Flight below minimum altitude occurrences, 40 km south of Cairns Airport, Queensland, on 24 and 26 October 2022
Final report
Report release date: 08/08/2023
Executive summary
What happened
24 October 2022
On the evening of 24 October 2022, a Virgin Australia Airlines Boeing 737-800, registered VH‑VUT, operated a passenger transport flight from Brisbane to Cairns, Queensland.
At 1945 local time, as the aircraft was cruising in darkness, air traffic control (ATC) provided a clearance for the HENDO 8Y arrival via the BARIA transition. The flight crew entered this arrival, transition and the following required navigation performance (RNP) Y instrument approach for runway 33 at Cairns Airport into the flight management computer (FMC). However, an approach transition was not selected resulting in a discontinuity being presented in the FMC’s programmed flight path between the HENDO arrival waypoint and the approach intermediate fix (IF) waypoint CS540. The flight crew resolved the FMC discontinuity by linking the 2 waypoints resulting in the 6,800 ft descent altitude constraint associated with HENDO in the RNP approach programming not being loaded into the programmed flight path.
As the aircraft approached HENDO, the captain selected the approach’s minimum descent altitude of 800 ft in the autopilot mode control panel and soon after, the aircraft descended below 6,800 ft and then below the minimum sector altitude of 6,500 ft. ATC alerted the crew and issued instructions to climb. The crew climbed the aircraft above 6,800 ft and commenced a missed approach before conducting a second approach and landing without further incident.
26 October 2022
On the morning of 26 October 2022, a Qantas Airways Boeing 737-800, registered VH-VZA operated a passenger transport flight from Brisbane to Cairns.
At 0739, in daylight, while the aircraft was in cruise to the south of Cairns, ATC provided the crew with clearance to conduct the Cairns HENDO 8Y arrival via the BARIA waypoint transition. The flight crew entered this arrival, transition and the following Cairns RNP Y runway 33 approach into the FMC.
The crew did not select an approach transition as they believed they had not yet received clearance for the HENDO approach transition. Consequently, the FMC presented a discontinuity between the HENDO arrival waypoint and the approach IF waypoint, CS540. The crew noted that required waypoints CS522 and CS523 were missing from the track presented on the navigation display, but as the track from HENDO to CS540 passed over those waypoints, the crew linked HENDO to CS540 and proceeded with the approach. This resulted in the 6,800 ft descent altitude constraint associated with HENDO in the RNP approach programming (as well as those associated with CS522 and CS523) not being loaded into the FMC.
As the aircraft approached HENDO, the captain selected 5,500 ft in the autopilot mode control panel and the aircraft subsequently descended below 6,800 ft, and shortly after, below 6,500 ft. Air traffic control contacted the crew and subsequently provided clearance for a visual approach. The aircraft landed at Cairns without further incident.
What the ATSB found
The ATSB found that on both occasions the flight crews did not recognise that an approach transition selection was required in the aircraft’s FMC. Consequently, no approach transition selection was made, and both crews resolved the resulting programmed flight path discontinuity by manually linking the HENDO waypoint associated with the arrival programming to waypoint CS540. This resulted in the removal of descent altitude protections associated with the HENDO waypoint in the approach programming and the resulting programmed flightpaths led to both aircraft descending below the minimum safe altitude.
The ATSB also identified that the Jeppesen RNP Y runway 33 approach chart used by both crews did not include the waypoints HENDO, CS522 and CS523 in the chart’s vertical profile depiction. Furthermore, the map presented the information associated with those waypoints over dense topographical information which limited the ability of both crews to identify the omitted descent restrictions associated with those waypoints. Additionally, the briefing conducted by the flight crews did not identify that data entry errors had removed some altitude protections.
Finally, the ATSB found that on each occasion, air traffic control quickly identified the incidents and took appropriate resolving actions.
What has been done as a result
Two days after the incident, Virgin Australia published a safety update for all flight crew providing contextual information of the occurrence and highlighting the missing waypoints in the vertical profile depiction on the Jeppesen Cairns RNP Y runway 33 chart. The safety update emphasised the requirement for an approach transition selection and was supported by an operational notice to Boeing 737 flight crews for operations into Cairns. The notice highlighted the complex nature of the HENDO 8Y arrival and Cairns RNP Y runway 33 procedure pairing and provided instruction for correct FMC data entry.
The day after the incident, Qantas Airways issued an internal notice to flight crew highlighting that many arrival and approach pairings require the selection of both an arrival transition and approach transition. The notice also described the effects of a non-selection of an approach transition with the information in the notice later incorporated into the Cairns Airport Route Manual Supplement. The details of the incident were also disseminated to all flight crew in a fleet newsletter and incorporated into Qantas’ evidence based training program.
Safety message
These occurrences highlight the risks associated with data entry errors that result in incomplete or incorrect information being entered in flight management systems. While no-one is immune from these errors, the risk can be significantly reduced through thorough and independent cross-checks between pilots and effective:
- communication
- operating procedures, and
- aircraft automation systems and software design.
The occurrences
24 October 2022
On the evening of 24 October 2022 a Virgin Australia Airlines Boeing 737-800, registered VH‑VUT, operated a passenger transport[1] flight from Brisbane to Cairns, Queensland. The captain was acting as pilot flying from the right control seat while the first officer was undertaking command training and operating as pilot monitoring in the left control seat.[2]
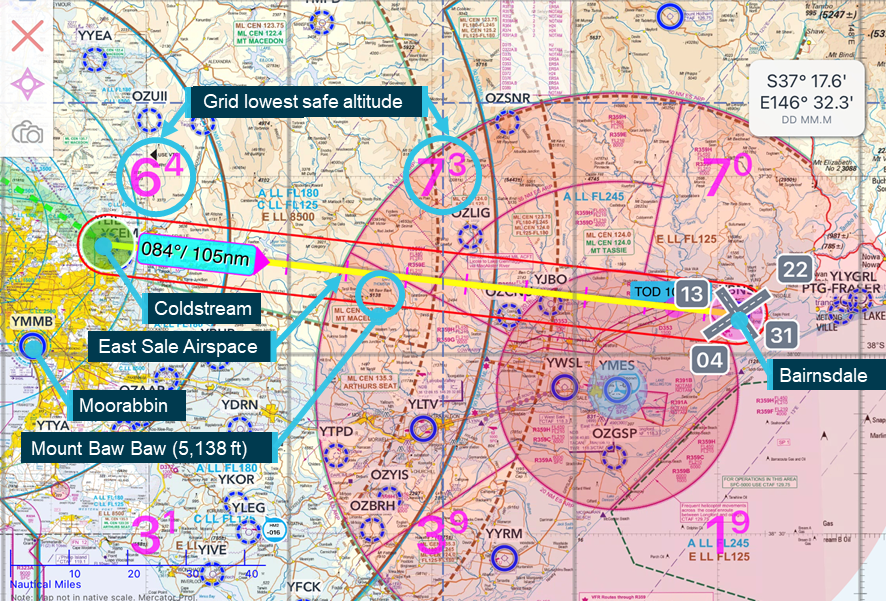
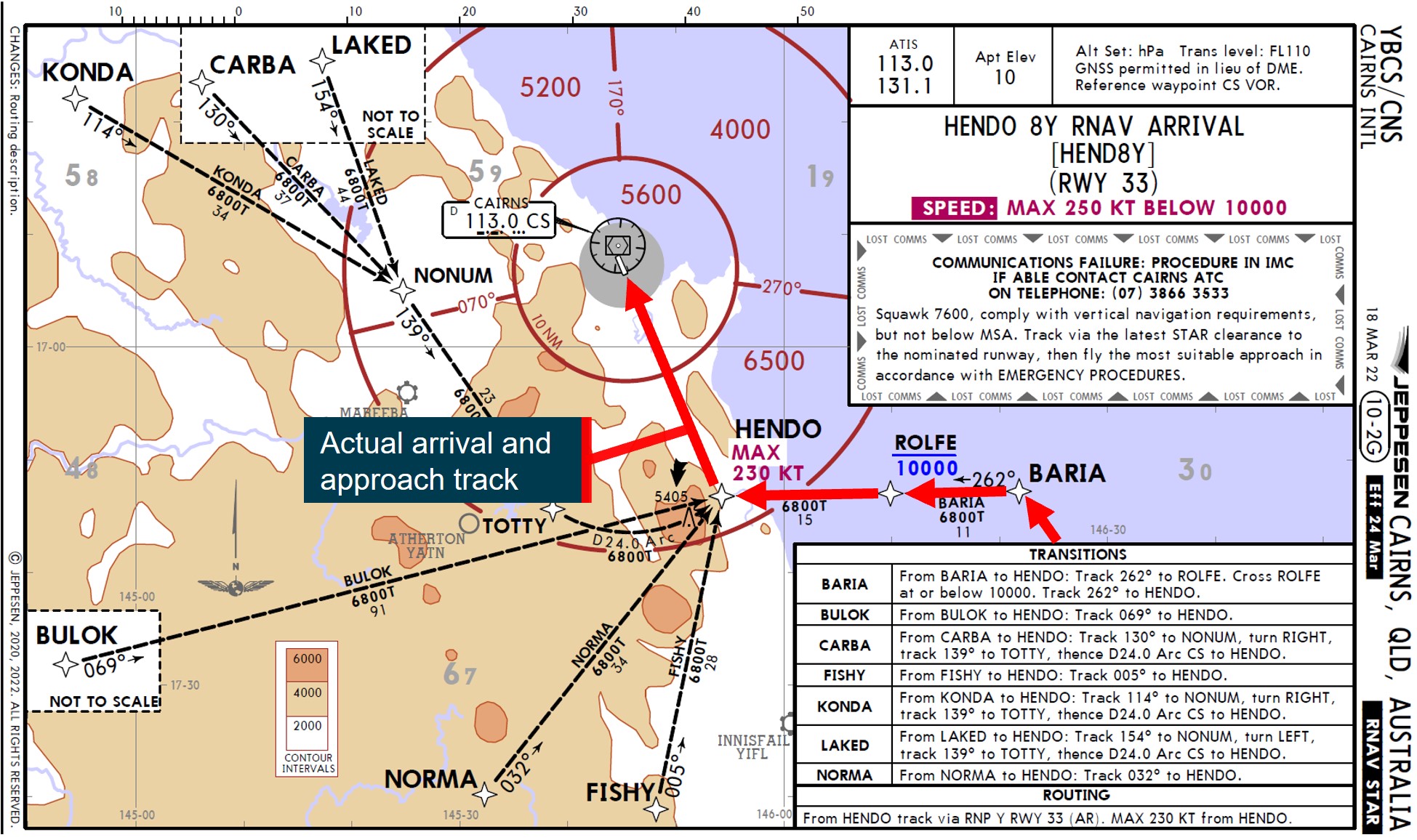
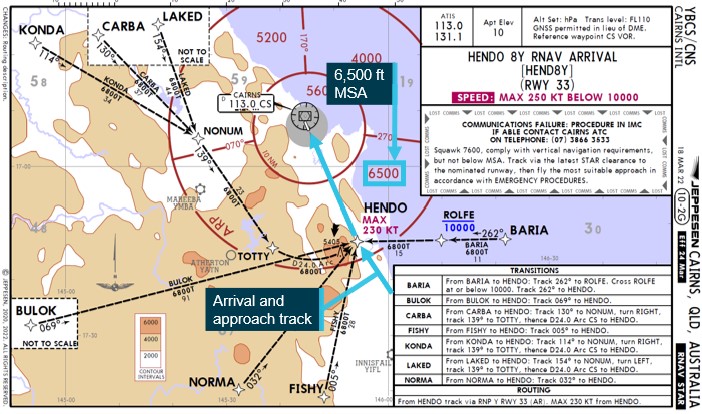
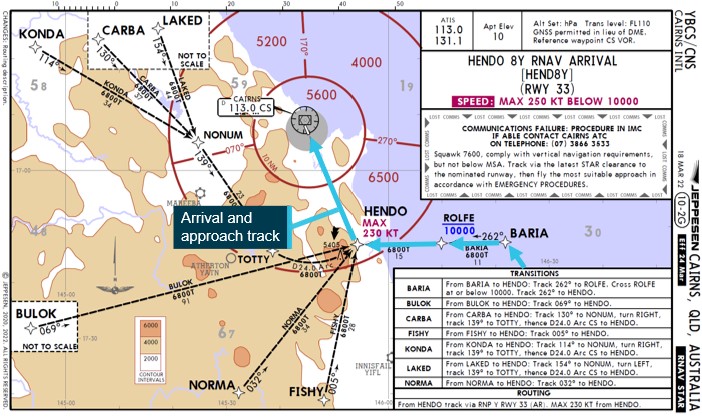
At 1945 local time, the aircraft was cruising in darkness at flight level (FL)[3] 380 about 215 NM to the south of Cairns. At that time, air traffic control (ATC) provided the crew with clearance to conduct the Cairns HENDO 8Y standard arrival via the BARIA waypoint[4] transition (Figure 1).
Figure 1: Jeppesen HENDO 8Y standard arrival – VH-VUT
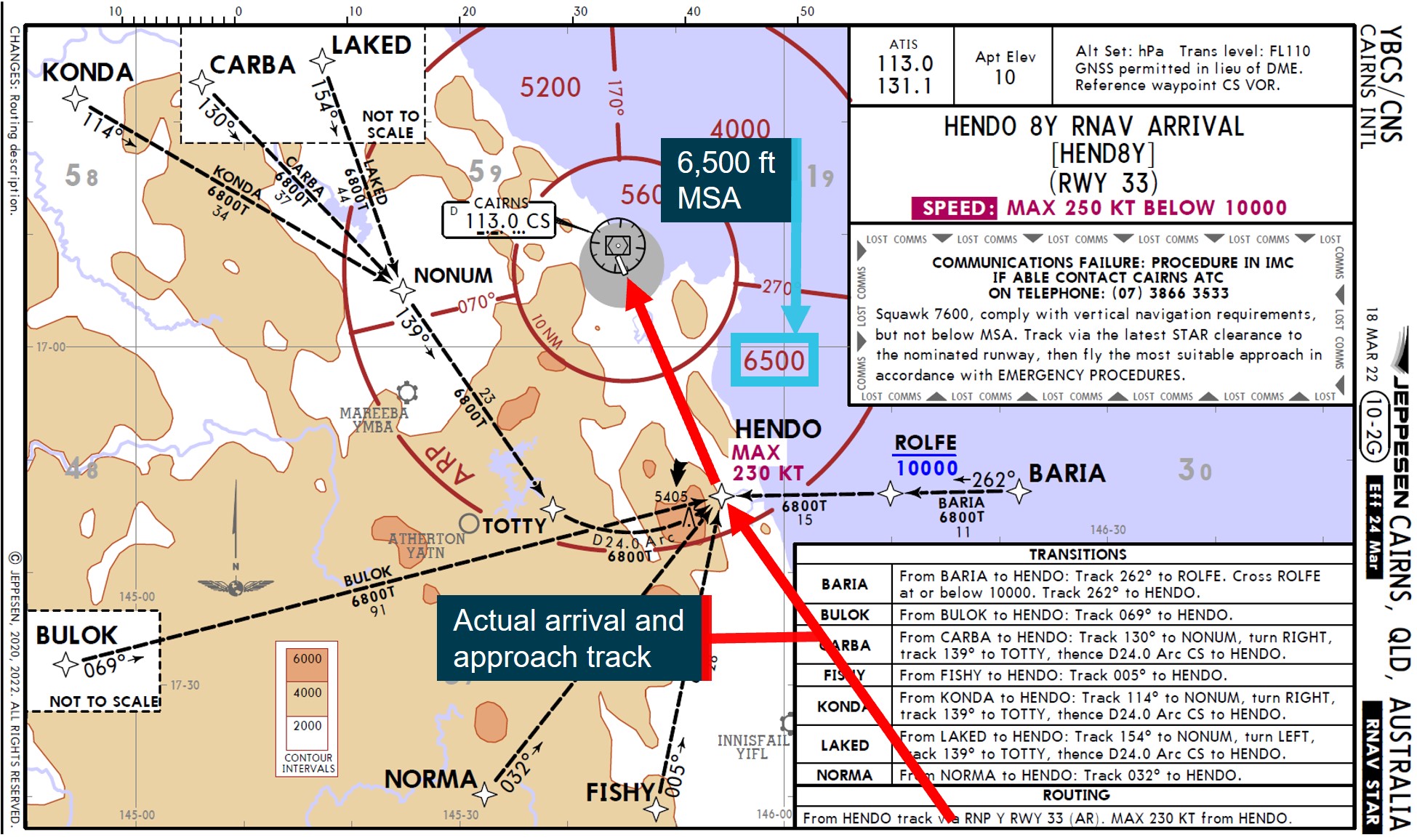
Note: Both Virgin Australia and Qantas Airways (see 26 October occurrence) were using procedure charts provided by Jeppesen.
Source: Virgin Australia, annotated by ATSB
The flight crew entered the HENDO 8Y arrival into the flight management computer (FMC) and selected the BARIA transition. The HENDO 8Y arrival progressed into the required navigation performance (RNP) Y instrument approach for runway 33 at Cairns Airport. While clearance for the approach had not been provided at that time, the crew anticipated the clearance and loaded the approach into the FMC. The HENDO waypoint was located within the 6,500 ft minimum sector altitude (MSA)[5] segment to the south of Cairns and from HENDO, the minimum altitude for commencing the RNP Y approach was 6,800 ft above mean sea level (AMSL).
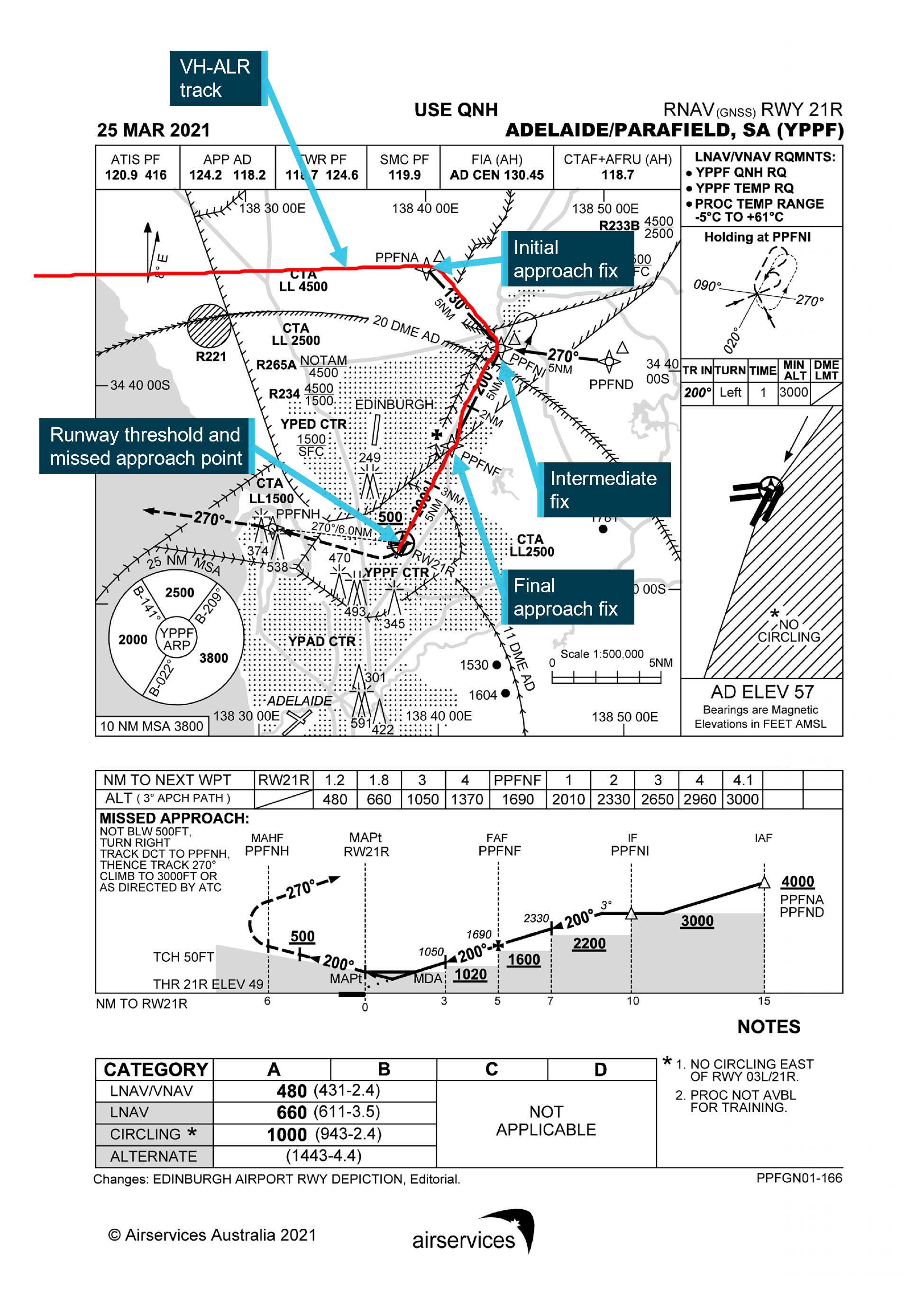
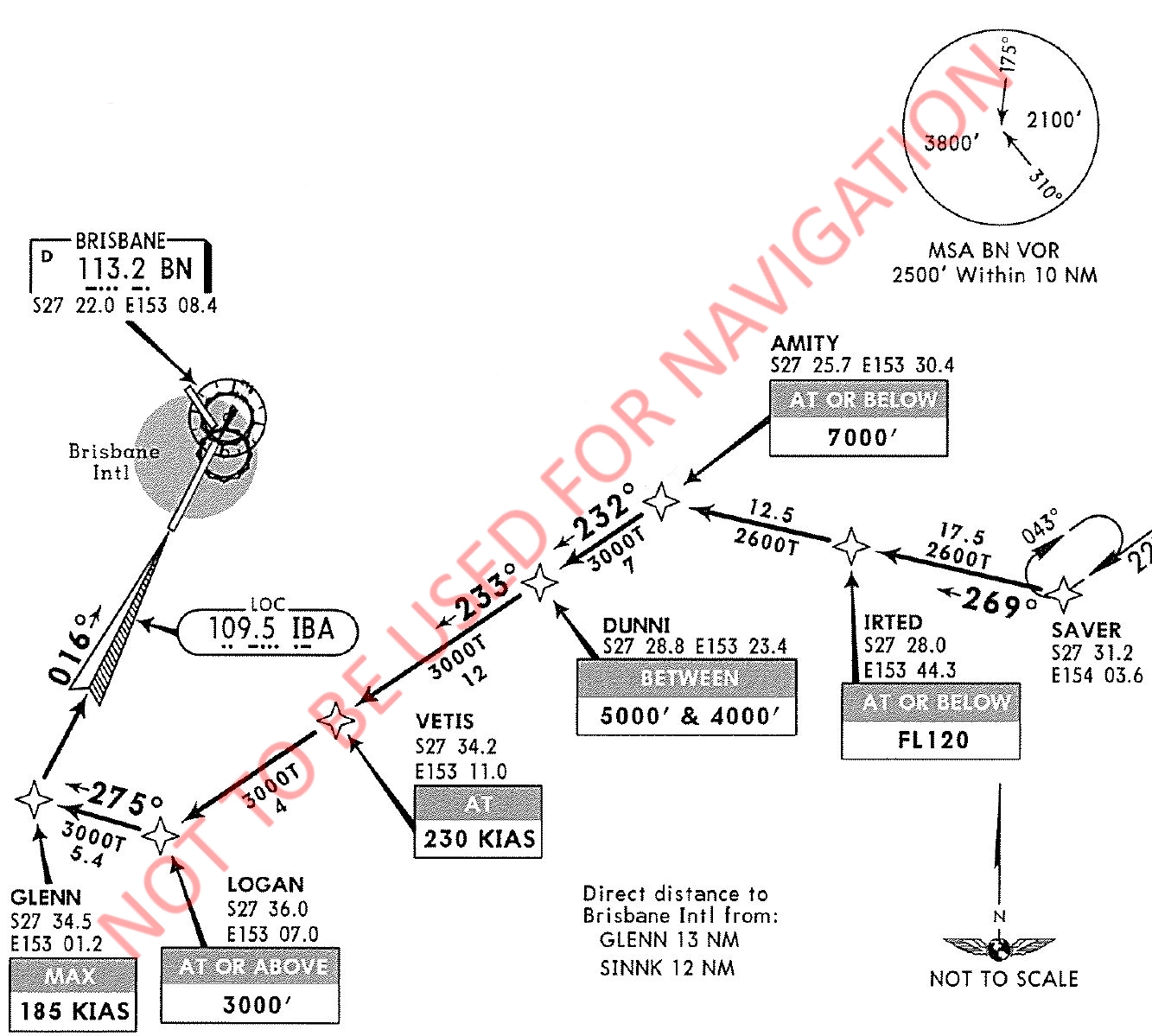
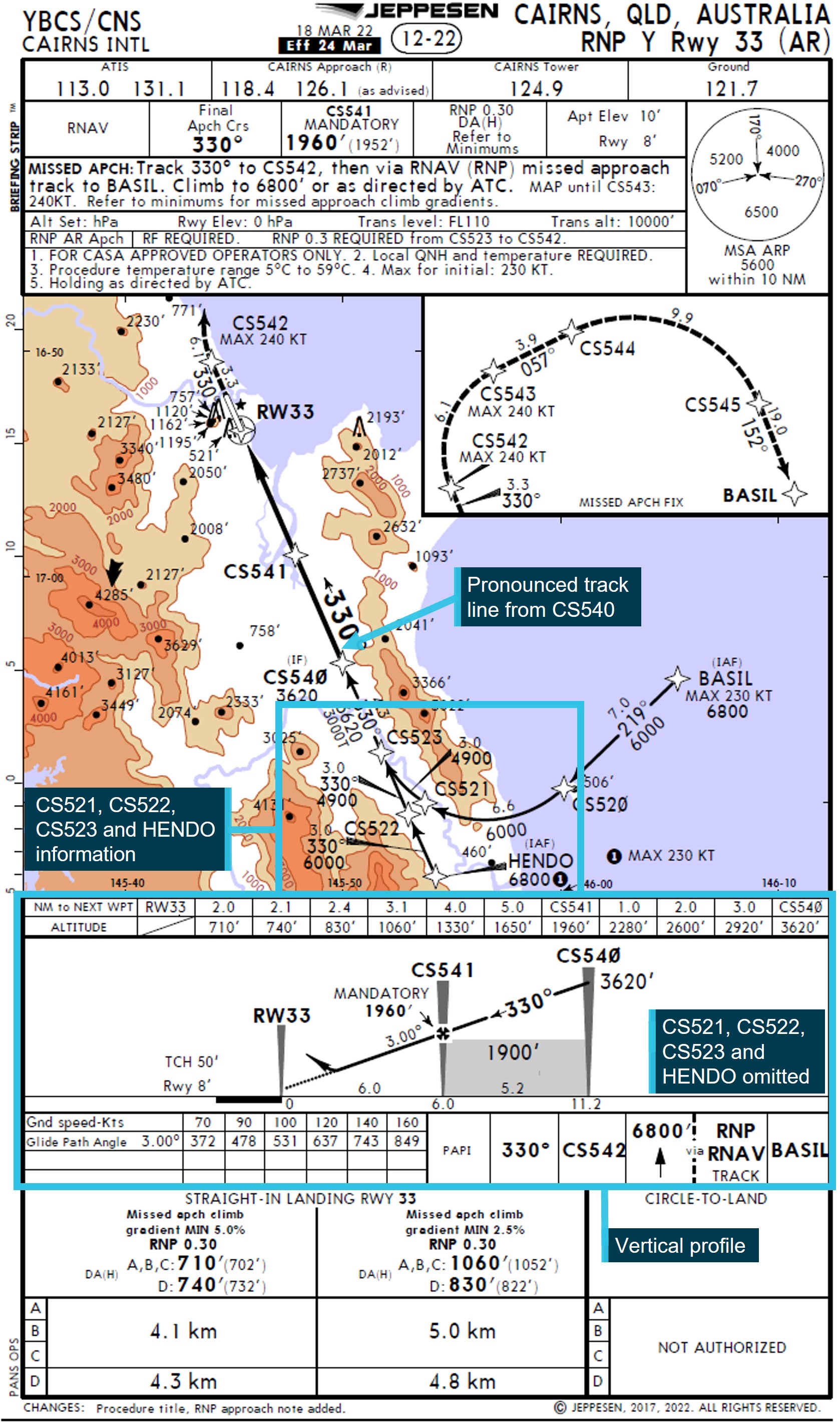
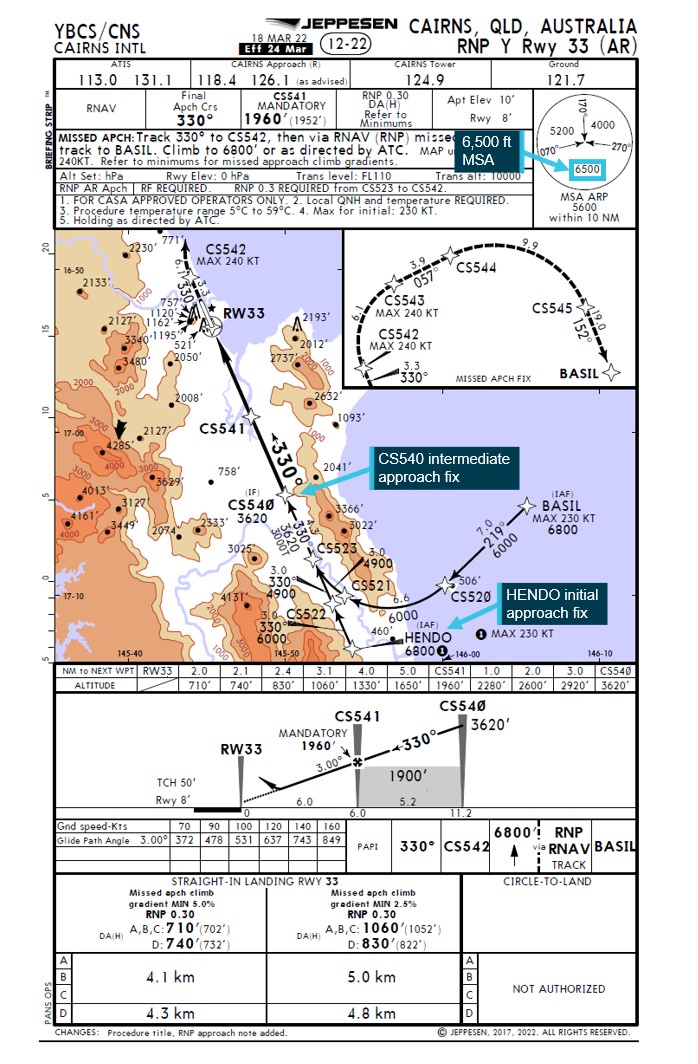
The approach procedure had 2 different initial approach fixes (IAF) (Figure 2) with associated paths to a common intermediate fix (IF) at waypoint CS540. From the BASIL IAF, the approach proceeded via CS520, CS521 and CS523, and from the HENDO IAF via CS522 and CS523. In order to load either path into the FMC, the flight crew needed to select one of the 2 approach transitions, BASIL or HENDO (see the section titled Flight management computer).
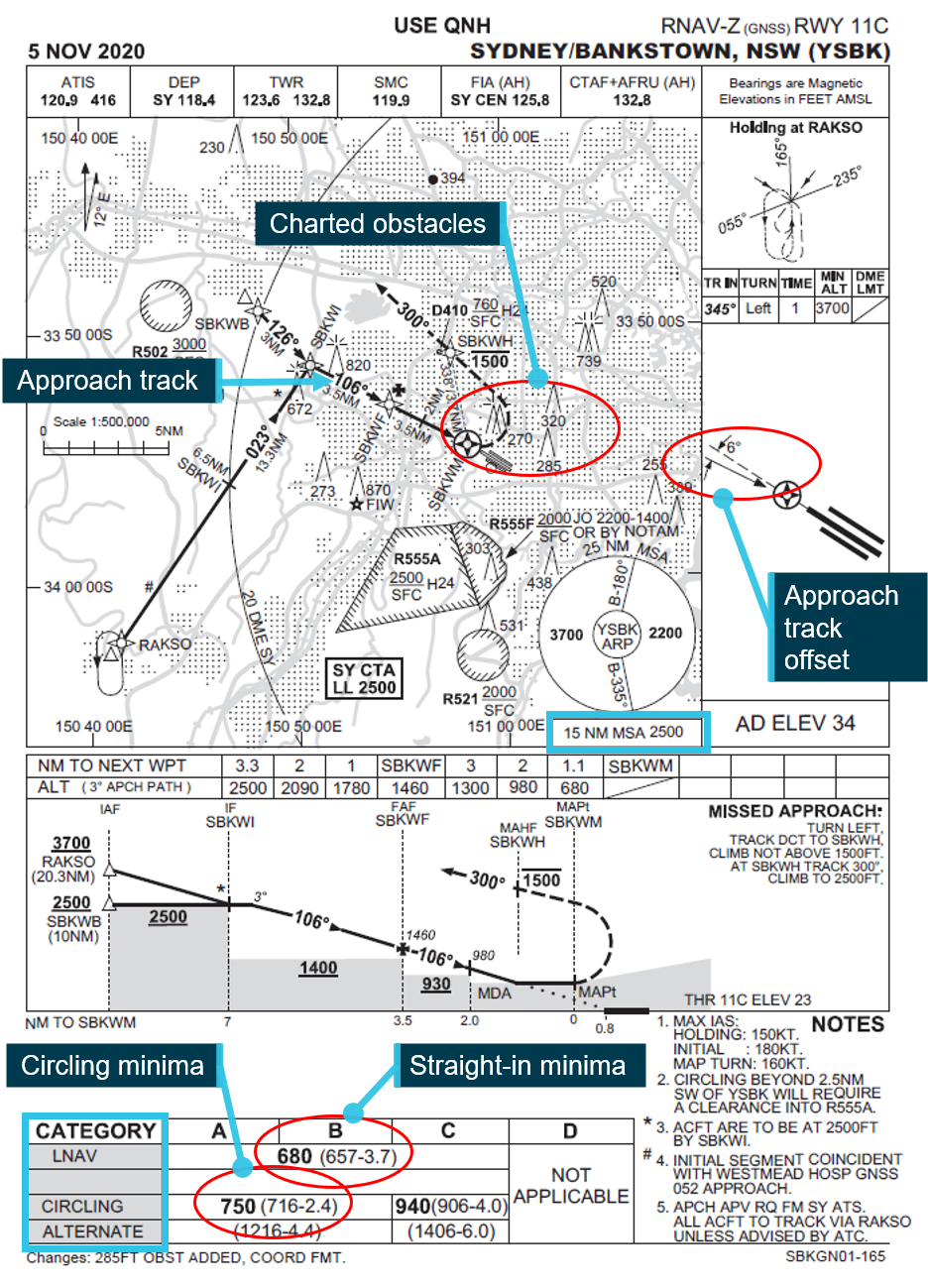
Figure 2: Jeppesen Cairns RNP Y runway 33 approach chart
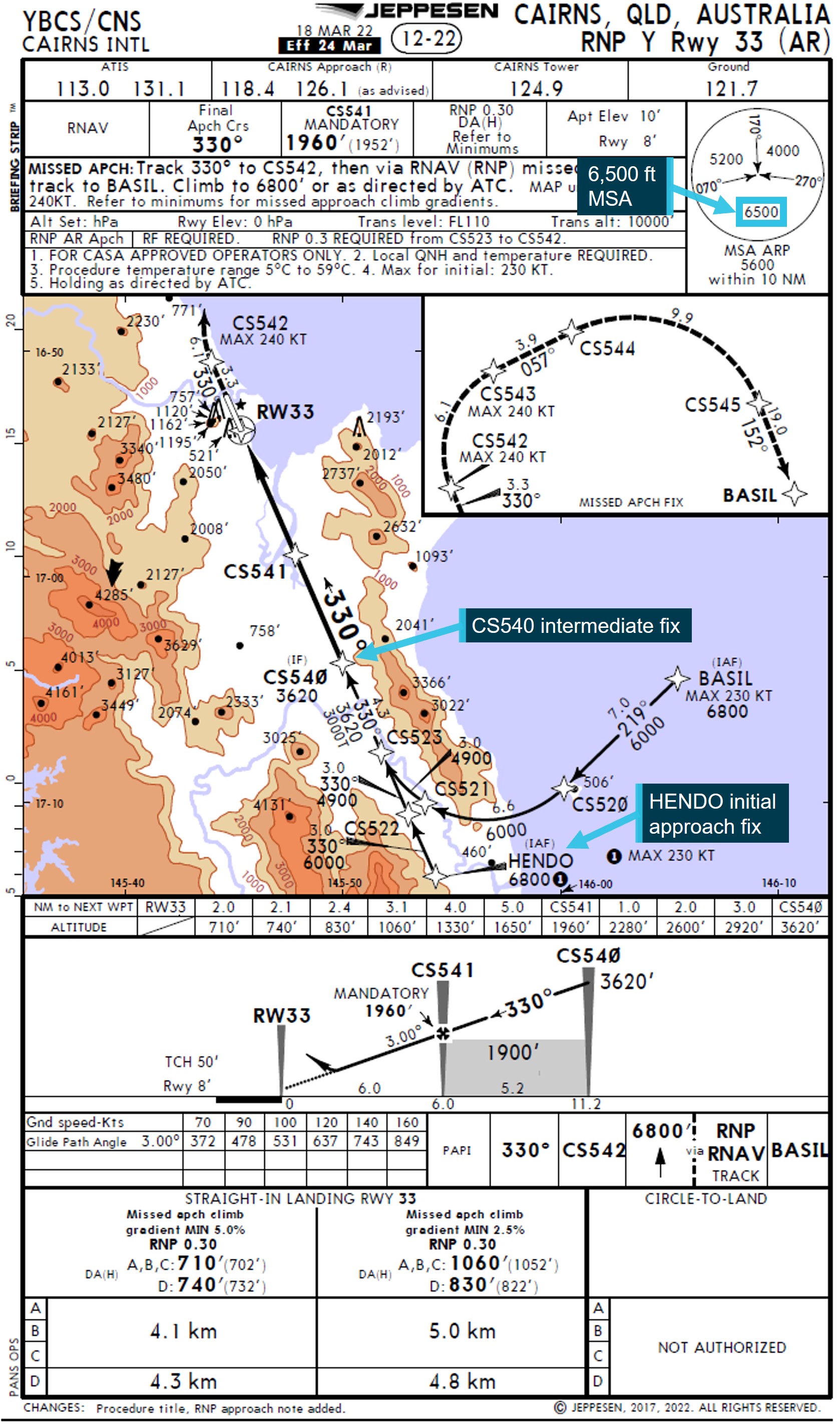
Source: Virgin Australia, annotated by ATSB
The flight crew did not recognise that an approach transition selection was required and consequently did not select one. As a transition had not been selected, the FMC presented a discontinuity in the entered flight path from the HENDO waypoint (see the section titled Flight management computer). The flight crew misidentified the approach IF, CS540, as the IAF and resolved the FMC discontinuity by connecting the HENDO arrival waypoint to CS540. This selection meant that the 6,800 ft descent altitude constraint associated with HENDO in the RNP approach programming was not loaded in the FMC.
At 1954, when the aircraft was 136 NM south of HENDO, ATC cleared the flight to track direct to the HENDO waypoint and 6 minutes later the crew commenced descending the aircraft. At 2010:51, when the aircraft was about 11 NM south‑east of HENDO, ATC provided the crew with clearance to conduct the RNP Y runway 33 approach.
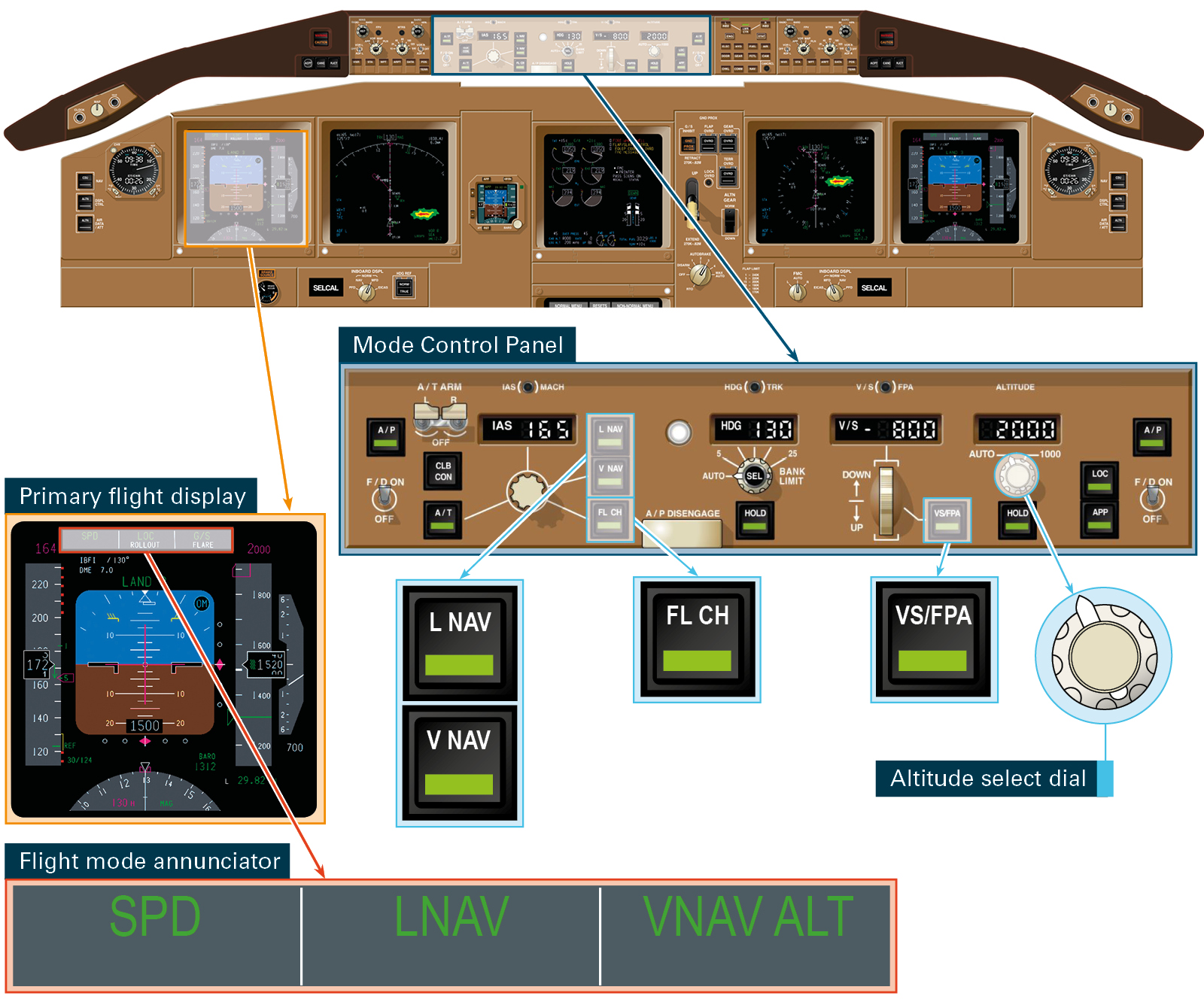
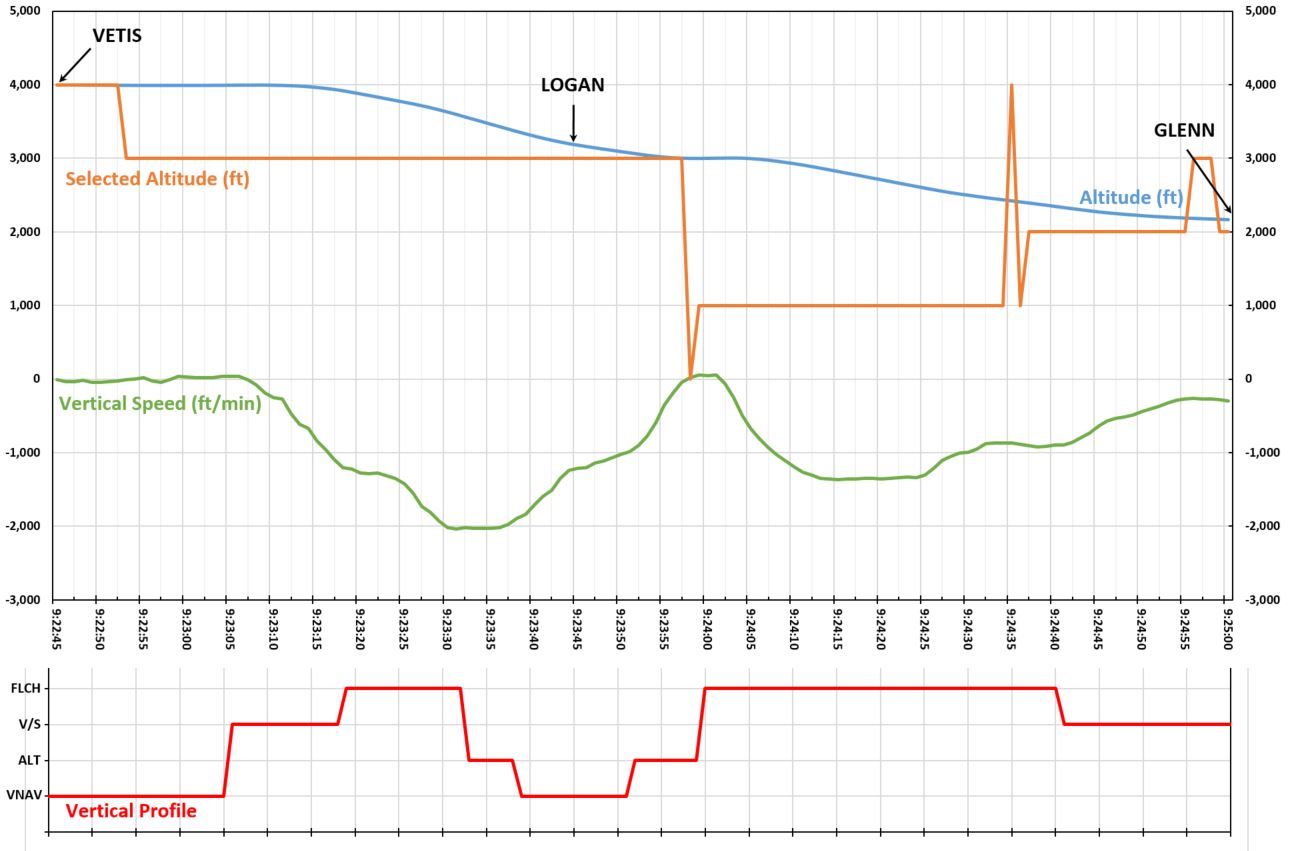
As the aircraft approached HENDO, it descended through about 7,300 ft with the autopilot engaged and the HENDO minimum safe altitude of 6,800 ft selected in the autopilot mode control panel. The captain then selected the approach’s minimum descent altitude of 800 ft on the autopilot mode control panel, but sensed that this selection was incorrect and therefore re‑selected an altitude of 6,800 ft. The captain then reviewed the approach briefing, confirmed that the aircraft was tracking as intended, that the vertical navigation autopilot mode[6] was active and then re-selected 800 ft.
At 2011:38, about 7 NM prior to crossing HENDO, the aircraft descended below 6,800 ft (Figure 3) and 9 seconds later descended below the 6,500 ft MSA. Six seconds later, at 2011:53, ATC observed that the aircraft had descended below 6,800 ft and contacted the crew to confirm the aircraft’s altitude. The captain then reselected 6,800 ft and manually arrested the descent. ATC then issued a low altitude alert to the crew and advised them to climb immediately. Three seconds later, at 2012:07, the aircraft stopped descending at about 6,048 ft and then commenced a climb. At 2012:28, the aircraft climbed back above 6,800 ft. No ground proximity warning system alerts were generated during the incident.
A missed approach was then commenced. During preparations for the second approach, the crew recognised that an approach transition selection was required and correctly loaded the RNP Y runway 33 approach using the BASIL transition. The crew then conducted the approach and landed without further incident.
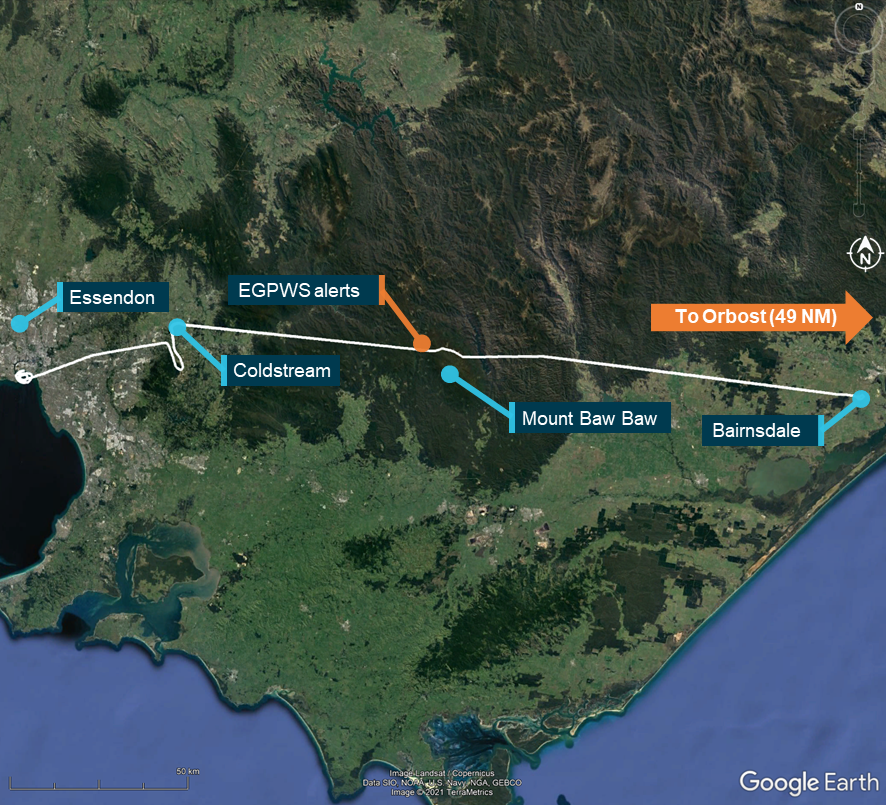
Figure 3: Flight path of VH-VUT
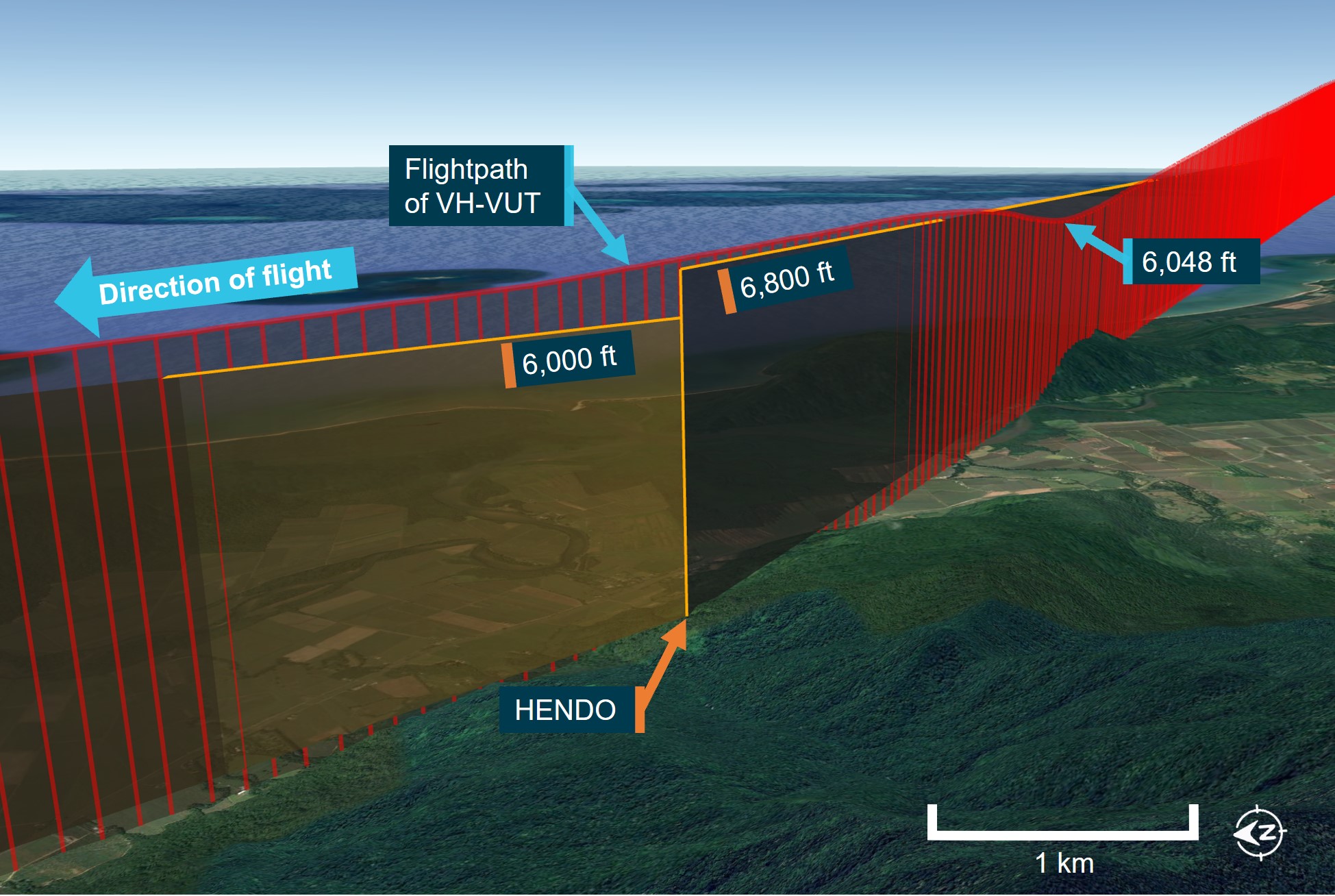
Source: Virgin Australia, Airservices Australia and Google Earth, annotated by ATSB
26 October 2022
On the morning of 26 October 2022 a Qantas Airways Boeing 737-800, registered VH-VZA, operated a passenger transport flight[7] from Brisbane to Cairns. The captain was acting as pilot flying, and the first officer was acting as pilot monitoring.
At 0739, in daylight, while the aircraft was in cruise at FL 380 about 225 NM to the south of Cairns, ATC provided the crew with clearance to conduct the Cairns HENDO 8Y arrival via the BARIA waypoint transition (Figure 4).
Figure 4: Jeppesen HENDO 8Y standard arrival – VH-VZA
Source: Virgin Australia, annotated by ATSB
The flight crew entered the HENDO 8Y arrival into the FMC and selected the BARIA transition. While clearance for the RNP Y runway 33 approach had not been provided at that time, the crew anticipated the clearance and loaded the approach. The crew believed that they had only been cleared for the BARIA arrival transition and had not yet received clearance for the HENDO approach transition, and therefore did not select that transition. As the selection had not been made, the FMC did not load the instrument approach segment from the IAF to the IF and presented a discontinuity between the waypoint HENDO and the IF waypoint CS540 (see the section titled Flight management computer).
The crew noted that the waypoints CS522 and CS523 were missing from the track presented on the navigation display and contacted ATC to request confirmation of the arrival clearance. ATC then provided a clearance for the HENDO 8Y arrival with a FISHY transition. The crew reviewed the arrival chart and assessed that they could not achieve the required descent profile to proceed via FISHY and requested clarification of the arrival transition. ATC then confirmed the arrival transition was via BARIA.
The flight crew noted that the track from HENDO to CS540 passed over the locations of CS522 and CS523. As there was no cloud along the flight path and terrain was visible, the crew were not reliant on FMC programming for terrain clearance. As such, the crew decided to join the discontinuity at HENDO to CS540 and proceed with the approach. The captain also selected the HENDO minimum safe altitude of 6,800 ft in the autopilot mode control panel.
At 0808:20, when the aircraft was 18 NM east of HENDO with the autopilot engaged and descending through about FL110, ATC provided the crew with clearance to conduct the RNP Y runway 33 approach.
At 0810:42, when the aircraft was about 7 NM east of HENDO, the crew noted that the approach vertical profile presented on the primary flight display showed the aircraft to be above the programmed descent path. During the crew’s investigation into the profile deviation, the captain selected 5,500 ft in the autopilot mode control panel. Without the 6,800 ft HENDO descent altitude programmed into the FMC, the aircraft commenced descending below 6,800 ft, and 34 seconds later below the 6,500 ft MSA.
The aircraft passed HENDO at 0811:56 at an altitude of 6,129 ft (Figure 5). The crew recognised that the aircraft had descended early and selected the altitude hold (ALT HLD) autopilot function to stop further descent. Eleven seconds after the aircraft crossed HENDO, ATC contacted the crew to verify that the aircraft had passed HENDO at the correct altitude. ATC then confirmed with the crew that the flight was operating in visual conditions and provided clearance for a visual approach.
The aircraft landed at Cairns without further incident. After landing, the flight crew discussed the incident and recognised that an approach transition selection was required. The crew then reloaded the approach using the HENDO transition and observed that all waypoints and altitude constraints were correctly programmed.
Figure 5: Flight path of VH-VZA
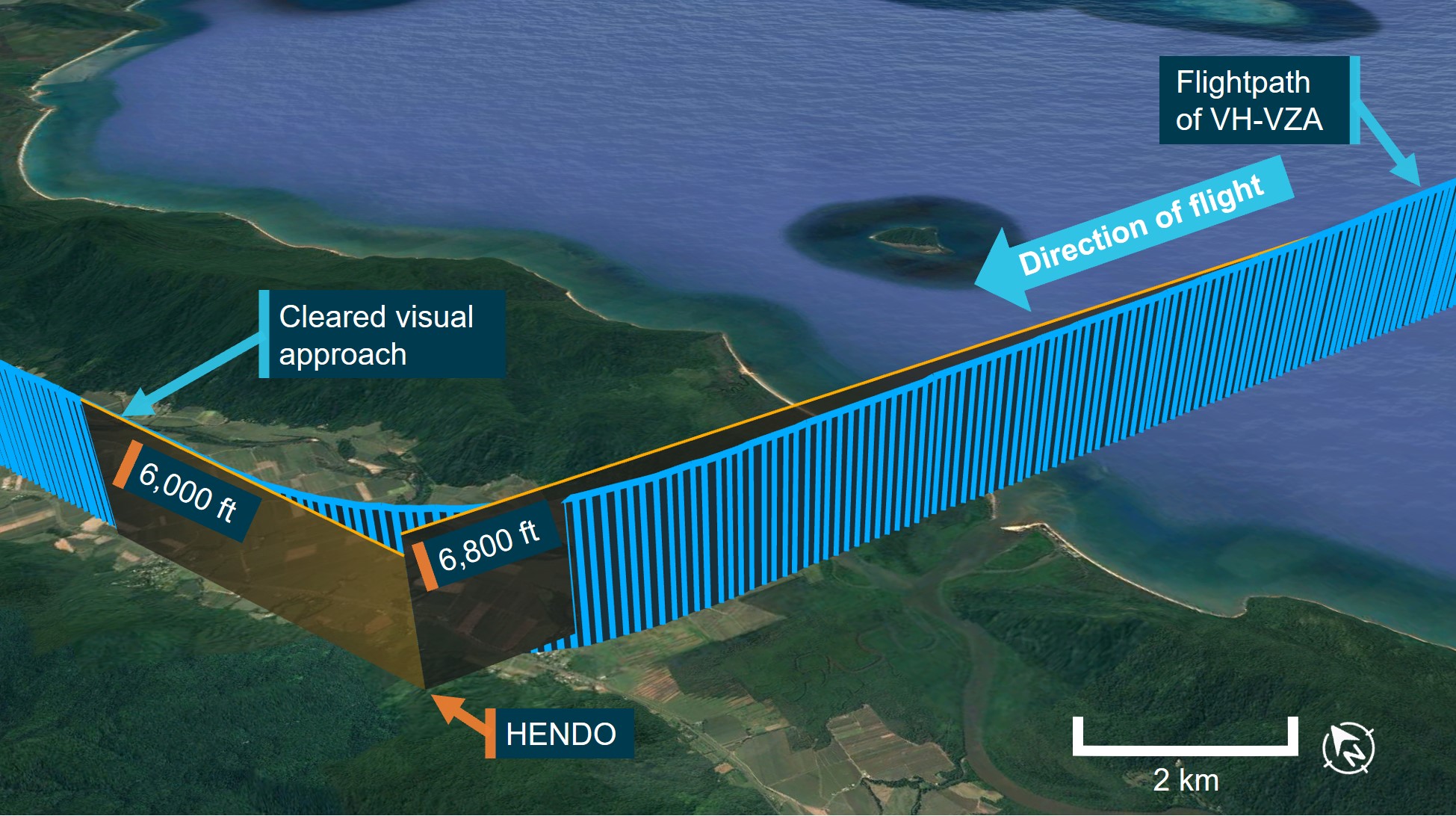
Source: Qantas, Airservices Australia and Google Earth, annotated ATSB
Context
Crew details
VH-VUT
The captain operated the flight as a training captain from the right control seat. The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate and had over 8,000 hours of flying experience, of which over 3,100 were on the Boeing 737.
The first officer was undergoing command upgrade training and operating the flight from the left control seat. The first officer held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate and had over 8,600 hours of flying experience, of which over 5,200 were on the Boeing 737.
VH-VZA
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had over 13,800 hours of flying experience, of which over 7,400 were on the Boeing 737.
The first officer held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had over 8,700 hours of flying experience, of which over 1,000 were on the Boeing 737.
Fatigue
The ATSB found no indicators that any of the flight crewmembers on either flight were experiencing a level of fatigue known to affect performance.
Meteorology
24 October 2022
The approach was conducted at night and terrain was not visible to the flight crew.
At 2010, 1 minute before VH-VUT descended below the HENDO altitude constraint, the Bureau of Meteorology (BoM) automatic weather station at Cairns Airport recorded the wind as 7 kt from 333° magnetic. Two cloud layers were also present: scattered[8] at 1,710 ft and broken at 2,110 ft above mean sea level (AMSL).
26 October 2022
The approach was conducted during daytime with no cloud and excellent visibility.
At 0800, 10 minutes before VH-VZA descended below the HENDO altitude constraint, the BoM automatic weather station at Cairns Airport recorded the wind as 2 kt from 213° magnetic. No cloud was recorded.
Arrival and approach procedures
Arrival naming
The HENDO 8Y standard arrival procedure included 7 individual transitions which led to a common waypoint, HENDO. The procedure was named after HENDO as the first (and only) common waypoint. The HENDO waypoint was also 1 of 2 initial approach fixes (IAF) for the Cairns RNP Y runway 33 approach. The other IAF, BASIL, was used for a different arrival procedure or following a missed approach.
The HENDO 8Y arrival led to the HENDO IAF and the arrival charts included the wording ‘from HENDO track via RNP Y RWY 33 (AR)’.
Approach transition selection
The two different IAFs of the RNP Y runway 33 approach procedure had associated paths to a common intermediate fix (IF) (CS540): from BASIL through waypoints CS520, CS521 and CS523, or from HENDO through CS522 and CS523. As there were 2 available options, the flight crew needed to select the required approach transition.
Selecting the RNP Y approach procedure in the flight management computer (FMC) provided the final approach procedure path, from CS540 through the final approach fix CS541, toward the runway and, if required, the missed approach procedure. The loaded data also included any associated altitude and speed limitations. To load the approach procedure from the IAF to the IF, the flight crew were required to select an approach transition. Selecting the HENDO transition would have loaded the track from HENDO to CS540, via CS522 and CS523, as well as any associated altitude constraints and speed limitations.
Cairns RNP Y runway 33 procedure chart
Airservices Australia and Jeppesen (an approved data service provider) published charts for the Cairns RNP Y runway 33 procedure. The charts produced by both organisations were designed and published in accordance with International Civil Aviation Organisation (ICAO) guidance.[9] Both of the aircraft involved in these occurrences used arrival and approach charts provided by Jeppesen.
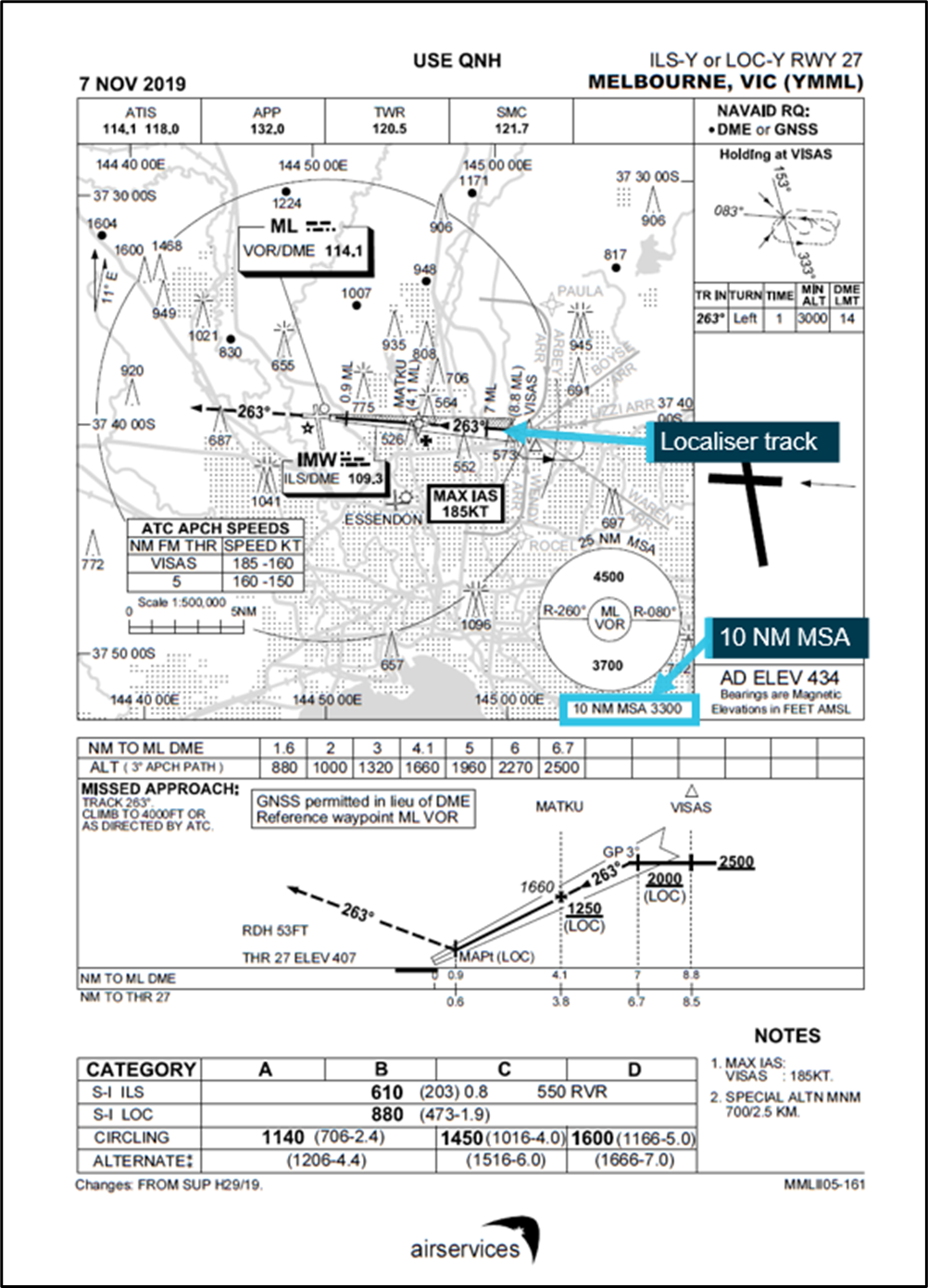
The Airservices Australia chart vertical profile presentation included the full approach including the waypoints CS521, CS522 and HENDO (Figure 6).
Figure 6: Airservices Cairns RNP Y runway 33 approach chart
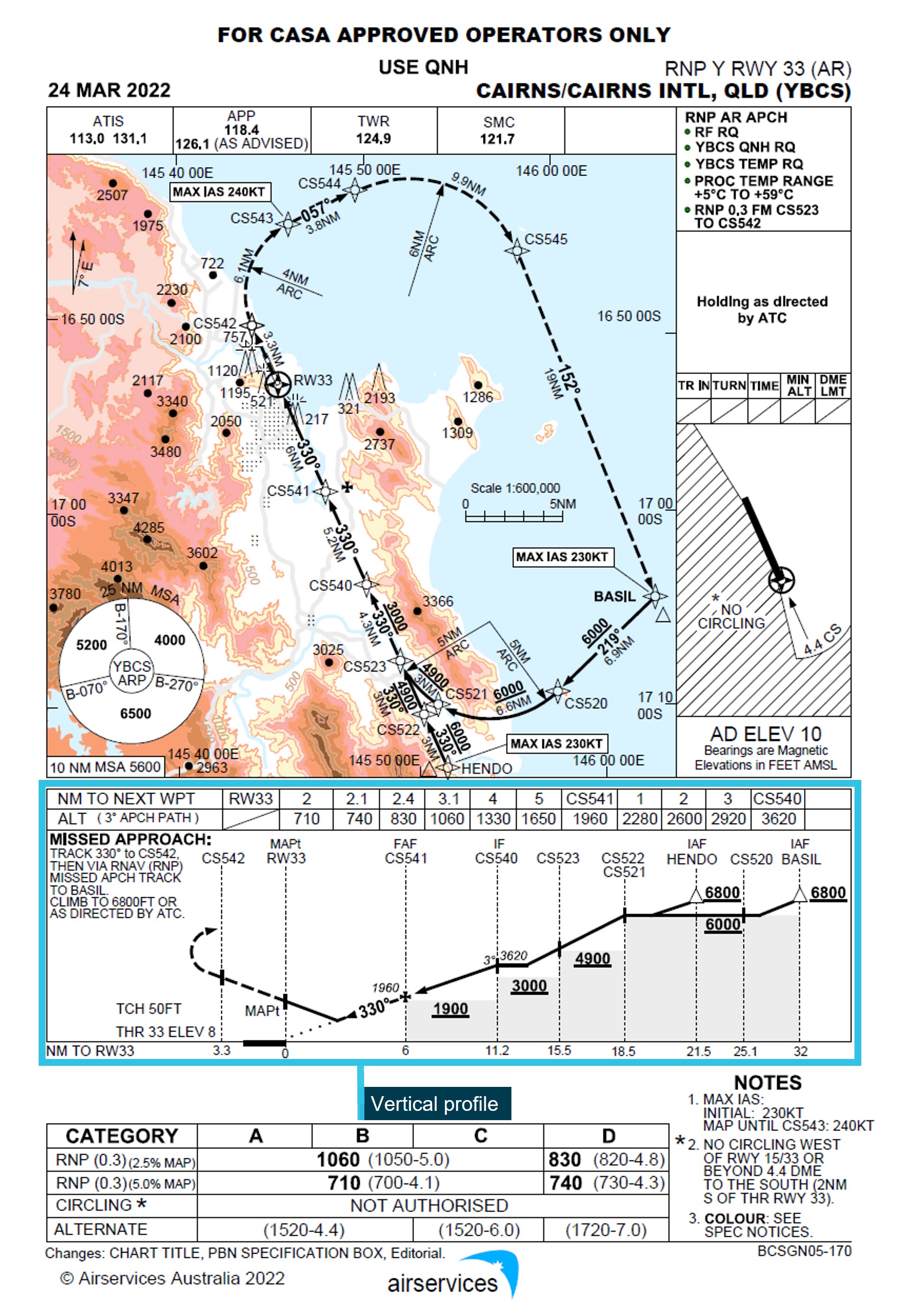
Source: Airservices Australia, annotated by ATSB
The Jeppesen chart (Figure 7) vertical profile did not include the waypoints CS521, CS522, CS523 and HENDO. The chart's vertical profile commenced at waypoint CS540 and approach track information on the map was emphasised with a broader line from this waypoint. The information (including altitude constraint information) relating to waypoints CS521, CS522, CS523, HENDO and their associated segments was presented on the map over shaded topographical information and with an arrow to the associated item.
Figure 7: Jeppesen Cairns RNP Y runway 33 approach chart
Source: Virgin Australia, annotated by ATSB
To provide a standardised presentation of aeronautical data for Jeppesen charts worldwide, Jeppesen chart design specifications directed that the vertical profile commence at the IF when an approach has multiple transitions. Jeppesen noted that this was the most common worldwide depiction of profile information. As the Cairns RNP Y approach had multiple transitions leading to the CS540 IF, the vertical profile commenced at that waypoint.
Flight management computer
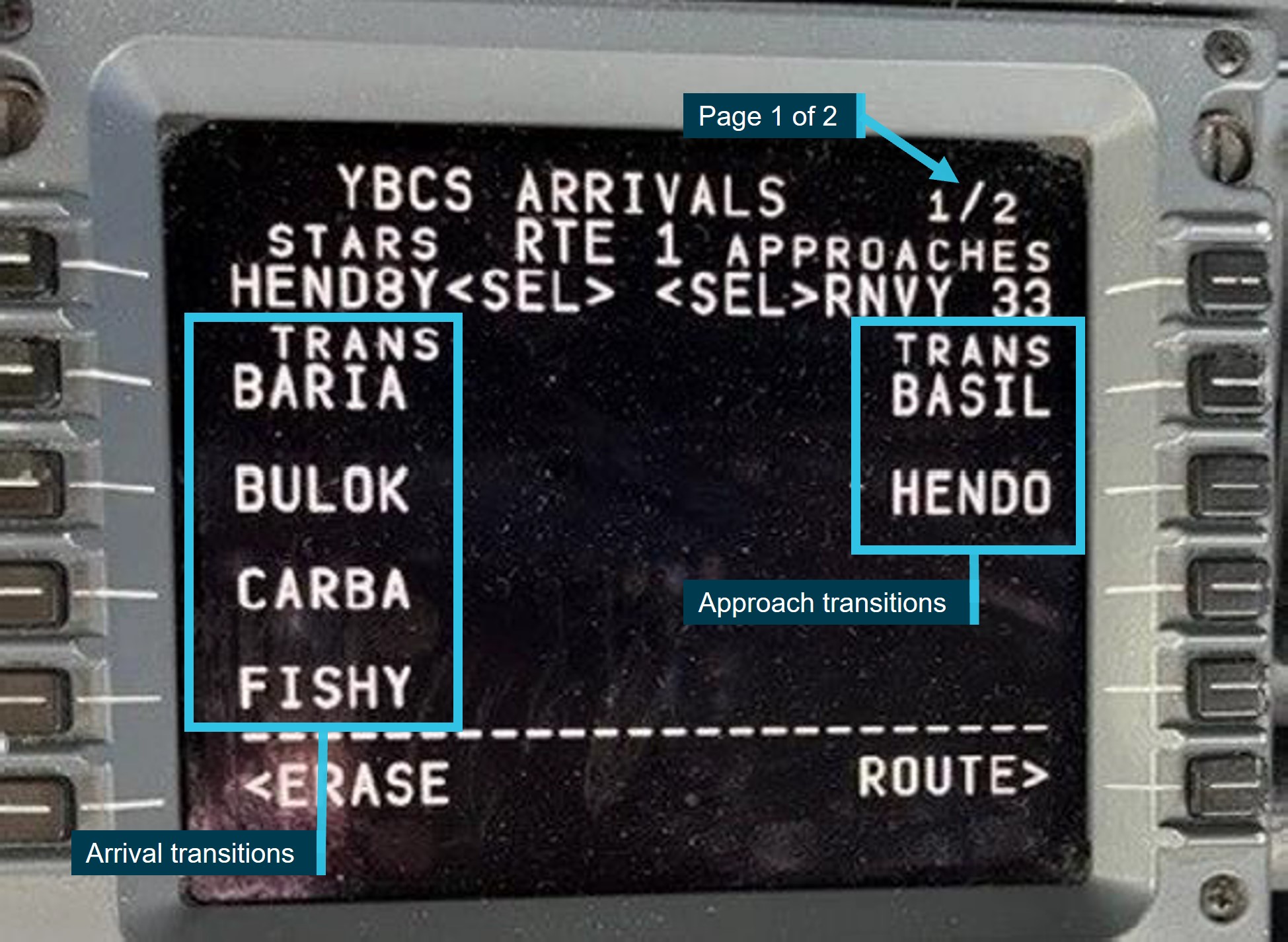
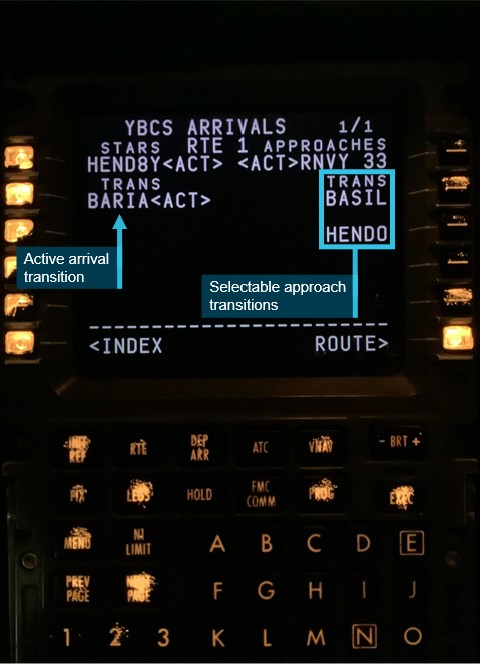
The arrival and approach transitions were both presented on the same FMC Arrivals page (Figure 8). In the case of the HENDO 8Y arrival, the number of available selection lines on the screen was limited to only display 4 of the 7 available transitions. The remaining 3 available arrival transitions were displayed on a second arrivals page. This second page was indicated by a ‘1 / 2’ (page 1 of 2) at the top right of the screen.
The 2 approach transitions were presented on the right side of the arrivals screen. The crews of both aircraft did not recognise that the right column were approach transition selections.
Figure 8: Flight management computer transitions
Source: Virgin Australia, annotated by ATSB
If an approach transition was not selected, the segment of the approach from the IAF to the IF, and the associated altitude constraints, would not be loaded in the FMC.
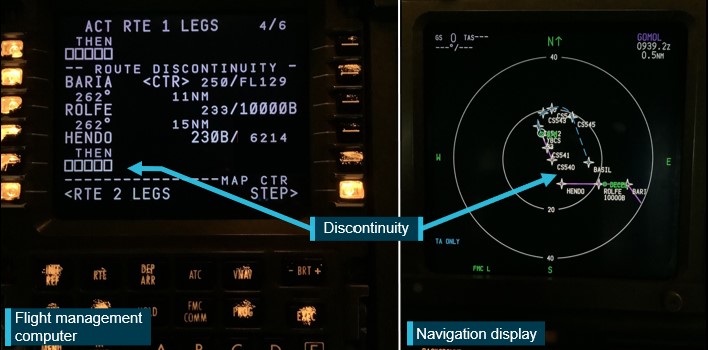
As the crews did not select an approach transition, a discontinuity was created at the HENDO waypoint associated with the HENDO 8Y arrival (Figure 9). Both crews resolved this discontinuity by connecting the waypoint HENDO from the arrival procedure to the waypoint CS540 in the approach procedure. As waypoint HENDO in the FMC arrival procedure did not have the 6,800 ft descent altitude constraint (the constraint was only associated with the HENDO approach waypoint), this altitude constraint was not loaded into the FMC. Similarly, the segment minimum safe altitudes associated with waypoints CS522 (6,000 ft) and CS523 (4,900 ft) were not loaded.
Figure 9: Flight management computer (left) and navigation display (right) showing the discontinuity
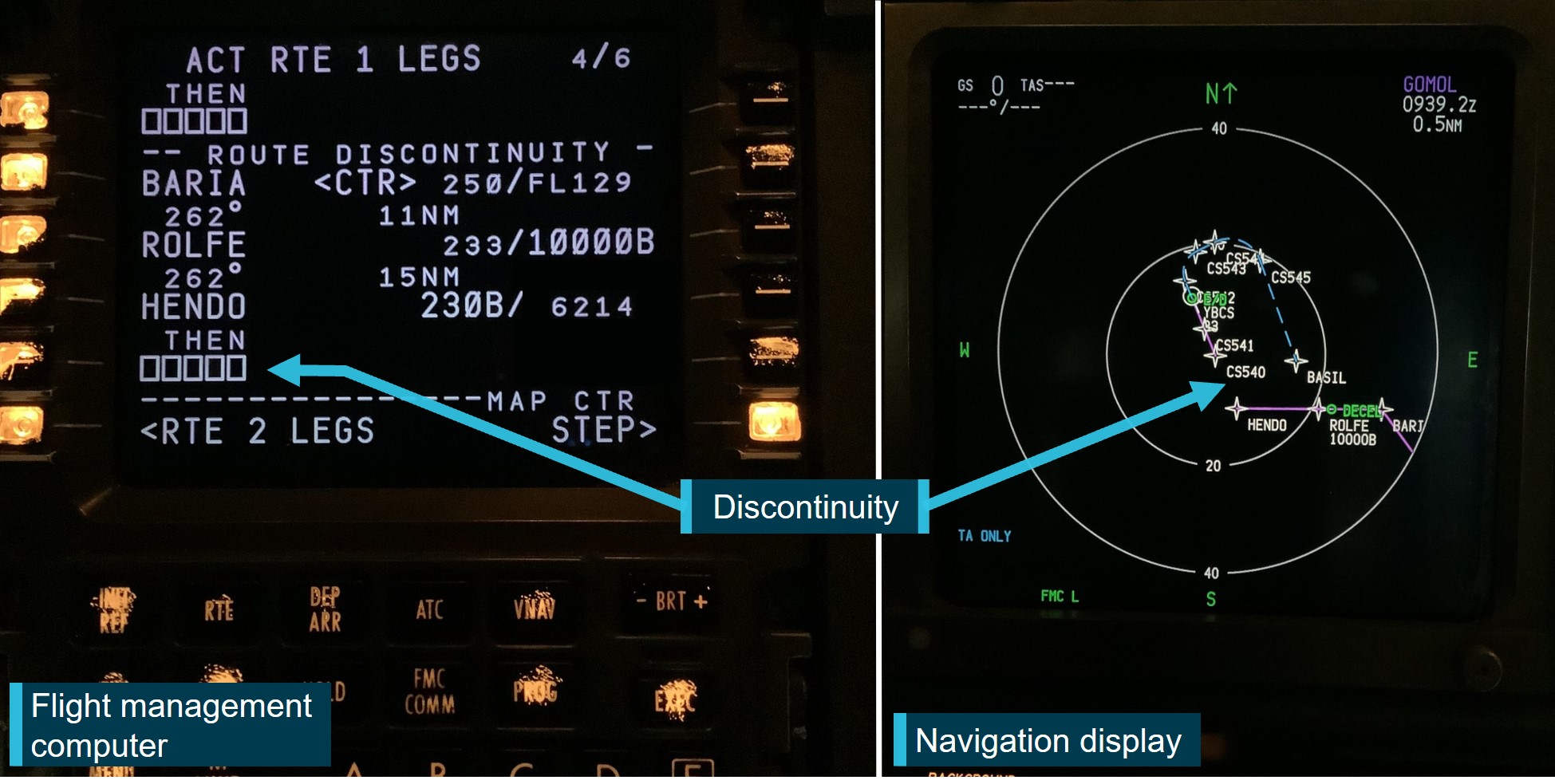
Source: Virgin Australia, annotated by ATSB
Approach briefings
The objective of an approach briefing is to ensure all flight crew understand and share a common mental model for the proposed plan of action. This briefing was normally performed by the pilot flying with the pilot monitoring checking the data entered into the FMC. Both operators provided requirements across training and operation manuals for crews to ensure effective cross checking of data entered into the FMC.
VH-VUT
The Virgin Operating Policies and Procedures Manual provided the following relevant guidance for approach briefings:
The captain of VH-VUT advised that, when conducting the approach briefing, they normally prioritised the vertical profile. The captain later reported that the absent waypoints in that profile, along with the thicker map line from CS540, may have contributed to their misidentification of CS540 as the IAF.
The captain did not announce the absent waypoints during the briefing. When confirming the data entered into the FMC, the first officer did not independently review the chart and therefore similarly did not identify the missing waypoints and altitude constraints.
During the briefing and check of the entered data, the pilot monitoring (first officer) became confused as to where in the sequence of the data being read the pilot flying (captain) had progressed to. The pilot monitoring sought clarification from the pilot flying, who advised that the brief had moved to the missed approach, a number of waypoints ahead of the pilot monitoring’s anticipated location. The crew did not further investigate the misunderstanding and continued the brief from the missed approach.
VH-VZA
The Qantas Flight Administration Manual provided the following relevant guidance for approach briefings in Boeing aircraft:
During the approach briefing the flight crew identified the 2 missing waypoints between HENDO and CS540. However, the captain did not note the altitude restrictions at CS522, CS523 and HENDO and did not announce them during the briefing. Furthermore, the first officer did not independently review the chart, removing an opportunity to identify the missing altitude constraints.
Airways clearances
Both crews were provided with the same approach clearance from air traffic control:
This clearance required the crews to adhere to all approach tracking and associated altitude constraints.
The clearance phraseology was consistent with Aeronautical Information Publication[10] guidance in not including reference to the HENDO approach transition. However, for VH-VUT, because a clearance had previously been provided direct to HENDO, the approach clearance should have been prefixed with ‘when established’. As the approach clearance was provided after the FMC data error had already been made and was unlikely to highlight any error, the incorrect phraseology did not contribute to the occurrence.
The air traffic control provider, Airservices Australia, advised that both aircraft had a route clearance to Cairns Airport. This was included in the arrival instruction ‘from HENDO track via the RNP Y runway 33’. For the RNP Y runway 33 approach, the IAFs HENDO and BASIL are subject to the same concept as other RNP approaches with multiple IAFs (for example EA, EB or EC). Therefore, the IAF did not need to be specified with the approach clearance.
Similar occurrences
The HENDO 8Y arrival and RNP Y runway 33 approach were introduced in August 2017, 5 years prior to the occurrences. At the time of the release of this report, the only recorded occurrences involving a descent below minimum altitude in the vicinity of HENDO are the 2 occurrences in this report.
A previous ATSB investigation involving a similar occurrence is summarised below:
ATSB investigation AO-2017-026
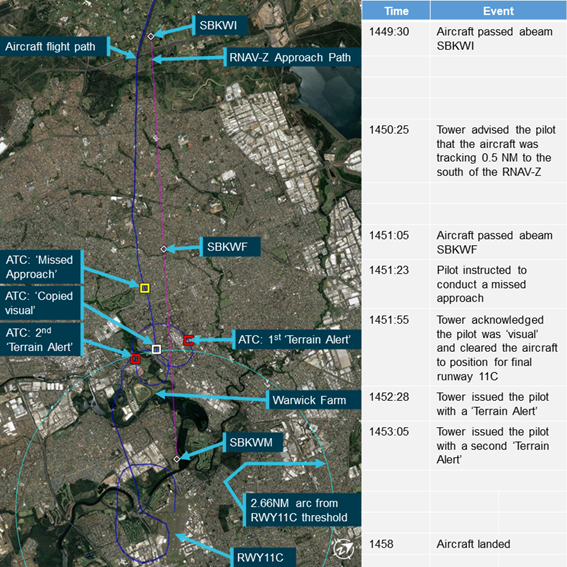
On the morning of 22 February 2017, a Singapore Airlines Boeing 777-212, registered 9V-SRP, operated scheduled flight SQ291 from Singapore to Canberra, Australian Capital Territory. Prior to descent, the flight crew prepared to conduct the POLLI FOUR PAPA arrival and associated RNAV-Z approach. As the aircraft descended, ATC instructed the flight crew to conduct the POLLI FOUR BRAVO arrival. As the 2 arrivals were very similar, the flight crew elected to reprogram the POLLI FOUR BRAVO arrival into the FMC while keeping the RNAV-Z approach, creating a discontinuity in the programmed FMC flight path. The captain resolved this discontinuity by manually connecting the arrival waypoint MENZI to the approach at waypoint SCBSI. In doing so, the approach waypoint SCBSG was erased from the programmed FMC approach. The captain manually re-entered SCBSG into the FMC without detecting that an associated 7,500 ft altitude constraint was now missing.
As the aircraft continued the approach it twice descended below minimum safe altitudes before being provided with clearance to complete a visual approach.
Safety analysis
Introduction
On the evening of 24 October 2022, a Boeing 737-800 operated by Virgin Australia Airlines operated a night air transport flight from Brisbane to Cairns, Queensland. On the morning of 26 October 2022, a Boeing 737-800 operated by Qantas Airways operated the same route in daylight. During both flights, the crews did not recognise that an approach transition had to be selected when entering approach data into the flight management computer (FMC) and no selection was made.
This analysis focuses on the reasons for the crews not making the approach transition selection or identifying the data entry error prior to it resulting in both aircraft descending below the minimum safe altitude.
Transition selection
The Cairns HENDO 8Y arrival procedure had 7 arrival transitions and was named after the last waypoint in the procedure (the first common waypoint for the transitions), which was relatively uncommon. The HENDO waypoint was also one of 2 initial approach fixes (IAF) and was therefore also the name of a transition for the approach. The 2 approach transition options were presented on the right-hand side of the same FMC page as the arrival transitions, with 4 arrival transitions on the left-hand side of the same page and the remaining 3 on the next page. The crews of both aircraft did not recognise that the transitions on the right related to the approach and consequently, the requirement to select an approach transition was not immediately apparent to them.
For the crew of VH-VUT, this perception was compounded by the misidentification of the waypoint CS540 as the IAF (see the section below titled Approach chart). Separately, the crew of VH-VZA were influenced by an expectation that the wording of the approach clearance would include the nomination of a transition. However, as an airways clearance to Cairns via the HENDO 8Y arrival and RNP Y approach had been provided, no separate nomination of the approach transition was required or provided.
Ultimately, these factors resulted in both flight crews not recognising that an approach transition selection was required and consequently, none was selected. Not selecting the approach transition resulted in a discontinuity between the waypoints HENDO and CS540 in the programmed flight path.
Discontinuity resolution
Having misidentified CS540 as the IAF, the captain of VH-VUT resolved the discontinuity by manually linking HENDO from the arrival to CS540 in the approach. This presented an approach track that closely aligned with the crew’s expectations, but with the omission of the altitude constraints associated with the approach waypoints HENDO, CS522 and CS523.
On board VH-VZA, after entering the approach without selecting a transition, the crew identified that waypoints were missing from the approach. As the programmed flight path continued along the same track, the crew elected to continue the approach without the entering the waypoints into the FMC and linked the waypoint HENDO from the arrival to CS540 in the approach. This decision was possibly influenced by the fact that the aircraft was operating in visual conditions and the crew were not reliant on the FMC programming for terrain clearance. However, the crew did not identify that altitude constraints associated with the unprogrammed waypoints were omitted from the programmed flight path.
In each case, this led to the approaches continuing with the altitude constraints removed and when an altitude below the minimum safe altitude was selected, the aircraft commenced automatically descending to that altitude. This resulted in both aircraft descending below the approach altitude constraints and then the minimum sector altitude. This was contrary to air traffic control clearances and, for VH-VUT, also reduced obstacle clearance assurance as the flight was conducted in darkness.
Approach chart
The HENDO 8Y arrival and Cairns RNP Y runway 33 approach were a complex procedure pairing with similarly complex charts.
In addition, the Jeppesen approach chart used by both crews was designed and published in accordance with ICAO guidance, but did not include the waypoints HENDO, CS522 and CS523 on the vertical profile depiction. This information was included on a comparable chart produced by Airservices Australia. Had those waypoints been included on the vertical profile of the Jeppesen chart, the likelihood of the descent restrictions being identified would have been increased.
The missing waypoints on the vertical profile and thicker track line from CS540 on the approach chart likely contributed to the captain of VH-VUT misidentifying that waypoint as the IAF. These missing waypoints were also the waypoints omitted from the FMC programming if an approach transition was not selected. Therefore, their omission was not an immediate indicator of a data entry error.
Furthermore, the Jeppesen chart presented the information (including the altitude constraints) associated with the missing waypoints and segments over topographical information on the map and separated from the relevant waypoints and segments. This reduced the readability of the information and may have contributed to the crews not associating the relevant information with their respective waypoints and segments thereby further reducing the crews’ ability to identify the associated altitude constraints.
Approach Briefing
Both operators required the approach briefing to ensure that the data entered into the flight management computer included all relevant waypoints and altitude constraints from the procedure chart.
In each case, the pilot flying read from the procedure chart while the pilot monitoring reviewed the data in the FMC. This method was not fully independent and relied on the pilot flying to identify all applicable details. The missed altitude constraints (and waypoints in the case of VH-VUT) were not read out by the pilot flying and therefore, their omission was not identified by the pilot monitoring’s check. The pilot monitoring’s assessments of the correct data input was also supported by the navigation display map view tracks closely aligning with expectations.
During the approach briefing conducted by the crew of VH-VUT an opportunity was presented to pause the brief and identify the data entry error. This occurred when the pilot monitoring became confused as to the sequence of the data being read by the pilot flying. The pilot monitoring sought clarification from the pilot flying. This likely occurred as the data entered was not complete and should have acted as a trigger for reassessment of that data.
In the case of VH-VZA, the crew did identify the missing waypoints but did not fully consider the altitude constraint implication associated with these waypoints. A comprehensive brief would probably have identified these missing constraints. While the terrain was visible to the crew and they were not reliant on FMC programming for terrain protection, the airways clearance did require adherence to the limiting altitudes.
In summary, the approach briefs conducted by the crews did not ensure that the charts, and the programmed approach flight path, were fully and independently assessed. Therefore, the data entry errors leading to the removal of the altitude protections were not detected.
Air traffic control intervention
On each occasion, air traffic control quickly identified the aircraft descending below the 6,800 ft altitude constraint and immediately contacted the crews. As the VH-VUT incident was at night and not in visual conditions, the controller issued a low altitude alert to the crew and advised them to climb immediately.
The conditions were clear and during daylight for the crew of VH-VZA and therefore air traffic control was able to provide a clearance for a visual approach.
Air traffic control acts to coordinate the flow of aircraft arriving at an airport, but also plays an important role in identifying risks to aircraft. On these occasions, air traffic control intervened quickly and appropriately to resolve the risks of each descent below the minimum safe altitude.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the flight below minimum altitude occurrences, 40 km south of Cairns Airport, Queensland on 24 and 26 October 2022.
Contributing factors
- Both flight crews did not recognise that an approach transition selection was required in the aircraft’s flight management computer. Not selecting the approach transition resulted in a programmed flight path discontinuity between the waypoints HENDO and CS540.
- The flight crews of both aircraft resolved the discontinuity by manually linking the HENDO waypoint associated with the arrival programming to waypoint CS540. This selection removed the 6,800 ft descent altitude constraint associated with the HENDO waypoint in the approach programming. With the altitude constraint removed, the programmed flightpaths led to both aircraft descending below the minimum safe altitude.
- The vertical profile depiction on the Jeppesen RNP Y runway 33 approach chart did not include the waypoints HENDO, CS522 and CS523 and the map presented the information associated with those waypoints over dense topographical information. This likely limited the ability of both crews to identify the descent restrictions associated with those waypoints.
- Both operator’s instrument approach briefing procedure included a requirement to ensure all necessary waypoints and operational constraints were included in the procedures loaded into the flight management computer. However, the briefing conducted by the flight crews did not identify that data entry errors had removed some altitude protections.
Other findings
- On each occasion, air traffic control intervened quickly and appropriately to resolve the risks of each descent below the minimum safe altitude.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety actions in response to this occurrence. |
Safety action not associated with an identified safety issue
Proactive safety action by Virgin Australia Airlines
| Action number: | AO-2022-051-PSA-01 |
| Action organisation: | Virgin Australia Airlines |
Two days after the incident, Virgin Australia published a safety update for all flight crew regarding the occurrence on 24 October 2022. This update provided contextual information on the occurrence and highlighted the missing waypoints in the vertical profile depiction on the Jeppesen Cairns RNP Y runway 33 chart. The update also emphasised the requirement for an approach transition selection.
Virgin Australia also supported the safety update with a flight crew operational notice to 737 flight crew for operations into Cairns. The notice highlights the complex nature of the HENDO 8Y arrival and Cairns RNP Y runway 33 procedure pairing and provides instruction for correct FMC data entry.
Proactive safety action by Qantas Airways
| Action number: | AO-2022-051-PSA-02 |
| Action organisation: | Qantas Airways |
The day after the incident, Qantas Airways issued an internal notice to flight crew highlighting that many arrival and approach pairings require the selection of both an arrival transition and approach transition. This notice also described the effects of a non-selection of an approach transition with the information in the notice later incorporated into the Cairns Airport Route Manual Supplement. The details of the incident were also disseminated to all flight crew in a fleet newsletter and incorporated into Qantas’ evidence based training program.
Proactive safety action by Airservices Australia
| Action number: | AO-2022-051-PSA-03 |
| Action organisation: | Airservices Australia |
To ensure that consistent and correct phraseology is used when providing approach clearances at Cairns, Airservices Australia has issued a standardisation directive to the air traffic control unit.
Glossary
AIP Aviation information publication
AMSL Above Mean Sea Level
ATC Air traffic control
CASA Civil Aviation Safety Authority
CASR Civil Aviation Safety Regulations
FMC Flight Management Computer
IAF Initial Approach Fix
IF Intermediate Fix
MSA Minimum sector altitude
RNP Required navigation performance
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Airservices Australia
- Virgin Australia Airlines
- Qantas Airways
- Jeppesen
- the flight crews of both aircraft
- Civil Aviation Safety Authority
- recorded aircraft data from VH-VUT and VH-VZA.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- Airservices Australia
- The United States National Transportation Safety Board
- Virgin Australia Airlines
- Qantas Airways
- Jeppesen
- the flight crews of both flights.
Submissions were received from:
- Airservices Australia
- Qantas Airways
- the flight crew of VH-VZA.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[2] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 380 equates to 38,000 ft.
[4] Waypoint: A defined position of latitude and longitude coordinates, primarily used for navigation.
[5] Minimum sector altitude (MSA) and lowest safe altitude (LSALT) are calculated to provide 1,000 ft obstacle clearance for instrument flight rules flights and are published on aeronautical charts and in the Aeronautical Information Publication (AIP) for pilot and controller reference.
[6] Vertical navigation (VNAV): This autopilot mode commands the auto flight system to follow the flight management system generated vertical navigation flight path including altitude constraints.
[7] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[8] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered.
[9] International Civil Aviation Organization 2016, Aeronautical Chart Manual third edition, document 8697.
[10] Aeronautical Information Publication General section 3.4 paragraph 6.14 – Approach and Area Control Services
Interim report
Report release date: 28/02/2023
| This interim report details factual information established in the investigation’s evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrences
24 October 2022
On the evening of 24 October 2022, a Virgin Australia Airlines Boeing 737-800 registered VH-VUT operated a flight from Brisbane to Cairns, Queensland. The captain was acting as pilot flying from the right flight crew seat, the first officer was undertaking command training and operating as pilot monitoring in the left flight crew seat.[1]
At 1945 local time, the aircraft was cruising in darkness at flight level (FL)[2] 380 about 215 NM to the south of Cairns. At that time, air traffic control (ATC) provided the crew with clearance to conduct the Cairns HENDO 8Y standard arrival (STAR) via the BARIA waypoint[3] transition (Figure 1).
Figure 1: Jeppesen HENDO 8Y standard arrival – VH-VUT
Note: Both Virgin Australia and Qantas (see 26 October occurrence) were using procedure charts provided by Jeppesen.
Source: Virgin Australia, annotated by ATSB
The flight crew entered the HENDO 8Y STAR into the flight management computer (FMC) and selected the BARIA transition. The HENDO 8Y STAR progressed into the required navigation performance (RNP) Y instrument approach for runway 33 at Cairns. While clearance for the approach had not been provided at that time, the crew anticipated the clearance and loaded the approach into the FMC. From HENDO, the minimum altitude for commencing the RNP Y approach was 6,800 ft above mean sea level (AMSL). The HENDO waypoint was located within the 6,500 ft minimum sector altitude (MSA)[4] segment to the south of Cairns.
The approach procedure had two different initial approach fixes (IAF) (Figure 2) with associated paths to a common intermediate fix (IF) at waypoint CS540. From the BASIL IAF, the approach proceeded via CS520, CS521 and CS523, and from the HENDO IAF via CS522 and CS523. In order to load either path into the FMC, the flight crew needed to select one of the two approach transitions (see the section titled Flight management computer).
Figure 2: Jeppesen Cairns RNP Y runway 33 approach chart
Source: Virgin Australia, annotated by ATSB
The flight crew did not recognise that an approach transition selection was required and consequently did not select one. As a transition had not been selected, the FMC presented a discontinuity in the entered flight path at the HENDO waypoint (see the section titled Flight management computer). The flight crew misidentified the approach IF, CS540, as the IAF and resolved the FMC discontinuity by connecting HENDO to CS540. This selection removed the 6,800 ft descent altitude constraint associated with HENDO in the RNP approach programming.
At 1954, when the aircraft was 136 nm south of HENDO, ATC cleared the flight to track direct to the HENDO waypoint and 6 minutes later the crew commenced descending the aircraft. At 2010:51, when the aircraft was about 11 NM southeast of HENDO, ATC provided the crew with clearance to conduct the RNP Y runway 33 approach.
One minute later, the aircraft approached HENDO descending through about 7,300 ft with the autopilot engaged and an altitude of 6,800 ft selected in the autopilot mode control panel. At about that time, the captain selected the approach’s minimum descent altitude of 800 ft, but sensed that this selection was incorrect and therefore reselected an altitude of 6,800 ft. The captain then reviewed the approach briefing, confirmed that the aircraft was tracking as intended and the vertical navigation autopilot mode was active and again selected 800 ft.
At 2011:38, about 7 NM prior to crossing HENDO, the aircraft descended below 6,800 ft (Figure 3) and 9 seconds later descended below the 6,500 ft MSA. Six seconds later, at 2011:53, ATC observed that the aircraft had descended below 6,800 ft and contacted the crew to confirm the aircraft’s altitude. The captain then reselected 6,800 ft and manually arrested the descent. ATC then issued a low altitude alert to the crew and advised them to climb immediately. Three seconds later, at 2012:07, the aircraft stopped descending at about 5,920 ft and then commenced a climb. At 2012:28, the aircraft climbed back above 6,800 ft. No ground proximity warning system alerts were generated during the incident.
A missed approach was then commenced, and the crew conducted a second approach without further incident.
Figure 3: Flight path of VH-VUT
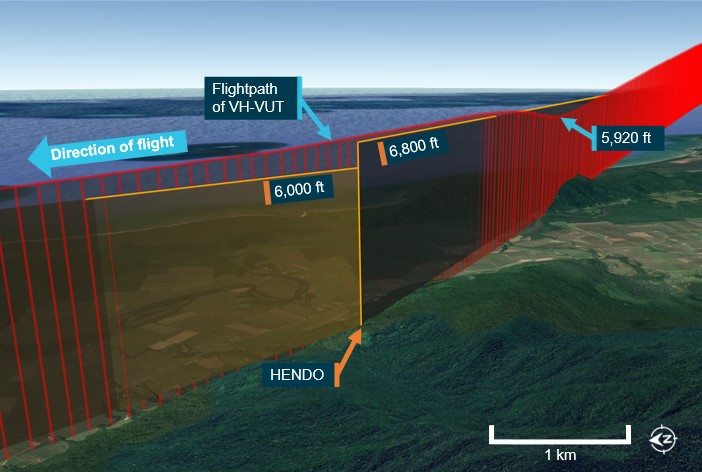
Source: Virgin Australia, Airservices and Google Earth, annotated by ATSB
26 October 2022
On the morning of 26 October 2022, a Qantas Airways Boeing 737-800 registered VH-VZA operated a flight from Brisbane to Cairns. The captain was acting as pilot flying, and the first officer was acting as pilot monitoring.
At 0739, in daylight, while the aircraft was in cruise at FL 380 about 225 NM to the south of Cairns, ATC provided the crew with clearance to conduct the Cairns HENDO 8Y STAR via the BARIA waypoint transition (Figure 4).
Figure 4: Jeppesen HENDO 8Y standard arrival – VH-VZA
Source: Virgin Australia, annotated by ATSB
The flight crew entered the HENDO 8Y STAR into the FMC and selected the BARIA transition. While clearance for the RNP Y runway 33 approach had not been provided at that time, the crew anticipated the clearance and loaded the approach. The crew believed that they had only been cleared for the BARIA STAR transition and had not yet received clearance for the HENDO approach transition, and therefore did not select that transition. As the selection had not been made, the FMC did not load the instrument approach segment from the IAF to the IF and presented a discontinuity between HENDO and the IAF waypoint CS540 (see the section titled Flight management computer).
The crew noted that the waypoints CS522 and CS523 were missing from the track presented on the navigation display and contacted ATC to request confirmation of the STAR clearance. ATC then provided a clearance for the HENDO 8Y STAR with a FISHY transition. The crew reviewed the STAR chart and assessed that they could not achieve the required descent profile to proceed via FISHY and requested confirmation of the STAR transition. ATC then confirmed the STAR transition was via BARIA.
The flight crew noted that the track from HENDO to CS540 passed over the locations of CS522 and CS523. As there was no cloud along the flight path and terrain was visible, the crew were not reliant on FMC programming for terrain clearance. As such, the crew decided to join the discontinuity at HENDO to CS540 to proceed with the approach. The captain also selected an altitude 6,800 ft in the autopilot mode control panel.
At 0808:20, when the aircraft was 18 NM east of HENDO with the autopilot engaged and descending through about FL110, ATC provided the crew with clearance to conduct the RNP Y runway 33 approach.
At 0810:42, when the aircraft was about 7 NM east of HENDO, the captain selected 5,500 ft in the autopilot mode control panel and the aircraft descended below 6,800 ft, and 34 seconds later below the 6,500 ft MSA.
The aircraft passed HENDO at 0811:56 at an altitude of about 6,125 ft (Figure 5). Eleven seconds later, ATC contacted the crew to confirm that the aircraft had passed HENDO at the correct altitude. ATC then confirmed with the crew that the flight was operating in visual conditions and provided clearance for a visual approach. The aircraft landed at Cairns without further incident.
Figure 5: Flight path of VH-VZA
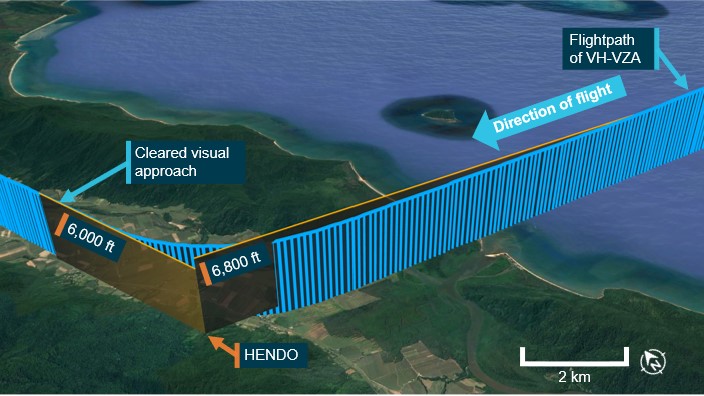
Source: Qantas, Airservices and Google Earth, annotated ATSB
Flight management computer
The approach procedure (Figure 2) had two different IAFs with associated paths to a common IF (CS540), from BASIL through waypoints CS520, CS521 and CS523, or from the HENDO through CS522 and CS523. Therefore, the flight crew needed to select one of the two approach transitions (Figure 6). If a transition was not selected, the segment of the approach from the IAF to the IF would not be loaded (the component of the instrument approach from the common IF onwards was automatically loaded).
Figure 6: Flight management computer approach transitions
Source: Virgin Australia, annotated by ATSB
As the crews did not select an approach transition, a discontinuity (Figure 7) was created at the HENDO waypoint associated with the HENDO 8Y STAR. Both crews resolved this discontinuity by connecting HENDO to CS540. This selection removed the 6,800 ft descent altitude constraint associated with HENDO in the RNP approach programming. The segment minimum safe altitudes associated with waypoints CS522 (6,000 ft) and CS523 (4,900 ft) were also removed.
Figure 7: Flight management computer (left) and navigation display (right) showing the discontinuity
Source: Virgin Australia, annotated by ATSB
Safety action
The ATSB has been advised of the following proactive safety action in response to these occurrences.
Virgin Australia
Virgin Australia updated flight crew operation notice information for Cairns with detailed guidance for the conduct of the HENDO 8Y arrival and RNP Y runway 33 approach. Virgin Australia also provided guidance to all Boeing 737 flight crew for the conduct of arrivals and approaches where the selection of an approach transition was required.
Qantas
Qantas issued an internal notice to flight crew providing guidance for the conduct of arrivals and approaches where the selection of an approach transition was required.
Further investigation
To date, the ATSB has:
- interviewed the involved flight crews
- examined recorded flight data
- reviewed recorded air traffic control audio and surveillance data
- reviewed operator and air traffic control procedures
The investigation is continuing and will include further review and examination of:
- flight crew actions and recency
- recorded flight data
- operator and air traffic control procedures
- instrument procedure and waypoint naming processes and standards
- arrival and approach chart information and presentation
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so that appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 380 equates to 38,000 ft.
[3] Waypoint: A defined position of latitude and longitude coordinates, primarily used for navigation.
[4] Minimum sector altitude (MSA) and lowest safe altitude (LSALT) are calculated to provide 1,000 ft obstacle clearance for instrument flight rules flights and are published on aeronautical charts and in the Aeronautical Information Publication (AIP) for pilot and controller reference.
Occurrence summary
| Investigation number | AO-2022-051 |
|---|---|
| Occurrence date | 24/10/2022 |
| Location | 40 km south of Cairns Airport |
| State | Queensland |
| Report release date | 08/08/2023 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Flight below minimum altitude |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8FE |
| Registration | VH-VUT |
| Serial number | 36608 |
| Aircraft operator | VIRGIN AUSTRALIA AIRLINES PTY LTD |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Brisbane Airport, Queensland |
| Destination | Cairns Airport, Queensland |
| Damage | Nil |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-838 |
| Registration | VH-VZA |
| Serial number | 34195 |
| Aircraft operator | QANTAS AIRWAYS LIMITED |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Brisbane Airport, Queensland |
| Destination | Cairns Airport, Queensland |
| Damage | Nil |