On 15 April 2025, an Embraer ERJ 190-100, registered VH-UZD, was conducting a passenger transport flight from Sydney, New South Wales, to Launceston, Tasmania. After commencing approach to Launceston, the flight crew received multiple caution messages including a SLAT FAIL caution. The flight crew discontinued their approach and after completing the relevant checklists elected to divert to Melbourne, Victoria, as it was the longest available runway in the region. The remainder of the flight was uneventful, and the aircraft landed safely.
Post-flight troubleshooting determined that a torque tube in the left wing slat drive system had disconnected as it had been incorrectly assembled when it was last refitted.
What the ATSB found
The ATSB identified a similar occurrence with another of the operator’s Embraer ERJ 190‑100 aircraft, VH-UYB, where a torque tube in the left wing flap drive system had disconnected as it had been incorrectly assembled when it was last refitted.
The occurrences were similar in that the locking bolts that secured the torque tubes to their actuators had not been fitted correctly into the holes of the splined shafts, since the torque tubes had been incorrectly positioned during installation.
In both occurrences, those carrying out and certifying for the torque tube installations did not identify that they had been incorrectly assembled.
These errors occurred at different maintenance providers, and reportedly from January 2005–August 2011 in the worldwide fleet of Embraer 170, 175, and 190 aircraft (all sharing similar componentry), there have been 5 similar occurrences related to incorrect torque tube installation.
What has been done as a result
The operator, Alliance Airlines, issued a maintenance notice that detailed the flap torque tube disconnect affecting VH-UYB and the slat torque tube disconnect affecting VH-UZD. This notice reiterated the aircraft maintenance manual information for the correct installation of flap and slat torque tubes.
The maintenance organisation added an additional task card that is automatically issued when work is scheduled on the E190 slat system torque tubes that provides guidance in addition to the aircraft maintenance manual to mitigate the incorrect assembly of torque tubes on their splines. A similar additional task card was being developed for the E190 flap system torque tubes.
Safety message
Historical occurrence and technical information provide an opportunity to review known errors prior to commencing particular maintenance activities, thereby reducing the possibility of further errors occurring. When an error does occur, this information also provides a means to bolster the actions taken to prevent re-occurrences.
This information can be available from multiple sources including the manufacturer, national aviation authorities (such as CASA or the FAA), accident investigation authorities, and the safety management systems of operators and maintenance organisations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Previous maintenance
In November 2024, an Embraer ERJ 190-100 aircraft, registered VH-UZD and operated by Alliance Airlines, commenced a heavy maintenance[1] check by Rockhampton Aviation Maintenance in Rockhampton, Queensland. A team comprising 2 aircraft maintenance engineers (AMEs) was tasked with inspecting and lubricating the leading-edge slat drive system (see Embraer E190 slats and flaps). This involved removing, cleaning, lubricating, and refitting each slat torque tube in turn. A licensed aircraft maintenance engineer (LAME) briefed the AMEs on what was required.[2] The LAME was familiar with the task but was unaware of any historical issues with the task (see Maintenance requirements). The work was carried out in a new facility with good lighting. Access to the components was good, and a purpose-built platform allowed the work to be carried out with the relevant components at eye level.
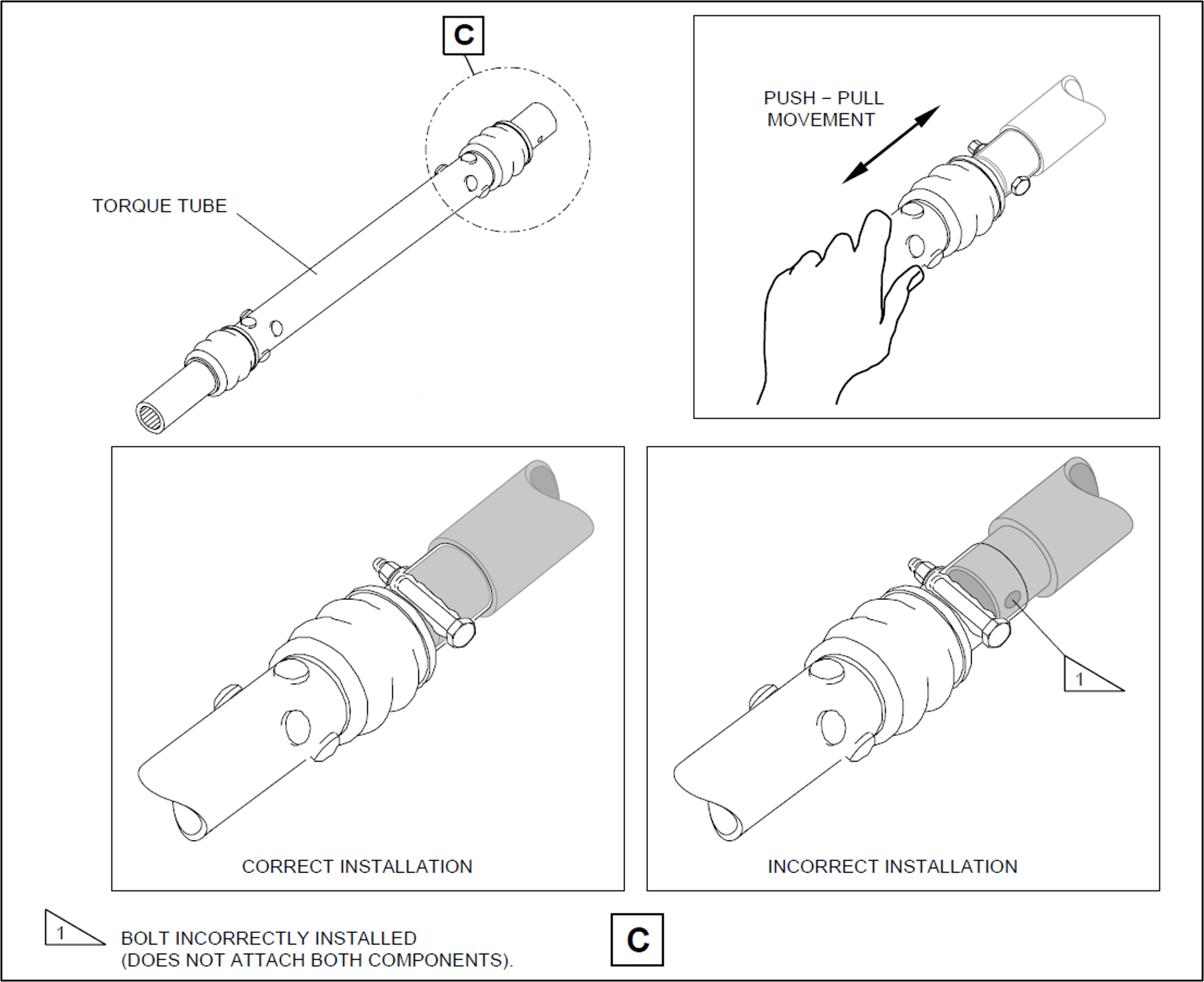
Prior to commencing work, brakes internal to the power drive units (PDUs) (which drive the flap and slat torque tubes) were electrically released as required by the aircraft maintenance manual (AMM) procedure. The AMEs printed a copy of the relevant AMM procedure, and worked together on the torque tube driving the left-wing outboard actuator for slat number 4. The PDU brakes were also required to be released prior to installing the torque tubes, however, it could not be established whether this took place (the PDU brakes reapply when power is removed). After refitting the outboard actuator torque tube, a push-pull check was carried out to ensure it was locked in place, as required by the AMM. Unknown to the AMEs, when this torque tube was refitted, it had not been positioned far enough onto the actuator’s splined shaft for the locking bolt to secure it (Figure 1, lower right). The locking bolt was inadvertently installed beyond the end of the spline (shown in grey) rather than through the hole as required.
One AME then continued work on the left wing and the other moved to the right wing slat drive system to work alone. The remaining slat torque tubes were correctly fitted.
After this work was completed, the LAME inspected the installation of the torque tubes and their locking bolts, and a second LAME carried out an independent inspection[3] of the work. The heavy maintenance check was completed in March 2025, and the aircraft was returned to service.
On 15 April 2025, 50 flights after returning to service from heavy maintenance, the aircraft was being operated on a passenger transport flight from Sydney, New South Wales, to Launceston, Tasmania, by Alliance Airlines for QantasLink. After commencing approach to Launceston, the flight crew received multiple caution messages[4] on the aircraft’s engine indicating and crew alerting system (EICAS) including a SLAT FAIL caution. The flight crew discontinued the approach and requested clearance from air traffic control for vectors[5] so they could action the relevant quick reference handbook (QRH) checklists for the caution messages.
The flight crew completed the QRH checklist. As the slat failure would require landing with the slats and flaps up, the flight crew elected to divert to Melbourne Airport, Victoria, as it had the longest available runway in the region. The flight crew declared a PAN PAN[6] and commenced the diversion to Melbourne. After climbing to 19,000 ft the aircraft was flown to Melbourne at 220 kt as required by the QRH because of the slat failure. The aircraft landed at Melbourne without further incident.
Post-flight inspection
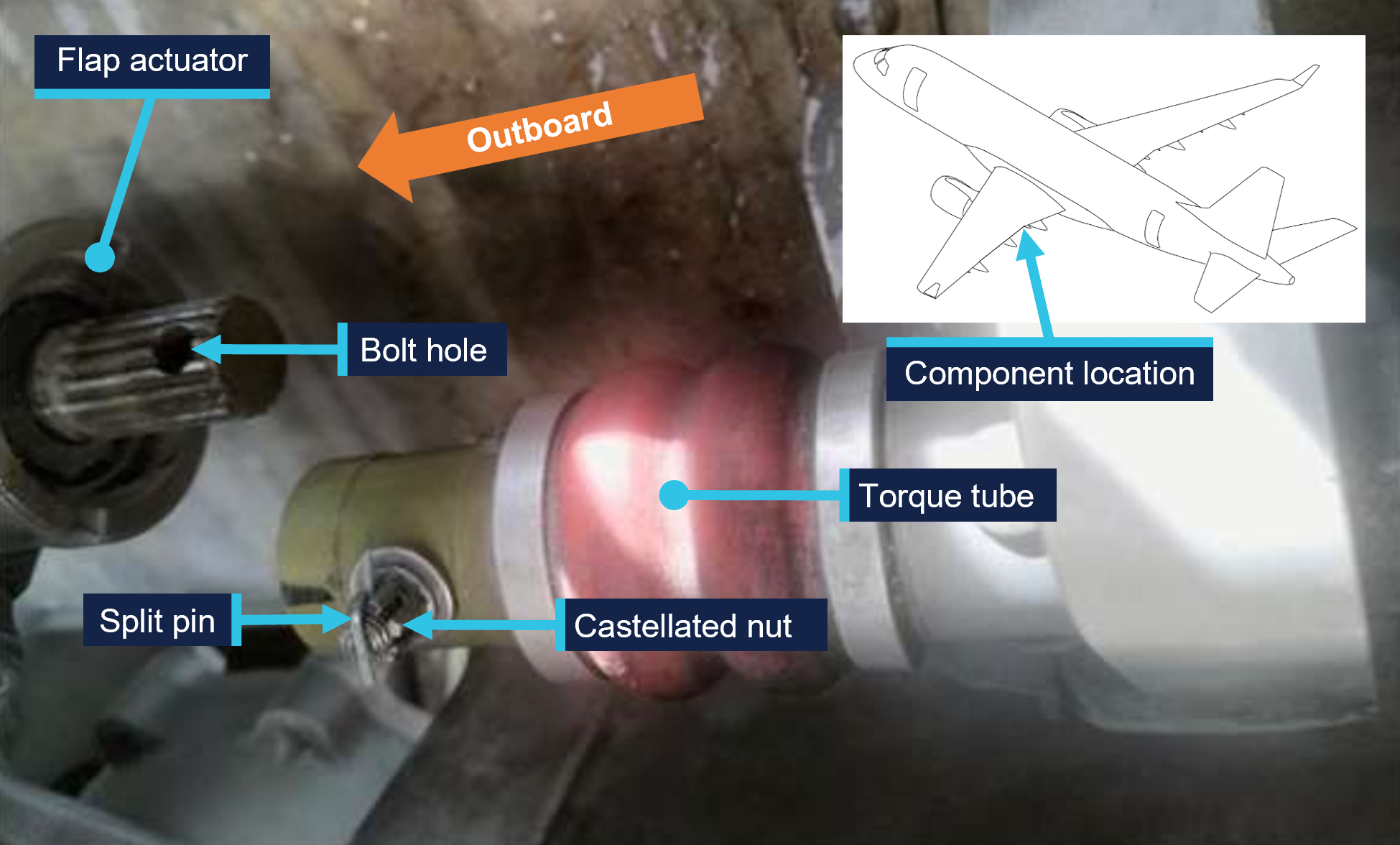
Post-flight inspection determined that the torque tube for the left wing slat number 4 outboard actuator had disconnected as the locking bolt fitted to the torque tube had not passed through the corresponding hole in the actuator’s splined shaft when it was last refitted (Figure 2).
Figure 2: VH-UZD left wing outboard actuator for slat number 4 and torque tube, shown disconnected after the occurrence flight
Source: Alliance Airlines, annotated by the ATSB
Context
Aircraft information
The Embraer ERJ 190-100 IGW (E190) is a narrow-body aircraft used for air transport operations and powered by 2 General Electric CF34-10E5 turbofan engines. VH-UZD was manufactured in Brazil in 2008 and registered in Australia on 31 January 2022.
Embraer E190 slats and flaps
The E190 is fitted with devices to increase the lift produced by its wings during take-off and landing. On the leading edges of the wings there are 8 slat panels and on the trailing edges of the wings there are 4 flap panels (Figure 3), where each set (slats/flaps) extends and retracts together.
Figure 3: Embraer E190 slats and flaps
Source: Embraer, annotated by the ATSB
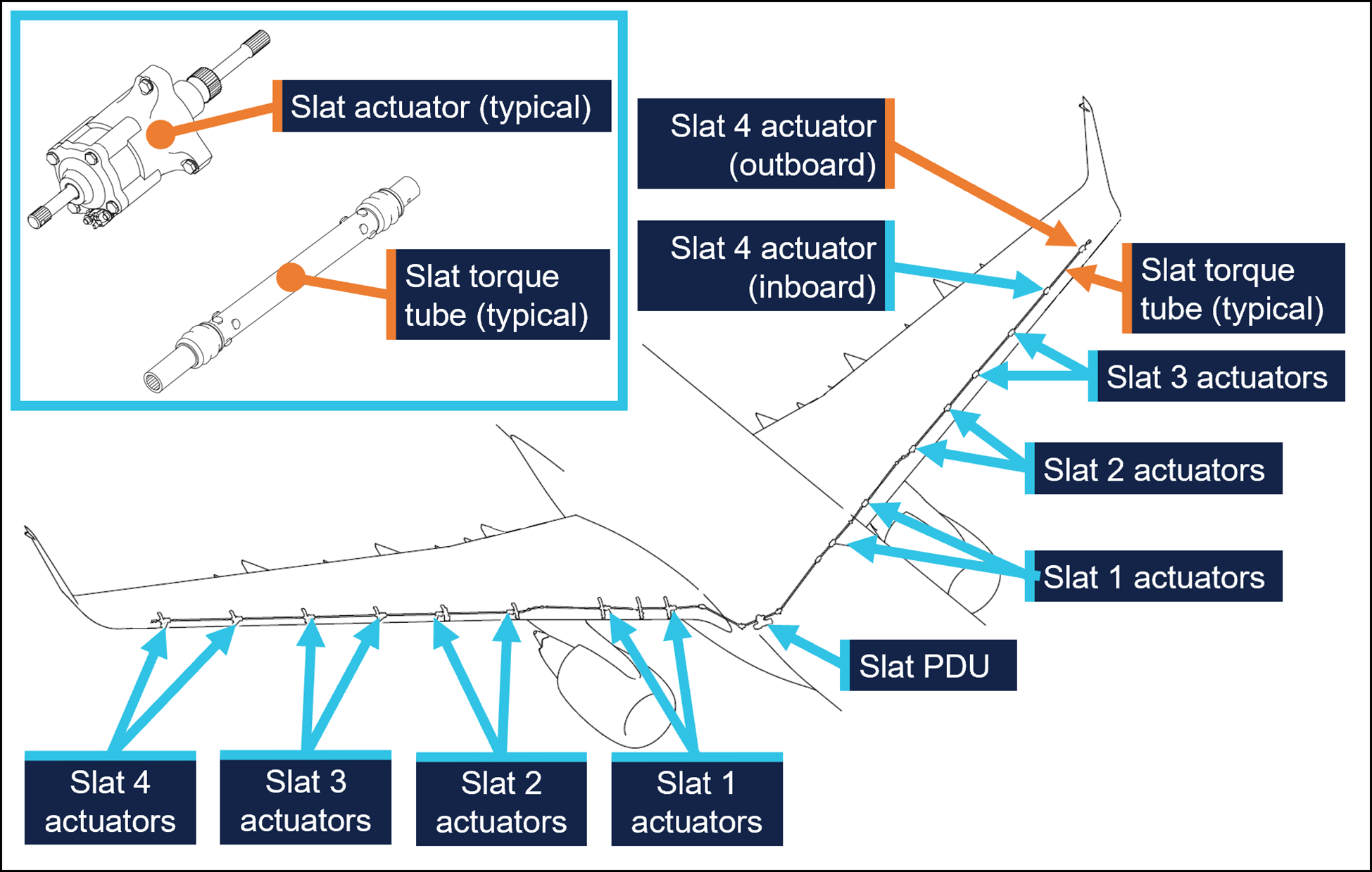
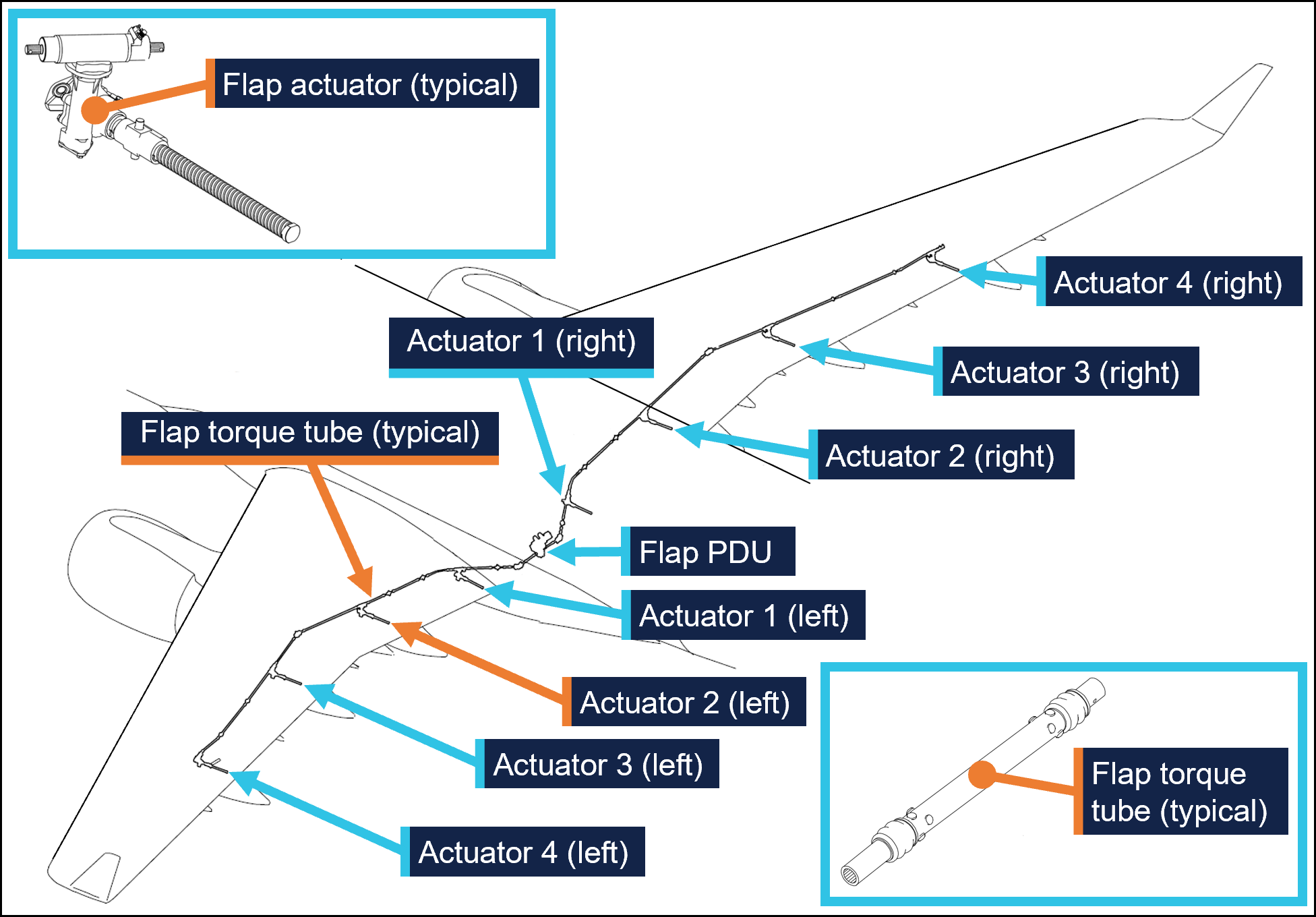
Slat and flap extension and retraction is controlled from the cockpit by using the slat/flap control lever (SFCL). When the SFCL is moved from its 0 (up) position,[7] the flap and slat power drive units (PDUs) drive torque tubes which in turn drive actuators, transferring the rotary motion of the torque tubes to linear motion that extends the slats and flaps (Figure 4 and Figure 5).
Each PDU has 2 internal brakes that are engaged under spring force and released electrically, such that the brakes would re-engage when power is removed. There are 26 torque tubes in the slat drive system and 22 torque tubes in the flap drive system.
In the event of a slat or flap failure, redundant detection and protection systems prevent them operating in such a way that may compromise safety of flight.
Figure 4: Embraer E190 slat drive system
Source: Embraer, annotated by the ATSB
Figure 5: Embraer E190 flap drive system
Source: Embraer, annotated by the ATSB
Maintenance requirements
The slat and flap torque tubes are removed periodically for the actuator splines to be lubricated with grease. They may also need to be removed to replace associated components. A detailed visual inspection of the slat and flap drive system is also carried out periodically and includes a requirement to check that the torque tubes are correctly secured in place by their locking bolts. No detailed visual inspections of the slat system had been required between the heavy maintenance in November 2024 and the occurrence flight.
The procedure to remove and install the slat and flap torque tubes is detailed in the aircraft maintenance manual (AMM). As part of this procedure, the slat or flap PDU brakes are disengaged electrically to eliminate any residual torque in the system that may impede (through friction) the removal of the torque tubes. For the same reason, the brakes must also be disengaged for their installation.[8] Embraer advised the ATSB of the importance of removing residual torque for the installation.
Rockhampton Aviation Maintenance noted during its investigation into the occurrence that excessive amounts of grease on the actuator splines can produce hydraulic resistance to re-assembly of the torque tube and therefore no more than what is required to lubricate the splines should be applied. It could not be determined whether this occurred during the maintenance of VH-UZD. The installation procedures for torque tubes in the AMM requires the old grease to be removed, new grease to be applied, and any unwanted grease to be removed prior to assembly.
The torque tubes interface with other components via splined shafts and are secured by locking bolts in conjunction with castellated nuts and split pins to prevent their inadvertent disconnection. There are 24 locking bolts in the slat drive system and 18 locking bolts in the flap drive system, all with this configuration.
The AMM describes and illustrates a ‘push-pull’ check to determine the locking bolt has been correctly installed and had showed representative examples of correct and incorrect installation (Figure 1).
The torque tube locking bolts pass through holes close to the end of each actuator’s splined shaft. A correctly installed torque tube is visually apparent by less exposed splines (Figure 6). If a slat torque tube is incorrectly positioned[9] on a slat actuator the locking bolt will not capture the splined shaft and can lead to the torque tube disconnecting and slat failures.
Figure 6: Exemplar slat torque tube correctly fitted (upper image) and incorrectly fitted (lower image) to a slat actuator
A slat actuator and torque tube were correctly and incorrectly assembled on a workbench to create these images. Source: The maintenance organisation, annotated by the ATSB
Actions taken to prevent installation errors
In 2010 the AMM was amended to include the previously mentioned illustration (Figure1) showing the correct and incorrect installation of slat and flap torque tubes along with the push-pull test. This revision also added the requirement to release the PDU brakes.
Embraer communicated these changes by publishing a service newsletter SNL 190‑27‑0050 noting reports of incorrect slat or flap torque tube installation, advising that the AMM had been revised to mitigate future occurrences, and provided an overview of the revisions. This information was also published in Embraer’s safety magazine[10] (available to operators of E190s) and was contained in a document[11] published by the National Civil Aviation Agency of Brazil.
In October 2017 Embraer published an update on the issue in a document[12] that reiterated the previous actions taken to mitigate these occurrences. This document noted that from January 2005–August 2011 in the worldwide fleet of Embraer ERJ170, 175, 190, and 195 aircraft[13] there were 483 reports of slat or flap system failures. Of these, 5 were occurrences related to incorrect torque tube installation. Additionally, the document stated that the subject of incorrect torque tube installation was presented to civil aviation authorities in Europe and the Americas. It was concluded that no additional actions were required, as there were a small number of exposed aircraft, and there had been no reported events since the AMM was revised in 2010, and the manufacturer considered the issue closed.
Related occurrences
Incorrect flap torque tube installation
In late 2024, an Embraer ERJ 190-100 aircraft, registered VH-UYB and operated by Alliance Airlines for QantasLink, commenced a heavy maintenance check at a facility in Singapore. The torque tube driving the left wing flap actuator number 2 (see Embraer E190 slats and flaps) was removed to carry out flap actuator torque limiter checks. When fitted, the torque tube had not been positioned far enough onto the actuator’s splined shaft for the locking bolt to secure it.
On 10 November 2024, 35 flights after returning to service from heavy maintenance, the aircraft departed for a passenger transport flight. After take-off, the flight crew received a FLAP FAIL caution on the EICAS as the flaps were retracting. The flight crew initiated a turnback and the aircraft landed safely.
Engineering personnel later found that the locking bolt for the left wing flap actuator number 2 torque tube had not passed through the corresponding hole in the actuator splined shaft when it was last refitted (Figure 7).
Figure 7: VH-UYB left wing flap actuator 2 and torque tube
Source: Alliance Airlines, annotated by the ATSB
Other flight control event involving VH-UZD
On 18 April 2025, VH-UZD was operating from Adelaide, South Australia, to Canberra, Australian Capital Territory. When flaps were selected down, the slats began to extend but the flaps did not deploy, and the crew received multiple failure warnings. The flight crew diverted to Melbourne. Post-flight troubleshooting determined that the flap power drive unit (PDU) torque limiter had tripped, which is a problem unrelated to the investigation occurrence or the recent heavy maintenance check.
Safety analysis
Incorrect fitment of actuator torque tubes
When the torque tube for the left wing slat number 4 outboard actuator was refitted to VH-UZD in November 2024, it had not been positioned far enough onto the actuator’s splined shaft for the locking bolt to secure it in place. After re-entering service and conducting 50 flights, the torque tube disengaged from the actuator, and the slat system failed. Protection systems ensured the safety of flight was minimally affected.
Similarly, when another E190, VH-UYB, was under heavy maintenance at a different facility at around the same time, the torque tube driving the left wing flap actuator number 2 was incorrectly assembled in that the locking bolt had not passed through the hole in the actuator’s splined shaft. The torque tube disengaged 35 flights after the aircraft re-entered service and the flap system failed.
Non-detection of the error
The 2 AMEs who fitted the torque tube in VH-UZD did not identify that the torque tube had been incorrectly fitted. Further, the LAME checking this work and the second LAME carrying out the independent inspection of this work did not identify that it had been incorrectly assembled. The similar error affecting VH‑UYB also apparently remained undetected by those carrying out and certifying for the work.
As far as could be established, there were no physical or environmental factors that may have influenced the incorrect assembly of the torque tube. The work on VH-UZD was carried out in a new facility with good lighting, and access to the work area was good and could be carried out with the relevant components at eye level.
Ultimately, it is likely that not knowing the subtle difference in appearance of an incorrectly assembled slat torque tube (that is, as little as about 6.35 mm more of the actuator spline visible) contributed to the error not being detected by the 2 AMEs and the 2 LAMEs involved. Further, the remaining torque tubes in the slat drive system were correctly assembled, however their subtly different appearance did not trigger recognition that the original torque tube had been incorrectly assembled.
Available relevant information
Installation of the slat and flap drive system torque tubes is a simple task, but errors have occurred. Embraer noted that from January 2005–August 2011 in the worldwide fleet of Embraer 170, 175, 190 aircraft (all sharing similar componentry) there were 5 occurrences related to incorrect torque tube installation. The Embraer 190 has 24 locking bolts in the slat drive system and 18 in the flap drive system representing a total of 42 opportunities to incorrectly secure the torque tubes.
In 2010, Embraer made amendments to the aircraft maintenance manual to reduce the possibility of assembly errors. These were intended to remove any residual torque loads during removal and installation (by releasing the PDU brake), highlight the possibility of error with an illustration, and through the addition of the push-pull check, provide a means to detect an installation error.
These changes were communicated in multiple documents, such as a service newsletter, that were available to operators and maintainers of E190s. Review of such documents can assist in highlighting known issues and thereby prevent reoccurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight control event involving Embraer E190, VH-UZD, 29 km south-east of Launceston Airport, Tasmania, on 15 April 2025.
Contributing factors
During scheduled maintenance, the locking bolt for the left outboard slat torque tube was not passed through the hole in the actuator’s splined shaft as the torque tube had been incorrectly positioned. The aircraft was released from maintenance, and 50 flights later, the torque tube disconnected, causing the slat system to fail.
Both licensed aircraft maintenance engineers inspecting the left outboard slat torque tube did not identify that it had been incorrectly assembled.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action taken by Alliance Airlines
On 17 April 2025, Alliance Airlines issued a maintenance notice that detailed the flap torque tube disconnect affecting VH-UYB on 11 November 2024 and the slat torque tube disconnect affecting VH-UZD on 15 April 2025. This notice reiterated the aircraft maintenance manual information for the correct installation of flap and slat torque tubes.
Safety action taken by Rockhampton Aviation Maintenance
The maintenance organisation added an additional task card that is automatically issued when work is scheduled on the E190 slat system torque tubes. This task card provides guidance in addition to the aircraft maintenance manual to highlight the possibility of hydraulic lock caused by lubricant and the importance of releasing the PDU brake. Additionally, this task details a dimensional check to confirm the correct installation of torque tubes on their splined shafts. A similar additional task card was being developed for the E190 flap system torque tubes.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Alliance Airlines
Centro de Investigação e Prevenção de Acidentes Aeronáuticos (Brazil)
Civil Aviation Safety Authority
Embraer
Rockhampton Aviation Maintenance
licenced aircraft maintenance engineer that made the final certification of the work
both aircraft maintenance engineers.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Alliance Airlines
Centro de Investigação e Prevenção de Acidentes Aeronáuticos (Brazil)
Civil Aviation Safety Authority
Embraer
Rockhampton Aviation Maintenance
licenced aircraft maintenance engineer that made the final certification of the work
both aircraft maintenance engineers.
Submissions were received from:
Embraer
Rockhampton Aviation Maintenance.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Heavy maintenance is typically when an aircraft is removed from service for a period of time for more extensive inspections, checks, servicing, and modifications to be carried out.
[2]One of the AMEs had carried out this task previously. The other had experience maintaining E190s including slat and flap drive systems however had they had not previously removed and installed slat and flap torque tubes.
[3]Civil Aviation Regulation (CAR) 42G required independent inspections to be carried out on flight control systems when they were disturbed during maintenance.
[4]The caution messages presented were SLAT FAIL, SHAKER ANTICIPATED, and AOA [angle of attack] LIMIT FAIL.
[5]In this context, a vector is a heading given by air traffic control to a flight crew for navigation guidance.
[6]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[7]The SFCL has 7 positions ranging from up (retracted) to fully extended slats and flaps.
[8]Embraer advised the ATSB that in a scenario where the PDU brakes had been released, and power was subsequently removed from the aircraft (thus reapplying the PDU brakes) this would not be expected to generate any residual torque in the slat or flap drive system. However, Embraer reiterated the importance of the PDU brakes being released when carrying out these tasks.
[9]These dimensions are for the slat actuator and torque tube interface. Dimensions vary for other components in the slat and flap systems.
On the morning of 1 September 2024, the pilot of a Cessna U206F, registered VH-TDQ and operated by Fly Esperance, departed a private aircraft landing area 21 NM (39 km) southeast of Moora, Western Australia (WA) with 5 passengers onboard for a 15-minute local area flight. On return to the landing area, the aircraft bounced twice on landing before the pilot attempted a go‑around. During the go-around, the pilot incorrectly set the flap, and the aircraft lost height impacting its right wing with terrain, resulting in minor damage. The aircraft then touched down on the landing gear in a field adjacent to the runway.
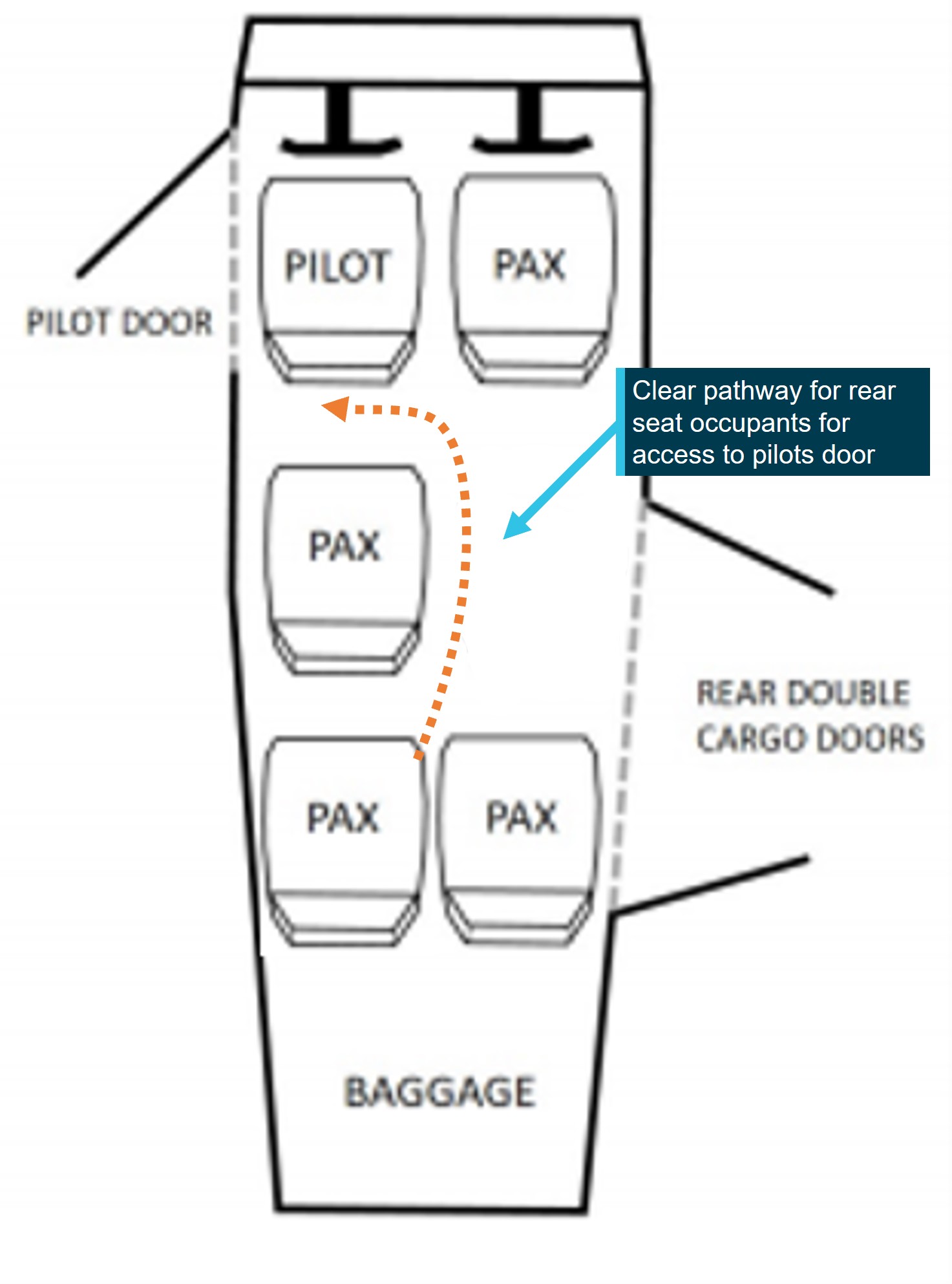
The pilot then evacuated the passengers. The front seat and middle row passengers egressed through the pilot’s forward left cabin door. The pilot then proceeded to assist the egress of 2 passengers seated in the rear seat row of the aircraft through the right-side cargo door emergency exit. The aircraft’s flaps remained extended in the 10° position which blocked the forward half of the cargo door emergency exit. The pilot was unable to retract the flaps and the passengers, an older person and child, were then forced to climb over the middle row of seats and egress through the pilot’s forward left cabin door. None of the occupants reported injuries.
What the ATSB found
On return to the aircraft landing area, the pilot conducted a non-standard approach to join the circuit. This reduced the time available for the pilot to configure the aircraft, manage the airspeed and prepare for a short field landing.
As a result of excess speed on approach for a full flap, short field landing, the aircraft landed long and bounced twice, at which point the pilot elected to conduct a go-around. As the aircraft began to climb away, the pilot retracted the flap further than intended and as a result, the aircraft could not achieve adequate climb performance.
The rear emergency exit was the double cargo doors, which required the forward half of the door to be opened before the rear door could be opened. With the flaps extended in the 10° position when the aircraft came to rest, the full opening of the forward cargo door was not possible. The forward door could still be made ajar with the flaps extended, enough to reach and operate the rear door handle. However, the rear seat passengers were not fully aware how to do this and were unable to open the rear cargo door to enable an emergency exit.
The pilot attempted to assist the rear seat passengers’ egress from outside the aircraft, however they were unaware that the rear cargo door on the Cessna 206 could be opened from the outside when the front cargo door was blocked by the extended flaps. After the pilot unsuccessfully attempted to retract the flaps, they instructed the passengers to climb over the middle row seats to egress via the pilot’s forward left cabin door.
The ATSB found that the operator’s pre-flight passenger briefing did not include the demonstration of, and pilots were not trained how to operate, the emergency exit via the cargo door with the flaps extended.
Similar to previous ATSB and international investigations involving Cessna 206 accidents requiring emergency egress, it was found that without the installation of optional cargo door modifications or a reduction in passenger seats, the emergency egress of rear seat passengers was impeded when the flaps are extended. The difficulty in egressing via the cargo door emergency exit (when flaps were extended) increases risk to passenger survivability in the event of a post-accident fire or water ditching. This has been formally recognised in Canada where cargo door modifications are compulsory unless middle row passenger seating is reduced. However, this is not the case in the United States, where the Cessna 206 was certified, nor in Australia.
What has been done as a result
To advise Cessna 206 pilots and operators of the difficulties occupants have encountered egressing the rear cargo door as identified in several transport safety investigations, the ATSB issued safety advisory notice (AO-2024-049-SAN-001). The safety advisory notice encourages pilots and operators to ensure a thorough pre-flight passenger demonstration is conducted of the rear cargo emergency exit egress when the wing flap remains extended.
Fly Esperance Pty Ltd also advised that a staff training exercise had been conducted to demonstrate the process for operating the rear door in the event of post-landing flap extension and has advised that this procedure is to be emphasised on all pre-departure passenger briefings. The ATSB will monitor this safety action until the adoption of procedural changes to staff training and operational pre-flight safety briefings.
Furthermore, a second safety advisory notice was issued to strongly encourage operators and owners to review Transport Canada Airworthiness DirectiveCF-2020-10, and consider either the removal of a middle row seat to improve rear seat occupants’ access to the pilot’s forward left cabin door or the fitment of approved Cessna 206 emergency exit modifications to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo doors during an emergency exit.
Fly Esperance Pty Ltd advised it is in the process of investigating the various STCs mentioned in the report, to see which will be best suited to VH-TDQ in order to improve egress from the aircraft in the event of flaps being deployed.
After the occurrence, the operator conducted an internal review and has made the following amendments to the company operations manual:
Added pictorial for non-controlled aerodrome circuit procedure to clarify the joining procedure at non-controlled aerodromes.
To assist pilots to identify a stable approach an aircraft landing weight table has been added, indicating the recommended speeds for landing with aircraft flaps retracted and extended.
Company aircraft will now have portable GPS tracking devices improving the visibility of the aircraft when away from base.
The operator also reported that a greater emphasis will be placed on pilots-in-command under supervision training prior to a company line check, highlighting what can happen when standard procedures are not followed.
The operator advised that its updated operations manual had been provided to CASA for approval.
Safety message
This occurrence further demonstrates the difficulty occupants of the Cessna 206 face during an emergency egress via the cargo door, when the wing flaps remain extended. This highlights the importance of Cessna 206 pre-flight passenger briefings incorporating a demonstration of the limitations of the cargo door as an emergency exit with the flaps extended.
Furthermore, owners and operators of Cessna 206 aircraft are encouraged to review and assess changes to the aircraft passenger configuration implemented by Transport Canada with Airworthiness Directive CF-2020-10. As an alternative, several acceptable means of compliance for the Airworthiness Directive exist, providing modifications to the emergency exits of the aircraft and thereby improving the survivability in the event of an incident or accident.
Summary video
The occurrence
The day before the accident
On 31 August 2024, the pilot of a Cessna U206F, registered VH-TDQ and operated by Fly Esperance, departed Esperance Airport, Western Australia (WA). The aircraft was ferried to a private aircraft landing area (ALA), 50 NM (93 km) north‑west of Esperance to conduct a non‑scheduled air transport flight to a private ALA about 21 NM (39 km) south‑east of Moora. The 3 passengers and pilot would spend the night at the property with the intention of returning the following day.
On the first arrival at the destination ALA, the pilot made an approach to the westerly runway and configured the aircraft with 20° flap[1] for landing. During the first landing attempt, the aircraft bounced and the pilot conducted a go-around.[2] On the second landing attempt, the pilot configured the aircraft in a 40° full-flap configuration and landed without incident.
Accident flight
On the morning of 1 September 2024, the customers requested two 15-minute local flights for the family members they had been visiting. The pilot consulted the operator’s chief pilot by phone who approved the flights. The pilot then collected the passenger’s weights and assigned them to each flight.
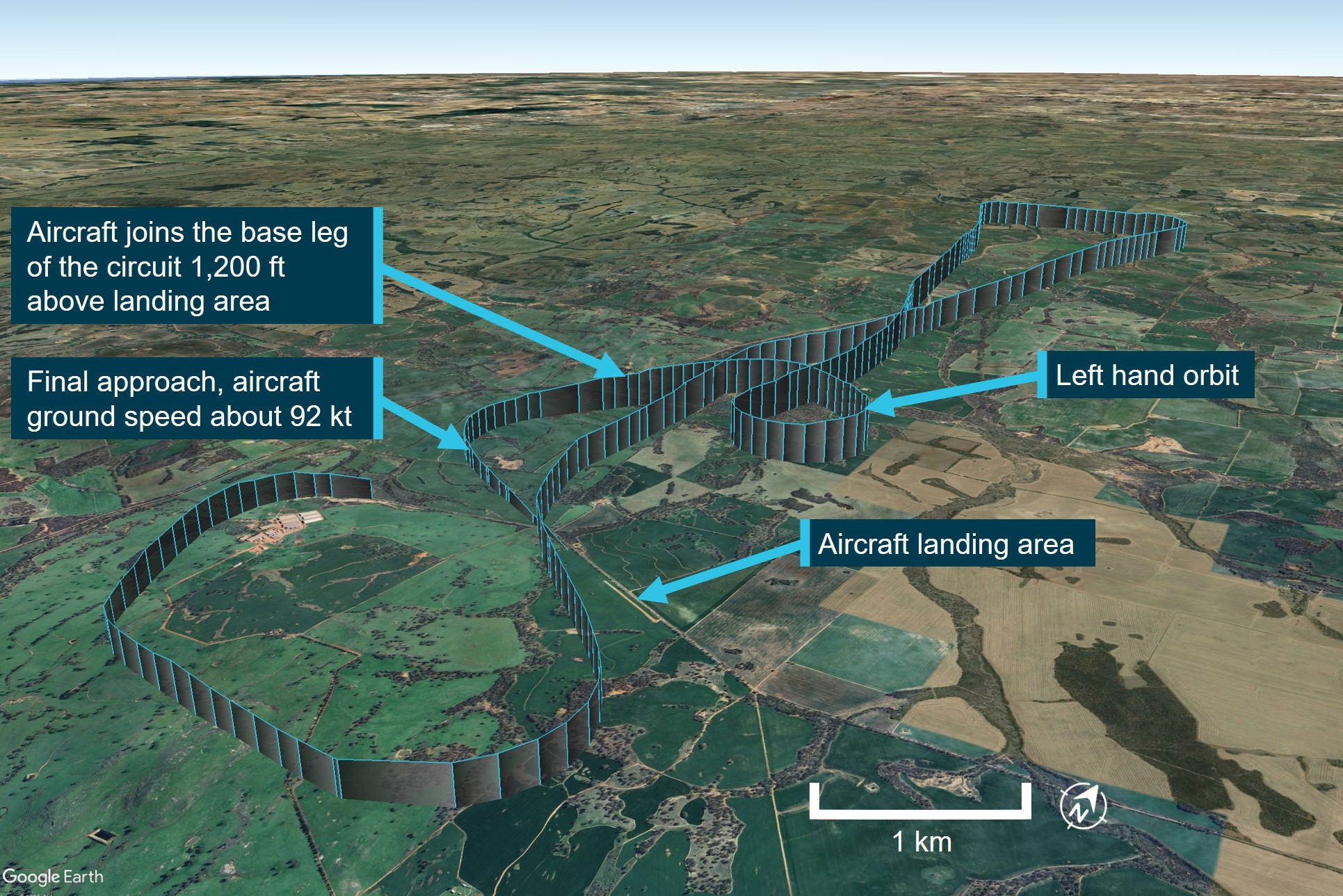
The pilot gathered the passengers of both flights together and conducted a group safety briefing before the passengers on the first flight boarded the aircraft. With 5 passengers on board, the pilot took off on the western runway and departed about 1050 local time, tracked to the north before returning to the ALA a short time later (Figure 1). About 2 NM (3.7 km) north and within sight of the ALA, the pilot assessed that the aircraft was too high and conducted a left orbit to reduce height.
The pilot reported they were advised the previous day by the local agricultural pilots to utilise the uphill slope for landing using the easterly runway and recalled, as there were no other aircraft in the vicinity, directly joining the base leg of the circuit for the easterly runway. They observed a 75 kt airspeed on final approach before configuring the aircraft for a full flap final approach for landing.
Figure 1: VH-TDQ flight track
Source: Google Earth, annotated by the ATSB
The pilot landed the aircraft about 80 m (Figure 2) past the end of the easterly runway and bounced twice before they applied full power and commenced a go-around. The pilot was unable to recall their airspeed at the time of the flap reduction, however reported that the aircraft had probably dissipated a considerable amount of speed during the bounces prior to initiating a go‑around. As the aircraft began the initial climb the pilot reduced the flap setting, unknowingly mis-selecting the 10° setting.
Figure 2: Aircraft landing area
Source: Google Earth, annotated by the ATSB
As the flap retracted, the aircraft lost height and the pilot was unable to maintain control. The aircraft dropped the right wing and the right wingtip grazed the ground in the adjacent field.
The right wingtip then raised above the crop height, however the propeller and landing gear remained partially in the crop (Figure 3) increasing drag and reducing speed. Shortly after, the aircraft touched down on its landing gear with the propeller making full contact with the crop and stopping the engine. The aircraft came to a stop upright, about 250 m from the runway, with the flaps extended in the 10° position. The pilot recalled at this point they switched off the aircraft’s fuel and electrics.
Figure 3: Aircraft landing gear marks in field adjacent to the runway
Source: Fly WA Group, annotated by the ATSB
The pilot then checked on the welfare of the passengers and as a precaution, instructed them to evacuate the aircraft.
The pilot successfully egressed the front seat and middle-row passengers through the forward left cabin door. They then proceeded to the right side of the aircraft to assist the 2 passengers in the rear seats egress through the right-side cargo doors.
On approaching the rear of the aircraft, the pilot observed that the extended flap had blocked the forward half of the cargo door and therefore believed they would not be able to open the rear half of the cargo emergency exit. After an unsuccessful attempt to retract the flaps, the pilot reported they were no longer operational. They did not attempt to open the rear cargo door further and instructed the rear seat passengers, an older person and young child, to egress over the middle row seat and then through the pilot’s forward left cabin door.
The aircraft received minor damage to the right fibreglass wingtip and aileron. No injuries were reported, and all passengers successfully evacuated the aircraft.
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane), issued in August 2016. At the time of the accident, the pilot had about 390 hours of total flying experience, with 134.4 hours as pilot in command and about 30 hours on the Cessna 206. The pilot had operated for 49.4 hours in the last 90 days and held a current class 1 medical certificate that was valid until 29 July 2025.
The pilot was employed by the operator in June 2024 and had flown scenic flights from Jandakot, Western Australia (WA), before gaining full time employment with the same operator to conduct flights from the operator’s Esperance base, where the pilot had been located since August 2024.
During their initial employment with the operator, the pilot received about 13 hours of line training. The training included:
emergency procedures
remote airfields
short fields
maximum all-up weight flight.
The pilot’s logbook indicated a check flight was conducted by the operator’s chief pilot on 19 July 2024. They then began commercial flights for the operator about 1 week later.
Although they had held a commercial licence since 2016, this was the pilot’s first aviation employment, having completed training and private flying before gaining employment with the operator. The logbook also indicated that prior to the pilot’s employment with the operator, limited flying was conducted, with a total of 4.2 hours flown in the 12 months before commencing with the operator.
Aircraft information
General information
The Cessna U206F is a single piston engine, high winged, 6-seat, unpressurised aircraft with fixed landing gear. The aircraft was powered by a Teledyne Continental IO-520 engine.
VH-TDQ was manufactured in the United States in 1975 and first registered in Australia in August 1975. Fly Esperance became the registration holder on 29 April 2023.
Cessna 206 variants
The Cessna 206 was produced between 1963 and 1986. In 1998, Cessna restarted production of the Cessna 206 and the aircraft remains in production.
The original model, named the Cessna 206 Super Skywagon, was produced between 1963 and 1965 and featured the rear right side double cargo doors. Subsequent models (Table 1)were also manufactured with the double cargo doors and included numerous different models between 1963 and 1986. Cessna aircraft company halted production of 206 aircraft between 1987 and 1997. Production resumed in 1998 with the current model 206H.
Table 1: Cessna 206 models manufactured with the double cargo doors
Year
Cessna 206 model name
1963/65
206 Super Skywagon
1966*
U206A 206 Super Skywagon
1967*
U206B Super Skywagon
1968*
U206C Super Skywagon
1969*
U206D Super Skywagon
1970/71*
U206E Skywagon 206/Stationair
1972-76*
U206F Stationair
1977-86*
U206G Stationair
1998-current*
206H Stationair
* Indicates model was also manufactured with a turbo variation
Aircraft flaps
The Cessna 206 has an electrically‑controlled flap system. This requires the battery master[3] to be on and also requires the cargo doors to be completely closed. Closed cargo doors trigger a micro‑switch, located in the doorframe, which completes the electrical circuit and then allows flap movement. As the Cessna 206 flaps extend across the closed forward cargo door (see Cabin layout and exits), this provides a protection so the flaps cannot be inadvertantly extended into an open cargo door and damage the aircraft.
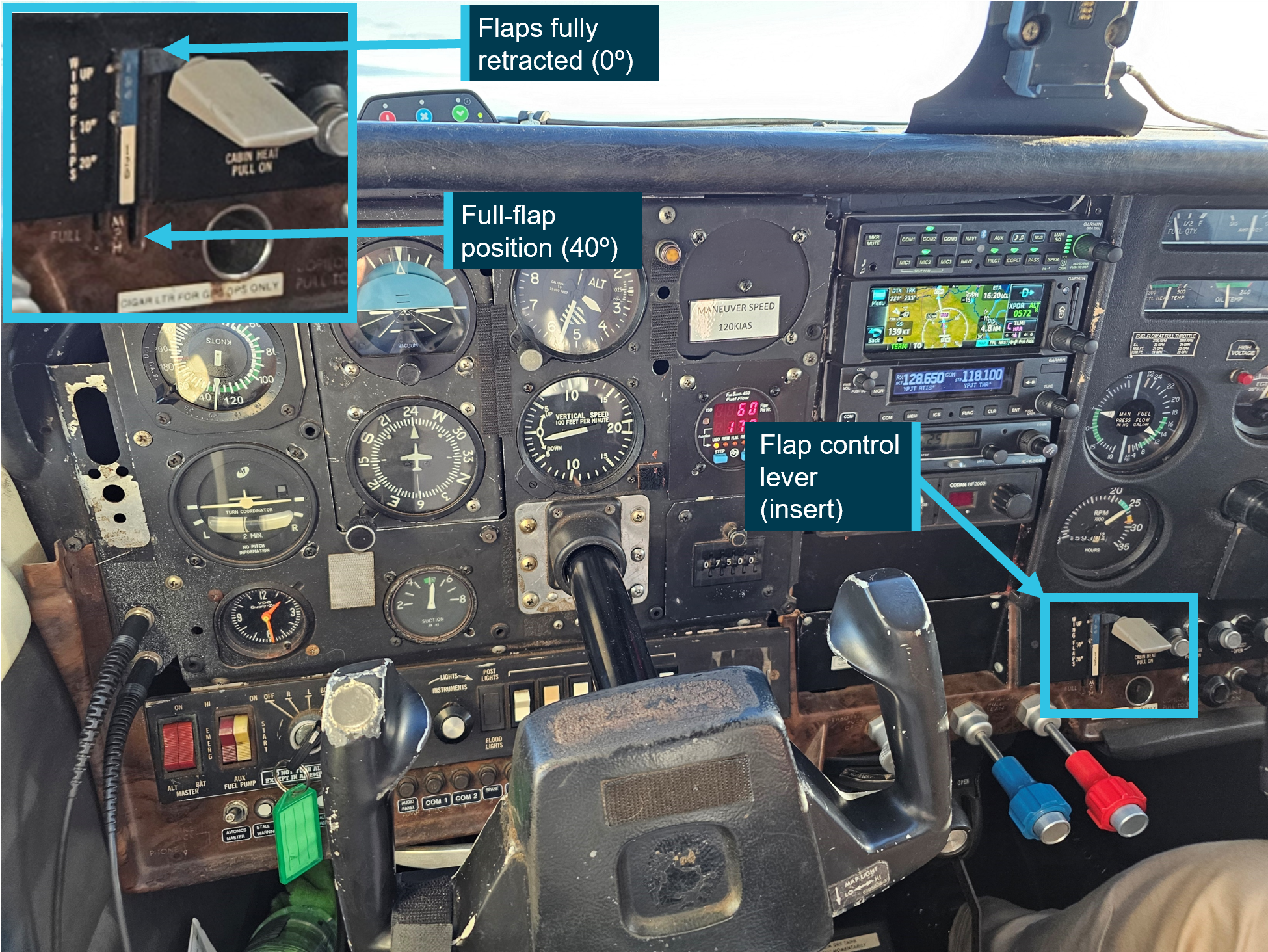
The flap control lever in the Cessna U206F is located on the pilot’s right side (Figure 4) and is clearly visible from the pilot’s seat. The lever allows the flaps to be set in any position between 0° (flaps fully retracted) and 40° (full-flap extension) with an adjacent placard marking the flap position.
The pilot described on numerous occasions during an interview with the ATSB ‘hitting or flicking’ the flap selector lever, identifying that the flap selection was sometimes made without the time taken to confirm the flap selection was in the correct position.
The operator’s chief pilot reported they had not observed the pilot manipulating the lever like this during the 13 hours of in command under supervision (ICUS) flying they completed with the pilot.
Figure 4: Cessna U206F cockpit
Source: Pilot, annotated by the ATSB
Cabin layout and exits
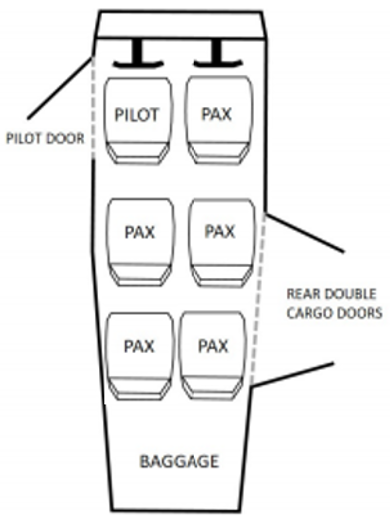
VH-TDQ was operated in a 6-person configuration with 2 front row (pilot) seats, 2 middle row seats and 2 rear seats (Figure 5).
Figure 5: Cessna 206 standard cabin seating configuration
Source: TSB investigation report A18W0129,adapted by ATSB to match occurrence aircraft
VH-TDQ included 2 emergency exits, the pilot’s forward left cabin door and a double ‘clam shell’ style cargo door located at the rear right of the aircraft cabin. Passengers seated in the middle row seats are able to access the pilot’s forward left door when the pilot’s seat is moved into a forward position. The forward part of the cargo door overlaps the rear cargo door as a preventative measure to stop the rear door (rear hinged) from opening in flight and damaging the aircraft. The rear cargo door cannot be opened independently of the front cargo door.
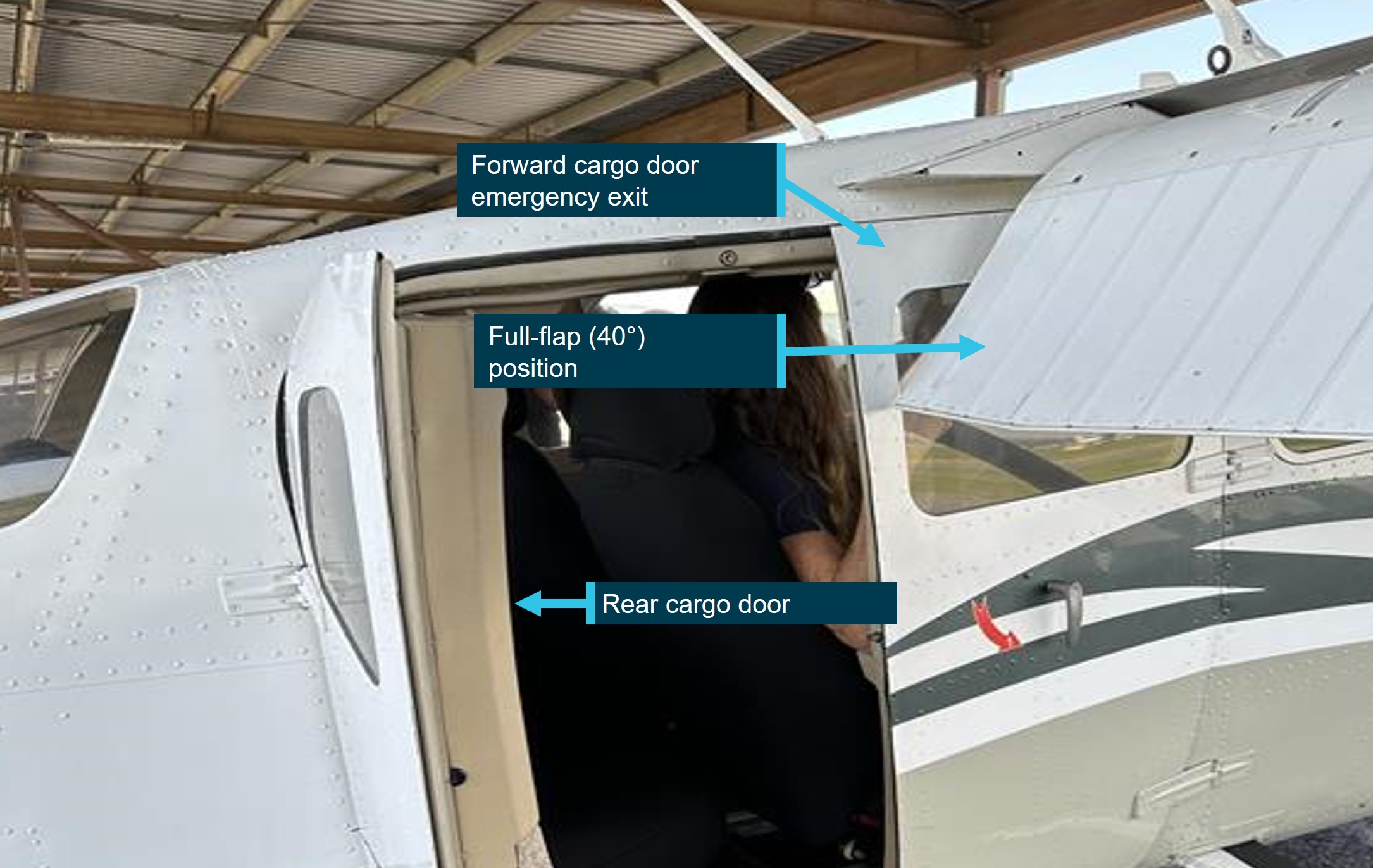
Wing flap extension greater than 10° results in the flap blocking the forward part of the cargo door (Figure 6) and restricts the opening to about 8 cm. When the aircraft wing flaps remain extended, the forward cargo door must be opened as far as possible to then allow the rear door to be opened. Further detail is discussed below in Cessna 206 rear passenger emergencyegress.
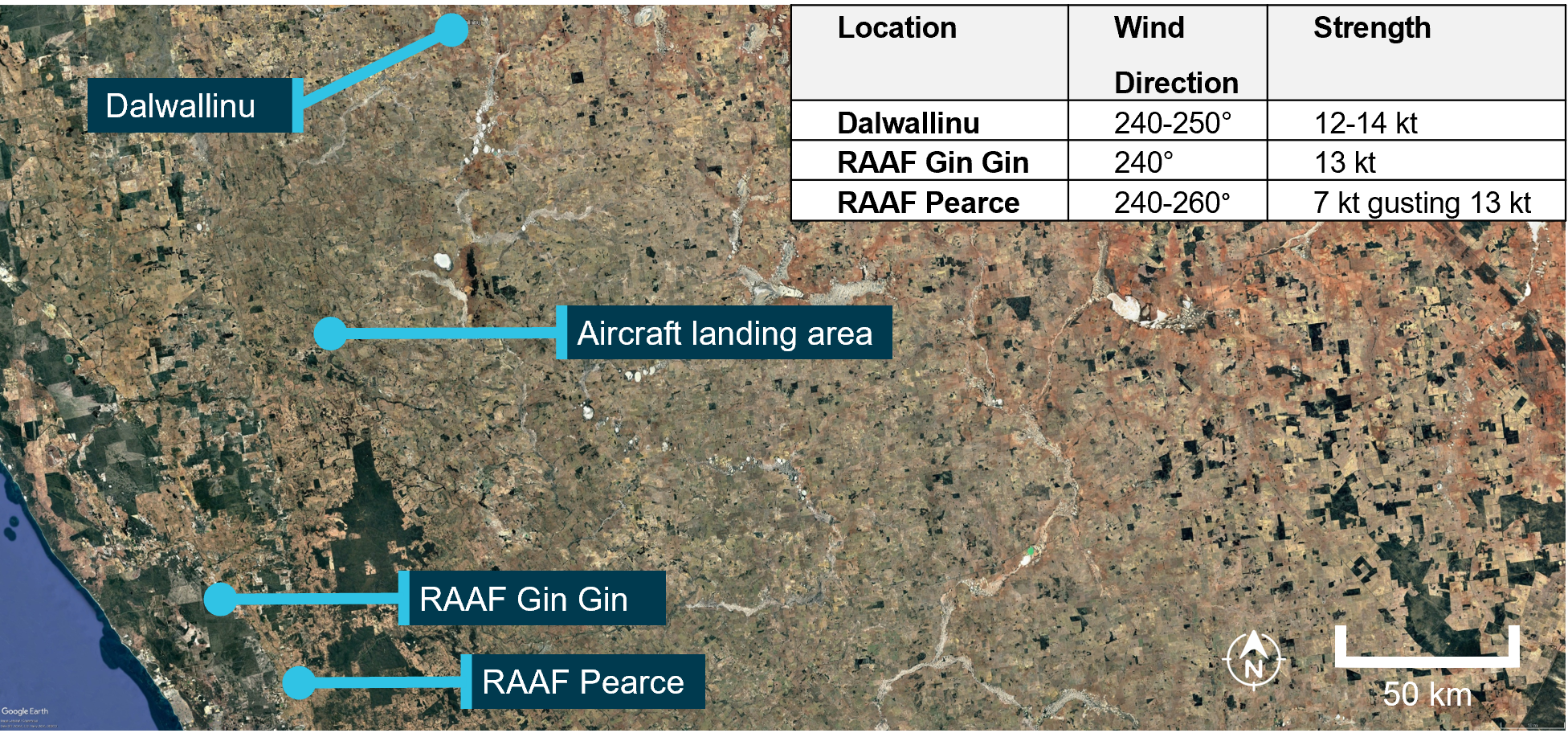
The pilot reported that they assessed the local weather conditions via their NAIPS[4] account on the morning of the occurrence flight and recalled that the predicted wind at the aircraft landing area (ALA) was calm.
Bureau of Meteorology data from the nearest recorded locations at the time of the occurrence indicated local winds between 12–14 kt in a south-westerly direction (Figure 7).
Figure 7: Weather reporting locations in relation to the private aircraft landing area
Source: Google Earth, annotated by the ATSB
Aeroplane landing area information
The ALA was on privately‑owned farming land and was regularly used by agricultural pilots to conduct spraying of crops in the local area. The elevation of the ALA was about 800 ft above mean sea level (AMSL) and the runway orientation was about 120/300°[5] and had a gradual slope that increased towards the east, rising about 40 ft over the length of the runway. It was surrounded by waist-high crops, had a gravel surface and a useable length of about 570 m. The ALA did not have a windsock, nor was there a wind indicating device located nearby.
Prior to operating at the ALA, the operator spoke with the landowners to gain understanding of the recent landing area conditions, as they had not flown to the location previously. They were put in contact with the agricultural pilots who had been recently operating from the field and received a landing area condition report. The operator assessed that the area was suitable for the Cessna 206.
Standard circuit pattern
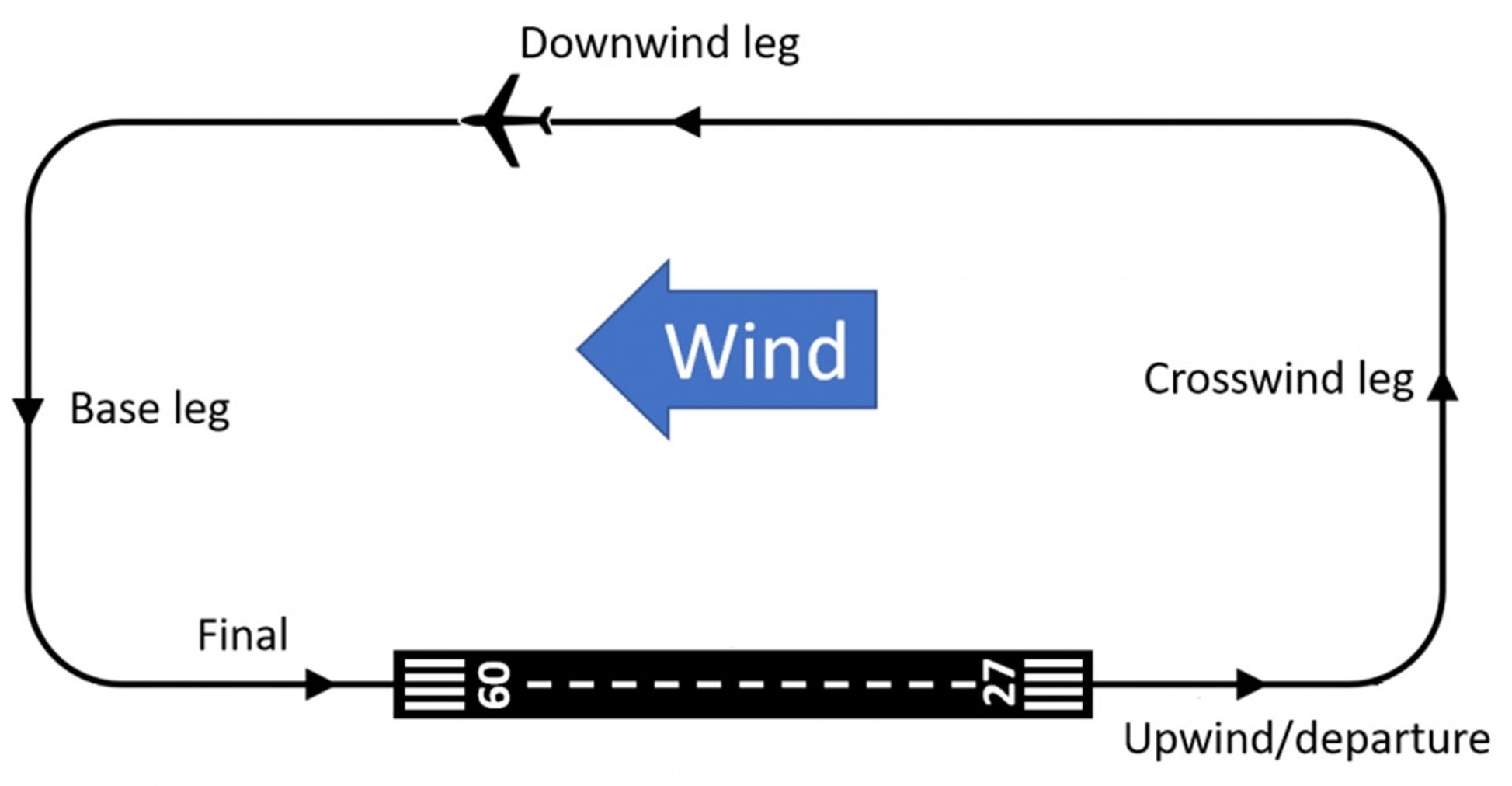
A circuit is the specified path to be flown by aircraft operating in the vicinity of an aerodrome (Figure 8). It comprises of upwind, crosswind, downwind, base and final approach legs.
Figure 8: Standard left-hand circuit pattern
Source: SKYbrary, modified by the ATSB
The Civil Aviation Safety Authority (CASA) Advisory Circular AC 91-10v1.3 advised pilots that joining a base leg of a circuit is not a standard procedure. Stating:
CASA recommends that pilots join the circuit on either the crosswind (midfield) or downwind leg. However, pilots who choose to join on base leg should only do so if they have familiarised themselves with the weather conditions to be expected and aerodrome serviceability.
The AC advised that pilots who join the base leg of the circuit increase the risk of a downwind landing and may conflict with other traffic using the into-wind runway. It also stated that late go‑around decisions and landings on a closed runway were more common.
Recorded data
Flight Radar 24 data[6] indicated that when the pilot commenced the left-hand orbit approaching the ALA, that the aircraft was about 2,000 ft AMSL and at the conclusion of the orbit, as the aircraft joined the base leg, it remained at about 2,000 ft AMSL, about 1,200 ft above the ALA. As the aircraft became established on final approach for the easterly runway, the aircraft height was recorded as 1,500 ft AMSL, 700 ft above the ALA and 1.6 NM from the runway threshold.
Flight Radar 24 showed that the aircraft’s ground speed had slowed to around 75 kt on the base leg of the approach to landing. As the aircraft turned onto final approach the ground speed increased, reaching 92 kt and indicated about 85 kt ground speed at the last data recording on short final for the easterly runway.
Video footage from a passenger seated in the rear left seat was obtained by the ATSB. Video footage showed that the initial touchdown point (Figure 2) was about 80 m past the runway threshold, reducing the remaining runway length to about 490 m. The footage also showed that during the go-round, the aircraft began to lose height shortly after the flaps were retracted and that this was followed by a roll to the right.
Operator’s internal review
On the day of the accident, the operator’s chief pilot attended the accident site, gathered images, reviewed the aircraft damage and debriefed with the pilot.
The chief pilot advised that post‑accident aircraft testing was carried out later that day and the flaps were tested and found to be operational.
From the pilot’s report, flight data and images gathered, the operator completed a detailed internal review of the accident. A summary of the findings included:
• the aircraft’s approach became unstable due to the excess speed
• the speed was more appropriate for a 20° flap setting
• the excess speed likely resulted in the aircraft ‘floating’ and landing long on the runway
• after an initial bounce on landing the pilot continued the approach to land before a second bounce
• inadvertent incorrect flap setting reduced the aircraft climb performance.
Cessna 206 procedures
Unstable approach procedure
The Cessna 206F aircraft flight manual (AFM) advised pilots that the approach speed for a full‑flap, short field landing should be 75 mph (65 kt).
The operator’s exposition stated that the airspeed for the stabilised approach criteria below 1,000 ft is not more than VREF[7] (65 kt) + 5 kt.
Data from Flight Radar 24 showed the aircraft ground speed had slowed to 75 kt on the base leg of the circuit, before increasing to 92 kt ground speed on final approach. The pilot reported the airspeed on final was 75 kt prior to selecting full flap for the landing.
Go-around procedure
The Cessna 206F AFM emergency section provided the balked landing (go-around) procedure:
Power – Full throttle and 2850 RPM
Wing Flaps – Retract to 20°
Airspeed 90 MPH (78 kt)
Wing flaps – Retract slowly
Cowl flaps – Open.
Additionally, the AFM provided further detail when conducting a go-around:
In a go-around climb, the wing flap setting should be reduced to 20° immediately after full power is applied. After all obstacles are cleared and once a safe altitude and airspeed are obtained, the wing flaps should only then be retracted further.
On initiating the go-around the pilot inadvertently reduced flap to the 10° setting resulting in a reduction of lift produced by the wing.
Ditching and forced landing procedure
The Cessna 206 ditching and forced landing procedure described in the AFM instructed pilots to configure the aircraft to the full-flap position so as to impact with water or terrain at the slowest possible speed. This procedure did not mention the retraction of the flaps on completion of the ditching or forced landing
Operator’s passenger safety briefing
The operator’s exposition stated that pilots shall brief passengers about the following matters and confirm they have an understanding:
• the pilot in command is responsible for passenger safety
• safety instructions and directions from the pilot in command must be followed
• smoking tobacco, electronic cigarettes or any other substance on the aircraft is prohibited
• when seatbelts are to be worn, and how to use them
• seat backs are to be upright during take-off and landing
• how and when to adopt the brace position
• how to approach and move away from the aircraft
• entry and egress from the aircraft, including in emergency situations
• where and how to stow baggage and personal effects
• use of survival equipment / ELT as appropriate
• use of life jackets and life rafts (if carried for the operation) and that life jackets must not be inflated inside the aircraft
• restriction on the use of PEDs (personal electronic devices) and when they can be used
• communications and headset use
• if the passenger is in a flight crew seat, the requirement to ensure controls are not manipulated or interfered with
• the location of the Safety Briefing Card located at each seat.
The pilot recalled that they conducted a group briefing of the passengers prior to the first planned local area flight, with the intention of providing the passengers for the second flight an additional briefing before they boarded.
The pilot reported they briefed the passengers on the aircraft’s seatbelts, location of the fire extinguisher, life jackets, first-aid kit and provided instruction to the front seat passenger regarding remaining clear of the flight controls. They also explained the use of both the forward left cabin door and the double cargo emergency exit doors, highlighting the red handle to open the rear cargo door. The pilot did not indicate that the passengers were briefed on actions in the event of the emergency exit being obstructed.
The adult passenger seated in the rear seat recalled seeing the handle for the forward cargo door, however they were unsure if the rear cargo door had a handle. As discussed (see Cessna 206 rear passenger emergency egress), the emergency handle is not readily visible from the rear seats in older Cessna 206 aircraft when the cargo doors are closed.
Regulatory information on emergency egress
The Cessna 206 was first certified in 1963 by the United States (US) Federal Aviation Administration (FAA). FAA regulation 14 CFR 23.2315 stated that an aeroplane is designed to:
(a)(2) Have means of egress (openings, exits, or emergency exits), that can be readily located and opened from the inside and outside. The means of opening must be simple and obvious and marked inside and outside the airplane.
There have been a number of revisions made to this FAA design standard over the years. However, once an aircraft has been certified, the design standard under which it was certified continues to apply.
Part 90 of Civil Aviation Safety Regulations (CASR) 1998 - Additional airworthiness requirements Subpart 90.005 sets out the airworthiness requirements for an aircraft that are in addition to the type certification basis for the aircraft.
Under regulation 90.020 of CASR 1998, the Manual of Standards (MOS) sets out the additional airworthinessstandards required for CASR Part 90 including, access to emergency exits.
Part 90 of the MOS stated that the minimum opening of an emergency exit must be unobstructed at all times.
CASR 90.135 stated that each passenger must have access to at least one exit that meets the requirements prescribed by Part 90 of the MOS.
Cessna 206 rear passenger emergency egress
Background
When configured as a 6 seat-passenger aircraft, the cargo door provided the closest emergency exit for passengers seated in the rear seats and an alternate exit if the pilot’s left front cabin door became obstructed.
As discussed above in Aircraft information, when the flaps are extended, they physically block the forward cargo door from being opened beyond about 8 cm, not enabling egress.
The internal forward cargo door handle has 3 positions:
when the lever is horizontal (with the lever facing forward), the door is locked
turned clockwise 90° to the vertical position, the door is closed
turned clockwise another 30°, the door is opened.
With the forward door handle in the locked position the door is unable to be opened from the outside. The pilot reported that the rear seat passengers attempted to open the forward cargo door, however due to the extended flap were unable to push the door open. As the passengers were unaware of the location of the rear door handle (see Operator’s passenger safety briefing), no attempt was made to open the rear cargo door.
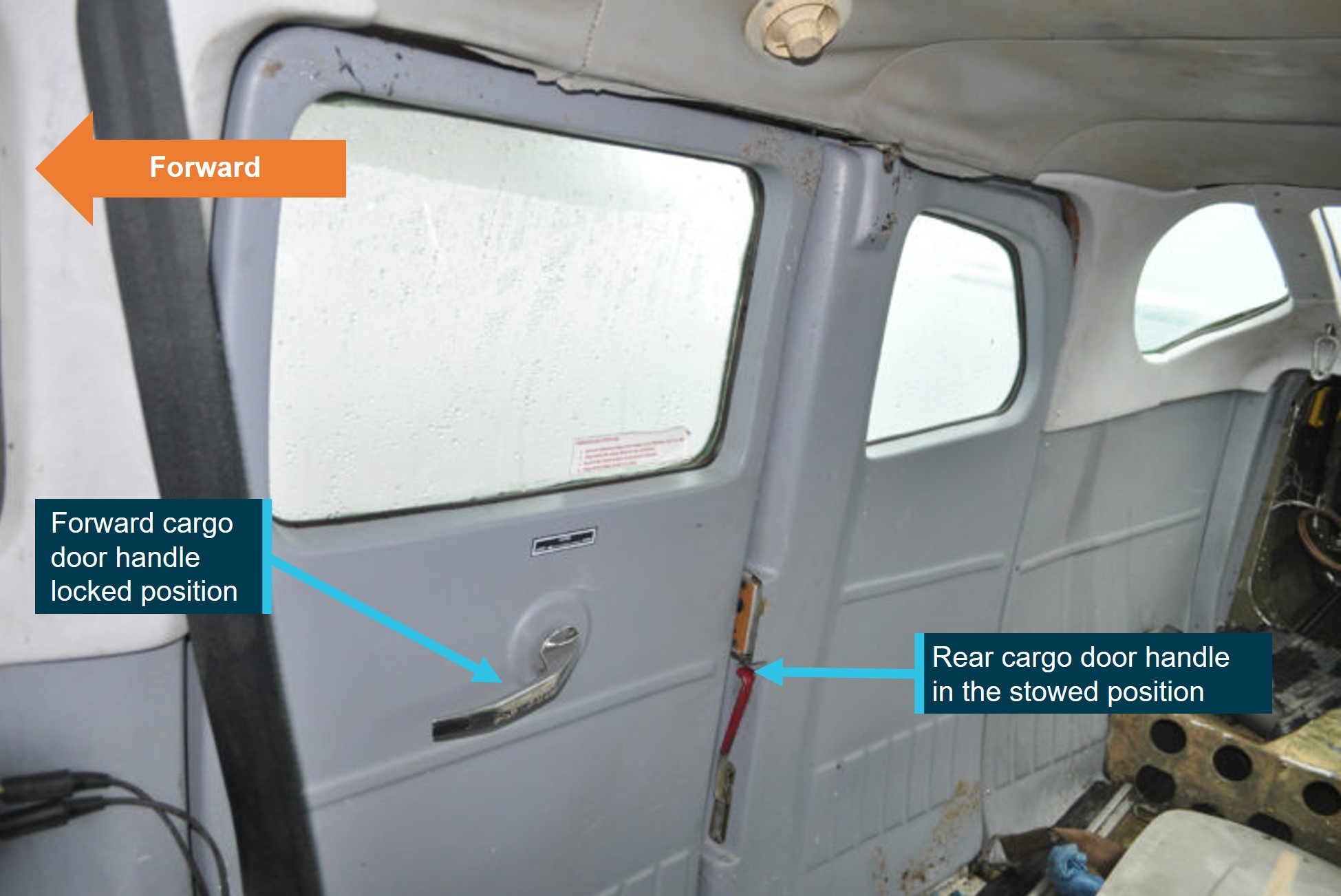
For the earlier models (pre-H model), including VH-TDQ, the rear door handle is a red lever (Figure 9) located in the leading edge of the rear door, which is rotated forward (to horizontal position) to open. When the forward cargo door is blocked by the flaps and the rear door handle is in the horizontal position, the rear door can only be partly opened as the horizontal handle cannot pass the forward door. The handle must then be re-stowed in the vertical position to allow the rear cargo door to pass the obstructed forward cargo door. In an emergency situation, this can and has delayed or prevented egress from the aircraft. Once the forward cargo door is slightly opened, it is possible to access the rear door handle from outside the aircraft and open the door using this process.
The pilot advised the ATSB they were aware that the forward cargo door became blocked with the flaps in an extended position. They also advised that they were aware of the requirement to open the forward cargo door before the rear door could be opened and understood the operation of both the cargo door handles. However, the pilot believed that when the flaps remained extended and blocked the forward cargo door, that the rear cargo door was unable to be opened.
The operator’s chief pilot also reported that if the forward cargo door was blocked by the flap that passengers would be forced to egress the aircraft via the pilot’s forward left cabin door, which would be difficult for passengers seated in the rear seats.
Figure 9: Cessna U206G Cargo door
Source: TSB investigation report A18W0129, annotated by the ATSB
Cessna 206F aircraft flight manual
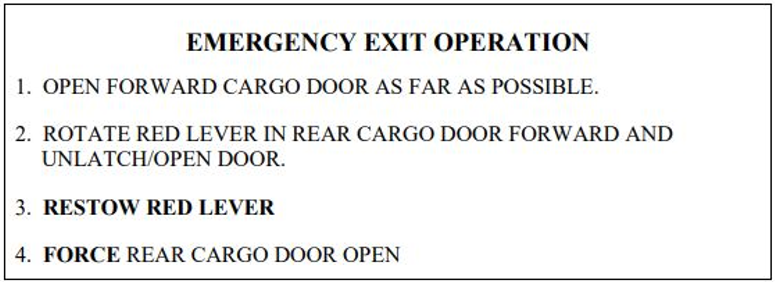
The emergency section of the aircraft’s flight manual contained instructions for the operation of the cargo door emergency exit which stated:
If it is necessary to use the cargo door as an emergency exit and the wing flaps are not extended, open the forward door and exit. If the wing flaps are extended, open the door in accordance with the instructions on the placard [see Figure 10] which is located on the forward cargo door.
Cessna cargo door latch service bulletin
In 1991, to assist in operating the rear cargo door from inside the aeroplane during night operations, Cessna issued Service Bulletin SEB 91-4 Cargo door latch improvement. The service bulletin recommended the installation of a return spring in the rear cargo door handle, automatically returning the handle to the closed position after opening. This assisted the rear cargo door to move freely past the blocked forward cargo door.
The service bulletin was not mandatory and was not installed on VH-TDQ.
Placard alternative
Prior to the service bulletin, due to demonstrated difficulties opening the cargo doors when the aircraft flaps remained extended during emergency situations in both Australia and overseas, the Civil Aviation Authority (CAA)[8] issued Airworthiness Directive 206/47 in 1988 that required the improvement of existing emergency exit placards for Cessna 206 aircraft in Australia (Figure 10). The placard drew attention via bold letters to step 3, to ensure the rear door handle was returned to the original position (vertical) before attempting to open the rear door (step 4).
In 1991, when Cessna issued Service Bulletin SEB 91-4, the CAA issued Airworthiness Directive Cessna 206/47 amendment 2, which allowed SEB 91-4 to be an alternate means of compliance to the CAA emergency exit placarding.
In 2011, CASA subsequently issued Airworthiness Directive Cessna 206/47 amendment 3, which clarified which Cessna 206 models the airworthiness directive applied to. This was due to SEB 91‑4 being incorporated by the manufacturer in some newer models, and because other models did not have the cargo door. SEB 91-4 remained as an alternate means of compliance.
The placard was installed on VH-TDQ.
Figure 10: Forward cargo door placard
Source: CASA Airworthiness Directive 206/47 Amendment 3
Canadian type certificate and airworthiness directive
In 1998, Cessna resumed manufacturing the 206 model aircraft with the 206H. The H model featured larger and more visible cargo door handles and incorporated SEB 91-4 for the return spring in the rear cargo door handle into the design. The forward cargo door remained blocked with flaps extended on this variant.
The 206H was certified under the US Federal Aviation Regulations 23.807. Transport Canada (TC) disagreed with the certification, stating that:
The design of the doors did not satisfy the (FAA) certification requirements that the method of opening the doors be simple and obvious and the door be readily opened, even in darkness.
As a result, in 2000 TC issued a type certificate reducing the Cessna 206H occupancy to 5 passengers.
In 2019, the Transport Safety Board of Canada issued safety advisory A18W0129-D1-A1 that stated that between 1999 and 2003, TC, the FAA and Cessna, had worked together in an effort to come up with a design change that could be applied to the Cessna 206H, which could also be used to retrofit older models of the Cessna 206 fleet. However, the matter remained unresolved and no acceptable solution was found.
In 2020 TC issued Airworthiness Directive CF-2020-10, applicable to Cessna 206 models that featured the double cargo door, stating that:
Earlier versions of the model 206 registered in Canada that feature the cargo doors have not been subject to occupancy limits, other limitations or corrective action requirements related to the cargo doors. These earlier versions of the model 206 have continued to operate in Canada without corrective or mitigating action despite the fact that the method of opening the cargo doors is essentially the same as the method for the 206H and T206H models. There is objective evidence that difficulty opening the cargo doors has contributed to fatalities during accidents in Canada involving the model 206.
The AD CF-2020-10 limited earlier model Cessna 206 to 5 occupants and required the removal of one of the middle row seats if either rear seat was to be occupied. The removal of a middle row seat provided access for passengers seated in the rear seats to the pilot’s forward left cabin door (Figure 11) for evacuation in the event the rear cargo door could not be opened quickly enough for egress. The AD also clearly stated that the vacant space left by the removal of a middle row seat must not be used for storage of cargo or baggage.
Figure 11: Seating configuration for Canadian Cessna 206
Source: TSB investigation report A18W0129, adapted to indicate seat removal, annotated by the ATSB
The AD also provided an alternative means of compliance through a supplemental type certificate (STC),[9]STC SA1470GL, for the installation of an additional door, on the forward right side of the cabin and was applicable to all models of the Cessna 206. This commercially available alternative means of compliance allowed Canadian registered aircraft to remain in the original 6‑seat configuration. If installed, the additional door provided immediate egress option for the passenger in the front right seat and an additional emergency egress for passengers seated in the middle row.
Australian acceptance of type certificate and supplemental type certificates
Since 1990 CASA has provided for the automatic acceptance of foreign aircraft type certificates and STC’s issued by a national aviation authority of recognised countries[10] including European Union Aviation Safety Agency (EASA).
CASA has accepted the type certificate of the national aviation authority issuing state (United States), for the following models of the Cessna 206: 206, P206, P206A, P206B, P206C, P206E, U206, U206A, 206H, U206B, U206C, U206D, U206E, U206F, U206G, T206H, TU206A, TU206C and TU206G (P206 models are not manufactured with the double cargo door).
ATSB safety recommendation
In 2020, after ATSB investigation (AO-2020-010), into an accident involving a Cessna U206G on Fraser Island, Queensland, the ATSB issued CASA with safety recommendation AO-2020-010-SR-018 recommending that CASA take safety action to address the certification basis for the design of the cabin doors in the Cessna 206, as wing extension beyond 10° will block the forward portion of the rear double cargo door, significantly hampering emergency egress.
In response CASA issued Airworthiness Bulletin 52‑006 in 2021, with a subsequent reissue in 2025. The bulletin advised pilots and operators of the impeded access from the cargo door emergency exit with the flaps extended and made recommendations that:
• Pilots should be aware that lowering the flaps may obstruct this exit and significantly increase the difficulty of opening the forward door section of the rear cargo door. All passenger pre-flight briefings should include a practical demonstration of how to open and egress the aircraft through a flap obstructed cargo door. This will require a demonstration with flaps lowered to at least 20 degrees to demonstrate the condition. Care should be taken to not damage the flap or door during this demonstration.
• Additionally, in the event that an emergency landing or water ditching is required, pilots should consider retracting the flaps if possible after the emergency landing or if operationally feasible, limit the amount of flap extension to a maximum of 10 degrees. This would of course be a judgement made by the pilot in command based on operational factors, severity of the emergency/damage to aircraft and if there are occupants seated in the rear of the aircraft.
• It is strongly recommended that registered operators and operators of affected Cessna 206, T206, TU206 and U206 aircraft series, review TC AD CF-2020-10 and give due consideration to compliance with the intent of this document, however compliance is not mandatory under CASR Part 39, because the AD is not from the state of design.
The ATSB investigation also issued Cessna a safety recommendation AO-2020-010-SR-017. The safety recommendation was to address the concern that although the Cessna 206 AFM ditching procedure required pilots to extend the flaps to the full-flap position, which resulted in a slower landing speed, this significantly impeded the emergency egress via the cargo door emergency exit and there was no warning in the AFM of the additional risk. In response, Cessna provided a temporary revision to only the Cessna 206H model AFM, providing a warning stating:
FLAP POSITIONS OF 10 DEGREES OR GREATER MAY IMPEDE EVACUATION FROM THE CARGO DOOR. FAILURE TO ADHERE TO ALL SAFETY INSTRUCTIONS CAN RESULT IN BODILY INJURY OR DEATH.
Cessna advised the warning would be incorporated into the next revision of the Cessna 206H AFM and a placard, with the same warning would be produced for older Cessna 206 models that featured the double cargo doors. In November 2024, mandatory service bulletin SEB-11-05 was released for all Cessna 206, and U206 models prior to the 206H, for the installation of the placard on the cockpit instrument panel or another location directly visible to the pilot. The service bulletin had not been released at the time of the occurrence.
Cessna 206 modifications to allow cargo door to open with flaps extended
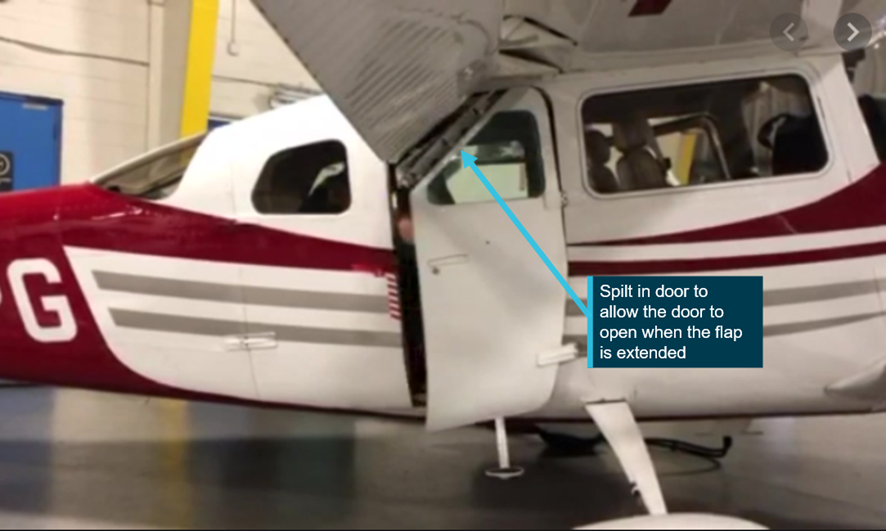
Since the release of AD CF-2020-10, in 2020 TC also approved STC SA20-34 which allows the forward cargo door corner to be hinged (Figure 12). This allows the door to fold on a hinge and fully open with flap extended in any position and therefore creating no restriction to the rear cargo door.
Figure 12: Cessna split cargo door
Source: Coast Dog Aviation, annotated by the ATSB
Additionally, on 2 May 2023, TC approved STC SA23-21 to provide an additional handle that is installed internally on the forward cargo door. The handle is accessible to the rear seat passengers, which, when activated jettisons the front cargo door from the aircraft. The removal of the door provided egress to the middle row occupants when flaps remained extended. The release of the door from the aircraft also improved visibility of the rear cargo door handle and simplified opening the rear cargo door for occupants seated in the rear seats.
Both STC SA20-34 and STC SA23-21 are approved as alternative means of compliance to TC CF-2020-10 and allowed Canadian registered aircraft to retain the 6 seat configuration.
VH-TDQ was not modified with the approved STC’s for the cargo door and a second forward right side door was not fitted (STC SA1470GL) and the aircraft remained in the original 6 seat configuration.
Related occurrences
ATSB conducted a search of aviation investigation databases and other sources to identify accidents involving Cessna 206 aircraft (Appendix 1 – Cessna 206 occurrences). This search specifically looked at accidents where the impact was considered likely survivable, however where difficulties opening the cargo door resulted in significant delays during the emergency egress, or the cargo door had not been opened.
The ATSB identified 10 occurrences that included 23 fatalities between 1985 and 2020 globally. Highlighted during the search were multiple occurrences of Cessna 206 accidents that involved fatalities when Cessna 206 aircraft were equipped with floats and operated on water.
In March 1999, near Pitt Island, New Zealand, a Cessna 206 had an engine failure and ditched in the sea. The pilot was aware of the issue with the extended flap blocking the cargo doors and ditched the aircraft with the flaps retracted. Consequently, all the occupants escaped from the aircraft and swam to shore (New Zealand Transport Accident Investigation Commission, investigation report 99‑001) .
In January 2020, during a landing at a beach landing area on Fraser Island, Queensland, the Cessna U206G aircraft veered significantly to the left. Once airborne it was identified that the rudder was jammed in the full‑left position and the pilot had to apply full opposite aileron to maintain control. Shortly after, possibly due to fuel starvation the aircraft collided with water. Unable to open the pilot’s door the trainee pilot kicked the cargo door to force it open past the extended flap (ATSB investigation AO-2020-010).
Safety analysis
Introduction
On the morning of 1 September 2024, the pilot of a Cessna U206F, registered VH-TDQ, departed a private aircraft landing area (ALA), 21 NM (39 km) southeast of Moora, Western Australia (WA) with 5 passengers on board for a 15-minute local area flight. On return to the ALA the pilot conducted a full flap landing on the easterly runway and bounced twice. The pilot then commenced a go-around, however as the aircraft began the initial climb, the pilot inadvertently reduced the flap setting 10°. The aircraft lost height and the right wing dropped, making contact with terrain, removing the right wing tip and damaging the right aileron. The aircraft then lost speed and landed upright in a field adjacent to the runway.
Unstable approach
As the pilot approached the ALA and was about 2 NM (3.7 km) north, they assessed that the aircraft was too high and elected to conduct a left orbit with the intention of reducing the aircraft’s height. However, no reduction in height was recorded during the orbit.
The pilot conducted a non-standard approach to the easterly runway by joining the circuit on a base leg. This resulted in a reduction of available time for the pilot to assess the vertical descent profile effectively and likely contributed to the pilot mis-managing the short field landing with additional speed and height on the final approach.
Contributing factor
The pilot conducted a non-standard base leg join to the circuit for landing. This reduced the time available for the pilot to configure the aircraft, reduce the airspeed and prepare for a short field landing.
A combination of additional speed on final approach, the effects of a tailwind and the aircraft in the full-flap landing configuration, likely extended the aircraft’s flare. This resulted in the aircraft landing past the intended touchdown point. This also contributed to the aircraft bouncing on landing and further reduced the runway available to safely stop and likely resulted in the pilot‘s decision to go-around.
Contributing factor
Due to excessive speed on approach for a full flap, short field landing, the aircraft landed long and bounced twice.
Go-around
After the aircraft bounced a second time, the pilot commenced a go-around and applied full power to climb away. As the aircraft increased speed and began the climb out, the pilot intended to reduce the flap setting to 20° to reduce drag, but inadvertently reduced the flap setting to 10°. This resulted in a flap configuration below the prescribed setting for the aircraft’s balked landing (go‑around) procedure.
The aircraft had not achieved the required airspeed for the lower than intended flap setting and this developed into a lack of sufficient lift and a loss of climb performance. This resulted in the aircraft losing height and directional control which caused right wingtip contact with the ground.
Contributing factor
The pilot mis-selected the flap setting during the attempted go-around. As a result, the aircraft could not achieve adequate climb performance.
Passenger evacuation
After the aircraft came to a stop, the pilot instructed the passengers to evacuate. The front seat passenger and middle row passengers were able to egress through the pilot’s forward left cabin door. However, due to the flaps remaining extended in the 10° position, the forward half of the right-side cargo door (emergency exit) could not be fully opened. While the rear cargo door could have been opened (either from the inside or the outside), the blocking of the forward door increased the difficulty of opening the rear cargo door and caused confusion about how to evacuate the rear seat passengers.
From the inside, the rear door handle was not easily visible to passengers in the rear seats due to its obscured position and location relative to the middle row seats and the forward cargo door only able to be partially opened. Although the pilot reported providing a safety briefing to the passengers, and an aircraft placard provided instructions for the operation of the cargo door emergency exit when the flaps remained in an extended position, the adult rear seat passenger was not fully aware of the location of the rear cargo door handle.
Due to the forward cargo door being blocked by the extended wing flaps, and a rear door handle that was not easily accessible to the pilot outside the aircraft and not easily visible to passengers in the rear seats, the 2 rear seat passengers could not enact the opening of the rear emergency exit, and ultimately were required to climb over the middle row seats and egressed via the pilot’s forward left cabin door.
While this delayed a timely evacuation, in this case the rear passengers were an older adult and a young child but both capable of climbing over seats, and the pilot was able to assist from outside the aircraft. However, in emergency situations where the passengers may be less able-bodied or the pilot is incapacitated or unable to assist, the functioning of aircraft emergency exit systems must be quickly apparent and passengers must have enough awareness of their operation to ensure timely and unassisted evacuation.
Other factor that increased risk
With the flaps extended in the 10° position when the aircraft came to rest blocking the full opening of the forward cargo door, the rear seat passengers were unable to open the rear cargo door to enable an emergency exit.
In this case, there was an additional chance to evacuate via the rear emergency exit as the pilot could walk around to the outside of that exit.
As pilots of small passenger aircraft are responsible for the emergency egress of passengers, it is essential that the pilot has a full understanding of the operation of the emergency exits. Instructions for the operation of cargo door emergency exit when the flaps remained in an extended position were available on an aircraft placard.
The pilot understood that the operation of the rear cargo door was reliant on the forward door being open, and was also aware that extended flaps may block the forward cargo door. However, the pilot was unaware the rear cargo door could be opened after the forward cargo door had been made ajar (blocked by flaps). As a result, the pilot first tried (unsuccessfully) to retract the flaps, even though this was not required to open the rear cargo door. When that failed, likely due to the door remaining ajar preventing the micro‑switch activation of power to the flap system as designed, the pilot instructed the occupants to egress via the forward cargo doors over the middle row seats.
In this case, as the aircraft was not on fire nor floating on water, this lack of knowledge did not result in a worse consequence. However, in other circumstances, the inability to egress rear seat passengers from the rear emergency exit could have serious consequences.
Other factor that increased risk
The pilot was unaware that the rear cargo door on the Cessna 206 could be opened from the outside when the front cargo door was blocked by the extended flaps.
Previous ATSB and international investigations have highlighted the difficulty occupants of the Cessna 206 face egressing via the cargo door emergency exit when the aircraft flaps remain extended. While it is possible to open the rear cargo door from outside the aircraft when the forward door is blocked by the extended flaps, without training or demonstration the process is not simple or obvious. The pilot had limited experience on the aircraft type and was unaware of the process.
Although CASA Airworthiness Bulletin 52-006 advised operators to brief passengers on emergency egress with flaps blocking the forward cargo emergency exit, the chief pilot also was unaware it was possible to open the rear cargo door when the forward cargo door was blocked by the flaps. This meant that they were unable to educate company pilots on the additional complexity operating the rear cargo door with flaps extended.
Although the company operations manual stated that pilots were required to brief passengers entry and egress from the aircraft, including in emergency situations, the operator did not provide further documentation to pilots that the passenger briefing should also demonstrate the cargo door operation with the flaps extended as recommended by CASA Airworthiness Bulletin 52-006.
The knowledge involved to demonstrate this would have provided the pilot with the correct understanding of the operation of those doors as was needed in this case. Further, had such a demonstration been conducted, it is likely that passengers seated in the rear of the aircraft would have also been aware of the location of the rear cargo door handle and process when the flaps remained extended.
Passenger briefings therefore lacked in this regard, and in an emergency event where passengers were required to open the rear cargo/emergency doors quickly with the flaps extended, this increased the risk that the rear seat passengers would not be able to egress at all or quickly enough to escape injury.
Other factor that increased risk
The operator’s pre-flight passenger briefing did not include the demonstration of, and pilots were not trained how to operate, the emergency exit via the cargo door with the flaps extended. (Safety Issue)
Safety advisory notice
The Australian Transport Safety Bureau advises Cessna 206 pilots and operators that due to the difficulties occupants have encountered egressing the rear cargo door as identified in several transport safety investigations, to ensure they are familiar with CASA‑issued Airworthiness Bulletin 52‑006, and ensure passengers are provided with a thorough safety briefing demonstrating the cargo door emergency egress when the wing flaps remain in the extended position.
Cessna 206 emergency egress
The Cessna 206 cargo door emergency exit has featured in numerous transport safety investigations across the world. To date, Transport Canada remains the only regulatory body that has made significant changes that improve the ease of use during an emergency.
Transport Canada’s decision to issue an amended type certificate for the Cessna 206H when production was restarted, limited the aircraft to 5 occupants, with the required removal of a middle row seat if either rear seat was to be occupied. The subsequent release of the airworthiness directive CF-2020-10 mandated the same limitations and meant that occupants of older model Cessna 206 aircraft, particularly those seated in the rear seats, had improved access to the pilot’s forward left cabin door emergency exit. The removal of the middle row seat also improved the visibility and access to both cargo door handles for middle and rear seat occupants.
The Civil Aviation Safety Authority (CASA) required that the aircraft emergency exits remain unobstructed at all times. Passengers seated in the rear seats of the Cessna 206 with the double cargo door are obstructed by either:
the middle row seats, when attempting to access the pilots forward left cabin door
the flap blocking the forward cargo door when the flaps remain extended.
The majority of aircraft accidents happen during take-off or approach and landing phases of flight. During normal operation, these phases of flight usually require an amount of flap extension, therefore it becomes likely that, in the event of an accident or incident, the flaps would remain extended and hinder the use of the cargo door emergency exit.
Previous investigations into the Cessna 206 that included fatalities of pilots who had a required knowledge of the use of an emergency exit, have found that the extended flaps blocking the cargo door contributed to the occupant’s inability to exit the aircraft during emergency egress.
The successful ditching of a Cessna 206 in New Zealand in 1999 indicated the increased occupant survivability potential when both emergency exits are clear of any obstruction.
Transport Canada has approved several modifications that provided an exemption to the occupancy limitations set out by the type certificate and airworthiness directive. This allowed the aircraft to maintain its intended 6 passenger configuration. The modifications are commercially available and improve the functionality of the emergency exits and provide access to an alternative or unobstructed emergency exit with the flaps extended.
The extended flap blocking the forward cargo door has contributed to fatalities in previous accidents. The Cessna 206 ditching and forced landing procedure both prescribe a full-flap landing. However, unless the pilot is able to retract the flaps after the ditching or landing, the flaps would remain extended blocking the forward cargo door.
Transport Canada’s required restriction of the Cessna 206 occupancy, or the approved emergency exit modifications, reduces the risk created by the extended flaps preventing the immediate and unobstructed use of the rear cargo door emergency exit. This significantly improves the occupant’s likelihood of successful egress, during an emergency.
In Australia, CASA has provided warnings regarding the obstruction of the emergency exit and strongly recommended operators to comply with the changes that Transport Canada made. However, the aircraft’s certifying state (United States) has not mandated these changes.
The ATSB and international transport safety investigations have highlighted the increased difficulty faced by occupants attempting to egress the Cessna 206 when the flaps remain extended. Existing approved emergency exit modifications are available to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo emergency exit.
The approved modifications for the cargo door emergency exit would likely have resulted in occupants of the rear seats successfully opening the forward cargo door and therefore improving the ease of operation of the rear cargo door handle for the occupants or pilot. Alternatively, with a middle row seat removed, rear seat occupants’ path to the forward left cabin door would have been unobstructed.
Other factor that increased risk
The aircraft did not have the modifications detailed by CASA for Cessna 206 emergency exits, increasing the likelihood of impeded egress during emergency situations. (Safety Issue)
Safety advisory notice
The Australian Transport Safety Bureau strongly encourages operators and owners review Transport Canada Airworthiness DirectiveCF-2020-10, and consider either the removal of a middle row seat to improve rear seat occupants’ access to the pilot’s forward left cabin door or the fitment of approved Cessna 206 emergency exit modifications to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo doors during an emergency exit.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain during go‑around involving Cessna U206F, VH-TDQ, 39 km south-east of Moora, Western Australia, on 1 September 2024.
Contributing factors
Due to excessive speed on approach for a full flap, short field landing, with a tail wind component, the aircraft landed long and bounced twice.
The pilot conducted a non-standard approach to the landing area by conducting a base leg join to the easterly runway which had a gradual upslope. This reduced the time available for the pilot to configure the aircraft, reduce airspeed and prepare for a short field landing.
The pilot mis-selected the flap setting during the attempted go-around. However, the aircraft could not achieve adequate climb performance.
Other factors that increased risk
The aircraft did not have the modifications recommended by CASA for Cessna 206 emergency exits, increasing the likelihood of impeded egress during emergency situations. (Safety issue)
The operator’s pre-flight passenger briefing did not include the demonstration of, and pilots were not trained how to operate, the emergency exit via the cargo door with the flaps extended. (Safety issue)
The pilot was unaware that the rear cargo door on the Cessna 206 could be opened from the outside when the front cargo door was blocked by the extended flaps.
With the flaps extended in the 10° position when the aircraft came to rest blocking the full opening of the forward cargo door, the rear seat passengers were unable to open the rear cargo door to enable an emergency exit.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The operator’s pre-flight passenger briefing did not include the demonstration of, and pilots were not trained how to operate, the emergency exit via the cargo door with the flaps extended.
Safety advisory notice to operators and pilots of Cessna 206
SAN number:
AO-2024-049-SAN-001
The Australian Transport Safety Bureau advises Cessna 206 pilots and operators that due to the difficulties occupants have encountered egressing the rear cargo door as identified in several transport safety investigations, to ensure they are familiar with CASA issued Airworthiness Bulletin 52‑006, and ensure passengers are provided with a thorough safety briefing demonstrating the cargo door emergency egress when the wing flaps remain in the extended position.
Safety issue description: The aircraft did not have the modifications recommended by CASA for Cessna 206 emergency exits, increasing the likelihood of impeded egress during emergency situations
Safety advisory notice to operators and pilots of Cessna 206
SAN number:
AO-2024-049-SAN-002
The Australian Transport Safety Bureau strongly encourages operators and owners review Transport Canada Airworthiness DirectiveCF-2020-10, and consider either the removal of a middle row seat to improve rear seat occupants access to the pilots forward left cabin door or the fitment of approved Cessna 206 emergency exit modifications to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo doors during an emergency exit.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Fly Esperance Pty Ltd
Following the occurrence Fly Esperance has made the following amendments to its operations manual:
Added CASA pictorial publication ‘non-controlled aerodrome circuit procedures’ to its Circuit and landing procedures and uncontrolled aerodromes section to better clarify the process.
Added a table to show the recommended aircraft speed and landing weight with the flaps retracted and extended.
Pilots will now carry portable GPS aircraft tracking devices to improve aircraft tracking when outside ADSB coverage.
Greater emphasis on training including ICUS training, highlighting what can happen when standard procedures are not followed.
The changes to the company operations manual are part of a larger amendment that will be under review by CASA in due course.
Glossary
AD
Airworthiness Directive
AFM
Aircraft flight manual
ALA
Aircraft landing area
AMSL
Above mean seal level
ATSB
Australian Transport Safety Bureau
AWB
Airworthiness Bulletin
CAA
Civil Aviation Authority (Australia)
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
FAA
Federal Aviation Association
ft
Feet
kt
Knots
MOS
Manual of Standards
NAIPS
National Aeronautical Information Processing System
NM
Nautical miles
SEB
Service Bulletin
STC
Supplemental type certificate
VREF
Landing reference speed
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight
Fly WA Group
the chief pilot of Fly WA Group
Civil Aviation Safety Authority
passengers of the accident flight
Textron Aviation
Bureau of Meterology
Flight Radar 24
accident witnesses
video footage of the accident flight and other photographs and videos taken on the day of the accident
United States Federal Aviation Administration
Transport Canada
Transport Safety Board of Canada
References
Australian Transport Safety Bureau. (2021). Collision with water involving Textron Aviation Inc. (Cessna) 206, VH-AEE, near Happy Valley, Fraser Island, Queensland, on 29 January 2020. Retrieved from /publications/investigation_reports/2020/aair/ao-2020-010#safetysummary0
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
Fly Esperance chief pilot
Textron Aviation
Civil Aviation Safety Authority.
Submissions were received from:
the pilot of the accident flight
Fly Esperance chief pilot
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix 1 – Cessna 206 occurrences
Year
Injuries
Summary
Link
Country of Occurrence
2020
2 Persons on board
(pob)
2 minor injuries
During a landing at a beach landing area on Fraser Island, Queensland, the Cessna U206G aircraft veered significantly to the left. Once airborne it was identified that the rudder was jammed in the full‑left position and the pilot had to apply full opposite aileron to maintain control. The engine subsequently stopped, possibly due to fuel starvation and the aircraft collided with water. Unable to open the pilots door the trainee pilot kicked the cargo door to force it open past the extended flap.AO-2020-010
During a landing on water, a float equipped U206G nosed over. The pilot and one passenger survived. The three remaining passengers, who received no injuries during the accident, were unable to escape the fuselage and drowned. The passengers were found with their seatbelts unfastened but had not opened the cargo door, which was blocked by 20˚ flap.
During a landing on water, the float equipped 206 nosed over. The flaps were extended blocking the cargo door. The pilot and three passengers escaped by bending the cargo door. The fourth passenger, found in her seat with the seatbelt on, likely died through injuries caused by the accident.
During cruise, the engine failed, and the pilot conducted a ditching into Lake Michigan. The pilot did not lower the flap; however, the cargo door had not been opened. The pilot survived. Two passengers were found outside the aircraft however, their life jackets had failed. Of the two passengers found inside the cabin, one had removed their seatbelt.
During the landing on water, the float equipped 206 flipped over. Contrary to instructions provided by the pilot, the passenger made their way to the rear of the aircraft, was unable to exit, and drowned.
TSB aviation occurrence A03Q0083
Canada
2001
5 pob
1 fatality
During the landing, the aircraft collided with a hole in the runway, nosed over and slid into a river. The pilot and three passengers escaped with minor injuries, however, one of the passengers drowned trying to escape the aircraft.
During an aerial surveillance air transport flight around Pitt Island, New Zealand the aircraft had a sudden engine failure and ditched in the sea. The pilot and four passengers escaped from the aircraft and swam to shore without the aid of life-jackets. Aircraft flaps were not extended during the ditching.
Transport Accident Investigation Commission, New Zealand 99-001
New Zealand
1997
3 pob
2 fatalities
During the landing on water, the float‑equipped aircraft flipped as the landing gear had not been retracted. Two passengers were unable to exit the aircraft and drowned. The door handle was found in the upright closed position.
TSB Aviation investigation report A97C0090
Canada
1996
6 pob
4 fatalities
During the take-off on water, the aircraft capsized. The pilot and three passengers drowned in the rear of the aircraft, when the pilot could not open the cargo door. Two passengers escaped through the pilot door. There was evidence that an adult had attempted to open the cargo door.
During the landing on a dam, the float‑equipped 206 nosed over as the landing gear had not been retracted. The pilot and one passenger survived, but three passengers were fatally injured.
During the landing on a dam, the float‑equipped 206 nosed over as the landing gear had not been retracted. The pilot and one passenger survived, but three passengers were fatally injured.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Flap: lift devices mounted on the wing trailing edge.
[2]Go-around: a flight path taken by an aircraft after an aborted approach to landing.
[3]Battery master: provides electrical power from the battery to the aircraft systems.
[4]NAIPS: National Aeronautical Information Processing System
[5]Runway direction indicating a magnetic heading.
[6]Flight Radar 24 height data is accurate to within 100 ft.
[9]A supplementary type certificate (STC) is a form of regulatory approval of the design of a major modification, or collection of changes, to a type certificated aircraft, aircraft engine or propeller.
[10]Recognised countries include Canada, Federal Republic of Germany, New Zealand, The French Republic, Kingdom of the Netherlands, The United Kingdom and The United States of America.
Occurrence summary
Investigation number
AO-2024-049
Occurrence date
01/09/2024
Location
39 km south-east of Moora
State
Western Australia
Report release date
30/06/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Control issues, Incorrect configuration, Missed approach
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
U206F
Registration
VH-TDQ
Serial number
U20602807
Aircraft operator
Fly Esperance Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
On 18 February 2023, a Boeing Company 787-9, registered VH-ZNJ, was being operated on a scheduled passenger flight between Santiago, Chile, and Sydney, Australia. At 1639 Sydney local time, prior to the top of descent, the flight crew requested and received, via the aircraft communication and addressing system (ACARS), the weather forecast (TAF 3) for Sydney, Melbourne, and Canberra airports in preparation for their planned arrival time of 1820. The flight crew also requested and received the forecast for Christchurch, New Zealand.
The Sydney TAF3 for their arrival stated clear skies and wind from 040° True with a speed of 22 knots. The forecast also stated that from 1900, for periods of up to 60 minutes, there would be a 30% probability of wind being variable at 20 knots gusting to 40 knots, along with thunderstorms and rain in which visibility would reduce to 2,000 m.
Due to the forecast thunderstorm having only a 30% probability and not commencing until 40 minutes after their planned arrival time, there was no company or CASA procedural requirement for the flight crew to discontinue the approach to Sydney Airport or to plan for an alternate destination. However, during the descent, the flight crew requested and received the forecast for Williamtown Airport, New South Wales, which stated clear skies and wind from 060° True at 14 knots.
An aerodrome warning was subsequently issued for Sydney Airport at 1735 by the Bureau of Meteorology for a squall line ahead of the storm commencing at 1845, again after the planned arrival time of VH-ZNJ. At 1745 the flight crew received the Automatic Terminal Information Service data (ATIS) which provided current information and conditions at Sydney Airport. The ATIS stated that at 1732 wind was from 020° True at 22 knots, visibility was greater than 10 km, and there were thunderstorms to the north. The ATIS also contained a significant weather caution for a possibility of turbulence on runway 34 right final.
At 1818, 2 minutes before VH-ZNJ arrived overhead Sydney Airport, the TAF 3 forecast was amended stating that from 1830, the forecast wind would be from 230° True with an average velocity of 25 knots gusting to 45 knots and that, from 1800 (retrospectively applied), there would be periods of up to 60 minutes of wind being variable at 30 knots gusting to 50 knots, along with thunderstorms and hail, visibility reducing to 1,000 m with scattered cumulonimbus at 600 feet above ground level.
At 1820, the aircraft arrived overhead Sydney Airport and conducted a left turn to position the aircraft on downwind for runway 34 left. Shortly after, moderate turbulence and high wind conditions were encountered leading to an unstable approach. In response, the crew conducted a missed approach and advised air traffic control of minimum fuel conditions. The captain later reported to the ATSB that the aircraft was down to approximately 60 minutes of fuel. Due to this quantity being insufficient to hold while the thunderstorm passed, the flight crew diverted the aircraft to Williamtown, where an uneventful landing was conducted.
Following notification of the occurrence, the ATSB initiated an investigation.
As part of its investigation, the ATSB:
interviewed the captain and the first officer
analysed:
recorded data from the aircraft’s flight data recorder
the ACARS flight log
the weather reports and forecasts from the Bureau of Meteorology
reviewed company planning and diversion procedures.
ATSB comment
The available evidence indicated that, prior to the top of descent, the flight crew of VH-ZNJ collated all necessary and available information required for a decision to be made for their arrival to Sydney Airport.
The Sydney TAF 3 was amended 2 minutes prior to VH-ZNJ being overhead due to the thunderstorm arriving earlier than forecast. The flight crew, already in visual range with the airport, had no requirement to collect or review the amended forecast. Additionally, until the 1818 amended TAF3 was issued with a retrospective forecast of deteriorating conditions, there was no requirement for the flight crew to make provision for holding or diversion to an alternate airport.
The retrospective application of periods of temporary or intermittent deteriorating conditions within a current TAF 3 validity is due to the format being unable to provide detail to the nearest minute. Amendments to a TAF are issued as soon as the need is recognised and when a TAF 3 is amended at a time between whole hours, the commencement of its validity is ordinarily the next hour. However, as was the case with the 1818 forecast detailed above, the TAF 3 may be amended from the preceding hour if the amendment criteria are expected to be met before the next hour.
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues or important safety lessons. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any similar occurrences that may indicate a need to undertake a further safety investigation.
Occurrence summary
Investigation number
AO-2023-009
Occurrence date
18/02/2023
Location
Sydney Airport
State
New South Wales
Report release date
29/05/2023
Report status
Discontinued
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Discontinued
Mode of transport
Aviation
Aviation occurrence category
Missed approach
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
787-9
Registration
VH-ZNJ
Serial number
66074
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
The aircraft was forced to go around from short final after three fire tenders were unable to vacate the runway as instructed. Four fire tenders were previously cleared to enter the movement area in order to conduct a response time test to the threshold of runway 33. The controller permitted the exercise after considering the aircraft traffic in the area. His expectation was that the tenders would would be able to clear the runway (to grassed areas outside the flight strip) immediately when requested. When the controller instructed the tenders to vacate the runway he was advised that they were restricted to operations on the sealed areas only. The surrounding ground was too soft.
The aircraft landed safely a short time later, after the fire vehicles had moved to the taxiways.
Notification procedures were then put in place at Cairns, so that air traffic control staff would be made aware of any restrictions to the movement of fire vehicles due to surface conditions.
At 0027 Western Standard Time on 1 June 2012, a Boeing 717 aircraft, registered VH-NXO and operated by Cobham Airline Services, was conducting an instrument approach to land on runway 03 at Perth Airport after a flight from Paraburdoo, Western Australia.
The approach was being conducted in instrument meteorological conditions. When the aircraft was at the decision altitude, the crew initiated a missed approach procedure as they had not obtained visual reference with the runway. Almost immediately, the crew obtained visual reference with the runway, discontinued the missed approach procedure and landed.
What the ATSB found
The onset of fog at Perth Airport at the estimated time of arrival was not forecast until after the aircraft had passed the point in the flight when it had insufficient fuel remaining to divert to a suitable alternate aerodrome. Before that point, there had been no requirement for the aircraft to carry fuel to continue to a suitable alternate.
Under the circumstances, the flight crew considered that the better option was to discontinue the missed approach procedure and land, in spite of the aircraft being in an unstable condition due to the initiation of the missed approach.
Safety message
This occurrence highlights that during a flight, the forecast weather at the destination may change and the advisability of obtaining the most up-to-date weather forecasts. However, pilots should be alert to the fact that the actual weather can differ significantly from forecasts.
The occurrence also highlights the risk of an unstable approach from not following a missed approach through to its conclusion. Unstable approaches are a frequent factor in approach and landing accidents, including controlled flight into terrain. The Flight Safety Foundation has developed an Approach and Landing Accident Reduction Tool Kit aimed at reducing the risk of approach and landing accidents. The toolkit can be found at Flight Safety Foundation website.
Context
Pilot information
The flight crew consisted of two pilots who held endorsements on the aircraft type.
The captain had been flying with the operator for 17 years and had a total of about 17,000 hours aeronautical experience in a range of different aircraft types. The captain had been flying this aircraft type for about 18 months, and a different jet airliner type for 8 years before that.
The first officer (FO) had been with the operator for about 5 years and had a total of about 10,000 hours aeronautical experience, with about 2,500 hours on this aircraft type. Before then, he had been flying turboprop aircraft.
Meteorological information
When planning for the return flight at Paraburdoo, the Perth aerodrome forecast (TAF)[7] and the trend forecast (TTF) did not contain any forecast operational requirements for this aircraft to carry sufficient fuel to fly to an alternate aerodrome. At 2300, 5 minutes after take-off, the Perth TTF changed with the forecast onset of fog 65 minutes after the estimated time of arrival (ETA).
At 0010, which was about the time when the aircraft commenced its descent and shortly before the aircraft no longer had sufficient fuel to divert safely to a suitable landing aerodrome, the Perth TAF was amended to indicate a requirement for the carriage of sufficient fuel to divert to an alternate airport on the basis of more than four OKTAS[8] of cloud with a base below the alternate minimum of 700 ft above the aerodrome reference point. The forecast also predicted that 35 minutes after the aircraft’s ETA, there was a 30 per cent probability of fog reducing the visibility to 300 m, which was below both the alternate and landing minimums for runway 03.
Soon after, at 0014, a TTF SPECI[9] was issued for Perth Airport indicating that the visibility had reduced to 7,000 m and the airport was partially covered in fog. The observed visibility, as reported on the TTF SPECI issued at 0030, which was soon after the aircraft’s landing time, was 900 m in fog.
Operational information
Information sources relating to alternate aerodrome requirements
Aeronautical Information Publication Australia (AIP) section ENR 1.1, 58.2 Weather conditions, paragraph 58.2.9 related to the application by crews of forecast weather conditions when determining the need to allow for an alternate aerodrome. In this regard the AIP stated that:
Flights which will be completed within the time of validity of the TTF may be planned wholly with reference to the destination TTF.
Operator procedures relating to fuel flight planning
The operator’s procedures for domestic operations for planning minimum fuel requirements were based on Civil Aviation Advisory Publication (CAAP) 234-1 (1) Guidelines for Aircraft Fuel Requirements. Those procedures allowed for fuel remaining to be recalculated before an aircraft passed its diversion point to a suitable alternate aerodrome. If crews undertook this calculation they were then authorised to continue to their destination if sufficient fuel remained to meet all of the fuel requirements for the contemplated flight at that time.
Specifically, section 5.17.2 of the operations policy and administration manual, titled Fuel Requirements stated, in part that an aircraft may continue:
…to the destination aerodrome from the diversion point only after it has been determined that the fuel on board the aircraft at that point is sufficient, in accordance with the fuel requirements detailed above [allowing for the recalculation of fuel remaining], to enable to aircraft to complete the flight to that destination aerodrome.
The flight crew reported reviewing the forecast weather at the destination before take-off by obtaining the most recent trend forecast for Perth Airport.
Alternative landing options at Perth
AIP section ENR 1.5, 1.10 Missed Approach – Standard Procedures paragraph 1.10.1 listed the circumstances in which an instrument approach was to be discontinued and a missed approach carried out. In the case of a runway approach at Perth such as the runway 03 instrument landing system (ILS) approach, these included:
the pilot not having clear visibility of the runway threshold, or approach lighting or other markings identifiable with the runway
once an aircraft reached the decision altitude of 320 ft, a visibility of less than 1,500 m.
ILS approaches were also available for use on runways 21 and 24 at Perth. These approaches could be accomplished in slightly worse weather conditions than for a runway 03 ILS, with a minimum visibility requirement of 800 m once reaching the decision altitude of 250 ft and 260 ft respectively. Unlike runway 03, runways 21 and 24 were also equipped with high intensity approach lighting that would have helped the crew obtain visual reference with the runway.
It would have taken some time to manoeuvre to conduct an ILS approach to a different runway, and there were a number of aircraft in the vicinity also intending to land, which could have delayed any subsequent approaches. In the event, when the aircraft landed after discontinuing the missed approach, it was carrying about 30 minutes more fuel than the operator’s minimum planned fuel for arrival at Perth.
Operator’s missed approach criteria
A missed approach procedure is initiated by conducting a go-around. During a go-around a number of actions are coordinated by the flight crew to reconfigure the aircraft and its systems for a climb away from the airport. The operator’s operating procedures for this aircraft type stated:
A go around can be as a result of not being visual at the missed approach point of an instrument approach or if the approach is not stable or becomes destabilised.
and that:
Before committing to a further approach following a Missed Approach/Go Around, the crew must review the factors that led to the preceding Missed Approach/Go Around and ensure that those factors are alleviated in the subsequent approach.
Approach and landing Accident Reduction Tool Kit
The Flight Safety Foundation has developed a tool kit to help manage the risks of approach and landing accidents. The kit highlights that unstabilised approaches were a factor in a high proportion of approach and landing accidents,[10] and recommends the use of stabilised approach criteria to mitigate this risk.
The criteria for a stabilised approach promoted by the Flight Safety Foundation were the same as those specified in the company’s operational procedures. In respect of the risk of continuing an unstable approach, the operator’s procedures stated:
In order to provide maximum opportunity for a well executed landing to be completed, a consistent and stable approach path is necessary. Continuing to land from an unstable approach has been shown to be the precursor of many landing accidents.
The initiation of the missed approach procedure by the captain resulted in the aircraft being outside the operator’s parameters for a stabilised approach. Continuing the landing from this profile increased the risk to the aircraft during the landing sequence.
Previous occurrences
The following occurrences were investigated by the ATSB and are available for download at ATSB website. Together with the crew’s experience in this occurrence, each provides an example of the landing risks/threats associated with bad/deteriorating destination weather and its management.
On 16 September 2006 at 0038 Western Standard Time, an Airbus A330 landed on runway 21 at Perth Airport in weather conditions that were below the applicable landing minima. The aircraft, registered VH-QPJ, was being operated under the instrument flight rules on a scheduled passenger flight from Singapore to Perth.
Before departure from Singapore, the TAF for Perth Airport predicted a 30 per cent probability of fog after 0200. The aircraft was due at Perth at 0020 so, in accordance with the operator's fuel policy, fuel was not specifically carried for a diversion from Perth to an alternate aerodrome. While the aircraft was in cruise, the TAF was revised to forecast fog from 2400, but the TTFs that superseded the TAF trended fog from 0030.
At about 2350, when the flight crew commenced descent, the aircraft passed the point where it had sufficient fuel to divert to Learmonth, Western Australia. About 10 minutes later, the TTF was amended to forecast fog before the aircraft's arrival time. The fog occurred at about 0015. The crew attempted two ILS approaches before they used autoland to land on runway 21 in weather conditions that were below the prescribed landing minima for the ILS.
The aircraft was certificated to conduct an autoland and the flight crew held the necessary qualifications. However, the airport’s ILS facilities were not approved for autoland operations in low visibility conditions. At that time, there were no autoland capable airports in Australia.
On 23 September 1999, a Boeing 747 was landing in adverse weather conditions at Bangkok Airport, Thailand. Shortly before touchdown, a missed approach was initiated but the aircraft’s wheels contacted the runway. The missed approach procedure was then discontinued, with a lack of clarity between the flight crew. The sequence of control inputs by the crew meant that not all the available aircraft equipment and systems that might have assisted its deceleration on the runway were operating to their maximum efficiency. In this configuration, there was insufficient runway remaining to stop and the aircraft overran the runway.
From the evidence available, the following findings are made with respect to the weather-related operational event involving a Boeing 717, registered VH-NXO, which occurred at Perth Airport on 1 June 2012. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The weather forecast for Perth Airport was amended to include the requirement to carry sufficient fuel to divert to a suitable alternate aerodrome when the aircraft no longer had that amount of fuel remaining.
The captain, as the flying pilot, continued an approach to land after the approach had been destabilised by initiating a go-around procedure.
Other factors that increased risk
The flight crew did not update the weather forecast for Perth Airport en route which, although in this instance did not indicate an operational requirement, was a missed opportunity to update pertinent operational information prior to the aircraft being committed to its destination.
Other findings
Given the circumstances, when confronted by a choice between completing the missed approach with an indeterminate outcome and landing from a discontinued missed approach, the captain chose the option that was considered to represent lower risk.
The operator’s procedures in the case of an unstabilised approach were unambiguous and reflected those promoted by the Flight Safety Foundation.
Safety analysis
Introduction
The flight proceeded normally until just after commencing descent to Perth Airport, when visibility reduced due to the rapid onset of fog. This deterioration in the weather conditions occurred after the last diversion point to a suitable alternate aerodrome for the flight and resulted in the crew being committed to landing the aircraft at Perth. The following analysis will consider the role of weather and procedural factors in this occurrence and assess the safety implications for future operations in similar conditions.
Weather factors
The aerodrome and trend forecasts for Perth Airport did not predict weather conditions that required the carriage of sufficient fuel to fly to a suitable alternate landing airport, until after the aircraft no longer had sufficient fuel to divert to a suitable alternate aerodrome. This committed the crew to landing at Perth where a safe landing could no longer be assured.
In the few minutes before landing, the flight crew observed a rapid deterioration in the weather conditions, and their observations were reinforced by information heard on the aircraft radio. The flight crew were confronted with rapidly deteriorating unforecast weather conditions, and uncertainty about how much further the weather might deteriorate.
Procedural factors
The crew updated their knowledge of the weather observations for Perth Airport as soon as the broadcast of those observations from the airport could be received. Observations with a trend forecast appended were available previously from the automatic en route information service facility at Meekatharra. However, the delay normally encountered by the captain in obtaining updated weather from this facility and the timing of this particular flight influenced the captain to not access that information in this case.
Weather observations do not predict expected weather conditions. In contrast, a weather forecast is intended to provide the best approximation of future weather conditions. Knowledge of any changes to forecast weather at the destination is assured when flight crews request or obtain the latest version of the relevant forecast. For safety purposes, the most relevant time to ensure that the destination’s forecast weather remains suitable for an assured landing is shortly before the aircraft no longer carries sufficient fuel to divert to an alternate aerodrome where a landing can be assured.
The crew had a reasonable knowledge of the point in the flight when they were committed to a landing in Perth because of the fuel remaining, and an amended forecast was not issued for Perth Airport before this time. However, by not confirming the latest weather forecast for Perth, and its potential effect on the flight, the crew could not assure themselves of the validity of that understanding.
Conduct of the approach and landing
The flight crew commenced the instrument landing system (ILS) approach to runway 03 and encountered unforecast and rapidly deteriorating weather, the extent and duration of which was unknown. Similar instrument approaches were available to runways 21 and 24 that allowed for landing in slightly worse weather conditions, but the time taken to change to either of these approaches would, given the traffic situation, have impacted further on the crew’s now less-than-ideal fuel situation.
In the event, the captain was confronted with a short-notice choice between completing the missed approach, with an indeterminate outcome, and landing from a discontinued missed approach. He was aware of the risk associated with continuing the landing in what amounted to an unstabilised configuration, but considered this option represented lower risk.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
flight crew of VH-NXO
Cobham Airline Services (Cobham).
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew, Cobham and the Civil Aviation Safety Authority.
Submissions were received from the aircraft captain, first officer, Cobham and the Civil Aviation Safety Authority. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
On 1 June 2012 at 0027 Western Standard Time,[1] a Boeing 717 aircraft, registered VH-NXO and operated by Cobham Airline Services, landed from a runway 03 instrument landing system (ILS)[2] approach at Perth Airport, Western Australia. The flight crew had initiated a missed approach procedure, due to visual reference not being established at the decision altitude, but discontinued this procedure and landed after the pilot flying (PF)[3] saw the runway.
The previous evening, the aircraft was flown from Perth to Paraburdoo, Western Australia and the occurrence took place on the return flight to Perth. Shortly before departure from Paraburdoo for the 90-minute flight to Perth, the flight crew obtained a trend forecast (TTF)[4] for Perth. They reported assuring themselves that based on this forecast, there was no weather-related requirement to carry sufficient fuel to divert from Perth Airport to an alternate aerodrome.[5] The aircraft took off from Paraburdoo at 2255.
Despite the lack of a requirement to provide for an alternate for Perth, the aircraft was carrying sufficient fuel to allow for the flight to be diverted to Kalgoorlie until shortly after commencing descent into Perth. Beyond that time, the aircraft was no longer carrying sufficient fuel to divert to another suitable aerodrome.
During the flight, the flight crew did not seek or obtain an amended or updated forecast for Perth. The captain reported that he normally obtained the latest TTF for Perth when overflying the automatic en route information service (AERIS) at Meekatharra, about 360 NM (667 km) north-north-east of Perth. However, the timing of the flight and the delay normally encountered in updating the available weather information on the AERIS meant that he did not expect to obtain the latest TTF at that time. When the aircraft was about 240 NM (440 km) from Perth, the crew obtained the latest automatic terminal information service (ATIS)[6] weather observation for Perth, which provided no indication of deteriorating weather.
After the aircraft descended below 11,000 ft, air traffic control (ATC) notified the crew of deteriorating visibility at Perth Airport, and the first officer (FO) observed a thin layer of cloud between the airport and the coast. ATC notified the crew of continuing reducing visibility as they manoeuvred the aircraft for a runway 03 ILS approach. While manoeuvring the flight crew heard on the radio that another aircraft had conducted a missed approach procedure from this approach.
As the aircraft started the ILS approach, it flew through small patches of cloud until it descended below 1,000 ft, when it entered continuous cloud. At the decision altitude of 320 ft the FO, who was the pilot monitoring (PM) called ‘nil sighting’. That statement indicated that the FO had not obtained visual reference with the runway. The captain, who was the PF, called ‘going around’ and initiated a missed approach procedure by pressing the go-around switches and advancing the thrust levers. It was reported that the captain had not initiated the next actions for the missed approach procedure when the aircraft flew clear of cloud and both crew members obtained visual reference with the runway. The captain called ‘landing’, disconnected the autopilot and the autothrottle, and manually landed the aircraft without exceeding any flight or landing tolerances (Figure 1).
Figure1: Plot of selected aircraft parameters during the approach and landing
Source: ATSB
The captain later reported being concerned about the unforecast weather deterioration with limited fuel remaining, and not knowing if the weather would deteriorate further after going around and repositioning for a second attempted approach and landing. He reported that this concern influenced his decision to land after initiating the missed approach, during which the aircraft exceeded the operator’s stabilised approach criteria for a landing.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
While VH-JJT was backtracking on runway 13 at Gove after conducting an instrument approach, VH-NJN became visual on final approach, also for runway 13. The airport safety officer reported that NJN continued the approach until very late final before executing a missed approach.
The crews of both aircraft were in radio contact with each other on the Gove MBZ frequency. After landing, the crew of JJT advised the crew of NJN that JJT was backtracking on runway 13 and would shortly be clear of the runway. The pilot in command of NJN elected to continue the approach, anticipating that JJT would clear the runway in sufficient time to permit NJN to land. When it became apparent that JJT would not be clear of the runway, the pilot in command of NJN discontinued the approach.
Examination of the Flight Recorder data from NJN revealed that the vertical separation between the aircraft during the missed approach was not less than 300 ft.
Occurrence summary
Investigation number
199901622
Occurrence date
16/04/1999
Location
Gove, Aero.
State
Northern Territory
Report release date
05/05/1999
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Missed approach
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
British Aerospace
Model
BAe 146
Registration
VH-JJT
Sector
Jet
Operation type
Air Transport High Capacity
Departure point
Darwin, NT
Destination
Gove, NT
Damage
Nil
Aircraft details
Manufacturer
British Aerospace
Model
BAe 146
Registration
VH-NJN
Serial number
Air Transport, Domestic, High Capacity, Passenger, Scheduled