Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
Source: Operator
What happened
On 30 January 2026 at about 1205 local time, the pilot and sole occupant of a Cessna U206F departed from an Emu Point aircraft landing area, Northern Territory, en route to Darwin Airport.
Prior to departure the pilot conducted a pre-flight inspection and reported that the aircraft departed with 190 L of fuel. No abnormalities were observed during the take-off or the initial climb. The aircraft levelled off at about 2,000 ft above mean sea level (AMSL) and the pilot conducted the cruise checklist, with no issues identified. Shortly after this, the pilot observed an engine RPM overspeed. The pilot reduced the propellor pitch lever, but this had no effect, so they reduced the throttle to maintain an appropriate RPM.
Shortly after this, the engine began running rough, accompanied by increasing vibration and a reduction in engine power. Almost immediately, smoke began entering the cockpit via the cabin air vents, which the pilot closed. The engine performance continued to degrade to the extent that the aircraft was unable to maintain straight and level flight. The pilot observed smoke and oil spraying onto the airframe and windscreen, reducing forward visibility. They reported that the engine vibrations increased violently, to the point that the entire airframe was shaking.
The pilot selected an area of open grassland interspersed with trees and termite mounds beyond a heavily wooded area and prepared to conduct a forced landing.
Figure 1: Aircraft wreckage
Source: Operator, annotated by the ATSB
Prior to landing, the pilot conducted final checks, unlatched their door and maintained what power was available to assist in clearing the tree line. However, prior to touchdown, the aircraft collided with several trees before rotating left, impacting the ground heavily and coming to a stop (Figure 1).
The pilot reported a brief period of unconsciousness and after ‘coming to’, turned off the ignition and checked that the ELT[1] had activated. The pilot exited through the shattered cockpit windscreen and moved to a safe distance from the wreckage, returning briefly to retrieve a handheld VHF radio and a personal mobile phone. The pilot’s initial attempts to coordinate emergency assistance were unsuccessful. Shortly after, they established radio contact with another aircraft that relayed a MAYDAY call. A rescue aircraft with an emergency response team arrived about one hour later.
The pilot was medically assessed and later admitted to hospital with minor abrasions and a broken collarbone requiring surgery.
The aircraft was significantly damaged and, at the time of publishing, the remote location, terrain and weather conditions have prevented aircraft recovery. Consequently, the likely cause of the reported engine failure remains undetermined.
Safety message
In-flight engine failures and partial power loss in single-engine aircraft require pilots to exercise effective and timely decision-making to reduce the severity of injuries and damage. These events often result in the pilot experiencing high workload and time pressure, where preparedness is critical. Deciding on responses to a partial engine power loss before the flight will reduce your workload during the event and assist you in taking some form of considered action.
When experiencing a rough running engine, pilots should focus on flying the aircraft and continually assess landing options. The ‘aviate, navigate and communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies. Acting in the appropriate order of priority improves situation awareness and supports coordinated responses in a dynamic environment.
recommends that scanning the environment should take 85% of the time available, 10% on checking aircraft attitude including lookout, and 5% of the time scanning of the altitude and airspeed indications.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Electronic Locator Transmitter (ELT): an aviation safety device installed in aircraft that automatically or manually transmits a distress signal via satellites.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-010
Occurrence date
30/01/2026
Location
102 km east-north-east of Port Keats Aerodrome
State
Northern Territory
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Smoke
Highest injury level
Serious
Brief release date
20/02/2026
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
U206F
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Emu Point Aircraft Landing Area, Northern Territory
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. About 10 minutes prior to landing in Hobart, one cabin crew member was checking the cabin was secure for landing when they identified smoke and flames coming from the top of an overhead locker. When the overhead locker was opened, a passenger’s backpack was found to be on fire. The cabin crew doused the flames with a fire extinguisher, and with the assistance of some passengers, poured water on the bag until no smoke was emitted. The aircraft landed without further incident.
After landing, aviation rescue firefighters retrieved a burnt power bank from inside the backpack.
What the ATSB found
The ATSB found that the lithium-ion battery in a power bank experienced a thermal runaway, resulting in a fire in the overhead locker inside a passenger’s bag. Due to the timing of the fire, when the aircraft was already close to landing, the cabin crew had limited time to complete the lithium battery firefighting procedure.
It was also identified that, while the cabin crew attempted to use the protective breathing equipment provided by the operator, difficulties during its fitment meant that they did not find it effective in this incident.
What has been done as a result
Following this incident, Virgin Australia Airlines reviewed its policy regarding the carriage of power banks and spare batteries. As of 1 December 2025, guidance provided to passengers stated:
Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that were damaged, swollen, leaking, recalled, showing signs of defects, or had been repaired or modified, could not be carried in either checked or carry-on baggage.
Safety message
Passengers often travel with multiple devices that contain lithium batteries, including laptop computers, mobile phones, headphones, and power banks. To reduce the risk associated with lithium battery fires, passengers should ensure their devices are packed safely, easily accessible in the cabin and are not carried on board an aircraft if they show signs of damage or deterioration.
The thermal runaway of a lithium battery can be difficult to manage, particularly when the aircraft is airborne. In-flight fires pose a significant risk to the safety of an aircraft if not managed quickly and appropriately. An operator’s procedure to manage battery fires is designed to limit the risk and reduce the likelihood of re-ignition of the battery until the aircraft can land. However, it requires the batteries to be out of a bag and accessible to be easily completed.
Passengers are encouraged to review their airline’s website, and check the Civil Aviation Safety Authority ‘Pack Right’ website to confirm that equipment they are planning to take on board an aircraft is permitted and packed safely.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. There were 2 flight crew, 4 cabin crew (comprised of a cabin manager under training (‘1L’), a cabin crew trainer (‘1R’), and 2 cabin crew (‘2L’ and ‘2R’) and 149 passengers on board. The first officer was pilot flying and the captain was the pilot monitoring.[1]
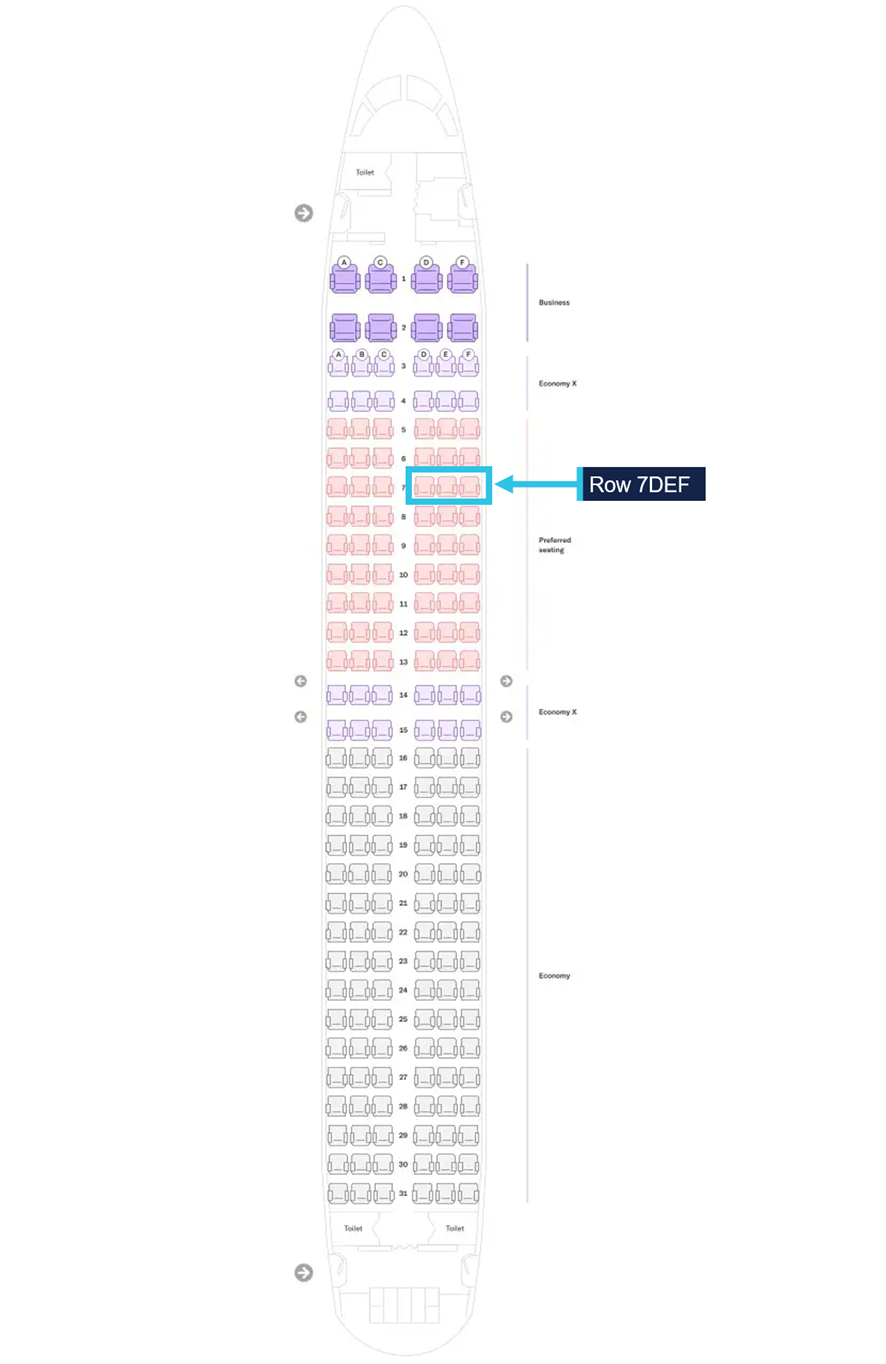
At about 0901 local time, as the aircraft descended through 10,000 ft with the seatbelt sign illuminated, the cabin crew began their final checks on the cabin prior to landing at Hobart. While near the front of the cabin, the 1R heard a sound that they described in their interview with the ATSB as a popping and hissing sound. On looking, they saw white smoke, then flames, emanating from the overhead locker above row 7DEF (Figure 1). They immediately instructed the passengers seated in both sides of rows 6,7 and 8 to move away from the area and into other seating in the aircraft. The 1R then retrieved a fire extinguisher, the portable breathing equipment (PBE), and water from the forward galley.
The 1L made a call from the front galley to the other cabin crew for assistance. The 2 rear cabin crew brought more water and another fire extinguisher forward. The 1R and 2R attempted to don the PBE around the same time, however, one was unable to stretch the neck ring sufficiently to don the PBE, and the other, after donning the PBE felt it restricted their ability to see and communicate effectively so decided to remove it.
Figure 1: Aircraft seat plan showing the location of the overhead locker where flames and smoke were observed
Source: Virgin Australia Airlines, modified by the ATSB
When the overhead locker was opened, flames and smoke were observed emanating from a backpack. Although they could not see what was causing the fire, from their training, the cabin crew suspected it was from a portable electronic device overheating. The 1L discharged a fire extinguisher into the locker until the flames were extinguished. The 1L and 1R then poured water over the bag, with the assistance of the 2R and passengers. To reduce the risk of re‑ignition, a second fire extinguisher was discharged into the locker. The cabin crew instructed passengers to keep their heads down and cover their nose and mouth to avoid inhaling smoke. They also asked the passengers who was the owner of the bag but did not receive a response at the time.
While the other cabin crew managed the fire, the 2L called the flight deck. The captain recalled in interview that, prior to the call, they detected a smoky odour in the flight deck, which they thought was ozone. The 2L advised the captain there was a fire in an overhead locker, which was extinguished, but there was still smoke, and the 1L was dousing the bag with water. They also stated that there were still passengers standing. On ending the call, the captain asked the 2L to ensure everyone was seated for landing.
Following receipt of this information, at 0905:17, just prior to descending through 5,100 ft, the captain made a ‘PAN PAN’[2] call to the Hobart approach air traffic control to advise of a possible fire in the cabin, and that they would require assistance on landing. The captain also asked to speak to the tower controller earlier to request clearances. The approach controller coordinated to get the tower controller on frequency.
The captain decided to take control of the aircraft for landing due to the emergency. At 0906:00, the aircraft was cleared to land on runway 30 by the tower controller. At this time, the first officer also asked to cancel the approach they had been previously cleared for and to instead conduct a visual approach. This change was permitted. At 0906:28, air traffic control contacted the aviation rescue and firefighting service at Hobart Airport, which deployed in preparation for the aircraft landing.
The 2L then retrieved gloves and the portable electronic device fire containment bag and took it to the other cabin crew, intending for the burnt device to be placed in the bag, and the bag stored in the rear lavatory, as per procedure. The backpack was too large to fit in the fire containment bag and there was difficulty in locating the device inside the backpack. Given the short amount of time remaining before landing, the decision was made by the 1R to keep the device inside the backpack in the overhead locker above row 7. It was identified by the cabin crew that the rounded shape of the overhead locker retained the water that had been poured on the backpack, which kept the bag soaked, and would help reduce the risk of re‑ignition during landing. The cabin crew planned to keep the overhead locker open, with the 1R seated in seat 7C adjacent to the locker to monitor the device during landing, with water to use if necessary. The cabin crew also directed the passengers standing to be seated immediately, even if it required 4 passengers to be in a row.
As recalled by the captain in interview with the ATSB, the first officer contacted the 1L just prior to the aircraft turning onto the final approach. This was likely just prior to 0909, with the aircraft between 1,500 ft and 1,000 ft. The 1L confirmed the fire was out, and the passengers were seated, but that the cabin crew were still standing. They assured the first officer the cabin crew would be seated for landing.
The 1L, 2L and 2R secured the final items for landing and seated themselves in their designated seats, except for 1L who sat in 1R’s seat to maintain better visibility of the cabin. On their way to their seat at the front, the 1L checked the overhead lockers around row 7 for heat or any developing hot spots. Once all the cabin crew were seated, the 1L signalled to the flight crew the cabin was secure. The 1L made a final announcement to passengers to ensure their seatbelts were fastened, to remain seated for landing and follow instructions of crew following the landing.
Flight data provided by Virgin Australia showed that the aircraft touched down at Hobart at 0910:29 (Figure 2).
Figure 2: Flight path with key events
Source: Google Earth, annotated by the ATSB
The captain stopped the aircraft on the taxiway and exited the flight deck to speak to 1L and observed the cabin to determine whether an evacuation was required. As the fire appeared to be contained, the captain taxied the aircraft to the parking bay. At 0919, the aviation rescue and firefighting personnel boarded the aircraft and removed the backpack from the overhead locker. They confirmed the origin of the fire was a lithium power bank, stored in one of the backpack’s front pockets (Figure 3).
Figure 3: Backpack containing the power bank
Source: Airservices Australia
The passengers were cleared to disembark normally at 0927. After disembarkation, one cabin crew member (2L) was treated by paramedics. It was unknown if this was due to the effects of smoke as they had been unwell throughout the flight prior to the fire commencing. No other crew or passengers reported to the operator about seeking medical attention from the effects of the smoke. The fire caused minor damage to the overhead locker above row 7/8 DEF (see section Aircraft damage).
Context
Cabin crew information
The flight comprised of 4 cabin crew, 2 located at the front set of aircraft doors (called ‘1L’ and ‘1R’) and 2 at the rear of the aircraft (called ‘2L’ and ‘2R’). Each cabin crew member had designated roles on the flight, based on which door they were operating. On this flight, the 1L position was filled by a trainee cabin manager who had previous experience in this role working for other airlines, but was completing their first flight as a cabin manager under training for this operator. The 1L was supervised by a cabin crew trainer in the 1R position.
Each of the cabin crew had between 1 and 17 years of experience as cabin crew. They had all completed their annual emergency procedures training between November 2024 and June 2025. This training included both theoretical information and a practical review of the lithium battery firefighting procedure. All cabin crew reported having completed simulated scenarios where the fire occurred either during cruise or on the ground, where there was plenty of time to complete the firefighting procedure, and store the damaged battery appropriately. None of the cabin crew had completed a simulated scenario involving a time‑pressured situation.
Aircraft cabin information
VH-YFY was a Boeing 737-800 aircraft, with a single aisle in the cabin and seating for 182 passengers. In economy, where this fire occurred, there were 3 seats on either side of the aisle.
The cabin on this aircraft was fitted with the Boeing 737 sky interior design. In this design, the overhead lockers lowered from the ceiling, creating a contained basket for the bags to sit in. In comparison, the doors in other locker designs would open upwards.
Lithium batteries
Overview
There are 2 primary types of lithium batteries – lithium metal and lithium-ion. Lithium metal batteries cannot be recharged and are designed to be disposed of once their initial charge has been used, whereas lithium-ion batteries are rechargeable. Compared to lithium metal, lithium-ion batteries store a high amount of energy and are commonly found in many portable electronic devices (PEDs) such as smartphones, tablets, cameras, laptops, and power banks.
Guidance on the safe carriage of lithium-ion batteries on board aircraft
Lithium batteries are classified by the United Nations as dangerous goods. As such, the International Civil Aviation Organization’s Technical Instructions for the Safe Transport of Dangerous Goods by Air (2025-2026 Edition) stated that lithium batteries, including power banks must be carried as carry-on baggage only.
The Civil Aviation Safety Authority stated that spare batteries and power banks should be packed in carry-on baggage only, so that trained aircrew can manage any issues quickly and safely. Their Pack right website provided safety tips when travelling with lithium batteries:
These simple steps help keep you and your fellow passengers safe:
• choose reputable suppliers when buying devices and spare batteries
• follow airline and manufacturer rules for carrying and charging lithium batteries
• keep spare batteries with you in the cabin and protect them from damage
• stop using or charging batteries that show signs of damage, overheating, or swelling
To prevent short circuits, protect spare battery terminals by:
• keeping them in original packaging
• covering terminals with tape
• placing each battery in a separate plastic bag or case.
At the time of the incident, the operator’s policy permitted power banks to be carried in the cabin only, but they could be stored inside a bag and there were no restrictions on their use on board. Advice on the carriage of power banks and other electronic devices was provided to passengers on the operator’s website and during check-in.
Thermal runaway
Thermal runaway is a rapid and uncontrolled increase in temperature and occurs when the internal cell(s) of a lithium battery become damaged for reasons including:
internal short circuits
breakage from dropping or crushing
exposure to excessive heat
failure of the battery cell due to manufacturing defects.
The operator’s Aircrew Emergency Manual stated that crew should be alert not just for signs of smoke or fire in the cabin but also to the smell of overheating electronic devices.
The smell of overheating may be the first sign of an impending lithium battery/PED fire. PEDs approaching a thermal runaway start initially displaying hissing, crackling sounds, as well as bubbling or blistering casings.
Once a lithium battery cell thermal runaway starts, it quickly leads to the failure of adjacent cells in a chain reaction that can produce fire, which is especially difficult to extinguish. A fire caused by lithium batteries can produce a fire burning with a temperature as high as 1,000°C, explosions releasing toxic gases and flammable electrolytes as well as shrapnel from damaged PED casings. The manual also stated that in some cases, the explosive force of the venting gasses could be significant enough to cause spikes in cabin pressure.
Managing lithium battery fires
The operator’s Aircrew Emergency Manual stated a general risk about onboard fires was that:
Any fire, no matter how small, may rapidly become out of control if not combatted quickly. Research has shown that if left uncontained, a smoke-filled cabin can be consumed by fire in as little as 6-10 minutes. The first priority shall always be to put the fire out.
In order to manage the risk, the manual outlined 3 important principles of firefighting:
Immediately locate the source of fire, smoke or fumes. Specific to lithium battery fires, all smoke or fire events occurring in baggage within an overhead locker should be assumed to be a PED/lithium battery fire until the source is positively confirmed.
Aggressively attack and extinguish the fire using all available resources, which can include able bodied persons.
Communicate to other crew and the flight crew, as soon as possible, specifying the location and source of fire.
Furthermore, the manual also guided crew that:
It is important to protect yourself from the effects of smoke and fumes while attempting to flight a fire. In some circumstances it may be safe and thus more important to attack a fire first than fitting of PBE [portable breathing equipment]. PBE should be worn by at least one person when a team is formed to flight a fire and anytime by the primary firefighter when they are in smoke, a confined space of affected by fumes.
In regard to managing a lithium battery fire, the manual stated:
The primary method for stopping a lithium battery from thermal runaway or overheating is to cool it down by pouring water or other non-flammable liquid on the battery or device. This should be done once any flames have been extinguished and continued until the device is cooled and there is no evidence of smoke, heat, crackling or hissing sounds usually associated with an overheating lithium battery. This could take as long as 10–15 minutes.
Another recommendation in the emergency procedures manual was a suggestion not to open any baggage if there was smoke or flames emanating from it, unless it was required to get a fire extinguisher and liquid onto an identified battery. Once the device was cooled, it could then be placed in a fire containment bag or other suitable container.
Aircraft firefighting equipment
Overview
The operator fitted the Boeing 737 aircraft with firefighting equipment. In addition to this designated equipment, the cabin crew were taught to use other equipment available on board as required, such as drinks used in the cabin service as well as wet blankets and pillows to smother a fire.
Fire extinguishers
The aircraft had 4 bromochlorodifluoromethane (BCF)/halon fire extinguishers. These fire extinguishers are designed to be used on all types of fires by discharging a colourless, odourless, non-corrosive, liquified gas. This gas is not cooling, meaning that further steps are required in fighting a lithium battery fire.
Fire protection gloves
Fire protection gloves were designed to protect the wearer’s hands when fighting fires, including lithium battery incidents. The emergency procedures also suggested that crew should use gloves whenever fighting fires, including using oven gloves if the fire protection gloves were not available.
The L2 retrieved the fire protection gloves from the galley with the intention to move the power bank once the fire was suppressed, but the gloves were not used during the firefighting process.
Portable breathing equipment
Portable breathing equipment (PBE), commonly referred to as a smoke hood, was provided for each cabin crew member on board. The PBE supplied was designed to protect the wearer from fumes and smoke by forming a secure seal using an elastic neoprene neck ring (Figure 4). An oxygen generator on the nape provided oxygen to the wearer.
Figure 4: Exemplar PBE, showing how to open the neck ring (left) and when donned (right)
Source: Virgin Australia Airlines, modified by the ATSB
Operator procedures recommend PBE should be used by at least one person involved in firefighting, or when one person was fighting a fire in an enclosed environment. Although, consideration was given that the first person to a fire might need to immediately attend to the fire while others gathered and donned the PBE.
The 2 cabin crew who attempted to use the PBE stated that the equipment provided in training was much easier to don as the neck ring was stretched from repeated usage.
In October 2025, the Airbus Safety First magazine contained an article about PBE, reviewing a case study where 7 cabin crew had difficulties using the PBE provided. The analysis indicated that, similar to this incident, despite having regular training in the use of PBE, the cabin crew found it difficult to use the PBE in a real emergency. The article recommended that ‘dummy’ PBE used in training may not represent the equipment found on board.
Fire containment bags
There were 2 sizes of fire containment bags carried on the operator’s Boeing 737 aircraft. The smaller sized bag, designed to fit an iPad, was carried in the flight deck in the event of a thermal runaway involving one of the flight crew’s electronic flight bags.
A larger bag, designed to fit a device the size of a laptop, was carried in the aircraft cabin (Figure 5). The purpose of this bag was to place the device in after it was cooled post‑fire, so that it could be stored in a water filled container in a secure place.
Figure 5: Fire containment bag
Source: Virgin Australia Airlines
Damage to the power bank
The power bank was inspected by the aviation rescue firefighters after being removed from the aircraft.
The power bank had a rated output of 37 watt hours and had both USB‑A and USB‑C charging ports. It was not charging a device when the fire started, but there was a cable plugged into the USB‑A charging port. When orientated with the manufacturer’s label facing up, most of the damage was observed along the top and right side of the power bank. The damaged right end contained the USB-C charging port. External observations suggest that the power bank contained 2 internal cells, of which only 1 was affected by the thermal runaway by the time the fire was extinguished (Figure 6). The power bank was not protected from short circuits as it did not appear to have the terminals covered and was not separated from other items in the bag by being placed in a protective pouch or the original packaging. The backpack was reported by the operator to be substantially damaged by the fire.
The owner of the power bank advised the operator that it was purchased in 2024 and:
it had no pre-existing damage
was fully charged the day prior to the incident, and there were no previous issues during charging or use
it was not dropped, exposed to moisture or heat prior to the incident.
Figure 6: Power bank showing damage from the back (left) and side view (right)
Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Aircraft damage
An inspection of the aircraft found fire damage in the panels above and behind the overhead locker above row 7 and 8 DEF. The passenger service unit containing the reading lights, call bell and information signals under this locker also sustained fire and water damage. The overhead locker needed to be replaced post-fire (Figure 7).
Figure 7: Overhead locker above row 7DEF where the smoke and flames were observed (left) and area behind the overhead locker showing fire damage (right)
Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Related occurrences
Australian data
This incident was the first reported power bank-related in-flight fire either in Australia or on an Australian‑registered aircraft. A review of the ATSB’s occurrence database identified 3 previous incidents where smoke was reported emanating from a power bank in the aircraft’s cabin, but no fire occurred:
OA2025-01608: On 20 January 2025, a Boeing 737 aircraft was being operated on a flight from Brisbane, Queensland, to Melbourne, Victoria. During cruise, a power bank overheated in the cabin, and smoke was observed emanating from the attached charging cable. The power bank and cable were placed in a container and stowed in the rear lavatory for the remainder of the flight.
OA2019-04325: On 28 May 2019, an Airbus A330 aircraft was being operated on a flight from Melbourne, Victoria, to Hong Kong. During cruise, smoke was detected emanating from a passenger's power bank.
OA2019-02629: On 15 April 2019, an Airbus A330 aircraft was being operated on a flight from Hong Kong to Melbourne, Victoria. During passenger disembarkation, smoke was observed emanating from a passenger's power bank. The crew doused the power bank in water.
ATSB records showed that, in the past 10 years, there were 4 in-flight fires resulting from mobile phones, 3 of which occurred after the mobile phone was crushed in the seat mechanism, damaging the lithium battery contained inside. The reason for the fourth fire was unknown.
International incidents
While this was the first reported incident in Australia, there have been a number of significant fires resulting from power banks, including:
In January 2025, an Air Busan A321 aircraft was preparing for flight at Busan, South Korea. Prior to taxi, a power bank fire started in an overhead locker. The fire spread, resulting in an evacuation. The aircraft was destroyed.
In March 2025, a Hong Kong Airlines A320 aircraft diverted after a power bank experienced a thermal runaway. The fire was extinguished.
In October 2025, an Air China A321 aircraft had to divert after a battery caught fire in an overhead locker.
The United States Federal Aviation Administration recorded 8 in‑flight fire incidents involving power banks occurring in the past 10 years.
Safety analysis
Power bank thermal runaway
For unknown reasons, one of the cells in a lithium-ion power bank stored in an overhead locker failed during the descent into Hobart. In this case, there was no reported pre‑existing damage, or any other identified problems with this power bank prior to flight. However, the power bank was stored with a cable in it and the ports uncovered, both factors which can increase the risk of a fault.
Inspection of the power bank post-flight, combined with the cabin crew reports of sounds they were trained to expect in the event of a lithium battery fire, suggested that the fire was characteristic of a thermal runaway. As the temperature of the power bank continued to increase, smoke, followed by flames resulted.
Completion of firefighting procedures
As described in the operator’s procedures, fires on board aircraft can spread quickly. As the aircraft was already on descent when the smoke was initially observed, there was limited time for the cabin crew to manage the power bank fire by completing all the procedures they were trained to do in response to an in-flight fire. In addition, they had the responsibility to ensure the cabin was secure for landing.
In less than 8 minutes, the cabin crew worked together to identify a fire, gather the required equipment, and aggressively fight the fire to a point where the fire appeared suppressed. In addition, they communicated the problem with the flight crew and managed moving passengers to alternative seating.
While the cabin crew had received emergency procedures training, they had never trained for a lithium battery fire in a compressed time. They completed as many of the procedures as they were able to in the available time, but by the time the fire was considered controlled, there was only around 90 seconds for the cabin crew to clear up the cabin and be seated for landing. Besides the logistics and risk that would result from handling the power bank to remove it from the backpack and place it in a fire containment bag, there was no time available.
The cabin crew identified an alternate solution to moving the burnt power bank. While the overhead locker held the water poured on the backpack, there was no assurance that the power bank was going to remain fully submerged for landing, in accordance with the operator’s procedures, or isolated from other lithium battery devices. Although there was no consequence as a result of the power bank remaining in the overhead locker, there was an increased risk of cabin occupant injury and aircraft damage if the power bank re‑ignited due to further exposure to fire and smoke.
Protective breathing equipment
Protective breathing equipment (PBE) was available for cabin crew to use if deemed necessary in preparation to fight a fire, and all crew were trained in their use. Two of the cabin crew attempted to use the PBE, but did not find it effective due to fitment and communication/visibility issues. As the cabin crew were unable to use the PBE, they had no protection from the smoke and were placed at an increased risk of smoke inhalation. While these cabin crew did not experience any residual effects from the smoke, any protective equipment provided should be efficient to don and wear continuously while managing an emergency situation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the in-flight fire involving Boeing 737, VH-YFY, 56 km north‑north‑east of Hobart Airport, Tasmania, on 21 July 2025.
Contributing factors
During the descent, a passenger's lithium-ion power bank, located in the overhead locker, overheated due to thermal runaway and began to emit flames and smoke.
Other factors that increased risk
Due to the timing of the fire starting on descent, the cabin crew had limited time to complete the procedure for managing a lithium battery fire.
The cabin crew attempted to use the protective breathing equipment provided by the operator but did not find it effective when managing the lithium battery fire.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Virgin Australia Airlines
Virgin Australia Airlines advised it has reviewed its policy regarding the carriage of power banks in the cabin. As of 1 December 2025, guidance provided to passengers stated:
Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that are damaged, swollen, leaking, recalled, showing signs of defects, or have been repaired or modified, cannot be carried in either checked or carry-on baggage.
It has updated the cabin crew’s pre-flight announcement and website to inform passengers of the revised policy.
Virgin Australian Airlines has also acknowledged that, while it made changes to its policy, there are challenges in monitoring passengers’ compliance with these measures. It also stated that greater awareness about the risks of travelling with lithium batteries should be delivered by all airlines and airports.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the cabin crew
the flight crew
Virgin Australia Airlines
Airservices Australia
Civil Aviation Safety Authority.
Submissions were received from:
Virgin Australia Airlines
2 cabin crew members
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
Occurrence summary
Investigation number
AO-2025-043
Occurrence date
21/07/2025
Location
56 km north-north-east of Hobart Airport
State
Tasmania
Report release date
18/12/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Fire, Smoke
Occurrence class
Serious Incident
Highest injury level
Unknown
Aircraft details
Manufacturer
The Boeing Company
Model
737-800
Registration
VH-YFY
Serial number
41016
Aircraft operator
Virgin Australia Airlines
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory, with a pilot and one passenger on board. As the helicopter neared the destination, the pilot felt the onset of severe airframe vibration. The pilot elected to conduct a precautionary landing in an area of open farmland, resulting in a hard landing. The pilot and passenger were uninjured, and the helicopter sustained minor damage.
What the ATSB found
The helicopter’s engine was found to have suffered a mechanical failure due to in-service loosening of the nuts on the connecting rod bolts, leading to separation of one of the connecting rods from the crankshaft. The reason the nuts became loose was not determined.
While there was no indication of influence on this occurrence, independent inspection of the connecting rod attaching hardware performed during the overhaul of the engine did not involve a physical torque check of the connecting rod bolts. While the inspection was not a regulatory requirement, this was a missed opportunity to verify the installation torque.
During the most recent periodic inspection the helicopter maintenance provider did not refit the spark plugs using new gaskets, as required by the spark plug manufacturer. It was also found that the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent in this respect.
What has been done as a result
The Civil Aviation Safety Authority acknowledged the inconsistent information contained within the 2 airworthiness bulletins. CASA advised that Airworthiness Bulletin AWB 20‑001 is scheduled for cancellation and Airworthiness Bulletin AWB 85-023 is to be amended to reflect current recommendations.
The helicopter maintenance provider advised the ATSB it now installs new gaskets when refitting spark plugs.
Safety message
This incident highlights the importance of managing inflight anomalies through a comprehensive understanding of aircraft systems and the application of emergency procedures. The pilot’s timely actions following the onset of the vibrations ensured a safe outcome for the occupants and resulted in minimal damage to the helicopter.
The incident also emphasises the importance of adhering to manufacturer requirements when installing aircraft components, as well as the additional assurance provided by a thorough independent inspection of completed work.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
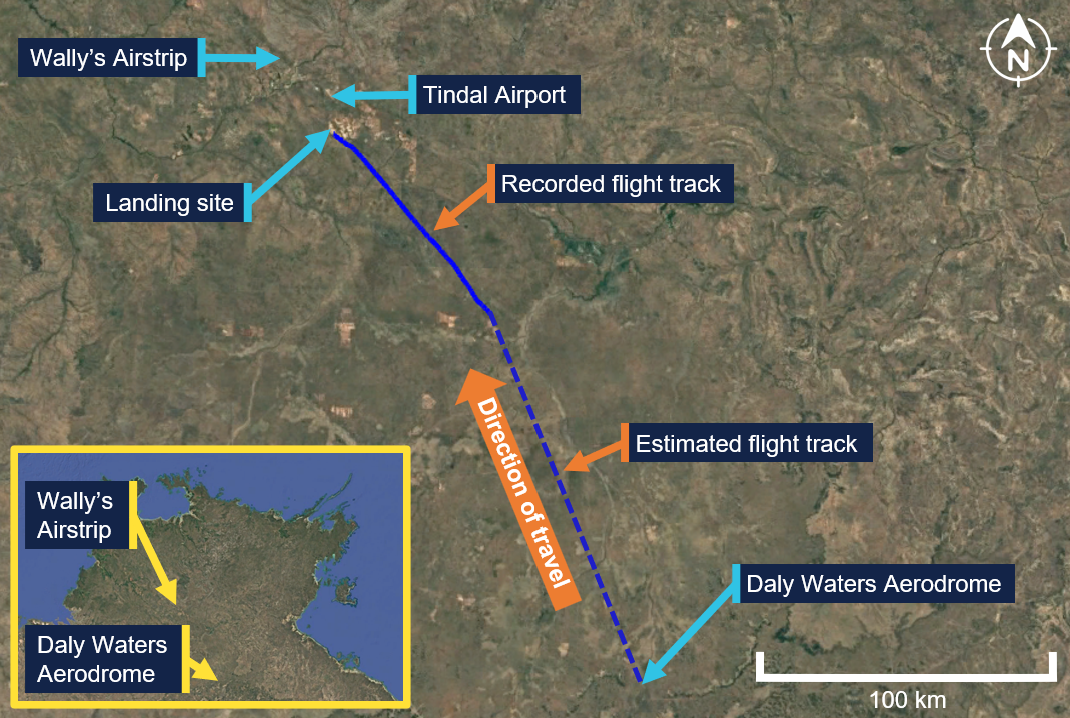
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight with a pilot and one passenger on board. The flight was conducted under the visual flight rules,[1] and the planned route was from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory (NT) (Figure 1).
On the morning of the flight, the pilot completed their pre-flight inspection and refuelled the helicopter. Shortly after starting the engine, the pilot recalled sensing an unusual sound and vibration through the helicopter, but it resolved when the engine speed was increased. The pilot completed their pre-take-off checks, and the helicopter departed Daly Waters Aerodrome at about 0900 local time. The pilot did not recount any issues with the helicopter’s performance during the take-off, climb or initial cruise.
Figure 1: VH-OOE flight track
Source: Google Earth, annotated by the ATSB
At about 1015, when the helicopter was about 46 km to the south‑east of Wally’s Airstrip, the pilot contacted Tindal Airport air traffic control (ATC). Several exchanges with Tindal Airport ATC took place, during which the pilot was instructed to follow a railway line and maintain an altitude not above 1,500 ft above mean sea level. The pilot complied with these instructions and continued towards their destination. At about 1020, when the helicopter was at an altitude of about 1,100 ft, the pilot felt the onset of severe airframe vibration. They recalled initially thinking the helicopter tail may had been struck but later discounted that possibility when they identified they still had directional control. The pilot was unable to diagnose the cause of the vibration and decided to undertake a precautionary landing.
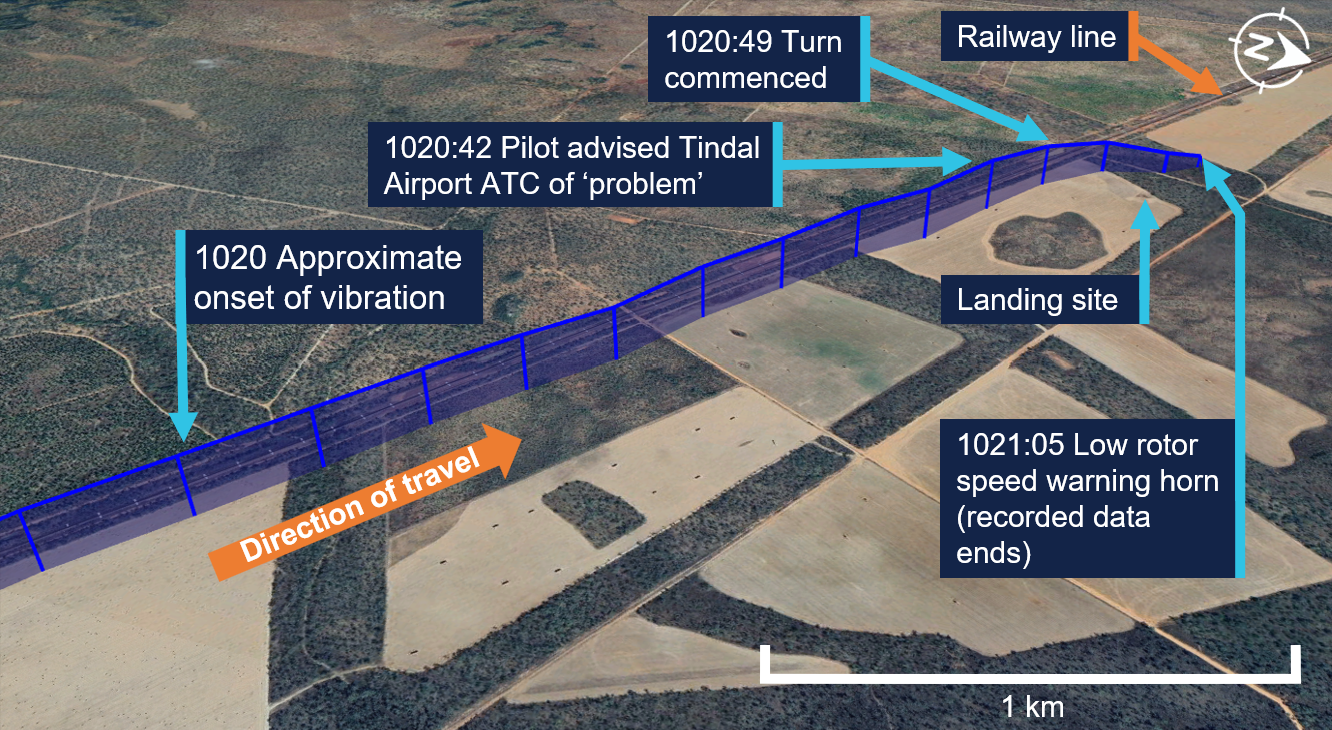
At 1020:42, and an altitude of about 1,100 ft, the pilot alerted Tindal Airport ATC that they had a ‘problem’ (Figure 2). The pilot selected a paddock for the landing that had recently been harvested of its crop and commenced a right turn towards the landing location at 1020:49. At 1020:52, they communicated that operations were not normal, and at 1021:00 they advised Tindal Airport ATC that they would be landing immediately. The pilot recalled noting the engine gauges and the rotor and engine speed indications at that time were normal.
Figure 2: VH-OOE flight path from the onset of vibrations until landing
Source: Google Earth, annotated by the ATSB
At 1021:05, and an altitude of 700 ft, the pilot made a transmission to Tindal Airport ATC during which a low speed warning horn could be heard in the background (see Low rotor speed). The pilot did not recall hearing the horn. At about 150 ft above ground level, the pilot recalled noting a low oil pressure light on the helicopter’s caution warning panel (see Oil warning caution light). They continued the approach and, as the helicopter slowed for landing, they observed smoke blowing forward from the rear and recalled having concerns about a fire.
The helicopter landed heavily in the paddock. The pilot recalled that the landing was probably completed ‘quicker’ and with a lower tail position than normal, due to their concerns about a fire. Once the helicopter had landed, the pilot instructed the passenger to exit and run forward. They then shut down the helicopter’s engine, and at 1021:41 advised Tindal Airport ATC that they had landed and were safe. The pilot then exited the helicopter. Both occupants were uninjured, and the helicopter sustained minor damage.
Context
Pilot information
The pilot held a valid Commercial Pilot Licence (Helicopter) with single engine and low‑level ratings. The licence was issued on 6 June 2025 following the successful completion of a commercial pilot licence flight test in May 2025. The pilot had held a Private Pilot Licence (Helicopter) since October 2023. They also held a current class 1 aviation medical certificate valid to 6 August 2025. At the time of the incident, they had a total flying time of 194 hours of which 118 hours were on the Robinson R44.
Helicopter information
General information
The Robinson R44 Raven I is a 4-place helicopter with a 2-bladed main rotor system and a conventional 2-bladed tail rotor. VH-OOE was manufactured in the United States in 2008 and first registered in Australia in July 2008. At the time of the incident, the helicopter had accumulated 1,995 hours total time in service.
It was powered by a Lycoming O-540-F1B5, 6-cylinder, horizontally opposed piston engine that is naturally aspirated and rated at 235 horsepower. The overhauled engine was installed in September 2022 and had operated for 291 hours at the time of the incident, with a total time of about 1,614.6 hours. The last periodic inspection was undertaken on 6 May 2025, and the helicopter had flown about 25 hours since that inspection.
Airworthiness and maintenance history
Recent maintenance
The last periodic inspection was undertaken by Platinum Helicopters on 6 May 2025. During the inspection, the Champion REM38E spark plugs fitted to the engine were removed, inspected and then refitted by the maintenance engineer. The maintenance engineer recalled that it was not their practice to fit new spark plug washers (gaskets) when refitting the spark plugs, instead electing to use annealed[2] gaskets (see Spark plug maintenance).
Engine overhaul
In September 2022, VH-OOE underwent a 12 year/2,200 hour inspection. During the inspection, the engine was removed and an overhauled engine was fitted to the helicopter. This engine had been salvaged from a Robinson R44, and was overhauled by South West Aviation, a CASA‑approved maintenance organisation.
During the overhaul of the engine, additional components were used to replace some aspects, including:
6 new cylinder kits
new connecting rod hardware (bolts and nuts) with parts manufacturer approval[3]
a crankshaft that had been salvaged from a different Robinson R44.
Records show all salvaged components were inspected and tested to assess serviceability prior to fitment. Once the engine overhaul had been completed, it underwent ground runs and checks prior to being installed in VH-OOE.
Records show that independent inspections were undertaken during the engine overhaul of the engine fitted to VH-OEE. The purpose of an independent inspection is to verify that a maintenance task has been completed correctly. The inspection is undertaken by an appropriately authorised person who did not undertake the original activity. While there was no regulatory requirement for the independent inspection of maintenance work carried out on engine systems, South West Aviation had included these inspections as part of the organisation’s worksheets for engine overhaul.
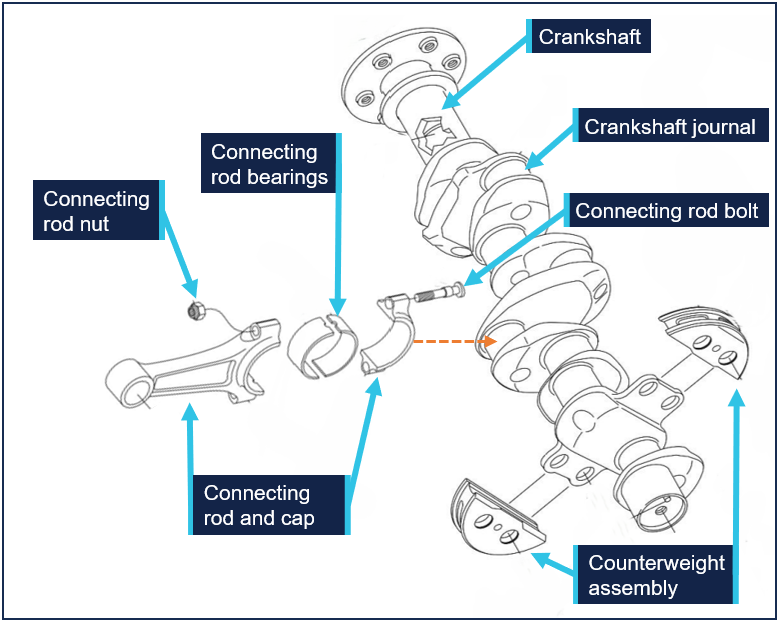
The worksheets for the engine overhaul stated that an independent inspection of the engine sub-assembly was completed during the engine rebuild. Figure 3 shows the sub‑assembly of the crankshaft and the connecting rods, which were secured to the crankshaft by 2 connecting rod bolts and nuts. The crankshaft has 2 dynamic counterweight assemblies fitted, which assist in removing torsional vibration during engine operation.
Figure 3: O-540 crankshaft and connecting rod sub-assembly
Source: Lycoming O-540-F1B5 Illustrated Parts Catalogue, annotated by the ATSB
During interview, when asked about a torque check of the connecting rod nuts, the engineer who conducted the independent inspection stated they would check the torque was set correctly on the tooling that had been used, but it was not their normal procedure to physically check the torque on each nut. South West Aviation did not have a documented procedure that detailed how the independent inspection of the connecting rod hardware should be conducted.
Helicopter systems and procedures
Vibration
The Robinson R44 pilot operating handbook (POH) contained advice for the management of vibration, and stated:
A change in the sound or vibration of the helicopter may indicate an impending failure of a critical component. If unusual sound or vibration begins in flight, make a safe landing and have the aircraft thoroughly inspected before flight is resumed.
Low rotor speed
The helicopter was fitted with a low rotor speed horn. The activation of the horn indicated that rotor speed may be below safe limits (97%). Power available from the engine is directly proportional to rotor speed. With less power the helicopter will start to sink. If the collective is raised to stop it from descending, the rotor speed will reduce even further causing the helicopter to sink faster. To restore rotor speed, the Robinson R44 POH stated that a pilot should lower the collective, roll throttle on and, in forward flight, apply aft cyclic.
Oil warning caution light
The helicopter was fitted with an oil warning caution light. The illumination of the light indicated a loss of engine power or oil pressure. The Robinson R44 POH stated the actions to take in response should be to check the engine tachometer for power loss and the oil pressure gauge. If oil pressure loss was confirmed, the POH stated the pilot should land immediately. Continued operation without oil pressure causes serious engine damage and engine failure can occur.
Spark plug maintenance
The Champion Aviation Service Manual,[4] which included recommended service, handling and reconditioning practices for Champion spark plugs stated:
Always install both new and reconditioned Champion aviation spark plugs with a new copper gasket.
Gaskets that have become too hard with normal usage won’t “hold torque” correctly, and spark plugs can come loose with disastrous results. An annealed gasket will not meet new specifications.
The maintenance engineer stated they carried out the periodic inspection in accordance with the Lycoming O-540 Operator’s Manual.[6] However, this manual, which covered both the O-540 and IO-540 engines, contained no information regarding spark plug gasket fitment. The guidelines for the installation of spark plugs were contained in Lycoming service instruction 1042 Approved Spark Plugs, which stated:
Always install a spark plug with a new gasket.
The Civil Aviation Safety Authority (CASA) had produced 2 advisory airworthiness bulletins (AWBs) that included information on spark plug fitment. However, the advice within these 2 documents was not consistent.
AWB 20-001 Spark Plug Care, issued in September 2001, stated:
Most modern spark plugs have a solid copper gasket that requires annealing prior to spark plug installation to ensure a tight, gas sealed fit. The maintainer should check that the spark plug has only one washer, is of correct dimensions and is annealed. If the engine is equipped with a thermocouple probe in the form of a spark plug gasket, a normal gasket is not required.
Whereas AWB 85-023 Piston Engine Spark Plug Cracking, issued in June 2021, stated:
Always install a new spark plug gasket when servicing spark plugs or installing new spark plugs. Failure to install a new spark plug gasket may result in incomplete sealing of the combustion chamber, loss of heat transfer with spark plug overheating leading to possible pre-ignition.
Meteorological information
The weather at the time of the incident, recorded at Tindal Airport around 13 km to the north of the landing site, captured a wind of between 9–13 kt from the east, clear skies and a temperature of 23°C.
Recorded information
The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the incident flight, data was being transmitted by the helicopter’s transponder. This data, recorded by ground-based receivers, captured the aircraft’s position, altitude, and groundspeed during the final 25 minutes of the flight. All radio communications made and received by Tindal Airport ATC throughout the flight were recorded.
Helicopter damage
The ATSB did not attend the landing site. A post-incident inspection of the helicopter was completed by a maintenance organisation located at Wally’s Airstrip, NT. This inspection identified:
damage to the engine with scattered material within the cowling
damaged and displaced drive belts
impact damage to the engine oil cooler caused by engine material
engine oil on external areas of the engine and airframe
the skid landing gear was spread outwards (Figure 4).
The engine and a selection of components were removed for a detailed examination by the ATSB.
Figure 4: VH-OOE shortly after landing showing oil leak and smoke haze
Source: Supplied, annotated by the ATSB
Engine examination
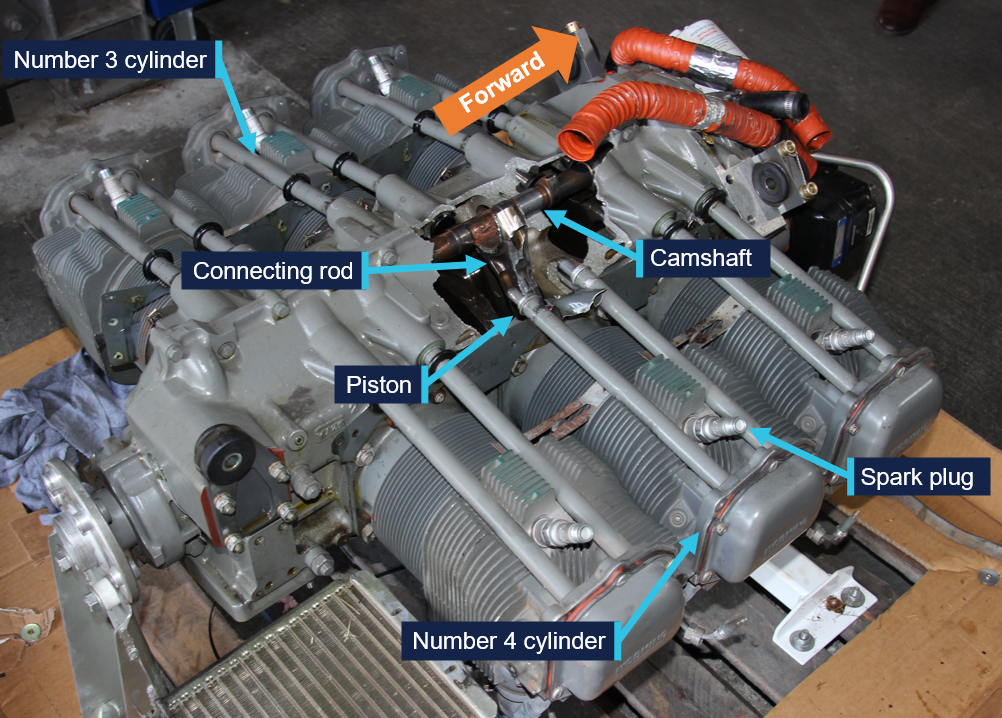
The engine was disassembled and examined at a CASA‑approved engine overhaul facility under the supervision of the ATSB. The examination found that the number 4 connecting rod had separated from the crankshaft journal, resulting in mechanical damage to the internal engine components and fracture of the adjacent crankcase. Both connecting rod bolts had been fractured, with one connecting rod nut missing and the other unwound (see Component examination). There were also witness marks from impact between the number 4 piston crown and cylinder head.
Prior to removal of the remaining connecting rods, the nuts were checked for torque. The check found that the number 3 cylinder connecting rod nuts were at 20 ft/lb, while numbers 1, 2, 5 and 6 connecting rod nuts were at the correct torque of 40 ft/lb.
The number 4 cylinder spark plugs were found loosened, but the spark plug leads were attached tightly. Subsequent testing of the spark plugs found both were serviceable. Figure 5 depicts the engine prior to disassembly.
Figure 5: Engine assembly showing damage
Source: ATSB
Component examination
Several components were retained from the engine disassembly and were examined at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
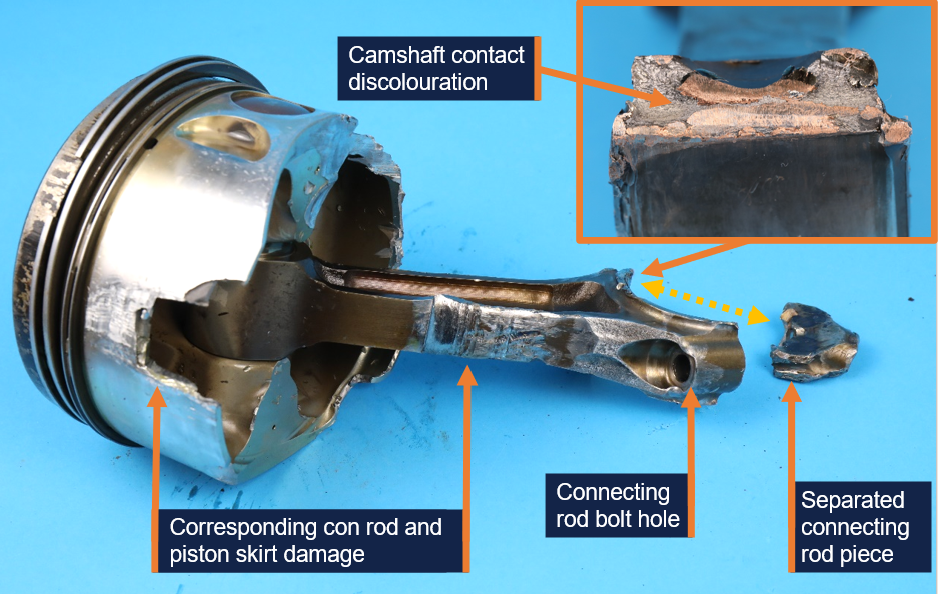
Extensive deformation and fracture of the number 4 connecting rod (Figure 6) and deformation of the crankshaft journal, was consistent with initial separation of the connecting rod, followed by repeated impacts to the connecting rod by the still-rotating crankshaft.
Figure 6: Number 4 cylinder connecting rod and piston
Source: ATSB
This resulted in significant damage to the adjacent cylinder wall, piston skirt, camshaft and the hole in the crankcase. The fractured connecting rod showed no evidence of fatigue cracking or other defect.
The number 4 connecting rod bearings were deformed due to contact with the moving internal engine components but were found to be the correct parts and did not exhibit any abnormal signs of wear. Bearings from some of the other connecting rods displayed minor surface wear, which was attributed to low engine oil volume during the final part of the flight.
There were visibly fewer combustion deposits on the number 4 piston crown, compared to the remaining pistons. However, a considerable amount of sand-like contamination was recovered from the number 4 cylinder during engine disassembly, which was found to be chemically similar to the piston deposits. There was no evidence of destructive combustion issues such as pre-ignition or significant detonation.
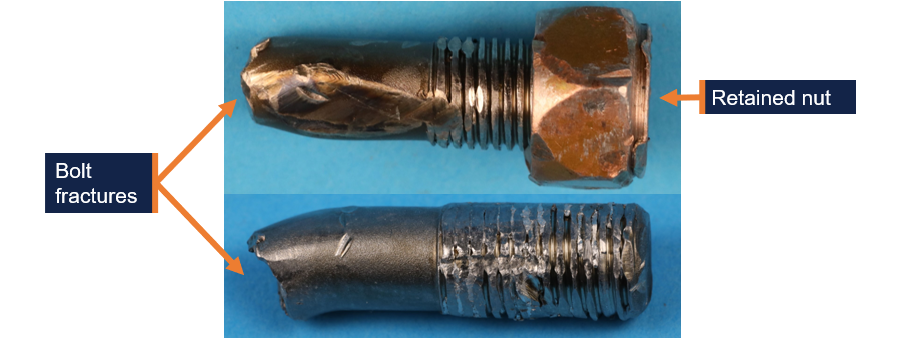
The connecting rod was secured to the crankshaft by 2 connecting rod bolts (Figure 3). Both number 4 cylinder connecting rod bolts were fractured in approximately the same location (Figure 7). The fracture surface features of both bolts and deformation of the adjacent shank were consistent with overstress failures.
Figure 7: Cylinder number 4 connecting rod bolts
Source: ATSB
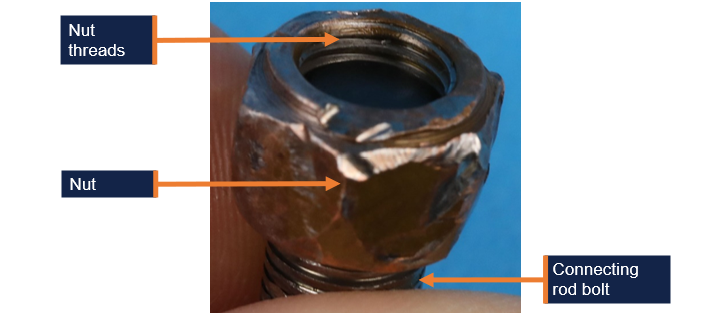
One of the cylinder 4 connecting rod bolts had no nut and heavily damaged threads. The nut was not located. The other connecting rod bolt had a partially unwound nut retained on the threads (Figure 8).[7] The exposed threads were damaged. The nut could not be further unwound by hand, likely due to impact damage. The bolts and nut material was in accordance with their specification. The extent of deformation precluded a detailed inspection of the threads; however, the threads were not stripped and the remnants of a compound consistent with thread lubricant was identified.
Figure 8: Number 4 cylinder connecting rod bolt showing position of retained nut
Source: ATSB
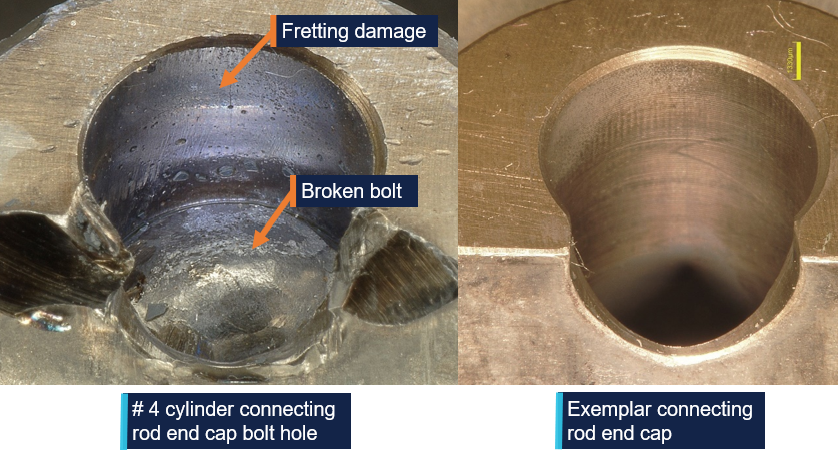
The examination also identified evidence of abnormal fretting[8] wear in the number 4 cylinder connecting rod bolt holes. A comparison between the number 4 cylinder and number 6 cylinder connecting rod bolt holes is depicted in Figure 9.
Figure 9: Number 4 cylinder connecting rod end cap bolt hole fretting wear and exemplar
Source: ATSB
The abnormal fretting wear indicated relative movement (micro-slip) between the bolted surfaces during operation, which would occur if the bolt tension was insufficient to restrain movement under normal operational loads. The missing nut from one of the bolts, and the other nut retained in an improper position on the fractured bolt, was also an indicator that the nuts had loosened in-service.
Possible mechanisms that could result in the in-service loosening of the nuts included:
Abnormal loading or vibration from engine overspeed or abnormal combustion that could lead to bolt stretch and nut loosening.
Variations in thread condition or installing the threads dry versus lubricated could produce a lower bolt stress than desired.
Unintended deformation due to improper or defective parts leading to reduced bolt stress over time.
Microscopic surface deformation and fretting at contact interfaces could reduce clamping force by a small margin over time, which could then make the nut susceptible to further loosening during service.
Inadequate torque applied to the nuts during installation that could lead to relative movement between the clamped surfaces and nut loosening during normal operation.
Related occurrences
In 2007, the ATSB published a research and analysis report (B20070191) into aircraft reciprocating (piston) engine failures. The report examined 20 high-power[9] piston engine structural failure occurrences in Australia, between 2000 and 2005. The report focused on failures of the combustion chamber, connecting rods and crankshaft assemblies. It included several engine failure investigations, including investigation 200105866 (below).
On 14 December 2001, a Piper PA31-350 aircraft, registered VH-JCH, was in cruise flight at 8,000 ft when the flight crew noticed that the propellers went out of synchronisation. Adjustments were made to correct the problem but were unsuccessful. Following right engine speed fluctuations, the crew shut the engine down, feathered the propeller and conducted a single‑engine landing.
During the subsequent disassembly of the engine, the crankshaft was noted to have fractured at the number 6 connecting rod journal, and the number 6 connecting rod big end had separated from the crankshaft and impacted the camshaft. The separation of the number 6 big end permitted the piston to strike the top of the combustion chamber with sufficient force to deform the top of the piston.
The number 6 connecting rod disconnection from the crankshaft was due to the loosening of the nuts on the connecting rod bolts, and eventual loss of one nut. Evidence of nut loosening, leading to fretting wear damage, was observed on the bolt threads and the connecting rod cap bolt hole locations. The reason for the loosening of the number 6 connecting rod nuts could not be determined.
The damage of these components was almost identical to the damage noted in the engine from VH-OOE.
Safety analysis
The ATSB examination of the engine components determined that the engine failure resulted from mechanical damage caused by the separation of the number 4 cylinder connecting rod from the crankshaft.
The initiating factor of the separation was almost certainly the in-service loosening of the connecting rod nuts of the number 4 cylinder. This was evidenced by the fretting wear in the connecting rod bolt holes, which was illustrative of engine operation after a loss of bolt tension, allowing relative movement between the bolts and holes. The absence of one of the associated nuts, and the opposite one mostly unwound was also evidence of the nuts loosening prior to the engine failure. There was also an absence of fatigue cracking of the number 4 bolts or connecting rod that might otherwise account for the component fractures and separation of the connecting rod.
Of the possible mechanisms identified that could have led to the connecting rod nuts loosening:
Abnormal loading or vibration: there was no evidence of engine overspeed, or of piston melting or structural damage consistent with severe abnormal combustion. There was no evidence that the spark plugs, found loose during the disassembly, had any negative impact on the engine performance.
Variation in thread condition and lubrication: this could not be fully assessed due to thread damage and the absence of one of the nuts.
Improper or defective parts: the connecting rod bolts and nut material was correct; however, a full assessment of their original condition was not possible.
Embedding (microscopic deformation): it is possible that the initial bolt tension reduced by a small margin due to microscopic deformation of the clamping or thread surfaces, which would then make the nut more susceptible to further loosening during service.
Inadequate installation torque: like the above, it was possible that the nuts were slightly under-torqued during installation and progressively loosened during the subsequent 291 hours of operation. The number 3 connecting rod nuts being found at the incorrect torque value during the engine disassembly further supports this scenario.
Given most of the possibilities above could not be definitively ruled out, the reason for the nuts loosening was ultimately not determined.
Despite this, it was identified that during the overhaul of the engine fitted to VH-OOE, the independent inspection of the engine sub-assembly did not involve a torque check of the connecting rod nuts. While there was no evidence of influence on this occurrence and while the inspection was not a regulatory requirement, the ATSB considered it a missed opportunity to positively verify the installation torque.
Additionally, during the engine examination, both spark plugs in the number 4 cylinder were found to be loose. The reason for the loose spark plugs was not determined and, as above, there was no evidence identified to indicate influence on the engine failure. However, it was identified that during the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the engine and spark plug manufacturer.
On the same subject, the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances.
The unusual sound and vibration noted by the pilot during engine start was possibly a precursor to the eventual failure inflight, however the vibration disappeared when engine speed was increased. In response to the onset of severe vibration inflight, the pilot assessed the controllability of the helicopter and noted there were no abnormal engine indications at that time. In accordance with the Robinson R44 POH, the pilot conducted a precautionary landing in a suitable location. They also communicated the issue to Tindal Airport ATC, which increased the likelihood of a timely emergency response had one been necessary.
During the late stages of the approach, the low rotor speed warning horn and low oil pressure caution light activated. Both indicated a reduction in power, almost certainly due to the mechanical failure, resulting in less power than normal to arrest the rate of descent in the final stages of landing. This, in combination with the pilot’s concern about a possible fire and recollection of landing ‘quicker’ than normal, likely resulted in the helicopter landing heavily which spread the landing gear skids.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine failure and forced landing involving Robinson R44, VH-OOE, 13 km south of Tindal Airport, Northern Territory, on 11 June 2025.
Contributing factors
In-service loosening of the connecting rod nuts resulted in the eventual separation of the connecting rod from the crankshaft and the mechanical failure of the engine. The reason for the nuts loosening was not determined.
During the engine overhaul, the torque on the connecting rod nuts was not physically checked as part of the independent inspection of the engine assembly. This was a missed opportunity to verify that the installation of the connecting rod nuts had been completed correctly.
Other findings that increased risk
During the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the spark plug manufacturer. This increased the risk of loosened spark plugs, insufficient heat transfer and pre-ignition.
The Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances. The inconsistency in this guidance could have led to incorrect procedures being performed which were not in accordance with spark plug maintenance requirements.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Civil Aviation Safety Authority
The Civil Aviation Safety Authority acknowledged the inconsistency between Airworthiness Bulletin AWB 20-001 (that stated that annealed gaskets could be used) and Airworthiness Bulletin AWB 85-023 (that stated new gaskets must be used in all circumstances) and advised the ATSB that AWB 20-001 will be cancelled and AWB 85‑023 will be amended to reflect current recommendations.
Safety action by Platinum Helicopters
Platinum Helicopters advised the ATSB that new spark plug gaskets are now fitted each time spark plugs are reinstalled.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Australian Government (2021), Aircraft Reciprocating-Engine Failure: An Analysis of Failure in a Complex Engineered System, Australian Transport Safety Bureau, Canberra, ACT. /publications/2007/b20070191
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of VH-OOE
Civil Aviation Safety Authority
the maintenance provider
the engine overhaul organisation
Textron Lycoming
Robinson Helicopters
National Transportation Safety Board (NTSB).
Submissions were received from:
the pilot of VH-OOE
the maintenance provider
the engine overhaul organisation
Textron Lycoming
Robinson Helicopters.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]Annealing: the process of heating a metal to a cherry red colour and them immersing into water to soften the material.
[3]A parts manufacturer approval (PMA) is a combined design and production approval for modification and replacement articles. It allows a manufacturer to produce and sell these articles for installation on type certificated products.
[4]Champion Service Manual AV6-R, revised August 2014.
[5]Champion Aviation Technical Bulletin 95-11, Aviation Spark Plugs – New and Reconditioned Should Always be Installed with a New Gasket, published November 1995.
[7]When installed correctly, 2–3 bolt threads would protrude from the edge of the nut. In this case 2–3 nut threads were visible on the end of the bolt.
[8]Fretting refers to wear involving small amplitude relative movement or vibration between contact surfaces.
[9]The high-power engines analysed as part of the study were Lycoming TIO-540 and IO-540, and Continental TSIO-520 and GTSIO-520 engines.
Occurrence summary
Investigation number
AO-2025-029
Occurrence date
11/06/2025
Location
13 km south of Tindal Airport
State
Northern Territory
Report release date
30/03/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Smoke
On 24 January 2025, a Cirrus SR22, VH-DCB, was conducting a private flight from the Gold Coast, Queensland, to Mildura, Victoria with the pilot and one passenger on board.
About 2 hours and 43 minutes into the flight, while approaching the Mitchell Highway to the east of Nyngan, New South Wales, the pilot observed a cautionary alert, advising of low engine oil pressure. The pilot diverted to Nyngan Aerodrome and a short time later, the engine subsequently sustained an in-flight mechanical failure and engine fire. The aerodrome was beyond the aircraft's glide range at the time and the pilot elected not to deploy the Cirrus Aircraft parachute system, but to perform a forced landing on the Mitchell Highway.
The pilot conducted a successful forced landing, both pilot and passenger were uninjured and the aircraft sustained only minor damage.
What the ATSB found
The engine lost oil pressure during flight and sustained an in-flight mechanical failure, prompting the pilot to declare an emergency. The pilot exercised timely and effective decision‑making, which mitigated the risk of injury to the occupants and further damage to the aircraft. The pilot then promptly executed a successful forced landing on a nearby highway, while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin.
Safety message
In-flight engine failures in single-engine aircraft require pilots to exercise effective and timely decision-making to reduce the severity of injuries and damage. These events often result in the pilot experiencing high workload and time pressure, where preparedness is critical.
The ‘aviate, navigate and communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies. Taking action in the appropriate order of priority improves situational awareness and supports coordinated responses in a dynamic environment.
Scenario-based training should reinforce these principles by developing both technical and non-technical skills, helping pilots become familiar with the appropriate responses and techniques required during high‑stress situations.
Decision-making tools also enables pilots to take a structured approach to problem‑solving which enhances safety by minimising the risk of errors during emergencies.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 25 January 2025, the pilot of a Cirrus SR22, registered VH-DCB, planned to conduct a private flight from Gold Coast, Queensland, to Mildura, Victoria. The aircraft departed Gold Coast Airport with the pilot and one passenger at about 0735 AEST.[1]
At 1018, while cruising at an altitude of about 8,000 ft above mean sea level (AMSL), the engine oil pressure decreased below the normal operating limits for the engine, 30 pounds per square inch (psi), and the pilot recalled an engine oil pressure alert. The pilot identified that Nyngan Aerodrome was the nearest aerodrome, about 15 NM (28 km) to the north-west. At 1019, the pilot diverted directly to Nyngan with the aid of the autopilot (Figure 1).
Figure 1: VH-DCB flight track and key events taken from recorded data
Source: Google Earth, annotated by the ATSB
The pilot calculated the distance, altitude and glide ratio[2] of the SR22 and concluded that they would likely not make it to Nyngan in the event that the engine failed. They continued towards Nyngan but began to look around for suitable landing sites and identified the Mitchell Highway on the left side of the aircraft.
After checking the engine indications and confirming the engine oil pressure was below normal operating limits and continuing to decrease, the pilot made a PAN PAN[3] broadcast to air traffic control (ATC), advising they were losing engine oil pressure and would be tracking directly to Nyngan. During this broadcast, the pilot recalled the engine began to ‘rev up’ which was followed by an audible ‘bang.’
The pilot then made a MAYDAY[4] broadcast to ATC, advising that the engine had experienced a mechanical failure and they would be making an emergency landing on the highway. As ATC acknowledged the broadcast, the pilot observed flames ‘pouring’ from the top of the cowl.
At 1020 the pilot began a controlled descent towards Nyngan and the Mitchell Highway (Figure 1), and they selected idle power, mixture to cut off and turned off the fuel pump. They attempted to switch the fuel selector lever to off, but they were unable to, recalling that they required both hands to do so. At this time their forward visibility became partially obscured by engine oil on the windscreen.
The pilot reported being concerned that the fire was fuel related and elected to continue with a forced landing rather than deploying the airframe parachute system fitted to the aircraft (see Cirrus airframe parachute system). The pilot was also aware of the increased risk of fire damage to the aircraft rescue system and potential injuries during a parachute‑assisted landing to the passenger, who was pregnant.
At 1023, the pilot commenced a left turn at about 5,000 ft in the direction of the Mitchell Highway. The pilot elected to ‘dive the plane down’ to supress the fire, and increased the rate of descent to over 3,600 ft/min (see Appendix A, Figure A1) and then set up for an immediate forced landing on the highway.
The pilot recalled that the fire appeared to extinguish as the aircraft descended through 4,000 ft and reported they were able to switch the fuel selector off at about 3,250 ft. However, they recalled smoke began to enter the cockpit at about 3,000 ft as the aircraft continued to descend. The pilot selected the first stage of flap and lined up on a section of the Mitchell Highway in a south‑easterly direction. On final approach, the pilot had to adjust the emergency landing flightpath to avoid 2 motor vehicles on the highway and safely conducted the emergency landing, vacating the highway onto a dirt access road at about 1024 (Figure 2).
The pilot recalled that, during the emergency, they had continuously tried to anticipate the next event or action, then evaluated the best course of action and confirmed their decision before proceeding.
The aircraft sustained minor damage to several components on the left wing as a result of colliding with roadside guideposts during the landing roll (Figure 2 right insert) and the pilot and passenger were uninjured. The New South Wales rural fire service attended the scene shortly after the aircraft had safely landed.
Figure 2: VH-DCB alongside Mitchell Highway and minor damage to left wing
Source: Operator, annotated by the ATSB
Context
Pilot information
The pilot held a Commercial Pilot Licence (aeroplane) with an instrument rating and a class 1 aviation medical certificate. They had 3,496 flight hours, including about 1,900 hours on the Cirrus SR22 and had recently logged about 40 hours on type in the last 90 days.
The pilot reported sleeping about 9 hours the night before the occurrence and had been awake for about 5 and a half hours at the time of the occurrence. They further reported that they felt ‘fully alert and wide awake’ on the day of the occurrence and were not tired or fatigued.
Aircraft information
The Cirrus Design Corporation SR22 is a low wing general aviation aircraft with 5 seats and a single piston engine, driving a constant speed propeller. The aircraft was registered as VH-DCB in Australia on 9 November 2018 to the pilot, who was the registered operator. The aircraft was certified for day and night VFR[5] and IFR[6] operations.
Powerplant
The SR22 is equipped with a single Continental Motors Inc. IO-550-N engine. The engine oil used for lubrication and cooling is drawn from an 8-quart capacity sump located in the engine crankcase. The engine had a total time in service of 1,678.5 hours and the manufacturer‑approved time between overhaul[7] was 2,200 hours total time in service.
Engine oil system
The aircraft’s pilot operating handbook required an engine oil level between 6 and 8 quarts for normal operation, with the manufacturer recommending a pre-flight dipstick indication of 7 quarts for extended flights. On the day of the occurrence, the pilot recalled that the engine dipstick was reading 8 quarts prior to departure.
Cirrus airframe parachute system
The Cirrus airframe parachute system (CAPS) was designed to lower the aircraft and its passengers to the ground in the event of a life-threatening emergency and is operated by the pilot. The CAPS system consists of a parachute, a solid-propellant rocket used to deploy the parachute, an activation handle, and a parachute harness embedded within the fuselage structure.
Maintenance history
Immediately prior to the occurrence, the aircraft had undergone a 50‑hour inspection at a Cirrus‑authorised service centre. No engine‑related defects were recorded in the aircraft maintenance certification log.
Prior to that, on 23 October 2024 at the same service centre, the engine had been inspected during an annual inspection and was certified in accordance with approved maintenance data as airworthy at a total time in service of 1,637.6 hours.
All records of inspections and maintenance tasks obtained by the ATSB in the course of the investigation were certified as being conducted in accordance with the latest revisions of the Cirrus airplane maintenance manual and the Continental maintenance manual.
The pilot recalled that they had completed the daily inspection prior to the flight, with no identified issues before certifying the daily inspection on the aircraft maintenance release.
Meteorological information
The Bureau of Metrology aviation meteorological information report, which included the graphical area forecast[8] encompassing Nyngan Aerodrome at the time of the occurrence, contained the following:
visibility greater than 10 km
nil significant weather or cloud
moderate turbulence below 7,000 ft in dust devils and thermals north of Dubbo Airport.
At the time of the occurrence, the pilot stated that the weather was generally fine with good flying conditions and ‘not a cloud in the sky.’
Post-incident inspection
The pilot inspected the aircraft engine after the serious incident and found the crankcase had ruptured adjacent to cylinder 6 (Figure 3 right insert) below the induction duct assembly. They recovered a connecting rod that had separated from the crankshaft (Figure 4) and identified that the air filter was visibly damaged as a result of a fire (Figure 3 left insert). The pilot recalled performing a post‑landing dipstick check and observed that about 6 quarts of oil remained in the engine.
Figure 3: VH-DCB engine bay and damage to the air filter and crankcase
Source: Operator, annotated by the ATSB
Figure 4: Fractured connecting rod recovered from VH-DCB
Source: Operator, annotated by the ATSB
Due to the remoteness of the location, the aircraft was secured on a nearby property and the engine was retained with the fuselage until a replacement was fitted to the aircraft. Following the subsequent removal of the engine, a disassembly and inspection had not been conducted at the time of publication of this report. As a result, the ATSB was unable to determine the root cause for the loss of oil pressure or the mechanical failure of the engine.
Aircraft manufacturer’s emergency procedures
The emergency procedures section of the Cirrus SR22 pilot’s operating handbook (POH) prescribes procedures for handling emergencies and critical flight situations that may occur while operating the aircraft. The POH states:
Although this section provides procedures for handling most emergencies and critical flight situations that could arise in the aircraft, it is not a substitute for proper flight training, thorough knowledge of the airplane, and recognised piloting techniques and standards.
Additionally, the POH recommends 4 basic actions that can be applied to any emergency which include:
maintain aircraft control
analyse the situation
take appropriate action
land as soon as conditions permit.
In cases when a procedure directs a pilot to ‘land as soon as possible’, the POH states:
Land without delay at the first site at which a safe landing can be made. Continued flight beyond an available airfield at which a safe landing can be made will result in increased risk and shall not be attempted.
Loss of engine oil pressure in-flight
When engine oil pressure decreases below 10 psi the aircraft’s crew alerting system[9] (CAS) will annunciate ‘oil pressure’ in red text on the primary flight display which is accompanied by a repeating double chime audio alert. The alert prompts the pilot to carry out the following procedure contained in the emergency procedures section of the POH:
a. Power..........REDUCE TO MINIMUM FOR SUSTAINED FLIGHT
b. Land as soon as possible.
(1) Prepare for potential engine failure
Procedure Complete
Engine fire in-flight
In cases of smoke and fire, the CAS will not alert the pilot to this condition. When a pilot identifies an engine fire in-flight, they must action the following items by memory:
The POH also contained a note which suggested that in the case of a wing fire in-flight, ‘putting the airplane into a dive may blow out the fire.’
During the occurrence, the pilot carried out their actions by memory and stated that they were unable to refer to checklists during the serious incident due to the lack of time. Although the ‘engine fire in-flight’ procedure did not direct the pilot to dive, the pilot decided that diving the aircraft would assist in extinguishing the fire in this case.
The pilot also stated that they encountered difficulty switching off the fuel selector while simultaneously flying the aircraft during the glide approach and managing the emergency. The POH stated ‘to select off, first raise the fuel selector knob release and then rotate the knob to off.’ This is not performed during normal operations which meant the pilot was not familiar with the action. The pilot also recalled turning the ignition switch off after the aircraft had landed.
Cirrus airframe parachute system deployment
The emergency section of the POH contains procedures regarding the deployment of the ballistic parachute in-flight. This section contains the following explanatory notes:
It should also be used in other life threatening emergencies where CAPS deployment is determined to be safer than continued flight and landing. Expected impact in a fully stabilised deployment is equivalent to a drop from approximately 13 feet.
A cautionary note also explains that ‘CAPS deployment will likely result in damage or loss to the airframe.’
The POH identifies several possible scenarios for deploying the CAPS:
midair collision
structural failure
loss of control
landing in inhospitable terrain
pilot incapacitation.
No specific guidance is contained in the POH regarding the use of the CAPS in cases of in-flight smoke and fire.
Recorded information
The Garmin avionics suite installed in the SR22 included a flight data logging feature that automatically stored critical flight and engine data on a removable data card.
The ATSB was provided with the data card installed in the aircraft at the time of the occurrence. The data on the card was downloaded by the ATSB and confirmed to have contained flight data recorded during the occurrence on 24 January 2025.
Recorded data
The recorded flight data captured parameters such as engine parameters, altitude, airspeed, vertical speed, bank angle and various avionics functions (Appendix A – Recorded data). This data enabled a detailed reconstruction of the flight, providing insights into the aircraft’s performance and pilot actions during the occurrence (Figure A1).
Prior to the occurrence, the recorded flight data (Figure A2) indicated that all recorded engine parameters were within normal operating limits outlined in the powerplant limitations section of the pilot’s operating handbook prior to the loss of engine oil pressure. Table 1 depicts the normal and recorded ranges of each engine parameter from the time the aircraft became airborne at 0733:21 until the engine oil pressure decreased below the normal range of 30 psi at 1018:46.
Table 1: Recorded in-flight range prior to loss of engine oil pressure
Recorded in-flight range inclusive of cylinders 1 – 6
[2]Recorded in-flight range inclusive of cylinders 1 – 6
Source: Operator supplied flight data card, tabulated by the ATSB
Related occurrences
The following ATSB investigations highlight the risks associated with encountering engine failures in flight, demonstrating the importance of effective decision‑making.
On 21 November 2012, a Cirrus SR22 aircraft, registered VH‑WYH, departed Emerald, Queensland for Dubbo, New South Wales, on a private flight conducted under instrument flight rules. The pilot and one passenger were on board.
During the flight, the oil pressure annunciation illuminated, and the engine oil pressure indicated 30 pounds per square inch (psi). As the oil pressure continued to slowly drop, the pilot became increasingly concerned and tracked via Gilgandra, New South Wales. They overflew Gilgandra and continued on towards Dubbo, at which point the oil pressure gauge indicated about 12 psi.
Two hours and 39 minutes after the oil pressure light illuminated, the engine failed. When it became evident that a landing at Gilgandra aerodrome was not achievable, the pilot deployed the ballistic parachute. The aircraft impacted the ground and was substantially damaged with the pilot receiving minor injuries while the passenger was uninjured. The pilot reported that the oil pressure indication dropped very gradually giving a false sense of security.
On 6 November 2020, the pilot of a S.E.D.E. Morane-Saulnier MS.893A (Rallye) aircraft, registered VH‑UQI, was conducting a private flight from Moruya, New South Wales, to Archerfield, Queensland. About 22 km south‑west of Archerfield Airport, the engine began running rough before eventually failing.
The pilot elected to conduct a forced landing into an open but slightly undulating paddock. The approach direction resulted in a tail wind landing. The aircraft over‑ran the open area before it impacted with a grove of trees, significantly disrupting the aircraft structure. A post‑impact fire consumed most of the fuselage. The pilot was seriously injured, and the aircraft was destroyed.
The pilot was ferrying the aircraft on behalf of the owner and had limited aircraft type experience and knowledge of its performance capabilities, and it was found that the pre‑flight planning was limited.
Safety analysis
During the investigation, the ATSB was unable to determine the initiating factor that led to the loss of oil pressure and subsequent mechanical failure of the engine. However, the recorded data from the occurrence revealed that all engine parameters were within normal operating limits prior to the loss of engine oil pressure and subsequent in‑flight mechanical failure of the engine.
After observing the oil pressure caution message, the pilot made a timely decision to divert to Nyngan Aerodrome. Being aware of the aircraft’s gliding capabilities and after the oil warning alert, they were immediately able to determine that the aircraft did not have sufficient altitude to safely conduct a forced landing at the aerodrome. They then identified the Mitchell Highway as the most suitable landing site before investigating the engine parameters.
When the engine experienced a mechanical failure, the pilot was able to immediately enact their pre‑planned forced landing procedure, declare the emergency and communicate their intention to land on the Mitchell Highway.
After observing flames and oil coming from the engine cowl, which obscured their visibility, the pilot made a timely decision and elected not to deploy the aircraft’s ballistic parachute. This was due to the pilot’s concern that the fire was fuel‑related and may affect the deployed parachute system as well as the potential risk of injury to the passenger, who was pregnant, and aircraft damage associated with a parachute‑assisted landing.
The pilot began an emergency descent, putting the aircraft into a ‘dive’ in an attempt to put out the fire. Once the fire self-extinguished, smoke entered the cockpit. However, the pilot proceeded to navigate the aircraft to land on the highway among traffic for a successful forced landing with no injuries and only limited damage.
The ATSB research report Engine failures and malfunctions in light aeroplanes, 2009 to 2014 (AR-2013-107) indicated that although engine failures are relatively rare, they do happen. Given the potential severity of the consequences of an engine failure or power loss in a single‑engine aircraft, such occurrences therefore need to be planned for and managed appropriately.
On this occasion, the pilot made effective and timely decisions to manage the evolving emergency and appropriately prioritised their actions. Their decision‑making was likely supported by their experience on the aircraft type and knowledge of the performance capabilities. This enabled prompt and appropriate responses from the pilot, which contributed to a safe outcome.
Additionally, the pilot’s methodical approach during this occurrence highlights the importance of decision-making tools to aid pilots to mitigate the possibility of errors and ensure a considered approach in resolving issues or problems (Civil Aviation Safety Authority, 2019).
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine failure involving Cirrus SR22, VH-DCB, 29 km east-south-east of Nyngan, New South Wales, on 24 January 2025.
Contributing factors
The engine lost oil pressure during flight, leading to an in-flight engine failure and fire.
Other findings
The pilot exercised timely and effective decision making in flight to divert and then identify a safe forced landing area.
The pilot successfully executed an immediate forced landing on a nearby highway while experiencing fire and reduced visibility from oil over the windscreen and smoke entering the cabin. This resulted in no injuries to the 2 occupants and only minor additional aircraft damage.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the serious incident flight
maintenance organisation
Civil Aviation Safety Authority
United States National Transportation Safety Board
Cirrus Design Corporation
Continental Motors Incorporated.
Submissions were received from:
pilot in command/operator
Cirrus Design Corporation
Continental Motors Incorporated.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Recorded data
Figure A1: In-flight data and key events after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Figure A2: In-flight engine parameters after loss of engine oil pressure
Source: Operator supplied flight data card, annotated by the ATSB
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
An explanation of terminology used in ATSB investigation reports is available here.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Local time was Australian Eastern Standard Time (AEST), which is Coordinated Universal Time (UTC) +10 hours. Times in this report are AEST unless otherwise noted.
[2]Glide ratio: the glide ratio of an aircraft is the distance of forward travel divided by the altitude lost in that distance. The Cirrus SR22 pilot’s operating handbook stated the maximum glide ratio for the aircraft was 8.8:1.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[5]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions
generally clear enough to allow the pilot to see where the aircraft is going.
[6]Instrument flight rules (IFR): rules which allow properly equipped aircraft to be flown under instrument meteorological
conditions
[7]Time between overhaul: is a time limit specified by the engine manufacturer for a specific engine in a specific installation, after which overhaul is either recommended or mandated depending on how the aircraft is used.
[8]Graphical area forecast (GAF) is a combination of graphical and textual information. The graphic is divided into areas that share common weather characteristics which are detailed in an associated table.
[9]Crew alerting system (CAS): aircraft annunciations and alerts are displayed in the CAS window located to the right of the altimeter and vertical speed indicator. Aircraft annunciations are grouped by criticality and sorted by order of appearance with the most recent message on top.
[10]Cylinder head temperature (CHT): CHT is measured by a temperature-sensing probe located at the cylinder head, and it measures heat energy wasted during the power stroke, when the cylinder is under maximum stress from high internal pressures and temperatures.
[11]Exhaust gas temperature (EGT): is a measurement of the temperature of the exhaust gases at the exhaust manifold.
On 15 August 2024, a Fairchild SA227-DC Metroliner 23, operated by Skippers Aviation, departed Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA, with 12 passengers and 2 flight crew on board. As the aircraft climbed, the crew noted high-temperature air and light smoke emanating from flight deck air vents.
As the smoke quickly increased, the crew commenced actioning the ‘smoke in aircraft’ checklist but required items of the checklist were not completed – the first officer did not don an oxygen mask due to difficulty with its usage, and the left bleed air system was not selected ‘off’. Instead, the crew commenced preparations for a return to Perth and subsequently, the left wing overheat light illuminated. The crew then actioned the ‘wheel well and wing overheat’ checklist and selected the left bleed air system ‘off’, which stopped the smoke ingress into the cabin, but elected not to complete the required action of extending the landing gear.
During the return to Perth, the aircraft deviated both above and below the altitude assigned by air traffic control including a descent to 639 ft below the lowest safe altitude. The crew then completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
What the ATSB found
The ATSB found that a failure within the left air cycle machine prior to departure resulted in hot engine bleed air and smoke entering the cabin and that items on the ‘smoke in aircraft’ checklist were not completed. Consequently, the smoke ingress into the cabin continued and during the return, the left air conditioning duct overheated, and the wing overheat light illuminated. Furthermore, the first officer’s decision not to don an oxygen mask increased their risk of impairment or incapacitation. A later decision not to extend the landing gear, as required by the response checklist, had the potential to increase risk if the wing overheat indication had been associated with a brake fire or wheel well overheat.
The ATSB determined that the workload associated with the in-flight response to the smoke in the cockpit and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision making.
During the return to Perth, the first officer readback an air traffic control altitude instruction as 2,000 ft AMSL instead of 2,800 ft AMSL. The controller did not identify or correct the error however, following a query from the crew, this was later corrected. Finally, after the assigned altitude had been confirmed by the crew, the aircraft descended below the lowest safe altitude. While the crew were advised of the deviation by air traffic control, the required ‘safety alert’ wording was not used.
What has been done as a result
Following the occurrence, the operator conducted a refresher training course for flight crew on emergency response briefings and a theory examination for flight crew on bleed air, pneumatics, pressurisation and fire warning systems. Practical training sessions were also held for flight crew on revised emergency procedures and the use of the crew oxygen system.
The operator also changed the Metroliner 23 flight crew training program to include a revised Line Oriented Flight Training (LOFT) program including more comprehensive oxygen system training and a presentation on the Metroliner 23 oxygen system.
Safety message
This occurrence highlights the importance of careful and methodical checklist completion. In this case, not completing a checklist resulted in increased risk to the flight and an avoidable increase to an already high workload. This in turn led to later decision-making and flight path management errors.
Additionally, the incident also emphasises the importance of flight crew familiarising themselves with the operation and use of the onboard emergency equipment. When exposed to an environment of smoke and fumes, flight crew must ensure that emergency breathing equipment is correctly utilised.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 15 August 2024, the crew of a Fairchild SA227-DC Metroliner 23 aircraft operated by Skippers Aviation, registered VH-WBQ and callsign ‘Skippy 5003’, taxied the aircraft to runway 24 at Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA. There were 12 passengers on board and the flight crew comprised the captain acting as pilot flying,[1] and the first officer acting as pilot monitoring.
As the aircraft taxied to the runway, the first officer noted that the cabin temperature was unusually warm and selected ‘full cold’ on the temperature selector.
At 0746, the aircraft departed runway 24 and turned left turn following the REPOK 1 standard instrument departure. As the aircraft climbed above about 1,500 ft above mean sea level (AMSL), the captain noted that the cabin temperature was warm and asked the first officer to select full cold on the temperature selector. The first officer responded by advising that full cold was already selected.
As the aircraft climbed above about 3,000 ft AMSL, the first officer attempted to reduce the high cabin temperature by selecting ‘auto’ on the temperature controller before then reselecting ‘full cold’. At about this time, the crew noted that vents on the captain’s (left) side of the flight deck (Figure 1) were blowing very hot air while the vents on the first officer’s (right) side blew the expected cool air.
Figure 1: Exemplar Metroliner 23 flight deck
Source: Matt Hayes, annotated by the ATSB
In response, the captain attempted to close the vent but found it too hot to touch. At the same time, they observed light smoke emanating from the vent. The smoke quickly increased, and the crew commenced the quick reference handbook (QRH) ‘smoke in aircraft’ checklist memory items.[2]
These memory items required the crew to don oxygen masks, establish communications (see the section titled Crew oxygen system) and consider donning smoke goggles. As the smoke was not impacting their vision, both flight crew members elected not to don smoke goggles. The captain donned an oxygen mask and made the required audio selections to establish communications using the mask.
The first officer encountered difficulties in adjusting the mask straps and could not get the mask to fit. They also did not make the required selections to establish communications using the mask, which resulted in the first officer hearing breathing noses through the headset and not being able to communicate using the oxygen mask microphone. As a result of these difficulties, the first officer elected not to wear the mask at that time.
The first officer retrieved the QRH ‘smoke in aircraft’ checklist to confirm the required memory actions had been completed and complete the remaining items of the checklist. For smoke emanating from a bleed air source, such as the air-conditioning system, the checklist required selecting the appropriate bleed air system ‘off’ (see the section titled Quick reference handbook). Before completing those checklist actions, the crew made a PAN PAN[3] broadcast advising air traffic control that there was smoke in the cockpit and that a return to Perth was required. The crew then began preparing for the return to Perth and did not complete the remaining items of the checklist at that time.
At 0751, the Perth Departures air traffic controller acknowledged the PAN transmission and instructed the crew to turn to a heading[4] of 360° and descend to 3,000 ft AMSL to commence the return. At this time, air traffic control also activated the Perth Airport emergency services.
Shortly after, the controller handed the crew over to the Perth Approach controller. One minute later, the approach controller instructed the crew to turn to a heading of 240° and descend to the lowest safe altitude of 2,800 ft AMSL. The first officer incorrectly read back the descent altitude as 2,000 ft AMSL, however the controller did not identify the error (Figure 2). The crew subsequently began descending the aircraft.
Figure 2: Flight path of VH-WBQ
Source: Airservices Australia and Google Earth, annotated by the ATSB
As the aircraft descended, the captain assisted the first officer with donning the oxygen mask and making the required audio selections to establish communications. From this time on, the use of the oxygen mask significantly reduced the intelligibility of the first officer’s radio broadcasts.
At 0756, the crew levelled the aircraft at 2,800 ft AMSL and contacted the controller to confirm the assigned altitude. The controller confirmed the altitude was 2,800 ft AMSL and the assigned heading as 180°. The first officer readback the altitude and heading instructions correctly.
At 0756, as the aircraft turned to the assigned heading, a descent commenced from 2,800 ft AMSL (Figure 3). About 50 seconds later, having observed the descent, the air traffic controller advised the crew to maintain 2,800 ft AMSL and that 2,800 ft AMSL was the lowest safe altitude. The crew immediately commenced climbing the aircraft, having descended to 2,338 ft AMSL (about 1,600 ft above ground level (AGL)).
Figure 3: Flightpath of VH-WBQ after the incorrect readback
Source: Airservices Australia and Google Earth, annotated by the ATSB
In response to the air traffic control instruction, the first officer replied stating ‘unable, Skippy 5003’ intending to convey that the crew were ‘unable’ to clearly hear the instructions. The controller interpreted the statement to mean that the crew were unable to maintain 2,800 ft AMSL and queried if the crew were in visual conditions. The first officer replied that the aircraft was not visual. At the same time, the air traffic control system generated a cleared level adherence monitoring (CLAM) alert for the aircraft. The controller, believing that the aircraft could not maintain altitude and aware that the Perth runway 24 instrument landing system (ILS) provided the lowest available minimum safe altitude, provided the crew with heading instructions directly to the ILS localiser.
While tracking toward the localiser, the aircraft continued climbing until 0757:57 when it reached 2,717 ft AMSL, before it once again commenced descending. At about this time, the crew returned to the ‘smoke in aircraft’ QRH checklist to complete the remaining items, but before these could be completed, the left wing overheat light illuminated continuously (see the section titled Quick reference handbook). The crew then actioned the relevant memory items of the ‘wheel well and wing overheat’ QRH checklist, including switching off the left bleed air system. Soon after switching off the bleed air, the crew noted that the smoke ceased. The checklist also required the crew to extend the main landing gear. As the aircraft was descending at a speed of over 220 kt (in excess of the 175 kt maximum landing gear extension speed), and wanting to expedite the return, the crew decided not to extend the landing gear at that time.
The aircraft continued descending and at 0758:23 reached 2,161 ft AMSL (about 1,200 ft AGL) before recommencing a climb. The air traffic controller observed the aircraft descend below the minimum safe altitude and, shortly after, a second CLAM alert was generated. The controller did not advise the crew of the low altitude as they believed the crew were unable to maintain altitude and that contacting them would only increase their workload.
At the same time, the crew commenced a right turn to intercept the ILS localiser and 12 seconds later, while still wearing the oxygen masks, the crew contacted the controller to request airport emergency services. The controller did not comprehend the broadcast and asked the crew to repeat the request. The crew repeated the request, but the controller again could not understand it. The controller did not query the crew further and commenced coordinating the handover of the aircraft to the Perth Tower controller. During this period, the left wing overheat light extinguished.
At 0758:41, the aircraft crossed the ILS localiser while climbing above about 2,800 ft AMSL. The climb and right turn continued until the aircraft levelled at about 3,000 ft AMSL for 7 seconds before recommencing a descent. The aircraft descended to 2,751 ft AMSL, before again climbing. The right turn continued for a further short period, followed by the aircraft commencing an intercept of the localiser from the left side. The aircraft climbed for a final time to 2,947 ft AMSL before again commencing a descent and levelling at 2,800 ft AMSL about 10 seconds later. The aircraft then maintained 2,800 ft AMSL until intercepting the localiser at 0800.
The crew completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
Context
Crew details
The captain held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The captain commenced flying with Skippers Aviation as a first officer in May 2022 before progressing to captain in April 2024 and had 1,484 hours of flying experience, of which 1,270 hours were accrued in the Metroliner.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer commenced flying with Skippers Aviation in April 2024 and had 509 hours of flying experience, of which 247 hours were obtained in the Metroliner.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Aircraft details
The Fairchild SA227-DC Metroliner 23 is a twin-engine turboprop regional airliner and an enhanced version of the Metroliner series that initially entered service in 1972. The aircraft was fitted with an analogue cockpit and was not equipped with an autopilot or flight director. VH-WBQ (Figure 4) was configured with 2 crew seats and 19 passenger seats.
Figure 4: VH-WBQ
Source: Lloyd Cartwright
Crew oxygen system
The aircraft was fitted with oxygen masks for use by the flight crew during a smoke event. After donning the masks, the following steps were to be followed to establish communications between the crew members and when using the aircraft radios:
select the microphone switch at the rear of the cockpit side panel from ‘boom’ to ‘mask’
deselect the cockpit button on the audio panel
to communicate with the other flight crew member, use the intercom push-to-talk button on the front side of the control column
to transmit using the radio use the push-to-talk button on the reverse side of the control column as normal.
If these steps were not fully followed, breathing noises would be heard through the crew’s headsets that could distract from, and disrupt, normal communications.
Air conditioning system
The aircraft was fitted with 2 identical air conditioning systems, one associated with each engine, and feeding conditioned air to the associated side of the flight deck and cabin. Each air conditioning system was supplied with hot, high pressure bleed air from the engine compressor through a shut‑off valve to the air cycle machine. The air cycle machine used ambient air to cool the bleed air and incorporated a mixing valve (for cabin temperature control).
An engineering evaluation of the left engine air cycle machine, conducted after the flight, found that it had overheated and that the cooling turbine was expelling oil. The hot air mixing valve was also found to be operating intermittently and sticking in various positions.
Quick reference handbook
The operator’s Metroliner 23 Flight Operations Manual included quick reference handbook (QRH) checklists with memory items specified within red brackets. This manual provided the following guidance for usage:
In a situation where the PM has had to reference the QRH to cross check correct memory item completion they will then announce to the PF that he/she is “Standing by with the ……..checklist”…Both pilots will then silently carry out the circuit breaker check at this point after which the PF then commands “Continue” when he/she is ready, and the checklist is read from the beginning.
The checklist must be announced by title and checklist notes must be read before proceeding with the checklist. A checklist is not completed until stating, “…. checklist complete”.
QRH items shall be read and actioned (any memory items will just be checked for completion) by the PM (where practical). A self-challenge and response technique is required.
Most of the PF attention should be directed at flying the aircraft; however, he must also be kept informed with the management process of accomplishing the appropriate procedures/checklist.
It would be appropriate for the PM to delay reading of the checklist procedure until the PF is in a position to monitor and assist if required. Confusion is often a problem area when conducting QRH procedures. Checklist procedures must not be rushed. It is important crews conduct checklists in a careful and controlled manner.
To stop smoke ingress into the aircraft from a bleed air source such as the air conditioning system, the ‘smoke in aircraft’ checklist required the crew to select the affected bleed air system ‘off’ (Figure 5).
Figure 5: Smoke in aircraft QRH checklist
Source: Operator, annotated by the ATSB
The wing overheat annunciator illuminated with either a steady or flashing indication. A steady light indicated a brake fire, wheel well or air conditioning duct overheat condition. A flashing light indicated a wing leading edge bleed air line failure or an overheated generator wire. The QRH checklist for a steady indication (Figure 6) required the crew to extend the landing gear to reduce the risk of a brake or tyre fire, overheat condition or a tyre explosion.
Figure 6: Wheel well and wing overheat, steady light QRH checklist
Source: Operator
Smoke and fumes exposure
The United States Federal Aviation Administration pilot safety brochure Smoke toxicity highlighted that smoke inhalation should be recognised as a very real danger. It also stated that ‘smoke gas levels do not need to be lethal to seriously impair a pilot’s performance’.
ATSB research report AR-2013-213 Analysis of fumes and smoke events in Australian aviation from 2008 to 2012: A joint initiative of Australian aviation safety agencies found that over 1,000 fumes/smoke events were reported to the ATSB and the Civil Aviation Safety Authority in the period from 2008–2012. The report highlighted that fumes associated with these events may have the potential to pose a health risk through eye/skin irritation, difficulty in breathing, incapacitation or illness. This was especially the case if the fumes were associated with particulates (smoke) or fire. However, while occurrences involving smoke were more likely to result in an outcome than a fumes‑only event, the research also found that ‘very few led to a serious consequential event (such as a forced landing) or outcome such as fire or crew incapacitation’.
Air traffic control safety alert
The air traffic control manual of air traffic services provided the following guidance for issuing a safety alert:
Unless the pilot has advised that action is being taken to resolve the situation or that the other aircraft is in sight, issue a safety alert prefixed by the phrase 'SAFETY ALERT' when you become aware that an aircraft is in a situation that places it in unsafe proximity to:
a) terrain;
b) obstruction;
c) active Prohibited/Restricted/Military Operating Areas; or
d) other aircraft.
As the crew prepared the aircraft for the return to Perth, it descended below the 2,800 ft altitude assigned by the air traffic controller. The controller identified the aircraft descending below the assigned altitude and contacted the crew stating, ‘maintain 2,800, 2,800 lowest safe’, but the broadcast was not prefixed by the required statement ‘safety alert’.
Meteorology
From soon after take-off until after the aircraft was established on the ILS approach, the flight was conducted in instrument meteorological conditions.[5]
At 0800, the Bureau of Meteorology (BoM) automatic weather station at Perth Airport recorded the wind as 5 kt from 222° magnetic. Cloud cover was recorded as few[6] at 1,267 ft above mean sea level (AMSL), scattered at 1,867 ft AMSL and broken at 3,067 ft AMSL. Visibility was recorded as 9,000 m in light rain showers.
Recorded data
Airservices Australia provided recorded air traffic control audio and surveillance data.
During maintenance actions following the occurrence, the aircraft electrical system was powered‑up and the cockpit voice recording of the incident flight was overwritten.
Flight data recorded by the aircraft’s flight data recorder, combined with recorded surveillance and audio data is presented in Figure 7.
Figure 7: Recorded flight data from 0756 to 0800
Source: ATSB
Safety analysis
Air conditioning pack failure and checklist error
The unusually high temperature noted by the first officer during the taxi to the runway, combined with the findings of the post‑event engineering examination, indicated that the left air cycle machine (ACM) failed prior to departure. This failure resulted in oil being expelled from the ACM cooling turbine and unconditioned hot bleed air entering the air conditioning system. This in turn resulted in the temperature control difficulties faced by the crew and, after take-off, smoke being emitted from the left side flight deck and cabin vents.
In response to the smoke, the crew actioned the memory items of the ‘smoke in aircraft’ checklist. This included donning oxygen masks however the first officer had difficulty in fitting the mask and establishing communications with the mask in use. As a result, the first officer elected not to wear the mask. This exposed the first officer to potentially harmful smoke and fumes. While the first officer reported no adverse effects from this exposure, it did increase the risk of impairment and incapacitation.
After completing the checklist memory items, the crew were required to action the complete ‘smoke in aircraft’ quick reference handbook (QRH) checklist to ensure all required actions had been completed. However, before completing the checklist, the crew commenced the actions required to return to Perth as they assessed that task was of higher priority. Had the QRH checklist been subsequently fully completed, the left bleed air would have been selected ‘off’ and this would have stopped the smoke ingress into the cabin. This action would also have likely prevented the later overheating of the air conditioning duct that triggered the ‘wheel well and wing overheat’ annunciation.
Workload and unsafe descents
The aircraft was equipped with analogue instrumentation with no flight automation to reduce flight crew workload and the smoke was detected immediately after take-off while the aircraft was operating in instrument flight conditions. These factors combined to create a high workload period for the relatively inexperienced crew.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing a take-off). These resources can change given the individual’s experience and training and the level of stress and fatigue being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternately, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
Examples of errors associated with excessive workload include:[7]
Flight crew may mishear, misunderstand or miss setting an air traffic control clearance provided during a period of high workload, leading to:
A deviation from assigned altitude (level bust)
controlled flight into terrain (CFIT)
loss of separation from other aircraft, or
an unstabilised approach.
The pilot becoming distracted from primary tasks resulting in an error in handling or managing the aircraft.
In response to the smoke and due to the high workload, the crew initially omitted or missed required checklist items (donning the oxygen mask and completing the ‘smoke in aircraft’ checklist). Had the checklist been completed with the left bleed air selected ‘off’ and the oxygen mask fitted, with communications correctly established, the additional workload associated with returning the aircraft to Perth would have been reduced. Furthermore, the increased distraction and workload associated with the response to the subsequent wing overheat annunciation would have been avoided.
Later, when the crew returned to complete the ‘smoke in aircraft’ checklist, they were interrupted by the wing overheat annunciator illuminating. The required response actions further compounded their workload and this likely influenced the decision error to leave the landing gear retracted. While the crew elected not to extend the gear due to their desire to expedite the return, the decision was not fully considered and would have exposed the aircraft to increased risk if the overheat condition had been associated with the landing gear.
The significant workload that the crew were subject to also adversely affected the crew’s management of the aircraft’s flight path. Without automation to reduce workload and support flightpath management, the aircraft deviated above and critically, twice considerably below the assigned and lowest safe altitude. The aircraft also passed through, and then deviated significantly left of, the localiser before the crew recovered and completed the approach.
Air traffic control factors
The clearance to descend to 2,800 ft was incorrectly readback as 2,000 ft by the first officer (who was not wearing the oxygen mask at that time), but this error was not identified by the air traffic controller. The purpose of a clearance readback is to ensure that the clearance has been correctly received and provides the controller an opportunity to correct any errors. As this error was not identified, there was increased risk of the crew descending the aircraft below the minimum safe altitude while still operating in instrument meteorological conditions. However, despite reading back the clearance incorrectly, the crew initially levelled the aircraft at 2,800 ft before querying and confirming the assigned altitude as 2,800 ft. Therefore, the non-identification of the readback error did not contribute to the aircraft descending below the lowest safe altitude.
Despite obtaining confirmation of the assigned altitude, very soon after, the aircraft began descending. The controller identified the aircraft descending below the assigned altitude and contacted the crew, advising them to maintain 2,800 ft as that was the lowest safe altitude. However, this broadcast was not prefixed by the required statement ‘safety alert’. Commencing such a broadcast with the phraseology ‘safety alert’ is designed to alert crews to safety critical information to ensure a response is prioritised and is particularly important during times of high crew workload. Despite the correct phraseology not being used, the broadcast achieved the desired crew response. The recorded data showed that immediately after the controller contacted the crew, the descent was stopped, and the aircraft commenced climbing. As such, the absence of a safety alert did not contribute to the occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the smoke in the aircraft and descent below lowest safe altitude involving Fairchild Industries SA227-DC, VH-WBQ, 25 km north-east of Perth Airport, Western Australia on 15 August 2024.
Contributing factors
A failure within the left air cycle machine resulted in hot engine bleed air and smoke entering the cabin soon after take-off. In response, the crew elected to return to Perth.
After commencing the ‘smoke in aircraft’ checklist memory items, the quick reference handbook checklist was not completed, and the left engine bleed air system was not selected off. As a result, during the return, the left air conditioning duct overheated, and the wing overheat light illuminated.
The workload associated with the in-flight response to the smoke in the aircraft and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision‑making.
On several occasions during the return to Perth Airport, the aircraft deviated above and below the assigned and lowest safe altitude. These deviations included a descent to 639 ft below the lowest safe altitude.
Other factors that increased risk
Following the smoke entering the cabin, the first officer initially elected not to wear the oxygen mask due to difficulties in donning the mask and then establishing communications. This increased their risk of impairment or incapacitation.
An incorrect altitude readback from the flight crew was not identified or corrected by air traffic control. Later, after the assigned altitude had been communicated, when the aircraft first descended below the lowest safe altitude, the crew were advised of the deviation by air traffic control, but the required ‘safety alert’ was not issued.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action taken by Skippers Aviation
Line oriented flight training
Action number:
AO-2024-048-PSA-01
Action organisation:
Skippers Aviation
In response to this incident, Skippers Aviation:
revised the Line Oriented Flight Training (LOFT) program to include more comprehensive oxygen system training
conducted the following refresher training for Metroliner 23 flight crew:
emergency response briefings
theory examination for the Metroliner 23 bleed air, pneumatics, pressurisation and fire warning systems.
practical training of the crew oxygen system
revised emergency procedures
updated the aircrew initial and recurrent training to include a presentation on the Metroliner 23 oxygen system.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
the aircraft operator
Civil Aviation Safety Authority
Airservices Australia
recorded data from VH-WBQ.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078-1084
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
the flight crew
the air traffic controller
Airservices Australia
Civil Aviation Safety Authority.
A submission was received from Airservices Australia. The submission was reviewed and did not result in any amendment to the report.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Memory items are checklist items required to be committed to memory to allow an immediate response to high priority abnormal events.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[5]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[6]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
On the morning of 23 April 2023, a Saab 340A, registered VH-KDK and owned by Pel-Air Aviation, was being operated by Regional Express Airlines (Rex) for a non-revenue flight from Wagga Wagga, New South Wales, to Charleville, Queensland. While in cruise at 22,000 ft and passing to the east of Cobar, New South Wales, the flight crew received a cargo smoke indication on the central warning panel. As a precaution, the crew fitted their oxygen masks and smoke goggles. Shortly after, the cockpit filled with smoke.
The captain commenced a diversion to Cobar while the first officer made a PAN-PAN[1] call to Melbourne Centre. Thick smoke then filled the flight deck preventing the crew from effectively seeing external visual references or the aircraft’s flight instruments. While completing the emergency checklists, the crew received further warnings for avionics smoke, followed by a cabin depressurisation, and then a right engine fire detection fail indication. The crew landed at Cobar and elected to stop on the runway and evacuate the aircraft.
Shortly after landing, Fire and Rescue New South Wales personnel arrived from the Cobar station and located a heat source at the air cycle machine and in the associated wiring. After gaining access to the cabin underfloor area, the source of the heat was doused with water. An internal inspection of the aircraft found fire damage in the area around the right recirculating fan. The aircraft was substantially damaged, and the crew were not injured.
What the ATSB found
The ATSB found that a likely failure of the right recirculating fan electronic box sub-assembly resulted in an in-flight fire under the cabin floor. The fire filled the cabin with smoke, which then entered the flight deck due to asmoke barrier curtain not being fitted in place and the flight deck door being open.
When the crew fitted their oxygen masks, it was found that the first officer’s mask microphone was not working correctly, which delayed emergency checklists being actioned. The fire also caused substantial structural damage and led to a breach of the fuselage, resulting in a depressurisation of the aircraft.
It was also found that the Rex flight crew had not been trained or had knowledge of the differences in the cargo‑configured Saab 340 aircraft, leading to them having nofamiliarity with specific systems fitted. This prevented them from completing some of the required steps in the emergency checklists.
The flight crew did not receive training on the cargo‑configured aircraft differences prior to conducting freight operations. Further, the operator’s flight crew operating manuals did not reflect the differences in the cargo‑configured aircraft interior checklists, which may have alerted the flight crew to these differences during pre-flight preparation. Additionally, the manufacturer did not have any specific pre-flight check for correct fitment of the smoke barrier curtain for cargo‑configured aircraft preparation.
What has been done as a result
On 13 May 2023, Rex issued an Operations Notice to all pilots, highlighting the guidance on the cross-valve handle as outlined in the Saab Aircraft Operating Manual (AOM). Furthermore, this guidance has been incorporated into the Rex Flight Crew Operating Manual (FCOM).
On 13 November 2024, Rex amended the internal inspection checklist that is contained in their Saab 340 FCOM. The amendment now requires flight crews verify the position of the cross‑valve handle during the pre-flight checks.
Rex have also updated the training information delivered in their ground school to include the cross-valve system for the cargo‑configured Saab 340 aircraft into the training syllabus.
Rex indicated they are implementing a fleetwide inspection of the recirculating fan assemblies at the next aircraft heavy maintenance cycle, with a focus on the electronic sub-assembly module.
Pel-Air have included a revision to their flight crew operating manual with a caution that the smoke barrier curtain must be installed whenever combustible material is carried in the cargo compartment. Due to contract completion, Pel-Air have ceased conducting freight operations using the Saab 340 aircraft and have since sold the aircraft.
Saab has revised their preparatory and walk-around pre-flight checklists to include the fitting of the smoke barrier curtain when carrying cargo in the cargo‑configured aircraft.
Safety message
It is essential for operators to ensure that flight crew are conversant with differences in aircraft configurations when required to conduct operations on aircraft they may be unfamiliar with. It is important that information is readily available and accessible and be delivered in a manner to inform flight crews on the operational requirements of the aircraft.
Operator flight crew operating manuals need to be relevant for the aircraft configuration being utilised. Further, manufacturer checklists for pre-flight inspections are required to cover the modifications fitted, so that this is available to operators to enable them to write the appropriate documentation for their flight crews.
The occurrence
History of the flight
On the morning of 23 April 2023, a Pel-Air Aviation cargo‑configured Saab 340A, registered VH‑KDK and operated by Regional Express Airlines (Rex), was being prepared for the first stage of a non-revenue freight flight from Wagga Wagga, New South Wales, to Charleville, Queensland. The purpose of the flight was to pre‑position a Rex Saab 340 engine to Cairns, Queensland, utilising a Rex crew, consisting of a captain and first officer (FO), and operating under the Part 91 flight rules.
The crew had flown the aircraft from Cairns the previous day, and were tasked to fly the return leg, including a refuelling stop at Charleville. The flight crew arrived at the aircraft at about 0830 local time and conducted their pre-flight checks. The captain performed the interior checks while the exterior walk around checks were conducted by the FO. The aircraft departed Wagga Wagga at about 0949, tracking for Charleville, and cruising at FL 220.[1] The captain was the pilot flying (PF), and the FO was pilot monitoring (PM).[2]
In-flight fire and diversion
At about 1052, the crew was alerted by a cargo smoke detection warning[3] on the central warning panel. They began to manage the warning by identifying and cancelling the indication. The crew then donned their oxygen masks and smoke goggles. However, once fitted, the crew had difficulty communicating due to the FO’s mask microphone not functioning correctly and being very faint. A review of the cockpit voice recorder (CVR) recording showed it took another 57 seconds for the crew to establish effective communications with each other before they could commence the emergency checks.
At 1055 the crew received a right (engine) fire detection fail caution light, followed shortly after by an air conditioner caution light. This was due to the detection of a right distribution duct over temperature which automatically closed the right engine low pressure bleed valve. The crew initially detected no smoke or fumes, however within about 60 seconds, thick black smoke began filling the cockpit.
During the process of establishing the nature of the warnings, the flight crew discussed which airport would best suit their needs for the emergency, and opted to divert to Cobar, New South Wales (Figure 1). The captain had flown to this airport on several previous occasions and was familiar with it, and from their position, they could conduct a direct approach with minimal manoeuvring.
Figure 1: VH-KDK flight overview
Source: Google Earth and Flightradar24, annotated by the ATSB
At 1056, the FO gave a PAN PAN[4] radio call and advised air traffic control (ATC) that they were diverting to Cobar. ATC arranged for emergency services to meet the aircraft upon arrival into Cobar. Due to the radio coverage in the Cobar area, ATC utilised an overflying aircraft to relay communications as the diversion progressed.
While descending through FL 160, the crew received a cabin pressure failure warning, indicating that the aircraft had lost pressurisation. This occurred 4 minutes after the initial warning of the cabin smoke. The cabin depressurisation led to the crew increasing their rate of descent to get below FL 100.
At approximately 1058, they commenced the ‘cargo compartment smoke’ emergency checklist. The CVR indicated the crew completed the first checklist item, which called for the left bleed valve to be closed. The checklist then called for closing the cross-valve handle, however the crew was unable to locate it, with the CVR recording indicating the crew tried to find it for 61 seconds before resuming the checklist flow without actioning the cross-valve handle closure. The crew completed the cargo compartment smoke checklist as visibility on the flight deck reduced to less than 10 cm. The captain recalled sliding their seat forward to enable them to see the instrument panel through the thick smoke.
Five minutes after the PAN PAN call, the crew commenced the checklist for ‘avionic or electrical smoke or fire’.[5] The crew then conducted the ‘smoke removal’ checklist to clear the smoke from the flight deck.
One requirement of the smoke removal checklist called for aircraft speed reduction to below 160 kt, and to open a crew hatch to aid in smoke removal. Due to the unknown severity of the on‑board fire, the crew decided to maintain their speed and not complete all the checklist items as required, enabling them to expedite their landing.
As the crew continued their approach, the volume of smoke in the flight deck began to dissipate. This allowed them to navigate using external visual cues and conduct a visual approach for the landing. Because of the unknown source of the fire, upon arrival in Cobar, the crew elected to stop the aircraft on the runway and evacuate the aircraft.
As part of the emergency evacuation procedure, the crew activated the fire extinguisher system[6] on both engines after shutting down, and then exited the aircraft. The incident had taken 22 minutes from the first smoke warning to landing.
After evacuation, the crew noted smoke to be coming from the vicinity of the right air cycle machine at the right wing root. Shortly after landing, Fire and Rescue New South Wales personnel arrived from the Cobar station and assessed the aircraft. After gaining access to the cabin underfloor area, an electrical harness was initially found melted and smoking. Consequently, the area was doused with water.
Further inspection of the aircraft found significant fire damage concentrated in the area around the right recirculating fan. The right recirculating fan was also significantly fire damaged. An assessment of the right engine found no evidence of a fire. The aircraft underfloor structure was substantially damaged, and the crew were not injured.
Context
Aircraft information
The Saab 340A[7] is a twin-engine turboprop aircraft designed and initially produced by Saab and Fairchild Aircraft. It is designed to seat 30–36 passengers in standard configuration and is powered by 2 General Electric CT7-5A2 turboprop engines.
VH-KDK was manufactured in Sweden in 1984 and first registered in Australia in February 1985. It was operated in passenger configuration by Regional Express Airlines (Rex), before being modified to cargo configuration in 2009. VH-KDK was then owned and operated by Pel‑Air Aviation.[8]
At the time of the accident,[9] VH-KDK had accrued a total time in service of 48,130.6 hours and 60,046 landings and had flown 13.5 hours since the last maintenance.
Flight crew information
Captain
The captain held an air transport pilot licence (ATPL) (Aeroplane), and a valid Class 1 aviation medical certificate. They reported a total flying time of 7,579 hours with about 5,070 of those being on the Saab 340. They had flown for the operator for about 10 years, and previously had flown for another regional airline and had operated into Cobar airport on numerous occasions.
The captain had previously flown the Saab 340A in a passenger configuration but had not flown either the Saab 340A or B variant in a cargo configuration.
First officer
The first officer (FO) held an ATPL (Aeroplane), and a valid Class 1 aviation medical certificate with a restriction for vision correction. They had reported a total flying time of about 18,297 hours, having flown about 1,480.9 in the Saab 340B. The FO had not previously flown any Saab 340 variants in a cargo configuration.
Meteorological conditions
Graphical area forecasts provided by the Bureau of Meteorology (BoM) stated that generally good weather conditions, with little cloud, and visibility greater than 10 km existed during the flight. The terminal area forecast for Cobar indicated light winds from the east at about 10 kt with the flight crew reporting CAVOK[10] conditions existing for the time of the diversion.
Cargo configuration
VH-KDK cargo conversion
The cargo conversion modification was carried out in accordance with Saab service bulletin (SB) 340-25-280. As an overview, the SB involved removal of the passenger fit‑out and replacing it with an interior cargo liner, blanked over windows, additional cargo barrier nets, and a floor roller system (Figure 2). In conjunction with this SB, other SBs were incorporated on the cargo version, which modified the air conditioning system. This was done by removing the left recirculating fan and introducing a cross-valve handle.
A removable smoke barrier curtain was added at the forward section of the cargo compartment. The fire extinguishing system for the passenger cargo area at the rear of the cabin (zones C1 and C2) was also removed, and additional smoke detectors were added to the cabin.
Figure 2: Cargo configuration modification
Source: Saab, annotated by the ATSB
Smoke curtain
A removable smoke barrier curtain was designed to be installed between compartment A and the front-left fuselage (Figure 2). The purpose of the curtain was to provide containment of smoke and fire within the cargo compartment in the event of an on-board fire and prevent smoke ingress to the flight deck (Figure 3). The aircraft carried a placard at the top of the entrance stairs which stated:
Smoke barrier must be installed for all cargo operation flights.
The smoke barrier was constructed of a fibreglass impregnated vinyl which was secured in place by a Velcro perimeter and metal press studs. The aircraft owner stated that the standard procedure was that it would be left attached by the left side attachment points and secured in place by the freight handlers after loading of cargo. It was then to be checked by the FO prior to flight.
During interview, the flight crew stated that they were not aware of the use of the smoke barrier, and that it had been located after the incident in compartment A of the cargo area, and that it was not in place on the left of the cabin. The ATSB did not determine why the engineers who loaded the engine into VH-KDK had not secured the smoke curtain.
Figure 3: Smoke barrier curtain location in exemplar aircraft
Source: Saab, annotated by the ATSB
Air conditioning system
In passenger configuration, the Saab 340 air conditioning system is comprised of a left and right air conditioning pack (ACP) which is supplied by bleed air from its respective engine. Each ACP is mounted externally under a fairing on the lower fuselage near the rear of each wing. The system has 2 recirculating fans under the adjacent cabin floor, ducting for the cabin and flight deck conditioned air supply and return, temperature sensors and controls, and cabin and flight deck air outlets.
The left and right ACPs supply conditioned air to the cabin, and a portion of the right ACP conditioned air is supplied to the flight deck. The left recirculating fan returns the air to the left ACP from the aircraft cabin, while the right fan extracted air from the flight deck. The avionics fan draws air for cooling the avionics from the cabin conditioned air supply. The air is then expelled under floor.
As part of the modification from passenger to cargo configuration, the left recirculating fan and ducting were removed. This resulted in limited extraction and recirculation of any contaminated air from the cabin interior, while the right recirculating fan would extract and recirculate air solely from the flight deck.
Cross-valve handle
In the cargo configuration, a cross-valve and handle were added to the air conditioning system ducting between the left and right ACP (Figure 4), with the manual operating handle being located at floor level, next to the FO seat. Closing of the left bleed valve and cross-valve in accordance with the emergency checklist would isolate the supply of air to the cabin in the event of cargo smoke or fire, and the right ACP would supply only to the flight deck. As part of the emergency checklist for ‘cargo compartment smoke’, the left ACP would also be isolated from supplying the cabin.
Figure 4: Schematic of modified air conditioning system
Source: Saab, annotated by the ATSB
Recirculating fan
The right recirculating fan was a centrifugal impeller type fan and was driven by an AC motor. The fan had an in‑built inverter, supplied by 28-volt DC. The majority of the electronics for the fan unit were contained in the box sub-assembly. This included the inverter, an electromagnetic interference (EMI) filter unit and the electronic card sub-assembly. The box sub-assembly controlled the fan operation, including the thermal control. Each electric motor was equipped with:
a thermal switch[11] located in the cooler which guarded against an abnormal temperature increase. This switch would cut off the power if the motor temperature exceeded 110°C +/− 5° (230°F +/− 41°). The fan would start again when the temperature decreased to 65°C +/− 5° (149°F +/− 41°)
a speed sensor which guarded against an abnormal decrease of nominal speed. If the speed fell below 80% of nominal speed for more than 17 seconds, the fan would be stopped.
In 1987, Saab released a service bulletin which gave operators the option to install an upgraded recirculating fan. The original fan was a brush type motor which required regular maintenance, including brush replacement when they had worn from use. Saab had received reports of smoke and burning smells which were attributed to brushes that were incorrectly installed. The brushless fans were introduced to help eliminate this issue and also required less maintenance.
The fan installed in VH-KDK was the new brushless fan, manufactured in 1990 and fitted in April 1996. The fan history prior to installation was unknown by the operator. The fan accrued 27,585 hours while fitted to VH-KDK.
Recirculating fan examination
Fire damage was found in the area around the right recirculating fan and on the fan itself (Figure 5). There were no other components in the vicinity of the fan with significant fire damage. As such, it is likely the right recirculating fan was the source of the fire.
Figure 5: Damaged recirculating fan
Source: ATSB
An examination of the recirculating fan was conducted at the ATSB’s technical facilities in Canberra. The examination found that the fire damage was most significant at the externalbox sub‑assembly which housed the EMI filter, the resistor support plates and electronic card sub‑assembly. The aluminium cover of the box sub-assembly had melted, the electrical wiring was damaged, and some terminals had disconnected as a result of the fire damage. There was heavy soot and melting of solder in the cooler assembly.
The electronic card sub-assembly was made up 3 circuit boards, mounted to the resistor support plate. The function of the circuit boards was for motor speed detection, timer control, and a logic card. The damage exhibited on the circuit boards showed significant burning, consistent with the other components within the aluminium cover.
The electromagnetic interference (EMI) filter sub-assembly had considerable damage to the filter itself and to the mounting plate with signs of melting and heat tinting of the steel plate structure, indicating a significant heat source. The heat tint was indicative of temperatures of approximately 310° to 330°C.
Of note, the fire did not appear to be associated with the motor and there was no indication of damage to the internal components of the fan and was able to rotate freely. There was carbon and soot observed on the external surface on the motor. The crew stated that there had been no circuit breakers tripped that would be associated with the failure of the electronic card sub‑assembly.
The ATSB examination of the recirculating fan could not determine the cause of the failure of the electronic components attached to the assembly.
Pressurisation system
The Saab 340 cabin is pressurised by the 2 air conditioning packs. The pressurisation system uses bleed air drawn from each engine and was either automatically controlled by a pressurisation controller, or manually controlled by a control valve operated by the flight crew from the flight deck.
Pressure is able to be regulated by the opening and closing of 2 outflow valves, located in the empennage. The primary outflow valve is electro-pneumatically operated by the pressurisation controller, while the secondary outflow valve is pneumatically controlled from the cockpit and used as a manual standby system.
When emergency pressure relief is required, the primary outflow valve is able to be opened with the emergency pressure dump switch. When the crew of VH-KDK experienced the smoke in the cabin and flight deck, dumping cabin pressure as stated in the ‘smoke removal’ emergency checklist was the method used to assist in rapid removal of the smoke.
Aircraft depressurisation
The severity of the fire resulted in significant damage to the surrounding underfloor furnishings, ducting and airframe structure. The damage was then sufficient to rupture the skin (Figure 6) and caused a subsequent depressurisation of the aircraft.
Figure 6: Underfloor fire damage showing fuselage hole
Source: Operator, annotated by the ATSB
Checklists
The pre-flight procedures for the Saab 340A aircraft, including cargo configuration aircraft, were covered by the Aircraft Operations Manual (AOM) normal procedures, produced by the aircraft manufacturer. The AOM pre-flight normal checklist contained a check of the cross-valve handle position prior to flight but did not include a specific check for correct fitment of the smoke barrier curtain.
A flight crew operating manual (FCOM) was carried on board VH-KDK which was developed by Pel-Air, based on the aircraft manufacturer’s AOM. Unlike the aircraft manufacturer's AOM, the pre-flight checks in the operator's FCOM did not contain any reference to the cross-valve handle. Consistent with the aircraft manufacturer’s AOM, the operator’s FCOM also did not include a specific pre-flight check for correct fitment of the smoke barrier curtain. The weight and balance chapter of the FCOM did show a diagram of the smoke curtain fitted but did not include a requirement to ensure the smoke curtain was in place.
The manufacturer had an airplane flight manual supplement in place, implemented as part of the cargo configuration SB, which included fitting the smoke barrier as a limitation (Figure 7 left). There were no identified interior checks in this supplement, which included the checking of the cross-valve handle prior to flight.
The aircraft manufacturer did have emergency checklists specific to cargo‑configured aircraft. These were compiled into the quick reference handbook (QRH) which was available to flight crew in the aircraft (Figure 7 right).
Figure 7: Flight manual supplement (left) highlighting smoke curtain use and QRH checklist (right) highlighting cargo cross-valve handle and cockpit door
Source: Saab, annotated by the ATSB
Flight deck door
The Pel-Air FCOM stated in the Operating Limitations section that during flight, the flight deck door must be kept closed and locked at all times. It is further listed in the engine start checklist that all doors are closed before engine start.
Evidence from the accident flight, however, shows that before the fire, the crew were operating with the cockpit door open. During interview, the flight crew indicated they closed the door, whilst performing the cargo compartment smoke checklist. This was further supported by the CVR review, where the crew were heard to state the door was to be closed as per the checklist steps, which was followed by the sound of the door shutting.
Flight crew training
Rex conducted a ground school, including simulator training, for their new Saab 340 flight crew. Under a commercial agreement, Pel-Air flight crews were also trained by Rex. The ground school covered the 340 variants of A, B and B WT. The aim of the ground school was to provide pilots from both operators with the necessary knowledge to gain a Saab 340 type rating. The type rating covered all Saab 340 aircraft and did not distinguish between any variant or configuration of the aircraft.
Following the Rex ground school, Pel-Air then conducted further training through its line training program for its flight crews allocated to freight operations. Delivery of this training was in a practical environment, with pilots learning the systems and differences of the cargo‑configured Saab 340. This included the use of the smoke barrier and the operation of the cross-valve handle.
The ATSB asked what the process was for Rex pilots to receive this training and knowledge. Pel‑Air advised that a pilot employed by Rex would only receive this if they were to transition to freight operations with Pel-Air in a permanent role.
Crew familiarity of cargo aircraft
The flight crew operating VH-KDK were both Rex pilots, who were normally rostered for passenger operations. The night before the flight to Wagga Wagga, they were rostered to fly the cargo‑configured 340A. The captain recalled asking the scheduler if they needed a briefing for flying the cargo 340A, and was told that they did not, but it could be arranged if needed.
The captain decided to speak to a Rex colleague who had flown the cargo‑configured 340A several times previously. They were told there were no differences other than the removal of the seats and a freight interior being fitted and that there were no special procedures to be aware of.
Both Rex and Pel-Air advised that their respective operations could roster a crew to fly either operator’s aircraft if it was available. Crewing arrangements were such that there was never any mixing of crew, that is that the flight crew would consist of either 2 Rex or 2 Pel-Air flight crew on any flight.
Oxygen mask
The flight crew fitted their oxygen masks and smoke goggles shortly after receiving the cargo smoke warning and smelling the smoke. The FO conducted the functional tests after fitment and found their microphone was barely readable by the captain. The cockpit voice recorder (CVR) indicated that, although muffled, the speech from the FO was recorded and they were also able to be heard by air traffic control (ATC) throughout the emergency.
The pre-flight checks relating to the crew oxygen system were conducted as part of the interior checklist. The FCOM detailed the checks as:
RIGHT OXYGEN MASK .................................................................................CHECKED
Check flight crew oxygen mask and microphone in accordance with the following:
• set BOOM - MASK switch back to the BOOM position, ….
The check on the left oxygen mask was to be performed in the same manner. Although not detected on the CVR, the captain advised the masks were both tested prior to departure.
Aircraft damage
The damage caused by the underfloor fire was substantial. The fire had damaged underfloor air conditioning ducting and electrical wiring (Figure 8).
Figure 8: Underfloor fire damage
Source: Operator, annotated by the ATSB
Structural components in the surrounding area had been distorted by the extreme heat, including the floor panels, which had collapsed when fire crews entered the aircraft and inadvertently walked over the affected area. The seat track support structure had distorted, and the fuselage was weakened by the fire which breached the outer skin, preventing the aircraft from remaining pressurised (Figure 9).
Figure 9: Fuselage skin breach
Source: Operator, annotated by the ATSB
The fuselage in the immediate area above and below the cabin floor was buckled and delaminated. The heat from the fire most likely travelled between the interior panels and freight lining, leading to the damage observed (Figure 10). Following an engineering inspection of the fire damage, the aircraft was withdrawn from service and not repaired.
Figure 10: Right side delamination on fuselage
Source: Operator, annotated by the ATSB
Recorded data
The ATSB was supplied raw data by the operator from the flight data recorder (FDR). This data was analysed and was found to include the previous 4 flights.
The recorded data from the occurrence flight showed that at about 59 minutes after becoming airborne at Wagga Wagga, the FDR stopped recording. The recording stopped at about the same time as the initial smoke indication. This was most likely due to fire damage to the electrical wiring which controlled the FDR.
Flight track information was also obtained from FlightRadar24, which showed the entire flight, including the diversion and landing at Cobar (Figure 11).
Figure 11: VH-KDK flight track and diversion
Source: Google Earth and Flightradar24, annotated by the ATSB based on CVR recordings
The CVR was removed and sent to the ATSB technical facilities in Canberra. The CVR data was downloaded, with the recovery of 4 channels of audio data of about 120 minutes duration which included the in-flight fire event. Reviewing the recorded CVR data also revealed that coincidentally, just prior to the indication of the cargo smoke caution, the flight crew had been discussing alternate airports in the area, and which one they would select if they had a need to divert.
The recording contained information from the end of the previous flight, and from the day of incident. It included the:
flight crew’s initial reaction to the caution warning for the smoke in the cabin
conduct of the emergency checklists
additional warnings as they occurred
crew intercom and communications with Melbourne Centre
landing at Cobar and subsequent exiting of the aircraft.
The recording also revealed that while conducting the emergency checklist for ‘cargo compartment smoke’ the crew closed the cockpit door as a loud bang was heard, indicating it was open during the flight.
Safety analysis
Introduction
On 23 April 2023, the Regional Express (Rex) Airlines flight crew operating a Pel-Air Aviation Saab 340A, registered VH-KDK were conducting an internal revenue cargo flight from Wagga Wagga, New South Wales, to Charleville, Queensland. About 1 hour into the flight, the crew experienced an in-flight fire and diverted to Cobar, New South Wales. After experiencing thick smoke on the flight deck and then a cabin depressurisation, the crew performed a safe landing at Cobar. The aircraft was substantially damaged, and the flight crew were not injured.
This analysis will explore:
origin of the in-flight fire
aircraft preparation for the flight
oxygen mask use and technical problem of the microphone
cabin depressurisation
flight crew knowledge of aircraft systems
flight crew operating with the cockpit door open
Pel-Air and Rex flight crew operating manual information deficiencies
training of Rex flight crews
Saab pre-flight inspection checklists
Rex crew familiarity of cargo aircraft.
Origin of the in-flight fire
The source of the in-flight fire was traced to the right recirculating fan assembly. Although the fan was not damaged internally, the fire damage was most significant at the box sub-assembly, which was mounted external to the fan and housed the electrical control circuit boards. It is likely that an electrical component or components within the box sub-assembly failed, resulting in the underfloor fire. The fire damaged underfloor insulation and plastic air conditioning ducting components, which led to thick smoke filling the cabin and cockpit and aircraft structural damage.
The avionics warning received by the crew during the diversion was most likely associated with the avionics cooling air that was being drawn from the now smoke-filled cabin. This was also stated in the ‘cargo compartment smoke’ checklist.
The ATSB examination of the recirculating fan could not determine a cause for the failure in the electronic control cards which led to the fire.
When the crew received the air conditioning system right duct over temperature caution light, it was most likely due to the distribution duct over temperature being affected by the fire and the melting which occurred as a result. When the over temperature was sensed, the right bleed valve closed automatically as a function of system logic for over temperature protection.
Smoke barrier curtain
Cargo operations can have a greater fire risk than passenger operations due to the carriage of cargo that could be the source of a fire and the lack of cabin crew available to fight a fire. As such, additional protection was available to minimise flight crew exposure to cabin smoke in the form of additional smoke detectors and a smoke curtain.
However, the smoke curtain was not installed into position by anyone involved in the flight preparation. The flight crew, who normally operated the same aircraft type but in a passenger configuration, did not notice there was a placard at the aircraft entrance stating the smoke curtain was to be fitted for all cargo flights. The flight crew remained unaware of the smoke barrier curtain and its use for cargo operations. Further, the engine being transported was positioned in the cargo area of VH-KDK, on both occasions, by Rex engineers. As the curtain was usually installed by freight handlers during normal cargo operations, it is possible the Rex engineers were also unaware of its requirement to be fitted.
In this accident, the source of the fire was an aircraft component rather than the cargo being carried. If a similar fire occurs in a passenger‑configured Saab 340 aircraft, then the smoke curtain would not be in place. However, the smoke curtain was available and was required for use for this flight, so its non-use increased risk for this event.
The flight deck door was not closed during flight as prescribed in the operator’s FCOM operating limitations and checklists. Having the door closed would have likely prevented the smoke being able to flow into the flight deck.
The result of not having the smoke barrier fitted and the flight deck door closed as part of the aircraft pre-flight preparation was that smoke from the fire was not contained to the cabin area and was able to move forwards toward the flight deck.
Oxygen mask fault
The flight crew fitted their oxygen masks and smoke goggles when alerted of the presence of smoke by the central warning panel. This decision may have prevented the crew from being overcome by smoke and fumes in the cockpit in the next several minutes. However, once fitted, the crew had difficulty communicating with each other, as a result of the mask microphone being very faint and difficult for the captain to hear the first officer (FO). This appeared to be an internal fault only, as the cockpit voice recording (CVR) showed that the FO was able to be adequately heard by ATC.
This breakdown of communication delayed the crew by 57 seconds, in which emergency checks were not initiated due to the breakdown of communication. It created confusion and distraction between the crew while trying to execute the emergency checklist.
A review of the CVR captured prior to flight could not positively determine if the pre-flight check action in relation to the oxygen mask was performed. This is an important check of the emergency communication system whilst on oxygen and was designated as a mandatory check item for a daily inspection as required by the Rex and Pel-Air FCOM.
Cross-valve handle
While the flight crew were conducting the emergency checklist items for cargo compartment smoke, they were unable to locate the cross-valve handle. This was due to the combination of the thick smoke obscuring their vision and their lack of knowledge of the differences in the cargo‑configured aircraft.
Had the location and function of the cross-valve handle been known by the flight crew, the time taken to identify it during completion of the emergency checklist would have been minimised, which would have limited the delay of smoke removal from the flight deck.
In this case, the subsequent depressurisation resulted in the smoke dissipating even in the absence of the cross-valve.
Cabin depressurisation
The weakening of the fuselage structure due to the underfloor fire resulted in a breach of the fuselage skin, which led to a subsequent depressurisation of the aircraft during the descent. Although adding to another caution alert indication for the flight crew and subsequent checklist to be conducted, it also benefited in the removal of smoke from the cabin and flight deck.
At the time of the depressurisation, VH-KDK was at FL 160 and descending. The crew, when alerted to the depressurisation, increased the rate of descent to below 10,000 ft. The cabin depressurisation occurred 4 minutes after the initial smoke warning occurred.
Due to the size of the hole created, the smoke removal most likely occurred at a greater rate than using the aircraft pressurisation outflow valves alone. The resulting fortuitous reduction in the amount of smoke in the flight deck improved visibility and allowed the crew to carry out a safe landing into Cobar.
Crew familiarity of cargo‑configured aircraft
The flight crew had not flown or had any prior training on the cargo‑configured Saab 340 and were not familiar with the differences of the passenger configuration. The captain chose to liaise with a colleague to gain information on the cargo‑configured aircraft instead of accepting the company offer for a briefing.
This non-formal approach to understanding the differences between the 2 aircraft types ultimately did not pass on the required operational differences and potential safety aspects of the change of aircraft configuration.
Rex and Pel-Air manuals
Both operators (Rex and Pel-Air) manuals, which were designed to provide essential information to flight crews, did not include the required information to enable the pre-flight checks to be conducted adequately. While the weight and balancechapter of the FCOM showed the smoke barrier curtain location, there was no information on its importance to cargo operations, and as the crew had not been informed of any differences, they would not have been expecting that this section contained this information. The smoke barrier curtain installation information that was contained in the Saab service bulletin and flight manual supplement was not included in the pre‑flight checklists. As a result, the flight crew did not have awareness of its use.
The operators' manuals also did not have a check to verify the position of the cross-valve handle. As discussed above, when the checklist called for the crew to use this handle when the aircraft was already filling with smoke, the crew could not locate it.
Flight crew training
The Rex ground school provided type rating training on the Saab 340 series aircraft to both Rex and Pel-Air pilots. This training was based on the passenger‑configured aircraft. Pel-Air pilots undertook further training which gave them the knowledge and skills for the cargo‑configured aircraft.
In scheduling their flight crews to operate the cargo‑configured Saab 340, Rex did not have a process to ensure that the additional training or knowledge sharing for their crews in the differences applicable to aircraft operated by Pel-Air was delivered.
Saab pre-flight checklists
As discussed above, both operators’ manuals had no inclusion of a pre-flight interior check for the smoke barrier curtain or the cross-valve handle. Likewise, there was no pre-flight interior check for these items in the manufacturer’s documentation. Saab confirmed that there were no checks in the pre-flight checklist for the crew to specifically verify that the smoke barrier curtain was correctly fitted.
The result of the manufacturer’s pre-flight and interior checklists not detailing information for the smoke curtain was that the operator did not detail these in their own FCOM. This information was not available for the flight crew who, even without prior knowledge of the cargo‑configured variant, would have been alerted to these changes while conducting these pre-flight checks in accordance with the FCOM.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the in-flight fire and cabin smoke involving a Saab 340A, VH‑KDK, 114 km east-north-east of Cobar, New South Wales, on 23 April 2023.
Contributing factors
It was likely that an electrical component of a control circuit board on the recirculating fan failed, resulting in an in‑flight fire under the cabin floor.
The smoke curtain was not fitted as required for the cargo configuration, and the flight deck door was open, which allowed smoke from the in‑flight fire to enter the flight deck.
The underfloor fire caused weakening of the fuselage structure, which led to a subsequent depressurisation of the aircraft during the descent. However, the depressurisation aided in the removal of enough smoke from the flight deck on approach to allow an unhindered visual approach at Cobar.
Crew were not familiar with the cargo configuration and were unaware of the smoke curtain requirements and location of the cross-valve handle.
The Pel-Air and Rex Saab 340 flight crew operating manuals did not include reference to the location and operation of the cross-valve handle or the operation and use of the smoke curtain. (Safety issue)
Rex did not ensure its flight crews received training in the differences between passenger and freight‑configured Saab 340 aircraft, prior to being scheduled to fly freight operations. (Safety issue)
Saab did not include the smoke curtain fitment in pre-flight documentation for the cargo‑configured Saab 340 aircraft to inform flight crew of this difference from the passenger-configured version. (Safety issue)
Other factors that increased risk
When the flight crew donned their oxygen masks, the first officer's oxygen mask microphone did not function correctly. This led to difficulty in communication between the flight crew and a delay in responding to the emergency.
Due to the combination of the smoke density and lack of prior knowledge, the flight crew were unable to locate the cross-valve handle during the emergency, therefore delaying the removal of smoke from the flight deck.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description:Saab did not include the smoke curtain fitment in pre-flight documentation for the cargo‑configured Saab 340 aircraft to inform flight crew of this difference from the passenger‑configured version.
Safety issue description: The Pel-Air and Rex Saab 340 flight crew operating manuals did not include reference to the location and operation of the cross-valve handle or smoke curtain.
Safety issue description: Rex did not ensure its flight crews received training in the differences between passenger and freight‑configured Saab 340 aircraft, prior to being scheduled to fly freight operations.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Regional Express
Rex advised that it is implementing a fleet‑wide inspection of the flight deck and passenger compartment recirculation fans at the next aircraft heavy maintenance visit. The inspection will be focused on the electronic sub-assembly module of the recirculation fan due to this component being identified to have the most significant fire damage on the fan assembly removed from VH‑KDK.
Glossary
AC
Alternating current
ACP
Air conditioning pack
AOM
Aircraft operating manual
ATC
Air traffic control
ATPL
Air transport pilot licence
BoM
Bureau of Meteorology
CASA
Civil Aviation Safety Authority
CVR
Cockpit voice recorder
DC
Direct current
FCOM
Flight crew operating manual
FDR
Flight data recorder
FL
Flight level
FO
First officer
INT/SPKR
Intercom/Speaker
PF
Pilot flying
PM
Pilot monitoring
QRH
Quick reference handbook
SB
Service bulletin
Sources and submissions
Sources of information
The sources of information during the investigation included:
the crew of VH-KDK
Regional Express Airlines
the chief pilot of Pel-Air Aviation
the manager training and checking and head of operations for Regional Express Airlines
Civil Aviation Safety Authority
Bureau of Meteorology
Fire and Rescue New South Wales
Saab
Airservices Australia
the cockpit voice recorder and flight data recorder
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Airservices Australia
Crew of VH-KDK
Regional Express Aviation
Pel-Air Aviation
Swedish Accident Investigation Authority (SHK)
Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA).
Submissions were received from:
the captain of the crew
Regional Express Aviation
Pel-Air Aviation
Swedish Accident Investigation Authority (SHK)
Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA).
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 220 equates to 22,000 ft.
[3] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach, and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[4]Warnings and cautions: give pilots aural and visual alerts for abnormal conditions. Warnings are highest priority which require immediate action. Cautions are the second priority and give advisory information to pilots.
[5]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[6]The avionics smoke indication was a result of the avionic bay drawing in smoke from the cargo area.
[7]Activating the fire extinguisher system also closes the fuel shut‑off valves, which removes all supply of fuel to the engines. The fire bottles are then operated, extinguishing fire within the engine cowlings.
[8]Saab manufactured the 340 in A, B and B WT variants.
[9]Both Rex Airlines and Pel-Air were wholly owned subsidiaries of Regional Express Holdings Limited (REX).
[10]Although VH-KDK landed safely, the extent of the damage from the fire is classified by ICAO Annex 13 as an accident due to the nature of major repair work required to the airframe.
[11]CAVOK: Conditions and visibility good, nil significant cloud and excess of 10 kilometres visibility
[12]The thermal switch is designed to detect an overheat of the cooler only. It is not configured or located where it would detect the overheating of the electronic card sub-assembly.
[13]Quick change aircraft are designed so that they can be operated in a passenger configuration and then quickly changed to then operate in a freighter configuration, depending on operator requirements.
On 16 March 2020 a Bombardier DHC-8-402 registered VH-QOE, departed Jacksons International Airport, Port Moresby, Papua New Guinea. Shortly after take-off, the flight crew detected fumes in the cockpit. Passing FL 100 on climb, the fumes became stronger and the cabin crew also reported detecting a fume smell in the cabin.
The flight crew donned oxygen masks and levelled off at FL 180. The first officer then made a PAN call and requested a return to Port Moresby. After switching off the number one bleed air, as per the quick reference handbook for smoke and fumes, the flight crew observed smoke emanating from the air vents. The crew switched off the number 2 bleed air and depressurised the cabin once the aircraft had descended below FL 100, and the smoke dissipated.
The Papua New Guinea Accident Investigation Commission (AIC) investigated the incident and requested assistance from the Australian Transport Safety Bureau (ATSB).
To facilitate this work the ATSB initiated an external investigation under the provisions of the Transport Safety Investigation Act 2003.
The ATSB has now concluded its involvement in the investigation.
The AIC is responsible for and will administer the release of the final investigation report into this incident.
On 14 October 2017, a Boeing 777-300 aircraft, registered A6-ETR and operated by Etihad Airways, was on a scheduled passenger service from Abu Dhabi, United Arab Emirates (UAE) to Sydney, New South Wales. An augmented flight crew, consisting of two pilots in each crew (crew A and crew B) conducted the flight.[1]
At about 0407 Central Daylight-saving Time,[2] while in the cruise and with flight crew B flying the aircraft, the flight crew noticed a burning smell coming from an air vent. In an attempt to establish the source of the smell, they requested that cabin crewmembers check the forward galley. The cabin crew confirmed that the forward galley was clear of any burning smells or smoke. The flight crew then requested two other cabin crewmembers enter the flight deck, who confirmed the burning smell. Around this time, the aural fire bell activated, a master warning light illuminated and a warning message ‘FIRE CARGO FWD’ was displayed on the engine-indicating and crew‑alerting system.
In response, the flight crew actioned the non-normal checklist, which included arming the forward cargo fire switches located in the flight compartment overhead panel. This action resulted in numerous mechanical and electrical actions, including de-energising the recirculation fan[3] and closing the air vents in the forward cargo compartment. The flight crew then selected the cargo fire discharge switch, which discharged the two fire extinguisher bottles located in the forward cargo compartment.[4] The flight crew declared a MAYDAY[5] to air traffic control and advised of their intention to divert to Adelaide Airport, South Australia, as it was the nearest suitable airport for the aircraft type.
Flight crew A had just completed their scheduled rest period and entered the flight deck where they were briefed by flight crew B of the situation. Flight crew A assumed control of the aircraft as they were the designated crew for landing. Flight crew B remained on the flight deck to provide assistance. A rapid descent to flight level (FL)[6] 125 was conducted and the aircraft was diverted to Adelaide.
During the remainder of the flight, the cabin crew, operator and passengers were informed of the situation and the diversion. The flight crew also advised air traffic control that, if smoke or fire from the forward cargo compartment was confirmed by emergency services upon landing, they would evacuate the aircraft on the runway.
At 0455, the aircraft landed uneventfully. The emergency services advised the flight crew that they did not observe any smoke or fire emanating from the aircraft. The aircraft was taxied from the runway to taxiway ‘F6’, where the emergency services inspected the aircraft externally with a thermal imaging camera. They confirmed that there were no identified hot spots indicating an on‑going fire in the forward cargo compartment. Based on this information, as a precaution, the crew decided to conduct a rapid deplane of the passengers through passenger door 5L using mobile boarding stairs. All passengers and crew disembarked in a controlled manner and were transported to the passenger terminal. Nil injuries were reported during the disembarkation.
Initial engineering inspection
Once the forward cargo compartment was emptied of cargo, maintenance engineers inspected the cargo hold for evidence of fire. A small quantity of soot was identified in the cargo ceiling area, between the fiberglass ceiling panel and fiberglass joint sealing tape about aircraft body station (BS) 508 (Figure 1).
Figure 1: Illustration showing aircraft structure in the forward cargo hold in relation to heat damage from electrical arcing about BS 508
Source: The Boeing Company, modified by the ATSB
The ceiling panels were removed where soot was identified in the area between the lower side of the cabin floor and the upper side of the cargo-ceiling panel (Figure 2). Inspection of that area found heat damage and chafed 115-volt electrical wire in wiring loom P/N W5279-3002R-12 (W5279), which supplied power to the right lower recirculation fan. The chafing enabled the wire core to come in contact with a cargo ceiling panel retainer screw where the short circuited wire tracked through the polyetheretherketone resin (PEEK) stand-off brackets and carbon fibre floor beam.
Figure 2: Damaged floor beams, webs and wiring covered in soot with ceiling panel opened
Source: Etihad Airways, modified by the ATSB
In consultation with Boeing and operator’s aviation regulator, the United Arab Emirates General Aviation Authority, the operator temporarily repaired the wiring and the damage to the floor beams were evaluated. The operator conducted a non-revenue flight (nil passengers) where they flew the aircraft back to the UAE for the purpose of further inspections and permanent repairs.
Detailed engineering inspection
A detailed inspection between the forward cargo ceiling and passenger floor was conducted at the operator’s maintenance facility in the UAE. Wire bundle W5279, located at about BS 508 was found to have been incorrectly routed. Consequently, the wires had come into contact with screws and nutplates used to close out the cargo-ceiling panel to the ceiling standoff clips.
Over a prolonged period of time, the 115V recirculation fan wire located within that bundle chafed through the insulation coating, allowing the wire to short circuit. The electrical wiring and fourteen of the cargo ceiling panel standoff clips manufactured from PEEK were heat damaged. Sections of the carbon fibre beam web and beam flange at BS 508 between the left buttock[7] lines 40 to 60 were also found to be heat damaged and delaminated between 6 and 7 percent in three locations where the current tracked (Figure 3).
Figure 3: Boeing 777 aircraft showing the approximate location of the heat damaged ceiling panel, soot and heat damaged wiring loom
Source: The Boeing Company, modified by the ATSB
Boeing determined that the wiring loom W5279 was likely to have been incorrectly positioned during the aircraft build in 2013. Boeing reported that this was the fifth reported incident involving wire chafing and arcing in the cargo area of a Boeing 777 aircraft. However, this was the first event that triggered the cargo fire warning system and that had been detected in flight. In all of these cases, the wiring loom had been installed incorrectly during manufacture, allowing screws to chafe wires and short circuit.
Recirculation fan wiring protection system
The 115V recirculation fan wiring system is protected by an electrical load control unit (ELCU) that is located in the aircraft’s main equipment centre. The ELCU is designed to protect the electrical circuit from over-current or differential loads by automatically opening (‘tripping’) to remove power. In this incident, despite the damage sustained to recirculation fan wiring it was reported that the ELCU did not open.
The circuit was tested during the repair of the wiring loom where it was identified that the ELCU functioned as designed. Boeing surmised that in this case, it was possible that the chafed wire may have been intermittently shorting to earth through the PEEK stand-off brackets. It is likely that the insulation properties of the PEEK prevented sufficient current draw to trip the ELCU.
Boeing also surmised that it was likely that the crew’s action of arming the forward cargo fire switches de-energised the chafed wire within loom W5279, thereby preventing further current flow and short circuit.
Cargo compartment fire protection
Materials used in the construction of passenger compartment interiors and in the space between the cabin floor and cargo ceiling are required by the United States Federal Aviation Administration to be self-extinguishing (i.e. stop burning after the heat source has been removed) or better. For example, electrical wire and cable insulation must be self-extinguishing. Cargo liners form part of the passive fire protection feature. In addition, the primary purpose of a cargo liner is to prevent a fire, originating in a cargo compartment, from spreading to other parts of the aircraft and to seal the compartment to help contain the suppression agent in that area.
In Class C cargo compartments, which include the lower cargo compartments of all passenger aircraft, the sidewall and ceiling liner panel installations are fire tested to determine flame penetration resistance. All other materials must be self-extinguishing.
Safety analysis
The flight crew identified a burning smell in the flight deck and completed the appropriate actions to manage the situation. By arming the forward cargo fire suppression system, electrical power was removed from the recirculation fans, which prevented further arcing and damage to the structural carbon fibre beam, support brackets and wiring. Even though there was a significant amount of soot and electrical arcing, de-energising the electrical circuit manually before sufficient current went to ground negated the electrical load control unit from tripping. It was likely that, once the electrical current was deactivated by arming the forward cargo fire switches, the smoke had also stopped. Discharging the fire bottles in the forward cargo space, even though procedurally correct, had nil effect on this occasion as the source of the electrical arcing was in the sealed zone between the cargo ceiling panel and the passenger floor compartment, not in in the cargo compartment.
A post-incident inspection of the aircraft found an electrical wiring harness (W5279) was in an incorrect location. Consequently, one of the forward cargo ceiling liner retainer screws chafed on the wires, which resulted in the electrical current from the chafed wire dispersing through the passenger floor carbon fibre beam about body station 508. That electrical current generated significant heat where 14 of the cargo ceiling polyetheretherketone resin standoff brackets were heat damaged and several areas of the structural carbon fibre beam were chafed and delaminated. The smoke generated from the arcing was of a magnitude that it migrated through the forward cargo ceiling liner into the forward cargo compartment and activated the forward cargo fire detection system.
This incident was the fifth reported case where damage to the wire bundles in the forward (and aft) cargo compartment of a Boeing 777 aircraft has occurred from chafing on a ceiling liner screw and/or nutplate. This was the first event that triggered the cargo fire warning and the only event to have been detected in air. A subsequent investigation conducted by Boeing found that the wire bundle W5279 had been incorrectly routed, likely during aircraft manufacture, and had not been installed as per the design drawings. Slight variations of the wire bundle position allowed it to run directly above the screw and nutplate, which chafed the wire bundle over time.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
During cruise, a burning smell was detected in the flight deck and the forward cargo compartment fire warning activated. The flight crew armed and set the forward cargo fire suppression system and diverted the aircraft to the nearest airport for a safe landing.
A wiring loom situated above the forward cargo compartment about body station 508 was incorrectly routed, likely during manufacture of the aircraft. Over several years, wires in that loom chafed against the support structure and short circuited. Electrical arcing created smoke that activated the forward cargo smoke detector.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB was advised of the following proactive safety action in response to this occurrence.
Aircraft manufacturer
As a result of this occurrence, Boeing advised the ATSB that they have taken the following safety actions:
Fleet communication
Boeing issued a ‘Fleet Communication’, 777-FTD-24-18001 to all Boeing 777 aircraft operators informing them of this issue:
Boeing has received reports of five separate in-service events where a ceiling liner screw in the forward cargo compartment was found in contact with a wire bundle, resulting in a short to ground that damaged cargo ceiling standoffs, the wire bundle, and the floor beam in some cases.
Wire installation inspections
Boeing recommend interim action:
Operators can choose to inspect the wire bundle runs in the forward cargo compartment and locate instances where the ceiling liner screws and nutplates are in contact or do not have 0.13 Inch clearance with the wire bundle. Wire harnesses should have a minimum separation distance of 0.13 inch to sharp edges of structure and equipment per SWPM (D6-54446), Sec 20-10-11 Page 39, table 21 ‘Minimum Clearance’. If a riding condition is found, Boeing can provide technical assistance if required to provide corrective action. The wire routing installation drawings can be reviewed to determine the correct routing of wire bundles in the cargo compartment.
In addition, Boeing has issued Service Bulletin 777-24-0157, which would require operators to inspect for and correct similar conditions that led to this occurrence. Service Bulletin 777-24-0157 relate to all Boeing 777-200,777-200LR, 777-300ER aircraft line numbers 1-1527 inclusive.
Boeing Engineering performed an investigation of all cargo ceiling wire bundle installation engineering drawings. Boeing will add additional spacing as a precaution when wire bundles are in close proximity to ceiling liner screws.
…inspect and made changes to wire bundles near ceiling liner nutplate locations, in the forward and aft cargo compartments. If this service bulletin is not done, wire chafing can result in a short circuit and a system failure.
There have been five reports of wire chafing on ceiling liner screws or nutplates. Several ceiling liner support standoffs were damaged by heat which was caused by the grounding path. The floor beam was also damaged. Wire bundles near heat damaged ceiling liner support standoffs have also been damaged. The wire bundles that do not have the correct clearance from the ceiling liner screws, can result in chafing causing exposed conductors and shorting.
Boeing has also taken action in their production line by inspecting aircraft from line number 1529 for correct installation. Boeing are also considering installation and design changes to new production aircraft to alter the position of the effected wiring loom to prevent recurrence.
Safety message
Despite complex systems of design and manufacturing, training, and quality control, errors do occur during manufacturing that may not be apparent for some time. In this case, the aircraft was manufactured 4 years prior to the incident.
While this was a serious incident, the severity of the damage sustained was minimised through regulatory design requirements, material composition, system protections and crew actions. In response to this, and four other incidents, the aircraft manufacturer utilised their system of communication to alert all operators of the issue and took actions in an effort to prevent reoccurrence. Regardless of this, operators and maintenance providers are another line of defence for detecting errors. Due diligence during scheduled aircraft maintenance and defect rectification will assist with ensuring that aircraft systems meet the design intent and function accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 23 June 2017, at about 1549 Central Standard Time,[1] a QantasLink Bombardier DHC-8-315 aircraft, registered VH-TQH, was being operated on a scheduled passenger service from Port Lincoln to Adelaide, South Australia. There were two flight crew, two cabin crew and 46 passengers on board. The captain was designated as the pilot monitoring and the first officer (FO) was the pilot flying.[2]
When on final approach to runway 23 at Adelaide, at about 300 ft, the captain noticed fumes in the cockpit and mentioned this to the FO, who did not notice the smell. Shortly after, at about 200 ft, both crew detected the fumes, which smelt like electrical/chemical burning. They looked down at the centre console and noticed light grey smoke coming from the switch on the aileron/rudder trim control panel. The captain instructed the FO to focus on the landing and that they would manage the problem when they were on the ground. The captain notified air traffic control of smoke in the cockpit and requested emergency services. The controller considered this a ‘PAN PAN’[3] call.
After landing, the aircraft was stopped on the taxiway and the captain called for the Smoke checklist from the Quick Reference Handbook to be completed. This involved donning oxygen masks, switching the microphone to mask, and turning the recirculation fans off to prevent the smoke being circulated within the aircraft. The smoke had dissipated from the cockpit, but fumes were still present.
Air traffic control called back to ask if the flight crew could continue taxiing. The FO responded they were using oxygen masks and would be shutting down on the taxiway. The captain delivered a public address to the passengers advising there was an issue and to await further instructions. The captain then made a call to the cabin crew to inform them of the smoke, that they were using oxygen, and were planning to do a precautionary disembarkation. The cabin crew member indicated that passengers seated in rows 4 and 5 could also smell the fumes, but there was no smoke.
The FO retrieved the On ground non-normal checklist. The captain completed the checklist and made the ‘precautionary disembarkation’ public address to the passengers. The FO exited and directed the passengers outside to an area away from the aircraft. The cabin crew cleared the cabin to ensure all the passengers had disembarked and the captain switched off all power before they exited as per the Precautionary disembarkation and Evacuation checklists.
The captain spoke to the airport fire personnel and provided them a description of the issue and where it occurred. The fire personnel assessed the situation and determined there was no fire risk.
The captain briefed the passengers on the incident, describing what happened and why they disembarked. There were no reported injuries or ill effects from the smoke and fumes, and the aircraft was not damaged.
Aileron/rudder trim control panel inspection
Following the incident, engineers removed the aileron/rudder trim control panel for inspection. That inspection identified visible damage underneath the rudder trim switch. Specifically, the rudder trim potentiometer[4] was blackened and burnt (Figure 1). The trim control panel was subsequently replaced.
Figure 1: Burnt potentiometer in the aileron/rudder trim control panel (circled in red)
Source: Operator, modified by the ATSB
Additional comments
The following additional comments were made by the captain and operator:
When the smoke and fumes were detected, the aircraft was about 1 minute from landing. Consequently, the captain elected to continue the landing, rather than action the appropriate checklist. The captain reported that, if the checklist was commenced during the approach, the aircraft’s controls would have been handed between the crew while donning masks. The captain considered this to be dangerous while hand flying the aircraft and when close to landing.
While the crew were disembarking, the aviation rescue and firefighting personnel attempted to enter the aircraft, but unintentionally blocked the exit. This resulted in a minor delay for crew exiting.
The aviation rescue and firefighting personnel did not allow the cabin crew to remove the first aid kit from the aircraft, which contradicted the operator’s emergency procedures.
The operator reported that communications throughout the incident were well managed and the crew were commended for their response to the incident.
Airservices Australia comments
Airservices advised that the airport fire personnel were present at the exit only after all the passengers had disembarked and then attempted to enter the aircraft to talk to the crew and assess the internal conditions. The request not to remove the first aid kit was made in consideration that fire personnel carry first aid kits at all time. In addition, it was standard practice when securing a site not to remove anything from the aircraft until an internal assessment had been made. Airservices were not aware that it was company policy to remove the first aid kit.
Previous occurrences
A search of the ATSB’s database found the following occurrences involving smoke or fumes in DHC-8 aircraft originating from in the cockpit:
On 29 July 2013, the crew of a Bombardier DHC-8-315 were en route from Sydney to Wagga Wagga, New South Wales (ATSB investigation AO-2013-120) when they noticed a blank area in the centre of the flight management system screen. About 10 minutes later, the screen went completely blank and thick, light-grey smoke was observed coming from the unit. Examination of the unit found that two capacitors failed, resulting in the smoke and failure of the unit.
On 8 June 2014, the crew of a Bombardier DHC-8-202 were on take-off at Cairns, Queensland (ATSB occurrence 201405530). During the take-off, the FO’s electronic displays failed and fumes were detected in the cockpit. The take-off was rejected and the aircraft returned to the bay. An engineering inspection revealed water contamination to the No.2 symbol generator.
On 10 November 2016, the crew of a Bombardier DHC-8-315 were on approach to Adelaide, South Australia (ATSB investigation AO-2016-151). At about 9,000 ft, the FO noticed the captain’s electronic attitude director indicator screen had gone blank and the crew conducted the display failure checklist. After the crew were cleared to descend, they noticed an electrical smell, which was suspected to originate from the failed screen. The crew actioned the fuselage fire or smoke checklist and made a ‘PAN PAN’ call to air traffic control. After landing, a precautionary disembarkation on the taxiway was conducted. An engineering inspection found the fumes were caused by damage to a circuit card assembly due to a blown resistor on the video driver.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The rudder trim potentiometer burnt in-flight, resulting in fumes and smoke in the cockpit during a critical phase of flight.
Shortly after landing, the crew conducted a precautionary disembarkation on the taxiway, which reduced the risk of fumes exposure to the aircraft’s occupants.
Safety message
This incident highlights the effective flight crew management of an in‑flight issue during a critical phase of flight. The ATSB has published a research report, An analysis of fumes and smoke events in Australia from 2008 to 2012, which found that, from a flight safety perspective, the majority of fumes/smoke events were minor in consequence and the most common source was aircraft systems issues. The research also identified that fumes and smoke events were generally appropriately managed by flight and cabin crew due to effectiveness of crew training and operational procedures, such as using checklists.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 22 February 2017, at 1433 Eastern Daylight-saving Time (EDT), a Virgin Australia ATR 72-212A aircraft, registered VH-VPJ, departed Port Macquarie Airport, New South Wales (NSW) to operate scheduled flight VA1188 to Sydney, NSW. There were four crew and 23 passengers on board.
At 1453:35, during cruise at Flight Level (FL) 180,[1] the Centralized Crew Alerting System (CCAS) alerted the flight crew to a failure of the number one static inverter (Figure 1).[2] The CCAS then displayed multiple messages indicating a loss of power to systems associated with the number one static inverter. The aircraft electrical system power transfer function automatically transferred these systems to the number two static inverter and the CCAS warnings extinguished.
At 1453:43, the cockpit master warning activated and the CCAS displayed an electrical smoke warning. The flight crew immediately donned their oxygen masks and enacted the smoke checklist memory items. As the flight crew fitted the oxygen masks, they detected a strong electrical type burning odour and observed faint wispy smoke within the cockpit. After conducting the memory items, the flight crew then completed the electrical smoke checklist. The checklist included selecting the avionics vent exhaust mode to overboard. After completing this selection, the flight crew reported the smoke quickly dissipated. Flight data shows the electrical smoke warning extinguished at 1454:56.
After completing the electrical smoke checklist, the captain identified Williamtown Airport about 65 km (35 NM) south-east of the aircraft and elected to divert the flight to Williamtown.
At 1455, the captain contacted air traffic control (ATC) and declared a MAYDAY.[3] The captain advised that they intended to divert to Williamtown Airport. ATC cleared the flight to descend and track directly to Williamtown.
After contacting ATC, the captain requested that the senior cabin crew (SCC) report to the aircraft interphone using the cabin public announcement system. The SCC heard the announcement, but due to muffling caused by the captain’s oxygen mask, they did not understand the request. The second cabin crewmember heard the announcement more clearly and communicated the request to the SCC. The SCC contacted the flight deck using the aircraft interphone. The captain advised them of the emergency and that the flight was diverting to Williamtown. The SCC advised the other cabin crewmember of the diversion and commenced securing the cabin.
After securing the cabin, the SCC returned to their seat and contacted the flight deck. The captain provided them with a full briefing, advising the nature of the emergency and to expect a precautionary disembarkation[4] after landing. Recognising the high workload of the flight crew, the SCC advised the captain that they would conduct the passenger briefing tasks on behalf of the flight crew. The captain instructed the SCC to begin the precautionary evacuation once the seat belt sign extinguished after landing.
As the aircraft descended through 10,000 ft, the flight crew removed their oxygen masks. The captain found the remaining odour very strong and elected to refit the oxygen mask. The captain identified that the aircraft was too high to commence an approach to Williamtown and conducted a descending orbit to lose height prior to commencing a visual approach for runway 12. While approaching runway 12, the captain found the oxygen mask blurred their vision. The captain briefly handed control of the aircraft to the first officer and removed the oxygen mask.
At 1512, the aircraft landed on runway 12. After landing, ATC instructed the flight crew to taxi the aircraft to Bay 11. Once the aircraft stopped and the flight crew shut the engines down and extinguished the seat belt sign, the SCC initiated the precautionary disembarkation. The SCC used the cabin public address system to direct passengers to disembark the aircraft using the cabin door. Emergency services personnel met the disembarking passengers and guided them clear of the aircraft to a safe area.
After shutting down the engines, the flight crew noticed the smell intensifying. The captain elected to immediately vacate the flight deck. The flight crew followed the last passenger and the cabin crew in vacating the aircraft through the cabin door.
The aircraft was not damaged, and no persons were injured during the incident.
Figure 1: Number one static inverter
Source: Operator
Captain comments
The captain provided the following comments:
Time was lost due to difficulties with the first officer refitting their headset after donning the oxygen mask. The oxygen mask also created difficulties in communication between the flight crew and cabin crew. Managing these communication difficulties added to the flight crew workload during the emergency.
While the company did not operate the ATR 72 to Williamtown and the captain had not previously operated there, the captain commented that the best place for an aircraft with smoke in the cockpit is on the ground. The long runway, available emergency services and clear weather between their position and the airport enabled the captain to quickly elect to divert to Williamtown.
Senior cabin crew member comments
The senior cabin crew (SCC) provided the following comments:
They had not expected and were not prepared for the communications difficulties caused by the flight crew’s use of oxygen masks. Their voices were heavily distorted which led to difficulty in understanding information. After the initial briefing from the captain, the SCC did not realise there was a smoke issue and believed the aircraft was experiencing an unspecified ‘leak’. After the initial briefing, they began to prepare the cabin for a possible depressurisation.
Due to the communications difficulties caused by the flight crew oxygen masks, the SCC did not realise that they were being requested to contact the flight crew and did not immediately respond.
The aircraft interphone does not allow the flight deck to address all cabin crew at the same time. Therefore, the SCC was required to relay information to the other cabin crewmember. This made it difficult for the other cabin crewmembers to be fully aware of the progress of the incident and increased the SCC’s workload.
Cabin preparation procedures for the precautionary disembarkation require that the SCC use designated Cabin Preparation cards. These cards provide guidance for full and reduced cabin preparation procedures and associated passenger briefings. The cards were located under the SCC’s seat and were inaccessible while seated. As the SCC was unable to leave their seat during the period between receiving the full briefing from the captain and landing, they were unable to access these cards.
Engineering examination
The manufacturer of the static inverter conducted an engineering investigation of the failed static inverter. The investigation found that the failure of the number one static inverter and associated smoke and odour was caused by a failure of a C60x series capacitor within the number one static inverter.
The aircraft manufacturer also noted that the operator experienced two previous static inverter failures in November and December 2016. These failures were also caused by failure of a C60x series capacitor.
Vendor Service Bulletin
On 22 June 2016, the manufacturer of the static inverter released vendor service bulletin
This service bulletin identified an issue with capacitor C311 which led to instances of reduced reliability and premature failure, sometimes with associated smoke emission. As part of this service bulletin, the C311 capacitor is replaced with a modified capacitor of increased reliability.
The service bulletin recommended that the modification be incorporated at the next shop visit for the static inverter units. After completion of the service bulletin modifications the static inverters are designated as ‘Amendment E’ status.
From October 2016, a retrofit campaign was undertaken by the static inverter manufacturer to refit all in-service static inverters to ‘Amendment E’ standard.
In December 2016, the aircraft manufacturer advised operators of the vendor service bulletin. The bulletin was classified as a minor change and did not imply safety concerns.
Continued static inverter issues
Following reports of failures of ‘Amendment E’ static inverters, the aircraft manufacturer identified an issue with additional capacitors within the static inverter. These capacitors are of the C60x (C601 through C605) series. Failures of these capacitors also led to failure of the static inverter unit and associated smoke emission.
Static inverter failure
In the event of failure of a static inverter, the power transfer function automatically transfers power of the associated electrical systems to the second static inverter.
The operator’s Minimum Equipment List allows dispatch of an aircraft with an unserviceable static inverter for a period of up to two days.
Safety analysis
A C60x series capacitor within the number one static inverter failed in a manner consistent with other C60x series capacitor failures. Failure of the capacitor resulted in failure of the static inverter and smoke being emitted into the cockpit.
Difficulties in communication with the flight deck led the SCC to initially believe the flight crew were managing an unspecified ‘leak’. Therefore, the SCC began preparing for a possible depressurisation. However, as the required actions were similar to those required for the smoke event in progress, the misunderstanding did not impact on the management of the cabin during the incident.
The Cabin Preparation cards were inaccessible during the period that procedures directed the SCC to use them. However, as the SCC was able to complete the required actions without reference to the cards this did not impact on their ability to prepare the cabin for landing and the precautionary disembarkation.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
A C60x series capacitor within the number one static inverter failed leading to failure of the static inverter and associated smoke.
Difficulties in communication caused by oxygen mask use led to misunderstandings between the flight crew and cabin crew and increased flight crew workload.
The Cabin Preparation cards were inaccessible to a seated cabin crewmember.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Verifying the integrity of the Power Transfer function across the ATR fleet. The operator advised that after completing this campaign no adverse findings were reported.
The operator has initiated a retrofit campaign to route all in-service static inverters to the vendor to have the modification to both the C311A and the C60x capacitors completed (‘Amendment E’ and ‘Amendment F’ (see Aircraft manufacturer) standard).
The operator has initiated a fleet wide inspection and operational test of the oxygen mask integrated microphone.
The operator has undertaken a risk assessment for single and dual static inverter failure.
Aircraft manufacturer
As a result of this occurrence, the aircraft manufacturer has advised the ATSB that they are taking the following safety actions:
Short term actions:
Replacement of C311 capacitor resulting in service units being modified to Amendment E standard. New production units have been modified and the retrofit process is on-going.
Change in the manufacturing process with ‘burn in’ test on C60x capacitors resulting in units being modified to ‘Amendment F’ standard. New production units have been modified. The retrofit process is being prepared.
Mid-term actions:
A design change is under development including the replacement of the C60x capacitors. The redesigned unit will be identified with a new part number. The design change certification expected to be complete before the end of quarter 2, 2017.
Safety message
This incident underlines the value of effective training and procedures. Despite the communications difficulties and the inaccessible cabin preparation cards, the cabin crew were able to effectively prepare the cabin during the diversion and manage the subsequent precautionary disembarkation. This enabled all aircraft occupants to disembark the aircraft quickly and without injury.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.