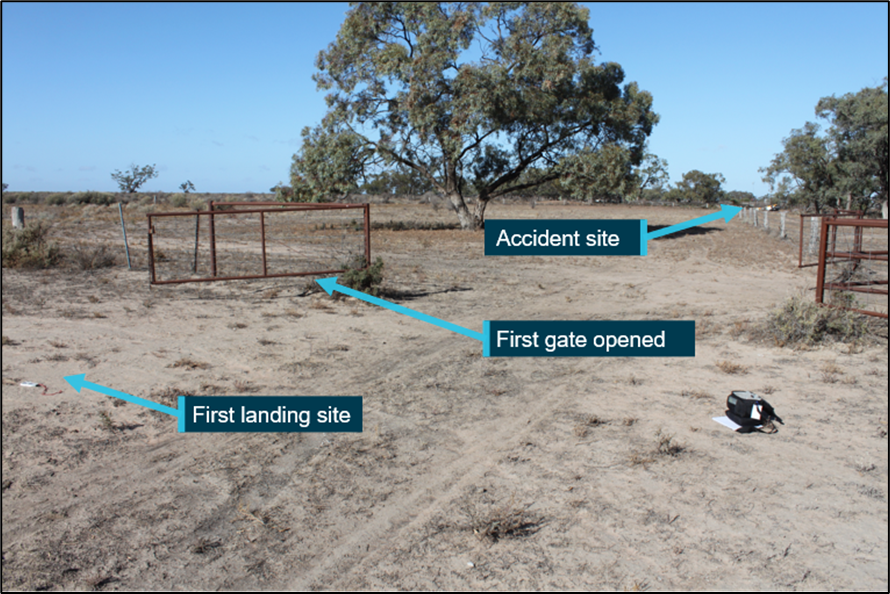
At about 1150 Eastern Standard Time,[1] the pilot was moving a small group of cattle along a fence line to yards, where they were to be loaded on to a truck and removed from the property. The pilot flew ahead of the cattle to open the gates to the yard, with witnesses observing the helicopter as it passed their house. The pilot landed and exited the helicopter, then opened the first gate at the entrance to the yards (Figure 2).
Figure 2: First landing site
Source: ATSB
A short time later, a witness at the house heard the helicopter take-off and, very soon after, heard a loud bang. Suspecting that the helicopter had crashed, they drove to the yards and found the helicopter on its side. First aid was rendered to the pilot however, they sustained fatal injuries. The helicopter was substantially damaged.
Context
Flight data
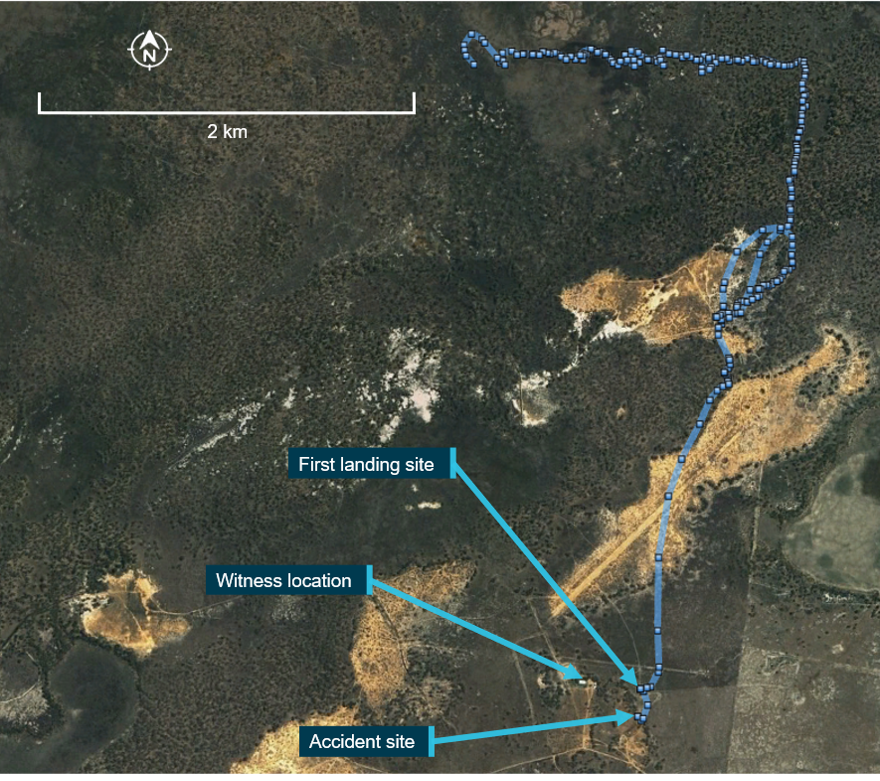
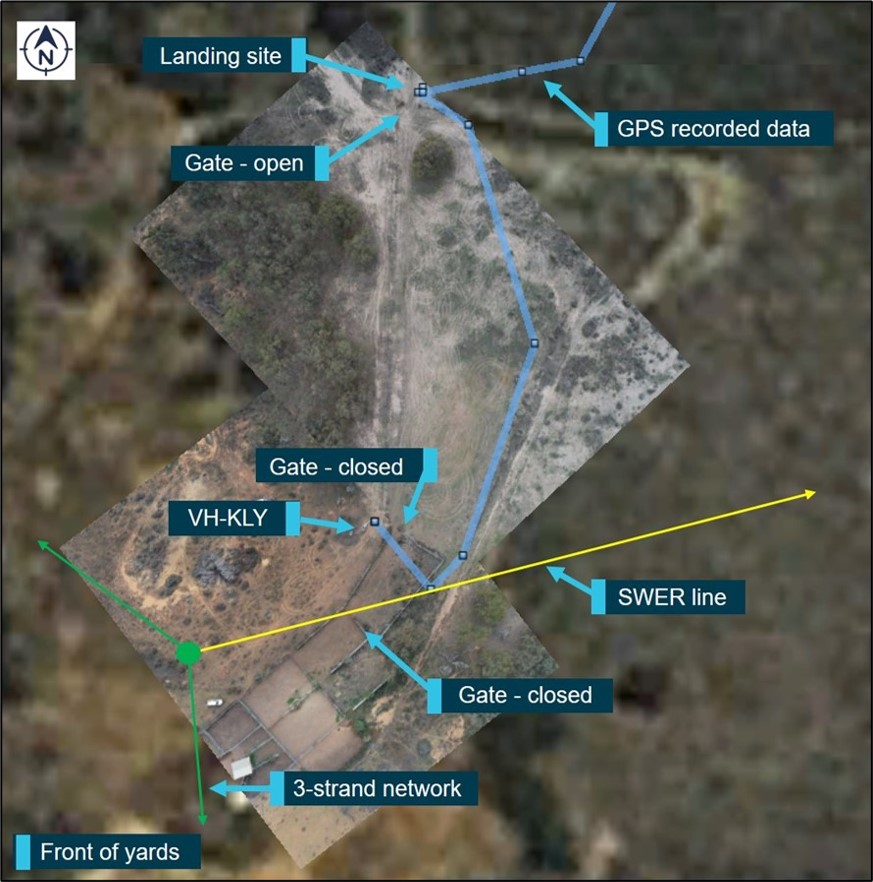
Analysis of recorded flight data indicated KLY took off from the landing site at the first gate and flew in a southerly direction toward the yards at between 20–30 ft (6–9 m) above ground level (AGL) and up to 27 kt (Figure 3). The track then turned slightly towards a gate which was required to be opened to allow the cattle through. This gate is adjacent to the accident site.
Figure 3: KLY flight data
Source: Google Earth, annotated by the ATSB
Wreckage information
All of the major aircraft components were accounted for at the site. Examination of the aircraft’s flight controls, engine and aircraft structure did not identify any pre‑existing defects. However, there was evidence of wire strike marks on the front of the helicopter’s left skid (Figure 4).
Figure 4: Wire strike marks on left skid
Source: ATSB
Powerline
A single wire earth return (SWER) line runs across the yard (Figure 3). This line runs from a power pole adjacent to the yards to a pole approximately 351 m away. The wire is attached to the power pole closest to the yards at 34 ft (10 m) AGL and the minimum height of the wire as it spans between power poles is 24 ft (7 m) AGL. The helicopter came to rest about 27 m from the wire.
Ongoing investigation
The investigation is continuing and will include examination of:
aircraft maintenance documentation and operational records
recorded data
weather information
wire visibility
accident survivability
pilot qualifications and experience.
Should any safety critical information be discovered at any time during the investigation, the ATSB will immediately notify operators and regulators so appropriate and timely safety action can be taken.
A final report will be published at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 26 May 2021, the pilot of a Robinson R22 Beta helicopter, registered VH-KLY and operated by Stock & Station Aviation, was conducting mustering operations on a property 75 km west‑north‑west of Hay, New South Wales. The pilot was the only person on board. As the helicopter was flown towards cattle yards, it struck a powerline and collided with terrain. The pilot was fatally injured.
What the ATSB found
The ATSB found that, as it was not originally planned for the pilot to muster cattle to the yard, they did not do an aerial inspection and the hazards at the yard were likely not considered. During a turn most likely associated with an approach to land, the helicopter contacted a single wire earth return line, which was very difficult to detect. Control was subsequently lost, and the helicopter collided with terrain.
The ATSB also found the emergency locator transmitter (ELT) did not activate as the transmitter was selected to OFF. As the accident was witnessed, this did not affect the response.
Safety message
Mustering operations around yards and buildings are inherently dangerous due to low‑level hazards including powerlines. According to the ATSB’s Avoidable Accidents No. 1 - Low-level flying research report, about 63% of pilots involved in wirestrike accidents reported they were aware of the powerlines but had forgotten about them before they were struck.
As such, the Aerial Application Association of Australia has been working with landowners and energy suppliers to install markers on powerlines through their Powerline Safety Program. In addition, a number of power companies are making these markers available at reduced cost.
Operators are also reminded of the importance of regularly conducting a self-test of the emergency locator transmitter (ELT) system. Having a working ELT increases the likelihood that an aircraft and its occupants will be located quickly in the event of an accident.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of resource required to obtain a safety benefit from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On Wednesday 26 May 2021, the pilot of a Robinson Helicopter Company R22 Beta helicopter (Figure 1), registered VH-KLY (KLY) and operated by Stock & Station Aviation, was conducting mustering operations on a property 75 km west‑north-west of Hay, New South Wales. The pilot was the only person on board.
Figure 1: Exemplar R22 helicopter
Source: Archangel12. Used under the Creative Commons Attribution 2.0 Generic license. Registration and company branding removed.
The pilot had arrived at the property on the preceding Sunday afternoon, to assist with a wild goat muster. This was to be conducted over a number of days, during which the mustering crew were staying at a house on the property. The goats were to be mustered to a set of temporary yards.
The muster began on the Monday and, during the day, the pilot observed a small herd of cattle, which were required to be removed after the completion of the goat muster. The following day, the weather deteriorated during the morning and the muster was called off early, with the pilot returning to the house at about lunchtime.
On Wednesday the muster re‑commenced and, at approximately 0707 Eastern Standard Time,[1] the pilot flew to the temporary yards, landed the helicopter and shutdown. The goats were being drafted[2] before being loaded on to trucks and the helicopter was not required for that work.
After a few hours, the pilot had a brief discussion with the lead contractor and a stockperson, following which the contractor instructed the pilot to find the previously detected cattle and direct the stockperson to them. The pilot was then to return to their accommodation, before beginning another muster on a different area of the property. The stockperson was instructed to move the cattle to the main yards on the property. Prior to this, there had been no plan to use these yards during the muster.
The helicopter took off at 1032 and, as the pilot was locating the cattle, they detected a second larger herd. The pilot advised the stockperson over the UHF radio and directed them to these cattle. The pilot then advised the stockperson that they would locate and move the original small herd to the main yards using the helicopter.
The pilot subsequently located the cattle and began moving them along a fence line toward the yards. They then flew ahead to open the gates to the yard. At about 1150, a witness located near the yards, observed the helicopter as it passed (Figure 2). The pilot landed the helicopter, exited and opened the first gate at the entrance to the yards.
Figure 2: Last section of flight from recorded GPS data
Source: Google Earth with data from onboard GPS, annotated by ATSB
A short time later, the witness heard the helicopter take-off and, very soon after, heard a loud bang. Suspecting that the helicopter had crashed, they drove initially to the front of the yards and, when they did not find it, they then drove around to the back of the yards and found the helicopter on its side. Shortly after, two more people arrived and first aid was rendered, however the pilot sustained fatal injuries. The helicopter was substantially damaged, with indications that it had sustained a wirestrike.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) and a class 1 aviation medical certificate, with no restrictions. They also held a single‑engine helicopter rating with grade 3 instructor rating, an aerial application rating with fire endorsement, and a low-level rating with sling and mustering endorsements.
An assessment of their logbook revealed the pilot had accrued approximately 3,017 flying hours with 2,525 on the Robinson R22. They had flown approximately 128 hours in the previous 90 days and 30 hours in the previous 30 days.
The pilot had completed a crew resource management, hazards and human factors course with the Aerial Application Association of Australia in 2018. This course covered the hazards involved in low level flying, including operations around powerlines.
The pilot was reported to be fit and healthy and there was no indication they were experiencing a level of fatigue known to affect performance.
Medical and pathological informational
The forensic pathologist who conducted the post-mortem examination concluded that the pilot succumbed to injuries sustained during the accident sequence. At the time of publication of this report, the finalised post-mortem and toxicology report were unavailable to the ATSB.
Aircraft Information
VH-KLY (KLY) was a two-seat Robinson Helicopter Company (RHC) R22 Beta helicopter, serial number 4424, and was powered by a Textron Lycoming O-360-J2A, four-cylinder piston engine. It was manufactured in 2009 and registered in Australia the same year. It was purchased by Stock & Station Aviation in July 2017 and had been maintained by the same maintenance organisation since that time.
The helicopter was maintained in accordance with the manufacturers’ maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever came first. A periodic inspection was completed on 13 May 2021 and a review of the maintenance release issued at that time indicated no outstanding maintenance requirements or serviceability issues. KLY had accrued 2,633.4 total time in service.
The helicopter did not have wirestrike protection equipment fitted, nor was it available for this helicopter type due to a lack of securing structure. In addition, KLY was being operated with the doors removed.[3]
Flight data
The helicopter had a Garmin 660 GPS unit and a TracPlus surveillance system installed. TracPlus provided real-time tracking through a satellite or mobile phone network. It reported position, altitude, and speed at set time periods, in this case every 15 seconds.
Analysis of the recorded flight data indicated KLY took off from the first gate at the yards and flew in a southerly direction, towards the second gate, at between 16–33 ft (5–10 m) above ground level (AGL) (Figure 3). The recorded groundspeed was about 22 kt, slowing to 15 kt[4] as the helicopter turned towards a closed gate adjacent to the accident site. This gate was required to be opened to allow the cattle access to the yards.
Analysis of the flight tracks flown during the previous days identified that the helicopter flew past the main yards once on the first day. On that flight, they flew in a northerly direction about 370 m east-south-east of the yards, passing over a single wire earth return (SWER) line (see the following section titled Powerline information) at approximately 280 ft AGL and at a speed of approximately 65 kt.
Figure 3: Flight track and powerline
Source: Google Earth, annotated by ATSB
Note: GPS data was recorded every 15 seconds so the line between track points was not necessarily representative of the actual flight path.
Powerline information
A power pole (green dot in Figure 3) was located about 75 m west-south-west of the accident site. It had one network consisting of 3-strands, which ran along the front of the yards. Above this, a SWER network ran across the northern side of the yards. The single strand was attached at the top of the pole at 10.48 m (34.4 ft) above the ground.
A SWER line is a single line of intertwined narrow-gauge steel wires. It spanned approximately 351 m to the next pole in the network. The minimum ground clearance of the SWER line was 7.23 m (23.7 ft). There were no markers or other devices installed on the powerline to enhance its visibility, nor was there a requirement to install such devices.
The power company advised there were no interruptions or surges reported in the electricity system at the time of the accident.
Visual cues during low-level flying
A key influence on the risk of a wirestrike when flying at low level is a pilot’s visual acuity in the given environmental conditions. According to Veillette (2015), the near invisibility of wires results from a number of factors including the:
size of the wire
viewing angle
sun position
condition of the aircraft’s transparencies (windscreen)
camouflaging effect of nearby vegetation.
Visibility of the powerline
Using a remotely piloted aircraft system (RPAS), the ATSB recreated the approximate flight path of the helicopter at about the time of day the accident occurred. The RPAS was flown at a similar speed and height above the ground to provide an appreciation of the pilot’s perspective (Figure 4).
Figure 4: Image taken by RPAS along approximate helicopter flight path
Image source: ATSB
Figure 5: Approximate helicopter flight path perspective with the SWER marked
Image source: ATSB
Weather and sun position
The Bureau of Meteorology graphical area forecast for NSW–West valid at the time of the occurrence indicated that from 1200, the forecast visibility was greater than 10 km with scattered[5] cloud between 4,000 and 8,000 ft. The relevant grid point wind and temperature chart valid at the time, forecast a wind from 250° at 31 km/h (17 kt). Witnesses reported that there was no cloud cover and very little wind at the time of the accident.
At 1200 that day, the altitude[6] of the sun was about 34° and its azimuth[7] was about 005°. During the flight, the pilot was wearing an aviation helmet, fitted with a retractable sun visor, designed to reduce glare. It was reported the pilot was not using the visor however, given the position of the sun, there was minimal potential for it to have been a factor in the wirestrike.
Previous operations at the yards
It was reported that the pilot had first worked at the property in May 2020. Prior to beginning that muster, the pilot and the lead contractor flew over the yards noting the hazards, including both sets of powerlines. They had then mustered cattle to the yards over the following days, reportedly flying in from multiple directions.
The pilot had worked at the yards again in February 2021, mustering cattle to the yards over 3‑4 days. It was reported that during that muster, the pilot had been reminded of the SWER line while cattle were being mustered in the same direction as the accident flight.
Wreckage and impact information
The wreckage was located on a dirt access road, just outside the fence at the north-west corner of the main yards. The area was clear flat ground with little grass and small shrubs (Figure 3). There was no evidence of a tree or bird strike, either on the helicopter, nor in the surrounding area.
All components of the helicopter were identified at the accident site. Examination of the site and wreckage indicated the helicopter collided with terrain largely inverted. Damage to the right side of the landing gear was consistent with a significant secondary impact, right side low and slightly nose up, before the helicopter came to rest on its right side, about 6 m from the initial impact point. The wreckage was located about 17 m from the SWER line.
Examination of the site and wreckage identified:
dirt embedded in the main rotor head assembly, the top and leading edge of one blade and the trailing edge of the second blade, along with ground scars consistent with the main rotor head and blades
the main rotor pitch links had failed in overstress
main rotor blade strike to the tail cone
no pre-existing defects with the rotors, drivetrain or flight controls that would have prevented normal flight
several indicators that the engine was providing power at the point of impact
the left skid, forward of the crosstube, had marks consistent with a wirestrike.[8] The marks indicated that the relative contact had been both towards, and away from, the front crosstube (Figure 7)
the right skid had collapsed under the fuselage.
The windshield was noted to be clean and in good condition, thereby not hindering the pilot’s view. In addition, it was noted that the ELT transmitter was selected to the ‘OFF’ position (see the section titled Emergency locator transmitter).
Figure 6: VH-KLY
Source: ATSB
Figure 7: Landing gear front left skid
Source: ATSB
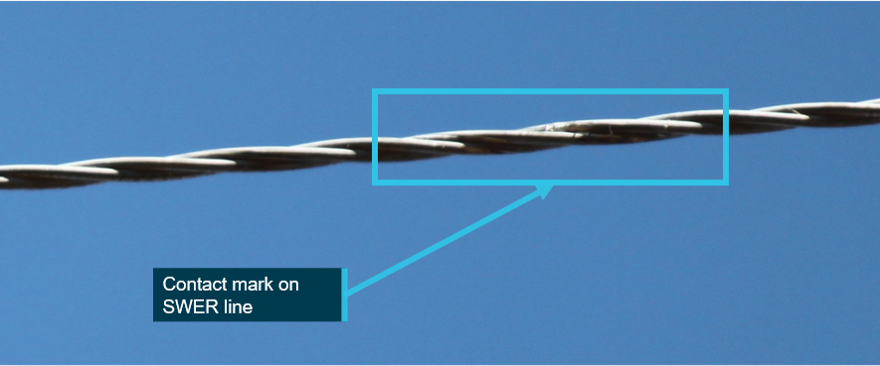
The SWER line was found intact and the insulators on the power poles at either end of the span were undamaged. A polished area was observed on the SWER line in the approximate location of the flight path, consistent with it being contacted (Figure 8). Equipment available to the ATSB during the initial site visit was not sufficient to enable a close inspection of the wire. This mark was not visible when the ATSB returned to the accident site approximately 4 weeks later.
Figure 8: Contact mark on SWER line
Source: ATSB
Survival aspects
The survivable space within the helicopter cabin was maintained throughout the accident sequence (Figure 6). The right (pilot) seat displayed minor creasing on the right side. The storage under the right seat was filled to the volumetric capacity,[9] however, as the helicopter was inverted when it collided with terrain, this was not considered to have contributed to the pilot’s injuries.
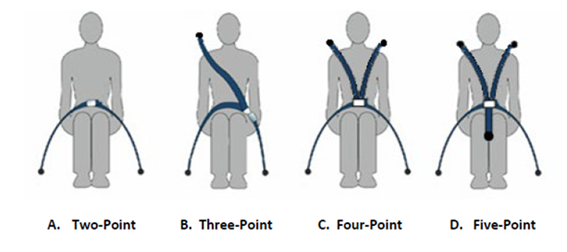
The pilot was wearing a three-point harness and aviation helmet, both of which were reported to have been fastened correctly.
There was evidence that the pilot may not been fully restrained within the structure of the helicopter during the accident sequence. The ATSB examined the pilot’s helmet at its Canberra technical facility and determined that it was structurally intact with no sign of cracking or fracturing of the composite outer shell and no damage to the inner shell. Dirt was identified on the back of the helmet with scratch marks which appeared to be recent, however it could not be established how or when they occurred.
Emergency locator transmitter
The optional emergency locator transmitter (ELT) fitted to the helicopter consisted of the transmitter, located in the main transmission bay and a remote switch/annunciator, which was located in the cabin, left of the cyclic. The ELT transmitter is normally selected to ‘ARM’.[10] With the transmitter selected to ARM, the three-position remote switch/annunciator, with indicator light, operated as follows:
ON – ELT activated
ARM – permitted ELT activation when subjected to high ‘G’ load
Test/RESET – allowed brief functional testing of the ELT or reset in case of inadvertent activation
Light – red light illuminated when the ELT was transmitting.
RHC recommended following the ELT manufacturer’s documentation for installation, operation and maintenance. The ELT manufacturer recommended a self-test ‘once a month but not more than once a week’. The ELT transmitter battery was to be replaced every 6 years, with the unit subject to specialised inspection and testing at the same time. The RHC periodic inspection included, ‘ELT (if installed): inspect condition and verify security’.
The maintenance organisation acknowledged that the ELT should be checked routinely during a maintenance inspection. They advised that they normally checked the security of the unit, battery expiry date, and conduct a self-test of the system. For reasons that could not be determined, the ELT had not been inspected by the maintenance organisation during the time they had maintained the helicopter.
Wreckage examination identified the remote switch/annunciator was in the ARM position and the transmitter was selected OFF. The position and orientation of the transmitter meant the switch position was unlikely to be discovered without performing a self-test. While it could not be determined if the pilot performed a self-test, it is most likely they did not as the test would have failed.
Testing of the ELT at the ATSB technical facilities, determined it was capable of activation and transmission. However, it was also determined that due to the angle the helicopter collided with terrain, it was possible the ELT would not have activated.
Calculations by the ATSB indicated the helicopter was within the prescribed weight and balance limits for the flight.
Related occurrences
A review of the ATSB database identified that, between 1 January 2010 and 31 December 2020 there were 350 reports of aircraft collisions with powerlines. Of these 12 resulted in fatal accidents, with an additional 25 accidents resulting in serious injuries.
Significantly, analysis of wirestrike accidents reported to the ATSB between 2001‑2010, showed that 63 per cent of the time pilots were aware of the presence of the wire before they struck it but had momentarily forgotten about it. Two such examples are detailed below.
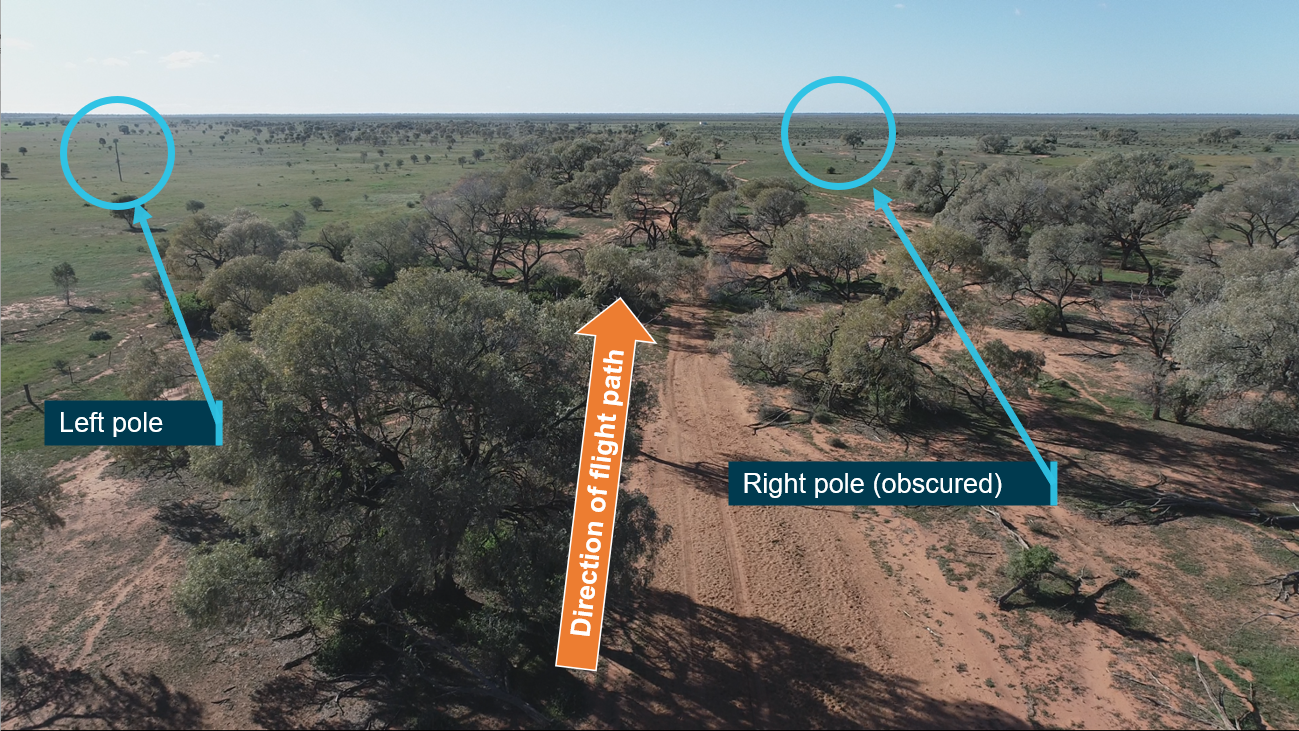
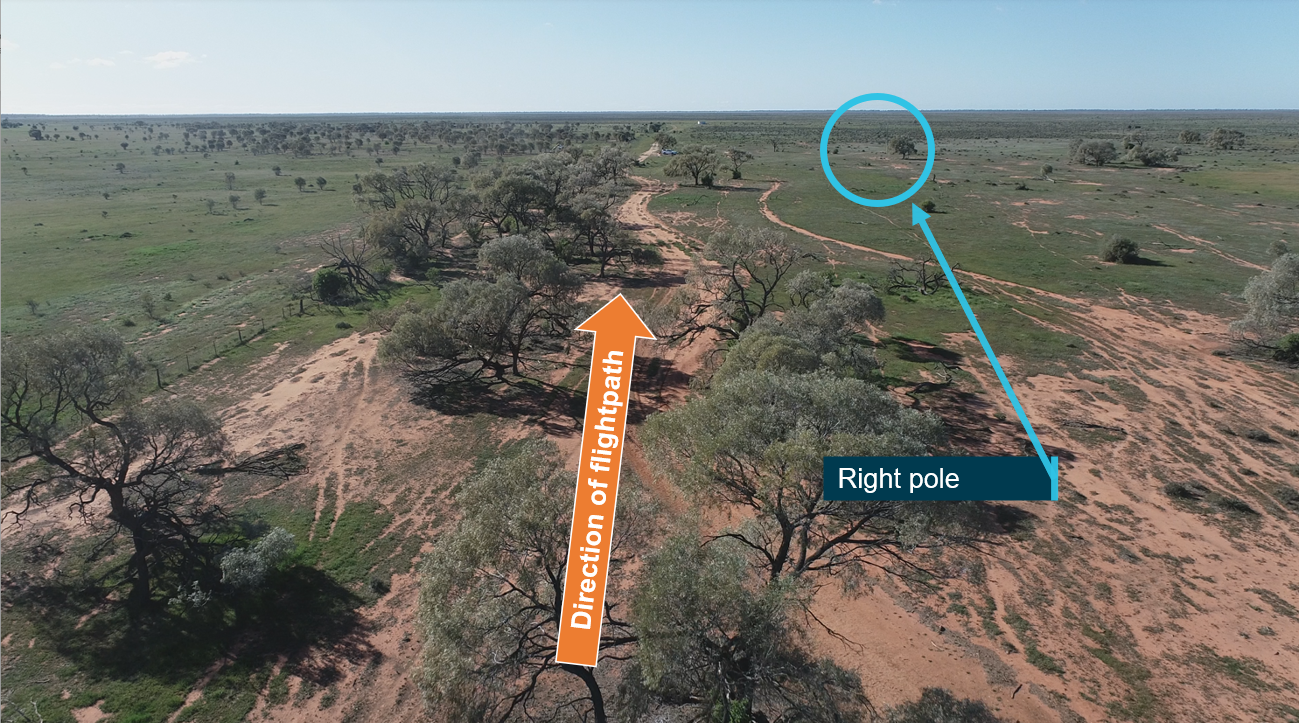
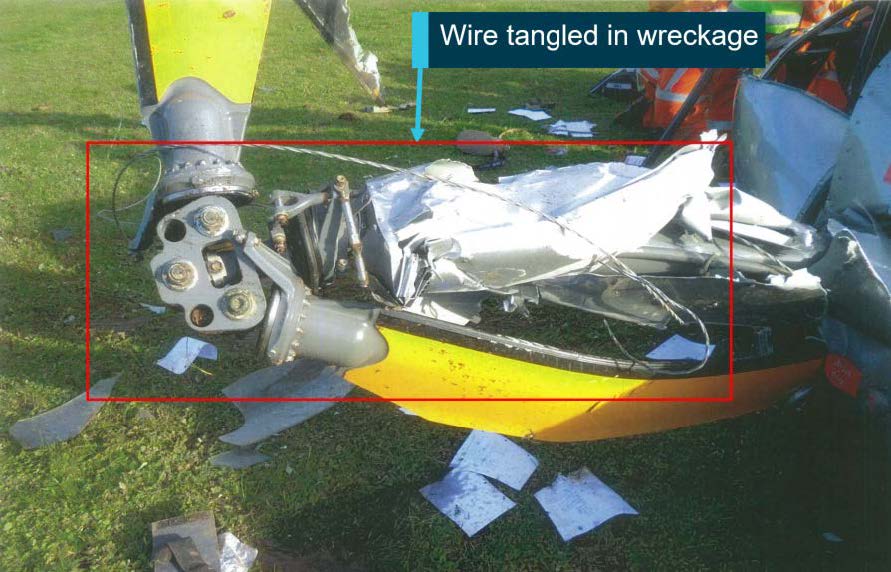
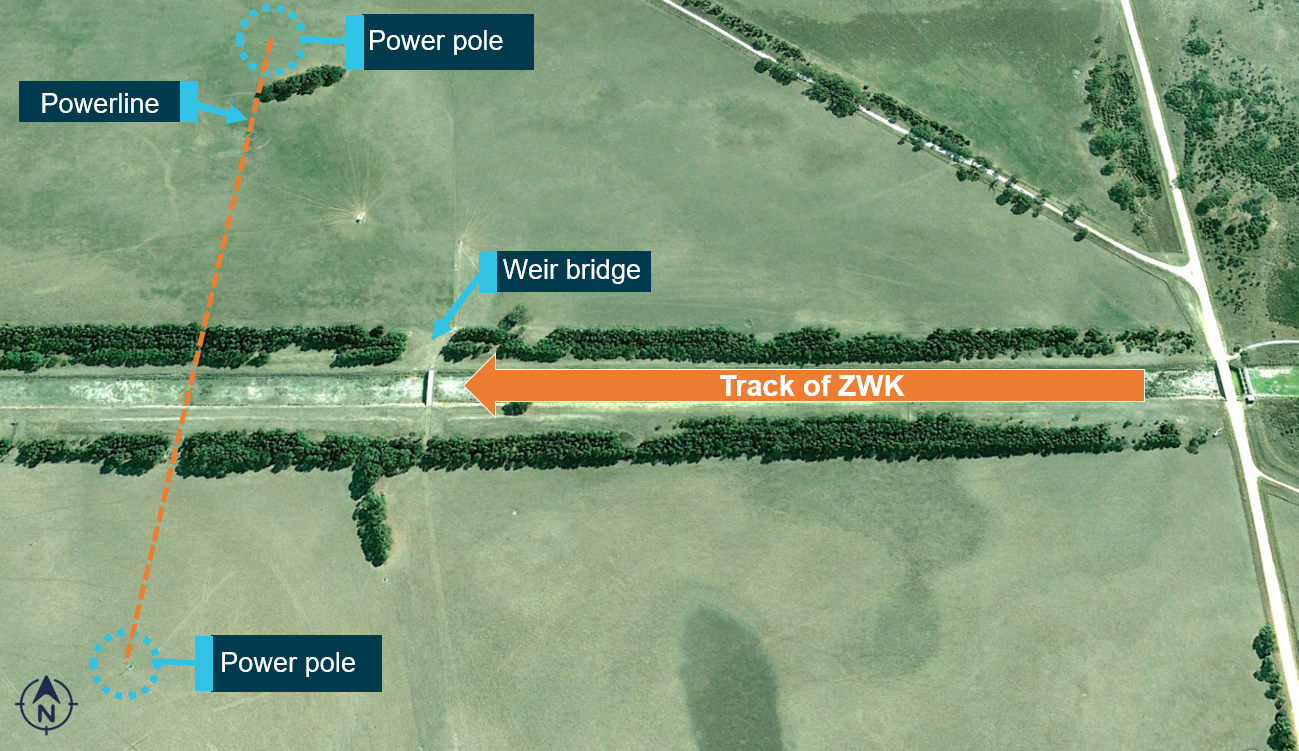
On 13 March 2019, a Robinson R44 helicopter, registered VH-ZWK, was conducting aerial spraying operations at Bool Lagoon, around 20 km south of Naracoorte, South Australia. While spraying along a drainage channel, the pilot momentarily lost awareness of the powerline while manoeuvring over a bridge. Nearby vegetation, which reduced the pilot’s ability to see the power poles and visually identify the powerline, probably reduced the pilot’s ability to maintain this awareness. The helicopter was destroyed, and the pilot sustained minor injuries.
On the morning of 20 February 2016, the pilot of a Robinson R22 helicopter, registered VH-LYW, was conducting aerial cattle mustering operations on a property about 88 km north‑east of Roma, Queensland. The pilot had mustered in that paddock several times previously and was aware of a set of high voltage transmission wires that had been erected across the property in the previous 12 months.
Prior to commencing mustering, the pilot overflew the paddock, sighted the powerlines and formed a plan to muster the cattle from north to south, giving due consideration to the wires running east‑west. The pilot then mustered the mob from north to south, and the helicopter remained above the wires during that time. The pilot then saw another vegetated area near the dam, where cattle may have been hidden from view, and flew the helicopter towards it. While the pilot’s focus was on searching for cattle in the scrub below, the helicopter neared the powerlines. The pilot’s attention suddenly returned to the wires, sighting them close in front at the same level. The pilot attempted to avoid the wires however, the tail rotor struck the earth wire. The helicopter sustained substantial damage and the pilot was seriously injured.
These investigations, and others, highlight the dangers posed by powerlines during low-level operations. They emphasise importance of pre-flight planning and continual reassessment of where an aircraft is in relation to the wires.
Safety analysis
The pilot had been tasked to direct a stockperson to a small herd of cattle and then return to base. However, during the flight, the pilot changed this plan due to the identification of further cattle and decided they would muster the original herd to the main yards. The ATSB Avoidable accidents No.2 - wirestrikes involving known wires: A manageable aerial agricultural hazard advised pilots to reassess risks when plans are changed.
The pilot was aware of the powerline locations at the main yards from their previous operations however, that was a significant period of time before so their presence is unlikely to have been front of mind for the pilot as they flew towards the yard. Additionally, while the recorded flight data showed that the helicopter had passed the yards once in the previous days, it is considered unlikely that the pilot was assessing the hazards as there was no plan to use the yards during this muster and the helicopter overflew at a height significantly above the wire. Further, there was no indication of any subsequent flights over, or around, the yards that may have provided an opportunity to reassess known hazards, including during the accident flight.
On the accident flight, the pilot flew in a southerly direction from the entrance of the yards, most likely with the intention of landing and opening a second gate to allow cattle to enter the yard. The SWER line, which crossed the yard, was very difficult to detect due to the:
lack of contrast to the background
next power pole in the SWER network being outside the pilot’s normal field of view in the direction of flight
absence of markers on the SWER line to increase the line’s visibility.
In addition, the power poles from the 3-strand network were in the pilot’s forward view. While also difficult to detect, if the pilot had seen them, it may have given them a false assurance that the powerlines were not in their immediate operating area.
The direction of the marks on the left skid indicate that the left skid contacted the SWER line on an oblique angle. The marks indicated the wire had rubbed along the skid toward the front crosstube, and then away from the tube. This, and the relatively low forward airspeed, likely contributed to the SWER line not being severed. It could not be determined if the pilot had observed the wire prior to contact and was trying to avoid it, or if they reacted as the wirestrike occurred.
After contacting the wire, the helicopter collided with terrain in an inverted position. It then rolled over with the front of the right skid collapsing under the fuselage while coming to a rest on its right side.
The ELT remote switch in the cabin was in the ARMED position and, as such, it is likely the pilot would have believed the system was operational, unaware the transmitter was selected to OFF. Why the transmitter was deactivated, and not detected via periodic self-testing, could not be determined. In this instance however, there was no effect to the outcome as wreckage was located quickly due to the nearby witness.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving Robinson Helicopter Company R22, VH-KLY, 75 km west‑north‑west of Hay, New South Wales on 26 May 2021.
Contributing factors
The helicopter struck a powerline which was very difficult to detect, resulting in a loss of control and collision with terrain.
As there was no plan for the pilot to muster cattle to the main yard and they did not conduct an aerial inspection, it is likely the hazards around the yard had not been considered.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the lead contractor for the muster
Stock and Station Aviation Pty Ltd
Robinson Helicopter Company
the maintenance organisation for VH-KLY
Civil Aviation Safety Authority
New South Wales Police Force
witnesses
recorded data from the helicopter.
References
Gibb, R., Scharff, L. and Gray, R., 2010. Aviation Visual Perception: Research, Misperception and Mishaps (Ashgate studies in human factors for flight operations). Ashgate Publishing Group.
Veillette, P., 2015. Wire wary: what you don't see can kill, and does. Business and commercial aviation.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
lead contractor for the muster
Civil Aviation Safety Authority
Robinson Helicopter Company
United States National Transportation Safety Board.
A response was received from the Robinson Helicopter Company. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 31 July 2020, the pilot of a Robinson R44 Raven 1 helicopter, registered VH-HNF and operated by Riverina Helicopters, was preparing to conduct aerial weed spraying at Steam Plains, 69 km south-east of Hay Airport, New South Wales.
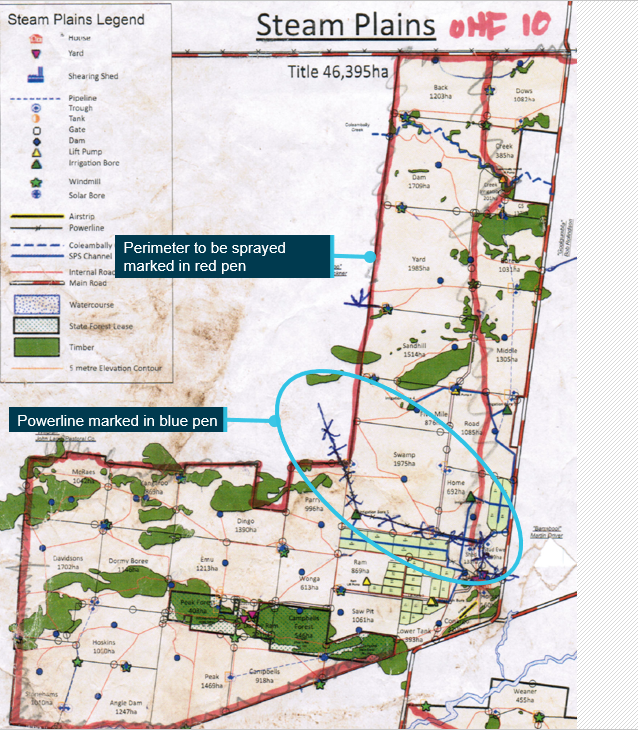
Prior to commencing the day’s flying, the pilot briefed with the helicopter owner/operator, who was performing the role of ground crew and responsible for loading the helicopter with chemical. The briefing included a review of the day’s tasking, maps of the property and hazards associated with the operation. The identified hazards included a 19.1 kV single wire earth return powerline, which crossed the property fence line about 5 m above the ground. The powerline had been marked on the pilot’s map during initial planning with the property manager 2 days prior.
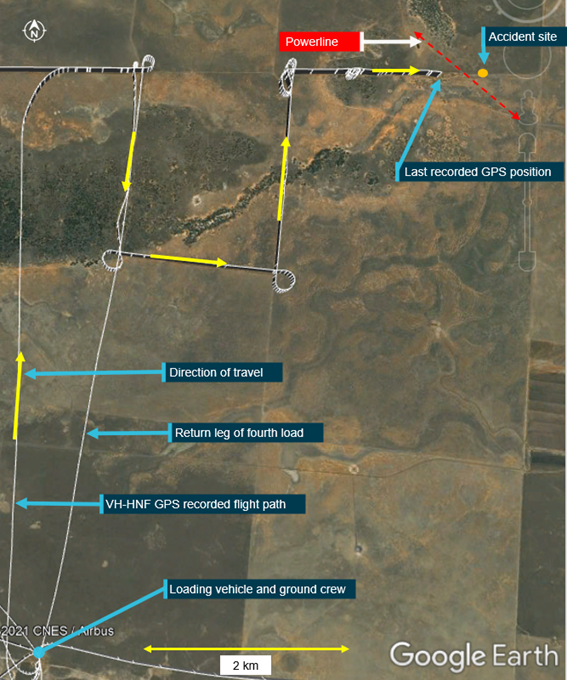
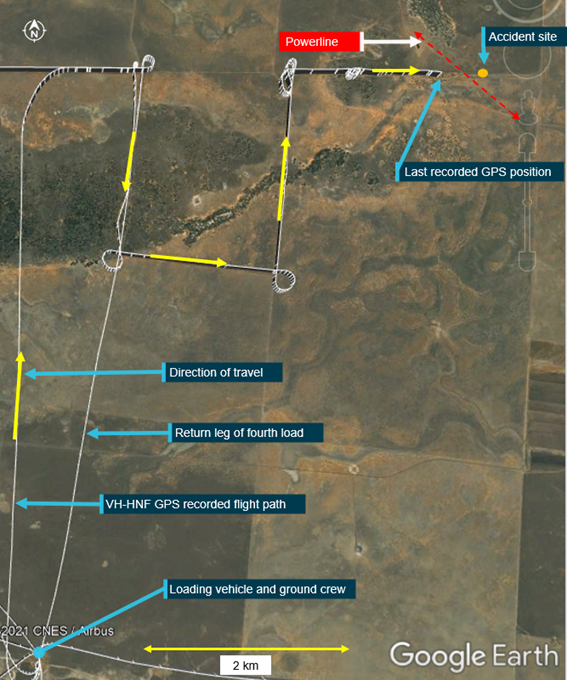
The ground crew then loaded the helicopter with chemical from a centrally-located vehicle. According to recorded GPS data from the helicopter, after loading, the pilot flew the helicopter to the property boundary to spray along the fence line, 2.5-5 m above the ground, before returning to the loader (Figure 1). The pilot sprayed four loads over an 80-minute period and departed with the fifth load at about 1050 Eastern Standard Time.[1]
The GPS data showed that the pilot flew the helicopter to the property boundary and began spraying the fifth load. About 350 m before reaching the position where the previously-identified powerline crossed the fence line, the pilot manoeuvred the helicopter to climb over an area of trees 12-15 m high, before descending to continue spraying. During the descent, the helicopter struck the powerline. The electricity provider reported that the fault to the powerline occurred at 1057. This was consistent with the time of the last recorded GPS position, about 300 m prior to the powerline.
The helicopter subsequently collided with terrain about 120 m beyond the powerline, resulting in fatal injuries to the pilot. The helicopter was substantially damaged.
Figure 1: VH-HNF flight path for fifth spray load
Source: Google Earth and GPS data, annotated by the ATSB
Site and wreckage examination
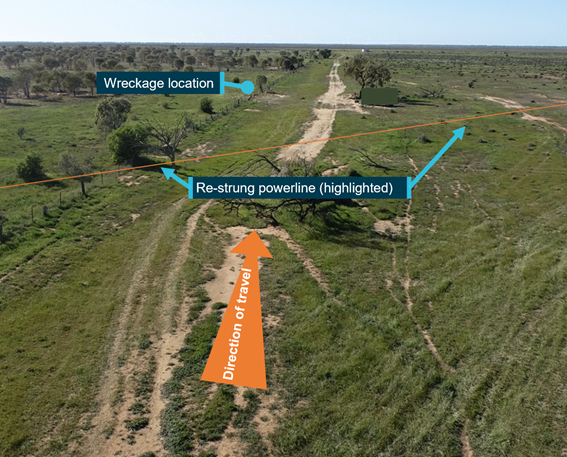
The accident site was located in flat and open farmland (Figure 2), about 7 km north-east of the loading vehicle. The ATSB conducted an examination of the site and wreckage, and identified:
the main wreckage was located about 120 m beyond the powerline in the direction of travel
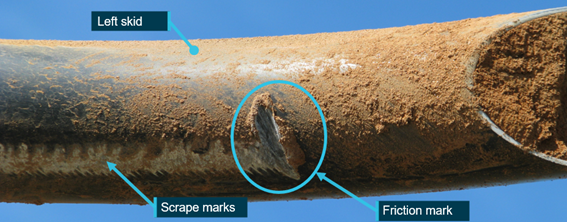
the powerline remained entangled in the wreckage, with evidence of wire contact on the front of the left skid
significant structural deformation, consistent with heavy impact on the left side of the helicopter
the helicopter was fitted with bladder fuel tanks, which had ruptured but there was no fire
flight control continuity was established
there were no pre-existing issues identified with the helicopter that would have precluded normal operation.
Figure 2: Drone image of accident location, taken at 1028 on 4 August 2020
Source: ATSB
Further investigation
The investigation is continuing and will include:
review of pilot qualifications, experience and medical information
review of operational procedures
review of environmental conditions
consideration of powerline visibility
examination of survivability aspects
review of similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 31 July 2020, the pilot of a Robinson R44 Raven I helicopter, registered VH-HNF and operated by Riverina Helicopters, was conducting aerial weed spraying at Steam Plains, 69 km south-east of Hay Airport, New South Wales.
During the fifth spray load of the morning, the pilot turned the spray off and conducted a climb to clear a stand of trees. At 1057 Eastern Standard Time, as the helicopter descended to continue spraying, the top of the left skid struck a powerline that crossed the flight path.
The helicopter entered uncontrolled flight and collided with terrain about 120 m beyond where it struck the wire, resulting in fatal injuries to the pilot. The helicopter was substantially damaged.
What the ATSB found
The ATSB found that the pilot knew the wire existed and overflew a small section of the target area earlier that morning but did not conduct an aerial inspection to identify hazards and verify the location of the powerline on the accident flight. Without the aerial hazard check, the pilot was reliant on seeing the wire during the flight but was unable to do so in time to avoid the wirestrike.
The pilot's injuries were consistent with flailing due to the left-side impact, but it could not be determined whether the pilot slipped out of, or was not wearing, the shoulder sash portion of the 3-point harness.
Although the pilot was wearing a helmet, it did not attenuate the impact to survivable levels. Either the impact forces exceeded the helmet design specifications, or the helmet was not fitted, worn or maintained correctly.
The pilot was not effectively managing severe obstructive sleep apnoea, which has been shown can cause impairments in cognitive functions including attention and short-term memory and increased the risk of the pilot suffering the effects of fatigue. It could not be determined whether the pilot was experiencing any impairments associated with the condition. The condition had also not been disclosed to the Civil Aviation Safety Authority, which prevented oversight of any ongoing safety risk associated with the condition.
What has been done as a result
The ATSB has released a safety advisory notice to strongly encourage pilots conducting low-level operations to wear a flight helmet, ensuring that it is:
fit for purpose
custom fitted to the pilot’s head
properly secured by using the chin strap
maintained in accordance with the manufacturer’s instructions.
Safety message
The risk of wirestrike in low-level operations is well-documented. Uncontrolled flight often follows a wirestrike, which increases the risk of serious and fatal injuries. For pilots conducting low-level operations, pre-flight identification of hazards is essential. As more up-to-date mapping and powerlines data is made available, and more wires carry visible markers, pilots have improved access to tools for planning and strike prevention. The ATSB encourages landowners who engage pilots to conduct aerial application operations to mark powerlines that may pose a hazard.
However, only by conducting an aerial inspection at a safe height, can the pilot be assured of the location of hazards.
Although planning for hazard avoidance is key, pilot limitations remain, including the ability to see a wire or obstacle, attention, memory and distraction. In these situations, survivability features including 4-point pilot seat restraints and flight helmets, significantly improve survivability of helicopter accidents and should be used. It is also important to remember that a helmet will only meet its design specifications if it is fitted properly, worn correctly and maintained in accordance with manufacturer’s instructions.
Common symptoms of obstructive sleep apnoea (OSA) include snoring, excessive daytime sleepiness and poor concentration. It can also have complex and significant physiological, neurological, cognitive and psychological impacts, and increases the risk of accidents. The Civil Aviation Safety Authority’s Obstructive sleep apnoea and aviation safety fact sheet advises pilots who have symptoms of OSA or suspect they may have it, to see a general practitioner. A diagnosis of OSA must be reviewed by a Designated Aviation Medical Examiner.
The occurrence
What happened
On 31 July 2020, the pilot of a Robinson R44 Raven I helicopter, registered VH-HNF and operated by Riverina Helicopters, was preparing to conduct aerial weed spraying along a perimeter fence and adjacent track at Steam Plains Station, 69 km south-east of Hay Airport, New South Wales.
At 0911 Eastern Standard Time,[1] the pilot ferried the helicopter from the station airstrip to the loading site, where the loading truck was positioned. The Riverina Helicopters’ chief pilot was performing the role of loader for the day, transferring chemical from the truck into the helicopter’s spray tank.
Prior to loading the helicopter with chemical for the first load, the loader briefed with the pilot. The briefing included a review of the day’s task, the map of the property and hazards associated with the operation. The identified hazards included a 19.1 kV single wire earth return powerline, which crossed the perimeter fence line once in the target area. The powerline had been identified as a hazard and highlighted on the pilot’s map during initial planning with the station manager 2 days prior.
After loading at 0931, recorded GPS data indicated the pilot flew the helicopter to the property boundary to spray the track adjacent to the fence line, operating 2.5 to 5 m above the ground, before returning to the loader. The pilot sprayed four loads over a 76-minute period and departed with the fifth load at 1047 (Figure 1).
The GPS data showed that the pilot flew the helicopter to the fence line and began spraying the fifth load. About 370 m before reaching the position where the previously-identified powerline crossed the fence, the pilot turned the spray off and manoeuvred the helicopter to climb over an area of trees 12 to 15 m high. At the end of the treed area, the helicopter descended, likely to recommence spraying. During the descent, the helicopter struck the powerline. The electricity provider reported that the fault to the powerline occurred at 1057. This was consistent with the time of the last recorded GPS position of the helicopter, about 300 m prior to the powerline.
The helicopter subsequently collided with terrain about 120 m beyond the powerline, resulting in fatal injuries to the pilot. The helicopter sustained substantial damage.
Post-accident actions
At 1140, the loader contacted the station manager and reported the helicopter overdue from the last load. Aware that the helicopter was operating in the vicinity of the powerline, the station manager drove to the accident site, advised the loader of the accident, and called emergency services. The station manager advised the emergency services call operator that the powerline was coiled over the fence and the helicopter, and requested the power be switched off as a priority. From a distance, the station manager assessed that the pilot was breathing but unconscious.
The emergency services operator advised Essential Energy and the system controller isolated that section of the electrical network. Field workers were dispatched to check power to the area had been effectively isolated and to ensure it was safe prior to first responders accessing the site.
Police and ambulance crews arrived on the scene and about 1 hour later, the Essential Energy workers arrived and tested the wires to verify they were not live. The pilot was then extricated from the helicopter and airlifted to hospital, where they remained on life support until the morning of 3 August.
Figure 1: VH-HNF flight path for fifth spray load
Source: Google Earth and GPS data, annotated by the ATSB
The pilot held a Commercial Pilot Licence (Helicopter) and a Private Pilot Licence (Aeroplane) issued under Civil Aviation Safety Regulations Part 61 on 10 February 2015, granted on the basis of Civil Aviation Regulations Part 5 licences issued in 2010. The pilot held the following helicopter ratings: single engine class, aerial application, low level, sling and aerial mustering.
The pilot’s Class 1 Medical Certificate was valid to 27 August 2020. At the pilot’s last medical examination with a Civil Aviation Safety Authority (CASA) Designated Aviation Medical Examiner in August 2019, no issues were raised by the pilot or apparent to the doctor. Following issue of the medical certificate, there was no further communication between CASA and the pilot.
The pilot was inducted into Riverina Helicopters in July 2015 with about 2,000 hours of aeronautical experience, 1,600 of which was in Robinson R22, and 30 was in R44 helicopters.
The pilot’s Aerial Application Association of Australia (AAAA) Spraysafe accreditation was current and in June 2019, the pilot had successfully completed the association’s Crew resource management, hazards and human factors course. In August 2019, the pilot had completed an annual CASA flight review/proficiency check.
On 27 May 2020, the chief pilot of Riverina Helicopters conducted an (annual) agricultural pilot and air work proficiency check and assessed the pilot ‘competent to carry out Agricultural and Aerial Work operations for Riverina Helicopters’. According to the pilot’s logbook, as of that date the pilot had accrued 3,730.3 hours of aeronautical experience and there were no further entries.
72-hour history
On 29 July, the pilot had left Griffith at about 0700 and driven the loading truck 1.5 hours to the Steam Plains property. That day, the pilot had been performing the loader duties (not flying) from 1138 to 1715. The pilot and chief pilot had stayed in accommodation at the property for the next 2 nights, going to sleep at about 2130 each night.
On 30 July, the pilot woke up at 0700 and conducted the daily inspection on the helicopter. The pilot started the helicopter at 0917 and commenced spraying operations at 0925 on the neighbouring property, finishing there at 1413. The loader then relocated the vehicle, and the pilot ferried the helicopter to Steam Plains, commencing spraying operations there at 1501. The pilot finished the day’s work and shut down the helicopter at 1743.
On the morning of the accident flight, the chief pilot reported that they had woken up at about 0700 and there had been no hurry in getting started as there was dew and they had to wait for the vegetation to dry before spraying.
Obstructive sleep apnoea
On 23 January 2020, the pilot attended a sleep clinic and completed a sleep study. On referral, the pilot had a STOP-Bang score[2] hat indicated a high risk of obstructive sleep apnoea (OSA) and an Epworth Sleepiness Scale[3] score in the higher normal range for daytime sleepiness. At that time, the pilot’s only reported symptom was loud snoring. The resulting polysomnography report identified fragmented sleep with oxygen saturation reducing to a minimum of 81 per cent. The diagnosis was severe OSA, with accompanying moderate oxygen desaturations.
The diagnosis of OSA is made when repetitive pauses in breathing occur during sleep, last at least 10 seconds, and occur due to the airway collapsing. These pauses reduce blood oxygen levels and lead to awakening or shifting into a lighter sleep.
The severity of OSA is based on the number of partial or complete pauses in breathing per hour. Severe OSA is defined as more than 30 events per hour. The pilot recorded 42.5 events per hour on average during the study. In response, the reviewing specialist recommended an urgent trial of a continuous positive airway pressure (CPAP) machine. A CPAP machine provides pressurised air, which opens the airway to ensure adequate delivery of oxygen. However, it does not cure OSA and compliance is a known limitation with CPAP treatment (Caldwell 2006).
CASA’s Obstructive sleep apnoea and aviation safety fact sheet stated that a CPAP should be used at least 5 hours per night for 6 nights per week and ‘must be used during the sleep period just prior to flight’. CASA may issue or reissue medical certification where compliance and effectiveness of CPAP treatment can be used to demonstrate control of OSA.
The ATSB obtained a detailed compliance report of sleep data automatically uploaded from the pilot’s CPAP machine. Between 21 February and 16 July 2020, the pilot had used the CPAP machine for at least 4 hours on 71 per cent of nights. The pilot’s CPAP usage had been frequent in March and April, then decreased. The CPAP had not been used between 8 and 15 July and the last recorded use was 16 July, 15 days prior to the occurrence flight. The pilot had not taken the CPAP machine to the accommodation at Steam Plains.
The effects of sleep apnoea on aviation outlined in the CASA fact sheet included reduced attention and concentration, and degraded cognition.
Fatigue risk
The US Federal Aviation Administration (FAA) pilot safety brochure Fatigue in aviation stated that typically fatigue ‘occurs with someone who does not get sufficient sleep over a prolonged period of time (as with sleep apnoea, jet lag, or shift work) or someone who is involved in ongoing physical or mental activity with insufficient rest’. It further stated:
Any fatigued person will exhibit the same problems: sleepiness, difficulty concentrating, apathy, feeling of isolation, annoyance, increased reaction time to stimulus, slowing of higher-level mental functioning, decreased vigilance, memory problems, task fixation, and increased errors while performing tasks.
Research has also found that sleep deprivation can impair decision making and increase risk-taking behaviour to avoid additional effort (Shingedecker and Holding 1974 as cited in Battelle Memorial Institute 1998; Harrison and Horne 2000; Killgore and others 2006). If a person has 20 or more apnoeas per hour, both health and daytime alertness will suffer (Caldwell 2006). When present, excessive daytime sleepiness is inversely correlated with vigilance, but not all people with OSA display excessive daytime sleepiness (Seda and Han 2020).
Circadian rhythms are the body’s internal clock that regulates the sleep-wake cycle and repeats roughly every 24 hours. An individual’s alertness, sleep tendency and human error have been shown to follow this 24-hour pattern (CASA 2016). According to the International Civil Aviation Organization’s Fatigue management guide for airline operators (ICAO 2015), there are two times of peak sleepiness within 24-hour cycle. The main peak is in the early morning between 0300-0500 known as the window of circadian low, another smaller peak is around 1500-1700 known as the afternoon nap window. During the afternoon nap window, someone who has had restricted or disturbed sleep can find it harder to stay awake.
Other factors that can increase the fatigue risk level include early shift start times (before 0600), when regular breaks have not been taken, and when shifts are longer than 8 hours (CASA 2012). Twenty per cent of accidents where fatigue was attributed were in the 10th or more hour of duty (Goode 2003).
Effects of sleep apnoea
Sleep apnoea can have significant physiological, neurological, cognitive and psychological impacts, and can affect multiple cognitive domains (Seda and Han, 2020). Several studies have shown that OSA has an adverse effect on inductive and deductive reasoning, attention, vigilance, learning, and memory (Lal and others 2012). These impairments are measurable in neurological and cognitive assessments, but they may not be readily evident during flying operations or medical examinations. Deficits in neurocognitive functioning have been shown to occur with a high frequency in OSA sufferers, but the exact prevalence is unknown.
Investigation findings regarding sleep apnoea
A search of the US National Transportation Safety Board database revealed 29 aviation accidents between 1997 and 2019 with ‘sleep apnea’ included in the analysis text, with 9 accidents where it was concluded that OSA had some contribution.
There were 8 accidents in which a pilot had OSA, and the OSA itself or in combination with other diseases and medications contributed to the accident. A further accident involved a fuel truck driver with OSA who fell asleep, and the truck collided with an aircraft.
In one investigation there was no evidence that the pilot suffered sleep apnoea, in another it was unlikely that the pilot’s effectively treated OSA contributed to the accident. For the other 17, the pilot either had, or was at risk of, OSA but it could not be determined whether the pilot was suffering from any effects of OSA and/or whether these contributed to the accident.
The Transportation Safety Board of Canada published a list of all their investigations with fatigue‑related findings from 1990 to 2018. One of 34 aviation occurrences where fatigue was listed as a causal or contributory factor or a source of risk, mentioned OSA. Following diagnosis of OSA and initial effective CPAP treatment, the pilot subsequently rarely used CPAP therapy. The investigation found that although the pilot was therefore at risk of fatigue, there was no indication that fatigue contributed to the occurrence.
One ATSB investigation report into a fatal accident involving a collision with terrain during landing practice in a solo training flight (AO-2016-112) identified that the pilot had ‘a history of health and chronic pain issues including sleep apnoea’. The investigation found that:
Fatigue and level of experience likely affected the pilot's ability to respond to the demands required to correct the aircraft's departure from controlled flight during the landing attempt and subsequent go‑around.
Post-mortem and toxicology results
The post-mortem report documented multiple impact-related injuries, including spinal fractures, with the cause of death identified as severe traumatic head injury. This was as a result of diffuse cerebral injuries, while only relatively superficial contact injuries to the head were noted. These included bruising consistent with a left-side impact to the head. There was also bruising consistent with the pilot being restrained during the accident by the lap belt, but not from the accompanying shoulder sash.
The only substance identified in toxicological examination was almost certainly administered by emergency/hospital personnel.
Aircraft information
VH-HNF was a Robinson Helicopter Company R44 Raven I helicopter, powered by a six-cylinder Lycoming O-540-F1B5 engine, manufactured in 2018 and first registered in Australia in April 2018.
The helicopter’s current maintenance release was issued on 21 January 2020 and was valid for 12 months or 100 hours, whichever occurred sooner. A 50-hourly inspection had been conducted on 26 March 2020, at 353.8 hours, and no defects were recorded on the maintenance release. Prior to the commencement of flying on 31 July 2020, the aircraft had accrued 388.5 hours total time in service.
The helicopter was fitted with a Helipod III Agricultural Spray System, which included a single fibreglass belly tank attached to the landing gear and a spray boom and nozzle arrangement located towards the front of the helicopter. Pilot control of the system was via a cyclic-mounted switch. For the system fitted, the maximum chemical tank load was 285 L or 285 kg. With the Helipod system installed, the helicopter was to be operated in the Restricted category and in accordance with a special certificate of airworthiness.
The exact quantity of fuel and chemical on board at the time of the accident was unable to be determined. However, the helicopter would have been within the weight and balance limitations through the range of empty to full fuel and spray tanks.
The R44 helicopter was not fitted with wirestrike protection. The most common aircraft-mounted wirestrike protection systems (WSPS) are passive and comprise deflectors to guide a struck wire to a fixed wire cutter consisting of sharpened blades. They are designed to reduce the likelihood of adverse outcomes resulting from a wirestrike, including entanglement, damage to flight controls, the airframe and injuries to occupants. To be effective, the system relies on the wire entering the cutter with sufficient force and at a suitable angle to cut it. ATSB research report
stated that smaller rotary-wing aircraft including Robinson (R22 and R44) helicopters ‘generally have no structural hard points to fit a WSPS and are generally too light and, in many instances, travel too slowly for WSPS to be effective’.
Meteorological information
Witness reports indicated the weather was fine and sunny with calm to mild winds. Bureau of Meteorology observations at 1100, from the nearest recorded weather stations, indicated the temperature was between 10 °C and 12 °C and the wind 0 to 4 kt.
Site and wreckage examination
Powerline
The 19.1 kV single wire earth return powerline spanned 305 m and was supported by two power poles, one located 144 m north-west and the other 161 m south-east of the fence. It crossed the fence line at a gate. Between the poles, the wire drooped parabolically from about 10 m at the pole to 6 m mid span when new but had likely stretched due to its age and was therefore about 5 m above the ground mid span, where it was struck. The wire was pulled off several poles and broken in two places.
The powerline was not marked and was not required to be, according to Australian Standards 3891.1 and 3891.2.[4] Following a wirestrike of a powerline owned by Essential Energy, field workers assess the risk of another strike. If it is considered likely, at least one aerial marker (Figure 2) is fitted to the wire. It was assessed at the time that a subsequent wirestrike was unlikely to occur due to the remoteness of the location and because the helicopter was spraying weeds along the perimeter fence rather than crop spraying. As a result, no markers were fitted to the wire when it was restrung or subsequently.
Figure 2: Example of a wire aerial marker
Source: Balmoral Engineering
Accident site
The accident site was in flat, open farmland, about 7 km north-east of the loading vehicle. The main fuselage was located about 120 m beyond the powerline, in the direction of travel.
Wire abrasion marks were evident down the front of the forward left strut and along the top of the left skid, ending with a distinct friction mark near the tip of the skid (Figure 3). The powerline remained entangled in the wreckage.
Examination of the ground scars, damage and distribution of the wreckage indicated:
the main rotor had impacted the tail boom during the accident sequence, resulting in loss of control of the helicopter
the helicopter collided with the ground on its left side in a nose-down attitude of about 30°
the main rotor blade and landing gear dug into the ground, resulting in the helicopter bouncing, rotating about 180°, and coming to rest on the right side.
Figure 3: Wire marks on VH-HNF’s left skid
Source: ATSB
The ATSB examined the helicopter and did not identify any evidence of in-flight breakup, birdstrike, or pre-existing defects that may have contributed to the wirestrike. Consistent with normal agricultural operations, the pilot door was not fitted at the time of the accident. Significant structural deformation of the helicopter’s left front quarter and seat was consistent with a heavy impact on that side, to the extent that there was no occupiable space for the front left seat. On the right (pilot’s) side, there was crushing of the seat lower box section (as designed, to absorb vertical impact loads) and some right-side roof deformation, associated with the left-front impact. Although compromised, occupiable space on the right side of the fuselage remained.
There were no issues identified with the flight controls, and examination of the engine found no anomalies that would have affected the engine’s performance. Evidence that the main rotor was being driven under power included that one of the main rotor blades showed significant chordwise bending and, from the other blade, a section of blade tip, measuring 850 mm and weighing 5.3 kg had fractured as a result of ground impact and was thrown approximately 300 m from the accident site.
The loader had recorded uplift of 40 L of Avgas prior to the start of the fifth load. A large quantity of fuel remained in the left fuel tank, and testing indicated no evidence of water or contaminants. There was no post-impact fire.
The chemical holding tank had been compromised and no visible herbicide remained, but a strong odour indicated that a quantity had leaked and soaked into the ground where the aircraft had come to rest. The pilot-controlled spray switch was in the on position.
Operational information
Helicopter operator
Riverina Rotor Work, trading as Riverina Helicopters, was the registered owner and operator of VH-HNF. Riverina Helicopters held a CASA-issued Air Operator’s Certificate to conduct aerial work and aircraft charter operations. Of relevance to this occurrence, the Riverina Helicopters Operations Manual included:
Protective helmets shall be worn for all specialised operations.
Low level operations
Before descending to conduct low level operations, the pilot in command shall conduct a reconnaissance of the area and identify the hazards noted from the study of the charts and to make a note of other hazards not indicated on the charts.
Agricultural operations – helicopters
The Company shall be responsible for supplying pilots with up-to-date maps and charts of the various treatment areas, clearly displaying all hazards associated with those areas. However, prior to the commencement of operations, the pilot in command shall become familiar with the task by personal inspection and briefing by drawing a ‘field map’ of each area to be treated. Pilots should be aware that any locally supplied information is often incorrect but it does at least provide a guide and can be verified during aerial inspection of the area. A copy of the applicable field map(s) should be taken by the pilot on each sortie…agricultural pilots are required to carry out a preliminary aerial inspection of the area to be treated including the adjacent manoeuvring areas in all directions, paying particular attention to the location of obstructions including those, if any, outside the actual treatment area.
In addition, the operator’s Management System procedure – Conduct an application, included that:
The pilot will conduct a pre-application aerial inspection of the target ensuring that they have confirmed the following with their work order:
iii. Power Lines, Towers, Aerials, moisture probes & other obstacles are located and identified.
Steam Plains task
The station manager had previously engaged Riverina Helicopters for aerial work in 2010, 2012, 2016 and March 2020. Commencing on 29 July 2020, the station manager had contracted Riverina Helicopters to spray weeds along the fence and adjacent track at Steam Plains and a neighbouring property as a firebreak. The pilot conducted the same task during the 2016 engagement.
Pre-flight planning
On the morning of 29 July (day 1 of the 3-day task), the chief pilot was delayed leaving Griffith in the helicopter due to fog. The pilot drove the loading truck and the station manager reported that it arrived at about 0800. The station manager met the pilot at the truck and gave the pilot a briefing of the task. This briefing included discussing the chemicals that would be used for spraying, the application rate of the chemicals, areas to be sprayed, flight path and hazards. The station manager provided the pilot with maps of Steam Plains and the adjacent property. The maps had been provided to the property owner on purchase in 2008, at which time the property owner had assessed by ground vehicle that the markings on the maps appeared to be correct.
The spray application path had been drawn on the map in red marker pen by the station manager. Using the map, the station manager briefed the pilot about the location of crops, stock and people working in the area. The pilot used a blue pen to over-mark the powerlines (Figure 4). When the chief pilot arrived later that morning, the pilot passed on the details from the briefing, including the powerlines.
The station manager met with the pilot and chief pilot on the morning of 31 July, at about 0650. They discussed the day’s plan including reviewing the map. Before commencing operations, the pilot and chief pilot briefed on the day’s operation again, including the task, map and powerline location.
Prior to the fifth (accident) load, the pilot fuelled the helicopter and discussed with the chief pilot the shape of the boundary fence to be sprayed on the next sortie and the location of the powerline.
Figure 4: Map of Steam Plains Station showing spray path (red) and powerline (blue)
Source: Station owner, marked by the station manager and pilot, and annotated by the ATSB
Mapped powerline location
Figure 5 shows a comparison between the powerline marked on the pilot’s map and its actual location taken from Essential Energy’s Look-up-and-live app. On the pilot’s map (left image), the powerline is depicted close to the fence corner and beyond the (marked) gate. The powerline’s actual location was exactly overhead the gate and about 300 m further west of the fence corner than depicted on the pilot’s map.
In addition to the commentary in the Riverina Helicopters Operations Manual about the possibility of incorrect locally-supplied information, training also emphasised possible inaccuracies. The instructor who conducted the pilot’s annual flight review and proficiency check in 2019 commented that pilots are trained to expect that planning information may be inaccurate, and reinforced the importance of verifying it by conducting an aerial inspection.
Figure 5: Map location compared with actual powerline location
Source: Helicopter operator, Google earth and Essential Energy, annotated by the ATSB
Spraying procedures
The AAAA Aerial Application Pilots Manual (AAAA 2011:166) advised that:
all application pilots should be trained to carry out an extra “wind and wires” check before commencing each run, to refresh short-term memory and refocus on any wires.
When spraying a crop or paddock, hazards in the whole area are identified before spraying and the hazards then generally remain fixed. However, the operator reported that, to retain identified hazards in working memory when spraying along a fence line on a large property, a pilot may conduct an aerial reconnaissance of a section of the target spray path before spraying that section, then repeat as the helicopter progresses along the fence line.
In addition, the AAAA Aerial Application Pilots Manual (AAAA 2011:151) stated:
Recollection of precise locations of power lines based on the [application management plan] AMP and a confirming aerial survey is critical to safe application. High situational awareness and an accurate mental map of the treatment area must remain front of mind for the pilot throughout the application…The aerial inspection is the last chance for the pilot to build defences and manage risk.
Aerial inspection and GPS data
Two GPS systems recorded data from the helicopter for the accident flight: Spidertracks and TracMap. Spidertracks data was recorded at 2-minute intervals. The TracMap GPS data associated with the spraying system included speed, altitude and whether the spray system was on or off. Due to buffering from incomplete shutdown associated with the collision, the last TracMap data that was recorded was above the trees with the spray off, before the helicopter descended and about 300 m before it struck the wire.
The TracMap data was compared for the 3 days of the task.
On the first day, the chief pilot reported conducting short inspection flights in the target area ahead, then spraying that section with a good understanding of the hazards present. This was evident in the GPS data for the day, where most tracks were flown twice – once 50 to 100 ft higher with the spray off, then from a lower height with the spray on. Where the intended spray path was along or across a powerline, the helicopter tracked to the wire with the spray off before descending and commencing spraying.
On the day prior to the accident, the pilot was operating on the property neighbouring Steam Plains and the chief pilot was performing loader duties. The GPS data showed that on that day, the helicopter had overflown a powerline several times, including before descending to spray along the wire and perpendicular to it. This was consistent with what the chief pilot observed when the helicopter was operating in sight of the loading truck – short inspection flights conducted before spraying.
On the accident day, the GPS data showed only one small segment of the southern perimeter was flown twice – at the end of the first and start of the second loads. There was no further duplication of any of the tracks and no aerial inspection conducted. The helicopter had not overflown the powerline before the wirestrike.
Previous wirestrike
In 2018, the pilot was operating a helicopter that struck a powerline during spraying operations. The pilot conducted an aerial inspection prior to commencing the task and was aware of the powerline. However, a moisture probe that stood above the crop canopy momentarily distracted the pilot’s awareness of the powerline.
The day after that occurrence, the chief pilot had a debrief with the pilot and recalled discussing the sequence of events leading up to the accident, the wirestrike and the post-accident period. A subsequent follow-up discussion with the pilot included techniques to remain situationally aware and understanding the danger of distraction. Following the accident, the pilot completed an AAAA course in cockpit resource management and wire awareness, and a Robinson Helicopter Safety course.
Survivability aspects
The following section is largely based on a report provided by The Royal Australian Air Force Institute of Aviation Medicine. The report included advice regarding the use of helmets and restraints in helicopter accidents and their role in reducing the risk of fatal injuries in an otherwise survivable accident, as well as analysis specific to this accident.
Survivability and injuries
The FAA report Analysis of rotorcraft crash dynamics for development of improved crashworthiness design criteria (Coltman and others 1985) defined a survivable accident as one in which the acceleration forces were within the limits of human tolerance and sufficient occupiable space remained for well-restrained occupants. Accidents in which impact injuries of the head or upper torso resulted from striking a surface, and could have been prevented by proper restraint, were deemed potentially survivable.
Injuries from aircraft accidents arise from three distinct sources:
excessive acceleration forces (internal injuries)
direct trauma from contact with hard surfaces
exposure to environmental factors such as fire, smoke, water, and chemicals.
Acceleration forces
Significant research has been conducted into human tolerance of impact forces. Survivable velocity/acceleration envelopes have been determined based on analyses of helicopter accidents, including the injuries sustained by occupants, and the vertical, longitudinal and lateral impact forces (Coltman and others 1989, Coltman and others 1985). A large proportion of the studied US civilian helicopter wirestrike accidents (1974–1978) were classified as non-survivable due to the uncontrolled flight that followed the strike, and 65 per cent of the wirestrike accidents resulted in serious or fatal injuries.
Due to the compound forces on the helicopter (VH-HNF) when it impacted the ground, including a vertical component that resulted in seat crushing (as designed), lateral impact on the left front side and rotational forces, the ATSB was unable to accurately determine the velocities in each plane, to assess whether the acceleration forces were survivable.
Trauma injuries
In US Army helicopter accidents from 1979 to 1985, trauma injuries from striking the aircraft structure occurred at least five times more frequently than acceleration injuries (Shanahan and Shanahan 1989). The potential for trauma injuries can be reduced by using restraint systems that decrease the area the body can move around in. That is, by reducing the ‘flail zone’ or ‘strike envelope’.
Restraints
The Australian Civil Aviation Safety Order 20.16.3 required at least one pilot crew member to wear a seat belt or safety harness at all times during flight. Civil Aviation Safety Regulation Part 137.225 required fitment of a 4-point harness to fixed-wing aeroplanes operating in the Restricted category – for example, when fitted with ‘role equipment’ such as a spray system – however, this requirement did not apply to helicopters operating in the Restricted category. CASA advised that a proposal to amend Part 137 to include Rotorcraft was expected to commence by the end of 2022. Civil Aviation Safety Regulations Part 90.105 required helicopters to be fitted with a safety harness that ‘must consist of a lap belt and at least 1 shoulder strap’ (3-point harness). Figure 6 illustrates 2-, 3-, 4- and 5-point harnesses.
Figure 6: Aviation restraint types
Source: Aircraft Crash Survival Design Guide, US Army Aeromedical Research Laboratory, annotated by the ATSB
The US Federal Aviation Regulation 137.31 for helicopters conducting aerial application was consistent with Australian regulations in requiring a minimum of a lap belt and shoulder harness for pilots. Some operators have higher standards to reflect their risk associated with their type of operation. For example, the US Department of the Interior, responsible for a large fleet of aircraft conducting land-management-related tasks, required the use of a 4-point restraint (with an inertia reel) for front seat occupants of helicopters. Military standards in the US and Australia mandate the use of a 5-point harness,[5] due to the risks associated with their requirement to fly at low altitudes, in close proximity to obstacles and hazards.
Upper torso restraints serve two purposes: to reduce upper body flailing and subsequent contact with aircraft structures and strike hazards, and to distribute acceleration forces across a larger body area to reduce local transmission of force. Although the shoulder sash of a 3-point harness (the design basis for the common seat belt in cars) provides restraint in a forward direction, it provides lateral restraint in only one direction. If the occupant moves in a lateral or diagonal direction away from the shoulder restraint, it is possible to slip out of the shoulder sash.
The limited aviation research for occupants in 3-point restraint systems subjected to oblique impact forces, indicates a risk of head and abdominal injuries from deceleration forces (Snyder and others 1969). Automotive accident research indicates the potential for greater flailing in oblique (60°) impacts compared to completely lateral (90°) impacts due to torso rotation and reduced engagement of the shoulder (Forman and others 2013). Therefore, if deceleration forces have large lateral or oblique components on the opposite side of the 3-point harness, there would likely be reduced protection provided to the upper torso and head in that direction. In a helicopter accident, crash deceleration forces on the occupant may be from multiple directions as the helicopter impacts the ground and rotates.
The front seats of VH-HNF were fitted with 3-point harnesses. The pilot’s shoulder sash was installed to cover the right shoulder. After the initial front-left impact, the helicopter rotated and came to rest on its right side. The pilot was found in the right seat, with the lap belt still attached across the waist, but the pilot’s upper body was outside the right side of the cabin, in front of (unrestrained by) the shoulder sash. The seat and seat belt were intact. This suggests the pilot may not have been wearing the shoulder sash at the time of the accident. Alternatively, the pilot may have slipped out of it during the uncontrolled flight following the wirestrike or during the crash sequence. In the latter case, the pilot would also have had to slip back underneath the sash to end up in front of it. The operator reported that the company pilots always wore the fitted restraint and specifically that they had observed this pilot to always wear the restraint correctly. However, it could not be determined whether the pilot was wearing the shoulder sash at the time of the accident.
A comparison between the flail zone for an occupant wearing a lap belt only (2-point harness) and a 4-point harness is depicted in Figure 7. These images show that the maximum head strike distance is reduced to 50 per cent with the 4-point restraint. Reducing the flail zone significantly reduces injury risk by reducing the number of objects that could cause strike injuries. In particular, this reduces the risk of potentially fatal head injuries, which was the most common cause of death in aircraft accidents (Crowley and others 1992).
Figure 7: Lap belt only (2-point harness) and 4-point harness flail zone
Source: Aircraft Crash Survival Design Guide, US Army Aeromedical Research Laboratory, annotated by the ATSB
Flight helmets
Benefits and requirements
Helicopter accident investigations conducted by the US Army in the 1980s determined that aircrew lives were being lost to head injury in otherwise survivable accidents (where the deceleration forces were within human tolerance). The outcome of this was the introduction and ongoing development of helmet standards. In an analysis of ‘severe accidents’, it was determined that occupants not wearing a helmet were significantly more likely to sustain severe and fatal head injuries (Crowley and others 1992). This finding was also consistent in civilian flying studies (Taneja and Wiegmann 2003). The introduction of protective helmets into military aviation has significantly reduced the incidence of head injury (Lewis 2006).
The Civil Aviation Safety Regulations did not require pilots to wear flight helmets. However, it was often mandated by aircraft operators for pilots engaged in aerial work, and necessary to meet federal- and state-legislated workplace, health and safety requirements. The AAAA code of conduct required a commitment to wear suitable personal protection equipment including a flight helmet. The pilot of VH-HNF was a member of AAAA and the company operations manual required a flight helmet to be worn.
Standards
Helmets are designed primarily to provide impact protection – attenuating force and distributing it over a larger surface area – and penetration resistance. Helmets primarily consist of a composite shell that encases an ‘impact cap’, made from a layer of rigid foam that crushes on impact, and an inner liner/padding for fitment and additional energy absorption. The helmet should also include support for the retention system (including chin strap), visor(s) and communication equipment, as well as noise attenuation. The helmet must be retained on the head following an impact to protect against injury in subsequent impact/s.
There are specific standards for each of these domains and many commercially available helmets for civilian helicopter operators meet these to varying degrees. There was no Australian Standard for flight helmets, however helmet manufacturers used relevant standards that included the US Department of the Interior (DOI)/US Forest Service (USFS) Aviation Helmet Standard, US Military Standard and the European Standard (EN-966) Helmets for Airborne Sports.
The pilot of VH-HNF wore a MSA LH250 helmet (Figure 8). The manufacturer’s brochure indicated that the helmet was for pilots/flight crew of helicopters, transport and training aircraft without ejection seats. The helmet was reported to meet or exceed:
impact resistance to US Air Force (USAF) MIL-DTL-87174A, DOI/USFS Aviation Helmet Standard
penetration resistance to USAF MIL-DTL-87174A EN-966, DOI/USFS Aviation Helmet Standard
retention to EN-966:2012 and EN-966:2006, DOI/USFS Aviation Helmet Standard.
The US military standards had different requirements for helmets used in helicopters and aeroplanes. Helicopter and aeroplane helmets were required to be impact tested at five sites (front, rear, left and right sides, crown), but helicopter helmets also required impact testing at two additional sites: the left and right ear cups. The MIL-DTL-87174A standard described helmet performance for use in fixed wing aircraft (aeroplanes) and therefore helmets qualified to that standard may not provide adequate protection for helicopter occupants.
Figure 8: MSA LH250 helmet
Source: Flight Helmets Australia
To meet the specifications a helmet is designed for, it must be fitted correctly, worn properly and maintained in accordance with the manufacturer’s requirements. The manufacturer of the pilot’s MSA LH250 helmet advised wearers of the following.
- To provide sufficient protection, the helmet must be fitted and adjusted to the head size of its wearer.
- The helmet is made in such a way that any energy received during an impact is absorbed by the destruction of or partial damage to the shell and impact cap; even if this damage is not immediately apparent, replacement of the whole helmet is recommended after a major impact.
- The helmet must be inspected for damage after obvious or suspected impact, or where routine maintenance reveals indications that suggest impact damage may have occurred. Helmet users are responsible for reporting known or suspected damage to helmets and to arrange further assessment, including if the helmet had sustained any impact in a previous accident. If the helmet has sustained a major impact, it should be replaced even if damage is not apparent.
Fitment and maintenance
The pilot purchased the helmet new in 2010. The shell was within its 15-year warranty period at the time of the accident. The pilot had purchased a new chin strap and edge roll (padding) in 2015, and earcup pieces and edge roll in 2017. There was no evidence of the helmet having been serviced by the distributor from which it was purchased.
The LH250 helmet comes in two shell sizes, which can be personalised with pads to fit the wearer’s head. The manufacturer advised that the pads degrade over time and should be replaced to ensure optimum fit. The fit of the helmet was not able to be assessed in this instance. The helmet was fitted with a chin strap and locking buckle, which met US DOI and US Military standards. The chin strap was noted by the ATSB to be worn and frayed (Figure 9). This was indicative of the chin strap being worn securely fastened over a long time.
The pilot had very likely been wearing the same helmet during a helicopter accident in 2018, in which the pilot sustained facial injuries. It could not be determined whether the helmet sustained an impact in that accident, or whether any subsequent inspection or maintenance was conducted, although it was confirmed that the helmet had not been sent to the distributor from which it was purchased.
Figure 9: Helmet chin strap
Source: ATSB
Effectiveness
The helmet was found at the accident site, on the ground on the left side of the helicopter, the opposite side to the final resting position of the helicopter on its right side and the pilot in the right seat. The helmet sustained extensive structural damage, with significant cracking of the shell on the top and on the left side. The structure around the left ear and visor attachment was crushed and there was a dent in the shell above the left eye. Most of the outer visor and track had broken off from the right side, and there was paint transfer and scrape marks on the top of the helmet.
The chin strap was found undone with dirt lodged in the clasp. The chin strap fastened on the right-hand side of the helmet (Figure 10). The post-mortem report did not identify chin injuries to indicate that the helmet had been forcibly removed with the chin strap properly adjusted and secured. However, any such injuries may have been obscured by facial hair. Post-accident testing of the helmet by the ATSB found it was possible to undo the clasp with a relatively small ‘bump’ applied to the clasp. As the clasp was on the right side, this force needed to be applied opposite the (left) side of the initial impact. Although there was no evidence of damage to the clasp or scuff marks near the latch to indicate contact, the damage to the right side of the helmet was consistent with a secondary impact on that side. There was also no documented history of this latch coming undone in accidents.
Figure 10: Helmet clasp and buckle
Source: ATSB
Risk of injuries
The ATSB considered whether wearing a helmet may increase the risk of cervical spine injury, given those sustained by the pilot in this accident. The Royal Australian Air Force Institute of Aviation Medicine indicated that there was limited data on this specific risk from helicopter accidents, however the considerable data from motorcycle and all-terrain vehicle accidents demonstrated clear benefits for helmet use in reducing head injury and no difference in regard to neck injuries.
Wirestrikes
Visibility of wires and poles
Powerlines, particularly unmarked wires, may be impossible to see due to the size of the wire, camouflage with the background and limitations of the eye.
Imagery taken from the ATSB’s remotely piloted aircraft (RPA), while following the helicopter’s estimated flight path at about the same time on a subsequent day, found that the wire would have been extremely difficult to see (Figure 11 and Figure 12).
Figure 11: RPA image 50–75 m prior to the powerline showing the accident location, taken at 1028 on 4 August 2020, with powerline highlighted
Source: ATSB
Figure 12: RPA image 50–75 m prior to the powerline showing the accident location, taken at 1028 on 4 August 2020, noting powerline visibility
Source: ATSB
During agricultural operations, pilots must retain the position of a powerline in their memory and are taught to use other visual indications of the presence of a wire, such as a group of trees, power pole, building or feature. The AAAA Aerial Application Pilot’s Manual (AAAA 2011:151) stated:
…the background to the wires – trees, hills etc. – may often provide a poor contrast. Poles may be concealed by intervening obstacles or by being located so far towards the periphery of the pilot’s visual field that they are not noticed.
Figure 13 shows the two closest power poles located either side of the helicopter’s flight path. From ATSB RPA footage taken along the estimated flight path, at times, both poles were obscured by trees and lacked contrast and texture variation from their background (Figure 14 and Figure 15). The two power poles should have been visible within the pilot’s peripheral vision, however it is likely that the pilot’s visual acuity was affected by contrast sensitivity, resulting in the pilot being unable to discriminate the poles from their background. Additionally, based on the powerline’s location on the pilot’s map, the pilot may not have been looking for cues at that time.
Figure 13: Power poles either side of flight path
Source: lookupandlive app annotated by the ATSB
Figure 14: RPA footage of reconstructed flight path showing location of poles left and right of track from about 160 and 350 m respectively
Source: ATSB
Figure 15: RPA footage of reconstructed flight path showing right pole from about 240 m
Source: ATSB
Similar occurrences
Research conducted for the ATSB publication Wirestrikes involving known wires: A manageable aerial agriculture hazard found that there were 180 wirestrike accidents in the ATSB database for the period between 2001 and 2010. During that period, 55 wirestrikes involved helicopters, 30 of which resulted in an accident and 25 were serious incidents. Of the 55 helicopter wirestrikes, 20 occurred during aerial agricultural operations. Particularly relevant to this accident, the report reminded pilots to:
have an up-to-date and detailed map with powerlines and other hazards clearly marked
obtain network maps from the power company if available
not rely solely on maps and pre-flight briefing
always conduct an aerial reconnaissance to confirm wire locations and detect other hazards.
For the 10-year period from 2010 to 2020, there were 67 wirestrikes involving helicopters recorded in the ATSB occurrence database, 54 of which were conducting aerial work – 30 of which were during aerial agricultural operations. Of the aerial work occurrences, 23 were classified as accidents and 9 resulted in serious or fatal injuries to the occupants.
The pilot had been employed by the operator since 2015 and was experienced, trained and qualified to conduct the spraying operation. After being involved in a wirestrike 2 years earlier, the pilot underwent additional training and checking with no issues identified.
The weather on the accident day was sunny with mild temperatures and very light winds. After a delayed start because of dew, the pilot had been flying for less than 2 hours, during which time the helicopter had landed five times to reload with chemical and fuel. The pilot appeared in good health and there was no indication of any performance issues with the helicopter.
Aerial inspection and hazard identification
Due to a lack of contrast between the wire and the vegetation as the pilot looked down from the helicopter towards the fence line below and with no markers fitted to the wire, it would have been very difficult for the pilot to visually detect the powerline with sufficient time to avoid the wirestrike.
Had the pilot been relying on the powerline’s location depicted on the map, the helicopter would have encountered the wire earlier than expected. Therefore, the remaining defence available to the pilot would have been visual cues along the spray path. In this case, the power poles would likely have been visible, had the pilot been looking for them either side of the flight path. However, as the helicopter approached the wire, the poles would have been difficult to detect in the pilot’s peripheral view, if looking straight ahead.
It was clear that the pilot was aware of the powerline from pre-flight planning, and the chief pilot reported having discussed the powerline with the pilot on multiple occasions, including while loading the helicopter prior to the last take-off. However, despite being aware of the wire, and for reasons that were not determined, the pilot had not completed an aerial hazard inspection of the spray path, other than overflying a small section of the southern perimeter at the start of the second load. Doing so would have provided a clearer mental model of the wire’s exact location and better equipped the pilot to avoid it.
Pilot restraint
The helicopter was fitted with a 3-point harness, consisting of a lap belt and shoulder sash. The pilot’s torso had not been effectively restrained by the shoulder sash as evidenced by:
the pilot’s head injury and damage to the helmet indicating a left-side impact
the pilot was found secured in the lap belt but positioned out (and in front) of the shoulder sash
an absence of bruising caused by the shoulder sash.
Based on the pilot’s final position in front of the shoulder sash, it was possible that the shoulder sash had not been worn at the time of the wirestrike, although the operator had always observed the pilot to wear it correctly. A right-seat shoulder sash is designed to restrict movement in the forward and right diagonal directions. Its effectiveness for restraint is likely to be significantly reduced with movement to the left. With the initial force sending the pilot leftwards, it is possible that the pilot came out of the sash. If so, the resultant flail zone would have been similar to wearing a 2-point harness (lap-belt only). Either way, not being restrained by the shoulder sash significantly increased the risk of strike injuries and injuries due to the pilot not being retained within the occupiable space.
Had the pilot been wearing a 4- or 5-point harness, which provide lateral stability to the upper torso in both directions, the risk of strike injuries, particularly to the head, would have been reduced. Additionally, the risk of deceleration injuries would also have reduced due to the decrease in relative impact forces for an occupant with the upper torso restrained.
Helmet effectiveness
The damage to the helmet and superficial contact injuries including bruising to the pilot’s left cheek, in the absence of skull and facial fractures, indicated that during the initial impact with terrain, the pilot was wearing the helmet and it had protected the head from significant blunt force trauma. Following the initial impact, the helmet completely came off the pilot’s head, increasing the risk of injury from subsequent impacts, and potentially reducing its effectiveness in attenuating the initial impact forces.
The chin strap was found intact and attached to the helmet but undone. It could not be determined whether the chin strap came undone during the accident sequence or was not secured at the time. Although the primary impact was on the left side of the helmet, there was also some damage to the right side of the helmet and visor and the chin strap clasp was on the right side. However, there was no visible damage to, or in the vicinity of, the clasp. Although the ATSB found that the clasp could come undone with a direct ‘bump’ force applied to it, there were no witness marks to indicate the clasp was opened from being caught on something during the impact sequence or directly impacted or bumped. The poor condition of the chin strap may also have resulted in it being uncomfortable to wear secured under the chin. Its poor condition was, however, consistent with the pilot having regularly worn it secured in the past.
It was very likely that the same helmet had been worn in an accident 2 years prior, and the helmet’s effectiveness would have been reduced had it sustained damage during that occurrence. There was no evidence to indicate that was the case, however there was also no evidence that the helmet had been inspected or serviced following that accident. An inspection would have provided an opportunity to identify any damage or items requiring maintenance to ensure that the helmet was continuing to function in accordance with its design specifications.
In any event, the diffuse brain injuries sustained by the pilot indicate the helmet did not attenuate the acceleration forces to the brain to a survivable level. It was not possible to determine if the impact forces exceeded the helmet’s specifications and/or whether the helmet’s effectiveness was compromised by any of the above considerations. However, it is important for pilots to remember that to be fully effective, a helmet must be fitted properly, worn correctly and maintained in accordance with manufacturer instructions.
Obstructive sleep apnoea
Following diagnosis of severe obstructive sleep apnoea (OSA) in February 2020, the pilot had initially managed the condition using a continuous positive airway pressure (CPAP) machine. However, over time, there had been reduced compliance with the treatment, and the CPAP machine had not been used for 2 weeks prior to the accident.
There was no evidence of the pilot having consulted a general practitioner or specialist physician since the diagnosis. This was a missed opportunity for a professional to ensure the CPAP machine’s efficacy in the pilot’s sleep quality. The pilot had also not reported the condition to a Civil Aviation Safety Authority designated aviation medical examiner, which prevented oversight of any ongoing safety risk associated with the condition.
Untreated, the pilot’s condition increased the risk of experiencing the effects of fatigue. However, the pilot had not reported excessive daytime sleepiness at the time of diagnosis. The pilot also had not stayed up late or awoken early and had been operating the helicopter for only about 1.5 hours that morning. Further, the time of day at which the accident occurred, 1057, was not a period of increased risk of fatigue based on the pilot’s reported sleep/wake times.
Even in the absence of fatigue, untreated severe OSA can cause inattention and impaired cognitive function and is linked with several other conditions. However, there is no evidence that cognitive impairment affects everyone with OSA or that the severity of OSA predicts its impact (or associated risks). Therefore, although the pilot was at an increased risk of cognitive impairment due to not using the CPAP to treat the severe OSA in the 2 weeks before the accident, it could not be concluded that the pilot was affected by this at the time of the accident.
Further, the ATSB assessed whether the pilot’s actions may have been indications that the pilot was experiencing the possible effects of OSA. It was possible that cognitive impairment led to the pilot inadvertently omitting the inspection, however, while the pilot had conducted an inspection the previous day, it could not be determined why the pilot did not do so on the accident day. Having briefed about the location of the wire in pre-flight planning and again immediately prior to the accident load, impaired memory and inattention may have affected the pilot’s recollection of the location of the wire and ability to identify it. However, it was equally possible that the pilot recalled the wire hazard but simply did not see the wire or poles. Additionally, numerous wirestrike accidents have occurred in the absence of OSA, in which the pilot was aware of the wire and/or where a hazard inspection was not conducted (ATSB 2006, 2014).
There is limited evidence of aircraft accidents in Australia and the US in which OSA was a contributing factor. This is at least in part because it is extremely difficult for investigators to assess what a pilot’s cognitive state was at the time of an occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving a Robinson R44 helicopter, registered VH-HNF, at Steam Plains, New South Wales, on 31 July 2020.
Contributing factors
The pilot did not conduct an aerial inspection to verify the location of hazards including the powerline identified during pre-flight planning. As the wire was very difficult to see, the pilot was unable to see and avoid the wire before the helicopter struck it.
The pilot's injuries were consistent with flailing due to the left-side impact, but it could not be determined whether the pilot was not wearing, or slipped out of, the shoulder sash portion of the 3-point harness.
Other factors that increased risk
The pilot was not effectively managing severe obstructive sleep apnoea, which had not been disclosed to the Civil Aviation Safety Authority. This prevented its oversight of any ongoing safety risk associated with the condition.
Other findings
The pilot’s helmet did not attenuate the impact to survivable levels. Either the impact forces exceeded the helmet design specifications, or the helmet was not fitted, worn or maintained correctly.
Untreated severe obstructive sleep apnoea can increase the risk of fatigue and impairment of neurological and cognitive functions which can include impaired memory, vigilance and decision-making.
Safety actions
Safety advisory notice to helicopter pilots and operators
Battelle Memorial Institute (1998) An Overview of the scientific literature concerning fatigue, sleep, and the circadian cycle, prepared for the Office of the Chief Scientific and Technical Advisor for Human Factors, United States Federal Aviation Administration.
Caldwell JL (2006) ‘Physiology of sleep and wakefulness, sleep disorders, and the effects on aircrew’, in Gradwell DP and Rainford DJ (eds) Ernsting’s Aviation Medicine, 5th edn, CRC Press, London, United Kingdom.
CASA (Civil Aviation Safety Authority) (2012) Fatigue Management Strategies for Aviation Workers: A Training & Development Workbook, CASA, Australian Government, accessed 25 September 2021.
Coltman JW, Bolukbasi AO, Laananen DH (1985) Analysis of rotorcraft crash dynamics for development of improved crashworthiness design criteria, United States Department of Transportation, Federal Aviation Administration.
Coltman JW, Van Ingen C, Johnson NB and Zimmerman RE (1989) Aircraft crash survival design guide: Volume II – Aircraft design crash impact conditions and human tolerance, United States Army Aviation Applied Technology Directorate.
Crowley JS, Licina JR and Bruckart JE (1992) ‘Flight Helmets: How they work and why you should wear one’, Journal of Air medical Transport, 11(8):19-23.
DOI and USFS (Department of the Interior and United States Forest Service) (2021) Interagency Aviation Life Support Equipment Handbook/Guide, Revision 3.0, United States.
Forman JL, Lopez-Valdes F, Lessley DJ, Riley P, Sochor M, Heltzel S, Ash J, Perz R, Kent RW, Seacrist T, Arbogast KB, Tanji H, Higuchi K (2013) ‘Occupant kinematics and shoulder belt retention in far-side lateral and oblique collisions: a parametric study’, Stapp Car Crash Journal, 57:343-85.
Gibb R, Scharff L and Gray R (2010) Aviation Visual Perception: Research, Misperception and Mishaps(Ashgate Studies in Human Factors for Flight Operations), Ashgate Publishing Group, Routledge, England, United Kingdom.
Goode JH (2003) ‘Are pilots at risk of accidents due to fatigue?’, Journal of Safety Research, 34:309-313.
Harrison Y and Horne JA (2000) ‘The Impact of Sleep Deprivation on Decision Making: A Review’, Journal of Experimental Psychology, 6:236-249.
Killgore WSS, Balkin TJ and Wesensten NJ (2006) ‘Impaired decision making following 49 h of sleep deprivation’, Journal of Sleep Research, 15:7-13.
Lal C, Strange C and Bachman D (2012) ‘Neurocognitive impairment in obstructive sleep apnea’. Chest, 141(6):1601–1610.
Lewis, ME (2016) ‘Head injury and protection’, in Gradwell DP and Rainford DJ (eds) Ernsting’s Aviation Medicine, 5th edn, CRC Press, London, United Kingdom.
Royal Australian Air Force Institute of Aviation Medicine (unpublished), Support to ATSB AO-2020-040 Accident involving R44 helicopter, vicinity Steam Plains, NSW 31 July 2020, Royal Australian Air Force Institute of Aviation Medicine, Australia.
Seda G, Han TS (2020) ‘Effect of Obstructive Sleep Apnea on Neurocognitive Performance’. Sleep Med Clin. March 15(1):77-85. doi: 10.1016/j.jsmc.2019.10.001. Epub 2019 Nov 26. PMID: 32005352.
Shanahan DF (1993) Basic Principles of Helicopter Crashworthiness, United States Army Aeromedical Research Laboratory (USAARL 93-15), United States.
Shanahan DF and Shanahan M (1989) ‘Injury in U.S. Army helicopter crashes October 1979 –September 1985’, Journal of trauma, 29(4):415–423.
Snyder RG, Snow CC, Young JW, Crosby WM and Price GT (1969) Pathology of trauma attributed to restraint systems in crash impacts, US Federal Aviation Administration Civil Aerospace Medical Institute (DOT/FAA/AM-69/3), United States.
Szczecinski G and Cable G (n.d.), Aviation Medicine for Aircrew, Royal Australian Air Force Institute of Aviation Medicine, Australia.
Taneja N and Wiegmann DA (2003) ‘Analysis of injuries among pilots killed in fatal helicopter accidents’, Aviation Space and Environmental Medicine, 74(4):337–41.
US FAA (Federal Aviation Administration) Pilot safety brochure Fatigue in aviation, FAA, United States, accessed 22 August 2021.
US FAA (Federal Aviation Administration) Sleep apnoea in aviation, FAA, United States, accessed 29 December 2021.
Veillette P (2015) ‘Wire wary: what you don't see can kill, and does’, Business and commercial aviation, October pp.24–28.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Riverina Helicopters
Steam Plains station manager and owner
the Civil Aviation Safety Authority
Essential Energy
the helicopter maintainer
Royal Australian Air Force Institute of Aviation Medicine.
Submissions were received from
Riverina Helicopters
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Glossary
AAAA
Aerial Application Association of Australia
ATSB
Australian Transport Safety Bureau
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CPAP
Continuous positive airway pressure
DOI
Department of the Interior
EN
European Standard
FAA
Federal Aviation Administration
OSA
Obstructive sleep apnoea
RPA
Remotely piloted aircraft
US
United States
USAARL
United States Army Aeromedical Research Laboratory
USAF
United States Air Force
USFS
United States Forest Service
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 July 2019, the pilot of a Robinson Helicopter Company R44 helicopter, registered VH-KCH, was conducting a private flight from a property near Mansfield, Victoria, with one passenger on board. Shortly after take-off, the helicopter struck a powerline and subsequently collided with terrain resulting in serious injuries to the passenger and minor injuries to the pilot.
What the ATSB found
The pilot obtained some information from the landowner about powerlines on the property from where the helicopter took off, and a neighbouring property. However, he did not identify the presence of powerlines during the flight planning process and he did not see the wires or the associated poles during the shallow departure. The wires were strung across a valley with a span of 560 m, which the helicopter struck 158 ft above the ground. The wire did not have aircraft warning markers and did not require marking in accordance with Australian Standard 3891.
The ATSB also identified that, unlike other states of Australia, electricity network information was not readily available in Victoria to aid pilots during the flight planning process.
Safety message
The ability of pilots to detect powerlines depends on physical characteristics such as the spacing of power poles, the orientation of the wire, and the effect of weather conditions. Depending on the environmental conditions, powerlines may not be contrasted against the surrounding environment. In addition, the size of the wire and limitations of the eye can mean that it is actually impossible to see the wire.
watch for power poles and fly directly over them when crossing powerlines
constantly scan the terrain on either side of your flight path for poles/towers
always maintain at least 500 feet above ground level except during take-off and landing.
The Aerial Application Association of Australia Powerline Safety Program aims to encourage and facilitate power companies to improve aviation safety. The program involves the provision of mapping information of powerline networks and the marking of powerlines by network operators wherever it is requested by a pilot, aviation company or landholder.
In summary, effective wire avoidance can be achieved using a combination of:
available wire location information
wire marking
avoidance of unnecessary low flying, especially flight below the height of surrounding higher terrain where wire spans may be present.
The occurrence
What happened
At 1259 Eastern Standard Time[1] on 6 July 2019, a Robinson R44 Raven 1 helicopter departed Moorabbin Airport, Victoria, for a private flight to a rural property near Mansfield, Victoria. The 128 km flight was conducted under the visual flight rules[2] with the pilot and one passenger on board.
At about 1400, the helicopter landed at the property in a westerly direction.
After spending about 1 hour at the property, the pilot and passenger boarded the helicopter for the planned return flight to Moorabbin. The pilot assessed there was a light breeze and elected to depart in a north-westerly direction, over different ground to that overflown during the arrival.
Shortly after 1505, the helicopter lifted off and climbed gradually. The pilot reported that he focused on clearing two trees on the departure path, and that he did not notice a powerline pole on the nearby hilltop (Figure 1). The helicopter accelerated to an airspeed of at least 50 kt and travelled about 400 m from the take-off site.
Figure 1: Helicopter shortly after take-off (hilltop pole visible from that location)
Source: Provided to the ATSB
At 1506, the helicopter struck a two-wire powerline, 158 ft above ground level (Figure 2). The pilot reported that he did not see the wires, but felt a jolt and observed that the windscreen had cracked. He did not identify that the helicopter had struck a powerline, and focused on controlling the helicopter to a run-on landing. The helicopter descended rapidly, travelling about 400 m after the wirestrike, in which time the pilot felt another jolt. The aircraft collided with the ground in an upright position before it spun around and rolled over. The pilot sustained minor injuries and the passenger was seriously injured. The helicopter was substantially damaged (Figure 3).
Figure 2: Overview of the accident location
Source: Victoria Police, annotated by ATSB
Figure 3: Accident site showing wire tangled in the wreckage
Source: Victoria Police, annotated by ATSB
A witness standing under the powerline heard and saw the helicopter take‑off. He reported that the powerline was ‘very hard to see’ and that he saw a flash (arcing) when it was struck by the helicopter.
Pre-flight planning
The pilot contacted the property owner prior to the flight and was advised that the property had solar power and no powerlines. The property owner did not know the contacted powerline ran across the valley and he could not see the wires from his property.
The pilot had visited the property and the neighbouring one many times by car and knew of powerlines and poles at the neighbouring property, which were about 26 ft (8 m) high. However, he was not aware of the distribution powerline that the helicopter struck and stated that he had not expected to encounter powerlines more than 150 ft above the ground.
Powerline
The single phase, two wire (conductor) 22 kV powerline was strung across the spur line. It traversed a valley from a pole on the top of a hill to a pole located near the main road. The span ran perpendicular to a line of poles leading to a neighbour’s house. The span length was 559 m between poles and the maximum clearance above the valley was 48.1 m (158 ft).
Following the wirestrike, the helicopter pulled the two wires off the pole, which then parted and fell to the ground. Some of the wire remained attached to the helicopter (Figure 3) with the rest of the span on the ground and resting in trees.
Mapping
Energy companies in New South Wales and Queensland provide general aviation pilots (including those conducting authorised low-level operations) with access to network maps of high voltage electricity transmission lines and lower voltage distribution lines. The information is provided with a caveat that it may not be current and accurate.
Similar access to network maps is not provided by Victorian energy companies although the Victorian Department of Environment, Land, Water and Planning has a Spatial Datamart, which includes high-voltage transmission network information. The data does not contain information on the lower voltage distribution network. Additionally, use of the data for flight planning purposes requires extraction of the powerline information from a large dataset and processing to present it in a readily usable format such a map overlay.
conducting a pre-flight briefing and reconnaissance
applying appropriate flying techniques
reading the physical structure indicators, e.g. poles and insulators
knowing the location of powerlines on and around the property or the area you are flying in.
Marking
Wire markings enhance the visibility of wires. The requirements for marking powerlines and their supporting structures were published in Australian Standard AS 3891 Part 1, Permanent marking of overhead cables and their supporting structures for other than planned low-level flying and Part 2, Low levelaviation operations.
The powerline associated with this accident was not considered to be in an area involved in planned low-flying operations as described in AS 3891.2, although it was reported that aerial agricultural operations had previously occurred in the vicinity of the powerline. Additionally, the helicopter landing site was not an authorised landing area as defined in Part 1, nor did the cable height exceed 90 m or span exceed 1.5 km. The powerline therefore did not require marking in accordance with either Australian Standard.
The ATSB publication Avoidable Accidents No. 2 - Wirestrikes involving known wires: A manageable aerial agriculture hazard states that ‘even in cases where the criteria of AS 3891.1 do not apply, there may be an obligation on the owner of the wire to mark the wire. This could be the case if there is a high level of risk in the particular circumstances associated with the visibility of the wire. If you consider that a wire creates an unacceptable level of risk you should tell the owner of the wire (and the property owner if they are not the same person).’
After this accident, local landowners advised the ATSB that the powerline was erected in the 1970s, and that an aircraft conducting aerial agriculture had struck it in the 1980s. They reported that following that past incident, orange plastic marker balls had been fitted to the wires, however, they had perished over time and not been replaced.
No other wirestrikes involving this powerline were known to have occurred, and the energy transmission company had no record of any wirestrikes.
Weather
Footage of the take-off showed a sunny day with clear sky with some scattered high-level clouds, no wind and visibility greater than 10 km.
The United States Federal Aviation Administration (FAA) Safety Study of Wire Strike Devices Installed on Civil and Military Helicopters found from 1970-1979 and 1986-1996 clear skies and unlimited visibility conditions during most reported wire strikes and from 1994-2004, 86 per cent of the fatal wirestrike accidents occurred in day visual meteorological conditions.[3]
Pilot experience
The pilot had 73.8 hours total aeronautical experience and attained his Private Pilot (Helicopter) Licence in April 2019. The pilot had completed 5.2 hours in an R44 helicopter in the 90 days prior to the accident flight.
The FAA study referenced above found that most of the helicopter wirestrikes occurred with experienced pilots. The study found that in the United States, between 1994 and 2004, there were 124 wirestrike accidents involving civil helicopters, of which 41 were fatal. About 60 per cent were general aviation operations, while agricultural operations accounted for about 27 per cent of the accidents. The average rotorcraft flying experience of the pilots was about 4,000 hours.
Previous occurrences
Between July 2003 and June 2011, a total of 166 aircraft wirestrikes were reported to the ATSB. Electricity distribution and transmission companies identified an additional 101 wirestrikes that occurred during the same period that were not reported to the ATSB. Further information is in ATSB report from 2011, Under reporting of aviation wirestrikes.
According to ATSB publication Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004, 15 per cent of wirestrike accidents occurred in aircraft conducting private operations. Of those accidents, 61 per cent occurred in the vicinity of the landing area. These included take-off, approach, landing and conducting an aerial inspection of the landing area.
Safety analysis
As part of his pre-flight planning, the pilot sought and obtained some information about hazards, including powerlines, from the property owner. However, the owner was not aware of the distribution powerline strung across the valley. Additionally, and unlike other states, readily usable electricity network maps were not available to assist the pilot’s planning. Such maps provide valuable safety information to aid pilots in planning flights, and assist the visual identification of hazards, such as wires and poles. From past visits to the property by road, he knew of some low powerlines at a neighbouring property however that knowledge did not assist identification of the airborne wire hazard.
The pilot elected to depart in the same direction as the helicopter landed. Therefore, he had not overflown the powerline when arriving, depriving him of an opportunity to visually identify it. Additionally, he did not conduct aerial reconnaissance of the take-off and departure track that might have helped identify the powerline’s poles and wires. Consequently, when the pilot departed from the property he was unaware of the presence of the distribution powerline across his intended flight path.
Powerlines at significant heights above the ground can be expected in valleys as they are often strung across them to use the terrain to reduce the number of poles and the need to clear vegetation below the wires. However, the pilot reported that he did not expect any powerline at a height of more than 150 ft above the ground. The pole on the hill was visible from the take-off site, but the pilot did not see it. Nor did he see (or expect) the powerline wires, which are inherently difficult to sight and had no markers to increase their visibility. Consequently, as the pilot conducted a shallow departure climb down the valley the helicopter struck the powerline about 400 m from the take‑off site.
The circumstances of this accident highlight that the most effective means of preventing wirestrike can be achieved using a combination of:
available wire location information
wire marking
avoidance of unnecessary low flying, especially flight below the height of surrounding higher terrain where wire spans may be present.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The helicopter’s track down the valley and a shallow climb gradient resulted in controlled flight into the unseen powerline that was not fitted with visual markers.
The pilot’s pre-flight planning had not identified the powerline that was unknown to the property owner of the take-off site, and detail of the powerline network was not available to the pilot.
Acknowledgements
The ATSB acknowledges the assistance provided by Victoria Police during this investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 13 March 2019, a Robinson R44 helicopter, registered VH-ZWK and operated by Helifarm, was conducting aerial spraying operations at Bool Lagoon, around 20 km south of Naracoorte, South Australia.
While spraying along a drainage channel, the helicopter pilot momentarily forgot about the location of a powerline spanning the channel, as he manoeuvred the helicopter over a bridge. The helicopter collided with the powerline, then crashed into the ground. The helicopter was destroyed, and the pilot sustained minor injuries.
What the ATSB found
The helicopter pilot momentarily lost awareness of the powerline as he manoeuvred over the bridge. Nearby vegetation, which reduced the pilot’s ability to see the power poles and visually identify the powerline, probably reduced the pilot’s ability to maintain this awareness. The operator had a number of policies and procedures to support pilots’ powerline awareness, and it may not be possible to completely mitigate the risk of wirestrike during repeated low-level flying near powerlines.
As a result of this momentary loss of awareness, the helicopter collided with the powerline, which led to a collision with terrain. The bladder-type fuel tank installed in the accident helicopter, as compared to an all-aluminium fuel tank, probably reduced the risk of a post-accident fire.
What's been done as a result
The operator has implemented new policies and procedures to increase pilots’ awareness of powerlines during spraying operations, particularly spraying of drains. These include improved maps and other planning documents for drain spraying operations involving flying near powerlines, and increased training of helicopter pilots engaged in these operations.
Safety message
This accident provides another reminder of the dangers posed by powerlines during low-level spraying operations.
The ATSB has released, in association with the Aerial Application Association of Australia (AAAA), an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains numerous wirestrike accidents and lessons learned from them. The AAAA has now launched its Powerline Safety Program that aims to encourage and facilitate power companies to improve aviation safety. The program includes marking of powerlines by powerline network operators (with a marker in accordance with Australian Standard AS 3891-2) wherever it is requested by a pilot, aviation company or landholder.
As this accident highlights, there may be limits to the extent to which operators can mitigate the risk of wirestrike during repeated low-level operations near powerlines. Helicopter wirestrike protection (WSPS) can provide a last line of defence in the event of a wirestrike. Some aircraft selected for aerial agriculture operations can be configured to include WSPS. However, this technology is not currently available on smaller helicopters such as the R44.
Pilots and operators involved in low-level spraying are also reminded that flight helmets can reduce the risk of serious injury in the event of an accident.
The occurrence
What happened
On 13 March 2019, a Robinson R44 helicopter, registered VH-ZWK and operated by Helifarm, was conducting aerial spraying operations at Bool Lagoon, around 20 km south of Naracoorte, South Australia. The operations involved spraying weeds in Bool Lagoon, then in the drain at the western edge of the lagoon. The pilot was the sole occupant of the helicopter.
At the start of the day, the pilot met with a representative of the client organisation, the operations manager of Helifarm, and the Helifarm ground crew who would be in charge of loading the helicopter with spray. Discussions included reviewing the planned spraying job, maps of the area, and a job safety analysis for the spraying work. The risk of colliding with powerlines was noted during the meeting.
Spraying operations involved loading the helicopter with spraying chemicals from a loader vehicle. The pilot would then conduct spray flights before returning and reloading.
After spraying the lagoon in the morning, the loader was relocated in preparation for the remaining work around the drain. The pilot flew towards the new loading point and, prior to landing, conducted a brief reconnaissance flight around the drain. During this flight, the pilot sighted several hazards, including a weir bridge and a single-wire powerline spanning the drain.
After landing at the new loading site, the pilot rested for around 15 minutes before resuming operations at around 1400 Central Daylight-saving Time (CDT). The pilot then conducted another reconnaissance flight and sprayed two loads of chemicals in the drain area. The pilot passed under the powerline on three occasions during the two spray flights.
The pilot commenced another spray flight at around 1430. The pilot started the spray run from a public road at the eastern end of the drain section, flying west towards the weir bridge and the powerline (Figure 1). The pilot recalled that, as he commenced this run, he reminded himself of the presence of the powerline further along the drain. The pilot turned on the spray nozzles, then looked at the nozzles and spray pressure gauge to confirm the spraying equipment was functioning as expected.
As ZWK flew along the drain, the pilot engaged in a visual scan both inside and outside of the helicopter. This included looking outside at where the helicopter was going, monitoring the track of the helicopter using a satellite track display, and monitoring the spraying equipment. This scan reflected the pilot’s normal practice and he had no particular concerns about the performance of the aircraft or the equipment.
When ZWK was around 50-100 m before the weir bridge, the pilot looked at the spray nozzles, as part of his scanning sequence. When the pilot looked up and outside the helicopter, he noticed that ZWK was slightly lower than intended, in terms of achieving adequate clearance over the bridge.
The pilot manoeuvred the helicopter in order to pass over the weir bridge. The control inputs caused the helicopter to ‘balloon’ over the bridge. The pilot reported that this manoeuvre meant the helicopter was higher than it would otherwise have been as it passed over the weir bridge. The pilot then applied control inputs to move the helicopter back down to the desired altitude. The pilot characterised these control inputs as ‘smooth’, noting that it was his preference and normal practice to not manoeuvre the aircraft aggressively unless necessary.
The pilot reported that it was his plan was to fly over the weir bridge and under the powerline. However, as he adjusted the flight path of ZWK over the bridge, he momentarily forgot about the powerline. The pilot noted that if he had been aware of the powerline at that moment, he would have descended more aggressively.
Figure 1: Accident location
The image shows the track of ZWK, the location of weir bridge, and the location of power infrastructure. Source: Google Earth, modified by ATSB
Shortly after passing the weir bridge, ZWK struck the powerline. The helicopter’s ground speed was around 60 kt at the time of impact.
The initial impact occurred around the centre of the front windscreen, just above the helicopter’s headlights. The powerline wire then cut into the helicopter, slowing its forward movement. The wire cut up into the helicopter cabin and the control instruments.
The pilot reported that that he retained some control of the aircraft following the impact, and was able to partially cushion the landing. However, the helicopter landed hard on the bank of the drain. The pilot exited the helicopter with minor injuries. There was no fire, but the helicopter was destroyed (Figure 2).
Figure 2: Helicopter wreckage
The image shows the helicopter wreckage, drainage channel and weir bridge. Source: SA police, modified by ATSB
Context
Pilot information
The pilot of ZWK was experienced in agricultural spraying operations at low levels, including using the R44. In the 90 days prior to the accident, the pilot had conducted around 150 hours flying, including 36 hours in an R44.
The pilot had conducted spraying operations in the area previously, including the drain where the accident occurred. The most recent time was around a year before the accident.
The pilot had all required approvals for conducting agricultural spraying operations. The pilot had conducted SpraySafe training, and had current accreditation issued by the Aerial Application Association of Australia.
The pilot did not wear a helmet during flying operations that day. The pilot reported he would typically wear a helmet. However, he was wearing a standalone headset due to problems with the headset in his helmet.
Powerline information
The powerline struck by ZWK was a single-wire earth return (SWER) line, which consisted of a single line of intertwined narrow-gauge steel wires. The powerline spanned 244 m, and the approximate point of contact was 60 m from the nearest power pole. At the approximate point of contact, the powerline was about 8.9 m high, above the edge of the drain bank. There were no markers or other devices installed on the powerline to enhance its visibility, nor was there any requirement to install such devices.
Location information
The drainage channel was about 30 m wide, with a further 10-15 m clear bank on each side before a tree-lined boundary. This tree-lined boundary obscured visibility of the power poles from within the drainage channel (Figure 3). It is likely that this reduced the ability of the pilot to use the power poles as visual cues for the position of the powerline.
The weather the time of the accident was clear, a temperature of about 20 °C, and a light breeze from the north-west. The pilot described the conditions as fine and said that wind had no effect on the handling of the helicopter.
Figure 3: Powerline and drain boundary
Shows powerline in profile view, and vegetation obscuring power pole beyond edge of the drain. Source: SA Power Networks. Annotated by ATSB
Helicopter information
The Robinson R44 helicopter is a single-engine, four-seat light helicopter produced by Robinson Helicopter Company.
For this accident, there was no evidence to suggest any defects or anomalies were contributory to the wirestrike.
Helicopter operators who routinely engage in low-level operations can have wirestrike protection systems (WSPS) installed on the helicopter. Helicopter WSPS commonly include cutting blades, which can provide a recovery defence when helicopters come into contact with wires. There was no WSPS installed on ZWK and no commonly available system available for the R44. The nature of these systems is such that their fitment on the outside of an aircraft is not typically possible for smaller helicopters, such as the R44.
R44 helicopters with all-aluminium fuel tanks are susceptible to post-accident fuel leaks increasing the risk of a potentially fatal post-impact fire following a collision with terrain. In 2012, the manufacturer issued a service bulletin requiring R44 helicopters with all-aluminium fuel tanks be retrofitted with bladder-type tanks as soon as practical. The ATSB issued a Safety Advisory Notice on 9 March 2012, advising of the potential dangers of the all-aluminium fuel tank. This followed from ATSB Safety Investigation Loss of control involving Robinson R44 helicopter (AO-2012-021).
ZWK had been fitted with a bladder-type fuel tank.
Helifarm risk management procedures
Helifarm utilised several procedures and other defences in order to manage the risks associated with low-level aerial application flying, particularly risks related to wirestrike. These included a requirement for:
Pilots engaged in aerial application to have current ‘SpraySafe’ accreditation with the Aerial Application Association of Australia, as well as other licences, ratings and endorsements.
Pilots to study maps and note the location of wires and other hazards.
Pilots to conduct reconnaissance flights prior to commencement of operations and prior to any clean up runs.
Helifarm and the pilot associated with this accident had complied with these procedures.
Related occurrences
The ATSB has reviewed trends in wirestrike accidents in several research reports, including Under Reporting of Aviation Wirestrikes (AR-2011-004) and Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004 (B2005/0055). This research has shown that many wirestrike accidents involve aerial agriculture operations.
The ATSB has also released, in association with the Aerial Agriculture Association of Australia, an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains numerous wirestrike accidents and lessons learned from them.
Reduced visibility of powerlines due to nearby vegetation has been noted in other wirestrike accident investigations. An investigation of an accident involving a Bell 206B JetRanger found that power poles were obscured by nearby trees, reducing the ability of the pilot to identify the powerline.[1] Similarly, an investigation of a wirestrike accident involving an Eagle DW1 found that a line of trees obscured vision of power poles.[2]
While the pilot knew about the location of the powerline spanning the drainage channel and had flown under it earlier that day, while manoeuvring over a bridge, he momentarily forgot and lost awareness of the powerline. As a result of this momentary loss of awareness, the pilot unintentionally flew the helicopter into the powerline, resulting in ZWK colliding with terrain.
Immediately before the wirestrike, the pilot’s attention was diverted towards flying and other equipment for the spraying activity. This was normal and required.
Native vegetation near the power poles obscured additional visual cues for the presence of the powerline. The powerline was narrow-gauge and had no markings. Due to the limits of the human eye, powerlines can be very difficult to see, particularly in low level flight.[3]
Humans have a limited capacity for working memory. Situational requirements to attend and respond to immediate and/or unexpected demands can mean that awareness and memory of other hazards can be lost. Other ATSB published wirestrike occurrence briefs and investigation reports have shown how awareness of powerlines can slip when pilots respond to demands such as unexpected obstacles[4] and checking a GPS display.[5]
Flying at low altitudes, particularly around powerlines, means that pilots must contend with many demands on their attention. The nature of low-level operations also means that there are very low margins for recovery from even momentary losses of awareness.
For this accident, once the pilot lost awareness of the powerline as he manoeuvred the helicopter over a bridge, it was difficult for him to regain awareness visually, as there were limited prompts for the position of the powerline.
Defences against wirestrike accidents
The operator’s defences against wirestrike sought to reduce the likelihood of aircraft colliding with powerlines by supporting pilots’ awareness of powerlines. The nature of spraying around powerlines is such that demands on attention are high and the ability to recover from any lapse in awareness is relatively low. It may not be possible to completely mitigate the risk of collision in this context. However, there may be some control measures that might reduce the potential consequence.
WSPS can provide an effective last-line of defence in the event of a wirestrike accident,[6] reducing the likelihood of a subsequent crash. However, these systems cannot typically be fitted to smaller helicopters, such as the R44. Helmets provide another valuable defence in the event of a crash, reducing the risk of more serious injury.[7] The ATSB noted in this accident, that the pilot was not wearing a helmet.
R44 Bladder Tank
Although the helicopter in this accident collided with terrain and was destroyed, there was no post impact fire. The helicopter had been fitted with a bladder-type fuel tank, and there was no indication of a fuel leak. The bladder-type fuel tank probably reduced the likelihood of a fuel leak and post-impact fire following the collision.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The helicopter pilot momentarily lost awareness of the position of an overhead powerline as he adjusted the track to navigate over a bridge during low-level aerial agriculture flying. It is likely that nearby vegetation contributed to the pilot’s reduced awareness of the powerline.
The helicopter collided with the overhead powerline, which led to a collision with terrain.
The installation of a bladder-type fuel tank in the R44 helicopter reduced the risk of a post-impact fire.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety actions in response to this occurrence.
Safety action by Helifarm
Helifarm advised that as a result of this accident, they have implemented the following actions in order to reduce safety risk:
Discussing the accident in team meetings, in order to increase focus on key hazards and risks.
Providing pilots conducting future spraying operations at the Bool Lagoon with georeferenced maps of the area.
Introducing additional company documentation for drain spraying to further document site-specific hazards prior to the start of each job.
Making human factors training mandatory for pilots conducting aerial application. This training intends to increase pilot awareness in the wire and low-level environment.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
At about 1728 Central Standard Time,[1] on 3 July 2018, a Cessna 172RG aircraft, registered VH‑LCZ, commenced circuit operations at Parafield Airport, South Australia (SA) with the pilot as the sole occupant. The flight commenced in day conditions and transitioned to operation under the night VFR[2] after last light, which occurred at 1743.
There were no identified aircraft defects and it was fully refuelled immediately prior to the flight. The pilot reported that he had conducted a post‑refuel drain and that there was nothing abnormal in any of the fuel samples.
At about 1748, the pilot performed a touch and go landing, and departed the runway for the sixth, and intended final, circuit. The pilot recalled that the engine ‘coughed’ once as the aircraft accelerated along the runway. He noted no other abnormalities and continued the take-off normally. About 10 minutes later, the pilot received air traffic control (ATC) clearance to land. He turned the aircraft onto final at an altitude of about 500 ft approximately 1,500 m from the runway threshold, and configured it for landing (full flap and landing gear extended).
On descent through 450 ft, the pilot observed the propeller speed reduce from 1,800 to 1,300 rpm. He selected the carburettor heat, increased the throttle and changed the position of the fuel selector from BOTH to LEFT. The pilot reported that, with the exception of this troubleshooting, he did not apply carburettor heat during any of the previous circuits. The engine did not respond to the pilot’s carburettor nor fuel selection inputs and the propeller speed remained constant at 1,300 rpm. The pilot then deselected the carburettor heat and moved the fuel selector back to its original position. A short time later, he assessed that the aircraft did not have sufficient altitude to reach the runway and that a forced landing would be necessary.
At about 1758, the pilot declared a PAN[3] and informed ATC that he was unable to make the runway. The pilot recalled that he had sighted an unlit area ahead, which he assumed to be an open space. He turned the aircraft towards that area and pitched the nose down to achieve the airspeed associated with the maximum glide distance. The pilot reported that, as the aircraft approached the open space, he heard the fuselage hitting treetops. Seconds later, the aircraft stopped abruptly as the nose wheel struck a power line and it then collided with the ground (Figure 1).
After the collision, the pilot attempted to switch off the master switch but was unable to do so due to distortion of the instrument panels. He then swiftly exited the aircraft through the co-pilot’s side window and moved away from the wreckage. Emergency services attended the scene shortly after. The pilot sustained minor injuries and the aircraft was substantially damaged.
Figure 1: Aircraft wreckage (note power line fouling the nose wheel)
Source: South Australia Police
Carburettor icing
Induction icing, often referred to as carburettor icing, is the accumulation of ice within the induction system of an engine fitted with a carburettor. This ice forms as the decreasing air pressure and introduction of fuel reduces the temperature within the system. The temperature may reduce sufficiently for moisture within the air to freeze and accumulate. This build-up of ice restricts airflow to the engine, leading to a reduction in engine performance and possible engine failure. Environmental conditions influence the likelihood of carburettor ice forming.
Weather observations recorded by the Bureau of Meteorology at Parafield Airport indicated a temperature of 12.2° C and a dew point[4] of -0.6° C at the time of the accident. Figure 2 (see annotation in yellow) shows that these meteorological conditions presented a risk of moderate icing when using cruise power and serious icing when using descent power. At the time of the power loss, the engine was operating at descent power.
Figure 2: Carburettor icing probability
Source: CASA, annotated by the ATSB
The Cessna 172RG pilot operating handbook (POH) provided the following guidance for carburettor icing:
before landing, switch carburettor heat to ON to prevent ice formation
in the event of a rough engine running or loss of power:
An unexplained drop in manifold pressure and eventual engine roughness may result from the formation of carburettor ice. To clear the ice, apply full throttle and pull the carburettor heat knob out until the engine runs smoothly; then remove carburettor heat and re-adjust the throttle.
Safety analysis
A post-accident examination of the engine was not conducted and therefore the possibility that a mechanical defect contributed to the accident could not be ruled out. However, the ATSB assessed the evidence with respect to some common known causes for an engine power loss. The evidence indicated that fuel contamination, fuel exhaustion and aircraft maintenance issues were unlikely.
Contrary to the guidance in the POH, the pilot reported that he did not apply carburettor heat while descending to the runway during any of the circuits. This combined with weather conditions conducive to severe carburettor icing at descent power made it likely that the power loss was due to the accumulation of carburettor ice.
The POH listed carburettor icing as a cause of the engine running rough or losing power. The actions listed in the POH to clear carburettor ice, however, do not clear ice immediately as it takes some time for the heat to take effect. The pilot first observed a reduction in propeller speed just after the turn onto final. Although he responded by applying carburettor heat, the short time between troubleshooting the engine power loss and conducting the forced landing meant there was probably insufficient time to clear enough ice for the engine to recover.
The pilot completed the turn onto final at an altitude of about 500 ft approximately 1,500 m from the runway threshold, which is within the normal profile for a powered approach. After troubleshooting the engine issues, the aircraft had already descended to about 450 ft. The POH indicated that, in ideal conditions, a maximum glide distance of about 1,500 m could be achieved from an altitude of 500 ft. However, a turn onto the final approach at that position is unlikely to permit an aircraft configured for landing to glide to the runway in the event of a power loss.
Consideration of a flight profile that balances the requirement for a stable approach while increasing the likelihood of being able to reach the runway in the event of a power loss is particularly important when flying in night VFR conditions. Selection of a suitable unprepared landing site is more difficult at night due to reduced visual discrimination. In this instance, the selected large unlit area was assumed to be clear but obstructions, such as the power lines, were not discernible.
Following the partial engine failure, the pilot resisted the temptation to lift the nose of the aircraft in an attempt to stretch the glide to the runway. That decision, to follow his training and pitch the nose of the aircraft down to establish the optimum glide speed, enabled him to maintain control of the aircraft. That action likely prevented a low altitude stall and uncontrolled collision with terrain.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
On final approach, the engine of VH-LCZ failed, likely due to carburettor icing.
The engine failed at a position during the final approach that did not permit the aircraft to glide to the runway and afforded limited alternative landing area options.
While descending during the forced landing at night, the aircraft struck a power line and then collided with terrain, resulting in minor injury to the pilot and substantial damage to the aircraft.
Safety message
Engine failure during single-engine aircraft operations is by far the most serious night time emergency. The Civil Aviation Safety Authority (CASA) advisory circular,
, provides useful recommendations for minimising risk during night visual flight rules (VFR) operations, including:
planning to fly at a higher altitude will increase the options available
planning the descent onto the base leg so that the aircraft is positioned to start the turn onto final at about 600 ft to 700 ft above ground level.
The routine application of carburettor heat during the period between the base turn point and late in the final approach will significantly reduce the potential for an ice-related power loss. More information regarding carburettor icing can be found in the ATSB report, The ongoing danger of carburettor icing.
While a successful landing was not achieved in this instance, the pilot's actions after realising he would not reach the runway closely followed the guidance in the Federal Aviation Authority pilot’s handbook (
). Flying in a controlled manner, wings level and at the recommended glide speed has a better survivability outcome than when control of the aircraft is lost. The pilot’s actions in maintaining control of the aircraft maximised the likelihood of a successful forced landing.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 5 September 2016, at about 0737 Central Standard Time (CST), a Cessna 441 aircraft, registered VH-NAX (NAX), departed from Adelaide Airport on a charter flight to Coorabie aircraft landing area (ALA), South Australia. On board were the pilot and nine passengers.
At about 30 NM from Coorabie, the pilot of NAX broadcast on the common traffic advisory frequency advising that they were inbound to the aerodrome. The pilot of another aircraft operated by the same company, that had landed some minutes earlier on runway 14 at Coorabie ALA, responded to the broadcast, advising the pilot of NAX to use runway 32 due to the downwards slope on runway 14 (Figure 1). The pilot of NAX had not previously operated into Coorabie ALA, but had studied prior to the flight the information provided by the operator (see Pilot hazard awareness below) with respect to any hazards associated with their landing. In addition, as the other company aircraft had landed safely, they elected to conduct a straight-in approach to runway 32. The pilot then positioned the aircraft on about a 10 NM final to runway 32.
Figure 1: Coorabie ALA facing south
Source: ALA operator
At about 0900, when the aircraft was on final approach to runway 32, the pilot reported that the aircraft decelerated suddenly (from about 120 to 110 kt). At the same time, there was a slight shudder of the right engine and a change in the sound of the propeller pitch. The pilot immediately increased the power to both engines and levelled the aircraft off. The pilot checked the engine instruments and the annunciator panel, and there were no abnormal indications.
The pilot then conducted a go-around and a left circuit at about 1,100 ft above ground level. The aircraft subsequently landed on runway 32. While back-tracking, the pilot sighted a power pole on a hill beyond the runway 32 threshold (in the direction from which the aircraft had just approached). After shutting the aircraft down, the pilot noticed damage to the right propeller blades and suspected that the aircraft had struck a powerline (Figure 2). Witnesses on the ground confirmed that they had seen and heard the aircraft strike the powerline.
The pilot and passengers were not injured. The aircraft sustained minor damage.
Figure 2: Coorabie ALA showing the powerline 370 m from the threshold
Source: ALA operator
Pilot comments
The pilot of NAX had planned to overfly the runway, inspect the landing area and then join the circuit on the downwind leg for runway 14. The pilot commented that if they had overflown the airstrip prior to commencing the approach, they may still not have identified the powerline as the poles and wire were difficult to see. There was one pole near a house and the next pole was some distance away on terrain rising from the runway threshold. The company pilot who had landed before NAX did not sight the powerline during their strip inspection (overflying the runway).
The pilot further commented that if they had conducted a steeper approach they may not have struck the powerline.
Pilot hazard awareness
The pilot reported that they had not been alerted to the presence of the wire before operating at the aerodrome. The pilot had reviewed the company strip guide information for Coorabie ALA and photos of the runway provided by the aerodrome operator.
The information provided included a sketch of the runway and its direction (14/32), the latitude and longitude, length (900 m), width (25 m), elevation (75 ft) and under Special procedures: ‘Slight rise to NW end Small hill’.
Wire marking standards
The requirements for mapping and marking powerlines and their supporting structures were published in Australian Standard AS 3891.1, Part 1, Permanent marking of overhead cables and their supporting structures and AS 3891.2, Part 2, Marking of overhead cables for low level flying. The ALA was not used as described in Clause 3.2 of AS 3891.1 nor were the powerlines in an area involved in planned low-flying operations as described in AS 3891.2. The powerlines did not require marking in accordance with either Australian Standard.
Advisory material
The Civil Aviation Advisory Publication (CAAP) 92-1(1)
, provided guidance on how pilots may determine the suitability of an aeroplane landing area (ALA) such as the recommended obstacle clearance standards and suggested landing area markings. The CAAP defined an obstacle free area to mean ‘there should be no wires or any other form of obstacles above the approach and take-off areas, runway, runway strips, fly-over areas or water channels’. The minimum landing area physical characteristics recommended in the CAAP for aircraft (other than single-engine and centre-line thrust aeroplanes not exceeding 2,000 kg maximum take-off weight) for day operations is depicted in Figure 3. This shows the approach and take-off area should be clear of wires within 900 m of the runway ends above a 5 per cent (3°) slope.
Figure 3: Recommended landing area characteristics
Source: Civil Aviation Safety Authority
Powerline
The powerline was located about 370 m from the runway threshold and about 7.5 m above ground level. The powerline was below the recommended slope gradient of 5 per cent (Figure 3).
The operator of the ALA reported that they had spoken to a representative from the aircraft operator and advised them of the existence of the powerline prior to the flight. The ALA operator had identified the powerline as a hazard and reported that they had requested the infrastructure provider to fit markers to the powerline about 12 months prior to the incident.
The power insfrastructure provider advised the ATSB that the ALA operator had enquired with the then distribution licensees about the fitting of markers to the powerline in 2012 and 2015. In 2012, the distribution licensee investigated and determined that the span of the powerline was too long to take the additional load of the markers. In 2015, the request for the markers was raised again by the ALA operator in conjunction with a request for a quote on a transformer upgrade. There was no follow-up with the provider about these requests.
Runway illusions
The profile of Coorabie ALA runway 32 and the approach area of 900 m (based on the recommended dimensions specified in Figure 3), obtained from Google earth, is depicted in Figure 4. The cleared area commencing from the runway threshold was about 1,170 m in length. Along that length, the profile rose from 9 m (30 ft) to 22 m (72 ft) elevation at the nominated runway length of 900 m, with higher ground rising to about 29 m (90 ft) beyond 900 m. The information provided to the operator by the ALA operator was that the runway length was 900 m, suggesting that the rising terrain beyond that point was not part of the runway. The stated runway elevation was 75 ft (23 m).
As can be seen in Figure 4, the terrain at the powerline was about the same height as the runway 32 threshold, with a dip in between. The glide path from a powerline 7.5 m above the terrain to the runway threshold was about 1°. A normal approach path is about 3°.
Runway slope is one environmental condition that can affect a pilot’s perception of the aircraft’s position relative to a normal approach profile. Flight Safety Foundation Approach and landing accident reduction tool kit briefing note 5.3 –
stated that an uphill slope creates the illusion of being too high. That illusion may induce the pilot to ‘correct’ the approach resulting in a lower flight path, or may prevent the pilot from detecting when the aircraft is too low during the approach.
The briefing note advises that to reduce the effects of visual illusions, flight crews should assess approach hazards and be trained to recognise and understand the factors and conditions that cause visual illusions.
Figure 4: Coorabie ALA runway 32 and 900 m approach area profile
Source: Google earth annotated by ATSB
ATSB comment
It is essential for pilots to be aware of hazards prior to operating into an aerodrome. The location of known hazards and obstacles such as powerlines should be included in aerodrome information that is provided to pilots and aircraft operators who are permitted to operate at the airfield. As runway slope can result in visual illusions that may affect a pilot’s judgement of the approach profile, runway slope information should also be included in operational information.
stated that straight-in visual approaches are not a recommended standard procedure. They can be conducted provided certain conditions are met, including that pilots must be able to assure themselves of the aerodrome’s serviceability and that hazards have been identified.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Powerline owner
Following the incident (at the time of repairing the wire), the infrastructure provider marked the wire with three round orange markers (Figure 5).
Figure 5: Powerline with orange markers
Source: ALA operator
Aircraft operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Notice to operational crew
The company issued the following directives in a notice to operational crew:
Operations to new ALAs require specific chief pilot approval.
ALAs that have not been used by company aircraft for more than 12 months are treated as new.
All operations to ALAs require an overhead join to check the runway.
Straight-in approaches to ALAs are not permitted.
Safety message
Research conducted by the ATSB found that 166 aircraft wirestrikes were reported to the ATSB between July 2003 and mid-June 2011 and another 101 occurred and were unreported but identified by electricity distribution and transmission companies. The majority of wirestrike occurrences were associated with aerial agriculture operations, however, 22 occurrences (8 per cent) involved private operations. Further information is in the research report, Under reporting of aviation wirestrikes.
The ability of pilots to detect powerlines depends on the physical characteristics of the powerline such as the spacing of power poles, the orientation of the wire, and the effect of weather conditions, especially visibility.
Depending on the environmental conditions, powerlines may not be contrasted against the surrounding environment. Often the wires will blend into the background vegetation and cannot be recognised. In addition, the wire itself can be beyond the resolving power of the eye: that is, the size of the wire and limitations of the eye can mean that it is actually impossible to see the wire. As such, pilots are taught to use additional cues to identify powerlines, such as the associated clearings or easements in trees or fields that can underlie the powerline, or the power poles and buildings to which the powerlines may connect.
Risks associated with operations to private airstrips can be mitigated by ALA owners assessing their airstrips against the guidance in CAAP 92-1(1)
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.