Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 9 December 2025, an Ayres Thrush S2R-T34was being used to conduct agricultural spraying, which involved multiple circuits and landings to pick up and disperse approximately 40 loads.
During landing, before picking up the final load for the day, the pilot observed a vehicle approaching the landing strip towards the loading area. The pilot applied additional braking to avoid a possible collision with the vehicle and the aircraft subsequently veered towards a drainage channel adjacent to the landing strip.
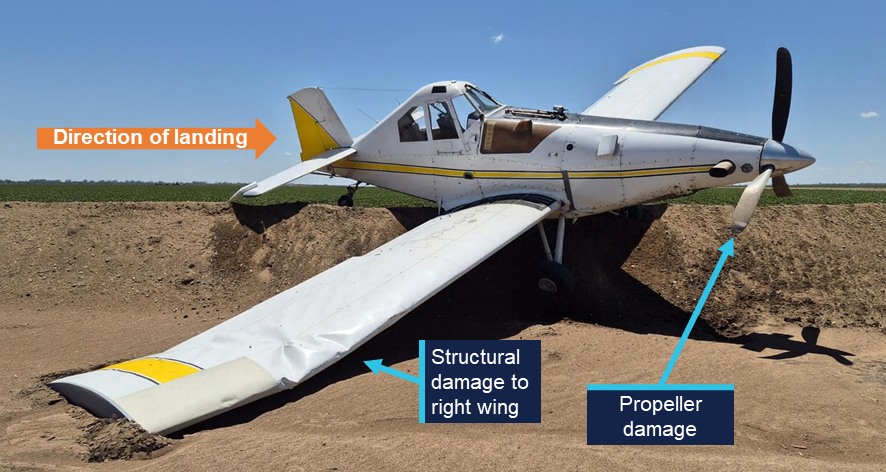
While the pilot monitored the approaching vehicle, the aircraft continued towards the end of the landing strip and the drainage channel. The pilot subsequently attempted to correct the aircraft to remain on the strip however there was insufficient distance and time, and the aircraft entered the channel. There were no injuries to the pilot, and the aircraft was substantially damaged.
Figure 1: Aircraft damage
Source: operator, edited by the ATSB
Safety message
In this occurrence the distraction of the vehicle approaching the landing strip diverted the pilot’s attention from monitoring the landing roll, resulting in a loss of situational awareness.
This type of distraction is more likely to impact performance due to the cognitive demands of one spatial visual scanning task (i.e. monitoring landing roll) being interrupted by another spatial task (i.e. a vehicle moving towards the aircraft’s projected path), particularly during a critical phase of flight where there is very little time to assess the situation.
Concurrent task management depends on the pilot’s ability to effectively prioritise tasks and appropriately time share tasks by rapid switching, whereby attention quickly shifts between tasks. This is essential when the pilot is dealing with multiple tasks, which are all critical to flight safety.
The ability to appropriately prioritise and use rapid switching may be affected by workload and fatigue, which can be a factor during operations involving large numbers of short, similar flights in quick succession. Effective use of rapid switching can also be improved through experience as well as specific task management training.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 22 December 2025 at 1640, a pilot was conducting circuit operations with one passenger on board a Cessna 150H at West Sale Airport, Victoria.
In contrast to the recorded weather conditions, the pilot identified a left-hand crosswind via the aerodrome windsock for the one runway available. Alternate grass runways were unavailable due to rain in the preceding 24 hours.
During landing in the crosswind on runway 27, the pilot ‘crabbed’ by yawing[1] the nose of the aircraft into the wind to prevent the aircraft from drifting off the centreline. The pilot assessed that the approach was stable and proceeded to touch down. During rollout, after the flare, the aircraft encountered a gusting wind, resulting in the aircraft ballooning[2] and yawing to the right. In response, the pilot attempted to counteract with a left yaw. However, the conditions exceeded the aircraft’s capabilities and the aircraft was carried to the right, and the right wheel contacted the runway surface. The right main landing gear collapsed, and the right wing tip struck the ground before the aircraft veered off the runway.
The pilot and passenger exited the aircraft without injuries, and the aircraft was substantially damaged (Figure 1).
Figure 1: Damage to the Cessna 150H right landing gear
Source: Aircraft owner
Safety message
Crosswind gusts during the later stages of landing can present challenges for pilots. Depending on the magnitude and direction of the gust, there may be insufficient time to apply corrective controls before the aircraft deviates from the intended path.
Once the aircraft wheels touch down, it's important to remain focused and use your rudder to keep the aircraft straight, even after you have touched down, to retain control and stability.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Yawing: the motion of an aircraft about its vertical or normal axis.
[2]Coequally a sudden unwanted gain in height of aircraft that can occur on approach and landing.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 4 December 2025, at 1720 local time, an Air Tractor AT-802A was preparing to conduct aerial firefighting operations from Linga Airbase, Victoria. Before departure the pilot briefly consulted electronic maps for Linga Airbase, however, did not observe that runways 17 and 19 were 2 separate runways with runway 19 commencing at the end of runway 17 rather than a single longer runway (Figure 1). After loading the aircraft with fire retardant, the pilot commenced taxi for runway 17, believing they were backtracking to use the entire length of runways 17 and 19. The pilot completed their take-off checks and commenced the take-off roll.
The pilot reported that during the take-off run, due to the upslope on runway 17, they were unable to see the threshold of runway 19 until the aircraft had crested the rise towards the end of runway 17. Unaware of the 20° right turn, on becoming visual with runway 19, the pilot assessed the turn was too sharp to navigate and the aircraft was travelling too fast to stop and not yet fast enough to become airborne.
Figure 1: Linga Airbase, Victoria
* Wind direction was recorded 82 km away at Hopetoun, Victoria. Source: Google Earth, annotated by the ATSB
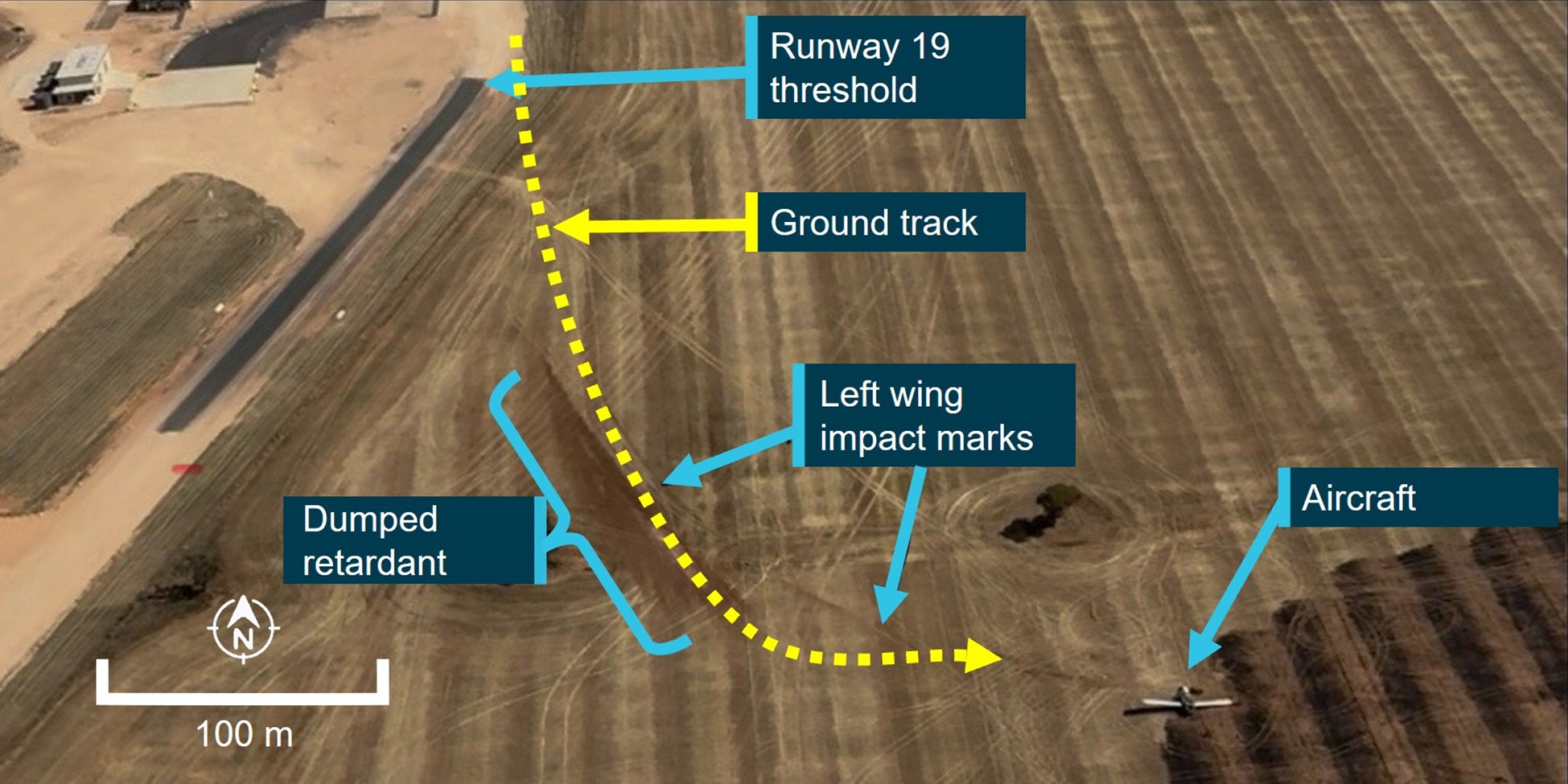
The pilot maintained the runway 17 heading, and the aircraft overran the end of runway 17 into a field, impacting a fence, before becoming airborne. The pilot intended to release the load of fire retardant to reduce weight, however, due to their unfamiliarity with the location of the load release switch in that aircraft, instead activated the aircraft lights, before locating the correct switch and dumping the load. Images show the left-wing tip dragged along the surface of the field while the load was dumped. A witness reported the aircraft briefly became airborne with a nose high attitude and left wing down in a left turn before the left wing again contacted the ground and pulled the aircraft to the ground before coming to a stop (Figure 2).
Figure 2: Occurrence aircraft impact marks and final position
Source: Operator, annotated by the ATSB
The impact was sufficient to liberate the engine and propeller from the aircraft which subsequently set fire to the field (Figure 3). The local airbase manager and 2 other state government employees attended the scene and were able to put the fire out in the vicinity of the aircraft and were then able to assist the pilot to egress the aircraft.
The pilot sustained minor injuries and was admitted to Mildura hospital. The aircraft was substantially damaged.
Figure 3: Occurrence aircraft
Source: Operator
The pilot reported that they had not previously operated from Linga Airbase, and earlier when arriving in the circuit they joined a midfield crosswind leg for runway 01 before landing, and had not observed the angle of the adjoining runways from the air.
The airbase manager reported other firefighting aircraft had been using runway 19 throughout the day. Linga Airbase runway 17 was about 660 m in length and joined the northern end of runway 19 which measured about 1,000 m in length. The aircraft was loaded with retardant to the western side of where runways 17 and 19 met.
The pilot reported the wind direction during the take-off roll was a crosswind. Conditions around the time of the occurrence recorded at Hopetoun, Victoria indicated temperature of 38°C with winds gusting between 16–33 kt from the north-west.
The aircraft loading log for the day of the occurrence indicated it was loaded with about 2,300 L of fire retardant. This gave the aircraft a take-off weight of about 6,900 kg, which was below the aircraft’s maximum take-off weight for the conditions. The operator reported the aircraft’s performance in the hot conditions required a take-off ground roll distance of about 1,000 m.
Although they were an experienced agricultural pilot, they had not previously operated from that airbase. Although the pilot observed other aircraft depart using runway 19 while reloading, they assumed they were not using the entire length of the runway, and by taxiing and backtracking to the threshold of runway 17 believed they were increasing their take-off roll distance. Performance calculations indicated that due to the air temperature, weight of the aircraft and wind conditions, the aircraft would have required the full length of the longer runway 19 to become airborne.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. As a result of the aircraft’s sudden stop the pilot’s flight helmet was damaged in the occurrence and they suffered a laceration to their head. Therefore, it was likely the pilot’s helmet prevented a more serious head injury.
Thorough pre-flight planning is essential to safe flight and is especially important when operating from unfamiliar airports. A clear understanding of the take-off distances available and runway configuration improves pilots’ situational awareness, reducing the possibility of the unexpected during higher risk stages of flight such as take-off and landing.
Aerial firefighting operations are often conducted in conditions of extreme heat and wind; accurate performance calculations including take-off weight and available runway distance are essential for safe operations in challenging conditions.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the afternoon of 12 November 2025, an American Champion Aircraft Corp 7GCBC with a tailwheel landing gear was conducting a dual training flight with an instructor and a student on board. After completing air work at a different location, the aircraft approached runway 24 at Camden Airport, New South Wales, for circuit training.
During approach, instruction was provided to the student until the aircraft reached 600 ft, at which point the instructor then took over the controls. After conducting a standard approach, the pilot flared the aircraft as it reached the threshold. A gust of wind occurred just prior to contact with the runway resulting in the aircraft being pushed to the right.
One main wheel struck the runway and the instructor reported that it seemed to ‘dig in’, resulting in the aircraft turning to the right significantly. The right wheel contacted the grass next to the runway and the instructor attempted to return the aircraft to the centreline, however the aircraft swung to the left resulting in a ground loop on the runway.
The aircraft sustained substantial damage to the right wing, fuselage and landing gear.
Safety message
Tailwheel aircraft are more susceptible to the effects of wind gusts during landing and can be more difficult for pilots to maintain directional control. If environmental conditions during the approach become challenging or unfavourable, initiating an early go-around will allow time to plan for how to manage the landing conditions and reconfigure the aircraft for a second approach.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-059
Occurrence date
12/11/2025
Location
Camden Airport
State
New South Wales
Occurrence class
Accident
Aviation occurrence category
Hard landing, Loss of control, Runway excursion
Highest injury level
None
Brief release date
15/12/2025
Aircraft details
Manufacturer
American Aircraft Corp
Model
7GCBC
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 19 August 2025, a Cessna 180 with a tailwheel landing gear was approaching runway 20 at Borroloola Aerodrome, Northern Territory, in variable, moderate crosswind conditions. There were 2 pilots and 1 passenger on board. Just after touchdown, the aircraft turned into the wind and started to veer left off the runway. The pilot in command initiated a go-around and as the aircraft began to lift off, it continued drifting off the runway.
The left wheel struck a mound of dirt beside the runway and the wheel departed the aircraft, causing the aircraft to rotate, collide with the ground and skid sideways, subsequently striking a concrete culvert before coming to rest (Figure 1). The aircraft was substantially damaged during the accident, however the 3 people on board were uninjured.
Figure 1: Aircraft damage
Source: Borroloola Aerodrome operator
Safety message
This accident provides a reminder for pilots to be prepared to conduct a missed approach, particularly in tailwheel aircraft during crosswind conditions. Tailwheel aircraft have less directional stability on the ground due to the location of the centre of gravity behind the main wheels. They are more susceptible to the effects of crosswind and the tail can have a tendency to swing sideways on the ground. They require more active input to maintain directional control and any yaw needs to be corrected immediately as it can quickly lead to a large swing and potential loss of control. If conditions during approach are challenging, an early go-around can provide an opportunity to reassess the landing options and make a reasoned decision about whether to attempt another approach and plan for how to manage the conditions.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
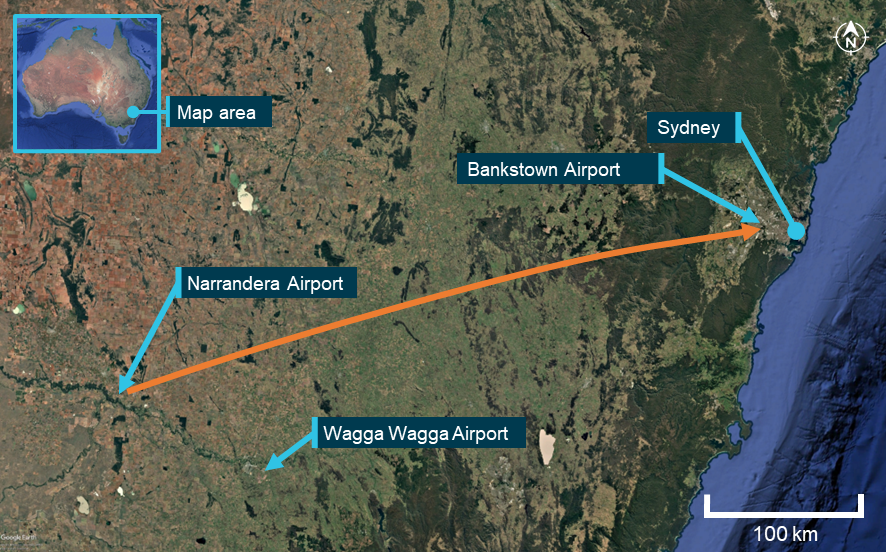
On 4 August 2025, an amateur-built Lancair IV departed Orange Airport, New South Wales, at 0652 local time, intending to fly to Bankstown Airport.
During cruise, the aircraft sustained an electrical system failure, resulting in numerous electrically driven systems failing. The pilot then made the decision to conduct an air return to Orange Airport, rather than continue the flight towards Bankstown.
Orange Airport consists of primary runway 11/29 which is 2,213 m long and is a sealed surface with a secondary runway 04/22 which is a 964 m long unsealed surface.
Due to the electrical malfunction, several systems of the aircraft were impacted, including the landing gear and VHF radio communication systems. The pilot used their mobile phone to communicate with a ground station to aid in facilitating their arrival at Orange Airport.
As the landing gear system is electrically controlled and hydraulically operated, due to the electrical failure, the primary method of the gear extension was not functional.
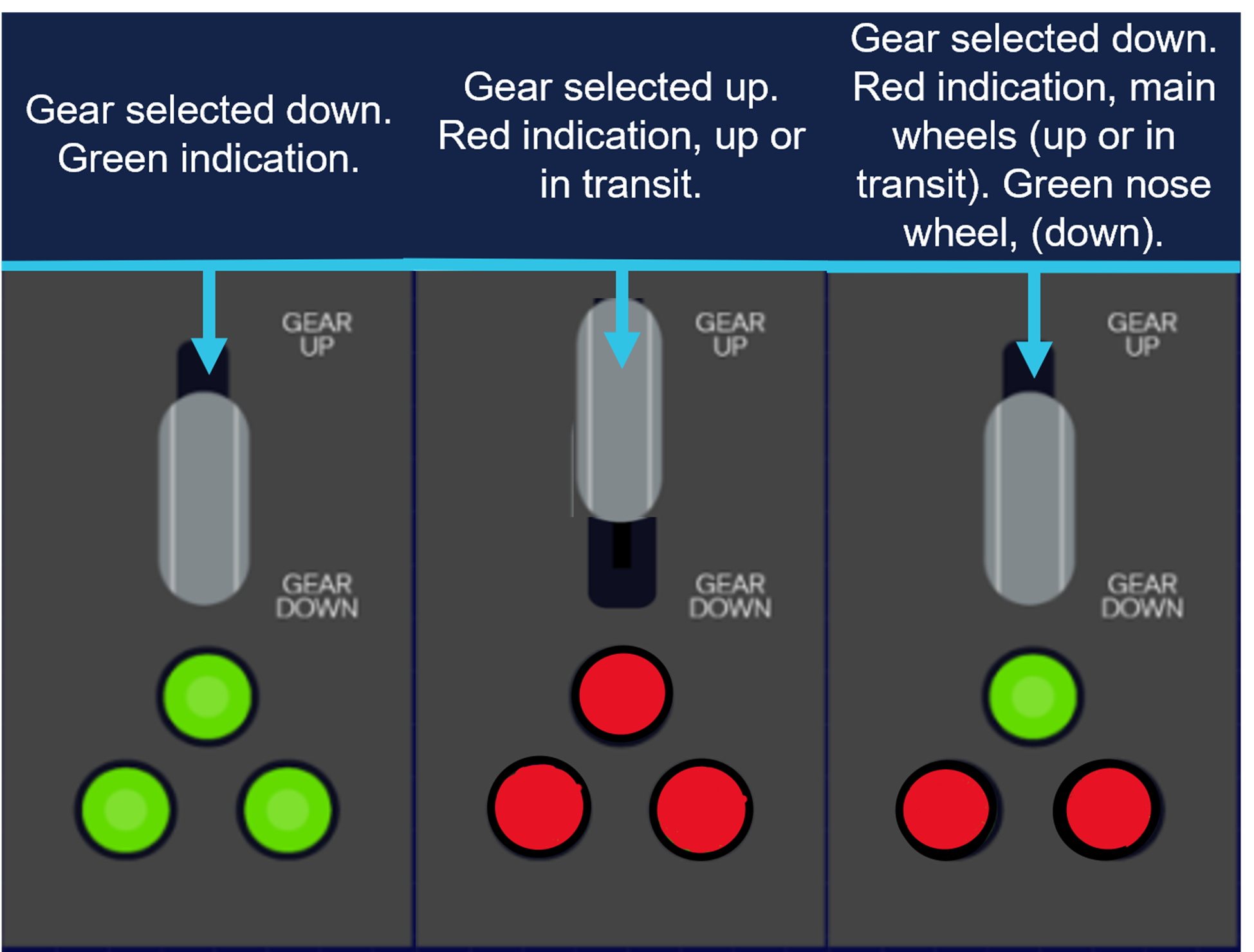
During the initial approach to the primary runway, the pilot manually selected the landing gear ‘down’ to extend the landing gear. Once manually selected ‘down’, the undercarriage extension indicator showed that only the nose gear had locked ‘down’, indicating (green), with the main gear, not indicating that it had ‘locked’ down (Figure 1).
Figure 1: Generic representation of landing gear selection
Source: ATSB representation of landing gear selection and indication. May not be indicative to type of aircraft.
The pilot proceeded to conduct several low passes of the runway to try to ascertain the condition of the landing gear with people on the ground.
However, after not being able to confirm the gear was fully down and locked, the pilot then made the decision to conduct a precautionary landing on the non-sealed cross strip, runway 04.
The pilot conducted the approach and landed, however on touchdown the main undercarriage legs collapsed, and the aircraft slid on the nosewheel (front of the aircraft) and rudder (rear of the aircraft) before coming to rest at the fence at the end of the runway.
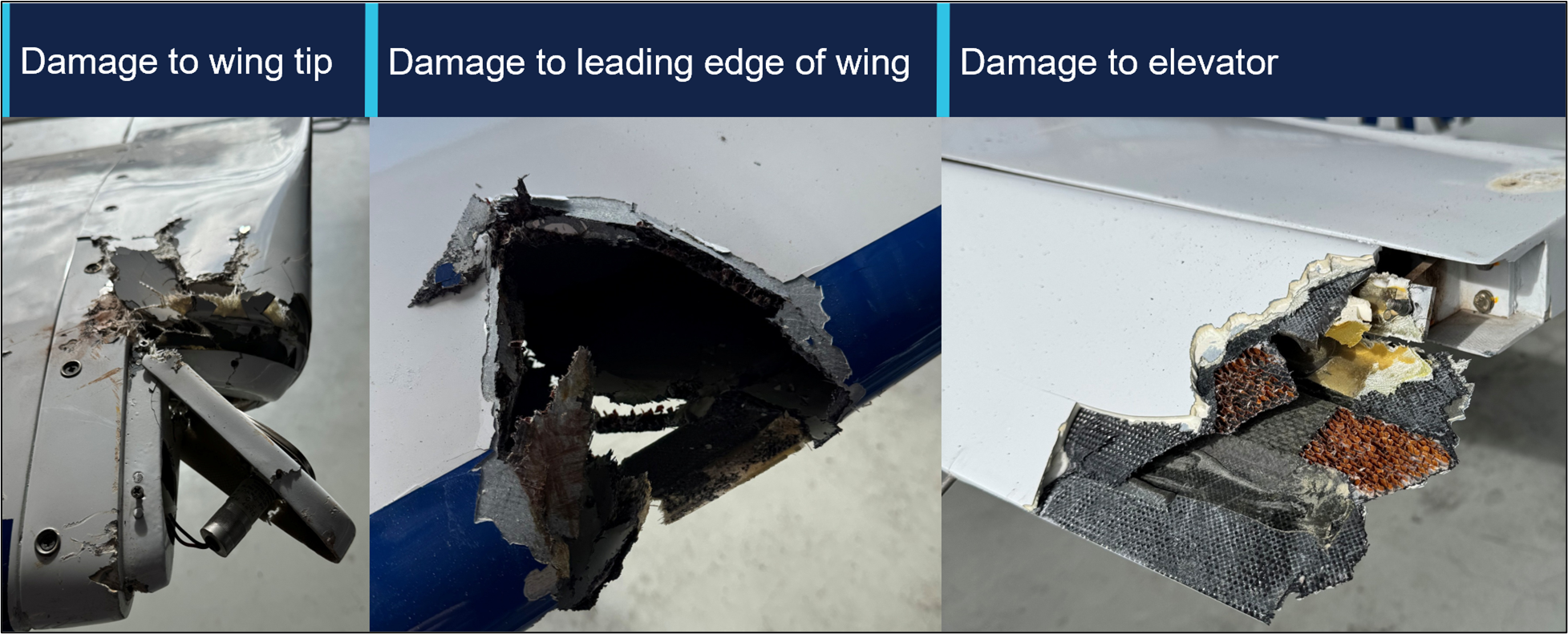
The aircraft incurred some minor damage (Figure 2) to the wingtip and elevator with no injuries to the pilot.
Figure 2: Damage to aircraft
Source: Operator, annotated by the ATSB
Subsequent engineering inspections found the electrical system had failed due to a defective voltage regulator.
Safety message
This occurrence illustrates that a good knowledge of aircraft systems coupled with sound decision‑making can help facilitate a positive outcome to an emergency.
Aircraft rely on hydraulic or electrical systems to extend and retract the landing gear. Should any component in these systems fail, pilots may be left with no choice but to manually extend the undercarriage or potentially execute a wheels-up landing.
Applying a structured and proactive approach to identifying and managing threats and errors, influences the safety of the flight.
In this instance, the pilot was able to identify the aircraft system failure and make several calculated risk-based decisions to manage the emergency. This was achieved by using various resources at their disposal, such as their mobile phone, to seek ground assistance in the absence of normal VHF radio.
In emergency situations, pilots need to utilise all the available resources at their disposal. Maintaining a degree of flexibility and adapting to select the most appropriate landing area can minimise risk, limit damage and maximise survivability.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-039
Occurrence date
04/08/2025
Location
Orange Airport
State
New South Wales
Aviation occurrence category
Collision with terrain, Diversion/return, Electrical system, Landing gear/indication, Runway excursion, Wheels up landing
On 29 May 2025, a Cessna 310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was conducting a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory. On board were the pilot and 4 passengers.
During the approach at Lake Evella Aerodrome, recorded data indicated that the aircraft touched down just prior to halfway along the runway. The pilot subsequently applied braking, but the aircraft did not decelerate as expected. This resulted in a runway excursion and the aircraft subsequently collided with a perimeter fence which substantially damaged the left wing. The pilot and 4 passengers were uninjured.
What the ATSB found
The ATSB found that the pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in the aircraft floating during the landing flare for a prolonged period in ground effect, and a landing beyond the planned touchdown point. After the aircraft touched down, the pilot subsequently commenced braking about halfway along the runway. The long landing reduced the available distance to decelerate on the runway.
At the aircraft’s landing weight, the remaining runway length should have provided sufficient stopping distance, but degraded braking capacity meant the aircraft could not be stopped before the runway end and it subsequently departed the runway.
During a scheduled maintenance event prior to the occurrence, a licensed aircraft maintenance engineer believed an apprentice had replaced the main-wheel brake pads. An inspection after the occurrence found that the right brake reservoir was empty and that the right pads were worn beyond limits, which reduced braking capacity on that side.
The ATSB also identified that the operator’s procedures allowed the use of self-reported passenger weights without additional allowances, and that the electronic weight and balance system had been configured with higher maximum weights applicable to a modification not fitted to this aircraft. In combination with calculation errors on the day, this resulted in the aircraft being operated above the maximum permitted ramp and take‑off weights.
What has been done as result
Marthakal Yolngu Airline advised that all references to the use of self-reported passenger weights for the purposes of weight and balance calculations will be removed in the next amendment of the operations manual.
The operator also advised that the electronic weight and balance system will be amended to reflect the correct maximum weights for VH-NXA prior to its return to service.
The safety manager briefed company personnel about the proposed changes and advised existing pilots that actual weights for passengers must be used for all flights.
The ATSB will monitor these safety actions until the proposed changes to the operations manual and weight and balance system have been formally implemented.
D & T Aircraft Engineering advised that, following the occurrence, a debrief with maintenance personnel highlighted the importance of increased vigilance during inspections conducted after maintenance tasks, and that the organisation also identified opportunities to improve internal processes following similar occurrences.
Safety message
Factors such as additional airspeed over the threshold can result in a landing beyond the intended touchdown point, increasing the risk of a runway overrun excursion. While adherence to a pre-determined stabilised approach criteria can effectively mitigate such risks, pilots should always exercise vigilance and ensure the aircraft is flown within the assumed conditions used to calculate landing performance.
Pilots are therefore encouraged to continue to actively monitor the flight path using cockpit instrumentation and external visual cues until a safe landing is assured. This should include identifying and nominating an appropriate touchdown point on the runway to ensure a go‑around can be executed if a touchdown beyond this point is likely to occur.
Additionally, maintenance organisations should ensure that effective systems are in place to disseminate important information to all maintenance personnel, so that emerging defects are identified and rectified before they affect flight operations.
The occurrence
Pre-flight preparation
On the morning of 29 May 2025, a Cessna C310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was being prepared for a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory.
When the pilot arrived at the airport, they observed a licensed aircraft maintenance engineer (LAME) and their apprentice performing maintenance on the aircraft braking system. During this period the pilot prepared their flight plan and when they returned to the aircraft, the LAME and the apprentice had completed the maintenance.
The pilot, who was operating their first flight as pilot in command of a multi-engine aircraft, commenced their pre-flight checks. Due to the recent work on the braking system, they taxied to an aircraft bay to conduct a static engine run-up.[1]
With both engines at 1,700 RPM, they recalled that the aircraft moved forward slightly with the brakes applied. They physically increased their braking pressure, after which, the aircraft remained stationary. After completing the run-ups, the pilot taxied back to the terminal where the passengers were waiting. At this time, they also discussed the brakes with another C310 pilot who advised them that quite a lot of brake pressure was required during run-ups.
The pilot reported feeling rushed, and elected to use the self-reported passenger and baggage weights prior to boarding for weight and balance calculations, which were recorded on the manifest. These weights were entered into an electronic weight and balance system, which indicated that the planned load complied with the aircraft weight and balance limitations. The passengers were then taken to the aircraft where the pilot conducted a safety briefing before they boarded.
Occurrence flight
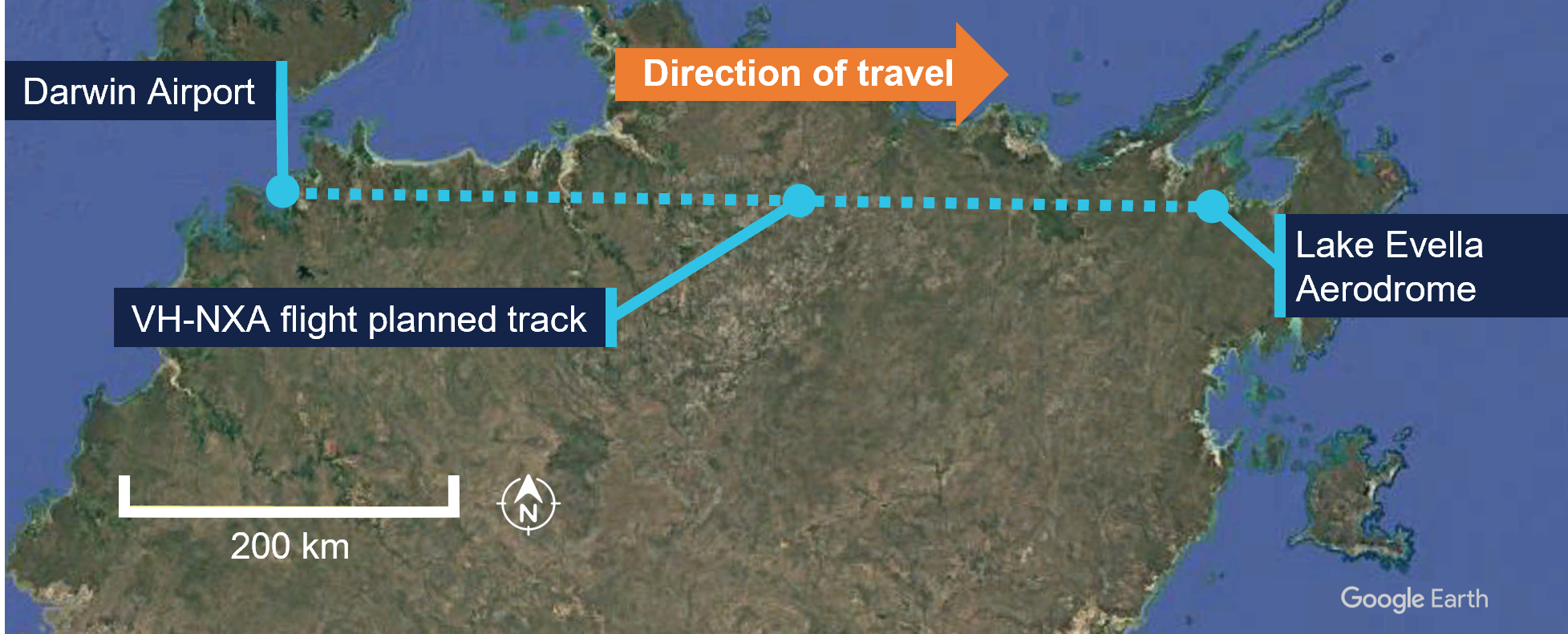
At 0857 local time, VH-NXA departed from Darwin Airport with the pilot and 4 passengers on board for Lake Evella (Figure 1). When approaching the Lake Evella Aerodrome, the pilot reported becoming visual with runway 08 at about 15 NM (28 km) and tracked for a straight in approach. At 1051, the aircraft was established on final approach for runway 08.
Figure 1: VH-NXA flight planned track
Source: Google Earth, annotated by the ATSB
The pilot recalled that there was a south-easterly wind between 8–10 kt for the approach, with a right crosswind component. Another pilot, who arrived at Lake Evella about 3 minutes after VH-NXA, recalled the wind was from an easterly direction at about 10 kt.
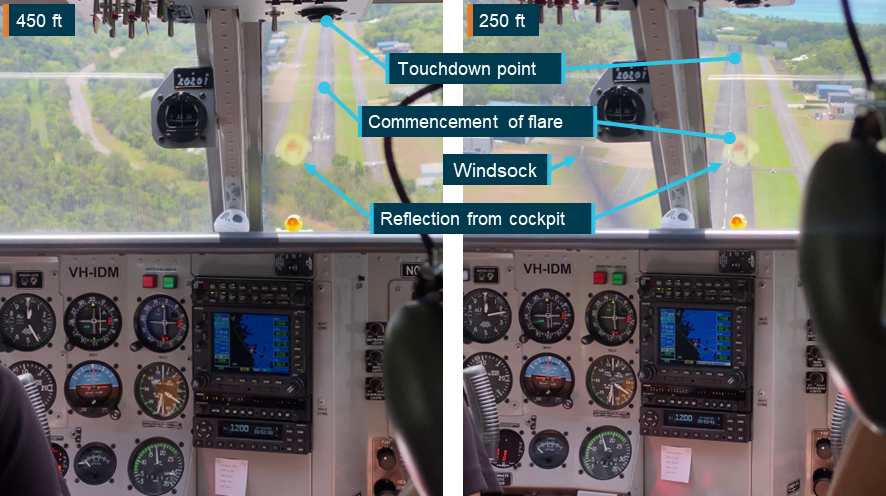
The pilot of VH-NXA recalled that the approach ‘seemed stable,’ (see Stabilised approach criteria) and stated that they generally used the runway threshold as their aiming point. They estimated crossing the threshold at their calculated approach speed of 90 kt or ‘just above.’
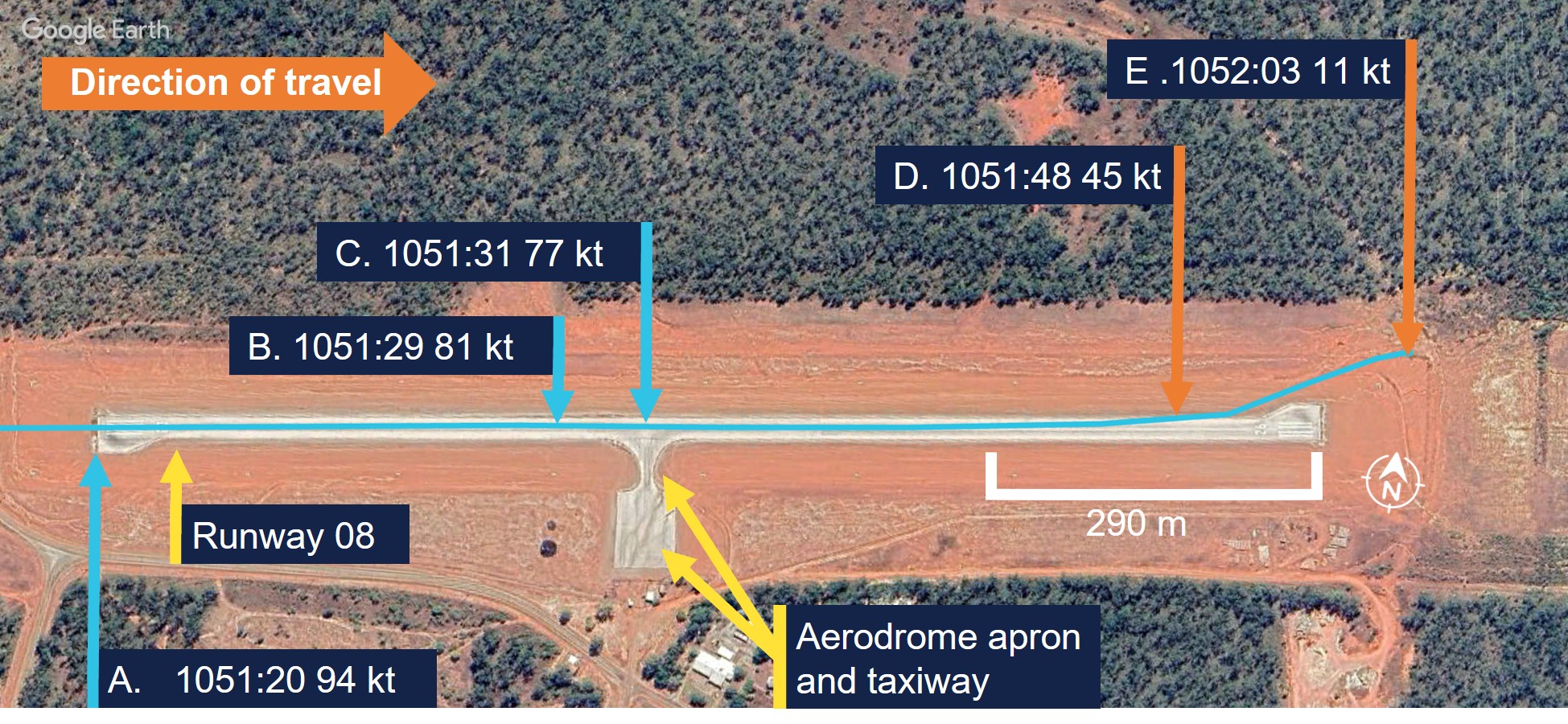
A navigational application (OzRunways) [2] was installed on a tablet computer and an Android phone on board the aircraft and broadcast flight data (see Recorded information). The OzRunways data taken from the Android phone, overlaid on a Google Earth image (Figure 2), showed the aircraft crossing the runway threshold at a height of 55 ft with a ground speed of 94 kt (Figure 2, A). The runway in Lake Evella was not equipped with visual slope guidance and the pilot relied on their visual assessment of ‘how the runway should look at certain height.’
Figure 2: VH-NXA ground speed at key points in landing sequence
Source: Google Earth, annotated by the ATSB
The pilot and the passenger seated directly behind them estimated that the aircraft touched down approximately 200 m past the threshold. ATSB analysis of recorded data indicated touchdown at 1051:29 (the corrected altitude of the aircraft matched the terrain elevation of runway 08), which was 402 m past the threshold (Figure 2, B). The passenger seated in the front row beside the pilot recalled passing the taxiway immediately after touchdown (Figure 2, C).
Another pilot on the ground standing at the apron who witnessed the landing reported observing VH-NXA a few feet above the ground in the ‘flaring attitude’ about a third of the distance along the runway. They also recalled that the aircraft was travelling faster than what they thought was normal and landed just beyond the taxiway (Figure 2, C).
The pilot reported that after touchdown, they applied the brakes passing the apron area about halfway along the runway (Figure 2, C). At that point, they reported that the aircraft did not appear to be slowing as expected and the passenger in the last row recalled the aircraft passing the apron ‘very fast’.
The pilot recalled increasing their braking pressure and when they saw the end of the runway approaching, they shut both engines down by selecting the mixture controls to idle cut-off. The pilot then elected to steer the aircraft to the left of the runway centreline to increase the runway distance for the deceleration required.
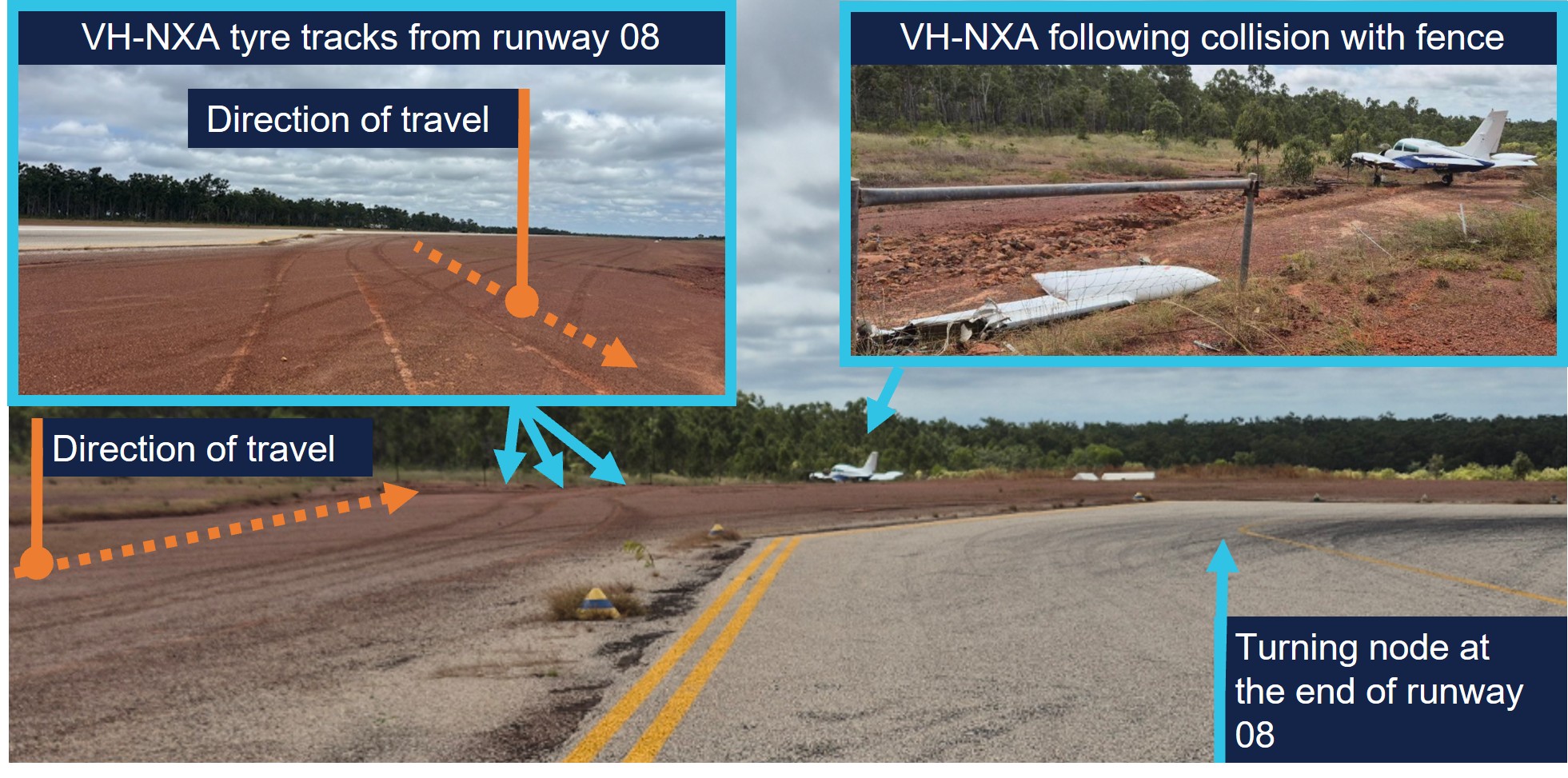
The aircraft departed the left side of the runway, 118 m from the runway end (Figure 2, D) (Figure 3, inset left), while the passenger seated beside the pilot verbally prompted the passengers to ‘brace.’ Recorded data indicated the aircraft was travelling at 45 kt at this point. The left wing subsequently collided with a fencepost (Figure 2, E) (Figure 3, inset right) located 193 m from the point the aircraft departed the runway.
Figure 3: VH-NXA ground roll following runway excursion
Source: Marthakal Yolngu Airline, annotated by the ATSB
Following the collision, the aircraft came to a stop and the pilot and passengers disembarked through the right cabin door. There were no injuries to the pilot or passengers, however the aircraft sustained substantial damage (see Post-accident inspection).
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) issued in 2021 and a class 1 aviation medical certificate. They also held a multi-engine aircraft class rating, which was issued in 2022 and renewed with a flight training organisation on 24 May 2025.
The pilot had accumulated 1,066 hours of total aeronautical experience, which included 71 hours of multi-engine time accumulated under the supervision of an instructor.
They reported they had flown about 70 hours in the last 90 days, including a total of 11.7 hours on the Cessna C310R, which was conducted during the course of their training.
The pilot’s training was conducted by a flight training organisation (FTO) in Darwin, on behalf of Marthakal Yolngu Airline. FTO training records detailed that the pilot commenced line training for the C310R on 15 May 2025.
This line training took place over 9.8 flight hours, after which they were assessed as proficient by a flight examiner during a combined line check and operator proficiency check for the C310R on 24 May.
The pilot had not operated the C310R to Lake Evella Aerodrome during the course of their training and had not operated there in any aircraft type prior to the occurrence. They reported sleeping about 8 hours the night before the occurrence and had been awake for about 7 hours at the time of the occurrence and feeling ‘fully alert.’
Aircraft information
The Cessna 310R is a twin-engine, low-wing (with a wingspan of 11.3 m), 6-seat, unpressurised aircraft equipped with retractable landing gear and powered by 2 Continental IO-520 piston engines. VH-NXA was manufactured in the United States in 1978 and first registered in Australia in 1989. A maintenance organisation located in Darwin became the registration holder on 4 March 2020.
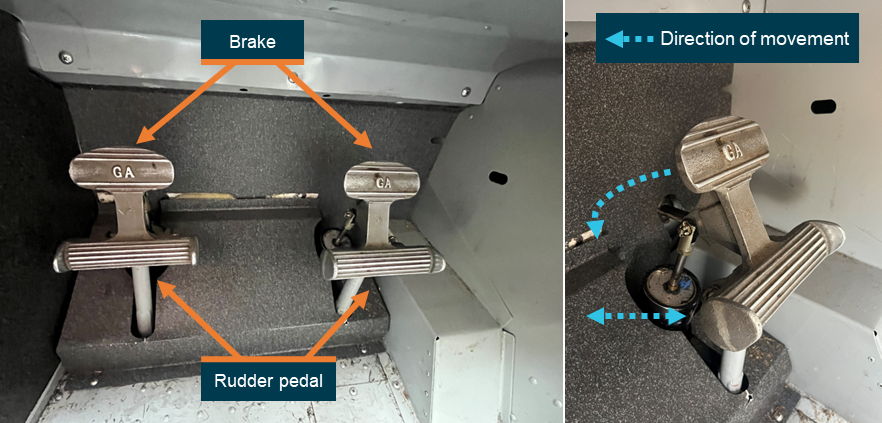
Braking system
Section 7 of the Cessna 310R Pilots operating handbook (POH) contained the following description of the braking system:
The airplane is provided with an independent hydraulically actuated brake system for each main wheel. A hydraulic master cylinder is attached to each pilot’s rudder pedal. Hydraulic lines and hoses are routed from each master cylinder to the wheel cylinder on each brake assembly. No manual adjustment is necessary on these brakes. The brakes can be operated from either pilot’s or co-pilot’s pedals.
Meteorological information
The graphical area forecast and the applicable grid point wind and temperature forecast for the flight indicated:
prevailing visibility greater than 10 km
scattered cloud[3] with bases 1,500 ft above mean sea level (AMSL)
isolated areas of smoke reducing visibility to 5,000 m
isolated rain showers and thunderstorms reducing visibility to 2,000 m and 1,000 m respectively, and broken cloud with bases 800 ft above AMSL
moderate turbulence below 4,000 ft in thermals and dust/sand whirls (dust devils)
wind 130° at 21 kt and temperature of 24°C at 1,000 ft above AMSL.
Aerodrome information
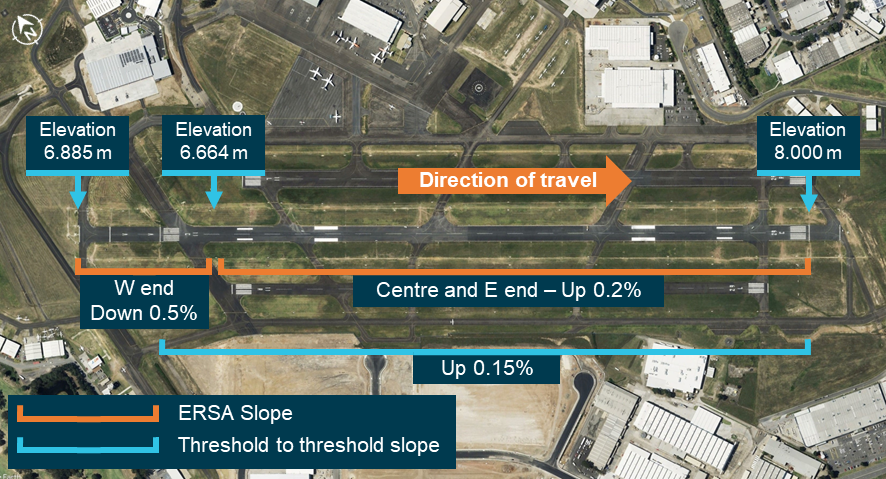
Lake Evella Aerodrome (YLEV) is situated at an elevation of 278 ft AMSL and comprised of a single sealed runway, 08/26, measuring 1,065 m in length and 18 m in width and was sloped 0.5% up toward the east. The aerodrome is uncontrolled and operated on a dedicated CTAF,[4] and is subject to animal hazards.
Maintenance information
Aircraft maintenance manual
The Cessna 310R Aircraft maintenance manual (AMM) contained a troubleshooting guide to assist maintenance personnel to rectify defects relating to systems fitted to the aircraft. The section that covered the wheels and brakes included the following information (Table 1):
Check for brake linings worn beyond limits. Replace linings as required
Air in brake system
Check for air trapped in brake system. Bleed the brakes
Brakes spongy
Air in brake system
Check for air trapped in brake system. Bleed the brakes
The AMM also described the brake wear limits on the C310R, which included:
Check back plate and pressure plate linings for wear. If worn to a thickness of 0.125 to 0.100 inch, the linings should be replaced.
Scheduled maintenance
The aircraft was flown to Darwin on 15 February 2025, where the authorising licensed aircraft maintenance engineer (LAME) planned to conduct a corrosion inspection at their maintenance facility. The LAME also performed a ‘check 1’ inspection, which they stated was the equivalent of a 100-hour inspection.
During the inspections, additional maintenance was conducted due to leaking brake callipers, which was common to the brakes on the C310 according to the LAME. This involved the removal, bleeding, resealing and refitting of both callipers and was performed by an apprentice. It was also the LAME’s expectation that the brake pads would be replaced during this maintenance task because this was routine practice, although not in the procedure.
As part of the 100-hour inspection, the LAME performed an engine run-up and observed the aircraft did not hold under brakes at this time. Believing that they had been replaced, they believed that the new brake pads needed to be bedded or burnt in. The AMM stated ‘brake burn in is required to minimize glazing of the friction surfaces’ when new brakes are installed. They subsequently completed the engine run up on one engine at a time, which allowed the aircraft to remain stationary.
Following the completion of the inspections and associated maintenance tasks, including the additional work carried out on the brakes, the LAME certified the aircraft maintenance logbook on 26 May 2025.
The authorising LAME later stated that new brake pads should have been installed before the callipers were refitted to the landing gear, however they did not verify that this had occurred. They reported that the brake pads were last changed on 15 December 2023 and had 494 landings prior to the occurrence.
Pre-departure maintenance
The aircraft underwent a post‑maintenance verification flight the day prior to the accident flight, with a flight instructor and the occurrence pilot as an observer. After the flight, the instructor advised the LAME by text message that the brakes felt ‘spongy.’
On the morning of 29 May, prior to the accident flight, the LAME checked the aircraft brakes, reporting that they were acceptable, even though the brake pedal travel felt more than usual. The decision was made to bleed the brakes to remove any air or water in the brake lines and top up the brake fluid. With assistance from an apprentice during this process, the LAME reported that hydraulic fluid spilled onto the right tyre and was subsequently wiped down. The aircraft was then released back to service.
Post-accident inspection
Following the occurrence, the LAME inspected the aircraft at Lake Evella Aerodrome on 18 June 2025 and documented the aircraft damage. The aircraft had sustained significant damage to the left wing (Figure 4), which separated from the fuselage outboard of the left engine nacelle. The pitot tube, right tip tank, propeller and nose gear door were also damaged following the runway excursion.
Figure 4: VH-NXA damaged left wing
Source: Aircraft maintainer, annotated by the ATSB
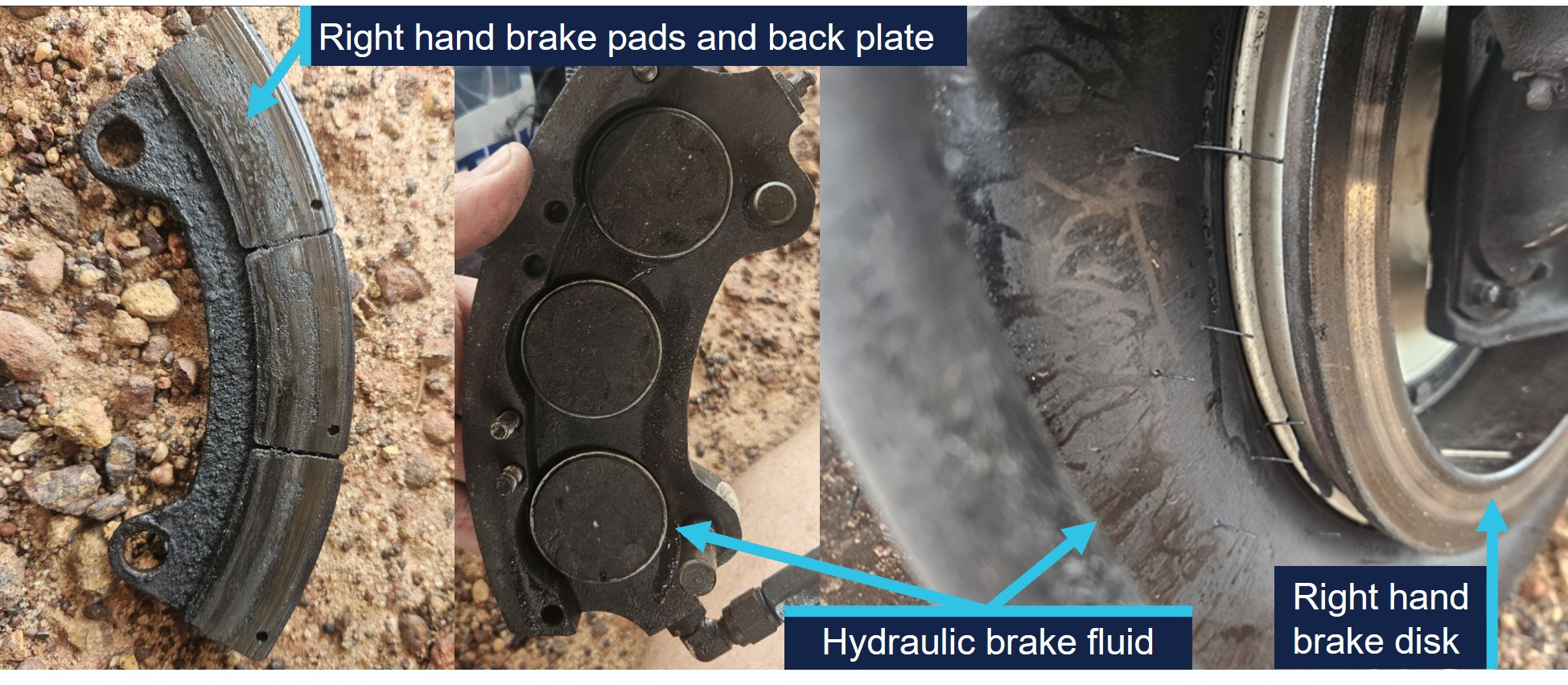
The LAME found that the right brake reservoir was empty, with evidence of hydraulic fluid leakage on the right tyre, however stated that the right brake disc was serviceable.
They identified that the right brake pads were ‘heavily worn.’ Images supplied by the LAME also indicated the presence of hydraulic brake fluid, originating from the brake piston adjacent to the brake line (Figure 5). They also indicated that the hydraulic fluid on the tyre may have been from fluid spilling when the brakes were topped up on the morning of the occurrence flight.
Figure 5: VH-NXA right hand brake components and hydraulic brake fluid
Source: Aircraft maintainer, annotated by the ATSB
No defects were identified on the left brake system and the right brake calliper was removed and tested in Darwin by the LAME. The right brake calliper was bolted onto a brake disc with sufficient pressure applied to prevent calliper movement. After 13 days, sufficient hydraulic fluid had leaked, which allowed the calliper to be moved in relation to the brake disc. The LAME subsequently disassembled the right brake calliper and identified a ‘very small’ hydraulic fluid leak, which they did not consider was the cause of the fluid loss during the occurrence.
Operational information
Weight and balance
The operator’s standard operating procedures(SOP) stated that during the conduct of air transport operations, prior to each sector, the pilot in command must complete an aircraft load and trim sheet.
An operator‑approved electronic load sheet was available to pilots for the purpose of completing weight and balance calculations in accordance with the POH weight and balance limitations.
The operator’s Cessna 310R Flight crew operating manual (FCOM) included the following statement regarding the possible modification of company operated aircraft:
The Company operates C310R aircraft in several possible modification states, which may affect limiting weight.
The only modification listed in the FCOM that affected the weight limitations for VH-NXA was the fitment of a vortex generator (VG)[6] kit. The FCOM also contained information relating to the fitment of the VG kit including increased weight limitations, changes to various airspeeds and stated:
If less than 84 vortex generators are in place or undamaged, the aircraft must be operated in accordance with the original AFM performance data (ie nil VGs).
Electronic weight and balance system
The electronic weight and balance system was developed by a third party to calculate the weight and balance for each flight. In the system, each aircraft was configured with a weight and moment arm[7] when empty.
The pilot would enter the pilot and passengers’ weights, their seating positions and fuel to calculate both the weight and centre of gravity of the aircraft at take-off and landing. The system was designed to alert the user if any weight and balance limitations were exceeded.
For VH-NXA, the electronic weight and balance system incorporated an increase in weight in accordance with a supplemental type certificate number for a C310R VG modification. However, the maintenance organisation that owned and maintained the aircraft stated that VH-NXA had not been fitted with the VG modification, and they were not aware of any modifications that increased the standard maximum permitted weights as prescribed in the POH.
As a result, the weight and balance system contained the following increases to the standard POH weight limitations which were not applicable to the aircraft (Table 2):
Table 2: Cessna 310R maximum weights
POH limitation
Standard weight (kg) applicable for VH-NXA
C310R with VG kit (kg) as listed for VH-NXA
Maximum zero fuel weight
2,222
2,386
Maximum ramp weight
2,510
2,586
Maximum take-off weight
2,494
2,563
Maximum landing weight
2,449
2,449
Passenger-declared weights
The operator’s SOP stated that for the purposes of calculating the aircraft’s weight and balance, ‘passenger weights must be actual, or self-reported.’ Following the occurrence, a passenger reported that their body and baggage weights were requested without the use of a calibrated scale. The pilot did not indicate that any adjustments of additional amounts were applied to the passenger reported weights.
The CASA multi-part AC 121-05, AC 133-04 and AC 135-08 – Passenger crew and baggage weights, described acceptable weight calculation methods that could be defined in operating procedures. The circular stated that:
The use of actual weights is the most accurate method of maximising payload capacity. Appropriately calibrated weighing scales should be used. Actual weighing is more commonly used by Part 133 [helicopter passenger transport] and 135 [smaller aeroplane passenger transport] operators. This is, in part, due to the smaller number of passengers being carried, which makes this option less disruptive than it is for Part 121 [larger aeroplane passenger operations] operators.
Operators should have procedures to identify when passenger-declared weights are not appropriate, such as when operating close to limitations. Under these circumstances, the use of actual weights may be required to ensure limitations are not exceeded.
Passenger-declared weights have inherent inaccuracies as passengers may not know their actual weight, especially when fully dressed. An adjustment allowance should be added to any passenger-declared weight, as a factor or a fixed additional amount.
Weight and balance calculations
Following a review of documentation provided by the operator and pilot, the ATSB identified several discrepancies contained in the operational documentation from the day of the occurrence.
The passenger and baggage weights recorded in the manifest by the pilot indicated a combined weight of 387 kg. However, the corresponding load sheet indicated a combined passenger and baggage weight of 337 kg (excluding the pilot).
Additionally, the fuel plan prepared by the pilot indicated a total fuel figure of 441 kg. By comparison, the fuel figure on the load sheet was recorded as 432 kg.
Due to the identification of the combined discrepancy of 59 kg, the ATSB recalculated the aircraft’s weight and balance for the flight. This identified the following updated weights and exceedances (Table 3) prescribed in the POH for aircraft not fitted with a VG kit.
Table 3: VH-NXA calculated weights and exceedances
Item
POH weight limitation (kg)
Pilot-calculated weight (kg)
ATSB-calculated weight (kg)
ATSB-calculated exceedance (kg)
Zero fuel weight
2,222
2,087
2,137
Nil
Ramp weight
2,510
2,519
2,578
68
Take-off weight
2,494
2,510
2,569
75
Landing weight
2,449
2,339
2,367 [1]
Nil
[1] The re-calculated landing weight was based on pilot reported fuel remaining added to the ATSB calculated zero fuel weight.
Landing performance calculations
The operator’s SOPs stated that company aircraft are subject to the requirements of Civil Aviation Safety Regulations Part 135 Manual of Standards (MOS) with respect to take-off and landing performance requirements. Chapter 10 of the Part 135 MOS stipulated ‘that the aeroplane crosses the runway threshold at a height of 50 ft’ unless an approved short landing operation was being conducted. Additionally for landing, the FCOM stated that the reference landing approach speed (Vref)[8] should be achieved at 50 ft above the landing surface.
For aeroplanes, take-off and landing distance calculations to determine maximum take‑off weight or the maximum landing weight are achieved through a manual calculation using the limitations given in the POH for the specific aircraft type, taking into account:
environmental conditions
runway length.
The FCOM also required pilots to apply landing distance factoring of 1.20 for all calculations. The pilot stated they had calculated their landing performance based on the aircraft’s maximum landing weight and calculated a factored landing distance of 680 m on the flight plan with a Vref of 90 kt for their landing at Lake Evella.
Calculations using the ATSB recalculated landing weight and the estimated ambient conditions at the time of the occurrence determined that the required landing distance (with the 1.20 factoring) with a 50ft threshold crossing height was 659 m. This figure included a landing ground roll distance of 195 m and a corresponding Vref of 91 kt.
Stabilised approach criteria
The SOPs stated that, ‘unless the aircraft meets stabilised approach criteria at the specified altitude, a missed approach must be executed.’
A stabilised approach was described in the SOPs as an approach to land that met a number of criteria by 300 ft above the runway during a visual approach. These included the following:
• the aircraft is on the correct flight path
• only small changes in heading & pitch are required to maintain the correct flight path
• the aircraft speed is Vref to Vref +20 kt
• sink rate is not greater than 1,000 fpm or pre-briefed limits.
Recorded information
The pilot used a flight planning application (OzRunways) on an iPad and an Android phone for en route flight planning and navigation. The flight planning software provider was an approved source of electronic aeronautical charts, however the application could not be used as a primary means of GPS-based navigation as the iPad and Android phone GPS did not meet certification for aviation use. The pilot reported that the iPad was placed on the floor for the approach while the Android phone was in their chest pocket. By examining the combination of groundspeed and derived deceleration data, in addition to the best direct line of sight to satellites, it was assessed that the Android data had the highest positional accuracy.
The recorded data had limitations due to an altitude resolution of 100 ft, while filtering and adjustments were also applied to smooth the data and are known to affect the accuracy of small sections. Additionally, the altitude data of VH-NXA was corrected to match the terrain elevation during the landing ground roll (Figure 6).
Based upon the operator’s stabilised approach criteria, the decision to continue the approach, or conduct a go-around, became applicable by the time the aircraft reached 300 ft above the runway.
The following recorded parameters were observed from below 300 ft to the threshold:
the aircraft crossed the threshold of runway 08 at a height of 55 ft
aircraft speed remained within Vref to Vref +20 kt
sink rate (vertical speed) less than 1,000 fpm.
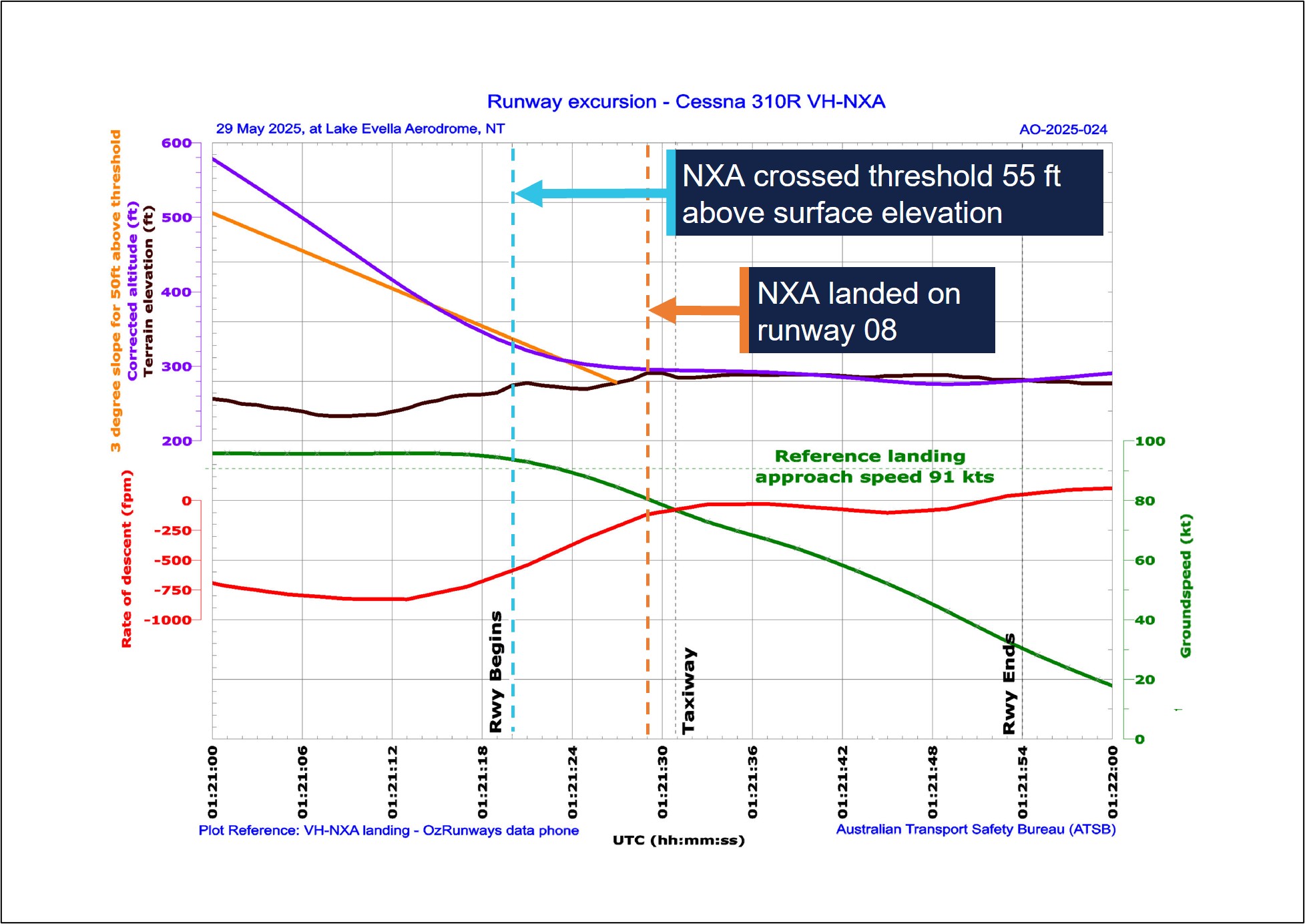
The recorded data indicated (purple line in Figure 6) that at the 300 ft (578 ft corrected altitude) stabilised approach gate, the aircraft was about 42 ft above the normal 3 degree slope (orange line), and remained above it until reaching 104 ft above the aerodrome elevation. During this period, the sink rate exceeded 800 fpm for 8 consecutive seconds between 1051:06 and 1051:14 local time.
At 1051:20, the aircraft crossed the threshold with a groundspeed of 94 kt. The pilot reported the wind component during the approach was a south-easterly wind between 8–10 kt, which would have resulted in a 3–4 kt headwind component. Accordingly, the aircraft’s airspeed was likely around 97–98 kt as it crossed the runway threshold, which was 6–7 kt above the Vref of 91 kt.
At 1051:29, the corrected altitude of the aircraft matched the terrain elevation, which indicated that the aircraft landed 402 m along the runway with a groundspeed of 81 kt. The pilot reported applying brakes as the aircraft passed the apron area, which occurred about 2 seconds after touchdown. Following a ground roll distance of about 540 m, the aircraft decelerated to a groundspeed of 45 kt when it vacated the left side of the runway at 1051:48.
Figure 6: VH-NXA approach and landing
All times are coordinated universal time (UTC). Local time was Central Standard Time (CST), which was UTC +9 hours and 30 minutes. The aerodrome elevation is 278 ft. Source: ATSB, data provided by OzRunways and Google Earth
On 2 November 2024, a GippsAero GA8-TC Airvan, was being used to conduct a scenic flight from Whitsunday Airport (Shute Harbour), Queensland. During the landing the aircraft departed the upwind end of the runway before entering marshy ground and coming to a stop in a ditch.
The ATSB investigation identified that the aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go-around, resulting in a landing beyond the planned touchdown point. The ATSB also identified that the operator’s weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with its procedures.
Safety analysis
On the morning of 29 May 2025, a Cessna 310R, registered VH-NXA, was being operated by Marthakal Yolngu Airline on a non-scheduled air transport flight from Darwin to Lake Evella, Northern Territory, with a pilot and 4 passengers on board.
During a straight-in visual approach, without visual slope guidance to runway 08 at Lake Evella, the pilot assessed that the approach was stable and continued with the landing. After the aircraft crossed the runway threshold, it floated for a prolonged period and subsequently landed before reaching a taxiway located about halfway along the runway.
When the pilot applied braking passing the airport’s apron area, the aircraft did not decelerate as expected. The aircraft subsequently overran the runway and collided with a fence. The pilot and passengers were uninjured, however, the aircraft sustained substantial damage.
This analysis examines how the condition of the aircraft braking system, and the conduct of the approach and landing, contributed to the runway excursion. It also explores the operator’s self-reported passenger weight procedures and electronic weight and balance system, and how the latter, in combination with incorrect pre-flight weight calculations, led to the aircraft being operated above the weight limits specified in the pilot’s operating handbook.
Pre-flight maintenance
Maintenance which was completed on the aircraft 3 days before the occurrence involved numerous concurrent tasks. These were conducted by a licensed aircraft maintenance engineer (LAME) with the assistance of an apprentice. One of the tasks involved the apprentice conducting maintenance on the braking system due to leaking brake callipers. It was the LAME’s expectation that the apprentice had replaced the main wheel brake pads during this maintenance task.
This expectation influenced their assessment that the aircraft rolled forward during post‑maintenance engine run-ups, due to the new brakes requiring ‘burning in.’ In this case, a physical verification of the brake pads was not conducted as a result.
On the morning of the occurrence, the LAME carried out corrective maintenance in response to the flight instructor text message report of ‘spongy brakes’ the day prior. While the occurrence pilot was aware of this report, they were not aware of the LAME’s experience with the aircraft rolling forward during the engine run-up.
When the pilot commenced the pre-flight engine run-up for the occurrence flight, the brakes failed to keep the aircraft stationary. The pilot physically increased the brake pressure and successfully kept the aircraft stationary, but did not advise maintenance personnel. The pilot’s limited experience on multi-engine aircraft led them to consider that this might be normal, which was reinforced during a brief discussion with another Cessna 310 pilot.
Gaps in communication and incorrect assumptions allowed a latent defect to persist into operation, contributing to the runway overrun in this occurrence.
Contributing factor
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
Approach
Lake Evella Aerodrome was not equipped with visual slope guidance, and as a result, the pilot relied on their assessment of visual cues of the runway itself to assess whether they were on the correct approach path while they typically used the runway threshold as their aiming point.
Recorded data from the pilot’s Android phone indicated that the aircraft was higher than the usual 3 degree ‘correct flight path’. The rate of descent exceeded 800 fpm for a period of 8 consecutive seconds until the aircraft descended below 140 ft relative to the runway. At the time, the pilot recalled the approach ‘seemed stable,’ while the operator’s stable approach criteria permitted rates of descent up to 1,000 fpm.
The aircraft subsequently crossed the threshold of runway 08 at a height of 55 ft with a ground speed of 94 kt. ATSB analysis concluded that the aircraft’s airspeed was likely 6–7 kt above the Vref for the recalculated landing weight 91 kt.
When the aircraft neared the point of touchdown, it was subjected to ground effect, which meant that excess airspeed at the point of flare would result in a considerable float distance due to the reduction in drag and lack of power-off deceleration in ground effect (Federal Aviation Administration, 2023).
Additionally, landing distances provided in the aircraft flight manual are based on the aircraft achieving Vref (plus wind and gust additives) at 50 ft above the runway surface. As a result, any additional airspeed will result in a later touchdown and reduce the remaining landing distance available (Federal Aviation Administration, 2023).
In this case, the additional airspeed crossing the threshold likely resulted in a prolonged float in ground effect. This resulted in the aircraft touching down 402 m beyond the runway threshold which was the pilot’s usual aiming point. Subsequently, the pilot applied braking about 2 seconds after the touchdown, at which point, there was about 585 m of remaining distance available to decelerate on the runway.
Contributing factor
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Excursion
The pilot first became aware of an issue with the braking system when they applied brake pressure during the landing roll with about 585 m of runway remaining. Witness accounts recalled the aircraft was travelling at high speed as it passed the taxiway and apron area without any significant deceleration. Additionally, recorded data showed the aircraft only slowed from 81 kt at touchdown to 45 kt when it vacated the left side of the runway following a ground roll distance of about 540 m.
At the aircraft’s landing weight, the ATSB calculated ground roll distance required was 195 m, which was sufficient to bring the aircraft to a stop within the remaining length of the runway had the brakes been functioning correctly. However, the loss of hydraulic brake fluid and the worn brake pads on the right-hand brake reduced the available braking capacity. As a result, the braking capacity was insufficient to arrest the aircraft’s forward momentum before the end of the runway. The pilot attempted to increase the available stopping distance by steering left and departing the runway, however it was insufficient, and the aircraft subsequently collided with the perimeter fence.
Contributing factor
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Passenger weights
The operator’s exposition permitted the use of self-reported passenger weights for weight and balance calculations, without requiring the application of additional allowances or validation. This practice introduced errors into the weight and balance data used for pre-flight planning.
Research has found that people tend to underestimate the weights of themselves and others. Further, people are less accurate at estimating the weight of others than they are of themselves.[9] To cater for the variation in weight, it is recommended that operators weigh passengers or apply adjustment factors to self-reported values (Civil Aviation Safety Authority, 2025). In contrast, the operator’s reliance on unadjusted self-reported passenger and carry-on baggage weights provided no systematic mitigation for potential inaccuracies, which increased the likelihood that the aircraft would be operated overweight or at centre of gravity limits outside the manufacturer’s requirements.
Other factor that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safety issue)
Electronic weight and balance
The operator used an electronic weight and balance system to calculate aircraft loading data for each aircraft in operation. In that electronic system, VH-NXA had been configured with the higher maximum weight limits applicable to aircraft fitted with a vortex generator (VG) modification. However, the aircraft did not have the specified modification installed. Consequently, the programmed maximum zero-fuel, ramp and take-off and weights in the system exceeded those authorised in the aircraft’s POH.
This configuration error meant the electronic weight and balance system allowed VH‑NXA to be loaded in excess of the certified weight limitations, while still indicating that the loading complied with those limitations. This created an ongoing risk that the aircraft could be operated above the approved maximum weights.
Other factor that increased risk
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safety issue)
Weight exceedances
During the occurrence flight, the aircraft was operated above the certified maximum ramp and take-off weights due to cumulative errors in the pilot’s weight and balance calculations. As a result of the configuration errors in the electronic weight and balance system, no alert to the overweight condition was made.
The pilot, who was conducting their first multi-engine command flight, reported feeling rushed during pre-flight preparation, which likely reduced the opportunity for careful verification of passenger weights, totals and data entry. Review of the weight and balance documentation from the occurrence identified multiple inaccuracies, indicating that the overweight condition arose from a breakdown in the usual cross-checking processes rather than a single isolated error.
Although the overweight condition did not result in the aircraft exceeding its maximum landing weight, operating above certified weight limits is known to increase take-off and landing distances and degrade braking performance. Additionally, excessive weight reduces the available safety margin if an in-flight emergency condition should arise (Federal Aviation Administration, 2016).
Other factor that increased risk
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion involving Cessna 310, VH-NXA, at Lake Evella Aerodrome, Northern Territory, on 29 May 2025.
Contributing factors
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Other factors that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safey issue)
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safey issue)
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations.
Safety issue description: Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by D & T Aircraft Engineering
D & T Aircraft Engineering advised that, following this occurrence, a debriefing was conducted with maintenance personnel to discuss key learnings. It was acknowledged that increased vigilance would be exercised in the future to ensure that aircraft components are carefully inspected and confirmed to be in a serviceable condition following the completion of maintenance tasks. Additionally, the organisation stated that it would prioritise accessing the aircraft at the earliest opportunity in the future to assist in identifying potential causes of component failure, particularly in cases where perishable evidence plays a critical role in determining the cause.
Glossary
AFM
Aircraft flight manual
AMM
Aircraft maintenance manual
AMSL
Above mean sea level
CASA
Civil Aviation Safety Authority
FCOM
Flight crew operating manual
FTO
Flight training organisation
LAME
Licensed aircraft maintenance engineer
MOS
Manual of Standards
POH
Pilots operating handbook
RPM
Revolutions per minute
SOP
Standard operating procedures
VG
Vortex generator
VMC
Visual meteorological conditions
VREF
Reference landing approach speed
Sources and submissions
Sources of information
The sources of information during the investigation included:
Ramos , E., Lopes, C., & Barros , H. (2009). Unawareness of weight and height – the effect on self-reported prevalence of overweight in a population-based study. The Journal of Nutrition, vol. 13, pp.310–314.
Reed, D., & Price , R. (1998). Estimates of the heights and weights of family members: accuracy of informant reports. International Journal of Obesity, vol. 22, pp.827–835.
Shapiro , J. R., & Anderson, D. A. (2003). The effects of restraint, gender, and body mass index on the accuracy of self-reported weight. International Journal of Eating Disorders, vol. 34, pp.177–180.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
the operator
maintenance organisation
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
pilot of the accident flight
the operator maintenance organisation
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Run-up: a high power run-up check is carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take off.
[2]OzRunways is an approved data provider for Australian pilots for flight planning and in-flight navigation.
[3]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered
[4]Common traffic advisory frequency (CTAF): A designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome or within a broadcast area.
[5]Brake linings: brake linings, often referred to as brake pads, are the friction material that, when pressed against the brake discs, slows and stops the aircraft. Over time and with use, these linings wear down and require replacement.
[6]A vortex generator installation typically offers the advantages of reduced stall speeds, reduced minimum single engine control speed (Vmc), improved take-off and landing performance and increased maximum take-off weight.
[7]Moment arm: the horizontal distance from a reference datum to the centre of gravity of an item.
[8]Reference Landing Approach Speed: The airspeed used on approach down to 50 ft above the runway when determining landing distances which is normally 1.3 times the stall speed.
[9]For example, see Ramos and others (2009), Reed and Price (1998), Sahyoun and others (2008) and Shapiro and Anderson (2003).
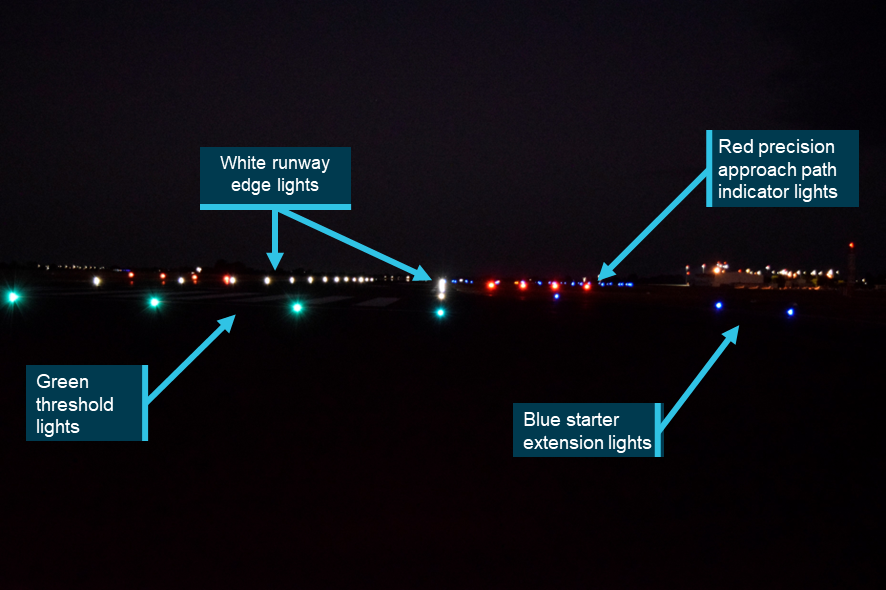
On 25 February 2025, a QantasLink DHC-8-315 aircraft, registered VH-TQM, was being operated on a scheduled passenger transport flight from Mildura to Melbourne Airport, Victoria. The flight crew commenced taxiing the aircraft prior to first light. The aircraft was backtracked on runway 09 and taxied past the threshold into the starter extension bypass pad to turn around and line up. The flight crew inadvertently lined up the aircraft with the right runway edge lights and commenced taking off from this position.
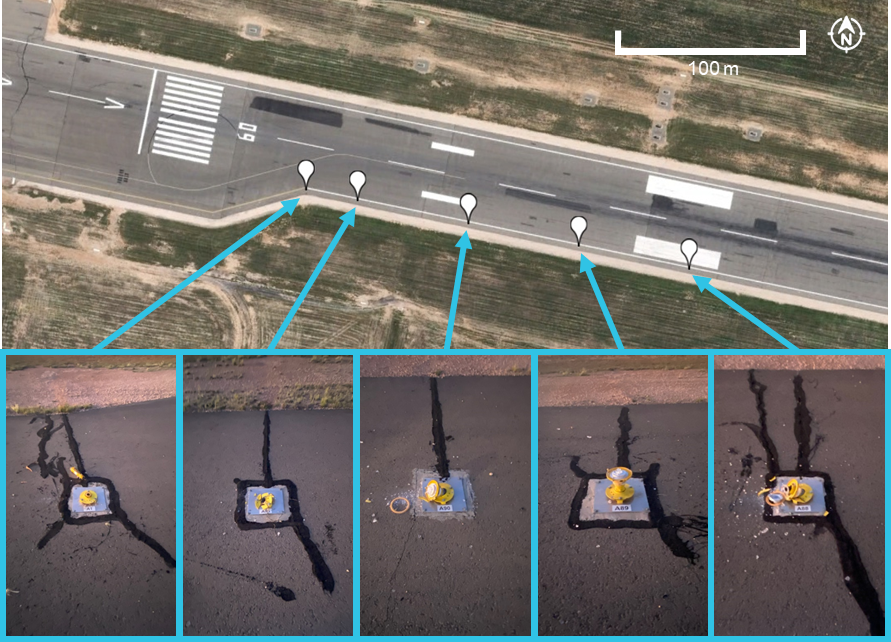
During the take-off roll, the nose landing gear contacted and damaged 5 runway edge lights. Although the flight crew heard some external noises, neither recognised this as contact with the runway edge lights. The captain, however, identified that the aircraft was not on the centreline and manoeuvred towards the centreline and continued the take-off. During the initial climb, the flight crew realised that the aircraft had contacted the runway edge lights.
The flight crew conducted a low pass at Melbourne to facilitate a visual inspection of the landing gear by air traffic control. This did not identify any issues and the aircraft landed without incident. An inspection of the aircraft found minor damage to the nose landing gear, fuselage and right propeller blade.
What the ATSB found
The ATSB found that the incident took place in dark ambient conditions and that the taxi guidance line markings were not followed for the turn to line up. Instead, the aircraft was turned tighter, which positioned it closer to the right edge of the runway. Also, the flight crew’s attention was focused on conducting checks during the turn and on completion of the turn. However, as the flight crew believed they were correctly aligned with the runway centreline, they commenced the take-off roll.
It was also established that, when conducting the low pass of the Melbourne air traffic control tower, the aircraft was not maintained at the briefed height of 200 ft above ground level and descended to 134 ft for a short period. It was noted that the flight crew did not seek advice on the low pass nor did the operator provide supporting procedures for this.
Further, during post‑incident drug and alcohol testing, the captain tested positive for a non-prescribed medication. However, impairment was not expected given the reported dosage and time elapsed since taken.
What has been done as a result
QantasLink advised that human factors and non-technical skills training on the threat awareness of factors that have contributed to misaligned take-offs was included for wider flight crew recurrent training. Supporting documentation for Mildura Airport was updated to include information on the runway 09 starter extension for increased awareness along with education material being distributed regarding flight crew briefings and identifying relevant threats.
A safety alert was issued to prohibit the conduct of checks during runway end turns. This was incorporated into the Flight Crew Operating Manual. QantasLink also introduced policy aligned with Qantas Group operators regarding the risks associated with air traffic control tower fly pasts.
Safety message
A number of factors known to influence misaligned take-off occurrences were identified in this investigation. Dark ambient conditions have been consistently identified in similar occurrences and can reduce the visual cues available. This may limit the ability of flight crew to identify their position when lining up.
Although the completion of checks are a necessary part of a flight, they may result in a diversion of attention towards the checks at the expense of another task such as lining up. Pilots must consider the timing for conducting checks in situations where monitoring their external environment is important.
The incident further highlighted that, in non-normal situations for which there is no documented procedure, pilots should consult all available sources including their operator for assistance. Lastly, pilots should exercise caution when taking any medications and should be discouraged from taking prescription medications without medical supervision. Many prescription (and non-prescription) medications are not safe for use while conducting aviation activities and are therefore not permitted for use.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Flight schedule
On 24–25 February 2025, a QantasLink DHC-8-315 (Dash 8) aircraft, registered VH‑TQM, was operated on scheduled passenger transport flights over the 2 days, which consisted of 5 sectors on the first day and 3 sectors the following morning.1 The crew consisted of 2 flight crew and 2 cabin crew.
On 24 February, the flight crew signed on at 1040 local time in Melbourne, Victoria, and completed 2 return flights to Devonport, Tasmania, and Wagga Wagga, New South Wales. For the final sector to Mildura, Victoria, the aircraft departed Melbourne at about 1922 and arrived at 2045. The crew signed off from duty at 2100 and arrived at their accommodation about 15 minutes later.
On 25 February, at about 0545, the crew departed their accommodation and signed on for duty at 0600 for a 0630 scheduled departure from Mildura to Melbourne. The captain was the pilot flying (PF) and the first officer (FO) was the pilot monitoring2 for this sector. There were 50 passengers on board.
Taxi to runway 09
The captain commenced taxiing the aircraft before first light at about 0631. Closed-circuit television (CCTV) footage showed the aircraft taxi light was on, illuminating a portion of the tarmac ahead of the aircraft. The captain reported that they had also selected the approach lights to ‘on’ to provide greater illumination of the runway surface during the taxi. CCTV footage also showed that the taxiway, runway and starter extension bypass pad3 lighting was active.
After entering the runway, the aircraft was backtracked along the centreline. CCTV footage showed that, when the aircraft approached the runway 09 threshold, the approach lights were selected on. The aircraft was taxied past the threshold and into the runway starter extension bypass pad to turn the aircraft around and line up. The captain reported that the starter extension was not required for performance, but their preference was to use the full runway length where possible. They also stated that the wider extension area would provide more room for the turn around.
The recorded flight data4 showed that the aircraft path followed the taxi guideline marking into the starter extension but was turned right, prior to the end, and away from the guideline, which led to the extended centreline. The captain explained that their initial intent was to use the complete starter extension. However, once established in the extension, they chose not to do so to avoid inadvertently exiting the pavement in the dark conditions. The FO reported that this was not communicated to them at the time nor were they aware that the aircraft had been turned earlier. The aircraft path during the turn remained to the right of the extended centreline, resulting in it being positioned close to the right edge of the runway (Figure 1).
During the turn, the flight crew conducted the ‘ready checks’ and the associated checklist, during which time they both reported being focused within the flight deck on the conduct of the checks. The captain also reported being distracted by either smoke or mist outside the left window. On completion of the turn, the captain stated they were drawn to the white right runway edge lights, believing them to be runway centreline lights. The captain also indicated that the flight director and heading bug confirmed that the aircraft was aligned with the runway direction. The FO reported that they observed the runway 09 threshold markings, which they equated as the aircraft being in the correct position to line up. They did not recall noticing any lights ahead of their position. Once lined up, both flight crew believed they were aligned on the centreline of runway 09.
Take-off on runway 09
The captain recalled that, when they commenced the take-off roll, they advanced the power levers as close to the required power setting as possible, then called ‘set power’. At this point, the FO checked the power setting and adjusted the levers to ensure the exact power required was set. The FO reported their attention was predominantly focused inside the flight deck from this time. The captain identified that the take-off roll was ‘rough’, explaining that this was not unusual for an early morning first flight of the day for that aircraft type.
The captain recalled that, about the time the FO called ‘70 kt’, the sounds and sensations became more intense and identified that the aircraft was on the runway edge (Figure 1). They then manoeuvred the aircraft to its correct position along the centreline.
The FO reported hearing ‘1 or 2 thuds’ at about the time that they called ‘70 kt’. The FO also explained becoming momentarily distracted with the storm light5 on their side of the flight deck, which had unexpectedly turned on. The FO continued their scan between airspeed and ahead of the aircraft and shortly after made the calls ‘V1’ and ‘rotate’.6
The FO stated that they had not become aware of the misaligned take-off until after the captain had already begun manoeuvring the aircraft toward the runway centreline.
The captain continued the take-off, recalling that the aircraft had operated normally, and that the abnormal sounds and sensations had ceased. Once airborne, the ‘after take-off’ procedures were completed, as required.
Figure 1: Flight tracking data for the take-off with the starter extension inset
The aircraft track (within the inset) at the end of the starter extension shows a sharply clipped turn, which is due to the fidelity of the data. Source: Google Earth, with aircraft flight data overlaid and annotated by the ATSB
During the initial climb, the flight crew realised that they may have contacted the runway edge lights. The FO contacted the Mildura Airport aerodrome reporting officer and advised them of this. They requested the area be inspected and for them to report back on any debris located. The flight crew were subsequently advised that there was damage to 5 lights on the right edge of runway 09 (Figure 2). No aircraft debris was identified.
Figure 2: Damaged runway edge lights (inset) on runway 09
Source: Google Earth and Mildura Airport, annotated by the ATSB
After take-off inspections
The flight crew reported that following discussion about what had occurred, they considered the possibility that the landing gear had not been damaged as the remainder of the take-off roll occurred normally and the landing gear retracted without fault. They consulted the Quick Reference Handbook, however, there was no procedure to assist them with assessing the landing gear status. They then discussed and assessed the potential risks for landing with potential damage to the aircraft, and that a visual inspection of the landing gear would be required.
The captain explained that after the landing gear was extended, the main gear would become visible from the passenger cabin. The captain had briefed a cabin crew member that the landing gear would be extended earlier than normal for them to inspect. The captain asked them to check for any signs of fluid or tyre damage and whether the gear had deployed correctly. The cabin crew were to use the cabin ready button to signal if the landing gear appeared okay, otherwise they were to call the captain if they had concerns. Although the cabin crew were able to inspect the main landing gear, they could not view the nose landing gear. QantasLink advised that, during this time there was no contact for assistance between the flight crew and its operations centre.
The FO contacted Melbourne Centre air traffic control (ATC) and requested to conduct a low pass on their arrival at Melbourne Airport to facilitate a visual inspection of the landing gear. ATC was requested to focus their inspection on the nose landing gear. On advice from ATC, the flight crew briefed to complete the pass at approximately 200 ft above ground level (AGL), which would place the aircraft at an equivalent level to the controller who was in the control tower. The captain set the radar altimeter to 150 ft AGL to assist them in maintaining the aircraft at 200 ft AGL. As the landing gear and flaps would be extended, the captain planned to fly the aircraft at 120–130 kt. During the low pass, the captain reported that the height was adjusted to enable ATC to inspect the landing gear and that they received a minimums audio alert, signifying that the aircraft had descended below 150 ft AGL. The flight data identified the aircraft had descended at its lowest to a height of 134 ft AGL at which point the speed was 122 kt.
The inspection of the main landing gear was completed by a cabin crew member and they pushed the cabin ready button to advise the flight crew that the gear appeared satisfactory. Similarly, ATC did not observe any anomalies of the landing gear, advising the flight crew that the gear appeared correctly aligned and the tyres appeared in satisfactory condition. Following the low pass, the landing gear was raised and a missed approach conducted. The flight crew completed another approach, and the aircraft was landed without further incident.
Context
Flight crew information
Qualifications and experience
The captain held an Air Transport Pilot Licence (Aeroplane) and a valid class 1 aviation medical certificate. They had a total of 19,000 hours flying experience of which 935 hours were on the Dash 8. The captain had flown 107 hours on the Dash 8 in the previous 90 days.
The FO held a Commercial Pilot Licence (Aeroplane) and a valid class 1 aviation medical certificate. They had a total of 3,386 hours flying experience of which 773 hours were on the Dash 8. The FO had flown 45 hours on the Dash 8 in the previous 90 days.
The captain’s logbook identified they had operated at Mildura on numerous occasions in the previous few months. None of those flights were at night or before first light. The FO reported they last operated in similar light conditions at Mildura in September 2024.
Flight crew fatigue assessment
The captain reported going to bed at around 2230 after arriving in Mildura and waking at around 0500 the next morning. The noise from the hotel had interrupted their sleep and they recalled feeling ‘a little tired, less than fresh’, to, ‘moderately tired’7 at the time of the incident. In total, the captain reported obtaining around 6 hours sleep in the previous 24 hours and around 13 hours in the previous 48 hours.
The FO reported they went to sleep at around 2200, woke around 0500, and obtained a ‘good’ sleep. During interview, the FO described that they did not feel ‘match fit’, as they had not operated a 5-sector overnight duty for some time. They also reported feeling ‘okay, somewhat fresh’7 at the time of the incident. In total, the FO reported obtaining around 7 hours sleep in the previous 24 hours and around 14.5 hours in the previous 48 hours.
Aside from the usual workload associated with a take-off in the dark, neither of the flight crew reported any additional fatigue‑related factors on the incident flight.
The ATSB assessed the flight crew’s sleep opportunity, actual sleep obtained, and quality of sleep leading up to the flight as well as other fatigue‑related factors. A number of factors were present that could have increased the risk of fatigue, including a minimum rest period that was provided after a 5-sector day, and a slight reduction of sleep hours and poor-quality sleep in the previous 24 hours (for the captain). However, given the total hours of sleep obtained, time awake, time on duty, and time of the incident, it was unlikely the flight crew was experiencing a level of fatigue known to have an adverse effect on performance.
Drug and alcohol test results
In accordance with the QantasLink drug and alcohol management plan, the flight crew underwent a post-incident alcohol breath test and urine drug test. The FO returned a negative result, however, the captain’s drug test was non-negative. When the test was administered the captain declared that on consecutive days during the prior weekend they had taken a prescription medication that was not prescribed to them.
As there was a non-negative result, a second test of the sample was conducted at a laboratory. The presence of a testable substance above the cut-off level was confirmed.
QantasLink confirmed that the captain had returned a positive test result and that they had been stood down pending further assessment in accordance with company policy. Their medical review officer explained that, while the test result confirmed the presence of a testable substance above the cut-off level, the testing could not indicate when or what dosage was taken, nor could it indicate if there were any effects. They further explained that the medication was not currently permitted for use by pilots, it had an effective period of about 10 hours, and there would be no lingering effects expected unless there was an adverse reaction.
The captain reported to the ATSB they did not experience any effect from the medication at the time it was taken, nor did they experience any side effects. The FO and cabin crew members reported not noticing anything of concern regarding the captain nor their fitness for duty on that morning.
The ATSB engaged a forensic pharmacologist to review the test results. They stated that the concentration detected was consistent with the reported dosage self-administered by the captain on the weekend prior to the incident flight.
The pharmacologist noted numerous potential adverse effects of the medication that included: insomnia, loss of appetite, restlessness, euphoria, dizziness, dyskinesia (involuntary, repetitive and or jerky movements), tremor, dysphoria and with higher doses personality changes, irritability, hyperactivity and psychosis. It may produce peripheral effects such as increasing blood pressure and heart rate, palpitations, increased sweating and hyperthermia (increased temperature). The manufacturer’s consumer medication information stated that the medication should not be taken by persons with known cardiovascular disease. Additionally, the information advised consumers to not drive or operate machinery until they know how the medication affects them. The pharmacologist advised it was possible that the non-therapeutic use of the medication could result in some impairment and potentially, in some cardiovascularly susceptible persons, serious harm.
The pharmacologist further noted it was not possible to determine the likelihood of impairment from a urine sample. There were no studies that have established any relationship between urine concentration of the medication and psychomotor skills performance. For a person using a non-prescribed medication and who has not developed a tolerance, they indicated that impairment could not be excluded as being possible. However, based on the reported dosage, the specialist assessed that impairment would not have been expected on the day of the incident.
Aircraft information
General
The aircraft was a Bombardier DHC-8-315 (Dash 8) twin turbo-propeller regional aircraft capable of carrying 50 passengers and normally crewed by 2 flight crew and 2 cabin crew. It was manufactured in 2004 (serial number 604) and first registered in Australia in 2004.
Post‑incident maintenance
Following the incident, the operator conducted a towing assessment and general visual inspection of the aircraft, with particular attention paid to the landing gear, engines, propellers and fuselage. More detailed inspections of the nose and right main landing gear also took place. In addition, the aircraft manufacturer requested an unscheduled engine inspection.
Damage was identified to the nose landing gear, including both tyres, the cover for the weight on wheels sensor, and the trailing arm (Figure 3). The lower fuselage skin sustained minor impact damage (to 17 areas) and there was minor impact damage to the leading edge sheath of a right propeller blade. Both tyres, the weight on wheels sensor cover and the nose landing gear trailing arm were replaced. The remaining damage was assessed to be within the limits in accordance with manufacturer guidance.
Figure 3: Nose landing gear damage
From left to right: trailing arm impact damage, tread cuts and chunking, tyre impact damage, tyre sidewall slice. Source: QantasLink
Meteorological information
The captain described the weather as good with no fog or rain, although it was dark at the time as their departure was before first light. They specifically noted that the conditions were very dark and the area was poorly lit when conducting the turn to line up. Similarly, the FO reported that it was clear but very dark.
Data from the Bureau of Meteorology showed that the weather at Mildura was fine and clear of any cloud or significant phenomena that may have reduced visibility. The aerodrome weather information service recorded visibility in excess of 10 km at the time of the incident. The wind was generally from 170° (southerly) around 5 kt in the 10 minutes prior.
Information from Geoscience Australia identified that the incident was 14 minutes prior to first light and 40 minutes prior to sunrise.8 CCTV footage showed that the conditions were dark and the sun had not yet risen.
Airport information
Mildura Airport was a certified, non-controlled aerodrome and had 2 sealed runways, aligned 09/27 and 18/36. Runway 09/27 was 45 m wide and included a starter extension bypass pad at the western end of the runway. The starter extension bypass pad provided an additional surface of 117 m in length available for take-off from runway 09. It also provided an additional 23 m in width to turn an aircraft around.
The extension included taxi guideline markings with turn guidance to realign the aircraft with the centreline. It also had arrows aligned with the runway centreline and pointing to the runway threshold (Figure 4).
Figure 4: Runway 09 starter extension bypass pad
Source: Google Earth, annotated by the ATSB
The airport was equipped with airfield lighting, which included elevated white omni‑directional runway edge lights, inset green and red bi-directional runway threshold lights9 and elevated blue omni-directional taxiway edge lights on taxiways C and D only. The starter extension also had elevated blue edge lights. Runway 09/27 did not have, nor was it required to have, runway centreline lighting. Runway 09 also included precision approach path indicator10 lighting on both sides of the runway. CCTV footage obtained from Mildura Airport confirmed that the airfield lighting was active at the time of the incident. Although the foreground was not illuminated by an aircraft taxi light, Figure 5 is indicative of the view that was likely available to the flight crew after lining up on the right edge of runway 09.
Figure 5: View of the runway 09 lighting that was available to the flight crew when lined up with the right edge of the runway
Source: Mildura Airport, annotated by the ATSB
Operational information
Runway alignment
The Operations Manual OM 1 section 6.13.1.2 Navigation and monitoring of taxi routes stated that:
During taxi, the PM is to monitor aircraft location and provide proactive guidance to the PF on the taxi route.
Section 6.13.5.1 Takeoff also required that:
Prior to commencing the takeoff the Pilot in Command and the First Officer shall check the aircraft position is on the runway centreline and either at the correct runway threshold or other designated takeoff position (e.g. intersection).
Similarly, section 2.8 Takeoff of the Flight Crew Operating Manual 300 (FCOM) also indicated that the captain shall align the aircraft with the runway centreline prior to take‑off.
‘Ready’ and take-off procedures
The FCOM included a ‘Ready and Line Up’ procedure. Although it directed flight crew to conduct the associated checks at an appropriate time, the FCOM did not provide detail as to when was appropriate. However, the captain reported that they would not normally conduct the ready checks during a turn to line up, explaining that some runways they operated on were 30 m wide and the tight turn required was not compatible with the conduct of the ready checks. They further explained that runway 09 at Mildura was 45 m wide, with an even wider starter extension, and they felt comfortable that this would allow them the appropriate time and area to conduct the checks concurrent with the turn.
The FCOM also included a rejected take-off procedure in section 3.4.1. The procedure stated that the take-off should be rejected for a critical malfunction (for example, a master warning, engine failure or directional control issue) when between 70 kt and V1. At and after V1, the take-off must be continued. Neither the captain nor FO reported anything meeting the rejected take-off criteria. The captain did, however, discuss in hindsight that they possibly should have rejected the take-off.
Low flying
Section 4.4.4 Low Flying Operations in the Operations Manual OM 1 stated:
A company aircraft shall not be flown below 500’ AGL in day VMC [visual meteorological conditions],11 below LSALT [lowest safe altitude] at night or in IMC [instrument meteorological conditions],12 or below 1000’ over a built up area, unless it is:
• An emergency,
• To takeoff or land,
• Part of a published instrument approach,
• In accordance with ATC instructions, or
• Specifically authorised.
There was no guidance provided on conducting a low pass for the purposes of an external visual inspection of the aircraft.
Airport guidance
Qantaslink provided additional operational guidance for Mildura Airport, which included:
The standard position for RWY [runway] 09 take-off is on the threshold lines. An alternate start position is available which includes the runway starter extension.
However, guidance on how or when flight crew could use the starter extension for runway 09 was not included.
Misaligned take-offs
Previous research
When pilots taxi and take-off during daylight conditions, they normally have a wide range of visual cues by which they can navigate and verify their location. At night, however, the amount of visual information available is markedly reduced. Pilots rely more on the taxiway and runway lighting patterns presented to them and what can be seen in the field of the aircraft’s taxi and landing lights.
The ATSB research report Factors influencing misaligned take-off occurrences at night (AR-2009-033) was published in 2010 following the review of 24 misaligned take-offs that occurred at night in Australia and overseas. The report identified 8 common and recurring factors that contributed to misaligned take-offs at night, as presented below (Figure 6).
Figure 6: Factors contributing to misaligned take-off occurrences
Source: ATSB
Environmental factors were the predominant contributors, which included physical features such as the runway layout, line markings and lighting. Weather and visibility were also considerations. The report identified that confusing runway entry, lighting or taxiway layout/lighting were the most frequent factors and that additional areas of pavement around taxiway entry and runway threshold areas could provide erroneous cues for pilots at night.
Human factors were the next most common contributor, in particular, flight crew distraction, divided attention, workload and fatigue. Flight crew distraction upon entering, or just prior to entering the runway was frequently identified as a factor. The report described distraction as the drawing away or diverting attention, or an action that divided attention. This was reported to have occurred for numerous reasons including the performance of checklists, setting power or checking instruments.
The report explained that:
…distraction comes about when multiple stimuli or tasks make simultaneous demands for attention.Generally, distraction results from one of these competing stimuli or tasks interfering with or diverting attention from the original task or focus of an individual.
Part of the problem with distraction is the resulting divided attention of the flight crew, with a focus on tasks inside the cockpit being at the expense of accurately assessing the external environment. This often occurs during taxi, when flight crew need to be ‘eyes inside’ the cockpit for significant periods of time. That is, instead of maintaining a visual look out from when they enter the runway, their attention is drawn inside for some reason such as checking instruments, confirming aircraft configuration or performing checklist items. While multi-crew operations partially mitigate this risk by articulating and dividing aircraft handling and monitoring roles between the pilots, there are still times when both crew members may not be processing the external environmental cues accurately. This divided attention is often a necessary part of lining up or beginning the take-off roll, but occasionally the attention of the flight crew will be diverted for longer than normal in response to an unusual event or problem. It is often attention to this non-standard action or item that contributes to line-up error events.
Operational factors were also identified such as air traffic control clearances and intersection departures were examples and in some cases they either contributed to, precipitated and/or exacerbated the environmental and human factors that were present.
Related occurrences
A review of the ATSB occurrence database identified a previous QantasLink misaligned take-off, which was investigated by the ATSB in 2009. ATSB investigation AO-2023-027 detailed 3 misaligned take-offs at Perth Airport in 2023 and 2024, and a number of other related occurrences were discussed in that report.
On 11 February 2009, at about 1922 local time, a Bombardier DHC-8-315 aircraft, commenced the take-off roll on runway 01 at Townsville Airport for Cairns, Queensland. During the take-off, the captain realised that the aircraft was aligned with the left runway edge. The aircraft was manoeuvred to the centre of the runway and the take-off rejected. It was later determined that the aircraft’s left mainwheel had damaged a runway edge light. There were no injuries to the 34 passengers or 5 crew members and no damage to the aircraft.
The investigation found a number of factors that may have led to the captain not aligning the aircraft on the runway centreline for the take-off. Those factors included misinterpreting the normal runway cues, time pressure to depart, the weather conditions at Townsville Airport and the associated delays during the aircraft’s arrival, landing and departure.
Between June 2023 and April 2024, 3 misaligned take-offs occurred at Perth Airport, Western Australia. Each occurred before first light and in all 3 incidents, when entering runway 06 from taxiway V, the pilots taxied past the turn onto the centreline and lined the aircraft up along the runway edge lighting on the far side of the runway to where they entered. The investigation found that, in each incident, the pilots believed they had correctly aligned the aircraft with the runway centreline, prior to taking off. Several factors known to increase the risk of a misaligned take-off in the dark were identified from the investigation:
In terms of the runway environment, there was an unlit and unmarked extended pavement area on each side of runway 06, which made the runway appear wider.
In relation to the available airport lighting, the lead-on lights from the taxiway continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway’s centreline.
Recessed edge lights at the start of runway 06 could be mistaken for centreline lighting.
There was limited ambient airport lighting around taxiway V and runway 06 to enhance visibility.
The taxi lighting on one of the aircraft was reported by the pilots as being of limited benefit.
The required runway markings were reported by 2 of the incident pilots to be difficult to see at night.
In one of the incidents, the flight crew’s attention was diverted to completing pre-take-off tasks and their take-off clearance while lining up on the runway. This divided their attention between the flight deck and the monitoring of the external environment.
Safety analysis
Diverted attention
The starter extension included a taxi guideline that curved around towards the extended centreline. The guideline was likely visible to the crew as the flight data showed that the aircraft was taxied along the line from the time it entered the starter extension bypass pad until the time it commenced the right turn to line up on runway 09. The captain reported that, although their intention was to use the full length of the extension, it was not required and due to the dark, ambient conditions, they did not want to continue that plan and risk exiting the pavement. As such, they turned the aircraft early.
The flight crew reported that the ready checks were conducted while turning the aircraft to line up for departure. The Flight Crew Operating Manual stated that ready checks could be conducted at a time appropriate for the anticipated take-off. However, the manual did not provide any guidance as to when an appropriate time was during this process. Therefore, the decision was at crew discretion and dependent on the circumstances at the time.
The FO and captain had predominantly focused their attention inside the flight deck while conducting the ready checks. The captain also reported becoming momentarily distracted looking out the side window. This was at a time when they would also be required to monitor the aircraft’s taxi path. The data showed that the aircraft was turned tightly to the right of the extended centreline and was no longer following the line markings for guidance.
Barshi and others (2009) discuss that it was easy for attention to become absorbed in one or more tasks, allowing another task to drop from awareness. Therefore, it can be concluded that, during the turn to line up, the flight crew's attention was diverted to completing the ready checks, likely reducing their monitoring of the aircraft position within the starter extension, and resulted in it being close to the edge of runway 09. This was consistent with the ATSB research report (2010), which discussed flight crews becoming focused on other tasks upon entering the runway or just prior to entering the runway, and that this was a frequently cited factor in misaligned take-off occurrences.
Misaligned take-off
Although not required for performance, using the starter extension allowed for additional take-off distance and a wider turn than was normally available at airports where the aircraft was mostly operated. However, as identified through ATSB research (2010) and related investigations, additional pavement on one or both sides of the runway has been known to provide erroneous visual cues for pilots. This potentially gives the impression that the additional pavement is part of the runway and that the runway is wider than it is.
Then, following completion of the ready checks and when the aircraft neared completion of the turn to line up, the captain reported being drawn to a row of white lights, believing them to be centreline lights, even though such lights were not fitted to runway 09. With reduced visual cues available due to the dark conditions, a distinct visual indicator such as the white runway edge lights was likely to have been an influence in their belief that it was the runway centreline. Such dark ambient conditions have been consistently cited in the research and similar occurrences. The FO reported looking up but also believed the aircraft was correctly lined up, having associated their observation of the runway threshold markings as being in the correct position to line up.
However, imagery of runway 09 in similar conditions to the incident flight did show that the runway threshold lights, edge lights and right side precision approach path indicator lights would have been visible to the crew from their line‑up position. Confirmation bias is the tendency for people to seek information and cues that confirm their tentatively held hypothesis or belief (Wickens et al, 2022). As the flight crew believed they were correctly aligned with the runway centreline, they commenced the take-off roll.
Low pass
The flight crew noted no indications of a landing gear malfunction or failure, and the gear was retracted without issue following the misaligned take-off. They also received advice from the Mildura Airport aerodrome reporting officer that no aircraft parts or debris were identified along the runway. As the aircraft documentation did not provide guidance for such an incident, and to further assess the condition of the landing gear, the flight crew decided that a visual inspection via a low pass of the Melbourne Airport ATC tower was necessary.
The flight crew did not contact QantasLink operations for assistance regarding the landing gear or the conduct of the low pass. This prevented QantasLink from providing input into the decision-making process. Further, while a visual inspection (using binoculars) by ATC from the tower may give a general assessment of the landing gear, it was not likely to have identified specific damage that would have otherwise been visible at close proximity during a ground inspection.
A flight at low altitude, and at a low speed with the landing gear and flaps extended may introduce a number of risks. Notably, the low pass was conducted lower than the briefed low pass height. As this was not a procedure within the operations manuals, there was no assurance that all potential risks had been identified and mitigated.
Unauthorised/unsupervised use of prescription medication
Post‑incident drug and alcohol screening of the flight crew detected the presence of a medication, which the captain reported was not prescribed to them. The medication had been taken in the days prior to the incident flight, and although the substance was above the permitted threshold for detection, the results could not be used to assess any level of impairment. Independent analysis by a forensic pharmacologist indicated any effects from the medication could not be completely ruled out, however, impairment was not expected given the reported dosage and time elapsed.
The medication taken could only be dispensed with a prescription, and its consumer medicine information sheet highlighted this requirement and several cautions and potential side effects. Although it was a strictly controlled, commercially produced medication, the absence of medical supervision meant there was no assurance that the captain would not experience any adverse effects or impairment that may have impacted their ability to safely operate the aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the misaligned take-off involving Bombardier DHC-8-315, VH-TQM, at Mildura Airport, Victoria, on 25 February 2025.
Contributing factors
During line‑up, the aircraft was taxied off the starter extension guidance line and the flight crew’s attention was diverted to completing the ready checks. This likely reduced their monitoring of the aircraft's position within the starter extension and resulted in it being positioned close to the right edge of runway 09.
The flight crew commenced the take-off from a misaligned position resulting in damage to the aircraft and runway edge lights.
Other factors that increased risk
The flight crew conducted a low pass to facilitate a visual inspection of the landing gear by air traffic control. There were no supporting procedures for the low pass or visual inspection, nor did the flight crew contact the operator to seek assistance.
The presence of a prescription medication was detected in the captain's post‑incident drug and alcohol test that was not prescribed for them. While they were unlikely to have been impaired by the medication, there was no assurance that the captain would not experience any adverse effects or impairment that may have impacted their ability to safely operate the aircraft.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by QantasLink
QantasLink advised the ATSB of the following safety actions:
Targeted human factors/non-technical skills training on the threat awareness of factors that have contributed to misaligned take-offs has been included in wider flight crew recurrent training.
Further information and a diagram was added to QantasLink operational documentation for Mildura Airport, specifically for the runway 09 starter extension to improve flight crew familiarity and situation awareness.
Educational material regarding departure briefings and identifying relevant threats was included in various mediums available to flight crew.
A safety alert was issued to flight crew soon after the incident with a new policy that prohibits ‘ready checks’ being completed during runway end turns. This was incorporated permanently in the Flight Crew Operating Manual to ensure that during runway turns the flight crew’s attention was not divided externally between aircraft manoeuvring and internally on checklist completion.
A policy was introduced to outline the risks associated with an ATC tower fly past published in the operations manual and aligned with other operators in the Qantas Group.
A risk review was conducted on reduced sleep opportunity during overnights, fatigue reporting trends, risk controls and mitigators currently used in fatigue risk management.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
the cabin crew
QantasLink
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meteorology
Mildura Airport
recorded data from the aircraft
the consultant forensic pharmacologist.
References
Australian Transport Safety Bureau. (2010). Factors influencing misaligned take-off occurrences at night, Australian Transport Safety Bureau, Australian Government.
Civil Aviation Safety Authority. (2024). Civil Aviation Safety Regulations 1998 Part 99-Drug and alcohol management plans and testing, Civil Aviation Safety Authority, Australian Government.
Civil Aviation Safety Authority. (2019). Part 139 Manual of Standards for Aerodromes, Civil Aviation Safety Authority, Australian Government.
Dawson, D., Sprajcer, M., & Thomas, M. (2021). How much sleep do you need? A comprehensive review of fatigue related impairment and the capacity to work or drive safely. Accident Analysis & Prevention, 151, 105955. doi: 10.1016/j.aap.2020.105955.
Goode J.H. (2003). Are pilots at risk of accidents due to fatigue?’ Journal of Safety Research, 34(3), 309–313. doi: 10.1016/s0022-4375(03)00033-1.
Dawson, D., Sprajcer, M., & Thomas, M. (2021). How much sleep do you need? A comprehensive review of fatigue related impairment and the capacity to work or drive safely. Accident Analysis & Prevention, 151, 105955. doi: 10.1016/j.aap.2020.105955.
Loukopoulos, L. D., Dismukes, R. K., & Barshi, I. (2009). The multitasking myth: Handling complexity in real-world operations. Routledge.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew
cabin crew
QantasLink
Civil Aviation Safety Authority
consultant forensic pharmacologist.
Submissions were received from:
the flight crew
QantasLink.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Footnotes
1
Although the crew was scheduled for 3 sectors the following morning, the captain was only rostered to fly the first sector back to Melbourne.
2
Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
3
Starter extension bypass pad: a runway starter extension may be established where additional take-off distance, take‑off run or accelerate-stop distance is required (Civil Aviation Safety Authority advisory circular AC 139.C-09 v1.0). It may also incorporate a bypass pad, which resembles a runway turn pad except that it is part of the runway starter extension and allows an aircraft to go around the declared end of the runway and runway end lights before turning around 180° to use the runway in a reciprocal direction.
4
The flight data for the incident was downloaded by the operator and provided to the ATSB for analysis. The cockpit voice recorder was removed from the aircraft and downloaded by the ATSB. However, a combination of the 1 hour and 45-minute flight time and delays in the isolation of the recorder resulted in the incident flight being overwritten.
5
The storm light is part of the flight deck lighting, which will illuminate the instrument panel when on.
6
The 70 kt and V1 calls were procedural calls that served as a confirmation of the indicated airspeed (70 kt) and as a decision point for the flight crew. Below 70 kt, the take-off was to be rejected for any failure, malfunction or caution/warning light. Between 70 kt and V1, the take-off was to be rejected for a critical malfunction or malfunction that was deemed to make the aircraft not flyable. Above V1, the take-off was to be continued.
7
Responses based on the Samn-Perelli 7-point scale which asks people to rate their fatigue at a point in time: 1 = fully alert, wide awake; 2 = very lively, responsive, but not at peak; 3 = okay, somewhat fresh; 4 = a little tired, less than fresh; 5 = moderately tired, let down; 6 = extremely tired, very difficult to concentrate; 7 = completely exhausted, unable to function effectively.
8
Morning civil twilight or first light is defined as the instant in the morning when the centre of the Sun is at a depression angle of 6° below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible. The brightest stars and planets can be seen and for navigation purposes at sea, the sea horizon is clearly defined. Sunrise is defined as the instant in the morning under ideal meteorological conditions, with standard refraction of the Sun's rays, when the upper edge of the Sun's disk is coincident with an ideal horizon.
9
Runway threshold lights: When viewed approaching the start of a runway, the threshold lights will be green, with red showing at the end of the runway.
10
Precision approach path indicator: a ground based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach.
11
Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
12
Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules, rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
Occurrence summary
Investigation number
AO-2025-008
Occurrence date
25/02/2025
Occurrence time and timezone
0636 EDT
Location
Mildura Airport
State
Victoria
Report release date
12/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Runway excursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Bombardier Inc
Model
DHC-8-315
Registration
VH-TQM
Serial number
604
Aircraft operator
Eastern Australia Airlines Pty Ltd operating as QantasLink
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
On 11 January 2025, a Cessna 510, registered VH-SQY and operated by AirMed Australia (AirMed), was being used to conduct a non-emergency medical air transport flight from Narrandera Airport to Bankstown Airport, New South Wales. On board were a pilot, a flight nurse and a patient.
At 1103 local time, the aircraft departed Narrandera and approximately 30 minutes later commenced descent into Bankstown. Weather information at Bankstown reported variable wind conditions and that the runway was wet. During the landing, the pilot experienced reduced braking performance and the aircraft overran the end of the runway into muddy ground. None of the occupants were injured and the aircraft was undamaged.
What the ATSB found
The ATSB determined that during the approach, an undetected tailwind was encountered and the aircraft landed with a groundspeed higher than the minimum aquaplaning speed. In addition, there was likely standing water on the runway and the aircraft’s main landing gear tyres were worn to limits resulting in reduced braking performance. Subsequently, the pilot cycled the anti‑skid system, likely further decreasing braking performance. In combination, these factors resulted in the aircraft departing the end of the runway.
The ATSB also identified that AirMed required pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. In addition, the type rating training provided by Air Link, a company associated with the operator, taught pilots to apply the same incorrect landing distance factor. Furthermore, AirMed’s procedures were unclear on how the factor should be applied, when the assessment should be conducted and how runway surface condition should be considered.
Finally, when determining the required landing distance at Bankstown, the pilot applied the incorrect landing distance factor prescribed by the operator. Subsequently, prior to descent and after obtaining the actual conditions at the aerodrome, the pilot did not identify that the landing distance available was insufficient for the landing.
What has been done as a result
AirMed updated its operations manual to require the use of a 60% landing distance factor and additional factoring for wet runway operations. Additionally, it introduced the requirement to conduct a landing distance calculation both before take-off and prior to landing, and included guidance on the applicability of options when using either tabulated data or flight planning software.
AirMed also provided training to all crew addressing the effects of tailwind, correct anti‑skid use, tyre limits and landing technique. In addition, it updated defect reporting procedures to encourage earlier reporting of anticipated maintenance requirements, and implemented a policy of tyre replacement when tread reaches 2 mm, representing 80% tyre wear.
Air Link amended training material for the C510 type rating to ensure that the correct landing distance factoring was applied and taught. In addition, past students were contacted to ensure that they understand performance requirements relating to the C510. Furthermore, it is in the process of including a new section in the endorsement training around wet weather operations, and has also implemented a policy of tyre replacement when tread reaches 2 mm.
Bankstown Airport amended the runway 11C/29C longitudinal slope information in the aerodrome manual to align with the En Route Supplement Australia slope values. Finally, while not in response to this occurrence, the Civil Aviation Safety Authority subsequently amended the performance section of the Part 121 guidance material as part of its continuous improvement process. These changes included:
the addition of a section specifying that landing performance must be checked both pre‑flight and in-flight
advice that actual landing distance data cannot be used to satisfy in-flight replanning operations
provision of a list of known aircraft types, including the C510, that must not use actual landing distance data for in-flight landing distance calculations.
Safety message
The use of safety margins on top of calculated take-off and landing distances provides mitigation for a wide range of issues that impact aircraft performance, including unexpected environmental conditions. Operators must be familiar with any factoring applicable to their operation and should adjust procedures appropriately when regulations change. For private pilots, while not mandated, the use of safety margins is highly recommended. These recommended safety margins can be found in the Civil Aviation Safety Authority (CASA) Advisory Circular (AC) 91-02 Guidelines for aeroplanes with MTOW not exceeding 5 700 kg - suitable places to take off and land, and should be applied in conjunction with any guidance given in the aircraft flight manual.
This occurrence also highlights the limitations on accurate and timely reporting of runway surface condition, particularly following a period of intense rainfall. Only 3 mm of standing water is required for a runway to be considered contaminated, and this depth of water can accumulate rapidly before the runway surface condition is able to be assessed. Furthermore, when landing on an un‑grooved runway, braking may be degraded when the runway is very wet but not yet classified as contaminated, with significant additional stopping distance required.
The occurrence
On 11 January 2025, a Cessna 510, registered VH‑SQY and operated by AirMed, was being used to conduct a non‑emergency medical air transport flight from Narrandera Airport to Bankstown Airport, New South Wales (Figure 1). On board were a pilot, a flight nurse and a patient.
Figure 1: Incident flight
Source: Google Earth, annotated by the ATSB
The aircraft had been repositioned earlier that morning from Wagga Wagga Airport to Narrandera Airport, where the flight nurse and patient boarded for the flight to Bankstown. Prior to departure from Wagga Wagga, the pilot obtained a weather forecast for both Narrandera and Bankstown (see the section titled Meteorology) and added sufficient fuel for both flights. The forecast conditions for Bankstown indicated rain and possible thunderstorms (see the section titled Forecast conditions) and the pilot determined that the aircraft would be below the maximum landing weight permitted in these conditions by the landing distance available charts (see the section titled Pilot assessment of landing distance available).
The aircraft departed Narrandera at 1103 local time and, approximately 30 minutes later, the pilot obtained the automatic terminal information service (ATIS)[1] information ‘Echo’ for Bankstown, prior to commencing descent. The pilot conducted the instrument approach procedure for runway 11C[2] and reported becoming visual with the runway at around 800–900 ft. The pilot recalled that the runway appeared wet, however they did not see any indications of standing or pooled water. Additionally, while they did not recall seeing the windsock, they reported that they did not feel as though there was a tailwind.
The aircraft commenced the round out for landing at 1156:32, and the pilot reported touching down firmly within the touchdown zone, deploying the speed brake and lowering the nose wheel prior to applying the brakes. The pilot stated that, despite braking, no deceleration or braking action was felt. They continued to hold brake pressure, expecting the anti‑skid system to activate (see the section titled Anti‑skid system), however the lack of discernible braking continued.
By this point, the pilot considered that the aircraft had passed the point on the runway where a go‑around could be safely conducted. Observing no system failure or warning indications in the cockpit, the pilot elected to cycle the anti‑skid system. They turned the anti‑skid system off, released and re‑applied the brakes. With no change in braking action the pilot again released the brakes, turned the anti‑skid back on, then re‑applied and held the brakes.
Realising that the aircraft would not stop prior to the end of the runway, the pilot advised air traffic control (ATC) that they could not stop. They then steered the aircraft slightly to the right to avoid the lights at the end of the runway. Departing the end of the runway at a groundspeed of 28 kt, the aircraft entered muddy ground and travelled another 30 m in a right turn before coming to a stop (Figure 2). The aircraft was undamaged and the pilot, flight nurse and patient were uninjured. After advising ATC of the situation and shutting down the aircraft, the patient was transferred to ground transport and the aircraft was recovered to a hanger.
Figure 2: VH-SQY after runway excursion
Source: Supplied
Context
Pilot
The pilot held an air transport pilot licence (aeroplane) issued in 2017 and a class 1 aviation medical certificate. They had accumulated 6,954 flight hours, of which 133 hours were operating the Cessna 510. In the previous 90 days, the pilot had accumulated 128 hours, all in the Cessna 510. The pilot had completed a type rating for the aircraft and an instrument proficiency check in October 2024 with Air Link, a company associated with the operator. The pilot had also completed line training with Air Link and had conducted operations for them, prior to commencing operations for AirMed.
Aircraft
General information
VH-SQY was a Cessna 510 Citation Mustang equipped with 2 Pratt & Whitney Canada PW615F‑A turbofan engines. The aircraft was manufactured and first registered in 2010 and was registered with the operator in 2019. It was in medical configuration, in which 2 seats and a cabinet in the main cabin were replaced with a stretcher and medical equipment.
At the time of the incident, the aircraft had accumulated 5,721 hours total time in service and was being maintained in accordance with the Cessna 510 maintenance manual. The last periodic inspection was conducted in December 2024, and the maintenance release showed no outstanding items.
Main landing gear tyres
VH-SQY was equipped with 2 Michelin main landing gear (MLG) tyres. Maintenance records showed that both MLG tyres were last replaced in October 2024, after conducting 255 landings. Since that time, the aircraft had conducted 239 landings including the incident flight.
The manufacturer required the MLG tyres to be inflated to a loaded pressure of 88 PSI. Both the maintainer and the pilot reported that, while the tyre pressure was not recorded or checked, the pressure appeared to be normal with no signs of over or under inflation.
The tyre manufacturer provided guidance on tyre removal criteria (Figure 3) which stated:
Removal criteria for normal wear is based on remaining tread rubber as determined by groove depth or exposure of textile/steel ply material… NORMAL REMOVAL WEAR LIMIT: Remove the tire when the wear level reaches the bottom of any groove at one point up to a maximum 1/8 of the circumference. NOTE: When the NORMAL REMOVAL limit is reached, the tire should be replaced. If it is necessary to continue the tire in service beyond the normal wear limit, the tire should be removed either at the next maintenance base or upon reaching the EXPOSED CORD LIMIT, whichever occurs first. At the EXPOSED CORD LIMIT the tire should be removed and replaced.
Figure 3: Michelin tyre wear guidance
Source: Michelin, annotated by the ATSB
During the post-incident inspection, the maintainer determined that both main landing gear tyres were worn to limits (Figure 4) and identified evidence of flat spotting, potentially due to the wheels previously locking up under braking. The maintainer further advised that the tread remaining on the left and right MLG tyres was measured to be 0.013 inches (0.3 mm) and 0.019 inches (0.5 mm) respectively. Comparatively, the tread of a new tyre was reported to be 0.26–0.29 inches (about 7 mm), indicating that 4–7% of the original tread was remaining. Both tyres were subsequently replaced before the aircraft was released back to service.
Figure 4: VH-SQY main landing gear tyres post‑incident
Source: Supplied, annotated by the ATSB
The pilot reported that they had inspected the condition of the tyres as part of the daily inspection of the aircraft prior to commencing operations for the day. They further reported that, while they identified that the centre tread on the tyres was low, they considered that as there was sufficient depth on the outside tread with no exposed cord the tyres were serviceable.
Anti‑skid system
The aircraft was equipped with an anti‑skid system to provide maximum braking efficiency across all runway surfaces and conditions. The anti‑skid system detects if the speed of any main landing gear wheel was too slow for the aircraft’s speed and released the brake momentarily to allow the wheel rotation to increase, preventing it from skidding. Anti‑skid systems are designed to reduce landing distance and minimise the potential tyre damage which can occur when a wheel is locked.
The aircraft was also equipped with a cockpit warning message to indicate when the anti‑skid was inoperative. While landing with anti‑skid inoperative was permitted, pilots were advised that doing so required the landing distance to be increased by between 39–45%.
In a normal landing with the anti‑skid system operative, the aircraft flight manual (AFM) advised pilots to apply brakes after nose wheel touchdown. The AFM further advised that:
to make sure of proper braking on water, snow, and ice-covered, hard-surfaced runways, and all unimproved surfaces, it is necessary for the pilot to apply maximum effort to the brake pedals throughout the braking run. When the system detects a skid and releases the applied brake pressure, any attempt by the pilot to modulate braking can result in an interruption of the applied brake signal and may increase stopping distance significantly.
The manufacturer advised that the anti‑skid system was not certified for turning off then on during a landing. They further advised that turning the system off during a landing roll may result in flat spotting the tyres if the anti‑skid was actively controlling a skid, especially on a wet runway. Additionally, when the system was powered on, it took several seconds to self‑test, during which time it would not function.
Meteorology
Forecast conditions
The Bureau of Meteorology (BoM) issued both a Graphical Area Forecast (GAF) for the area including Bankstown Airport and a terminal area forecast (TAF) for the aerodrome that covered the pilot’s expected landing time. The GAF was initially issued at 0308 that morning and described the weather to expect around Bankstown as including:
periods of scattered rain showers with towering cumulus clouds and broken cloud at 500 ft
isolated thunderstorms with heavy rain, becoming occasional from 1300.
The GAF was re‑issued as part of the regular cycle at 0926 with no changes, other than that the thunderstorms were no longer expected to produce heavy rain and were expected to remain isolated.
The TAF for Bankstown Airport was issued and then amended at 0352. It described the weather at the airport for the expected arrival time as:
wind from 050°M at 14 kt, light showers of rain and broken cloud at 2,000 ft
periods of up to 60 minutes of showers of rain with wind gusting 15–25 kt, broken cloud at 800 ft and visibility reduced to 2,000 m
possibility of thunderstorms for periods up to 60 minutes with variable strong winds, broken cloud at 500 ft and visibility reduced to 1,000 m.
A new TAF was issued at 1026, with the only change being that the wind was now expected to be from 060°M at 10 kt.
Reported conditions
Prior to descent, the pilot reported that they listened to the automatic terminal information service (ATIS)[4] information ‘Echo’ for Bankstown Airport to obtain the reported conditions at the airport. The information included that:
runway 11 left, centre and right were in use
runway surface condition code was 5,5,5. Whole runway was wet (see the section titled Assessment of runway surface condition)
wind was variable at 8 kt
visibility reduced to 3,000 m in rain
cloud was scattered at 800 ft, scattered at 1,200 ft and broken at 2,000 ft
The BoM weather station at Bankstown Airport recorded the mean direction of the wind at 1‑minute intervals in addition to the minimum, mean and maximum wind strength. Additionally, the standard deviation of the wind direction was recorded as a measurement of the variability of the wind direction within each minute.
The mean wind direction varied significantly between 1130–1215 (Figure 5). The recorded wind changed from a headwind to a tailwind on runway 11C, 6 minutes prior to VH-SQY landing. However, at around this time, the variability of the wind direction increased. At the time of the landing, the mean wind was recorded as a 6 kt tailwind. Subsequently, the tailwind further increased slightly before decreasing again, becoming a headwind again 14 minutes after the landing.
Figure 5: Runway 11C mean tailwind and wind direction variability 1130–1215
Source: ATSB
Rainfall
BoM observations recorded that Bankstown Airport received 2.8 mm of rain from 0900–1130 that morning. At 1133, heavy rain began to fall and continued to fall until 1155, 1 minute prior to the aircraft landing (Figure 6). During this 23‑minute period, 15 mm of rain was recorded. This represented a rainfall rate of 39 mm/hr, significantly higher than the threshold of 10 mm/hr required to be classified as heavy rain. Satellite imagery and CCTV footage confirmed that significant rain was observed at and around the aerodrome prior to the aircraft landing.
Figure 6: Bankstown Airport recorded rainfall 1130–1215
Source: ATSB
Runway surface condition
While the runway surface condition was reported as wet on the ATIS, the ATSB identified evidence of standing water on the runway at the time VH‑SQY landed. CCTV footage recorded the latter portion of the landing, during which spray was observed being ejected from beneath the aircraft during its ground roll (Figure 7).
Figure 7: CCTV images of water spray during landing
Source: Google Earth and Bankstown Airport, annotated by the ATSB
Additionally, a photograph of runway 11C taken at 1202, 6 minutes after the runway excursion, showed water on the runway (Figure 8). A subsequent photograph taken 9 minutes later showed that the amount of water on the runway had visibly reduced over this time.
Figure 8: Runway 11C surface after incident
Source: Supplied, annotated by the ATSB
Air traffic control observations
Air traffic control did not advise the pilot of any tailwind when giving an initial landing clearance at 1154 or when a subsequent landing clearance was given at 1155. After the incident, the next aircraft to arrive at Bankstown was advised of an occasional tailwind of 5 kt prior to receiving a landing clearance for runway 11L at 1159.
While the ATSB did not interview the air traffic controllers who were on duty at the time, Airservices Australia advised that an internal occurrence review was conducted into the incident which reported that a tailwind was not observed by the controller at the time that a landing clearance was given to VH‑SQY. They further advised that it was likely that controllers were using instantaneous wind readings in conjunction with visual observations to inform their assessment of wind conditions.
Recorded data
The ATSB analysed flight data recorded by the aircraft’s Garmin G1000 avionics. This data recorded specific flight and system parameters every 1–2 seconds throughout the flight, including during the landing and runway excursion. The aircraft was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to have them installed.
The data from the G1000 showed that on final approach, the aircraft was at 50 ft above ground level (AGL) approximately 240 m before the displaced threshold before arriving at an aim point short of the first touchdown marker (Figure 9).
Figure 9: VH-SQY flight path and landing
Source: Google Earth, annotated by the ATSB
At 1156:32 the aircraft commenced the round out and flare approximately 135 m past the displaced threshold at which point the aircraft’s groundspeed was 102 kt. The recorded data did not contain a specific data point to indicate when the aircraft was on the ground, however a positive G indication, consistent with a touchdown, was recorded at 1156:38, 430 m past the displaced threshold. At this time, the aircraft’s groundspeed had decreased to 93 kt. The aircraft’s groundspeed continued to decrease with no discernible change to the deceleration rate until 1156:58, at which time 140 m of the pavement remained. Subsequently, the aircraft departed the end of the runway at 1157:05 at a groundspeed of 28 kt.
The data recorded both the indicated airspeed and groundspeed of the aircraft, enabling the headwind and tailwind component of the wind to be determined (Figure 10). At approximately 550 ft, the aircraft was experiencing a headwind of 9 kt. As the aircraft descended on the approach, the headwind decreased prior to switching to a tailwind at approximately 250 ft. As the aircraft continued its descent, the tailwind increased up to a maximum of 6.3 kt when the aircraft was 50 ft AGL, consistent with the wind recorded at the airport. After peaking at 50 ft, the tailwind decreased throughout the remainder of the landing.
Figure 10: VH-SQY calculated wind on final approach and landing
Source: ATSB
Bankstown Airport
Runway environment
Bankstown Airport’s runway environment consisted of 3 parallel runways. The centre runway, 11C/29C, was the longest runway. It was typically used for arrivals and departures under the instrument flight rules (IFR) due to associated instrument approach and standard instrument departure procedures. The runway was un-grooved, and the runway surface was asphalt.
The En Route Supplement Australia (ERSA) provided information on Bankstown Airport, including runway dimensions, take-off and landing distances, runway slope and local procedures for operating at the aerodrome. The ERSA advised that runway 11C had a displaced threshold of 97 m and a landing distance available (LDA) of 1,259 m. The pavement surface continued for a further 60 m, however this section was not permitted to be used for either take-off or landing. The reciprocal runway 29C had no displaced threshold and a LDA of 1,356 m.
Runway longitudinal slope
The ERSA described the longitudinal slope of the runway as:
Slope W end 0.5% down to E. Centre 0.2% up to E. E end 0.2% down to W
The ERSA did not contain information on how this description should be used to determine a runway slope value for landing and take-off performance calculations. Bankstown Airport survey information detailed how the slope described in the ERSA was constructed (Figure 11). The survey information identified that the threshold‑to‑threshold slope was 0.15% up to the east. This would have been the runway slope applicable to performance calculations for an aircraft landing on runway 11C.
Figure 11: Runway 11C longitudinal slope
Source: Google Earth, annotated by the ATSB
Bankstown Airport maintained an aerodrome manual, as required under Part 139 (Aerodromes) of the Civil Aviation Safety Regulations (CASRs). The manual included technical information regarding the longitudinal slope of runway 11C/29C and reported:
The runway slope was 1.12% slope to the south-west.
In a different section of the manual, the runway was a code 3 non‑precision approach runway with an overall longitudinal slope of 1.34%, whereby the current standard was 1%. This was identified as non‑compliant with the current standards, however, was being used under grandfathering provision of the regulations.
An independent aerodrome technical inspection (ATI) was conducted for the aerodrome in December 2023. The inspection included a visual inspection of all movement area pavements to appraise compliance with CASR Part 139. The inspection reported that the overall longitudinal slope of runway 11C/29C was 1.34%, consistent with one of the statements in the aerodrome manual, but not consistent with survey information.
The ATSB sought clarification from Bankstown Airport regarding the variation between the runway 11C/29C longitudinal slopes reported in the ERSA, aerodrome manual, ATI and survey documentation. Airport personnel advised that the survey information was correct and that the aerodrome manual and ERSA would be amended.
Runway transverse slope and drainage
The aerodrome manual stated that the transverse slope values required by the CASR Part 139 Manual of Standards (MOS) had not been exceeded for runway 11C/29C.
The ATI did not contain a statement regarding assessment of the transverse slope of the runway. However, it did state that the drainage infrastructure of the runway:
appeared to be operating effectively at the time of inspection within minimal areas of ponding observed.
The ATSB was advised by Bankstown Airport that the ATI offered only a visual inspection of the transverse slope and that the slope was typically determined during the runway design process. Both the pilot and the operator reported that discussions had occurred between representatives of the operator and the airport regarding what they considered to be poor runway drainage. Bankstown Airport management advised that they were not aware of any conversations where this was discussed.
Assessment of runway surface condition
Bankstown Airport had procedures for assessing and reporting runway surface conditions and associated braking action under the global reporting format (GRF). The procedures defined the steps required to determine the runway condition report (RCR), a standardised report relating to runway surface conditions, and their effect on an aircraft’s landing and take-off performance.
The RCR was provided in 2 parts, a runway condition code (RWYCC) and a surface description. Additionally, each runway was divided into approximate thirds, with an RCR being determined separately for each of these thirds. The RWYCC was initially assigned based on a runway surface description (Table 1).
Table 1: Runway surface description to assign initial RWYCC
Runway surface description
Applicable runway condition code (RWYCC)
Braking action
Dry
6
N/A
Wet (The runway surface is covered by any visible dampness or water up to and including 3 mm depth)
5
Good
Wet (‘Slippery Wet’)
3
Medium
Standing Water (Depth more than 3 mm)
2
Medium to Poor
After initial assignment of an RWYCC from the runway surface description, receipt of 2 or more pilot reports of braking action less than that expected, could result in the description being downgraded.
During tower hours, ATC was trained to determine if the runway was completely dry or wet and could create the RCR when conditions were dry or wet for the whole runway. Further to this, ATC was able to request the aerodrome reporting officer (ARO) to conduct a runway inspection to assess the runway surface. AROs were also required to carry out inspections after severe weather events, so long as the weather conditions would not pose a safety hazard.
The assessed RCR was advised on the ATIS. Additionally, if the runway surface condition was determined to be slippery wet, or had standing water, a NOTAM[6] was required to be submitted containing details of the adverse RCR.
The ATIS ‘Echo’ current at the time of the incident contained an RCR of 5,5,5, whole runway wet (see the section titled Reported conditions). ATC did not report having received any reports of adverse braking from other pilots prior to the incident that would have required the RCR to be amended. After the incident, while attending to VH‑SQY, the ARO advised the tower controller that there was no observed standing water on runway 11C. Subsequently, when the ATIS was updated to ‘Foxtrot’ at 1213 to advise of a disabled aircraft, the RCR remained the same.
Air traffic control requirements
Airservices Australia’s Manual of Air Traffic Services (MATS) included procedures for ATC relating to the issuing of an ATIS, and the conditions under which it should be revised. These procedures required that an ATIS include:
Surface wind direction and speed, including significant variations
Wind direction was further required to be reported as one of:
SINGLE MEAN DIRECTION;
TWO VALUES representing variation in wind direction, whenever: i) the extremes in wind direction vary by 60 degrees or more; or ii) the variation is operationally significant (e.g. the variation is less than 60 degrees, but the variation from the mean results in either a tailwind, and/or significant crosswind component on a nominated runway) (e.g. WIND VARYING BETWEEN [DIRECTION] AND [DIRECTION]);
VARIABLE, where it is not possible to report a mean wind direction, such as: i) in light wind conditions (3 kt or less); or ii) the wind is veering or backing by 180 degrees or more (e.g. passage of thunderstorm, or localised wind effect).
The wind component of the ATIS was also required to:
Quote significant crosswind and any tailwind as: a) MAXIMUM CROSSWIND (speed) KNOTS [RUNWAY (number), if applicable]; and b) MAXIMUM TAILWIND (speed) KNOTS [RUNWAY (number), if applicable].
MATS also advised on wind limitations when nominating a runway. When the runway was dry, a runway could not be nominated for use when the tailwind exceeded 5 kt. When the runway was not completely dry, a runway could not be nominated for use when there was any tailwind component.
ATC was required to revise an ATIS and assign a new code letter when certain items changed and were expected to remain that way for at least 15 minutes. This included changes to an RCR or when wind direction varied by 10°.The CASR Part 179 (Air Traffic Services) MOS also required that:
Changes to ATIS wind information must be provided to pilots with a take-off or landing clearance if it is considered that it would be of significance to the aircraft operation.
Landing performance
Aircraft flight manual
Landing performance data
The Cessna 510 AFM contained performance data for use in calculating the landing distance required (LDR) at a destination aerodrome. This data was contained in 2 sections. The first section provided data to calculate the landing distance when the runway was forecast to be dry. This section of the AFM was marked as approved by the United States Federal Aviation Administration (FAA), the organisation that originally issued the aircraft’s type certificate. The performance data was based on several assumptions including:
the landing was on a paved, dry runway
landing preceded by a steady 3° angle approach down to the 50 ft height point with airspeed at VREF[7] in the landing configuration
maximum wheel braking was initiated immediately on nose wheel contact and continued throughout the landing roll
winds were to be taken as the tower winds 32.8 ft (10 m) above runway surface
factors of 50% of the headwind, and 150% of the tailwind had been applied to winds.
The second section of the AFM provided performance data for landing on wet, slush, snow‑ and ice‑covered runways. This section was marked as advisory information and stated that:
The following information is considered the most accurate and practical guidance material available for wet and contaminated runway operations. This advisory information is not FAA approved.
The section also stated that:
The published limiting maximum tailwind component for this airplane is 10 knots, however, landings on precipitation covered runways with any tailwind component are not recommended.
Advisory and unapproved information
The Civil Aviation Safety Authority (CASA) Advisory Circular (AC) 21‑34Aircraft flight manuals contained information relating to approved and unapproved sections of an AFM and advised that:
- Approved parts of the AFM are approved by the applicable national aviation authority (NAA), based on the type certification requirements effective at the time of certification.
- Unapproved parts of the AFM are provided by the manufacturer additionally, as deemed necessary for the safe operation of the aircraft, and cannot conflict with approved parts of the AFM. Each approved part of the AFM is clearly distinguished from any unapproved part of that AFM.
CASA also published Civil Aviation Safety Regulation (CASR) Part 135 Acceptable means of compliance and guidance material (AMC/GM) - Australian air transport operations—smaller aeroplanes which provided guidance on complying with required performance data calculations. It stated that:
Some performance information presented in AFM or AFM supplements may be advisory information only and should not be used to determine performance in compliance with the provisions of regulations 135.345 and 135.350 [Take-off performance and Landing performance]. Caution should be exercised when using advisory material or when using third-party performance calculations as the results may not be based on the required AFM provided certification data.
Similar advice was contained in CASR Part 121 Acceptable means of compliance and guidance material (AMC/GM) - Australian air transport operations—larger aeroplanes.
The ATSB sought clarification from CASA as to the applicability of data from unapproved sections of an AFM for use in flight planning. They advised that this data could not be used for performance planning, in part because the advisory information was not developed in accordance with standardised conditions.
Landing distance requirements
Safety Margins
Take-off and landing performance data contained in an AFM was obtained through formal testing using specific criteria. It was therefore unlikely that a pilot could replicate the testing performance during normal flying conditions. For this reason, additional distance was added to the calculated distance to provide a safety margin. While only recommended for private operations, the use of safety margins was required when conducting air transport operations.
CASA AC 91-02 provided guidance on the purpose of safety margins including that:
These additional safety margins mitigate risks associated with a range of issues that impact on aircraft performance, including but not limited to:
- pilot inaccuracies compared to performance flight testing (excess landing speed, excess height over threshold, increased float before touchdown, delayed use of braking and deceleration devices, inaccurate application of maximum braking techniques)
- runway characteristics
- aerodrome density altitude
- changed external drag configuration of the aeroplane
- underperforming engine compared to that used for performance testing.
Landing distance factor
CASR Part 135 - Australian air transport operations—smaller aeroplanes, under which this flight was conducted, prescribed certain landing performance requirements. As part of these requirements, if the aircraft was a jet‑driven, multi‑engine aircraft with a maximum take‑off weight (MTOW) of greater than 2,722 kg, such as the Cessna 510, then the performance calculations were required to be conducted in accordance with CASR Part 121, the regulations for larger aeroplanes.
CASR Part 121 required that a pilot determine that the runway at the planned destination aerodrome had sufficient landing distance available (LDA) to bring the aircraft to a stop. For a jet‑engine aeroplane, such as the Cessna 510, the aircraft was required to be shown to able to stop within 60% of the full LDA (Table 2). This calculation was required to be conducted both prior to departure using forecast conditions and in‑flight when actual aerodrome conditions were obtained.
If the runway surface condition was expected to be wet or contaminated, an additional 115% factor was required to be applied as a further safety margin. If the AFM contained landing performance data specific to wet or contaminated runways an alternative calculation was available. However, if this data was contained in an advisory or unapproved section of the AFM, as it was for the Cessna 510, it was not eligible to be used (see the above section titled Advisory and unapproved information).
Table 2: Summary of landing distance required calculations
Runway surface condition
Landing distance factor
Additional factor
Dry
60%
-
Wet
60%
115%
Contaminated
60%
115%
The regulations stated conditions to be considered when calculating LDR, which included:
runway surface condition
forecast wind speed and direction. Unless otherwise accounted for in the performance data in the AFM, 50% of the headwind and 150% of the tailwind
expected runway to be used
expected landing weight
aerodrome elevation
runway slope if greater than 1%.
Actual landing distance data
CASR Part 121 allowed a single, less restrictive landing distance factor of 15% to be used when determining LDR in‑flight for aircraft where the AFM contained actual landing distance (ALD) data. CASR Part 121 AMC/GM listed key points surrounding the use of ALD including:
- Actual landing distance information is intended to show landing performance that can realistically be achieved by flight crews in commercial operations.
- This is distinct from landing performance demonstrated by test pilots during flight tests for aircraft type certification.
The AMC/GM also stated that to be classified as ALD data, performance data was required to be accordance with International Civil Aviation Organisation (ICAO) Annex 8 standards and that:
the applicability is also limited to aeroplanes intended for the carriage of passengers or cargo or mail in international air navigation. These are known in some States as transport category aeroplanes. This has resulted in some aeroplanes that are seemingly captured by the requirements of ICAO Annex 8 Part IIIB not having performance data that is required to be in accordance with those requirements.
CASA confirmed that performance data in the Cessna 510 AFM did not constitute ALD data.
Landing in very wet conditions
CASA guidance material contained advice for operators and flight crew on landing in very wet conditions which stated:
Operators and flight crews should be aware that the landing distance factors mentioned above – whether based on type certification testing or actual landing distance data provided by OEMs [original equipment manufacturer] separately – may not provide adequate stopping distance in very wet but not yet contaminated runway surface conditions.
Issues that contribute to such incidents include runway conditions such as texture (polished or rubber contaminated surfaces), drainage, puddling in wheel tracks and active precipitation. For un-grooved runways, wheel braking may be degraded when the runway is very wet. Research conducted by the FAA has indicated that 30 to 40 percent of additional stopping distance may be required in certain cases where the runway is very wet, but not yet classified as contaminated.
In order to manage some of the risks associated in operating to very wet runways, it is recommended that operators consider the landing safety factor of 1.15 (which is the difference between 1.67 and 1.92 for type certification data and the value mentioned in the actual landing distance data) to be a minimum value.
Flight planning software
The operator utilised third party flight planning software from Aircraft Performance Group (APG) for performance calculations. Access to this software and underlying performance data was available to pilots through the following means:
the APG iPreFlight App available on the pilot’s tablet
the APG Atlas website, available via a computer with an internet connection
tabulated data for individual aerodromes, available as PDF documents via the electronic flight bag (EFB) on the pilot’s tablet.
The APG iPreFlight App and APG Atlas website provided an interface into which pilots entered the destination airport and runway, forecast or actual conditions and estimated landing weight. Additionally, options were available to configure how the landing distance was calculated which included:
landing distance factor: 60%, 80% or unfactored
wet runway calculation method: 115% or use of AFM advisory data
other runway surface conditions: including 0.125 inches (3 mm) of water, snow and slush.
Of these options, 80% landing distance factor was selected by default.
The tabulated data provided both take-off and landing performance data for an individual airport. The landing performance data (Figure 12) was presented as a maximum landing weight (MLW) permitted and the LDR required at this weight, across a discrete set of temperature and wind conditions. Tables for both dry and wet (115%) runway conditions were provided, with 60%, 80% landing distance factors in addition to unfactored data. If the landing distance required for the selected runway was not available, then ‘NA’ was listed as the MLW and the actual distance required was specified.
Figure 12: Extract of tabulated landing performance data for runway 11C
Source: Supplied, annotated by the ATSB
Type rating training
The pilot completed a type rating for the Cessna 510 with Air Link, a company related to the operator. The ground school component of the type rating contained a section on aircraft performance, which included the calculation of landing distance required. The trainer reported that this training included:
a review of relevant CASR Part 135 and CASR Part 121 requirements for landing distance calculation
use of the advisory section of the AFM to calculate landing distance required under CASR Part 135 on a wet and contaminated runway
use of the APG flight planning software on a company EFB to conduct the same landing distance calculation.
The pilot recalled that, during ground training and during the type rating test, an 80% landing distance factor was used. The trainer confirmed that use of an 80% landing distance factor was taught during the type rating. Air Link advised that this factor was adopted as a safety margin in consultation with CASA when both Air Link and AirMed were initially approved under previous regulations as there was no factoring required under the previous legislation.
Operator procedures
Procedures for determining landing distance available
The operator advised the ATSB that, consistent with the training provided by Air Link, pilots were required to apply an 80% landing distance factor when determining LDA. The pilot also reported that they consistently used an 80% factor.
The operator’s procedures contained requirements for pilots when determining landing distance and advised that:
The means to determine maximum allowable take-off and landing weights are based upon:
- airport characteristics consisting of airport elevation, runway gradient and length, runway contaminants, obstructions within the take-off path,
- airport/environmental conditions consisting of temperature, wind and pressure altitude
- aircraft configurations consisting of power settings, flap settings, bleed configurations and MEL [minimum equipment list] inoperative components.
- specified factoring (set by company, in accordance with CAO 20.7.1 [historical regulation])
The procedures further stated that:
The calculation of aircraft performance must be considered prior to dispatch, as part of the pre-flight planning process.
Additional procedures for landing on a wet runway
The operator provided additional guidance for operating on wet or contaminated runways which stated:
Due to the large number of variables involved no exact formula has so far been found, but an empirical result of a 15% increase in the overall distance required has been accepted in the US [United States] and in other countries as providing an acceptable correction for landing.
It is desirable to apply some correction for take-off when the runway is considered to be significantly wet, so as to provide a distance margin to offset the reduced braking likely to arise in the accelerate-stop manoeuvre, whenever the take-off is likely to be distance limited. For take-off and landing, the 15% increase is considered to be appropriate.
It also provided the following guidance for adjusting landing distance available when expecting to land on a wet runway:
Obtain the LDA, and using only 0.85 X LDA as the effective distance available, derive a ‘wet’ length limited landing weight from the general chart in the manual.
Derive the approach climb limit in the usual way, and observe this and the structural limit.
If the ‘wet’ length limit is the most restrictive consider using another runway to provide better protection.
Note: That in both the take-off and landing cases, the use of 1.67% of the overall distance will provide an acceptable margin in that portion of the distance used. In most cases, the distance available for decelerating will be approximately doubled by this means.
Stabilised approach criteria
The operator’s procedures contained requirements for a stabilised approach that stated:
An approach to land must be stabilised by the FAF [final approach fix] in IMC [instrument meteorological conditions] and by 300 ft above the airport elevation in VMC [visual meteorological conditions]. An approach is stabilised when all of the following criteria are met:
- The aircraft is on the correct flight path.
- Only small changes in heading and pitch are required to maintain the correct flight path.
- The aircraft speed is not more than VREF +15 IAS [indicated airspeed] and not less than VREF +5.
- The aircraft is in the correct landing configuration.
- The sink rate is no greater than 1,000 ft/min.
- Power setting is appropriate for the configuration.
- All briefings have been conducted.
The operator further advised that the expectation was for pilots to fly the aircraft within the specified range as they approach the field, reducing airspeed so that the aircraft was at VREF at touchdown.
Pilot assessment of landing distance available
Pre-departure
The pilot reported that prior to departure, as part of their pre-flight planning process they assessed the landing distance available at Bankstown using the APG tabulated landing distance data. Given the forecast conditions (see the section titled Forecast conditions), they determined that the runway would likely be wet on arrival, therefore they consulted the section of the data for a wet runway. Rather than using the wind forecast from the TAF, they used for a more conservative 5 kt tailwind on arrival. Using the 80% landing distance factor in accordance with operator procedures, a more conservative temperature of 29° and interpolating between the values for nil wind and a 10 kt tailwind, they determined that the maximum landing weight was approximately 7,700 lb for runway 11C at Bankstown (Figure 13).
The pilot had also determined that the landing weight of VH‑SQY was expected to be 7,089 lb based on calculated take‑off weight and anticipated fuel consumption. Therefore, as the aircraft was expected to be below the maximum landing weight, the aircraft could depart.
In-flight
The pilot reported that upon receiving the ATIS they again conducted an assessment of the landing distance available at Bankstown using APG tabulated data and the reported conditions (see the section titled Reported conditions). Considering that the variable 8 kt wind reported could be all tailwind, the pilot used a more conservative 10 kt tailwind. Again, using the 80% landing distance factor in accordance with operator procedures, the pilot determined that the maximum landing weight was 7,401 lb. The pilot recalculated the estimated landing weight with the current fuel load as approximately the same as that estimated prior to take‑off.
As the aircraft was expected to be below the weight assessed in the chart, they determined that the landing could be conducted. In addition, the pilot advised that they had decided that if they observed a tailwind greater than 5 kt during the approach, they would request to land on the reciprocal runway 29C. At this point, the pilot also determined 89 kt as the required VREF for the aircraft, for the expected landing weight.
ATSB assessment of landing distance required
The ATSB calculated the landing distance required using the 60% landing distance factor required for operating the Cessna 510. A pre‑departure assessment was conducted using conditions from the TAF available prior to departure from Narrandera. An in‑flight assessment using the conditions reported on the ATIS prior to descent was also performed (Table 3). The calculations were conducted using APG flight planning software, software from the manufacturer and using performance data from the AFM with the results consistent across the 3 methods. The pre‑departure calculation determined that a landing distance of approximately 1,230 m was required on runway 11C, less than the 1,259 m available. However, the in‑flight calculation determined that approximately 1,530 m was required, greater than that available.
Table 3: ATSB assessment of landing distance required
Dynamic aquaplaning (also known as hydroplaning) can occur when an aircraft lands on a runway contaminated with standing water, slush or wet snow. Above a certain groundspeed and with sufficient contaminant, the tyre is lifted off the runway surface. This can have serious adverse effects on ground controllability and braking efficiency.
The depth of standing water required for dynamic aquaplaning to occur is generally accepted to be 3 mm (approximately 0.125 inches). This is also the depth required for a runway surface condition to be considered contaminated rather than wet.
The minimum speed above which dynamic aquaplaning can occur is a function of tyre pressure. Two different speeds are often quoted depending on whether the tyre is rotating. A lower speed is considered for a non‑rotating tyre as is the case immediately on touchdown (Table 4).
Table 4: Generally accepted Cessna 510 main landing gear aquaplaning speeds
Tyre state
Formula
Speed
Rotating tyre
9 x √PSI
84 kt
Non-rotating tyre
7.7 x √PSI
72 kt
The operator’s procedures contained guidance for pilots regarding aquaplaning and stated:
The formula used to determine the speed at which a tyre is likely to hydroplane [aquaplane] after touchdown on a wet runway is: Hydroplane speed = 7.7√𝑇𝑦𝑟𝑒𝑃𝑟𝑒𝑠𝑠𝑢𝑟𝑒𝑃𝑆𝐼
From the above formula, the Citation Mustang’s nose gear hydroplane speed is about 86 knots and the main gear about 72 knots. Above these speeds hydroplaning may occur.
The manufacturer advised that the aircraft’s minimum aquaplaning speed for performance calculations was 84 kt. The operator’s speed was consistent with that for a non‑rotating tyre, while the manufacturer’s speed was consistent with that for a rotating tyre.
Recorded data showed that the groundspeed of the aircraft was above both the rotating and non‑rotating tyre minimum aquaplaning speed until approximately 360 m of LDA remained (Figure 14).
Figure 14: Recorded groundspeed of VH‑SQY during landing
Source: Google Earth, annotated by the ATSB
Effect of reduced tyre tread
The ATSB reviewed research to assess the effect of reduced tyre tread on braking effectiveness when landing on a wet or contaminated runway. Research conducted by Leland & Taylor (1965) An investigation of the influence of aircraft tire-tread wear on wet‑runway braking concluded that:
On the wet runway, a gradual degradation in braking effectiveness was experienced up to about the 80 percent worn tire tread condition, where the wet-runway friction coefficients dropped markedly.
The completed worn tire was observed to develop, at higher speeds, only about one‑half the braking effectiveness of a new tire.
The research from O’Callaghan (2023) Wet‑runway overruns: still a slippery problem included consideration of the effect of tyre wear on braking performance and stated that:
For the aircraft operator, tire wear is a most important factor … the available 𝜇𝐵 [coefficient of braking] in wet conditions decreases as a tire wears. For a typical aircraft-type, rib-tread tire, when groove depths have been reduced to about 20% or less of the unworn value, the remaining tread may be ‘flattened out’ under load and the tire may then behave as if smooth
Additionally, the research paper Aircraft tyre hydroplaning and how to analyse it in runway excursion events, van Es (2018) discussed the effect of tyre tread on the depth of water required for aquaplaning to occur and stated:
The tyre tread grooves act similar to the pavement macrotexture in draining the bulk water. When there is sufficient macrotexture on the surface and/or the tyre has a sufficient number of deep circumferential grooves, full dynamic hydroplaning will normally not occur, unless the water depth is at a level that both tyre grooves and runway macro texture cannot drain the water sufficiently quick enough…
Smooth tread tyres operating on smooth pavements surfaces require the smallest fluid depth for dynamic hydroplaning, whereas rib treads tyres operating on an open textured or grooved-pavement surface require the largest fluid depths.
Related occurrences
Australia
The ATSB occurrence database contained 263 instances of runway excursions on landing in Australia between 2020–2024. The majority of these involved the aircraft veering off the runway rather than overrunning.
Of these occurrences, 3 included mention of standing water leading to aquaplaning, one of which involved a Cessna 525 operated by Air Link landing on runway 11C at Bankstown in 2022. The ATSB did not investigate these occurrences.
In 2020 the ATSB investigated the runway excursion of a Fokker 100 landing at Newman, Western Australia (AO‑2020‑002). It was found that poor braking effectiveness in wet conditions resulted in the aircraft overrunning the runway.
In 2008, the ATSB published a two‑part research report (AR‑2008‑018) titled Runway Excursions with the objective of analysing international and Australian trends in runway excursions. Part 1 of the report explored the contributing factors associated with runway excursions between 1998 and 2007. Water‑affected and contaminated runways was one of the contributing factors identified.
International
The ATSB identified the following occurrences of runway excursions associated with a wet or contaminated runway:
Runway excursion of a Beech 95-C55 on 12 January 2023 (NTSB WPR23LA089)
During the landing roll, the pilot applied the brakes but discovered that there was more standing water on the runway than expected, resulting in the airplane aquaplaning. It was determined that the wet runway contributed to the aircraft overrunning the runway.
Runway excursion of a Learjet 36 on 9 September 2022 (NTSB WPR22LA344)
During a landing following recent rainfall, the pilot reported that the aircraft did not decelerate normally and subsequently overran the runway. It was determined that a fast landing on a wet runway resulted in the airplane aquaplaning during the landing roll.
Safety analysis
Introduction
On the morning of 11 January 2025, a Cessna 510, registered VH‑SQY, was being used to conduct a medical air transport flight from Narrandera Airport to Bankstown Airport, New South Wales. During the landing at Bankstown, the pilot experienced reduced braking performance, and the aircraft overran the end of the runway.
This analysis will discuss the operator’s procedures for determining landing distance and the pilot’s use of these procedures. The environmental conditions at the time and the actions performed during the landing are also examined. Additionally, the analysis will consider the reporting of conditions at Bankstown Airport and the airport’s runway environment.
Pilot training
The pilot completed a type rating for the Cessna 510 with Air Link, a company related to the operator. The performance component of the ground school incorporated the use of Part 135 regulations.
These regulations required the application of a 60% landing distance factor for a twin‑engine jet aircraft over 2,722 kg, such as the Cessna 510, when determining the landing distance required at a destination aerodrome. However, pilots were taught to use an 80% landing distance factor for this calculation. Use of this factor reduced the safety margin applied to mitigate issues that impacted the aircraft’s ability to achieve published landing performance. Furthermore, pilots were taught to use the aircraft flight manual (AFM) wet runway performance data for wet runway landing distances. However, this data was not permitted to be used for flight planning as it was from an advisory section of the AFM.
Contributing factor
The type rating training provided by Air Link taught pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. (Safety Issue)
Operator procedures
Both the operator and the pilot reported that, consistent with the type rating training, a landing distance factor of 80% was used when determining the required landing distance. However, a 60% factor was required for these types of operations.
The operator’s procedures contained guidance for calculating the required landing distance during the pre‑flight planning. However, while they referred to the application of specified factoring when determining landing distance available, they did not define what this factoring was. Additionally, the procedures did not advise that a landing distance assessment was required in‑flight in addition to prior to departure.
Furthermore, the operator’s flight planning software provided 2 options for determining the landing distance required: 60% and 80% landing distance factors. However, the 80% option was incorrectly selected by default when using the APG iPreFlight App. In addition, an option to use the AFM advisory wet runway performance data was also available on the App. However, the operator’s guidance did not specify that this was not permitted to be used for flight planning.
Contributing factor
AirMed required pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. Furthermore, its procedures were unclear on how the factor should be applied, when the assessment should be conducted and how runway surface condition should be considered. (Safety Issue)
Flight planning
Pre departure planning
Prior to departure, the pilot assessed the landing distance available at Bankstown Airport using tabulated data extracted from the flight planning software. Using the Terminal Area Forecast (TAF) at Bankstown Airport, they determined that the runway would likely be wet. While the TAF forecast a headwind on runway 11C, the pilot used a more conservative assumption of a 5 kt tailwind, despite the aircraft flight manual (AFM) stating that landing with a tailwind was not recommended on a wet runway.
The pilot used an 80% landing distance factor, as they had been taught, and determined that sufficient landing distance was available under these conditions. However, the use of a 60% factor was required for this flight.
The ATSB calculated the landing distance required using the conditions forecast in the TAF and the required 60% landing distance factor. It was determined that sufficient landing distance did exist at Bankstown due to the forecast headwind on runway 11C. Therefore, while incorrect data was used to conduct the assessment, the pilot correctly determined that a departure was possible.
In-flight planning
Prior to descent, the pilot obtained aerodrome conditions from the Automatic Terminal Information Service (ATIS). This information included that the wind was variable at 8 kt, the runway 11C was in use and the whole runway was wet. Using this information, the pilot again consulted the 80% landing distance factor tabulated data and determined that there was sufficient landing distance available to attempt a landing with up to a 10 kt tailwind.
However, this assessment also required that a 60% factor was used. Use of this factor would have identified that insufficient landing distance was available to plan for a landing on runway 11C.
If the pilot had determined that insufficient landing distance was available to attempt the landing, options were available to hold for the weather to improve or request more up‑to‑date weather information from air traffic control (ATC).
Contributing factor
When determining the required landing distance at Bankstown, the pilot applied the incorrect landing distance factor prescribed by the operator. Subsequently, prior to descent and after obtaining the actual conditions at the aerodrome, the pilot did not identify that the landing distance available was insufficient for the landing.
Landing and runway excursion
Tyre condition
During the daily inspection of the aircraft, the pilot inspected the aircraft’s main landing gear (MLG) tyres and assessed them as serviceable. However, an inspection after the incident identified that the tyres were below the tyre manufacturer’s guidance for normal removal wear, and less than 10% of the tread was remaining.
Research showed that the braking performance of an aircraft on a wet runway degraded as its tyres wore, with a marked increase in effect when reaching 20% of the original tread depth. Additionally, the depth of tread on a tyre influenced the amount of standing water required to support aquaplaning. Consequently, while permitted for flight, the low tread on the aircraft’s MLG tyres likely had an adverse effect on the aircraft’s braking performance when landing on a wet or contaminated runway.
Meteorology
Rainfall and standing water
At Bankstown Airport there was a period of very heavy rain which continued until 1 minute prior to the landing. Given the intense nature of this rainfall, it is likely that parts of the runway were contaminated with standing water. Furthermore, video and photographic evidence showed that the aircraft encountered standing water during the landing roll. The pilot was not aware of the recent rainfall and had assessed the runway surface as wet but not contaminated, observing no standing water. This was consistent with the runway surface condition reported by the Automatic Terminal Information System (ATIS). Standing water on the runway provided an environment for aquaplaning. In addition, guidance material advised that when landing in very wet conditions degraded wheel braking may require an additional 30–40% of stopping distance.
Tailwind
The ATIS reported that the wind was variable at 8 kt. The pilot recalled that they considered this and had planned to use the reciprocal runway if they observed a tailwind greater than 5 kt. The pilot further reported that they did not observe, nor were they advised by air traffic control (ATC), of a tailwind. However, while the wind was initially a headwind during the approach, this headwind decreased and became a tailwind as the aircraft approached the runway and commenced the landing.
Landing with a tailwind increased the landing distance required. Additionally, while the recorded tailwind was below the maximum permitted by the aircraft flight manual (AFM), landing with any tailwind component was not recommended by the manufacturer when landing on a wet or contaminated runway.
Landing sequence
The aircraft conducted the final portion of the approach to an aim point short of the first touchdown marker. At 50 ft AGL, the indicated airspeed was within 5 kt of the VREF and within the operator’s stabilised approach criteria. However, due to the tailwind encountered, the aircraft’s groundspeed was higher than the airspeed and above both the rotating and non‑rotating dynamic aquaplaning speeds during the touchdown. Consequently, the aircraft likely experienced dynamic aquaplaning when encountering standing water on the runway. Throughout the landing roll, the aircraft’s groundspeed did not decrease below the non‑rotating minimum aquaplaning speed of 72 kt until approximately 900 m into the landing roll.
During the landing roll, due to the lack of braking performance, the pilot elected to release and reapply the brakes and cycle the anti‑skid system. While well intentioned, this action likely further decreased braking performance as brake pressure was released for portions of the landing, and the anti‑skid system was momentarily not operational while a self‑test was conducted. Furthermore, this was not in accordance with the AFM which required that maximum braking was maintained throughout the landing roll. Damage observed on the main landing gear tyres was consistent with them having locked up under braking.
In summary, while the individual contributions of standing water, tailwind, tyre condition and pilot braking action could not be ascertained, the combination of these factors resulted in the aircraft’s reduced braking performance and subsequent runway excursion.
Contributing factor
During the approach, an undetected tailwind was encountered and the aircraft landed with a groundspeed higher than the minimum aquaplaning speed. In addition, there was likely standing water on the runway and the aircraft’s main landing gear tyres were worn to limits resulting in reduced braking performance. Subsequently, the pilot cycled the anti‑skid system, likely further decreasing braking performance. In combination, these factors resulted in the aircraft departing the end of the runway.
Bankstown Airport
Reported conditions
Wind and nominated runway
The ATIS reported the wind as variable at 8 kt with runway 11C nominated for use and no maximum tailwind advised. The Manual of Air Traffic Services (MATS) did not permit the nomination of a runway when there was a tailwind component with a wet runway. Recorded data showed that a mean tailwind had been recorded during the 6 minutes prior to landing. However, the wind direction was highly variable over this time. MATS required that ATIS information be updated when changes to meteorological conditions were expected to remain for 15 minutes, supporting the decision to report the wind as variable, and maintain runway 11C as the nominated runway. It was also required that wind significant to aircraft operation was provided to pilots with a landing clearance. However, at the time the landing clearance was given, the instantaneous wind observed by air traffic control (ATC) may not have indicated a tailwind.
Runway condition code
The ATIS reported the runway condition code as ‘whole runway wet’, however it was likely that sections of the runway were contaminated with standing water. Had the runway condition included sections reported as 2/standing water, the pilot would have been alerted to the potential for reduced braking performance.
However, ATC observations could only be used to declare a runway as fully dry or wet. Downgrading the runway surface condition required either 2 less-than-good braking reports from pilots or physical inspection of the runway surface by the aerodrome reporting officer (ARO). On this occasion, no braking reports had been received, and the ARO had not inspected the runway. After the incident, the ARO reported that there was no standing water observed. However, some water had likely drained away by this time.
Runway environment
Runway slope and drainage
Survey information showed that the longitudinal slope was approximately 0.15% up when landing on runway 11C. While the aerodrome manual and the aerodrome technical inspection (ATI) report contained conflicting information, Bankstown Airport advised that the surveyed slope was correct.
The En Route Supplement Australia (ERSA) entry provided runway slope information expressed by dividing the runway into 3 sections and reporting the slope for each section individually. As a result, it was unclear how to use runway slope values for performance planning. However, as the reported slopes, and the actual surveyed slope were not greater than 0.5%, use of one or a combination of these values would have had little, if any, effect on landing distance calculations.
The ATSB was advised of previous discussions regarding poor runway drainage at Bankstown Airport. However, an aerodrome technical inspection had assessed that the drainage of the runway was operating effectively. In addition, the aerodrome manual stated that the runway slope was designed in accordance with regulatory requirements. Furthermore, while standing water was likely present during the landing, no standing water was observed by the ARO after the incident. Therefore, it was likely that the runway drainage was operating effectively.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion involving Cessna 510, VH-SQY, at Bankstown Airport, New South Wales, on 11 January 2025.
Contributing factors
During the approach, an undetected tailwind was encountered and the aircraft landed with a groundspeed higher than the minimum aquaplaning speed. In addition, there was likely standing water on the runway and the aircraft’s main landing gear tyres were worn to limits resulting in reduced braking performance. Subsequently, the pilot cycled the anti‑skid system, likely further decreasing braking performance. In combination, these factors resulted in the aircraft departing the end of the runway.
The type rating training provided by Air Link taught pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. (Safety Issue)
AirMed required pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. Furthermore, its procedures were unclear on how the factor should be applied, when the assessment should be conducted and how runway surface condition should be considered. (Safety Issue)
When determining the required landing distance at Bankstown, the pilot applied the incorrect landing distance factor prescribed by the operator. Subsequently, prior to descent and after obtaining the actual conditions at the aerodrome, the pilot did not identify that the landing distance available was insufficient to attempt the landing.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The type rating training provided by Air Link taught pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome.
Safety issue description: AirMed required pilots to apply an incorrect landing distance factor, which reduced the safety margin when determining the required landing distance at a destination aerodrome. Furthermore, its procedures were unclear on how the factor should be applied, when the assessment should be conducted and how runway surface condition should be considered.
Safety action not associated with an identified safety issue
Additional safety action by Air Link Pty Ltd
Air Link is in the process of including a new section in the endorsement training around wet weather operations, including the associated limitations and the effect of worn tyres on aircraft performance. In addition, it has implemented a policy of tyre replacement when tread reaches 2 mm, representing 80% wear.
Additional safety action by AirMed
The operator conducted the following additional proactive safety action:
Provided training to all crew addressing the effects of tailwind, correct anti‑skid use, tyre limits and landing technique.
Updated defect reporting procedures to encourage earlier reporting of anticipated maintenance requirements.
Implemented a policy of tyre replacement when tread reaches 2 mm.
Safety action by Bankstown Airport
Bankstown Airport amended the runway 11C/29C longitudinal slope information in the aerodrome manual to align with the En Route Supplement Australia depiction of runway slope.
Safety action by the Civil Aviation Safety Authority
While not in response to this occurrence, the Civil Aviation Safety Authority subsequently amended the performance section of the Part 121 guidance material as part of its continuous improvement process. These changes included:
the addition of a section specifying that landing performance must be checked both pre‑flight and in‑flight
advice that actual landing distance data cannot be used to satisfy in-flight replanning operations
provision of a list of known aircraft types, including the C510, that must not use actual landing distance data for in-flight landing distance calculations.
Glossary
AC
Advisory circular
AFM
Aircraft flight manual
AGL
Above ground level
ALD
Actual landing distance
AMC/GM
Acceptable means of compliance / guidance material
APG
Aircraft performance group
ARO
Aerodrome reporting officer
ATC
Air traffic control
ATI
Aerodrome technical inspection
ATIS
Automatic terminal information service
BoM
Bureau of Meteorology
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulation
EFB
Electronic flight bag
ERSA
En Route Supplement Australia
FAA
Federal Aviation Authority
GAF
Graphical area forecast
GRF
Global reporting format
ICAO
International Civil Aviation Organisation
IFR
Instrument flight rules
LDA
Landing distance available
LDR
Landing distance required
MATS
Manual of Air Traffic Services
MEL
Minimum equipment list
MLG
Main landing gear
MLW
Maximum landing weight
MOS
Manual of standards
MTOW
Maximum take-off weight
NOTAM
Notice to airmen
OEM
Original equipment manufacturer
RCR
Runway condition report
RWYCC
Runway condition code
TAF
Terminal area forecast
Sources and submissions
Sources of information
The sources of information during the investigation included:
O’Callaghan, J. (2023, August). Wet-runway overruns: still a slippery problem. Presentation to the International Society of Air Safety Investigators (ISASI), Nashville, Tennessee, USA.
Van Es, G. (2018). Aircraft tyre hydroplaning and how to analyse it in runway excursion events. Presentation to the International Society of Air Safety Investigators (ISASI), Dubai, United Arab Emirates.
Leland, T. J., & Taylor, G. R. (1965). An investigation of the influence of aircraft tire-tread wear on wet-runway braking (Vol. 2770). National Aeronautics and Space Administration, Washington, D.C., USA
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and operator
the manufacturer
Air Link
Civil Aviation Safety Authority
Bankstown Airport
Airservices Australia
Aircraft Performance Group
National Transportation Safety Board.
Submissions were received from:
the pilot
the operator
Air Link
Bankstown Airport
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[2]Runway number: the number represents the magnetic heading of the runway. C specifies the centre runway when there are parallel runways available.
[3]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[4]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[5]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[6]Notice to Airmen (NOTAM): a notice containing information or instructions concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to persons concerned with flight operations.
[7]VREF: landing reference speed. The airspeed equal to the landing 50-foot point speed with the aircraft configured for landing.
Occurrence summary
Investigation number
AO-2025-002
Occurrence date
11/01/2025
Location
Bankstown Airport
State
New South Wales
Report release date
02/10/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
510
Registration
VH-SQY
Serial number
510-0343
Aircraft operator
AirMed Australia Pty Ltd
Sector
Jet
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 2 November 2024, a GippsAero GA8-TC Airvan, registered VH-IDM and operated by Wave Air, was being used to conduct a scenic flight from Whitsunday Airport (Shute Harbour), Queensland. On board were a pilot and 7 passengers. During the landing the aircraft departed the upwind end of the runway before entering marshy ground and coming to a stop in a ditch. Neither the pilot nor any of the passengers were injured and the aircraft was substantially damaged.
What the ATSB found
The ATSB identified that the aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go‑around, resulting in a landing beyond the planned touchdown point. Additionally, despite having sufficient landing distance remaining, the pilot did not apply sufficient braking to prevent the aircraft departing the runway
It was also determined that the training, supervision and checking flights conducted by Wave Air did not identify that an excessive approach speed was routinely being used by the pilot. Additionally, the pilot’s initial training was not fully completed, and they were not assessed on several abnormal and emergency procedures prior to operating unsupervised.
The ATSB also identified that Wave Air’s weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with its procedures. Finally, it was determined that the decision height for assessing whether an aircraft met Wave Air’s stabilised approach criteria was too low.
What has been done as a result
Wave Air has taken the following proactive safety action:
The operations manual was modified to require that the stabilised approach criteria be met by 300 ft above airport elevation in visual meteorological conditions and 500 ft in when operating under instrument flight rules.
The empty weight moment arm of the aircraft was corrected in the weight and balance system and the data of other aircraft was reviewed.
Passenger scales have been serviced and made accessible for routine passenger weighing in accordance with the operator’s procedure.
The training and checking manual has been updated to more precisely detail training criteria.
A new head of training and checking has been appointed.
Pilots are required to complete examinations prior to commencing in command under supervision (ICUS) training and operating unsupervised.
Updates have been made to the remedial training processes.
6-month flight reviews are now required for all pilots.
Safety message
Pilots should always be prepared to promptly execute a go-around if an approach for landing does not proceed as expected. Accurate knowledge of the aircraft’s reference speeds, in addition to having pre‑determined stabilised approach criteria, assist the assessment of whether an approach should be discontinued. Furthermore, routine practice of this manoeuvre will ensure that it can be performed safely when needed.
The occurrence
On 2 November 2024, a GippsAero GA8-TC Airvan, registered VH-IDM and operated by Wave Air, was being used to conduct a scenic flight with a pilot and 7 passengers on board. At 1120 local time, the aircraft departed from Whitsunday Airport (Shute Harbour), Queensland in‑company[1] with another of the operator’s aircraft as part of the same tour (Figure 1). Approximately one hour after departure, the 2 aircraft returned to the airport, joining the base leg of the circuit for a landing on runway 32.[2] VH‑IDM was leading the company and the pilot made positional broadcasts on behalf of both aircraft on the common traffic advisory frequency (CTAF).
Figure 1: Scenic flight route
Source: Google Earth, annotated by the ATSB
The airport did not have a dedicated Bureau of Meteorology (BoM) weather station, however the pilot recalled a cloud base at about 2,500 ft above ground level (AGL) and a 3–5 kt wind. Footage of the windsock at the time showed a light headwind on runway 32.
The pilot advised that, as the aircraft proceeded on the final approach to landing, they intended to maintain an airspeed of 80 kt and a flight path to arrive at the runway past the displaced threshold due to trees in the runway undershoot (see the section titled Whitsunday Airport (Shute Harbour)). However, the pilot reported that the aircraft did not descend as expected, resulting in it being above the intended approach path. In response, the pilot lowered the nose to increase the descent rate and regain the approach path, but as a result the airspeed increased from 80 to 90 kt.
At about this time, the trailing company aircraft contacted the pilot on the company frequency to request that they roll through to the end of the runway to exit after landing rather than backtracking. This was to avoid obstructing their landing. Because VH‑IDM could only broadcast on one of its 2 radios, the pilot selected the standby frequency (that was selected to the company frequency) on that radio, replied that they would roll through, and then reselected the CTAF frequency.
The aircraft continued the approach (Figure 2), remaining above the desired approach path while the airspeed varied between 85–95 kt. The aircraft passed over the displaced threshold of the runway at approximately 100 ft AGL. The pilot commenced the flare about 300 m beyond the displaced threshold, at an airspeed of approximately 90 kt. The aircraft then floated for about 640 m before touching down at a groundspeed of 65 kt with 370 m of runway remaining. The pilot recalled that throughout the approach and landing they did not consider conducting a go‑around[3] and were focused on landing the aircraft.
Figure 2: VH-IDM flight path and landing roll
Source: Google Earth, annotated by the ATSB
After touching down, the pilot retracted the flaps and recalled attempting to apply full braking pressure. They further recalled that the brakes did not perform as expected and they were unable to bring the aircraft to a stop. Subsequently, veering slightly right, the aircraft departed the end of the runway at a groundspeed of 24 kt. The aircraft travelled briefly across grass before entering marshy ground and coming to rest in a ditch, as the propellor struck the ground. Neither the pilot nor any of the passengers were injured and the aircraft received damage to the propellor and firewall (Figure 3)
Figure 3: VH-IDM damage
Source: Wave Air
After verbally confirming with the passengers that they were uninjured, the pilot advised the pilot of the trailing company aircraft via radio of the accident, before exiting and assisting the passengers to evacuate the aircraft. The trailing aircraft landed at approximately the same time as VH‑IDM came to a stop and taxied to the terminal after confirming the safety of the pilot and passengers of VH‑IDM.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) issued in 2020 and a class 1 aviation medical certificate. They had accumulated 1,103 hours, of which 15 hours were operating the GA8‑TC Airvan and 225 hours were operating the non‑turbocharged GA8 Airvan. In the previous 90 days, the pilot had accumulated 170 hours, all in the GA8 and GA8‑TC. The pilot had been flying with the operator since June 2024 and had flown almost exclusively from Whitsunday Airport (Shute Harbour). The pilot had last conducted a flight review as part of an instrument proficiency check in December 2022.
While the pilot reported having limited sleep in the 24 and 48 hours prior to the accident, the ATSB examined the possible effect of fatigue and determined that they were not experiencing a level of fatigue known to affect performance.
Aircraft information
General information
VH-IDM was a GippsAero GA8-TC Airvan fitted with a Lycoming TIO‑540‑AH1A turbocharged piston engine. The aircraft was manufactured and first registered in 2009 and at the time of the accident had accumulated 1,240 hours total time in service.
A service bulletin that allowed an increased maximum take‑off weight of 1,905 kg and maximum landing weight of 1,860 kg had been completed on the aircraft. The aircraft was being maintained in accordance with the GA8‑TC‑320 maintenance schedule. A periodic inspection had been completed the morning of the accident and the maintenance release showed no outstanding items. The accident flight was the first flight following the inspection. The pilot advised that a different aircraft had originally been scheduled to be used for the occurrence flight, however the operator substituted VH‑IDM at the ‘last minute’.
Brake system
The aircraft’s brake system included toe brakes incorporated into the rudder pedals. Each rudder pedal was connected hydraulically to a brake unit on the corresponding main landing gear wheel and was engaged by applying pressure to the top of the pedal (Figure 4). During flight, a pilot’s feet rested on the floor in contact with the lower part of the rudder pedals to control the rudder. On the ground, a pilot would move their feet up on the pedal so that the top of the foot could be used to apply brake pressure. The heel was then used to maintain rudder control and nosewheel ground steering.
Figure 4: GA8-TC rudder pedals and brakes
Source: ATSB
The pilot did not report any issues with the braking performance of the aircraft prior to take‑off, and the ATSB was advised that no fault was found with the brakes during the post‑accident inspection. Additionally, there were no marks observed on the runway to indicate that the wheels had locked up and the aircraft had skidded. The pilot also advised that their seat position had been adjusted appropriately and that all controls, including the rudder pedals, could be used effectively.
Whitsunday Airport (Shute Harbour)
Whitsunday Airport (Shute Harbour) was a privately‑owned, uncertified airport (aircraft landing area) located in hilly terrain onshore from the Whitsunday Islands. The airport had a single sealed runway 14/32, which was 1,410 m long and 15 m wide (Figure 5). Runway 32 had a displaced threshold due to trees in the undershoot, which reduced the runway available for landing to 1,310 m. The displaced threshold and departure end of the runway were at elevations of approximately 80 ft and 20 ft respectively, giving it a downslope of approximately 1.4%.
Figure 5: Whitsunday Airport runway environment
Source: Google Earth and passenger video footage, annotated by the ATSB
The airport’s management published a Visiting pilot’s guide that provided information regarding operating at the airport and procedures for approaching and departing each runway. The arrival procedure for runway 32 specified that:
A straight in approach requires a slight right hand dog leg on final to maintain terrain clearance. After following the centre of Shute Harbour water in towards the valley, a right hand dogleg should be made prior to crossing Shute Harbour Road. When necessary to join base for runway 32, keep south of the Shute Harbour Jetty. Land after the displace threshold - this applies to both ends.
The airport management also had a website which contained the above information but also included detail that the:
Touchdown aiming point (Displaced Landing Threshold) is no shorter than the windsock on the lefthand side of the runway.
The pilot advised that landing on runway 32 required modifications to a standard approach. Firstly, as described in the pilot’s guide, high terrain to the south‑west required an oblique approach before aligning with the runway centreline to maintain terrain clearance. Secondly, trees near the arrival end of the runway necessitated a higher approach and could result in visual contact with the displaced threshold being lost. Lastly, due to the downslope of the runway it was necessary to touch down as early as possible to avoid an extended float. The pilot advised that due to the combination of the trees and the downslope they were required to get over the trees and then ‘chop the power’. The pilot of the trailing company aircraft provided similar advice regarding these considerations when landing on runway 32.
As an uncertified airport, Whitsunday Airport was not required to comply with any obstacle or terrain clearance standards. The Civil Aviation Safety Authority (CASA) Advisory Circular (AC) 91‑02 Guidelines for aeroplanes with MTOW not exceeding 5,700 kg - suitable places to take off and land providedguidance for pilots when determining the effect of obstacles on, and in the vicinity of, an uncertified aerodrome:
Pilots should be aware that uncertified aerodromes may declare an available runway length that begins and ends directly at an obstacle. Common examples might be small trees at the beginning or the end of the runway surface.
During landing, high ground or obstructions in the approach area can cause a pilot to adopt a higher than normal approach path to avoid the obstacle, but still achieve a touchdown early in the available runway length…In all cases, the likely outcome is a long landing and the subsequent psychological effect of continuing a landing from an unusual situation outside the experience of the pilot.
Recorded data
VH-IDM was equipped with ADS‑B out capability however flight data was not available for the approach and landing portion of the flight. Two passengers took video recordings of the landing and runway excursion on their mobile phones. Both passengers were seated on the right of the aircraft, one in the first row behind the pilot, and the second one row further back. The recordings showed the view through the front of the aircraft, as well as sections of the instrument panel and certain actions conducted by the pilot (Figure 6).
Figure 6: Passenger video footage
Note: Altitude is above mean sea level (AMSL). Adjustment of 30 ft applied to aircraft altimeter. Source: Passenger video annotated by the ATSB
From the passengers’ videos, the ATSB was able to determine the flight path and speed of the aircraft throughout the approach and landing. While the pilot advised their intended aim point was just past the displaced threshold, the aircraft maintained an average descent path of approximately 7° towards a landing spot 300 m beyond the displaced threshold. Overhead the displaced threshold, the aircraft was approximately 100 ft above ground level. Throughout the approach, the navigation unit displayed the groundspeed as between 90–95 kt. The airspeed indicator was also periodically visible and showed readings up to 95 kt.
After the commencement of the flare, the aircraft floated for approximately 640 m. During the float, the aircraft decelerated and with about 560 m of runway remaining was at the landing approach speed of 71 kt (see the section titled Landing Performance). Subsequently, the main wheels contacted the ground with approximately 370 m of runway remaining at a groundspeed of 65 kt. The aircraft took 18 seconds to reach the end of the runway, during which the groundspeed slowed from 65 kt to 24 kt.
The pilot was observed to reduce the throttle at several points during the final approach with the last reduction observed just prior to the flare. This indicated the approach was conducted with some power. The pilot was also observed to interact with the radio unit during the final approach, which was likely when responding to the trailing aircraft. The video confirmed that the flaps were set to 38° for landing and were retracted immediately upon touchdown. Also on touchdown, the pilot’s feet moved upwards on the rudder pedals and pressure was applied against the pedals during the landing roll. However, it could not be ascertained whether the pressure was maintained throughout the landing roll, or whether the pressure was being applied to the top of the pedals to apply brakes or to the bottom of the pedals for rudder and steering.
Weight and balance
Software
The operator used a third‑party system to calculate the weight and balance for each flight. In the system, each aircraft was configured with the weight and moment arm[4] when empty. Subsequently, for each flight, the fuel onboard, the pilot and passengers’ weights and their seating positions were recorded to calculate both the weight and centre of gravity of the aircraft at take‑off and landing. The system would provide an alert if the limits prescribed in the aircraft flight manual (AFM) were exceeded. A paper copy of the weight and balance calculation was provided to the pilot before each flight.
Aircraft empty weight
VH-IDM was last weighed on 12 August 2024 and the empty weight was determined to be 1,058 kg, with an empty weight moment arm of 1,202 mm. The operator advised that the aircraft was weighed in the freight configuration, therefore they added the weight of the operational equipment required for passenger carrying from the AFM, establishing the weight as 1,110.6 kg. The operator further advised that to provide a safety margin, a higher weight of 1,134 kg was configured in the system.
The ATSB identified that the empty weight moment arm was not adjusted to account for the added passenger operational items, with the freight configuration arm of 1,202 mm being used. Additionally, the operator had inadvertently added the weight of one passenger seat to each row, rather than 2. The ATSB calculated that the actual empty weight of VH-IDM in passenger configuration was 1,131.3 kg, with an empty weight moment arm of 1,275 mm. This was 2.7 kg less than the empty weight and 73 mm aft of the empty weight moment arm compared to that configured in the operator’s weight and balance system (Table 1).
Table 1: Operator vs ATSB empty weight and arm
Item
Operator weight (kg)
ATSB‑calculated weight (kg)
ATSB‑calculated moment arm (mm)
Aircraft empty weight (freight)
1,058
1,058
1,202
Passenger operational equipment
52.6
73.3
2,329
Aircraft empty weight (passenger)
1,110.6 (1,134 used)
1,131.3
1,275
Passenger weights
The operator’s standard operating procedures (SOPs) required that in determining the weight and balance of an aircraft:
Actual weights will be determined by weighing all occupants, equipment and other baggage.
The operator’s website also required that:
Full names and exact weights per passenger must be advised when booking due to flight weight availability.
The passengers reported that their weight was requested at the time of booking, but they were not weighed prior to the flight.
The CASA Multi-part AC 121‑05, AC 133‑04 and AC 135‑08 – Passenger crew and baggage weights described acceptable weight calculation methods that could be defined in operating procedures. The circular stated that:
The use of actual weights is the most accurate method of maximising payload capacity. Appropriately calibrated weighing scales should be used. Actual weighing is more commonly used by Part 133 and 135 operators. This is, in part, due to the smaller number of passengers being carried, which makes this option less disruptive than it is for Part 121 operators.
Operators should have procedures to identify when passenger-declared weights are not appropriate, such as when operating close to limitations. Under these circumstances, the use of actual weights may be required to ensure limitations are not exceeded.
Passenger-declared weights have inherent inaccuracies as passengers may not know their actual weight, especially when fully dressed. An adjustment allowance should be added to any passenger‑declared weight, as a factor or a fixed additional amount.
Take-off and landing weight
The ATSB requested actual weights from the pilot and passengers including the baggage they took with them on the flight. Using this information, in conjunction with the revised empty weight and moment arm, the take‑off and landing weight and balance of the aircraft was calculated and compared to that calculated by the operator (Table 2).
Table 2: Operator‑ vs ATSB‑calculated take‑off and landing weight – accident flight
Item
Operator‑calculated weight (kg)
Operator‑calculated moment arm (mm)
ATSB‑calculated weight (kg)
ATSB‑calculated moment arm (mm)
Aircraft empty weight
1,134
1,202
1,131
1,275
Row 1 (pilot row)
117
965
122
965
Row 2
135
1,772
132
1,772
Row 3
148
2,523
154
2,523
Row 4
150
3,247
146
3,247
Fuel
215
1,715
215
1,715
Take-off weight (Maximum 1,905 kg) (Allowable moment arm range 1,446 mm – 1,626 mm)
1,899
1,550
1,900
1,592
Fuel Used
41
1,715
41
1,715
Landing weight (Maximum 1,860 kg) (Allowable moment arm range 1,435 mm – 1,626 mm)
1,858
1,547
1,859
1,589
While the take‑off and landing weight differed by 1 kg, the actual moment arm was 42 mm aft of that calculated by the operator. This was still less than the maximum of 1,626 mm specified in the AFM. However, the ATSB identified loading scenarios where the operator’s configuration would present the weight and balance as acceptable, when the actual moment arm was aft of this limit (Table 3).
Table 3: Operator‑ vs ATSB‑calculated take‑off weight – aft centre of gravity limit scenario
Item
Operator‑calculated weight (kg)
Operator‑calculated moment arm (mm)
ATSB‑calculated weight (kg)
ATSB‑calculated moment arm (mm)
Aircraft empty weight
1,134
1,202
1,131
1,275
Row 1 (pilot row)
96
965
96
965
Row 2
100
1,772
100
1,772
Row 3
100
2,523
100
2,523
Row 4
259
3,247
259
3,247
Fuel
215
1,715
215
1,715
Take-off weight (Maximum 1,905 kg) (Allowable moment arm range 1,448 mm – 1,626 mm)
1,904
1,625
1,901
1,670 (44 mm aft of the allowable limit)
Pilot training
Operator proficiency check
Prior to conducting scenic flights unsupervised, the operator’s SOPs required the pilot to successfully complete an operator proficiency check (OPC). The flight component of the OPC was conducted without passengers and provided an assessment of the pilot’s competency in normal, abnormal and emergency procedures when operating the aircraft.
Upon starting with the operator, the pilot conducted a one‑hour supervised flight in a non‑turbocharged GA8 with the head of flying operations (HOFO),[5] where initial handling training was conducted. This was the pilot’s first flight operating a GA8. The pilot recalled that the flight included conducting steep turns, stall recovery and several circuits on runway 14 at Whitsunday Airport. They reported being uncertain whether a go‑around or a short field landing was conducted during that flight. The pilot also did not recall that they had practiced applying maximum braking, nor that they had done so subsequently.
At the conclusion of the flight, the HOFO completed an OPC assessment, which recorded that several items had been assessed as ‘competent’ including a go‑around and a short field landing. However, several items were marked as ‘not yet competent’ including low‑level flying, flapless landing, basic instrument flying, engine failure and forced landing and aircraft system malfunctions as these items were not conducted during the flight. While the OPC was not completed, no subsequent OPC was conducted prior to the pilot operating unsupervised.
The operator advised the ATSB that due to the nature of some of the flight sequences, a flight training organisation (FTO) had been engaged to conduct OPCs. The FTO had last conducted training and assessment for a group of the operator’s pilots in March 2024, prior to the accident pilot’s commencement with the operator. The operator further advised that due to the timing of their commencement, the pilot had not conducted an OPC with the FTO and that this was an oversight.
Line training and line check
The operator’s line training consisted of a series of flights with a supervising pilot, with passengers on board. Following line training, a line check was conducted, after which a pilot could operate unsupervised if an OPC had also been completed. Training records and the pilot’s logbook showed that 9 supervised flights totalling 9.9 hours were conducted in June 2024 prior to a line check flight. The flights were supervised by 3 different pilots including the HOFO. Following a line check conducted by the HOFO, the pilot commenced operating unsupervised.
General emergency training
The operator required the pilot to successfully complete a general emergency procedures competency check for the aircraft type being flown. This consisted of ground‑based topics and an in‑water practical component. While training records were not available, both the operator and the pilot recalled that the ground‑based training had been completed. However, the in‑water practical component was not conducted. The operator advised that the most recent in‑water training session had occurred in May 2024, prior to the pilot commencing, and that this was also an oversight.
The pilot reported that they had completed in‑water practical training with 2 previous operators, initially in August/September 2022 and subsequently in September/October 2023. They also completed the training with the current operator after the accident and advised that the training provided by all operators involved donning and inflating a lifejacket while in water. They also reported that the while the training conducted by the previous operators was conducted in a swimming pool, the training with the current operator was conducted in open water and included carrying an injured passenger and discussion of survival skills.
Differences training
The SOPs required that differences training was conducted prior to operating an aircraft of the same type with performance differences. Additional training was therefore required prior to operating a turbocharged GA8-TC, such as VH‑IDM, when initial training had been conducted in a non‑turbocharged GA8.
The operator had provided documentation to the pilot on the differences in operating the GA8‑TC and a supervised flight was conducted with the HOFO in October 2024, prior to operating the aircraft type unsupervised.
Recognition of prior learning
The operator’s procedures allowed flight crew members who had completed training with other operators to be eligible for recognition of prior learning (RPL). The procedures further advised that the training needed to have been completed within the previous 6 months, and could be applied to the following training events:
general emergency training
differences training
line training.
Approach speed
The operator reported that pilots were taught to conduct the final approach to land at an airspeed of 70 kt with 500 ft/min descent rate. They also advised that there was no difference between the approach and landing speeds when operating the GA8 compared to the GA8‑TC. Additionally, the operator’s SOPs stated that:
During the approach phase the pilot-in-command shall ensure that the aircraft is flown at the approach speeds (VREF) provided in the Aircraft Flight Manual for the aircraft being flown.
The FTO advised that pilots were taught and assessed in the non‑turbocharged GA8 on establishing a reference airspeed (VREF)[6] of 71 kt on final as per the AFM. They also advised that no training or assessment had been conducted in the GA8‑TC.
The pilot reported that they considered 80 kt as the appropriate final approach speed. However, they also stated that, following discussions with other pilots after the accident, they now understood that 70–75 kt was an appropriate final approach speed. The ATSB was also advised that the pilot had been observed landing long on previous occasions, however this had not been communicated to the operator or discussed with the pilot.
The pilot of the trailing aircraft reported they typically aimed for 80 kt on final and were ‘happy to get it down to about 75 [kt] on runway 32’. They also reported that for a short field landing they used 70–75 kt on final.
Landing Performance
The AFM provided performance charts to calculate the expected landing distance and ground roll. At a landing weight of 1,860 kg with a runway slope of −1.4% and the atmospheric conditions present at the time of the accident, the expected landing distance required was calculated to be 480 m, including a ground roll of 210 m. The AFM further described the reference speed and technique for achieving this performance:
airspeed at 50 ft of 71 kt
power off, 7° approach profile
38° (full) flap
aircraft approaches with idle power at the given airspeed appropriate to weight
after touch down maximum wheel braking is used to bring the aircraft to a stop
for maximum braking effectiveness the wing flaps should be retracted and back pressure applied to the control column.
The AFM also stated that:
Care must be taken to ensure airspeed is accurately maintained during the final landing approach. Timely and appropriate use of power should be exercised to maintain the desired flight path and airspeed. Excessively high approach speeds will result in prolonged floating and increased landing distance.
The AFM also provided performance charts for a 3° approach angle with power. In this circumstance the landing distance was expected to be higher due to the lower approach angle, with the ground roll remaining approximately the same.
Stabilised approach criteria
The operator’s procedures specified that aircraft should be on a stabilised approach as early as practical on the final approach path and that the following criteria were required for an approach to be stable:
• the aircraft is on (or close to) the correct flight path, only small changes in heading and pitch being required to maintain that path
• the aircraft speed is not more than Vref + 20 kt and not less than Vref
• the aircraft is in the proper landing configuration (except that full flap should not be selected until committed to land)
• sink rate is maximum 1,000 ft/min
• power setting appropriate to the configuration but not below any minimum power for approach specified in the Aircraft Flight Manual
• all briefings and checklist items have been performed.
In visual conditions, if these criteria were exceeded below 100 ft above airport elevation, the pilot was required to execute a go‑around.
The ATSB calculated that if an aircraft was 20 kt above the landing reference speed at the 100 ft decision height, in a power off 7° approach descent, the pilot had 2.7 seconds to reduce their speed to the landing reference speed. By comparison, a decision height of 300 ft would increase this time to 13.3 seconds while a decision height of 500 ft would increase the time to 23.9 seconds.
CASA provided guidance in AC 91‑02 on initiating go‑arounds in response to an unstable approach, stating that:
Pilot training emphasises that a safe landing is the result of a stabilised approach. If pre-determined stabilised approach criteria are exceeded, then a safe landing is not assured. The decision to execute a go-around should be made as early as possible to maximise the safety outcome. At the conclusion of an effective go-around, the pilot will then have an opportunity to consider what options are available to conclude the flight.
Additionally, the Flight Safety Australia article Quantifying the go-around (CASA, 2021) highlighted the importance of practicing go‑arounds:
It’s not enough to pass the test and fly a go-around only every couple of years when tasked by an instructor. Consciously ask yourself if you’re in the slot, judging your aeroplane’s state and trend all the way down final. By quantifying your performance, you can make the go-around decision before you are at the highest risk of loss of control.
Going around is as natural a part of flying as landing itself – or it will be, if you evaluate landing criteria every time and occasionally practice the go-around task.
The pilot advised that, in addition to not considering a go‑around during this approach, they could not recall having previously conducted a go‑around outside of training.
Related occurrences
The ATSB occurrence database contained 200 other reported occurrences of runway excursions during landing in Australia between January 2021 and December 2024. Of these, 12 resulted in injuries to the pilot and/or passengers, including 2 where the injuries were serious.
Included in these occurrences were 2 other runway excursions involving a GA8 Airvan, both of which were investigated by the ATSB:
Runway overrun involving GippsAero GA8, VH-WSB on 26 December 2021 (AO-2022-001)
During the landing, the aircraft floated significantly beyond the intended landing point. The pilot did not recognise the risk of a runway overrun and did not conduct a go‑around or apply sufficient braking to stop the aircraft on the remaining runway.
Runway excursion involving GippsAero GA8, VH-TBU on 6 April 2023 (AO-2023-016)
During the landing, the aircraft floated for a significant time and touched down approximately halfway down the runway, with insufficient remaining runway to stop. While the pilot recognised opportunities to conduct a go-around when they determined they were not on the correct approach profile, this was not conducted.
Safety analysis
Pilot actions
Approach and landing
During the approach to land, the aircraft’s flight path was significantly above that intended, with an aim point approximately one third down the runway. While the deviation was likely influenced by the associated terrain and obstacles, the pilot had conducted this approach regularly and was familiar with the required approach path to land safely. The deviation was also possibly influenced by distraction when interacting with the radio to respond to the pilot of the trailing aircraft and by implied pressure to minimise the time spent on the runway.
Attempting to regain the intended flight path, the pilot lowered the nose, but did not reduce the power to idle. Subsequently, the aircraft’s airspeed increased to approximately 95 kt. While the pilot planned 80 kt as the airspeed on final, the approach airspeed required by the operator was 70–71 kt. This approach speed was also the reference landing approach speed (Vref) in the aircraft flight manual (AFM). Therefore, the aircraft’s airspeed deviation was about 24 kt.
While recognising that the aircraft was above the intended flight path and faster than the intended airspeed, the pilot continued the approach. The operator’s procedures required a go‑around to be conducted when the aircraft was not on the correct flight path or was more than 20 kt faster than the landing approach speed below 100 ft. While the airspeed was within this limit based on the pilot’s incorrect understanding that the approach speed was 80 kt, the aircraft was not on the correct flight path and therefore a go‑around was required. However, the pilot did not consider a go‑around and commenced the flare well beyond the planned touchdown point at a high airspeed. Due to the high airspeed and the downslope of the runway, the aircraft floated significantly before touching down with less than a third of the runway remaining.
Contributing factor
The aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go‑around, resulting in a landing beyond the planned touchdown point.
Landing roll and braking
Despite the reduced runway available, performance calculations determined that sufficient runway remained for the aircraft to stop if maximum braking was applied. However, although the pilot was observed retracting the flap and applying pressure to the rudder pedals, the aircraft did not decelerate as expected. Given the braking system was functional prior to take‑off and after the accident and there was no indication that the aircraft skidded, maximum braking application was likely not conducted effectively. Subsequently, due to the insufficient braking, the aircraft departed the end of the runway.
Contributing factor
Despite having adequate landing distance remaining, the pilot did not apply sufficient braking to prevent the aircraft departing the runway.
Training and assessment
Initial training
The ATSB considered the effect of the training the pilot received from the operator prior to the accident. Given the elapsed time since their last flight review, additional training from a flight training organisation would have given them opportunity to practice procedures such as go‑arounds and short field landings. In addition, the operator did not complete the operator proficiency check and as a result the pilot was not assessed on several abnormal and emergency procedures in the GA8. However, the pilot was assessed as competent in both go‑arounds and short field landings during the initial handling training and had completed a number of line training flights that would have given them time to practice basic handling skills.
The general emergency training required an in‑water practical exercise that was not conducted. While recognition of prior learning was able to be applied to this training event, training with another operator was completed more than 6 months prior and so was not applicable. However, given the pilot had received this training twice in the preceding 26 months from other operators and the training was similar, it was likely that the pilot was competent in this area.
Other factor that increased risk
The pilot’s initial training was not fully completed, and they were not assessed on several abnormal and emergency procedures prior to operating unsupervised.
Approach speed
The pilot had received initial handling training and conducted line training flights supervised by 3 different pilots. They had also passed a line training check and had recently received differences training in the GA8‑TC. Notwithstanding this, the pilot’s pattern of using the incorrect approach speed was not identified or corrected.
Contributing factor
The training, supervision and checking flights conducted by Wave Air did not identify that an excessive approach speed was routinely being used by the pilot during the final approach to land. (Safety issue)
Weight and balance
The ATSB determined that the empty weight for the aircraft was calculated incorrectly, however as the operator had increased the weight in the system as a safety buffer, this did not have an effect. Additionally, the empty weight moment arm used to calculate if the aircraft’s centre of gravity was within the allowable limits, was not adjusted for the additional operational items. As a result, the system calculated the aircraft’s centre of gravity forward of the actual position. While the actual weight and centre of gravity of the accident flight was within limits for both take‑off and landing, the incorrect empty weight moment arm permitted the aircraft to be loaded in a way that the centre of gravity was aft of the limit, while presenting to the pilot as within.
Furthermore, passengers were not weighed prior to flight and instead passenger‑declared weights were used. This was not in accordance with the operator’s procedures and was not recommended when operating close to the weight limitations of the aircraft.
Other factor that increased risk
Wave Air's weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with their procedures. (Safety issue)
Stabilised approach criteria
It was determined that the decision height for assessing if the aircraft met the operator’s stabilised approach criteria was too low. As in this case, where an aircraft’s airspeed was 20 kt faster than Vref at 100 ft (the decision height), it was very unlikely that the aircraft could be slowed to the reference landing approach speed in 2.7 seconds, most likely leading to a go‑around.
While go‑arounds are a normal aspect of flying, as stated in AC 91‑02, ‘the decision to execute a go‑around should be made as early as possible to maximise the safety outcome’. However, in this case the pilot did not consider the operator’s stabilised approach criteria in their decision‑making.
Other factor that increased risk
The decision height for assessing whether an aircraft met Wave Air’s stabilised approach criteria was too low. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion involving GippsAero GA8-TC, VH-IDM, at Whitsunday Airport (Shute Harbour), Queensland on 2 November 2024.
Contributing factors
The aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go-around, resulting in a landing beyond the planned touchdown point.
Despite having adequate landing distance remaining, the pilot did not apply sufficient braking to prevent the aircraft departing the runway.
The training, supervision and checking flights conducted by Wave Air did not identify that an excessive approach speed was routinely being used by the pilot during the final approach to land. (Safety issue)
Other factors that increased risk
The pilot’s initial training was not fully completed, and they were not assessed on several abnormal and emergency procedures prior to operating unsupervised.
Wave Air's weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with their procedures. (Safety issue)
The decision height for assessing whether an aircraft met Wave Air’s stabilised approach criteria was too low. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The training, supervision and checking flights conducted by Wave Air did not identify that an excessive approach speed was routinely being used by the pilot during the final approach to land.
Safety issue description: Wave Air's weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with their procedures.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and operator
Whitsunday Airport (Shute Harbour)
Civil Aviation Safety Authority
Submissions were received from:
the pilot
the operator
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]In-company: a group of aircraft that navigate and communicate as a single unit. Each aircraft self-separates from other aircraft within the group.
[2]Runway number: the number represents the magnetic heading of the runway.
[3]Go-around: a standard aircraft manoeuvre that discontinues an approach to landing.
[4]Moment arm: the horizontal distance from a reference datum to the centre of gravity of an item.
[5]The same person held the roles of HOFO and the head of training and checking for the operator.
[6]Reference Landing Approach Speed: the airspeed equal to 1.3 stall speed, and is the airspeed used on approach down to 50 ft above the runway when determining landing distances.
Occurrence summary
Investigation number
AO-2024-056
Occurrence date
02/11/2024
Location
Whitsunday Airport (Shute Harbour)
State
Queensland
Report release date
07/05/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Gippsland Aeronautics Pty Ltd
Model
GA8-TC320
Registration
VH-IDM
Serial number
GA8-TC 320-08-137
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes