In-flight fire involving Boeing 737, VH-YFY, 56 km north-north-east of Hobart Airport, Tasmania, on 21 July 2025
Final report
Report release date: 18/12/2025
Investigation summary
What happened
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. About 10 minutes prior to landing in Hobart, one cabin crew member was checking the cabin was secure for landing when they identified smoke and flames coming from the top of an overhead locker. When the overhead locker was opened, a passenger’s backpack was found to be on fire. The cabin crew doused the flames with a fire extinguisher, and with the assistance of some passengers, poured water on the bag until no smoke was emitted. The aircraft landed without further incident.
After landing, aviation rescue firefighters retrieved a burnt power bank from inside the backpack.
What the ATSB found
The ATSB found that the lithium-ion battery in a power bank experienced a thermal runaway, resulting in a fire in the overhead locker inside a passenger’s bag. Due to the timing of the fire, when the aircraft was already close to landing, the cabin crew had limited time to complete the lithium battery firefighting procedure.
It was also identified that, while the cabin crew attempted to use the protective breathing equipment provided by the operator, difficulties during its fitment meant that they did not find it effective in this incident.
What has been done as a result
Following this incident, Virgin Australia Airlines reviewed its policy regarding the carriage of power banks and spare batteries. As of 1 December 2025, guidance provided to passengers stated:
- Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
- Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
- Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
- Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
- Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
- Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that were damaged, swollen, leaking, recalled, showing signs of defects, or had been repaired or modified, could not be carried in either checked or carry-on baggage.
Safety message
Passengers often travel with multiple devices that contain lithium batteries, including laptop computers, mobile phones, headphones, and power banks. To reduce the risk associated with lithium battery fires, passengers should ensure their devices are packed safely, easily accessible in the cabin and are not carried on board an aircraft if they show signs of damage or deterioration.
The thermal runaway of a lithium battery can be difficult to manage, particularly when the aircraft is airborne. In-flight fires pose a significant risk to the safety of an aircraft if not managed quickly and appropriately. An operator’s procedure to manage battery fires is designed to limit the risk and reduce the likelihood of re-ignition of the battery until the aircraft can land. However, it requires the batteries to be out of a bag and accessible to be easily completed.
Passengers are encouraged to review their airline’s website, and check the Civil Aviation Safety Authority ‘Pack Right’ website to confirm that equipment they are planning to take on board an aircraft is permitted and packed safely.
Summary video
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. There were 2 flight crew, 4 cabin crew (comprised of a cabin manager under training (‘1L’), a cabin crew trainer (‘1R’), and 2 cabin crew (‘2L’ and ‘2R’) and 149 passengers on board. The first officer was pilot flying and the captain was the pilot monitoring.[1]
At about 0901 local time, as the aircraft descended through 10,000 ft with the seatbelt sign illuminated, the cabin crew began their final checks on the cabin prior to landing at Hobart. While near the front of the cabin, the 1R heard a sound that they described in their interview with the ATSB as a popping and hissing sound. On looking, they saw white smoke, then flames, emanating from the overhead locker above row 7DEF (Figure 1). They immediately instructed the passengers seated in both sides of rows 6,7 and 8 to move away from the area and into other seating in the aircraft. The 1R then retrieved a fire extinguisher, the portable breathing equipment (PBE), and water from the forward galley.
The 1L made a call from the front galley to the other cabin crew for assistance. The 2 rear cabin crew brought more water and another fire extinguisher forward. The 1R and 2R attempted to don the PBE around the same time, however, one was unable to stretch the neck ring sufficiently to don the PBE, and the other, after donning the PBE felt it restricted their ability to see and communicate effectively so decided to remove it.
Figure 1: Aircraft seat plan showing the location of the overhead locker where flames and smoke were observed
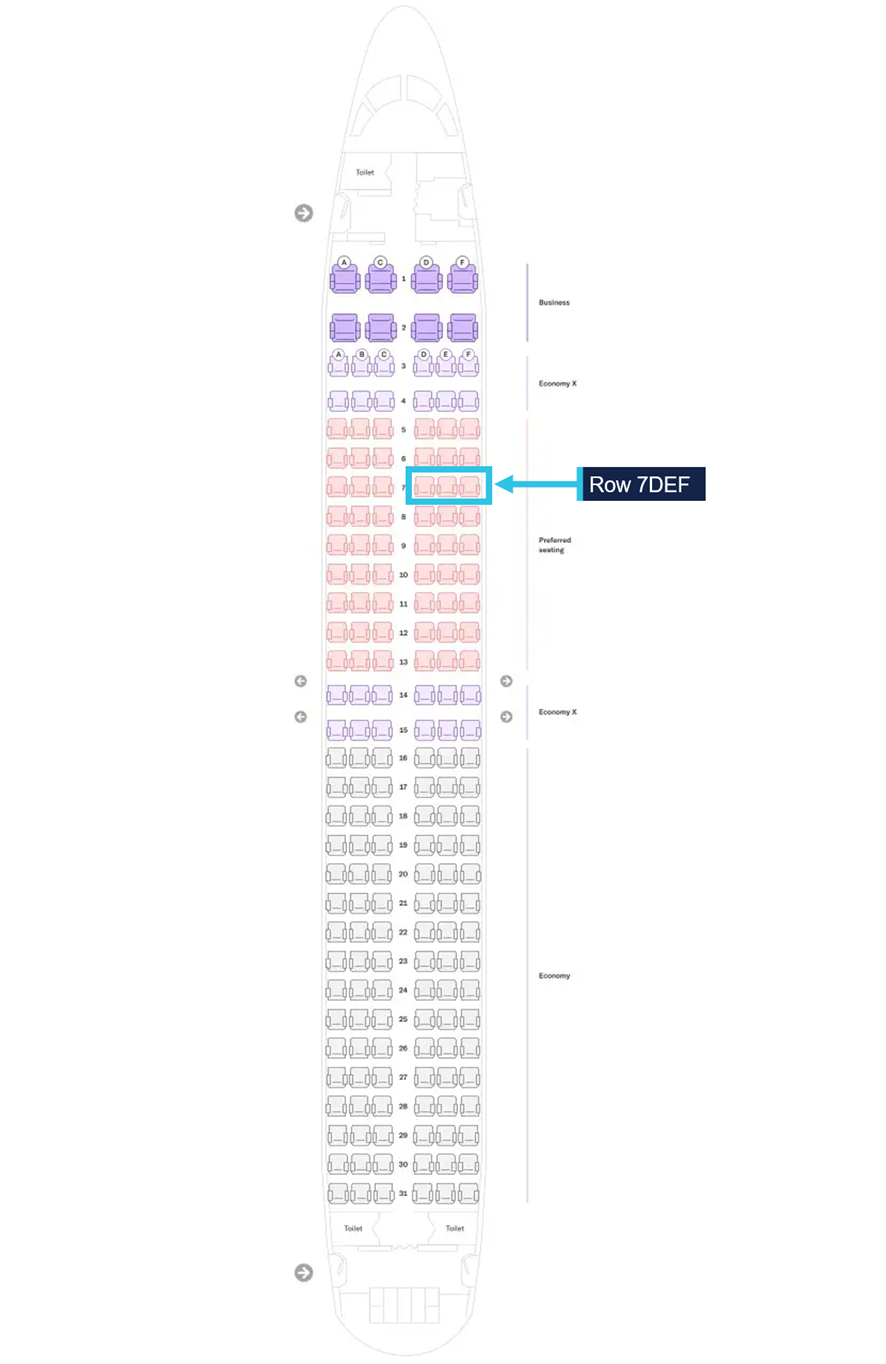
Source: Virgin Australia Airlines, modified by the ATSB
When the overhead locker was opened, flames and smoke were observed emanating from a backpack. Although they could not see what was causing the fire, from their training, the cabin crew suspected it was from a portable electronic device overheating. The 1L discharged a fire extinguisher into the locker until the flames were extinguished. The 1L and 1R then poured water over the bag, with the assistance of the 2R and passengers. To reduce the risk of re‑ignition, a second fire extinguisher was discharged into the locker. The cabin crew instructed passengers to keep their heads down and cover their nose and mouth to avoid inhaling smoke. They also asked the passengers who was the owner of the bag but did not receive a response at the time.
While the other cabin crew managed the fire, the 2L called the flight deck. The captain recalled in interview that, prior to the call, they detected a smoky odour in the flight deck, which they thought was ozone. The 2L advised the captain there was a fire in an overhead locker, which was extinguished, but there was still smoke, and the 1L was dousing the bag with water. They also stated that there were still passengers standing. On ending the call, the captain asked the 2L to ensure everyone was seated for landing.
Following receipt of this information, at 0905:17, just prior to descending through 5,100 ft, the captain made a ‘PAN PAN’[2] call to the Hobart approach air traffic control to advise of a possible fire in the cabin, and that they would require assistance on landing. The captain also asked to speak to the tower controller earlier to request clearances. The approach controller coordinated to get the tower controller on frequency.
The captain decided to take control of the aircraft for landing due to the emergency. At 0906:00, the aircraft was cleared to land on runway 30 by the tower controller. At this time, the first officer also asked to cancel the approach they had been previously cleared for and to instead conduct a visual approach. This change was permitted. At 0906:28, air traffic control contacted the aviation rescue and firefighting service at Hobart Airport, which deployed in preparation for the aircraft landing.
The 2L then retrieved gloves and the portable electronic device fire containment bag and took it to the other cabin crew, intending for the burnt device to be placed in the bag, and the bag stored in the rear lavatory, as per procedure. The backpack was too large to fit in the fire containment bag and there was difficulty in locating the device inside the backpack. Given the short amount of time remaining before landing, the decision was made by the 1R to keep the device inside the backpack in the overhead locker above row 7. It was identified by the cabin crew that the rounded shape of the overhead locker retained the water that had been poured on the backpack, which kept the bag soaked, and would help reduce the risk of re‑ignition during landing. The cabin crew planned to keep the overhead locker open, with the 1R seated in seat 7C adjacent to the locker to monitor the device during landing, with water to use if necessary. The cabin crew also directed the passengers standing to be seated immediately, even if it required 4 passengers to be in a row.
As recalled by the captain in interview with the ATSB, the first officer contacted the 1L just prior to the aircraft turning onto the final approach. This was likely just prior to 0909, with the aircraft between 1,500 ft and 1,000 ft. The 1L confirmed the fire was out, and the passengers were seated, but that the cabin crew were still standing. They assured the first officer the cabin crew would be seated for landing.
The 1L, 2L and 2R secured the final items for landing and seated themselves in their designated seats, except for 1L who sat in 1R’s seat to maintain better visibility of the cabin. On their way to their seat at the front, the 1L checked the overhead lockers around row 7 for heat or any developing hot spots. Once all the cabin crew were seated, the 1L signalled to the flight crew the cabin was secure. The 1L made a final announcement to passengers to ensure their seatbelts were fastened, to remain seated for landing and follow instructions of crew following the landing.
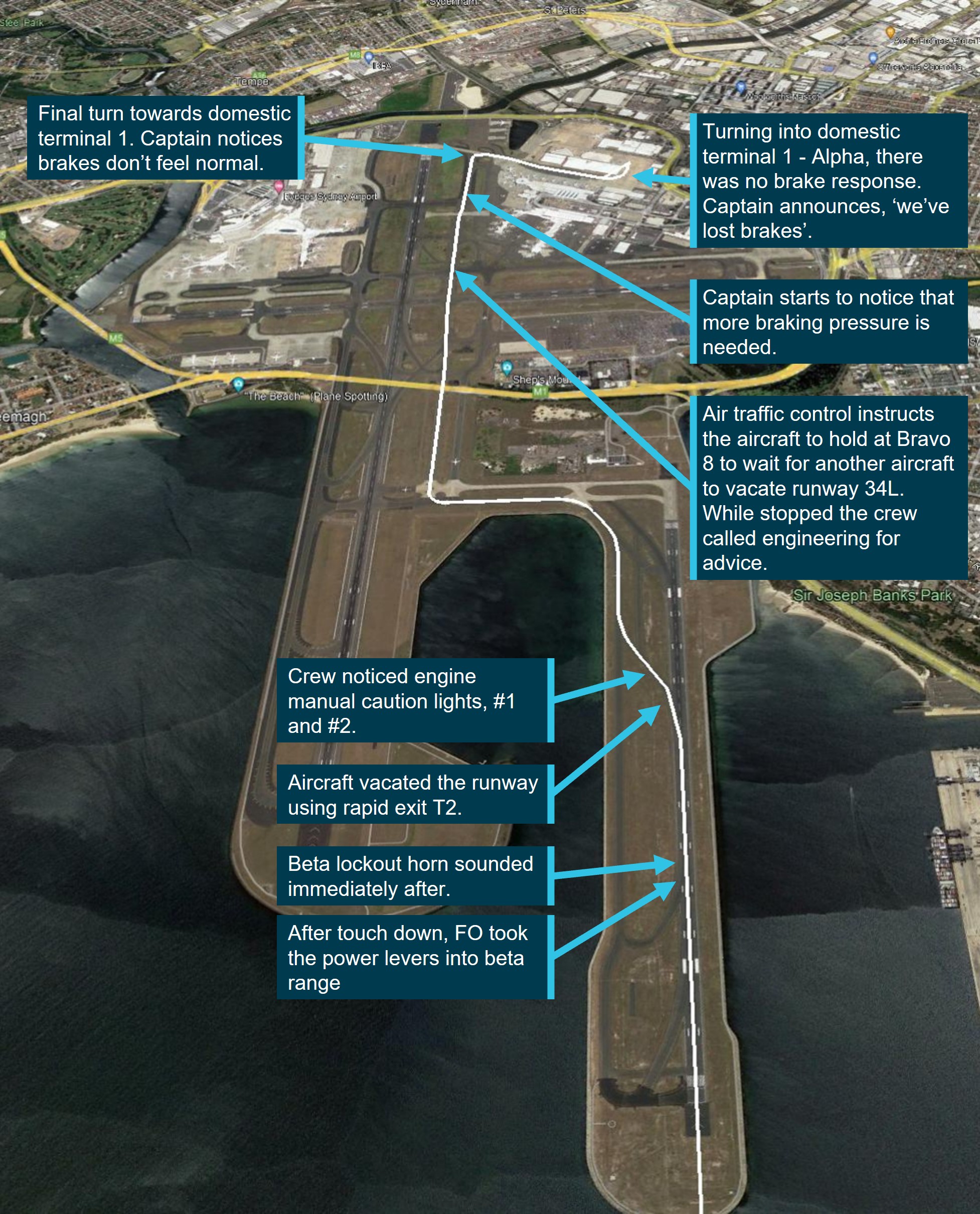
Flight data provided by Virgin Australia showed that the aircraft touched down at Hobart at 0910:29 (Figure 2).
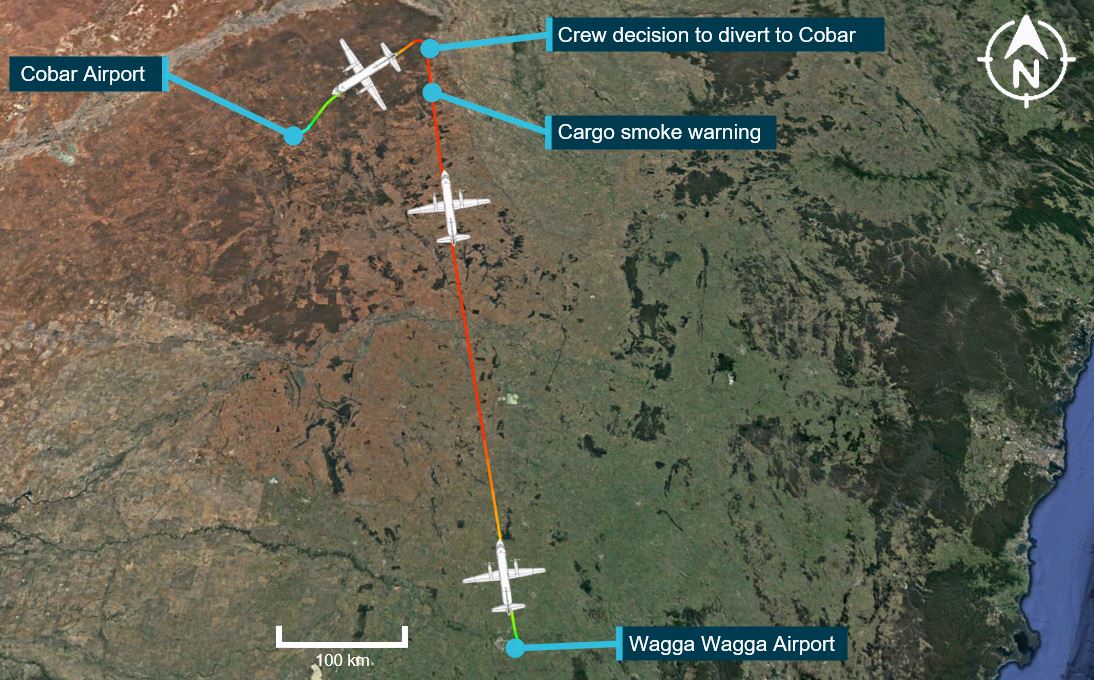
Figure 2: Flight path with key events

Source: Google Earth, annotated by the ATSB
The captain stopped the aircraft on the taxiway and exited the flight deck to speak to 1L and observed the cabin to determine whether an evacuation was required. As the fire appeared to be contained, the captain taxied the aircraft to the parking bay. At 0919, the aviation rescue and firefighting personnel boarded the aircraft and removed the backpack from the overhead locker. They confirmed the origin of the fire was a lithium power bank, stored in one of the backpack’s front pockets (Figure 3).
Figure 3: Backpack containing the power bank

Source: Airservices Australia
The passengers were cleared to disembark normally at 0927. After disembarkation, one cabin crew member (2L) was treated by paramedics. It was unknown if this was due to the effects of smoke as they had been unwell throughout the flight prior to the fire commencing. No other crew or passengers reported to the operator about seeking medical attention from the effects of the smoke. The fire caused minor damage to the overhead locker above row 7/8 DEF (see section Aircraft damage).
Context
Cabin crew information
The flight comprised of 4 cabin crew, 2 located at the front set of aircraft doors (called ‘1L’ and ‘1R’) and 2 at the rear of the aircraft (called ‘2L’ and ‘2R’). Each cabin crew member had designated roles on the flight, based on which door they were operating. On this flight, the 1L position was filled by a trainee cabin manager who had previous experience in this role working for other airlines, but was completing their first flight as a cabin manager under training for this operator. The 1L was supervised by a cabin crew trainer in the 1R position.
Each of the cabin crew had between 1 and 17 years of experience as cabin crew. They had all completed their annual emergency procedures training between November 2024 and June 2025. This training included both theoretical information and a practical review of the lithium battery firefighting procedure. All cabin crew reported having completed simulated scenarios where the fire occurred either during cruise or on the ground, where there was plenty of time to complete the firefighting procedure, and store the damaged battery appropriately. None of the cabin crew had completed a simulated scenario involving a time‑pressured situation.
Aircraft cabin information
VH-YFY was a Boeing 737-800 aircraft, with a single aisle in the cabin and seating for 182 passengers. In economy, where this fire occurred, there were 3 seats on either side of the aisle.
The cabin on this aircraft was fitted with the Boeing 737 sky interior design. In this design, the overhead lockers lowered from the ceiling, creating a contained basket for the bags to sit in. In comparison, the doors in other locker designs would open upwards.
Lithium batteries
Overview
There are 2 primary types of lithium batteries – lithium metal and lithium-ion. Lithium metal batteries cannot be recharged and are designed to be disposed of once their initial charge has been used, whereas lithium-ion batteries are rechargeable. Compared to lithium metal, lithium-ion batteries store a high amount of energy and are commonly found in many portable electronic devices (PEDs) such as smartphones, tablets, cameras, laptops, and power banks.
Guidance on the safe carriage of lithium-ion batteries on board aircraft
Lithium batteries are classified by the United Nations as dangerous goods. As such, the International Civil Aviation Organization’s Technical Instructions for the Safe Transport of Dangerous Goods by Air (2025-2026 Edition) stated that lithium batteries, including power banks must be carried as carry-on baggage only.
The Civil Aviation Safety Authority stated that spare batteries and power banks should be packed in carry-on baggage only, so that trained aircrew can manage any issues quickly and safely. Their Pack right website provided safety tips when travelling with lithium batteries:
These simple steps help keep you and your fellow passengers safe:
• choose reputable suppliers when buying devices and spare batteries
• follow airline and manufacturer rules for carrying and charging lithium batteries
• keep spare batteries with you in the cabin and protect them from damage
• stop using or charging batteries that show signs of damage, overheating, or swelling
To prevent short circuits, protect spare battery terminals by:
• keeping them in original packaging
• covering terminals with tape
• placing each battery in a separate plastic bag or case.
At the time of the incident, the operator’s policy permitted power banks to be carried in the cabin only, but they could be stored inside a bag and there were no restrictions on their use on board. Advice on the carriage of power banks and other electronic devices was provided to passengers on the operator’s website and during check-in.
Thermal runaway
Thermal runaway is a rapid and uncontrolled increase in temperature and occurs when the internal cell(s) of a lithium battery become damaged for reasons including:
- internal short circuits
- breakage from dropping or crushing
- exposure to excessive heat
- failure of the battery cell due to manufacturing defects.
The operator’s Aircrew Emergency Manual stated that crew should be alert not just for signs of smoke or fire in the cabin but also to the smell of overheating electronic devices.
The smell of overheating may be the first sign of an impending lithium battery/PED fire. PEDs approaching a thermal runaway start initially displaying hissing, crackling sounds, as well as bubbling or blistering casings.
Once a lithium battery cell thermal runaway starts, it quickly leads to the failure of adjacent cells in a chain reaction that can produce fire, which is especially difficult to extinguish. A fire caused by lithium batteries can produce a fire burning with a temperature as high as 1,000°C, explosions releasing toxic gases and flammable electrolytes as well as shrapnel from damaged PED casings. The manual also stated that in some cases, the explosive force of the venting gasses could be significant enough to cause spikes in cabin pressure.
Managing lithium battery fires
The operator’s Aircrew Emergency Manual stated a general risk about onboard fires was that:
Any fire, no matter how small, may rapidly become out of control if not combatted quickly. Research has shown that if left uncontained, a smoke-filled cabin can be consumed by fire in as little as 6-10 minutes. The first priority shall always be to put the fire out.
In order to manage the risk, the manual outlined 3 important principles of firefighting:
- Immediately locate the source of fire, smoke or fumes. Specific to lithium battery fires, all smoke or fire events occurring in baggage within an overhead locker should be assumed to be a PED/lithium battery fire until the source is positively confirmed.
- Aggressively attack and extinguish the fire using all available resources, which can include able bodied persons.
- Communicate to other crew and the flight crew, as soon as possible, specifying the location and source of fire.
Furthermore, the manual also guided crew that:
It is important to protect yourself from the effects of smoke and fumes while attempting to flight a fire. In some circumstances it may be safe and thus more important to attack a fire first than fitting of PBE [portable breathing equipment]. PBE should be worn by at least one person when a team is formed to flight a fire and anytime by the primary firefighter when they are in smoke, a confined space of affected by fumes.
In regard to managing a lithium battery fire, the manual stated:
The primary method for stopping a lithium battery from thermal runaway or overheating is to cool it down by pouring water or other non-flammable liquid on the battery or device. This should be done once any flames have been extinguished and continued until the device is cooled and there is no evidence of smoke, heat, crackling or hissing sounds usually associated with an overheating lithium battery. This could take as long as 10–15 minutes.
Another recommendation in the emergency procedures manual was a suggestion not to open any baggage if there was smoke or flames emanating from it, unless it was required to get a fire extinguisher and liquid onto an identified battery. Once the device was cooled, it could then be placed in a fire containment bag or other suitable container.
Aircraft firefighting equipment
Overview
The operator fitted the Boeing 737 aircraft with firefighting equipment. In addition to this designated equipment, the cabin crew were taught to use other equipment available on board as required, such as drinks used in the cabin service as well as wet blankets and pillows to smother a fire.
Fire extinguishers
The aircraft had 4 bromochlorodifluoromethane (BCF)/halon fire extinguishers. These fire extinguishers are designed to be used on all types of fires by discharging a colourless, odourless, non-corrosive, liquified gas. This gas is not cooling, meaning that further steps are required in fighting a lithium battery fire.
Fire protection gloves
Fire protection gloves were designed to protect the wearer’s hands when fighting fires, including lithium battery incidents. The emergency procedures also suggested that crew should use gloves whenever fighting fires, including using oven gloves if the fire protection gloves were not available.
The L2 retrieved the fire protection gloves from the galley with the intention to move the power bank once the fire was suppressed, but the gloves were not used during the firefighting process.
Portable breathing equipment
Portable breathing equipment (PBE), commonly referred to as a smoke hood, was provided for each cabin crew member on board. The PBE supplied was designed to protect the wearer from fumes and smoke by forming a secure seal using an elastic neoprene neck ring (Figure 4). An oxygen generator on the nape provided oxygen to the wearer.
Figure 4: Exemplar PBE, showing how to open the neck ring (left) and when donned (right)

Source: Virgin Australia Airlines, modified by the ATSB
Operator procedures recommend PBE should be used by at least one person involved in firefighting, or when one person was fighting a fire in an enclosed environment. Although, consideration was given that the first person to a fire might need to immediately attend to the fire while others gathered and donned the PBE.
The 2 cabin crew who attempted to use the PBE stated that the equipment provided in training was much easier to don as the neck ring was stretched from repeated usage.
In October 2025, the Airbus Safety First magazine contained an article about PBE, reviewing a case study where 7 cabin crew had difficulties using the PBE provided. The analysis indicated that, similar to this incident, despite having regular training in the use of PBE, the cabin crew found it difficult to use the PBE in a real emergency. The article recommended that ‘dummy’ PBE used in training may not represent the equipment found on board.
Fire containment bags
There were 2 sizes of fire containment bags carried on the operator’s Boeing 737 aircraft. The smaller sized bag, designed to fit an iPad, was carried in the flight deck in the event of a thermal runaway involving one of the flight crew’s electronic flight bags.
A larger bag, designed to fit a device the size of a laptop, was carried in the aircraft cabin (Figure 5). The purpose of this bag was to place the device in after it was cooled post‑fire, so that it could be stored in a water filled container in a secure place.
Figure 5: Fire containment bag

Source: Virgin Australia Airlines
Damage to the power bank
The power bank was inspected by the aviation rescue firefighters after being removed from the aircraft.
The power bank had a rated output of 37 watt hours and had both USB‑A and USB‑C charging ports. It was not charging a device when the fire started, but there was a cable plugged into the USB‑A charging port. When orientated with the manufacturer’s label facing up, most of the damage was observed along the top and right side of the power bank. The damaged right end contained the USB-C charging port. External observations suggest that the power bank contained 2 internal cells, of which only 1 was affected by the thermal runaway by the time the fire was extinguished (Figure 6). The power bank was not protected from short circuits as it did not appear to have the terminals covered and was not separated from other items in the bag by being placed in a protective pouch or the original packaging. The backpack was reported by the operator to be substantially damaged by the fire.
The owner of the power bank advised the operator that it was purchased in 2024 and:
- it had no pre-existing damage
- was fully charged the day prior to the incident, and there were no previous issues during charging or use
- it was not dropped, exposed to moisture or heat prior to the incident.
Figure 6: Power bank showing damage from the back (left) and side view (right)

Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Aircraft damage
An inspection of the aircraft found fire damage in the panels above and behind the overhead locker above row 7 and 8 DEF. The passenger service unit containing the reading lights, call bell and information signals under this locker also sustained fire and water damage. The overhead locker needed to be replaced post-fire (Figure 7).
Figure 7: Overhead locker above row 7DEF where the smoke and flames were observed (left) and area behind the overhead locker showing fire damage (right)

Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Related occurrences
Australian data
This incident was the first reported power bank-related in-flight fire either in Australia or on an Australian‑registered aircraft. A review of the ATSB’s occurrence database identified 3 previous incidents where smoke was reported emanating from a power bank in the aircraft’s cabin, but no fire occurred:
- OA2025-01608: On 20 January 2025, a Boeing 737 aircraft was being operated on a flight from Brisbane, Queensland, to Melbourne, Victoria. During cruise, a power bank overheated in the cabin, and smoke was observed emanating from the attached charging cable. The power bank and cable were placed in a container and stowed in the rear lavatory for the remainder of the flight.
- OA2019-04325: On 28 May 2019, an Airbus A330 aircraft was being operated on a flight from Melbourne, Victoria, to Hong Kong. During cruise, smoke was detected emanating from a passenger's power bank.
- OA2019-02629: On 15 April 2019, an Airbus A330 aircraft was being operated on a flight from Hong Kong to Melbourne, Victoria. During passenger disembarkation, smoke was observed emanating from a passenger's power bank. The crew doused the power bank in water.
ATSB records showed that, in the past 10 years, there were 4 in-flight fires resulting from mobile phones, 3 of which occurred after the mobile phone was crushed in the seat mechanism, damaging the lithium battery contained inside. The reason for the fourth fire was unknown.
International incidents
While this was the first reported incident in Australia, there have been a number of significant fires resulting from power banks, including:
- In January 2025, an Air Busan A321 aircraft was preparing for flight at Busan, South Korea. Prior to taxi, a power bank fire started in an overhead locker. The fire spread, resulting in an evacuation. The aircraft was destroyed.
- In March 2025, a Hong Kong Airlines A320 aircraft diverted after a power bank experienced a thermal runaway. The fire was extinguished.
- In October 2025, an Air China A321 aircraft had to divert after a battery caught fire in an overhead locker.
The United States Federal Aviation Administration recorded 8 in‑flight fire incidents involving power banks occurring in the past 10 years.
Safety analysis
Power bank thermal runaway
For unknown reasons, one of the cells in a lithium-ion power bank stored in an overhead locker failed during the descent into Hobart. In this case, there was no reported pre‑existing damage, or any other identified problems with this power bank prior to flight. However, the power bank was stored with a cable in it and the ports uncovered, both factors which can increase the risk of a fault.
Inspection of the power bank post-flight, combined with the cabin crew reports of sounds they were trained to expect in the event of a lithium battery fire, suggested that the fire was characteristic of a thermal runaway. As the temperature of the power bank continued to increase, smoke, followed by flames resulted.
Completion of firefighting procedures
As described in the operator’s procedures, fires on board aircraft can spread quickly. As the aircraft was already on descent when the smoke was initially observed, there was limited time for the cabin crew to manage the power bank fire by completing all the procedures they were trained to do in response to an in-flight fire. In addition, they had the responsibility to ensure the cabin was secure for landing.
In less than 8 minutes, the cabin crew worked together to identify a fire, gather the required equipment, and aggressively fight the fire to a point where the fire appeared suppressed. In addition, they communicated the problem with the flight crew and managed moving passengers to alternative seating.
While the cabin crew had received emergency procedures training, they had never trained for a lithium battery fire in a compressed time. They completed as many of the procedures as they were able to in the available time, but by the time the fire was considered controlled, there was only around 90 seconds for the cabin crew to clear up the cabin and be seated for landing. Besides the logistics and risk that would result from handling the power bank to remove it from the backpack and place it in a fire containment bag, there was no time available.
The cabin crew identified an alternate solution to moving the burnt power bank. While the overhead locker held the water poured on the backpack, there was no assurance that the power bank was going to remain fully submerged for landing, in accordance with the operator’s procedures, or isolated from other lithium battery devices. Although there was no consequence as a result of the power bank remaining in the overhead locker, there was an increased risk of cabin occupant injury and aircraft damage if the power bank re‑ignited due to further exposure to fire and smoke.
Protective breathing equipment
Protective breathing equipment (PBE) was available for cabin crew to use if deemed necessary in preparation to fight a fire, and all crew were trained in their use. Two of the cabin crew attempted to use the PBE, but did not find it effective due to fitment and communication/visibility issues. As the cabin crew were unable to use the PBE, they had no protection from the smoke and were placed at an increased risk of smoke inhalation. While these cabin crew did not experience any residual effects from the smoke, any protective equipment provided should be efficient to don and wear continuously while managing an emergency situation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the in-flight fire involving Boeing 737, VH-YFY, 56 km north‑north‑east of Hobart Airport, Tasmania, on 21 July 2025.
Contributing factors
- During the descent, a passenger's lithium-ion power bank, located in the overhead locker, overheated due to thermal runaway and began to emit flames and smoke.
Other factors that increased risk
- Due to the timing of the fire starting on descent, the cabin crew had limited time to complete the procedure for managing a lithium battery fire.
- The cabin crew attempted to use the protective breathing equipment provided by the operator but did not find it effective when managing the lithium battery fire.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Virgin Australia Airlines
Virgin Australia Airlines advised it has reviewed its policy regarding the carriage of power banks in the cabin. As of 1 December 2025, guidance provided to passengers stated:
- Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
- Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
- Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
- Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
- Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
- Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that are damaged, swollen, leaking, recalled, showing signs of defects, or have been repaired or modified, cannot be carried in either checked or carry-on baggage.
It has updated the cabin crew’s pre-flight announcement and website to inform passengers of the revised policy.
Virgin Australian Airlines has also acknowledged that, while it made changes to its policy, there are challenges in monitoring passengers’ compliance with these measures. It also stated that greater awareness about the risks of travelling with lithium batteries should be delivered by all airlines and airports.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the cabin crew
- the captain
- Virgin Australia Airlines
- Airservices Australia
- Civil Aviation Safety Authority.
References
Airbus. (2025). Focus on protective breathing equipment. https://safetyfirst.airbus.com/focus-on-protective-breathing-equipment/
Civil Aviation Safety Authority. (n.d.). Lithium batteries. Retrieved 25 July 2025, from https://www.casa.gov.au/packright/lithium-batteries
International Civil Aviation Organization (2025). Technical instructions for the safe transport of dangerous good by air 2025-2026. https://www.icao.int/Dangerous-Goods/Technical-Instructions
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the cabin crew
- the flight crew
- Virgin Australia Airlines
- Airservices Australia
- Civil Aviation Safety Authority.
Submissions were received from:
- Virgin Australia Airlines
- 2 cabin crew members
- Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
Occurrence summary
| Investigation number | AO-2025-043 |
|---|---|
| Occurrence date | 21/07/2025 |
| Location | 56 km north-north-east of Hobart Airport |
| State | Tasmania |
| Report release date | 18/12/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Fire, Smoke |
| Occurrence class | Serious Incident |
| Highest injury level | Unknown |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-800 |
| Registration | VH-YFY |
| Serial number | 41016 |
| Aircraft operator | Virgin Australia Airlines |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Sydney Airport, New South Wales |
| Destination | Hobart Airport, Tasmania |
| Damage | Minor |










![Figure 1: ADS-B[5] derived flight data showing the approximate location of the radio altimeter failure on approach to Sydney](/sites/default/files/inline-images/AO-2022-056%20Figure%201.jpg)