Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At around 0537 local time (before sunrise) on 13 May 2024, an Aero Commander 500-S (AC500) was taxied for departure at Brisbane Airport, Queensland on a regular scheduled freight flight to Dalby Airport, Queensland. The pilot was the sole person on board.
The aircraft was cleared for a departure from runway 01R[1] at the intersection of taxiway A7, and the pilot taxied to this holding point. While turning onto the runway, the pilot inadvertently lined up along the left side runway edge lighting instead of the runway centreline.
During the take-off run, it became increasingly apparent to the pilot that the aircraft was to the left of the centreline, and they took corrective action to reposition the aircraft centrally on the runway and continued with the take-off. The aircraft rotated[2] and departed without further incident. The pilot later advised that they had mistaken the runway edge lights for centreline lighting and although after completing the turn onto runway 01R they noticed something ‘didn’t feel right’ with the position of the aircraft, they thought that the left wheel of the aircraft was to the right of the lights and so the aircraft was on the runway.
Around 10 minutes after take-off, the pilot contacted Brisbane ground controllers to report a possible ‘bump on the runway’ during the departure and advised of the need to conduct a runway inspection. An airport vehicle was sent to the intersection to investigate but no damage was identified at that time, and this information was relayed back to the pilot and the operator. A routine inspection of the runway was conducted at first light,[3] and this inspection also did not identify any damage at that intersection.
Four hours later at around 0934, another runway inspection was conducted for an unrelated matter. During this inspection multiple broken runway edge lights near the intersection with taxiway A7 were identified (Figure 1). The runway was briefly closed to traffic while standard procedures were followed to assess and clear the damage. CCTV footage was subsequently reviewed by the airport operator, and it was determined that the damage to the runway edge lights had been caused by the AC500 several hours earlier.
Figure 1: Damage to runway lighting at intersection of taxiway A7 and runway 01R
Source: Supplied, annotated by the ATSB
It was later established that the runway stop bars and all runway and taxiway lights were operational when the AC500 departed. Weather conditions were CAVOK[4] with no known limitations on ground visibility. A total of 3 runway edge lights were damaged. The operator reported some damage to the underside of the aircraft, but no injuries were reported.
Intersection lighting and markings
Markings
Taxiway
The taxiway had a single yellow unbroken centreline with a black border up to the runway holding point at A7, after which the line continued as an unbroken yellow line going straight across the runway. The holding point was marked with 2 solid lines and 2 broken lines. The taxiway edge was marked by a double yellow line, which intersected with the white runway edge line (Figure 2).
Runway
The runway centreline is a broken white line for the length of the runway. There were also 2 yellow taxiway lead-off lines (for the reciprocal runway) which led to holding point A7. The runway edge markings were solid white unbroken lines that run continuously for the length of the runway, except across intersecting taxiways.
Adding to the complexity of the layout at this intersection, is a pair of runway touchdown zone markings, which consist of thicker solid white lines that are between the runway edge lines and the runway centreline.
Figure 2: Overview of the markings at the intersection of taxiway A7 and runway 01R
Source: Google Earth, annotated by the ATSB
Lighting
Runway 01R had medium-intensity, omni-directional white runway edge lights and white centreline lighting. The A7 holding point had elevated flashing yellow runway guard lights, and a stop bar in the form of a row of red lights. The taxiway centreline lights were green. Videos were provided to the ATSB to illustrate the visual and lighting conditions at night at the intersection, and screenshots were taken from those videos to provide a visual representation. The taxiway lights and runway stop bar lights are shown in Figure 3.
Figure 3: Lighting on taxiway A7 approaching the stop bars prior to runway 01R
Source: Supplied, annotated by the ATSB
Once pilots are cleared to enter or cross runway 01R from holding point A7, the red stop bars were deactivated and the green lead-on lights activated as shown in Figure 4.
Figure 4: Lighting on taxiway A7 after clearance given to cross or enter runway 01R
Source: Supplied, annotated by the ATSB
Figure 5: Lighting and markingsat intersectionafter clearance given to cross or enter
Source: Supplied, annotated by the ATSB
Figure 6shows the likely position of the aircraft on the runway immediately prior to commencing the take-off run, and highlights the risk of not following the green taxiway lights onto the runway.
Figure 6: Likely line-up of AC500 on runway 01R immediately prior to take-off
Source: Supplied, annotated by the ATSB
Similarities to previous incidents
The misaligned take-off on 13 May 2024 was not the first such incident at that location. In October 2016, the ATSB investigated a near-identical occurrence involving a misaligned take-off and runway excursion from the same intersection at night.[5] On that occasion, pilot distraction at a critical moment prior to take-off contributed to them not noticing that the aircraft was incorrectly positioned on the runway. Another contributing factor was the darkness of the intersection and low visibility of the taxiway centreline markings. The pilot reported feeling that ‘something was not right’ and realigned the aircraft during the take-off run. The pilot did not believe they had hit any objects, but a subsequent inspection by ground personnel located several damaged left side runway edge lights. Since this incident, runway stop bars and lead-in lights have been introduced at Brisbane Airport as a visual aid to assist pilots.
Safety action
Following the incident, the operator issued a notice to their pilots in response to several incidents involving Aero Commander 500 aircraft at Brisbane Airport. This document noted that the AC500 ‘has the lowest taxiing pilot eye-height of any aircraft regularly using the airport’. This has resulted in pilots having difficulty with distance judgement and aircraft positioning on very wide taxiways and runways.
The document also advised pilots that the centreline of runway 01R, when viewed from taxiway A7, is raised to allow lateral water drainage. From the cockpit, the far side of the runway can be difficult to see, and pilots can mistake the runway centreline lights for the far side edge lights.
The operator also emphasised that AC500 pilots must follow the green ‘lead-on’ lights (see Figure 4) when lining up on the runway.
Safety message
This incident highlights the need for pilots to maintain situational awareness and avoid distractions when entering an active runway particularly at night. This is especially important in the seconds between receiving a clearance to enter the runway and completing the turn onto the runway. Radio calls, conflicting traffic, or the completion of standard checklist items such as the activation of landing and strobe lights can cause task-saturation and divert a pilot’s attention at a critical moment. In some circumstances, risk may also be reduced by limiting intersection departures to daylight hours only. This ensures that all aircraft departing between last light[6] and first light enter the active runway and commence their take-off run from the runway threshold where lighting and markings are most prominent.
The ATSB produced a research report, Factors influencing misaligned take-off occurrences at night, which outlines a series of conditions that are known to contribute to misaligned take-offs. Intersection departures were identified as one of 8 common factors which increased the risk of a misaligned take-off or runway excursion, with poor visibility and factors relating to lighting also contributing to past incidents.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]Rotation: the positive, nose-up, movement of an aircraft about the lateral (pitch) axis immediately before becoming airborne.
[3]First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions.
[4]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud, and no other significant weather. [AIP GEN 3.5 – METEOROLOGICAL SERVICES, Section 4 METEOROLOGICAL REPORTS, paragraph 4.4.1, subparagraph g; and Section 12 AERODROME WEATHER AND FORECAST DECODE, paragraph 12.13 CAVOK.]
[5]Misaligned take-off involving Beechcraft B200, VH-XGV, Brisbane Airport, Queensland, on 26 October 2016 (AO-2016-142)
[6]Last light: the time when the centre of the sun is at an angle of 6° below the horizon following sunset. At this time, large objects are not definable but may be seen and the brightest stars are visible under clear atmospheric conditions. Last light can also be referred to as the end of evening civil twilight.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-026
Occurrence date
13/05/2024
Location
Brisbane Airport
State
Queensland
Occurrence class
Incident
Aviation occurrence category
Runway excursion
Highest injury level
None
Brief release date
30/07/2024
Aircraft details
Manufacturer
Aero Commander
Model
500-S
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 8 June 2024, a de Havilland Canada DHC-6 Twin Otter, registered P2-BBM, had a runway excursion at Kikori Airstrip, Papua New Guinea.
The Papua New Guinea Accident Investigation Commission (AIC) is investigating the occurrence. AIC has requested assistance from the ATSB to decompress recovered flight data.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The ATSB provided the decompressed file to the AIC on 19 June 2024.
Any enquiries relating to the investigation should be directed to AIC.
Occurrence summary
Investigation number
AA-2024-007
Occurrence date
08/06/2024
Location
Kikori Airstrip, Papua New Guinea
State
International
Investigation type
Accredited Representative
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
The Transport Accident Investigation Commission (TAIC) of New Zealand has commenced an investigation into a runway excursion involving an Airbus A320, registered VH-VFF, at Christchurch Airport, New Zealand, on 30 May 2024.
During descent while conducting a passenger flight from Auckland, New Zealand, to Christchurch, the crew received a warning for one of the hydraulic systems, affecting the nose wheel steering. On landing, the aircraft had a runway excursion and made contact with a runway sign causing damage to the right engine. There were no reported injuries to crew or passengers and minor damage to the aircraft.
The TAIC requested assistance and the appointment of an accredited representative from the ATSB. To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of Annex 13 to the Convention on International Civil Aviation and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 19 March 2026, the TAIC released the final investigation report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation. A copy of the report can be obtained from the TAIC at: https://taic.org.nz/inquiry/ao-2024-004.
Any enquiries relating to the investigation should be directed to the Transport Accident Investigation Commission at https://taic.org.nz/.
Occurrence summary
Investigation number
AA-2024-005
Occurrence date
30/05/2024
Location
Christchurch Airport, New Zealand
State
International
Investigation type
Accredited Representative
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Serious Incident
Aircraft details
Manufacturer
Airbus
Model
A320-232
Registration
VH-VFF
Serial number
5039
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 11 April 2024, a flight instructor and student pilot were conducting a dual training flight under the instrument flight rules in a Beechcraft E55 aircraft, registered VH-OMD and operated by Fly Oz. The aircraft departed from Cowra Airport, New South Wales, and conducted instrument approaches to Goulburn and Canberra Airports, before returning to Cowra.
As the aircraft tracked over the Cowra non-directional beacon (NDB) to conduct a practise instrument approach to runway 15, the instructor simulated a failure of the left engine by moving the mixture lever to the idle cut-off position. The student continued the approach with the left engine inoperative and the propeller windmilling, then joined the circuit for runway 33 on the crosswind leg.
During the landing flare, the instructor initiated a go-around. The aircraft rapidly yawed and rolled to the left and impacted the ground in an almost vertical nose-down attitude before coming to rest inverted. The flight crew sustained minor injuries and the aircraft was substantially damaged.
What the ATSB found
The ATSB found that the instructor moved the left engine mixture lever to idle cut-off to simulate an engine failure over the navigation aid, and it was likely that they unintentionally did not subsequently move the lever to rich and ensure the engine was restarted and available for instant use, when attempting to set zero thrust on the downwind leg of the circuit. As a result, the instructor initiated a go-around below the minimum control speed, unaware the left engine was inoperative, resulting in an asymmetric loss of control.
The ATSB also found that Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. The use of the throttle to simulate an engine failure ensures the engine is available for immediate use, whereas using the mixture control increased the risk of an undetected inoperative engine during descent and landing, and the associated loss of control.
What has been done as a result
Fly Oz amended its multi-engine training to simulate engine failures only using throttle at any height. It has also taken the following proactive safety action:
Following a simulated engine failure, zero thrust is to be set immediately after the student has completed the engine failure drills.
The instructor standardisation manuals were being updated to include a requirement that both the student and instructor confirm that the pitch, power and mixture controls are set back to normal 2‑engine configuration during checks on final. This is now a call out item, ensuring that both pilots are satisfied with the correct settings.
Safety message
In conventional twin-engine aeroplanes, loss of power on one engine can lead to a loss of directional control and an accident if there is insufficient height above the ground to recover.
Aircraft manufacturers’ procedures for one engine inoperative training should be followed in the first instance. In this case, the manufacturer required the throttle be used to simulate an engine failure. In addition to the manufacturer’s procedures, Civil Aviation Safety Authority guidance recommended using the throttle rather than the mixture to simulate an engine failure when at low level – such as asymmetric instrument approaches. This ensures power can quickly be restored if needed.
Accidents as a result of engine malfunctions in twin-engine aeroplanes are rare, but often fatal. As such, training to manage one engine inoperative flight is important, but should not introduce unnecessary risks.
The occurrence
On 11 April 2024, a student pilot and flight instructor were conducting a dual instructional flight in a Beechcraft E55 aircraft, registered VH-OMD and operated by Fly Oz. The flight was the student’s third multi-engine aeroplane navigation exercise. The flight was to be conducted under the instrument flight rules,[1] from Cowra, New South Wales (NSW), to Canberra, Australian Capital Territory, and return. As the flight was conducted almost entirely in visual meteorological conditions,[2] the student wore a view limiting device or ‘hood’, to simulate flying in cloud or poor visibility.
OzRunways[3] flight path data showed that the aircraft departed Cowra Airport at 1156 local time. En route to Canberra, the student conducted an instrument approach[4] to Goulburn Airport, NSW, but did not land there. The student then conducted an instrument approach to Canberra, landed and taxied to the general aviation apron. After a short break, and without shutting down the engines, the aircraft departed Canberra Airport at 1323 via a standard instrument departure. The aircraft climbed to 10,000 ft above mean sea level (AMSL), tracked via waypoint AVBEG and commenced a descent when 35 NM from Cowra (Figure 1).
Figure 1: VH-OMD track from Cowra to Goulburn, Canberra and return via AVBEG
Source: OzRunways data overlaid on Google Earth, annotated by the ATSB
At 1404, the aircraft passed over the Cowra non-directional beacon (NDB)[5] at about 3,600 ft AMSL (2,600 ft above ground level) and commenced the NDB approach to runway 15. The instructor then simulated an engine failure, by pulling the left engine mixture control lever to the idle cut-off position. In that position, no fuel would flow from the injectors to the engine, but the magnetos would continue generating spark, and the propeller blades would windmill[6] unless feathered.[7]
In response, the student conducted initial engine failure checks and identified that the left engine was inoperative. At that time, the flight crew did not complete the operator’s one engine inoperative procedure to either feather the left propeller or set zero thrust to simulate a feathered propeller (see the section titled Simulated one engine inoperative – Fly Oz procedures). The flight path data showed that, consistent with the simulated left engine failure, the aircraft deviated left of the published outbound track, and tracked outbound on the published inbound track for about 2 minutes, before starting to correct to the right (Figure 2).
Figure 2: VH-OMD track overlaid on published Cowra NDB approach
Source: OzRunways and Airservices Australia data overlaid on Google Earth, annotated by the ATSB
About 4 minutes after passing over the NDB, the aircraft commenced a left inbound turn and was established within the required 5° tolerance of the published inbound track about 5 NM from the threshold of runway 15.
The Cowra Airport common traffic advisory frequency (CTAF) was not recorded. However, the student reported making the standard radio calls, including broadcasting when inbound and on downwind, and using the word ‘asymmetric’ in their calls to alert others that they were practising one engine inoperative procedures. The instructor reported communicating with the pilots of 2 other aircraft operating in the circuit at the time. Those 2 aircraft were operating on runway 33, which was the most into wind runway. To sequence with the circuit traffic, the instructor advised the student they were now ‘visual’ and could lift the hood and track to join the crosswind leg of the circuit for runway 33.
The instructor thought that they had set zero thrust either when inbound on the instrument approach or on the downwind leg of the circuit, and recalled first asking the student whether they wanted zero thrust set. However, the student recalled prompting the instructor to set zero thrust on downwind. The instructor reported that their normal procedure for setting zero thrust was to bring the propeller pitch lever to the feather detent, then push the mixture lever forward to rich and gradually move the left throttle lever forward until the manifold pressure gauge read about 10 inches Hg.[8] The instructor reported that, although they usually moved the engine/propeller controls slowly, there would be a detectable yaw[9] associated with returning power to the inoperative engine.
The student and instructor both reported that the student’s normal downwind checks included checking both mixture levers were in the fully rich position, but neither could recall when the checks were done. The student recalled extending the landing gear either just before, or when turning onto, the base leg of the circuit. Neither the instructor nor the student recalled when the student extended the approach (15°) stage of flaps. After turning onto final, the student reported completing their pre-landing checks by pushing both pitch levers forward to the full fine position, checking they had 3 green lights, which indicated the landing gear was down and locked, and electing not to extend full (30°) flap for landing.
A review of recorded flight data identified that the aircraft crossed the runway threshold at 1416:01 aligned with the runway centreline. The instructor reported that the student commenced the flare[10] a bit high and therefore directed them to add some power to cushion the landing. The instructor further reported that when the student added power, the aircraft immediately yawed significantly to the left such that it was no longer aligned with the runway. In response, the instructor called for a go-around. The student could not recall being asked to add power and reported that the main landing gear touched down on the runway before the instructor initiated the go-around. However, the instructor recalled that the wheels did not touch down and that the go-around commenced about 30–50 ft above the runway.
OzRunways data showed that the aircraft started to deviate left of the runway centreline at 1416:14 at 69 kt ground speed, but there was insufficient recorded information to determine whether or not it touched down prior to that occurring. The instructor reported taking control of the aircraft from the student and verifying that both throttle levers were fully forward. Assessing that the yaw was due to left rudder input by the student, the instructor called for the student to let go of the controls and applied right rudder, but was unsuccessful in regaining control of the aircraft. A witness facing away from the runway heard what they assessed as one engine power up and turned to see the aircraft 10–20 ft above the runway, pitched 10–12° nose-up, and in a rapid left roll (Figure 3).
Figure 3: VH-OMD track along the runway, accident site and witness location
Source: OzRunways data overlaid on Google Earth, annotated by the ATSB
The aircraft collided with the ground in a nearly vertical nose-down attitude and came to rest inverted (Figure 4). The student and instructor sustained minor injuries and it is possible that their recollection of events may have been affected by trauma associated with the collision. The aircraft was substantially damaged.
Figure 4: VH-OMD accident site
Source: Cowra Council
Context
Personnel information
The student was enrolled in Fly Oz’s commercial pilot licence (aeroplane), multi-engine aeroplane class and command instrument rating integrated flight training course. At the time of the accident, the student held a private pilot licence (aeroplane) and had accrued 247 hours of flying time, 11 of those in VH-OMD (all in the last 90 days), with 7 hours recorded as instrument flight time.
The instructor held a commercial pilot licence (aeroplane), with multi-engine aeroplane class and command instrument ratings, which they had attained at Fly Oz. The instructor had accrued 850 hours of flying time, of which 82.8 were in VH-OMD (70.3 of those in the last 90 days and 43.5 hours recorded as instrument flight time).
Aircraft information
General
VH-OMD was a Beechcraft E55 (serial number TE-970), manufactured in the United States (US) in 1974 and first registered in Australia in 1990. Fly Oz was not the registered operator[11] of VH‑OMD but hired the aircraft and had been using it for training and charter operations for about 6 months.
The aircraft was powered by 2 Continental IO-520-C 6-cylinder, horizontally‑opposed, fuel‑injected engines rated at 285 hp at 2,700 RPM and fitted with 2 Hartzell 3-bladed full‑feathering constant speed propellers (PHC-C3YF-2UF).
The maintenance release[12] current on the accident day showed that the aircraft was approved to operate under instrument flight rules and charter categories. The maintenance release was issued on 9 April 2024 with an aircraft total time in service of 4,622.1 hours. Since then, 2 flights totalling 8.8 hours flight time had been conducted prior to the accident day. There were no recorded defects or outstanding maintenance.
The aircraft departed with a take-off weight of 2,190 kg and operated within the approved weight and balance envelope during the flight, at mid-range centres of gravity.
Fuel system
The fuel system included multiple individual fuel cells with a total capacity of 651 L. The fuel cells had elastomeric liners capable of tolerating large deformation without rupture. In an impact, this reduced the likelihood of an explosive fuel-air mist compared with unlined metal tanks. The fuel selector was an OFF-ON-CROSSFEED arrangement for each engine with the selector panel located on the floor.
Each engine had a 2-speed electric (auxiliary) fuel boost pump, which could be selected at HIGH pressure, OFF or LOW pressure. High was used for providing fuel pressure to prime the engine before start and provided near maximum engine performance should the engine‑driven pump fail. The airplane flight manual (AFM) stated that the ‘high pressure position should not be selected while the engine is operating except in the event of engine driven pump failure since the high pressure mode supplies a greater pressure than can be accepted by the injector system for a reduced power condition’.
Front seats and restraints
The front seats were fitted with 4-point restraints, each consisting of 2 lap straps connected to the seat frame and 2 shoulder harness straps connected via a Y belt to an inertia reel attached to the upper cabin structure. The inertia reel was designed with a locking device that would secure the shoulder straps in the event of sudden forward movement or impact. The seats could be adjusted forward or aft, with the seat guides sliding along 3 seat rails: 2 main (aft) and 1 centre (forward) (Figure 5). The seat is retained at the desired adjustment by a spring-loaded locking pin engaging in one of the forward centre rail holes. Shims could be added to the inside of the guide to ensure locking pin alignment.
Figure 5: Seat rails
Left seat position depicted in image, right seat rails identical. Source: ATSB and Beechcraft, annotated by ATSB
Meteorological information
The Bureau of Meteorology graphical area and grid point wind and temperature forecasts covering Cowra Airport for the accident time predicted primarily clear skies, visibility greater than 10 km and a light northerly wind.
Consistent with the forecasts, Cowra Airport’s recorded meteorological conditions[13] at 1400 included wind at 3 kt from 010°, and at 1430 the wind was 5 kt from 310°. At both those times, there was no cloud, the temperature was 21 °C and QNH 1019 hPa.[14]
Recorded data
OzRunways[15] data from the student’s electronic flight bag application contained aircraft track, altitude and ground speed. The ATSB also obtained flight data from the aircraft’s Garmin electronic flight instrument (EFI), which included 40 data parameters. Figure 6 shows key parameters from the EFI data, with the following observations.
From 1404:07, after passing over the NDB, there were heading changes, yaw (evident as lateral accelerations) and a sudden left roll[16] followed by a 10–15 kt reduction in airspeed, consistent with a left engine power loss.
Between about 1408:12 and 1409:27, during the turn from the outbound to the inbound tracks of the NDB instrument approach, the aircraft descended, climbed and descended again, at vertical speeds exceeding 1,000 fpm. During that period the airspeed varied between about 120–150 kt, with left roll angles up to 34°.
The aircraft was on the downwind circuit leg between about 1413:26 and 1414:14, during which time there were no significant changes in lateral acceleration, roll, heading or performance (speed or height).
The aircraft crossed the runway threshold at 1416:01 at 98 kt airspeed aligned with the runway centreline. The last position recorded by the EFI was at 1416:09, at which time the aircraft’s nose had pitched[17] up 6.5°, the airspeed had reduced to 79 kt and the ground speed was 77 kt, indicating a 2 kt headwind. The OzRunways recorded ground speed at the same time was 76 kt.
The OzRunways data showed the aircraft started to deviate left of the runway centreline at 1416:14 at 69 kt ground speed, which would equate to an airspeed of about 71 kt for the same headwind component. The final OzRunways data point recorded before the fence, where the impact with terrain occurred, was at 1416:18 at a ground speed of 65 kt.
Figure 6: Selected parameters from the Garmin electronic flight instrument
Source: ATSB analysis of Garmin data
Site and wreckage
The aircraft impacted the ground nose-down and inverted about 75° from the horizontal, resulting in crushing of the 2 m‑long nose structure (Figure 7). It collided with a fence and came to rest about 66 m left of the runway centreline and about 700 m beyond the runway threshold. The landing gear was extended, and the flaps were in the approach position.
Both engines had folded backwards around the wing leading edge, which pulled the engine control cables such that the engine control levers were no longer representative of the pre‑impact positions. Damage to the wing leading edge resulted in fuel leaking, but there was no post-impact fire. The aircraft departed with full fuel, and had approximately 400 L of fuel remaining on board at impact. Both fuel selectors were set to ON. Flight control continuity was established.
Figure 7: Impact damage to VH-OMD
Source: Supplied, annotated by the ATSB
The left propeller flange fractured resulting in the propeller assembly detaching from the engine crankshaft and coming to rest spinner-down embedded in the dirt. The propeller manufacturer advised that the damage to the blades was consistent with the propeller either windmilling or not rotating at impact. The left spinner was indented with the counterweight, showing that the propeller was in fine pitch and not feathered.
The right propeller remained attached to the right engine with evidence of being driven by significant engine power. Fence wire was wrapped around the engine and propeller, which had dug into the ground and first responders reported evidence of dirt having been flung from the hole by the rotating blades.
Examination of the left engine found no evidence of mechanical failure or any pre‑existing fault. The fuel filters and air induction system were clear. The spark plugs were removed with no evidence of fouling from oil or carbon deposits and there were no visible defects with the ignition leads. Borescope examination of the cylinders found no damage or abnormal appearance of the internal surfaces. The fuel distributor manifold was empty of fuel and the diaphragm was undamaged. When electrical power was applied to the starter motor, the engine turned over normally with no evidence of loss of compression in the cylinders.
The 2 front (crew) seats had separated from their track assemblies, although the shoulder harness inertia reels of both seats remained attached to the upper cabin structure. The instructor and student remained partially secured in their seats via the lap straps attached to the seat frame, The instructor came to rest in their seat outside the aircraft cabin following the opening of the cabin door during the accident sequence.
Damage and distortion to the seat rails and seat guides was consistent with forward and right forces sustained during the impact sequence. Both seats’ centre rails exhibited distortion and smearing on the forward edge from the locking pins being forced from their rail holes. The left seat locking pin was bent rearward, and the right seat alignment pin had sheared. Figure 8 shows spreading of one of the seat guides and the associated damage to the seat rails.
Figure 8: Spreading of one seat guide (left) and associated damage to the rails (right)
Source: ATSB
A post-impact photograph showed the left engine auxiliary pump in the high position (Figure 9). However, as the entire panel had come adrift, there was dirt adjacent to the switch, and most of the switches in the row beneath it had broken off, its post-impact position was not considered reliable evidence of its position at the time of the accident. The switch panel location was also consistent with injury to the student’s knee. Additionally, the student reported that the pump had been used only for priming prior to engine start then confirmed to be off and not used again during the flight. The metal fuel pump switches were also by design unlikely to be confused with the smaller plastic light switches in the row below and inadvertently selected. It was therefore unlikely to have been on prior to the accident.
Figure 9: Panel showing post-impact switch positions and disruption
Source: Fly Oz, annotated by the ATSB
Asymmetric flight
Asymmetric control
In conventional light twin-engine aeroplanes with one engine inoperative, asymmetric thrust will cause the aeroplane to yaw (rotate about its vertical axis) towards the inoperative engine. As a secondary effect of yaw, it will also roll. The yawing needs to be countered by deflection of the rudder and a small aileron deflection to raise the inoperative engine’s wing, in order to maintain balanced flight. At maximum power on the operative engine, the amount of rudder deflection needed increases as airspeed reduces, to a minimum control speed, below which the rudder is unable to maintain directional control.
Below the minimum control speed, the pilot must reduce power on the operative engine to reduce the asymmetric force, and/or lower the aircraft nose to increase airspeed, to prevent a loss of control. If directional control is lost, the aircraft will yaw and then roll and descend rapidly. Controlled flight may be recovered if enough height is available, by reducing power and lowering the nose.
Minimum control speed
The Civil Aviation Safety Authority’s (CASA) Civil Aviation Advisory Publication (CAAP) 5.23‑1(2) Multi-engine aeroplane operations and training, defined minimum control speed (VMC) as:
a speed that is associated with the maintenance of directional control during asymmetric flight. If the pilot flies below this speed the tail fin and rudder are unable to generate enough lift to prevent the aircraft from yawing. If uncorrected, the yaw causes roll, the nose drops, the aircraft rapidly assumes a spiral descent or even dive, and if the aircraft is at low altitude, it will impact steeply into the ground. This type of accident is not uncommon in a multi-engine aircraft during training or actual engine failure.
There is both a ground value (VMCG) and an airborne value (VMCA), but for simplicity, VMC usually refers to VMCA. The VMC is designated by the red radial on the airspeed indicator. The AFM specified VH-OMD’s VMCA as 79 kt indicated airspeed. That value is determined by US Federal Aviation Regulations (FAR) as the minimum airspeed at which it is possible to recover directional control of the aircraft within 20° heading change, and thereafter maintain straight flight, with no more than 5° of bank toward the operating engine following the sudden failure of one engine with:
take-off power on both engines
rearmost allowable centre of gravity
flaps in the take-off position
propeller windmilling in take-off pitch configuration.
However, the actual VMC will vary depending on the configuration, conditions and pilot technique (FAA, 2021). The CASA CAAP 5.23-1(2) stated that flight tests conducted in a Cessna Conquest aircraft, which had a published VMC of 91 kt, found that if the wings were held level instead of the inoperative engine wing raised 5°, the actual minimum control speed was 115 kt – an increase of 24 kt. Other light twin-engine aeroplanes would similarly show an increase in actual minimum control speed without bank towards the operative engine. The American Bonanza Society Air Safety Foundation advised that in Baron aircraft types (including the E55), actual VMC is about 15 kt higher than the published VMC if the wings are held level instead of the inoperative engine wing raised, and the slip/skid ball remains centred instead of deflected towards the operative engine.
At speeds below the actual VMC, with one engine inoperative and the other at take-off power, the aircraft will lose directional control – yaw, roll towards the inoperative engine and descend steeply.
Best rate of climb one engine inoperative airspeed
The best rate of climb speed with one engine inoperative (single-engine) (VYSE) is denoted by a blue line on the airspeed indicator and therefore also known as ‘blue-line speed’. It represents the single-engine best rate of climb speed at maximum weight. The AFM for VH-OMD specified the VYSE was 99 kt. Pilots often use blue-line speed as a safety margin above VMC for initiating a simulated engine failure and assume that if blue-line speed is maintained, there is sufficient margin above VMC to prevent an asymmetric loss of control.
Simulated one engine inoperative
Aircraft manufacturer’s procedures
The AFM emergency procedures section included the following procedure titled Determining inoperative engine:
The following checks will help determine which engine has failed.
1. DEAD FOOT – DEAD ENGINE. The rudder pressure required to maintain directional control will be on the side of the good engine.
2. THROTTLE. Partially retard the throttle for the engine that is believed to be inoperative; there should be no change in control pressures or in the sound of the engine if the correct throttle has been selected. AT LOW ALTITUDE AND AIRSPEED THIS CHECK MUST BE ACCOMPLISHED WITH EXTREME CAUTION.
Do not attempt to determine the inoperative engine by means of the tachometers or the manifold pressure gages. These instruments often indicate near normal readings.
The AFM further described the following procedure titled Simulated one engine inoperative:
Zero thrust (simulated feather)
Use the following power setting (only one engine at a time) to establish zero thrust. Use of this power setting avoids the difficulties of restarting an engine and preserves the availability of engine power.
The following procedure should be accomplished by alternating small reductions of propeller and then throttle, until the desired setting has been reached.
Propeller lever – RETARD TO FEATHER DETENT
Throttle lever – SET 12 in. Hg MANIFOLD PRESSURE
NOTE: This setting will approximate zero thrust using recommended one-engine inoperative climb speeds.
Fly Oz procedures
Fly Oz provided a document detailing its simulated engine failure procedure for the Beechcraft E55 aircraft. The procedure was for the instructor to reduce the mixture on one engine to idle cut‑off when above 1,000 ft. Once a student completed the initial checks, identified and verified the inoperative engine, the flight crew must decide whether to ‘fix’ the engine (if en route), or ‘feather’ the engine (‘at critical stages of flight’). If they elect to feather the engine:
… the student will articulate to the instructor which engine they determine has failed and the instructor will set zero thrust.
Fly Oz also provided a copy of their Multi Engine Training Approval Standardisation Manual, which it advised was written for operating Beechcraft Model 76 Duchess aircraft, but was also applicable to the Beechcraft E55. The manual included an Engine failure recovery sequence, describing the 3 stages of a student’s mastery in handling an engine failure. For that sequence, the instructor was to ‘fail an engine by closing the mixture’ [their emphasis]. This was followed by completing the ‘engine out checks’, identifying and verifying the failed engine, then either feathering or troubleshooting to ‘fix’ the failed engine. That procedure did not mention its applicability to asymmetric instrument approaches.
The standardisation manual also had an Asymmetric circuits one engine inoperative procedure, which included 2 notes:
• Never fail an engine below 500 ft AGL.
• Always use the throttle to fail engines in the circuit so you can immediately add power if required.
For that procedure, the instructor was to set zero thrust once the student had identified the correct engine to feather by touching the corresponding pitch lever. The asymmetric circuit procedure also mentioned conduct of an instrument approach and stated:
During an instrument approach a power setting of 20”MP [manifold pressure] with gear down should provide similar performance to the standard 15”MP with both engines operating. Gear should remain down if performance can be adequately maintained.
Additionally, the student or instructor was to include in the radio transmissions that they were ‘asymmetric’ to ‘allow other pilots to keep a safe distance and not try and push in on you in the circuit’.
Fly Oz also provided the ATSB with a copy of the Beechcraft Pilot Proficiency Program Instructor Standards Manual (American Bonanza Society, 2020), which it reported provided best practice guidance for operating the aircraft. The manual stated not to use the mixture to simulate an engine failure in single engine aircraft types. However, it did not stipulate how to simulate an engine failure in multi-engine aeroplanes, and included the following guidance on simulating zero thrust:
set the throttle to 10-12” MP, minimum governing RPM and mixture for ~ 6-7 GPH.
Fly Oz advised the ATSB that it was common industry practice in both flight training and CASA flight testing to use the mixture to shut down an engine particularly when above circuit height. They further advised that their interpretation of the Beechcraft E55 AFM was that it did not specify how a simulated engine failure should be initiated.
Guidance material
The US Federal Aviation Administration (FAA) publication Flying light twins safely (P-8740-066) advised pilots to ‘become thoroughly familiar with the AFM/POH recommended procedures’. Further, it recommended that simulated engine failures below 3,000 ft above ground level (AGL) should be accomplished by smoothly retarding the throttle (FAA, 2008). This was reiterated in the FAA’s Airplane Flying Handbook (FAA-H-8083-3C), Chapter 13: Transition to multiengine airplanes, which stated:
The FAA recommends that all in-flight simulated engine failures below 3,000 feet AGL, be introduced with a smooth reduction of the throttle. Thus, the engine is kept running and is available for instant use, if necessary. Smooth throttle reduction avoids abusing the engine and possibly causing damage.
The handbook also advised that the AFM/POH takes precedence, and that for engines equipped with dynamic crankshaft counterweights, it was essential to make throttle reductions smoothly.
The United Kingdom Civil Aviation Authority’s Aeronautical Information Circular (Pink) 2008-P-064 also advised pilots to refer to the engine manufacturer’s recommendations for simulating engine failures. It recommended that engine failures after take-off ‘should be simulated only by reducing power and never by complete shutdown of the engine until recommended minimum heights at paragraph 9.4 have been achieved’. The referenced paragraph 9.4 recommended minimum safe heights for complete shutdown of power plants for training purposes of 3,000 ft AGL for twin engine piston and turboprop aeroplanes with a maximum take-off weight not exceeding 5,700 kg.
Transport Canada’s Instructor Guide – Multi-engine class rating (TC, 2010), stated:
Actual engine shutdowns for training purposes are not recommended, as the training value is not worth the added safety risk and abuse of engines and airframe…
Simulate the engine failure by reducing the throttle to idle, while calling out "simulated". Complete the engine failure drill in accordance with the [pilot’s operating handbook] POH or the procedures outlined on the previous page.
When these checks have been completed, and you are ready to simulate feathering the propeller, adjust the manifold pressure and rpm to simulate by setting zero thrust. Consult the POH for zero thrust power settings prior to flight. Complete the engine securing items by referring to the appropriate emergency checklist.
The CASA CAAP 5-23-1(2) Multi-engine aeroplane operations and training advised instructors to consult the aircraft flight manual or pilot’s operating handbook for the recommended method of simulating an engine failure. It recommended:
Do not simulate an engine failure using procedures that may jeopardise the restoration of power. It is not recommended to simulate an engine failure at low level by selecting the mixture to idle cut-off or turn the fuel selector off. These procedures would be more appropriate at higher altitude.
Further, the CAAP stated:
6.5.4 Slowly closing the throttle is one of the methods used to simulate an engine failure. Although selecting idle cut-off may be kinder to an engine, the engine or aircraft manufacturer may not permit it. So slowly closing the throttle to idle or zero thrust is unlikely to harm the engine and allows for immediate restoration of power.
…
6.8.1 Flight instructors often simulate an engine failure by rapidly closing the throttle or moving the mixture control to idle cut-off. The latter method should never be used at low altitude.
American Bonanza Society Air Safety Foundation recommendation
The American Bonanza Society Air Safety Foundation recommended multi-engine instructors simulate an engine failure by smoothly reducing the throttle to idle, then block throttle movement on the simulated inoperative engine while the pilot receiving instruction (PRI) completes actions from the POH Engine failure in flight checklist. When the PRI gets to the checklist item ‘Propeller – Feather’, the instructor takes over the power controls and sets zero thrust in accordance with the BE55 POH/AFM.
The American Bonanza Society Air Safety Foundation recommended not simulating engine failure by turning off the fuel selector or pulling the mixture control to cutoff, consistent with FAA guidance.
Lycoming service bulletin
In April 1987, engine manufacturer Lycoming issued Service Bulletin No. 245D, Dynamic counterweight system detuning, which affected 9 Lycoming 6-cylinder engine models. The service bulletin explained that when the inertia force on an engine (which increases with engine speed), or the expansion force (manifold pressure), is suddenly changed, the engine counterweight system can ‘detune’. Damage to the counterweights, rollers and bushings could result, culminating in engine failure.
The service bulletin listed 4 operating conditions that could cause the counterweight system to detune: rapid throttle operation, high engine speed and low manifold pressure, excessive speed and power, and propeller feathering. The bulletin stated:
To avoid detuning during simulated engine failure, use the mixture control to shut off the engine and leave the throttle in normal open position until the engine has slowed down because of lack of fuel.
Fly Oz reported being unaware of the bulletin at the time of the accident. Additionally, Fly Oz reported that its procedures had been written for the Beechcraft 76 (Duchess) aircraft type, which were fitted with 4-cylinder Lycoming O-360 engines, and therefore not affected by the service bulletin. Finally, VH-OMD was not fitted with Lycoming engines and there was no comparable service bulletin or known issue associated with Continental engines.
Checklists
The student’s normal checklists are listed in the following tables.
Table 1: Downwind checklist
Item
Action
Brakes
Pressure and off
Undercarriage
Down
Mixture
Rich
Fuel
On and sufficient
Instruments
Indicating normally
Switches
As required
Hatches and harnesses
Secure
Table 2: Final checklist
Item
Action
Pitch
Full fine
Undercarriage
Down and 3 greens
Flap
As required
Fuel
Sufficient for a go-around
Workload
The student described the flight as ‘quite busy’, that they were ‘learning a lot of things’, and ‘a little overwhelming but normal for that stage of flying’. The student rated their workload on final as moderate (about 6/10).
The instructor described that the student had been performing really well that day, asymmetric work and checks were good, and overall the student was a good pilot. The instructor also assessed that the student ‘got a bit distracted on the outbound’ leg of the approach, was a ‘little slow’ getting established on the inbound track, and there was some distraction due to circuit traffic operating on the opposite runway. The instructor reported that the student was ‘wrestling’ the aircraft on inbound or downwind, which prompted the instructor to ask whether the student wanted zero thrust set.
The instructor rated their workload as moderate (5/10) and reported that for every landing, they had their seat fully forward, feet on the pedals and was alert and ready to intervene if necessary.
Survivability
The student sustained a cut under the chin, a small fracture in the right hand, and lacerations to the left knee. The instructor had a deep laceration to the chin and one arm and bruising to the knees. Both sustained additional cuts and bruises, including bruising from the lap belt and shoulder harnesses.
The certification basis of the aircraft was US Civil Air Regulation 3. The certification standards required that for a standard weight person (77 kg), the seat must withstand flight, ground, and emergency load conditions. For the seats, the critical conditions were 9 G forward, 3 G upwards and 1.5 G sideways, with the seat attachments to withstand 133% of those requirements.
ATSB analysis of the wreckage and accident site found that the impact deceleration likely exceeded 30 G in a principally forward direction. This significantly exceeded the 9 G forward requirement and the 12 G requirement for the seat attachments. The stable collapse of the airframe structure forward of the occupants aided their survivability.
Similar occurrences
ATSB occurrences
The ATSB occurrence database contained 16 twin-engine aeroplane loss of control occurrences during simulated engine failures since 1978. Two of those occurred in the last 10 years and resulted in fatal accidents in which the loss of control resulted from a simulated engine failure using a method and/or height contrary to manufacturers’ guidance. Key findings of these 2 investigations are as follows.
Loss of control and collision with terrain involving Cessna 441, VH-XMJ, 4 km west of Renmark Airport, South Australia on 30 May 2017 (AO-2017-057)
The flight departed Adelaide, South Australia, at about 1524 local time and flew to the Renmark area for exercises related to the check flight, followed by a landing at Renmark Airport. After a short period of time running on the ground, the aircraft departed from runway 25 at about 1614.
The ATSB determined that, following a simulated failure of one of the aircraft’s engines at about 400 ft above the ground during the take‑off from Renmark, the aircraft did not achieve the expected single engine climb performance or target airspeed. As there were no technical defects identified, it is likely that the reduced aircraft performance was due to the method of simulating the engine failure, pilot control inputs or a combination of both.
It was also identified that normal power on both engines was not restored when the expected single engine performance and target airspeed were not attained. That was probably because the degraded aircraft performance, or the associated risk, were not recognised by the pilots occupying the control seats. Consequently, about 40 seconds after initiation of the simulated engine failure, the aircraft experienced an asymmetric loss of control.
The single engine failure after take‑off exercise was conducted at a significantly lower height above the ground than the 5,000 ft recommended in the Cessna 441 pilot’s operating handbook. This meant that there was insufficient height to recover from the loss of control before the aircraft impacted the ground. The 3 occupants were fatally injured.
The operator’s training and checking manual procedure for simulating an engine failure in a turboprop aircraft was inappropriate and increased the risk of asymmetric control loss.
Loss of control and collision with terrain involving Angel Aircraft Corporation 44, VH-IAZ, near Mareeba Airport, Queensland, on 14 December 2019 (AO-2019-072)
On 14 December 2019, 2 pilots were conducting a private flight in an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ, at Mareeba, Queensland. An instructor seated in the right pilot seat was conducting a flight review of the pilot (and aircraft owner) in the left seat.
After the aircraft took off from Mareeba Airport, witnesses reported hearing one of the engines hesitating and backfiring, accompanied by a sooty smoke trail from the right engine. The aircraft operated in the training area until returning to the airport circuit area. Witnesses observed the aircraft touch down on the runway, accelerate and take off again. After take-off, the aircraft climbed to about 100–150 ft above ground level before entering a right descending turn. The aircraft was airborne for about 20 seconds before witnesses observed it rolling rapidly to the right and impacting terrain in a cornfield 475 m north of the runway. The pilots sustained fatal injuries and the aircraft was destroyed.
The ATSB found that shortly after take-off, the flight instructor very likely conducted a simulated failure of the right engine in environmental conditions and a configuration in which the aircraft was unable to maintain altitude with one engine inoperative. Power was not immediately restored to the right engine to discontinue the exercise and the pilots were unable to maintain altitude or heading, particularly with the aircraft banked towards the inoperative engine. The pilots did not reduce power and land ahead, as required by the Airplane Flight Manual, resulting in a loss of directional control and roll. The loss of control occurred at a height too low to recover and the aircraft impacted terrain.
United States occurrences
A search of the US National Transportation Safety Board’s (NTSB) database for investigations involving twin engine aeroplanes, with the words ‘engine’ and ‘simulated’ in the probable cause text, yielded 37 investigations since February 1989,13 of which occurred in the last 10 years. Two of those provide some context relevant to this occurrence:
Piper PA-34, N88AG, Miami, Florida, US on 11 September 2018
The flight instructor in the multi-engine aeroplane reported that the pilot under instruction was conducting a simulated instrument approach in visual flight rules conditions. The instructor placed the left engine fuel selector in the ‘off’ position to simulate an engine out, and the pilot under instruction initiated the left engine failure procedure by placing the engine and propeller levers in a simulated feathered zero-thrust configuration. The instructor became distracted by traffic and failed to place the left engine fuel selector back to the ‘on’ position.
With full flaps and the landing gear extended and while about 250 ft above ground level, the instructor terminated the simulated instrument approach and instructed the pilot to land visually; however, the airspeed decreased below safe limits, and the instructor directed the pilot to increase the airspeed. The pilot increased power on both engines; however, the left engine power did not increase, and the aeroplane rolled to the left about 45°. The instructor took the controls and applied right aileron and rudder, but the aeroplane settled down in a level attitude in a shallow lagoon on the left side of the runway.
Probable cause: The pilot under instruction’s failure to maintain the twin-engine airplane’s minimum control airspeed with one engine inoperative and the flight instructor’s distraction when reconfiguring the airplane following the simulated engine failure, which resulted in no power being available to the left engine and a loss of control during landing when the throttles were advanced to increase airspeed.
Cessna 402C, N2714B, Hyannis, Massachusetts, US on 26 April 2021
A flight instructor and a new-hire trainee pilot were practising instrument approach procedures in the multi-engine aeroplane. On climb-out, the flight instructor reduced power on the left engine to simulate an engine failure on take-off. The pilot then ran the memory items for an engine failure, which included turning the left engine auxiliary fuel boost pump to high. They then conducted an instrument approach. When the aircraft was about 50 ft above the runway, the flight instructor called for a 2-engine go-around. The pilot brought both throttles to full power and retracted the flaps and gear. The flight instructor reported that the aircraft yawed left, and the airspeed was about 80 kt, well under the aircraft’s best single engine rate of climb speed of 95 kt. The flight instructor took control of the aircraft and called for the gear to be extended. The aircraft landed hard and the nose and left main landing gear collapsed, resulting in substantial damage to the left engine and wing. Prior to exiting the aircraft, the pilot turned the left engine auxiliary boost pump from the high position to the off position.
The flight instructor reported that turning the boost pump to high while the engine was still operating could flood the engine with excess fuel and cause it to lose power. The instructor reported that they normally reminded pilots not to turn the pump to high during a simulated engine failure in flight, but neither flight crewmember recalled it being mentioned during the accident flight. Post-accident examination of the left engine revealed no mechanical discrepancies that would have precluded normal operation. As a result, it was most likely that when the boost pump was turned to high, it flooded the engine with excess fuel, resulting in loss of engine power while attempting to go around.
Probable cause: The flight instructor’s failure to confirm the position of the left engine’s auxiliary fuel boost pump switch during a simulated engine out procedure, which resulted in an excess amount of fuel in the engine and subsequent partial loss of power during a go-around/rejected landing. Contributing to the accident was the flight instructor’s failure to maintain control of the airplane, which resulted in a hard landing.
Engine control standardisation
VH-OMD was certified to the 1956 US Civil Air Regulations. The NTSB special study General Aviation Accidents involving fuel starvation 1970–1972 identified design-associated and pilot‑associated factors that influenced or caused ‘operational problems’ in fuel starvation accidents. As a result, the NTSB issued several recommendations. One was for the FAA to issue an advisory circular including ‘to warn certificated flight instructors of the danger associated with simulation of emergency engine failure by positioning the fuel selector valve to “off” or the mixture control to “idle cutoff”’. Another recommendation, A-74-38, was for the FAA ‘to amend the regulations to include specifications for standardizing powerplant control location, visual and tactile appearance, and mode of actuation’.
In 1976, in response to NTSB recommendation A-74-38 regarding fuel control standardization, the US General Aviation Manufacturers Association (GAMA) proposed to the FAA changes to FAR 23.777 through 23.781. It prescribed left to right throttle, propeller and mixture controls, landing gear to the left of the throttle or pedestal centreline, and flap to the right, and included recommended shapes and colours (Figure 10). The FAA’s General aviation (FAR 23) cockpit standardization analysis (FAA-NA-77-38) recognised that ‘increased standardization of cockpit systems can reduce cockpit workload, reduce the potential for habit interference when transitioning to another type aircraft, and provide for application of the best and most error‑resistant designs’ (FAA, 1978).
However, regarding the subsequent FAR amendment 23–33 1986, the FAA stated, ‘that color of control knobs is not a safety issue and will not adopt the proposed color requirement’. As a result, the recommended black throttle control knob and blue propeller control knob standard was not incorporated into FAR 23. A mixture lever was considered an ‘emergency control’ and therefore under FAR 23.1555(e)(2) must be red. The landing gear lever (left) and flap lever (right) requirement was incorporated in FAR 23.777 (f) and (g)).
Figure 10: Recommended control standardisation shapes and colours
Source: US Federal Aviation Administration
Figure 11 is a post-accident photo of VH-OMD’s engine control levers, which are all black, the throttle pair is in the middle and each pair has different shaped knobs. Additionally, the landing gear selector was to the right of the centre console and the flaps to the left. As VH-OMD was certified prior to the standardisation requirements, it was not required to comply with subsequent FARs.
In this case, as the instructor primarily flew VH-OMD, and it was the only twin engine aeroplane the student had flown (other than a simulator), habit interference was unlikely. However, the lack of colour differentiation in the levers, and particularly not having red mixture control levers, may have reduced the opportunity for rapid visual identification of the mixture lever position.
Figure 11: VH-OMD engine control levers
Source: Fly Oz, annotated by the ATSB
Safety analysis
Introduction
When overhead the Cowra Airport navigation aid at the commencement of an instrument approach, at about 2,600 ft above ground level, the instructor simulated a failure of the left engine. After the student conducted the instrument approach and had visually established the aircraft on final approach to the runway, the instructor initiated a go-around at a low height above the runway. Control of the aircraft was lost as it rapidly yawed and rolled left and impacted the ground in an almost vertical nose-down attitude, before coming to rest inverted.
Wreckage examination determined that the left engine was not producing power and the right engine was making significant power at impact. Additionally, there was no evidence of any defect in the left engine or airframe that could have contributed to the accident.
The following analysis will consider why the left engine was not operating at impact and why the go‑around was attempted with one engine inoperative. Additionally, operational procedures associated with simulated engine failures and related risk controls, including their potential to influence future operations will be discussed.
Left engine not restarted
The instructor followed their normal method of simulating an engine failure in accordance with the operator’s stated procedure for the aircraft type by moving the left engine mixture control lever to the idle cut-off position, thereby rendering the engine inoperative.
The required response was for the student to maintain directional control of the aircraft and complete the engine failure checks. Once the student had identified which engine was inoperative, they were to either complete troubleshooting checks to ‘fix’ the failed engine when en route or feather the propeller at a critical stage of flight.
In a training scenario, once the student had identified the inoperative engine correctly, the instructor would normally set zero thrust to simulate a feathered propeller. Their process for setting zero thrust included returning the mixture control to full rich, thereby restarting the engine. However, for reasons that could not be determined, zero thrust was not set at that stage, the mixture remained at idle cut-off with the left propeller windmilling.
The windmilling propeller increased drag and the likelihood of a loss of control, particularly during the left turn towards the inoperative engine. Although the student did not report experiencing a high workload, the approach was not flown within prescribed tolerances and included significant changes in airspeed and altitude. Given the benign weather and light winds at the time, these deviations were likely a result of pilot handling, not environmentally induced. The subsequent improvement in tracking accuracy evident when the aircraft turned to join the circuit, was consistent with the student lifting the hood and resuming flight with external visual reference.
Whether the instructor or student prompted the setting of zero thrust could not be resolved. Given that the instructor recalled setting zero thrust either on inbound or downwind and the student recalled this occurred on downwind, downwind was considered more likely as it was consistent with both recollections. There was no change in heading or increase in performance evident in the recorded data to indicate power was restored to the left engine on downwind, although any such change may have been negligible at the relatively low power settings.
As the manifold pressure would essentially read normally with the propeller windmilling, the stated practice of the instructor of moving the throttle lever forward to achieve the target manifold pressure for setting zero thrust would not confirm the engine was operating. It was for this reason that the Beechcraft E55 Airplane Flight Manual (AFM) cautioned against using manifold pressure indications to assess engine power. In the context of this accident, the observed (and expected) variation of manifold pressure with throttle movement supported an assessment that the engine had been restarted and was capable of normal operation.
Prompting and attempting to set zero thrust on downwind may have interrupted the student’s completion of the downwind checks, which should have included moving both mixture levers to the full rich position. Additionally, the student did not complete the previous checklist item of extending the landing gear, electing to defer doing so until turning onto the base leg and potentially interrupting the checklist flow. As the student had broadcast that they were operating in asymmetric configuration, they were not anticipating the conduct of a go-around. There was no check conducted by either crewmember, or required by procedure, that would verify the engine had restarted and was making power.
The initial small increase in power to the right engine and associated yaw prior to the go-around, as reported by the instructor, was not evident in the data. However, the recorded data showed the aircraft veered off the runway within 3 seconds of the initial deviation from the runway centreline, and the yaw and roll continued to impact. This was consistent with significant asymmetric thrust due to the left engine being inoperative, as evidenced by the absence of rotation when the propeller blades subsequently impacted the ground.
As there was also no evidence of any engine failure mechanism and although the mixture lever position prior to impact could not be determined, the ATSB found that the left mixture lever likely remained in the idle cut-off position from shortly after commencing the instrument approach and the engine was unintentionally not restarted.
Go-around and loss of control
The instructor was unaware they had not returned power to the left engine, and therefore when they instructed the student to commence a go-around, it was based on a belief that symmetrical power was available. This misunderstanding meant the instructor's initial actions in response to the left yaw were to verify the throttle levers were fully forward and to call for the student to let go of the controls, while attempting to correct with rudder. At that stage the only way to avoid the loss of control would have been to reduce power on the right engine and land.
The last recorded airspeed from the electronic flight instrument data, prior to the yaw was 79 kt, which was the published minimum control speed (VMC). The OzRunways data showed the ground speed reduced another 7 kt before the yaw commenced, and the airspeed likely similarly reduced. Additionally, the actual VMC may have been higher, as the wings were probably levelled for landing, rather than having the inoperative engine wing raised 5°, as required to achieve the optimum published VMC. As the aircraft was almost certainly below actual VMC when the go-around commenced, there was insufficient rudder authority to maintain control, and the loss of control occurred at a height too low to recover.
The low height at which the loss of control commenced, estimated to be about 20 ft above the runway, and the crushing of the aircraft’s structure on impact, contributed to the accident’s survivability. The impact forces exceeded the certification requirements of the seats, which detached from their rails, but the flight crew were initially restrained by 4-point harnesses. Significantly, as the aircraft was fitted with fuel cells, despite disruption to the wing leading edge and fuel slowly leaking post impact, there was no explosive fuel-air misting or post-impact fire.
Fly Oz simulated engine failure procedure
The Beechcraft E55 AFM included a procedure for simulating one engine inoperative. The procedure was to set zero thrust, which involved retarding the propeller lever to the feather detent and the throttle lever to set 12 inches of manifold pressure. The flight manual stated that the purpose of the procedure was to ‘avoid difficulties of restarting an engine and preserve the availability of engine power', which would be associated with cutting off the mixture and/or selecting the fuel off.
Fly Oz’s procedure for simulating an engine failure in the Beechcraft E55 aircraft was to move the mixture to idle cut-off to simulate an engine failure, when above 1,000 ft, which was contrary to the AFM procedure to use throttle. It was also contrary to guidance not to use mixture to simulate engine failures when below 3,000 ft above ground level from the aviation regulators in the United States, United Kingdom, and Canada. The Australian Civil Aviation Safety Authority’s guidance did not specify a height below which mixture cut-off should not be used. However, it advised not to simulate an engine failure ‘using procedures that may jeopardise the restoration of power’. Further, that slowly closing the throttle allows for immediate restoration of power.
As the conduct of an asymmetric instrument approach may include one or more legs of a circuit and end in a landing, there is a potential need for immediate restoration of power close to the ground. Therefore, the use of throttle to simulate an engine failure for conduct of an instrument approach could be inferred from the CASA guidance. The guidance also included the need to consult the aircraft flight manual for the manufacturer’s recommended method of simulating an engine failure.
Fly Oz’s Multi Engine Training Approval Standardisation Manual also included a procedure to simulate an engine failure that involved moving the mixture to idle cutoff. However, consistent with the AFM, it also contained a procedure that stipulated the use of throttle to simulate engine failures in the circuit (under which it included the conduct of asymmetric instrument approaches). Fly Oz stated that, while the manual had been written for a different aircraft type, it provided a description of the procedure applicable to VH-OMD. Despite that, on the day of the accident the instructor used the Fly Oz Beechcraft E55 specific procedure in use at the time and simulated the engine failure using the mixture control. That procedure did not contain a requirement or process to verify the engine was subsequently restarted and available for instant use.
This likely resulted in the inoperative engine being undetected by the flight crew, while operating at low power during the approach and landing. Ultimately this resulted in the loss of control during initiation of a go-around.
The ATSB occurrence database held 2 fatal accidents in the last 10 years that resulted from a loss of control following a simulated engine failure using a method and/or height contrary to guidance. Although there was no data available for the number of simulated engine failures conducted and by what method, the frequency of loss of control accident types and likelihood of fatality indicated that these posed a significant risk.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Beech E55, VH-OMD, at Cowra Airport, New South Wales on 11 April 2024.
Contributing factors
The instructor moved the left engine mixture lever to idle cut-off to simulate an engine failure overhead the navigation aid, and it was likely that they unintentionally did not subsequently move the lever to rich and ensure the engine was restarted and available for instant use.
The instructor initiated a go-around below the air minimum control speed unaware the left engine was inoperative, resulting in an asymmetric loss of control.
Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. This increased the risk of undetected asymmetric operation during descent and landing and the associated loss of control. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation, industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Operator’s procedure to use mixture to simulate engine failure
Safety issue description: Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. This increased the risk of undetected asymmetric operation during descent and landing and the associated loss of control.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Fly Oz
Fly Oz has taken the following proactive safety action:
Following a simulated engine failure, zero thrust is to be set immediately after the student has completed the engine failure drills.
The instructor standardisation manuals were being updated to include a requirement that both the student and instructor confirm that the pitch, power and mixture controls are set back to normal 2‑engine configuration during checks on final. This is now a call out item, ensuring that both pilots are satisfied with the correct settings.
Glossary
AFM
Airplane Flight Manual
AGL
Above ground level
AIP
Aeronautical information publication
AMSL
Above mean sea level
CAAP
Civil Aviation Advisory Publication
CASA
Civil Aviation Safety Authority
CTAF
Common traffic advisory frequency
EFI
Electronic flight instrument
FAA
(US) Federal Aviation Administration
FAR
Federal Aviation Regulations
METAR
Meteorological conditions at an aerodrome
NDB
Non-directional beacon
NSW
New South Wales
NTSB
(US) National Transportation Safety Board
QNH
The altimeter barometric pressure subscale setting used to indicate the height above mean seal level
TIS
Time in service
US
United States
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight instructor and student pilot
the maintainer of VH-OMD
Fly Oz
Civil Aviation Safety Authority
New South Wales Police Force
the aircraft, propeller and engine manufacturers
Bureau of Meteorology
OzRunways
accident witnesses
photographs and videos taken on the day of the accident and for subsequent examination
recorded data from the GPS unit on the aircraft.
References
American Bonanza Society, BPPP Instructor Standards Manual, Revision 10, July 2020.
Civil Aviation Safety Authority, Civil Aviation Advisory Publication 5.23-1(2) Multi-engine aeroplane operations and training, September 2015.
United Kingdom Civil Aviation Authority, Aeronautical Information Circular, 64/2008 (Pink 142) 17 July 2008. Accessed 10 May 2024: Pink 142.qxp (ead-it.com)
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight instructor and student pilot
Fly Oz
Civil Aviation Safety Authority
the maintainer of VH‑OMD
American Bonanza Society Air Safety Foundation
the aircraft, engine and propeller manufacturers.
Submissions were received from:
the flight instructor and student pilot
Fly Oz
Civil Aviation Safety Authority
American Bonanza Society Air Safety Foundation.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[3]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[4]Instrument approach procedure: A series of predetermined manoeuvres by reference to flight instruments that provides specified protection from obstacles.
[5]NDB: a ground-based radio transmitter that provides a reference point to navigate by.
[6]Windmilling: a rotating propeller being driven by the airflow rather than by engine power, and results in increased drag at normal propeller blade angles.
[7]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[8]Manifold pressure gauge measures the absolute pressure in the intake manifold of an engine, expressed in inches of mercury (in. Hg). Normal operating range (green arc) was 15 to 29.6 in. Hg.
[9]Yawing: the motion of an aircraft about its vertical or normal axis.
[10]Flare: the final nose-up pitch of a landing aeroplane used to reduce the rate of descent to about zero at touchdown.
[11]A registered operator is responsible for airworthiness and maintenance control of the aircraft (CASA).
[12]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[13]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour. Winds use true north as the reference.
[14]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[15]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It also provides the option for live flight tracking by transmitting the device’s position and altitude.
[16]Rolling: the movement of an aircraft about its longitudinal axis.
[17]Pitching: the motion of an aircraft about its lateral (wingtip-to-wingtip) axis.
Occurrence summary
Investigation number
AO-2024-011
Occurrence date
11/04/2024
Location
Cowra Airport
State
New South Wales
Report release date
22/08/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control, Runway excursion
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Beechcraft
Model
E55
Registration
VH-OMD
Serial number
TE-970
Aircraft operator
Fly Oz Cowra
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On 8 January 2024, a Cessna 208B Grand Caravan, registered VH‑NWJ and operated by East Air, departed Lizard Island Airport, Queensland on a non‑scheduled passenger service to Cairns Airport, with the pilot and 9 passengers on board. During the climb, at approximately 3,400 ft, the pilot observed the engine speed and thrust increase uncommanded, and the engine instrumentation indicated numerous parameters were exceeded or were not indicating at all. The pilot returned to land but due to the uncontrollable excessive power being generated by the engine, they conducted a high‑speed approach, touched down long on a short runway, overran the end, and the aircraft flipped over. All occupants received minor injuries, and the aircraft was substantially damaged.
What the ATSB found
The ATSB determined that the fuel control unit of the Pratt & Whitney Canada PT6A‑114A engine very likely malfunctioned due to internal or external influences. This resulted in the engine speed accelerating uncommanded and exceeding numerous engine limitations, including the gas generator speed and interstage turbine temperature. The ATSB was not able to determine the exact nature of the fault.
In accordance with the aircraft flight manual procedure, pilots of PT6A turbine engine aircraft are trained for ‘roll back to idle’ malfunctions, including the use of the manual override or emergency power lever where fitted. However, there was no such procedure for an uncommanded engine acceleration malfunction or inability to reduce power, although this type of event occurred at a rate higher than any other fuel control unit related malfunction or failure mode. As such, ATSB’s consultation with training organisations for the Cessna Caravan aircraft identified that the nature of the fuel control unit malfunction was not widely understood by pilots, operators or the pilot training industry.
What has been done as a result
As a result of this accident, East Air has published a temporary revision to its Quick Reference Handbook for the Cessna 208B aircraft to include an emergency item for 'Unscheduled power increase during flight (High Torque, Ng, ITT and/or Fuel Flow)'.
The ATSB has issued safety advisory notice AO‑2024‑001‑SAN‑001 in conjunction with this investigation report. The SAN raises awareness of engine acceleration events on PT6A powered aircraft and encourages operators to consider the potential responses to this type of failure for different phases of flight, to document appropriate actions, and to train pilots to ensure that operations are performed correctly and consistently.
Safety message
Procedures are widely recognised as being basic to safe aircraft operations. They are designed to assist with reducing variation within a given process and ensure operations are performed correctly. Without procedures, pilots are required to exercise judgement based on their experience, skills and knowledge. When details regarding certain non‑normal or emergency scenarios are not contained in an aircraft flight manual, air transport operators should consider customising their exposition and providing appropriate training to ensure that their pilots are adequately prepared for such an event.
Summary video
The occurrence
On 8 January 2024, at about 0646 local time, a Cessna 208B Grand Caravan, registered VH‑NWJ and operated by East Air, departed Lizard Island Airport, Queensland on a non‑scheduled passenger service to Cairns. On board the aircraft were the pilot and 9 passengers.
After take-off from runway 12, the pilot turned right, tracked south‑south‑west and made a departure call to Brisbane Centre air traffic control (ATC).[1] At 1,750 ft above mean sea level, the pilot turned left onto the departure track in a cruise climb and engaged the autopilot.
At 0652, passing 3,400 ft at an indicated airspeed of 102 kt, the pilot noted a change to the engine sound and that the aircraft was accelerating (Figure 1, ‘Exceedance event’). The pilot checked the engine gauges on the Garmin G1000 multifunction flight display. They noted the values indicated on both the engine torque and interstage turbine temperature gauges were above the redline and the gas generator speed and fuel flow were not indicating, being marked with a diagonal red cross through the gauge locations. The propeller revolutions per minute was high but within the green operating range.
Within 10 seconds, the pilot initiated a left turn with the purpose of returning to Lizard Island and broadcast a PAN PAN call[2] on the area frequency advising their intentions. Despite trying to arrest it, the aircraft continued to climb and accelerate over the next 2 minutes reaching 4,000 ft and 166 kt.
The pilot started troubleshooting the issue by moving the power, propeller control and emergency power levers with the only response coming from the propeller control lever. The pilot also partially moved the fuel condition lever through the gate[3] from low idle to cut‑off and noted the engine power cutting in and out and returned the condition lever to low idle. At the same time, the pilot conducted a large orbit around the island attempting a shallow descent while the engine continued to produce excessive power. Further manipulation of the propeller control lever somewhat reduced the engine thrust. The pilot updated ATC on their situation and progressively deployed the flaps to create drag in an attempt to slow the aircraft.
After one orbit of the island, the pilot felt they were low enough to attempt a landing with a 2 NM (4 km) final approach to runway 12 and notified ATC of their intentions. The pilot reported they were concerned with the populated resort accommodation and maintenance buildings on the approach end of the runway and the possibility of injury to those on board and on the ground if the aircraft did not have the energy to make the runway. To ensure they cleared potential obstacles, the pilot elected to perform a powered‑on approach.
The pilot continued to adjust the propeller lever in an attempt to reduce the engine thrust. The final approach was started at 147 kt (the pilot operating handbook stated the normal approach speed with full flaps was 75–85 kt). The pilot was able to reduce the airspeed to 123 kt by the runway threshold and reported attempting to shut down the engine. The aircraft floated along the down‑sloping runway, bouncing and touching down at around 100 kt, an estimated two‑thirds of the way along the runway.
The pilot applied maximum braking, but the aircraft exited the end of the runway at 92 kt. The aircraft continued across undulating sandy soil and low vegetation before the left wingtip struck the ground, which spun and flipped the aircraft, coming to rest inverted, 127 m from the end of the runway.
Figure 1: Flightpath of VH-NWJ
Source: Google Earth, annotated by the ATSB
After the aircraft had stopped, most passengers started evacuating the aircraft through the cargo (rear left) door. The pilot, after completing shutdown actions, exited through the front left door, followed by other passengers. Upon exiting, the pilot noticed a small fire had started at the front of the engine. After ensuring the passengers were still evacuating successfully, the pilot returned to the cockpit to retrieve a fire extinguisher, then discharged it into the engine cowling. The fire was extinguished but continued to smoulder.
Once all passengers had evacuated, the pilot moved them to the end of the runway where they were met by Lizard Island resort staff who raised the alarm with emergency services. Concurrently, ATC tried to contact the pilot but received no response. They engaged another pilot flying in the area to make contact, but that pilot was also unsuccessful in receiving a response. ATC then called the island resort and were advised the aircraft had overturned off the end of the runway. ATC then advised the Australian Maritime Safety Authority Joint Rescue Coordination Centre which coordinated the emergency response.
All aircraft occupants were flown to Cairns Hospital with the pilot and 9 passengers receiving minor injuries. The aircraft was substantially damaged.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) with a single-engine class rating and tailwheel, retractable undercarriage, gas turbine engine and manual propeller pitch control design feature endorsements. The pilot had 3,706 hours total aeronautical experience, of which 2,431 hours were on the C208 type. All the pilot’s recent flying had been on the C208B. The pilot held instrument and flight instructor operational ratings.
The pilot held a valid class 1 aviation medical certificate and reported being well rested and fully alert for the flight. The pilot was required to wear distance vision correction.
Airport information
Lizard Island Airport was a restricted access airfield servicing a resort and marine research centre. It had one sealed asphalt 15 m wide runway aligned to 120/300° of 980 m length. The runway rises and falls through approximately 5 m over its length.
Aircraft information
General
The Cessna 208B Grand Caravan was a high‑wing aircraft powered by a single Pratt & Whitney Canada (P&WC) PT6A‑114A turboprop engine and McCauley Propeller Systems feathering 3‑bladed metal propeller. VH‑NWJ was first registered in Australia in April 2023 and had accumulated about 8,765 hours total time in service at the time of the accident. It was configured with a cargo pod and a 14‑seat interior layout.
Engine limitations
The P&WC PT6A-114A turboprop engine is managed by a Honeywell DP‑F2 fuel control unit (FCU) controlling and limiting the gas generator speed (Ng), interstage turbine temperature (ITT) and engine torque. Ng and ITT are controlled by the rate of fuel consumption, while engine torque is controlled by a combination of fuel consumption and propeller pitch. The associated limits for the engine and propeller are listed in Table 1.
Table 1: Powerplant limitations for PT6A-114A as installed in the Cessna 208B
Instrument
Normal operating limit (caution range)
Permitted transient exceedance (time)
Engine power (shaft horsepower)
675
-
Engine torque (ft-lb)
1,865/1,970[1]
2,400 (20 s)
Interstage turbine temperature (°C)
765 (805)[2]
850 (2 s)
Gas generator (% RPM)
101.6
102.6 (2 s)
Propeller speed (RPM)
1,900
2,090 (2 s)
[1] Engine torque has a moving limit. If maximum torque is used, propeller rpm must be set so as not to exceed power limitations.
[2] 5-minute limitation.
Source: Pilot’s operating handbook for Cessna Model 208B G1000 aircraft
Engine controls
In the C208 aircraft, the engine and propeller are controlled principally by 3 levers, the power lever, propeller lever, and fuel condition lever. The power lever primarily controls the amount of power the engine generates. The propeller lever controls the propeller speed (Np) by biasing a constant speed governor. However, in beta mode,[4] the power lever also directly controls the propeller blade angle. The condition lever provides 2 idle speeds for the engine but is there principally as a fuel control to permit starting or stopping the engine.
Engine power is controlled by the power lever that, through FCU fuel scheduling, controls the gas generator speed. Excess energy generated by the engine core is used to turn the power turbine which, via a gearbox, turns the propeller. The propeller thrust generated is controlled by the propeller rotational speed in combination with the propeller blade angle. The propeller blade angle is adjusted by the propeller speed governor to maintain a constant propeller speed that can be biased by the propeller lever.
A fourth control is provided on the C208 for emergency purposes. The emergency power lever (EPL) can be used to manually override control of the FCU, which can be effective during certain fuel control malfunctions[5] (refer to section titled Malfunction conditions).
Fuel control unit basic operation
The FCU receives 2 inputs directly from the engine, Ng and compressor discharge air pressure (P3). P3 air passes through 2 metering orifices to the pneumatic section of the FCU. Air from both the first and second pneumatic meterings are used as part of the fuel control and are labelled Px and Py respectively (Figure 2). A flyweight governor driven by the compressor turbine pushes against spring‑loaded levers, which open a bleed valve to Py (governor valve).
The Py and Px air lines connect to the governor bellows, which controls a liquid metering valve in the fuel side of the FCU. Px and an ambient pressure line are connected to a second bellows (acceleration bellows), which also connects to the governor bellows shaft and is used to provide smooth changes to the fuel scheduling.
The fuel side of the FCU is supplied with unmetered fuel from the fuel pump. The metering valve, controlled by the governor and acceleration bellows, meters fuel to the flow divider and fuel nozzles.
Figure 2: Fuel control unit schematic
Source: Pratt & Whitney Canada, annotated by the ATSB
In normal operation when a power increase is requested, the power lever moves the speed set lever in the FCU, which biases the spring pressure to close the governor valve, increasing Py causing the governor bellows to compress, opening the metering valve and increasing fuel flow. As Ng accelerates, P3 increases (and in turn Px and Py) allowing the acceleration bellows to compress, further opening the metering valve. However, the engine does not continue to accelerate as the increase in Ng also increases the flyweight governor force on the governor valve, thereby opening it and reducing Py. This slight reduction finds a new equilibrium in the governor bellows and maintains the metering valve position until another input changes.
In summary, the power lever indirectly controls the fuel flow to the engine. The governor bellows initiates acceleration, deceleration, and controls the Ng steady state. Increasing Py pressure causes Ng to increase, and vice versa, a decrease in Py reduces Ng. The power lever only biases the governor spring and lever to alter the rate of Py bleed.
In the case of an FCU malfunction, an EPL is provided to the pilot to manually override the automated fuel scheduling. In practice, moving the EPL drives a shaft in the FCU, which presses on the end of the governor bellows, compressing it and the acceleration bellows mechanism, which in turn opens the fuel metering valve. As such, the feature is used to maintain engine functionality when the engine experiences a power rollback (usually to idle). As the EPL linkage is not directly attached to the governor bellows and can only push on it, the EPL can only be used to increase fuel flow to the engine above what the FCU is scheduling (either in normal use or during a malfunction). The EPL cannot be used to reduce fuel flow and thus cannot control an engine experiencing an uncommanded engine acceleration event.
Meteorological information
There was no Bureau of Meteorology weather station at Lizard Island. The nearest station was at Cape Flattery, 20 NM (37 km) south‑south‑west, which reported winds of 7 kt at 120° and a temperature of 30°C. The pilot reported there was little cloud and light winds of about 5 to 6 kt from the south‑east. Video taken by a witness of the final approach showed greater than 10 km visibility, few cumulus clouds[6] at lower levels and scattered cirrus cloud at high levels suitable for a visual approach.
Wreckage and impact information
Site information
While there was no evidence of the touchdown point on the runway, a skid mark, identified to be from the right main tyre, started about 110 m before the end of the runway asphalt. The skid mark disappeared and reappeared multiple times towards the end of the runway and was determined to be evidence of wheel brake modulation by the pilot.
Low foliage disruption showed the aircraft track through about 100 m of scrub after it had exited the end of the runway. The aircraft came to rest inverted with the aircraft nose pointing to the west (Figure 3). There was evidence of a small fire on the underside of the engine cowl in the vicinity of the exhaust duct and areas of the engine were found to have a coating of dry powder extinguishant.
Figure 3: Wreckage position in relation to the runway
Source: East Air, annotated by the ATSB
Wreckage examination
The outboard 1.5 m of the left-wing leading edge was crushed down and back (Figure 4). The left‑wing front spar fuselage attachment had failed in tension and the rear spar fuselage attachment had pushed into the adjacent fuselage wall. In addition, the wing strut had failed at the fuselage end fitting. The vertical stabiliser and rudder were bent to the left with downward bending damage to the tailcone.
The nose wheel strut had collapsed rearward. The propeller blades were bent in a manner that indicated they were in the feathered[7] position at the time of impact with the ground.
The engine cowl side doors had been removed. The engine mount was distorted downwards and to the right, and there was minor creasing of the firewall. All engine controls and rigging, sense lines, piping and hoses were checked and found to be secure and intact. All secured connections were found to be lock wired or pinned. The oil tank lid was latched and secure.
Figure 4: Aircraft wreckage
Source: Queensland Police Service, annotated by the ATSB
The wing fuel tank selectors were both off. Battery and avionics switches were off, and no circuit breakers were identified as tripped. The following centre console control positions (Figure 5) were found:
fuel shutoff: in (on)
wing flaps selector and indicator: FULL
fuel condition lever: just above LOW IDLE
prop RPM lever: FEATHER
power lever: IDLE
emergency power lever: one third of the way between IDLE and MAX
elevator trim: a quarter from NOSE DOWN.
Cockpit engine controls were exercised and, despite some distortion and damage in the engine bay, moved as expected through their ranges of motion.
Figure 5: Centre console as found after the accident
Source: ATSB
The cabin was intact except for the left wall adjacent to the wing where the incursion of the wing had created slightly reduced space for one passenger in the fourth row. All seats were attached to the floor and not deformed.
Fuel control unit examination
No pre-existing damage or faults were found with the aircraft during the wreckage examination, and so the other plausible explanation for the engine acceleration was an internal issue with the FCU. During ATSB attendance at the accident site, the FCU was retrieved from the engine. The FCU mates with the fuel pump and shares a common driveshaft from the compressor turbine via a gearbox. The FCU and fuel pump were separated to determine the condition of the drive coupling, a possible failure location associated with uncommanded engine acceleration. The input drive shaft to the FCU and the drive coupling were both found serviceable and in good condition (Figure 6).
The P3 compressor discharge air hose and P3 inline filter were checked and found to be clean and clear of debris.
Arrangements were then made for the FCU to undergo a specialised inspection by Pratt & Whitney Canada on behalf of the ATSB. The FCU was dispatched from the ATSB Brisbane office as an international air freight consignment but it was lost in transit. Extensive checking and investigation by the freight provider to locate the tracked consignment was unsuccessful. Consequently, any internal mechanical faults, such as component failures, material degradation, or contamination of pneumatic passageways in the FCU could not be determined. Should the FCU ever be recovered, this report will be amended to reflect any findings of the subsequent analysis.
The FCU had been removed from the aircraft and sent to TAE Aerospace 3 weeks before the accident. Work packs showed the unit was bench flow tested to confirm the operator‑reported high cut‑off angle and was adjusted. The FCU was not disassembled during the procedure.
Figure 6: Fuel control unit and fuel pump
Source: ATSB
Recorded data
Garmin G1000
The aircraft was fitted with a Garmin G1000 electronic flight instrument system consisting of 2 primary flight displays and one multi-function display. The G1000 had a 58 channel, 1 Hz, flight and engine parameter, flight data logging capability. Crew alerting system messages were not recorded in the flight data log. An SD memory card was retrieved from the device, which contained recorded data from multiple flights, including the accident flight.
The data indicated at 0652:00 there was a sudden change in fuel flow and consequential increase in Ng, ITT and engine torque (the exceedance event). There was an associated momentary 25 rpm increase in Np but it returned to its prior setting of ~1,868 rpm immediately (Figure 7). After the exceedance event, fuel flow and Ng both appeared to increase to such an extent that the values went outside the range of sensor capabilities. This aligned with the pilot’s recollection that these parameter indications blanked on the G1000 display and were replaced by a red cross indication.
While flight and engine control positions were not recorded, engine parameter changes could be associated with certain inputs of the propeller and condition levers. Particularly, on short finals when the aircraft was approaching the runway threshold, a marked reduction in fuel flow, Ng, ITT, propeller speed and engine torque over 6 seconds was identified, indicative of an attempted engine shutdown. However, all these parameters then slowly increased over the next 18 seconds until about the time the aircraft overturned. The engine manufacturer could not understand the slow response without inspecting the FCU and advised that in throttle slam testing, the PT6A takes approximately 3–4 seconds to reach maximum power.[8]
Figure 7: Garmin G1000 recorded data for accident flight
Source: ATSB
Powerplant parameters
A review of the data showed that for the exceedance event, engine torque, ITT, and Ng all exceeded the upper limits including permitted transient periods and values. The variation in all 3 parameters were characterised by a step change in value over a 3 second period.
The Ng parameter recorded periods of valid and invalid data. Analysis of the data appeared to indicate periods where sensor values surpassed the limits of the recordable range. This interpretation would indicate Ng exceeded 105.16% for 2 minutes initially, with additional shorter exceedance periods also noted. Hence, the maximum Ng during the flight could not be determined. Regardless, assuming the invalid data were out‑of‑range values, the Ng exceeded the normal operating limit for a total period of more than 8 minutes.
ITT exceeded the normal operating limit from the exceedance event until approximately the time of the flare for landing (almost 10 minutes). The maximum recorded temperature was 885°C.
At the time of the exceedance event, engine torque increased from 1,700 ft-lb to ~2,080 ft-lb. In an attempt to control the engine and reduce propeller thrust, the pilot progressively coarsened the propeller pitch. This had the effect of increasing engine torque. The maximum engine torque recorded was 2,483 ft-lb.
Propeller speed was within limits for the entire flight except for a small, permitted transient event that occurred during initial power application at the start of the take‑off. Other engine parameters such as oil pressure and temperature remained within limits for the entire flight.
Fuel control unit
Malfunction conditions
There are at least 3 ways in which an FCU malfunction is known to affect engine performance:
engine power rolls back to idle
an inability to change the power setting, or
induce uncommanded engine acceleration.
A roll back to idle can result from Py leaks or governor spring failures. The EPL is provided for this situation and if used, can command more fuel as described above.
An inability to change power usually results from a control (power lever) disconnect. If more power was required than what was set at the time of the disconnect, the EPL could be used to achieve that. However, there is no way to reduce power other than to shut down the engine, that is, zero power.
An uncommanded acceleration can result from multiple sources in either the pneumatic or fuel side of the FCU. In the pneumatic side of the FCU, cap bearing distress, a sheared drive coupling, Py bleed blockage (multiple causes), drive body contamination, or split governor bellows can result in engine acceleration. The fuel side of the FCU includes possible failures such as splitting of the metering valve seat or bypass valve seal failure. Such failures will command the equivalent of pushing the power lever fully forward, or for some failure modes, possibly higher power levels.
Malfunction rates
FCU failure and malfunction rate information of PT6A engines was sought from the engine manufacturer. P&WC reported 13 uncommanded acceleration or the inability to reduce power events over a 10‑year period (2014–2024) for the C208/C208B Caravan and 19 similar events for other single‑engine aircraft types using a similar FCU configuration. The manufacturer also supplied 5‑year (2019–2024) malfunction rate data shown in Table 2. The data provided events in different classifications as well as malfunction rates over an equivalent period for power rollback events.
It was shown that half of all reported Honeywell FCU malfunctions on single‑engine aircraft, including the Cessna Caravan, were uncommanded engine acceleration or inability to reduce power situations. While this malfunction rate met acceptable levels of reliability for component part certification, the rate for uncommanded engine acceleration or inability to reduce power situations was higher than any other type of event and equated to 0.9 events per million flight hours as shown in Table 2 for PT6A‑114/114A engines fitted to the Cessna Caravan.
Table 2: 5-year malfunction rate (events per million flight hours)
Event type
All PT6A equipped with Honeywell FCU single‑engine
PT6A‑114/114A (Cessna Caravan)
All FCU events
2.2
1.8
Power roll back to idle
0.3
0.2
Uncommanded acceleration/ inability to reduce power
1.1
0.9
Source: Pratt & Whitney Canada
Operational information
Operator information
The aircraft operator, East Air, was conducting a non‑scheduled passenger service under Part 135 of the Civil Aviation Safety Regulations (1998) ‘Australian air transport operations – smaller aeroplanes’. The operator conducted multiple flights most days between Cairns and Lizard Island carrying passengers as required to and from the resort island.
Engine emergency scenarios
All Cessna 208/208B pilot’s operating handbooks and flight manuals incorporate emergency checklists and expanded procedures that include engine scenarios such as engine fire or engine failure. Specifically, the flight manual for the accident aircraft included engine failure emergency checklist procedures for 4 different phases of flight.
The manual also included 3 engine malfunction procedures including ‘Loss of Oil Pressure’, ‘Fuel Control Unit Malfunction in the Pneumatic or Governor Sections (Engine Power Rolls Back To Idle)’, and ‘Emergency Power Lever not Stowed’ at engine start, along with some related fuel system procedures. The FCU malfunction in the pneumatic or governor sections provided instruction, among other things, on the use of the EPL.
There was no procedure for an uncommanded engine acceleration or inability to reduce power. The ATSB sought the aircraft manufacturer’s (Textron Aviation) advice as to why there was no procedure for this type of malfunction. Textron Aviation advised that at the time of the aircraft’s certification, the flight manual was reviewed and approved by the United States Federal Aviation Administration and subsequently accepted by the Civil Aviation Safety Authority. It also advised that it was not aware of any single‑engine aircraft with a procedure for what to do if a pilot finds that they do not have control over an engine.
The ATSB sought the engine manufacturer’s (Pratt & Whitney Canada) advice as to why there was no procedure for an uncommanded engine acceleration or inability to reduce power malfunction. P&WC advised that, while it is the engine manufacturer, the aircraft manufacturer is responsible for developing the aircraft handling procedures, which are documented and approved through the aircraft flight manual. P&WC advised it would support any manufacturer in the development of suitable procedures.
The ATSB reviewed pilot operating handbooks and aircraft flight manuals for many PT6A powered single‑engine aircraft as well as those powered by other makes of turbine engines. While some aircraft types had propeller overspeed procedures, the only PT6A powered single‑engine aircraft identified that had a procedure that mentioned excessive power was the PA46‑600TP. This procedure stated that, for excess power when performing a manual [fuel] override operation, pitch up and deploy the landing gear and flaps. This was followed by an instruction to land as soon as possible and when landing was assured, to bring the condition lever to cut‑off/feather.
The C208B flight manual emergency procedures for engine failure and engine fire, as well as the normal procedure for engine shutdown, all called for the propeller to be feathered before the fuel condition lever was moved to the cut‑off position. In the event of an uncommanded engine acceleration, feathering a propeller prior to moving the fuel condition lever to cut‑off would increase the risk of overstressing the engine or airframe structures.
Training requirements
Parts 119 and 135 of the Civil Aviation Safety Regulations (1998) and the Part 135 Manual of Standards contained requirements for operator training of flight crew including proficiency checks in non‑normal and emergency procedures. As a Part 135 operator using a prescribed single‑engine aeroplane[9] they were required to have procedures in their exposition for engine malfunction or failure for certain phases of flight, for example, during the take‑off roll, take‑off below turnback height, and take‑off above turnback height. The standards also required procedures for other phases of flight in visual[10] and instrument meteorological conditions,[11] and further delineated between phases of flight above and below 1,000 ft above ground level.
Most relevant, the operator had to establish procedures to address certain defined engine failure and malfunction scenarios including ‘the exceeding of an engine performance parameter’. Advisory circular 135‑13 v1.0 Prescribed single‑engine aeroplanes, further explained this requirement and advised that these items would normally be addressed in the aircraft’s flight manual. However, if the detail in the flight manual was insufficient, operator customisation of their exposition was encouraged, provided that the mandatory matters of the flight manual were still included in the correct order.
The operator reported that it was previously unaware that the PT6A engine could malfunction in such a way as to produce an uncommanded acceleration. Hence, no training was conducted within the organisation for that type of failure, nor was there a procedure in the company’s exposition for the C208 aircraft.
Industry knowledge of uncommanded acceleration events
An ATSB review of selected training organisations in Australia conducting initial and conversion training for the Cessna Caravan, and similar types, identified limited industry knowledge of this type of engine malfunction. Those organisations had a range of knowledge on uncommanded engine acceleration malfunctions varying from:
no knowledge of the malfunction and thus no inclusion in their training syllabus
some knowledge of certain events and included a ‘discussion’ during class‑based training
knowledge of multiple events and inclusion of a procedure to follow in such situations.
Only one training organisation covered an uncommanded acceleration malfunction as part of its training syllabus. Its inclusion was based on the organisation having experienced such an event with one of its own aircraft. The emergency procedure was developed by the organisation and was based on its incident experience.
The pilot of this accident reported they had no knowledge that an uncommanded engine acceleration was a possible malfunction of the FCU, and they had subsequently talked to other pilots who also had not heard of such malfunctions.
Passenger safety
A passenger survey was conducted post‑accident with a 66% response rate. All respondents reported they received a safety briefing from the pilot before the flight, which included information about lifejackets, seatbelts, exits and fire extinguishers. Most respondents reported that they were aware of exit locations because of the briefing. Passengers were also asked about seatbelt fitment, with all of those that responded advising that they wore both the lap belt and shoulder harness. Two passengers reported the belts were ‘snug’. One passenger reported the shoulder harness was difficult to fit initially but was resolved and fitted correctly prior to take‑off.
The pilot recalled that, when the engine malfunction occurred, they turned to the passenger behind them and said, ‘we've got an engine issue, we've got to go back to Lizard [Island]’. While a passenger at the front of the aircraft reported they were alerted to an issue by the pilot, and they passed that information to some passengers behind, other passengers did not realise there was a problem until the aircraft was coming into land.
Three passengers reported that the pilot told them to brace for impact. After stopping, one passenger reported difficulty releasing their seatbelt due to them being upside down. Four respondents reported they were instructed to leave the aircraft, and 2 passengers reported the pilot gave instructions to move away from the wreckage once they had evacuated. Three passengers reported they left the aircraft by the rear left exit, which was opened by one of those passengers, and it was identified that 3 other passengers left by following the pilot out the front left door. One passenger got stuck exiting via the pilot’s door and required assistance from other passengers. Estimations by the passengers on time to evacuate ranged from ‘approximately 30 seconds’ to ‘less than a couple of minutes’.
Injuries reported by the passengers included bruising, cuts and abrasions, stiffness and soreness to joints and muscles. One reported receiving a seatbelt burn to their left shoulder. The most severe passenger injury was a laceration to the side of the head.
Related occurrences
A review of the ATSB’s aviation occurrence database between 2010 and 2024 involving aircraft with P&WC PT6A engines showed that there was one related occurrence during that period. Additionally, the Transport Canada Web Service Difficulty Reporting System[12] was also searched for power runaway events between 2014 and 2024. One defect in this system was also identified on the Transportation Safety Board of Canada investigation website. The following occurrences are a selection of those found as part of this search.
ATSB occurrence (OA2011-08920)
On 23 December 2011, while in cruise flight, the engine of a Cessna Caravan went uncommanded to full power and was unresponsive to power lever inputs. The aircraft was climbed to a safe height and the crew shut down the engine and glided to the destination airport. Recorded data indicated at times the ITT exceeded 920°C, Ng exceeded 112% and engine torque exceeded 2,300 ft‑lb. While the fault could not be replicated in bench tests of the FCU, an inspection revealed non‑required grease on the P3 air adapter mating face could have made its way to, and temporary blocked, the Py air bleed orifice, leading to the metering valve moving towards the maximum fuel stop.
Transport Canada defect report (20140908003)
The pilot of a Cessna 208 reported that, while flying, the power lever was moved to the idle position but there was no change in engine power. Engine torque stayed between 1,250 and 1,400 lbs. The FCU manufacturer found a cracked governing bellows.
Transport Canada defect report (20141218004)
On 4 December 2014, a Cessna C208B, experienced a runway overrun upon landing and came to rest in water. The aircraft sustained substantial damage, and the 6 occupants on board were not injured. The engine was reported to have had an uncommanded and uncontrollable acceleration.
Transport Canada defect report (20141218009)
After landing, during the engine shutdown procedure, the pilot of a Cessna 208B reported that the engine remained at flight [sic] idle even when the fuel condition lever was placed at ground idle [sic]. When they slightly moved the power lever, the engine experienced an uncommanded acceleration. After some manipulation of the condition and power levers, the pilot successfully shut down the engine.
Transport Canada defect report (20171103016)
During taxi, the pilot moved the fuel condition lever from low to high and noticed engine torque and Ng reached the upper limit, with the ITT crossing the red line. The pilot returned the condition lever back to the initial position, but the engine did not respond, with no changes to the indicated parameters. The crew attempted to maintain control but due to the aircraft’s speed, the aircraft flew to 100 ft off the ground. The crew elected to shut down the engine and landed uneventfully.
Transport Canada defect report (20190906001)
On 25 August 2019, while the aircraft was on approach for landing, the pilot reduced the power lever and reported that the torque did not reduce. The pilot elected to perform an in‑flight shutdown and landed uneventfully. The maintenance repair overhaul service provider performed an engine ground run, which was found satisfactory and elected to perform a flight test. During the flight test, the engine behaved as previously, and the pilot elected to perform a second in‑flight shutdown and landed again uneventfully. The failed part was reported as a cracked bellows in the FCU.
Transport Canada defect report (20210721007)
On 15 June 2021, when climbing through 2,500 ft above ground level, the engine tone on a Cessna 208 aircraft changed, and all engine parameters started increasing. The power lever was retarded, but the engine parameters such as propeller speed, engine torque, and ITT all increased continuously. All indications on the primary flight display for the engine turned red. The pilot declared an emergency and made a 180° turn back to the runway. To prevent damage to the engine, or possible catastrophic failure, the engine was shut down and a safe landing was made down wind.
Transportation Safety Board of Canada (A24C0004)
On 10 January 2024, the pilot of a De Havilland DHC‑3T Turbo Otter was unable to reduce engine power shortly after take‑off. The pilot activated the emergency power lever, but it had no effect. The pilot initiated a climb in an attempt to manage the airspeed. The flight proceeded to its destination, however, the airspeed increased to over 140 miles per hour, and the pilot’s side window shattered. When within range of the airport at approximately 4,000 ft, the pilot shut down the engine with the condition lever. The aircraft decelerated more quickly than anticipated and struck trees on final approach. The aircraft came to a stop beside the runway, sustained substantial damage but there were no injuries.
Safety analysis
Introduction
On 8 January 2024, a Cessna 208B Grand Caravan with a pilot and 9 passengers on board departed Lizard Island Airport to Cairns, Queensland. Shortly after take‑off, the aircraft experienced an uncommanded and uncontrolled engine acceleration. The pilot elected to return to Lizard Island where a high‑power, high‑speed landing was conducted that resulted in a runway overrun and the aircraft flipping over.
This analysis reviews the reason for the engine acceleration and the resulting effect on the flight. It also examines the aircraft procedures for Pratt & Whitney Canada PT6A engines, and industry awareness and training on experiencing an uncommanded engine acceleration event.
Uncommanded engine acceleration
Shortly after take-off, the engine experienced an uncommanded acceleration, which was detected by the pilot as a change to the engine sound and that the aircraft was accelerating. The pilot confirmed a malfunction by the available engine parameter displays, which were either beyond limits or not indicating. The pilot attempted to diagnose the malfunction but had no ability to correct the situation and thus elected to return to the departure airport. Recorded data reviewed by the ATSB confirmed the engine malfunction and engine parameter exceedances.
With no other pre-existing damage or faults found with the aircraft, the fuel control unit (FCU) was the only component that could produce such a malfunction. It was removed from the aircraft wreckage for further examination. The ATSB determined that the input drive shaft and drive coupling was serviceable. Unfortunately, further analysis by the manufacturer was unable to be conducted. Irrespective, and consistent with other related occurrences, an internal failure or foreign object contamination of the FCU was the only plausible explanation for the uncommanded engine acceleration, although the definitive reason for the malfunction could not be determined.
Contributing factor
Shortly after departure, the fuel control unit very likely malfunctioned resulting in an uncommanded engine acceleration event beyond limits, necessitating a return to the airport.
Runway overrun
The pilot, faced with an aircraft producing excessive power and thrust, inhospitable terrain, populated areas under the approach path, and a short runway, elected to perform a power on approach to land to enable them to control their final flightpath.
The pilot reported moving the fuel condition lever to cut‑off when the aircraft was on short finals and making the runway was assured. While the recorded data showed the engine parameters dropped significantly, the engine then accelerated slowly over the next 18 seconds to again exceed limits. The pilot recalled attempting to shut the engine down, however, the emergency power and condition levers were not found in their expected positions post‑accident. This, in addition to the flight data, showed that the engine had not been successfully shut down as intended. The slow response of the engine returning to excessive power could not be explained and was possibly associated with an FCU malfunction.
Due to the excessive speed and the downslope of the runway, the aircraft touched down about two‑thirds along the runway. Despite brake application, the aircraft left the end of the runway crossing uneven terrain with low foliage before a wingtip caught the ground and the aircraft flipped upside down.
Contributing factor
The engine power was unable to be reduced and the engine was not successfully shut down on final approach. As a result, the aircraft could not be slowed sufficiently to prevent a runway overrun.
Limited pilot and operator awareness
While the aircraft flight manual provided a procedure for scenarios such as an engine failure and FCU malfunction resulting in a roll back to idle power, there was no equivalent procedure for an uncommanded engine acceleration. Therefore, there was no documented procedure or troubleshooting information available to the pilot for this type of malfunction. Instead, the procedural options available were for an engine failure or fire, or the normal procedure for engine shutdown. However, for an uncommanded engine acceleration event, the steps in an engine shutdown procedure would have to occur in a different order so as not to overstress the engine or airframe structures.
Both the pilot and operator indicated that, prior to the event, they were not aware the FCU could malfunction in such a manner. There was also a mixed understanding from the flight training organisations consulted. While one organisation specifically trained for uncommanded engine acceleration malfunctions (based on directly having experienced the problem), the majority did not, though some did informally discuss the issue with trainees while not providing a procedure for handling the situation.
For Pratt & Whitney Canada PT6A engines, data provided by the manufacturer showed an uncommanded engine acceleration or inability to reduce power event occurred at a rate of 0.9 events per million flight hours. While this malfunction rate met acceptable levels of reliability for component part certification, the rate for uncommanded engine acceleration or inability to reduce power situations was higher than any other type of event, including roll back to idle events, for which a specific procedure existed. It is acknowledged that every type of event cannot be accounted for in an aircraft flight manual or the pilot’s operating handbook. However, given the likelihood of this type of event, it is important that pilots are aware that the event can occur and how best to manage such a situation.
As the pilot had intended to shut down the engine, it could not be determined if a lack of procedure and training influenced the accident. However, awareness and training for an uncommanded engine acceleration event will prepare pilots, ensure operations are performed correctly and consistently, and should result in a better outcome. As noted in the Civil Aviation Safety Authority advisory circular for prescribed single‑engine aeroplanes, it would also be beneficial for operators to develop strategies to manage this type of malfunction in the absence of a flight manual procedure. Otherwise, without formal procedures, pilots are required to exercise judgement and innovate in a highly stressful situation, based on their experience, skills and knowledge.
Other factor that increased risk
While uncommanded engine acceleration or inability to reduce power events occur at a higher rate than any other type of fuel control unit malfunction in Pratt & Whitney Canada PT6A single‑engine aircraft, there were no flight manual procedures addressing this type of occurrence. Consequently, there was limited awareness by pilots and operators on how to identify and safely respond to an uncommanded engine acceleration event.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the engine malfunction and runway overrun involving Cessna 208, VH-NWJ, at Lizard Island, Queensland on 8 January 2024.
Contributing factors
Shortly after departure, the fuel control unit very likely malfunctioned resulting in an uncommanded engine acceleration event beyond limits, necessitating a return to the airport.
The engine power was unable to be reduced and the engine was not successfully shut down on final approach. As a result, the aircraft could not be slowed sufficiently to prevent a runway overrun.
Other factors that increased risk
While uncommanded engine acceleration or inability to reduce power events occur at a higher rate than any other type of fuel control unit malfunction in Pratt & Whitney Canada PT6A single‑engine aircraft, there were no flight manual procedures addressing this type of occurrence. Consequently, there was limited awareness by pilots and operators on how to identify and safely respond to an uncommanded engine acceleration event.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions will be provided separately on the ATSB website on release of the final investigation report, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website after the release of the final report as further information about safety action comes to hand.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by East Air
As a result of this accident, East Air published a temporary revision to its Quick Reference Handbook for the Cessna 208B to include an emergency item for 'Unscheduled power increase during flight (High Torque, Ng, ITT and/or Fuel Flow)'.
Safety advisory notice to operators of PT6A engine aircraft
SAN number:
AO-2024-001-SAN-01
SAN release date:
22 August 2025
In the absence of a flight manual procedure and with limited industry awareness, the ATSB encourages operators of single‑engine PT6A powered aircraft to consider potential responses to an uncommanded engine acceleration event for different phases of flight, and to document and train pilots on appropriate actions to ensure operations are performed correctly and consistently.
Glossary
ATC
Air traffic control
EPL
Emergency power lever
FCU
Fuel control unit
ITT
Interstage turbine temperature
Ng
Gas generator speed. The rotational speed (depicted as a percentage of nominal speed) of the core compressor in a turbine or turboprop engine.
Np
Propeller speed. The rotational speed (depicted in revolutions per minute) of the propeller of a turboprop engine.
P&WC
Pratt & Whitney Canada
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passengers
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
Transport Canada
Transportation Safety Board of Canada
Queensland Police Service
recorded data from the primary flight display unit on the aircraft.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
United States National Transportation Safety Board
Transportation Safety Board of Canada.
Submissions were received from:
the pilot
East Air
Textron Aviation
Pratt & Whitney Canada
Civil Aviation Safety Authority
Transport Canada Civil Aviation.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
[1]The Australian flight information region is split into 2 geographical areas each controlled by Brisbane Centre and Melbourne Centre. Each centre provides regional air traffic services.
[2]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[3]A gate is a second motion, additional lever or button that is required to be actioned in order to progress the movement of the lever. It is designed to prevent inadvertent progression of a lever to a position usually commanding a mode change or exceeding a limit.
[4]Beta mode is a range of propeller pitch angles that typically result in zero to negative thrust. Beta is used selectively for all ground operations aside from take-off.
[6]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
[7]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[8]Throttle slam testing involves moving the power lever from the idle position to maximum power position rapidly, and measuring the response time of the engine.
[9]Prescribed single-engine aeroplanes (PSEA) are single-engine aeroplanes that are approved, if suitably equipped, to perform passenger carrying air transport operations under instrument flight rules or visual flight rules at night. Pre‑2 December 2021, these aircraft were referred to as approved single-engine turbine powered aeroplanes (ASETPA).
[10]Visual meteorological conditions: an aviation flight category in which visual flight rules flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[11]Instrument meteorological conditions: weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules, rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[12]This system contains reports submitted to Transport Canada, the United States Federal Aviation Administration and the Civil Aviation Safety Authority defect reporting systems. It also contained defects occurring in countries outside these systems as P&WC submitted defects reported to them by operators worldwide.
Occurrence summary
Investigation number
AO-2024-001
Occurrence date
08/01/2024
Location
Lizard Island Airport
State
Queensland
Report release date
22/08/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Engine failure or malfunction, Runway excursion
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
208B
Registration
VH-NWJ
Serial number
208B2161
Aircraft operator
Townsville Airlines Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 21 July 2023 at 0119 local time, an Airlink Piper PA-31 taxied at Essendon Fields Airport, Victoria for a departure to Bankstown, New South Wales. The pilot received an airways clearance and was asked by air traffic control if they could accept a departure from runway 26. After reading back the clearance and accepting the departure runway, the aircraft was taxied and prepared for take-off.
After commencing the take-off run, the pilot heard multiple loud noises, rejected the take-off and exited the runway. Inspection of the aircraft upon return to the apron identified a damaged main landing gear tyre and brake caliper.
What the ATSB found
The ATSB found that during a period of high workload, the aircraft was misaligned with the runway edge lighting, resulting in minor damage during the take-off run.
What has been done as a result
Airlink advised the ATSB of the following proactive safety action, involving reviews of the:
fatigue management of aircrew conducting night operations, including setting mandatory ‘out of contact’ hours
night proficiency checks for pilots and how regularly these occur
airport familiarisation process for pilots conducting night operations, including developing a clear procedure on aspects to be considered when inducting aircrew at new ports
current simulator set up to determine the potential for simulator training and checks to support practical assessment, including night checks
fatigue management plan to identify areas of improvement for night flights and variances against Civil Aviation Safety Authority Civil Aviation Order 48.1 regulations.
Safety message
This investigation highlights the importance of reducing distractions during critical stages of flight. Pilots should consider having a sterile cockpit rule at those times to reduce the chance for distractions to occur. In addition, the conduct of checklists during ground operations should, where possible, be done when the aircraft is stationary.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 21 July 2023, a Piper Aircraft PA-31-350, registered VH-XMM and operated by AirLink, taxied at Essendon Fields Airport, Victoria for a departure to Bankstown, New South Wales. The pilot was the only person on board and was conducting a freight charter flight under the instrument flight rules.
At 0109 local time, VH-XMM taxied from the southern apron where they had been parked, with the airport lighting energised. The pilot contacted Melbourne Centre air traffic control (ATC) and relayed their taxi intentions, to which the controller responded asking if they could accept runway 26[1] for departure. The pilot accepted and over the next 10 minutes taxied the aircraft via taxiway Papa and November, crossing runway 17, (Figure 1). They completed their pre-departure checklists, engine run-up checks[2] and obtained an airways clearance during the taxi. After they arrived at the holding point of runway 26, the pilot reported ready for departure and received departure instructions from the controller.
Figure 1: Aircraft taxi route
Source: Airservices Australia, annotated by the ATSB
As they entered the runway, the pilot completed the departure flight logs, read back the departure instructions to ATC and conducted the line-up checklist. After they commenced the take-off run, they heard multiple loud noises and, in response, rejected the take-off at 77 kt by closing the throttles and applying the brakes. As the aircraft’s speed reduced, the pilot felt abnormal braking pressure on the right main landing gear. The aircraft subsequently veered to the left side of the runway and the pilot continued the aircraft‑induced left turn to complete a full 360° turn before exiting the runway at taxiway Hotel. The pilot contacted the controller at 0122 and advised that they were vacating the runway and cancelled their departure instructions. The aircraft was returned to the southern apron for further inspection.
On inspection of the aircraft, the pilot determined that the right main landing gear brake caliper was leaking fluid and a cut in the tyre was observed. The pilot sought the advice of a senior base pilot who was on site at the time however, it was not clear at this time exactly how the aircraft came to be damaged. The pilot entered a defect into the aircraft maintenance release and arranged another aircraft to complete the flight.
During a subsequent inspection of the runway, damage to multiple runway lights was detected and foreign object debris was found scattered across the runway.
Figure 2: Damaged runway lights
Source: Airport operator, annotated by the ATSB
Context
Pilot experience
The pilot attained their commercial pilot licence (aeroplane) in 2018 and completed a satisfactory instrument proficiency check on a multi engine aircraft in January 2023. Both a line check and proficiency check for Airlink were completed on 21 July 2022, where the pilot was assessed as competent for charter and regular public transport flights.
At the time of the incident, the pilot had 1,540 total flight hours and 532 hours on Piper PA-31-350 type aircraft, with approximately 400 hours accrued at night.
Fatigue
The Melbourne‑based pilot routinely flew the night sector between Essendon and Bankstown. They had conducted a similar flight on the previous night where they had encountered a mechanical issue on the aircraft they were flying. A replacement aircraft could not be found and therefore the duty period had ended in Bankstown. A rest period away from base was utilised where the pilot received 6 hours of sleep. The pilot awoke at 0630 the following day and repositioned via a commercial flight to Melbourne. Due to the pilot’s late-night roster, their normal wake-up time was around 1000.
After arriving in Melbourne, the pilot was provided with an off-duty period of 12 hours between 1130 and 2330 however, they were discussing weather conditions with the company for the upcoming flight and advised they received 1-hour of sleep during this period.
Initially the pilot advised they did not feel fatigued during the incident flight, however after the pilot reviewed their disrupted sleep pattern and the discussion held during their off-duty period they reported that they considered fatigue was a contributing factor.
Aircraft information
VH-XMM is a Piper Aircraft Corporation PA-31-350 type aircraft fitted with 2 Textron Lycoming TIO-540-J2BD piston engines, each driving a 3‑bladed Hartzell propellor. The aircraft was manufactured in the United States in 1979 and issued serial number 31-8052020. VH-XMM was first registered in Australia in 1986 and Airlink became the registered operator in July 2021.
After the occurrence, the aircraft was inspected by engineers. Further damage was found to the main fuselage which was consistent with the aircraft striking the runway lights (Figure 3).
Figure 3: Damaged sustained by VH-XMM
Source: Airport operator
Aerodrome information
The airport lighting was energised without interruption during the course of the aircraft’s taxi out, take-off run, aborted take-off and return taxi until after shut-down. The airport lighting de-energised at 0129.
The airport is equipped with green taxiway centreline lighting and runway 26 has a lit lead in taxi line with painted yellow markings. The runway edge lighting provided for runway 26 includes medium and high intensity lighting at 58 metre intervals along the runway edge (Figure 4).
Figure 4: Runway 26 lights and markings
Source: Google earth, annotated by ATSB
The aerodrome inspection carried out on the evening prior to the incident, did not note any defects or damage to the airport lighting system.
The airport operator provided the ATSB with ADS-B movement data which showed the position of the aircraft, and further ADS-B data was obtained from publicly‑available, third-party websites (Figure 5).
Figure 5: VH-XMM take-off path with damaged light positions
Source: Google earth, annotated by ATSB
Standard operating procedures
As the pilot was lining up, they were also completing the line-up checklist. The Airlink standard operating procedure was for pilots to complete the checklist from memory via a flow method and then confirm by referring to a checklist. The line-up checklist required the pilot’s attention to ensure the correct position of multiple items. Figure 6 shows the required checklist flow of an exemplar aircraft, which highlighted the pilot’s attention being drawn from outside the aircraft into the cockpit to identify and confirm specific switches. In addition to the checklist, the pilot also reported checking the extended runway 26 approach for traffic.
Figure 6: Exemplar aircraft showing the line-up checklist flow
CCTV footage showing the runway was obtained to confirm if the runway lights were energised during the take-off. From the footage, an aircraft could be seen conducting a take-off run from runway 26 at 0119 and during the take-off, one of the runway lights extinguished as the aircraft passed over it.
Figure 7: CCTV before and after take-off run
Source: Airport operator, annotated by the ATSB
Safety analysis
The pilot of VH-XMM was conducting a flight from Essendon to Bankstown and taxied to runway 26. Recorded position data from the aircraft confirmed that the aircraft was aligned with the runway edge lighting during the line-up.
CCTV footage confirmed that the aerodrome lights were energised and an aircraft was observed to conduct a take-off run along runway 26 at the time of VH‑XMM’s departure. As the aircraft moved along the northern runway edge lights were observed to extinguish. In addition, after the aircraft returned to the apron, the damage was detected, which was consistent with striking the runway lights.
During the interview, the pilot confirmed that while entering the runway, they checked the runway approach for traffic, filled out flight departure times and confirmed the line-up checklist was completed by using a physical checklist. These actions diverted the pilot’s attention from outside into the cockpit. In addition to the refocusing of attention, the pilot also advised that runway 26 was not a frequently used runway for operations. A combination of the high workload, unfamiliarity with the runway and night operations increased the risk of runway misalignment.
Due to the time of the occurrence and pilot’s belief that fatigue was a contributing factor, the ATSB conducted an analysis of the pilot’s fatigue level. This analysis showed that, based on the information known in relation to the pilot’s previous sleep and work roster, it is unlikely that the pilot was experiencing a level of fatigue known to have an effect on performance at the time of the incident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the misaligned take‑off involving Piper PA-31-350 VH-XMM at Essendon Fields Airport, Victoria on 21 July 2023.
Contributing factors
The pilot had a high workload during runway line up and subsequently aligned the aircraft with the northern edge lighting, resulting in minor damage during the take‑off run.
Safety action
Airlink advised the ATSB of the following proactive safety action, involving reviews of the:
fatigue management of aircrew conducting night operations, including setting mandatory ‘out of contact’ hours
night proficiency checks for pilots and how regularly these occur
airport familiarisation process for pilots conducting night operations, including developing a clear procedure on aspects to be considered when inducting aircrew at new ports
current simulator set up to determine the potential for simulator training and checks to support practical assessment, including night checks
fatigue management plan to identify areas of improvement for night flights and variances against Civil Aviation Safety Authority Civil Aviation Order 48.1 regulations.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot and operator
Airservices Australia.
Essendon Field Airport operator.
CCTV footage of the incident flight.
recorded data from the aircraft.
Airlink Standard Operating Procedures
PA-31-350 pilot operating handbook
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot in command
Airlink
Civil Aviation Safety Authority
A submission was received from:
pilot in command
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2] Run-up checks: a high-power run-up check carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take-off.
Occurrence summary
Investigation number
AO-2023-035
Occurrence date
21/07/2023
Location
Essendon Airport
State
Victoria
Report release date
17/11/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-31-350
Registration
VH-XMM
Serial number
31-8052020
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Between June 2023 and April 2024, 3 misaligned take-offs at Perth Airport, Western Australia, were reported to the ATSB. Each incident occurred before first light and involved the pilots inadvertently lining the aircraft up with the edge lighting, rather than the centreline, on runway 06 prior to take-off.
On 12 June 2023, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-IWQ, was being operated on a regular passenger transport flight from Perth, Western Australia, to Sydney, New South Wales. During the take-off roll, the flight crew identified that the aircraft was aligned with the left edge lights of the runway and manoeuvred to the centreline. The flight continued without further incident. A subsequent aircraft and runway inspection did not find any damage.
On 10 August 2023, a Western Sky Aviation Cessna Conquest 441, registered VH‑NSA, was being operated on a passenger charter flight from Perth to Southern Cross, Western Australia. During the take-off roll, the pilot detected an impact with the aircraft. After take‑off, the pilot returned to Perth and a subsequent inspection found no aircraft damage, but identified several damaged runway edge lights.
On 4 April 2024, VH‑NSA was again operating a passenger charter flight from Perth to Southern Cross. During the take-off roll, the pilot (different to the previous incident) heard an unusual noise but believed it originated from inside the cabin. As all engine indications were normal, they continued the departure. A runway inspection conducted by the aerodrome operator later that morning found several damaged runway edge lights. The pilot identified minor damage to the propeller on the right engine after returning to Perth Airport.
What the ATSB found
The ATSB found that, in all 3 incidents, when entering runway 06 from taxiway V, the pilots taxied past the turn onto the centreline and lined the aircraft up along the runway edge lighting on the far side of the runway to where they entered. In each incident, as the pilots believed they had correctly aligned the aircraft with the runway centreline, they commenced the take-off.
Several factors known to increase the risk of a misaligned take-off in the dark were identified as present in all 3 incidents. In terms of the runway environment, there was an unlit and unmarked extended pavement area on each side of runway 06, which made the runway appear wider. In relation to the available airport lighting, the lead-on lights from taxiway V continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway’s centreline; recessed edge lights at the start of runway 06 could be mistaken for centreline lighting, and there was limited ambient airport lighting around taxiway V and runway 06 to enhance visibility. The taxi lighting on one of the aircraft was reported by the pilots as being of limited benefit. Additionally, the required runway markings were reported by 2 of the incident pilots to be difficult to see at night.
One factor specific to the flight crew in incident 1 was their attention was diverted to completing pre-take-off tasks and their take-off clearance while lining up on the runway. This divided their attention between the flight deck and the monitoring of the external environment.
The ATSB also identified differences in how the pilots responded to the misaligned take‑off. In the first incident, the flight crew identified that they had lined up in the incorrect position, manoeuvred the aircraft onto the centreline, and continued the take-off and flight. The pilot of the second incident detected an impact during the take-off roll and decided to conduct a return to Perth for further inspection. The pilot of the third incident was not aware the aircraft was misaligned on the runway edge and damage to the propeller blade was not detected until several flights later.
What has been done as a result
After the incidents in August 2023 and April 2024, Western Sky Aviation distributed notices to its flight crew that included strategies to check runway alignment prior to take‑off, including the use of an electronic flight bag aerodrome chart and integrated landing systems, where available.
Perth Airport requested an update to the Aeronautical Information Publication supplement, effective November 2023, to identify a misaligned take-off hotspot on runway 06, and highlight to pilots that runway 06 did not have centreline lighting and that there was extra pavement on either side of the runway. The En Route Supplement Australia was updated to reflect the misaligned hotspot area in March 2024. Further, in works to repaint the runway markings, completed in April 2024, Perth Airport also painted chevrons on the extra pavement on either side of runway 06 to delineate this area from the useable runway to assist pilots with determining their position prior to commencing take-off.
Following the incident in June 2023, Virgin Australia Airlines completed a number of safety actions, including:
added caution notes to its Perth Airport supplementary port information about centreline misidentification on runway 06
revised the before take-off procedure to reallocate tasks earlier in the taxi to reduce flight crew workload during line-up.
developed case studies involving this event, which were incorporated into non‑technical skills training.
Safety message
The features of airport runways and taxiways can vary, and the combination of these features or lack of guidance to assist pilots to navigate or confirm their aircraft’s position can increase the risk of runway misalignments. Further, this can be exacerbated at night‑time where the amount of visual information available is markedly reduced. These reduced visual cues can affect pilots even when they are familiar with the airport. It is important for all pilots to thoroughly brief themselves with the local conditions to increase their awareness of the environment. Pilots are also encouraged to report any circumstances where they believe they may have conducted a misaligned take-off, to limit the risk to their aircraft and others subsequently using the same runway. This would also allow aerodrome operators to identify any trends or emerging misaligned take-off hotspots to consider mitigations.
Summary video
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrences
Between June 2023 and April 2024, 3 misaligned take-off events occurred at Perth Airport, Western Australia. Each incident occurred prior to first light and involved the pilots inadvertently lining the aircraft up with the runway 06 edge lighting, rather than the centreline, prior to take‑off.
Incident 1
On the morning of 12 June 2023, the captain and first officer (FO) of a Virgin Australia Airlines Boeing 737-800, registered VH-IWQ, prepared for a regular passenger transport flight from Perth, Western Australia, to Sydney, New South Wales.
At 0600 local time, the aircraft was pushed back from the bay and the captain switched on the aircraft navigation lights and logo lights. The FO obtained a taxi clearance from air traffic control, and the captain switched on the taxi lights before taxiing the aircraft to runway 06 using taxiway ‘V’ (Figure 1).[1] Around 12 minutes later, as they approached the holding point[2] on taxiway V from the south, the FO reported to the controller that they were ‘ready’ [for take-off]. At this time, the flight crew commenced the ‘before take-off’ procedure (see Incident 1 Virgin Australia procedures). When they arrived at the holding point, the captain turned off the taxi light to avoid stunning the flight crew of another aircraft on the opposite taxiway.
At 0616, after the controller provided a line-up clearance, the flight crew taxied the aircraft onto runway 06 and switched on the taxi lights, landing lights, and strobe lights. Prior to entering the runway, the flight crew recalled crosschecking the runway number to assist with positioning the aircraft, as per the procedure. The captain did not recall whether there were lead-on lights to the runway.[3]
The FO reported that the markings that would lead into the runway centreline were not followed but believed the captain was trying to maximise the take-off distance on the runway. The captain reported in interview that maximising take-off distance was their general practice. The FO also recalled that they were completing the line-up scan inside the flight deck during the turn onto the runway. Recorded flight data showed the aircraft was taxied past the runway centreline and lined up on the left edge lights of runway 06 (Figure 1). Both flight crew believed they were lined up on the runway centreline lights.
At 0616:50, as the aircraft was lined up, the controller issued a take-off clearance to the flight crew, and the FO focused on preselecting the next radio frequency for departure. At this time, the captain handed over control of the aircraft to the FO, who was the designated pilot flying[4] for the sector. At 0617:18, the captain set take-off thrust. In interview later, the FO reported that, during the commencement of the take-off roll they noticed a raised edge light and realised the aircraft was lined up on the runway edge. In response, they manoeuvred the aircraft toward the centreline as evidenced by the right rudder pedal input at 0617:20. Shortly after, at 0617:24 the aircraft was aligned with the runway centreline. The FO recalled asking the captain to confirm whether to continue with the take-off, which the captain confirmed as they believed they were above the take‑off decision speed.[5]
Figure 1: Overhead of Perth Airport and showing the aircraft’s line up on runway 06 with key events during the take-off for incident 1
Taxi and take‑off roll during the departure is shown in green. Source: APS Aerospace Flight Animation System based on flight data recorder from the aircraft, annotated by the ATSB
The continuation of the take-off and departure was normal. Once airborne, the flight crew discussed the incident. As they believed they did not strike the runway lights they decided to continue the flight and reported the incident after arriving in Sydney around 4 hours later. After the incident, a runway inspection was conducted, which identified no damage to the runway lights. The operator completed an engineering inspection and found there was no damage to the aircraft.
Incident 2
On the morning of 10 August 2023, the pilot of a Cessna 441 aircraft, registered VH-NSA and operated by Western Sky Aviation, prepared for a passenger charter flight from Perth to Southern Cross, Western Australia.
At around 0500, when at a parking bay at the terminal, the pilot completed the taxi checklist, which included switching on the navigation light, taxi light, and beacon light. In interview later, the pilot commented that the environment appeared dark, even with the aircraft lighting on. At 0508, the pilot received a taxi clearance from air traffic control and taxied to taxiway V towards runway 06.
The pilot recalled that, while at the northern runway holding point, lights from what they assumed to be another aircraft stunned them, affecting their vision. Three minutes later, at the runway holding point, the pilot was cleared to line up and wait on runway 06 until another aircraft had departed. Prior to entering the runway, the pilot completed the line‑up checklist, which included switching on the anti‑collision lights and landing lights.
Air traffic control recorded data showed that the aircraft taxied past the centreline of the runway and lined up along the right edge lighting (Figure 2). During interview, the pilot recalled that the runway markings were ‘scuffed’ and difficult to see, but they believed they were lined up on the runway centreline lighting. They also noticed ‘plenty’ of runway to their right and reported not realising there were no centreline lights on runway 06.
At 0512, the aircraft was cleared for take-off. During the take-off roll, the pilot heard an impact outside the aircraft and suspected a birdstrike had occurred. The pilot decided they were above the rejected (decision) take-off speed so continued with the take-off, but manoeuvred the aircraft to the left, toward the centreline. After the aircraft was airborne, the pilot contacted air traffic control to request a return to Perth. A runway inspection identified damage to several runway edge lights. There was no damage to the aircraft.
Figure 2: Overhead of Perth Airport showing the aircraft’s line up and take-off on runway 06 for incident 2
Taxi and take‑off roll during the departure is shown in red. Source: Google Earth, annotated by the ATSB
Incident 3
On the morning of 4 April 2024, VH-NSA was again prepared for a passenger charter flight from Perth to Southern Cross, Western Australia. During preparation, the pilot[6] reviewed the relevant Notices to Airmen[7] that stated, due to runway resealing works the centreline lights on taxiway V, the runway 24 to taxiway V lead-off lights, and taxiway V stop bar[8] were unserviceable. Temporary blue edge lighting was provided on taxiway V while the resealing work was completed.
At around 0500, while at the parking bay at the terminal, the pilot completed their taxi checklist, which included switching on the navigation light, taxi light, and beacon light. In interview, the pilot commented that they felt the aircraft lights did not appear to illuminate the environment well, so they switched the lights off and on again to confirm their operation. At 0509, the pilot taxied to taxiway V, noting that the northern corner between taxiway V and runway 06 appeared darker than usual, and there was little ambient light in the area.
At 0519, the pilot called ‘ready’ [to take off] to air traffic control and 2 minutes later received a clearance to line up on runway 06. Prior to entering the runway, the pilot completed the line‑up checklist, which included switching on the anti-collision lights and landing lights. To assist with runway alignment, the pilot reported that they would normally taxi between the runway number and the gap between the threshold markings (see Markings). The pilot reported they lined up with a white line, which they assumed was the runway centreline marking. They also recalled that the runway markings appeared to be ‘scuffed’ and were difficult to see. They also checked for the runway edge lights on both sides and believed they were aligned with the runway centreline.
Air traffic control recorded data showed that the aircraft taxied past the runway centreline and lined up along the edge lighting on the right side of the runway (Figure 3). At 0523, air traffic control issued the take-off clearance. During the take-off roll, the pilot reported hearing a noise and believed that the sound originated within the cabin, so continued the take-off. They also reported that they checked their engine indications, which were normal. The pilot departed and completed the planned flight.
Figure 3: Overhead of Perth Airport showing the aircraft’s line up and take-off on runway 06 for incident 3
Taxi and take‑off roll during the departure is shown in orange. Source: Google Earth, annotated by the ATSB
The pilot conducted a flight back to Perth from Southern Cross and then flights from Perth to Cue and return. After each of these flights, the pilot conducted a walk around the aircraft. This involved the pilot using the torch from their phone when conducting the aircraft inspection in the dark. The first inspection was conducted in the dark, and the others were during daylight. The inspection involved the pilot walking in a clockwise direction around the aircraft and included an examination of the propellers for damage. A checklist was reviewed afterwards to ensure all the components were checked.
Later in the morning, Perth Airport contacted the operator to advise that several runway edge lights were damaged, which they determined were coincident with the aircraft’s departure based on recorded departures and closed-circuit television footage. At 1208, the aircraft returned to Perth and during the walk around inspection, the pilot noticed damage to one propeller blade on the right engine (Figure 4).
Figure 4: Damage to propeller blade on right engine
Source: Operator
Context
Pilot information
All the pilots held the appropriate licences and qualifications to conduct their respective flights. ATSB analysis of sleep and roster information obtained from each of the pilots found that, despite the early morning departure time, there was a low likelihood any individual was experiencing a level of fatigue known to adversely affect performance.
The ATSB also considered whether pilot familiarity with the airport played a role in the incidents. Both pilots involved in the first incident were based in Sydney. The captain last operated from Perth one month prior to the incident, while the FO last operated from Perth one week prior. The pilots involved in the second and third incidents were both employed by a Perth-based operator, and therefore familiar with the airport. The operator reported that the third incident pilot was advised of the hazards around runway 06 during their line training.
Environmental conditions
During interview, all the pilots described the lighting conditions during the taxi to the runway as dark. Information from Geoscience Australia found that the first incident occurred around 1 hour prior to sunrise and the second and third incidents occurred around 1.5 hours prior to sunrise. All the incidents occurred before morning civil twilight, also known as first light.[9]
Perth Airport information
Runways
Perth Airport has 2 runways, 03/21 and 06/24 (Figure 5). Both runways are 45 m wide but runway 06/24 is shorter than 03/21. All pilots involved in the incidents reported that runway 03/21 was the runway they would use most frequently on departure.
Prior to the construction of taxiway V in 2012, there was a turning bay at the beginning of runway 06 to allow pilots to backtrack their aircraft and line-up to use runway 06. As a result, extra pavement remained on either side of the runway. The width of this extra pavement was 34 m from either side of the runway edge at the widest part, which is where each of the aircraft were aligned. The extra pavement tapers, where the widest part was closest to the runway end. At the time of each of the incidents, this extra pavement was not lit or marked, and there was no regulatory requirement to do so.
Taxiway V crossed the end of runway 06 and could be used to enter the runway from either the right (south) or left side (north). The flight crew from the first incident entered runway 06 from the right of taxiway V, and lined up on the left edge lights, while the pilots from the second and third incidents entered from the left and lined up on the right edge lights.
Figure 5: Perth Airport runways
Source: Google Earth, annotated by the ATSB
Lighting
The Civil Aviation Safety Regulations Part 139 Manual of Standards (MOS) for Aerodromes stated the requirements for runway and taxiway lights and markings for Australian airports.
Runway centreline lights
When installed, runway centreline lights were inset in the runway, and would be white and omnidirectional, apart from lights towards the end of the runway, which were required to be red.
Runway 03/21 was fitted with centreline lights (Figure 6). Runway 06/24 did not have centreline lights, and was not required to as per MOS 139.
Runway edge lights
The MOS stipulated that a permanent runway edge lighting system was required to be installed on runways intended for use at night. The edge lighting system should be comprised of 2 parallel rows of lights, equidistant from the runway centreline. The lights may be elevated (raised) or recessed (inset) and would be situated along the declared edge of the runway to delineate the area available to pilots for landing and take-off at night in reduced visibility. Consistent with the MOS requirements, the runway 06/24 edge lights were white (Figure 6 shows these lights for runway 03). The first 2 edge lights on runway 06 were inset into the runway, and the remainder of the lights were elevated (Figure 7).
Figure 6: Runway centreline lights and edge lights on runway 03
Source: Perth Airport, annotated by the ATSB
Figure 7: Runway 06 edge lighting (left side)
Source: Perth Airport, annotated by the ATSB
Taxiway centreline lights
The MOS also stated that, where taxiway centreline lights were used for both runway exit and runway entry purposes, the colour of the lights viewed by the pilot must be green for entering the runway and alternately green and yellow for exiting the runway. Taxiway V had lights from the centreline of the runway to the centre of the taxiway (Figure 8). These lights were alternating yellow and green unidirectional lights visible only when exiting the runway, known as lead-off lights. Lights visible when entering the runway were known as lead-on lights. Taxiway V did not have lead-on lights that joined from the taxiway to the runway centreline, but there were green bi-directional taxiway centreline lights spanning across the runway threshold in the middle of taxiway V (Figure 8 top and bottom).
Figure 8: Runway centreline lights (top), view from the runway centreline of runway 06 (middle) and view from taxiway V holding point, facing towards the opposite side of the taxiway (bottom)
Source: Google Earth (top image) and Perth Airport (middle and bottom images), all images annotated by the ATSB
Markings
MOS 139 stipulated the characteristics of aerodrome markings, including runway and taxiway markings. Runway markings were required to be white (on paved runways) and included runway designation, runway threshold, centreline markings, and edge markings (also known as side-stripe markings). Runway designation markings were the 2-digit runway number, determined from the approach direction, indicating the magnetic heading of the runway. Runway threshold markings identified the beginning of the runway that was available for landing and take-off using ‘piano key’ markings. They consist of a white line across the width of the runway and a series of white longitudinal stripes of uniform dimensions. Runway centreline markings were a line of uniformly spaced stripes and gaps that identify the centre of the runway and provide the pilot alignment guidance during take-off and landing. Runway edge markings were required to be continuous white lines on both sides of the runway. Taxiway markings were required to be yellow and provided on all sealed, concrete or asphalt taxiways for continuous guidance between the runway and the apron.[10]
Runway 06 had runway markings as per the MOS requirements. The runway edge markings were an unbroken white line and centreline markings were broken white lines. The markings were painted with non-reflective paint. There was no regulatory requirement to use reflective paint for runway markings. All taxiways including taxiway V had continuous yellow taxi centreline markings (Figure 9).
Figure 9: Runway markings on Runway 06 (as of March 2023)
Source: Perth Airport, annotated by the ATSB
Alternate runway markings to assist with visibility
There was no requirement for runway markings to be painted using reflective markings in Australia, but other countries use reflective paint to increase visibility and contrast in the dark. For example, the International Civil Aviation Organization recommended that aerodromes where operations take place at night, pavement markings should be made with reflective materials to enhance the visibility of markings. The United States Federal Aviation Administration (FAA) includes the use of retroreflective airport markings with glass beads in paint to improve conspicuity of markings at night, during low visibility conditions or when the pavement is wet. The Federal Aviation Administration also stated that runway shoulder stripes may be used to supplement runway edge stripes to identify pavement areas contiguous to the runway sides that are not intended for use by aircraft. Runway shoulder stripes were to be painted yellow.
Air traffic control information
Airservices Australia provided the ATSB with the air traffic control data for each of the incidents. The data included a recording of the tower controller’s screen from the Advanced Surface Movement Guidance and Control System, which showed the position of aircraft and ground vehicles. For all 3 of the incidents, the recording showed the respective incident aircraft lining-up and taking off from the edge of runway 06.
When asked whether a tower controller could detect misaligned take-offs, Airservices Australia advised that the scale setting and margin of error on the screens may make it difficult for controllers to detect a misaligned take-off. Further, the tower controller’s role was to look outside, and they may not be using the screen to check the runway alignment of an aircraft.
Operational information
Incident 1
Virgin Australia procedures
The Virgin Australia Policy and Procedures Manual stated that during take-off, flight crew must:
Use all available cues to ensure the aircraft is on the correct runway (including runway numbers, localizer, etc)
Ensure the take-off roll is only commenced when the aircraft is aligned.
The Flight Crew Operations Manual included as part of the ‘before take-off’ procedure a runway verification check, which included runway take-off position (Figure 10).
Figure 10: Excerpt of the ‘before take-off’ procedure
Source: Virgin Australia
Take-off decision speed
Based on the airspeed calculations for the flight on the take-off and landing card, the decision speed (V1) was 139 kt. The flight data showed that, when the aircraft was manoeuvred from the runway edge to the centreline, the groundspeed was 44 kt. As there were no significant winds in the area at the time affecting the aircraft’s speed, it was likely that a rejected take-off could have occurred.
Incidents 2 and 3
The pilots from the 10 August 2023 and 4 April 2024 incidents recalled that they would use the runway markings, including the centreline and runway threshold markings, to assist with alignment. They would also check that the runway edge lights were on either side of the aircraft when lining up on the runway.
Misaligned take-offs
Previous research
When pilots taxi and take-off during daylight conditions, they normally have a wide range of visual cues by which they can navigate and verify their location. At night, however, the amount of visual information available is markedly reduced. Pilots rely more on the taxiway and runway lighting patterns presented to them and what can be seen in the field of the aircraft’s taxi and landing lights.
In 2010, the ATSB published a research report titled Factors influencing misaligned take‑offs at night (AR-2009-033) which reviewed several Australian and international occurrences. The report identified several factors that increased the risk of a misaligned take-off. The most prevalent factors that contributed included environmental factors such as the physical layout of the runway and/or airport. Examples included a wide runway and/or extra pavement near the runway or confusing taxiway marking and/or lighting, such as recessed lighting at the runway’s edge and/or the absence of centreline lighting.
Areas of additional pavement around the taxiway entry and runway threshold area can provide erroneous visual cues at night and pilots can believe that they are in the centre of the runway when they are actually lined up on the edge. Recessed (inset) lighting, particularly at the taxiway entry to the runway, was often quoted as an influencing factor in reports relating to lining up incorrectly. Centreline lighting, when it was present, was always recessed to allow aircraft to safely travel over the centreline during take-off. However, runways will often have recessed lights at the runway edge where the taxiway meets the runway. Therefore, recessed runway edge lighting can act as confirmation that the flight crew have lined up on the centreline, when this is not actually the case. Similarly, the degradation of airport markings can provide erroneous cues to the pilots of the aircraft’s position on the runway.
The next most common factors were human factors such as flight crew distraction (divided attention). Divided attention results in a focus inside the flight deck at the expense of monitoring the external environment. An example was flight crew performing checklist items or setting power/checking instruments/readings. Completing checklists were a normal and necessary part of the departure, however, can be a distraction during a critical time, such as while lining up. Another factor was a lack of familiarity with the runway at night, as it can present an additional demand during taxi and line-up.
The last group of factors were operational factors, such as air traffic control clearances, which can provide a distraction to flight crew depending on the timing. They can also contribute to, precipitate, and/or exacerbate the presence or impact of other factors such as workload, distraction, or a lack of visual cues to assist the crew in lining up the aircraft on the runway centreline.
Previous safety recommendations
Previous investigations conducted by the United Kingdom Air Accident Investigation Branch (UK AAIB) and Dutch Safety Board, involving misaligned take-off incidents in 2015 and 2018 respectively, have included safety recommendations to the International Civil Aviation Organization (ICAO). These recommendations proposed that ICAO should develop runway design standards that would prevent pilots misidentifying runway edge lighting as centreline lighting. ICAO reviewed these safety recommendations and determined that guidance included in the Procedures for Air Navigation Services (PANS) – Aerodromes (Doc 9981) provided strategies to address misaligned take-offs. The guidance included considerations for aerodrome operators, such as conducting safety assessments as part of the risk management process. An example of an item to be considered in this process was aerodrome/runway layout.
In 2021, the Global Action Plan for the Prevention of Runway Excursions was published and included addressing misaligned take-off incidents. Specifically, the report stated there should be measures for preventing visual confusion during line-up between runway edge and centreline lights leading to misalignment with the runway centreline. The measures should also take into account the effects of low visibility and runway contamination and the effect of using various light colours and patterns to differentiate the runway centreline and edge lighting systems.
Related occurrences
A review of the ATSB occurrence database found 3 reported incidents of misaligned take-offs in the 5 years prior to April 2024. These incidents, along with 2 similar international incidents are as follows.
On 20 April 2021, at 1854 local time, the pilot of a Fairchild SA227 aircraft taxied at Townsville Airport for a freight charter flight to Brisbane, Queensland. While lining up for take-off on runway 01, air traffic control advised that the aerodrome QNH[11] had changed. During this time, the pilot became aware that the aircraft had deviated from the lead-on line and started correcting the turn to realign with the centreline. During the take-off roll, the aircraft struck a runway edge light resulting in minor damage to the propeller.
A number of factors that contributed to the misaligned take-off included the wider paved section at the end of the runway, no centreline lights on the runway, recessed edge lighting, and taxiway lead-on lights not visible when entering the runway. It was also found that there was reduced visibility prior to departure due to the rain and time of day.
On 21 July 2023, at 0109 local time, the pilot of a Piper PA-31 aircraft taxied at Essendon Fields Airport, Victoria for a freight charter flight to Bankstown, New South Wales. After reading back their clearance from air traffic control and accepting the departure from runway 26, the aircraft was taxied and prepared for take-off. The pilot was completing checklists, which required attention to be focused within the aircraft. After commencing the take-off run, the pilot heard multiple loud noises, rejected the take-off and exited the runway. Inspection of the aircraft upon return to the apron identified a damaged main landing gear tyre and brake calliper. An inspection of the runway found damage to multiple runway lights and foreign object debris scattered across the runway.
On 13 May 2024, at 0537 local time, the pilot of an Aero Commander 500-S aircraft taxied for departure at Brisbane Airport on a regular scheduled freight flight. The aircraft was cleared for a departure from runway 01 at the intersection of taxiway A7, the pilot taxied to this holding point. While turning onto the runway, the pilot inadvertently lined up along the left side runway edge lighting instead of the runway centreline. During the take‑off roll, the pilot recognised the aircraft was left of the centreline and took corrective action to reposition the aircraft on the runway. The underside of the aircraft had minor damage and several runway lights were also damaged.
The brief highlighted the complexity of the intersection with multiple lead-off lines into the runway as well the runway touchdown zone markings near the runway centreline markings that were both broken white lines.
German Federal Bureau of Aircraft Accident Investigation BFU20-0251-EX
On 27 April 2020, at 0353 local time, the flight crew of a ATR72-212 aircraft prepared for take-off on a freight flight from Cologne Airport, Germany, to Sofa Airport, Bulgaria, in the dark. After receiving their taxi clearance, the flight crew taxied the aircraft to the centreline of runway 24 towards the turn pad (paved area next to the runway for turning) for runway 06 (the reciprocal runway). The flight crew completed the before take-off checklist during taxi. At this time, the flight crew heard a sound in the cockpit and determined it was from the captain’s bag falling from the chair. When the turn pad was reached the aircraft initially followed the yellow taxiway markings to turn 180°. The captain completed the turn and aligned the aircraft with the row of lights ahead, believing they were the centreline lights. During the take-off roll, the flight crew felt and heard an impact to the aircraft, so the captain aborted the take-off. The aircraft had minor damage to the nose landing gear and propeller blades.
Factors identified that contributed to the misaligned take-off related to the runway environment and distraction. The runway edge marking on the turn pad was a broken white line, which was similar to the centreline markings. Due to the viewing angle from the cockpit to the runway edge and centreline lighting they were difficult to differentiate, especially in the dark without any other visual refences. The width of the turn pad including the runway was also identified as a factor. Another factor was flight crew distraction during the turn due to determining the sound in the cockpit. The report had a safety recommendation (07/2020) to ICAO:
The International Civil Aviation Organization (ICAO) should modify the standard recommendations regarding runway edge lighting in Annex 14 Volume 1 Aerodrome Design and Operations to ensure clear distinction of other airport lightings (sic).
Transportation Safety Board of Canada investigation A23F0062
On 16 February 2023, at 1817 local time, the flight crew of a Boeing 737 aircraft taxied to runway 01R in Nevada, United States, to Edmonton, Canada, on a scheduled passenger flight. The flight crew taxied the aircraft along the taxiway centreline until reaching the right runway edge marking, turned to the right and entered and lined up with what was believed to be the runway centreline. The aircraft took off while aligned with the right edge of runway 01R, and its nosewheel contacted 8 runway edge lights. During the take‑off roll, both the flight crew heard sounds and felt vibrations but believed it was the runway centreline lights. The flight crew were unaware of the misaligned take-off and the flight was continued. The aircraft had minor damage to the right tyre on the nose landing gear and there was damage to several runway lights.
The investigation identified several factors that contributed to the misaligned take-off. The factors included the high workload between the flight crew at the time of departure where the FO was focused on a task within the cockpit and the captain’s perceived time pressure to depart. Other factors included the visual cues in the runway environment. The taxiway centreline lighting on the taxiway used for departure terminated at the runway edge markings and the runway did not have centreline lighting.
Safety analysis
Runway environment resulting in the misaligned take-off
On runway 06, there was extra pavement on either side of the runway where each aircraft lined up for take-off. As there were no markings or lighting to delineate this area, there were no visual cues to assist the pilots to identify the extra pavement was adjacent to the runway. Consequently, this area likely appeared to be an extension of the usable runway. This was consistent with the pilot’s observation in incident 2 where they reported seeing ‘plenty’ of runway to their right when lined up on the right runway edge.
Although the runway had all the required markings in accordance with regulations, they were reported by 2 of the pilots as being difficult to see at night and were ‘scuffed’, thereby reducing the contrast and visibility of the markings. It was also noted that, while not required, reflective paint was not used for the markings to improve conspicuity at night.
While there were taxiway centreline markings, there were no lead-on lights from the taxiway to the runway centreline. Although there were lead-off lights, these were unidirectional and designed to only be visible when exiting the runway. Therefore, at night, the pilots had limited cues to assist them while navigating from the taxiway to ensure they would turn the aircraft into the centre of the runway.
Runway 06 did not have centreline lighting. However, the first 2 edge lights on either side were white and inset within the runway, which were the same characteristics for centreline lighting. Given that all the pilots indicated they would use runway 03/21 more frequently for take‑off, which was fitted with centreline lights, this potentially influenced them misidentifying the edge lights as centreline lights.
The pilots of the 2 incidents operating the Cessna 441 also commented that although the aircraft lighting was switched on, the environment appeared dark. One of these pilots also reported that there was limited ambient lighting at the intersection of taxiway V to runway 06. The combination of the reduced visual cues and runway features that can be misidentified may have also given the impression that the aircraft were aligned with the runway centreline and increased the risk of a misaligned take-off. These characteristics were evident in many previous similar investigations.
Consistent with the ATSB’s research, the extra pavement area, the absence of lead-on lights and runway centreline lights, and some degraded markings, were all factors that influence misaligned take-offs at night, where visual information may be markedly reduced. A combination of these factors in each incident supported the pilots’ belief that the aircraft were correctly aligned with the centreline when they were positioned on the runway edge lighting. Confirmation bias is the tendency for people to seek information and cues that confirm the tentatively held hypothesis or belief (Wickens et al 2022). As they believed they were correctly aligned with the runway centreline, the pilots in each occurrence commenced the take-off roll.
Flight crew focus of attention
In incident 1, the flight crew divided their attention between pre-take off tasks being completed in the flight deck and monitoring the environment. Additionally, the flight crew also received their take-off clearance during the turn onto the runway, requiring the FO to communicate with air traffic control. While these are normal and a required part of the departure, they can divert the flight crew’s attention away from the external environment at a critical time, such as while lining up. Barshi and others (2009) state that during busy periods, it is easy for attention to be absorbed in one task, which can divert attention from other important tasks, such as monitoring.
Pilots’ response to the misaligned take-off
The pilots’ responses to each misaligned take-off incident were different. During the take‑off roll, the flight crew in the June 2023 incident identified that they had lined up on the runway 06 edge lighting and manoeuvred the aircraft toward the centreline and continued the take-off. However, believing they had not struck the runway lights, the misalignment of the take-off was not reported to the operator or to airport personnel until the flight had arrived in Sydney, around 4 hours later. Although the subsequent aircraft and runway inspections did not identify any damage, there was the risk that unrecognised debris could have affected the safety of other aircraft using the same runway or the flight continuing with unknown damage.
The pilot in the August 2023 incident detected an impact during take-off, though did not initially notice the aircraft was aligned with the runway edge lighting. As they had detected a problem, the pilot returned to the airport to ensure there was no damage to the aircraft and provided the opportunity for a runway inspection to occur to check for damage. The pilot’s decision was important as damage to the aircraft (which was carrying passengers) and debris on the runway can affect flight safety.
The pilot in the April 2024 occurrence did not identify they had lined up the aircraft on the runway edge lighting and subsequently completed multiple flights. As a result of the misaligned take-off, the aircraft had sustained damage to the right propeller and several runway lights were damaged, which was not detected until later that day. Damage from a foreign body impact to a propeller blade could lead to gouges, dents and deformation, or cracks and blade failure if left undetected (Federal Aviation Administration 2005), although in this instance there was no reported effect on flight from the sustained damage.
Overall, misaligned take-offs can increase the risk of damage to aircraft and lighting given that raised runway lighting, unlike recessed runway lighting, is more likely to sustain an impact. Given the risk, it is important to promptly communicate the incident, for example to air traffic control or airport personnel, to provide the opportunity for inspections to be conducted. The outcome of these inspections allows pilots to make more informed decisions on whether to continue the flight, return or divert to a closer location.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the 3 misaligned take-off occurrences on runway 06 at Perth Airport, Western Australia.
Contributing factors
On runway 06 at Perth Airport, features of the runway environment included extra pavement, degraded markings, and reduced lighting. As a result, the pilots in 3 separate occurrences misidentified this runway's edge lighting for centreline lighting and commenced take-off from this position.
During the turn onto the runway in incident 1, the flight crew were focussed on completing pre-take off tasks within the flight deck, and communicating with the air traffic controller about their take-off clearance. These actions diverted their attention away from monitoring their position on the runway.
Other factors that increased risk
After the misaligned take-offs, the 3 pilots responded differently. This increased the risk of damage, to aircraft or runway lighting, remaining undetected.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Perth Airport Pty Ltd
After the first 2 misaligned take-off incidents, Perth Airport submitted a notice to Airservices Australia requesting an update to the Aeronautical Information Publication about the misaligned take-off risk on runway 06. Subsequently, this update was included in an Aeronautical Information Publication supplement H78/23 effective November 2023 containing an update to the ground and movement charts for Perth Airport. The new aerodrome chart highlighted there was a ‘misaligned take-off hot spot’[12] at the intersection of taxiway V and runway 06. The supplement detailed that runway 06 had wider shoulders due to previously being used as a turn pad, had no centreline lights, and that, when lining-up on the runway from taxiway V, pilots should ensure that the aircraft was aligned with the runway centreline. In March 2024, Airservices Australia updated the En Route Supplement Australia to reflect this change.
Perth Airport conducted airport works in late March to early April 2024 to repaint all markings on the runway and taxiway. As part of this work, they also painted chevron markings on the extra pavement next to runway 06 to prevent future misalignment.
Safety action by Western Sky Aviation
As a result of the incident on 10 August 2024, the operator issued a notice to aircrew to highlight the importance of vigilance by confirming the nominated runway position. For runways with an instrument landing system (ILS), the operator encouraged pilots to line up and tune the ILS and dial up the course to check the course deviation indicator is centred. For runways with no ILS (such as runway 06), the operator encouraged pilots to crosscheck the runway heading with the GPS position of the aircraft overlaid on the aerodrome map display in the OzRunways software on tablets in the aircraft.
After the April 2024 incident, a second notice to aircrew was distributed, emphasising the importance of situational awareness with runway identification when preparing for take‑off. The notice specified that pilots must confirm they are on the runway centreline and ensure the runway number is identified, either through the runway markings or association with the heading displayed by an aircraft instrument. For night take-offs specifically, pilots were instructed to self-brief the expected runway to familiarise with the specific characteristics of the runway such as whether it has centreline lighting or not, and to ensure that they have both the sides of the runway lighting visual before commencing the take-off roll.
Safety action by Virgin Australia Airlines
Virgin Australia Airlines added caution notes to its Perth Airport supplementary port information about centreline misidentification on runway 06 due to the environment, such as no centreline lighting during night or in poor visibility conditions. They also revised the before take-off procedure to reduce flight crew workload during line‑up by reallocating items (setting the weather radar) to earlier in the taxi. Finally, case studies involving this event were incorporated into non-technical skills training.
Sources and submissions
Sources of information
The sources of information during the investigation included:
pilots from the 3 incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Airservices Australia.
References
Airservices Australia. (2023). A pilot’s guide to runway safety, Airservices Australia.
Australian Transport Safety Bureau. (2010). Factors influencing misaligned take-off occurrences at night, Australian Transport Safety Bureau, Australian Government.
Barshi, I., Loukopoulos, L.D. and Dismukes, R.K. (2009). The multitasking myth: Handling complexity in real-world operations. Ashgate Publishing.
Civil Aviation Safety Authority. (2019). Part 139 Manual of Standards for Aerodromes, Civil Aviation Safety Authority, Australian Government.
Federal Aviation Administration. (2005). Advisory Circular AC20-37E Aircraft Propeller Maintenance, US Department of Transportation, United States.
Wickens, C.D., Helton, W.S., Hollands, J.G., and Banbury, S. (2022). Engineering psychology and human performance, 5th edn, Routledge, doi: 10.4324/9781003177616.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots from the 3 incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Airservices Australia
Civil Aviation Safety Authority.
Submissions were received from:
a pilot from one of the incidents
Virgin Australia Airlines
Western Sky Aviation
Perth Airport
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway (for example, runway 06 is orientated 60º magnetic). The runway identification may include L, R or C as required for left, right or centre. Runways 06/24 were reciprocal runways.
[2]Holding point: designated point for holding on airfield, especially before entering active runway.
[3]Lead-on lights: green unidirectional taxiway centreline lighting that extends into the runway.
[4]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path. On the Boeing 737, the captain taxis the aircraft as the steering is on the left side.
[5]Take-off decision speed (V1): the critical engine failure speed or decision speed required for take-off. Engine failure below V1 should result in a rejected take off; above this speed the take-off should be continued.
[6]The pilot in incident 3 was a different pilot to incident 2.
[7]Notice to Airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[8]Stop bars are a series of unidirectional red lights embedded in the pavement, at right angles to the taxiway centreline, at the associated runway holding point. They are intended to provide additional protection of runway/taxiway intersections to reduce runway incursions.
[9]First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions.
[10]Apron: large paved area of airfield for such purposes as: loading and unloading of aircraft; aircraft turnaround operations; aircraft modification, maintenance or repair; any other approved purpose other than flight operations.
[11]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[12]Hot spot: a location on an aerodrome movement area with a history of potential risk of collision or runway incursion, and where heightened attention by pilots / drivers is necessary.
Occurrence summary
Investigation number
AO-2023-027
Occurrence date
12/06/2023
Location
Perth Airport
State
Western Australia
Report release date
20/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Runway excursion
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8SA
Registration
VH-IWQ
Serial number
44225
Aircraft operator
Virgin Australia Airlines Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Perth Airport, Western Australia
Destination
Sydney Airport, New South Wales
Damage
Nil
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
441
Registration
VH-NSA
Serial number
441-0087
Aircraft operator
Western Sky Australia Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
On the morning of April 6 2023, a chartered GippsAero GA8 Airvan, registered VH‑TBU and operated by Shine Aviation Services, took off from Geraldton Airport to Rat Island aircraft landing area in the Houtman Abrolhos Islands, Western Australia. A pilot and 6 passengers were on board.
During the landing on runway 18, the aircraft did not stop before the edge of the island and tipped into shallow seawater. The pilot and passengers were uninjured. The aircraft was substantially damaged.
What the ATSB found
The ATSB found that the aircraft was unstable during the approach due to excessive height and airspeed. During the landing, the aircraft floated for a significant time and touched down approximately halfway down the runway, with insufficient remaining runway to stop. While the pilot recognised opportunities to conduct a go-around when they determined they were not on the correct approach profile, this was not conducted.
Finally, the ATSB found that the pilot was possibly experiencing fatigue at a level known to affect human performance, due to a combination of restricted sleep and insufficient sustenance.
What has been done as a result
Shine Aviation Services has taken safety action to improve pilot landing and late‑stage go‑around training for their single‑ and multi‑engine piston aircraft. An increased oversight program has also been implemented to provide more regular mentoring for junior flight crew.
Safety message
This incident highlights how an unstable approach can contribute to the risk of a runway excursion. Pilots should be prepared to conduct a go-around if the stabilised approach criteria are not met. The later the decision to go-around is made, the more likely that additional hazards will be present for pilots to manage.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 6 April 2023, a GippsAero GA8 Airvan registered VH-TBU and operated by Shine Aviation Services was being used on a chartered passenger flight. The aircraft departed Geraldton, Western Australia at 0814 local time on a flight to Rat Island in the Houtman Abrolhos Island chain, Western Australia (Figure 1). Onboard were the pilot and 6 passengers.
Figure 1: Flight track of VH-TBU
Source: Google Earth and flight track, annotated by ATSB.
After cruising at 2,600 ft, the aircraft approached Rat Island and joined an extended base leg of the circuit for runway 18.[1] The pilot made a left turn onto final and extended the flaps to 38°.[2] Coming out of the final turn, the pilot noticed that the aircraft was higher than normal. Consequently, they reduced the engine power to idle and lowered the nose of the aircraft to intercept the normal approach profile. The pilot advised the aircraft’s airspeed increased to approximately 85 kt at this stage, before reducing to a little higher than normal over the threshold (see the section titled Stabilised approach criteria).
During the landing, the aircraft floated significantly more than the pilot expected, with the aircraft touching down about 247 m beyond the threshold (Figure 2). The pilot recalled ‘jumping on the brakes’ as soon as they touched down, and then realised that the aircraft could not be stopped before the runway end. In response, they applied left rudder in an attempt to avoid entering the water in the overshoot. The aircraft traversed the runway overshoot area, coming to rest on the island’s edge, before tipping forward into shallow seawater at about 0841 (Figure 3).
Figure 2: Rat Island runway and flight path of VH-TBU
Source: Google Earth and flight track, annotated by ATSB.
Water entered the cockpit to about ‘shin-height’ and the passenger seated in the rear left seat opened the emergency exit upon recalling the instructions from the safety briefing. All 6 passengers evacuated the aircraft through the rear left door. The pilot evacuated through the left cockpit door, walking across the wing strut onto land (Figure 3).
Neither the pilot nor 6 passengers were injured during the landing or evacuation. The aircraft sustained substantial damage to the nosewheel, propellor, right landing gear and cargo pod, and remained partially submerged for several days before being airlifted back to Geraldton.
Figure 3: VH-TBU accident site
Source: Shine Aviation Services, annotated by ATSB.
Context
Pilot information
The pilot held a commercial pilot license (aeroplane) with an instrument rating, and a class 1 aviation medical certificate. They had a total of 789.7 hours flying experience, of which 157.4 hours were operating the GA8 Airvan. The pilot had experience flying a variety of single‑ and multi-engine piston aircraft during island operations. They had been flying for the operator for about 12 months and had flown to Rat Island many times.
The pilot had passed an instrument proficiency check (IPC) in February 2023 and operator proficiency check (OPC) in September 2022, which included satisfactory results in conducting a missed approach/go‑around. [3]
Aircraft information
The GA8 Airvan is a single engine aircraft manufactured by GippsAero[4] of Victoria, Australia. It is fitted with a Textron Lycoming IO-540-K1A5 piston engine and can seat up to 8 people, including the pilot. VH-TBU was manufactured and registered in 2002. It was owned and maintained by the operator.
The aircraft was maintained in accordance with the GA8 service manual and had a current maintenance release. The last periodic inspection was in March 2023, and the aircraft had accumulated about 3,256.7 total hours in service.
The aircraft’s maintenance records showed an open observation recorded 2 weeks prior to the occurrence that the pilot seat was difficult to adjust. Prior to the flight, the pilot had detected this and decided it would not affect their ability to control the aircraft. During the flight, the seat was set fully aft, 1–2 increments further back than the pilot’s normal seat position. They later observed that, with the seat further rearward than normal, they could not fully depress the brake pedals.
After the accident, the ATSB received photographs of the aircraft and identified evidence of previous low hydraulic fluid in the left brake master cylinder. This was recorded to have been topped up 3 weeks prior to the occurrence, after a report of sponginess [5] on the left brake. It was unclear if this was the case at the time of the accident, although evidence of wheel skidding was observed on the runway surface after this occurrence.
Rat Island aircraft landing area
Rat Island aircraft landing area (ALA) was managed by the Western Australian Department of Biodiversity, Conservation and Attractions (DBCA). It had one unsealed runway aligned 180/360° and was about 517 m long and 30 m wide, with no significant slope. The windsock was located at the northern end, and there was a 20 m rocky overrun area at the end of runway 18. DBCA reported that improvements had been made to the overrun surface area in August 2022. The airstrip was suitable for GA8 operations.
Meteorological information
Rat Island did not have a dedicated Bureau of Meteorology (BOM) weather station. Weather observations at North Island weather station, about 50 km north of Rat Island, showed that 10 minutes prior to the runway excursion, winds were 110°, varying between 9 to 13 kt.
The pilot reported that the conditions on Rat Island favoured runway 18 with a slight headwind, which was usual for this area. They were unable to recall the direction of the windsock, and it was not captured on the passenger video recording (see the section titled Recorded data). The runway was dry.
Stabilised approach criteria
The operator required that if a VFR aircraft was not stable by 500 ft above the touchdown point a go‑around was to be conducted. The following stabilised criteria was outlined in their policy and procedures manual:
the aircraft is on the correct lateral and vertical flight path
descent rate is less than 1,000 ft per minute
bank angle is less than 10°
the aircraft is in the correct landing configuration
the aircraft is at approach speed (Vref to Vref +10) [6]
power setting is appropriate for the configuration
conditions landing checklist has been completed
The operator’s policy and procedures manual also stated:
If at 50 ft altitude, the aircraft airspeed is in excess of the planned threshold speed plus 10 kts then a go-around is mandatory.
The GA8 flight manual noted that for approach and landing:
Excessively high approach speeds will result in prolonged floating and increased landing distance.
The pilot reported being familiar with the stabilised criteria, and a general rule of thumb to conduct a go-around if the wheels had not touched down by the first third of the runway when using a shorter runway.
The standard approach into Rat Island for the GA8 at maximum take‑off weight was a standard approach angle of 7° at idle power. Pilots were instructed to employ a short-field landing to cross the threshold at a maximum airspeed of 70 kt, and upon touchdown, retract the flaps, applying firm brake application and back pressure on the control column to allow the full weight of the aircraft onto the runway for maximum braking effectiveness. Calculations for the distance required to land a GA8 aircraft with a 3 kt headwind indicated that from 50 ft overhead the threshold, it would need 410 m of runway to stop, including a ground roll of 170 m.
Recorded data
The operator supplied flight data and a passenger took a video recording of the landing and runway excursion on their mobile phone. This passenger was sitting in the front right seat, and primarily videoed in the direction of travel out the lower right corner of the windscreen. This information was used to conduct a flight path analysis of the approach and landing. The flight analysis revealed that from the start of the video recording to the 50 ft point on the approach, the average approach angle was about 10º.
At 50 ft altitude on final, and about 70 m from threshold, the aircraft was travelling at a groundspeed of 88 kt. At the runway threshold (about the landing aim point), the aircraft was about 21 ft above ground level (AGL) and was travelling at a groundspeed of 86 kt. After the flare, the aircraft floated for about 170 m, and touched down approximately 247 m beyond the threshold, travelling at a groundspeed of 77 kt. It was at this point that the pilot reported that the airspeed was slightly below the aircraft’s Vref speed of 70 kt. The aircraft exited the overrun area at a groundspeed of about 43 kt. Full flaps remained deployed during the landing sequence.
Work schedule
The pilot was rostered for a flight duty period (FDP) [7] between 0530–1800, with a split-duty rest period from 1000–1400 for sleep at home, which was 15 minutes commuting time away. They were to then sign on again at 1530. They had flown a return trip from Geraldton to East Wallabi Island earlier that morning, and had flights scheduled at 1600 and 1700 later that day. They were working their third day after 3 days off.
Fatigue
The pilot reported waking at 0400 that morning after about 5.5 hours of sleep, and about 11 hours of sleep in the previous 48 hours. The pilot had been awake for about 5 hours prior to the occurrence. Usually, they would be asleep by 2200 for this sort of work schedule, but they reported that on that night they struggled to fall asleep until about 2230.
The pilot reported their mental fatigue at the time as ‘a little tired, less than fresh’, and that while they had packed a banana and muesli bar to eat that morning during their shift, they had left them behind. They reported having had their last meal around 1700 the day before.
Previous similar occurrences
There have been 62 runway excursions in the last 4 years at ALAs across Australia. 11 of these occurrences resulted in 14 injuries: 9 minor injuries to crew, 1 serious injury to a passenger and 4 minor injuries to passengers. Of these, 2 occurrences were at the Abrolhos Islands.
The ATSB investigated 6 of these 11 occurrences.
Safety analysis
Despite the pilot identifying that the approach profile was steeper than normal and taking action to remedy the situation, flight analysis indicated that the aircraft arrived at the threshold both high and fast. The ATSB considered whether the seating position may have affected the pilot’s approach perspective. However, given they identified the steep profile, any significant effect was considered unlikely. The aircraft then touched down well into the runway at a recorded groundspeed of 77 kt, with the pilot recalling that the aircraft’s airspeed was slightly below Vref (70 kt). This indicated that the landing was conducted with a tailwind component.
It was considered unlikely that the braking capacity of the aircraft was affected by the seating configuration or low hydraulic fluid in the brake master cylinder. There were skid marks along the runway surface where the brakes had been applied and locked the wheels. While this indicates that full brake application was available, the locked wheels would have provided less stopping effectiveness than if the braking had been modulated to remain on the threshold of locking and the flaps retracted on touchdown. These elements, in combination with the long landing and groundspeed detailed above, meant that the pilot was unable to stop the aircraft before it entered the water.
There were opportunities to conduct a go-around prior to landing and during touchdown. The pilot recalled considering a go-around as they pushed the nose down to intercept the approach profile and the speed increased more than expected, however they advised that they expected to regain the correct profile and airspeed prior to landing. They also considered conducting a go‑around as the wheels made contact with the runway. However, having assessed that the airspeed was below the take-off speed of 70 kt, they were concerned that there was a risk of stalling over the water.
Fatigue is a known factor that can impair decision making and reduce reaction time. There was evidence that the pilot was possibly experiencing mild to moderate acute fatigue at the time of the occurrence. This was due to a combination of some restricted sleep in the previous 24 and 48 hours, and lack of sustenance that morning. However, it is difficult to conclude whether fatigue impaired the pilot’s actions in response to identifying the unstable approach and electing not to conduct a go-around. The ATSB reviewed the operators’ procedures for sleep arrangements during split shift duty periods and found that sign-on and sign-off times accounted for commuting time and aircraft preparation between scheduled departures.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion, involving GippsAero GA8 registered VH-TBU, that occurred at Rat Island, Western Australia on 6 April 2023.
Contributing factors
The aircraft was unstable during the approach and landed approximately halfway down the runway with insufficient remaining runway to stop.
The pilot did not conduct a go-around, as required by the operator, when they identified the aircraft was not stabilised during the latter stages of the approach.
Other findings
The pilot was possibly experiencing fatigue at a level known to affect human performance, due to a combination of restricted sleep and insufficient sustenance.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Shine Aviation Services
As a result of this occurrence, the operator has advised the ATSB that they have taken the following actions:
implemented late stage go-around training for pilots operating to the Abrolhos Islands
implemented an increased oversight program for junior pilots and reviewed the non-technical skills syllabus
amended training packages to clarify the aircraft flap retraction policy upon landing
implemented anti-skid training into an appropriate location within training material
included aircraft performance items into the line training syllabus for their single‑ and multi‑engine aircraft
reviewed average pilot commuting times to improve the scheduling of rest periods and sleep periods for split duty times
improved operational procedures to clearly define minimum turnaround times, minimum sign‑on and sign-off times
reviewed the aircraft performance manual to ensure referenced material was up to date
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight.
a passenger of the accident flight.
video footage of the accident flight and other photographs and videos taken on the day of the accident.
recorded data on the aircraft.
Shine Aviation Services.
Bureau of Meteorology (BOM).
References
Gippsland Aeronautics (2019). GA8 Flight Manual. CASA Amendment 54. C01-01-03
Gunston, B. (2004). The Cambridge aerospace dictionary. Cambridge University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Shine Aviation Services
Civil Aviation Safety Authority
United States National Transportation Safety Board
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway number: the number represents the magnetic heading of the runway.
[2] This was the full flap setting required for the GA8 to achieve the factored landing roll required for Rat Island at the maximum landing weight of 1,814 kg.
[3] Go-around: A standard aircraft manoeuvre that discontinues an approach to landing.
[4] The manufacturer was previously known as Gippsland Aeronautics.
[5] Compressibility within the braking system requiring greater‑than‑expected pedal application to achieve effective braking.
[6] Vref: the reference landing approach speed. For the GA8 at idle power and full flap this was 70 kt.
[7] Flight Duty Period (FDP): A period of time that starts when a person is required, by an operator, to report for a duty period in which they undertake one or more flights as part of an operating crew and ends at the later of either the person’s completion of all duties associated with the flight, or the last of the flights; or 15 minutes after the end of the person’s flight, or the last of the flights.
Occurrence summary
Investigation number
AO-2023-016
Occurrence date
06/04/2023
Location
Abrolhos Rat Island
State
Western Australia
Report release date
25/10/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Gippsland Aeronautics Pty Ltd
Model
GA-8
Registration
VH-TBU
Serial number
GA8-02-011
Aircraft operator
Shine Aviation
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 30 November 2022, a Boeing 737, registered VH‑YFH and operated by Virgin Australia, commenced its take-off roll from the A3 intersection of Brisbane Airport’s runway 19L. During the take‑off the aircraft briefly entered, and became airborne in, the section of the runway that was closed due to the runway works. The aircraft completed the departure and continued onto its destination where a maintenance inspection subsequently cleared the aircraft of any damage.
What the ATSB found
The ATSB found that the briefing package for the aircraft’s previous sector from Melbourne to Brisbane included:
a dispatcher’s note which stated that Brisbane RWY 01R had a displaced threshold, but without any resultant landing weight performance limitation
a notice to airmen (NOTAM) with the headline RWY 01R THR DISPLACED, which identified reduced runway distances for take-off and landing on Brisbane’s runways (RWY) 01R/19L
critical performance data appended to the displaced threshold NOTAM.
The captain misinterpreted the dispatcher’s note to mean that there were no performance requirements for operations on RWY 19L. The captain reviewed the NOTAMs and, based on this misunderstanding, dismissed the NOTAM as not being relevant for their operation. There was uncertainty about whether the first officer reviewed the dispatcher’s note and NOTAMs in Melbourne, but if they were, the relevance of the note and this NOTAM was probably missed. As such, neither crew member identified the critical performance data appended to this NOTAM.
The NOTAMs were not reviewed en route or as part of the approach briefing prior to descent into Brisbane, as required by the operations manual. Additionally, the automatic terminal information service (ATIS) advice of the reduced landing distance for RWY 19L was not identified and accounted for in the performance calculations for the landing (or subsequent departure) on that runway. Fortunately, this did not affect the landing as the landing’s stopping solution was based on the aircraft exiting the runway well before the closed section. The flight crew’s misunderstanding was reinforced by the absence of any visible runway works or other indications of restrictions on the runway during the landing.
Due to the now‑established belief that there were no performance requirements for operations on RWY 19L, together with time pressures and distractions from prioritising training needs, the flight crew used the full runway length in the performance data calculation for departure, instead of the reduced length identified in the ATIS and NOTAM. This resulted in a departure with insufficient runway available due to the aircraft being overweight for that reduced runway length.
Finally, contrary to the requirements of Part 139 Manual of Standards, the A3/19L intersection departure point take-off run available Movement Area Guidance Sign presented a take-off distance that was more than that available, creating the potential to mislead flight crews about the status of the runway when conducting a departure from that point.
What has been done as a result
Virgin Australia implemented a number of safety management, procedural and information‑based changes designed to improve flight crew awareness of changes to runway configuration and related aircraft performance criteria.
Brisbane Airport Corporation implemented several safety actions to reduce the risk associated with this type of occurrence. These included:
changes to departure and arrival procedures associated with runway works
redrafting of the NOTAM to clarify the operational changes to both runways 01R and 19L, and the procedures to ensure correct runway distance was displayed on movement area guidance signs
publication of an aeronautical information circular supplement for the works.
Safety message
Flight crews must ensure they consider possible variations to take-off and/or landing dimensions when determining runway performance data. While this operator’s procedures accounted for such changes through notification of performance requirements within their NOTAM system, due to a combination of distraction and incorrect assumption, they were not identified.
When presented with many NOTAMs, flight crews need to be aware that dismissing them based on the headline alone increases the risk that safety relevant data may be overlooked. As an additional defence, flight crews should ensure that the data input into that calculation is in conformance with other relevant information, such as the ATIS.
The occurrence
Overview
On 30 November 2022 a Boeing 737-8FE (B737), registered VH‑YFH and operated by Virgin Australia as flight number VA324, commenced its take-off roll from the A3 intersection of Brisbane Airport’s runway 19L. The take-off thrust and speeds set by the flight crew for the take‑off from A3 were based on the full runway length from that intersection being available. However, unrecognised by the crew, the take-off distance available for runway 19L had been reduced at the upwind (01R threshold) end by 871 m due to runway works. As a result, the thrust set for the take‑off was insufficient for the actual runway length available and the aircraft briefly entered, and became airborne in, the section of the runway that was closed due to the runway works. The aircraft completed the departure and continued on to its destination where a maintenance inspection subsequently cleared the aircraft of any damage.
The sequence of events that resulted in the runway excursion commenced earlier the same day, during flight planning for the previous sector from Melbourne to Brisbane.
Melbourne
Arrival
VH-YFH arrived in Melbourne as flight number VA254 from Canberra at 0846 EDT,[1] about 10 minutes behind schedule. The aircraft was scheduled to depart Melbourne for Brisbane as flight number VA319 at 0910 EDT. The flight crew consisted of a training captain (captain) and a first officer (FO). The captain had been assigned a number of ‘line flying under supervision’[2] sectors with the FO over the previous 2 days as part of the FO’s conversion onto the B737.
Pre‑flight
Flight planning package
Shortly after arriving, the flight crew received the flight planning package[3] (see the section titled Flight planning) for the flight from Melbourne to Brisbane. This package included the operational flight plan (OFP),[4] NOTAMs[5] for the sector and flight operations engineering (FOE) data appended to the relevant NOTAMs. The captain recalled that the package was initially missing a part of the NOTAMs section, although a full reprint was subsequently received prior to departure.
The OFP commenced with a section titled ‘Dispatcher Notes to Crew’ (Figure 1), which included a note from the dispatcher that stated:
YBBN RWY 01R DISPLACED BY 921M. NO LDW PERF LIMITATION.
The flight crew expected the approach and landing into Brisbane would be on runway (RWY) 19L. The captain incorrectly interpreted the dispatcher’s note to mean that the displaced threshold of RWY 01R did not have associated performance requirements for runway 19L (see the section titled Flight dispatch). The captain then reviewed the Brisbane NOTAMs, which included a NOTAM (NOTAM YBBNC1174/22) with the headline ‘RWY 01R THR DISPLACED’. This NOTAM was dismissed as it referred to the displaced runway threshold in the dispatcher note, and because the headline did not include any reference to RWY 19L (which was the expected landing runway).
Figure 1: Dispatcher notes for VA319 (Melbourne to Brisbane)
Source: Virgin Australia
FOE requirements for RWY 19L
The NOTAM section of the flight planning package also included a company notice, titled ‘VOZ FOE COMPANY REMARK’, appended to the displaced threshold NOTAM YBBNC1174/22 (see the section titled VA319 (Melbourne to Brisbane) flight planning package). This notice included specific data required to be used for both landing and take‑off performance data calculations when using Brisbane RWY 01R and RWY 19L. The captain did not identify the company notice associated with NOTAM YBBNC1174/22. There was uncertainty about whether the FO read the dispatcher notes and NOTAMs prior to departure from Melbourne, but if they did, the relevance of the dispatcher’s displaced threshold note and NOTAM was probably missed. As a result, both flight crew were unaware of the performance data calculation requirements for operations at Brisbane’s RWY 01R and RWY 19L.
En route to Brisbane
The aircraft departed Melbourne at 0940 EDT with the flight to Brisbane expected to take about 2 hours. The FO conducted the pilot flying (PF)[6] duties for the sector, while the captain was the pilot monitoring (PM). The intention was to reverse these roles for the later return flight to Melbourne. Available spare time during the cruise portion of the flight was used to cover training‑related matters.
As the aircraft approached Brisbane, the crew completed arrival preparations, which included recording the Brisbane automatic terminal information service (ATIS),[7] calculating the landing performance data, and briefing for the approach and landing. The ATIS stated that arrivals were being conducted onto RWY 19L and RWY 19R, and that RWY 19L had a reduced length with the landing distance available being 2,689 m.[8]
The flight crew did not review the Brisbane NOTAMs inflight or as part of arrival preparations.
While the crew completed the landing performance data calculations based on the full length of RWY 19L being available, and not the reduced length as stated on the ATIS, the stopping solution (see the section titled Enroute landing performance calculator) was based on the aircraft exiting the runway at the A6 taxiway.
Brisbane
Arrival
VH-YFH landed on Brisbane’s RWY 19L at 1050 EST[9] and exited the runway using the A6 rapid exit taxiway located about 850 m from the displaced threshold at the end of RWY 19L.[10] The flight crew stated that they did not observe any runway works activity or markers indicating works on the runway during the landing roll and exit from the runway.
Post-flight
VH-YFH was scheduled to arrive at the gate in Brisbane at 1020 and depart for Melbourne as VA324 at 1055. The aircraft arrived at the gate 34 minutes behind schedule, at 1054.
Following completion of post-flight duties, the flight crew did not immediately commence preparation for VA324. The captain’s observations of the FO’s performance as PF for the landing into Brisbane identified a need to alter the intended flight crew duties for the VA324 sector and assign the FO the PF role once again. To support this decision, the captain allocated time to debrief the FO on their performance during the completed sector and to provide training support for the return flight. During those training discussions the crew received the flight planning package for the return flight to Melbourne.
Pre-flight
The training discussions were put on hold while the flight crew reviewed the OFP and dispatcher notes and determined the fuel order for the VA324 sector. The OFP included a dispatcher’s note that stated:
YBBN RWY 01R THR DISPLACED 29/2100-30/0630Z
The flight crew understood that this note was in reference to the same runway matter identified by the dispatcher in the previous sector’s OFP and was dismissed.
The captain then finalised the training discussion and, at its completion, the FO exited the flight deck to conduct an exterior inspection of the aircraft while the captain commenced pre‑flight duties. The captain later estimated that around 5 minutes of the turnaround was spent in the training discussion.
As part of the pre‑flight duties, the captain obtained a hard copy of the ATIS from the ACARS,[11] and used that data to fill out the relevant fields of the take-off data card (TODC). The captain made a handwritten entry ‘2689 TORA’ in the remarks section at the bottom of the card (see the section titled Pre‑flight procedures and the performance data calculation). The take-off performance data was then determined using the onboard performance tool (OPT).[12] The captain decided to use the taxiway A3 intersection with RWY 19L as the take-off commencement point (Figure 2). The power setting, take-off speeds and other data relevant to this take-off commencement point were then calculated using the OPT’s runway selection that related to the normal runway length from A3 rather than the reduced available length. The resultant calculated data was then transcribed onto the TODC.
Figure 2: VA324 departure
A Google Earth image of Brisbane Airport with the departure track of VA324 overlaid. The image shows location and timestamps for specific points of the departure. Source: Google Earth, modified by ATSB
After completing the exterior inspection, the FO returned to the flight deck and commenced their pre‑flight checks. This included a required independent calculation of the take-off performance data using the OPT. The FO conducted the calculation using data from the TODC (previously filled out by the captain). The FO stated that they did not see the captain’s annotation of ‘2689 TORA’ in the remarks section.
On completion of the performance calculation, both flight crew cross-checked and confirmed agreement on the calculated data using the OPT cross-check function. The subsequent pre‑flight procedures and checklists then confirmed that the data entered into the flight management computer was in agreement with that on the TODC. The FO then conducted a departure briefing, which included stating that the take-off was planned to commence from the A3 intersection for RWY 19L. The aircraft was then prepared for push back from the gate.
It is likely that the NOTAMs were not reviewed by either pilot during the turnaround and that while the specific reasons could not be determined, it may have been due to a combination of distraction, time pressure and a previously‑formed view of the NOTAM content.
Departure
The flight crew commenced push-back at 1139 and, at 1143, requested a taxi clearance from air traffic control (ATC), advising that ATIS information D had been copied, and that an A3 departure could be accepted. ATC cleared the aircraft to taxi to the A3 runway holding point. As the aircraft approached the holding point, ATC cleared the aircraft for take-off from RWY 19L. On passing the runway distance signs (see the section titled Movement area guidance signs) at the A3 holding point at about 1147, the flight crew completed the take-off performance check (see the section titled Runway entry performance check) and, with all checks completed, the aircraft entered the runway. Both flight crew later recalled that the runway looked clear with no markers or obstructions visible from their take-off commencement point.
The crew performed a rolling take-off, with take-off power being applied at 1148. The captain later recalled that, following the power application, their attention was mostly inside the aircraft performing PM duties and that they did not observe any obstructions or cones on the runway during the take-off.
The FO recalled that:
at an airspeed of about 100 kt, they observed cones positioned in a line across the runway
while they considered the cones an immediate threat, they estimated that the aircraft would become airborne before the cones and, as the aircraft’s airspeed had exceeded 80 kt, they continued the take-off
they did not verbally notify the captain of sighting the cones as it was assessed that the aircraft would clear them
they commenced the take-off rotation before the cones and as the aircraft climbed through about 50 to 70 ft above the runway, the cones were observed to pass underneath.
Recorded audio[13] from the ATC tower identified that, during the aircraft’s take-off run, when it was about midway between the runway intersections of taxiways A6 and A7, the tower controller commented on whether the aircraft was going to rotate. As the aircraft passed over the cones, the tower controller remarked that the aircraft had passed very close over the cones. ATC immediately called a ground vehicle on the tower frequency to inspect the cones. The aircraft’s flight crew heard this exchange before transferring to the departure frequency. Shortly after, the ground vehicle reported that, while the cones did not appear to have been struck, 3 cones had been blown from their original position.
About midway through the climb out of Brisbane, ATC informed the flight crew of the cones being blown over during their departure. The flight crew discussed the departure, noted that the aircraft was handling normally and continued to monitor the aircraft’s instruments for abnormal indications. Shortly after, the captain contacted Virgin maintenance to report that they may have struck cones during departure and organised an inspection on arrival. The aircraft proceeded on to Melbourne without further incident and landed safely at 1441 EDT. The aircraft was subsequently cleared of any damage by a maintenance inspection in Melbourne.
Context
Pilot information
Both the captain and the first officer held Air Transport Pilot Licences (Aeroplane) with Class 1 aviation medical certificates and were appropriately qualified for the flight. The ATSB found no indicators that increased the risk of the flight crew experiencing a level of fatigue known to affect performance.
The captain had accumulated about 9,000 hours of flight experience, of which about 5,500 hours were on the Boeing 737 (B737). In the previous 90 days, the captain had flown 73 hours on B737 type aircraft. The first officer had accumulated about 13,000 hours of flight experience, of which about 9,200 hours were on the B737, with 77 hours flown in the previous 90 days.
Flight planning
Flight plan manager
Flight crews were provided with all required pre‑flight briefing material in a single document – the flight planning package (FPP).The FPP was generated by flight dispatch using the Flight Plan Manager (FPM), a flight planning software package used by Virgin Australia to automate the collation of flight planning data and the production of briefing material for flight crews. The FPP comprised the operational flight plan (OFP),[14] weather data, route plots and NOTAMs for the sector.
NOTAMs were automatically received and imported into the FPM database. For a particular FPP, the FPM software would filter the NOTAMs, presenting only those relevant to that sector, format that NOTAM data into a form usable in a pre-flight information bulletin (see the section titled Notice to Airmen), and attach any company remarks applicable to that NOTAM.
Flight dispatch
Virgin flight dispatch was responsible for the maintenance of the FPM database and the production of the FPP, including the acquisition, collation and evaluation of NOTAM, meteorological and other operational information in support of flight planning activities. Flight dispatch was also responsible for the distribution of NOTAM data to relevant specialist functions within Virgin, such as flight operations engineering (FOE).
As part of the flight planning process, flight dispatchers were required to establish whether the runway, environmental and aircraft performance conditions required a reduction in the normal aircraft limit weights—that is, whether there was any performance limitation to the aircraft’s weight, such as for take-off and/or landing. This was done through calculations using the onboard performance tool (OPT) (see the section titled Performance calculators).
In determining whether there was a limiting weight to be applied, dispatch used weather conditions sourced from TAF[15] data, and were required to ensure consistency of that weather data with other data sources such as METAR[16] and automatic terminal information service (ATIS). Flight dispatch was also required to apply any FOE-determined performance requirement in the limiting weight calculation. When the calculation determined that a weight restriction was to be applied, that limiting weight (or performance limitation) was to be input into the FPM and applied to the overall plan. Any performance limitation was to be noted in the FPP, and the parameters used for the calculation provided in the OFP. The dispatcher was also required to ensure that flight crew were aware of the performance restriction.
Flight operations engineering
On receipt of a NOTAM from flight dispatch, FOE were required to determine whether the NOTAM had a performance impact on operations. For NOTAMs impacting performance, FOE would input the required performance response into the FPM as a company remark, as well as amend the OPT database with the relevant input options applicable to that NOTAM. Where FOE determined that there was no performance impact associated with a received NOTAM, an FOE company remark with a statement such as ‘NO PERFORMANCE IMPACT’ would be input into the FPM.
The flight planning package
Operational flight plan
The FPP’s operational flight plan (OFP) component contained a synopsis of data critical to the conduct of the planned flight. It included information such as the dispatch message, fuel and weight data,[17] the navigation log[18] and any applicable performance restrictions.[19] The dispatch message comprised dispatcher notes to the crew, aircraft discrepancy items and the filed air traffic services[20] flight plan.
Dispatcher notes were required for every flight, and were used by dispatchers to notify flight crew of all decisions pertaining to the preparation of the briefing package and any other information that could assist in the safe conduct of the flight. The notes could also be used to provide flight crew with an overview of the flight planning requirements or any special considerations.
NOTAMs
The FPP was the primary source of NOTAM information for flight crews, and the only source of information for FOE performance requirements. NOTAMs provided as part of the FPP by flight dispatch were stated to be the latest available for departure and arrival ports and, as a general rule, were valid for 30 minutes prior to the estimated time of departure and for 4 hours after the estimated time of arrival.
The National Aeronautical Information Processing System (NAIPS)[21] was an alternative source of NOTAM information available to flight crew and was accessible through the flight crew’s electronic flight bag (EFB).[22] Unlike the FPP NOTAM data, NAIPS NOTAMs were unfiltered and did not have FOE company remarks data attached.
VA319 (Melbourne to Brisbane) flight planning package
The VA319 flight dispatcher determined that there was no landing weight performance limitation for the Melbourne to Brisbane sector resultant from the displaced threshold for Brisbane’s RWY 01R. This was notified to the flight crew through a remark in the ‘Dispatcher notes to crew’ section of the FPP (see Figure 1) as follows:
YBBN RWY 01R DISPLACED BY 921M. NO LDW PERF LIMITATION
The absence of any performance weight limitation was also identifiable from the aircraft limit weights section of the OFP (Figure 3), where the limit weights listed were maximum weights for those conditions in the aircraft’s flight manual. While the dispatcher’s note identified that there were no performance weight limitations, the OFP did not present the specific parameters used in the limit weight calculations (see the section titled Flight dispatch). However, flight crew could ascertain the parameters from various parts of the FPP.
Figure 3: VA319 limit weights
An image of the limit weight section of VA319 OFP. Source: Virgin Australia, annotated by ATSB
VA319 NOTAMs
The VA319 FPP consisted of 33 pages, of which 18 contained the sector’s NOTAMs. There were about 120 individual NOTAMs within the package.
The first of the Brisbane NOTAMs listed was NOTAM YBBNC1174/22 with the headline ‘RWY 01R THR DISPLACED’ (Figure 4 – broken blue box highlighting added by the ATSB). This NOTAM appeared on page 5 of the NOTAMs section and detailed the reduction in length for runways 01R (RWY 01R) and 19L (RWY 19L) due to aerodrome works being conducted around the RWY 01R threshold. Appended to the end of this NOTAM was a company remark titled ‘…>>> VOZ FOE COMPANY REMARK <<<…’. This remark was to notify the flight crew of FOE-required modifications to the take-off and landing performance data calculations for Brisbane RWY 01R and RWY 19L as a consequence of NOTAM YBBNC1174/22.
Figure 4: Page 5 of the NOTAM package, highlighting NOTAM YBBNC1174/22 and its associated FOE performance requirement
An image of page 5 of the VA319 NOTAMs, with YBBN NOTAM 1174/22 highlighted. Source: Virgin Australia, annotated by ATSB
VA324 (Brisbane to Melbourne) flight planning package
Similar to VA319, the VA324 flight dispatcher determined that there were no performance weight limitations for the return sector to Melbourne as a result of the displaced threshold, and while the OFP did not include a direct statement of the parameters used in that determination, those parameters could be ascertained from data within the FPP.
The VA324 flight dispatcher stated that one of the roles of the Dispatcher Notes was to highlight to flight crew any information considered critical by the dispatcher, such as NOTAM YBBNC1174/22. Further, given the short turnarounds often associated with multi-sector flights, the dispatcher intended to direct the flight crew’s attention to this NOTAM through inclusion of the following statement in the dispatcher notes:
YBBN RWY 01R THR DISPLACED 29/2100-30/0630Z.
VA324 NOTAMs
The VA324 FPP consisted of 30 pages, 13 of which contained the sector’s NOTAMs. There were about 80 individual NOTAMs within the package.
The YBBNC1174/22 NOTAM was the first of the NOTAMs included within the VA324 NOTAM package and included an attached FOE company remark. The presentation of the NOTAM and its FOE remark directly reflected the VA319 presentation (Figure 4), but was split over 2 pages, with the FOE remarks appearing on the second page.
FOE conspicuity
The operator’s internal investigation into the event noted that performance critical NOTAMs with associated FOE data were presented in the FPP in the same typeface as less critical NOTAMs, and that there was ‘little to draw the reader’s attention’ to something that was critical to safety of flight. The investigation noted that, in a high workload environment with many distractions, it was ‘…not difficult to miss text that looks the same’.
The VA319 FPP contained 8 NOTAMs with FOE remarks attached, while the VA324 FPP contained 5 NOTAMs with FOE remarks attached. For both FPPs, only 2 of the FOE notices contained performance requirements, while the rest were notifications that the NOTAM had no performance effect. The ATSB also noted that FOE remarks were highlighted via a unique banner (Figure 4) intended to increase their conspicuity to flight crew.
Notice to Airmen
Notification of aerodrome facilities
Airport operators were required to report detailed information about their various aerodrome facilities to Airservices. This information was then published in the Aeronautical Information Publication (AIP). Short-term changes to these facilities were also required to be notified to Airservices. Users of those facilities were then advised of these short-term changes through the NOTAM system.
NOTAM standards
CASR Part 175 prescribed standards covering when NOTAMs were to be issued and how they were to be structured and formatted. A detailed examination of those standards, and the documents in which they are found, is at Appendix – NOTAM standards and related guidance materials.
A NOTAM issued by Airservices was required to meet a prescribed format and contain specific information about the matter being reported. That format comprised multiple fields that not only provided a description of the matter(s) being reported—referred to as the free text section—but also contained coding that enabled both the automatic classification and filtering of that NOTAM, The NOTAM content presented to the flight crew in the FPP was limited to the free text section.
As well as meeting the format and content requirements, a NOTAM was also to adhere to various rules. These are covered in detail at Appendix – NOTAM standards and related guidance materials, but can be summarised under the following 4 basic principles:
A NOTAM shall deal with only one subject and one condition of that subject. It shall be as brief as possible and compiled such that the meaning is clear, and without the need to refer to another document.
The subject matter and related condition shall be determined in accordance with specific coding procedures and tables found in the International Civil Aviation Organization (ICAO) Document 8400.[23]
The code identifying the subject or denoting its status of operation is, whenever possible, self‑evident. Where more than one subject could be identified by the same self-evident code, the most important subject is chosen.
The content of the free-text section of the NOTAM shall be based on the selected code, be clear and concise and if possible limited to 300 characters—to facilitate use in a Pre‑flight Information Bulletin (PIB).[24]
Of the various standards-defining documents identified in CASR Part 175, only ICAO Document 8126[25] included material on circumstances where multiple NOTAMs could be combined and reported in a single NOTAM. The document stated:
The NOTAM Code selected describes the most important status or condition to be promulgated.
Although not included in CASR Part 175 as a standards document, EUROCONTORL[26] guidance material on NOTAMs included the following caution on combining NOTAMs:
The negative impact on end-users caused by NOTAM proliferation is not to be solved by including more information in a single NOTAM, but that this fact further increases the difficulty for end-users. More information in one NOTAM makes the message less readable and essential information more difficult to detect.
Assessment of NOTAM YBBNC1174/22
The ATSB sought advice from both ICAO and the Civil Aviation Safety Authority (CASA) regarding NOTAM YBBNC1174/22 and its adherence to the applicable standards. ICAO and CASA acknowledged the guidance with regard to NOTAM content being limited to one subject matter and one condition of that subject matter, but differed in the application of this limitation with respect to related content.
CASA advised that the most important status or condition being reported in this NOTAM was the displaced threshold, and that the matters being reported within the free text section were the result of the changed condition of that subject matter. Further, the additional matters being reported were information necessary for the safe conduct of flight. As an overall assessment, CASA stated that the NOTAM met the standards as required under CASR Part 175. On whether the NOTAM’s headline should have contained reference to ‘RWY 19L’, CASA stated that this could not be the case as there was no displacement of that runway’s threshold.
ICAO stated that, as per PANS-AIM, matters not directly related to the subject matter and related conditions should not be included within the free text section, but that there also needed to be a balance between usability and convenience while adhering to the guidance principles. ICAO nevertheless advised that the free text section of the NOTAM held critical information interspersed with less critical information, and that the critical information should have preceded the less critical information. While ICAO indicated that the NOTAM complied with ICAO guidance principles, the information concerning the runway lighting, and probably the taxiway information, should have been published as separate NOTAMs.
Brisbane Airport
Runway works
The Brisbane NOTAM YBBNC1174/22 was published as notification of scheduled works around the threshold of RWY 01R. Those scheduled works were part of a larger programme of works documented in a Method of Working Plan (MOWP) YBBN 22/07,[27] published by Brisbane Airport Corporation (BAC) in August 2022. The works were to be staged over about a year to minimise disruption to operations at the airport. In accordance with the Civil Aviation Safety Regulations (CASR) Part 139, the MOWP detailed the timing, scope of the works and specific aerodrome facilities that would be affected. The MOWP also identified how the individual work stages affected aircraft operations, and listed any NOTAM to be issued, where required, for each stage.
The works around the threshold of RWY 01R were scheduled to commence on 30 November 2022. After being notified of these works by BAC, on 23 November Airservices issued the predecessor of YBBNC1174/22. As a result of some minor changes, that original NOTAM was modified, and on 30 November YBBNC1174/22 was published by Airservices.
Runway distance information
NOTAM C1174/22 included runway distance data under the title DECLARED DISTANCE AND GRADIENT CHANGES. The information immediately below this line provided runway distance measurements used in the calculation of aircraft runway performance data.
Part 139 Manual of Standards (Part 139 MOS) required aerodrome operators to report various runway distances for publication in the AIP. The following ‘declared distances’, as defined in Part 139 MOS, were to be notified by aerodrome operators (Figure 5):
Take-off run available (TORA). The length of runway declared available and suitable for the ground run of an aeroplane taking off. The take-off run available may include additional length available from a starter extension if provided, but neither stopway (SWY)[28] nor clearway (CWY)[29] were included in the take-off run available.
Take-off distance available (TODA). The length of the take-off run available plus the length of the clearway, if provided.
Accelerate-stop distance available (ASDA). The length of the take-off run available plus the length of the stopway, if provided.
Landing distance available (LDA). The length of runway which is declared available and suitable for the ground run of an aeroplane landing.
Figure 5: Runway declared distances
A diagram identifying the various components of a runway’s declared distances, and their relationships to the physical dimensions of the runway. Source: ICAO Annex 14, modified by ATSB
The various take-off and landing distances applicable to RWY 19L[30] and the A3 intersection with RWY 19L, while in unrestricted use and when the displaced threshold was in effect (as notified by NOTAM C1174/22), are stated in Table 1.
Table 1: Runway 19L distances
Departure designation
TORA
TODA
ASDA
LDA
19L
3560
3620
3560
3560
19L/A3
2781
2841
2781
-
19L-WIPS
2689
2749
2689
2689
19L/A3-WIPS
1910
1970
1910
-
Movement area guidance signs
Movement area guidance signs (MAGS) were installed at the taxiway A3 holding point for entry to RWY 01R/19L. MAGS may be either mandatory instruction signs or information signs. Instruction signs used white lettering on a red background, while information signs used black lettering on yellow background. There were 2 types of MAGS installed abeam that runway holding point (Figure 6):
a runway designation sign that identified the taxiway and runway, located to the left of the taxiway and adjacent to the holding point
2 take-off run available (TORA) signs located either side of the taxiway that stated the TORA distances available in the identified direction from that runway entry point.
The flight crew stated that these signs were not obscured at the time of VA324’s departure. Brisbane Airport personnel advised that the TORA MAGS would not normally be covered or obscured when there was variation in the runway length due to works.
Figure 6: MAGS situated at the A3 holding point for 01R/19L
An image showing the movement area guidance signs at the A3 intersection to runway 01R/19L. Source: BAC
Part 139 MOS paragraph 8.27(4) stated:
If:
(a) a movement area guidance sign (MAGS) displays declared distance information; and
(b) because of a period of temporary threshold displacement the MAGS information is incorrect for the period;
the MAGS must be obscured until the permanent threshold is reinstated.
The MOWP did not include any instruction for obscuring the TORA MAGS located at the A3 holding point.
OPT calculated runway performance data
Introduction
The Onboard Performance Tool (OPT) was developed by Boeing as the application to be used by flight crew for calculating take-off and landing performance. While the primary source of B737 aircraft performance data was the Airplane Flight Manual (AFM),[31] the OPT provided data equivalent to the AFM and met all take-off and landing regulatory requirements. It was accessed through the Electronic Flight Bag (EFB).
OPT database
The OPT used a database of airports and runways available for use by the operator’s flight crew. That database was maintained by flight operations engineering (FOE). Changes to an airport’s runway data, such as a reduction in runway length notified through NOTAM, required FOE to determine how aircraft performance was affected and what additional runway data was to be included within the OPT database. As part of their response, FOE would amend the database to include a temporary runway identifier with the modified runway data relevant to this change. The requirement to use this temporary identifier would be notified to flight crews through the VOZ FOE COMPANY REMARK notice attached to the relevant NOTAM in the FPP. Updates to the OPT database were automatically sent to the EFB. Prior to the first use of the day, the user was required to ensure that the OPT database version was the latest, as listed within the company NOTAMs. Virgin stated that quality control procedures established within FOE ensured that flight crew were not required to independently verify runway data used by the OPT.
Performance calculators
Introduction
In setting up the OPT for performance calculation, the user was required to select the relevant airframe registration and airport from the database. There were 3 types of performance calculators available:
take-off performance
landing performance
en route landing performance.
Take-off and landing performance calculators
The take-off and landing performance calculators enabled determination of take-off and landing performance data as well as the performance limited weights for take-off and landing. The performance limited weight feature of both the take-off and landing performance calculators were primarily used by flight dispatch during flight planning to determine whether the sector had limiting weight considerations. The take-off performance calculator was used by flight crew for calculating take-off performance data as part of the preliminary pre‑flight procedure (Figure 7).
An exemplar image of the OPT take-off performance calculator, with the data inputs in green and, in the lower third, the calculator’s take‑off performance data. Source: Virgin Australia
When used by flight crew for take-off or landing performance data calculation, the user was required to input data into the various fields, and if a valid performance solution was possible, the application would provide performance data for those parameters. For a take‑off calculation, a valid performance solution would provide data that included the relevant take-off speeds and any available thrust derate.[32] An invalid performance solution would clearly advise the flight crew that a take-off using those parameters was not permitted. With respect to the landing calculator, the performance results included the landing limit weight and relevant landing speed for the selected flap setting at that weight.
En route landing performance calculator
The en route landing performance calculator was the primary landing data calculator used by flight crew (Figure 8). It provided data based on an input landing weight and selected environmental and aircraft configuration inputs. If a valid landing performance solution was possible, the calculator would provide landing performance data that included the landing speed and stopping distances for the various braking selections available. That stopping data could be displayed in both tabular and graphic form. The selected runway’s landing distance available (LDA) was displayed as a product of the landing data solution.
Figure 8: Exemplar OPT en route landing performance calculator
An image of the OPT en route landing performance calculator, extracted from the Virgin manual. The calculations are for Coolangatta, with the data inputs in green and, in the lower third, the calculated landing performance data. The image also shows the calculated stopping solution in graphic form. Source: Virgin Australia
Runway distance data
While runway distance data was displayed in the calculation results for the en route landing performance calculator (displayed as the Landing Distance Available), it was not displayed as part of the calculated take-off performance data. However, runway data was available in all OPT calculators through the ARPT Info tab (see Figure 7 and Figure 8). Selecting the ARPT Info tab (Figure 9) provided database details for the airport and runway that were selected as inputs. Intersection details relevant to that runway data was then available through a further selectable option. However, to determine the TORA for an intersection departure, the flight crew needed to manually calculate it using the displayed information.
Figure 9: OPT airport information
An image showing access to runway data through the Airport Info tab in the various OPT calculators. Source: Virgin Australia modified by ATSB
VA319 landing performance data
For the VA319 landing, the runway (RWY) input for Brisbane Airport (YBBN/BNE) had several selectable options available through a drop-down box. These were, in order, 01L, 01R, 19L, 19R, 01R WIP-S and 19L WIP-S (Figure 10). The 2 WIP-S runway options were the required selections for those runways based on the FOE remark in the VA319 FPP while NOTAM 1174/22 and the RWY 01R threshold displacement was in effect.
As part of their landing performance calculations for arrival into Brisbane, the flight crew selected the 19L option. The calculator provided a stopping solution based on the full runway length, and the other selectable variables input by the flight crew. The displayed landing solution included the LDA for RWY 19L, which was 3,560 m, while the available stopping solutions were based on this full runway length.
While the stopping solution for the landing in Brisbane was based on an incorrect runway length, the landing was not affected by this error. The aircraft was able to exit the runway using the using the A6 rapid exit taxiway, which was about 850 m short of the displaced threshold.
Figure 10: Runway input selection
An image of the OPT take-off performance calculator with the runway options displayed for the VA324 departure. Source: Virgin Australia modified by ATSB
VA324 take-off performance data
For the VA324 departure, the selectable YBBN/BNE runway inputs were those as stated for the VA319 arrival. However, on selecting the runway, the user was then also able to select various intersection (INTX) departure points available for that runway. While the normal RWY 19L configuration had the FULL and A3 INTX (intersection) options available, FOE had removed the A3 INTX option for RWY 19L WIP-S, and therefore the A3 intersection departure was not an available input.
For the VA324 take-off performance calculation, the flight crew selected the 19L option as the departure runway and A3 as the intersection departure. The OPT provided take-off performance and thrust derate based on the TORA of 2,781 m.
As part of its internal investigation, Virgin calculated the VA324 take-off performance data using the same inputs as the flight crew, but with the 19L WIP-S runway option and an A3 INTX selection (an A3 intersection departure). The OPT displayed an invalid take-off performance solution, with the following message being displayed:
No takeoff allowed. Planned weight exceeds max allowable weight of 67350 KG.
This result indicated that, even with maximum take-off thrust, the aircraft was overweight for a departure from A3 on runway 19L with the reduced runway length due to the displaced RWY 01R threshold.
Operator’s policies and flight procedures
Operations manual requirements
The operations manual detailed the operator’s general policies and specific procedures that governed the conduct of safe flying operations. With respect to the approach and pre‑flight phases of operations, it contained both common and specific requirements relevant to both. While the aircraft captain was accountable for the aircraft’s safety, and to obtain and check all available relevant information, the first officer was also required to be able to assume pilot in command duties should the aircraft captain become incapacitated. To meet this requirement, the first officer was to actively participate in the preparation and conduct of the flight, and in particular regarding flight preparation, to be familiar with all relevant operational information, including NOTAMs.
The operations manual also required both flight crew to independently review the weather information to be used in the departure and arrival preparations, such as that sourced from the ATIS. This independent review required each pilot to listen to the source information, or, if the source was a printed readout, independently read that data. That review was required to include verification of the information recorded on the take-off data card (TODC).
Flight crews were also required to be alert for NOTAMs that may have performance effect, but which did not have an FOE remark attached. The absence of the FOE remark identified that the NOTAM had not been assessed by FOE, and in such cases flight crews were required to contact flight dispatch and initiate an assessment of the NOTAM.
The manual also included a requirement for departure and arrival briefings. These briefings, which were normally conducted by the PF, had explicit content requirements, but both specifically included applicable NOTAMs. There was also a general threat and error management component to be addressed in these briefings.
Departure specific requirements
The pilot-in-command was responsible for ensuring that the aircraft’s gross weight was such that the flight could be conducted in compliance with the AFM, and similarly that the aircraft did not exceed take-off performance limitations. For take-off performance calculations, the operations manual required compliance with procedures that ensured an adequate independent cross-check be conducted with respect to several factors, including the input data used for the calculation. These independent cross-check procedures were detailed in the FCOM and the Performance and Loading Manual. Finally, the operations manual required specific items to be included within the departure briefing, when applicable. These items included any NOTAMs that were relevant to the departure.
Approach specific requirements
Before landing, the pilot in command was required to determine that the landing distance available (LDA) was sufficient and with an adequate safety margin. The operations manual provided 3 methods through which this determination could be made.
The first 2 methods were based on the dispatcher’s pre‑flight calculation of the landing weight limit for the sector. This limit was stated as the maximum landing weight (MLDW) in the limit weight (LIMIT WT) section of the OFP (Figure 3). If the aircraft’s landing weight was less than this MLDW:
and there had been no adverse changes to the environmental conditions, aircraft configuration or runway of intended use, or
having considered any changes to the environmental conditions, aircraft configuration and/or runway of intended use and found them to have no adverse effect,
then the landing distance requirement was met. Both MLDW methods were reliant on the flight crew knowing the variable parameters of environmental conditions, aircraft configuration and runway of intended use, that the dispatcher used in the MLDW calculation. Generally, dispatchers did not declare the parameters used in the MLDW determination within the OFP (see the section titled Flight planning). However, the dispatcher’s manual stated how these variable parameters were to be determined and flight crew could ascertain them from various parts of the FPP.
The third method required the flight crew to calculate an operational landing distance using maximum manual braking and factored by 1.15, and then ensuring that this landing distance was less than or equal to the LDA. The operations manual also required a stopping solution be determined when the LDA was sufficient. An operational landing distance calculation was made as part of the OPT’s en route landing performance solution (see the section titled En route landing performancecalculator). Therefore, the sufficient LDA determination was met as part of the stopping solution calculation.
Training manual requirements
As the occurrence flight was also being used to support a training function (line flying under supervision), it was necessary to examine relevant training policy and guidance to determine any likely effect on the conduct of normal operations. The operator’s training manual stated that safety remained the primary objective of all training events, and that:
The safe conduct of our flying operations and all supporting activities relies on our systems, our operating procedures, and most importantly in the way we think and act.
The manual further stated that:
All flight crew and Training and Checking personnel engaged in … training and assessment activities are required to ensure that safety remains at the forefront of all actions and decisions. This is especially important for training conducted in the aircraft, where Trainers … must always ensure that the safety of the aircraft and its occupants is never compromised.
The training manual also stressed that training pilots should conclude all training events with some degree of debrief.
Flight procedures
Introduction
The procedures required of the flight crew for the various phases of flight were contained in the operator’s Flight Crew Operating Manual (FCOM). These procedures were to be performed by memory and ensured that operational systems were correctly configured for the relevant phase of flight, and data for the flight management systems was entered and correct. Pre and post‑flight duties were divided between the captain and first officer, while phase of flight duties were divided between the PF and PM.
The procedures required of the flight crew as part of the approach preparation for VA319, and those required as part of the departure preparation for VA324, are addressed separately. The FCOM procedures for both the approach and departure preparation required calculation of performance data. Those calculations, which were made using the OPT, were to be completed using procedures and guidance found in the aircraft Performance and Loading Manual.
Pre‑flight procedures and the performance data calculation
Take-off performance data calculations were part of the FCOM flight management computer’s (FMC) data entry procedure that was conducted in parallel with the captain and FO pre‑flight procedure. This procedure required the determination of input data for the performance calculation, recording of that data on the TODC, and entry of that data into the OPT. These procedures and method of calculation using the OPT were prescribed by the Performance and Loading Manual.
The pilot not performing the exterior inspection was required to complete the TODC. The weather conditions for the departure, such as that reported by the ATIS, and the input variables for the OPT calculation were to be determined and recorded onto the TODC. These included items such as:
the relative wind (headwind or tailwind component)
adjusted ambient temperature
runway data to be used
aircraft configuration data, such as the relevant weights, fuel on board, engine thrust rating, and the intended take-off flap setting.
These variables were then entered into the OPT and if a valid take‑off performance solution was calculated, the various take-off speeds, any take-off thrust derate (if applicable), and other performance data provided by the OPT calculation were to be recorded on the TODC (Figure 11).
Figure 11: A partial replication of the VA324 TODC
A partial replication of the VA324 TODC archived record, showing the recorded ATIS, aircraft weights, departure point and take-off performance data. Source: Virgin Australia modified by ATSB
The take-off performance data was entered into the FMC as part of the data entry component of the pre‑flight procedure. The other pilot was then required to independently calculate the take-off performance data as part of their pre‑flight procedures.
Validating performance data calculations
The OPT had a ‘compare calculation’ function to compare the performance calculations made by 2 EFB devices connected through wi-fi. This ‘compare calculation’ function operated as the independent cross-check of input data required by the operations manual for all take-off performance calculations. The ‘compare calculation’ function displayed a comparison of the performance results and checked for any differences in the user inputs. Any discrepancies were notified to the user. Where no differences existed, both devices displayed a ‘check complete’ and ‘no mismatches found’ message.
Runway entry performance check
The FCOM’s before take-off procedures required the flight crew to verify that the runway about to be used for the take-off and the runway take-off position were correct. This was triggered when the aircraft was approaching the take-off position. It required, among other things, that the flight crew confirm that the runway location used for the performance calculation was coincident with the aircraft’s actual location.
Landing performance calculations
The OPT’s Landing En route Performance calculation, using the actual landing weight and the relevant weather components drawn from the ATIS, provided the operational landing distance for the various braking options (see the section titled En route landing performance calculator).
The landing distance available was also displayed, however, flight crews were not required to confirm that a changed landing distance available notified on the ATIS matched the landing distance available displayed on the OPT. This assurance was met through flight crew awareness and selection of the appropriate runway selection from the runway drop-down options in the OPT, which in turn was dependent on timely FOE updates to both the OPT database and notification to flight crew through the FPP.
Pre‑flight tasks and turnaround schedules
The operator provided a synopsis of the normal turnaround tasks and timings for a B737 flight crew. A turnaround was allocated 40 minutes from arrival to departure from the gate. The tasks required to be performed during the turnaround were estimated to take about 30 minutes, of which 4 minutes was assigned to planning the next sector. The operator noted that sector patterns were arranged such that ports were revisited, thereby enabling a significant part of the briefing process to be covered during an earlier cycle.
Air traffic control information
VA324 departure
Airservices Australia stated that several aircraft departed via the A3 intersection prior to the VA324 departure, and that there were no restrictions on doing so. The airport operator had installed several cones across the runway about 200 m south of the A7 taxiway intersection with the runway (Figure 12). VA324’s nose wheel was observed by the tower controller to lift at about taxiway A7 and the main wheels were observed to have passed extremely close to the displaced threshold cones. Several of the cones were blown over, and the airport operator advised that one cone was damaged.
In its internal investigation report, Virgin identified that some tower controllers were heard on the day, advising other flights that the runway was operating with a reduced length. Further, while acknowledging this was a non-standard radio call, the internal report also stated that consideration should be given to enhancing this radio call.
The ATSB determined that absence of such an alert for the VA324 departure was not contributory to the overrun occurrence. The shortened runway was included within the ATIS, which the flight crew acknowledged receipt of. Nevertheless, the inclusion of limiting runway conditions such as a shortened runway within the take-off clearance would enhance flight crew awareness of those conditions.
ATIS information
The ATIS information for both the arrival of VA319 and the departure of VA324 was ‘D’, which stated:
EXPECT INSTRUMENT APPROACH RWY 19L AND R FOR ARRIVAL AND DEPARTURES INDEPENDENT PARALLEL DEPARTURES IN PROGRESS REDUCED RUNWAY LENGTH IN OPERATION RWY 19L, LANDING DISTANCE AVAILABLE 2689 M, TAKE OFF RUN AVAILABLE 2689 M WIND 140 DEG, MIN 8 KT MAX 20 KT, CROSSWIND MAX 20 KT VISIBILITY GREATER THAN 10 KM SHOWERS IN AREA CLOUD FEW 1500 SCT 3500 TEMPERATURE 22 QNH 1014
Recorded data
Recorded data from the aircraft’s flight data recorder, Automatic Dependent Surveillance Broadcast (ADS-B) data from Airservices Australia, and video from various aircraft gates around the airport, enabled the ATSB to determine where VA324 became airborne. The relationship between the point where the aircraft’s main wheels left the runway and the cones, as well as the declared distances stated in NOTAM YBBNC1174/22 are identified in Figure 12.
Figure 12: Runway 19L configuration for VA324 take-off
An image showing the location of the cones on runway 01R/19L, and also displaying the various distances notified through NOTAM YBBN 1174/22. Specific locations of VA324’s take-off are also displayed.
Source: ATSB
The Global Action Plan for the Prevention of Runway Excursions
In May 2021, EUROCONTROL, with the support of the Flight Safety Foundation, published the Global Action Plan for the Prevention of Runway Excursions (GAPPRE). This publication was the result of contributions from multiple international public and private organisations with the goal of enhancing the safety of runway operations. The GAPPRE recommendations represent industry best practice which extend beyond regulatory compliance.
As part of its examination of take-off performance data calculations, the GAPPRE made the following observations:
Many runway safety events stem from erroneous or inadequate take-off performance calculations.
While the independent take-off performance calculations by all active crew members, which are subsequently cross-checked, can be time consuming, it is highly recommended.
EFB solutions incorporating navigational charts and applications for flight planning such as take-off and landing performance calculation programs not only save costs but also can simplify processes for flight crews. However, if threats such as runway shortening are not incorporated in time into the database used for performance calculations, the probability of the flight crew failing to detect such errors is high, especially as current NOTAM format and presentation in aviation in combination with fatigue, time pressure or complacency may lead to flight crews sometimes not reading or checking NOTAM information properly.
Visualisation in particular is a great tool to enable flight crews to easily build a correct risk picture for their take‑off in terms of runway excursion prevention. Being aware of the additional stop margin resulting from their calculation and being able to easily cross‑check that the take‑off position and line-up procedure used for the calculation matches the one expected or used is key for flight crews’ safety-relevant decision-making (e.g. deciding on a re-calculation or accepting or rejecting line-up clearances). If technically feasible, visualisation of this information should therefore combine results of performance calculations and airport layouts.
These, and other observations with respect to the calculation of performance data, led to several recommendations, including that aircraft operators develop policies or standard operating procedures that require flight crews to perform independent performance calculations. This should include an independent cross-check of actual TORA/TODA from the AIS with the TORA/TODA used to calculate the take-off performance.
The implementation of this recommendation included a strategy that the actual TORA/TODA, especially if being altered by NOTAM, should be checked against the value used in the take-off performance program individually and independently by each flight crew member. If it is not technically feasible to combine the results of take-off performance calculations and airport/runway layout in one visualisation, at least the EFB solution should make it possible to visualise the available stop margin in relation to the TORA.
Operator processes
Virgin’s procedures did not require flight crew to confirm that the runway distance used in the performance calculation matched that stated on the aerodrome ATIS. The operator advised that the OPT and gross error checking systems currently used were satisfactory for runway performance calculations.
While the operator’s dispatch NOTAM update service and FOE review provided the latest information available for flight crew for use in runway performance calculations, it did not mitigate inadvertent flight crew error where FOE performance requirements were not identified as part of the briefing process. Further, while extremely remote, there is also the likelihood of late changes in runway configuration being reported on ATIS but being outside of any update to the NOTAM package being provided to flight crew. Both could lead to miscalculation of runway performance data, which could be mitigated through procedure requiring confirmation of an ATIS reported change in runway data being confirmed and matched to the data used in the performance calculation.
Similarly, tools that enable the visualisation of the relevant performance distances, and in particular the stopping margins available for the take-off, are of great value in enabling flight crews to easily build a correct risk picture for their take-off in terms of runway excursion prevention. While these visual tools were available for the OPT’s en route landing calculator, there was not an equivalent visual tool available for use in the take-off calculator.
The first part of this 2-part ATSB research and analysis report presented a worldwide perspective of accidents and incidents involving take-off performance parameter errors. The report noted that, despite advanced aircraft systems and robust operating procedures, accidents continued to occur during the take-off phase of flight. The report documented accidents and incidents that resulted from take-off performance parameter data being incorrectly calculated or entered into aircraft systems.
It was found that calculation and entry of erroneous take-off performance parameters had many different origins, and that many factors were identified at all levels of influence. Due to the immense variation in the mechanisms involved in making take-off parameter calculation and entry errors, the report stated that there was no single solution to ensure that such errors were always prevented or captured. The report did, however, discuss several error capture systems that airlines and aircraft manufacturers can explore.
On 14 October 2013, a B737 aircraft departed from runway 11 intersection B2 at Darwin Airport using take-off performance data for the full runway length. The flight crew had prepared performance data for both a B2 intersection departure and a full-length departure and entered data for the full‑length departure into the flight management computer. As the aircraft taxied for a full-length departure, ATC advised of delays for a full-length departure due to arriving aircraft, but that an immediate departure was available from B2. The flight crew elected to use the B2 departure and reprogrammed the flight management computer. After a normal take-off, the flight crew identified that they had used the full-length data to reprogram the flight management computer, and that the aircraft had taken off with incorrect performance data.
During the month of September 2021, a NOTAM advised flight crew that Darwin Airport runway 29 had a displaced threshold due to runway works. Two flight crews, the first on 3 September and the second on 19 September, misinterpreted the NOTAM to mean that runway 11 threshold was displaced. Both flight crews planned for a displaced threshold landing on runway 11, and both crews subsequently landed long with reduced runway available for the landing roll. Further, both flight crews misinterpreted the aerodrome ATIS, which stated the active runway as being 11 and that the runway had reduced length.
On 7 July 2017, an Airbus A320 was cleared to land at San Francisco airport runway 28R. The aircraft, which was conducting a visual approach to the runway, was lined up with the parallel taxiway C and not the runway. There were 4 air carrier aircraft waiting clearance to take off that were occupying taxiway C. The A320 descended to an altitude of 100 ft AGL before initiating a go‑around, during which the aircraft descended to 60 ft and overflew a number of the waiting aircraft, narrowly missing one of the waiting aircraft.
The flight crew aligned the aircraft with the taxiway on an incorrect understanding that the lights to their left were for the parallel runway 28L. That runway, however, was closed and not lit. A NOTAM stating the closure of runway 28L was included within the flight crew’s briefing package. The NTSB found several contributing factors to the runway misalignment, including that the flight operations information provided to the flight crew needed more effective presentation of information to optimise pilot review and retention of relevant information, particularly given the large volume of data presented to flight crew.
Safety analysis
Introduction
At 1148 on 30 November 2022, a Boeing 737-800 flight from Brisbane to Melbourne, operating as VA324, commenced its take-off run from the A3 intersection of runway 19L (RWY 19L) at Brisbane Airport (BNE). While the aircraft’s flight crew were aware of the upwind threshold being displaced, they were not aware that the take-off distance available for runway 19L had also been significantly reduced due to that displacement and that there were cones across the runway to mark the closed end of the runway.
Consequently, the performance data used for the take-off was incorrectly based on a normal length runway being available. This resulted in insufficient power being applied at the commencement of the take-off for the aircraft to complete the take-off in the declared distance available. This analysis will examine the factors that led to this serious incident and the opportunities to have corrected the misunderstanding of the runway status.
Flight planning in Melbourne
Incorrect mental model for runway 19L
Before the departure from BNE RWY 19L, the flight crew operated a sector from Melbourne (MEL) to BNE as VA319. The VA319 operational flight plan (OFP) component of the flight planning package (FPP) included a dispatcher’s note that identified that the threshold for BNE RWY 01R was displaced, but also contained the statement ‘NO LDW PERF LIMITATION’. This was intended to inform the flight crew that the displaced threshold had not led to any change to the aircraft’s maximum landing weight limitation for the landing into BNE.
The captain, however, misinterpreted this to mean that the displaced threshold had no performance effect for operations on runway 19L, that is, that flight operations engineering (FOE) had determined that there were no specific requirements with respect to the onboard performance tool (OPT) data input due to the threshold displacement. This misunderstanding led to a mental model that the displaced threshold for RWY 01R had no effect on performance requirements for RWY 19L.
Dismissing NOTAM YBBNC1174/22
The operator’s turnaround time between flights was generally scheduled at 40 minutes, of which about 5 was allocated to planning for the next sector. During this short period, there was typically a large volume of NOTAM data to be reviewed and flight critical data identified and actioned. While the grouping of sectors, revisiting of ports, and the use of a dispatcher to provide support, enabled efficiencies related to briefing, the aircraft captain retained overall responsibility for being aware of all relevant data.
To achieve this in the limited time available, the occurrence captain used NOTAM headlines as a guide to the content when assessing the relevance of a NOTAM. The scanning of NOTAMs using their heading is a practice often used by flight crew to enable large volumes of NOTAMs to be reviewed quickly. While the one subject matter and one condition standard for NOTAM construction generally supports this practice, there may be instances where a NOTAM’s headline does not fully reflect data contained within the free text section. NOTAM YBBNC1174/22 was one such NOTAM.
The 33-page VA319 FPP, which was presented to the flight crew in Melbourne, contained 120 NOTAMs over 18 pages. The NOTAMs for BNE included NOTAM YBBNC1174/22 with the headline RWY 01R THR DISPLACED. That NOTAM detailed the reduction in the runway length for operations on 01R/19L, data that was critical for the arrival into Brisbane. During review of the sector’s NOTAMs, the captain sighted the NOTAM headline and identified the NOTAM as being the matter to which the dispatcher had referred to in the note. However, the captain incorrectly dismissed this NOTAM as not being relevant to the flight because they:
had previously incorrectly interpreted the dispatcher note on the performance effect of the displaced threshold, and therefore this NOTAM, as having no impact on their operations
expected a landing on RWY 19L in Brisbane and the NOTAM headline made no reference to RWY 19L.
The ATSB was unable to conclusively determine whether the first officer reviewed the dispatcher’s notes and sector NOTAMs prior to departure from Melbourne, however, if they did, they missed the relevance of the note, the NOTAM and its attached FOE data.
FOE data not identified
The FPP was the only source available to the flight crew for notification of FOE data changes. Any performance calculation made without the use of the applicable FOE data had an elevated potential to be incorrectly applied. The FOE remark attached to YBBNC1174/22 contained the data necessary to select the correct OPT inputs and correctly calculate aircraft performance data when using the reduced length of runway 01R and 19L in Brisbane.
During the VA319 pre‑flight at MEL, the flight crew did not identify the FOE data applicable to operations on Brisbane’s RWY 19L during the review of the NOTAMs. The FOE data appended to NOTAM YBBNC1174/22 was either missed or dismissed due to an expectation that there was no performance effect.
The operator found that performance critical NOTAMs were presented in the same typeface as less critical NOTAMs and that this was contributory to the flight crew not identifying the FOE remark. While this is possible, it was also noted that the remarks were distinguished by a unique heading banner. The ATSB assessed that the incorrect mental model established by the captain was probably the overriding factor which influenced the dismissal of the NOTAM and its associated FOE remark.
Finally, the ATSB considered the possibility that the delayed issue of the complete FPP to the flight crew in Melbourne impacted the crew’s ability to effectively review NOTAMs and associated FOE. However, a full reprint of the FPP’s NOTAMs was available to the crew before departure and the preparations for arrival into Brisbane including the arrival briefing offered another opportunity to review the NOTAMs and identify applicable FOE data.
The Brisbane arrival
Readdressing the NOTAM
The operations manual requirements for an arrival briefing specified runway conditions and applicable NOTAMs for the arrival as items to be addressed in the briefing. It also included a general threat and error assessment for the arrival and landing. NOTAM YBBNC1174/22 contained critical information that merited review under both the briefing and the threat and error assessment.
However, contrary to these requirements, NOTAMs were not reviewed before arrival, nor were they reviewed when the time and opportunity was present during the en route phase of flight between MEL and BNE. While this time was likely allocated to training, the flight crew’s primary responsibility for safety of flight necessitated that, at a minimum, this NOTAM be reviewed. As a result, another opportunity to correct the captain’s (crew’s) mental model of BNE RWY 19 was missed.
ATIS and incorrect landing performance
While the BNE ATIS stated that the runway length of RWY 19L was reduced and specified the reduced landing distance available (LDA), the flight crew did not consider this notification to be relevant to the approach preparations. This was probably a result of the continuation of the misunderstanding of the dispatcher’s note regarding the performance requirements for RWY 19L. This resulted in the flight crew selection in the OPT of the full runway length for the runway input criteria, instead of the reduced length option. While the OPT landing performance data was based on an incorrect runway landing distance available, the calculated stopping solution was based on exiting the runway well before the closed section. Therefore, the landing was not affected by the incorrect runway data input. Further, the aircraft performed in accordance with the calculated data, exiting the runway normally using the planned rapid exit taxiway. The flight crew also did not see any visible restrictions or obstructions either on or around the runway which further supported their incorrect mental model.
While the LDA used in the landing performance calculation was displayed as part of the OPT en route landing performance calculation, the operator’s procedures did not require flight crews to crosscheck the LDA presented by the OPT with any notification of LDA change, such as that stated on the ATIS. Such a check, as recommended by the GAPPRE, could have provided an additional defence to capture the flight crew’s incorrect mental model and landing performance error.
The Brisbane departure
The pre‑flight
The flight crew commenced the pre‑flight preparations for VA324 with an understanding that YBBNC1174/22 did not impose any limitation on RWY 19L operations. Due to a combination of time pressures and distractions, particularly the delayed arrival into Brisbane and the initial prioritisation of training requirements during departure preparations, the flight crew had reduced time for their review of the VA324 FPP. As a result, the captain dismissed the dispatcher's note alerting the flight crew to the displaced threshold and, while the flight crew reviewed the OFP component of the briefing package prior to departure, they likely did not review the NOTAM package.
Take-off data error
Despite reviewing the ATIS content, due to an enduring belief there were no runway restrictions, the captain used an incorrect normal runway length input to determine the take-off performance figures for the BNE departure. This error was not identified as the first officer used the captain’s input data from the take-off data card (TODC), contrary to the independent take-off performance calculation procedures, resulting in the same incorrect figures.
Due to the use of the full runway length option as the basic runway configuration, the OPT calculator enabled a departure from the A3 intersection with a power derate. However, had the actual reduced runway length option (19L-WIPS) been used, the OPT would have excluded an A3 departure as the aircraft was overweight for such a departure, even with full take-off power. Further, had the A3 intersection departure selection been available for the 19L-WIPS option, the OPT would have notified the flight crew that a take-off from that point on the runway was not permitted.
Due to the incorrect take-off performance calculation, the aircraft did not meet the required performance for its departure from the A3 intersection of RWY 19L. The effect of this meant that the aircraft may have been unable to stop within the declared TORA if the take-off had to be rejected at high speed, and a runway excursion would have occurred. In addition, in the event of engine failure at high speed, the aircraft would probably have been unable to achieve its required performance.
Misleading MAGS
The Part 139 Manual of Standards required that movement area guidance signs (MAGS) located at runway intersection holding points be obscured when a temporarily displaced runway threshold altered the distance displayed by the MAGS. This did not occur while NOTAM YBBNC1174/22 was in effect. The signs presented a take-off distance that was in excess of that available, creating the potential to mislead flight crews about the status of the runway and the distance available when conducting a departure from that point.
While the operator’s procedures required the conduct of a performance data check at the holding point, they did not require consideration of the MAGS data in relation to that check. However, as MAGS were not required by Part 139 at all departure holding points, the mandating of a MAGS check as standard procedure would not have been possible. Nevertheless, obscuring the signs or including an indication of works in progress on the signs, had the potential to alert flight crews to changed conditions and trigger crews to confirm that correct runway data was being used for the take-off performance calculation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the incorrect calculation of take-off performance data by the flight crew of VH-YFH on 30 November 2022 that led to a runway excursion on Brisbane Airport runway 19L.
Contributing factors
For the Melbourne to Brisbane sector, the dispatcher notes in the operational flight plan stated that Brisbane runway 01R displaced threshold had no landing weight performance limitation. The captain misinterpreted that note to mean that there were no performance requirements limits for operations on runway 19L.
While the Brisbane NOTAM with the headline RWY 01R THR DISPLACED contained data concerning a significant reduction in the length of runways 01R/19L, the previously established misunderstanding of this NOTAM and the absence of any reference to 19L in the heading resulted in the captain incorrectly dismissing this NOTAM, which was also probably missed by the first officer.
The flight crew did not identify the critical performance data that was appended to the Brisbane NOTAM that stated the runway length reduction for 01R/19L prior to the departure from Melbourne.
The ATIS notification of the reduced length of runway 19L was not recognised or accounted for in the performance calculations for operations on that runway, likely due to the captain’s established belief that there were no performance requirements for runway 19L and the absence of the required independent check by the first officer.
Due to time pressures and distractions from prioritising training requirements during the preparation for departure from Brisbane's runway 19L, and a previous assessment that it was not relevant, the flight crew dismissed a dispatcher's note alerting the crew to the RWY 01R THR DISPLACED NOTAM. Also, while the crew reviewed the operational flight plan component of the briefing package prior to departure, they probably did not review the NOTAM package.
Unaware of the reduced available length of the departure runway, which was reinforced by the absence of any visible runway works or restrictions during the previous landing on 19L, the flight crew miscalculated the aircraft's take-off performance data. That resulted in a departure with insufficient available runway due to the aircraft being overweight for that reduced runway length.
Other factors that increased risk
Having not reviewed the NOTAMs as part of the approach briefing prior to descent into Brisbane, contrary to the requirements of the operations manual, or on an opportunity basis en route, the flight crew missed an opportunity to correct the incorrect mental model developed for Brisbane's RWY 19L during the turnaround in Melbourne.
Contrary to the requirements of Part 139 Manual of Standards, the A3/19L intersection departure point take-off run available Movement Area Guidance Sign (MAGS) presented a take-off distance that was more than that available, creating the potential to mislead flight crews about the status of the runway when conducting a departure from that point.
Safety actions
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Virgin Australia
Virgin Australia (VA) advised the ATSB of several changes and improvements made as a result of learnings from an examination of the occurrence. These included:
The introduction of threat-based standard dispatcher notes, with enhanced engagement between VA fight dispatch and flight operations in identifying impactful NOTAMs, while also constructing standard dispatcher notes that focus on the threat presented to flight crew.
An operational performance tool (OPT) update to bring runway options with a WIP designator ahead of the normal runway selection options.
A focus on standard operating procedure changes to limit pilot distraction at the runway entry point and to remove scan items requiring action below the glareshield.
Enhanced engagement between Brisbane Airport and VA on safety initiatives.
The risk assessment methodology for runway displacements has been adapted from a general risk model to an airport‑specific risk analysis, as well as a monthly runway works risks review meeting being established by Flight Operations Quality Assurance.
A flight operations STOP PRESS Safety Update relating to the occurrence event was issued by the chief pilot on 5 December 2022.
Flight operations now provide enhanced guidance for flight crew for runways with displacements through easy to read and digest marked-up runway diagrams.
In response to a holistic review of communication to flight crew regarding significant events, flight operations introduced a monthly Safety Town Hall to better communicate current issues, trends, and events. These have been in place and running every calendar month since February 2023.
In response to a number of events that had contributing factors of distraction/situational awareness, VA conducted an independent human factors review through a specialist third party. A number of findings and actions were issued as a result and are now being tracked through safety governance.
Additional safety action by Brisbane Airport Corporation
Brisbane Airport Corporation implemented several changes to reduce the risk associated with this type of occurrence. The changes included:
adjustments to departure and arrival procedures associated with runway works
redrafting of the NOTAM to clarify the operational changes to both runways 01R and 19L, and procedures to ensure correct runway distance was displayed on take-off run available movement area guidance signs
publication of an aeronautical information circular supplement for the works.
Glossary
ACARS
Aircraft Communications, Addressing and Reporting System
ADS-B
Automatic dependent surveillance - broadcast
AFM
Airplane Flight Manual
AIC
Aeronautical information circular
AIP
Aeronautical information publication
AIS
Aeronautical information service
ASDA
Accelerate stop distance available
ATC
Air traffic control
ATS
Air traffic services
ATIS
Automatic terminal information service
B737
Boeing 737
BAC
Brisbane Airport Corporation
BNE
Brisbane
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
EDT
Eastern daylight-saving time.
EFB
Electronic flight bag
EST
Eastern Standard Time
FCOM
Flight crew operations manual
FMC
Flight management computer
FO
First officer
FOE
Flight Operations Engineering
FPP
Flight planning package
FPM
Flight plan manager
GAPPRE
Global Action Plan for the Prevention of Runway Excursions
GM-AIS
Guidance Manual for Aeronautical Information Services
ICAO
International Civil Aviation Organization
LDA
Landing distance available
MAGS
Movement area guidance signs
METAR
Aviation routine weather report
MOS
Manual of standards
MLDW
Maximum landing weight
MOWP
Method of working plan
NAIPS
National aeronautical information processing system
NOTAM
Notice to airman
OFP
Operational flight plan
OPADD
Operating Procedures AIS Dynamic Data
OPT
Onboard performance tool
PANS-ABC
Procedures for Air Navigation Services – Abbreviations and Codes
PANS-AIM
Procedures for Air Navigation Services – Aeronautical Information Management
PIB
Pre-flight information bulletin
PF
Pilot flying
PM
Pilot monitoring
SARP
Standard and Recommended Practice
TAF
Aerodrome forecast
TODA
Take-off distance available
TODC
Take-off data card
TORA
Take-off run available
UTC
Coordinated Universal Time
YBBN
Brisbane Airport
YMML
Melbourne Airport
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew and dispatchers
Virgin Australia Airlines
Civil Aviation Safety Authority
International Civil Aviation Organization
Airservices Australia
Boeing
Brisbane Airport Corporation
recorded data from the aircraft and Airservices Australia.
References
Civil Aviation Safety Authority. (2020). Manual of Standards Part 139 - Aerodromes. Canberra: Civil Aviation Safety Authority.
EUROCONTROL and Flight Safety Foundation. (2021). Global Action Plan for the Prevention of Runway Excursions. Brussels, Belgium: EUROCONTROL.
International Civil Aviation Organization. (1951). Annex 15 (Aeronautical Information Services) to the Convention on International Civil Aviation (16th ed.). Montreal, Canada: International Civil Aviation Organization.
International Civil Aviation Organization. (2018). Doc 10066, Procedures for Air Navigation Services — Aeronautical Information Management (1st ed.). Montreal, Canada: International Civil Aviation Organization.
International Civil Aviation Organization. (2021). Doc 8126, Aeronautical Information Services Manual (7th ed.). Montreal, Canada: International Civil Aviation Organization.
International Civil Aviation Organization. (2016). Doc 8400, Procedures for Air Navigation Services (PANS) - ICAO Abbreviations and Codes (9th ed.). Montreal, Canada: International Civil Aviation Organization.
International Civil Aviation Organization. (2002). Guidance manual for Aeronautical Information Services (AIS) in the Asia/Pacific Region (1st ed.). Bangkok, Thailand: International Civil Aviation Organization Asia and Pacific Office.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
Virgin Australia
Brisbane Airport Corporation
Airservices Australia
United States National Transportation Safety Board, and Boeing
Civil Aviation Safety Authority
International Civil Aviation Organization.
Submissions were received from:
Civil Aviation Safety Authority
Virgin Australia
Brisbane Airport Corporation
the flight crew.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix – NOTAM standards and related guidance materials
Introduction
The following sections discuss the various types of aeronautical information and the role of NOTAM within this scheme. The sources of NOTAM standards are identified, and each of these examined for their contribution. Other authoritative source material that provided guidance on NOTAM structure and content is also examined. In examining these standards and guidance materials, NOTAM C1174/22 will be used as an example of their application. To provide some background into the reasons for issuing C1174/22, the origins of that NOTAM will also be examined.
Types of aeronautical information
CASR Part 139 required airport operators to provide detailed information about various aerodrome facilities, such as movement areas, lighting systems and other facilities that were available for use by aircraft at that airport. That aeronautical information was to be sent to relevant aeronautical information service (AIS) providers for publication. Airport operators were also required to notify users of any changes or limitations to that published information, such as that caused by aerodrome works.
The AIS provider, Airservices Australia, collated aeronautical data concerning airspace, navigation aids and other facilities provided by airport operators and other sources. That information was published in:
the aeronautical information publication (AIP) and supplements
notices to airmen (NOTAM)
aeronautical information circulars (AIC).
The AIP was the primary aeronautical information document, containing current information of a lasting character that was essential for air navigation. AIP supplements provided a means to publish information of a temporary nature but of a long duration. The NOTAM system was designed to provide immediate distribution of information of direct operational significance that was of short duration. Information that did not qualify for publication within the AIP or as a NOTAM, but which related to flight safety or other aviation activities, was published as an AIC.
The RWY 01R displaced threshold NOTAM
The Brisbane Airport MOWP YBBN 22/07 included scheduled work segments for the replacement of various runway and approach lighting power cables. This required working near the RWY01R threshold and the consequent need to displace that runway’s threshold. The works also resulted in the temporary disabling of various runway lighting systems.
After submission to Airservices of data detailing facilities that would be affected by these works, NOTAM C1139/22 was issued. Due to minor changes in the taxiway availability and the relocation of the displaced threshold markers, C1139/22 was amended and reissued as C1174/22. The full published version of NOTAM C1174/22 stated:
C1174/22 NOTAMR C1139/22 Q) YBBB/QMTCM/IV/NBO/A/000/999/2723S15307E005 A) YBBN B) 2211292100 C) 2211300630 E) RWY 01R THR DISPLACED RWY 01R/19L 871M SOUTH END NOT AVBL DUE WIP OBST WORKERS AND EQPT 16FT AGL ON RCL 2889M FM START OF TKOF RWY 19L EFFECTIVE RWY LEN AVBL 2689M THR RWY 01R DISPLACED 921M MARKED BY FIVE GREEN LGT AND RWY THR IDENT LGT (RTIL) EACH SIDE OF RWY DECLARED DISTANCE AND GRADIENT CHANGES RWY TORA TODA ASDA LDA 01R 2689 2809(1.6) 2749 2579 19L 2689 2749(3.6) 2689 2689 SUPPLEMENTARY TKOF DISTANCES RWY19L- 2577(1.6) 2626(1.9) 2662(2.2) TWY A7 AVBL FOR RWY 01R INTL DEP RWY 01R PAPI, HIGH INTENSITY APCH LGT (HIAL) AND RCLL NOT AVBL HIGH INTENSITY RWY LGT (HIRL) NOT AVBL RWY 01R TEMPO PAPI LEFT SIDE 3.0 DEG 75FT AVBL REFER METHOD OF WORKING PLAN YBBN 22/07
Aeronautical information standards
CASR Part 175 (Regulation.175.105) required aeronautical information published through the AIP, NOTAM and AIC to meet standards established under specific publications as follows:
Part 175 Manual of Standards (MOS)
Annex 15 to the Chicago Convention – Aeronautical Information Services
International Civil Aviation Organization (ICAO) Document 10066 Procedures for Air Navigation Services – Aeronautical Information Management (PANS-AIM)
ICAO Document 8126 Aeronautical Information Services Manual (Doc 8126)
other AIS-applicable ICAO documents.
The CASR dictionary included a definition for ‘other AIS applicable ICAO documents’. That definition identified those documents, which included ICAO Doc 8400 ICAO Procedures for Air Navigation Services – Abbreviations and Codes (PANS-ABC).
Regulation 175.105 also stated that, when standards established under one document contradicted those stated in another, then the standards in the first listed document were to apply.
At the time of the occurrence, Part 175 MOS had not been published. Annex 15 did not contain any standards relevant to the structure and required content of NOTAM. The principal document for those standards was PANS-AIM, which also made direct reference to PANS-ABC on matters relating to a specific but critical component of the NOTAM. Doc 8126 provided guidance material on the requisite components of the NOTAM Format.
PANS-AIM
PANS-AIM contained the following basic principles governing NOTAMs:
A NOTAM shall contain information in the order stated in the NOTAM Format, a template that set out communications handling instructions and the required content for a NOTAM. That required content was structured around various fields labelled as Item ‘Q)’ and Items ‘A)’ through ‘G)’. Each field had a specific structure and required content, as designated by the NOTAM Format.
ATSB Observation
These fields can be identified in the following extract from C1174/22:
Q) YBBB/QMTCM/IV/NBO/A/000/999/2723S15307E005 A) YBBN B) 2211292100 C) 2211300630 E) RWY 01R THR DISPLACED
Each field had a specific structure and required content, as designated by the NOTAM Format.
A NOTAM shall deal with one subject and one condition of that subject only. It should be as brief as possible and compiled such that the meaning is clear.
ATSB Observation
NOTAMs advise flight crews of information that has direct operational significance. In the case of C1174/22, this was the displacement of RWY 01R threshold. For this NOTAM, the runway threshold was the subject matter, while its displacement the condition.
The subject matter and related condition shall be reported through coding contained within Item Q). The components of that coding are to be selected from NOTAM Code tables published in PANS-ABC.
ATSB Observation
For C1174/22, the Q-Code was stated in the 5 letters QMTCM, the second field in the Q) line. The first letter, Q, identified that the field is the Q-Code field, the second and third letters MT stated the subject matter, which was decoded as Threshold (specify runway). The fourth and fifth letters CM stated the condition of that subject matter, which was decoded as Displaced.
The content of the free-text section of the NOTAM, Item E), shall be based on the decoded NOTAM code, also called the code’s signification, supplemented where necessary by ICAO abbreviations and other identifiers and designators. The content of Item E) is to be sufficiently clear and concise so as to facilitate its use in a Pre-flight Information Bulletin (PIB).
ATSB Observation
The NOTAM content for C1174/22 printed in the VA319 FPP (Figure 4) was an example of a PIB version of a NOTAM. Similarly, NOTAMs published by NAIPS use the PIB version of the NOTAM. Essentially, for a PIB, the NOTAM is stripped of all detail except the free text Item E) content.
PANS-ABC
PANS-ABC is the principal document for the NOTAM code, which is reported in the Item Q) line as the NOTAM’s Q-code. The NOTAM’s Q-code is a comprehensive description of the information contained in the NOTAM. In combination with the other information presented in the Item Q) line, it provides a means of determining the operational significance of the information and a method for storage and retrieval of information. Further, the Q-Code is a method for standardisation of information presented in item E).
PANS-ABC details procedures used to select the code reported in item Q). The code’s subject matter and status/condition components are derived from separate tables within PANS-ABC. With respect to selection of the code letters, PANS-ABC stated:
The code identifying the subject or denoting its status of operation is, whenever possible, self-evident. Where more than one subject could be identified by the same self-evident code, the most important subject is chosen.
The code components listed in these tables have an associated standardised plain language text, referred to as the code’s signification, or decode, which forms the basis for the NOTAM’s free text section, Item E.
With respect to C1174/22, and the PIB content of that NOTAM found in the VA319 and VA324 FPPs, the free text section contained items of information that were reportable under various subject matter codes listed in the PANS-ABC tables. These subject matter codes were:
Movement and landing area subject matters
MD, Declared distances for RWY 01R and RWY 19L
MT, Threshold for RWY 01R
MX, Taxiway A9 and A7
Lighting facilities subject matters
LC, Runway centre line lights
LH, Runway high intensity lights
LI, Runway end identifier lights
LP, Precision approach path indicator lights.
ICAO Doc 8126
While this document re-affirmed that a NOTAM was to be limited to one subject matter and one condition related to that subject matter, it also included the statement that:
The NOTAM Code selected describes the most important status or condition to be promulgated.
This indicated that more than one status or condition of a specific subject matter could be reported in a NOTAM. There was nothing further in Doc 8126 to support how, or under what circumstances, such combinations of status or conditions were to be made.
With respect to Item E), the free text section of the NOTAM, Doc 8126 stated that the information was to be kept as short as possible, preferably not exceeding 300 characters, containing all the essential information and ready for inclusion in PIB.
ICAO APAC GM-AIS
The Asia and Pacific office of ICAO had produced a guidance material document that provided States with a single source manual, the Guidance Manual for Aeronautical Information Services (AIS) in the Asia/Pacific Region (GM AIS).[33] The GM-AIS repeated much of what was provided in the above source documents. It also contained a significant amount of data extracted from the EUROCONTROL Operating Procedures AIS Dynamic Data (OPADD), which was stated to contain best practice material for AIS support.
The GM-AIS contained more specific guidance on how and when to combine multiple NOTAMs into a single NOTAM. It stated that combining NOTAMs may be appropriate when they are directly related to each other; however, the choice of subject matter was critical, in that the selected subject matter must enable all elements to be reported to be included within Item E) of the NOTAM. Further, the GM-AIS stated:
While selecting the most precise code enables quick information identification, in some cases a more general approach provides the end-user with sufficient relevant information in a single NOTAM with no negative impact on briefing. For example, if a displaced threshold results in a change in declared distances, it may be more appropriate to use the code QMDCH (rather than QMTCM) and include in Item E) the information on the displaced threshold and declared distances.
This guidance had direct relevance to the codes chosen for C1174/22 as it indicated a preference for coding using QMDCH (decoded to Declared distances (specify runway) and Changed) over QMTCM for a displaced threshold.
The GM-AIS also cited other situations that enabled the combining of NOTAMs into a single NOTAM, including when:
there was more than one occurrence of one subject matter
a facility consisting of several elements had all elements unserviceable then a single NOTAM covering the combined facility could be used.
EUROCONTROL OPADD
The OPADD was specifically designed to document and harmonise operating procedures for AIS dynamic data (primarily NOTAMs). It was designed as supporting guidance for NOTAM operations, but also contained enhanced explanations to take into account identified deficiencies reported by users of PIB content.
The following statement from the OPADD was relevant to combining NOTAMs:
To avoid excessive publication of NOTAM, the listed events in ICAO SARPs for which a NOTAM shall be issued must be strictly adhered to. Issuance of unnecessary or irrelevant NOTAM contributes to a greater pressure on the end-user and NOTAM providers during the filtering stage, generating a growing risk of missing vital information that could have a flight safety impact.
Note: The negative impact on end-users caused by NOTAM proliferation is not to be solved by including more information in a single NOTAM, but that this fact further increases the difficulty for end-users. More information in one NOTAM makes the message less readable and essential information more difficult to detect.
Automated NOTAM systems
PANS-ABC described the code in the NOTAM’s item Q) field as a means of enabling storage and retrieval of information and being designed for easy adaptation to automated systems to enable filtering of NOTAMs. The Virgin Australia operations manual identified the adoption of automated NOTAM filtering, through the use of the Flight Plan Manager (FPM) software which automatically imported the NOTAMS and displayed or supressed them based on their code—that is the coding presented in Item Q).
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Eastern Daylight-saving Time (EDT): Coordinated Universal Time (UTC) + 11 hours.
[2]Following the completion of the flight training and checking part of the operator’s conversion course, supervised line flying exposes flight crew to the operator’s line operations, while also attaining the experience requirements required under the Civil Aviation Safety Regulations. A pilot is considered to be inexperienced until they have achieved a certain number of hours and/or sectors under the supervision of a flight crew member nominated by the operator.
[3]The flight planning package was a paper-based briefing document.
[4]The Virgin OFP provided fuel, weight and route data necessary for pre‑flight planning purposes.
[5]Notice to Airmen (NOTAM): A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[6]Pilot flying (PF) and Pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[7]Automatic terminal information service: The provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[8]See the section titled Air traffic control informationfor the full ATIS data.
[9]Eastern Standard Time (EST): Coordinated Universal Time (UTC) + 10 hours. Unless otherwise indicated, all times in this report are EST.
[10]A rapid exit taxiway is a taxiway connected to a runway at an acute angle, designed to allow landing aircraft to turn off the runway at higher speeds than are achieved on exit taxiways, thereby minimising runway occupancy times.
[11]Aircraft Communications, Addressing and Reporting System, a datalink system for message exchange connecting aircraft and ground services.
[12]See the section titled OPT calculated runway performance data.
[13]In accordance with international standards, ATC units, including tower operations, are equipped with devices that record radio and background communications as well as the aural environment at ATC workstations.
[14]The Virgin OFP included the fuel and weight plan, wind data, alternate summary, critical fuel summaries and the navigation log.
[15]Aerodrome Forecast (TAF): a statement of meteorological conditions expected for a specific period of time in the airspace within a radius of 5 NM (9 km) of the aerodrome reference point.
[16]METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[17]The fuel and weight plan was primarily used during pre‑flight to determine various aircraft and payload weights and fuel uplift.
[18]The navigation log was used during flight for route segment information and to monitor the flight’s progress and fuel usage.
[19]The post-flight copy of the OFP was retained as the formal record of the flight.
[20]Air Traffic Service: a generic term meaning variously, flight information service, alerting service, air traffic advisory service, air traffic control service (area control service, approach control service or aerodrome control service).
[21]NAIPS is a computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots. It is accessed through the Airservices Australia website.
[22]Electronic flight bag (EFB): an electronic device or set of devices containing applications used for flight planning, such as take-off performance calculations.
[23]Procedures for Air Navigation Services – ICAO Abbreviations and Codes (PANS-ABC).
[24]The PIB is a cutdown version of the original NOTAM, where the content is limited to the free text section of the NOTAM.
[25]Titled the Aeronautical Information Services Manual, 7th Edition, 2022.
[26]EUROCONTROL is a pan-European, civil-military organisation, governed by an international convention that supports European aviation and is mostly comprised of ATS providers.
[27]Method of Working Plan YBBN 22/07, Brisbane Airport: AGL Cable Upgrade Phase 2 – Pillars 1, 2, 3C, 4, 5, and 7.
[28]A defined rectangular area on the ground at the end of the take-off run available prepared as a suitable area in which an aircraft can be stopped in the case of an abandoned take-off.
[29]A defined area at the end of the take-off run available, under the control of the aerodrome operator, that is selected or prepared as a suitable area over which an aeroplane may make a portion of its initial climb to a specified height.
[30]The Departure designation column uses the OPT nomenclature to identify the various RWY 19L conditions and departure points. 19L identifies the full length of RWY 19L, while 19L-WIPS identifies the reduced runway length due to NOTAM C1174/22. 19L/A3 is the A3 intersection of RWY 19L take-off commencement point.
[31]The AFM is part of the certification documentation for the aircraft type. It contains the operating data, limitations and procedures necessary for safe flight and operation of the aircraft.
[32]A derated thrust, or reduced thrust, take-off is a take-off that is accomplished utilising less thrust than the engines can produce under the existing conditions of temperature and pressure altitude. Designed to reduce engine wear and maintenance costs, the amount of thrust reduction is dependent on regulatory requirements and variables such as the runway length and weather conditions.
[33]The GM-AIS was designed to assist states in the development and implementation of AIS systems.
Occurrence summary
Investigation number
AO-2022-064
Occurrence date
30/11/2022
Location
Brisbane Airport
State
Queensland
Report release date
05/11/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8FE
Registration
VH-YFH
Serial number
40996
Aircraft operator
Virgin Australia Airlines Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 5 October 2020, a Hawker 850XP conducted a passenger flight from Bangkok Don Muang International Airport to Pattani Airport. On landing the aircraft had a runway excursion and sustained damage, the 3 crew and 4 passengers were uninjured.
The Ministry of Transport, Thailand – Aircraft Accident and Incident Investigation Commission requested assistance from the Australian Transport Safety Bureau (ATSB) to download the aircraft’s cockpit voice recorder (CVR) and flight data recorder (FDR) to assist their investigation.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003. The CVR and FDR were couriered to the ATSB technical facilities arriving on 29 September 2022. The ATSB has completed its work downloading the CVR and FDR.
Preliminary data was provided to The Ministry of Transport, Thailand – Aircraft Accident and Incident Investigation Commission on 19 December 2022, with a copy of the data, animation of the occurrence and a report detailing the work undertaken by the ATSB provided on 24 April 2023.
Any enquiries relating to the accident investigation should be directed to Office of the Aircraft Accident and Incident Investigation Commission, Office of the Permanent Secretary of Transport, Ministry of Transport, Thailand.

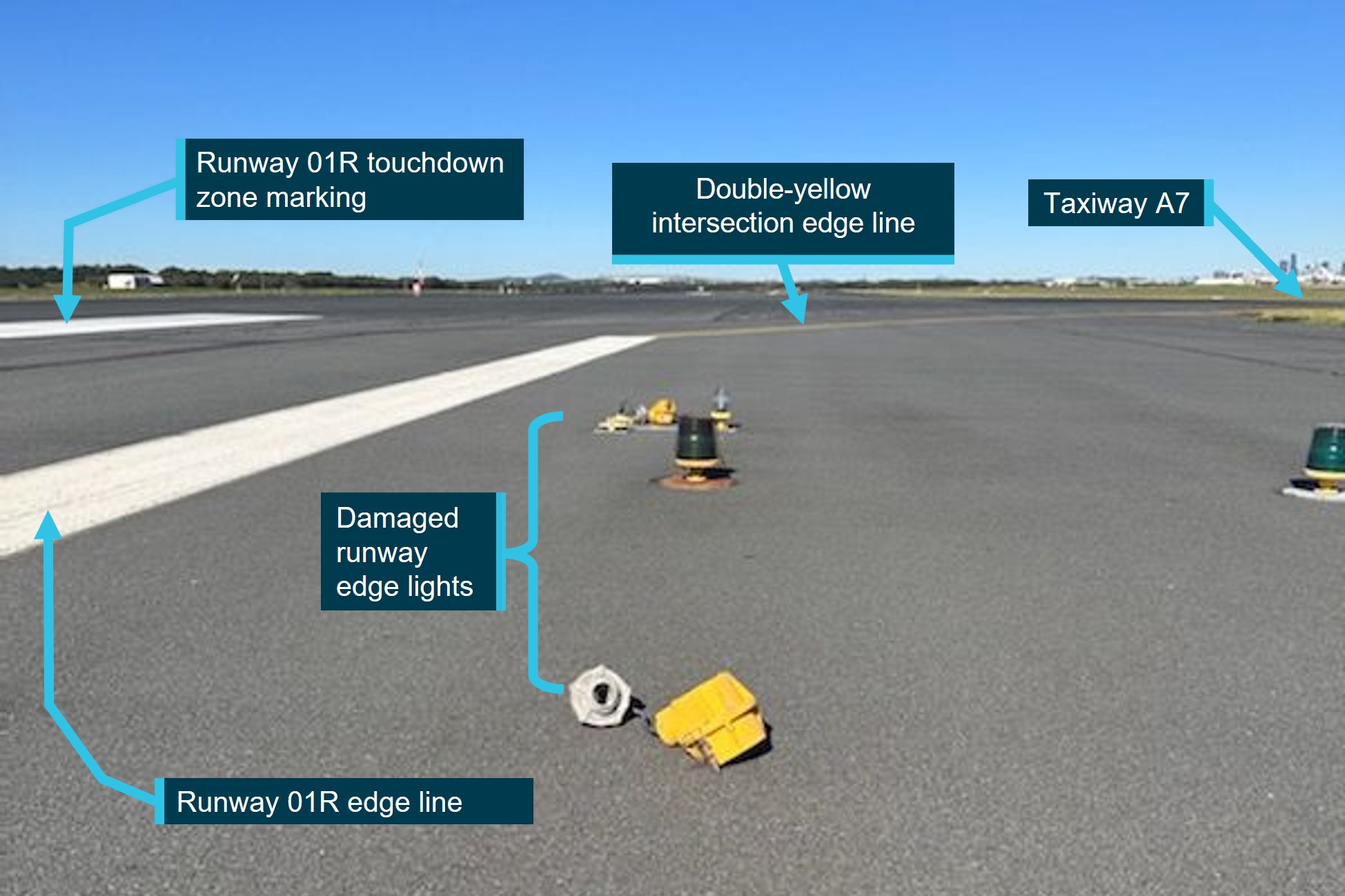
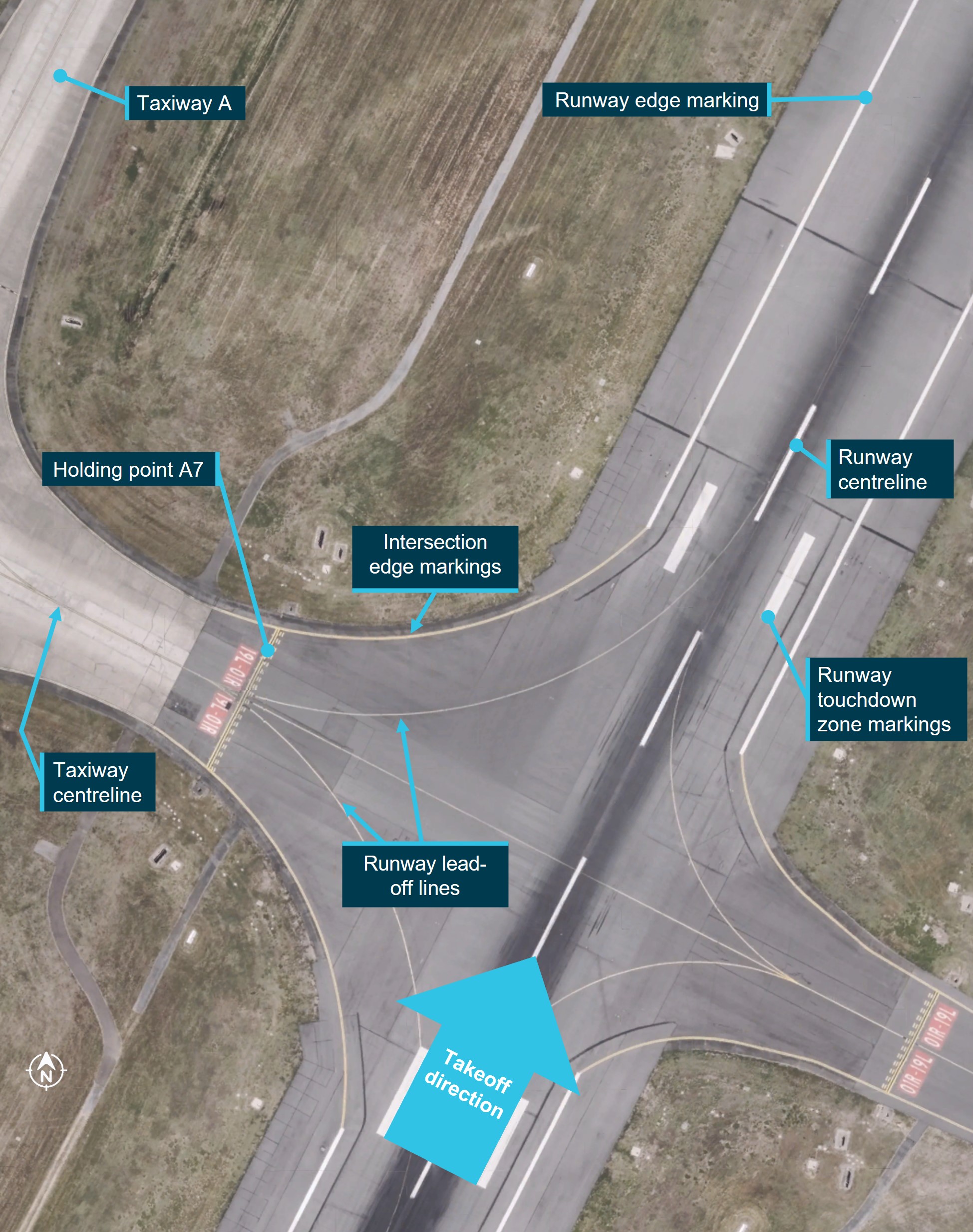
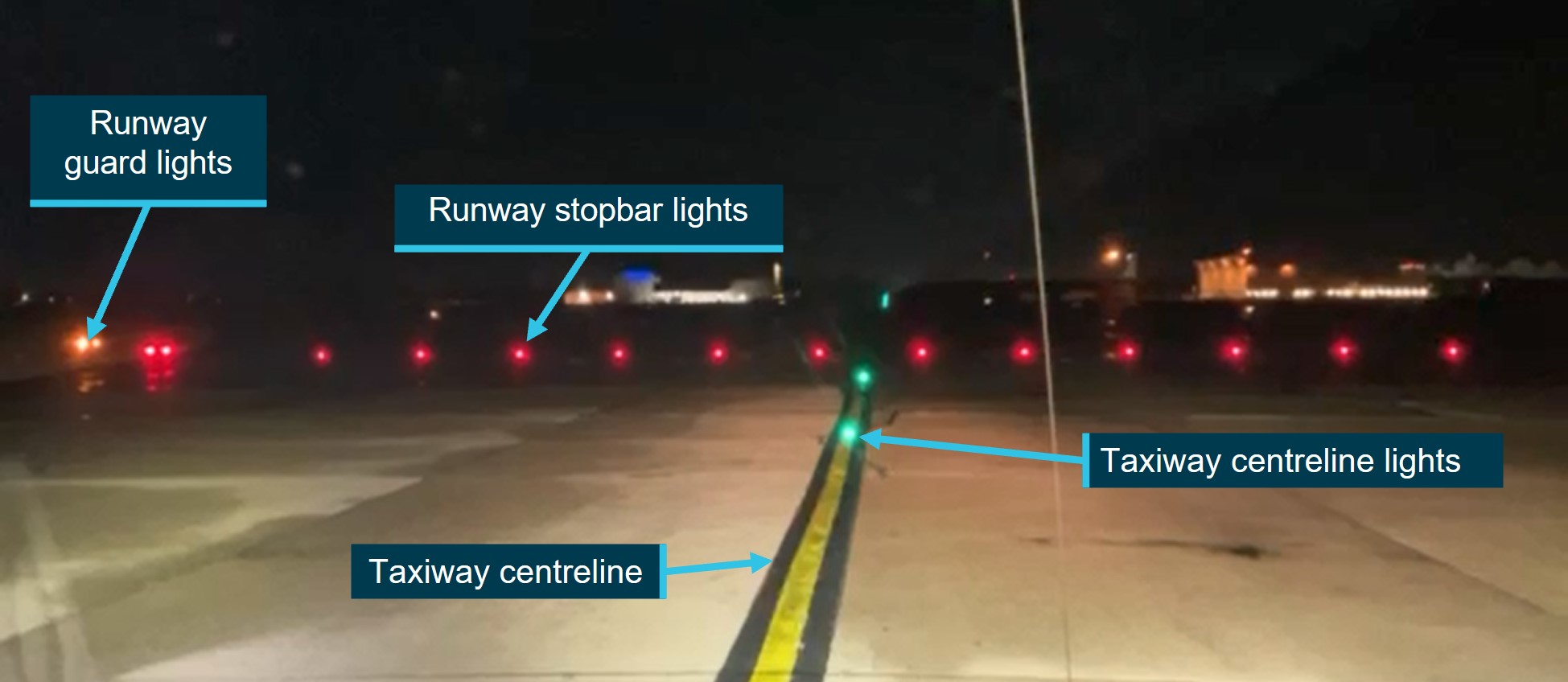

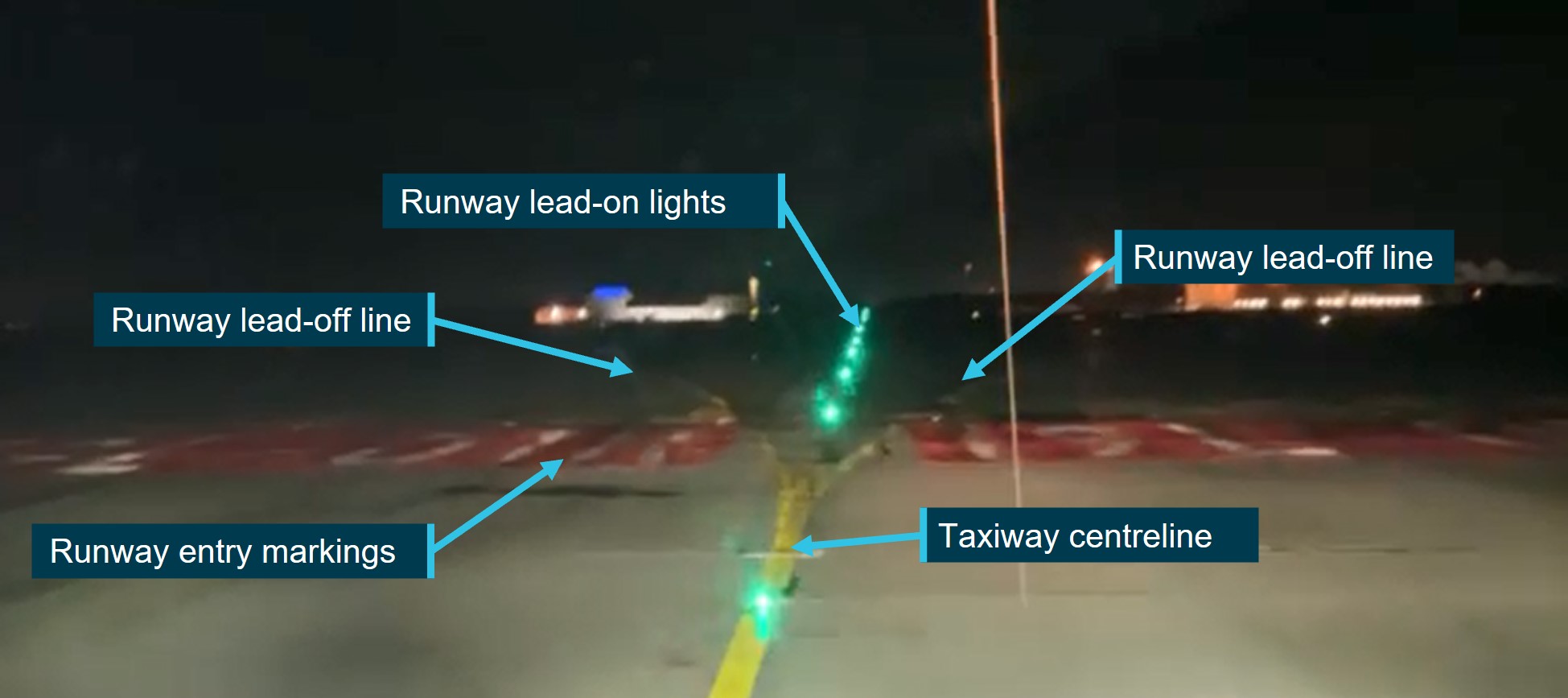


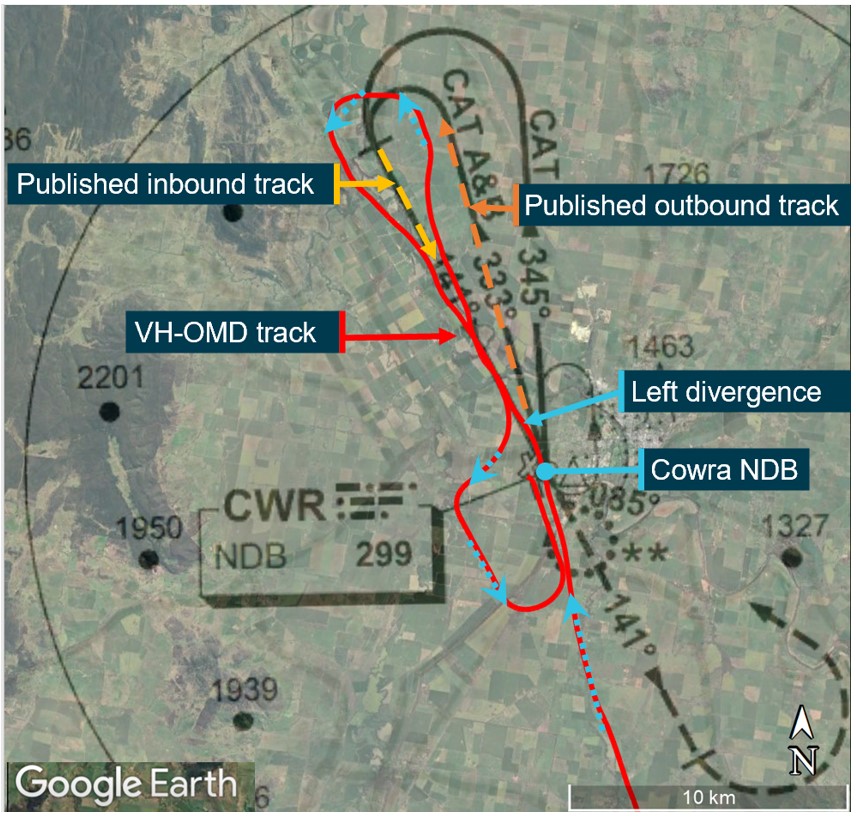


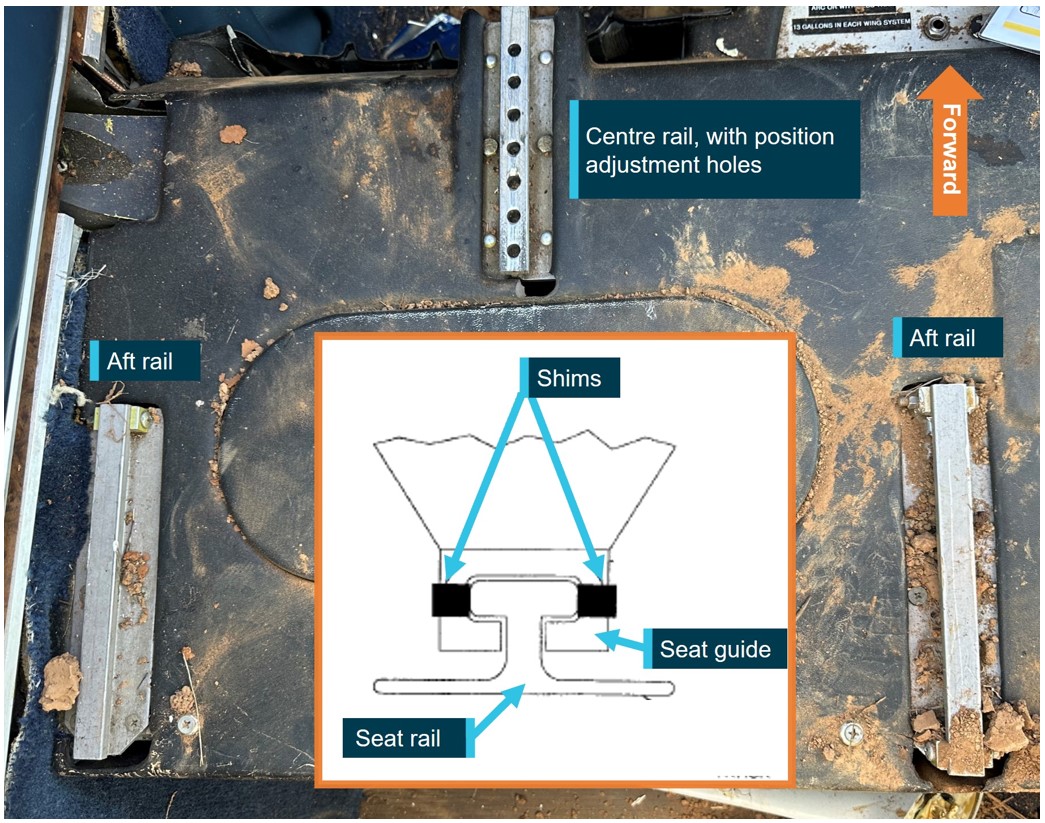
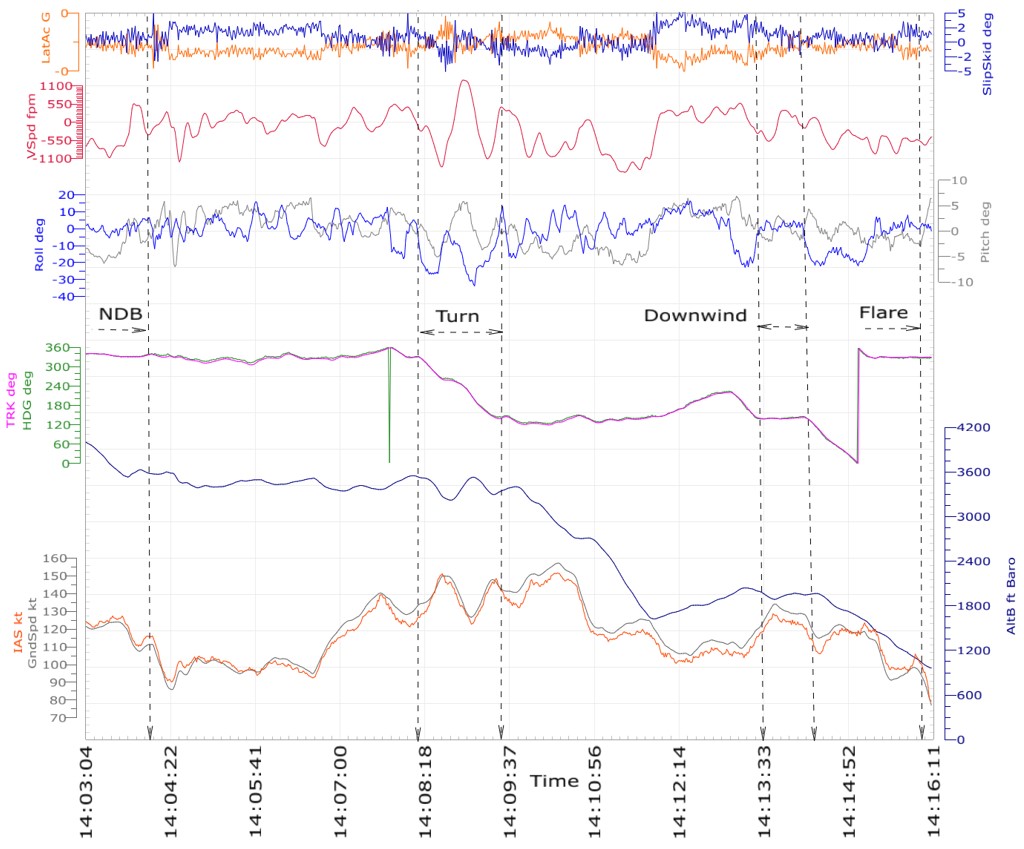
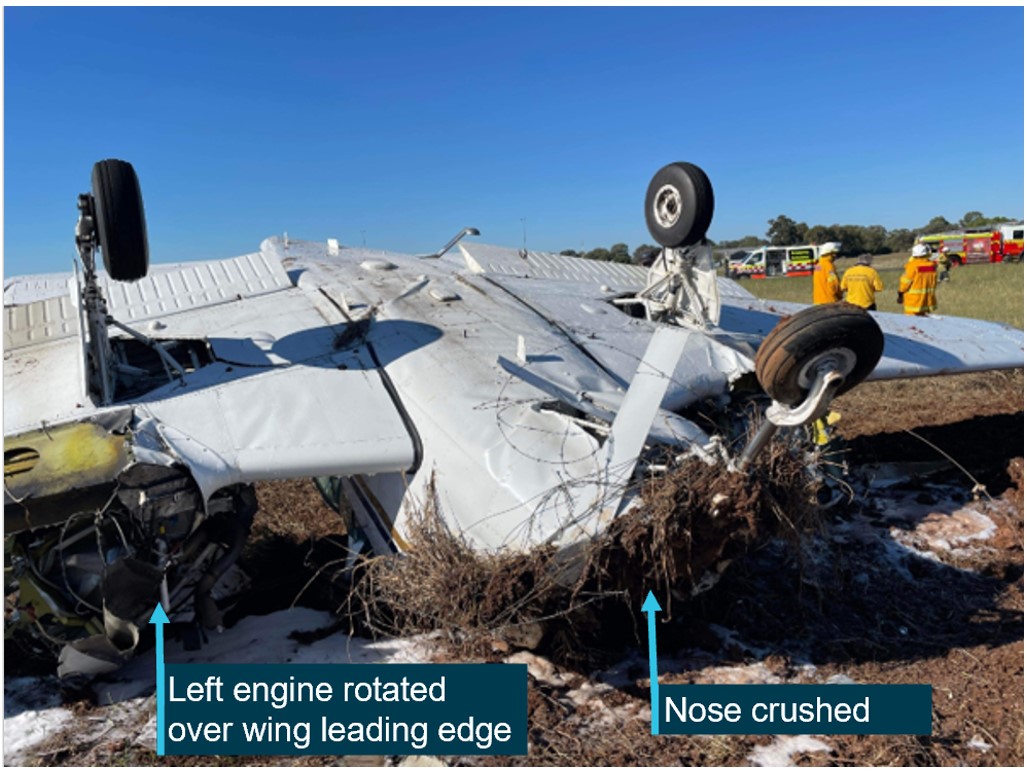
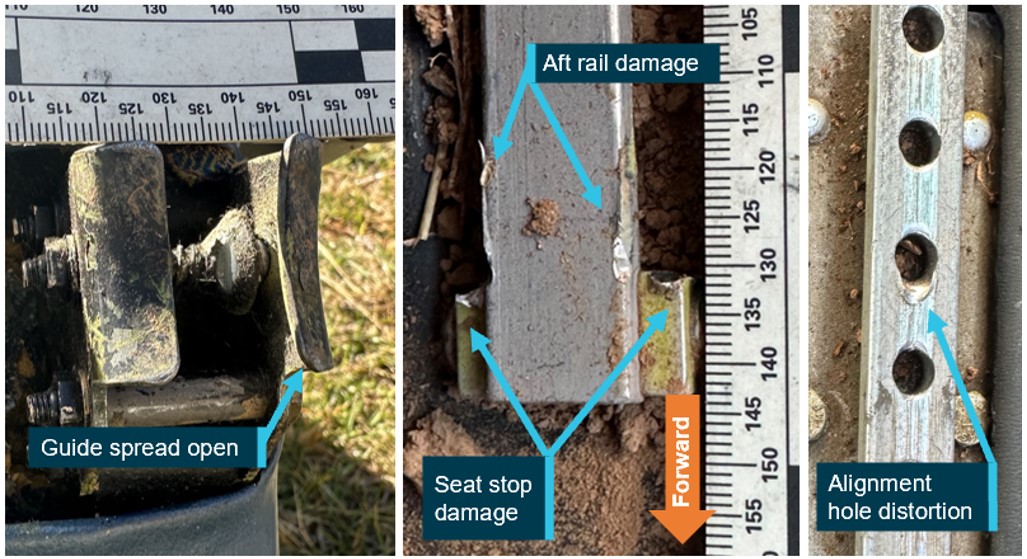
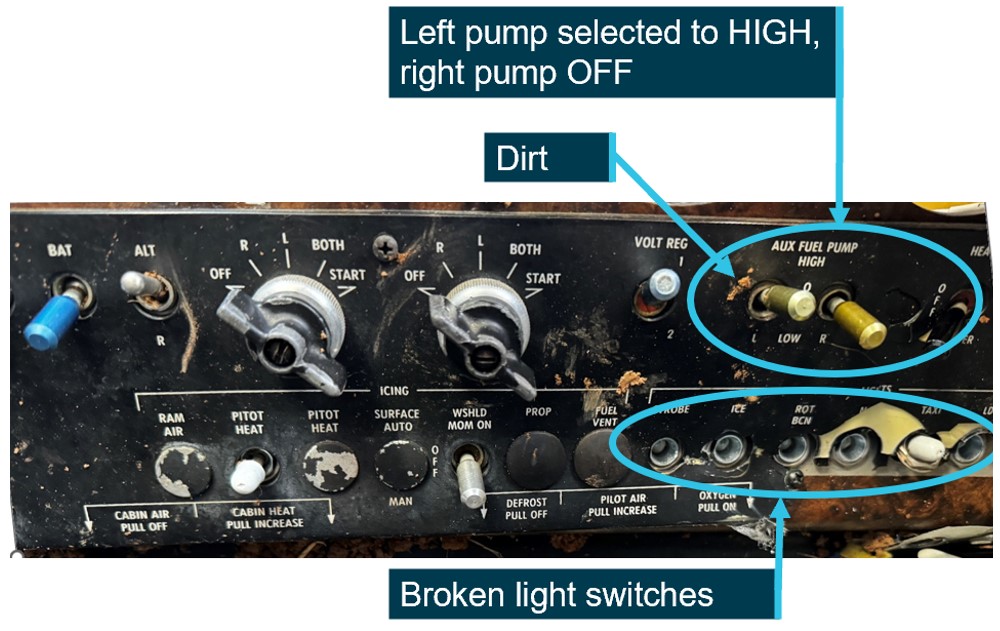
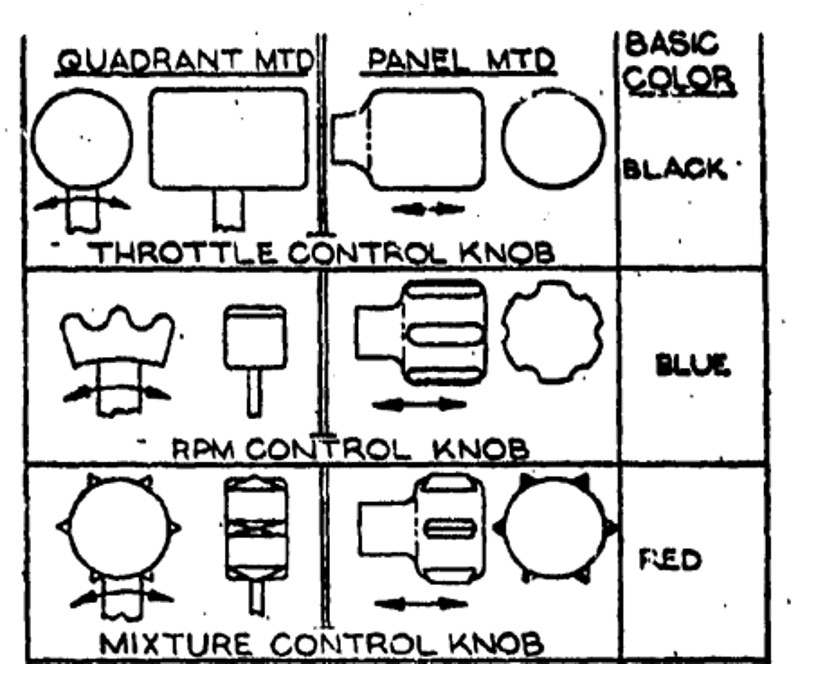
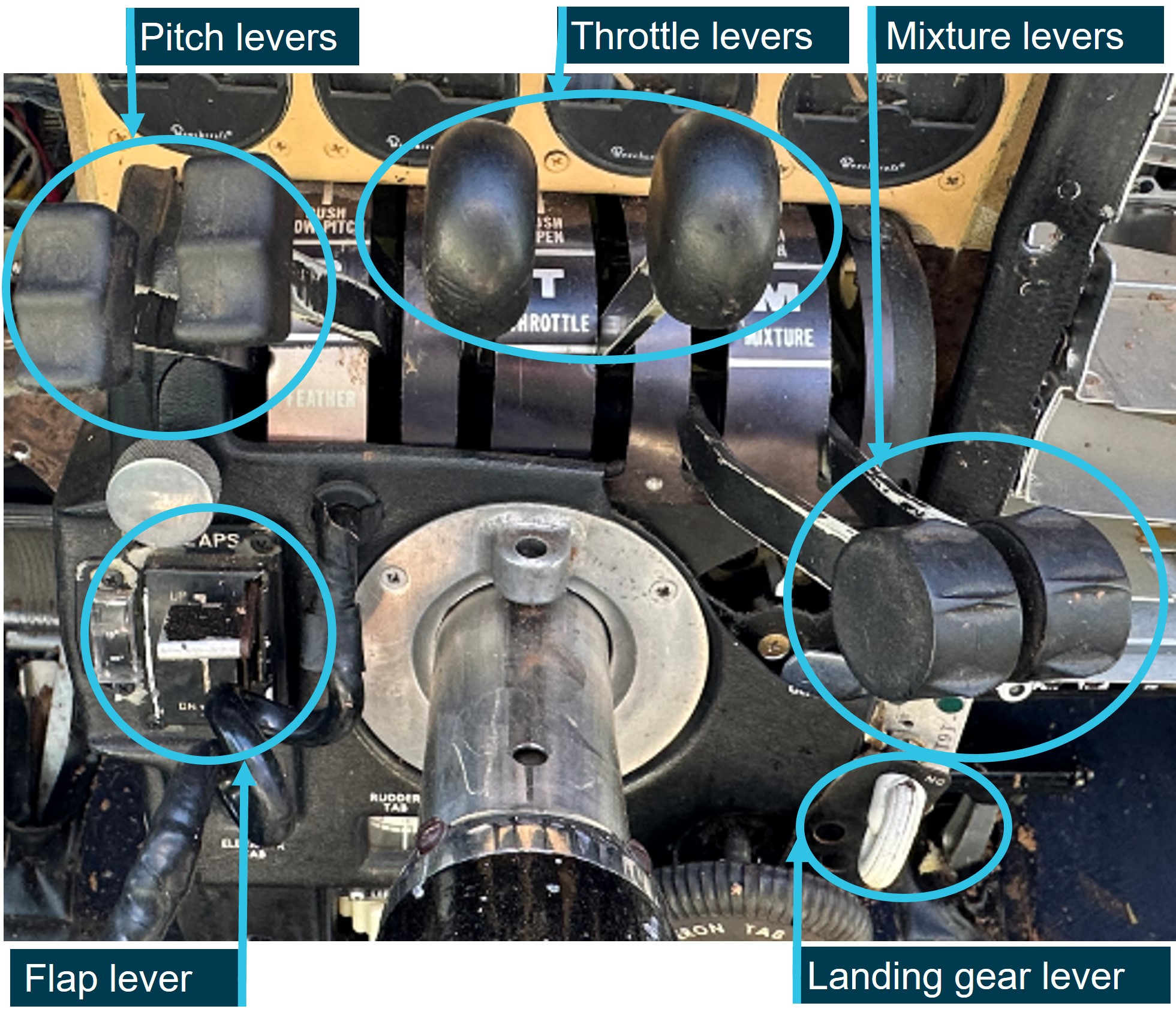

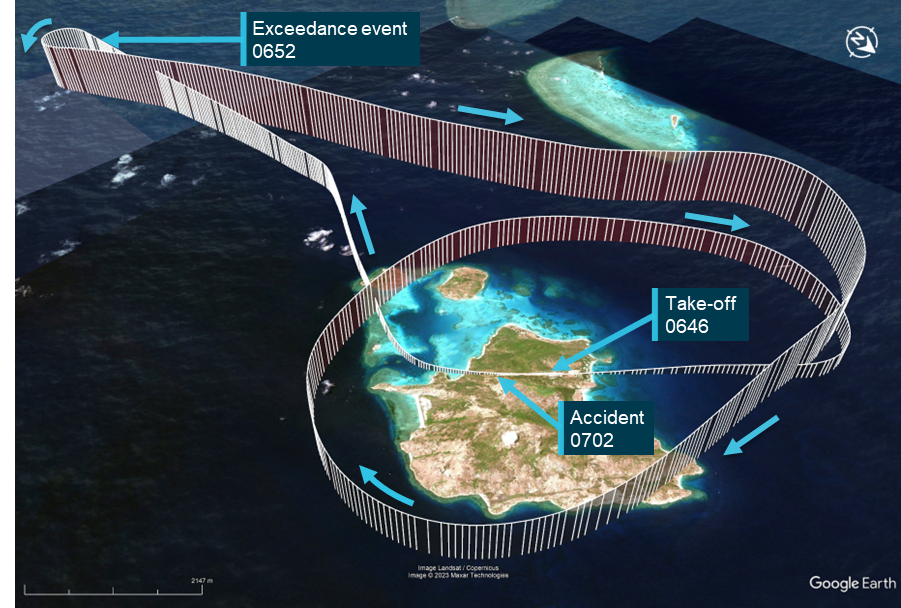
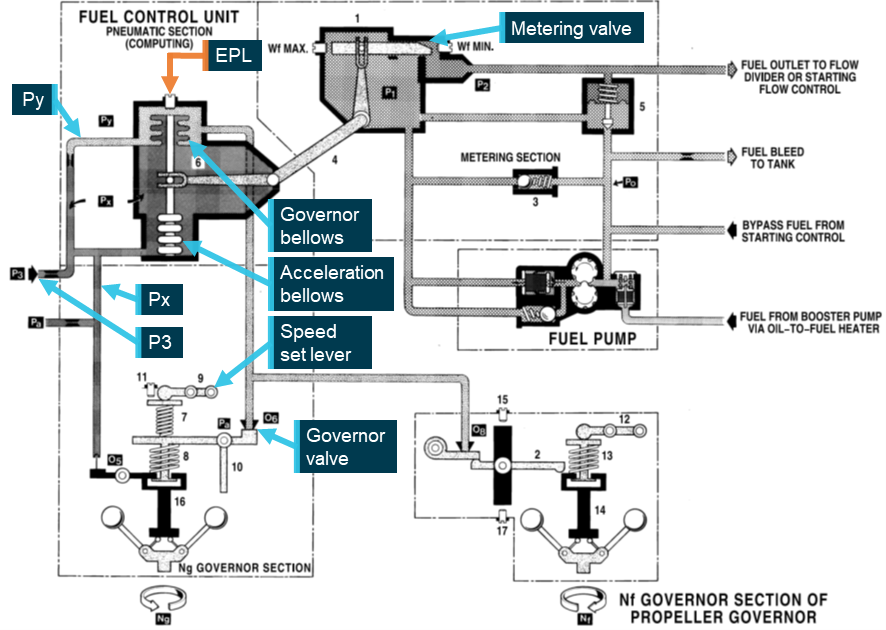

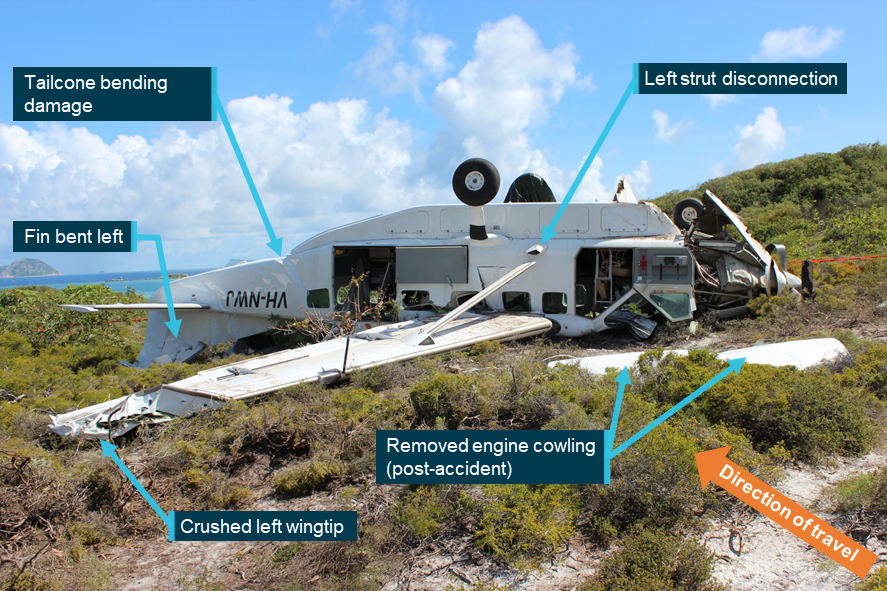
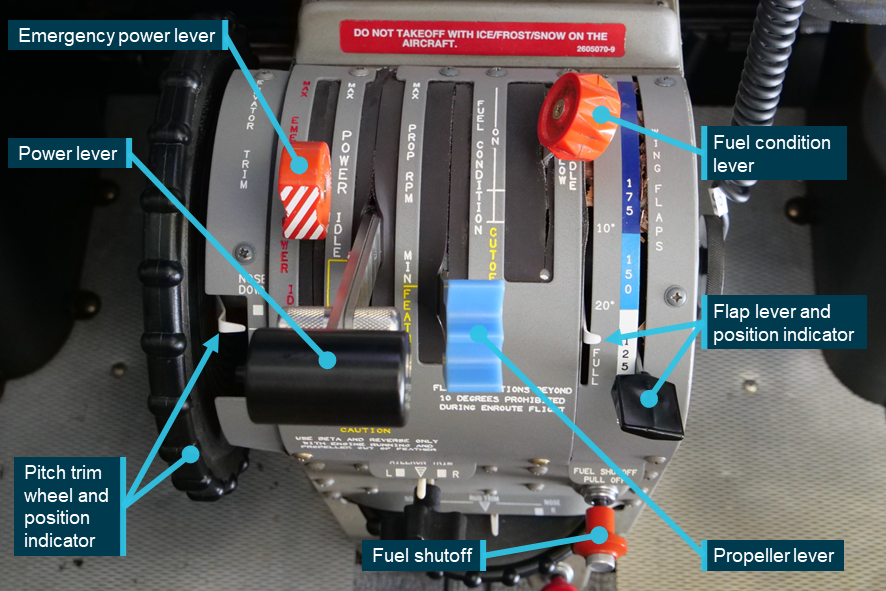
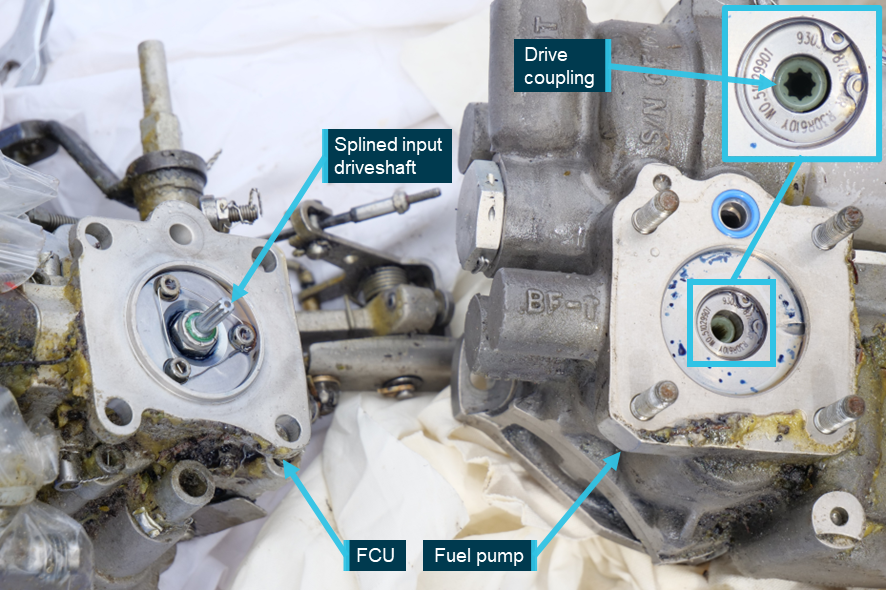
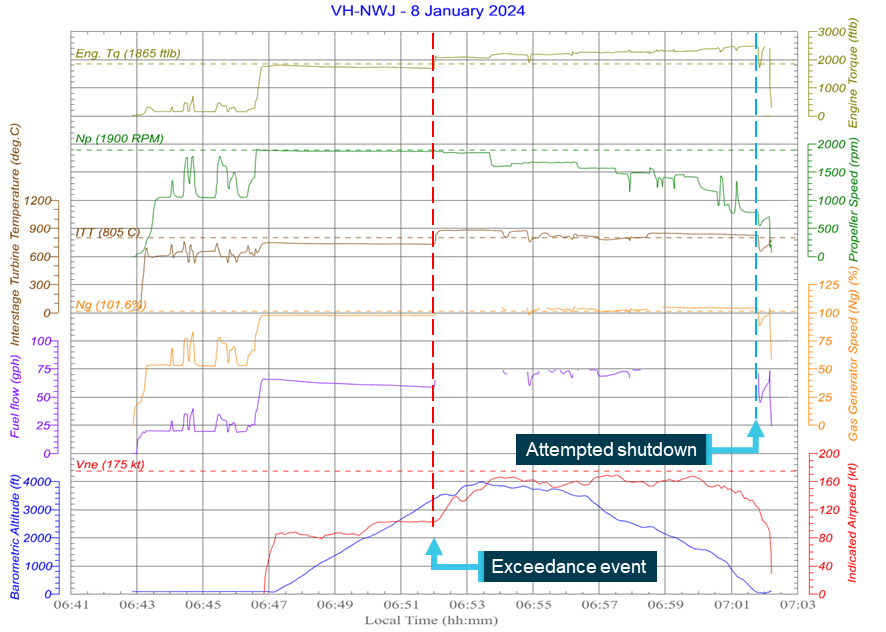
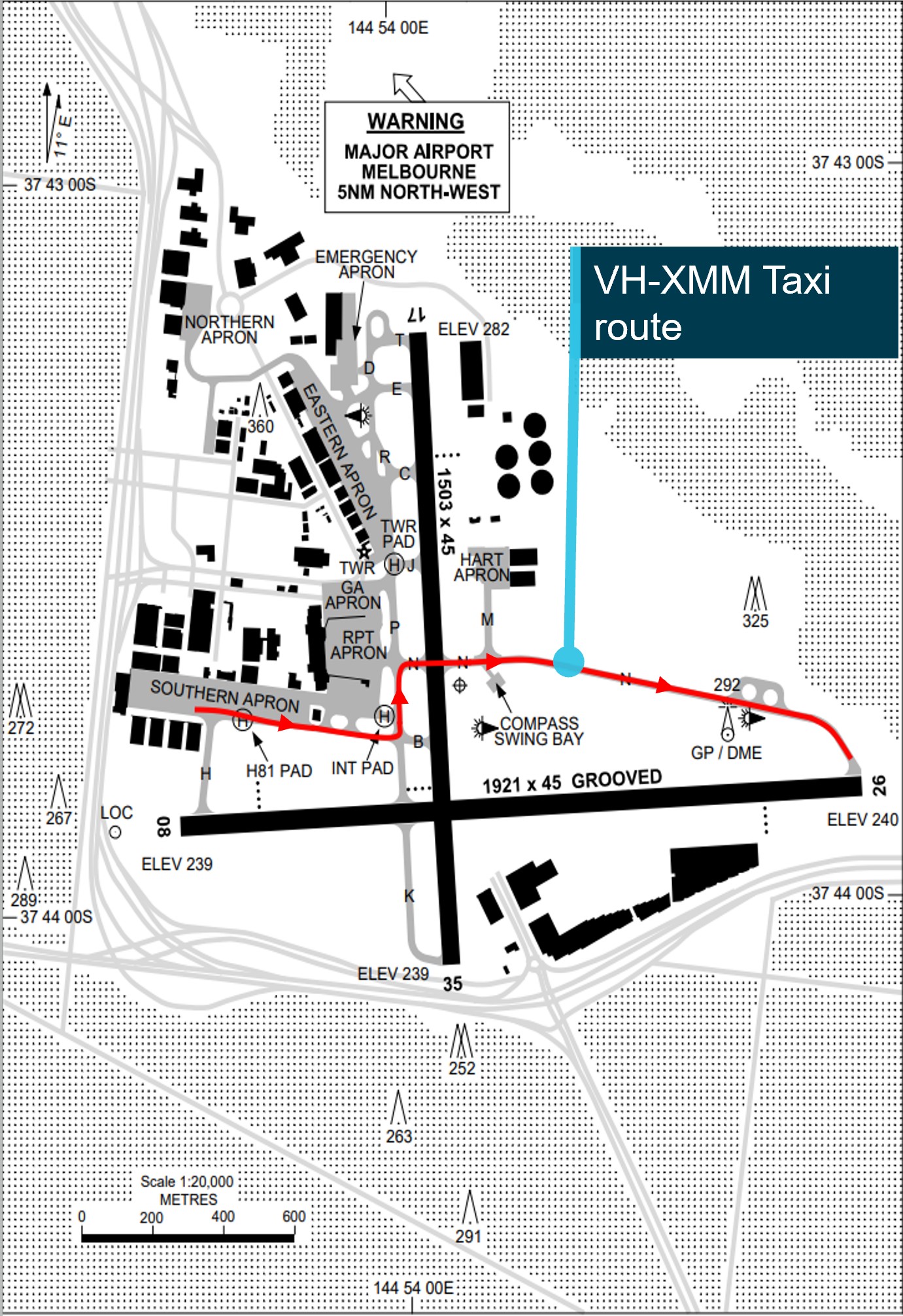




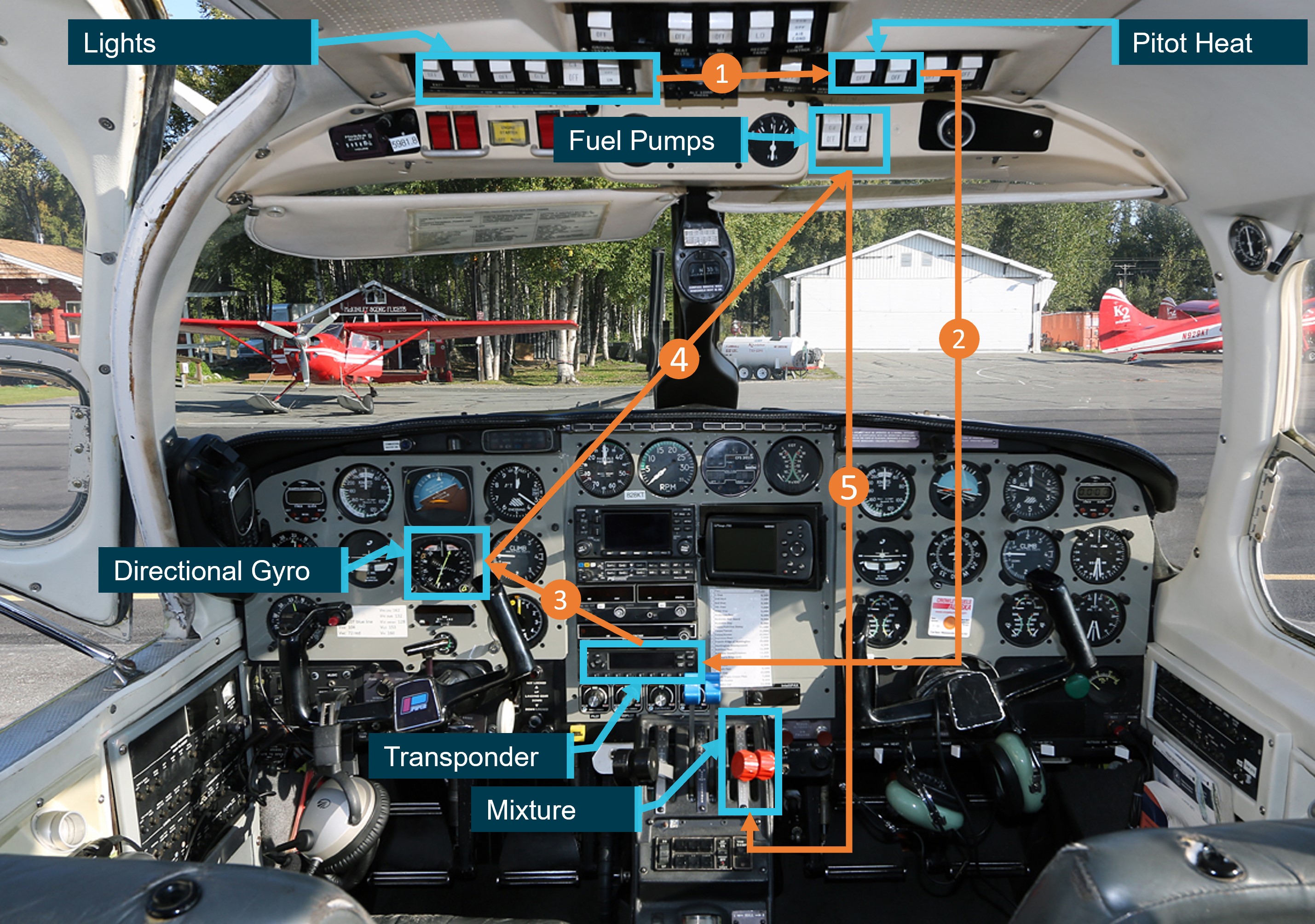
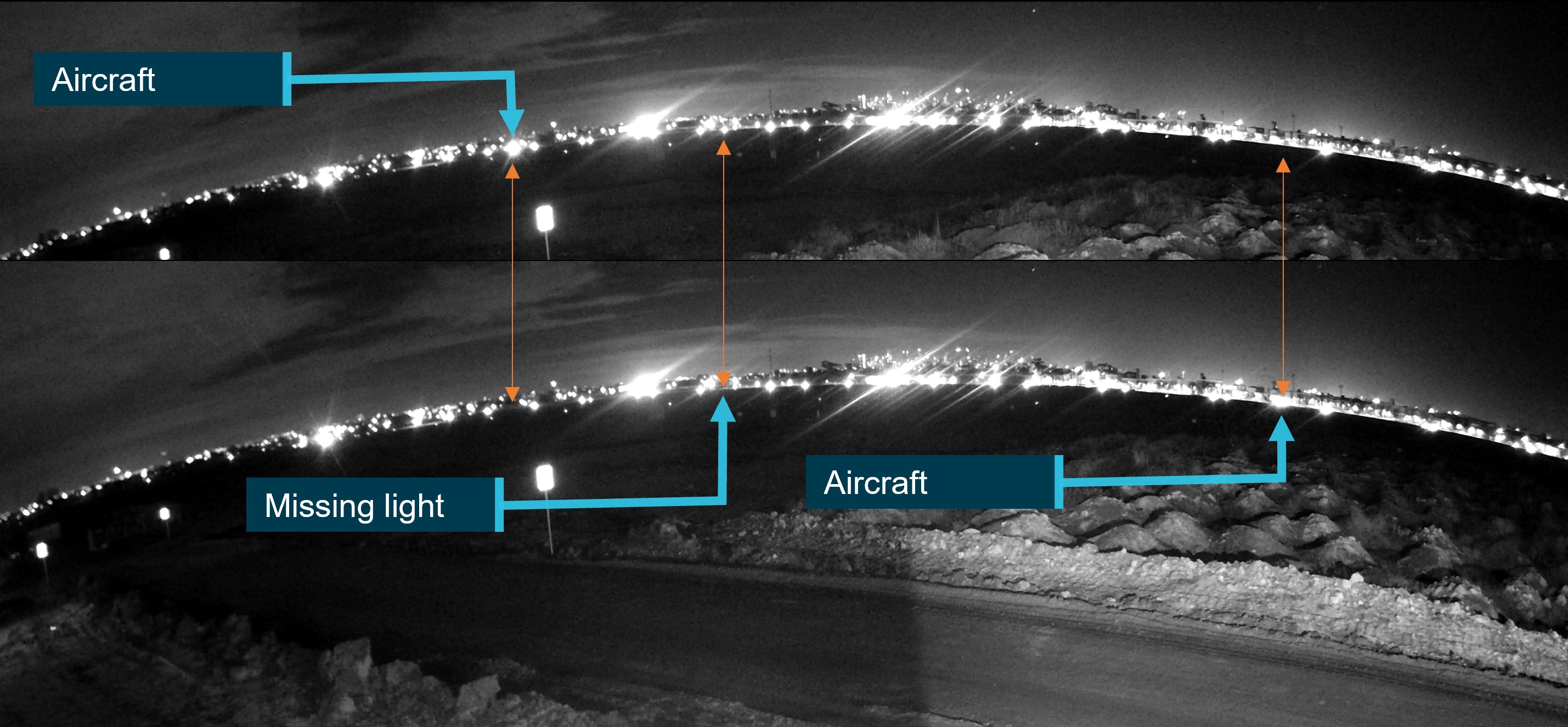


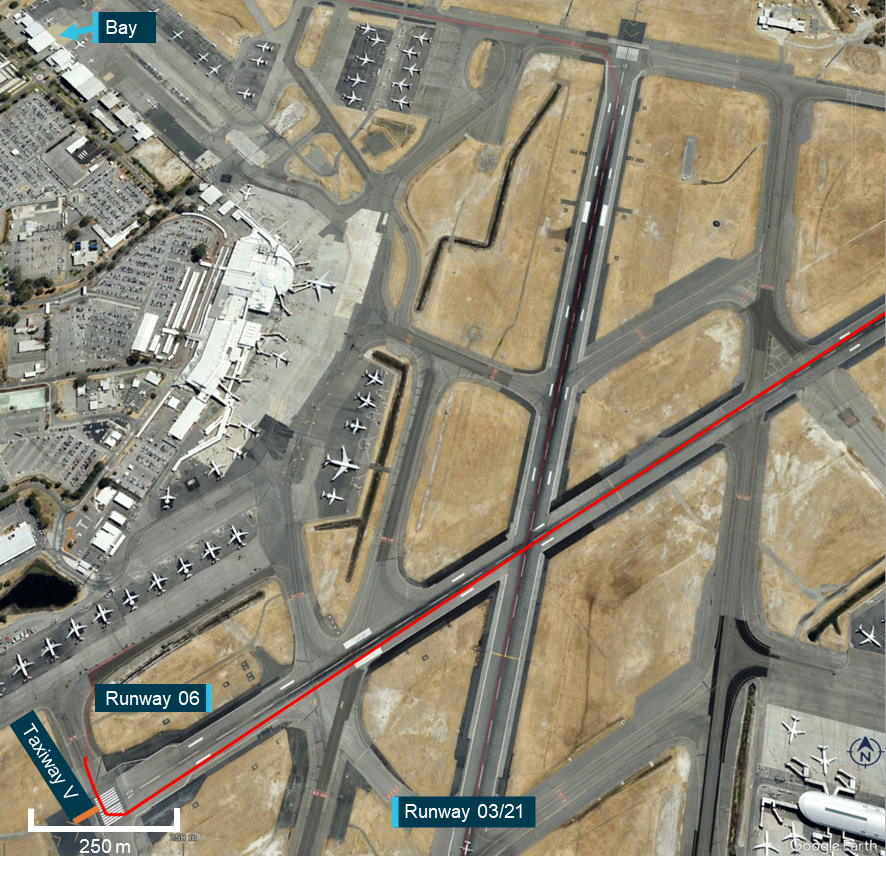




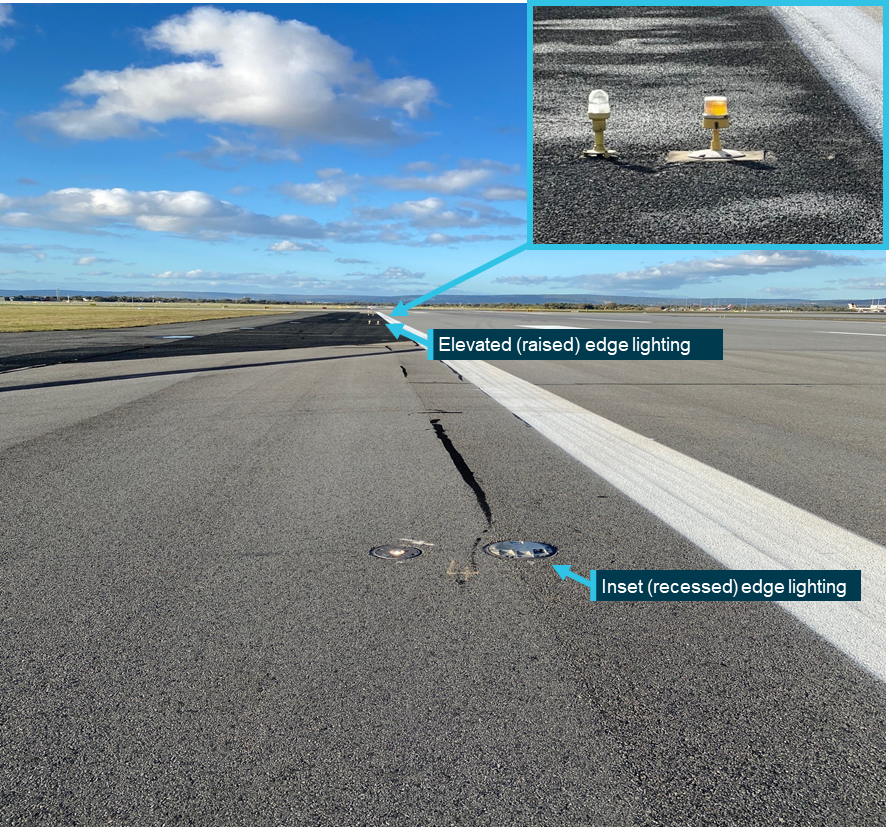
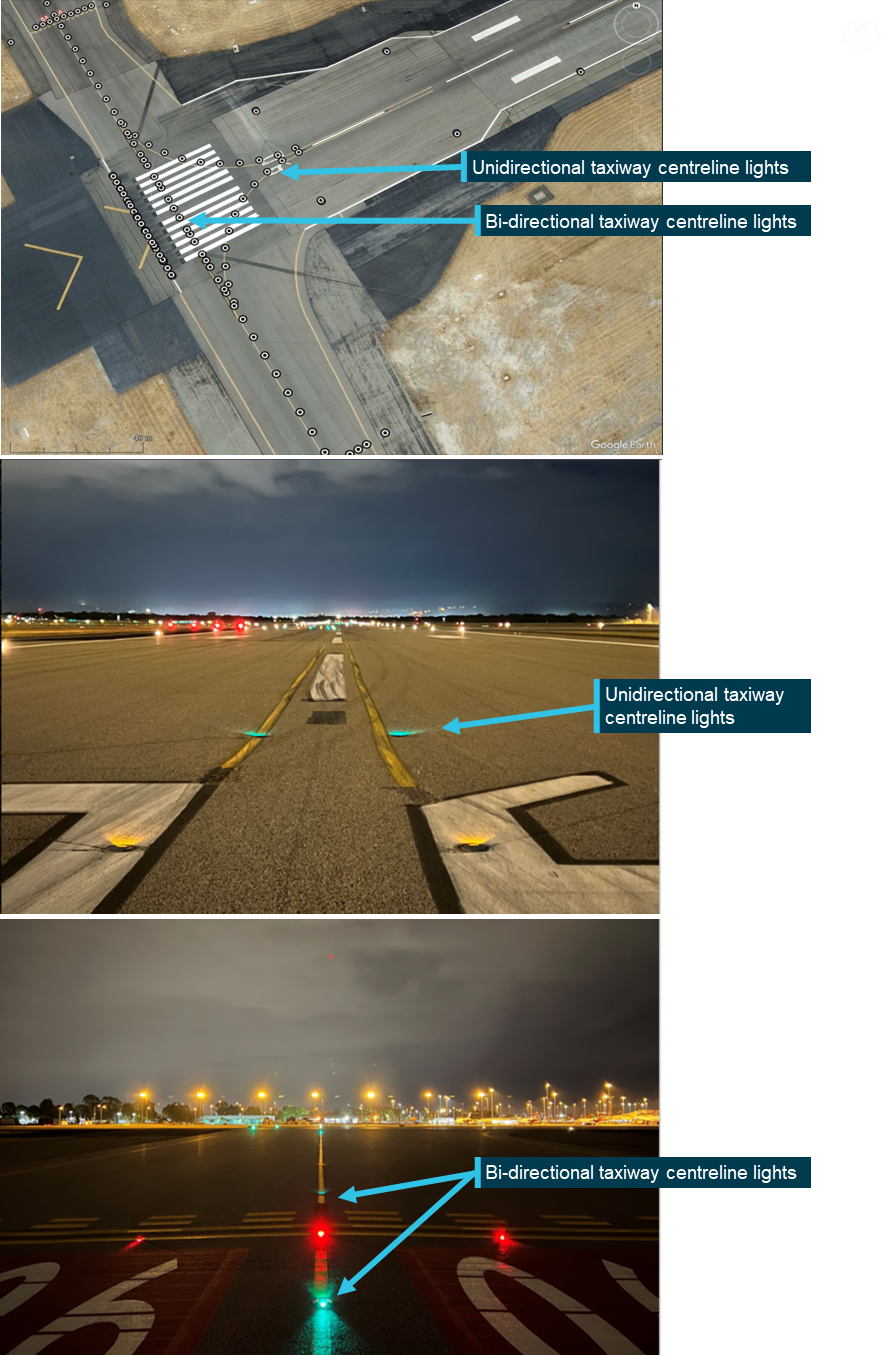
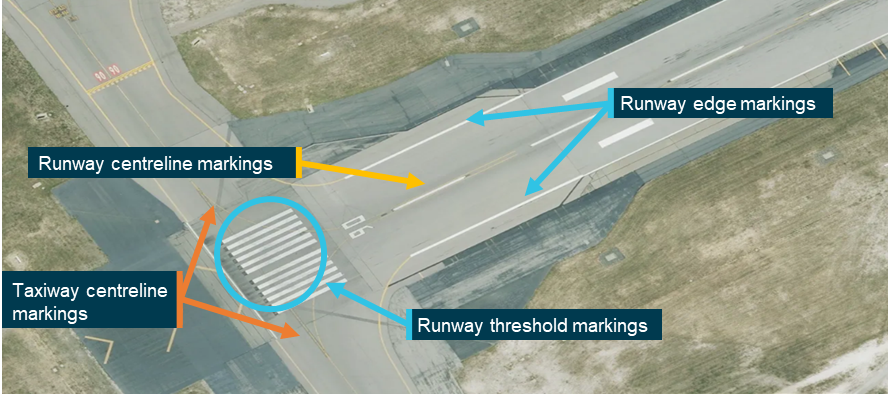
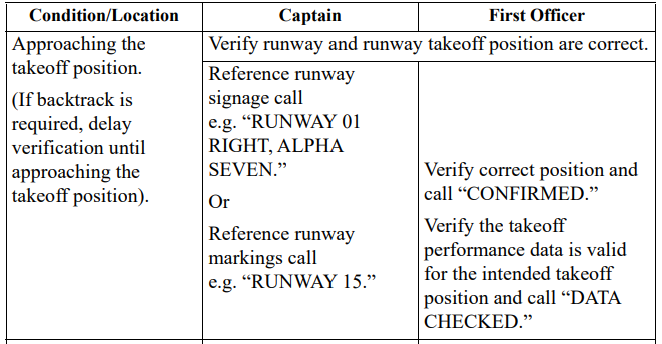

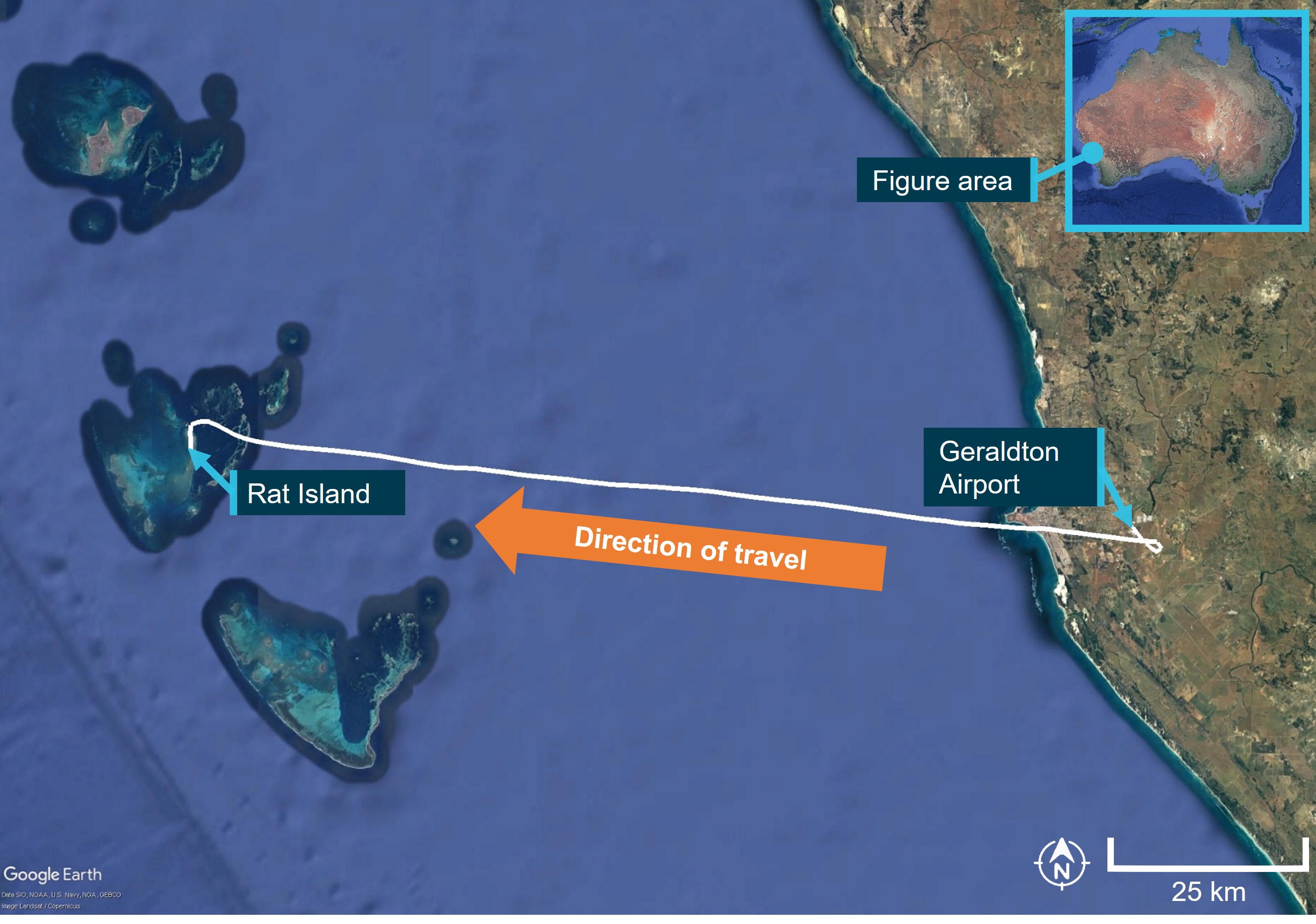


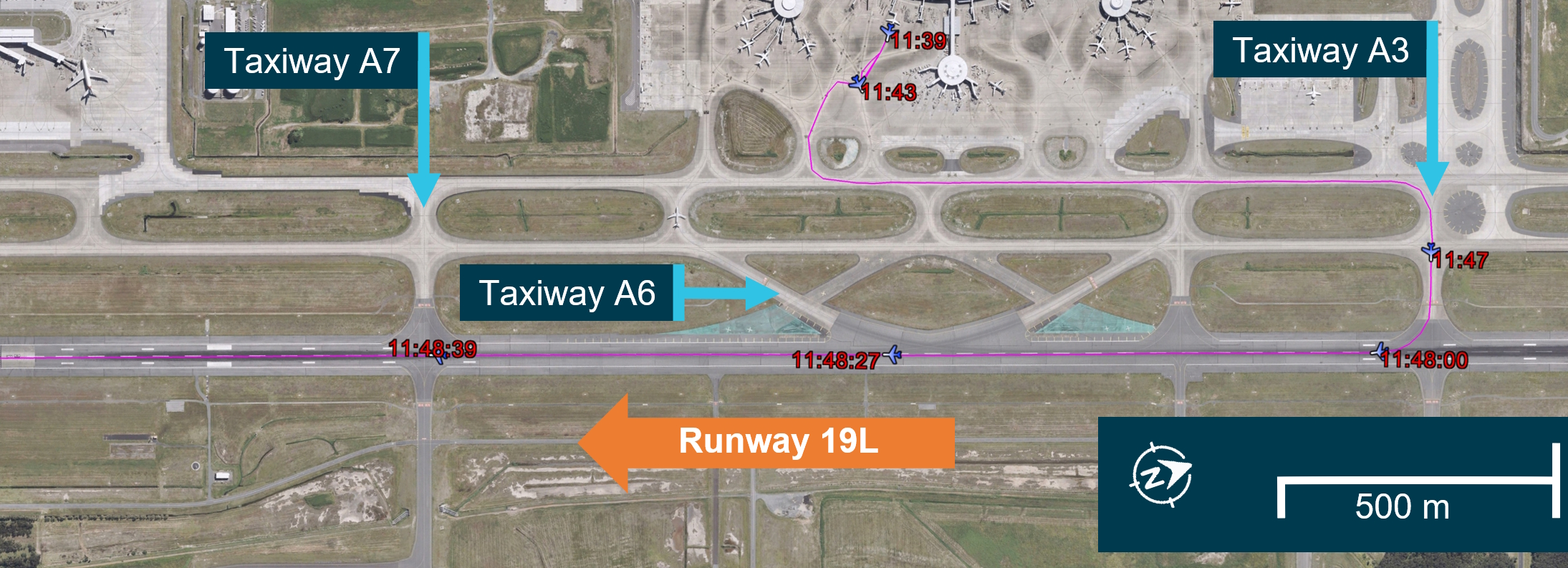
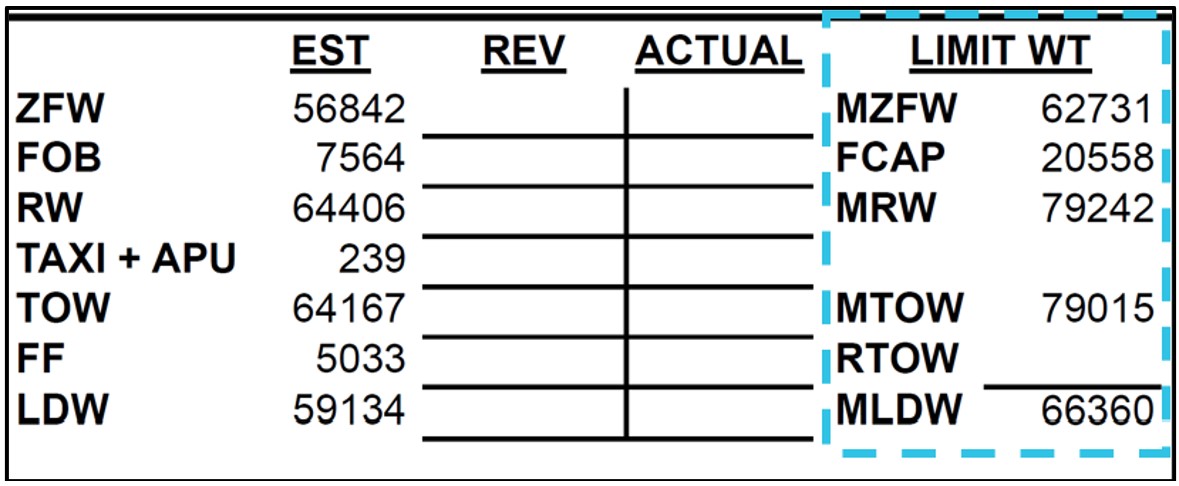
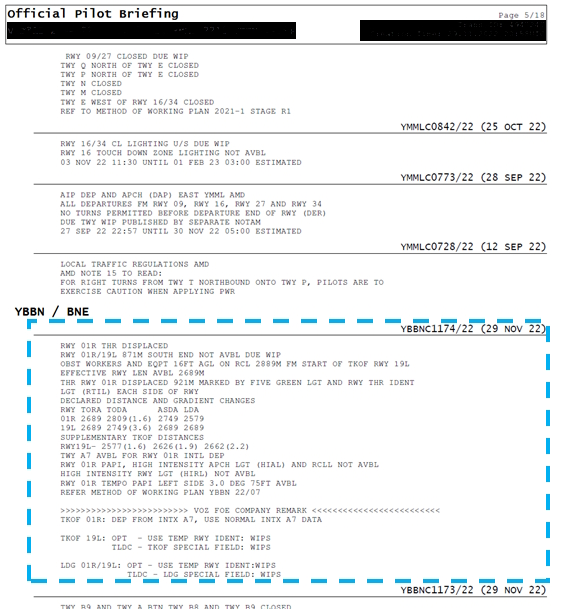
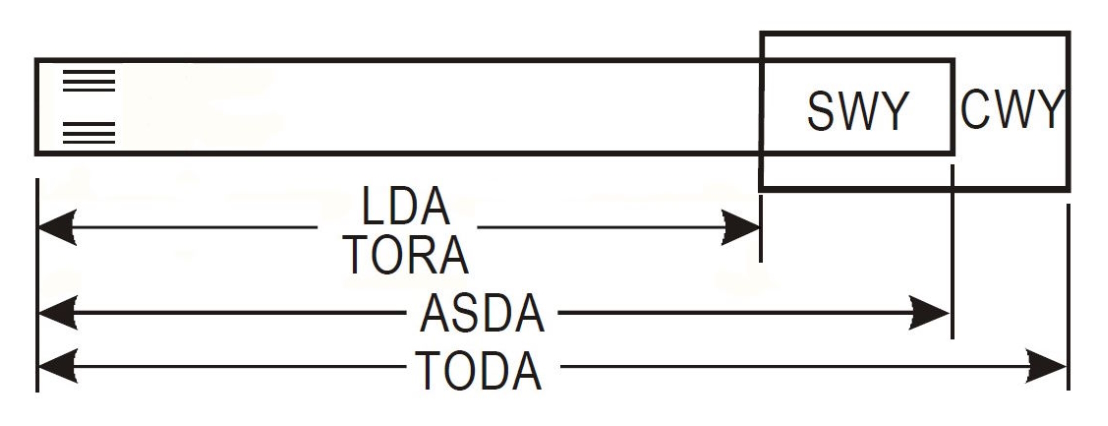

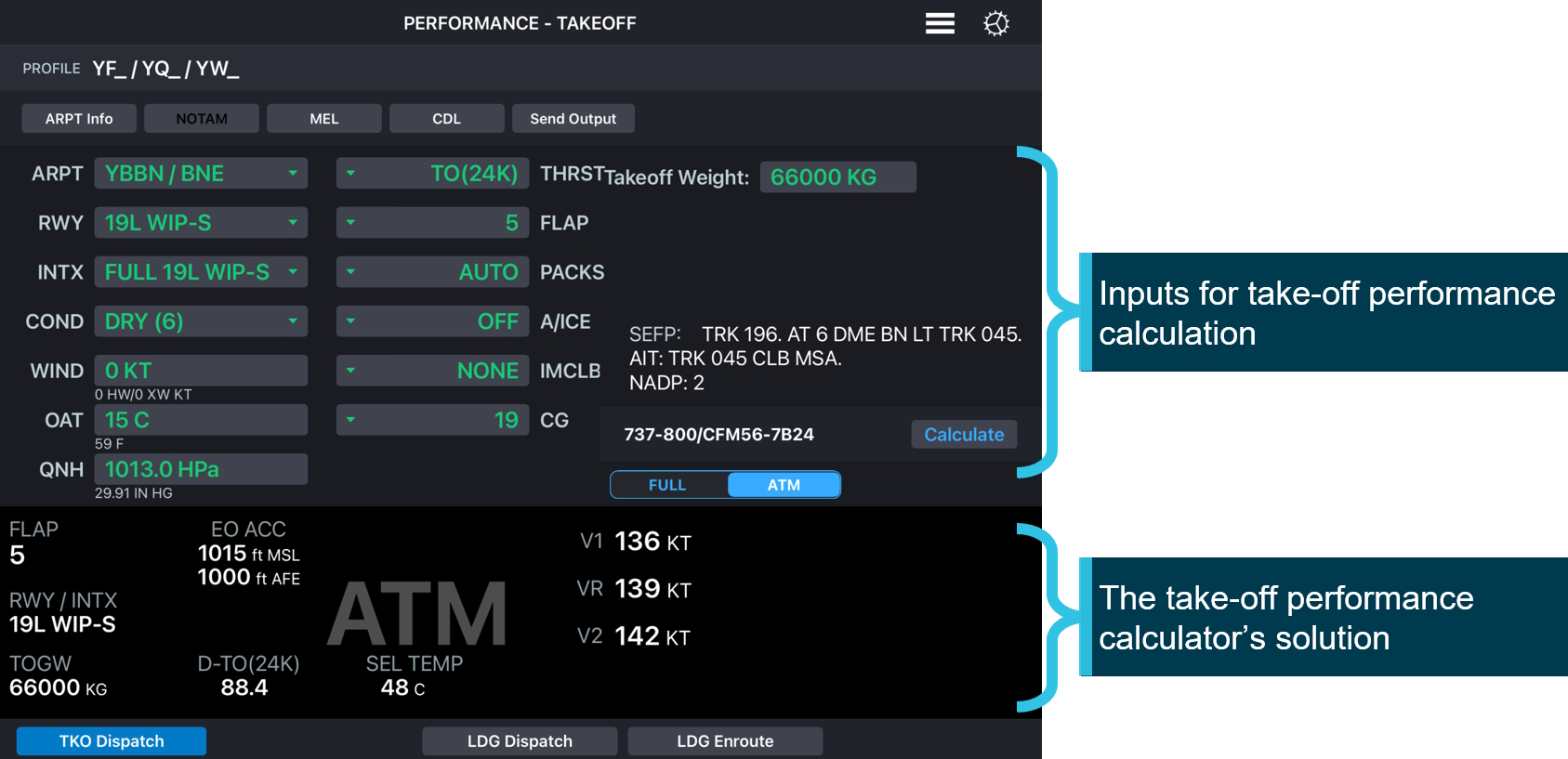
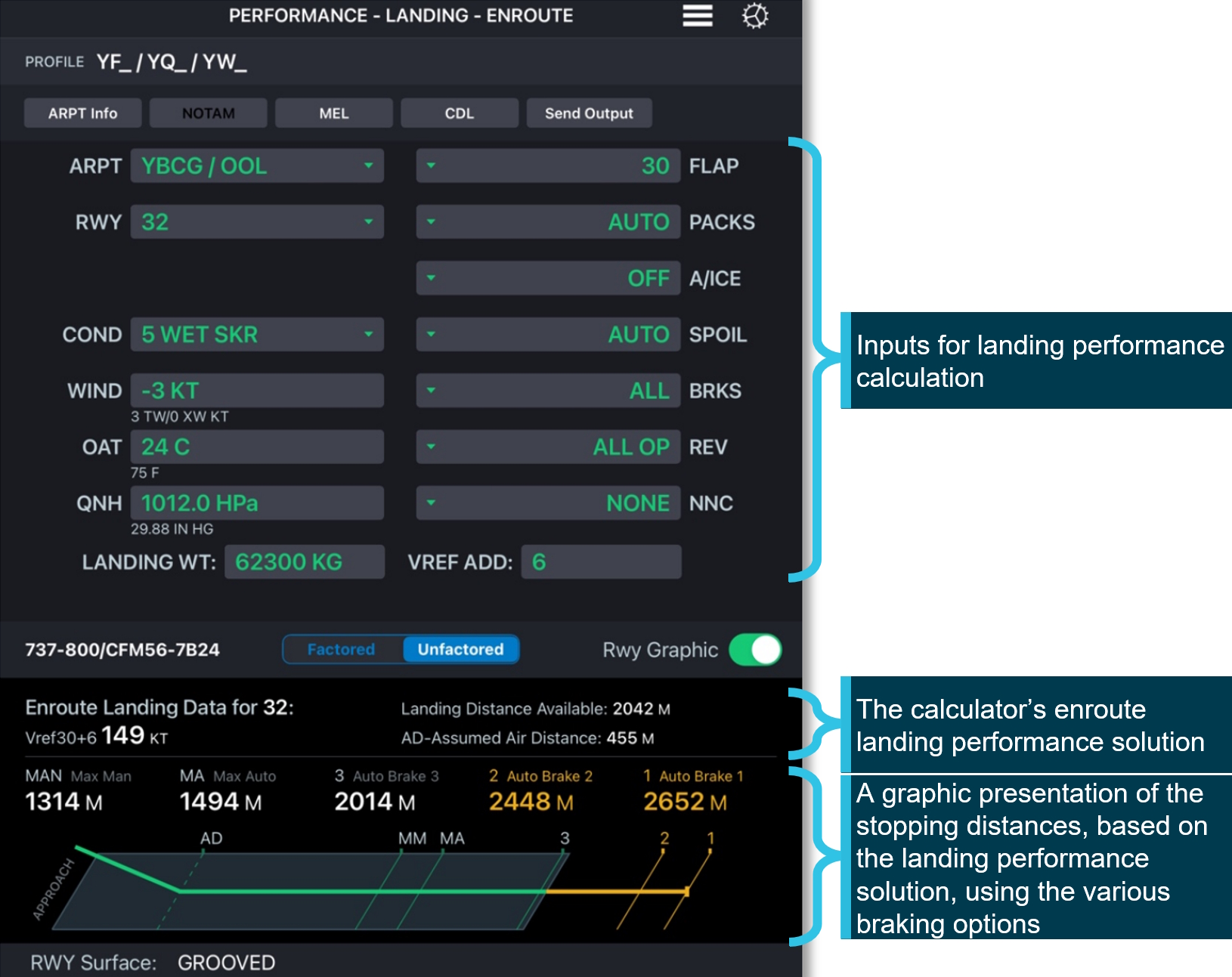
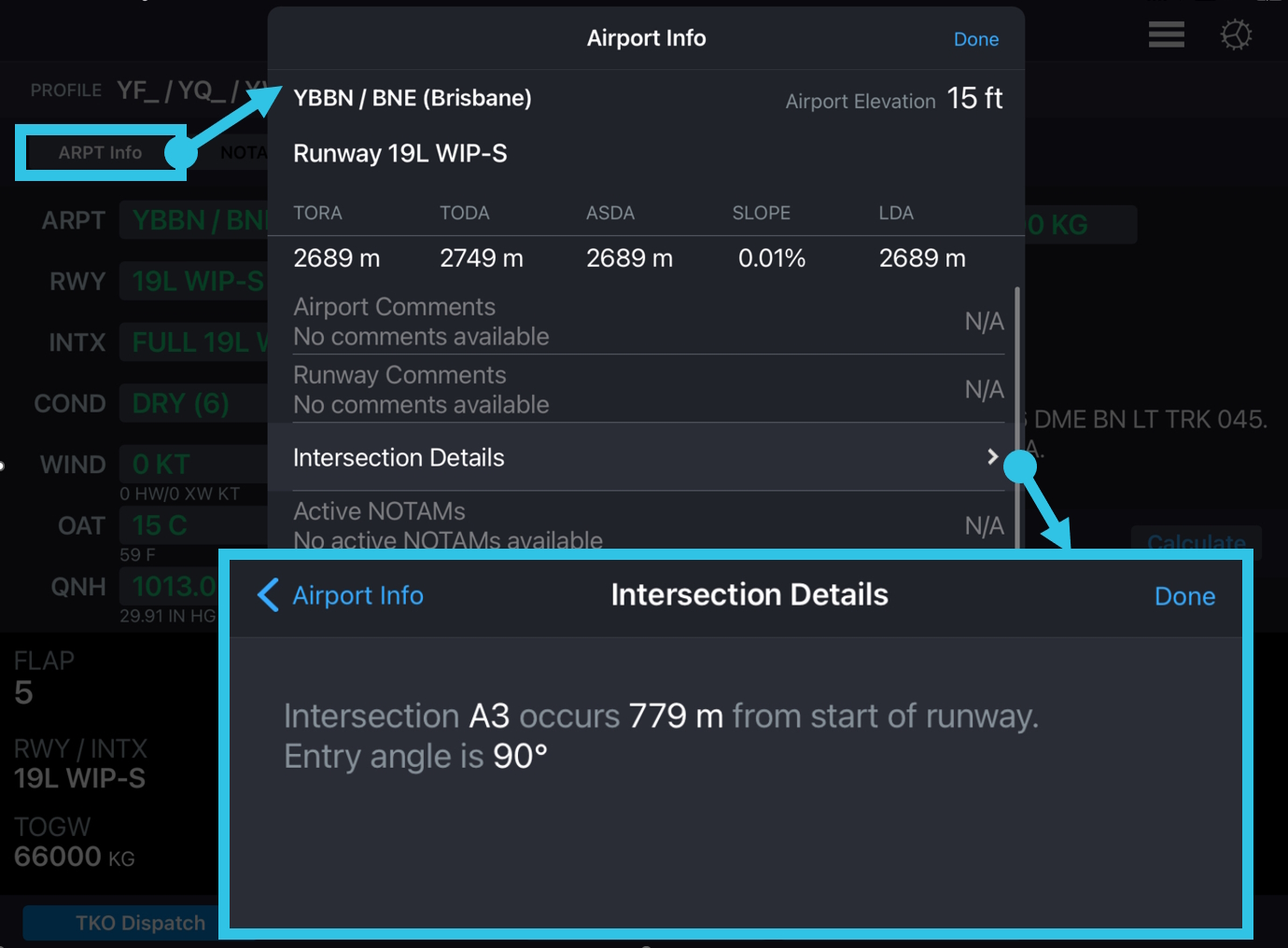
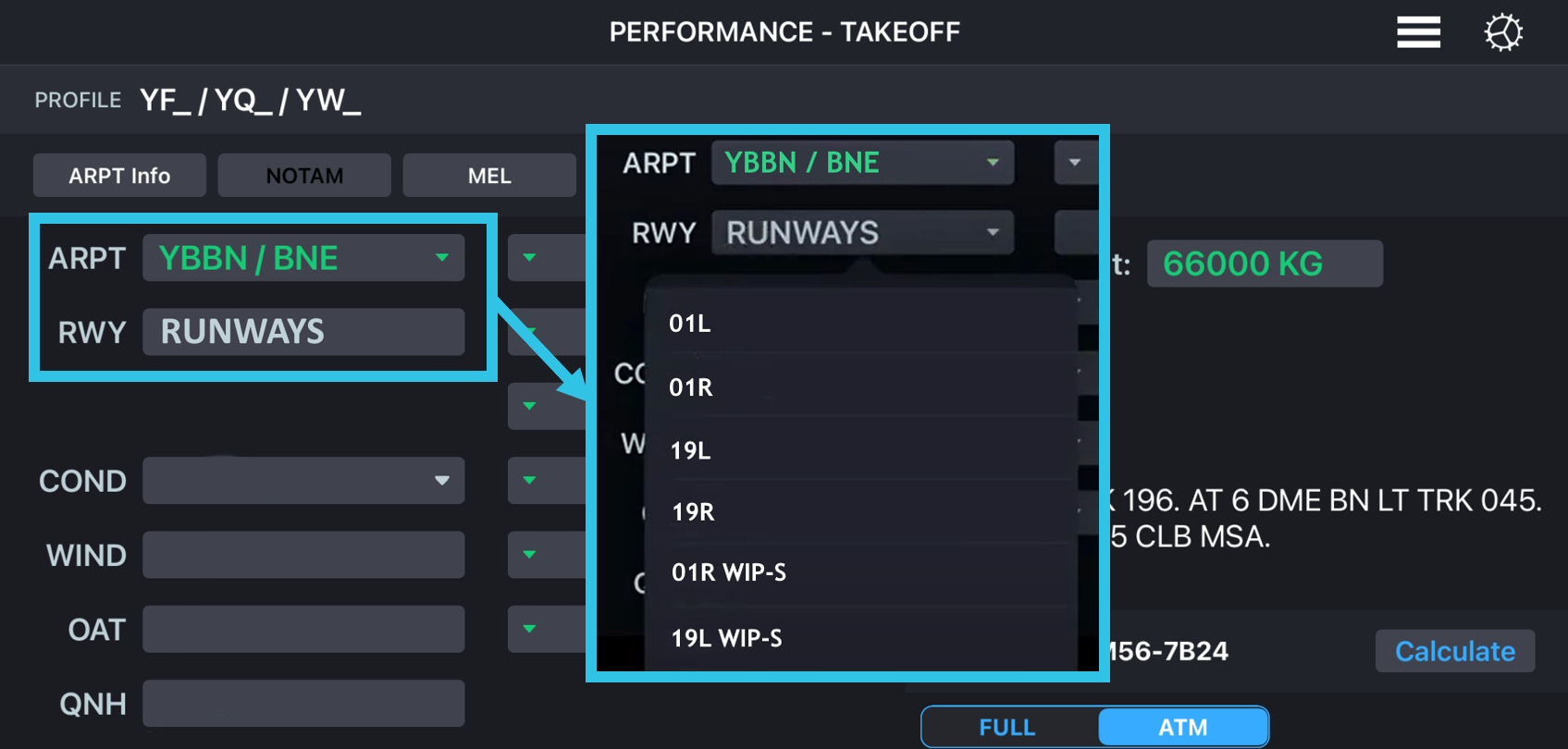
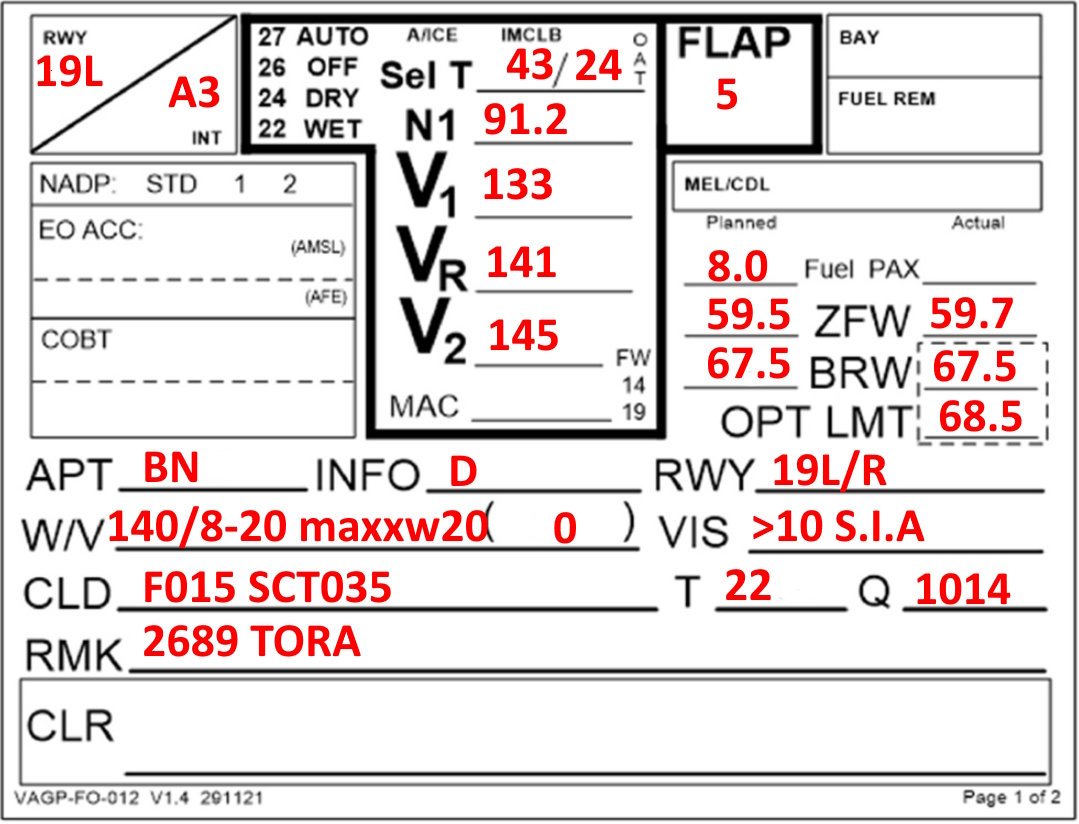
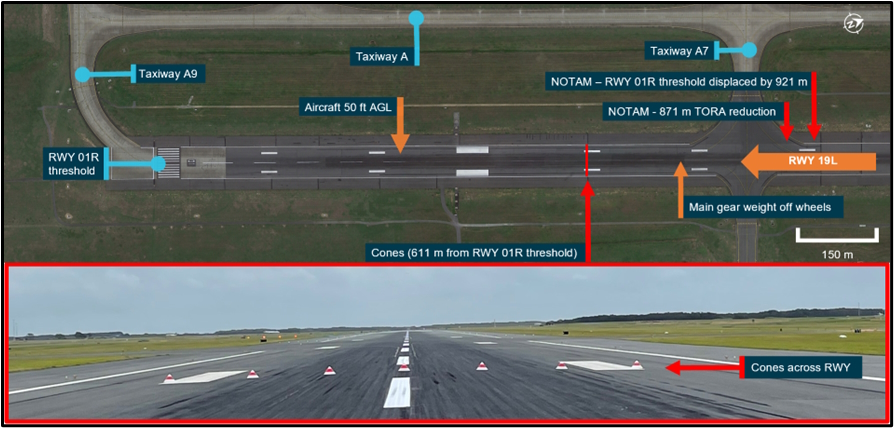

.jpg){kind=link}