Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 12 July 2025, at approximately 0940 local time, an Airbus A380 was parked at Sydney Airport, New South Wales. Once boarding of the aircraft’s upper deck had been completed and the upper main left door was closed by the customer service supervisor (inside the aircraft) assisted by the customer service agent (outside the aircraft), the agent returned to the double doors located inside of the aerobridge cabin.
The supervisor requested that the agent retract the aerobridge that was attached to the upper main left door. The agent reported having difficulty closing the aerobridge double doors prior to retraction, only closing the right door after the fourth attempt. When the agent then swiped on at the aerobridge operating panel to begin retracting the aerobridge, they heard alarms sounding. The agent returned to the double doors on the aerobridge to see if this was the source of the alarms and reported that they assessed the alarms as being associated with the nearby lower deck aerobridge attached to the aircraft.
With the alarms still sounding, the agent then attempted to retract the aerobridge straight back multiple times without success. Believing that a straight back retraction could be achieved if the aerobridge was moved slightly to the right, they proceeded with this aerobridge movement. However, while moving to the right, the aerobridge contacted with the number 2 engine (Figure 1). The aircraft sustained minor damage.
Figure 1: Aerobridge contact with no 2 engine
Source: Media, annotated by the ATSB
Safety message
A 2010 ATSB research study into Ground operations occurrences at Australian airports found approximately 28 per cent of all ground operations occurrences happened while the aircraft was parked at the gate. Collision or contact with an aircraft by a vehicle, including aerobridges, was the most common gate event reported to the ATSB.
There are many risk controls in place at airports and within ground handling companies and airlines to help minimise the hazards associated with airport ground operations. The ATSB reminds all ground handling personnel operating airside vehicles that if an abnormal situation should occur, such as the audible alarms in this incident, to cease operations immediately and request assistance. Effective communication is vital to reduce the risk of ground operations occurrences.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-033
Occurrence date
12/07/2025
Location
Sydney Airport
State
New South Wales
Occurrence class
Incident
Aviation occurrence category
Ground handling
Highest injury level
None
Brief release date
03/09/2025
Aircraft details
Manufacturer
Airbus
Model
A380-842
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, from 2 separate airlines, intended to drive the aerobridge parallel to the parked aircraft on the bay from the aerobridge home position prior to docking. However, the aerobridge moved diagonally towards the aircraft until the bottom right corner of the aerobridge impacted the aircraft and broke through the aircraft cockpit windshield. The collisions resulted in minor damage on both occasions with no recorded injuries.
What the ATSB found
Visibility of narrow-body aircraft was restricted from the aerobridge home position due to the required parking location of narrow-body aircraft, to the far right of the aerobridge home position. In addition, the design of the aerobridge cab walls, which lacked viewing windows installed in some other aerobridges at the airport, also limited direct visibility.
Both operators did not have visual reference of the aircraft prior to the collisions but expected to gain visibility following aerobridge extension. This expectation was reinforced by previous successful operations and was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft.
Both operators had moved the joystick to a 3 o’clock position and believed they were moving the aerobridge parallel to the aircraft. However, the aerobridge moved diagonally towards the aircraft. Both operators had rotated the cab left and were unaware that this orientation changed the direction of travel of the aerobridge. The operators were not alerted to the diagonal movement because they could not see the aircraft and perceived no other information to challenge their spatial orientation.
The ATSB identified that Brisbane Airport Corporation’s training material and in-cab instructions did not provide direction to operators to gain and maintain visibility of the aircraft from the home position, before moving the aerobridge.
Safety features designed to prevent collisions and damage to aircraft did not activate due to the approach angle of the aerobridge.
In the first occurrence an engineer on the ground activated the aerobridge emergency stop button to prevent further damage to the aircraft.
What has been done as a result
Following the occurrences in August 2025, Brisbane Airport Corporation (BAC) disseminated a safety notice to all operators that emphasised the requirement to rotate the cab towards the aircraft, always maintain positive line-of-sight with the aircraft, and cease operations if visual reference is lost.
BAC also reviewed the operator training material and identified gaps and an opportunity to be more specific in the process to safely attach aerobridges (similar to aerobridge 82) to aircraft. The training was updated in January 2026. Obsolete and inconsistent in‑cab instructions are in the process of being removed and will not be replaced in the aerobridge cabs.
BAC also created a new role focused on airside performance of assets and operators, including aerobridges, and all supporting infrastructure tools the operators use. Quality assurance activities have commenced with the role in place.
An aerobridge replacement program will renew 8 aerobridges at Brisbane Airport, including the aerobridge at Gate 82, commencing in 2026 at the International Terminal. BAC will review safety features and narrow-body visibility will be reviewed as part of this program. BAC is also planning to trial automated docking of aerobridges in the first half of 2026.
Fiji Airways has temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Safety message
There are many risk controls in place at airports and within ground handling companies and airlines to help minimise the hazards associated with airport ground operations.
Visibility of aircraft is critical for safe aerobridge operations. Aerobridges should be designed to maximise visibility and aerobridge training should reinforce visibility as a critical step in safe operations.
Aerobridge training and operational documentation should also highlight the mental rotation required for operators when joystick movement is relative to the orientation of the cab and not fixed to the direction of the aerobridge tunnel, or other stationary visual references outside the aerobridge.
The occurrences
Aerobridge operation – both occurrences
On 2 separate occasions, during aircraft arrival at the bay at night, prior to passenger disembarkation, the aerobridge at Gate 82 of the international terminal at Brisbane Airport collided with 2 different aircraft, resulting in minor damage to the cockpit windshields.
The first aircraft was a B737-838 narrow-body operating as Qantas flight QF186 (VH‑VZG), from Queenstown, New Zealand, on 18 June 2025.
The second aircraft was a B737-8 MAX narrow-body operating as Fiji Airways flight FJ923 (DQ-FAE), from Nadi, Fiji, on 26 July 2025.
On both occasions, the aircraft were correctly parked in the designated marshaller’s position[1] for a Boeing 737 (Figure 1), in line with the visual docking guidance system (VDGS).
Figure 1: Overview of aerobridge operational area
Source: Brisbane Airport Corporation
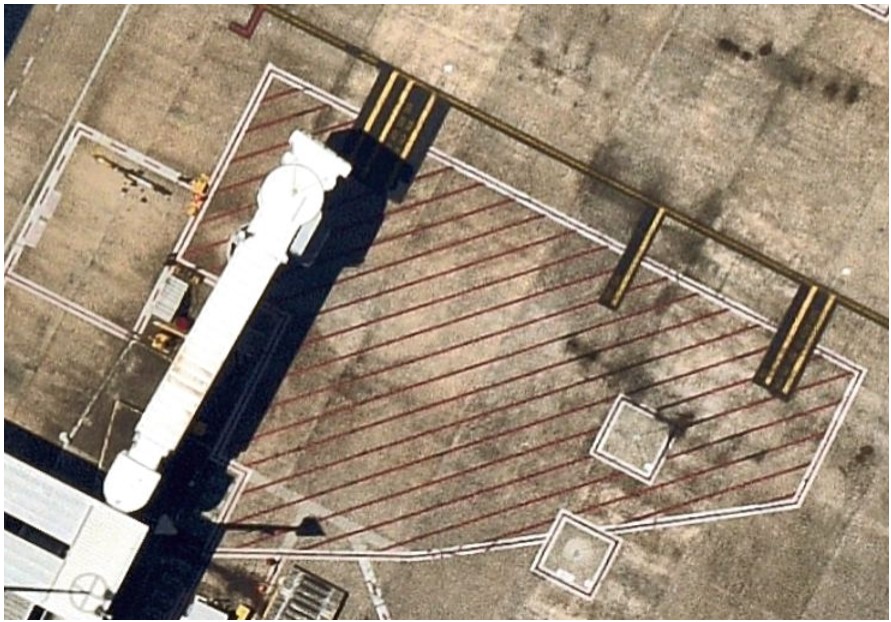
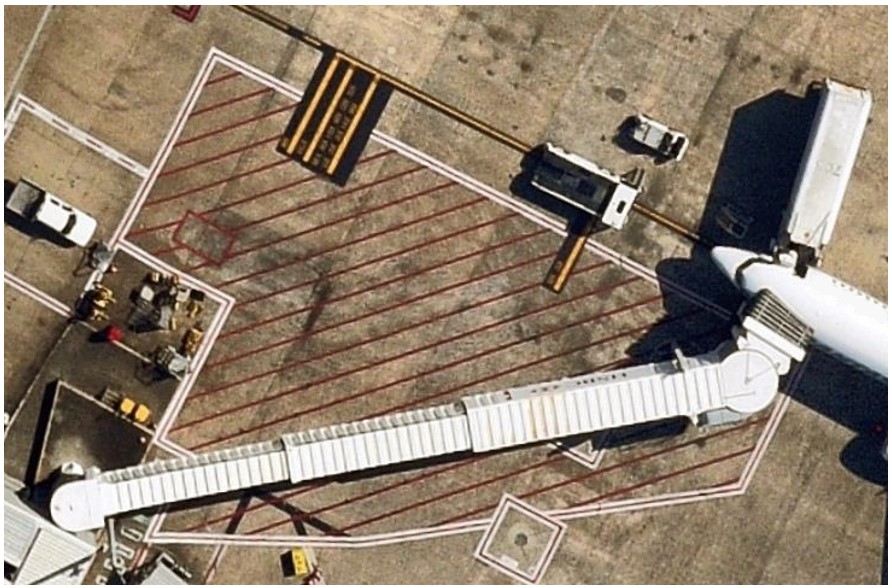
On both occasions, the aerobridge was operated at night (Figure 2). Rain was present in the area prior to the second event on 26 July 2025, with water visible on the ground (Figure 2, right).
After receiving visual confirmation from ground staff to indicate the wheels were chocked and the park brake was released, both operators activated the aerobridge by swiping their security identity card at the operator console and then initiated movement from the default home position (Figure 2).
Figure 2: Home position of aerobridge with parked QF186 (left) and FJ923 (right)
Source: Brisbane Airport Corporation
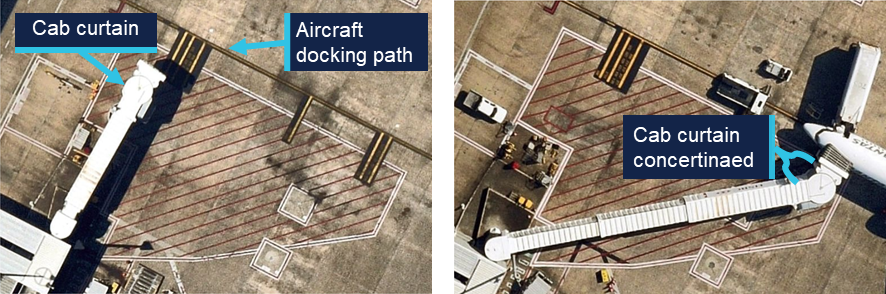
Closed circuit television (CCTV) showed that at about 30 seconds into the aerobridge extension (halfway through), and while moving diagonally, the aerobridge cab was rotated to the left as identified by contraction of the concertinaed side curtain (Figure 3).
Figure 3: Left orientation of cab at 1845, 18 June 2025 (left) and 2304, 26 July 2025 (right)
Source: Brisbane Airport Corporation, annotated by the ATSB
During this time, the aerobridge continued to move diagonally towards the aircraft before the bottom right corner of the aerobridge impacted the aircraft windshield.
Both operators expected to gain visibility of the aircraft from the cab window during the aerobridge extension from the home position. They both reported previous successful operations where gaining visibility of the aircraft was delayed, but always occurred, and both stated that they were surprised by the unexpected collision.
While glass fragments entered the cockpit, and a jolt occurred, no injuries resulted to crew or passengers on either occasion. The aircraft windshields were subsequently replaced, and pressurisation was checked before both aircraft continued operations. The aerobridge was also assessed, however no faults were identified, and a return to service check was conducted before further operations on each occasion.
Occurrence 1 details
At 1845 on 18 June 2025, aerobridge 82 was being operated by a Qantas customer service agent (Operator 1) to disembark QF186 (VH-VZG), a B737-838 narrow-body aircraft after arrival from Queenstown, New Zealand.
At 1846 the right aircraft windshield was impacted by the front right aerobridge corner (Figure 4, left). A licensed aircraft maintenance engineer (LAME) was on the ground assessing the aircraft following a potential bird strike. They detected abnormal operation of the aerobridge and attempted to alert the aerobridge operator by hand gestures before activating the on-ground emergency stop at the same time as the impact.
From the cockpit, 2 flight crew members noticed the aerobridge approaching the aircraft from a high angle and further towards the nose of the aircraft than usual. The captain pressed the ground call switch on board to contact engineering or other ground staff to advise them of their urgent concern that the aerobridge was likely to impact the aircraft.
The crew were unable to make contact with engineering or ground staff before the aerobridge collided with the first officer’s windshield, shattering the glass (Figure 4, right). Although the glass fragments landed on the first officer, they were uninjured. The flight crew reported a jolt at impact, however, no passengers or cabin crew were injured.
Figure 4: Collision and damage to QF186
Source: Qantas
Occurrence 2 details
At 2304 on 26 July 2025, aerobridge 82 was being operated by a Fiji Airways customer service agent (Operator 2) to disembark FJ923 (DQ-FAE), a B737-8 MAX narrow-body aircraft after arriving from Nadi, Fiji.
At 2305 the left aircraft windshield was impacted by the front right aerobridge corner (Figure 5, left). From the cockpit, 2 flight crew members noticed the unusual movement of the aerobridge towards the aircraft, aligned with the windshield (rather than the side of the fuselage). They expected the movement to stop, but it continued until impact.
Although glass fragments and the corner of the aerobridge partially entered the cockpit (Figure 5, right), the captain was able to move out of their seat and they were uninjured. The flight crew reported a jolt at impact; however, no passengers or cabin crew were injured.
Figure 5: Collision and damage to FJ923
Source: Brisbane Airport Corporation
Context
Personnel information
Both aerobridge operators were airline customer service agents employed directly by airlines. Their normal tasking involved customer-facing pre-flight and post-flight services as well as ground operations support.
Operator 1 (Qantas) was certified in January 2024, and Operator 2 (Fiji Airways) was certified in June 2024, both were certified to operate international aerobridges, including aerobridge 82. At the time of the occurrences Operator 1 had 17 months experience and Operator 2 had 13 months experience in operating aerobridges.
Operator 1 had controlled aerobridge 82 within 3 months of the occurrence and Operator 2 had controlled aerobridge 82 within 2 months of the occurrence.
Both operators reported adequate prior sleep and recalled feeling fully alert at the time of the occurrences.
Aircraft information
Both aircraft were Boeing B737 narrow-body aircraft. VH-VZG (QF186) was a Boeing 737‑838 and DQ-FAE (FJ923) was a B737-8 MAX.
Meteorological information
Dark night conditions were present in both occurrences, and the operational area was illuminated with bright lights (Figure 2).
No significant weather was recorded prior to the first occurrence on 18 June 2025. In contrast, rain occurred at Brisbane Airport on 26 July 2025, and precipitation was present in the area prior to the second occurrence.
Aerobridge information
An aerobridge (or passenger boarding bridge) is an enclosed, elevated passageway which extends from an airport terminal gate to an aircraft.
Five types of aerobridges were in operation at Brisbane Airport across the international and domestic aprons, these ranged from fixed or pedestal aerobridges to moveable or apron drive aerobridges.
Aerobridge 82
The aerobridge at Gate 82 of the Brisbane international terminal was a Jetway Apron Drive Aerobridge. It was installed in 1995 and was in continued service for 30 years at the time of both occurrences.
As a telescopic bridge, aerobridge 82 was used for a wide range of aircraft and parking positions. The aerobridge could swing up to 180 degrees (clockwise and counterclockwise) across the bay and extend, raise or lower depending on the aircraft size. Fiji Airways used aerobridge 82 mostly for narrow-body aircraft, while Qantas used aerobridge 82 for mostly wide-body aircraft, and narrow-body aircraft on occasion.
A prime factor determining the parking position of the aircraft and therefore the required orientation and extension length of the aerobridge was maintaining aerobridge slope as close to the design limit of 1:14. For example, if the aerobridge was to rise 1 m, then it also needs to extend by 14 m to maintain suitable slope.
Another factor determining the parking position of the aircraft was the aircraft length forward from the wings (Figure 6):
Wide-body aircraft fuselage length from the wings forward is relatively long. The designated parking position provided sufficient clearance for the wings from the aerobridge passenger tunnel. When in the designated parking position, the left‑front door lined up with the aerobridge and the required aerobridge extension was minimal.
Narrow-body aircraft fuselage length from the wings forward is relatively short and require parking further from the aerobridge home position to maintain clearance of the left wing and the aerobridge passenger tunnel. The aerobridge required further extension to the right to line up with the left-front door of the aircraft for aerobridge attachment.
Figure 6: Schematic drawing showing aerobridge movement in relation to a wide-body and narrow-body aircraft
Source: Brisbane Airport Corporation, modified by the ATSB
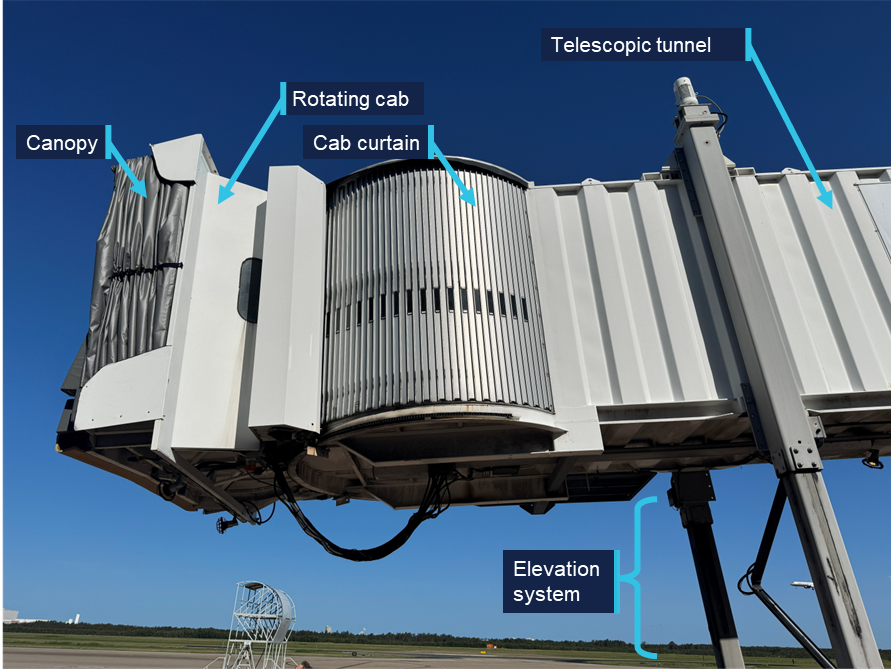
The aerobridge was formed by the following main elements (Figure 7 and Figure 8):
rotunda with column
canopy (which closes on to aircraft once the aerobridge is docked)
bumper with bumper proximity switches
slow down sensor located under the cab floor
rotating cab and cab curtain
telescopic tunnels (which extend and retract)
elevation and traveling systems.
Figure 7: Front view of aerobridge 82 in the home position
Source: ATSB
An external/on ground emergency stop button was located above the aerobridge wheels (Figure 7).
Figure 8: Side view of aerobridge 82 in the home position
Source: ATSB
Home position
Before and after aerobridge operations, the aerobridge returned to a default home position (Figure 7) where the:
wheels faced forward within a red home position box marked on the ground
telescopic tunnel retracted and sat perpendicular to the passenger walkway
rotating cab faced directly forward
height was set to 3.57 m.
The home position ensured safe clearance for parking aircraft wing tips, engines and fuselage. Pre-positioning of aerobridge 82 prior to aircraft arrival was previously considered by BAC, however, was removed following safety concerns.
Operator console
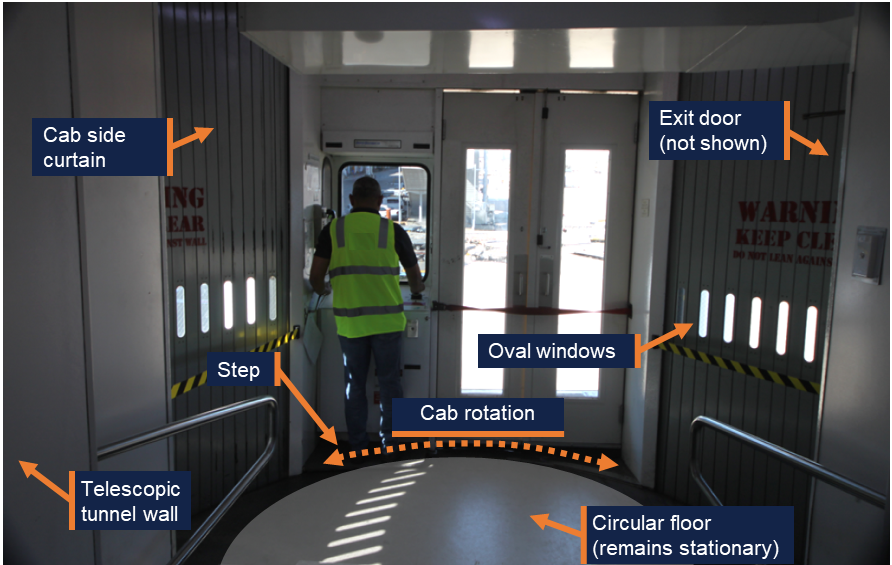
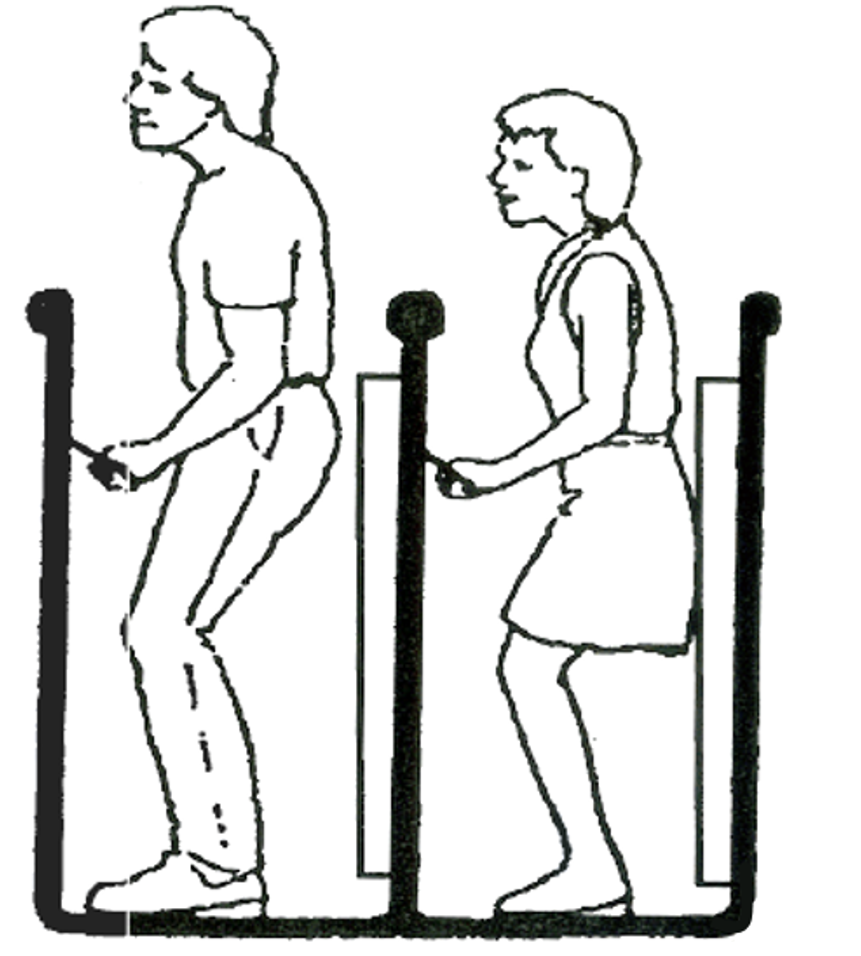
The aerobridge was operated using controls mounted on a console on the left side of the cab (Figure 9). The console was positioned and orientated to provide the operator a clear view of aircraft in front during final aerobridge manoeuvring and docking. The operator stood on a slightly raised step below the console.
The step and the console moved together left or right as the cab was rotated, while the circular cab floor remained stationary,[2] and the cab side curtains concertinaed (folded in) or expanded (folded out).
Figure 9: Example operator standing at operator console
Note: The footprint of circular floor has been exaggerated by the ATSB to illustrate cab rotation around the stationary floor. Source: ATSB
Visibility of narrow-body aircraft
From the home position, wide-body aircraft were visible to aerobridge operators standing at the operator console (Figure 6). However, narrow-body aircraft fell outside the operator’s field of view at the console as the designated parking position was to the far right of the aerobridge. The operator’s view of narrow-body aircraft was blocked by protruding walls inside and outside the right side of the cab (Figure 7 and Figure 9).
For aerobridge 82, oval shaped windows interspersed on the right curtain below the operator’s eye height provided very limited visibility unless the operator left the operating console and bent down to establish visibility directly through the section of window. However, full visibility was not possible while operating the aerobridge and manoeuvring to narrow-bodied aircraft (Figure 9).
Similarly, the operator could exit the cab to view the aircraft via a service door on the far‑right of the cab. This was done on occasion to obtain visual confirmation from the ground crew prior to operation, but the operator could not operate the aerobridge unless they returned to the console.
Some other aerobridge types had been designed with large windows on the right side of the cab at eye level and below, such as the aerobridge at Gate 44 of the Brisbane Domestic terminal (Figure 10).
Figure 10: Right side windows on aerobridge at Gate 44 of the Brisbane Domestic terminal
Source: Brisbane Airport Corporation
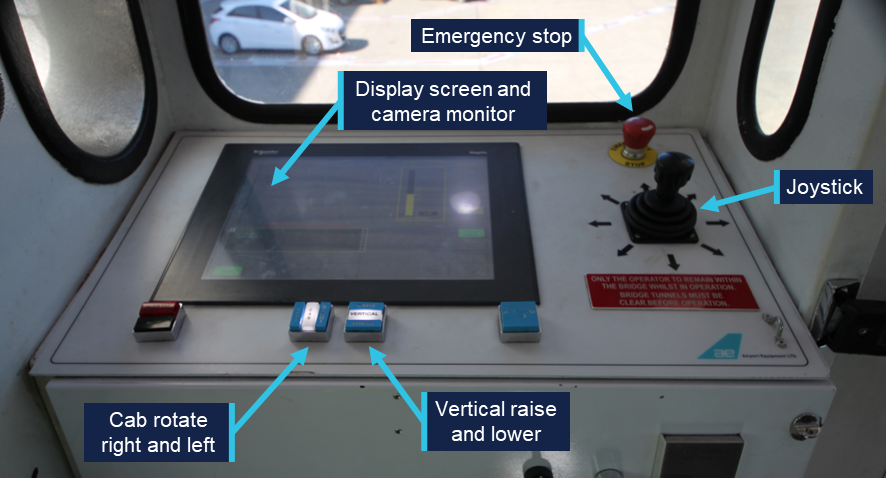
Control panel
The control panel contained the required switches, buttons and control sticks to operate the aerobridge (Figure 11). By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions to align with the aircraft door. Operators reported it was normal practice to do so.
Figure 11: Aerobridge control panel
Source: Brisbane Airport Corporation, annotated by the ATSB
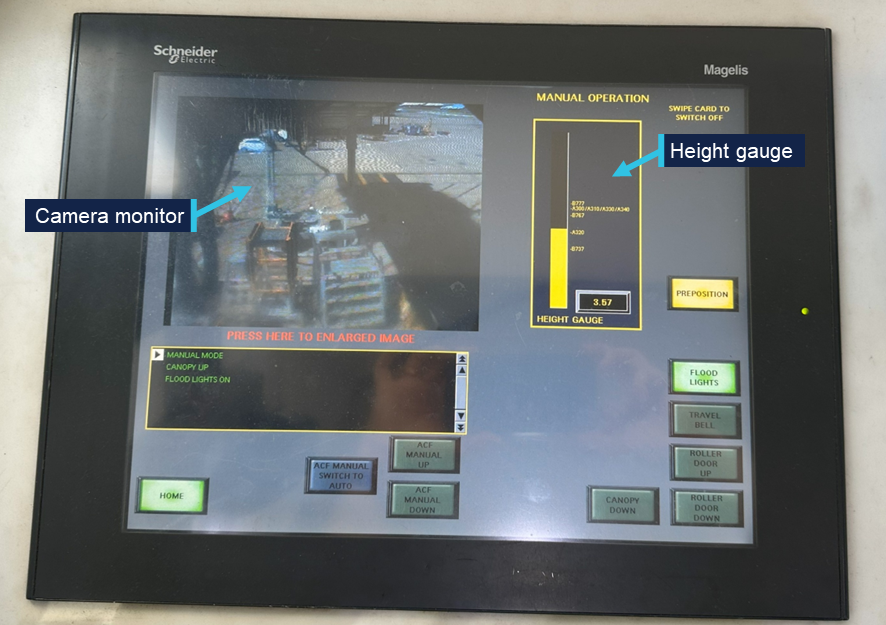
Vertical control
Aerobridge height could be adjusted via the vertical raise and lower buttons (Figure 11) to meet the height requirements of each aircraft type. The current height of the front bumper was displayed to the operator via a height gauge on the display screen (Figure 12). The gauge also showed 8 different aircraft types for reference.
Figure 12: Display screen and camera monitor
Source: ATSB
The default home height of 3.57 m was suitable for attaching aerobridge 82 to the door of an Airbus A320 aircraft, however the aerobridge needed to be lowered to meet the door height of a Boeing 737.
Cab rotate right and left
To attach the aerobridge to the aircraft door, operators were required to orient the rotating cab, using the left and right buttons (Figure 11) to ensure the cab was parallel to the fuselage (or the aircraft docking path). As the home position of the cab faced directly forward, the cab also needed to be rotated left to attach to a 737 (Figure 13), demonstrated by the concertinaed cab curtain.
Operators reported it was normal technique to pre-emptively rotate the cab to the left while moving the aerobridge horizontally or laterally.
Figure 13: Aerobridge in home position (left) and correctly attached to a 737 (right)
Source: Qantas
Joystick
The joystick controlled the aerobridge’s direction of travel and could be moved 360 degrees about its central point (Figure 11). The aerobridge drive wheels oriented to the desired direction of travel when the operator pushed the joystick in the required direction.
Speed of aerobridge movement and extension was controlled by the amount of pressure the operator applied to the joystick. The further control input, the faster the aerobridge would move. Movement stopped when the operator released the joystick (following a short delay which was perceived as a minor jolt to operators) and the joystick returned to the central neutral position.
The joystick was designed to move relative to the orientation of the cab. Specifically, relative to the forward-facing window (and therefore the direction the operator was normally facing) and not the direction of the tunnel. If the orientation or rotation of the cab changed, so did the direction of travel.
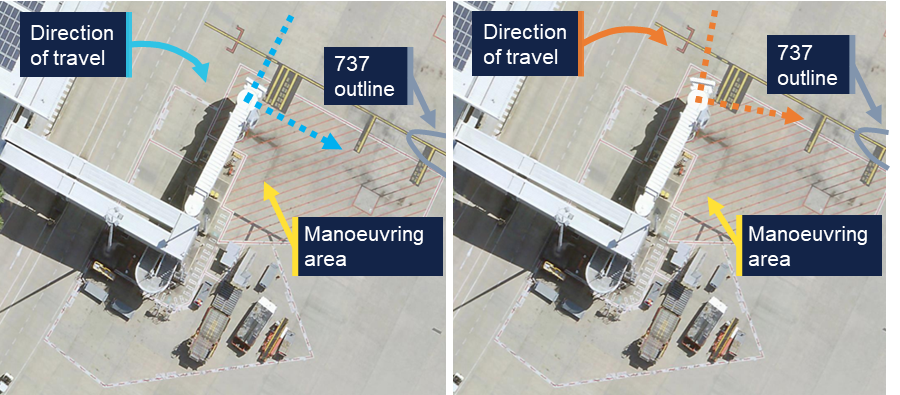
From the home position, the operator could move the joystick to a 3 o’clock direction, and the wheels would orient to travel right (Figure 14, left), and the aerobridge would travel to the right, parallel to the parked aircraft.[3]
If the operator rotated the cab slightly left from the home position (Figure 14, right), and pushed the joystick to a 3 o’clock position, as the movement of the aerobridge would be relative to the direction the cab was orientated, the aerobridge would travel diagonally towards the parked aircraft.
Figure 14: The operator’s 3 o’clock direction from home position (left) versus the operator’s 3 o’clock direction when the cab rotated slightly left (right)
Note: Right image was edited to replicate left cab rotation. Source: Brisbane Airport Corporation, annotated by the ATSB
To anticipate the direction of travel, operators were therefore required to mentally rotate[4] the direction of travel relative to the orientation of the cab. Visible stationary references outside the cab would likely aid operators to orient the direction of travel during aerobridge movement (and correct any potential orientation errors).
Camera monitor
A front facing CCTV view of the area underneath the cab (around the wheels) was presented to the operator as a safety control to prevent contact between the elevation and travel systems (Figure 7) and any person or object inside the aerobridge manoeuvring area marked by red hatching (Figure 14).
Operators reported, and the ATSB observed, that perceptibility of the CCTV could be reduced by glare and shadows (Figure 12).
The aerobridge operator of the second occurrence reported additional blurriness on the monitor, potentially due to condensation following rain in the area prior to the event.
Safety features
The following safety features were installed on aerobridge 82 to prevent collisions with aircraft:
A slow down sensor (or slow down beam) located under the cab floor was used to detect aerobridge proximity to the aircraft fuselage. When the ultrasonic sensor detected an obstruction directly in front of the cab, the horizontal speed slowed.
Four bumper switches (or bumper proximity switches) located in the bumper of each aerobridge were designed to detect when the aerobridge bumper contacted an aircraft. Four spring loaded probes stopped bridge extension if activated by forward touch, while the outer 2 probes also prevented cab rotation if activated by forward touch.
Neither proximity nor bumper switches activated during the 2 occurrences.
More sophisticated anti-collision systems were installed on 7 multi-bridge[5] aerobridges at Brisbane Airport. These anti-collision systems were designed to avoid collision with other aerobridges or aircraft in front of, and either side of, the aerobridges. However, these were not equipped on single aerobridges like aerobridge 82.
Separate to the camera monitor which showed the wheel area, no other CCTV cameras were installed. Additional camera views had been discussed and considered by Brisbane Airport Corporation (BAC) for aerobridge 82, however were not installed. Further, these camera views were for inside the cab to view operator functions, not as additional visibility for the operator.
While alarms (and alerts via the display screen) were frequently presented to operators of aerobridge 82 to help operators troubleshoot common faults or issues, no alarms or alerts activated prior to the collisions.
Maintenance
Aerobridge 82 was maintained by a third party service provider, Alstef Group on behalf of BAC.
Onsite technicians responded to phone calls and callouts to address issues, faults and alarms that could not be addressed by aerobridge operators. Operator training highlighted the reporting process (and 24/7 phone number) for faults, error messages and persistent alarms. A phone was installed on the wall near the operator console for maintenance provider contact.
Preventative maintenance inspections were carried out at 3, 6, and 12 months in line with the Operating and maintenance manual[6] using standardised checklists. Weekly inspections were conducted as an additional control for aerobridge serviceability and operation. A weekly cab curtain serviceability check was also added following a fall from height occurrence at Sydney Airport in 2025.
Return to service inspections were conducted following both occurrences, with no significant damage and no faults identified.
Aerobridge operator training
BAC was responsible for the aerobridge operations at Brisbane Airport. BAC held the responsibility for operator training, operational procedures and instructions and governed user access. However, the day-to-day operation was performed by airline staff or contracted to third party service providers (e.g. ground handlers).
Certification
BAC required aerobridge operators to be trained and certified for the appropriate aerobridge type. Training involved e-learning modules, in-person demonstrations and assessment by certified aerobridge trainer/assessors for competency.
E-learning
Operators were required to successfully complete a general aerobridge e-learning module (updated in June 2022) and at least one other aerobridge specific e-learning module for each aerobridge type.
The specific module that was applicable to aerobridge 82 was the Jetway Apron Drive (International) module (updated in September 2023). The training content of this module was relevant to 3 different Jetway Apron Drive aerobridges in use at Brisbane Airport, with different control panels, but similar functionality. The training material broadly covered operations for both wide and narrow-body aircraft but did not specify individual instructions for different aircraft types.
Both the general and specific modules included online assessments that required a 100% pass mark. Ten questions were provided for the general module and 5 questions for the Jetway Apron Drive (International) module.
The training content was based on Airport Equipment (New Zealand) Limited Operation and Maintenance manuals, particularly the standard operating procedures for manual docking.
The training modules contained clear safety messages about the operation of aerobridges. Safety risks (and controls) were emphasised for:
movement of aircraft once docked (use of auto lever and safety shoe)
contact with the elevation and travel systems (visual check of the control area to ensure no person or obstruction is present)
injury due to moving machine parts (one operator permitted in cab (unless training))
risk of falls from height (use of safety straps and curtain gap checks)
loss of control during operation (emergency stop button).
The general module also contained case studies of previous safety occurrences to communicate safety lessons.
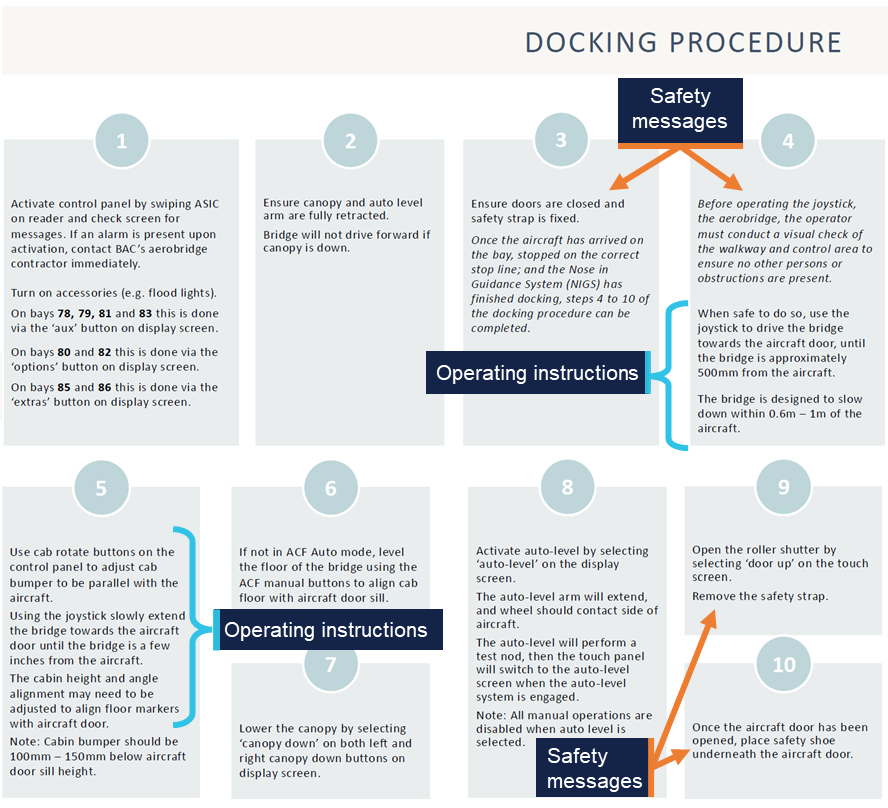
The BAC docking procedure detailed in the training module (Figure 15) instructed operators to:
first use the joystick to drive towards the aircraft door until approximately 500 mm (Step 4)
then use the cab rotate buttons to ensure the bumper was parallel with the aircraft (Step 5)
then use the joystick to extend further (Step 5)
further adjust the cabin height and angle to align the with the aircraft door (Step 5).
Figure 15: Docking procedure from the Jetway Apron Drive (International) module
Source: Brisbane Airport Corporation
The docking procedure did not detail rotation of the cab to obtain visibility of the aircraft prior to movement, or to stop movement if visibility was lost. Also, visibility of aircraft was not explicitly mentioned elsewhere in the 2 modules or online assessments.
ATSB review of available training material from other airports showed that at least one other Australian international airport emphasises visibility in aerobridge operator training and assessment material.
Interviews with involved personnel (including Operator 1 and 2) did not highlight that joystick operation was relative to the operator’s front facing window. The operator training and instructions were also silent on this feature of the joystick.
Train-the-trainer
BAC provided train-the-trainer service to designated airline staff (such as experienced airline aerobridge operators), who would then internally train and assess airline aerobridge operators. The train-the-trainer service was provided by a third party contractor, Aviator Operator Solutions, which was contracted by Airport Equipment (New Zealand) Limited, which in turn was contracted by Alstef, on behalf of BAC.
Trainers completed a train-the-trainer session every 2 years to maintain approved trainer/assessor status.
The training involved 2 days of classroom theory and concluded with an in-person demonstration and assessment.
Both operator 1 and 2 received in-person practical training and assessment by trainer/assessors from their company airline.
Operator assessment
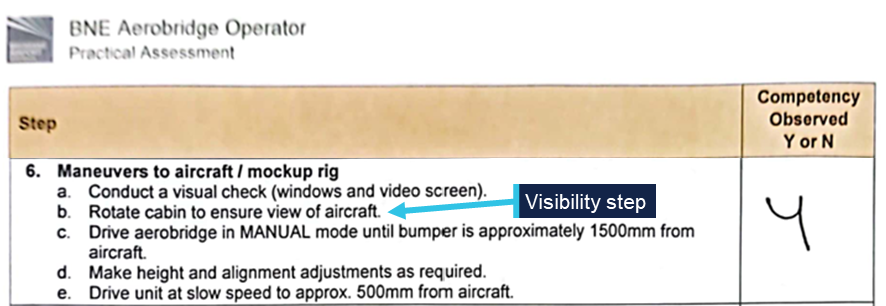
Assessment was conducted by an approved trainer/assessor using the BNE Operator Practical Assessment form (updated on 1 July 2022).
An operator was deemed competent once14 steps were observed by the trainer/assessor. Each step contained several sub-steps, however full competency was recorded (yes or no) for the full step (Figure 16).
One item, step 6b, of the assessment form required operators to rotate the cab to ensure view of the aircraft (Figure 16).
Once assessed as competent under the BNE Operator Practical Assessment, competency was valid for a maximum of 2 years before the operator would need to be reassessed.
Operator recency
Where an operator had not operated an aerobridge for 6 months, e-learning refresher training was required. The BAC security card system would automatically revoke the operator’s access if operator recency was not up to date.
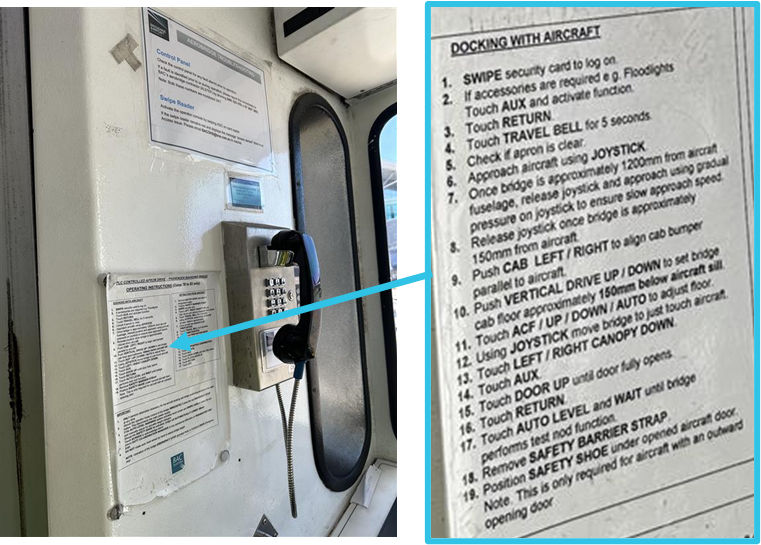
Aerobridge operating instructions
Laminated operating instructions were stuck to the cab wall next to the operator console (Figure 17). Step 6 of the instructions stated: ‘approach aircraft using joystick’ and steps 7–12 contained instruction to continue docking with control movements once the aerobridge was within 1.2 m of the aircraft.
These instructions did not require operators to obtain visibility of the aircraft, rotate the cab prior to movement or to stop movement if visibility was lost.
Figure 17: Laminated operating instructions
Source: ATSB
Visibility requirements for safe operation
Interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not widely understood as a critical safety step prior to the occurrences.
Both operators reported multiple previous successful aerobridge dockings, including at aerobridge 82, where they did gain visibility of the aircraft prior to docking, but not prior to initial aerobridge movement.
Insufficient visibility from the driving or operating position is recognised as an ergonomic hazard in the European design standard used for Australian aerobridges (EN 12312‑4:2024).
External visual reference points
While not formally documented or trained, both operators reported using alternate visual reference points. Operator 1 reported using the CCTV camera monitor (Figure 12) briefly to view the nose of the aircraft prior to the collision. Operator 2 reported using the ‘red line’ aircraft docking path (Figure 13) to help orient their direction of travel on occasion during normal operations, but not on this occasion. The height of the cab during operation may restrict visibility of these ground reference points, depending on the position of the aerobridge and the height of the operator.
Recorded information
BAC automatically recorded each time an operator swiped their aviation security identity card (ASIC) to activate an aerobridge at Brisbane Airport.
BAC also recorded Gate 82 aerobridge operations from a CCTV camera mounted on the terminal building (view shown in Figure 2 and Figure 3).
No cameras were installed inside the aerobridge cab and the CCTV camera monitor showing the underneath wheel area of the aerobridge was not recorded. The aerobridge 82 control system did not log or record specific user actions or system output while the bridge was in operation.
Regulatory information
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (the Part 139 MOS) required aerodrome operators to ensure that the apron safety management procedures were followed by any organisation that conducts operational activities on the apron. Where operations on an apron are controlled by third parties, such as airline operators, ground handling agents or other parties, the responsibility of apron safety remains with the aerodrome operator. Further guidance is available at Advisory Circular 139.C-13 v1.0.
Related occurrences
Two similar occurrences have been recorded at Brisbane International Airport Gate 82, occurring on 3 March 2011 and 19 February 2012.[7]
On 3 March 2011, the lower, right-hand corner of the aerobridge contacted the nose cone of a Boeing 737-800 during aerobridge docking. An internal investigation by the aircraft operator identified several contributing factors, including:
The aerobridge operator’s visual reference was impeded.
The slowdown sensors fitted to the aerobridge did not detect/sense the aircraft due to the approach angle of the aerobridge.
On 19 February 2012, the lower, right-hand corner of the aerobridge contacted the forward upper fuselage of a Boeing 737-800 aircraft during docking, penetrating the skin forward of the windscreen. The internal investigation by Brisbane Airport Corporation identified an option of determining via a risk management process whether retrofitting the existing aerobridges with extra sensor equipment at the side will minimise future impacts with aircraft fuselage.
Safety analysis
Introduction
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, employed by 2 separate airlines, intended to dock with the parked aircraft on the bay. However, the aerobridge collided with the aircraft cockpit windshield resulting in minor damage on both occasions with no recorded injuries.
This analysis will explore the visibility of narrow-body aircraft, the training provided to operators, the design of the joystick operation, the required mental rotation for operators to orient movement, and aerobridge safety features.
Visibility of narrow-body aircraft
From the home position, with the default home cab orientation, operators standing at the operational console have clear visibility directly in front via the front-facing cab windows. As such, there was good visibility of wide-body aircraft parked to the right of the aerobridge. However, due to the parking location of narrow-body aircraft on the bay and the design of the aerobridge 82 walls and windows, there was limited visibility of narrow‑body aircraft for an aerobridge operator at the control console prior to aerobridge movement.
Aerobridge 82 also lacked viewing windows that were available on some other aerobridges at Brisbane Airport. Such windows may have given the operators visibility towards aircraft parked in the narrow-body parking position. Without such windows, the operator was effectively restricted to seeing only what was in front of the cab.
This created a hazard for the safe operation of the aerobridge and increased the risk of an aerobridge collision with narrow-body aircraft.
Contributing factor
The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge.
Normal operations
While not explicitly emphasised in their training, both aerobridge operators understood that visibility of the aircraft prior to docking was required for safe operation. They reported that gaining visibility was immediate for wide-body aircraft from the home position and normally delayed for narrow-body aircraft. Both operators expected to gain visibility of the narrow-body aircraft following aerobridge movement. Their normal steps included simultaneous actions of rotating the cab, lowering the bridge, and moving toward the aircraft.
Both operators did not expect their actions to result in a collision and they did not believe their technique was incorrect or that it differed from other aerobridge operators.
The operators understood they were required to rotate the cabin left to dock successfully and likely pre-emptively rotated the cab left while moving the aerobridge, further reducing visibility. They did not believe that rotating the cab (to the right) to gain and maintain visibility was a critical step before moving from the home position. While there was an opportunity for the operators to become aware of the critical step when they completed their practical assessment, the step was not explicitly trained or emphasised via in-cab instructions.
Contributing factor
It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions.
Object orientation and mental rotation
The aerobridge operators believed that they were extending the aerobridge parallel to the aircraft. However, it is certain that both operators rotated the cab left from the home position during aerobridge extension, and this changed the aerobridge travel direction from parallel to diagonal towards the aircraft.
Due to the design of the joystick, cab rotation required operators to mentally rotate, and account for, the expected aerobridge movement. Both operators were unaware that their 3 o’clock frame of reference had rotated (after rotating the cab left) and did not perceive other visual information to make them aware of the diagonal movement.
The operators reported that the movement did not feel different to normal, and that they expected to gain visibility of the aircraft imminently.
However, in the absence of any contradictory feedback, the operators proceeded with an incorrect awareness of the aerobridge directional movement. It was likely that the complexity of the mental rotation required, was not widely understood by the operators and that the task complexity likely increased prior to both collisions because the cab was simultaneously orientated to the left during aerobridge extension, further blocking the operator’s already limited view of the aircraft on the bay.
Contributing factor
Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task.
Diagonal movement
Both operators reported pushing the joystick right (to a 3 o’clock position) to move the aerobridge parallel to the aircraft and did not perceive any conflicting information (in what they heard, saw, or felt).
Following the occurrences, one operator believed that the aerobridge system had performed an incorrect movement and was faulty (whereby the operator’s action of pushing the joystick right did not match the system behaviour). However, the system did not record user input (or system output) and no relevant pre-occurrence faults were recorded. Post-occurrence return to service inspections also found no faults.
CCTV footage of the occurrences shows that the aerobridge moved diagonally from the home position towards the aircraft at a 2 o’clock angle. The operators did not gain visibility of the aircraft because the cab had been rotated left (away from the aircraft), and because they did not perceive conflicting information, they were unaware of the parallel movement toward the aircraft.
Contributing factor
The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision.
Operator training and instruction gaps
Operator training material and in-cab instructions contained clear safety messages regarding the operation of aerobridges. The operator training material also included case studies of previous safety occurrences to communicate safety lessons. However, the importance of initial visibility was not highlighted in the safety messages and the case studies did not mention limited visibility operations, particularly due to the parking position of narrow-body aircraft at Gate 82 and some other international gates at Brisbane Airport.
By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions. The operator training material and in-cab instructions provided specific instructions for how to operate the aerobridge to successfully dock with aircraft, however omitted instructions to gain and maintain visibility of the aircraft as a critical first step.
While gaining and maintaining visibility of the aircraft may not be explicitly trained or emphasised via instructions, there was an opportunity for the step to be raised with operators at the time they were assessed. The practical operator competency assessment required operators to ensure aircraft visibility from the home position, before moving the aerobridge.
However, interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not understood as a critical safety step prior to the occurrences and it was normal to rotate the cab left while moving the aerobridge horizontally and laterally.
Contributing factor
The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue)
Safety features
The slow down and bumper contact sensors installed on the aerobridge were designed to aid docking and prevent damage to the aircraft when the aerobridge approached the aircraft from a forward direction (normal operations). The sensors would either slow or stop movement. There were no similar sensors installed on the side of aerobridge 82, therefore no sensors activated prior to the collisions when the side of the aerobridge and the corner of the cab approach the aircraft windshields.
Further, no alarms or alerts were presented to the users prior to the collisions, and no side cameras were installed to aid outside visibility of the aircraft blocked by the right side of the cab.
Contributing factor
Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side.
Emergency stop
An engineer on the ground at the time of the first occurrence detected the abnormal operation of the aerobridge and immediately attempted to alert the aerobridge driver (via hand signals) before activating the ground emergency stop button. Activation of the emergency stop button was a positive action to prevent further damage to the aircraft.
Other finding
In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the Ground handling events involving Boeing 737-838, VH-VZG, and Boeing 737-8 MAX, DQ-FAE, at Brisbane Airport, Queensland, on 18 June and 26 July 2025.
Contributing factors
The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge.
It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions.
Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task.
The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision.
The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue)
Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side.
Other findings
In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by Fiji Airways
Fiji Airways temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Glossary
ASIC
Aviation security identify card
BAC
Brisbane Airport Corporation
BNE
Brisbane
CASA
Civil Aviation Safety Authority
CCTV
Closed-circuit television
LAME
Licensed Aircraft Maintenance Engineer
Sources and submissions
Sources of information
The sources of information during the investigation included:
Brisbane Airport Corporation
the aerobridge operators and aerobridge trainer/assessors
Qantas Airways
Fiji Airways
Civil Aviation Safety Authority
Airport Equipment (New Zealand) Limited
video footage of the occurrences and other photographs and videos taken on the day of the accident
recorded data from the aerobridge access security card system.
References
CASA (Civil Aviation Safety Authority), (2023), Part 139 Apron safety management, Advisory Circular AC 139.C-13 v1.0, CASA
European Committee for Standardisation, (2024), Aircraft ground support equipment - Specific requirements - Part 4: Passenger boarding bridges (European standard EN 12312-4:2024). CEN.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Aerobridge operator 1
Aerobridge operator 2
Brisbane Airport Corporation
Qantas Airways
Fiji Airways
Civil Aviation Safety Authority
Airport Equipment (New Zealand) Limited
National Transport Safety Board.
Submissions were received from:
Brisbane Airport Corporation
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] The marshaller’s stop line indicates the designated position where the aircraft’s nose wheel must stop.
[2]The circular cab floor remained stationary unless the bridge was moving horizontally or laterally at the same time (separate operations to cab rotation).
[3]If the operator continued with the cab in the home orientation, with no rotation, and continued to hold the joystick at 3 o’clock, the aerobridge would continue to arc around to the right.
[4]The cognitive ability to rotate 2-dimensional or 3-dimensional mental representations of objects in one’s mind.
[5]Feature multiple and independent walkways, tunnels or arms that connect to an aircraft at different doors simultaneously.
[6]Jetway Systems Apron Drive 2 & 3 tunnel computerized smart bridge manual, June 1994.
[7]Note that the incident described in this report as ‘Occurrence 1’ was originally published as an ATSB Occurrence Brief (AB-2025-025).
Occurrence summary
Investigation number
AO-2025-047
Occurrence date
26/07/2025
Location
Brisbane Airport
State
Queensland
Report release date
02/04/2026
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Ground handling
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VZG
Serial number
34201
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 18 June 2025 at approximately 1845 Eastern Standard Time, a Boeing 737 was parked at gate 82 at Brisbane International Airport Terminal, Queensland, with the crew preparing the aircraft for disembarkation.
After the wheels were chocked and the park brake was released, the 2 flight crew members noticed that the aerobridge was approaching the aircraft from a high angle and further towards the nose of the aircraft than usual. The captain pressed the ground call switch on board, in an attempt to contact the engineer or other ground staff to advise them of their urgent concern that the aerobridge was likely going to impact the aircraft. As the engineer was no longer in the vicinity, they were unable to make contact before the aerobridge collided with the first officer’s windscreen, shattering the glass (Figure 1 left and right). Although the glass fragments landed on the first officer, they were uninjured in the incident. The flight crew reported that the ‘jolt of the impact was significant’, however, no passengers or cabin crew were injured.
Figure 1: Aerobridge position and impact with aircraft
Source: Operator
The aircraft operator provided the ATSB with images showing the aerobridge home position (Figure 2) and the aerobridge docked to a Boeing 737 (Figure 3). The bridge must be moved approximately 30 metres laterally from the home position and lowered to gain visibility of the aircraft prior to forward movement.
Figure 2: Aerobridge home position
Source: Operator
Figure 3: Aerobridge docked to a Boeing 737 aircraft
Source: Operator
The aircraft operator is conducting an internal investigation to determine factors that may have influenced the incident.
The ATSB notes that a second ground handling incident involving a different airline occurred at Brisbane International Airport Terminal, gate 82 on 26 July 2025 in which an aerobridge collided with a parked Boeing 737 during passenger disembarkation.
Safety message
This incident highlights that when in close proximity to an aircraft, the aerobridge must be moved with clear visual reference to the aircraft to prevent damage or injury.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-025
Occurrence date
18/06/2025
Location
Brisbane Airport
State
Queensland
Occurrence class
Serious Incident
Aviation occurrence category
Ground handling, Windows
Highest injury level
None
Brief release date
07/08/2025
Aircraft details
Manufacturer
The Boeing Company
Model
737-800
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 16 March 2019, two passengers were seriously injured when the basket of a Kavanagh B‑400 hot‑air balloon tipped over during vehicle-assisted deflation.
Prior to the accident, the balloon, operated as a scenic charter flight, landed without incident at a private property near Coldstream, Victoria.
Due to a lack of wind and the large size of the envelope, the crew elected to use the retrieval vehicle to assist by pulling the envelope over (by the crown line) during the deflation.
During this process, with 16 passengers and the pilot on board, the vehicle assisting inadvertently pulled the basket over, seriously injuring two passengers.
What the ATSB found
The ATSB found that the operator had not conducted a risk assessment around the use of a vehicle to assist in the deflation process. Although not required by regulations, the lack of a risk assessment likely left the operator and crew unaware of the risks associated with the vehicle-assisted deflation, and without appropriate procedures to control those risks. Consequently, a communication breakdown between the pilot and vehicle driver led to the basket tipping, and the passengers were unprepared and not in landing positions during the deflation process - increasing their likelihood of injury.
The ATSB also found that the Civil Aviation Safety Authority had not provided guidance to commercial balloon operators concerning the risks associated with vehicle‑assisted deflation. This likely contributed to the limited awareness commercial operators had of the risks associated with vehicle‑assisted deflation. Further, with substantial growth in the number of large, Australian-registered balloons requiring vehicle-assisted deflation, this is an ongoing safety risk.
What's been done as a result
The operator has updated their procedures to reduce the probability of a communication breakdown during the deflation process and is requiring the pilot to instruct passengers to assume landing positions during any vehicle-assisted deflations.
CASA has indicated they will publish an advisory circular, which will include guidance on deflation of hot air balloon envelopes using a vehicle to assist.
The ATSB has released a safety advisory notice (AO-2019-014-SAN-014) to all commercial balloon operators about the risks associated with vehicle‑assisted deflation, as identified in this report.
Safety message
This investigation highlights that gradual changes to operational procedures, while possibly perceived as inconsequential, have the potential to conceal new or emerging safety risks. A thorough assessment of any introduced changes should identify these new risks and allow their mitigation or reduction to an acceptable level.
This investigation also highlights that an increase in the number of aircraft and occupants (passengers and crew) exposed to a hazard has a compounding effect that, in a relatively brief period, can increase the overall risk significantly.
Context
Balloon deflation
All hot air balloons have a load ring known as a crown ring at the top of the envelope. Attached to the crown ring is a crown line, which is long enough to reach to the balloon’s basket. During envelope deflation, a vent at the top of the balloon is opened progressively to release hot air. To prevent the envelope collapsing on top of the basket in light wind conditions, a force is applied to the crown line to pull the envelope down and away from the basket.
For smaller balloons (generally less than 350,000 ft3), one or two persons can provide enough force by pulling on the crown line and walking away from the basket. For large balloons, the crown line can be attached to the rear of a vehicle that then drives slowly away from the basket pulling the envelope as it deflates.
Crew experience
The pilot obtained a private balloon pilot certificate in 1997 and commercial balloon pilot licence in 2000. At the time of the accident, the pilot had just over 2,000 hours (10 hours in the previous 90 days) as pilot in command.
The ground crew member driving the vehicle during the deflation had around 20 years’ experience as a ground crew member for Picture This Ballooning (PTB). The other ground crew member had been working in this position for the operator for around 4.5 years.
Aircraft information
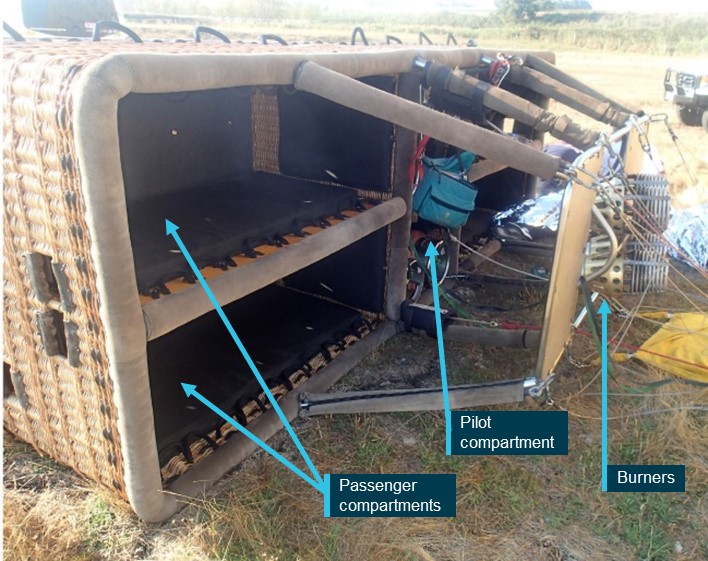
VH‑LNB was a Kavanagh Balloons B‑400 hot‑air balloon designed and manufactured in Australia with an envelope air capacity of around 400,000 ft3. The balloon was certified to carry up to 22 passengers and the basket had capacity to accommodate 20 passengers within four passenger carrying compartments, and a pilot in the central compartment (Figure 1). Heat was produced by a four‑burner liquefied petroleum gas system.
Meteorological information
The pilot reported reviewing several weather forecasts for the intended flight time, on the night before the flight and again on the morning before the flight. In addition, prior to, and during the flight, the ground crew launched pibals (pilot balloons) to check the prevailing wind speed at different altitudes. This information was communicated to the pilot.
The ATSB obtained weather data from the Bureau of Meteorology for Coldstream Airport (approximately 5 km from the accident site). It included observations recorded at 1‑minute intervals between 0700 and 0900 on 16 March 2019 (at ground level). Across that period, the winds were calm (0 kt) with no gusts.
Organisational information
Picture This Ballooning
Picture This Ballooning (PTB) was a charter balloon operator that had been operating for around 22 years. It had 15 balloons in their fleet, of which 11 were used for passenger charter operations. The operator had two balloons (one Kavanagh B‑350 and a B‑400) with envelope sizes of 350,000 ft3 or more. Sizes below this were less likely to require a vehicle to assist during deflation. PTB began using a vehicle to assist with in the deflation of their two large balloons about 12 months prior to the accident.
Communications procedures
The operator’s Operations manual (OM) contained the following procedure for radio communications:
Communication with retrieve crew will be via UHF radios with mobile phones as back up. Prior to launch the pilot must conduct a UHF radio check with the crew to ensure two-way communication is possible. During flight both parties shall maintain a continuous watch.
The operator’s crew procedures and training manual contained additional information regarding radio failure:
Use of mobile phone as back up
Recognise that the radio is not working if you are not receiving instructions
Pilot has a crew number and vise [sic] versa
Stay near the balloon and do not get too far in front
Try a second radio
It’s not that big a deal so long as you think what the pilot would want you to do.
Although not documented prior to the time of the accident, the process during vehicle‑assisted deflation, as reported by the pilot and the ground crew member driving, was that once the instruction to drive forward was given, the driver would continue until the pilot commanded them to stop.
Following the accident, the pilot identified that putting down the handheld radio and not maintaining communication throughout the entire process was a likely contributor to the accident.
Passenger safety briefings
The operator’s procedures contained in the OM required the pilot in command to conduct passenger briefings:
as to correct inflation procedures
inside basket on landing positions prior to lift off.
The OM also contained the following information regarding briefing of passengers:
Passengers are to be briefed on the ballooning experience in general and safety aspects of ballooning (e.g. the fan, landing positions, exiting the basket, etc). Pilots should make use of the PTB checklists and briefing cards found on board all PTB balloon basket.
Further, the OM contained the following information regarding the positioning of passengers in basket:
A physical demonstration of landing positions by the passengers must be conducted before take-off on each flight.
The pilot and a passenger reported that a safety briefing was conducted, upon arrival at the launch site, primarily regarding the hazards associated with the inflation fans (pre-boarding). Another briefing was conducted in the basket prior to launch (pre-flight) which included passengers demonstrating they could correctly assume landing positions. A final briefing, primarily concerning landing positions, was also conducted by the pilot around 10 minutes prior to landing (pre-landing).
In addition to the safety briefings, the balloon had safety cards on board that also contained safety information including a pictorial representation of the body position when in the landing position (Figure 2).
Figure 2: Picture This Ballooning’s on-board safety briefing cards
Source: Picture This Ballooning
Landing position
The Kavanagh Balloons Flight Manual contained procedures for fast landings, including:
When a high horizontal landing speed is expected, passengers should be made aware that the basket will tip forward and they should take a lower-than-normal landing positions to avoid being thrown out of the basket.
The pilot reported that during the vehicle‑assisted deflation the passengers were not in the landing position.
Crew’s awareness of the risk of tipping during vehicle‑assisted deflation
The pilot reported that at the time of the accident not noticing that there was a problem until the basket began to tip. In addition, while having previously observed baskets tipping due to wind, the pilot had not considered that the deflation vehicle could produce the same outcome. Further, the ground crew member driving the vehicle also reported not expecting anything to go wrong during the deflation process.
Civil Aviation Safety Authority
The Civil Aviation Safety Authority (CASA) is an independent statutory authority with the primary functions of conducting safety regulation of civil air operations in Australia and the operation of Australian aircraft overseas.
Passenger safety briefings
CASA’s Civil Aviation Advisory Publication: Passenger safety information: Guidelines on content and standard of safety information to be provided to passengers by aircraft operators (CAAP 253-02 V2.0), included specific guidance for balloon operators regarding passenger safety briefings during pre‑boarding, pre‑flight, pre‑landing final approach and landing.
The guidance did not contain information regarding passenger safety briefings during the deflation process.
Safety management system
CASA regulations did not require operators of balloon aerial work and charter operations to have a safety management system (SMS).
CASA have proposed Civil Aviation Safety Regulation (CASR) Part 131, which was available as an exposure draft until 30 September 2019, and scheduled to commence on 2 December 2021. Part 131 would have required balloon transport operators (currently charter operations) to have an SMS that is ‘…appropriate for the size, nature and complexity of the operator’s balloon transport operations’. The SMS must include:
…a safety risk management process, including:
(i) Hazard identification processes; and
(ii) Safety risk assessment and mitigation processes
In addition, the proposed Part 131 also contained the requirement for balloon transport operators to have a safety manager with
…sufficient relevant safety management experience to capably lead, manage and set standard to enable the operator to safely implement the operator’s safety management system…
and the responsibility for
…managing the operation of the safety management system including managing corrective, remedial and preventative action in relation to the system…
In a 22 November 2019 update, CASA provided a summary following the consultation period for Part 131:
To provide additional time to consult with industry on the requirements related to safety management systems and training and checking systems, CASA has removed the proposed regulations related to safety management systems (SMS) and training and checking systems for balloon transport operators (including the requirement for the two associated key personnel – the head of training and checking and the safety managers).
Large balloons in Australia
Multiple ground crew and pilots reported to the ATSB that the use of the vehicle‑assisted method is only used for balloons with envelope sizes of 350,000 ft3 or greater (some reported 400,000 ft3 as the minimum size). Balloons with smaller envelope sizes are more likely to be collapsed by hand in low wind conditions.
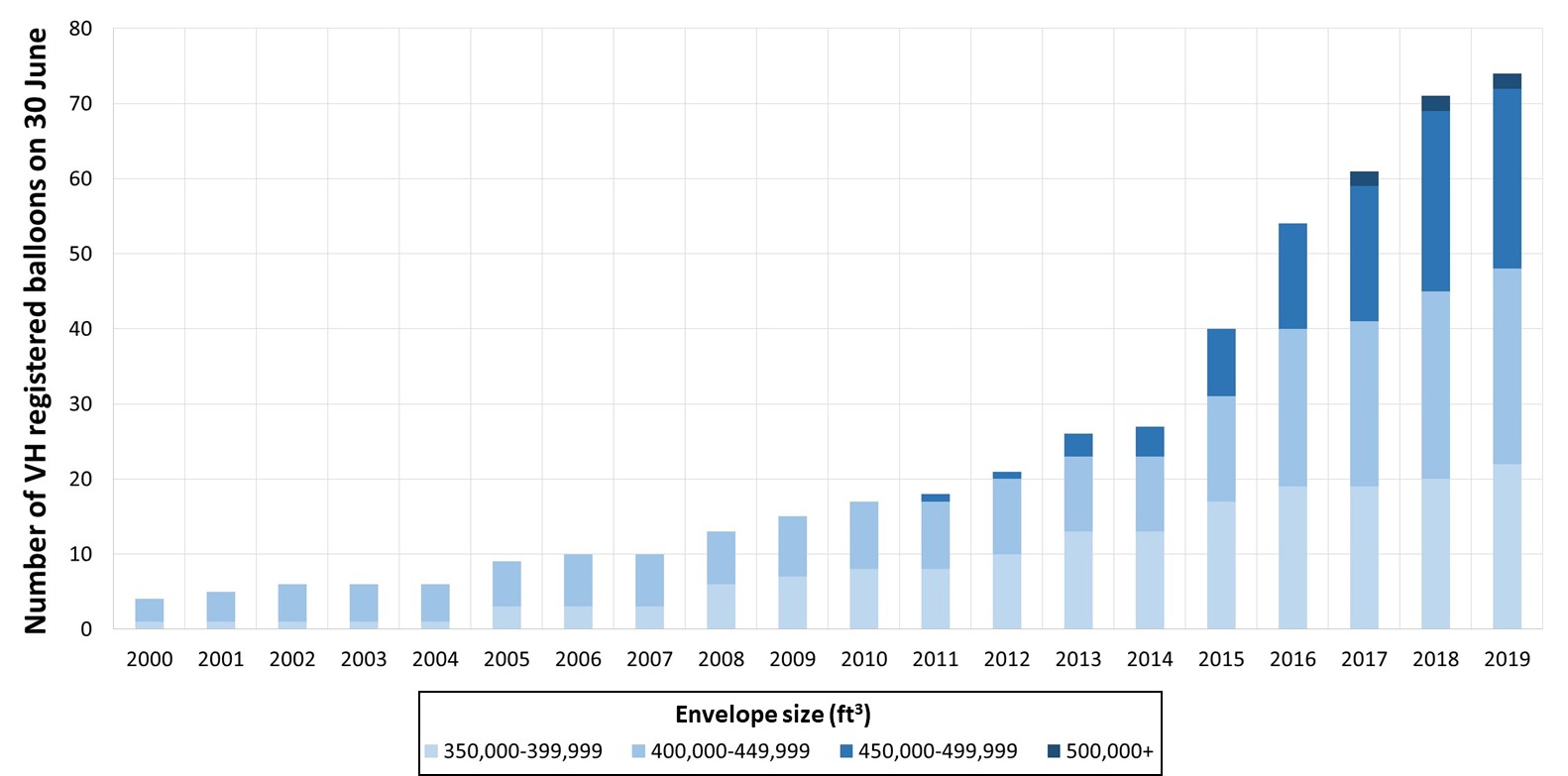
Figure 3: Number of large VH-registered balloons on 30 June between 2000 and 2019
The ATSB conducted an analysis of the trend in the risk associated with vehicle‑assisted deflation. This was based on vehicle-assisted deflation only being used for balloons with a capacity of 350,000 ft3 or greater.
Over the period mid‑2015 to mid‑2019, the number of large balloons registered in Australia increased by around 8-9 more balloons each year (Figure 3).
Given this trend, it is likely that the use of vehicles to assist during deflation will continue to increase over the period 2020–2022. In addition, the average size of these balloons (350,000 ft3 or greater) has also increased and accordingly, the average number of passengers per larger balloon flight has also increased.[6] It follows then, that, the number of passengers potentially exposed to injury associated with vehicle‑assisted deflation per flight will also probably increase.
Related occurrences
A review of the ATSB occurrence database found the following ground handling occurrences involving the use of a vehicle to assist in the deflation process:
Occurrence 201600589
At 0700 on 22 April 2016, the pilot of a Kavanagh Balloons B‑425 was seriously injured when the basket tipped during a vehicle‑assisted deflation. During the deflation, the pilot dropped the radio resulting in a communication breakdown with the driver of the vehicle. The pilot was then unable to command the driver to stop, resulting in the vehicle driving too far, causing the basket to tip. At the time of the accident, there was probably only one passenger still on board the balloon.
Following that occurrence, the operator involved implemented new procedures intended to reduce the likelihood and consequences of a communication breakdown during vehicle‑assisted deflation. This included the following information:
Communication needs to be very clear not only on the radio but visually as well. This is where the second crew member is vitally important, if for whatever reason radio comms are lost between the PIC [pilot in command] and vehicle this crew member needs to be able to convey information between basket and vehicle. Whilst anyone is pulling over an envelope, please limit radio transmissions in other balloons and retrieve vehicles, multiple people using the same channel will cause cancelling of transmissions, PIC and driver only to use radio during the pull-down procedure with the vehicle driver “reading back” instructions, this ensures the information is correct and understood. If multiple balloons are about to begin collapsing their envelopes using mobile phones is preferred to ensure continuous communication. Discuss hand signals between crew members before commencing procedure and if at any-time communication either visual or verbal is lost STOP and wait until comms are restored.
The new procedure also contained information intended to reduce the consequence of a similar accident:
While collapsing envelope the pilot is to remain inside basket and passengers are to adopt landing positions.
Occurrence 201809492
At 0630 on 31 December 2018, a passenger on board a Kavanagh Balloons B‑400 sustained a minor injury when the basket tipped during a vehicle‑assisted deflation. During the deflation, radio interference resulted in a communication breakdown between the pilot and the driver of the vehicle. The driver was unable to hear the pilot’s command to stop, resulting in the vehicle driving too far, causing the basket to tip. At the time of the occurrence there were 18 passengers on board the balloon.
From the evidence available, the following findings are made with respect to the ground handling event involving a Kavanagh B‑400 balloon, registered VH-LNB, near Coldstream, Victoria on 16 March 2019. Two passengers were seriously injured when, during deflation, the balloon’s basket was inadvertently tipped by the vehicle assisting with deflation of the envelope. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The pilot put down the handheld radio to operate the vent line, and the second ground crew member was not in an observable position for the driver, which led to a communications breakdown and limited their opportunity to promptly command the driver to stop to avoid the basket tipping.
The majority of the passengers were not in the landing position when the basket tipped, increasing their probability for injury.
Picture This Ballooning did not have any procedures for conducting vehicle‑assisted deflation. [Safety issue]
The pilot and ground crew were unaware of the risk of the basket tipping from the vehicle pulling the envelope during vehicle-assisted deflation.
Picture This Ballooning's safety risk management processes and practices were not sufficient to facilitate the identification of key operational risks associated with vehicle‑assisted deflation. [Safety issue]
Other factors that increased risk
The Civil Aviation Safety Authority provided no guidance for operators concerning the risks associated with vehicle‑assisted deflation. [Safety issue]
The occurrence
What happened
On 16 March 2019, at about 0700 Eastern Daylight‑saving Time,[1] a Kavanagh B‑400 hot‑air balloon, registration VH‑LNB and operated as a scenic charter flight by Picture This Ballooning, was being prepared for departure from a private property near Dixons Creek, Victoria.
The balloon operating crew conducted passenger safety briefings:
at the meeting point (including equipment that can be carried on board and what to expect during the flight)[2]
on the bus during the transit from the meeting point to the launch site (including conditions at the launch site and the inflation procedure), and
at the launch site prior to the passengers entering the basket.
Prior to take‑off, with the passengers positioned in the basket, the pilot also conducted a safety briefing which included the risks associated with a layover landing in windy conditions, and having all the passengers demonstrate they could correctly assume the landing position.[3] The two ground crew assisted the pilot by checking the passengers had understood the briefing and could physically adopt the landing position.
At around 0720, after the pilot and ground crew conducted pre‑flight and radio checks, the balloon lifted off with 16 passengers and the pilot on board.
During the flight, the ground crew were in communication with the pilot by radio to coordinate arrival at the planned landing site. At the landing site, prior to the arrival of the balloon, the ground crew launched a pibal[4] and observed that there was nil wind below 300 ft above ground level. This information was communicated to the pilot.
About 10 minutes prior to landing, the pilot conducted another passenger briefing concerning safety during landing. This included the requirement for the passengers to assume the landing position.
The balloon landed without incident at a private property near Coldstream, Victoria at about 0820, with the passengers all satisfactorily adopting the landing position.
Following the landing, the pilot began to shut down the burner system and waited for the two-ground crew to prepare to deflate the envelope. Due to a lack of wind and the large size of the envelope, the crew elected to use the retrieval vehicle to assist by pulling the envelope over (by the crown line) during the deflation. Then, by radio, the pilot instructed the driver in the vehicle to drive forward. The vehicle started to slowly move forward, at less than walking pace, pulling the envelope. The driver’s vision of the balloon’s basket was obstructed by the collapsing envelope. During this process, the second ground crew member (located next to the basket) and the driver could not see each other.
The pilot then put down the handheld radio to operate the vent line, which required both hands. The envelope began to deflate faster than anticipated and the fabric started to collapse directly on top of the basket and burners. The second ground crew member assisted by lifting the fabric away from the burners and passengers. The pilot picked up the radio and instructed the driver to ‘drive a little bit faster’. The pilot then put the radio back down on the top of one of the fuel tanks and proceeded to operate the vent line and talk with the passengers. The driver proceeded for another 5 to 6 m then started to slow down.
Shortly after, at around 0830 (10 minutes after landing), the basket began to tip (Figure 1). The pilot instructed the passengers to ‘hang on as best they could’ and did not have the opportunity to use the radio to command the driver to stop.
The second ground crew member jumped out of the way of the tipping basket. The pilot’s radio landed at second ground crew member’s feet. The second ground crew member then communicated with the driver to stop and quickly get back to assist.
The driver, unaware of what was happening with the basket, heard unintelligible sounds from the radio and decided to stop the vehicle.
Two of the 16 passengers were seriously injured[5] when they were propelled out of the basket as it tipped over. One of the passengers sustained two broken ribs and another was knocked unconscious for around 10 minutes.
The pilot and second ground crew member, who had both received first aid training about 8 weeks prior, began administering first aid to the injured passengers and called an ambulance. The driver, also trained in first aid, took control of the injured passengers and continued to administer treatment. Around 15 minutes after the basket tipped, an ambulance arrived, and the injured passengers were taken to Maroondah hospital. Both were discharged later that day.
The sources of information during the investigation included:
Picture This Ballooning
The Civil Aviation Safety Authority
The Bureau of Meteorology
Witnesses
Victoria Police.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Picture This Ballooning and the Civil Aviation Safety Authority.
Submissions were received from Picture This Ballooning and the Civil Aviation Safety Authority. There submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Safety issues and actions
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
Depending on the level of risk of the safety issue, the extent of corrective action taken by the relevant organisation, or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue safety recommendations or safety advisory notices as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description:Picture This Ballooning's safety risk management processes and practices were not sufficient to facilitate the identification of key operational risks associated with vehicle-assisted deflation.
Safety issue description: The Civil Aviation Safety Authority provided no guidance for operators concerning the risks associated with vehicle‑assisted deflation.
Additional safety actions
ATSB safety advisory notice to all commercial balloon operators
To accompany this report and encourage proactive safety action, the ATSB has released a safety advisory notice to all commercial balloon operators informing them of the risks associated with vehicle‑assisted deflation.
The ATSB advises all commercial balloon operators utilising vehicle‑assisted deflation methods to review their current operational practices in light of the findings in the ATSB investigation report AO-2019-014 with the aim of mitigating the risks associated with the procedure. This review should be conducted with emphasis on:
reducing the risks associated with a communications breakdown between the pilot and vehicle driver, and
include a review of the positioning of occupants within the basket to minimise the likelihood of injury if the basket tips during the vehicle‑assisted deflation.
Future study proposed by Picture This Ballooning
Action number: AO-2019-014-NSA-015
Picture This Ballooning has informed the ATSB that, at the earliest practical date, they intend to study the forces present during the vehicle‑assisted deflation process and to pass these results to other commercial ballooning operators.
Safety analysis
This analysis will discuss how and why the basket tipped over during the vehicle‑assisted deflation and the effect of the passengers not being in the landing position. The risk management of vehicle-assisted deflation will also be analysed from both the balloon operator’s perspective and the commercial balloon industry and regulator more broadly.
Communication breakdown and procedures
During the vehicle-assisted deflation, the driver did not have vision of the basket and the pilot (in the basket) put the hand-held radio down. Subsequently, the pilot was unable to pick up the radio in time to order the driver to stop the vehicle when it became apparent that the basket would tip. In addition, the second ground crew member was not in a position to effectively communicate with the driver during the deflation. The scenario collectively meant that no one could quickly communicate with the driver to prevent the basket tipping.
Picture This Ballooning (PTB) did not have specific procedures for vehicle-assisted deflation or communicating during the process. The general loss of communication (radio failure) procedure was not suitable during vehicle‑assisted deflation because there was no time in which to access an alternative means of communication in the event of a communication breakdown.
The normal communication practice for vehicle-assisted deflation was for the driver to continue until the pilot instructed them to stop. However, the pilot could have a very short time to instruct the driver to stop if they approached the point where the basket tips. This would require continuous radio communication between the pilot and the driver, which was lost when the pilot put down the radio to open the vent. While the communications procedure in the company’s operations manual required pilot and ground crew to ‘maintain a continuous watch’ during flight, it did not stipulate the same during deflation. However, if the pilot needed two hands to open the vent, an alternative means of communicating with the driver was required.
The vehicle-assisted deflation process did not effectively utilise the second ground crew member and that person was not required to be in a position to be able to communicate with the driver by an alternative means such as shouting or signalling.
The pilot and ground crew did not use standard communication phraseology during the vehicle‑assisted deflation. The lack of standard phraseology can increase the likelihood of miscommunication or delayed actions.
Use of passenger landing position
The landing position was designed to reduce the likelihood and severity of injury during layover landings. ATSB analysis concluded that the injury profile of passengers within a basket that tips during a vehicle‑assisted deflation would be similar to when a basket tips during a fast landing.
PTB did not have specific passenger positioning procedures for vehicle-assisted deflation, nor was there a specific passenger briefing for this process. In addition, the pilot was unaware there was a risk of the basket tipping, and accordingly, did not instruct the passengers to assume the landing position during the vehicle‑assisted deflation. As such, most of the passengers were not in the landing position during the deflation and were thus exposed to a greater risk of injury when the basket tipped.
Awareness of tipping risk
The pilot and ground crew was unaware that there was a risk of the basket tipping during the vehicle‑assisted deflation. A greater awareness of the risks associated with vehicle‑assisted deflation would likely have prompted greater vigilance during the process and thus a reduced probability of the basket tipping. Further, the pilot would have been more likely to brief passengers on the risk and instruct on use of the landing position.
Operator’s safety risk management processes
Before the accident, the operator had not conducted a safety risk assessment of deflation techniques, nor were they required to by current regulations or their own management processes and practices. As a result, the operator had not properly considered the risks of vehicle-assisted deflation and so had not considered writing specific safety procedures to ensure it was done safely and the crew was aware of the risks.
Following a similar accident, another operator working under similar conditions developed a new procedure for deflation. This included measures to reduce the likelihood of a communication breakdown[7] during vehicle‑assisted deflation and having passengers in the landing position during the process. This further indicates that if a risk assessment had been conducted by PTB, it is probable they would have identified communication breakdown and the risk of injury to passengers (if the basket tipped) as key operational risks requiring mitigation.
CASA guidance material
Guidance material produced by CASA did not contain information regarding passenger safety briefings during the deflation process.
Prior to the subject event, there had been two related accidents with similar contributing factors. More generally, the ATSB found limited awareness of any risks associated with vehicle‑assisted deflation in the commercial ballooning industry. It is likely that if guidance material had been issued by CASA on the risks associated with vehicle‑assisted deflation, it would have increased awareness of the associated risks with operators introducing large balloons to their charter operations.
As balloon charter operators are not presently required by regulation to have a safety management system (SMS), there was, and remains, a lower likelihood of these operators conducting risk assessments for changes in operations. Given another operator involved in a similar accident reported that they had not conducted a formal risk assessment of vehicle‑assisted deflation prior to the accident, guidance material from CASA could have drawn attention to the risks for these operators.
With the increase in the numbers of larger balloons registered in Australia, it is expected that the use of the vehicle-assisted deflation practice will similarly increase and will likely be used by a greater number of operators over time. Further, with larger envelope and basket capacities comes an increase in the numbers of passengers exposed to injury risk in the event of a basket tipping during a vehicle-assisted deflation. As such, this guidance will be important for helping educate other operators as they move to larger balloon operations in the future.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 31 March 2016, an Airbus A330-323, registered 9M-MTB and operated by Malaysia Airlines Berhad (Malaysia Airlines), was being prepared and boarded for a flight from Melbourne Airport, Victoria, to Kuala Lumpur, Malaysia. The captain engaged the aircraft’s park brake before carrying out an external inspection of the aircraft. The resulting lit park brake indicator light on the nose landing gear led the aircraft maintenance engineer to assume that the park brake would remain on. Thinking that the aircraft would remain secure, the maintenance engineer removed the main landing gear chocks out of sequence with the relevant procedure and without informing the others in the ground crew. The ground crews did not check the main gear chocks before removing the nose gear chocks to attach the tow tractor to the nose gear. Unaware that no chocks were in place, and out of sequence with the relevant procedure, the captain released the park brake on return to the flight deck. The aircraft rolled back about 3 m and struck the aerobridge. The aircraft’s forward-left door and hinges, and the aerobridge were damaged. There were no injuries.
What the ATSB found
The ATSB found that the ground and flight crew procedures were not well harmonised, leading to reduced cohesion between the crews, and that the tractor operator’s procedures did not match the way tasks were carried out locally. These problems reduced the likelihood that the respective procedures would be followed correctly. In addition, the flight crew and engineers did not explicitly convey their actions and intentions to the others, resulting in a number of missed opportunities to discover the resulting procedural errors.
What's been done as a result
The engineering company, tractor operator and Malaysia Airlines each planned or initiated safety action in response to this occurrence. The engineering company introduced standard procedures and initiated periodic operational safety inspections at all ports. The tractor operator developed a written procedure to incorporate local differences in work practices and improve coordination. Malaysia Airlines reported that it was planning to amend its procedures so that flight crews advise ground crews whenever the park brake is about to be released. As an interim measure, Malaysia Airlines sent A330 flight crews a reminder to communicate with ground crews before releasing the park brake to verify that chocks are in place.
Safety message
The ATSB stresses the importance of organisations ensuring that ground and flight crew procedures are harmonised to increase the likelihood that potential problems or mistakes are detected before causing harm. It is also important that local variations to procedures are formalised to reduce the risk of the inconsistent completion of tasks, and to improve the organisation’s ability to identify and address potential safety concerns. In addition, the ATSB encourages crews to highlight any procedural problems to their operator in order for them to be reviewed and enhanced as appropriate.
Importantly, when about to perform a key action like removing chocks or releasing the park brake, crews should consider checking with others to identify potential conflicts between tasks. This can reduce the risk of unintentional aircraft movement.
The occurrence
Sequence of events
On 31 March 2016, an Airbus A330-323, registered 9M-MTB and operated by Malaysia Airlines Berhad (Malaysia Airlines), was being prepared and boarded for a flight from Melbourne Airport, Victoria, to Kuala Lumpur, Malaysia. The aircraft had been parked in the bay for several hours following its previous flight, and was secured using wheel chocks under the left main and nose landing gears.
An engineering company provided an aircraft maintenance engineer (AME) and a licenced aircraft maintenance engineer (LAME) to prepare the aircraft for departure. A third company provided a towbarless tractor[1] and driver for pushback.[2] A technician was also refuelling the aircraft using a fuel truck parked under the aircraft’s wing. Ground crews could communicate with the flight crew via a headset.
At 0037 Eastern Daylight-saving Time[3], the aircraft captain engaged the park brake before disembarking to perform a pre-flight external inspection of the aircraft. The park brake had to be set to check the brake wear indicators and could only be controlled from the flight deck. A closed-circuit television recording showed the captain performing the inspection from 0043 to 0048.
Shortly after the captain checked the main landing gear chocks, the AME removed them from the left main landing gear in preparation for pushback. The AME was aware that this step was not in accordance with the normal sequence for pushback with a towbarless tractor, but thought that the aircraft would be secure because the:
nose landing gear chocks were installed
park brake indicator light on the nose landing gear had been on when it was recently checked by the AME, consistent with the brake being engaged (Figure 1).
Figure 1: Nose landing gear showing the aircraft’s park brake indicator light (note the wheel chocks in place)
Source: ATSB
Shortly after, the tractor driver arrived at the bay and boarded the tractor. The driver prepared the vehicle for docking to the aircraft’s nose landing gear. The tractor driver reported being unable to see whether the main landing gear chocks were in place due to the shadowing under the aircraft.
At 0051:03, the LAME started to remove the nose chocks so that the towbarless tractor could be docked. The AME assisted the LAME and together they finished removing the chocks at 0051:14. Both then moved off under the aerobridge, which was still in use by boarding crews and passengers. The closed-circuit television recording showed the refueller disconnecting the refuelling equipment from the aircraft’s under-wing filler point at about the same time as the nose chocks were removed.
The driver began to move the towbarless tractor into position to engage the nose landing gear at 0051:18. The closed-circuit television recording showed that the park brake indicator light turned off at 0051:21. This aligned with the flight crew’s recollection that the captain released the park brake on return to the flight deck. The captain later reported always doing this, expecting that the ground crews would inform him when it was necessary to apply the brake.
At 0051:27, as the towbarless tractor moved towards the nose landing gear, the aircraft began to move very slowly backwards. The refueller lowered the fuel truck’s lift a few seconds after the aircraft started moving. The towbarless tractor driver did not notice the aircraft’s movement at first. He continued forward and stopped when the tractor made contact with the aircraft’s nose gear tyres, then drove forward for another 3 seconds. This second movement was probably because the driver noticed the increasing distance between the tractor and the aircraft and automatically tried to bring them closer. The driver did not initially recognise that the situation was abnormal.
The aircraft’s slow movement was not immediately obvious to the flight or ground crews. The aircraft stopped after coming into contact with the aerobridge, having rolled backwards about 3 m in 22 seconds. Hearing the noise and realising that the aircraft had moved, the LAME radioed the flight crew to set the park brake. The captain completed this action at 0052:09.
The aircraft’s forward-left door was dislocated by the contact with the aerobridge (Figure 2). The door, hinges, and aerobridge were damaged and there was slight indentation of the fuselage skin forward of the door. There was no major structural damage. There were no injuries.
Figure 2: The aircraft’s forward fuselage showing the dislocated forward-left door. The slight indentation in the fuselage skin forward of the door is not visible. The aerobridge is shown retracted from its position when struck by the aircraft
Source: Melbourne Airport, modified by the ATSB
Pushback procedures
Engineer procedures
The engineering company used Malaysia Airlines procedures for ground handling. The procedure for the departure stage of a transit check included a step to remove all of the chocks after the aerobridge is detached from the aircraft. The procedure for pushback stated that ‘Chocks should not be removed from the main-gear until the tractor is fully secured to the nose‑gear’. It did not contain guidance for coordinating with a tractor driver.
Tractor operator procedures
The tractor operator used a set of written procedures as the basis for activities that varied across the organisation depending on local arrangements. Workers were trained according to these local requirements.
The written procedure for pushback with a towbarless tractor showed photographs of the pushback activity that included steps for a ‘walk-around check’. It also included confirming that the:
‘main gear [was] chocked’ prior to docking the tractor with the aircraft’s nose wheels
‘Chocks should not be removed from the main-gear until the tractor is fully secured to the nose-gear and brakes on [the] tractor set.’
At Melbourne Airport, these steps were omitted in practice, because the tractor operator’s work arrangements there did not include management of the wheel chocks. The procedure did not describe how a driver should coordinate with other ground crews when docking the tractor to the aircraft.
Flight crew procedures
The flight crew procedures included steps to:
set the park brake before carrying out an external inspection of the aircraft
check the park brake is set and release it only if the brakes are hot (that is, soon after landing) and chocks are in place
release the park brake after all aircraft doors are closed, pushback clearance is received from air traffic control and ground crew readiness is confirmed.
The procedures did not provide guidance or instruction on how to coordinate park brake release with ground crews.
The aircraft’s park brake was set for the captain’s external inspection of the aircraft. The resulting illumination of the park brake indicator light on the nose landing gear led the aircraft maintenance engineer to assume that it would remain set, though this was not confirmed with the flight crew. Thinking that the aircraft would remain secure, the aircraft maintenance engineer removed the main landing gear chocks.
Subsequently, the ground crews did not check the main landing gear chocks before the engineers removed the nose landing gear chocks to dock the towbarless tractor. The tractor operator’s written procedure included a step to check the main landing gear chocks, but in practice, the step was omitted at Melbourne Airport because of a local variation in the way the work was conducted. In addition, there was no corresponding step in the engineers’ procedures. As a result, the absence of main gear chocks remained undetected.
Separately, the aircraft captain was unaware that the docking process was underway and that no chocks were in place. Although the flight crew procedures stated that the park brake should only be released when the wheel brakes were hot (generally only shortly after landing), or after the aircraft doors were closed and with ground crew clearance, the captain released the park brake on return to the flight deck. In the absence of any braking mechanism, the aircraft commenced moving until it struck the aerobridge.
Lessons for effective teamwork
This occurrence highlights the importance of organisations ensuring that ground and flight crew procedures are harmonised to increase the likelihood that potential problems or mistakes are detected before causing harm, and of affected crews applying those procedures consistently. In addition, it is important that local variations to procedures are formalised to reduce the risk of the inconsistent completion of tasks, and improve the organisation’s ability to identify and address potential safety concerns.
Also highlighted is the importance of crews, when about to perform a key action, considering a check with others to identify potential conflicts between tasks. In this instance, such a check before removing chocks or releasing the park brake would likely have reduced the risk of unintentional aircraft movement.
Findings
From the evidence available, the following findings are made with respect to the ground handling occurrence involving Airbus A330, registered 9M-MTB and operated by Malaysia Airlines Berhad, which occurred at Melbourne Airport, Victoria on 31 March 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The aircraft maintenance engineer removed the main landing gear chocks before the towbarless tractor was secured to the aircraft and out of sequence with the normal operating procedures.
Consistent with local practices, neither the engineers nor the tractor driver checked that the main landing gear chocks were in place before attempting to dock the towbarless tractor to the aircraft.
The aircraft captain released the park brake out of sequence with the normal operating procedures.
Other factors that increased risk
The procedures provided to ground and flight crews by Malaysia Airlines Berhad and the towbarless tractor operator did not provide clear guidance or instruction on coordinating activities related to pushback and, in the case of the tractor operator, were informally replaced by local procedures. [Safety Issue]
Safety issues and actions
The safety issue identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The ATSB expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
The procedures provided to ground and flight crews by Malaysia Airlines Berhad and the towbarless tractor operator did not provide clear guidance or instruction on coordinating activities related to pushback and, in the case of the tractor operator, were informally replaced by local procedures.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk.
Action number: AO-2016-028-NSA-001
On 10 June 2016, the ATSB was advised by Aircraft Maintenance Services Australia (AMSA), the engineering organisation, of the following proactive safety action in response to this occurrence:
The engineering team that day received retraining in pre-departure and pushback operations. This included refamiliarisation with documented procedures, practical assessment and a requirement to perform a team safety brief on lessons learned.
AMSA began introducing standard aircraft arrival, turnaround and departure procedures to all ports. This will ensure that practices are standardised and that they are over and above client’s requirements.
AMSA commenced periodic operational safety inspections at all ports. These inspections include assessments of the standard procedures to identify opportunities for improvement.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
A passenger reported that incorrect techniques were used when refuelling the aircraft, with respect to the earthing of the aircraft. The report was correct, however, investigations revealed that the petroleum company and the CAA were in the final stages of negotiation to change the relevant Civil Aviation Orders (CAO's). Although not in accordance with the CAO's, the procedure used was not dangerous, according to the petroleum company representative and was acceptable to the CAA.
On 5 October 2010, at 2115 Eastern Standard Time, a Boeing Company 737-8FE, registered VH-VUR, had completed push back from parking bay 47 at Brisbane aerodrome, Queensland. The handling engineer disconnected the power push unit (PPU) from the aircraft and the pilot in command (PIC) received clearance from air Traffic Control (ATC) to taxi via taxiway C6.
As the aircraft moved away from the disconnect point on the apron, the PIC steered the aircraft to the left instead of right. This required the PIC to make a tight 2700 turn to continue along the apron to taxiway C6. During the 2700 turn, the dispatch engineer had to quickly manoeuvre the PPU to avoid a collision with the aircraft and, at the same time, avoid the hot exhaust emissions from the aircraft turbine engines.
This occurrence reinforces the importance of the flight crew maintaining situational awareness when manoeuvring aircraft.
As a result of this occurrence, the aircraft operator notified their flight crew and issued a flight crew operational notice.
On 1 June 2010, an Airbus A320-232 aircraft, registered VH-VQL, was being operated on a scheduled passenger service from the Gold Coast, Queensland (Qld) to Sydney, New South Wales (NSW). On arrival at Sydney the passengers commenced disembarking through the aircraft's forward and rear doors. During this time, a ground handler drove a cargo loader towards the rear cargo door of the aircraft in preparation for unloading baggage and cargo.
When the loader was about 3 m away from the aircraft, the ground handler stopped the loader, completed the relevant safety checks and then commenced moving towards the aircraft. After moving forward about 0.3 m the loader unexpectedly accelerated towards the aircraft. The ground handler reported he was unable to stop the loader or turn it away from the aircraft prior to it impacting the aircraft just forward of the rear cargo door. The aircraft, cargo loader and rear passenger stairs sustained serious damage. No one was injured in the incident.
A subsequent inspection by the operator identified that when the throttle pedal was depressed to the full open position, the pedal would intermittently become caught on the throttle stop due to a missing striker plate on the back of the pedal assembly.
As a result of this incident, the operator inspected all their cargo loaders of the same model to ensure they were not missing the striker plate. One loader was found to be missing a striker plate and this has since been repaired.
On 20 September 2009, at about 1630 Western Standard Time, a Boeing 737-400 (737) aircraft, had been pushed back from the domestic terminal onto the taxiway at Perth Airport, Western Australia (WA), when a technical fault was experienced. The aircraft remained in position to allow the flight crew to examine the fault. At the same time, a Boeing 717- 200 (717) aircraft, located in an adjacent bay, requested a pushback clearance from the surface movement controller (SMC). The SMC advised the 717 flight crew to contact their ground crew to discuss suitable pushback options. The 717 was pushed back with the aircraft kept as close to the terminal as possible. A clearance marshaller was located next to the left wing of the 717.
The flight crew of the 737 and the ground engineer for the 717 estimated that the wing of the 717 and the nose of the 737 were 11 m apart. However, the ground engineer for the 737 reported that the distance between the two aircraft was within 1 m and that as a result, he and another ground engineer with him may have been placed within the inlet and exhaust hazard area of the 717.
It was not possible to reconcile the differing accounts of aircraft proximity. However, the incident highlights the potential dangers associated with ground operations around jet aircraft and the need for particular care and attention when dealing with dynamic traffic situations.
As a result of this occurrence, the aircraft operator advised the Australian Transport Safety Bureau that it would:
align all documents defining the marshalling process to comply with the International Civil Aviation Organization standard and issue instructions to staff to ensure compliance
use marshalling equipment when it is available
recommend to the airport operator that parking bays be renamed.
In addition, The Civil Aviation Safety Authority advised that it will take the following action:
ascertain if any airports have procedures that require aircraft to reverse park on a bay
determine if any other airports use the term 'reverse bay'
ensure that the term 'reverse bay' is discontinued
discuss with operators the use of marshalling bats
ensure all operators use standard marshalling signals in accordance with CAO 20.3.
Analysis
Although uncertain as to the meaning of 'reverse bay', the flight crew thought the term was used to indicate the method of positioning the aircraft on the bay. Any uncertainty about the reverse manoeuvre should have been resolved by the crew before the aircraft was reversed.
The stop signal used by the marshaller was ambiguous as the arms were repeatedly crossed at chest height and not over the head. The operator's ground handling manuals included information that the use of marshalling bats would minimise the risk of misidentification. The opportunity for any misinterpretation of the stop signal used may have been minimised if marshalling bats had been used in this instance.
The intervention of the off-duty marshaller was timely and appropriate. Had he not taken this action, it is likely that the aircraft would have collided with the terminal building. The crew's uncertainty with parking on a reverse bay, and the marshaller's use of an unfamiliar hand signal combined to create doubt in the minds of the crew as to what the marshaller's intentions were.
Factaul Information
On 19 February 2005 at 1310 Eastern Daylight-saving Time, a de Havilland Canada DHC-8-102 aircraft, registered VH-TQR, was being operated on a scheduled regular public transport service from Canberra, ACT, to Sydney, NSW. On arrival at the terminal the crew was given marshalling instructions from ground staff to taxi onto bay 57R and stop. The pilot in command (PIC) then reversed the aircraft until instructed to stop by an off-duty marshaller who had seen that the tail of the aircraft was very near to the Terminal 2 building.
While en route to Sydney, the crew had contacted the operator's movement control officer to request a parking bay and to advise that the weather radar was unserviceable. The crew were advised to expect a 'reverse bay'. The crew discussed the requirement to park on a reverse bay. They were uncertain if the aircraft was to be reversed onto the correct stopping point. There was no discussion about the marshalling signals they would expect to see. The PIC referred to the aircraft's parking bay diagrams (see Appendix A) and was satisfied that the lead in lines painted on the tarmac and the signals of the marshaller would provide sufficient guidance.
After vacating runway 34 left, the crew was advised by the operator to park on bay 57 reverse (57R) so that engineers could repair the weather radar. Bay 57R is located near the southern end of Terminal 2 Pier B (see Figure 1) and required aircraft to park with the nose pointing away from the terminal.
Figure 1: Parking bay 57 (for illustrative purposes only)
The bay is also marked 57A for aircraft parked facing the terminal. Bay 57R was used to park aircraft in conditions of strong westerly winds, or if engineering staff required the nose of the aircraft to be facing away from the terminal building. The bay was commonly referred to by both ground staff and flight crew as 57 reverse or a reverse parking bay.
The PIC taxied the aircraft to Bay 57R, where it was marshalled into position and stopped by the crew when they observed the marshaller cross his arms once at approximately chest height. The position of the aircraft at that stage was correct for Bay 57R. However, the crew were concerned that the aircraft was positioned too close to a vehicle access road marked on the movement area and after briefly discussing between themselves the meaning of the signal used by the marshaller, decided that the instruction was to reverse. The PIC then reversed the aircraft and anticipated that the marshaller would signal them to stop at the correct point. The crew noted that the marshaller was walking toward the aircraft as it reversed, using hand signals which they interpreted as confirmation of the reverse manoeuvre, but which the marshaller intended as a signal to stop.
The marshaller had been told that the aircraft had a problem with the weather radar, which required that the ground power unit (GPU) be positioned away from the aircraft's nose. When the aircraft started to reverse the marshaller thought the crew were also positioning the aircraft away from the GPU.
Three off-duty marshallers were in a lunchroom, adjacent to bay 57R, when the shift supervisor observed the aircraft being marshalled onto the bay. He then saw the aircraft reversing and alerted the other two marshallers in the room to the situation. They observed the aircraft marshaller signal the PIC to stop the aircraft, by crossing his arms repeatedly at chest height. One of the off-duty marshallers ran out onto the tarmac to the aircraft's two o'clock position1 and signalled the crew to stop by crossing his arms over his head. The tail of the aircraft was estimated by that off-duty marshaller to be within 1 m of the terminal. The shift supervisor also went onto the tarmac and marshalled the aircraft forward to the correct bay 57R stop position.
The on-duty aircraft marshaller had received training on aircraft ground marshalling in accordance with the operator's ramp handling course document. The description for 'stop' in that document was in accordance with the Civil Aviation Safety Authority Civil Aviation Order (CAO) 20.3 Issue 5, Air Service Operations, Marshalling and Parking of Aircraft.
Stop is indicated by the arms to be repeatedly crossed above the head. (the rapidity of the arm movement related to the urgency of the stop, ie. the faster the movement the quicker the stop).
Other documentation used by the operator that included marshalling signals were a Customer Service Ground Handling Manual and a Flight Deck Engineering Manual that both stated:
Arms extended to full length above head in vertical position with bats or wands held steady. Widely accepted signal for use when there is no urgent stop requirement.
Although not in accordance with CAO 20.3, this signal was recognised by ground staff and by flight crew to indicate stop.
All of the manuals reviewed as part of the investigation stated that marshalling bats should be used to minimise the risk of misinterpretation. However, marshalling conducted by the operator during daylight was conducted without the use of marshalling bats.
1.The numbers on a clock are used to describe relative position, where 12 o'clock is directly in front. For example, a person or object observed abeam to the left of an aircraft would be said to be at 9 o'clock.
Summary
On 19 February 2005 at 1310 Eastern Daylight-saving Time, a de Havilland Canada DHC-8-102 aircraft, registered VH-TQR, was being operated on a scheduled regular public transport service from Canberra, ACT, to Sydney, NSW. On arrival at the terminal the crew was given marshalling instructions from ground staff to taxi onto bay 57R and stop. The pilot in command (PIC) then reversed the aircraft until instructed to stop by an off-duty marshaller who had seen that the tail of the aircraft was very near to the Terminal 2 building.
Occurrence summary
Investigation number
200500778
Occurrence date
19/02/2005
Location
Sydney, Aero.
State
New South Wales
Report release date
13/09/2005
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Ground handling
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada