On 3 October 2014, at about 0900 Western Standard Time, a Jabiru J230 aircraft, registered 24-7491, departed Cape Leveque for Broome, Western Australia, with a pilot and one passenger on board. When at about 5 NM from Broome Airport, an air traffic controller cleared the aircraft to join a right circuit for runway 28. The pilot reported that the approach and landing were normal and the aircraft touched down on runway 28 just beyond the threshold.
During the landing roll, the pilot was focused on looking for the correct taxiway to exit the runway for the itinerant parking bay. The aircraft was decelerating normally and the pilot did not apply brakes due to the length of runway remaining. The pilot detected the right wing rising slightly, possibly due to a crosswind. He then looked straight ahead and realised that the aircraft had veered off the runway centreline to the left. He applied right rudder in an attempt to return to the centre of the runway, but the aircraft continued towards the edge of the runway and taxiway A. He sighted a grass area and a drainage ditch ahead just off the runway which he wanted to avoid, along with a Fokker 100 aircraft that was stationary on taxiway A at the holding point for runway 28. The pilot elected to apply full left rudder to turn the aircraft around and remain on the sealed area.
The Jabiru aircraft’s propeller and right wingtip struck the ground and the aircraft came to rest upright and facing in the opposite direction to the landing and about 20 m from the Fokker 100. The pilot and passenger were uninjured.
On 3 July 2014, a Piper Aircraft Corp PA-28-161, registered VH-TEK, was returning from the training area via the 2RN reporting point to Bankstown Airport, New South Wales. The student pilot was the only person on board. The flight was conducted in visual meteorological conditions.
The student tracked from the 2RN reporting point and joined downwind for a touch-and-go landing on runway 29L. The student turned onto base and then final and the Bankstown tower gave the student a clearance to conduct a touch-and-go clearance. The student reported that the approach and landing were normal. As soon as the student felt the aircraft wheels were on the ground, he reached down to the flap lever and selected the flaps to the retracted position.
The aircraft veered slightly to the right and then quickly to the left, departing the runway and onto the grass strip. The student regained control of the aircraft and informed the tower of what happened, reporting that he did not require assistance. The student then taxied onto taxiway B, between taxiway B4 and B3, passing about 20 metres in front of a taxiing Cessna 150. TEK taxied to the flying school without further incident. The student pilot was uninjured, and the aircraft was not damaged.
On 10 May 2014, an accredited Cirrus salesman conducted a sales demonstration flight of a Cirrus SR22 aircraft, registered N802DK, in the local training area, from Bankstown Airport, New South Wales, with a pilot (and potential aircraft buyer) seated in the front left seat and one passenger on board. At about 1330 Eastern Standard Time, the aircraft departed Bankstown and the salesman, as pilot in command (PIC) elected to track towards Katoomba at about 6,000 ft above mean sea level.
After demonstrating a series of turns and a straight and level stall, the PIC selected 50% flap, rolled the aircraft into a left turn at about 25° angle of bank, reduced the power to idle, and raised the nose of the aircraft. The right wing dropped rapidly, and the aircraft entered a spin to the right. When about 2,000 ft above ground level, the PIC was unsure whether he then had enough height remaining to recover control of the aircraft, and elected to deploy the aircraft’s parachute. The rocket fired, the aircraft initially pitched up slightly and then as the parachute deployed, the aircraft pitched down rapidly into a nose low attitude. About 6 seconds after the rocket fired, the right snub line of the parachute released, followed by the left snub line, which then established the aircraft in a wings level attitude.
The aircraft narrowly avoided powerlines, collided with branches of a tree, and came to rest on a fence in the garden of a residential dwelling.
This incident provides a reminder to pilots to know your own limitations and those of the aircraft.
On 15 January 2014, the pilot of a Piper PA‑28 aircraft, registered VH‑HVX, was undergoing a Commercial Pilot Licence test flight with a testing officer on board. At about 1500 Eastern Daylight-savings Time, the aircraft landed at Orange Airport, New South Wales. The aircraft had encountered moderate turbulence during the flight from Bankstown and the pilot reported a slight overshoot on landing at Orange due to fluctuating wind conditions.
During the time on the ground, the pilot observed the wind varying from an easterly to a westerly direction and the speed fluctuating from 0 to about 15 kt. The temperature at Orange was about 33 ºC, and the aerodrome elevation was 3,115 ft. The pilot had calculated the density altitude at Orange to be about 5,725 ft.
At about 1530, the pilot observed the wind to be from 110º at about 10-15 kt and configured the aircraft for a short field take-off from runway 11, selecting two stages of flaps. During the take-off run, the pilot and testing officer observed the aircraft performing normally and the pilot rotated the aircraft at about 55-60 kt indicated airspeed (IAS). The pilot then established the aircraft in an attitude to achieve a best angle-of-climb speed of about 72 kt IAS. The pilot reported that the stall warning horn sounded momentarily during the take-off due to turbulence.
When at about 50 ft above ground level (AGL) and about 65-70 kt IAS, the testing officer reduced the engine power to idle and stated “simulated engine failure”. The pilot immediately lowered the nose of the aircraft in an attempt to increase the airspeed and selected the third stage of flaps. At about 10 ft AGL, the pilot reported the aircraft was sinking and flared the aircraft for landing. However, the aircraft continued to sink and landed heavily. The pilots reported that the stall warning did not sound during the descent and that a shift in the wind direction was the most likely cause of the accident.
This incident highlights the critical importance of considering local conditions such as wind, elevation and temperature, as well as the inherent risks of conducting simulated engine failure at low altitude.
On 7 December 2013, the pilot of a Cessna 182 aircraft, registered VH-LMA, departed Albury, New South Wales on a private flight to the Tyabb aeroplane landing area (ALA), Victoria. The flight was being conducted under the instrument flight rules (IFR), and on board were the pilot and one passenger.
After the aircraft had left controlled airspace and with about 6 NM to run, the pilot levelled the aircraft at 1,100 ft to prepare to join the circuit on an extended left base leg for runway 17.
When on final approach, he checked the secondary windsock and noted the wind was predominantly crosswind from the right, gusting around 5-10 knots. With the final stage of flap selected, the aircraft touched down on the main wheels about 20-30 metres past the runway threshold, close to the centreline. The pilot estimated the aircraft speed at touchdown was about 65 knots. During the landing roll, he applied a small amount of right aileron to counter the crosswind.
When the aircraft had slowed he began to apply the brakes. At about the same time, a gust of wind pushed the aircraft to the left. The pilot applied right rudder in an attempt to steer the aircraft back to the centreline, but stated the aircraft pulled to the left and felt like the left brake had locked. The aircraft rapidly decelerated, and continued along a path through the wet grass a few metres to the left of the sealed runway. As it stopped, the aircraft nosed forward, and then tipped over onto its back.
The pilot and his passenger were hanging upside down in their seatbelts. A person who had been waiting for the aircraft to arrive assisted the young passenger and then the pilot. The pilot and passenger sustained minor injuries, and the aircraft was substantially damaged.
A search of the ATSB database for fixed wing, private operation accidents, 2004 to 2013 found the landing phase accounted for 33% of all accidents. The take-off and initial climb phases together accounted for 25% of accidents from this group.
On 8 December 2013, at about 1430 Eastern Daylight-savings Time, a Eurocopter EC-120B helicopter, registered VH‑VMT, departed from a property 16 km north of the Ballina/Byron Gateway Airport, New South Wales for a local flight.
At about 1555, the helicopter returned to the property from the north, overflew and approached to land on a heading of about 340º. The pilot reported that the wind was from the north, at about 20 kt.
When about 3 ft above ground level, the pilot reported that he entered the hover. Immediately after, the helicopter began to yaw left. The pilot applied right rudder pedal to counteract the yaw and reduced the engine power to idle. The helicopter continued to yaw left and the pilot applied full right rudder pedal, but was unable to arrest the rotation. The helicopter rotated left about 90° before the left skid lowered and contacted the ground. It continued to rotate around and rolled onto its right side. The helicopter was substantially damaged, and the passengers were uninjured.
The pilot believed that a combination of main rotor downwash and a wind gust contributed to a loss of tail rotor effectiveness. By maintaining an awareness of the wind and its effect on the helicopter, pilots can significantly reduce the exposure to LTE.
On 31 October 2013, a Cessna 172 aircraft, registered VH-IGS, departed Parafield, on a private flight to the Gum Creek area near Clare, South Australia. The pilot was the sole occupant on board.
The pilot had flown to Parafield earlier in the morning to pick up a part needed to repair a hay cutting machine. The pilot felt pressure to get the part back to the property and repair the machine so that the harvest could continue.
At about 1300 central daylight time, the aircraft arrived overhead a back road the pilot had selected in the Gum Creek area. His intention was to land as close as possible to the hay machine. After conducting two precautionary searches over the road and identifying some powerlines, he commenced the approach onto the road.
Just as the aircraft was touching down, a gust of wind struck the aircraft from the right, moving it rapidly to the left. The pilot attempted to initiate a go-around, but the aircraft continued further left. The left wing struck a large tree and was severed, and the aircraft was further damaged as it continued through a gate and fence. The pilot sustained minor injuries, and the aircraft was substantially damaged.
On 21 October 2013, an Air Tractor AT-502B aircraft, registered VH-FLH, was conducting rice sowing operations north-east of Deniliquin, New South Wales. At about 1145 Eastern Daylight-savings Time (EDT), the pilot was conducting his fourth landing for the day onto the property airstrip located about 11 NM north-east of Deniliquin Airport.
The pilot reported that the approach was normal, at an airspeed of about 58-60 kt, with a predominately south-west wind of about 5-8 kt. The wind fluctuated between the west and south, but remained light.
During the landing, the main wheels touched down first, followed by the tail, which was locked into place. Shortly after, the aircraft suddenly veered right about 45°. The pilot considered a go around, but was concerned that the aircraft would not clear the boundary fence running along the side of the runway. Consequently, he elected to continue the landing and selected reverse thrust, applied left brake, left rudder and left aileron in an attempt to re-align the aircraft with the runway.
The wheels began to grab and the left undercarriage leg detached causing the aircraft to swing facing about 90 ° from the runway.
The pilot was not injured, but the aircraft was substantially damaged. An investigation could not determine what led to the loss of ground control, however a wind gust may have been a contributing factor.
On the morning of Saturday 5 October 2013, the pilot of a Rand Robinson KR-2 aircraft, registered VH-CTE, took off from an airstrip on private property 12 km west of Tumut, New South Wales. The pilot was reported to have intended flying to Holbrook, New South Wales, and return home the following evening.
When the pilot had not returned by early Sunday evening, authorities were notified. A search located the aircraft wreckage in the early morning on 7 October 2013. The wreckage was found about 450 m east-north-east of the departure airstrip. The pilot was fatally injured, and the aircraft was destroyed by impact forces.
What the ATSB found
Data from a global positioning system receiver recovered from the wreckage identified that the pilot turned back towards the departure airstrip shortly after take-off. During the attempt to land back on the airstrip, the aircraft likely entered a stall. The pilot was unable to recover the aircraft before impacting terrain.
The ATSB’s examination of the wreckage found that a spark plug had been ejected from its respective cylinder head mount. The failure of the cylinder head spark plug mount was probably the result of an incorrectly installed thread insert. There were reports and evidence that the pilot maintained and modified the aircraft, despite not being qualified or authorised to do so. As well, in the previous 2 years, an authorised maintainer had not completed the required regular aircraft maintenance.
The pilot’s decision not to have proper maintenance performed on the aircraft most likely contributed to the ejection of the spark plug, resulting in the accident.
Safety message
Unauthorised maintenance increases the risk of mechanical failure. This, in turn, reduces the level of safety and increases the risk of injury or death.
Authorised aircraft maintenance is mandated to assure a level of safety for aircraft operations. That directive also identifies the requisite qualifications for the maintainer.
As well, managing airspeed and bank angle is critical to preventing an aerodynamic stall following partial engine failure after take-off. Research shows partial engine power loss is more complex and more frequent than a complete engine power loss. These accidents are typically a result of the aircraft entering an aerodynamic stall from a height where recovery is not possible.
On the morning of the accident, it was reported that the pilot arose at 0600 and had breakfast, then left for the airstrip. Reports state that the pilot was in good health, was not on any medication and had recently completed a medical examination required for drivers of commercial coaches.
Pilot licences and certificates
The pilot held a Private Pilot (Aeroplane) Licence issued by the Civil Aviation Safety Authority on 26 February 1990. The licence included an endorsement for single-engine aeroplanes below 5,700 kg. Additionally, the pilot held a special design feature endorsement for manual propeller pitch control. The pilot did not hold the special design feature endorsement for tail wheel or for retractable landing gear, which were required for operation of an Australian (VH) registered aircraft with those features, such as the KR2. The pilot held a valid Class 2 medical certificate with a restriction that reading correction must be available while flying.
Before flight as pilot in command in an Australian registered aircraft, Civil Aviation Regulation 5.81 required that a pilot holding a private (aeroplane) pilot’s licence must successfully complete an aeroplane flight review within the period of 2 years immediately before the day of the proposed flight. The last Aeroplane Flight Review recorded as being completed by the pilot was on 20 August 2009.
The pilot also held a Recreational Aviation Australia (RA-Aus) pilot certificate. This certificate included endorsements for high-performance aircraft, tail wheel aircraft, and in-flight adjustable pitch propeller. The certificate did not include an endorsement for retractable landing gear. The certificate recorded the date of the last RA-Aus flying review as 18 November 2012. The pilot had previously held a senior instructor qualification for flight training in RA-Aus-administered aircraft.
Flight experience
The pilot’s logbook contained a record of the pilot’s flying from 1989 to November 2012. The logbook recorded the pilots total flying time as 988 hours. The last entry in the logbook was the Biennial Flight Review in a RA-Aus-administered aeroplane on 18 November 2012. From 2003, nearly all of the pilot’s logged flying time was in RA-Aus-administered aeroplanes, a considerable amount of which was logged as instructional flight. The last recorded flight in an Australian registered aircraft was an Aeroplane Flight Review on 20 August 2009.
Meteorological information
The weather conditions in the Tumut area on the morning of the accident were reported to be fine, with a light to moderate westerly wind. Recorded weather observations in the region of the planned flight also identified fine weather conditions with good visibility and light winds below 5,000 ft. Weather was not considered to be a contributing factor.
Wreckage information
The aircraft, a Rand Robinson KR-2 (KR-2), impacted terrain about 450 m to the east-north-east of the northern end of the Adelong airstrip (Figure 2).
Figure 2: Overview of accident site looking south, away from the direction of take-off
Source: NSW Police Force
Examination of the aircraft wreckage (Figure 3) determined the following:
All components of the aircraft were located at the impact site.
The aircraft was in a left wing low, steep nose-down attitude and heading in a south-westerly direction on impact.
Damage to the landing gear was consistent with the landing gear being extended at impact.
The position of the flap could not be determined.
All flight controls appeared to be intact and securely connected at impact. The position of the aircraft’s electrical elevator trim at impact could not be determined.
The engine was producing low or no power at impact.
The engine controls were disrupted by the impact and their position at impact was uncertain.
There appeared to be sufficient fuel remaining on board the aircraft at impact.
The number three cylinder upper spark plug (No.3 upper) was dislodged from its cylinder head hole. The spark plug remained attached to the engine through the spark plug lead and the engine cylinder head temperature gauge wiring. The dislodgment was not a result of impact forces.
Shaped aluminium panels with fire-resistant material attached were located in a shed adjacent to the airstrip. These panels were probably cooling air baffles previously fitted to the aircraft’s engine.
Figure 3: Aircraft wreckage
Source: ATSB
A number of aircraft components were removed from the accident site for testing and more detailed examination. The following additional evidence was determined from this examination:
Six of the eight spark plugs were of the type originally fitted by the builder of the aircraft (builder). The remaining two spark plugs, which included the dislodged No. 3 upper spark plug, were of a different type.
All engine cylinder lower spark plug holes were fitted with heli-coil inserts.
Both right hand cylinder upper spark plug holes, which included the No. 3 cylinder, were fitted with threaded inserts.
The No. 3 upper spark plug displayed evidence of having been blown out from its cylinder head hole before the aircraft impacted terrain. The failure of the cylinder head spark plug hole thread was probably the result of an incorrectly installed thread insert.
The fuel system and ignition system components tested normally.
The engine was disassembled and found to be in good condition with no mechanical defects.
The airspeed indicator displayed an impact witness mark at 48 kt.
The vertical speed indicator displayed an impact witness mark at 1,850 ft/min rate of descent.
The aircraft was fitted with a stall warning indicator. The stall warning sensor was significantly damaged by the impact with terrain. It was not possible to determine the stall warning system’s serviceability before the accident.
The engine manufacturer advised that the ejection of one spark plug from the cylinder head mounting would result in a loss of power in the order of 30 per cent.
Aircraft information
Construction, certification and registration
The KR-2 was an amateur-built, two-place, low-wing monoplane aircraft with retractable landing gear. The airframe was constructed of wood, foam and fibreglass composite. The builder purchased a partially completed KR-2 kit with a Revmaster engine in 1994.
The Sport Aircraft Association of Australia (SAAA) provided oversight and supervision of the construction of amateur built and kit aircraft. The builder registered with the SAAA in 1995.
The aircraft was fitted with a 4 cylinder, horizontally opposed, air-cooled Revmaster 2100D engine and a fixed-pitch, 2-blade, wooden propeller. The Revmaster 2100D engine was a modified Volkswagen automotive engine. Regulations required that, prior to fitment, this engine type be dismantled and inspected. The engine was dismantled, inspected and rebuilt at an authorised facility in Australia in 1990, before being fitted to the aircraft.
The builder entered the aircraft onto the Australian register on 31 March 2000. On 18 March 2001, a Civil Aviation Safety Authority (CASA) delegate issued a Special Certificate of Airworthiness (SCOA) for the aircraft to enable flight testing. The SCOA was in the Experimental airworthiness category for Amateur Built Aircraft and had an unlimited expiry date. Attached to the SCOA was an annex that caused the SCOA to expire in March 2003. That annex permitted operation of the aircraft for flight-testing only and limited those test flights to a specified restricted area. The issue of a second annex to the SCOA on 12 March 2003 identified the successful completion of the test flight programme. The second annex returned the SCOA to an unlimited status, but included a number of conditions attached to the operation and maintenance of the aircraft. The maintenance conditions included that:
The aircraft shall not be operated unless within the preceding 12 calendar months it has a Condition Inspection performed in accordance with the relevant CASA maintenance schedule.
Condition inspections may be performed by a Licenced Aircraft Maintenance Engineer (LAME) or by the builder.
In January 2012, the builder sold the aircraft to the pilot. The pilot transferred the aircraft’s registration into their name in January 2012. The pilot had discussed the possibility of transferring the aircraft from the Australian register to the RA-Aus register. However, this process had not been commenced prior to the accident.
Transport, maintenance and modification
The pilot was reported to have transported the aircraft by road to Tumut, New South Wales. Transporting the aircraft required the removal of the wings and disconnection of the aileron flight control system. At Tumut, the pilot had the aircraft repainted and on completion, the aircraft was reassembled. The reassembly required re-rigging the wings and reattachment of the flight control system. The first flight recorded by the pilot in VH-CTE (CTE) was on 4 August 2012.
The builder stated that the aircraft that was sold to the pilot in the following condition:
All spark plugs were of the same type.
Neither heli-coils nor the threaded inserts were fitted into the engine cylinder head spark plug holes.
The aircraft was fitted with a mechanical elevator trim system of a type similar to that fitted to DH82 Tiger Moth aircraft.
The builder also stated that the aircraft’s engine cooling system was specially designed to overcome cooling problems often experienced by aircraft fitted with Volkswagen-type engines. Finally, it was reported that during the builder’s ownership of CTE, the engine temperatures were normal at all times.
It was reported to the ATSB that the pilot began discussing high temperature issues with the aircraft’s engine in the months leading up to the accident. When discussing the problem, the pilot believed that the high temperatures were the result of the aircraft’s engine cooling system configuration, and that this would be corrected through modifying the cooling system to a more conventional layout. The pilot removed the cooling baffling and modified the engine cowl. The modified engine cowl was returned from repainting the day before the accident flight.
The aircraft’s maintenance documentation did not have any record of any of the above maintenance actions or aircraft modifications.
The builder completed and signed the last recorded Maintenance Release (MR) on 30 October 2010.
Authorisation to conduct maintenance
Civil Aviation Regulation 42ZC stated that the holder of a Certificate of Registration for an Australian aircraft must ensure that maintenance on that aircraft is conducted by a person authorised by that regulation. This obligation also applied to the pilot of that aircraft. The regulation then identified the class of persons authorised to conduct maintenance on certain types of aircraft.
With respect to CTE, that class of person included a LAME and a person authorised in writing by CASA. CASA normally issues written authorisations through the publication of an instrument. In March 2013, CASA published an instrument, CASA 33/13, which authorised certain persons who were not a LAME to carry out maintenance on amateur-built aircraft with special certificates of airworthiness. That instrument also authorised those persons to issue maintenance releases. To qualify as a person, other than a LAME who could conduct maintenance on CTE, that person was required to have been the primary builder of CTE, or an aeroplane that was essentially similar to CTE. The pilot did not meet these criteria.
GPS data
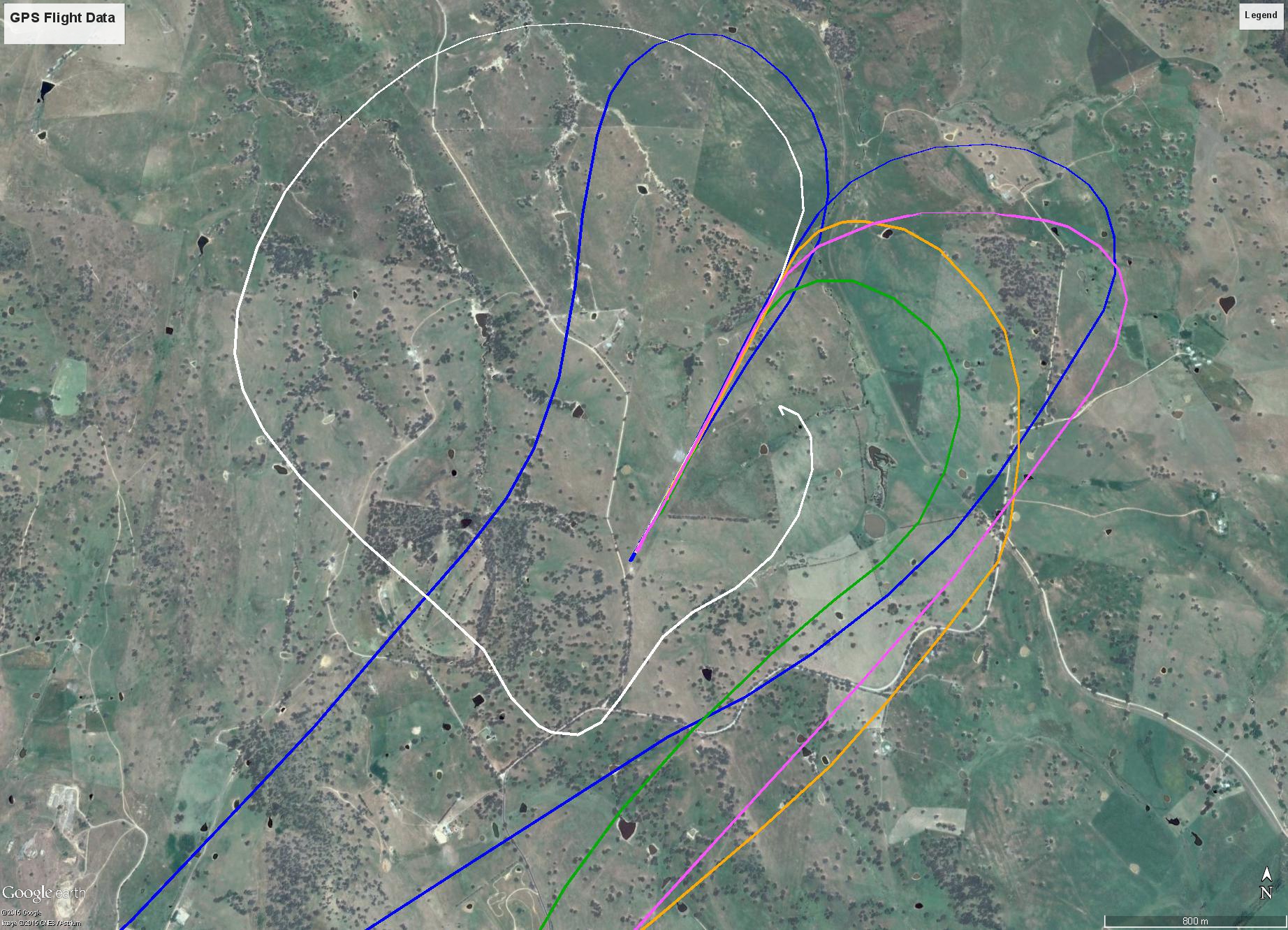
The GPS unit found in the wreckage contained data for a number of flights. These recorded flights were consistent with reports and observations of flights that the pilot conducted in CTE. The data included the accident flight. The flight recordings identified that the pilot would depart the Adelong airstrip to the north-east before turning left and setting heading for Holbrook. For the return legs, the pilot would position the aircraft for a left hand circuit to land to the south-west. A comparison of the recorded circuits for landing at the Adelong airstrip is at Figure 4. The flight profiles are for flights that departed Holbrook and landed at Adelong, with the following exceptions:
the accident flight (white)
a flight that departed Adelong and then turned back to the Adelong airstrip from a position near Holbrook (blue).
Figure 4: GPS flight data with accident flight shown as the white track
Source: Google earth modified by ATSB.
The data for the accident flight was analysed to determine the aircraft’s flight profile. The data is presented at Table 1 and graphically presented in Figure 5. The following conditions and limitations apply to this data:
There was no vertical component (altitude) in the GPS data.
The positional data with associated time enables ground speed to be determined. The actual airspeed may be greater or lesser due to wind as well as any vertical component of the aircraft’s velocity vector.
The wind component is unknown, however, the meteorological data and local reports identify that the wind was probably calm.
The track, groundspeed and bank angle values are derived values based on the latitude/longitude and time data provided by the GPS.
Based on the GPS data, the estimated time of impact was at 0859:55.
Table 1: GPS data
Position Number
EST
Track (Degrees)
Ground speed (kt)
Bank Angle (Degrees)
1
08:59:42
18
62
11
2
08:59:47
358
62
20
3
08:59:51
330
57
28
4
08:59:54
295
54
19
5
08:59:55
283
29
42
6
09:04:46
155
0
0
Figure 5: Accident flight with final data points from Table 1
Source: Google earth modified by ATSB.
The aircraft’s maintenance logbook recorded the stall warning system as being set to activate at 45 knots indicated airspeed (KIAS). The builder stated that the aircraft stalled at about 40 KIAS. Table 2 contains data for the stall warning activation speed when the aircraft is in a level turn at various angles of bank.
Table 2: Stall speed for angle of bank
Angle of Bank (Degrees)
Airspeed KIAS
0
45
20
46
30
48
37
50
45
54
60
64
The following observations in relation to the accident flight are also of note. The ground speed for the majority of the flight was between 58 kt and 70 kt, except for the last 8 seconds of flight. The average angle of bank remained below 10°, except:
when the pilot turned towards the north-east onto a downwind heading, where the bank angle increased to just under 25°
during the last 13 seconds of flight.
Survivability
To assist an emergency response in the event of an accident, the Aeronautical Information Publication Australia, En Route section 1.10 paragraph 2.11 stated the criteria under which a VFR flight was required to submit flight notification. That requirement could be met through the notification of SARTIME[2] to Air Traffic Services, or the use of a Flight Note. For the accident flight, the pilot was not required to and did not notify a SARTIME, or leave a Flight Note.
In addition, the aircraft was not equipped with an emergency locator transmitter (ELT), nor did the pilot carry an approved substitute for the ELT. The carriage of an ELT or substitute was not required.
The accident was not considered to have been survivable due to the magnitude of the impact forces during the collision with terrain.
Previous occurrences
ATSB research report AR-2007-043(2), published 26 March 2013 made the following conclusions in relation to amateur built aircraft accidents:
Between 1988 and 2010, amateur-built aircraft on the Australian VH-register had an accident rate three times higher than comparable VH-registered factory-built aircraft conducting similar flight operations.
The fatal and serious injury accident rate was more than five-times higher in amateur-built aircraft than similar factory-built aircraft.
Loss of aircraft control led to 25 per cent of all amateur-built accidents; slightly more than for factory-built aircraft accidents, however, the loss of control accident rate was over four times higher. Against factory built aircraft, serious injury was three times more likely after loss of control in amateur-built aircraft accidents. In respect of amateur-built aircraft, loss of control accidents were more likely to arise from aircraft handling issues where pilots had comparatively lower levels of experience on the aircraft type. Similarly, loss of control was more likely to occur in the initial climb phase of flight.
Amateur-built aircraft pilots involved with accidents were significantly more experienced overall than factory-built aircraft accident pilots. However, they were significantly less experienced on the aircraft type that they were flying at the time of the accident, compared to both pilots of factory-built aircraft accidents and amateur-built aircraft owners in general. Twenty per cent of amateur-built aircraft accident pilots had less than 10 hours experience on the accident aircraft type.
Engine failures and partial power loss occurrences were twice as likely in amateur-built aircraft accidents (accounting for 30 per cent of accidents) when compared with factory-built aircraft accidents.
This analysis will examine the operational and maintenance factors surrounding the accident. Evidence from the accident site as well as data from the pilot’s global positioning system receiver indicate that the pilot most likely lost control of the aircraft while approaching to land back at the Adelong airstrip. The pilot was unable to recover the aircraft before colliding with the ground. The departure from controlled flight was consistent with a probable aerodynamic stall. The analysis will consider the development of circumstances that preceded that event.
Partial engine failure
Shortly after departing the Adelong airstrip, the pilot turned back towards the airstrip. The turn back was probably the result of the loss of power caused by the ejection of the number three cylinder upper spark plug. While the engine manufacturer indicated that the ejection of a spark plug would result in a loss of power in the order of 30 per cent, the investigation was unable to determine whether any power was available to the pilot post the engine failure event. Analysis of the wreckage indicated that the engine was producing low or no power at impact.
The aircraft maintained a relatively stable ground speed during the return to land and manoeuvring onto downwind. It is probable that the aircraft was at a low altitude when it probably entered an aerodynamic stall as it turned towards the runway. The following evidence supports this conclusion:
the rapid speed loss during the last 8 seconds of flight, combined with
the short time duration from the point of rapid speed loss until the aircraft impacted terrain.
The recorded data, instrument witness marks, the aircraft’s impact attitude and finally the wreckage distribution are all consistent with the aircraft having entered an aerodynamic stall in the last seconds of the flight.
Unapproved modifications and maintenance
The pilot had reported that the aircraft was operating at high engine temperatures. The pilot attempted to correct the problem through self-diagnosis and maintenance action. However, the pilot did not have the requisite qualifications nor authorisation to conduct the necessary maintenance action to correct the reported temperature problems.
The attempt by the pilot to correct the temperature problem was not the only conduct of unauthorised maintenance or modifications on the aircraft. There is sufficient evidence to identify that the pilot also conducted a number of other unauthorised maintenance and modification actions on the aircraft, including the fitment of an electric trim system and the rigging of the aircraft wings and flight controls.
In addition, the aircraft’s maintenance release (MR) had expired almost 2 years prior to the accident flight.
There were a number of missed opportunities where qualified maintenance action could have identified and corrected the impending failure of the number three cylinder upper spark plug mount. These opportunities were the conduct of regular MR maintenance action, as well as specific maintenance action to address the engine temperature issues. The pilot's decision not to have qualified engineers perform maintenance action on the aircraft prior to the accident flight therefore likely contributed to the partial engine failure that triggered the accident sequence.
Flight notification
The pilot did not use a recognised method of flight following, or search and rescue alerting through the use of an emergency locator beacon or recognised substitute. This resulted in significant delays before the authorities were notified that the pilot was missing, and search and rescue action initiated. However, due to the significant impact forces evident from the aircraft’s collision with terrain, these factors did not affect the survivability of the accident.
Currency and qualifications
The pilot had not completed the required aeroplane flight review within the requisite period before the flight. Nor had the pilot obtained the required endorsements to command an aircraft of the KR-2 type with retractable undercarriage and tailwheel. The pilot held a pilot’s certificate to operate a similar type of aircraft using the Recreational Aviation Australia (RA-Aus) based system. The pilot also had considerable experience in similar types of aircraft under the RA-Aus system before the accident. Therefore, the pilot’s lack of qualification and experience were not determined to have contributed to the accident; however, these matters were significant breaches of the Civil Aviation Regulations.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot’s family members
previous aircraft owner/builder
the engine manufacturer
other pilots
NSW Police Force
State Coroner of NSW.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority and the previous aircraft owner/builder.
Submissions were received from the previous aircraft owner/builder. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
At about 0855 Eastern Standard Time[1] on Saturday, 5 October 2013, the pilot and owner of a Rand Robinson KR-2, registered VH-CTE (CTE) took off from an airstrip on private property near Adelong and 12 km west of Tumut, New South Wales (NSW). Reports stated that the pilot intended to fly to Holbrook, NSW, for the weekend. The pilot was due to return home on the evening of Sunday, 6 October. Holbrook is 89 km to the south-west of the departure airstrip.
The pilot’s family reported the pilot missing early on the evening of 6 October. A search commenced, but was suspended due to darkness without locating the pilot or the aircraft. On recommencing early the following morning, the wreckage of the aircraft was found about 450 m east-north-east of the airstrip. The pilot was located in the aircraft wreckage and was fatally injured. The aircraft was destroyed by impact forces. There was no fire.
A portable Garmin Pilot III global positioning system (GPS) satellite navigation receiver was found in the wreckage. The GPS held recorded data for a number of flights, including flight path data for the day of the accident (Figure 1). The accident data started at 0853:21. It recorded the aircraft departing the airstrip towards the north-east before turning left onto a south-westerly heading. At a point adjacent to the downwind threshold of the airstrip the aircraft turned left 90° and tracked south-east. The aircraft then turned left again to make what appeared to be a close-in left downwind leg. This appears consistent with positioning to land toward the south-west, the opposite direction to that used for the take-off. The data showed that in the last 20 seconds of the flight, the aircraft’s groundspeed was steady at about 63 kt before rapidly decreasing during the final left turn. The recorded data indicated that the aircraft impacted terrain at about 0900.
From the evidence available, the following findings are made with respect to the loss of control following partial engine failure involving the amateur-built Rand Robinson KR-2, registered VH-CTE that occurred near Tumut, New South Wales on 5 October 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Shortly after take-off the number three cylinder upper sparkplug was ejected from the cylinder head hole, resulting in a significant loss of engine power. This failure was the result of an incorrectly installed spark plug thread insert.
While positioning VH-CTE for a return landing onto the departure airstrip after the power loss, the aircraft probably entered an aerodynamic stall from which the pilot was unable to recover before the aircraft impacted terrain.
The pilot's decision not to have qualified engineers perform maintenance action on the aircraft, both with respect to regular maintenance action as well as corrective maintenance action regarding engine overheating problems, represented missed opportunities to identify and correct the impending failure of the number three cylinder upper spark-plug mount.
Other factors that increased risk
During the period that the aircraft was owned by the accident pilot, there were a number of unauthorised modifications and maintenance actions carried out on VH-CTE. None of these maintenance actions were recorded in the aircraft’s maintenance documentation.
The pilot did not use a recognised method of flight notification or search and rescue alerting, resulting in significant delay before authorities were alerted that the pilot was missing.
The pilot had not completed an aeroplane flight review within the requisite period before the flight, and was not endorsed to fly an Australian registered aircraft with tailwheel or retractable landing gear.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 15 September 2013, the pilot of a Robinson R44 helicopter, registered VH-NUZ, was flying passengers on a private scenic flight over the Montgomery Reef and Buccaneer Archipelago area of Western Australia. The pilot had completed several take-offs and landings at that site already on the day.
After a routine landing at the reef, the pilot shut down the engine. The passengers had disembarked and were standing about 20 to 30 m away.
At about 1530 Western Standard Time the pilot, who was the sole occupant, then started the helicopter’s engine and completed the pre-flight checks. When the pilot raised the collective to bring the helicopter into a hover, it suddenly rotated three times while airborne. The pilot could not regain control and elected to land immediately, however the helicopter landed heavily. The pilot shutdown the engine and exited the helicopter.
The direction that the helicopter rotated could not be ascertained by the pilot or witnesses. The pilot and bystanders were not injured but the helicopter sustained substantial damage as a result of the hard landing.
Based on the information provided, the Australian Transport Safety Bureau (ATSB) was unable to determine what led to the loss of control.
During the investigation, the ATSB was made aware that instances of ‘sudden and violent yawing in forward flight’ had occurred on other ‘low time’ R44 helicopters, being attributed to a ‘sticky inlet valve’, with no recurrence after maintenance rectification.
There were no Service Difficulty Reports (SDR) regarding this issue in the Civil Aviation Safety Authority’s SDR database, making it difficult to pursue this line of enquiry.
The ATSB encourages reporting of occurrences to the ATSB and defects to CASA to allow for continued improvements to aviation safety.