Hydraulic leak involving Boeing 787, 9V-OFG, Melbourne Airport, Victoria, on 8 September 2016
Final report
What happened
On 7 September 2016 at 1720 UTC,[1] Scoot Airline flight TZ026, a Boeing 787 aircraft, registered 9V‑OFG, departed Singapore on a scheduled passenger transport flight to Melbourne, Victoria.
Flight TZ026 made an approach to Melbourne Airport runway 34 and landed without incident at 0021 UTC on 8 September 2016. During the landing roll, the flight crew used maximum reverse thrust in order to vacate runway 34 at Taxiway F (Figure 1). After the aircraft exited the runway onto Taxiway F, air traffic control (ATC) instructed the flight crew to change radio frequency to the ATC Ground frequency. The surface movement controller (SMC) then provided the flight crew with their taxi instructions.
The flight crew proceeded to taxi the aircraft from Taxiway F, right onto Taxiway T, then another right onto Taxiway A. As they started to taxi down Taxiway A, they heard a comment on the Ground frequency about smoke. The flight crew were unsure if the comment was in reference to their aircraft, so they queried the SMC. The SMC responded that flight TZ026 had smoke coming from their right engine. The captain elected to stop the aircraft on the taxiway and request an inspection from the aviation rescue and fire-fighting (ARFF) services.
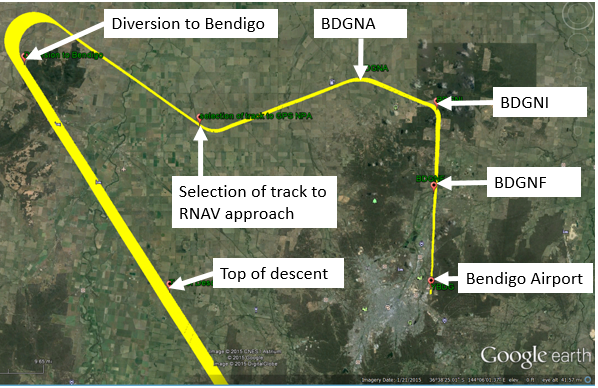
Figure 1: Aircraft ground track at Melbourne Airport
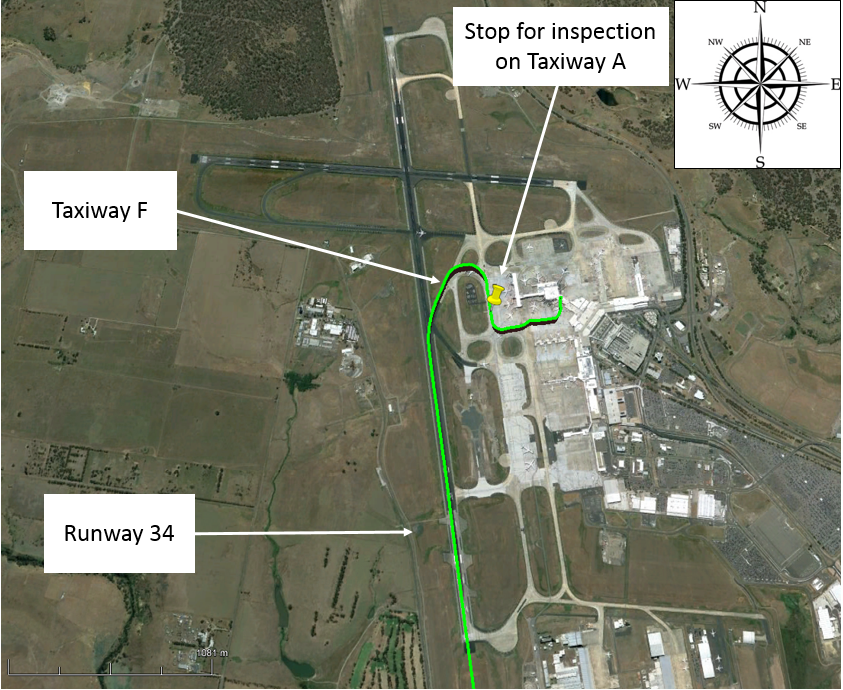
Source: Google earth, annotated by ATSB
The ARFF vehicles arrived in front of the aircraft on Taxiway A and an ARFF officer communicated their observations of the right engine to the SMC. The SMC directed the flight crew to monitor the frequency in use by the ARFF. Consequently, the flight crew heard the ARFF officer report to the SMC that the smoke they saw ‘appeared to be normal’. The aircraft captain was aware that the aircraft engines can emit smoke from the engine oil system and cross-checked their engine indications. There were no abnormal indications present and therefore the captain elected to taxi the aircraft to their allocated parking bay and conduct a normal shut down with ARFF in attendance. The aircraft was shut down without further incident.
Maintenance fault finding
After the passengers had disembarked, the captain informed one of the company maintenance engineers that smoke had been observed coming from the right engine after landing, but all engine indications were normal. The engineer conducted a general visual inspection of the engine and reported to the captain that there was no obvious sign of a fault. The captain documented the incident in the aircraft technical log and signed-off duty.
During the turn-around inspection, another company maintenance engineer noted that the right hydraulic system was at the refill level. The engineer conducted leak checks on the right hydraulic system and found a damaged hydraulic hose in the right engine pylon hydraulic bay (Figures 2 and 3). The damaged hose was located downstream of the right engine thrust reverser stow line.
Figure 2: Location of aircraft hydraulic systems and leak
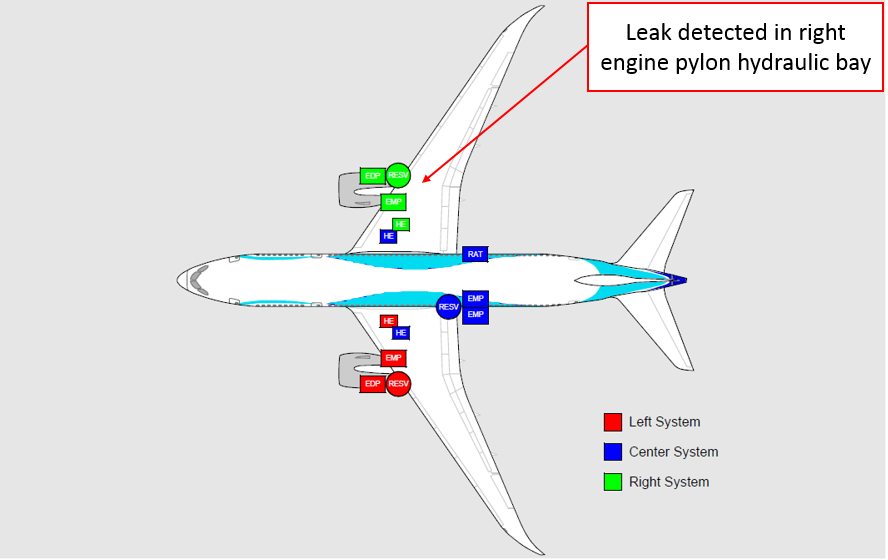
Source: Boeing, annotated by ATSB
Figure 3: Location of hydraulic hose
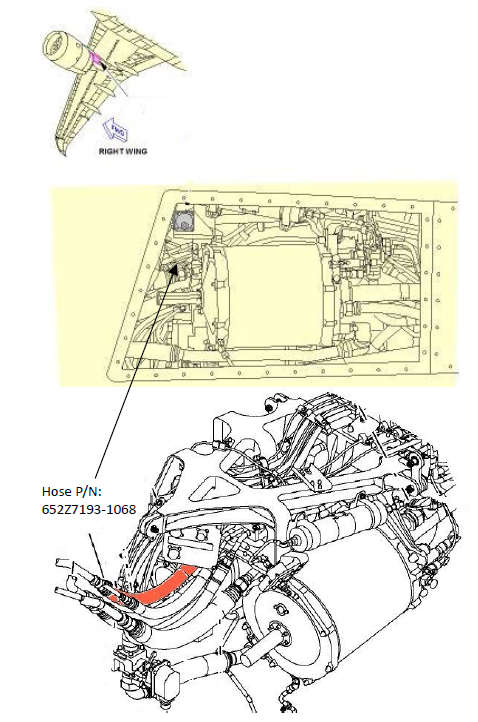
Source: Boeing
Flight data recorder
The engine thrust reversers are electrically controlled, but hydraulically powered systems. The right hydraulic system powers the right engine thrust reverser and the left system powers the left engine thrust reverser. Flight data recorder information indicated that the three hydraulic systems were at the same quantity when the aircraft landed. When the thrust reversers were applied to assist braking, the left and right hydraulic system quantities reduced, as required, to power the thrust reverser actuators. However, when the thrust reversers were stowed only the left hydraulic system returned to the normal quantity. The right system quantity continued to reduce, which was consistent with a leak in the hydraulic system.
Aircraft manufacturer findings and recommendations
The failed hose was part of the thrust reverser retraction circuit and is otherwise isolated during flight. The thrust reverser circuit is the only location where this part is installed on the aircraft. Boeing note that the leak has previously been observed either as drip from the aft fairing of the engine pylon after flight, or during landing as a mist sprayed from the engine exhaust during thrust reverser retraction. Boeing has advised operators to heighten their awareness of the issue, and in the event of an observed leak at the aft pylon fairing module, to check the incident part number hose for a rupture. Boeing has recorded several in-service failures of this part number hose and investigated the fault with the part manufacturer.
Engine manufacturer findings
During development testing of the engine, the manufacturer, Rolls Royce, identified the potential for a visible white-coloured mist from the engine oil breather to occur at any stage of engine operation. They stressed that this is a normal characteristic of the engine, which is a result of incomplete air/oil separation, and ‘does not represent an increase in engine oil consumption.’
Aircraft captain comments
The captain noted that during the inspection from the ARFF services, the flight crew were asked by the SMC to monitor the ARFF frequency, but they were not allocated a discrete frequency for communications with ATC. This resulted in interruptions from other traffic using Ground frequency for routine communications and at times the captain felt they could not immediately relay information to ATC.
Airservices comments
Airservices noted the captain’s comment regarding the need for a discrete frequency. This is currently not standard practice and has the potential to create confusion for ATC at times of high workload. The use of a published frequency can aid in situational awareness for other operators and ARFF services throughout the emergency.
Safety analysis
Hydraulic leak
During the turn-around inspection of the aircraft, the right hydraulic system fluid level was found to be low due to a ruptured hydraulic hose. This hydraulic hose is only installed in the engine thrust reverser retraction circuit and is otherwise isolated inflight. The flight data indicated that the reduction of fluid in the right hydraulic system, consistent with a hydraulic fluid leak, coincided with the thrust reverser retraction after landing.
Engine smoke
At the time that the aircraft stopped for a visual inspection by ARFF, what was reported as smoke appears to be mist emanating from the vicinity of the engine oil breather (Figure 4). The presence of mist is consistent with the Boeing investigation into the failures of the affected hydraulic hose that indicates a rupture of this hose. However, the location of the mist suggests the source could have been (by itself or in addition to the hydraulic fluid) due to the engine oil breather. This is because the mist was also consistent with what Rolls Royce had previously noted as a visible white-coloured mist that can be observed emanating from the engine oil breather as a result of incomplete air/oil separation.
Figure 4: Aircraft stopped for inspection

Source: Melbourne Airport
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
- The hydraulic hose in the right engine thrust reverser retraction circuit ruptured when the right engine thrust reverser was retracted on landing.
- The reported engine smoke was probably mist from the right hydraulic system leaking hydraulic fluid into the engine exhaust, or mist from the engine oil breather as a result of incomplete air/oil separation, or a combination of both conditions.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Aircraft manufacturer
As a result of this occurrence and previous occurrences, Boeing has advised the ATSB they have taken the following safety action:
A ‘capture and control in production’ process was introduced. This process has identified and screened out defective parts. Their own investigation has identified the likely root causes of the failures and identified the population of hoses affected. They have communicated recommended actions to aircraft operators, which describes how to identify and replace potentially affected hoses.
Aircraft Operator
As a result of this occurrence, Scoot Airlines has advised the ATSB they are taking the following safety action:
As per the aircraft manufacturer’s recommendations, a 787 fleet check was conducted, potentially affected hoses identified, and replacement hoses ordered.
Safety message
At each stage during this incident: after the aircraft had landed, when the engineering inspection detected a low hydraulic system fluid level, and subsequently when the manufacturer received the failed part, the exact nature of the problem was unclear. However, at each stage, precautionary action was taken to investigate the problem, which mitigated the risk to the safety of personnel and serviceability of the aircraft.
Short Investigations Bulletin - Issue 55
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016

Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
__________
Occurrence summary
| Investigation number | AO-2016-114 |
|---|---|
| Occurrence date | 08/09/2016 |
| Location | Melbourne Airport |
| State | Victoria |
| Report release date | 14/12/2016 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Smoke |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 787-8 |
| Registration | 9V-OFG |
| Serial number | 37123 |
| Aircraft operator | SCOOT |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Singapore |
| Destination | Melbourne, Vic. |
| Damage | Nil |