Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
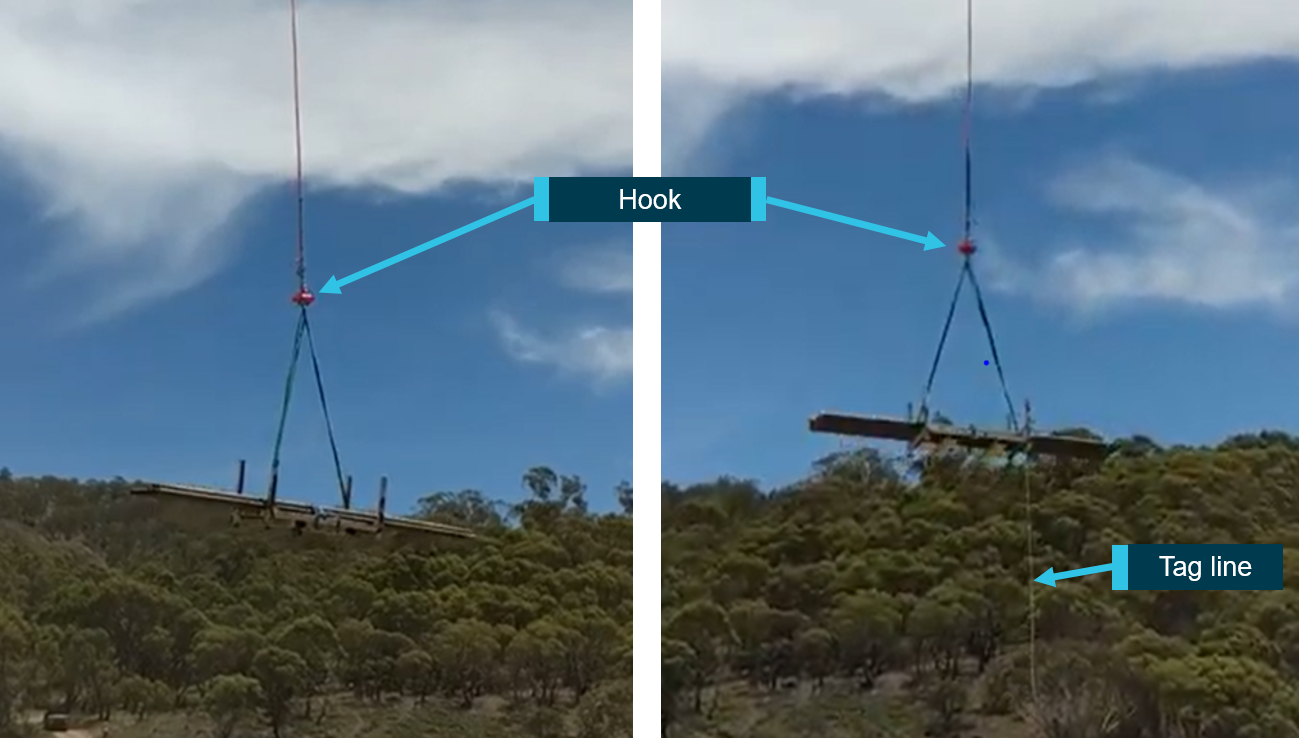
At around 1209 local time on 14 October 2025, a Eurocopter AS350, with only the pilot onboard, was carrying an externally slung load between 2 sites in regional Western Australia, located approximately 6 km apart. The load weighed around 800 kg, and was secured using 4 strops, each rated to carry 3,000 kg.
The helicopter was transiting at around 60 kt, about 1,000 ft above ground level. Approximately midway through the flight, with the load stable, the pilot heard a sudden loud thud and felt the helicopter vibrate. At the same time, without the pilot’s command, the helicopter pitched forward into a nose down attitude. The pilot attributed this to a large change in the aircraft’s centre of gravity. In response, they immediately jettisoned the load, which restored full control of the helicopter. The pilot continued the short flight to the intended destination and landed without further incident.
The jettisoned load was later located and inspection revealed that one of the lifting strops had been severed by jagged metal material contained in the load. This resulted in a sudden and significant shift in the load’s orientation beneath the helicopter, leading to the uncommanded pitch change.
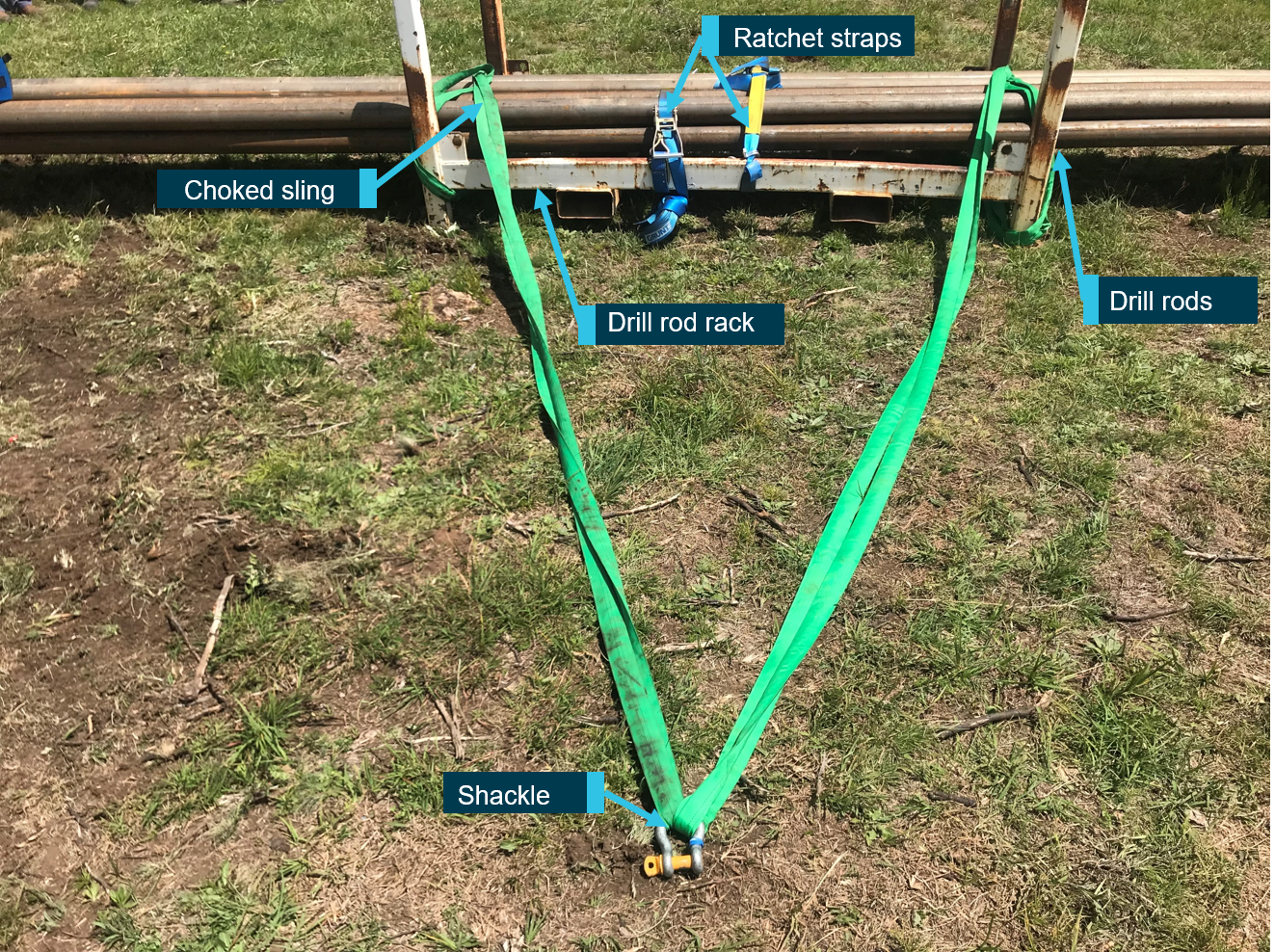
Figure 1: Load and lifting strop condition post-occurrence
Image shows the load as it was found after being jettisoned and the condition of the severed lifting strop. Source: aircraft operator
Safety action
The operator has initiated a review of its risk assessment for sling load activities, which will incorporate information learned from this occurrence. It also produced internal recommendations to avoid loads from shifting in flight or damaging lifting equipment including:
using protective measures, such as rubber matting or edge protectors, wherever slings contact sharp or potentially abrasive surfaces
testing the structural integrity of loads prior to lifting, including an inspection process for loads that may have structural weaknesses, fatigue, or brittle components.
Safety message
This incident highlights the importance of detailed consideration when preparing external loads for lifting. The nature of aerial construction/deconstruction work can make it difficult for pilots to conduct a detailed inspection of the prepared load prior to each lift operation. Operators are encouraged to ensure effective risk control processes are in place for load preparation, especially with irregularly shaped loads. On this occasion the flight was operating in a remote area and the consequence of jettisoning the load was relatively benign. However, falling loads have the potential to cause catastrophic/fatal outcomes, and the risk must be appropriately mitigated.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 21 October 2025, a Robinson R22 helicopter with one pilot on board was conducting a private flight from Jimboomba to Southport, Queensland.
Prior to departure, the pilot loaded a box of freight, approximately 1,000 mm long, 350 mm wide and 400 mm deep, weighing 10 kg, onto the passenger seat and secured it by wrapping the seatbelt around the box. The flight departed Jimboomba at 1033 local time with a flight time of approximately 12 minutes.
As the pilot turned onto the base leg for final approach to runway 01 at Southport, the box on the passenger seat shifted and interfered with the cyclic[1] control resulting in the helicopter being unable to turn left. The helicopter then veered to the right and as the pilot focused their attention on moving the box, they lost control of the helicopter which came into contact with trees before colliding with terrain, resulting in substantial damage (Figure 1). The pilot sustained serious injuries in the accident.
Figure 1: Post-impact damage
Source: Queensland Police, annotated by the ATSB
Safety message
Pilots must adhere to CASA Regulation 91.610 (2) (b) Carriage of cargo – unoccupied seats, which states that the cargo, and the means of restraint of the cargo, must not interfere with the safe operation of the aircraft.
The ATSB has had 3 occurrences reported in a 15-year period involving Robinson R22 helicopters carrying cargo on the passenger seat which has interfered with the helicopter’s flight controls. All 3 of these occurrences resulted in a collision with terrain and substantial damage.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-057
Occurrence date
21/10/2025
Location
Southport Aerodrome
State
Queensland
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Flight control systems, Loading related, Loss of control, Unrestrained occupants/objects
On 29 May 2025, a Cessna 310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was conducting a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory. On board were the pilot and 4 passengers.
During the approach at Lake Evella Aerodrome, recorded data indicated that the aircraft touched down just prior to halfway along the runway. The pilot subsequently applied braking, but the aircraft did not decelerate as expected. This resulted in a runway excursion and the aircraft subsequently collided with a perimeter fence which substantially damaged the left wing. The pilot and 4 passengers were uninjured.
What the ATSB found
The ATSB found that the pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in the aircraft floating during the landing flare for a prolonged period in ground effect, and a landing beyond the planned touchdown point. After the aircraft touched down, the pilot subsequently commenced braking about halfway along the runway. The long landing reduced the available distance to decelerate on the runway.
At the aircraft’s landing weight, the remaining runway length should have provided sufficient stopping distance, but degraded braking capacity meant the aircraft could not be stopped before the runway end and it subsequently departed the runway.
During a scheduled maintenance event prior to the occurrence, a licensed aircraft maintenance engineer believed an apprentice had replaced the main-wheel brake pads. An inspection after the occurrence found that the right brake reservoir was empty and that the right pads were worn beyond limits, which reduced braking capacity on that side.
The ATSB also identified that the operator’s procedures allowed the use of self-reported passenger weights without additional allowances, and that the electronic weight and balance system had been configured with higher maximum weights applicable to a modification not fitted to this aircraft. In combination with calculation errors on the day, this resulted in the aircraft being operated above the maximum permitted ramp and take‑off weights.
What has been done as result
Marthakal Yolngu Airline advised that all references to the use of self-reported passenger weights for the purposes of weight and balance calculations will be removed in the next amendment of the operations manual.
The operator also advised that the electronic weight and balance system will be amended to reflect the correct maximum weights for VH-NXA prior to its return to service.
The safety manager briefed company personnel about the proposed changes and advised existing pilots that actual weights for passengers must be used for all flights.
The ATSB will monitor these safety actions until the proposed changes to the operations manual and weight and balance system have been formally implemented.
D & T Aircraft Engineering advised that, following the occurrence, a debrief with maintenance personnel highlighted the importance of increased vigilance during inspections conducted after maintenance tasks, and that the organisation also identified opportunities to improve internal processes following similar occurrences.
Safety message
Factors such as additional airspeed over the threshold can result in a landing beyond the intended touchdown point, increasing the risk of a runway overrun excursion. While adherence to a pre-determined stabilised approach criteria can effectively mitigate such risks, pilots should always exercise vigilance and ensure the aircraft is flown within the assumed conditions used to calculate landing performance.
Pilots are therefore encouraged to continue to actively monitor the flight path using cockpit instrumentation and external visual cues until a safe landing is assured. This should include identifying and nominating an appropriate touchdown point on the runway to ensure a go‑around can be executed if a touchdown beyond this point is likely to occur.
Additionally, maintenance organisations should ensure that effective systems are in place to disseminate important information to all maintenance personnel, so that emerging defects are identified and rectified before they affect flight operations.
The occurrence
Pre-flight preparation
On the morning of 29 May 2025, a Cessna C310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was being prepared for a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory.
When the pilot arrived at the airport, they observed a licensed aircraft maintenance engineer (LAME) and their apprentice performing maintenance on the aircraft braking system. During this period the pilot prepared their flight plan and when they returned to the aircraft, the LAME and the apprentice had completed the maintenance.
The pilot, who was operating their first flight as pilot in command of a multi-engine aircraft, commenced their pre-flight checks. Due to the recent work on the braking system, they taxied to an aircraft bay to conduct a static engine run-up.[1]
With both engines at 1,700 RPM, they recalled that the aircraft moved forward slightly with the brakes applied. They physically increased their braking pressure, after which, the aircraft remained stationary. After completing the run-ups, the pilot taxied back to the terminal where the passengers were waiting. At this time, they also discussed the brakes with another C310 pilot who advised them that quite a lot of brake pressure was required during run-ups.
The pilot reported feeling rushed, and elected to use the self-reported passenger and baggage weights prior to boarding for weight and balance calculations, which were recorded on the manifest. These weights were entered into an electronic weight and balance system, which indicated that the planned load complied with the aircraft weight and balance limitations. The passengers were then taken to the aircraft where the pilot conducted a safety briefing before they boarded.
Occurrence flight
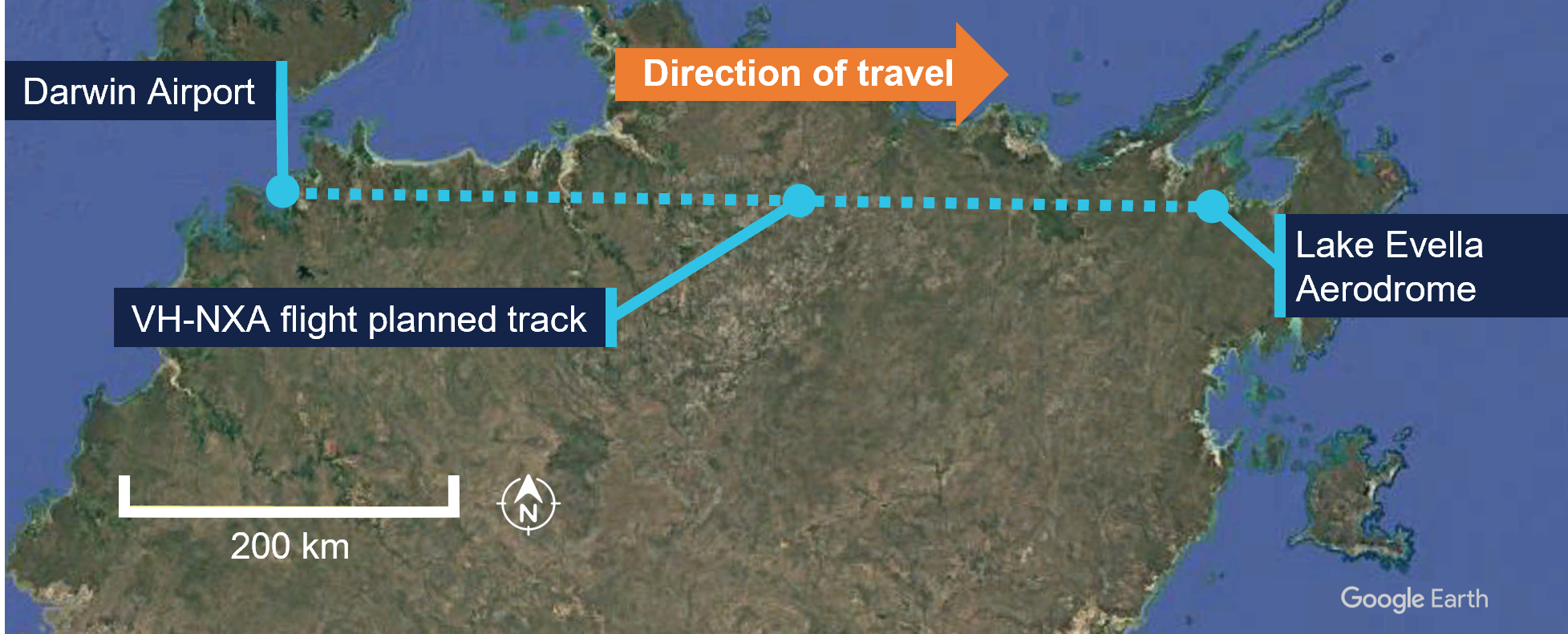
At 0857 local time, VH-NXA departed from Darwin Airport with the pilot and 4 passengers on board for Lake Evella (Figure 1). When approaching the Lake Evella Aerodrome, the pilot reported becoming visual with runway 08 at about 15 NM (28 km) and tracked for a straight in approach. At 1051, the aircraft was established on final approach for runway 08.
Figure 1: VH-NXA flight planned track
Source: Google Earth, annotated by the ATSB
The pilot recalled that there was a south-easterly wind between 8–10 kt for the approach, with a right crosswind component. Another pilot, who arrived at Lake Evella about 3 minutes after VH-NXA, recalled the wind was from an easterly direction at about 10 kt.
The pilot of VH-NXA recalled that the approach ‘seemed stable,’ (see Stabilised approach criteria) and stated that they generally used the runway threshold as their aiming point. They estimated crossing the threshold at their calculated approach speed of 90 kt or ‘just above.’
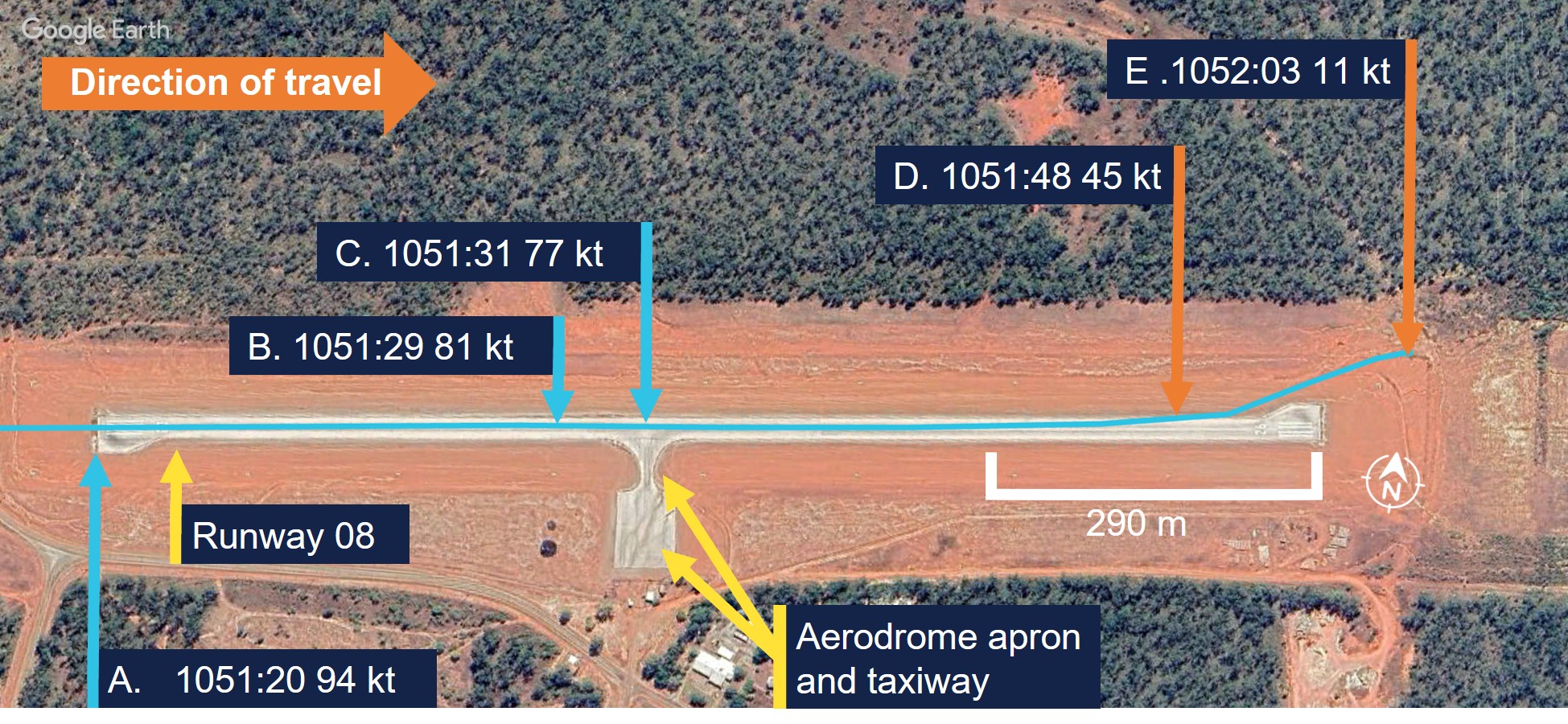
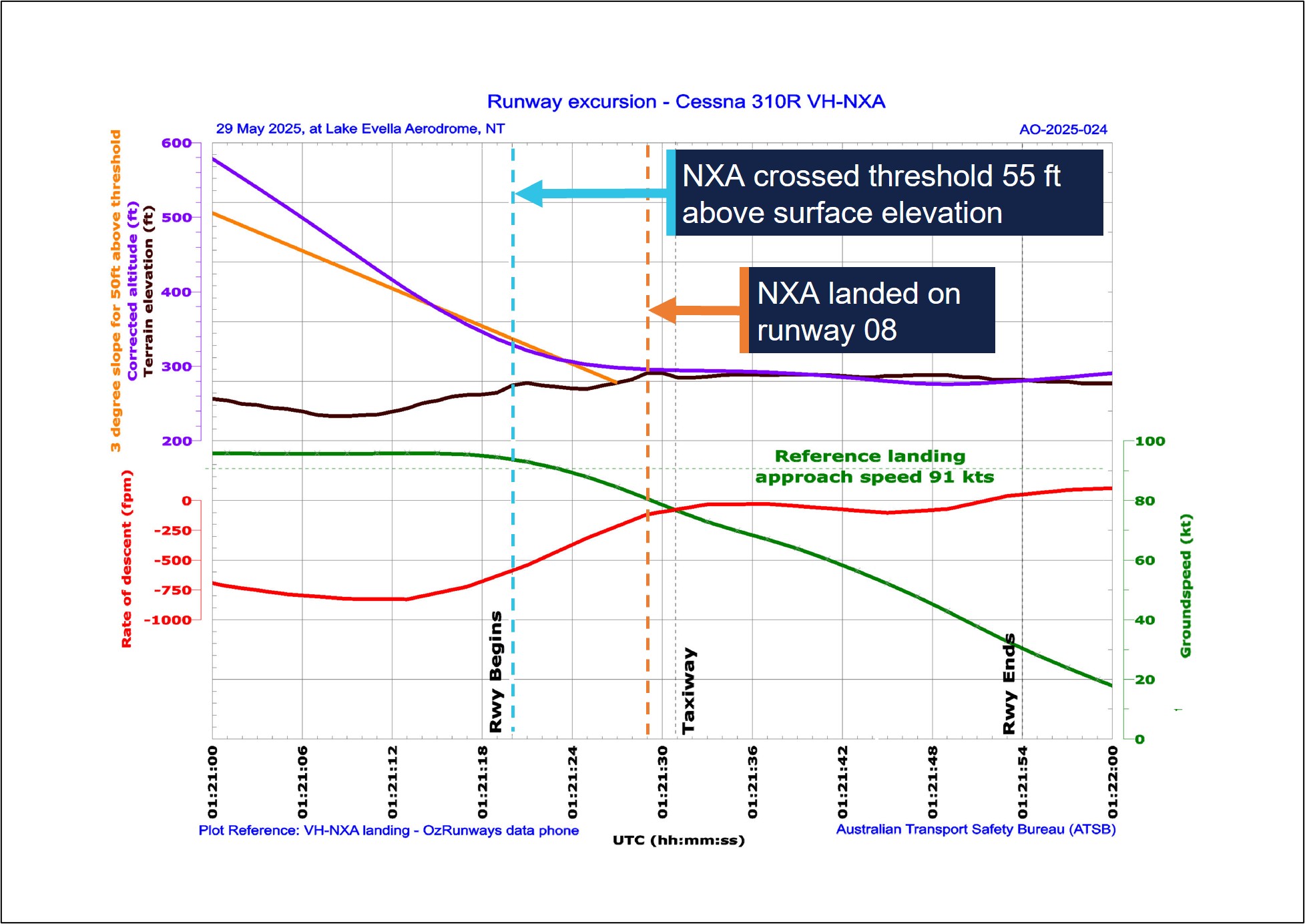
A navigational application (OzRunways) [2] was installed on a tablet computer and an Android phone on board the aircraft and broadcast flight data (see Recorded information). The OzRunways data taken from the Android phone, overlaid on a Google Earth image (Figure 2), showed the aircraft crossing the runway threshold at a height of 55 ft with a ground speed of 94 kt (Figure 2, A). The runway in Lake Evella was not equipped with visual slope guidance and the pilot relied on their visual assessment of ‘how the runway should look at certain height.’
Figure 2: VH-NXA ground speed at key points in landing sequence
Source: Google Earth, annotated by the ATSB
The pilot and the passenger seated directly behind them estimated that the aircraft touched down approximately 200 m past the threshold. ATSB analysis of recorded data indicated touchdown at 1051:29 (the corrected altitude of the aircraft matched the terrain elevation of runway 08), which was 402 m past the threshold (Figure 2, B). The passenger seated in the front row beside the pilot recalled passing the taxiway immediately after touchdown (Figure 2, C).
Another pilot on the ground standing at the apron who witnessed the landing reported observing VH-NXA a few feet above the ground in the ‘flaring attitude’ about a third of the distance along the runway. They also recalled that the aircraft was travelling faster than what they thought was normal and landed just beyond the taxiway (Figure 2, C).
The pilot reported that after touchdown, they applied the brakes passing the apron area about halfway along the runway (Figure 2, C). At that point, they reported that the aircraft did not appear to be slowing as expected and the passenger in the last row recalled the aircraft passing the apron ‘very fast’.
The pilot recalled increasing their braking pressure and when they saw the end of the runway approaching, they shut both engines down by selecting the mixture controls to idle cut-off. The pilot then elected to steer the aircraft to the left of the runway centreline to increase the runway distance for the deceleration required.
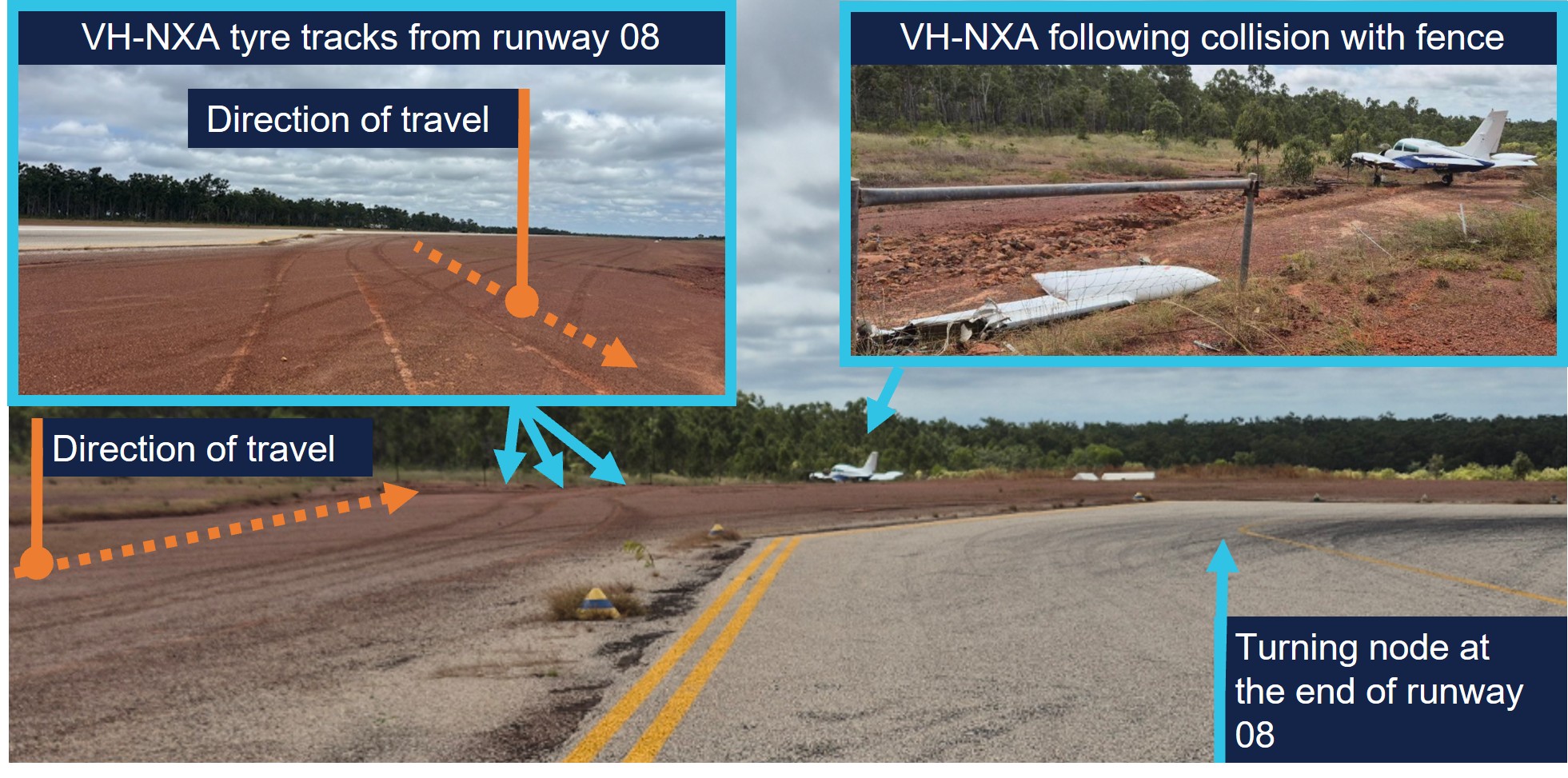
The aircraft departed the left side of the runway, 118 m from the runway end (Figure 2, D) (Figure 3, inset left), while the passenger seated beside the pilot verbally prompted the passengers to ‘brace.’ Recorded data indicated the aircraft was travelling at 45 kt at this point. The left wing subsequently collided with a fencepost (Figure 2, E) (Figure 3, inset right) located 193 m from the point the aircraft departed the runway.
Figure 3: VH-NXA ground roll following runway excursion
Source: Marthakal Yolngu Airline, annotated by the ATSB
Following the collision, the aircraft came to a stop and the pilot and passengers disembarked through the right cabin door. There were no injuries to the pilot or passengers, however the aircraft sustained substantial damage (see Post-accident inspection).
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) issued in 2021 and a class 1 aviation medical certificate. They also held a multi-engine aircraft class rating, which was issued in 2022 and renewed with a flight training organisation on 24 May 2025.
The pilot had accumulated 1,066 hours of total aeronautical experience, which included 71 hours of multi-engine time accumulated under the supervision of an instructor.
They reported they had flown about 70 hours in the last 90 days, including a total of 11.7 hours on the Cessna C310R, which was conducted during the course of their training.
The pilot’s training was conducted by a flight training organisation (FTO) in Darwin, on behalf of Marthakal Yolngu Airline. FTO training records detailed that the pilot commenced line training for the C310R on 15 May 2025.
This line training took place over 9.8 flight hours, after which they were assessed as proficient by a flight examiner during a combined line check and operator proficiency check for the C310R on 24 May.
The pilot had not operated the C310R to Lake Evella Aerodrome during the course of their training and had not operated there in any aircraft type prior to the occurrence. They reported sleeping about 8 hours the night before the occurrence and had been awake for about 7 hours at the time of the occurrence and feeling ‘fully alert.’
Aircraft information
The Cessna 310R is a twin-engine, low-wing (with a wingspan of 11.3 m), 6-seat, unpressurised aircraft equipped with retractable landing gear and powered by 2 Continental IO-520 piston engines. VH-NXA was manufactured in the United States in 1978 and first registered in Australia in 1989. A maintenance organisation located in Darwin became the registration holder on 4 March 2020.
Braking system
Section 7 of the Cessna 310R Pilots operating handbook (POH) contained the following description of the braking system:
The airplane is provided with an independent hydraulically actuated brake system for each main wheel. A hydraulic master cylinder is attached to each pilot’s rudder pedal. Hydraulic lines and hoses are routed from each master cylinder to the wheel cylinder on each brake assembly. No manual adjustment is necessary on these brakes. The brakes can be operated from either pilot’s or co-pilot’s pedals.
Meteorological information
The graphical area forecast and the applicable grid point wind and temperature forecast for the flight indicated:
prevailing visibility greater than 10 km
scattered cloud[3] with bases 1,500 ft above mean sea level (AMSL)
isolated areas of smoke reducing visibility to 5,000 m
isolated rain showers and thunderstorms reducing visibility to 2,000 m and 1,000 m respectively, and broken cloud with bases 800 ft above AMSL
moderate turbulence below 4,000 ft in thermals and dust/sand whirls (dust devils)
wind 130° at 21 kt and temperature of 24°C at 1,000 ft above AMSL.
Aerodrome information
Lake Evella Aerodrome (YLEV) is situated at an elevation of 278 ft AMSL and comprised of a single sealed runway, 08/26, measuring 1,065 m in length and 18 m in width and was sloped 0.5% up toward the east. The aerodrome is uncontrolled and operated on a dedicated CTAF,[4] and is subject to animal hazards.
Maintenance information
Aircraft maintenance manual
The Cessna 310R Aircraft maintenance manual (AMM) contained a troubleshooting guide to assist maintenance personnel to rectify defects relating to systems fitted to the aircraft. The section that covered the wheels and brakes included the following information (Table 1):
Check for brake linings worn beyond limits. Replace linings as required
Air in brake system
Check for air trapped in brake system. Bleed the brakes
Brakes spongy
Air in brake system
Check for air trapped in brake system. Bleed the brakes
The AMM also described the brake wear limits on the C310R, which included:
Check back plate and pressure plate linings for wear. If worn to a thickness of 0.125 to 0.100 inch, the linings should be replaced.
Scheduled maintenance
The aircraft was flown to Darwin on 15 February 2025, where the authorising licensed aircraft maintenance engineer (LAME) planned to conduct a corrosion inspection at their maintenance facility. The LAME also performed a ‘check 1’ inspection, which they stated was the equivalent of a 100-hour inspection.
During the inspections, additional maintenance was conducted due to leaking brake callipers, which was common to the brakes on the C310 according to the LAME. This involved the removal, bleeding, resealing and refitting of both callipers and was performed by an apprentice. It was also the LAME’s expectation that the brake pads would be replaced during this maintenance task because this was routine practice, although not in the procedure.
As part of the 100-hour inspection, the LAME performed an engine run-up and observed the aircraft did not hold under brakes at this time. Believing that they had been replaced, they believed that the new brake pads needed to be bedded or burnt in. The AMM stated ‘brake burn in is required to minimize glazing of the friction surfaces’ when new brakes are installed. They subsequently completed the engine run up on one engine at a time, which allowed the aircraft to remain stationary.
Following the completion of the inspections and associated maintenance tasks, including the additional work carried out on the brakes, the LAME certified the aircraft maintenance logbook on 26 May 2025.
The authorising LAME later stated that new brake pads should have been installed before the callipers were refitted to the landing gear, however they did not verify that this had occurred. They reported that the brake pads were last changed on 15 December 2023 and had 494 landings prior to the occurrence.
Pre-departure maintenance
The aircraft underwent a post‑maintenance verification flight the day prior to the accident flight, with a flight instructor and the occurrence pilot as an observer. After the flight, the instructor advised the LAME by text message that the brakes felt ‘spongy.’
On the morning of 29 May, prior to the accident flight, the LAME checked the aircraft brakes, reporting that they were acceptable, even though the brake pedal travel felt more than usual. The decision was made to bleed the brakes to remove any air or water in the brake lines and top up the brake fluid. With assistance from an apprentice during this process, the LAME reported that hydraulic fluid spilled onto the right tyre and was subsequently wiped down. The aircraft was then released back to service.
Post-accident inspection
Following the occurrence, the LAME inspected the aircraft at Lake Evella Aerodrome on 18 June 2025 and documented the aircraft damage. The aircraft had sustained significant damage to the left wing (Figure 4), which separated from the fuselage outboard of the left engine nacelle. The pitot tube, right tip tank, propeller and nose gear door were also damaged following the runway excursion.
Figure 4: VH-NXA damaged left wing
Source: Aircraft maintainer, annotated by the ATSB
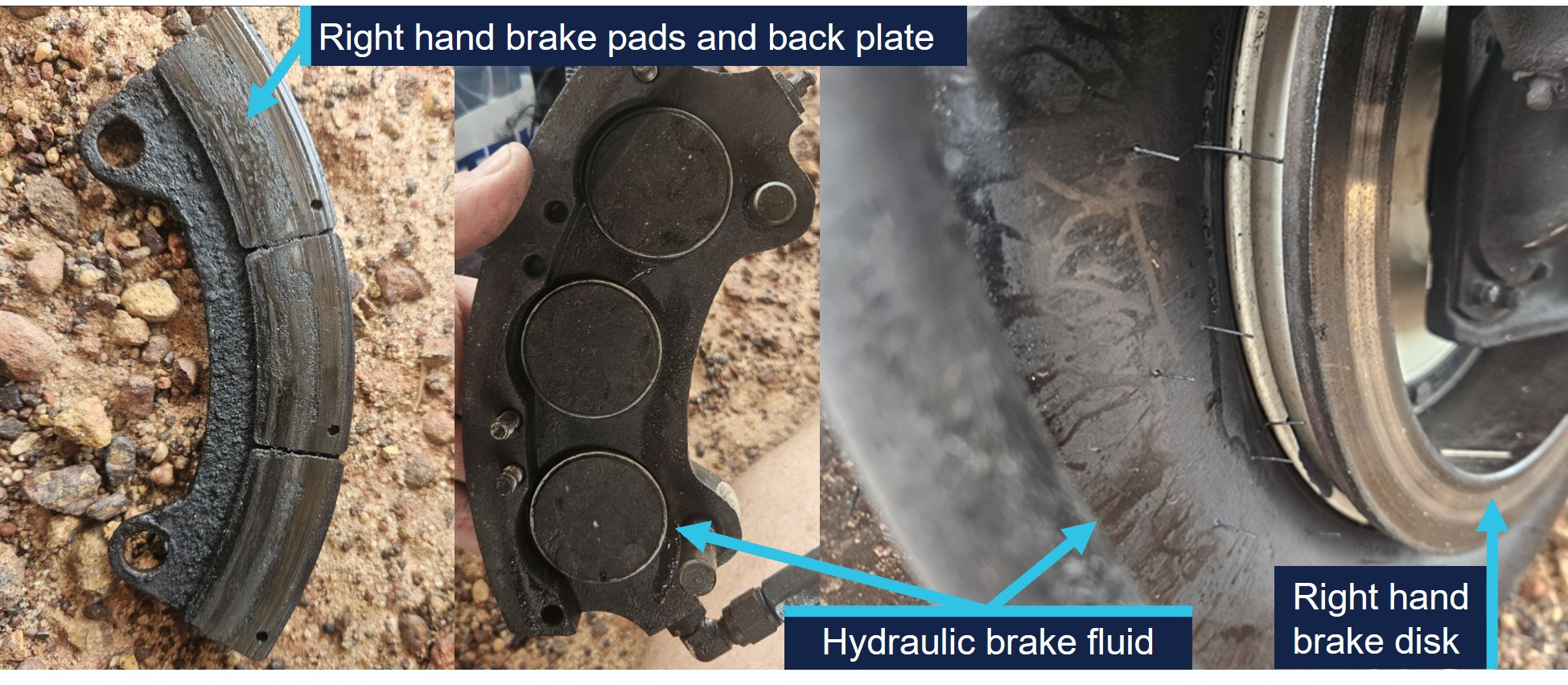
The LAME found that the right brake reservoir was empty, with evidence of hydraulic fluid leakage on the right tyre, however stated that the right brake disc was serviceable.
They identified that the right brake pads were ‘heavily worn.’ Images supplied by the LAME also indicated the presence of hydraulic brake fluid, originating from the brake piston adjacent to the brake line (Figure 5). They also indicated that the hydraulic fluid on the tyre may have been from fluid spilling when the brakes were topped up on the morning of the occurrence flight.
Figure 5: VH-NXA right hand brake components and hydraulic brake fluid
Source: Aircraft maintainer, annotated by the ATSB
No defects were identified on the left brake system and the right brake calliper was removed and tested in Darwin by the LAME. The right brake calliper was bolted onto a brake disc with sufficient pressure applied to prevent calliper movement. After 13 days, sufficient hydraulic fluid had leaked, which allowed the calliper to be moved in relation to the brake disc. The LAME subsequently disassembled the right brake calliper and identified a ‘very small’ hydraulic fluid leak, which they did not consider was the cause of the fluid loss during the occurrence.
Operational information
Weight and balance
The operator’s standard operating procedures(SOP) stated that during the conduct of air transport operations, prior to each sector, the pilot in command must complete an aircraft load and trim sheet.
An operator‑approved electronic load sheet was available to pilots for the purpose of completing weight and balance calculations in accordance with the POH weight and balance limitations.
The operator’s Cessna 310R Flight crew operating manual (FCOM) included the following statement regarding the possible modification of company operated aircraft:
The Company operates C310R aircraft in several possible modification states, which may affect limiting weight.
The only modification listed in the FCOM that affected the weight limitations for VH-NXA was the fitment of a vortex generator (VG)[6] kit. The FCOM also contained information relating to the fitment of the VG kit including increased weight limitations, changes to various airspeeds and stated:
If less than 84 vortex generators are in place or undamaged, the aircraft must be operated in accordance with the original AFM performance data (ie nil VGs).
Electronic weight and balance system
The electronic weight and balance system was developed by a third party to calculate the weight and balance for each flight. In the system, each aircraft was configured with a weight and moment arm[7] when empty.
The pilot would enter the pilot and passengers’ weights, their seating positions and fuel to calculate both the weight and centre of gravity of the aircraft at take-off and landing. The system was designed to alert the user if any weight and balance limitations were exceeded.
For VH-NXA, the electronic weight and balance system incorporated an increase in weight in accordance with a supplemental type certificate number for a C310R VG modification. However, the maintenance organisation that owned and maintained the aircraft stated that VH-NXA had not been fitted with the VG modification, and they were not aware of any modifications that increased the standard maximum permitted weights as prescribed in the POH.
As a result, the weight and balance system contained the following increases to the standard POH weight limitations which were not applicable to the aircraft (Table 2):
Table 2: Cessna 310R maximum weights
POH limitation
Standard weight (kg) applicable for VH-NXA
C310R with VG kit (kg) as listed for VH-NXA
Maximum zero fuel weight
2,222
2,386
Maximum ramp weight
2,510
2,586
Maximum take-off weight
2,494
2,563
Maximum landing weight
2,449
2,449
Passenger-declared weights
The operator’s SOP stated that for the purposes of calculating the aircraft’s weight and balance, ‘passenger weights must be actual, or self-reported.’ Following the occurrence, a passenger reported that their body and baggage weights were requested without the use of a calibrated scale. The pilot did not indicate that any adjustments of additional amounts were applied to the passenger reported weights.
The CASA multi-part AC 121-05, AC 133-04 and AC 135-08 – Passenger crew and baggage weights, described acceptable weight calculation methods that could be defined in operating procedures. The circular stated that:
The use of actual weights is the most accurate method of maximising payload capacity. Appropriately calibrated weighing scales should be used. Actual weighing is more commonly used by Part 133 [helicopter passenger transport] and 135 [smaller aeroplane passenger transport] operators. This is, in part, due to the smaller number of passengers being carried, which makes this option less disruptive than it is for Part 121 [larger aeroplane passenger operations] operators.
Operators should have procedures to identify when passenger-declared weights are not appropriate, such as when operating close to limitations. Under these circumstances, the use of actual weights may be required to ensure limitations are not exceeded.
Passenger-declared weights have inherent inaccuracies as passengers may not know their actual weight, especially when fully dressed. An adjustment allowance should be added to any passenger-declared weight, as a factor or a fixed additional amount.
Weight and balance calculations
Following a review of documentation provided by the operator and pilot, the ATSB identified several discrepancies contained in the operational documentation from the day of the occurrence.
The passenger and baggage weights recorded in the manifest by the pilot indicated a combined weight of 387 kg. However, the corresponding load sheet indicated a combined passenger and baggage weight of 337 kg (excluding the pilot).
Additionally, the fuel plan prepared by the pilot indicated a total fuel figure of 441 kg. By comparison, the fuel figure on the load sheet was recorded as 432 kg.
Due to the identification of the combined discrepancy of 59 kg, the ATSB recalculated the aircraft’s weight and balance for the flight. This identified the following updated weights and exceedances (Table 3) prescribed in the POH for aircraft not fitted with a VG kit.
Table 3: VH-NXA calculated weights and exceedances
Item
POH weight limitation (kg)
Pilot-calculated weight (kg)
ATSB-calculated weight (kg)
ATSB-calculated exceedance (kg)
Zero fuel weight
2,222
2,087
2,137
Nil
Ramp weight
2,510
2,519
2,578
68
Take-off weight
2,494
2,510
2,569
75
Landing weight
2,449
2,339
2,367 [1]
Nil
[1] The re-calculated landing weight was based on pilot reported fuel remaining added to the ATSB calculated zero fuel weight.
Landing performance calculations
The operator’s SOPs stated that company aircraft are subject to the requirements of Civil Aviation Safety Regulations Part 135 Manual of Standards (MOS) with respect to take-off and landing performance requirements. Chapter 10 of the Part 135 MOS stipulated ‘that the aeroplane crosses the runway threshold at a height of 50 ft’ unless an approved short landing operation was being conducted. Additionally for landing, the FCOM stated that the reference landing approach speed (Vref)[8] should be achieved at 50 ft above the landing surface.
For aeroplanes, take-off and landing distance calculations to determine maximum take‑off weight or the maximum landing weight are achieved through a manual calculation using the limitations given in the POH for the specific aircraft type, taking into account:
environmental conditions
runway length.
The FCOM also required pilots to apply landing distance factoring of 1.20 for all calculations. The pilot stated they had calculated their landing performance based on the aircraft’s maximum landing weight and calculated a factored landing distance of 680 m on the flight plan with a Vref of 90 kt for their landing at Lake Evella.
Calculations using the ATSB recalculated landing weight and the estimated ambient conditions at the time of the occurrence determined that the required landing distance (with the 1.20 factoring) with a 50ft threshold crossing height was 659 m. This figure included a landing ground roll distance of 195 m and a corresponding Vref of 91 kt.
Stabilised approach criteria
The SOPs stated that, ‘unless the aircraft meets stabilised approach criteria at the specified altitude, a missed approach must be executed.’
A stabilised approach was described in the SOPs as an approach to land that met a number of criteria by 300 ft above the runway during a visual approach. These included the following:
• the aircraft is on the correct flight path
• only small changes in heading & pitch are required to maintain the correct flight path
• the aircraft speed is Vref to Vref +20 kt
• sink rate is not greater than 1,000 fpm or pre-briefed limits.
Recorded information
The pilot used a flight planning application (OzRunways) on an iPad and an Android phone for en route flight planning and navigation. The flight planning software provider was an approved source of electronic aeronautical charts, however the application could not be used as a primary means of GPS-based navigation as the iPad and Android phone GPS did not meet certification for aviation use. The pilot reported that the iPad was placed on the floor for the approach while the Android phone was in their chest pocket. By examining the combination of groundspeed and derived deceleration data, in addition to the best direct line of sight to satellites, it was assessed that the Android data had the highest positional accuracy.
The recorded data had limitations due to an altitude resolution of 100 ft, while filtering and adjustments were also applied to smooth the data and are known to affect the accuracy of small sections. Additionally, the altitude data of VH-NXA was corrected to match the terrain elevation during the landing ground roll (Figure 6).
Based upon the operator’s stabilised approach criteria, the decision to continue the approach, or conduct a go-around, became applicable by the time the aircraft reached 300 ft above the runway.
The following recorded parameters were observed from below 300 ft to the threshold:
the aircraft crossed the threshold of runway 08 at a height of 55 ft
aircraft speed remained within Vref to Vref +20 kt
sink rate (vertical speed) less than 1,000 fpm.
The recorded data indicated (purple line in Figure 6) that at the 300 ft (578 ft corrected altitude) stabilised approach gate, the aircraft was about 42 ft above the normal 3 degree slope (orange line), and remained above it until reaching 104 ft above the aerodrome elevation. During this period, the sink rate exceeded 800 fpm for 8 consecutive seconds between 1051:06 and 1051:14 local time.
At 1051:20, the aircraft crossed the threshold with a groundspeed of 94 kt. The pilot reported the wind component during the approach was a south-easterly wind between 8–10 kt, which would have resulted in a 3–4 kt headwind component. Accordingly, the aircraft’s airspeed was likely around 97–98 kt as it crossed the runway threshold, which was 6–7 kt above the Vref of 91 kt.
At 1051:29, the corrected altitude of the aircraft matched the terrain elevation, which indicated that the aircraft landed 402 m along the runway with a groundspeed of 81 kt. The pilot reported applying brakes as the aircraft passed the apron area, which occurred about 2 seconds after touchdown. Following a ground roll distance of about 540 m, the aircraft decelerated to a groundspeed of 45 kt when it vacated the left side of the runway at 1051:48.
Figure 6: VH-NXA approach and landing
All times are coordinated universal time (UTC). Local time was Central Standard Time (CST), which was UTC +9 hours and 30 minutes. The aerodrome elevation is 278 ft. Source: ATSB, data provided by OzRunways and Google Earth
On 2 November 2024, a GippsAero GA8-TC Airvan, was being used to conduct a scenic flight from Whitsunday Airport (Shute Harbour), Queensland. During the landing the aircraft departed the upwind end of the runway before entering marshy ground and coming to a stop in a ditch.
The ATSB investigation identified that the aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go-around, resulting in a landing beyond the planned touchdown point. The ATSB also identified that the operator’s weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with its procedures.
Safety analysis
On the morning of 29 May 2025, a Cessna 310R, registered VH-NXA, was being operated by Marthakal Yolngu Airline on a non-scheduled air transport flight from Darwin to Lake Evella, Northern Territory, with a pilot and 4 passengers on board.
During a straight-in visual approach, without visual slope guidance to runway 08 at Lake Evella, the pilot assessed that the approach was stable and continued with the landing. After the aircraft crossed the runway threshold, it floated for a prolonged period and subsequently landed before reaching a taxiway located about halfway along the runway.
When the pilot applied braking passing the airport’s apron area, the aircraft did not decelerate as expected. The aircraft subsequently overran the runway and collided with a fence. The pilot and passengers were uninjured, however, the aircraft sustained substantial damage.
This analysis examines how the condition of the aircraft braking system, and the conduct of the approach and landing, contributed to the runway excursion. It also explores the operator’s self-reported passenger weight procedures and electronic weight and balance system, and how the latter, in combination with incorrect pre-flight weight calculations, led to the aircraft being operated above the weight limits specified in the pilot’s operating handbook.
Pre-flight maintenance
Maintenance which was completed on the aircraft 3 days before the occurrence involved numerous concurrent tasks. These were conducted by a licensed aircraft maintenance engineer (LAME) with the assistance of an apprentice. One of the tasks involved the apprentice conducting maintenance on the braking system due to leaking brake callipers. It was the LAME’s expectation that the apprentice had replaced the main wheel brake pads during this maintenance task.
This expectation influenced their assessment that the aircraft rolled forward during post‑maintenance engine run-ups, due to the new brakes requiring ‘burning in.’ In this case, a physical verification of the brake pads was not conducted as a result.
On the morning of the occurrence, the LAME carried out corrective maintenance in response to the flight instructor text message report of ‘spongy brakes’ the day prior. While the occurrence pilot was aware of this report, they were not aware of the LAME’s experience with the aircraft rolling forward during the engine run-up.
When the pilot commenced the pre-flight engine run-up for the occurrence flight, the brakes failed to keep the aircraft stationary. The pilot physically increased the brake pressure and successfully kept the aircraft stationary, but did not advise maintenance personnel. The pilot’s limited experience on multi-engine aircraft led them to consider that this might be normal, which was reinforced during a brief discussion with another Cessna 310 pilot.
Gaps in communication and incorrect assumptions allowed a latent defect to persist into operation, contributing to the runway overrun in this occurrence.
Contributing factor
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
Approach
Lake Evella Aerodrome was not equipped with visual slope guidance, and as a result, the pilot relied on their assessment of visual cues of the runway itself to assess whether they were on the correct approach path while they typically used the runway threshold as their aiming point.
Recorded data from the pilot’s Android phone indicated that the aircraft was higher than the usual 3 degree ‘correct flight path’. The rate of descent exceeded 800 fpm for a period of 8 consecutive seconds until the aircraft descended below 140 ft relative to the runway. At the time, the pilot recalled the approach ‘seemed stable,’ while the operator’s stable approach criteria permitted rates of descent up to 1,000 fpm.
The aircraft subsequently crossed the threshold of runway 08 at a height of 55 ft with a ground speed of 94 kt. ATSB analysis concluded that the aircraft’s airspeed was likely 6–7 kt above the Vref for the recalculated landing weight 91 kt.
When the aircraft neared the point of touchdown, it was subjected to ground effect, which meant that excess airspeed at the point of flare would result in a considerable float distance due to the reduction in drag and lack of power-off deceleration in ground effect (Federal Aviation Administration, 2023).
Additionally, landing distances provided in the aircraft flight manual are based on the aircraft achieving Vref (plus wind and gust additives) at 50 ft above the runway surface. As a result, any additional airspeed will result in a later touchdown and reduce the remaining landing distance available (Federal Aviation Administration, 2023).
In this case, the additional airspeed crossing the threshold likely resulted in a prolonged float in ground effect. This resulted in the aircraft touching down 402 m beyond the runway threshold which was the pilot’s usual aiming point. Subsequently, the pilot applied braking about 2 seconds after the touchdown, at which point, there was about 585 m of remaining distance available to decelerate on the runway.
Contributing factor
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Excursion
The pilot first became aware of an issue with the braking system when they applied brake pressure during the landing roll with about 585 m of runway remaining. Witness accounts recalled the aircraft was travelling at high speed as it passed the taxiway and apron area without any significant deceleration. Additionally, recorded data showed the aircraft only slowed from 81 kt at touchdown to 45 kt when it vacated the left side of the runway following a ground roll distance of about 540 m.
At the aircraft’s landing weight, the ATSB calculated ground roll distance required was 195 m, which was sufficient to bring the aircraft to a stop within the remaining length of the runway had the brakes been functioning correctly. However, the loss of hydraulic brake fluid and the worn brake pads on the right-hand brake reduced the available braking capacity. As a result, the braking capacity was insufficient to arrest the aircraft’s forward momentum before the end of the runway. The pilot attempted to increase the available stopping distance by steering left and departing the runway, however it was insufficient, and the aircraft subsequently collided with the perimeter fence.
Contributing factor
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Passenger weights
The operator’s exposition permitted the use of self-reported passenger weights for weight and balance calculations, without requiring the application of additional allowances or validation. This practice introduced errors into the weight and balance data used for pre-flight planning.
Research has found that people tend to underestimate the weights of themselves and others. Further, people are less accurate at estimating the weight of others than they are of themselves.[9] To cater for the variation in weight, it is recommended that operators weigh passengers or apply adjustment factors to self-reported values (Civil Aviation Safety Authority, 2025). In contrast, the operator’s reliance on unadjusted self-reported passenger and carry-on baggage weights provided no systematic mitigation for potential inaccuracies, which increased the likelihood that the aircraft would be operated overweight or at centre of gravity limits outside the manufacturer’s requirements.
Other factor that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safety issue)
Electronic weight and balance
The operator used an electronic weight and balance system to calculate aircraft loading data for each aircraft in operation. In that electronic system, VH-NXA had been configured with the higher maximum weight limits applicable to aircraft fitted with a vortex generator (VG) modification. However, the aircraft did not have the specified modification installed. Consequently, the programmed maximum zero-fuel, ramp and take-off and weights in the system exceeded those authorised in the aircraft’s POH.
This configuration error meant the electronic weight and balance system allowed VH‑NXA to be loaded in excess of the certified weight limitations, while still indicating that the loading complied with those limitations. This created an ongoing risk that the aircraft could be operated above the approved maximum weights.
Other factor that increased risk
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safety issue)
Weight exceedances
During the occurrence flight, the aircraft was operated above the certified maximum ramp and take-off weights due to cumulative errors in the pilot’s weight and balance calculations. As a result of the configuration errors in the electronic weight and balance system, no alert to the overweight condition was made.
The pilot, who was conducting their first multi-engine command flight, reported feeling rushed during pre-flight preparation, which likely reduced the opportunity for careful verification of passenger weights, totals and data entry. Review of the weight and balance documentation from the occurrence identified multiple inaccuracies, indicating that the overweight condition arose from a breakdown in the usual cross-checking processes rather than a single isolated error.
Although the overweight condition did not result in the aircraft exceeding its maximum landing weight, operating above certified weight limits is known to increase take-off and landing distances and degrade braking performance. Additionally, excessive weight reduces the available safety margin if an in-flight emergency condition should arise (Federal Aviation Administration, 2016).
Other factor that increased risk
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion involving Cessna 310, VH-NXA, at Lake Evella Aerodrome, Northern Territory, on 29 May 2025.
Contributing factors
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Other factors that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safey issue)
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safey issue)
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations.
Safety issue description: Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by D & T Aircraft Engineering
D & T Aircraft Engineering advised that, following this occurrence, a debriefing was conducted with maintenance personnel to discuss key learnings. It was acknowledged that increased vigilance would be exercised in the future to ensure that aircraft components are carefully inspected and confirmed to be in a serviceable condition following the completion of maintenance tasks. Additionally, the organisation stated that it would prioritise accessing the aircraft at the earliest opportunity in the future to assist in identifying potential causes of component failure, particularly in cases where perishable evidence plays a critical role in determining the cause.
Glossary
AFM
Aircraft flight manual
AMM
Aircraft maintenance manual
AMSL
Above mean sea level
CASA
Civil Aviation Safety Authority
FCOM
Flight crew operating manual
FTO
Flight training organisation
LAME
Licensed aircraft maintenance engineer
MOS
Manual of Standards
POH
Pilots operating handbook
RPM
Revolutions per minute
SOP
Standard operating procedures
VG
Vortex generator
VMC
Visual meteorological conditions
VREF
Reference landing approach speed
Sources and submissions
Sources of information
The sources of information during the investigation included:
Ramos , E., Lopes, C., & Barros , H. (2009). Unawareness of weight and height – the effect on self-reported prevalence of overweight in a population-based study. The Journal of Nutrition, vol. 13, pp.310–314.
Reed, D., & Price , R. (1998). Estimates of the heights and weights of family members: accuracy of informant reports. International Journal of Obesity, vol. 22, pp.827–835.
Shapiro , J. R., & Anderson, D. A. (2003). The effects of restraint, gender, and body mass index on the accuracy of self-reported weight. International Journal of Eating Disorders, vol. 34, pp.177–180.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
the operator
maintenance organisation
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
pilot of the accident flight
the operator maintenance organisation
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Run-up: a high power run-up check is carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take off.
[2]OzRunways is an approved data provider for Australian pilots for flight planning and in-flight navigation.
[3]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered
[4]Common traffic advisory frequency (CTAF): A designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome or within a broadcast area.
[5]Brake linings: brake linings, often referred to as brake pads, are the friction material that, when pressed against the brake discs, slows and stops the aircraft. Over time and with use, these linings wear down and require replacement.
[6]A vortex generator installation typically offers the advantages of reduced stall speeds, reduced minimum single engine control speed (Vmc), improved take-off and landing performance and increased maximum take-off weight.
[7]Moment arm: the horizontal distance from a reference datum to the centre of gravity of an item.
[8]Reference Landing Approach Speed: The airspeed used on approach down to 50 ft above the runway when determining landing distances which is normally 1.3 times the stall speed.
[9]For example, see Ramos and others (2009), Reed and Price (1998), Sahyoun and others (2008) and Shapiro and Anderson (2003).
In the early morning of 27 March 2025, rapidly rising floodwater started surrounding the Queensland town of Adavale, flooding homes and requiring people to seek refuge on their roofs.
The planned Queensland Fire Department swift water rescue team were unable to deploy to Adavale, so Channel Country Helicopters, a local helicopter mustering company, was requested to assist with the evacuation of the town as a mercy flight. They agreed and subsequently dispatched three Robinson R22 helicopters to Adavale.
When the second helicopter arrived overhead the town, the pilot spotted a person on the roof of a demountable building with a strong flood current flowing around it. The pilot assessed the situation as critical and proceeded to land on a flat roof section to pick up the passenger. The pilot was not sure whether the roof could hold the weight of their helicopter, they kept the aircraft in a flying condition with the skids resting lightly on the roof.
After the passenger climbed in, the pilot took off from the roof and attempted to depart upwind. As the helicopter cleared the demountable roof it was no longer in ground effect and available performance was insufficient for level or climbing flight. The lack of available power caused the rotor RPM to decay, activating the ‘low RPM’ warning horn. The pilot then immediately realised the criticality of the situation, identified a sheltered landing spot and conducted a controlled ditching into chest-high floodwater in the lee of a nearby building.
The pilot and passenger then safely exited the helicopter into the water but were unable to climb to the roof of the building. The pilot then attempted to retrieve a ladder from the take-off site but was washed away by the current. They found shelter in a tree about 900 m downstream of the ditching site and was later rescued by another helicopter. The passenger avoided the strong current by standing close to the helicopter, but sustained significant chemical burns due to the fuel seeping out of the helicopter’s tank.
The helicopter was substantially damaged by the floodwater.
Source: Photo received from operator
What the ATSB found
After the embarkation of the passenger on the roof, the helicopter was overloaded to an extent that prevented flight out of ground effect, with insufficient clear space available to accelerate to an airspeed to obtain translational lift. Once this was recognised by the pilot, they conducted a successful ditching into floodwater. The pilot’s choice of landing site in the only sheltered area available allowed for the helicopter to remain upright in the otherwise fast‑flowing water. Additionally, their rapid and correct application of the helicopter manufacturer’s low RPM recovery procedures resulted in a controlled ditching which allowed both pilot and passenger to exit the helicopter without injury.
The pilot’s decision‑making was affected by the heavy workload of conducting a rescue operation, for which they were not prepared, in a light helicopter. The pilot conducted an unfamiliar and demanding rescue operation which likely overwhelmed their decision‑making capacity while the passenger was boarding the helicopter. This heavy workload, in addition to the rotor operating at high power, prevented the pilot from verbally briefing the passenger on seatbelt use and other safety information. The passenger was subsequently unrestrained during the flight.
Once committed to the rescue, under high workload and the perception of imminent danger of staying on the roof, the pilot continued with the plan and did not reassess the feasibility of the flight once they realised that helicopter performance was going to be marginal with the heavier than expected passenger on board.
The helicopter operator was aware that the requested flight was outside of their normal scope of operations. However, they felt a moral obligation to act due to their perception of being the only people that could help preserve life. This meant that they agreed to conduct mercy flight operations to attempt rooftop rescues for which they were not trained or equipped.
Safety message
Many aspects of emergency response in Australia rely on volunteers, both by organised groups and ad-hoc by people who happen to be in the right position to help. These ad‑hoc or bystander rescues save many lives when dedicated, trained assistance is not available. However, when responding to an emergency it is of paramount importance to stop and take a moment to assess risk to the rescuers before assisting others. This applies in any emergency context, not just aviation, and is strongly reinforced in training for surf rescue, medical first aid, fire-fighting and marine rescue operations.
In the aviation context, mercy flights are by definition outside the scope of the normal operations of the involved pilots and operators. This places a high burden on pilot and operator to assess risks that may be out of their area of expertise. Where possible it is important for all involved to take the time to reassess the risk of (continuing) the proposed flight and consider any alternatives. This may include discontinuing a rescue and waiting for additional assistance, as continuing may expose the crew and the people being assisted to much greater risks.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 27 March 2025, widespread rain associated with a passing surface trough was causing catastrophic flooding in Queensland’s channel country region. In particular, the small rural town of Adavale, about 89 km north of Quilpie, was most heavily affected. Telephone communication had been lost the previous day, but during the night reports reached authorities indicating that the town was rapidly flooding and that some people in lower lying areas had sought shelter on roofs.
At around 0630,[1] an aerial work operator, Channel Country Helicopters, dispatched a Robinson R22 helicopter, registered VH-KNG, from Quilpie with the pilot and a police officer on board to assess the situation in Adavale. The officer had tried to reach Adavale in the days before but had found the roads impassable. A helicopter flight was previously arranged but had not been possible due to the heavy rain until the operator noted an improvement of weather conditions.
On arrival in Adavale at 0721, the pilot and the police officer found the situation in the town critical, with fast‑flowing floodwaters throughout the town. This limited landing access, with the only dry place available at the town waste disposal site, about 1 km to the north‑east. After disembarking the police officer, the pilot returned to Quilpie and refuelled the helicopter.
Around 0915, the helicopter operator received a phone call from the local disaster management group asking ‘if they were able to conduct a mercy flight’[2] as there were people reported on the roofs of buildings in Adavale and no other rescue assets were available. The operator assessed that the weather was not suitable for VFR flight at the time, but agreed to send its helicopters when able. The operator then briefed its pilots on some of the risks involved, including the possibility of overloading roofs when landing and the need to pay special attention to powerlines and other overhead obstructions that were expected in the town.
Once the weather cleared, the operator mobilised the first 2 Robinson R22 helicopters, shortly followed by a third helicopter.
The first helicopter that arrived in Adavale touched down on a roof of a demountable building, boarded a resident who was waiting on the roof, and departed to a nearby cattle station.
At around 1115, the second helicopter, VH-KNG (flown by the pilot who had ferried the police officer to Adavale that morning), which had stopped en route to avoid flying through rain showers,[3] was back overhead Adavale where the pilot observed that the fast-flowing water was ‘pushing around a parked semi‑trailer road‑train’, reinforcing a sense of urgency to evacuate residents. The pilot then spotted a person on the same roof and elected to conduct a rooftop rescue.
On approach to the rescue site, the pilot recalled that they assessed that the building was at immediate risk of being washed away, and that the roof strength was insufficient to carry the full weight of the helicopter. The pilot then opted to maintain lift on the main rotor while picking up the passenger to reduce the load on the roof sheeting. The helicopter touched down on the flat roof between the two demountable buildings (Figure 1). The pilot kept the helicopter flying throughout the passenger embarkation, with only part of the skids lightly touching the roof.
Figure 1: View underneath roof
Source: Video still from passenger, annotated by the ATSB
The passenger boarded the helicopter from the left side, into the left seat, wearing a rain jacket with some personal effects. During the rapid boarding and take-off, the noise of the engine running at full power did not allow verbal communication with the boarding passenger. The passenger did not attempt to secure their seat belt prior to take‑off.
The pilot reported realising the passenger was heavy, but being confident that the helicopter would be able to fly away after building up airspeed to obtain translational lift.[4] The pilot lifted off the helicopter (in ground effect[5] over the roof) and immediately departed into wind. However, once clear of the roof with reduced ground effect, the helicopter was no longer able to sustain level flight. As rotor speed decayed below 97%, the low rotor RPM light and horn alarms activated in the cockpit.
The pilot lowered the collective[6] and applied aft cyclic[7] and quickly concluded that the helicopter would not be able to clear approaching obstacles such as trees, buildings and powerlines during the take‑off run. They then selected an area sheltered from the floodwater current, behind a building about 60 metres away, and conducted a controlled ditching.
Figure 2: Overview of flight
Source: Google Earth, annotated by the ATSB
After ditching, the helicopter became submerged in floodwater, stopping the engine. Due to the lee of the building protecting the helicopter from the main current, it remained upright, allowing both the passenger and pilot to egress into the chest deep water.
There was no access to the roof of the building, so the pilot attempted to return to the take-off site to retrieve a ladder. However, the pilot was swept away by the current before finding shelter in a tree about 900 metres downstream, where they were later rescued by a larger helicopter.
The passenger stayed in the lee of the building, in the sheltered water near the helicopter, and was later transported to a temporary shelter on a roof by the police officer, who had commandeered a small motorboat.
The pilot was unhurt, but the passenger sustained serious chemical burns due to exposure to the fuel leaking from the submerged helicopter’s tank. The passenger was treated for their injuries by the swift-water rescue team and later in hospital.
No further rooftop rescues were conducted by the operator, instead company helicopters guided motorboat and swift-water rescue teams to people in need of rescue.
Figure 3: Adavale flood in the afternoon after the accident
Source: Nathan Covey
Context
Pilot information
The pilot held a Commercial Pilot Licence (CPL) for helicopters and aeroplanes, a valid class 2[8] aviation medical certificate and a low‑level mustering endorsement for helicopters.
The pilot reported having flown for about 25 years, first in fixed wing aircraft and then operating helicopters for the last 3 years, mostly in support of cattle mustering operations.
At the time of the accident, the pilot had accumulated about 11,400 hours aeronautical experience, of which about 800 hours were on R22 helicopters. The pilot had flown about 30 hours in the preceding 90 days but had not flown for 5 days prior due to the poor weather conditions.
The pilot was very familiar with the area, having flown there for most of their career, and felt well rested on the day of the accident. They reported that they started work at about 0600 for the initial flight to Adavale with the police officer, and that they were not experiencing any effects of fatigue.
Aircraft information
General information
The Robinson Helicopter Company R22 Beta II helicopter is powered by a Textron Lycoming O‑360‑J2A 4‑cylinder piston engine. The R22 has 2 seats, with the pilot flying from the right seat, with each seat fitted with a 3‑point, inertia reel shoulder strap seatbelt, similar to those used in motor vehicles.
The R22 is commonly used for helicopter flight training, private flight and livestock mustering operations. It has a payload capacity of about 215 kg and a maximum seat limit of 109 kg (including any items in the small luggage compartment under the seats).
VH-KNG
VH-KNG was manufactured in the US in 2001 and first registered in Australia in October 2011. The helicopter had undergone a periodic inspection on 21 February 2025 with a total time in service of 13,424.2 hours.
The current maintenance release was not located and was likely lost in floodwaters. There were no indications of any mechanical issues with the aircraft before the accident.
Figure 4: VH-KNG after the accident
Source: Channel Country Helicopters
Weight and balance
During the last maintenance period the aircraft was weighed, and empty weight was recorded as 405 kg. The helicopter was used in mustering operations, and had both doors removed. This reduced the empty weight by about 5 kg, increasing the total payload to about 222 kg for a maximum take‑off weight of 622 kg.
With full fuel when it departed Quilpie, the ATSB calculated, based on the flying time from departure in Quilpie, the helicopter had approximately 70 L or 50 kg of 100LL Avgas[9] on board on arrival in Adavale. The pilot reported their weight was 78 kg. As can be seen in Table 1, that left an available load of about 94 kg.
The passenger reported their weight as around 130 kg with an estimated additional 10 kg for their wet clothing and essential medical equipment also carried. This resulted in the helicopter being about 46 kg overweight.
Table 1 VH-KNG calculated take-off weight
Item
Weight (kg)
Basic Empty weight
405
Removed doors left and right
-5
Fuel (avgas 70 litres)
50
Pilot
78
Total
528
Maximum all up weight
622
Available margin on landing
94
Passenger weight
130
Passenger personal effects /clothing
10
Total
668
Available margin on take-off
-46
Helicopter performance
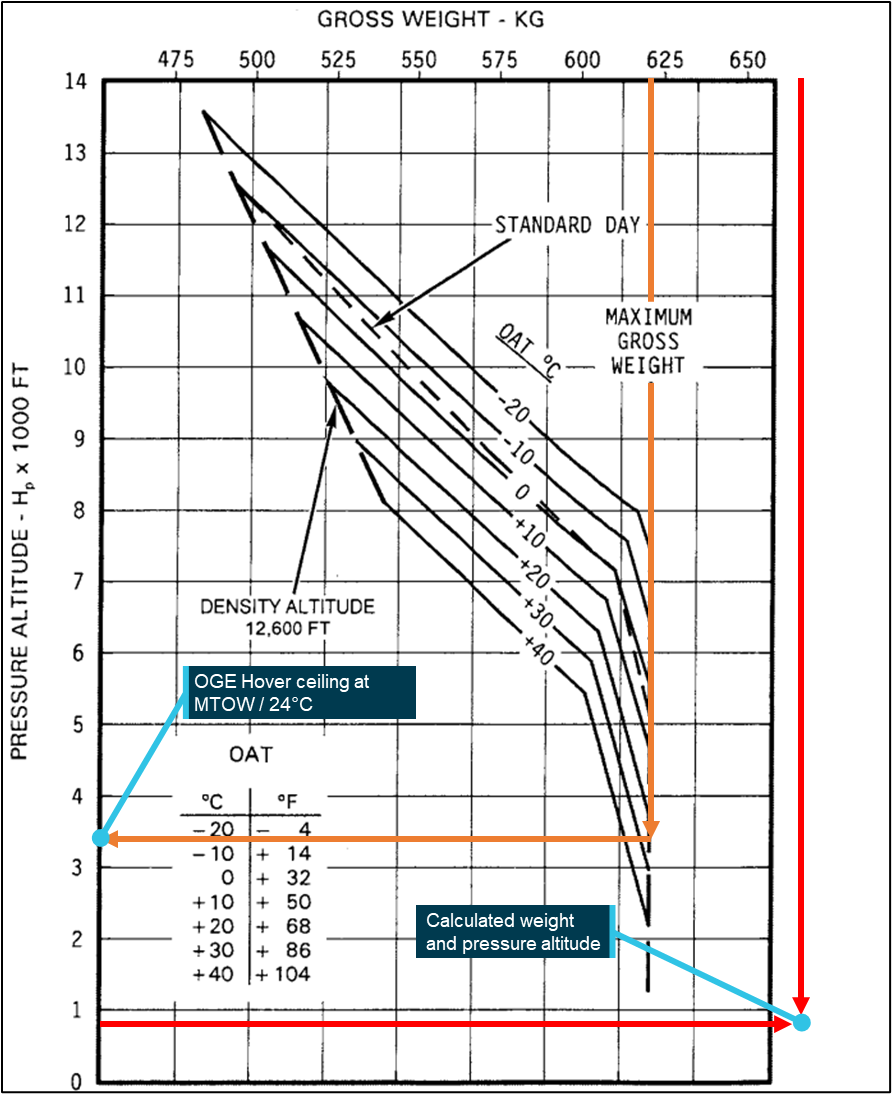
Performance data provided by the Robinson R22 pilot’s operating handbook (POH) indicated that, at its maximum take‑off weight (MTOW) of 622 kg and the temperature at the time of the accident of 24°C (see Meteorological conditions), the helicopter should have had sufficient available performance to hover in ground effect (IGE) up to a pressure altitude of about 7,900 ft and an out of ground effect (OGE) up to a pressure altitude of about 3,400 ft (Figure 5).
This performance is based on ‘ideal conditions’, however, in this case, high humidity would likely have further decreased the available performance by as much as 3 or 4% (FAA, Federal Aviation Agency, 2021). However, this should still have allowed OGE hover at maximum take‑off weight, at the calculated pressure altitude of 811 ft at the time and location of the accident.
No performance data was available for the helicopter outside its maximum allowed take‑off weight and the manufacturer advises against exceeding limits due to possible overloading of the rotor drive components.[10]
Figure 5 shows the maximum pressure altitude for flight out of ground effect at maximum take‑off weight (orange line) and the calculated helicopter weight and actual pressure height (red line).
The pilot recalled that they thought that the helicopter performance would be ‘marginal’ on take‑off, but believed they would be able to climb out using translational lift after take‑off.
Figure 5: OGE hover ceiling vs gross weight
Source: Robinson R22 Pilot’s operating handbook, annotated by the ATSB
Power check
To confirm sufficient power is available for hover out of ground effect, the Robinson flight training guide (Robinson Helicopter Company, 2019) recommends conducting a power check before committing to a take‑off requiring OGE hover performance:
…Perform a takeoff to a 2 foot IGE hover and complete a hover check to confirm available power. The [OGE] maneuver should not be attempted unless the IGE hover manifold pressure is 2 inches below the maximum takeoff power (5 minute) limit…
The pilot did not conduct a power check but they stated that they were aware the helicopter was heavily loaded and that they had to take off straight away as the building was ‘highly likely to be washed away’.
Confined area take-off
The manufacturer’s recommend take-off profile, as defined in the POH (Figure 6), involves accelerating in ground effect before pitching up into a climb. This technique ensures sufficient energy and reaction time available at any stage of the take‑off to enter autorotation in case of an engine or tail‑rotor failure. For the R22, this required acceleration to 45 kt indicated airspeed in ground effect before starting to climb.
Figure 6: Height velocity diagram Robinson R22
Source: R22 Pilot’s operating handbook, annotated by the ATSB
When operating from unprepared landing areas, physical space may not be available to follow the recommended take‑off profile. As this forces the helicopter to climb out of ground effect before obtaining translational lift, the pilot must ensure that the helicopter’s weight is below the OGE limit before attempting a confined area take‑off.
The Civil Aviation Safety Authority (CASA) has published advisory circular 91‑29 (AC 91‑29): Guidelines for helicopters – suitable places to take‑off and land (CASA, 2023). Section 11.1.1 provided the following description of a ‘confined area’:
An unprepared landing site that has obstructions that require a steeper than normal approach, where the manoeuvring space in the ground cushion is limited, or whenever obstructions force a steeper than normal climb-out angle is often defined as ‘Confined Area’.
Photos, video and satellite imagery of the take‑off site show several obstructions in the form of power lines and trees in the departure direction (Figure 2). These obstructions were high enough to limit departure using the recommended take‑off profile and to require a confined area take‑off.
Low RPM recovery
The lift produced by a helicopter rotor is determined by a combination of rotor RPM, and the angle of attack of the rotor blades. The pilot controls the amount of lift by using the collective lever to vary the pitch angle of the blades. As the pitch increases, the governor increases the engine throttle to maintain a constant rotor RPM. When the governor has fully opened the throttle, any further increase of collective pitch will result in the rotor RPM reducing, progressively reducing lift and resulting in a loss of climb performance or a descent.
Further increasing the collective pitch will force the blades to reach their critical angle of attack (around 15°) and airflow will separate from the blades resulting in aerodynamic rotor stalling.
As per Robinson Safety Notice 24:
The stall causes a sudden loss of lift and an increase in drag, slowing down rotor RPM further. As the helicopter begins to fall the upward moving air through the rotor increases angle of attack further making recovery virtually impossible, even with full down collective.[11]
And Robinson Safety Notice 10:
No matter what causes the low rotor RPM, the pilot must first roll on throttle and lower the collective simultaneously to recover RPM before investigating the problem. It must be a conditioned reflex. In forward flight, applying aft cyclic to bleed off airspeed will also help recover lost RPM.[12]
A low RPM light and warning horn are fitted in the R22 to warn the pilot of this condition; both activate when the rotor RPM decays below 97%.
The R22 pilot’s operating handbook states:
LOW RPM HORN
[…] The horn activates simultaneously with the LOW RPM caution light and indicates rotor speed below 97% RPM. To restore RPM, lower collective, roll throttle on and, in forward flight, apply aft cyclic. [..]
The R22’s light weight and low inertia rotor system means that rapid pilot intervention is required before control is lost.
Meteorological conditions
No weather forecast was available for either Quilpie or Adavale, a grid point wind and temperature forecast for southern Queensland showed winds near Adavale at around 6 kt at 010°, which is consistent with the pilot’s reported observations of a light northerly wind and localised showers. Temperature was reported at 24°C. No humidity observations were available for Adavale, but given the inclement weather and flooding conditions, it was expected to be high.
The nearest reported QNH,[13] at Charleville, about 175 km away, was reported as 1012 hPa. Adavale lies at an elevation of 781 ft which resulted in a pressure altitude of 811 ft and a density altitude of 2,048 ft.
Operator information
The helicopter was operated by Channel Country Helicopters (CCH), which was based at Quilpie Airport and held a Civil Aviation Safety Regulation 1998 (CASR) Part 138 aerial work certificate. It operated 3 Robinson R22 helicopters used primarily for mustering and agricultural aerial work.
While a CASR Part 138 aerial work certificate does not allow the operator to carry passengers as part of air transport operations, it did permit carriage of ‘aerial work passengers’ on operations which are aerial work operations.
These included aerial work passengers such as:
persons rescued as part of search and rescue operations
emergency service operation personnel carried as part of an aerial work operation that is also an emergency service operation.
Disaster response management
Managing disaster response in Australia is primarily a matter for the individual states and territories. To provide for disaster response and recovery at an appropriate level, Queensland has plans in place at local, district and state levels.
The disaster response for the flooding in south‑west Queensland was managed at a district level by the district disaster coordinator (DDC) in Charleville, guided by the district disaster management plan (DDMP), and locally in Quilpie council led by the local disaster coordinator (LDC), following the local disaster management plan (LDMP).
Flooding in the area had severely affected the roads around the region in the days before the accident, this was followed by a loss of phone coverage in both Quilpie and Adavale the day before the accident, which meant that only limited satellite communication was available.
However, the LDC had maintained some contact with Adavale residents and identified that overnight reports indicated that flooding was becoming more widespread and that the town of Adavale was at risk of severe flooding with residents beginning evacuation to the roofs of their dwellings.
Queensland Fire Department
As flooding had been anticipated in the wider region due to the expected heavy rains, a swift-water rescue team (SRT)[14] had been pre-positioned in Charleville in anticipation of the floods. This consisted of specially trained Queensland Fire Department personnel with an inflatable rescue craft (Figure 7) being transported by a chartered heavy‑lift helicopter to the site of the rescue. This helicopter was not equipped or crewed for instrument or night flying conditions and so could only be used during daylight and in visual meteorological conditions (VMC).[15]
As the only dedicated rescue asset available in the area, the SRT was planned to be used for life threatening situations only, under direction of the DDC.
The LDC in Quilpie contacted the DDC in Charleville for urgent assistance in the early hours of the morning of the accident. However, due to a combination of inclement weather conditions and a technical fault on the heavy‑lift helicopter, the SRT was not immediately available to deploy.
Figure 7: QFD swift-water rescue team and volunteer boats at Adavale
Source: Queensland Fire Department
Queensland Police Service
The Queensland Police (QPS) operational procedures manual (OPM) chapter 2.21.2 addresses helicopter use in search and rescue as well as disaster management situations. These procedures required approval from the DDC before tasking helicopters. The OPM specified that privately owned helicopters could be used if no other options were available, but did not include directions on the identification of hazards or the management of risk when using privately owned helicopters.
Disaster management plans
Neither the DDMP, LDMP nor the local evacuation sub‑-plan contained references to evacuation by helicopter. Adavale residents were anticipated to use their own means of transport to get to the evacuation centre.
The residents trapped on their roofs were unable to make their own way to higher ground due to the fast‑flowing floodwaters. As the SRT was unable to immediately deploy, and no other rescue assets were available at short notice, the DDC requested that the LDC check if local helicopters were available to conduct rescues.
Mercy flight
Although the term ‘mercy flight’ is no longer defined in aviation regulations, the Civil Aviation Safety Authority (CASA) recognises that there may be times when it is necessary for pilots to not follow aviation safety rules in order to respond to a sudden or extraordinary emergency.[16] The legal basis for this is the provision in section 10.3 of the Commonwealth Criminal Code Act 1995 which states that:
a person is not criminally responsible for an offence [in response to a] sudden or extraordinary emergency . . . if committing the offence is the only reasonable way to deal with the emergency.
CASA makes it clear that these provisions are a last resort option. For example, a pilot can get people to emergency medical treatment or out of a life‑threatening situation if there is no other (legal) way to do so. Before declaring a mercy flight, CASA states that pilots and operators should consider if the flight itself gives rise to equally serious or greater risks to safety and to manage those risks accordingly (CASA, 2025).
Tasking of local helicopters
The deputy LDC contacted the CCH chief executive officer (CEO) at Quilpie Airport at about 0915 on the morning of the accident and requested ‘mercy flight’ operations with their helicopters to rescue people from roofs in the Adavale township. Although outside the scope of their normal operations, the CEO recognised the urgency of the request and the need to provide immediate help to the people trapped in the floodwater and informed the deputy LDC that they would send out helicopters as soon as the weather cleared enough to conduct safe operations.
Operator processes
Pilot briefing
The CEO of Channel Country Helicopters (CCH) contacted the chief pilot, who was unable to get to Quilpie due to the floods. They discussed the mercy flight request and the need to conduct operations that were outside the scope of their normal operations in an effort to save lives. They agreed to assist in the rescue operation and identified a number of hazards to be mitigated.
The CEO then informed the pilots of the need to conduct rooftop rescues and provided a briefing which included:
risks of placing too much helicopter weight on temporary roof structures, which would require pilots to continue to fly the helicopter while boarding passengers
risks associated with power lines in close proximity to the township, which would restrict landing and take-off areas.
Task familiarity
In the course of their normal employment, the operator’s pilots mostly conducted low level flight and aerial stock mustering. The pilots were not familiar with rescue operations, particularly those requiring special landing techniques, passenger onboarding during flight and in‑flight risk assessment of rescue operations at low level during emergencies.
The accident pilot stated that they had never conducted rescue operations and had never landed on a structure before.
Pilot expectations
The pilot was well aware of the extent of the flooding due to the previous operations that morning and understood that there was little other external help available. They recalled that this set an expectation that they were the only available assistance at the time to evacuees in Adavale.
They reported that when asked to conduct a rescue flight, they felt compelled to assist due to the urgency of the natural disaster and the imminent risk to life.
STEP landing
The technique used for landing on rooftops is defined as ‘Single-Skid, Toe-in and Hover Exit/Entry Procedure’ or STEP landing. STEP landings are commonly used in military, search and rescue, helicopter skiing, or any operation where a helicopter is unable to fully set its full weight down on its landing gear due to uneven or soft terrain.[17]
The conduct of a STEP landing requires the pilot to keep most of their focus on controlling the helicopter throughout the boarding process. This was particularly important as any inadvertent interference with the controls by a boarding passenger into a small helicopter cabin could lead to uncontrolled helicopter movement.
While this manoeuvre is conducted routinely in certain types of operations, it is not commonly required during cattle mustering operations, and the pilot was not familiar with it.
Safety analysis
Introduction
On 27 March 2024, a Robinson Helicopter Company R22 Beta, registered VH-KNG, was being used to conduct rooftop rescue of residents of the township of Adavale, Queensland, during large scale flooding. After picking up a passenger from a rooftop, the pilot assessed during take-off that they did not have the required performance to continue flight and conducted a controlled ditching into floodwaters.
This analysis will explore the operational considerations pertaining to helicopter loading, take‑off performance, the pilot’s decision‑making and factors affecting the controlled ditching and survivability of the occupants.
Decision‑making processes
Pilot workload
Once committed to the rooftop landing, the pilot faced an increased workload due to a combination of factors which likely negatively affected their decision‑making processes.
While the pilot had significant aeronautical experience, including considerable recent experience flying the Robinson R22, they had never landed on top of a structure or conducted, or ever trained for, any type of rescue operations. The accident flight was their first attempt at a rescue operation and as such, it is likely that the pilot was under significant workload.
The high degree of concentration required likely limited the pilot’s cognitive capacity to assess the weight or brief the passenger prior to take‑off. Similarly, the lack of full consideration for the aircraft’s performance limitations were likely due to the narrowed attentional focus on the immediate control demands required in the confined area.
Plan continuation
Plan continuation is described as when pilots decide to continue with the original plan of action despite the presence of cues or information that suggests changing the course of action would be the safer (Orasanu, Fischer, & Davison, 2002)
Furthermore, as workload increases, the stimuli or conditions will appear obvious to people external to the situation; however, it can be very difficult for a pilot caught up in the plan to recognise the saliency of the cues and the need to alter the plan (Skybrary); (TSBC).
Plan continuation bias is often associated with situations involving dynamically changing risk and pilots underestimating the risk (Wiegmann, Goh, & O'Hare, 2002) as well as in high‑pressure environments where altruistic or time critical factors are present (Nadri and others 2024; Orasanu & Martin 1998)
The need to identify and control rapidly changing risks in emergency flights is emphasised in the procedures used by dedicated SAR operations and firefighting aircraft. For example, the AMSA ‘rotorcraft rescue standards and procedures manual’ chapter 1.6 (AMSA, 2025) contains procedures for dynamic risk assessment process that involves the whole crew of the aircraft and is repeated at critical points in the mission.
As the only crew member on an ad hoc search and rescue mission, the pilot did not have training in these specialised procedures nor the support of additional crew members to alert them to the emerging indications of increased risk. Additionally, their understanding at this point that the passenger was in grave danger, made it likely that the pilot did not consider disembarking the passenger as a possibility.
Consequently, although the pilot was aware that the helicopter weight (and consequently performance) was ‘marginal’, their perception of imminent danger of roof collapse meant they did not change their plan and continued the take‑off without considering an alternative course of action.
Helicopter performance
On conducting the rooftop landing and passenger loading, the pilot was unable to calculate the gross weight of the helicopter before conducting the take‑off. Their estimation of the passenger weight was likely hampered by the bulky raincoat the passenger was wearing and the focus of the pilot on controlling the aircraft during an operation that they were not specifically trained or experienced in.
Weight data supplied to the ATSB by the accident pilot and passenger and a calculation of the remaining fuel load indicated that the helicopter was likely at least 46 kg over its maximum allowable take‑off weight (MTOW).
Being significantly overweight, when the helicopter became airborne in ground effect over the building, there was no assurance that it could achieve the required performance that was needed to clear nearby obstacles during take‑off.
This could have been ascertained if the helicopter pilot had performed a power check while still above the building, however because the position of the helicopter on the roof was precarious with the passenger onboarding and the pilot held concerns that the structure would not support the helicopter weight or last much longer in the floodwater, this was not conducted.
Moral obligation to conduct rescue operations
After receiving a phone call from the deputy local disaster coordinator informing them of the emergency in Adavale and requesting urgent assistance, the CEO of Channel Country Helicopters likely felt a moral obligation to assist in the rescue of evacuees facing extreme danger in the flood zone.
The request for mercy flight operations reinforced the urgency of the request and the need to assist even though it was outside the scope of their normal operations. This moral obligation was likely also passed to the pilots conducting the operations and would have been a strong influence in their acceptance of additional risk to their normal operations.
Controlled ditching
While embarking the passenger, the pilot initially felt confident that the helicopter performance was adequate to obtain translational lift. However, once it cleared the roof and lost ground effect, the helicopter was no longer able to sustain level flight or climb.
The pilot applied the correct recovery technique for low rotor RPM, selected the only sheltered location available, next to a building about 60 m from the take‑off site and conducted a controlled ditching of the helicopter with very little lateral speed.
It is common for helicopters to roll over in emergency landings, especially when ditching. In this case, the identification of a sheltered landing site, and the correct emergency technique, allowed the helicopter to remain upright after landing. This made it possible for both the pilot and passenger to safely exit the helicopter.
Survivability
The pilot’s workload during the boarding of the passenger likely limited the pilot’s cognitive capacity to brief the passenger. Furthermore, the high noise levels in the cockpit would have made a normal passenger safety briefing very difficult. Consequently, the passenger was not made aware of the use of the seatbelt, the weight limit of the seat, exit procedures and the possibility of inadvertent interference with the aircraft controls.
The incorrect (or lack of) use of seatbelts has been identified by the ATSB as a factor affecting survivability in several light aircraft incidents.[18] Inadvertent interference with helicopter flight controls by passengers has been identified as an issue in several incidents and is the subject of a Robinson Helicopters safety notice.[19]
If the pilot had continued the flight while building up airspeed in ground effect, there would have been a high risk of a forward impact with an obstacle or the floodwater. In that case the lack of seatbelt would have likely resulted in severe injuries to the unrestrained passenger.
In this accident the correctly applied forced landing technique by the pilot meant that the passenger was not exposed to forces large enough to require a seatbelt and their lack of restraint may have made their exit from the small helicopter cabin easier.
Exposure to fuel
After exiting the helicopter, the passenger witnessed the pilot being washed away in the floodwater. Recognising the danger of entering the floodwater current, they stayed in the sheltered area near the submerged helicopter. This exposed the passenger to AVGAS floating on the water, causing significant chemical burns that were subsequently treated in hospital.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the ditching in floodwater involving Robinson R22 Beta, VH‑KNG, at Adavale, Queensland, on 27 March 2025.
Contributing factors
The pilot conducted an unfamiliar and demanding rescue operation which likely overwhelmed their decision‑making capacity. Under time pressure due to the perceived imminent risk of a roof collapse, the pilot did not assess available performance after boarding a heavier than expected passenger and committed to the rescue with an immediate take‑off.
The pilot departed with the helicopter significantly overweight. As a result, it did not have available performance to conduct a confined area take‑off.
The CEO and pilot felt a moral obligation to conduct a rescue operation for which they were neither trained nor equipped.
Other factors that increased risk
The passenger was not briefed before the flight, consequently they did not wear the fitted 3‑point seatbelt, which increased their risk of injury.
Other findings
After take-off, the pilot immediately realised the helicopter could not maintain altitude and, following the correct procedure for low rotor RPM, made a controlled landing in the only sheltered area available, allowing the pilot and passenger to exit safely.
Flood currents around the ditching site prevented the passenger from seeking shelter away from the helicopter while waiting to be rescued. This caused an extended exposure to fuel floating on the water, resulting in serious chemical burns.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
passenger the accident flight
CEO of Channel Country Helicopters
Queensland Police Service
Queensland Fire Department
maintenance organisation for VH-KNG
Bureau of Meteorology
photographs and videos taken on the day of the accident
district disaster management plan for Charleville region
local disaster management plan for Quilpie.
References
AMSA, Australian Maritime Safety Authority. (2025). Rotary Wing Search and Rescue standards and procedures manual (Version 8 ed.). Canberra.
FAA, Federal Aviation Agency. (2021). Helicopter Flying Handbook. United States of America: Simon and Schuster.
Nadri, C., Regalado, J., Ferris, T., & Zahabi, M. (2024). Cognitive Biases in Commercial Aviation: Empirical Review of Accident Reports. Proceedings of the Human Factors and Ergonomics Society Annual Meeting.68, pp. 56-60. Los Angeles: SAGE publications.
Orasanu, J. &. (1998). Errors in aviation decision making: A factor in accidents and incidents. Proceedings of the workshop on human error, safety, and systems development, (pp. 100-107).
Orasanu, J., Fischer, U., & Davison, J. (2002). Risk perception: A critical element of aviation safety. 15th IFAC World Congress (pp. 50-51). Barcelona: Elsevier.
Wiegmann, D. A., Goh, J., & O'Hare, D. (2002, 6). The role of situation assessment and flight experience in pilots' decisions to continue visual flight rules flight into adverse weather. Human Factors, 189-197.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident aircraft
the operator of the accident aircraft
Charleville district disaster coordinator
Quilpie local disaster coordinator
Civil Aviation Safety Authority
Robinson Helicopter Company
A submission was received from the Civil Aviation Safety Authority.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]All times referred to in this report are local time, Coordinated Universal Time (UTC) + 10 hours.
[2]By declaring a mercy flight, a pilot can operate beyond some of the usual regulatory constraints, for example to transport someone who needs lifesaving medical help or to evacuate someone from an emergency such as flood or fire.
[3]Apart from the requirements to maintain VMC visibility, flying through rain has a strong corrosive effect on the main and tail rotor blade’s leading edges of helicopters and is generally not recommended.
[4]Translational lift occurs when clear, undisturbed air, flows through the rotor system from wind or forward speed.
[5]When hovering within about one rotor diameter of the ground, the performance of the main rotor is affected by ground effect. A helicopter hovering in-ground-effect (IGE) requires less engine power to hover than a helicopter hovering out‑of-ground-effect (OGE).
[6]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[7]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[8]Commercial pilots with a Class 2 medical certificate can fly commercial flights without passengers if the maximum take‑off weight is less than 8,618 kg (CASA).
[9]Avgas 100LL: leaded gasoline fuel for reciprocating piston engine aircraft.
[13]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[14]Swift-water rescue teams are part of Queensland Fire Department (QFD) and consist of a team of specially trained firefighters equipped with either paddled or motorised inflatable craft.
[15]Minimum visibility requirements for VFR flight in helicopters are a horizontal visibility of 800 m and clear of cloud (Part 91 MOS 2.07).
On the afternoon of 1 December 2024, a Boeing 737-838, registered VH-XZK, was being operated by Qantas on a scheduled passenger service from Perth, Western Australia, to Sydney, New South Wales. As the aircraft neared Sydney the flight crew were advised that the airport was not accepting arrivals due to storms in the area. The flight crew diverted to Canberra Airport, Australian Capital Territory, with the intention of continuing to Sydney once the airport reopened.
After the aircraft arrived in Canberra, an error was made within the Qantas departure control system that resulted in 51 passengers being incorrectly listed as not on board the aircraft. A loadsheet[1] was created using the incorrect passenger information that contained a weight that was 4,291 kg less than the actual weight of the aircraft. The erroneous loadsheet was issued to the flight crew who used it to make performance calculations for the take-off. The flight crew were not advised of the error until after the aircraft had departed Canberra.
What the ATSB found
The ATSB identified that a minor data input error resulted in an automatic, and undetected, reduction in the number of passengers allocated to the flight. This error cascaded and erroneous passenger information was used by Qantas airport personnel to close the flight, and Qantas load control personnel to create the loadsheet.
Qantas airport personnel had later identified the issue but were unable to rectify the passenger error and did not advise load control. It was also found that although load control personnel held concerns about the validity of the data, and had attempted to understand it, the erroneous loadsheet was issued to the flight crew without resolution.
The error was identified by load control personnel before the aircraft had departed, and they raised the error with Qantas airport movement control. After that point communication procedures were not followed, and Qantas airport personnel were not successful in communicating the error to the flight crew prior to departure.
What has been done as a result
Qantas has amended its procedures to include a requirement for airport personnel to conduct a headcount when a passenger discrepancy is identified. Qantas has also revised its procedures for communicating critical flight information to flight crew and will implement a new procedure that allows load control personnel to contact flight crew directly via the aircraft communications addressing and reporting system when a loadsheet error is identified. Additionally, local briefings have been issued to Canberra Airport personnel communicating handover requirements, and diversion flight handling scenarios.
Safety message
This occurrence highlights the importance of proactively identifying, addressing, and, when necessary, escalating unusual situations. It is not sufficient to rely on downstream controls or other functions to intervene or trap errors. It also reinforces the value of clear and effective communication with feedback, and adherence to defined procedures.
Demonstrating the value of prudent flight planning, the safety margins built into the performance calculations by the flight crew meant that their reliance on the incorrect data did not lead to an adverse outcome.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Diversion to Canberra
On the afternoon of 1 December 2024, a Boeing 737-838, registered VH-XZK, was being operated by Qantas on a scheduled passenger service from Perth, Western Australia, to Sydney, New South Wales. There were 2 flight crew, 4 cabin crew and 172 passengers on board.
Figure 1: Boeing 737-838 VH-XZK
Source: Victor Pody
As the aircraft neared Sydney Airport, the flight crew were advised that the airport would not be accepting arrivals for about one hour due to storms in the vicinity. Rather than holding until the storms cleared, the flight crew diverted to Canberra Airport, Australian Capital Territory, with the intention of continuing to Sydney Airport once it reopened. The passengers would remain on board the aircraft in Canberra, and it would be refuelled for the short flight to Sydney.
At about 1516, the aircraft arrived at gate 9 at Canberra Airport. On arrival it was identified that there were 17 passengers whose final destination was Canberra. These passengers were permitted to disembark the aircraft, leaving 155 passengers remaining on board for the flight to Sydney.
The flight from Canberra to Sydney required the operator to update flight information within their departure control system. That information was to be provided to the flight crew for flight planning.
Canberra to Sydney flight creation
For the aircraft to continue to Sydney, a customer journey lead (CJL) needed to issue a new flight, known as an ‘addstop’, for the Canberra to Sydney sector in the Altéa Inventory (inventory) system[2] (see Departure control system and Customer journey management).
When issuing the addstop for the flight, the CJL identified that it did not have an assigned aircraft configuration code. As a result, they looked up the code for the Boeing 737, which was 73RA01, but they inadvertently entered the code for the Boeing 717, which was 71RA01, and committed (locked) the flight. The Boeing 737 had a maximum seating capacity of 176 passengers, which was composed of 12 business seats and 164 economy seats, and the Boeing 717 had a maximum seating capacity of 125 passengers with no business seating.
There were 11 business and 161 economy passengers on board the aircraft when it arrived in Canberra. When the CJL committed the flight with the incorrect configuration code, the system automatically offloaded[3] all 11 business class passengers and placed between 40 and 57 passengers[4] on standby[5] due to the reduced capacity of the Boeing 717.
The CJL recalled that they knew the Boeing 737 was the correct aircraft for the flight, and the incorrect code was the result of a typing error. They also recalled experiencing a high workload at the time due to an unusually large number of diversions and they felt pressure to complete the addstop ‘as quickly as possible’.
Prior to committing the flight, the system would have presented the CJL with a dialogue box, caused by the Boeing 717 not having business seating, that required them to check and acknowledge the change (Figure 2). While the CJL recalled that the inventory system would present a number of automated pop-ups that needed to be accepted, they did not specifically recount sighting or accepting the class matching dialogue box.
Figure 2: Amadeus Altea Inventory system class change dialogue box
Source: Qantas
The CJL identified the aircraft configuration code error almost immediately after committing the change, and they escalated the matter to their manager, and then to the load control systems manager (LCSM) to unlock the flight. The LCSM was the only person within the organisation who held the necessary permissions to unlock the inventory system.
At about 1526, the CJL contacted the LCSM and requested assistance to unlock the system so that the correct aircraft configuration code could be entered. The CJL contacted the LCSM again at about 1532. The LCSM was off duty at the time and away from their home. The LCSM returned home and unlocked the system using their laptop.
The CJL corrected the aircraft configuration code for a Boeing 737 and re-committed the flight. However, the CJL had not realised that the inventory system had automatically offloaded some passengers from the flight and placed others on standby due to the reduced passenger capacity of the Boeing 717 (see Customer journey management).
Canberra Airport activities
The Qantas airport duty manager (ADM), who was overseeing the ground activities for the aircraft in Canberra, noticed that the new addstop flight to Sydney was unusually slow to show in the Altéa Customer Management (CM) system (see Departure control system). Between 1519 and 1600, the ADM attempted to establish the status of the addstop by calling the CJL, the load control operations leader (LOCO), and the integrated operations centre (IOC) and was advised that there was an issue with the flight in the system.
At about 1632, the ADM was advised by the IOC that the issue had been partially resolved. Once the Canberra to Sydney addstop flight became available to the ADM in the CM system, they made adjustments to reflect the offloaded 17 passengers who were disembarking the aircraft in Canberra, all of whom had occupied an economy seat. The ADM then undertook a ‘mass boarding’[6] of the remaining passengers, in accordance with Qantas procedures, and closed the flight. At about 1646, the ADM issued the ‘passenger clearance’ for the flight and the ‘ramp clearance’ was issued at about the same time (see Ramp and passenger clearance).
A short time later, an airport customer service agent (CSA 1) advised the ADM that there were passengers listed as standby for the flight. The ADM recalled that it was unusual for a diversion flight to have standby passengers and they were not aware of this when they closed the flight. At that time, 11 passengers had been offloaded, and 40 were listed as standby, resulting in a total of 51 passengers not recorded as on board the aircraft when the flight was closed.
The ADM recalled attempting to onboard the standby passengers within the CM system but was not successful. They recalled assuming the problem was related to the earlier issues with the addstop flight. They also recalled thinking that load control would already be aware of the issue, based on earlier telephone conversations with the LOCO where they had discussed the number of disembarking passengers, and that they would be able to rectify the problem prior to issuing the loadsheet. The ADM did not contact the LOCO.
Load control activities
The LOCO commenced the creation of the addstop loadsheet within the Altéa Flight Management (FM) system once the correct aircraft configuration code had been entered by the CJL (see Departure control system). At that time, the LOCO was in contact with the LCSM by telephone and they soon identified that the incorrect code had caused changes to be made to the loading documentation for the aircraft. This had resulted in a significant discrepancy between the number of passengers on board the flight from Perth and the number of passengers on the addstop flight to Sydney.
Over a period of about 35 minutes, both the LOCO and the LCSM attempted to understand the information. This included contacting the Canberra ADM to confirm the number of passengers that had disembarked the aircraft as well as the fuel usage for the previous flight. The LOCO recalled they did not understand the issue or how to resolve the discrepancy and discussed the matter with the LCSM. They recalled the LCSM advised them to go with the passenger figure within the system as it had been confirmed by Qantas airport personnel.
At about 1702, the LOCO issued the flight crew the provisional loadsheet and the final loadsheet for the flight simultaneously despite having ongoing concerns about the validity of the information (see Loadsheet). About one minute later the LCSM, who was still examining the loading information for the flight, identified the standby passengers within the system and advised the LOCO of the error.
Communication of loadsheet error
The LOCO initially attempted to contact the captain by mobile phone to inform them of the loadsheet error, but the call went unanswered. At about 1704, the LOCO contacted the Canberra airport movement control officer (MOCO) and advised them that the loadsheet was incorrect and the aircraft was not to depart (see Load control loadsheet error communication procedures).
The MOCO recalled that they attempted to contact the flight crew via radio, but they did not receive a response. The captain recalled they turned off the company frequency on receipt of the final loadsheet to reduce distractions while they entered the data and generated the take-off speeds.
The MOCO then radioed a customer service agent (CSA 2), who was at the aircraft door with the flight’s customer service manager (CSM) at the time. The CSA 2 recalled discussing the loadsheet with the CSM, and they believed the CSM had also overheard the radio communications about the matter. The CSA 2 also recalled seeing the CSM enter the flight deck shortly after the discussion and believed the message had been passed to the flight crew.
A short time later the CSM advised the CSA 2 that the doors could be closed, and the aircraft would be departing. However, the CSM reported that they did not receive a message from the CSA 2 about the loadsheet and, as a result, had not advised the flight crew of an error.
At about 1705, after providing instructions to the CSA 2 to contact the crew, the MOCO went on a scheduled break when advised to do so by the ADM. No handover was completed prior to the MOCO going on break as they believed the ADM was already aware of the loadsheet issue. However, the ADM recalled they had no awareness of the error at that time.
Aircraft departure
The error in the final loadsheet resulted in a calculated weight that was 4,291 kg less than the actual weight of the aircraft. The flight crew used this erroneous weight to make performance calculations for the take-off (see Loadsheet error and performance implications).
The captain noted that the passenger figure within the loadsheet had reduced from the flight from Perth, but recalled that the CSM had made them aware that some passengers would be leaving the aircraft as their final destination was Canberra. They also recalled observing a line of people departing the aircraft. On receipt of the final loadsheet, the captain believed the reduced passenger figure reflected the number of people that had left the aircraft. Other than the passenger figure within the loadsheet, the flight crew were not advised of the final number of passengers that had disembarked the aircraft, nor was there a procedural requirement to do so.
At 1712 the aircraft doors were closed. At 1714, the aircraft pushed back from gate 9 and it became airborne at about 1721. The captain recalled that during the take-off the aircraft was slightly slow to accelerate but they did not experience any controllability issues.
At 1737, when the aircraft was in cruise at 15,000 ft, the flight crew received an aircraft communications addressing and reporting system (ACARS)[7] message that load control were working to correct the loadsheet. On receipt of the ACARS message, the flight crew radioed the port controller and were advised that the loadsheet that had been issued to them contained an incorrect passenger figure. The flight crew placed the aircraft in a hold[8] while the correct weights were established. The aircraft later landed at Sydney Airport without further incident.
Context
Departure control system
Qantas utilised the Amadeus Altéa Departure Control information technology system to manage operational activities. The system was composed of various integrated components including:
Altéa Inventory (inventory) – which was used to manage flight schedules, passenger seating and flight disruptions.
Altéa Customer Management (CM) – which was used to carry out the management of customers including monitoring cabin seating configurations, boarding activities, baggage, and acceptance figures.
Altéa Flight Management (FM) – which was used to perform load control functions for aircraft and create the necessary documents for flight.
Customer journey management
Qantas customer journey personnel were responsible for the issuance of a new flight following a diversion to an alternate airport. These new flights, called ‘addstops’, were managed within the inventory system.
When issuing a new addstop flight, customer journey personnel would make manual amendments as required, including adding or changing the aircraft configuration code. If a change was made that resulted in the allocation of an aircraft with a smaller seating capacity than the original aircraft, it would cause the system to automatically either offload or place on standby the excess number of passengers. While the offloading of passengers was an automatic function, any further amendment to an aircraft with a larger capacity required the user to manually transfer the passengers back onto the flight.
Airport passenger management
Qantas airport personnel were responsible for the arrival and dispatch of the diversion flight, including oversight of the refuelling and passenger management. During this process, airport personnel utilised the CM system to manage passenger information. In normal circumstances, as passengers boarded a Qantas aircraft, their boarding passes were scanned, and the CM system was updated automatically with passenger boarding information. However, as this was a diversion flight which involved the majority of the passengers remaining on board, airport personnel were required to manually update this information within the CM system.
Loadsheet
General
A loadsheet is a document created for each flight that contains details such as the quantity and distribution of fuel, cargo, baggage, crew and passengers on board the aircraft. It is used to calculate aircraft weight and balance parameters, and performance requirements. Load control personnel were responsible for the creation of loadsheets using the FM system.
A provisional and a final loadsheet were required to be created for all flights. The provisional loadsheet detailed the anticipated configuration of the aircraft. The final loadsheet contained the confirmed aircraft configuration and could only be issued after the passenger and ramp clearances were received from the departure airport personnel.
Ramp and passenger clearance
Ramp clearance was a report issued by the airport loading supervisor[9] to load control personnel indicating the completion of loading, including final baggage numbers. The data contained within the ramp clearance was then used for loadsheet computation.
Passenger clearance was a report issued by departure airport personnel to load control personnel indicating that no further passengers were to be accepted for the flight, with the majority of passengers on board and the remaining passengers’ exact location known.
Communication of loadsheet errors
Load control loadsheet error communication procedures
In scenarios where an error was identified in the final loadsheet after it had been issued to the flight crew, but before the aircraft had departed from the gate, the Qantas Weight and Balance Manual required the load control operations leader (LOCO) to contact the movement control officer (MOCO) in Canberra and for them to notify the flight crew of the nature of the discrepancy.
Airport communication procedures
The procedures to be used by Qantas airport personnel to contact the flight crew prior to an aircraft having departed the gate were documented in the Qantas Canberra Airport Movement Control Operating & Training Manual (version 1.2 dated September 2024). That stated:
Contacting a [flight] crew is to be done via ground to air radio in the first instance.
If contact is not made, then an agent is sent to ask the crew to contact MOCO.
If agent is unable (due door closed/aerobridge disconnected), engineer/pushback on headset to request crew contact MOCO.
Flight crew communication procedures
The procedures to be used by flight crew when maintaining radio communications with the airport personnel were contained in the Qantas Flight Administration Manual (dated 1 August 2024) which stated:
Subject to operational requirements, flight crew should maintain a listening watch on company frequency and interphone during transit.
It also stated:
For domestic operations, the frequency for the [port controller] must be monitored from [estimated time of departure]-5 minutes until pushback commences.
Loadsheet error and performance implications
Loadsheet information
The passenger composition and aircraft zero fuel weight (ZFW)[10] as documented in the loadsheet for the previous flight, and the erroneous and corrected loadsheet for the incident flight are contained in Table 1.
Table 1: Loadsheet information
Sector
Loadsheet
Passengers
Zero fuel weight
Perth – Sydney
(diversion to Canberra)
Final version 1
11 business class
161 economy class
61,264 kg
Canberra – Sydney
Final version 1
0 business class
104 economy class
55,539 kg
Canberra – Sydney
Final version 2
11 business class
144 economy class
59,830 kg
Loadsheet error
The erroneous loadsheet issued to the flight crew listed the total number of passengers on board the aircraft as 104, whereas the actual number of passengers on board was 155. This resulted in a ZFW of 55,539 kg when the actual ZFW of the aircraft was 59,830 kg.
The Qantas Flight Administration Manual contained a caution note to flight crew that stated:
Following a diversion the ZFW and passenger numbers on the loadsheet for the subsequent sector must be reconciled against those for the preceding sector. The new ZFW should be the same unless passengers disembark or pantry is changed.
For a change in passenger load allow 100 kg per passenger when reconciling ZFW values. e.g. if 20 pax disembark the new ZFW should be approximately 2,000 kg less than previous.
The error within the loadsheet resulted in a ZFW difference between the subsequent and preceding sectors of 5,725 kg, with 68 passengers captured as having disembarked the aircraft. This reduction in weight was more conservative than the formula contained within the Qantas Flight Administration Manual, which equated to about 6,800 kg. While the captain recalled being aware of the reduced passenger figure, they did not recount having undertaken the ZFW reconciliation calculation.
Performance implications
The flight crew used the incorrect loadsheet to calculate aircraft performance. This resulted in the generation of take-off speeds 3–4 kt less than those applicable to the aircraft’s actual weight. This increased the risk of degraded performance and unanticipated handling characteristics during the take-off. However, the flight crew elected to use the full length of the runway for the take-off, and did not apply the headwind component, which added an increased safety margin for take-off performance.
Independent passenger number verification
The Qantas Cabin Crew Operations Manual (dated 1 October 2024) contained a process for an independent verification of passengers on board an aircraft. It stated:
Security requires that where positive accountability of passengers is not possible during boarding, the number of passengers must be verified by a headcount prior to departure. The headcount is to ensure that the correct number of passengers have entered the aircraft, via the tarmac.
However, the process was not required for scenarios involving the partial disembarkation at a diversion airport.
Related occurrences
Aircraft loading and confirmation processes involve a number of people fulfilling different functions. Errors can be introduced at any point and carried through various interfaces.
At Sydney Airport in 2017, an Airbus A330 departed overweight after a required cargo variation was not actioned by ground crew (ATSB investigation AO-2018-003). A decision by the flight crew to carry additional fuel led to a requirement to reduce the weight of freight on board the aircraft. A 2,005 kg freight pallet was to be replaced with a lighter unit weighing 1,130 kg. The cargo variation was not actioned by the loading supervisor as electronic messages associated with the revised loading instruction were acknowledged without being correctly interpreted. That was probably influenced by the supervisor’s experience that load changes were accompanied by verbal advice, and that did not occur on this occasion.
In the East Midlands, UK, in 2023 a Boeing 737 tail strike resulted from the provision of 2 different load data sheets (AAIB investigation AAIB-29762). One was correct and the other, a remnant from the previous flight, was incorrect for the next flight. The incorrect data was used for performance calculations, and the aircraft weight was calculated to be around 10,000 kg lighter than the actual weight. This led to the take-off being 15 kt too slow on rotation and the tail struck the ground.
Five passenger loading events that occurred in Australia over the period 2015–2017 were investigated (ATSB investigation AI-2015-139).On these five separate occasions the aircraft were loaded with incorrect passenger distributions or with incorrect passenger numbers used to determine the aircraft's weight and balance. This placed increased operational pressure on flight and cabin crews and, on at least one occasion, adversely affected aircraft performance during take-off.
Safety analysis
Incorrect aircraft configuration code
The customer journey lead (CJL) entered the incorrect aircraft configuration code when creating the ‘addstop’ flight for the Canberra to Sydney sector. This error was consistent with a skill-based ‘slip’, where an individual’s intentions are correct, but the action is incorrectly completed (Tsang and Vidulich 2003). In this case, the CJL entered one incorrect digit.
The CJL also described a high workload environment at the time due to the number of diverted flights, and that they felt a time pressure to complete the addstop task. According to Orlady and Orlady 1999, workload within the aviation environment can be considered as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. It represents the cost incurred by the human operator in achieving a particular level of performance’. Increases in workload during abnormal situations have been linked to an increase in error rates in individuals (Johannsen and Rouse 1983). Consequently, it is possible that the CJL’s input error was influenced by the increased workload they were experiencing at the time.
The CJL committed the flight in the Altéa Inventory system prior to identifying the error. When doing so, the CJL would have been presented with a pop-up that highlighted the business class seating issues. However, they did not specifically recount sighting or acknowledging the pop-up. This was probably due to ‘expectation bias’ which involves an individual observing what they expected to occur, rather than what actually occurred (Flight Safety Foundation 2014). It is therefore likely that the CJL acknowledged the pop‑up, without considering the contents of the message, due to their expectation that the flight information was correct.
Having later identified and corrected the aircraft configuration code, the CJL did not identify that the system had made automatic changes to the passenger composition of the flight. This was also likely due to expectation bias as the CJL believed the correction had fully addressed the issue. Consequently, some passengers who were on board the aircraft were offloaded, or listed as standby, and not reallocated to the flight.
Contributing factor
After correcting a minor data input error, the customer journey department did not notice that an automatic reduction in the number of passengers allocated to the flight had occurred. As a result, some passengers who were on board the aircraft were not reallocated to the flight.
Flight closed with incorrect passenger data
The Qantas airport duty manager (ADM) at Canberra closed the flight without identifying the 51 offloaded and standby passengers. As a result, these passengers were recorded as not being on board the aircraft. The ADM recalled that it was unusual for standby passengers to be listed for a diversion flight, and they did not see them within the Altéa Customer Management (CM) system. The ADM’s recollections were consistent with expectation bias, where the ADM’s prior experience with diversion flights influenced their ability to identify the unusual scenario.
Having closed the flight, the ADM was made aware of the standby passengers by a customer service agent. The ADM attempted to onboard these passengers within the CM system, but when this proved unsuccessful the ADM took no further action to address the issue. The ADM recalled assuming the standby passenger issue was a manifestation of the earlier problems with the addstop flight, and that load control were aware of the issue and would resolve it prior to publishing the loadsheet. As a result, they did not consider communicating the matter to load control.
Contributing factor
Qantas airport personnel inadvertently used the erroneous passenger data within the scheduling information to close the flight. The issue was identified after the flight was closed, but airport personnel did not ensure Qantas load control were aware of the matter.
Erroneous loadsheet issued
The load controller’s (LOCO) decision to issue the loadsheet to the flight crew, despite having ongoing concerns about the validity of the information, was likely influenced by several factors including the closure of the flight and issuance of the passenger clearance by the ADM. In accordance with Qantas procedures, the ADM’s passenger clearance confirmed to the LOCO that the number of people listed as on board the aircraft in the Altéa Flight Management (FM) system, was correct. However, as stated above, the ADM had later become aware that there were additional passengers listed as standby for the flight but did not communicate this information to the LOCO.
The LOCO had also exhausted their ability to identify the reason for the anomalies and resolve the issue, and they communicated their concerns to the load control system manager (LCSM). In response, the LCSM advised the LOCO to issue the loadsheet using the information within the FM system, which the LOCO then did. It is possible this outcome was a result of a phenomenon known as ‘risky shift’. Risky shift means it is easier for a group to make a decision involving a greater acceptance of risk than an individual would on their own due to a variety of factors including the diffusion of responsibility (Smith and Radinsky 1970).
The result was the provision of an erroneous loadsheet to the flight crew that contained a weight that was 4,291 kg less than the actual weight of the aircraft. Shortly after the loadsheet was issued to the flight crew, but before the aircraft had departed, the LCSM identified the standby passengers within the FM system and advised the LOCO.
Contributing factor
Although Qantas load control personnel held concerns about the validity of the data, and had attempted to understand it, the concerns were not resolved and the erroneous loadsheet was issued to the flight crew. The error was identified by load control after it had been provided to the flight crew, but before the aircraft had departed.
Communication of loadsheet error
Once the LOCO was made aware of the error within the loadsheet, they took immediate action to inform the flight crew of the issue. When the captain did not answer their mobile telephone, the LOCO communicated the error to the airport movement control officer (MOCO) in accordance with Qantas procedures. Having done so, it was reasonable for the LOCO to believe the flight crew would be informed of the error and the aircraft would not be permitted to depart.
On receipt of the information from the LOCO, the MOCO attempted to contact the flight crew via radio, but they had deselected the company frequency. This took place about 10 minutes prior to pushback at a time when Qantas procedures required the flight crew to maintain a listening watch on the company frequency, subject to operational requirements. The captain recalled that the radio was deselected to reduce distractions while they entered the loadsheet data and generated the take-off speeds. This reason for deselecting the company frequency was likely consistent with the ‘operational requirement’ caveat of the procedures. However, it limited the ability of Qantas airport personnel to communicate directly with the flight crew in the lead up to departure.
Having been unable to contact the flight crew via radio, the MOCO radioed the customer service agent (CSA 2) and instructed them to inform the flight crew that the loadsheet contained an error. This did not conform with Qantas procedures which required the flight crew to be instructed to contact the MOCO and communicate directly with them. Doing so would have ensured that the flight crew received the information and closed the communication loop with the MOCO.
The CSA 2 did not inform the flight crew. The CSA 2 reported that at the time the MOCO contacted them by radio the CSA 2 was with the customer service manager (CSM) at the aircraft door. The CSA 2 believed the CSM overheard the MOCO’s radio call and that the CSM would tell the flight crew.
However, The CSM could not recall either being advised of a loadsheet error or overhearing the radio communications about the matter. It is likely that the CSM would have advised the flight crew had they heard of the problem. The flight crew were not informed of the loadsheet error.
While the procedure was for the MOCO to request direct communication from the flight crew, shortly after divesting responsibility to the CSA 2, the MOCO went on break as instructed by the ADM. No one was allocated the responsibility of ensuring resolution prior to departure as the MOCO believed the ADM was already aware of the loadsheet issue. However, the ADM reported they had no awareness of the error at that time. The MOCO did not return from break until after the aircraft had departed.
The procedural and communication breakdown meant that while Qantas’ airport personnel were aware of problems with the loadsheet, no-one communicated directly with the flight crew or made certain that the flight crew understood that there was a problem. As a result, the aircraft departed with 4,291 kg more weight than anticipated by the flight crew. The flight crew’s prudence in applying safety margins to their departure profile avoided adverse outcomes for the flight.
Contributing factor
The flight crew were not informed of the identified loadsheet error before the aircraft departed. This was due to:
the flight crew had deselected the ground communication frequency and were therefore not contactable by radio
after instructing the customer service agent to contact the flight crew in person, there was no further follow-up or communication with the flight crew made by the movement controller
the customer service agent was not instructed to advise the flight crew to contact the movement controller via radio when attempting to pass the information on in person
the customer service agent understood that they had informed the cabin crew of the loadsheet error, and believed they would inform the flight crew.
Independent process to confirm actual number of passengers on board aircraft
Qantas did not have an independent process to confirm the actual number of passengers on board an aircraft following partial disembarkation at a diversion airport. In these scenarios the final passenger figure within the loadsheet relied exclusively on the accuracy of the transposed data from the previous flight and any manual amendments made by Qantas airport personnel. Other than the figure within the loadsheet, Qantas had no other mechanism to advise the flight crew of the number of passengers that had disembarked the aircraft. Consequently, the absence of an independent process to confirm the actual number of passengers on the aircraft, such as a headcount, could limit a flight crew’s ability to verify the information contained within a final loadsheet and identify any passenger number error.
Other finding
Qantas did not have an independent process to confirm the actual number of passengers onboard an aircraft following partial disembarkation at a diversion airport. This could limit a flight crew’s ability to verify the information contained within a final loadsheet and identify any passenger number error.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the passenger loading event involving Boeing 737-838, VH-XZK, Canberra Airport, Australian Capital Territory, on 1 December 2024.
Contributing factors
After correcting a minor data input error, the customer journey department did not notice that an automatic reduction in the number of passengers allocated to the flight had occurred. As a result, some passengers who were on board the aircraft were not reallocated to the flight.
Although Qantas load control personnel held concerns about the validity of the data, and had attempted to understand it, the concerns were not resolved and the erroneous loadsheet was issued to the flight crew. The error was identified by load control after it had been provided to the flight crew, but before the aircraft had departed.
Qantas airport personnel inadvertently used the erroneous passenger data within the scheduling information to close the flight. The issue was identified after the flight was closed, but the airport personnel did not ensure Qantas load control were aware of the matter.
The flight crew were not informed of the identified loadsheet error before the aircraft departed. This was due to:
the flight crew had deselected the ground communication frequency and were therefore not contactable by radio
after instructing the customer service agent to contact the flight crew in person, there was no further follow-up or communication with the flight crew made by the movement controller
the customer service agent was not instructed to advise the flight crew to contact the movement controller via radio when attempting to pass the information on in person
the customer service agent understood that they had informed the cabin crew of the loadsheet error, and believed they would inform the flight crew.
Other factors that increased risk
Qantas did not have an independent process to confirm the actual number of passengers on board an aircraft following partial disembarkation at a diversion airport. This could limit a flight crew’s ability to verify the information contained within a final loadsheet and identify any passenger number error.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Qantas
The Qantas load control diversion checklist has been amended to include a requirement for airport personnel to conduct a headcount when a passenger discrepancy is identified.
The Qantas airport product and service manual has been amended to contain a procedure for scenarios where critical flight information needs to be communicated to the flight crew, but they are uncontactable. This includes contacting air traffic control to prevent the aircraft from departing and requiring closed loop communications to confirm receipt of critical information. Qantas will also implement a procedure that allows load control personnel to contact flight crew directly via the aircraft communications addressing and reporting system when a loadsheet error is identified.
A local brief was issued to Canberra Airport personnel that defined the requirements for a handover, when going on break, to ensure critical information is communicated. A local brief was also issued that outlined the requirements for handling an inbound diversion, including ‘all possible scenarios regarding passengers disembarking/remaining onboard’.
Sources and submissions
Sources of information
The sources of information used during the investigation included:
Qantas
captain and first officer
customer service manager
airport duty manager
customer service agent
officer movement control
load control operations leader
customer journey lead
load control systems manager
Bureau of Meteorology
References
Flight Safety Foundation. (2014). A practical guide for improving flight path monitoring, final report of the active pilot monitoring working group. Available from https://flightsafety.org.
Johannsen, G. and Rouse, W. (1983). Studies of planning behavior of aircraft pilots in normal, abnormal, and emergency situations. Systems, Man and Cybernetics, IEEE Transactions on, (3), pp.267-278.
Orlady, H. and Orlady, L. (1999). Human factors in multi-crew flight operations. Ashgate, Aldershot, UK p.203.
Smith, G. and Radinsky, T. (1970). The Effect of Diffusion and Concentration of Responsibility on the Risky Shift Phenomenon in a Two-choice Situation. Proceedings of the Iowa Academy of Science, 77(1), 308-314.
Tsang, O. and Vidulich, M. (2003). Principles and practice of aviation psychology. Lawrence Erlbaum Associates, Mahwah, New Jersey.
Wickens, C. Hollands, J. Banbury, S. & Parasuraman, R. (2013). Engineering psychology and human performance (4th edition). Pearson, Boston.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Qantas
captain and first officer
customer service manager
Canberra Airport duty manager
Canberra Airport customer service agent
Canberra Airport officer movement control
load control operations leader
customer journey lead
load control systems manager
Civil Aviation Safety Authority
Submissions were received from:
Qantas
Civil Aviation Safety Authority
load control operations leader
Canberra Airport officer movement control.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Loadsheet: a document provided to pilots that details the distribution and weight of passengers and freight on board an aircraft for use in performance calculations for the flight.
[2]Altéa Inventory system: a revenue and schedule management system with passenger and seat availability functions,
On 20 October 2023 the pilot of a Cessna 208 aircraft, registered VH‑UMV and operated by Experience Co, was conducting parachute operations at Barwon Heads Airport, Victoria with 16 parachutists on board. Passing about 500 ft on climb, the pilot detected a partial power loss consistent with a previously‑encountered transient power reduction.
Expecting the power to return immediately, the pilot did not lower the aircraft’s nose to maintain airspeed. The airspeed continued to reduce until the stall warning horn sounded and, due to the low height, low engine power and low airspeed, the pilot attempted to conduct a forced landing. However, the aircraft collided with water before continuing onto the riverbank and ground for approximately 50 m before coming to rest.
The aircraft was substantially damaged, 6 of the parachutists received serious injuries, 8 sustained minor injuries, and 2 were uninjured. The pilot also sustained minor injuries.
What the ATSB found
The ATSB found that passing about 500 ft on climb, the power reduced likely due to abnormal activation of an engine torque and temperature limiting system. Expecting the power to return quickly and surge, and in preparation for turning off the system, the pilot moved the power lever aft to reduce the power setting and delayed lowering the aircraft’s nose to maintain airspeed, resulting in a stall warning and subsequent collision with water.
The ATSB also found that Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the engine limiting system, but did not specify a minimum safe height at which to do so. This increased the risk of a loss of control and/or ground collision.
Further, the ATSB found that the operator's weight and balance calculation for the accident flight did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity, therefore, although it did not contribute to the accident, the weight and balance was inaccurate for the intended flight. Additionally, the software used to calculate aircraft weight and balance did not provide a warning if individual aircraft zones were overloaded.
Finally, the ATSB found that Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
What has been done as a result
At the time of writing, Experience Co was re‑developing its sport skydivers safety video to include emergency procedures. Additionally, the following proactive safety actions have been taken:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet-wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the single red line/torque and temperature limiter malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed Cessna 208 and Cessna 208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the supplemental type certificate (STC) holder to be followed at or above 1,000 ft above ground level.
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of its aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Finally, the Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Lower the nose to maintain the glide speed of the aircraft. If turning is conducted, keep in mind an increased bank angle will increase the stall speed of the aircraft.
Maintain glide speed and assess whether the aircraft is maintaining, gaining or losing height to gauge current aircraft performance.
Fly the aircraft to make a landing, given the aircraft’s height and performance, and the pre-planned routes for the scenario.
If time permits, moving the power lever through the full range may result in increased power available to climb and/or create the time to diagnose the issue.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. This incident highlights the importance of passengers being appropriately briefed on the brace position and use of emergency exits. It also illustrates the higher injury risk associated with the carriage of parachutists, due to the increased number of occupants and inferior restraints compared to being secured in a certified seat.
The occurrence
Early on the morning of 20 October 2023, the pilot of a Cessna 208 aircraft, operated by Experience Co and registered VH-UMV, refuelled and inspected the aircraft in preparation for parachuting operations from Barwon Heads Airport, Victoria. No defects, including any fuel debris or contaminants, were identified.
The pilot’s first flight of the day was to carry 16 sport parachutists for a parachute jump from 15,000 ft. At about 0750 local time, the parachutists boarded the aircraft. The pilot recalled that the conditions were CAVOK,[1] with a light wind from the north. They taxied the aircraft to runway 36 for a northern departure.
A review of OzRunways[2] flight data, recorded at 5-second intervals, showed the aircraft commenced the take-off roll at 0757. The pilot reported moving the power lever forward until the engine reached 100% torque, and then reducing the power slightly during the take-off roll. Camera footage showed that the aircraft became airborne at 0757:22.
The pilot reported that, as the aircraft climbed and the airspeed increased, they retracted one stage of flap passing through 85 kt and another at about 95 kt. At 0757:47, climbing through about 400 ft, the aircraft reached its maximum recorded ground speed of 95 kt. The pilot reported that as the aircraft approached 500 ft above ground level and they reached for the flap lever to retract the last stage of flap, they heard a reduction in engine noise, and felt a deceleration.
The pilot initially associated the loss of power with activation of the torque and temperature limiter (TTL) (see the section titled Torque and temperature limiter), which they had previously experienced in that aircraft. Consistent with the previous TTL activation, the pilot expected the power to quickly return, and reported reducing power slightly to prevent the engine surging[3] as power was restored.
The reduction in engine power, combined with the climb pitch attitude, resulted in the airspeed reducing and activation of the stall warning horn. On hearing the stall warning, the pilot lowered the aircraft’s nose to reduce the angle of attack[4] and increase the airspeed.
At 0757:57 the aircraft reached the highest recorded altitude of about 700 ft at 88 kt ground speed and, 5 seconds later, had descended to 600 ft and the ground speed reduced to 71 kt, then to 69 kt 5 seconds later. This flight path was consistent with video camera footage of the aircraft’s flight path (Figure 1). At 0758:08 the ADS-B[5] data recorded a descent rate of 3,520 ft/m passing an altitude of approximately 400 ft.
Figure 1: VH-UMV flight path captured by the airport camera
The ATSB combined multiple images together to show the flight path of the aircraft as captured by a local video camera. Source: Airport operator, annotated by the ATSB
The pilot reported that, as the aircraft descended, they observed the engine torque indication reducing through approximately 30% and attempted to switch off the TTL in accordance with the operator’s Engine Power Loss checklist. Due to the aircraft’s low height above the ground, and the pilot’s assessment that there was an engine issue, the pilot then selected a field in which to conduct a forced landing.
The pilot turned to the loadmaster[6] seated beside them and called out ‘gear-up’, to alert parachutists to be ready to exit the aircraft. In response, the loadmaster began directing parachutists to open the roller door, secure their harnesses, and brace for landing. The roller door was opened, but not secured in that position.
The pilot selected a forced landing location in a clearing beyond a river. However, less than 1 minute after becoming airborne and unable to maintain altitude, the aircraft impacted the water short of the clearing, resulting in water entering the cabin and forcing the unsecured roller door closed. The aircraft continued onto the riverbank where the main landing gear detached, then travelled along the ground for about 50 m before coming to rest (Figure 2).
The pilot sustained minor injuries, 6 parachutists sustained serious injuries, 8 sustained minor injuries and 2 were uninjured. The aircraft was substantially damaged.
Figure 2: VH-UMV flight path
Source: ADS-B exchange flight data overlaid on Google Earth and image of accident site provided by operator, annotated by the ATSB
Context
Pilot information
The pilot held a commercial pilot licence (aeroplane) and a current class 2 aviation medical certificate. On 19 April 2023, the pilot completed their gas turbine engine design feature endorsement and single engine aircraft flight review in a Cessna 208 aircraft.
At the time of the accident, the pilot had accrued approximately 220 hours of total flight experience, which included 38 hours on the Cessna 208 aircraft type. Of those hours on type, 36 had been accrued in the previous 90 days.
The pilot reported that they were familiar with VH-UMV, having conducted multiple flights in it prior to the accident flight. The pilot was also aware of operator-specific engine operating limitations for VH-UMV, and reported having previously experienced an engine surge at 5,000 ft (see the section titled Engine surging).
Aircraft information
Certification details
The Cessna Aircraft Company 208 (C208) is an all-metal, high-wing aeroplane with tricycle landing gear and designed for general utility usage. The aircraft type certificate data sheet (TCDS) A37CE described the C208 as an ‘11-place closed land monoplane’, and under the heading ‘No. of seats’, provided a centre of gravity range for seating for one or 2 pilot seat locations and referenced the current Pilot’s Operating Handbook (POH) and United States (US) Federal Aviation Administration (FAA) Airplane Flight Manual (AFM) for passenger seat arrangements for seats 3 to 11.
The C208 POH Section 2 – Limitations – Maximum passenger seating limits stated that up to 11 seats, including the pilot’s seat/s, may be installed.
VH-UMV, serial number 20800077, was manufactured in 1986 and first registered in Australia in 2005. At that time, the aircraft was issued 2 certificates of airworthiness, one for normal category[7] operations and one for restricted category[8] operations for the purpose of carrying people for parachute jumping.
Operating in the restricted category required several conditions, including removal of the cabin seats, compliance with a specific engineering order and readily visible restricted category placards, none of which were in place on the accident flight. Additionally, under Civil Aviation Safety Regulations (CASR) current at the time of the accident (CASR 91.845, 91.025, 135.030), aircraft operating in the restricted category were not permitted to conduct air transport operations (carriage of passengers or cargo for hire or reward).
In 2017, the aircraft’s Pratt & Whitney PT6A-114 gas turbine engine was replaced with a Honeywell International Incorporated TPE331-12JR-704TT gas turbine engine that drove a 4‑bladed, constant‑speed, full‑feathering,[9] reversible[10] Hartzell HC-E4N-5KL propeller with hydraulically‑operated variable‑pitch control. The engine modification was completed under the Texas Turbine Conversions supplemental type certificate (STC) SA10841SC, with an associated AFM Supplement. Under the heading ‘Maximum passenger seating limits’, the AFM supplement stated ‘No changes’ (from the C208 AFM).
The aircraft was also modified in accordance with STC SA01180SE, which increased the original maximum take-off weight from 3,628 kg to 3,792 kg. Both STCs were approved by the US FAA and therefore accepted in Australia and taken as having been issued by CASA in accordance with CASR Part 21 regulation 21.114.
Three modifications made to VH-UMV and other aircraft in the operator’s fleet were completed under engineering orders in accordance with the CASR Part 21 regulation 21.437 Grant of modification/repair design approvals—grant by authorised person or approved design organisation:
ESE-C208-25-001—Rework of interior for parachute operations
ESE-C208-25-007—Installation of parachute bench seating
ESE-C208-95-003—Installation of Go-Pro cameras.
Torque and temperature limiter
VH‑UMV was fitted with a switch‑activated torque and temperature limiter (TTL) system designed to prevent these parameters exceeding specified limits. Where an exceedance of the allowable torque or exhaust gas temperature (EGT) was detected, the TTL computer restricted fuel flow to the engine. The maximum allowable fuel reduction of a normally-functioning bypass was about 68 L/hour (125 lbs/hour), resulting in a reduction of the torque output from 100% to about 62% (due to the approximate 25% reduction in fuel flow).
Texas Turbine Conversions advised that, when functioning normally, the system would maintain the lower of the allowable torque or EGT limits and if the TTL bypassed the maximum allowable fuel, it would be felt immediately. In that case, the appropriate pilot response was to switch off the TTL.
The aircraft’s engine monitoring system included a single red line (SRL) controller, associated with the EGT limit. Like the TTL, the SRL was switch‑activated and deselection of the SRL also deactivated the TTL.
The allowable EGT limit was dependent on the phase of flight. Specifically, the operating margin from the EGT limit in the climb phase was reduced in the cruise phase. The phase was dependent on the position of the speed lever. Therefore, if the speed lever was moved aft during take-off or climb, the EGT limit also reduced and could result in activation of the TTL. The operator reported that the speed lever was fully forward throughout the short flight, and therefore the climb EGT limit applied.
Operating limits
The AFM supplement for the Honeywell engine specified operating limits. With the SRL and TTL on, those limits included a maximum EGT of 650 °C, maximum 100% torque and maximum of about 101% RPM during take-off and climb. The supplement also provided an EGT table with limits for operating with the SRL off or inoperative, or ‘manual mode’. The limits were provided for operating at 100% RPM or 96% RPM based on the outside air temperature in 5 °C increments from −60 to +60 °C.
The AFM defined take-off power as the lower of 100% torque or 650 ºC EGT (SRL ON), whichever is reached first at 100% engine RPM.
Engine surging
On 17 October 2023, the pilot submitted an internal safety report relating to an uncommanded engine surge, which they experienced at an altitude of approximately 5,000 ft. The pilot report stated:
Torque roll back for a split second, noticeable reduction in power and deceleration.
The pilot reported reducing the power then slowly increasing it while monitoring engine parameters in response to the event.
Although not recorded on the aircraft’s maintenance release (MR),[11] reportedly due to their transient nature, pilots submitted 7 other internal safety reports between July and October 2023 of engine surging in VH‑UMV, assessed as being due to the TTL.
A review of maintenance recorded in VH-UMV’s engine logbook for the previous 12 months showed that the TTL controller was replaced ‘for fault isolation’ following the first reported surging occurrence on 3 April 2023. A further logbook entry on 18 September 2023 recorded that the EGT harness was replaced in response to reported engine surging at take-off power.
The engine surging safety reports indicated troubleshooting test flights were also conducted. A series of test flights on 7 September 2023 was able to replicate the previously‑reported surging.In addition, a test flight following the EGT harness replacement noted that the surging was still present. One of the experienced surges resulted in a torque value of 62% and fuel flow reduced by approximately 72 L/hour (128 lbs/hour). The MR current at the time of the accident identified that the aircraft operated over 90 flights prior to the next reported surge event on 17 October 2023. On that day, the aircraft operated 6 flights, and one surge occurrence was reported. According to the MR, 12 flights were conducted over the next 2 days (18–19 October), with no reports of engine surging submitted. However, the ATSB was also advised of an engine surge on 18 October, which was not recorded.
The MR current at the time of the accident recorded 257 flights over 3 months, during which there were 6 reported surging events. That frequency illustrated the intermittent nature of the anomaly, which likely hindered troubleshooting.
As a result of the internal reports, on 21 July 2023, pilots were advised to operate VH-UMV under a set of unique operating conditions to avoid the TTL scheduling a significant bypass of fuel and subsequent notable drop in available power. These were limitations of 95% torque and 640 °C EGT.
A review of the operator’s safety reports also identified that surging events were reported on 3 other company aircraft. For those aircraft, maintenance actions rectified the cause of each event and there were no subsequent surging events reported.
Minimum equipment list
Experience Co’s minimum equipment list (MEL) specified permissible unserviceable items with which the aircraft was permitted to operate temporarily under the stated procedures, conditions and limitations. The MEL included that both the SRL computer system and TTL ‘may be inoperative provided inoperative SRL system procedures and limits are observed’. In that case, it was also required that an MEL placard be fitted adjacent to the TTL or SRL switch for the inoperative system/s. There was no MEL placard for the TTL nor was it listed as inoperative at the time of the accident.
Engine power loss checklist
The Texas Turbine Conversions AFM supplement provided checklists for engine failures, but not for partial engine power loss. The operator’s ‘Engine Power Loss’ checklist for the C208 with the Honeywell engine (Figure 3), required pilots to first control the aircraft by moving the elevator control forward to lower the aircraft’s nose if climbing. After completing initial checks, if the RPM was above 60% or the engine was surging, the pilot was to move the power lever to ½ inch (12.7 mm) forward of the flight idle position, in preparation for turning off the TTL, so as not to produce a transient exceedance of the EGT.
Figure 3: Engine power loss checklist
Source: Aircraft operator
Weight and balance
Aircraft moment arms
To enable calculation of the aircraft’s weight and balance, the C208 POH included a 2-place seating option, which divided the cabin into 7 zones (zones 0–6) (Figure 4). The flight manual supplement for the Texas Turbine Conversions STC did not include changes to the zones or seating configuration, therefore the POH applied.
Source: Cessna 208 Pilot’s Operating Handbook, annotated by the ATSB
Accident flight weight and balance
Prior to departure, a member of the parachuting operations team calculated the weight and balance for the proposed flight using the IBIS Technology flight planning module software (Table 1).[12] The moment arms from the POH were used for the calculations. Zone 6 was not used.
Table 1: Planned weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272.152
1,273.672
Zone 0 [1]
3,442
272
936.142
Zone 1
4,277
218
932.386
Zone 2
4,948
318
1,573.464
Zone 3
5,613
173
971.049
Zone 4
6,261
404
2,529.444
Zone 5
6,896
173
1,193.008
Total
3719.152
17,307.075
Centre of gravity
4,653
The operator’s weight and balance used the crew seat arm as the zone 0 arm.
The calculated weight and balance resulted in a take-off weight of approximately 3,719 kg and the aircraft’s centre of gravity located at 4,653 mm aft of the datum. To remain inside the operating limitations, the maximum allowable weight was 3,792 kg. Additionally, the aircraft needed to remain within the centre of gravity envelope, which had an aft limit of 4,680 mm and the forward limit varied with the operating weight. Each zone had a maximum allowable weight limit, and the maximum for zone 0 was 159 kg. However, the calculation software did not provide a warning to notify the user a zonal limit had been exceeded.
Information provided by the parachutists included the position they were seated at the time of the accident. Those positions did not match the original seating positions on the planned weight and balance sheet provided to the pilot prior to departure. The operator calculated a revised weight and balance based on the probable parachutist seating positions, which moved the aircraft’s centre of gravity 5 mm aft, although still within the allowable envelope (Table 2). It also showed that zone 0 was under the allowable weight limit.
Table 2: Revised weight and balance for accident flight
Item
Arm (mm)
Weight (kg)
Moment (kg-mm)
Aircraft basic empty weight
4,181
1,889
7,897.909
Fuel
4,680
272
1,272.960
Crew seat
3,442
92
316.664
Zone 0
3,472
80
277.760
Zone 1
4,277
349.4
1,494.384
Zone 2
4,948
271.4
1,342.887
Zone 3
5,613
334.4
1,876.987
Zone 4
6,261
197
1,233.417
Zone 5
6,896
233
1,606.768
Total
3,718.2
17,319.746
Centre of gravity
4,658
Aircraft basic empty weight
A weigh of VH‑UMV on 17 October 2017 identified that the aircraft’s basic empty weight was 1,889 kg in the single pilot seat configuration (Figure 5).
Figure 5: VH-UMV configuration on date of reweigh
The image meta-data showed the image was taken on 17 October 2017 – the reweigh date. Source: AeroWeigh.
The aircraft seating configuration at the time of the accident is shown in Figure 6.
Figure 6: VH-UMV cabin seating arrangement
Source: Aircraft operator, annotated by the ATSB
The basic empty weight of the aircraft did not include the flooring, or the 36 kg bench seating installed under engineering order ESE-C208-25-007. The engineering order provided the moment arms and weights shown in Table 3.
Table 3: ESE-C208-25-007 Parachute bench seating options – bench seat weight and arm
Item
Arm (mm)
Weight (kg)
Forward seat & backrest right-hand side only – option 2, without oxygen bottle mount.
3,556
7.82
Centre cabin bench seats both left-hand and right-hand sides (2 x 10.92 kg)
5,003
21.84
Aft bench seat right hand side only
6,553
6.36
Total of unaccounted weight for bench seating
36.02
Using the operator’s revised weight and balance calculation that reflected the likely positions of the parachutists, and the additional weight of the bench seating, the ATSB determined the probable take-off weight was 3,754 kg and the centre of gravity was 8 mm aft of the originally calculated centre of gravity (4,661 mm).
The operator subsequently weighed the aircraft’s jump mat, single point restraints, rubber matting, and portable oxygen tank. The total of these items was 30.2 kg, increasing the probable take-off weight to 3,784 kg.
Weight and balance implications
Regarding the importance of accurate weight and balance, the FAA Pilot’s handbook of aeronautical knowledge stated:
An overloaded aircraft may not be able to leave the ground, or if it does become airborne, it may exhibit unexpected and unusually poor flight characteristics.
Changes of fixed equipment have a major effect upon the weight of an aircraft. The installation of extra radios or instruments, as well as repairs or modifications, may also affect the weight of an aircraft.
Loading in a nose-heavy condition causes problems in controlling and raising the nose, especially during take-off and landing. Loading in a tail-heavy condition has a serious effect upon longitudinal stability and reduces the capability to recover from stalls and spins. Tail heavy loading also produces very light control forces, another undesirable characteristic. This makes it easy for the pilot to inadvertently overstress an aircraft.
Recorded data
The ATSB obtained OzRunways and third-party ADS-B recorded data for the accident flight. That data was compared with flight data for the flight conducted by the same pilot in the same aircraft on 17 October 2023, which was the day the pilot reported engine surging at about 5,000 ft. The comparison did not show significant performance difference from take-off to about 500 ft between the 2 flights.
Although the aircraft had an engineering order to fit GoPro cameras, they were not in place for the accident flight. The operator reported that these were only used during the creation of promotional footage and not during day-to-day operations. There was also no video footage from inside the aircraft, but the airport operator provided video footage from cameras located at the airport. One of those cameras recorded the accident flight footage (Figure 1) and provided audio for analysis.
The recorded audio included the aircraft noise and the nearby road and wind noise. The camera was stationary, therefore as the aircraft departed its sound signature reduced. Analysis of the audio conducted by Honeywell found that the engine RPM was approximately 99% throughout the take-off and initial climb. However, the engine noise was not discernible from the background sounds recorded at the time of the reported engine surge.
Site and aircraft examination
Site assessment
The ATSB did not attend the accident site, but the aircraft operator and Victoria Police attended shortly after the accident and provided the ATSB with photos of the aircraft and cockpit. A review of the images showed that the:
flaps were fully retracted
power lever was in the max reverse position
speed lever was in the minimum position
condition lever was in shutoff/feather position.
Those positions were consistent with the pilot’s reported actions to secure the engine after the impact. Additionally, one image appeared to show the TTL switch ON and the SRL switch OFF, indicating that the pilot may have inadvertently selected the SRL OFF instead of the TTL.
Engine and accessories assessment
The aircraft’s engine was recovered by the operator and sent to the Honeywell Investigation Laboratory in the US. On behalf of the ATSB, the US National Transportation Safety Board (NTSB) arranged independent oversight of the engine examination that was conducted between 3–5 January 2024.
Honeywell and the NTSB subsequently oversighted inspection and testing of removed components at various technical facilities. The Honeywell investigation report, provided to the ATSB and aircraft operator, detailed the observations and findings from the engine and associated component examinations, as follows.
The SRL and TTL were tested on 27 February 2024. Although some test points were not within the specified test tolerances, both units were found to be functional. However, further examination of the fuel bypass valve conducted by Woodward Inc. on 5 November 2024, resulted in a maximum bypass flow of 110 L/hour (194.5 lbs/hour), which exceeded the maximum flow test range of 68–74 L/hour (120–130 lbs/hour). At take-off power, a normal fuel flow was approximately 312 L/hour (550 lbs/hour). Therefore, if a bypass of 110 L/hour occurred during the accident flight with take‑off power set, the fuel flow would have reduced by about 35%.
Initial inspection of the fuel bypass valve’s outer casing revealed impact markings (Figure 7). When the protective cover plate was removed, the pole associated with the impact side was found in contact with the armature. When a 4.5 kg (10 lb) force was applied to each of the poles, there was no visible movement. The armature was cut away from the spade to determine if the armature screws were loose. The armature screws were found to be suitably tightened, and the armature was not bent.
The findings of the inspection showed the out‑of‑limit test results were due to impact damage resulting from the accident. As such, the higher fuel bypass identified in the test was not considered to be contributory.
Figure 7: Fuel bypass valve
Source: Woodward Inc, annotated by the ATSB
The fuel control unit (FCU) was examined and tested between 26–27 March 2024. The FCU tested values were either within specified ranges or marginally outside of tolerance limits for new or overhauled components. The test results may have been affected by procedures for adjusting an in-service FCU defined in the engine maintenance manual.
On 11 January 2024, a computed tomography scan of the propeller governor was conducted by Honeywell. Between 26–27 March 2024, the propeller governor was subject to functional testing by the manufacturer. While there were abnormalities identified with the magnetic pickup voltage and RPM maximum/minimum speeds, no contributing anomalies were noted. It was then disassembled, inspected and reassembled, followed by an additional functional test. The results from both functional tests were consistent with expected parameters of various operational modes.
The fuel pump was functionally tested on 2 May 2024, and found to be operating within specifications.
The Honeywell investigation found that the damage was indicative of an engine that was rotating and operating at the time of impact. It found no pre-existing condition that would have prevented normal operation.
Photos of the propeller were provided to Hartzell for analysis. As the propeller was of composite material, on impact it fractured into parts rather than deforming the propeller shape. From the limited fragments that were retrieved, Hartzell concluded the blades were likely rotating under low power at the time of the accident.
The ATSB considered whether the pilot had moved the power lever to beta range, reversing the propeller, but Hartzell found it likely that the propeller was forced to a low pitch angle during the initial impact.
Carriage of parachutists
Cabin configuration
The aircraft was configured for skydiving such that:
the cargo door was replaced with a vertical sliding door (made of nylon, polycarbonate and aluminium)
the passenger seats and lap belts were removed
bench seating and 17 single point restraints were installed.
The restraints attached to the parachute harness and parachutists could be seated either on the bench seating or floor, facing toward the aft of the aircraft.
The associated flight manual supplements for the parachute configuration were:
cargo doors removed kit
in-flight openable cargo door
in-flight opening of doors
oxygen system
skydiving jump light
external mounted GoPro cameras.
Aircraft modifications
Classification of design changes
CASA stipulated regulations for modification of an aircraft from the original manufacturer specifications. CASA Advisory Circular (AC) 21-12 Classification of design changes provided different processes for modifying aircraft, depending on the type of change being made. These changes were classified as either major or minor.
A minor modification was anything that was not considered to be a major modification and could be completed by a CASA-authorised person under CASR Part 21.M. Any modification with a significant effect on airworthiness – structural, weight and balance, systems, operational or other characteristics, were classified as major. Additionally, any alteration to the type certificate datasheet was classified as a major change.
A major modification was further classified into a substantial change or a significant change. A significant change required a supplemental type certificate application to be completed with CASA’s involvement. A substantial change required a new type certificate application, which also involved CASA. The AC provided the following example of a significant change to a small aircraft:
Changes in types and number of emergency exits or an increase in maximum certificated passenger capacity.
The notes associated with that example were:
Emergency egress certification specifications exceed those previously substantiated. Invalidates assumptions of certification.
CASA advised that the modifications would be considered a major change if the number of persons was increased above that permitted by the aircraft type certificate data sheet. This was consistent with the US FAA Advisory Circular 105-2E – Sport Parachuting, which included:
The approved number of skydivers that each aircraft can carry for parachute operations will most commonly be found on FAA Form 337, Major Repair and Alteration (Airframe, Powerplant, Propeller, or Appliance), used for field approvals, or an aircraft Supplemental Type Certificate (STC).
In its submission to the draft report, CASA advised that it considered that the legal basis for conducting parachuting flights with a greater number of passengers than the TCDS specified may be met if the aircraft was modified appropriately by a suitably authorised person and there was an associated aircraft flight manual supplement.
In determining whether the parachuting configuration modification was major or minor, the CASA‑authorised design engineer assessed that it was minor as it had no significant effect on:
structure
cabin safety
flight
performance or function of:
systems
propellers
engines or powerplant installation
environment.
The engineer also assessed that the design did not:
alter airworthiness or operating limitations
require an adjustment of the type-certification basis
Technical assessment of modifications
Aircraft modifications must meet the airworthiness requirements of the aircraft’s certification basis. According to the type certificate data sheet, VH-UMV was certified under FAR 23 amendments 23-1 through 23-28. Modifications were required to comply with standards from that or subsequent amendments. Technical assessments of the modifications detailed in the engineering orders nominated FAR 23 amendment 62 as the certification basis for the parachuting configuration modifications, including the roller door, bench seating and oxygen system.
The technical assessments included a design compliance matrix, with the following key comments by the design engineer of relevance.
Weight and balance
The engineering order was to include that:
It is the operator’s responsibility to accurately update the aircraft’s load data sheet to reflect the quantity and positioning of oxygen bottles as this may vary dependant on the number of parachutists on a given high altitude drop.
Structure
Standard aircraft hardware is used to secure items of mass installed as part of the parachute fit out modifications. This modification does not alter or effect the strength of the aircraft structure to support all normal aircraft loads. All materials & fasteners used as part of this design package have been selected to have adequate structural properties for their intended use.
Flight loads
The document package includes instructions to ensure the Cessna standard Flight Manual Supplement for operations with the cargo door open/removed is in the Flight Manual.
Oxygen
The engineer assessed the oxygen requirements for conducting flights above 14,000 ft in an unpressurised aircraft, stating:
…The operators (max) occupant capacity for the 208 & 208B model aircraft is x16 & x20 occupants respectively. As such these aircraft must be fitted with a minimum of 2x oxygen dispensing face masks if more than x15 occupants are carried…
Emergency landing conditions
Engineers assessed that the oxygen cylinder restraints were adequate in all load cases. They also rated the seats to at least 170 lb (77 kg) as required by FAR 23.785.
Regarding the installation of the oxygen bottle the engineers provided the following:
…the seat base and surrounding structure is adequate to support the small increase in weight due to the installation…there is no risk of the installation coming loose and inflicting serious injury on the cabin occupants.
Control systems
The design package included instructions for the removal of the copilot control wheel and column in accordance with the aircraft maintenance manual, to configure the aircraft for parachuting operations. There was no change to the design or functionality of the pilot's primary flight controls.
Doors
The number and arrangement of doors was not altered by the modifications. Regarding ‘vibration and buffeting’, the parachute door had a proven service history, with no reported issues since the design was originally implemented in June 2012. Further, the roller-style parachute door was commonly installed on parachuting aircraft and Cessna had an approved roll-up door as part of the production standard design.
Operation of the roller door was ‘simple and obvious’, easily operable from inside and outside the aircraft. The door was held in place by gravity and friction and could not be accidentally opened. Decals specific to the operation of the parachute roller door were installed.
Seats and restraints
The single point restraints for the parachutists were previously approved for use by ‘Air Safety Solutions’.
The aircraft certification did not require dynamic testing of the seats and, although the bench seating was not tested, the design engineer referenced FAA AC 105-2E Sport parachuting, which stated:
1. Straddle benches can offer more occupant crash protection than floor seating since they can be designed to provide significant vertical energy absorption.
Emergency exits
For reference, FAR 23.807 required:
In addition to the passenger-entry door, for an airplane with a total passenger seating capacity of 16 through 19, three emergency exits, as defined in paragraph (b) of this section, are required with one on the same side as the passenger entry door and two on the side opposite the door.
(b) Emergency exits must be movable windows, panels, canopies, or external doors, openable from both inside and outside the airplane, that provide a clear and unobstructed opening large enough to admit a 19-by-26-inch ellipse. Auxiliary locking devices used to secure the airplane must be designed to be overridden by the normal internal opening means. The inside handles of emergency exits that open onward must be adequately protected against inadvertent operation. In addition each emergency exit must:
• be readily accessible, requiring no exceptional agility to be used in emergencies;
• have a method of opening that is simple and obvious;
• be arranged and marked for easy location and operation, even in darkness;
• have reasonable provision against jamming by fuselage deformation; …
(c) The proper functioning of each emergency exit must be shown by tests
The design engineer commented that there was no change to the number of emergency exits and that the ‘steps, handles, bench seats etc. installed for this modification met the requirements for egress in an emergency as specified by this regulation’. Additionally, as there was no change to the door functionality or positioning, no additional emergency testing was required.
The unmodified rear right passenger door met the requirements of the regulation in that a 19" x 26" (48 x 66 cm) ellipse may be passed through the door un-obstructed. However, the rear right bench seat extended across the door at a height of 10” (25.4 cm). The design engineer commented that access to the door handles/operation and decals was not obstructed, and no exceptional agility was required to exit through that door in an emergency.
The roller door was also required to meet the emergency exit criteria, including ‘reasonable provisions against jamming by fuselage deformation’, and that ‘proper functioning of each emergency exit must be shown by tests’. However, this was not documented.
The parachuting configuration detailed in the engineering orders enabled seating and single-point restraints for 17 parachutists, in addition to the fitted pilot seat and 5-point restraint. The design engineer had not intended to explicitly increase the seating capacity above the 11 specified in the TCDS, as the number of parachutists that could be carried was an operational consideration. The design engineer provided comment on a technical assessment provided to CASA in 2017 regarding maximum passenger seating configuration, that the aircraft operator’s understanding was:
it is the pilots [sic] responsibility to ensure the aircraft is loaded within the weight and balance and centre of gravity limitations of the aircraft at all times. From these calculations the maximum safe number of parachutists to carry on the Cessna 208 Caravan is 17...
Regulatory requirements
Part 105 of the CASR came into effect in December 2021 and set out the operational requirements for aircraft used to facilitate parachute descents. Civil Aviation Order (CAO) 20.16.3 paragraph 15 Carriage of parachutists was in force at the time of the accident, and the following regulations were relevant to the aircraft parachuting configuration:
CASR 91.200 Persons not to be carried in certain parts of aircraft permitted a person to be carried in ‘a part of the aircraft that is not designed to carry crew members or passengers’, if the aircraft was being operated for a parachute descent and met the Part 105 MOS.
CAO 20.16.3 required parachutists to wear a seatbelt, shoulder harness or approved single point restraint (except when about to jump). Similarly, CASR Part 105 section 105.105 required parachutists who were not flight crew to be provided with a seatbelt, shoulder harness or approved single-point or dual-point restraint.
The Part 105 Manual of Standards (MOS) came into effect on 2 December 2023, 44 days after the accident, and specified requirements in greater technical detail. CASA advised that the Part 91 Manual of Standards will be amended to remove ambiguity about approved passenger restraints being permitted in lieu of seatbelts.
Maximum passenger seating configuration
In drafting CASR Part 105, the number of parachutists that could be carried was a significant point of discussion between CASA and the parachuting industry.
In 2006, CASA proposed Civil Aviation Safety Regulation 105.140 paragraph 3.5.20 which stated:
Proposed CASR Part 105 seeks to provide clarity to the parachuting industry that operating a parachuting aircraft with more parachutists than the normal published aircraft seating capacity in passenger-carrying operations is acceptable, provided weight and balance and other manufacturer’s limitations for the aircraft are observed.
A subsequent notice of proposed rulemaking indicated that the following may be included in the proposed CASR Part 105.140 – Number of parachutists in aircraft:
(1) A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and…
When the above proposed rule was not incorporated into draft CASR Part 105 or MOS, as detailed in meeting minutes of the technical working group that reviewed the 30 August 2022 draft Part 105 MOS, they proposed to meet with CASA’s Airworthiness and Engineering Branch to discuss:
possible options for parachuting aircraft to operate with seats removed, to carry more passengers than currently permitted by the aircraft’s type certificate or flight manual and regulatory support mechanisms for modifications (doors, handles etc.) that support safe parachuting operations.
The ATSB was unable to determine whether this discussion took place, however no related changes were incorporated into the regulations or MOS, noting that the MOS had not come into effect at the time of the accident.
In response to the ATSB’s request for clarification of CASA’s expectation for the number of parachutists that could be carried, CASA advised that:
The legal basis for conducting parachuting flights with a greater number of passengers than the TCDS is met where the aircraft has been modified appropriately by a suitably authorised person and the aircraft’s flight manual has been modified accordingly.
CASA has been aware for multiple decades that parachuting aircraft were carrying a maximum number of passengers greater than the TCDS maximum number of dedicated passengers.
CASA understood that the increase in passenger capacity for parachuting aircraft was achieved by operators through legitimate aircraft modification processes that removed the normal passenger seats and modified the aircraft for parachute‑specific operations.
CASA did not identify any immediate safety of flight issues.
In its submission to the draft report, CASA advised that it was ‘considering the issue of a legislative instrument to remove any doubt that an approved aircraft modification which replaces normal seating with appropriate alternative seating and restraint arrangements is explicitly permitted’.
Supplemental type certificate application
In April 2017, the design engineer applied to CASA on behalf of the aircraft operator for a supplemental type certificate based on the engineering order for the addition of bench seating. The STC application submitted to CASA included details and images of aircraft that already had modifications completed under an engineering order and did not include an increase in the seating capacity.
After several communications and iterations of the documents provided, in August 2017, CASA highlighted 2 areas directly related to safety of parachutists: the rear exit crashworthiness and the increase of maximum passenger capacity to 17.
In July 2020, the STC application was withdrawn by the applicant.
Other parachuting configuration supplemental type certificates
Cessna 182 models E to R
In 1996, CASA issued STC-214 to the APF. The STC background explained the application was the result of a CASA ramp check, which identified that there were 6 persons on board without single point restraints while conducting parachute operations, where the TCDS stated it was a 4‑seat aircraft.
The STC assessed the floor loading capacity of the aircraft to carry 6 persons (including the pilot) for the purpose of parachute operations. It concluded:
The floor was analysed and substantiated for parachutist loads. The hard points for the approved single point restraints were determined, analysed and substantiated for parachute loads... The aircraft loading is such that no special loading system needs to be devised as the aircraft will always be within the approved centre of gravity range.
The original C182 TCDS 3A13 showed ‘No. of seats 4’.
The amended TCDS for the STC showed ‘No. of seats 1, Parachutist 5’.
Cessna 208, 208B
In 2018, the US FAA issued supplemental type certificate SA04352CH, which incorporated many similar modifications made to model 208 and 208B aircraft certified under A37CE. The modifications included the installation of:
wind deflector
benches
external assist handle
internal assist handle
jump exit control light
external step
wind block (sliding parachute door).
The STC limitations and conditions included:
(3) This modification does not install Title 14 [US Code of Federal Regulations] CFR part 23 compliant seating and is therefore zero occupancy.
(4) The left and right hand benches are compliant as monuments and are not certified to carry any items of mass. Testing performed during certification would be sufficient for gust loading or seven evenly distributed masses of 215 pounds (97.5 kg) each…
Australian Parachute Federation
The APF is the peak body for the administration and representation of Australian Sport Parachuting. With the approval of the Civil Aviation Safety Authority, the APF:
applies the standards of operation
conducts competitions
issues parachuting licences, certifications and instructor ratings
conducts exams
distributes publications to keep its members informed of events and safety standards.
The APF organisation had over 55 group members also known as member organisations, 3,000 licenced members, and engaged with the operators of nearly 100 aircraft conducting parachute operations. As detailed above, the APF held an STC for parachuting operations in Cessna 182 models E through R for parachuting 6‑person operations. The associated supplemental type certificate data sheet amended the aircraft configuration to 1 seat and 5 parachutists from the 4‑seat configuration stated on the type certificate data sheet.
Aircraft operators that conducted parachuting operations as a member of the APF did so in accordance with the APF regulations. This included adhering to the APF Jump Pilot Manual. The Jump Pilot Manual Version 01-2023, in force at the time of the accident, stated:
5.3.3 Loading – Balance/C of G
A parachuting aircraft may carry more occupants than the maximum number that is specified in the aircraft’s flight manual only if the aircraft is loaded in accordance with the following requirements and limitations set out in the flight manual or the certification data for the aircraft:
(a) the weight and balance requirements; and
(b) any other limitations related to the provision of:
(i) adequate structural support for restraint of occupants; or
(ii) supplemental oxygen for the flight.
For paragraph 5.3.3 (b), the limitations do not include those that are solely related to the number of seats or seating positions that are, or are normally, fitted in the aircraft.
If an aircraft does not have a flight manual, then any information supplied by the manufacturer that relates to the matters mentioned above or is included in the aircraft’s airworthiness certificate, is taken to be the flight manual.
Balance must be a consideration for all aircraft involved in parachuting operations and can be especially critical during climb-out and exit, when changes occur. Know the operational limitations of your aircraft!
Under the Loadmaster’s supervision, the parachutists will normally load the aircraft in the reverse order of the exit.
The Jump Pilot Manual was accepted by CASA and CASA personnel reported having reviewed the manual. Regarding the wording that a parachuting aircraft could carry more occupants than the maximum specified in the AFM, CASA reported that they understood that only applied to Cessna 182 models E through R, for which the APF held a supplemental type certificate that permitted the carriage of 6 persons. CASA personnel also reported that the manual wording was ‘never intended to serve as a quasi-engineering approval’.
At the time of writing, CASA and the APF were engaged in ongoing discussions, including the carriage of occupants in excess of the number detailed in the TCDS without the necessary modification approvals.
Survivability
Passenger briefing requirements
The CASA Multi-Part Advisory Circular – Passenger safety information, stated:
2.1.1 In addition to certification standards for the crashworthiness of the aircraft and cabin crew evacuation procedures, well-informed and knowledgeable passengers contribute to survivability in an aircraft accident or incident. There are multiple factors that affect survivability. Physical factors include adopting the correct brace position for impact, the correct use of seatbelts, as well as the location and operation of all emergency exits.
2.1.2 Accident investigations have shown that survival rates are improved when passengers are provided with accurate and effective information about the correct use of equipment such as seatbelts, and the actions they should take in a life-threatening situation such as how to adopt the brace position.
A pilot in command was in contravention of regulation 91.565 if an aircraft commenced a flight and the passengers had not been given a safety briefing and instructions as prescribed by the Part 91 MOS, unless:
(a)the passenger has been previously carried on the aircraft; and
(b)the passenger has previously been given a safety briefing and instructions in accordance with this regulation; and
(c)in the circumstances it is not reasonably necessary to give the same safety briefing and instructions.
The CASR Part 91 MOS provided a list of items that must be covered in a passenger safety briefing and instructions before an aircraft takes off for a flight. Relevant to this occurrence, the list included:
(c) when seatbelts must be worn during the flight, and how to use them;
(f) how and when to adopt the brace position;
(g) where the emergency exits are, and how to use them;
(s) for a flight of a jump aircraft — the physical location(s) within, or on, the aircraft that the passenger must occupy during the flight in order to ensure the aircraft is operated within the aircraft’s weight and balance limits during the flight.
Operator’s safety briefing
The aircraft operator had 2 videos, one of which was shown to parachutists depending on whether they were conducting a tandem jump or a sport jump. The sport jump video was specific to the Barwon Heads operation and included:
aircraft climb performance
17 single point restraints, which were to be worn up to 2,000 ft
sport jumpers were to listen to the pilot in command in the event of an emergency
location of the door securing clip (but not instructions for use).
The video shown to tandem jump parachutists provided specific aircraft safety information including:
how to approach the aircraft
the use of single point restraints
the location of fire extinguishers
how to brace
how to egress
the requirement not to smoke
the use of life jackets where required.
For the accident flight, the pilot reported that they did not provide a safety briefing, and multiple parachutists reported not having received a safety briefing prior to flight. There was no procedure in the operations manual that waived the pilot’s responsibility to provide parachutists with a safety briefing. The pilot reported that they understood that the drop zone safety officer ensured everyone was briefed on emergency situations before jumping and a video briefing was provided to tandem parachutists.
The operations manual provided the following guidance for providing a safety briefing during an emergency landing with parachutists on board:
It will be the Load Masters responsibility to assist the pilot in ensuring;
1. Parachutists are briefed on and instructed to assume the BRACE position prior to touchdown.
2. Emergency Exits are opened and secured (where possible) prior to touch down.
3. Single point restraints are utilised by all occupants.
The aircraft also had a sign on the rear wall of the internal cabin, detailing the in-flight emergency plan (Figure 8). The sign stated that single point restraints were required as directed by the pilot and at all times below 1,500 ft, differing from the 2,000 ft stipulated in the sport jump video.
The APF Jump Pilot Manual required that restraints were utilised by all occupants below 1,000 ft, or as directed by the pilot.
Figure 8: In-flight emergency plan
Source: Victoria Police and the aircraft operator
Parachutist preparedness
After the accident, in response to an ATSB survey, parachutists reported a lack of awareness of how to brace and the location of emergency exits that were available if the main roller door became damaged and unavailable for use in an evacuation. On this occasion the clip that secured the roller door in the open position was not used, which resulted in it closing on impact. Fortunately, the parachutists were still able to successfully evacuate the aircraft via that door. As detailed further below, several of the parachutists also reported that their restraints were not taut prior to the ground collision.
Some parachutists recalled receiving aircraft-specific emergency information during their initial parachuting training. However, in some cases, several years had passed without receiving a refresher. Furthermore, some had conducted their initial training on different aircraft types.
Injuries and seating positions
The pilot wore a 5-point restraint, and the 16 parachutists each had a single-point restraint attached to their parachute. The probable seating arrangement at the time of the accident was determined based on the recollections of parachutists who responded to ATSB’s request for information (Figure 9). There were 4 parachutists seated on the floor, 4 on the left bench seat and 8 on the right bench seat. The parachutists were facing aft and those on the bench seats were seated between each other’s legs.
Injury information was obtained for the pilot and 14 of the 16 parachutists, with the other 2 assumed to have no injuries (Table 4). The injury mechanisms included deceleration, flail and impact with the aircraft or other occupants.
Figure 9: Seating positions
The seating positions in the image are referenced in Table 4: Injuries sustained. Source: Texas Turbines Cessna 208 pilot operating handbook, annotated by the ATSB
Table 4: Injuries sustained
Image reference
Injuries sustained
ATSB injury classification
Survivability Comments
A. (Pilot)
Cut on forehead, bruising, whiplash, bruised sternum, and difficulty talking/breathing
Minor
5-point safety harness; likely impact with control column/dash
B.
Pulmonary contusion, fifth and sixth rib fractures, psychological trauma, and lower back pain
Serious
Slipped off the end of the bench seat and ended up squashed against the ladder or back of the pilot seat due to a loose restraint
C.
No reported injuries
No injuries
D.
Tears to both rotator cuffs, tear to sternocleidomastoid muscle, and nerve damage to left arm and shoulder
Serious
E.
Broken ribs and internal bleeding to the chest.
Serious
Loose restraint
F.
Whiplash, fractured L4 transverse process, and nerve pain in right shoulder and leg
Serious
Loose restraint, seated on floor; adjacent end of bench seat
G.
Whiplash, bruising, and headaches
Minor
Seated on floor
H. (Loadmaster)
Cut injury to right leg requiring stitches, and sore back
Minor
I.
Strained back, cuts, and bruising
Minor
J.
Whiplash, cuts, and bruising
Minor
Loose restraint
K.
Whiplash, cuts, and bruising
Minor
Loose restraint
L.
Cuts to head, face, internal chest cuts, and bruising
Minor
Tight restraint
M.
Broken tailbone, bruising
Serious
Tight restraint
N.
Concussion, and bruising
Minor
O.
Swollen knee, bruised kidney, bruised vertebrae, and strained neck ligaments
Minor
Loose restraint
P.
Internal abdomen bleeding, Internal hematoma inner right leg, cuts, bruising, whiplash, and back pain.
Serious
Loose restraint; inappropriate structures around/in front
Q.
No reported injuries
No injuries
The single point restraints could not be adjusted, but an occupant could potentially position themselves such that the restraint was taut. Nine parachutists provided information about the tightness of their restraint; 7 reported their restraints were loose and 2 reported tight restraints. Of those with loose restraints, 3 sustained minor injuries and 4 sustained serious injuries. Of the 2 parachutists who reported having tight restraints, one sustained minor injuries and the other sustained serious injuries.
Of the 4 parachutists seated on the floor, 2 sustained serious injuries, one sustained minor injuries, and another was reported to have been uninjured. The other serious injuries were sustained by 2 parachutists on the left bench seat and one on the right bench seat.
The parachutist who sustained the most injuries of the highest severity was at the front of the left bench seat. As that bench seat did not have a seatback, the parachutist came off the forward end of the bench between the bench and pilot seat and contacted the back of the pilot’s seat and/or ladder adjacent to the seat. The injuries were likely also increased by the mass of the 3 other parachutists on that bench moving forward during the impact sequence.
The ATSB compared the injuries sustained by the pilot and parachutists of VH-UMV with those involved in 2 survivable accidents involving C208 aircraft, assessed as likely to have been subjected to similar impact forces (AO-2016-007 and AO-2024-001). In the 2 comparative accidents, some of the occupants sustained minor injuries while others were uninjured. The pilot and front seat passengers had 5-point restraints, and in the 2016 accident the other passengers wore lap belts. In the more recent accident, the other passengers wore 3-point restraints.
ATSB investigation AO-2014-053 found that single point restraints were less effective than dual restraints in mitigating injury for parachutists. This was consistent with the US FAA’s technical report – Evaluation of Improved Restraint Systems for Sport Parachutists, which found that dual straps attached to the parachute harness provided better restraint and produced less flailing and bending of the body than single point restraints (FAA 1988). The following loading of aft‑facing passengers was found to increase restraint effectiveness:
• the person most forward in the cabin should be leaning against a bulkhead or other substantial support to limit flailing and head impact.
• each parachutist’s restraint should be anchored to the floor aft of his/her pelvis (relative the aircraft’s orientation) at a point on the floor near the middle of the thigh. The restraint should be taut to reduce forward motion, and the loads transmitted to the person behind.
• the proper brace for impact position would be to lean toward the front of the aircraft onto the person or bulkhead behind them.
The US FAA AC 105-2E Sport parachuting also stated that single point restraints were ‘not very effective’, and that dual point restraints offered ‘superior restraint’.
The ATSB assessed that the increase in number and severity of injuries of the parachutists compared to passengers seated and restrained in seats, was probably a result of single-point restraints being less effective and less cushioning due to being seated on the floor or bench.
Related occurrences
National Transportation Safety Board Special investigation report
The US National Transportation Safety Board (NTSB), Special investigation report on the safety of parachute jump operations (2008), found that between 1980 and 2008 in the US, 32 accidents involving parachute aircraft resulted in fatal injuries of 172 people, most of whom were parachutists. Acknowledging risks associated with parachuting, the report stated:
Although parachutists, in general, may accept risks associated with their sport, these risks should not include exposure to the types of highly preventable hazards that were identified in these accidents and that the parachutists can do little or nothing to control. Passengers on parachute operations aircraft should be able to expect a reasonable level of safety that includes, at a minimum, an airworthy airplane, an adequately trained pilot, and adequate Federal oversight and surveillance to ensure the safety of the operation.
Of the 32 accidents, 8 involved exceedances of the aircraft’s weight and balance, and 21 resulted from inadequate airspeed or stall situations, and in 6 accidents, both were factors. There was one accident involving a Cessna 208, which resulted in 17 fatalities.
The report also acknowledged that parachuting is typically a revenue operation where a participant pays for a jump and receives the flight as part of that service, it stated:
Most parachute operations flights are operated under the provisions of 14 Code of Federal Regulations (CFR) Part 91 and are typically revenue operations; parachute jump operators provide the flights as part of their services to parachutists who pay to go skydiving, or parachutists pay dues for membership in parachuting clubs. The risks of parachuting are generally perceived to involve the acts of jumping from the aircraft, deploying the parachute, and landing; parachutists are aware of and manage these risks. However, a review of accident reports reveals that traveling on parachute operations flights can also present risks.
The report highlighted the potential for paying participants to be unaware of the risks they were accepting when they boarded a parachute aircraft.
The report identified the following recurring safety issues:
• inadequate aircraft inspection and maintenance;
• pilot performance deficiencies in basic airmanship tasks, such as preflight inspections, weight and balance calculations, and emergency and recovery procedures; and
• inadequate FAA oversight and direct surveillance of parachute operations.
Recent accidents
The following 3 more recent accidents involved aircraft conducting parachuting operations and resulted in injuries to the occupants.
Loss of engine power after take-off involving Cessna 208B, PH-FST, West of International Airport Teuge, Netherlands, on 25 June 2021 (2021062)
On 25 June 2021 at 0932 local time, a Cessna 208B with a pilot and 17 parachutists on board departed from International Airport Teuge. During the initial climb, the aircraft suddenly lost engine power after which the pilot made an emergency landing in a field close to a motorway. The aircraft was substantially damaged, and one parachutist sustained minor injuries.
Accident involving GA8-TC-320 Airvan, SE-MES, Storsandskär, Västerbotten, Sweden, on 14 July 2019 (RL 2020:08e).
The purpose of the flight was to drop 8 parachutists from an altitude of 13,000 ft. On the drop run, the pilot lost control of the aircraft. The parachutists were unable to evacuate the aircraft resulting in fatalities of the 9 persons on board.
The investigation found that control of the aeroplane was probably lost due to low airspeed. Other contributing factors were that the aeroplane was unstable as a result of a tail-heavy loading, weather conditions, and a high workload in relation to the pilot’s knowledge and experience.
Loss of control involving Cessna U206G, VH-FRT, Caboolture Airfield, Queensland, on 22 March 2014 (AO-2014-053)
On 22 March 2014, a Cessna U206G aircraft was being used for tandem parachuting operations at Caboolture Airfield, Queensland. At about 1124 local time, the aircraft took off from runway 06 with the pilot, 2 parachuting instructors and 2 tandem parachutists on board. Shortly after take-off, witnesses at the airfield observed the aircraft climb to about 200 ft above ground level before it commenced a roll to the left. The left roll steepened, and the aircraft then adopted a nose‑down attitude until impacting the ground in an almost vertical, left-wing low attitude. All the occupants on board were fatally injured. A post-impact, fuel-fed fire destroyed the aircraft.
The ATSB identified that the aircraft aerodynamically stalled at a height from which it was too low to recover control prior to collision with terrain. The reason for the aerodynamic stall was unable to be determined. Extensive fire damage prevented examination and testing of most of the aircraft components. Consequently, a mechanical defect could not be ruled out as a contributor to the accident.
A number of safety issues were also identified by the ATSB. These included findings associated with occupant restraint, modification of parachuting aircraft and the regulatory classification of parachuting operations.
Safety analysis
Introduction
On the morning of 20 October 2023, the pilot of a Cessna 208, registered VH-UMV, commenced take-off for a planned climb to 15,000 ft to drop 16 parachutists. Passing about 500 ft on climb, the pilot detected a partial power loss, consistent with an abnormal activation of the torque and temperature limiter (TTL). The pilot reduced the power to prevent the engine surging, but the combination of low power and airspeed resulted in the aircraft colliding with water before continuing into a field.
Six of the parachutists sustained serious injuries and the pilot and 8 parachutists sustained minor injuries. The aircraft was substantially damaged.
This analysis will discuss the TTL activation and response actions. The aircraft’s seating configuration, weight and balance and occupant safety will also be examined. Additionally, the analysis will consider the number of parachutists on board, and operational guidance from the Australian Parachute Federation manual approved by the Civil Aviation Safety Authority (CASA).
Operator’s prescribed actions
Normal operation of the TTL permitted reduction in the fuel flow to the engine to maintain the lower of 100% torque or 650 °C nominal exhaust gas temperature (EGT). However, the TTL manufacturer advised that the limiter was capable of restricting fuel flow sufficiently to reduce the maximum power to about 62% torque. A noticeable power reduction, followed quickly by a power increase, had been reported by the operator’s pilots as engine surging events associated with the TTL. However, maintenance actions had been unable to identify or resolve the cause of 6 reported engine surging events in VH-UMV over a 5‑month period.
Unable to resolve the intermittent excessive TTL response, the aircraft operator had advised pilots to limit torque to 95% and EGT to 640°C to prevent TTL activation. Although well intentioned, that was contrary to the aircraft flight manual supplement, which defined take-off power as 100% RPM and 100% torque or 650°C EGT, whichever was reached first. The operator had not assessed the TTL and single red line (SRL) systems as inoperable, which would have required pilots to manually ensure torque and temperature limits were not exceeded. Power reductions resulting from TTL activations were reported to be momentary and power returned to the previous level after the torque or EGT limit reduced below the limit.
Additionally, in the absence of an aircraft manufacturer’s checklist for partial power loss, the operator had created an engine power loss checklist. The first item was to immediately move the elevator control forward if climbing to prevent airspeed decay. After other initial actions, the checklist then instructed pilots to significantly reduce power if the engine RPM was above 60% or surging, in preparation for switching off the TTL. While that was intended to ensure engine limits would not be exceeded when the pilot subsequently reintroduced power, the operator did not specify a minimum height at which it was appropriate for a power reduction to be made.
Such a significant power reduction close to the ground increased the risk of a loss of control and/or ground collision.
Contributing factor
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Pilot actions
At the commencement of the take-off roll, in accordance with normal and the manufacturer’s procedures, the pilot reported applying full power – initially reaching 100% torque for take-off, before reducing power slightly in an attempt to remain under the operator‑specific torque limit of 95%. Whether the torque or temperature limit were reached during the initial climb could not be determined as these parameters were not recorded. However, the pilot detected a power reduction consistent with an abnormal TTL activation.
As shown by previous safety reports, in the event of TTL activation, the maximum power available may have been approximately 62%. Such a significant power reduction would have required the pilot to lower the aircraft’s nose attitude to prevent an aerodynamic stall, consistent with the operator’s engine power loss checklist.
However, the pilot did not initially lower the aircraft’s nose, instead they moved the power lever aft, reducing the power setting. This was in accordance with the operator’s procedure in preparation for switching off the TTL. Although the as‑found switch positions indicated that the pilot may have inadvertently selected the SRL switch instead of the TTL, in either event the TTL would have been deactivated. However, as the pilot had not lowered the aircraft’s nose, the aircraft approached an aerodynamic stall, and the stall warning horn sounded.
In response, the pilot lowered the aircraft’s nose and, due to the low height above terrain, low airspeed and low power, searched for a suitable field for landing. Although the pilot only reported reducing the power slightly, as the post-accident inspections found the engine was capable of producing normal power, and there were no pre-existing conditions that would have prevented normal operation, the low power was likely a result of the pilot reducing power to a level insufficient to maintain height in the climb attitude, and not restoring it.
At the low height above the ground at which the power loss occurred, the above factors led to the collision with water.
Contributing factor
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Weight and balance
The aircraft had all the aircraft’s certified seating removed other than the pilot’s seat, following which the aircraft was weighed, and a basic empty weight established. However, that weight did not include the bench seating, parachute restraints, floor matting or oxygen bottles which were fitted to the aircraft at the time of the accident. Although the weight and moment arm of the bench seating had been provided with the engineering order, it was not accounted for in the IBIS Technologies weight and balance calculation software used by the operator.
As a result, the bench seating and other aircraft fixtures were not accounted for in the accident flight weight and balance calculation. Additionally, parachutists did not sit in the positions used for the weight and balance calculations for the accident flight. Therefore, the calculated weight and balance was inaccurate.
Although the operator’s post-accident calculations found that the aircraft was almost certainly operating within the weight and balance limitations throughout the flight, an accurate weight and balance assessment prior to take-off to ensure the flight will operate below the maximum take-off weight is essential for the structural integrity of the aircraft. Operating outside the centre of gravity limits increases the risk of a loss of control. Exceeding weight and balance limitations has previously resulted in fatal accidents involving aircraft conducting parachute operations.
Other factor that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
IBIS Technologies flight planning module
When conducting post-accident weight and balance calculations using the operator’s IBIS Technologies flight planning module, the ATSB identified that, while warnings were provided when the aircraft was outside the overall weight or centre of gravity limit, there was no warning when the weight for a zone within the cabin exceeded the limit. This increased the likelihood of an aircraft being loaded contrary to zone limitations.
The lack of an alert did not contribute to this accident and, as noted above, the aircraft was not loaded in accordance with the planned overall or zonal distributions. However, the software used to calculate the aircraft weight and balance was used by many operators and overloading a zone limit could result in damage to the aircraft.
Other factor that increased risk
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Safety briefings
To maximise survivability in the event of an emergency, pilots are required to ensure aircraft occupants receive a safety briefing and instructions including in the correct use of restraints, emergency exits and adopting the brace position. However, a pilot is not required to brief passengers on every flight, if they have previously been on the aircraft and are likely to be familiar with safety information.
The pilot understood that this responsibility had been delegated to the drop zone officer and that the parachutists had received the required safety briefing and information. However, there was no record of which parachutists had been briefed or when. Additionally, as none of the parachutists on board were tandem jump parachutists, they were unlikely to have viewed the operator’s video that included use of single point restraints, how to brace or exit the aircraft in the event of an emergency.
Although some of the parachutists on board had previously received a safety briefing, it had not necessarily been in the accident aircraft type or recently. Additionally, an ‘in-flight emergency plan’ printed on the rear of the cabin advised parachutists to remain seated with single point restraints attached and brace for an emergency landing when below 500 ft, but did not specify how to brace or exit the aircraft. As a result, some of the occupants were unaware of essential safety information regarding brace position and emergency exits.
Although the aircraft’s roller door closed on impact and water entered the cabin, all 17 occupants evacuated with no difficulties reported. The ATSB was unable to determine whether the absence of a safety briefing increased the severity of the injuries sustained by parachutists. However, adopting the correct brace position for impact, the correct use of restraints, and knowledge of the location and operation of all emergency exits, are factors demonstrated to increase survivability.
Other factor that increased risk
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Seating configuration
The operator routinely conducted parachuting operations in Cessna 208 aircraft with the pilot and up to 17 parachutists on board. This was based on the CASA-accepted Australian Parachute Federation Jump Pilot Manual, which stated that the aircraft could carry as many parachutists as there were restraints and provided the aircraft was operated within the weight and balance limitations.
The aircraft’s cabin was configured with a roller door, oxygen system, bench seating and single‑point restraints for parachuting operations under an engineering order by a CASA‑authorised person. Although the configuration nominally provided restraints and seating (including on the floor) for up to 17 parachutists, this was not formally documented in the aircraft flight manual or a supplement. The engineer also assessed and modified the aircraft to supply oxygen for 16 occupants to meet the operator’s requirements of their intended operation.
CASA assessed that increasing the number of persons carried above that stated on the type certificate data sheet (TCDS) required a supplemental type certificate (STC) as it was a major modification. In this case the TCDS stated that the aircraft had a maximum seating capacity of 11, but the aircraft was modified to supply oxygen for an intended 16 occupants. As such, the CASA‑authorised engineer incorrectly assessed that the modifications they were approving were minor and conducted them under engineering orders. The ATSB considered whether conducting the modifications in that manner increased safety risk.
As part of the assessment of an STC application for the same modifications submitted by the design engineer in 2017, CASA questioned the modified rear exit crashworthiness and increased number of occupants. Specifically, it was noted that the effect of increased occupancy on speed and ease of emergency egress had not been established, nor had it been demonstrated that the roller door would be unlikely to jam in the event of fuselage deformation.
As that STC application was never finalised, the safety of egress via the modified exit was not verified. However, in this accident, all the occupants evacuated the aircraft through the roller door after impact. As such, while the STC process was not followed when modifying the aircraft, there was no evidence that it increased the safety risk on this occasion. Additionally, CASA advised that the legislative requirements would likely be met if a modification conducted by an authorised person (under an engineering order) included an associated aircraft flight manual supplement.
The expectation for parachuting operations was that the parachutists would jump from a planned height, or be able to exit the aircraft in the event of an emergency when above a safe height. However, they would be inside the aircraft during take-off, at low level, and if unable to exit in the event of an emergency. In those phases of flight or conditions, increasing the number of occupants increased the number of people exposed to the risk of harm in the event of an accident. In this accident, as the aircraft was too low for parachutists to exit airborne, 15 of the 17 occupants sustained injuries, some of which probably occurred due to impact with each other.
Although the parachuting configuration was assessed as compliant with the required airworthiness standards, parachutists were exposed to greater risk of harm than if they were passengers in certified seats with adequate restraints. Those seated on the floor did not have the benefit of a seat to absorb impact forces and the bench seating had not been shown to optimally absorb impact forces. Additionally, the lack of a seatback on the left bench seat likely increased the injuries sustained by the forward-most parachutist seated on that side. The parachutists were also using single-point restraints, demonstrated to be less effective than dual restraints.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the partial power loss and collision with terrain involving Cessna 208, VH-UMV near Barwon Heads Airport, Victoria on 20 October 2023.
Contributing factors
Experience Co’s engine power loss checklist instructed pilots to significantly reduce power in preparation for deactivating the TTL, but did not specify a minimum safe height at which to do so. This increased the risk of loss of control and/or ground collision.
Passing about 500 ft on climb, the power reduced likely due to abnormal activation of the torque and temperature limiter (TTL). Expecting the power to return quickly, and in preparation for deactivating the TTL, the pilot further reduced the power and delayed lowering the aircraft’s nose to maintain airspeed. This resulted in a stall warning and subsequent collision with water.
Other factors that increased risk
The operator's weight and balance calculation for the accident flight was inaccurate as it did not include the bench seating weight or moment, and the loadmaster did not load parachutists in positions used for the calculation of the centre of gravity.
The IBIS technologies software used to calculate aircraft weight and balance did not provide a warning if individual zones were overloaded.
Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety issue description: Experience Co did not ensure sport parachutists received essential safety information about emergency exits, restraints and brace position, prior to take-off.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Proactive safety action taken by Experience Co
Experience Co has taken the following proactive safety actions:
A safety communique was developed and circulated at each drop zone reminding parachutists to be seated in accordance with their manifested location.
Chief instructors, drop zone safety officers and loadmasters were reminded of the loadmasters’ responsibilities to ensure parachutists were seated in accordance with the weight and balance calculation.
Skydive Operations Manual was amended to clarify the loadmasters’ responsibilities.
Additional training was provided for manifest staff.
A fleet‑wide audit was undertaken to ensure all aircraft had accurate basic empty weight figures.
A prompt was added to the internal reporting software to confirm an entry has been made to the aircraft’s maintenance release when submitting a maintenance‑related internal safety report.
Briefings that cover essential safety information about emergency exits, restraints, and brace position, are now required annually by sport skydivers.
Additional pilot training relating to the SRL/TTL malfunctions has been developed and was scheduled to be delivered to all pilots.
Emergency exit signs in all aircraft were being assessed for compliance and effectiveness, and updated if necessary.
Engineering personnel have undertaken specialised TPE331 Powerplant and Systems training.
Information circulars were provided to company pilots about the proper defect reporting requirements using the aircraft maintenance release.
Experience Co was updating advice as to the altitude at which seatbelts must be worn.
Experience Co has developed C208 and C208B aircraft flight manual supplements, which outline the carriage of 17 parachutists and 21 parachutists respectively.
An additional support bracket has been designed to be fitted to the end of the bench seats in aircraft and will be installed once formally approved.
A new engine power loss checklist was developed in cooperation with the STC holder to be followed at or above 1,000 ft above ground level.
Proactive safety action taken by IBIS Technologies
IBIS Technologies amended its software to include an alert that will be flagged to the staff member in charge of manifesting the flight load if a zone exceeds zonal weight limits.
Proactive safety action taken by the Australian Parachute Federation
The Australian Parachute Federation (APF) has taken the following safety action:
The APF will ensure skydivers and pilots review their aircraft emergency procedures on a regular basis. Recommended topics are likely to include:
general safety around aircraft
hot loading
door activation
achieving correct restraint fitment
emergency landings
brace position
emergency exit altitudes and which parachute to use
communication during an emergency
for coastal operations, life jacket use in a ditching.
Each parachuting aircraft operator will conduct a thorough assessment of their aircraft to ensure single point restraints are properly installed, to prevent parachutists from moving outside their designated seating positions and to maintain the aircraft’s weight and balance.
The APF will review global data on the use of dual-point restraints to gather insights from other national parachuting organisations regarding their experiences with this system.
The APF examined aircraft flight manual wording of all aircraft currently conducting parachute operations in Australia to identify which aircraft would require a short-term CASA exemption to permit operations with the number of passengers onboard in excess of those able to occupy the normal seats under the type design. They identified 22 aircraft requiring an exemption, spanning 5 operators.
The APF added the following statement to the participant waiver form: ’parachuting aircraft are not operated to the same safety standards as a normal commercial passenger flight’.
Proposed safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority advised that it is developing the following:
An exemption, for pilots or operators of parachuting aircraft who may be unable to comply with elements of the aircraft flight manual, is expected to be completed by mid‑2025.
CASA stated that it was satisfied that reasonable steps had been taken by the APF to ensure that a level of safety, commensurate with the risks involved in the parachuting activities in which participants engage, was provided to those participants in the interim while the exemption was being developed.
An amendment to the Civil Aviation Safety Regulations Part 21 Manual of Standards to specify the standards required for the modifications made to parachuting aircraft. This proposed action is expected to be finalised by the end of 2025.
Additional guidance to support aircraft owners and operators seeking to make an approved modification.
Glossary
AC
Advisory circular
ADS-B
Automatic dependent surveillance broadcast
AFM
Airplane Flight Manual
APF
Australian Parachute Federation
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CAVOK
Conditions and visibility okay
EGT
Exhaust gas temperature
FAA
(United States) Federal Aviation Administration
FCU
Fuel control unit
MEL
Minimum equipment list
NTSB
(United States) National Transportation Safety Board
POH
Pilot’s Operating Handbook
RPM
Revolutions per minute
SRL
Single red line
TCDS
Type certificate data sheet
TTL
Torque and temperature limiter
US
United States
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and sports jump parachutists
Experience Co
Civil Aviation Safety Authority
Australian Parachute Federation
Victoria Police
Textron Aviation
Honeywell International Inc
OzRunways
Barwon Heads Airport
Texas Turbine Conversions
References
Federal Aviation Administration (2023). Pilot’s handbook of aeronautical knowledge. FAA-H-8083-25C.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Textron Aviation
Honeywell International Inc
Texas Turbine Conversions
Bowden Engineering solutions.
Submissions were received from:
the pilot and aircraft operator
Australian Parachute Federation
Civil Aviation Safety Authority
Honeywell International Inc.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather (Source: Airservices Australia).
[2]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[3]Engine surging as reported by the pilots of VH-UMV was a power reduction followed quickly by an increase in the power level.
[4]Angle of attack: the relative angle between the chord line of the wing and the relative airflow.
[5]Automatic dependent surveillance-broadcast (ADS-B) is a surveillance system that broadcasts the precise location of an aircraft through a digital data link.
[6]Loadmaster: a person nominated by the drop zone safety officer who is performing duties for a parachute descent.
[7]Normal category applies to aircraft which are intended for non-acrobatic operation, having a seating configuration (excluding pilot seats) of 9 seats or less, and a maximum take-off weight of 5,700 kg or less.
[8]Restricted category applies to aircraft which may carry out certain special purpose operations, but may not carry passengers or cargo for hire or reward.
[9]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[10]The propeller can move to reverse when the engine is operating in beta mode, which results in thrust acting in the opposite direction of the aircraft. In beta mode, the propeller blade pitch is controlled by the power lever.
[11]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[12]The parachutist’s names, weights, and seating locations removed.
Occurrence summary
Investigation number
AO-2023-049
Occurrence date
20/10/2023
Location
Near Barwon Heads Airport
State
Victoria
Report release date
14/03/2025
Report status
Final
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Incorrect configuration, Loading related
In the evening on 15 January 2021, a QantasLink Bombardier Dash-8-315 aircraft, registered VH‑TQE, was being prepared for a scheduled passenger service from Tamworth to Sydney, New South Wales. There were two flight crew, two cabin crew and 29 passengers on board. During the pre‑flight preparations, the flight crew misread the aircraft’s fuel tank gauges and interpreted the total fuel on board to be about 340 kg more than the actual quantity.
The incorrect fuel figure was subsequently used to complete pre-flight documentation and data entry inputs, and the aircraft departed Tamworth with inaccurate load, take‑off and fuel management data. The error was not detected by the flight crew until the aircraft reached its cruise level, when it was corrected, and the flight continued without further incident.
What the ATSB found
The ATSB found that the captain and first officer were distracted by the circumstances associated with the Tamworth arrival and this probably influenced the inaccuracy of the initial fuel check. Having made the initial error, the flight crew formed an incorrect mental model of the aircraft fuel state that persisted throughout the pre-flight preparations. The crew identified the error when seeking out new fuel‑related information during the cruise procedural check.
What has been done as a result
Following this incident, QantasLink provided internal communications to flight crew on checklist usage and cross checking of data. QantasLink also intends using the incident as a case study in its human factors/non-technical skills training program.
Safety message
Data input error is one of the ATSB’s SafetyWatch priorities. Flight crews can guard against errors similar to those in this incident by applying effective threat and error management strategies that recognise when such threats may arise and put in place suitable actions to minimise error potential. These actions include the strict adherence to standard operating procedures, clear and concise communication and independent cross checks between pilots.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 1658 Eastern Daylight-saving Time[1] on 15 January 2021, a QantasLink Bombardier Dash-8-315 aircraft, registered VH-TQE (Figure 1), arrived at Tamworth Regional Airport, New South Wales. The aircraft was operating as a scheduled passenger service from Sydney to Tamworth with 23 passengers, and then returning to Sydney with 29 passengers at a planned departure time of 1740. The crew comprised the captain, first officer (FO) and two cabin crew. The captain was pilot flying (PF) and the FO was pilot monitoring for both sectors.[2]
Figure 1: VH-TQE
Source: Supplied
Shortly after parking the aircraft at Tamworth, the captain left their seat and stood at the doorway between the flight deck and cabin. There had been thunderstorms while approaching Tamworth and the captain thought the disembarking passengers might have questions about the arrival.
The FO remained on the flight deck and finalised the records for the completed flight. As part of this task, the FO read the analogue gauges of the two fuel tanks as indicating a total remaining fuel quantity of 3,830 pounds (see the section titled Fuel gauges). The FO recorded this quantity as the shutdown fuel in the flight record without completing the required fuel quantity validation check (see the section titled Standard operating procedures).
Soon after, the FO provided the captain with the flight record to cross check the information entered. The captain recalled checking the fuel gauges and mentally calculating the total fuel to be about 3,820 pounds. The captain also omitted the fuel quantity validation check, and the FO then submitted the flight record electronically.
Shortly afterwards, the flight crew started completing the flight record for the return flight to Sydney and, as the aircraft did not require refuelling, entered a fuel figure of 3,830 pounds. The FO and captain then began their assigned ‘before start' checks. One of the captain’s assigned checks was to physically verify the fuel quantity. The captain, however, recalled the fuel quantity from memory and entered that figure (3,820 pounds) into the aircraft’s flight management system (FMS)[3] without verifying it.
The captain later completed the departure briefing using the same fuel figure. Following the departure briefing, the captain and FO undertook the ‘before start' checklist. This involved cross checking items, with the FO reading each item in the checklist and the captain actioning them. The captain recalled looking at the fuel gauges for the fuel quantity check but again relied on memory to read out the fuel figure.
As the aircraft’s load sheet weight data was in kilograms, the flight crew converted the fuel figure into kg (3,820 pounds to 1,733 kg). The load sheet for the return flight was submitted at 1714, recording a total fuel on board of 1,733 kg and a take‑off weight of 16,908 kg. The flight crew then used this take‑off weight to calculate the aircraft’s take‑off data, and at 1735, the aircraft departed Tamworth (see the section titled Load, take‑off and fuel management data).
At about 1750, the aircraft reached its assigned cruise level. Shortly after, the flight crew identified a fuel data mismatch during the procedural fuel check for that stage of the flight. They soon established that the fuel quantity used for all pre-flight activities and tasks had been incorrect (the correct fuel figure had been about 3,081 pounds). The fuel figure within the FMS was then amended, the aircraft load data recalculated, and sufficient fuel for the flight was verified.
The aircraft completed the flight to Sydney without further incident and the fuel figure error was reported by the flight crew on arrival. The fuel remaining on board the aircraft in Sydney was reconciled correctly and no defect with the fuel system or instrumentation was identified.
Context
Flight crew
The captain held an Airline Transport Pilot (Aeroplane) Licence and had recently been promoted to that position. The captain had a total flying time of 2,650 hours, having flown 86 hours in the previous 90 days. The captain’s total time included 83 hours on the Bombardier Dash-8-315 (Q300) aircraft and 1,205 hours as a FO on the Bombardier Dash-8-400 (Q400).
The FO held a Commercial Pilot (Aeroplane) Licence and a total flying time of 1,706 hours, having flown 67 hours in the previous 90 days. The FO had accrued a total of 346 hours on the Q300.
Both the captain and FO reported experiencing a high level of workload in the final phase of the Sydney to Tamworth flight due to thunderstorms in the vicinity of the airport. They also stated that, once the aircraft had landed, they both experienced a stress response to the high workload arrival. The captain stated that ‘the adrenaline was still coming from the previous flight making us do things quicker’. As such, it is likely that the flight crew’s attentional focus was reduced during the pre-flight preparations for the return to Sydney.
The ATSB found no indicators that increased the risk of either the captain or FO experiencing a level of fatigue known to have an effect on performance.
Fuel gauges
The Q300 aircraft has two analogue fuel quantity gauges located on the lower part of the engine instrument panel (Figure 2). The gauges fitted to VH-TQE indicated the quantity of usable fuel in each of the two main tanks in pounds. The flight crew needed to add these quantities to determine the total fuel on board.
Figure 2: Q300 fuel gauge layout
Source: QantasLink, adapted and annotated by the ATSB
The captain had only recently commenced operating the Q300 and had significantly more experience on the Q400 aircraft. In the Q400, the fuel quantity is presented on the aircraft’s multi‑function display and includes a digital readout of the total fuel quantity, removing the need for any calculation (Figure 3).
Figure 3: Q400 fuel gauge layout
Source: QantasLink, adapted and annotated by the ATSB
Standard operating procedures
QantasLink procedures required the flight crew to check or confirm the fuel on board the aircraft on five separate occasions prior to departure. Had these procedures been followed properly, the incorrect fuel figure would most probably have been identified. However, on each occasion the flight crew either did not complete the required procedure or did so erroneously (see Table 1).
Table 1: Standard operating procedures (fuel) and crew actions comparison
Procedure
Procedural requirement(s) – fuel
Flight crew action(s)
Flight record (QL-2)
‘check actual fuel burn against the estimated fuel burn from the nav log’
‘fuel at shutdown must be verified against fuel gauges’
‘all entered fields need to be cross checked by both crew members’
an incorrect shutdown fuel figure was identified and recorded by the FO
neither the captain nor the FO checked the actual fuel burn against the estimated fuel burn from the nav log
the captain’s cross check of the fuel gauge readings did not identify the incorrect fuel figure
Before start checks
captain to ‘confirm the fuel quantity is correct, adequate for the planned flight(s) as cross checked with the OFP [operational flight plan]’
the captain recalled the incorrect fuel figure from memory rather than reading the fuel gauges
the captain did not check the fuel quantity against the OFP
Departure briefing
PF to verbally confirm ‘the fuel on board meets requirements as per before start checks’
the captain verbally restated the incorrect fuel figure
Before start checklist
‘ensure that the fuel on board has been checked against the fuel required on the OFP. State the fuel quantity currently on board as indicated on the fuel gauges’
‘the person reading the checklist should also confirm each checklist item called is configured correctly as the checklist is read’
the captain recalled the incorrect fuel figure from memory rather than reading the fuel gauges
the captain did not confirm the fuel on board had been checked against the fuel required on the OFP
the checklist compliance and fuel figure error was not identified by the FO
Load sheet
Cross check ‘fuel – ramp fuel weight’
the captain and FO both entered the incorrect fuel figure in their independent load sheets
the cross check did not identify the incorrect fuel figure
Load, take‑off and fuel management data
The load sheet submitted by the flight crew before departing Tamworth incorrectly recorded the aircraft’s ramp fuel as 1,733 kg (3,820 pounds). As a result, the calculated take‑off weight of 16,908 kg was also incorrect. The flight crew then used the incorrect take‑off weight to determine the take‑off data, resulting in higher than required V speeds.[4] Additionally, the fuel figure entered into the FMS by the captain during the pre-flight activities was also incorrect. Consequently, the fuel data presented to the flight crew during the early stages of the flight were erroneous.
Safety analysis
Both the captain and FO described experiencing a physiological response to the Tamworth arrival, which persisted throughout the pre-flight preparations for departure. This physiological distraction probably degraded their attentional focus and resulted in the initial misinterpretation of the fuel gauges. Additionally, the captain had limited experience on the Q300 aircraft in which the flight crew was required to mentally calculate the total fuel on board. This additional cognitive step probably increased the chance of the error and made it more difficult to identify the error once it had occurred.
As a result of the actions during the initial fuel quantity identification, the captain and FO formed an incorrect mental model of the aircraft’s fuel state. This, coupled with ongoing reduced attentional focus, probably led them to recall the incorrect fuel figure during subsequent pre-flight activities. The same factors probably influenced the flight crew’s cross checks and contributed to the captain and FO omitting procedural checks aimed at capturing fuel quantity errors. Consequently, neither identified the error until the aircraft was airborne, when they followed procedures by seeking out new information during the cruise fuel check.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel data event involving Bombardier Dash-8-315, VH-TQE at Tamworth Regional Airport, on 15 January 2021.
Contributing factors
The flight crew misread the aircraft’s fuel gauges after arrival at Tamworth probably as a result of distraction. This created an inaccurate mental model of the fuel quantity on board which, in turn, hampered identification of this error during subsequent pre-flight preparations for departure.
The incorrect fuel figure was used in pre-flight documentation and data entry inputs resulting in the aircraft departing Tamworth with inaccurate load, take‑off, and fuel management data.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by QantasLink
Following this incident, QantasLink provided internal communications to flight crew on checklist usage and cross checking of data. QantasLink also intends using the incident as a case study in its human factors/non-technical skills training program.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-TQE
QantasLink
Avdata
Airservices Australia
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew of VH-TQE and QantasLink.
A submission was received from QantasLink.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 11 May 2020, a Fairchild SA227-DC Metro 23 (Metro) aircraft, registered VH-HPE and operated by Toll Aviation, was being loaded for its scheduled freight service from Townsville to Rockhampton then Brisbane, Queensland. The pilot was the only person on board.
The pilot completed a load and trim sheet, which indicated that the planned load was not within the allowable centre of gravity limits. It was agreed that 126 kg of freight would be moved from compartment three to the nose compartment. The revised load and trim sheet indicated the centre of gravity to be within the limits. During the flight to Rockhampton, the pilot observed that the aircraft felt tail heavy, but did not experience any controllability issues.
Due to the concern of an aft centre of gravity, the additional freight loaded at Rockhampton was limited, which was still within the calculated allowable centre of gravity limits. On take-off from Rockhampton, the pilot reported that the aircraft had a strong pitch-up tendency and that strong forward pressure on the flight controls was required to maintain the correct pitch attitude. During the cruise, the autopilot would not consistently maintain level flight. The pilot disconnected the autopilot and with full nose-down trim applied, the pilot had to maintain forward pressure to control the pitch attitude of the aircraft. The aircraft continued to Brisbane and the pilot reported that no problems were experienced during the approach and landing.
What the ATSB found
The ATSB found that, the ground handlers at Townsville did not accurately weigh the freight relocated into the nose compartment, but rather, it was estimated by feel. This resulted in an inaccurate load and trim sheet, and the centre of gravity being further aft than expected. Therefore, when additional freight was loaded in Rockhampton, this unknowingly moved the centre of gravity beyond the rear limit, leading to the pitch-up tendency experienced by the pilot.
Although not contributory, the operator’s paper-based load planning tool used by ground handlers for the Metro did not account for the centre of gravity position. Rather, this was later determined by the pilot on the load and trim sheet, which was potentially completed after loading had commenced. This increased the chance of freight having to be relocated and the potential for loading errors to occur.
It was also identified that the operator’s ground handling manual did not contain sufficient procedural detail to facilitate the accurate redistribution of freight. In particular, there was no guidance on conducting last-minute changes or taking into account the centre of gravity when preparing a load plan to ensure that an aircraft would be correctly loaded.
What has been done as a result
Following the incident, the operator amended their ground handling processes and included increased direction to ensure that freight would be accurately redistributed in the event of a last-minute change. The operator has since relinquished their Civil Aviation Safety Authority’s Air Operator’s Certificate and divested their flying operations to another operator. The new Metro aircraft operator also considered the findings of this investigation, reviewed their ground handling manual and incorporated amendments to ensure that an aircraft would be correctly loaded.
Safety message
This incident demonstrates the critical nature of load control and the requirement to ensure an aircraft is correctly loaded and the centre of gravity is within the allowable limits. It also emphasises the importance of providing ground handlers with sufficient and detailed procedures to allow them to accurately conduct load control duties and minimise the potential for error.
The occurrence
Townsville–Rockhampton
On 11 May 2020, a Fairchild SA227-DC Metro 23 (Metro) aircraft, registered VH-HPE and operated by Toll Aviation, was being loaded for its scheduled freight service from Townsville to Rockhampton then Brisbane, Queensland. The pilot was the only person on board.
The pilot signed on for duty at 1700 Eastern Standard Time[1] and shortly after commenced pre‑flight preparations of the aircraft. The loading process had already commenced by that time and was about half complete when the ground handlers provided the load plan to the pilot.
The pilot then completed a load and trim sheet and ascertained that the planned load was aft of the rear centre of gravity limit. The pilot advised the ground handlers that the load was too heavy in compartment (zone) three and that some of that freight be moved to the nose compartment.
A team of four ground handlers were loading the aircraft, none of which were designated as a supervisor. One ground handler suggested to the pilot that 126 kg could be moved from compartment three into the nose compartment, leaving 300 kg in zone three. The pilot agreed, provided this could be achieved, having noted that the nose compartment was much smaller than the remaining compartments in both size and weight limit (Figure 1).
The ground handler contacted their supervisor who was at the freight depot. The supervisor had completed and signed the load plan, and advised the ground handler to carry out the pilot’s request to move the load. The ground handler commenced loading freight into the nose compartment. The ground handler recalled that ‘the nose is small in space’ and that it will ‘only fit a certain amount of things in there’, so only loaded as many bags as they could, filling the nose to volume capacity. This freight was not weighed, but rather, estimated by feel as there were no scales available at the aircraft. The ground handler explained that the load change took place at about 1745 and that the aircraft was scheduled to depart at 1800.
The pilot asked the ground handler if the freight had been moved as requested and the ground handler confirmed it had been. Believing that the load distribution was correct as amended from the original plan, the pilot completed a new load and trim sheet, which indicated the centre of gravity to be within the limits.
Shortly after, the aircraft departed Townsville. During the flight to Rockhampton, the pilot indicated that the aircraft felt tail heavy, but did not experience any controllability issues.
Figure 1: VH-HPE freight compartment configuration and weight limits
Source: Toll Aviation, modified by the ATSB
Rockhampton–Brisbane
On arrival in Rockhampton, the pilot discussed the load with ground handlers. The ground handlers had already reviewed the load plan from Townsville and were aware that the aircraft was relatively heavy. As a result, they had transferred most of the freight to another carrier for transport.
The ground handler at Rockhampton noticed that the aircraft appeared to be sitting ‘tail heavy’, and due to the pilot’s concern regarding an aft centre of gravity, the aircraft was only loaded with 111 kg in compartment three and 3 kg in compartment five. While the pilot believed the aircraft could still be loaded with more, they both agreed to minimise additional load.
On take-off from Rockhampton, the pilot reported the aircraft had a strong pitch-up tendency and rotated without input. The pilot had to apply strong forward pressure on the flight controls to maintain the correct pitch attitude and the pressure required to do so increased with altitude. Concerned with maintaining sufficient air density[2] to maintain control effectiveness, the pilot reduced the planned cruising altitude to flight level (FL)[3] 130.
After establishing the aircraft in the cruise, the pilot observed that the autopilot would not consistently maintain level flight. The aircraft would ‘porpoise’ as the autopilot tried to correct the pitch-up tendency. The pilot disconnected the autopilot from controlling the pitch of the aircraft, keeping it in GPS steer mode (lateral guidance only). Full nose-down trim had already been applied and the pilot then manually controlled the pitch attitude of the aircraft.
The pilot found that constant application of forward pressure was required, though noted that the force needed was ‘only a couple of kilograms’. The pilot did not observe any other controllability issues and was satisfied that control of the aircraft could be maintained.
The aircraft continued to Brisbane and the pilot reported that no problems were experienced during the approach and landing. The pilot had contacted operations prior to arrival, explained their observations regarding pitch control, and was met on the ground by maintenance engineers.
The pilot held a valid Commercial Pilot Licence (Aeroplane) and multi-engine command instrument rating. The pilot had over 3,000 hours in total, with about 2,500 hours in command and about 700 hours on the Metro 23 aircraft. The majority of their flying experience was in overnight freight (single pilot operations). The pilot had been flying for Toll Aviation (Toll) for about 1 year.
Ground handler 1 (Townsville)
Ground handler 1 had been a Toll employee for a combined total of 11 years. In addition to ground handling duties, they conducted other freight related duties including deliveries via motor vehicle.
Ground handler 2 (Townsville)
Ground handler 2 had been a Toll employee for almost 10 years in a variety of roles with the last six in operational roles. Their current position was supervisory in nature and oversaw freight related duties. Mostly located in the depot, they did not normally carry out actual loading duties, but were responsible for the preparation of, and signing of load plans.
Ground handler 3 (Rockhampton)
Ground handler 3 had 13 years at Toll and was in a supervisory role similar to ground handler 2. They had about 10 years’ experience with loading the Fairchild SA227 (Metro) aircraft, and often carried out both load planning and actual loading tasks.
Organisational information
Toll Aviation was part of the Toll group of companies and provided air freight capability to Toll Express Parcels. Toll Express Parcels provided ground handling services to Toll Aviation at some of its ports but was not a full-time aviation ground handling organisation. Ground handling in Townsville and Rockhampton was undertaken by Toll Express Parcels, but Brisbane was handled by Toll Aviation.
Ground handling staff explained that they were a mix of Toll employees and contract delivery drivers who were trained in aviation ground handling duties. When not conducting aircraft related duties, the ground handlers undertook road deliveries/pickup.
Aircraft information
VH-HPE was a Fairchild SA227-DC Metro 23, twin turboprop engine regional aircraft, which had been configured for freight operations. Freight could be loaded into the nose compartment, or the main fuselage compartment, which had been divided into five zones (compartments) (Figure 1). The zones had a webbing style net for segregation of freight between compartments. Heavy, bulkier freight could be physically restrained to the compartment floor.
Table 1: VH-HPE aircraft weight limits
Weight limit
lb
kg
Maximum ramp weight
16,566
7,530
Maximum take-off weight
16,500
7,485
Maximum landing weight
15,675
7,110
Maximum zero fuel weight
14,500
6,580
An aircraft must be operated within prescribed weight and balance limits. That is, it should not be loaded above the maximum weight limitations (Table 1) and the position of the aircraft load (fuel, passengers, cargo etc.) should be such that the centre of gravity is within lateral and longitudinal limits (balance). Maintaining this balance is critical to stable, controllable flight. A pilot is to use the approved loading system for the aircraft to ensure that the weight and balance is within the approved envelope, either manually (graphical) or electronically.
The approved loading system for the Metro operated by Toll utilised a graphical method (load and trim sheet) for determining the centre of gravity position. The pilot was required to complete the load and trim sheet once all the weight information (freight, fuel, passengers) had been obtained. Freight loads were provided on the load plan (Appendix A). The operator had a load and trim sheet that was specific to VH-HPE (Appendix B).
The load and trim sheet considered weight and position when graphically determining centre of gravity. Load placed closer to the front (nose compartment) or rear (compartment five) of the aircraft would have greater effect on centre of gravity than load placed near the middle of the aircraft (compartment two). Load placed in compartment two had negligible effect on the aircraft’s centre of gravity. Load placed in the nose compartment and in compartment one shifted the centre of gravity towards the front of the aircraft. Load placed in compartments three‑five shifted the centre of gravity towards the rear of the aircraft.
Post-incident inspection/actions
Freight reweighed
Following arrival in Brisbane, the pilot discussed the incident with the maintenance engineers. This resulted in the freight being reweighed as it was unloaded from the aircraft. When compared to the load plan used to complete the load and trim sheet, there was a significant difference in the weight distribution. Notably, only 65 kg was in the nose compartment and an extra 64 kg was in compartment three. All other compartments had more weight than planned. However, the individual compartment weights were not exceeded. The planned and actual weights are shown in Table 2, representing the load for the flight from Rockhampton to Brisbane.
The pilot subsequently completed a new load and trim sheet using the actual weights and the centre of gravity was found to be aft of the rear limit (outside of the limits) (Appendix C).
Table 2: Aircraft load (reweighed) for Rockhampton to Brisbane
Compartment
Load plan (kg)
Actual weights (kg)
Weight difference (kg)
Nose
126
65
-61
1
527
545
+18
2
582
606
+24
3
411
475
+64
4
219
225
+6
5
90
103
+13
The weight of the additional freight loaded at Rockhampton was subtracted to determine the actual weight and distribution of freight for the flight from Townsville to Rockhampton. The actual weights did not correspond to the load plan but did not exceed individual compartment limits. Table 3 shows the weights on the original load plan during aircraft loading and the revised plan after moving some freight from compartment three to the nose compartment, compared with the actual weights.
A load and trim sheet with the actual weights determined that the load from Townsville was still within limits but the centre of gravity was much further aft than originally calculated. The recalculated load and trim sheet also revealed that the aircraft departed Townsville about 6 kg above its maximum take-off weight (Appendix D). A lower fuel load on departure from Rockhampton meant that the aircraft was within the take-off weight limits. However, the additional freight loaded in Rockhampton shifted the centre of gravity position beyond the rear limit.
Table 3: Aircraft load for Townsville to Rockhampton
Compartment
Original load plan (kg)
Revised load plan (kg)
Actual weights (kg)
Nose
0
126
65
1
527
527
545
2
582
582
606
3
426
300
364
4
219
219
225
5
87
87
100
Scales at Townsville
The operator’s internal investigation report stated that the scales used in Townsville were calibrated on 27 June 2019 and were due to be recalibrated in June 2020. They also verified that these scales were reporting an accurate weight.
Flight controls inspections
To confirm the serviceability of, and their potential to have contributed to the pitch control issues, the operator replaced the pitch servo and pitch flight guidance computer. Maintenance logs showed that replacement parts were fitted and tested serviceable. There was no evidence to suggest the components were malfunctioning or contributory.
Aircraft loading process
Townsville
On the day of the incident, items for air freight began arriving at the depot around 1600 and aircraft load preparations commenced at that time. Individual freight items were weighed with smaller envelope style parcels placed in consolidation bags, to a limit of 14 kg per bag. As each item was weighed, it was allocated to an aircraft compartment. The Townsville supervisor reported that, compartment allocation was based on the size or volume of the freight item and the experience of the ground handler to get an even distribution of freight. The supervisor said it was normal to prioritise freight to compartments one and two (toward the front of aircraft), to enable later ports to add freight to the rear.
Each aircraft compartment had its own ‘barrow’ (or area in a truck) to ensure segregation and facilitation of loading onto the aircraft. All weights were written on a load sheet, which upon completion, was presented to the supervisor.
Normally, consigned items already had a weight annotated on them. However, if found to be different when weighed prior to compartment allocation, it did not appear that these items were annotated with their correct weight. Consolidation bags did not have total weights annotated on the bag, nor was there a requirement to do so.
The supervisor stated that the load was driven to the aircraft as soon as preparations had completed.
Despite not taking part in the load preparation, the supervisor completed and signed the load plan in addition to other freight paperwork. The supervisor explained that the paperwork was then delivered to the pilot by one of their staff who was not on the load team. The supervisor stated they did not have an opportunity to verify if the load matched the plan or make changes prior to the load being delivered to the aircraft. They then forwarded a copy of the load plan to the Rockhampton supervisor to enable them to begin their load preparations.
The ground handler contacted the supervisor and was advised to amend the load as directed by the pilot.
The supervisor indicated that, on this particular night the freight allocation was much bigger than normal. Further, in general, it was a rare occasion in which the pilot requested freight to be moved once the load plan had been completed.
Rockhampton
The load process at Rockhampton was described as being similar to Townsville. Due to Rockhampton being a smaller depot, a distinct difference was the supervisor being more involved in the loading process and physically participated in all aspects. The supervisor at Rockhampton also stated that it was a rare occasion for a pilot to request changes to the load plan.
Load control policy and procedures
The operator’s load control policy and procedures were contained in numerous manuals within their operations manual suite. These are described in the following sections.
Flight operations
The flight operations manual stated that:
Responsibility for load control of Toll Aviation aircraft lies with the Pilot-in-Command for the particular flight.
The Pilot-in-Command shall ensure that a load sheet is completed prior to departure of the aircraft on each stage of every flight.
The Pilot-in-Command will advise Toll Aviation Operations or the Supervisor/Load Controller of the maximum payload for the particular flight as this will allow loading to commence. During the loading and unloading of freight on company aircraft, the Pilot-in-Command shall monitor the operation and location of loading vehicles and equipment by ground handling staff to ensure the aircraft is not damaged.
The Pilot-in-Command may delegate this duty to a person identified as an employee to a client freight organisation, trained in loading procedures for the aircraft.
Before each flight, the Pilot-in-Command shall ensure that the aeroplane is loaded within the prescribed centre of gravity limits as determined by the current approved loading system specified in the AFM for that aircraft.
As stated above, the pilot was ultimately responsible for load control, despite not physically undertaking load duties. Ground handlers carried out the bulk of load control duties on behalf of the pilot.
The pilot reported that it was not possible to physically confirm the load was accurate (for example, confirming correct weights). Similarly, although present at the aircraft for part of the loading, the pilot was not able to closely supervise the process. As these tasks were delegated to ground handlers, the pilot relied on the ground handlers providing an accurate load plan, so the pilot could complete the load and trim sheet and fulfil their requirement to ensure the aircraft was loaded within the prescribed centre of gravity limits.
Ground handling operations
The operator’s ground handling manual (GHM) covered the requirements for all organisations conducting ground handling for Toll Aviation. Section 2.4.4 was titled Ready reference and stated:
This manual is intended for use by Toll Aviation employees, contractors, freight forwarders and ground handlers involved in any way with the air transport process and specifically in relation to acceptance, handling, loading, carriage or consignment of cargo on Toll Aviation aircraft.
The ATSB’s review of the load control aspect of the GHM identified that it was focused on policy and procedural inclusions that were primarily related to load plan preparation. There was no other document or manual containing procedures or work instructions relating to load control.
Allocation of responsibilities
The GHM indicated that responsibility for load control was assigned to the pilot in command, reiterating the requirements of the flight operations manuals as:
2-4-6 Pilot-in-Command
…the Pilot-in-Command shall at all times:
b. take all reasonable steps to ensure that the:
1. load is properly distributed and safely secured
2. aircraft weight and balance is within the calculated limits for the operating conditions.
3-1-2 Pilot-in-Command responsibilities
Responsibility for Load Control of Toll Aviation aircraft lies with the Pilot-in-Command for the particular flight.
The Pilot-in-Command shall ensure that:
a. a Load and Trim Sheet is completed prior to departure of the aircraft for each stage of every flight
3-1-24 Pilot-in-Command approval
Prior to departure, a completed Loading Plan signed by the person responsible for loading the aircraft shall be provided to and shall be approved by the Pilot-in-Command
The GHM did not specify a similar assignment of responsibility for ground handlers undertaking load duties.
Supervision
The GHM did not specify a requirement for a supervisor to be included in the load team and none of the ground handlers in the load team at Townsville were assigned as a supervisor. The supervisor at Townsville said that, as the supervisor for all depot operations, they were not always able to attend the aircraft. Furthermore, there was not a leading hand position or similar that was part of the load team.
Weighing freight
The GHM directed that:
All freight loaded at any port shall be weighed and the weight shall be measured in kilograms to the nearest kilo using calibrated scales.
Ground handlers at both Townsville and Rockhampton confirmed that, upon arrival at the depot, all freight items were weighed. However, once weighed, items were not annotated with their verified weight, nor was there a requirement to do so.
Load plan preparation
The GHM included procedures for the preparation of a load plan and a generic load plan procedure.
3-1-22 Preparing the Loading Plan
The Departure Port Supervisor/Responsible person or PIC [pilot in command] shall be responsible for preparing the Loading Plan. He/she shall:
a. obtain the maximum payload figure from the Pilot-in-Command
b. using the excel Loading Plan spreadsheet, freight is allocated to particular zones on the aircraft (taking into account the maximum weight for floor loading limits for the zone). This information is then transferred to a Loading Plan form.
c. complete Loading Plan on the day departure including information at the end of the Loading Plan, REGO = Aircraft Rego, FROM = departing port, TO = NEXT port aircraft will land, DATE = Date of departure, Loaders name = Person responsible for completing Loading Plan on day of departure, Signature = of person responsible for Loading Plan
d. provide a copy of the Loading Plan to the Loader
e. transmit a copy of the Loading Plan to the Supervisor/responsible person at each transit port.
The load plan tool used by the operator for the Metro was a manual, paper-based tool. A diagram of each aircraft and their compartment layouts were annotated with the applicable weight limits. This tool did not account for how the position of freight may affect the resultant centre of gravity (Appendix A).
Load and trim sheet
The subsequent completion of the load and trim sheet was the only means to calculate the centre of gravity position. This was the responsibility of the pilot, since ground handlers were not required to undertake this task. To complete the load and trim sheet, the pilot was wholly reliant on the information provided on the load plan by ground handlers.
Freight loading and last-minute changes
The GHM did not provide guidance on how to distribute freight across the aircraft compartments. As previously discussed, the distribution of freight was highly dependent on the experience of the ground handler conducting the task. According to the pilot and the ground handlers, it appeared that, in most cases, the planned allocation rarely required changes to be made and the load plan was usually within the centre of gravity limits. The redistribution of freight requested by the pilot was considered a last-minute change (LMC). The GHM only referred to LMCs as follows:
Any last-minute change to the freight load shall be approved by the Pilot-in-Command
The operator stated that this scenario was trained for, and that in a situation like the incident, freight was to be returned to the depot to be reweighed before loading. This was not documented in any manual, nor was it included in the training presentations. Further, ground handlers were not able to weigh the freight at the aircraft as scales were not available to the load team at the aircraft.
Ground handler 1 at Townsville inferred that, if 10-20 kg needed to be moved then estimating the weight by feel would be sufficient. However, if 150 kg needed to be moved, this would require taking freight back to the depot to reweigh. The ground handler could not explain why the 126 kg LMC for this incident was any different.
Ground handler 3 at Rockhampton explained that, if freight needed to be moved, they would attempt to move an entire compartment allocation (a known weight) or only move items that had weights annotated. Although not explicitly stated, the ground handler inferred that, if either of those options were not feasible, then they would return to the depot to reweigh the freight.
A procedure or explanation regarding a LMC was not detailed in the GHM. However, ground handlers appeared to have been provided some training/guidance for handling an LMC. The operator advised that, returning to the depot to reweigh freight was taught but conceded this was not documented anywhere.
Ground handling training
The operator’s ground training program included several presentations covering all aspects of load control. This was supplemented by practical instruction and formal assessment. Recurrent training was required every 24 months.
Module 3 of the training covered load control and discussed its critical nature. It emphasised the requirement for accurate loading of the aircraft and that the pilot was reliant on ground handlers to provide accurate information to complete the load and trim sheet. The module provided examples of the consequences of incorrect loading to reinforce this message. The ATSB noted that this information was not explicitly included in the GHM.
The operator advised that ground handlers were taught that freight was to be returned to the depot to be reweighed in the event of LMCs such as this incident. They acknowledged that this was not documented in any manual (it was also not in module 3 of the training).
The operator also reported that, about 3 years prior, several issues covering the delivery of, and management of ground handling training had been identified. As a result, the operator received board approval for additional resources to revise their training structure and improve those issues. They advised that, at the time of this incident, remedial action was in progress to amend training documentation and provide greater scrutiny over training activity.
The supervisor at Townsville was the designated trainer, but had not completed recurrent training. The supervisor explained that, training had been deficient for about 4 years since the branch manager had left the organisation. The supervisor also reported that significant catch-up had been required to get all staff up-to-date. Rockhampton did not appear to have such training issues.
The ATSB reviewed training as a possible contributing factor to the incident. However, when considering the lack of procedural guidance for load control duties, the ATSB assessed that effective training could not take place without robust documented procedures to train for, therefore did not consider training aspects any further.
On 30 January 2013, a Toll Fairchild SA-227AC Metro aircraft, registered VH-UUO, departed Melbourne Airport, Victoria for Launceston Airport, Tasmania on a scheduled freight flight. The pilot was the only person on board.
During the take-off, the pilot reported that they needed more forward elevator trim than usual to climb out at a 10° nose-up attitude. The pilot noticed that, in straight-and-level flight, the aircraft had full nose-down trim, but flying at a 5° nose-up attitude. When the autopilot was engaged, the pilot stated that the autopilot struggled to maintain straight-and-level flight, explaining that the aircraft ‘porpoised’. The pilot conducted a normal landing at Launceston.
The operator determined that, although the loading plan for the aircraft indicated 100 kg of freight in the nose locker, one of the loaders had removed about 70 kg of freight from the nose locker and moved it to the rear of the aircraft. The operator identified that there was no formalised approach to the loading and unloading of the aircraft.
In addition, as the freight for the aircraft was not reweighed at Launceston, it was not possible to determine the exact centre of gravity that existed at the time of take-off from Melbourne. However, the flight characteristics of the aircraft suggested that it was either at the most rearward centre of gravity position, or just outside the rear centre of gravity limit.
The operator identified a lack of formal training for ground handlers and a lack of general procedures for them to follow. They also noted that there was insufficient oversight of the loading process and that the load plan for the Metro did not take centre of gravity position into account. Actions proposed by the operator included a review of, and publishing revisions to the GHM and the development of a ground handling training manual.
Operator comments
The operator’s investigation for this incident also identified that there was a lack of procedural guidance in the ground handling manual to support ground handlers in their duties. They stated that:
The Ground Handling Manual provides limited information on practical application of safe loading procedures for the Metro Aircraft and instead relies on input from the Pilot in Command.
The ATSB noted similarities between the two occurrences (albeit 8 years apart) and sought additional information regarding the status of safety actions from the 2013 incident. The operator’s safety manager was not able to provide any additional information relating to the previous occurrence as it was before their tenure and there was no record within their safety management system. Therefore, the ATSB was unable to explore any potential links between the two occurrences.
Safety analysis
Introduction
During the dedicated freight flight from Townsville to Rockhampton, Queensland, the pilot of VH‑HPE noted that the aircraft felt tail heavy, but did not experience any controllability issues. On the subsequent flight from Rockhampton to Brisbane, the aircraft had a strong pitch-up tendency, and the pilot was required to apply strong forward pressure on the flight controls to maintain the correct pitch attitude. The aircraft continued to Brisbane and the pilot reported that no problems were experienced during the approach and landing.
This analysis will examine the planned and actual load distribution and corresponding centre of gravity position for the flights from Townsville to Rockhampton and then to Brisbane. It will further discuss the operator’s load planning tool and ground handling procedures regarding the redistribution of freight.
Inaccurate load
After receiving the load plan from the ground handlers at Townsville, the pilot completed the load and trim sheet, and identified that the aircraft’s centre of gravity was aft of the rear limit. Consequently, it was agreed that 126 kg of freight was to be relocated to the nose compartment.
As there were no scales available at the aircraft, the ground handler estimated the amount of freight to be moved based on feel. However, the reweigh of the load post-incident established that the aircraft was not loaded in accordance with the revised load plan. Therefore, the completed load and trim sheet did not reflect the actual load distribution. Although the load distribution was not as planned, it was still within centre of gravity limits, albeit more toward the rear than expected. As this was not known, any additional load would not have been accurately reflected on the load and trim sheet and was potentially out of limits.
Centre of gravity out of limits
At Rockhampton, additional freight was loaded based on the load and trim sheet prepared at Townsville. However, since the load and trim sheet did not accurately reflect the actual load distribution, the additional freight moved the centre of gravity rearward, beyond the rear limit. As a result, the aircraft was operated outside of its centre of gravity limitations.
The centre of gravity envelope is established to provide a pilot with the allowable distribution of weight, within which the aircraft will have longitudinal stability and allow the pilot to have full control of the aircraft. Although the aircraft was still controllable in this case, the pilot had used full nose‑down trim and the auto pilot was not able to maintain level flight. This required the pilot to apply constant forward pressure to manually control pitch and reduced the options available to the pilot to maintain full control of the aircraft.
Load plan did not account for centre of gravity position
The paper-based load planning tool utilised by Toll Aviation (Toll) for its Metro aircraft only accounted for compartment weight limits and did not provide information on the resultant centre of gravity position. This was later determined on completion of the load and trim sheet, which was a pilot responsibility. Ground handlers were not trained to, nor were they required to, complete the load and trim sheet. Further, there was no documented guidance for the distribution of freight within the aircraft and it was dependent upon an individual ground handler and/or supervisor’s training, experience and knowledge of the aircraft.
Loading was often commenced prior to the pilot being able to complete the load and trim sheet. Consequently, loading may be quite advanced if not already completed by the time the pilot has determined that the load plan was not within limits. While in this case and for the 2013 incident, the loading error occurred due to the freight not being weighed, this could necessitate additional workload and delay. As there was no ability to weigh freight at the aircraft and no documented procedure to guide such a reasonably foreseeable situation, this increased the chance of freight having to be relocated, thereby creating opportunities for errors to occur.
Ground handling procedures
According to the operator’s flight operations and ground handling manuals (GHM), the pilot was ultimately responsible for load control. However, practically, a significant portion of the load process was delegated to the ground handlers. The GHM detailed the requirements for conducting ground handling operations, including the loading of freight. However, the procedures were primarily related to the preparation of a load plan, with no other routine tasks or reasonably expected contingency tasks included. Further, there was no other documents or manuals that contained work instructions for ground handling operations.
Specifically, the GHM did not provide details on how to take centre of gravity into account when preparing a load plan, to minimise the potential for last-minutes changes. Also, the GHM did not include any instructions for the conduct of last-minute changes to ensure the aircraft was loaded correctly. For such situations, ground handlers were taught that the freight was to be returned to the depot to be reweighed, however, this instruction was not documented. The operator also identified that there was limited information in the manual regarding safe loading procedures.
In this incident, the ground handlers involved had different views on what was required when faced with a similar situation. Ground handler 1 at Townsville displayed an understanding of what should have occurred with regard to moving the freight, specifically mentioning that an amount of 150 kg would require return to the depot for reweigh, although they could not answer why 126 kg was different. Ground handler 3 at Rockhampton displayed a higher understanding and had numerous options available to consider when redistributing freight, none of which were documented in the GHM.
In the absence of clear, documented procedures, ground handlers were effectively put into situations where they had to rely on their own judgement and experience, and possibly utilise other procedures, which may not necessarily be appropriate for the task. Robust documented procedures create predictable standards and expectations and provide a solid foundation for training. This will enable staff to undertake tasks, identify errors and ensure consistent, safe outcomes.
Load awareness
The ground handler’s recognition that the aircraft was relatively heavy on arrival at Rockhampton and the decision to make alternative arrangements for freight to minimise the additional load demonstrated a high level of situational awareness. While they were not to know that the aircraft was incorrectly loaded and that additional load would result in the centre of gravity being out of limits, their actions limited the potential severity of the situation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the aircraft loading and in-flight controllability issue involving Fairchild SA227, VH-HPE, Rockhampton Airport, Queensland, on 11 May 2020.
Contributing factors
Ground handlers did not accurately weigh the freight relocated to the nose compartment at Townsville. This resulted in an inaccurate load record on the load and trim sheet, with the centre for gravity further aft, though still within limits.
Additional freight was loaded in Rockhampton as per the load and trim sheet. However, due to inaccuracies in the load and trim sheet (ex. Townsville), the additional load unknowingly moved the centre of gravity aft of the rear limit (out of limits). This resulted in the aircraft exhibiting a strong pitch-up tendency, requiring the pilot to apply constant forward pressure to maintain aircraft control.
Other factors that increased risk
The load planning tool used by the operator for the SA227-DC Metro 23 aircraft did not account for the centre of gravity position. This increased the chance of freight having to be relocated once the pilot completed the load and trim sheet and increased the potential for loading errors to occur.
The operator's ground handling manual did not contain detailed procedural guidance for facilitating accurate redistribution of freight to ensure that an aircraft would be correctly loaded. (Safety Issue)
Other findings
Ground handlers at Rockhampton assessed the aircraft as relatively heavy and took action to minimise additional load. On arrival, it was agreed with the pilot to limit the additional freight. These actions reduced the severity of the centre of gravity being out of limits.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The operator's ground handling manual did not contain detailed procedural guidance for facilitating accurate redistribution of freight and ensure that an aircraft would be correctly loaded.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action Toll Aviation
Soon after the incident, Toll Aviation advised that:
An outcome discussion was conducted with all ground handlers regarding the actions taken on the day of the incident and their responsibilities under the ground handling manual.
Human Factors for Ground Handlers training had been finalised and was being implemented in stages across Toll Air Express.
An electronic load tool (Excel) had been devised for the Metro aircraft, to provide the ground handlers with a guide for the position of the index units when determining freights loaded into each compartment. This tool was in the stage of testing and quality review prior to formal change management process and implementation.
A weight and balance review of VH-HPE was conducted by the weight control officer. The load and trim sheet has been revised and was undergoing testing and quality review prior to formal change management process and implementation.
Glossary
EST Eastern standard time
FL Flight level
GHM Ground handling manual
GPS Global positioning system
LMC Last-minute change
Sources and submissions
Sources of information
The sources of information during the investigation included the:
the pilot
the ground handlers (Toll Express Parcels)
the operator (Toll Aviation).
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the ground handlers (Toll Express Parcels)
the operator (Toll Aviation)
the Civil Aviation Safety Authority.
Submissions were received from:
the pilot
the ground handlers (Toll Express Parcels)
the operator (Toll Aviation)
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Metro 3/23 load plan
Source: Toll Aviation
Appendix B – VH-HPE load and trim sheet
Source: Toll Aviation
Appendix C – Centre of gravity (CoG) position (Rockhampton to Brisbane)
Source: Toll Aviation, annotated by the ATSB
Appendix D – Centre of gravity (CoG) position (Townsville to Rockhampton)
Source: Toll Aviation, annotated by the ATSB
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the 10 January 2019, a Bell Helicopter 205A-1, registered VH-HUE (HUE), was being used for external sling loading operations near Talbingo, New South Wales with the pilot as the sole occupant. As the helicopter approached the drop‑off site, the load unexpectedly disconnected from the remote cargo hook. One of two ground personnel was struck and seriously injured by the falling load.
What the ATSB found
Despite examination of the involved components, the reason why the load disconnected unexpectedly from the remote cargo hook could not be determined. However, the ATSB found that the loadmasters were not maintaining a safe distance from the load. Their positioning, in combination with the significant movement of the load as it contacted the ground, resulted in one of them being struck and seriously injured.
What's been done as a result
As a result of this accident, all contractors involved reviewed the procedures being used for helicopter lifting operations during this project. They have reviewed the risk controls for receipt and positioning of loads, based on the positioning precision required.
The operator who supplied the loadmasters has reviewed and updated their procedures. They have identified a ‘dynamic exclusion zone’ as a position above a person’s head height that is in the pathway of a potential uncontrolled load that may drop and impact onto a person. In recognition that the zone may vary due to a number of variables, specific guidance will be provided as part of pre‑activity briefings.
The lead contractor is overseeing a range of initiatives, including a behavioural safety review of the project with the intention to implement an appropriately designed program to positively influence behaviours across their projects.
Safety message
This incident highlights the dangers associated with external sling load operations. Unexpected events can occur and ground personnel should ensure they maintain their separation from external slung loads that are above head height. Each sling load operation can be unique, with different locations, load shape and environmental conditions creating different safety considerations. As a consequence, clear written procedures and detailed discussions prior to commencement of each operation are essential to ensure all participants are aware of the unique dangers of the operation.
Transport Canada commissioned a video titled ‘Keep your eyes on the hook’, which shows some of the dangers for ground crew when working around helicopters and longline loads.
The occurrence
What happened
On the 10 January 2019, a Bell Helicopter 205A-1, registered VH-HUE (HUE), was being used for external sling loading operations near Talbingo, New South Wales with the pilot as the sole occupant. As the helicopter approached the receiving site, the load unexpectedly disconnected from the remote cargo hook. One of two loadmasters assisting on the ground, was struck and seriously injured by the falling load.
Preparation for the operation
There were a number of different organisations involved in lifting operations on the day. The lead contractor had sub‑contracted two helicopter operators to move the equipment from a staging area near Tantangara Dam to a drilling site about 3 km away. The three organisations had conducted this type of work together a number of times. One helicopter operator (operator A) supplied an AS350B3 helicopter, long line, remote cargo hook, lifting equipment and three experienced loadmasters. The second operator (operator B) supplied HUE, a long line and remote cargo hook.
At around 0800 Eastern Daylight Time,[1] two of the loadmasters arrived at the staging site to begin preparations for the day. Both helicopters and the third loadmaster were delayed due to fog. The loadmasters checked all the lifting equipment, including the slings and shackles, for integrity and ensured they had been checked during the last routine equipment inspection. They then began working with the drilling crew to organise, weigh and rig the loads to be moved by the helicopters. The third loadmaster arrived after the fog had lifted, and they all worked together to finish rigging the loads.
Among the loads were three lots of drill rods on drill racks (Figure 1). The loadmasters decided not to use the lift points on the drill racks, as the lift points were not rated or stamped. Working together, the loadmasters ensured the weight of the loads were equal, secured the drill rods to the rack and rigged the slings, so the loads would be balanced during flight. To do this, they used two 6 m round slings, rated to carry 2,000 kg, choked at either end of the rod rack. The slings were then attached to a shackle, which connected directly to the remote cargo hook. A 5.6 m tag line was attached to the load, to assist with manoeuvring the load into the required position at the receiving site. The loadmasters rigged the loads a number of times before they were happy with the rigging.
Figure 1: Drill rods ratcheted to the rack and slings attached
The figure shows the drill rods ratcheted to the drill rod rack and the slings which are choked at the ends of the drill rack.
Source: NSW police, annotated by ATSB
After all the loads were rigged to their satisfaction, the pilots and loadmasters then held an aviation briefing where they discussed a helicopter lift plan. One of the loadmasters then led a toolbox talk, with all people involved in the day’s operations. They discussed every item on their company’s safe work method statement, which included known hazards. It was reported that the discussion clearly identified:
safe sites for people not involved in the helicopter lifting operations
the routes the helicopters would be taking
being mindful of avoiding the ‘crush zone’.
Inside the ‘crush zone’ there was an injury risk from contact with the external loads. There was no definition for the extent of the crush zone.
The loadmaster also highlighted that:
as taglines were being used, people should not become fixated on getting hold of them
ground personnel should not put themselves in a dangerous position and were to remain within the view of the pilot at all times.
The lead contractor then conducted a third briefing, which discussed their company’s expectations including radio communications, transfer of crew between the loading and receiving zone, staff resourcing of both the loading and receiving areas, and emergency procedures. It was reported that all three briefings were done methodically, with clear instructions and time for all involved to ask questions and understand their role.
The people who were being flown to the drill site were then given a helicopter induction. While this was occurring, inspections of the helicopter's cargo hook on the underside of the helicopter, long lines and remote cargo hook connections were conducted. This involved a number of release and reattachments of the long line to the cargo hook on the underside of the helicopter and a number of pilot-operated releases and manual releases by the loadmasters of the remote cargo hook. After the loadmasters had checked the shackles to ensure they fitted in the cargo hook throat (Figure 2), the group split up and went to their designated areas. One loadmaster went to the loading site and two went to the drill site, which was receiving the equipment. At the drill site, the supervisor identified the designated safe zone ensuring all personnel not involved in the lifting operations were within this zone and placed the emergency equipment to ensure easy access if required.
Figure 2: Cargo hook
Source: ATSB
Lifting operations
Operations commenced after lunch with a check of the radios. The loadmasters had VHF radios in their helmets, which they used to communicate with each other at the drill site and with the helicopter pilots. The pilot of HUE conducted the first lift and, having requested to start with a light load, moved an 800 kg load to the drill site with no issues. Loadmaster 1 conducted all radio communications with the pilot at the drill site. He reported that when the helicopter was clear of all obstacles along the approach path, he advised the pilot and then gave directions to position the load where it was required, with clear advice of the height of the load above the ground.
It was reported that one load carried by the AS350B3 was spinning on arrival at the drill site. In response, the pilot touched the load to the ground away from the loadmasters to stop the spin. The helicopter then lifted the load off the ground to about knee height and the loadmasters manoeuvred the load to its position on the site while directing the pilot.
Accident load
After moving two lighter loads, the pilot of HUE requested a heavier load be connected. The loadmaster selected one of the drill rod racks, weighing about 1,200 kg, and connected the shackle to the hook. As the load lifted, it was slightly uneven and the loadmaster instructed the pilot to return the load to the ground, so he could re-adjust the slings. The pilot lowered the load and placed the hook on the load. After adjustment to the sling, the load lifted evenly and was flown to the drill site (Figure 3).
Figure 3: Images showing the occurrence load during departure from loading site
The image on the left shows that on departure the load was slightly uneven, the image on the right shows the load after loadmaster had adjusted the slings.
Source: Helicopter Operator A, annotated by the ATSB
As the helicopter approached the drill site, the pilot contacted the loadmasters and advised them that he was carrying the drill rods. Loadmaster 1 told him that the load was to go to a different area of the site and advised that the wind had dropped to around 3–5 km/h (0.5–1.5 kt). Loadmaster 1 subsequently told the pilot that they could see the helicopter and gave him advice on directions and distance to run to the drill site. He then advised the pilot he could descend, calling out the load’s height above the ground. The loadmasters began to approach the load when it was at about 7 m above the ground. Loadmaster 1 later advised that the plan was to lower the load to touch the ground and then raise it to knee level before moving it to its final resting position. Both loadmasters were reportedly careful to maintain clearance with the area under the load and stood at 45° to the load. They were both on the same side of the load. It was reported that the load was steady as it was flown in to the drill site.
The load was moved very slowly down to an area having an estimated 10˚ slope, with loadmaster 1 being downhill of loadmaster 2. Loadmaster 1 observed loadmaster 2 step toward the load, reach up, take hold of the tagline and immediately step back out to regain their 45˚ spacing. Loadmaster 1 reported that the load was about 5 m above the ground at this stage and the pilot reported that the end of tagline appeared to be near the ground.
Loadmaster 1 reported that as loadmaster 2 returned to their position, the slight forward motion of the load stopped and the load moved back slightly towards the rising ground. As the load moved back, the load detached unexpectedly from the hook.
It was reported that as the load fell, it seemed like one end of the load fell faster than the other and after it struck the ground, the load either bounced or pivoted around. Both loadmasters had to scramble backwards away from the load but the movement resulted in loadmaster 2 being struck by the drill rods and knocked to the ground under the load.
The pilot reported that he felt the helicopter ‘pop up a bit’ and thought that a sling had snapped as he had not released the load. Loadmaster 1 advised that he did not hear the ‘clack’ sound associated with the solenoid release of the hook (see the section titled RemoteCargo hook). He advised that the sound of the solenoid activation was audible over the helicopter noise and while wearing a helmet.
Loadmaster 1 spoke to the helicopter pilot on the radio and advised him that the sling had not separated, the hook was useable and to bring the helicopter back to lift the load. The pilot re‑positioned the helicopter and loadmaster 1 re‑connected the load, which was then lifted off the seriously injured loadmaster.
Remote cargo hook
The remote cargo hook used by the operator of HUE was a TALON 6K half-cage cargo hook (Figure 2). This was the first operational use of this hook following a recent overhaul and was also the first time the helicopter (HUE) was used with this long line and remote hook combination.
The load beam on the remote cargo hook can be made to release by two methods:
a pilot-activated switch on the cyclic, which activated a solenoid in the hook to release the load beam
a manual release on the hook itself.
The hook and long line inspections conducted prior to the flight, included a number of activations of both of these release systems.
The pilot advised that, due to a previous injury to his hand, he had to deliberately move his hand to the top of the cyclic and move the switch sideways to activate the hook. As such, unintended load release by that mechanism was considered very unlikely. The ATSB viewed video footage of the helicopter pilot operating the switch at the top of the cyclic, which supported that conclusion.
The keeper was designed to allow items to enter the hook throat but not return. It opened toward the inside of the load beam and had a spring-loaded automatic return to the closed position.
Loading equipment examination
The slings, shackle and hook were examined by the ATSB. The inspection of the slings determined they were intact. To check that the load had not released through dynamic rollout,[2] the ATSB ensured that the hook and shackle combination did not allow the shackle to pass the end of the load beam. The cargo hook owner’s manual specified that the shackle used with this hook should have an inside diameter less than 11.4 cm. The internal diameter of the shackle used was 5.5 cm. A physical examination of the hook was conducted and it was determined that the manual release and the keeper worked as expected. The ATSB did not dismantle the hook or connect the hook to an electrical supply.
The ATSB examined video footage of the helicopter lifting the load from the loading site. It showed that the ‘D’ shackle was behind the keeper (Figure 4) when the helicopter departed and that the load was evenly balanced as the helicopter flew towards the drill site (Figure 3).
Figure 4: Image shows that the ‘D’ shackle was behind the keeper
The image shows that on departure after the load had been adjusted, the ‘D’ shackle was behind the keeper.
Source: Helicopter operator A, annotated by the ATSB
Electromagnetic interference
The ATSB also considered whether electromagnetic interference (EMI) could have resulted in the inadvertent release of the load. While this accident occurred in an area which has high voltage power lines from the Tumut 3 power station, the aircraft was about 35 km from the power station and 10 km from the closest high voltage power lines. Research suggests that magnetic radiation returns to normal levels at about 150 m from power lines.
A licenced aircraft maintenance engineer inspected the electrical system used on the helicopter to control the hook release mechanism and they reported that the system was working as expected. It was reported that there were no exposed wires within the system that could have resulted in a short circuit if exposed to electromagnetic interference from equipment in the aircraft. The helicopter operator also reported that the system has not had any issues with the hook release system since the accident.
Procedures used for this operation
The ATSB reviewed the procedures used by the different operators involved on the project on the day. The lead contractor had conducted a risk assessment of the overall project, which involved all of the contractors involved.
Operator A had completed a helicopter lift plan for the day and a safe work method statement that identified hazards and the mitigations for lifting operations. There were a number of areas in the procedures indicating that no one should be located below the suspended load. The procedures also specified that people should not be within the ‘crush zone’ but did not identify where the crush zone was. The operator advised that the crush zone was dependent on a number of job-specific variables, including the load shape and size, and the length of sling required. While there was no specific section in the safe work method statement to prompt this discussion, the loadmasters worked together to rig the loads, adding tag lines where required, and so were aware of the individual load’s size, shape and aerodynamic stability.
Safety analysis
The ATSB considered a number of inadvertent load release mechanisms, including:
the pilot release system
dynamic rollout
failure of the manual load release
electromagnetic radiation
failure of the hook mechanism.
A previous injury meant that accidental release by the pilot was unlikely and the loadmaster did not hear the audible ‘clack’ of the solenoid, associated with operation of the pilot‑activated release.
The shackle was the appropriate size, to ensure a dynamic rollout would not occur. The video footage shows that the ‘D’ shackle was securely behind the keeper as the helicopter departed from the loading area.
While flying in an area of electricity production, the helicopter was 35 km from the closest power station and around 10 km from the closest power lines. The wiring was also checked and there were no bare or loose wires in the system. If the load had released through EMF activation of the release system, the loadmasters would have heard the ‘clack’ of the solenoid releasing.
There were no indications that the remote hook release mechanism was faulty after the previous overhaul and the pilot and loadmasters conducted an operational check of the mechanism before operations began on the day. It also successfully lifted the two previous loads and lifted the load off the loadmaster after the incident. In addition, the manual release mechanism operated correctly at the ATSB facility and an examination of the hook release electrical system in the helicopter did not reveal any faults. Despite this, a transient hook fault that resulted in an inadvertent release of the load could not be ruled out.
In summary, based on the available evidence, the mechanism that led to the release of the load could not be determined.
Immediately prior to the accident, the load was being positioned without needing to be adjusted. The plan was that it would touch the ground and then be lifted to knee height before being moved to its final position. Therefore, being in the vicinity of the load when it was above head height was an unnecessary risk.
When the load released, one end fell first and there was likely a movement back toward the rising ground. The loadmasters were reportedly standing to the side and at 45˚ angles from the load, but they were still close enough for one of them to be struck when the load pivoted.
The procedures and briefings for the operation contained several references for individuals not to place themselves in a dangerous position with respect to the load. While the extent of the crush zone was not defined in general, there were a number of variables unique to each job that made this difficult. The opportunity to discuss these aspects was during the briefing, although there was no discussion on the specific loads in this instance. Despite this, the loadmasters did discuss and adjust the different loads, adding tag lines where required. This would imply they were aware of the load size, weights and aerodynamics of specific loads for this job.
ATSB comment
In response to a previous accident, CASA released Airworthiness Bulletin, AWB 25-006 Issue 2, which provided advice to operators involved in sling load operations. While not directly relevant to this occurrence, it details important information relating to external sling load operations. This included information related to the inadvertent release of the load through the use of the incorrect shackle size and electromagnetic radiation (EMI).
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The load released from the hook unexpectedly for reasons that were not determined.
The loadmasters were not maintaining a safe distance from the load. Their positioning, in combination with the significant movement of the load as it contacted the ground, resulted in the loadmaster being struck and seriously injured.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
As a result of this accident, all the contractors jointly reviewed the processes used on this project. They determined that the existing documentation contained sufficient warning for personnel to not enter the ‘crush zone’ or ‘work under loads’, but also identified enhancements to the existing processes. This included a control that removed all people (including loadmasters) from the receiving area where there was no requirement for precision in the placing of the load and increased controls where a precision placement of the load was required.
Helicopter operator who supplied the loadmasters
Operator A advised the ATSB that they have reviewed their own safe work method statement and made changes including identifying a ‘dynamic exclusion zone’[3] under the moving helicopter. Recognising that the zone may vary due to a number of variables, the intention is that specific guidance will be provided as part of pre‑activity briefings.
Lead contractor
The lead contractor is overseeing a range of initiatives, including a behavioural safety review of the project with the intention to implement an appropriately designed program to positively influence behaviours across their projects.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the Australian Transport Safety Bureau (ATSB) to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
On 6 February 2018, the ATSB commenced an investigation into an aircraft loading event involving a Qantas Boeing 737, VH-VYE, at Brisbane Airport, Queensland that occurred on 1 February 2018.
During takeoff, the first officer, in their role as pilot flying, noted that the aircraft rotated at a slower rate than expected with a resultant higher than normal initial climb speed. The crew later observed a large tour group of children/adolescents onboard, seated together primarily aft of the over wing exits. The crew did not know the age of the passengers in the group or if they were recorded correctly for weight and balance purposes.
The ATSB obtained additional information from the operator that confirmed a tour group of 96 passengers was onboard. The age of the group ranged between 14-16 years old, which classified them as adults in the operator’s load control system. The operator confirmed that the loading, take-off performance figures, and speed/trim settings were correct for the conditions of that flight. The operator noted however that it was possible the positioning of the tour group of adolescents, with slight frames, likely affected the feel of the aircraft on rotation. The operator and pilot confirmed the aircraft was at all times controllable, however increased backpressure was required to rotate the aircraft.
The ATSB reviewed the additional information provided by the operator into this occurrence as well as information relating to previous loading occurrences involving the operator. Based on this review, the ATSB considered it was very unlikely that further investigation would identify any systemic safety issues. Consequently, the ATSB has discontinued this investigation, but will continue to monitor loading occurrences involving all operators.
____________ The information contained in this web update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this web update. As such, no analysis or findings are included in this update.
Initial summary
The ATSB is investigating a loading event involving a Boeing 737, VH-VYE at Brisbane Airport, Queensland, on 1 February 2018.
During takeoff, the aircraft rotated at a slower rate and required a high initial climb speed than normal. The crew detected that a number of child passengers had been incorrectly recorded as adults for weight and balance purposes.
As part of the investigation, the ATSB will interview airline staff, review recorded data, and gather additional information.
A final report will be released at the end of the investigation.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify those affected and seek safety action to address the issue.