The ATSB is investigating a near collision involving Cessna 172S, VH-KOJ, and Cirrus SR22, VH-XC5, about 22 km south-south-east of Melbourne Airport, Victoria, on 22 January 2026.
During cruise, the crew of the Cessna 172S detected the Cirrus SR22 in close proximity on a crossing track. The pilot of the SR22 also identified the conflict and conducted a descent below the lowest safe altitude to increase separation.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB investigation has included:
interviewing involved parties
reviewing recorded data
examination of other relevant documentation.
The continuing investigation will include examination and analysis of:
operational documentation
recorded data
related occurrences.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-007
Occurrence date
22/01/2026
Occurrence time and timezone
21:50 Australian Eastern Daylight Time
Location
About 22 km south-south-east of Melbourne Airport
State
Victoria
Report status
Pending
Anticipated completion
Q2 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Flight below minimum altitude, Near collision
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cirrus Design Corporation
Model
SR22
Registration
VH-XC5
Serial number
9217
Aircraft operator
Reserve Corporation Pty Ltd
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Sport and pleasure flying-Pleasure and personal transport
Departure point
Essendon Airport, Victoria
Destination
Essendon Airport, Victoria
Injuries
None
Damage
Nil
Aircraft details
Manufacturer
Textron Aviation Inc.
Model
172S
Registration
VH-KOJ
Serial number
172S12147
Aircraft operator
Oxford Aviation Academy (Australia) Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
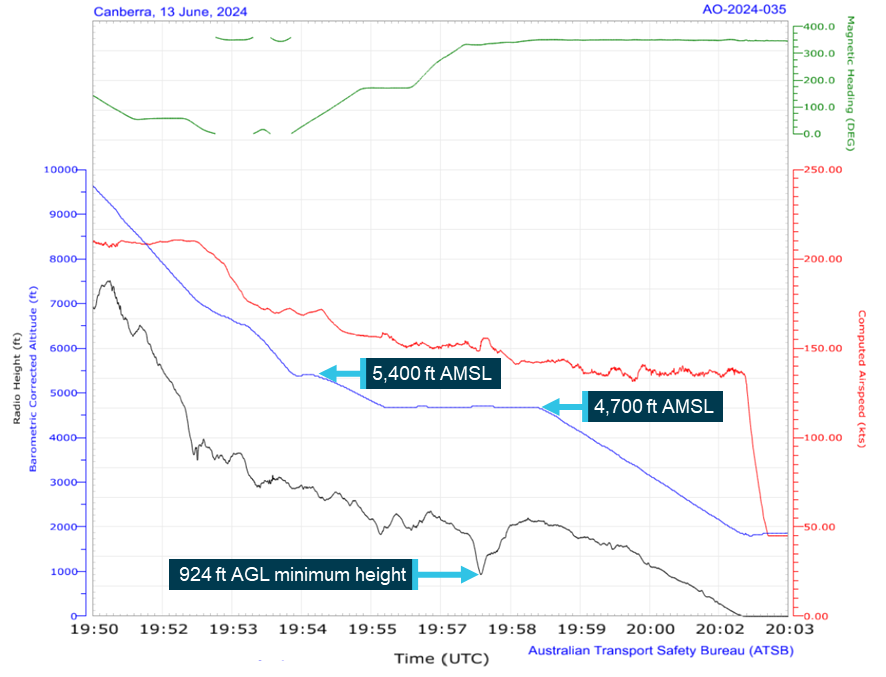
The ATSB is investigating a flight below minimum altitude involving Cirrus SR22T, VH-XXO, 10 km east of Canberra Airport, Australian Capital Territory, on 2 October 2025.
The aircraft did not adhere to the height or tracking requirements during approach and subsequently descended below the minimum safe altitude. The controller issued a safety alert, followed by a visual approach that did not meet the requirements of operations after last light.
To date, the ATSB investigation has included:
analysis of recorded and air traffic surveillance data
interviewing the pilot
reviewing weather and environmental conditions
reviewing operational documentation
reviewing related occurrences.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
The ATSB is investigating a descent below minimum safe altitude involving Boeing 767, VH‑XQU, 16 km north of Sydney Airport, New South Wales, on 10 September 2025.
During approach, the aircraft descended below the minimum safe altitude. The approach controller received a minimum safe altitude warning (MSAW) and issued a safety alert. The crew subsequently conducted a missed approach.
In the course of the investigation, the ATSB identified potential limitations in risk controls / organisational factors relevant to the occurrence that potentially contributed to the occurrence. Examination of these factors represent a significant increase in the scope of this investigation, and it has been upgraded from Short to Defined as a result (the ATSB's different levels of investigation are detailed here).
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
The ATSB is investigating a descent below minimum safe altitude and ground proximity alert involving a Cessna 560, registration VH-OHE, 23 km north-east of Perth Airport, Western Australia, on 13 August 2025.
Prior to commencing an instrument approach for runway 24 at Perth Airport, the aircraft descended below the minimum safe altitude. During this time flight crew reported that the autopilot disengaged and recalled observing an autopilot fail message on the primary flight displays.
The aircraft continued descending, and the flight crew subsequently received a terrain alert from the enhanced ground proximity warning system fitted to the aircraft. After responding to the alert, the flight crew continued the instrument approach and landed on runway 24.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
On 24 July 2025, a Cessna 206G, VH-ARS, taxied for departure shortly before last light for a flight from Archerfield Airport, Queensland, to Rockhampton with a flight instructor and pilot under training on board. The pilot was a qualified private pilot conducting training for a private instrument rating.
The flight was planned under the instrument flight rules, but the pilot informed air traffic control that they would conduct a visual flight rules departure. Air traffic control informed the pilot of the last light time and requested they confirm their departure would be before last light, which they did. However, shortly after departure, air traffic control issued them with a terrain alert and requested they expedite their climb. The pilot acknowledged and complied, and the flight continued without further incident.
What the ATSB found
The ATSB found that flight instructor elected to conduct a visual departure just prior to last light, which resulted in the aircraft operating below the minimum altitude after last light and the issuing of a terrain alert by air traffic control.
Safety message
The importance of planning, particularly around times when rules change, such as the transition from day to night, was previously promoted by the ATSB in the safety message for AO-2022-061. In this case the aircraft departed later than planned on a visual departure, rather than climbing within the circling area to the required safety height, which resulted in the terrain alert after last light.
Additionally, during the investigation the ATSB became aware of a potential conflict point overhead Archerfield Airport for instrument flight rules departures from Archerfield with arrivals to Brisbane Airport runway 01 right, currently being managed by ATC. This was known by the involved parties, with a project underway to develop a procedural instrument departure from Archerfield Airport.
The ATSB encourages the parties involved in this project to implement it as soon as reasonably practicable in order to provide improved traffic deconfliction.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 24 July 2025, at 1732 local time, a Cessna 206G, registered VH-ARS, taxied for departure from Archerfield Airport, Queensland, bound for Rockhampton with a flight instructor and pilot under training on board. The pilot was a qualified private pilot conducting training for a private instrument rating and was making all the radio calls. A flight plan had been submitted for the flight under the instrument flight rules[1] (IFR) with a departure time of 1730. The Archerfield air traffic control (ATC) tower had closed at 1700 and common traffic advisory frequency (CTAF) procedures applied.
The pilot requested their aircraft transponder code for the flight from Brisbane Centre (Centre) at 1732:57, to which Centre initially responded with their allocated code and other IFR traffic, and then queried if they would depart before 1739, which was last light. The pilot confirmed they would depart before 1739 and were ‘happy’ to do a visual flight rules[2] (VFR) departure to the north (see the section titled Departure from Archerfield – En route Supplement Australia), which Centre acknowledged. The instructor reported at interview that they were aware that last light was at 1739.
At 1736:01, the pilot reported on the CTAF that they were entering and rolling runway 28 right for departure to the north not above 1,000 ft. At 1736:50, Centre attempted to contact the aircraft to request they report at the runway holding point so that they could be transferred to Brisbane Departures (Departures) before take-off. However, noting that the aircraft had become airborne, they ceased their transmission.
The pilot made a departure call on CTAF and, at 1737:15, they reported to Centre that they were airborne in a right turn towards the Walter Taylor Bridge. Centre acknowledged their airborne report and instructed them to verify their altitude and remain clear of controlled airspace, to which the pilot reported they were passing 400 ft and climbing to 1,000 ft. At 1737:56, Centre instructed them to contact Departures for their clearance to enter controlled airspace.
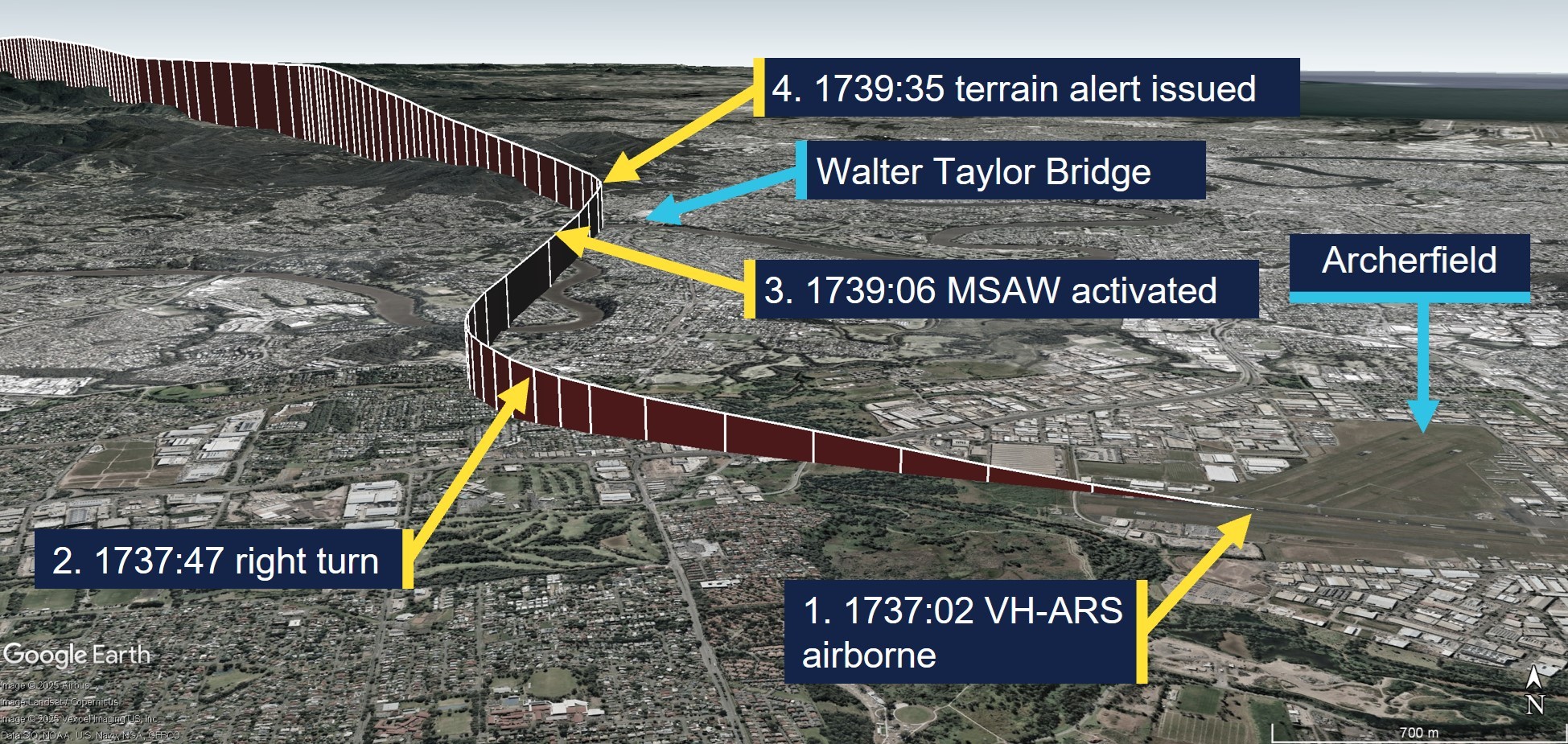
The pilot contacted Departures, and at 1738:39 received an initial clearance to climb to 3,000 ft on their flight planned route, which was then followed by a clearance to climb to 4,000 ft. At 1739:06, a minimum safe altitude warning (MSAW) activated for the aircraft on the ATC radar display. At 1739:35, the ATC radar indicated the aircraft was at 1,200 ft and Departures issued the pilot with a terrain alert due to the aircraft operating below the minimum altitude in their area (2,900 ft) after last light and requested they expedite their climb to ‘at least 3,000 ft’, which the pilot acknowledged and complied with. The flight continued without further incident and the departure flight path and key events are depicted in Figure 1.
Figure 1: Departure flight path from Archerfield with key events
Source: ADS-B Exchange and Google Earth, annotated by the ATSB
Context
Flight crew information
Flight instructor
The flight instructor held an air transport pilot licence (aeroplane) with multi-engine and single-engine class ratings, and a Grade 1 instructor rating with endorsements for instrument rating and night VFR training. The instructor’s last flight review was an instructor proficiency check on 25 March 2025, and they held a Class 1 aviation medical certificate, valid until 14 December 2025.
Pilot under training
According to the flight instructor, the pilot under training, who was also the aircraft owner, held a commercial pilot licence (helicopter) and a private pilot licence (aeroplane). They were studying for their private instrument rating, command instrument rating and night VFR rating exams at the time of the incident.
Meteorological information
The Archerfield Airport METAR[3] reports for 1700, 1730 and 1800 recorded light wind conditions, greater than 10 km visibility and no cloud detected. The aerodrome forecast was for CAVOK[4] conditions. The forecast and recorded conditions were consistent with the instructor’s report of clear sky conditions and they surmised that the good visual conditions might have influenced their decision to proceed with a VFR departure.
Recorded data
The ATC radar data indicated the aircraft was at 1,100 ft when the MSAW activated at 1739:06 and it had reached 1,200 ft when Departures issued them with their terrain alert. Recorded data, retrieved from ADS-B (automatic dependent surveillance-broadcast) Exchange indicated that the aircraft’s speed initially reduced from 125 kt to 120 kt after the clearance from Brisbane Departures to climb to 3,000 ft. The speed then reduced to 80 kt after the terrain alert was issued until the aircraft reached 3,000 ft, and then the speed trend reversed and recovered to about 100 kt as the aircraft reached 4,000 ft. The aircraft took about 5 minutes to reach 3,000 ft after take-off.
Departures from Archerfield
En Route Supplement Australia
The En Route Supplement Australia entry for Archerfield Airport included the following flight procedures and notes:
IFR ACFT [aircraft] departing YBAF [Archerfield Airport] directly into Brisbane Class C airspace [controlled airspace] may EXP [expect] delays due terminal area traffic density. VFR ACFT DEP [departure] after last light may also EXP delays.
Pilots electing to commence or terminate an IFR flight under the VFR should communicate such intention at the earliest possible time to ensure their arrival or departure is processed efficiently.
Departure from the Archerfield CTR [control zone] shall be 1,000 ft.
For a planned DEP [departure] track BTN [between] 310 and 019 DEG MAG [degrees magnetic]: - Depart via “Northern DEP” – track via Walter Taylor (Indooroopilly) Bridge [about 8 km north-north-west of Archerfield];
By day VFR ACFT (and IFR ACFT conducting a VFR DEP) are to depart via the following procedures:
- Advise intended DEP procedure (Northern, Southern, Eastern or Western) on TAX [taxi].
- IFR ACFT conducting a VFR DEP will receive a directed FREQ [frequency] transfer from AF TWR [Archerfield Tower – Brisbane Centre outside tower hours].
The instructor reported that they were aware of a history of delays for IFR departures from Archerfield and that they believed ATC preferred them to depart VFR and then request a change to IFR. They reported that they were in visual conditions and could see obstacles on the ground along their flight path when Brisbane Departures provided their clearance to resume their flight planned track and climb to 3,000 ft.
Standard instrument departure
For an IFR departure from Archerfield there were 2 options, which were the Archerfield standard instrument departure (SID – radar) or a climb within the circling area[5] to the required safety height for the departure track. The instructor reported that a clearance from ATC would be required to climb above 1,500 ft and that a SID would have been their preferred option for an IFR departure, which they believed that they could have done.
The Archerfield SID instructions for runway 28 right were to maintain the runway track until at or above 900 ft, then turn to the ATC assigned heading, and to maintain a minimum climb gradient of 4.3% to 1,900 ft. The SID indicated the 10 NM minimum sector altitude was 2,900 ft.
Airservices Australia procedures
Following external review of the report, Airservices Australia provided the following procedural information:
Its manual of air traffic services prohibits vectoring aircraft outside controlled airspace except when warranted by an emergency.
Consistent with the above, the Brisbane local procedures prohibit use of the Archerfield radar SID outside of tower hours. However, Airservices Australia is developing a procedural SID for Archerfield that will be available all hours. The project for the Archerfield procedural SID commenced in 2019 to facilitate improved deconfliction of IFR departures from Archerfield with IFR arrivals to Brisbane runway 01 right.
IFR arrivals to Brisbane runway 01 right pass overhead Archerfield at 3,000 ft (4,000 ft for runway 01 left), which is the same altitude ATC need IFR departures from Archerfield to climb to in the circling area before departing, which creates a potential traffic conflict point for ATC to manage. In addition, there is a wake turbulence hazard for light aircraft departing overhead Archerfield between jet aircraft arrivals at Brisbane. Furthermore, the known delays for IFR departures from Archerfield may pressure pilots to depart VFR in marginal weather conditions.
The reason for the attempt to transfer the incident aircraft to Brisbane Departures before take-off was to provide a clearance to become airborne and climb in the circling area to above the radar lowest safe altitude while ensuring separation of the IFR departure from Archerfield with traffic arriving and/or departing from Brisbane Airport.
Safety analysis
The flight from Archerfield to Rockhampton was planned as an IFR training flight with a flight instructor and pilot-under-training on board. Despite the IFR plan, the instructor elected to conduct the VFR Northern departure instead of conducting an IFR departure because they believed it was the preferred method for Brisbane ATC traffic management. While it was feasible that the aircraft would reach the required minimum altitude before last light based on their flight plan departure time of 1730, take-off actually occurred 7 minutes later than what was flight planned.
While the aircraft was taxiing for departure, ATC queried the pilot, who was making the radio calls, as to whether they would depart before last light. This query from ATC provided a prompt for the instructor and pilot to reconsider their plan. However, they elected to continue with the VFR Northern departure at 1,000 ft, which took the aircraft out of the circling area and into the 10 NM minimum sector altitude of 2,900 ft. Lift‑off occurred 2 minutes prior to last light and consequently they were below the 10 NM minimum altitude after last light and outside the circling area, which triggered a terrain alert from ATC.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight below minimum altitude involving Cessna 206G, VH-ARS, 6 km north-west of Archerfield Airport, Queensland, on 24 July 2025.
Contributing factors
The flight instructor elected to conduct a visual departure just prior to last light, which resulted in the aircraft operating below the minimum altitude after last light and the issuing of a terrain alert by air traffic control.
Sources and submissions
Sources of information
The sources of information during the investigation included:
ADS-B Exchange
Airservices Australia
Bureau of Meteorology
Civil Aviation Safety Authority
the flight instructor of the incident flight.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Airservices Australia
Civil Aviation Safety Authority
the flight instructor.
A submission was received from:
Airservices Australia
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[4]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[5]The circling area is determined by drawing an arc centred on the threshold of each usable runway and joining these arcs by tangents. For Archerfield Airport, the radius for each arc was 2.59 NM (4.8 km) and the circling altitude was 1,010 ft.
Occurrence summary
Investigation number
AO-2025-045
Occurrence date
24/07/2025
Location
6 km north-west of Archerfield Airport
State
Queensland
Report release date
24/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Flight below minimum altitude
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
U206G
Registration
VH-ARS
Serial number
U20606898
Aircraft operator
Peace Aviation Rockhampton
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On 15 August 2024, a Fairchild SA227-DC Metroliner 23, operated by Skippers Aviation, departed Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA, with 12 passengers and 2 flight crew on board. As the aircraft climbed, the crew noted high-temperature air and light smoke emanating from flight deck air vents.
As the smoke quickly increased, the crew commenced actioning the ‘smoke in aircraft’ checklist but required items of the checklist were not completed – the first officer did not don an oxygen mask due to difficulty with its usage, and the left bleed air system was not selected ‘off’. Instead, the crew commenced preparations for a return to Perth and subsequently, the left wing overheat light illuminated. The crew then actioned the ‘wheel well and wing overheat’ checklist and selected the left bleed air system ‘off’, which stopped the smoke ingress into the cabin, but elected not to complete the required action of extending the landing gear.
During the return to Perth, the aircraft deviated both above and below the altitude assigned by air traffic control including a descent to 639 ft below the lowest safe altitude. The crew then completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
What the ATSB found
The ATSB found that a failure within the left air cycle machine prior to departure resulted in hot engine bleed air and smoke entering the cabin and that items on the ‘smoke in aircraft’ checklist were not completed. Consequently, the smoke ingress into the cabin continued and during the return, the left air conditioning duct overheated, and the wing overheat light illuminated. Furthermore, the first officer’s decision not to don an oxygen mask increased their risk of impairment or incapacitation. A later decision not to extend the landing gear, as required by the response checklist, had the potential to increase risk if the wing overheat indication had been associated with a brake fire or wheel well overheat.
The ATSB determined that the workload associated with the in-flight response to the smoke in the cockpit and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision making.
During the return to Perth, the first officer readback an air traffic control altitude instruction as 2,000 ft AMSL instead of 2,800 ft AMSL. The controller did not identify or correct the error however, following a query from the crew, this was later corrected. Finally, after the assigned altitude had been confirmed by the crew, the aircraft descended below the lowest safe altitude. While the crew were advised of the deviation by air traffic control, the required ‘safety alert’ wording was not used.
What has been done as a result
Following the occurrence, the operator conducted a refresher training course for flight crew on emergency response briefings and a theory examination for flight crew on bleed air, pneumatics, pressurisation and fire warning systems. Practical training sessions were also held for flight crew on revised emergency procedures and the use of the crew oxygen system.
The operator also changed the Metroliner 23 flight crew training program to include a revised Line Oriented Flight Training (LOFT) program including more comprehensive oxygen system training and a presentation on the Metroliner 23 oxygen system.
Safety message
This occurrence highlights the importance of careful and methodical checklist completion. In this case, not completing a checklist resulted in increased risk to the flight and an avoidable increase to an already high workload. This in turn led to later decision-making and flight path management errors.
Additionally, the incident also emphasises the importance of flight crew familiarising themselves with the operation and use of the onboard emergency equipment. When exposed to an environment of smoke and fumes, flight crew must ensure that emergency breathing equipment is correctly utilised.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 15 August 2024, the crew of a Fairchild SA227-DC Metroliner 23 aircraft operated by Skippers Aviation, registered VH-WBQ and callsign ‘Skippy 5003’, taxied the aircraft to runway 24 at Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA. There were 12 passengers on board and the flight crew comprised the captain acting as pilot flying,[1] and the first officer acting as pilot monitoring.
As the aircraft taxied to the runway, the first officer noted that the cabin temperature was unusually warm and selected ‘full cold’ on the temperature selector.
At 0746, the aircraft departed runway 24 and turned left turn following the REPOK 1 standard instrument departure. As the aircraft climbed above about 1,500 ft above mean sea level (AMSL), the captain noted that the cabin temperature was warm and asked the first officer to select full cold on the temperature selector. The first officer responded by advising that full cold was already selected.
As the aircraft climbed above about 3,000 ft AMSL, the first officer attempted to reduce the high cabin temperature by selecting ‘auto’ on the temperature controller before then reselecting ‘full cold’. At about this time, the crew noted that vents on the captain’s (left) side of the flight deck (Figure 1) were blowing very hot air while the vents on the first officer’s (right) side blew the expected cool air.
Figure 1: Exemplar Metroliner 23 flight deck
Source: Matt Hayes, annotated by the ATSB
In response, the captain attempted to close the vent but found it too hot to touch. At the same time, they observed light smoke emanating from the vent. The smoke quickly increased, and the crew commenced the quick reference handbook (QRH) ‘smoke in aircraft’ checklist memory items.[2]
These memory items required the crew to don oxygen masks, establish communications (see the section titled Crew oxygen system) and consider donning smoke goggles. As the smoke was not impacting their vision, both flight crew members elected not to don smoke goggles. The captain donned an oxygen mask and made the required audio selections to establish communications using the mask.
The first officer encountered difficulties in adjusting the mask straps and could not get the mask to fit. They also did not make the required selections to establish communications using the mask, which resulted in the first officer hearing breathing noses through the headset and not being able to communicate using the oxygen mask microphone. As a result of these difficulties, the first officer elected not to wear the mask at that time.
The first officer retrieved the QRH ‘smoke in aircraft’ checklist to confirm the required memory actions had been completed and complete the remaining items of the checklist. For smoke emanating from a bleed air source, such as the air-conditioning system, the checklist required selecting the appropriate bleed air system ‘off’ (see the section titled Quick reference handbook). Before completing those checklist actions, the crew made a PAN PAN[3] broadcast advising air traffic control that there was smoke in the cockpit and that a return to Perth was required. The crew then began preparing for the return to Perth and did not complete the remaining items of the checklist at that time.
At 0751, the Perth Departures air traffic controller acknowledged the PAN transmission and instructed the crew to turn to a heading[4] of 360° and descend to 3,000 ft AMSL to commence the return. At this time, air traffic control also activated the Perth Airport emergency services.
Shortly after, the controller handed the crew over to the Perth Approach controller. One minute later, the approach controller instructed the crew to turn to a heading of 240° and descend to the lowest safe altitude of 2,800 ft AMSL. The first officer incorrectly read back the descent altitude as 2,000 ft AMSL, however the controller did not identify the error (Figure 2). The crew subsequently began descending the aircraft.
Figure 2: Flight path of VH-WBQ
Source: Airservices Australia and Google Earth, annotated by the ATSB
As the aircraft descended, the captain assisted the first officer with donning the oxygen mask and making the required audio selections to establish communications. From this time on, the use of the oxygen mask significantly reduced the intelligibility of the first officer’s radio broadcasts.
At 0756, the crew levelled the aircraft at 2,800 ft AMSL and contacted the controller to confirm the assigned altitude. The controller confirmed the altitude was 2,800 ft AMSL and the assigned heading as 180°. The first officer readback the altitude and heading instructions correctly.
At 0756, as the aircraft turned to the assigned heading, a descent commenced from 2,800 ft AMSL (Figure 3). About 50 seconds later, having observed the descent, the air traffic controller advised the crew to maintain 2,800 ft AMSL and that 2,800 ft AMSL was the lowest safe altitude. The crew immediately commenced climbing the aircraft, having descended to 2,338 ft AMSL (about 1,600 ft above ground level (AGL)).
Figure 3: Flightpath of VH-WBQ after the incorrect readback
Source: Airservices Australia and Google Earth, annotated by the ATSB
In response to the air traffic control instruction, the first officer replied stating ‘unable, Skippy 5003’ intending to convey that the crew were ‘unable’ to clearly hear the instructions. The controller interpreted the statement to mean that the crew were unable to maintain 2,800 ft AMSL and queried if the crew were in visual conditions. The first officer replied that the aircraft was not visual. At the same time, the air traffic control system generated a cleared level adherence monitoring (CLAM) alert for the aircraft. The controller, believing that the aircraft could not maintain altitude and aware that the Perth runway 24 instrument landing system (ILS) provided the lowest available minimum safe altitude, provided the crew with heading instructions directly to the ILS localiser.
While tracking toward the localiser, the aircraft continued climbing until 0757:57 when it reached 2,717 ft AMSL, before it once again commenced descending. At about this time, the crew returned to the ‘smoke in aircraft’ QRH checklist to complete the remaining items, but before these could be completed, the left wing overheat light illuminated continuously (see the section titled Quick reference handbook). The crew then actioned the relevant memory items of the ‘wheel well and wing overheat’ QRH checklist, including switching off the left bleed air system. Soon after switching off the bleed air, the crew noted that the smoke ceased. The checklist also required the crew to extend the main landing gear. As the aircraft was descending at a speed of over 220 kt (in excess of the 175 kt maximum landing gear extension speed), and wanting to expedite the return, the crew decided not to extend the landing gear at that time.
The aircraft continued descending and at 0758:23 reached 2,161 ft AMSL (about 1,200 ft AGL) before recommencing a climb. The air traffic controller observed the aircraft descend below the minimum safe altitude and, shortly after, a second CLAM alert was generated. The controller did not advise the crew of the low altitude as they believed the crew were unable to maintain altitude and that contacting them would only increase their workload.
At the same time, the crew commenced a right turn to intercept the ILS localiser and 12 seconds later, while still wearing the oxygen masks, the crew contacted the controller to request airport emergency services. The controller did not comprehend the broadcast and asked the crew to repeat the request. The crew repeated the request, but the controller again could not understand it. The controller did not query the crew further and commenced coordinating the handover of the aircraft to the Perth Tower controller. During this period, the left wing overheat light extinguished.
At 0758:41, the aircraft crossed the ILS localiser while climbing above about 2,800 ft AMSL. The climb and right turn continued until the aircraft levelled at about 3,000 ft AMSL for 7 seconds before recommencing a descent. The aircraft descended to 2,751 ft AMSL, before again climbing. The right turn continued for a further short period, followed by the aircraft commencing an intercept of the localiser from the left side. The aircraft climbed for a final time to 2,947 ft AMSL before again commencing a descent and levelling at 2,800 ft AMSL about 10 seconds later. The aircraft then maintained 2,800 ft AMSL until intercepting the localiser at 0800.
The crew completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
Context
Crew details
The captain held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The captain commenced flying with Skippers Aviation as a first officer in May 2022 before progressing to captain in April 2024 and had 1,484 hours of flying experience, of which 1,270 hours were accrued in the Metroliner.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer commenced flying with Skippers Aviation in April 2024 and had 509 hours of flying experience, of which 247 hours were obtained in the Metroliner.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Aircraft details
The Fairchild SA227-DC Metroliner 23 is a twin-engine turboprop regional airliner and an enhanced version of the Metroliner series that initially entered service in 1972. The aircraft was fitted with an analogue cockpit and was not equipped with an autopilot or flight director. VH-WBQ (Figure 4) was configured with 2 crew seats and 19 passenger seats.
Figure 4: VH-WBQ
Source: Lloyd Cartwright
Crew oxygen system
The aircraft was fitted with oxygen masks for use by the flight crew during a smoke event. After donning the masks, the following steps were to be followed to establish communications between the crew members and when using the aircraft radios:
select the microphone switch at the rear of the cockpit side panel from ‘boom’ to ‘mask’
deselect the cockpit button on the audio panel
to communicate with the other flight crew member, use the intercom push-to-talk button on the front side of the control column
to transmit using the radio use the push-to-talk button on the reverse side of the control column as normal.
If these steps were not fully followed, breathing noises would be heard through the crew’s headsets that could distract from, and disrupt, normal communications.
Air conditioning system
The aircraft was fitted with 2 identical air conditioning systems, one associated with each engine, and feeding conditioned air to the associated side of the flight deck and cabin. Each air conditioning system was supplied with hot, high pressure bleed air from the engine compressor through a shut‑off valve to the air cycle machine. The air cycle machine used ambient air to cool the bleed air and incorporated a mixing valve (for cabin temperature control).
An engineering evaluation of the left engine air cycle machine, conducted after the flight, found that it had overheated and that the cooling turbine was expelling oil. The hot air mixing valve was also found to be operating intermittently and sticking in various positions.
Quick reference handbook
The operator’s Metroliner 23 Flight Operations Manual included quick reference handbook (QRH) checklists with memory items specified within red brackets. This manual provided the following guidance for usage:
In a situation where the PM has had to reference the QRH to cross check correct memory item completion they will then announce to the PF that he/she is “Standing by with the ……..checklist”…Both pilots will then silently carry out the circuit breaker check at this point after which the PF then commands “Continue” when he/she is ready, and the checklist is read from the beginning.
The checklist must be announced by title and checklist notes must be read before proceeding with the checklist. A checklist is not completed until stating, “…. checklist complete”.
QRH items shall be read and actioned (any memory items will just be checked for completion) by the PM (where practical). A self-challenge and response technique is required.
Most of the PF attention should be directed at flying the aircraft; however, he must also be kept informed with the management process of accomplishing the appropriate procedures/checklist.
It would be appropriate for the PM to delay reading of the checklist procedure until the PF is in a position to monitor and assist if required. Confusion is often a problem area when conducting QRH procedures. Checklist procedures must not be rushed. It is important crews conduct checklists in a careful and controlled manner.
To stop smoke ingress into the aircraft from a bleed air source such as the air conditioning system, the ‘smoke in aircraft’ checklist required the crew to select the affected bleed air system ‘off’ (Figure 5).
Figure 5: Smoke in aircraft QRH checklist
Source: Operator, annotated by the ATSB
The wing overheat annunciator illuminated with either a steady or flashing indication. A steady light indicated a brake fire, wheel well or air conditioning duct overheat condition. A flashing light indicated a wing leading edge bleed air line failure or an overheated generator wire. The QRH checklist for a steady indication (Figure 6) required the crew to extend the landing gear to reduce the risk of a brake or tyre fire, overheat condition or a tyre explosion.
Figure 6: Wheel well and wing overheat, steady light QRH checklist
Source: Operator
Smoke and fumes exposure
The United States Federal Aviation Administration pilot safety brochure Smoke toxicity highlighted that smoke inhalation should be recognised as a very real danger. It also stated that ‘smoke gas levels do not need to be lethal to seriously impair a pilot’s performance’.
ATSB research report AR-2013-213 Analysis of fumes and smoke events in Australian aviation from 2008 to 2012: A joint initiative of Australian aviation safety agencies found that over 1,000 fumes/smoke events were reported to the ATSB and the Civil Aviation Safety Authority in the period from 2008–2012. The report highlighted that fumes associated with these events may have the potential to pose a health risk through eye/skin irritation, difficulty in breathing, incapacitation or illness. This was especially the case if the fumes were associated with particulates (smoke) or fire. However, while occurrences involving smoke were more likely to result in an outcome than a fumes‑only event, the research also found that ‘very few led to a serious consequential event (such as a forced landing) or outcome such as fire or crew incapacitation’.
Air traffic control safety alert
The air traffic control manual of air traffic services provided the following guidance for issuing a safety alert:
Unless the pilot has advised that action is being taken to resolve the situation or that the other aircraft is in sight, issue a safety alert prefixed by the phrase 'SAFETY ALERT' when you become aware that an aircraft is in a situation that places it in unsafe proximity to:
a) terrain;
b) obstruction;
c) active Prohibited/Restricted/Military Operating Areas; or
d) other aircraft.
As the crew prepared the aircraft for the return to Perth, it descended below the 2,800 ft altitude assigned by the air traffic controller. The controller identified the aircraft descending below the assigned altitude and contacted the crew stating, ‘maintain 2,800, 2,800 lowest safe’, but the broadcast was not prefixed by the required statement ‘safety alert’.
Meteorology
From soon after take-off until after the aircraft was established on the ILS approach, the flight was conducted in instrument meteorological conditions.[5]
At 0800, the Bureau of Meteorology (BoM) automatic weather station at Perth Airport recorded the wind as 5 kt from 222° magnetic. Cloud cover was recorded as few[6] at 1,267 ft above mean sea level (AMSL), scattered at 1,867 ft AMSL and broken at 3,067 ft AMSL. Visibility was recorded as 9,000 m in light rain showers.
Recorded data
Airservices Australia provided recorded air traffic control audio and surveillance data.
During maintenance actions following the occurrence, the aircraft electrical system was powered‑up and the cockpit voice recording of the incident flight was overwritten.
Flight data recorded by the aircraft’s flight data recorder, combined with recorded surveillance and audio data is presented in Figure 7.
Figure 7: Recorded flight data from 0756 to 0800
Source: ATSB
Safety analysis
Air conditioning pack failure and checklist error
The unusually high temperature noted by the first officer during the taxi to the runway, combined with the findings of the post‑event engineering examination, indicated that the left air cycle machine (ACM) failed prior to departure. This failure resulted in oil being expelled from the ACM cooling turbine and unconditioned hot bleed air entering the air conditioning system. This in turn resulted in the temperature control difficulties faced by the crew and, after take-off, smoke being emitted from the left side flight deck and cabin vents.
In response to the smoke, the crew actioned the memory items of the ‘smoke in aircraft’ checklist. This included donning oxygen masks however the first officer had difficulty in fitting the mask and establishing communications with the mask in use. As a result, the first officer elected not to wear the mask. This exposed the first officer to potentially harmful smoke and fumes. While the first officer reported no adverse effects from this exposure, it did increase the risk of impairment and incapacitation.
After completing the checklist memory items, the crew were required to action the complete ‘smoke in aircraft’ quick reference handbook (QRH) checklist to ensure all required actions had been completed. However, before completing the checklist, the crew commenced the actions required to return to Perth as they assessed that task was of higher priority. Had the QRH checklist been subsequently fully completed, the left bleed air would have been selected ‘off’ and this would have stopped the smoke ingress into the cabin. This action would also have likely prevented the later overheating of the air conditioning duct that triggered the ‘wheel well and wing overheat’ annunciation.
Workload and unsafe descents
The aircraft was equipped with analogue instrumentation with no flight automation to reduce flight crew workload and the smoke was detected immediately after take-off while the aircraft was operating in instrument flight conditions. These factors combined to create a high workload period for the relatively inexperienced crew.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing a take-off). These resources can change given the individual’s experience and training and the level of stress and fatigue being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternately, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
Examples of errors associated with excessive workload include:[7]
Flight crew may mishear, misunderstand or miss setting an air traffic control clearance provided during a period of high workload, leading to:
A deviation from assigned altitude (level bust)
controlled flight into terrain (CFIT)
loss of separation from other aircraft, or
an unstabilised approach.
The pilot becoming distracted from primary tasks resulting in an error in handling or managing the aircraft.
In response to the smoke and due to the high workload, the crew initially omitted or missed required checklist items (donning the oxygen mask and completing the ‘smoke in aircraft’ checklist). Had the checklist been completed with the left bleed air selected ‘off’ and the oxygen mask fitted, with communications correctly established, the additional workload associated with returning the aircraft to Perth would have been reduced. Furthermore, the increased distraction and workload associated with the response to the subsequent wing overheat annunciation would have been avoided.
Later, when the crew returned to complete the ‘smoke in aircraft’ checklist, they were interrupted by the wing overheat annunciator illuminating. The required response actions further compounded their workload and this likely influenced the decision error to leave the landing gear retracted. While the crew elected not to extend the gear due to their desire to expedite the return, the decision was not fully considered and would have exposed the aircraft to increased risk if the overheat condition had been associated with the landing gear.
The significant workload that the crew were subject to also adversely affected the crew’s management of the aircraft’s flight path. Without automation to reduce workload and support flightpath management, the aircraft deviated above and critically, twice considerably below the assigned and lowest safe altitude. The aircraft also passed through, and then deviated significantly left of, the localiser before the crew recovered and completed the approach.
Air traffic control factors
The clearance to descend to 2,800 ft was incorrectly readback as 2,000 ft by the first officer (who was not wearing the oxygen mask at that time), but this error was not identified by the air traffic controller. The purpose of a clearance readback is to ensure that the clearance has been correctly received and provides the controller an opportunity to correct any errors. As this error was not identified, there was increased risk of the crew descending the aircraft below the minimum safe altitude while still operating in instrument meteorological conditions. However, despite reading back the clearance incorrectly, the crew initially levelled the aircraft at 2,800 ft before querying and confirming the assigned altitude as 2,800 ft. Therefore, the non-identification of the readback error did not contribute to the aircraft descending below the lowest safe altitude.
Despite obtaining confirmation of the assigned altitude, very soon after, the aircraft began descending. The controller identified the aircraft descending below the assigned altitude and contacted the crew, advising them to maintain 2,800 ft as that was the lowest safe altitude. However, this broadcast was not prefixed by the required statement ‘safety alert’. Commencing such a broadcast with the phraseology ‘safety alert’ is designed to alert crews to safety critical information to ensure a response is prioritised and is particularly important during times of high crew workload. Despite the correct phraseology not being used, the broadcast achieved the desired crew response. The recorded data showed that immediately after the controller contacted the crew, the descent was stopped, and the aircraft commenced climbing. As such, the absence of a safety alert did not contribute to the occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the smoke in the aircraft and descent below lowest safe altitude involving Fairchild Industries SA227-DC, VH-WBQ, 25 km north-east of Perth Airport, Western Australia on 15 August 2024.
Contributing factors
A failure within the left air cycle machine resulted in hot engine bleed air and smoke entering the cabin soon after take-off. In response, the crew elected to return to Perth.
After commencing the ‘smoke in aircraft’ checklist memory items, the quick reference handbook checklist was not completed, and the left engine bleed air system was not selected off. As a result, during the return, the left air conditioning duct overheated, and the wing overheat light illuminated.
The workload associated with the in-flight response to the smoke in the aircraft and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision‑making.
On several occasions during the return to Perth Airport, the aircraft deviated above and below the assigned and lowest safe altitude. These deviations included a descent to 639 ft below the lowest safe altitude.
Other factors that increased risk
Following the smoke entering the cabin, the first officer initially elected not to wear the oxygen mask due to difficulties in donning the mask and then establishing communications. This increased their risk of impairment or incapacitation.
An incorrect altitude readback from the flight crew was not identified or corrected by air traffic control. Later, after the assigned altitude had been communicated, when the aircraft first descended below the lowest safe altitude, the crew were advised of the deviation by air traffic control, but the required ‘safety alert’ was not issued.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action taken by Skippers Aviation
Line oriented flight training
Action number:
AO-2024-048-PSA-01
Action organisation:
Skippers Aviation
In response to this incident, Skippers Aviation:
revised the Line Oriented Flight Training (LOFT) program to include more comprehensive oxygen system training
conducted the following refresher training for Metroliner 23 flight crew:
emergency response briefings
theory examination for the Metroliner 23 bleed air, pneumatics, pressurisation and fire warning systems.
practical training of the crew oxygen system
revised emergency procedures
updated the aircrew initial and recurrent training to include a presentation on the Metroliner 23 oxygen system.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
the aircraft operator
Civil Aviation Safety Authority
Airservices Australia
recorded data from VH-WBQ.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078-1084
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
the flight crew
the air traffic controller
Airservices Australia
Civil Aviation Safety Authority.
A submission was received from Airservices Australia. The submission was reviewed and did not result in any amendment to the report.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Memory items are checklist items required to be committed to memory to allow an immediate response to high priority abnormal events.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[5]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[6]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
On 1 July 2024, a Cessna 310R, registered VH-ZMB, was returning to Alice Springs from Willowra aircraft landing area, Northern Territory (NT), with only the pilot on board.
During an instrument approach in instrument meteorological conditions, the pilot reported receiving false indications from the attitude indicator and directional gyroscope. The aircraft deviated from the published approach path and tracked perpendicular to the approach track, below minimum sector altitude (MSA).
The pilot notified air traffic control at Alice Springs tower of the situation, before obtaining a clearance to track from their present position back to the initial instrument landing system approach point, for a subsequent attempt at landing.
A second approach was then flown, followed by a successful landing at Alice Springs Airport.
What the ATSB found
The ATSB found that the pilot, whilst established on the ILS approach to Alice Springs, likely experienced spatial disorientation that led to an undesired flight path, below the MSA.
In their state of distress, the pilot did not broadcast a PAN PAN call notifying air traffic control of their situation. Further, air traffic control did not issue a safety alert, which would have alerted the pilot that they were in unsafe proximity to terrain and needed to climb immediately. This was also influenced by the pilot not broadcasting a PAN PAN, but could have been made independently.
Once the pilot was outside of the required tolerances for the instrument approach and below the MSA, the pilot did not conduct a missed approach, remaining below minimum sector altitude for an extended period.
Other factors that increased the risks identified in this investigation include post‑occurrence fault finding that found the artificial horizon exhibited deviations outside the manufacturer’s required tolerances. Additionally, the pilot’s choice to not make use of the autopilot for the approach may have increased their workload and the subsequent risk of spatial disorientation during the instrument approach procedure.
What has been done as a result
The operator has since introduced an automation policy for the use of autopilot in instrument meteorological conditions and in high workload single-pilot operations.
Safety message
Pilots should not hesitate to report an urgent condition when encountering situations that may not be immediately perilous but significantly increase risk. Broadcasting a PAN PAN call when there is uncertainty about the safety status of the aircraft will alert ATC to the need for immediate assistance.
Air traffic control has a duty of care to provide safety alerts to pilots on becoming aware that an unsafe situation such as proximity to terrain has, or may, occur.
Once an aircraft is no longer on an established approach path and doubt exists as to its lateral position and location, a missed approach should be conducted, including an immediate climb to achieve a safe altitude, clear of terrain.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 1 July 2024, a Cessna 310R, registered VH-ZMB, conducted a passenger transport flight[1] to Willowra aircraft landing area, NT, and was repositioning[2] to Alice Springs, NT, with only the pilot onboard.
At approximately 1020 local time, the pilot commenced an instrument landing system (ILS) approach[3] for runway 12 at Alice Springs Airport. This approach was manually flown (not utilising the autopilot system), in instrument meteorological conditions.[4]
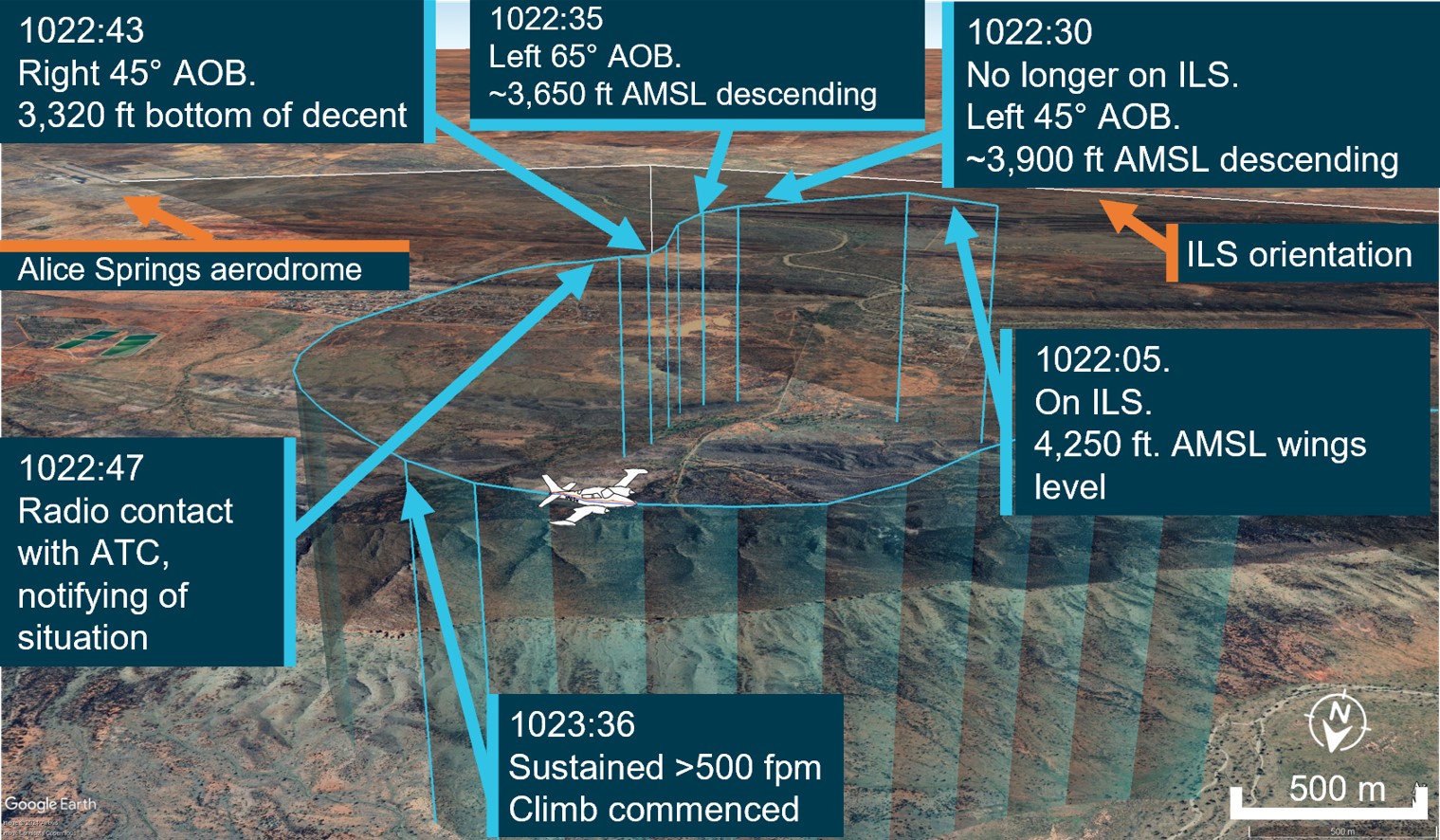
At 1022:05, the aircraft was established at 4,250 ft above mean sea level (AMSL) on the approach into Alice Springs Airport on the published ILS approach profile. About 25 seconds later, the pilot recalled receiving erroneous instrument indications from the artificial horizon (AH). At 1022:30, flight data showed the aircraft departing the ILS to the left, and tracking at a perpindicular direction from the approach path with unusual aircraft bank angles (AOB) (Figure 1).
Figure 1: VH-ZMB flight path
Source: ATC recordings and recorded flight data, overlaid on Google Earth and annotated by the ATSB
At 1022:47, the pilot contacted air traffic control (ATC), using their callsign twice. The pilot reported an issue with the instruments and requested clearance to commence a second approach. The ATC controller observed, and ATC recordings indicate, a level of stress in the voice of the pilot at this time.
ATC subsequetly cleared the pilot to climb to 5,500 ft and to track directly to the initial approach fix for the ILS (position LISZT).
At 1023:36, nearly a minute after obtaining a clearance from air traffic control and over a minute from leaving the ILS profile, the pilot commenced a sustained climb.
Recorded flight data indicated that during this time, the aircraft was below the minimum sector altitude of 4,300 ft and tracking towards rising terrain. The aircraft came within its closest proximity to terrain as it passed the ridgeline at about 810 ft above ground level.
At 1024:30 the pilot acheived an altitude of 4,300 ft enroute to position for a second approach.
A subsequent ILS approach was then flown into Alice Springs, followed by a successful landing.
Table 1: Sequence of events
Time: local
Description of event
1022:05
On ILS, wings level, 4,250 ft. Standard rate of descent (ROD)
1022:30
No longer on localiser (LOC), AOB 45° left, ~3,900 ft, descending
1022:35
Tracking greater the 90° off LOC, AOB 65° left, ~3,650 ft descending
1022:43
Tracking greater than 90°of LOC, AOB 45° right, bottom of descent ~3,320 ft
1022:47
ZMB – Tower broadcast
VH-ZMB: ‘ZMB, ZMB we’ve got incorrect AH [artificial horizon] information we have lost glidepath request tracking direct to LISZT…Currently at 3,700…’
ATC: ‘Climb to 5,500 track direct to LISZT’
1023:16
Closest point of approach to the terrain was approximately 810 ft recorded
1023:36-38
Sustained climb begun with >500 fpm climb. Sustained 15° AOB left (controlled), ~3,800 ft
1024:30
10 NM minimum sector altitude (MSA) achieved 4,300 ft
Source: ATC recordings and recorded positional data tabulated by the ATSB
Context
Pilot qualifications and experience
The pilot held a commercial pilot licence (aeroplane) and a valid class 1 aviation medical certificate. The pilot reported a total flying time of 386 hours with about 66 of those being on the Cessna 310. The pilot obtained a multi-engine aeroplane instrument rating in February 2024. The pilot reported accruing 27.3 total hours of instrument flight time with 5.7 hours being accrued in the last 90 days. The pilot had been employed with the operator since April 2024 and had completed their Operator Proficiency Check – IFR [5], on 17 May 2024.
Aircraft
The Cessna 310R is a twin-engine, low-wing, 6-seat, unpressurised aircraft equipped with retractable landing gear. The aircraft was manufactured in 1976 and had greater than 16,600 hours recorded on the maintenance release. VH-ZMB was fitted with Garmin 430W avionics, coupled with a traditional avionics suite (Figure 2).
Figure 2: Photo of cockpit instruments from perspective of left (pilot) seat
Source: Operator annotated by the ATSB
The pilot reported that placement of the standby artificial horizon on the far right‑hand side of the instrument panel (Figure 2) precludes the pilot from observing angles of bank (especially to the left). However, the pilot also reported utilising the standby AH as the primary means of spatial orientation, both during the occurrence and post‑occurrence to fly the second approach and identified that recovery to a safe altitude was ultimately slowed by the significant workload of stabilising the aircraft on a limited instrument panel.
Weather conditions
Weather conditions in the Alice Springs terminal area at the time of the occurrence were identified as a moderate south-easterly wind of 10 kt, with greater than 10 km of visibility. The cloud was reported as scattered (between 3–4 oktas[6]) at 900 ft, broken (between 5–7 oktas) at 1,300 ft and overcast (8 oktas) at 2,400 ft above ground level. The pilot reported the approach was conducted in instrument meteorological conditions and recalled being in stratiform cloud [7] from 7,000 ft to 2,500 ft AMSL.
Instrument landing system approach
The Alice Springs ILS runway 12 initial approach fix is a waypoint designated as LISZT which is about 15 NM (27.8 km) from the end of runway 12. The approach descent commences at 11.5 NM (21.2 km) from the runway 12 threshold, on a standard 3° descent profile. The missed approach procedure is to track 116° magnetic and climb to 5,500 ft AMSL.
Minimum sector altitude
Minimum sector altitude (MSA) is the lowest altitude which will provide a minimum clearance of 1,000 ft above all objects located within a specified area. This specified area is contained within a circle, or a sector of a circle of 25 NM (46.3 km) or 10 NM (18.5 km) radius centred on a significant point.
In the case for Alice Springs, the significant point being used as the datum reference point is the Alice Springs VHF Omni Directional Range (VOR) station[8].
The 10 NM MSA in the area around Alice Springs Airport is 4,300 ft AMSL.
Missed approach procedures
The missed approach procedure plays a pivotal role in instrument approach safety. It provides a standardised procedure for managing an aborted approach and landing attempt, ensuring appropriate terrain clearance to safely conduct flight operations in diverse environmental conditions.
Section 15.11 of the Part 91[9] Manual of Standards contains specific circumstances where a missed approach must be conducted.
A summary of these circumstances is as follows:
during the final segment of an instrument approach, where the aircraft is not maintained within the applicable navigation tolerance for the aid in use
when the required visual reference is not established at or before reaching the missed approach point from which the missed approach procedure commences
when a landing cannot be made from a runway approach, unless a circling approach can be conducted in weather conditions equal to or better than those specified for circling
when visual reference is lost while circling to land from an instrument approach.
Procedures outlined in the Aeronautical Information Publication (AIP) state that a missed approach must be conducted under certain conditions if the aircraft is below MSA. These conditions include, but are not limited to:
• issues arising with the radio aid,
• visual reference not being established, and
• a landing cannot be effected from the runway approach.
Operational procedures require that during a missed approach manoeuvre, an immediate climb is carried out to achieve an altitude that will remove the aircraft’s exposure to the risks of collision with terrain.
Instrument approach procedures
An instrument approach or instrument approach procedure (IAP) is a series of predetermined manoeuvres for the orderly transfer of an aircraft operating under instrument flight rules from the beginning of the initial approach fix to a landing, or to a point from which a landing may be made visually.
An IAP enables a descent below the MSA, positioning the aircraft to safely approach and land.
Operations below MSA increase the risk of collision with terrain or obstacles which are an immediate threat. Maintaining the published instrument approach path assures the pilot of obstacle clearance below the MSA. Outside of these areas, while below the MSA and in instrument meteorological conditions (IMC), separation from terrain and obstacles cannot be guaranteed and the pilot must conduct a missed approach procedure.
Recorded data
Automatic dependant surveillance broadcast (ADS-B) Exchange and Flightradar24 data was collected by the ATSB and was supplemented with OzRunways data provided by the pilot.
ATSB analysis combined the ADS-B flight data and the OzRunways aircraft track data to ascertain the track position and orientation of the aircraft during the occurrence.
At 1022:30 the aircraft deviated significantly to the left of the approach path resulting in the aircraft no longer being established on the ILS approach. The aircraft was below the MSA at 3,900 ft and continued to descend to the lowest point of 3,320 ft.
About 35 seconds later the aircraft crossed a ridgeline, further reducing the vertical separation with terrain to 810 ft above ground level.
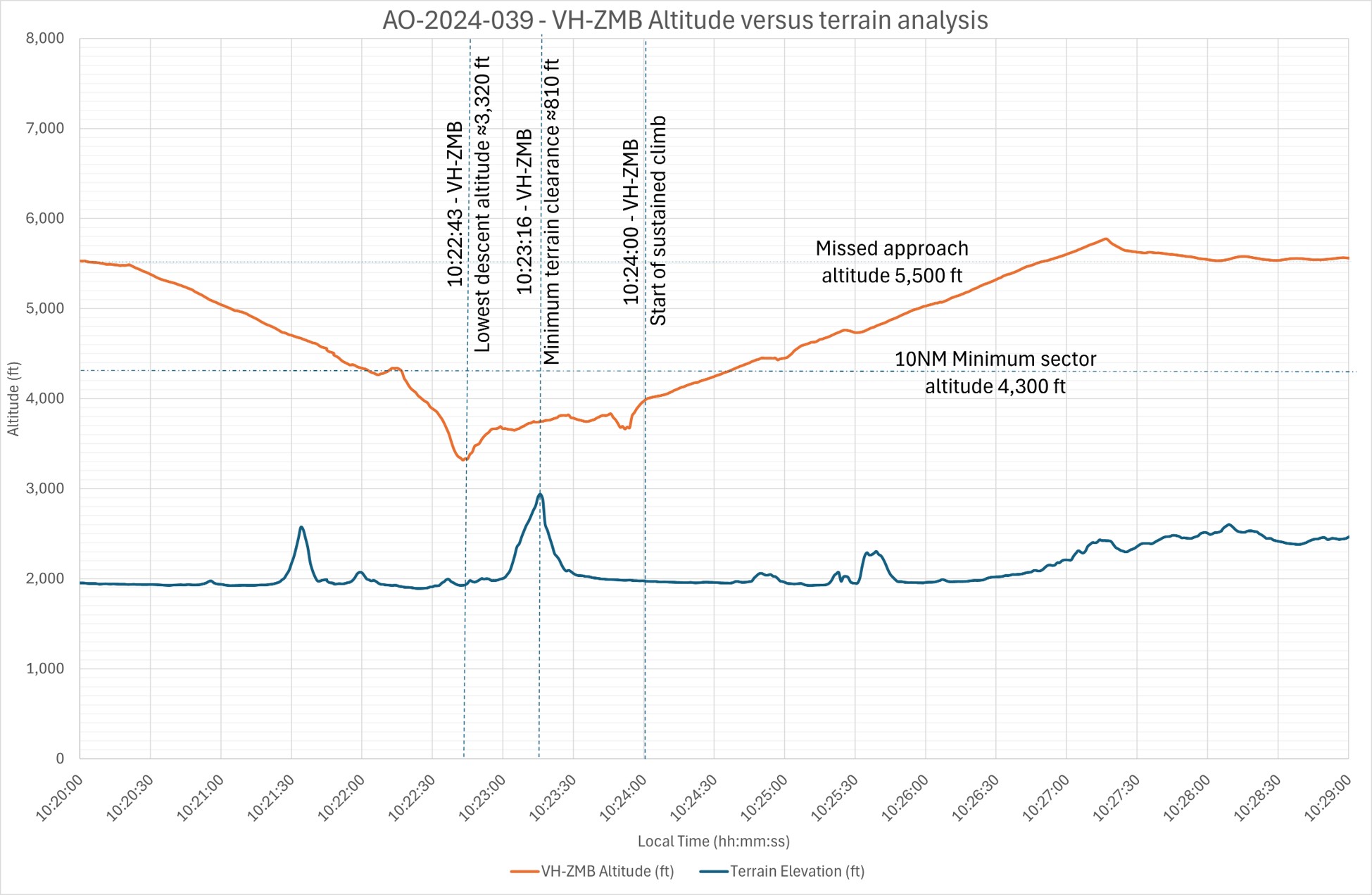
Recorded data indicated (Figure 3) that 30–40 seconds after speaking to ATC and approximately 70 seconds after leaving the ILS approach profile, the pilot commenced a sustained climb and began tracking to the initial approach fix of LISZT. During this time the aircraft was operated below the MSA.
Figure 3: Aircraft vertical profile
Source: ADS-B Exchange, Flightradar24 and OzRunways data analysed and annotated by the ATSB
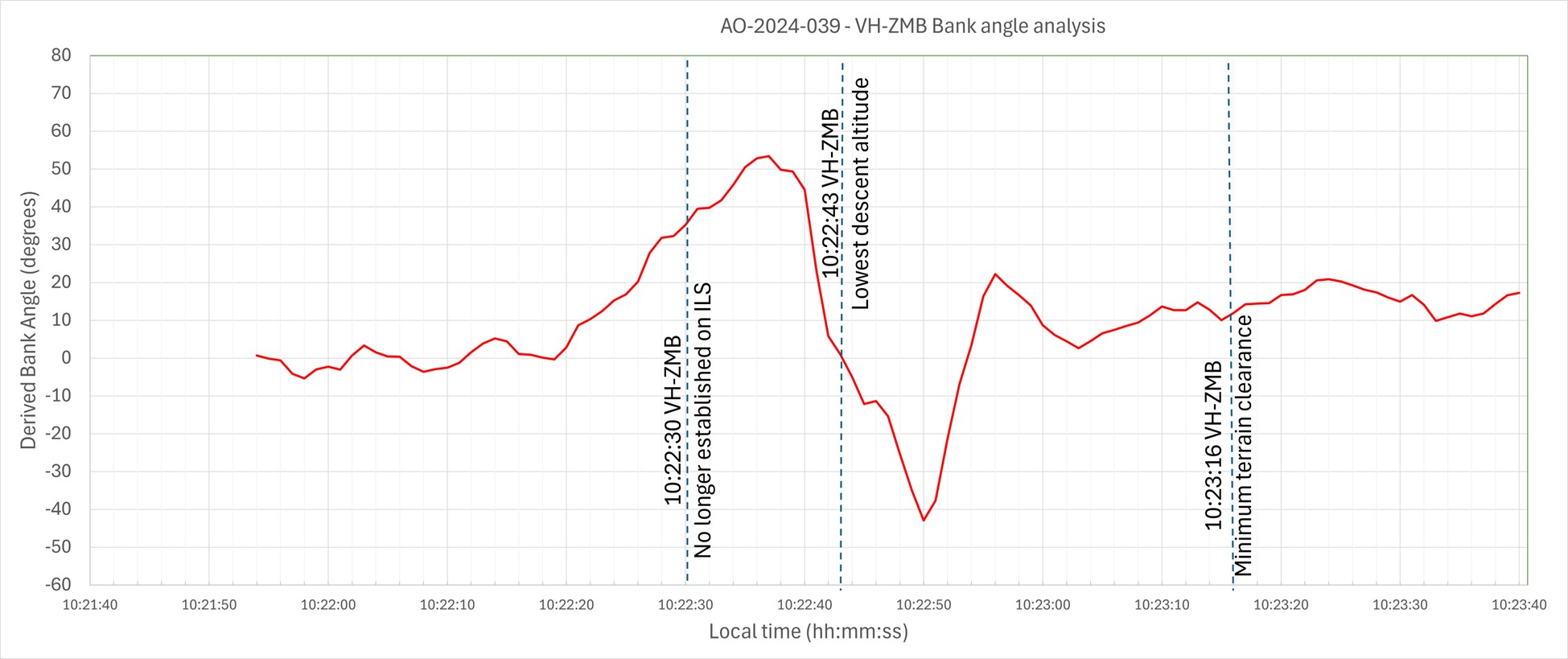
Recorded data identified a significant left turn, greater than 60° AOB, with a subsequent bank to the right of greater than 40° AOB and a further left correction (Figure 4). These occurred while the aircraft was still descending. The descent was arrested, at an altitude of about 3,320 ft. With minimal climb observed for about 30 seconds before approaching rising terrain, the aircraft then passed over the ridgeline at a height of approximately 810 ft (Figure 3). (Note: Graphical figures contain smoothed data profiles that may not precisely reflect the exact data point at an exact period).
Figure 4: VH-ZMB bank angles
Source: ADS-B Exchange, Flight Radar 24 and OzRunways data analysed and annotated by ATSB
The Cessna 310R is fitted with gyroscopic instruments[10] including an artificial horizon (AH), heading indicators and turn coordinators (turn and bank).
The vacuum system instruments on the Cessna 310R consist of 2 directional gyros, 2 AH gyros and the suction gauge.
The artificial horizon is the main instrument pilots use to fly through IMC. This instrument is considered a master instrument because it presents pitch and bank attitude information directly against an artificial horizon. It is a critical instrument to allow pilots to fly through non-visual and low-visibility conditions. It indicates the aircraft's orientation relative to the earth, expressed in pitch, roll, and yaw.[11]
Figure 5: Generic example of an artificial horizon
Source: Wikipedia
The gyroscopic instruments are powered by the vacuum system, consisting of a vacuum pump on each engine, pressure relief valve for each pump, a common vacuum manifold, vacuum air filter and suction gauge. Air pressure is used to rotate vanes to spin the instrument gyroscopes thus utilising gyroscopic forces as a mechanism that keeps the instrument level with respect to the direction of gravity. The AH gyro is mounted in a double gimbal, which allows the aircraft to pitch and roll as the gyro stays vertically upright.
The pilot reported that during the approach they noticed that the suction gauge was indicating ‘low pressure’. A partial blockage or issue in the pilot suction line, immediately after the air filter, could affect the pilot (left-side) AH and the suction gauge, with nil effect on the copilot (right-side) gauges.
However, post‑occurrence maintenance inspections and ground runs could not identify any abnormalities in the vacuum system.
Figure 6: Example of the suction gauge
Source: ATSB
Post occurrence maintenance testing of the artificial horizon identified a gradual drift in pitch, up to 7°, and up to 4° drift in the roll axis over a period of 20 minutes. The AH deviations were gradual, inconsistent and outside the manufacturer’s required tolerances.
Flight automation and operator policy
Flight automation, such as an approved autopilot, utilises different control systems and technologies that reduce the requirements of human interaction.
An autopilot system can reduce the pilot’s workload. This is achieved by the automation taking over routine tasks such as maintaining altitude, heading, and airspeed. Subsequently allowing the pilot mental capacity to focus on other critical aspects of the flight, such as monitoring systems, flight path, weather conditions and communicating with air traffic control. This is particularly useful in times of a high workload environment.
The operator’s policy did not detail requirements on when it was appropriate or required to use the autopilot.
PAN PAN call
A ‘PAN PAN’ transmission is used to describe an urgent situation, but one that does not require immediate assistance. Examples of such situations include instrument malfunctions, deviation from route or entering controlled airspace without a clearance.
When an air traffic controller receives a PAN PAN call from an aircraft, the controller will declare an alert phase.[12] The Safety bulletin What happens when I declare an emergency, released by Airservices Australia, stated that ATC may provide a range of support services including:
• passing information appropriate to the situation, but not overloading the pilot
• allocating a priority status
• allocating a discrete frequency (where available) to reduce distractions
• notifying the Joint Rescue Coordination Centre (JRCC), appropriate aerodrome or other agency
• asking other aircraft in the vicinity to provide assistance.
An aircraft is in an urgency condition the moment that the pilot becomes doubtful about position, fuel endurance, weather, or any other condition that could adversely affect flight safety. The time for a pilot to request assistance is when an urgent situation may or has just occurred.
No ‘PAN PAN call was made by the pilot during the occurrence.
Air traffic control safety alert
A safety alert issued by air traffic control is instructions prefixed by the phrase 'SAFETY ALERT'. The AIP outlines a safety alert as:
ATC will issue a Safety Alert to aircraft, in all classes of airspace, when they become aware that an aircraft is in a situation that is considered to place it in an unsafe proximity to:
1. terrain;
2. obstruction;
3. active restricted areas; or
4. other aircraft.
A safety alert should trigger an appropriate response from the pilot to address and resolve the undesirable state.
When the pilot made contact with ATC, the controller reported observing a level of stress in the pilot’s voice and noticed the pilot tracking perpendicular to the approach path for the runway 12 ILS, below the MSA, towards rising terrain.
No safety alert was made by air traffic control during the occurrence.
Spatial disorientation
Spatial disorientation (SD) occurs when a pilot has a false perception of the motion or orientation of the aircraft with respect to the Earth (Ledegang & Groen, 2018), subsequently incorrectly interpreting the aircraft attitude, altitude or airspeed.
The ATSB publication Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions (AR-2011-050) explains the basis of SD.
In order to correctly sense the orientation of the body relative to its environment, a pilot relies on a number of sensory systems in order to establish or maintain orientation: » the visual system » the vestibular system, which obtains its information from the balance organs in the inner ear » the somatic sensory system which uses the nerves in the skin and proprioceptive senses in our muscles and joints to sense gravity and other pressures on the body.
The visual system is by far the most important of the three systems, providing some 80 per cent of the raw orientation information. In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
The ATSB research report, An overview of spatial disorientation as a factor in aviation accidents and incidents (B2007/0063)identified that spatial disorientation is a very common problem and estimates that the chance of a pilot experiencing SD during their career is in the order of 90 to 100%. This report also detailed several international studies showing that SD accounts for some 6 to 32% of major accidents, and some 15 to 26% of fatal accidents. The report also identified that the true prevalence of SD events is almost certainly underestimated.
The FAA Advisory Circular, Pilot’s spatial disorientation (FAA AC60-4A) discussed the challenges associated with recovering from spatial disorientation. The results of a test conducted with qualified instrument pilots found that it took as much as 35 seconds to establish full control by instruments after a loss of an applicable visual reference.
Safety analysis
This analysis will explore the factors that involved aircraft directional changes, resulting in the aircraft deviating from the published ILS approach. The deviations occurred whilst the pilot was manually flying, in instrument meteorological conditions. The consequence of this deviation led to extended flight below the minimum sector altitude with increased pilot workload prior to recovering to a safe altitude.
The pilot reported being concerned with the aircraft’s location in relation to terrain, however, believed the aircraft was under control, attributing the unusual attitudes indicated on the artificial horizon to an instrument error rather than the aircrafts attitude.
The pilot reported that, at the time, false indications by the vacuum instruments were incorrectly indicating a turn to the right, which the pilot believed to be a consequence of erroneous instrument indications. The pilot recalled that their initial response to correct this was a turn to the left and believed that the vacuum instruments were still incorrectly indicating a level of bank even though the aircraft was level.
ATSB analysis of the recorded data reviewed the aircraft pitch and bank angles, descent and climb profiles, and aircraft tracks and timings confirmed that the instrument indications (at this time) correlated with high levels of bank and the aircrafts track.
Furthermore, although the pilot remembered observing a low vacuum pressure indication, a post‑incident system inspection indicated no identified problems with vacuum pumps or the check valves.
As such, it is almost certain that there was no instrument malfunction to the extent believed by the pilot. Rather, with no visual cues due to the IMC, the pilot likely became spatially disorientated and interpreted the real instrument indications as false as they mismatched the pilot’s sensed orientation.
As is common in spatial disorientation, the pilot likely followed their sense of direction rather than the (perceived faulty) instruments, leading to directional changes of up to 90° from the approach track as well as left and right angles of bank up to 65°, whilst continuing to descend.
However, post‑occurrence maintenance fault‑finding of the artificial horizon did identify a gradual drift in pitch, (up to 7°) and roll, (up to 4°) over a period of 20 minutes. While this may have indicated a degree of unserviceability of the instrument, this was not consistent with the reported sudden and absolute failure reported by the pilot.
Prior to the deviations on approach in IMC, the pilot descended below the minimum sector altitude. However, after deviating from the approach and no longer meeting approach tolerances, the pilot did not conduct a missed approach as quickly as practicable to achieve an altitude that would remove the aircraft’s exposure to the risks of collision with terrain.
Subsequently, the pilot was below MSA and no longer offered the protection of being on the approach. This situation was further exacerbated by the aircraft being in unusual attitudes and tracking perpendicular to the approach path, without intent. If this high-risk situation had been identified either by ATC issuing a safety alert or the pilot issuing a PAN PAN call, (a PAN PAN call should have triggered a safety alert to climb), a climb could have been expedited and the risk of proximity to terrain removed sooner than was the case.
Pilots should not hesitate to report an urgent condition when encountering situations that may not be immediately perilous but significantly increase risk.
ATC recordings indicated that the pilot notified ATC that they had incorrect artificial horizon information and had lost glidepath guidance. The pilot used their callsign twice, (which can often precede a distress call), and other verbal cues were also identified by the controller to indicate the pilot was under a level of stress. Being below the MSA and off the ILS, with indications of stress, was an opportunity for the controller to issue a safety alert to the pilot to climb immediately.
In an urgent situation such as this where the safety of the aircraft was uncertain, the broadcast of a PAN PAN call would have been appropriate. Had a PAN PAN call been broadcast, ATC would have almost certainly issued a safety alert. This would have required the pilot to conduct an immediate climb, removing their subsequent risk exposure to collision with terrain.
Flight data and recordings indicated that the aircraft was below MSA, from leaving the approach profile to commencing a sustained climb to a safe altitude, for greater than one minute. Additionally, the time elapsed from notifying ATC (below MSA), to commencing a sustained climb to a safe altitude, was greater than 30 seconds. During this time, in IMC, the aircraft came within 810 ft of terrain.
Instrument flight can be considered one of the more challenging operational environments to which a pilot can be exposed. Single-pilot operations have the potential to increase pilot workload (ALPA 2019).
Manually flying a single pilot approach in IMC increases the workload of any pilot. In this occurrence, the suspected loss of a primary instrument during an instrument flight rules approach, departing the ILS approach, experiencing unusual aircraft attitudes in IMC, and subsequently conducting a second approach all increased the workload of the pilot. Use of the autopilot system has the potential to significantly reduce the workload on pilots during this approach. This is achieved by the autopilot taking over routine tasks such as maintaining altitude, heading and airspeed. Thus, allowing the pilot to focus on other critical aspects of the flight. Whilst compliant with operator procedures at the time, use of the autopilot may have reduced the risk of spatial disorientation of the pilot on approach. The pilot reported that the autopilot could not be engaged post the occurrence, when positioning for the second approach.
Use of automation can afford the pilot spare mental capacity to recognise and address navigational deviations and tolerances. Thus, aiding the pilot to respond to the operational demands of the flight in a correct and timely manner.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight below minimum sector altitude involving Cessna 310R, VH-ZMB, 14 km west-north-west of Alice Springs Airport, Northern Territory, on 1 July 2024.
Contributing factors
At about 8 NM from Alice Springs whilst established on the ILS approach in instrument meteorological conditions, the pilot likely experienced spatial disorientation that led to directional changes of up to 90° from the approach track as well as left and right angles of bank up to 65°, whilst continuing to descend.
The pilot did not maintain track or glidepath and deviated from instrument landing system below the minimum sector altitude. Once outside of the required tolerances, the pilot did not conduct a missed approach, which increased the risk of collision with terrain.
Air traffic control did not issue a safety alert. This would have alerted the pilot that they were in unsafe proximity to terrain and needed to climb immediately.
The pilot did not broadcast a PAN PAN call notifying air traffic control and other traffic of their situation, leading to the pilot remaining below minimum sector altitude for an extended period without air traffic control instruction to climb.
Other factors that increased risk
Post occurrence fault‑finding of the artificial horizon, identified gradual and inconsistent deviations outside the manufacturer’s required tolerances.
The pilot did not utilise the autopilot for the approach even though they were in a high workload environment. The appropriate use of autopilot can reduce workload and subsequent risk of spatial disorientation such as during an instrument approach.
Safety actions
Safety action by Avcharter
The operator has since introduced an automation policy for the use of autopilot in conditions applicable to instrument meteorological conditions (IMC) and in high workload single-pilot environments.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the flight
the head of flight operations for the operator
Civil Aviation Safety Authority
the aircraft manufacturer
the maintenance organisation for VH-ZMB
independent avionics specialists
Airservices Australia
recorded data from the GPS unit on the aircraft.
References
Airservices Australia. (2024) Aeronautical Information Publication Australia.
Airline Pilots Association International (ALPA) (2019) The dangers of single pilot operations Retrieved from
Bailey, R. E., Kramer, L. J., Kennedy, K. D., Stephens, C. L., & Etherington, T. J. (2017, September). An assessment of reduced crew and single pilot operations in commercial transport aircraft operations. InN2017 IEEE/AIAA 36th Digital Avionics Systems Conference (DASC) (pp. 1‑15). IEEE.
Barnum, F., & Bonner, R. (1971). Epidemiology of USAF spatial disorientation aircraft accidents, 1 Jan 1958-31 Dec 1968. Aerospace Med, 42, 896-898.
Braithwaite, M., Durnford, S., & Crowley, J. (1998b). Spatial disorientation in US Army rotary-wing operations. Aviation Space Environ Med, 69, 1031-1037.
Cessna 1976, Pilot’s Operating Handbook, Cessna 310 Skyhawk, model C310R
Cheung, B., Money, K., Wright, H., & Bateman, W. (1995). Spatial disorientation implicated accidents in the Canadian forces, 1982-92. Aviation Space Environ Med, 66, 579-585.
Civil Aviation Safety Authority. (2020) Part 91 (General Operating and Flight Rules) Manual of Standards.
Federal Aviation Authority. (1983). Advisory Circular AC60-4A: Pilot’s spatial disorientation
Gillingham, K., & Previc, F. (1996). Spatial orientation in flight. In R. DeHart (Ed.), Fundamentals of aerospace medicine (2nd ed., pp. 309-397.). Baltimore: Williams & Wilkins
Hixson, W., Niven, J., & Spezia, E. (1972). Major orientation error accidents in regular Army UH-1 aircraft during FY 1969. Accident factors report namrl1169. Pensacola, FL: Naval Aerospace Medical Research Laboratory.
Knapp, C., & Johnson, R. (1996). F-16 class a mishaps in the U.S. Air Force, 1975- 93. Aviat Space Environ Med, 67, 777-783
Ledegang, W. D., & Groen, E. L. (2018). Spatial disorientation influences on pilots’ visual scanning and flight performance. Aerospace medicine and human performance, 89(10), 873-882.
Lyons, T., Ercoline, W., O’Toole, K., & Grayson, K. (2006). Aircraft and related factors in crashes involving spatial disorientation: 15 years of U.S. Air Force data. Aviat Space Environ Med, 77, 720-723.
Moser, R., Jr. (1969). Spatial disorientation as a factor in accidents in an operational command. Aerospace Med, 40, 174-176.
Singh, B., & Navathe, P. (1994). Indian Air Force and world spatial disorientation accidents: A comparison. Aviation Space Environ Med, 65, 254-256.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a peon receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
The pilot of the flight
The operator
Air traffic controller
Airservices Australia
Civil Aviation Safety Authority
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Flight operated under Part 135 of the Civil Aviation Safety Regulations. Part 135 of the Civil Aviation Safety Regulations (CASR) covers the air transport rules for smaller aeroplanes.
[2]Flight was operated under Part 91 of Civil Aviation Safety Regulations. Part 91 of the Civil Aviation Safety Regulations (CASR) – General operating and flight rules, sets out the general operating rules for all pilots and operators. It consolidates all of the general operating and flight rules for Australian aircraft.
[3] Instrument Landing System (ILS) approach is defined as a precision runway approach aid based on two radio beams which together provide pilots with both vertical and horizontal guidance during an approach to land.
[4]Instrument meteorological conditions (IMC) means meteorological conditions other thanvisual meteorological conditions.
[5] Instrument proficiency check means an assessment, against the standards mentioned in the Part 61 Manual of Standards, of a pilot’s competency to pilot an aircraft under the IFR
[6] Total cloud amount measured visually by the fraction (in eighths or oktas) of the sky covered by clouds.
[7] Stratus clouds tend to be featureless, low altitude clouds that cover the sky in a blanket of white or grey.
[8] VHF Omni Directional Range (VOR) navigation consists of a ground-based component, called VOR stations, (as well as receivers installed in the aircraft). VOR stations are infrastructure, often located at terminal areas, to aid in navigation and approaches.
[9] Part 91 of Civil Aviation Safety Regulations, General operating and flight rules.
[10]Gyroscopic flight instruments are instruments which have a mechanical gyroscope incorporated into their design.
[11]Rotation around the front-to-back axis is called roll. Rotation around the side-to-side axis is called pitch. Rotation around the vertical axis is called yaw.
[12]Alert phase: a situation where apprehension exists as to the safety of an aircraft and its occupants (this generally equates to a PAN PAN).
On the evening of 13 June 2024, a Batik Air Boeing 737-800, registered PK-LDK, departed I Gusti Ngurah Rai (Denpasar) International Airport, Bali, Indonesia for the inaugural passenger transport flight of a new service to Canberra, Australian Capital Territory. While en route, the flight crew noted that the estimated time of arrival into Canberra was prior to 0600 local time on 14 June, when Canberra Tower and Approach air traffic control began providing services for the day. The crew elected to proceed without any delays and prepared for an arrival without those air traffic control services, using the Canberra Airport common traffic advisory frequency (CTAF).
As the aircraft was descending toward uncontrolled airspace and tracking direct to Canberra along the flight path cleared by air traffic control, the crew deviated from the cleared track by commencing the AVBEG 5A standard arrival route (STAR). The duty air traffic controller intervened and provided altitude instructions to maintain separation from an en route restricted area. This intervention resulted in the aircraft becoming higher than the desired descent profile and the crew decided to use the holding pattern at the approach waypoint of MOMBI to reduce altitude. While flying the holding pattern at MOMBI, the aircraft was descended to 4,700 ft above mean sea level (AMSL), significantly below the holding pattern minimum safe altitude of 5,600 ft AMSL. The aircraft’s recorded radio height subsequently reduced to a minimum of 924 ft above ground level before the approach was recommenced from 4,700 ft AMSL, below the 5,400 ft AMSL minimum altitude for that segment of the approach.
The Canberra Approach controller who took over management of the airspace while the aircraft was in the holding pattern identified that the aircraft was operating below the minimum altitude, contacted the crew to provide a safety alert and advised the crew to contact Canberra Tower. The approach continued using controlled airspace procedures and the aircraft landed shortly after without further incident.
What the ATSB found
The ATSB found that the MOMBI holding pattern was not correctly flown by the crew and resulted in the aircraft descending significantly below the minimum safe altitude. The Canberra CTAF was also not selected by the crew, and the appropriate radio broadcasts were not made. This prevented the crew from receiving the oncoming Canberra tower controller's safety alerts, being able to illuminate the runway lights and increased the risk of conflict with other traffic.
Prior to commencing the approach, when the crew deviated from the cleared track to Canberra by commencing the AVBEG 5A STAR, the air traffic controller did not advise them of the deviation or provide a safety alert. Instead, the controller provided instructions that contributed to the crew becoming confused regarding the airspace classification for the arrival and approach.
The Melbourne Centre controller providing the flight information service for the aircraft was not, and was not required to be, aware of the holding pattern minimum altitudes. Therefore, the controller did not issue a safety alert when the aircraft descended below the minimum safe altitude.
The ATSB also found that Batik Air's change management processes were not effective at fully identifying and mitigating the risks associated with the commencement of the Denpasar to Canberra route. Batik Air also did not ensure that the crew had completed all CTAF training prior to them operating flights into Australia where the use of these procedures could be required.
The investigation also determined that during a 2022 review of Canberra runway 35 instrument landing system approaches, an obstacle evaluation error led to Airservices Australia increasing the MOMBI holding pattern minimum altitude from 5,100 ft to 5,600 ft. This increase resulted in a transition from the holding pattern to the approach glideslope that increased the risk of unstable approaches and sudden pitch ups. After conducting a revalidation test flight of the holding pattern minimum altitude increase, the Civil Aviation Safety Authority advised Airservices Australia that the increased minimum altitude did not provide an appropriate transition to the approach glideslope and recommended modifications to the holding pattern design. Despite Airservices Australia receiving this advice, no changes were made, and the increased holding pattern minimum altitude was maintained.
What has been done as a result
Following the incident, Batik Air has implemented several proactive safety actions including:
Revising the Canberra Airport Briefing document to include detailed information on Canberra air traffic control hours, CTAF procedures, holding requirements and guidance for adherence to lowest safe altitude requirements.
Issuing internal notices to flight crew highlighting the importance of a comprehensive approach briefing, adherence to air traffic control instructions and altitude awareness. These notices also provided information on CTAF and traffic information by aircraft (TIBA) procedures and highlighted the additional risks and absent protections when operating in uncontrolled airspace. Batik Air also disseminated details of the incident to all flight crew and conducted a special flight crew briefing with event details and lessons.
Completing practical and theoretical CTAF training for all flight crew assigned to Australian operations and incorporating this training into its annual training program.
Issuing an internal notice highlighting the mandatory Risk Management Review (RMR) process for all new routes and other significant operational changes. This notice intends to ensure comprehensive hazard identification, detailed risk assessments and an evaluation of the need for route proving flights or additional crew familiarisation.
Adjusting the flight schedule for the Denpasar to Canberra flight to ensure that early arrivals occur during Canberra Tower and Approach air traffic control operating hours.
In December 2024, Airservices Australia reassessed the MOMBI holding pattern and reduced the minimum holding altitude back to 5,100 ft.
Safety message
This incident underlines the need for operators to ensure that they have comprehensive and effective change management processes in place to identify all foreseeable risks relevant to a new route and implement appropriate mitigations to ensure the safe operation of these routes. In this case, the unfamiliar operating environment included the potential for operations using a CTAF, an uncommon operating procedure for non‑Australian operators and crews. Comprehensive and regular crew training is vital in ensuring that crews can effectively manage the risks inherent in the use of unusual procedures.
Additionally, the investigation highlights the importance of suitably designed and appropriate instrument flight procedures for safe air transport operations. In this case, the error made in the holding pattern design was not identified before it was published and while the error did not contribute to this occurrence, it introduced the potential for an unstable approach and/or a sudden pitch up risk to flight crews using the procedure.
The occurrence
On the evening of 13 June 2024, a Batik Air Boeing 737-800, registered PK-LDK, departed I Gusti Ngurah Rai (Denpasar) International Airport, Bali, Indonesia for the inaugural passenger transport flight of a new service to Canberra, Australian Capital Territory. The flight was operating with an enlarged flight crew, the captain was acting as pilot flying, the first officer was acting as pilot monitoring[1] and a second captain was occupying the flight deck jump seat.[2]
As the aircraft climbed to the cruising level of flight level 350,[3] the crew input forecast en route winds, which included strong tailwinds, into the aircraft’s flight management system. The crew noted that the estimated time of arrival into Canberra was prior to 0600 local time on 14 June, when Canberra Tower and Approach air traffic control began providing services for the day (see the section titled Canberra Airport and airspace). The crew elected to continue to Canberra without any en route delays and prepared for an arrival without those air traffic control services, using the Canberra Airport common traffic advisory frequency (CTAF).
As the aircraft descended towards Canberra in darkness, the flight was cleared by air traffic control (ATC) to track via the waypoint AVBEG direct to Canberra Airport and to descend to FL 120. During the descent, the crew prepared to conduct the AVBEG 5A standard arrival route (STAR) (see the section titled AVBEG 5A standard arrival route and restricted areas)but did not make a request to track via the STAR to the Melbourne Centre air traffic controller managing the airspace.
At 0541 local time, as the aircraft approached AVBEG, ATC cleared the crew to leave controlled airspace descending. The aircraft crossed AVBEG while descending below FL 205 and commenced tracking via the AVBEG 5A STAR.
At 0543, the controller managing the airspace handed over management of the airspace to a controller commencing work. This oncoming controller identified that the Batik Air flight was deviating from the cleared track (direct to Canberra) presented in the ATC system while still in controlled airspace. The oncoming controller was unsure if the aircraft was deviating from its clearance or if it had been provided the clearance by the outgoing controller and that clearance had not been entered into the ATC system. The controller also noted that the aircraft was descending toward an active restricted area (Figure 1).
The controller did not query the crew’s deviation or provide a safety alert (see the section titled Safety alerts) but instead asked the crew if they were going to remain clear of the restricted area 17 NM to the south of their position. The crew advised the controller that they were tracking via the AVBEG 5A STAR.The controller acknowledged the tracking advice and instructed the crew to maintain 10,000 ft above mean sea level (AMSL) to remain above the restricted area. After receiving this instruction, the crew became uncertain as to whether the aircraft would be operating within, or outside of, controlled airspace during the STAR and approach.
Figure 1: Overview of the descent
Source: Google Earth, recorded flight data, Airservices Australia and ATSB
The crew levelled the aircraft at 10,000 ft AMSL with the autopilot engaged and the aircraft passed over the restricted airspace. As was required by ATC procedures, the controller waited until the aircraft was observed to be more than 2.5 NM past the restricted area before instructing the crew to continue the descent to leave controlled airspace. The crew responded by advising that they would descend and continue tracking via the STAR. At about this time, the crew noted that the aircraft was about 1,300 ft above the desired descent profile for the arrival.
At 0551, the crew requested confirmation from ATC that they had clearance to conduct the instrument landing system (ILS) approach to runway 35 at Canberra. The controller responded by advising that the Canberra control tower was closed and that CTAF procedures applied for that airspace. At 0551:38, the aircraft descended below 8,500 ft AMSL, outside controlled airspace (into class G airspace).
As the aircraft was higher than the desired flightpath, the captain decided to conduct a holding pattern at the approach waypoint of MOMBI to reduce altitude and the first officer requested ATC clearance to hold at MOMBI. The controller responded by providing traffic information for the MOMBI holding pattern. At 0552:56, the crew again requested confirmation that they had clearance to conduct the ILS approach and the controller responded by advising that clearance was not required, the crew were now in class G (non-controlled) airspace and that the crew must broadcast their intentions on the Canberra CTAF.
At 0553:10, the aircraft passed the ILS initial approach fix waypoint MENZI (Figure 2) while descending below 6,720 ft AMSL and soon after, made another request to hold at MOMBI. The controller provided traffic information for the hold and requested that the crew make a right‑hand orbit to remain clear of the restricted airspace, now to the west of the aircraft.
Figure 2: Overview of arrival
Source: Google Earth, recorded flight data, Airservices Australia and the ATSB
As the aircraft approached MOMBI, the captain entered 5,400 ft AMSL (the approach’s minimum safe altitude before intercepting the ILS glideslope) into the autopilot mode control panel (MCP) and at 0554:15, the aircraft descended below the minimum holding altitude of 5,600 ft AMSL (see the section titled Instrument landing system approach) before levelling at 5,400 ft AMSL.
The captain then used the heading select function to make a right turn to a heading of 170°[4] and the aircraft commenced turning prior to crossing MOMBI. At 0554:30, the aircraft passed MOMBI at a speed of 172 kt (2 kt above the maximum speed for the 5,600 ft AMSL minimum holding altitude).
The captain then asked the first officer to enter a holding pattern into the aircraft’s flight management system (FMS) at MOMBI. As the aircraft had already passed MOMBI, the waypoint had dropped off the FMS track and the first officer was required to manually re‑enter the waypoint into the FMS planned track. As the turn continued, the speed reduced below 170 kt, the captain selected 4,700 ft AMSL (the crew’s intended MOMBI crossing altitude) on the autopilot MCP and the aircraft commenced descending to that altitude. During this time, the Melbourne Centre controller did not identify that the aircraft was operating below the minimum holding altitude of 5,600 ft AMSL.
The aircraft turned to a heading of 170° and continued descending until levelling at 4,700 ft AMSL at 0555:59. As the aircraft tracked south, the oncoming Canberra Approach air traffic controller prepared to take control of the Approach airspace (see the section titled Canberra Tower and Approach) and commenced a handover with the Melbourne Centre controller.
The aircraft continued south and at 0556:25, proceeded beyond the 14 distance measuring equipment (DME) limit for the 5,600 ft AMSL minimum holding altitude. At or before that DME limit, an inbound turn back to MOMBI needed to be commenced, or the minimum holding altitude had to be increased to 6,000 ft AMSL to maintain clearance from higher terrain further to the south. By that time, the first officer had completed re‑entering MOMBI into the FMS and the captain then used the lateral navigation autopilot mode to commence a right turn toward the waypoint.
As the aircraft was turning back toward MOMBI, at 0556:58, the incoming Canberra Approach controller completed their handover with the Melbourne Centre controller and took over the airspace as well as the Melbourne Centre radio frequency that the aircraft was using (this frequency then became a Canberra Approach frequency).
At the same time, the Canberra Tower air traffic controller preparing to commence the tower service observed that the aircraft was operating below the minimum holding altitude and made multiple attempts to contact the crew on the Canberra CTAF. At that time, the crew had not selected the Canberra CTAF and did not receive these broadcasts. As the Tower controller did not have a direct means of communication with the Melbourne Centre controller, the Tower controller contacted a Melbourne Approach air traffic controller to relay their concerns to the Melbourne Centre controller.
The aircraft continued turning toward MOMBI (Figure 3) and as it crossed over the eastern slopes of Mount Campbell at 0557:46, the recorded radio height reduced to a minimum of 924 ft above ground level. The aircraft did not penetrate the ground proximity warning system activation envelope and no alert was generated. At 0558:21, the aircraft rejoined the ILS approach.
Figure 3: Overview of MOMBI hold
Source: Google Earth, recorded flight data, Airservices Australia and the ATSB
The Melbourne Approach controller contacted the Melbourne Centre controller to relay the Canberra Tower controller’s concerns about the aircraft’s altitude and the Melbourne Centre controller responded by advising that the airspace was now being controlled by Canberra Approach.
At about the same time, the Canberra Approach controller also identified that the aircraft was operating below the minimum altitude. The controller contacted the crew and provided a safety alert, querying whether the crew were ‘visual’. The crew responded advising that they were ‘visual with the runway’ and continued the approach. The Approach controller then advised the crew to contact Canberra Tower and the approach continued using controlled airspace procedures. The aircraft landed at 0602 without further incident.
Context
Canberra Airport and airspace
Canberra Tower and Approach
On the day of the incident, the operating hours of controlled airspace associated with Canberra Airport were 0600 to 2300 local time. During these hours, Canberra Airport was within class C airspace, with airspace bases that increased as the airspace fanned out at increasing distances from the airport (Figure 4). The Canberra Tower and Approach air traffic control (ATC) services controlled the class C airspace within 30 DME of Canberra and below 8,500 ft above mean sea level (AMSL). Control services for the airspace above 8,500 ft AMSL were provided by a Melbourne Centre controller at all times during the flight’s descent and approach.
Figure 4: Canberra airspace when Tower and Approach were operating
All altitudes and elevations are above mean sea level. Source: ATSB
Outside of the Canberra Tower and Approach operating hours, the base of the Class C airspace was 8,500 ft AMSL. Below this was class G, non‑controlled airspace (Figure 5). Within class G airspace, flight crews could manoeuvre aircraft as required to position for an approach and were responsible for maintaining adequate terrain clearance. ATC was unable to issue STARs or approach clearances within class G airspace.
Figure 5: Canberra airspace when Tower and Approach were not operating
All altitudes and elevations are above mean sea level. Source: ATSB
Common traffic advisory frequency
When the Canberra Approach and Tower services were not operating, flight crew used a common traffic advisory frequency (CTAF) to make positional radio broadcasts and coordinate self‑separation with other traffic. The CTAF used the same frequency as Canberra Tower (when it was operational).
Pilot‑activated lighting
When Canberra Tower services were not available, the runway and movement area lighting was activated using a pilot-activated lighting system. The lighting was activated by a series of timed transmissions on the CTAF and remained active for 30 minutes.
Aviation rescue firefighting service
Canberra Airport aviation rescue and firefighting services operated only during times advised by NOTAM.[5] On the day of the incident, category 7 rescue and firefighting services[6] were provided from 0540 until 2225. Outside of these hours, no rescue or firefighting service was provided at the airport.
Air traffic control procedures
Manual of air traffic standards
Safety alerts
Airservices Australia’s manual of air traffic standards stated that an air traffic controller must issue a safety alert as soon it is recognised that an aircraft has deviated from an air traffic control clearance and will enter an active restricted area or is operating in unsafe proximity to terrain.[7] Additionally, if possible, a controller was required to provide an alternative clearance.
Track deviation
When observed, air traffic controllers were required to advise flight crews of flight path deviations.[8]
Controller knowledge
When the aircraft descended below the MOMBI holding pattern minimum altitude, the aircraft was operating in non‑controlled airspace. Within that airspace, aircraft operating under the instrument flight rules, such as the incident flight, were only provided with a flight information service.
The Melbourne Centre controller providing the flight information service for this airspace held an area radar control rating. This rating did not require a controller to have knowledge of STAR altitude restrictions and minimum holding altitudes associated with instrument approaches to airports located in non‑controlled airspace, nor did it require controllers be trained to provide specific instructions or corrections to pilots conducting instrument arrivals. The appropriate instrument flight procedure charts were available to the controllers using electronic displays at the control console, but area radar‑rated controllers were not required to know the details of the charts and only required to have awareness of broader lowest safe altitudes within that airspace.
Controllers providing an approach service within controlled airspace (such as the airspace that became active as the aircraft rejoined the approach) were trained to have more detailed knowledge of instrument approach procedures within the airspace. In addition, automated minimum safe altitude warning alerts were generated by the air traffic control system within that airspace.
When the aircraft descended below the minimum safe altitude of the MOMBI holding pattern, the Melbourne Centre controller providing the flight information service was not aware that this had occurred and therefore did not provide a safety alert. The oncoming Canberra Approach and Tower controllers both identified the aircraft operating below the minimum safe altitude. The Tower controller tried several times to contact the crew, but the crew did not have that frequency selected. The Approach controller issued a safety alert to the crew at the earliest available opportunity.
Canberra instrument flight procedures
AVBEG 5A standard arrival route and restricted areas
South‑west of Canberra Airport, restricted areas of airspace (R430 A‑C) encompassed the Canberra Deep Space Communication Complex at Tidbinbilla. The uppermost of these restricted areas (R430C) had a radius of 10 NM and a ceiling of 10,000 ft AMSL. The AVBEG 5A standard arrival route (STAR) (Figure 6) passed over this restricted area and had a 10,000 ft AMSL descent restriction at the waypoint LANYO which prevented aircraft descending via the STAR from entering the restricted area.
Figure 6: AVBEG 5A standard arrival route
Source: Batik Air and Navblue, annotated by the ATSB
Instrument landing system approach
An instrument landing system (ILS) is an instrument approach procedure that provides lateral (localiser) and vertical (glideslope) position information using angular deviation signals from the localiser antennas (located past the upwind end of the runway) and the glideslope antennas (located approximately 1,000 ft from the runway threshold).
The AVBEG 5A STAR connected with the Canberra runway 35 ILS Y approach at the initial approach fix waypoint MENZI. The minimum crossing height for MENZI was 5,400 ft AMSL. The ILS approach from MENZI included a 3° glidepath to the runway which crossed MENZI at 6,040 ft and the approach waypoint of MOMBI at 4,760 ft AMSL.
The approach included a right turn, 1-minute holding pattern at the approach waypoint MOMBI (Figure 7) available for use if required. The minimum holding altitude at MOMBI was 5,600 ft AMSL. To use that minimum altitude, the crew was required to adhere to a maximum speed of 170 kt and a 14 DME limit from the Canberra DME for commencing the inbound turn back to MOMBI. A higher minimum holding altitude of 6,000 ft AMSL could also be used which allowed for a higher maximum speed of 210 kt with no DME limit.
Figure 7: Canberra runway 35 instrument landing system approach
Source: Airservices Australia, annotated by the ATSB
Increase to MOMBI holding pattern minimum altitude
Incorrect assessment area
In March 2022, Airservices Australia undertook a required 3-yearly review of Canberra instrument flight procedures. During this review, the reference file for the MOMBI holding pattern could not be retrieved within the procedure design software. To conduct the review, the reviewing designer imported a new procedure template and assessed the relevant terrain and obstacles for the holding pattern. This assessment unintentionally omitted the area reduction associated with the 14 DME limit for the outbound leg of the holding pattern. Therefore, the assessed area was larger than necessary and included higher obstacles that necessitated an increase from the existing 170 kt speed‑limited minimum holding altitude of 5,100 ft to 5,600 ft. The minimum altitude for the 210 kt speed‑limited pattern remained 6,000 ft. These 170 kt and 210 kt speed‑limited minimum altitudes were respectively 840 ft and 1,240 ft above the unchanged 4,760 ft glidepath crossing height at MOMBI. The assessment and increased holding altitudes underwent an internal review, but the error was not identified. Airservices Australia then published the increase in the MOMBI holding pattern minimum altitude (Figure 8) via NOTAM.
Figure 8: Approach charts showing the increase to the MOMBI minimum holding altitude
The 23 March 2023 version of the approach chart was the last version to include the 5,100 ft minimum altitude, but from May 2022, the minimum altitude had been increased to 5,600 ft by NOTAM. Source: Airservices Australia, annotated by the ATSB
Glideslope intercept
Intercepting an ILS glideslope is normally accomplished from below as intercepting the glideslope from above requires high descent rates, increasing the risk of an unstable approach. Furthermore, the ILS ground equipment can also emit false glideslopes at steeper than normal glideslope angles. The Airservices Australia Aeronautical Information Publication cautioned that these false glideslopes could lead to a severe and sudden pitch up when intercepting a glideslope from above and that caution should be exercised in such situations, particularly for autopilot coupled approaches.[9]
The lowest of these false glideslopes typically occurs at an angle of about 9° to 12°, well above the flightpath of PK‑LDK during the incident approach.
Flight revalidation
In April 2022, the instrument flight procedure underwent a periodic revalidation flight by the Civil Aviation Safety Authority (CASA). For this revalidation, Airservices Australia provided CASA with the results of the 3‑yearly review including the increased minimum holding altitudes. On 19 May 2022, following the revalidation flight, CASA provided the flight report to Airservices Australia. The report’s findings stated that:
the suitability of the holding procedure design was unsatisfactory
the holding altitude at MOMBI did not allow for an appropriate transition to the ILS glidepath
the flyability of the ILS approach procedure was satisfactory
modification of the procedure was desirable.
The report also recommended moving the holding point to the waypoint KATIA (if design requirements allowed).
Following receipt of the report, the findings were not incorporated into the associated instrument flight procedures and, on 30 November 2023, updated instrument flight procedures were published without modification, with the increased minimum holding altitude.
The Airservices Australia procedure design manual stated that upon receipt of an instrument flight procedure revalidation report, the chief designer would assign the report to the designer who compiled the relevant revalidation pack. Any issues identified by the report were required to be addressed and advice of any action taken needed to be provided to the chief designer. Airservices Australia advised that for the MOMBI holding pattern flight revalidation report, internal records of correspondence regarding the possible relocation of the holding pattern were located, but the record of the outcome could not be found.
CASA surveillance of instrument flight procedure design
CASA conducts regular surveillance of instrument flight procedures, including approach design. The surveillance included a review of the incorporation into flight procedures of relevant revalidation flight findings and recommendations. However, the surveillance was conducted on a sampling basis and therefore did not include every revalidation report finding. CASA surveillance activities did not include the MOMBI holding pattern findings and therefore it was not identified that these had not been incorporated into the published instrument approach procedure.
Action following Batik Air incident
In December 2024, following ATSB enquiries into the MOMBI holding pattern design, Airservices Australia conducted a review of the 2022 design changes. This review found that when the 14 DME limit was correctly incorporated into the terrain and obstacle assessment area, the higher terrain that caused the minimum altitude increase from 5,100 ft to 5,600 ft was excluded. This assessment also determined that the minimum altitude for the 210 kt speed limit could be reduced and, on 20 December 2024, Airservices Australia published a NOTAM reducing the MOMBI minimum holding altitudes to 5,100 ft for the 14 DME‑limited and 170 kt speed‑limited holding pattern and 5,600 ft (from 6,000 ft) for the 210 kt speed‑limited holding pattern.
Pilot details
The captain was an instructor pilot with Batik Air and held an Indonesian air transport pilot licence (aeroplane) and the required aviation medical certificates and operational ratings to undertake the flight. The captain had a total flying experience of 10,508 hours of which 7,772 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 164 hours, all in the Boeing 737.
The first officer held an Indonesian commercial pilot licence (aeroplane) and the required aviation medical certificates and operational ratings to undertake the flight. The first officer had a total flying experience of 6,843 hours of which 6,688 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 159 hours, all in the Boeing 737.
The second captain held an Indonesian air transport pilot licence (aeroplane) and the required aviation medical certificates and operational ratings to undertake the flight. The second captain had a total flying experience of 11,295 hours of which 11,018 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 191 hours, all in the Boeing 737.
From 1998 to 2010, the captain was a pilot in the Indonesian military and, in that role, had conducted operations in non‑controlled airspace. In 2010, the captain commenced employment with Batik Air’s parent company Lion Air and moved to Batik Air in 2013. From 2010, the captain had not undertaken any flights within non‑controlled airspace. The first officer and second captain reported having no experience operating in non‑controlled airspace. All crewmembers had previously operated flights to Australian destinations, but not to Canberra.
Batik Air
Batik Air began operations in 2013 as a subsidiary of Lion Air and commenced flights to Australia in 2016. At the time of the incident, Batik Air operated to 2 Australian destinations: Perth, Western Australia, and Canberra, Australian Capital Territory. The airline operated 46 Airbus A320 series aircraft, 22 Boeing 737‑800s and 1 Airbus A330‑300. All of Batik Air’s scheduled flights were undertaken in controlled airspace, except for any early Canberra arrivals (before 0600) and potential diversions from Perth Airport to the operator‑nominated diversion destination of Kalgoorlie, which operated using a CTAF at all times.
In October 2024, unrelated to this occurrence, Batik Air ceased operating the Denpasar to Canberra route.
Denpasar to Canberra route preparation
Prior to commencing the Denpasar to Canberra route, Batik Air conducted the required process to risk assess and obtain approval to commence the new route. This included conducting a risk management review and publishing a company airport briefing document.
Risk Management Review
The risk management review identified several risks and associated mitigations that were relevant to the incident including the items shown in Table 1 below:
Table 1: Relevant risk management review items
Identified risk
Mitigation
Unfamiliarity with new route and new airport
During the initial flight of any new route, provide the crew with all data available.
If available, the initial flight is to be flown by a pilot who has previously had experience on the route. If such pilot is unavailable, an instructor captain shall operate the initial flight.
High obstacle standard instrument departure
Create a specific one engine inoperative standard instrument departure procedure.
Ensure the one engine inoperative standard instrument departure procedure is included in the company airport briefing document.
CTAF operations in non-controlled airspace/airports
Ensure the crew is familiar with and understands CTAF operations.
Ensure guidance of CTAF operations is included in the company airport briefing.
Airport area surrounded by obstacles.
Publish a company airport briefing and train crew for special airports.
The risk management review did not identify that Canberra Airport aviation rescue and firefighting services operated only during times advised by NOTAM. Batik Air’s minimum permissible category of rescue and firefighting (RFF) services for 737‑800 operations was RFF category 7. On the day of the incident, this category of service began 13 minutes before the aircraft commenced the approach. Before that time, the available category of RFF was less than that permitted by Batik Air’s operations manual.
Company airport briefing
The company airport briefing document provided to the crew for the inaugural flight was incomplete. Specifically, in the airport information section the:
radio frequency for company operations was listed as ‘TBA’ (to be advised)
airport operating hours were listed as ‘24’, but the operational hours of air traffic control services were not provided
aviation rescue and firefighting information provided did not state that services were only provided during hours advised by NOTAM, nor was it advised that outside of these hours, the available level of rescue and firefighting was less than that required for the 737‑800 by Batik Air.
The CTAF information and high obstacle standard instrument departure risk mitigations required by the risk management review were also not included in the briefing.
Common traffic advisory frequency procedures and training
Operations manual
Batik Air’s operations manual noted that Australian routes may require the use of non‑controlled aerodromes as alternate airports and that these airports did not provide 24‑hour air traffic control services. The manual did not provide information advising that Canberra, a destination airport, could also be non‑controlled at times. The manual provided adequate procedures for an arrival to a non‑controlled airport (destination or alternate), including the use of pilot‑activated lighting and guidance for appropriate CTAF procedures and radio broadcasts.
CTAF training
Prior to commencing operations into Australia, Batik Air flight crew were required to complete a module of online training for CTAF operations. All flight crew had completed this training prior to operating the incident flight.
Batik Air also incorporated CTAF use into one simulator session (session 15) of its recurrent training program. This session simulated a flight from Denpasar to Perth, Western Australia and included a diversion from Perth to Kalgoorlie, where pilots were trained in the use of CTAF procedures for the arrival into Kalgoorlie.
Session 15 had last been incorporated into Batik Air’s training program in 2020, 4 years prior to the incident flight. The captain last undertook this training in May of 2020 and the second captain in March of 2020. The first officer commenced employment with Batik Air in 2021 and had therefore not undertaken session 15.
Crew training before route commencement
Prior to commencing the Canberra route, Batik Air reviewed the route and associated operational requirements. Batik Air assessed that a proving flight on the route or simulator training were not required as the new destination did not involve any significant operational complexities, and the aircraft type had demonstrated the required performance capabilities when operating similar routes.
To prepare the crew for the new route, the chief pilot had provided an in-person briefing to the operating crew on the day of the flight.
CASA route approval process
In March 2023, Batik Air applied to CASA to extend its Australian services beyond Perth to 3 additional airports – Adelaide, Brisbane and Canberra.
CASA conducted a desktop review of the application that included examination of Batik Air’s organisational structure, operational certificates and manuals, infrastructure and operational approvals to ensure that the required items were in place. This included an assessment of Batik Air’s CTAF procedures and guidance. CASA did not review Batik Air’s risk management review or the company airport briefing for Canberra, nor was it required to.
International Civil Aviation Organization guidance
The International Civil Aviation Organization (ICAO) publication Annex 6 to the convention on international civil aviation, Operation of Aircraft provided guidance for appropriate flight crew qualification and training standards for international air transport operations.[10] This stated that an operator shall not utilise a pilot as pilot‑in‑command of an aeroplane on a route for which that pilot was not qualified until the pilot has demonstrated adequate knowledge of relevant operational details for the route including:
terrain and minimum safe altitudes
communication and air traffic facilities, services and procedures
rescue procedures
arrival, departure, holding and instrument approach procedures
applicable operating minima.
This demonstration relating to arrival, departure, holding and instrument approach procedures could be accomplished in an appropriate training device, such as a simulator.
The guidance also stated that a pilot shall have made an actual approach into each aerodrome of landing on the route accompanied by a pilot who is qualified for the aerodrome unless:
• the approach to the aerodrome is not over difficult terrain and the instrument approach procedures and aids available are similar to those with which the pilot is familiar, and a margin to be approved by the State of the Operator is added to the normal operating minima, or there is reasonable certainty that approach and landing can be made in visual meteorological conditions; or
• the descent from the initial approach altitude can be made by day in visual meteorological conditions; or
• the operator qualifies the pilot-in-command to land at the aerodrome concerned by means of an adequate pictorial presentation; or
• the aerodrome concerned is adjacent to another aerodrome at which the pilot-in-command is currently qualified to land.
It was also recommended that a pilot be requalified if more than 12 months had elapsed and the pilot ‘had not made a trip on the route or a route in close proximity and over similar terrain and had not practised such procedures in a training device’.
The ICAO publication Guidance on the Preparation of an Operations Manual provided further guidance for these operations.[11] This document noted that it was common practice for operators to apply similar requirements to all pilots (not just the pilot in command). Depending on the complexity of the area or route and aerodrome, this may require in‑flight familiarisation or familiarisation using a training device. This document also stated that it was normal practice to give each pilot a general route or line check at least every 12 months.
Collision avoidance at non‑controlled aerodromes
Non‑controlled aerodromes cater for flights conducted by a broad mix of aircraft under both the instrument flight rules and the visual flight rules, including:
larger turboprop, jet and powered lift aircraft
smaller aircraft operated both commercially and privately
agricultural aircraft
military aircraft
various sport and recreational aircraft.
This presents many challenges to pilots operating into, out of, or in the vicinity of these aerodromes including collision avoidance. The Civil Aviation Safety Authority advisory circular AC91-14 pilots’ responsibility for collision avoidance describes the 2 methods of collision avoidance for aircraft operating in the vicinity of non‑controlled aerodromes.
Unalerted see‑and‑avoid:
Unalerted see-and-avoid relies totally on the crew – with no other assistance – to visually detect other aircraft that are on a conflicting flight path. Unalerted see-and-avoid is only viable in a minority of circumstances when all the following factors are present to defend against a mid-air [collision]:
• horizontal closure rates are slow enough for human reaction
• vertical closure rates are slow enough for human reaction
• aircraft are of sufficient profile to be seen with the available ambient light, or are made sufficiently conspicuous using artificial lighting
• aircraft and/or the ground are sufficiently well lit or ambient light provides sufficient contrast
• the aircraft structure is such that the pilot’s visibility is unhindered in all directions (a near practical impossibility)
Alerted see‑and‑avoid:
As aviation developed, with increasing aircraft performance, traffic density and flight in non-visual conditions, it became apparent that unalerted see-and-avoid had significant limitations. The need to enhance a pilot’s situational awareness led to the principle of ‘alerted see-and-avoid’. The primary tool of alerted see-and-avoid is radio communication. Radio allows for the communication of information to the pilot from the ground or from other aircraft.
Other tools of alerted see‑and‑avoid include airborne collision avoidance systems, but the equipment required for these systems to provide effective alerting were not required for all aircraft types using non‑controlled aerodromes.
The advisory circular describes accurate provision and interpretation of traffic information for the purposes of separation to or from another aircraft as an essential pilot skill and stated that effective training in the use of radio procedures is vital to ensure crews can effectively operate at non‑controlled aerodromes using common traffic advisory frequencies. Without understanding and confirming the transmitted information, the potential for alerted see‑and‑avoid is reduced to the less safe situation of unalerted see‑and‑avoid.
Light and meteorology
The approach was conducted in clear night conditions. On the morning of 14 June 2024, first light[12] was at 0641, 39 minutes after the aircraft landed. The moon was below the horizon. At 0554, when the aircraft descended below the minimum holding altitude, the Bureau of Meteorology (BoM) automatic weather station at Canberra Airport recorded the wind as 1 kt from 141° magnetic. The station recorded that there was no cloud cover, and visibility was greater than 10 km.
Recorded data
Quick access recorder
The aircraft’s quick access recorder data was provided to the ATSB by Batik Air. This data captured the aircraft’s descent commencing from 10,000 ft AMSL at 0550:20, 2.3 NM after passing LANYO. It then continued descending past the waypoints of HONEY at 9,184 ft AMSL, DALEY at 7,104 ft and MENZI at 6,720 ft (680 ft above the ILS glideslope).
At 0554:15, while approaching MOMBI at a speed of 171 kt, the aircraft descended below 5,600 ft AMSL and 2 seconds later, 0.6 NM before crossing MOMBI, the aircraft commenced a right turn from the approach track into the holding pattern at a speed of 172 kt. At 0554:24, the aircraft levelled at 5,400 ft AMSL and 6 seconds later passed MOMBI at a speed of 169 kt while continuing the right turn.
At 0554:51, the aircraft commenced descending from 5,400 ft AMSL and 4 seconds later, airspeed increased to 172 kt, before reducing to 170 kt, 4 seconds later. Speed remained at or below 170 kt for the remainder of the flight.
At 0555:44, the aircraft turned to and maintained a heading of 170° and 15 seconds later levelled at 4,700 ft AMSL (Figure 9). At 0556:25, the aircraft proceeded beyond 14 DME from the Canberra DME before commencing the right turn toward MOMBI 4 seconds later. During this turn, the lowest recorded radio height was 924 ft above ground level (AGL). No ground proximity alerts were recorded.
The aircraft passed KATIA at 0557:53 at an altitude of 4,700 ft AMSL (700 ft below the ILS approach minimum altitude at that waypoint) while tracking back toward MOMBI and rejoined the approach about 12 NM from the Canberra DME at 0558:19.
At 0558:48, the aircraft began descending from 4,700 ft along the runway 35 glidepath (Figure 9).
Figure 9: Recorded quick access data
All times are coordinated universal time (UTC). Local time was Australian Eastern Standard Time (EST), which was (UTC) +10 hours. Source: Quick access recorder from PK-LDK, annotated by the ATSB
Air traffic control
Recorded air traffic control surveillance and communications audio data was provided by Airservices Australia. The recorded audio showed that:
the crew did not request, and were not provided with, a clearance to track via the AVBEG 5A STAR
no safety alert was provided by the Melbourne Centre controller
no broadcasts were made by the crew on the Canberra CTAF
at 0547, and again at 0555, the Canberra runway lighting system was activated using the pilot‑activated lighting. The Batik Air crew did not have the CTAF selected at that time and the only other recorded transmissions on the CTAF at around those times were from a ground vehicle and another aircraft preparing to taxi for departure
at 0558, the Canberra Approach controller established communication with the Batik Air crew and provided a safety alert.
Safety analysis
Deviation from clearance and controller response
While en route to Canberra, the flight crew were provided with a tracking clearance from the waypoint AVBEG direct to Canberra Airport and instructed to leave controlled airspace by descending below the 8,500 ft above mean sea level (AMSL) controlled airspace base along that track.
The crew’s normal practice for arrivals was to use a standard arrival route (STAR), and they prepared for the arrival at Canberra using the AVBEG 5A STAR. However, the crew did not request or receive a clearance to descend via the STAR and with Canberra Approach air traffic control (ATC) services not yet active, this clearance could not have been provided. Therefore, when the aircraft crossed AVBEG and commenced tracking via the STAR, it deviated from the provided clearance.
From AVBEG, this STAR deviated from the aircraft’s cleared track by turning south and crossed restricted areas R430A, B and C. The AVBEG 5A STAR included a 10,000 ft AMSL descent limitation until past the waypoint LANYO to ensure that crew using the STAR did not enter the uppermost of these restricted areas. The descent clearance for the direct track provided to the crew did not have a descent restriction and the controller was unaware that the AVBEG 5A STAR included a descent restriction to prevent the aircraft entering the restricted areas. Therefore, the controller was required to issue a safety alert as it appeared to them that the aircraft’s deviation would take the aircraft into the active restricted areas. However, at that time, the controller had only recently taken over management of the airspace and was unsure if the crew were deviating from the cleared route, or if a clearance had been provided which hadn’t been correctly entered in the air traffic control system and was therefore not visible to the controller. Additionally, the controller noted that the aircraft was still 17 NM from the restricted area and therefore, instead of advising the crew of the clearance deviation and issuing a safety alert, the controller intervened by issuing a descent altitude restriction.
The crew believed that they were correctly following the AVBEG 5A STAR into non‑controlled airspace and when they received the descent restriction from the controller, they became confused as to whether the approach would be conducted within, or outside of, controlled airspace. Despite the controller stating that the approach would take place outside of controlled airspace and that clearances were not required for the manoeuvring associated with the approach, the crew remained confused and made several clearance requests when operating in non‑controlled airspace. This confusion was only resolved when Canberra Approach and Tower services commenced, and the approach continued using those services.
A ‘safety alert’ is designed to alert crews to safety critical information to ensure a response is prioritised. The controller’s decision not to issue the safety alert and not to alert the crew to the deviation were missed opportunities to draw the crew’s attention to the situation and may have helped avoid the later confusion about the airspace classification.
Furthermore, the controller needed to wait until the aircraft was observed to be 2.5 NM beyond the restricted area before further descent clearances could be provided and by the time this clearance was issued, the aircraft was about 1,300 ft above the desired STAR profile.
Contributing factor
While descending and tracking direct toward Canberra in controlled airspace, the flight crew were provided with a clearance to leave the controlled airspace by continuing to descend on that track. The flight crew then deviated from the cleared track by commencing the AVBEG 5A standard arrival route (STAR).
Contributing factor
The air traffic controller did not advise the flight crew of the track deviation or provide a safety alert but provided altitude instructions to maintain separation from a restricted area (a separation built into the AVBEG 5A STAR). This intervention resulted in the aircraft becoming higher than the desired descent profile and the crew becoming confused regarding the airspace classification for the arrival and approach.
Descent below minimum altitude
Incorrectly flown holding pattern
Following the controller’s descent clearance after crossing the restricted area, the crew did not re‑establish the desired descent profile prior to commencing the approach. Consequently, the aircraft passed the instrument landing system approach’s initial approach fix waypoint MENZI about 680 ft higher than the glideslope and the captain decided to use the approach holding pattern at MOMBI to descend to the desired descent profile. This decision was made late during the arrival and the crew did not identify that the holding pattern minimum altitude (5,600 ft) was unusual in being significantly higher than the waypoint glideslope crossing altitude (4,760 ft). As a result, the captain referenced the 4,760 ft AMSL glideslope crossing altitude for MOMBI and selected 4,700 ft for the holding altitude.
The crew also did not begin to enter the pattern into the flight management system until after MOMBI had already dropped from the programmed track. As a result, the first officer had to manually enter the holding waypoint. When entering the holding waypoint, the first officer did not enter minimum altitude constraints associated with the holding pattern.
While the first officer entered the holding waypoint, the captain used the heading select function and altitude window to enter the holding pattern. In doing so, the captain did not adhere to several holding pattern requirements. The turn to enter the pattern commenced prior to the aircraft crossing MOMBI resulting in less distance being available to complete the outbound leg of the holding pattern. The maximum speed for the 5,600 ft minimum altitude was marginally exceeded and the aircraft then descended below the 5,600 ft minimum altitude to the commanded altitude of 4,700 ft. As the pattern continued, the inbound turn to MOMBI then did not commence until after the aircraft had proceeded beyond the 14 DME limit. As the aircraft was operating below both the 6,000 ft minimum altitude of the non‑distance restricted holding pattern and the 7,500 ft 25 NM minimum safe altitude, obstacle and terrain clearance was not assured.
As the aircraft turned toward back toward MOMBI at an altitude 900 ft below the minimum safe altitude, it crossed over terrain at a height of 924 ft above ground level. The aircraft did not penetrate the enhanced ground proximity warning system envelope and no alert was generated. Furthermore, as the aircraft then turned to rejoin the approach, it was now positioned about 700 ft below the minimum altitude for that segment of the approach, which also reduced obstacle clearance assurance during this part of the flight.
Contributing factor
The aircraft passed the initial approach fix for the instrument landing system approach about 680 ft higher than the glideslope and the crew intended to use the holding pattern at the approach waypoint of MOMBI to reduce altitude. However, the holding pattern was not correctly flown, and the aircraft was manoeuvred significantly below the minimum safe altitude. The approach was then recommenced from an altitude about 700 ft below the minimum altitude.
Low altitude safety alerts
Unlike approach controllers, area radar controllers providing the flight information service for the non‑controlled airspace were not required to know the details of instrument flight procedures for airports in that airspace. Therefore, the controller providing the flight information service was not aware of the minimum holding altitudes associated with the MOMBI holding pattern.
Air traffic control procedures required the controller to issue a safety alert as soon as they became aware that the aircraft was in unsafe proximity to terrain. However, the controller was unaware of the minimum holding altitudes and descending below the broader lowest safe altitudes was inherent to the progress of a flight following an instrument approach. Therefore, the controller did not become aware that the aircraft was operating below the minimum safe altitudes and did not issue a safety alert. Had an alert been provided when the aircraft first descended below the minimum altitude, this would have occurred prior to the aircraft turning toward the high terrain, reducing the risk of collision with terrain.
The Canberra Tower and Approach controllers both recognised that the aircraft was operating below the minimum safe altitude. The Tower controller attempted to contact the crew however, as the crew had not selected the CTAF, these broadcasts were not received. After the aircraft rejoined the approach, the Approach controller took over the airspace and immediately provided a safety alert to the crew, but by this time the aircraft was re‑established on the approach and within the associated protected area.
Other factor that increased risk
The Melbourne Centre air traffic controller providing the flight information service for the aircraft was not, and was not required to be, aware of the holding pattern minimum altitudes. Therefore, the controller did not issue a safety alert when the aircraft descended below the minimum safe altitude.
Common traffic advisory frequency use and training
Non-use of Canberra common traffic advisory frequency
During the arrival and approach, the crew were confused about the airspace classification and despite attempts by the controller to clarify this, the confusion was not resolved. As the aircraft approached Canberra Airport the crew did not select the Canberra common traffic advisory frequency (CTAF) but remained on the Melbourne Centre frequency.
As a result, the crew could not have activated the runway lights, nor could they make the required radio broadcasts to ensure separation with other traffic using the airspace. However, at the time the aircraft approached Canberra, another CTAF user had illuminated the runway lights and there was no conflicting traffic using the CTAF.
More importantly however, as the crew had not selected the CTAF, they did not receive the oncoming Canberra Tower controller’s broadcasts attempting to alert them to their low altitude.
Contributing factor
The Canberra common traffic advisory frequency was not selected by the crew, and the appropriate radio broadcasts were not made. This prevented the crew from receiving the oncoming Canberra tower air traffic controller's safety alerts, being able to illuminate the runway lights and increased the risk of conflict with other traffic.
Batik Air common traffic advisory frequency training
Batik Air’s operations manual included guidance on CTAF operations. While this guidance was focused on a Kalgoorlie diversion scenario, this guidance was also suitable for an early morning Canberra arrival.
Australian flights are the only flights in Batik Air’s route network where CTAF operations may have been required and Batik Air required that crew complete online CTAF training before operating to Australia. A simulator training session had also been developed that included CTAF operations, but this had last been incorporated into Batik Air’s recurrent training program 4 years prior to the incident, in 2020. The captain and deadheading captain had completed this session over 4 years before the incident, but the first officer had joined Batik Air after this date and had not undergone the training. None of the crew had previously operated into a non‑controlled airport as an operating crew of an air transport flight.
International Civil Aviation Organization (ICAO) guidance recommended that a pilot acting as pilot‑in‑command undergo training and demonstrate the required knowledge relevant to an intended operation within 12 months of undertaking that operation. Furthermore, this guidance stated that it was commonplace to ensure that all flight crew (not just the pilot‑in‑command) were trained and demonstrated similar operation knowledge.
Operating to a non‑controlled airport in an air transport aircraft while using CTAF procedures is a complex task. The crews of these aircraft may be faced with managing separation with smaller commercial and private aircraft as well as agricultural, military or sport and recreational aircraft. In addition, these aircraft may be operating to either the visual or instrument flight rules and many of these aircraft are not required to be fitted with the equipment required to enable effective alerting using airborne collision avoidance systems. Furthermore, these crews may be required to manage additional tasks like activating the runway lighting when arriving at night.
Effective training in the use of CTAF procedures is vital to ensure crews can effectively and safely operate using these procedures, in particular for crews who may not have previously used them or seldom used them. Batik Air had identified this risk for its Australian operations and developed training to mitigate the risk. However, this training was not conducted regularly, and Batik Air processes did not ensure that all flight crew members had completed the training before undertaking operations to Australia. This was inconsistent with the standards set out by ICAO guidance and increased the risk that crews would be inadequately prepared to manage this task.
After the crew deviated from the airways clearance, the controller’s intervention resulted in the crew becoming confused as to the classification of the airspace for the arrival and approach. This may have contributed to the crew’s non‑use of the CTAF. However, as the non‑use of CTAF procedures did not lead to the descent below minimum altitude, the inadequate CTAF training was not considered contributory to the incident.
Other factor that increased risk
Batik Air did not ensure that flight crew completed all common traffic advisory frequency (CTAF) training prior to them operating flights into Australia where the use of these procedures could be required. (Safety issue)
Route commencement process
Prior to commencing the Denpasar to Canberra route, Batik Air completed the required process to receive approval to commence flights on the route. This included a risk management review for the intended operation which identified a number of risks and associated mitigation actions that were relevant to the operation. However, a number of mitigations were not implemented such as the absence of CTAF guidance and a one engine inoperative standard instrument departure in the company airport briefing document. Other mitigations that were implemented, such as the inclusion of an instructor pilot on the flight and the publication of an (incomplete) company airport briefing document were ineffective at mitigating the risk of operating to an unfamiliar airport. Furthermore, the risk presented by airport fire and firefighting services being unavailable at times was not identified and therefore, no mitigating action was implemented.
ICAO guidance stated that an operator should not utilise a pilot as pilot‑in‑command of an aeroplane on a route for which that pilot was not qualified until the pilot had demonstrated adequate knowledge of relevant operational details. This could be conducted in a number of ways including self‑briefing, operator briefing, undertaking a route proving flight or by using an adequate training device.
Batik Air assessed that a proving flight or simulator training for the route were not required as the new destination did not involve any significant operational complexities and the aircraft type had demonstrated the required performance capabilities when operating similar routes. Instead, the crew were briefed on the operation by the Chief Pilot on the day of the flight.
However, the route did involve several significant operation complexities. The scheduled arrival time for the flight was during night hours; Canberra is surrounded by mountainous terrain and may have required the use of CTAF procedures. Furthermore, the runway 35 instrument landing system approach included significant and unusual complexities as demonstrated by the MOMBI holding pattern glideslope transition.
Recognising that a briefing was provided by the Chief Pilot to the crew prior to the flight, it did not achieve its aim of adequately preparing them for the route. A route proving flight, or the use of a suitable training device, would likely have provided more effective crew preparation in accordance with ICAO guidance, giving them greater awareness of the terrain, airspace and instrument flight procedure complexities of Canberra and may have avoided the descent below the minimum safe altitude.
Contributing factor
Batik Air's change management processes were not effective at fully identifying and mitigating the risks associated with the commencement of the Denpasar to Canberra route. (Safety issue)
Holding pattern to glideslope transition design
During a required, periodic review of the Canberra runway 35 ILS approach procedure by Airservices Australia, a new procedure template was imported to assess the approach including the MOMBI holding pattern as the existing design could not be uploaded to the procedure design software. The lower of the existing holding pattern’s 2 minimum altitudes (5,100 ft AMSL) required a crew to turn inbound from the outbound course before reaching 14 DME from Canberra. This distance limitation reduced the size of the pattern’s terrain and obstacle consideration area. When conducting the review, this 14 DME distance limitation was not included when determining the assessment area and therefore an area larger than required was assessed. This larger area included higher terrain and obstacles that required a 500 ft increase to the minimum altitude, raising it to 5,600 ft AMSL. The error in this assessment was not identified during internal reviews by Airservices Australia and the increased holding altitude was then published via NOTAM.
The approach glideslope crossed MOMBI at 4,760 ft AMSL, 840 ft below the minimum holding altitude. Consequently, to rejoin the approach from the holding pattern, crews could be required to intercept the glideslope from significantly above it, increasing the risk of sudden pitch ups. To achieve this could also require significant descent rates, increasing the risk of unstable approaches.
This was identified when the Civil Aviation Safety Authority (CASA) conducted a revalidation flight of the holding pattern and determined that the transition from the pattern to the glideslope was not appropriate and the design was unsatisfactory. This feedback was provided to Airservices Australia and despite Airservices Australia’s internal processes requiring this feedback to be addressed, the approach procedure with the increased altitude was published without any further modification.
The erroneous minimum altitude remained in place for over 2 years until a review following the Batik Air incident. This review identified the assessment area error and resulted in the minimum altitude being lowered back to 5,100 ft AMSL. While this minimum altitude remains above the MOMBI glideslope crossing altitude, the 500 ft reduction allows crews to appropriately transition to the glideslope while on the inbound leg of the holding pattern.
While the transition increased the risk of unstable and sudden pitch ups approaches, it did not contribute to the incident as the captain had manually selected a holding altitude of 4,700 ft AMSL on the flight management system, which in turn descended the aircraft below the lower and more appropriate 5,100 ft AMSL minimum altitude.
Other factor that increased risk
During a 2022 review of Canberra runway 35 instrument landing system approaches, an obstacle evaluation error led to Airservices Australia increasing the MOMBI holding pattern minimum altitude from 5,100 ft to 5,600 ft. This increase resulted in a transition from the holding pattern to the approach glideslope that increased risk of unstable approaches and sudden pitch ups.
Other factor that increased risk
After conducting a revalidation test flight of the holding pattern minimum altitude increase, the Civil Aviation Safety Authority advised Airservices Australia that the increased minimum altitude did not provide an appropriate transition to the approach glideslope and recommended moving the holding location to the waypoint KATIA. Despite Airservices Australia receiving this advice, the holding waypoint remained at MOMBI and the increased minimum holding altitude was maintained.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight below minimum altitude involving Boeing 737‑800, PK-LDK, 19 km south of Canberra Airport, New South Wales on 14 June 2024.
Contributing factors
While descending and tracking direct toward Canberra in controlled airspace, the flight crew were provided with a clearance to leave the controlled airspace by continuing to descend on that track. The flight crew then deviated from the cleared track by commencing the AVBEG 5A standard arrival route (STAR).
The air traffic controller did not advise the flight crew of the track deviation or provide a safety alert but provided altitude instructions to maintain separation from a restricted area (a separation built into the AVBEG 5A STAR). This intervention resulted in the aircraft becoming higher than the desired descent profile and the crew becoming confused regarding the airspace classification for the arrival and approach.
The aircraft passed the initial approach fix for the instrument landing system approach about 680 ft higher than the glideslope and the flight crew intended to use the holding pattern at the approach waypoint of MOMBI to reduce altitude. However, the holding pattern was not correctly flown, and the aircraft was manoeuvred significantly below the minimum safe altitude. The approach was then recommenced from an altitude about 700 ft below the minimum altitude.
The Canberra common traffic advisory frequency was not selected by the flight crew, and the appropriate radio broadcasts were not made. This prevented the crew from receiving the oncoming Canberra tower air traffic controller's safety alerts, being able to illuminate the runway lights and increased the risk of conflict with other traffic.
Batik Air's change management processes were not effective at fully identifying and mitigating the risks associated with the commencement of the Denpasar to Canberra route.(Safety issue)
Other factors that increased risk
Batik Air did not ensure that flight crew completed all common traffic advisory frequency (CTAF) training prior to them operating flights into Australia where the use of these procedures could be required. (Safety issue)
During a 2022 review of Canberra runway 35 instrument landing system approaches, an obstacle evaluation error led to Airservices Australia increasing the MOMBI holding pattern minimum altitude from 5,100 ft to 5,600 ft. This increase resulted in a transition from the holding pattern to the approach glideslope that increased risk of unstable approaches and sudden pitch ups.
After conducting a revalidation test flight of the holding pattern minimum altitude increase, the Civil Aviation Safety Authority advised Airservices Australia that the increased minimum altitude did not provide an appropriate transition to the approach glideslope and recommended modifications to the holding pattern design. Despite Airservices Australia receiving this advice, no changes were made and the increased minimum holding altitude was maintained.
The Melbourne Centre air traffic controller providing the flight information service for the aircraft was not, and was not required to be, aware of the holding pattern minimum altitudes. Therefore, the controller did not issue a safety alert when the aircraft descended below the minimum safe altitude.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Batik Air common traffic advisory frequency training
Safety issue description: Batik Air did not ensure that flight crew completed all common traffic advisory frequency (CTAF) training prior to them operating flights into Australia where the use of these procedures could be required.
Safety issue description: Batik Air's change management processes were not effective at fully identifying and mitigating the risks associated with the commencement of the Denpasar to Canberra route.
Proactive safety action not associated with a safety issue
Action number:
AO-2024-035-PSA-03
Action organisation:
Batik Air
Action status:
Closed
Batik Air adjusted the flight schedule for the Denpasar to Canberra flight (6015) to ensure that all Canberra arrivals occur during Canberra Tower and Approach air traffic control operating hours.
Glossary
AGL
Above ground level
AMSL
Above mean sea level
ATC
Air traffic control
CASA
Civil Aviation Safety Authority
CTAF
Common traffic advisory frequency
DME
Distance measuring equipment
FL
Flight level
FMS
Flight management system
ICAO
International Civil Aviation Organization
ILS
Instrument landing system
MCP
Mode control panel
NOTAM
Notice to airmen
PF
Pilot flying
PM
Pilot monitoring
STAR
Standard arrival route
TIBA
Traffic information by aircraft
Sources and submissions
Sources of information
The sources of information during the investigation included:
Batik Air
the flight crew
the air traffic controller
Civil Aviation Safety Authority
Airservices Australia
recorded flight data from PK-LDK
Bureau of Meteorology.
References
International Civil Aviation Organization 2018, Annex 6 to the Convention on International Civil Aviation, Operation of Aircraft, Part 1 International Commercial Air Transport — Aeroplanes Eleventh Edition.
International Civil Aviation Organization 2023, Doc 10153, Guidance on the Preparation of an Operations Manual.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Batik Air
the flight crew
the air traffic controller
Civil Aviation Safety Authority
Airservices Australia
National Transportation Safety Committee of Indonesia.
Submissions were received from:
Batik Air
Civil Aviation Safety Authority
Airservices Australia
National Transportation Safety Committee of Indonesia.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and Pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Jump seat: an auxiliary seat on the aircraft flight deck.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 350 equates to 35,000 ft.
[5]NOTAM: a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[6]Airservices Australia’s levels of aviation rescue firefighting services available at Australia’s 26 busiest airports range from category 6 to category 10 services with the categories dictating number of response personnel, response times, water discharge rates and the required amount of water and foam that is needed to be carried. The category of service provided was determined by the size (length and width) of the largest aircraft serving an airport.
[7]Manual of air traffic standards, 4.2.21.1 Entering an active Restricted/Military Operating Area and 9.1.4.3 Issuing a safety alert.
[8]Manual of air traffic standards, 9.7.12.4 Flight path deviation.
[9]Aeronautical Information Publication En Route section 7 - Precision Approach Operations, paragraph 7.1.3.
[10]Annex 6, Operation of Aircraft, 9.4.3 Qualifications.
[11]ICAO document 10153, Guidance for the preparation of an operations manual, 4.6 Route and aerodrome qualifications.
[12]First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions.
Preliminary report
Report release date: 04/09/2024
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the evening of 13 June 2024, a Batik Air Boeing 737-800, registered PK-LDK, departed Denpasar International Airport, Indonesia for the inaugural passenger transport flight of a new service to Canberra, Australian Capital Territory. The captain was acting as pilot flying, and the first officer was acting as pilot monitoring.[1] A second captain was also on board, acting as a relief crewmember, occupying the flight deck jump seat located behind the flight crew during the arrival and approach.
As the aircraft climbed to the cruising level of flight level 350,[2] the crew input forecast winds, which included strong tailwinds, into the aircraft’s flight management computer. The crew noted that the estimated time of arrival into Canberra was prior to 0600 local time on 14 June, when Canberra Tower and Approach air traffic control began providing services for the day (see the section titled Canberra Tower and Approach). The crew elected to continue to Canberra without any en route delays and prepared for an arrival without those air traffic control services, using the Canberra Airport common traffic advisory frequency (CTAF).
As the aircraft descended towards Canberra in darkness, the flight was cleared by air traffic control (ATC) to track via the waypoint AVBEG direct to Canberra Airport and to descend to FL120. During the descent, the flight crew prepared to conduct the AVBEG 5A standard arrival route (STAR) but did not make a request to track via the STAR to the Melbourne Centre air traffic controller managing the airspace.
At 0541 local time, as the aircraft approached AVBEG, ATC cleared the crew to leave controlled airspace descending. The aircraft crossed AVBEG while descending below FL205 and commenced tracking via the AVBEG 5A STAR. The Melbourne Centre air traffic controller identified that the Batik flight was deviating from the cleared track (direct to Canberra) and noted that the aircraft was descending toward a restricted area (Figure 1).
The controller did not query the flight crew’s deviation, but asked the crew if they were going to remain clear of the restricted area. The crew advised the controller that they were tracking via the AVBEG 5A STAR (see the section titled AVBEG 5A standard arrival route and restricted areas). The controller acknowledged the tracking advice and instructed the crew to maintain 10,000 ft above mean sea level (AMSL) to remain above the restricted area. After receiving this instruction, the flight crew became uncertain as to whether the aircraft would be operating within, or outside of, controlled airspace during the STAR and approach.
Figure 1: Overview of the descent
Source: Google Earth, recorded flight data, Airservices Australia and ATSB
The crew levelled the aircraft at 10,000 ft AMSL with the autopilot engaged and the aircraft passed over the restricted airspace. As was required by ATC procedures, the controller waited until the aircraft was observed to be more than 2.5 NM past the restricted area before instructing the crew to continue the descent to leave controlled airspace. The crew responded by advising that they would descend and continue tracking via the STAR. At about this time, the crew noted that the aircraft was about 1,300 ft above the desired descent profile for the arrival.
At 0551, the crew requested ATC clearance to conduct the instrument landing system (ILS) approach to runway 35 at Canberra. The controller responded by advising that the Canberra control tower was closed and that CTAF procedures applied for that airspace. At 0551:38, the aircraft descended below 8,500 ft AMSL, outside controlled airspace (class G).
As the aircraft was higher than the desired flightpath, the captain decided to conduct a holding pattern at the approach waypoint of MOMBI to reduce altitude and the first officer requested ATC clearance to hold at MOMBI. The controller responded by providing traffic information for the MOMBI holding pattern. The crew then again requested clearance for the ILS approach and the controller responded by advising that clearance was not required and that the crew must broadcast their intentions on the Canberra CTAF.
At 0553:10, the aircraft passed the arrival waypoint MENZI (Figure 2) while descending below 6,720 ft AMSL and soon after made another request to hold at MOMBI. The controller provided traffic information for the hold and requested that the crew make a right-hand orbit to remain clear of the restricted airspace, now to the west of the aircraft.
Figure 2: Overview of arrival
Source: Google Earth, recorded flight data, Airservices Australia and ATSB
As the aircraft approached MOMBI, the captain entered 5,400 ft AMSL (the approach’s minimum safe altitude before intercepting the ILS glideslope) into the autopilot mode control panel (MCP) and at 0554:15, the aircraft descended below the minimum holding altitude of 5,600 ft AMSL (see the section titled Instrument landing system approach) before levelling at 5,400 ft AMSL.
The captain then used the heading select function to make a right turn to a heading of 170°[3] and the aircraft commenced turning prior to crossing MOMBI. At 0554:30, the aircraft passed MOMBI at a speed of 172 kt (2 kt above the maximum speed for the 5,600 ft AMSL minimum holding altitude).
The captain then asked the first officer to enter a holding pattern into the aircraft’s flight management system (FMS) at MOMBI. As the aircraft had already passed MOMBI, the waypoint had dropped off the FMS track and the first officer was required to manually re-enter the waypoint into the FMS planned track. As the turn continued, the speed reduced below 170 kt, the captain selected 4,700 ft AMSL (the crew’s intended MOMBI crossing altitude) on the autopilot MCP and the aircraft commenced descending to that altitude. During this time, the Melbourne Centre controller did not identify that the aircraft was operating below the minimum holding altitude of 5,600 ft AMSL.
The aircraft turned to a heading of 170° and continued descending until levelling at 4,700 ft AMSL at 0555:59. As the aircraft tracked south, the incoming Canberra Approach air traffic controller prepared to take control of the Approach airspace (see the section titled Canberraairspace) and commenced a handover with the Melbourne Centre controller.
The aircraft continued south and at 0556:25, proceeded beyond the 14 distance measuring equipment (DME) limit for the 5,600 ft AMSL minimum holding altitude. At or before that DME limit, an inbound turn back to MOMBI needed to be commenced, or the minimum holding altitude increased to 6,000 ft AMSL. By that time, the first officer had completed re-entering MOMBI into the FMS and the captain then used the lateral navigation autopilot mode to commence a right turn toward the waypoint.
As the aircraft was turning back toward MOMBI, at 0556:58, the incoming Canberra Approach controller completed their handover with the Melbourne Centre controller and took over the airspace and the Melbourne Centre radio frequency that the aircraft was using (this frequency then became a Canberra Approach frequency).
At the same time, the Canberra Tower air traffic controller preparing to commence the tower service observed that the aircraft was operating below the minimum holding altitude and made multiple unsuccessful attempts to contact the crew on the Canberra CTAF frequency. As the Canberra Tower controller did not have a direct means of communication with the Melbourne Centre controller, the Tower controller contacted a Melbourne Approach controller to relay their concerns to the Melbourne Centre controller.
The aircraft continued turning toward MOMBI (Figure 3) and as it crossed over the eastern slopes of Mount Campbell at 0557:46, the recorded radio height reduced to a minimum of 924 ft above ground level. At 0558:21, the aircraft rejoined the ILS approach.
Figure 3: Overview of MOMBI hold
Source: Google Earth, recorded flight data, Airservices Australia and ATSB
The Melbourne Approach controller contacted the Melbourne Centre controller to relay the Tower controller’s concerns about the aircraft’s altitude and the Melbourne Centre controller responded by advising that the airspace was now being controlled by Canberra Approach.
At about the same time, the Canberra Approach controller also identified that the aircraft was operating below the minimum altitude. The controller contacted the crew to provide a safety alert and asked the crew if they were ‘visual’. The crew responded advising that they were ‘visual with the runway’ and continued the approach. The aircraft landed at 0602 without further incident.
Context
Pilot details
The captain was an instructor pilot with Batik Air and held an Indonesian air transport pilot licence (aeroplane) and the required medical certificates and operational ratings to undertake the flight. The captain had a total flying experience of 10,508 hours of which 7,772 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 164 hours, all in the Boeing 737.
The first officer held an Indonesian commercial pilot licence (aeroplane) and the required medical certificates and operational ratings to undertake the flight. The first officer had a total flying experience of 6,843 hours of which 6,688 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 159 hours, all in the Boeing 737.
The relief captain held an Indonesian air transport pilot licence (aeroplane) and the required medical certificates and operational ratings to undertake the flight. The relief captain had a total flying experience of 11,295 hours of which 11,018 were on the Boeing 737 aircraft type. In the previous 90 days, they had flown 191 hours, all in the Boeing 737.
From 1998 to 2010, the captain was a pilot in the Indonesian military and, in that role, had conducted operations in uncontrolled airspace. In 2010, the captain commenced employment with Batik Air’s parent company Lion Air and moved to Batik Air in 2013. From 2010, the captain had not undertaken any flights within uncontrolled airspace. The first officer and relief captain reported having no experience operating in uncontrolled airspace. All crewmembers had previously operated flights to Australian destinations.
Operator details
Batik Air was a subsidiary of Lion Air and commenced operations in 2013 and operated to 2 Australian destinations: Perth, Western Australia, and Canberra. The airline operated 46 Airbus A320 series aircraft, 22 Boeing 737-800s and 1 Airbus A330-300. All of Batik Air’s scheduled flights were undertaken in controlled airspace, with the exception of any early Canberra arrivals (before 0600) and potential diversions from Perth Airport to the operator nominated diversion destination of Kalgoorlie, which operated as a CTAF at all times.
Light and meteorology
The approach was conducted in night conditions. On the morning of 14 June 2024, first light[4] was at 0641, 39 minutes after the aircraft landed. The moon was below the horizon.
At 0554, when the aircraft descended below the minimum holding altitude, the Bureau of Meteorology (BoM) automatic weather station at Canberra Airport recorded the wind as 1 kt from 141° magnetic. The station recorded that there was no cloud cover, and visibility was greater than 10 km.
Canberra airspace
Canberra Tower and Approach
On the day of the incident, the operating hours of Canberra Tower and Approach controlled airspace were 0600 to 2300. During these hours, Canberra Airport was within class C airspace, with airspace bases that increased as the airspace fanned out at increasing distances from the airport (Figure 4). The Canberra Tower and Approach air traffic control (ATC) services controlled the class C airspace within 30 DME of Canberra and below 8,500 ft above mean sea level (AMSL). Control services for the airspace above 8,500 ft AMSL were provided by a Melbourne Centre controller at all times during the flight’s descent and approach.
Figure 4: Canberra airspace when tower and approach were operating
All altitudes and elevations are above mean sea level.
Source: ATSB
Outside of the Canberra Tower and Approach operating hours, the base of the Class C airspace was 8,500 ft AMSL. Below this was class G, non‑controlled airspace (Figure 5). Within class G airspace, aircraft crews could manoeuvre as required to position for an approach and were responsible for maintaining adequate terrain clearance. ATC was unable to issue STARs or approach clearances for the class G airspace.
Figure 5: Canberra airspace when tower and approach were not operating
All altitudes and elevations are above mean sea level.
Source: ATSB
When the tower was not operating, Canberra Airport operated using a common traffic advisory frequency (CTAF). When operating using a CTAF, pilots make positional radio broadcasts to coordinate self-separation with other traffic.
AVBEG 5A standard arrival route and restricted areas
South‑west of Canberra Airport, restricted areas of airspace (R430 A-C) encompassed the Canberra Deep Space Communications Complex at Tidbinbilla. The uppermost of these restricted areas (R430C) had a radius of 10 NM and a ceiling of 10,000 ft AMSL. The AVBEG 5A STAR (Figure 6) passed over this restricted area and had a 10,000 ft AMSL descent restriction at the waypoint LANYO which prevented aircraft descending via the STAR from entering that area.
Figure 6: AVBEG 5A standard arrival route
Source: Batik Air and Navblue, annotated by the ATSB
Instrument landing system approach
An instrument landing system (ILS) is an instrument approach procedure that provides lateral (localiser) and vertical (glideslope) position information using angular deviation signals from the localiser antennas (located past the upwind end of the runway) and the glideslope antennas (located approximately 1,000 ft from the runway threshold).
The AVBEG 5A STAR connected with the Canberra runway 35 ILS Y approach at the initial approach fix waypoint MENZI. The minimum crossing height for MENZI was 5,400 ft AMSL. The approach included a 3° glidepath to the runway which crossed the approach waypoint of MOMBI at 4,760 ft AMSL.
The approach included a right turn, 1 minute holding pattern at the approach waypoint MOMBI (Figure 7). The minimum holding altitude at MOMBI was 5,600 ft AMSL. To use that minimum altitude, the crew was required to adhere to a maximum speed of 170 kt and a 14 DME limit from the Canberra DME for commencing the inbound turn back to MOMBI. A higher minimum holding altitude of 6,000 ft AMSL could also be used which allowed for a higher maximum speed of 210 kt with no DME limit.
Figure 7: Canberra runway 35 instrument landing system approach
Source: Airservices Australia, annotated by the ATSB
Recorded data
Air traffic control
Recorded air traffic control surveillance and communications audio data was provided by Airservices Australia. The recorded audio showed that:
the crew did not request, and were not provided with, a clearance to track via the AVBEG 5A STAR
no broadcasts were made by the crew on the Canberra CTAF
no safety alert was provided by the Melbourne Centre controller.
Quick access recorder
The aircraft’s quick access recorder data was provided by Batik Air. This data captured the aircraft’s descent commencing from 10,000 ft AMSL at 0550:20, 2.3 NM after passing LANYO. It then continued descending past the waypoints of HONEY at 9,184 ft AMSL, DALEY at 8,608 ft and MENZI at 6,688 ft.
At 0554:15, while approaching MOMBI at a speed of 171 kt, the aircraft descended below 5,600 ft AMSL and 2 seconds later, 0.6 NM before crossing MOMBI, the aircraft commenced a right turn from the approach track into the holding pattern at a speed of 172 kt. At 0554:24, the aircraft levelled at 5,400 ft AMSL and 6 seconds later passed MOMBI at a speed of 169 kt while continuing the right turn.
At 0554:51, the aircraft commenced descending from 5,400 ft AMSL and 4 seconds later, airspeed increased to 172 kt, before reducing to 170 kt, 4 seconds later. Speed remained at or below 170 kt for the remainder of the flight.
At 0555:44, the aircraft turned to and maintained a heading of 170° and 15 seconds later levelled at 4,700 ft AMSL (Figure 8). At 0556:25, the aircraft proceeded beyond 14 DME from Canberra DME before commencing the right turn toward MOMBI 4 seconds later. During this turn, the lowest recorded radio height was 924 ft above ground level (AGL). No ground proximity alerts were recorded.
The aircraft passed KATIA at 0557:53 at an altitude of 4,700 ft AMSL while tracking back toward MOMBI and rejoined the approach about 12 NM from the Canberra DME at 0558:19.
At 0558:48, the aircraft began descending from 4,700 ft along the runway 35 glidepath.
Figure 8: Recorded quick access data
All times are coordinated universal time (UTC). Local time was Australian Eastern Standard Time (EST), which was (UTC) +10 hours.
Source: Quick access recorder from PK-LDK, annotated by the ATSB
Safety actions
Following the occurrence, Batik Air implemented several safety actions:
The Canberra Airport flight crew briefing document was revised to include more detailed information on Canberra air traffic control hours, common traffic advisory frequency (CTAF) procedures, holding requirements and guidance for adherence to lowest safe altitude requirements.
Internal flight crew notices were also issued to highlight the importance of a comprehensive approach briefing, adherence to air traffic control instructions and altitude awareness. These notices also provided information on CTAF and traffic information by aircraft (TIBA) procedures and highlighted the additional risks and absent protections when operating in non‑controlled airspace. Details of this incident were also disseminated to all flight crew and Batik Air conducted a special flight crew briefing with event details and lessons.
Batik Air also adjusted the flight schedule for the Denpasar to Canberra flight (ID6015) to ensure that arrivals occur during Canberra Tower and Approach air traffic control operating hours.
Further investigation
To date, the ATSB has:
examined recorded flight and air traffic control data
interviewed the flight crew and air traffic controller
obtained Batik Air operational procedures and route implementation processes
collected operational and airport information.
The investigation is continuing and will include further review and examination of:
recorded flight and air traffic control data
Batik Air operational procedures and training
Batik Air route implementation processes
air traffic control procedures and training.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is improving risk management associated with change.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and Pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 350 equates to 35,000 ft.
[4]First light: when the centre of the sun is at an angle of 6° below the horizon before sunrise. At this time the horizon is clearly defined but the brightest stars are still visible under clear atmospheric conditions.
On 30 August 2023, the flight crew of an Alliance Airlines Fokker 100 aircraft, registered VH-FGB, was operating scheduled passenger flight VA1388 from Brisbane, Queensland to Adelaide, South Australia. At about 1048 local time, the aircraft commenced the standard instrument arrival into Adelaide. During the arrival with the auto‑flight system engaged, the aircraft descended below a segment minimum safe altitude of 3,800 ft.
Observing the deviation, the captain commanded the aircraft to hold its current altitude. However, the first officer observed that the aircraft continued to descend, and in response, disconnected the autopilot and initiated a climb.
The auto-flight system then captured the lateral track of the localiser and intercepted the instrument landing system (ILS) glideslope when the autopilot was subsequently reconnected. The aircraft continued the ILS approach and landed at about 1100.
What the ATSB found
The ATSB found that, for an undetermined reason, the FMS did not capture the selected altitude. This resulted in the aircraft descending about 480 ft below the segment minimum safe altitude.
Safety message
This incident highlights the importance of flight crew continuously monitoring auto-flight systems and reacting quickly when the aircraft is not on the expected flight path to ensure that limits are not exceeded.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 30 August 2023, an Alliance Airlines Fokker 100 aircraft, registered VH-FGB, was operating scheduled passenger flight VA1388 from Brisbane, Queensland to Adelaide, South Australia. The first officer was the pilot flying and the captain was the pilot monitoring.[1]
Prior to departure from Brisbane, the flight crew entered the planned route, arrival, and approach procedures into the flight management computer. The flight crew selected the vertical navigation profile (PROF) mode, which was then armed to automatically capture the altitude at which the climb thrust was reduced (see the section titled Automated flight). The PROF mode is a flight management system (FMS) managed mode, in which the FMS controls the aircraft’s vertical path. However, an altitude selected by the flight crew at the flight mode panel (FMP) (Figure 1) takes precedence over PROF commands. The flight crew also selected and armed the FMS-managed lateral navigation (NAV) mode.
Figure 1: Flight mode panel
Source: Fokker, annotated by the ATSB
The aircraft took off at about 0900 Brisbane local time. Recorded flight data showed that passing about 90 ft above mean sea level (AMSL) on climb, the lateral NAV mode activated. A review of flight data identified that, at that time, both the vertical and lateral modes were FMS‑managed, and the armed vertical mode was altitude hold (ALT HOLD). The No. 2 (right) autopilot was engaged passing 574 ft on climb, consistent with the first officer as pilot flying.
When the aircraft reached the cruising altitude of flight level (FL) 320,[2] the active vertical mode changed to FMS-managed altitude hold (ALT HOLD). Apart from during a 30-second period in which the aircraft commenced a climb to a new cruising altitude of FL 340, the selected modes remained unchanged for the cruise phase of the flight.
The flight crew had entered the expected Adelaide BLACK 3A standard instrument arrival (STAR) and instrument landing system (ILS) – Z for runway 23 into the FMS. For that STAR, there were FMS-coded altitude restrictions at waypoints PLEZN (at or below 9,000 ft) and KERRS (at or above 5,000 ft) (Figure 2). The aircraft was required to remain at or above the segment minimum safe altitude of 3,800 ft until reaching GULLY. There was no altitude restriction and therefore no FMS-coded altitude for waypoint GULLY on the STAR (Figure 2). However, the ILS had the FMS‑coded altitude constraint at GULLY as depicted on the ILS chart (Figure 3).
Figure 2: Extract of BLACK 3A standard instrument arrival chart
Source: Airservices Australia, annotated by the ATSB
Figure 3: Extract of ILS-Z Runway 23 Adelaide chart
Source: Airservices Australia, annotated by the ATSB
At about 1036 Adelaide local time, the aircraft commenced descent from FL 340. The selected altitude was set to 9,000 ft, consistent with the air traffic control clearance, the lateral mode remained FMS-managed NAV and the vertical mode became FMS-managed DESCENT.
At 1048:03, the aircraft passed waypoint BLACK at the commencement of the STAR, descending through 13,600 ft. The altitude was then selected to 5,000 ft. About 1 minute later, APP mode was selected on the right electronic flight information system panel in preparation for the ILS.
At 1051:17, the aircraft passed the next waypoint on the STAR (PLEZN), descending through 8,090 ft barometric altitude,[3] thereby meeting the altitude requirement to be at or below 9,000 ft. About 1 minute later, the selected altitude was set to 3,800 ft. The flight crew reported that, in accordance with standard procedure, when they received air traffic control clearance to descend to 3,800 ft, the first officer set that altitude at the FMP and checked that it annunciated on the primary flight display. The first officer reported that they read aloud ‘3,800’ and the captain crosschecked that was the altitude set at the FMP and on the primary flight display. Shortly afterwards, the selected airspeed was reduced from 250 kt to 193 kt.
At 1053:19, descending through 5,377 ft, the recorded flight data showed the FMS-managed vertical mode changed from DESCENT to ALT HOLD, consistent with the auto-flight system reducing the descent rate to meet the altitude constraint at KERRS. The aircraft then passed waypoint KERRS at about the required 5,000 ft altitude, still descending. Shortly afterwards, the vertical mode reverted to FMS-managed DESCENT. About 10 seconds later, the APP mode was selected on the left electronic flight information system panel in preparation for the ILS.
Recorded flight data showed that an altitude alert activated as the aircraft descended through 4,562 ft, consistent with the aircraft being about 750 ft above the selected altitude (of 3,800 ft). The alert ceased as the aircraft passed 4,062 ft, still descending.
At 1054:43, the aircraft was 1.7 NM prior to waypoint GULLY and descending at about 1,100 ft per minute, when it descended below the selected altitude of 3,800 ft, which was the segment minimum safe altitude. The flight crew were monitoring the altitude and noticed that the FMS did not capture the selected altitude. In response, the captain pressed the altitude control knob to command the aircraft to hold the current altitude[4] and the FMS-managed mode was disconnected. The flight crew reported that the aircraft was in and out of cloud at that time, but they had sufficient visibility with the ground and terrain to assess that adequate separation existed. As the aircraft continued to descend through 3,631 ft, the selected airspeed was increased from 193 kt to 206 kt and the selected altitude was then increased to 4,700 ft by the first officer in an attempt to make the auto-flight system commence a climb.
Assessing that the aircraft was continuing to descend, 8 seconds later the first officer disconnected the autopilot, and initiated a climb. The aircraft was then at 3,487 ft. About 15 seconds later, the aircraft passed GULLY at 3,321 ft, descending at 704 ft per minute. The aircraft then entered a gradual climb, but as the aircraft had passed GULLY, the minimum safe altitude was 3,200 ft and no further climb was necessary. The flight crew reported selecting the approach mode (LAND on the FMP), and the aircraft captured the lateral track of the localiser. The autopilot was reinstated 40 seconds later, at which time the aircraft intercepted the ILS glideslope. The aircraft continued the ILS approach and landed at about 1100.
Context
Automated flight
The aircraft was fitted with an automatic flight control and augmentation system (AFCAS), consisting of the automatic flight control, autothrottle and flight augmentation systems. The automatic flight control system (AFCS) provided flight director guidance, autopilot control and altitude alerting. Two flight control computers provided the calculations for the AFCS. AFCS outputs were connected to the electronic flight instrument system (EFIS), autopilot servos for the ailerons, rudder and elevator, and to the flight management system (FMS) and flight warning computer. AFCS modes, speed, altitude, heading and bank limit could be selected at the flight mode panel (FMP), which also had autopilot engage (and an alternate autopilot disconnect).
The AFCAS could be operated in 2 basic states – programmed by the FMS with lateral and vertical navigation modes (NAV/PROF mode), or through flight crew manipulation of the FMP, referred to as AFCAS mode. The flight crew had received training in operating PROF and AFCAS states. The captain reported a preference for AFCAS mode, which required more manual inputs. The first officer, as pilot flying, elected to operate the flight in PROF mode. The flight crew also reported being aware that very rarely, the aircraft did not behave as expected when in PROF mode. As such, the training included monitoring and the importance of reverting to the manual mode if the auto-flight system was not behaving as expected.
The Alliance Airlines Operations Policy and Procedures Manual, section Flight Techniques stated:
The use of PROF mode in certain approach conditions creates extra workload.
Disconnect the PROF mode in cases where:
• Radar headings and/or speed restrictions are given.
• The NAV mode is not used for other reasons.
• Late clearances are given.
• Operationally not acceptable speed targets are issued by FMS.
• PROF should not be used when NAV is not engaged.
None of these listed conditions existed on the incident arrival/approach.
Recorded data
Recorded flight data from the incident flight is depicted in Figure 4. ATSB analysis of the recorded data was unable to determine the reason for the descent below the selected altitude. The ATSB therefore requested assistance from Fokker and Honeywell, as the manufacturer of the flight management computer.
Fokker advised that the flight data recorder only showed No. 1 (left side) parameters. As the first officer was the pilot flying, the aircraft was flying on autopilot No. 2. Therefore, it was possible that the systems were in independent operation and that there was a difference between the 2 systems. However, Alliance Airlines advised that the flight management systems were operating in cross-talk configuration, so both side parameters should have been evident in the recorded data.
Fokker also observed that when the flight crew changed the selected altitude to 3,800 ft, they initially wound the dial down to 3,500 ft before selecting 3,800 ft. Fokker advised that had the system been in altitude hold mode at the time, it would have captured 3,500 ft. However, it was in descent mode at that time and the recorded selected altitude was 3,800 ft. Fokker advised that the alert would activate about 750 ft above the selected altitude and the alert commenced as the aircraft descended through 4,562 ft, supporting that 3,800 ft was selected.
Honeywell was also unable to provide any reason for the occurrence and advised that they reviewed their problem reports and did not identify any similar occurrences.
Alliance Airlines analysed flights that tracked to Adelaide via GULLY from August 2023, and found that the incident flight was the only Alliance Airlines flight below the segment minimum safe altitude at GULLY. Alliance Airlines also provided additional flight data from VH-FGB, which included 4 flights from Brisbane to Adelaide in October 2023. In 2 of those, the arrival and approach were not conducted in FMS-managed mode and in another flight, the FMS‑managed mode was disconnected at about KERRS (the 5,000 ft altitude constrained waypoint).
In data from a flight on 15 October 2023, the auto-flight system entered altitude hold mode and levelled the aircraft at about 4,500 ft halfway between KERRS and GULLY, with the selected altitude of 3,800 ft. No difference was identified in the data to explain why that flight met the minimum safe altitude requirement, and the incident flight did not.
Figure 4: Recorded flight data for the incident flight showing selected parameters
Safety analysis
During the standard instrument arrival to Adelaide Airport, the aircraft was operating in an automated flight mode, in which the flight management system controlled the flight path. Approaching waypoint KERRS, although the automatic flight system entered altitude hold mode, the aircraft continued to descend, but met the 5,000 ft minimum altitude restriction at KERRS. The automatic flight system then returned to the descent mode and did not capture the selected 3,800 ft altitude, which was the segment minimum safe altitude between KERRS and waypoint GULLY.
Despite the ATSB consulting with the aircraft manufacturer, Fokker, and the flight management computer manufacturer, Honeywell, the reason the aircraft did not level at the selected altitude could not be determined.
Fortunately, in this incident the flight crew were monitoring the instruments and disconnected the automatic flight system when they detected the descent below the selected altitude and initiated a climb. By the time the flight crew had completed resolution actions and reinstated the automatic flight system, the aircraft had passed GULLY and intercepted the lateral localiser track. During that period, the aircraft was in and out of cloud and the flight crew were able to visually assess terrain clearance. When the flight crew reconnected the autopilot, the aircraft intercepted the glideslope and completed the instrument landing system approach.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the descent below the segment minimum safe altitude involving Fokker 100, VH-FGB, near Adelaide Airport, South Australia on 30 August 2023.
Contributing factors
For reasons that could not be determined, the flight management system did not capture the selected altitude. This resulted in the aircraft descending about 480 ft below the segment minimum safe altitude.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
the aircraft operator and manufacturer
the flight computer software manufacturer
Airservices Australia
recorded flight data from the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew
Alliance Airlines
Fokker
Honeywell
United States National Transportation Safety Board
Civil Aviation Safety Authority.
Submissions were received from:
Honeywell
Fokker
Alliance Airlines.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 320 equates to 32,000 ft.
[3]Barometric altitude was pressure altitude corrected for QNH, which was 1018 hPa. Subsequent heights all reference barometric altitude.
[4]The Fokker 100 Aircraft Operating Manual stated that when the ALT control knob is pushed during climb or descent, the aircraft will overshoot the altitude at which it is selected by approximately 10% of the vertical speed.
Occurrence summary
Investigation number
AO-2023-041
Occurrence date
30/08/2023
Location
10 NM from Adelaide Airport
State
South Australia
Report release date
12/04/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Flight below minimum altitude
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Fokker B.V.
Model
Fokker 100
Registration
VH-FGB
Serial number
11446
Aircraft operator
Alliance Airlines Pty Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 16 November 2022, a non-scheduled passenger transport flight was conducted in a Cessna Citation Mustang, registered VH-IEQ, between Young Airport and Bankstown Airport, New South Wales. On board were a pilot and one passenger.
As the aircraft approached Bankstown Airport to land under the instrument flight rules, about 10 minutes after last light, the pilot established contact with air traffic control (ATC), where a ‘visual’ approach was requested. ATC approved the pilot to fly directly toward final approach for runway 11 centre. Immediately after this clearance, the pilot started tracking toward final approach for this runway and descended to a height of 1,000 ft, which was about 800 ft below the lowest safe altitude for the area. ATC subsequently issued a terrain safety alert. An uneventful landing was conducted at 2020 local time.
What the ATSB found
The ATSB found that the pilot had submitted a flight plan earlier in the day for an arrival after last light, when more stringent rules applied than day operations. However, the pilot followed the rules applicable to day operations as there was still some ambient light available to allow features on the ground to be visually identified and avoided. This resulted in the pilot descending below the lowest safe altitude applicable for operations at night.
Safety message
This incident highlights the importance of planning, particularly around times when rules change, such as the transition from day to night. In this case, the pilot reported that flying a published instrument approach procedure, rather than declaring ‘visual’ would have been a more suitable plan for this flight.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
In the late afternoon of 16 November 2022, a non-scheduled passenger transport flight was conducted in a Cessna Citation Mustang, registered VH-IEQ (IEQ) between Young Airport and Bankstown Airport, New South Wales (Figure 1). On board were a pilot and one passenger.
This was the fourth and final flight of the day, with the pilot completing 3 earlier flights in the aircraft. National Airspace Information Planning System records indicated that the pilot submitted all flight plans for these flights at about 0448 local time, with this plan showing a planned departure from Young at about 1945 for the incident flight. This flight was planned to follow flight routes under the instrument flight rules (IFR)[1] and arrive at Bankstown at about 2014.
Figure 1: Flight path of VH-IEQ and incident location
Image showing flight path of aircraft (red line) on a map, with take-off, arrival and location of flight below lowest safe altitude.
Source: Google Earth and Geoscience Australia, annotated by the ATSB
Flight data recorded by the GPS navigation unit onboard the aircraft indicated that a take-off was commenced from Young on runway 19 at about 1946. After take-off, the aircraft started tracking to the east and climbed to a cruising altitude of flight level (FL)[2] 230 by about 1956.
At about 2001, the aircraft started to descend, continuing to track toward IFR waypoint WATLE. During this descent, at about 2004, last light[3] for Bankstown occurred. Six minutes later, the aircraft arrived overhead WATLE and proceeded to follow the planned IFR route denoted ‘Y20’, directly toward Bankstown Airport, 28 NM (52 km) to the east. At 2014:48, at waypoint NOLEM (Figure 2), the aircraft levelled out at 2,000 ft[4] above mean sea level and continued to track toward Bankstown. At this time, the pilot established first contact with Bankstown Tower air traffic control (ATC) near waypoint NOLEM (Figure 2), with the following communication exchange:
2014:48 IEQ: ‘Bankstown tower IEQ is 11 miles west 2,000 with Quebec visual inbound’
2014:59 BANKSTOWN TOWER: ‘IEQ BK TWR Join Final Runway 11 centre’
2015:08 IEQ: ‘Join Final 11 centre IEQ’
Immediately after responding to ATC, flight data indicated that the aircraft began a left turn onto a track of approximately 060° (true). Near the completion of the left turn, at 2015:22, the aircraft began to descend from 2,000 ft (labelled ‘left turn toward final approach and start of descent below 2,000 feet’ in Figure 2). The aircraft continued to descend on this track, levelling out at 1,000 ft at 2016:20. Around this time, ATC identified that the aircraft was ‘too low’, and issued a ‘Terrain’ safety alert at the location marked in Figure 2. The communication exchange for the safety alert between ATC and the pilot were as follows:
2016:30 BANKSTOWN TOWER: ‘IEQ Safety Alert Terrain QNH[5] is 1012’
2016:38 IEQ: ‘Roger copy 1012 IEQ I'm ahh visual’
2016:43 BANKSTOWN TOWER: ‘IEQ’
At the time the safety alert was issued and while maintaining at 1,000 ft, flight track data showed that the aircraft started to change track to the right by 15° to 075° for about 2 NM (3.7 km). The aircraft then changed track again to the right toward the intersection of the Bankstown Airport control zone and the extended centreline of runway 11 centre. Just prior to entering the control zone at 2017:55, Bankstown Tower provided the aircraft with a clearance to land, which was acknowledged by the pilot. At this time, the aircraft turned toward runway 11 centre and started to descend from 1,000 ft. An uneventful landing on runway 11 centre was conducted at 2019:56.
Figure 2: Flight path of VH-IEQ showing descent to 1,000 ft and approach to land
Note: Image showing flight path of aircraft (red line) on a low level enroute chart (right) and from the perspective of the approach from the NOLEM waypoint (left).
Source: Google Earth and Airservices Australia, annotated by the ATSB
Context
Meteorological information
The meteorological report (METAR)[6] for Bankstown Airport released at 2000 local time indicated the following weather conditions for the aircraft’s arrival:
winds at 6 kt from the north-west
visibility greater than 10 km
3 layers of cloud, comprising scattered[7] at 5,100 ft and at 7,000 ft, and broken at 8,200 ft above the ground
the QNH was 1012 hPA.
Images from weather cameras at the time of the incident located at Camden and Sydney Airports facing the direction of the aircraft and Bankstown Airport are shown in Figure 3. The images show that less than half of the sky is covered by cloud, with the cloud tops illuminated by the sun. There were no weather cameras operating at Bankstown Airport.
The Bureau of Meteorology advised that these weather cameras were configured 'to work in low light and will use the light available to provide the best image’, that is, the images shown in Figure 3 ‘look brighter than the actual conditions experienced by the pilot’. However, relatively clear atmospheric conditions are shown by the images, with well-defined silhouettes of ground‑based features.
Figure 3: Images from weather cameras at Camden and Sydney Airports
Source: Bureau of Meteorology, annotated by the ATSB
Visual approach to Bankstown Airport
During the approach, the pilot advised ATC that they were ‘visual’. This transmission signified that the requirements for a visual approach under the IFR could be met. ATC responded providing an instruction to ‘join final 11 centre’, which constituted a clearance to enter the Bankstown control zone on the centre line of runway 11 centre, tracking toward that runway.
As last light was at 2004 and this instruction was provided at 2014, this meant that the visual approach requirements for IFR flights by night applied.
To assist with conducting the visual approach, runway 11 centre was equipped with a precision approach path indicator system.[8]
Required actions by pilot following instructions from ATC
AIP ENR 1.1 paragraph 2.2.7.2[9] (Operations in Class D Airspace)[10] stated that in circumstances where ATC responds with the aircraft callsign and instructions, the pilot must comply with ATC instructions. It also states that ‘when no level instruction is issued’, the pilot may ‘descend as necessary to join the aerodrome traffic circuit’. In this case, ATC had instructed the pilot to join final runway 11 centre without a level instruction. The instructions meant that the pilot was required to fly the aircraft to enter the Bankstown control zone on the extended centreline for runway 11 centre. However, minimum height requirements applied to the flight as discussed in the next section.
Minimum height requirements during a visual approach for an IFR flight at night
During a visual approach at night, subparagraph 91.305(3)(b)(i) of the Civil Aviation Safety Regulations 1998 (CASR 91.305(3)(b)(i)) allowed an IFR flight to descend below minimum stipulated heights if the aircraft was being flown in accordance with:
…requirements relating to visual approach or departure procedures published in the authorised aeronautical information for the flight.
AIP ENR 1.5 section 1.14 articulated these requirements. AIP ENR 1.5 paragraph 1.14.6(b)[11] was relevant to this flight and included the provision that the pilot may visually approach the aerodrome by night when at an altitude not below the lowest safe altitude (LSALT)[12] or minimum sector altitude (MSA)[13] for the route segment, if the aircraft was established:
(1) clear of cloud;
(2) in sight of ground or water;
(3) with a flight visibility not less than 5,000M; and
(4) subsequently can maintain (1), (2) and (3) at an altitude not less than:
…
(ii) one of the following:
Route segment LSALT/MSA; or…
Based on the reported weather conditions, clauses 1, 2 and 3 noted above were achieved when the request for a visual approach was made by the pilot to ATC. Further, the AIP stipulated one of the conditions allowing an aircraft to descend below LSALT was when the aircraft was:
Within 5NM (7NM for a runway equipped with an ILS/GLS) of the aerodrome, aligned with the runway centreline and established not below “on slope” on the T-VASIS or PAPI;
Based on the ATC clearance provided to the pilot, and runway 11 centre being equipped with a PAPI, this meant that the aircraft could descend below LSALT once aligned with the runway centreline and not below on-slope of the PAPI and within 5 NM (9.3 km) of the PAPI.
Calculation of the lowest safe altitude
Flight data showed that after the initial climb from Young Airport, the aircraft had been above the published LSALT for the duration of the flight until reaching waypoint NOLEM.
AIP GEN 3.3 section 4 defined how to calculate the LSALT. Specifically, paragraph 4.2 stated:
For routes and route segments not shown on AIP aeronautical charts, the lowest safe altitude must not be less than that calculated in accordance with para 4.3 within an area defined in the following paras 4.6, 4.7, 4.8 and 4.9.
For this flight, paragraph 4.3 clause 4.3(a) stated the LSALT was to be calculated using the following method:
Where the highest obstacle is more than 360FT above the height determined for terrain, the LSALT must be 1,000FT above the highest obstacle; …
Additionally, paragraph 4.5 stated:
If the navigation of the aircraft is inaccurate, or the aircraft is deliberately flown off-track, or where there is a failure of any radio navigation aid normally available, the area to be considered is a circle centred on the DR position, with a radius of 5NM plus 20% of the air distance flown from the last positive fix.
Paragraph 4.5 applied to the incident flight after the pilot intentionally flew off-track toward final approach for runway 11 centre with the last positive fix being the waypoint NOLEM. Based on this, the ATSB calculated the LSALT for the aircraft between NOLEM and being aligned with runway 11 centre. An extract of the visual terminal chart applicable to the area is shown inFigure 4.
The aircraft was equipped with an approved global navigation satellite system, which was being used for navigation under RNP 2[14] meaning that the aircraft remained with a positive fix for the duration of the flight. For RNP 2 operations, AIP GEN 3.3 paragraph 4.7 required the following area to be considered for LSALT calculations:
…within an area of 5NM [9.3km] surround and including the departure point, the destination and each side of the nominal track.
This area is shown for the incident between the red circle labelled ‘Lowest safe altitude area at turn’ and the magenta circle labelled ‘Lowest safe altitude area from final intercept’ inFigure 4. Calculations were also performed in the circumstance where the aircraft flew to an extended 5 NM final for runway 11 centre, the earliest point of descent when using the PAPI, and this is depicted by the green circle labelled ‘Lowest safe altitude area from 5 NM final’ in Figure 4.
Figure 4 also shows 2 charted obstacles in the area. This indicated that paragraph 4.3(a) from AIP GEN 3.3 applied to this part of the flight. The highest obstacle in the area to be considered for LSALT was the tower ‘TWO RN’ at 870 ft above mean sea level, located about 2.5 NM (4.6 km) to the right of track, as labelled in Figure 4. Another tower was present about 2.5 NM (4.6 km) to the left of track at a height of 813 ft. Based on this, the LSALT for the aircraft during this segment of the flight was 1,870 ft.
Figure 4: Area applicable to lowest safe altitude calculations for VH-IEQ between flight path deviation and the extended centreline of runway 11 centre at Bankstown Airport
Source: Airservices Australia, annotated by the ATSB
Lowest safe altitude for a visual approach during the day
AIP ENR 1.5 section 1.14 paragraph 1.14.6(b) stipulated the same requirements for a visual approach by an aeroplane in the day, except for clause (4)(ii), which required pilots to maintain an altitude not less than:
The minimum height prescribed by CASR 91.265 or 91.267 as relevant to the location of the aircraft.
For the location of this incident, regulation 91.265 for flights over ‘populous areas and public gatherings’ applied. This stipulated that the aeroplane must be flown more than 1,000 ft above the highest feature or obstacle within a horizontal radius of 600 m of the point on the ground or water immediately below the aeroplane. Based on this, the height flown by the aircraft was above that required for an IFR visual approach during the day.
Decision to descend below lowest safe altitude
During an interview with the ATSB, the pilot recalled the following observations about the navigation conditions during the approach:
It was a light evening with plenty of twilight allowing the ground to be seen clearly.
The light was sufficient to see a clear horizon.
Ground features were able to be clearly seen, sufficient to identify the aircraft’s precise position.
All known obstacles could be seen.
Based on these observations, the pilot reported deciding to ‘call visual’.
The pilot’s description of the weather conditions was consistent with those recorded by the Bureau of Meteorology.
The pilot stated that, during a self-briefing prior to departure, the time of last light had been recorded for Young Airport and not Bankstown Airport as intended. The pilot also reported reviewing the last light time prior to descent to Bankstown Airport. Last light at Young Airport occurred about 12 minutes later than Bankstown Airport due to it being further west. The pilot later stated that recording the last light time for Young instead of Bankstown in the briefing sheet possibly contributed to the decision to descend and conduct the approach flown.
The pilot stated that descending to 1,000 ft assisted with meeting the stabilised approach criteria, which was:
“in a landing configuration with gear down, full flap, the sink rate … under 1,000 feet per minute and the checklists … completed…by 1,000 feet”.
The pilot stated that a challenge with using the PAPI was not being able to descend until 5 NM (9.3 km) from the runway, and that this was up to 1,000 ft higher than the ideal glideslope of about 1,600 ft at that location if the minimum sector altitude of 2,500 ft was used. The pilot also stated:
“the aircraft will then give you a lot of warnings about sink rate and terrain which can be very stressful… for passengers”.
For these reasons, the pilot stated:
“that is why I elected to descent to make sure that I was able to get that stabilised approach criteria. And …, it only worked because I had such good visibility in the twilight, I was able to see the ground, and I was able to see visually where I was.”
The pilot also stated that a motivation for declaring visual was to ‘fit in’ with the other traffic in the Bankstown area. However, the pilot stated that, on reflection, flying an instrument approach (specifically the RNP approach, rather than declaring visual) would have been a better solution for arriving close to or after last light for the aircraft stating:
“the only way to do it to achieve the stabilised approach is by the RNP”.
Fatigue considerations
The ATSB evaluated the likelihood that the pilot was fatigued at the time of the incident. Some areas of increased risk of fatigue potentially relevant related to:
continued period of wakefulness/length of duty period
split duty and efficacy of naps
quantity of sleep, particularly relating to early starts.
The pilot reported obtaining 7.5 hours of sleep immediately prior to the incident, and 8 hours for each of the 2 nights prior to that. The pilot submitted a flight plan at 0448 and was likely awake for some time prior to this. The pilot’s flight duty period (FDP) for the day started at 0630,[15] had a split duty rest period between 1030 and 1730 that included a 1-hour nap, and then was on duty again until 2100. As the incident occurred at 2016, the pilot’s total FDP was 14 hours and 30 minutes, which was 30 minutes over the maximum allowed under Appendix 4 of Civil Aviation Order 48.1 for single-pilot air transport operations, or to an approved fatigue risk management system. However, section 5.3 of Appendix 4 stated:
Despite the FDP limits provided in the operations manual, in unforeseen operational circumstances at the discretion of the pilot in command, the FDP limits in the operations manual may be extended by up to 1 hour.
The pilot reported having a discussion with the chief pilot about extending the FDP limits due to floods in the area delaying the departure time for the flights. However, the final flight of the day arrived within 5 minutes of the planned time.
Based on the reported sleep obtained, the pilot was likely not fatigued at the time of the incident.
Safety analysis
After last light, the pilot contacted Bankstown Tower declaring that they were ‘visual’ at 2,000 ft. This signified to ATC that requirements for a visual approach at night under the IFR could be achieved. The controller’s subsequent instruction to join final runway 11 centre indicated that the pilot could track toward the extended centreline for that runway.
The clearance from ATC did not specify an altitude, allowing the pilot to descend to the LSALT until established within 5 NM (9.3 km) of the PAPI for runway 11 centre. However, immediately after this clearance, the pilot descended to 1,000 ft, below the LSALT of 1,870 ft. This LSALT applied due to the 2 towers in the area rising to a height of 870 ft about 2.5 NM (4.6 km) from the aircraft. Analysis by the ATSB showed that flight above the LSALT could have been achieved by maintaining altitude between the point of diversion until being aligned with the extended centreline of runway 11 centre within 5NM (9.3 km) of the PAPI.
The pilot reported that the actual approach flown was as they had planned and declared ‘visual’ as they could ‘see the obstacles’. Weather camera imagery showed that the conditions were consistent with the pilot’s description. However, the camera imagery was likely brighter than that experienced by the pilot from altitude looking down on the obstacles and terrain. In this case, the flight path flown by the pilot was applicable and suitable for operations in the day. However, both the planned and actual times when the flight below LSALT occurred were after last light, based on the elapsed time between first contact with ATC and landing. Further, the pilot also reported incorrectly recording a later time for last light than actual, based on Young instead of Bankstown. The additional perceived duration of usable light possibly contributed to the decision to conduct the approach flown. The pilot reported that, on reflection, a better option would have been to fly an instrument approach procedure when planning to arrive at Bankstown just prior to or after last light. This indicated that these requirements could have been considered prior to the flight and represented a missed opportunity during flight planning.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight below minimum altitude involving Cessna Citation 510, VH-IEQ, 13 km west of Bankstown Airport, New South Wales, on 16 November 2022.
Contributing factors
While conducting a visual approach to Bankstown Airport, the aircraft descended 800 ft below the lowest safe altitude for operations at night, reducing the assurance for separation from terrain and ground-based obstacles.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
Airservices Australia
recorded data from the GPS unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Navair Flight Operations Pty Ltd
the Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from:
the pilot
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 230 equates to 23,000 ft.
[3]Last light is defined as the end of evening civil twilight, marking the commencement of night. The end of evening civil twilight occurs when the Sun’s centre is 6° below the horizon.
[4]This was also the published lowest safe altitude between IFR waypoint NOLEM and Bankstown Airport.
[5]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[6]METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
[7]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
[8]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach.
[9]AIP ENR 1 GENERAL RULES AND PROCEDURES, section 1.1 GENERAL RULES, subsection 2 OPERATIONS IN CONTROLLED AIRSPACE, sub subsection 2.2 Air Traffic Control Clearances and Instructions
[10]Class D: This is the controlled airspace that surrounds general aviation and regional airports equipped with a control tower. All flights require ATC clearance.
[11]AIP ENR 1 General Rules and Procedures, section 1.14 Visual Approach Requirements for IFR flights, subsection 6, sub subsection 6(b) Visual approach by Night, dated 02 DEC 2021.
[12]Lowest safe altitude (LSALT): The lowest altitude that provides safe terrain clearance at a given place.
[13]Minimum sector altitude (MSA): The lowest altitude that will provide a minimum clearance of 1,000 ft above all objects located in an area contained within a circle or a sector of a circle of 25 NM (46 km) or 10 NM (19 km) radius centred on a significant point.
[14]Required navigation performance (RNP) levels refer to the performance required from the navigation system. RNP 2 is primarily used in continental airspace where there is some ground navigation aid infrastructure.
[15]A flight duty period starts when ‘a person is required by an AOC [Air Operator’s Certificate] holder to report for a duty period in which 1 or more flights as an FCM [flight crew member] are undertaken’. The flight plan submission at 0448 was therefore not counted as duty (only time awake).
Occurrence summary
Investigation number
AO-2022-061
Occurrence date
16/11/2022
Location
15 km west of Bankstown Airport
State
New South Wales
Report release date
05/06/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Flight below minimum altitude
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Textron Aviation Inc.
Model
510
Registration
VH-IEQ
Serial number
510-0462
Aircraft operator
NAVAIR FLIGHT OPERATIONS PTY LTD
Sector
Jet
Operation type
Part 135 Air transport operations - smaller aeroplanes