Detachment of the actuator from the nose landing gear leg may result in flight control interference.
What happened
On 29 April 2026, a pilot and instructor commenced a training flight in a Diamond DA42 twin‑engine aircraft at Parafield Airport, South Australia. After take-off, the nose landing gear (NLG) remained extended after the main gear was retracted. The aircraft veered left, before it banked left wing down and began a steep descent. The aircraft subsequently collided with a hangar, fatally injuring the pilot and instructor.Nine people were reported to be taken to hospital.
Why did it happen
Onsite aircraft wreckage analysis found that the NLG actuator rod end had fractured, with preliminary ATSB examination identifying indications of progressive (fatigue) cracking. The ATSB identified 2 Diamond Aircraft Industries (DAI) mandatory service bulletins, issued in 2013 (MSB 42‑099/1, also published in European Union Aviation Safety Agency (EASA) airworthiness directive (AD) 2013-0121) and 2019 (MSB 42-136/1, also published in EASA AD 2019-0066), which described the potential for an NLG actuator to become separated from the gear leg and interfere with the nose wheel steering/rudder control mechanism. In one instance, it was reported this interference forced the rudder control into a left-hand deflection, which was rectified by the pilot re-extending the landing gear, after which full rudder control was regained.
Safety advisory notice
AO-2026-074-SAN-001: The ATSB encourages operators of Diamond DA42 aircraft to review the Diamond Aircraft Industries mandatory service bulletins, and associated airworthiness bulletins, and be aware that there is the potential for a fractured NLG actuator to interfere with the rudder controls during landing gear retraction.
Considering all options
While there are many reasons that pilots may experience difficulty with directional control on take-off, including an engine failure, an unusual reason to consider is flight control mechanism interference. Re‑extending the landing gear after take-off would not be a usual action considered by pilots, but as noted in the previous occurrence, this unexpected response allowed the pilot to regain aircraft control in this instance.
Friction locks fitted on the Beechcraft King Air series aircraft require careful adjustment to prevent the power levers migrating rearwards to the idle position, particularly during take-off.
What happened
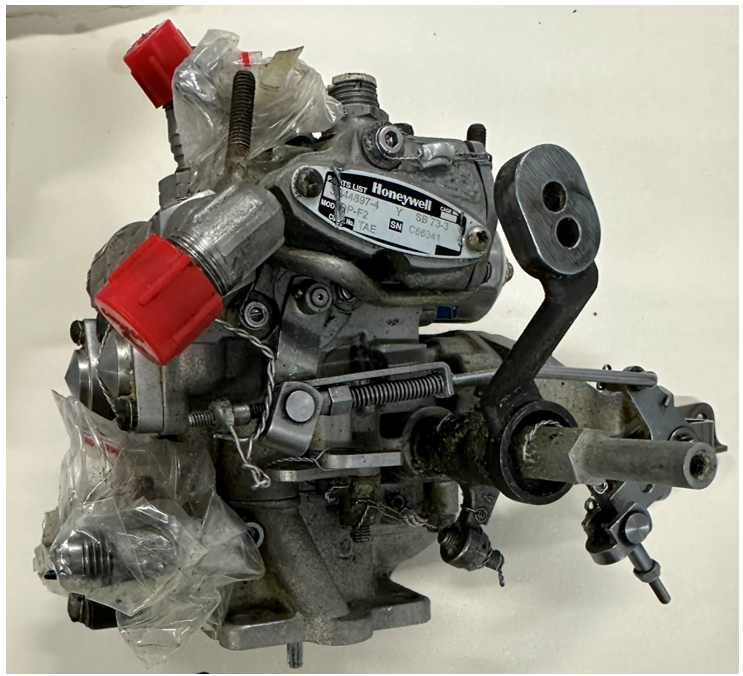
On the night of 19 August 2021, the pilot and medical crew of a Hawker Beechcraft King Air B200C aircraft, registered VH‑VAH, departed Essendon Fields Airport, Victoria on a patient retrieval flight. During the take-off, there was a loss of left engine power and an uncommanded left yaw. The pilot initially managed the situation as an engine power loss situation. However, shortly after, they identified that the left engine power lever had migrated rearwards to the idle position. The pilot moved the power lever back to take-off power and adjusted the friction lock to prevent further movement. The flight continued without further incident.
Power levers and friction locks
(Source: Operator, modified by the ATSB)
Why did it happen
The left engine power lever had migrated rearwards as the friction lock had not been sufficiently adjusted during pre-flight checks.
The cockpit to engine nacelle power lever control cables in King Air series aircraft were spring loaded towards idle. This was to protect the engines in the event of any power lever cable issues, and to reduce the effect of hysteresis (or backlash) in the system. The effect of the springs migrating the power levers was managed by adjusting the friction locks. The left engine was more susceptible to power lever migration as its cable connecting it to the engine was shorter when compared with the right engine.
When correctly set, the friction locks provided adequate resistance for the power levers to remain in position. However, if not adequately set, power lever migration could occur. This was typically experienced when the pilot removed their hand from the levers during take-off and could lead to the aircraft yawing towards the engine experiencing the power lever migration, a significant reduction in power, and the auto‑feather system disarming.
A characteristic of the King Air friction locks was that they required careful adjustment as some aircraft had a narrow range between no friction and too much friction. In addition, the desired resistance could be inconsistent between power levers in the same aircraft and other aircraft, and this could change over time due to wear. This characteristic has been experienced among different King Air operators and pilots and has also been considered as a potential factor in several fatal accidents.
Safety advisory notice
AO-2021-034-SAN-01:
The Australian Transport Safety Bureau advises pilots and operators of the King Air series aircraft (c90, 200, and 300) that the power lever friction locks require careful adjustment to prevent power lever migration towards the idle position, particularly during take-off. Inadvertent migration of one power lever towards idle can result in power reduction and yaw that, when occurring at low height, can result in catastrophic outcomes. Operators should ensure pre-flight checks provide opportunities to confirm friction lock settings before the take-off run, and ensure pilots have adequate knowledge of friction lock sensitivity to help prevent and recover from inadvertent power lever migration.
Correct operation of approved mode S transponders can significantly improve situational awareness of other traffic on the ground. Electronic surveillance information is an effective trigger to alert pilots of other ground traffic. Early use of mode S transponders before taxi assists the process of ‘alerted see‑and‑avoid’ to identify and avoid traffic conflict.
What happened
On 15 July 2024, a De Havilland Aircraft of Canada Limited DHC-8 (Dash 8), registered VH-QOD, entered runway 05 at Wagga Wagga, unaware that a Piper PA-28, registered VH-XDK, was commencing its take-off roll from the reciprocal runway 23. The Dash 8 pilots did not detect the PA-28 until the crew of a third aircraft broadcast that there was an aircraft taking off.
Why did it happen
The pilot of the PA-28 reported selecting the mode S transponder mode to ON/ALT prior to entering the runway. This was in compliance with their operations manual and standard operating procedures. However, this meant that the aircraft would not be electronically conspicuous to other traffic in the vicinity of the aerodrome, prior to entering the runway.
While not a formalised procedure for the Dash 8 crew, electronic surveillance equipment could be used as an aid to identify potential conflicting ground movements. The crew of the Dash 8 reported that transponder information was used to identify potential traffic at the time to develop their mental model.
Safety advisory notice
AO-2024-041-SAN-001: The effective use of mode S transponders from the first movement of the aircraft can serve as an effective tool in adding another layer of collision avoidance between aircraft at a non‑controlled aerodrome. Using the mode S transponder, particularly if the aircraft has ADS-B OUT capability, is the most effective way of making an aircraft electronically conspicuous and delivering maximum interoperability with other aircraft as well as the ground traffic environment. The ATSB advises pilots and operators to review their procedures to ensure that mode S transponders are on from first movement of the aircraft, particularly at non-controlled aerodromes.
Use of mode S transponders during taxi
At non-controlled airports, maintaining awareness of other traffic is critically important. Good airmanship dictates that all pilots should be looking out and using all available resources at their disposal. Pilots can guard against the issues highlighted by this incident by utilising all available tools at their disposal.
Turning your mode S transponder on prior to taxi will increase your electronic conspicuity to other aircraft, enhancing their situation awareness and alerted see and avoid practices. Likewise, using an electronic flight bag at a non‑controlled aerodrome can enhance your awareness of other traffic in the vicinity when they are using mode S transponders or ADS-B.
To operators of single-engine PT6A powered aircraft
Increased awareness and training for pilots in uncommanded engine acceleration events involving PT6A engines will improve outcomes for such malfunctions.
What happened
On 8 January 2024, a Cessna 208B Grand Caravan, departed Lizard Island Airport, Queensland on a flight to Cairns with the pilot and 9 passengers on board. During the climb, the pilot observed the aircraft’s speed and thrust increase uncommanded, and some engine parameters were exceeded or were not indicating. The pilot returned to land but due to the uncontrollable excessive engine power, they conducted a high-speed approach, touched down long on a short runway, overran the end, and the aircraft flipped over. All occupants received minor injuries.
Why did it happen
The ATSB’s examination determined that the uncommanded engine acceleration was very likely associated with an engine fuel control unit (FCU) malfunction. It was identified that there was no documented procedure or troubleshooting information available in the aircraft flight manual and there was limited industry awareness of this type of event and how it should be managed in-flight.
Safety advisory notice
AO-2024-001-SAN-001: In the absence of a flight manual procedure and with limited industry awareness, the ATSB encourages operators of single-engine PT6A powered aircraft to consider potential responses to an uncommanded engine acceleration event for different phases of flight, and to document and train pilots on appropriate actions to ensure operations are performed correctly and consistently.
Awareness and training
Many single-engine PT6A powered aircraft have a procedure for when the engine rolls back to idle power. Some aircraft also have a manual override or emergency power lever to handle this situation and pilots are trained in this. However, there was no such procedure for when the engine accelerated to, or beyond, engine limitations, which occurred more often than any other type of FCU malfunction. Without a formal procedure, pilots are required to exercise judgement based on their experience, skills and knowledge.
ATSB consultation with Cessna Caravan training organisations found that there was limited awareness of such an event. While not as immediately dire as an engine failure or roll back to idle event, an uncommanded engine acceleration is alarming and requires prompt action to control the aircraft and prevent overstress of the engine and airframe. Awareness and training of this type of event will prepare pilots and should result in a better outcome.
The removal of a middle row seat or approved cargo door modifications can improve the survivability for occupants of the Cessna 206.
What happened
On the morning of 1 September 2024, the pilot of a Cessna U206F took off from a private aircraft landing area, 40 km south-east of Moora, Western Australia, to conduct a local scenic flight with 5 passengers on board. On return to the landing area, after bouncing twice on landing, the pilot then attempted to conduct a go-around. However, an incorrect flap setting resulted in the aircraft not climbing, impacting the right wing with terrain before coming to a stop in an adjacent field.
The rear seat passengers, an older person and a child, were unable to egress the aircraft via their closest emergency exit (the cargo doors). The pilot tried assisting them but found that the forward cargo door was blocked due to the flap extension and was unaware how to open the rear cargo door with the forward cargo door blocked by the flap. The pilot attempted to retract the flaps so the door could be opened, but they would not retract. The pilot then instructed the passengers in the rear seats to climb over the middle row of seats so they could exit through the left forward cabin door. This ultimately increased the time taken to evacuate the aircraft and further increased the risk of passenger injury and post-impact survivability, such as if fire or ditching had been a factor.
Why did it happen
The Cessna 206 is a 6‑seat, high wing aircraft with a forward cabin door on the pilot’s side and a double cargo ‘clam-shell’ style door on the rear right hand side of the aircraft. When the aircraft flaps are extended 10° or more, this prevents the forward, overlapping part of the cargo door from opening, requiring a multi-step process to open the rear part of the door to exit the aircraft.
In response to a fatal Canadian Cessna 206 accident in 2018, Transport Canada issued
requiring Canadian registered Cessna 206 aircraft to have one of the second row (middle row) seats removed if passengers were to be seated in the rear seats of the aircraft. The airworthiness directive was introduced due to aircraft occupants being unable to evacuate the aircraft during an emergency and allowed the rear seat passengers easier access to the forward cargo door. At the time, the Canadian airworthiness directive did provide for an alternative means of compliance to the removal of a middle row seat with a supplemental type certificate (STC) STC SA1470GL(Opens in a new tab/window), for the installation of a second forward cabin door located adjacent to the forward right seat.
In 2020, STC SA20-34(Opens in a new tab/window) was approved as an alternative means of compliance, which allowed the forward cargo door corner to be hinged so the door corner can fold and the door fully open with flap extended in any position and without any restriction to the rear cargo door.
In 2023, Transport Canada also approved STC SA23-21(Opens in a new tab/window) to provide an additional handle that is installed internally on the forward cargo door. The handle is accessible to the rear seat passengers, which, when activated, jettisons the front cargo door from the aircraft. The removal of the door provided enhanced egress to the middle row occupants when flaps remained extended. The release of the door from the aircraft also improved visibility of the rear cargo door handle and simplified opening the rear cargo door for occupants in the rear seats.
, and consider either the removal of a middle row seat to improve rear seat occupants’ access to the pilot’s forward left cabin door or the fitment of approved Cessna 206 emergency exit modifications to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo doors during an emergency exit.
Cessna 206 emergency egress modifications
The additional complexity involved with opening the rear cargo door of the Cessna 206 when the flaps remain extended requires a multi-step process that is not intuitive or simple.
Transport Canada made significant changes to the aircraft configuration mandating the removal of a middle row seat and therefore providing access for passengers in the rear seats and improved access to the pilot’s forward left door. As an alternative to the removal of a seat, Transport Canada also approved modifications that either provided an additional exit or modification to the cargo door, so as the extended flap does not block the forward cargo door exit.
Australian operators of Cessna 206 aircraft that feature the double cargo door are strongly encouraged to review the changes Transport Canada has mandated, or the approved modifications, and consider implementing the improvements for the survivability for passengers during emergency egress in the Cessna 206.
Emergency egress from the rear cargo doors becomes more complex with flaps extended.
Ensure passengers have a thorough understanding of the use of emergency exits.
What happened
On the morning of 1 September 2024, the pilot of a Cessna U206F took off from a private aircraft landing area, 40 km south‑east of Moora, Western Australia, to conduct a local scenic flight with 5 passengers on board. On return to the landing area, after bouncing twice on landing, the pilot then attempted to conduct a go‑around. However, an incorrect flap setting resulted in the aircraft not climbing, impacting the right wing with terrain before coming to a stop in an adjacent field.
The rear seat passengers, an older person and a child, were unable to egress the aircraft via their closest emergency exit (the cargo doors). The pilot tried assisting them but found that the forward cargo door was blocked due to the flap extension and was unaware how to open the rear cargo door with the forward cargo door blocked by the flap. The pilot attempted to retract the flaps so the door could be opened, but they would not retract. The pilot then instructed the passengers in the rear seats to climb over the middle row of seats so they could exit through the left forward cabin door. This ultimately increased the time taken to evacuate the aircraft and further increased the risk of passenger injury and post-impact survivability, such as if fire or ditching had been a factor.
Why did it happen
The Cessna 206 is a 6‑seat, high wing aircraft with a forward cabin door on the pilot’s side and a double cargo ‘clam-shell’ style door on the rear right hand side of the aircraft. When the aircraft flaps are extended 10° or more, this prevented the forward, overlapping part of the cargo door from opening, requiring a multi-step process to open the rear part of the door to exit the aircraft.
The pilot reported they provided the passengers with a pre-flight briefing that included the operation of both the forward and rear cargo doors, however the briefing did not include a demonstration of the operation of the cargo door emergency exit with the flaps extended.
The emergency exit placard located on the forward cargo door states:
Open forward cargo door as far as possible
Rotate red lever in rear cargo door forward and unlatch/open door
Restow red lever
Force rear cargo door open
During landing and take-off, it is likely there will be flap extension and therefore also likely that the flaps would remain extended after a forced landing, ditching or accident, making the egress via the rear cargo doors more difficult for passengers.
The newer Cessna 206H model incorporates the improvements that were made with the 1991 Cessna service bulletin SEB 91-4 Cargo door latch improvement applicable to all models prior to the Cessna 206H. The service bulletin recommended modifying the rear door handle to include a spring to ensure that the handle would return to the stowed position after opening, this improved the ease of opening the rear cargo door when the flaps remained extended. The service bulletin was not a mandatory modifcation.
In 2021, the Civil Aviation Safety Authority (CASA) issued Airworthiness Bulletin 52‑006(Opens in a new tab/window) recommending that pilots demonstrate the operations of the cargo door emergency exit with the flaps in an extended position. This was further revised by CASA in January 2025 to detail advice on placarding or fitment of the ‘return spring’ on the emergency release handle.
Safety advisory notice
AO-2024-049-SAN-001: The Australian Transport Safety Bureau advises Cessna 206 pilots and operators that due to the difficulties occupants have encountered egressing the rear cargo door as identified in several transport safety investigations, to ensure they are familiar with CASA‑issued Airworthiness Bulletin 52‑006(Opens in a new tab/window), and ensure passengers are provided with a thorough safety briefing demonstrating the cargo door emergency egress when the wing flaps remain in the extended position.
Cargo door emergency egress briefing
The emergency egress via the cargo door is hampered by the extension of flaps and the process to evacuate when the flaps are extended is neither simple nor obvious. The ATSB has identified that this presents a high risk to passengers, particularly those seated in the rear of the aircraft.
Pilots and operators are encouraged to ensure passengers of Cessna 206 aircraft with the standard double cargo doors are provided a pre-flight safety briefing that demonstrates the emergency egress process required to use the cargo doors when the flaps are in the extended position. Operators are encouraged to develop safety briefing cards with imagery clearly depicting the process as well as incorporating into the passengers’ pre-flight briefing. The incident also highlights the responsibilities of pilots to ensure passengers have a thorough understanding of the use of emergency exits.
To operators of De Havilland Aircraft of Canada Limited DHC-8 aircraft
Reduced quality of radio signal reception and transmission on De Havilland Aircraft of Canada Limited DHC-8 (Dash 8) aircraft during ground-based communication
What happened
On 29 September 2023, a Lancair Super ES taxied for runway 36 at Mildura, Victoria at about the same time a Dash 8 began to taxi for runway 09.
Both aircraft gave taxi, entering and backtracking calls on the local common traffic advisory frequency. The Dash 8 crew did not hear the calls from the Lancair, nor did the Lancair pilot hear the calls from the Dash 8. The crew of the Dash 8 gave a rolling call and had commenced their take-off on runway 09. Shortly after, the pilot of the Lancair gave a rolling call on runway 36. This call was received by the Dash 8 just prior to rotating for take-off, with the crew responding for the Lancair to hold on the runway. Another aircraft taxiing behind the Lancair for runway 36, advised the Lancair to hold position while the Dash 8 departed. The Dash 8 crossed the runway 09/36 intersection while the Lancair remained on the threshold of runway 36.
Why did it happen
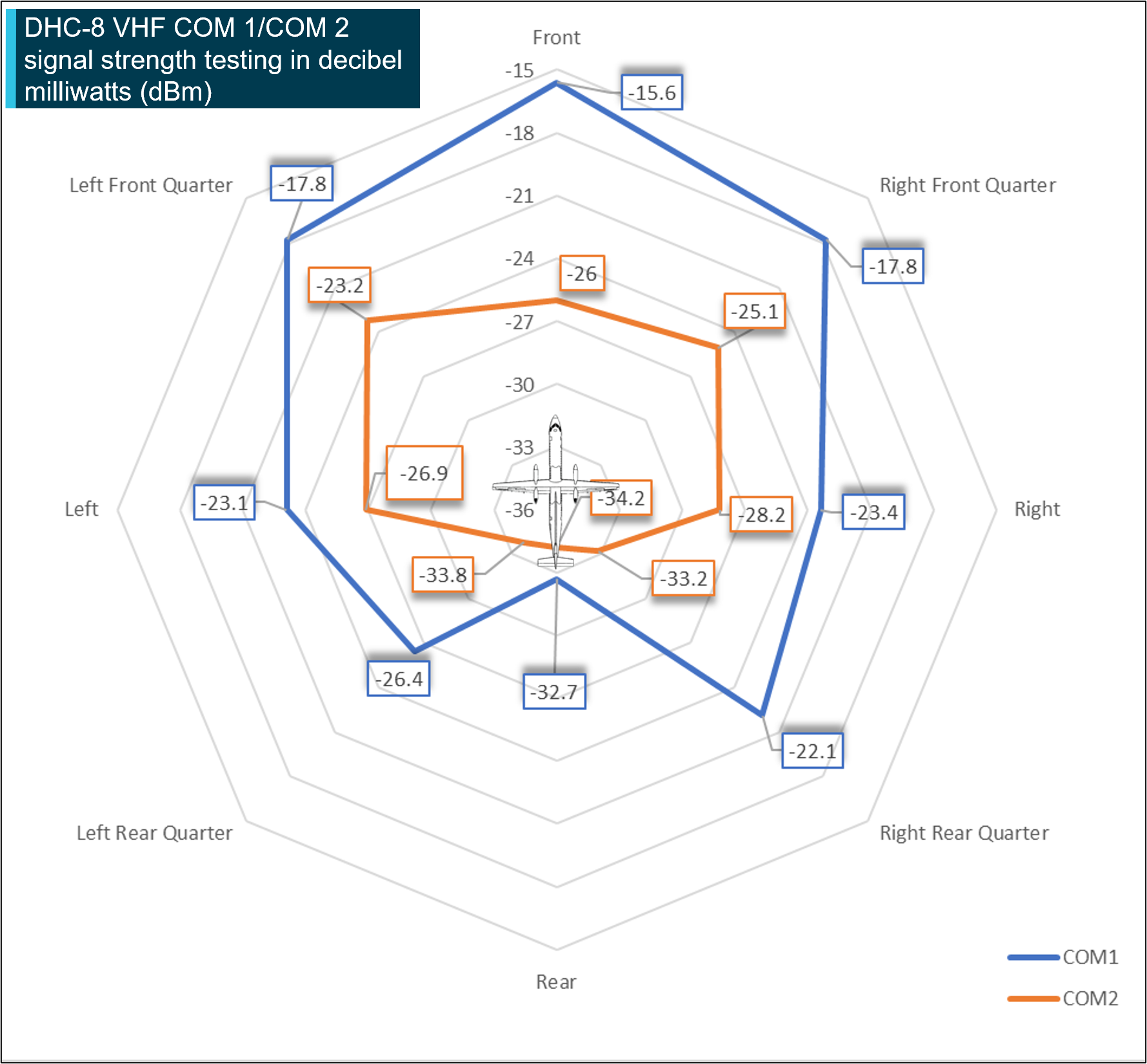
The Dash 8 series of aircraft has a VHF antenna for the COM 1 radio on the upper fuselage, and a VHF antenna for the COM 2 radio on the lower fuselage.
Radio frequency interference testing at Mildura Airport was completed by the ATSB, the Australian Communications and Media Authority (ACMA), Mildura Airport management, Airservices and QantasLink in March 2024. Testing identified reduced radio signal transmission and reception quality on a Dash 8 300 aircraft while using VHF COM 2 for ground-based very high frequency (VHF) communications.
Reduced signal strength reception and transmission was identified during ground-based communications on VHF COM 2 when compared to VHF COM 1. This was identified as a factor leading to incomplete, unintelligible or non‑receipt of VHF positional radio broadcast information at non‑towered aerodromes. These broadcasts are normally used to enhance the alerted see‑and‑avoid situational awareness of flight crew and other pilots in the vicinity.
This was of particular importance at Mildura Airport as aircraft positioned on runway thresholds may not be visible to the pilots from each respective aircraft.
Aircraft radio shielding on all Dash 8 aircraft variants can occur during ground operations due to the close proximity of the VHF COM 2 antenna to the ground and airframe shielding which is likely to affect communications resulting in reduced signal strength, reduced clarity of transmissions and impair reception of other radio calls. This can be further exacerbated by physical obstacles, such as hangars and terrain. Furthermore, negative effects on ground‑to‑ground based communications are exacerbated by increased distance between the aircraft.
De Havilland Aircraft of Canada Limited reviewed the testing and on 6 December 2024, issued twoflight operations service letters relating to radio communications, with one covering Dash 8 100‑300 series aircraft and the other covering the Dash 8 400 series aircraft. The service letters remind operators that ground based VHF communications are affected by line of sight and can be impacted by buildings, terrain or aircraft structures and that use of VHF COM 1 is more effective for ground‑based communications with other aircraft.
Communications at non‑towered aerodromes
Pilots are responsible for making themselves aware of nearby aircraft and maintaining separation at non‑towered aerodromes. Traditionally, VHF radio broadcasts are made at non‑controlled aerodromes to provide situational awareness, traffic separation and deconfliction to other traffic in the vicinity of the aerodrome.
Broadcasting to other traffic in the vicinity of a non‑controlled aerodrome is known as radio‑alerted see‑and‑avoid and assists by supporting the pilot’s situational awareness. Positional broadcasts rely on the ability of other traffic receiving, comprehending and reacting to this information.
In some aircraft, using an antenna that is positioned underneath the aircraft may not have optimal ground‑based transmission or reception strength and clarity due to airframe shielding. Positional broadcasts are a one‑way communication, so they do not imply receipt of information by other parties unless direct radio contact is made between stations. As a result, in some circumstances, broadcasts may be missed without either pilot realising it, and this affects their shared understanding of the traffic in the vicinity.
Safety advisory notice
AO-2023-050-SAN-01: The Australian Transport Safety Bureau advises all operators and crew of De Havilland Aircraft of Canada Limited DHC-8 (Dash 8) aircraft to consider the use of VHF COM 1 radios for ground‑based communication while operating at non‑controlled aerodromes, to improve radio transmission and reception with other stations.
Research and testing required for fitment of constant wear lifejackets with multipoint seatbelts.
Occupants in helicopter tourism operations worldwide are at risk of increased injury in an accident due to inadvertent incorrect use of seatbelts. There is no guidance available on correct use of constant wear lifejackets with multipoint seatbelts and research and testing is needed.
What happened
On 2 January 2023, while conducting short scenic flights, 2 Eurocopter EC130 B4 helicopters collided midair at the Gold Coast, Queensland. One helicopter proceeded to a controlled landing on a sandbar; the pilot and 2 passengers were seriously injured. The other helicopter was uncontrollable and fell to the edge of the sandbar. Three passengers were seriously injured and the pilot and 3 passengers were fatally injured.
What was identified
Passengers from both helicopters were found to be inadequately restrained from incorrect fitment of their seatbelt. This was due in part to the placement of constant wear lifejackets that were being worn. The ATSB was unable to determine the level of contribution of incorrect restraint to the injuries sustained by the passengers.
Australian regulations for scenic flight operations over water require passengers to be wearing lifejackets in addition to seatbelts in a helicopter. This is to ensure that passengers can access this piece of equipment in a timely manner. To comply with the regulation most operators provide their passengers with pouch style constant wear lifejackets. While these 2 pieces of equipment were commonly used together there was no available guidance about how to integrate them while maintaining their functionality. Manufacturer instructions for fitment of all pouch style constant wear lifejackets requires them to be worn around the waist and positioned at the middle of the body. However, this interferes with the correct fitment of a multipoint seatbelt.
The correct fitment of any seatbelt requires the lap portion to be worn low and tight across the hips. The operator’s ground and flight crew were not aware of how to integrate the constant wear lifejacket with seatbelts without affecting correct fitment of the seatbelt. This led to inadvertent incorrect fitment of passenger seatbelts.
However, no readily available guidance exists from lifejacket manufacturers or regulatory authorities for use by aircraft operators regarding the fitment of multipoint seatbelts with constant wear lifejackets.
Safety advisory notice
AO-2023-001-SAN-002: The ATSB encourages those organisations capable of research to determine a correct method of wearing a constant wear lifejacket with a multipoint seatbelt, while ensuring the correct function of each.
Research and testing required
Having access to a lifejacket in the case of ditching is important and reduces the risk of drowning, which is why the use of a constant wear lifejacket is required for certain overwater operations. However, an occupant must survive the impact and therefore correct fitment of their seatbelt is vital to ensure the restraints and energy attenuating features of seats work as designed.
The ATSB issued AO-2023-001-SAN-001, which provided information on the correct fitment of multipoint restraints and called for guidance to be developed by lifejacket manufacturers and/or certifying authorities. This notice acknowledges that those parties would benefit from research organisations’ investigation and validation so that appropriate guidance on the correct fitment of multipoint restraints and constant wear lifejackets can be developed.
The outcomes of the research and testing will contribute to a solution for the widespread problem of inconsistent and frequently incorrect wearing of seatbelts. Development of guidance and procedures for aircraft operators to correctly integrate constant wear lifejackets with a multipoint seatbelt will benefit passengers across helicopter tourism operations worldwide.
Crashworthiness of some DHC-1 Chipmunks may be compromised by incorrect specification rivets.
What happened
On the afternoon of 26 April 2024, the pilot of a DHC‑1 Chipmunk took off from Jandakot Airport, Western Australia. The engine cowling on the left side had not been fastened prior to take-off and began to open and close in flight. The aircraft turned to the left at low height near the end of the runway, with an increasing angle of bank, before descending and colliding with terrain. The pilot was transported to hospital and later succumbed to injuries.
What increased risk
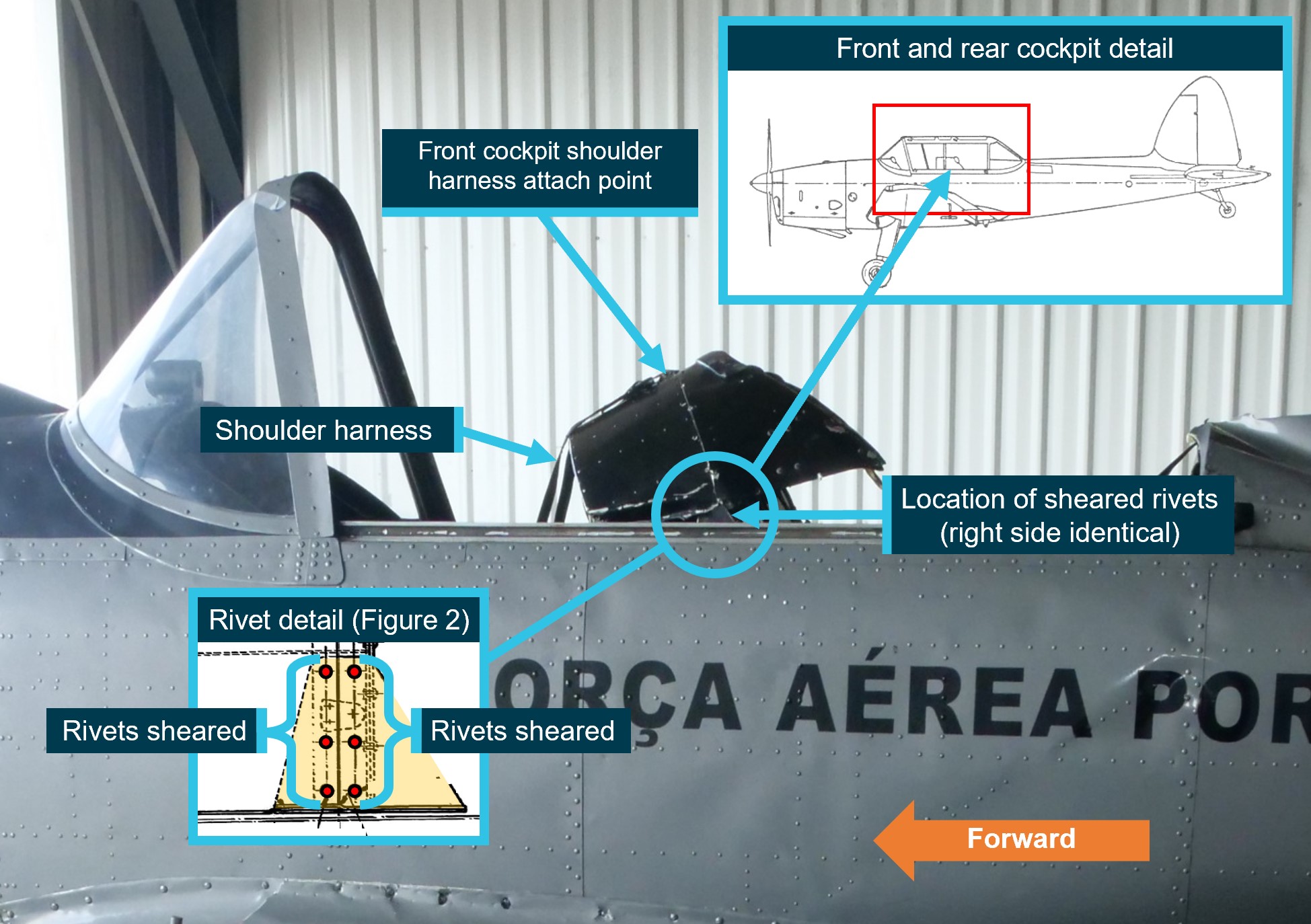
The DHC-1 Chipmunk is a low-wing aircraft designed for military flight training. It has 2 seats that are arranged in tandem (one cockpit behind the other). The front cockpit shoulder harness is attached to the upper structure between the front and rear cockpits.
The ATSB found that on impact the upper structure between the front and rear cockpits, corresponding to the attach point for the front cockpit shoulder harness, was torn away from its mountings. Most noteworthy, all 12 rivets (6 per side) that attached the structure to the mountings had sheared (Figure 1).
Image source: ATSB, de Havilland Support Ltd, annotated by the ATSB.
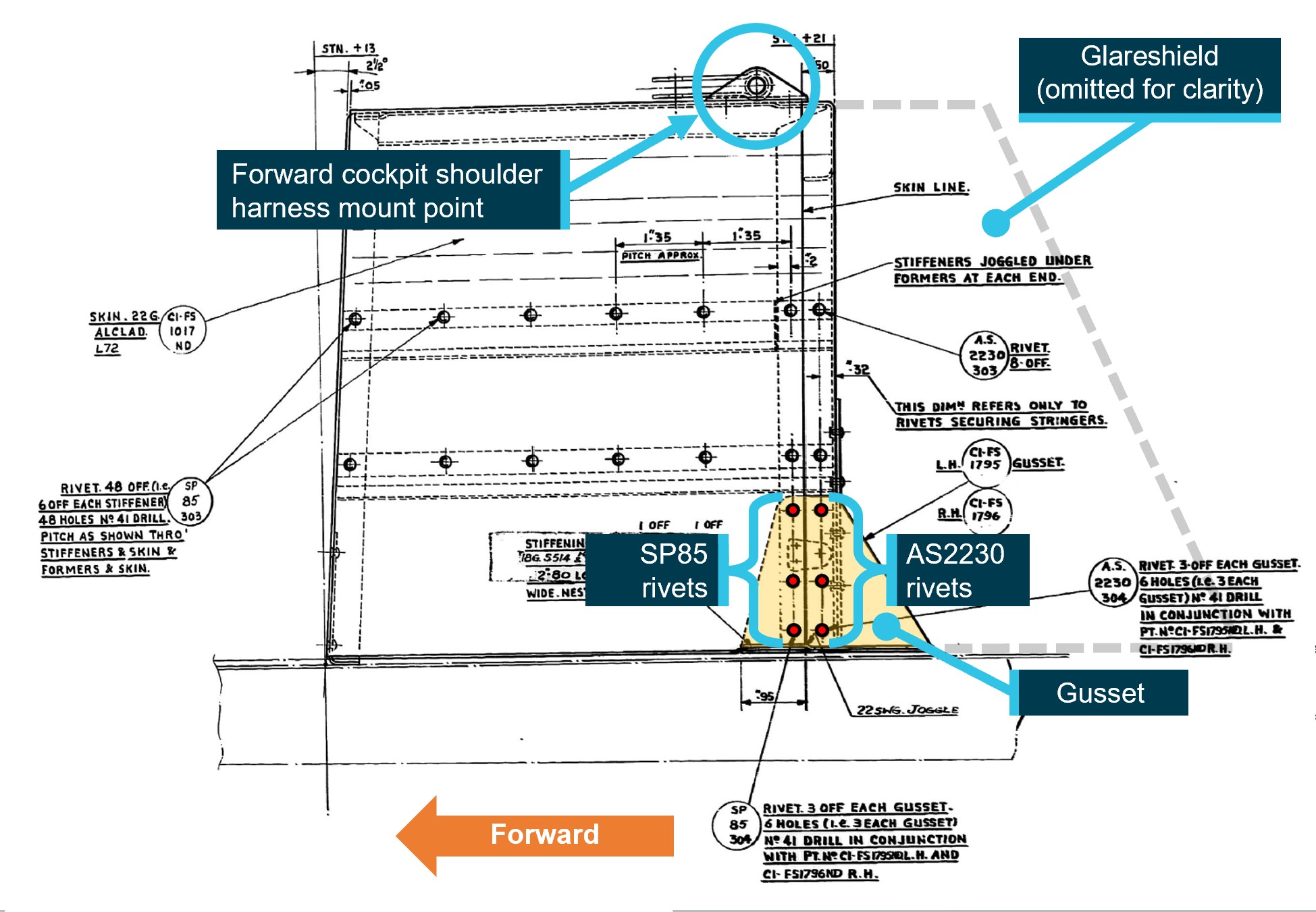
The 2 mountings, called gussets, were installed as modification H.268. This modification was issued by Hawker Siddeley in 1966 to replace the original aluminium alloy gussets with high‑tensile steel. The modification required the forward row of rivets attaching the structure to the gussets to be part number SP85 mushroom head rivets, and the rear row to be part number AS2230 countersunk rivets (Figure 2).
Image source: ATSB, de Havilland Support Ltd, annotated by the ATSB.
Both part number SP85 and AS2230 rivets were required to be manufactured to British standard L.86, which was an aluminium alloy that included copper and magnesium (with international equivalences of Alloy Designation 2117, US specification AMS7222, and European specification ENAW-AlCu2.5Mg). The standard also specified that the rivets were to be anodised (a surface treatment) and coloured violet.
The sheared rivets were examined by the ATSB using metallurgical equipment and it was determined that:
The rear row of countersunk rivets appeared to be pure or near-pure aluminium and therefore the incorrect specification. Testing indicated a significant reduction in strength (estimated to be about one-third of the specification strength).
The forward row of mushroom head rivets appeared to be an alloy consistent with L.86. The rivets were coated with a gold-coloured chromate conversion coating instead of violet anodising. ATSB testing indicated that the strength of the rivets met or exceeded literature values for L.86 alloy.
The ATSB has not determined when or where modification H.268 was embodied, or whether the rivets had been replaced since the modification.
The presence of the non-conforming rivets significantly reduced the integrity of the structure retaining the front cockpit restraint, and thereby compromised the crashworthiness of the aircraft. This non-conforming modification may be present in other Chipmunk aircraft, in which case it would likely affect survivability in an accident.
Crashworthiness design
One element of aircraft crashworthiness is the ability of a restraint system to restrain the occupant within the aircraft’s ‘living space’ throughout a crash. The use of upper torso restraints such as a shoulder harness can further prevent the occupant from striking the surrounding structure during an accident. All components forming part of the restraint system (including the structures to which they are attached) need to be to defined specifications.
Safety advisory notice
AO-2024-013-SAN-01: The ATSB advises DHC‑1 Chipmunk maintainers and owners to be aware that fitment of incorrect specification rivets where the upper structure between the front and rear cockpits attaches to the gussets on either side could significantly compromise the crashworthiness of the aircraft.
Those conducting work on aircraft must ensure modifications are carried out to the required specification, or during maintenance returned to that specification.
A recent ATSB / OTSI investigation has found issues with the assessment of rail safety worker competence. These issues have involved both vocational education and training (VET) and enterprise‑based qualifications.
What happened
The Office of Transport Safety Investigations (OTSI) has completed an investigation into an accident, on behalf of the ATSB, where 3 locomotives located at the rear of a loaded grain train separated from the lead portion of the train in transit. Shortly afterwards, the lead portion of the train stopped and the 3 now detached locomotives at the rear collided with the stationary lead portion. This resulted in significant damage to the rear wagon and a locomotive.
What increased risk
The investigation found that the train crew had not performed a ‘stretch test’ after completing shunting duties at Werris Creek, which contributed to the incident. It also found that while the train crew had been assessed as competent in shunting during both VET and enterprise-based assessments on several occasions, the supporting evidence collected was usually limited to a single check box that the task had been ‘performed correctly’.
Safety advisory notice
RO-2022-001-SAN-02: The Australian Transport Safety Bureau strongly encourages rail transport operators, and registered training organisations acting on their behalf, to review and validate their rail safety worker competency assessments. This is to ensure these assessment tools, processes and judgements are reliably meeting the principles and requirements of competency-based training and assessment.
Assessment of competence
The competence of rail safety workers is critical to safe railway operations. Where competency assessments are aligned to the Australian Qualifications Framework (AQF), i.e. VET, certain standards must be met. These include, in part, that sufficient assessment evidence is collected to ensure a sound, reliable and consistent competency decision is made, irrespective of the assessor. For example, for practical assessments well-described skills, observable behaviours and underpinning knowledge of the task being performed should be assessed and recorded.
Where complying with the AQF is not reasonably practical, for example, a suitable unit of competency or qualification is not available, enterprise-based assessments should still follow these same principles of competence-based training and assessment.
Practical guidance to assist rail transport operators in meeting their obligations include those from the Australian Skills Quality Authority (Users’ guide to the standards for registered training organisations 2015) and the Office of the National Rail Safety Regulator (Application of the AQF to rail safety worker competence assessment).